488 DR CRAIG ARMSTRONG OF HOUSTON AWARDED THE TDA GOLD MEDAL FOR DISTINGUISHED SERVICE
496 AN UNRELENTING SORE THROAT A CASE REPORT
JOHN J. BURDITT, DDS, FACD
500 FBI: FOUND BUT NOT IDENTIFIED (YET)
KATHLEEN A. KASPER DDS, D-ABFO
507 ASK THE POWERS CENTER
MARIA GONZALEZ, DDS, MS
ROSALIE NGUYEN GULLA, DDS, MS
Anesthesia
Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
HIGHLIGHTS
495 In Memoriam
Oral and Maxillofacial Pathology: Case of the Month
Oral and Maxillofacial Pathology: Case of the Month Diagnosis and Management
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
John J. Burditt, DDS,
Kathleen A. Kasper DDS, D-ABFO
507 ASK THE POWERS CENTER
Maria Gonzalez, DDS, MS
Rosalie Nguyen Gulla, DDS, MS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 141 | No. 8
Texas Dental Association 8701 W Hwy 71, Ste 201-M Austin, TX 78735
Phone: 512-443-3675 • FAX: 512-443-3031
Email: tda@tda.org • Website: www.tda.org
Texas Dental Journal (ISSN 0040-4284) is published monthly except January-February and August-September, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2024 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement included in the online September Annual Membership Directory or on the TDA website: tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
Get unmatched coverage. Practice more safely. Your good name is protected.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).
Contact
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PAST PRESIDENT Duc “Duke” M. Ho, DDS 281-395-2112, ducmho@sbcglobal.net
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
Adam S. Awtrey, DDS 314-503-4457, awtrey.adam@gmail.com
SENIOR DIRECTOR, NORTHEAST
Drew M. Vanderbrook, DDS 214-821-5200, vanderbrookdds@gmail.com
DIRECTOR, SOUTHEAST Ron Hill, DDS 713-626-8343, rhilldds@gmail.com
DIRECTOR, SOUTHWEST
Oshmi Dutta, DDS 210-888-0700, odutta@gmail.com
DIRECTOR, NORTHWEST
Annie C. Wilson, DDS 817-860-4343, annie@anniewilsondds.com
DIRECTOR, NORTHEAST
Shane A. Ricci, DDS 972-381-1888, riccidds@hotmail.com
SECRETARY-TREASURER*
Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN**
Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR**
Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL
Carl R. Galant
EXECUTIVE DIRECTOR
Linda G. Brady CAE 512-443-3675, lbrady@tda.org
*Non-voting member **Non-voting
•
•
•
•
•
•
Jerry E. Bouquot, DDS, MSD Ngozi N. Nwizu, BDS, MMSc, PhD Kalu U.E. Ogbureke, BDS, DMSc, JD, MSc Nadarajah Vigneswaran, DMD, DrMedDent
Craig Armstrong, DDS, of Houston is this year’s recipient of the TDA Gold Medal for Distinguished Service, the highest achievement within the Association. Dr Armstrong is the 28th TDA member to be so honored by his peers. TDA President Dr Cody Graves presented the award to Dr Armstrong, saying he represented the best of TDA for his commitment, strength, and vision.
Dr Craig Armstrong of Houston Awarded the TDA Gold Medal for Distinguished Service
The Texas Dental Association awarded Dr Craig Armstrong of Houston with the Association’s highest honor, the TDA Gold Medal for Distinguished Service, at the House of Delegates in May 2024. The award was a surprise to Dr Armstrong and his wife Lana who were in the audience, and it recognizes his commitment and involvement in organized dentistry.
Dr Armstrong’s road to dentistry began across the world. He was born in Verdun, France, in 1960 to a military family. His father was an Army First Sergeant, and the family moved every 3 years or so, living in Frankfurt, Germany, and Edinburgh, Scotland, before heading to the states to move to Arizona, Georgia, and finally Texas.
He says the frequent relocation taught him the art of making friends quickly. “It provided me with a unique perspective on diverse cultures, cuisines, and people, that very few get to experience.”
He and his 2 brothers found ways to stay busy during their childhood, whether it was delivering newspapers, running a lawn care service, or sacking groceries at the base commissary. He played baseball and basketball throughout high school, which helped him build lasting connections, he says.
Dr Armstrong’s father died tragically on active duty at 46 years old. His mother was 42, a stay-at-home mom, and he says her sacrifices laid the foundation for his journey.
“After his death, she stepped into the role of a bookkeeper in a small family business, demonstrating incredible strength and resilience,” he says. “Despite the challenges, she was determined to ensure that her 3 sons attended college. I proudly became the first in my family to earn a college degree, a testament to my mother’s unwavering commitment to our education and future.”
It was his mother who influenced his decision to become a dentist. When she immigrated to the United States from Scotland at 21 years old, she found a job working at a dental office which she loved.
“She spoke often of that job and how great it would be for one of her children to become a dentist. It was always a subject in a conversation,” Dr Armstrong recalls. “When I was 12 years old, I was living in Scotland and wrote an essay about becoming a dentist and years later, that dream came true.”
Dr Armstrong received his dental degree in 1989 from the University of Texas School of Dentistry in Houston. He was a D2 student when he volunteered for the Star of the South dental meeting in Houston and got his first taste of organized dentistry. Now, he has been a member of ADA for almost 36 years.
“Dr Ed Sauer introduced me to my first dental meeting, and I immediately knew I wanted to be part of this vibrant community,” he says. “At that time, opportunities for young dentists were limited, but I was fortunate to serve on the Greater Houston Dental Society’s (GHDS) Committee for Young Professionals—now known as the New Dentist Committee. That experience was my launching pad.”
From there, he soared. He served on several committees at GHDS and eventually became president. When he became president of TDA, he said he truly discovered his passion for service.
“I recognized areas within TDA that could benefit from change and was eager to contribute to that transformation,” Dr Armstrong says. “My tenure as president of TDA served as a springboard for my role as the ADA’s 15th District trustee. Representing Texas at the national level has been an incredible experience, made even more meaningful by the remarkable individuals I have met along the way.”
Representing the state on a national level is among his proudest moments in organized dentistry. When he was
appointed by Dr Jerry Long to serve on the ADA’s Council on Dental Practice, he found himself on a subcommittee that reviewed current workplace policies in dentistry. The committee ultimately recommended allowing non-dentists, or midlevel providers, to perform surgical and irreversible procedures. In a striking vote, Dr Armstrong was the lone dissenting voice.
“When the proposal was presented to the full council, it passed with a majority vote of the full council. I felt a deep disappointment, recognizing the potential implications for our profession. Seeking guidance, I contacted the ADA attorney to understand my options as a council member who disagreed with a council’s majority decision.”
Encouraged by the attorney’s suggestion at drafting a minority report, Dr Armstrong collaborated with TDA Senior Policy Manager Diane Rhodes to submit it to the ADA Board of Trustees along with the council’s recommendation.
“I worked diligently behind the scenes, rallying support from allied organizations like the ASDA, NDA, and AGD, ensuring that our voices were heard at the reference committee,” recalls Dr Armstrong. “It was a surreal moment watching as members of my own council testified in favor of the resolution while 20 to 30 of us stood in line at the microphone to speak against it.”
