• 4 Tier Rates Nationwide—No age rating, no census needed and no medical underwriting
• Coverage cannot be denied. (No pre-existing limitations)
• In-network coverage in all 50 states, plus DC and Puerto Rico
• ACA Compliant health benefits available
• Concierge access and support
Members can enroll THE FIRST DAY OF ANY MONTH with open enrollment.
Enrollment needs to be completed no later than 30 days in advance.
TDA members enjoy an average savings of $6,496 (27%) per year on credit card processing costs by switching to Best Card.
Options include:
• Countertop, portable, and Clover card readers; Dial, IP, Wi-Fi
• BCPay, an online system offering recurring payments, text-to-pay, card vault, and automatic posting to popular dental software.
Best of all, Best Card is renowned for its exceptional customer service. Chat with its friendly experts to see how much you could save and why TDA members across the state rave about this program.
Ready to discover your savings?
Send a recent processing statement to Compare@BestCardTeam.com or fax it to (866) 717-7247 for a no-obligation analysis.
Marat Wartanovic
João Carlos Roque, PhD
James Choi, CDT
Luis Felipe Rondón, DDS
Abdulkareem Alhumaidan, BDS, MSD
Faisal al-Qarni, BDS, MS, PhD
Mishali AlSharief, BDS, MSD, DScD
Baneen AlShammasi, BDS
Zainab Albasry, BDS
Editorial Staff
Jacqueline M. Plemons, DDS, MS, Editor
Juliana Robledo, DDS, Associate Editor
Nicole Scott, Managing Editor
Barbara Donovan, Art Director
Lee Ann Johnson, CAE, Director of Member Services
Editorial Advisory Board
Ronald C. Auvenshine, DDS, PhD
Barry K. Bartee, DDS, MD
Patricia L. Blanton, DDS, PhD
William C. Bone, DDS
Phillip M. Campbell, DDS, MSD
Michaell A. Huber, DDS
Arthur H. Jeske, DMD, PhD
Larry D. Jones, DDS
Paul A. Kennedy, Jr., DDS, MS
Scott R. Makins, DDS, MS
Daniel Perez, DDS
William F. Wathen, DMD
Robert C. White, DDS
Leighton A. Wier, DDS
Douglas B. Willingham, DDS
The Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 142 | No. 1
Texas Dental Journal (ISSN 0040-4284) is published monthly, except January-February, March-April, July-August, and November-December, which are combined issues, by the Texas Dental Association, 8701 W Hwy 71, Ste 201-M Austin, TX 78735, 512-443-3675. Periodicals Postage Paid at Austin, Texas, and at additional mailing offices. POSTMASTER: Send address changes to TEXAS DENTAL JOURNAL, 8701 W Hwy 71, Ste 201-M, Austin, TX 78735. Copyright 2025 Texas Dental Association. All rights reserved. Annual subscriptions: Texas Dental Association members $17. In-state ADA Affiliated $49.50 + tax, Out-of-state ADA Affiliated $49.50. In-state Non-ADA Affiliated $82.50 + tax, Out-of-state Non-ADA Affiliated $82.50. Single issue price: $6 ADA Affiliated, $17 Non-ADA Affiliated. For in-state orders, add 8.25% sales tax. Contributions: Manuscripts and news items of interest to the membership of the society are solicited. Electronic submissions are required. Manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the Instructions for Contributors statement at tda.org. All statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the Texas Dental Association, unless such statements have been adopted by the Association. Articles are accepted with the understanding that they have not been published previously. Authors must disclose any financial or other interests they may have in products or services described in their articles.
Advertisements: Publication of advertisements in this journal does not constitute a guarantee or endorsement by the Association of the quality of value of such product or of the claims made.
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
NOW Available: In-Office ACLS & PALS renewals; In-Office Emergency Program Live Programs Available Throughout Texas
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner. WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE Requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs:
Principles of Pain Management Fulfills rule 104.1 for all practitioners
Use and Abuse of Prescription M edications and Provider Prescription Program Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2
(ONLINE, LIVE WEBCAST AND IN CLASS)
ONLINE LEVEL 3 AND 4 SEDATION REPERMIT AVAILABLE! (Parenteral Review) Level 3 or Level 4 Anesthesia Programs (In Class, Webcast and Online available): American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs
NOTE: ACLS or PALS Renewal can be completed by itself at any combined program Combined ACLS-PALS-BLS and Level 2, 3 and
4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214-384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the course.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels.
Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedation permits. AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs. Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
JKJ Pathology
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports
¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface Professional, reliable service with hightechnology solutions so that you can better serve your patients. Call or email for free kits or consultation. jkjpathology.com 281-292-7954 (T) 281-292-7372 (F) johnkacher@jkjpathology.com
Board of Directors Texas Dental Association
PRESIDENT Georganne P. McCandless, DDS 281-516-2700, gmccandl@yahoo.com
PRESIDENT-ELECT Glen D. Hall, DDS 325-698-7560, abdent78@gmail.com
VICE PRESIDENT, SOUTHEAST Laji J. James, DDS 281-870-9270, lajijames@yahoo.com
DIRECTOR, NORTHWEST Annie C. Wilson, DDS 817-860-4343, annie@anniewilsondds.com
DIRECTOR, NORTHEAST Shane A. Ricci, DDS 972-381-1888, riccidds@hotmail.com
SECRETARY-TREASURER* Carmen P. Smith, DDS 214-503-6776, drprincele@gmail.com
SPEAKER OF THE HOUSE* Gregory W. Rashall, DDS 936-336-5171, rashdent@sbcglobal.net
PARLIAMENTARIAN** Jodi D. Danna, DDS 972-377-7800, jodidds1@gmail.com
EDITOR**
Jacqueline M. Plemons, DDS, MS 214-369-8585, drplemons@yahoo.com
LEGAL COUNSEL Carl R. Galant *Non-voting member **Non-voting
Those in the dental community who have recently passed
David Bennett Campbell
Dallas
2/28/45–2/14/24
Good Fellow: 2002 Life: 2010
Howard Talley Graff Hamshire
3/24/31–11/11/24
Good Fellow: 1983
Life: 1996
Fifty Year: 2008
Norman Irwin Schneidler
Houston
10/21/33–12/2/24
Good Fellow: 1990
Life: 1998
Fifty Year: 2015
James Gordon Price Corsicana
11/23/34–11/15/24
Good Fellow: 1986
Life: 2000
Fifty Year: 2011
Joe Chris Freeman
Tyler 10/16/42–12/4/24
Life: 2018
Ronald G Presswood
Houston
12/21/40–11/8/24
Good Fellow: 1994
Life: 2005
Fifty Year: 2015
Charles E Campbell Pearland 3/17/50–12/14/24
Good Fellow: 2001 Life: 2015
Malpractice insurance that’s all about you .
As a dentist, you face unique challenges every day. That’s why at MedPro Group, we created an industry-leading malpractice policy that keeps you safe. Here’s what else you can expect with MedPro on your side.
You’ll get great coverage at a great price. We also offer policy options that others don’t — including Occurrence and a pure consent clause, which gives you more control during a claim. Get unmatched coverage.
With 24/7 access to our free risk resources and on-staff experts, you and your practice will be better prepared for every day challenges. We don’t just defend claims, we help you avoid them.
The average dentist is sued at least once in their career, which is why we’re in your corner when it matters most. We lead the industry with a 95% dental trial win rate (plus 8 out of 10 claims close without payment).
OFFICIAL CALL FOR NOMINATIONS
OFFICIAL CALL FOR CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS: SPEAKER OF THE HOUSE, SECRETARY-TREASURER, AND EDITOR
OFFICIAL CALL FOR SPEAKER OF THE HOUSE CANDIDACY
ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of Texas Dental Association (TDA) Speaker of the House may be submitted to TDA Secretary-Treasurer Dr Carmen P Smith for the upcoming 2025 House elections. Only an active, life, or retired member in good standing of this Association shall be eligible. A curriculum vitae (CV) must be submitted, and the candidate will also have to sign a conflict of interest statement. Nominations are in order at the first meeting of the House of Delegates and remain open until the close of the second meeting of the House of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility may be verified. To become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the House of Delegates. Please see the Manual on Caucus, Campaigns, Nominations and Elections at tda.org for full details.
Duties of the Speaker of the House are enumerated in the Bylaws and include the following (excerpt):
1. To serve as an ex-officio member of the Board of Directors without vote or the privilege of proposing resolutions.
2. To serve as an ex-officio member of the Executive Committee without vote or the privilege of proposing resolutions.
3. To preside at all meetings of the House of Delegates.
4. To determine the order of business for all meetings, subject to the approval of the House of Delegates, in accordance with Section 140B of this chapter.
5. To appoint tellers to assist him/her in determining the result of any action taken by vote.
6. To appoint members of reference committees in consultation with the president, president-elect, and the immediate past president by the Board of Directors’ first meeting of the calendar year.
7. To notify the divisional officers and the Committee on Credentials, Rules and Order, prior to the annual session, the number of delegates and alternates necessary to constitute a quorum.
8. To meet with the divisional officers prior to the meeting of the divisional caucuses at the annual session to review the Rules for Caucus Procedures, Nominations, And Elections.
9. To appoint a parliamentarian pro tem, should it become necessary for the parliamentarian to be absent during a session of the House of Delegates.
10. To serve as presiding officer of the TDA Candidates Forum, unless the Speaker is in a contested race, at which time the Speaker Pro-tem will preside.
11. To be a certified parliamentarian or be in the process of certification
Candidacy announcements are to be mailed to TDA Secretary-Treasurer Dr Carmen P. Smith, Texas Dental Association, 8701 W Hwy 71 Ste 201-M, Austin, Texas 78735; or, emailed to TDA Executive Director Linda Brady: lbrady@tda.org.
(See TDA Bylaws, Chapter IV, House of Delegates—Sections 100 (Officers), 110A (Duties), 150C(3), 150D, Chapter V, Board of Directors—Sections 10 (Composition); TDA House Manual; Speaker Manual).
OFFICIAL CALL FOR SECRETARYTREASURER CANDIDACY
ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of Texas Dental Association (TDA) Secretary-Treasurer may be submitted to TDA Secretary-Treasurer Dr Carmen P Smith for the upcoming 2025 House elections. Only an active, life, or retired member in good standing of this Association shall
be eligible. A curriculum vitae (CV) must be submitted, and the candidate will also have to sign a conflict of interest statement. Nominations are in order at the first meeting of the House of Delegates and remain open until the close of nominations at the end of the second meeting of the House of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility can be verified. To become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the House of Delegates. Please see the Manual on Caucus, Campaigns, Nominations and Elections at tda.org for full details.
Duties of the TDA Secretary-Treasurer are enumerated in the Bylaws and include the following (excerpt):
1. To serve without vote as member of the Board of Directors and the House of Delegates.
2. To serve without vote as chair of the Budget Committee.
3. To examine the income and expenses of this Association and report at each meeting of the Board of Directors.
4. To ensure that the minutes of the House of Delegates and the Board of Directors be maintained.
5. To be responsible and perform such other duties as shall be specified by the Board of Directors and the Bylaws
Other duties as Secretary include the following:
• Serve as recording officer and custodian of the records of the House of Delegates and the Board of Directors.
• Serve as secretary to the Executive Committee, without the right to vote.
• Serve as secretary to the House of Delegates.
• Serve as the secretary of the American Dental Association Fifteenth Trustee District Delegation.
Candidacy announcements are to be mailed to TDA Secretary-Treasurer Dr Carmen P. Smith, Texas Dental Association, 8701 W Hwy 71 Ste 201-M, Austin, Texas 78735; or, emailed to TDA Executive Director Linda Brady: lbrady@tda.org.
