Chester County Medicine is a publication of the Chester County Medical Society (CCMS). The Chester County Medical Society’s mission has evolved to represent and serve all physicians of Chester County and their patients in order to preserve the doctorpatient relationship, maintain safe and quality care, advance the practice of medicine and enhance the role of medicine and health care within the community, Chester County and Pennsylvania.
The opinions expressed in these pages are those of the individual authors and not necessarily those of the Chester County Medical Society. The ad material is for the information and consideration of the reader. It does not necessarily represent an endorsement or recommendation by the Chester County Medical Society.
Contents
Every Issue
ESPRING 2025 PRESIDENT’S MESSAGE
A PIECE OF MY MIND
BY DAVID E. BOBMAN, MD PRESIDENT OF CHESTER COUNTY MEDICAL SOCIETY
ntering the final several months of my term as President of the Chester County Medical Society has led to introspection as I review the successes and failures we have had. Medical school taught me a lot about how to treat patient illness but nothing about how I, as a practicing physician, can contribute to the profession of Medicine. In my many years with the Chester County Medical Society, I have learned how little I originally knew about the political and medicolegal machinery that shapes the way we practice- not only in how we care for patients, but also the way we stay up to date on our fund of knowledge and medical expertise, the practice of defensive medicine, the financial and lifestyle pros/cons of different types of practice situations (eg. private practice, hospital-based medicine, etc.).
There have been seismic shifts in our daily routines. When I began practicing medicine, I recall having an entire hour-long lunch each day, much of which would be shared with other physicians in the hospital cafeteria. This was a great opportunity to connect with colleagues and led to a terrific camaraderie. It also provided a nexus for sharing ideas and information amongst the physicians. As time has elapsed, this has disappeared and many physicians neither come to the hospitals nor even have time for more than a quick lunch bite squeezed between patients’ phone calls and other administrative responsibilities.
Reimbursements have suffered with physicians having to work far harder to maintain income levels and lifestyle, all the while maintaining near perfection in quality of care- lest the threat of litigation and negative online patient reviews. Red tape and increased paperwork requirements have added to this burden.
Bottom line, my emotions have ranged from frustration, a sense of futility, and at times even anger, all of which contribute to
a sense of job burnout. In part, it was these emotions as well as a sense of wanting to correct these issues that led me to get involved with the Chester County Medical Society.
I recognize that the following thoughts are my own, will be controversial, and do not necessarily represent the thoughts of our other Medical Society members.
Through the years, I have tried to motivate others and enlist help in trying to reverse this trend. On multiple occasions, I have heard pushback that little has gotten accomplished by our Medical Societies. There are a few points to be made in this regard. While I do not feel our overall situation has improved, I believe that the Medical Society’s (both PA Medical Society’s and the Chester County Medical Society’s) efforts have reduced a potentially worse situation and there have been some successes. Despite this, much like sandcastles at the beach, there is constant erosion of our efforts which require repeated reinforcement and updating. This is tiresome and labor intensive.
I do believe that through the years our Medical Societies have been significantly weakened for a number of reasons. First, the adage of “divide and conquer” has been largely true of the medical community. We are no longer a cohesive group of private practitioners, but rather a hodgepodge of physicians working in different situations with different needs and goals. For instance, many are now hospital employed, are employed by private equity, are university or pharmaceutical researchers, with a few remaining private practitioners, among others. Many doctors have put more emphasis on their specialty societies which more directly serve their specialty’s interests; however, by their very nature, tend to be smaller and therefore less influential than the larger medical societies.
Bigger is better when it comes to political clout. Nowadays, only a minority fraction of physicians are members of their respective Medical Societies. I have noticed that many physicians involved with the Chester County Medical Society are older, and when looking at our Board of Directors, many are at or about retirement age. It seems to me that younger physicians do not get involved. I remain at a loss to understand why this is the case as the future of medicine will impact them far more than older physicians. This may be a generational difference with attitudes to work-family balance having gradually changed through the years. My worry is that unless the younger physicians step up, who will be left to represent their interests in the years to come? We are actively looking for a few leadershiporiented younger physicians to join our board- both to maintain leadership for the next generation of physicians and to help us better understand and strategize to meet the needs and wants of the younger generation of physicians.
In the next couple of weeks, we will be hosting an informational meeting for Chester County Medical Society members to explore the formation of a physician guild, in essence a separate entity that is part of the AFL-CIO. I have mixed feelings about this step. It saddens me to think that apathy and declining physician involvement has led to the point that we alone do not have the ability to make our needs known in a meaningful manner with our politicians. On the other hand, I think it may be a very necessary step to strengthen our bargaining position- both politically and with the employers that many physicians now are contracted with- so that we as practicing physicians, are in a better position to maintain or even further the great quality of care that Chester County physicians are known for. I encourage all to attend this meeting and seriously consider the pros (and cons) of this step. If you cannot attend, we will provide information on our website. On the brighter side, in order to increase connectedness, we have been trying to have more social events. Many of these are planned with the goal of having events that the whole family can enjoy, including the very young. To that end, late this Spring we will hosting another family picnic at East Goshen Park which will include many activities and food/refreshments for all. In early September, we will be hosting what we hope to be the first annual Chester County Medical Society golf outing to be held at Concord Country Club. Not long after, our annual Physician’s Appreciation Dinner will be held, also at Concord Country Club. The dinner will include an exciting keynote speaker that promises to be both entertaining and informative.
In summary, the Chester County Medical Society is working hard in the best interests of all Chester County physicians. I encourage every physician residing or working in Chester County to join as members, as there is “strength in numbers”. This alone would help the collective good of all physicians in the County. As above, we are looking for a few younger physicians who would like to help lead this effort and get involved at the board level with the Chester County Medical Society. As I stated above, these views are my own and I am confident that others may well disagree with my thoughts. I would welcome feedback from anyone who would like their voice to be heard and I will have them published in our next newsletter. Responses can be sent to OurCCMS@gmail.com
Sincerely,
David E Bobman, MD President, Chester County Medical Society
Out & About
with Mian A. Jan, MD
Drs. Mian and Ambereen Jan with Senators Carolyn Comitta, Sharif Street and their spouses at a charity event for breast cancer awareness.
Chester County Medical Society and Hospital staff physicians February SCRUM at Dressler Estate Cidery in Downingtown.
Dr. Mian Jan with Coach Dick Vermeil and Senator John Kane at a charity event arranged by Coach Vermeil.
CHASING IMMORTALITY: THE SCIENCE AND REALITY OF LONGEVITY
BY MIAN A. JAN, MD, FACC, FSCAI, AND TALHA FAROOQ
“Is this the land that has the Fountain of Youth? For remember he was seeking this fountain but never found it.” - Juan Ponce de Leon
Spanning generations, humanity’s enduring fascination with longevity mirrors Juan Ponce de León’s quest for the Fountain of Youth. Despite myriad efforts, akin to his fruitless search, the secret to everlasting vitality remains elusive. This universal longing underscores a timeless desire to defy aging’s inevitability. As we examine the mysteries of longevity, we recognize its profound societal and individual implications. With global life expectancy on the rise, understanding aging mechanisms and practicing healthy aging strategies becomes paramount
WHY WE AGE
However, before we look to increase our longevity, we must consider why we age. Modern-day research suggests a multitude of possible causes and explanations for why we age. Of these causes, the most prominent is the shortening of telomeres, which are DNA-protein structures located at the ends of chromosomes. Telomeres are primarily responsible for preserving chromosomal stability and preventing chromosomal degradation. In our bodies, cells continuously undergo the cell cycle throughout our lives, dividing and replicating themselves so the body can develop and repair itself. With each cell division, a small part of each telomere is lost until the telomeres are too short to protect the DNA on their chromosomes, resulting in DNA damage. When this point is reached, cells undergo either senescence (cells can no longer divide or grow) or apoptosis (programmed cell death).
Because of this, telomeres can be considered as a sort of biological clock that can be used to predict an organism’s lifespan. The rate at which telomeres shorten varies for each individual with current research estimating that humans lose approximately 25 to 200 base pairs of telomeric DNA per year. Factors such as smoking and alcohol consumption, obesity, environment, diet, and exercise play a major role in determining each individual’s rate.
Figure 1: Juan Ponce de Leon Juan Ponce de León was a Spanish explorer known for discovering and exploring Florida in 1513, naming it “La Florida.” He also sought the legendary Fountain of Youth during his expeditions in the Americas, contributing to early Spanish colonization efforts in the region.
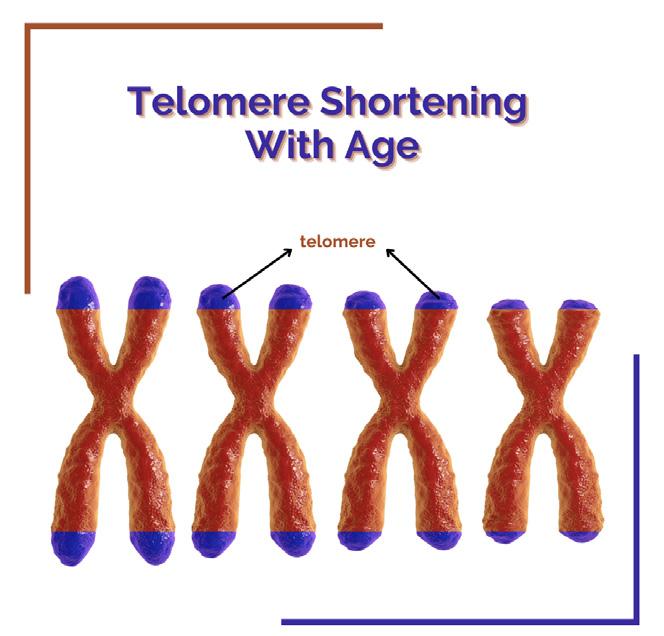
2: Telomere Shortening
The shortening of telomeres as one ages is pictured in Figure 2. The telomeres are the blue caps at the end of each chromosome. From left to right, the telomeres shorten as one ages.
