

WWW.PHYSICIANOUTLOOK.COM | 1 | VOLUME 9 | 2022 PHYSICIAN OUTLOOKMAGAZINE 2022: THE YEAR WE START ANEW WWW.PHYSICIANOUTLOOK.COM PUBLICATION DEDICATED SOLELY TO PHYSICIANS AND THEIR PATIENTS Cover Artists: Moritz Albrecht, MD and Marwen Eid, MD Po


LIFE CHANGER byAmandaDunec,MD/p.4-5
TECHOS DE CRISTAL by MarleneJ.Wüst-Smith,MD/p.6
THE PHOENIX byEdenCourville,BA/p.8-9
TWO CENTS ON PHYSICIAN UNITY byDanaCorriel,MD/p.10
ALTRUISM IN MARRIAGE? byGeorgeP.Naum,MD& VanessaNaum/p.11
RECOVERING FROM COVID byRoxanneBruce,MBA,DrBA/p.12-13
THE BEST DOG EVER byPeterCoffman,MD,FAPA/p.14-15
FIGHTING FOR THE HEALTH OF OUR COMMUNITIES byKristineScheer,SHRM-SCP/p.17
EVERYDAY IS AN INTERVIEW byRileySnowden& MaryAnneVaccaro,BFA/p.18
LET’S TALK ABOUT WOMEN AND SEXUAL DYSFUNCTION byRileySnowden/p.23
DEFENDING THE OATH I TOOK byDianaBlum,MD/p.24-25
RACHAEL DENHOLLANDER VS. LARRY NASSAR byRileySnowden/p.26-27
LIGHTS, CAMERA, ACTION! byRileySnowden/p.28
WE NEED TO STOP CALLING IT BURNOUT byAndrewJ.Sauer,MD/p.29
@THEMODELSURGEON byEdenCourville,BA& SheilaNazarian,MD,MMM/p.30-32
BE BRAVE ENOUGH TO SPEAK UP! byMyieshaD.N.Taylor,MD/p.33

I want to take a moment to say thank you to all of our readers! Thank you for sticking with us, for supporting us, and for understanding as we work hard to improve our magazine. We admit that 2021 brought us some challenges. From print house issues to staff changes, it has been a wild ride.
At Physician Outlook we provide a safe space for learning and mentorship opportunities for students who are working towards a future in journalism, marketing, and/or healthcare. This issue has several articles from our rockstar intern Riley Snowden, a Public Relations major at Penn State University class of 2022. She did a fantastic job and we wish her the best luck in all of her future endeavors.
Featured in this issue are speakers from the Brave Enough Conference, a life changing women’s conference created by cardiac anesthesiologist Dr. Sasha Shillcutt. If you are wondering why your calendar is full but your heart is empty, it probably has a lot to do with your needs. Brave Enough helps thousands of women find clarity, set boundaries, and gain control of their lives.
“You just have to be brave enough to take that first step...”
Also featured is the first of many articles from Fair in Medicine. FAIR in Medicine is a nonpartisan professional network dedicated to advancing the highest ethical standards in medical practice, and to promoting a common medical culture based on critical thinking and the pursuit of excellence in all medical endeavors.
Fair in Medicine is an extension of The Foundation Against Intolerance and Racism (FAIR), a nonpartisan organization dedicated to advancing civil rights and liberties for all Americans, and promoting a common culture based on fairness, understanding and humanity.

Respectfully,
Roxanne Bruce, MBA, DrBA Managing EditorBerkeley photos courtesy of Peter Coffman, MD, FAPA
My first thought when I received the Brave Enough Conference pictures was — Dr. Sasha Schoville Shillcutt is someone to whom I want to dedicate an entire post.
She has changed my life.
I feel like a broken record on this topic but it’s true. And so I will say it over and over again. The power of 1.
She is 1.
Not only has she changed my life, but she has changed the lives of so many others. So many women I now get to do life with. Being in the public eye comes with tremendous pressure and responsibility. She shoulders that every day.
I am grateful she does because without her leadership and vision, I’d be in a different place. Many people reach out to me in different ways sharing the impact I have on their lives (which I always much appreciate). Sasha and BE are part of the reason I get to do what I do. This is how the chain works. Everyone tries their best, it makes an even larger splash. To anyone who thinks their impact isn’t great enough — nonsense.
Show up. Rise up. Level up.
You never know who is watching. You never know who needs exactly you. Sasha takes away from her family and herself to be a leader. It can be lonely in moments at the top. So today, I toast Sasha. And all the visionaries who choose others in many moments over themselves. And I believe this deeply: in our choosing of others, we ultimately choose ourselves!
Written by Amanda Dunec, MD
For
more information, head to www.physicianoutlook.com
Dr. Sasha Shillcutt - Featured in this issue
Mrs. Aimee Lowe
Rachael Denhollander - Featured in this issue
Dr. Julie Freischlag
Cy Wakeman
Alli Worthington
Ms. Hilary Blair - Featured in this issue
Dr. Lyndsay Harper - Featured in this issue
Dr. Erica Howe
Dr. Annaheita Kalatari
Dr. Tiffany Love
Dr. Howard Liu
Dr. Ed Mariano
Dr. Sheila Nazarian - Featured in this issue
Dr. Amy Shah - Featured in a future issue
Mary Anne Vacarro - Featured in this issue
Dr. Tom Varghese
Dr. Nneka Unachukwu
A defining moment of my childhood was when my Cuban-born “Papi” recommended that I choose medicine “so I would never have to financially depend on a man” (Iwas then a naïve career-planning 2nd grader torn between a “well-paying” career as a pediatrician (HaHa!--joke is on me!) vs. becoming a teacher with summers off and lots of free time for my future children.
Even as a child I recognized my father’s counsel to be very powerful yet dichotomous advice. I was used to watching “I Love Lucy” on television and knew that my father was his own special brand of “Ricky Ricardo” -- charming, but somewhat culturally bred to be chauvinistic. Yet. . . he wanted for me, his first-born daughter, to have a career that would never leave me wanting or needing a man for support. He was an early feminist of sorts, but one who also revels -- even to this day (he just turned 85) -- in being awkwardly and inappropriately flirtatious around pretty women. He has always been a “womanizer” who is “a lot of talk” and no action.
friends were getting married and starting their families, I spent my 20’s and 30’s studying hard, working long shifts, and barely meeting anyone outside of medicine. I had very little time left for dating. In my mind I had very high standards for who I wanted as a life-partner, and was very suspicious of anyone who DID want to date me. I also had a very unfortunate knack for choosing poorly in my younger days. I went from almost marrying a cardiac surgeon who (unlike my dad was more action than talk in his womanizing ways) to becoming engaged to a nearly homeless recovering alcoholic HarleyDavidson aficionado. I recognize now that low self-esteem and “settling” were strong motivators for my poor choices.
It was emotionally very difficult to be a pediatrician to everyone else’s children,
to connect with families and patients who could not possibly imagine that I was “THE” doctor.
A few years ago I read an article about Chelsea Batista1, a Dominican medical student who, like me, was accepted to almost every medical school to which she had applied. Naysayers attributed both of our success to “affirmative action” programs, but she made a powerful statement to which I can relate:
“At some points, i hAd to remind myself thAt i eArned these Accomplishments thAt i worked just As hArd As those Around me And thAt i hAd to breAk through A prominent glAss ceiling to get here. i hAd to remind myself thAt i wAs not chosen becAuse i Am A hispAnic womAn who fulfills the requirements i wAs chosen becAuse As A hispAnic womAn, i hAd to struggle through more obstAcles And resistAnce thAn the typicAl medicAl school ApplicAnt And i still mAnAged to excel.”


