The synergy of orthodontics and myofunctional therapy
Dr. Maria Sokolina
ADD and ADHD in children
Drs. Peter J. Catalano and John Walker
Single visit regenerative endodontics using the GentleWave ® Procedure
Dr. Lauren Tink
Scan for exclusive offers!
pulpdent.com/activademo
MERGING RESTORATIVE AND PREVENTIVE DENTISTRY
ACTIVA™ KIDS is an esthetic, BioACTIVE resin restorative that stimulates apatite formation and the natural remineralization process with release and recharge of calcium, phosphate and fluoride. It is an opaque white shade ideally suited for pediatric dentistry. Scan the QR code to schedule an in-person or virtual demo today.
Photos courtesy of Dr. Leon Katz
Life-changing diagnostics
What a journey you are about to embark on with each page turn of the fall issue of this magazine! I was fortunate enough to be asked to write the intro letter to what has proven to be a leading source of information in pediatric dentistry. Where else are you finding up-to-date research on pediatric sleep-related breathing disorders (SRBDs), myofunctional therapy, and restorative techniques? We are long overdue to have OSA/SRBDs at the forefront of our conversations in pediatric dentistry.
Recognizing the signs
While dentists are not the parents’ first-line consult for ADHD/ODD conversations, we should be, because what you will find in this population of patients is underdeveloped jaws, large overjets, mouth breathing, and extremely sad children.”
I am constantly verbalizing the need for dentists to recognize the signs of adult and pediatric SRBDs. I feel it’s fairly well known now that snoring, tooth grinding, tongue ties, and mouth breathing should equate to more questions from providers regarding a child’s sleep. However, behavioral disorders are not translating well as being a symptom of sleep apnea for dentists to consider, one of which I want to discuss today: Oppositional Defiant Disorder (ODD). While dentists are not the parents’ first-line consult for ADHD/ODD conversations, we should be, because what you will find in this population of patients is underdeveloped jaws, large overjets, mouth breathing, and extremely sad children.
Dr. Kalli Hale
I have treated numerous children with ODD over my career, and they nearly all present the same — they will not make eye contact with me, they will not talk to me, and they have not only fear, but intense frustration for life. The parents are completely
Kalli Hale, DDS, MPH, D.ABDSM, D.ABSB, is passionate about how our teeth affect our systemic health — the link between chronic jaw infections, periodontal disease, and subsequent heart problems. Her training in obstructive sleep apnea has transformed both her personal and professional career. Dr. Hale is a Clinical Advocate for VIVOS Therapeutics and works with dentists around the country to develop clinical protocols for the treatment of mild-to-moderate obstructive sleep apnea and sleepdisordered breathing. Her work in pediatric expansion and sleep-disordered breathing catapulted her speaking career, and she lives by the slogan, “We have to stop getting it wrong, for our kids.” She is faculty for the Dental Success Network, a key-opinion leader for Candid, and the Chief Dental Officer for Toothpillow. She travels monthly across the U.S. and abroad to teach dentists about Obstructive Sleep Apnea. Follow her on social media @theairwaycentereddentist. Learn more about her sleep mentorship program at https://sleepwelljourney.com/.
distraught and end up in my office after exhausting years of medical treatments, unsuccessfully. To give an example, a recent patient presented at 6 years old, struggling intensely with ODD and bedwetting. This small child was being treated with Desmopressin for bedwetting, which the parents had recently discontinued on their own because of its lack of efficacy. The only reason the mother sought my opinion was because she happened to see a reel on Instagram discussing myofunctional therapy and bedwetting! She was absolutely shocked to know there could be a correlation between those two topics, which led her to seek a consult with a myofunctional therapist, who then referred her to me. Imagine her heartbreak at the number of medical visits, psychology appointments, money spent, and dead ends reached, only for a social media algorithm to be how she found this information. Her child had maxillary and mandibular hypoplasia, a 7 mm overjet, and a tongue tie; the sleep study revealed an AHI of 4 with hypoxemia and numerous wakes. If we are medicating our children, there should not be a stone unturned to ensure we have the right diagnosis! In cases of ODD, a sleep study should be prescribed to rule out obstructive sleep apnea.
As a result of reading this message, I hope you will learn more about attention and behavior disorders, so you can educate your patients and offer the most important appointment they will have: a dental airway exam. As dentists, we need to do our part to decrease the burden of pediatric behavior disorders by recommending sleep studies and airway exams to rule out OSA/SRBDs, which will be a life changing diagnostic test for these patients.
Respectfully,
Kalli Hale, DDS, MPH, D.ABDSM, D.ABSB
Dr. Jennifer Villalta is an active advocate for pediatric patients
Cover image of Dr. Jennifer Villalta courtesy of NuSmile.
Dr. Maria Sokolina
Dr. Lauren Tink treats an anxious
• No gr i t, no st icki ness, no tac ki nes s
• No c lumpi ng…instead an easi l y sp readab l e m ater i al that , like a l ubricant , will mi grate into c rev i ce s
• A materia l that w ill stay on t he brush until i t is sp read on teet h
• App l y wet or d ry… .m uch eas i er for children
• Pl easant B er r y and Mint flavo rs…and an Unfla v ored that tastes j ust li ke t he pat i ent ’ s sa liv a…no taste !
• No more clogged e v acuat i on lines… . and many more benefit s
ADD and ADHD in children: the answer is right in their nose
Drs. Peter J. Catalano and John Walker discuss the consequences of sleep-disordered breathing and how dentists can help
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager
Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Sales Assistant & Client Services
Melissa Minnick melissa@medmarkmedia.com
PRODUCT PROFILE
Breakthrough: HealthyStart introduces new innovative technology of the FasTrack system ............. 22
PRODUCT SPOTLIGHT Optimizing pediatric dental care in the OR
Shaun Valentine, VP of Product at Zyris Isolite, visits the Carmel Ambulatory OR Center with Dr. Ana Vasquez of Fishers Pediatric .............................................................. 24 PRODUCT PROFILE A truly “Universal” bonding agent Kerr Dental’s OptiBond™ Universal 360 streamlines workflows ......................................... 26 PRODUCT PROFILE How I overcame dreading patients with braces as a hygienist
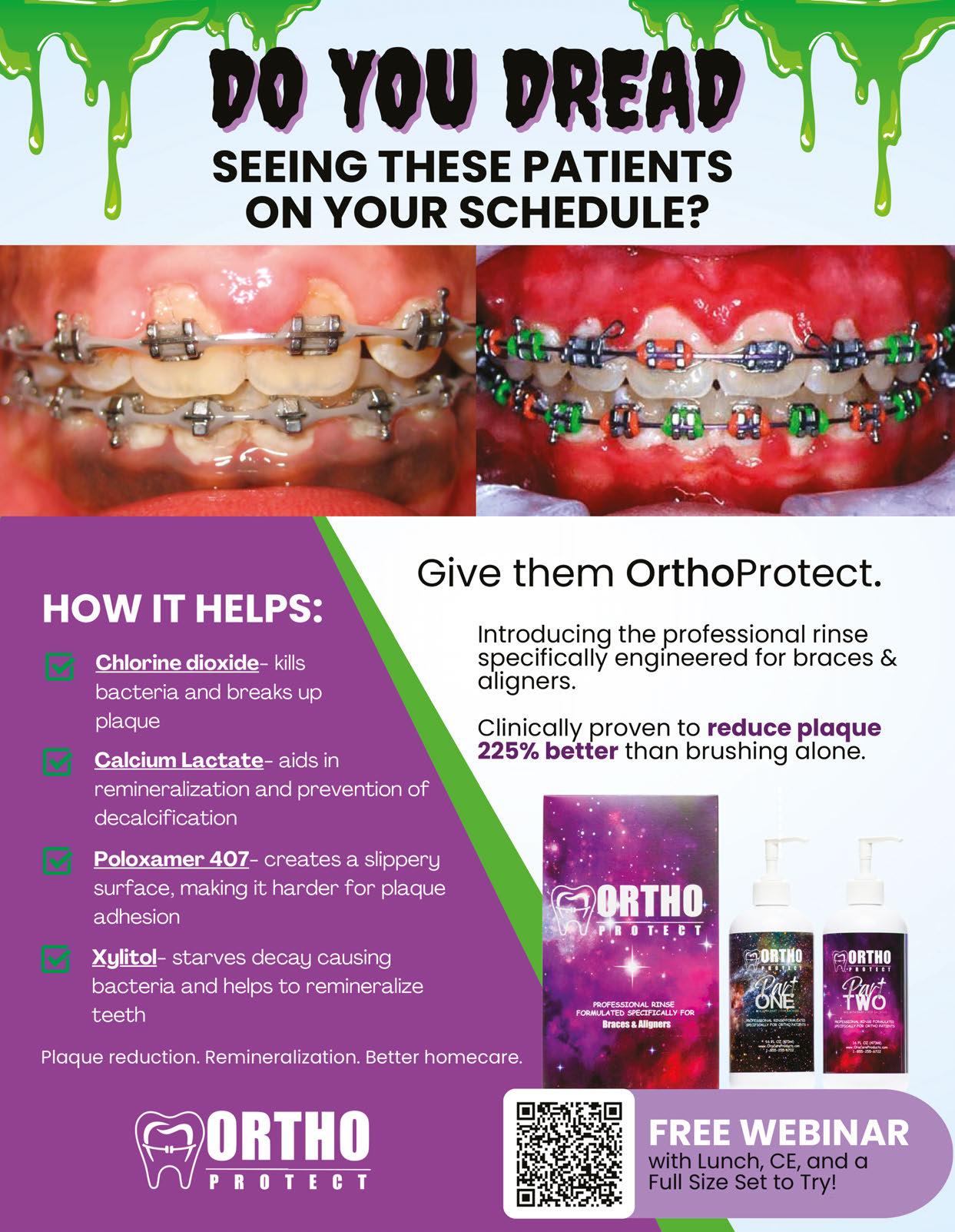
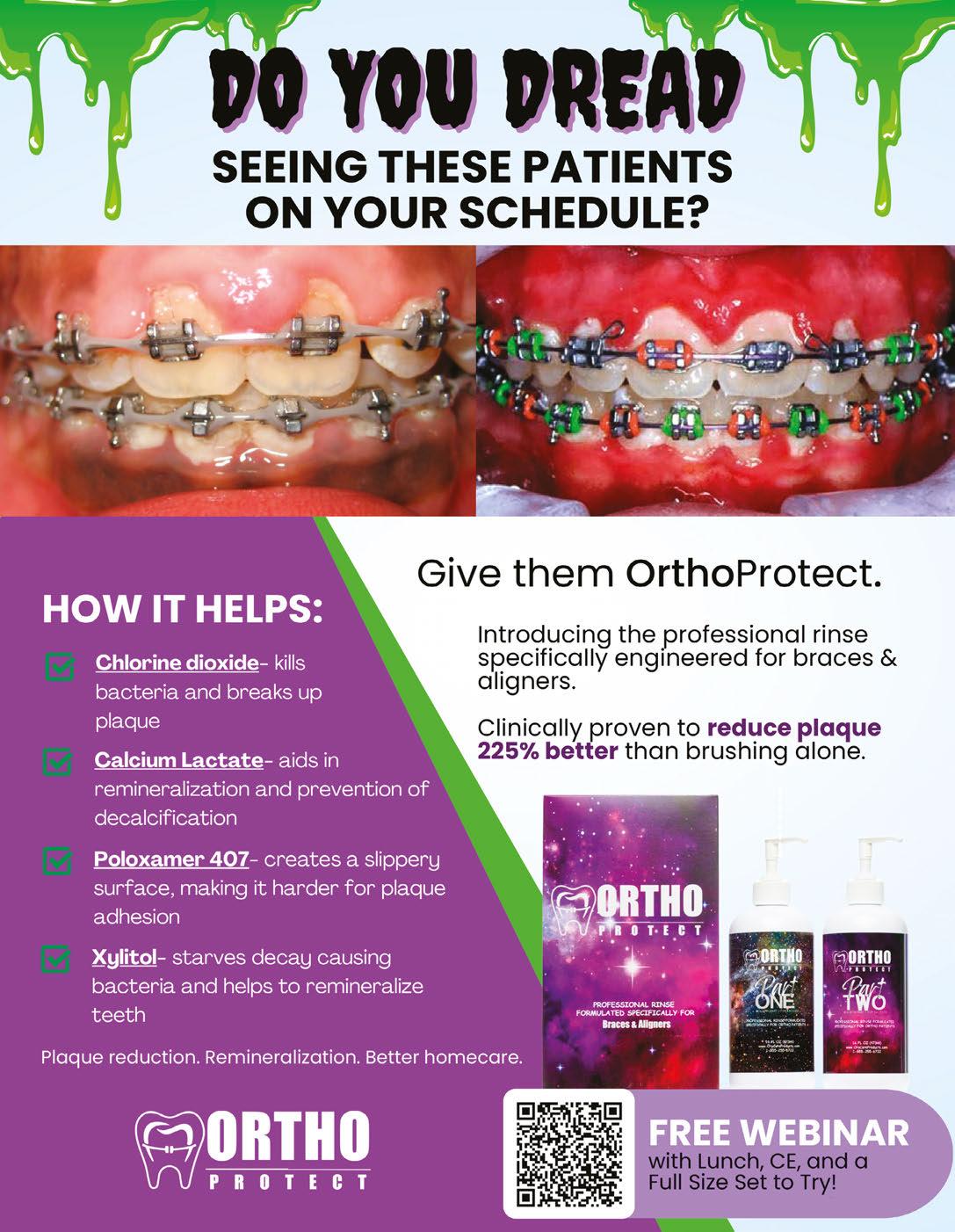
Kristin Sheridan, RDH, discusses a mouth rinse that promotes patients’ oral health ................... 28
PROFILE Why thousands of pediatric specialists have quietly partnered with IDSOs
Chip Fichtner discusses the benefits of a large silent partner 30
Social Media Manager Felicia Vaughn socialmedia@medmarkmedia.com
Website Support
Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC
15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260
Tel: (480) 621-8955
Toll-free: (866) 579-9496
www.medmarkmedia.com
www.pediatricdentalpractice.com
SimpliShade™ Self-Adhesive Flow
“By changing nothing, nothing changes.”
Change is hard — some days it feels like fate is not satisfied with any stable situation that makes us comfortable and secure. Sure, no one can dispute the serenity of “business as usual” in the midst of ever-changing world issues, politics, and everyday craziness. Instead of losing sleep or stomach lining over change, let’s consider the positive aspects of being open to expanding our comfort zones, living in the moment, and having a mindset of “faith over fear.” As the title quote from Tony Robbins suggests, you have to build up some momentum in order to actually get somewhere. Let’s hear from some successful and inspirational people on how change can bring positive movement to our lives.
