CLINICAL FOCUS 2022
Glaucoma Innovations

JULY 1, 2021 — JUNE 30, 2022
Moran Eye Center at a Glance
RESEARCH GRANTS: $9.57 Million

CLINICAL TRIALS/STUDIES: 90+
PUBLICATIONS: 270+

SURGERIES PERFORMED: 7,999
• Cataract – 4,117
• Pediatric – 1,002
• Retina - 856
• Oculoplastic - 715
• Other - 695
• Glaucoma – 362
• Cornea – 252
Best Hospitals for Ophthalmology No. 10 Nationwide
Other: 13,744
Uveitis: 4,898
Best Overall Program 2021 No. 11 Nationwide
B est Residency Program No. 10 Nationwide
B est Clinical Care Program No. 11 Nationwide
Residency Education No. 5 Nationwide No. 1 in the West
Low Vision: 1,693
Pediatric: 15,767 Retina: 20,390
153,369
TOTAL PATIENTS VISITS By Specialty
Cornea/Refractive: 19,502 Glaucoma: 17,930
Neuro-Ophthalmology: 3,027
Comprehensive Ophthalmology/Cataract: 16,899
Oculoplastic: 6,819
Optometry: 32,700
ON THE COVER
In this cross-section of the back of the eye, the optic nerve (shown in purple) sends information from the retina to the brain to create sight. Credit: Drs. Alejandra Bosco and Monica L. Vetter, University of Utah.

Dr. Zabriskie is a glaucoma specialist and division chief of glaucoma at the John A. Moran Eye Center. He is professor, vice-chair and medical director of clinical services, and executive director of clinical operations.

Doing Our Best for Patients
Treating glaucoma can be one of the most challenging yet rewarding opportunities in ophthalmology.
We see our patients regularly, talk with them about their goals and concerns, and help them weigh the risks and benefits of different therapies to treat a lifelong condition that can be quite unpredictable. It’s a special relationship. Our patients trust us to not only provide excellent care presently but also to innovate better modalities going forward.
This edition of Clinical Focus highlights many ways our team at the John A. Moran Eye Center is advancing glaucoma care and research.
You’ll find an overview of our Alan S. Crandall Center for Glaucoma Innovation, led by Iqbal “Ike” K. Ahmed, MD, FRCSC. If anyone has championed innovation for the benefit of their patients, it has been Dr. Ahmed—widely known as one of the top ophthalmic surgeons in the world and at the forefront in the development of micro-invasive glaucoma surgery (MIGS).
Dr. Ahmed highlights potential new devices utilizing the supraciliary space while other Moran physicians discuss their approaches to care in complex cases. Craig Chaya, MD, reviews an aniridia-associated case, while Austin Nakatsuka, MD, looks at the use of topical netarsudil in multiple situations.
Other members of our team of eight specialists share innovative new technology-based approaches to glaucoma management. Brian Stagg, MD, discusses a computer-based prototype for managing care; Barbara Wirostko, MD, highlights the value of adding at-home self-tonometry to care models; and Susan Chortkoff, MD, shares the increased role of optical coherence tomography (OCT) in glaucoma diagnosis and treatment. Rachel Simpson, MD, delivers keys to use when talking with patients about MIGS. You’ll also find details on our expanded online glaucoma education at morancore.utah.edu.
I hope you will find this edition of Clinical Focus useful as we all continue to do our very best for our glaucoma patients.
Sincerely, Norm A. Zabriskie, MD

Alan S. Crandall Center for Glaucoma
Innovation: Doing Glaucoma Differently
Studies are beginning to demonstrate the longitudinal success of an interventional glaucoma treatment approach rooted in micro-invasive glaucoma surgery (MIGS).
Scientists are translating bench discoveries about the pathophysiology of the disease into potential neuroprotective therapies.
Low-resource care paradigms and devices that have decreased the global burden of cataracts are models for what can be done with glaucoma.
New virtual reality-based visual field testing and surgical simulation technologies are coming of age.
Crandall Center Director Ike Ahmed, MD, speaks with Moran colleague Liliana Werner, MD, PhD, co-director of the Intermountain Ocular Research Center.

These collective advances show the timing could not be better for a quantum leap forward in glaucoma treatment and care, says Ike Ahmed, MD, FRCSC, director of the Moran Eye Center’s new Alan S. Crandall Center for Glaucoma Innovation.
“I truly believe we can create a radically different future for glaucoma patients,” says Ahmed. “The Crandall Center is aimed at supercharging our efforts in a way that hasn’t been done before.”
Four Crandall Center initiatives bring to bear unique resources and talent.
Glaucoma Therapeutics
Director: Ike Ahmed, MD, FRCSC
Goal: Develop safer and more effective surgical therapeutics.
Method: Assist companies with device development, testing, and research by conducting independent preclinical, clinical, complications-related, and comparative studies. Ahmed draws upon his unique expertise as a consultant to over 50 medical companies. He is principal investigator for numerous research studies and clinical trials, including the recent HORIZON randomized trial for a Schlemm’s Canal microstent in combination cataract and glaucoma surgery. The initiative is modeled after Moran’s renowned Intermountain Ocular Research Center, which vets new intraocular lens technology and complications.
Neuroprotection-Based Therapies
Director: David Krizaj, PhD
Goal: Develop new therapies to restore or regenerate the optic nerve, damaged by high intraocular pressure associated with glaucoma.
Method: Bring together top neuroprotective researchers and investors to fund their work. Studying how the trabecular meshwork senses pressure to regulate the flow of aqueous humor, Krizaj has targeted Transient Receptor Potential Vanilloid 4 (TRPV4), an ion channel that can sense tiny changes in pressure and translate them into cellular responses. He has developed a potential eye drop therapy that inhibits TRPV4 to increase outflow. The treatment also appears to be neuroprotective. Fiona McDonnell, PhD, joined the Crandall Center in October to work with this initiative, studying meshwork exosomes and their potential for use in new therapies and as disease biomarkers.
Translational Research
Director: Gregory S. Hageman, PhD
Goal: Understand the biology and genetics of glaucoma to develop new treatments.
Method: Use Moran’s Sharon Eccles Steele Center for Translational Medicine’s (SCTM) model of establishing partnerships among academia, philanthropists, and private industry to fast-track drug development. Researchers can use a collection of nearly 10,000 donor eyes and glaucoma patients already enrolled in an SCTM macular degeneration clinical study that collects genotype, phenotype, and retinal images. They also can cross-reference data with the Utah Population Database, which contains genealogical, public health, medical, and environmental exposure records for more than 20 million people. Moran’s Utah Retinal Reading Center, directed by SCTM scientist Steffen Schmitz-Valckenberg, MD, will analyze disease progression and the best time to administer new therapies.
Scan to learn more about the Alan S. Crandall Center for Glaucoma Innovation at crandallcenter.org.