He had two very strong sisters (my aunts) who were trail-blazers and role models for me. His oldest sister, Ana Maria, who we all called “Tia China” qualified for the Cuban Women’s Olympic Basketball team as a college student. She went on to study chemistry and later become a college professor. His other sister, Miriam (who raised me as her own daughter) worked at a Cuban law firm as a paralegal before coming to the United States, and then went on to become a teacher at our elementary school. Both aunts eventually married and raised families, staying at home when we children were young.
I did not have that luxury as a woman in medicine. While my high school and college
suspecting that I, myself, would never be able to fulfill my lifelong dream of becoming a wife and mother. Very few men seemed interested in dating female medical students or doctors, and I felt that being Latina was an added burden. I dreaded the label “solterona” (Spanish for an older unmarried woman or “Old Maid”).
Lady physicians often complain that patients and staff frequently mistake them for nurses, even when they introduce themselves as “doctor.” My brown skin, my large derriere, and my ability to speak fluent Spanish often led patients and staff members to mistake me for a hospital cleaning lady, cafeteria worker, or an orderly. I sometimes used this familiarity to my advantage, and although discriminatory, I was often much better able
Spoiler alert:
I eventually did meet and marry my “Prince Charming,” when I was almost 35, introduced by his 3 year old niece Ryan, who was one of my first pediatric patients when I started in private practice. Together, we fulfilled my life-long dream of becoming a mother to our wonderful daughter, Madison, on my 37th birthday. Jim and I recently celebrated our 22nd wedding anniversary.
Dreams DO come true, and glass ceilings are meant to be broken.



A songbird.
I flew freely across the skies, singing as my wings glided easily through the air.
I wanted the world to hear my song. Upon the ground, a man beckoned to me “songbird please come grace me with your voice,” My heart fluttered and I flew down to get a closer look, cautious but not enough to fly away.
I sang for him and his eyes lit with wonder. I was delighted to share my song. He asked me to stay with him telling me I could fly off as I wanted to share my song with the world, and I agreed, wanting to make him happy.
I continued to sing for him many times and it always brought him joy, which brought me joy. I began to feel restless on his perch and asked him if I could fly off to share my song with others, but he denied me saying he didn’t want them to hear because it was special to him. I accepted this for a while but soon I continued to ask, desperate to spread my wings and spread my song, and his responses became irate.
He would tell me my voice wasn’t good enough for others and sometimes rip off my feathers in anger. I realized I would need to fly away by myself, and plotted my time to fly away.
He noticed this change in me however and at night he held me and clipped my wings so I could no longer fly. And with that, my song died.
Another found me and though I had dyed my feathers black to appear perhaps as a Raven instead, he approached “you’re not a Raven you’re a songbird.”
I was alarmed but he touched my feathers gently to wash away the black and told me that just because my wings were clipped did not mean I couldn’t sing. “If you sing your song for me I will fix your wings so you can fly,” I spent a long time singing by his side a darker melody than before.
He cared for me at first, lightly touching my feathers, listening in fascination. However, he began to grow bored of my song, and he began to tell me I was worthless, that my singing was deafening. I was no good and no one should have to hear or see how ugly I was. However cruel his words got, I endured because I was nothing without him.
I woke one night to find he was plucking my feathers as I slept in an attempt to make sure no one found me beautiful. Despair plagued me at the realization of the damage he had done, and when I begged him to stop he took out a match to set my feathers on fire.
I was consumed by flames, smothered by the smoke as I watched him disappear in the blinding black. My eyes opened and I emerged from the ashes alive. I realized that I was never just a songbird. My singing wasn’t made just to entertain others. The flames burn, but in the end, I only come back stronger than before. My new wings spread and carefully I taught myself how to fly.
“I’mnotjustanysongbird,” I thought as I sang into the night, I’m a Phoenix.
Written by Eden Courville, BA Artwork courtesy of author
The last decade has brought about astounding growth in the number of entrepreneurial physician leaders who have incredible ideas, many of whom have actually put foot to pedal and opened up online spaces and communities for physicians to engage in and collaborate with one another.
In a world where physicians are increasingly isolated from one another, these groups have become invaluable sources for “finding our people.”
Physicians who individually innovate in today’s world, however, face a major pain point: they work hard to build and nurture their groups, but they sometimes struggle getting visibility for them. So growth can be painstakingly slow.
Conversely, physicians who are looking for groups to join (particularly social media “newbies” who are just dipping their toes into a digital world) are becoming easily duped and disappointed when they realize that some of the groups they have joined and invested time in are nothing more than self-serving businesses for their physician founder.
The unsuspecting and trusting physician who is looking for camaraderie, support, advice and a sense of community can easily fall victim to leadership and an organization that are not measurably different from the bureaucratic employed hospital models that many in medicine are fleeing. There’s nothing wrong with these groups and leaders, other than the fact that they are not being transparent.
WE’RE CHANGING THAT.
At SoMeDocs, we believe in getting Facebook groups (as well as other social media platforms) the visibility they deserve. We have formed an interactive space-- a physician “United Nations” of sorts-- that functions on one simple premise: experts want to collaboratively grow. We bring together like-minded individuals who are interested in collaborating with other hard working administrators and physician-members.
We have created a unique and inclusive online space at www. DoctorsOnSocialMedia” that is called “Physician Interactive Spaces” where doctors can click in and see from a “30,000 foot view,” who’s running what
physician group, and how that group is run/what the purpose is/what the rules are.
We are categorizing these interactive spaces, so that you and I, and all of our colleagues, can finally be made aware of all the many groups are out there. There is strength in numbers, and in order to effect change, and to break up some of the “same” we are seeing and giving fuel to the “little guy” who is just starting out.
If you are a physician “doer” and the administrator of a Facebook group (or other social media community) please join our collaborative at SoMeDocs. If you are a physician member of a group that we don’t know about, please encourage the founders and/or administrators to contact us.
doctorsonsocialmedia.com/submissioncommunities
If you are a physician and haven’t claimed YOUR free profile do so today! doctorsonsocialmedia.com/claim-myprofile
 Written by Dana Corriel, MD View this author’s profile on www.doctorsonsocialmedia.com
Written by Dana Corriel, MD View this author’s profile on www.doctorsonsocialmedia.com

