A COMPARISON OF THE CARIES RISK BETWEEN PATIENTS WHO USE VAPES OR ELECTRONIC CIGARETTES AND THOSE WHO DO NOT A CROSS-SECTIONAL STUDY
KARINA F. IRUSA, BDS, MS
MATTHEW FINKELMAN, PHD
BRITTA MAGNUSON, DMD
TERENCE DONOVAN, DDS
STEVEN E. EISEN, DMD
407
ASK THE POWERS CENTER
STEPHEN J. CHU, DMD, MSD, CDT
ADAM J. MIELESZKO, CDT
GUEST EDITOR:
RADE D. PARAVINA, DDS, MS, PHD
408 ETHICS CORNER: THE ETHICS OF THE UNEXPECTED LOSS OF A PRACTITIONER
KAREN DIANE FOSTER, DDS
412 FBI: FOUND BUT NOT IDENTIFIED (YET)
KATHLEEN A KASPER, DDS, D-ABFO
You proactively recommend the CareCredit credit card to patients. Have patients scan your custom link QR code where they can privately see if they prequalif y, apply and pay with CareCredit.
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
FEATURES
400 A COMPARISON OF THE CARIES RISK BETWEEN PATIENTS WHO USE VAPES OR ELECTRONIC CIGARETTES AND
Reprinted with permission from the American Dental Association.
Karina F. Irusa, BDS, MS
Matthew Finkelman, PhD
Britta Magnuson, DMD
Terence Donovan, DDS
Steven E. Eisen, DMD
407 ASK THE POWERS CENTER
Stephen J. Chu, DMD, MSD, CDT
Adam J. Mieleszko, CDT
Guest Editor Rade D. Paravina, DDS, MS, PhD
Reprinted with permission from the American Dental Association.
Karen Diane Foster, DDS
Kathleen A Kasper, DDS, D-ABFO
HIGHLIGHTS
418 Oral and Maxillofacial Pathology: Case of the Month
Oral and Maxillofacial Pathology: Case of the Month Diagnosis and Management
In Memoriam
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 141 | No. 7
Texas Dental Journal (ISSN 0040-4284) is published monthly except January-February and August-September, which are combined issues, by the Texas Dental Association, 1946 S IH-35, Austin, TX, 78704-3698, 512-443-3675. PeriodicalsPostage Paid at Austin, Texas and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 1946 S IH 35 Ste 400, Austin, TX 78704. Copyright 2023 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. Instate ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax.
Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement included in the online September Annual Membership Directory or on the TDA website: tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PAST PRESIDENT Cody C. Graves, DDS 325-648-2251, drc@centex.net
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
System’s Annual Insurance & Coding Course is coming to
Friday, October 25, 2024
9am-4pm
• Gain insight into various insurance plans, translating benefits & COB rules.
• Review the upcoming 2025 CDT code changes
• Assess Procedures Requiring Pre-Certification
• Discuss HCFA 1500 Claim Form Basics
• Hands-on/Mock Coding of Claims
• Translate Medical Insurance Terminology
• Select Medical Codes for Dental Procedures (exercise)
• Review Sample Letters of Medical Necessity with handout
• Learn effective systems for efficient revenue cycle management
• Classify Dental Procedures considered to be Medically Necessary
If planning a t am building trip discount d room rat includ s up to 4 gu sts to wat rpark. Email S minar@IAPlus.com or call 800-683-2501 for mor d tails
and
There are options for spa experiences, bowling, shopping, zip lines, live entertainment, restaurants, escape room, plus an indoor water park with a 900 foot lazy river and adult swim up Grotto Bar Includes 6 CE Credits and hot lunch buffet.
Anne Cale Jones, DDS and Juliana Robledo, DDS
3001 Kalahri Blvd | Round Rock, TX 78665
Guest Speaker: Leslie Icenogle, an industry expert in the field of dental
medical billing.
Hieu Huynh, DDS, JD
LAW OFFICES OF MARK J. HANNA
Mark J. Hanna JD
Former General Counsel, Texas Dental Association
• Representation Before the Texas State Board of Dental Examiners
Electronic cigarettes (e-cigarettes) were introduced to the US market in 2006 as a safer alternative to conventional cigarettes, as well as a smoking cessation tool.1
Up to 4.7% of middle school students and 19.6% of high school students have been reported to be using e-cigarettes.2 Vaping has received attention internationally as a result of the outbreak of deaths due to e-cigarette, or vaping, product use–associated lung injury in 2019.3 The Centers for Disease Control and Prevention’s statistics placed the total number of deaths due to e-cigarette, or vaping, product use–associated lung injury in the United States at 68 as of February 18, 2020, with a total of 2,807 hospitalizations.3
Vaping entails the use of an electronic device that heats vaping liquid, producing an aerosol. This aerosol is then inhaled and some of its components will adhere to the hard and soft tissues of the oral cavity.
Vaping liquids typically contain a base, which includes propylene glycol and glycerin, nicotine, and flavors. The viscous aerosol produced during vaping has been found to not only increase microbial adhesion and biofilm
ABSTRACT
Background
Evidence on the potential oral health effects of vaping is scarce and there are limited data on possible links to both caries and periodontal disease. The authors assessed the association between electronic cigarette (e-cigarette) or vape use and caries risk level. The Caries Management by Risk Assessment tool was used.
Methods
A cross-sectional study of patient records was conducted; 13,098 patients who attended the dental school clinics from January 1, 2019, through January 1, 2022, were included in the study. Mann-Whitney U test and multivariable ordinal logistic regression were used to assess the rela- tionship between use of e-cigarettes or vapes and caries risk level.
Results
Data from 13,216 patients were included in the data set initially; 13,080 responded “no” when asked whether they used e-cigarettes or vapes (99.3%), and 136 responded “yes” (0.69%). There was a statistically significant difference (P < .001) in caries risk levels between the e-cigarette or vape group and the control group; 14.5%, 25.9%, and 59.6% of the control group were in the low, moderate, and high caries risk categories, respectively, and 6.6%, 14.3%, and 79.1% of the e-cigarette or vape group were in the low, moderate, and high caries risk categories, respectively.
Conclusions
In this study population, there was an association between use of e-cigarettes or vapes and caries risk level of patients; vaping patients had a higher risk of developing caries.
Practical Implications
Within the study limitations, it was recommended that use of e-cigarettes or vapes should not only be included in the routine dental-medical history questionnaire, but also among the risk factors that increase a patient’s caries risk level.
Key words
Vaping; e-cigarettes; caries; caries risk level. formation, but also allow Streptococcus mutans to adhere to enamel.4 The flavors are typically composed of sucrose, and the results of in vitro studies have shown that this can substantially increase biofilm formation, as well as enamel demineralization.5 Flavored vaping liquids have also been found to be detrimental to the growth of commensal oral bacteria and, as a result, pose a potential risk to the health of the oral cavity.6,7
In an in vitro study, researchers found that 38 of 45 e-cigarette liquids tested had a relatively low pH of less than 5.5.8 Although the results do not directly implicate the erosive potential of these liquids, they do raise concerns.
The oral health effects of vaping relating to gingival and periodontal health have been investigated and both vaping and tobacco use have been negatively associated with periodontal health.9-12 It has also been found that clinical and radiographic periimplant parameters are compromised due to an increased inflammatory response in people who vape.12
Vaping has been marketed as a safe alternative to cigarette smoking, and information on the potential cariogenicity of vaping is limited. Our study provides some additional information on the potential association between using e-cigarettes or vapes and caries risk.
Research on the effects of vaping and e-cigarette use on caries prevalence remains scarce. The first clinical report on this topic was a case series in which researchers highlighted 3 patients seeking treatment at a private practice who had an atypical patterns of caries. All 3 patients admitted to being vapers using tetrahydrocannabinol-containing vaping liquids.13
In a 2021 cross-sectional study, researchers assessed 4,618 records from the 2017-2018 National Health and Nutrition Examination Survey.14 They concluded that both participants who smoked e-cigarettes and dual smokers (that is, those who smoked conventional cigarettes and e-cigarettes) were more likely to have untreated caries than nonsmokers and non–dual smokers.14
Caries has been defined as a biofilm-mediated, diet-modulated, multifactorial, noncommunicable, dynamic disease resulting in net mineral loss of dental hard tissue.15 The categorization of patients into different caries risk levels dictates the management of the disease, as well as the frequency of follow-up required. The Caries Management by Risk Assessment (CAMBRA) philosophy was developed in 2007.16,17 The level of risk is determined by means of assessing the balance among the disease indicators, risk factors, and protective factors. Disease indicators are the presence of inter-proximal lesions, restorations in the past 3 years, and presence of white-spot lesions. Risk factors include visible heavy plaque on teeth, frequent snacking, inadequate saliva, deep pits and fissures, and recreational drug use. Protective factors include use of fluoridated toothpaste or mouthrinse and living in a fluoridated community.16 Because risk level is the determinant of caries management protocols, we focused on this as an outcome variable.