Global Care
Director: Craig J. Chaya, MD
Goal: Change the trajectory of glaucoma in low-resource nations where the rates of detection and treatment are low.
Method: Leverage Moran Global Outreach Division partnerships with providers worldwide to find new ways to detect glaucoma earlier, create systems where local health care workers can screen for glaucoma, and develop affordable surgical devices to preserve vision. Working in more than 20 countries, the division builds sustainable access to high-quality eye care through teaching and training doctors, nurses, and medical personnel. It is a North American academic partner of India’s Aravind Eye Care System, renowned for its unique ability to manufacture safe, effective, low-cost surgical devices.
New Approaches in Supraciliary MicroInvasive Glaucoma Surgery (MIGS)
BY IKE AHMED, MD, FRCSC
The supraciliary space has been untapped in the last few years since the CyPass Micro-Stent (Alcon) was withdrawn from the market in 2018 due to long-term endothelial cell loss.
This is an aqueous outflow space with vast potential; there is no episcleral venous floor, so the potential to lower pressure is quite great. It is freely accessed and a large, absorptive space that we can take advantage of because the gradient from the anterior chamber to the suprachoroidal space allows for filtration as well.
The question in this space has always been, can we balance safety and efficacy to achieve outcomes? The biggest challenge is controlled outflow and dealing with wound healing that can prevent success and cause failure.
Targeting Suprachoroidal Flow and Gradient
We know the CyPass was, of course, a suprachoroidal MIGS procedure combined with phaco and a pressure-lowering stand-alone procedure. We also know the problems we had with CyPass. Most of us believe it’s not necessarily an issue with the supraciliary space; the issue was more the device itself and placement of the device.
Dr. Ahmed is a fellowship-trained glaucoma, cataract, and anterior segment surgeon with clinical and research focuses on managing glaucoma, complex cataracts, and intraocular lens complications. He has done pioneering work in innovative glaucoma therapeutics and coined the term MIGS as a new genre of surgical approaches and devices. He is director of Moran’s Alan S. Crandall Center for Glaucoma Innovation.
W hen we were developing the CyPass, we debated how stiff or soft the implant should be. We chose to use a stiff, non-conformable implant we felt allowed tenting of the space, and this device had a lumen designed to drain aqueous. We are moving away from these singlelumen stiff devices.
We know the suprachoroidal space has outflow. We know that devices can drain aqueous. But we also know the concerns around implantable hardware. While I am certainly not opposed to implantable hardware, there is always a concern about its effect on the tissue surrounding the implant. The more similar an implant is to surrounding tissue, the less likely it is to have a foreign body reaction. High stiffness and less homologous tissue are likely to elicit more macrophages and fibrosis.
Advancing Device Technology
Two new approaches in the supraciliary space are the iStar Medical MINIject and the Iantrek AlloPass.
The MINIject (Figure 1) is a very soft silicon sponge. Stenting opens the supraciliary space to allow flow around and through the device, which acts like a wick. We have already published early results of a two-year study.1 On a cursory look, I would say the pressure lowering seems more effective than what we have seen with trabecular procedures, although it is not as much as bleb-forming procedures.
The AlloPass BioTissue device uses sclera inside the eye (Figure 2)
We have a lot of experience managing sclera. It’s homologous, porous, hydrophilic, and readily available in terms of access. What are some of the device’s features? It’s conformable; there’s no hardware; the device can be placed with adequate depth with the right injector and hydrate and adhere to surrounding tissue. Sclera shows very good permeability, potentially allowing this to act as a wick for the aqueous into the supraciliary space from the anterior chamber.




The AlloPass can be placed with direct viewing of the angle or with a gonio-free approach. Early results from 10 patients over 12 months show fairly good pressure lowering down into the low- to mid-teens, with fortunately no serious adverse events (Figures 3, 4). Combined and stand-alone procedures have shown similar effects. So far, we have seen 10% endothelium loss combined with phaco, which is not too different from other devices in this space.
So, we’ll have to see where these types of devices fit in the zone of pressure lowering and risk. Can we go beyond what we see with MIGS and micro-invasive bleb surgery? Perhaps the suprachoroidal space may provide this middle ground of efficacy balancing with safety.
INANCIAL DISCLOSURE
 R EFERENCE
1. Denis P, Hirneiss CW, Durr GM, et al. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br J Ophthalmology. 2022;106(1):65-70.
F
R EFERENCE
1. Denis P, Hirneiss CW, Durr GM, et al. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br J Ophthalmology. 2022;106(1):65-70.
F
Improving Quality of Vision and Life in a Patient with Aniridia-Associated Glaucoma
BY CRAIG J. CHAYA, MDAnna, an 11-year-old with aniridia, was referred to the glaucoma service for poorly controlled intraocular pressure (IOP) despite maximal medical therapy. Her aniridia was familial, with her father having the same condition. Her best-corrected visual acuity was 20/250 in both eyes, and her IOP was 39 mmHg in the right eye and 28 mmHg in the left eye on Latanoprost, Brimonidine, and Dorzolamide/Timolol. She had moderate-to-severe light sensitivity at a baseline that had worsened over the last year. Because of her nystagmus, she had difficulties performing visual fields or optical coherence tomography (OCT) scans.
Treatment Plan
We performed an examination under anesthesia, which revealed peripheral iris stumps with evidence of progressive angle closure. Fortunately, her optic nerves appeared healthy, with no significant cupping in either eye. In addition, her corneas were clear without evidence of significant limbal stem cell deficiency. However, she had moderate cortical cataracts in both eyes.
Dr. Chaya specializes in anterior segment ophthalmology and surgery, focusing on the medical and surgical management of routine/ complex cataracts and glaucoma. He serves as medical director of Moran’s Global Ophthalmology Division.

