Luis Alzate-Duque, MD’14, and his canine sidekick, Nacho
KEITH B. BRATCHER, JR.
At Rutgers New Jersey Medical School, our standard of excellence in clinical care is second to none. As physicians and educators, we seek out and integrate the latest tools and technology to ensure we are providing the absolute best in patient care. But it’s not only about tools and technology. Hand in hand with this expertise is our commitment to humanistic, compassionate care.
This issue of Pulse shines a light on the many innovations in clinical care we are now using at NJMS. You’ll read about how our cardiology team is using artificial intelligence, or AI, in cardiovascular imaging. This high-tech tool enables cardiologists to see the intricacies of the heart like never before, making their diagnoses and treatments more accurate and efficient, and making prevention of future heart disease a reality.
The Global Tuberculosis Institute at NJMS is now using the latest smart technology to make TB treatment—which is usually many months long— far more convenient for patients. They no longer need to wait for a case manager to visit them at home or work with their medications.
Women’s health is also advancing at NJMS with the launch of a new center for the management of high-risk pregnancies. The Early Pregnancy As -
A Message from the Dean
sessment Clinic at University Hospital’s Ambulatory Care Center provides much-needed services to treat a variety of complications.
We are also doing pioneering work in the treatment of orthopaedic cancer. Read about a patient who developed a serious osteosarcoma in his leg at age six that spread to his arm. Through life-saving care from NJMS experts, he is now a happy, thriving college student.
While we are extremely proud of our technological advances to clinical care, humanism and compassion continue to be at the core of everything we do. Our students and physicians care about their patients as much as they care for them. They know that compassion is a powerful catalyst for healing.
Please take the time to read this issue of Pulse, and I’m sure you’ll agree that NJMS never stops striving to help patients in every way possible.
Robert L. Johnson, MD, FAAP’72
The Sharon and Joseph L. Muscarelle Endowed Dean Rutgers New Jersey Medical School
DEAN
Robert L. Johnson, MD, FAAP’72
The Sharon and Joseph L. Muscarelle Endowed Dean, Rutgers New Jersey Medical School
ASSOCIATE EDITOR
LaCarla Donaldson
Manager, Marketing and Communications
SENIOR EDITOR
Mary Ann Littell
CONTRIBUTING WRITERS
Ty Baldwin
Merry Sue Baum
Amanda Castleman
Nancy A. Ruhling
DESIGN
Sherer Graphic Design
PRINCIPAL PHOTOGRAPHERS
Keith B. Bratcher, Jr
John Emerson
KEEP IN TOUCH
Pulse is published twice a year by Rutgers New Jersey Medical School. We welcome letters and suggestions for future articles.
Send all correspondence to: Marketing and Communications
Rutgers New Jersey Medical School
ADMC Building 11, Suite 1110 30 Bergen Street Newark, NJ 07107 or via email to: njmsmarketing@njms.rutgers.edu
ON THE COVER
Luis Alzate-Duque, MD’14, came to the U.S. as a child, speaking no English. Now he gives students the same educational support he received.
Get Social with Rutgers NJMS
PHOTO BY KEITH B. BRATCHER, JR.
KEITH B. BRATCHER, JR.
FY i
Liver Transplant Program Again Ranked a Top Leader
Kudos to the NJMS/University Hospital liver transplant team! The Center for Liver Transplantation at UH has again been recognized as the nation’s top leader in three-year liver transplantation survival. The Scientific Registry of Transplant Recipients (SRTR), a federally supported research group, identified the Rutgers-UH center as the national leader, boasting an estimated three-year survival rate of 97.36 percent. The center outpaced the national rate by nearly 12 percent.
“The institutional focus on liver transplantation at Rutgers and University Hospital allows our multidisciplinary team to stay on the cutting-edge of technology and advance clinical research to improve short- and long-term safety outcomes,” said James V. Guarrera, MD, NJMS professor and chief of transplant and hepatobiliary surgery and the UH director of the liver transplant program. “We are grateful to the dozens of organ donors, families, and organizations that have given the gift of life to our patients.”
Excellence Awards for NJMS Faculty Members
Our NJMS faculty does outstanding work to improve the health and lives of countless patients. Read about two faculty members who received high recognition for their contributions to research and health care.
Marc Klapholz, MD, MBA, professor and chair of medicine, was one of three heart specialists honored at the American Heart Association’s (AHA) 2024 New Jersey Heart Ball held in June. He received the Researcher of the Year Award for his contributions to the field of congestive heart failure. A principal investigator on more than 100 clinical trials in heart failure and other cardiovascular diseases, Klapholz’s research interests include the evaluation of novel therapeutic agents and devices for the treatment of heart failure. He serves on numerous research and grant review committees and the editorial boards of several journals, and has authored and co-authored numerous articles,
book chapters, monographs, and reviews in cardiovascular disease.
Klapholz is also the recipient of the EJI Physician’s Award in this year’s 2024 EJI Excellence in Medicine Awards, presented in May 2024. He was recognized for his contributions to the training of next-generation physicians, for pioneering new and innovative health care, and for leading research and discovery to expand the cutting edge of medicine.
Matthew Neiditch, PhD, NJMS professor of microbiology, biochemistry, and molecular genetics, was also honored at the EJI Excellence in Medicine Awards ceremony. Neiditch received the EJI Outstand-
ing Scientist Award for his studies of bacterial cell-cell signaling, also known as quorum sensing, which enables communities of bacteria to coordinate their gene expression, and in turn, phenotypes such as virulence and antibiotic resistance. His lab employs a powerful combination of diverse methods, including biochemical, genetic, computational, and biophysical techniques, to study fundamentally important cellular processes in bacteria.
EJI Excellence in Medicine promotes excellence through its awards program and by providing scholarships to New Jersey residents who are in medical, dental, pharmacy, and physician assistant programs.
Marc Klapholz, MD
Matthew Neiditch, PhD
Members of the award-winning liver transplant team, left to right: Paul J. Gaglio, MD, medical director; James V. Guarrera, MD, director; and Joel Lindower, assistant director of liver transplantation.
KEITH B. BRATCHER, JR.
Neonatology Team is ‘Poster Child’ for Maternal/Fetal Health
Exposure to lead and mercury can be harmful to both mothers and babies, causing a myriad of health issues. To combat this problem, NJMS and University Hospital are collaborating with the NJ Department of Health on a biomonitoring program to provide protection from lead and mercury exposure.
The program offers free prenatal screening for lead and mercury, working with hospitals that treat people from underserved communities. Patients have blood tests to evaluate levels of lead and mercury. When high levels are detected, mothers in the program are educated about ways to reduce exposure. To date, more than 17,000 samples have been screened. “The project is a maternal-infant dyad approach to improving perinatal health, given the shared causal pathways and overlapping burden of maternal and infant health disparities,” notes Onajovwe Fofah, MD, NJMS chair of pediatrics.
At NeoFORUM 2024, a conference held in June, the NJMS neonatology team presented a poster about their work.
Vocal Chords Bring Cheer Through Music
Meet the NJMS Vocal Chords: a group of students who share a love of music. With their incredibly busy schedules, they carve out time to come together and perform, enchanting audiences at NJMS, University Hospital, and beyond. Some members sing, some play instruments, and many do both, gathering weekly for practices and impromptu jam sessions.
“The group is composed of some 20 students with different musical interests,” explains second year NJMS student Ronald Bangiyev, part of the Vocal Chords’ fivemember executive board. “Students play various instruments—I play the saxophone and drums. There’s a jazz group and an a capella group. It’s both an outlet for artistic expression, and a respite from the demands of medical school.”
The Vocal Chords perform throughout the year for hospital staff, patients, faculty, and students, and at various events at NJMS, including the White Coat Ceremony, convocation, and Follies,
the fabled annual celebration for fourth-year students. “We do three concerts in December, one an a cappella sing-along, and perform at a few events off campus, including a spring concert for the NJ chapter of the American Academy of Pediatrics,” says Bangiyev.
Rehearsals are held Wednesday evenings in the group’s dedicated rehearsal space on B-level. The jam group meets on Fridays; it’s less structured, for those who want to play, sing, and hang out.
The Vocal Chords’ faculty advisor is Manasa Ayyala, MD, associate professor of medicine and director of the Healthcare Foundation Center for Humanism and Medicine at NJMS. “We appreciate all the help we receive from Dr. Ayyala, Tanya Norment, the Humanism Center, and our other supporters,” says Bangiyev. “They do so much for us. Right now they’re helping us remodel our rehearsal room.”
He adds: “We contribute to the culture of the school through our performances. Students look forward to hearing our music and having a good time. For us, it’s a way of giving back to students, and they in turn give back to us, through their enjoyment.”
Above, Harpreet Kaur, MD, pediatric section chief (right), and NJMS student Osogieahon Ewanehi accepting an award for best poster.
WATCH
THE VIDEO
a closer look The Continuing Story of TB
BY MERRY SUE BAUM
Preventable, curable, but largely forgotten. That’s been the common description of tuberculosis (TB) in the U.S. since the 1940s. While it may be controlled in some areas, globally there are nearly 11 million TB cases reported every year. Institutions around the world are working to eradicate this deadly disease, including the Global Tuberculosis Institute (GTBI) at NJMS.
One of only four CDC-funded TB Centers of Excellence (COE) in the U.S., the GTBI was established more than 30 years ago. “We are extremely proud of our work here,” says Alfred Lardizabal, MD, GTBI’s executive director. “We provide patient-centered care and treatment, develop education and training programs, and contribute to ground-breaking research. It’s all vital to accelerating our goal of TB elimination.”