(Ref. TDA Bylaws, Chapter IV, House of Delegates—Sections 70A-B (Notice and Publication-Official Call & Publication of Actions, 110B (Duties); Chapter V, Board of Directors—Sections 10 (Composition), 80B (Officers-Secretary); Chapter VI, Elective Officers—Section 90G (Duties); Chapter VIII, Fifteenth Trustee District American Dental Association Delegates and Alternate Delegates—Section 80 (Delegation Secretary); Board Manual; Secretary-Treasurer Manual).
OFFICIAL CALL FOR EDITOR
CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of Texas Dental Association (TDA) Editor may be submitted to TDA Secretary-Treasurer Dr Carmen P. Smith for the upcoming 2025 House elections. Only an active, life, or retired member in good standing of this Association shall be eligible. A curriculum vitae (CV) must be submitted, and the candidate will also have to sign a conflict of interest statement. Nominations are in order at the first meeting of the House of Delegates and remain open until the close of nominations at the end of the second meeting of the House of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility can be verified. To become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the House of Delegates. Please see the Manual on Caucus, Campaigns, Nominations and Elections at tda.org for full details.
Duties of the editor are enumerated in the Bylaws and include the following (excerpt):
1. To be editor-in-chief of all journals and publications of the Association and exercise full editorial control over such publications, subject only to policies established by the House of Delegates, Board of Directors, and these Bylaws and provided such content is not in conflict with or contrary to the TDA’s established policies, legislative agenda, or advocacy efforts.
2. To control the selection of scientific material published in the Journal. The editor may appoint associate editors, with the concurrence of the Board of Directors, to gather and/or review material for publication. Such associate editors shall serve as long as the editor deems necessary; but never longer than the term of the editor.
3. To attend all open meetings of the Board of Directors and the House of Delegates of this association, and the annual session of the American Dental Association.
4. To hold no other office in this association or the American Dental Association while serving as editor, except the editor may be elected as delegate or alternate delegate to the ADA House of Delegates from his/her respective division.
5. To cooperate with his/her successor upon termination of the Editor’s term of office.
Candidacy announcements are to be mailed to TDA SecretaryTreasurer Dr Carmen P. Smith, Texas Dental Association, 8701 W Hwy 71 Ste 201-M, Austin, Texas 78735; or, emailed to TDA Executive Director Linda Brady: lbrady@tda.org.
Why send your patient to the endodontist when you can bring the endodontist to your patients?
EndoConnect partners with dentists to provide specialty endodontic care in your office.
• No hidden costs
• State-of-the-art equipment
ACCESS SPECIALIZED EQUIPMENT & EXPERTISE
• A par tnership for success
• Increased production
COLLABORATE TO CREATE BETTER PATIENT OUTCOMES
INCREASE YOUR PRACTICE’S REVENUE
BECOME A PARTNER TODAY!
Call us at 214.797.5131 or scan the QR code to visit our website at EndoConnect.net.
P R E V I E W
SPEAKER
Joshua austin, dds, magd
will be presenting 4 sessions at the TDA Meeting: What’s New? Materials and Tech that Expedite Excellence
Thursday, May 8, 8:30 AM – 11:30 AM
The New Glass Ionomer: A Hands-on Experience!
Thursday, May 8, 1:00 PM – 4:00 PM
Expedited Excellence Hands-on: Increase Your Efficiency & Predictability with Direct Restorations
Friday, May 9, 8:00 AM – 11:00 AM
The Mental Dental Connection: The Secret to Being a Better Clinician and Leader
Friday, May 9, 1:30 PM – 4:00 PM
There is no dental meeting closer to my heart than the TDA Meeting. It just feels like home. It was the first dental meeting I ever attended, starting during my days in dental school at UT Health San Antonio. It is always great to see old friends from my time in Texas Dental Association leadership. I also get to catch up with former classmates and connect with the Texas dentists that time has let drift away. In addition, I don’t have to get on an airplane, which is so nice! The truth is, I would gladly fly across the world for the TDA Meeting, which is why it is such an honor to present there in 2025.
The 4 sessions we have planned at the TDA Meeting 2025 are varied and diverse! We have 2 lecture style courses and 2 participation courses. Participation courses are clinical in nature, while one of the lecture topics is a little different. All the sessions will be fast paced, fun and packed with pragmatic, useful pearls for restorative dentists.
Starting with the participation courses, we will be covering differing aspects of direct restorative dentistry. While attending Expedited Excellence hands-on: Increase Your Efficiency & Predictability with Direct Restorations, we will be focusing on getting faster and more predictable with the most common procedure in general and restorative dentistry… the posterior composite. Most of us fill our days with these procedures, performing multiple per day. The problem is they are difficult, timeconsuming and barely profitable. My insurance reimbursement rates have hardly raised on these procedures, despite numerous increases in the “costs of doing business.” The only way for us to remain profitable with these restorations is to work faster and have fewer post operative issues. That’s what this workshop will focus on! After this course, you will feel faster and more confident in all the kinds of posterior direct restorations and ready to go back to your practice with those skills.
The second hands on course, The New Era of Glass Ionomer: A HandsOn Experience, focuses on a topic that gets little attention at continuing education courses…glass ionomer. There has been a dramatic shift in the properties of glass ionomers available on the market. These materials have a place in your practice…whether they be for pediatric patients, geriatric patients, or even high caries risk patients. Glass ionomer materials are severely under-utilized in dentistry today. After attending this workshop, dentists will become knowledgeable about which glass ionomers to use in which clinical situations and how to place them!
The first lecture program on the agenda is What’s New? Materials & Tech That Expedite Excellence. This lecture will cover the newest in dental technology like digital scanning, 3D printing, and artificial intelligence. We will examine how technology can help us in diagnosis and treatment planning, as well as executing and delivering treatment. Digital technology is an amazing thing that can change your practice. Most of us under-utilize it and therefore don’t see the full benefit. This course will help you realize the full benefit of digital technology in your practice!
The second lecture program is perhaps a little bit different. This course, The Mental Dental Connection: The Secret to Being a Better Clinician & Leader, will cover 2 tracks of information. Firstly, the struggle that many dentists have, including myself. Anxiety and depression are rampant in our industry. In part of this course, I will share my journey through discovering my issues and working to treat them. We will also discuss how best we, as clinicians, can treat patients with mental disease. These 2 tracks will weave together and end with an uplifting message for us all. Despite the heavy subject matter, this course is funny and inspiring.
During my dental career in my private practice in San Antonio, I have learned a few things I would like share with other members of the Texas Dental Association. These topics will be touched on in greater depth at the TDA Meeting, but until then, here are some tips:
1. Use your intraoral scanner in the hygiene room. We all know what a scanner can do to replace impression material, but it can be
so much more. It can be the patient communication tool that rules them all. A patient cannot say yes to what they don’t see and understand. That is the true value of the intraoral scanner. Use it in new patient visits. Use it in recall visits. Use it anytime you need to talk to a patient about treatment they need!
2. A sectional matrix system is a must when using resin composite. The days of Tofflemire bands have gone the way of amalgam. Modern materials require modern matricides. There is no more difficult routine procedure than back-to-back class IIs. Sectional matrix systems do not make them easy…but they do make them easier!
3. Take care of yourself. You can’t be the best servant for others unless you remember to serve yourself too. As dental clinicians, we are all givers. We give of ourselves unto others. We do so all day until there is nothing left to give. Leave some in the tank for the people that matter and remember to refill that tank early and often! Whether that be through time off, exercise, meditation or just a night out with friends, fellowship is vitally important.
With that final tip, now’s the perfect time to add the 2025 TDA Meeting to your schedule. Join your peers and colleagues, bond with your team, and refuel your tank!
See you in San Antonio, May 8-10, 2025!
MCNA Insurance Company is pleased to be a benefits administrator for the Texas Medicaid and CHIP program.
MCNA is a provider-centered organization committed to helping dentists serve Medicaid and CHIP enrollees. We provide dentists with leading-edge technology and superb customer service support to reduce missed appointments and encourage patients to seek timely dental care.
For more information, visit us online at: www.mcnatx.net
PRELIMINARY PROGRAM
INSPIRATION AWAITS
SAN ANTONIO MAY 8–10, 2025
JOIN US!
Welcome to the 2025 Texas Dental Association Meeting! Join us at the Henry B. Gonzalez Convention Center along the picturesque San Antonio Riverwalk from May 8-10, 2025. Our dedicated Council on the Annual Meeting and Continuing Education Programs, along with the professional staff of the TDA, have worked tirelessly to create an engaging and unparalleled educational experience. We invite dentists and their entire team there’s something for everyone at the 2025 TDA Meeting!
This year’s educational presentations will feature some of the nation’s leading speakers. Over three days, attendees can access diverse courses tailored for dentists, hygienists, assistants, and office managers. We’re excited to welcome both new speakers and favorites from previous years. The Council has also ensured that essential licensing courses are included, covering critical topics such as opioids, sleep dentistry, sedation, and human trafficking. Plus, we’ll offer hands-on workshops that allow participants to practice and reinforce their skills, enabling them to return to their patients with fresh techniques. Our CE Express will feature many new emerging speakers from around the state. We can’t wait to showcase new talent in these quick, low-cost courses.
MEET THE COUNCIL ON THE ANNUAL MEETING AND CONTINUING EDUCATION PROGRAMS
TDA’s Council on the Annual Meeting and Continuing Education Programs (CAMCEP) is comprised of six members, one new dentist representative, and one consultant. They meet quarterly to plan all continuing education programs with TDA staff.
Throughout the year, they attend dental meetings nationwide to discover new speakers, exhibitors, and cutting-edge ideas. Their hard work behind the scenes ensures that each meeting and program exceeds expectations and provides the best experience for attendees. Look out for them at the meeting in their navy blue coats and be sure to say hi!
The Exhibit Hall will again serve as the vibrant hub of the meeting, featuring hundreds of exhibitors showcasing the latest materials, equipment, and technology. Connect with colleagues and join us for the “I Want My TDA Totally 80s Party” on Thursday. Lace up your skates and take a spin around the roller skating rink and dance to your favorite 80s music.
Don’t forget to download the TDA Meeting App to help navigate your experience. The app includes the CE schedule and verification, along with real-time updates on specials and news. To register for the meeting and view a complete schedule of events, please visit tdameeting.com. Register early to take advantage of our Early Bird Discounts!
While you’re in San Antonio, take the time to explore the Riverwalk, admire the art and historic architecture, and indulge in the city’s award-winning dining. Consider taking a river taxi to explore the vibrant Pearl Brewery, with its bars, restaurants, shops, and live entertainment. Bring your team to enjoy camaraderie beyond the classroom.
Whether you’re looking to expand your technical skills, empower your team, or focus on your own well-being, there is something for everyone. So, gather your team, colleagues, and friends, and get ready for the best TDA meeting experience in San Antonio. We can’t wait to see you there!
Katie Stuchlik, DDS and Elizabeth Jaynes, DDS 2025 TDA Meeting Co-Chairs
Brought to you by the Texas Dental Association 8701 W. Highway 71, Ste. 201-M Austin, TX 78735
(512) 443-3675
tda@tda.org
tdameeting.com
8:30 am – 4:30 pm, Monday-Friday (Central Time)
TDA MEETINGS STAFF
This department is responsible for the organization, coordination, and council support of the TDA Meeting, conferences, regional events, and online continuing education programs.
Shannan Cook, CMP Director of Meetings and Continuing Education scook@tda.org
Henry B. Gonzalez Convention Center 900 E. Market Street, San Antonio, TX 78205
2025 REGISTRATION AND HOUSING SERVICES
Eleventh & Gather is the official registration and housing provider for the 2025 TDA Meeting. Please do not call the hotel directly to make reservations, as TDA has secured special rates. For any questions about registration or hotel accommodations, please contact them using the information below:
Eleventh & Gather 170 Depot St., Unit 1A, Blue Ridge, GA 30513
678-341-3039
tda@prereg.net prereg.net/2025/tda
9:00 am – 4:00 pm, Monday-Friday (Eastern Time)
Beware of scam emails trying to sell you registration lists or discounted hotel rates.
