
































































Experience a whole new dimension in treatment comfort. KaVo ESTETICA® E70 KaVo Dental GmbH · D-88400 Biberach/Riß · Telefon +49 7351 56-0 · Fax +49 7351 56-1488 · www.kavo.com Simply comfortable. Comfortably simple. The new KaVo ESTETICA® E70: More comfort – with the new intuitive operation More comfort – with the ergonomic suspended chair More comfort – with customisable and expandable equipment More comfort – with integrated, automatic hygiene functions The new KaVo ESTETICA® E70. Treatment comfort redefined. www.kavo.com/E70
Putting people at the centre
The new Programat ceramic furnaces are focussed on you, the user.
The combination of timetested technology and innovation allows you to achieve the best possible firing results.

The range of second-generation furnaces is now complete. All G2 furnaces are equipped with power saving technology and numerous technological innovations.
www.ivoclarvivadent.com Ivoclar Vivadent AG Bendererstr. 2 | 9494 Schaan | Principality of Liechtenstein | Tel.: +423 / 235 35 35 | Fax: +423 / 235 33 60 P500 P300 Programat® A STORY OF SUCCESS
P700 Multimedia
Color



zmack® system

zmack® comp shades: A1; A2; A3; A3.5; A2-O; A3.5-O; B1; B2; B3; C3
*For zmack® intro kits content, contact your local dealer or visit www.zhermack.com
YOUR SMART CHOICE TO CREATE SMILES
Zhermack presents zmack® system, the new universal light-cured composites line for conservative restoration that has been studied to solve everyday needs of dental practitioners and patients of any age. Born today, as the result of our laboratory experience and know how.
Specially designed to mimetically blend with the surrounding tooth structure, zmack® comp shades become imperceptible, for very natural, aesthetic and lasting results.


* + Tel. +39 - 0425 597611 - Fax +39 - 0425 597645 comm.expo@zhermack.com - www.zhermack.com
® system HIGH QUALITY FAIR PRICE TOTAL CAMOUFLAGE!
zmack
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona
Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob,
Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz
COORDINATOR
ART DEPARTMENT
SUBSCRIPTION
ADVERTISING
PHOTOGRAPHY
TRANSLATION
DIRECTOR ISSN
Suha Nader
Ibrahim Mantoufeh
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim, Marielle Khoury Tony Dib 1026-261X
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg. POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com www.facebook.com/dentalnews1
INTERNATIONAL REVIEW BOARD
Pr. M.A. Bassiouny BDS, DMD, MSc, Ph.D. Director International Program, Temple University, Philadelphia, USA.
Pr. N.F. Bissada D.D.S., M.S.D Professor and Chairman, Department of Periodontics, Case Western Reserve University, USA.
Pr. Jean-Louis Brouillet D.C.D, D.S.O. Chairman, Department of Restorative Dentistry, Aix-Marseille II, France. Pierre Colon D.C.D., D.S.O. Maître de conférence des universités, Paris, France.
Pr. Gilles Koubi D.C.D., D.S.O. Department of Restorative Dentistry, Aix-Marseille II, France.
UK.
Pr. Dr. Klaus Ott, Director of the Clinics of Westfälischen Wilhelms-University, Münster, Germany.
Pr. Dr. Alfred Renk, Bayerische Julius-Maximilians-University, Würzburg, Germany.
Pr. M. Sharawy B.D.S., Ph.D. Professor and Director, Department of Oral biology, Medical College of Georgia, Augusta, Georgia, USA.
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC. Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
www.facebook.com/dentalnews1
twitter.com/dentalnews
Dental News App on both Appstore & Google play
How Prepared Are You for a Medical Emergency?
Dr. Catharine Goodson.
Comparison of Short Term Effectiveness of Four Different Tooth Whitening Systems
Dr. Faraj. A. Behbehani, Dr. Jaber Akbar, Dr. Yacoub Altarakemah, Dr. Prem Sharma.
Use Of Glass Ionomer Cements In Paediatric Dentistry: Clinical Cases of Application in Primary Teeth
Dr. Elisabeth Dursun, Dr. Lucile Goupy, Dr.Frédéric Courson, Dr. Jean Pierre Attal.
Gastro Esophageal Reflux Disease (Gerd) And Tooth Erosion; Statistical Study Of 100 Cases
Dr. Ines Kallel, Pr. Nabiha Douki, Dr. Hajer Turki, Pr. Salem el Ajmi.
The Esthetic Anterior Restoration
Dr. Mayada Jemâa, Pr. Neila Zokkar, Dr. Amine Jenhani, Pr. Lotfi Bhouri, Pr. Sonia Zouiten, Pr. Nabiha Douki, Pr. MS Belkhir.