Figure
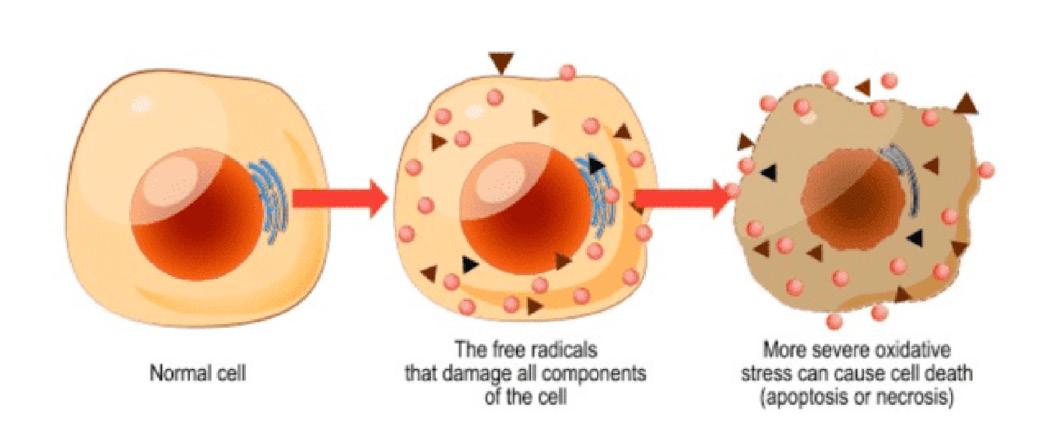
Figure 3: Oxidative Stress
Pictured here is accumulation of free radicals and reactive oxygen species, resulting in high oxidative stress.
SMOKING/ALCOHOL
Smoking is associated with accelerated shortening of telomeres, demonstrating a dose-dependent relationship. A study has found that smoking a pack of cigarettes each day results in the loss of an additional 5 base pairs of telomeric DNA per year. It is estimated that smoking one pack of cigarettes a day for 40 years is equivalent to losing about 7.4 years of life in terms of telomere shortening. Furthermore, smoking can cause oxidative stress in the body; oxidative stress is the disparity between the generation of reactive oxygen species (ROS) and the body’s capacity to remove these reactive intermediates from the body or repair any damage they may have caused. Oxidative stress can damage telomeres and accelerate the rate at which they are shortened. Cigarette smoke has a high concentration of ROS and free radicals that bring oxidative stress into the body’s lungs and bloodstream, thereby accelerating the shortening of telomeres. Smoking also triggers inflammation in the body, which increases as one ages. Chronic inflammation contributes to the breakdown of tissues and organs, accelerating the aging process and possibly contributing to the emergence of age-related illnesses. Like smoking, excessive alcohol consumption has been found to increase oxidative stress and cause inflammation, resulting in the shortening of telomeres.
OBESITY
Obesity is associated with elevated levels of ROS in plasma and urine. This suggests that obesity is linked with increased oxidative stress. This correlation is likely due to the uncontrolled production of adipocytokines, which are created by adipose (fat) tissue. Adipocytokines are signaling molecules that help regulate metabolism, inflammation, and immune function. In the case of obesity, they trigger and increase inflammation. Additionally, BMI is strongly correlated with biomarkers of DNA damage, regardless of age, indicating that obesity itself contributes to DNA damage. Researchers have found that compared to lean women in the same age group, obese women have substantially shorter telomeres. An 8.8-year reduction in life expectancy was associated with excessive telomere shortening in these obese individuals.
ENVIRONMENT: AIR POLLUTION
Air pollution is one of several environmental factors that play a role in telomere shortening. Pollutants such as particulate matter and nitrogen dioxide induce oxidative stress and inflammation by generating free radicals in the body. As previously described, oxidative stress leads to DNA damage and the shortening of telomeres. Toxins from industrial processes and pesticides, heavy metals, and pollutants from household cleaning items and paints are all contributors to oxidative stress, typically through prolonged exposure. Studies have shown that traffic police officers exposed to traffic pollution (toluene
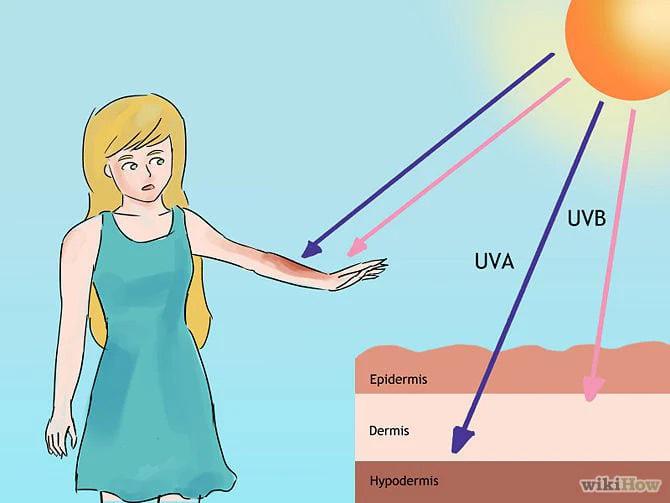
and benzene) exhibited shorter telomeres in their leukocytes as compared to office workers. Ultraviolet (UV) radiation, especially UVA and UVB rays, directly damages DNA, including telomeric regions, leading to telomere shortening. UV radiation impairs DNA repair mechanisms and accelerates skin aging, contributing to the overall aging process by promoting telomere dysfunction and cellular damage.
Figure 4: Ultraviolet Radiation Penetration on Human Skin UVA rays have longer wavelengths and penetrate deeper into the dermis (middle layer of skin), contributing to skin aging, skin wrinkling, and the development of skin cancer. UVB rays have shorter wavelengths and are almost entirely absorbed by the epidermis (outer layer of skin), contributing to sunburn, skin aging, and the development of skin cancer.
ENVIRONMENT: STRESS
The body releases cortisol and other stress hormones when stress triggers the “fight or flight” response. Chronically high cortisol levels can lead to inflammation and oxidative stress, both of which contribute to telomere degradation. Additionally, stress may impact the activity of telomerase, an enzyme involved in maintaining telomere length. One study examining the psychological stress of women in their daily lives found that women with higher levels of perceived stress exhibited shorter telomeres in some cells, decreased telomerase activity, and elevated oxidative pressure in comparison to women with low levels of stress. The difference in telomere length was found to be the equivalent of 10 years of aging, suggesting that chronic stress accelerates cellular aging. Fostering strong social connections, reducing stress, and maintaining good mental health are crucial components of increasing longevity. By nurturing relationships through regular communication and social engagement, individuals can combat feelings of loneliness and promote emotional resilience. Additionally, prioritizing mental health by cutting out unnecessary stressors, such as excessive social media use, and practicing mindfulness exercises like breathing techniques can alleviate anxiety and improve cognitive function. These small actions, which have the potential to improve mental, emotional, and social well-being, add to a comprehensive strategy for longevity and overall health.
ENVIRONMENT: GEOGRAPHY
Another aspect of the environment to consider is geography, as different regions vary in socioeconomic status; areas with lower socioeconomic status may have higher exposure to stressors, limited healthcare, and poorer nutrition, all of which can contribute to accelerated telomere shortening. Furthermore, different geographical locations have different cultural and social norms that impact stress levels and lifestyle choices. The Blue Zones are regions of the world where people live longer than the average population, likely due to their healthy lifestyle habits.
continued on next page >
Figure 5: The Blue Zones
Blue Zones are regions where people live longer, healthier lives, identified as Okinawa (Japan), Sardinia (Italy), Nicoya (Costa Rica), Ikaria (Greece), and Loma Linda (USA). Common factors include a plant-based diet, regular physical activity, strong social ties, a clear sense of purpose, and stress reduction practices.
Water, especially the ocean, holds profound potential for enhancing longevity. Its therapeutic effects, such as promoting relaxation and improving sleep quality, are well-documented. Exposure to sunlight near water boosts essential vitamin D levels crucial for immunity and bone health. Clean coastal air supports respiratory wellness, while saltwater benefits various skin conditions. Moreover, the meditative calm of ocean living promotes emotional well-being. Integrating water into daily life offers holistic health benefits, making it a cornerstone of longevity practices and promoting a vibrant and prolonged lifespan.
SLEEP
Sleep plays a crucial role in influencing the length of telomeres. Research suggests that longer sleep duration is associated with longer telomeres, while shorter sleep duration is linked to shorter telomeres. Telomere length maintenance may be aided by the body’s vital processes that occur while we sleep, such as cellular renewal and repair. On the other hand, insufficient or poor sleep may accelerate telomere shortening by raising oxidative stress and inflammation. According to a study analyzing data from the National Health Interview Survey, individuals with optimal sleep habits, including ideal sleep duration, minimal difficulty falling and staying asleep, absence of sleep medication use, and feeling wellrested upon waking, were 30% less likely to die from any cause and had a significantly reduced risk of cardiovascular disease and cancer-related mortality. Moreover, those with all five quality sleep measures enjoy a notable increase in life expectancy, with men gaining an additional 4.7 years and women 2.4 years compared to those with fewer favorable sleep factors. These findings emphasize the significance of prioritizing restorative sleep as a cornerstone of longevity-promoting strategies.
DIET
Unhealthy diets increase oxidative stress and inflammation, accelerating telomere shortening. High-sugar and saturated lipid diets that include red meat, processed meats, alcohol, and sugar-sweetened beverages are associated with the shortening of telomeres as well as cardiometabolic diseases. A diet focused on high fiber and unsaturated lipids is optimal for telomere health; foods such as legumes, nuts, fruits, dairy products, and coffee fall into this category. The Mediterranean diet is one of the most recommended models because of its antioxidant and anti-inflammatory properties. This diet features legumes, nuts, fruits, vegetables, fish, grains, olive oil, and a consistent but reasonable consumption of alcohol, particularly wine.
Figure 6: The Mediterranean Diet Pyramid
The Mediterranean Diet Pyramid is pictured in Figure 6, describing what kinds of foods and drinks to have as well as how often they should be consumed.
EXERCISE
Exercise is another vital factor in aging. Intense physical activities, like running, have been linked with longer telomere length as they increase telomerase activity and reduce oxidative stress. Current research has demonstrated that aerobic exercise for more than 6 months slows the degradation of telomeres. A study performed by Professor Larry Tucker of Brigham Young University found that adults who ran at least 30 to 40 minutes a day, 5 days a week, had a 9-year age advantage at the cellular level over those who are relatively inactive as well as a 7-year advantage over those who are moderately active.