We considered addressing the cataract and glaucoma separately or simultaneously. After discussing several options with Anna and her family, we planned to address the glaucoma first. We chose the XEN Gel Stent procedure because of her early age, difficulty managing a trabeculectomy in the setting of nystagmus, and the need for substantial IOP lowering.
In early 2020, she underwent a XEN Gel stent augmented with mitomycin C and Ologen collagen matrix. She recovered well from the surgery and had excellent IOP reduction in both eyes.
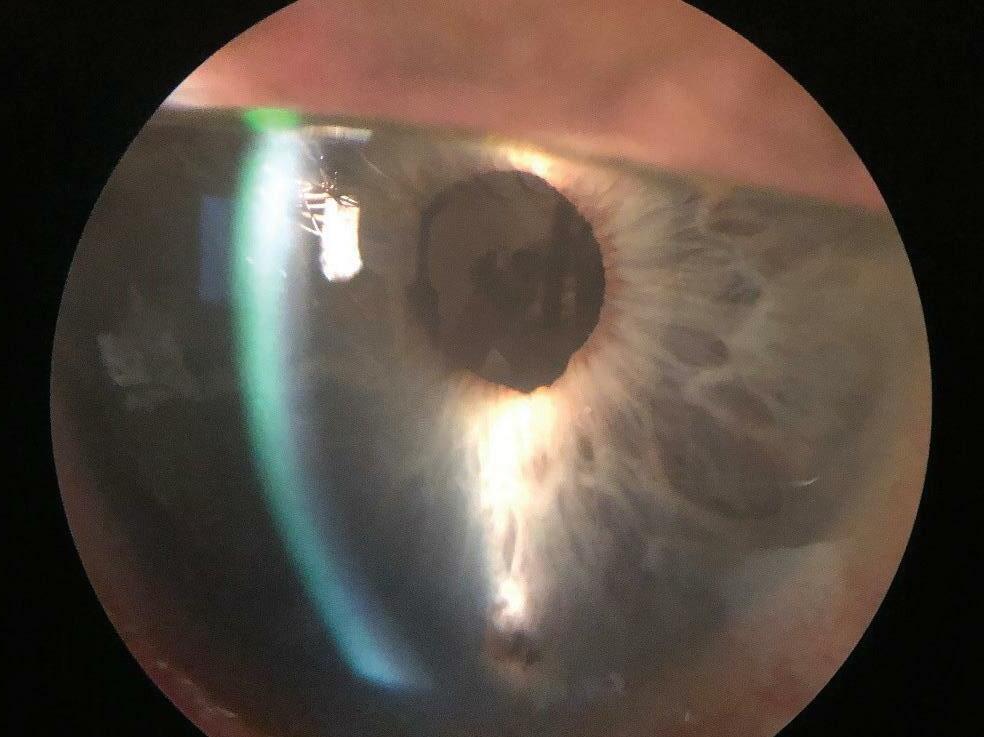
The next phase of her therapy focused on improving her vision. Anna’s cataracts had progressed. We considered the option of simultaneous cataract surgery and placement of an iris prosthesis to reduce glare and improve the quality of her vision. Anna was excited about this option and submitted a picture of an iris with her desired color, which was used as a template to custom-make her prostheses. In 2021, Anna underwent successful cataract surgery, with an IOL and iris prosthesis in each eye (Figures 1-3)
James Gilman, CRA, FOPS, project administrator of Moran’s Ophthalmic Imaging, scans the patient’s eyes following her iris prosthesis surgery.

About Aniridia
Aniridia is a condition with near-total or total absence of iris tissue. The condition can be inherited or acquired in cases of severe penetrating injury or during complicated anterior segment surgery. Inherited cases are bilateral and arise from defects in the PAX6 gene that is responsible for normal ocular development. This may result not only in aniridia but also in abnormalities of the cornea (limbal stem cell deficiency), fovea (hypoplasia), optic nerve (hypoplasia), and lens (cataracts). Sporadic aniridia may also be associated with non-ocular abnormalities such as a renal tumor known as a nephroblastoma (Wilms’ tumor). The condition requires vigilant screening.




In 2016, the FDA approved the XEN 45 Gel Stent as the first subconjunctival soft implant for refractory glaucoma. It is composed of pliable gelatin that allows it to conform to the contours of the eye. Its internal lumen is 45 microns in diameter and 6 mm in length. Although not wellstudied in children, the implantation of the XEN 45 Gel Stent is less invasive than traditional glaucoma surgery. In addition, the first FDA-approved silicone iris prosthesis, the CUSTOM FLEX ARTIFICIALIRIS, became available to treat all types of aniridia in 2018. The CUSTOM FLEX is color-matched to the unaffected iris or can be made to a patient’s desired color. In a study of aniridic patients,1 over 95% reported an improvement in glare and photophobia. In addition, there were no major adverse events or increases in post-operative complications.
Case Discussion
Anna’s case illustrates the complexity of caring for aniridic patients who may be suffering from multiple issues like glaucoma, cataracts, and glare simultaneously.

For Anna, a staged approach was critical. First, we needed to manage her glaucoma to mitigate irreversible optic nerve damage. Then, we needed to remove her cataracts and place an iris prosthesis in the capsular bag to complete her anterior segment reconstruction. Placing both her IOL and iris prosthesis in the capsular bag would reduce the risk of long-term corneal decompensation.
Her specific vision goals and timely technology anchored our approach.
REFERENCE
1. Figueiredo GB, Snyder ME. Long-term follow-up of a custom-made prosthetic iris device in patients with congenital aniridia. J Cataract Refract Surg. 2020 Jun;46(6):879-887.
F INANCIAL DISCLOSURE
Dr. Chaya has served as a consultant and received research funding from AbbVie, the maker of the XEN 45 Gel Stent. He has nothing to disclose regarding HumanOptics, maker of the CUSTOMFLEX ARTIFICIAL IRIS prosthesis.
Figure 1. The patient’s right eye before (left) and after iris prosthesis surgery. Figure 2 The patient’s left eye before (left) and after iris prosthesis surgery. Figure 3. The patient picked the color for the custom-made iris prosthesis in each of her eyes.Dr. Nakatsuka specializes in glaucoma and anterior segment conditions. He completed a fellowship at Moran in glaucoma and advanced cataract and iris surgery, training extensively with the late Alan S. Crandall, MD. Before that, he completed a fellowship in cornea and refractive surgery at Moran.

