3 3 www.yourexpertwitness.co.uk






4 4 www.yourexpertwitness.co.uk 29 26 15 contents IN THIS ISSUE 2YWV Copyright Your Expert Witness. All rights reserved. No part of this publication may be copied, reproduced or transmitted in any form without prior permission of Your Expert Witness. Views expressed in this magazine are not necessarily those of the publisher. Printed in the UK by The Magazine Printing Company Plc www.magprint.co.uk Your Expert Witness Suite 2, 61 Lower Hillgate, Stockport SK1 3AW Advertising: 0161 710 3880 Editorial: 0161 710 3881 Subscriptions: 0161 710 2240 E-mail: ian@dmmonline.co.uk 7 Opening Statement NEWS 9 Bond Solon conference returns as a hybrid event 9 Leading judge opens proceedings at EWI conference 11 Legal Services Bill draws plaudits and brickbats from Scottish lawyers VIEWPOINT 12 Back to basics – when and how to use your expert FORENSIC ACCOUNTANCY 15 New guidance reflects changes to solicitors’ anti-money laundering rules 15 HMRC names firms penalised for breaching money laundering rules 17 The cliché ‘variety is the spice of life’ certainly applies to the work of an expert! 18 Convictions top-off NCA operation against cash smuggling gang 19 Why would you use a forensic accountant to challenge a POCA? 20 Freezing order issued on land in NI 20 HMRC issues new scam alert TRANSLATION & INTERPRETATION 21 Translation organisations come together 21 Inaugural awards celebrate police interpreters 23 Translation myths LEGAL ISSUES IN CONSTRUCTION 25 Construction-related pipeline incidents spiralling, report finds 25 HSE’s message is that Dust Kills FIRE INVESTIGATION 26 Fire risk benchmark gets a warm welcome from the industry 27 Experience and scientific knowledge combine to offer an expert’s view HEALTH & SAFETY 28 Slip or trip: however you fall it may be avoidable ROAD TRAFFIC INCIDENTS 29 Young drivers admit to not wearing seat belts, survey finds 29 E-scooters: provisional accident figures released TREE CARE 30 Where is the evidence taking me? A to Z WEBSITE GUIDE 32 Our A to Z guide to the websites of some of the country’s leading expert witnesses. EXPERT CLASSIFIED 77 Expert Witness classified listings 82 Medico-legal classified listings EXPERTS FOR MEDIA 31 Our new section for experts wishing to offer their expertise to the vast range of print and broadcast media
MEDICAL ISSUES
35 Medical Notes
NEWS
37 Mesothelioma claim fails on exposure levels
37 Leaflets share learning on medication errors
39 GMC gives two cheers to proposed reform
41 Missed opportunities led to untimely death
DIABETES
43 The hot topics and difficult areas in diabetes

PAIN
45 Specialists caution against stigmatisation of patients using dependency drugs
45 US researchers generate objective pain indicators for first time
CONSENT
47 Can ‘material risk’ ever be defined?
NOISE INDUCED HEARING LOSS
49 HSE updates NIHL stats
49 Campaign targets hearing risk at music venues
ORTHOPAEDICS
51 Orthopaedic hospital continues its expansion
51 Research highlights radiation risk to female surgeons
53 Study shows need for co-operation in trauma treatment
53 Training course helps orthopaedic surgeons deal with the law
55 Six MSK projects share near-£2m pot
CARDIOLOGY
57 AI could soon be used to diagnose heart attacks

VASCULAR SURGERY
58 Limb ischaemia: when can the leg be saved?
PSYCHIATRIC & PSYCHOLOGICAL ISSUES

61 Psychiatrists ‘surprised and concerned’ by Met police no-show threat
61 Government should resentence IPP prisoners, report finds
DELIRIUM
63 What are the medicolegal challenges posed by delirium in an ICU?
PLASTIC, RECONSTRUCTIVE & HAND SURGERY
65 Council takes action against buttock filler business
67 Plastic and bariatric societies voice concerns over ‘surgical tourism’
67 Hand surgeons across the world meet in Wales
DENTISTRY & MAXILLOFACIAL SURGERY
69 GDC publishes registration and fitness to practise figures
69 Research on ‘dental deserts’ shows only part of the picture, dentists say
OPHTHALMOLOGY & OPTOMETRY

73 Optometrists respond to reports of ‘forever chemicals’ in lenses
74 What are the medicolegal trends in injectable facial aesthetics and eyelid surgery?
76 MPs’ eye health debate draws on ophthalmologists’ research
5 5 www.yourexpertwitness.co.uk 57
43 www.yourexpertwitness.co.uk
76

Opening Statement
[TWO THREADS run through the first part of this issue of Your Expert Witness: the divergence of the role of expert witnesses and the large part played by the accountancy profession in the rule of law in this country. Both areas are brought together by regular contributor Chris Makin, a forensic accountant of some standing and an expert witness for many years. He is also an entertaining raconteur on the subject. In this issue he goes through some of the points to bear in mind when instructing any expert.

The many and varied areas of law requiring the attention of a financial expert are also related by another regular, Fiona Hotston Moore, whose expertise has been deployed in resolving disputes ranging from valuing businesses to investigating allegations of financial wrongdoing – even assessing the possibility of professional negligence by a law firm (surely not!).
• The work of the forensic accountant only comes to the attention of the public when there is either a huge amount of money involved, along with a famous personality, or the money concerned has been criminally acquired. The latter has been the case with a number of recent high-profile successes by both HMRC and the National Crime Agency The latter has most recently reported the breaking up of a courier ring involved in the transferring of funds, believed to be derived from drug dealing, abroad for laundering. At the same time HMRC has sanctioned a number of financial firms for a lack of attention to the possibility money is being laundered via their accounts.
• In many cases, where crime has resulted in profit for the criminals, those profits are required to be handed over to the public purse by a Proceeds of Crime (POCA) order. But the way those funds are calculated has itself to be fair and legal: the interests of justice are not served when funds are seized that are not the proceeds of crime. Keeping that balance is the subject addressed by chartered accountant Lennie Harris.
• Alongside the financial experts, there is a sometimes bewildering variety of subject areas which require an expert witness to ensure the court is properly informed. We hear from experts in arboriculture and fire risk assessment.
• Ensuring that the complexities of a legal document are intelligible when everything is expressed in one language is one thing; bringing complex detail together when a number of different languages are involved is quite another. Hitherto in this country, there has been no standardised format for translations of legal documents – leading to confusion and even miscarriage of justice. Now, however, the professional bodies involved in translation have come together to ensure a common standard. In addition to the technical jargon which all specialities by their nature generate, justice demands that anyone involved in legal proceedings is able to understand what is going on. That is where the interpreter comes in. In April the best of those unsung heroes were honoured at the inaugural National Police Interpreter of the Year Awards.
• With the plethora of experts in all their different fields it is sometimes hard to identify a common thread; but such a thread does exist, and there are shared areas of interests for all experts. Those areas of interest are debated and expounded at the various expert witness conferences. We hear both preview and review of two of the most notable of those annual events.
• Away from the legal arena, the opinion and experience of experts across a wide range of subjects is in constant demand by the press, broadcast media and dramatists. For those who wish to make their expertise available to those professions we are offering a new billboard. q
Ian Wild
Ian Wild, Director of Business Development Your Expert Witness
7 7 www.yourexpertwitness.co.uk
8 8 www.yourexpertwitness.co.uk
BOND SOLON CONFERENCE RETURNS AS A HYBRID EVENT
THIS YEAR’S Bond Solon annual Expert Witness Conference –the UK’s largest gathering of expert witnesses – returns on 3 November as both an in-person and virtual event. The in-person event will be taking place as in previous years at Church House Conference Centre in Westminster. This year’s keynote speaker will be the president of the Law Society, Lubna Shuja.
Mark Solon said of the event: “One of the main considerations for many experts is their working relationship with solicitors. The president of the Law Society will be talking to you about how crucial this partnership is. We have done many surveys of experts over the years and issues such as solicitors putting pressure on experts to change their opinion and problems over the payment of fees often come up. So, let’s see what the president has to say.”
Other highlights include an address by a senior lawyer from
Dentons on how artificial intelligence is changing the legal landscape and from an experienced IT expert witness on how experts can work safely and effectively in the ever-changing digital environment.
Mark Solon continued: “We have again organised a debate between two King’s Counsels this year, on whether there should be an independent accreditation system for experts to ensure high standards or if the current safeguards are sufficient.”
Those attending in person will also be able to celebrate commitment to excellence at the Cardiff University Bond Solon Expert Witness Certificate Awards Ceremony and complementary drinks reception. q
• For further information and to book places, both in-person and virtually, visit ewc.bondsolon.com
LEADING JUDGE OPENS PROCEEDINGS AT EWI CONFERENCE
[THE ANNUAL Conference of the Expert Witness Institute (EWI) was once more held online this year, on 12 May. The conference provided essential insight and practical advice to help expert witnesses develop their knowledge and skills.
The event began with a keynote speech from Lady Justice Simler discussing what makes an excellent expert witness and how experts can increase their credibility in the eyes of the court.
Dame Simler emphasised the importance of the expert witness role within the legal profession. “There is strong public interest in the work performed by experts”, she said. “The justice system depends on expert evidence being the highest quality it can be.”
Emma Mitra of the EWI noted: “And, at a time when many disciplines are lacking a wide pool of high-quality experts, Lady Justice Simler praised the training and support on offer by organisations like the Expert Witness Institute as an integral way for professionals to access invaluable guidance, retain experts and raise the profile of the expert witness field.”
Following a number of absorbing debates, the closing address was delivered by EWI chair Sir Martin Spencer.
Reviewing the conference, barristers Phillip Taylor MBE, head of Richmond Green Chambers, and Elizabeth Robson Taylor wrote: “It feels like the online conferences are now here to stay. They do work. We were very fortunate this year to have such a high powered judicial
and legal line-up which allowed for contributions from those in busy practices. Although some miss direct face-to-face contact, virtual sessions are here to stay as a consequence of COVID. Thank you to everybody who participated as we realise that our system of justice depends on expert evidence.” q
9 9 www.yourexpertwitness.co.uk
[

10 10 www.yourexpertwitness.co.uk
LEGAL SERVICES BILL DRAWS PLAUDITS AND BRICKBATS FROM SCOTTISH LAWYERS
[THE LAW SOCIETY OF SCOTLAND has warned that proposed new powers allowing Scottish Ministers to intervene and direct regulators of legal services in the country are ‘deeply alarming’ and risk seriously undermining the independence of legal regulation from the state.
The Regulation of Legal Services (Scotland) Bill would for the first time make it possible for complaints to be made against those who provide legal services to the public but who are not regulated. The appeal process for complaints about poor service will be simplified in line with an ‘ombudsman approach’, helping to make the system more accessible and affordable.
The Scottish Government says that the Bill, if passed by the Scottish Parliament, would also place legal duties on the profession’s current regulators – the Law Society of Scotland, the Faculty of Advocates and the Association of Commercial Attorneys – to be more transparent and accountable in their regulatory work. They will be required to protect the principle that consumers should be treated fairly at all times and have access to a range of legal services which are affordable and suited to their needs.
Government Ministers will also be able to launch a review of the regulators and require them to make improvements or impose financial sanctions if they fail to regulate in the public interest.
Voicing the concerns of the Law Society of Scotland, its president Murray Etherington commented: “Some aspects of the proposed Bill are deeply alarming. One of the most important roles of the legal sector is to challenge government on behalf of clients and hold it to account.
“The proposed new power allowing Scottish Ministers to intervene directly in regulation risks seriously undermining the independence of the legal profession from the state. This is clearly unacceptable and needs to be removed from the Bill by the Scottish Parliament as the Bill progresses.”
There was support for other measures in the Bill. Murray Etherington continued: “Maintaining professional standards and protecting clients is some of the Law Society’s most important public interest work. However, much of the existing legislation on regulation is now over 40 years old and is simply unfit for today’s modern and diverse legal sector. This is why we went to the Scottish Government
almost a decade ago, asking for change.
“The complaints system in particular needs reforming to make it quicker and simpler for the benefit of all involved. There is also a chance to better protect consumers from unqualified providers of legal services, especially when things go wrong."
The Scottish Government is currently consulting on the proposals.
Kaukab Stewart MSP, convener of the Equalities, Human Rights and Civil Justice Committee, said: “This new bill aims to modernise the legislation covering the regulation, which is now over 35 years old. There have been several calls for change over the past decade. Through our scrutiny, we want to ensure that this new Bill delivers on its aims.
“We would like to hear views from across the legal sector and public bodies as we seek to understand how the current regulatory landscape is viewed. We also want to get an understanding of what impact the changes in the Bill would have on consumers of legal services. To share your views on the Bill with the committee please complete our call for views.”
The consultation closes on 9 August. q
11 11 www.yourexpertwitness.co.uk
BACK TO BASICS –WHEN AND HOW TO USE YOUR EXPERT
By CHRIS MAKIN chartered
accountant, accredited civil mediator and accredited expert determiner

WHAT FOLLOWS should be familiar to all solicitors engaged in contentious work, but it does no harm to remind ourselves of the basics. How can I, a humble chartered accountant, feel able to propound on such matters?

Because I have practised for over 30 years as an expert witness; also for many years as a mediator and expert determiner. I have written many hundreds of expert and valuation reports, given expert evidence over 100 times, and conducted more than 120 mediations and 45 expert determinations.
I served for 14 years on the ICAEW forensic committee and then for six years on the ethics committee. I am a fellow at the Academy of Experts, one of only about 60 worldwide, where I am chief examiner in expert determinations and assessor for membership from accountants and similar. In a word, I’ve been round the houses a few times.
But more particularly, in going round the houses I have seen too many of my professional colleagues get it wrong at court. That is why, when on the forensic committee, I helped devise a scheme of accreditation for expert accountants. The list can be viewed on their website at www.icaew.com/learning-and-development, and it
About Chris Makin
CHRIS MAKIN was one of the first 30 or so chartered accountants to become an Accredited Forensic Accountant and Expert Witness –see www.icaew.com/about-icaew/find-a-chartered-accountant/find-anaccredited-forensic-expert
He is also an accredited civil and commercial mediator and an accredited expert determiner. Over the last 30 years he has given expert evidence at least 100 times and worked on a vast range of cases. For CV, war stories and much more go to the website at www.chrismakin.co.uk – now with videos! q

is noteworthy that there are currently only 63 chartered accountants of that high standard out of a total English and Welsh membership of about 155,000. These are the accountants who have bothered to train in their second profession of expert witness, and these are the accountants who are unlikely to let you down at court.
A quick story. Some years ago, I was the expert in a case where my opponent was a local chartered accountant who was highly regarded as a general practitioner. I don’t think he had been in a courtroom before. His expert report was delusionary.
The judge was HHJ Behrens. As he sat down, the first thing he said was: “I see that one of the experts is Mr Makin. I have often relied on Mr Makin’s expertise when I was at the bar. If that is a problem to anyone, I will recuse myself. I will rise for five minutes.” Within three minutes, the other side had thrown in the towel and agreed to pay significant costs. That did their side, justice and the reputation of the ICAEW no good at all.
So when you need an expert, don’t engage a wannabe or an enthusiastic amateur!
How then do you choose and instruct an expert accountant? Let us first take a step back.
Terminology
First, terminology. Disputes come in many forms and there are rules to match. We have the Civil Procedure Rules (CPR), the Family Procedure Rules (FPR) and – you’ve guessed it – in criminal cases it’s the Criminal Procedure Rules (CrimPR). There are other rules for specialist courts and for the various arbitration bodies. It is essential that you, and particularly your expert, are familiar with the relevant rules.
When a dispute arises
Before considering use of an expert, have a good think about the best way to resolve the dispute. There is a good guide in my blog chrismakin.co.uk/how-many-routes-to-resolution/
In criminal cases you have plea bargaining – as well as a jolly good defence; in family it’s resolution, mediation with a MIAM and then the FDR; and in civil we have early neutral evaluation, Part 36 offers, mediation again, arbitration or just going the distance. And don’t forget expert determination, which can be much cheaper and quicker than arbitration and remarkably versatile.
Of course, there’s always talking to the other side – useful in the early stages, but not so when positions have become entrenched after aggressive letters have been sent and received.
Do you really need an expert?
This may be a strange thing for me to say, but it is wise to have an expert whom you trust, who can cast their eye over your case at an early stage. Their advice may well be that an expert is not
12 12 www.yourexpertwitness.co.uk
[
[
needed, or that a case may have really interesting legal aspects but negligible quantum, or a Pyrrhic victory.
Set up a relationship with an expert who will look at a case and not charge you if the case doesn’t proceed. See my terms on my website at chrismakin.co.uk/fees-and-gdpr/.
How do you choose an expert?
Sign in a cobblers’ window in Boston, Mass: ‘ High Quality – Low Price – Fast Service: choose any two ’.
Is that how you choose your expert? Or, worse still, do you ask the office junior or a new trainee to find one? Wrong! It’s your case, you know what you need, so you should choose this very important member of your team.
Except, of course, that the expert isn’t on your team, or any team. See this at CPR Part 35 at 35.3:
(1) It is the duty of experts to help the court on matters within
(1) their expertise.