Neurologist and psychologist Viktor E. Frankl said, “When we are no longer able to change a situation, we are challenged to change ourselves.” Some people just need a bigger push to get moving. Taking the easy route and sticking with “the familiar” is only possible until the stress of the known outweighs the fear of the unknown. So, sticking with only the activities or mindsets that are within your safety zone will eventually leave you watching others who have the ambition and confidence to move forward. You don’t want to look around in a few years and see your friends and peers busy and fulfilled with new possibilities that can change your community or your world. There is a lot of competition out there, and being a pioneer or game changer may be a challenge at first, but will head off the future frustration of a stagnating life.
going to get the best fruit.” Overcoming fear of making the wrong decision or failing can feel daunting. But, there are a lot of ways to build your confidence, such as talking to friends, mentors, experts, attending conferences, reading MedMark publications, and listening to those who bring you inspiration. There will be learning curves and maybe even some speed bumps, but most times, innovation will lead to new and exciting ways to grow.
Our fall issue is filled with innovation and information to create productive change. In our Cover Story, Dr. Jennifer Villalta redefines pediatric dentistry with innovation, compassion, and esthetic excellence that she achieves, in part, thanks to NuSmile crowns. In our Case Study column, Dr. Lauren Tink shows how GentleWave can be used as an efficient endodontic treatment option for cleaning and disinfection of the root canal on an anxious pediatric patient. Also, Dr. Maria Sokolina shows how orthodontics and myofunctional therapy can combine to treat sleep apnea.
Lisa Moler Founder/Publisher, MedMark Media
World famous performer Robin Williams said, “No matter what people tell you, words and ideas can change the world.” Don’t leave your success to chance. Change your ideas into action. Innovation will create a happier you, family, and work life. When you embrace change, the benefits will spread throughout your world!
To your best success,
Actress Sarah Parish noted, “Living with fear stops us from taking risks, and if you don’t go out on the branch, you’re never
Lisa Moler Founder/Publisher MedMark Media
The Problem: Mouth breathing can lead to underdevelopment of the upper jaw and restricted forward growth of the lower jaw. This can cause crowding and restriction of the airway. Left untreated, the child may develop Sleep Disordered Breathing (SDB).
The Solution: Whole team education and training from Nexus.
Helping you grow healthy kids. Join us: nexusdentalsystems.com/pediatrics/
Standing out by delivering an outstanding experience for patients and parents
Dr. Jennifer Villalta is an active advocate for pediatric patients
Nestled within the bustling streets of Southern California’s Playa Vista, Dr. Jennifer Villalta is redefining pediatric dentistry with a blend of innovation, compassion, and a keen eye for esthetic excellence. The Baby Teeth Studio practice isn’t just a dental office; it’s a sanctuary where children rediscover their self-esteem, parents discover peace of mind, and smiles are transformed.
“Nobody does it that way”
That’s what the office design group of one of the world’s largest dental products distributors told Dr. Villalta when she shared her dreams for her new pediatric dental practice. What they didn’t know is that Dr. Villalta had never blindly accepted the status quo or given in when facing adversity. She was firmly committed to her vision for how pediatric dental patients and their families should be treated, and so she simply found another design firm that shared that vision.
An unconventional entrée into dentistry — for an unconventional dentist
Dr. Villalta’s road to becoming a dental practice owner and industry thought leader was, to say the least, a road less travelled. She was introduced to the dental profession at the age of 16, when she started working as a dental sterilization technician. Within a year, she obtained her Registered Dental Assistant (RDA) license. She began working full-time while taking night classes at Santa Rosa Junior College. She then transferred to UCLA, where she was awarded an academic scholarship and earned a B.S. degree in Physiological Sciences. While attending UCLA, she continued to work as a RDA at a federally qualified health center (FQHC) serving children from under-resourced
Dr. Jennifer Villalta is a board-certified pediatric dentist known for her exceptional, personalized care and dedication to making children smile. Dr. Villalta started her career working full-time at an orthodontic practice while attending Santa Rosa Junior College in the evenings. Her determination led her to UCLA on an academic scholarship, where she earned a B.S. in Physiological Sciences. After a gap year dedicated to humanitarian missions with the U.S. Navy and other military branches, and backpacking through Southeast Asia and Europe, she completed her dental education at the UOP Arthur A. Dugoni Dental School. She then obtained a Pediatric Dental Specialty certificate and a Master of Public Health from UCLA. Bringing her rich experiences and deep compassion to her practice, Dr. Villalta inspires her young patients and their families with health and confidence. Celebrating over 20 years in the field, she proudly owns a boutique startup dental office, fulfilling her dream of creating a positive impact in pediatric dentistry.
Disclosure: Dr. Villalta serves as a Key Opinion Leader for NuSmile.
Dr. Villalta in her boutique dental office she always dreamed of
communities. There she noticed that not all pediatric patients had esthetic options for restoring their teeth as most patients had silver crown full-coverage restorations, even for anterior teeth.
Dr. Villalta went on to complete her residency at UCLA, where she hoped to learn more about esthetic restorative options for her young and often economically disadvantaged patients. However, because financial and educational limitations prevent most residency programs from being able to teach esthetic
dentistry, Dr. Villalta knew she would have to seek this education on her own.
To that end, she attended the California Society of Pediatric Dentistry’s Annual Conference, where she first encountered NuSmile®. “NuSmile’s RESTORE workshop really opened my eyes to advanced techniques beyond stainless steel crowns and fillings,” Dr. Villalta recounts. The workshop exposed her to the technical aspects of modern pediatric dentistry and to a community of like-minded professionals eager to push the boundaries of traditional care. “It felt like a mini-residency,” she recounts, “and equipped me with not just new clinical skills, but a mindset focused on patient self-esteem, comfort, and esthetics.”
Dreaming big — and making the dream come true
With a little over a year of practice experience under her belt, Dr. Villalta — “Dr. Jen” to her patients and their parents — founded The Baby Teeth Studio as a place where dental care transcends the technical and embraces the artistic. “Most people, especially kids, hate going to the dentist,” she asserts. “So why not make them feel like they’re about as far away from a dental office as they could possibly be?”
She adds, “I serve a diverse population of patients, ranging from kiddos who live in foster care to kiddos with affluent parents who have high health IQs. One thing that connects all families is that they almost always prefer esthetic options for their kids.” The Baby Teeth Studio quickly became known for its ability to offer better esthetic alternatives in an upbeat environment.
Empowering parents with choices: the social media effect
Dr. Villalta’s impact extends far beyond her studio walls, thanks to her active presence on social media platforms like Instagram and TikTok. “I started sharing educational content online during the pandemic,” she explains. “It became a way to connect, educate, and empower parents to make informed decisions.”
Dr. Villalta’s commitment to esthetic dentistry is about dignity, not just appearance. She passionately advocates for using the best possible products to ensure that every child leaves her office with a smile they’re proud of.