The ADA House of Delegates overwhelmingly defeated the measure by approximately 86%. “I felt a sense of vindication, knowing I had acted in the best interest of our profession, bolstered by the unwavering support of the TDA and Texas dentists. This experience stands as my proudest accomplishment in dentistry.”
Another significant event in his professional life happened in May 2024 when the TDA awarded Dr Armstrong with the Gold Medal, though by surprise as the announcement is designed.
“Having the president read out the recipient’s accomplishments, only to realize they are your own, is
Dr Ed Sauer introduced me to my first dental meeting, and I immediately knew I wanted to be part of this vibrant community.
a moment when time seems to stand still. The list of previous Gold Medalists is short, populated by individuals who embody a Hall of Fame in dentistry—a humbling legacy that inevitably makes you reflect on your own worthiness of such an honor.”
He credits his mentors with the honor and thanks them for their guidance and support. “Although I never anticipated receiving the Gold Medal, it is an honor I carry home—not just for myself, but as a tribute to the incredible servant leaders who paved the way before me. They recognized potential in a young dentist and encouraged me to engage, speak up, and always ask, ‘Why?’”
When Dr Armstrong is not practicing dentistry, he enjoys life to the fullest with Lana and their daughters and grandchildren. “Natalie lives in Austin with her husband Craig—affectionately known as OC (for “Other Craig”)—and they have 2 adorable kids, Sadie and Finn. Meanwhile, Tammy resides in Chicago with her husband, Andrew, and their 2 wonderful children, Connor and CeCelia. Our family is spread across 2 vibrant cities, and we cherish every moment spent with our grandchildren, creating memories that bridge the distance.”
Dr Armstrong and Lana enjoy hitting the trails and cycling in a shared love of the outdoors. When he retired,
Dr Armstrong is pictured with his wife Lana after receiving the Gold Medal for Distinguished Service Award in May.
Pictured are Dr Armstrong and Lana with their grandchildren Sadie and Finn.
Dr Armstong is pictured with his grandchildren Connor and CeCe.
he was able to spend time on another hobby.
“After I retired, I could not resist the allure of a Porsche 911 Cabriolet. There is nothing quite like cruising the scenic roads of Austin with the top down on a sunny day,” he says. “And when it comes to family fun, my bright yellow 1971 Super Beetle convertible is a favorite for taking my grandkids on adventures. Whether we are exploring the city or
just enjoying a leisurely drive, those moments create memories that will last a lifetime.”
Dr Armstrong’s adventure in dentistry had several more stops along the road, though the key to its fulfillment was the remarkable people who accompanied him.
I have been fortunate to be mentored by giants in our profession—many of
About the Gold Medal Presentation
whom are no longer with us—but their influence continues to resonate within me and hopefully extends to those I have had the honor of mentoring along the way.”
His advice for dentists starting their new journey. “I urge each of you to get involved and to remain curious—never stop asking, ‘Why?’ You never know when you might be called upon to craft your own ‘minority report.’”
Owing to its stature, the TDA president presents the award before the House of Delegates. The name of the recipient is not revealed to anyone, including the recipient, until the actual presentation takes place. The Awards Committee works behind the scenes with the recipient’s family members to make sure they are in attendance without alerting the recipient. In 2006 the TDA commissioned nationally renowned Texas artist Ronadró to design a unique award piece to represent the Association. The result is a beautiful bronze relief depicting a dentist caring for a patient. This sculpture was adopted for the Gold Medal award in 2008. Inset into the shadowbox are custom designed medallions: the TDA seal and the gold medal.
About the Past Recipients
To date, there have been 27 previous recipients of the Gold Medal: Drs John D. Wilbanks, Michael D. Vaclav, O.V. Cartwright, H.M. “Mit” Sorrels, Jack H. Harris, James E. Bauerle, Robert V. Walker, Frank K. Eggleston, Robert M. Anderton, Rene M. Rosas, Richard M. Smith, Sam W. Rogers Jr, Stephen F. Schwartz, John S. Findley, S. Jerry Long, Patricia L. Blanton, Paul E. Stubbs, Richard C. Black, Michael L. Stuart, Hilton Israelson, Thomas Harrison, J. Preston Coleman, Larry W. Spradley, Rita M. Cammarata, John Purdy, Jacqueline M. Plemons, and Rise’ Martin. By the judgment of their colleagues, they represent the best of the TDA; dentists who have dedicated their lives to the Association and profession, and have advanced both through their commitment, strength, and vision.
The family visited Disney World in October 2023 after the ADA Meeting in Orlando.
Dr Armstrong and his wife Lana are pictured with their daughters, sons in laws, and grandchildren at grandson Connor’s Bar Mitzvah in December 2023.
1. Do you have or have you considered an exit strategy?
2. How long do you plan on being a practice owner? If your health allows, would you like to continue practicing after that point?
3. Do you know what your practice is worth today? How do you know? When was your last Practice Valuation done?
4. Have you met with a financial planner and have a documented plan? Have you established a liquid financial resources target that will enable you to retire with your desired lifestyle/level of income?
Henry Schein Dental Practice Transitions has your best interests has your in mind throughout your career. Schedule a complime a complimentary consultation with your local Transition Sales Consultant today! If you answered no or do not know to any of these questions, let’s have a conversation!
LAW OFFICES OF MARK J. HANNA
EXPERIENCED LEGAL REPRESENTATION FOR TEXAS DENTISTS
Mark J. Hanna JD Former General Counsel, Texas Dental Association
• Representation Before the Texas State Board of Dental Examiners
Those in the dental community who have recently passed
Jerry Allyn Marshall Rotan
6/27/38–10/13/24
Good Fellow: 1988 • Life: 2003 • Fifty Year: 2013
Robert B. Verduzco Granbury 7/1/44–10/4/24
Good Fellow: 2000 • Fifty Year: 2009
George Robert Bradley Boerne 10/28/62–10/11/24
Good Fellow: 2014 • Fifty Year: 2021
James Richard Carroll Jr Sherman 1/10/46–10/12/24
Good Fellow: 1999 • Life: 2011 • Fifty Year: 2023
Carter Edmond Karr Amarillo 3/5/34–11/3/24
Good Fellow: 1984 • Life: 2000 • Fifty Year: 2009
Hieu Huynh, DDS, JD
An Unrelenting Sore Throat
A Case Report
John J. Burditt, DDS, FACD
During a new patient exam for routine dental care, a 78-year-old female mentioned that she had been experiencing chronic sore throat for several years and was continuing to have almost unbearable pain when swallowing. She reported that many months of treatment for the throat pain and swallowing discomfort with many courses of antibiotics had been ineffective. Also, she reported that she had used throat lozenges and other over the counter measures for sore throat relief, but over time, the pain had increased, especially upon swallowing.
Oral exam revealed 2 dime-sized mirror-imaged ulcerations of the soft palate just posterior and medial to the hamular notch (Figure 1). Palpation of the very tender ulcers divulged the sharp tip of the hamular processes on both the right and the left sides. The fact that these lesions were matching and bilateral suggests that abnormal anatomical structures could be a contributing factor to this very painful condition. Consultation with the oral surgeon confirmed the probability of bilateral elongated hamular processes.