(2) This duty overrides any obligation to the person from whom
(2) experts have received instructions or by whom they are paid.
That independence is at the root of the expert’s duties. An expert can be civil and helpful, but don’t expect him to be your bestie!
The Ikarian Reefer: [1993] 2 Lloyd’s Reports 68
Do you know what a reefer is? For a long time I thought it was a cannabis cigarette, and it may be – though I won’t participate, thank you – but recently I learned it is a refrigerated ship.
Back in April 1985 at around 23:00 the Ikarian Reefer, travelling from Kiel to Abidjan, ran aground off the coast of Sierra Leone. Fire broke out in the engine room, the crew abandoned ship and the vessel sank. The ship owner claimed a total loss under the marine policy whilst the insurer alleged that following the owner’s instructions the vessel had been deliberately set on fire.
The dispute came before Cresswell J in the Queen’s Bench Division. His judgment in favour of the owner was appealed and subsequently overturned by the Court of Appeal in December 1994.
The outcome is not relevant for the purposes of this article, but during the hearing the judge was rightly concerned by the parlous standard of the expert witness evidence that had been given. He also believed this caused the trial to take much longer than it should have done. He took the opportunity to set out clear guidance as to an expert’s duties and responsibilities.
Those principles are now explicitly stated in the rules of each court and the various arbitration bodies. Every expert must know them. Here is the first, which first appeared in a House of Lords judgment ( Whitehouse v Jordan ) from Lord Wilberforce:
“The report of the expert must be, and be seen to be, the independent product of the expert, uninfluenced as
to form or content by the exigencies of litigation.”
You see, independence really matters.
For your further delectation
I have made reference to some blogs on my website. There are a great many more – on litigation, mediation and expert determination – and I have tried to make them light-hearted and easy to digest. So indulge! There is much to learn on the perils of choosing the wrong expert, but I draw your attention to one on a different subject.
Some years ago I had the great privilege to co-mediate a professional negligence dispute with Sir Alan Ward, recently retired as Lord Justice Ward of the Court of Appeal. He had been so scathing in his judgments to parties who had refused to mediate that, when he retired, he felt honour bound to become a mediator himself.
This was his first mediation, so I led him – amazing – and he was wonderful. But just for fun, have a look at this from Sir Alan’s judgments: chrismakin.co.uk/the-bon-mots-of-sir-alan/ Enjoy! q
13 13 www.yourexpertwitness.co.uk

NEW GUIDANCE REFLECTS CHANGES TO SOLICITORS’ ANTI-MONEY LAUNDERING RULES
[THE Legal Sector Affinity Group (LSAG) – part of the Solicitors’ Regulation Authority (SRA) – has published the latest update to its HM Treasuryapproved guidance on preventing money laundering in the legal sector.
The changes reflect the recent amendments to the Money Laundering, Terrorist Financing and Transfer of Funds (Information on the Payer) Regulations 2017.
In a statement the Law Society of Scotland said: “The changes include guidance on the new requirement to carry out proliferation financing risk assessments, either as part of the firm’s existing practice-wide risk assessment or as a standalone document, and changes to the duty to report discrepancies to company registries – from 1 April 2023, these will only need to be made in certain defined circumstances.”
HMRC NAMES FIRMS PENALISED FOR BREACHING MONEY LAUNDERING RULES
HIS MAJESTY’S REVENUE AND CUSTOMS has named hundreds of businesses which have been fined a total of £3.2m for breaching anti-money laundering regulations. The 240 supervised businesses named on 8 June were fined between 1 July and 31 December 2022 by HMRC for breaching the regulations aimed at preventing criminals from exploiting illicit cash.
In addition to the named businesses, another 179 companies received smaller fines totalling more than £200,000 for rule breaches.
The largest fine – £1.4m – was handed out to Xpress Money Services Ltd, based in London. The penalty was for failing to carry out risk assessments, not having appropriate anti-money laundering controls and failing to conduct proper due diligence checks.
Of the 219 businesses in England fined, 114 were based in London and the South East. In addition, 12 were based in Northern Ireland, six in Wales and three in Scotland.
HMRC’s work with other enforcement agencies and government departments to tackle economic crime and crack down on breaches is working to drive non-compliant firms out of business. That means that the number of money service businesses has fallen by around a third from 1,508 in 2020 to 1,049 in 2023, and the number of money service business agents has reduced from 35,507 to 30,217 in the same period.
Nick Sharp, deputy director of economic crime at HMRC’s Fraud Investigation Service, said: “Money laundering is not a victimless crime. We are here to help businesses protect themselves from criminal attacks and will continue to tackle the minority of businesses which do not comply with the Money Laundering Regulations.
“Serious and organised crime costs the UK billions of pounds every year and our anti-money laundering supervision is a vital tool in combatting that.”
Money service businesses provide vital services to the community, HMRC said, offering currency exchange, money transmission and cheque cashing. However, they can be exploited by criminals to launder the proceeds of crime, so must have a robust risk assessment and policies, controls and procedures to prevent that.

HMRC supervises tens of thousands of businesses across the UK under Money Laundering Regulations, and helps these firms protect themselves from criminals who seek to launder cash or finance terrorism. q
According to the Law Society of England and Wales, proliferation financing is broadly defined by the SRA as: “…the act of providing funds or financial services for use, in whole or in part, in the manufacture, acquisition, development, export, transshipment, brokering, transport, transfer, stockpiling of, or otherwise in connection with the possession or use of, chemical, biological, radiological or nuclear weapons, including the provision of funds or financial services in connection with the means of delivery of such weapons and other CBRN-related goods and technology, in contravention of a relevant financial sanctions obligation.”
The circumstances in which the duty to report discrepancies to company registries now applies are if the business relationship being established is with:
• A company
• A limited liability partnership
• A Scottish partnership
• A trust which is required to register with HMRC’s trust registry
• An overseas entity that needs to register due to ownership of UK
• real property
• The discrepancy is ‘material’ – not a typographical or minor spelling
• mistake
• The discrepancy ‘by its nature and having regard to all the
• circumstances, may reasonably be considered’ to be linked to
• money laundering or terrorist financing, or conceal details of the
• customer’s business. q
15 15 www.yourexpertwitness.co.uk
[
THE OLD CLICHÉ THAT VARIETY IS THE SPICE OF LIFE CERTAINLY APPLIES TO THE WORK OF AN EXPERT!
Forensic accountant and accredited expert witness Fiona Hotston Moore , of FRP Advisory, reflects on a number of recent cases.
[
THE PAST FEW MONTHS have been particularly varied and interesting in terms of the matters on which I have been instructed as an expert witness. I am fortunate to be assisted by an experienced team of forensic accountants, which enables us to accept a number of instructions – from large fraud investigations and professional negligence cases through to smaller matrimonial matters.
Here are just a few of our recent cases highlighting what we found particularly interesting or challenging.
Instruction as party expert to assess a warranty claim and to determine the value of any loss arising
I was instructed as party expert by a transport technology company to review and give an opinion on a warranty claim arising in respect of buying a business for which the sale completed in 2021. I was instructed to review the completion accounts and to give a view on the warranty claim and the potential loss arising.
We reviewed the completion accounts and management accounting, with particular reference to the recognition of income on the customer contracts. In our opinion the completion accounts materially overstated the income and there was a claim under the warranties.

Following the preparation and disclosure of our report and correspondence between the parties, the matter settled in favour of our client and therefore on that occasion avoided protracted and costly litigation.
A particular challenge in this case was to determine an approach that enabled us to focus our review on the key contracts, ensuring that our work was cost proportionate.
Instruction as an expert witness in a professional negligence claim against a firm of solicitors
The client, a business providing services in the construction sector, was involved in a professional negligence claim against a firm of solicitors, arising from the advice given in relation to the corporate finance transaction regarding the disposal of the business.
The company was claiming for a resulting loss, as the sale consideration was substantially less than was anticipated. I was engaged as party expert witness to give a valuation of the company at the time of the sale, which had taken place around 10 years earlier. We prepared financial and market analysis, looking at the information available at the time of the sale. My valuation considered the relevance of alternative methodologies and explored the value that an alternative purchaser might have placed on the company. Following the valuation, a joint report was prepared, combining our team’s findings with the findings from the other party’s expert, who provided an alternative view. The matter was settled just prior to the court hearing, in favour of our client. The lawyers said the work undertaken by us had placed the client in a good position to negotiate the deal achieved.
A key issue in this case was to assess the market value of the company at a point 10 years earlier, based on the information that would have been available at that time; so avoiding tainting my view with the benefit of hindsight.
Engagement to undertake a financial investigation following a whistleblower report
Following a report by a whistleblower, I was engaged to undertake a financial investigation into the financial reporting, corporate governance and internal controls of a fast-growing entrepreneurial business in the technology sector. The engagement required a rapid deployment of our forensic services team to complete the investigation, as the matter had a potentially significant impact on business operations.
We were appointed as forensic accountants to undertake an indepth investigation, including a review of financial records, interviews of company staff and the investigation of electronic records. Our forensic services staff were deployed from our Cambridge, Norwich and Birmingham offices alongside our forensic technology team and worked on the investigation with the instructed lawyers. Our review initially identified over 240,000 documents and the team was able to refine those to a subset of 15,000 potentially relevant items that were included in our investigation.
FRP’s engagement was concluded – and a full report including recommendations issued – within 10 weeks. The client and instructing lawyers were pleased with the efficiency and thoroughness of our team’s investigation. Following the issue of our report the investigation was concluded and the company was able to share the executive summary with relevant parties.
The key challenge in this case was to sift through 240,000 documents, using search methodology to reduce the documents to a manageable number that could be reviewed by the team q

17 17 www.yourexpertwitness.co.uk
CONVICTIONS TOP-OFF NCA OPERATION AGAINST CASH SMUGGLING GANG
[THE NATIONAL CRIME AGENCY has dismantled a network of criminal cash couriers that laundered more than £100m by smuggling it out of the UK to Dubai in the UAE.

Guilty verdicts returned in the trial of Beatrice Auty, Jonathan Johnson, Jo Emma Larvin and Amy Harrison at Isleworth Crown Court on 25 April brought the number of couriers convicted to 11. Their network smuggled more than £104m from the UK to Dubai during 83 separate trips between November 2019 and October 2020. The operation was overseen by ringleader Abdullah Alfalasi, who was jailed for more than nine years in July last year.
Adrian Searle, director of the National Economic Crime Centre at the NCA, said: “The laundering of such vast quantities of cash around the globe enables organised criminals and corrupt elites to clean or hide their ill-gotten gains.
“Cash smugglers typically work on behalf of international controller networks, who move the finances of the international drug trade, people traffickers, fraudsters and other criminal groups, making the source of the money difficult to trace. The criminality this enables costs the UK billions every year, causes misery and ruins lives across the world.
“This case demonstrates the continued commitment by the NCA to crackdown on money laundering and close the vulnerabilities being exploited.”
The couriers, who were paid around £3,000 for each trip and would be booked on business class flights due to the extra luggage allowance, communicated on a WhatsApp group entitled ’Sunshine and lollipops’.
The network collected cash from criminal groups around the UK, which is believed to be the profits of drug dealing, and took it to counting houses, usually rented apartments in central London. The money was then vacuum packed and separated into suitcases, which would typically each contain around £500,000 and weigh around 40 kilos. They were sprayed with coffee or air fresheners in an effort to prevent them being found by Border Force detection dogs.
NCA senior investigating officer Ian Truby explained: “These couriers were important cogs in a large money laundering wheel. The crime group they belonged to was responsible for smuggling eye-watering amounts of criminal cash out of the UK. This simply wouldn’t have been possible without couriers doing their bidding, in return for a sunshine holiday and a slice of the profit.
“Cash is the lifeblood of organised crime groups, which they re-invest into activities such as drug trafficking. This fuels violence and insecurity around the world, which is why our investigation into other cash couriers continues.”
Five other couriers had pleaded guilty at previous hearings and will be sentenced at a later date, along with those convicted on 25 April. Other couriers remain under investigation. q
18 18 www.yourexpertwitness.co.uk
WHY WOULD YOU USE A FORENSIC ACCOUNTANT TO CHALLENGE A POCA?
by Lennie Harris, Chartered Accountant at HCA Consultancy

[USING A FORENSIC ACCOUNTANT makes perfect sense when there is a need to understand the financial figures relating to particular litigation, to evaluate losses relating to claims, provide second opinions, challenge other parties’ claims and ultimately, when required, provide expert opinion in court.
In my experience, especially when dealing with Proceeds of Crime (POCA) orders, the amounts demanded by the court can be arbitrary and bare no relation to the actual money gained through crime.
My independent reports have been successful in helping many prisoners faced with such problems, as I know what I am looking for in the books and records: simply producing invoices will not help in the same way. To get the full benefit of using a forensic accountant it is necessary to bring him or her in early, rather than simply request permission from the court to use them during the trial proceedings as an expert witness.
With POCAs I’m frequently retained by legal firms to guide their clients through the confiscation proceedings. During the sentencing hearing a timetable will be set, which will outline various dates for the service of statements by you as defence solicitor and the prosecution.
The POCA timetable will set out the date for service of your client’s Section 18/16/17 Statements. That is the order in which the statements will be served. The Section 18 Statement served by you will outline your client’s available assets. That can be anything from property and cash to cars, jewellery and savings. It will also show exactly what available assets can be sold to pay off the Confiscation Order.
The prosecution will then serve the Section 16 Statement. That outlines the prosecution’s case against your client, showing what financial benefit was gained as a result of the crime, and the assets available to repay it. It is prepared by a financial investigator for the prosecution, who will go through the bank accounts, highlighting any unidentified credits that he believes came from criminal conduct. He can go back six years.
When you see the statement you may be surprised by the size of the benefit figure. That is where close examination and discussion of the entries with a forensic accountant can help to reduce the amount substantially. It is my job to work closely with you as part of your team.
Your client is obliged to provide the evidence to challenge the prosecution’s case. You will then serve the Section 17 Statement, showing what assets your client actually has. That must be prepared very carefully. You may want to challenge the prosecution’s valuations of assets such as property by obtaining expert valuation reports.
Family members may believe that there are assets which belong to them, or that they are entitled to an interest in them as they are not the proceeds of the crime. That can be the basis of a separate application to court.
Once the statements have been served there is usually some discussion between the parties to try to reach a fair settlement without the need to approach the judge. I will usually be involved in those discussions, as a forensic accountant’s contribution can help achieve a reduced settlement.
Once the case has concluded, a
Confiscation Order will be made which will outline the concluded benefit figure and the amount that is available. Those assets will be listed and a deadline given for the amount to be paid. That is usually three months, but can be extended by a further three months. Once the six months are up, interest will accrue daily. If the client is unable to pay the amount after that, the time in prison will increase.
With such a tight timetable, it is very important to seek professional advice from an experienced forensic accountant as soon as dates have been determined. I’m often approached directly by the accused to recommend a solicitor who is experienced in the field. I am then available, with the court’s agreement, to act as an expert witness during the court proceedings. q
• For further information call Lennie on 0845 8623260 or email info@hcaconsultancy.com.
19 19 www.yourexpertwitness.co.uk
FREEZING ORDER ISSUED ON LAND IN NI
[A PROPERTY FREEZING ORDER has been issued for a plot of land in County Armagh in Northern Ireland as part of an on-going civil recovery investigation. The order was granted to the National Crime Agency at Belfast High Court on 22 May as it is suspected the land, in Blackwatertown, was purchased for £100,000 using money obtained from fraud and money laundering offences.
The order will prevent anyone from selling or transferring ownership of the land while the investigation continues into the source of the funds used to make the purchase. If unlawful conduct is found, the NCA may seek the recovery of the land.
NCA’s regional head of asset denial Rob Burgess said: “The NCA works to tackle organised crime gangs at all levels in order to frustrate, disrupt and ultimately dismantle them.
“Our civil recovery powers play an integral role and we are committed to working closely alongside partners in the Joint Agency Task Force to prevent those engaged in criminal activity from benefitting financially from their illegal actions. We will continue to use these powers to pursue the assets of criminals, no matter how carefully they have been hidden.”
Detective Superintendent Emma Neil, from the Police Service of Northern Ireland’s Organised Crime Branch, added: “Working with our partner agencies, we are committed to tackling and disrupting the activities of organised crime groups.
“These groups use whatever means possible – from drug dealing to money laundering – to line their own pockets and, sadly, it’s often at the expense of the most vulnerable members of our society.
“This is an excellent example of working in partnership. We’re also grateful for the support of local people, and would appeal to anyone with information or concerns to contact us on 101.” q
HMRC ISSUES NEW SCAM ALERT
[HMRC has published details of a number of new scams reported that aim to trick people into handing over money or personal information.

The scammers use deadlines such as the tax credits renewal deadline on 31 July to target their victims and the department is warning around 1.5 million tax credits customers to be alert to scams that mimic government communications to make them appear genuine.
Typical scams outlined by HMRC include:
• Emails or texts claiming an individual’s details aren’t up to date
• and that they risk losing out on payments that are due to them
• Emails or texts claiming that a direct debit payment hasn’t
• ‘gone through’
• Phone calls threatening arrest if people don’t immediately pay
• fake tax owed
• Claims that the victim’s national insurance number has been used
• in fraud
• Emails or texts offering spurious tax rebates or bogus grants
• or support
Myrtle Lloyd, HMRC’s director general for customer services, said: “Tax scams come in many forms and we’re urging customers to be alert to the tactics used by fraudsters and never to let yourselves be rushed. If someone contacts you saying they’re from HMRC and asks you to give personal information or urgently transfer money, be on your guard. Search ‘HMRC scams’ advice on GOV.UK to find out how to report scams and help us fight these crimes.”
According to the National Cyber Security Centre, HMRC was the third most spoofed government body in 2022, behind the NHS and TV Licensing. HMRC is also urging tax credits customers to be alert to misleading websites or adverts asking them to pay for government services which are free, often by charging for a connection to HMRC helplines. q
20 20 www.yourexpertwitness.co.uk
TRANSLATION ORGANISATIONS COME TOGETHER
THOSE WHO TRANSLATE official documents for use by the UK’s public sector, government agencies or for businesses in the UK know that there are differences in the expectations and requirements for certified translations. There are also differences in how certified translations are produced, laid out and certified by translators and translation companies in the UK.
In Europe and around the world practice varies greatly, with most countries having clearer standards and more requirements than in the UK. The UK is unusually deregulated by international standards.
Those variations can cause confusion and delays in translation and certification processes and can make it challenging for translators and translation companies to confidently provide a service that they know will be accepted by the receiving organisation.
Now, the Chartered Institute of Linguists (CIOL) is working with the Institute for Translation and Interpreting (ITI) and the Association of Translation Companies (ATC) to harmonise best practices around the certification of translations in the UK. All three leading associations now recognise and endorse each other’s certification guidelines and practices.
CIOL chief executive John Worne explained: “The diverging practices stem from the fact that, unlike in many other countries, no sworn or state-authorised system for certifying translations exists in the UK – and this landscape is unlikely to change. Working together with the ITI and the ATC, we will promote the use of properly qualified and accredited professional translators and quality assured translation companies, for the benefit of both the users
INAUGURAL AWARDS CELEBRATE POLICE INTERPRETERS
ON 28 APRIL the first National Police Interpreter of the Year Awards were held at the National Police Language Services Conference, organised by the police’s national lead for language services, the Leicestershire Police.

Baroness Coussins, vice president of the Chartered Institute of Linguists, delivered the keynote address congratulating the winners. The awards ceremony celebrated and was a powerful reminder of the extraordinarily important and challenging work public service interpreters do within the criminal justice system.
The winner of Spoken Interpreter of the Year for 2023 was Samira Hajmi, with Shefki Bytyqi the runner-up. The Simon Cole Award for Excellence in Police Interpreting went to Karina Stefanescu (pictured, right, with Baroness Coussins). Awards were also given for NonSpoken Interpreter of the Year to Alison Gilchrist and runner-up Lesley Weatherson.
A special mention went to Ian Fraser and Mark Lewis of Leicestershire Police for their work in supporting police interpreting nationally and for conceiving and managing the awards.
In her address Baroness Coussins paid tribute to the work of police interpreters: “The strategic importance of linguists goes largely
and producers of these translations.”
ITI chief executive Paul Wilson added: “Our members regularly report on issues with authorities whose requirements on producing certified translations can vary greatly. Through this initiative we will guide public authorities towards qualified and accredited members and partners who can provide a true, complete and accurate certified translation.”
The ATC’s CEO Raisa McNab welcomed the collaboration: “Uncertainty serves no one,” she asserted. “No one benefits from translations carried out by a next door neighbour who has an 'A’ Level in French.
“Our aim is to ensure that certified translations in the UK are produced by suitably qualified, registered translators and reputable translation companies, and we look forward to working with the ITI and the CIOL on this initiative.” q
unnoticed and unsung, especially in your field of law enforcement and the administration of justice, despite being so vital – vital to the quality of public services, to the quality of justice and to human rights. You can almost count on headlines when things go wrong, but the daily competent exercise of your specialist and professional skills is largely hidden and yet every year in England and Wales public service interpreters attend about 66,000 face-to-face assignments for police forces, often in out of the way places at unsociable times.” q
21 21 www.yourexpertwitness.co.uk
[
[

TRANSLATION MYTHS
by Hayley Cowle of Translate Hive
[ IN TODAY’S highly culturally diverse society, the demand for experienced and qualified linguists is increasing. Reliable translation has become very important to each and every case.
Without translation the world would be a very different place. How else would we communicate effectively with each other when the spoken language is a barrier? How else can we ensure that all measures have been taken to guarantee that the content and context of a matter have been fully conveyed and understood?
The law and the legal system underpin pretty much everything we do. Making sure that everyone understands all the legal documents and surrounding information they need is vital.
Often translation is taken for granted and overlooked. As a result, the work behind such assignments and the need for it can go unseen and misunderstood, creating many misconceptions and assumptions about translators and the work that they do. The importance of that work only becomes apparent when things goes wrong – usually at the most inconvenient times, which can affect court deadlines and hearing procedures.