Let’s start by defining the word. Altruism, according to Webster’s Dictionary is, “the belief or practice of self-less interest and concern for the well-being of others”.
Studies have shown that there are brain-based rewards in being altruistic. Hormones such as oxytocin and neurotransmitters like dopamine provide us with, like the old saying says, “a good feeling all over”. The good feeling brought about by altruism provides us with better health (stable blood pressure, less heart disease, and less stress), better wellbeing in the form of increased happiness and finally a better sexual relationship as arousal and desire are known to increase as a result of altruistic actions.
As physicians, we have chosen a profession that has historically been seen as an altruistic profession. It was the driving force that made me want to become a doctor. My vision was altruistic and my desire was to have a positive impact on peoples’ lives for a purpose greater than my own.
Now, think about this for a moment, what if we apply those same principles of altruism to our marriage much like we do to our practice of medicine? So doc, do you really practice self-less interest and concern for the wellbeing of your partner? Let us begin by examining our actions. Then, be the force of good for a greater purpose in our marriage.
Marital altruism calls for actions made for the higher purpose of the marriage itself. The marriage is greater than the sum of its parts. Putting this into practice, I am concerned about the health and welfare of my wife in every respect, as well as her emotional, physical, psychological, intellectual and spiritual needs, and I know she reciprocates.
Is it possible to be altruistic all of the time? After all, let’s face it, we are human and we have our own needs and desires. But, being a believer of the phrase “what we put into the lives of others comes back into our own” makes me confident that putting it into practice in my marriage will
be an example that will be reciprocated. In most relationships, this is an ideal or something we would like to see happen. I urge you to adopt it as a value and make it happen because the sum will be greater than its two parts.
I invite you to practice altruism within your marriage and watch. . . what you put into the life of your partner will come back into your own. And, it will be multiplied!
 Written by George P. Naum, MD and Vanessa Naum
For more information, head to www.physicianoutlook.com
Written by George P. Naum, MD and Vanessa Naum
For more information, head to www.physicianoutlook.com
In April of 2021, I started to feel ill, but then my husband tested positive for COVID-19 and we figured that I probably had it too. That is when the worrying started as I have Multiple Sclerosis and a compromised immune system from my bi-annual infusions. You might ask why I didn’t run to get the vaccine, and the answer is pretty simple.
The doctors didn’t think it would work! I had a small window just before my infusions that we stood a chance for my body to create antibodies and we weren’t there yet. You see, COVID-19 got me before I had a chance to go out and get a vaccine to stop it. After 7 days in the ICU fighting to survive, I was sent home on oxygen at 8L and told to do a series of exercises to work on my legs and my lungs.
After months of hard work, it appeared that I was getting better. Better to the point where I no longer needed the oxygen and could go back to life as normal. Well, as normal a life as someone with a chronic illness can get.
Let me share my thoughts on what worked and what didn’t work as well. Feel free to share it with other folks struggling with postCOVID recovery. My solution will not work for everyone, but it is certainly something that everyone can talk to their doctors about. Having backup plans to backup plans makes all the difference. I noticed that as my care was passed from group to group, first the ICU, then the home health staff, then my PCP, there was a lack of coordinating care to help me get back to normal. So what you read here is a combination of advice from multiple providers as well as what I tested on my own.
I came home from the ICU on oxygen 24/7 at a rate of 8L. There were few instructions on how to wean off of oxygen. The nurses said that my body would need it to heal my lungs, the doctors agreed with that sentiment as well. I was provided with a machine to help train my lungs and instructed to use that daily! I went from being able to pull 250ml of air into my lungs to be able to pull almost
2,500ml of air over a 3 week period. Still, I was on the oxygen, though I had lowered it to 4L because my nose was constantly cracking and bleeding even with the humidifier.
By week 4 the nurses and I were talking about possible ways to reduce the oxygen and how to go off of it completely. Many of the places that I wanted to go would have required 2-4 tanks of oxygen just for the car trip! Living in farm country is great until you need medical care, then everything is far, far away. The home health staff and I discussed tactics of going off cold turkey for a few hours a day or lowering the output by .5L every 3 days. Let me explain what did and didn’t work.
Going off of it for 15-minute intervals, worked for 1x per day, but the 2nd or 3rd time I tried to go off oxygen, my O2 fell and took a while to come back up. My little finger blood ox reader was beeping like a maniac!
Going down .5L every 3 days wasn’t super reliable. It worked towards the end, but in the beginning, 3 days wasn’t enough. For the first 2 weeks, I put 6 days between each .5L drop.
Switching from the nasal cannula to a mask and vice versa. It was only after family and friends pointed out that the reason the hospital was able to send me home with a mask was that I was on 8L of oxygen. The mask isn’t safe below that because the air exchange made it so that there was too much CO2. I am sure the hospital staff told me that too, but I was way too sick to remember and we (neither them nor I) wrote it down.
Trying to do stuff on hot humid days is still a total bust. It gets hard to breathe, I get exhausted, and even with dragging around the oxygen tank, it just doubles down on the exhaustion. Just don’t do it yet! Even in July, months after I first got sick, the hot and humid days were too much for my lungs.
Eating a full meal! When your belly is full, it feels like (I don’t know if there really is) a lot less room for your lungs. It is especially hard if you need to lay down. So just eat several small meals at first until you know that you can manage a big meal.






Burnout. Moral injury. Emotional exhaustion. Anger, and frustration, that makes us question our choices, ourselves, and others when faced by the day-to-day stressors in our professional lives as physicians. Navigating the inconsistencies, the changing environments, the overwhelming demands, and the forced injustices we face daily in the realms of modern healthcare brings so many of us to the brink in our professional and personal lives.
Those of us lucky enough to find the means of making our profession less chaotic, less toxic to ourselves and our loved ones, and heel the galloping madness that is the profession of medicine in this era, are the ones who find solace in healthy outlets and supports.
Until we lose one of those supports.
As a practicing psychiatrist, I have been fortunate enough to have a constant companion and support, my dog Berkeley. A therapy dog, he has been a fixture in my office for the past three or so years, with my current organization fully supportive of his daily presence. Adored by patients and loved by my staff of therapists and office personnel, his was a bright presence bringing calm, and joy, and peace to so many.
So many young trauma victims, so reluctant to talk of what befell them, would hug and hold Berkely (or Barkleby, or Barks, or Berks, or Sparkly, or whatever
the other dozen or so nicknames he responded to. . .) and feel so much safer Patients, visitors, pharma reps. . . all looked forward to seeing him and his bright presence and his “Joker dog smile”.
Every morning, I would let him off the leash so he could trot down the hall to hurry to make his ‘rounds’, stopping for treats in different offices, his nails clicking so jauntily on the wood flooring. Berkeley was also known in the community: more than once, an employee has told me that people in the community recognize our organization as “the place where Berkeley works”. So many people described him as “remarkable”, “refined”, “unique”, and so many other words that described Berkeley as a person, which he was. . . he was more earnestly human than many other persons I have known, and in entirely good ways.
Mostly, however, his greatest role was in helping me maintain my equilibrium and equanimity with his presence, either lying in his dog bed under my desk, or on the carpet by my feet. During administration meetings, he would sit upright in a chair next to me, and look around at everyone, as if listening and participating, and likewise in my group supervisions with the therapy staff. As I adored Berkeley, he did me, as well. That rush of oxytocin that flooded my brain, and likewise his when our gaze met, his tail wagging furiously, fueled me with elation.
Our conversations on the drive to and from work, despite being primarily onesided, were extensive. . . when he did speak, it was often quite profound yet succinct. . .
When my mom passed away a few years ago, he was there, letting me cry my eyes out into his fur. When I was deathly ill when he was a puppy, he stayed by my side until the ambulance took me away in hypovolemic shock.
During other emotionally taxing periods in my life, he was my steady best friend. When I used to drive my Armada to visit my family in Louisville, he would spend the entire trip sitting on the broad armrest next to me, never laying down, and maintaining a constant eye on everything around me, as if he were my navigator. Riding in the convertible, he would not stick his nose into the wind; instead, he would lay with his head upon my arm. A comfort to both of us.
Doesn’t matter what kind of shitty day I might have had, Berkeley always made it better. He was Krypto to my Superman (and I have the statues of both in my office to prove it). He lay in his dog bed that resembled Captain Kirk’s command chair from the bridge of the USS Enterprise while I worked on the computer in my home library, a constantly reassuring presence.

The worst day ever.
We lost him August 1st, 2021 around 9AM, and very suddenly. He had been severely ill in late May/early June, and I thought we were losing him then. But he bounced back from diabetic ketoacidosis/ pancreatitis and surgery (splenectomy for tumors that were benign). The past week or so, he developed labored breathing and was lethargic, and started on ABX for a UTI. He perked up fro 2-3 days prior to his passing, bright and happy and had his sparkling smile back. On the last day of July, I woke up and he was laying next to me. He perked up when I said it was time to go out, seemed excited. We would let out.
We walked down the stairs, passed through the dining room to the kitchen. . . yet he did not follow. I turned back to the dining room, where he was on his side, seizing. He stopped breathing and expireddespite attempts to provide doggy CPR, check serum glucose, etc. . . Based on everything, I believed he had a stroke and died. We held him all day after he died. He appeared peacefully asleep, but from a slumber from which he could never awaken.
The next morning we took him to be cremated, saying goodbye on his final car ride. . .
I am devastated, and heart broken. I am one of those people who believes dogs are special beings, the co-evolution of humans and canines over the past 20,000-40,000 years forging a unique interspecies bonding not achievable between humans and other animals. And Berkeley was (to me) the pinnacle of that co-evolutionary process. The bond we shared was nothing like any other dogs I have had, or ever hope to have again, I fear. He will be painfully missed. I dreaded returning to the office to be consoled by the staff and by patients, for I know they loved Berkeley, and knowing just how many lives he touched makes it that much harder to accept his loss. My best friend has died.
Berkeley. . . . THE BEST DOG EVER. 2/15/2011-8/01/2021

