
221 TDA
Journal JUNE 2024 232 2024 ANNUAL SESSION AWARD HIGHLIGHTS ADDRESSES TO THE 2024 TEXAS DENTAL ASSOCIATION HOUSE OF DELEGATES 234 DR GEORGANNE P. MCCANDLESS INCOMING TDA PRESIDENT 240 DR CODY C. GRAVES OUTGOING TDA PRESIDENT 246 DR RITA CAMMARATA ADA 15TH DISTRICT TRUSTEE COVER DR GEORGANNE P. MCCANDLESS Incoming TDA President
Texas Dental
practice solutions
Dental practice financing1
Our practice specialists can help you achieve your goals

We’ll work with you to determine the financing solutions that best fit your plans, and help guide you through the process.
New office startups
Get started with up to 100% project financing.¹
Practice sales and acquisitions
Benefit from our many years of experience helping clients purchase practices.
Business debt consolidation¹
Let us help you restructure your debt and improve your cash flow.
Office improvement and expansion
Enjoy competitive terms when you remodel or expand.
Commercial real estate ²
Buy, refinance¹ or relocate with conventional or Small Business Administration (SBA)³ loan options.
Equipment financing
Choose from a variety of options and flexible terms tailored to meet your needs.
To learn more, call 800.428.2847 to talk to a practice specialist, or visit bankofamerica.com/practicesolutions.
Bank of America can also help you with cash management, employer solutions and your personal banking and financial needs.
Proudly endorsed by:

1 All programs subject to credit approval, and loan amounts are subject to creditworthiness. The term, amount, interest rate, and repayment schedule for your loan, and any product features, may vary depending on your creditworthiness and on the type, amount, and collateral for your loan. Bank of America may prohibit use of an account to pay off or pay down another Bank of America account. Repayment structure, prepayment options and early payoff are all subject to product availability and credit approval. Other underwriting standards and restrictions may apply. Products and restrictions are subject to change.
2 Owner occupied commercial real estate will be determined in underwriting and requires occupancy by the borrower/guarantor. Please note SBA guidelines require at least 51% occupancy to be considered Owner Occupied.
3 Small Business Administration (SBA) financing is subject to approval through the SBA 504 and SBA 7(a) programs. Loan terms, collateral and documentation requirements apply. Actual amortization, rate and extension of credit are subject to necessary credit approval. Bank of America credit standards and documentation requirements apply. Other restrictions may apply.
All promotional and marketing materials are Bank of America Practice Solutions property and, as such, cannot be changed, altered or modified, orally or in writing. All questions regarding these materials should be directed or referred to a Bank of America Practice Solutions Sales Associate.
Sponsorship of endorser’s products and services is not an expressed opinion or approval by the Bank.
Bank of America and the Bank of America logo are registered trademarks of Bank of America Corporation. Bank of America Practice Solutions is a division of Bank of America, N.A. ©2023 Bank of America Corporation. MAP6112413 | 11/2023 | AD-11-23-0365.A
222 Texas Dental Journal | Vol 141 | No. 5
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and 4
Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
www.tda.org | June 2024 223
Approved PACE Program Provider FAGD/MAGD Credit. Approval does not imply acceptance by a state of provincial board of dentistry or AGD endorsement. 8/1/2018 to 7/31/2022. Provider ID# 217924
246 15TH DISTRICT TRUSTEE, AMERICAN DENTAL ASSOCIATION, ADDRESS TO THE 2024 TEXAS DENTAL ASSOCIATION HOUSE OF DELEGATES DR RITA M. CAMMARATA
251 ASK THE POWERS CENTER
Guido Fichera DMD, MSc
Claudia Mazzitelli DMD, MSc, PhD
Vincenzo Picciariello DMD
Tatjana Maravic DMD, PhD
Uros Josic DMD, PhD
Annalisa Mazzoni DMD, PhD
Lorenzo Breschi DMD, PhD
Guest Editor Rade D. Paravina, DDS, MS, PhD
252 FBI: FOUND BUT NOT IDENTIFIED (YET)
Elif D. Aksoylu, DMD, MPH
HIGHLIGHTS
226 In Memoriam
258 Oral and Maxillofacial Pathology: Case of the Month
260 Oral and Maxillofacial Pathology: Case of the Month Diagnosis and Management
262 Value for Your Profession: Making Sense of Capnography in Your Dental Office 264 Classifieds 270 Index to Advertisers
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 141 | No. 5
Texas Dental Association
1946 S IH-35 Ste 400, Austin, TX 78704-3698
Phone: 512-443-3675 • FAX: 512-443-3031 Email: tda@tda.org • Website: www.tda.org
Texas Dental Journal (ISSN 0040-4284) is published monthly except January-February and August-September, which are combined issues, by the Texas Dental Association, 1946 S IH-35, Austin, TX, 78704-3698, 512-443-3675. PeriodicalsPostage Paid at Austin, Texas and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 1946 S IH 35 Ste 400, Austin, TX 78704. Copyright 2023 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. Instate ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax.
Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement included in the online September Annual Membership Directory or on the TDA website: tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
224 Texas Dental Journal | Vol 141 | No. 5
contents
FEATURES 232 2024 TDA MEETING AWARD HIGHLIGHTS 234 TDA INCOMING PRESIDENT’S ADDRESS TO THE 2024 TEXAS
HOUSE
DR GEORGANNE
PRESIDENT’S ADDRESS
2024
ASSOCIATION HOUSE OF DELEGATES DR
DENTAL ASSOCIATION
OF DELEGATES
MCCANDLESS 240 TDA OUTGOING
TO THE
TEXAS DENTAL
CODY C. GRAVES














www.tda.org | June 2024 225 Content on the Texas Health Steps Online Provider Education website has been accredited by the UTHSCSA Dental School Office of Continuing Dental Education, the Texas Medical Association, American Nurses Credentialing Center, National Commission for Health Education Credentialing, Texas State Board of Social Worker Examiners, Accreditation Council for Pharmacy Education, and Continuing Education for multiple disciplines will be provided for some online content. Join 250,000+ professionals who get free Continuing Education (CE) with Texas Health Steps Online Provider Education. Choose from a wide range of courses developed by trusted Texas experts, for dental experts like you. Courses such as caries risk assessment and dental quality measures are available 24/7. Texas Health Steps is health care for children from birth through age 20 who have Medicaid. Learn more at TXHealthSteps.com Practical dental CE, at your pace.

JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface Professional, reliable service with hightechnology solutions so that you can better serve your patients.

Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
Board of Directors Texas Dental Association
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PAST PRESIDENT Cody C. Graves, DDS 325-648-2251, drc@centex.net
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
VICE PRESIDENT, SOUTHWEST Krystelle Anaya, DDS 915-855-1000, krystelle.barrera@gmail.com
VICE PRESIDENT, NORTHWEST Stephen A. Sperry, DDS 806-794-8124, stephenasperry@gmail.com
VICE PRESIDENT, NORTHEAST Mark A. Camp, DDS 903-757-8890, macamp1970@yahoo.com
SENIOR DIRECTOR, SOUTHEAST Matthew J. Heck, DDS 210-393-6606, matthewjheckdds@gmail.com
SENIOR DIRECTOR, SOUTHWEST Melissa Uriegas, DDS 956-369-9235, meluriegas@gmail.com
SENIOR DIRECTOR, NORTHWEST Adam S. Awtrey, DDS 314-503-4457, awtrey.adam@gmail.com
SENIOR DIRECTOR, NORTHEAST Drew M. Vanderbrook, DDS 214-821-5200, vanderbrookdds@gmail.com
DIRECTOR, SOUTHEAST Ron Hill, DDS 713-626-8343, rhilldds@gmail.com
DIRECTOR, SOUTHWEST Oshmi Dutta, DDS 210-888-0700, odutta@gmail.com
DIRECTOR, NORTHWEST Annie C. Wilson, DDS 817-860-4343, annie@anniewilsondds.com
DIRECTOR, NORTHEAST Shane A. Ricci, DDS 972-381-1888, riccidds@hotmail.com
SECRETARY-TREASURER* Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN** Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR** Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL Carl R. Galant
*Non-voting member **Non-voting
Those in the dental community who have recently passed
Olen R Allred Beaumont 9/1/32–3/24/24
Good Fellow: 1982
Life: 1997
Fifty Year: 2007
Kent J Hinrichsen Georgetown 10/3/42–1/11/23
Good Fellow: 2010
Life: 2007
226 Texas Dental Journal | Vol 141 | No. 5
patients, limiting
your liability
in memoriam
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
Get unmatched coverage. Practice more safely. Your good name is protected.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).



www.tda.org | June 2024 227
All data is derived from MedPro Group records and calculations; claims data range is 2012-2021 unless otherwise indicated. MedPro Group is the marketing name used to refer to the insurance operations of The Medical Protective Company, Princeton Insurance ompany, PLI O, Inc. and MedPro RRG Risk Retention Group. All insurance products are administered by MedPro Group and underwritten by these and other Berkshire Hathaway affiliates, including National Fire & Marine Insurance Company. Product availability is based upon business and/or regulatory approval and may differ among companies. © 2023 MedPro Group Inc. All Rights Reserved. Dental-230228 Ready to get the best protection for you? Contact us for your free custom quote and see how much you could save! 800.4MEDPRO x119660 | dental@medpro.com medprodental.com/TXDA
































228 Texas Dental Journal | Vol 141 | No. 5 www.TexasDentistLawyer.com Not Board Certified by the Texas Board of Legal Specialization Principal Office Houston, TX 713-622-1111 Dental entity structuring Dental practice sales and purchases Associate, employment, and partnership agreements Lease and real estate transactions Texas Attorney and Dentist 7670 Woodway Drive, Suite 342 Houston, TX 77024 Dental practice consulting Insurance audit and defense duly licensed
Hieu Huynh, DDS, JD

As a Practice Owner, You Should be Able to Answer the Following Questions:
1. Do you have or have you considered an exit strategy?
2. How long do you plan on being a practice owner? If your health allows, would you like to continue practicing after that point?
3. Do you know what your practice is worth today? How do you know? When was your last Practice Valuation done?
4. Have you met with a financial planner and have a documented plan? Have you established a liquid financial resources target that will enable you to retire with your desired lifestyle/level of income?