Translate Hive have been witness to several cases where hearings have been adjourned due solely to poorly conducted translations submitted as evidence by non-qualified or inexperienced interpreters.
A few of the misconceptions that translators and linguistic agencies face are:
Anyone who speaks a language can automatically write a report in that language
That is simply not the case. All our translators have expertise in specific fields, not every field. It is important to use the correct translator for the specific source text in question. Most often, translators will hold qualifications in the legal or medical sector as well as their own language field.
Translation and interpreting are the same thing
That couldn’t be further from the reality: they are two completely different processes that require different education, knowledge and skills:
Translation is the written transmission of any text in a source language to a target language.
Interpreting is transmission of verbal statements and speeches from one language to another in real time and usually simultaneously.
Translation is basically a word for word re-write of the original source document
Quite the contrary: translation isn’t just about words, it’s also about concepts and context. We are all familiar with idioms
and plays on words that do not always translate accurately.
All languages have completely different vocabularies, grammar and sentence structure, and in order to provide a superior and professional translation service it’s important to know both languages perfectly and not just translate the words, but take into account the main sense of a sentence.
There could be words and phrases that have no correspondent in another language; therefore, it will be necessary to convey the meaning. An experienced translator will have that skill and can provide a high-quality translation.
It’s impossible to translate the material without understanding it. Translating words is not enough for people to be able to understand a text. Very often it contains some professional or cultural nuances. In order to explain those details to readers or listeners it’s obligatory for a professional to understand all concepts, terms, linguistic nuances and so on.
The need for translators is decreasing
The truth is very much the opposite. As machine translation is not nearly accurate enough for legal requirements, human translators are sought after to complete translations for the legal sector. The need for fully-qualified translators is not only important for the integrity of the document itself, but also for the submission of evidence to the courts. Human translators can keep up to date with the ever-evolving vernacular phrases that a machine translation just cannot do – through refresher courses and day-to-day contact with other persons from the same and similar cultures.
Certified translation is the same as basic translation
Another misconception: fully-qualified translators can provide certification for all work carried out. A certified translation means that the translator must legally acknowledge and confirm that the translation is an accurate and truthful representation of the source document, which keeps the original meaning intact. That usually means that the translator must have certain qualifications and must provide a signed statement confirming that the new document is an authenticated translation of the original. Documents deemed certified are vital for many official purposes and there can be detrimental effects if it is not completely correct. There are many misconceptions about professional translators and interpreters that many people still believe. Translators and interpreters are qualified people with relevant education, experience, certification and deep language knowledge; and not every person can provide quality translation or interpreting services.
23 23 www.yourexpertwitness.co.uk
q


24 24 www.yourexpertwitness.co.uk
CONSTRUCTION-RELATED PIPELINE INCIDENTS SPIRALLING, REPORT FINDS
THE NUMBER OF TIMES construction workers and developers were found to be working too close to high-pressure oil, gas and chemical pipes without the owner’s permission increased by 57% last year, according to Linewatch, the pipeline safety and awareness group. Of the 316 incidents reported, 127 (40%) were caused by contractors and developers.
Murray Peat, manager of Linewatch, commented: “Construction workers have historically been some of the worst offenders when it comes to damaging or operating too close to the UK’s underground network of high-pressure oil, gas and chemical pipelines. Although reporting took a major step forward in 2022, a 57% increase is significant. It highlights that there is still plenty of educational work to do, engaging with developers and contractors up and down the country.”
An infringement can range from someone working near an oil, gas or chemical pipeline without the proper permissions or the owner’s awareness, through to them actually striking or damaging a pipe.
Linewatch's annual Infringement Report states that close to half
of infringements occurred even though the person responsible for the incident was already aware of the pipeline’s existence. That is a 15% increase on 2021 and highlights a distinct casualness in some quarters about the dangers of working near pipelines.
Murray Peat expressed concern at the situation: “There is an assumption that high-pressure pipelines carrying flammable oil, gas and chemicals are buried too deep underground to hit. This is far from the truth; in fact, they can be buried as little as three feet below the surface. Given that hitting one of these pipes can cause serious injuries and fatalities, as well as irreversible environmental damage with commensurate fines, it is clear why searching before digging is so important.”
He concluded: “There are no signs of digging slowing down as the government commits to kickstarting the UK economy to regain control over spiralling inflation. It is therefore more important than ever that the correct digging procedures are followed.”
To download the full 2022 Infringement Report visit the Linewatch website at www.linewatch.org.uk q

HSE’ MESSAGE IS THAT DUST KILLS
[THE Health and Safety Executive (HSE) is currently engaged on a campaign targeting construction sites to get the message across that failure to prevent lifethreatening diseases caused by dust at work is unacceptable.
The site visits are in support of HSE’s Dust Kills campaign, which provides free advice to businesses and workers on the control measures required to prevent exposure to dust.

Each year in the construction industry there are thousands of preventable cases of irreversible lung disease due to past exposure to dust at work. Those diseases often have a life-changing impact and can result in an early death.
HSE’s chief inspector of construction Michael Thomas explained: “Every year we see construction workers die from diseases caused or made worse by their work. This is unacceptable in the 21st century, when
occupational lung disease is preventable.
“We are urging employers and workers to take the necessary precautions today to protect their long-term lung health, to avoid them and their families suffering from the devastating impact that can result.”
Inspectors are checking the control measures in place to protect workers from inhaling construction dusts, including respirable crystalline silica and wood dust. They will also seek assurances that asbestoscontaining materials have been identified and removed or managed where necessary to prevent or reduce exposure.
The primary aim of the inspections is to ensure workers’ health is being protected. However, if safety risks or other areas of concern are identified, inspectors will take the necessary action to deal with them.
Michael Thomas continued: “Through engaging with those on site, we can make sure they have considered the job from start to finish, have considered the risks at each stage and are managing the risks with effective measures in line with the broad hierarchy of control options such as water suppression, extraction and as a last resort respiratory protective equipment.” q

25 25 www.yourexpertwitness.co.uk
[
FIRE RISK BENCHMARK GETS A WARM WELCOME FROM THE INDUSTRY
[ THE FIRE SECTOR FEDERATION (FSF) has published a new Industry Benchmark Standard for Fire Risk Assessors to provide practical guidance for assessors who want to understand the application of fire risk assessment across a range of buildings. The document was launched on 20 March.
The aim is to support the delivery of comparable standards across the sector. The standard has been developed by the federation’s Fire Risk Assessors Working Group and identifies criteria reflecting individual
competency at three distinct core levels: Foundation, Intermediate and Advanced. It offers increasing levels of skill, knowledge, experience and behaviour to form a competency-based progression route for fire risk assessors, spanning a clear career pathway for individuals from entry through continuing personal development to the highest levels of competency achievable.
It is unique in that it also seeks to match the three core levels of competency to the fire risk presented in three general types of buildings.
Dennis Davis, executive officer of the Fire Sector Federation, who led the working group, commented: “This Benchmark Standard has been developed by the federation’s Fire Risk Assessors Working Group to expand and complement our previous work on competency. It supports the need for a systematic assessment of fire risk followed by the implementation of recommended appropriate controls, mitigation and continuous management of fire safety.
“Our aim is to raise the professional status of the important work undertaken by fire risk assessors. We also wish to engage with all those proficient assessors, operating without formal or recognised competency assurances, to help them seek appropriate independent accreditation.
The document is available to download from the FSF website at www.firesectorfederation.co.uk
The work undertaken by the federation’s working group will shortly move on into a new phase of development through BSI’s new Competence in the Built Environment Committee CPB/1 to create a British Standard Code of Practice.
The document was welcomed by the Institution of Fire Engineers (IFE). The IFE says it has reviewed the standard and is supportive of its content, which will become central to its own fire risk assessor registration process moving forward.

IFE chief executive Steve Hamm said: “The FSF’s benchmark aims to raise the professional status of the valuable work fire risk assessors undertake and we echo the federation’s commitment to promoting competency.
“A number of our own members have been involved in the competency steering group work tasked with developing the principles that underpin this standard and we have aligned our internal processes to ensure that future applicants to join the IFE’s Fire Risk Assessors Register will be assessed in line with this newly-launched benchmark standard.
“This will enable those seeking a competent fire risk assessor to benefit from the assurance provided by the rigorous IFE registration processes.”
As the global professional body for the fire sector, the IFE is committed to shaping a future world that is safer from fire. Its Fire Risk Assessors Register is a good example of that work.
The register is not just designed to benefit those seeking a fire risk assessment; it provides its member network with independent validation of their services and a marketing tool to support opportunities for business. It is one of a number of initiatives developed by the IFE to help give members the platform, resources or opportunity to drive advantage within increasingly competitive markets. q
26 26 www.yourexpertwitness.co.uk
EXPERIENCE AND SCIENTIFIC KNOWLEDGE COMBINE TO OFFER AN EXPERT’S VIEW
[ JASON HILL is a Chartered Engineer (CEng) registered through the Institution of Fire Engineers (IFE), a Chartered Engineer (CABE CBuild E MCABE) registered through Chartered Association of Building Engineers and a Chartered Engineer Member of Engineering New Zealand (CMEngNZ). He is also a Fellow of the IFE (FIFireE), a member of the United Kingdom Association of Fire Investigators (MFireInv) and a student with the Royal Institution of Chartered Surveyors (RICS).
He has a First Class Bachelor of Science Degree (BSc Hons) in Fire Safety Engineering studied at the University of Wales, Newport and a Master of Science Degree (MSc) in Fire Explosion and Fire Investigation studied at Leeds University.
Jason has worked as an engineer for over 25 years and specialises in matters relating to fire safety engineering and fire risk assessment. He was a member of the UK Government working groups following the Grenfell fire to assist in the authorship of the competency criteria for fire risk undertaking and also an IFE comember of the PAS9980:2021 fire risk appraisal and assessment of external wall construction and cladding: Code of Practice (PAS9980) Technical Steering Group.

He also has experience of working with British Standards Institute (BSI) for PD 7974-6:2019 – Application of fire safety engineering principles to the design of buildings. Human factors: Life safety strategies – occupant evacuation, behaviour, and condition (Sub-system 6) and was a technical steering group member for means of escape for disabled people and technical
steering group member for construction technologies, design and usage.
Jason established Fire Investigation Risk Evaluation (F.I.R.E.) Consultancy Ltd in 2014 to provide a specific, bespoke and high-quality service worldwide, and gained valuable experience representing a leading expert witness business as their technical expert. He has worked within highly-regulated industries to establish analytical thinking to review evidence, conduct investigations, liaise with authorities and identify relevant standards, regulations and other published guidance for each case. The output provides clients with timely verbal or written advice that can be readily understood by a layperson.
In the sphere of education, he has developed platforms and tools such as FRED (Fire Related Educational Development) talks aimed at providing detailed understanding though discussion and experiments – each talk is accredited with CPD through the IFE – and produced a YES (Young Engineer and Scientist) Journal, aimed at helping students aged 5-18 relate STEM (Science, Technology, Engineering & Mathematics) to industry. The content explores everyday engineering problems to show the application of STEM in industry.
Jason commented: “F.I.R.E. Consultancy would like to be your aid in determining key factors in a case, for which we will demonstrate the required appropriate knowledge and understanding to examine the evidence: the output from which can be used as a healthy challenge to the other experts’ opinion.”
27 27 www.yourexpertwitness.co.uk
q
SLIP OR TRIP: HOWEVER YOU FALL IT MAY BE AVOIDABLE
[SLIPS, TRIPS AND FALLS are often seen as minor incidents, or even funny. In truth, they are a significant cause of serious injuries and fatalities in the workplace, public spaces and the home. In 2021/22, slips, trips and falls accounted for 30% of all non-fatal reportable workplace injuries. There are several challenges which can make investigating those incidents –and correctly managing risk – difficult.
• When describing a fall, the terms ‘slip’ and ‘trip’ are often used interchangeably to describe a loss of balance. Slips and trips have different root causes and each will require different controls to be implemented in order to prevent falls.
• When investigating a fall it is easy to assume that the sole root cause is human error. Although all falls will involve an error by the pedestrian in maintaining a safe walking gait, the likelihood of that error is influenced by a range of environmental and task-based factors. Assuming that a fall is purely due to human error without identifying those additional root causes prevents an organisation learning from the incident and making relevant improvements to prevent similar falls in the future.
• Falls are typically seen as simple incidents. However, while the solutions required to prevent slips, trips and falls are often simple, without good root cause analysis that considers all the risk factors it is difficult to identify a suitable intervention that will genuinely reduce risk. That is made more difficult by the poor standard tests which are in common use for assessing the slip resistance of flooring and footwear, and often lead to
inappropriate solutions being specified. The causes of slip, trips and falls have been the topic of many scientific studies and understanding the science helps to provide a more robust and reliable assessment of risk and identify appropriate interventions to prevent falls. Examples of the important considerations for slip, trips and stair falls are:
Slips
The key contributing factors to slips are presented in the Health and Safety Executive’s slip potential model, which is illustrated below.
Minimum toe clearance (MTC) is defined as the minimum vertical distance between the lowest point under the front part of the foot and the ground during the mid-swing phase of pedestrian gait. Understanding MTC helps to determine the risk posed by an underfoot obstacle.
In addition, local lighting levels and the visibility of the hazard, as determined by light reflectance value contrast, as well as the age and visual acuity of the pedestrian, will all influence the risk of trips.
Stair falls
A fall on stairs, particularly on descent, often leads to serious injury and stair falls cause many fatalities each year.
Understanding the tribology of the foot-floor interface with different contaminants is critical in making a robust assessment of slip risk. That requires appropriate information from a relevant test when assessing flooring, footwear or both. Human factors will also play an important role, especially in the efficacy of the cleaning process.
Trips
There are two common factors that contribute to trips: they are an obstacle in the walking route and a failure by the pedestrian to clear the obstacle with their foot – which is influenced by the size of the obstacle and whether they have seen it.
Falls on stairs are often seen as purely human error. In reality, however, stair design has a huge influence on the likelihood of someone making a mistake when using the stair. Human behaviour is hard to control, but good stair design reduces the risk of falls for all stair users. Critical areas of stair design include:
• The dimensions of the stair
• The consistency of the dimensions
• The design of the treads
• The availability, design and visibility of
• handrails
Slips, trips and falls frequently cause serious injury. While the solutions to minimise risk are often simple, a robust understanding of the root causes is needed in order to identify appropriate controls. There is a lot of misinformation in the public domain from standards and ‘expert consultants’ that can make the process more difficult. q

28 28 www.yourexpertwitness.co.uk
YOUNG DRIVERS ADMIT TO NOT WEARING SEAT BELTS, SURVEY FINDS
[ALMOST TWO IN FIVE (38%) of 25 to 34-year-old drivers admit they do not always wear a seat belt when on the road, according to a report published in March by road safety charity Brake in partnership with Direct Line and Green Flag.
The report, which surveyed 2,004 drivers, also found almost a third (29%) of drivers aged 18-24, and more than a quarter (26%) of those aged 35-44, do not always belt up in cars. That is in stark contrast to older drivers: just 4% of those aged 55 or above and 6% of those aged between 45 and 54 say they do not always belt up.
The proportion of car occupants killed who were not wearing a seat belt has remained consistently above 20% in the past six years. Studies show seat belts reduce both fatal and non-fatal injuries by 60% for front seat passengers, and by 44% for rear seat passengers.
Other findings from the report include:
• More than one in 10 (12%) car passengers admit they wouldn’t
• speak out if the driver was speeding – with those aged 45-52
• most likely to stay quiet (14%) and those aged 25-34 least likely
• to do so (8%).
• Male passengers are twice as likely as female passengers to not say
• anything if the driver was breaking the speed limit (16% versus 8%).
• A quarter (25%) of drivers said they have knowingly driven the

• morning after drinking, even though they may still be over the limit.
• Only two-thirds (66%) check the weather forecast before making a
• long journey.
• If it was snowing, more than one in 10 (13%) of drivers would still
• make a non-urgent trip.
• More than eight in 10 drivers (85%) check the pressure of their
• tyres less frequently than once a week.
The report was published to promote the Roadmap to Safe and Healthy Journeys project, an online resource that enables people to learn about, and commit to making, safe and healthy journey choices – including always wearing a seat belt.
Jason Wakeford, head of campaigns at Brake, said: “We all have a responsibility to follow safety rules and help others to be safe on roads. Brake is urging people to visit the roadmap for information and resources to help them stay safe, and to pledge to play their part in reducing deaths and serious injuries on our roads.” q
E-SCOOTERS: PROVISIONAL ACCIDENT FIGURES RELEASED
[IN MAY the Department for Transport published a factsheet of provisional data on the number and severity of collisions involving e-scooters and consequent casualties.
E-scooter users, the DfT says, comprise one of the most vulnerable user groups. They are not protected by a vehicle body in the same way car users are and tend to be harder for drivers to see on the road. They are, therefore, particularly susceptible to injuries.
The factsheet is based on provisional data supplied by police forces up to 5 May this year. No estimation is made for any missing data, so the provisional estimates are likely to slightly underestimate the final number of e-scooter collisions and casualties for the year. Final figures and underlying data are due to be published in September.
The provisional data shows that, in 2022, there were 1,369 collisions involving e-scooters, compared to 1,352 in 2021. Of those, 342 included only one e-scooter with no other vehicles involved in the collision, compared to 324 in 2021. There were 1,458 casualties, compared to 1,434 in 2021: 1,117 were the e-scooter users, compared to 1,102 in 2021.
There were 12 people killed in collisions involving e-scooters, 11 of whom were e-scooter riders.
In terms of severity of injury, the best estimate, after adjusting for changes in reporting by police, is that there were 421 seriously injured and 1,025 slightly injured in collisions involving e-scooters. That compares to 418 and 1,006 respectively in 2021.
However, the DfT concedes: “It should be noted that a considerable percentage of non-fatal casualties are not reported to the police. Nonfatal casualties for e-scooter users are amongst the most likely to be under-reported in road casualty data since they have no obligation to inform the police of collisions. This should be borne in mind when analysing and interpreting the data.” q