Meeting Parking
Parking is available at area hotels for overnight guests. In addition, there are multiple parking garages available within walking distance of the convention center. Visit www.sahbgcc.com/Visit-Us/Location-Directions-Parking for more information.
2025 TDA MEETING SCHEDULE OF EVENTS
All events will be held at the Henry B. Gonzalez Convention Center unless otherwise noted.
THURSDAY, MAY 8
7:00 am – 5:00 pm Onsite Registration
8:00 am – 5:00 pm Continuing Education Courses
8:30 am – 8:30 pm Alliance of the TDA Program, Grand Hyatt
10:00 am – 6:00 pm Exhibit Hall
4:30 pm – 6:00 pm TDA Totally 80s Party – Exhibit Hall
FRIDAY, MAY 9
7:00 am – 5:00 pm Onsite Registration
8:00 am – 7:00 pm TDAA Program, Marriott Riverwalk Hotel
8:00 am – 5:00 pm Continuing Education Courses
8:00 am – 11:00 am TDA House of Delegates
8:30 am – 4:30 pm Alliance of the TDA Program, Grand Hyatt
10:00 am – 5:00 pm Exhibit Hall
11:00 am Reference Committees
5:30 pm Divisional Caucus Meetings
SATURDAY, MAY 10
7:00 am – 8:30 am TDA Past Presidents & Past Vice-Presidents Breakfast
8:00 am – 10:00 am Onsite Registration
8:00 am – 12:00 pm Continuing Education Courses
8:00 am – 12:00 pm TDA House of Delegates
8:00 am – 5:00 pm TDAA Program, Marriott Riverwalk Hotel
1:30 pm – 2:30 pm TDA House of Delegates
3:00 pm – 4:00 pm TDA House of Delegates
2025 TDA MEETING MEETING SPONSORS AND DONORS
Thank you to our TDA Meeting Sponsors. Their generous support and donations help us provide you with cutting-edge education and one of the best dental meetings in the country.
The TDA regrets the omission of any sponsors or donors due to print deadlines.
GOLD BRONZE
EDUCATIONAL FUNDING PROVIDED BY:
Align Technology
Alliance of the TDA
Bank of America
Brasseler USA
Clinician’s Choice
CloSYS
DenMat
Dentsply Sirona
Dove Dental Products
Electro Medical Systems
Hager Worldwide
Nobel Biocare
Q-Optics
Solmetex
Texas Dental Association Smiles Foundation
Beverly Bane Lecture Series
VOCO
REGISTRATION INFORMATION
REGISTRATION OPENS JANUARY 6, 2025
Early Bird Registration
Register before February 14!
Register between January 6 and February 14 and SAVE!
TDA members and their staff register for FREE!
Pre-Registration
Register before March 31!
Register between February 15 and March 31.
Registration fees go up slightly.
Standard Registration
Register after April 1st!
Register between April 1 and May 10.
Full-price registration fees apply.
Register online at www.tdameeting.com from January 6 to May 10, 2025. Seats in continuing education courses are first-come, first-served, so register early to save money and secure your spot in popular courses!
Eleventh & Gather is our official registration provider. They will manage online and onsite registration of attendees and exhibitors. Be cautious of fraudulent companies that might try to contact you for registration or to sell attendee lists. Please note that the Texas Dental Association does not sell attendee lists or handle registration or hotel bookings through third parties.
For registration inquiries, please contact Eleventh & Gather at: 678-341-3039
tda@prereg.net prereg.net/2025/tda 9:00 am – 4:00 pm, Monday-Friday (Eastern Time)
CANCELLATION POLICY
A full refund (less a 20% administrative fee) will be issued if cancelled on or before April 10, 2025. No refunds will be approved after this date. In the event of an emergency or death, cancellations will be reviewed on an individual basis.
REGISTRATION POLICIES:
• Dentists may not register under any category other than “dentist”.
• You must be registered under a dentist or team member registration category in order to earn CE credits.
• Photo identification is required for onsite registration.
• 2025 TDA dues must be paid before you can attend the meeting at the member dentist rate.
• The deadline for early bird discounted registration is February 14, 2025.
• The deadline for pre-registration is March 31, 2025.
• Register on or before April 20 to receive your badge by mail. After this date, registration materials may be picked up onsite in registration.
• By registering for the meeting, you authorize the TDA to add you to their email marketing list to receive convention updates for 2025 and subsequent years. You can opt-out at any time, but you will not receive pertinent information regarding your registration.
2025 REGISTRATION FEES
HOTELS
TDA MEETING HOTELS
Support TDA by booking your room within the annual session hotel room block. TDA has secured special discounted rates with these official hotels.
Eleventh & Gather is the official housing provider for the 2025 TDA Meeting.
170 Depot St., Unit 1A, Blue Ridge, GA 30513 678-341-3039
tda@prereg.net
prereg.net/2025/tda
9:00 am – 4:00 pm, Monday-Friday (Eastern Time)
Beware of fraudulent companies who may reach out to you to reserve hotel rooms or sell attendee lists. Eleventh & Gather is the only authorized company to solicit hotel reservations.
Open Monday, January 6
RESERVE YOUR ROOM
https://www.prereg.net/2025/tda
THURSDAY
PROGRAM AT-A-GLANCE
OSHA Dewhirst Annual OSHA Training and Update: Are You Safe Enough?
Practice Mgmt Garofolo Twenty
T27 Pediatrics Rodriguez Pediatric Medical Emergencies and What the Dental Team Should Know
T30 Human Trafficking Swarthout In Plain Sight: Confronting the Human Trafficking Crisis in the Dental Setting
T31 Pharmacology Viola I Haven't Got Time for This Pain: Dental Pain Management for the Entire Dental Team
F02 Hygiene Auger What Lies Beneath: Treating Periodontal Disease Systemically
F03 Esthetics Austin Expedited Excellence Hands-on: Increase Your Efficiency & Predictability with Direct Restorations
F04 Nutrition/Health Austin The Mental Dental Connection: The Secret to Being a Better Clinician and Leader
F05 Lasers Bock Laser Integration in Hygiene: Principles, Protocols and Practical Applications
F06 Dental Assisting Brinker Creating the Digital Workflow Practice Workshop
F07 Dental Assisting Brinker Fundamentals of Aligner Therapy: Hands-on Workshop
F08 Team Building Christopher Are We Having Fun Yet? Attitude, Humor and Peak Performance in Your Practice
F09 Infection Control Dewhirst Infection Control Workshop - What Works?
F10 Technology Duplantis The 3D Experience: An Introduction to CBCT for the Dental Practitioner
F11 Technology Duplantis The 3D Experience Workshop: An Introduction to CBCT for the Dental Practitioner
F12 Oral Surgery Edwab Oral Surgery Workshop for the General Practitioner
F13 Insurance Garofolo AP Insurance
F14 Oral Medicine Gonzales Emerging Trends in the Diagnosis & Treatment of Chronic Orofacial Pain Management
F15 Oral Pathology Gonzales Epithelial Pathology from Aphthae to Zoster
–
Anesthesia Luce Minimal (Lvl 1) Enteral Sedation Review Course
Insurance Patel Demystifying Dental Insurance for the New Dentist and Practice Owner
F28 Practice Mgmt Patel How to Juggle it All and Still Stay Sane: Smart Organization and Life Skills for Dentists and their Teams
F29 Occlusion Peppard Splints: Diagnostic vs. Therapeutic and Their Role in Comprehensive Dentistry
F30 Practice Mgmt Phillips Newland Your Patients Expectations: Ditch the Rose Colored Glasses
Medical Emergencies Read-Fuller Avoiding Disasters: Emergency Management in the Dental Office
F32 Communication Reisman Communicate Like Duct Tape: Gain Traction With Your Patients, Team and Colleagues
F33 Periodontics Saltz When Bad Things Happen to Good Implants
F34 Periodontics Saltz Biofilm Therapy: A New Team Approach to an Age-Old Enemy
F35 Marketing Sampat 30 Dental Marketing Ideas in 90 Minutes: From Engagement to Conversion
F36 Marketing Sampat Comprehensive Marketing for Dentists: From Campaigns to Communication
F37 Marketing Sampat Social Media for Dentists: From Engagement to Conversion
F38 Anesthesia Viola I Have Become Profoundly Numb: An Update on Local Anesthetics , Vasoconstrictors and Clinical Dental Considerations
F39 Hygiene Void-Holmes/ Paveletz Precision Power Prevention: Advanced Hands-on Workshop Part 1
F42 Networking Panel Dental School Admissions Panel
–
–
–
FRIDAY – SATURDAY
Oral Medicine Velemati When Doing Everything Right Still Goes Wrong: Neuropathic Pain Following Dental Trauma
EXP07 Esthetics Najafi Mastering Smile Design: A Multidisciplinary Approach to Crown Lengthening and Lip Repositioning
SATURDAY
CE EXPRESS: INDUSTRY INSIGHTS THURSDAY PROGRAM AT-A-GLANCE
TOPICS BY DAY
See the chart below for a full list of CE topics offered at the 2025 TDA Meeting, organized alphabetically. Scan across to find each session’s day and speaker’s last name.
Topics Thursday Friday Saturday
Anesthesia/Sedation Luce Viola Luce
Caries Paveletz
Communication/Team Building Christopher Christopher Reisman
Cosmetics/Esthetics Austin Austin CE Express Duplantis
Practice Management Garofolo Phillips Newland CE Express Kleive Patel Phillips Newland Bank of America Smith
Radiology CE Express
Restorative Kleive CE Express
Sleep Medicine Hale Hui/McDavid Hui/McDavid
Technology Stanley CE Express Duplantis CE Express
GOVERNANCE
The House of Delegates convenes four sessions during the Annual Session of the Texas Dental Association.
PRELIMINARY HOUSE OF DELEGATES SCHEDULE*:
*The start time of any meeting of the House may be changed by the TDA Speaker with House approval, depending on the extent of House business being considered.
TDA MEMBERS – GET INVOLVED
The House of Delegates is the legislative and supreme governing body of the TDA. The 2025 House of Delegates is composed of 134 voting members, which includes duly elected and installed delegates from each of the 26 components of the Texas Dental Association and the 15 voting members of the Board of Directors. The Speaker of the House of Delegates is the presiding officer and is without vote. The TDA SecretaryTreasurer is also a non-voting office of the House of Delegates and serves as the Secretary of the House. Finally, there are four student delegates, each elected and installed by their respective dental school; student delegates have full privilege and access to the floor of the House of Delegates but are without the right to vote and may not introduce resolutions.
HOUSE MATERIALS
Delegates and alternates will receive their House book in a searchable PDF format. Reference committee reports will be emailed in PDF format to all participants and these reports can be downloaded from any location with internet access.
For more information, contact TDA Governance Manager, Amy Gamber at agamber@tda.org or (512) 443-3675, ext. 150.
ADA/TDA LEADERSHIP CANDIDATES FORUM
Friday, May 9 4:00 pm – 5:30 pm
In the event there are no contested TDA statewide elections and no participation by candidates for ADA elected offices, the candidate’s forum will not be held.
CAUCUS MEETINGS
Friday, May 9 5:30 pm
Get involved by attending divisional caucus meetings and selecting your representatives on the state and national levels. ADA delegates and alternates from your division and the divisional directors of the TDA Board of Directors are nominated in this forum.
