TDA’S 2025 LEGISLATIVE AGENDA: SHAPING THE FUTURE OF DENTISTRY IN TEXAS! DR MATTHEW B. ROBERTS, CHAIR, COUNCIL ON LEGISLATIVE, REGULATORY, AND GOVERNMENTAL AFFAIRS
540 THE POWER YOU HAVE IN TEXAS POLITICS
DR R. LEE CLITHEROE, DENPAC CHAIR
542
SUPPORTING DENTISTS: THE TEXAS DENTAL ASSOCIATION’S WORK WITH THE TEXAS STATE BOARD OF DENTAL EXAMINERS
550 OFFICE OF INSPECTOR GENERAL DENTAL CASE REVIEW AND ANALYSIS
554 2025 TDA MEETING PREVIEW
ADAM SALTZ, DMD, MS, MPH
565 ASK THE POWERS CENTER
MARTA REVILLA-LEÓN, DDS, MSD, PHD
JONATHAN M. ZEITLER
JOHN C. KOIS, DMD, MSD
GUEST EDITOR RADE D. PARAVINA, DDS, MS, PHD
Anesthesia
Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management
Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
532 TDA’S 2025 LEGISLATIVE AGENDA: SHAPING THE FUTURE OF DENTISTRY IN TEXAS!
Dr Matthew B. Roberts, Chair, Council on Legislative, Regulatory, and Governmental Affairs
534 TDA’S 89TH LEGISLATIVE SESSION AGENDA 540 THE POWER YOU HAVE IN TEXAS POLITICS
Dr R. Lee Clitheroe, DENPAC Chair
SUPPORTING DENTISTS:
554 2025 TDA MEETING PREVIEW:
Adam Saltz, DMD, MS, MPH
565 ASK THE POWERS CENTER
Marta Revilla-León, DDS, MSD, PhD
Jonathan M. Zeitler
John C. Kois, DMD, MSD Guest Editor Rade D. Paravina, DDS, MS, PhD
HIGHLIGHTS
560 Oral and Maxillofacial Pathology: Case of the Month
562 Oral and Maxillofacial Pathology: Case of the Month Diagnosis and Management
566 Value for Your Profession: Protecting Your Practice from Supply Chain Attacks
Classifieds 574 Index to Advertisers
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 141 | No. 8
Texas Dental Association 8701 W Hwy 71, Ste 201-M Austin, TX 78735
Texas Dental Journal (ISSN 0040-4284) is published monthly except January-February and August-September, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2024 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement included in the online September Annual Membership Directory or on the TDA website: tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service with hightechnology solutions so that you can better serve your patients.
Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com Protecting your
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
PAST PRESIDENT Duc “Duke” M. Ho, DDS 281-395-2112, ducmho@sbcglobal.net
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
Adam S. Awtrey, DDS 314-503-4457, awtrey.adam@gmail.com
SENIOR DIRECTOR, NORTHEAST
Drew M. Vanderbrook, DDS 214-821-5200, vanderbrookdds@gmail.com
DIRECTOR, SOUTHEAST Ron Hill, DDS 713-626-8343, rhilldds@gmail.com
DIRECTOR, SOUTHWEST
Oshmi Dutta, DDS 210-888-0700, odutta@gmail.com
DIRECTOR, NORTHWEST
Annie C. Wilson, DDS 817-860-4343, annie@anniewilsondds.com
DIRECTOR, NORTHEAST
Shane A. Ricci, DDS 972-381-1888, riccidds@hotmail.com
SECRETARY-TREASURER*
Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN**
Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR**
Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL
Carl R. Galant
EXECUTIVE DIRECTOR
Linda G. Brady CAE 512-443-3675, lbrady@tda.org
*Non-voting member **Non-voting
INSPIRING DREAMS
Michelle Phillips, D.D.S. Luis Ortega Regueira, Sr., D.M.D.
Asra S. Hashmi, D.D.S. & Zayd M. Hashmi, D.M.D.
We
Practices For Sale
FANTASTIC TEXARKANA LOCATION: GP in a bustling retail center with great visibility. The office has 3 ops, digital X-ray, and paperless patient charts. The practice has over 1,200 active patients that are a mixture of 20% FFS and 80% PPO. The seller refers out most specialties, and the practice operates on 3.5 doctor days and 4 hygiene days, leaving ample room for growth. Opportunity ID: TX-02243
FANTASTIC RETAIL LOCATION: Plano GP that is highly visible in a retail center. This practice operates with the owner and 1 PT associate, is open 7 days a week and provides regular dental care as well as emergency services. The practice has over 1,750 active patients who are 20% FFS, 70% PPO, and less than 10% Medicaid. The office has 4 ops and is in excellent condition. This is a great opportunity for growth by capitalizing on the existing patient base and expanding services. Opportunity ID: TX-02219
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Excellent opportunity for growth by adding a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02171
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS with a small amount of PPO. The office collected over $876K in a four-day workweek. Opportunity ID: TX-02041
TDA’s 2025 Legislative Agenda: Shaping the Future of Dentistry in Texas!
Dr Matthew B. Roberts, Chair, Council on Legislative, Regulatory, and Governmental Affairs
The 89th Regular Legislative Session begins on January 14, 2025. However, at the Texas Dental Association (TDA), the work has already begun. TDA’s legislative team, together with the Council on Legislative, Regulatory, and Governmental Affairs, is already advocating for your interests and keeping a close watch on activities at the Texas Capitol.
Let’s start by examining how the elections will influence the political dynamics. In the Senate, Republicans secured the only competitive seat, giving them a 2011 majority. However, the main focus is on the Texas House, where Republicans will hold 88 of the 150 seats. While this doesn’t mark a major change in numbers, the arrival of many new members could significantly influence the direction House Republicans take in the upcoming speaker’s race.
The new freshman class of 26 Republican lawmakers is the largest since 2013, giving the party’s far-right faction an exceptional level of influence in the upcoming legislative session. When discussing Republican gains
during this election cycle, Governor Abbott was quoted as saying, “Texans sent a clear message: they want safer streets, a secure border, a strong economy, and the opportunity to choose the best school for their children.”
The legislative session’s political dynamics are influenced not just by the individuals involved but also by the key issues at play. Governor Greg Abbott and Lieutenant Governor Dan Patrick have emphasized that school vouchers will be a top priority. Additionally, prefiled bills suggest other prominent topics will include reducing property taxes, addressing specific social issues, further dismantling diversity and inclusion programs in higher education, enhancing border security, and tackling problems related to power grid reliability.
How does this impact the TDA’s legislative agenda? It means that getting dentistry’s priorities noticed by lawmakers will be a challenge. However, the TDA excels in advocacy and has already begun its efforts to ensure that legislators are well aware of the issues that matter most to dentists across Texas.
TDA’s 89th Legislative
Session Agenda
Increasing Medicaid Dental Funding: Expanding Care for Texans
TDA recognizes that meaningful improvements to Medicaid dental reimbursements depend on the Texas Legislature increasing General Revenue (GR) funding for Medicaid dental services.
To address this, TDA is advocating for a $250 million annual GR increase to restore Medicaid dental fees to their 2007 levels, adjusted for inflation. This funding is critical to ensure that dentists can continue participating in the Medicaid program and that all Medicaid patients have access to quality dental care.
In preparation for difficult Medicaid budget discussions, TDA is simultaneously working on a secondary funding proposal asking for targeted fee increases for 30 Medicaid dental codes equating between $30-$35 million in GR annually.
Additionally, TDA will support legislative initiatives to reduce administrative burdens for dentists in Medicaid-managed care. These efforts include improving the efficiency of claims administration and enhancing the reimbursement process for participating dentists.
Dental Insurance Reform: Limiting Bundling and Downcoding
TDA is pursuing legislation limiting the circumstances where state-regulated dental plans can bundle and downcode dental codes. Insurance companies sometimes adjust the dental procedure codes submitted by dentists; a practice known as “downcoding.” This happens when the insurer reviews the dentist’s submitted codes for the patient’s treatment and decides the original coding was either incorrect or unnecessarily broken into smaller parts (called “unbundling”).
Downcoding can harm dental practices by reducing the payments dentists receive for the dental care they provide. This forces dentists to accept less money than they should, making it harder to cover their business expenses. In the long run, this could negatively impact patients’ quality of care.
For patients, downcoding increases out-of-pocket expenses, making dental care less affordable. Additionally, it can damage the trust between patients and their dentists. When dental procedures are downcoded, patients may feel that they are receiving less care than they are entitled to, leading to dissatisfaction and a weakened dentistpatient relationship.
Furthermore, TDA will strongly oppose any legislative efforts that would allow third-party payers to interfere in the direct relationship between dentists and their patients. Protecting the integrity of this relationship is essential to ensuring that patients receive the best care possible.
Fair Dental Coverage:
Monitoring Dental Loss Ratios
TDA conducted extensive research and engaged in detailed discussions about the potential benefits of pursuing a Dental Loss Ratio (DLR) in Texas. Several factors were taken into account, including the absence of state-specific data due to Texas not having a reporting requirement. After careful consideration, the decision was made to monitor the progress of DLR legislation. Additionally, TDA will keep track of DLR developments in other states and reassess its stance if necessary.