29 29 www.yourexpertwitness.co.uk
WHERE IS THE EVIDENCE TAKING ME?
role
the

[I HAVE BEEN an accredited expert witness for more than a decade and it is two decades since my first case as the expert. My role as an expert, which was emphasised during my training, is that my duty is to the court. With every case I need to remain independent and impartial.
One common theme I am encountering is how limited the evidence is for many cases I am instructed to review. In part that is because arboriculture is an unregulated profession and some individuals – presenting themselves as experts – are lacking the skills, training, experience and mindset for the role. I covered that problem in the last issue of Your Expert Witness. There is also a risk of becoming emotionally involved with a case.
Often I am presented with a professionally-presented report; and yet when I begin to explore the evidence, I find all is not as it may initially seem. In my first case as an expert that required my attendance at court, a local authority was seeking to enforce what they considered to be a breach of a Tree Preservation Order. I was left distinctly underwhelmed by the evidence presented. The officers presented a series of photographs of tree stumps as evidence that the landowner had been busy felling trees in a woodland. As I looked at the plethora of images I saw a theme of dead stumps, some with decaying fungi present – which is evidence that the host tree was already dead or dying.
At the Meeting of Experts the lead officer conveyed an air of confidence in the merits of their case: ‘We’ll see you in court’ being their informed view. There was little in common with our views and I watched as the case soon unravelled. The local authority had become emotionally involved and focused on prosecuting a landowner who they were convinced was up to no good. The feeling was mutual. Unfortunately, in their desire to ‘get their man’, the local authority had lost focus and was left with little but experience and a large bill for costs.
More recently, I was asked to investigate a case where a tree had broken and caused a road traffic accident. The defendants confidently presented their case that the tree had broken in a storm and its failure was not foreseeable. They had a tree expert within their team to support that view.
It took a quick online search of weather for the time of the incident to conclude that there was no storm – just a wet morning. Another online search soon revealed that the ‘expert’ was only qualified to use a chainsaw and the ‘detailed tree survey’ had been a walk around the grounds of the property with the owner to discuss a schedule of works.
The confidence with which the case had been presented soon dissipated. I duly submitted my report and awaited a call to attend court. It was a bittersweet moment when, soon after, I was informed that the defendant had settled on reading my report.
Sometimes there is evidence of foreseeability, but it may be difficult
to find and may require a degree of intentionality. I found that when investigating the failure of a tree felled by Storm Arwen. That particular case demonstrates that the evidence may not be clear-cut and one should consider nuances when presenting a view.
An ash tree was blown over in the storm, causing damage to a nearby property. The tree was on the edge of a field opposite the property – and possibly on third-party land. At the base of the tree, on the field side, were fungi indicating decay. If the insurer had commissioned a tree report as part of offering insurance, then either the presence of the decay or its potential should have been highlighted. However, in mitigation, the evidence was difficult to locate and the storm was northerly in direction and unexpectedly strong, causing widespread damage. Had the tree been blown over in more typical conditions it would probably have landed in the field rather than on the building!
It can be interesting when investigating a case that has also been considered by an experienced fellow professional. I had that experience more recently. The expert for the claimant could cite a Master’s degree, which focused on tree failure assessments. Two trees had been uprooted in inclement weather, causing damage to a vehicle. The owners of the vehicle were seeking compensation. The two trees were in a group of more than a dozen and the owner, a local authority, had an inspection programme in place.
As I explored I soon realised that the expert had no training in tree inspections, no training in the protocol of being an expert witness and they had focused only on the two trees that failed. Decay was evident. However, when investigating it is important to place oneself in the position of the inspector. As I inspected the remaining trees I found them all to be in a good condition. The claimant’s expert, who had no experience of managing a large population of trees, considered that if the inspector had undertaken a decay assessment using appropriate equipment, then the decay would have been identified. I felt this to be unrealistic.
We had a Meeting of Experts, where my fellow arborist informed me that he ‘knew where I was coming from and the differences between us were small’. He considered ‘it was clear that the inspector should have undertaken a more detailed inspection of the two trees that failed’. I politely declined to concur.
His CV was notable for an absence of some core training in tree safety protocol which many professionals, myself included, have. I queried this. My fellow expert informed me that he didn’t have much time for such courses, they were run when he did his training. He had a Master’s degree and his thesis, on tree safety, had won an award!
His summary of our meeting, extending over more than a dozen pages, indicated that he was not fully acquainted with the protocol of the role: the summary should be just that, only a couple of pages in length.
My day in court was duly booked when I got the update that, based on my own report, the case had been settled, largely in favour of the defendant.
I have come under pressure from clients to emphasise the merits of their case, to emphasise foreseeability when it was to their benefit, or confirm negligence. I need to be polite but firm: if the evidence does not support that, I need to follow the evidence. I also need to consider being cross-examined on such matters. My clients may not appreciate that, but it ensures the merits of a case are succinctly presented.
Sometimes, I don’t progress beyond the initial feasibility assessment. When I do, all parties can be assured that there is a case, and with care it can be resolved efficiently. However, I don’t bluff – and if my day in court is needed, I’ll be there. q
30 30 www.yourexpertwitness.co.uk
The
of
accredited arboricultural expert witness is explained by Mark Chester of Cedarwood Tree Consultants.
EXPERTS FOR MEDIA
The following experts offer their expertise to the media
Professor Charles Davis MBBS FRCS Consultant Neurosurgeon



Professor Charles Davis acts as an expert witness with very extensive experience in cases relating to neurosurgery, including the preparation of medico-legal reports and appearing in court. Speedy reporting, free advice and screening.
Contact: Marlene Scruton T: 01772 761150 F: 01772 761150
E: marlene.scruton@talktalk.net
Dr Emma Ferriman MBChB MRCOG FRCOG Consultant Obstetrician and Fetal Medicine Specialist

Medical negligence cases involving:
• multiple pregnancy and high
• risk obstetrics including intra
• partum complications and
• birth asphyxia
• prenatal diagnosis
• obstetric ultrasound
• first trimester screening
T: 07812 353820 E: emmaferriman@doctors.org.uk
W: www.emmaferriman.co.uk
Mr Robert Hensher
FRCS FDSRCS
Consultant Oral and Maxillofacial Surgeon
EXPERTS FOR MEDIA is a new section in Your Expert Witness for experts who wish to offer their views and the benefit of their experience to the vast range of print and broadcast media.


Ever wondered how news teams find the experts they consult to explain the ramifications of breaking news stories, seemingly at the drop of a hat? Or how the producers of TV drama series ensure their stories are accurate and reflect the realities of the professions they portray?
The fact is that researchers consult registers of experts and expert periodicals just as lawyers do. In fact, Your Expert Witness is receiving an increasing number of enquiries from media researchers and public relations agencies looking to locate appropriate experts to inform their clients.
Experts for Media is therefore an ideal space to attract their attention. For prices and to book your space, contact Ian on 0161 710 3880 or via ian@dmmonline.co.uk

Mr Hensher’s subspeciality interests include dental implantology, facial injury and temporomandibular joint replacement. He prepares over 50 reports yearly including negligence and criminal cases.
E: jackiesorrell@kingedwardvii.co.uk M: 07947445414
E: roberthensher@kingedwardvii.co.uk M: 07836540457
Mr Panayiotis Kyzas
FRCS(OMFS) PhD MBBS BDS FST
Consultant OMFS Head & Neck Surgeon
Mr Panayiotis Kyzas is a Consultant OMFS Head and Neck Surgeon who specialises in major oncological head and neck cancer surgery. Mr Kyzas can take instructions on behalf of either claimant or defendant or as a Single Joint Expert.

T: 07505 402640 E: kyzasp@icloud.com
Dr Ian C Perry
MBBS MFOM DAvMED(Lond) CFIOSH FCIM MA Consultant in Occupational Medicine
Clinical negligence and personal injury cases on behalf of claimant, defendant or as a Single Joint Expert. Specialist areas of expertise include work related accidents and injuries – most notably in the aviation industry – and those due to long term exposure to chemicals, noise and vibration.
T: 07836 664670 E: ian@ianperry.com W: www.ianperry.com
31 31 www.yourexpertwitness.co.uk
Welcome to our A to Z guide of the websites of some of the Expert Witness field’s leading players.
If you are one of our many online readers simply click on any of the web addresses listed below and you will be automatically directed to that particular website.
To get your website listed on this page just give us a call on 0161 710 3880 or email ian@dmmonline.co.uk
DentoLegal Ltd – Gary M Simon
Translations and Interpreting for the Legal Profession since 1997. Specialists in Personal Injury and Clinical Negligence. www.abc-translations.co.uk
Salam Alaswad LLM PGDip BSc
• Financial derivatives • Contracts for Difference (CFD)
• Forex fraud • Financial crimes • Pre-action assessment
• Charts and diagrams for complex cases www.fxandcfd.com/expert-witness
Dr Paul Baskerville MA DM FRCS
Expert witness instructions in cases relating to all aspects of vascular disease. Can act on behalf of claimant, defendant or as Single Joint Expert. www.baskervilleclinic.com
Mr Timothy Burge MBChB FRCS FRCS(Plast) DMCC MSc
Consultant Burns & Plastic Surgeon
• Cosmetic and aesthetic surgery of the breast and trunk
• Burns • Trauma • Scars www.clifton-plastic-surgery.co.uk
Professor Frank Chinegwundoh MBE

Consultant Urological Surgeon specialising in Personal Injury and Medical Negligence cases on behalf of either claimant or defendant or as a Single Joint Expert. www.urologyconsultant.co.uk
Clarke Gammon
Chartered Surveyors with experience in All Aspects of Property
• Residential property values
• Asset valuations • Land values and more www.clarkegammon.co.uk

D & HB Associates Ltd

Experts in Road Traffic Offences
• Accident investigation and reconstruction
• Tachograph analysis
DentoLegal specialises in the preparation of evidencebased Breach of Duty & Causation and Condition & Prognosis Dental Reports on the instruction of solicitors. www.dentolegal.com

DRC Forensics Limited
DRC Forensics Limited offers the complete range of forensic accounting & litigation support: • Fraud • Money laundering

• Partnership disputes • Loss of profit
• Professional negligence www.drcforensics.co.uk
Mr Roger Emmott CEng BSc(Hons) MSc/MBA MA FCMI FIC Steel and iron ore expert with international arbitration and cross-examination experience in complex disputes


• Pricing • Contractual matters • Valuations
T: 07974 351704 E: roger@rogeremmottassociates.com www.rogeremmottassociates.com

FHDI - Kathryn Thorndycraft-Pope
Examining documents & handwriting • to determine authenticity • to expose forgery • to reveal aspects of origin. Electro Static Detection Apparatus and Mi-Scope used. www.forensichandwriting.co.uk
Forensic Collision Investigation & Reconstruction Ltd

Specialists in the analysis of road traffic collisions
• Collision Reconstruction • Expert Witness
• Vehicle Examinations
www.FCIR.co.uk
Fiona Hotston Moore (FRP Advisory)
Fiona is a partner of FRP’s Forensic Services practice specialising in share and business valuation cases, commercial and tax disputes and professional negligence. www.frpadvisory.com/people/people-profiles/fiona-hotston-moore/

Mr Kim Hakin FRCS FRCOphth
Consultant Ophthalmic Surgeon and Expert Witness on ophthalmological matters
• Stolen vehicle examination and identification
• Statement Taking www.dandhb.com
Dr Lars Davidsson MRCPsych MEWI
Consultant Psychiatrist and Accredited Mediator Reports within most areas of general adult psychiatry. Specialist in PTSD, anxiety disorders & mood disorders. www.angloeuropeanclinic.co.uk

Chris Dawson MS FRCS LLDip
Consultant Urologist with over 19 years experience of medico legal report writing and expert witness work in personal injury and clinical negligence cases. www.chrisdawson.org.uk





www.kimhakin.com
Haydn Jones MEng DipLaw FIET
Data Technologist & Digital Regulation Expert
• Injunctive relief
• Money laundering
• Digital currency theft
• Counter funding of terrorism haydn@blockchainhub.com
Dr Raj Kumar – Dental Expert

Causation and Liability and Condition and Prognosis Reports
• General dentistry
• Cosmetic dentistry

• Dental implantology
• Orthodontics
www.dentalexpert.me
• Patient consent
• Facial aesthetics
32 32 www.yourexpertwitness.co.uk
Kulvinder Lall Consultant Cardiothoracic Surgeon

Instructions taken in cases relating to cardiac and thoracic surgery, including aspects relating to surgical care and those following trauma to the structures of the chest.
www.kulvinderlall.com
Mr Chris Makin
• Chartered Accountant • Accredited Civil Mediator
• Accredited Expert Determiner
www.chrismakin.co.uk
Martyn Slyper Consultancy
Expert Witness in Assistive Technology
• Personal Injury • Clinical Negligence • Industrial Injury
E: ms@martynslyperconsultancy.co.uk
www.martynslyperconsultancy.co.uk
Professor Christopher Raine MBE Specialist in paediatric and adult otology





• Medical negligence • Personal injury cases involving noise induced hearing loss.
www.profchrisraine.co.uk
Mr Sameer Singh MBBS BSc FRCS Orth
Consultant Orthopaedic Surgeon • All aspects of trauma – soft tissue and bone injuries
• Upper and lower limb disorders and injuries
• Whiplash injuries
• Expert Witness for defence and claimant Clinic locations – London, Milton Keynes and Bedford

www.orthopaedicexpertwitness.net
Dr Elizabeth J. Soilleux MA MB BChir PhD FRCPath PGDipMedEd
Expert Witness Pathologist with a particular interest in haematopathology. Short reports on specimens, full court compliant reports and expert biopsy reporting. www.expertwitnesspathologist.co.uk

Mr Bernard Speculand MDS FDS FFD FRACDS (OMS)
Consultant Oral and Maxillofacial Surgeon. Personal injury and clinical negligence cases for claimant, defendant and as Single Joint Expert. Special interest is TMJ Surgery.
Yvette Young (Secretary) T: 0121 605 1884
E: info@medsecadmin.co.uk www.birminghamtmj.co.uk
Myles J O Taylor BA(Oxon) PhD FRCOG
Expert witness specialising in: • General obstetrics & gynaecology • Fetal Medicine • Multiple pregnancy
– including twin to twin transfusion syndrome, intrapartum care and general gynaecology.
www.mylestaylor.co.uk
Vincent Theobald-Vega
Health and Safety expert • Asbestos management & removal

• Construction design and management • Laboratories
• Biological & chemical safety and much more.
www.safety4hed.co.uk

33 33 www.yourexpertwitness.co.uk

MEDICAL NOTES

[ IF BEING the subject of a satirical debate on the BBC’s News Quiz is an indicator for the importance of a news story, then the report that the Metropolitan Police are set to refuse to attend calls involving mental illness is one of the big stories of recent weeks. The move, according to leaked documents published in The Guardian, was prompted by impatience on the part of Met Commissioner Sir Mark Rowley with progress in implementing an approach to responses called ‘Right Care, Right Person’.
As with most of these stories, the background somewhat dilutes the headline. The approach has been in place in a number of trial areas for some time, with a measure of success.
• New approaches to treatment are a perennial element in medical advances, whether in the field of new drugs or in therapies to replace drugs in the treatment of certain conditions. Chronic pain is one condition where the medication needed to treat the condition has traditionally been addictive or dependence inducing. Recent approaches to the treatment of pain have focused on alternatives to opioids and the like, with support to counter the effects of withdrawal being offered.
The Faculty of Pain Medicine, while welcoming the offer of alternatives and support to withdraw, has cautioned against the stigmatisation of patients whose treatment still depends on powerful pain killers as the only defence.
• Pain has hitherto been a difficult condition to quantify, being entirely dependent on subjective measurement – I refer readers to a previous column relating my own post-operative experience. A breakthrough in San Francisco has indicated for the first time that pain can be measured by using implants in the brain to measure the brain’s response to pain.
The news is one more instance of technology being the conduit for medical advance. Another has been reported closer to home. In Scotland researchers have developed a method of diagnosing heart attacks quicker and more accurately by means of an algorithm developed using artificial intelligence.
• A technology that has been around for a little longer than AI is the use of ionising radiation in both diagnostics and treatment. Orthopaedic surgeons are one group using such treatment routinely, and there is concern that female surgeons can be at a raised risk of breast cancer as a result. A working group of the BOA has expressed concerns at the level of protection provided by current PPE for women. One of its members is articulating those concerns effectively.
• While risks associated with the workplace can be identified and legislated for, the many risks associated with cut-price cosmetic or bariatric surgery abroad are less easy to guard against. Even the very act of returning home after surgery can present serious dangers, such as DVT. Two associations representing aesthetic and bariatric surgeons respectively have voiced their concerns about what they term ‘surgical tourism’. Their message is to ‘Consult a UK surgeon first’ – and ideally stay in the UK for your procedure.
The many advantages of consulting a well-regarded surgeon in this country are explained by two leaders in the field.
• Being able to give informed consent is one of the pitfalls of surgical tourism: if much of the protocols surrounding the procedure is in a foreign language, how do you know if you are getting what you expected?
The issue is complex enough at home, where the patient’s consent may be based on an appreciation of the risks associated with a procedure. Case law is its usual dense quagmire in that area, as elucidated by a senior ophthalmologist. q
35 35 www.yourexpertwitness.co.uk
36 36 www.yourexpertwitness.co.uk
MESOTHELIOMA CLAIM FAILS ON EXPOSURE LEVELS

[A RECENT ‘Case of Note’ described by NHS Resolution has highlighted the complexities in pinpointing responsibility for contracting mesothelioma –the cancer caused by asbestos exposure which is invariably fatal.
The case was that of a Mr White, who died on 8 April 2020 from mesothelioma at the age of 87. His estate claimed that his death had been caused through wrongful exposure to asbestos dust while working at Sefton General Hospital in Liverpool between 1949 and 1960, when he was a junior laboratory technician, and between 1973 and 1992, when he worked as a senior biochemist. The Secretary of State was the defendant, having inherited liabilities from bodies running Sefton Hospital at the relevant times.
LEAFLETS SHARE LEARNING ON MEDICATION ERRORS
[NHS RESOLUTION has published a suite of seven information leaflets relating to medication errors in order to share learning from clinical negligence claims with healthcare professionals.
It describes medication errors as ‘any patient safety incidents where there has been an error in the process of prescribing, preparing, dispensing and administering, monitoring or providing advice on medicines’. Such errors can occur at many steps in patient care, from ordering the medication to the time when the patient is administered the drug.
From 1 April 2015 to 31 March 2020 NHS Resolution received 1,420 claims relating to errors in the medication process. Of those claims 487 were settled with damages paid, costing the NHS £35m, excluding legal costs.
Initial data for medication errors indicates that anticoagulants, opioids, antimicrobials, antidepressants and anticonvulsants are the most common medications to be implicated in incidents.
The seven information leaflets, published in the Did You Know series cover:
• Anti-infective medication errors
• Extravasation
• General practice medication errors
• Heparin and anticoagulants
• Insights into medication errors
• Maternity
• Paediatric medication errors
The leaflets can be downloaded from resolution.nhs.uk q
The NHS Resolution report said: “Cause of death was not disputed. Symptoms commenced in about July 2019 and a formal diagnosis of mesothelioma was made in September that year. However, the defendant argued that Mr Wilson was exposed to extremely low levels of asbestos dust while working at the hospital, at a time when the risk of injury from such limited exposure was not generally known.”
Prior to his death Mr Wilson had made a statement in which he described the use of asbestos mats in the laboratory. He categorised them as ‘very fragile’ and said: “…they would simply break and the edges would be flaky. If you placed the board down onto the desk heavily it would just break into pieces and cause so much dust to emerge.”
The defendant engaged an occupational hygiene expert witness, whose opinion was that the level of exposure during Mr White’s second spell at the hospital as a senior biochemist was minimal. During his first spell there the exposure was higher but still low. During that time the risks of low exposure were not known. It was only in 1965 that a paper was published exposing the risk.
The judge concluded that, during his first period in the laboratory Mr Wilson was exposed to very low levels of asbestos dust. Since the entirety of this period was before publication of the key paper in 1965, it was not foreseeable to the hospital authorities that there was a risk the deceased might develop mesothelioma or some other malignant disease from very low level exposure to asbestos dust. During the second period of employment, the degree of exposure was very low indeed. Consequently, although causation had been accepted, it was not foreseeable to the employers at the time that Mr White might be exposed to a risk which they had a duty to guard against. Judgment was therefore given in favour of the Secretary of State. q
37 37 www.yourexpertwitness.co.uk