Art Science and Dentistry, Saint Joseph University, Beirut, Lebanon. May 31 June 1-2, 2012

Europerio 7, june 6-7, 2012 Vienna, Messe Wien

Dental News, Volume XIX, Number III, 2012 3 13 22 34 42 46 52 54 Volume
2012
XIX, Number III,
CONTENTS


WIEDOO
Trident
Verdi, 20
20090 ASS
is a trade mark of
S.r.l. - via
-

SSAGO - ITALY
www.trident-dental.com - info@trident-dental.com sole worldwide distributor edoo
-
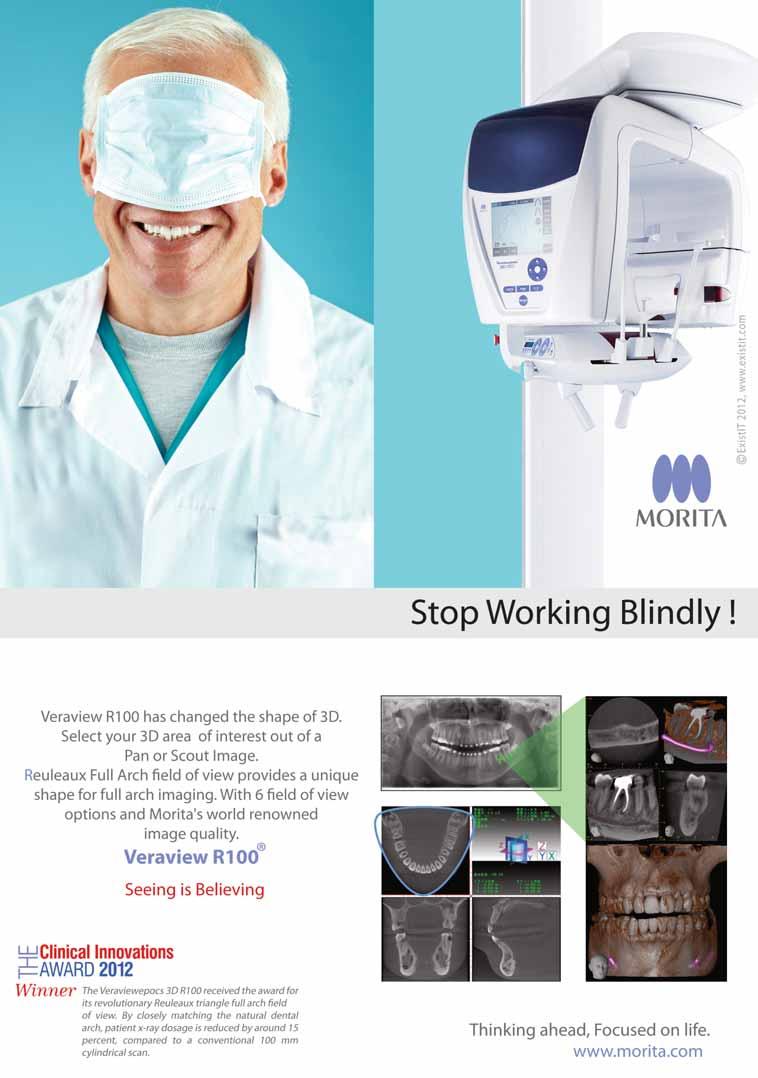
More precise than the eye: digital determination and verification of all tooth shades
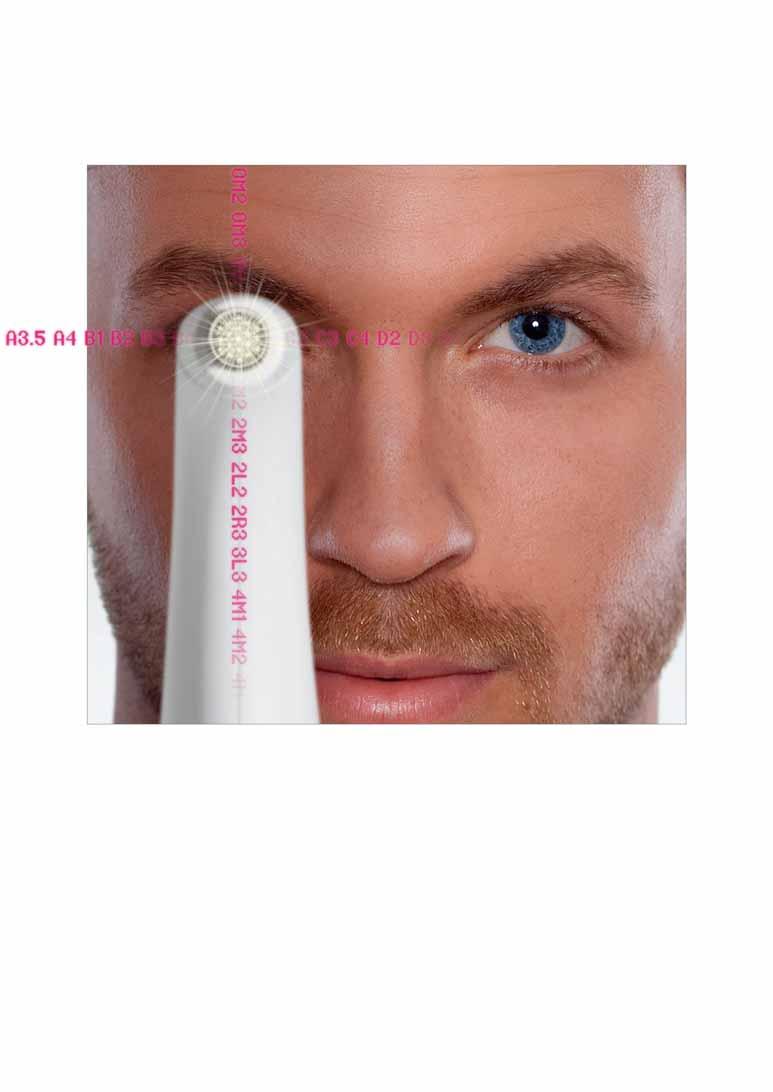