Friday, May 9 8:00 am – 11:00 am
Saturday, May 10 8:00 am – 12:00 pm 1:30 pm – 2:30 pm 3:00 pm – 4:00
REFERENCE COMMITTEES
Reference committee hearings offer an opportunity for any member to participate in the TDA policy-making process. All members are encouraged to attend the hearings scheduled on Friday, May 9. All 2024-2025 resolutions will be discussed in up to potentially five Reference Committees before presentation to the 2025 TDA House of Delegates for policy-making decisions.
Reference Committee Hearings will begin at 11:00 AM or 15 minutes after the adjournment of the first meeting of the House of Delegates.
Reference Committee assignments and starting times are subject to change, please visit www.tda.org for the latest information.
EXHIBIT HALL
Explore the TDA Meeting Exhibit Hall to connect with your favorite dental reps, discover the latest products and services for your practice, and find career solutions all while having some fun!
Be sure to stop by the 600-aisle, featuring our TDA Perks Program partners, to learn about member-exclusive discounts and resources. Whether it’s compliance, supplies, insurance, marketing, finance, or real estate you’ll find everything you need to support your practice.
EXHIBITOR LIST AND FLOOR PLAN
Plan your visit and search for products or services to maximize your time in the hall!
Explore the exhibitor list and interactive floor plan at tdameeting. com or by scanning the QR code.
EXHIBIT HALL HOURS
Thursday, May 8 10:00 am – 6:00 pm
Friday, May 9 10:00 am – 5:00 pm
EXHIBIT HALL
DON’T MISS OUT ON THE FUN…
ROLLER SKATING
We’re bringing the FUN to the exhibit hall with a roller-skating rink! Lace up your skates and join us for some retro vibes, networking, and a chance to unwind between sessions. It’s the perfect way to add some excitement to your day see you on the rink!
Thursday, 2:00 pm – 6:00 pm
Friday, 10:00 am – 2:00 pm All skating equipment will be provided
I WANT MY TDA TOTALLY 80s PARTY
Get your neon ready and tease up that hair it’s time to party 80s style! Join us for the Totally 80s Party on Thursday, May 8 from 4:30 pm – 6:00 pm.
Special thanks to TDA Perks for making this rad event possible.
ARCADE GAMES
Take a trip down memory lane with classic arcade games! Whether you’re a Pac-Man pro or just want to relive the glory days, we’ve got all your favorites ready for some fun and friendly competition. Play, unwind, and enjoy the 80s vibes!
Thurs. MAY 8, 2025 4:30 –6:00 pm
Mark your calendars for a totally rad party in the Exhibit Hall!
Thurs. MAY 8, 2025 4:30 – 6:00 pm
Mark your calendars for a totally rad party in the Exhibit Hall!
Practices For Sale
FANTASTIC TEXARKANA LOCATION: GP in a bustling retail center with great visibility. The office has 3 ops, digital X-ray, and paperless patient charts. The practice has over 1,200 active patients that are a mixture of 20% FFS and 80% PPO. The seller refers out most specialties, and the practice operates on 3.5 doctor days and 4 hygiene days, leaving ample room for growth. Opportunity ID: TX-02243
FANTASTIC RETAIL LOCATION: Plano GP that is highly visible in a retail center. This practice operates with the owner and 1 PT associate, is open 7 days a week and provides regular dental care as well as emergency services. The practice has over 1,750 active patients who are 20% FFS, 70% PPO, and less than 10% Medicaid. The office has 4 ops and is in excellent condition. This is a great opportunity for growth by capitalizing on the existing patient base and expanding services. Opportunity ID: TX-02219
HUGE OPPORTUNITY FOR GROWTH: Dallas GP in a professional building with great accessibility. The office has 3 ops and is in good condition. Currently using paper charts and is non-digital. The practice operates on 4 doctor days per week. Excellent opportunity for growth by adding a hygienist, new procedures, current marketing and/or extending hours. The practice has over 1,200 active patients who are a blend of 10% FFS, 50% PPO, and 40% Medicaid. Opportunity ID: TX-02171
FANTASTIC HIGH-END OPPORTUNITY: L.V.I. trained GP located in a Houston retail center with great visibility and a very popular anchor store next door. This office has 6 fully equipped ops and one unequipped but plumbed. The office equipment includes digital X-ray and Pano and has paperless charts. The practice is 90% FFS with a small amount of PPO. The office collected over $876K in a four-day workweek. Opportunity ID: TX-02041
Narrative Review
Surgical guides for esthetic crown lengthening procedures:
Dr Alhumaidan is an assistant professor, Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Dr al-Qarni is an assistant professor, Department of Substitutive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Dr AlSharief is an assistant professor, Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Address correspondence to Dr AlSharief, Department of Preventive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, PO Box 1982, Dammam 31441, Saudi Arabia, email msalsharief@iau.edu.sa.
Dr AlShammasi is a dentist, Ministry of Health, Saudi Arabia.
Dr Albasry is a teaching assistant, Department of Substitutive Dental Sciences, College of Dentistry, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Disclosures. None of the authors reported any disclosures.
ABSTRACT
Background. In patients with gingival exposure on smiling due to altered passive eruption, esthetic crown lengthening is often indicated. Meticulous planning and surgical precision are key for successful outcomes. Surgical guides are helpful tools that are seldomly reported on in the literature related to esthetic crown lengthening procedures.
Types of Studies Reviewed. The authors searched the literature for articles that described the planning, tools, and execution related to esthetic crown lengthening procedures.
Results. Several techniques have been reported to guide the esthetic crown lengthening procedure, ranging from direct bone level measurement to 3-dimensional printed surgical guides.
Practical Implications. This review serves the clinician as an aid in the decision-making process for esthetic crown lengthening procedures and available surgical guide options, including computer-based guides.
Our review aims to shed light on available options and serve as a guide in the planning and decision-making process when the esthetic crown lengthening procedure is indicated owing to altered passive eruption (APE).
An evolution in patient demands has reached an unprecedented level of exactness. Patients are even more demanding when it comes to restoring nonesthetic areas than esthetic areas. This increase in esthetic demand does not go unjustified. There is a relationship between a person’s physical appearance and their self-esteem. Researchers have found that a person’s face is the primary source of determining physical attractiveness.1,2
Increased gingival exposure on smiling, termed excessive gingival display (EGD) has been an ongoing point of concern for both the patient and clinician. Patients will often refer to this as a “gummy smile.” The clinician must fully understand the multifactorial nature of this situation to provide patients with a satisfactory solution. A thorough examination, an accurate diagnosis, and proper planning are imperative for achieving predictable and esthetically superior results.
Several conditions are known to cause EGD, including vertical maxillary excess, hypermobile or short upper lip, dentoalveolar extrusion, gingival overgrowth, and altered passive eruption (APE).3 Management depends primarily on the underlying cause. If EGD is due to vertical maxillary excess, orthognathic surgery is often indicated to correct the skeletal anomaly. Hypermobile or short upper lip can be corrected by means of lip repositioning surgery or temporarily by means of botulinum toxin injections. Another etiologic factor is dentoalveolar extrusion, which is usually corrected with orthodontic intrusion. Furthermore, in cases of gingival overgrowth, external bevel gingivectomy is often sufficient. Finally, EGD might be due to APE, which requires an esthetic crown lengthening procedure. Because combined etiologies more commonly underlie EGD, multitreatment interdisciplinary approaches are frequently indicated.3
Despite major esthetic advances in periodontal therapy, the preservation of a sound periodontium remains a prerequisite of a successful esthetic and functional restoration. Thorough knowledge of anatomy and the interplay between a restoration and the periodontium is essential for achieving a successful and predictable esthetic outcome. Communication between the prosthodontist and periodontist is a crucial factor in the treatment of such cases.
Surgical guides can be useful in properly executing the planned outcome. Although numerous articles and case reports have used surgical guides of one form or another, literature focusing on discussions of them is scarce. Our review aims to shed light on available options and serve as a guide in the planning and decision-making process when the esthetic crown lengthening procedure is indicated owing to APE.
PRESURGICAL DETERMINATION OF THE CEMENTOENAMEL JUNCTION AND THE ALVEOLAR BONE LEVEL
One of the most important parameters to be evaluated before performing an esthetic crown lengthening procedure is the location of the cementoenamel junction (CEJ), which ultimately dictates clinical crown length.4 Under normal circumstances, the gingival margin is located 1 through 2 mm coronal to the CEJ and follows its outline.5 Furthermore, the location of the alveolar crest and its thickness determine whether to perform a gingivectomy procedure with or without resective osseous surgery.6 Another critical factor is understanding the interplay between the position of gingival margin and CEJ relative to the alveolar crest.7 Failure to establish optimal distances between the CEJ and alveolar crest could result in possible relapse or undesired exposure of root surfaces.8
Clinical Assessments CEJ
The CEJ can be visualized clinically as a demarcating line in the presence of gingival recession.7 The CEJ can be also located subgingivally using a periodontal probe or an explorer to feel a catch as the instrument shifts from the smoother enamel surface to the rougher cementum surface.7 Detecting the exact location of CEJ is subject to errors that are related to either visual assessment or tactile sensation.8 Deep subgingival location of the CEJ or the presence of subgingival calculus or restorations are factors that hinder identification of the CEJ.8,9
Alveolar Crest
Direct bone level (DBL) measurement obtained after surgical flap reflection is considered the most accurate method and the reference standard for detecting alveolar crest location.10,11 However, it is an invasive procedure that causes discomfort to patients and might not always be applicable in the presurgical diagnostic and planning phases.10,11
Bone sounding, also known as transgingival probing (TGP), aims to detect the osseous structures underneath the gingival tissues and determine the proximity of the alveolar crest relative to the gingival margin, as well as the thickness of soft tissues.12,13 This was described in detail by Coslet and colleagues6 in 1977 and later by Kois and colleagues in 1994.14
Several authors compared TGP with DBL measurements for various purposes.15-19 All studies reported good agreement between the 2 methods and concluded that TGP could be used for an accurate assessment of alveolar crest level. It is considered a simple, less invasive, and reliable alternative to DBL measurement. The reported overall agreement between TGP and DBL measurements in those studies ranged from 83.2% through 91.9%.15-19
Factors that affect the clinical assessment of the alveolar crest level by means of bone sounding include root surface anatomy, cervical crown contour, health of the gingival tissues, presence of calculus, facial infrabony defects, tip diameter of the periodontal probe, and experience of the clinician.19 Furthermore, the presence of a thin buccal osseous plate or bone dehiscence hinders precise identification of alveolar bone crest. On the contrary, a thick gingival phenotype and buccal plate result in a more accurate assessment.13
Radiographic Assessment
2-Dimensional Radiography
The use of intraoral periapical (PA) and bite-wing radiographs to detect CEJ and alveolar bone levels has been reported.20,21 They also serve as tools aiding in the diagnosis and treatment planning of APE cases.22 Zanatta and colleagues compared the accuracy of PA and bite-wing radiographs and TGP in the planning of crown lengthening procedures with the DBL measurement.23 All methods had statistically significant differences and were inferior in accuracy compared with the reference standard. Measurements obtained via TGP were the closest in accuracy compared with the reference standard, followed by bite-wing radiograph. PA radiographs were the least accurate among the methods investigated.23
Parallel Profile Radiograph
Alpiste-Illueca suggested the use of parallel profile radiograph technique for measuring the dentogingival unit of anterior teeth. This technique was found to be reproducible and useful in planning esthetic crown lengthening surgery, especially in APE cases, as it allows the evaluation of alveolar crest morphology and location relative to the CEJ.24
Parallel profile radiograph is obtained from a lateral projection using a long cone parallel technique and using 2 auxiliary elements. A lead plate evaluates any dimensional distortion in the radiograph obtained, as it demarcates the gingival tissues. Then gutta-percha is inserted into the gingival sulcus and extended from the bottom of the sulcus apically to the gingival margin coronally. In the radiograph obtained, the CEJ is visualized clearly as it lies between the radiopaque enamel surface that becomes thinner cervically to meet the more radiolucent dentin. Beyond the CEJ, the alveolar crest and buccal bone plate can be visualized as radiopaque structures surrounding the radiolucent periodontal ligament space. The image is then digitized and imported into software to allow for measurements to be obtained.24
Cone-Beam Computed Tomography
Cone-beam computed tomography (CBCT) has become an essential tool in the field of dentistry, as it offers a highquality, 3-dimensional (3D) image.25 It is superior to bone sounding and conventional 2-dimensional radiography in the assessment of CEJ and bone morphology, as well as detecting abnormal root anatomy and bony dehiscence or fenestrations.13 Furthermore, it is more comfortable for patients and less invasive than bone sounding.26 Leung and colleagues reported on the greater accuracy of CBCT in identifying the CEJ than identifying alveolar bone margin.26 This was due to the fact that the CEJ is the junction between enamel and cementum, which have different densities, and the latter is the interface between cementum and bone, which have similar densities. In addition, greater accuracy was reported in detecting bone fenestration than dehiscence.