The Doctor Jekyll and Mr. Hyde Story of Topical Netarsudil
BY AUSTIN S. NAKATSUKA, MDTopical netarsudil 0.02% (Rhopressa, Aerie Pharmaceuticals) is an FDA-approved rho-kinase (ROCK) inhibitor for reducing intraocular pressure (IOP) in patients with ocular hypertension or open-angle glaucoma. ROCKs are enzymes with effector roles in the Rho pathway, a group of proteins that regulate cell structure, motility, and destruction. ROCKs are present in many tissue types, including the cornea, trabecular meshwork, and Schlemm’s canal. Clinically, ROCK inhibition has been utilized effectively in glaucoma and corneal pathology. Currently, the use of Rhopressa for corneal pathology is off-label. We present three short case presentations showing beneficial and adverse effects of topical netarsudil treatment.
Case Presentation 1
A 66-year-old aphakic patient with steroid-response glaucoma is referred for secondary intraocular lens (IOL) placement and possible corneal transplant for chronic corneal edema. We started him on netarsudil nightly. After one month, visual acuity improved from 20/60 to 20/40, corneal thickness decreased from 675 to 587 microns, and slit lamp examination revealed a clear cornea with minimal edema. We decided to defer corneal transplantation due to significant improvement.
Case Presentation 2
A 63-year-old patient with severe primary open-angle glaucoma and a history of Descemet’s stripping endothelial keratoplasty (DSEK) is started on netarsudil/latanoprost (Rocklatan) nightly. The patient has a history of a failed trabeculectomy, two Ahmed glaucoma tube shunts, and micropulse diode treatment. Twelve days after starting Rocklatan, the patient is noted to have focal honeycomb subepithelial changes with corneal edema most prominently in the area of his corneal graft.
Case Presentation 3
A 78-year-old patient with moderate primary open-angle glaucoma is started on netarsudil nightly in both eyes. She had been on latanoprost monotherapy due to systemic effects of other drops. Although IOP decreased to low teens with the addition of netarsudil, the patient reported vision loss and BCVA decreased from 20/20 to 20/25- OU. We found marked corneal verticillata and decided to stop netarsudil. Shortly after, the verticillata resolved and visual acuity returned to baseline.
Case Presentation 4
A 60-year-old patient underwent Descemet’s membrane endothelial keratoplasty (DMEK) and started on netarsudil after 1 month to expedite corneal clearing and offset steroidrelated IOP spikes. A few days after we initiated treatment, the cornea cleared and IOP was controlled, but we noted mild honeycomb changes peripheral to the graft.
Case 2. Focal honeycomb subepithelial corneal changes adjacent to an endothelial graft.
Discussion:
Topical netarsudil is a versatile treatment option for glaucoma and corneal pathology and may be even more beneficial in cases where a combination of these diseases exist in the same eye. Because of the ubiquitous nature of ROCKs in the human body, there is evidence to suggest that ROCK inhibition may affect the episcleral venous network, leading to an IOP-lowering effect downstream of the trabecular meshwork. This may mimic the IOP results of filtering surgeries such as trabeculectomy. In this author’s experience, netarsudil has been able to lower patients’ IOP to single digits even after the failure of multiple glaucoma drop classes, preventing larger glaucoma surgeries in highrisk patients.
This has also been the case for clearing corneal edema and preventing corneal transplants. Topical netarsudil has been successfully used off-label as an adjunct to Descemet’s stripping without endothelial keratoplasty where corneal clearing is achieved despite no corneal graft being placed. Nevertheless, the adverse effects of netarsudil can be debilitating. Besides frequent complaints of conjunctival hyperemia and discomfort, punctal stenosis has been reported as a reversible effect in a recent Ophthalmology publication.1 In this author’s experience, hyperemia is common, but patients are often willing to overlook cosmetic changes if they have significant improvements in IOP. However, visually significant verticillata and honeycomb edema can be difficult to predict, and the author has had to suspend treatment for these reasons on more than one occasion.
Case 3. Right and left eyes with marked corneal verticillata or whorl-like keratopathy.

Case 4. Slit lamp photo showing a clear DMEK graft with mild honeycomb supbepithelial corneal changes peripheral to the graft.



More studies are needed to determine the full capabilities of this unique ophthalmic medication. This treatment has yet to be studied in pregnant women or patients with congenital glaucoma, where systemic side effects from other medication classes can be prohibitive. Perhaps a different route of administration, including intracameral or intravitreal, may mitigate many of the adverse effects. Netarsudil has promising results in treating retinal pathology and may even have a role in optic nerve protection.


REFERENCE
1. Meirick TM, Mudumbai RC, Zhang MM, Chen PP. (2022). Punctal Stenosis Associated with Topical Netarsudil Use. Ophthalmology, 129(7), 765–770. https://doi.org/10.1016/j.ophtha.2022.02.025.
FINANCIAL DISCLOSURE
Dr. Nakatsuka has no financial interest in any of the products mentioned in this article.
Case 1. Aphakia and a clear cornea with minimal residual corneal folds following treatment with topical netarsudil.Dr. Chortkoff specializes in the management and treatment of glaucoma as well as comprehensive ophthalmology. She is a member of the American Glaucoma Society and the American Academy of Ophthalmology.

