FORENSIC ACCOUNTANCY
using an employment expert
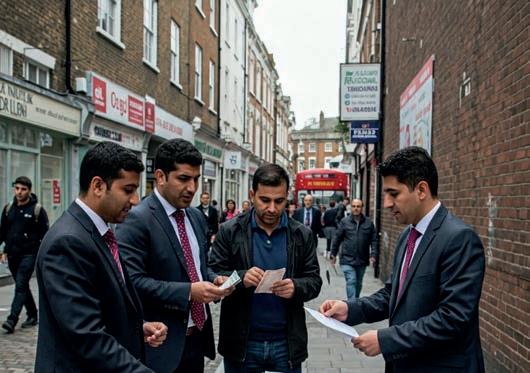
15 Hawaladars warned against infiltration by people smugglers
17 SFO utilises new court order in Schools case 17 Govt acts to address umbrella company anomalies 19 Offender must pay more under PoCA
19 Pair arrested for financial crime in recycling industry
PROPERTY, CONSTRUCTION & ENGINEERING
21 Industry unites in welcoming Rayner’s Grenfell response
22 Proposals to digitalise home buying welcomed by lawyers
22 Institutions combine to create HRB register
IRON & STEEL
23 In complex industrial disputes, engage your expert early
GEOTECHNICAL ENGINEERING
24 Who do you turn to when the earth moves beneath your feet?
25 Developer loses damages case against ground engineers
25 BGS dataset maps groundwater flood risk
THE OIL & GAS INDUSTRY
27 Offshore safety benefits from HSE involvement
27 Well-plugging technology goes on show in Aberdeen
28 Ruling pauses production but allows development of new North Sea fields
HEALTH & SAFETY
29 PI lawyers back MP’s bid to repeal Section 69
29 Video shows moment man is crushed by loading bucket
FIRE INVESTIGATION
30 Fire chiefs call for co-ordinated remediation strategy
31 Are you forewarned if gas ignites?
TREE CARE
32 When investigating tree-related claims, being ‘The Tree Detective’ is an important skill
ENVIRONMENTAL ISSUES
33 How the climate change expert witness is becoming key to everyday cases
35 Speed is of the essence when managing a spillage claim
35 Day of action nets a clutch of waste criminals
TRANSLATING & INTERPRETING
37 How a human-AI combination delivers seamless, high-quality translations
FORENSIC DOCUMENT INVESTIGATION
38 Forensic handwriting analysis: it’s a very modern science and it’s happening now
38 What handwriting can – and cannot – reveal



NEWS
49 Royal College exam gaff stirs up condemnation from doctors’ bodies
51 Infected Blood Inquiry to publish further report following criticism of govt response
53 GPs’ body reacts to GP registration cancer screening errors
53 Behind the headlines: what the abolition of NHS England means
55 Doctors discuss AI in practice for new research
57 Home-grown blood plasma starts to flow again after 23-year ban
57 CQC publishes providers’ responses to assessment concerns
THORACIC MEDICINE
59 Study identifies safety failings in pleural procedures
59 Lung charity warns of lack of capacity for testing
59 Experts should be hands-on
NEUROSURGERY & NEUROLOGY
61 Post-concussion syndrome: what are the medicolegal implications?
UROLOGY
63 Targeted prostate screening can save lives and have socio-economic benefits
RADIOLOGY
64 Radiologists cry foul over recruitment freezes
COLORECTAL SURGERY
65 How do we approach delays in the diagnosis of colorectal cancer?
67 Intestinal surgical disaster: who’s to blame?
NEPHROLOGY
68 What does a nephrologist do and when is their expert opinion needed?
CARDIOLOGY
69 Heart care waiting lists rise, although ambulance response times fall
71 AI can be used to identify women at risk from heart disease, study finds
OBSTETRICS & GYNAECOLOGY
73 ONS figures on endometriosis and earnings are ‘staggering’, RCOG says
74 Midwives welcome govt response to Lords preterm birth report
NURSING
75 HSE issues guidance for nitrous oxide exposure
77 RCN urges govt to support Bill to protect title ‘nurse’
77 Regulator reports progress on reform of FtP processes
VASCULAR SURGERY
78 Iatrogenic vascular problems: how surgery can lead to further injury
A&E MEDICINE
81 A&E medics hit out at near record number of patients on corridors in Scotland
PLASTIC, RECONSTRUCTIVE & HAND SURGERY
83 Scar free charity takes 3D ear-printing to Parliament
83 BAPRAS welcomes Royal visitor at Congress
OPHTHALMOLOGY & OPTOMETRY
85 Consent is the conversation topic at anniversary celebration
85 New optical standards came into force in January
87 New data tool predicts increases in eye health conditions
DENTISTRY & MAXILLOFACIAL SURGERY
89 Extra 700,000 appointments only covers third of need, BDA says
89 GDC falls below standard on fitness-to-practice timeliness
89 Letter calls for GDC chair to be a registrant
ORTHOPAEDICS
93 New scanning technique can detect early signs of osteoarthritis
95 Health professional to stress work as an aid to good MSK outcomes
PHYSIOTHERAPY
96 Why I put my expertise at the disposal of the courts
PAIN MEDICINE
97 Pain doctors comment on reports of forced opioid reduction
PSYCHIATRIC & PSYCHOLOGICAL ISSUES
99 What are the medicolegal implications of a suicidal patient?
101 The Neurodiversity Series: complimentary ADHD and autism webinars now available
103 Blame culture contributes to inability to learn from deaths
103 Psychiatrists call for end to child OAPs
104 Transparency in family courts can be a tightrope for experts


[ AS WITH JUST ABOUT every publication, climate change and the environment take up column inches in this issue. While environmental concerns feature in many areas of our reporting, we also take a look at the issue as a specific subject. All areas of life are affected, from national planning and the role of the expert in policy formulation to the street-level effects of individual polluters. Who knew that the effect of climate change on weather patterns across the globe would affect the time it takes for a flooded road to return to normal?
• As with climate change, many areas of the expert’s work are of a technical nature, and instructing an expert in such subject areas as steel and heavy engineering, geotechnology and the offshore oil and gas industries takes a high level of expertise itself. We are lucky in having experts in their own field offering advice to the confused lawyer on what to look for. What comes across in all cases is that the expert should be engaged at an early stage to ensure they are properly acquainted with the nuances of the case in point.
• The highest aspiration in almost any dispute of a technical nature (or non-technical, for that matter) is for it to be resolved without going to court. The new version of the Arbitration Act will help to make that aspiration a reality for many. It will also, according to the government, make the UK an even more attractive place to do business when it comes to legal matters. International arbitration is big business and the UK has a healthy slice of that cake.
• We are also lucky in having a leading mediator as a regular contributor. Chris Makin’s sideways views on life as an expert always make interesting reading, and his comparison of mediators in commercial disputes with hostage negotiators is a fascinating one. Chris has a mnemonic that serves for both jobs: MORE PIES. Yes please!
• While most disputes over contracts tend to centre on the wording and the actual terms of the contract – and whether they have been adhered to – the actual validity of the document can be another bone of contention. Signatures can be forged, be it on a contract, a divorce settlement or a will. Handwriting experts are remarkably adept at spotting such anomalies and will soon expose a cheat in that respect.
• More sophisticated ploys than simply forging signatures are employed in the murky world of money laundering. A particularly cynical manifestation of the practice is the taking of cash from would-be immigrants and handing it over to people smugglers once the deed has been done. That was the crime of one Iranian national who is currently serving an eight year prison sentence. He laundered the money through his work as a Hawaladar: a system of transferring goods and value without cash. Other Hawaladars are being cautioned against their businesses being infiltrated by other people smugglers.
• Even when they have been caught, money launderers can still pull the wool over the eyes of even seasoned investigators. Such was the case with Simon Mason, who found himself back in court after Environment Agency investigators discovered that his assets far exceeded the eight thousand and some pounds he had been presumed to have. He now has to pay more than a quarter-of-a-million pounds in proceeds of crime. That sum is what he pocketed from an illegal waste disposal operation.
• In February the Grenfell Tower Inquiry formally closed. There followed the government’s official response, which was striking in its acceptance of all the recommendations. That itself drew plaudits from many organisations involved in both construction and building safety. We at this publication do not want to be carrying news on any similar inquiries in the future. q
Ian Wild, Director of Business Development Your Expert Witness


[THE ARBITRATION ACT, which received
Royal Assent on 24 February, will re-enforce Britain’s position as the best place to resolve disputes without having to go to court, the government says.
The process to reform the Arbitration Act 1996 began in 2023 when recommendations were made by the Law Commission. The new law makes measured amendments to the 1996 Act which will make arbitration fairer and more efficient by simplifying procedures to reduce costs and protecting arbitrators from unreasonable lawsuits. It also strengthens the courts’ powers to support emergency arbitration so time-sensitive decisions can be made more easily.
The new Arbitration Act will:
• Clarify which law underpins individual
• arbitration agreements, thereby improving
• legal certainty and speeding up arbitrations
• Empower arbitrators to speed up decisions
• on issues that have no real prospect of
• success to make arbitration more efficient
• Introduce a duty on arbitrators to tell parties
• any circumstances which could cast
• reasonable doubt on their impartiality in
• deciding an outcome of a dispute
• Empower the court to better support
• arbitration through orders supporting the
• actions of emergency arbitrators to enhance
• their effectiveness, and orders against third
• parties (those not involved in the
• proceedings) to, for example, preserve
• evidence or take witness evidence
• Extend arbitrator immunity against liability for
• resignations and the costs of the application
• to court for their removal, to support
• arbitrators to make impartial decisions
• Simplify court procedures related to
• arbitration to increase clarity as well as
• reduce delays and costs for parties.
According to the Ministry of Justice, modernising arbitration law will ensure the UK remains the global destination of choice for the legal sector, outstripping competitors such as Singapore, Hong Kong and Paris. That will help generate greater employment in the sector to bring even more investment into the UK.
The Minister for Courts and Legal Services, Sarah Sackman KC MP, said: “The UK’s legal sector contributes billions to the economy and employs hundreds of thousands across the country. Companies from across the world look to the UK for our legal services and dispute resolution. This new Act ensures that arbitration law keeps this country ahead of the rest and supports economic growth as part of this government’s Plan for Change.” q
[THE LAW SOCIETY OF SCOTLAND will ensure a Holyrood inquiry understands the extent of the crisis in civil legal aid, and the changes required to restore the system.
On 13 March the Scottish Parliament’s Equalities, Human Rights and Civil Justice Committee launched a call for views as part of a new inquiry into civil legal aid. The Holyrood committee has indicated the inquiry has been launched on the basis of evidence already presented showing significant issues making it difficult for people to access civil legal assistance.
The Law Society said last month that a discussion paper and other limited measures announced by the Scottish Government fail to reflect the urgency and scale of the crisis in legal aid.
The co-convener of the society’s Legal Aid Committee, Pat Thom, said: “This Holyrood inquiry is a welcome chance to highlight the problems with civil legal aid, the unacceptable impact that is having on access to justice in Scotland and what the potential solutions are to restore the system.
“Solicitors have been warning for years that Scotland’s legal aid system is under enormous pressure. In this civil context vulnerable people are being forced to deal with traumatic legal situations across critical parts of their lives, including their housing, relationships and work.
“We hope that people and organisations with first-hand knowledge of the civil legal aid system will contribute to this inquiry, including solicitors, law centres and the growing number of people facing legal
challenges without the expert advice they need.
“Without action solicitors will continue to turn away from civil legal aid work. Around a third of Scotland’s legal aid solicitors are approaching retirement age, and many younger solicitors cannot see legal aid work being part of their working lives.” q

By CHRIS MAKIN chartered accountant, accredited civil mediator and accredited expert determiner
[YOU MAY BE TEMPTED to reverse the question and ask what are the similarities between the two. Surely there can’t be any? But read on. I recently attended the advanced mediation training course run by the Association of Northern Mediators up near Malham Tarn, in the rugged but beautiful North Yorkshire. It’s been run for 23 years, I have attended all but a couple of them, and we get some amazing speakers.
This time we had Phil and Damien, who had recently retired from the Metropolitan Police as negotiators with hostage takers. What a job! Remember the Balcolme Street siege? The Spaghetti House restaurant siege? How about the Iranian Embassy, where WPC Yvonne Fletcher was murdered? If you are old enough, you will undoubtedly remember watching the action on live TV where the SAS belayed down from the roof, threw stun grenades through the windows and retook the premises.
Well, this was not a failure in negotiation, since some situations are intractable and violence has to be used, but our guys are the ones who talk to the hostage takers (or those threatening suicide) to defuse the situation, make them appreciate their position is hopeless, and persuade them to surrender whilst releasing the hostages unharmed. Many of these situations we don’t even hear about.
How is it done? By active listening. Let me digress for a moment.
When I was taking advanced driving lessons, I was taught that many skills are remembered through mnemonics. For example, the things
[ CHRIS MAKIN was one of the first 30 or so chartered accountants to become an Accredited Forensic Accountant and Expert Witness –see www.icaew.com/about-icaew/find-a-chartered-accountant/find-anaccredited-forensic-expert
He is also an accredited civil and commercial mediator and an accredited expert determiner. Over the last 30 years he has given expert evidence at least 100 times and worked on a vast range of cases. For CV, war stories and much more go to the website at www.chrismakin.co.uk – now with videos! q


you have to check before driving away are POWER: that’s Petrol, Oil, Water, Electrics and Rubber (tyres). Similarly, with negotiation the mnemonic is MORE PIES. And, remarkably, this is where mediation comes in, because the effectiveness of active listening is identical in hostage taking as in mediation. It’s remarkable, but true. So let’s look at active listening in detail.
With hostage taking, there will usually be a telephone line between the leader of the hostage takers and the police negotiator, who will have a team working silently to help him. With mediation, we have had the joint session at the start, and when I see the parties separately in their rooms, when I feel I have their confidence (it may be in the first meeting or a later one) I ask the magic question: “What do you seek to achieve today that you don’t have right now?” And the reply is usually surprising, and nothing to do with the formal case. These, then, are the techniques which the mediator (and the hostage negotiator) must use to find out what the other party really wants:
M = Minimal encouragers. Make short noises (hmmm, ahh, I see, go on) or smile and nod. I remember giving a couple of interviews for BBC’s File on Four (about rogue landlords and the British National Party, since you ask) and I talked too much and too fast. The interviewer actually conducted me with her eyebrows, and I made a much better job of it.
O = Open questions. A closed question invites only a yes or no answer; you don’t learn much. But with an open question such as “Tell me, then what happened?” you encourage a full answer.
R = Reflection. Repeat some of the words they use, to show that you understand and to encourage them to say more.
E = Emotional labelling. Hear the emotion and express it back. Closely allied with reflection. Don’t worry if you express it wrongly; they will correct you and this all helps to build empathy.
P = Paraphrasing. Hear their words and give back the same, but more briefly. Again, this builds empathy because, whether or not you agree with them (and who would agree with a hostage taker or a party in mediation with a hopeless case?) they will tell you their true needs.
I = I-messages. ‘You’ is accusatory; ‘I’ allows you to say the same thing in a less provocative way. For instance, if you suggest the person is lying, don’t say “You are a liar” which is likely to end the conversation, but “I am confused; you said before X but now I’m hearing you say Y. How is that?”
E = Effective pause or silence. When they stop talking, perhaps to think or because they don’t want to say any more, don’t be tempted to fill that silence with your own words. Silences are unnatural, so wait silently and they will be tempted to speak, and perhaps reveal something really valuable.
S = Summarising. Summarise what has been said, at more length than with paraphrasing. Use some of their words; they will see that you have understood what they were trying to tell you.
So this gives you an insight into what goes on in those private rooms in a mediation. Hostage negotiators bear huge responsibility in life or death situations, and I admit that mediation is seldom a matter of life or death. But it is hugely important to the parties, so the mediator carries huge responsibilities too. We are not just having a cosy chat with your clients; we are highly trained (well, most of us are!) and we have tools we can use to help them.
As May LJ said in Egan v Motor Services (Bath) Ltd [2007] EWCA Civ 1002: “Mediation is a perfectly proper adjunct to litigation. The skills are now well developed. The results are astonishingly good. Try it more often.” q

[A MAJOR INJURY that derails your client’s career is a disaster that can affect every aspect of their life. But it can be even worse for them if potential lost earnings are calculated incorrectly, which could leave them thousands of pounds out of pocket.
Too often, settlements for loss of earnings are assessed using ‘typical’ salaries and career paths. But few if any of us are typical, especially with the rise of portfolio careers, side hustles and regular vocational changes.
An employment expert can help the court see the whole picture and ensure an individual receives fair and accurate compensation for lost earnings.
Clydebank-based Employment Experts have been working in this field for 30 years, bringing a vast amount of knowledge and expertise to the process. They have a team of experts with years of specialist experience and insightful knowledge of their industry. For instance, they have experts who have been HR directors and others with a background in occupational psychology. Crucially they match the expert with the type of job your client did and may be expected to have in the future.
Employment Experts director Lee Fish explained: “We can bring a much more certain figure to the claim. We can be more nuanced.
“We really come into our own with difficult to value cases where the person has, for example, been in a self-employed profession or one with highly variable earnings.
“That also extends into the corporate world. You can be a bank manager running a very small rural branch, earning £30,000 a year. You can have the same job title but be a commercial manager in a head office, earning
£150,000 with big bonuses. So again, we can bring much more nuance and specificity.”
This can be particularly useful for people in the early stage of their careers.
“We also deal with abuse claims, where perhaps people have gone on to have mental health issues, or drug and alcohol addiction caused by this mistreatment,” added Lee. “We’re very well equipped to give much better life-long predictions over a variety of scenarios.”
In addition to experts, they have their own research team who work extensively with employment statistics, adding an extra layer of informed knowledge to their reports.
Many people who have been injured are assessed by their doctor as being ‘capable of sedentary work’. But a claim for lost earnings needs to look realistically at what that means, what skills they have and whether they could learn new ones.
To find the answers, Employment Experts work hand-in-hand with their sister company, Novo Therapy and Care, whose trained expert therapists conduct functional capacity evaluations on claimants.
Lee Fish continued: “We have a specialist suite with equipment to evaluate the likes of mobility, motor skills, fitness, stamina, strength, agility, coordination and dexterity. We modify the studio so it mirrors a claimant’s former workplace; if they were a decorator, we’ll check how well they can climb a ladder or use a paint roller.
“Via video-link, our employment experts, who are based all around the country, watch
the tests and can actively ask the person to try different activities, giving them first hand insight into each individual’s capabilities. They will gather more information via additional video calls.
“Our experts will report what sort of work the individual could do and whether there will be any suitable jobs. It means we can be robust when it comes to evaluating their earning potential.
“It’s not just asking whether they can do something, It’s can they work five full shifts back-to-back? Can they only do one day and then need two days off? And then is there likely to be an employer who would employ them based on that sort of capacity? We bring answers to those questions.”
The armed services have a particularly complicated pay structure which can greatly affect potential earnings as people gain extra qualifications.
The company’s team includes the former head of army personnel, as well as a current RAF wing commander who was responsible for re-writing the pay structure. It means they have the best possible experts who can help to deal with claims in this field.
Using an employment expert means we can lighten a solicitor’s load, often at a favourable rate, while adding an extra layer of expertise. q
• To find out more visit employconsult.com , email on info@employconsult.com or call 0141 488 6630

[ NATIONAL CRIME AGENCY (NCA) OFFICERS have warned registered Hawaladars in the UK of the consequences of being involved in organised immigration crime. Hawaladar systems serve entirely legitimate purposes, but are known to be exploited by criminals looking to move criminal cash, including from small boat people smuggling activity.
Visits to 44 businesses across the UK were carried out by the NCA, in co-ordination with HMRC, over the course of two days, the 25 and 26 February. The visits were also attended by officers from nine forces: a show of joint commitment to increase intelligence on financial flows linked to those who facilitate and enable people smuggling.
Hawala is a type of informal value transfer system that operates on a basis of transfer of value without actual movement of money. It relies heavily on trust – between Hawaladars and their customers, and within the networks themselves. The systems are used for a wide variety of reasons – such as cheaper or faster money transmission, cultural preference, lack of confidence in banks or because they are the only channel through which funds can be transmitted in certain conflict regions.
In the UK they are subject to regulations and standards. They must be compliant with the Money Laundering, Terrorist Financing and Transfer of Funds Regulations, and are legally required to report anything suspicious to the NCA.
Those who do not do so risk criminal charges, heavy fines, business closures and severe reputational damage. Those who take payment from people smuggling activity, whether willingly or unwittingly, are helping to fuel a crime that endangers the lives of thousands.
Alex Murray, director of threat leadership at the National Crime Agency, commented: “Organised immigration crime is a deadly threat that led to more than 70 fatalities in the Channel last year alone. Criminal gangs are behind these crossings.
“The National Crime Agency has around 70 on-going investigations into people smuggling networks, and we are determined to do all we can to target those involved – including those who enable, support and financially benefit from this criminal activity.
“Money service businesses provide an important service, and the vast majority are compliant with regulation; however, it is absolutely key that all those who work in this sector remain vigilant, report suspicious activity and play their part to stop this horrific crime. Those who don’t will be pursued and prosecuted as harshly as those directly involved in organising the crossings.”
Last year, following a National Crime Agency investigation, Iranian Hawaladar Asghar Gheshalghian was sentenced to eight years in jail after being convicted of running an unregistered money services business that served people smuggling networks. Gheshalghian acted as a trusted middleman, accepting payments from migrants or their families and then releasing money to the criminal gangs following the completion of their journeys to the UK, charging a commission at the same time.
Louise MacDonald, deputy director of economic crime at HMRC’S Fraud Investigation Service, said: “Businesses who fail to comply with money laundering regulations leave themselves, and the UK economy, open to attacks by criminals, including those involved in organised immigration fraud.
“We know many registered Hawaladars provide vital and legitimate services to scores of communities. That’s why we’re working with partners at the NCA to help protect them from criminals who would prey on their services, and we will use all our powers to tackle those who fail to meet their legal obligations.”
February§’s activity was designed to emphasise the importance of vigilance, signpost reporting mechanisms and warn all those working
in the sector that a failure to comply with legislation will result in serious consequences. It will be paired with further activity over the coming months.
Minister for Border Security and Asylum, Dame Angela Eagle, added: “Law-abiding Hawaladars have a responsibility to report suspicious activity, and as this warning makes clear we will not hesitate to prosecute those who enable people smugglers to profit from putting countless lives at risk.
“This government continues to combat organised immigration crime and tackling illicit finance is a priority as we work to secure the UK’s borders and deliver the Plan for Change.” q


[ON 17 JANUARY the Serious Fraud Office (SFO) secured its first Unexplained Wealth Order (UWO) at the High Court, as it seeks to recover a Lake District property believed to have been purchased with the proceeds of a £100m fraud.
The property is valued at around £1.5m and is owned by Claire Schools: the ex-wife of the convicted solicitor Timothy Schools, who was sentenced to 14 years in prison in 2022.