Grimard and colleagues reported a strong correlation between CBCT and direct surgical measurements of the hard tissues.27 Although CBCT was found to underestimate the distance from CEJ to the base of bone defect, it precisely estimated the distance between CEJ and alveolar crest. In contrast, intraoral PA radiographs were found to be less reliable than CBCT, as they underestimated the measurements of all investigated parameters considerably.27 Batista and colleagues suggested the use of CBCT for the diagnosis and presurgical planning of APE cases, as it provides accurate measurements related to the CEJ and alveolar bone crest, in addition to the actual anatomic crown length.4
SURGICAL GUIDES FOR ESTHETIC CROWN LENGTHENING PROCEDURE
Below we describe various techniques used to guide surgical crown lengthening. A decision tree is provided in Figure 1 to help choose the best guide on the basis of clinical presentation as well as clinician’s preference.
Bleeding Points (bone sounding)
The esthetic crown lengthening procedure has traditionally been guided on the basis of clinical evaluation of parameters using direct visual assessment and bone sounding.28 The clinician pierces through the gingival tissues with a periodontal probe, thereby creating bleeding points (Figure 2). These points are then connected in a scalloped fashion to represent the future gingival outline.28,29 Soft tissue can
Tooth preparation and temporization
Conventional/digital surgical guide fabrication
Esthetic crown lengthening based on existing finish line
Esthetic crown lengthening based on the surgical guide
Definitive restorative treatment Tooth preparation and temporization (intraoperative, early or delayed)
Figure 1 A decision tree illustrating various surgical guide options.
Figure 2. Bleeding points as a guide.
be removed with either a surgical blade or using laser technology, which might be advantageous in achieving better hemostasis, especially in cases of external bevel gingivectomies. A flap is then elevated to preform resective osseous recontouring, rendering the bone crest 2 through 3 mm from the newly outlined gingival margins and thereby limiting the amount of gingival rebound.28 The amount of bone resection should be gradually reduced toward the line angles to avoid loss of interdental attachment and resulting in black triangles.
Chu Proportion Gauges
Chu proportion gauges were introduced by Stephen Chu in 2007.30 He proposed the use of 2 different proportion gauge tipsdthe T-bar (Figure 3) and in-line gauges. They determine the ideal clinical crown length to width ratio following a predetermined proportion of 78%, for which the appropriate gingival margin
position and tooth dimension could be anticipated without a subjective estimation.30 This technique relies on the following clinical parameters: gingival width, gingival margin position relative to the CEJ, crown width, clinical crown length, anatomic crown length, and distance between the CEJ and alveolar crest.30,31
The osseous level is assessed before flap elevation on the basis of the measurements obtained by means of bone sounding technique or gauge.28,32,33 After the flap is elevated, the appropriate proportion of supracrestal attached tissue and amount of osseous resection can be planned and carried out using a periogauge or crown lengthening gauge.29,32 Such gauges estimate the desired crown length and enable the clinician to determine the future location of the alveolar crest to be 3 mm away from the CEJ facially, tapering toward the interdental area.29,32
The esthetic crown lengthening procedure guided by Chu proportion gauge has been found to achieve predictable and stable postsurgical outcomes related to supracrestal attached tissue and gingival margin position.33 In addition, it overcomes the disadvantages of additional cost and dental visits required to fabricate a surgical stent. However, the practical use of proportion gauges cannot be applied to worn or modified dentition, as the presence of intact incisal edges is crucial for successful outcomes.34
Existing Restorative Margins
For situations in which APE is present concomitant with existing prostheses or compromised tooth conditions such as wear, caries, large restorations, or trauma, prosthetic rehabilitation is necessary to achieve satisfactory results. When restorative treatment is indicated, the presurgical plan begins with determining the proposed incisal
Figure 3. Chu proportion gauge (T-bar).
edge position on the basis of tooth display in repose and during smiling.35 Once established, the mean length to width ratio is calculated, and the level of the future gingival margin is determined accordingly. Such measurements are transferred to stone casts and diagnostic waxing is performed to predict the final crown dimensions.
The restorative dentist can then prepare teeth and place artificial crown margins at the level of the proposed gingival margin before the actual crown lengthening surgery. The prepared finish lines will serve as a surgical guide from which the periodontist will apically position the alveolar bone crest by 3 mm.
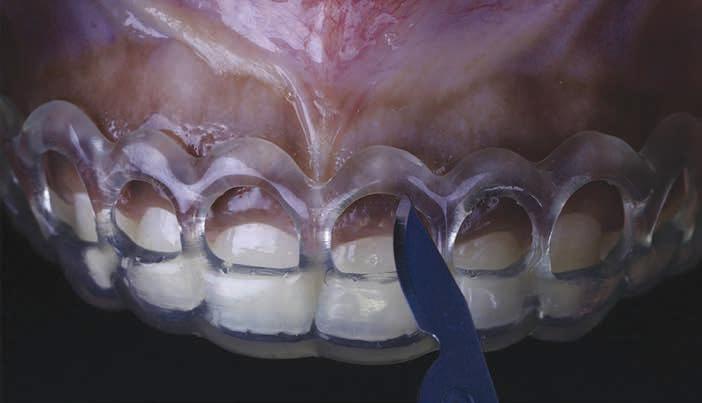
Laboratory-fabricated Surgical Guides
When indicated, surgical guides can be fabricated indirectly using vacuform shells or polymethyl methacrylate resin on the basis of diagnostic waxing. The table below summarizes the advantages and disadvantages of the material options. The surgical incision is then outlined following the surgical guide, followed by osseous recontouring if needed. Tooth preparation can be performed at the time of surgery, 3 weeks after surgery, or after 6 through 12 months, when soft-tissue stability is achieved.36 This technique is especially indicated in patients with severe wear of anterior teeth, when it might be challenging to prepare teeth and
DigitalDesigned3-DimensionalPrinted Best fit Expensive
Easeoffabrication Quickest
Guidessoftandhardtissues
Table. Material options and characteristics for laboratory-fabricated surgical guides.
place provisional crowns before crown lengthening owing to lack of adequate retentive and resistance form.37 Laboratory-fabricated surgical guides can also be beneficial in cases that do not require restorative treatment (Figure 4).
3D Printed Surgical Guides
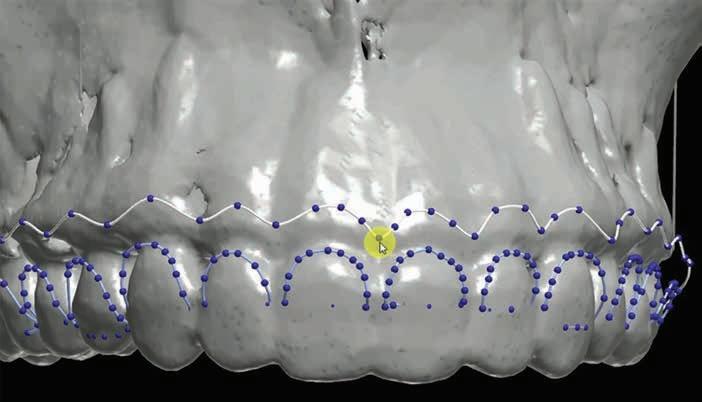
The use of a digital workflow to treat patients with APE has been proposed in situations with restorative treatments, as well as when no restorative treatment is anticipated.38,39 In this method, a CBCT scan is acquired to analyze the level of the alveolar bone crest in relation to the CEJ. An intraoral scan is acquired to aid in fabricating a surgical guide. Digital Imaging and Communications in Medicine files obtained from the CBCT are converted to Standard Tessellation Language format and then superimposed with Standard Tessellation Language files acquired from the intraoral scan. The level of the CEJ is then marked (Figure 5) to guide the gingivectomy incision line, followed by a second line 3 mm apical to the CEJ line to guide the bone resection.
TessellationLanguageformatandthensuperim posedwithStandardTessellationLanguage fi les acquiredfromtheintraoralscan.TheleveloftheCEJisthenmarked(Figure5 )toguidethe gingivectomyincisionline,followedbyasecondline3mmapicaltotheCEJlinetoguidethe boneresection.
Figure 4 Surgical guide made with tooth-colored acrylic resin placed on teeth.
Figure 5. After superimposition of the cone-beam computed tomographic scan and intraoral scan, the cementoenamel junction and future bone level are marked. Reproduced from Alhumaidan A, Alqahtani A, al-Qarni F. 3D-printed surgical guide for crown lengthening based on cone beam computed tomography measurements: a clinical report with 6 months follow up. Appl. Sci. 2020;10(16):5697, CC-BY 4.0. https://doi. org/10.3390/app10165697.39
Figure 6. Surgical incision based on the guide. Reproduced from Alhumaidan A, Alqahtani A, al-Qarni F. 3D-printed surgical guide for crown lengthening based on cone beam computed tomography measurements: a clinical report with 6 months follow up. Appl. Sci. 2020;10(16):5697, CC-BY 4.0. https://doi.org/10.3390/app10165697.39
Figures 5-7 are reprinted with approval from the authors.
Figure 7. Surgical guide placed to determine level of osteoectomy. Reproduced from Alhumaidan A, Alqahtani A, al-Qarni F. 3D-printed surgical guide for crown lengthening based on cone beam computed tomography measurements: a clinical report with 6 months follow up. Appl. Sci. 2020;10(16):5697, CC-BY 4.0. https://doi.org/10.3390/app10165697.39
The virtual design of the surgical guide is performed accordingly. Data are transferred to a 3D printer, and the guide is printed. After placing the guide in the patient’s mouth, an internal bevel incision is made following the upper border of the window of the guide (Figure 6). The guide is then removed, and a second sulcular incision is made. The secondary flap is removed while visualizing the new crown lengths. A full-thickness mucoperiosteal flap is elevated and the surgical guide is then placed again to determine the extent of osteoectomy needed (Figure 7). An osteoectomy is then performed, followed by osteoplasty to finalize buccal bone thickness. The guide is then positioned for a final check before sutures are placed, and hemostasis is ensured.
This technique provides guides for both gingival and bone resection, facilitating the surgical procedure and providing predictable outcomes. Using a precise outline of the anatomic CEJ location can compensate for the variability among patients and reduce the chance of
under- or overcontouring hard and soft tissues.
CONCLUSIONS
A surgical guide used to perform esthetic crown lengthening is a time-efficient tool that facilitates predictability and reproducibility. After assessing the location of the alveolar bone and the CEJ, several techniques can be used to guide the surgical procedure. These include bleeding points, Chu proportion gauge, and laboratory-fabricated surgical guides. When restorative treatment is indicated, esthetic crown lengthening can, alternatively, be guided by existing teeth preparation finish lines. The use of digital technologies simplifies fabricating surgical guides and minimizes clinical time.