DELRP Funding:
Helping Dentists Serve Texans in Need
TDA supports reinstating GR funding to the Dental Education Loan Repayment Program (DELRP) for 400 dentists to earn up to $200,000 over 4 years in loan repayment assistance for practicing in rural and underserved areas of Texas.
According to the most recent Health Resources and Services Administration’s Quarterly Summary, as of September 30, 2024, 367 dentists are needed across the designated areas of Texas to eliminate all of Texas’ Dental Health Professional Shortage Area designations (DHPSAs).1 Texas can effectively redistribute the dental workforce to rural and underserved areas by reinstating funding for the DELRP.
Improving Oral Health Access:
Strengthening Texas Public Health Dental Programs
TDA will advocate for legislation that ensures the Oral Health Improvement Program (OHIP) at the Texas Department of State Health Services is led by a Texas-licensed dentist. Additionally, TDA will push for the restoration of state GR funding for OHIP.
TDA strongly supports maintaining a strong dental public health safety net in Texas, which includes programs that assist populations with limited access to dental care. A key component of this safety net is the OHIP.
TDA is only as successful as your support. We need every member dentist engaged in TDA’s legislative agenda. If you can, please give to DENPAC. If you are interested in helping TDA achieve its legislative goals, become a key contact dentist by emailing Staci Rives at srives@tda.org for more details.
By having a dentist lead the OHIP, the program will be better positioned to operate effectively. Restoring state funding will help ensure that each dental health region is adequately staffed and will allow the OHIP to expand its services, providing low-cost or free direct dental care to Texans who depend on the dental safety net.
Supporting the TSBDE:
Ensuring Resources for Public Safety
It is a long-standing tradition that TDA supports adequate funding for the Texas State Board of Dental Examiners (TSBDE). The TSBDE needs adequate funding to effectively fulfill its responsibilities of safeguarding public health and maintaining high standards in dental care.
Investing in Dental Education:
Building Texas’ Oral Health Future
TDA supports the 3 legacy dental schools’ clinic operations proposal for at least $6 million per biennium for each school. The Texas Tech University Health Sciences Center El Paso Woody L. Hunt School of Dental Medicine
received a dedicated clinic operations funding increase during the 2023 legislative session.
TDA will also support funding to Texas’ dental schools to help lower tuition costs for dental students. This will help Texas dental students enter the workforce with less concern about high student loan debt.
Preserving Dentists’ Independent Professional Judgement
TDA will continue working with lawmakers to determine if additional steps are needed to address patient safety issues with certain types of dental practice models. TDA embraces innovation and diversity among dental practice models in Texas. However, each model must comply with Texas laws and regulations.
Maintaining Texas Standards:
Opposing Dental Licensure Compacts
TDA will oppose legislation creating licensure compacts for dentists and dental hygienists. While TDA acknowledges the difficulty in recruiting and retaining qualified dental healthcare professionals in Texas, no evidence supports that a licensure compact would result in dentists and dental hygienists practicing in rural and underserved areas of Texas.
Texas licenses a significant number of new dentists and dental hygienists each year and provides for expedited licensure of military personnel, veterans, and their spouses. The workforce issue in Texas is not the lack of dentists but having them practicing in Texas’ rural and underserved areas.
TDA understands the challenges many dentists face in hiring dental hygienists. TDA supports proven efforts to increase the number of dental hygienists working in Texas. This includes increased state funding to help dental hygiene education programs expand class size as well as potentially brining new dental hygiene education programs to Texas.
These incentives encourage more people to enter the profession while maintaining Texas’ educational and licensing criteria.
Empowering Dentists:
Supporting Botox Administration for Better Patient Care
TDA will pursue legislation authorizing any Texas-licensed dentist to use a neuromodulator that is derived from Clostridium botulinum or is biosimilar to or the bioequivalent of such a neuromodulator for solely aesthetic purposes.
Dentists are uniquely qualified to administer neuromodulators due to their extensive knowledge of facial anatomy, including the muscles, nerves, and tissues involved in cosmetic procedures. Dentists possess the expertise to safely perform such injections. This expertise is crucial for ensuring patient safety, as improper injection techniques can lead to complications such as muscle weakness, nerve damage, or undesirable cosmetic outcomes.
Preserving Quality Care: Opposing the Dental Therapist Model in Texas
TDA will oppose legislation creating a dental therapist in Texas. TDA is committed to identifying and advancing solutions that meaningfully address barriers to oral health care for Texans. Helping all Texans attain the optimal oral health they deserve is a core commitment of the TDA. Every Texan deserves comprehensive care provided by a dentist.
As we enter the 89th legislative session, TDA’s strong advocacy efforts will continue to fight for the interests of Texas dentists. With a clear focus on key issues, a dedicated team, and unwavering support from our members, we are confident that our collective efforts will drive meaningful change.
TDA Ignites Momentum for the 89th Legislative Session
As you can see, despite the political challenges TDA will likely face in 2025, TDA is committed to having a robust legislative agenda that supports dentists and the patients they serve. TDA is only as successful as your support. We need every member dentist engaged in TDA’s legislative agenda. If you can, please give to DENPAC. If you are interested in helping TDA achieve its legislative goals, become a key contact dentist by emailing Staci Rives at srives@tda.org for more details.
We will keep you informed throughout the legislative session by emailing you The Root. If you have questions, do not hesitate to reach out to me or TDA’s Public Affairs Director Mr Jess Calvert, at jcalvert@tda.org.
As we enter the 89th legislative session, TDA’s strong advocacy efforts will continue to fight for the interests of Texas dentists. With a clear focus on key issues, a dedicated team, and unwavering support from our members, we are confident that our collective efforts will drive meaningful change. Together, we will ensure that Texas dentistry thrives and that our profession remains well-supported and protected throughout this session and beyond.
Resources
1. Bureau of Health WorkforceHealth Resources and Services Administration. Designated Health Professional Shortage Areas Statistics. Third Quarter of Fiscal Year 2024. Designated HPSA Quarterly Summary as of September 30, 2024. Accessed November 20, 2024.
The Power You Have
Dr R. Lee Clitheroe, DENPAC Chair
It’s not what you know, it’s who you know. You’ve heard that saying, right? Well, it’s true, especially in politics. Two things matter most when it comes to being influential in politics—relationships and resources. Luckily for you as a Texas dentist, the Texas Dental Association prioritizes both on your behalf. But it’s not that simple, because TDA doesn’t have either without the involvement of members like you.
That’s where DENPAC and its “key contact” dentist program comes in. Key contact dentists are TDA members who have a relationship with their state senator and/or state representative. They volunteer their time and resources to help advance TDA’s legislative and regulatory agendas. These key contacts may be asked to reach out to the legislator in their district when legislative issues affecting dentistry arise. And because these key contacts have already established a relationship with their legislator, they are more effective at influencing and achieving success.
Put yourself in a lawmaker’s shoes. If you were them, and there was a bill before you that you needed to vote on, but it was on a subject matter that was completely out of your wheelhouse, who would you trust for guidance? Would it be a random lobbyist who walked into your office, issuing impersonalized pleas, or would it be a constituent who lives and works in your district, who you know has the personal knowledge and experience to provide wise counsel on this subject? I think the choice is clear.
Ready to get involved? Whether it’s by making a phone call, sending an email, attending a meet-and-greet, or volunteering at a campaign event, there’s one more piece of the puzzle for you to consider. While you work on establishing a one-on-one relationship, TDA still needs to establish and maintain relationships with hundreds of state candidates and officials. And that takes resources.
As a political advocacy arm of the TDA, DENPAC uses voluntary contributions from member dentists to support election campaigns of state candidates who are friends to TDA—meaning they are supportive of access to care, oral health, and organized dentistry. The financial support that DENPAC provides allows TDA’s legislative team to foster close relationships with these lawmakers and is a crucial part of the continued legislative achievements TDA has been able to attain.
But DENPAC can’t continue to foster political relationships without contributions from members like you. Especially in times like this most recent election cycle where at the state level in Texas we saw a record number of turnovers, meaning there will be dozens of new faces at the Capitol when the 89th Legislature begins in January. None of those new legislators are dentists—they don’t know TDA, and they certainly don’t know what issues you’re facing and what is important to you, your practice, or your patients.
We need you. Every contribution, regardless of size, makes a difference. Will you donate today? Visit denpac.org to learn more and make an investment now.
Want to learn more about being a key contact dentist? Email Staci Rives at srives@tda.org for more information.
Thank you to all our current DENPAC members and key contact dentists. Your investments and involvement are making a difference in our profession both now and for future generations.
Scan to join Now
in Texas Politics
DENPAC
Supporting
Every 2 years, the Texas Legislature dives into a whirlwind 140-day session, sifting through thousands of proposed bills. Only a small number make it through to become law. For dentistry, the spotlight lands on the Occupations Code, where most dental laws find their home. The Texas Dental Practice Act is outlined in Chapters 251 through 267 of the Texas Occupations Code, laying out the statutes for dentistry.
Under the Texas Constitution, the power to create laws—like the Dental Practice Act (DPA)—rests solely with the state legislature. Thanks to the DPA, the Texas State Board of Dental Examiners (TSBDE) takes the lead in enforcing state laws and its own regulations. The TSBDE has the authority to investigate licensed dental professionals, impose sanctions, and write binding rules regulating the dental profession.