Our objective was to examine a limited researched topic that is of clinical importance given what is known so far. None of the researchers in the published studies had specifically evaluated caries risk as an outcome variable, despite caries risk being the key determinant in caries management, according to risk assessment protocols. The aim of our study was to assess the association between vaping or e-cigarette use and caries risk.
The null hypothesis was that there was no difference in caries risk between vaping or e-cigarette using and nonvaping or non–e-cigarette using patients.
METHODS
Ethical approval was obtained from the Tufts University Health Sciences Institutional Review Board (00002288). An electronic search was then performed on axiUm electronic records.
Inclusion criteria were patients from January 1, 2019 through January 1, 2022 who were older than 16 years, had received a diagnosis of caries, had a caries risk assessment on record, and who answered “yes” or “no” to use of e-cigarettes or vapes in a health history questionnaire. Exclusion criteria were patients who answered “yes” to recreational drug use, unless the drugs were consumed as part of vaping or e-cigarette use (for example, tetrahydrocannabinol), and patients who had not received a caries diagnosis.
The CAMBRA form included the following 7 questions:
• Are there new or active or progressing visible cavitated carious lesions, radiographic radiolucencies in dentin?
• Are there restorations or extractions due to caries within the past 3 years or since the previous caries risk assessment?
• Is there visible heavy biofilm?
• Are there new or active or progressing initial occlusal, smooth surface, or radiographic proximal lesions not in dentin?
• Is there inadequate saliva flow per observation or measurement?
• Does the patient have a diet high in carbohydrates, sugar, acids, or frequent snacking?
• Is the patient at risk of erosion?
Patient records software then generates a risk-level category on the basis of a predetermined algorithm, resulting in a low, moderate, high, or extreme
categorization. The high and extreme categories were combined into a single category called high.
A query was made in axiUm using Current Dental Terminology18 codes D0120 (periodic oral evaluationestablished patient) and D0150 (comprehensive oral evaluation, new or established patient). The data retrieved were the patient’s caries risk assessment status, axiUm record number, age, sex, date of examination, and the patient’s response to whether they used e-cigarettes or vapes. Once data were retrieved, participants were assigned identification codes to ensure the confidentiality of patient records in the data set. The included participants were also categorized into the following 3 age groups: 16 through 25 years, 26 through 40 years, and older than 40 years.
A convenience sample of patients who attended the dental clinic at Tufts University School of Dental Medicine from January 1, 2019, through January 1, 2022, with a CAMBRA form on record was obtained. Descriptive statistics (frequencies, percentages) were calculated. Bivariate analyses were conducted via Mann-Whitney U test. Multivariable analyses were also conducted via ordinal logistic regression to adjust for sex and age category as potential confounding variables. The significance level was set at α = .05. SPSS, Version 26 (IBM) was used in the analysis.
RESULTS
Data for 13,216 patients were initially included in the data set; 13,080 responded “no” to questions about the use of e-cigarettes or vapes (99.3%), and 136 responded “yes” (0.69%). Of the total number of patients, 47.9%
were male and 52.1% were female. Of the 13,216 patients, 6.4% were aged 16 through 25 years, 32.8% were aged 26 through 40 years, and 60.7% were older than 40 years. The distribution of caries risk level within the entire sample was 14.5% in the low-risk category, 25.8% in the moderate-risk category, and 59.7% were in the high-risk category. A total of 118 patients had missing data on caries risk level, leaving 13,098 patients who met the inclusion criteria (13,007 reported that they did not use e-cigarettes or vapes, and 91 reported that they did).
Among the patients who did not use e-cigarettes or vapes, 6.3% were aged 16 through 25 years, 32.6% were aged 26 through 40 years, and 61.1% were older than 40 years. The age distribution for the e-cigarette or vape group was 19.1% in the age category of 16 through 25 years, 52.9% in the age category of 26 through 40 years, and 27.9% in the age category of older than 40 years.
Results of Mann-Whitney U test showed significantly lower caries risk levels for the control group compared with the e-cigarette or vape group (P < .001), with 14.5%, 25.9%, and 59.6% of the control group in the low, moderate, and high caries risk categories, respectively, and 6.6%, 14.3%, and 79.1% of the e-cigarette or vape group in the low, moderate, and high caries risk categories, respectively (Table 1).
A multivariable ordinal logistic regression model adjusting for both age group and sex also found a statistically significant difference (P < .001) in caries risk level between the control group and the e-cigarette or vape group. The control group again exhibited lower caries risk levels than the e-cigarette or vape group, with an odds ratio of
0.36 (95% CI, 0.22 to 0.60) for the control group when using the e-cigarette or vape group as a reference category. The age groups 16 through 25 years and 26 through 40 years had lower caries risk levels than the group older than 40 years when adjusting for vaping and sex. These results were statistically significant (P ¼ .005 and P < .001, respectively). Male patients had a significantly higher caries risk level (P < .001) than female patients when adjusting for vaping and age group (Table 2).
DISCUSSION
There was a statistically significant difference in caries risk levels between the e-cigarette or vape group and the control group; the former had a higher caries risk level. The null hypothesis was therefore rejected. Results of an in vitro study showed that e-cigarette aerosols hindered the growth of commensal oral bacteria, such as Streptococcus sanguinis and Streptococcus gordonii; growth of S mutans was not affected.7 In fact, S mutans exhibited higher hydrophobicity and coaggregation ability with increased biofilm formation.7 This may provide some justification for the increased caries risk in patients using e-cigarettes or vapes. In a cross-sectional study, researchers reviewed the records of 4,618 patients and found that those who used e-cigarettes were more likely to have untreated caries.14 Although the researchers did not specifically assess caries risk level in these patients, their results support our study’s results.
Vaping has been marketed as a safe alternative to cigarette smoking, and information on the potential cariogenicity of vaping is limited. Our study provides some additional information on the potential association between using e-cigarettes or vapes and caries risk.
The limitations of our study include the fact that this was a cross-sectional study design dependent on patient records. A total of 118 patients were excluded from our study because of some missing records. The percentage of patients who responded “yes” to use of e-cigarettes or vapes was only 0.69% of the entire sample size, which may have skewed the results of the statistical analysis, making extrapolation of the results difficult. Small sample sizes may make it difficult to assess whether a finding is true and may increase the likelihood of a type II error occurring. Among the nonvaping and non–ecigarrette using patients, most (59.6%) were in the high caries risk category. There is a risk that the proportion of high caries risk patients in the vaping and e-cigarette group (79.1%) was increased due to difference in the sample sizes between the 2 groups (test, control). Social desirability bias may have also played a role in the low number of vaping and e-cigarette using patients, as this was dependent on self-reported data. Although data on the duration, frequency, and quantity of e-cigarette and vape use were extracted, no valid conclusion could be made after analysis of these data due to the small number of patients who responded “yes” to e-cigarette and vape use. Drug use in general has been linked to a variety of unhealthy behaviors, such as poor oral hygiene and increased sugar intake. These unhealthy behaviors may be potential confounding variables.19-22 Finally, caries risk level is influenced by means of various socioeconomic factors, which could not be accounted for in our study.
The CAMBRA tool has been validated for use in children aged 0 through 5 years, as well as those 6 years and older.16,17,23 Several assessments have found a clear relationship between CAMBRA levels of low, moderate, high, and extreme and cavitation or radiographic lesions into dentin.24-26
Table 1. Cross-tabulation of e-cigarette or vaping group and caries risk level*
Although validated, results of these studies also showed that CAMBRA is approximately 70% predictive of actual caries outcomes for high-risk patients.16 The inaccuracy of this caries risk assessment tool is another limitation of our study. Finally, caries outcome was not assessed in our study, and the correlation between caries risk and outcome is not perfect.
CONCLUSIONS
Within the limitations of our study, it was concluded that in our study population, use of e-cigarettes or vapes was associated with caries risk level; vaping and e-cigarette using patients had higher caries risk. It is therefore suggested that the use of e-cigarettes or vapes should not only be included in the routine dental-medical history questionnaire, but also among the risk factors that increase a patient’s caries risk level. Patients who engage in e-cigarette or vape use may benefit from a more rigorous caries management protocol. A longitudinal assessment is highly recommended as a continuation of our study.