The Rise of OCT to Detect and Treat Glaucoma Earlier
BY SUSAN CHORTKOFF, MDLike many of you, I am a clinician seeing many new and established glaucoma patients to diagnose disease so that treatment can be initiated and detect progression so that treatment can be advanced to prevent functional impairment.
The diagnosis of glaucoma is not based on a pathognomonic test or symptom but a compendium of tests and observations. These include history, assessment of risk factors, findings of intraocular pressure, corneal thickness, gonioscopic findings, optic nerve features, nerve fiber layer defects and hemorrhages, and testing that includes perimetry and imaging. Historically, optic nerve photographs served to document glaucomatous features and their change over time.1
Testing Improvements
Over the last 20 years, objective imaging and measurements of ocular structures have dramatically improved our ability to assess structural changes in glaucoma. While many other technologies have contributed to the development of imaging as a key determinant in diagnosing glaucoma and glaucomatous progression, optical coherence tomography (OCT) has risen to the forefront. It has brought us the ability to examine structural changes within the optic nerve head, the nerve fiber, and macular ganglion cell layers. This technology has given us unprecedented ability to detect early glaucoma development and progression even if we don’t fully understand the underlying pathogenesis of these changes. However imperfect, never before have we been able to correlate so closely the structural and functional relationships that result in glaucomatous damage.
Finding theFix in Visual Loss Indicators
We know that the presence of visual field loss on initial evaluation is highly associated with the development of blindness.2,3 Macular ganglion cell and circumpapillary retinal nerve fiber layer thickness (RNFL) measurements are mutually predictive of visual field progression and are relevant to facilitating early detection of disease deterioration.4 And while it has yet to be proven that detecting and treating early progressive glaucomatous change results in functional benefits to patients or prevents blindness,5-7 it allows us to discuss with patients the expanding surgical and non-surgical treatment options for their care while balancing potential risk and burden of treatment and its impact on quality of life.8 Using complementary diagnostic techniques to “find” patients with rapid rates of progression can help us determine those in which a more aggressive “fix” is warranted to prevent blindness.5
Comparing OCT Platforms, Combining Strategies
Over 100 companies offer OCT technology. Our glaucoma service primarily uses the Heidelberg Engineering imaging platform, which, along with the Glaucoma Premium Edition Software, allows measurement of progressive change in the circumpapillary RNFL, optic nerve structure, and ganglion cell layer. It is important to recognize that while diagnostic abilities of most OCT platforms are comparable, data is not transferrable 9-11 and that when we change technologies, our ability to measure progression is interrupted until we obtain new baselines. In addition, we must carefully analyze results to identify potential pitfalls in diagnosis and progression analysis. Artifacts from segmentation error, inadequate image acquisition, poor signal strength (dry eye, cataract, nystagmus, strabismus), and
6
1
coexisting ocular pathologies (myopia, peripapillary atrophy, epiretinal membranes, vitreous traction, and macular degeneration) may confound our ability to measure and follow one or another area of the pathways involved in glaucoma. The disease stage may also influence which testing modalities offer the most reliable and accurate assessment of progression. For example, progressive structural loss in the peripapillary region predicts future functional losses at earlier stages of disease, whereas visual fields and measurement may better evaluate increased disease severity in the ganglion cell layer within the macula.

In all cases, visual field testing continues to be paramount in evaluating glaucoma, and metrics that combine testing strategies in glaucoma are being designed to achieve greater power than each test can alone.
Case Study in Structure-Function
We followed a 71-year-old woman with ocular hypertension for eight years without progression until December 2019. At that time, we noted significant thinning (-57um inferior temporal and -8um global) on OCT RNFL imaging of the right eye, along with a corresponding large area of arcuate thinning on the macular thickness map change report. Treatment of intraocular pressures had been initiated before these changes and escalated after these changes occurred. Although initially, progression continued in the inferior RNFL and macular region, OCT measurements have now stabilized. (See figures at left.) Visual field testing five months prior to these findings was completely normal in the involved eye, with only very subtle changes on visual field testing first being noted six months after OCT progression was first noted, with definitive progression in the superior paracentral field lagging until May 2021.
REFERENCES
. Yuksel Elgin C, Chen D, Al-Aswad LA. Ophthalmic imaging for the diagnosis and monitoring of glaucoma: A review. Clin Exp Ophthalmology. 2022;50(2):183-97.
2 . Chen PP. Blindness in patients with treated open-angle glaucoma. Ophthalmology. 2003;110(4):726-33.
3 . Hattenhauer MG, Johnson DH, Ing HH, Herman DC, Hodge DO, Yawn BP, et al. The probability of blindness from open-angle glaucoma. Ophthalmology. 1998;105(11):2099-104.
4 . Hou HW, Lin C, Leung CK. Integrating Macular Ganglion Cell Inner Plexiform Layer and Parapapillary Retinal Nerve Fiber Layer Measurements to Detect Glaucoma Progression. Ophthalmology. 2018;125(6):822-31.
5 . Johnson DH. Progress in glaucoma: early detection, new treatments, less blindness. Ophthalmology. 110. United States2003. p. 1271-2.
. Yu M, Lin C, Weinreb RN, Lai G, Chiu V, Leung CK. Risk of Visual Field Progression in Glaucoma Patients with Progressive Retinal Nerve Fiber Layer Thinning: A 5-Year Prospective Study. Ophthalmology. 2016;123(6):1201-10.
7. Miki A, Medeiros FA, Weinreb RN, Jain S, He F, Sharpsten L, et al. Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes. Ophthalmology. 2014;121(7):1350-8.
8

. Gracitelli CP, Abe RY, Tatham AJ, Rosen PN, Zangwill LM, Boer ER, et al. Association between progressive retinal nerve fiber layer loss and longitudinal change in quality of life in glaucoma. JAMA Ophthalmology. 2015;133(4):384-90.
9 . Lee ES, Kang SY, Choi EH, Kim JH, Kim NR, Seong GJ, et al. Comparisons of nerve fiber layer thickness measurements between Stratus, Cirrus, and RTVue OCTs in healthy and glaucomatous eyes. Optom Vis Sci. 2011;88(6):751-8.

10 Kanamori A, Nakamura M, Tomioka M, Kawaka Y, Yamada Y, Negi A. Agreement among three types of spectral-domain optical coherent tomography instruments in measuring parapapillary retinal nerve fibre layer thickness. Br J Ophthalmology. 2012;96(6):832-7.





11 Koh KM, Jin S, Hwang YH. Cirrus high-definition optical coherence tomography versus spectral optical coherence tomography/scanning laser ophthalmoscopy in the diagnosis of glaucoma. Curr Eye Res. 2014;39(1):62-8.