The TSBDE doesn’t wait 2 years to make changes like the Texas Legislature; its rulemaking process is continuous. Texas dentists need to keep up with the new and changing rules and how they affect dental practice in the state. Staying informed can be tough, but Texas Dental Association (TDA) members have a clear edge. Through its advocacy, TDA represents member dentists at both the state capitol and the dental board, ensuring their voices are heard.
TDA ensures its members stay informed about TSBDE rule updates through various channels, including written publications, emails, and social media postings. Additionally, TDA offers personalized support for regulatory and compliance issues. Members can easily get help with specific legislative or compliance questions by simply reaching out via phone or email. There is also a designated webpage on tda.org for all things TSBDE. Go to Advocacy > Texas State Board of Dental Examiners.
Dentists:
Individual TSBDE Regulatory Compliance Assistance
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
The Texas Dental Association’s Work with the Texas State Board of Dental Examiners
Individual TSBDE Regulatory Compliance Assistance
TDA provides individualized help for member dentists who need TSBDE assistance. Call or email Senior Policy Manager Diane Rhodes at drhodes@tda.org or 512-443-3675 ext 122.
Governor Appoints New Dental Board
In December 2023, Governor Greg Abbott appointed 4 new TSBDE members. The governor appointed Dr Brady Morehead, a general dentist from San Antonio, and reappointed Dr Bryan Henderson, a dentist anesthesiologist from Dallas. Additionally, Governor Abbott reappointed Ms Lori Jones, RDH, from Magnolia, and appointed a new public member, Ms Sarah Lamb of Dallas.
Important TSBDE Rule Changes for 2024
Registered Dental Assistants: Retire Registration
Registered Dental Assistants (RDAs) in Texas can now apply for retired registration status with the TSBDE, with the option to reinstate it later.1 RDAs with a valid registration can request retired status using the TSBDE form before their registration expires. Applications will be denied if there are current or pending complaints or disciplinary actions.
Once approved, retired status waives licensure fees and continuing education requirements for the duration of retirement. While on retired status, an RDA cannot engage in any activities regulated under the Texas Occupations Code. The TSBDE will send confirmation of the RDA’s retired status through an RDA’s online licensing account.
For more information and to access the RDA retirement form, go to TSBDE’s designated webpage titled, “Retire a Registration,” at https://tsbde.texas.gov/licensing/dentalassistants/requirements-to-retire-a-registration/.
Changes to Electronic Prescribing Waivers
The TSBDE simplified the electronic prescribing waiver process by removing the need for dentists to provide a written statement and supporting documents explaining their need for a waiver. Dentists can simply attest to the circumstances requiring a waiver, reducing the administrative burden when asking for a waiver.
In February 2024, the TSBDE published an updated Electronic Prescribing Waiver Form, which dentists must use when applying for a waiver. Dentists can access the form from the TSBDE’s website at https://tsbde.texas.gov/e-prescribing-waiver/.
To find your waiver’s expiration date, visit the TSBDE Public License Search at https:// ls.tsbde.texas.gov/. Approved waivers will display their expiration date under “Electronic Rx Waiver Expiration Date.”
TDA Triumphs in Advancing Local Infiltration Rule for Dental Hygienists
TDA’s advocacy helped shape the TSBDE rule governing dental hygiene local infiltration anesthetic.3 The rule finalized TDA’s historic legislative effort during the 2023 legislative session—House Bill 3824—authorizing properly trained and educated dental hygienists to administer local infiltration anesthetic to patients under certain conditions.
The rule outlines the procedures and requirements for dentists in Texas to delegate the administration of local infiltration anesthetic to dental hygienists holding a TSBDE-issued local anesthetic certificate.
Remember that delegating local anesthetic to a dental hygienist is limited to:
• Infiltration only;
• To non-sedated patients or patients only sedated with nitrous oxide/oxygen inhalation; and
• Only when the hygienist is providing hygiene services within the dental hygiene scope of practice.
A rule summary can be accessed on tda.org at Advocacy > Texas State Board of Dental Examiners > TSBDE Rule Updates > May 2024.
TDA Supports Amended Coronal Polishing Rule for Dental Assistants
The TSBDE amended the coronal polishing rule for dental assistants.4 Thanks to TDA’s support, dentists can more easily delegate coronal polishing to dental assistants.
A Texas-licensed dentist may delegate coronal polishing to a dental assistant if the assistant (1) works under the direct supervision of the dentist; and (2) meets the dental board’s education requirements. A dental assistant does not have to hold an RDA from the TSBDE to perform coronal polishing, but the dental assistant must meet the TSBDE’s coronal polishing rule requirements.
When delegating coronal polishing to a dental assistant, TDA recommends that the delegating dentist maintain documentation showing that the dental assistant met the TSBDE’s education and training requirements for coronal polishing.
Dental Assistants Graduating: CODA-Accredited Dental Assisting Program
A dentist can immediately delegate coronal polishing to a dental assistant who completed their dental assistant training at a CODA-accredited dental assistant program that included specific didactic education and clinical training in coronal polishing.
Dental Assistants Not Graduating: CODA-Accredited Dental Assisting Program
Dental assistants who did not graduate from a CODA-accredited dental assisting program must have 1 year of experience as a dental assistant before completing the required minimum 8 hours of clinical and didactic education in coronal polishing taken through a CODA-accredited dental, dental hygiene, or dental assisting program. The course taken must meet the requirements for coronal polishing education specified in the dental board’s rule.4
The rule finalized TDA’s historic legislative effort during the 2023 legislative session— House Bill 3824— authorizing properly trained and educated dental hygienists to administer local infiltration anesthetic to patients under certain conditions.
A rule summary can be accessed on tda. org at Advocacy > Texas State Board of Dental Examiners > TSBDE Rule Updates > June 2024.
Essential TSBDE Insights: What Every Dentist Should Know
TDA Helps Members Understand TSBDE Continuing Education Requirements
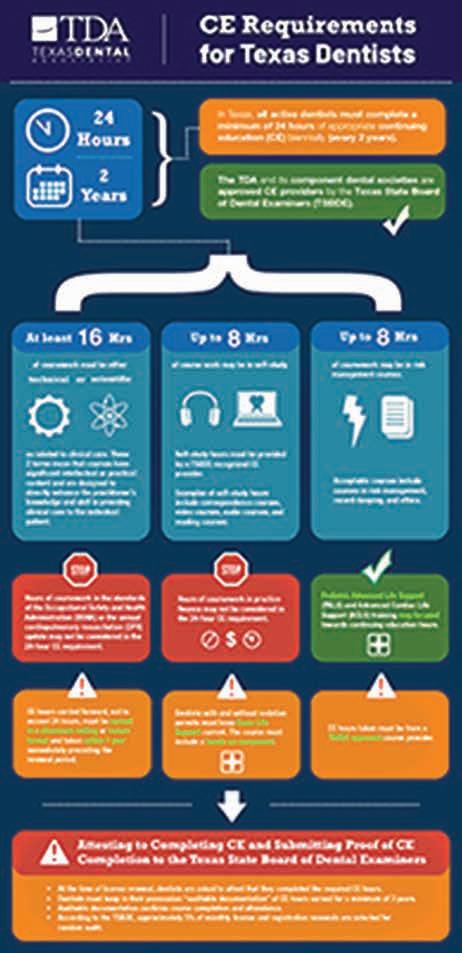
Texas dentists must complete a specific number of continuing education (CE) hours to renew their dental licenses. The required hours and topics can vary depending on the dentist’s role and activities. How do dentists keep track of what’s needed, know where to focus, and what CE the TSBDE accepts?
TDA made it simple by creating an easy-to-read infographic. Visit tda. org > Member Center > select “CE Requirements for Texas Dentists and Staff.” This resource allows dentists to verify their CE requirements, and staff can also find information on CE needed for dental hygiene licenses or dental
TDA CE Infographic
As a Texas dentist, you are required to take a certain amount of CE to renew your dental license. And depending on what you do, the specifics of what CE you need can change. How do you keep track of the hours you need, in what areas, and what’s acceptable by the Dental Board?
PLEASE NOTE: This is only an excerpt of the infographic, and does not show the full requirements. To view the full infographic, go to tda.org > Member Center > click on “CE Requirements for Texas Dentists and Staff.”
Simplify CE for the whole team.
Dentists, hygienists, and RDAs can track and submit CE hours with the TDA Dental Concierge app.
And you can start right now.
Scan here:
assistant registrations. The infographic is regularly updated to stay current with CE regulation changes.
For even more convenience, TDA offers the Dental Concierge CE tracking app. This app lets dentists track CE hours and securely store CE certificates in the cloud. A personalized dashboard helps dentists monitor what courses and hours are needed to renew their license. It also provides access to affordable, high-quality CE courses and lets dentists set reminders for important tasks like license renewal and nonTSBDE requirements, such as x-ray equipment inspections.
Sign up at tdadentalconcierge.com, and download the app on the Apple App Store or Google Play to get started.
TDA Supports Efforts to Focus on the Importance of Mental Health and Well-being
The well-being of dentists and their team members is essential to providing quality patient care, maintaining a healthy work environment, and ensuring the long-term success of dental practices.