VITA Easyshade Advance features cutting-edge spectrophotometric shade measurement technology with an integrated light source. As a result, it is entirely independent of ambient conditions and delivers shade results in VITA
VITA shade, VITA made.
SYSTEM 3D-MASTER, VITA classical A1–D4 and VITABLOC shades in a matter of seconds. Increase your reliability and profitability – very easily and entirely digitally with Easyshade Advance. / www.vita-zahnfabrik.com
VITA Easyshade® Advance – To err was human! 3421E













































Whatever happens:
With W&H restoration and prosthetic instruments you are always prepared.






























Now at your dental supplier or at wh.com









































TAKARA BELMONT CORPORATION Tel. +81 (0)6 6213 5945 Fax. +81 (0)6 6212 3680 e-mail : belmont_d7@belmont.jp http://www.takara-net.com


philipsoralhealthcare.com.







The #1 patient-requested professional whitening system* is now better than ever. New Philips Zoom offers advanced light technology that gives you more control
patients even greater results. And
worldwide public awareness campaign to drive patients to you
new programs to help you easily integrate
light-activated whitening into your practice, you’ll have
answer to the confident, beautiful smile your patients are asking for.
new
WhiteSpeed today. Call +1.310.845.8260 or visit
EGYPT Elsafaa Tel: 2 (0) 10 1466997 JORDAN Al Ghad Medical Supplies Tel: +962 6 552 6358 KUWAIT Alpha Medical Co. Tel: +965 2247 8611 LEBANON G. Tamer Holding Tel: 961 1 694000 MOROCCO Ortho-Rama Tel: +21 2 22862086 SAUDI ARABIA Bashir Shakib Al Jabri & Co. Ltd. Tel: +966 26700430 TUNISIA MSI Tel: +216 73 449 401 UNITED ARAB EMIRATES Al Hayat Pharmaceuticals Tel: +971 6 5592 481 *In the United States. Philips is a registered trademark of Koninklijke Philips Electronics N.V. ©2012 Discus Dental, LLC. All rights reserved. To be dispensed by or on the order of a dental professional only. ADV-3539ARA 053112
and your
with a
and
Philips Zoom WhiteSpeed
the
Ask about the
Philips Zoom
Electropolish: Provides a protective sheet against corrosion and a professional appearance

Efficient Hole Pattern: Protects instruments from protrusion while allowing for enhanced cleaning and sterilisation

Durable Silicone Rails: Specifically designed to safeguard instruments from damage during processing
Smooth Round Corners and Slotted Edges: Increase drainage and reduce drying time
Functional Accessory Area: Includes built-in needle cap holder and winged syringe slot for optimized positioning (available in some models)


Positive Locking Mechanism: Provides a visual indication that cassette is locked for safety


IS NOT JUST A BOX...

HU-FRIEDY CASSETTES





























The Hu-Friedy INSTRUMENT MANAGEMENT SYSTEM was specially designed to help you increase the produc tivity of your practice, guarantee the safety of your patients and staff and extend the life of your instruments. With IMS you can save up to 70 minutes per day in hygiene and sterilisation procedures giving you more time for your patients and staff.

IMS is a complete system for managing, cleaning and organising the instruments you need — saving you time and money while facilitating infection control and prevention techniques.
Plus, IMS reduces the risk of injury to your patients and dental team, keeping everyone safe and happy.
To discover IMS, please contact your local Hu-Friedy dealer.

Please visit our website hu-friedy.eu or contact us by e-mail: info@hu-friedy.eu
How the best perform
©2012 Hu-Friedy Mfg. Co., LLC. All rights reserved.
THIS
BUSINESS SOLUTION BY HU-FRIEDY!
THIS
IS A
October 6 - 7, 2012
7th CAD/CAM & Computerized Dentistry International Conference at The Marina Bay Sands Hotel, Singapore
Email: info@cappmea.com Website: www.capp-asia.com
October 9 - 12, 2012
The Jordanian International Dental Conference under the title: Dentistry, much is Possible. Organized by the Jordan Dental Association at the Land Mark Hotel Amman, Jordan. Email: conference@jda.org.jo Website: www.conf.jda.org.jo
October 11 - 13, 2012
The European Association for Osseointegration will meet in Copenhagen, Denmark - 11 to 13
October 2012 . 20 years, what have we learned?
Email: eao@congrex.com Website: www.eao.org
November 7 - 11, 2012
Alexandria International Dental Congress
Email: azaher@idsc.net.eg Website: www.aidc-eygpt.com
November 9 - 10, 2012
4th Dental - Facial Cosmetic International Conference, Jumeirah Beach Hotel, Dubai, UAE
Tel: +971 4 3616174
Email: info@cappmea.com Website: www.cappmea.com
November 21 - 23, 2012
Arab Dental Federation Conference Sanaa, Yemen.
Email: adf.yemen@gmail.com
November 27 - 30, 2012
Le congrès 2012 se tiendra du 27 Novembre au 1er Décembre 2012 au Palais des Congrès de Paris,
Email: adf@adf.asso.fr Website: www.adfcongres.com