One family’s experience highlights the transformative impact of Dr. Villalta’s approach. Xio’s mom stumbled upon Dr. Villalta’s TikTok page in a moment of desperation when searching for a way to restore her child’s smile and confidence after she had stainless steel crowns placed on her anterior teeth.
Upon Xio’s first visit to The Baby Teeth Studio, Dr. Villalta and her team immediately recognized the emotional toll the previous treatment had taken on the young girl. “Xio was
Dr. Villalta puts Brooklyn at ease prior to her procedure
Dr. Villalta connects with Xio and Brooklyn before their appointments
apprehensive, extremely nervous, anxious, and withdrawn,” Dr. Villalta remembers. “It was heartbreaking to see how much her selfesteem had been affected. Her parents mentioned Xio stopped smiling like she used to prior to the placement of silver crowns on her front teeth.”
We replaced SSC with NuSmile Zirconia Anterior Crowns. The transformation was incredible with her appearance, comfort, and confidence.”
Dr. Villalta devised a treatment plan that not only addressed Xio’s dental needs, but restored her confidence. “We replaced Xio’s stainless steel crowns with NuSmile ZR Anterior Zirconia Crowns,” she explains. “The transformation was incredible with her appearance, comfort, and confidence.” Xio’s mom also noticed an immediate change in her daughter. “She couldn’t stop smiling and showing off her new teeth,” she reports. She was also struck by the contrast between their initial traumatic experience at the prior dental practice, which she described as “literally like an assembly line,” and the personal, compassionate treatment they received at The Baby Teeth Studio.
Xio’s sister Brooklyn soon became a patient as well. “At first, she was just as anxious and scared as Xio had been,” recalls Dr. Villalta. In keeping with her philosophy of tailoring treatment to each patient’s unique needs, Dr. Villalta readily accommodated Brooklyn’s parents’ requests to avoid stainless steel crowns, general anesthesia, and anything else that might further traumatize her. She chose a new posterior crown from NuSmile called BioFlx® due to it’s esthetics and ease of placement to complete Brooklyn’s treatment with the use of nitrous over multiple visits. According to her mom, “Brooklyn now loves coming to the dentist, so much so that she pretends to be Dr. Jen when she and her sisters play dentist at home.”
The power of community and transparency
Beyond clinical excellence, Dr. Villalta stands out for her transparency and community engagement. Her robust social media presence, including her popular “Tuesday Tips” collaboration with NuSmile, has become a trusted resource for parents and dentists seeking dental advice and insights. Her postings are not just informative but empowering, demystifying dental procedures and fostering a sense of community among parents and dental professionals alike.
As a NuSmile Key Opinion Leader, she is able to learn about the latest products on the market from the other members of the NuSmile family of pediatric dentists around the world. “I’m so fortunate to be able to get their expert opinions on what works, how they use it, how their patients like it, and what the ROI is,” she says. And she repays the favor by sharing her insights as well.
Dare to be different — and to make a difference
“My whole life, I’ve been told, ‘You’re too over the top,’ ‘You can’t talk that way’ and ‘You can’t dress that way,’” says Dr. Villalta. “Well, guess what? When you dare to be different, people might find it to be refreshing, fun, and appealing. And it helps you stand out from the crowd, which is what any dental practice — any business, period — needs to do.”
Dr. Villalta understands that many young dentists would like to have the autonomy that comes with running their own practice, but they’re afraid to make what feels like a risky leap. “I get it. I’m still scared every day,” she says. “But I’m so thankful that I can sleep well every night knowing that I’m providing the care I want, using the products I want, in the way I want for my patients and their parents. And in the morning,” she adds, “I can’t wait to get up and get to my practice.”
Conclusion
At The Baby Teeth Studio, having a range of restorative products plays a pivotal role in Dr. Villalta’s practice. “The versatility of NuSmile products ensures that we have tailored solutions for every child,” Dr. Villalta explains. “These products aren’t just about esthetics; they’re about functionality, comfort and self-esteem.”
As Dr. Villalta continues to expand her influence through social media and innovative dental procedures, her commitment to children’s dental health remains unwavering. “Every smile transformed is a testament to the power of choice and education,” she says.
In the ever-evolving landscape of pediatric dentistry, The Baby Teeth Studio stands out as a beacon of innovation and compassion. Dr. Villalta continues to comfort and empower patients, transform smiles, and redefine what it means to provide outstanding dental care for children. PD
Xio pre-op and 3-month post-op with NuSmile ZR Crowns
Xio (left) and Brooklyn (right) proudly showing their new smiles to the camera
How to submit an article to Pediatric Dental Practice US
Pediatric Dental Practice US is a peer-reviewed, biannual publication containing articles by leading authors from around the world. Pediatric Dental Practice US is designed to be read by pediatric dentists and GPs performing pediatric dental techniques.
Submitting articles
Pediatric Dental Practice US requires original, unpublished article submissions on pediatric topics, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,000 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Pediatric Dental Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to pediatric dentistry. Clinical and continuing education articles include an abstract of up to 250 words. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple)
Doe JF
Permissions
Doe JF, Roe JP
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased at any time.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to:
Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Single visit regenerative endodontics using the GentleWave ® Procedure: a pediatric case report
Dr. Lauren Tink treats an anxious pediatric patient using an efficient treatment
Introduction
Recent advancements in endodontic techniques have revolutionized our ability to manage pediatric patients with complex cases. Traditionally, cases with wide open apices presented significant challenges. These cases often required multiple visits in order to achieve optimal outcomes.
However, contemporary approaches have provided more efficient treatment options, leading to improved clinical results and patient satisfaction.
Apexification has been the treatment of choice for teeth with open apices, aiming to induce the formation of an artificial apical barrier. While effective, apexification has its limitations as there is no potential for further root development.1 The emergence of regenerative endodontics has offered a paradigm shift in the management of these cases.2 This technique not only addresses the underlying pathology but also allows for continued root growth, ultimately leading to a more functional and resilient dentition.3
The implementation of traditional pulpal regeneration protocols in pediatric patients can be challenging, especially in cases with limited cooperation. Conventional approaches often require multiple visits,4 increasing the burden on both the patient and the clinician.
Single visit regenerative endodontics, coupled with advanced disinfection techniques, have emerged as a promising solution. This approach requires fewer visits, allows for enhanced disinfection, and promotes optimal blood clot formation in the canal. By eliminating the need for multiple visits, single visit regenerative endodontics offers a patient-centered approach that prioritizes both clinical outcomes and patient comfort.
Lauren Tink, DMD, was born and raised in Montreal, Canada. She attended McGill University and earned her doctoral degree in 2014. Following graduation, Dr. Tink moved to New York City and furthered her training at NYU Lutheran Medical Center’s Advanced Education in General Dentistry residency program. Subsequently, she attended Nova Southeastern University where she earned her postdoctorate degree in Endodontics. During her training at Nova, Dr. Tink participated in a surgical externship in Barcelona, Spain at the Universitat Internacional de Catalunya, performing a variety of specialized surgical procedures. She is currently in private practice at Weston Endodontic Care in Weston, Florida.
Disclosure: Dr. Tink reports no financial or other interests regarding any of the products mentioned in this article.
Figure 3 (left): Preoperative CBCT scan of tooth No. 20 showing evidence of a wide open apex. Figure 4 (right): Bleeding noted in the canal immediately after removing the GentleWave platform
In this case report, we present a 10-year-old patient with a wide open apex and a dens evaginatus.5 This case was successfully managed with single visit regenerative endodontics using the GentleWave® System (Sonendo®).6 The outcomes demonstrate not only the feasibility but also the efficacy of this approach in achieving favorable clinical and radiographic results in pediatric patients.
Case report
A 10-year-old female patient with a history of swelling and pain associated with tooth No. 20 was referred to our office. The patient exhibited severe dental anxiety. Upon clinical evaluation, a dens evaginatus was noted on the occlusal surface of the tooth (Figure 1). The tooth was sensitive to percussion, palpation, and bite stick while cold testing yielded no response. A periapical radiograph and CBCT scan (Carestream 9600) revealed a wide open apex and evidence of apical periodontitis, leading to the
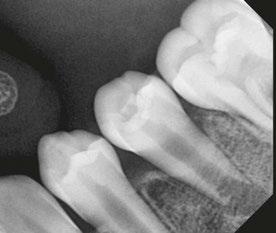
Figure 1 (left): Dens evaginatus noted on the occlusal surface. Figure 2 (right): Preoperative periapical radiograph of tooth No. 20 showing evidence of apical periodontitis and a wide open apex
diagnosis of a necrotic pulp and symptomatic apical periodontitis of tooth No. 20 (Figures 2 and 3).
Given the presence of a wide open apex, traditional root canal therapy was not possible in this case. Treatment options such as apexification and regenerative endodontics were discussed along with the risks and benefits of both modalities. With apexification, placing the apical plug would present a challenge since there would be a risk of extruding the material past the apex. In addition, this option would present no opportunity for increasing the root width and length. For these reasons, it was determined that pulpal regeneration would be the ideal approach. The goals of the pulpal regeneration procedure would include facilitating root formation while eliminating apical periodontitis and achieving an asymptomatic and functional outcome for the patient. Traditionally, pulpal regeneration would be completed over the course of two visits with interim calcium hydroxide or triple antibiotic paste. However, this 10-year-old patient was severely anxious. Her parents requested for her to be treated under IV sedation. By maintaining the traditional protocol for pulpal regeneration, the patient would have to undergo IV sedation twice at two separate visits.
scan showed no evidence of apical periodontitis (Figure 10). Thickening of the radicular walls was noted, and a calcific barrier was noted to be forming mid-root. She will continue to be recalled in another 6 months to continue monitoring the healing of this case.
Summary
An alternative approach of single visit regenerative endodontics was employed utilizing the GentleWave system to facilitate disinfection and blood clot formation. After the IV was placed, local anesthesia was administered using 3% mepivacaine. No vasoconstrictor was used so as not to inhibit blood flow to the tooth. After isolating with a rubber dam, the tooth was accessed. A necrotic pulp was noted. No endodontic files were used for instrumentation. Flowable dam material (EndoSequence® , Brasseler USA) was used to build a platform and create a seal for the GentleWave CleanFlow™ procedure instrument (Sonendo). The full GentleWave cycle was run using NaOCl and EDTA as irrigants with a final water flush. Once the platform was removed, bleeding was immediately noted in the canal (Figure 4). A microsuction tip was used to control the bleeding to below the level of the CEJ. A piece of collagen tape (HeliCote® Collagen Dressing by Integra Miltex) was placed over the blood clot (Figure 5). Bioceramic putty (EndoSequence BC RRM Fast Set Putty) was placed on top of the collagen tape (Figures 6 and 7). The chamber was then etched and bonded and restored using Luxacore build up material (LuxaCore Z Dual Cure) and light-cured resin composite (Clearfil Majesty™ Composite, Kuraray) (Figures 8 and 9).