John J. Burditt, DDS, FACD Director of Dental Services
Texas
Kerrville State Hospital, Kerrville,
The bony projections of the pterygoid hamulus as shown on the dry skull reveals the size and proximity of the bony tips to the approximate locations of the ulcerations (Figure 2).
The patient had quite an extensive medical history with many long-term medications including antibiotics, steroids, chemotherapy, and immunosuppressive drugs. Another interesting aspect in this patient’s history was that she was a former U.S. Army nurse and had been a prisoner of war for 2 years. Her knowledge as a nurse had her believing that her chronic throat condition was related in some way to her years in the tropics under less-than-ideal conditions.
After much thought, surgical reduction of the bony processes seemed to be the only reasonable solution. Under IV sedation and local anesthesia an elliptical incision was made around the ulcerated area and blunt dissection was used to expose and identify the hamular process. Using rongeur forceps, approximately 8 millimeters of the tip of the hamular processes were removed on both right and left sides.
Bony edges were smoothed with a fine bone rasp. Tissue edges were closed in a normal fashion. Healing of the area was uneventful. The patient was totally free of throat pain by day 2 of recovery. At the 1 week follow up visit, the patient had no adverse effects with swallowing, breathing, or speech.
Figure 2. Photo showing the pterygoid hamular processes
Figure 1. Photo showing bilateral ulcerations of the soft palate
Bibliography
1. Hertz, Robert S. Pain Resulting From Elongated Pterygoid Hamulus, J. Oral Surg, March 26, 1986, pp 209-210.
2. Wooten, J. W., Tarsitano, J. J., and Reavis, D. K. The Pterygoid Hamulus: A Possible Source of Swelling, Erythema and Pain: Report of Three Cases, J. Am. Dent. Association. 87: pp 688-690. 1970.
3. Gores, R. J. Pain Due to Long Hamular Process in the Edentulous Patient. Applied Therapeutics, Vol. 7, pp 1128. Dec. 1975.
The conclusion was that the pterygoid hamular process was elongated, causing mucosa over the soft palate to be thinned, giving rise to increased pressure, irritation, and trauma, resulting in erythema swelling and ulceration (Figure 3). There are several predisposing or etiologic factors in this case other than elongated hamular process.
1. The patient had continuously sucked throat lozenges in an attempt to soothe her pain while inflicting trauma from the oral side
2. The patient’s medications including steroids, chemotherapy and immunosuppressive drugs could be related to the slow healing
3. The patient had received long-term antibiotic therapy which did not relieve her swallowing pain
We could speculate that the mechanical action of the throat lozenges and hard candy had likely abraded the mucosa over the hamular processes. The immunosuppressive and chemotherapy drugs possibly affected the long-term ability of the healing process. Also, antibiotic use possibly disrupted the balance of oral flora, allowing fungal overgrowth and infection. In this case, surgical intervention resulted in complete resolution of the pain and resulted in a very happy patient.
This case falls into one of the very rare categories of pain in the oral cavity and reminds us to remember the location of the hamular processes and its possibility to cause pain. As previously stated by Wooten, Tarsitano, and Reavis: “the pain, erythema, and swelling that result from this condition may be difficult to diagnose if the anatomy is not considered.”
4. Giansarti, J. S., Cramer, J. R, and Weathers, D. R. Palatal Erythema, Another Etiologic Factor, Oral Surg, Oral Med, Oral Path. 40: pp 379381. 1975
5. Charbeneau, T. O., Blanton, P. L. The Pterygoid Hamulus: A Consideration in the diagnosis of Posterior Palatal Lesions. Oral Surg, Oral Med, Oral Path 52. Pp 574-576. 1981.
Figure 3. Photo of elongated hamulus before excision
FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Kathleen A Kasper, DDS, D-ABFO
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than 1 year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after 1 year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive and expensive, and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long-term unidentified in Texas is that one of the many Texas dentists who read the Texas Dental Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical Examiner’s Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
By far Latent Prints (finger, palm, sole), are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, incinerated, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers), require knowing what hospital/physician placed the device to get the matching serial number, which can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent; however, success depends on a presumptive identity and availability/existence/ quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/ profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
Anthropologic Methods will use skeletal features to make a positive identification.
Author
Kathleen A. Kasper, DDS, D-ABFO
Dr Kasper has been practicing general dentistry in Carrollton, Texas, for 29 years. She is a graduate of the University of Iowa College of Dentistry.
She provides 3 counties in the Dallas-Ft. Worth Area with forensic dental services. These include Collin, Dallas, and Tarrant Counties. She is currently the only active board certified forensic dentist in north Texas.
She received her formal forensic odontology training at the University of Texas Health Science Center San Antonio, Texas, Center for Education and Research in Forensics (CERF) in 2003-2004.
Dr Kasper obtained Board Certification from the American Board of Forensic Odontology in 2010.
She is a fellow of the American Academy of Forensic Sciences, a member of the American Board of Forensic Odontology, and a member of the American Society of Forensic Odontology.
She is the current American Board of Forensic Odontology Dental Age Assessment Committee Chair.
Dr Kasper is also a published author in the Journal of Forensic Sciences and coauthor of a chapter in each of 3 forensic textbooks.
Perhaps one of her greatest undertakings was chairing a working group for the American Dental Association that has published the “Technical Report” for Forensic Dental Age Estimation which went on to become a “standard” for the Organization of Scientific Area Committees (OSAC) for Forensic Science.
DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from family members or multiple family members if known. If no matches are obtained, then:
DNA Samples are submitted to CODIS (Combine DNA Index System), which is a computer program that operates local, state, and national databases of DNA profiles from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long-term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may still remain unidentified once completed. This is the proverbial end of the road; therefore, all Texas Dentists, Dental Auxiliaries, and Staff: Can you help the Tarrant County Medical Examiner’s Office give a name to the unidentified male decedent described below?
The Unidentified Individual:
Southwestern Institute of Forensic Sciences at Dallas County Medical Examiner (DCME)
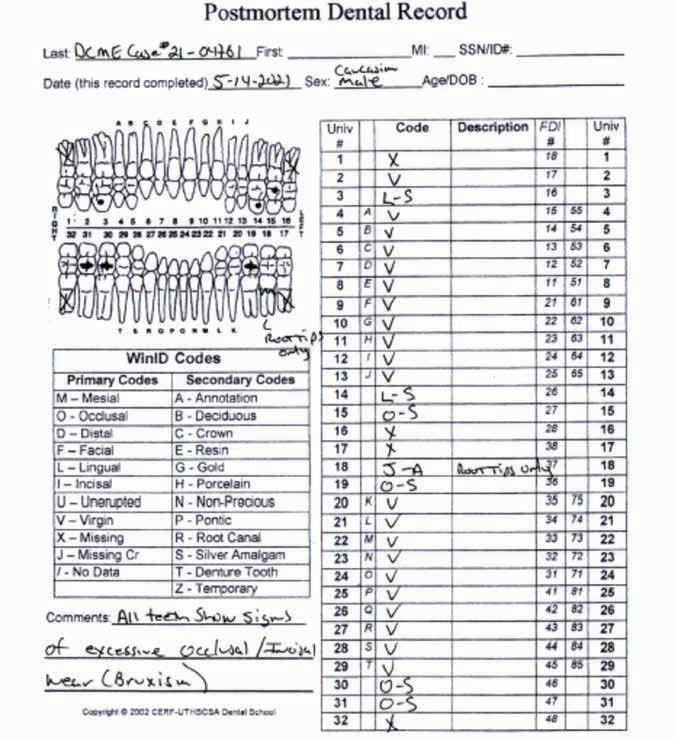
Case #IFS-21-04761
Date of Death (Decedent found): March 2, 2021
Cause of Death: Hypothermia in conjunction with the toxic effects of methamphetamine
Manner of Death: Accident
Body Condition: Decomposed
Sex: Male
Ancestry: Caucasian (White)
Age: 42-59 years based upon anthropological methods which included analysis of the sternal rib ends and the pubic symphysis.