Amee Patrawalla, MD, MPH, medical director of the Waymon C. Lattimore Practice and patient-care arm of GTBI, explains that there was a decline in TB cases for three decades, but the rate in the U.S. has been increasing since 2020. “This trend is concerning,” she says. “But if you look at the timeline over the last century, we’re still far better off.”
Most TB diagnosed in the U.S. is found in people who were not born here. “Risk of contracting TB depends on where a person has lived, whom they have contact with, and their own health,” says Patrawalla. “Most have what’s known as a latent TB infection that does not produce symptoms and can’t be spread. Some with latent TB develop active TB. People with diabetes or compromised immune systems, for example, are at higher risk of the disease progressing if they do get infected.” She adds that the rate of active TB in New Jersey is higher than the national average, and Newark’s rate is more than double the national average.
TB can be underrecognized, leading to delays in diagnosis. Brooklyn native Kate O’Brien
is a perfect example. When she was two months pregnant, she began feeling what she describes as “absolutely horrible.”
The mother of a two-year-old, Kate knew the illness wasn’t related to her pregnancy. She had the classic symptoms of active TB disease: extreme lethargy, night sweats and coughing up blood. Physicians were reluctant to do a chest x-ray because of the pregnancy. She went from doctor to doctor, to no avail. “I got a different diagnosis
from each one,” she says. “It was everything from pneumonia and an eating disorder to my favorite, histrionic mother.” Because O’Brien didn’t have any of the risk factors, the doctors didn’t consider TB. While she doesn’t know exactly where she got it, the TB strain was unique to New York City.
Diagnosing TB is now much faster and more efficient. There are now blood tests that can detect if a person is infected, though they do not differentiate active from latent TB. A molecular test, the Xpert MTB/ RIF Assay, is primarily used on sputum to rapidly diagnose active pulmonary TB. David Alland, MD, MSc, professor and chief of the Division of Infectious Diseases, Department of Medicine, is internationally known for leading the effort that resulted in this new test, which is now
recommended by the World Health Organization and used in 130 countries.
Not all the tests in use today were available when O’Brien was sick. She was finally diagnosed after her obstetrician admitted her to a hospital in New York City. Hospitalized for more than two months, she then completed her treatment with Patrawalla and the staff at the Lattimore Practice. Care is provided through a multidisciplinary team approach, using what’s known as Directly Observed Therapy (DOT). At that time, a public health representative visited O’Brien every day at her home and watched her take her medication. While the institute still uses DOT, technology has made it more convenient. Patients
available for in-person DOT, based on patients’ circumstances and preferences.
Along with using the latest methods of diagnosis and treatment, the GTBI exchanges information and ideas throughout the northeastern U.S. Using the web-based platform ID Crowd, health care professionals can get help with TB issues and questions. Along with a team of TB experts, GTBI also provides advice to other clinicians.
GTBI is also involved in research. In the past, the institute was part of the CDC’s TB Trials Consortium, and now scientists there are looking at new methods of diagnosing the disease and improving outcomes.
Education is another important piece of what GTBI does. As the CDC-funded TB COE for the northeastern U.S., the institute’s team of educators plans and implements regional training courses and conferences and trains more than 3,000 health care workers annually, both in-person and online. Survivors are invited to share their stories to foster a better understanding of the physical and emotional
impacts of TB and encourage patientcentered approaches to care.
There is still a stigma attached to the disease, so having survivors who are willing to talk about their experiences is invaluable. O’Brien is one of them. She speaks across the country to educate others and give support to those who have the disease. She is also an active member and leader of We Are TB, a national TB survivor’s network advocating for better diagnostics, treatment regimens, and support to U.S.-based public health programs. The network provides a forum for patients, survivors and their families to share their struggles and their triumphs and offers free, confidential online support groups in English and Spanish.
“I really appreciated how the Lattimore team spent time with me during my treatment and truly listened to my concerns and questions,” O’Brien says. “I had so many concerns for myself and my baby, and they really tried to support me.” ●
Did You Know?
● There are about 9,000 cases of active TB in the US.
● Although it is less common, people can get TB of the lymph nodes, joints and spine.
● Not everyone who gets TB has symptoms. Someone with what’s known as latent TB will be asymptomatic. Symptoms only arise if the TB is reactivated.
● Only about five to 10 percent of people with TB become ill.
● The bacterium that causes TB dies when it hits surfaces outside the body. It is only spread by close contact with someone who has the disease.
● TB is not as contagious as a cold or the flu.
now download a cellphone app that videos them taking their medications and sends it to the institute. If the patient is not near an internet connection, the videos are stored, and the patient sends them when he or she can. Staff are readily
● TB is one of the oldest and deadliest diseases in human history. It earned several ominous names. In the 1700s it was known as “the white plague,” in the 1800s it was called “consumption,” and in the 1900s it was referred to as “the robber of youth.”
After successful treatment for TB (while pregnant, no less), Kate O’Brien became an advocate for others struggling with this debilitating disease.
a closer look
Help Early, Help Often: New Early Pregnancy Assessment Clinic
BY AMANDA CASTLEMAN
Anew clinic is addressing a critical gap in pregnancy care: the first trimester, when 80 percent of miscarriages occur. It often takes two months to secure a first obstetrics visit, so many patients turn to emergency rooms for concerns that could be safely triaged in outpatient settings that provide more support. But Marianne DiNapoli, MD—assistant professor of obstetrics, gynecology, & reproductive health—is now charting a better course at NJMS.
In October 2023, she launched the Early Pregnancy Assessment Clinic (EPAC), held weekly on Monday afternoons at University Hospital’s Ambulatory Care Center. It treats patients who have pregnancies with uncertain viability. This includes people experiencing bleeding, cramping, and possible ectopic pregnancies, plus those seeking care after pregnancy losses. “The ER is a hard place to
build rapport,” she notes. “In the ambulatory setting you have time to sit down and talk in a calm environment. It builds trust.”
This “one-stop shop” avoids the traditional approach to care, which tends to be heavily siloed. Instead, the EPAC expedites the provision of patient-centered early pregnancy care. DiNapoli explains: “If you’re having a miscarriage, we’ll offer same-day treatment. If you have a viable pregnancy, I’ll offer lab work and referrals to prenatal care. And if you want to terminate your pregnancy, I will do that right then and there.”
The EPAC can also provide exams, ultrasounds, contraception and pregnancy planning, and grief counseling. That’s especially important, as 10 to 20 percent of people experience depression after a miscarriage, DiNapoli notes. The rate’s “exceedingly high” and the mental health risks increase for patients of color... the same BIPOC patients who comprise up to 71 percent of the ER visits for early pregnancy complications.
The EPAC’s clinical model emphasizes protocols, which can help negate implicit bias. “It potentially takes race out of the equation, treating all patients the same to eliminate health care disparities and miscarriage management,” she says. “It’s very important to me to help potentially marginalized patients access high-quality, evidence-based care.”
This approach has been common in the U.K. since the early 1990s, but only gained traction here in the last five years. The University of Pennsylvania’s clinic, PEACE, reports it saves patients $500 to $1,000 per case, while eliminating an average 3.5 hours of ER personnel time. It also decreases steps, allowing for swifter resolutions.
Originally from upstate New York, DiNapoli practiced in Ohio after her residency. NJMS offered her
the opportunity to teach, while working with medically underserved patients without insurance and those with insufficient coverage.
“I also wanted a place to further develop my career interest in family planning,” she says. “It was a pretty ideal fit.”
She joined the OB/GYN team in August 2023, and the clinic launched two months later. Within weeks, the clinic had 17 patients scheduled for the half-day session, based just from internal referrals. “This was before any marketing and I don’t think it’s even built into the call-center algorithm yet,” she says.
None of this swift success surprised her colleagues, including Lauren Naliboff, MD, MPH, assistant professor of obstetrics, gynecology and reproductive health. “Dr. DiNapoli is an excellent addition to the department and provides compassionate and innovative care,” she says. “This clinic increases access and improves the quality of care for patients with concerns in early pregnancy.”
Currrently DiNapoli is the EPAC’s only attending physician. She has occasional help from a chief resident and medical students, plus usually one or two support staff, often a medical assistant or licensed practical nurse.
“Right now it’s a small team,” she says, “but hopefully one that will grow.
“With time, if other folks are interested, it would be ideal to have this clinic two or three times a week,” DiNapoli says. “Then patients would only have to wait a maximum of two days, instead of six now.” ●
Addiction Treatment Programs Hailed as ‘Model for the Nation’
BY AMANDA CASTLEMAN
The White House has praised New Jersey’s care for incarcerated people with opioid use disorders. Rahul Gupta, MD—the first physician to lead the Office of National Drug Control Policy—called the state’s medication-focused efforts a “model for the nation.” All 122 federal prisons will adopt the lifesaving approach, one already enacted in New Jersey county correctional facilities with the help of an NJMS team.
The urgency is rising. The opioid crisis has increased sixfold since 1999 and kills someone every five minutes. People who are incarcerated remain especially vulnerable: 65 percent have active substance use disorders. Treatment within the correction system reduces addiction and crime when patients return to the community.
Medications for opioid use disorder (MOUD)—such as buprenorphine, methadone, or naltrexone—help sustain recovery. These work on the brain’s opioid receptors, preventing euphoria and diminishing cravings and withdrawal symptoms. They can reduce overdose deaths by 38 to 59 percent.