If you answered no or do not know to any of these questions, let’s have a conversation!

Henry Schein Dental Practice Transitions has your best interests has your best in mind throughout your career. Schedule a complime a complimentary consultation with your local Transition Sales Consultant today!


Practices For Sale
FANTASTIC TYLER LOCATION: Discover an exceptional GP practice, strategically situated in a bustling retail center with superb visibility along a high-traffic thoroughfare. This digital office boasts 4 furnished ops and one additional that is plumbed, with the majority of equipment being a mere 6 years old. Catering to over 1,600 active patients from a FFS, PPO, and 28% Medicaid mix, this practice thrives on 4 doctor days per week and produced more than $528K in 2023. Opportunity ID: TX-02053
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano, and has paperless charts. The practice is 90% FFS patients with a small amount of PPO. The office collected over $876K on a four-day workweek. This is a fantastic practice with the potential to grow for a motivated purchaser. Opportunity ID: TX-02041
MULTI-MILLION DOLLAR OPPORTUNITY: Large GP located north of Houston is available with real estate. The office is in a stand-alone building with 8 ops and is in excellent condition. It has digital X-rays, Pano, and paperless charts. The office operates 45 hours per week with 3 clinicians. There is over 6,500+ active patients, 70% Medicaid & 30% PPO/FFS, with an average of 96 new patients per month. Opportunity ID: TX-01979
FANTASTIC RETAIL LOCATION: Cypress GP in a busy retail center with great visibility and foot traffic. This 3,000 sq. ft. office has 8 ops, 6 are equipped with 2 additional plumbed and ready for expansion. The office is all digital with paperless patient files and Open Dental operating software. With over 1,200 active FFS/PPO patients, this practice has the location and potential to be a huge collectin office with the right motivated purchaser. Opportunity ID: TX-01929
www.tda.org | June 2024 229
C ll: 866-335-2947 © 2024 Henry Schein, Inc. No copying without permission. Not responsible for typographical errors. 23PT2801 www.henryscheinDPT.com 866-335-2947 n C C n n B Y Since 1968
Go to our website or call to request information on other available practice opportunities! 800.232.3826 Practice Sales & Purchases Over $3.5 Billion www.AFTCO.net We are pleased to announce... Mark Malone, D.D.S. has acquired the practice of have acquired the practice of Houston, Texas Fort Worth, Texas We are pleased to have represented all parties in these transitions. & David C. Sun, D.D.S.
P. Kuruvilla, D.D.S. Hulen Dental Veronica Y. Chen, D.D.S.
Jini
Free Dental Practice Valuation Take the 1st step in selling your dental practice. Contact us to receive a free practice valuation. Terry Watson, D.D.S. Jeremy Brown, J.D. Frank Brown, J.D., LL.M. WatsonBrownSales.com 469-222-3200 * Call us for details on this offer.
LAW OFFICES OF MARK J. HANNA

Mark J. Hanna JD
Former General Counsel, Texas Dental Association
• Representation Before the Texas State Board of Dental Examiners
• Medicaid Audits and Administrative Hearings
• Employment Issues—Texas Workforce Commission Hearings
• Administrative (SOAH) Hearings and Counsel
• Professional Recovery Network (PRN) Compliance
• Employment/Associateship Contract Reviews
• Practice Acquisition and Sales
• Business Organizations, PAs, PCs, and PLLCs
• Civil Litigation
Email: mhanna@markjhanna.com
• Conventional biopsy
• Cytopathology
• Histochemistry
• Immunohistochemistry
• Direct immunofluorescence testing
www.tda.org | June 2024 231 713.486.4411 go.uth.edu/Pathology • Complimentary biopsy kits • Delivery via FedEx, local courier or USPS • Diagnosis within two business days of receiving most biopsy specimens. • UT M.D. Anderson Cancer Center and UTHealth Medical School available for consultations as needed.
Affiliated with UT School of Dentistry at Houston. Our Pathologists: Specializing in:
•
testing
Jerry
Ngozi N. Nwizu, BDS, MMSc, PhD
E. Bouquot, DDS, MSD
Kalu U.E. Ogbureke, BDS, DMSc, JD, MSc Nadarajah Vigneswaran, DMD, DrMedDent
2414
•
78703 •
Exposition Blvd., Suite A1
Austin, Texas
Phone: 512-477-6200 • Fax: 512-477-1188 •
Not Board Certified by the Texas Board of Legal Specialization
LEGAL
EXPERIENCED
REPRESENTATION FOR TEXAS DENTISTS

AWARD HIGHLIGHTS
Photos by Kayla Prasek Photography
TDA Awards Committee
Chair Dr Krystelle Anaya, Dr Mark A. Camp, Dr Laji J. James, Dr Stephen A. Sperry

Rising Star of the Lone Star: Dr Akshay Thusu
2024 Rising Star of the Lone Star recipient, presented by 2023-24
TDA President Dr Cody Graves.
Gold Medal for Distinguished Service:
Dr Craig S. Armstrong
2024 recipient of the Gold Medal of Distinguished Service Award, presented by 2023-24
TDA President Dr Cody Graves.



Outgoing Council Members, 2023:
Drs Susan L. Putthoff, J. Michael Wedin, Gregory W. Rashall, Wade R. Barker, Gabrielle Dizon, Paul M. McLornan, and Sara Ehsani, who served the Association as Council Members.
10-Year, Good Fellow, Life, 50-Year, and 60-Year Membership Awards
The recipients of the 10-year, Good Fellow, Life, 50-Year, and 60-Year Membership Awards will be featured in the July 2024 Texas Dental Journal.
Outgoing Vice Presidents
Drs Shailee J. Gupta, Summer Ketron Roark, Jodi D. Danna, Richard M. Potter
232 Texas Dental Journal | Vol 141 | No. 5

Incoming President Award:
Dr Georganne McCandless of Tomball assumes the presidency of the TDA at the Saturday afternoon House of Delegates. Turning the office over to her is Outgoing TDA President Dr Cody C. Graves of Goldthwaite.

Outgoing President Award:
Dr Cody C. Graves of Goldthwaite receives the Outgoing President’s award from Incoming TDA President Dr Georganne McCandless of Tomball at the Saturday afternoon House of Delegates.
TDA Service Recognition Awards:
Dr John W. Baucum III in recognition of his steadfast commitment and thoughtful leadership as speaker of the house. His dedicated service has made a lasting impact, and TDA is deeply grateful for his tireless efforts, shaping policy, and representing the voices of the people with integrity and compassion. Thank you for your exemplary service and unwavering dedication to the Texas Dental Association.

Dr Carmen P. Smith
with deep appreciation for her unwavering dedication and tireless efforts as secretary-treasurer. Her steadfast commitment to financial stewardship and strategic planning has been instrumental in ensuring the prosperity and stability of our association. Thank you for your exceptional service, integrity, and diligence in safeguarding our resources and advancing our mission.
Certificates of Merit:
Gino R. Garza, RDH MEd, MAADH, in recognition of his efforts to serve the dental health and welfare of the disadvantaged population in the San Antonio area, be awarded a 2024 Texas Dental Association Certificate of Merit.
North Dallas Shared Ministries, in recognition of its efforts to serve the dental health and welfare of the disadvantaged population of the Dallas area, be awarded a 2024 Texas Dental Association Certificate of Merit.
The Bethesda Health Clinic, in recognition of its efforts to serve the dental health and welfare of the disadvantaged population of East Texas, be awarded a 2024 Texas Dental Association Certificate of Merit.
Outgoing Alliance of the TDA Service Recognition: Mrs Angela Estes, Outgoing Alliance President
Outgoing Past President Award:
Dr Duc “Duke” M. Ho of Katy received the Outgoing Past President’s award from the Awards Committee at the Friday afternoon House of Delegates. Dr Ho served as president-elect, president, and past president from 2021 to 2024.
President’s Recognition Awards:

TDA Secretary-Treasurer Dr Carmen Smith (pictured) and the TDA Accounting Department, TDA Director of Finance Kelly Doolittle (pictured), AP Accountant Barb Carlson (not pictured), and GL Accountant Arlene Knox (not pictured) for their outstanding service and dedication to the financial well-being of the Association.