2. Patzer GL. Understanding the causal relationship between physical attractiveness and self-esteem. J Esthet Dent. 1996;8(3):144147.
3. Dym H, Pierre R. Diagnosis and treatment approaches to a “gummy smile.”. Dent Clin North Am. 2020; 64(2):341-349.
4. Batista EL, Moreira CC, Batista FC, de Oliveira RR, Pereira KK. Altered passive eruption diagnosis and treatment: a cone beam computed tomography-based reappraisal of the condition. J Clin Periodontol. 2012;39(11): 1089-1096.
6. Coslet JG, Vanarsdall R, Weisgold A. Diagnosis and classification of delayed passive eruption of the dentogingival junction in the adult. Alpha Omegan. 1977;70(3): 24-28.
7. Vandana KL, Haneet RK. Cementoenamel junction: an insight. J Indian Soc Periodontol. 2014;18(5):549-554.
8. Bennani V, Ibrahim H, Al-Harthi L, Lyons KM. The periodontal restorative interface: esthetic considerations. Periodontol 2000. 2017;74(1):74-101.
9. Watts T. Constant force probing with and without a stent in untreated periodontal disease: the clinical reproducibility problem and possible sources of error. J Clin Periodontol. 1987;14(7):407-411.
10. Suomi JD, Plumbo J, Barbano JP. A comparative study of radiographs and pocket measurements in periodontal disease evaluation. J Periodontol. 1968;39(6):311-315.
11. Kim HY, Yi SW, Choi SH, Kim CK. Bone probing measurement as a reliable evaluation of the bone level in periodontal defects. J Periodontol. 2000;71(5):729-735.
12. Lee EA. Aesthetic crown lengthening: classification, biologic rationale, and treatment planning considerations. Pract Proced Aesthet Dent. 2004;16(10):769-778.
13. Abduo J, Lyons KM. Interdisciplinary interface between fixed prosthodontics and periodontics. Periodontol 2000. 2017;74(1):4062.
14. Kois J. Altering gingival levels: the restorative connection, part I: biologic variables. J Esthet Restor Dent. 1994;6(1):3-7.
15. Greenberg J, Laster L, Listgarten MA. Transgingival probing as a potential estimator of alveolar bone level. J Periodontol. 1976;47(9):514-517.
16. Isidor F, Karring T, Attström R. Reproducibility of pocket depth and attachment level measurements when using a flexible splint. J Clin Periodontol. 1984;11(10):662-668.
17. Ursell MJ. Relationships between alveolar bone levels measured at surgery, estimated by transgingival probing and clinical attachment level measurements. J Clin Periodontol. 1989;16(2):81-86.
18. Perez JR, Smukler H, Nunn ME. Clinical evaluation of the supraosseous gingivae before and after crown lengthening. J Periodontol. 2007;78(6):1023-1030.
19. Kan JY, Kim YJ, Rungcharassaeng K, Kois JC. Accuracy of bone sounding in assessing facial osseousgingival tissue relationship in maxillary anterior teeth. Int J Periodontics Restorative Dent. 2017;37(3):371-375.
20. Schuller AA, Holst D. Testing the consistency of measurements of the distance between the cementoenamel junction and the alveolar bone crest on bitewing radiographs. J Clin Periodontol. 1996;23(11):977-981.
21. Persson RE, Hollender LG, Persson GR. Assessment of alveolar bone levels from intraoral radiographs in subjects between ages 15 and 94 years seeking dental care. J Clin Periodontol. 1998;25(8):647-654.
22. Levine RA, McGuire M. The diagnosis and treatment of the gummy smile. Compend
23. Zanatta FB, Giacomelli BR, Dotto PP, Fontanella VR, Rosing CK. Comparison of different methods involved in the planning of clinical crown lengthening surgery. Braz Oral Res. 2010;24(4):443-448.
24. Alpiste-Illueca F. Dimensions of the dentogingival unit in maxillary anterior teeth: a new exploration technique (parallel profile radiograph). Int J Periodontics Restorative Dent. 2004;24(4):386-396.
25. White SC, Pharoah MJ. The evolution and application of dental maxillofacial imaging modalities. Dent Clin N Am. 2008;52(4):689-705.
26. Leung CC, Palomo L, Griffith R, Hans MG. Accuracy and reliability of cone-beam computed tomography for measuring alveolar bone height and detecting bony dehiscences and fenestrations. Am J Orthod Dentofacial Orthop. 2010;137(4 suppl):S109-S119.
27. Grimard BA, Hoidal MJ, Mills MP, Mellonig JT, Nummikoski PV, Mealey BL. Comparison of clinical, periapical radiograph, and cone-beam volume tomography measurement techniques for assessing bone level changes following regenerative periodontal therapy. J Periodontol. 2009;80(1):48-55.
28. Aroni MAT, Pigossi SC, Pichotano EC, de Oliveira GJPL, Marcantonio RAC. Esthetic crown lengthening in the treatment of gummy smile. Int J Esthet Dent. 2019;14(4):370-382.
29. Fletcher P. Biologic rationale of esthetic crown lengthening using innovative proportion gauges. Int J Periodontics Restorative Dent. 2011;31(5):523-532.
30. Chu SJ. A biometric approach to predictable treatment of clinical crown discrepancies. Pract Proced Aesthet Dent. 2007;19(7):401-409.
33. Nautiyal A, Gujjari S, Kumar V. Aesthetic crown lengthening using Chu aesthetic gauges and evaluation of biologic width healing. J Clin Diagn Res. 2016;10(1): ZC51-ZC55.
34. Chu SJ, Hochman MN, Fletcher P. A biometric approach to aesthetic crown lengthening, part II: interdental considerations. Pract Proced Aesthet Dent. 2008;20: 529-536.
35. Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51(1):24-28.
36. Marzadori M, Stefanini M, Sangiorgi M, Mounssif I, Monaco C, Zucchelli G. Crown lengthening and restorative procedures in the esthetic zone. Periodontol 2000. 2018;77(1):84-92.
37. Scutella F, Landi L, Stellino G, Morgano SM. Surgical template for crown lengthening: a clinical report. J Prosthet Dent. 1999;82(3):253-256.
38. Passos L, Soares FP, Choi IGG, Cortes ARG. Full digital workflow for crown lengthening by using a single surgical guide. J Prosthet Dent. 2020;124(3):257261.
39. Alhumaidan A, Alqahtani A, al-Qarni F. 3D printed surgical guide for crown lengthening based on cone beam computed tomography measurements: a clinical report with 6 months follow up. Appl Sci. 2020; 10(16):5697.
LAW OFFICES OF MARK J. HANNA
JD Former General Counsel, Texas Dental Association
• Representation Before the Texas State Board of Dental Examiners
Introducing a novel approach to dental color reproduction using AI technology
Marat Wartanovic Awdaljan, MDT, João Carlos Roque, PhD, James Choi, CDT, Luis Felipe Rondón, DDS
Read this article in full at: https://onlinelibrary.wiley.com/doi/10.1111/jerd.13300
Objective
This article aims to describe a systematic method for tooth color reproduction with ceramics restorations employing artificial intelligence (AI) software named Matisse. It provides a comprehensive analysis of the entire process, beginning with shadetaking and extending to ceramic application in a complex clinical case in the anterior region—specifically, a single central restoration supported by an implant.
Clinical Considerations
The clinical case presented highlights the potential of Matisse software for generating ceramic (inSync-Jensen Dental, USA) and staining (Miyo-Jensen Dental, USA) recipes over a zirconia abutment (Katana-Noritake Dental, Japan). This approach achieves an optimal single central restoration utilizing CADCAM and layering techniques.
Conclusions
The systematic method employing the Matisse software achieved accurate color reproduction for a single central restoration supported by an implant. This result was achieved by the dental ceramist within the first attempt and without seeing the patient in the entire process.
Clinical Significance
The Matisse AI-assisted protocol offers a systematic and scientifically grounded method for color reproduction in dentistry.
Guest Editor Rade D. Paravina, DDS, MS, PhD
Figure 1. The Color checker depicts color differences by thirds of the stained framework and the target tooth.
Figure 2. Immediate outcome following implant restoration placement and X-ray displaying the final condition of the case.
Hieu Huynh, DDS, JD
ORAL and maxillofacial
pathology
case of the month
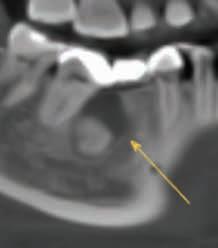
Case History
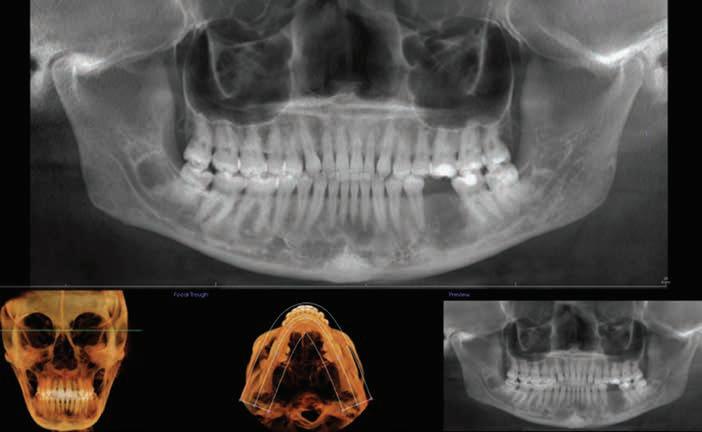
A 44-year-old female presented to a dental office for a routine cleaning and periodic exam, during which an incidental finding was noted (see below). The patient was asymptomatic, and the duration of the condition was unclear. The patient’s medical history was insignificant. The clinician requested an updated cone beam computed tomography (CBCT) scan (Figure 1) due to a suspected lesion at the apex of the right mandibular first molar. Upon review, a lesion was immediately noted at the extraction site of the missing left mandibular first molar. It was reported that the left mandibular first molar had been extracted sometime between 2011 and 2017 at a different office.
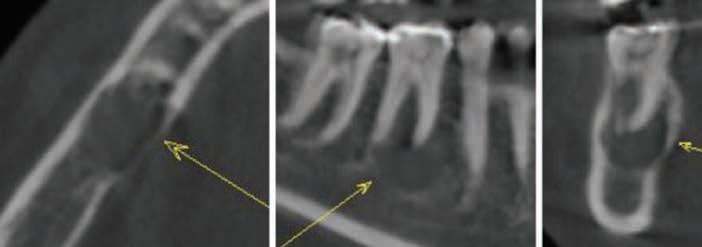
No findings were noted on intraoral-examination. CBCT (Figure 2) imaging showed a mixed-density lesion with focal internal radiopacities in the area of the missing left mandibular first molar. There is thinning and expansion of the cortical plates, as well as superior displacement of the adjacent crestal bone. The lesion partially surrounds the roots of the adjacent teeth and the left mandibular canal, without any evidence of canal displacement.
What is your differential diagnosis?
See page 48 for the answer and discussion.
AUTHORS
Karan Dharia, CEO, DDS
Maxradpath
Madhu Shrestha, DDS
Clinical Assistant professor, Department of Diagnostic Sciences, Texas A&M University School of Dentistry, Dallas, Texas.
Ajay Shakya, DDS
Post-doctoral Fellow, Department of Biomedical Sciences, Texas A&M University School of Dentistry, Dallas, Texas.
Figure 1. Panoramic reconstruction from the CBCT.
Figure 2. Axial, sagittal and coronal sections of the mixed density area in the area of the missing left mandibular 1st molar from the CBCT.