The patient was recalled 6 months later and showed promising results. She was asymptomatic and functional. The CBCT
In conclusion, this case report highlights the successful management of an anxious pediatric patient with a wide open apex using single visit regenerative endodontics, incorporating the GentleWave procedure. By circumventing the need for multiple visits and integrating advanced disinfection techniques, this approach not only expedited treatment but also optimized disinfection and facilitated blood clot formation in the canal. The favorable clinical and radiographic outcomes observed underscore the efficacy and feasibility of single visit regenerative endodontics as a patient-centered approach for addressing challenging cases in pediatric patients with limited cooperation and severe dental anxiety.
PD
REFERENCES:
1. Rafter M. Apexification: a review Dent Traumatol. 2005 Feb;21(1):1-8.
2. Diogenes A, Ruparel NB, Shiloah Y, Hargreaves KM. Regenerative endodontics: A way forward. J Am Dent Assoc. 2016 May;147(5):372-380.
3. Lin J, Zeng Q, Wei X, Zhao W, Cui M, Gu J, Lu J, Yang M, Ling J. Regenerative Endodontics Versus Apexification in Immature Permanent Teeth with Apical Periodontitis: A Prospective Randomized Controlled Study. J Endod. 2017 Nov;43(11):1821-1827.
4. American Association of Endodontists. AAE Clinical Considerations for a Regenerative Procedure: Revised 5/18/2021. https://www.aae.org/specialty/wp-content/uploads/sites/2/2021/08/ ClinicalConsiderationsApprovedByREC062921.pdf. Accessed May 17, 2024.
5. Lerdrungroj K, Banomyong D, Songtrakul K, Porkaew P, Nakornchai S. Current Management of Dens Evaginatus Teeth Based on Pulpal Diagnosis. J Endod. 2023 Oct;49(10):1230-1237.
6. Sigurdsson A, Garland RW, Le KT, Woo SM. 12-month Healing Rates after Endodontic Therapy Using the Novel GentleWave System: A Prospective Multicenter Clinical Study. J Endod. 2016 Jul;42(7):1040-1048.
Figure 5 (left): Collagen tape was placed directly over the blood clot. Figure 6 (center left): Bioceramic putty was placed directly over the collagen tape. Figure 7 (center right): Periapical radiograph showing the placement of the bioceramic putty in the canal. Figure 8 (right): Restored access
Figure 9 (left): Immediate postoperative periapical radiograph of tooth No. 20. Figure 10 (right): 6-month recall CBCT scan showing no evidence of apical periodontitis and a calcific barrier forming mid-root
The synergy of orthodontics and myofunctional therapy
Dr. Maria Sokolina discusses a game-changer in long-term stability and sleep apnea treatment
Abstract
Orthodontic treatments often face challenges related to longterm stability. This article discusses the connection between orthodontic relapses and orofacial myofunctional habits, especially among sleep-breathing disorder patients. Recognizing this link, the author integrated myofunctional therapy (MFT) into orthodontic treatment. The combination of clear aligners and MFT not only improves orthodontic outcomes but also addresses related issues, notably in sleep-breathing disorders treatment. This holistic approach offers potential for enhanced orthodontic results and overall patient well-being.
Introduction
Having embarked on a journey in orthodontics with clear aligner therapy since 2002, I’ve had the privilege of witnessing numerous cases and their outcomes. Over time, I observed a recurring theme that left me both intrigued and concerned — the long-term stability of orthodontic treatments.1 Some patients adhered rigorously to retainers and still experienced relapse or changes in teeth position after several years, while others seemingly defied the odds, maintaining their results without retention.2 This inconsistency in outcomes piqued my curiosity.
Orofacial myofunctional therapy (OMT) has a rich history dating back to the early 1900s. It emerged as a response from the orthodontic field to restore normal muscle function, alleviating unintentional pressure on dental structures. OMT was initially developed by orthodontists with the goal of enhancing orthodontic outcomes and preventing relapses.
The roots of OMT trace back to the late 1800s when Dr. Edward Angle made a pivotal observation — he recognized that
Maria Sokolina, DDS, is founder and CEO of Harmony Dental Arts. She emigrated from Russia with her first medical degree and later received her DDS degree from New York University College of Dentistry. Upon graduation, Dr. Sokolina pursued specialized skills in different areas of dentistry such as implants, cosmetic dentistry, full mouth rehabilitation, and orthodontics. As part of her practice, Dr. Sokolina became an active explorer of the world of Dental Sleep Medicine, treating sleep apnea with dental appliances and myofunctional therapy. Dr. Sokolina is a lecturer and Diplomate of American Academy of Dental Sleep Medicine and a Board member of the American Academy of Dental Sleep Medicine as well as TEDx. Dr. Sokolina spends much of her professional time trying to spread knowledge with lectures about sleep, breath, and wellness among the general population as well as in the medical community. She may be contacted through her website at https://www. harmonydentalarts.com/.
issues such as mouth breathing and improper tongue resting posture played a primary role in hindering orthodontic results. However, the turning point came in the early 1900s with the pioneering work of Dr. Alfred Rogers.
Dr. Rogers, born in 1873 and a prominent orthodontist, made significant contributions to the field. He acknowledged not only the impact of dental issues but also the role of soft tissue dysfunction on the oral skeletal system. He was a distinguished figure, serving as the President of the American Association of Orthodontists (AAO) and playing a pivotal role in the formation of the American Board of Orthodontics.
Dr. Rogers was among the first to develop a treatment program focusing on orofacial muscular exercises. This therapy aimed to stimulate desirable growth in the maxillofacial region, which he termed “Myofunctional Therapy in Orthodontics.” As early as 1918, he began disseminating this concept through articles and presentations, including the annual meeting of the AAO.
Dr. Rogers emphasized that orthodontists should not solely concentrate on straightening teeth but must also consider the function of oral facial muscles. He asserted that alterations in the functional activity of the oral cavity could lead to malocclusion, thus highlighting the profound impact of muscular functioning on oral facial growth, development, and overall whole-body health.
This historical perspective underscores the enduring significance of OMT and its role in understanding the influence of orofacial myofunctional habits, including mouth breathing, on orthodontic outcomes and overall well-being.
The turning point in my exploration came when I delved into cases related to dental sleep medicine. During my initial evaluations of sleep apnea patients, I noticed a striking connection between their orthodontic history and their malocclusions. Issues such as crowding, spacing, open bites, Class II, and Class III malocclusions were prevalent among these patients.3 What intrigued me even more was the correlation between their malocclusions and their tongue, lip, and cheek function, especially during swallowing, as well as their breathing patterns. Most of these individuals weren’t even aware of how they breathed, and it became evident that their orofacial myofunctional habits were closely linked to their orthodontic relapses and the success of my sleep-breathing disorder treatment plans.
The myofunctional connection
As I delved deeper into this intriguing correlation, I began to understand the profound influence of orofacial myofunctional habits on the longevity of orthodontic treatment results. It was clear that addressing these myofunctional issues was paramount
to ensuring the stability of orthodontic outcomes. Furthermore, I realized that integrating myofunctional therapy into orthodontic treatment4 could offer a holistic solution to not only enhance the results of orthodontics but also to address a range of other concerns.
Embracing myofunctional therapy
To equip myself with the necessary skills and knowledge, I decided to pursue a myofunctional5 course from Myomentor Sarah Hornsby. Armed with this additional expertise, I could now offer my patients orthodontic treatment in conjunction with myofunctional therapy. This innovative approach aimed to increase the longevity of orthodontic treatment results,7 correct orofacial myofunctional habits, and tackle various related issues head-on.
Case presentation
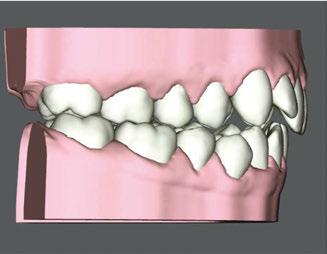
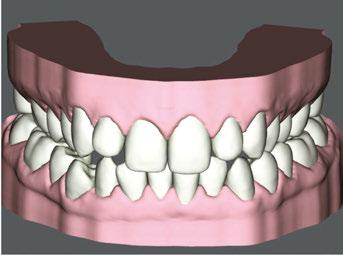
Patient J, a 39-year-old female, (Figures 1, 2, 3, 4, 5, 6) came to the office with concerns about difficulties chewing food and experiencing dry mouth upon waking up in the morning. Additionally, her partner was disturbed by her snoring. Upon examination, several issues came to light:
1. An open bite in the anterior region and a posterior crossbite
2. Breathing through the nose 10% of the time.
3. Lips and cheek muscles actively helping with swallowing food and drinks
4. Lips open 100% of the time
5. Tongue cannot maintain position on a spot, moves between teeth upon swallowing
6. Tongue thrust
7. Weak control over soft palate
Muscle tension around the temporomandibular joint (TMJ) was also evident5 as well as mandibular bilateral lingual torus as response to constant occlusal pressure applied during bruxism.
To address her concerns and provide comprehensive care, I presented a treatment plan that combined clear aligners with Myofunctional Therapy (MFT). The main goals of MFT for Patient J were as follows:
• Improving oral functionality: One of the primary aims of MFT was to enhance Patient J’s oral functionality. This included improving her ability to chew food effectively. By addressing any dysfunctional orofacial muscle patterns, we aimed to help her achieve more efficient and comfortable chewing.
• Alleviating dry mouth: Patient J’s complaint of dry mouth in the morning was a concerning symptom that could be related to mouth breathing during sleep.
MFT would focus on retraining her to breathe through her nose, promoting better oral and nasal hygiene, and potentially reducing dry mouth symptoms.
• Reducing snoring: Snoring can be associated with improper tongue and airway positioning during sleep. MFT aimed to address this issue by working on tongue posture, lip seal, and overall orofacial muscle tone. These improvements could contribute to a reduction in snoring, potentially improving her partner’s sleep quality and overall well-being. I recommended that the patient
proceed with a sleep study to eliminate the possibility of sleep apnea, but the patient refused to proceed with my recommendations.
• Correcting open bite and crossbite: The clear aligners were a crucial component of the treatment plan, primarily focusing on the correction of the open bite in the anterior region and the posterior crossbite. MFT would complement these efforts by ensuring that the corrected bite alignment was maintained through improved tongue and muscle function.
• Relieving muscle tension: The muscle tension observed in the TMJ area needed attention to prevent further dis-
Figure 1: Swallowing with tongue trust
Figure 2: Anterior view before treatment
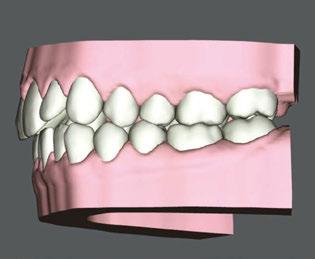
Figures 3 and 4: 3. Right side before treatment. 4. Left side before treatment
Figures 5 and 6: 5. Upper arch before treatment. 6. Lower arch before treatment
comfort and complications. MFT would involve exercises and techniques to relax and balance the orofacial muscles, reducing tension in the TMJ region.