The SFO obtained an order to freeze the property to ensure that, if sold, the proceeds are secured. Ms Schools has also been ordered to produce information about how the property was obtained within 28 days. The SFO may use that information to bring a case to seize the house at a later date.
The order follows the confiscation of a further £1m from Schools in a hearing at Southwark Crown Court earlier in the month.
A UWO is an investigative tool used to determine the source of funding for an asset, where there is reasonable suspicion that it was acquired with the proceeds of crime. If the recipient fails to prove that the asset was acquired legitimately, the SFO may apply to seize it at the High Court. This is the first UWO used by the SFO since they were introduced by parliament in 2017.
The SFO is the second law enforcement authority to ever use the tool.
Nick Ephgrave QPM, director of the Serious Fraud Office, commented: “This is a milestone case for the SFO and follows on from last week’s successful £1m recovery to go back to the victims in this case. Wherever criminal assets have been hidden or dispersed, we will progress our investigations with determination and explore new methods to recover funds for victims and the public purse.” q
[THE GOVERNMENT has confirmed that it will take forward plans to regulate umbrella companies for the purposes of employment rights and that it will continue to review further policy options.
An umbrella company is an intermediary which typically employs workers on behalf of an employment agency. The temporary workers are then supplied to end clients. The umbrella company model can provide a useful employment solution for all parties, enabling flexible, temporary work while managing the administration, compliance and tax obligations. However, it has often been abused and used for tax avoidance purposes.
Government estimates for 2022/23 indicate that umbrella companies were used to engage at least 700,000 temporary workers in the UK. Of those workers, at least 275,000 were engaged by umbrella companies that failed to comply with their tax obligations, and approximately £500m was lost to disguised remuneration tax avoidance schemes, almost all of which was facilitated by umbrella companies.
The previous government launched a consultation on tackling noncompliance in the umbrella company market in summer 2023. That was informed by an earlier call for evidence. The government has now published an outcome of the consultation, setting out how it intends to proceed.
It has announced that it will amend the Employment Rights Bill to bring umbrella companies within the definition of employment businesses. The government says that this will allow for the regulation of umbrella companies and bring them within the scope of the Employment Agency Standards Inspectorate’s – and subsequently the Fair Work Agency’s – remit.
The consultation had invited views on measures to address abuse of the VAT flat rate scheme and the employment allowance, and had proposed the introduction of mandatory due diligence within the labour supply chain. The government will not proceed with those measures; however, it will continue to monitor levels of abuse and may consider taking action in the future.
In the Autumn Budget 2024 the government announced that it will legislate to move the responsibility for accounting for Pay as You Earn
and National Insurance from the umbrella company to the recruitment agency, or the end client If there is no recruitment agency involved in the supply chain. The changes are expected to apply from April 2026. q
[ A CONVICTED waste offender must pay hugely increased proceeds of crime after the Environment Agency (EA) re-opened an inquiry into his finances and discovered he had undeclared assets.
On 27 February, at Lincoln Crown Court, Simon Mason of St Johns Chase in March, Cambridgeshire was ordered to pay an additional £278,492 on top of the £8,317 he paid after being sentenced in 2021.
Mason’s case was re-opened after the Environment Agency learned of changes in his financial position. It was discovered that he owned a property that he had not declared at the time of his sentencing, when only £8,317 was recovered from him because it was believed he had limited means.
Mason was originally prosecuted in the summer of 2021 for waste crime offences. He was given a suspended prison sentence for storing and burning waste illegally at
a site in Holbeach, Lincolnshire – despite repeated warnings from the Environment Agency. A number of fridges were found on the site, which are classed as hazardous waste and require specialist disposal.
At court on 27 February it was recalculated that Mr Mason benefited from his illegal waste activities by £286,809. He was given three months to pay the remainder or serve five years imprisonment, and was ordered to make a £1,500 contribution towards the Environment Agency’s costs.
Peter Stark, Environment Agency enforcement team leader, said: “Waste criminals should be aware how seriously we take their offending, including the benefit they obtain from their illegal activities. They won’t get away with concealing information or their assets, and due to the EA’s hard work, justice was served.”
During the initial investigation, Environment Agency officers visited the
Holbeach site on six occasions and told Mr Mason verbally and in writing to stop bringing waste to the site and burning it. However, on returning to the site, Environment Agency officers found more waste had been brought to the site and burned.
Waste observed at the site during the numerous visits included household waste, furniture, mattresses, clothing, paint cans, toilets, televisions and fridges. Some of the rubbish had been burned, prompting neighbours to complain about the smoke generated. Fridges are classed as hazardous waste and require specialist disposal.
The Environment Agency stated that it works to stop illegal waste activities and support legitimate business while protecting communities and nature from harm. The Environment Agency takes illegal waste activity very seriously and will not hesitate to disrupt activity and prosecute those responsible. q
[ TWO MEN WERE ARRESTED for fraud and money laundering in Greater Manchester on 12 March as part of an on-going investigation into illegal recycling of export paperwork. Officers from the Environment Agency and North West Regional Organised Crime Unit worked together to secure the arrests and custody of the suspects following an extensive investigation which found packaging export notes – used by law-abiding firms exporting waste to cover recycling costs – were unlawfully sold for £747,000.
A 45-year-old man was arrested at a property in Rusholme, while a 43-year-old man was detained in Stretford. Both have now been interviewed and released on bail, while evidence gathered by the Environment Agency during the arrests will support the next part of their investigation.
Vernon Smith, acting deputy director for environmental markets and regulation at the Environment Agency, said: “Fraud in the recycling industry is waste crime. It undercuts legitimate businesses investing in growth in the circular economy, impacting the environment we are striving to protect. The Environment Agency is determined to clamp down on it.
“Working with the North West Regional Organised Crime Unit, these arrests are a significant milestone for our extensive investigation. Our teams will now examine the evidence gathered to bring these individuals to justice and end their fraudulent activities once and for all.”
The Packaging Producer Responsibility Regulations were introduced to oblige the producers of waste packaging such as plastic, glass and cardboard to contribute towards the financial cost of recycling and disposing of the waste.
Businesses that meet the criteria are required to prove they have made a financial contribution by purchasing credits, known as Packaging Export Recovery Notes, from waste reprocessors or exporters. The credits have a monetary value which means organised criminal gangs can look to infiltrate the sector and engage in high-value fraud and money laundering. q

[ THE PUBLICATION of the government’s response to the Grenfell Inquiry report drew responses itself from a number of the professional bodies in the construction industry.
Although the inquiry’s Phase Two Report was published last September, the government’s response was published on 26 February, following the formal winding up of the inquiry on 10 February.
Speaking for the RICS, its head of professional practice Gary Strong commented: “RICS welcomes the UK Government’s statement on the Grenfell Tower Inquiry Phase 2 Report, and we look forward to continuing to support these crucial reforms going forward. A new, dedicated construction sector regulator and Chief Construction Adviser is welcome, and RICS will continue to offer its expertise to the government to support plans for the new regulator as it takes shape.
“New rules on product safety should further raise manufacturing standards, whilst new laws empowering tenants in the social housing sector will help protect some of the most vulnerable. It is reassuring that the government plans to provide updates every quarter and RICS will support the implementation of these reforms every step of the way.”
In its response the government accepted all of the inquiry’s recommendations – 49 of them in full and the other nine in principle.
Presenting the response, Deputy Prime Minister Angela Rayner said: “We must face the stark reality that the failings that led to the events on 14 June 2017 were not unique to Grenfell Tower. Thousands of people are still living in buildings with combustible cladding across the country. The impact on their lives is completely intolerable and the speed at which this has been addressed has been too slow.”
National Fire Chiefs Council chair, Mark Hardingham, said: “We strongly welcome the government’s acceptance of the Phase 2 recommendations in full, their commitment to introducing tough reforms to fix building safety, their promise to hold industry to account, and their support in fire and rescue service improvement and reform.”
RIBA’s chair of the board Jack Pringle said: “Many actions the Deputy Prime Minister outlined echo those which we have also called for, including the need to review the definition of higher-risk buildings, regular updating of Approved Document B, and appointing a Chief Construction Adviser.
“Now the work continues, we are committed to engaging across the sector and with the government to create buildings and homes that are safe and high quality for all.”
The Construction Products Association (CPA) referenced the ensuing Construction Products Reform Green Paper, published on

the same day as the government’s response and currently out for consultation.
Announcing the Green Paper, Angela Rayner said: “The inquiry’s report was clear that one very significant reason why Grenfell Tower came to be clad in combustible materials was systematic dishonesty on the part of those who made and sold the rainscreen cladding panels and insulation products.
“The government is taking action. The construction products regime must include deterrents to prevent the behaviours we saw as part of the refurbishment of Grenfell Tower. Having committed to reform in September 2024, our construction products green paper includes proposals to strengthen sanctions, penalties and liabilities against manufacturers.”
In a statement the CPA said: “The Construction Products Association therefore welcomes the government’s publishing of the Construction Products Reform Green Paper – its ambition, clarity and direction of travel for the construction products sector has been long awaited.
“As with the two independent reviews overseen by Dame Judith Hackitt and Morrell/Day, we will work with our members and wider industry to provide our full support and response during the Green Paper’s consultation. We are already pleased to note in the paper the recognition and support from government for our work in developing the Code for Construction Product Information as a positive industry initiative to raise standards in product information and marketing.” q
[GOVERNMENT PLANS to make home buying and selling easier and quicker have been welcomed by the Law Society of England and Wales.
The proposed reforms will look to modernise the conveyancing process, including increased digitalisation in order to reduce transaction delays, as well as cutting down the number of transactions falling through altogether.
Announcing the reforms on 9 February, the MHCLG said: “One of the key reasons the buying and selling process can be long and frustrating is a lack of digitalisation and join up in the sector, which is why the government is opening up key property information, ensuring this data can be shared between trusted professionals more easily, and driving forward plans for digital identity services to slash transaction times.”
The ministry estimates that so-called ‘fall throughs’ affect around one third of all transactions, costing £400m, on top of four million working days lost by conveyancers and estate agents.
Housing and Planning Minister Matthew Pennycook said: “We are streamlining the cumbersome home buying process so that it is fit for the 21st century, helping homebuyers save money, gain time and reduce stress while also cutting the number of house sales that fall through.”
Currently, information such as building control and highways information is predominantly paper-based or recorded in non-machinereadable formats. On top of that, where data is available electronically, there are not established protocols for accessing, sharing and verifying that data which leads to more delays. The new proposals will see the process fully digitalised.
Law Society vice president Mark Evans commented: “The Law Society is committed to improving the home-buying experience for consumers and others involved in the conveyancing process, including solicitors.
“It is encouraging to see that the government will invest time, money and energy into making transactions smoother for buyers and sellers and the professionals they work with.
“While not a silver bullet, because there are many other aspects of the home moving process that need improvement, digitalisation could be transformative in this work over time.
“We look forward to examining the government’s plans in detail, working with them on these reforms, and ensuring the voices of our members, who play a key role in the conveyancing process, are heard.” q
[THE Institution of Structural Engineers (IStructE) and the Institution of Civil Engineers (ICE) are managing a new competency register for their professionally qualified members to ensure the safety of higher-risk buildings (HRBs).
Professionally qualified IStructE and ICE members, who have at least five years experience following their professional registration, can now submit applications to join the register, which will be held by the Engineering Council. The institutions were granted a joint licence by the Engineering Council to manage the application process for the HRB (Structures) Register.
Yasmin Becker, CEO of IStructE, commented: “This development is an excellent example of structural and civil engineering bodies working together for the benefit of structural safety. With some 12,500 HRBs to be assessed by 2029, competent engineers are and will be in demand. We therefore welcome applicants to be tested in this specialist discipline.”
To join the register, eligible engineers will be assessed on five key competence areas – knowledge and understanding; design, development and solving engineering problems; responsibility, management and leadership; communication and interpersonal skills; and personal and professional commitment – with 21 sub-competences.
Dr Janet Young, director general of the ICE, explained: “As civil, infrastructure and structural engineers, we are committed to ethical practice. An essential part of this is putting safety at the heart of everything we do. This register is an important step to increase public transparency in how critical infrastructure is managed. We’re pleased to be working with the Engineering Council and IStructE to deliver this essential register.”
Applicants need to submit an application form, their CV and an experience report form for each of the competences, alongside a portfolio of evidence. They will then be interviewed by assessors who will submit a final report to the IStructE/ICE HRB Joint Committee for the final stage of the registration process. IStructE is managing the process for both bodies. q

By Roger Emmott, managing director of Roger Emmott Associates Ltd
[IN DISPUTES INVOLVING INDUSTRIES such as steel production, mining and metallurgical processes, expert witnesses play a vital role. Those fields are highly technical and expert insights are often key to shaping arguments, interpreting evidence and presenting complex issues clearly. However, experts are frequently brought in late, which can hinder case preparation and weaken legal strategies. Experts can provide much more support than just writing reports.
Involving an expert early in arbitration or litigation offers significant advantages. Legal teams must focus on legal arguments at the outset, but in technical disputes it is essential to integrate expert insights into foundational documents such as statements of claim, response or rebuttal.
Experts provide the technical accuracy and context needed to ensure those documents are robust. Misunderstanding technical issues early on can lead to vulnerabilities that opposing counsel may exploit later. Early involvement allows the expert to work alongside the legal team to build a strong, cohesive case from the beginning.
When experts are brought in late they often face tight deadlines to review extensive case materials and produce detailed reports. That compressed timeline increases the risk of missing critical details or failing to explore alternative perspectives that could strengthen the case.
Late involvement also limits collaboration with the legal team. Experts can provide valuable input during the early stages, such as reviewing technical evidence, identifying gaps and ensuring that arguments are based on sound technical foundations. Without that input, legal strategies may need costly revisions later.
Early integration of experts enables a more collaborative approach, ensuring that legal and technical perspectives align. Key benefits include:
• Pre-filing analysis – experts can assess technical evidence,
• highlight strengths and weaknesses, and refine arguments.
• Document review – input from experts ensures technical accuracy
• in key documents like statements of claim or response. Involving
• experts at this stage can highlight critical areas of focus. It also
• builds the case team dynamic: an area frequently overlooked.
• Anticipating counterarguments – experts help identify and address
• potential rebuttals from opposing witnesses.
• Efficient evidence gathering – experts can prioritise relevant
• technical data early, avoiding delays or disputes later.
Proactive collaboration ensures that technical evidence is clear, compelling and presented effectively to arbitrators or courts. That approach strengthens the case while saving time and resources.
Industries such as steel and mining are complex, requiring a deep understanding of technical processes, global standards and operational practices. Experts in those fields must navigate intricate details while considering broader commercial and regulatory contexts.
Early involvement allows experts to address those complexities comprehensively. For instance, in disputes over metallurgical failures or mining operations, early analysis can pinpoint root causes, assess compliance with standards and clarify contributing factors. Those insights can shape the case narrative and provide a stronger foundation for legal arguments or settlement negotiations.


In short, expert witnesses in specialised fields do more than provide technical testimony: they are critical to building strong, effective legal strategies. Early involvement allows experts to collaborate with legal teams, ensuring technical evidence is accurately represented and integrated into case preparation. Conversely, late involvement can limit an expert’s effectiveness, introducing risks that may weaken the case. In disputes involving complex industries, early expert involvement is not just beneficial – it is essential. By engaging experts at the start, legal teams can develop stronger, more cohesive cases that stand up to scrutiny and deliver fair outcomes. q
[NO LEGAL DISPUTE generates as much heat with so little light as one involving the very earth beneath our feet. When the very foundations of our lives and homes is threatened the stakes are high indeed.
It is also an issue needing a high level of expertise to resolve. That is where geotechnical engineers come in. They play a crucial role in legal cases involving soil, foundation stability and earth-related construction disputes. They may have expertise in soil mechanics, rock behaviour and structural stability, making them invaluable in determining causes of failure and supporting litigation processes.
Geotechnical engineers specialise in analysing soil, rock and groundwater conditions to ensure safe and stable infrastructure. Their knowledge extends to foundation design, slope stability, retaining walls and excavation support. In legal cases, they provide technical evaluations, forensic investigations and expert testimony.
One of the primary roles of geotechnical engineers in legal disputes is to conduct forensic investigations. In cases involving construction failures, landslides or structural collapses they identify root causes by
analysing soil samples for composition, strength and moisture content.
They also evaluate site conditions, drainage patterns and previous geological studies to determine if soil conditions were adequately considered in the project's design. For example, in a case where a building's foundation cracks, a geotechnical engineer may conclude that poor soil preparation, inadequate compaction, or water infiltration was the primary cause.
Geotechnical engineers are frequently called upon to provide expert testimony. In that role they translate complex engineering principles into clear language for judges and juries. Their testimony often involves explaining technical aspects of soil mechanics, presenting findings from forensic investigations and reconstructing the sequence of events that led to a structural failure. That testimony is crucial in informing court decisions, particularly when liability or negligence is in question.
Geotechnical engineers are also involved in mediation and consultation. By offering impartial technical advice, they help resolve disputes without the need for costly litigation. Their insights can guide settlement negotiations by establishing technical facts that support or

challenge claims made by either party.
To carry out their investigations, they rely on specialised techniques and tools. Soil sampling and laboratory testing provide critical data on soil density, moisture levels and shear strength. Ground penetrating radar is used to identify subsurface anomalies without excavation. Engineers also use slope stability analysis software to simulate soil behaviour and predict potential failures. Finite element analysis is another essential tool, used to model stress distribution in foundations and retaining structures.
In short, geotechnical engineers are indispensable in legal cases involving soil, foundation and structural disputes. Their expertise provides essential insights for legal professionals and clients. By clarifying the technical causes behind construction issues, they play a pivotal role in achieving fair and informed outcomes in legal proceedings. q

[A PROPERTY DEVELOPER lost a legal case for £7.5m of damages against two engineering firms whose ground investigations failed to identify a high risk of ground dissolution beneath a proposed development site near Reading.
The company, Darcliffe Homes Ltd, claimed the damages in the Technology and Construction Court from engineering firms Glanville and Ground and Water Ltd (GWL) for their ‘erroneous advice’ provided by geoenvironmental surveys and site investigations at the site.
Darcliffe had alleged that Glanville and GWL failed to disclose in their reports that the proposed development site was at high risk of ground dissolution due to the presence of chalk beneath it. As a result, Darcliffe had to pay substantial remediation costs when constructing the development.
However, a High Court judge ruled that the erroneous findings of the investigations had little impact on the property developer’s decision to purchase and develop the site, and therefore dismissed the claim.
The trial was heard in the High Court in October 2024, with closing submissions delivered on 22 November. The proceedings were against Glanville only, as Darcliffe had settled all their claims against GWL before the trial began.
Discussing the outcome in a post in February, Iain Drummond and
Alejandro Coghill from law firm Shepherd and Wedderburn commented: “Glanville did not need to do much more in order not to be held negligent. The court was persuaded by expert evidence that all Glanville had to do to avoid breach of its duties was provide a ‘single simple warning about the potential for deep weathering and chalk dissolution’.
“Importantly, Glanville did not suggest there was no risk at all; Glanville had indicated that the site’s geology was at a ‘low risk’ of ground dissolution, which the expert cited by Darcliffe accepted was ‘probably correct’. The court noted this was potentially within the realm of non-negligent advice.”
Crucially, the judge ruled that Darcliffe would not have acted differently if it had been given non-negligent advice.
The lessons to be learned from the case, the team from Shepherd and Wedderburn concluded, are: “Depending on the facts of the case, a desktop ground investigation may not give rise to liability where the ground conditions are not as stated. This is particularly so where there is little evidence of reliance on the investigation report; and the desktop analysis precedes intrusive investigations.
“For a claimant to recover loss in respect of negligent advice in a report, there must be evidence that the claimant relied on the report and would have acted differently had the report been non-negligent.” q
[ THE British Geological Survey (BGS) has published a new dataset mapping the areas of Great Britain most susceptible to groundwater flooding.
According to the BGS, groundwater flooding occurs when the water table rises to meet the ground surface. The hazard often goes unnoticed because it commonly occurs alongside river and surface water flooding.
“Without dramatic images of burst river banks or breached sea defences, groundwater flooding rarely makes the headlines,” said the BGS, “yet in England and Wales it is estimated that groundwater flooding accounts for on average £530m in damage per year. This represents 30% of the total national annual economic loss due to flooding.

“Generally, the water table response to rainfall is much slower than rivers. Persistent rainfall over weeks and months can raise groundwater levels to a tipping point, where even a short period of low-intensity rainfall can unexpectedly trigger a flooding event. The mechanics of groundwater flooding also result in flood water lingering for longer than other forms of flooding as the water table slowly recedes, causing an estimated 2.5 times greater damage than that incurred from other flood types.”
The BGS Groundwater Flooding Susceptibility dataset highlights which areas of England, Scotland and Wales are most susceptible to groundwater flooding, based on geological and hydrogeological conditions at a 50m resolution. Models of groundwater flooding originating from both superficial and bedrock aquifers are combined creating zones of susceptibility which are classified as:
• The potential for groundwater flooding to occur at surface
• The potential for groundwater flooding of property situated below ground
• level (basements, etc)
• Limited potential for groundwater flooding to occur
A complementary dataset providing a measure of confidence in the susceptibility classification (based on the hydrogeological setting) is included, which considers the groundwater flooding mechanism, susceptibility class and locations of previous groundwater flooding. The
data is recommended as a screening tool for scoping and planning rather than for site-specific risk assessments.
Many home insurance providers do not provide cover for the effects of groundwater flooding and ensuring awareness of an area’s susceptibility to the hazard is an essential component of any property conveyancing report. q

[AN INSPECTION PROGRAMME by Britain’s workplace regulator has led to major safety improvements in the offshore industry. The Health and Safety Executive (HSE) inspected 13 production operators between January 2022 and May 2024 as part of its Process Safety Leadership Principles (PSLP) programme.
In addition to their inspections, HSE inspectors were also engaging with senior leaders at offshore firms and industry groups as they determined how PSLP was being embedded across the United Kingdom Continental Shelf.
The programme was launched by HSE after it noted a stagnating safety record in the offshore industry. A report on the PSLP programme was published on 6 February.
Samantha Peace, director of the energy division at HSE, said: “One of the main successes from our PSLP programme is that offshore companies are now engaging with one another on an unprecedented level. We found that firms were looking at themselves, identifying areas of improvement, engaging with other companies and, above all, finding solutions.”
That has led to developments in process safety leadership, major accident hazard (MAH) management and performance, workforce
engagement and utilisation of their Elected Safety Representatives.
While there were successes from the programme, HSE found cumulative risk continues to be a challenge among offshore companies, with the regulator also noting that the industry is prepared to accept a greater degradation of MAH barriers, rather than fixing them.
The programme also identified that a reduction in headcount has consequently led to a decrease in skills, knowledge and competency in the industry.
“Although the programme has now finished, we will continue to challenge industry,” Samantha Peace added. “We will continue to question companies on how they are implementing PSLP and whether they are still collaborating with other firms on the same level we witnessed during the programme.
“We will also focus on the challenges we have identified in the industry, such as risk management and risk tolerance. It is not just down to HSE to develop safety standards in these areas, however; companies will need to drive their own self-improvement. The PSLP programme shows that this can be done through collaboration, engagement and application – industry now needs to continue along this path.” q
[NEW TECHNOLOGIES to improve and speed up well plugging and abandonment (P&A) are crucial to cementing the UK’s position as worldleader in cost-effective decommissioning.
That’s why UK and international operators and supply chain companies convened at an event in Aberdeen in January to hear how smart decommissioning technologies have been piloted and rolled out in the United Kingdom Continental Shelf (UKCS) in recent years, helping the sector build its reputation for innovation and cost-efficiency. However, despite progress, many more are waiting for all-important field trials.
More than 20 technology providers were on display at the showcase event at Aberdeen’s Union Kirk, which was attended by around 20 international operators and organised by the North Sea Transition Authority (NSTA) and the Net Zero Technology Centre.
The event aimed to raise awareness of the technologies and encourage operators to facilitate more field trials every year. Technologies included alternative materials with the potential to create barriers in the well, such as resins, polymers and bismuth, and logging and perforating tools designed to make the P&A process more efficient.
Around 1,500 wells will be due for decommissioning in the UKCS between 2026 and 2030: a golden opportunity to test innovative well P&A technologies, demonstrating how they can save operators time and money.
Well P&A is the most expensive stage of the decommissioning process, and there is significant scope for further cost reductions. Delivering savings also benefits the UK by lowering the cost of tax reliefs to the Exchequer. Furthermore, innovative technologies have an important role to play
in ensuring operators comply with their regulatory obligation to fully decommission wells which have permanently ceased production within set timeframes.
In addition to highlighting useful solutions through events and its Technology Insights Reports, the NSTA is using data, guidance and regulatory levers, including disputes and sanctions powers, to improve compliance with well abandonment deadlines. q


[
OFFSHORE ENERGIES UK has underlined that a robust process for Environmental Impact Assessments must be delivered at pace for two proposed new oil and gas fields. The statement was in response to the decision in the Court of Session in Edinburgh that new permissions must be sought for the Rosebank oil and Jackdaw gas fields.
The judge ruled that the two North Sea projects can continue development works while the arrangements for a revised environmental impact assessment are completed; however, production from the fields cannot begin until revised environmental consents are in place for each project.
The UK Government is looking to finalise its guidance on environmental impact assessments, following the Finch Ruling last summer, which requires so-called ‘downstream’ emissions to be taken into account.
Organisations on both sides of the dispute over the fields announced themselves pleased with the ruling for different reasons. Environmental campaigners from Greenpeace and Uplift, which brought the action, argued it should lead to a refusal of consent, while industry bodies welcomed the fact that development could continue.
Offshore Energies UK (OEUK) pointed out that the UK offshore oil and gas industry was one of the first sectors to make a commitment to net zero by 2050 and remains committed to that goal. It has already reduced production emissions by 28% since 2018 and is on track to deliver reductions of 50% by 2030.
Commenting on the decision, OEUK chief executive David Whitehouse said: “Today the court has confirmed that these projects can now move forward according to due process. Development work can continue; however, production from these fields will not begin until revised environmental consents are in place for each project.
“The revised environmental impact assessment process which manages these consents must be robust and must be delivered at pace.
“Our domestic oil and gas remain a strategic asset for the UK. Industry takes its environmental responsibilities and the goal of net zero seriously which is why we need a robust process which provides clarity to investors, enables timely and predictable decisions and provides certainty.
“We still have significant oil and gas reserves in our offshore waters and we should use them responsibly alongside renewable energy. Unlocking an additional four billion barrels adds over £200bn to our economy, supports our jobs and supports our world-class supply chain with lower emissions than imports.
“If we do not produce it here in the North Sea, we will simply import it –paying less tax to the Treasury and creating a higher carbon footprint.
“As a society we are in a critical period for shaping the future of the North Sea, the UK’s energy system, the future of those working in the sector, the communities that depend on those jobs and the wider UK economy. We must get this right.” q
[A BID TO REVERSE Coalition Government legislation which led to increased complexity and uncertainty in workplace injury claims has been launched by a Scottish MP. Dundee Central’s Chris Law MP has tabled an amendment to the Employment Rights Bill to repeal Section 69 of the Enterprise and Regulatory Reform Act 2013.
“Until the 2013 Act, injured workers had the statutory right to claim compensation if their employers had breached health and safety regulations. But Section 69 of the Act took this route to compensation away,” explained Gordon Dalyell, treasurer of the Association of Personal Injury Lawyers (APIL).
“Injured workers must now rely almost exclusively on the common law instead, which means they have to demonstrate that negligence has taken place. This is especially challenging in the workplace, where employers always have the upper hand. They control the workplace, the equipment, the systems, and hold all the information,” he went on.
APIL opposed Section 69 in the strongest terms at the time and has briefed Mr Law on the issues. “Recent judicial decisions have highlighted the increased complexity in some employers’ liability cases and the increasing uncertainty for people who suffer injuries at work since Section 69 came into effect. There is a real concern that many people who suffer harm in the workplace may not be getting as far as establishing a claim,” Gordon Dalyell explained, adding: “Mr Law’s amendment to repeal Section 69 is a chance to right a wrong.”
APIL analysis of data from the Compensation Recovery Unit and the Health and Safety Executive found that between 2018 and 2024 there was a 16% increase in the number of workers with injuries which required more than seven days absence, or who became ill because of their work. In the same timeframe, employers’ liability compensation claims plummeted by 50%. q
[CCTV HAS BEEN issued of the moment a welder was crushed while working at a shipyard in Sunderland. David Vinsome sustained multiple rib fractures as well as internal injuries, including an abdominal wall burst, following the incident at Pallion Shipyard on 18 Oct 2022.
The 37-year-old from North Shields was crushed between an excavation bucket and a fabrication table. Following an investigation by the Health and Safety Executive, Midland Steel Traders Ltd has been fined £100,000.
At the time of the incident welders had been using an overhead gantry crane and a fork lift truck in tandem to rotate a large excavator bucket. David Vinsome was crushed as he attempted to attach the chains from the overhead crane to the bucket, and a fork lift truck started the lifting operation, unaware of his position behind it.
In a victim statement, the father-of-one, recalls how he spent nine days in hospital, before returning home. “When I did come home, I was in bed for about a month before I tried to get down the stairs,” he said. “My partner is a NHS nurse, so she helped a lot.
“I am still suffering a lot of pain with my shoulder. I have a daughter and I cannot do the school run anymore or take her out for meals or ice cream. I am worried about getting back to work. I don’t know when that will be or how I will manage. I don’t think I will go back to welding.”
Midland Steel Traders Ltd of Portobello Ind Est, Chester le Street pleaded guilty to breaching Sections 2(1) and 3(1) of the Health and Safety at Work etc. Act 1974. The company was fined £100,000 and told to pay £4,916 costs at Newcastle Magistrates Court on 13 Feb 2025. q