Dr Irusa is an assistant professor, Department of Comprehensive Care, Tufts University School of Dental Medicine, Boston, MA. Address correspondence to Dr Irusa, Department of Comprehensive Care, Tufts University School of Dental Medicine, 1 Kneeland St, Boston, MA 02111, email karina.irusa@tufts.edu.
Dr Finkelman is an associate professor, Department of Public Health and Community Service, Tufts University School of Dental Medicine, Boston, MA.
Dr Magnuson was an associate professor, Department of Diagnostic Sciences at Tufts University School of Dental Medicine, Boston, MA, when the work described in this article was conducted. She is now an independent researcher.
Dr Donovan is a professor, Division of Comprehensive Oral Health, University of North Carolina at Chapel Hill, Chapel Hill, NC.
Dr Eisen is an associate professor, Department of Comprehensive Care, Tufts University School of Dental Medicine, Boston, MA.
Disclosures. None of the authors reported any disclosures.
ORCID Numbers. Karina F. Irusa: https://orcid.org/0000-0003-35675860; Matthew Finkelman: https://orcid.org/0000-0002-3136-0389; Britta Magnuson: https://orcid.org/0000-0002-6490-0863. For information regarding ORCID numbers, go to http://orcid.org.
Table 2. Results of the multivariable ordinal logistic regression model including e-cigarette or vaping group, age, and sex as factors and caries risk level as the outcome.
References
1. Singh T, Arrazola RA, Corey CG, et al. Tobacco use among middle and high school students: United States 2011-2015. Morb Mortal Wkly Rep. 2016;65(14):361-367.
2. Wang TW, Neff LJ, Park-Lee E, Ren C, Cullen KA, King BA. E-cigarette use among middle and high school students: United States, 2020. Morb Mortal Wkly Rep. 2020;69(37):1310.
3. Outbreak of lung injury associated with the use of e-cigarette, or vaping, products. Centers for Disease Control and Prevention. Updated February 25, 2020. Accessed October 11, 2022. https:// www.cdc.gov/tobacco/basic_ information/e-cigarettes/severelung-disease.html.
4. Ruddick JA. Toxicology, metabolism, and biochemistry of 1,2-propanediol. Toxicol Appl Pharmacol. 1972; 21(1):102-111.
5. Kim SA, Smith S, Beauchamp C, et al. Cariogenic potential of sweet flavors in electroniccigarette liquids. PLoS One. 2018;13(9):e0203717. https://doi. org/10.1371/ journal.pone.0203717
6. Fischman JS, Sista S, Lee D, Cuadra GA, Palazzolo DL. Flavorless vs. flavored electronic cigarettegenerated aerosol and e-liquid on the growth of common oral commensal Streptococci. Front Physiol. 2020;11:585416.
7. Catala-Valentin A, Bernard JN, Caldwell M, Maxson J, Moore SD, Andl CD. E-cigarette aerosol exposure favors the growth and colonization of oral Streptococcus mutans compared to commensal Streptococci. Microbiol Spectr. 2022; 10(2):e0242121. https://doi. org/10.1128/spectrum.02421-21
8. Afrashtehfar KI. Vape labelling fails to report possible dental erosion and caries induced by e-cigarette fluids. Br Dent J. 2021;231(11):700.
9. Vora MV, Chaffee BW. Tobaccouse patterns and self-reported oral health outcomes. JADA. 2019;150(5): 332-344.
10. Akinkugbe AA. Cigarettes, e-cigarettes, and adoles- cent’s oral health: findings from the Population Assessment of Tobacco and Health (PATH) study. JDR Clin Trans Res. 2018;4(3):276-283.
11. Wadia R, Booth V, Yap HF, Moyes DL. A pilot study of the gingival response when smokers switch from smoking to vaping. Br Dent J. 2016;221(11):722- 726.
12. Al-Aali KA, Alrabian M, ArRejaie AS, Abdajabbar T, Vohra F, Akram Z. Peri-implant parame- ters, tumor necrosis factor-alpha, and interleukin-1 beta levels in vaping individuals. Clin Implant Dent Relat Res. 2018;20(3):410-415.
13. Irusa KF, Vence B, Donovan T. Potential oral health effects of e-cigarettes and vaping: a review and case re- ports. J Esthet Dent. 2020;32(3):260-264.
14. Vemulapalli A, Mandapati SR, Kotha A, Aryal S. Association between vaping and untreated caries: a cross- sectional study of National Health and Nutrition Exami- nation Survey 2017-2018 data. JADA. 2021;152(9):720-729.
15. Pitts NB, Zero DT, Marsh PD, et al. Dental caries. Nat Rev Dis Primers. 2017;3(1):1-6.
16. Featherstone JD, Chaffee BW. The evidence for caries management by risk assessment (CAMBRA®). Adv Dent Res. 2018;29(1):9-14.
17. Featherstone JD, DoméjeanOrliaguet S, Jenson L, Wolff M, Young DA. Caries risk assessment
in practice for age 6 through adult. J Calif Dent Assoc. 2007;35(10):703707, 710-713.
18. CDT 2022. Current Dental Terminology. American Dental Association; 2021.
19. Reece AS. Dentition of addiction in Queensland: poor dental status and major contributing drugs. Aust Dent. J. 2007;52(2):144-149.
20. Picozzi A, Dworkin SF, Leeds JG, Nash J. Dental and associated attitudinal aspects of heroin addiction: a pilot study. J Dent Res. 1972;51(3):869.
21. Shekarchizadeh H, Khami MR, Mohebbi SZ, Virtanen JI. Oral health behavior of drug addicts in withdrawal treatment. BMC Oral Health. 2013;13:11.
22. Zador D, Lyons Wall PM, Webster I. High sugar intake in a group of women on methadone maintenance in south western Sydney, Australia. Addiction. 1996;91(7): 1053-1061.
23. Ramos-Gomez F, Crall J, Gansky SA, Slayton RL, Featherstone JD. Caries risk assessment appropriate for the age 1 visit (infants and toddlers). J Calif Dent Assoc. 2007; 35(10):687702.
24. Doméjean-Orliaguet S, Gansky SA, Featherstone JD. Caries risk assessment in an educational environment. J Dent Educ. 2006;70(12):1346-1354.
25. Doméjean S, White JM, Featherstone JD. Validation of the CDA CAMBRA caries risk assessment: a six-year retrospective study. J Calif Dent Assoc. 2011;39(10):709- 715.
26. Chaffee BW, Cheng J, Featherstone JD. Baseline caries risk assessment as a predictor of caries incidence. J Dent. 2015;43(5):518-524.
Clinical
management of vital and non-vital discolored tooth preparation stump shades: A clinical case series
Stephen J. Chu, DMD, MSD, CDT; Adam J. Mieleszko, CDT; Guest Editor Rade D. Paravina, DDS, MS, PhD
Read this article in full at: https://onlinelibrary.wiley.com/doi/full/10.1111/jerd.13184
Objective
Traditional and modern-day laboratory techniques can be used to mask vital and non-vital discolored teeth.
Clinical Considerations
Two clinical case reports are presented showing different treatment approaches to differing clinical scenarios of partial coverage veneer and full coverage crown restorations, respectively.
Conclusions
Case: A 43-year-old Caucasian male patient presented with a history of trauma to his maxillary central incisor teeth, which had discolored over time. His chief complaint was not only the discoloration of the central incisor teeth but also the shape, form, and facial contour that had been attempted with composite resin restorations. (A) After crown removal of #7, the metal post was covered with a white composite resin core material; (B) A gold post foundation restoration was used on tooth #10; (B) Stump shade photographs were taken after tooth preparation; (C) The intaglio surface of the crown restorations with the white opaque liner added short of the cervical margin; and (D) Extraoral smile view of the patient demonstrating esthetic integration of the crown restorations.
Feldspathic ceramics should be considered when customization of stump shade correction and equalization is required with minimum facial reduction with veneer restorations. Translucent zirconia (5 mol% Y2O3) can be used to mask metal posts and core restorations on non-vital teeth using an opaquer material that is infused into the intaglio surface in the green state.
Clinical Significance
Different clinical scenarios will present to the clinician in regard to discolored stump shades where understanding what laboratory material treatment options are available that will help guide definitive restoration types and ultimately tooth preparation design.
ethics corner
TDA Council on Ethics and Judicial Affairs
The ethics of the unexpected loss of a practitioner
QThe dentist returns to her personal office in between patients and notices her cell phone ringing. The caller ID indicates it is the associate’s spouse calling. The news of the call was that the associate unexpectedly passed away overnight. What are the ethical considerations when a dental care practitioner passes away unexpectedly?