In the TSBDE’s August 2024 newsletter, TSBDE Secretary Dr Robert McNeil wrote an article about the importance of mental health and well-being in the dental community. To support that effort, the dental board removed “stigmatizing
DENTAL CONCIERGE
The Dental Concierge is an app and learning management system commissioned by TDA and TDA Perks Program that allows its users to keep track of CE courses taken, which requirements are outstanding, and easily access CE documentation in the event of a TSBDE audit.
tdadentalconcierge com
TDA is dedicated to supporting its members by promoting prodentistry legislation and regulations while keeping you informed about state legislative and regulatory developments.
questions” from its licensing and renewal applications “to remove barriers to seeking help.”
In that article, the TSBDE announced that it was recognized as a 2024 Wellbeing First Champion for ALL IN: Wellbeing First for Healthcare! This annual designation recognizes the TSBDE for removing stigmatizing or intrusive language about mental health from licensure applications.
TDA supports the TSBDE’s efforts to create a safe environment where dental professionals can seek the mental health care they need without fear of jeopardizing their license or employment.
TDA wants you to know that if you are struggling with mental health or substance abuse issues, YOU’RE NOT ALONE. The TDA Council on Professions and Trends created an easy-to-access toolkit to provide members with a diverse supply of resources. Visit https://www.tda.org/member-center/mental-health-resources to access the toolkit.
REMINDER: Requirement to Post License/Registration
Licensees and registrants are required to display their license/registration in every location where the individual is practicing dentistry, dental hygiene, and registered dental assisting.5 If your license/registration expires, immediately stop practicing until your license/registration is active.
Foreign Trained Dentists Working as Dental Hygienists
Only licensed hygienists may perform hygiene services in Texas. While graduates of a non-accredited dental school/program are allowed to perform hygiene services in certain states, this is not allowed in Texas.6
Your Voice is Our Mission:
TDA Advocating for Dentistry at the TSBDE
TDA is dedicated to supporting its members by promoting pro-dentistry legislation and regulations while keeping you informed about state legislative and regulatory developments. TDA actively engages with regulatory and legislative proposals that affect dentistry in Texas, ensuring your voice is heard. Rest assured, TDA will not stand by quietly as decisions are made that could impact your dental practice.
References
1. 22 Texas Administrative Code §114.8, Retired Registration Status
5. 22 Texas Administrative Code §§108.11(a), 114.2(g), Professional Conduct, Registration of Dental Assistants
6. 22 Texas Administrative Code §103.1, General Qualifications for Licensure
Dental Case Review and Analysis
The Texas Health and Human Services Office of Inspector General works with Medicaid dental providers to prevent waste and wrongdoing in Medicaid and CHIP services delivery. Through educational articles and informational presentations, the OIG’s efforts help ensure dental providers and professionals have the latest information on compliant and effective service delivery.
The OIG has worked on a variety of investigations involving dental providers. Many cases concerned illegal solicitation, recordkeeping, mishandling of anesthesia and sedation—which we previously covered—and quality of care concerns. This article breaks down 2 recent cases to examine the underlying regulations and how the problem could have been avoided.
Please note that this material is provided for general informational purposes only and is not intended to present an official position of the OIG or legal advice. The facts and circumstances of any particular question should be verified independently. It is vital that dentists and their staff stay abreast of updates and ensure proper delivery of services.
Case No. 1: Improper recordkeeping
The OIG reached a settlement with a Houston dentist to resolve 4 investigations involving insufficient or incomplete patient records and billing for services not provided. The provider failed to produce 86 out of the 120 records requested. Of the 34 records produced, the investigation revealed poor quality and non-diagnostic X-rays, missing or incomplete documentation, insufficient documentation of medical necessity, and errors or inconsistencies between the services documented and the corresponding billing for those services.
The provider settled with the OIG for $66,804, almost half of which consisted of penalties, and was excluded from Medicaid for 2 years.
Analysis
Without adequate records, the OIG cannot establish whether the services allegedly provided were billed properly or ever performed. Additionally, without documentation of medical necessity or diagnostic quality X-rays, the OIG has no basis to determine whether the services provided were necessary or met the standard of care.
Prevention
To avoid record-related issues, providers must thoroughly understand their responsibilities. The Texas State Board of Dental Examiners addresses these requirements in Texas Administrative Code, Title 22, Section 108.8. Providers may review grounds for OIG enforcement actions related to records and documentation in Texas Administrative Code, Title 1, Section 371.1667. Additionally, the August 2024 Texas Medicaid Provider Manual (TMPPM) covers such requirements in sections 1.10, 1.7.12, 3.2.3.5 and 3.3.
The Texas Medicaid Healthcare Partnership (TMHP) offers workshops and training sessions to stay up to date on program requirements. Dentists should also review TMHP provider notifications for recent changes.
Potential consequences
Failure to keep adequate records may result in recoupment, including any overpayments determined through statistical sampling and extrapolation; interest and penalties; suspension or restriction of Medicaid payments; cancellation of the Medicaid provider agreement; exclusion for a specified period, permanently or indefinitely, which also includes all programs under Titles V and XX of the Social Security Act; or criminal or civil actions through the Office of Attorney General if the recordkeeping violations are an intentional act to defraud the State.
Case No. 2: Illegal dental solicitation
The OIG executed a settlement agreement with a Dallas-Fort Worth area dentist after an investigation found that the dentist employed a marketer to pay “educators” a perperson fee for each patient brought to the dentist’s practices for care. As a result of the settlement, the dentist voluntarily accepted a 10-year exclusion from participating in Texas Medicaid, CHIP and other HHS programs.
Analysis
Texas Medicaid providers are prohibited from engaging in any marketing activity that involves unsolicited personal contact with a Medicaid client or the client’s parent or is directed at them solely because they receive Medicaid benefits and is intended to influence their choice of provider.
Medicaid providers cannot offer to pay another person in exchange for soliciting a patient for the provider. Further, providers are prohibited from offering cash, gifts or other items to Medicaid clients to influence their health care decisions. Providers may not offer, and clients may not accept:
• Cash, cash equivalents or gift cards in any amount.
• Transportation, unless it’s properly arranged through the Medicaid Transportation Program
• Free or discounted services for a family member to influence their health care decisions.
Providing goods or services of any value could be considered a violation, but that would typically not be true for non-cash, low-cost items customarily distributed at appointments, such as toothbrushes or dental floss valued at less than $10.
Prevention
To avoid issues involving dental solicitation, providers must understand and adhere to the provisions of Texas Occupations Code, Chapter 102, as well as Texas Administrative Code Title 1, Sections 354.1452, 371.1669, and 371.27.
The Texas Health and Human Services Commission also provides marketing guidelines, which include information on an optional process where providers can submit marketing materials to the agency for review and approval.
Potential consequences
A provider who solicits Medicaid clients may face a class A misdemeanor—or a third-degree felony if they were previously convicted of illegal dental solicitation or were employed by the federal, state or local government at the time. Further, the provider may be subject to disciplinary action by the Texas State Board of Dental Examiners, an injunction, civil penalties of up to $10,000 and possible exclusion from Medicaid.
Working with the OIG
Providers who discover their own discrepancies are encouraged to self-disclose the matter to the OIG by visiting ReportTexasFraud.com or calling the OIG Fraud Hotline at 800-436-6184.
By self-disclosing potential violations, dentists can potentially reduce their legal and financial exposure by avoiding prolonged investigations or litigation. Download the OIG’s Quick Guide to Self-Disclosing Errors or visit the OIG provider resources page to learn more.
LAW OFFICES OF MARK J. HANNA
• Representation Before the Texas State Board of Dental Examiners
asaltz@me.com will be presenting 3 sessions at the TDA Meeting: When Bad Things Happen to Good Implants
Friday, May 9, 8:00 AM – 11:00 AM
Biofilm Therapy: A New, Team Approach to an Age-Old Enemy
Frida, May 9, 1:00 PM – 4:00 PM
Thread Lightly: Assessment, Maintenance and Homecare of Dental Implants
Saturday, May 10, 8:30 AM – 11:30 AM
It’s a full circle moment for me at this year’s TDA Annual Meeting. I graduated from the periodontal program at the UT Health San Antonio School of Dentistry in 2020 and I’m excited to return to Texas after a long, cold winter in Maine. I hope to share innovative ways to treat and maintain ailing teeth and implants over my 3 sessions. Together, we can improve oral and overall health outcomes using evidence-based materials, techniques, and homecare regimens.
When Bad Things Happen to Good Implants
FRIDAY, MAY 9
8:00 AM - 11:00 AM
We’ll kick off Friday morning with one of my favorite courses. We have confidently treated hard and soft tissue changes around teeth for over a century but are still lacking in our handling of peri-implant disease. Dental implants do fail, and fast.
To prevent this, we must first understand the etiologies that illicit these destructive sequelae, even in the most ideal situations. Implants do not behave like teeth and must be treated and maintained as such. We will explore these nuances, emphasizing strategies for risk management on a local, patient, and esthetic level.