[A CENTRALLY CO-ORDINATED programme is urgently needed to address barriers to remediating unsafe buildings, the National Fire Chiefs Council (NFCC) has said.
Writing on the publication of a new Industry White Paper on Remediation on 24 February, NFCC said that, despite progress being made, there are longstanding challenges yet to be addressed. The paper sets out some of the barriers to meeting the government’s targets – including significant difficulties in identifying and inspecting affected buildings and tackling workforce shortages.
Fire chiefs are also calling on the government to step up efforts to manage the risk for those currently living in affected buildings, by increasing the use of sprinklers in existing residential buildings over 11 metres, based on risk assessment.
Since the Grenfell Tower fire in 2017, fire and rescue services have played a crucial role in identifying unsafe buildings, supporting enforcement and ensuring the immediate safety of residents. But NFCC says that fire and rescue services are under pressure to balance that work against other key priorities – including protecting people in other high-risk buildings, such as care homes and hospitals – while having to manage increasing funding pressures, workforce shortages and increased costs.
The government published its Remediation Acceleration Plan in December, committing to completing remediation of all buildings over 18m in height within government-funded initiatives by the end of 2029. For buildings over 11m with safety defects, remediation is intended to be complete or have a clear timeline for completion by the end of 2029. The Ministry of Housing, Communities and Local Government estimates that up to 12,000 buildings over 11 metres need to be remediated, with 60% of affected buildings still to be identified.
Fire and rescue services already face many pressures due to their evolving role in protecting communities, including the increasing frequency of extreme weather events, alongside on-going inflationary pressures. Most will have their funding cut in cash terms under next year’s local government financial settlement.
However, NFCC says that, even with more funding in place, hitting remediation targets would be hindered by significant workforce challenges in the construction and fire safety sectors. Training fire engineers takes three to five years, with many leaving the public sector for better-paid private sector roles and the limited pool of professionals causing wage inflation. Slow progress in improving competency and capacity across fire
engineering and fire risk assessment is also being compounded by a decline in STEM skills and an aging construction workforce. NFCC is urging the government to establish a crossdepartmental Construction Skills Strategy to address chronic shortages in fire engineers, fire risk assessors and other key professionals.
The paper also calls for the government to deliver on recommendations from the Grenfell Tower Inquiry Phase 2 report regarding occupational regulation and competency, and in relation to the building regulations guidance, not facilitating compliance with the Building Regulations 2010.
NFCC chair, Mark Hardingham, said: “The Grenfell Tower fire was a national tragedy; and yet, nearly eight years on, not enough progress has been made in addressing issues in the built environment. We need to put the proper processes in place now to fully identify and remove the barriers to remediation, to manage risk and ensure people are protected.
“This means a centrally co-ordinated programme, a serious plan to tackle workforce shortages and joined up strategic direction to manage other crucial priorities. Unless we get these foundations right, we risk repeating the mistakes of the past and leaving thousands of people living in unsafe buildings for many years to come.” q

[IN INDUSTRIAL SETTINGS safety is paramount, especially in environments where flammable or toxic gases are present. A robust gas detection system is an important line of defence, but it’s not the whole story. Integrating flame detection into your safety setup can create a safer and more reliable environment.
The role of gas and flame detection systems
Gas detection systems are designed to identify harmful gases in the air, whether combustible, toxic or asphyxiating. They provide early warnings, helping to enable preventive action before conditions become dangerous. However, gas detection alone doesn’t account for what happens when a gas leak ignites.
Flame detection systems complement gas detectors by identifying the presence of fire, which may occur even where gas concentration hasn’t yet reached detectable levels. Together, these systems can contribute to a more comprehensive safety net that addresses both potential and actual hazards.
Combining gas and flame detection creates a more resilient safety framework that reduces the likelihood of accidents and enables a quicker recovery in the event of an incident. This reliability is key to maintaining trust and productivity.
Despite its importance, users might hesitate to include flame detection in their safety systems due to perceived challenges such as cost, complexity, or maintenance. Users may also assume that gas detection alone is sufficient for preventing incidents, underestimating the speed at which a leak can escalate into a fire. Addressing those misconceptions and highlighting the critical role of flame detection in mitigating catastrophic events is key to overcoming reluctance and ensuring comprehensive safety solutions.
Safety in industrial environments is not about choosing between gas or flame detection: it’s about understanding the benefits of both to build a layered defence. While gas detectors prevent potential hazards by identifying leaks, flame detectors act as a safeguard when ignition occurs.
By integrating flame detection into your gas detection system, you help to ensure that your operations are protected from the full spectrum of potential hazards, safeguarding lives, assets and your reputation.
For further information visit gb.msasafety.com q

By Mark Chester, of Cedarwood
[I HAVE BEEN WORKING as a Cardiff University-accredited expert witness (CUEW) for more than a decade and it is more than 20 years since my first case. Increasingly, I am asked to comment on cases where the evidence is limited, and I need to be a detective. That includes exploring the evidence and knowing what questions to ask. Sometimes the key issues are not actually tree related!
A key element is assessing the competency and skills of other parties involved. Arboriculture is not a regulated industry, and so often individuals can be instructed as experts who lack specialist skills. In one case, where trees had been felled for power line clearance and the felling, of mainly alder, had exceeded the agreed brief, the claimant presented a claim for extensive landscaping of the affected site.
The limitation was that their ‘expert’ was a landscape contractor who was experienced in using machinery to regrade landscapes. However, plant knowledge was notably lacking, including removing stumps with a digger and planting new alder trees. A pathogen that kills alder was present on the site and an alternative tree was needed to replace the damaged trees.
In another case, where a tree had split in two, causing a road accident, the defendants, who had employed a land agent to manage the site, confidently presented their defence and the opinion of their ‘expert’. The land agent provided reassurance that they only worked with qualified specialists. The tree had been damaged in a storm and trees across the site had been surveyed. There was no case to answer. The insurance company for the claimant was reassured. However, they sought my opinion to demonstrate to the claimant that they had fully investigated.
It was soon evident to me that the ‘expert’ was not as qualified and experienced as presented by the land agent. The storm cited had not passed through the area and the absence of a formal report seemed a notable omission. Within one week of receiving the report, the defendants settled the claim.
Weather forecasts, police reports where there may have been a road traffic accident, and even the absence of evidence can be integral in appraisal the merits of a claim.
It is important, when investigating, to remain impartial, otherwise perspective can be affected. In one case, where a tree had been uprooted in a storm damaging a vehicle and the insurers of the vehicle sought to recover costs, the opinion of a local specialist was sought. Lacking training in the protocol of the expert witness, their specialist persuaded the claimants that they had a case. The specialist was convinced that the owners of the tree, a local authority, had been negligent.
My investigations showed that the local authority had a defendable

position, and that the tree specialist was lacking in training in tree risk management. The claim was settled before the expected court hearing being pursued by the claimant, with my report being significant in identifying key issues and the limitations of the specialist.
Arboriculture contains a range of specialist areas. They include tree safety, trees and planning, Tree Preservation Orders, amenity tree valuation, trees and damage to property and trees within the utility sector. I can advise on all of those. I can advise on some aspects of woodland management and forestry. Specific timber mensuration and valuation are not within my expertise. Other experts may have similar experience, but that is not always the case.
In one case, where the claimant was of the opinion that tree clearance within woodland, under a power line, had been excessive, the skills of an arboricultural expert were sought. The limitation for the claimant was that the expert they engaged had experience mainly in trees and planning. The claim was based on replacing the felled trees, using specimen trees typically planted in landscaping schemes. They were both inappropriate for the woodland setting and not suited for planting under a power line.
Sometimes, I am looking for evidence – or its absence. In one case, where a tree had been uprooted during Storm Arwen, my persistence identified the fungus that had weakened the trunk. Was it foreseeable? With care, yes.
Often, the work of the expert witness, when relating to trees, is a limited snapshot. It can be easy to draw incomplete conclusions. In one case the expert for the claimant saw a hollow by an uprooted tree, filled with water, and assumed it was a ditch; and possibly the cause of the tree being uprooted. When I visited later, I found the hollow was dry and unrelated. Sometimes, it is the absence of evidence that is key, or an incomplete appraisal. In a case where a woodland owner was facing enforcement action for the alleged felling of protected trees, I was able to identify that several of the ‘felled’ trees were actually pruned branches at the base of the tree being buried under soil. In another case, the presence of decay within the stump of the fallen tree, of a type which does not result in the host tree responding, supported the view of the landowner that failure had not been foreseeable.
Sometimes, the presence of evidence is itself evidence of insufficient attention by the tree owner. That may be the case where dead wood is retained on site even if there is a safety issue. Sometimes, the failure of the tree was foreseeable, but only if the surveyor was able to access third party land. In such scenarios, I need to remain objective.
I don’t always know the background details of a case. In one case the instructing party considered a tree failure was due to negligence by the landowner. As I walked the site, the landowner giving me the tour explained how they had a tree management programme. I mentioned in passing that the evidence for the claimant seemed limited. The landowner observed that two other expert witnesses, instructed by other parties, had reached the same conclusion.
Usually I visit a site unaccompanied or guided by the landowner. It is unusual for a legal guide to be present; however, for one claim the instructing solicitor was present. A boundary hedge had been damaged and we were trying to determine the cause of the damage. Chemical damage was one possible cause. I was not convinced. The solicitor had concluded otherwise, and informed me that if I was unwilling or unable to state that in my report, another expert would be appointed who was more amenable. The claimant then identified mechanical damage as a possible cause. The evidence supported that and I was able to proceed with my report, reputation intact!
As an expert, I need to know what evidence I am looking for, and where to find it. Absence of evidence may be integral to a claim. The mindset of being ‘The Tree Detective’ is important in my work. q
[THE ISSUE OF CLIMATE CHANGE impinges on all aspects of modern life. Dealing with its effects, and our attempts to reverse it, inform government policy and decisions at all levels.
Similarly, the effects of climate change are becoming an increasingly significant factor in legal disputes – particularly when apportioning responsibility for damage caused. Whether bringing or defending a claim, engaging a climate change expert witness can be crucial to achieving a fair and equitable outcome.
Scientific credibility is a key reason to instruct such an expert. Climate science is complex, and courts rely on expert testimony to interpret data and explain the links between human activity, environmental policies and climate-related impacts. A well-qualified expert can present clear, authoritative evidence, ensuring arguments are based on facts rather than conjecture.

Another area where the analysis of an expert witness is invaluable is that of legal and regulatory compliance. There have been many cases involving allegations that businesses or public bodies have failed to meet their environmental obligations – whether that be emissions standards or sustainability commitments. An expert witness can assess compliance and provide testimony on whether legal responsibilities have been upheld or breached.
Causation and liability are often central to climate-related disputes. When events such as flooding, wildfires or coastal erosion occur, expert evidence
in subsequent inquiries can help determine the role of climate change in those events. Establishing such connections is often key to determining whether there is any responsibility on the part of individuals or corporations – and consequently any scope for compensation claims.
In insurance disputes climate experts assess the extent to which climate change has contributed to damage affecting property or business operations. Their analysis ensures claims are grounded in sound scientific evaluation, benefiting both insurers and claimants.
Beyond individual cases, climate change expert witnesses are frequently called upon in public interest and policy disputes. As governments and corporations face increasing scrutiny over their environmental impact, expert testimony can influence legal precedents and shape future regulations.
In the UK, the government’s commitment to net-zero by 2050 to help reverse climate change has led to a reliance on renewable energy sources. The multitude of planning inquiries that have resulted have emphasised the importance of expert evidence in balancing local and global priorities.
Given the growing role of climate change in legal proceedings, instructing a knowledgeable expert witness provides the scientific foundation and credibility needed to enable the courts to come to their decision. Their insights can be pivotal in proving claims, refuting allegations or shaping policy decisions with far-reaching consequences. q


RSK Raw and Ecologia are two of the leading companies supplying environmental consultancy, remediation and spill response services to the UK insurance industry. Both are part of RSK Group and they have come together to explain the need for speed when dealing with environmental claims.
[ENVIRONMENTAL CLAIMS may not be the most common reason for a policyholder to pick up the phone to their insurer; however, when they do arise, they can be far more complex than other claims to manage. If not handled effectively, an environmental claim may become protracted and costly, and can easily leave the customer feeling let down.
Many environmental claims result from leaks and spills of liquids – most typically heating oil or agricultural slurries. Part of the difficulty in managing such a claim is that there may be many stakeholders involved, including the regulators and the professionals supporting the claim within an insurer’s supply chain. Even a modest spill can significantly impact human health, building structures, contents, third-party receptors and, of course, our wider environment.
The speed of response, the appointment of experienced and technically competent consultants and contractors, and effective, informed decision-making are key to reducing the lifecycle of claims and the subsequent collective impact on the environment, consumer duty and costs.
experts on the ground quickly
Environmental claims often involve pollution events, hazardous material spills or other incidents with potential to harm the environment, building structures and human health. Delayed action in the initial stages of
an incident will have a significant impact on eventual claim quantum. Looked at another way, dealing effectively with a spill at the outset will achieve the greatest degree of cost and time mitigation for the smallest financial outlay.
Appointment of an ISAS-accredited contractor at the first notification of loss, even before policy cover is fully established, is likely to benefit all parties by:
• Containing the spill or pollution, thus
• mitigating against further damage
• Preventing the contamination spreading
• to impact third parties, such as into
• groundwater or onto neighbouring
• properties
• Limiting harm to wildlife and natural
• resources
• Ensuring that claimants feel supported
• during high-stress situations, thus
• establishing a positive relationship with
• 0the insured and fulfilling consumer duty Obviously, an insurer or claims professional needs time to ensure that the costs and scope of any proposed works are appropriate. However, we have seen cases where extended decision-making, or breakdown in communications, have resulted in hugely, and unnecessarily, increased spend.
It’s not all about oil Leaks and spills of heating oil (kerosene)
and other fuels are the most frequent type of incident resulting in an environmental claim in the UK, and they can be particularly devastating in a domestic property. However, the need for speed is just as critical in relation to commercial and agricultural claims.
Farm slurries, or even apparently innocuous substances such as milk, can have a devastating impact on water quality and aquatic ecology if released into rivers, streams or groundwater. Dissolved oxygen concentrations can deplete rapidly, resulting in significant environmental damage and, potentially, fish kills on a huge scale. Urgent oxygenation of the water can be expensive to deploy, but can save thousands of pounds in regulatory fines and fish restocking costs.
Prompt decision-making and experienced site assessment is crucial in the initial stage of incidents to contain the situation, avoid escalation and provide reassurance to policyholders and affected third parties.
Following emergency works, a competent, experienced response contractor can then work with insurers and policyholders to plan and undertake further remedial works proportionate to risks, and to minimise disruption, alternative accommodation and business interruption costs.
In short, the benefits of experience, prompt informed decision-making, and the right ‘team’ to manage a claim are widespread, varied and key to controlling costs. q
[A SUCCESSFUL DAY of action against waste crime led to vehicle seizures and prevented illegal waste dumping across Lincolnshire. Operation Clean Sweep took place on 6 March, with roadside inspections in Boston and site visits in Skegness conducted by the Lincolnshire Environmental Crime Partnership.
The multi-agency operation was led by the Environment Agency and involved Lincolnshire Police, British Transport Police, Boston Borough Council, East Lindsey District Council and the Driver and Vehicle Standards Agency (DVSA) working together to detect and disrupt illegal waste activities.

In Boston a number of teams conducted roadside stops and inspections of vehicles capable of carrying waste, with 25 vehicles inspected in total. Of the six vehicles found carrying waste, five were doing so unlawfully. Some had no explanation for their final destination, while two were carrying hazardous waste insecurely.
Boston Borough Council issued six £300 fines for waste offences and six notices to produce documents. Lincolnshire Police issued seven fines, 19 traffic offence reports, one summons and one
caution. The DVSA issued 11 prohibition notices preventing onward journeys. At the same time, two waste sites were visited in Skegness. One site was found breaching scrap metal legislation designed to prevent metal theft, while the other was identified as an illegal waste site.
Stuart Hoyle, an Environment Agency waste crime specialist, said: “Large scale waste crime and fly-tipping can only happen through the use of vehicles, which is why operations such as Clean Sweep are vital for tackling waste crime. Last week’s operation uncovered crime, prevented offences and gathered a wealth of intelligence to aid future investigations.”
Callum Butler, environmental portfolio holder at Boston Borough Council, said: “Tackling waste crime is a priority for our borough, and Operation Clean Sweep demonstrates the power of partnership working in keeping our community clean and safe. By bringing together multiple agencies, we can identify and disrupt those who fail to dispose of waste responsibly, ensuring that those who follow the rules are protected.” q
[IN A WORLD where the legal industry needs fast, accurate translations, Translate Hive has emerged as a leading solution. By leveraging cutting-edge artificial intelligence (AI) to streamline workflows and combining it with the expertise of NRPSI-qualified human translators, Translate Hive ensures precision, cultural accuracy and efficiency in every project.
That unique approach makes it easy for clients to access reliable translations while maintaining the nuances that automated systems often miss.
The best of both worlds: AI and human expertise
Many translation services rely solely on machine translation, which can often produce awkward or incorrect phrasing. Conversely, human-only translation can be time consuming and costly. Translate Hive bridges that gap by integrating AI-driven automation with skilled linguists, ensuring speed without compromising on quality.
Translate Hive employs artificial intelligence to optimise the translation workflow. That includes:
Automated file handling: AI analyses and organises content before human translators begin their work, ensuring they focus on translation rather than administrative tasks.
Pre-translation assistance: The system pre-translates simple and repetitive content, allowing human translators to refine and enhance the text rather than starting from scratch.
Smart terminology management: AI detects industry-specific terminology and ensures consistency across large projects by offering translation memory and glossaries.
Project allocation: The platform automatically assigns tasks to translators with the most relevant expertise in the target language, ensuring efficiency and accuracy.
Quality control checks: AI tools flag potential errors in grammar, terminology or formatting before final human review – reducing revisions and improving turnaround time.
These AI-driven efficiencies help Translate Hive complete projects faster, while human expertise ensures that every translation is contextually accurate and natural.
The role of human translators
While AI accelerates the process, Translate Hive recognises that true linguistic quality comes from human intuition and cultural understanding. Expert witness translators ensure that:
Context and nuance are preserved: Idioms, colloquialisms and cultural references are accurately translated.
Technical accuracy is maintained: In specialised industries such as legal, medical and technical fields, human experts ensure precise terminology.
Final reviews ensure perfection: Human linguists conduct thorough proofreading and editing to guarantee fluency and coherence.
By balancing AI-driven efficiencies with human expertise, Translate Hive provides translations that are not only fast but also of the highest quality.
One of Translate Hive’s biggest strengths is its seamless user experience. The platform is designed for ease of use, whether for an individual, a small business or a large corporation. Here’s how simple it is to get started:
Upload your content: Clients can upload text, documents or multimedia files directly onto the platform.

Select language and specialism: Choose the target language and specify any industry-specific requirements.
AI prepares the translation: The AI-driven system processes the text, pre-translating standard phrases and structuring the document.
Human experts refine and perfect: Professional translators review, edit and ensure the text maintains its original intent and readability.
Quality assurance checks: AI tools and human proofreaders perform a final check before delivery.
Receive your completed translation: Clients receive their completed translation in the desired format, ready for immediate use.
This streamlined workflow ensures a hassle-free experience while guaranteeing accurate, high-quality translations.
Translate Hive also offers professional interpretation services, blending AI-assisted scheduling and human interpreters for real-time communication. Whether for court, legal proceedings or medical consultations, clients can easily book interpreters through the platform. AI optimises scheduling and matches interpreters based on expertise, ensuring a seamless and efficient process.
Translate Hive is trusted by businesses worldwide for its commitment to:
Accuracy: Combining AI precision with human expertise ensures exceptional translations.
Speed: AI-powered automation reduces turnround time without sacrificing quality.
Consistency: Translation memory and terminology management maintain uniformity across documents.
Ease of use: The intuitive platform simplifies the process for businesses of all sizes.
By using AI to streamline workflow while maintaining human oversight, Translate Hive offers a translation service that is not only effective but also incredibly easy to use. Whether for legal contracts, marketing materials, technical manuals or live interpretation, Translate Hive delivers a seamless solution for all translation needs. q
[IT SOUNDS LIKE something from an Agatha Christies novel: the will, leaving the deceased’s entire fortune, was a forgery. The signature had been forged by the person who stood to inherit. How could our intrepid detective tell?
In reality, such determinations are the everyday work of the forensic handwriting expert. They are the diligent examiners who use meticulous analysis to provide evidence in the many cases that come to court dealing with disputed documents. Aside from the obvious disputed will cited above, they may comprise disputed commercial contracts, marriage certificates, birth certificates or documents pertaining to divorce settlements.
There are also celebrated cases where extensive documents such as whole diaries have been proved to be forgeries. The most famous case was the fiasco of the so-called Hitler Diaries: 60 volumes purporting to be the journals of Adolf Hitler purchased for £2m by German news magazine Stern, which then sold circulation rights to numerous other publications including the Sunday Times. In fact the diaries were the work of forger Konrad Kujau, as forensic analysis proved.
Even the recently concluded police investigation into the Scottish National Party, Operation Branchform, contained allegations of signature forgery on financial documents.
The US-based Expert Institute describes the discipline of forensic handwriting analysis thus: “Forensic handwriting analysis is based on the premise that no two individuals have identical handwriting. Each person will produce letters of slightly different shapes, making different grooves, indentations and other identifying features as they do.
“Handwriting expert witnesses apply pattern-based scientific principles
to their work, analysing letter formations, line quality, alignment of letters, and the spacing and placement of writing. They also compare handwriting samples to determine whether the two came from the same source.
“Handwriting experts typically express their results on a nine-point scale developed by experts within the field. The scale ranges from ‘Identification’, a definite positive conclusion, to ‘Elimination’, a definite negative conclusion. Most results fall somewhere within these extremes.”
British expert Kathryn Thorndeycraft-Pope uses latest technology for her work, in the form of a palm-held microscope.
A darker side of life that has light shed on it by handwriting experts is the identifying of anonymous communications such as poison pen letters and other threats. Even the perpetrators of graffiti can be identified.
All this is a world away from the popular perception of the perceptive sleuth noticing the irregular slant of the ‘t’ in the will. q
[FORENSIC HANDWRITING ANALYSIS should not be confused with graphology – a method of deriving a person’s personality and other traits from analysing their handwriting.
The British Institute of Graphology describes the practice thus: “Graphology analyses the patterns and strokes of handwriting to uncover hidden personality traits and gain insights into how someone thinks, feels and behaves. The way we write can reveal a great deal about us, sometimes more than we’d like others to know. This is because handwriting is as uniquely personal as our fingerprints and DNA.”
According to Britannica: “The theory underlying graphology is that handwriting is an expression of personality; hence, a systematic analysis of the way words and letters are formed can reveal traits of personality.” It also cautions: “In general, the scientific basis for graphological interpretations of personality is questionable.”
Despite the absence of any scientific evidence that graphology has any accuracy – The British Psychological Society ranks it alongside astrology with a ‘zero validity’ rating – a number of businesses and other organisations use the technique to evaluate candidates for senior positions. Graphologists will also advise on compatibility, child development and even offer to interpret doodles. q




