Dr Wade Barker for donating time, talent, and outstanding service to the TDA Smiles Foundation through Texas Missions of Mercy in 2024.

Dr Susan Jolliff for donating time, talent, and outstanding service in many capacities within the TDA in 2024.
www.tda.org | June 2024 233

234 Texas Dental Journal | Vol 141 | No. 5
TDA Incoming President’s
Address to the 2024 Texas Dental
Association House of Delegates
TDA INCOMING PRESIDENT
DR GEORGANNE MCCANDLESS
Mr Speaker, Board of Directors, Members of the House of Delegates, and esteemed guests:
I am honored to be speaking to you today as your next Texas Dental Association President and feel very humbled for the opportunity to be serving you and our Association over the next year.
My journey into organized dentistry started a long time ago, but I just hadn’t realized it back then. Growing up I always wanted to be a dentist. I landed in my orthodontist’s chair at age 12 and proudly announced I wanted to be a dentist. Not only did my orthodontist encourage me to go into dentistry but years later when we were in this very House of Delegates as colleagues, he told me he expected me to go into leadership one day. That orthodontist was Dr Rick Black, a past TDA president himself. It was a full-circle moment for me.
Like Dr Black, there are many people who have helped me during my professional journey that I’d like to acknowledge. Thank you to Dr Cody Graves for your encouragement and patience. You’ve taught me to never assume, and I will take that lesson with me. Dr Duke Ho—we’ve known each other for more than 25 years. You have always supported me and cheered me on. It’s all about relationships as you always say.

Drs Duc Ho, Georganne McCandless, and Cody Graves are pictured at ADA Dentist & Student Lobby Day in Washington, DC.
www.tda.org | June 2024 235


Thank you to our amazing TDA Board. They are single-handedly the most disciplined, professional and smartest group of people to work with. And to our TDA staff under the direction of our executive director, Ms Linda Brady—they are a group of dedicated individuals that work tirelessly on our behalf. And to my staff—without them, I wouldn’t be able to serve in this capacity.
A very special thank you goes out to my best friend, my sister, and my travel buddy—Dr Rita Maxine Cammarata. She hates it when I use her middle name. She isn’t here, so don’t tell her.
We met casually in dental school, but it was one fateful elevator ride in particular, in the first few months of our Pediatric residency, that we became fast friends. If you want the story behind that elevator ride, just ask one of us later. This is not the place for that story.
Rita has continually challenged me out of my comfort zone and her encouragement and mentorship have led me to where I am right now, standing here as your TDA president. I have always looked up to her and I am forever grateful for that elevator ride.
When I think about what organized dentistry has meant to me, I have to go back to why I joined, to begin with. My friend Rita joined the Dental Health committee and invited me to go with her. On that committee, I found other colleagues with the same concerns and issues as mine. Back then it was trying to find the right job, trying to decipher employment contracts, and how to pay back our student loans. We had a shared experience
When I volunteered for the Star of the South dental conference, I ran into old classmates. We reminisced about dental school days.
236 Texas Dental Journal | Vol 141 | No. 5
A very special thank you goes out to my best friend, my sister, and my travel buddy—Dr Rita Maxine Cammarata.
We took continuing education courses that advanced our knowledge base. We discussed challenges regarding patient care. We were trying to find a work-life balance. We had a shared experience
When I got involved in my local Legislative Action committee and later the House of Delegates, legislative issues and the importance of advocacy with one big voice became our shared experience
So, what is your shared experience with your colleagues? Actively finding that shared experience is our duty and what I hope to highlight as TDA president.
Defining and focusing on those shared experiences are important to growing membership. We are combating a real societal shift when it comes to memberships writ large. Membership is about a personal connection. We all joined because someone invited us. We must continue to invite them and emphasize our shared experiences and find ways to use those shared experiences to learn and grow.
With our DSO colleagues for example that say they don’t feel welcome, we can find common ground in everyday practice concerns such as third party payor issues, the burden of increasing student debt and patient care concerns.
For our smaller components that are struggling with bringing continuing education programs to their members, we can offer the regional meetings or continuing education through our CE concierge.

So, what is your shared experience with your colleagues? Actively finding that shared experience is our duty and what I hope to highlight as TDA President.
www.tda.org | June 2024 237


For our early career dentists, they need mentorship and mentorship is the fastest way to TDA membership. We can only continue to grow as an organization by counseling those young dentists just starting out and who need a guiding hand or sometimes just an ear that will listen to them.
I was one who benefited from that guidance as a younger dentist. Years ago, when I was a young delegate in the TDA House of Delegates, I was asked to serve on a reference committee. It was an intimidating appointment, and I was nervous the entire time. But the committee chair kept reassuring me and kept guiding the rest of us. The chair of that reference committee was Dr Jerry Hopson. And where is he today? Right here in this House of delegates continuing to mentor and guide not only me, but all of our members. Thank you, Dr Hopson!
Fast forward and earlier this year I received a very heartfelt handwritten note of thanks from one of our youngest members. In her note, she expressed thanks that TDA is making room for everybody at the table, both young and I won’t say old, but more seasoned dentists. That young dentist is Dr Yeri Guak. And where is she today? She is here, serving on our CAMCEP team, which works hard all year long to bring us this exceptional meeting.
Communication will be key to growing our ranks and fortifying the membership we already have. It will also be key to letting our members know what it means to be a part of TDA, and why it’s important to their individual practices but also to the profession as a whole. We need to adopt a messaging strategy that is a
238 Texas Dental Journal | Vol 141 | No. 5
Dr Tommy Harrison, Dr Debrah Worsham, Dr Georganne McCandless, Dr Jon Vogel, Dr Rita Cammarata, Dr Rob Neal in Washington DC advocating for the dental profession.
Dr McCandless and Dr Cody Graves serving the underserved at a recent Texas Mission of Mercy event.
new way to think about creating, sharing, and consuming information in our cluttered and noisy digital world. If what we are communicating is not being read, we need to adjust this. By adopting a smart communications strategy, we can positively impact membership.
Governmental affairs and advocacy is and will always be the hallmark of what TDA does for us. For years we have successfully protected this profession and our patients through the guidance of this House of Delegates and the efforts of CLRA. As we move into the next legislative session, we must continue those efforts. These include issues such as dental loan repayment, the burden of increasing student debt, and workforce shortages.
Before I close, I’d like to say a special thank you to my husband Skip Fortune. You are my golden hour, and you make all things possible.
Dentistry has been good to me, and that’s in large part due to organized dentistry. When I look back at that 12-year-old girl who wanted to be a dentist, I can’t believe I’m standing here, helping guide professionals who are part of the third-largest state dental association in the US. I find it incredibly rewarding to work on behalf of our essential profession. TDA is invested in the success of every dentist, and I hope to help educate people that we are the trusted source for dentists across their careers, no matter the practice setting, no matter if they are just starting out or have helped make smiles brighter over a long career.
Thank you.

www.tda.org | June 2024 239
Dr McCandless is pictured with her husband Skip Fortune

240 Texas Dental Journal | Vol 141 | No. 5
TDA Outgoing President’s
Address to the 2024 Texas Dental
Association House of Delegates
TDA OUTGOING PRESIDENT DR CODY C. GRAVES
Thank you, Mr Speaker. Good morning, TDA House. Welcome to all delegates, alternate delegates, distinguished leaders of today and previous years, TDA staff members, and guests.
It’s my honor to stand in front of you again and be humbly reminded of how nerve-racking it is to stand in front of a big group like this.
If you don’t recall, I talked about working together “like a village” to accomplish goals. There is really no “I’m just one member”. We all can make a difference. I believe this past year shows that. So, indulge me a few minutes to give you a recap.
Starting off this past year, dental hygiene anesthesia was passed by the state legislature and will be implemented soon in State Dental Board rules. TDA Board and staff heard your voices last year and with some great help, accomplished something that has been at times very controversial in these houses for years.
TDA and our legislative team also supported the creation of the bill (Multiple Employment Welfare Agreement). This, once the Texas Department of Insurance approves it, will create a partnership with another state association to give TDA members access to PPO health insurance plans and potentially decrease premiums. This could be one of those “sticky” products that could help entice membership.
www.tda.org | June 2024 241