INTERNATIONAL CALENDAR
December 7 - 8, 2012
ITI Congress Middle East, Abu Dhabi, United Arab Emirates Organized by the “ITI International Team for Implantology”
Email: events@iticenter.ch
Website: www.iti.org
January 28 - 30, 2013
Saudi Dental Society
24th Saudi Dental Society International Dental Conference at the Riyadh International Exhibition Center.
Website: www.sds.org.sa
February 5 - 7, 2013
AEEDC
The 17th edition of the UAE International Dental Conference & Arab Dental Exhibition – AEEDC Dubai 2013 will take place at the state-of-the-art Dubai International Convention & Exhibition Centre (DICEC).
Website: www.aeedc.com
February 21 - 23, 2013
Midwinter Meeting
2013 Midwinter Meeting will take place in Chicago for three days where lectures, demonstrations and participation courses coincide with three days of the latest commercial exhibits.
Email: rgrove@cds.org
Website: www.cds.org/mwm
March 12 - 16, 2013
IDS 2013
35th International Dental Show in Cologne, Germany at the Koelnmesse.
Website: www.ids-cologne.de
ADVERTISING INDEX
Dental News, Volume XIX, Number III, 2012 11
ACTEON 25 - A-DEC 47 - AL TURKI 40 - BELMONT 8 - BIEN AIR 19 - BISCO 65 - CARESTREAM 15, 51, 74, 75 - CAVEX 33 - COLTENE 53
DURR 55 - EMOFORM 67 - GC 35 - GSK 29, 49, 61,
HU FRIEDY
MEGA 23 - MORITA 12 - NSK C1 - PLANMECA 43 - SDI 75 - SOREDEX 37 - SULTAN 67
- VOCO 17 - W&H 7 - ZHERMACK 2 -ZIMMER 69 www.dentalnews.com GET YOUR ISSUE ONLINE www.dentalnews.com Tel: 961-3-30 30 48 Fax:961-1-38 46 57 Email: info@dentalnews.com Volume XIX, Number III, 2012 www.facebook.com/dentalnews1 GETYOURISSUEONLINE
- DENTSPLY 21DEPURDENT 76 - DENTAURUM 54 - DISCUS PHILIPS 9 - DMG 73 -
C3 -
10 - IDEM 4-5, IVOCLAR 1, C4 - KAVO C2 - KERR 31 - MEDESY 20 - MECTRON 39 - MICRO
THOMMEN 27 - TEBODONT 66 - TRIDENT 71 - ULTRADENT 41 - VITA 6