EFFECTS OF TELOMERE SHORTENING
Maintaining a healthy lifestyle is crucial, as the shortening of telomeres puts individuals at higher risk for heart failure, coronary heart disease, diabetes, osteoporosis, and several cancers (lungs, bladder, head and neck, renal cell, and gastrointestinal). An accelerated rate of telomeric shortening is associated with early onset of these diseases.
GENETICS
Other factors that play a role in cellular aging are genetics and gender. Genetics accounts for about 25% of the variation in human longevity. Individuals inherit telomere length from their parents. Studies have shown that telomere length primarily follows a paternal inheritance pattern. Certain mutations can cause genetic disorders, such as Dyskeratosis Congenita, and directly affect telomeres, resulting in rapid shortening and premature aging.
GENDER
Women typically have longer telomeres than men, partly because of estrogen, a hormone that acts as an antioxidant and enhances telomerase activity, protecting telomeres from oxidative stress. Differences in lifestyle factors likely play a role as well, as men experience higher rates of smoking and alcohol consumption than women, contributing to shorter telomere length in males. Other lifestyle factors, such as work environment and stress levels, are thought to have some influence on the gender disparity as well.
HOW WE AGE: INDIVIDUAL PARTS OF THE HUMAN BODY
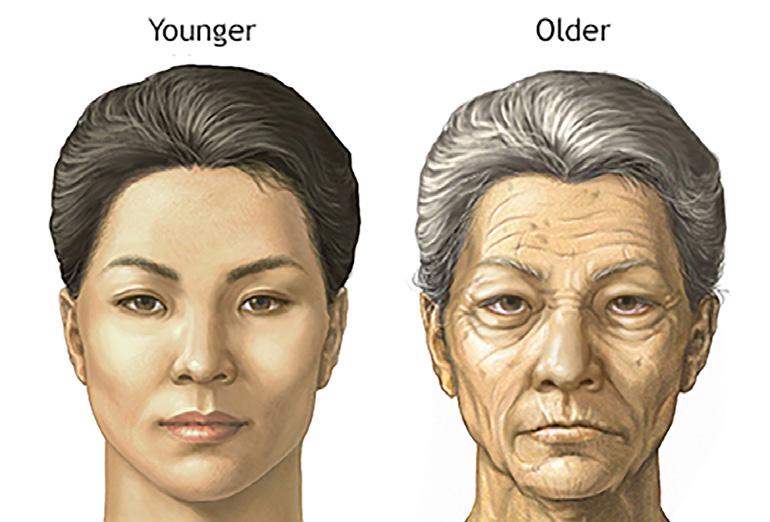
Examining how we age is also a necessary component of understanding how to increase longevity because it allows for targeted prevention and treatment strategies. The different parts of the human body age in different ways. For example, as we age, our skin becomes thin, wrinkly, fragile, and age spots begin to form due to reduced oil production and exposure to the sun. Our hair grays because of a lack of melanocytes, thins, and becomes brittle. With age, our faces lose muscle tone
resulting in sagging, our lips appear shrunken, our lower jaw loses bone mass, and our eyes look sunken because fat from the eyelids settles into the eye sockets.
Figure 7: Aging of the Face
Figure 7 displays the difference in one’s face as a result of aging. As previously described, our skin wrinkles and age spots began to form. Our faces lose muscle tone, our lips appear to shrink, our lower jaw loses bone mass, and our eyes look sunken.
Our hearts may slow, increase in size, develop arrhythmias, or experience valve stiffness. The brain and nervous systems lose nerve cells and weight, messages are passed slower, waste accumulates, reflexes and senses are reduced, and cognitive function declines. Bones become less dense and more brittle, lean body mass decreases, muscles become rigid, and joints become stiff. Lung tissue loses elasticity, the ribcage does not expand and contract as well, and the diaphragm weakens, all of which reduce respiratory efficiency. Furthermore, kidney, bladder, and liver function weakens as we age. The lenses of the eyes become less flexible, resulting in diminished visual acuity. Hearing loss is also common as the inner ear structure degenerates. In the digestive system, metabolism slows and digestive tract function decreases. Women experience a loss of fat, tissue, and mammary glands in their breasts. In the reproductive system, fertility declines, menopause occurs in women, and men may experience reduced testosterone levels and changes in sexual function. The immune system responds slower, the body heals slower, and autoimmune disorders may develop.
HOW TO INCREASE LONGEVITY
Now that we have examined why and how we age, we can review how to live longer. Advances in medicine, public health, and living standards have caused a significant increase in life expectancy. The global average life expectancy has increased from 32 years in 1900 to 71 years as of 2021. In the United States, the average life expectancy has risen from 47 years in 1900 to 76.4 years as of 2021 with the average lifespan being 73.5 years for men and 79.3 years for women.
As American comedian Aries Spears aptly stated, “To sustain longevity, you have to evolve.” In line with this wisdom, our approach to longevity must change as modern medicine and health practices do. This will ensure that individuals can thrive and experience prolonged periods of health and vitality by continuously adapting to new information and technological advancements. However, several lifestyle habits have consistently been found to be effective in increasing longevity. Eat a healthy and balanced diet that features foods rich in fiber and unsaturated fats as well as antioxidant and anti-inflammatory properties. Avoid smoking and limit alcohol consumption. Stay fit and in shape by exercising regularly, including both aerobic and strength-training exercises. Minimize exposure to environmental toxins, air pollution, and excessive UV exposure. Managing stress, getting adequate sleep, and staying mentally active by engaging the brain are also important habits as are regularly receiving health checkups, maintaining social connections, and having a positive outlook on life. Following these
practices will help slow the shortening of telomeres, reduce oxidative stress, lower disease risk, and slow aging at the cellular level. These strategies have been proven to be effective. One such example is Dr. Howard Tucker, the oldest practicing doctor in the world. Born in 1922 when the average life expectancy in the U.S. was 58 years for men and 61 years for women, Dr. Tucker is a 101-year-old neurologist who is still practicing today.
Pictured here is Dr. Howard Tucker when he was young (left) and how he currently looks (right).
His wife, Dr. Sara Siegel, is 89 years old and still practicing psychoanalysis and psychiatry. Dr. Tucker has credited his longevity to his genes and a few lifestyle practices he has consistently practiced over the years. These practices include continuing to work to reduce the risk of cognitive decline, exercising regularly (swimming, jogging, hiking, skiing), avoiding smoking, living in moderation, particularly in diet, and teaching the younger generations.
In summary, although no one has found Ponce de Leon’s fountain of youth, we have attempted to describe the mechanism and pathophysiology of aging and things we can do to prolong healthy life. A plant-based diet, avoiding smoking and alcohol, exercise, enough sleep, reducing stress, and finding joy in life are all pillars of longevity. It is also essential to remember the words of Martin Luther King, Jr., who wisely remarked, “The quality, not the longevity, of one’s life is what is important.” While longevity is undoubtedly valuable, it’s equally crucial to prioritize the quality of life, ensuring that extended years are characterized by vitality, purpose, and fulfillment.
This article was a collaboration between Mian A. Jan, interventional cardiologist practicing in Chester County, and
Figure 8: Dr. Howard Tucker
Talha Farooq, who is a student at Temple University
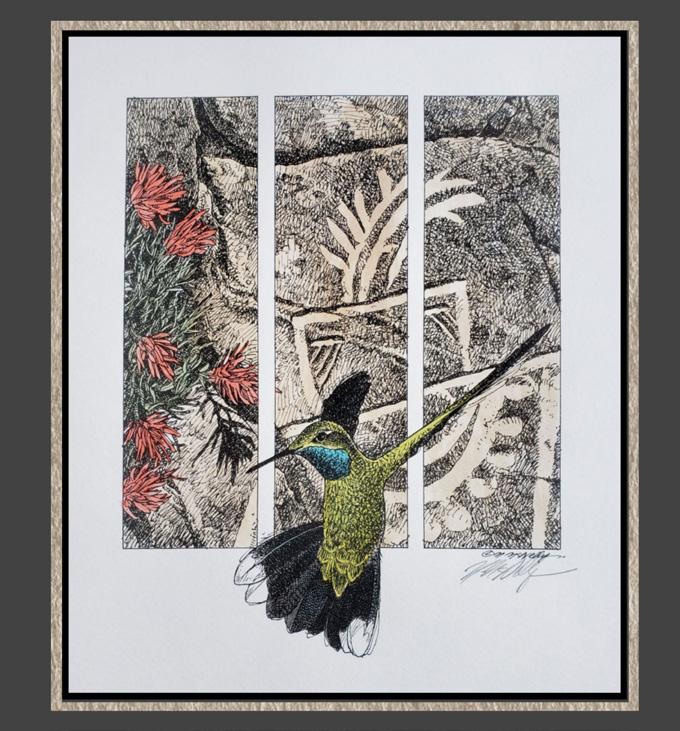
Michael mcnelly
BY BRUCE A. COLLEY, DO
I was lucky to meet with Michael on a bright sunny February day at his studio. I have met, interviewed and featured dozens of artists for our journal in the past 10 years, all exceptionally talented and unique in their approach to their craft and diverse in their oeuvres. Michael did not disappoint. Immediately upon entering his studio I was given a whirlwind tour and synopsis of his wide-ranging artistic endeavors. They include illustrations, sculpture and a recent addition to his artistic endeavors, something called gourd art. Michael uses a wide variety of media, including pencil, oil, acrylic, polychromal pencils, and watercolor. Moreover, he uses many natural materials as his canvas, such as stone, tile, petrified wood, and, as noted, gourds.
Early on in my interview with Michael I noted that with each question I asked, he answered with passion and energy. He would then have questions for me. I soon found the table being turned where the interviewer became the interviewee. Probing my interest in art, among many things, he asked, “What kind of art do you do? Why are you interested in art?” I responded that I have no talent in art whatsoever, but my mother was a pretty good artist, and my son and grandchildren seem to have a talent for it. Michael then casually mentioned that he was an art teacher at one point in his career. Then with infectious passion he launched into a tutorial encouraging me to draw. “Just draw! It doesn’t matter what it looks like, but it helps one think out of the box, improve and polish your thinking skills and catalyze your creativity.” Then with another mini lesson he explained many techniques to help our grandkids learn to enjoy art and encourage their creativity. I was reminded of my father, a professor of education who told me, while I was teaching chemistry for a few years before I went into medicine, that “The heart is the teacher.” The lesson being that it is ideal to be good at what you do but also to love what you do, and that passion will teach for you. There is certainly no question as to Michael’s love of art.