ORAL
and maxillofacial pathology
diagnosis and management—from page ///
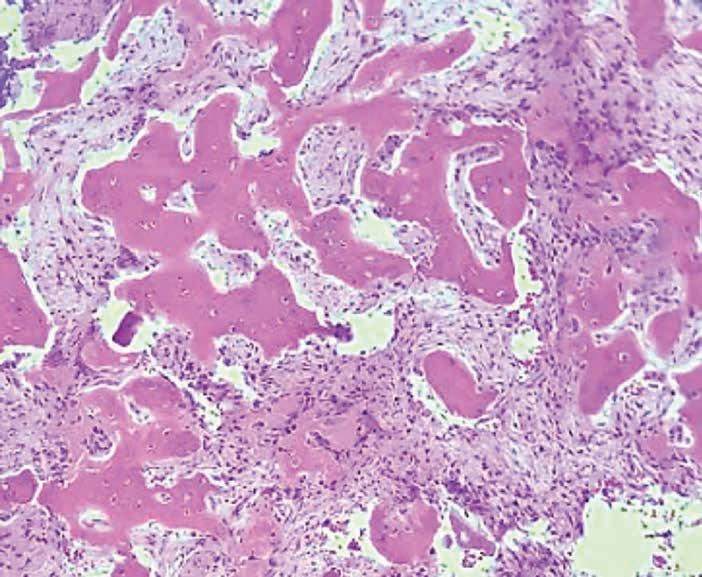
Diagnosis: Cemento-osseous dysplasia
Discussion
Due to suspicion of an ossifying fibroma, the lesion was biopsied. Histologic evaluation depicted fibrous connective tissue with variable amounts of mineralized and calcified bone and cementum like material (Figure 3). The histomorphology combined with the radiographic presentation is consistent with a diagnosis of cementoosseous dysplasia.1 The purpose of this report is to raise awareness of the radiographic differentials of cementoosseous dysplasia (COD) and its varied
Figure 3. Biopsy results demonstrating histology of Cemento osseous dysplasia.
presentations based on its different stages.2 Cemento-osseous dysplasia is a benign fibro-osseous condition that occurs in the gnathic bones, most commonly at the apices of mandibular and maxillary teeth. It is characterized by the replacement of normal bone with fibrous connective tissue, which subsequently calcifies into osseous and cementum-like material.3 This process is typically asymptomatic and does not require clinical intervention. However, if symptoms are present, secondary infection should be considered. Biopsy of COD can lead to low-grade osteomyelitis; thus accurate diagnosis based on clinical and radiographic findings is essential to avoid complications and unnecessary treatment.4 COD has been observed with higher frequency in AfricanAmerican, Hispanic and Asian populations.5,6
Cemento-osseous dysplasia progresses through various stages, with the first stage appearing radiolucent. This is followed by the development of internal radiopacities, eventually leading to a predominantly radiopaque appearance as the fibrous connective tissue is mostly replaced by osseous and cementum-like material. The radiographic appearance varies by stage and may present as a mixed-density lesion, as demonstrated in the case described.3
Cemento-osseous dysplasia is almost always seen superior to the mandibular canal and rarely causes root resorption. It is classified as focal, periapical, or florid based on its location and the number of quadrants involved. When confined to the anterior teeth, it is termed periapical. A single location in the posterior mandible or maxilla is referred to as focal. In cases involving two or more quadrants, the term florid is used.7
Due to its varying stages, differentiating cemento-osseous dysplasia from other conditions—such as inflammatory lesions, cementoblastoma, ossifying fibroma, and benign cystic lesions—can be challenging radiographically. In these scenarios, clinical evaluation and prior or follow up imaging are essential to provide additional clues for an accurate diagnosis.4,8,9
For inflammatory lesions, vitality testing is imperative, as teeth remain vital in cases of COD.8 If an area of COD is suspected and there is concurrent pain or symptomology, the possibility of an overlapping inflammatory process should be considered. Early lesions of COD can be mistaken for inflammatory processes due to their similar radiolucent appearance at the apices of maxillary and mandibular teeth.9
A cementoblastoma is a neoplasm derived from cementum and can be mistaken for COD in cases where cementum-like material fuses to the roots of maxillary or mandibular teeth.10 The thin radiolucent halo surrounding the cementum-like material can be mistaken for the fibrous periphery as seen in cementoblastoma.11 Differentiating these lesions is crucial, as COD fused to the root does not require clinical intervention.
An ossifying fibroma is a neoplasm that can grossly enlarge, displace, and impinge on adjacent structures.12 Ossifying fibromas continue to grow in a symmetrical fashion, similar to the presented case, but they cause displacement of adjacent structures and are typically seen with a thin radiolucent band on imaging.13 Ossifying fibromas require surgical intervention, making it essential to differentiate them from COD.1,14
ORALand maxillofacial pathology
Benign cystic lesions can mimic COD in their early stages, similar to inflammatory lesions, due to their uniform radiolucent appearance and the possible expansion or thinning of adjacent cortical plates. After the early stage of COD, radiopacities may appear internally, also mimicking mixed-density lesions, as fibrous connective tissue is replaced by cementum - or osteoidlike material(3). However, on interval
imaging, the radiolucent areas in COD will mature further, and the appearance will become a homogenous radiopacity.
Osteosclerosis is an area of increased osseous density, typically with little to no clinical significance.15 These areas can mimic late-stage COD, especially when significant calcified tissue is deposited and a thin radiolucent rim, pathognomonic for COD, is not
visible. This can be further complicated in situations where both COD and osteosclerosis are present in a single area.
The radiographic appearance of COD varies across stages (Figure 4 A-F). Early stages appear radiolucent, middle stages have a mixeddensity appearance, late states are predominantly radiopaque.16 These radiopaque areas can fuse to the surfaces of the roots. COD can also be seen surrounded by osteosclerosis, and in 37% of cases, causes mild cortical thinning and expansion.
Figure 4A. Early-stage COD mimicking a periapical cyst (axial, sagittal and coronal sections).
Figure 4B COD mixed density stage.
Figure 4C. COD late stage.
Figure 4D. COD associated with a simple bone cyst.
References
1. Su L, Weathers DR, Waldron CA. Distinguishing features of focal cemento-osseous dysplasia and cemento-ossifying fibromas. II. A clinical and radiologic spectrum of 316 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Nov;84(5):540–9.
2. Kawai T, Hiranuma H, Kishino M, Jikko A, Sakuda M. Cementoosseous dysplasia of the jaws in 54 Japanese patients: a radiographic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Jan;87(1):107–14.
3. Alsufyani NA, Lam EWN. Osseous (cemento-osseous) dysplasia of the jaws: clinical and radiographic analysis. J Can Dent Assoc. 2011;77:b70.
4. Decolibus K, Shahrabi-Farahani S, Brar A, Rasner SD, Aguirre SE, Owosho AA. Cemento-Osseous Dysplasia of the Jaw: Demographic and Clinical Analysis of 191 New Cases. Dent J. 2023 May 19;11(5):138.
5. Neville BW, Damm DD, Allen CM, Chi AC. Oral and Maxillofacial Pathology-E-Book: Oral and Maxillofacial Pathology-E-Book. Elsevier Health Sciences; 2015.
6. Shafer WG, Hine MK, Levy BM. A
textbook of oral pathology. In: A textbook of oral pathology. 1963. p. xv, 768–xv, 768.
7. Olgac V, Sinanoglu A, Selvi F, SolukTekkesin M. A clinicopathologic analysis of 135 cases of cementoosseous dysplasia: To operate or not to operate? J Stomatol Oral Maxillofac Surg. 2021 Jun 1;122(3):278–82.
8. Melrose RJ. The Clinico-Pathologic Spectrum of Cemento-Osseous Dysplasia. Oral Maxillofac Surg Clin N Am. 1997 Nov 1;9(4):643–53.
9. Brody A, Zalatnai A, Csomo K, Belik A, Dobo-Nagy C. Difficulties in the diagnosis of periapical translucencies and in the classification of cemento-osseous dysplasia. BMC Oral Health. 2019 Jul 10;19:139.
10. Maxillofacial fibro-osseous lesions: classification and differential diagnosis - PubMed [Internet]. [cited 2024 Nov 27]. Available from: https://pubmed.ncbi.nlm.nih. gov/8734416/
11. Chrcanovic BR, Gomez RS. Cementoblastoma: An updated analysis of 258 cases reported in the literature. J Cranio-Maxillofac Surg. 2017 Oct 1;45(10):1759–66.
12. Jih MK, Kim JS. Three types of ossifying fibroma: A report of 4
cases with an analysis of CBCT features. Imaging Sci Dent. 2020 Mar;50(1):65–71.
13. Hall G, Wright J. 8 - Bone Lesions. In: Gnepp DR, Bishop JA, editors. Gnepp’s Diagnostic Surgical Pathology of the Head and Neck (Third Edition) [Internet]. Third Edition. Oxford: Elsevier; 2021. p. 689–742. Available from: https:// www.sciencedirect.com/science/ article/pii/B9780323531146000080
14. Hoe SV, Bladt O, Steen KVD, Eynde HV den. Sclerotic Lesions of the Jaw: A Pictorial Review. J Belg Soc Radiol [Internet]. 2021 Apr 8 [cited 2024 Nov 27];105(1). Available from: https://jbsr.be/ articles/10.5334/jbsr.2208
15. Bartl R, Frisch B. Osteosclerosis. In: Bartl R, Frisch B, editors. Biopsy of Bone in Internal Medicine: An Atlas and Sourcebook [Internet]. Dordrecht: Springer Netherlands; 1993 [cited 2024 Nov 27]. p. 121–9. Available from: https://doi. org/10.1007/978-94-011-2222-1_11
16. Benign fibro-osseous lesions: a review of current concepts. PubMed [Internet]. [cited 2024 Nov 27]. Available from: https://pubmed.ncbi.nlm.nih. gov/11345237/
Figure 4E. COD with surrounding osteosclerosis.
Figure 4F. Two cases of COD mimicking a cementoblastoma.
Swallowing and Aspiration Events— A Growing Area of Concern
By Marc Leffler, DDS, Esq.
Dental Risk Solutions Lead, MedPro Group Head, Dental Advisory Board, MedPro Group
One of the more frequent, and growing, areas of claimed dental malpractice involves the swallowing or aspiration of just about anything that a dentist places into or works on inside of a patient’s mouth. Objects swallowed or aspirated include burs thrown from handpieces, endodontic files, rubber dam clamps, implants, implant instruments, pieces of teeth/ restorations, and many others.
As a refresher, an object is swallowed if it makes its way to and into the GI tract (esophagus, stomach, and beyond), whereas an object is aspirated if it enters the respiratory tree (trachea, bronchi, lungs). Swallowed objects are sometimes allowed to (hopefully) pass in stool, but many are retrieved by way of endoscopy; some situations involve the object lodging in the intestines or even appendix, thereby requiring abdominal surgery for removal. Aspirated objects cannot be left in place in that dead-end organ system, but must be removed by bronchoscopy or, rarely, by open chest surgery.
Prevention is the risk management key here: if appropriate mechanisms are established by the dentist such that nothing can pass into, behind and below the oropharynx, swallowing and aspiration events are stopped before they happen. How is that done? By employing any of multiple ways: use of rubber dam whenever possible (as objectionable as that might sound, both to dentist and patient); tying dental floss through holes in instruments or around others, with the free end of the floss remaining under the dentist’s control always; commercially available “gripping” instruments; positioning patients so that gravity helps objects fall to the floor of the mouth rather than to the throat; active and attentive suctioning; maintaining extra vigilance when sedation or general anesthesia is involved (because some physiological protective reflexes are muted or eliminated); and placing oropharyngeal drapes.