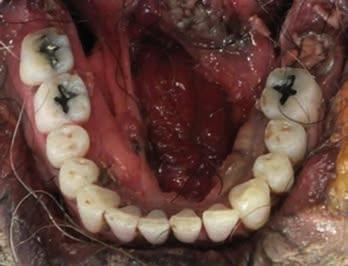
Scene Description: An unknown White male was found unresponsive in the back of an empty commercial box truck by an Enterprise Rent A Car lot near Dallas-Ft Worth (DFW) Airport. The decedent was found lying supine in the back of a box truck and was nude. Decomposition, skin discoloration, and marbling were apparent. There were no visible signs of foul play or trauma. Clothing was present in the truck and was retained by DFW Airport Department of Public Safety. There was no identification found and the decedent may have been homeless. Tattoos were also visible to the arms and posterior left leg. A black tattoo depicting a spider web is on the right elbow. A black tattoo depicting “COWBOY UP” with a lasso is on the dorsal left upper arm. A black tattoo depicting “JUANITA” is on the left calf.
Dental Evidence Recovered: Maxilla and Mandible.
Frontal View
Right Left
Right Lateral View
Left Lateral View
Right Left Right Left
Maxilla
Mandible
Closing
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans, or other dental information regarding the unidentified male decedent described above as DCME Case #21-04761, please contact the Southwestern Institute of Forensic Sciences at Dallas County Medical Examiner’s Office, phone 214-9205900, Press 1, and ask for Steven Kurtz, Chief Medicolegal Death Investigator, or Keara St Louis, Deputy Chief Medicolegal Death Investigator.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/ services/cjis/ncic.
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International.
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021.
Practices For Sale
Since 1968
FANTASTIC TEXARKANA LOCATION: GP in a bustling retail center with great visibility. The office has 3 ops, digital X-ray, and paperless patient charts. The practice has over 1,200 active patients that are a mixture of 20% FFS and 80% PPO. The seller refers out most specialties, and the practice operates on 3.5 doctor days and 4 hygiene days, leaving ample room for growth. Opportunity ID: TX-02243
FANTASTIC RETAIL LOCATION: Plano GP that is highly visible in a retail center. This practice operates with the owner and 1 PT associate, is open 7 days a week and provides regular dental care as well as emergency services. The practice has over 1,750 active patients who are 20% FFS, 70% PPO, and less than 10% Medicaid. The office has 4 ops and is in excellent condition. This is a great opportunity for growth by capitalizing on the existing patient base and expanding services. Opportunity ID: TX-02219
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Excellent opportunity for growth by adding a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02171
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS with a small amount of PPO. The office collected over $876K in a four-day workweek. Opportunity ID: TX-02041
Enhancing Dentistry: The Power of Dental Mock-up Previews
This case report reviews the advantages of utilizing mock-up prior dental treatment in the esthetic zone.
Case Report
The patient initially reported the CC of “My teeth are breaking”. Upon assessment, notable findings included erosion of the lingual surfaces of anterior teeth and fractured incisal edges. Diagnostic casts were made, and a comprehensive digital smile design was completed. Subsequently, a 3D printed model was generated and a PVS matrix was fashioned to create a mock-up, providing the patient with a visual representation of the proposed treatment plan. Recognizing the need to increase the clinical crown, crown lengthening was determined necessary. Following this procedure, crown preparations were completed. Provisional restorations were fabricated based on mock-up template, allowing the patient to preview the anticipated outcome. After ensuring optimal occlusion through final adjustments, the patient was scanned with the temporaries in place. This scan was then forwarded to the dental laboratory for the fabrication of the definitive restorations.
Advantages
Mock-ups may be digital or physical representation of the proposed dental.
1. Visual aid: This visual aid helps patients to envision the outcome clearly, which can alleviate uncertainties or concerns they may have.
2. Customization: Dentists can customize mock-ups to meet the specific needs and preferences of each patient, by adjusting the shape, size, color and contour the dentist can tailor the final restorations to achieve the desired result.
3. Trial Run: Mock-ups allow the patient to “try-on” their new smile before permanent alterations are made to their teeth.
4. Communication: They facilitate communication between dentists and patient and dental technicians by providing a common reference point.
Conclusions
Mock-ups play a crucial role in the dental treatment process by helping to visualize the final restorations, customize treatment plans, facilitates communication with the dental laboratory and ensure patient satisfaction. Incorporating mock-ups in the dental practice can enhance the patient experience and achieve optimal treatment outcomes.
Maria Gonzalez, DDS, MS; Rosalie Nguyen Gulla, DDS, MS
Left: Figure A. Pre-op, Figure B. Chairside mock-up, Figure C. Crown lengthening procedure. Right: Figure D. Crown preparations, Figure E. Provisional restorations, Figure F. Final restorations.
ORAL and maxillofacial
pathology
case of the month
Clinical History
A 68-year-old female presented to an oral and maxillofacial surgeon with a complaint of a lesion on her upper lip, which she had noticed for 4 years. She reported that the lesion had slowly increased in size. Additionally, she complained that the lesion occasionally itched and caused minor discomfort. The patient had a history of type II diabetes mellitus, hypertension, hyperlipidemia, and hyperthyroidism, all managed with medications. She had no known drug allergies.
AUTHORS
Sehrish Javaid, BDS, MS, PhD
Associate Professor, Woody L. Hunt School of Dental Medicine, Texas Tech University Health Sciences Center El Paso, El Paso, Texas.
Arshad Kaleem, DMD, MD, FACS Oral and Maxillofacial Surgeon, High Desert Oral and Facial Surgery, El Paso, Texas.
Angela C. Chi, DMD Professor, Woody L. Hunt School of Dental Medicine, Texas Tech University Health Sciences Center El Paso, El Paso, Texas.
Disclosures: None
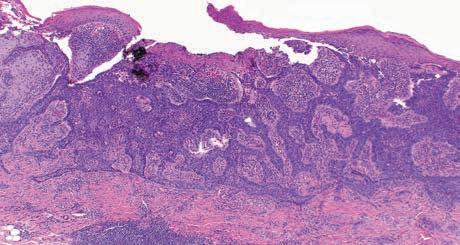
Figure 1. Clinical photograph showing an ulcerated, crusted, and erythematous lesion on the skin adjacent to the upper lip.