 Written by Peter Coffman, MD, FAPA Photos provided by author For more information, head to www.physicianoutlook.com
Written by Peter Coffman, MD, FAPA Photos provided by author For more information, head to www.physicianoutlook.com

In early 1990, I was newly married, finishing my undergraduate degree, and taking home a part-time income cashiering and bagging groceries. I was also pregnant with my first child, and over the course of the next two years become a parent to two young girls.
Giving birth was my first adult encounter with the healthcare system. After experiencing birth complications with one delivery, I realized how disparate the standards of care were at different hospitals using different doctors.
Fast forward to 2017. I was working in the health insurance industry as a broker, designing and managing plans for employers. Access to high quality healthcare varied radically in the U.S., even for those covered by insurance, and American health metrics were low compared to those in other developed nations. Healthcare had become a mega money industry where consolidated health systems, insurers, and venture capital
firms were making big bucks off the backs of hard-working Americans and their employers. How could our country be spending more on healthcare than any nation in the world yet have such poor health?
I co-founded K2 Strategic LLC in 2017 to be part of the solution. Quality, affordable healthcare should be a right, not a privilege. We partner with like-minded physicians, nurses, and administrators to design employer-sponsored health plans that deliver higher quality health care at
Restoring health and financial dignity to Americans and their employers is our mission.
Fighting for the health of our communities against the big business of healthcare is a daily battle.
I do it for people like 1990s me who had no idea where to turn to get quality care at an affordable price. Aligning my an entrepreneur is the hardest yet best
For more information, head to

Growing up, I have always been told by my mother, “Every day is an interview.” If you are unsure what she means by this, my mother emphasized that I should always look my best going out because I never knew who I would run into out and about. I have always questioned this as a child, thinking if I go out to the grocery store or post office, who am I trying to impress? If I see someone I know or meet someone new, they should accept me for who I am.
Well, I have learned my lesson in my late teen years and early 20’s that mothers, in fact, do know best. I live by this statement now in a slightly different way, that even though I am not trying to impress anyone going out to certain places, I still want to look the best for myself, to make myself feel good and improve my performances for any type of activity.
In an article published by The Huffington Post, Dr. Audrey Tang, a psychologist and member of the British Psychological Society, says that by dressing up, we “walk taller,” meaning we make our posture better. Good posture has a surprising effect on one’s mood to make someone feel more confident in themselves, which in results makes the person more confident in how they look too.
So why do I bring this up? Because none other than award-winning designer Mary Anne Vaccaro can make us feel the best AND more confident in her couture clothing when we are feeling the desire to dress up. Vaccaro, located in Omaha, Nebraska, has been a designer for over 40
years and has styled anything from bridal gowns, suits, and dresses for those who are looking to enhance their look.
Mary Anne began designing at a young age, learning how to create patterns, as well as cut and sew from her grandmother who was a seamstress. Vaccaro studied at Minneapolis College of Art and Design and the University of Nebraska at Omaha, receiving a BFA in Fine Art, Art History, and Theatre Costuming.
The renowned designer has owned multiple businesses, specifically Mary Anne Vaccaro Design, which she has been running for over 37 years. In her role at Mary Anne Design she has been a business owner, production manager, designer, speaker, and image stylist. Vaccaro has created wear for the New York Bridal industry, being the first designer to create bridal and bridesmaid separates in the 1980s for Bill Levkoff in New York. In addition, she is a stylist for Carlisle in New York and ran a Fashion Advertising business for several years for over 50 stores in 5 states.
To add the cherry on top, Vaccaro has her own business for cooking wear, called Invisible Apron, creating clear, invisible aprons to show off your style while making the most delicious meals.
Vaccaro has designed for those of the highest caliber, creating coronation gowns for three queens of Ak-Sar-Ben, as well as the gowns of their princesses, countesses, and courtesans. By now, I am sure you
are already able to see that Vaccaro has a unique and keen sense for design.
Her style is intricate and custom made, creating pieces that will suit and please just about anyone. Vaccaro has been recognized by Town and Country Magazine for her evening and cocktail wear, as well as her Ready-to-Wear Collections. The Durham Museum praised Vaccaro for her work in 2009 and even created an exhibit for her gowns.
Due to the exposure of design at such a young age, Vaccaro has been able to make herself a self-made, successful designer. She has been recognized nationally and talked highly of by many. Her passion and love for the industry has made her career all the more rewarding and has opened many different avenues, such as her many businesses and collaborations. So, the next time you are wanting to get dressed up and make yourself feel great, reach out to Mary Anne Vaccaro, I am positive you will not be disappointed.
Written by Riley Snowden and Mary Anne Vaccaro, BFA
Thank YOU (yes, YOU!)
It is because of subscribers, contributors, advertisers, and sponsors like YOU that Physician Outlook has continued to grow and flourish in the “medical magazine” space. We highlight the beauty, artistry, and humanity of our profession like no other publication in existence. We give a voice to patients and physicians alike!
OUR MISSION IS TO TAKE BACK MEDICINE ONE ISSUE AT A TIME! WITH YOUR HELP, IN 2022, WE WILL HELP EVEN MORE PEOPLE FIND THEIR VOICE.
Our print magazines, with stunning physician art, have become coveted collector’s items, and readers tell us that PO is one of the few publications they actually enjoy cover-to-cover.

As we approach our 2-year anniversary, we wanted to let you know about some exciting changes in store for 2022:
• We are adding Patient-created art alongside our Physician-created art
• Help us help others! We will be working with Let’s Rethink This and RIP Medical Debt to take a portion of each subscription and use it to eliminate medical debt.
• Premium subscription pricing for regular contributors, sponsors, and referral sources (our prices are going up in 2022 to keep up with the rising costs of producing, publishing, and mailing print magazines, but we vow to remain affordable for physician entrepreneurs, authors, podcasters, coaches and others who do not have ties to (or the deep pockets of) big Pharma/Hospital/Insurance. Lock in your Subscription and/or Advertising Package before our prices go up on 2/22/22!
• A unique Job Board complete with “side hustle”, locum, telemedicine, consulting opportunities, and so much more will go live in early 2022.
• We will be bringing our readers Direct Primary, Specialty Care, and affordable insurance models (resources for physicians and patients)
• We want to welcome students, researchers, and doctors to submit their studies for peer review and publication

Dear fellow Healthcare Professional,

This is just a little note and THANK YOU from the team at Physician Outlook Magazine. We know that the COVID-19 pandemic has taken a toll on our medical community. While we can’t make the pandemic go away, we CAN give you a break from the “everyday” with a little light reading and some physician-created art through our unique national publication.
Our print magazines are sent out bi-monthly. As a subscriber you will also have access to the full magazine as a digital download on our website and to all the great articles we have online. An annual subscription is just $250 per year (a $50 savings from our usual $25/monthly plan) and includes our print magazines and access to our dynamic and unique digital content on www.physicianoutlook.com.
We will be adding some additional benefits in 2022 and those include an online job board for physicians by physicians. We will have opportunities for physicians to advertise their books, coaching, DPC and other services in bonus issues throughout the year.
We actively encourage our subscribers to share content with us. We welcome ALL physician perspectives, and we let our readers pick and choose which authors resonate with them. In 2022 we are actively reaching out to patients to tell THEIR stories, especially ones which are appreciative of the special impact physicians have had on their lives.
Please share YOUR work, whether it be a written article, a poem, original artwork or a photograph. If you prefer, schedule a time to be interviewed and Physician Outlook can feature you in a video or a podcast. Let's make 2022 the year that more physician and patient voices are heard.