How Prepared Are You for a MedicalEmergency?
Dr Catharine Goodson
catharine@catharinegoodsondds com www portable iv.com
In March 2011 what was supposed to be a routine wisdom tooth extraction on a 17- year-old girl from Woodstock, Maryland, went horribly wrong Jenny Olenick had been given the standard dose of anesthesia, but it didn’t sedate her adequately The anesthesiologist administered more, and the procedure began Then Jenny began experiencing bradycardia, or a slowing heart rate, and the oxygen saturation in her blood started dropping Soon she went into hypoxic arrest
Emergency responders were called and restored Jenny’s pulse within four minutes of their arrival, but the damage had been done Jenny was rushed to the hospital, where she died after being in a coma for a week The autopsy showed that Jenny had brain edema and acute hypoxic-ischemic encephalopathy due to lack of oxygen The death was ruled accidental, but Jenny’s parents sued the anesthesiologist and oral surgeon for medical malpractice
No one likes to think that a dental medical emergency will happen in their office But as professionals we need to realize that a single dental medical emergency can alter the course of our professional careers and the lives of our patients forever
As a dentist, my defining emergency lived in the body of an outof-control asthmatic with a less-than-truthful medical history Her dental treatment was being performed with the use of IV sedation The first 60 minutes of the procedure were uneventful, with stable vitals and no indication of what was yet to come
As we began the second hour of what we hoped would be a three-hour full mouth restorative treatment, she began to experience respiratory distress that initially exhibited as slight wheezing When I first noticed her labored breathing, I called for an inhaler, repositioned her into a more comfortable, upright breathing position and encouraged her to assist me with inhaling the Albuterol Her attack progressed from mild wheezing to a high-pitched crowing, accompanied by an obviously more occluded airway It was apparent the inhaler was not providing any relief of the attack
One day you will wake up and there won’t be any more time to do the things you’ve always wanted Do it now
and this was much more severe asthma than she indicated on her medical history
She become combative due to her restricted airway and my mind began to race What do I do next? My thoughts were disorganized and chaotic. But one thought predominated all others: How did this happen? What did I miss?
Research done at the University of Texas Health Science Center San Antonio reveals that every practicing U.S. dentist will face approximately eight potentially life-threatening medical emergencies in their offices every 10 years That means there will be approximately 150,000 dental medical emergencies in the U.S. every year
More and more dental emergencies are due to unanticipated interactions between sedation and the medications a patient is taking According to the AMA, in 2010 the average American between the ages of 35 and 50 was currently taking seven prescribed medications (an increase from four in 2002) These drugs are primarily used to treat hypertension, diabetes, high cholesterol and cancer-related illnesses And since the five leading causes of death in the U.S. as released from the CDC’s National Center for Health statistics are heart disease, cancer, stroke, respiratory disease and accidental death, the average American is taking seven medications that are used to treat the five leading causes of death
How does this affect you and your practice? Medical emergencies due to adverse drug reactions have dramatically increased Every year in the United States, 30 million prescription-dispensing errors out of 3 billion prescriptions filled occur at outpatient pharmacies, according to the National Patient Safety Foundation The number of pharmacy errors has increased due to a greater quantity of medical services being rendered outside the hospital-type setting Most errors are minor and are recognized by the patient, but the more serious errors cause drug interactions that can be potentially fatal
Dental News, Volume XIX, Number III, 2012 13 Med i cal Emergency MEDICAL EMERGENCY
Paulo Coelho
MEDICAL EMERGENCY
Imagine the compound effect of administering local anesthetics or providing sedation to a patient possibly taking the wrong medication, or with a potentially fatal interaction of medications
If you’re not adequately prepared, you, your patients, and your practice could be in for significant problems How confident are you that your current medical history accurately captures the medications your patients are taking? And are you (and your team) ready to deal with a life-threatening medical emergency like the one I faced?
In that emergency 10 years ago, after I administered the Albuterol, I knew time was of the essence My reaction involved two primary responses: first, assist her respiratory efforts Second : Mobilize the staff to summon emergency assistance
The next five minutes were a technical blur We located our emergency drug kit, but which drug should I request? The inhaler I used previously was an easy find it was hers! Did I ask someone to phone 911 or did I just think I did? Where was the ambu bag? Should I reverse the sedation? My rote learning from ACLS that accompanied my IV sedation training reminded me to use an epi pen I administered it through her pant leg, and this provided her a slight amount of relief But she struggled so violently for breath, it was impossible for her to assist with the placement of any positive pressure oxygen supplementation measures
I’d like to say this story ended wonderfully, but that wouldn’t be the truth The paramedics arrived in approximately 10 minutes (ADA average is 11 how nice to be below average!) She was intubated in the ambulance and remained intubated for 3 days in ICU, during which time it was determined that she was pregnant While I was at the hospital with her family, they tried to console me by telling me this wasn’t my fault and this kind of episode had occurred twice before! When I asked them why she didn’t tell me during our pre-treatment consultation, they said she was afraid I wouldn’t treat her
I returned to the office later that evening to examine the disaster I left behind that afternoon: the operatory, the emergency equipment, the tapes from the EKG I couldn’t rest until I dissected this tragedy into its basic components And I decided that this would never happen to me again.
The incident with the asthma patient almost 10 years ago began with an inadequately designed medical history That small piece of paper altered my life and my practice completely I re-defined my mission in dentistry and began a quest to design a better emergency system for dentists—an area of dentistry that has been neglected
“Medical Emergency Mastery” was designed to take the guesswork out of emergency preparedness It empowers general dentists and their staffs to recognize and manage medical emergencies in their office through (1) an expertly crafted medical history, (2) a targeted emergency drug kit specifically for general dentists and (3) staff emergency training that is reproducible for staffs of
any size This three-pronged approach will prepare you to proactively lead your staff, protect your patients and give you the peace of mind you have earned
Component #1: A properly constructed Medical History
The composition of a thorough medical history is the single most significant diagnostic tool we possess In my emergency, a wellcrafted medical history may not have alleviated the severity of the emergency but would have helped me determine the ability of this patient to tolerate routine dental treatment The majority of dentists purchase pre-packaged medical questionnaires that are far too generic and ask questions in an alphabetic type order (such as asthma, allergy, angina etc.). These questions require the practitioner to look at each question, determine if the response is acceptable and then ask an appropriate follow-up question
- What if we forget the next right question?
- What if we don’t know the next question?
- What if we’re too busy?
The medical history should be constructed to include questions that you believe are relevant to your patient population, asked in a way that will give you maximum access to the information I’ve designed the “Dental Safety” medical history to ask questions in a sequential order by systems—for example, all the questions regarding cardiac concerns are grouped together This computergenerated system follows the patient’s positive responses: he or she completes the questionnaire on the computer and a positive response generates the next series of questions By asking the questions in a systems format, you are able to follow a logical progression of questions and answers to achieve a greater understanding of your patients’ health
I’ve divided the questions into three sections: (1) physical systems, (2) psychological systems and (3) dental experiences
Examples of questions that relate to a physical system would include: Asthma-related questions:
- When was your asthma diagnosed?
- When was your last attack?
- Do you consider your asthma controlled?
- How often do you have an attack?
- When was your last medical evaluation of your asthma?
- Have you been hospitalized due to your asthma?
- Do you carry an inhaler with you?
- When was the last time you replaced your inhaler?
- What causes your asthma attacks?
- What medications do you take for asthma?
- Have you ever had an attack in the dental office?
- Do you leave your inhaler in the car?
- How often do you replace your inhaler?
Examples of questions that relate to psychological system assessment include:
- Are you under the care of a psychiatrist of psychologist?
Dental News, Volume XIX, Number III, 2012 14 Med i cal Emergency
How has stepping up our expertise over the last 100 years made us who we are today?