Michael was born and raised in Chester, Pennsylvania, then worked in many locations nationwide (see his artist statement). Michael then moved to Chester County about 20 years ago, attracted as are many artists to the wide-ranging and dynamic art community here. Since living in Chester County, Michael has concentrated on fine art. Though influenced by many artists, Jamie Wyeth and Peter Sculthorpe are two Chester County artists he finds especially talented and inspiring. Michaels’s career as an illustrator and commercial artist has given him clients as diverse as The Rolling Stones Magazine, Philadelphia Magazine, and TV Guide, as well as the Philadelphia 76er’s organization and an illustrator of many children’s books. Please take a moment to enjoy Michael’s breathtaking talent.
Hawk with Polychromal Pencil
Mouse 2 on Petrified Wood
ARTIST STATEMENT
“As an artist I explore and celebrate the natural world through a combination of ideas, concepts and images. We can all agree that our natural heritage deserves our protection, sharing my visions with society may perhaps bring the beauty of our planet to light.” Living in Chester County, Pennsylvania, my lifelong interest in art and nature has culminated into a career that is very fulfilling.
Upon graduation from Philadelphia’s Hussian School of Art in 1976, I embarked on a career in illustration. Some of my clients included the New York Times, The Jaques Cousteau Society, The Audubon Society, The World Wildlife Fund, The Sierra Club and The Nature Conservancy. While I still accept an occasional illustration assignment, my focus tor the last thirty-five years has been fine arts.
My travels in the Americas, from Alaska to the Amazon jungle, have deepened a strong interest in the natural world and its inhabitants. Banding raptors with the Raptor Trust, monitoring bluebird boxes for the Tyler Arboretum, and volunteering at the Tri-State Bird Rescue and Research Center have enhanced that passion. In addition, monies raised by the sale of my art helped to fund a publication entitled The Effects of Oil on Wildlife for a Washington, DC symposium. I have donated works in support of many organizations throughout the world. In addition, Penn State University, National Wildlife Federation and Bird Watcher’s Digest commissioned me for limited edition prints.
I have been fortunate enough to receive many awards over the years, such as The Philadelphia Academy of Natural Science’s Award of Excellence and purchase awards including University of Pennsylvania. My work is represented by numerous galleries nationwide and can be found in private and corporate collections throughout the United States and overseas.
Fawn in Spring
Man in the Moon
Cat on Ceramics
Hummingbird
Sunflower Saw
BUILDING HEALTHIER COMMUNITIES: CHRISTIANACARE’S WEST GROVE CAMPUS AIMS TO TRANSFORM LOCAL CARE
VINAY MAHESHWARI, M.D., MHDCS; HUGH R. SHARP, JR., CHAIR OF MEDICINE AND PHYSICIAN EXECUTIVE, THE MEDICAL GROUP OF CHRISTIANACARE
At ChristianaCare, we continually strive to meet the evolving health care needs of the communities we serve.
A key part of our strategy involves neighborhood hospitals, such as the facility we are building on our West Grove campus in southern Chester County in partnership with Emerus Holdings, Inc., the nation’s leading developer of neighborhood hospitals.
In recent years, many communities in southeastern Pennsylvania have faced hospital closures and reduced access to critical emergency care and other services. To address these challenges, neighborhood hospitals offer a sustainable and right-sized approach to providing high-quality care tailored to the needs of local communities.
Construction is underway on the 20,000-square-foot hospital at West Grove, which is expected to open in the summer of 2025.
The hospital will operate 24 hours a day, seven days a week. It will feature a 10-bed inpatient unit for overnight stays, observation care and testing. The emergency department will address urgent care needs such as falls, injuries, heart attacks and strokes. Additionally, the hospital will benefit from virtual consultations in specialties such as neurology and cardiology to enhance support services.
Patients arriving at the hospital will receive appropriate care for their needs. Those requiring complex, acute care or surgical intervention will be assessed and transferred to a larger hospital equipped for intensive care or surgical services.
Our goal is to make health care accessible and convenient for residents of southeastern Pennsylvania. We have also announced plans to build two neighborhood hospitals in Delaware County, including one in Aston and another at a site yet to be determined. Together, these three new hospitals will provide a new layer of care for the community.
The neighborhood hospital model brings several key advantages:
• Sustainability and scalability: These hospitals are designed to meet the needs of smaller communities efficiently.
• Efficiency and streamlined operations: Patients benefit from faster treatment and shorter wait times.
• Short-stay and outpatient focus: Advances in technology and treatment have reduced the need for extended hospital stays, making this model ideal.
• Personalized care experience: By building strong relationships within the community, these hospitals address unique health needs.
The neighborhood hospitals will be staffed by emergency physicians, hospitalists, radiologists, nurses and ancillary support staff. The three hospitals—one in Chester County and two in Delaware County— will share staffing and resources to ensure sustainable operations and support recruitment and retention of top talent.
In each of these communities, ChristianaCare will also provide outpatient services tailored to community needs. These include primary and specialty care practices along with a variety of other clinical services.
For physicians, these facilities and services offer opportunities for collaboration and coordinated care. ChristianaCare’s emphasis on integrated health services ensures seamless communication between the neighborhood hospitals and primary care providers, specialists and other health care resources. This approach minimizes care fragmentation and enhances continuity, supporting better outcomes for patients.
ChristianaCare is grateful to our Pennsylvania community partners for their feedback and support as we develop the new West Grove campus. The West Grove project is funded in part through generous grants from the Commonwealth of Pennsylvania and from the Chester County Board of Commissioners—Josh Maxwell, Marian Moskowitz and Eric Roe.
ChristianaCare has a long history of serving the residents of southeastern Pennsylvania. Today, we provide primary care at three Chester County locations: Jennersville, West Grove, and Kennett Square. Additionally, Concord Health Center in Chadds Ford, Delaware County, offers services such as primary care, women’s health, sports medicine, and behavioral health. Altogether, ChristianaCare serves as the medical home for 25,000 residents in these communities, reinforcing our commitment to delivering highquality, accessible care.
For more information about our West Grove Campus and services within the region, sign-up for our enewsletter at https://christianacare.org/us/en/facilities/west-grove-campus.
EVIDENCEBASED EXERCISE FOR OSTEOPENIA:
A SOLUTION YOU CAN RECOMMEND
As physicians, we know the importance of addressing osteopenia early to reduce the risk of fractures and improve patients’ quality of life. At Kinetic Physical Therapy, we’ve designed our Freedom Barbell classes using current research to help individuals with osteopenia safely improve Bone Mineral Density (BMD) and functional strength.
Using progressive resistance training, our classes incorporate barbell exercises such as the back squat, deadlift, bench press, and overhead press, all of which have been found to be key in addressing BMD in high-fracture areas including the spine, femoral neck, and wrists.
Our upcoming article in the CCMS magazine will highlight the current research that strongly supports the benefits of resistance training for improving BMD in older adults. For example,
• Harvard et al. (2024) This is tremendously useful to help offset age-related declines in bone mass as strength training, in particular, has bone benefits beyond those offered by aerobic weight bearing exercise.
• O’Bryan et al. (2022) found that progressive resistance training leads to simultaneous increases in muscle strength and BMD high risk fracture areas in older adults.
• Hejazi et al. (2022) demonstrated that exercise interventions, particularly those involving resistance training, significantly improve BMD in postmenopausal women.
At Kinetic, our Freedom Barbell Classes are designed by Doctors of Physical Therapy and supervised by experienced trainers who ensure individualized customization, proper technique, and progression tailored to each participant’s needs. These classes provide an empowering and safe environment for patients to combat bone loss and regain strength.
HOW TO REFER PATIENTS:
Referring your patients is easy—simply provide them with our contact information below, or use the referral pad we’ve included with this email. For more information on our program, please contact Dr. Gabriel Kresge at gabek@kineticptpa.com.
CONTACT US: 610-424-1100
LOCATION: Eagleview, 640 Rice Blvd., Suite 102, Exton, PA
WEBSITE: www.kineticptpa.com
Help your patients take the first step toward stronger bones and a healthier future. Thank you for supporting innovative, evidence-based care!
Best regards,
Dr. Gabriel Kresge, PT, DPT Kinetic Physical Therapy
INCREASING BONE MINERAL DENSITY THROUGH RESISTANCE TRAINING: A POWERFUL TOOL IN COMBATING OSTEOPENIA
BY DR. GABE KRESGE, PT, DPT
AN INTRODUCTION TO OSTEOPENIA
Life expectancy has almost doubled over the last 100 years. By 2050, the global number of individuals over the age of 65 is projected to rise from 703 million to 1.5 billion! (O’Bryan et al. 2022) With this rise in life expectancy, we can also expect to see a sharp rise in disease states commonly present in aging adults, including Osteopenia, Osteoporosis and Sarcopenia.
Osteopenia, a precursor to osteoporosis, is marked by low bone mineral density (BMD) and increased fracture risk. This disproportionally affects women due to the loss of estrogen and progesterone following menopause. For example, while the annual loss in muscle strength is relatively the same for both men and women between the ages of 65 and 80, the decline in bone mineral density is accelerated in women at 1.3% vs. 0.25% for men annually. (O’Bryan et al. 2022)
Fractures of the spine, wrist, and femoral neck related to poor bone density impair quality of life and independence, particularly in older adults. While pharmacological interventions are necessary and common, they do not address the biomechanical deficits and functional limitations contributing to fracture risk.
An evidence-based approach—progressive resistance training—has emerged as a powerful tool to improve BMD in these high-risk areas. This is tremendously useful to help offset age-related declines in bone mass as strength training, in particular, has bone benefits beyond those offered by aerobic weight bearing exercise. (Harvard Health Pub 2024) By leveraging this well-researched tool, Doctors of Physical Therapy health care and fitness professionals can help reduce the risk of fractures and the sequelae that follow them.
THE ROLE OF PROGRESSIVE LOADING IN BONE HEALTH
Bone is a dynamic tissue that responds to mechanical stress. Progressive loading, characterized by gradually increasing weight or resistance, triggers osteogenesis by stimulating the activity of osteoblasts. This process strengthens bone, particularly in regions subjected to high stress, such as the spine, wrist, and femoral neck.