NJMS has expanded this approach and runs the Northern New Jersey Medication-Assisted Treatment Center of Excellence (NNJMATrx-COE). The center’s mission is to increase access to MOUD and recovery support services for with substance use disorders. Its director, Petros Levounis, MD, professor and chair of psychiatry, explains: “We provide support and education for our colleagues. We’ve made great strides in outpatient clinics, inpatient programs, our own University Hospital, and our fellowship in addiction medicine. But we found that correctional facilities needed more attention.”
The approach gained traction in New Jersey state institutions by late 2017, shortly before NNJ-MATrx-COE’s spring 2019 launch. The team then began spreading the word in
county correctional facilities. At first, they faced suspicion, fueled by misunderstandings about the chronic disease of addiction, says Levounis: “It can be seen as a moral failure, the inability to resist the temptations of opioids.”
The team presents workshops and training that delve into the neurobiology
“Providing support and education for our colleagues, we’ve made great strides in outpatient clinics, inpatient programs, University Hospital, and our fellowship in addiction medicine. But we found that correctional facilities needed more attention.”
PETROS LEVOUNIS, MD
of addiction, which weakens the prefrontal cortex controlling complex cognitive and social behaviors, unleashing compulsive behavior. They also share information and resources.
“Our educational workshops and training of MOUD bring county correctional providers and custodial staff together,” explains team member Pamela Valera, PhD, MSW, an assistant professor at Rutgers School of Public Health. Including custodial staff is important, since they work with medical providers. NJMS trainers spend a full day discussing what’s happening in each facility and the help that is
needed. Vendors from companies contracted to provide health care services in correctional facilities also join in the training.
Levounis says attitudes are shifting for the better: “I think it is because of the hard work that has been put into these programs, the Center of Excellence, the different grants, and all the work that has been done for medication-assisted treatment. We have seen a significant improvement in how these evidence-based and life-saving interventions are received.”
Continued on page 9
AI Gets to the Heart of the Matter
BY MERRY SUE BAUM
Not since the printing press has anything transformed our lives more than artificial intelligence (AI). It touches almost every facet of our daily lives. Nowhere has AI been more revolutionary than in medicine, particularly cardiology.
“In cardiac imaging, we’re using AI on a daily basis,” says Alfonso H. Waller, MD, associate professor of medicine and radiology and chief of the Division of Cardiology. “With recent advances in technology, computers can manage massive quantities of data quickly, with consistency and accuracy. We have leveraged that ability and now use it for acquiring data, interpretation, diagnoses and predicting of outcomes.”
He adds: “This tool has vastly improved the efficiency of performing and interpreting cardiac testing. That means we can do more procedures per hour, leaving us to spend more time with our patients.”
In machine learning, a branch of AI, there is a subset of deep learning in which the basic building blocks are neural networks. For example, a computer system is “trained” by analyzing hundreds of thousands of sets of similar readings. It becomes experienced in looking at a focused problem. The result is that an AI system can read a simple test, detect a heart condition, and predict probable future problems.
One area in which AI has proved particularly useful is in cardiac magnetic resonance imaging, or CMR, used to diagnose and treat patients with a variety of cardiovascular disorders. CMR uses radio waves and a strong magnetic field to create detailed images of the body’s interior. After images are taken, AI automatically identifies and sorts them. The software then presents the images in a standard format, optimizing the orientation, brightness and magnification, and it analyzes
the data before the physician even reviews the images. That task takes only a few seconds, compared to the 30-plus minutes it once took. There are several different MRI techniques. Some show if the patient has had previous heart attack(s), whether the heart is scarred, and if there is inflam mation. Additionally, AI can measure the amount of scarring and/or inflammation.
AI has also had a tremendous impact on the use of computed tomography imaging, or CT scans, a technique using radiation to create detailed images of the inside of the body. With
“In cardiac imaging, our use of AI has vastly improved the efficiency of cardiac testing. That means we can do more procedures per hour, leaving us to spend more time with our patients.”
ALFONSO H. WALLER, MD
AI, scans of the heart now automatically quantify the amount of calcium in the coronary arteries. “We can actually calculate the person’s risk of having a future heart attack, and change the treatment, if necessary,” says Waller. “AI can also help identify patients with calcium on the aortic valve and diagnose cases of aortic stenosis.”
An echocardiogram, commonly known as echo, is a type of ultrasound scan that uses sound waves to create a moving image of the heart and nearby blood vessels. Explains Waller: “With AI we can identify if someone with heart failure has a preserved ejection fraction, a measurement of how much blood the left ventricle pumps out with each
contraction.” An echo can now automatically measure the heart’s structures, as well as the blood flow through the different chambers of the heart, automatically quantifying several measurements. “These were tasks that took a great of manual effort,” says Waller. “AI is saving us huge amounts of time.”
A new development in echocardiography is benefiting the layperson: software with direct feedback that instructs someone other than a trained technician how to perform or optimize the scan. Besides easing the shortages of echo technicians, a person in a remote area could potentially have a relative or friend do an echo on him/her and send the results to the doctor.
Cardiologists have used electrocardiogram (EKG) since the early 1900s to measure the electrical activity of the heart. Advances in AI are now used to detect left ventricular dysfunction, silent or previously undocumented and asymptomatic atrial fibrillation (heart rhythm irregularities), and hypertrophic cardiomyopathy, a disease in which the heart
muscle becomes thickened, making it harder to pump blood. A person’s age, sex and race, among other characteristics, can also now be determined.
Waller has a wealth of expertise in clinical informatics, cardiovascular imaging and AI. He completed an advanced multimodality cardiovascular imaging fellowship at Brigham and Women’s Hospital/Harvard Medical School. After joining the Division of Cardiology at NJMS in 2014, he served as chief medical informatics officer for NJMS from 2016 to 2020. During that time, he was very involved in implementing an electronic health record in the faculty practices.
With the availability and use of large datasets, AI has the potential to accelerate the diagnosis and treatment of cardiovascular disease and improve patient care at every stage of the imaging chain. In addition to the benefits it offers to the here-and-now, “AI has also advanced our ability to diagnose and prevent future cardiovascular events,” says Waller. “It truly is a marvel.” ●
Treatment Programs
continued from page 7
The co-director of NNJ-MATrx-COE, assistant professor of medicine Amesika Nyaku, MD, MS, assistant professor of medicine, agrees and says a recent surge of funding also increased buy-in at county correctional facilities. “Now we’re saying, ‘Okay, great: you’re doing it! How can we help you?’
“We’re talking about how to maximize the benefits. Because this is not only about saving people’s lives and not having overdoses in a facility or when people return to the community. It also makes a difference in terms of the climate and culture of the facility. People going through withdrawal often have behavior issues that cause stress and disruptions.”
The program educates about how to support individuals with opioid use disorder after their release from incarceration. That’s a critical time when drug overdose is the leading cause of death. Within the first two weeks, their risk of death from drug overdose is 12.7 times higher than for the general population, according to a recent study.
NNJ-MATrx-COE advocates for Medicaid to help with these transitions. With recent legislative changes, 15 states will soon use the service to fund treatment for some people in custody. The changes will also help connect these patients with providers in their communities, creating care continuity as they’re released. Pilot programs in California and New Mexico show that this coordination leads to fewer repeat offenses and ER trips, plus more primary care visits. ●
Reach NNJ-MATrx-COE via sites.rutgers.edu/mat-coe or for immediate clinical concerns its 24/7 hotline: 1-844-HELP-OUD To get involved professionally, contact coe@njms.rutgers.edu.