AUnexpected loss of a dentist raises several ethical issues regarding sharing the news with the dental team and the patients, transfer of patient care, and caring for patients while grieving. Legal issues are beyond the scope of this article; only ethical issues will be discussed. The American Dental Association’s Principles of Ethics and Code of Professional Conduct (ADA Code) is 1 tool that provides helpful analysis of the possible dilemmas presented.1
What ethical responsibility does the surviving dentist have to inform the patients of the deceased dentist? Per the ADA Code section 1 principle: Patient Autonomy (“self-governance”), “The dentist has a duty to respect the patient’s rights to selfdetermination and confidentiality…Under this principle, the dentist’s primary obligations include involving patients in treatment decisions in a meaningful way, with due consideration being given to the patient’s needs, desires and abilities, and safeguarding the patient’s privacy.”1 This principle needs to be considered, because patients have the right to be involved in treatment decisions and need to be aware that the practitioner will no longer be available to continue care. Therefore, there is an ethical consideration to make sure the patients are informed about the loss of the dentist. When faced with this situation in my own practice, an email was sent to active patient families, a memorial sign was posted in the office, and a post was made on the social media page for the practice.
Ethically, what should be communicated to the team and the patients? According to the ADA Code section 5 principle: Veracity (“truthfulness”), “The dentist has a duty to communicate truthfully.”1 Per the American Medical Association, “The cause of death should only be disclosed if approved by the family or emergency contact person… Organizations have a responsibility to balance the need to be truthful with the community with the need to remain sensitive to the family’s preferences.”2 The loss of the dentist must be communicated truthfully to the team and patient community. Specific details of the death do not need to be communicated. If there are rumors about the cause of death, those should be redirected.
How long may the name of the deceased dentist be used by the practice? Under the principle of Veracity in the ADA Code, subsection 5.G. Name of Practice states, “Since the name under which a dentist conducts his or her practice may be a factor in the selection process of the patient, the use of a trade name or an assumed name that is false or misleading in any material respect is unethical.”1 The dentist who passed away would not be able to give permission for the use of his or her name. Appropriate notice should be provided to the public, and the use of the dentist’s name should be ceased.
Should the surviving dentist or team be considered impaired and not able to treat patients ethically? Subsection 2.D.1. Ability to Practice under the principle of Nonmaleficence (“do no harm”) of the ADA Code states, “A dentist who contracts any disease or becomes impaired in any way that might endanger patients or dental staff shall, with consultation and advice from a qualified physician or other authority, limit the activities of practice to those areas that do not endanger patients or dental staff.”1 Although this principle refers to chemical or other impairment, grief could be considered impairing. Per Lee and Neimeyer, “Though most mourners are resilient, a minority of the bereaved experience disabling grief accompanied by clinically significant impairment in important areas of functioning.”3 If any members of the office team experience impairing grief, they should limit activities of practice until they no longer would endanger the patient. In my experience, I was unable to return to patient care the day I learned my associate had passed away. The grief was overwhelming. I was able to contain it and return to patient care in the following days. My team preferred to work and welcomed the distraction from their grief. The
My team preferred to work and welcomed the distraction from their grief. The surviving dentist also should be cautious of potential burnout, as the loss of a provider in the practice leads to additional work for the surviving dentist.
surviving dentist also should be cautious of potential burnout, as the loss of a provider in the practice leads to additional work for the surviving dentist.
Who is ethically responsible for the care of the patients of the deceased? Per the ADA Code, 2.F. Patient Abandonment, “Once a dentist has undertaken a course of treatment, the dentist should not discontinue treatment without giving the patient adequate notice and the opportunity to obtain the services of another dentist.”1 Under this principle, the office must continue the care for the patients of the lost associate so the patients’ care is not abandoned. If the surviving dentist does not have the skills to provide the treatment or the patient wishes to have a different provider, the practice should help facilitate the transfer of the patient’s care to another dentist. This could have financial ramifications for the surviving dentist. If the dentist is not able to complete work that was paid for, a complete refund would be appropriate to allow for the patient to receive care from a different provider.
When a practitioner is lost unexpectedly, there are guidelines provided by the ADA Code. If an unexpected loss occurs in a dental practice, truthful, compassionate care must be taken when informing the practice and patients and in the steps that follow. The ADA offers additional resources at ada.org/wellness.
https://doi.org/10.1016/j.adaj.2023.02.011
Copyright ª 2023 American Dental Association. All rights reserved.
Dr Foster is a full-time faculty member, Pediatric Dental Residency and Internship, Denver Health, Denver, CO, a member of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs, and a wellness ambassador, American Dental Association. Address reprint requests to the American Dental Association Council on Ethics, Bylaws and Judicial Affairs, 211 E Chicago Ave, Chicago, IL 60611.
Disclosure. The author did not report any disclosures.
Ethical Moment is prepared by individual members of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs (CEBJA) or guests of CEBJA, in cooperation with The Journal of the American Dental Association. Its purpose is to promote awareness of the American Dental Association Principles of Ethics and Code of Professional Conduct. Readers are invited to submit questions to CEBJA at 211 E Chicago Ave, Chicago, IL 60611, email ethics@ada.org.
The views expressed are those of the author and do not necessarily reflect the opinions of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs or official policy of the ADA.
References
1. Principles of Ethics and Code of Professional Conduct, with Official Advisory Opinions Revised November 2020. American Dental Association. Accessed January 6, 2022. https://www.ada.org/ en/about-the-ada/principles-of-ethics-code-of-professional-conduct.
2. After a physician suicide: responding as an organization toolkit. American Medical Association. Accessed February 2, 2023. https://www.ama-assn.org/practicemanagement/ama-steps-forward/ after-physician-suicide-responding-organization-toolkit.
3. Lee S, Neimeyer RA. Grief Impairment Scale: a biopsychosocial measure of grief-related functional impairment. Death Stud. 2023;47(5): 519-530.
Hulen Dental
Mark Malone, D.D.S. has
Veronica Y. Chen, D.D.S.
& David C. Sun, D.D.S.
Jini P. Kuruvilla, D.D.S.
We
Practices For Sale
FANTASTIC OPPORTUNITY FOR GROWTH: Dallas GP in a beautiful retail center off a busy thoroughfare. The office is all digital with 4 ops and is in excellent condition. The practice collected over $466K on 4 doctor and hygiene days a week, plus 1 to 2 Saturdays a month. There are over 1,200 active patients that are a blend of 15% FFS, 80% PPO, and 5% children’s Medicaid. The seller refers out most specialties, leaving ample room for growth. Opportunity ID: TX-02114
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Very real opportunity for growth by adding: a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02061
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS patients with a small amount of PPO. The office collected over $876K in a four-day workweek. This is a fantastic practice with the potential to grow for a motivated purchaser. Opportunity ID: TX-02041
MULTI-MILLION DOLLAR OPPORTUNITY: Large GP located north of Houston is available with real estate. The office is in a stand-alone building with 8 ops and is in excellent condition. It has digital X-rays, Pano, and paperless charts. The office operates 45 hours per week with 3 clinicians. There is over 6,500+ active patients, 70% Medicaid & 30% PPO/FFS, with an average of 96 new patients per month. Opportunity ID: TX-01979
FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Kathleen A Kasper, DDS, D-ABFO
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than 1 year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after one year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive and expensive, and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long-term unidentified in Texas is that one of the many Texas dentists who read the Texas Dental Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical
Examiner’s
Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
By far Latent Prints (finger, palm, sole), are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, incinerated, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers), require knowing what hospital/physician placed the device to get the matching serial number, which can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent, however, success depends on a presumptive identity and availability/ existence/quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
Anthropologic Methods will use skeletal features to make a positive identification.
Author
Kathleen A. Kasper DDS, D-ABFO
Dr Kasper has been practicing general dentistry in Carrollton, Texas, for 29 years. She is a graduate of the University of Iowa College of Dentistry.
She provides 3 counties in the Dallas-Ft. Worth Area with forensic dental services. These include Collin, Dallas, and Tarrant Counties. She is currently the only active board certified forensic dentist in north Texas.
She received her formal forensic odontology training at the University of Texas Health Science Center San Antonio, Texas, Center for Education and Research in Forensics (CERF) in 2003-2004.