• Enhancing overall quality of life: Ultimately, the goal of this comprehensive treatment plan was to enhance Patient J’s overall quality of life. By addressing her functional issues, improving her sleep quality, and correcting her bite problems, we aimed to provide her with a more comfortable and satisfying daily experience.
By combining clear aligners with MFT and tailoring our approach to address Patient J’s specific concerns and goals, we aspired to provide her with a holistic treatment that would not only enhance her oral health but also contribute to her overall well-being and happiness.
Here’s a concise summary of the treatment plan for Patient J: MFT sessions were scheduled every two weeks, totaling 12 sessions. After each session, the patient received videos of exercises and detailed instructions for continued practice.
1. Active exercise: 5 minutes in the morning, 5 minutes during the day, and 5 minutes at night of active breathing exercises. During these sessions, the patient should practice controlled nasal inhalation and exhalation while using a mirror to monitor her progress.
2. Passive exercise: Introduce passive exercises using orthodontic elastics to help improve tongue position and encourage proper tongue posture on the roof of the mouth. Start with 5 minutes a day and gradually increase the duration to 1 hour over time.
3. Nose breathing: The treatment plan focused on establish-
ing nose breathing through exercises, nose rinses, and conscientious breathing for at least 30 minutes a day. The use of Mute inserts (a soft, pliable polymer stent that dilates the nose) may have been recommended to assist in promoting nasal breathing.
4. Lip seal: To ensure that the mouth remained closed during both daytime and nighttime, the patient was guided to establish a proper lip seal with different exercises to improve muscle strength of lips, self-applied massages and stretching exercises.
5. Tongue posture: The plan included training the tongue to rest on the roof of the mouth, encouraging proper tongue posture.
6. Swallowing pattern: The patient was coached to develop a swallowing pattern that relied solely on tongue movement without assistance from the lips or cheeks.
Clear Aligner Therapy (Figures 7, 8, 9)
Our orthodontic goals were the following:
1. Expand upper arch, correct crossbite
2. Close anterior open bite
3. Correct crowding
Patient J was prescribed a series of 43 aligners, with each aligner being worn for 20 hours a day for 1 week.
This comprehensive approach combining aligner therapy and MFT aimed to correct oral dysfunction, enhance breathing patterns, and ensure the long-term stability of orthodontic treatment. It combined clear aligners with MFT to address both the esthetic and functional aspects of the patient’s oral health.
Figure 7: Digital view of right side before treatment
Figure 8: Digital anterior view before clear aligner treatment
Figure 9: Digital view of left side before treatment. Anterior open bite
Figure 10: Anterior view with elastic buttons to close open bite in conjunction with clear aligners
Figure 11: Right side with elastic buttons for treatment in conjunction with clear aligners
16:
Table 1
Treatment progress
Patient J wore her aligners for 20 hours a day, using the lingual edge of the aligners as a guide for her tongue position. However, when it came to her exercises, she found it challenging to adhere strictly to her routine. Due to this difficulty, I observed that even though progress was made in improving her swallowing pattern without requiring her to forcefully push her tongue through her teeth on the left side, she still pushed it on the right side. To address her open bite on the right side, I introduced elastics (Figures 10, 11) in addition to clear aligner therapy. During each MFT session, I asked the patient to grade the percentage of time she achieved Breathing Through the Nose (BTN), Tongue on a Spot (TOS), and Lips Together (LT).
Treatment results
Upon completion of MFT and active treatment phase with clear aligners (Figures 12, 13, 14, 15, 16), the patient revealed that snoring significantly reduced, her partner does not complain anymore, and she is breathing through the nose 75% of the time. The patient is holding her lips together 75% of the time and is able to keep her tongue on the spot 50% of the time.
I recommendeded that the patient wear her retainers every night, continue with her MFT exercises, and have recall visits for MFT every 3 months to continue to improve her tongue strength, lip seal, and nose breathing capabilities.
Conclusion
The synergy of orthodontics and MFT has been transformative in my practice. It has not only provided long-term stability7 to orthodontic treatments but has also become a valuable asset in addressing a myriad of concerns, particularly in the context of sleep apnea treatment. This journey has reinforced the notion that the holistic approach of combining orthodontics and MFT can indeed be a game-changer, leading to healthier,9 more stable, and happier smiles for my patients.
REFERENCES
1. Takahashi O, Iwasawa T, Takahashi M. Integrating orthodontics and oral myofunctional therapy for patients with oral myofunctional disorders. Int J Orofacial Myology. 1995 Nov;21:66-72.
2. Smithpeter J, Covell D Jr. Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy. Am J Orthod Dentofacial Orthop. 2010 May;137(5):605-614.
3. Benkert KK. The effectiveness of orofacial myofunctional therapy in improving dental occlusion. Int J Orofacial Myology. 1997;23:35-46.
4. Daglio S, Schwitzer R, Wüthrich J. Orthodontic changes in oral dyskinesia and malocclusion under the influence of myofunctional therapy. Int J Orofacial Myology. 1993 Nov;19:15-24.
5. Mills CS. International Association of Orofacial Myology History: origin - background - contributors. Int J Orofacial Myology. 2011 Nov;37:5-25.
6. Magnusson T, Syrén M. Therapeutic jaw exercises and interocclusal appliance therapy. A comparison between two common treatments of temporomandibular disorders. Swed Dent J. 1999;23(1):27-37.
7. Toronto AS. Long-term effectiveness of oral myotherapy. Int J Oral Myol. 1975 Oct;1(4):132-136.
8. Ohno T, Yogosawa F, Nakamura K. An approach to open bite cases with tongue thrusting habits with reference to habit appliances and myofunctional therapy as viewed from an orthodontic standpoint. Int J Orofacial Myology. 1981;7(1):3-10.
9. Daglio SD, Schwitzer R, Wüthrich J, Kallivroussis G. Treating orofacial dyskinesia with functional physiotherapy in the case of frontal open bite. Int J Orofacial Myology. 1993 Nov;19:11-14.
Figure 12: Anterior view upon the completion of active treatment
Figure 17: Smile upon the completion of active treatment
Figures 13 and 14: 13. Right side upon the completion of active treatment. 14. Left side upon the completion of active treatment
Figures 15 and
15. Occlusal view upon the completion of active treatment. 16. Lower occlusal view upon the completion of active treatment
Dentsply Sirona and TeamSmile partnership delivers free dental care to Charlotte children
Dentsply Sirona, the world’s largest manufacturer of dental products and technologies, partnered with TeamSmile to organize a free dental clinic for underprivileged children from local Boys and Girls Clubs and other organizations in Charlotte, North Carolina. The event, held at Truist Field at the end of July, aimed to provide much-needed dental care and oral health education to the youth.
Children attending the clinic received a range of free dental services, including X-rays, cleaning, fillings, sealants, and extractions, with a total estimated value of almost $26,000. In addition to receiving dental care and free oral health education, the young patients had the opportunity to meet Homer the Dragon, the Official Mascot of the Charlotte Knights baseball team, along with other TeamSmile mascots. The event also featured face painting to create a fun and memorable dental treatment experience for the children. Increasing access to oral health and achieving 25 million healthy smiles by 2025 are core commitments of Dentsply Sirona’s mission and sustainability program, “BEYOND: Taking Action for a Brighter World.”
Align Technology launches integrated consumer campaign and #Invisisforkids to drive awareness of how the Invisalign® Palatal Expander System is a better option for expanding a child’s narrow palate to make room for adult teeth
Align Technology, Inc. announced the “Better Way” new advertising campaign for the Invisalign brand featuring the “Invis is for Kids” tagline and hashtag. The “Better Way” campaign, launched across the United States and Canada, informs parents of a new and better option for expanding a child’s narrow palate that is safe, clinically effective, and without the pain and anxiety of traditional appliances. The integrated campaign will include targeted messages and materials for consumers and for doctors to drive awareness of early orthodontic intervention and that “Invis is for Kids.”
For more information on Dentsply Sirona, visit www. dentsplysirona.com. For more on TeamSmile, go to https://team smile.org/.
DEXIS™ launches DEXIS Connect Pro, a new proactive service platform for DEXIS CBCT and intraoral sensor devices, focused on increasing device uptime
DEXIS™ Connect Pro proactively monitors the health of DEXIS CBCT and intraoral sensor devices through IoT technology and can automatically arrange support or equipment replacements if performance issues are detected, allowing customers’ DEXIS products to stay up and running more consistently. DEXIS Connect Pro arms 100+ DEXIS technical support agents with insights into client equipment performance in order to deliver issue resolution efficiently, as device status is remotely monitored. DEXIS devices compatible with DEXIS Connect Pro include ORTHOPANTHOMOGRAPH™ OP 3D™ LX, i-CAT™ FLX V-Series, DEXIS™ Ti2 Sensor, DEXIS™ IXS Sensor, and DEXIS™ Titanium Sensor.
For more information, visit DEXIS.com.
The Invisalign Palatal Expander System is a modern and innovative direct 3D printed device based on proprietary and patented technology. Invisalign Palatal Expanders are intended for use in rapid expansion and subsequent holding of skeletal and/or dental narrow maxilla (upper jaw) with primary, mixed, or permanent dentition during treatment of patients. Combined with Invisalign First™ aligners, Invisalign Palatal Expanders provide doctors with a full early intervention treatment solution for Phase 1 treatment, an early interceptive orthodontic treatment for young patients. Phase 1 treatment is traditionally done through arch expanders or partial metal braces, before all permanent teeth have erupted — typically at ages 6 through 10.
For more information, visit www.invisalign.com.
Overjet for Kids: dental AI that parents need
Overjet, dental AI company has launched Overjet for Kids, the only technology cleared by the U.S. Food and Drug Administration (FDA) to detect, outline, and quantify tooth decay in children ages 4 and above, a critical time to prevent future problems. Overjet for Kids helps pediatric dentists build trust with patients by catching subtle tooth decay in X-rays before children feel pain, and by better explaining their recommendations to parents. In a rigorous clinical study conducted for the FDA, 100% of dentists were more accurate in detecting cavities when using Overjet for Kids, compared to their evaluations without it. The AI is trained to analyze both primary and permanent teeth, which allows Overjet to highlight its findings with colorful outlines that kids and parents can understand. Overjet’s artificial intelligence provides dentists with the first objective standard that quantifies pathologies like tooth decay, down to the millimeter.
The launch of Overjet for Kids comes at a time of rapid growth and innovation for the company. On March 5, Overjet announced it had raised $53 million of Series C funding, the largest investment in the history of dental AI. This funding will fuel the development of products that extend its AI platform to more patients and use cases. For more information, visit overjet.ai.