Research consistently demonstrates the effectiveness of progressive resistance training (PRT) in increasing BMD. O’Bryan et al. (2022) conducted a systematic review and meta-analysis of PRT in older adults and found significant improvements in both muscle strength and BMD. Importantly, these gains were most pronounced in weight-bearing and at high-risk fracture sites including the wrist and femoral necks of individuals participating in the studies.
Similarly, Hejazi et al. (2022) analyzed randomized controlled trials examining exercise in older postmenopausal women and reported notable BMD improvements in the lumbar spine and hip. While this research highlights the positive effects of progressive loading, the fact remains that both patients and practitioners are often unclear on the best modality to receive the effects. In order to see BMD gains in highrisk areas and at the magnitude that instills a protective response, an understanding of proper loading exercises and techniques is required.
TARGETING HIGH-RISK AREAS FOR FRACTURE
According to Wolff’s Law, bones adapt to mechanical load. Mechanical load can come in the form of gravitational forces and muscle contractions. Progressive loading is particularly effective when applied to high-risk fracture sites.
These include:
1. Spine
Spinal fractures often lead to pain, deformity, and reduced mobility. Nguyen (2021) highlighted the critical role of axial loading exercises, such as squats and deadlifts, in maximizing BMD at the thoracic and lumbar spine. Axial loading refers to placing load on the spine in a vertical fashion, or in other words, placing load down through your spine while in a standing position. Examples of axial loading exercises include deadlifts, overhead presses and farmer’s carries.
2. Wrist
Wrist fractures are common in falls. Weight-bearing exercises, such as the bench press, overhead press, push-ups and weighted carries, place compressive forces on the radius and ulna, promoting bone remodeling and increased density. Incorporating dynamic movements improves wrist stability and reduces the risk of fallrelated injuries.
3. Femoral Neck
The femoral neck is a critical area for maintaining mobility and independence. Nguyen (2021) Fractures here often result in longterm disability or mortality. Exercises like the back squat, lunges, split squats, and step-ups target this region by generating high mechanical stress, encouraging bone growth and strengthening. As an added bonus, these movements have all been shown to increase functional strength and significantly contribute to activities of daily living (ADLS) and independence as aging progresses.
THE NEED FOR EXPERT GUIDANCE IN RELATION TO WEIGHTLIFTING
Unfortunately, due to a combination of factors including an increased sedentary lifestyle and a reduction in daily activities that require compound movements like squatting, pushing and pulling, many of us have lost the range of motion and motor control needed to perform these movements. This ability to simply “move” effectively must be established before implementing these compound movements under external load. Once the ability to perform these movements with bodyweight is achieved, the following principles are implemented:
• Axial Loading: Movements such as deadlifts, back squats, and overhead presses are essential for any BMD building program. These exercises have the greatest ability to affect BMD in the spine, femoral neck, and wrists.
• Progressive Loading: Prioritize incremental increases in resistance to match individual capabilities, ensuring a balance between challenge and safety. O’Bryan (2022) found that external load (%1 Rep. max.) of 75-80% 1 RM seemed better for improving BMD. This indicates that compound lifts utilizing higher weight and lower reps are the most beneficial for achieving desired BMD changes.
• Expert Guidance: Knowledge on compound lifting requirements and technique is essential in order to ensure proper form is being emphasized to reduce injury risk.
• Targeted ProgrammLing: Workouts and classes focused on functional movements should mimic real-world activities to enhance bone strength and overall functional capacity. Furthermore, progressive loading principles including using enough load to create healthy stress is key. If it doesn’t challenge you, it doesn’t change you.
EVIDENCE-BASED SUCCESS
In an effort to provide our community with a safe and effective program to combat osteopenia, Kinetic Physical Therapy has designed a classbased program using current evidence called Freedom Barbell. Freedom Barbell is designed by Doctors of Physical Therapy and has been operating since 2022.
Participants in Freedom Barbell classes have consistently demonstrated increased strength, improved posture, and greater confidence in their ability to perform daily activities—all indicators of enhanced bone and functional health.
“I was diagnosed with low bone density a year and a half ago, specifically in my femoral neck. As someone active in my sixties, this diagnosis came as a huge shock. I began researching ways to reverse bone density decline, which eventually led me to the team at Kinetic and their Freedom Barbell classes.
“I started slowly, focusing on light weights and technique, and the results have been transformative! Within just a few months, I saw significant improvements in my overall strength and balance. This program has truly been life changing.”
– SRC (current Freedom Barbell member)
IMPLEMENTATION IN CLINICAL PRACTICE
For medical doctors managing patients with osteopenia, referring to evidence-based programs like Freedom Barbell offers a practical, non-invasive option to complement pharmacological treatments. Collaboration between healthcare providers, physical therapists and strength coaches ensures a cohesive care plan, optimizing patient outcomes.
Key considerations for implementation include:
1. Patient Selection: Ideal candidates are those with osteopenia who are medically cleared for exercise. Individuals with contraindications, such as unstable fractures or severe cardiovascular conditions, should be evaluated carefully. Individuals with osteoporosis should be referred to Physical Therapy.
2. Customized Programming: Tailored exercise plans based on initial strength assessments and risk factors are critical.
3. Ongoing Monitoring: Regular reassessments of BMD and functional outcomes ensure the program remains effective and safe.
CONCLUSION
Progressive loading through resistance training offers a powerful, evidence-based solution for improving BMD in individuals with osteopenia. By targeting high-risk fracture sites—the spine, wrist, and femoral neck—this approach not only strengthens bone but also enhances overall physical function and quality of life.
At Kinetic, our Freedom Barbell classes exemplify how structured, progressive resistance training can transform osteopenia management. For physicians seeking effective, multidisciplinary solutions for their patients, integrating such programs into care plans represents a proactive step toward reducing fracture risk and promoting long-term musculoskeletal health. For more information on Kinetic, Freedom Barbell and ways to refer, physicians are encouraged to reach out to Dr. Gabe Kresge, PT, DPT, at gabek@kineticptpa.com.
REFERENCES
1. O’Bryan, S.J., Giuliano, C., Woessner, M.N. et al. Progressive Resistance Training for Concomitant Increases in Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis. Sports Med 52, 1939–1960 (2022).
2. Hejazi, K., Askari, R. & Hofmeister, M. Effects of physical exercise on bone mineral density in older postmenopausal women: a systematic review and meta-analysis of randomized controlled trials. Arch Osteoporos 17, 102 (2022).
3. Nguyen VH. Exercises aimed to maximize lean mass and bone mineral density at the hip and lumbar spine. Osteoporos Sarcopenia. 2021 Mar;7(1):42-43. doi: 10.1016/j.afos.2021.03.001. Epub 2021 Mar 18.
4. Harvard Health Publishing. Staying Healthy; Strength Training Builds More Than Muscles. 2024, Jan 16.
POSITION OF CHESTER COUNTY DEPARTMENT OF DRUG AND ALCOHOL SERVICES ON THE STATEWIDE LEGALIZATION OF CANNABIS
Adopted from PACDAA position paper March 6, 2024
The Pennsylvania Association of County Drug and Alcohol Administrators (PACDAA), an affiliate of the County Commissioners Association of Pennsylvania (CCAP), is a professional association representing the 47 Single County Authorities (SCA’s) across the Commonwealth. SCA’s receive state and federal dollars to plan, coordinate, and manage, fiscally and programmatically, the delivery of drug and alcohol prevention, intervention, treatment, case management, and recovery support services at the local level.
SCA’s have a keen interest in the current discussions regarding potential legalization or decriminalization of cannabis. We believe that any changes to public policy or law should be based on research and evidence, not public opinion polling. Our hope is that public health concerns will drive the conversation and the subsequent policy decisions. We believe that SCA’s and the prevention and treatment community need to be key stakeholders in the process and welcome the opportunity to participate in the discussion.
PACDAA employs the term ‘cannabis’ as a comprehensive descriptor that encompasses marijuana products and other related substances. This terminology reflects the diverse array of products derived from the cannabis plant, which are utilized for medicinal, recreational, or industrial applications.
The consensus of PACDAA members is to oppose full, statewide legalization and the creation of a new industry for distribution and sale of cannabis. In the situation where the Commonwealth proceeds with legislation allowing the legalization of cannabis, we are adamant that certain structures and plans be implemented to protect vulnerable populations. We offer the following concerns as areas that are critical to consider in these discussions:
• There are concerns with the legalization of cannabis use, including those related to overall public health and safety, the unintended impact on youth, a negative impact on mental health, impaired driving, and the continued prevalence of the illicit use. Additional consideration must be given to the type and manner of taxation and the ethical delegation of the tax revenue.
• Public health and safety concerns exist pertaining to the number of accidental poisonings1 and the interaction between cannabis and other medications,2 both of which can lead to an increased number of emergency department visits.
• The commercial cannabis industry has developed much more potent forms of cannabis. Between 1995 and 2015, THC content in the cannabis flower has increased by 212%.3 The emergence of edible cannabis products with high THC content presents new concerns regarding addiction potential and safety, including overconsumption, inconsistent labeling and formulation, accidental consumption, and products that may appeal to children.4
• Proximity to a medical cannabis dispensary has been associated with a four- to six-times larger usage of cannabis and higher positive expectations of cannabis.5
• The connection between cannabis use and a variety of mental health concerns cannot be disregarded. Research suggests that there may be a connection between cannabis use and psychosis/psychotic
like experiences,6 anxiety disorders,7 and suicide.8 9 Community healthcare facilities and emergency departments must learn more and be prepared to address episodes of cannabis-induced psychosis and other mental health conditions that may be related to cannabis use.
• The concerns for the adolescent population do not end at accidental poisonings10 and mental health conditions, such as psychotic disorders and psychotic-like experiences.11 Research of the impact of increased access to cannabis on youth and the developing brain must be involved in any public health discussion.