If those precautions are taken, then even unforeseen events like earthquakes or construction debris flying through a dentist’s window (yes, those things have happened) will not lead to a swallowing or aspiration episode.
If a dentist loses sight of any object which ought to be accounted for, then it should be assumed that the missing object was swallowed or aspirated, until proven otherwise. At that point, time is of the essence in getting the patient into the care of medical colleagues who can locate and treat (or refer for treatment), before an object travels too deeply into the GI tract or wedges itself into lung tissue, complicating what might otherwise be a fairly straightforward procedure. The time saved by temporizing a restoration in progress, as compared
Objects swallowed or aspirated include burs thrown from handpieces, endodontic files, rubber dam clamps, implants, implant instruments, pieces of teeth/restorations, and many others.
with finishing it before referral, is often the difference between simple and complex treatment.
Patients do not expect to have an endoscopy, bronchoscopy or chest/abdominal surgery due to having dentistry performed. Because it is almost always preventable.
For more information regarding MedPro Group, please call (800) 677-8644 or visit tdamemberinsure.com (Go to: For Dentists, Business, Professional Liability).
Note that this case presentation includes circumstances from several different closed cases, in order to demonstrate certain legal and risk management principles, and that identifying facts and personal characteristics were modified to protect identities. The content within is not the original work of MedPro Group but has been published with consent of the author. Nothing contained in this article should be construed as legal, medical, or dental advice. Because the facts applicable to your situation may vary, or the laws applicable in your jurisdiction may differ, please contact your attorney or other professional advisors if you have any questions related to your legal or medical obligations or rights, state or federal laws, contract interpretation, or other legal questions.
Opportunities Online at TDA.org and Printed in the Texas Dental Journal
CLASSIFIEDS INFORMATION
DEADLINE
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of November 20.)
MONTHLY RATES
PRINT: First 30 words—$60 for ADA/TDA members and $100 for non-members. $0.10 each additional word.
ONLINE: $40 per month (no word limit). Online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
SUBMISSION
Ads must be submitted, and are only accepted, via www.tda.org/MemberResources/TDA-Classified-Ads-Terms. By official TDA resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”). Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
ALL
TEXAS
LISTINGS
FOR
MCLERRAN
&
ASSOCIATES.
AUSTIN (ID #662): Large, general dentistry practice (with a recent focus on implants) located in a free-standing building with great visibility in north Austin. Large facility with 8 fully equipped operatories, digital radiography, an iTero digital scanner, and a 3D CBCT unit. FFS/PPO patient base, over 2,000 active patients, and has a stellar reputation. The owner invested heavily in growing the implant side of the business. AUSTIN (ID #691): Unique opportunity to purchase a GD practice with two locations in the Austin area. The offices have a total of 10 operatories with computers in each room and digital radiography. The offices serve a large FFS/PPO patient base with a healthy new patient flow and strong hygiene recall with over 20-25% of total annual production coming from the hygiene department. AUSTIN (ID #708): Growing practice, turn-key office, with strong cash flow located in one of Austin’s busiest neighborhoods. Modern office with state-ofthe-art equipment/technology, including a cone beam CT and iTero digital scanner. The practice treats a robust FFS/PPO patient base and boasts a near-perfect Google rating across 300+ reviews. DALLAS-PEDO/ORTHO (ID #665): Legacy pedo/ ortho practice in the heart of north Dallas. Thriving practice, large fee-for-service patient
base, revenue of 7 figures. Over 2,800 sq ft, fully digital with computers in the operatories, digital radiography, and a digital pano. DALLAS (ID #706): Legacy, GD practice located in a highly sought after north Dallas community with room to grow. Newly renovated office building situated off of a heavily trafficked thoroughfare. Features 2,400 sq ft with 5 fully equipped ops (plumbed for nitrous), computers throughout, digital pano, intra-oral cameras, and paperless charts. This practice serves a multi-generational patient base, relies mostly on word-of-referrals with limited marketing/advertising activities, has a robust hygiene recall program with 40% of total office production coming from the hygiene department, and they refer out many specialty procedures.
DALLAS/FORT WORTH-ORAL SURGERY (ID
#711): Legacy oral surgery practice located in a bustling suburb between Dallas and Fort Worth. A heavily tenured team, large patient base, and a fantastic reputation in the local community. 3,300 sq ft office in an easily accessible medical office park, 4 fully equipped operatories, two plumbed operatories for future expansion, computers throughout, digital X-ray sensors, and a 3D cone beam CT. With over 7 figures in 2023 revenue and profit margins trending at 50%, the foundation for a successful future has already been laid with abundant upside potential available. If you are looking to hit the ground running in a turn-key, stable, and highly profitable business,
reach out for details. HOUSTON-SOUTH
(ID
#682): Established, multi-specialty dental office in a suburb appromimately 20 miles south of Houston. Large (4,000 sq ft), easily accessible office condo with 13 equipped operatories, computers throughout, CBCT, and digital scanner. Massive PPO/FFS patient base (3,000+) with over 50 new patients visiting the office per month. The practice revenue averages over 7 figures annually with strong net cash flow, and there is room for expansion through enhancing the hygiene recall and focusing on standardizing the procedural mix. With approximately 55% of the dentistry being
McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered.
PRACTICE SALES
DSO C S
PRACTICE APPRAISALS
Austin 512-900-7989
DFW 214-960-4451
Houston 281-362-1707
San Antonio 210-737-0100
South Texas 361-221-1990
Email: texas@dentaltransitions.com
www.dentaltransitions.com
classifieds
restorative, 25% pediatrics, 10% ortho, and 10% OMS, the office is on a stable foundation with the opportunity to take it in whatever direction you choose.
HOUSTON-NORTH (ID #712):
Established, GD office located north of Houston. Six fully equipped operatories, digital X-rays, a CBCT, a digital scanner, and a CAD/CAM milling unit. PPO/FFS patient base, over 1500+ active patients, and boasts a near-perfect Google rating across 100+ reviews. Strong net cash flow in 2024 and a robust hygiene recall program with over 20% of production coming from the hygiene department annually.
SAN ANTONIO-TX HILL
COUNTRY (ID #685): Well-established dental practice and real estate nestled in the hill country north of San Antonio. The office relies mostly on word-of-mouth referrals with limited marketing/ advertising activities, has a robust hygiene recall program with over 40% of total office production coming from the hygiene department, and refers out many specialty procedures leading to upside potential for an incoming buyer. The practice saw strong revenue growth in 2023 and the trend has continued into 2024.
SOUTH
TEXAS
(ID #651):
General dentistry practice located in south Texas. This state-of-the-art office occupies 3,500 sq ft with room for 10 total operatories, is fully digital with CBCT, a digital scanner, handheld X-ray units, and a 3-D printer. The practice serves a
large PPO/Medicaid patient base with over 3,000 active patients seen over the last 24 months with a strong monthly new patient flow. TO REQUEST MORE INFORMATION ON MCLERRAN & ASSOCIATES’ LISTINGS: Please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@dentaltransitions.com.
AUSTIN: Fee-for-service private practice, 46 years same location with a 10-15 mile panoramic view over the downtown Austin skyline. Associate to buy with a preferred long transition for the senior doctor. Eight years remaining current lease with option to extend. Tremendous amount of residential growth immediately outside our huge windows. Ideally a GP interested in learning fullscale orthodontics. Please email for information: info@austinskylinedental.com.
AUSTIN: Looking for a doctor interested in starting with an associate relationship that could lead to ownership. Two merged practices, 1 in Lakeway and the other in north Austin on Highland Mall Boulevard, across from Austin Community College Highland campus, are looking for an associate willing to work 2 full days a week at each practice. The 2 practices have been open, each in the same location, 32 and 46 years respectively. The Austin practice will come up
for sale over the next few years with the senior doctor in his 70s. Both are non-network, fee-forservice practices with attractive numbers. Those interested call 512-452-9547 or send email to info@austinskylinedental.com.
CENTRAL
TEXAS HILL COUNTRY: For sale by owner, thriving fee-for-service general dental practice. Established rural 4 operatory dental practice for sale in the heart of the beautiful Texas hill country. This all-digital practice with a new pano produces mid-6 figure income with just 2 days per week of operation, offering great room for expansion and growth. The recently renovated real estate which offers a modern, welcoming environment for patients is also for sale. This is a perfect opportunity for a dentist looking to step into a successful, modern and established dental practice with plenty of room to expand. Contact dentalofficesale2024@gmail.com for more information and showings.
EAST TEXAS: Exceptional practice opportunity in Troup, Texas. Seeking associate to join high quality, well-established dental practice with a long history of excellence. This is an exceptional opportunity to move into ownership after a successful initial employment phase. Must be committed to providing optimal patient care
with exceptional technical skills, strong people skills, personal integrity, honesty and a passion for excellence. This practice has a dynamic, experienced team and a strong emphasis on Christian values and professional growth. Our office expansion should be complete mid to late September 2024, but the new associate could begin in August if he/she would like. Please reply in confidence with your CV and a letter outlining your future objectives and goals to: drmay@ troupfamilydental.com or call our office at 903842-4600.
HOUSTON: General practice (reference: “Southwest”) in the southwest area practice near a main highway in Houston. Collections in mid6 figures. Production is growing. Practice in a strip shopping center. The office is 1,475 square feet with 3 total operatories: 2 for dentistry and 1 for hygiene. Please let me know if you need anything else from me. A fourth operatory area is plumbed. Contains reception area, dentist office, sterilization area, lab area. Majority of patients are 30 to 65 years old. Practice has operated at this location for over 35 years. Practice sees patients about 16 to 19 days per month. Collection ratio of 99%. Practice is a fee-for-service and PPO practice. Contact Christopher Dunn at 800-930-8017 or Christopher@DDRDental.com.
classifieds
HOUSTON: Houston Metro periodontal practice for sale: 5 operatories, 7-figure collections, $245K EBITDA, 1,555 active patients, and strong growth potential. Contact Bailey Jones at bailey@ professionaltransition.com or 719-694-8320. #TX101624.
NEW BRAUNFELS: Dental practice for sale in high traffic area and very visible building. Beautifully renovated recently, with 3 operatories, movein ready, with 1,250 sq ft. No HMO or DMO. If interested, please email to salemydentalpractice@ yahoo.com or leave message on landline, 830606-4544.
SAN ANTONIO: General practice, 42 years established generational, exceptional patients in growing southwest San Antonio, with 2000+ active patients, 25/30 N.P. monthly. Exceptionally trained team. High 6-figures revenue, based on a 4-day work week, with high collections rate and low overhead. Range of services include: restorative, endo, restore implants, CB, removables, oral surgery, non-surgical perio. Patients primarily FFS, PPO, cash pay, 6% Medicaid. Great potential for expansion of services would include, molar endo, ortho, implant placement, perio surgery, and hygiene expansion, open up Fridays and
Saturdays. Physical plant consists of a 5,300 sq ft free standing corner lot building on a busy street. Six operatories are in use, the facility is plumbed for 11 operatories. Tech includes: CBCT, scanner, digital X-ray units, computers/TV’s in ops, phone system. Doctor is willing to work part time for transition as associate. Practice is for sale, real estate is available as well or long-term lease. Interested buyers please contact Kaylor Karlin at 210-500-3431, kaylorkarlin@kw.com.
WATSON BROWN PRACTICES FOR SALE: Practices for sale in Texas and surrounding states, For more information and current listings please visit our website at www.adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
INTERIM SERVICES
HAVE MIRROR AND EXPLORER, WILL TRAVEL: Sick leave, maternity leave, vacation, or death, I will cover your general or pediatric practice. Call Robert Zoch, DDS, MAGD, at 512-517-2826 or drzoch@yahoo.com.