The answer is the Carestream Dental Factor




The Carestream Dental Factor is all about showing you how we care. It’s about challenging dentistry today and building on three main cornerstones – diagnostic excellence, workflow integration and humanized technology. It’s about empowering you as an oral health professional to make the best use of your expertise and ultimately enhance patient care.
Let’s continue to work closely together.
Let’s keep challenging what’s possible.
Let’s redefine expertise.
Workflow integration






LET’S REDEFINE EXPERTISE
Humanized technology Diagnostic excellence Explore it here carestreamdental.com/factor © Carestream Health, Inc. 2012
MEDICAL EMERGENCY
- Does a psychiatrist prescribe medications to you?
- What medications have been prescribed to you?
- How long have you been taking medications?
- What is your diagnosis?
- Have you been hospitalized in relation to mental health issues?
- Do you drink alcohol?
Examples of questions that relate to dental experiences include:
- At what age did you have your first dental exam?
- When was the last time you were at the dentist?
- Do you have specific fears concerning dental treatment?
- Do you have a strong gag reflex?
- What did you like most about your last dentist? The least?
- Is there anything we should know about your previous dental experience that would help us understand you better?
The patient is requested to complete their form prior to the first visit, so the dentist has adequate time to review it. (If the patient doesn’t have a computer or doesn’t have the opportunity to complete it, the information can be obtained in the office ) The dentist or reviewing staff member is able to review the completed health history, highlight areas of concern and question the patient in greater detail prior to the initiation of dental treatment This allows you to assess the overall health of your patients more effectively, and prevent potential medical emergencies
Component #2: A properly constructed Emergency Drug Kit
As a provider of in-office I.V. moderate conscious sedation in the practices of my colleagues, I have had the unique opportunity to examine many commercially prepared emergency drug kits The large majority of these kits have far too many components that general dentists aren’t qualified or comfortable using And many specialists currently not providing sedation are uncomfortable using any kind of injectable emergency drugs My goal became quite simple: Construct an emergency drug kit specifically for general dentists or specialists not providing sedation I simplified the components of this drug kit to reflect the drugs used to treat the seven most commonly occurring medical emergencies in the dental office: syncope, hypoglycemia, asthma, mild allergic reaction, severe allergic reaction, angina, and heart attack
The current kits include:
- Ammonium ampules (x3)
- Benadryl (50 mg) tabs x 100
- Epi Pen ( 3mg) single use pen or Twin Jet pen
- Glucose substitute (name brand)
- Nitro Tabs ( 4mg) / nitro spray ( 4mg)
- Albuterol inhaler/ Proventil inhaler
- Aspirin (81 mg) (aka baby aspirin)
Each drug is in a waterproof pouch and labeled individually with its name, the medical and laymen’s terms for the emergency that it is used to treat, and directions for its use In my discussions with my colleagues one theme was consistent: they knew what the
drugs are used for in theory, but they were afraid they wouldn’t remember what and how to administer the drugs in an emergency My packaging and directions solved that problem! The drugs are kept together along with an emergency manual that outlines the signs, symptoms and treatments for the most commonly occurring emergencies, including ones that don’t require medical intervention For example, if your patient begins to experience chest pains (angina), the manual outlines the possible causes of the pain and which emergency drugs would be used to treat it. The directions for the nitro tab administration are clearly indicated on the label as well This removes any “guesswork” from administration You are now able to consult a chairside guide to provide your patient the best medication to treat any possible emergency A properly stocked drug kit is essential, no doubt But of much greater significance is the awareness that the majority of our patients’ emergency needs will be those that require knowledge of airway management With this in mind, I developed an inventory of the necessary equipment and supplies required to provide airway maintenance By creating spreadsheets to inventory emergency equipment and supplies, your team can methodically review the use of equipment and inventory their supply in as little as 15 minutes a month (Fig. 1)
Component #3: A properly trained and empowered staff
The most integral component of the Dental Safety system is the staff training We all know we have amazing staff members, so why not let them shine? Each team member has specific duties and responsibilities to assist us chair-side, maintain office equipment and supplies; why not apply that to emergency preparedness?
That is exactly what I decided to do We started our training with the premise that we would stop being afraid of what could go wrong and start being positive about what could go right I designed specific roles for staff members that could be modified for a staff with as few as three members Included is the exact text for a 911 call, a method for documentation of an emergency incident as well as flow sheets for staff review
The most simplistic system is one that requires the fewest staff members but is adaptable for large practices This training regimen requires three team members, not including the Doctor Two of the team members will have the predominance of the roles and the third will primarily summon emergency assistance (This staff member may be non-clinical if necessary.)
The Doctor’s primary role is to remain with the patient, direct the response efforts, maintain the patient’s airway, administer CPR, if necessary, and direct the administration of emergency drugs