• The presence of cannabis retailers and cannabis advertising affects children’s perception of cannabis. A 2017 study in Oregon correlated exposure to the cannabis retail environment and adolescent cannabis use and beliefs, specifically noting that cannabis use in younger students was linked to the exposure to cannabis advertising and cannabis use in older students were more common for students whose schools were within a mile of a cannabis retailer.12
• Impaired driving remains a significant concern. Substantial evidence has shown a statistical association between cannabis use and an increased risk of motor vehicle crashes.13
Tetrahydrocannabinol (THC) impacts driving ability, specifically reaction time, lane position, and lane weaving.14 A national study examined impaired driving and found that risky driving behaviors were higher in states that legalized cannabis than states that did not legalize cannabis.15
• Discussions that legalization of cannabis is a solution to social justice issues have been disproven. Crime data in states that have legalized cannabis demonstrates how minority communities continue to be disproportionately affected in terms of arrests, justice system involvement, negative social and economic consequences, and public health impacts.16
• Diversionary programs (as opposed to/in conjunction with legalization/decriminalization) for specific levels of offenses (like ARD) are seen as an opportunity to utilize intervention and treatment services to reduce and/or prevent cannabis use disorder and other substance use disorders. Diversionary programs could decrease the costs to the criminal justice and other state and local systems and communities. 17
• Legalization of cannabis does not eradicate an illicit market. A study in CA found that the number USPIS cannabis seizures were greater in states that allow for medical and recreational cannabis than for states that criminalize cannabis.18 A February 2024 bipartisan letter from more than 50 members of Congress was sent to the Attorney General to express concern over reports of Chinese nationals cultivating cannabis illegally in the United States.19
• Legalization of cannabis can both positively and negatively impact the local economy. One study found that “post-legalization, average state income grew by 3 percent, housing prices by 6 percent, and population by 2 percent. However, substance use disorders, chronic homelessness, and arrests increased by 17, 35, and 13 percent, respectively.”20
• There are a wide variety of approaches to how to tax cannabis, including a percentage of price tax, a weight-based tax, and a potency-based tax. Each comes with its own pros and cons. The cannabis tax cannot be so high that users choose to purchase cannabis illegally, nor can it be too low and potentially limit the revenue to the state. Additionally, the question of where the revenue from cannabis tax should be dedicated must be carefully considered. If the amount of cannabis purchased and sold within the state decreases, how will these programs and services funded by the revenue from cannabis tax be affected?21
• There remain many unanswered questions and consequences regarding public health impacts of the legalization and use of medical cannabis, including in law enforcement, employment/ hiring practices, medical issues, and others that we see as the priority to focus on at this point.
SCA’s agree there is a need to discuss these critical issues with community stakeholders before the enactment of any new legislation. There are also diverse opinions regarding diversion, decriminalization, and enforcement efforts; current practice has resulted in inconsistencies in enforcement and penalties. PACDAA members support addressing social justice in a comprehensive approach that includes key stakeholders and is based on research that truly reflects this issue. Significant discussion needs to take place to whether counties and/or municipalities should retain the option to regulate cultivation, sale, delivery, security, inventory control and/or use of cannabis within their jurisdictions. Any local regulation should be opt-in rather than opt- out and counties and/ or municipalities must be able to create more stringent requirements than the state’s law if they so choose.
SCA’s and the prevention, intervention, treatment, and recovery communities must be key players in the process.
1 Hughes, A. R., Grusing, S., Lin, A., Hendrickson, R. G., Sheridan, D. C., Marshall, R., & Zane Horowitz, B. (2022). Trends in intentional abuse and misuse ingestions in school-aged children and adolescents reported to US Poison Centers from 2000-2020. Clinical Toxicology, 61(1), 64–71. https:// doi.org/10.1080/15563650.2022.2120818
2 Han, B. H., Brennan, J. J., Orozco, M. A., Moore, A. A., & Castillo, E. M. (2023). Trends in emergency department visits associated with cannabis use among older adults in California, 2005-2019. Journal of the American Geriatrics Society, 71(4), 1267–1274. https://doi.org/10.1111/jgs.18180
3 Stuyt E. (2018). The Problem with the Current High Potency THC Marijuana from the Perspective of an Addiction Psychiatrist. Missouri medicine, 115(6), 482–486.
4 Barrus, D. G., Capogrossi, K. L., Cates, S. C., Gourdet, C. K., Peiper, N. C., Novak, S. P., Lefever, T. W., & Wiley, J. L. (2016). Tasty THC: Promises and Challenges of Cannabis Edibles. Methods report (RTI Press), 2016, 10.3768/rtipress.2016.op.0035.1611. https://doi.org/10.3768/ rtipress.2016.op.0035.1611
5 Shih, R. A., Rodriguez, A., Parast, L., Pedersen, E. R., Tucker, J. S., Troxel, W. M., Kraus, L., Davis, J. P., & D’Amico, E. J. (2019). Associations between young adult marijuana outcomes and availability of medical marijuana dispensaries and storefront signage. Addiction (Abingdon, England), 114(12), 2162–2170. https://doi.org/10.1111/ add.14711
6 Sideli, L., Quigley, H., La Cascia, C., & Murray, R. M. (2020). Cannabis Use and the Risk for Psychosis and Affective Disorders. Journal of dual diagnosis, 16(1), 22–42. https://doi.org/10.1080/15504263.2019.1 674991
7 Myran, D. T., Harrison, L. D., Pugliese, M., Tanuseputro, P., Gaudreault, A., Fiedorowicz, J. G., & Solmi, M. (2024). Development of an anxiety disorder following an emergency department visit due to cannabis use: A population-based Cohort Study. eClinicalMedicine. https://doi. org/10.1016/j.eclinm.2024.102455
8 Doucette, M. L., Borrup, K. T., Lapidus, G., Whitehill, J. M., McCourt, A. D., & Crifasi, C. K. (2021). Effect of washington state and Colorado’s cannabis legalization on death by suicides. Preventive Medicine, 148. https://doi.org/10.1016/j.ypmed.2021.106548
9 Hammond, C. J., Hyer, J. M., Boustead, A. E., Fristad, M. A., Steelesmith, D. L., Brock, G. N., Hasin, D. S., & Fontanella, C. A. (2024). Association between marijuana laws and suicide among 12- to 25-year-olds in the United States from 2000 to 2019. Journal of the American Academy of Child & Adolescent Psychiatry, 63(3), 345–354. https://doi.org/10.1016/j.jaac.2023.06.014
10 see note 1 above
11 Kapler, S., Adery, L., Hoftman, G. D., Amir, C. M., Grigoryan, V., Cooper, Z. D., & Bearden, C. E. (2023). Assessing evidence supporting Cannabis Harm Reduction Practices for adolescents at clinical high-risk for psychosis: A review and clinical implementation tool. Psychological Medicine, 54(2), 245–255. https://doi.org/10.1017/s0033291723002994
12 Firth, C. L., Carlini, B., Dilley, J., Guttmannova, K., & Hajat, A. (2022). Retail cannabis environment and adolescent use: The role of advertising and retailers near home and school. Health & place, 75, 102795. https://doi.org/10.1016/j.healthplace.2022.102795
13 National Academies of Sciences, Engineering, and Medicine. 2017. The Health Effects of Cannabis and Cannabinoids: The Current State of Evidence and Recommendations for Research. Washington, DC: The National Academies Press. https://doi.org/10.17226/24625.
14 Sevigny E. L. (2021). Cannabis and driving ability. Current opinion in psychology, 38, 75–79. https://doi.org/10.1016/j.copsyc.2021.03.003
15 Lensch, T., Sloan, K., Ausmus, J., Pearson, J. L., Clements-Nolle, K., Goodman, S., & Hammond, D. (2020). Cannabis use and driving under the influence: Behaviors and attitudes by state-level legal sale of recreational cannabis. Preventive medicine, 141, 106320. https://doi.org/10.1016/j. ypmed.2020.106320
16 Sabet, K., & Jones, W. (2019). Marijuana Legalization in the United States: A Social Injustice. University of Pennsylvania Journal of Law and Public Affairs, 5(1), 15–23. https://doi.org/https://scholarship.law.upenn. edu/jlpa/vol5/iss1/3
17 Bernard, C. L., Rao, I. J., Robison, K. K., & Brandeau, M. L. (2020). Health outcomes and cost-effectiveness of diversion programs for low-level drug offenders: A model-based analysis. PLoS medicine, 17(10), e1003239. https://doi.org/10.1371/journal.pmed.1003239
18 Worrall, J. L., Han, S., & Mannumood, M. S. (2022). Marijuana Legalization and U.S. Postal Inspection Service Seizures: An exploration of black market activity. American Journal of Criminal Justice, 47(4), 617–636. https://doi.org/10.1007/s12103-022-09696-3
19 Sessions, P. (2024, February 2). Letter to Attorney General Garland Regarding CCP Affiliated Marijuana Farms. Retrieved February 28, 2024, from https://sessions.house.gov/_cache/files/2/6/26e3597f-1926-4b3c-afdf0ad74d4be61a/F237E75AF24FAF7F3301D05F24D04595.24.02.02--letter-to-ag-garland-regarding-ccp-affiliated-cannabis-farms.pdf.
20 Brown, J., Cohen, E., & Felix, A. (2023). Economic benefits and social costs of legalizing recreational marijuana. The Federal Reserve Bank of Kansas City Research Working Papers, 1–63. https://doi.org/10.18651/ rwp2023-10
21 Auxier, R. C., & Airi, N. (2022). (rep.). The Pros and Cons of Cannabis Taxes. Tax Policy Center. Retrieved February 28, 2024, from https://www. taxpolicycenter.org/publications/pros-and-cons-cannabis-taxes/full.
PIONEERING CARDIAC TREATMENTS FOR A HEALTHIER FUTURE
BASEL RAMLAWI, MD SYSTEM CHIEF, CARDIOTHORACIC SURGERY, AND CO-DIRECTOR, LANKENAU HEART INSTITUTE AT MAIN LINE HEALTH
Cardiac care has always been one of the most innovative fields in medicine because the heart is the engine of the body. As a cardiac surgeon with nearly twenty years of experience, I’ve witnessed first-hand how far we’ve come in the past decade—from the open-heart surgeries that took patients weeks to recover to the minimally invasive procedures that allow patients to leave the hospital the next day. Today, we aren’t just prolonging life; we’re enhancing the quality of life for patients in ways I couldn’t have imagined when I began my training.
The heart is at the core of everything we do—literally and figuratively. It supplies life to the brain, lungs, liver, and every cell in our bodies. Over the past ten years, technological advancements have transformed cardiac care, particularly in the way we treat heart valves and the aorta, the major blood vessel supplying the entire body. The ability to repair a valve or replace a section of the aorta through a tiny puncture, often while the patient is awake, is revolutionary. These innovations are not simply ensuring the survival of patients, they’re enabling them to carry on living with minimal pain and suffering, enjoying life better than before.