F INANCIAL DISCLOSURE
Dr. Chortkoff has no financial interest in any of the products mentioned in this article.
Dr. Wirostko treats glaucoma patients and specializes in clinical research. As a serial entrepreneur, she has large and small pharmaceutical company expertise and focuses on drug development for glaucoma pharmaceutical therapies. She recently co-founded MyEYES.net with a glaucoma patient to help patients access the iCare Home tonometer.

The Case for Adding Self-Tonometry into Care Models
BY BARBARA M. WIROSTKO, MD, FARVOGlaucoma is a leading cause of irreversible blindness worldwide and the second leading cause of blindness in the U.S. An estimated 53 million people in the world had open-angle glaucoma (OAG) in 2020, with a prevalence of 3% in the population aged 40–80 years.1 Prevalence studies suggest that OAG will increase by 50% worldwide as the population ages, impacting 79.8 million people by 2040.
Large prospective longitudinal studies have shown that OAG causes irreversible damage to the optic nerve, leading to visual field loss and eventual blindness. They also have revealed that glaucoma is a chronic progressive disease with inherent intraocular pressure (IOP) fluctuations. In fact, a CIGTs subgroup analysis at nine years found that the larger the range of IOP fluctuation and variability at baseline, rather than the mean and or maximum IOP, the greater the likelihood of substantial visual field loss and progression.2 Reducing IOP is the target of medical and surgical standard-of-care treatments shown to slow disease progression and prevent optic nerve damage.
So why are we not measuring IOP at various times of the day and night like other chronic diseases that demonstrate variability and fluctuation?
IOP Fluctuation Patterns
Studies have shown that diurnal and nocturnal IOP rhythms fluctuate, with spikes often occurring outside office hours and often in the early waking hours.3 In studies of IOP measured around the clock in hundreds of patients, peak IOP can occur during morning or night.4-5 In addition to elevations of more than normal IOP, wide fluctuations of IOP ranges have also been shown to contribute to glaucoma progression.2,6-7 IOP is known to fluctuate over 24 hours and longitudinally; yet, we rely on one IOP measurement every 3-4 months in the office for management decisions.
Self-Tonometry Tools Emerge
Home self-tonometry can provide robust measures of diurnal intraocular pressure, contributing to improved patient-level clinical management of IOP.
Self-tonometry is available with the iCare Home instrument. At the Moran Eye Center, my colleagues and I have been using this instrument to better diagnose and learn what a patient’s peak IOP is and to evaluate therapy responses to medications, lasers, and surgical interventions.8 By detecting changes in IOP and responses to treatments within a short period of monitoring, we can better determine and personalize what therapies are most effective.4 Self-tonometry assists us not only in determining what maximum IOP is, but also in monitoring patients at risk for progression. This may be due to diurnal fluctuation in IOP, which may be leading to damage and occurring outside of the office. Eventually, longitudinal studies will help determine if lowering that IOP spike and flattening variability can improve outcomes and reduce progression. Current data does suggest this.
Studies found that patients with glaucoma or ocular tension using home monitoring were able to detect fluctuation and patterns in IOP peak in eyes that showed progression in glaucoma despite stable in-office IOP measurement, and we are finding the same.4, 9
6
2
Discussion
In addition to in-office clinical IOPs, self-tonometry studies demonstrate a positive role in obtaining an accurate IOP assessment with data to better assist treatment decision-making.4 Studies found that a significant reduction in mean IOP after selective laser trabeculoplasty (SLT) could be detected when providing self-tonometry devices to patients after their procedure.10 The data from the six-year LiGHT study also found that SLT had slower progression as compared to topical drops.11
With the development of more sustained-release glaucoma drugs and devices (i.e., Durysta and the iDose), the use of an at-home device, like the iCare Home, can help determine when the drug effect is wearing off. I have found the iCare Home device invaluable for patients receiving the Durysta and who are not in close proximity to a clinic. These IOP monitoring devices are relatively easy to use for patients, and the data is available in the cloud for physician and patient review. Plus, I have found that self-tonometry empowers the patient to understand their disease better.

As we move toward more remote patient monitoring and a digital and virtual telemedicine healthcare delivery system, I believe that home IOP monitoring will become more integral for improved glaucoma care and better personalized patient care. It will teach us not only about the individual patient’s disease course but also about glaucoma in general.
REFERENCES
1. AAO Primary Open-Angle Glaucoma Preferred Practice Pattern 2020, p. 76.
. Musch DC, Gillespie BW, Lichter PR, Niziol LM, Janz NK. Visual field progression in the Collaborative Initial Glaucoma Treatment Study: the impact of treatment and other baseline factors. Ophthalmology. 2009;116(2):200-207.
3 . McGlumphy EJ, Mihailovic A, Ramulu PY, Johnson TV. Home Self-tonometry Trials Compared with Clinic Tonometry in Patients with Glaucoma. Ophthalmology Glaucoma. 2021 Nov-Dec;4(6):569-580.
4 . Levin AM, Vezina D, Wirostko BM. Home-Based Intraocular Pressure Measurements: Tracing a Parallel with Out-of-Office Blood Pressure Measurement. Ophthalmology Glaucoma. 2021 May-Jun;4(3):235-237.