While implant failures can seem catastrophic, simply removing them could be worse. A solid grasp of biology, risk assessment, and comprehensive treatment planning is essential for making informed choices. Non-invasive approaches, regenerative materials, and periodontal plastic surgery have improved the longevity of implants at a fraction of the cost of their replacement. It’s crucial to explore strategies for peri-implantitis and their related surgical and restorative complications to ensure that implants are properly maintained, treated, or removed when necessary.
Effective patient education and communication are also foundational to treatment success. A recent study presented the importance of providing detailed explanations to reduce anxiety about potential complications and individualized hygiene and recall regimens to limit etiology.1 We can empower patients to take an active role in their care to better outcomes and satisfaction.
This session is packed with case studies and real-world scenarios showcasing the good, bad, and ugly of implant dentistry.
Biofilm Therapy: A New, Team Approach to an Age-Old Enemy
FridaY, May 9
1:00 PM – 4:00 PM
The afternoon we’ll take a deep dive into the oral microbiome. Pathogenic bacteria, normally present in small amounts, can challenge the host-immune response in the right environment. The resulting biofilm potentiates periodontal destruction and implant surface corrosion. This course highlights the importance of a team-oriented approach between dentists and hygienists to eliminate these “bad actors” and ensure consistent messaging for patients with periodontal and/or peri-implant disease. Guided biofilm therapy (GBT) allows clinicians to implement a gentle yet effective method for biofilm removal that not only protects soft tissues but safeguards the integrity of the implant body, abutment, and crown.
Attendees will learn the exact workflow of GBT. We will review the specific powders, instruments, and accessories to remove biofilm in its entirety for non-surgical and surgical interventions. Understanding how to manage different systemic and environmental conditions before, during, and after treatment will reduce the overall inflammatory burden. Diabetes mellitus, cardiovascular disease, obesity, and other inflammatory conditions can contribute to the rate of disease progression and responsiveness to treatment.2 Compound these with cigarette smoking, vaping, or even marijuana use, and you have the “perfect storm” for bone and attachment loss.3
The literature continues to support GBT, demonstrating the dual benefits of biofilm removal with a more pleasant patient experience. Its emphasis on patient education and motivation improves oral hygiene compliance and recare adoption.4 Implementing this protocol will re-excite the entire clinical team in their management of the dental biofilm.
Thread Lightly: Assessment, Maintenance and Homecare of Dental Implants
Saturday, May 10
8:30 AM – 11:30 AM
We bring it all together on Saturday morning. As patients outlive their teeth, requiring single, multiple, or full-arch implant reconstructions, their maintenance needs change. This session highlights the specialized instruments and protocols to preserve implant health, particularly in cases of periodontal breakdown, where exposed roots and threads complicate homecare and prophylaxis. Attendees will learn to diagnose peri-implant conditions using the latest classification systems. We’ll discuss best practices for patient education, stressing the role of engagement, accountability, and risk evaluation at and between appointments.
Recent findings reinforce the importance of regular maintenance and clinical and radiographic monitoring of dental implants. Several studies have found that regular follow-up and personalized homecare can significantly reduce the incidence of peri-implant disease and the transformation from peri-implant mucositis to peri-implantitis.1,5 This underscores the necessity for dentists and hygienists to implement structured maintenance programs in their practices.
Key Takeaways
This year feels like a meaningful homecoming, as I complement the teachings from my residency with my experiences in practice. By integrating innovative and evidence-based techniques, we can better navigate the challenges posed by periodontal and peri-implant diseases. Ongoing education and tailored homecare regimens foster a proactive mindset among patients, leading to improved compliance and health. I look forward to our discussions!
References
1. Mombelli A. Maintenance therapy for teeth and implants. Periodontol 2000. 2019;79(1):190-199.
2. Monje A, Catena A, Borgnakke WS. Association between diabetes mellitus/hyperglycaemia and peri-implant diseases: Systematic review and meta-analysis. J Clin Periodontol. 2017;44(6):636-648.
3. Youssef M, Marzouk T, Abdelsalam H, Malmstrom H, Barmak AB, Fraser D, Tsigarida A. The effect of electronic cigarette use on peri-implant conditions in men: a systematic review and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol. 2023;135(4):492-500.
4. Herrera D, Berglundh T, Schwarz F, Chapple I, Jepsen S, Sculean A, Kebschull M, Papapanou PN, Tonetti MS, Sanz M; EFP workshop participants and methodological consultant. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50 Suppl 26:4-76.
5. Lin CY, Chen Z, Pan WL, Wang HL. The effect of supportive care in preventing peri-implant diseases and implant loss: A systematic review and meta-analysis. Clin Oral Implants Res. 2019;30(8):714-724.
Hieu Huynh, DDS,
» Histochemistry, immunohistochemistry, direct immunofluorescence, and Sjogrën syndrome focus scoring
» Free local courier or overnight FedEx service
» Most cases receive a diagnosis within 24-hours following receipt of specimen
A 13-year-old male was referred to an oral and maxillofacial surgeon based on radiographic findings observed during an evaluation for orthodontic care. The patient presented with a wellcircumscribed unilocular radiolucency containing radiopaque calcifications in the right posterior mandible around impacted tooth #32. The lesion had been present for an unknown duration of time, and the patient was asymptomatic. There were no signs of damage to the adjacent teeth, nerves, or blood vessels. The patient’s medical, social, surgical, and familial history were unremarkable. The clinical impression by the oral and maxillofacial surgeon was an odontoma, and the patient was scheduled for surgical excision of the lesion.
AUTHORS
Tyler Stevens, BS Fourth-Year Dental Student, School of Dentistry, UT Health San Antonio, San Antonio, Texas.
Anne Cale Jones, DDS UT System Distinguished Teaching Professor, Department of Pathology and Laboratory Medicine, UT Health San Antonio, San Antonio, Texas.
Grant K. Nakashima, DDS
Oral and Maxillofacial Surgeon, San Gabriel Oral & Maxillofacial Surgery Associates, Georgetown, Texas.
Juliana Robledo, DDS Assistant Professor/ Clinical, Department of Pathology and Laboratory Medicine, UT Health San Antonio, San Antonio, Texas.
Figure 1. Panoramic radiograph revealing a 2 x 2 cm mixed radiolucent/radiopaque lesion located around impacted tooth #32. Tooth #31 is displaced mesially.
A panoramic radiograph revealed a 2 x 2 cm well-defined, corticated, unilocular mixed radiopaque-radiolucent lesion in the right posterior mandible around the crown of underdeveloped impacted tooth #32. Tooth #31 was displaced mesially (Figure 1). Upon surgical excision, the size of the specimen was reassessed as 4.0 cm x 3.5 cm x 1.4 cm. The soft and hard tissues were submitted for histopathologic evaluation.
Pathological Findings
Multiple brown irregularly shaped fragments of soft and hard tissue were received. The specimen measured 4.0 cm x 3.5 cm x 1.4 cm in aggregate. Also received was the crown of an underdeveloped molar tooth. The tooth was submitted for gross examination only.
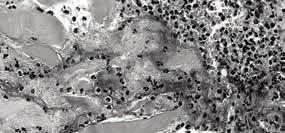
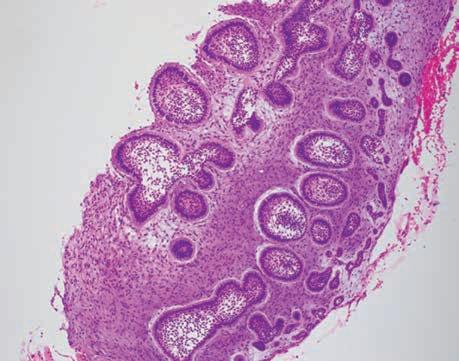
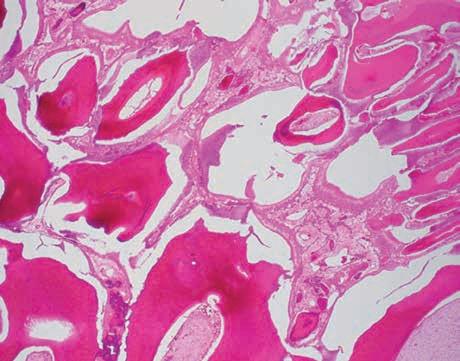
Histopathologic examination revealed sections of a specimen composed of islands and interconnecting strands of ameloblastic epithelium set in a loosely arranged connective tissue stroma resembling dental papilla. The ameloblastic epithelium exhibited a peripheral layer of columnar shaped epithelial cells demonstrating palisading and subnuclear vacuolization. The central portions of the epithelial islands were more loosely arranged and resembled stellate reticulum (Figure 2). Separate disorganized masses of dentin, cementum, enamel matrix, pulp, and reduced enamel epithelium were noted (Figure 3).
What is the most likely diagnosis?
See page 562 for answer and discussion.
Figure 3. Disorganized mass of dentin, cementum, enamel matrix, pulp, and reduced enamel epithelium (H&E: original magnification 10x).
Figure 2. Islands and interconnecting strands of ameloblastic epithelium set in a loosely arranged connective tissue stroma resembling dental papilla (H&E: original magnification 10x).
ORAL and maxillofacial pathology
diagnosis and management—from page 561
Diagnosis: Ameloblastic
Fibro-odontoma
Discussion
Based on the clinical and radiographic findings, a differential diagnosis includes: odontoma, adenomatoid odontogenic tumor, calcifying epithelial odontogenic tumor, and ameloblastic fibro-odontoma.