Have you ever experienced a lack of sexual desire, but for a long, LONG time? Maybe to the point where you’re concerned that you do not have any sexual interest at all? Well, if you have experienced this, you may be suffering from sexual dysfunction, or Female Sexual Arousal Disorder. This is exactly what it sounds like, in which someone has a lack of interest and arousal for sexual encounters. According to the book Our Sexuality , written by
RobertCrooks, Karla Baur, and Laura Widman, in order to be diagnosed with female sexual dysfunction, one must experience at least three of these symptoms on an ongoing basis: lack of interest for engaging in sexual activity, lack of sexual thoughts/fantasies, does not want to initiate sexual activity or turns it down when offered, lack of excitement during sexual activity, lack of sexual interest from external and internal cues, and lack of satisfaction from genital or non-genital stimulations in sexual activity.
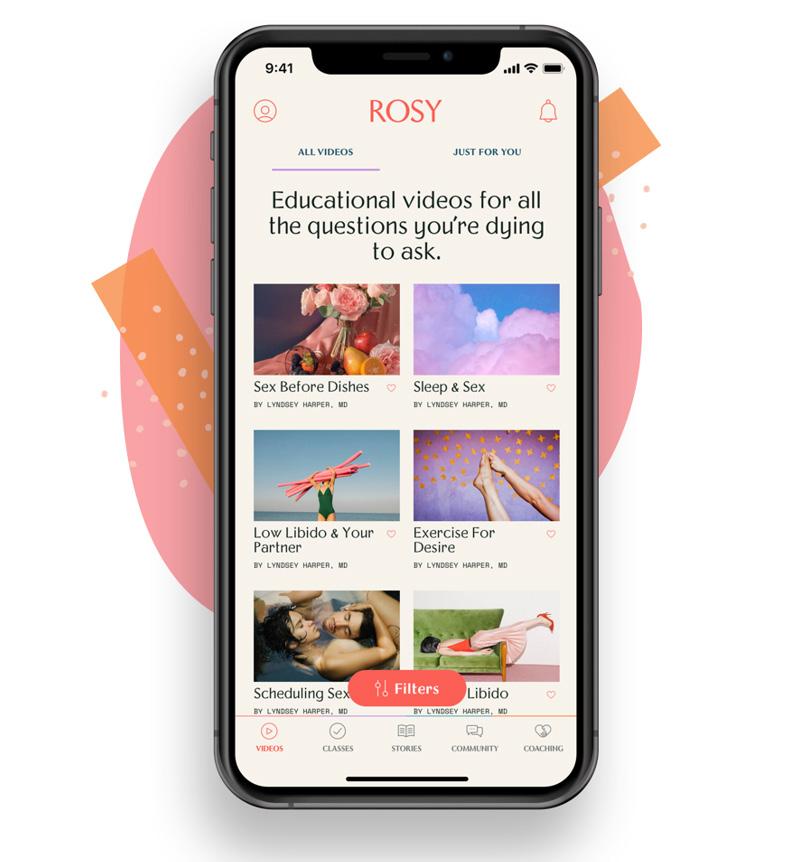
Don’t worry though! Low libido is something than can be easily cured through simple steps. Fortunately for women struggling with this, Dr. Lyndsay Harper, an Associate Professor of Ob/ Gyn for Texas A&M College of Medicine, has created a business that can help one’s sexual interest come back in a fun and holistic way. Rosy Wellness is a platform that provides educational videos, self-help classes, erotica and community to help talk about sexual health and wellness. Rosy Wellness also provides a telehealth service where women can get expert advice about their sexual health and treatment.
Rosy states that about 43% of women have sexual problems (so it is very likely you may know someone who struggles from one!). The sexual wellness business by Harper offers multiple platforms for women to educate themselves on sexuality and how to increase their low sex drive. The videos provided answer all your questions from pleasure, to low libido, to body image. The classes on Rosy are created by doctors and psychologists, offering tools and tips for women to excel in their sexual wellness journey. Erotica stories that range from sci-fi to romance can show every woman the amount of spice and warmth they need to help with their sexual desires in over 50 sexy stories. Lastly, all women are invited to join a community of thousands of females where they can ask questions, share stories, give tips, and help with any concerns regarding sexual health.
This all sounds so amazing, right? Well, there’s more! Rosy Telehealth helps over 84 million women struggling with sexual wellness problems and offers doctor or expert help. To get started, women
interested should download the app, Rosy-Women’s Sexual Health.
Once downloaded, create an account, and then choose treatment options you would like to pursue. These treatments can be anything from low sexual desire, menopause, trouble with orgasms, contraception, and more. From these options, Rosy will make a match based on your needs, or if that does not sound appealing, you can browse the app on your own. The final steps include making an appointment, then talking to your very own sexual health expert, and finishing off with supplemental appointments. Firsttimers can even receive $20 off their first appointment with the code MYFIRSTTIME.
With Rosy, there is no way one cannot overcome their low libido. The help and expertise provided offer a community that is supportive, friendly, and caring. Even if you aren’t struggling with sexual dysfunction, Rosy is a great way to explore your sexual life and find out pleasures that are right for you and your partner. So, what are you waiting for?
 Written by Riley Snowden
Written by Riley Snowden
I am a physician. I am also a refugee from the former Soviet Union and the granddaughter of Holocaust survivors. My parents were both physicians - something not easy to achieve as Jews in the USSRbut they gave up practicing medicine for freedom in America.
I grew up in San Francisco, watching my parents, as nurses, proudly caring for each individual patient, right in the thick of the HIV-AIDS epidemic of the 1980’s. They taught me that it is a privilege to care for human life, and becoming a physician always felt like a natural calling – an honor in line with my deeply cherished Jewish values.
My passionate concern is scientific, humanistic, and based on my clinical experience. I am a board-certified neurologist with a special interest in cognitive neuroscience (college research in implicit memory and role of emotions). I spent the past decade taking care of patients suffering from Parkinson’s Disease -- a disease that disconnects the brain from the body. In managing the many different symptoms this disease can present with, I learned the importance of understanding a dysregulated nervous system.
Dysregulation can occur for a variety of reasons and the most common in my experience is unprocessed trauma. No wonder our current civilization is exhibiting signs of “limbic hijack.” We are
living through a collective trauma and any individual perceived threat reflexively strengthens our tribal instincts.
It is with sadness and dismay that I reflect on what’s become of my once sacred profession. Even before the pandemic, moral injury spread throughout the house of medicine taking ~ 400 of my beloved colleagues’ lives each year to suicide. For over a decade, I witnessed corporate business influences destroy the sanctity of the doctor-patient relationship. Advocating for medically appropriate care has become nearly impossible. It’s no surprise that soaring costs and plummeting quality medical care have led to the morbid reality we are living through today.
We recently celebrated the Jewish New Year, and my Rabbi’s sermon was all about the importance of hope. Hope, after all, has guided the survival of my ancestors throughout time. I am grateful for the many inspirational physicians, who, over the past several years, have been replenishing my bucket of hope.
I have found the strength to fight back buoyed by my fellow healers who abide by the Oath of Hippocrates. In a variety of different ways, we have been exposing how conflicts of interests contribute to third-party intermediaries profiteering at the expense of our patients’ lives.
But this is only the beginning.
For hope to lead to profound transformation, we must strive to:
- Reveal the revolving door among media, academia, government, and corporate greed, and educate the public about how decisions are being made without regard to unintended consequences.
- Reaffirm medical ethics - those lessons from history we must not take for granted. Emphasize the merits of the scientific method without discounting the art of healing.
- Encourage civil discourse and honest logical debate in order to seek truth for the betterment of humanity.
At the start of the pandemic, I was encouraged by the hard work and achievements of my fellow practicing physicians when treating this “novel” coronavirus. Of unknown etiology and pathophysiology, we collaborated and took charge, just as our education and training prepared us to do and despite many “administrative suits” trying to get in the way. We found strength in knowing this was our calling and our chance to show why practitioners need a seat at the Healthcare decision table.
But just as the division in our country grew, so did division amongst ourselves. Ideology began influencing medical decisions and instead of focusing on addressing root causes of our problems,
we began arguing amongst ourselves and taking out frustrations on our patients (e.g., refusing to provide medical care based on vaccination status). It’s against this backdrop of chaos that poorly designed “anti-racist” policymaking in medicine has begun to spread, which should be alarming to us all.
While acknowledging disparities in health outcomes is imperative to achieving meaningful change, the “equity” not “equality” goals adopted by the AMA, among a growing number of academic institutions, is counterproductive and will ultimately cause more harm and division. Fortunately, organizations like the Foundation Against Intolerance & Racism (FAIR) are working to address this cultural shift, and instead promote a shared culture of fairness and understanding, rooted in our common humanity.
The “anti-racist” approach currently gaining momentum ignores confounding variables and inappropriately generalizes to solutions, relying on observed correlations as a substitute for analyzing and addressing root causations of perceived differences. As a result, conclusions, and the corresponding policy prescriptions, are fraught with error.
Proper tracking and analysis of potential harm doesn’t appear to even be considered. Moreover, negative unintended consequences can take decades to fully be appreciated, so needless suffering is currently being overlooked.
The growing division among physicians today regarding what is ethical antiracism is quite troubling. The discussions
regarding “Whiteness” seem no different than how my 100 year old grandpa describes his “Jewness” according to the Soviet and Nazi regimes, which he thankfully survived.
I understand the historical context differences, but respectfully argue that we are seeing a parallel dehumanization of the individual. It was wrong then, and it is wrong now, no matter the skin color or group identity to which a person is assigned.
I believe:
Medical Ethics, especially those reaffirmed after the atrocities of WW2, must be reiterated.
Medical Standards including what constitutes informed consent ought to be reasserted.
Transparency and Accountability in medical decision making, access, and cost should be demanded.
Trust in the doctor-patient relationship needs to be reestablished.
When we took the Hippocratic oath, we committed to putting each individual life we are caring for first, no judgements, only empathy and good will. The current version of our medical system is robbing our society by silencing its healers and denying what is bordering on basic human rights. Ignoring history and denying pain is driving fear, shame, and guilt, which further divides us into growing tribal silos of hate, resentment, and imagined superiority.
We must learn from the past, acknowledge and process our emotions, heal our wounds, and with kindness, proceed in repairing our sense of shared humanity, so our children don’t continue repeating our generational suffering.
Over the coming months, I look forward to drawing attention to the current barriers doctors face just trying to care for their patients. In doing so, I hope to inspire constructive dialogue on how we can deliver more humanistic, affordable, and easily accessible medical care.
 Written by Diana Blum, MD For more information, head to www.physicianoutlook.com
Written by Diana Blum, MD For more information, head to www.physicianoutlook.com