38 38 www.yourexpertwitness.co.uk
GMC GIVES TWO CHEERS TO PROPOSED REFORM
[ LEGISLATION PROPOSED BY the UK Government for the regulation of physician and anaesthesia associates (PAs and AAs) by the General Medical Council (GMC) has been welcomed by the regulator, although it fears some aspects will have unintended consequences.
The proposed reforms will allow the GMC greater flexibility to adapt policies and procedures to meet the needs of healthcare systems, registrants and patients. However, it says some areas, such as the grounds for fitness to practise action, need a rethink before they become law.
The GMC says the proposed legislation is a crucial step in enabling it to take a compassionate approach to regulation, with tangible benefits. They include:
• A simpler and streamlined regulatory framework, allowing fitness to practise cases to be resolved more quickly – for example, new powers to administratively remove people convicted of serious criminal offences from the registers.
• A faster and less adversarial process: where concerns are raised about an AA or PA that meet the threshold for investigation it will be possible, where appropriate, for them to be addressed through a process of ‘accepted outcomes’.
• An end to the ‘five year rule’. The GMC is currently unable to consider complaints relating to matters more than five years old, unless certain criteria are met. The rule will not apply to AAs and PAs and it is expected that, in future, it will not apply to doctors either.
• Greater autonomy: allowing the regulator to make and amend legally-binding rules that govern how it operates, balanced by a requirement to consult stakeholders.
Reform will also allow the GMC to support the UK’s health workforce by streamlining registration and making it more
accessible for those who want to work in the UK.
However, the GMC has raised some issues that it wants to be addressed before the proposals become law, including a plan to reduce the grounds on which fitness to practise action can be taken. There are currently six grounds, but the legislation would reduce that to just two: inability to provide care to a sufficient standard and misconduct.
The regulator argues that such a change, in particular dropping ‘adverse health’ as one of the grounds, risks unintended consequences, as the GMC would be required look at a person’s current ability to provide care rather than focus on risk. It argues that such a move would undermine a compassionate approach to managing registrants’ health concerns, and the practical effect could mean the GMC having to wait for harm to have occurred before it was able to intervene.
Charlie Massey, the GMC’s chief executive, said: “There are issues to address and it is important the government gets this right, but overall we welcome the proposals. We are pleased to be another step closer to having a framework for regulating AAs and PAs, which will enhance their professional standing and the contribution they make to health services and patient care.
“The government must continue to deliver on its commitment to prioritise this work. A more flexible and modern approach to regulation, so we can work ‘upstream’ to prevent harm from occurring, will allow us to devote our energies to the work of highest priority – supporting clinicians to deliver first-class care for patients.”
Following the outcome of the DHSC’s consultation the new legislation, the Anaesthesia Associates and Physician Associates Order, will be laid before UK legislatures before coming into effect. q
39 39 www.yourexpertwitness.co.uk
40 40 www.yourexpertwitness.co.uk
MISSED OPPORTUNITIES LED TO UNTIMELY DEATH
[ TRACEY ANN SOUTH was 51 years of age at the time of her death. Having suffered with spina bifida, she spent her life in a wheelchair. On 22 March last year she was admitted to King’s Mill Hospital in Nottingham following her carer’s concerns that she seemed weaker than normal and had fallen out of her chair.
She remained on Ward 34 until 26 April when she was transferred to an ‘outlier’ ward due to bed pressures, before being discharged home on 3 May 2022. At the time of her discharge Tracey had not been seen or reviewed by a doctor for five days.
The following day, 4 May 2022, Tracey was an emergency readmission back to King’s Mill Hospital and by the time she was properly reviewed she was deemed to be too unwell to be rescued. In short, Tracey was beyond medical help at that juncture. She tragically died on 9 May 2022, at King’s Mill Hospital, having been placed on an end-oflife pathway.
At an inquest on 19 April this year at Nottingham Coroner’s Court the coroner delivered a narrative verdict citing numerous
missed opportunities by medical staff between 27 April 2022 and 5 May 2022, leading to a failure to rescue the patient who would likely have lived longer had she received appropriate treatment.
In a statement, Rotheras Solicitors, who represented Tracey’s family, said: “It appears clear that there were a number of missed opportunities and failings by medical staff, which meant that they did not rescue Tracey. They had not recognised the key issues requiring urgent treatment and delayed in providing her with fluid resuscitation and other medication in good time.
“Despite her kidney injury, the acute kidney injury treatment bundle was not provided to her in a timely manner and there were a number of service delivery problems, including a failure to repeat bicarbonate levels, to repeat blood tests, a lack of consultant review and no highlighting of outstanding jobs at the times of transfer, which meant potentially lifesaving treatment was overlooked or delayed.
“Communication was also lacking and infrequent, both between staff and with
Tracey’s family, who were desperate for news of her health in a COVID era where visiting the ward was not routinely permitted.
“While her family note the recommendations made by King’s Mill Hospital following their own investigation into Tracey’s untimely death, they are keen that these lessons must be learnt, and her death must not be in vain. Acute kidney injury is a medical emergency and must be treated as such. Tracey’s family hope that the findings at inquest help to safeguard other vulnerable patients in the future.”
Julie Walker of Rotheras Solicitors said:
“Tracey’s family have shown great strength since her death. It has been a lengthy and difficult process for them. I am pleased that the coroner recognised that there were missed opportunities by King’s Mill, and I hope that lessons are now learnt.
“Ensuring that questions were answered at the inquest, and responsibility was taken, was the last thing which the family could properly do for Tracey. I hope that they now feel they have some of the justice which they deserve for her.” q
41 41 www.yourexpertwitness.co.uk

THE HOT TOPICS AND DIFFICULT AREAS IN DIABETES
The number of people with diabetes is growing and there is now estimated to be five million people with diabetes in the UK. That creates a considerable burden on the NHS budget, both in prescribing and in managing complications. This fourth article in his series on the subject by Dr Bobby Huda outlines new developments in diabetes and current areas where problems in management can arise.

Type 1 diabetes
People with type 1 diabetes are generally diagnosed as children or as younger adults. Type 1 diabetes can present later and may be initially mis-diagnosed as type 2 diabetes.
People with type 1 diabetes are now living longer due to significant improvements in their care. Those people usually produce very little or no insulin of their own – insulin is a hormone from the pancreas gland that is needed to keep blood sugar down. Without insulin they will eventually go into a coma and die from it. Thankfully, since the discovery of insulin that is now very rare.
People with type 1 diabetes usually give themselves insulin through injections into the skin. In the past 20 years many people have been giving insulin through an insulin pump – which is an automated device that is attached to their body by tubing and gives insulin under the skin. They usually need to test their blood glucose several times a day with a finger prick glucose meter, but more recently they can use a glucose sensor. That also sits under the skin and each sensor lasts up to two weeks.
The sensor tells them their glucose 24 hours a day, avoids the need for frequent glucose testing and alerts them when their blood sugar level is too low or too high. These sensors were traditionally quite expensive but the NHS is now funding more of them and availability has increased.
In the last five years, we now have devices where the pump and the sensor can talk to each other – and the pump will automate the amount of insulin given, depending on the glucose. It is almost an ‘artificial pancreas’ – but not fully as the user will still need to estimate how much food they are eating and enter the values into the pump. Nevertheless, it is a significant breakthrough and for the first time represents a partial ‘cure’ for type 1 diabetes. More people will
be using the devices as the NHS widens access to funding.
Type 2 diabetes
People with type 2 diabetes are usually older, overweight and have a family history of diabetes. They may be from an ethnic minority background. People with type 2 diabetes still produce insulin, but are insulin resistant due to their body weight and genetic profiles.
Insulin pumps can be used in people with type 2 diabetes but it is more common to focus on oral medications. There are some groundbreaking medications – SGLT-2 inhibitors (eg Forxiga) and GLP-1 agonist medications (eg Ozempic: the weight loss drug) – which reduce glucose and body weight and can reduce complications such as kidney and heart failure as well as overall mortality. Some of the medications can now be used outside of diabetes.

Inpatient diabetes
Up to 20% of hospital inpatients can have diabetes in the UK. That means that people with diabetes are often looked after by non-
specialists in diabetes. Most hospitals have diabetes inpatient teams and guidelines, protocols or education programs to upskill non-specialist staff; but unfortunately problems with care do still arise. That can be due to lack of glucose monitoring – often a result of understaffing on wards – or errors in insulin or drug administration.
Most hospitals take part in the National Diabetes Inpatient Audit (NaDIA), which has shown that on the whole errors in hospital are improving with better standards of care. Sub-optimal diabetes control can also lead to increased wound infections after surgery.
Rarely, people with diabetes can have a diabetes emergency while in hospital, including a severe hypoglycaemia episode (very low blood sugar) or develop diabetic ketoacidosis – usually where a person with type 1 diabetes has not received the correct amount of insulin. q
• To contact Dr Huda call 020 3594 6058 / 07919 924925, email bobby.huda1@nhs.net alternatively visit londondiabetes.com or clevelandcliniclondon.uk
43 43 www.yourexpertwitness.co.uk
44 44 www.yourexpertwitness.co.uk
PAIN SPECIALISTS CAUTION AGAINST STIGMATISATION OF PATIENTS WHO CONTINUE TO USE DEPENDENCY DRUGS
[THE FACULTY OF PAIN MEDICINE (FPM) has responded to the publication of the NHS England Document Optimising personalised care for adults prescribed medicines associated with dependence or withdrawal symptoms: Framework for action for ICBs and primary care, which was published in March.
The FPM – which is a faculty within the Royal College of Anaesthetists – says it is supportive of the overall scope of the document, which is to help Integrated Care Boards achieve their four key objectives: improving outcomes in population health and healthcare; tackling health inequalities in outcomes, experience and access; enhancing productivity and value for money; and helping the NHS support broader social and economic development.
The FPM highlights the statement in the document that reads:
US RESEARCHERS GENERATE OBJECTIVE PAIN INDICATORS FOR FIRST TIME
“Effective, personalised care should include shared decision-making with patients and regular reviews of whether treatment is working. Patients who want to stop using a medicine must be able to access appropriate medical advice and treatment and must never be stigmatised.”
It also cautions, however, that it is important to recognise that the reverse is also true, that the “effective personalised care with shared decision-making with patients and regular reviews of treatment” will also reveal a group of patients where medications associated with dependence or withdrawal symptoms will be providing a significant degree of pain relief and improvement in overall function and quality of life. That group of patients must also never be stigmatised and/or taken off their medication inappropriately, the FPM says.
The FPM “advocates personalised care and shared decision-making with each patient suffering from chronic pain, using multi-modal evidence-based pain management appropriately, and may often include using such medication. It is vital that such medication usage is regularly reviewed and only continued if there is evidence of improvement in pain, quality of life and level of function, always balanced against a clear understanding of potential risks or side effects associated with such medication.”
[
ONE OF THE perennial problems in determining compensation for pain is the subjective nature of the experience of pain and the hitherto impossibility of objectively assessing pain.
Recent research carried out at the University of California in San Francisco and published in Nature Neuroscience promises to make objective assessment of pain a possibility for the first time.
The researchers explain: “Pain severity is often measured through subjective report, while objective biomarkers that may guide diagnosis and treatment are lacking.”
According to a digest of the report: “Researchers have used a device implanted in the brain to record, for the first time, objective signs of chronic pain. Several times a day for up to six months, the implant recorded four people’s brain activity, which scientists matched to their self-reported symptoms.
“One participant had phantom pain from an amputated leg; the rest had unexplained sensations after a stroke. When participants felt chronic pain, brain activity in the orbitofrontal cortex was detected. A different region of the brain was active when they experienced pain from touching a hot object.”
One of the authors of the report, Prasad Shirvalkar, is reported as saying: “Chronic pain is actually its own separate disease that is not simply an extension of pain in general.” q

The faculty argues that the document “rightly advocates other treatment modalities, including exercise, self-management and psychological therapies to replace inappropriate medication”.
“It also highlights the need for services to help patients who may have developed drug dependence to be supported appropriately. Significant investment, workforce increase and upskilling of NHS health professionals will be essential to meet this demand.” q
45 45 www.yourexpertwitness.co.uk
46 46 www.yourexpertwitness.co.uk
CAN ‘MATERIAL RISK’ EVER BE DEFINED?
[ MONTGOMERY v LANARKSHIRE HEALTH BOARD has been a landmark case concerning the rights of patients and the responsibilities of clinicians in the consent process. Although the case provides some guidance for both patients and clinicians regarding the process of consent, many clinicians have felt that more issues have been raised than solved.
The term ‘material risk’ was born from the case and is deemed to be any risk that the consenting clinician felt the patient would attach significance to. There have been several cases since Montgomery which have put the issue back in the spotlight. Two cases stand out for having implications for clinicians.
Spencer v Hilingdon Hospitals NHS Trust 2015 relates to information provided to a patient post procedure and the potential implications of a lack of suitable post-procedure information. In that case the claimant underwent a hernia operation after which he was discharged from hospital. He was provided with a discharge leaflet which advised him to contact the hospital switchboard if he had any problems after surgery.
Three days later he developed calf pain and breathlessness, both of which he attributed to his recent inactivity. He was subsequently admitted to hospital with bilateral pulmonary emboli. The question asked was whether the hospital trust had given adequate information following discharge about the possibility of deep vein thrombosis and pulmonary embolism post hernia repair and the signs and symptoms of each.
The judge ruled that the trust was liable in that case, relating that the fatal nature of the complication, the improved prognosis with early treatment, the ease of giving the patient oral or written warnings as well as hospital and national guidelines on venous thromboembolism risk for such procedures, were relevant factors in ruling against the trust. The case brings to light the fact that information provided post-procedure is as important as the pre-surgery consent and can lead to negligence claims if deemed inadequate.
In Tasmin v Barts NHS Trust 2015 , the claimant developed cerebral palsy after sustained hypoxia during delivery. The claimant argued that she ought to have been delivered earlier by Caesarean section (C-section) in light of a pathological cardiotocography (CTG) trace during delivery.

The judge ruled against the claimant, suggesting that, in fact, rather than a C-section, a foetal blood sample was reasonable obstetric practice in that situation – in light of guidance from both the Royal College of Obstetrics and Gynaecology and the National Institute for Clinical Standards. Furthermore, the judge deemed that the risk of severe neurological injury from an abnormal CTG was approximately 1:1,000, which was deemed to be too low to be material; and thus such a risk was not obligated to be disclosed at that point, as per Montgomery. The claimant’s case was rejected on those grounds.
Those cases highlight that there is no specific test or standard, either written or numerical, by which doctors can appraise the details that any consenting process requires in a given situation. In Montgomery, the risk of shoulder dystocia was 1:10, with
subsequent prolonged hypoxia causing disability at approximately 1:1,000, which was ruled to have been a material risk.
However, in Tasmin, the same risk of 1:1,000 of neurological injury from an abnormal CTG trace was not deemed material. There is an interesting confoundment here suggesting that there is significant contextual judgment in every case which is not apparent when looking at numbers alone.
The question arises, therefore, as to whether Montgomery has raised more questions than it has answered for clinicians? Was the Bolam Principle a more standardised method of thinking about such problems? That is undoubtedly a complex area, and no single judgment will be able to cover the breadth and complexity of everyday clinical encounters between clinicians and patients.
It is certainly the case that every consent process needs to be tailored for every patient. It is, unfortunately, only test cases in the legal system which can bring on-going clarification of the principles underlying Bolam and Montgomery pertaining to material risk. q
47 47 www.yourexpertwitness.co.uk
Mr Huzaifa Malick MBChB, FRCOphth, PGCertMedEd, consultant ophthalmic surgeon and expert witness with Eye Law Chambers, looks at two cases with different outcomes that show the difficulties for clinicians in knowing what information is appropriate for a valid consent.
48 48 www.yourexpertwitness.co.uk
HSE UPDATES NIHL STATS
THE HEALTH AND SAFETY EXECUTIVE has published the latest available figures for people with work-related hearing problems.
According to HSE, there is limited information available on work-related noise induced hearing loss. HSE’s preferred data source is the Labour Force Survey (LFS), with the Industrial Injuries Disablement Benefit (IIDB) scheme providing a further source of information. Those sources present very different estimates, the HSE concedes.
According to the LFS there were an estimated 11,000 cases of hearing problems each year caused or made worse by work over the past three years (2019/20-2021/22). That was statistically significantly lower than the figure of 21,000 for the previous three-year period (2016/17-2018/19).
The IIDB figures shown on the graph paint a different picture, but include only annual new claims and are based on a much stricter definition of ‘deafness’ in which claimants must have a substantial measured loss of hearing in both ears (greater than 50 dB). The IIDB scheme will also tend to underestimate annual incidence for other reasons, including:
• Cases arising from circumstances other than those covered by the
• terms of the prescription
• Individuals being unaware of the possible occupational origin of
• their disease
• A lack of knowledge regarding the availability of compensation
• The scheme does not include self-employed workers.
Hence, HSE says, the LFS is the preferred source to judge the overall scale of the condition. In addition, assessments of new IIDB cases in 2020 were affected by the coronavirus pandemic and may also have been affected to some extent during 2021. q
CAMPAIGN TARGETS HEARING RISK AT MUSIC VENUES

ON 3 MARCH the Night Time Industries Association (NTIA) announced a partnership with the WHO’s Make Listening Safe campaign: an initiative to increase the awareness of avoidable risks to hearing and promote the WHO’s global standards on safe listening at venues and events.
According to WHO, 1.1 billion young people between 12 and 35 years of age are at risk of permanent hearing loss due to unsafe listening practices in a recreational setting: not in the workplace.
The NTIA’s CEO Michael Kill commented: “Losing the ability to listen to music is inconceivable, especially given that I have based my career on music and night time economy. Thousands of people across our sector suffer from hearing loss, and if we continue to dismiss the wider impacts thousands more will follow.
“When asked if we would like to work with WHO as part of our wider UK project to educate people on hearing loss and the potential impacts and the methods of protection, we grabbed the opportunity with both hands.”
A report from the Commission on Hearing Loss in 2014 calculated the cost of hearing loss to the UK economy at £24.8bn, which will potentially rise to £38.6bn by 2031. That is reduced economic output due to loss of productivity and unemployment due to hearing loss, and does not include the cost of healthcare, which is calculated at £450m annually to the NHS.
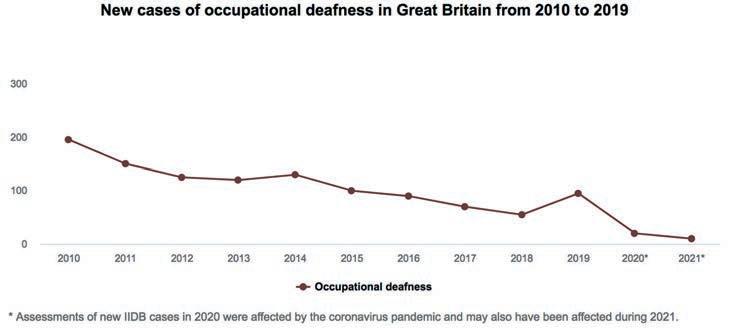
In addition, a paper published by The Lancet in 2000 proposed that hearing loss is the biggest modifiable factor in a person’s life course that will increase the risk of dementia.
Consultant audiologist Robert Shepheard explained: “Hearing loss and tinnitus is extremely common with people working in and enjoying musicrich environments. It is sometimes not fully understood the irreversible impact listening to loud sound can have on many aspects of our health. As audiologist for the NTIA it is so encouraging to see the industry taking such a proactive step to maintain the health of everyone involved.“
One in six people are impacted by hearing loss in the UK and the aim of the campaign, alongside partners and key stakeholders, is to reduce that number across the entertainment sector through awareness and education, so that people can listen to music safely within the workplace, social or personal environments.
Biff Mitchell of Glastonbury & Beautiful Days Festival said: “It’s time we went further than an earplug dispenser and a set of ear defenders on a sign as the only education given to staff in venues and concerts on the dangers of long exposure to loud music. In over 30 years working in the live sector I have seen people from all parts of the industry suffering from hearing problems and for some resulting in mental health problems – it’s time to educate.” q
49 49 www.yourexpertwitness.co.uk
[
[
ORTHOPAEDIC HOSPITAL CONTINUES ITS EXPANSION
[ THE ROYAL ORTHOPAEDIC HOSPITAL (ROH)
in Birmingham has officially opened its new outpatient physiotherapy and podiatry department at College Green, with a ribbon cutting event attended by GB athlete Hannah England.