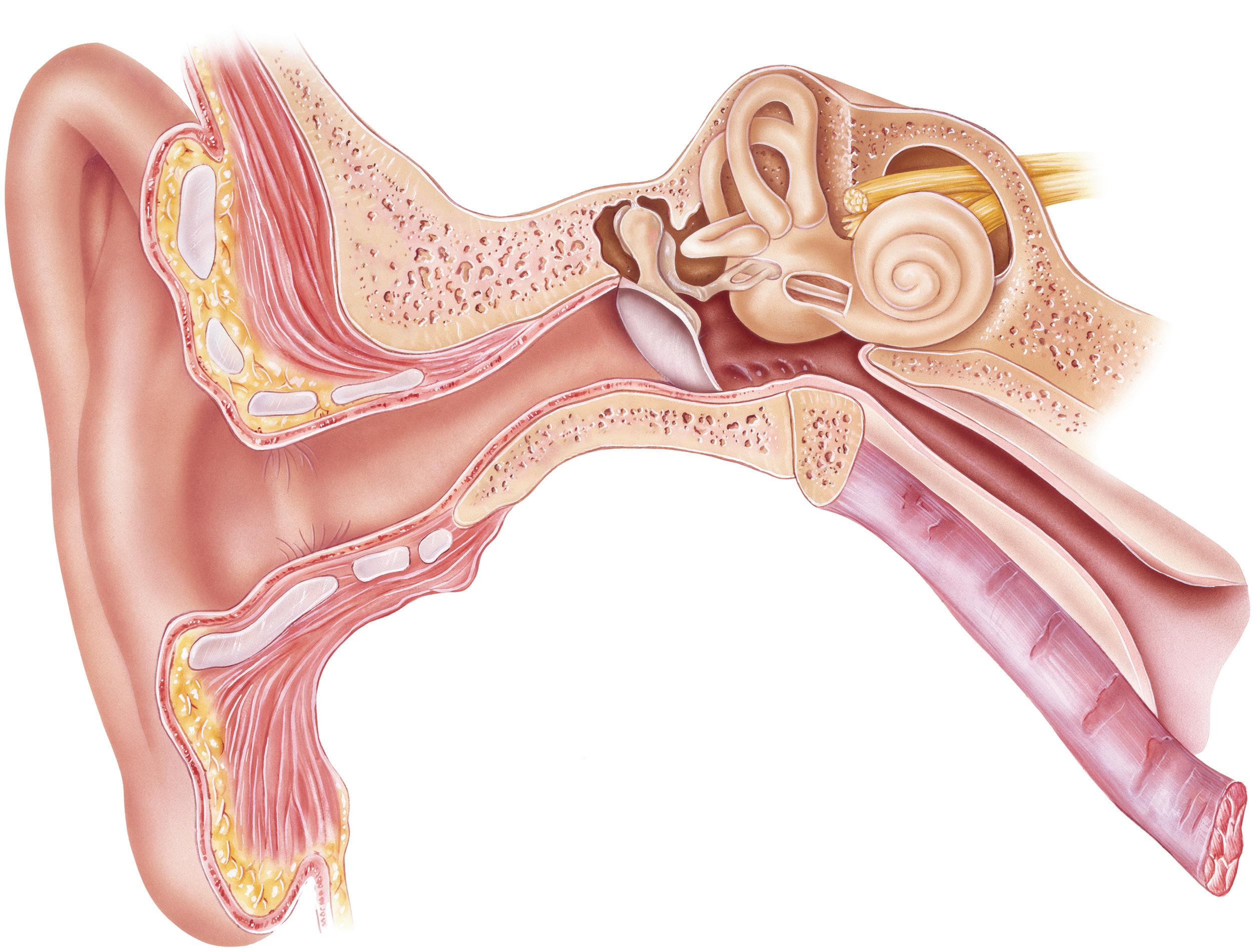
Cochlear Implant Center Celebrates 25 Years
BY MERRY SUE BAUM
Sound Giving Patients the Gift of
Giving the gift of sound to patients never gets tiresome for members of the Rutgers Cochlear Implant Center of New Jersey (CICNJ). For more than a quarter of a century, physicians and audiologists there have been helping patients as young as 8 months to as old as 97. When a patient hears for the first time, or regains his/ her hearing, it’s an emotional, heartwarming experience for everyone involved.
“I believe hearing is the ultimate sense that connects human beings,” says Robert Jyung, MD, associate professor and director of otolaryngology/neurology. “It’s one of the greatest privileges as a physician to be able to so dramatically improve a patient’s quality of life.”
To celebrate their 25 years, the entire team held a party and invited former and current implant patients and their families. Besides reconnecting with everyone, Jyung says it was also a day to remember the pioneers in the field, particularly otologist William House, MD, who is considered the father of the cochlear implant (CI). “He paved the way, and here we are today,” says Jyung. “We are considered the leading cochlear implant program in the state. We’re very proud of that.”
The CICNJ opened in 1999 at Newark’s University Hospital. At that time, cochlear implants did not have the widespread success
they do today.
Implantation criteria were more stringent, and the age requirement was higher. Nevertheless, Sujana Chandrasekhar, MD, associate professor of otolaryngology-head and neck surgery, and medical director of CICNJ at the time, and Lisa Bell, AuD-CCC-A, lead audiologist, took a leap of faith and established the center. Chandrasekhar placed the first adult implant in April 1999, and the first pediatric implant two years later. Over the years, more physicians joined the team, including Jyung, Jed Kwartler, MD (retired), and Yu-lan Mary Ying, MD, associate professor of otolaryngologyhead and neck surgery.
Lisa Bell leads a team of four audiologists in activating and programming implants. Together this talented team has placed and activated a total of 775 CIs and counting. The center places two types of implants: the CI, used for patients with sensorineural hearing loss who do not benefit from hearing aids; and the bone conduction implant.
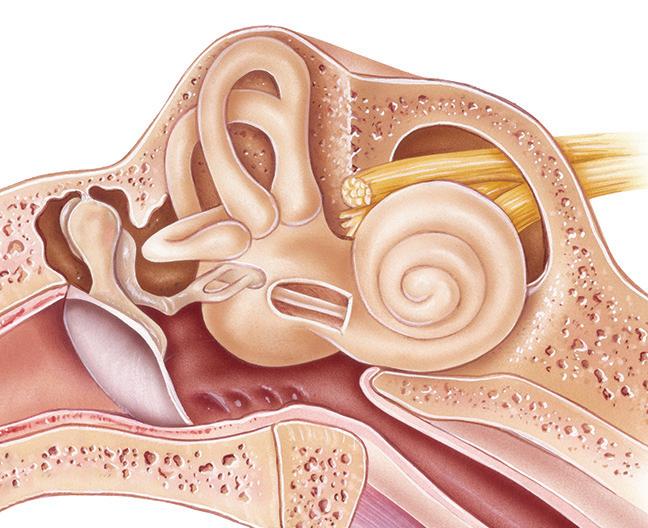
The CI procedure is done in the operating room under general anesthesia. The surgeon makes a small incision behind the patient’s
Sound
ear and creates an opening in the mastoid bone. He then guides the electrodes into the cochlea. The surgeon inserts the implant into a pocket between the muscle and bone behind the ear. The implant receives information from an external speech processor that is worn outside the skin.
About two weeks after surgery, the audiologist activates and programs the CI and shows the patient how to use the external processor. The goal is to stimulate the nerve of hearing to restore the ability to appreciate sound and improve communication. At the activation appointment, the patients are often overwhelmed, but so happy that they can hear. Patients then regularly return to the center for
fine-tuning of the de vice. The ability to hear improves over time with patience, perse verance and practice.
The second type of device, the bone conduction implant, amplifies sound via conduc tion, or vibrations, through the skull bones. The vibration directly stimulates a functioning cochlea. There are two types: nonsurgical devices and surgically implanted devices. The nonsurgical devices are worn on a headband or affixed to the skin with adhesive. The procedure for the implanted conduction device
begins with the surgeon making an incision behind the ear. A small hole is drilled in the mastoid bone and the titanium implant placed directly into it. A connector is attached to the implant, and the skin heals around it. A processor is later placed over the connector.
This type of amplification does not require any part of the device to be placed in the ear canal. “These are often used in children born with outer or middle ears that are closed,” explains pediatric audiologist Nicole Raia, ScD, CCC-A. “Unlike cochlear implants, these devices are like a light switch. The wearer begins to hear immediately.” Cochlear implants truly are life-changing. Says mom Heidi Shillabeer: “My son Travis was born in 2009, profoundly deaf in both ears. He had his right CI inserted in 2011 and the left inserted in 2014. I went from wondering if I would ever have a conversation with my child, to having a 15-year-old who can almost hear a pin drop. Travis has just entered high school, and I’m confident that he’ll reach his highest potential for the future, with the assistance of the implant team at University Hospital.”
Much has changed in 25 years. CIs now come from three companies rather than just one, giving patients more options. “It’s like using a particular type of iPhone or driving a certain kind of car,” Ying says. “Each one has certain features that people like or dislike.” Another change, she says, is the center will now implant only one CI if that is what’s indicated.
Continued on page 23
The cochlear implant team, left to right: Patricia Perez, patient navigator; James Dublin, AuD, CCC-A; Danielle Noll, AuD, CCC-A; Lisa Bell, AuD,, CCC-A; Yu-lan Mary Ying, MD; Robert Jyung, MD; Nicole Raia, ScD, CCC-A; Miranda Scalzo, AuD, CCC-A.
PHOTO: JOHN EMERSON; IMPLANT IMAGE COURTESY OF COCHLEAR AMERICAS
and
Saving Balance Lives Work-Life
A pioneering orthopedic surgeon inspires her colleagues, while restoring patients’ functionality with innovative approaches
BY AMANDA CASTLEMAN
At age six, Matias developed a “huge, abnormal-looking bump” on his knee and spent most nights in agony. A high-grade osteosarcoma had grown in his distal femur: a limb- and life-threatening condition. Despite chemotherapy, the bone cancer metastasized into his arm, making his prognosis even more challenging. “I wasn’t able to really go to school or eat or live normally,” he says. “I was confused about the situation; not understanding exactly what was happening.” He recalls a lot of fake smiles, silent crying and restless praying, but also finding joy in the support of his family, community, and care team.
Now 19, he just returned from traveling in his mother’s homeland of Peru and is about to start college at New Jersey’s Montclair State University. He credits his surgeon, NJMS professor of orthopaedics Kathleen Beebe, MD, with saving his life.
Initially, Matias was treated by an oncologist from the Valerie Fund Children’s Center in Morristown, NJ. This physician referred him to Dr. Beebe, saying if it were her child who
had cancer, that’s where she’d go. His family followed that advice, securing an insurance exemption so he could see her out of network. “The company said there wasn’t anyone better than her,” he recalls. “She’s the best, not just on a surgical level, but on a human one.
“She’s caring and kind, and wasn’t just there to fix a limb. She made a connection and saw me and my family through the hardest time. I’m truly in her debt.”
Patients with osteosarcoma have a fiveyear survival rate of 71 percent…unless they present with metastatic disease at diagnosis like Matias. Then it drops to 15 to 20 percent, Beebe notes. Thankfully, the young patient had her — and a multidisciplinary team — on his side. “We worked with pathologists to get the diagnosis and pediatric medical oncologists for treatment,” she says. Matias endured round after round of surgeries, followed by chemotherapy.