In June, TDA hosted a leadership conference in which leaders from around the state were able to come together in Austin to talk about their component’s strengths, weaknesses, goals, and other collaborative work. We also talked about what TDA can offer them, what resources TDA has available, what TDA has plans to do, and quite frankly we opened up the discussions on what TDA needs to do better.
In July, TDA joined forces with the South Plains Dental Society to have the first ever TDA Regional Meeting. The Overton Hotel was the gathering place for a one-day course, with vendors outside the classroom, where attendees could gather continuing education and have hands-on experience so close to their seats. This idea came from our Council on Annual Meetings and Continuing Education. And we are grateful to Lubbock for allowing us to kick this off in their town. This year, the TDA Regional Meeting will be happening in Beaumont on September 27th. So, if you are available and would like to join, additional details will be coming.
August was busy and hot. Not only was I preparing my oldest for her first day at college, but I was also attending the Southwest Dental Conference. Being a Baylor graduate, like my father, I’ve been going to that conference before I even decided I wanted to be a dentist. I would like to thank Ms Jane Evans for the continual invitation to that event. Oh, and this little organization known as TXDOT had all sorts of fun with our building, which others will give a report about today or this weekend.
Into September we see where strong relationships come into play. We had some of TDA’s leadership participate in the TAGD’s Lonestar Dental Conference. Not just because it is a similar type of
242 Texas Dental Journal | Vol 141 | No. 5
professional association, but to show support for our very own Dr Shane Ricci who was president of TAGD last year. I’ve known Shane for a few years now. I would personally like to praise Shane for the selfless work he has done for both associations throughout these years. TAGD is a great association and TDA appreciates the working relationship with them.
My first trip, that I can remember, to El Paso was the following weekend. Dr/Dean/past TDA president/past ADA trustee Rick Black graciously guided Ms Diane Rhodes and me around the Woody L. Hunt School of Dental Medicine. And wow what a campus. Dr Black and his team have constructed a curriculum that changes the way we think of educated future dentists. I can’t wait to see how this translates into success for those new dentists. On a side note, I was also able to attend, for a very very short time, my first El Paso Chihuahuas baseball game.
October was packed with ADA events, and I’ll let smarter, more experienced people talk about the ADA topics.
As a first of its kind for TDA, the TDA Dentist Symposium happened the first weekend in November at the Omni Barton Creek Resort & Spa in Austin. CAMCEP’s goal was to offer a “spa-like” experience similar to the ones some special associations offer their members. Mixing CEs with socializing was the key to this event. Believe it or not, this was some of the best “hotel buffet food” that I’ve ever had. And the CEs could be applied to any general dentist’s repertoire if applied appropriately.
While you might think December and January would be easy, well that’s when I was finally able to start talking about the potential for ADA credit union creation. Since June, an ADA task force was created to determine the potential need, structure, offering and financing of a credit union. If you don’t know this about me, I have a fondness for economics and finance. As you can imagine, I jumped at this opportunity because this falls into my big 3 wishes for membership value. Quick recap, I want:
1. TDA or ADA to have better health insurances options for our members.
2. Financial support or backing for dentists with better interest rates and products.
3. Be the leading provider of dental insurance in the US.
Back on topic, we are well along the road to creating this credit union and have submitted our application to the National Credit Union Administration. So hopefully by the time Dr McCandless gives her outgoing speech next year, she can discuss the credit union details.
Component visits really started picking up for me in January. There was one week where I had a meeting for 3 straight nights, 2 hours away, in opposite directions from me. Before I forget, I would really like to take this opportunity to say a big “thank you” for the kindness and hospitality I felt on all these visits. I apologize for those I could not make and for those I
TDA hosted a leadership conference in which leaders from around the state were able to come together in Austin to talk about their component’s strengths, weaknesses, goals, and other collaborative work.
www.tda.org | June 2024 243
From dentists, dental students, dental staff, and family members; this village still needs more help. That’s why we have legislative contacts, TDA staff members, ADA contacts, faculty members, lawyers (yes even you Mr Galant) to shore up the help we need with this profession. We tend to be known as the fixers, but we don’t know it all and can’t get to it all. So, take this from someone who is
known
to just do things myself, we need and must work together.
had to reschedule. Juggling everything became very difficult for some weeks. And a special thanks goes out to FWDDS for the invitation to help pass out “build-a-bears” to the kids at Cook’s Children hospital. My wife and I had such an emotional day. That same morning, she lost her young cousin, who was an SMU professor, to cancer. Words can’t express the emotional ride we had that day, but at the end of it, we were in a better place. So, thank you Dr Drennan for the invitation and others from the Ft. Worth District Dental Society.
In the middle of these visits, I had the opportunity to attend 2 TMOM events. One in Lumberton and one in El Paso. If you haven’t ever attended one of these events, I challenge you to do so. The experience will solidify how great our profession is and how important it is to our society. Get over the, “I don’t want to take a day or 2 off and do free dentistry.” “I do this all week long.” “These things make me uncomfortable.” Reach out to one of the many passionate volunteers for this charitable event and they will happily connect you to an area where you will feel comfortable and make a difference. I have said this many times over the past almost decade, the TDA Smiles Foundation and the TMOM events are the best advertising the TDA can do to the public. These volunteers, not just dentists but others as well, are great ambassadors to TDA, dentistry and just the givinglife and they are leading some incredible, life-changing events.
Speaking of leading, just a few months ago, the first TDA Leadership Institute was held in Rockwell. With collaboration with the ADA and its leadership institution, TDA was the pilot state to see if this type of experience would be worthwhile. If so, then can it be replicated throughout other states. The TDA board created a task force to develop this opportunity and we hope to continue to bring our members updates on this endeavor. Any questions or comments can be directed to Ms Lee Ann Johnson, our director for member services and administration (who shamelessly wanted a plug).
And to round out the multiple ways this membership can make a difference, in April, I attended the ADA Student and Dentist Lobby Day in Washington, DC. Around 50 dental students from 3 of the 4 dental schools attended this event and participated with experienced dentists to visit our legislators. This was a fantastic opportunity for these soon-to-be-dentists to discuss some hot topics and learn about the lobbying process. Grassroots efforts are still alive and working for our profession.
From dentists, dental students, dental staff, and family members; this village still needs more help. That’s why we have legislative contacts, TDA staff members, ADA contacts, faculty members, lawyers (yes even you Mr Galant) to shore up the help we need with this profession. We tend to be known as the fixers, but we don’t know it all and can’t get to it all. So, take this from someone who is known to just do things myself, we need and must work together. As you will probably know, our members’ desire instant response to their needs and wishes, our software systems all must be interlinked, and our communication needs to be specific and clear. And all that is just to be responsive to the new
244 Texas Dental Journal | Vol 141 | No. 5
generation embracing dentistry. We still must have personal service, and the communications and systems in place to handle everything the boomers need. The goal, one day, is to reach every dentist with the products and services they need to be successful in their life and career. Then it won’t be the value they are looking for, it will be ‘the want’. Do they, do YOU, want to join or stay a member of this association?
Lastly, I want to thank my wife and girls for putting up with my trips this year. My goal was to make it to all my girls’ events over these last 9 years. I was not perfect, but I was pretty darn close. And a special thanks to my staff…because these events are numerous and sometimes just pop up. They aren’t here this weekend, which makes it easier to talk about them, because my youngest daughter is graduating tonight. Don’t worry, I’m heading home right before Dr Smith starts talking about numbers. I will not be missing this occasion.
Thank you again for the privilege to represent this association over the past year. I look forward to seeing where we can go together and grow together.

www.tda.org | June 2024 245
Dr Graves’ family at the 2023 TDA House of Delegates.

246 Texas Dental Journal | Vol 141 | No. 5
15th district trustee, american dental association, Address to the 2024 Texas Dental Association House of Delegates
15TH DISTRICT TRUSTEE, AMERICAN DENTAL ASSOCIATION
DR RITA M. CAMMARATA
Good morning everyone, Mr Speaker, Mr President, Madame President-Elect, and my colleagues of the House. Everyone can put your credit cards away. I’m not asking for donations. I’ve turned that over to Dr Rob Neal, and today I address you as your 15th District Trustee to the ADA.
On several occasions as I have heard Dr Raymond Cohlmia speak he says, “If we want different results from our ADA, then we have to do something different at our ADA.” Rest assured ADA is changing and by changing we have the opportunity to grow our market share and membership numbers so we can continue to be the premier voice for dentistry for our patients and our profession.
Change is inevitable, and everyone is working at the ADA to create business values allowing us to become an organization that can adapt to change quickly and take advantage of opportunities as they emerge.
When Dr Cohlmia became executive director, he set up a 5 year timeline for change and we are currently in the third year, “The Implementation Year”.
www.tda.org | June 2024 247
ADA has spoken of the impending cliff of doom, which is less than 50% of market share. Well, Texas has already gone over the cliff, our current market share here in Texas is 44%. We all agree we must change, so what is currently changing at ADA?
So, what are we implementing? Only the most critical part of this 5-year process, changing our database to a new software, moving to Salesforce/Fontiva for each entity of the tripartite. ADA is supplying this software at no charge to all state and local organizations.
And why is it so critical? Because this new management software will allow our members to have a unique experience, customized to their wants and needs. We will no longer assume what they want to see but through this use of AI the member will see the content that is meaningful to them. It will be one database so each part of the tripartite has the same member information, at the same time, thereby improving our customer service capabilities.
SalesForce/Fontiva works off the same AI platform that is used by Amazon. This is the fundamental change we are making so we can begin to stop the continual fall in membership that is occurring, we all agree we must attempt a course correction. If this is the first you are hearing of Salesforce Fontiva, you need to go back to your local organization and ask what they are doing to train on this software changeover from Aptify. The change date is upcoming on this July 8th.
Why is this most critical? ADA has spoken of the impending cliff of doom, which is less than 50% of market share. Well, Texas has already gone over the cliff, our current market share here in Texas is 44%. We all agree we must change, so what is currently changing at ADA?
Here’s a list:
1. We are in our second year of the Strategic Forecasting Committee Program. It was slow to get off the ground, but remember this was a huge change to our governance structure. The sub-committees are working now to develop their forecast for the next 5 years. With the work of our members and our own Dr Graves, who is co-chairing one of the Tripartite subcommittee, SFC is working toward productive results for the sub-groups, councils and advancing our Association towards a sustainable future.
2. We are currently in the process of selling 2 of the buildings that ADA owns, one is the 12-story office building in DC on 14th Street, and the other is the flagship building in Chicago at 211 Chicago Ave. It is going through inspections, and closing should be finalized within the next few months. We will lease back needed space from the buyers for approximately 9-12 months, and then we will move to our new lease space at 401 Michigan Ave along the North River.
3. When we discuss creating value for our members, the number one item members ask for is financial services. Last month we filed for the charter for the America Dental Association Credit Union, solely owned and operated by the ADA. It is a startup, we are not partnering with any established entity. Dr Graves is serving on the Financial Services Task Force, and a complete credit union financial package offering will be forthcoming by 2025.
4. As you may know we merged ADASRI (the Science and Research Institute) with the Forsythe Institute creating the ADA Forsythe Institute or AFI. That merger will lead the way in building our global network along with growing the ADA Seal program and developing a new ADA Forsythe-certified program
248 Texas Dental Journal | Vol 141 | No. 5