The ROH has invested over £3.5m in relocating outpatient physiotherapy and podiatry services from the main hospital site on the Bristol Road to College Green at Bournville, where patients and staff will have easier access to new, upgraded equipment and facilities.
Nikki Mason, head of therapy services at the Royal Orthopaedic Hospital, commented: “It’s so exciting to see our new department open and ready for patients. The move provides opportunities for the ROH to engage with the wider local community to promote good musculoskeletal health.
“Many teams have worked together to create this new centre of
RESEARCH HIGHLIGHTS RADIATION RISK TO FEMALE SURGEONS
[THE PREDOMINANCE OF REPORTING of patient harm resulting from hospital treatment can obscure the fact that the hospital – and the operating theatre in particular – poses risks for those working in them in the same way as any other workplace.
That fact has been illuminated by a short-life working group created by the British Orthopaedic Association, which worked on identifying and understanding the risks and ways of providing better protection for female health workers from ionising radiation in the workplace. Their guidance has been published on the BOA website and recently its breast cancer risk section has been updated to highlight the best gowns to use for protection of the breast from irradiation. An editorial highlighting the risks and concerns was published by the BMJ on 13 April.
Working group member Hannah Sevenoaks has also shared her own personal thoughts around occupational radiation protection safety and why she felt health workers needed to demand better from their PPE. Her article A tipping point to improve radiation safety in orthopaedics has been published on the website Orthopaedics Online
Female breast tissue extends into the axilla and the majority of breast cancers occur in the upper outer quadrant (UOQ). Currently available PPE consists of tabard-style one-piece gowns or a twopiece skirt and vest. Simulated studies measuring dose exposure to the UOQ of the breast have shown that they provide inadequate protection. Dosimeters worn over those gowns showed the area next to the axilla and UOQ received the highest dose of radiation in the torso.
In her article Hannah Sevenoaks concluded: “This, and the work supported by the BOA to improve breast protection, highlights the tangible and easily measurable improvements we can make to radiation safety in orthopaedics with physical interventions.
“Ultimately, however, it is the more subtle, arguably mundane and probably more elusive changes in behaviour, attitude and culture that will protect everyone more than any amount of shiny new PPE. Hopefully by starting this conversation about radiation safety, we can generate a tipping point for the profession as a whole.” q
excellence in the community for our patients. There’s a dedicated paediatric area for our younger patients and the new space will be a fantastic environment for our colleagues to work in.”
Officially opening the new location, Hannah England commented: “As an athlete physiotherapy has been essential throughout my career. I am also aware of the massive difference it makes in restoring function and transforming lives. This is a fantastic assessment and rehabilitation facility with some amazing new equipment which will really benefit the patients who use it.”
Nearly a third of all primary care appointments are related to musculoskeletal conditions. Investing at the new location in the community at College Green means that patients can be treated in a specialist area away from the main hospital site, with parking and public transport services nearby. q
51 51 www.yourexpertwitness.co.uk
52 52 www.yourexpertwitness.co.uk
STUDY SHOWS NEED FOR CO-OPERATION
IN TRAUMA TREATMENT
ORTHOPOD is a multi-centre collaborative study investigating the performance of trauma services and the characteristics and distribution of injuries across the UK. It emerged out of growing concerns within the trauma community that injuries with recommended time-to-surgery windows were being missed and the delivery of trauma care within the nationalised health service was suboptimal.
The study ran for 10 consecutive weeks across 90 hospitals, including 23,138 general trauma cases and 709 weeks’ worth of theatre capacity entries. From that, two key pieces of work were produced.
The first paper described trauma performance in its generality. It highlighted significant variability in the delivery of trauma services, both operative demand and list provision. On average, 1.73 cases were completed per trauma theatre session. Those injuries associated with performance metrics and incentives, for example open and hip fractures, showed least variation and shortest time to surgery.
Patients waiting for surgery at the start of each week also fluctuated greatly within and between hospitals, highlighting an opportunity to develop intra-regional networks to better distribute trauma workload to effectively utilise all available trauma theatre capacity.
The second paper described day-case trauma services or lack thereof. Regular dedicated day-case trauma lists were rare – a national
TRAINING COURSE HELPS ORTHOPAEDIC SURGEONS DEAL WITH THE LAW

[THE BRITISH ORTHOPAEDIC ASSOCIATION has taken the legal bull by the horns and is running a training module for its members and other orthopaedic surgeons on Law for Orthopaedic Surgeons – Avoiding Jeopardy
The course is aimed at consultants, SAS doctors and orthopaedic trainees who wish to gain knowledge of the elements of law which underpin various aspects of contemporary surgical practice.
The course provides broad coverage of the interface between the law and the practice of orthopaedic surgery. It is specifically designed to highlight potential pitfalls in practice from the medico-legal perspective and to help steer surgeons away from potential jeopardy.
It includes:
• Practical advice on how to approach giving evidence in legal
• proceedings such as a coroner's court
• Advice on practical measures to avoid jeopardy with employers,
• the courts and the regulator
• A full delivery day of case-based discussion talks with Q&A,
• including a mock coroner's inquest
• Pre-recorded material to be watched in advance, which will be
• available six weeks prior to the course delivery day
The faculty delivering the course comprises experienced consultants in surgical specialties, all with extensive knowledge of the law relating to surgery, as well as practising barristers, coroners, assistant coroners and a representative from the Medical Protection Society.
The topics covered are of surgical relevance and include consent, gross negligence manslaughter, the Medical Practitioners Tribunal Service and the GMC, blood transfusion refusal, introduction to coronial law and the coroner’s court, confidentiality and data protection, clinical negligence and the pitfalls of social media. q
average of zero lists per week. Day-case trauma accounted for nearly one third (29.1%) of overall trauma burden, but only six hospitals had access to a daily day-case trauma list. That placed a heavy reliance on general trauma lists to manage inpatient and outpatient caseload. Furthermore, the day-case trauma patient was identified as disadvantaged as they typically waited longer for surgery and had higher cancellation rates compared to inpatients while still causing more disruption to scheduled elective operating.
There is, the researchers found, a common message in the two papers: the need for interconnectivity – whether it be an equitable distribution of general trauma between neighbouring trusts or regional collaborative effort at creating a hub-and-spoke model of dedicated day-case trauma centres and pooled day-case patients. More than ever, greater co-operation within the trauma community is needed to address the ever-expanding trauma burden. q
53 53 www.yourexpertwitness.co.uk
[


54 54 www.yourexpertwitness.co.uk
SIX MSK PROJECTS SHARE NEAR-£2M POT
[THE NUFFIELD FOUNDATION AND VERSUS ARTHRITIS have committed £1.94m of funding to six new research projects that aim to improve the wellbeing and working lives of people with musculoskeletal (MSK) conditions.
More than 20 million people –around a third of the UK population – have an MSK condition such as osteoarthritis, rheumatoid and psoriatic arthritis, back pain, fibromyalgia and rarer conditions such as lupus. They are the greatest cause of pain and disability in the UK, affecting people’s ability to work, care for a family and live independently. MSK conditions also have a profound impact on society and the economy, leading to 28.4 million lost working days a year and accounting for the third largest area of NHS programme spending.
The new research grants are the second round of awards from the Nuffield Foundation’s Oliver Bird Fund, which is dedicated to improving the lives of people with MSK conditions.
The charity Versus Arthritis, which is contributing £250,000, is calling for more research into addressing MSK health inequalities by striving for better MSK health and care at home, in leisure, at work and in communities under the Living Well ambition in the charity’s research strategy.
The six projects will help deliver that ambition, as well as the person-focused principle of ensuring people with arthritis are active partners in research.
The partnership between Versus Arthritis and the Nuffield Foundation will put lived experience at the heart of the six projects, which are being carried out in five universities.
People living with MSK conditions will advise across the lifetime of the projects, from helping to develop tools and interventions to guiding researchers’ understanding of the needs of underserved communities. This will ensure that the research is highly relevant to real-world needs and issues.
Colin Wilkinson, a research partner at Versus Arthritis, said: “It can be difficult to understand the variety and range of ways arthritis affects people in their everyday lives because the 200-plus musculoskeletal conditions are all so different, just as we are all different.”
The projects have a common theme of how MSK conditions impact on people’s ability to live and work well, to inform policy and practice responses. They are:
The PAW Trial: feasibility and acceptability of the Pain-at-Work Toolkit, led by Professor Holly Blake (University of Nottingham, £338,000)
Arthritis, work and well-being: A mixed methods study with policy recommendations, led by Dr Adam Martin and Dr Sarah Kingsbury (University of Leeds, £300,000)
Remote osteoarthritis peermentorship for socioeconomically underserved people, led by Professor Gretl McHugh (University of Leeds, £266,000)
The Psychological, Social and Economic Impact of Musculoskeletal Conditions, led by Professor Andrew Steptoe (University College London, £288,000)
Juvenile onset rheumatic diseases: Education, vocational readiness and employment, led by Professor Suzanne Verstappen (University of Manchester, £402,000)
Extending working lives for people with musculoskeletal conditions, led by Dr Ross Wilkie (University of Keele, £345,000)
Dr Catherine Dennison, lead for the Oliver Bird Fund Programme at the Nuffield Foundation, explained: “These six research projects align around issues that can make it very challenging for people with MSK conditions to enjoy full and rewarding lives. We are really delighted to be partnering again with Versus Arthritis to fund research that aims to address some of these barriers and find new and better ways to support people with MSK conditions.” q
55 55 www.yourexpertwitness.co.uk
56 56 www.yourexpertwitness.co.uk
AI COULD SOON BE USED TO DIAGNOSE HEART ATTACKS
[AN ALGORITHM developed using artificial intelligence could soon be used by doctors to diagnose heart attacks with better speed and accuracy, according to new research from the University of Edinburgh. The research, funded by the British Heart Foundation and the National Institute for Health and Care Research, has been published in the journal Nature Medicine

The effectiveness of the algorithm, named CoDE-ACS, was tested on 10,286 patients in six countries around the world. Researchers found that, compared to current testing methods, CoDE-ACS was able to rule out a heart attack in more than double the number of patients, with an accuracy of 99.6%.
That ability to rule out a heart attack faster than before could greatly reduce hospital admissions. Clinical trials are now underway in Scotland with support from the Wellcome Leap, to assess whether the tool can help doctors reduce pressure on our overcrowded EDs.
Tackling inequality
As well as quickly ruling out heart attacks in patients, CoDEACS could help doctors to identify those whose abnormal troponin levels were due to a heart attack rather than another condition. The AI tool performed well regardless of age, sex or pre-existing health conditions, showing its potential for reducing misdiagnosis and inequalities across the population.
The current gold standard for diagnosing a heart attack is measuring levels of the protein troponin in the blood; but the same threshold is used for every patient. That means factors such age, sex and other health problems which affect troponin levels are not considered, affecting how accurate heart attack diagnoses are.
That can lead to inequalities in diagnosis. For example, previous BHF-funded research has shown that women are 50% more likely to get a wrong initial diagnosis. People who are initially misdiagnosed have a 70% higher risk of dying after 30 days. The new algorithm is an opportunity to prevent that.
The research was led by Professor Nicholas Mills, BHF Professor of Cardiology at the Centre for Cardiovascular Science, University of Edinburgh. He explained: “For patients with acute chest pain due to a heart attack, early diagnosis and treatment saves lives.
“Unfortunately, many conditions cause these common symptoms and the diagnosis is not always straightforward. Harnessing data and artificial intelligence to support clinical decisions has enormous potential to improve care for patients and efficiency in our busy emergency departments.”
Professor Sir Nilesh Samani of the BHF added: “Chest pain is one of the most common reasons that people present to emergency
departments. Every day, doctors around the world face the challenge of separating patients whose pain is due to a heart attack from those whose pain is due to something less serious.
“CoDE-ACS, developed using cutting-edge data science and AI, has the potential to rule-in or rule-out a heart attack more accurately than current approaches. It could be transformational for emergency departments, shortening the time needed to make a diagnosis, and much better for patients.” q
57 57 www.yourexpertwitness.co.uk
LIMB ISCHAEMIA: WHEN CAN THE LEG BE SAVED?
By PHILIP COLERIDGE SMITH DM MA BCh FRCS Consultant Vascular Surgeon, Medical Director of the British Vein Institute and Emeritus Reader in Surgery at UCL Medical School
[LOWER LIMB ISCHAEMIA is a common problem, especially in elderly patients. Total disease prevalence has been evaluated in several epidemiological studies and is in the range of 3%-10%, increasing to 15%-20% in persons over 70 years. Modern surgical and endovascular treatments are available which will avoid amputation in patients with severe limb ischaemia.
The causes of limb ischaemia
Ischaemia most commonly affects the lower limb and usually arises as the result of atheroma (hardening) of the arteries. The main causes of this are a smoking history and diabetes. Diabetes currently affects about 4.9m people in the UK, 90% of whom have type 2 diabetes. This disease may lead to narrowing of the leg arteries, especially those vessels in the calf and foot. Poorly-controlled diabetes is more likely to cause narrowing of arteries than well-controlled diabetes. The calf is a region which is more difficult to treat than the proximal arterial system where techniques such as balloon angioplasty and open surgical bypass operations are effective in most cases.
Chronic limb ischaemia
The development of atheroma gradually narrows the affected arteries which eventually become blocked as thrombosis develops in the diseased vessels. Where arteries gradually become blocked there is an opportunity for an alternative circulation to develop to supply the limb. Less active patients may not notice the reduced blood flow but others may notice that they have developed pain in the calf on walking known as ‘intermittent claudication’. Surgical treatment is often not necessary for this condition which does not threaten the limb. It may progress to more severe arterial disease in about one quarter of cases.
Acute limb ischaemia
In some cases a blood clot forms within the vascular system and then detaches from its source to become an embolism. This travels with blood flow before blocking the artery where is comes to rest. Common sources of embolism include the heart where an irregular heart rhythm or recent heart attack may allow thrombus to develop on the wall of the
heart. Atheromatous arteries may also accumulate thrombus on their irregular walls.
The clinical presentation of embolism of thrombus into the leg arteries is often more dramatic than when arteries narrow gradually. Sudden occlusion of a major artery leads to acute limb ischaemia. The main presenting symptom is severe and excruciating pain, often not relieved by opiate analgesic drugs. The limb is described as painful, pale, pulseless, perishing with cold and paralysed.
Trauma to the limb may also give rise to disruption of the artery which supplies the leg. Arterial occlusions may occur with fractures of the lower limb or dislocation of the knee. Occasionally, the trauma can arise from iatrogenic sources such as following knee replacement surgery. Traumatic interruption of the blood flow to the leg can leave the limb in great jeopardy.
In contrast to patients in whom the arteries have narrowed gradually, no alternative circulation has had an opportunity to develop and the damaged vessel has to be repaired expediently before the limb is severely damaged by ischaemia.
Diagnosis of limb ischaemia
In general the diagnosis in patients presenting with acute limb ischaemia due to sudden cessation of blood flow in the limb is readily made. The patient complains of very severe pain in the limb, which is usually cold, white and pulseless. This problem commonly presents to doctors in A&E departments who are readily able to make the correct diagnosis based on clinical examination alone.
In patients who have a reduced level of consciousness the diagnosis may not be so obvious to the attending clinicians. Patients who have suffered multiple trauma and are sedated or unconscious may have loss of the lower limb circulation associated with lower limb fractures. Some patients remain sedated following major surgery and opiate analgesics are required to provide post-operative analgesia. Examples of this include lower limb arterial surgery, cardiac surgery and knee replacement surgery. Failure to check or regularly monitor the blood flow to the lower limb in these contexts may lead rapidly to severe ischaemic damage to the limb if the circulation fails following surgery.

58 58 www.yourexpertwitness.co.uk
I have advised in cases where failure to monitor the blood flow to the lower limb following vascular, cardiac and orthopaedic surgery permitted undetected limb ischaemia to develop. By the time the diagnosis was identified, the limb was beyond salvage.