“It was sort of one day at a time,” Beebe says. “String enough of those together and he grew into a long-term survivor. Really, it’s one of our miracles.”
Mathias’ treatment combined chemotherapy and reconstruction using endoprostheses (implanted internal devices).
The approach usually results in better mobility, stability,
and posture for patients.
Salvaging Life and Limb
As a young boy, Matias had several treatment options available, including amputation and rotationplasty. This rare procedure involves removing the cancerous bone, then attaching the lower leg to the thigh bone, essentially making the ankle into a knee joint. The backward position of the leg “makes patients a bit more functional, but it’s not cosmetically pleasing for everyone,” Beebe says. “That wasn’t something he or his mother wanted.”
Instead, they chose the dominant treatment paradigm: a combination of chemotherapy and reconstruction using endoprostheses (implanted internal devices). The approach usually results in better mobility, stability, and posture for patients, as well as an easier time returning to normal life.
Beebe explains: “You operate on the leg [to remove the cancerous bone] and it doesn’t grow anymore, but the other leg does. To make them equal, Matias needed a special expandable prosthesis, which was pretty new to the market at the time.”
The innovative implants offered a gradual, non-invasive way to extend his limbs. Inside, each contained two tubes and a compressed spring that expands, essentially “growing” along with the young patient. The endoprostheses slowly pushed apart skeleton segments, while stretching soft tissues like skin, muscles, nerves and blood vessels.
Previously, surgeons had to make incisions and physically crank implants to extend them. But Matias only had to insert his arm and leg in a donut-shaped device, which stretched his limbs about five millimeters, the width of a pencil’s eraser, over a few minutes. Depending on his growth rate, he needed lengthening every three to 12 months.
The salvage efforts paid off. Today his body appears almost even; his arm no longer needs lengthening, but Beebe is still finalizing adjustments to his adult leg prothesis.
Matias dislikes how weak these altered body parts are — as well as the discomfort, pain and stiffness — but still considers them a blessing. “I am thankful every day that I have my limbs,” he says. “The drawbacks are noth-
ing compared to the gift of feeling the ocean rush past my feet or the warmth of petting my dog or holding the hands of people I love.
“Even if it hadn’t turned out well and I had needed to give up my limbs, the opportunity to fight for them is a privilege.”
Physician, Heal Thyself
Beebe also changes lives outside the operating room. Representation matters — especially in a field where only six percent of practicing surgeons are women. That’s a steep drop from the 15 to 20 percent found in residency programs. “We lose a lot through attrition somehow,” notes the physician.
Some women shy away from a discipline that’s considered quite physical. Beebe disagrees. “There’s an (incorrect) myth that orthopedists are ‘strong as an ox and half as smart,’” she says. “When I hear that, I just laugh. I’m 5’2” and a little over 100 pounds. I’m
A huge proponent of work-life balance, Beebe finds her own balance outdoors, on running paths and tracks. This past summer, she competed in the World Masters Athletic Championship in Sweden.
not a big person. I just think about what needs to be done and how to get some mechanical advantage.
“It can be physically tiring being on your feet for 12 hours in the operating room. But you really don’t need that much brute force. Sometimes it’s about finesse. Be twice as smart and half as strong!”
Beebe started her medical career studying physical therapy instead of the usual biology or chemistry. After earning a BS at Hunter College, she worked for two years at Memorial Sloan Kettering Cancer Center. So she already had some oncology and patient care experience before attending medical school at Columbia University’s Vagelos College of Physicians and Surgeons. This unconventional path inspired an emphasis on function and rehabilitation, not just saving lives.
Her trajectory continued to soar: Beebe did her internship and residency at NJMS, before completing a fellowship in musculoskeletal oncology there (she created this program for her own training and now runs it). The surgeon is affiliated with University Hospital, Newark; Cooperman Barnabas Medical Center; Newark Beth Israel Medical Center; and Robert Wood Johnson University Hospital in New Brunswick.
“I came here and stayed,” she says. “So really, this has been my only job. I’ve been at this institution for 25 years now.” In particular, she praises the ease of interdisciplinary collaborations at NJMS, where she has teamed up with radiation oncologists and physical therapists, among others.
Beebe continues to inspire residents, as she works with them in the OR and clinic. And she tends to medical students, often helping with research about how equity influences different outcomes — for patients and the profession alike.
She’s also grown into a supporter of better work-life balance. Many surgeons overlook this, as they scramble to help an aging population despite burnout and an accelerating workforce shortage. Yet research shows doctors experience more depression and emotional exhaustion than average, and a disproportionate number struggle with alcohol,
opioids and stimulants too. Compounding the problems, many physicians refuse to seek help for mental health conditions, fearing professional consequences like losing their medical licenses.
“In residency, I had my first child, while working 80- to 90-hour weeks,” Beebe admits. “Back then, you could easily be away for a solid 36 hours. You came home and just slept. I didn’t really exercise.” The passionate surgeon didn’t mind at the time, but now she strives for more variety. She loves spending time out-
doors, and with her family and running clubs, since socialization can unlock a treasure trove of health benefits and cognitive perks.
“I think that the Millennials might have it right. We need to advocate for a little bit of balance. Some might say that’s a lazy or selfish attitude,” Beebe says. “But we send people the wrong message when we use that kind of language.
“If we’re going to take care of patients and help them get well, we need to be well ourselves,” she says. ●
people Rutgers Partnership Is Paving a Path for Tomorrow’s Biomedical Researchers
BY GREG BRUNO
New Jersey Medical School and Rutgers–Newark are helping biology students gain valuable hands-on laboratory experience
When Andrew Solomon transferred to Rutgers University–Newark from Middlesex College two years ago, he had no idea that biophysics was his calling. But once he settled on the science major, an obstacle stood in his way: a dearth of research opportunities on campus.
Determined to find time in a lab, Solomon spent a summer at Boston University, where he took part in BU’s Physics Research Opportunity Program. Then he applied to the Pathway for Junior Scientists program, a new Rutgers-Newark initiative partnering with NJMS designed to help undergrads like Solomon get the research hours they need— without leaving the city.
accommodate the 600 or so biology majors seeking appointments.
“Even if every lab took two undergraduate researchers, there would be hundreds left out,” said Nan Gao, PhD, professor of pharmacology, physiology and neuroscience at NJMS. “Most students at Newark don’t have the opportunity to participate in research.”
Working with William Gause, PhD, senior associate dean for research at NJMS, Gao and other Rutgers–Newark leaders partnered to find a solution. They didn’t have to look far. About a mile down the road, NJMS had the opposite problem as Rutgers–Newark: It boasts more than 100 NIH-funded labs but has few students available to run the experiments.
By matching undergrads with NJMS researchers, a perfect synergy emerged.
“At NJMS, we have research laboratories studying everything from infectious disease to neuroscience,” Gause says. “What we didn’t have before this program was easy access to students.”
“Ever since the program in Boston, I knew that research with cells was something that I wanted to do more of,” said Solomon, who was selected for the Rutgers-Newark program’s inaugural class of researchers. “You don’t simply learn about science. To really excel, you need to ‘do’ science.”
Of the 7,500 undergraduates studying at Rutgers–Newark, a few dozen can “do” research, a disconnect borne less of interest than opportunity. In the biological sciences, for instance, National Institutes of Health–funded labs at Rutgers–Newark are already saturated with college students and can’t
The program is particularly suited for students interested in a career in biomedical research, medicine, data science and related disciplines. Students are paid $800 per month and required to work a minimum of 10 hours per week in the laboratory. Since January, the first cohort has been working on research from pharmacology to pediatrics.
Solomon, who was among the first 20 fellows, spent the spring semester working for Samantha Bell, PhD, assistant professor of microbiology, biochemistry and molecular genetics, where he studies the bacterium that causes tuberculosis. Among his contributions: deploying a program he wrote in Python to do image analysis on cells.
Laura Oyuela, another program participant, was assigned to the lab of Robin Stephens,
Continued on page 19
Getting a Second Wind: Breathing Help for People With Neuromuscular Disorders
BY AMANDA CASTLEMAN
For most of us, breathing comes so naturally that we don’t pay any attention to it. Not so for people with Duchenne muscular dystrophy (DMD), amyotrophic lateral sclerosis (ALS), and other neuromuscular disorders that weaken muscles, including those needed for breathing. When these people get a cold, their muscles are too weak to cough effectively, so they can’t clear mucus from their airways. That leads to pneumonia and respiratory failure, which brings them to the hospital, explains John Bach, MD’76, professor of physical medicine and rehabilitation and neurology, and director of the Rutgers New Jersey Medical School Muscular Dystrophy Association clinic. And that’s when things really go wrong.
Patients with neuromuscular disorders who struggle to breathe, are commonly placed on oxygen, which makes things worse.
That’s why doctors at Bach’s clinic do things differently. Instead of invasive procedures, they provide air via simple mouth or nose pieces and ventilation belts, and use a medical “vacuum cleaner” to prevent pneumonias, called the CoughAssist. Ventilation belts are essentially girdles with an air sack inside that presses on the abdomen to move the diaphragm to regulate people’s breathing.
CoughAssist devices clear people’s airways by making them cough. “They give you a deep breath and then the pressure drops—and that simulates a cough, so you don’t get pneumonia,” explains Bach. “Your muscles rest, and breathe unaided, so you don’t lose strength.”