Extraoral examination revealed a 1-cm ulcerative lesion on the skin adjacent to the left upper lip with associated crusting and mild peripheral erythema (Figure 1). The lips showed signs of damage from chronic ultraviolet light exposure, including blended vermilion borders and perioral wrinkles. Additionally, an area of white surface change was noted on the lower lip.
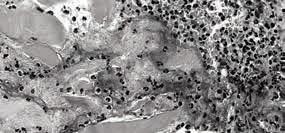
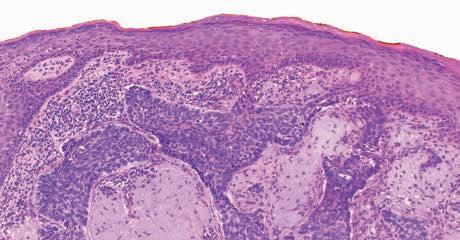
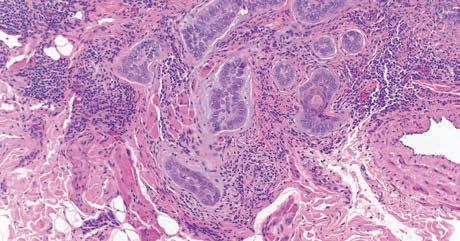
An excisional biopsy of the ulcerated lesion was performed. Microscopic examination showed a portion of skin and subcutis covered by stratified squamous epidermis with central ulceration (Figure 2A). The dermis demonstrated a proliferation of malignant basaloid epithelial cells arranged in islands, nests, and trabeculae. Some tumor islands were connected to the basal layer of the overlying epidermis (Figure 2B). Retraction artifact and myxoid change (stromal mucin) occasionally were observed in the connective tissue surrounding the tumor islands. The tumor cells exhibited nuclear enlargement, nuclear and cellular pleomorphism, frequent peripheral palisading, increased mitotic activity, and isolated keratinization. Tumor focally invaded the underlying skeletal muscle and fat (Figure 2C). Solar elastosis and scattered inflammatory cells were present in the background.
What is the diagnosis?
What is the most likely diagnosis?
See page 510 for the answer and discussion.
1B. Medium-power view showing tumor islands with focal connection to the basal cell layer of the overlying epidermis. The tumor cells exhibit peripheral paslisading, nuclear enlargement, and nuclear and cellular pleomorphism. Isolated artifactual retraction of the stroma surrounding the tumor islands also is seen. Inflammatory cells and solar elastosis are present within the background. (hematoxylin and eosin, original magnification 200x).
Figure 2. Photomicrographs of the excisional biopsy.
1A. Low-power view showing surface ulceration and an underlying proliferation of basaloid epithelial cells arranged in anastomosing trabeculae within the dermis (hematoxylin and eosin, original magnification 100x).
1C. High-power photomicrograph showing nests and small islands of tumor cells invading the underlying skeletal muscle and fat. A few of the tumor islands are surrounded by myxoid change (stromal mucin). (hematoxylin and eosin, original magnification 400x).
ORAL and maxillofacial pathology
diagnosis and management—from page 509
Diagnosis: Basal cell carcinoma
Discussion
Basal cell carcinoma (BCC) is the most common malignancy and the most common type of skin cancer. In the United States, approximately 2 to 2 million cases of BCC are diagnosed annually.1 The incidence has been increasing over the last several decades in many parts of the world.2,3 Males are affected more often than females, and increased age is an independent risk factor for lesion development.4 However, studies of various cohorts in the United States and Europe have reported a disproportionate increase in cases among females compared to males over the past several decades, and a trend toward younger age at diagnosis among cases in women.5-8 BCC is most frequently diagnosed in white patients, although it affects individuals across all racial groups.
The primary risk factor for BCC is sun exposure; therefore, most lesions are located on sun-exposed skin. There is also a strong, dose-related association between tanning bed use and BCC development.4,9 Intermittent UV light exposure (e.g., from recreational tanning or childhood sunburns) has been suggested to play a major role in lesion development, although chronic sun exposure contributes as well.4,10 Ultraviolet (UV) light induces DNA damage and causes mutations that initiate carcinogenesis.11 Additional risk factors for BCC include fair skin, red or blond hair, light eye color, prior radiation therapy, and certain rare heritable disorders (e.g., xeroderma pigmentosum, Li-Fraumeni syndrome, nevoid basal cell carcinoma syndrome.1,12,13 Patients with such heritable conditions tend to develop BCCs at a younger age compared to individuals without these conditions.
BCCs exhibit a marked predilection for the head and neck region, although trunk or limb involvement also is possible. As seen in the current case, lesions arising in the lip area most often involve the skin adjacent to the upper lip vermilion.14 Multiple lesions can be seen in the same patient.15 BCC can exhibit a wide range of clinical presentations. Many cases present as slow-growing, dome-shaped papules with telangiectatic vessels and central ulceration. Other examples may appear as scaly patches or scar-like lesions. Lesion color may be red, tan, brown, or black. Clinicopathologic variants include nodular, superficial, infiltrative, morpheaform
(sclerosing), pigmented, and fibroepithelial type.16 Individual lesions may exhibit features of more than one type.11 A biopsy is critical for diagnosis and ruling out other entities, such as cutaneous squamous cell carcinoma or melanoma.
Microscopic examination typically shows a proliferation of dark-staining, basaloid epithelial cells arranged in islands, trabeculae, nests, or strands. The tumor invades the connective tissue and often appears to arise from the basal cell layer of the epidermis. The tumor islands often exhibit peripheral palisading, artifactual retraction of the surrounding connective tissue, and surrounding stromal mucin (or “myxoid change). Necrosis and overlying ulceration or scale crust formation are variable findings. Solar elastosis (actinic damage of the stroma) is usually evident. There are multiple histopathologic subtypes of basal cell carcinoma (such as nodular, superficial, morpheaform/sclerosing, infiltrative, micronodular, and basosquamous).17 In the present case, the excisional biopsy showed a mixture of nodular and micronodular features (including solid tumor islands and small tumor nests).
BCC is classified as low- or high-risk for recurrence based on clinical and histopathologic features. Clinical features associated with increased risk for recurrence include head and neck location (especially in the “H-zone” or “mask area” of the face), ill-defined tumor borders, immunosuppression, underlying genetic syndromes, sites of prior radiotherapy, and already recurrent disease. Pathologic features associated with increased risk for recurrence include certain histopathologic subtypes (e.g., morpheaform/sclerosing, infiltrative,
micronodular, basosquamous) and perineural invasion.1,18,19 In our patient’s case, head and neck location as well as a micronodular component were identified as high-risk features.