Dr Kasper obtained Board Certification from the American Board of Forensic Odontology in 2010.
She is a fellow of the American Academy of Forensic Sciences, a member of the American Board of Forensic Odontology, and a member of the American Society of Forensic Odontology.
She is the current American Board of Forensic Odontology Dental Age Assessment Committee Chair.
Dr Kasper is also a published author in the Journal of Forensic Sciences and coauthor of a chapter in each of 3 forensic textbooks.
Perhaps one of her greatest undertakings was chairing a working group for the American Dental Association that has published the “Technical Report” for Forensic Dental Age Estimation which went on to become a “standard” for the Organization of Scientific Area Committees (OSAC) for Forensic Science.
DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from family members or multiple family members if known. If no matches are obtained, then:
DNA Samples are submitted to CODIS (Combine DNA Index System), which is a computer program that operates local, state, and national databases of DNA profiles from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long-term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may still remain unidentified once completed. This is the proverbial end of the road; therefore, all Texas Dentists, Dental Auxiliaries and Staff; Can you help the Tarrant County Medical Examiner’s Office give a name to the unidentified male decedent described below?
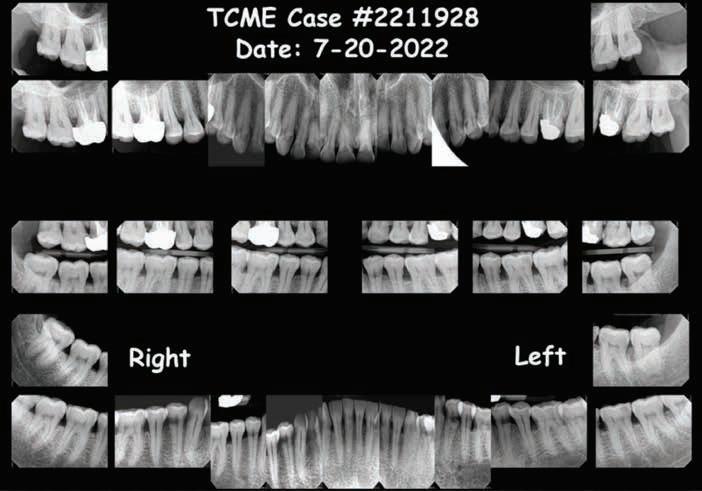
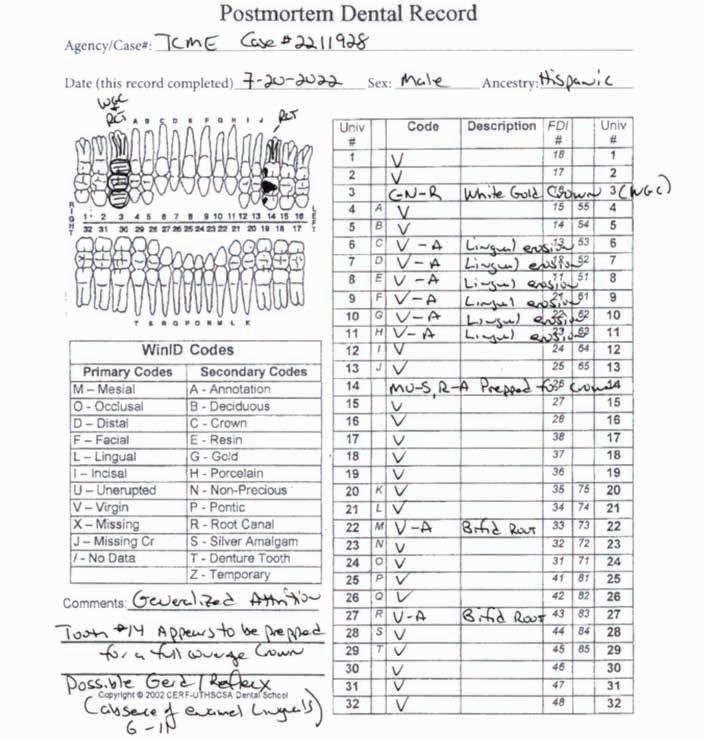
The Unidentified Individual: Tarrant County Medical Examiner (TCME) Case #2211928
Date of Death (Decedent found with lividity): June 28, 2022
Cause of Death: Hyperthermia
Manner of Death: Accident
Body Condition: Recent/Fresh
Sex: Male
Ancestry: Hispanic
Age: 40-60 years
Scene Description: An unidentified Hispanic male was found by a worker mowing grass near the back parking lot of a Domino’s restaurant in Ft. Worth, Texas, on 6-28-2022. The decedent was lying unresponsive in a supine position on the pavement between a dumpster and a cargo shipping container when Ft. Worth police arrived at the scene. Video surveillance obtained from the restaurant caught the decedent moving around on camera near the dumpster at 1800 hours on 6-28-2022. The decedent was clad in pants and a belt. No signs of medical intervention were observed, and brown emesis was present around the decedent’s mouth. No foul play was suspected.
Dental Evidence Recovered: Maxilla and Mandible
Right Left
Right Lateral View
Left Lateral View
Right Left Right Left
Periapical Tooth #3 (Root Canal Treatment)
Periapical Tooth #14 (Root Canal Treatment)
#3 #14
Dental
Closing
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans, or other dental information regarding the unidentified Hispanic male decedent described above as TCME Case #2211928, please contact the Tarrant County Medical Examiner’s Office, phone (817) 920-5700, extension 8387, ask for Chief of Human Identification Services Christian Crowder, PhD, D-ABFA.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/services/cjis/ncic
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021
ORAL and maxillofacial
pathology
case of the month
Case history
A 62-year-old male patient presented with a chief complaint of red, sore, and bleeding gums while brushing. The patient reported that he started noticing these symptoms approximately 2 years ago which has progressively worsened over time. The patient’s general dentist recommended deep cleaning, however that did not help resolve his problems. Subsequently, patient was referred to a periodontist for further evaluation and treatment. His initial periodontal therapy consisted of plaque control, scaling and root planing which resulted in limited improvement of his gingival condition. Patient could not recall taking any new medications or any other possible triggers for this condition. The patient’s medical history was unremarkable,
AUTHOR
Safia Durab, BDS, BSc, MSc.
Departments of Diagnostic and Biomedical Sciences, The University of Texas Health Science Center at Houston, School of Dentistry, Houston, Texas
Ida Varghese, BDS, DDS
Departments of Diagnostic and Biomedical Sciences, The University of Texas Health Science Center at Houston, School of Dentistry, Houston, Texas
Nadarajah Vigneswaran, BDS, DrMedDent, DMD
Departments of Diagnostic and Biomedical Sciences, The University of Texas Health Science Center at Houston, School of Dentistry, Houston, Texas
Figure 1. Maxillary and mandibular facial gingivae appear swollen and fiery red with sharp demarcation at the mucogingival margin.
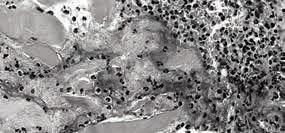
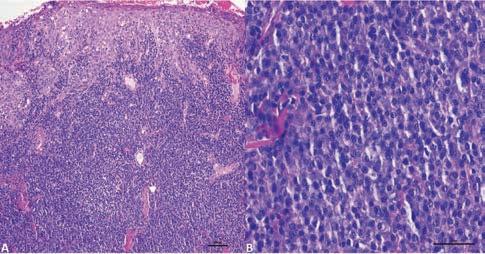
2. A: Microscopic examination of the H&E-stained sections of the biopsy reveals psoriasiform mucositis with spongiosis and neutrophilic exocytosis (A; x 40). The underlying lamina propria reveals an intense chronic inflammatory cell infiltrate (A; x 40) consisting exclusively of plasma cells (B; x 200).
3.
and he denied any current or past use of tobacco products. Patient reported he did not have any rashes or itchy areas on his skin or genital mucosa. Clinical examination revealed generalized, enlarged, edematous and erythematous maxillary and mandibular facial gingiva, predominantly the anterior region. The affected gingiva revealed sharp demarcation along the mucogingival margin and between involved and uninvolved gingiva (Figure 1). The affected gingiva appeared swollen, fiery red in color, with a shiny granular surface
expression
texture with loss of stippling (Figure 1). Affected gingiva was mildly tender to palpation, revealed no evidence of ulcerations or erosions and periodontal probing elicited profuse bleeding. Rest of the oral soft tissue examination was unremarkable. Given the clinical presentation, his periodontist suspected desquamative gingivitis secondary to autoimmune vesiculo-erosive diseases and took incisional biopsies from the affected gingiva and submitted routine histopathologic and direct immunofluorescence studies.