ADD and ADHD in children: the answer is right in their nose
Drs. Peter J. Catalano and John Walker discuss the consequences of sleepdisordered breathing and how dentists can help
Abetter understanding of ADD and ADHD symptoms and a new way to reverse them has given new found hope to the parents of children who struggle with behavioral issues and learning disabilities in school and at home. The solution, according to recent medical research, is surprisingly simple and yet frustratingly elusive: healthy, unbroken sleep.
The key word in that phrase is “unbroken.” While parents do commonly strive to ensure that their children sleep for the recommended 8 to 10 hours each night, very few can attest to the real quality of that sleep. Increasing evidence is now coming to light that certain children with attention-related or behavioral disorders can be treated without medication. The real culprits behind their behavior? Interrupted sleep due to nasal obstruction.
The key to great sleep is healthy breathing through the nose. Not all breathing is equal. Many children with narrow or blocked nasal passages are forced to breathe through their mouths all or part of the time. For many, the nasal obstruction only occurs at night. When the children lie down and fall asleep, their nasal tissues swell and their throat muscles relax making an already small airway even tighter. They don’t get the oxygen they need and effectively start to suffocate. The body goes into panic mode and partially reawakens not enough for the child to regain consciousness, but just enough for the throat muscles to reopen the airway.
The issue lies in the body’s need to arouse itself repeatedly throughout the night. When a sleeping child’s body reawakens, the child then gets the oxygen they need. The reawakening occurs in response to adrenaline, the body’s natural stimulant
Peter J. Catalano, MD, FACS, FARS, is the Chief of Otolaryngology at St. Elizabeth’s Medical Center and a Professor of Otolaryngology at Tufts University School of Medicine. He is a native of New York and graduated from Mount Sinai School of Medicine whereupon he completed his residency training in Surgery at Cedars-Sinai Medical Center (Los Angeles, CA) and Otolaryngology at Mount Sinai Medical Center (New York, NY). He is board certified in Otolaryngology He has served as Program Director since the Rhinology program’s inception while helping innovate many new technologies in the field of Otolaryngology. He has lectured throughout the world and published numerous journal articles and book chapters on many areas of Minimally-Invasive Rhinologic Surgery. His practice interests additionally include Pediatric Rhinology and Sleep Surgery.
John Walker, DMD, is an instructor of Orthodontics & Dentofacial Orthopedics at Boston University Henry M. Goldman School of Dental Medicine. He recieved his DMD from the College of Medicine and Dentistry of New Jersey in 1976 and his CAGS (Orthodontics) from Boston University School of Dental Medicine in 1978.
that can be secreted by our adrenal glands numerous times an hour in order to keep the child breathing. The child is forced into something called “sympathetic dystrophy,” which basically means that they become over stimulated. Hours of such chemical stimulation during sleep leads to an anxious, hyperactive, unfocused child during the day. This is why we commonly see young patients filled with nervous energy. Parents tell us that their son or daughter just can’t keep still. That’s the adrenaline at work; the repeated awakenings also cause the child to miss out on a complete sleep cycle. This happens over and over all night long. By morning, the child has failed to reach the deepest cycle of sleep, and over the years, this can have catastrophic consequences on behavior, physical health, and intellectual development.
ADD, ADHD, and the risk of misdiagnosis
This chronic sleep problem, known in the medical community as “Sleep-Disordered Breathing” (SDB), has begun to receive more and more attention in recent years as the number of ADD and ADHD diagnoses have skyrocketed. The symptoms of SDB in children are one cause of ADD and ADHD, and it is currently unclear how many children have sleep deprivation. For example, SDB symptoms can include problems such as hyperactivity, shorter attention spans, unexplained anger or depression, and poor school performance — all traditional hallmarks of ADD or ADHD. Children suffering from SDB may also exhibit other easily overlooked symptoms, including snoring, bed wetting, slouched posture, poor appetite, messy eating habits, headaches, and frequent open-mouth breathing.
Many children’s behavior-related struggles turn out to be a direct result of ongoing sleep deprivation. It is important to note that tiredness can also be a symptom of poor sleep, but it is mostly limited to older children and adults.
As years of improper sleep progress, a child’s symptoms can also begin to reveal more lasting damage. The deepest cycles of sleep are when a child’s body develops physically, emotionally, and intellectually. If enough time passes without healthy sleep, you can see issues like delayed cognitive development, stunted physical growth, and abnormal upper and lower jaw development. The latter ultimately leads to orthodontic and dental problems.
The surprising link between sleep and dentistry
New research coming out about sleep deprivation has emerged, surprisingly, from the field of dentistry or more specifically, from a dental subfield called “Airway Orthodontics.” Instead of simply correcting crooked teeth with braces and sending patients on their way, more and more orthodontists have begun to ask a previously unconsidered question: Why are teeth getting crooked in the first place? The answer, it turns out, is the same root cause behind sleepless nights: mouth breathing brought on by a blocked nasal passage. In fact, studies show that over 90% of children with crooked teeth, teeth-grinding issues, or poor jaw alignment also have compromised nasal breathing.
You really cannot overestimate the impact that nasal breathing has on facial development. Constant airflow through the mouth puts inward pressure on the jaw and teeth. This keeps the jaw from growing properly. Eventually, we end up with a child whose narrow jaw and face can’t hold all their adult teeth. From there, you can suffer from all types of orthodontic problems.
What does a narrow jaw have to do with sleep, though? Your jaw affects the size of your airway passage; thus if your jaw doesn’t develop to its proper width, then your airway is going to be too small for healthy breathing, especially when you lie down at night. Patients usually begin with a blocked nose and start mouth breathing at a young age (i.e., 1 year to 4 years old). By the time they require braces, they’ve effectively been damaging their bodies and their airway for years.
Finding a solution that’s right on the nose
The vast majority of children with SDB have nasal airway obstruction that results in mouth breathing that may be present day and night, or just when the child lies down. The latter occurs as fluid that had been drained out of the nasal tissues by gravity during the day, re-enters the nasal tissues when the child lies down and loses the benefit of gravity.
We are not supposed to breathe through our mouths at any time. Our noses have evolved to do a better job of breathing in almost every way from filtering impurities out of the air you breathe, to warming and humidifying the air for your body, to giving you a sense of smell. But when a child can’t breathe through their nose, they have no choice but to resort to mouth-breathing instead. From there, all sorts of problems arise.
The first step in helping a child, therefore, is to identify and correct any blockage in the nose. Possible reasons for nasal obstruction include anatomical deformities, septal deviations, enlarged septal swell bodies and/or turbinates, enlarged adenoids, or environmental allergies. It’s not uncommon for orthodontic patients to consult with other specialists depending on
what the dentist sees during their exam and sinus/airway CT scan. The latter is now commonplace in airway orthodontics. If the orthodontists see nasal and/or sinus problems, or large adenoids or tonsils, they will recommend an otolaryngology consult.
The correction of nasal obstruction in a child can be challenging due to the small size of the nasal passages and the severity of the intranasal deformities encountered. In addition, many ENT doctors simply focus on removing the child’s adenoids and/ or tonsils in an attempt to improve their breathing during sleep. However, studies have shown that only 1/3 of children with SDB are cured after T&A, with the rest requiring surgery on their nasal passages. We have pioneered many of the procedures to correct nasal obstruction using minimally invasive techniques that allow children and adults to return to school or work within 24 hours of surgery. There is no nasal packing or external evidence of surgery, and most children do not even require Tylenol after surgery. This newly developed ability to correct nasal obstruction in children, coupled with the breakthrough in understanding how ADD and ADHD develop from poor sleep, have revolutionized our treatment of this condition.
After healthy nasal breathing gets restored, the orthodontist then begins the second important aspect of treatment: ensuring proper jaw growth. The ideal time to help a child is before their jaw has finished growing. This allows the use of non-surgical and non-invasive methods to guide the jaw growth natural and wide enough to promote a healthy-sized airway.
Typical orthodontists don’t see a child until age 11 or 12, when their facial growth is already 90% complete. Airway Orthodontists argue that this is far too late. Even a 4-year-old has already completed 60% of their facial growth, thus the sooner a child can be seen, the easier it will be on them. However, this doesn’t mean hope is lost for a preteen, teenager, or even an adult with SDB. It’s never too late to address a breathing problem; it just may get more difficult to correct, but there are still treatment options.
The parent’s role in healthy breathing
While SDB has begun to receive more attention recently, only a small percentage of pediatric doctors are able to recognize the symptoms. We have amazing pediatric doctors out there taking care of children, but unfortunately they just haven’t been made aware of the opportunity to correct SDB through minimally invasive nasal surgery and proper orthodontic care. You combine that with the fact that SDB produces ADD or ADHD symptoms, and you end up with great doctors who are simply misdiagnosing some of their patients.
What can parents do in the meantime? “Keep an eye out for sleep deprivation symptoms in your child, and don’t be afraid to seek out a second or third opinion from an Airway Orthodontist or a pediatrician who keeps up with recent medical research on childhood sleep, especially if your child has been diagnosed with ADD or ADHD. There is a chance that your child’s issues are, in fact, reversible without needing medication or therapy. The improvements in these patients can be nothing short of life changing.
Republished with permission: Catalano PJ, Walker J. ADD & ADHD in Children: The Answer is Right in Their Nose. Am J Otolaryngol Head Neck Surg. 2018; 1(5): 1025.
Breakthrough: HealthyStart introduces new innovative technology of the FasTrack system
The FasTrack system introduces a significant advancement in effectiveness and compliance with the HealthyStart Pulsator device. No longer is daytime exercising required, but instead a 5-minute prior to sleep session and then nighttime wear are required. An additional proprietary development is a convenient direct-to-office customized adjunct device assessed and designed specifically for each patient. Both devices are integral parts of HealthyStart’s 5-Prong System called FasTrack.
HealthyStart’s FasTrack is a comprehensive and advanced system to tackle the root causes of sleep-disordered breathing (SDB) through a five-prong approach, which includes:
1. Comprehensive patient evaluation: This involves assessing potential patients for breathing, orthodontic, and sleep issues to identify underlying root causes of SDB.
2. Built-in myofunctional therapy: Activated by swallowing, this continuous therapy is designed to work throughout the night, improving overall oral function and airway health.
3. 5-Minute Pulsator compliance device: This innovation eliminates the need for daytime exercises, making therapy easier for patients to follow.
4. Customized adjuncts: These are tailored directly for each patient, with guidance and timing provided to ensure appropriate expansion and distalization.
5. Significant growth and development: Research has shown 54% more growth and development in HealthyStart patients compared to control groups, indicating the efficacy of their system.