DELIVERING BETTER CARE, MINIMALLY INVASIVE METHODS
One of the central challenges in cardiac surgery has always been the delivery. We have effective treatments, but how do we deliver them in ways that reduce the burden on the patient? Traditional open-heart surgery, while often effective, requires significant recovery time, and for many patients, the idea of such an invasive procedure can be daunting.
The shift towards minimally invasive techniques has not only made these treatments more accessible but has dramatically improved patient recovery. One example I often reflect on is a recent valve replacement I performed—through a small incision, while the patient chatted with me. A decade ago, this would have required a full sternotomy and several days of hospitalization. Today, patients are going home within 24 hours, ready to resume their lives. They are attending their grandchildren’s graduations or even taking long-planned trips just days after their procedures. This transformation embodies the true essence of innovation in cardiac care: extending lives while simultaneously enhancing their quality.
BALANCING INNOVATION WITH PROVEN OUTCOMES
Introducing these cutting-edge procedures is not without its challenges. As healthcare professionals, we must balance our excitement for innovation with the need for proven outcomes. The rigorous scientific method is the backbone of everything we do, ensuring that new treatments aren’t just effective in theory but bring meaningful results to patients’ lives. Large-scale clinical trials and ongoing data collection allow us to validate these innovations—and sometimes, we find that what seemed promising doesn’t work as well as we hoped. The key is to
adapt, to be both scientist and caregiver, and to always prioritize what’s best for the patient.
I’ll never forget an elderly patient in her late seventies who came to us with a complex aortic aneurysm. She had multiple comorbidities—bad lungs, kidney issues, a history of stroke—and had been turned down for surgery by several other specialists. Offering her a traditional openheart procedure would have likely led to months in the hospital, with a high risk of complications. Instead, we enrolled her in a trial for a new, less invasive approach. Through small incisions in her neck and leg, we replaced her entire aortic arch, without the prolonged recovery or significant health risks.
That patient walked out of the hospital days later, not weeks or months. To me, this is what cutting-edge cardiac therapy is all about: providing solutions that are specifically tailored to patients’ needs, allowing them to enjoy not just longer lives but better ones.
A HYBRID APPROACH TO CARDIAC CARE
The future of cardiac care, in my view, lies in a hybrid approach. We take what works from traditional, proven methods and combine it with the latest technological advancements to offer the best of both worlds. For example, integrating traditional surgical expertise with catheterbased techniques—where we guide thin, flexible tubes through blood vessels to treat heart conditions—allows us to tailor treatments to each patient’s unique needs. No two patients are the same, and the ability to customize treatment plans by drawing on multiple approaches ensures better outcomes.
Being a cardiac surgeon today is not about doing every procedure for every patient. It’s about being an expert in a specific disease, knowing when surgery is the right option, when a minimally invasive approach would be better, and when simply monitoring is in the patient’s best interest. Our goal is not only to extend life but to enhance its quality.
THE ROAD FORWARD
The heart surgery field is evolving, and so too must the role of the cardiac surgeon. We must embrace new technologies while remaining deeply connected to the tried-and-true methods that have served our patients well. The future is bright, and the advances on the horizon— from enhanced imaging technologies to more sophisticated hybrid procedures—will only continue to push the boundaries of what we can achieve.
For those of us at the forefront of cardiac care, the mission is clear: Innovate with purpose, treat each patient as an individual, and always strive to enhance both the length and quality of life.
For more information or to refer a patient for cardiac consultation or second opinion, please contact Dr. Basel Ramlawi at 484.476.5648 or RamlawiB@mlhs.org
HIGHLY PATHOGENIC AVIAN INFLUENZA A (H5N1) VIRUS UPDATE
BY WILLIAM F. KRAMER, D.O.
BACKGROUND
Highly Pathogenic Avian Influenza A, HPAI, are novel Influenza A viruses that are antigenically and genetically different from seasonal Influenza A viruses that circulate among humans. Influenza A viruses are categorized into subtypes based on two surface proteins: hemagglutinin (H) and neuraminidase (N). There are 18 known hemagglutinin subtypes (H1-H18) and 11 neuraminidase subtypes (N1-N11), leading to various H and N combinations. (VDH.VIRGINIA.GOV)
In humans, the primary subtypes responsible for seasonal flu are A(H1N1), the strain that emerged during the 2009 pandemic and has since become a regular human flu virus, and A(H3N2), another common subtype causing seasonal flu outbreaks. (WHO.INT) Influenza B is a less common seasonal flu strain.
Other subtypes, such as certain H5, H7, and H9 strains, primarily infect animals with occasional human infections noted after direct contact with infected animals. These human cases are rare and do not typically result in human-to-human transmission.
The panzootic of HPAI A(H5N1) viruses in wild birds has resulted in outbreaks among commercial poultry and backyard bird flocks and has spread to domesticated animals, notably dairy cattle. Sporadic human infections with HPAI A(H5N1) virus have been reported in 23 countries since1997, with a small number of cases since 2022. Human infections with H5N1 occur after unprotected exposure to sick or dead infected poultry or dairy cattle. Since April 2024, there have been 68 confirmed cases in the U.S. Most human infections with H5N1 in the U.S. are clinically mild, with one reported fatality. To date, there have been no cases in Chester County or Pennsylvania.
WHO IS AT RISK/PUBLIC RECOMMENDATIONS
Livestock farmers and workers handling poultry and dairy, Veterinarians and staff, food processing workers including slaughterhouse workers, animal health responders and laboratory personnel, and employees engaged in culling poultry all have increased risk of exposure to H5N1. Game bird hunters are at risk for exposure to sick birds as well. Personal protective equipment that includes an N-95 respirator, gloves, safety goggles, face shield, head cover, disposable coveralls, and shoe covers is recommended when direct or close contact is required by atrisk personnel.
The public should avoid exposure to sick or dead animals. Poultry, eggs, and beef should be cooked to a safe temperature. Raw (unpasteurized) dairy products like milk, cheese, and ice cream should be avoided. Pasteurized milk is safe.
RECOMMENDATIONS FOR CLINICIANS
H5N1 can present with symptoms similar to Influenza A(H1N1). Patients with symptoms of acute upper or lower respiratory tract infection, conjunctivitis, or gastrointestinal symptoms such as diarrhea may have HPAI A(H5N1). It is important to ascertain if the patient has had any contact with sick or dying poultry, dairy cattle, or wild birds, or has ingested raw dairy or poultry products within 10 days to the start of symptoms.
The state and local health departments should be notified immediately of any suspected cases of HPAI. Clinical specimens should be collected as soon as possible if HPAI A(H5N1) is suspected. If the patient has conjunctivitis, with or without respiratory symptoms, both a conjunctival swab and a nasopharyngeal swab and/or nasal swab combined with an oropharyngeal swab should be collected. The County Health Department should be notified if you suspect HPAI A(H5N1), and guidance for specimen collection and delivery of the specimens will be provided. Alerts from state and local health departments have been sent to urgent care facilities, hospitals and clinicians with guidance.
Patients hospitalized for suspected HPAI will have specimens collected and subtyping of Influenza A performed. This will help identify the involved strain in the infection.
Post exposure prophylaxis, PEP, can be given to patients who experience high risk exposure. Oseltamivir BID for 5 days is the preferred regimen. Longer treatment courses may be necessary for patients with compromised immune status. The same medication is employed for treatment. There is no available vaccine at the present time.
Asymptomatic patients who report exposure are reported to the Health Department and undergo monitoring for 10 days. Testing is performed if symptoms develop. Since Spring 2024, roughly 15,000 people have been monitored and more than 700 have been tested in the U.S. The current public health risk is considered low by the CDC.
Further detailed guidance is available on the CDC website.
CHAMPIONING WOMEN’S MENTAL HEALTH: THE WOMEN’S EMOTIONAL WELLNESS CENTER
Mental health is a critical aspect of overall well-being, yet women often face unique emotional and psychological challenges that require specialized care. The Women’s Emotional Wellness Center, part of Main Line Health, was established in 2015 to meet the distinct behavioral needs of women in the community. Expanding to Main Line Health King of Prussia in 2020, the Women’s Emotional Wellness Center continues its mission to provide comprehensive, compassionate and evidence-based mental health services tailored to women at all stages of life.
ADDRESSING THE UNIQUE MENTAL HEALTH NEEDS OF WOMEN
Women experience mental health challenges that can stem from biological, social, and cultural factors. Life transitions, hormonal changes, trauma, and the pressures of caregiving roles often contribute to increased rates of depression, anxiety and mood disorders among women. The Women’s Emotional Wellness Center recognizes these unique challenges and offers a supportive environment where women can receive individualized care.
Among the common mental health concerns addressed are:
• Depression, anxiety, and mood disorders
• Trauma and its lasting effects
• Adjusting to life’s transitions
• Work-life balance and stress management
• Relationship challenges
• Parenting concerns
• Grief and loss
• Unexpected medical outcomes
A COMPREHENSIVE RANGE OF MENTAL HEALTH SERVICES
The Women’s Emotional Wellness Center offers a full spectrum of outpatient behavioral health services designed to meet the diverse needs of women. Services include individual therapy, group therapy, and specialized treatment programs, all led by a team of experienced psychiatrists, therapists and behavioral health professionals. Key offerings include:
WOMEN’S PARTIAL HOSPITALIZATION PROGRAM (PHP)
One of the few women-only PHPs in the nation, this intensive program provides structured, short-term treatment for women requiring more support than traditional outpatient therapy but less than inpatient hospitalization. The PHP incorporates:
• Group psychotherapy
• Individual therapy
• Psychiatric care and medication management
• Dialectical Behavior Therapy (DBT) techniques
• Trauma-informed care and mindfulness-based interventions
WOMEN’S INTENSIVE OUTPATIENT PROGRAM (IOP)
Designed for women who need more than weekly therapy but do not require PHP-level care, the IOP offers structured group therapy sessions that focus on:
• Coping strategies for anxiety and depression
• Managing trauma and grief
• Enhancing self-esteem and resilience
• Navigating relationship and communication challenges
DIALECTICAL BEHAVIORAL THERAPY (DBT INTENSIVE OUTPATIENT PROGRAM (IOP)
DBT is an evidence-based approach that helps individuals regulate emotions, improve distress tolerance and develop interpersonal effectiveness. The DBT IOP provides:
• A structured curriculum focusing on emotional regulation
• Practical coping skills for stress management
• Supportive group settings to foster connection and healing
THE NEST PROGRAM: PRE- AND POSTNATAL MENTAL HEALTH SUPPORT
A standout offering is the Nest Program, which provides specialized support for women before, during and after pregnancy or adoption. Emotional challenges during the perinatal period are common but treatable with professional care. The Nest Program addresses:
• Anxiety and depression during pregnancy and postpartum
• Postpartum depression and adjustment difficulties
• Infertility-related grief and emotional distress
• Birth trauma and unexpected medical outcomes
• Emotional effects of NICU stays and special healthcare needs
• Adoption-related emotional challenges
The Nest Program also extends its support to spouses, significant others, grandparents and caregivers, ensuring that the entire family unithas access to care and resources.