Biopsy findings:
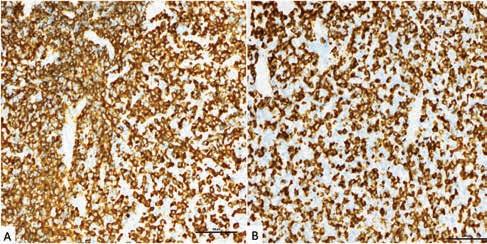
Light microscopic examination of the hematoxylin & eosin-stained sections revealed psoriasiform epithelial hyperplasia with spongiosis, neutrophilic exocytosis and micro-abscesses. The underlying connective tissue revealed numerous dilated vascular channels and dense sheets of chronic inflammatory cells infiltrate exclusively consisting of plasma cells (Figure 2). Further ancillary testing such as chromogenic RNA in situ hybridization studies revealed that the plasma cells were positive for both kappa and lambda light chain mRNA (Figure 3). Lack of light-chain restriction within the plasma cell infiltrate excluded plasma cells neoplasm (i.e. multiple myeloma/ plasmacytoma). Furthermore, direct immunofluorescence studies were negative for lichen planus, mucous membrane pemphigoid and pemphigus vulgaris.
What is your diagnosis?
See page 420 for the answer and discussion.
Figure
Chromogenic RNA in situ hybridization studies reveal the
of mRNA for both kappa (A) and lambda (B) light chains within the plasma cell infiltrate confirming their polyclonal nature (x 200).
Figure
ORAL and maxillofacial pathology
diagnosis and management—from page 419
Diagnosis: Plasma cell
gingivitis
Differential Diagnosis
The clinical differential diagnosis for a patient presenting with generalized, diffuse, erythema and edema of the gingiva which failed to respond to conventional periodontal therapy, can be broadly categorized under two groups based on their etiology:
1. Desquamative gingivitis associated with autoimmune vesiculo-erosive diseases:
• Lichen planus
• Mucous membrane pemphigoid
• Pemphigus vulgaris
2. Granulomatous and plasma cell gingivitis associated with contact hypersensitivity or systemic diseases.
• Sarcoidosis
• Crohn’s disease
• Granulomatosis with polyangiitis
• Foreign body gingivitis
• Idiopathic granulomatous gingivitis
• Plasma cells gingivitis
Discussion
Desquamative gingivitis associated with autoimmune vesiculo-erosive diseases:
Desquamative gingivitis (DG) is a clinical term to describe diffuse gingival erythema, edema with erosions/ulcerations with or without preceding vesicles or bullas. DG involves both free and attached facial gingiva and less frequently affects the lingual gingiva. This condition typically presents as red, swollen, and friable gums with a tendency to bleed easily. Lichen planus is the most common cause of DG followed by mucous membrane pemphigoid and pemphigus vulgaris.1 Other rare causes of DG include Graft versus Host Disease (GVHD) and lupus erythematosus. DG is a clinical description and is not the final diagnosis which needs biopsies of the affected and non-ulcerated gingiva for histopathologic and direct immunofluorescence studies.1
Lichen planus (LP) is a relatively common immunologically mediated mucocutaneous inflammatory and ulcerative disease affecting approximately 1-5 % of the adult population.2,3 Although LP is suspected to be an autoimmune disease, the target antigen is unknown.3 Mucosal LP most commonly affects the oral cavity and in rare instances may affect the oropharynx, esophagus and vulvovaginal mucosa.3 Oral LP usually develops in adults over the age of forty with a strong female predilection.3 The following intraoral sites are, in descending order, the most common sites of involvement for LP: gingiva, buccal mucosa, tongue, lips and palate.3 Oral LP has several clinical types that include reticular, erosive and ulcerative variants.3 The reticular variant is the most common clinical type of oral LP and presents as lacy white keratotic striae and patches. These lesions exhibit symmetrical distributions involving bilateral buccal mucosa, lateral and ventral surface of the tongue, and lips. The reticular variant of LP is asymptomatic and usually detected as an incidental finding during a routine oral examination. Erosive LP presents as painful, diffuse erosive and ulcerative areas of erythema with white striae and patches at the periphery. Erosive LP frequently affects the gingiva presenting as desquamative gingivitis.3 Lichen planus involving the gingiva tends to be more active in areas with fixed prosthesis (i.e. crown, bridges and dental implants) compared to natural teeth.3
Mucous membrane pemphigoid (MMP), also known as cicatricial pemphigoid, is a chronic autoimmune disease characterized by development of painful vesiculobullous lesions predominantly involving the mucosa.3 MMP is a humoral autoimmune
disorder in which affected patients have autoantibodies directed against specific adhesion molecules localized within the hemidesmosomes of the basal keratinocytes and in the lamina dura of the basement membrane.3 MMP is more common among women with a female to male ratio of 2:1 and frequently affects the elderly population (age range: 60-80 years).3 MMP may involve all mucosal sites but rarely affects the skin. Oral (90% of cases) and ocular mucosa (65% of the cases) are the most commonly affected sites.3 MMP patients with lesions limited to oral mucosa have a better prognosis compared to patients with MMP involving other mucosal surfaces.3 The most common oral manifestation of MMP is desquamative gingivitis.3 More than 85% of patients with MMP have gingival involvement.3 In contrast, only 25% of patients with oral lichen planus and 18% of patients with pemphigus vulgaris have gingival involvement.3
Pemphigus vulgaris (PV) is an extremely debilitating, potentially life-threatening vesiculobullous disease of the skin and mucous membrane.3 It is a humoral mediated autoimmune disorder caused by autoantibodies against desmosomal proteins, desmogleins 1 and 3, resulting in intraepithelial blistering.3 Paraneoplastic pemphigus (PNP), also known as paraneoplastic autoimmune multiorgan syndrome (PAMS) is a rare life-threatening autoimmune disease with mucocutaneous and multi-organ involvement seen in patients with lymphoproliferative malignancies (i.e., leukemia or lymphoma).3 PNP is a rare disorder that clinically and microscopically resembles PV. Although PV mainly afflicts adults between the ages of 40 to 60 years, it may be seen in children and young adults.3 PV does not have a gender predilection. The oral cavity is the primary and initial site of
disease manifestation in the majority of PV patients; skin lesions do not appear until months or even years later. Oral lesions of PV develop as vesicles or small bullae that burst rapidly leaving painful erosions and ulcers. Established PV lesions may resemble major aphthous ulcers or large superficial ulcers surfaced by a necrotic pseudomembrane with erythematous and irregular outlines mimicking pseudomembranous candidiasis. The most common intraoral sites affected by PV in descending order are soft palate, hard palate, buccal mucosa, ventral tongue and floor of the mouth.
Granulomatous gingivitis:
Chronic granulomatous inflammation is a distinctive type of inflammation characterized by the presence of epithelioid macrophages and multinucleated giant cells. Differential diagnoses for granulomatous gingivitis include foreign body reactions, Crohn’s disease, sarcoidosis, and Granulomatosis with polyangiitis also known as Wegener’s granulomatosus.4,5
For patients presenting with granulomatous gingivitis, microscopic examination of the H&E slides using polarized light can help to exclude foreign bodies within the granulomatous inflammation. Bacterial and fungal special stains are used to exclude systemic infections.4 If microbial and foreign body etiologies are excluded, clinical and laboratory evaluations should be conducted to rule out sarcoidosis, Crohn’s disease and granulomatosis with polyangiitis. Sarcoidosis is a multisystem granulomatous inflammatory disease of unknown etiology, primarily affecting the lungs, lymph nodes, skin, eyes, and salivary glands.4 Oral manifestations of sarcoidosis are submucosal masses, isolated papules, or ulcerations, most
commonly affecting the buccal mucosa, gingiva, lips, tongue, and palate. Elevated serum angiotensin-converting enzyme (ACE) levels and bilateral hilar lymphadenopathy on chest radiographs support the diagnosis of sarcoidosis. Crohn’s disease is a chronic inflammatory disorder of the gastrointestinal tract with multifactorial etiologies. Common gastrointestinal symptoms include abdominal cramping and pain, nausea, and diarrhea, sometimes accompanied by fever. Oral manifestations of Crohn’s disease include diffuse or nodular swelling of the oral and perioral tissues and deep granulomatous-appearing linear ulcers. Patchy erythematous macules and plaques on both attached and unattached gingivae, referred to as muco-gingivitis, may be among the more common lesions associated with Crohn’s disease.