An uncommon presentation of acute lower limb ischaemia is with sudden onset of paralysis in one or both limbs. Pain may not be reported by the patient because failure of blood flow to the main nerves supplying the limb prevents pain sensations being felt. This presentation occurs when the abdominal aorta or the iliac arteries in the pelvis are suddenly occluded.
If the emergency medical team does not consider limb ischaemia as a possible diagnosis and instead investigates the neurological system, severe ischaemic damage to the lower limbs may result before the correct diagnosis is established. The diagnosis is readily established by palpation of the lower limb pulses on initial hospital attendance. Failure to complete this part of the clinical examination may fall below an acceptable standard of medical care in such cases.
Critical limb ischaemia
In patients presenting with gradual and insidious occlusion of the lower limb vessels, the diagnosis may only be established after several consultations with doctors. Where much of the blood supply to the lower limb has been blocked off, the condition is referred to as ‘limb threatening ischaemia’ or ‘critical limb ischaemia’. The symptoms are gradual onset of pain in the toes and foot. This is worse a night and is relieved by hanging the affected leg out of bed. Ulceration of the foot and toes may also arise due to the ischaemia – see photo opposite.
Diagnosis of critical limb ischaemia
The diagnosis of critical limb ischaemia can be established by palpation of the lower limb pulses, which are absent in this condition and associated with a low blood pressure measured at the ankle. However, pain in the toes is sometimes misdiagnosed as gout or some other condition of the foot. In diabetic patients, ulceration of the feet or toes may be mistakenly thought to be the result of loss of sensation in the foot due to diabetic neuropathy. In critical limb ischaemia expediency of appropriate investigation and treatment is required.
However, the timescale over which this should be done is greater than for acute limb ischaemia. The Vascular Society recommends that patients with this condition should be investigated and treated within two weeks of diagnosis, where feasible. NICE Guideline 19 on the subject of diabetic foot ulcers advocates referral to a diabetic foot multidisciplinary team within 24 hours for patients presenting with the diagnosis of a new diabetic foot ulcer. Failure to comply with these recommendations may fall below an acceptable standard of care.
Patients with limb-threating ischaemia have a 80-90% chance of avoiding amputation within 30 days of treatment with referral before irreversible damage has arisen to the limb. Delayed treatment allows progressive ischaemic damage to arise which may be complicated by uncontrolled infection in diabetic patients. Delayed referral to a vascular service in such cases may be considered to comprise substandard care.
Can the leg be saved?
In patients presenting with acute limb ischaemia, especially in those where vascular trauma has occurred and there is no preceding arterial disease, the limb will survive 4-8 hours without severe damage commencing in the muscles and nerves of the limb. These patients require expedient diagnosis and treatment. This will usually lead to avoidance of the need for limb amputation. Substandard delays in diagnosis leading to delayed treatment and adverse outcomes, including the need for limb amputation, may lead to allegations of substandard care.
For patients with insidious onset of limb-threatening ischaemia, urgent management is required, preferably within two weeks of the onset of symptoms. Vascular surgery to improve the blood supply to the limb will lead to avoidance of the need for amputation in about 90% of cases providing that the limb is still viable at the time of consideration for surgery. This type of ischaemia may lead to extensive gangrene and limb amputation where delays in diagnosis and treatment have occurred.
Causation – the main issues
My experience is that delays in surgical or endovascular intervention being commenced leading to an amputation may lead to allegations of substandard care. However, these cases are usually defended on causation.
In some cases, tiny emboli travel to the foot and toes leading to ischaemia confined to the toes or forefoot. It may not be feasible to remove the emboli from such tiny arteries, even with the best of care. The toe or forefoot may already have become irreversibly ischaemic at the time of presentation. Amputation of the toes would always have been a likely outcome in such cases.
Patients with diabetes tend to have severe disease in the arteries below the knee and in the foot. Sometimes all of the three main arteries below the knee are occluded over most or all of their course. Modern endovascular treatments such as balloon angioplasty may be effective in a limited number of cases but severe distal arterial disease often limits the efficacy of treatment. It may not be possible to restore any useful blood flow in the leg where extensive disease is present. The surgeon has no alternative but to advise amputation in these cases. The defence advanced in these cases is likely to be along the lines that the arterial disease was untreatable with any currently available method and amputation was the only feasible treatment.
In cases where delayed diagnosis and treatment has resulted in extensive gangrene of the tissues, there is no prospect of saving the limb and amputation will be advised. In these cases the claimant can argue that the limb would have been saved with timely treatment. His case is likely to succeed in this scenario.
Conclusion
The modern vascular surgical team can offer several options to restore the blood flow to severely ischaemic limbs. Delays in referral to hospital prejudice the outcome since ischaemic limbs very rapidly become non-viable if neglected. However, not all limbs can be saved. Sometimes the arterial disease is too extensive or severe to permit restoration of blood flow and an amputation is the only solution. q
59 59 www.yourexpertwitness.co.uk
60 60 www.yourexpertwitness.co.uk
PSYCHIATRISTS ‘SURPRISED AND CONCERNED’ BY MET POLICE NO-SHOW THREAT

[THE Royal College of Psychiatrists (RCPsych) has responded to a report in The Guardian on 29 May, that the Met Commissioner Sir Mark Rowley has plans to order officers not to attend 999 calls about mental health incidents. It follows a lack of progress in implementing a procedure known as ‘Right Care, Right Person’ – a procedure already in place in some parts of the country.
The Guardian report quotes Sir Mark as saying: “In fact, we are failing Londoners twice. We are failing them first by sending police officers, not medical professionals, to those in mental health crisis, and expecting them to do their best in circumstances where they are not the right people to be dealing with the patient.
“We are failing Londoners a second time by taking large amounts of officer time away from preventing and solving crime, as well as dealing properly with victims, in order to fill gaps for others.”
The report says the Commissioner has given health and social care services in the capital a deadline of 31 August before the force starts its ban, which will only be waived if a threat to life is feared.
Commenting on the reports, RCPsych president Dr Adrian James said: “We have a great deal of sympathy with the Met police as their challenges mirror those of the mental health workforce. They are under a huge amount of pressure while at the same time being chronically under resourced. Therefore, while the best solution to many of the issues we both encounter is more resources, we do understand the need to make the best use of those that we have. However, in doing this we must all make sure we do not forget our duty to protect the most vulnerable in our society.
“That is why we are surprised and concerned by the unilateral declaration by Sir Mark Rowley to withdraw the police from attending emergencyrelated mental health incidents by the end of August. This presents a number of issues and concerns that simply cannot be resolved in this timescale. For example, the police are the only
service to hold certain legal powers to convey a disturbed person from public places to a place of safety and so they are likely to always be needed when people are in acute crisis.
“It is simply unhelpful and impractical to
make decisions like these before we have worked out what will happen in some very concerning situations, both for patients with mental illness, but also for the public and police officers alike.” q
GOVERNMENT SHOULD RESENTENCE IPP PRISONERS, REPORT FINDS
[THE British Psychological Society (BPS) and Probation Institute have expressed support for the findings of the Justice Select Committee inquiry report into Imprisonment for Public Protection (IPP) sentences.
The report recommended that every person still serving an IPP should receive a new sentence that balances justice with public protection. It also recommended reviewing people’s IPP sentences five years after release from prison. The government has rejected both recommendations.
The BPS and Probation Institute said they are ‘disappointed’ by that and are calling on MPs to support the re-sentencing of all prisoners subject to IPP sentences as soon as possible. The inquiry heard evidence about the psychological harm that is caused by indefinite imprisonment under a sentence that has been abolished in law, is wrongful and undermines rehabilitation and risk management efforts.
The report recommended greater planning and resources dedicated to the mental health, release and resettlement of people serving IPP sentences. The BPS and Probation Institute welcomed that, but have highlighted the potential impact of the changes on the staff who work in prisons, including psychologists and probation staff.
The organisations are calling for a clear strategy from the Ministry of Justice and HM Prison and Probation Service on improving access to mental health support for IPP prisoners, including transfers to secure hospitals and therapeutic settings. There also needs to be a fully-formed and costed strategy to address the large gaps in the workforce.
Dr Nic Bowes, chair of the BPS’s division of forensic psychology, said: “The report symbolises the restoration of hope for those who are on an IPP sentence. We know that IPP sentences cause acute harm to the mental health of those subject to them, fostering a lack of trust in the system that is meant to rehabilitate them.
“It is a welcome step towards reversing these harms, and creating a system that is focused on rehabilitation and values the mental health of prisoners. It is vital that the government accepts the report’s recommendations and commits to resentencing people on IPP sentences as a matter of urgency. We are cautious, however, about the increased demand this will place on psychologists working in the prison service and on probation staff, which is why the resources and workforce issues must be addressed as a matter of priority.”
Professor Loraine Gelsthorpe, chair of the Probation Institute, added: “The Justice Committee report outlines a group who have found themselves experiencing an unjust legacy, after a change in the law that was used to sentence them, but not a change in their circumstances.
“We urge the government to remedy the injustice in their situation and to ensure that probation staff are resourced to provide a professional service to them and to potential victims.” q
61 61 www.yourexpertwitness.co.uk

62 62 www.yourexpertwitness.co.uk
WHAT ARE THE MEDICOLEGAL CHALLENGES POSED BY DELIRIUM IN AN ICU?
By Dr Martin Stotz, consultant in adult intensive care and anaesthesia

[DELIRIUM IS A FORM of acute brain dysfunction – defined by acute disturbances in attention, awareness or cognition – that develops over hours or days and cannot be explained by an alternative diagnosis or comatose state. Patients who develop delirium are at an increased risk of complications, and the condition is also associated with longer hospital stays and increased healthcare costs.
Furthermore, delirium is a major risk factor for cognitive impairment following critical illness, which can be particularly debilitating, and the severity of the impairment is related to the severity of the delirium. Over half of all patients admitted to an intensive care unit (ICU) will develop delirium at some point during hospitalisation and in patients who are mechanically ventilated that proportion rises to around 75%. Known risk factors include old age, frailty, preexisting neurologic disease or cognitive impairment and comorbidities such as cardiac disease and hypertension.
or a lack of motivation to follow them due to a belief that doing so will not confer any meaningful benefit to the patient, are also barriers to diagnosis and treatment and should be addressed.
DELIRIUM
It is thought that those factors lead to a lower physical or cognitive physiological reserve, which appears to reduce the capacity to sustain normal brain functioning during the stress of critical illness. Various medications commonly used in the ICU setting, such as benzodiazepines, opiates, anticholinergic agents and corticosteroids may also represent significant co-factors in the development of delirium.
The cause of delirium is currently unknown, but it is likely that numerous brain pathways are affected during critical illness and combine to affect cognitive function. Proposed mechanisms include brain inflammation, poor cerebral blood flow, neurotransmitter imbalance and genetic disposition.
The manifestation of the condition varies and can be classified into one of three types: patients with hyperactive delirium are often agitated and restless, while those with hypoactive delirium are lethargic. When symptoms fluctuate over the course of the disease and show features of both hyperactive and hypoactive states, a diagnosis of mixed delirium is given. The latter two types are the most common and account for over 90% of all cases. Hypoactive delirium seems to be also associated with a higher mortality rate than the other types.
In order to minimise the long-term effects of delirium, early recognition is crucial. However, that can be very difficult in patients who are sedated to tolerate mechanical ventilation. Furthermore, delirium is often found in patients with existing neurological diseases such as dementia, traumatic brain injury and stroke, which can mask the symptoms and make diagnosis even more challenging. In order to improve diagnostic rates, validated assessment tools have been developed to screen patients for delirium and offer the best chance of improving diagnosis rates and patient outcomes
The CAM-ICU tool was specifically designed to assess patients receiving mechanical ventilation or who are sedated. However, the use of such tools is not uniform in all care centres, as some believe them to be too complex, too time-consuming or simply unnecessary. Instead, they rely on clinical observation. Not surprisingly, studies have shown that clinicians who do not use an assessment tool miss up to three-quarters of delirium days.
A lack of knowledge about delirium or lack of training in using the assessment tools can also impede diagnosis, as can the wrongful belief that the condition cannot be either prevented or treated. Unfamiliarity with existing guidelines concerning the management of patients with delirium,
Even if delirium is diagnosed, the management of those patients remains challenging, as there are few effective pharmacological treatment options. For years, antipsychotic medication was the therapy of choice; but recently it has been recognised that they confer little benefit and actually increase the mortality rate in elderly patients. However, they may have a role in reducing the agitation associated with hyperactive delirium that may result in patient harm. Dexmedetomidine, a new shortacting sedative, may shorten the duration of delirium but does not appear to prevent it developing, or reduce deliriumassociated mortality and longterm cognitive impairment. Due to their anti-inflammatory effects, statins have been postulated to be protective against delirium, although the results from randomised trials have failed to confirm that.
Due to the lack of effective medications, non-pharmacologic measures have become the cornerstone of delirium management. Those measures have been incorporated into a care package known as the ‘ABCDEF bundle’, which comprises:
• Assess, prevent and manage pain: uncontrolled pain is a risk factor
• for delirium
• Both spontaneous awakening trials and spontaneous breathing trials
• should be performed, ideally daily
• Choice of analgesia and sedation: assess medication regimens
• depending on the clinical context and patient characteristics
• Delirium: assess, prevent and manage by monitoring for early
• identification and risk factor modification where possible
• Early mobility and exercise, using a range of activities appropriate to
• the patient’s condition
• Family engagement and empowerment, which helps to improve team
• communication and cognitive rehabilitation of the patient
In conclusion, the long-term effects of delirium can have a significant impact on the patient’s life, as the resulting cognitive impairment may affect daily activities and employment. The effect of medication has failed to show clear beneficial effects in prevention of delirium and treatment of hypoactive delirium. Implementation of the ‘ABCDEF bundle’ in its entirety has been shown to significantly improve patient outcomes. Additionally, research into biomarkers may aid early diagnosis, leading in turn to better patient outcomes and reducing the risk of litigation. q
• Dr Martin Stotz is a consultant in adult intensive care and anaesthesia at St Mary’s Hospital in London, where he is the airway lead in a multidisciplinary team. St Mary’s Hospital, as part of Imperial College NHS Trust, is one of four major trauma centres in London and a tertiary vascular referral centre. Dr Stotz can provide expert opinion on a range of cases relating to the anaesthetic care and management of patients pre, during and post-operatively, and the clinical management of critically ill patients for both claimant and defendant.
63 63 www.yourexpertwitness.co.uk

64 64 www.yourexpertwitness.co.uk
COUNCIL TAKES ACTION AGAINST BUTTOCK FILLER BUSINESS
[CITY OF WOLVERHAMPTON COUNCIL has served a prohibition notice on a business offering non-surgical ‘Brazilian butt lifts’ (BBL’s) –making it the first local authority in England to take such action against premises offering such a procedure.
The notice was served on Clinique Modele Aesthetics. The premises offered non-surgical buttock augmentation injections with dermal filler, also commonly referred to as ‘body sculpting’ and ‘bum filler’.

Action was taken under the Health and Safety at Work etc Act 1974 to prevent the risk of serious personal injury and the potential for fatalities from the procedure when carried out by unsuitably trained practitioners. The prohibition notice was served following an assessment of the skills, knowledge and experience of those carrying out the procedure, a review of equipment available on site and expert opinion from a consultant plastic and reconstructive surgeon.
The expert’s report identified risks and complications associated with the procedure, including pulmonary embolism, sepsis, deep vein thrombosis and fat and skin necrosis.
Following an assessment, Clinique Modele Aesthetics was unable to show that its staff had enough training, skills and knowledge to undertake buttock augmentation, adequately recognise and deal with complications that may arise during the procedure and ensure adequate consent – including recognition of the need for psychological assessment of some individuals.
There was also no trained assistant during the procedure, no access to suitable equipment – including an ultrasound machine – and no ability to prescribe medication on site in the event of complications.
Clinique Modele Aesthetics is now prohibited from carrying out those activities from the premises in Wolverhampton and any other location in Great Britain. No appeal was made.
The popularity of surgical and non-surgical ‘BBLs’, which sees fat or dermal filler injected into the buttocks to change size or shape, has increased significantly over recent years. But there is currently no standard licensing scheme in England for businesses offering the procedure. A public consultation is due to be carried out under the Health and Care Act 2022 to give government powers to introduce such a scheme, but the timescale for it has yet to be determined.
Due to the serious risks involved, that particular procedure is likely to be excluded from the scheme unless it is carried out by someone listed on the General Medical Council Specialist Register.
Therefore, City of Wolverhampton Council took action using existing powers provided by the Health and Safety at Work etc Act 1974, with the aim of protecting residents from potential harm.
Cllr Steve Evans, City of Wolverhampton Council’s cabinet member for city environment and climate change, said: “We have based our decision to issue this prohibition notice on expert medical advice and with the aim of preventing any harm coming to our residents.
“The provision of these procedures is currently unlicensed and although work is underway to agree a standardised licencing scheme, it is not known how long this will take. Therefore, we have taken this action in the meantime as we believe people could be putting themselves at real risk.
“When it is not carried out with the required level of training and skills this type of procedure can cause serious injury, pain and even death. We do not want anyone to suffer these terrible outcomes.
“We are able to issue prohibition notices where we have concerns, and we will continue to take a pro-active approach. This will involve identifying and investigating other businesses offering this service.”
Marc Pacifico, consultant plastic surgeon and president of the British Association of Aesthetic Plastic Surgeons, said: “BAAPS seeks to promote patient safety in aesthetic procedures and surgery.
“We are fully supportive of the decisions taken by the City of
Wolverhampton Council. The risks involved in filler injection can be significant, especially when injected blindly into the buttocks.
“Furthermore, not being medically trained in both the procedure and in recognising and managing risks and complications, puts patients at significant risk of harm. We hope that other councils around the UK follow this example of decisive action to protect the public.” q
65 65 www.yourexpertwitness.co.uk

66 66 www.yourexpertwitness.co.uk
PLASTIC AND BARIATRIC SOCIETIES VOICE CONCERNS OVER ‘SURGICAL TOURISM’
[ THE British Association of Aesthetic Plastic Surgeons (BAAPS) and the British Obesity and Metabolic Surgery Society (BOMSS) – the aesthetic and bariatric UK surgical societies – have issued an unprecedented joint statement of their concern for patient welfare and safety in light of the significant increase in the number of patients travelling abroad for both aesthetic and bariatric (weight loss) surgery, which has been linked to serious complications and even deaths.
Both societies have previously warned about the risks of surgical tourism; however, due to economic pressures, concerted advertising and ready availability, there is a continuous and increasing stream of UK patients who choose to travel abroad for surgery.
In the statement the two societies said: “As professional societies we are concerned by the number of patients presenting with the complications of surgical procedures performed outside the UK. There is an assumption that the NHS will deal with any issues on return home and a significant financial cost can be attached to the management of complications. This cost
might well be down to the patient to pay, and must be considered in advance.
“BAAPS and BOMSS recognise that surgery in the independent sector in the UK is more expensive than in some other countries. The principal reason is that healthcare in England is tightly regulated by the CQC, in Scotland by the HIS and in Wales by HIW. This ensures quality, standards and ultimately safety are as good as possible. Not all countries have the equivalent to CQC regulation, and not all countries’ standards are at the high level of those in the UK.”
The statement listed specific concerns about people travelling overseas for surgery. They include:
• Lack of adequate expert pre-operative
• assessment, discussion and counselling
• Poor choice of procedure offered and the
• number of combined procedures offered in
• one surgical sitting
• Different procedures being performed from
• the one the patient expected, or the details
• of the procedure conducted being unknown
• Unknown quality and safety of the team
• providing surgery
HAND SURGEONS ACROSS THE WORLD MEET IN WALES
• Risks of long-distance travel immediately
• following surgery, for example developing
• a blood clot in the leg or lung, which can be
• potentially life-threatening
• Poor or non-existent access to routine
• post-operative follow-up care, increasing
• the possibility of outcomes such as weight
• regain and nutritional deficiencies in
• bariatric patients, and increasing the risks
• of sub-optimal outcomes and complications
• in plastic surgery patients
• No direct access to expert care if a
• complication occurs: most GPs are not
• trained in the care of patients who have
• had bariatric or plastic surgery
“Having surgery abroad is certainly less expensive than in the UK,” the statement continued, “but standards of healthcare regulation overseas often differ from the UK, which means the quality of surgical care can vary significantly. In the event of a problem, clinical and legal redress is much more difficult, leaving people exposed and unprotected.
“Therefore, both the BAAPS and BOMSS strongly urge caution to anyone considering surgical tourism – what cost is your health? Consult a UK surgeon first.” q
HAND SURGEONS from across the world gathered in Swansea in April for the spring conference of the British Society for Surgery of the Hand (BSSH). The city was chosen as the venue as the society’s president hails from there. Swansea Bay’s Clinical Director of Plastic Surgery, Dean Boyce, was elected by his peers in January and will serve 12 months in office.
Mr Boyce said: “It was a great pleasure to welcome The British Society for Surgery of the Hand and experts from all around the world: China, Australia, Holland and France.
“Swansea has a long and fascinating history dating from the ninth century, and it was a real pleasure to showcase my home town. I’m particularly glad to welcome Jin Bo, as Nantong is twin city to Swansea. Everyone has commented on what a great venue we have in Swansea.
“Outside of the speeches, lectures and demonstrations it has been a real privilege to show off our outstanding natural sights such as Gower, which they enjoyed very much.”
Professor Steven Hovius from Holland commented: “There’s an extraordinary faculty gathered here in Swansea and we are delighted to be here. This is a lovely venue and we have had an amazing conference.”
BSSH president Dean Boyce is pictured (second left) with, from left to right: Professor Steven Hovius (Holland), Professor Jin Bo Tang (China) and Professor Michael Tonkin (Australia). q

67 67 www.yourexpertwitness.co.uk
[
68 68 www.yourexpertwitness.co.uk
GDC PUBLISHES REGISTRATION AND FITNESS TO PRACTISE FIGURES
[THE GENERAL DENTAL COUNCIL (GDC) has published its annual registration and fitness to practise statistical reports for 2022. Both reports include comparison data from previous years to show any trends or changes over time.
The Registration Report shows that, overall, the number of registered dental professionals has remained stable, with a 0.6% increase compared to 2021. In December 2022 there were 44,000 dentists and 71,000 dental care professionals on the GDC register.
Of the new dentists who joined the register in 2022, 46% qualified outside the UK and there were 160 new dentists who joined the register through the Overseas Registration Exam route, which restarted in 2022.
Half of all newly registered dental hygienists and dental therapists were not UK qualified.
They were almost all overseas-qualified dentists who had applied for registration as a hygienist and/or therapist.