5 . Tan S, Baig N, Hansapinyo L, et al. Comparison of self- measured diurnal intraocular pressure profiles using rebound tonometry between primary angle closure glaucoma and primary open angle glaucoma patients. PloS One. 2017;12(3): e0173905.
. Hasegawa K, Ishida K, Sawada A, et al. Diurnal variation of intraocular pressure in suspected normaltension glaucoma. Jpn J Ophthalmology. 2006;50(5):449e454.
7. Gao F, Miller JP, Miglior S, et al. A joint model for prognostic effect of biomarker variability on outcomes: long-term intra- ocular pressure (IOP) fluctuation on the risk of developing primary open-angle glaucoma (POAG). JP J Biostat. 2011;5(2):73e96.
8
. Levin AM, McGlumphy EJ, Chaya CJ, et al. The utility of home tonometry for peri-interventional decision-making in glaucoma surgery: Case series. American Journal of Ophthalmology Case Reports. 2022. https://doi.org/10.1016/j.ajoc.2022.101689.
9 . Cvenkel B, Velkovska MA, Jordanova VD. Self-measurement with Icare HOME tonometer, patients’ feasibility and acceptability. Eur J Ophthalmology. 2020 Mar;30(2):258-263.
10 Awadalla MS, Qassim A, Hassall M, et al. Using Icare HOME tonometry for follow-up of patients with open-angle glaucoma before and after selective laser trabeculoplasty. JE.Clin Exp Ophthalmology. 2020 Apr;48(3):328-333.
11 Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. LiGHT trial: 6-year results of primary selective laser trabeculoplasty versus eye drops for the treatment of glaucoma and ocular hypertension. Ophthalmology. 2022 Sep 16;S0161-6420(22)00732-1.
FINANCIAL DISCLOSURE
Dr. Wirostko is co-founder and medical advisor to MyEYES but receives no financial compensation for her work.
A recent Glaucoma Research Foundation event conference-goer demonstrates an iCare Home device, shown below.Dr. Stagg specializes in the diagnosis and treatment of glaucoma. His research focuses on using modern technology to personalize glaucoma care to ensure that each patient gets appropriate treatment.

A New Computer-Based Tool for Managing Glaucoma Care
BY BRYAN C. STAGG, MDClinicians caring for patients with glaucoma must incorporate large amounts of longitudinal data from many sources accurately and efficiently to make critical decisions regarding patient care.1 Further complicating this decision-making process, clinicians must gather and synthesize this complex data amid busy clinics filled with competing distractions and pressures. The data are complex, with high test-retest variability and patient-specific variation.2
Advances in the field of predictive modeling and machine learning for glaucoma have the potential to help with physician information overload and improve patient care.3-4 However, for the results of these models to meaningfully improve clinical practice, the predictions need to be integrated into clinical workflow in a way that influences clinician and patient behavior.4-5 Optimized, workflow-appropriate clinical decision support (CDS) systems can help address this challenge.6
CDS Systems and Visual Field Testing
CDS systems are computer-based tools designed to improve clinician decision-making for individual patients at the point the decisions are made.7 However, not all CDS tools are effective.8 CDS systems are most effective when implemented within clinical workflow, developed using rigorous, user-centered iterative design principles, and integrated with the electronic health record using standards-based CDS technology that is scalable to other institutions.4-9
Optimal visual field testing frequency for an individual patient with glaucoma is a difficult clinical decision that could be dramatically improved with predictive modeling and effective CDS.3 Five to 30% of patients actively treated for glaucoma continue to have significant visual field loss and need additional eye pressure lowering.10-12 We periodically monitor visual function using visual field tests to identify patients who are being treated for glaucoma and continue to have progressive visual field loss to prevent blindness.
Visual field testing that isn’t frequent enough can lead to considerable delays in detecting glaucomatous progression and subsequent vision loss.13 For example, in many patients with a baseline mean deviation (MD) of -10 dB, annual visual field testing would take 12.7 years to detect glaucoma progression of -0.5 dB/year in 80% of eyes, at which point a patient could have lost 6.35 dB, resulting in significant disability.14
Determining the optimal testing frequency for an individual patient is complicated because visual field tests have high test-retest variability. The ability to detect progressive visual field loss depends on the test-retest variability (which varies between patients), the rate of visual field loss, and the number of tests performed over a given time.4
Figure 1 illustrates this with a hypothetical patient with rapid true visual field MD progression (-2 dB/year). In this case, because of test-retest variability, visual field progression is not detected until several years have passed. Annual testing would be insufficient for this patient. Testing that isn’t frequent enough risks unidentified vision loss, while testing that is too frequent is burdensome for patients and overuses resources.2
The frequency of visual field testing should vary based on patient characteristics.13 For example, to detect a MD change -1.0 dB/year in patients with baseline MD of -5 dB, standard automated perimetry testing approximately every 6 months was the average frequency needed to detect progression within 5 years in patients with high test variability
Figure 1 A hypothetical patient with a true visual field mean deviation (MD) loss of–2dB/year.
(>2 dB). Patients with low variability (<1 dB) in this same group needed testing approximately every 18 months to detect progression within 5 years on average.
I surveyed 105 clinicians who care for patients with glaucoma about clinical decision-making and interest in a CDS system for glaucoma.3 Clinicians identified visual field timing as a difficult clinical decision, and 90/105 (85.7%) felt that determining visual field timing would benefit from CDS. Overall, the clinicians expressed strong interest in using a CDS system for glaucoma, with 94/105 (89.5%) interested. This high level of interest increases the likelihood of successful CDS implementation.15
Using a statistical model that calculates a personalized frequency for visual field testing, I developed a prototype Glaucoma CDS System (Figure 2). Data from my survey guided this prototype.3 Most clinicians felt that automatic data entry, an easy-to-use interface, and minimal time to use the tool would be “very important.”
CDS systems such as this can potentially reduce clinician cognitive burden and improve patient care. As these systems are developed, it is important they are designed to be integrated within patient care to support rather than replace patient and clinician decision-making.
REFERENCES
1. Prum BE, Rosenberg LF, Gedde SJ, et al. Primary Open-Angle Glaucoma Preferred Practice Pattern(®) Guidelines. Ophthalmology. 2016;123(1):P41-P111.
2. Crabb DP, Russell RA, Malik R, et al. Frequency of Visual Field Testing When Monitoring Patients Newly Diagnosed with Glaucoma: Mixed Methods and Modelling. NIHR Journals Library; 2014. Accessed June 10, 2019. http://www.ncbi.nlm.nih.gov/books/NBK259972/.
3. Stagg B, Stein JD, Medeiros FA, Cummins M, Kawamoto K, Hess R. Interests and needs of eye care providers in clinical decision support for glaucoma. BMJ Open Ophthalmology. 2021;6(1):e000639.
4. Stagg BC, Stein JD, Medeiros FA, et al. Special Commentary: Using Clinical Decision Support Systems to Bring Predictive Models to the Glaucoma Clinic. Ophthalmology Glaucoma. Published online August 15, 2020.
5. Matheny ME, Whicher D, Israni ST. Artificial Intelligence in Health Care: A Report From the National Academy of Medicine. JAMA. Published online December 17, 2019.
6. Tcheng JE, National Academy of Medicine (U.S.), eds. Optimizing Strategies for Clinical Decision Support: Summary of a Meeting Series. National Academy of Medicine; 2017.
7. Berner E, ed. Clinical Decision Support Systems: Theory and Practice. 3rd Edition. Springer International Publishing; 2016.
8
. Bright TJ, Wong A, Dhurjati R, et al. Effect of Clinical Decision-Support Systems: A Systematic Review. Ann Intern Med. 2012;157(1):29.
9. Kawamoto K, Kukhareva P, Shakib JH, et al. Association of an Electronic Health Record Add-on App for Neonatal Bilirubin Management With Physician Efficiency and Care Quality. JAMA Netw Open. 2019;2(11):e1915343.
10. Chauhan BC, Mikelberg FS, Artes PH, et al. Canadian Glaucoma Study: 3. Impact of risk factors and intraocular pressure reduction on the rates of visual field change. Arch Ophthalmol. 2010;128(10):1249-1255.
11. Chauhan BC, Malik R, Shuba LM, Rafuse PE, Nicolela MT, Artes PH. Rates of Glaucomatous Visual Field Change in a Large Clinical Population. Invest Ophthalmology Vis Sci. 2014;55(7):4135-4143.
12. Heijl A, Buchholz P, Norrgren G, Bengtsson B. Rates of visual field progression in clinical glaucoma care. Acta Ophthalmology. 2013;91(5):406-412.
13. Stagg B, Mariottoni EB, Berchuck S, et al. Longitudinal visual field variability and the ability to detect glaucoma progression in black and white individuals. Br J Ophthalmology. Published online May 13, 2021.
14. Abe RY, Diniz-Filho A, Costa VP, Wu Z, Medeiros FA. Predicting Vision-Related Disability in Glaucoma. Ophthalmology. 2018;125(1):22-30.
15. Kawamanto K, Flynn MC, Kukhareva P, et al. A Pragmatic Guide to Establishing Clinical Decision Support Governance and Addressing Decision Support Fatigue: a Case Study. AMIA Annu Symp Proc. 2018;2018:624-633.
FINANCIAL DISCLOSURE
Dr. Stagg has no financial interest in any of the products mentioned in this article.
Dr. Simpson is associate program director of education. She specializes in the medical and surgical treatment of glaucoma and cataracts and advanced anterior segment surgeries.