An odontoma is the most common odontogenic tumor, with a higher prevalence than all other odontogenic tumors combined.1,2 Odontomas are usually discovered during the first two decades of life.3 Most patients are asymptomatic, and the lesions are detected on routine radiographic examination. Odontomas tend to be relatively small, but large examples of up to 6 cm or more have been identified.4 Odontomas may occur at any site but are more frequently found in the maxilla than the mandible.1 Odontomas are subdivided into two types: compound and complex. A compound odontoma is composed of small toothlike structures, sometimes referred to as “toothlets.”1 A complex odontoma is composed of a mass of enamel and dentin that does not anatomically resemble a tooth. Odontomas are not considered true neoplasms because they are not characterized by unlimited growth but represent an abnormal proliferation of tissue indigenous to the area. Thus, they are considered developmental anomalies, or hamartomas.3 Radiographically, a compound odontoma appears as multiple radiopaque toothlike structures surrounded by a radiolucent zone. A complex odontoma appears as a radiopaque mass with a radiodensity similar to a tooth and surrounded by a radiolucent zone.5 Both subtypes can prevent the eruption of an associated tooth. Histologically, a compound odontoma consists of multiple toothlike structures containing varying amounts of enamel, dentin, cementum, and pulp laid down in their appropriate anatomical relationships; thus, resembling small teeth.6 Complex odontomas consist of mature tubular dentin, enamel matrix, and cementum in which the dental hard tissues are laid down haphazardously.1,7 Odontomas are treated by local excision and have an excellent prognosis. Recurrence is rare.8
An adenomatoid odontogenic tumor (AOT) represents 2% to 7% of odontogenic tumors.9 AOTs are known as the “tumor of two-thirds,” because two-thirds are found
in the maxilla, in females, and in the second decade of life.10 Most cases are associated with maxillary canine.10 AOTs are relatively small and rarely exceed 3 cm in diameter.11 They are usually asymptomatic and are detected on routine radiographic examination. Radiographically, an AOT manifests as a well-circumscribed, unilocular radiolucency involving the crown of an unerupted tooth, most frequently a canine.12 The tumor often contains fine “snowflake” calcifications.13 Upon microscopic examination, spindleshaped epithelial cells form sheets, strands, or whorled masses throughout the tumor within a fibrous connective tissue stroma.1 Characteristic features of an AOT are tubular (duct-like) structures consisting of a central space surrounded by a layer of columnar or cuboidal epithelial cells.1 Distinct areas of calcification may be seen throughout the tumor as well.11 AOTs are treated by complete surgical enucleation, which is made easier due to their thick capsules.1 Prognosis is excellent, and the recurrence rate is as low as 0.2%.11
A calcifying epithelial odontogenic tumor (CEOT), also known as a Pindborg tumor, represents less than 1% of odontogenic tumors.14 CEOTs are most frequently identified in the third to fifth decades of life.15 Two-thirds of cases occur in the mandible, usually in the posterior region.16 There is no sex predilection.16 CEOT’s most commonly present clinically as a slow-growing, painless swelling.17 Radiographically, a CEOT manifests as unilocular or multilocular radiolucency.1 Radiopacities representing fine calcifications are commonly seen.1 A few cases of peripheral CEOTs have been identified, most frequently on the anterior gingiva with some examples causing cupped-out erosion of the underlying
bone.18 Histologically, CEOTs have distinct islands or sheets of polygonal epithelial cells in a fibrous connective tissue stroma.1 The tumor cells are often pleomorphic and giant nuclei and intercellular bridges may be seen.1 Large areas of eosinophilic, hyalinized extracellular (amyloid) matrix may be seen enclosed by the tumor islands, leading to a cribriform appearance.1 CEOT’s characteristically display multiple concentric rings known as Liesegang ring calcifications within the extracellular amyloid matrix.17 CEOTs are treated by conservative local excision including a thin rim of surrounding bone.19 The prognosis is good with a recurrence rate of about 15%.17 Some rare examples of malignant tumors with metastasis to regional lymph nodes and the lungs have been reported.17
Based on histopathologic examination, the definitive diagnosis in our case was an ameloblastic fibro-odontoma
(AFO). An AFO is a tumor with the characteristic histopathologic features seen in an ameloblastic fibroma but it also contains enamel and dentin, resembling an odontoma.20 AFOs are usually seen in children with an average age of 10 years old, and are rarely seen in adults.1 AFOs tend to occur in the posterior mandible, and an unerupted tooth is associated with the tumor in most cases.1,21 AFOs are usually asymptomatic and, like the previously mentioned lesions, tend to be discovered on routine radiographic examination or when determining the reason for failure of a tooth to erupt.22 If they become large, AFOs may be associated with painless swelling of bone in the affected area.1
Radiographically, an AFO most often appears as a well-circumscribed unilocular radiolucency with areas of radiopaque calcified material.23 The calcified regions may be observed as multiple small radiopacities or as one
large mass.1 Histologically, the soft tissue of the AFO is identical to an ameloblastic fibroma with narrow cords and islands of odontogenic epithelium within a loose primitive connective tissue that resembles the dental papilla.24 The hard tissue component of the AFO consists of enamel and dentin matrix.1 AFOs are usually treated by conservative curettage.25 The tumor is well-circumscribed and is usually easy to separate from the surrounding bone.1 The prognosis is excellent, with an estimated recurrence rate of around 7%.1
Our patient was treated with curettage and removal of the surgical specimen which consisted of multiple irregularly shaped fragments of soft and hard tissue. A panoramic radiograph two months post-surgery revealed no radiographic evidence of recurrence or persistent disease (Figure 4). An additional panoramic radiograph
Figure 4. Panoramic radiograph revealing 2 x 2 cm radiolucency 2 months post-surgery suggesting uneventful healing with no evidence of recurrence or persistent disease.
ORALand maxillofacial pathology
taken 8 months post-surgery showed bone regeneration with a normal trabeculation pattern throughout the surgical site and no radiographic evidence of recurrent or persistent disease (Figure 5).
References
1. Chi, Angela, Brad Neville, Douglas Damm, Carl Allen. Oral and Maxillofacial Pathology, 4th Edition. Saunders, 052015. VitalBook file.
2. Labib A, Adlard RE. Odontogenic Tumors of the Jaws. [Updated 2023 Jul 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
3. Satish V, Prabhadevi MC, Sharma R. Odontome: A Brief Overview. Int J Clin Pediatr Dent. 2011 Sep-Dec;4(3):177-85. doi: 10.5005/jp-journals-10005-1106. Epub 2011 Apr 15. PMID: 27678223; PMCID: PMC5034075.
4. Perumal CJ, Mohamed A, Singh A, Noffke CE. Sequestrating giant complex odontoma: a case report and review of the literature. J Maxillofac Oral Surg. 2013 Dec;12(4):480-4. doi: 10.1007/s12663-010-0148-y. Epub 2011 Feb 4. PMID: 24431893; PMCID: PMC3847030.
5. Cheng FC, Yu-Fong Chang J, Chen MH, Chen YC, Chen HY, Wang YL, Chiang CP. Radiographic characteristics of odontomas in patients in the National Taiwan University Children’s Hospital. J Dent Sci. 2023 Jan;18(1):392-399.
6. Nelson BL, Thompson LD. Compound odontoma. Head Neck Pathol. 2010 Dec;4(4):290-1. doi: 10.1007/s12105-010-01862. Epub 2010 Jun 9. PMID: 20533004; PMCID: PMC2996496.
7. Tyagi P, Singla S. Complex Composite Odontoma. Int J Clin Pediatr Dent. 2010 May-Aug;3(2):117-20. doi: 10.5005/jpjournals-10005-1066. Epub 2010 Aug 17. PMID: 27507924; PMCID: PMC4968180.
8. Mazur M, Di Giorgio G, Ndokaj A, Jedliński M, Corridore
D, Marasca B, Salucci A, Polimeni A, Ottolenghi L, Bossù M, Guerra F. Characteristics, Diagnosis and Treatment of Compound Odontoma Associated with Impacted Teeth. Children (Basel). 2022 Oct 2;9(10):1509.
10. Barnts K, Feng J, Qin C, Zhang H, Cheng Y. Adenomatoid odontogenic tumor: evidence for a mixed odontogenic tumor, Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, Volume 133, Issue 6, 2022, Pages 675-683, 11. More CB, Das S, Gupta S, Bhavsar K. Mandibular adenomatoid odontogenic tumor: Radiographic and pathologic correlation. J Nat Sci Biol Med. 2013 Jul;4(2):45762. doi: 10.4103/0976-9668.116965. PMID: 24082751; PMCID: PMC3783799.
12. Karam Genno N, Aoun N, El Toum S. Adenomatoid Odontogenic Tumor Associated with an Impacted Maxillary Lateral Incisor: A Case Report with Five-Year Follow-Up. Case Rep Dent. 2017;2017:1709492. doi: 10.1155/2017/1709492. Epub 2017 Oct 29. PMID: 29214083; PMCID: PMC5682065.