BCC is managed primarily by surgical excision. Head and neck lesions at high-risk for recurrence may be removed by Mohs surgery (which involves intraoperative, frozen section examination of mapped tumor margins to ensure complete removal). Alternative treatments include non-surgical methods, such as topical agents (e.g., 5-fluorouracil, imiquimod) or destructive therapy (e.g., cryotherapy, photodynamic therapy). Such non-surgical methods typically are reserved for low-risk lesions.1 A disadvantage of destructive therapy is that it does not allow for histopathologic examination.11 The 5-year recurrence rate is reported to range from 0.817.4% for surgically excised tumor.1
Metastasis and tumor-related deaths are extremely rare. However, lesions show not be left untreated because of the risk for locally aggressive behavior. Use of sunscreen and other sun preventive gear during peak sunlight hours is recommended for disease prevention.20 In the present case, a focally positive margin was noted on the initial excision, and so re-excision was performed to ensure complete tumor removal. The patient will continue to be monitored periodically for recurrence or development of new lesions.
References
1. Schmults, C. D., R. Blitzblau, S. Z. Aasi, et al., Basal Cell Skin Cancer, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw, 2023. 21(11): p. 11811203.
2. Lomas, A., J. Leonardi-Bee, and F. Bath-Hextall, A systematic review of worldwide incidence of nonmelanoma skin cancer. Br J Dermatol, 2012. 166(5): p. 1069-80.
3. Fagan, Jake, Jennifer Brooks, and Michael L Ramsey, Basal cell cancer. 2023.
4. Cameron, M. C., E. Lee, B. P. Hibler, et al., Basal cell carcinoma: Epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol, 2019. 80(2): p. 303-317.
5. Heaton, H. and N. Lawrence, Nonmelanoma skin cancer in women. Int J Womens Dermatol, 2019. 5(1): p. 2-7.
6. Flohil, S. C., I. Seubring, M. M. van Rossum, et al., Trends in Basal cell carcinoma incidence rates: a 37-year Dutch observational study. J Invest Dermatol, 2013. 133(4): p. 913-8.
7. Evans, S. S., M. H. Jih, L. H. Goldberg, et al., Increased burden of melanoma and nonmelanoma skin cancer in young women. Dermatol Surg, 2014. 40(12): p. 1385-9.
8. Muzic, J. G., A. R. Schmitt, A. C. Wright, et al., Incidence and Trends of Basal Cell Carcinoma and Cutaneous Squamous Cell Carcinoma: A Population-Based Study in Olmsted County, Minnesota, 2000 to 2010. Mayo Clin Proc, 2017. 92(6): p. 890898.
9. Tran, M. M., E. A. George-Washburn, J. Rhee, et al., A prospective cohort study exploring the joint influence of sunlight exposure and tanning bed use on basal cell carcinoma, squamous cell carcinoma, and melanoma risk. Arch Dermatol Res, 2024. 316(6): p. 281.
10. Firnhaber, J. M., Basal Cell and Cutaneous Squamous Cell Carcinomas: Diagnosis and Treatment. Am Fam Physician, 2020. 102(6): p. 339-346.
11. Peris, K., M. C. Fargnoli, C. Garbe, et al., Diagnosis and treatment of basal cell carcinoma: European consensusbased interdisciplinary guidelines. Eur J Cancer, 2019. 118: p. 10-34.
12. Juan, H. Y., A. E. Zhou, K. M. Hoegler, et al., Overview of familial syndromes with increased skin malignancies. Arch Dermatol Res, 2023. 315(4): p. 707-727.
13. Gold, N. B., I. M. Campbell, S. E. Sheppard, et al., Proposed criteria for nevoid basal cell carcinoma syndrome in children assessed using statistical optimization. Sci Rep, 2021. 11(1): p. 19791.
14. Neville, Brad W, Douglas D Damm, Carl M Allen, et al., Oral and Maxillofacial Pathology-E-Book: Oral and Maxillofacial Pathology-E-Book. 2015: Elsevier Health Sciences.
15. Castanheira, A., P. Boaventura, F. Vieira, et al., Clinicopathological features of head and neck cutaneous basal cell carcinoma observed at the Centro Hospitalar de Trás-os-Montes e Alto Douro ENT Department. Porto Biomed J, 2022. 7(5): p. e190.
16. Naik, P. P. and M. B. Desai, Basal Cell Carcinoma: A Narrative Review on Contemporary Diagnosis and Management. Oncol Ther, 2022. 10(2): p. 317-335.
17. McDaniel, Brianna, Talel Badri, and Robert B Steele, Basal cell carcinoma. 2024.
18. Zloty, D., L. C. Guenther, M. Sapijaszko, et al., Non-melanoma Skin Cancer in Canada Chapter 4: Management of Basal Cell Carcinoma. J Cutan Med Surg, 2015. 19(3): p. 23948.
19. Connolly, S. M., D. R. Baker, B. M. Coldiron, et al., AAD/ACMS/ASDSA/ ASMS 2012 appropriate use criteria for Mohs micrographic surgery: a report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J Am Acad Dermatol, 2012. 67(4): p. 531-50.
20. Jin, J., Screening and Prevention of Skin Cancer. Jama, 2023. 329(15): p. 1324.
value for
2025 Open Enrollment and ACA Update
By Eric Tiedtke, CFP
It’s that time of year again, and some changes are happening.
It looks like increased subsidies for Affordable Care Act (ACA) individual plans will be extended, which can help with the premiums for individual plans.
There are less companies offering plans in Texas and some new options to consider.
TDA Financial Services Insurance Program is here to keep you informed and to update you on the changing dynamics of health insurance for 2025 in the individual and small group markets.
Rate Changes
There
are small rate increases—and some rate decreases—for individual HMOs.
Small groups see slight increases.
If you have individual or small group coverage now, there are changes coming.
Filed rates are being reviewed to determine if proposed increases are based on reasonable cost assumptions and solid evidence. Final rates won’t be available until Nov. 1 when open enrollment starts, so you can’t really start comparing rates until then.
Individual Plans
Blue Cross and Blue Shield is the only company offering individual plans statewide in Texas. These Blue Cross and Blue Shield plans are HMO only, however they offer their Plus plan (or POS Plan), which is still an HMO but provides coverage outside the network. Blue Cross filed for a 6.7% increase on its most popular HMO.
The other plans offered in Texas—many that are regional or hospital specific—have filed for various rate increases, some as high as 27%; but also some rate decreases, so keep an eye out for your renewal.
In Texas, there are no ACA-compliant individual PPO plans available statewide. There are regional or local plans available—mostly HMOs—and in limited areas of the state where a hospital system has several facilities and offers a plan, such as Scott & White or Memorial Herman. And there are other companies offering plans in a few select regions, such as Molina, Oscar, Community Health, Imperial Health, and Sendero.
Blue Cross and Blue Shield is the only company offering individual plans statewide in Texas. These Blue Cross and Blue Shield plans are HMO only, however they offer their Plus plan (or POS Plan), which is still an HMO but provides coverage outside the network.
Keep in mind the network being offered, as it could have limited or no coverage in parts of the state.
Most plans are incorporating tele-med, direct primary care, or concierge medicine as part of the coverage. Tele-med allows for virtual visits with your physician; these may or may not have a copay. Direct primary care and concierge arrangements typically provide certain services—such as an annual physical exam and specified treatment for a specific condition—and often don’t qualify as insurance, as essentially you’re prepaying for a service. Virtual primary care sessions can include some prescriptions, durable medical equipment, lab tests, and diagnostic imaging.
Again, it’s very important to understand the scope of the networks, the coverage, and limitations—especially if you’re seeing specialists for an ongoing medical condition.