The Fitness to Practise Report shows that the GDC received 1,264 ‘concerns’ in 2022: down 7% compared to 2021. On average, of every 100 cases it received, 84% were closed through assessment and case examiner reviews, with only 16% progressing to a Practice Committee hearing.
The council held 84 Practice Committee hearings in 2022 – 31 fewer than in 2021. There were 18 dental professionals erased from its registers following a Practice Committee hearing, compared to 17 in 2021 and 25 in 2020.
The report also shows that dental professionals who live in London or the South East are more likely to have a fitness to practise
concern raised against them, compared to all other regions of the UK.
John Cullinane, executive director for fitness to practise, said: “These reports offer an interesting summary of two important facets of the GDC’s regulatory remit.
“This is the second year we have published EDI [equality, diversity and inclusion] data in the context of fitness to practise and we continue to look at how we can use this in our work to ensure there is no discrimination in any of our processes.
“What we do know is that EDI analysis is complex and I would ask you not to use the data in our reports in isolation to draw conclusions as many other factors may be relevant, such as practice location, size or local demographics.” q
RESEARCH ON ‘DENTAL DESERTS’ SHOWS ONLY PART OF THE PICTURE, DENTISTS SAY [
COMMONS LIBRARY RESEARCH commissioned by the Liberal Democrats shows that the rise in ‘dental deserts’ has left people struggling to get an appointment, with some areas now having over 3,000 people for every NHS dentist. Of 104 local areas in England, 65 have seen the number of people per dentist rise since 2019, the figures show.
However, the BDA – the professional body representing dentists – claims that official data is a work of fiction, given that the government has never attempted to collect data on how much NHS work those dentists perform.
Most dentists combine NHS and private work and officials have no estimate of the whole-time equivalent NHS workforce. The BDA's analysis of official data shows hundreds of dentists are doing the equivalent of a single NHS check-up a year. It says the number of dentists delivering a single unit of dental activity (UDA) in 2021/22 was over 500.
The Prime Minister has repeatedly claimed that there are 500 ‘new’ dentists practising in the NHS as a result of government reforms. The BDA says their data underlines the emptiness of those claims. Recent polls by the BDA indicate that over half of dentists in England (50.3%) report having reduced their NHS commitment since the start of the pandemic – by 27% on average.
That movement is not tracked in official workforce data, which counts ‘heads not commitment’ and where dentists doing one NHS check-up a year carry the same weight as an NHS full-timer. There are fewer dentists performing higher volumes of NHS dentistry in 2021/22 than in 2019/20, with the proportion performing over 5,000 UDAs falling by more than half.
Recent analysis undertaken by the BDA indicates unmet need for dentistry in 2022 stood at over 11 million people – almost one in four of England’s adult population. The professional body warned the Health and Social Care Committee last month that the government was just ‘rearranging the deck chairs on the Titanic while the service slowly slips into the sea’.
BDA chair Eddie Crouch said: “Dental deserts are on the rise, but the true scale of the exodus from the NHS is going untracked in official data.
“The Prime Minister keeps boasting of 500 ‘new’ dentists in the NHS. The
reality is we have 500 doing a single check-up a year.
“We need a reality check from government, together with honesty, ambition and investment.” q
69 69 www.yourexpertwitness.co.uk
72 72 www.yourexpertwitness.co.uk
OPTOMETRISTS RESPOND TO REPORTS OF ‘FOREVER CHEMICALS’ IN LENSES
[ THE COLLEGE OF OPTOMETRISTS has issued a statement in response to news reports that many soft contact lenses in the USA contain compounds called per- and polyfluoroalkyl substances (PFAS), dubbed ‘forever chemicals’ because of their persistence in the environment.

A report in the Daily Express in May quoted Mamavision, an eco-wellness product investigation community in the USA, as saying that: “…exposure to PFAS could cause lowered immunity, increased cholesterol levels, metabolic diseases like obesity and diabetes, cardiovascular disease, lowered fertility in men and women, increased risk of kidney and testicular cancers, and other side effects.”
The statement from the College of Optometrists says: “We are aware that PFAS are increasingly being detected as pollutants and some are linked to negative effects on human health. They are used in rigid gas permeable contact lenses in Europe, although the use of PFAS in the EU (including in medical devices) is currently under review.”
The college points out that there are currently no published case reports or formal safety alerts of direct harmful effects relating to PFAS in contact lenses, or peer-reviewed published studies on the release or absorption characteristics of the chemicals from a contact lens to the eye.
“We recognise the need to reduce the environmental impact of eye care, including contact lens manufacture and disposal,” the statement says, “while maintaining the quality and safety of patient care. We would strongly support the research and development of contact lens materials that offer high clinical performance, excellent patient safety and comfort, and environmentally sustainable manufacturing methods.”
In the meantime, the college says that current contact lenses, when worn and cared for according to recommendations by a contact lens practitioner, are considered very safe. Contact lens complications such as infections do occur but these are rare, with severe contact lensrelated infections affecting 2-4 people for 10,000 per year with typical daily wear. It is, therefore, important that contact lens wearers attend contact lens appointments as recommended by their practitioner, as that helps ensure their lenses remain suitable and their eye health can be assessed. q
73 73 www.yourexpertwitness.co.uk
WHAT ARE THE MEDICOLEGAL TRENDS IN INJECTABLE FACIAL AESTHETICS AND EYELID SURGERY?

GLOBALLY-LEADING DOCTORS EXPLAIN
 By Rachna Murthy BSc MB BS FRCOphth and Jonathan C P Roos MB BChir MA PhD FEBO FRCOphth
By Rachna Murthy BSc MB BS FRCOphth and Jonathan C P Roos MB BChir MA PhD FEBO FRCOphth
[ NUMBERS DON’T LIE: both by volume and money the aesthetics sector is booming and is the fastest growing area of private medicine. The face is the main target – after all, it is how we present ourselves and interact with the world. Facial neurotoxin injections, facial fillers and facial surgery together now surpass any other area of the body for enhancement or rejuvenation. But the aesthetics industry differs from other areas of medicine in terms of whom it attracts as both clinicians and patients, as well as the treatments offered.
What is different about the aesthetic industry practitioners?
In fact, not every aesthetic practitioner is a medically trained person. Self-proclaimed experts abound. In the UK – unlike in most other countries – fillers can be administered not just by doctors, nurses or dentists, but by anyone, including hairdressers, beauticians and those without any training at all.
Even the doctors may be unusual, many having had no clinical training beyond the mandatory foundation years or having dropped out of specialist registrar training early. Some will seek to upskill and sign up for a panoply of for-profit aesthetic training businesses which vary greatly in quality.
The clinics in which the work is performed also vary, of course, with some national chains offering high-volume low-cost treatments with little variation, despite differing patient needs. At the other end of the spectrum those treating celebrities may charge an order of magnitude more for the same treatments and without marked advantages.
Unlike those working in the NHS, whose salaries are unrelated to their clinical decision-making, the aesthetic industry is almost exclusively private, resulting in an incentive to over rather than under-treat.
What is different about the aesthetic industry patients?
The patient population is also different. The aesthetic industry has always attracted those wishing to reverse the signs of ageing
or to redress a disparity in their external appearance and sense of self. However, there are also now social media-driven facial trends, with younger people seeking ‘hunter eyes’ or ‘fox eyes’ and risking permanent facial disfigurement.
There has been an industry-wide push to identify those suffering from body dysmorphic disorder (BDD), where the actual appearance is not recognised, leading to excessive treatments and disfigurement
often with an alien-like appearance with exaggerated lip size. The BDD can affect the practitioner doing the treatment too.
The location of the chosen treatment is also different. While disease tends to warrant treatment near ones loved ones and carers, the aesthetics field is notable for medical tourism – most often driven by price. Until there is an untoward event many may not identify as patients, but as customers or clients.
What is different about the aesthetic industry products?
When a pharmaceutical product is brough to market, regulations are tight and clinical trials showing safety and efficacy are required. Except for botulinum toxins – which are only available on prescription – aesthetic injectable products are classed as devices or cosmetics and have a much lower standard for approval. That can lead to a delay in the identification of complications.
For example, around 20 years ago a novel French injectable was found to create granulomas, and the ensuing abscesses would erupt through the skin, expelling the product. The lack of safety studies also means that complications monitoring is performed by international groups of leading clinicians working as a team through IMCAS Alert, for example, or the companies producing the product themselves.
A more recent example involved the model Linda Evangelista, who claimed to have suffered a rare complication of fat over-production in her chin after a treatment intended to reduce that fat. Much in the industry is marketing rather than science led and exaggerated claims abound.
74 74 www.yourexpertwitness.co.uk
–
What is different about the medicolegal scene in aesthetics?
We run a London-based practice which frequently receives tertiary referrals for managing complications. Over the past few years we have noted a number of distinct trends. These most commonly include:
• Not listening to what patients want and giving treatments which the
• patient had not envisaged having: “I went for toxin for my wrinkles
• and they gave me fillers to my jowls”.
• Practising outside ones area of expertise: “I went for a breast lift but
• he offered to do my eyelids instead”.
• Doing a one-size-fits-all approach, which fails to recognise patients’
• unique wishes and facial appearances.
• Forcing patients to sign nondisclosure agreements.
• Punishing patients by refusing to see them again if they seek a
• second opinion from another doctor.
• Inflating credentials or awards, for example suggesting one is
• ‘Harvard trained’ after spending a medical school elective there
• observing, or suggesting one is a ‘consultant’ surgeon or
• anaesthetist when one has dropped out of registrar training prior
• to completion.
• Failing to recognise medical conditions such as thyroid eye disease,
• dry eyes or scarring disorders, which preclude certain procedures.
• Failing to recognise warning signs suggesting the patient may be
• unsuitable for treatments, such as having a psychological condition.
• Compounding of injuries by further treatments such as dissolving
• filler or doing further surgery with skin grafting which worsens the •
• appearance.
• Using inappropriate devices and in the wrong locations – there are
• different types of filler products and laser devices which can burn
• certain skin types or create granulomas and product migration if
• placed incorrectly.
• Failing to seek informed consent.
• Chain clinics altering surgical staff without notice and leading to less
• competent surgeons operating and removing excessive skin.
• Seeking to bribe patients when GMC referrals have been made. Vexatious complaints can be made by patients who regret spending money or who suffer with psychological dependencies, but the crux is that they are high-value procedures combined with sometimes relatively unskilled practitioners who are not adept at dealing with medical aspects of care, such as identifying psychological conditions or dealing with adverse events or reactions – including by listening. That compounds injury and leads to complaints and lawsuits.
We have found repeatedly that clinical photography pre and postprocedure is key to supporting either a claim or defence. Beauty is very subjective and memories of a prior appearance can be distorted or forgotten. q
• Rachna Murthy and Jonathan Roos are consultant ophthalmologists and eyelid surgeon specialists with decades of experience. They are globally recognised for their aesthetic and clinical work and have won many industry and academic prizes. Rachna was Consultant Surgeon of the Year 2022 and sits on Allergan’s UK complications board.
They contribute to the IMCAS Global Alert and teach for Allergan –a leading producer of injectable aesthetic treatments.
Both Dr Roos and Dr Murthy are invited lecturers at leading aesthetic events in the UK and internationally, and teach anatomy and safe injection techniques. They have published textbook chapters on the management of aesthetic complications and contributed to guidelines to minimise the risk of blindness and other filler and surgical-related complications.
They have Bond Solon accreditation and are now producing many medicolegal reports per year. They are increasingly the go-to experts when periocular surgery or facial filler has gone wrong and needs remedial treatment or a robust medico-legal opinion.
75 75 www.yourexpertwitness.co.uk
MPS’ EYE HEALTH DEBATE DRAWS ON OPHTHALMOLOGISTS’ RESEARCH

[IN MAY Members of Parliament debated the potential merits of a national eye health strategy at Westminster Hall. The debate, tabled by Marsha de Cordova MP, saw Parliamentarians from across the political spectrum cite recent statistics from the Royal College of Ophthalmologists (RCOphth) and explore several policy priorities advocated by the college.
They discussed how an eye care strategy, supported by investment and resourcing, could help facilitate solutions to the ophthalmology capacity challenge.
Marsha de Cordova MP stated that ‘nearly 80% of eye care units already do not have enough consultants to meet current demand’, while Dr Rupa Huq MP highlighted that 80% more eye units have become more reliant on multidisciplinary team (MDT) and allied health professionals (AHPs) compared to 12 months ago.
Labour’s Shadow Health Minister Karin Smyth MP linked the statistics to the impact on outpatient backlogs, citing census statistics showing 63% of eye units estimating it will take at least a year to clear and a quarter that it will take at least three years. Shadow Minister Smyth subsequently posted RCOphth census statistics on Twitter.
Increased delivery of NHS-funded ophthalmology care by independent sector providers (ISPs) was also a point of focus by Dr Huq. She drew attention to the Health Service Journal report on the RCOphth Workforce Census 2022, which found that 58% of eye units say ISPs delivering NHSfunded care in their area had a negative impact on patient care and their ophthalmology services. Dr Huq highlighted the specific focus by ISPs on the delivery of ‘low-risk, routine work’ such as cataracts which was leading
to sustainability and accessibility issues with local NHS services.
Responding on behalf of the government was Minister for Primary Care and Public Health Neil O’Brien MP, who stated that an expansion in training places would be made available in 2023 and met one of RCOphth’s policy calls by committing to “improved training for existing ophthalmology staff so they can work at the very top of their clinical licence”, including MDT and AHP staff.
Minister O’Brien publicly acknowledged for the first time the challenges associated with the lack of training opportunities provided by ISPs, while stressing the importance of the independent sector’s role in reducing backlogs more broadly.
He stated it is important to “ensure that trainees can get sufficient cataract surgery training and can have a broad range of clinical experiences as they are trained.”
The RCOphth said it believes that is an important acknowledgement and continues to work with NHS England and ISPs to resolve the challenge following publication of the blueprint for cataract training in the independent sector, co-created between RCOphth and NHS England.
Commenting on the proceedings, the RCOphth said: “The college believes that a national eye health strategy, if supported by effective investment and resourcing, would help increase ophthalmology capacity and enable more efficient eye care services, ensuring sustainable hospital eye services that can meet ever-growing patient need. We will continue to engage with politicians from across all parties to advocate for the solutions needed to fix ophthalmology capacity challenges.” q
76 76 www.yourexpertwitness.co.uk
AGRICULTURAL & HORTICULTURAL CONSULTANTS





ARTS & ANTIQUES SURVEYORS

BETTING & GAMING

77 77 www.yourexpertwitness.co.uk ACCOUNTANCY
BUILDING, PROPERTY & CONSTRUCTION




COLLISION INVESTIGATION & RECONSTRUCTION


COMPLIANCE CONSULTANTS



COMPUTER & MOBILE FORENSICS
78 78 www.yourexpertwitness.co.uk
ENERGY CONSULTANTS
CRIMINOLOGY

ERGONOMICS
DIAMOND & JEWELLERY VALUERS


FINANCIAL SERVICES



FORENSIC SERVICES


DIGITAL TECHNOLOGY

79 79 www.yourexpertwitness.co.uk
GEOTECHNICAL CONSULTANTS


POLICE CUSTODY
INSURANCE

MECHANICAL & PROCESS ENGINEERING


RISK MANAGEMENT

STEEL & IRON ORE
80 80 www.yourexpertwitness.co.uk






81 81 www.yourexpertwitness.co.uk
TRANSLATING & INTERPRETING
WOOD & TIMBER
TREE CONSULTANTS
MEDICO-LEGAL EXPERTS




ACCIDENT & EMERGENCY MEDICINE


CARDIOLOGISTS & CARDIOTHORACIC SURGEONS

ANAESTHESIA
82 82 www.yourexpertwitness.co.uk
DENTAL & ORTHODONTIC EXPERTS



ENDOCRINOLOGY
GASTROINTESTINAL & COLORECTAL SURGEONS



ENT CONSULTANTS
83 83 www.yourexpertwitness.co.uk
GENERAL SURGEONS
INTENSIVE CARE MEDICINE

LIVER SURGEONS & HEPATOLOGISTS


GERIATRICIANS

MEDICAL NEGLIGENCE


HAEMATOLOGY

MICROPIGMENTATION
84 84 www.yourexpertwitness.co.uk
NEUROLOGY
NEUROPSYCHOLOGISTS

NURSING & REHABILITATION CONSULTANTS




NEUROSURGEONS



85 85 www.yourexpertwitness.co.uk NEONATAL MEDICINE
OBSTETRICS & GYNAECOLOGY


ONCOLOGISTS
OCCUPATIONAL MEDICINE & THERAPY

OPHTHALMIC SURGEONS



86 86 www.yourexpertwitness.co.uk
ORAL & MAXILLOFACIAL SURGEONS
ORTHOPAEDIC SURGEONS






87 87 www.yourexpertwitness.co.uk
OSTEOPATHS


PAIN MEDICINE

PATHOLOGY
PHARMACOLOGY

PHYSICIANS
PLASTIC & HAND SURGEONS


88 88 www.yourexpertwitness.co.uk
PSYCHIATRISTS
PSYCHOLOGISTS







89 89 www.yourexpertwitness.co.uk
SPEECH & LANGUAGE THERAPY


REHABILITATION

TOXICOLOGY


90 90 www.yourexpertwitness.co.uk
SOCIAL CARE
UROLOGICAL SURGEONS


VASCULAR SURGEONS





91 91 www.yourexpertwitness.co.uk
TRICHOLOGY