CRIMINOLOGY

DIGITAL TECHNOLOGY

EMPLOYMENT

ENERGY CONSULTANTS


ENGINEERS












TRANSLATING & INTERPRETING






Translations and Interpreting for the Legal Profession since 1997. Specialists in Personal Injury and Clinical Negligence. www.abc-translations.co.uk
Andrew F Acquier BA FRICS
Chartered Art & Antiques Surveyor
Expert witness reports and representation at court for matters involving: • Divorce settlements • Insurance valuation disputes
• Arts litigation • Contentious Probate
www.andrewacquier.co.uk
David Berry PhD FRC Path MFSSoc MRSC
Independent Toxicology Consultant Specialist in Clinical and Forensic Toxicology with particular emphasis on drugs (both illicit and therapeutic) and alcohol. www.toxicologyservices.co.uk
Professor Paul J Ciclitira MB PhD FRCP MRCS FRCP AGAF
Professor of Gastroenterology with particular interest in food allergy, including Coeliac disease, peptic ulcer, inflammatory bowel disorder and hepatology. www.profpaulciclitira.co.uk
Dr Sarah Cockbill Expert Pharmaceutical Witness PhD BPharm MPharm LLM DAgVetPharm FRPharmS FVPA
• Pharmacology • Drug Interactions • Formulation
• Appropriate Dosage • Veterinary Pharmacy • Drug Licensing Instructions for claimant, defendant or as Single Joint Expert
E: cockbills1@gmail.com
Mr Philip Coleridge Smith DM MA BCh FRCS
Consultant Vascular Surgeon 20 years of:
• Defendant instructions • Claimant instructions
• Single joint expert • Court experience





www.adsummedicolegal.com & www.britishveininstitute.com
Clarke Gammon
Chartered Surveyors with experience in All Aspects of Property • Residential property values
Chris Dawson MS FRCS LLDip
Mr Roger Emmott CEng BSc(Hons) MSc/MBA MA FCMI FIC
Steel and iron ore expert with international arbitration and cross-examination experience in complex disputes
• Industry • Pricing • Contractual • Valuations
T: 07974 351704 E: roger@rogeremmottassociates.com www.rogeremmottassociates.com
Equip2Speak
Specialists in Brain and Spinal Injury. SLT & AT Consultants
• CUBS Certified Experts since 2012/2013 • Accident, Negligence and Criminal Cases • Experienced in High Value Claims
• Claimant/Defendant/Joint Instruction
www.equip2speak.co.uk
Face Restoration
• Complications of cosmetic eyelid surgery
• Brow lift surgery • Ptosis • Non-surgical aesthetics
• Orbital diseases • Watery eyes • Thyroid eye disease www.facerestoration.com
FHDI - Kathryn Thorndycraft-Pope





Examining documents & handwriting • to determine authenticity • to expose forgery • to reveal aspects of origin. Electro Static Detection Apparatus and Mi-Scope used. www.forensichandwriting.co.uk
Forensic Collision Investigation & Reconstruction Ltd
Specialists in the analysis of road traffic collisions
• Collision Reconstruction • Expert Witness
• Vehicle Examinations www.FCIR.co.uk
Formedecon Ltd
Forensic & Investigative Services to the Legal Profession
• All Aspects of Forensic Work Undertaken
• LAA and Privately Funded • Free Estimates www.Formedecon.com


Griffin Forensics eForensics and Data Recovery Experts
• CCTV Recovery and Analysis • Computer Media
Investigations • Mobile Phone Extraction and Analysis • Forensic Data Recoveries
www.griffinforensics.com

Mr Kim Hakin FRCS FRCOphth
Consultant Ophthalmic Surgeon and Expert Witness on ophthalmological matters
• Asset valuations • Land values and more www.clarkegammon.co.uk www.chrisdawson.org.uk

Consultant Urologist with 20 years experience of medico legal report writing and expert witness work and has completed over 1,850 reports. He also regularly completes Fitness to Practice reports for the General Medical Council.
DRC Forensics Limited


DRC Forensics Limited offers the complete range of forensic accounting & litigation support: • Fraud • Money laundering
• Partnership disputes • Loss of profit • Professional negligence www.drcforensics.co.uk
Mr Mark Duxbury MA (Oxon) DM FRCSEd (Gen Surg)
Consultant Hepatobiliary, Pancreatic & General Surgeon
• General & emergency surgery • Hernia surgery
• Liver & pancreatic surgery • Gallbladder & biliary surgery
• Laparoscopic surgery • Hepatobiliary surgery www.markduxbury.info/medicolegal

www.kimhakin.com
Haydn Jones MEng DipLaw FIET
Data Technologist & Digital Regulation Expert
• Injunctive relief • Money laundering
• Digital currency theft • Counter funding of terrorism E: h.jones@xchain.com
Atul Khanna FRCS (Plast)
Consultant Plastic, Reconstructive and Hand Surgeon
• Hand surgery • Soft tissue injury • Burns management
• Medical negligence in cosmetic surgery www.atulkhanna.co.uk/expert-witness/
Dr Raj Kumar – Dental Expert
Causation and Liability and Condition and Prognosis Reports
• General dentistry • Cosmetic dentistry • Patient consent
• Dental implantology • Orthodontics • Facial aesthetics
07802 456 804 | info@dentalexpert.me | www.dentalexpert.me




Kulvinder Lall Consultant Cardiothoracic Surgeon
Instructions taken in cases relating to cardiac and thoracic surgery, including aspects relating to surgical care and those following trauma to the structures of the chest. www.kulvinderlall.com
Maggie Sargent & Associates
Internationally renowned provider of detailed and independent medical expert witness reports. We consistently provide our solicitors with meticulously prepared and highly trusted reports that put the client at the centre.
www.maggiesargent.co.uk
Mr Chris Makin
• Chartered Accountant • Accredited Civil Mediator
• Accredited Expert Determiner www.chrismakin.co.uk



Mr Richard Matthews MB BS FRCS FRCSE MAE PLASTIC & HAND SURGEON
Mr Matthews is well versed in the provision of Medical Reports relating to Personal Injury ranging from scarring through trauma, including burns and scalds, to non-bony hand injuries.
www.richardmatthewsmedicolegal.uk
Mr Fredrik P Nath FRCS MBChB
Consultant Neurosurgeon • Head injury • Spinal injury
• Acoustic neuroma • Lumbar and cervical degenerative disease • Musculo-skeletal injury including whiplash www.neurosurg.co.uk
Mr Abraham Odumala
MBBS M.MedSci FWACS FRCS FRCS(Tr & Orth)
Consultant Orthopaedic Surgeon – Upper Limb Specialist. Expertise in all upper limb conditions and treatment. Shoulder, elbow, wristand hand injuries. www.yorkshire-upperlimb.co.uk
Dr Shanthi Paramothayan
BSc PhD MBBS LLM MScMedEd FHEA FCCP FRCP
Consultant Respiratory Physician specialising in negligence cases relating to all aspects of respiratory medicine. www.paramothayan.com
Dr Stuart Porter Chartered Physiotherapist
PhD MCSP HCPC BSc Hons Grad Dip Phys MLACP PgCAP Cert.MHS SFHEA Specialist areas of expertise include: • Clinical negligence
• Breach of duty • Allegations of inappropriate contact
• Assessment of adults and children • HCPC investigations. stuartbporter@aol.com
Simon Quinton Smith BSc FRICS MI Hort
Expert Witness to the Garden Centre & Horticultural Industry
• Rent Reviews
• Lease Renewals
• Valuation • Planning • Compensation • Tax Issues
www.quintonedwards.co.uk
Professor Christopher Raine MBE
Specialist in paediatric and adult otology






Andrew Smith FPC III CeMAP
Financial Conduct Authority Compliance & Risk Consultant Cases relating to FCA compliance in consumer credit and mortgage lending.
• Mediation • Arbitration • Adjudication • Expert Determination
www.paxen.co.uk

Prof. Elizabeth J. Soilleux MA MB BChir PhD FRCPath PGDipMedEd Expert Witness Pathologist with a particular interest in haematopathology. Short reports on specimens, full court compliant reports and expert biopsy reporting. www.expertwitnesspathologist.co.uk

Dr Ian Starke MSc MD FRCP
Stroke Medicine and Medicine for the Elderly Reports and examinations for clinical negligence and fitness to practise cases in stroke medicine and geriatric medicine www.expertwitnessinstrokes.co.uk
Mr David Anthony Sykes (Tony Sykes) BSc CEng CITP MBCS MIET FAE MEWI Specialist in IT and Telecommunications. Expert witness and consultancy services to lawyers, insurers and loss adjusters. Experience in international arbitrations and the High Court TCC.
www.rocksideconsultants.co.uk
Mr. William E G Thomas Bsc, MBBS, FRCS, MS
Consultant Surgeon specialising in general surgery, hernia surgery, gastrointestinal surgery, hepatobiliary-pancreatic surgery, laparoscopic surgery and endocrine surgery
T: 0114 262 0852 E: wegthomas@btinternet.com W: www.wegthomas.com




UK Ophthalmology Experts
Dr Ravinder Varaich Dental Expert
Mr Sameer Singh MBBS BSc FRCS Orth
Consultant Orthopaedic Surgeon • All aspects of trauma – soft tissue and bone injuries • Upper and lower limb disorders and injuries
• Whiplash injuries • Expert Witness for defence and claimant Clinic locations – London, Milton Keynes and Bedford
• Medical negligence • Personal injury cases involving noise induced hearing loss. www.profchrisraine.co.uk www.orthopaedicexpertwitness.net


BDS (University of Birmingham) MFGDP (RCS Eng) MAE
> Criminal cases > Personal injury > Clinical negligence

• Restorative dentistry • Periodontal disease • Endodontics • Dentures
• Oral surgery • Orthodontics • Cosmetic dentistry • Facial aesthetics
UK Ophthalmology Experts are a team of leading, independent ophthalmology experts covering all aspects of ophthalmology. ukophthalmologyexperts.co.uk www.dentalexpertreports.co.uk
DR S V MEDICALS (Mr Sen Venkat)
MSc Ortho (London) FRCS Consultant Orthopaedic Surgeon • Whiplash injuries • General trauma • Sports injuries
• Clinical negligence work • Joint replacement surgery of hip and knee • Hand, shoulder, elbow and wrist injury www.drsvmedicals.co.uk
WOODEXPERTS
Specialist Timber Consultancy and Training since 1991
• Site visits & investigations • Structural surveys
• Desktop analysis & review of documents
• Specialist reports • Species identification
www.woodexperts.com
Ms Leyla Ziyal MPhil AFBPsS CPsychol
HCPC Registered clinical Neuropsychologist
• Neuropsychological assessment and rehabilitation
• Depression • Occupational stress • PTSD • Anxiety www.accentpsychology.co.uk





[AT FIRST SIGHT the news was a stunner: the Prime Minister had announced that the government was to abolish NHS England. The headline writers began feverishly composing obituary notices for the health service as we know it. Then, after a few seconds of reflection the panic subsided. What was being abolished was not the NHS in England; it was the quango that had been created in 2013 as an experiment in distancing the running of the NHS from the government. Does that mean the Department of Health and Social Care is now going to take responsibility for failings in the running of the NHS? We’ll have to wait and see on that one.
• The manifold organisations running things in the NHS are quite capable of mucking things up without any help from politicians. Nearly 300 doctors who took the exam for the Royal Colleges of Physicians – a federation of non-surgical royal colleges – in 2023 were given the wrong results. Of those, 222 were told they had passed when they hadn’t and, maybe even worse, 61 were told they had failed when they had passed. The idea that we were being treated by doctors who didn’t have the level of expertise they thought they had is worrying; what is more worrying is that there are doctors who may have given up and left medicine who do have the skills and had been told they don’t.
• Failures of the past are still coming home to roost. Nobody is saying that, when batches of blood were imported from the USA all those years ago, the officials in charge knew they were infected with hepatitis and HIV. The fact that in the USA blood is a commodity should have raised concerns, but it didn’t. Those affected by the subsequent transfusions and their families have to live with the consequences of that negligence. That the government should be dragging its feet in compensating them is a national disgrace.
• As the Health Secretary contemplates life in direct charge of the NHS in England and Wales there are enough contemporary issues to keep him occupied. That includes dealing with the fact that around 10 people have died from cancer who were not screened because their GP registration was not completed properly. The error affected more than 5,000 people – of whom at least a further 10 have subsequently been diagnosed with the disease.
• Diagnosis of cancer and other life-threatening conditions is also being delayed by a lack of radiologists across the country. The Royal College of Radiologists has raised ‘urgent concerns’ over what it calls freezes in recruitment in the specialism across the NHS. They apply across the English regions and in all the devolved nations. It threatens government aspirations to reform elective surgery, the college says.
• Delays in diagnosis of colorectal cancer are also coming to public attention more, as a result of the widely publicised National Bowel Screening programme. More than half of those diagnosed with colorectal cancer present with the more advanced stages of the disease, which carries a commensurately greater risk of death. As our expert contributor points out, though, there have been significant recent advances in diagnosis and treatment.
• Not all is doom and gloom, however. The much-derided AI (by none more than me!) is enabling the detection of potential heart disease in women. By analysing the ECGs of women an AI algorithm can detect those whose patterns more closely match those of men. They, it emerges, are more likely to suffer heart disease.
AI is apparently being embraced by doctors, either for routine tasks or more complex diagnostics. I thought my GP sounded a bit strange on the phone the other day. I’ve no idea what they look like: never seen ‘em. q

[
DOCTORS’ LEADERS have written to Health Secretary Wes Streeting calling on him to take ‘urgent, co-ordinated action’ after it was revealed that hundreds of doctors had been incorrectly informed about the results of their MRCP (Membership of the Royal Colleges of Physicians) examinations.
The admission of error by the Federation of the Royal Colleges of Physicians (FRCP) of the UK came after an audit revealed 283 doctors received incorrect results for their MRCP exams taken in September 2023. The errors, which the BMA has described as ‘nothing short of catastrophic’, saw 222 doctors incorrectly informed that they had passed the exam, with a further 61 doctors erroneously advised they had failed.
In a letter to Mr Streeting, sent on 21 February, BMA council chair Philip Banfield stated that, while the incident had exposed the ‘serious deficiencies’ in the processes of the FRCP’s examination system, it was ‘unacceptable’ that mistakes had taken nearly 18 months to be uncovered.
The letter, which was co-signed by deputy council chair Emma Runswick, as well as the BMA council chairs for Scotland, Wales and Northern Ireland, emphasised that the failings will have affected the careers and mental wellbeing of hundreds of doctors.
The letter read: “This news is devastating for these doctors, and urgent co-ordinated action must be taken to provide assurances, compensation and pastoral support to those affected. The consequences of these errors are far-reaching, affecting the careers and mental well-being of these doctors. Some individuals who believed they had passed may have progressed in their careers, only to now face uncertainty and potential setbacks.
“Conversely, those who were incorrectly told they failed may have had to retake the exam at significant financial and emotional cost, delayed their training, or even left medicine entirely.
“This situation has highlighted serious deficiencies in the governance and audit processes of the FRCP’s examination system. It is unacceptable that such errors have taken so long to be identified, placing doctors' careers in jeopardy and affecting the future of patient care in the NHS. Rectifying this serious error will require a co-ordinated effort from different organisations.”
The BMA has called on Mr Streeting to use his powers to implement a raft of measures to support those affected by the MRCP debacle. They include:
• Ensuring that those doctors who began training be allowed to
• continue in their jobs without fear of punitive action being taken
• against them
• Offering immediate pastoral support and mentorship to any affected
• individuals and ensuring that all associated costs are met by
• colleges, employers or the NHS
• That all doctors impacted by the examinations error be
• compensated financially including, but not limited to, reimbursement
• for exam costs, lost earnings and potential lost earnings
In addition, the BMA is calling for an independent investigation to determine how mistakes in the grading process occurred, why they took so long to be identified and what decisions were taken by the FRCP once it became aware of errors.
The doctors’ regulation body, the General Medical Council (GMC), also expressed its consternation at the errors. In a letter dated 4 March the GMC wrote to the Academy of Medical Royal Colleges. In the letter the GMC set out the actions it now expects the FRCP to take. It also asked the academy how it intends to work with all medical royal colleges and faculties to make sure such an error doesn’t happen again.
The GMC stated: “We also set out our role in setting the standards for the design and development of postgraduate curricula and assessment. And we explain how they help us to make sure that doctors have the
appropriate skills and training to deliver high-quality care.
“We now need assurance from the academy, the federation and from the wider college community. Action must be taken by those accountable to make sure candidates are not put in this position again.”
In a statement on the issue, Professor Colin Melville, medical director and director of education and standards at the GMC, said: “Doctors who have been provided with the wrong exam result following a marking error by the Federation of the Royal Colleges of Physicians of the UK are, understandably, extremely distressed. The effect of this mistake on them is devastating and will have taken a significant emotional, mental and financial toll.
“We have asked the federation to provide a full report that explains what led to the marking error and the immediate improvements it will make to ensure this does not happen again. We have asked for regular updates from the federation against their proposed actions, including how they are involving the Academy of Medical Royal Colleges in this work.
“Doctors must have confidence that royal colleges can administer exams competently, and the public must have confidence that decisions made about assessment of doctors maintain patient safety.
“We have a statutory duty to approve the assessments designed and developed by royal colleges, but this is reliant on them maintaining the required standards. It is their responsibility, as the awarding bodies, to deliver assessments and quality manage their processes.
“Adhering to our standards provides confidence for patients and the public that doctors have the appropriate skills and training to deliver the high-quality patient care they rightly deserve.” q
[THE INFECTED BLOOD INQUIRY is to publish an additional report, it has announced. Since 20 May, when the report was published, the Inquiry has been contacted by many people infected and affected from across the UK. Long-standing campaigners, as well as many concerned individuals, have expressed their concerns about the way compensation is being implemented and the time it is taking.
On 13 March additional evidence was published: witness statements which highlight many of the issues that have been raised with the Inquiry. The statements come from 27 organisations, groups and individuals, as well as the Paymaster General and Minister for the Cabinet Office Nick Thomas-Symonds, James Quinault – the director general responsible for work within the Cabinet Office on infected blood compensation – and David Foley, interim chief executive of the Infected Blood Compensation Authority (IBCA).
The evidence the Inquiry received and published on 13 March included this from David Foley: “We [IBCA] are also working within timescales as agreed with the Cabinet Office, which are to pay the first infected person by the end of 2024, to pay the first affected person by the end of 2025, to pay the bulk of infected persons by the end of 2027 and to pay the bulk of affected persons by the end of 2029.”
One of the victims, campaigner Sean Cavens, wrote: “When the Inquiry final report was published on 20 May, I felt that the Inquiry had taken the time to listen to us and that we had been vindicated. The recent actions of Government make me feel as though they have not paid attention to the criticisms made in the report, to the point where I question whether they have even read it. I feel total despair.”
His comments were echoed by Samantha May of the Hepatitis C Trust: “The impact on the community has been absolutely devastating; it has caused upset, confusion, anxiety, fear, desperation and division unlike anything we have experienced so far in the 21 years of supporting them.”
In light of the gravity of the issues that have been raised with the Inquiry, the chair, Sir Brian Langstaff, said he intends to publish a further report, which will consider the timeliness and adequacy of the government’s response on compensation. He has not yet decided whether any further hearings are required.
Sir Brian said: “The distress and feelings of powerlessness expressed in many of these statements can neither be denied nor ignored. Our goal at the Inquiry is to identify whether there are practical measures that could be taken or changes made to address the concerns that have been brought to us. Our intention is for this to be a constructive process, and we are anxious not to contribute to further delay in individuals receiving compensation.”
The report will be published in line with Paragraph 5 of the Inquiry’s Terms of Reference. To inform the further report, the Inquiry is seeking

further evidence, including from the Cabinet Office and IBCA. In due course core participants to the Inquiry will be invited to make written submissions through their recognised legal representatives – where they are represented – in accordance with the Inquiries Act and Inquiry Rules. That has been said now so that those who intend to make written submissions may begin considering them in the interest of speed, even if they cannot be completed until all the further evidence has been gathered in.
The Inquiry expects to publish further statements in April. At that time, it will also announce whether additional hearings will be held, the timeframe for providing written submissions and for the publication of its further report. q

[ THE Royal College of General Practitioners has responded to the Ministerial Statement made by Public Health Minister Ashley Dalton regarding NHS screening and GP registrations, following revelations that over 5,000 people had missed cancer screening opportunities because their GP registrations had not been processed properly.
Professor Kamila Hawthorne, chair of the Royal College of GPs, said: “As GPs, the health and wellbeing of our patients is our number one priority, so it’s distressing to hear that some people may have missed health interventions as a result of inadvertent administrative errors.
“GP practices take the management of their patient records very seriously; but if mistakes happen, it's important robust safeguards are in place to identify and rectify them, so that patients can continue to receive the care and services they need.
“Now that the issue has been identified, serious action must be taken to contact those who have been affected – and we have been reassured this has already started – and ensure that steps are taken so that something similar cannot happen again.
“National screening programmes, which are evidence-based and approved by NICE and the UK National Screening Committee, have potentially saved millions of lives so it’s important that these are accessible for all patients who are eligible.”
On 11 March, Parliamentary UnderSecretary of State for Public Health and Prevention Ashley Dalton MP, made a Written Ministerial Statement to the House of Commons, in which she said: “I would like to inform the House that yesterday the NHS wrote to around 5,261 people who have not been invited for routine screening.
“This is because their General Practice registration process was not completed correctly, meaning their details were not passed to NHS screening systems. Those affected have now been added into relevant screening programmes and work is ongoing to ensure that this does not occur in the future.”
The Minister admitted that some patients who had not been screened had contracted cancer, of which a number had died.
“Records indicate that up to 10 patients have been diagnosed with a relevant cancer and were not invited for certain screening.
“NHS England are writing to these patients this week. The impact on these patients is not yet known and a clinical harm assessment process will be undertaken, based on expert clinical advice. It is with deep sadness that I must report that records also indicate that around 10 people who were not invited for screening may have died from a relevant cancer. NHS England will take appropriate action in these circumstances, based on expert clinical advice.”
Steve Russell, NHS national director for vaccinations and screening, said: “We would like to extend our sincere apologies to those affected for this error and any additional worry this may have caused – anyone who is concerned they may have missed an invitation to screening can call our dedicated helpline for support and further information.
“Around 15 million people are invited to NHS screening every year and it is important that everyone eligible can access these lifesaving programmes. The NHS has issued guidance to GP practices and integrated care boards to make sure all patient registrations are fully completed and has put in place new measures to ensure all eligible people are invited for screening.” q
[ DESPITE HEADLINES announcing the abolition of NHS England being framed as if the world was about to end, less excitable commentators reacted with a more measured tone – pointing out it was simply a 12-year-old arms-length quango that was going, not the NHS itself. The management of NHS services will continue to be provided by local trusts and the function of NHS England will be reabsorbed into the DHSC.
Responding to the announcement, Hugh Alderwick, director of policy at the Health Foundation, said: “Abolishing NHS England is a watershed moment in how the English NHS is governed and managed – and ends a 12-year experiment with trying to manage the NHS more independently from ministers.
“There is some logic in bringing the workings of NHS England and the government more closely together – for example, to help provide clarity to the health service on priorities for improvement; and in reality it is impossible to take politics out of the NHS. But history tells us that rejigging NHS organisations is hugely distracting and rarely delivers the benefits politicians expect.
“Scrapping NHS England completely will cause disruption and divert time and energy of senior leaders at a time when attention should be focused on improving care for patients. It will also eat up the time of ministers, with new legislation likely needed.
“Expected cuts to local NHS management budgets will add to the disruption, and may undermine the NHS’s ability to implement the government’s plans for improving the NHS. Reforming NHS bureaucracy is not the same as reforming patient care – and government must be careful that these changes don’t get in the way.”
Even UNISON, the trade union that represents large numbers of staff in the NHS and describes itself as the largest healthcare union in the UK, did not condemn the decision per se – despite the fact many jobs are at risk – but rather attacked the way the announcement was made as ‘shambolic’. Prime Minister Starmer revealed the plan in a speech on reforming the state on a visit to
a pharmaceutical company in Hull, leaving Health Secretary Wes Streeting to fill in MPs in Parliament.
Christina McAnea, UNISON’s general secretary, pointed out that the NHS needs to expand its workforce, adding: “But this announcement will have left NHS England staff reeling. Just days ago they learned their numbers were to be slashed by half, now they discover their employer will cease to exist.
“The way the news of the axing has been handled is nothing short of shambolic. It could surely have been managed in a more sympathetic way. Thousands of expert staff will be left wondering what their future holds. Wherever possible, their valuable skills must be redeployed and used to the benefit of the reformed NHS and patients.”
What the changes will mean for those who have reason to seek to hold the NHS to account will no doubt become clearer in the following weeks and months. q


[DOCTORS WHO USE artificial intelligence (AI) see benefits for their own efficiency and for patient care in a resource-stretched NHS and, although they recognise there are risks, they feel confident in managing them, according to a study published by the General Medical Council (GMC).
Researchers sought to find out more about the types of AI doctors are using, how well they understand the risks and what they do if they disagree with the output of an AI system. Doctors who had used AI in the past 12 months discussed the benefits, risks and their understanding of their professional responsibilities when using such technologies, in a series of in-depth interviews with researchers from Community Research.
Most saw benefits to their efficiency when using AI – seeing it as a way to save or make more use of their time. However, some queried that, saying they lacked confidence in the accuracy of some diagnostic and decision support systems and so spent more time checking the results they received.