Don’t forget about subsidies or premium credits.
The ACA’s health insurance premium subsidies—also known as premium tax credits—normally adjust each year to keep pace with premiums. For 2025, subsidies are again much higher than in past years. There is no “subsidy cliff” for this two-year period. Instead, nobody purchasing coverage through the marketplace has to pay more than 8.5% of their household income. And people with lower incomes are expected to pay a smaller-than-normal percentage of their income for the benchmark plan—as low as $0 for people with income that doesn’t exceed 150% of the poverty level.
The eligibility range was capped at household incomes of 400% of the federal poverty level (FPL), but that has changed. New legislation would substantially increase or eliminate the income cap for subsidy eligibility through 2025.
Small Group Plans
Small group plans continue to be the only option for getting true PPO plan options under the ACA.
Rate changes filed for small group plans range from less than .5% to as high as 13%, depending on the company. For 2025, it appears small group:
• PPO rates will again be slightly lower than individual HMO rates.
• HMO group rates will be 5-15% lower than individual plans (non-subsidized).
Of the major companies, we anticipate Blue Cross will have the lowest rates—their filed rate increase for the PPO and HMO is around 8.4%; followed closely by United Healthcare, Baylor Scott & White, and Memorial Herman. Aetna & Humana are no longer in the small group market in Texas.
Coverage Options
Small group plans are less expensive than individual plans and offer more options.
If you have a practice with at least one other full or part time employee, you should consider a small group plan. Depending on how your practice is structured, the other employee could be your spouse. Contact TDA Financial Services Insurance Program at (800) 677-8644 for details.
Why go through the additional paperwork and effort for a small group?
• Small group plans will be less expensive than unsubsidized individual plans, and you can still get a PPO.
• If you sign up during the special enrollment for new small groups (starting Nov. 1), the mandatory employer contribution towards employee premiums (as well as other requirements) are waived. This is a good way to attract and retain high-quality employees while offering a lot of flexibility on plan designs.
• If you payroll deduct the employee premiums, it saves the practice and employees on taxes.
• You can offer more than one plan within your group—a base plan that’s less expensive for employees (perhaps an HMO with an RX and office copay), and a PPO plan for you and your family..
We can start comparing rates for small group plans beginning October.
Here are the maximum out-of-pocket amounts for coverage in 2025:
In-network
• $9,200 for an individual
• $18,400 for a family
High-deductible plans intended to be HSA-compatible are subject to these out-of-pocket maximums:
• $8,300 for individual coverage
• $16,600 for family coverage
Out-of-network
If you have out-of-network expenses, the maximum can be double what’s listed above, or more. Or the out-of-network expenses might not even be covered. The plans with the lowest premiums will have the highest out-of-pocket expenses.
This is Important.
It is critical you check the network of the insurance company you select for 2025 and make sure your providers and hospitals are in-network. You need to know the company name and the network name. Some providers, for instance, might take a Blue Cross PPO but not Blue Cross HMO; or United Healthcare Choice Plus but not the Choice Network.
What other options do I have for health insurance in 2025?
Level-Funded plans
United Healthcare is going all in on level-funded plans and changed some of the requirements for smaller groups. If your practice and its employees are generally healthy and not big users of health care, you might consider a level-funded plan. These are underwritten based on the health of the group and can be as much as 10 to 25% lower than regular ACA small group plans.
Keep in mind only about 50% of groups will qualify based on underwriting, but the rate savings can be significant and worth considering. Also, these plans typically don’t qualify for the special enrollment, so the practice has to pay 50% of the employee premium and meet a participation requirement regarding the number of eligible employees that participate. There are other considerations, such as the different PPO networks, stop loss coverage, and just understanding how the plans work and what’s covered.
Faith-Based, Medi Share and Health-Share Groups
These types of plans are not insurance and should not be considered a substitute for insurance, but can be an option if you understand how they work. With these types of arrangements, you join a group and pay or contribute a monthly amount to a plan. After your deductible is met, you submit your medical bills and are reimbursed from the funds available or through others making additional contributions to cover your bill. Many have incorporated a PPO network so you can get the discounted amount when you have treatment. However, you’re still responsible for the bill—even if the health-share plan reimburses you.
These arrangements have stricter guidelines than traditional insurance companies and on which procedures are eligible for reimbursement or cost sharing. There’s normally a lifestyle guideline where a member agrees to live a certain way (abstain from illegal drug consumption, sex outside of marriage, tobacco use, and abuse of alcohol or prescription drugs).
The payments of medical bills through these arrangements are not guaranteed in any way. Each member is always solely responsible for the payment of his or her own medical bills.
If you understand how these plans work and their limitations, they can be a less expensive option than ACA plans.
Short Term Medical
We don’t recommend you go without insurance, so short-term health insurance can be an option if you’re without coverage because:
• Of a waiting period.
• You’re transitioning from one plan or coverage to another (e.g., in-between jobs).
• It’s outside the open enrollment period.
• Or you’re close to being eligible for Medicare.
These plans are exempt from the definition of individual health insurance coverage under ACA provisions, and usually don’t pay for pre-existing conditions. They’re designed to cover a new sickness or accident (with no treatment in the previous 5 years).
They also have limitations on coverage (e.g., no maternity coverage) and don’t have all the same mandates, such as unlimited-benefits maximums. These coverages don’t automatically renew, and you can typically only keep them for a maximum of 12 months.
Limited Benefit Sickness-and-Accident Plans
These plans are sometimes called “mini-med plans,” and are marketed as an ACA alternative with a PPO.
They may offer copays and RX benefits, however, they don’t include the “essential minimum health benefits” required by the ACA.
These also may include a PPO and provide a schedule of benefits that pay a certain amount per day or treatment, and are limited to a maximum amount. A company selling these plans will often address this limitation by selling additional coverage for critical or specified illness or accidents.
These plans are underwritten based on good health and have some form of preexisting condition limitation. The latter means anything you’ve previously been treated for is not covered for a period—normally 12 months. If the plan is guaranteed issue with no pre-existing condition, make sure you’re not just buying a discount plan.
These plans can be an option; however, you need to really understand the limitations and coverage, as you could be responsible for tens of thousands of dollars—even though you’re covered—if you have a major accident or illness.
Additional Options and Considerations
If you’re concerned about having a high deductible, limited, or no out-of-network coverage, you might consider a supplemental product for accidents or hospital confinements.
These types of plans pay you directly and in addition to your other coverage. They tend to be relatively less expensive and are a good option if you don’t want to self-insure high-deductible and outof-pocket expenses.
HSA Plans
If you haven’t looked at HSA plans or didn’t think they made sense previously, you should revisit them.
When picking a plan, you should keep the above numbers in mind; but also consider this: though prescription-drug and office-visit copays are convenient plan features, you need to know the combined cost of your total out-ofpocket exposure and your plan (the premium).
HSA plans offer the lowest premium and can be a great way to build up a self-funding account for current and future medical expenses. This can be especially important if you have to go out-of-network.
• Contributions are tax deductible (as much as $5,300 for an individual and $9,550 for a family with a catch-up contribution).
• Earnings and interest accumulate tax-free.