Granulomatosis with polyangiitis (GPA), an uncommon systemic disorder of unknown etiology, is characterized by necrotizing granulomatous inflammation with vasculitis involving the upper and lower respiratory tract and kidneys. The most characteristic oral manifestation of GPA is “strawberry gingivitis”, characterized by swollen, red and hemorrhagic gingiva with a granular or bumpy surface texture. The combination of the clinical manifestation and the microscopic findings of necrotizing and granulomatous vasculitis leads to the diagnosis of GPA.
Plasma Cell Gingivitis:
Plasma cell gingivitis (PCG) is a benign inflammatory condition of unknown etiology and hence considered as an idiopathic disorder, characterized by polyclonal plasma cell proliferation in the lamina propria of the gingiva6. PCG is suspected to be a contact
ORAL
and maxillofacial pathology
hypersensitivity (allergic) reaction to food additives and flavoring agents in chewing gum, toothpaste and mouth washes. Plasma cell gingivitis presents with a wide age range in both males and females. Patients present with the chief complaint of rapid onset of a “sore and red gums”, often exacerbated by dentifrices and hot or spicy food. Clinically, the anterior free and attached gingiva shows diffuse enlargement with fiery erythema and loss of normal stippling with a sharp demarcation at the mucogingival junction. The gingiva is usually painful and prone to bleed easily, especially while brushing. Occasionally, patients may present with similar lesions occurring over the mouth in addition to the gingivae which is designated as oral plasma cell mucositis.7 Interestingly, increased prevalence of plasma cell gingivitis and oral plasma cell mucositis is noted after COVD-19 pandemic based on the anecdotal evidence from oral pathology biopsy services and a recent published report.6
Most of the time, the typical clinical appearance is diagnostic, when accompanied by a history of possible association and temporal relation with an allergen such a new mouthwash, toothpaste etc., and may be treated when the possible allergen is eliminated. The final diagnosis of PCG relies on a robust clinical and histopathologic correlation, where the observed changes coincide with a rapid onset of mouth soreness that persists despite improved oral hygiene. Patients with this diagnosis should be advised to maintain a comprehensive dietary
history, documenting all oral intake including foods, dentifrice, mouthwash, tobacco, alcohol, chewing gum, candy, and medications. Spatial relationship with potential allergens is important to make an association. Management involves eliminating potential allergens and administering anti-inflammatory therapies. For patients where no underlying cause is found, various topical or systemic immunosuppressive medications have been tried with mixed results. These include corticosteroid oral rinses, topical corticosteroid gel or calcineurin inhibitors (i.e. pimecrolimus and tacrolimus) applied using the medication carrier trays. Despite thorough evaluations and therapeutic interventions, some patients remain unresponsive to treatment, and the cause of the disease remains unidentified.
Treatment and Follow Up of
the Current Patient
As first-line management, the patient’s plasma cell gingivitis was treated with systemic steroids along with antifungal prophylaxis. The patient responded well to this initial treatment. Following stabilization of the disease and alleviation of the worst symptoms, custom gingival medication trays were constructed for the topical application of steroid to the affected gingiva, on an as needed basis.
References
1. Suresh L, Neiders ME. Definitive and differential diagnosis of desquamative gingivitis through direct immunofluorescence studies. J Periodontol 2012;83(10):1270-8.
2. Cheng YS, Gould A, Kurago Z, Fantasia J, Muller S. Diagnosis of oral lichen planus: a position paper of the American Academy of Oral and Maxillofacial Pathology. Oral Surg Oral Med Oral Pathol Oral Radiol 2016;122(3):332-54.
3. Vigneswaran N, Muller S. Pharmacologic treatment of common oral mucosal inflammatory and ulcerative diseases. In: Jeske A, editor. Contemporary dental pharmacology; Evidencebased considerations. Second edition ed. Switzerland, AG: Springer Nature; 2024. p. 103-22.
4. H.E. J, R. B, M.E. W, Vigneswaran N. Oral and Maxillofacial Pathology Case of the Month: Orofacial granulomatosis associated with Crohn Disease. Texas Dental Journal 2019;136(8):456-65.
5. Mena C, Kiat-amnuay S, Chua S, Hasapes J, Vigneswaran N. Oral and Maxillofacial Pathology. Case of the Month. Limited granulomatosis with polyangiitis (Wegener’s granulomatosis). Tex Dent J 2016;133(1):14-5, 52-4.
6. Fitzpatrick SG, Alramadhan S, Islam MN, Bhattacharyya I. Increased frequency of oral plasma cell mucositis/plasma cell gingivitis after the COVID-19 pandemic: a 23-year retrospective analysis and review of diagnostic challenges relating to this condition. Oral Surg Oral Med Oral Pathol Oral Radiol 2024;137(2):153-60.
7. Coppola N, Cantile T, Canfora F, et al. Pitfalls and Challenges in Oral Plasma Cell Mucositis: A Systematic Review. J Clin Med 2022;11(21).
in memoriam
Those in the dental community who have recently passed
Curtis Lee Kaiser
College Station
8/31/68–6/27/24
Good Fellow: 2020
Gregory C. Schlimmer
Corpus Christi
1/18/72–7/22/24
David Charles Boyles
Alvin 10/5/26–7/18/24
Good Fellow: 1977
Life: 1991
Fifty Year: 2003
Hal Harrison Ramsey
Abilene
7/4/35–7/28/24
Good Fellow: 1985
Life: 2000
Fifty Year: 2011
Mark Steven Quagliotti
League City
11/22/57–4/14/24
Life: 2021
James H. Hailey
Longview
11/17/40–4/30/24
Good Fellow: 1990
Life: 2005
Fifty Year: 2015
Kenneth Edward Aboussie
Wichita Falls 11/25/44–6/21/24
Good Fellow: 1997
Life: 2009
Fifty Year: 2020
Thomas Michael Smith
Longview 5/171941–5/29/24
Good Fellow: 1991
Life: 2006
Fifty Year: 2016
James R. Mitchell
Wichita Falls 10/13/48–7/7/24
Good Fellow: 2006
Life: 2013
George Frederick Schudy
Houston 11/2/43–11/13/23
Good Fellow: 1997
Life: 2008
Fifty Year: 2021
value for your profession
Provided by:
PERKS
G R
A M
A Crash Course in Membership Plans
By Brett Wells, DDS; CEO, DentalHQ
Your patients are looking for the best possible option to have their dental needs taken care of. And you’re looking for patients who keep coming back to your practice. How do you have the best of both worlds?
Allow us to introduce membership plans.
What is a membership plan? And how does it work?
Your patients pay a monthly or annual membership fee for their plan’s services, and then you provide them with those services. That’s it.
Member benefits are most often preventive care—exams, cleanings, X-rays for the year; all that good stuff. Most practices give additional member benefits, like whitening treatments, fluoride, and members-only discounts on restorative treatment.
Why membership plans are attractive to patients
Pricing and services are transparent with membership plans. There are no complexities associated with insurance claims and coverage limitations. And there’s
no second-guessing what kind of care patients will receive, because it’s all in the plan.
With a clear understanding of the costs and services included in their plan, patients have more control over their treatment decisions and the services they receive and can better plan and budget for their dental care needs. Membership plans help remove the involvement of insurance companies, leading to a more personalized and tailored approach to dental care; something that’s been lacking in the dental insurance industry for some time now.
Getting your patients on board won’t be a problem.
Who are membership plans for?
A dental membership plan is typically designed for individuals and families seeking affordable dental care options—whether they’re uninsured or already have insurance.
Because they enable individuals and families to access dental services at discounted rates, they help subscribers receive the best care at an affordable price.
Don’t confuse dental membership plans with dental discount plans or dental savings plans. Dental savings plans are more like buyer’s clubs—offering discounts on care from various dentists. And they are nothing like dental insurance.
For individuals who don’t have dental insurance—such as selfemployed individuals, small business owners who lack access to employersponsored dental benefits, and retirees who no longer receive dental benefits from their former employers—membership plans are an easy alternative to traditional dental insurance.
Dental membership plans can also be great for individuals with dental insurance seeking to supplement limited coverage. Because membership plans often provide additional savings on services not covered by insurance—such as cosmetic dentistry or orthodontic treatments—patients enrolled in a plan alongside their insurance may further reduce out-ofpocket expenses and have access to a broader range of discounted dental services.
In short, anyone can benefit from them because there’s no downside.
What can a membership plan do for my practice?
Offering membership plans will likely mean a significant increase in patient membership and loyalty.