Many doctors felt that NHS IT systems would need to improve to pave the way for a broader roll out of AI technologies, noting that many are highly specialised and still in the development stage. Doctors who currently use generative AI, such as ChatGPT, often do so through a current interest in AI.
Researchers spoke to a variety of doctors at different career stages and across specialties, from doctors in training to consultants working in general practice, radiology, emergency medicine and more.
Three types of AI were discussed.
• Generative AI, which produces text or images following prompts
• Diagnostic and decision support systems (DDS), which aid the use
• of multimedia data; for example, by identifying the presence of
• tumour on an MRI scan. It also includes tools for supporting
• decisions, outlining risks and predicting patient outcomes.
• Systems efficiency systems (SES), which predict missed
• appointments, maximise staffing and resource allocations or
• optimise care pathways based on provided data
Doctors using generative AI often did so of their own accord, whereas those using DDS or SES did so through their workplace’s adoption of those technologies. The research found that many doctors were often unsure of which technologies constituted AI in their practice.
Those using generative AI had a keen interest in the technology and used it for a variety of reasons, including for administrative support, producing clinical scenarios and generating images for teaching.
However, doctors were careful to specify that they knew no confidential information could be inputted, instead using AI to generate templates with personal information omitted.
Doctors using DDS in primary care did so to help prioritise which patients to see, find medication conflicts in prescriptions and suggest diagnostic tests. In secondary care, some ways used included to assist in assessing stroke patients and administering local anaesthesia.
Further benefits of AI use shared by doctors included the potential to reduce risk of human error and reduce bias through judgments made on patient characteristics. They also identified the limitless capacity AI had to draw from wider research, data or guidance on a particular topic, compared to an individual.
But doctors interviewed also understood that the emergent technologies presented risks. They saw potential for AI-generated answers to be based on data that could itself be false or biased. They also acknowledged possible confidentiality risks in sharing patient data and the potential for over reliance and deskilling.
Many said they feel confident to override decisions made by AI systems if necessary, and that ultimately the responsibility of patient care remains with them. Some did speculate on whether that may change in the future as systems become more sophisticated, and looked to regulators like the GMC for more guidance going forward. q

[THE FIRST NHS PATIENTS in a generation have started to receive lifesaving plasma from the blood of UK donors, thanks to a partnership between NHS Blood and Transplant and NHS England.
Since a long-standing ban on UK plasma was lifted in 2021 the UK has been building its own supply of plasma medicines amid a global shortage. The reintroduction of the plasma will reduce reliance on imports, saving the NHS between £5m and £10m per year.
Around 17,000 NHS patients with immune deficiencies and rare diseases rely on vital human-donated plasma to save or improve their lives. It is also used in emergency medicine for childbirth and trauma care.

Health Minister Baroness Gillian Merron said: “This is a significant milestone for the NHS as we take a step towards UK self-sufficiency in these vital medicines. As part of our Plan for Change we are improving access to life-saving treatments for thousands of NHS patients and strengthening healthcare security. By sourcing our own medicine, we are
[LAST AUTUMN the Care Quality Commission (CQC) commissioned the Care Provider Alliance (CPA) to seek the views of adult social care providers on its single assessment framework, alongside the review undertaken by Professor Sir Mike Richards.
The CPA’s appraisal also raised provider concerns about assessment, registration and backlogs. The results were published in January and contained 11 recommendations.
Sir Julian Hartley, chief executive of CQC, commented “We welcome this report which has been instrumental in ensuring we hear the voices of a wide range of adult social care providers, as the findings are a robust reflection of their views and experiences.”
James Bullion, chief inspector of adult social care and integrated care, added: “This report gives us a practical agenda for change which we will incorporate into our urgent improvement work underway in CQC. Professor Vic Rayner, as chair of the CPA, met with me and my executive team colleagues and with the CQC board to discuss the findings of this report. She articulated a powerful message on behalf of providers, including in some cases the distressing impact of approaches to regulation and assessment on their organisations and mental wellbeing.
“We acknowledge too the strength of feeling from providers about the need to improve their experience of inspection. Underlying this report, but not looked at in detail, are the changes needed to improve our computer systems, portal arrangements and communications.
“CQC colleagues have themselves struggled with the challenges caused by the technology issues and rollout of the assessment framework, including the clarity of how the system worked, training, complexity of the approach and the consistency of approaches in different care sectors. CQC inspectors are skilled and dedicated to good regulation and have struggled to be effective because of these factors.”
Prior to the publication of the CPA report the CQC set the terms of reference for the second phase of the review of its assessment. That will also be conducted by Professor Sir Mike Richards with a further targeted programme of engagement with care providers led by the CPA. q
building a more resilient and domestic medical supply chain and boosting economic growth.”
Previously the NHS relied solely on imported plasma medicines due to a long-standing ban on using UK plasma. The ban was introduced in 1998 as a precautionary measure against variant Creutzfeldt–Jakob disease (vCJD), linked to mad cow disease.
In 2021, following rigorous scientific reviews, the Medicines and Healthcare Products Regulatory Agency confirmed that plasma from UK donors is safe, supported by robust safety measures. Decades of rigorous research showed no confirmed cases of vCJD transmission through plasma-derived medicines.
Sir Stephen Powis, national medical director of NHS England, added: “This landmark moment ensures patients relying on crucial plasma-derived medicines will always have access to the treatment they need. Thanks to NHS efforts, new plasma-derived products, owned from start to finish by the UK, will reduce our reliance on imported stock and boost the fortitude of hospital supplies.
“Thousands of people with serious and potentially life-threatening conditions rely on these products, and strengthening the supply chain of plasma-derived treatments through UK donations will help NHS clinicians ensure these vital medicines are available for all who need them.”
Dr Jo Farrar, chief executive of NHS Blood and Transplant, explained: “Plasma makes up 55% of our blood and contains antibodies, which strengthen or stabilise the immune system. It is used to save lives during childbirth and trauma and is used to treat thousands of patients with lifelimiting illnesses such as immune deficiencies.” q

[A NEW REVIEW has identified significant safety concerns in pleural procedures across the UK, identifying a need for better training, improved ultrasound use and clearer protocols.
The research, conducted by Dr Andrew E Stanton and colleagues, reviewed patient safety incidents from the National Reporting and Learning System between April 2018 and March 2022. Key findings from the research include:
• 21 pleural-related safety incidents were identified from 256 reports,
• including two deaths.
[NEW RESEARCH by Asthma + Lung UK shows a bleak picture of the state of respiratory care in England, because of an alarming lack of capacity for testing in local healthcare services.
Over half of the Integrated Care Systems (ICSs) in England that responded to a survey by the charity – 16 out of 27 – said they did not have enough spirometry testing capacity to meet the demand in their area, while only eight reported having enough capacity to carry out all the tests needed. That gap means hundreds of thousands of people with debilitating symptoms of chronic obstructive pulmonary disease may wait years for a diagnosis, or not get a diagnosis at all.
The data provides a vital snapshot of respiratory care across local health systems in England, from diagnosis and provision of basic care to hospital admissions. It also highlights the intrinsic link between poverty and poor lung health, showing worse outcomes for people with lung conditions in ICSs in areas with higher levels of deprivation.
Worryingly, the survey responses also reveal large gaps in data collection. Most of the ICSs that responded were unable to say how many referrals for spirometry tests they had received, or how many tests were performed in their area in the past year, making it impossible to gauge the true scale of the problem or resources needed to ensure everyone waiting for a diagnosis can be tested.
Sarah Sleet, chief executive of Asthma + Lung UK, said: “Lung conditions are the third biggest killer in the UK, the top cause of emergency hospital admissions and the driver behind the NHS winter crisis every year. It’s a scandal that they’re still not being prioritised in local health systems in half of the country: people who are struggling to breathe can’t even get the basic tests they need for a diagnosis.” q
[KNOWING WHICH EXPERT to instruct can be challenging for lawyers, especially in cases of personal injury due to trauma.
According to consultant thoracic surgeon Mr Vijay Joshi: “It is important to know that there are now more formalised pathways in trauma and only certain specialists will have on-going operative experience repairing chest wall injuries. Lawyers should be mindful of this and consider asking such experts for evidence of their role in their local trauma pathway for thoracic injuries.
“It may be that, although an expert may hold a general awareness of how such cases are managed, they may not be involved in actual patient-level decision making, which would also include operative planning, in their NHS practice. Furthermore, evidence from an operative logbook and/or recent appraisals may also help demonstrate that the expert is still maintaining ongoing competency in contemporary thoracic surgical practice.
“Such evidence can be a useful tool to help identify an appropriate expert in personal injury cases and can also be applied to clinical negligence cases.” q
• The most common error was organ puncture, particularly the liver
• – raising serious concerns about procedural accuracy.
• Documentation of ultrasound was often missing, or ultrasound may have
• been used inappropriately.
• Many incidents occurred outside respiratory environments, both during
• and outside normal working hours.
Reporting on the research, the British Thoracic Society (BTS) said: “The authors emphasise that improving patient safety requires a national focus to standardise best practice in pleural procedures. They underline that, as stated in the 2023 BTS Pleural Guidelines, ultrasound assessment should be mandatory before any pleural intervention involving fluid. Better training and clearer protocols are also needed to ensure that ultrasound is used appropriately and consistently across all clinical settings.
“To further reduce the risk of harm associated with emergency procedures performed by less experienced clinicians, access to trained pleural proceduralists should be available at all times.”
The authors also express support for the upcoming National Confidential Enquiry into Patient Outcome and Death (NCEPOD) study. That review hopes to identify underlying factors contributing to procedural risks and to drive meaningful improvements.
Dr Stanton commented: “We still don’t fully understand why these episodes of harm are occurring, so we welcome an upcoming NCEPOD study to understand this in much more detail. Importantly though this study highlights the importance for teams in all clinical areas treating pleural effusions that ultrasound must be fully embedded in clinical protocols and used appropriately to provide safe intervention, in line with national published British Thoracic Society guidance.”
Dr Stanton and colleagues stress that, while pleural procedures are essential for many respiratory patients, stronger adherence to safety protocols and improved training will be key to reducing patient harm. q

By Professor Upendra Chowdhary, Emeritus Professor of Neurosurgery
[THE POPULATION DEVELOPING post-concussion syndrome (PCS) can be divided into two major groups: those related to sports injuries and those related to accidental trauma. In this article I am going to discuss only the latter group.
The definition of PCS is somewhat confusing, but the best definition is from the World Health Organisation. It states that after traumatic brain injury patients have cognitive deficits in attention and memory and three or more of the following symptoms: headache, dizziness, fatigue, irritability, insomnia, apathy, balance problems or personality changes.
Concussion is the result of rapid deceleration of the brain within the cranial cavity, which produces shearing, torsional and stretching forces to the neural tissue, followed by metabolic changes and diffuse axonal injury, especially to the long white matter tracks. The metabolic changes are mostly related to a release of harmful chemicals, which lead to a cascade of events including changes in the neuronal membrane and reduced blood flow. In most of the cases those changes, and hence the symptoms and
clinical signs, are temporary and reverses to normality after a few days to a few weeks – but approximately 10% develop persistent symptoms and signs for a much longer period. In such patients sophisticated brain MRI protocols have shown structural evidence of diffuse axonal injury, blood-brain barrier disruption, reduced localised cerebral blood flow and, in the worst cases, focal cerebral neuronal cell death.
The Prague International Conference on Concussion classified concussion as simple or complex. A simple concussion resolves within seven to 10 days without any remaining symptoms or neurological deficits. In complex concussion the patients have persistent PCS symptoms and signs, or have developed additional neurological symptoms such as epilepsy.

In the medicolegal context most of the patients had suffered symptoms of PCS for longer than a few days, if we exclude sports-related PCS. In such patients, loss of employment and difficulty in leading a normal life leads to additional psychological symptoms of anxiety, depression and hopelessness. Ideally, those patients should receive immediate intensive supportive treatment, related to training to combat the effects of memory and attention deficits, delivered by consultants in neuropsychology, expert physiotherapists and occupational therapists, together with dedicated and targeted rehabilitation. That is likely to lead to faster and greater symptomatic recovery, near normalisation of day-to-day life and a return to, in a step-by-step fashion, productive employment.
Such treatment is likely to reduce the incidence and/or severity of the secondary psychological symptoms. It is also important that, when such psychological symptoms occur, immediate and effective treatment by a trained clinical psychologist is made available. There is no established pharmacological agent which would treat PCS. There has been research going on to see if drugs which alter some of the neurotransmitters – such as anticholinesterases, serotonin, norepinephrine and dopamine, and/or some of the anti-depressants –would be useful.
For the past dozen years or so there has been increasing constraint on all types of resources, more so in the treatment of non-life threatening conditions. Hence, patients with PCS have not, in my experience of being a neurosurgical expert witness since 2007, been able to access even a fraction of the treatment stated above, leading to destroyed life, family upheaval, unemployment, anxiety and depression, which then become a vicious cycle.
For the medicolegal expert dealing with PCS, the first thing is to get a diagnosis of the degree of head and brain injury, and then to have the diagnosis of PCS done properly. Some of those patients, especially those with severe and more persistent symptoms, should have a special protocol MRI scan of the brain carried out, with the aim of showing diffuse axonal injury and signs of neuronal cell death.
The other responsibility of such experts would be to strongly suggest to the legal entities that the multi-modality and intensive supportive treatments, as described already, are made available to such patients with prolonged PCS, through the NHS and/or private sector, with resources for the latter to be made available through the litigation system. q
[A NATIONAL prostate cancer screening programme applying new technologies could generate socio-economic benefits to the UK of over £200m, research has revealed.
Prostate Cancer Research (PCR), who commissioned the report, are calling for urgent improvements to screening provision to tackle rising prostate cancer deaths and health inequality in the UK.
The report launch coincided with an order from Health Secretary Wes Streeting for the NHS to review its guidance on prostate cancer screening, following calls from Sir Chris Hoy.
The introduction of a targeted national prostate cancer screening programme for high-risk groups using the current pathway could deliver around 650 earlier diagnoses annually for men with a family history of prostate cancer aged 45-69 and in the region of 170 for Black men aged 45-69. For those groups, almost 230 men with a family history of prostate cancer per year could be spared a stage 4 diagnosis, when prostate cancer becomes incurable. For Black men, 60 could have avoided stage 4 diagnoses.

rue a late diagnosis of prostate cancer ever again. We want to reduce the number of men diagnosed too late to be cured.”
New technologies could make universal screening viable for the first time
The report also explores the potential impact of introducing future improvements in testing technologies into a screening programme for the general population: those aged 50-69.
Oliver Kemp, CEO of Prostate Cancer Research, said: “Prostate cancer is taking too many lives, and our current system of ‘informed choice’ is failing those at greatest risk. Our report proves that targeted screening could save lives and alleviate the burden on our healthcare system by avoiding late-stage diagnoses and the associated treatments.
That would be achieved using current technologies and pathways, and by targeting men from high-risk groups: Black men and those with a family history of prostate cancer, including those with BRCA1/2 mutations.
Prostate cancer is the most common cancer diagnosed in UK men, with over 55,000 new cases reported annually, and the second most deadly cancer among men. The existing ‘informed choice’ system for requesting testing places the onus on men to understand their risk and actively seek testing. That system is both ineffective and inefficient and contributes to the fact that men from high-risk groups, particularly Black men, are more likely to be diagnosed late and are more than twice as likely to die from this disease.
The report details how replacing the existing system with a national targeted screening programme would reduce these late diagnoses and deaths. Additional analysis from PCR has found that it would move the UK from being one of worst OECD performers on prostate cancer to being one of the best.
The call for a targeted screening programme has been backed the British Association of Urological Surgeons (BAUS).
Vishwanath Hanchanale, chair of the Section of Oncology at the BAUS, said: “We welcome the backing of – and fully endorse – the development and implementation of a nationally-integrated, riskstratified early detection programme for prostate cancer in high-risk populations. This can only be achieved by working in partnership with others, including the urological, radiological and general practitioner communities to improve the diagnosis and treatment of prostate cancer, and to reach those who don’t come forward for testing at present.
“There is a need for a focus on PSA testing thresholds, early testing for high-risk communities, standardising MRI protocols to improve diagnostic accuracy and the use of MRI-targeted biopsies to reduce harmful overdiagnosis.
“We remain committed to the advancement of prostate cancer diagnostics and therapeutics through evidence-based research, clinical advocacy and equitable healthcare access.
“Our efforts are for all the fathers, brothers, sons, uncles, grandfathers – and their loved ones – to ensure that no one is left to
“We have also shown for the first time that a universal screening programme using existing technologies is within our grasp. It’s time we took concrete steps towards making that happen. It’s time to act and bring hope to thousands of men and their families across the UK.”
The full report can be accessed as a PDF via the website at www.prostate-cancer-research.org.uk q
[THE Royal College of Radiologists has raised urgent concerns about widespread recruitment freezes in cancer and diagnostic services across the NHS, undermining critical efforts to reduce delays for patients and improve early cancer diagnosis.
New analysis shows more than a fifth of NHS trusts have implemented recruitment freezes, across every English region and every UK nation. That halts workforce growth at a time of rising patient demand and persistent care backlogs.

It calls into question the feasibility of the government’s commitments to reform elective care, established in January – which includes bringing down diagnostic delays and delivering same-day results. Recruitment freezes put those ambitions at risk, the college says: to build diagnostic capacity, we must build the diagnostic workforce.
And with more than 80% of patient pathways in the NHS reliant on radiology, staff shortfalls can create a wider domino effect, as delays in scan reporting result in delayed treatment. A swift diagnosis is especially important for cancer, where a month’s delay in starting treatment can raise the risk of death by 10%.
The NHS sets itself a target that every scan should be reported within a month – but in the first half of 2024 alone, over 420,000 scans took more than a month to report.
The cause of the freezes is mixed. Some trusts are freezing or cutting posts in an effort to balance local budgets; others have been placed under freezes by national NHS bodies, preventing them from hiring new trainees, consultants or specialty and specialist doctors.
Shortfalls mean consultants already face heavy workloads and burnout, which exacerbates early retirement and compromises non-clinical responsibilities like training and service improvement. Shortfalls drive higher costs for the NHS, meaning demand must be managed through locums and outsourcing to private companies. Outsourcing is already widespread in radiology, with 99% of trusts unable to meet their reporting requirements on their own in 2023 – resulting in a national outsourcing bill of £276m: an amount that could pay the salaries of 2,690 consultants.
Newly trained consultants could struggle to find jobs
In 2024, funded vacancies for consultant radiologists dropped from 518 to 152 because of financial pressures. Doctors coming to the end of training could be unable to find work, with 264 radiologists completing their training last year. This would be a failure for those hard-working doctors, for patients and for the NHS, given the cost and time it takes to train specialist doctors.
Commenting on the analysis, Dr Katharine Halliday, president of the Royal College of Radiologists, said: “Recruitment freezes are a false economy, and it is patients who will pay the price. We are facing severe workforce shortfalls and rising demand, so all these freezes will achieve is to force departments to spend more on costly alternatives. We urge the government to make sure our cancer and diagnostics services can recruit the staff they need.” q
By Rakesh Bhardwaj MBChB MD FRCS FRCS (Ed) FRCS (Gen Surg) LLM Consultant colorectal surgeon
[ INSTRUCTIONS TO COLORECTAL SURGEONS often relate to delays in the diagnosis and treatment of colorectal cancer. In recent years there has been increased public awareness through the National Bowel Screening initiative and improved patient education. Despite that, many colorectal cancers are diagnosed in their later stages.
Instructions follow similar themes and instructing parties may ask the following questions:
• Was there an opportunity to make a diagnosis and initiate
• treatment earlier?
• If a diagnosis had been made earlier would the cancer have
• been caught at an earlier stage? What would be the burden of
• metastatic disease if the tumour had been caught earlier?
• If a diagnosis had been made earlier would the treatment have
• differed? How would that have impacted the patient?
• If the diagnosis had been made earlier would the outcome for
• the patient been different?
The current State of the Nation report from the National Bowel Cancer Audit showed that 35,779 patients were diagnosed with colorectal cancer in England and Wales between 1 April 2021 and 31 March 2022. Of those, 42% presented with stage I or II disease. So the burden of those with disease in stages III and IV is
still significant. The number of patients presenting with colorectal cancer has now returned to pre-pandemic levels.
Based upon data from Cancer Research UK in England for figures for people diagnosed between 2016 and 2020 and followed up until 2021, the five-year survival for stage I, II, II and IV disease is 90%, 85%, 65% and 10% respectively. Thus, survival is directly related to the stage of disease at diagnosis. It is therefore important to diagnose colorectal cancer at an early a stage as possible.
It must be stressed that there have been significant paradigm shifts in treatment of colorectal cancer in recent years. Enhanced diagnostic and staging imaging, newer oncological strategies and improved surgical techniques are changing the outcomes constantly. Caution must be applied, too: subgroup pathological analysis has highlighted stage-specific survival paradoxes, further complicating interpretation. Falsely interpreting the literature can also be hazardous and that could be reflected in a biased expert report. UK expert witnesses should restrict their evidence base to the standards applied in the UK.
Colorectal surgical experts should leave the interpretation of issues that arise from primary care to experts in primary care. There is evidence that delays in referral from primary care worsen survival for patients with colorectal cancer. In August 2023
NICE revised guidance for the recognition and referral of lower gastrointestinal tract cancers. That helps to act as a framework for referral and provide clarity of whom and when to refer a patient. It is vitally important that assumptions about health care are not translated into experts’ conclusions.
Assessing whether investigating a patient earlier would have resulted in an earlier stage at diagnosis requires an understanding of tumour growth characteristics. It is often a difficult area to draw firm conclusions from as there is a paucity of evidence in the literature. Tumour growth is not linear. Inference of stage migration from detailed radiological and pathological studies may provide some assistance to expert witnesses who wish to draw conclusions. The presence of metastatic disease, seemingly more present in the later stages of the disease, is of importance as the treatment strategies become increasingly complex when metastatic disease is identified.
The crucial question often posed by instructing parties is: would the survival outcome have been different if a diagnosis had been made earlier? On the surface it seems a simple question to answer: of course, there is a vast difference between the treatment and outcome of a stage I colorectal cancer and a stage IV colorectal cancer. But instructions often focus on delays of a matter of weeks and months. It is left for the expert to discuss whether such a delay does affect disease-free and survival outcome.
The literature is far from clear and may confuse the issue further. Heterogeneity from cancer analyses may complicate the interpretation of data, contributing to a lack of clarity. Often the expert’s clinical experience may allow further conclusions to be drawn.
Increasing burdens on primary and secondary health care may lead to diagnostic and treatment delays of colorectal cancer in the UK. Detailed evaluation of the medical records and careful interpretation of the literature is essential for a colorectal expert witness to be able to aid instructing parties. q
By RIchard Guy MBChB MD FRCS FRCS(Gen)
[ACCORDING TO the National Bowel Cancer Audit (www.nboca. org.uk) around 40,000 people in England and Wales are diagnosed with colorectal cancer (CRC) each year, of whom 50-60% undergo major resection. Outcomes for most patients are good: the death rate within 90 days of elective operation is around 3%, although it is 4-5 times higher for emergency operations.
Unplanned re-operation following CRC surgery occurs in around 6-8%, often for the consequences of a failed bowel anastomosis or join. For surgeons, a feared complication is anastomotic leak (AL) – a breach in that join, sometimes with catastrophic results. The prevalence of AL in colorectal surgery varies from 1-19%, the highest rates being for anastomoses in the pelvis, for example after the removal of rectal cancer.
Why are anastomotic leaks important?
An AL means a longer hospital stay at the least; but at worst more surgery, a permanent stoma, malnutrition, sepsis, multi-organ failure and death. Sepsis – life-threatening organ dysfunction caused by dysregulated response to infection – has a mortality rate of more than 10%. Septic shock – in which profound circulatory, cellular and metabolic abnormalities ensue –is associated with mortality rates of more than 40%.
AL may also increase the risk of cancer recurrence and reduce cancerspecific survival. Economic studies demonstrate a significant financial burden for hospital trusts when AL occurs.
Why do anastomotic leaks occur?
Surgeon factors
The exact causes and nature of ALs are uncertain. Bowel surgery, especially that undertaken for pelvic pathology, can be technically demanding. Various techniques are used – open, minimally invasive laparoscopic (‘keyhole’) and robotic surgery – all with advantages and disadvantages.
Regardless of approach, construction of a safe anastomosis is paramount – lack of accuracy is usually unforgiving. Surgeons need to be familiar with a range of anastomotic techniques, including hand-sewn methods and those using stapling devices – and what to do when an anastomosis goes wrong: should they repair or re-do the join, or ‘bail out’ and form a colostomy which may never be reversed, or for which reversal is potentially formidable?
A healthy anastomosis needs a good blood supply (perfusion) to both ends. Whilst this might partly depend upon a patient’s general health, the surgeon must be satisfied that there is adequate arterial flow: if not, the join is likely to fail. Furthermore, surgical manoeuvres that a surgeon may use to ensure that the bowel reaches the pelvis for a tension-free anastomosis may critically compromise perfusion.
Patient factors
UK society is ageing. A ‘frailty epidemic’ means that many patients having surgery for CRC are compromised by cardiac or respiratory disease, potentially affecting outcome. There is a linear relationship between increasing frailty and worse outcomes after surgical admission.
A less active, over-indulgent population has generated an ‘obesity epidemic,’ influencing surgical decision-making and operative ease. Expectations for a favourable outcome need adjustment for many individuals.
Diagnosis can be challenging: vigilance, recognition of illness and a high index of suspicion are required. Symptoms and signs may be

insidious, subtle and difficult to discriminate from other problems, such as pneumonia or heart failure. But early diagnosis of AL – including close monitoring of blood tests such as C-Reactive Protein (CRP) and timely radiological scanning – is more likely to permit successful treatment, including operative intervention and salvage of a leaking anastomosis.
Treatment of sepsis should start as early as possible. Delays in antibiotic administration show a linear increase in mortality: for every hour’s delay, mortality may increase by around 8% in shocked patients. Annual National Emergency Laparotomy Audits (NELA) consistently highlight antibiotic delays (www.nela.org.uk).
Many emergency operations are time-sensitive. Once a decision has been made for an unwell patient with AL to have surgery it should proceed promptly, according to guidelines from the National Confidential Enquiry into Perioperative Deaths (ncepod.org.uk/ classification.html). For patients with peritonitis a delay of a few hours can substantially increase the risk of death: each hour of delay is associated with more than a 2% decrease in 90-day survival.
NELA figures consistently show that patients requiring emergency surgery may experience considerable delays, with only around twothirds arriving in theatre within an appropriate time. Insufficient critical care capacity also means that only 80% of high-risk patients are admitted to that environment, potentially compromising recovery.
In my expert witness practice, unravelling cases of alleged clinical negligence where there has been a poor surgical outcome – and determining whether care has fallen below an expected standard –must consider all confounding factors in a complex landscape. Whilst there may be identifiable individual inadequacies, patient factors and system failures mustn’t be overlooked.
Surgical complications occur unexpectedly in the best hands: no surgeon intends to cause harm and most are adversely affected by a patient’s suffering. The Bolam and Bolitho tests provide some ‘protection’ for clinicians who make reasonable decisions in accordance with accepted guidelines and opinion. Assigning ‘blame’ for surgical misadventure to an individual may be inappropriate.
For me, the significance of complications lies not in their occurrence per se, or because a surgeon lacks necessary skills – although technical competence may need questioning – but owing to responses to operative difficulty or clinical scenarios in sick patients, including:
• Failure to recognise or accept that a problem has occurred and to
• deal with it – reflective of lack of vigilance and responsibility,
• preferring to ‘bury one’s head in the sand’.
• Failure to seek help or opinions from colleagues – reflective of
• surgical arrogance, blinkered practice and inability to work in a
• team.
• Failure of sound decision making – potentially resulting in an even
• worse clinical situation.
A combination of factors usually exists. A traditional surgical aphorism reads: “Good surgeons know how to operate, better ones know when to operate and the best know when not to operate.” Rushing back into an abdomen following AL, for example, may not be a sensible option.
Superior technical expertise is undoubtedly an advantage in some situations, but poor decision-making in the face of disaster may have catastrophic consequences. q