HealthyStart by OrthoTain has been a pioneer in creating devices to address orthodontic conditions for over 57 years. They have successfully treated over 5 million cases, gaining extensive research and a deep understanding of the breathing and sleep epidemic. The recent introduction of the Pulsator and the customized adjuncts aims to overcome previous barriers to patient success.
Key points from patient and doctor
feedback
• Difference from traditional orthodontic treatment: The FasTrack system assesses all issues, including habitual problems, growth and development deficiencies, and orthodontic conditions, which are often linked to SDB.
• Comparison with Rapid Palatal Expander (RPE): While an RPE can improve nasal breathing, it doesn’t aid in developing proper tongue posture and swallowing habits. The RPE does not correct mouth breathing and can interfere with tongue position, unlike HealthyStart’s approach.
• Arch-width expansion: Generic standards like a minimum 40-mm arch width can be misleading. Each patient
needs a customized assessment to avoid potential issues like teeth being forced outside the cortical bone and potential gum recession.
• Types of expansion: Understanding the differences between sagittal and transverse expansion and distalization is crucial. HealthyStart offers digital and live courses to educate providers on these concepts.
• Eliminating exercise stress: HealthyStart’s system integrates myofunctional therapy with the Pulsator, removing the need for additional exercises and reducing stress on children and parents.
Nationwide educational campaign
HealthyStart is launching a $1-million educational marketing campaign starting in September to raise awareness about SDB, which affects 40 million children in the US. The campaign aims to increase public interest, drive more inquiries to offices, and boost the number of provider requests. Current providers have received training, and new doctors can register for an upcoming digital course on October 28, with a special offer of $500 off and a free FasTrack treatment for one patient.
HealthyStart continues to lead the industry by continuously innovating and introducing new technology to improve treatment for sleep and breathing issues. Their mission is to ensure no child is left behind, and their investment in education aims to change the trajectory of SDB, leading to better health, breathing, and retention for children.
REFERENCES
1. Bergersen EO, Stevens-Green B, Rosellini E. Efficacy of Preformed Sleep and Habit Appliances to Modify Symptoms of Sleep-Disordered Breathing and Oral Habits in Children With Focus on Resolution of Mouth Breathing. Compend Contin Educ Dent. 2022 Jan;43(1):e9-e12.
2. Keski-Nisula K, Keski-Nisula L, Salo H, Voipio K, Varrela J. Dentofacial changes after orthodontic intervention with eruption guidance appliance in the early mixed dentition. Angle Orthod. 2008 Mar;78(2):324-331.
3. Bergersen EO, Stevens-Green. Mouth Breathing and Its Impact on Sleep-Disordered Breathing. Compend Contin Educ Dent. 2023; 44(4). PD
Optimizing pediatric dental care in the OR
Shaun Valentine, VP of Product at Zyris Isolite, visits the Carmel
Ambulatory OR Center with Dr. Ana Vasquez of Fishers Pediatric
Dr. Ana Vasquez is the founder of Fishers Pediatric, in Fishers, Indiana, just outside of Indianapolis. It is a large, thriving practice, serving thousands of patients, with a team of over 70 clinicians. Dr. Ana received her Doctor of Medicine Degree at the University of Puerto Rico School of Medicine and her Certificate in Pediatric Dentistry at the Indiana University School of Dentistry.
Dr. Ana sees the incidence rate of OR visits increasing for younger patients, which is why she believes clinicians need to be taught oral sedation in school. Right now, that is not the case, though they may get some IV sedation training. She views the OR as the safest option. There, she has a team of a pediatric anesthesiologists, nurses, and her staff all in a facility designed for these cases.
Typically, there are a few situations that lead to procedures being done in the OR under general anesthesia.
• Medically-compromised children
• Special needs adults and children
• Children with compliance issues
• Children who require far more work than can be done in the clinic without multiple sessions
With the help of the new Zyris Isolite Operating Room Adapter for Posterior Mouthpieces, Dr. Ana was able to successfully treat nine patients in 8 hours, ages 4-8 with an average of 8 crowns plus extractions. One patient had 18 cavities out of her total of 20 teeth! The single-use adapter enables quick operating turns by allowing everything from the vacuum canister to the mouthpiece to be disposed of.
Dr. Brian (Anesthesiologist) explains that when just throat packs and gauze are used, he sometimes needs to suction any
of the water/fluid that leaks into the patient’s stomach (OG suction) before waking the patient. This ends up being an additional procedure. Dr. Brian recommends doing that procedure using isolation with suction because it is a much cheaper alternative.
Dr. Ana has two dental assistants in the OR at the same time. In Figure 2, you can see Kassy at the end of the bed with a laptop. As Dr. Ana completes a step of the procedure, she calls out what she has completed, and Kassy immediately logs that information into the billing and insurance system. Dr. Ana’s other Dental Assistant, Amanda, keeps a smooth flow of materials and tools for Dr. Ana to keep procedures efficient.
As soon as the patient is out of the room, Kassy will begin setup of the tray for the next patient, and Amanda will turn the operatory. Kassy and Amanda rotate jobs with each new patient.
When the last patient is seen, they are done for the day. There is no additional paperwork to be done. Dr. Ana still has to call and log her notes with the insurance company, but the team’s work is complete. This team is awesome!
In the realm of pediatric dentistry, where the primary focus is on delivering gentle, efficient, and effective care, technological advancements play a crucial role. Among the latest innovations making waves in this field is the Isolite System. This device is revolutionizing pediatric dental practices by offering versatile solutions that cater to various clinical needs, from posterior cases to sealants, anterior treatments, and even complex operating room environments.
This information was provided by Zyris. PD
Figure 1: Zyris Isolite Operating Room Adapter used in conjunction with Isolite Posterior Mouthpiece and new HOOPLA Retractor
Figure 2: Dr. Ana Vasquez with one DA assisting and one transcribing procedures into billing and insurance system
14 Million Pediatric Patients Protected
“I could not do what I do as a pediatric dentist without it.”
-Dr. Anna Fencl
Discover why over 2,600 pediatric dentists use Zyris Isolite dental isolation in their practice.
True Shadowless Illumination for YOU and your TEAM– See More, Miss Less!
Dual-Channel Control with continuous hands-free saliva and water evacuation
Integrated Bite block and airway protection for patient comfort and safety
Two-Quadrant Isolation for faster and efficient procedures
Tongue and cheek retraction for better access and control
Matthew R. Miller, DDS, is a life-long learner. He is an active advisor in his local Seattle Study Club, a clinical ambassador for The Dental Advisor, and a board member on Kerr Dental’s endodontic advisory board and restorative advisory board. “Continuing my education and getting involved in clinical research gave me the opportunity to test different dental products and materials and to be involved in writing articles and even product development,” says Miller.
Miller played a role with Kerr’s restorative advisory board in developing OptiBond™ Universal 360, the next generation of the company’s best-selling OptiBond Universal bonding agent. He says, “One of my priorities is finding materials that allow for consolidation with other materials to reduce the steps involved in various techniques and workflows.”
Bond Universal 360 will play well with your other preferred products. This is also the first Kerr bonding agent that includes MDP, eliminating the need for a dedicated primer when bonding to metal and zirconia.”
OptiBond Universal 360 is specifically formulated to provide reliable bond strength to all surfaces and substrates, including zirconia, lithium disilicate, gold, base metal alloys, alumina, titanium, porcelain-fused-to-metal (PFM), and porcelain-fused-to-zirconia (PFZ). It does not require a separate ceramic or metal primer. Miller says. “We wanted OptiBond Universal 360 to be universal for all indications and to be universally compatible with other resins, including cements, core buildup materials, and composites.”
A one-bottle solution, OptiBond Universal 360 can be used in self-etch, selective-etch, and total-etch protocols for both direct and indirect restorations. Kerr’s patented GPDM, MDP, and proprietary ternary solvent system with water, acetone, and ethanol enables dental practices to reduce technique sensitivity and application time without compromising bond strength. “Universal bonding agents that are acidic can interfere with the bonding of another resin, so in many situations, you have to light cure your bond first,” Miller says. “OptiBond Universal 360 will self-cure with any dual-cure resin, so if you’re using a buildup material or cement, and your curing light won’t reach the bonding agent, there’s no worry. Furthermore, Opti-
OptiBond Universal 360 also features an all-new ergonomic bottle design that significantly improves ease of use. With an auto-open button, dental professionals need only one hand for opening, dispensing, and closing, and the dropper delivers a precise drop size at every application. Miller says, “When you are holding a few things and actively working on teeth, it can be cumbersome, so the auto-open feature is really neat.”
Miller also notes the improved film thickness of OptiBond Universal 360, which means that less is needed to cover teeth. Because OptiBond Universal 360 combines etching, priming, and bonding and works well with as little as one coat without auxiliary products, it can also help dental practices save on inventory costs. Also, the material doesn’t need to be refrigerated.
Miller also appreciates OptiBond Universal 360’s ability to bond in both wet-and-dry conditions. Miller says. “It is nice that you can bond to the tooth in dry, moist, or wet conditions, including to wet dentin. The material is hydrophilic in its application, but then as it dries and cures, it becomes hydrophobic to receive the resin.” This allows OptiBond Universal 360 to penetrate the tooth optimally, reducing the risk of postoperative sensitivity and increasing patient satisfaction.
With six full-time dentists and an orthodontist in his office, it is important to Miller that everyone approaches materials and workflow similarly, and as such, they use just one bonding agent for everything in the practice. Previously, that bonding agent was OptiBond Universal, but now his office will upgrade to OptiBond Universal 360 as soon as it is fully mass-marketed.
Excerpted from: Dr. Matthew Miller, “A Truly Universal Bonding Agent for All Procedures.” Inside Dentistry. Copyright 2024 to Conexiant LLC. All rights reserved. Used with permission of the publisher. This information was provided by Kerr Dental.
Matthew R. Miller, DDS
Kerr OptiBond™ Universal 360
OptiBond™ Universal 360
Single Component Universal Adhesive
Goes with anything.
Just as white paint seamlessly matches with any color, OptiBond Universal 360 goes with virtually all common substrates.
The only adhesive you’ll ever need, OptiBond Universal 360 delivers exceptional bond strength to substrates including zirconia, base metal alloys, alumina, lithium disilicate, titanium, PFM, and PFZ.
True single-bottle solution
Minimal post-op sensitivity
One-hand to open, dispense, and close
Build stronger bonds: Connect with OptiBond™ Universal 360 Today go.kerrdental.com/optibond360-lanmark
How I overcame dreading patients with braces as a hygienist
Kristin Sheridan, RDH, discusses a mouth rinse that promotes patients’ oral health
Iused to dread the arrival of children and teenagers with braces — shorter appointment times with more work to meticulously complete around brackets and wires. Still being young, many of them have yet to develop proper hygiene habits. And how do I get them to floss when I despise threading floss through? Good hygiene is incredibly important, especially for a positive outcome with braces. If they don’t properly care for their teeth during treatment, then we know the problems like extreme decalcification and decay occur. I even see heavy plaque build-up, decalcification, and decay with kids who are using clear aligners! Since they have not developed the proper skills, even with removable appliances, the issue persists. For most patients, regardless of their skill level, a good therapeutic rinse can be super beneficial. There are a few key ingredients to look out for to help with this and improve not only orthodontic patient’s oral health but the whole child in general.