for dental materials and we are taking advantage of opportunities in dental innovation through a program called DenTech. Think of Shark Tank with a dental twist. All of these and more will increase our opportunities for non-dues revenue on a potentially expansive scale.
5. ADA continues in its lawsuit against Delta Dental, currently still being in the yearslong discovery phase and completing final briefs on having a class action certified, which should be forthcoming in September of this year.
6. Actions from the ADA Board
a. We approved a Board resolution regarding Dental Benefits Annual Maximums, some of which hasn’t
increased since the 1960s for some insurance companies. The resolution directs i. investigation of data on annual benefit maximum usage, ii. developing policy drafts to support best practices, iii. and identifying legislative opportunities to support increasing yearly dental benefit maximums.
b. Another is regarding a task force Dr Edgar populated to address “Decreasing Dental School Tuition.” Dr Jon Vogel of Dallas is on that Task Force.
c. A Faculty Ambassador program in each of the 73+ dental schools in the US is
being developed to identify faculty members that can be the face and the voice of organized dentistry to the students and faculty they interact with daily.
d. Let’s not forget about SmileCon this year in New Orleans. Plan on attending this year and come to the Saturday night event sponsored by the ADA Foundation that will be held at the WW II museum honoring our veterans and supporting our Give Veterans a Smile Program. Monies raised during this event will be used to provide care to veterans in the surrounding New Orleans area.
www.tda.org | June 2024 249
What
are the metrics of success? Obviously increase in number of members and market share, continuing to be the voice of oral health in America, continuing to be financially stable, and most importantly having strong state and local association and societies that are the foundation to the success of the ADA and the tripartite.
7. The Membership Model Pilot program. We currently have 6 states engaging in the new Membership Model Pilot; this is a 3-year pilot program and it will allow us to gain data on the proposed new model and to measure its success.
This is the main take away you should leave here with regarding the new model, TEXAS is not affected by the pilot in anyway; our national, state and local dues and membership categories will remain as they are now. Our national dues amount and categories will not change in Texas, unless of course the 2024 ADA House would vote to increase or decrease ADA dues. Remember, the 2023 House voted to decrease dues last year. “Dues are too high” is the number one reason new dentists do not convert over to full paying members.
You might ask, “If the pilot model succeeds, what happens in the fourth year?” Well it will take a resolution and approval by the ADA HOD to change all states to the new ADA membership model.
Remember, what that model starts as may not be what it finishes as, which is why the pilot is happening so testing and tweaking of the model can occur.
What are the metrics of success? Obviously increase in number of members and market share, continuing to be the voice of oral health in America, continuing to be financially stable and most importantly having strong state and local association and societies, that are the foundation to the success of the ADA and the tripartite.
In closing, my commitment to you is to be your voice, to stay vigilant, and to make decisions to the best of my ability while on the ADA Board.
Please reach out if you have questions or comments and I appreciate all you do as a delegate to this House. And, Mr Speaker, if I may have a moment of personal privilege.
I would like to say “congratulations” to my dear friend Dr Georganne McCandless on her soon-to-be new position as Madame President of the TDA. Georgie I am so proud of you! And to my other good friend Dr Cody Graves, welcome to the club of the pastpresidents of Texas Dental Association, the best position to have. And, Mr Speaker, as you enter into your final House, a huge thank you for all you have done the past 12 years as Speaker of the House here in Texas. Job well done, John.
Thank you.
250 Texas Dental Journal | Vol 141 | No. 5
Structurally compromised teeth. Part I: Clinical considerations and novel classification proposal
Guido Fichera, DMD, MSc; Claudia Mazzitelli, DMD, MSc,PhD; Vincenzo Picciariello, DMD; Tatjana Maravic, DMD, PhD; Uros Josic, DMD, PhD; Annalisa Mazzoni, DMD, PhD; Lorenzo Breschi, DMD, PhD; Guest Editor Rade D. Paravina, DDS, MS, PhD
Read the article in full at: https://onlinelibrary.wiley.com/doi/epdf/10.1111/jerd.13117
Objective
To introduce the “Peripheral Build-Up technique — PBUt” as a foundation restoration strategy for structurally compromised teeth (SCT).
Clinical Considerations
Several strategies have been proposed over time (cervical marginal relocation, doughnut, and preformed ring techniques) to enable the management of restorative procedures in challenging situations such as the presence of deep subgingival defects. The PBUt is a versatile, completely additive direct technique that share some strategical concepts with these techniques to approach critical clinical situations while supplying a wider field of application thanks to distinct operative expedients. The clamp insertion modality, the extension of the proximal wall and the matrix customization/stabilization strategies adopted in PBUt endorse the possibility to manage the most apical and peripheral border of the residual tooth structure when located up to >1.5 mm above the bone crest. The periodontal response has to be then monitored over time. Moreover, thanks to the peripheral and apically-extended addictive approach, it allows a massive preservation of residual sound tooth structure and improves the resistance and retentive physical/geometrical features of the abutment tooth. The PBUt operative workflow is herein explained.




Clinical Significance
The Peripheral-Build-Up technique (PBUt) advocates some innovative clinical restorative steps for the management of SCT with coronal and deep subgingival defects.
Case: The lower left second premolar has the cervical structure, in one limited portion, apical to the gingival margin and to the tip of the proximal papilla, but coronal to the periodontal attachment (that is, the cervical structure is in the gingival sulcus). The most coronal location of the residual buccal/lingual structure was supragingival with no more than 1.5/2 mm height of residual tissues (absence of ferrule) (A). As the target tooth is the more distal element, the matrix stabilization was achieved by bonding flow resin composite on the distal clamp’s bow (B). Once the rubber dam was removed (C) a radiographic check was done (D).
www.tda.org | June 2024 251 A B C D