“Oxygen turns off the brain’s drive to breathe and only increases chances of ventilatory failure,” says Bach. “It’s like putting a Band-Aid on cancer.” When patients go into respiratory failure, they’re intubated and placed on ventilators, having a tube inserted down their throats for lung ventilation. That only perpetuates a vicious cycle, according to Bach. Using machines to help people breathe via invasive tubes causes the patients’ muscles to atrophy. Often, such patients can’t be taken off ventilators because they can no longer breathe on their own, due to the tubes. They are then urged to resort to a tracheotomy, in which surgeons make an incision in a patient’s neck to install a tube through it and into the trachea for air to be pumped in.
“Patients are told that’s the only option,” Bach says, “but who wants to live with an unnecessary tube through their neck?”
For people with neuromuscular disorders, Bach’s techniques are a game-changer. “I ask people, what would you prefer?” he says. “A permanent tube in your neck, or a girdle that presses on your belly to ventilate the lungs all day?” Not surprisingly, people choose noninvasive ventilatory support and a CoughAssist. It’s like getting a second wind. During his 50 year-long career, Bach had taken invasive airway tubes out of over 500 people. He has authored over 300 peer-reviewed papers and 12 medical textbooks. He teaches his methods at medical conferences around the world. More than 250 doctors and therapists from other countries have come to learn his techniques to practice them at their medical centers.
Unfortunately, in the U.S., Bach’s techniques aren’t as popular—a phenomenon he attributes to the skewed economics of the medical system. Complex procedures and equipment, like intubation and tracheotomies, allow providers to charge more money.
Hoping to improve this situation, Bach’s now outlining his techniques in a book for the general public. Its title was inspired by one of Bach’s patients who couldn’t be taken off a ventilator after a surgery—until he ended up in Bach’s clinic to remove his tracheostomy tube. “His doctors just kept asking him why he doesn’t want to breathe on his own,” Bach shares. “So my book is called, ‘Why don’t you want to breathe?’” He hopes it’ll create more public interest in less invasive medical care. ●
Bach’s book outlines his innovations in providing his patients the non-invasive breathing help they need.
Stopping Malaria Before It Starts
BY AMANDA CASTLEMAN
Each year, malaria sickens around 250 million people and kills 608,000 globally. Now an NJMS lab hopes to add a new approach to the treatment arsenal: limiting the life-threatening pathogen’s pathways inside the body.
The disease originated long before the human line, and transmits when female Anopheles mosquitoes bite and release single-celled Plasmodium parasites into the bloodstream. Roughly 95 percent of cases strike in Africa, with children under five accounting for almost three-quarters of fatal illnesses, according to the World Health Organization. Despite eradication efforts, the preventable and curable disease can progress to severe illness and death, especially if the deadliest strain to humans, P. falciparum, goes untreated.
Fighting malaria in the lab, left to right: Hanna Dhiyebi, PhD student; Aminata Mbaye, PhD, postdoctoral fellow; Anusha Thaniana, BA, research technician; Purnima Bhanot, PhD, associate professor; Jiapeng Liu, PhD, postdoctoral fellow; Shiny Joy, PhD, postdoctoral fellow; Camille Louvat, PhD, postdoctoral fellow
PHOTOS: KEITH B. BRATCHER, JR.
“It remains a pressing global health challenge,” says the research’s lead, Purnima Bhanot, PhD, an associate professor of microbiology, biochemistry and molecular genetics. “But it’s difficult to eradicate because of continual resistance to antimalarial drugs.
“Given the toll it takes on human health, there are proportionately insufficient research funds and attention paid to the disease,” she notes. “I want to work towards filling that gap. Also, the organism that causes malaria has some unique and fascinating biology.” She explains that the pathogen excels at cycling between humans and mosquitos: two very different environments. For example, the insects function best at 80°F, but Plasmodium can spark 104°F temperatures in warm-blooded humans. “And the single-celled organism evades immune responses, staying one step ahead of what we can throw at it,” Bhanot notes.
Vulnerable populations often rely on preventative doses of antimalarial medications, taken during high-risk periods like wet seasons. Current drugs treat the disease as symptoms like fevers and chills arrive, signaling the infection has reached red blood cells. But Bhanot and her team are looking upstream for another solution.
Highly motile Plasmodia enter blood vessels and spend one or two weeks multiplying in the liver, producing 10,000 to 30,000
other parasites. “It’s a clever strategy,” Bhanot explains. “For the immune system, looking for one infected cell is like searching for a needle in a haystack. And by the time the organism enters red blood cells, it looks very different, so the immune response has to retool and play catch-up.”
Instead, Bhanot wants to stop the pathogen from entering or exiting the liver, with a prophylaxis that blocks the enzyme, protein kinase G (PKG), facilitating this movement. “The slogan of our lab is ‘stopping malaria before it starts,’” she says. “Even if some parasites escape and enter the liver, the same drug would have a second opportunity to stop the pathogen as it tries to leave. Then the immune system can recognize and take care of the trapped parasites. We hope [the strategy] will be both elegant and effective.”
Her research lab at the International Center for Public Health is in the early lead-optimization phrase of drug discovery. But the team hopes to design pills with half-lives long enough to halt Plasmodium both coming and going from its breeding grounds in the liver. This “one shot, many kills” approach should help patients be more compliant than with the current daily or weekly doses, sometimes triggering severe side effects. It could also prevent P. vivax — the dominant parasite outside of sub-Saharan Africa — from forming dormant stages in the liver, which can reactivate, causing disease months and years after the initial infection.
The research involves a lot of iteration and multidisciplinary talent, including medical chemists John Gilleran, PhD, manager of Rutgers’ Wright Rieman Laboratories, and Jacques Roberge, PhD, director of the Molecular Design and Synthesis department, Office for Research. Bhanot remains grateful to them, as well as funding from the National Science Foundation, the National Institutes of Health (R1) and the Department of Defense.
It’s an endeavor calling for “really good chemistry, a healthy dose of luck and lots of elbow grease,” Bhanot says. ●
Rutgers Partnership
Continued from page 16
PhD, associate professor and director of neuroinflammation in the Department of Pharmacology, Physiology and Neuroscience at NJMS. Oyuela is studying immune responses to infection by Plasmodium chabaudi, a rodent strain of malaria.
“For my project, we are infecting mice with two strains of the Plasmodium species to evaluate immunity,” said Oyuela, a chemistry major at Rutgers–Newark. The goal, she said, is to try and find mechanisms that could trigger human immunity responses. “I’m passionate about how science contributes to health care. A lot of people think research is just doing the experiments, but as I’m learning, it’s so much more than that.”
Gause said these types of experiences are mutually beneficial for students and their mentors. Laboratories get the resources they need to conduct their work, he said, and students get a leg up on their peers.
“It’s a great opportunity for college students at Rutgers–Newark to explore possible career opportunities and get their feet wet in terms of conducting biomedical research, which could really help when they apply for graduate school or jobs,” notes Gause.
The inaugural cohort was so successful that Gause and Gao sought to expand, launching a summer research program for Newark-area high school students and science teachers. As with the undergraduate program, high schoolers will be paid to work in NJMS labs during the summer; high school teachers will volunteer their expertise.
Gause says the high school initiative is meant to create “more interactions with the community” and to serve as a “potent outreach program” for future Rutgers–Newark science students.
“For high schoolers, the pathway program may encourage them to go to college, and for college students, it may entice them to pursue careers in biomedical research,” Gause says. “It’s a win-win for everybody.” ●
Where Are They Now?
BY TY BALDWIN
It’s been 10 years since the integration of schools, hospitals, departments and divisions that became Rutgers Biomedical and Health Sciences (RBHS), and is now Rutgers Health, a hub of world-class research, outstanding educational programs and community partnerships. RBHS produced its first group of graduates in 2014, and they’ve gone off to make important contributions. Here, read the stories of two NJMS grads from the inaugural graduating class.
LUIS ALZATE-DUQUE, MD’14
Movin’ On Up: It Takes a Village
“Iwould not be where I am today without the support of the people around me,” says Luis Alzate-Duque, MD’14. “There’s no way that any one person gets to be successful without the support of a strong network. It’s through community connections—and, obviously, their own determination—but I think a lot of it is support, guidance, and mentorship. I want to acknowledge the people who supported me along the way.”
Alzate-Duque, assistant dean for student affairs and assistant professor of medicine and pediatrics, speaks from experience. His path to medical school was anything but straightforward.
“I was born in Bogotá, Colombia,” he says. “We lived near a park with a small nature reserve. There was a group called Park Guards, and they would teach you about environmental consciousness and protecting nature. I spent my summers with them, and I became really interested in science and ecology when I was about seven years old.”
When Alzate-Duque was eleven, his older brother contracted bacterial meningitis and required brain surgery. “He had an abscess in his brain and ended up in the ICU. He was intubated. There were times when the doctors didn’t know if he would make it, or what he could recover to be.”
Thankfully, Alzate-Duque’s brother made a full recovery. “The relief affected me profoundly,” he says. “Seeing the medical team engage and interact with our family sparked a desire in me. I thought, if I could bring that kind of relief to a family, similar to what that team brought to my family, I would be very fulfilled. That’s when I decided I wanted to become a doctor.”