15. Turatti E, Brasil J, de Andrade BA, Romañach MJ, de Almeida OP. Clear cell variant of calcifying epithelial odontogenic tumor: Case report with immunohistochemical findings. J Clin Exp Dent. 2015 Feb 1;7(1):e163-6. doi: 10.4317/ jced.51995. PMID: 25810830; PMCID: PMC4368006.
16. Vigneswaran T, Naveena R. Treatment of calcifying epithelial odontogenic tumor/Pindborg tumor by a conservative surgical method. J Pharm Bioallied Sci. 2015 Apr;7(Suppl 1):S291-5. doi: 10.4103/0975-7406.155961. PMID: 26015736; PMCID: PMC4439696.
17. Demian N, Harris RJ, Abramovitch K, Wilson JW, Vigneswaran N. Malignant transformation of calcifying epithelial odontogenic tumor is associated with the loss of p53 transcriptional activity: a case report with review of the literature. J Oral Maxillofac Surg. 2010 Aug;68(8):1964-73. doi: 10.1016/j.joms.2010.02.017. Epub 2010 Jun 9. PMID: 20542620; PMCID: PMC2906672.
18. Lee SK, Kim YS. Current Concepts and Occurrence of Epithelial Odontogenic Tumors: II. Calcifying Epithelial Odontogenic Tumor Versus Ghost Cell Odontogenic Tumors Derived from Calcifying Odontogenic Cyst. Korean J Pathol. 2014 Jun;48(3):175-87. doi: 10.4132/ KoreanJPathol.2014.48.3.175. Epub 2014 Jun 26. PMID: 25013415; PMCID: PMC4087130.
19. Silva AAM, Martins TA, Veronese HRM, Silva MI. Calcifying epithelial odontogenic tumor with maxillary sinus extension: Case report and therapeutic review. Int J Case Rep Images 2022;13(2):71–81.
20. Surej Kumar LK, Manuel S, Khalam SA, Venugopal K, Sivakumar TT, Issac J. Ameloblastic fibro-odontoma. Int J Surg Case Rep. 2014;5(12):1142-4. doi: 10.1016/j. ijscr.2014.11.025. Epub 2014 Nov 13. PMID: 25437658; PMCID: PMC4276268.
21. Sánchez-Romero C, Paes de Almeida O, BolognaMolina R. Mixed odontogenic tumors: A review of the clinicopathological and molecular features and changes in the WHO classification. World J Clin Oncol. 2021 Dec 24;12(12):1227-1243. doi: 10.5306/wjco.v12.i12.1227. PMID: 35070741; PMCID: PMC8716991.
22. Thulasirman SK, Thuasidoss G, Prabhu NK, Krishnakumar Raja VB. A Rare Case of Ameloblastic Fibro-Odontoma of Mandible with Literature Review. Ann Maxillofac Surg. 2018 Jul-Dec;8(2):324-326. doi: 10.4103/ams.ams_127_18. PMID: 30693255; PMCID: PMC6327819.
23. Divya Bharat, Jayesh Vahanwala, Ashok Dabir, Prachi Jobanputra, Ameloblastic fibro-odontoma in the mandible – Clinical, radiological and surgical aspect, Advances in Oral and Maxillofacial Surgery, Volume 2,2021, 100066, ISSN 2667-1476
24. Buchner A, Kaffe I, Vered M. Clinical and radiological profile of ameloblastic fibro-odontoma: an update on an uncommon odontogenic tumor based on a critical analysis of 114 cases. Head Neck Pathol. 2013 Mar;7(1):54-63.
25. Omar N, Ullah A, Ghleilib I, Patel N, Abdelsayed RA. A Locally Aggressive Ameloblastic Fibro-Odontoma: A Case Report and Literature Review. Cureus. 2021 Dec 12;13(12):e20366. doi: 10.7759/cureus.20366.
Figure 5. Panoramic radiograph eight months post-surgery: #32 area displays bone regeneration with normal trabeculation pattern throughout the surgical site.
Guest Editor Rade D. Paravina, DDS, MS, PhD
An overview of the different digital facebow methods for transferring the maxillary cast into the virtual articulator.
Marta Revilla-León, DDS, MSD, PhD; Jonathan M. Zeitler; John C. Kois, DMD, MSD
J Esthet Restor Dent. 2024;36:1675–1686
Objectives
The purposes of this study were to classify the described digital facebow techniques for transferring the maxillary cast into the semi-adjustable virtual articulator based on the digital data acquisition technology used and to review the reported accuracy values of the different digital facebow methods described.
Overview
Digital data acquisition technologies, including digital photographs, facial scanners, cone beam computed tomography (CBCT) imaging, and jaw tracking systems, can be used to transfer the maxillary cast into the virtual articulator. The reported techniques are reviewed, as well as the reported accuracy values of the different digital facebow methods.
Conclusions
Digital photographs can be used to transfer the maxillary cast into the virtual articulator using the true horizontal reference plane, but limited studies have assessed the accuracy of this method. Facial scanning and CBCT techniques can be used to transfer the maxillary cast into the virtual articulator, in which the most frequently selected references planes are the Frankfort horizontal, axis orbital, and true horizontal planes. Studies analyzing the accuracy of the maxillary cast transfer by using facial scanning and CBCT techniques are restricted. Lastly, optical jaw trackers can be selected for transferring the maxillary cast into the virtual articulator by using the axis orbital or true horizontal planes, yet the accuracy of these systems is unknown.
Clinical Implications
Digital photograph method for transferring the maxillary cast into the virtual articulator. (A) Standardized photograph obtained by using a reference glasses (Kois Reference Glasses; Kois Center). (B) Calibrating the digital photograph by using the known distance between the 2 optical markers of the reference glasses. (C) Alignment between digital photograph and maxillary scan. (D) Maxillary cast transferred into the virtual articulator.
Digital data acquisition technologies, including digital photographs, facial scanning methods, CBCTs, and optical jaw tracking systems, can be used to transfer the maxillary cast into the virtual articulator. Studies are needed to assess the accuracy of these digital data acquisition technologies for transferring the maxillary cast into the virtual articulator.
We know cyber threats are constantly evolving with attackers seeking new ways to access systems and networks. We’re also aware our security is only as strong as our weakest link. Health care supply chain attacks rely on that, and further, rely on vendor software being a blind spot.
As health care increasingly relies on technology, and with patient care and practice administration being paramount, many practices rely on the resources provided by software vendors to support everything from RCM and communications to health care workflows. With those reliances likely to increase, practices need to understand supply chain attacks and how to reduce their risk.
What is a Supply Chain Attack?
A supply chain attack is a cyberattack that targets an organization’s external vendors or service providers, exploiting security vulnerabilities within the supply chain to gain unauthorized access to the main network.
In a health care supply chain attack, rather than attacking a health care practice directly, cybercriminals focus on third-party vendors such as software providers, medical device manufacturers, or cloud service platforms, which may have weaker security controls. Once compromised, these trusted partners can serve as a gateway for attackers to infiltrate sensitive systems. Essentially, it can become like a chain of dominoes, toppling one system after another.
For health care practices, supply chain attacks pose a significant threat, not only to workflows but also to patient data and HIPAA compliance.
As an example, the Change Health Care of attack in 2023 highlighted the widespread and devastating impact of an attack on a supply chain. In that case, the consequences have been longlasting and may continue for years to come. The direct and immediate impact meant that not only could health care providers not access records or process payments, but patients were also unable to get necessary prescriptions.
As we saw with the Change Health Care attack, assaults on the supply chain can even prevent practices from conducting business, processing payments, and ensuring the financial security of their practice or organization.
In short, these attacks may not only lock down systems, but they can also expose EHRs, billing systems, and other critical data to malicious actors, and in some cases, the dark web or other hackers. Given the complexity of health care supply chains and the volume of external services used, the risk of attack is heightened, making it crucial to ensure all partners maintain rigorous security and compliance standards and practices utilize Business Associate Agreements (BAA).
To better protect your organization, it’s important to understand how supply chain attacks happen.
How Do Health care Supply Chain Attacks Happen?
One of the most common ways is through software updates. Vendors often push automatic updates to their products, and cybercriminals can compromise these updates to inject malicious code into health care systems. If a health care provider relies on an affected software platform, the malware gets installed without detection, opening pathways for data theft, ransomware, or system disruption. This is what occurred in a 3CX attack, where a compromised software update allowed attackers to access health care communications networks.
Similarly, vulnerabilities in cloud services and medical devices also create entry points for attackers. Many health care organizations rely on third-party cloud platforms for storing and managing patient data; and if these platforms have weak security protocols, they become prime targets for cybercriminals.
In the same way, connected medical devices that run on third-party software are vulnerable if they lack adequate encryption, authentication, or regular patching. The Philips Health Care Devices breach in 2023 highlighted this risk, as attackers exploited vulnerabilities in medical device software to access health care networks.
Other vulnerabilities include weak vendor cybersecurity policies, lack of regular security assessments, and insufficient monitoring of thirdparty access. If a vendor does not
adhere to strict security practices, it can expose the health care provider to risks like phishing, ransomware, or data breaches.