Note: this article contains graphic descriptions of sexual assault that may be offensive or painful to some readers.

What do you think is the greatest fear a woman may have? For some, it may be not being able to have a child. For others, it may be losing a loved one. Unfortunately for many women, it is being taken advantage of and not getting the justice they deserved. And I am not talking about money being stolen or being used to run errands for someone, I am talking about a woman’s dignity being taken away from them by offenders and perpetrators who want sex. This nightmare became a reality for Rachael Denhollander, a former USA gymnast who was part of one of the biggest sexual abuse sports scandals in history.
According to the National Sexual Violence Resource Center, about one in five women have experienced rape or an attempted rape each year, and about one in four college women experience rape or an attempted rape. This makes it almost impossible to not know someone in your
life affected by some form of sexual assault. Jim Hopper, a clinical psychologist and independent consultant who teaches at Harvard Medical School, states that four to sixteen percent of college males admit to rape. The even scarier fact is that about one-third of those men in smaller studies have admitted to committing rape more than once, where the average is about four times for each rapist.
But do you want to know what is the scariest fact of all? One man who has committed over 300 sexual assault acts. That’s unfortunately true in our world today. I am talking about Larry Nassar, a former USA Gymnastics and MichiganState University doctor/ educator, who had Rachael Denhollander as one of his many victims.
Not too long ago, we saw the United States compete in the 2020 Olympic
Games in Tokyo, Japan. Out of all the Olympic sports, one of the most beloved by all fans to watch is women’s gymnastics. We have seen so many success stories with these women, such as Simone Biles, Aly Raisman, Gabby Douglas, Jordyn Wieber, and more. Not only did all these gymnasts achieve Olympic medals in their time, but they also have something else in common. They were also all sexually assaulted by Larry Nassar.
Larry Nassar began working with the USA Gymnastics team as an athletic trainer in 1986. His first sexual assault dates back as early as 1992, according to SBNation. However, Nassar continued his career with the USA Gymnastics team, and eventually received his osteopathic medical degree from Michigan State University in 1993 and became the team physician and assistant professor for the school in 1997.
In 2000, Rachael Denhollander, at the age of 15, was sexually assaulted by Nassar as she got treatment for her wrist and lower back pain. IndyStar reports that all victims of Nassar had been “sexually penetrated when he put his fingers into their vaginas.” Denhollander reported that her mother was in the room at the time of these sexual assaults, but that Nassar positioned her and himself in a way where Rachael’s mother was not able to notice. Rachael says part of this is the reason why she kept quiet because she believed if her mother saw him “massaging internally” on Rachael, her mother would say something. Rachael also stated on her police report that she experienced penetration from her anus and her breasts were massaged, mentioned on IndyStar. His assaults would continue until 2016, and the youngest victim to date was six years old. It is said that Nassar never wore gloves during the assaults or as Nassar would call them, “examinations.”
With over 20 years of being an assaulter, the hope of these gymnasts and other athletes getting justice for their abuse seemed slim to none. Countless numbers of women reported their assaults to police, school/athletic authorities and other sources. Girls were told “Nassar is an Olympic doctor” and “he knows what he is doing,” or that “they must be misunderstanding what is actually going on.” However, in 2016, all that lost hope was about to change.
After police investigations and reports were made regarding Nassar and his sexual abuse in 2014, Rachael Denhollander was the first victim to speak up and pursue criminal charges against the former trainer of assaulting her back in 2000. Denhollander filed a police complaint on August 29, 2016, and on September 12, 2016, went alongside an Olympic gymnast to tell their stories of sexual assault and abuse, reported by SBNation.
In her interview with IndyStar, Denhollander said that what made Nassar able to perform these unforgivable acts was his ability to get people to trust him.
Rachael states that he was a very warm and caring person, which made it all the easier to be able to trust such a man. “Honestly, part of what grieves me so much is that he has everything he needs to be an incredible leader,” said Denhollander about Larry Nassar in her interview. “He has the personality, he has the skill, he has the knowledge, and he’s using that to prey on people. What a waste.”
Because of the courage and determination Denhollander had, she was able to use her activism to help over 300 women share their stories of sexual abuse that Larry Nassar committed. Of these 300 women, Olympic medalists like Simone Biles and Aly Raisman were able to speak up as well about their tragic history with Nassar.
Denhollander continued her work towards getting justice and helped reveal the underground secrets the USA Gymnastics team and Michigan State University had as well. Executives and other authorities in both organizations faced charges for keeping Nassar’s assaults a secret, and coercing victims into settling lawsuits without their attorneys present. As a result, Michigan State University awarded $500 million to victims and survivors of Nassar’s abuse in 2018. Finally in 2018, Nassar was sentenced to life imprisonment (up to 175 years) after pleading guilty to sexual assault under guise of medical treatment.
Due to her advocacy and bravery, Denhollander is now an attorney, author, educator, and mother. She continues to help the USA women’s gymnastics survivors in the USA Gymnastics’ bankruptcy. She has also published an autobiography in 2019 titled, “What is a Girl Worth?: My Story of Breaking the Silence and Exposing the Truth about Larry Nassar and USA Gymnastics.” Denhollander along with her autobiography released a children’s book called “How Much Is a Little Girl Worth?” in 2019, and in 2022 will release another children’s book called “How much Is a Little Boy Worth?”
If it wasn’t for Denhollander, we may have not seen Larry Nassar receive life imprisonment and we may have also not seen the courage of over 300 women speak up about their experiences of sexual abuse with the former doctor. Rachael states that communicating problems is the first step in taking action, specifically when it comes to sexual abuse. “If you cannot even acknowledge the problem, you cannot fix the problem . . . and that’s what communicates to survivors that they’re going to be heard and listened to, and it’s safe to speak up. If you did not communicate that, you haven’t done the most basic thing you need to start to change the culture around you.”
Written by Riley Snowden