FBI: Found But not Identified (yet)
A series of articles intended to assist Texas Medical Examiners in giving a name to “unidentified” individuals using postmortem dental evidence.
Do you recognize the dental work/conditions presented?
Elif D. Aksoylu, DMD, MPH
252 Texas Dental Journal | Vol 141 | No. 5
The Extent of the Problem
Over 600,000 individuals go missing in the United States every year. Fortunately, many missing children and adults are quickly found, alive and well. However, tens of thousands of individuals remain missing for more than 1 year—what many agencies consider “cold cases”.1
It is estimated that 4,400 unidentified bodies are recovered each year, with approximately 1,000 of those bodies remaining unidentified after one year.2
Medical examiner and coroner offices reported 11,380 unidentified remains on record as of 2018.3
The challenge in giving a name to these unidentified decedents is that the research and time invested can be extensive and expensive, and after normal protocols have been exhausted, many individuals still remain unidentified. The hope in writing this series of articles on long-term unidentified in Texas is that one of the many Texas dentists who read the Texas Dental Journal will recognize the dental work presented as theirs or possibly remember a dental condition or feature that can give a name to the unidentified and help bring closure to the family.
The Medical Examiner’s Protocol to Legally Identify Individuals
Medical examiners follow a specific protocol to identify individuals who are found without any presumptive identity. This protocol is described below and, in this order, depending on the condition of the body.
By far Latent Prints (finger, palm, sole), are the fastest and least expensive way to make a positive identification. This method of identification is not always possible if remains are severely decomposed, incinerated, or skeletonized.
Medically Implanted Devices (hip/joint replacements, pacemakers), require knowing what hospital/physician placed the device to get the matching serial number, which can be difficult.
Dental Records are also an easy, fast, and inexpensive way to identify a decedent, however, success depends on a presumptive identity and availability/existence/quality of those antemortem (before death) dental records. If all leads for a presumptive identity are exhausted, then a postmortem (after death) dental charting/profile is created and entered in the NamUs (National Missing and Unidentified Persons System) and NCIC (National Crime Information Center) databases.
 Author
Elif D. Aksoylu DMD, MPH
Author
Elif D. Aksoylu DMD, MPH
Dr Aksoylu practices general dentistry at a community health center in Winslow, Arizona and currently serves as a consultant forensic odontologist for Dallas and Tarrant Counties.
She completed her Bachelor of Science at the University of Washington, Doctor of Medicine in Dentistry at Arizona School of Dentistry and Oral Health, and Master of Public Health at A.T. Still University. She is also a graduate of the Forensic Dentistry Fellowship at Lincoln Memorial University.
Dr Aksoylu is a Member of the American Society of Forensic Odontology, an Associate Member of the American Academy of Forensic Sciences, and a Member of the International Association of Coroners & Medical Examiners.
www.tda.org | June 2024 253
Anthropologic Methods will use skeletal features to make a positive identification.
DNA samples are collected. This takes the longest period of time and is most expensive. Depending upon the individual, it may involve obtaining DNA samples not only from the decedent but also from family members or multiple family members if known. If no matches are obtained, then:
DNA Samples are submitted to CODIS (Combine DNA Index System), which is a computer program that operates local, state, and national databases of DNA profiles from convicted offenders, unsolved crime scene evidence, unidentified remains and missing persons. This is maintained by the Federal Bureau of Investigation. If this search fails then, the State of Texas requires medical examiners to submit a DNA sample from long-term unidentified decedents to the University of North Texas Center for Human Identification for additional genetic testing and comparison. This comparison may take up to a year to process, and a decedent may still remain unidentified once completed. This is the proverbial end of the road; therefore, all Texas dentists, dental auxiliaries and staff: Can you help the Dallas County Medical Examiner’s Office give a name to the unidentified male decedent described below?
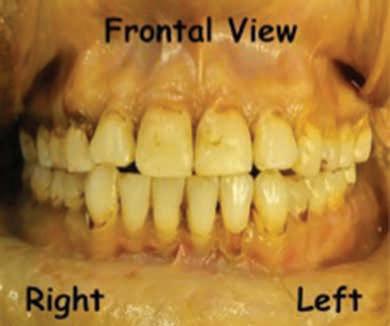
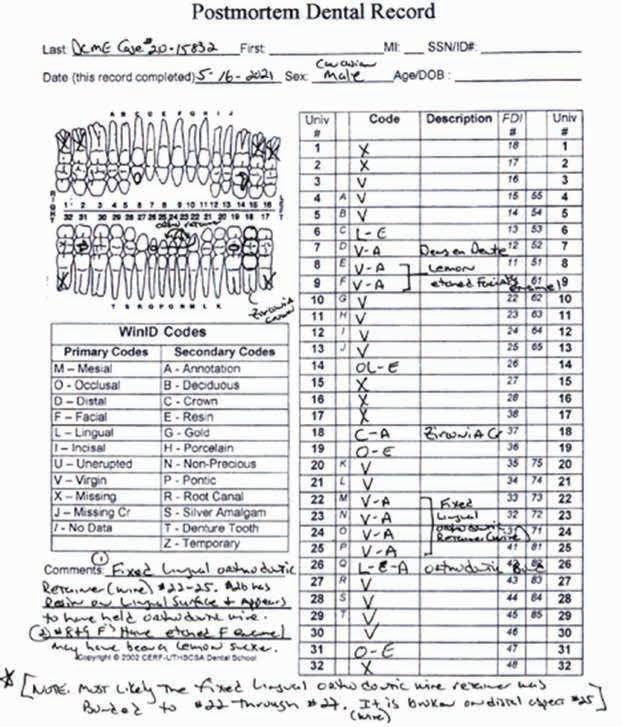
The Unidentified Individual: Dallas County Medical Examiner (DCME) Case #20-15832
Date of Death (Decedent found): August 26, 2020
Cause of Death: Methamphetamine Overdose
Manner of Death: Accident
Body Condition: Decomposed
Sex: Male
Ancestry: Caucasian
Age: 36 – 48 years
Scene Description: An unidentified male was found lifeless under a bridge during a welfare check by Emergency Medical Services in Dallas, Texas, on August 26, 2020. The decedent appeared to be homeless.
Dental Evidence Recovered: Maxilla and Mandible
254 Texas Dental Journal | Vol 141 | No. 5




www.tda.org | June 2024 255
Dental Postmortem Photographs DCME Case #20-15832
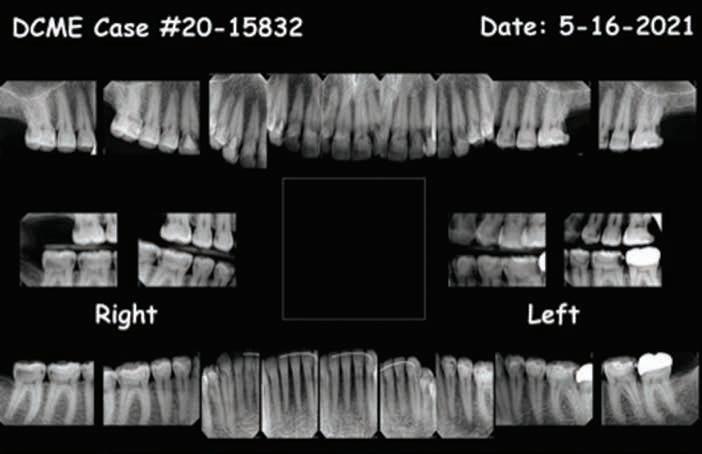

Note: The fixed mandibular lingual retainer is broken on the distal aspect of #25. It was most likely originally bonded from #22 through #27. Additionally, #7 presents with a dens en dente malformation (dens invaginatus).

256 Texas Dental Journal | Vol 141 | No. 5
Dental Postmortem Radiographs DCME Case #20-15832:
Dental Existing Conditions DCME Case #20-15832:
Closing
If you believe you have any dental records, dental radiographs, intraoral/extraoral dental photographs, dental scans, or other dental information regarding the unidentified male decedent described above as DCME Case #20-15832, please contact the Southwestern Institute of Forensic Sciences at Dallas County Medical Examiner’s Office at 214-9205900, Press 1, and ask for Steven Kurtz, chief medicolegal death investigator, or Keara St Louis, deputy chief medicolegal investigator.
Let’s give this individual a name!
References
1. Between 2007 and 2020, an average of 664,776 missing persons records annually were entered into the National Crime Information Center. See https://www.fbi.gov/ services/cjis/ncic
2. Medical Examiners And Coroners’ Offices, 2004. Matthew J. Hickman, Ph.D., Kristen A. Hughes, M.P.A., Bureau of Justice Statistics, Kevin J. Strom, Ph.D., Jeri D. Ropero-Miller, Ph.D., DABFT, RTI International
3. Medical Examiner and Coroner Offices, 2018. Connor Brooks, Bureau of Justice Statistics, November 2021
www.tda.org | June 2024 257
ORAL and maxillofacial
pathology
case of the month
clinical History
AUTHOR
 John E. Kacher, DDS Director, JKJ Pathology, Oral Medicine/ Oral Pathology, The Woodlands, Texas
John E. Kacher, DDS Director, JKJ Pathology, Oral Medicine/ Oral Pathology, The Woodlands, Texas
This case concerns a 39-year-old female patient who presents with an asymptomatic radiographic lesion discovered on a routine panoramic radiograph. A radiolucency was noted in the right posterior mandible in the furcation area of tooth #30. Also noted was spiking root resorption of the roots of #30 (Figure 1). The associated tooth was vital and non-mobile No

Figure 2. PA radiograph 3 years later demonstrating obvious enlargement of the radiolucency with increased root resorption of tooth #30.

258 Texas Dental Journal | Vol 141 | No. 5
L
Figure 1. Radiolucency of the right mandible in the furcation area of #30, with ill-defined margins and spiking resorption of the adjacent tooth roots.
buccal or lingual cortical plate expansion of the mandible was detected on the clinical exam.
The patient was referred to an oral surgeon for evaluation and a potential biopsy of the area; however, this referral was generated during the COVID-19 pandemic. Due to fear of both surgical treatment and coronavirus exposure, the patient failed to seek out any specialist care.
She returned to the clinic 3 years later for routine care and admitted to never having addressed the area or seeing the oral surgeon. A periapical radiograph revealed that the lesion had greatly expanded in size, and there was further resorption of the roots of #30 (Figure 2). Still, there was little evidence of expansion of the alveolus clinically at that time (Figure 3).
At this point, the patient did agree to see the surgeon and to undergo cone beam computed tomography (CBCT) imaging studies at that office. A panoramic view of the CBCT scans revealed the lesion to measure approximately 22-17mm (Figure 4). During surgery, tooth #30 was extracted, the lesional tissue was removed and submitted for histopathologic evaluation, and the site was thoroughly curetted. No graft material was placed due to the uncertain nature of the pathologic process at the site.
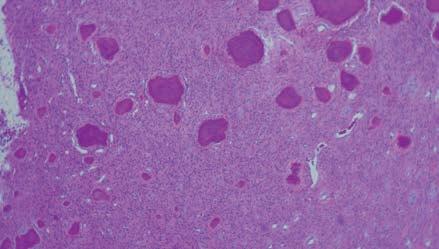
Microscopic examination reveals a cellular tumor composed of bundles of plump to spindle cells set within a fibrous matrix. Mitotic figures are rare. Round calcifications exhibiting concentric ring lines were noted scattered throughout the lesional tissue (Figure 5).
What is your differential diagnosis?
What is your final diagnosis?
See page 260 for the answer and discussion.