The Impact of Health care Supply Chain Attacks
Particularly in health care, supply chain attacks have emerged as a significant cybersecurity risk. With the increasing reliance on interconnected software platforms, medical devices, and cloudbased services, health care practices face greater vulnerability to such attacks. The protection of sensitive patient information and maintaining compliance with regulations, including HIPAA, are paramount.
One of the primary concerns in health care is the potential exposure of ePHI due to supply chain vulnerabilities. A compromised vendor can give cybercriminals access to the entire health care network, jeopardizing data such as patient records, billing information, and even clinical workflow systems. This not only puts the practice at risk of violating HIPAA regulations, which mandate strict data protection standards, but can also lead to hefty fines, legal liabilities, and a loss of patient trust.
As supply chain attacks grow more sophisticated, it’s essential for health care organizations to be proactive in managing their third-party relationships, ensuring every vendor adheres to stringent cybersecurity protocols. This is why BAAs are essential, though not a security guarantee. With health care already a high-value target for attackers, protecting the extended supply chain
is crucial for maintaining security and compliance.
Though supply chain attacks are on the rise and an increasing cybersecurity threat, they’re not a new phenomenon. Sadly, Change Health care is only one example out of many.
Supply Chain
Attacks in 2023: Were You Impacted?
MOVEit
MOVEit is a managed file encryption and transfer software used by many organizations. Cybercriminals exploited a vulnerability in the software to access and steal sensitive data from affected systems. Health care organizations relying on MOVEit for secure file transfers were compromised, leading to the exposure of protected health information (PHI) and other confidential data.
United Health care
In this supply chain attack, hackers targeted a third-party vendor United Health care used for secure file transfers: IBM’s Aspera. Exploiting a vulnerability in Aspera’s software, cybercriminals gained access to sensitive data, including personal health information (PHI) of United Health care members.
NextGen
A ransomware attack on a third-party vendor that provided services to NextGen Health care, a health care technology provider, led to the exposure of sensitive patient data, including protected health information (PHI). This breach potentially affected NextGen’s HIPAA compliance.
Philips Health Care Devices
This attack involved exploitation of vulnerabilities in software integrated into Philips medical devices. Attackers potentially accessed sensitive health care data and disrupted device functionality. As Philips devices are widely used in health care settings, the attack raised concerns about the security of Internet of Things (IoT) medical technologies and emphasized the risks posed by third-party software.
Brightline
A vulnerability in the platform of a thirdparty vendor was exploited, leading to exposure of sensitive patient data in the supply chain attack of Brightlane. Brightlane is a telehealth provider specializing in behavioral health care, and relied on this vendor for critical services. The breach compromised the protected health information (PHI) of numerous patients.
3CX
Hackers infiltrated a popular communications software, 3CX, injecting malicious code into the company’s software update mechanism. Health care organizations using 3CX for communication services were affected, as the malware provided attackers with access to sensitive information, which potentially included patient data.
Top Strategies to Decrease Your Risk
Protecting your practice from health care supply chain attack risks requires a multi-layered approach—addressing technical safeguards and vendor management practices.
Thankfully, there are critical strategies you can use to minimize the risks associated with supply chain attacks. Let’s go through them.
• Review third-party vendors’ security policies to ensure HIPAA compliance.
• Evaluate vendors’ incident response procedures and their ability to handle breaches.
• Require vendors to share their history of security breaches and corrective actions taken.
• Develop comprehensive Business Associate Agreements (BAA) to help protect ePHI and data.
2. Establish strong contracts with security clauses.
• Include clauses in vendor contracts that require adherence to your security policies.
• Mandate timely notification in the event of any data breaches or security incidents.
• Specify penalties for noncompliance with HIPAA and other data protection regulations.
3. Implement zero-trust architecture.
• Limit vendor access to your systems based on the principle of least privilege.
• Use network segmentation to minimize the spread of any potential breaches from vendor systems.
• Regularly audit user access and permissions granted to third-party vendors.
4. Enforce regular software updates and patching.
• Require vendors to provide regular updates and security patches.
• Establish a policy for timely internal patch management and system updates.
• Verify that medical devices and other vendor-supplied technology are regularly patched against the latest vulnerabilities.
5. Enhance encryption and data protection standards.
• Use end-to-end encryption for all data transfers between your practice and vendors.
• Require third-party systems to meet advanced encryption standards for sensitive data, especially patient health information.
6. Implement multi-factor authentication (MFA).
• Enforce MFA for any system access involving external vendors, especially those accessing sensitive patient data.
• Regularly review MFA logs and activity for any unusual or suspicious login attempts.
7. Conduct ongoing vendor monitoring.
• Continuously monitor vendor behavior for signs of malicious activity or unusual patterns.
• Conduct periodic security audits and assessments of your vendors’ networks.
• Leverage threat intelligence feeds to stay informed about vendor-specific risks.
8. Develop a vendor-specific incident response plan.
• Create incident response workflows that include steps for addressing vendor-related security incidents.
• Ensure vendors are aware of their role in your practice’s incident response plan.
• Regularly test your plan to ensure it’s effective and all parties know their responsibilities.
Following these strategies can help you significantly reduce the risks associated with a supply chain attack, maintain HIPAA compliance, and safeguard patient data. Additionally, working with software and platform providers that have health care expertise can be beneficial.
Two of the listed examples of supply chain attacks were related to filetransfer or exchange applications. With iCoreExchange, you can email other providers and send encrypted files, of any size, and know your files (and inbox) are safe. Similarly, a HIPAA risk assessment from iCoreHIPAA can help you identify potential vulnerabilities and develop a solid security plan and framework to ensure you’re decreasing any potential attack surface at your practice.
Whether you need secure HIPAA compliant software solutions or more support and expertise tailored to your practice and your needs, iCoreConnect can help. Learn more about iCoreConnect’s products at tdaperks.com (Compliance & Supplies).
classifieds
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/Member-Resources/TDAClassified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL TEXAS LISTINGS FOR MCLERRAN & ASSOCIATES. AUSTIN (ID #662): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business. AUSTIN (ID #691): Unique opportunity to purchase a GD practice with two locations in the Austin area. The offices have a total of 10 operatories with computers in each room and digital radiography. The offices serve a large FFS/PPO patient base with a healthy new patient flow and strong hygiene recall with over 20-25% of total annual production coming from the hygiene department. DALLASPEDO/ORTHO (ID #665): Legacy pedo/ortho practice in the heart of North Dallas. Thriving practice, large fee-for-service patient base, revenue of 7 figures. Over 2,800 sq ft, fully digital with computers in the operatories, digital radiography, and a digital pano. DALLAS (ID #706): Legacy, GD practice located in a highly sought after north Dallas community with
room to grow. Newly renovated office building situated off of a heavily trafficked thoroughfare. Features 2,400 sq ft with 5 fully equipped ops (plumbed for nitrous), computers throughout, digital pano, intra-oral cameras, and paperless charts. This practice serves a multi-generational patient base, relies mostly on word-of-referrals with limited marketing/advertising activities, has a robust hygiene recall program with 40% of total office production coming from the hygiene department, and they refer out many specialty procedures. HOUSTON-SOUTH (ID #682): Established, multi-specialty dental office in a suburb about 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over seven figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose. SAN ANTONIOTX HILL COUNTRY (ID #685): Well-established
dental practice and real estate nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouth referrals with limited marketing/advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023 and the trend has continued into 2024. SOUTH TEXAS (ID #651):
General dentistry practice located in south Texas. This state-of-the-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld X-ray units, and a 3-D printer. The practice serves a large PPO/Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions. com or contact us at 512-900-7989 or info@ dentaltransitions.com.
AUSTIN: Fee-for-service private practice, 46 years same location with a 10-15 mile panoramic view over the downtown Austin skyline. Associate to buy with a preferred
classifieds
long transition for the senior doctor. Eight years remaining current lease with option to extend. Tremendous amount of residential growth immediately outside our huge windows. Ideally a GP interested in learning full-scale orthodontics. Please email for information: info@austinskylinedental.com.
CENTRAL TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural 4 operatory dental practice for sale in the heart of the beautiful Texas hill country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail. com for more information and showings.
EAST TEXAS: Exceptional practice opportunity in Troup, Texas. Seeking associate to join high quality, well-established dental practice with a long history of excellence. This is an exceptional
opportunity to move into ownership after a successful initial employment phase. Must be committed to providing optimal patient care with exceptional technical skills, strong people skills, personal integrity, honesty and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on Christian values and professional growth. Our office expansion should be complete mid to late September 2024, but the new associate could begin in August if he/she would like. Please reply in confidence with your CV and a letter outlining your future objectives and goals to: drmay@troupfamilydental.com or call our office at 903-842-4600.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid-6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 sq ft with 3 total operatories: 2 for dentistry and 1 for hygiene. Please let me know if you need anything else from me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over
35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee-for-service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
NEW BRAUNFELS: Dental practice for sale in high traffic area and very visible building. Beautifully renovated recently, with 3 operatories, move-in ready, with 1,250 sq ft. No HMO or DMO. If interested, please email to salemydentalpractice@yahoo.com or leave message on landline, 830-606-4544.
WATSON BROWN PRACTICES FOR SALE:
Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
DSO C S PRACTICE SALES
Austin 512-900-7989 DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com PRACTICE APPRAISALS