In a world full of craziness, it is nice to have an outlet through entertainment. Movies and television have been a form of pleasure for citizens since as early as the 1890s, helping people escape their reality in times of war, disease outbreaks, and much more. Speaker Hillary Blair and renowned actress Mayim Bialik have provided us forms of entertainment and laughter, while also handling other fulltime jobs.
Hillary Blair, best known for being a well-regarded speaking, communication, and voice expert and coach for companies such as American Express, Maersk, Liberty Global and Hunter Douglas, has also created a career out of stage, film and voice-over acting. With over 30 years of experience, Blair is a professional voice-over artist for Commercial and Industrial Narration and has shared her knowledge through teaching and coaching people how to publicly speak. The voice actor holds an MFA from the National Theatre Conservatory and a BA from Yale University.
In addition to Blair, one of Hollywood’s beloved actresses, Mayim Bialik is not only known for her roles as Blossom Russo on Blossom, Amy Farrah Fowler on The Big Bang Theory, and becoming one of Jeopardy’s newest hosts, she is also a neuroscientist and author. Bialik studied at UCLA in 2000 to pursue a degree in neuroscience and has once stated that science did not come easy to her. Mayim worked hard for seven years, crediting her love for neuroscience to her biology tutor and her first semester at UCLA, and finally received her doctorate.
The actress shared her wonderful experiences of being able to play a role on The Big Bang Theory that incorporated her real-life job, and how Amy’s character portrayed neuroscience so well: “Being part of ‘The Big Bang Theory’ for gosh, almost a decade of my life, was a thrill, it was a real thrill as an actor to be employed for that long and to be employed at something that I enjoyed so much with people that I enjoyed working with so much. As a neuroscientist in real
life, I really enjoyed going to a job where our intellect is appreciated and our characters’ intellects were appreciated.” Bialik has also written over five books, ranging from talks about healthy diets to raising confident children.
The entertainment business can attract all different types of people, which is what makes the industry so unique. Both Blair and Bialik can appeal to all different types of audiences, with Blair’s ability to publicly speak to a variety of groups and Bialik’s creativeness in science, on stage and in her books. Due to their wide range of skills, anyone can appreciate their hard work ethic and dedication to the entertainment industry.
Written by Riley Snowden
Burnout. We need to stop calling it burnout. Actually, it’s moral injury.
It’s what happens to people on the front lines of clinical care who are forced to witness human
while feeling powerless and unable to do enough about it. 500,000 deaths from COVID alone and countless excess non-COVID deaths
America
to
quate access to cardiac care. Watching patients suffer and die during pandemic. Watching
patients experience complications of delayed care or minimized access to care
COVID this past year.
Are we surprised? It’s not burnout.
It is moral injury. It is a silent trauma. We need to be talking about it. Or we will
ment, or even suicide which is a legitimate under- appreciated epidemic
Please read, appreciate, and share this story.
By Andrew J. Sauer, MD Check out Dr. Sauer’s profile

Dr. Sheila Nazarian is a Board-Certified Plastic Surgeon who owns a private practice in Beverly Hills, California. In alignment with being a surgeon, she has a master’s degree in medical management from Marshall School of Business at USC and serves as an Assistant Professor in the Division of Plastic Surgery at the University of Southern California. Her practice extends to online as well as she is the founder of spa26.com and TheSkinSpot.com. Skin Decisions: Before and After, is a Netflix show that displays her client’s stories as well as the before and after results.

1. What inspired you to pursue this plastic surgery?
“I initially was looking into architecture or orthopedic history as I loved to design and build things ever since I was a child. When looking further into those professions, I realized I wouldn’t actually be building as an architect and orthopedics was not creative enough for me. Someone suggested I look into plastic surgery, and it was the perfect fit of art and science for me.”
2. What is the most common type of plastic surgery you perform?
“My practice is actually a 50/50 mix of surgery and non-invasive treatments with the aim of natural results, always. I perform the gamut of aesthetic surgeries, as well as use thirty devices in my practice. Optimal results usually come from a combination of treatments. For example, if I do a facelift and leave the skin wrinkled and full of sunspots, the results will not be in harmony and people will know my patient had work done. But when surgical and non-surgical treatments like lasers or injectables are used together, the results make sense, and no one can tell any work has been done.”
3. Would you say that the amount of people who seek plastic surgery in the Beverly Hills/Los Angeles area is much larger than other areas of the United States? (Due to the lifestyle and financial status of people living in LA/Beverly Hills)
“Sixty percent of my patients actually fly in to see me. I think plastic surgery is talked about more in certain age groups and geographical regions, but everyone is doing something these days. In my practice, I have three other physicians at lower price points to be able to accommodate most budgets.”
4. Although you are a plastic surgeon, do you promote the idea that women should accept who they are and love themselves, without any work done?
“I absolutely promote self-love and self-acceptance. However, to tell someone they should live with a pannus hanging over their pubis after massive weight loss, or a completely sun-damaged and aged face when they feel younger than they look is not optimal either. If a person is healthy, both physically and mentally, and they want to refresh their faces and bodies, and it is safe to do so, we should not make them feel guilty for it. We should empower them to live their most confident lives.”
5. Can you give women a piece of advice who may not be able to afford plastic surgery but are struggling with their image?
“Medical grade skincare products and devices have come a long way. I started TheSkinSpot.com 7 years ago to help women and men find the best products out there. Products that are backed by studies and proven to deliver results. Oftentimes, you can look so much better by just switching from store-bought brands to medical grade products.”
6. Have you done surgery on any celebrities?
“I have operated on celebrities. Celebrities seek me out because they don’t want anyone to know they have had anything done. #NaturalByNazarian and #SmallBreastQueen are two of my hashtags. I absolutely love natural results.”
7. Tell us about your website, TheSkinSpot.com.
“The Skin Spot is a skincare and wellness site I created 7 years ago. Products can be so confusing. Marketing, packaging, smells, and paid influencer recommendations are what most people go by when choosing their skincare products these days. I created the site to curate the best-of-the-best, medical-grade products that deliver on their promises. We have an awesome Skin Quiz to help newcomers figure out their exact regimen and a loyalty program as well to reward our customers for making smart choices when it comes to their skincare and wellness product choices.”
8. On TheSkinSpot.com, your products seem to be very high end. Who is our target audience since most of these products are very expensive?
“Our audience is typically a twenty-five- to fifty-five-year-old woman who wants products that deliver. Effective and proven ingredients will be more expensive than your drug store brands but our customers are willing to spend a bit more for products that actually work... not just smell good and have cute packaging. Our customers want results.”