Five Key Things I Tell Patients About MIGS
BY RACHEL G. SIMPSON, MDMicro-invasive glaucoma surgery (MIGS) is perhaps the fastest-growing surgical sphere in ophthalmology. The term applies to any surgical procedure designed to lower eye pressure that requires minimal tissue disruption, has a high safety profile, and can be completed quickly, sometimes as part of cataract surgery. As with any surgery, appropriate patient counseling is vital for the patient to understand what to expect with their MIGS procedure.
MIGS is a tool to treat glaucoma — not a cure. With any surgery, expectation management is important. I start by telling patients that the procedure is designed to give us an edge when treating their glaucoma, but it’s not a cure. Glaucoma is a chronic disease.
MIGS is quick, and so is the recovery.
One of the nicest things about MIGS procedures is that they can be quick. Unlike more traditional glaucoma surgeries that can take up to an hour, a typical MIGS procedure with cataract surgery adds only 3-4 minutes to the procedure. The recovery from MIGS, while a little longer than with cataract surgery alone, is also usually much faster than traditional glaucoma surgery.
MIGS is safe.
If there is one area where all glaucoma surgeons can agree, it’s that the risk posed by MIGS is minute compared to some of the more traditional glaucoma surgeries. The risk posed by MIGS is essentially equal to that of cataract surgery, and I usually counsel my patients as such.
MIGS might get patients off a drop (or two), but don’t count on it.
One of the major potential benefits of MIGS is the possibility of getting a patient off one or more of their prescription eye drops. However, outcomes vary. While I counsel this is a potential added benefit, I am sure to remind them it’s not the primary reason for surgery. Lower intraocular pressure is the hoped-for outcome. I usually tell them that, on average, about 50% of patients with mild or moderate glaucoma can reduce their use of drops.
MIGS is sometimes a one-chance-only opportunity.
Two of the most popular MIGS procedures, the Hydrus Microstent and the iStent inject, only have FDA approval to be implanted at the time of cataract surgery. Currently, insurance will only cover these stents when implanted during cataract surgery. For now, I tell my patients that if we decide not to place these stents during their cataract surgery, we can’t easily go back a few years later and implant them. Once that ship sails, it’s gone.
Moran’s online Clinical Ophthalmology Resource for Education (CORE), offering worldwide access to high-quality, peer-reviewed ophthalmic learning since 2015, recently expanded its glaucoma section.

The update includes new surgical videos and manuscripts, plus a more user-friendly outline, says Susan Chortkoff, MD, the glaucoma section editor.



The section has nine content areas covering everything from glaucoma classifications, patient evaluations, and disease management to epidemiology, genetics, and basic science.

Moran CORE has grown exponentially in recent years via the website and a YouTube channel, with more than 900 videos on various subjects from basic eye care training and surgery techniques to best practices for outreach work.
Moran produces the site in partnership with the Spencer S. Eccles Health Sciences Library at the University of Utah. Here’s a closer look at this invaluable learning resource.
John A. Moran Eye Center
65 Mario Capecchi Drive
Salt Lake City, UT 84132
moran.info@hsc.utah.edu
Resources for Physicians


Moran Eye Center
@ moraneyecenter
moran.eye.center
John A. Moran Eye Center
Refer a Patient 801-213-2001 healthcare.utah.edu/moran/refer-patient.php
Glaucoma Center
The Alan S. Crandall Center for Glaucoma Innovation crandallcenter.org
Moran CORE
Clinical Ophthalmology Resource for Education morancore.utah.edu

NOVEL
Neuro-Ophthalmology Virtual Education Library novel.utah.edu
W EBVISION
moraneyecenter.org
The Organization of the Retina and Visual System webvision.med.utah.edu
U.S. POSTAGE PAID

Permit No. 1529
Salt Lake City, Utah
issuu.com/moraneyecenter

CME Information medicine.utah.edu/cme