3 minute read
Accurate collimation


Accurate collimation reduces patient exposure by limiting the size and shape of the x-ray field to the area of clinical interest. Careful and accurate collimation is emphasized and demonstrated throughout this textbook. The adjustable collimator is used routinely for general diagnostic radiography. The illuminated light field defines the x-ray field on accurately calibrated equipment and can be used effectively to determine the tissue area to be irradiated. Safety standards require light field and x-ray field concurrence within 2% of the selected siD.
The concept of divergence of the x-ray beam must be considered for accurate collimation. Therefore, the illuminated field size as it appears on the skin surface appears smaller than the actual size of the anatomic area, which would be visualized on the IR. This is most evident on a projection such as lateral thoracic or lumbar spine (Fig. 1-177), in which the distance from the skin surface to IR is considerable. In such cases, the light field, when collimated correctly to the area of interest, appears too small unless one considers the divergence of the x-ray beam.
Advertisement
The practice of visible collimation on all four sides of a radiograph reduces patient exposure, improves image quality, and acts as a method to ensure that appropriate collimation did occur. If no collimation border is visible on the radiograph, evidence does not exist that the primary beam was restricted to the area of clinical interest. An added benefit of showing the extent of collimation on all four sides is the ability to check the final radiograph for correct central ray location. As described previously, this is done by imagining a large “X” extending from the four corners of the collimation field, the center of which is the CR location.
ColliMATion RUle
A general rule followed throughout this text indicates that collimation should limit the x-ray field to only the area of interest, and collimation borders should be visible on the iR on all four sides if the IR size is large enough to allow four-sided collimation without “cutting off” essential anatomy.
ColliMATion AnD TissUe Dose
Accurate and close collimation to the area of interest results in a dramatic drop-off in tissue dose as distance from the border of the collimated x-ray field is increased. For example, the dose 3 cm from the edge of the x-ray field is about 10% of that within the x-ray field. At a distance of 12 cm the reduction in dose is about 1% of that within the x-ray field.*
PosiTiVe BeAM liMiTATion (PBl)
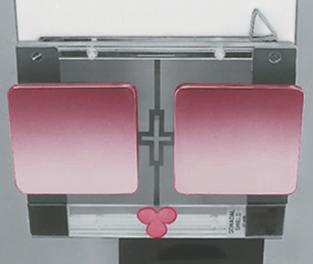
All general-purpose x-ray equipment built between 1974 and 1993 in the United States required collimators with positive beam limitation (PBL) that automatically adjusts the useful x-ray beam to the film size (this requirement became optional after May 3, 1993, as a result of a change in U.S. Food and Drug Administration [FDA] regulations). The PBL feature consists of sensors in the cassette holder that, when activated by placing a cassette in the Bucky tray, automatically signal the collimator to adjust the x-ray field to that film size. PBL can be deactivated or overridden with a key, but this should be done only under special circumstances, in which collimation by manual control is needed. A red warning light is illuminated to indicate that PBL has been deactivated. The key cannot be removed while PBL is overridden (Fig. 1-178).
MAnUAl ColliMATion
Even with automatic collimation (PBL), the operator can manually reduce the collimation field size. This adjustment should be made for every projection in which the IR is larger than the critical area to be radiographed. Accurate manual collimation also is required for upper and lower limbs that are acquired tabletop, in which PBL is not engaged. Throughout the positioning pages in this textbook, collimation guidelines are provided to maximize patient protection through careful and accurate collimation.
The practice of close collimation to only the area of interest reduces patient dose in two ways. First, the volume of tissue directly irradiated is diminished, and second, the amount of accompanying scattered radiation is decreased. Scatter radiation produced by additional tissue in the x-ray field from improper collimation or lack of shielding not only adds unnecessary patient dose but also degrades image quality through the “fogging” effect of scatter radiation. (This is especially true in high-volume tissue imaging such as abdomen and chest.)

Fig. 1-177 Close four-sided collimation. The collimated light field may appear too small because of divergence of x-rays.
Red light Key
*Keriakes JG, Rosenstein M: Handbook of radiation doses in nuclear medicine and diagnostic x-ray, Boca Raton, 1980, CRC Press. Fig. 1-178 Automatic collimation (PBL).