Alzate-Duque emigrated to the U.S. with his family when he was twelve. They settled in North Bergen. “I did not speak English at all,” he says. “I was supposed to go into seventh grade, but was pulled back a year.” His first
Luis Alzate-Duque, MD’14, with ‘man’s best friend’—his canine sidekick Nacho, PhDog’24
week of school just happened to be one for state exams. “They sat me down. It was like, ‘Okay, take this exam,’ which I don’t understand and which I can’t read or comprehend.” An aide sat with him, “but all they could do was read the question back to me in English. It just made me feel worse. Not only can I not read it, I also have someone reading me the exam, and I still can’t understand it. That was my experience starting education in the U.S.”
“My family was very blue-collar,” AlzateDuque adds. “My mother worked as a housecleaner and my stepfather was a welder, but they were a great support system. One of the things my parents imparted in me was the importance of schooling. My mom would tell me, your dad is very smart, but he never went to the university. And she was very smart, but her mom told her she needed to help out at home. For them, the dream was to continue their education. I remember overhearing conversations: ‘How do we pay rent?’ I realized that this is a problem that persists, but I can still go to school. The only way to exit this cycle of uncertainty and angst is to get an education.”
Throughout high school and college, at New Jersey City University, Alzate-Duque worked as a waiter. “I became sort of selfsufficient. Maybe not thriving, but I was able to overcome some barriers. I would think, I just need to live today and know that at some point I can achieve my dream.”
One challenge was his immigration status. “I was undocumented until I was twenty. I would work and save money, and then pay for my undergrad studies. I did that for three, four years, until I was able to adjust my status. Once I was able to do that, I knew there was nothing that could hold me back.”
“As an undergrad, I had the good fortune to have Dr. John Grew as my cell biology professor. He was one of the toughest professors, but he was tough because he cared about your education and wanted to challenge you and make sure that you learned.” Dr. Grew offered Alzate-Duque a position as a teaching assistant in his summer lab and encouraged him to apply for a joint internship with NJMS. “Fortunately, I got it.”
At NJMS, Alzate-Duque worked with Ana Natale-Pereira, MD’96, MPH, associate professor of medicine. “That was when I was first introduced to public health and the environment of social determinants,” he says. “How social factors affect access to health care, how language affects outcomes, how neighborhood safety contributes to unhealthy habits. She was looking at elderly Hispanic folks and the
“My family was very blue-collar. I remember overhearing: ‘How do we pay the rent?’ This is a problem that persists… and the only way to exit this cycle of uncertainty is to get an education.”
LUIS ALZATE-DUQUE, MD’14
He graduated in 2008, spent a gap year taking courses in public health, and matriculated at NJMS in 2010.
What he best remembers about his student days at NJMS was the continued mentorship. “Finding people here who were invested in my future, and who saw potential in me, that guided me through. Feeling like I belonged and that people believed in me really helped make my dream a reality.”
barriers to completing screening for cancer. My experiences were not just my own; other folks who looked like me and sounded like me had similar experiences, and those experiences affected their health. It sort of clicked: these are factors everyone may experience to one degree or another, yet marginalized communities experience to a greater extent.”
“One day I mentioned that my dream was to go to medical school and be a doctor, but because of my background and my social status—needing to work and provide for myself— I was considering physician assistant school, as it would be quicker. Dr. Natale-Pereira responded, ‘No, no, no. You can do this’—referring to attending medical school. She took the time to sit down with me and go through my options. She helped me see that medical school was something I SHOULD pursue.”
Alzate-Duque took the MCAT during his senior year. He hadn’t known to take the test when he was a junior so as not lose a year.
Alzate-Duque stayed at NJMS to do a residency in internal medicine and pediatrics. “I knew that the people here believed in the community, served the community, understood the community, and had a vested interest in the community. Why would I want to go somewhere else and maybe serve a different community, or find other mentors, when I already felt like I belonged here. This is where I needed to be.”
“After residency, I told everyone who would listen, ‘Hey, I want to stay.’ I had the opportunity to be part of the Hispanic Center of Excellence academic medicine fellowship, so I stayed another year working on that and in student affairs.”
A lot of students, he found, faced the same challenges he had, which reflected on or impacted their academic performance. “Whether it was economics or caring for family, housing insecurity or food insecurity, or believing in self,” there were a lot of barriers to student success. “I was versed on social determinants now because I had some academic experience, and I could also use my expertise in internal medicine and pediatrics to troubleshoot
for students in things like knowledge gaps, or how they can improve on test taking.”
Alzate-Duque’s work as assistant dean for student affairs involves collaborating with offices such as the offices of education, admissions, and student health services, among others, and engaging with students to improve on strategies and allocate resources that lead to academic excellence. “I like to think holistically,” he says. “Beyond you just doing well academically, what is happening around you? Whether it’s anxiety, or impostor syndrome, or perfectionism. Or if it’s financial issues, or someone in the family is sick and needs to be taken care of, or you are looking to improve on test-taking or learning strategies. How can we support you so you can excel?”
One of Alzate-Duque’s most important colleagues is Nacho (PhDog, NJMS’24), his fifteen-month-old German shepherd. “Nacho helps out as a support dog. He has open office hours on Mondays and Fridays from four to five o’clock. Students love it and so do staff.” People come by just to hang out with Nacho, and maybe scratch his ears. “Everyone asks, ‘When is he getting a white coat?’ I always say, ‘I have to speak with Dean Johnson and Dr. Soto-Greene to get the green light.’”
He notes that ultimately, whether with students or patients, it starts and ends with connection, humanity and building trust that enables the completion of common goal.
CHRISTIE BUONPANE, MD, NJMS’14
Creating a Path to Pediatric Surgery
Christie Buonpane, MD, NJMS’14, decided to become a doctor when she was in middle school. She still remembers that day.
“I had my heart set on NJMS,” says. “I grew up in Morris County—lived there my whole life. It was the cool thing to do—if you were going to medical school, you went to NJMS.”
Her initial inspiration was Jack, a family friend. “There were a bunch of families where the parents were all friends, and the kids were all friends,” she says. “Jack was a cardiologist, and I looked up to him so much. One day we were pumpkin picking, and someone had a medical emergency. He ran over to help, and I was just in awe of him. I told my parents I wanted to be a doctor.”
Buonpane, now an assistant professor of pediatric surgery at the University of Louisville School of Medicine, received her undergraduate degree at Villanova University, where she majored in biology, with minors in both sociology and Spanish. “Anytime I was on break, I would come back and talk with the admissions office at NJMS. I was overeager, like ‘Can we meet and talk about how I can improve my application?’” Buonpane laughs. “Mercedes Rivero (assistant director of admissions) might have thought I was stalking her. But she was really great and set me up with opportunities. We had a good relationship when I was in school.”
Jack passed away while Buonpane was taking the MCAT, so “he never knew I got into medical school,” Buonpane says, “but he knew he was my inspiration. When he died, his wife gave me his stethoscope.”
Arriving at NJMS, it was clear to Buonpane that her heart had been right all along. “One of the most appealing things was the school’s involvement with the community. It wasn’t just study, study, study. We had a program where we would go to a pregnancy crisis center and teach the women about different health topics: vaccines for their babies, or even simple things like how to change diapers or tell when your baby is sick.” The Student Family Health Care Center was also central to her education. “It was such a good experience to feel like you were making a difference even before you had finished med school. You got to build a good rapport with some of the patients because they would keep coming back, and you would be their point of continuity. I loved that.”
She adds that her class had a lot of camaraderie. “I’m still best friends with three of my friends from medical school. We all live far away from each other, but we talk every day,
“NJMS shaped my career and my outcomes. The people there are so supportive.”
CHRISTIE BUONPANE, MD’14
and the four of us meet every year and take a trip together.”
Buonpane did her residency in general surgery at Pennsylvania’s Geisinger Medical Center, and with the encouragement of her program director, took time off after third year to do two years of research (a requirement for pediatric surgery) at Lurie Children’s Hospital in Chicago. Buonpane returned to Geisinger for the fourth and fifth years of residency, and then matched into a two-year fellowship in pediatric surgery at Oklahoma Children’s Hospital. “They take one fellow per year, so you were on call every other day for two years. You don’t sleep, but you learn a lot. That was an amazing experience.”
When it came time to look for a job, Buonpane knew she wanted to go somewhere where she could work as a clinician and also have her own research lab. The University of
Louisville School of Medicine was a perfect fit. “I knew Dr. Cynthia Downard (director of pediatric surgery and surgeon-in-chief at Norton Children’s Hospital) from academic conferences, and she’d always been supportive, like an unofficial mentor.”
With her lab up and running, Buonpane is continuing her studies on necrotizing enterocolitis, a condition affecting some premature babies because their intestines aren’t fully formed. “They get really sick and part of their intestines can die,” she explains. “Some of these kids have issues with long-term nutrition. It’s a devastating disease.” Louisville also has a strong program in environmental science, and Buonpane wants to look at how exposure to heavy metals affects women’s breast milk, and what health impact that has during their pregnancies and for their babies.
Now beginning her second year at Louisville, Buonpane feels settled in and ready for the challenges ahead, and she is quick to credit NJMS for her success. “NJMS shaped my career and my outcomes,” she says. “The people there were so supportive. Mercedes Rivero connected me with an NJMS grad who was a pediatric surgeon. And all of the community involvement, all the volunteer activities—that’s what made my CV for residency, and for the rest of my career. I have only good memories of NJMS. It really was my foundation.” ●
Please support NJMS and our students.