The primary responder will be the staff member with the most dental or emergency experience She should have experience in recognizing the signs of an emergency and be knowledgeable in their treatment She will know the location of all the emergency drugs, equipment and their use This responder will follow only the Doctor’s direction After receiving instructions from the Doc-
Dental News, Volume XIX, Number III, 2012 16 Med i cal Emergency
MEDICAL EMERGENCY
tor, she will direct a second responder to be on standby to notify 911 and prepare for emergency intervention The call to 911 will be placed only when requested by the Doctor
Responder 2 will actually place the 911 call (The content of the call is scripted and the script remains at the front desk (Fig. 2).)
This staff member monitors treatment in adjacent rooms and surveys patients in the reception area to provide reassurance and dissipate any anxiety
Responder 3 remains chair-side with the Doctor to provide assistance with drug or equipment administration as needed She also will communicate with any staff as necessary and complete any documentation Her focus will remain on monitoring vitals and airway maintenance
In order to facilitate this training, I implemented a flow sheet for my staff that outlined each responsibility Written protocols ensured that emergency scenarios could be reviewed on a monthly basis: equipment maintenance sheets would only require about 15 minutes a month to monitor (Fig. 3) Cross training was essential to prevent any lack of knowledge due to absence or staff changes Initially, my staff felt awkward and clumsy when they spoke to each other, even slightly confused Combining the emergency protocol with the staff responsibilities caused frustrations and self-doubt in even the most talented members of the staff, but after a few sessions, the team was relieved that we had a system in place
The Dental Safety System in Action
To put my system to the test, I phoned a friend and requested she masquerade as a new patient with a complex medical history We decided she would feign syncope After two sessions of “verbal drills” and one “play date” of a reenactment with a non-clinical staff member, I thought surely syncope could be managed without any difficulty That proved to be incorrect
After the initial examination, diagnosis of a restoration and initiation of treatment, our “new patient” indicated she felt faint The ensuing few minutes found my staff primarily startled After the initial “shock” wore off, they first looked at each other and seemed to forget the patient I remained by the patient and initiated my chair-side responsibilities Once I began to instruct the first responder in their duties, a calm rhythm began Ever so slowly the staff began to move, like an inexperienced athlete beginning their first race I prompted, waited, praised and assisted them in their efforts When the emergency drug kit arrived with the ammonia, the patient recovered spontaneously My feelings of pride in a staff that just a month before had cried at the end of an asthma attack were beaming with pride. Syncope obviously paled in comparison to the more severe asthma attack, but nonetheless, the crisis had been averted by teamwork, knowledge and application of simple principles It wasn’t necessary to tell the team that this was “only a test ” They had passed! I shared my system with my colleagues, and this kit of simple tools worked incredibly well in practices of every size and composition
I constructed kit after kit, improving upon each with recommendations from my friends I began to share my experiences with doctors in their offices, training their staffs and empowering their teams The greatest satisfaction came in the feedback I received The office managers that phoned to report how they had handled an emergency without incident The doctors who remained calm as they requested the appropriate drug from their kit and their staff responded instantly “A real decision is measured by the fact that you’ve taken a new action If there’s no action, you haven’t truly decided” Tony Robbins It is impossible to predict what will occur in our practice on a daily basis: that is a given What I have learned to predict is that medical emergencies will happen to each one of us The shape, form and fashion will be unique to your patient population—but no matter what, you are responsible for your reaction to them I reacted to a horrific occurrence and moved toward a solution And I want to encourage you to be ready to respond long before you face a severe medical emergency in one of your patients
When evaluating the three integral components necessary for a well-established emergency preparedness protocol, ask yourself the following questions
o When did I last objectively review my medical history questionnaire?
o Do I know what question to ask next in response to a positive answer from a patient?
o Do I know how to effectively and correctly use all the drugs in my emergency drug kit?
oWhen was the last time I trained my staff in emergency scenarios? Do not delude yourself into thinking a medical emergency will never happen to you in some form or fashion Whether it’s a patient’s reaction to antihypertensives and local anesthesia, a hypoglycemic reaction or an anaphylactic shock, do you want to take the chance that your staff will forget their roles in an unfolding emergency?
Don’t wonder what the answer will be for one moment longer Assess and evaluate your present systems of emergency preparedness With a modest effort, a well-structured framework and an enthusiastic staff, your training protocol can reflect a comprehensive vision of patient care that has left no stone unturned
For additional information regarding training programs for your staff, contact Dr Goodson by email: catharine@catharinegoodsondds com or visit her website: www catharinegoodsondds com
REFERENCES
1) Equipment logs 2) Content of 911 call 3) Emergency scenario review
Dental News, Volume XIX, Number III, 2012 18 Med i cal Emergency





Medesy is glad to introduce GAMMAFIX ™, a new range of sterilization trays. The quality and functionality of these trays facilitate the cleaning and sterilization process. Their special shape allows an extremely safe handling of the surgical instruments during the washing and sterilization phases. We selected the finest stainless steel to withstand the thermal shock caused by the constant sterilization cycles.