By Dr Michael Robson BA(Oxon) MBBS PhD
[ A NEPHROLOGIST specialises in the diagnosis and treatment of conditions affecting the kidneys. They do not perform operations on the kidneys, as that is the remit of a urologist.
Acute kidney injury is a term used to describe a recent decline in kidney function, which may or may not be reversible. Causes include infections, gastrointestinal bleeds, heart attacks, autoimmune diseases and medication. If the cause is not clear, a kidney biopsy may be needed.
Chronic kidney disease refers to an established reduction in kidney function; and it is considered irreversible. Many patients with chronic kidney disease can be monitored in primary care.
Indications to see a nephrologist include the possibility of a treatable condition and kidney disease approaching a stage when planning for dialysis and transplantation is needed.
Nephrologists also provide what is known as ‘renal replacement therapy’ for patients with end-stage kidney disease. This comprises haemodialysis, peritoneal dialysis, preparation for renal transplantation and post-transplant care. The care of patients with end-stage kidney disease is multidisciplinary.
Nephrologists work closely with transplant surgeons, vascular surgeons and specialist dialysis nurses. Access to the circulation is needed for haemodialysis and that is usually achieved by surgically joining an artery and vein in the arm, known as an arteriovenous fistula. Surgeons also insert tubes into the abdomen for peritoneal dialysis and perform kidney transplants.
When a patient discovers their kidney function is reduced, they may ask if it could have been avoided. If they have previously seen doctors who were not nephrologists, questions on breach of duty will need to be posed to other experts. However, a nephrologist can still advise on causation: for example, if the claimant had been referred to a nephrologist at an earlier stage, would the outcome have been different?
There may be several factors leading to acute kidney injury or chronic kidney disease, and that can be a difficult question to answer. However, the job of a nephrology expert is to determine whether it is more likely than not that the outcome would have been different, and to explain their reasoning.
An opinion on the care of patients receiving renal replacement therapy may also be requested from a nephrologist. That may be regarding dialysis prescription, blood pressure control, arteriovenous fistula complications, preparation for renal transplantation or posttransplant care.
Nephrologists may provide condition and prognosis reports for people with kidney disease, or people who have sustained kidney damage. Irreversible kidney damage can occur if urine outflow is obstructed. That might be due to ureteric injury during pelvic surgery or other causes.
Such cases may require an opinion on breach of duty from a gynaecologist or urologist and an opinion on condition and prognosis from a nephrologist. Moderately reduced kidney function does not usually cause symptoms. However, patients on dialysis may be unable to work or perform other activities due to fatigue and the time needed for dialysis.
Furthermore, patients with end-stage kidney disease have a reduced life expectancy, primarily due to an increased risk of cardiovascular disease. That is more marked in people on dialysis compared to those with a kidney transplant. People with reduced kidney function who have not reached end-stage also have a decreased life expectancy and will be more likely to develop endstage kidney disease.
Conclusion
I hope this article has illustrated the varied nature of a nephrologist’s work. This is reflected in the instructions that I have received, which have covered the full range of acute and chronic kidney disease, dialysis and transplantation.
It may not always be clear to a solicitor if an opinion is needed from a nephrologist, a urologist, a transplant surgeon, a vascular surgeon or a dialysis nurse. It is important that a nephrologist only accepts cases within their expertise and advises the solicitor if the instruction should go to another expert. q
[THE HEART CARE waiting list rose in December last year, despite a fall in the overall list for treatment and care, latest figures show. Figures released by NHS England in February show that there were 423,245 people waiting for ‘routine’ cardiac care, up from 420,589 in November.
Since the start of 2024, the heart care waiting list had risen by 4% (17,285) and more than doubled since December 2020, when it stood at 197,938.
There was, however, a slight fall in the number of people waiting longer than 18 weeks – from 169,620 in November to 168,924 in December.
However, the proportion of people on the list who have been waiting over 18 weeks for time-sensitive cardiac care remains at 40%. There was also a fall in the number of people waiting over a year for cardiac care: to 9,009 in December, down from 9,885 in November. In February 2020, there were just 28 people waiting that long.
Dr Sonya Babu-Narayan, clinical director of the British Heart Foundation, said: “It’s frustrating to see yet another rise in the heart care waiting list, even though some progress has been made to reduce waits for other NHS treatment and care.
“Heart treatment is clearly time-critical and not a luxury people can live without. Long waits are dangerous: four in 10 people on the heart care list are waiting more than 18 weeks. This inevitably puts people at risk of avoidable heart attacks, heart failure and even premature death.
“We’re in the grip of a heart care crisis and it’s putting lives on the line. Heart patients need to see a National Cardiovascular Disease Plan to make emergency treatment and planned heart care fit for the future, and stop more people from getting heart disease in the first place.”
The same data set also revealed that average ambulance response times

for heart attacks and strokes were 36 minutes in January That is significantly down from the figure for December, which was 47 minutes: itself up from 42 minutes in November.
They nevertheless breached the current NHS England average response target for category 2 calls of 30 minutes. Before the pandemic the response target for category 2 calls – which includes suspected heart attacks and strokes – was an average of 18 minutes. However, the target was relaxed due to growing pressure on the NHS and not a change in clinical urgency.
Dr Babu-Narayan added: “Heart attacks and strokes are life-threatening emergencies. With each minute lost, the risk increases of permanent brain or heart damage and even death. We cannot accept such dangerous ambulance wait times as a new normal.
“This extreme disruption to emergency care reflects a broken pipeline of care for heart patients.” q
[AN ARTIFICIAL INTELLIGENCE (AI) MODEL
can identify women at higher risk of heart disease based on their electrocardiogram (ECG) readings, according to new research carried out at Imperial College London and funded by the British Heart Foundation. The researchers say that the algorithm, designed specifically for female patients, could allow doctors to identify women at high risk of heart disease at an earlier stage, allowing for better treatment and care.
An ECG is one of the most common medical tests and records the electrical activity of the heart. In their study, the researchers used AI to analyse over one million ECGs from 180,000 patients, over half of whom were female.
In the study, published in the journal Lancet Digital Health, researchers developed a score that measured how closely an individual's ECG matches ‘typical’ patterns of ECGs for men and women. They found that women whose ECGs more closely matched the typical ‘male’ pattern – such as having an increased size of the electrical signal – tended to have larger heart chambers and more muscle mass.
Those women were also found to have a significantly higher risk of cardiovascular disease, future heart failure and heart attacks, compared with women with ECGs more closely matching the ‘typical female’ ECG.
Last year, the researchers published a study suggesting that an AI-ECG risk estimation model – known as AIRE – can predict patients’ risk of developing and worsening heart disease from an ECG. They’re currently planning trials of AIRE at two NHS trusts in London, to begin later this year. This latest model, to identify women at higher risk of heart disease, will be trialled in conjunction with AIRE.
Dr Sonya Babu-Narayan, clinical director at BHF, commented: “Far too often women are misdiagnosed or even dismissed by healthcare professionals, thanks to the myth that heart disease is only a male issue. Even if they do receive the right diagnosis, evidence shows that women are less likely than men to receive recommended treatments.
“This study has applied powerful AI technology to ECGs: a routine, cheap and widely available heart test. Harnessing the potential of this

type of research could help better identify those patients at highest risk of future heart problems and reduce the gender gap in heart care outcomes. However, one test alone will not level the playing field. Ensuring every person gets the right heart care they need when they need it will require change in every part of our healthcare system.” q

[ THE Royal College of Obstetricians and Gynaecologists (RCOG) has responded to the latest Office for National Statistics (ONS) data on the impact of an endometriosis diagnosis on monthly employee pay and employee status.
Endometriosis is a condition where endometrial tissue, similar to the lining of the uterus, grows in other places, such as the ovaries and fallopian tubes. Common symptoms include chronic pelvic pain, fatigue, heavy menstrual bleeding, pain during or after sex, painful urination and bowel movements, and reduced fertility.
The data, released by the ONS on 6 February, revealed that there was a ‘statistically significant’ average decrease in monthly earnings among women aged 25 to 54 years in England from one to five years after a diagnosis of endometriosis between April 2016 and December 2022, compared with the two-year period before being diagnosed with the condition.
Among all women in the dataset, including both paid employees and those not in paid employment, monthly pay initially dropped on average in the first three months post-diagnosis, then returned to pre-diagnosis levels from four to 12 months. Afterwards, pay decreased on average each year, reaching a £130 monthly reduction in the four to five years post-diagnosis compared with the two years before diagnosis.
Dr Ranee Thakar, president of the RCOG, said: “These statistics are staggering and mirror the findings of our recent Waiting for a way forward report. Our report found that nearly seven in 10 of the women surveyed said their ability to take part in work and social
activities had been negatively impacted by their gynaecological condition.
“Endometriosis is a progressive gynaecological condition that becomes more complex to treat over time. The sooner we can see these women in our clinics, the sooner we can support them, prevent their conditions worsening and help keep them in work.
“We know that there are over 750,000 women and people currently waiting for hospital gynaecology care and the impact of these prolonged waits is affecting society as a whole and should concern all of us. Women play an extensive and important role in the economy, making up a significant portion of the UK workforce in key sectors, including health and social care, education and the civil service. It is simply unacceptable that women are having to work less, or being forced out of work altogether, because their gynaecological health needs are not being met.
“In its manifesto this government committed to prioritising women’s health. After missing a vital opportunity to do this last week in the NHS Operational Planning Guidance, we urge the government to take the health of 51% of the population into account when considering the upcoming Spending Review, the NHS 10-year plan and the future of the Women’s Health Strategy.
“This should include sustained investment in gynaecology services to ensure that all women can access diagnosis and treatment when they need it and allow them to continue to work and participate in society. This investment will not only benefit thousands of individual women, but the wider economy too.” q
[THE Royal College of Midwives (RCM) has said it is reassured that the government has acknowledged the issues raised by the House of Lords Preterm Birth Committee report, Preterm birth: reducing risks and improving lives – particularly as the focus of the inquiry is on improving care for groups most at risk.
Preterm birth, affecting 8.1% of all births in England in 2023, remained the leading cause of neonatal death and illness. While England’s preterm birth rate was lower than in some countries, inequalities persist, with Black and Asian women more likely to experience preterm births than white women.
Despite progress, the report emphasises persistent inconsistencies in care, workforce challenges and inadequate maternity infrastructure, which contributed to disparities and impacted service delivery. The government agreed with the report’s findings and recommendations, particularly regarding the need for improvements in care.
In its response to the report, the Department for Health and Social Care said: “We share the inquiry’s view that current and future action will not only improve outcomes for babies but the

experiences of families as they embark on this unexpected start of parenthood.
“As acknowledged in the report, the prediction and prevention of preterm birth is challenging due to the wide range of factors that contribute to a woman’s individual risk, and many women who have preterm births do not have apparent risk factors.
“While most babies born prematurely go on to do well, we know that reducing the incidence of preterm birth and improving outcomes for babies and their families would lead to significant health benefits and cost savings across healthcare, education and wider public sector.”
The RCM says it is a positive step from

government and it looks forward to working with it and other stakeholders to ensure women and families who experience preterm birth receive appropriate care and support. The RCM is also pleased that the House of Lords carried out the inquiry in the first place as it ensures the issue is on the political radar.
Clare Livingstone, professional advisor on policy and public health at the RCM, said: “There are multiple contributory factors which have been identified in relation to preterm birth and, given its complexities, the exact causes are often not fully understood. However, evidence shows that continuity of midwifery care and smoking are the two main factors.
“More support needs to be given to trusts to assess population groups who would most benefit from receiving continuity of care throughout the perinatal period. In addition, the college has previously called for more investment on multiple fronts to continue reducing smoking in pregnancy rates. Now we need action.”
The RCM has produced a Maternity Disadvantage Assessment Tool to support midwives and maternity support workers in assessing women’s needs. q
[ NEW GUIDANCE to protect Britain’s midwives from excessive nitrous oxide exposure has been published by the Health and Safety Executive (HSE). The guidance is aimed at those responsible for ensuring the safety of workers and new mothers on maternity wards.
More commonly known as ‘gas and air’ when mixed with oxygen, nitrous oxide is an invisible gas used widely in healthcare, including for pain relief during childbirth. Depending on how well exhaled gas from women in labour is controlled, midwives are at greater risk of exposure to higher levels of nitrous oxide due to the extensive time they spend working in labour rooms.
Over time, high levels of exposure can cause serious health effects, including neurological problems and anaemia, so it is important that levels are properly controlled.
Nitrous oxide is subject to the Control of Substances Hazardous to Health Regulations (COSHH). It has a long-term workplace exposure limit of 100ppm or 183mg.m3 8-hour time-weighted average. HSE advises that all hospitals using gas and air should carry out a COSHH risk assessment of each space in which it is used.
Helen Jones, head of HSE’s health and public services sector, said: “This is an essential piece of guidance. It should be taken on board by those responsible for managing health and safety in maternity units and for controlling the risks faced by staff who work with nitrous oxide. This should include consideration of workers who may be more vulnerable to the effects of exposure, such as those who are pregnant.
“Workers must also be fully consulted when it comes to monitoring how effective the control measures are, including how results are to be used. This will include how workers will be managed if results suggest their exposure should be reduced.”
There are three main types of control systems used in maternity wards:
• A demand valve and mouthpiece or facemask used by the patient
• which captures exhaled breath, ensuring it is not released into
• the room.
• An associated extraction or scavenging system with an extraction
• unit located close to the breathing zone of the patient.
• General ventilation.
The demand valve and mouthpiece or facemask system is the most effective method of control. That is because the exhaled air is not released back into the room, as long as the mouthpiece or facemask is not removed before the patient exhales.
General ventilation is least effective because it is located at a distance from the source – the exhaled air – and relies on the effectiveness of the room ventilation
It is important that exposure monitoring for any airborne contaminant includes the relevant contextual information for each sample taken. For nitrous oxide in a maternity department that would include:
• The time midwives and student midwives, doctors and/or support
• staff attend to the delivery of a child or children: the actual
• exposure time, assessed over a representative number of days
• An estimate of the level of demand by the expectant mother
• Any controls present, for example scavenging equipment
• Any other information that is likely to affect the exposure levels,
• such as movement of people or other activities in the room.
The new guidance on how gas and air should be used safely has been developed by HSE together with maternity specialists in the NHS and is also relevant for professionals working in other parts of the healthcare sector, outside of maternity wards. q

[THE Royal College of Nursing (RCN) has welcomed news that Dawn Butler MP introduced a Ten Minute Rule Bill in Parliament on 11 February that sets out to legally protect the title ‘nurse’. The proposal states only those registered with the Nursing and Midwifery Council as a registered nurse can use the title ‘nurse’ when working in health and social care.
If successful, the Bill would bring the UK in line with international best practices and give patients confidence that those providing their care meet professional standards.
In her speech Ms Butler emphasised that this is important for patient safety, highlighting cases where individuals have falsely portrayed themselves as qualified healthcare professionals.
The RCN is urging government and parties to get behind the campaign to ensure nursing gets the respect it deserves. The title ‘registered nurse’ is already protected in the UK in law.
RCN general secretary and chief executive Professor Nicola Ranger said: “Nursing is a safety-critical
profession, and the title ‘nurse’ needs to be protected. Patients deserve to know that when they are being treated by a registered nurse, they can trust the knowledge, professionalism and clinical expertise that brings. The changes in this bill will provide better legal protections for nursing. This includes preventing those who have lost the right to be called nurses from legally continuing to do so.
“We will continue to urge government and parties across the political spectrum to get behind this campaign, ensuring our highly-skilled profession gets the respect it deserves.”
The bill has been given a Second Reading date of 28 March 2025, but it is unlikely to be debated progress to the next stage unless the government allocates Parliamentary time. Therefore, the RCN is calling on the government to give the bill time for debate, so it has a chance of progressing further.
A resolution in favour of protecting the title ‘nurse’ was passed at RCN Congress in 2022, and it was union’s General Election 2024 manifesto priorities.

[THE Nursing and Midwifery Council (NMC) has issued an update on its fitness-to-practise plan, in which it reported that the average longevity of fitness-to-practise (FtP) cases continues to fall across several stages of the process, as it starts to reach quicker decisions.
But there is more to someone’s experience of such processes than timeliness alone, as the NMC acknowledges, and it is open about the fact it will take many months more progress before people start to see and feel a positive difference.
In its statement the NMC said: “We aim to conclude 80 percent of our cases within 15 months of the initial referral being made. We are seeing meaningful progress towards this target; between December 2023 and December 2024, 65.5 percent of cases were closed within 15 months.
“We are also making progress at the initial assessment stage – screening – where most of the caseload is held. In December 2024, 25% of our cases at this earliest point in our process were resolved within our two-month target. Additionally, the number of screening decisions we have been making in recent months has been exceeding the number of new referrals being made.”
While there are some early green shoots of progress, there is still a long way to go, the NMC said, with the total caseload increasing from 5,778 in January 2024 to 6,633 by that December – in part driven by high volumes of
referrals. The next step is the publication of the realigned FtP plan.
“We’re taking a step-by-step approach, with it being a long-term effort to make real improvements for everyone involved: our colleagues, the professionals on our register and the public. We are currently prioritising the stabilisation of our processes, with a focus on eliminating the backlog of cases at screening while also working to resolve older cases more swiftly. We will then aim to conclude cases faster and ensure fewer cases require high court extensions.”
Since the plan was launched in April the context has changed. Screening teams are receiving higher than expected volumes of referrals and an independent review of the NMC’s culture highlighted areas of operational performance that required immediate action to resolve, including within safeguarding.
“As we launch our realigned plan, we are acutely aware of the significant pressures across the entirety of our FtP process and the real impact this has on people,” the statement said. “Which is why the plan will remain responsive to a changing environment and continue to seek both internal and external views on further improvements that we can make.
“We are currently finalising further external specialist support to reinforce the plan. This will focus on relieving pressure at screening, and recommending further improvements to
regulatory processes across the NMC.”
Listening to the views of professionals and stakeholders about their FtP experiences has also been critical to shaping the plan’s development. That is in addition to the support and advice from external advisers Anthony Omo from the General Medical Council and former Professional Regulatory Adviser at the Scottish Government Professor Donna O’Boyle.
Lesley Maslen, executive director of professional regulation at the NMC, said: “Thanks to colleagues’ hard work, we’re starting to see some green shoots of progress from our fitness-to-practise plan. Recent months show early signs of improvement in our decisionmaking rates across several stages of the FtP process: one of the keys to a better experience for everyone involved.
“However, we’re under no illusion about the long journey ahead. The range of improvements we want to deliver are complex and will take time to embed. This means that many of the people involved in our processes will have yet to feel the positive impact of the operational changes we’re making.
“We need to keep investing in our people and in the tools they need to do their jobs well. We must also keep working to better understand people’s lived experiences of our processes. This is how we’ll achieve the step change in the experience of FtP that people inside and outside the NMC deserve.” q
By Philip Coleridge Smith DM MA BCh FRCS, Consultant Vascular Surgeon, Medical Director of the British Vein Institute and Emeritus Reader in Surgery at UCL Medical School
[THE BLOOD SUPPLY to all parts of the body is carried by arteries and veins and the normal functioning of blood vessels is essential to the wellbeing of the body. Vascular surgeons are sometimes asked to advise urgently when blood vessels have been damaged during routine operations involving a number of medical specialisms.
The cause of the damage may be attributable to poor surgical technique, or it may be a recognised and unavoidable adverse event of some surgical procedures. However, the response to the occurrence of an injury is critical in ensuring that the injured patient makes a satisfactory recovery.
Lower limb arterial injury
I have advised in a number of cases where orthopaedic surgery to the lower limb has caused damage to arteries. At the knee, the popliteal artery lies close to the knee joint, so may be damaged during operations such as knee replacement and tibial osteotomy.