TELEHEALTH AND EXPANDED ACCESS TO CARE
Recognizing the importance of accessibility, Women’s Emotional Wellness Center has integrated telehealth services to ensure women can receive care regardless of location or personal circumstances. Virtual therapy sessions and remote psychiatric care allow patients to connect with clinicians in a flexible and convenient manner, reducing barriers to mental healthcare.
A COMMITMENT TO COMPASSIONATE, EXPERT CARE
At the heart of Women’s Emotional Wellness Center is a team of highly skilled professionals dedicated to women’s mental health. The center’s staff includes board-certified psychiatrists, psychiatric nurse practitioners, licensed clinical social workers and therapists who specialize in women’s behavioral health. Their approach combines clinical expertise with deep compassion, creating a safe and nurturing environment for healing.
The Women’s Emotional Wellness Center stands as a beacon of support for women navigating mental health challenges. By providing specialized, evidence-based treatment in a compassionate and empowering setting, Women’s Emotional Wellness Center plays a vital role in enhancing the well-being of women and their families. As awareness of the importance of mental health continues to grow, the Women’s Emotional Wellness Center remains steadfast in its mission to ensure that every woman in the community has access to the care she deserves. For more information about Women’s Emotional Wellness Center and its services, visit mainlinehealth.org/wewc or to refer a patient contact 888.227.3898.
Scan this QR code to schedule an Office Visit or a Procedure (like a colonoscopy).
COLONOSCOPY CANCER
Colon cancer can be lethal if undetected. Colonoscopy has long been considered the Gold Standard in colon cancer detection and treatment. But today, US Digestive Health has set a higher standard in the detection and removal of cancerous polyps.
Introducing The Platinum Standard®
Combining an advanced AI-enabled technology with the experience of our gastroenterologists, USDH can now detect and remove more dangerous polyps and save more lives than ever before.
L to R: Dr. Katelyn Bradley, Dr. Maria DeMario, Dr. I. Dennis Holgado, Dr. Nicholas Kalman, Dr. John Khalifa, Stacey Yantis (CRNP), Dr. Stephen Belfiglio, Dr. Valerie McAuley, Dr. Michael McGuire, Elizabeth Facciolo (CRNP), Sarah Smith (CRNP), Dr. Lauren Kummer, Dr. Susan Leath, Dr. David Lewis, Carrie Karhnak-Glasby (CRNP), Suzannah Maynard (CRNP), Dr. Douglas Atlas, Dr. Sadaf Ausaf, Dr. Qurratulain Baig, Dr. Katherine Chin, Dr. Heather Lockner, Dr. Jane Sunoo, Dr. Mariele Briones, Dr. Christopher Bruno, Dr. Neema Chokshi, Dr. Matthew Kane, Dr. Arti Patel, Amy Knickerbocker (CRNP), Debbie Preble (CRNP), Dr. Susan Kohli, Dr. Monika Kumanova, Dr. Marianne Nikas, Dr. Drew Rowan, Dr. Gene Uhler, Dr. Alpa Vadher, Erin Lender (CRNP), Denise Meli (CRNP), Dr. Brian Boucher, Dr. Charles Catania, Dr. John Hornick, Dr. Sissy John, Dr. Sony John, Dr. Madeline Wood, Andrea Leffet (CRNP), Anita Snyder (CRNP), Sue Villarini (CRNP), Dr. Vitasta Bamezai, Dr. Harmony Bonnes, Dr. Francis Brennan, Dr. Victoria Brosius, Dr. Eric DiCicco, Dr. Laurie Gallagher, Dr. Neeraja Peri, Dr. Jessica Schleusner, Dr. Rannette Schurtz, Dr. Eric Yeh, Laurie Taylor (CRNP)
RECREATIONAL MARIJUANA: ITEMS TO CONSIDER
Marijuana, which can also be called cannabis, weed, pot, or dope, refers to the dried flowers, leaves, stems, and seeds of the cannabis plant. The cannabis plant contains more than 100 compounds (or cannabinoids). These compounds include tetrahydrocannabinol (THC), which is impairing or mind-altering, as well as other active compounds, such as cannabidiol (CBD). CBD is not impairing, meaning it does not cause a “high,” according to the Centers for Disease Control (CDC).
MARIJUANA FACTS:
The Centers for Disease Control has studied marijuana, and its impacts on public health.
• Marijuana is the most commonly used federally illegal drug in the United States; 48.2 million people, or about 18% of Americans, used it at least once in 2019.
• Recent research estimated that approximately 3 in 10 people who use marijuana have marijuana use disorder. For people who begin using marijuana before age 18, the risk of developing marijuana use disorder is even greater.
• Marijuana use directly affects the brain, specifically the parts of the brain responsible for memory, learning, attention, decisionmaking, coordination, emotion, and reaction time. Infants, children, and teens (who still have developing brains) are especially susceptible to the adverse effects of marijuana and THC.
• Long-term or frequent marijuana use has been linked to increased risk of psychosis or schizophrenia in some users.
• Using marijuana during pregnancy may increase the person’s risk for pregnancy complications. Pregnant and breastfeeding persons should avoid marijuana.
• Marijuana can make the heartbeat faster and can elevate blood pressure immediately after use. It may also lead to increased risk of stroke, heart disease, and other vascular diseases.
• Marijuana use has been linked to social anxiety, depression, and schizophrenia (a type of mental illness where people might see or hear things that aren’t there), but scientists don’t yet fully understand the relationships between these mental health disorders and marijuana use.
• Unintentional poisoning may occur; edibles, or food and drink products infused with marijuana, have some different risks than smoked marijuana, including a greater risk of poisoning. Children can mistake edibles for regular food or candy. Consuming marijuana can make children very sick. Since marijuana use has been legalized in some states, unintentional poisonings in children have increased, with some instances requiring emergency medical care.
BABIES’ HEALTH AND DEVELOPMENT:
Marijuana use during pregnancy may cause fetal growth restriction, premature birth, stillbirth, and problems with brain development, resulting in hyperactivity and poor cognitive function. Tetrahydrocannabinol (THC) and other chemicals from marijuana can also be passed from a mother to her baby through breast milk, further impacting a child’s healthy development.
IMPACTS ON DRIVING:
• States that have legalized marijuana have seen the impact of impaired driving.
• Marijuana, like alcohol, negatively affects several skills required for safe driving. It can slow reaction time and ability to make decisions.
• Marijuana can impair coordination and distort perception when driving.
• The use of multiple substances (such as marijuana and alcohol) at the same time can increase impairment.
• Some studies have shown an association between marijuana use and car crashes.
• Since recreational marijuana was legalized, traffic deaths where drivers tested positive for marijuana increased 138% while all Colorado traffic deaths increased 29%.
• Since recreational marijuana was legalized, traffic deaths involving drivers who tested positive for marijuana more than doubled from 55 in 2013 to 131 people killed in 2020.
• Since recreational marijuana was legalized, the percentage of all Colorado traffic deaths involving drivers who tested positive for marijuana increased from 11% in 2013 to 20% in 2020
COMMERCIALIZATION DELIVERS SOCIAL JUSTICE:
• According to “Lessons Learned, after 4 years of MJ Legalization (paper 2016) Smart Approach to Marijuana (SAM),” on the surface, legalizing marijuana might sound like a good way to address issues of systemic injustice. People of color are almost 6 times more likely to be arrested for all drugs, including marijuana, than whites.
• Drug and narcotics crime in Denver has increased at about 11% per year since marijuana legalization. While it is unclear if legalization has caused this increase, it does contradict promises of pro-legalization advocates that legalization would reduce such crime rates.
• Indeed, Denver’s overall crime rate has risen, as well as rates of serious crimes like murder, motor vehicle theft, aggravated assault, and burglaries. Many marijuanarelated offenses, such as public marijuana consumption, have also increased as use has trended upward.
IMPACTS ON EMPLOYMENT:
States that have legalized marijuana have seen impacts on employment.
• According to a study reported by the National Institute on Drug Abuse, employees who tested positive for marijuana had 55% more industrial accidents, 85% more injuries and 75% greater absenteeism compared to those who tested negative.
FIVE MAIN PRONGS TO
‘COMBAT’ THE NEGATIVE IMPACTS OF LEGALIZATION:
1. Require zoning restrictions (local ordinances regarding where shops can be located, density/ number of shops allowed in municipalities).
2. Require marketing restrictions (what ages can be targeted, what kinds of images can be used, what kinds of claims can be made). Those who are marketing the sale of marijuana should be required to uphold standards in various ‘truth in advertising’ laws and in the regulations surrounding the medicinal/healing claims that can be made.
3. Emphasize concurrent areas of restriction (employment impacts, job restrictions regarding use of machinery or access to certain work).
4. Emphasize potency restriction measures (if it does become legal, work on minimizing the amount of THC that is legal).
5. “Big Tobacco” has been justly criticized for employing an unethical marketing strategy that relied on cultivating lifelong addicted customers to ensure ongoing profits. A major part of this strategy focused on making tobacco use attractive to youth. Indications from states that have legalized marijuana for adult use is that “Big Marijuana” is employing the same playbook (PACDAA position paper March 2022).
OTHER LINKS:
• PA Department of Health oversees the MJ cards, doctors, and dispensaries in PA: https://www.pa.gov/guides/pennsylvaniamedical-marijuana-program/
• County Commissioners Association of Pennsylvania (CCAP’s) Medical Marijuana Task Force page: https://www.pacounties.org/GR/Pages/ MedicalMarijuanaTaskForce.aspx
• Permitting pot is one thing; promoting its use is another: https://www.newyorker.com/magazine/2019/01/14/ is-marijuana-as-safe-as-we-think