• You own and control the funds.
• HSA plans are not a use-it or-lose-it vehicle.
ICRA
Individual Coverage HRA (ICHRA) presents an opportunity for employers to take more control over their benefits spend. It allows employers to set aside tax-advantaged dollars to reimburse their employees for individual health insurance plans that are inflationresistant, compared to group plan premiums.
While ICHRA brings more cost control and less risk for the employer, it also provides more purchasing power and choice to employees. However, keep in mind individual health insurance plans offered are probably going to be HMO only; and individual HMO plans are 10-15% higher than the group HMO plan, if unsubsidized.
There’s also the administration and set-up involved with ICHRA, which is not particularly burdensome but adds administration on behalf of the practice.
HRAs
Use of Health Reimbursement Accounts (HRAs) has expanded because new regulations issued by the Departments of Labor, Treasury, and Health and Human Services, allow reimbursements for individual-market insurance premiums.
Before employers offer a benefit that includes individual HRAs, they should consider the following:
• The implications related to the (ACA) employer shared-responsibility mandate
• The ability of their employees to obtain a premium tax credit (PTC) or subsidy on the ACA marketplace.
The maximum new-contribution amount for an excepted benefit HRA (EBHRA) remained $2,150 for the 2025 plan year. An EBHRA may enable you to help reimburse your employees for certain health benefits such as vision or dental coverage—or for coinsurance, and copayments for individual coverage and shortterm health insurance.
2025 Landscape Review
If you want or need full coverage, the small group market is still the best way to get coverage with more options available at lower cost than in the unsubsidized individual market.
The alternative options discussed have a place at the table, but you need to make sure you understand plan limitations and risks before making a change to something less expensive. Stay informed and get ready to review and compare your options, and make a decision as soon as possible. You will be able to review individual plans and rates beginning Nov. 1, and small group plans and rates in early October.
Important Dates
The open enrollment period for health plans offered under ACA begins November 1, 2024, and ends January 15, 2025. For individual plans, you have until December 15 to pick or change to a new plan with a January 1 effective date; or until December 31, if your plan terminates December 31.
Disclaimer: This article was submitted the first part of September, so some information may have changed by the time this article is published.
If you would like to receive more information or discuss available insurance options, please feel free to contact TDA Financial Services Insurance Program at (800) 677-8644 or visit www. tdamemberinsure.com.
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #662): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business. AUSTIN (ID #689): Dynamite practice located in a high visibility retail center off a heavily trafficked highway that feeds into many of west Austin’s newest prominent subdivisions. Newly constructed office with a clean, modern aesthetic, and state of the art equipment/ technology (Pano, digital scanner, Cad/Cam, digital sensors). The practice treats a large, FFS/PPO patient base, has steady new patient flow at 40+/month, and consistent 7 figure revenue with 40% profit margins. AUSTIN (ID #691): Unique opportunity to purchase a GD practice with two locations in the Austin area. The offices have a total of 10 operatories with computers in each room and digital radiography. The offices serve a large FFS/PPO patient base with a healthy new patient flow and strong hygiene recall with over 20-25% of total annual production coming from the hygiene department. DALLAS-PEDO/ ORTHO (ID #665): Legacy pedo/ortho practice in the heart of north Dallas. Thriving practice, large fee-for-
service patient base, revenue of 7 figures. Over 2,800 sq ft, fully digital with computers in the operatories, digital radiography, and a digital Pano. DALLAS (ID #699): Well-established, highly profitable GD practice in a fast-growing location north of Dallas. The practice serves a large PPO/FFS patient base with virtually zero marketing or advertising. The 1,800+ sq ft office has 6 fully equipped operatories with computers in each op, digital X-ray units, intra-oral cameras, paperless charts, and a digital Pano. There is additional upside for anyone who desires to keep any specialty procedures in-house as nearly all endo, implant placement, oral surgery, and orthodontics are currently being referred out. HOUSTONSOUTHWEST (ID #627): Legacy GD practice with majority FFS patient base in a growing southwest Houston suburb. Located in a retail center on a busy intersection, this 1,200 sq ft office features 4 fully equipped ops plumbed for nitrous, computers throughout, digital radiography, a digital scanner, intraoral cameras, and paperless charts. HOUSTONSOUTH (ID #682): Established, multi-specialty dental office in a suburb approximately 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and
focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose. SAN ANTONIO-TX HILL COUNTRY (ID #685): Wellestablished dental practice and real estate nestled in the Hill Country north of San Antonio. The office relies mostly on word-of-mouth- referrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023 and the trend has continued into 2024. SOUTH TEXAS (ID #651): General dentistry practice located in south Texas. This state-of-the-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld X-ray units, and a 3-D printer. The practice serves a large PPO/Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow. SOUTH TEXAS (ID #668): Thriving south Texas practice (with real estate) that has established itself as the premier dentistry provider in the local community. This one-doctor practice has a massive active patient base, strong hygiene production, and generated revenue of 7 figures. The real estate is available for purchase and features 6 equipped operatories and state-of-the-
classifieds
art equipment (CBCT, digital intraoral scanner, and CAD/CAM milling unit). This may also be an ideal fit as an associate-run practice for a Texas-based group practice owner. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions. com or contact us at 512-900-7989 or info@ dentaltransitions.com.
AUSTIN: Fee-for-service private practice, 46 years same location with a 10-15 mile panoramic view over the downtown Austin skyline. Associate to buy with a preferred long transition for the senior doctor. Eight years remaining current lease with option to extend. Tremendous amount of residential growth immediately outside our huge windows. Ideally a GP interested in learning full-scale orthodontics. Please email for information: info@austinskylinedental. com.
CENTRAL TEXAS HILL COUNTRY:
For sale by owner, thriving fee-for-service general dental practice. Established rural 4 operatory dental practice for sale in the heart of the beautiful Texas Hill Country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a
dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail.com for more information and showings.
EAST TEXAS: Exceptional practice opportunity in Troup, Texas. Seeking associate to join high quality, well-established dental practice with a long history of excellence. This is an exceptional opportunity to move into ownership after a successful initial employment phase. Must be committed to providing optimal patient care with exceptional technical skills, strong people skills, personal integrity, honesty and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on Christian values and professional growth. Our office expansion should be complete mid-late September 2024, but the new associate could begin in August if he/she would like. Please reply in confidence with your CV and a letter outlining your future objectives and goals to: drmay@troupfamilydental.com or call our office at 903-842-4600.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 sq ft with 3 total operatories: 2 for dentistry and 1 for hygiene. Please let me know if you need anything else from
me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee-forservice and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
ROCKPORT: Practice for sale in Rockport. Two chairs, plumbed for 3. Currently being worked 3 days a week producing near mid-6 figures. Fee-forservice, no DMO, HMO or PPO contracts. Hygienist 3 days a week and will stay, been with practice since 2019. Digital X-rays, paperless, Newtom 3D/Panorex, 3 X-ray sensors. Practice is in older house, which can be leased or purchased. Great starter practice or for someone slowing down and wants to live on the coast. Send inquires to jim@jlongdds.com or call: 281-726-1812, leave message.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www.adstexas.com or call us at 469-2223200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.