www.tda.org | June 2024 259
Figure 3 Clinically, expansion of the right mandible is not appreciated.
Figure 4. Reconstructed panoramic radiograph from cone beam data, demonstrating the lucency measures approximately 22x17mm.
Figure 5. H&E section at 10x magnification exhibits a cellular lesion composed of plump spindle cells and interspersed psammoma body calcifications.
ORAL and maxillofacial pathology
diagnosis and management—from page 258
Diagnosis and Management:
Aggressive Ossifying Fibroma, Psammomatoid variant
Discussion
Aggressive ossifying fibroma (also termed “Juvenile ossifying fibroma”), is an uncommon tumor that can affect the jawbones or craniofacial skeleton and is known to possess the potential for rapid growth, high recurrence rate and destruction of local tissues and structures. Two known variants are recognized based on microscopic findings: trabecular and psammomatoid.
The psammomatoid variant outnumbers trabecular cases by a ratio of four to one. There are demographic differences in age between the variants, with the trabecular form typically being diagnosed in younger patients at 11 years of mean age. The mean age of the psammomatoid variant is 22 years. There is a predilection for occurrence in the maxilla, and slightly more cases occur in males than females.1
The psammomatoid variant is also reported to arise 70% of the time in the orbital and frontal bones and paranasal sinuses. Most frequently, aggressive ossifying fibroma is noted incidentally on radiographic exams. It may also be discovered due to complications secondary to tumor growth into adjacent structures. This may result in nasal obstruction, exophthalmos, or blindness if the tumor is adjacent to the optic nerves.
Although genetic studies of aggressive ossifying fibroma are not well established, non-random chromosome break points at Xq26 and 2q33 resulting in (X;2) translocation have been found. Also, alterations of the HPRT2 tumor suppressor gene have been identified in half of the cases.2
Treatment is complete local excision with thorough curettage for small lesions. Larger lesions may require resection. Recurrence rates of 30-58% have been noted in the literature, therefore close follow-up is mandatory. There are no reports of malignant transformation.3
Treatment is complete local excision with thorough curettage for small lesions. Larger lesions may require resection. Recurrence rates of 30-58% have been noted in the literature, therefore close follow-up is mandatory.
260 Texas Dental Journal | Vol 141 | No. 5
The differential diagnosis for this lesion includes conventional ossifying fibroma, cemento-osseous dysplasia, or metastatic disease. While conventional ossifying fibroma may also display root resorption and intra-lesional calcifications, the histology will lack the cellularity of the fibrous component as compared to aggressive ossifying fibroma. Cemento-osseous dysplasia would less commonly exhibit root resorption, and also be distinguishable on histologic examination. Metastatic disease would have notably different histology and additional studies would indicate the site of the primary tumor.
For this patient the site was never grafted but did demonstrate good bone fill in imaging done 6 months after surgery (Figure 6). Although the potential for placing an implant in the site was discussed, ultimately this was decided against due to the uncertain nature of aggressive ossifying fibroma. The patient may elect to do a bridge in the future to restore the missing tooth #30.
The clinical differential diagnosis for this case includes odontogenic keratocyst, ameloblastoma, myxoma, lymphoma, or metastatic tumor from a distant site.
Thanks to Dr Ryan Parnell for providing surgical care for this case.
References
1. Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology, 3rd edition. Philadelphia: WB Saunders Company 2009; location 26058.
2. Juvenile Ossifying Fibroma: A Clinicopathologic Study of 8 Cases and Comparison with Craniofacial Fibro-osseous Lesions, Park S et al, The Korean Journal of Pathology 2007; 41: 373-9.
3. Nelson, BL. Head and Neck Pathology, 3rd edition. Elsevier, 2019; under “Benign Neoplasms of the Gnathic Bones”.

www.tda.org | June 2024 261
Figure 6. Reconstructed panoramic radiograph from cone beam data after 6 months of healing, demonstrating adequate bone fill of the surgical site with no remaining radiolucent areas.
value for your profession
Provided


Making Sense of Capnography in Your Dental Office
By Rose Dodson, MSc, CEO; Sedation Resource, Inc.
Let’s Talk About Capnography in Dental Offices
Capnography stands out as an essential monitoring tool that is reshaping patient safety in dental practices, especially during sedation. Whether you are a seasoned dentist or a dental assistant looking to broaden your expertise, understanding how to use this monitoring tool can greatly enhance patient care.
This guide is tailored for the entire dental team, combining fundamental capnography principles with practical application. It is designed to bring clarity to this valuable technology and aims to equip every team member with the knowledge to effectively utilize capnography for enhanced patient monitoring and care.
262 Texas Dental Journal | Vol 141 | No. 5
by: PERKS P R O G R A M
The Role of Capnography in Monitoring Sedated Patients
Capnography measures the carbon dioxide that comes out when a patient exhales, giving us forewarning if they start having trouble while sedated. It is like getting a play-by-play of their breathing, which helps us evaluate how well their lungs are working when viewing the waveform patterns on the monitor’s screen. However, this is predicated on having accurate readings.
Overcoming the Challenge of Moisture
When a patient breathes out, there is always a bit of moisture mixed in with the air. Capnography devices require a moisture-free sample of breath to accurately measure CO2 levels. Each monitor has its own method of accomplishing this, either via a moisture trap or dehumidification tube. This not only ensures that the readings we get are accurate, but also helps in protecting the internal CO2 device from moisture exposure, which can extend the lifespan of the monitor.
The Right Sampling Strategy
Selecting the right sampling line is an important aspect of effectively monitoring CO2 levels. It is imperative to select the correct sampling lines based on your method of administering oxygen.
Oxygen Delivery via a Nitrous Hood:
• Nasal Sampling Cannula: The most accurate CO2 measurements for non-intubated anesthesia, like moderate sedation, are achieved with a nasal sampling cannula. When using nitrous oxide, this cannula’s thin-walled design allows it to fit comfortably under the hood.
• Straight Sampling Line Alternatives:
Trimming Method: Carefully maneuver the sampling line to run it alongside the nitrous hood. Then, tuck it under the nostril to ensure it is exposed to the patient’s exhaled breath, allowing the monitor to accurately detect CO2 levels.
Hood Puncture Method: Make a round opening in the nitrous hood for a nitrous hood adapter. Once the adapter is in place, the male luer on the sampling line can be securely attached to the female luer of the adapter. Inline Adapter: More recently, plastic adapters have been developed specifically to work with nitrous hoods. These are available in single lumen and double lumen formats.
Each option is tailored to effectively gather CO2 levels, while prioritizing the patient’s comfort during the entire sedation procedure. It is important to understand that scavenging can affect the monitor’s ability to capture a sample of the patient’s breath.
Oxygen Delivery via a Cannula:
The ideal configuration for administering oxygen and monitoring CO2 during sedation involves a cannula designed with a two-tube system. One tube connects to the oxygen supply, and the other attaches to the water trap on the capnography monitor.
Each prong of the cannula serves a specific purpose: one delivers oxygen, and the other samples the exhaled air. This arrangement prevents the mixture of fresh oxygen with exhaled CO2, ensuring a clear and accurate assessment of the patient’s breathing.
While some cannulas aim to deliver oxygen and measure CO2 through both nostrils simultaneously, this can sometimes compromise the accuracy of the CO2 readings. A cannula that separates these functions, assigning one to each nostril, ensures the patient receives consistent oxygen flow and CO2 measurements are as accurate as possible, which is crucial for patient care during sedation.
The Importance of Calibration
Calibrating your capnography monitor is like setting a scale to zero before you weigh something—it makes sure the readings are on point. Even though most monitors adjust themselves from time to time, doing a quick calibration check before each patient can make your equipment last longer and give you better results. It is a simple step, but it makes all the difference in getting accurate information for every case.
Conclusion
Capnography is an indispensable tool in the dental office, especially when providing sedation. It empowers both dentists and dental assistants with immediate feedback on the patient’s breathing and, ultimately, their safety. Embracing this technology means embracing a commitment to the highest level of patient care.
Sedation Resource, Inc. is endorsed by TDA Perks Program. It is dedicated to supporting dental professionals in providing safe and effective care with the help of advanced monitoring technologies. For more information regarding Sedation Resource, visit tdaperks.com (Compliance and Supplies) or call (903) 634-5333.
www.tda.org | June 2024 263
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN-NORTH (ID #604):
Legacy FFS practice with an impeccable reputation located in a budding community north of Austin. The office has relied solely on word-of-mouth referrals with very little marketing/advertising and refers out many specialty procedures leading to upside potential for an incoming buyer. The real estate is also available for purchase. AUSTIN (ID #636): Rare opportunity to purchase a turnkey, FFS/PPO general dentistry practice and real estate in Austin. This spacious 2,500 sq ft office features 4 operatories, digital radiography, iTero, and paperless charts. The practice is situated in a highly desirable Austin community. AUSTIN (ID #662): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business.
DALLAS-PEDO/ORTHO (ID #665): Legacy Pedo/ Ortho practice in the heart of north Dallas. Thriving practice, large fee-for-service patient
264 Texas Dental Journal | Vol 141 | No. 5
base, revenue of 7 figures. Over 2,800 sq ft, fully digital with computers in the operatories, digital radiography, and a digital Pano.
FORT WORTH (ID #664): Established, fee-for-service general dentistry practice in Fort Worth with computerized operatories, digital X-ray sensors, CBCT, and paperless charts. There is plenty of room to continue growing by adding several specialty procedures currently being referred out.
HOUSTON-SOUTHWEST (ID #627): Legacy GD practice with majority FFS patient base in a growing southwest Houston suburb. Located in a retail center on a busy intersection, this 1,200 sq ft office features 4 fully equipped ops plumbed for nitrous, computers throughout, digital radiography, a digital scanner, intraoral cameras, and paperless charts. HOUSTONSOUTHEAST (ID #644): 100% FFS, legacy practice in SE Houston. The 2,500+ sq ft office features 7 ops, computers throughout, digital pano, digital x-rays, digital scanner, intraoral cameras, and paperless charts. If you’re looking for a centrally located, profitable practice with a dedicated patient base and room to grow, call us now for more details.
HOUSTON-ORTHO (ID #673): Rare opportunity to purchase an orthodontic practice and real estate in a wellestablished north Houston suburb. State-ofthe-art facility, top-of-the-line digital technology,
including a digital pano and a digital iTero scanner. The practice has shown consistent annual growth over the past years on 3 doctor days per week. HOUSTON-SOUTHWEST (ID #674): Highly profitable, turn-key, PPO/ FFS general dentistry practice Southwest of Houston. High-visibility office, 4 computerized operatories, digital X-ray sensors, digital pano, Cerec scanner, Cerec milling unit and oven, and intraoral cameras. The practice has exceptional net cash flow. 1,400+ active patients, 20+ new patients per month, 30% hygiene production and exceptional net cash flow. The real estate is available for sale.
NORTHEAST TEXAS (ID #584): 100% FFS general dentistry practice in a desirable town in northeast Texas with 7 figures in revenue and strong net income. The turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCT, and a digital scanner. SAN ANTONIO (ID #654): PPO/FFS general dentistry practice in San Antonio. The 3,000+ sq ft office is prominently located on a busy street and features 6 computerized operatories, digital x-ray sensors, digital pano, digital scanner, intraoral cameras, and paperless charts. With 2,000+ active patients, 25+ new patients a month, and a stellar reputation, this practice is poised for continued
www.tda.org | June 2024 265
classifieds
success. SOUTH TEXAS (ID #651): General dentistry practice located in south Texas. This state-of-the-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld X-ray units, and a 3-D printer. The practice serves a large PPO/Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow.
SOUTH TEXAS (ID #668): Thriving south Texas practice (with real estate) that has established itself as the premier dentistry provider in the local community. This one-doctor practice has a massive active patient base, strong hygiene production, and generated revenue of 7 figures. The real estate is available for purchase and features 6 equipped operatories and state-of-the-art equipment (CBCT, digital intraoral scanner, and CAD/CAM milling unit). This may also be an ideal fit as an associaterun practice for a Texas-based group practice owner. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATESí LISTINGS: Please register at www.dentaltransitions. com or contact us at 512-900-7989 or info@ dentaltransitions.com.
EAST TEXAS: Exceptional practice opportunity in Troup, Texas. Seeking associate to join high quality, well-established dental practice with a
long history of excellence. This is an exceptional opportunity to move into ownership after a successful initial employment phase. Must be committed to providing optimal patient care with exceptional technical skills, strong people skills, personal integrity, honesty and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on Christian values and professional growth. Our office expansion should be complete mid to late September 2024, but the new associate could begin in August if he/she would like. Please reply in confidence with your CV and a letter outlining your future objectives and goals to: drmay@troupfamilydental.com or call our office at 903-842-4600.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 sq ft with 3 total operatories: 2 for dentistry and 1 for hygiene. Please let me know if you need anything else from me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to
266 Texas Dental Journal | Vol 141 | No. 5
19 days per month. Collection ratio of 99%. Practice is a fee for service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
ROCKPORT: Practice for sale in Rockport. Two chairs, plumbed for 3. Currently being worked 3 days a week producing near mid6 figures. Fee-for-service, no DMO, HMO or PPO contracts. Hygienist 3 days a week and will stay, been with practice since 2019. Digital X-rays, paperless, Newtom 3D/Panorex, (3) X-ray sensors. Practice is in older house, which can be leased or purchased. Great starter practice or for someone slowing down and wants to live on the coast. Send inquires to jim@jlongdds.com or call: 281-726-1812, leave message.
TRINITY: Six operatories, 3,700 sq ft office. Retired from practice established in 1973. No other practicing dentist in the county. Contact Dr Bubba Hirsch 936-594-2424 or drbubbahirsch@gmail.com.
WATSON BROWN PRACTICES FOR SALE:
Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
DSO C S PRACTICE SALES
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com PRACTICE APPRAISALS
www.dentaltransitions.com
www.tda.org | June 2024 267
268 Texas Dental Journal | Vol 141 | No. 5