The distance from the back of the knee joint to the artery is 5-10mm, so orthopaedic surgeons take great care to avoid injury to the vessels during that type of surgery.
In elderly patients arteries are often atheromatous and that can cause problems when a tourniquet is applied to the limb during knee replacement surgery. The tourniquet may fracture an atheromatous plaque, leading to thrombosis of the femoral artery. Where hip replacement surgery necessitates marked angulation of the hip, the atheroma may also be fractured, leading to thrombosis of the common femoral artery.
Vascular surgeons treating peripheral vascular disease due to atheromatous occlusion of arteries often see patients in whom the femoral and popliteal arteries have occluded. That often occurs without symptom. In those patients the arteries slowly narrow and a collateral circulation – an alternative blood supply – develops over several years. However, in patients who suffer sudden occlusion of one of the main lower limb arteries due to iatrogenic causes without prior atheromatous narrowing, the loss of blood flow leads to severe limb ischaemia necessitating urgent intervention to restore blood flow.
The diagnosis of limb ischaemia may not be clear from superficial clinical review of the limb. Patients are often sedated after surgery having received opiate analgesia. Where spinal anaesthesia has been used, the restoration of sensation in the lower limb may take several hours. Those factors conceal severe pain in the limb, the most common symptom arising from acute limb ischaemia. Unless objective assessment of the peripheral pulses by palpation or Doppler ultrasound is done, evidence of occluded arteries may be missed for several hours.
The limb is intolerant of ischaemia lasting more than about six hours; hence the need for the restoration of blood flow to the leg to be confirmed by objective means following completion of the surgical procedure. Early detection of loss of blood flow will allow transfer of the patient to the care of a vascular surgical team, often at a different hospital, in time to avoid severe ischaemic damage to the limb should
vascular injury have occurred. Without prompt intervention, muscle and nerve damage can occur, leading to loss of function, chronic pain syndrome or even limb amputation in severe cases.
In cases where occlusion of the lower limb arteries is suspected, emergency referral to a vascular service is mandatory. Delaying referral to observe a limb with suspected ischaemia in the hope that the blood flow will improve could be regarded as substandard care.
Blocked arteries rarely recover function without surgical intervention. The vascular surgical team will arrange vascular imaging with duplex ultrasonography and CT angiography, which will immediately indicate the nature and extent of the problem. Emergency open vascular surgery is usually required where direct injury to an artery has arisen. Repair or bypass of the damaged segment of vessel is usually required. In some cases endovascular techniques may be feasible; but this is not usually the case.
A successful outcome from iatrogenic blood vessel injuries requires rapid recognition and treatment of the damage. Monitoring of the blood flow to the leg when arthroplasty has been done, by clinical examination or Doppler ultrasound, should be standard practice. Failure to monitor the limb or delay in diagnosis leading to an adverse outcome of vascular injury may comprise substandard care. In addition, failure to make an emergency referral to a vascular service may also comprise substandard care.
I have advised in a number of cases where iatrogenic injury to the popliteal and femoral arteries has occurred. In general, delays may accumulate in the management of that complication. Some of them are non-negligent, arising for example from the need to transfer the patient to another hospital. However, delays in diagnosis and referral are usually more difficult to defend.
In the lower limb, inadvertent damage to arteries arising in the course of operations on the leg does not normally give rise to external bleeding from the legs. The most frequently damaged artery is the popliteal artery. Operations are usually carried out with a tourniquet applied to
the limb and therefore any bleeding is not obvious during the operation and may be concealed once the surgical incision has been closed. However, during laparoscopic surgery on the abdomen, laceration or puncture of the abdominal arteries may occur on rare occasions. Surgeons undertaking laparoscopic surgery are well aware of that hazard and take great care to avoid such injuries. The main arteries in the abdomen are very large and damage to one of those vessels may lead to substantial blood loss. The occurrence of such an injury is immediately apparent once a view of the abdomen is obtained with a laparoscope.
Spinal surgeons undertaking microdiscectomy to the lumbar spine may also damage major arteries in the abdomen. The common iliac artery lies in front of the intervertebral disc and can be damaged if a sharp instrument is allowed to pass beyond the anterior limit of the disc space.
In the event of an injury to the aorta or iliac artery it is essential that a surgeon undertakes emergency laparotomy without any delay. Loss of much of the circulating blood volume can occur within minutes, leading to loss of blood pressure and cardiac arrest. Fatal outcomes of such injuries have been reported. A vascular surgeon can then undertake a sutured repair of the injury with restoration of blood flow to the legs. Discussion of liability in such cases usually revolves around whether the operating surgeon took sufficient precautions to avoid a vascular injury.
In conclusion, injuries to blood vessels may occur during routine surgical procedures such as total knee replacement, laparoscopy and lumbar disc surgery. The most important determinant of the outcome appears to be the rapidity with which the injury is identified and treated. Delayed diagnosis of limb artery injuries can lead to loss of function of the limb or the need for amputation.
Fatal outcomes may occur in the case of damage to major intraabdominal arteries, which can lead to claimants bringing successful cases to the courts. The risk of losses can be mitigated by assiduous monitoring of patients after surgical intervention in the lower limb. q


[ AS SCOTLAND’S HOSPITALS experienced the second worst January on record for A&E performance, the Royal College of Emergency Medicine (RCEM) has told the government ‘we need more than apologies; we need action’.
Figures released on 4 March by Public Health Scotland (PHS) come after First Minister John Swinney and Health Secretary Neil Gray apologised to patients who have experienced extremely long stays in A&Es.
The PHS data, for the month of January, reveals 8,401 patients waited 12 hours or longer in an emergency department before being admitted, discharged or transferred.
Since January 2018 the number of people waiting 12 hours or more in major A&Es has increased 11-fold (767 to 8,401), eight hours or more sixfold (2,816 to 16,684) and four hours or more by 2.6 times (15,401 to 40,552).
Patients are often stuck in emergency departments, on trolleys in corridors, experiencing extremely long stays because there are no in-patient beds available. That is caused because people who are well enough to go home cannot be discharged, often due to a lack of social care support.
Therefore the system grinds to a halt, with ambulances queueing outside EDs, waiting to handover their vulnerable patients. Such socalled ‘delayed discharges’ meant that an average of 1,964 patients each day were in hospital waiting to be discharged, despite being deemed medically well enough to go home. That is the highest number since 2016, when guidelines changed.
Dr Fiona Hunter, vice-president of RCEM Scotland, said: “This data provides a glimpse into the levels of pressure major hospitals in Scotland were under during the depths of winter: each figure a person who was seeking urgent care in a system that is well off being described as ‘gold standard’.
“And behind each person is a team of hard-working and burnt-out emergency medicine clinicians who are trying to deliver the best care they can to patients who are often on a trolley in a corridor.
“The time for warm words and apologies from policymakers has passed; we need action. Long stays are not just inconvenient – they are dangerous. This is where the real harm lies for patient safety.
“The government’s operational improvement plan, set to be delivered this month, is a golden opportunity to detail how it will address this vitally important issue. Until a meaningful plan is put in place, staff and patients will continue to bear the brunt of a system that is in crisis.”
At the end of February the Scottish Liberal Democrats revealed that an 87-year-old woman waited around 12 hours at A&E on

separate occasions after she fell and broke her hip. Her experience was highlighted as the party released data showing 12,438 people aged over 85 waited more than 12 hours in A&E in 2024.
After hearing the patient’s experience, First Minister John Swinney apologised to her and her family for the wait.
Earlier that month, Health Secretary Neil Gray MSP apologised on BBC’s Reporting Scotland , stating: “Anybody that is waiting for too long to receive services, either in an accident and emergency department or waiting on elective procedure; I apologise to them. It’s not an acceptable situation.” q
[WHEN IS IT WORTH taking a £50,000 bioprinter on a 184-mile train journey? That was the question answered by the Scar Free Foundation and the Swansea University 3D Bioface team, who were invited to the House of Commons for the Association of Medical Research Charities 2025 Showcase to celebrate the collective impact of the UK’s medical research charity sector to an audience of MPs and Peers.
The Scar Free Foundation was one of five chosen to present their research interactively –and what better way to do that than print 3D ears in front of a live audience?

Patients who are born without ears, or who lose them later in life, have limited options. They can wear a plastic prosthetic, which needs to be fitted and replaced every year, or have surgery to remove cartilage from elsewhere on their body to reconstruct the missing body part. That is painful and invasive; and can cause further scarring.
Scientists in the 3D Bioface lab at Swansea University are developing new techniques to ‘print’ ears from a patient’s own cells. The researchers have developed a unique type of ‘bio-ink’ which encourages cartilage –a type of tissue that makes up our ears and noses – to grow. Combined with cells from the patient, the scientists can 3D-print a scaffold the size
and shape of the body part that’s missing.
Eventually, the patient’s cells will fill in the scaffold, leaving researchers with a custom ear or nose that can be surgically implanted into the patient. It is hoped that this will become the new gold standard in facial reconstruction.
Bringing this technology into a clinical setting will have a huge impact on the field of facial reconstruction. The tissue sample needed to make the bio-ink is tiny: about the size of a hole punch. That means patients will not have to undergo invasive, painful surgery.
Ears and noses could also be customised to match the patient’s features, helping patients adapt to having an altered appearance.
Simon Weston CBE, lead ambassador for the Scar Free Foundation, commented: “It’s fantastic that this research is taking place and what we are going to do is amazing. This new research – bioprinting ear cartilage made from the patient’s own cells – would have made a big difference to me.
“There simply wasn’t the research or capability at the time to rebuild my ears – I literally had to watch them fall off. This research also avoids the need for skin grafts taken from other parts of the body – a process which itself can be very painful and leaves behind new scars.” q

[THE British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) was delighted to welcome a visit from their Royal Patron, Her Royal Highness
The Princess Royal, on 6 December – the last day of the BAPRAS Congress 2024. The Princes Royal took over the role of patron in 2022, after the passing of her father the late Duke of Edinburgh, who held it for the previous 57 years.
BAPRAS, which represents the majority of reconstructive and aesthetic plastic surgeons providing services to patients in the UK today, held its 3-day Scientific Congress, themed International, at the International Convention Centre in Newport, South Wales. Her Royal Highness addressed an audience which included national and international plastic surgeons at all levels of their careers, as well

as nurses and allied healthcare professionals, to honour the history of plastic surgery.
The Princess Royal’s visit emphasised the specialty’s critical role within the NHS across numerous areas – such as congenital conditions treatment, post-cancer reconstruction, trauma surgery and complex wound management – and recognised BAPRAS’s role as a leader in training and educating plastic surgeons who are committed to the highest standards of care.
BAPRAS Congress 2024 brought together over 500 people from 20 different countries, fostering collaboration in creating a platform for advancing the speciality. The Congress also highlighted the impact of furthering global knowledge through the Journal of Plastic, Reconstructive & Aesthetic Surgery – the second largest journal of its kind –
and overseas education with the British Foundation of International Reconstructive Surgery and Training.
The visit reiterated BAPRAS’s mission of training and education in plastic surgery for the benefit of patients, and its role in bringing the international community together to promote innovation in teaching, learning and research.
Consultant plastic surgeon and BAPRAS president Mani Ragbir spoke on the visit, saying: “We were deeply honoured to receive a visit from our Royal Patron at this year’s Congress. The Princess Royal is regarded as one of the hardest working members of the royal family, and with her support for the military services we are thrilled she, as His Royal Highness the late Duke of Edinburgh did before her, feels a connection with the work and origins of our profession.” q
[LAST MONTH MARKED the 10th anniversary of Eye-Law Chambers. The chambers grew from a small fledgeling with two experts to a trusted group of nearly 20 medicolegal experts, who are also leaders in their area of expertise.
The landmark occasion was marked by a gathering of members and families, and a pleasant meal at the top of The Shard with wonderful views. As the evening progressed, the discussions on the table where Dr Ayman Khaier MB BS MSc FRCSEd FRCOphth was sitting were diverse, and the topic of consent in ophthalmology came up.
Dr Khaier is a consultant in paediatric and neuro-ophthalmology. He explained: “Many a time, patients find it difficult – and perhaps emotional – to make an educated assessment of the risks and benefits of ophthalmic procedures when faced with information and statistics given to them by their practitioner. A 2008 survey of cataract surgery patients found that 32% prefer not to know about the possible complications of surgery and trust their surgeon to decide on their behalf. In the era of Montgomery this is not admissible in a court of law. However, a degree of flexibility in the consent discussion is probably reasonable.
“The GMC guidance sets out that shared decision-making and consent are fundamental to good medical practice. It promotes taking a proportionate approach, exploring what matters to a patient, and discussing benefits and harm in a manner that is clear, up to date but also considerate to the patient. Clearly, the key word here is in it being a shared process, that allows the patient to make an educated decision about their treatment.”
That level of dialogue, together with shared opinion, is what makes Eye-Law Chambers more relevant than ever.
Dr Khaier continued: “The unique ability to share learning and expertise allows the medicolegal expert to provide a robust and nuanced assessment that is beneficial to the court, the solicitor and the client. Thus, adopting a group practice in ophthalmology does more than just elevate the professional standards; it nurtures a supportive environment that benefits all stakeholders.
“So, as we look forward to the next 10 years, Eye-Law Chambers intends to provide the context for the highest possible quality reports which meet the expectations of the judiciary. This will promote an effective relationship with solicitors and agencies and raise the practice standards across the ophthalmological medicolegal scene.” q
[FOLLOWING A PERIOD of consultation and feedback, the General Optical Council (GOC) has launched its new Standards of Practice for Optometrists and Dispensing Opticians, Standards for Optical Students and Standards for Optical Businesses. The changes came into effect from 1 January, coinciding with the start of the new CPD cycle.
The standards outline the behaviours, attitudes, conduct and professional practice expected of registrants. They describe the minimum standard of care which patients and the public can expect from optical professionals, and inform the GOC’s decision making about the fitness to practise of professionals.
The changes to the standards have been made after a period of extensive consultation with key stakeholders, including patients and the general public. The revised standards reflect developments in practice, such as the increased use of digital technologies, as well as the changing expectations of patients and the public, such as registrants identifying themselves and their role during a consultation.
The changes aim to improve the clarity and alignment of the GOC’s standards to ensure that they reflect emerging changes in the sector. It is important to note that most of the existing standards have not changed, the GOC says, but key changes that have been put in place address these issues:
• Delivering better care for patients in vulnerable circumstances
• Requiring registrants to identify themselves and their role, and
• advise patients who will provide their care
• Maintaining appropriate professional boundaries, including
• prohibiting conduct of a sexual nature with patients
• Promoting better workplace cultures by explicitly referencing
• inclusive behaviour between colleagues and ensuring employers
• support staff who have experienced discrimination, bullying or
• harassment in the workplace
• Keeping updated on developments in digital technologies and
• applying professional judgement when utilising the data they
• generate to inform decision making

• Maintaining confidentiality when sharing patient images online
• Demonstrating leadership in practice, for example by supporting the
• education and training of others.
Registrants have been required to utilise the new standards as of 1 January 2025. A short animation video outlining the changes has been produced and can be viewed at www.youtube.com/ watch?v=Ld5LaM9bmws q


[THE NUMBER OF PEOPLE with glaucoma, age-related macular degeneration (AMD) and cataracts is set to increase over the next 10 years. That is the prediction of the UK Eye Care Data Hub, a new online tool that is set to be a critical planning resource for commissioners and providers of eye health care.
Eye disease is a major contributor to National Health Service backlogs, and the number of cases is set to significantly increase with an ageing population. Organisations from across the UK’s eye care sector, led by The College of Optometrists, have collaborated to launch this new data tool to support health care commissioners and providers plan and design future eye care services.
The new data tool forecasts the number of people expected to have a wide range of eye diseases and conditions and models the future eye care workforce, by UK nation and region, over the next 15 years. The number of people with the following conditions are predicted to increase across the UK over the next 10 years:
• Late-onset AMD by 24.4%
• Primary open-angle glaucoma by 15.9%
• Vision impairing cataracts by 16.7%
The tool models over 40 eye conditions and more will be added in future updates to provide a comprehensive view of eye disease and conditions across the UK.
The UK Eye Care Data Hub allows users to calculate the future eye care workforce, spanning both primary and secondary eye care services. That vital insight will support eye care and service planners across the UK to understand how the workforce will change over time.
While the number of optometrists is forecast to increase by 38.2%, orthoptists by 50% and consultant ophthalmologists by 71.2% over the next 10 years, there is also projected to be a decrease in dispensing opticians (-11.7%) and nurses specialising in eye care (-33.3%).
Current hospital capacity is already failing eye care patients, with long waits across the UK and tens of thousands of patients waiting over a year for treatment: putting them at risk of irreversible sight loss. Even with a predicted increase in some areas of the eye care workforce, experts are worried that hospital capacity will not meet the level of demand forecast by the increase in prevalence of eye conditions and eye disease. That is why professional bodies representing the eye care workforce are calling for both greater investment in training and a recognition that services should be remodelled to make best use of the eye care expertise available in and out of hospitals.
The new open-access online tool has been designed to support all health systems across the UK, optimise the existing eye care workforce, address health inequalities, and identify priorities for future eye care workforce
education, training and development to support new models of care.
For eye care sector employers, the tool will enable them to make decisions about recruitment planning and investment in higher qualifications and training, informed by forecast future demand and trends in eye disease prevalence.
Dr Gillian Rudduck MCOptom, president of The College of Optometrists, commented: “With the launch of the UK Eye Care Data Hub, eye care commissioners and service planners across the UK will have access to critical data and insights to support them to plan services that meet the evolving needs of their local area more effectively. This will help ensure patients receive the right care, in the right place, at the right time, as well as reducing hospital waiting lists for the most urgent and complex cases.
“We believe that by commissioning more eye care services in primary care, health commissioners can provide more timely access to effective eye care for an ageing population and ultimately help prevent avoidable sight loss."
The College of Optometrists led the project to develop the tool on behalf of the UK’s eye care sector. The project was supported and cofunded by the Association of British Dispensing Opticians, the British & Irish Orthoptic Society, the Department of Health Northern Ireland, the Federation of Optometrists and Dispensing Opticians and The Royal College of Ophthalmologists.
The tool was developed by York Health Economics Consortium (YHEC) at the University of York. Eye disease prevalence and incidence data was compiled by 16 expert working groups of The Royal College of Ophthalmologists. YHEC led on all other aspects of the model, including workforce. q
[ THE BRITISH DENTAL ASSOCIATION (BDA) has reported that, while government has discovered the demand for urgent dental care to stand at 2.2 million people, it has covered less than a third of that total.
In an annex to a message sent by NHS England to Integrated Care Boards following the rollout of commissioning for Labour’s manifesto pledge of 700,000 urgent appointments, officials stated: “This calculation gives a total estimate of 2.2m people each year (3.5% of the population) who are currently unable to get an NHS dentist appointment, and who have a treatment need. It is assumed that these are the people who would require urgent care appointments.”
Revealing that information, the BDA says: “We are not surprised that, having discovered this level of need, officials stuck to a relatively modest level of delivery. Treasury pressure had already seen pledges of new money from the ‘non-dom’ squeeze dropped in October, with the 700,000 appointments paid for by recycling underspends in the dental budget, which are fuelled by on-going recruitment and retention problems.
“At the launch of this policy last week, we stressed the extra appointments would translate into each of the 24,200 dentists recorded as doing some NHS activity last year seeing the equivalent of little over two extra urgent cases a month. Our analysis of government data – the same data underpinning NHS England modelling for urgent care –shows total unmet need for NHS dental care in England amounts to
[ THE PROFESSIONAL STANDARDS AUTHORITY (PSA) annual review of the General Dental Council for 2023/24 found that the GDC met 16 out of 18 Standards of Good Regulation. Where the GDC fell short were on the standards for equality, diversity and inclusion (EDI) and fitness-to-practise timeliness.
This year the Standards for Registration were met, by reducing the backlog of overseas-qualified dentists who applied as dental care professionals (DCPs) significantly. The backlog of unworked DCP applications, which stood at 5,700 in April 2023 following a change in legislation, has now been eliminated, with all remaining applications scheduled to undertake a panel assessment by April 2025.
Key achievements highlighted in the review include reducing the average processing time for UK graduate registration to two weeks, enhanced support systems for those involved in fitness to practise (FtP) cases and strengthened stakeholder engagement and consultation processes.
Tom Whiting, chief executive of the GDC, said: “We welcome the PSA’s recognition of our progress across multiple areas, particularly in registration, while acknowledging there is more work to do. We remain firmly committed to improving fitness to practise processes and implementing our EDI strategy.
“Our priority is ensuring we deliver effective regulation that protects patients and supports dental professionals. We welcome close working with partners and stakeholder organisations to build trust in effective regulation and achieve a goal that we all share, which is patient safety and public confidence in the dental professions.” q
13 million, or one in four of the adult population.”
The BDA also called for Integrated Care Boards to build in capacity for follow-up care for high needs patients.
“Many patients will need further dental treatment once their immediate urgent care needs are met,” the BDA said. “Some existing local schemes allow flexibility for these patients to return for follow-up care and this good practice should be adopted elsewhere.”
The BDA quoted examples from around the country where lack of availability of dental care had led to medical emergency and even, in one case, death.
"So, it seems a new government discovered the need for urgent care, but chose just to cover a third of it,” said General Dental Practice Committee chair Shiv Pabary. "This is austerity on stilts. Rather than eliminating DIY dentistry, the Treasury is ensuring we keep seeing horrors that belong in the Victorian era.
"We are clear that ministers across England, Scotland, Wales and Northern Ireland have a moral responsibility to ensure no patient is ever left in this position.” q
[THERE WAS UNITY across the dentistry profession in calls for the new chair of the General Dental Council to be a dental registrant. As applications closed for the position on 24 February, professional bodies and specialist societies came together to sign an open letter to that effect.
From dental nurses to dental therapists, the message was signed by 11 bodies representing almost all the regulator’s registrant group, specialist bodies from gerodontology to perio and the full spectrum of NHS, private, routine and cosmetic dentistry.
The letter reads in part: “Lord Harris [the outgoing chair] has left a long lead time to ensure the right process is in place for selection of a successor. We want the right person for this role, and so we are united that the next Council Chair must be a registrant.
“Rebuilding trust is a journey, not a final destination. We want to ensure your next Chair can bring knowledge, insight and empathy from the coalface to the task ahead.” q

[A NEW IMAGING TECHNIQUE called field-cycling imaging (FCI) offers hope for earlier detection and improved monitoring of osteoarthritis, potentially transforming how clinicians understand and treat the condition.
Usually, the early signs of knee osteoarthritis (OA) go undetected until significant joint damage has occurred. Current detection methods are not sensitive enough to identify the condition in its early stages and clinicians lack clear indicators of its onset.
The early detection of knee OA is critical to slowing the disease's progression and improving people’s quality of life. Currently, there are no diagnostic methods that can reliably detect OA in its early stages, which means many people miss the opportunity for timely intervention.

The inability to detect changes in the knee at an early stage is partly the reason why there are still no treatments which can slow down the progression of OA. Being able to detect OA and monitor its progress may open the door to new treatment options before the disease progresses further.
A breakthrough in early detection
Previously, researchers at the University of Aberdeen discovered that a property of the cartilage of the knee which determines response to different magnetic fields, is starkly different in osteoarthritic cartilage compared to healthy cartilage. That finding could mark a key breakthrough in early detection. Identifying changes in how the cartilage responds to different magnetic fields before damage occurs could be a crucial indicator of OA onset. The discovery was made possible via FCI.
Developed at the University of Aberdeen, FCI follows in the footsteps of magnetic resonance imaging (MRI). The first MRI scanner was also invented at the University of Aberdeen around 50 years ago and has since gone on to save millions of lives.
FCI works similarly to MRI, but with one key difference: FCI can very quickly change the strength of the magnetic field during the scan.
Traditional MRI uses a constant magnetic field throughout the body to create images, while FCI can adjust the magnetic field at different points during the scan.
Dr James Ross from the University of Aberdeen explained: “Being able to change the strength of the magnet allows us to see how different tissues respond to different magnetic fields.
“We already know from our research that the way that tissues respond to different magnetic fields changes in disease, potentially at quite an early stage. Because these changes are sensitive to disease, this information might potentially be used as a new diagnostic ‘biomarker’ for many conditions, including osteoarthritis.
“It is exciting to be part of the team who brought MRI to the world and now with FCI technology, the possibilities are endless for disease detection and diagnosis”
PioKneering the future of knee osteoarthritis detection
Versus Arthritis has funded the PIOKNEER study, led by Professor Cosimo de Bari – who recently moved from the University of Aberdeen to the University of Edinburgh – to further investigate the potential of FCI to detect early knee OA. Previously, researchers had studied small samples of cartilage from people undergoing joint replacement surgery. With the PIOKNEER study they will move from these cartilage samples to scanning living people.
The researchers will track individuals who are experiencing knee pain but who have no visible signs of OA. Through annual FCI scans, researchers will look for early signs of disease progression, identifying the moments when FCI might be most useful for early diagnosis.
While FCI is a powerful new tool, it is not designed to replace traditional MRI or other imaging techniques. Instead, it complements existing methods by providing additional, unique insights that current technologies cannot capture. Just as ultrasound and X-rays offer different perspectives on a patient's health, FCI will add another layer of valuable information to help doctors understand knee OA in more detail.
The PIOKNEER study marks the beginning of a new era in understanding knee OA diagnosis and treatment. As researchers continue to study the effectiveness of FCI, the innovative technology has the potential to become a standard tool in clinical practice. The results from the study will be compared with similar research worldwide, ensuring that the best possible approaches to the early detection of OA are developed. q
[IMPROVING HEALTH AND WORK OUTCOMES for the over 20 million people with musculoskeletal (MSK) conditions in the UK forms a key part of the government’s mission to build an NHS fit for the future and kickstart economic growth. Healthcare professionals play a vital prevention and early intervention role in supporting people to self-manage their MSK condition and enabling them to work.
The 2025 Healthcare Professionals’ Consensus Statement for action on health and work – produced jointly by the Academy of Medical Royal Colleges, Royal College of Nursing and Allied Health Professions Federation – contains a commitment to work over the next five years to promote ‘good work as a health outcome’ across the health and care sector. It is intended to support patients, including those with MSK conditions, to return to and remain in ‘good work’. The statement has been endorsed by government.
The role of health professionals in keeping people well in work and enabling return to work
In addition to asking patients what they do for work, and how they are managing it, healthcare professionals may support people in their work as an integral part of patient care pathways. Healthcare professionals can also promote a culture where good work is seen as a benefit to people. Through promoting healthy life choices and lifestyles, healthcare professionals might also contribute to the prevention of ill health and injury, so reducing risk of people falling out of work, as well as supporting people to enter, remain in, or return to work.
The organisations behind the consensus have committed themselves to work over the next five years to support healthcare professionals to engage more proactively with, and to celebrate and advance the concept of, ‘good work as a health outcome’ across the health and care sector. They will work together, as individual organisations and collaboratively, to enable every healthcare professional to:
• Ask the work question – what do you do for work; how are you
• managing in work; and what may help you get back to work?
• Understand through training the importance of work as a health
• outcome; how health may be promoted through good work and where
• to signpost their patients who need further support.
• Be able to advise their patients through easy access to up-to-date
• guidance from government, professional bodies and health
• professionals on the impact of health conditions and treatment on their
• work, and on adjustments to assist those with disabilities.