Activated chlorine dioxide: Chlorine dioxide is exceptional at dissolving even the most resilient of biofilms without being caustic or harming the oral environment. It will eliminate the bacteria that cause gum disease and decay in addition to breaking up the plaque. Long-term usage of this safe and effective treatment can help patients maintain better overall oral health.
Calcium lactate: Enamel integrity needs to be strengthened in order to prevent cavities. This component, which is a bioavailable form of calcium, effectively contributes to the remineralization of tooth enamel, helping to repair early signs of tooth decay and strengthen teeth. Furthermore, by neutralizing pH levels and buffering oral acids, calcium lactate enhances saliva’s defensive properties.
Xylitol: This ingredient is most well-known for its capacity to reduce harmful decay-causing bacteria like Streptococcus mutans. The inability of the bacteria to digest this sugar alcohol interferes with their ability to function. It also restricts bacterial adhesion, and therefore helps to reduce plaque formation. When used with calcium lactate, xylitol can further improve teeth’s remineralization, strengthening teeth’s resistance to attacks from bacteria and acids. Additionally, it stimulates increased salivation, which aids in the natural removal of food particles. Since minerals are naturally found in saliva, it helps to remineralize the teeth.
Poloxamer 407: Poloxamers enhance the effectiveness of other ingredients in solutions. They do this by reducing surface tension and increasing the “spreading and wetting properties’’ of products. This also creates a “slippery” surface that plaque has trouble building on, thereby minimizing the amount of plaque accumulation on tooth surfaces and brackets and wires.
How can we get all four of these ingredients incorporated into an orthodontic patient’s homecare? The answer is a new professional rinse, Ortho Protect.
I’ve used rinses for years to help my patients take better care of their oral health, and I have seen dramatic improvements in a really short period of time. And even though I still sometimes cringe when an orthodontic patient is on my schedule, knowing they have good hygiene habits makes it a little easier to deal with.
This information was provided by OraCare. PD
Why thousands of pediatric specialists have quietly partnered with IDSOs
Chip Fichtner discusses
the benefits of a large silent partner
Over the last 5 years, thousands of pediatric specialists have quietly partnered with Invisible Dental Support Organizations (IDSO). An IDSO becomes a doctor’s silent partner by buying 51% to 80% of a practice for cash up front at today’s low tax rates. Doctors remain as owners, with their brand, team, and full autonomy for years or decades. Practice performance can be enhanced, and the upside in a doctor’s retained ownership can be far greater than competing alone.
IDSO partner practices benefit from the resources of a larger silent partner to reduce the administrative burdens of banking, payroll, accounting, benefits administration, compliance, credentialling, tax, and legal. Doctors can also access 30% lower costs on supplies. And many practices today benefit from their partner’s professional, full-time recruiting and marketing teams.
While there are now almost 1,000 IDSOs and DSOs in the U.S., in the last 3 years, many new dental trifecta IDSOs have been created to focus solely on pedodontics, orthodontics and OMS practices in the same regions. They are competing with pedodontists/orthodontists, multispecialty, and GP IDSOs for great pediatric practices nationally. In an LPS process, values are achieving new records, often with six or more eager, qualified bidders from which doctors can choose the right partner.
Tens of thousands of practices have quietly partnered with IDSOs over the last 35 years in all 50 U.S. states. Some may have only a few practice partners and others over 700. Their size also gives them leverage in payer negotiations and team benefit costs not available to independent dentists.
IDSOs are eager for growing pediatric practices with at least $1.5 million in collections, and the younger the doctor, the more valuable the practice. In LPS’ $1.0 billion of completed IDSO partnerships in the last 24 months, over $150 million have been for doctors in their 30s.
Chip Fichtner, co-founder of Large Practice Sales which completed over $1.0 billion of IDSO partnerships in 2022 and 2023. Over the past 40 years, he has built, bought, and sold public and private companies in a variety of industries, and has been featured in numerous media outlets. His tolerant wife of 34 years allows him to live on his airplane visiting clients every week.
The IDSOs act as a doctor’s silent partner. Their goal is to support a practice, not to micromanage it or homogenize a practice to meet some corporate standard. Doctors retain full autonomy, not just clinically, but also in how they hire, fire, and lead their teams. Supply, labs, and payers accepted decisions are made by the owner doctor, not the IDSO.
Ultimately, the IDSO can also provide doctors with a known exit strategy for retirement, years or decades in the future. Thousands of doctors have experienced dramatic increases in the value of their retained ownership over time. Some have experienced equity increases of 300%, 500%, 1,000%, or more when they selected the right IDSO partner.
Doctors today should understand the potential value of their practice in an IDSO partnership. Values achieved by LPS are often twice what a practice might achieve in a doctor-to-doctor sale or associate buy-in. Doctors who own their real estate also have two great options. They either have an AAA credit tenant for decades, or due to their new IDSO tenant, the value of the real estate increases in a sale to a Real Estate Investment Trust (REIT) now or in the future.
To learn more about IDSOs and receive a confidential, no cost, no obligation practice valuation, doctors can contact Large Practice Sales at 844-577-1057, pedo@largepracticesales.com, or by visiting www.LargePracticeSales.com.
This information was provided by Large Practice Sales.
Dental
Organizations (IDSO) become your silent partner by purchasing 51% to 80% of your practice for cash at today’s low tax rates.
Silent Partners Buy Part of Your Practice - IDSOs purchase 51% to 80% of practices for cash now at low tax rates. Doctors retain ownership and have significant upside in the equity value. Some LPS pediatric clients have achieved 3x to 7x equity returns in only three to five years.
Long-Term Wealth Building Partnership - Doctors continue to lead their practice with their brand, team and strategy for years or decades. Practices benefit from the resources of a larger, silent partner, but are not micromanaged or homogenized.
Six or More Choices in Partnership - LPS clients often have 6 to 10+ qualified bidders. LPS is the largest advisor which enables our clients to achieve record values that the little advisors cannot match.
Large Practice Sales Brings Multiple Bidders for the Highest Value in IDSO Partnerships Get Your No-Cost, No-Obligation Practice Valuation
Your Value in Today’s Consolidation Frenzy - You should understand the value of your practice in an LPS-advised process. Doctors who deal directly with IDSOs often leave millions on the table and do not get to consider ALL of their options.
Large Practice Sales (LPS) is the largest transaction advisor to pediatric, GP and all specialty practices in the U.S. and completed over $1 Billion of Invisible Dental Support Organization (IDSO) partnerships in the last 24 months.
“I am ecstatic! You guys got me DOUBLE the best offer I could get on my own! Have any doctor call me and I’ll tell them you can’t go wrong with LPS. Use my name. I am referring all my friends.”
-T.J., MD, DMD
View the LPS Library of Webinars LargePracticeSales.com/webinars
•IDSO: What’s Changed in 2024?
•Wealth Building Strategy for Doctors of All Ages
•Specialist Options Not Available to GPs
•Dental Trifecta: The Best IDSO Option for Pedo, Ortho & OMS
REMplenish Myo-Nozzle
Innovation in sleep and airway health
At REMastered Sleep, we are dedicated to improving the health and well-being of children and adults through innovative products that enhance sleep and airway health. We are excited to introduce our REMplenish™ Myo-Nozzle, a revolutionary product that aligns perfectly with the mission of pediatric dentists to promote better sleep, oral development, and airway health among their young patients.
Childhood airway and breathing-related sleep issues, including snoring, bed wetting, behavior, and cognitive struggles as well as obstructive sleep apnea, have become increasingly prevalent. These symptoms are commonly overlooked and can truly be devastating and lead to long-term health problems if left untreated. As healthcare providers, pediatric dentists play a crucial role in advocating for preventative measures to mitigate these issues early on.
The REMplenish Myo-Nozzle integrates passive exercise directly into a familiar object — a water bottle. Our innovative approach addresses common airway problems with a userfriendly solution. Children naturally gravitate toward drinking from water bottles, making this an accessible and non-invasive method to support their airway health and ultimately, better sleep.
One of the primary benefits of the REMplenish Myo-Nozzle is its ability to promote better breathing patterns during sleep. Children experiencing snoring or mild breathing difficulties can benefit significantly from using the Myo-Nozzle. By encouraging proper tongue positioning and jaw alignment, the REMplenish Myo-Nozzle can be used with children as young as 3 years old to help establish correct oral habits that will support their airway health for a lifetime of improved sleep, health, and wellness.
have the opportunity to benefit from improved airway function and better quality sleep.
From a dental perspective, proper airway growth and development is crucial for oral health and overall physical and mental wellness. Compromised airways in children may lead to dental issues such as narrow dental arches, crowded teeth, and improper bite alignment. Addressing these airway issues early can improve oral health outcomes and contribute to better overall facial development and alignment.
The REMplenish Myo-Nozzle is a cost-effective option for families aiming to improve their child’s sleep and airway health. Unlike more complex medical interventions, such as continuous positive airway pressure (CPAP) machines or oral appliances, the REMplenish Myo-Nozzle is affordable and easy to incorporate into a child’s daily routine. This accessibility ensures that all children
We believe in empowering healthcare providers like pediatric dentists with solutions that enable parents to take proactive steps toward their child’s health. The REMplenish Myo-Nozzle exemplifies this proactive approach by offering a preventative measure that is practical and effective. By incorporating this nozzle into their daily lives, parents can actively promote their child’s airway health, overall health, and well-being.
The REMplenish Myo-Nozzle is a valuable tool for promoting better breathing, improved sleep, and a healthier life. By addressing airway issues early and effectively, we can significantly impact the long-term health outcomes of young patients. We invite pediatric dentists to embrace this innovative solution and continue prioritizing preventive care measures that pave the way for healthier futures.
Together, we can make a difference—one good night’s sleep at a time.
Exclusive Bonus Workshop!
5000+ PEDIATRIC DENTISTS TRAINED IN NUSMILE WORKSHOPS
WHAT YOU’LL MASTER
•Crown placement and prep technique for BioFlx, SSCs, Pre-Veneered and Zirconia crowns
• Implement an easier and simplified solution using Universal Chairside Space Maintenance
•Modern pulp therapy using NeoLINER LC and NeoPUTTY
Explore the benefits of digital scanning with AS 200E scanner and intraosseous injections using SOAN and SleeperONE devices.
+3 Hrs CE
"Restore is like a mini-residency. It equipped me with new clinical skills and a mindset focused on patient selfesteem, comfort and esthetics.”