Recruit for Rewards Caring • Connections
• Create • Commitment
You know first-hand the value you receive from your ADA membership. Through the community and resources you’ve come to count on, the ADA provides the support you need to help achieve your goals. You can help colleagues and friends thrive by inviting them to join the ADA.

For every 5 new members
you recruit, you’ll receive a chance to win a 7-day interisland Hawaiian cruise* for you and a guest.
Eligibility
Who can recruit? Any ADA member dentist (including graduate student, resident, active licensed, active life, retired and retired life) is eligible to participate as a recruiter
Who can be recruited? Any degreed dentist who was not an ADA member in 2023 (including graduate students, residents)
Who is not eligible to be recruited for this program?
• A renewing member (someone who was a member in 2023)
• Dental students
• Retired dentists
How to Participate
• Newly recruited members are required to indicate the recruiter’s name and contact information as a referral on the membership application.
• ADA member recruiters will receive an email notification after the dentist referred has been accepted into membership.
• A raffle entry for quarterly drawings will be awarded for each new, active member recruited who pays national dues (as applicable) in the current year. Recruiters will receive a chance to win a 7-day Hawaiian cruise* for every five new recruited members who pay national dues (as applicable).
Recognition
• All recruiters will be recognized at SmileCon 2024. Top recruiters will receive additional recognition.
• Quarterly winners and top recruiters will be announced in ADA Morning Huddle.

For each new member
you recruit, you’ll be entered into a quarterly drawing for a chance to win $1,000 in prizes from ADA-endorsed providers or products from the ADA Store.
Program Rules
• This program will run January 1 – August 31, 2024.
• For each new, active member who joins in that timeframe, the referring member’s name will be entered into quarterly drawings for a chance to win $1,000 in prizes from ADAendorsed providers or products from the ADA Store. Referring members will also receive a chance to win a 7-day interisland Hawaiian cruise* for every five new, eligible members they recruit.
• Referring members will receive a qualifying entry each time their name is listed as the “referring member” on the new member’s application (one entry for quarterly drawings for every one member recruited, one entry for the grand prize drawing for every five members recruited). There is no limit to the number of new members who can be recruited or entries in the drawing.
• Referring members will automatically win a quarterly prize (up to $1,000 value) when they recruit 25 eligible new members. Quarterly prize winners are also eligible to win the grand prize should they recruit at least five new members.
• The grand prize drawing will take place at SmileCon® 2024 in New Orleans. SmileCon attendance is not required to win.
* The grand prize winner will receive a 7-day interisland Hawaiian cruise with a balcony room and airfare for two to be redeemed in 2025, an estimated value of $7,500. If winners do not wish to claim the Hawaiian cruise package, they are able to select another trip from AHI’s catalog at equal or lesser value, or take a cash prize option of $3,500. Learn more about the available cruises provided by ADA Member Advantage endorsed partner, AHI Travel.
The ADA Member Recruitment Initiative is subject to all applicable federal, state and local laws and regulations, and is void where prohibited by law. Visit ADA.org/R4R for more details.
www.tda.org | June 2024 269
© 2023 American Dental Association All rights reserved. Updated: 12/11/2023
270 Texas Dental Journal | Vol 141 | No. 5 YOUR PATIENTS TRUST YOU. WHOM CAN YOU TRUST? If you or a dental colleague experiences impairment due to substance use or mental illness, the Professional Recovery Network is here to provide support and an opportunity for confidential recovery. PRN Helpline (800) 727-5152 Visit us online www.txprn.com AFTCO .......................................................................... 229 Anesthesia Education & Safety Foundation, Inc. 223 Choice Transitions ............................ Inside Back Cover Henry Schein Financial Services .............................. 229 Huynh and Huynh PLLC 228 JKJ Pathology ............................................................... 226 Law Offices of Mark J. Hanna ................................... 231 McLerran & Associates.............................................. 267 MedPro Group............................................................ 227 Professional Recovery Network ............................... 270 Professional Services Technologies ......................... 228 Southwest Sedation Education 228 TDA Perks .......................................... Inside Front Cover Texas Health Steps .................................................... 225 UTSD Houston ............................................................ 231 Watson Brown ............................................................ 230 ADVERTISERS
Since 1996, our team of experts have provided successful transition services exclusively to dentists. Choice prides itself on its reputation for integrity, service and results.

Considering selling
Scan the QR code to watch a brief and informative video to help you decide.



www.tda.org | June 2024 271
C e.
) DSO-INF etr e walk oc t off ess str tia eceiv e f actice ver e o c ta es t g y fees! If y e c o a DSO y rec c ectly c s.
to a DSO?