Hearing a Community Need
When NJMS students Shrey Shah and Afash Haleem arrived on campus, they were struck by the clamor of the big city. Both grew up in a quieter environment, but they didn’t consider the noise an annoyance. Instead, they saw it as an opportunity. With the goal of helping Newark residents preserve their hearing, they established the Community Audiometry Screening Clinic, or CASC.
Haleem had done research in hearing loss at Massachusetts Eye and Ear Institute in Boston. He knew that along with impacting a person’s quality of life, hearing loss has many comorbidities. He and Shah took their idea of a screening clinic to otolaryngologists Yu-lan Mary Ying, MD, and Robert Jyung, MD, who helped the pair apply for funding from the Pozen Scholars program. The program gives grants for student projects that assist Newark residents. With their funding they bought a laptop, noisecancelling headphones and incidentals like otoscope tips, antibacterial wipes, etc.
The next step was finding a quiet space. The two partnered with the Newark Public Library’s main branch to set up shop.
Using a free app known as Hear Pro, they screened patients for general hearing loss as well as their ability to hear in noisy environments like a restaurant. They took turns spending two hours, one day each week doing screenings. By the end of their second year, they had screened 100 patients.
“We recently got word that the CASC has been approved as a Community Engaged Service Learning (CESL) program,” says Shah. “That means all first- and secondyear students who work at CASC will receive credit toward their required 40 hours of service learning,” adds Haleem.
Now in their third year, the students say they’ll run the clinic until they graduate. The two hope to expand to other Newark Public Library branches and possibly beyond.
“With all the new students who are interested, we’re well on our way,” says Shah.
To learn more about the CASC, please go to Instagram@NJMS_CASC.
To make a donation, scan the QR code here. Or if you would like to discuss making a gift to NJMS, contact Mary Ruotolo at mary.ruotolo@ rutgersfoundation.org. Stay in touch by writing to the NJMS alumni office at njmsalum@njms. rutgers.edu
Hear! Hear!
Continued from page 11
Implants are now Bluetooth-compatible and water-resistant, so a wearer can swim using an approved cover.
The number of CIs placed in a year has greatly increased as well. “From 1999 to 2012 we performed an average of 20 implants,” says Bell. “From 2013 to 2024 the average was 46 per year. And over the years our pediatric patients have gotten younger and
younger, and our adults have gotten older and older.” Another change is that the center is now placing two CIs at the same time instead of sequentially, and the implants are activated much sooner. Instead of waiting a month after surgery, they are usually turned on after two or three weeks.
What hasn’t changed is the center’s successes. “The children I saw when I first came here are now in high school,” Raia says. “It’s amazing to see what they’ve become. And the babies we implant learn to speak the same as any other child. It is truly life-changing.” ●
BY NANCY A. RUHLING
The idea of really making a difference in people’s lives is why Peter Attia decided to become a physician.
The third-year NJMS student is off to a stellar start: He just received a 2024 Alpha Omega Alpha Carolyn L. Kuckein Student Research Fellowship to support research on optimal methadone dosing for the treatment of opioid use disorder.
“We all need to help each other pull each other up,” says Attia, who has a bachelor’s degree in cellular biology and neuroscience, minoring in public health, from Rutgers University-New Brunswick.
The idea of being of service, though, remained somewhat abstract until he became a research assistant for NJMS professor of medicine Stanley H. Weiss, MD, who has been collaborating with medication-assisted treatment programs for some four decades.
Attia began working on one of Weiss’ studies on opioid use disorders that focused on methadone treatments, interviewing subjects and extracting and collating data from various treatment programs to create uniform databases in a comprehensive manner that had never been done before. For some subjects, more than 10 years of daily dosing data have
Student Wins Fellowship for Unique Methadone Study
been analyzed, in conjunction with admission and discharge records, drug toxicology testing, and medical information.
The unprecedented “treasure trove of data” Attia collected led to analyses suggesting that higher doses of methadone are needed for longer-term treatment success.
Led by Weiss, the research team, which includes assistant professor of medicine
Daniel M. Rosenblum, PhD, and Attia, recruited 325 subjects between 2016 and 2018 from four New Jersey programs, and has followed their progress through 2024. Some 20 percent of them, according to treatment histories, received a daily methadone dose of over 120 milligrams.
The project, which is believed to be the first to evaluate longitudinal methadone dosing in an observational study using electronic medical records, is groundbreaking because the Substance Abuse and Mental Health Services Administration provides only limited dosage guidelines. People generally begin on 30 milligrams of methadone, with gradual dosage changes to usually 60 to 120 milligrams. There is a need to understand dosing and the relationship to outcomes.
“It’s a totally unique observational, analytical, and epidemiological project with important ramifications, and Peter’s award is very
prestigious and recognizes that the preliminary data is significant,” said Weiss. “The first study of its kind, it required many skills and elements—medical knowledge, computer expertise, collaboration, data security and approval from institutional review boards because it has human subjects.”
He adds that the project “has a high probability of helping influence how we treat people with opioid use disorders.”
Noting that there may be additional factors, such as co-morbidities, that contributed to the results, Attia says, “We don’t have an answer yet, but we’re close to it because we have a stable cohort. We have to look at the whole person physically and psychologically—methadone is only one part of the treatment.”
Working on the study, whose results are being prepared for publication with Attia as the lead author, “changed my perspective of persons with opioid use disorder,” Attia says. “The stories they told me of their lives opened my eyes and made me appreciate the complexities behind substance use disorders. Understanding the patients will help me become a better clinician.”
Attia, who envisions a clinical and research career, adds that Weiss “pushed me to be the best researcher I can be; I would not be the researcher I am today without him. I was also fortunate to have Dr. James Hill and Dr. Robert Schwartz encourage me to apply for the fellowship grant.”
Attia says the $5,000 award is a “nice surprise that will help with the cost of medical school expenses.”
A medical school with an active Alpha Omega Alpha chapter may nominate at most one medical student each year, from its firstor second-year students, with the national association selecting the fellowship winners.
The additional $1,000 reimbursement for travel to present the study at a conference “offers me the opportunity to share the results with others in the field,” he says.
Noting that he found some of the study’s results “surprising,” Attia says that “I’m happy my work will have an impact. It’s one of the things that drive me forward.” ●
Peter Attia’s mentor: professor of medicine
Stanley H. Weiss, MD.
Offering Heartfelt Thanks to Whole-Body Donors
In January, NJMS held a ceremony that was both solemn and joyful. Students and faculty gathered to show their gratitude to total strangers—incredibly generous people who donated their bodies for medical education.
Part memorial, part celebration, it’s a scene that occurs at health science universities across the country, explains NJMS assistant professor of medicine Jeremy Grachan, PhD, who teaches anatomy to first- and second-year students. “Donor ceremonies are a way for students to show appreciation to the anonymous individuals who donated their bodies for education,” he says. “There is no greater gift you can give, and the students are mindful of that.”
NJMS students, under the current curriculum, take anatomy in their first and second years, January to January. “The students work in teams, studying the same donor for the entire year,” explains Grachan. “They spend a lot of time with that donor. Right after the last anatomy practical exam, we host the ceremony. The entire class of 2027 is invited to attend.”
January’s donor ceremony, the first one since the onset of COVID, was held in the NJMS lecture hall. Some students wrote essays and read them aloud. Grachan and George Holan, PT, DPT, GCS, NCS, director of anatomy teaching programs and assistant professor of surgery and medicine, also spoke, and members of the NJMS Vocal Chords and jazz ensemble performed. Students brought hand-written thank you notes and pinned them to a human body silhouette. Central to the ceremony was a depiction of a cherry blossom tree of life, where the students left their thumbprints. “It was a very meaningful event that we plan to repeat every January,” notes Grachan.
With the current shortage of human bodies donated to science, some medical schools lack access to donors. In that case, students learn anatomy virtually, and/or by studying plasticized human models. NJMS receives 15 donated bodies each year for the anatomy small group curriculum and anatomy dissection laboratory sessions. The donors are received through the Robert Wood Johnson Medical School Anatomical Association Body Program.
Grachan, who spent a considerable amount of time in a relative’s funeral home while growing up, has always been fascinated by human anatomy. But not all students share this keen interest. “Some students come with trepidations and are sensitive to working with donors,” says Grachan. “I understand where they’re coming from. At my first dissection in 2016, I had just lost a grandparent, and felt a mix of emotions. I tell students who are processing emotions that this lab is a safe space.”
Once the students move beyond any trepidations, they become absorbed in the learning process. “The
skills you acquire in anatomy lab go beyond anatomy,” says Grachan. “Working together, students acquire important teamwork and leadership skills. Clinicians come to speak, surgeons talk through surgical procedures, and other specialists share their knowledge. Students have the opportunity to build relationships with faculty.”
He adds: “Also, every body is different. When we find an anomaly or other unusual or unique attribute in a donor, we’ll use it as a teaching moment for the entire class.”
Following this year’s ceremony, the anatomy professors surveyed the students to learn what they thought of the experience. The response was positive, with many students noting they found the ceremony meaningful—not just marking the end of anatomy lab, but also the transition from a pre-clerkship to a clerkship student. “Spending a year with these deceased individuals, and learning from them, is a wonderful opportunity and moment,” sums up Grachan. “The ceremony provides a way for students to express their gratitude for the impact these donors will have on their future careers and lives as physicians.” — Mary Ann Littell
Top: Jeremy Grachan, PhD, organizer of the donor ceremony. Bottom: First- and second-year students offer heartfelt thanks to the generosity of donors.