9. On your Instagram you posted about Sheila’s Closet that is being sold on TheSkinSpot.com. Can you tell us a little bit about your line (what made you want to start selling clothing and accessories) and the Hope Foundation of Los Angeles? (Proceeds from purchases from this line are going to this foundation)
“I work with a stylist to edit my closet often. Instead of just donating my clothes, I decided to sell them on TheSkinSpot.com to my followers who watch our live edits and always ask if they could have the clothes, I was editing in. So, I thought, give the people what they want. All proceeds from my gently used or brand-new clothing go to the Hope Foundation of Los Angeles, who help indigent families in my community.”
10. What is the most rewarding part of being a plastic surgeon?
“The most rewarding part of my life is using my voice in activism. With my Instagram following and Netflix show, I have a platform to speak from and I use it to call out racism against my Jewish community. My family escaped Iran and came to America as refugees during the Iran/Iraq war. As Jews, we were persecuted and had to leave everything behind to come to America, not even speaking the language. Being a plastic surgeon has given me the opportunity to have a large platform and influence. I am so much more than just my job as I think all physicians are. We need to give ourselves permission to explore and nurture all aspects of ourselves creatively. I am exceedingly grateful to be in America where a refugee can, with hard work, perseverance, and talent, become nominated for an Emmy, and succeed as a plastic surgeon. The sky is the limit.”
Written by Eden Courville, BA and Sheila Nazarian, MD, MMMWhile I’m #storytelling, let me tell you about another patient that left her mark on my heart.
Raina is a 41 y/o Black woman with a PMH of left-sided breast cancer, diagnosed 2 years ago when it was discovered on her very first mammogram at age 39.
For her 39th birthday she decided to make an appointment with her doctor for a comprehensive physical exam including a pap and mammo. She diligently performed her BSE (breast self exams) as recommended and never felt any lumps. She has no 1st degree relatives with breast cancer, but her grandmother and her grandmother’s sister both died of breast cancer at young ages.
When she tried to obtain a mammogram at age 35, she was told ‘no’ by her primary doctors. “It is not indicated. . . dense breast tissue in young women. . . false positive. . . yadda yadda yadda.”
When she argued that she was ‘highrisk’ based on her family history she was informed that she, in fact, was *not* high risk since she has no *first-degree* relatives with breast cancer (mother, sister, daughter), nor did she have a personal history of breast cancer. She did not receive genetic testing for the same reasons. Since her HMO wouldn’t allow mammograms, unhassled, as screening for women such as herself - and since her PMD didn’t continue to actively advocate for this exam - nothing happened. . . and the cancer grew.
So after her very first mammogram, weeks before her 40th birthday, there it was “an abnormal density” in her left breast.

Ultrasound. Biopsy. Biopsy is “inconclusive.” Weeks pass. Finally another (larger core) biopsy reveals the cancer. She is *then* rapidly scheduled for a lumpectomy, XRT (radiation), and chemo.
She goes into remission.
Then, 2 years later, like clockwork, she goes to her PMD for a “check-up.” She is told “Everything is fine.” She is told she doesn’t need to come back as frequently. She is scheduled for a mammogram in 6 months.
6 months pass. Mammogram is abnormal. There is a density in the right breast. It is not calcified so the “suspicion for cancer is low.” She is scheduled for an ultrasound, and repeat mammogram in 3 months.
In the meantime she develops a cough. Then a fever. Then the cough becomes productive of yellow sputum. Then weakness and fatigue sets in. She sees her doctor. They do a CXR and see “an infiltrate.” It is diagnosed as pneumonia and treated with antibiotics. The HMO calls her to schedule her ultrasound, but she explains that she is too sick with ‘pneumonia.’ A note is made, but nothing was done.
She returns to the PMD when the ‘pneumonia’ persists despite a course of strong antibiotics. She is given another prescription for a different antibiotic, and sent home. This 2nd antibiotic causes her to have diarrhea, abdominal cramping, and eventually dehydration.
This is when she presents to me in our emergency department.
Chief complaint: nausea, vomiting, productive cough, shortness of breath, abdominal pain, and diarrhea for 1 week. Her husband is at the bedside holding her hand. Both look at me as I enter the room and through their tears they both start talking at once. . .
“Dr. Taylor please help us!” is how it begins. . .
[like before, I gotta run. I have a thing tonight. But I’ll be back with the conclusion soon!]
Oh. And while this story is shared with permission, her name is obviously not really Raina.
Written by Myiesha D. N. Taylor, MDTo read “Part Two” of Dr. Myeisha Taylor’s patient story, please visit www. PhysicianOutlook.com









Dr. Sasha Shillcutt is a physician, gender equity researcher, speaker, author, wife, mother to four amazing children and Founder/CEO of Brave Enough.
She founded Brave Enough after a successful career climb as a clinical scientist and national expert. Despite her professional success, she found herself empty and deeply lonely. She started a community, realizing that women need each other and are at their best when they show up for themselves and for each other.
Through her book, talks, courses, membership site, and in-person events, she has inspired tens of thousands of women to believe in themselves and their innate value.
She has taught women to take control of their time of their lives.
Dr. Schillcutt has published more than 50 peer-reviewed articles (including ones in JAMA & the NEJM), and is a TedX Speaker.
Her greatest passion is empowering and encouraging women to be #braveenough in their professional and personal lives.
Publisher: Marlene Wüst-Smith, M.D. Editor in Chief: Alicia Roselli Managing Editor: Roxanne Bruce, MBA, DrBA, VP of Advertising: Pamela Ferman Director of Art and Production: Tobias Sarrio Marketing/Copyright Editor/Journalism/Social Media
Interns: Riley Snowden, Dana Bushery, Madison Smith, Pennsylvania State University; Hannah Bushery, Hofstra University; Elizaben Egan, St. Bonaventure University Contributing Authors: Marlene J. Wüst-Smith, MD, Eden Courville, BA, Peter Coffman, MD, FAPA, Dana Corriel, MD, George P. Naum, MD & Vanessa Naum, Riley Snowden, Myiesha D. N. Taylor, MD, Kristine Scheer, SHRM-SCP, Diana Blum, MD, Mary Anne Vaccaro, BFA, Andrew J. Sauer, MD, Sheila Nazarian, MD, MMM, Amanda Dunec Cover Art: Moritz H. Albrecht, MD and Marwen Eid, MD
Published by “PhysicianOutlook Publishing” Editorial policy: PhysicianOutlook magazine is a national magazine dedicated to empowering physicians and their patients to improve the world of medicine together. Editorial decisions are based on the editor’s judgement of the quality of the writing, the timeliness of the content, and the potential interest to the readers of the PhysicianOutlook magazine. The magazine may publish articles dealing with controversial issues. The views expressed herein are of the authors and/or those interviewed, and may not reflect the official policy of the magazine. PhysicianOutlook neither agrees, nor disagrees with those ideas expressed, and no endorsement of those views should be inferred, unless specifically identified as officially endorsed by the magazine.
“Letters to the Editor” email: rbruce@physicianoutlook.com
Information on advertising, subscriptions, and job board email: hello@physicianoutlook.com
“PhysicianOutlook” is a registered trademark. Madison Baylock
The artwork consists of cardiac CT images. The artwork is the handy work of radiologist Moritz H. Albrecht, MD and preventive cardiologist Marwen Eid, MD.
Traditional radiology refers to diagnostic imaging. However, x-rays and magnetic resonance images, as well as computed tomography (CT) reconstructions can also be used in an artistic approach. Furthermore, painting or crafting artists may choose radiological subjects. The resulting modern artwork is referred to as Radiology-Art. The project Radiology-Art.com is part of the Techspressionism movement and was founded in 2017 by Moritz H. Albrecht. Albrecht, creative radiologist based in Frankfurt, Germany and www.techspressionism. com-indexed visual artist aims at providing a platform for radiology artists for showcasing their artwork in a permanent digital exhibition.
Do you have Radiology-Art you would like to share with the world? Follow them on Instagram @ artsyradiology