• Derive most value from the ‘Fit Note’ in primary care, hospitals and
• in the community, through training for health professionals and utilising
• updated easy-to-use guidance.
• Recognise their own role in supporting healthy and safe working
• environments, looking after their own health and wellbeing, and
• promoting the health and wellbeing of their colleagues within the
• organisations in which they work.
The full statement can be read on the website of the Academy of Medical Royal Colleges at www.aomrc.org.uk q
[I GRADUATED as a chartered physiotherapist in 1987 and undertook 17 years of clinical practice in rheumatology and orthopaedics. I now lecture at the University of Salford and worked as medical director for Chinese students attending Corpus Christi College, Cambridge between 2015 and 2019; I have also lectured in Brazil.
From 1990 to 1993 I was the physiotherapist for the women’s football ‘Lionesses’ squad and I am the author of 10 textbooks translated into 11 languages. I hold a PhD in rheumatology and am a member of the Medico Legal Association of Chartered Physiotherapists.
I began my medico-legal work roughly six years ago. While the learning curve was initially steep, it is now an extremely gratifying and fulfilling part of my career that allows me to maintain my CPD activity – and to give something back to the profession that has given me so much. While I had lectured theoretically about ethics, consent and scope of practice for many years, it is now extremely valuable to see those cases in real-life scenarios.
It is a two-way street, as the cases that I work on – anonymised for data protection – can now feed back directly into my teaching to inform the next generation of chartered physiotherapists.
I enjoy the attention to detail and the almost detective-like nature of the cases I am instructed on. It is also essential that I remember that, on occasion, people's careers are at stake; therefore, a balanced view presenting all possible aternative opinions is extremely important.
One of the most interesting parts of being a medico-legal expert witness is the wide scope of cases that come my way. Those cases range from clinical negligence to Health and Care Professions Council investigations for inappropriate behaviour and professional misconduct, and appeals to EHCP tribunals for children with disabilities. I have also worked on cases for the Ministry of Defence and undertaken prison visits. Each case is uniquely different, requiring great attention to detail all the time: remembering my duties are to the court and not to any particular side. In all the cases I have worked on, I have had complete respect from all parties I have dealt with. Also, our clinical interest group, the Medico Legal Association of Chartered Physiotherapists, has been a great

resource since it can be a rather lonely journey at the outset; and to call oneself an expert goes against all principles of humility instilled into us as healthcare professionals. The key is to recognise what cases I am qualified to take instruction on and what I am not.
Some cases I have worked on in the past include:
• Alleged inappropriate therapeutic touching by a sports coach
• Alleged clinical neglect post intravenous insertion, resulting in a skin
• flap and amputation in a minor
• Alleged lack of duty of care involving a fractured femur in a minor
• Assessment of care for a young adult with spastic quadriplegia
• Assessment of a minor with a chromosomal disorder
• Alleged failure by a physiotherapist to recognise compartment
• syndrome
• HCPC investigation of professional practice, including inappropriate
• behaviour, alleged assault and clinical negligence
• Alleged assault in prison resulting in a hand fracture
• Ministry of Defence: alleged neglect following a parachute accident
• Alleged inappropriate touching by a sports coach
• Alleged electrotherapy burns by a chartered physiotherapist
• Assessment of person in prison accused of assault/attempted
• murder
• Alleged mortality caused by inappropriate physiotherapy discharge
• post-spinal decompression surgery
Try not to think of yourself as an island; seek out the advice of other experts and listen carefully to the advice that they give. Be true to yourself and remember that your duty is to the court and that the instructing parties are genuinely interested in your opinions and will give you the respect that you deserve. q
[TOWARDS THE END OF LAST YEAR
the Faculty of Pain Medicine (FPM) of the Royal College of Anaesthetists reported it had received reports from doctors and patients that forced reduction of opioids is taking place in some parts of the UK in patients who have been taking opioids for pain for long periods of time with reported benefit. At its worst, that may involve no more than written notification that opioids are to be withdrawn by the prescriber as a one-size-fits-all policy decision.
The FPM stated: “We strongly advise against this unsafe practice – it is also contrary to current NHS and NICE Guidelines, which clearly state that ‘prescribing and deprescribing decisions should be made jointly with the patient’ and ‘dependence forming medicines should never be stopped abruptly unless they have been taken for only a short time’.
“There is compelling evidence that such action may lead to psychological destabilisation, self-harm and death. Rapid reduction is usually appropriate for those taking opioids in response to a resolving physical trauma such as pain after surgery, who have been recently started on opioids. It is both inappropriate and dangerous to adopt this approach more generally in patients
who are living and coping with chronic pain.”
The FPM said it was further aware that medico-legal, fitness-to-practise and coroner’s cases have scrutinised the decision-making process around opioid prescribing and most recently opioid reduction in both primary and secondary care.
“Adverse criticism is also to be expected with inappropriate, unsafe practice associated with rapid de-escalation/cessation of opioids in this manner,” the FPM said.
When healthcare professionals are engaged in opioid optimisation – the FPM preferred term – it is imperative that they are aware of the guiding principles and act accordingly, placing patient safety first. The FPM has produced publications to guide best practice in opioid prescribing, including Opioids Aware, which defines the principles that should be applied. They include:
• Individualised risk assessment on the
• benefits and harms of opioids.
• A comprehensive biopsychosocial
• assessment of pain.
• Decisions to reduce opioids to be
• undertaken within a comprehensive shared
• decision-making framework.
• Psychological assessment of risk with
• reduction.
• Appropriate management of patient non-
• engagement.
The usual clinical approach is to strive further for shared decision making by detailed explanation and careful management of patient concerns, and to avoid unilateral opioid reduction. The healthcare professional must have demonstrably exhausted all available avenues of patient engagement to consider opioid reduction in this extremely difficult circumstance. Infrequently, unilateral opioid reduction is desirable.
In summary, the opioid optimisation process requires meticulous individualised assessments and decision making, detailed documentation with regular and timely monitoring, assessment and review.
Specialist pain management units can provide expertise and clinical support in dealing with the most complex patients while recognising that much of this work is undertaken in community care by experienced general practitioners, dedicated pharmacists and other professionals. The principles of care outlined above are nevertheless the same. q


By Dr Priscilla Kent, consultant psychiatrist
[
EACH YEAR, over 5,000 people in the UK die by suicide; however, it is very likely that that figure underestimates the true picture. While women attempt suicide more frequently than men, men are more likely to be successful. Suicide may be precipitated by a number of factors, including illness which is not necessarily psychiatric in nature, loss of social support leading to isolation, relationship breakdown, economic catastrophe and underlying personality traits.
The loss of a family member by suicide is often extremely traumatic for those left behind and litigation in those circumstances is very common. Around 50% of families have considered consulting a lawyer following the suicide of a loved one, and 25% have actually done so. Should a lawsuit be successful, financial settlements can be substantial.
However, as with every medicolegal case, it is necessary to prove that the treating psychiatrist and/or hospital staff were negligent; and it was that negligence which led to the patient’s death.
The reasons cited for pursuing a claim for medical negligence following a patient suicide differ slightly depending on whether the suicide took place in a hospital or outpatient setting. In hospital situations the key management points are an assessment of suicide potential at the time of admission, the precautions taken or systems used to minimise suicide attempts while an inpatient, and any changes made in the management of the patient in accordance with their perceived suicide risk.

medical and employment records, personal journals and computer hard drives – and legal documents, such as wills and life insurance policies. In this way a picture of the patient’s own and family psychiatric history, personality and lifestyle characteristics can be built up, together with recent stressors or conflicts and the patient’s reaction to them, the quality of interpersonal relationships and plans for the future. From there an overall assessment of suicidal intention can be made.

A criticism of the psychological autopsy procedure is that it lacks reliability and validity. To address those concerns, the Empirical Criteria for Determination of Suicide screening instrument has been developed to directly assess the patient’s mental state at the time of their death. It assesses the pathological, toxicological, investigatory and psychological evidence indicative of selfinflicted death, and has proved to be remarkably accurate at distinguishing between a suicide and an accident.
Clearly, litigation could be avoided entirely if every suicide could be prevented. In reality that is almost impossible to achieve. Many patients who die by suicide are successful on their first attempt, and many have not expressed any suicidal ideation or sought any type of psychiatric help before they die. Therefore, even if all those who have previously attempted suicide could be prevented from doing so again, many suicides would still occur.
The usual accusations are that the psychiatrist failed to use appropriate clinical judgement or to conform to appropriate medical practice, while the hospital staff may be charged with failure to carry out medical orders, not following hospital policy or not reporting significant events to the medical staff.
Common allegations following an outpatient suicide include failure to adequately assess the patient’s mental state and evaluate for suicide risk, failure to correctly diagnose the patient’s symptoms, to establish a formal treatment plan, to properly evaluate the need for psychological or pharmacological intervention, maintain adequate observation and supervision of the patient, or to initiate hospitalisation if necessary.
Before a lawsuit can be launched it must be established that the patient’s death really was suicide. Therefore, as well as determining the cause of death, the mode of death – which relates specifically to the patient’s state of mind at the time of their demise – must be investigated. In the absence of a note, the motive of suicide can be difficult to prove. In some circumstances, including cases involving hanging or firearms, the intent is clear; but that is often less true for scenarios such as single car accidents, falls and cases involving alcohol or drugs. Thus, distinguishing between suicide, accident, homicide or natural causes presents a challenge.
In that respect a psychological autopsy can be helpful in determining the mode of death. That procedure attempts to determine the state of mind of the patient at the time of their death through in-depth interviews with family and friends and close scrutiny of relevant records – including
Attempts to develop screening tools to identify those at risk of suicide have proved unsuccessful. Most lack both sensitivity and specificity, meaning that the rates of both false-positive and false-negative results are high. Furthermore, without the correct resources in place, patients with positive screening results will remain untreated.
During their career, around half of psychiatrists will lose a patient to suicide; and there is a high chance that litigation will follow. In order to successfully defend a case, the defendant must show that they provided adequate, rather than perfect, care. Thus, comprehensive medical records, precise documentation of every decision taken –particularly those involving patient privileges – and adherence to clear hospital policies and procedures are vital.
The best strategy is prevention, but that is difficult to achieve as no universal screening tool exists. In addition, psychiatrists should be particularly careful when encountering patients who do not fit the typical profile not to dismiss the risk of suicide completely. q
• Dr Priscilla Kent is a consultant psychiatrist, currently providing clinical lead to a busy Community Mental Health Team in South Hackney, London. Her areas of expertise include the diagnosis and treatment of depression, anxiety, obsessive compulsive disorder, stress-related disorders, bipolar affective disorders, psychosis, personality disorders and adult ADHD. She is available for medicolegal consultations in London.
Visit www.medicolegal-partners.com/our-experts/dr-priscilla-kent/ to find out more, or email info@medicolegal-partners.com to discuss a case or to instruct Dr Kent.

[ EXPERT IN MIND , alongside its sister company, The ADHD Clinic, has announced another series of their complimentary CPDaccredited webinars, planned to take place throughout 2025. With a prestigious history spanning over 16 years, Expert in Mind has established itself as a leading expert witness firm specialising in mental health.
The company boasts a dedicated team of experienced psychiatrists and psychologists, whose in-depth knowledge and skills are crucial to the production of high-quality court reports for various legal areas, including family law, personal injury, clinical negligence, criminal cases, immigration and housing matters. Their webinars cover topics including but not limited to PTSD, Neurodiversity, Sex Offenders and Perinatal Psychiatry.
Responding to an increasing demand for expertly-handled ADHD assessments in a timely manner, Expert in Mind inaugurated The ADHD Clinic. Led by the esteemed Consultant Psychiatrist, Dr Sajid Suleman, the clinic has a team of 15 leading psychiatrists and psychologists, who collaborate with an efficient senior leadership and administrative team.
That collective effort ensures the provision of comprehensive and dependable services for both children and adults on their ADHD journey, offering assessments with short waiting times and treatments aligned with NICE guidelines. Additionally, the clinic provides expedited Autism Spectrum Disorder (ASD) assessments to meet the community’s pressing needs.
The ADHD Clinic not only provides assessments, but also focuses on comprehensive treatment plans that include medication management and psychosocial interventions for patients and their families. At the core of their business they uphold values that embody professionalism, knowledge, clarity and respect. That approach ensures that individuals receive the support necessary to improve their overall functioning and quality of life.
Dr Suleman (right), Clinical Lead at The ADHD Clinic and renowned medico-legal expert, has partnered with Dr Bhatnagar (below right), another highly experienced Consultant Adult Psychiatrist, expert witness and ADHD Clinic Clinician, to present this webinar on Autism in Adulthood on 13 June at 9am (1.5-hour duration).


This webinar will delve into key aspects of adult autism and cooccurring conditions such as ADHD.
It is an opportunity to have pressing questions answered by leading experts in the field and to receive a comprehensive exploration of adult autism – covering everything from diagnosis and treatment options to its impact on daily life, challenges and strengths.
Following the overwhelming success of his previous webinar on adult ADHD, Dr Nayrouz (right), an accomplished London-based Consultant Psychiatrist and Clinical Professor of Psychiatry, recently returned by popular demand with the highly anticipated session, Unlocking Focus Part 2, which is now available on-demand.

This engaging and informative webinar offers a valuable opportunity to expand understanding and enhance professionals’ ability to support clients with ADHD. Building on the insights from Part 1, this webinar delves deeper into the complexities of adult ADHD, offering advanced strategies to better understand and support clients navigating this often-misunderstood condition.
For those who missed Unlocking Focus Part 1, the team at The ADHD Clinic can provide access to watch it on-demand.
ADHD can significantly impact daily life, making it challenging to stay organised, maintain focus, meet deadlines and manage commitments. Procrastination, forgetfulness and difficulties in task completion are common struggles. Additionally, ADHD is often accompanied by psychiatric co-morbidities, including anxiety, depression, substance misuse and ASD.
When left undiagnosed or untreated, ADHD can contribute to lower academic achievement, employment instability, relationship difficulties and an increased risk of legal and safety issues.
Individuals with ADHD are also more likely to experience chronic sleep disturbances, heightened stress levels and persistent fatigue, further impacting their overall well-being. But ADHD and its associated symptoms are highly treatable, as Dr Nayrouz explained further.
Designed for legal and healthcare professionals, this session offers a well-rounded perspective on autism’s complexities and profound effects on adulthood. Autism Spectrum Disorder is a lifelong neurodevelopmental condition that affects social interaction, communication and behaviour in varying degrees. While it is often diagnosed in childhood, many adults remain undiagnosed or struggle to navigate life without adequate support.
Expert in Mind continuously offers a wide array of complimentary, insightful webinars throughout the year, covering various topics that are crucial for legal and healthcare professionals. These educational sessions are instrumental for anyone looking to expand their knowledge and make an effective impact on their professional fields.
Engaging with these educational opportunities enriches professional knowledge and significantly enhances the outcomes for individuals affected by mental health difficulties such as ADHD and autism. q
• For those interested in attending complimentary CPD-accredited webinars, the full 2025 schedule and access to those on-demand can be found at www.expertinmind.co.uk
For more information relating to The ADHD Clinic, or to book an assessment, visit wwww.theadhdclinic.co.uk ; tel 01424 533259; or email office@theadhdclinic.co.uk
[SIGNIFICANT SYSTEMIC ISSUES, lack of patient and family involvement and cultures of fear and blame contribute to mental health services not learning from inpatient deaths. That was the conclusion of a report from the Health Services Safety Investigations Body (HSSIB).
The report is the result of an investigation into how mental health providers learn from deaths in inpatient units and those up to 30 days after discharge.
According to the HSSIB: “Our comprehensive findings evidence significant challenges in maintaining safety, conducting effective and timely investigations and ensuring system-wide learning. We identified that, whilst investigations and patient safety event analysis aim for transparency and learning, they are often of variable quality. For example, local investigations often have incomplete information to inform the findings, or they do not routinely undertake observations of clinical work to understand how care is delivered in practice.”
A key finding in the investigation was that there is a culture of blame where individuals – including patients and families – and organisations fear safety investigation processes. The report highlights that patient safety investigations often do not consider the emotional distress experienced by all affected, resulting in compounded harm. Bereaved families described having to fight to be involved in investigations, with some describing the
investigation process as ‘worse than the actual death because they were reliving the death over and over again’.
Many families shared with HSSIB that they feel marginalised and excluded from the investigation process, experiencing them as a ‘tick box’ exercise and without a culture of transparency, learning and accountability.
Commenting on the report, the president of the British Psychological Society Dr Roman Raczka said: "The latest report from the Health Services Safety Investigations Body highlights the urgent need for joinedup care for those using mental health inpatient services, as well as those who have been recently discharged.
“Over 6 million referrals are made to NHS Talking Therapies and other mental health services every year in England alone. Service users deserve high-quality care in safe and compassionate environments whilst accessing inpatient services, and in the community upon discharge.
“There must be an opportunity to effectively learn from patient safety incidents; however, a long-term lack of investment in services is preventing this from happening. The government must properly fund mental health services and grow the workforce, while embedding a greater focus on prevention. Only then will mental health patients, and their families, get the expert support they need.” q
[ANALYSIS BY the Royal College of Psychiatrists (RCPsych) of NHS England data shows that 319 children and adolescents in England were forced to travel out of their area for mental health treatment from December 2023 to November 2024. That represents, as the RCPsych points out, nearly one child every day.
Those children and young people under 18 spent a total of 35,845 days away from their local area – known as inappropriate out-of-area placement (OAP) bed days – as a result of beds being unavailable in their local area.
The RCPsych is calling on the UK Government to set a target date to end OAPs in child and adolescent mental health services (CAMHS) across England.
Extremely vulnerable children and young people with serious mental illnesses, such as eating disorders, self-harm and psychosis, are being treated miles away from their loved ones and support networks, as a result of inappropriate OAPs. With family and friends having to travel so far, visiting often becomes impossible, which only leaves unwell children feeling more isolated and lonely, and can be harmful to their recovery. When a child or adolescent is treated as an inpatient in local CAMHS services, stays tend to be shorter.

Many children are being treated in paediatric wards, without access to specialist mental health services during their stay, or even after discharge. Those environments can feel overwhelming, particularly for those with neurodevelopmental conditions such as autism.
Dr Guy Northover, deputy chair of the Royal College of Psychiatrists’ Child and Adolescent Faculty, said: “It is unacceptable that sick and extremely vulnerable children and young people with mental illness are still being sent miles away from their family and friends, sometimes for months on end, simply because they need treatment that is either not available as community care or within a local inpatient setting. Although we know that some improvements have been made compared to last year these figures are still unacceptably high. One child being sent away from home almost every day is simply unacceptable.
“At a time when these children are having to cope with a mental illness,
the last thing they need is to be left isolated, lonely and unsupported. It is also counterproductive as it will take longer for them to recover, lengthening their stay out of area and putting more pressure on overstretched services.” q
By Lisa Crowther of Carter Brown
[IN RECENT YEARS the UK family courts have seen a shift towards increased transparency. That movement, aimed at making the family justice system more open and accountable, has profound implications for all involved, particularly expert witnesses.
From 27 January the reporting ‘pilot’ which commenced in 2023 has been extended across all courts, enabling journalists or accredited ‘legal bloggers’ access to all hearings heard by a judge within public law children’s (or care) proceedings and greater access to hearings in other types of family proceedings.
Experts, who play a crucial role in providing objective opinions on complex matters, such as where children live and who they spend time with, parenting capacity and all aspects of a parent’s functioning – including psychological and psychiatric assessments – face a challenging and changing landscape.
The increased push for transparency stems from a desire to ensure that the public has a clearer understanding of, and confidence in, how decisions are made and that the processes within family law are fair and consistent. Court hearings are now more open, and the publication of judgments online is encouraged within the judiciary. That has led to increased scrutiny of experts’ contributions to cases. There are both benefits and challenges tied to that shift.

For expert witnesses, transparency can lead to greater public confidence in their role within the family justice system. Knowing that their assessments and recommendations will be publicly accessible and reviewed should only encourage experts to ensure their work is thorough, objective and well documented. Within family proceedings there are clear quality standards that all experts should comply with, which cover all aspects of an expert’s work: from training and development to appropriate insurance, information security and safeguarding arrangements.
However, one key concern is the risk of misinterpretation. Expert evidence can be highly technical and difficult for those outside of the profession to fully understand. With judgments and expert reports being made publicly available, there is a real risk that expert opinions could be oversimplified or misunderstood by the public, potentially damaging the credibility of the witness, or misrepresenting their findings. Recent scrutiny of expert evidence in the Lucy Letby case shows that, even among experts, there can be disagreements over interpretation of information.
Moreover, increased transparency may influence experts’ willingness to take on contentious or sensitive cases. With a heightened risk of their work being exposed to public scrutiny, some experts might hesitate to offer their opinions in particularly high-profile or emotionally-charged cases. That could lead to a reduced pool of available experts, which could affect the quality of evidence presented in family law cases and the timeliness of disposal where appropriate experts are in short supply.
The push for transparency in the family courts requires a delicate balance. While it has the potential to enhance the accountability and integrity of the justice system, it also places increased pressure on expert witnesses. For family lawyers it is important to navigate this new landscape carefully, ensuring that expert evidence is presented in a way that maintains both its integrity and its accessibility to the public. q
ACCIDENT & EMERGENCY MEDICINE













MEDICAL NEGLIGENCE

MICROPIGMENTATION
NEONATAL MEDICINE








OBSTETRICS & GYNAECOLOGY





OPHTHALMIC SURGEONS




ORTHOPAEDIC SURGEONS











PHARMACOLOGY


PHYSICIANS






PSYCHOLOGISTS
RADIOLOGISTS



SKIN CAMOUFLAGE CONSULTANTS

SPEECH & LANGUAGE THERAPY




TRICHOLOGISTS

TOXICOLOGY





EXPERTS FOR MEDIA is a regular section in Your Expert Witness for experts who wish to offer their views and the benefit of their experience to the vast range of print and broadcast media.
Ever wondered how news teams find the experts they consult to explain the ramifications of breaking news stories, seemingly at the drop of a hat? Or how the producers of TV drama series ensure their stories are accurate and reflect the realities of the professions they portray?
The fact is that researchers consult registers of experts and expert periodicals just as lawyers do. In fact, Your Expert Witness is receiving an increasing number of enquiries from media researchers and public relations agencies looking to locate appropriate experts to inform their clients.
Experts for Media is therefore an ideal space to attract their attention. For prices and to book your space, contact Ian on 0161 710 3880 or via ian@dmmonline.co.uk
Mr Francis Michael Brooks BSc MBBS MD FRCS Consultant Orthopaedic Spinal Surgeon
Mr Brooks is experienced in the treatment of all degenerative adult spinal conditions as well as trauma and tumour. He undertakes instructions relating to personal injury claims in general orthopaedic, spinal and trauma injuries on behalf of either claimant or defendant.
T: 07732 989991 E: brooks.francis@gmail.com / spinalreports@gmail.com

Joanne Caffrey Expert Witness & Trainer
Ms Joanne Caffrey undertakes expert witness instructions in cases relating to the following police topics:
• Use of force
• Custody procedures
• Drink/drug driving
• Ligature deaths
T: 07528 800 720 E: joanne_caffrey@sky.com

Professor Paul J Ciclitira
MB PhD FRCP MRCS FRCP AGAF Professor of Gastroenterology
Professor Ciclitira has a particular interest in food allergy, including Coeliac disease, peptic ulcer, inflammatory bowel disorder and hepatology. He undertakes expert witness instructions in cases relating to all of these conditions, acting on behalf of either claimant or defendant or as a Single Joint Expert.

T: 0207 603 3594 E: gastropjc@gmail.com W: www.profpaulciclitira.co.uk
Mr Jeremy Crew
MA MD BChir(Cantab) FRCS(Urol) Consultant Urological Surgeon

Mr Jeremy Crew has offered a medicolegal service for over sixteen years. He provides expert medical opinion, medico-legal reports and court attendance on all aspects of urology including clinical negligence, personal injury and criminal matters.
T: 01865 307433 or 07508 617949 E: jeremycrew@urologyoxford.com W: www.oxfordurology.co.uk
Mr Robert Hensher
FRCS FDSRCS
Consultant Oral and Maxillofacial Surgeon
Mr Hensher’s subspeciality interests include dental implantology, facial injury and temporomandibular joint replacement. He prepares over 50 reports yearly including negligence and criminal cases.
E: jackiesorrell0101@gmail.com M: 07947445414
E: roberthensher@gmail.com M: 07836540457
Dr Dan Jones
PhD MSc BSc MA MEWI Cert Ecological Consultant - Japanese Knotweed


Chris Makin FCA FCMI FAE QDR MCIArb
Chartered Accountant • Accredited Civil Mediator • Accredited Expert Determiner
Chris Makin was one of the first chartered accountants to become an Accredited Forensic Accountant and Expert Witness. He is also an accredited civil and commercial mediator and an accredited expert determiner. Over the last 30 years he has given expert evidence at least 100 times and worked on a vast range of cases.
T: 01924 495888 or 07887 660072 E: chris@chrismakin.co.uk
W: www.chrismakin.co.uk

Mr Robert Marston
BSc(Hons) MBBS FRCS(Eng) FRCS(Edin) FRCS(ORTHO) Consultant Orthopaedic and Trauma Surgeon

Mr Marston has 25 years experience as an expert witness. His special interest is lower limb orthopaedics and trauma, particularly hip and knee arthroplasty, joint injuries and fractures. His main medico legal work is with alleged clinical negligence. He also takes on selected personal injury cases.
T: 07464 425 444 E: marstonmedicolegal@gmail.com W: www.marstonmedicalpractice.co.uk
Mr Luke Meleagros BSc MBBS MD FRCS
Consultant Surgeon
Mr Meleagros completes around 6-10 expert reports per month, the majority in medical negligence cases and a smaller number of personal injury cases. He has reported extensively on cases involving abdominal laparoscopy surgery and hernia surgery.
T: 0208 527 0977 E: L.Meleagros@btinternet.com
Sec: jawdobson@gmail.com

Dr Dan Jones undertakes expert witness instructions, including the preparation of expert reports and giving evidence in court, in civil claims relating to the growth and spread of all invasive plants. He can act on behalf of either claimant or defendant or as a Single Joint Expert.
T: 07967 408844 E: daniel@advancedinvasives.com W: www.advancedinvasives.com
Laird Assessors Automotive Expert
Laird Assessors are the UK’s leading independent automotive expert witness firm supporting claimant, defendant and criminal solicitors – from instruction to court. Laird provide intelligence to the automotive world predominantly relating to crashed vehicles.

T: 0151 342 9961 E: enquiries@laird-assessors.com W: www.laird-assessors.com

Materials and Structures
T: 01442 437500 E: info2@rsk.co.uk W: www.rskgroup.com RSK

RSK offers impartial specialist materials and structures expertise in support of legal matters. Our team of consultants can act as expert witnesses on behalf of either claimant or defendant or as a Single Joint Expert in a range of construction disputes.
Target Psychology Ltd
Providing Expert Witness Reports and Assessments
Target Psychology provide exceptional reports and their highly trained team of expert psychologists and psychiatrists regularly take instructions from solicitors and local authorities, providing assessments for families and individuals involved in legal proceedings.
T: 0161 425 1826 E: office@targetpsychology.co.uk
W: www.targetpsychology.co.uk