Because patients are already paying for their membership plan them through a subscription service, they’re more likely to make it to their appointments. Patients will be more likely to continue using your services and enjoy their accessibility to quality care. This boost in the number of loyal patients means increased revenue for your practice.
Because membership plans run on subscriptions, they simplify billing If you want to get ahead of the game, you can also automate your plans with membership plan automation software. These platforms can organize your plans, give you insights into your practice’s growth, handle payout reporting, and make the management of your members a lot easier.
Dental membership plans also establish a direct connection between your practice and your patient, which is something insurance can’t do. There’s no awkward, invisible middleman. Just you and the people you want to care for.
Finally, membership plans make it easier to provide preventive care to your patients. You’ll be able to detect issues early on and help patients avoid costly and extensive treatments in the future. Membership plans can help your patients prioritize their dental health, which contributes to their overall health.
In short, membership plans can help you help your patients and make it easier to grow your practice.
The leading platform for successful membership plans, DentalHQ enables practices to create, manage, and grow flexible and automated in-house membership plan programs. DentalHQ is endorsed by TDA Perks Program. For more information, visit tdaperks.com (Insurance, HR & Marketing) or call 833222-4748.
Find more articles by DentalHQ at https:// tdaperks.com/?s=dentalhq.
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES.
AUSTIN (ID #662): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business.
DALLAS-PEDO/ORTHO (ID #665): Legacy Pedo/Ortho practice in the heart of north Dallas. Thriving practice, large fee-for service patient base, revenue of 7 figures. Over 2,800 sq ft, fully digital with computers in the operatories, digital radiography, and a digital pano. HOUSTON-SOUTHWEST (ID #627): Legacy GD practice with majority FFS patient base in a growing southwest Houston suburb. Located in a retail center on a busy intersection, this 1,200 sq ft office features 4 fully equipped ops plumbed for nitrous, computers throughout, digital radiography, a digital scanner, intraoral cameras, and paperless charts. HOUSTON-SOUTHWEST (ID #674): Highly profitable, turn-key, PPO/FFS general dentistry practice southwest of Houston. High-visibility office, 4 computerized operatories, digital x-ray sensors, digital pano, Cerec scanner, Cerec milling unit and oven, and intraoral cameras. The practice has exceptional net cash flow. 1,400+ active patients, 20+ new patients per month, 30% hygiene production and exceptional net cash flow. The real estate is available for sale. HOUSTON-SOUTH (ID #682): Established, multi-specialty dental office in a suburb about 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong
net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose. HOUSTONNORTHWEST (ID #688): Well-established, profitable GD practice in northwest Houston in a great location with room to grow. 2,000+SF office, 5 fully equipped operatories, a digital pano, a digital scanner, intraoral cameras and digital radiography. Large majority PPO/FFS patient base and about 40+ new patients per month. There is additional upside for anyone who desires to keep specialty procedures in-house as the majority of endo, implant placement, and orthodontics are currently referred out. NORTHEAST TEXAS (ID #584): 100% FFS general dentistry practice in a desirable town in northeast Texas with 7 figures in revenue and strong net income. The turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCT, and a digital scanner. SAN ANTONIO (ID #681): GD practice and real estate in NW San Antonio. Legacy practice, 100% feefor-service, multi-generational patient base, stellar reputation. Four fully equipped operatories with digital radiography, computers and intraoral cameras throughout, and a digital Pano. The practice has consistently increased revenue year over year and has a strong hygiene recall program with nearly 30% of annual production coming from the hygiene department. SAN ANTONIO (ID #685): Well-established dental practice and real estate nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouthreferrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in
2023 and the trend has continued into 2024. SOUTH TEXAS (ID #651): General dentistry practice located in south Texas. This state-of-the-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld X-ray units, and a 3-D printer. The practice serves a large PPO/Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow. SOUTH TEXAS (ID #668): Thriving south Texas practice (with real estate) that has established itself as the premier dentistry provider in the local community. This one-doctor practice has a massive active patient base, strong hygiene production, and generated revenue of 7 figures. The real estate is available for purchase and features 6 equipped operatories and state-of-the-art equipment (CBCT, digital intraoral scanner, and CAD/CAM milling unit). This may also be an ideal fit as an associate-run practice for a Texas-based group practice owner. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-9007989 or info@dentaltransitions.com.
AUSTIN: Fee-for-service private practice, 46 years same location with a 10-15 mile panoramic view over the downtown Austin skyline. Associate to buy with a preferred long transition for the senior doctor. Eight years remaining current lease with option to extend. Tremendous amount of residential growth immediately outside our huge windows. Ideally a GP interested in learning full-scale orthodontics. Please email for information: info@austinskylinedental.com.
EAST TEXAS:
Exceptional practice opportunity in Troup, Texas. Seeking associate to join high quality, well-established dental practice with a long history of excellence. This is an exceptional opportunity to move into ownership after a successful initial employment phase. Must be committed
classifieds
to providing optimal patient care with exceptional technical skills, strong people skills, personal integrity, honesty and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on Christian values and professional growth. Our office expansion should be complete mid to late September 2024, but the new associate could begin in August if he/she would like. Please reply in confidence with your CV and a letter outlining your future objectives and goals to: drmay@troupfamilydental.com or call our office at 903-842-4600.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 square feet with 3 total operatories: 2 for dentistry and one for hygiene. Please let me know if you need anything else from me. . A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee-for-service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
KERRVILLE: Close to the Kerrville Medical Center, 1,300 sq ft. Hill country/contemporary style 3 operatories sterilization/lab: including sterilizer and basic lab equipment, business section, patient waiting area for 8. Private doctor’s office, patient and staff bathrooms (meeting ADA code), mechanical room with vacuum, staff lounge, private entrance/exit, Cone Beam CT machine available for use, computer system established and wired. Perfect for general dentist or specialist. Text 210-4162424 for information.
NORTH TEXAS: If you don’t want to deal with insurance, have the skillset to keep some specialty procedures in house, and want the autonomy to do things your own way, this is the practice for you. It’s located about two hours north of DFW. Weíre a completely OON office. Our staff is a great close knit group of people. Wonderful patient base. We do a little bit of everything from bread and butter crowns and fillings, to root canals, implants, and AOX and cosmetic/full mouth rehab stuff. We got in on scanning, milling, and printing pretty early and have an amazing workflow that lets us do a lot of our own custom lab work for a more aesthetic and personal touch. This includes 3D printing our own dentures, partials, and nightguards, as well as milling our own crowns and AOX prostheses. We have a lab grade 5-axis mill, 3D printer, IO scanner, CBCT machine, intraoral cameras, digital X-rays, etc. All brand new in 2022. 4 ops, 1 full-time hygienist and 1 parttime. Last year we did over 7 figures in collections and are on track to beat that this year. The practice is also newly remodeled. I would be willing to consider an immediate purchase or an associate with the option to buy me out after a smooth transition. If interested, please call/text Chandler at 801-895-0514.
ROCKPORT: Practice for sale in Rockport. Two chairs, plumbed for 3. Currently being worked 3 days a week producing near mid-6 figures. Fee for service, no DMO, HMO or PPO contracts. Hygienist 3 days a week and will stay, been with practice since 2019. Digital x-rays, paperless, Newtom 3D/Panorex, (3) x-ray sensors. Practice is in older house, which can be leased or purchased. Great starter practice or for someone slowing down and wants to live on the coast. Send inquires to jim@jlongdds.com or call: 281-726-1812, leave message.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www.adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
OFFICE SPACE
PLANO: Dental office space in Plano for rent or purchase: 2,978 sf space in the 75024 zip code. Plumbed for central nitrous for 4 ops. Large waiting area, front office, 4 enclosed ops, 1 consultation room, open hygiene bay (plumbed for 4 chairs), sterilization/lab room, X-ray room, manager’s office, doctor’s office, staff lounge with lockers and restroom, patient restroom, storage area, nitrous closet, equipment closet. Current tenant is a pediatric dentist. Space will be available in Dec 2024/Jan 2025. Interested tenants or buyers please message Dr Patel at 972-814-3545.
SAN ANTONIO: Ready to go dental space for lease with chairs and some equipment in place. Great northside location at Hwy 281 N and Brookhollow. The space is 1783 SF and rents for $2407/mo modified gross. Two restrooms in the suite, floor plan available. Broker is BK Properties 210-4900483 or 210-887-8828.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-5172826 or drzoch@yahoo.com.
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
DSO C S PRACTICE SALES
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com PRACTICE APPRAISALS