The “911” Call
When notified by the Team Leader, the responder will phone 911 and state the following.
1. State YOUR name, the name of The DOCTOR’S name, PRACTICE location, and crossroads
2. State the patients, SYMPTOMS, STATUS of the Patient, whether CONSCIOUS of UNCONSCIOUS, STABLE or UNSTABLE, ALERT, etc
3. State the ENTRANCE into the practice State whether the entrance is blocked, obstructed, etc
4. State that someone will greet them
5. Remember to stay on the phone until told to hang up!
6. Communicate to your team leader that EMS has been summoned and wait
Equipment Maintenance Log
- AED/ Batteries
- Oxygen tank
- E-cylinders/ number__
- Nasal Canula
- Ambu bag
- Face Mask
- Nitro Tab 4mg
- Nitro Spray 4mg
- Ammonia
- Benadryl (50mg ) tabs
- Epi Pen ( 4 mg)
- Albuterol
- Glucose Sub
- Aspirin (81 mg)
Monthly Emergency Simulation Practice
- Update Emergency Kit Contents
- Update First Aid Kit Contents
- Blood Pressure Technique, Pulse
- Airway Obstruction
- Syncope
- Hypoglycemia
- Anaphylactic Shock, or Severe Allergic - Rx
- MIld Allergic Reaction
- Asthma Attack
- Seizure




NEW GENERATION TRAYS
- Propanolol
- Ice Pack
- First Aid
- Expired Anesthetics
- MSDS Sheets
- OSHA Compliance
- Angina
- Cardiac Arrest
- Hypotension
- Hyperventilation
- Adverse Drug Reaction
- Staff Duties AED Use
- Eye Injury
- Needle Sticks
- 911 Call
- Fire Drill
Dental News, Volume XIX, Number III, 2012 20
Fig. 3
Fig. 1
Fig. 2
by
www.medesy.it 1670/1 DIAGNOSTIC SET






www.dentsplymea.com wave TM everything you like about x smart TM witha S P L WAVE ONE RECIPROCATING SYSTEM FILE AUTO REV DENTSPLY Limited | Building 1 | Aviator Park | Station Road | Addlestone | KT15 2PG | United Kingdom | +44 (0) 19 32 85 34 22 |
OPERATIVE DENTISTRY
Comparison of short term effectiveness of four different tooth
A Behbehani. DDS, MS, Jaber Akbar DDS, MS, Yacoub Altarakemah DDS, MS , Prem Sharma MSc, PhD
Abstract:
Statement of the Problem : Dental practitioners are faced with many materials and methods commercially available for tooth whitening This study aims to compare the short term effectiveness and major side effects of 4 popular bleaching systems in a relatively large sample
Materials and Methods: A sample of 300 subjects were divided equally into 4 groups and treated with (home bleaching - Opalescence 20%, in office – Bright Smile, in office - Zoom, and in office - Zoom plus home bleaching - Day White 9 5%)
Results: The four whitening systems were significantly effective at 3 days (T1) and 3 months (T2) after the whitening treatment At T2, there was no significant difference in whitening effectiveness among the four whitening systems Tooth sensitivity and gingival irritation were associated with the 4 whitening systems
Conclusion: The bleaching procedures tested in this study are equally effective with high satisfaction level and with self-limiting tooth and gingival sensitivity
Key words: Tooth bleaching, Vital, Hydrogen Peroxide, Carbamide Peroxide.
Introduction:
The shade of teeth is one of the main contributes to improve smiles 1,2 Television and magazines have influenced the general populations idea that whiter teeth are both healthier and more pleasing This has led to huge demand for teeth whitening procedures Consequently, dental practitioners are faced with a market flooded with many materials and methods catered to this demand The main ingredient of most bleaching products is carbamide peroxide with different concentrations (up to 35%) Questions regarding the most economical, effective, and conservative teeth whitening procedures are yet to be answered Attempts to bleach teeth were initiated more than a century ago and has since developed new methods and materials to make the
treatment procedure more effective, less time consuming and more convenient for both patient and dentist In-office bleaching has a wide variety of methods for application and activation Initially, heat was used in conjunction with hydrogen peroxide and ethyl ether on cotton to treat discolored teeth 4 In office teeth whitening procedures then evolved from a procedure performed over a span of multiple office visits into a technique that achieved the desired results in one or two visits Light-activation of high concentration hydrogen peroxide in the dental office emerged as an advanced technique to whiten all teeth simultaneously and became a prescribed method of whitening teeth 5, 6 10% carbamide peroxide was eventually discovered to whiten teeth when placed in orthodontic positioners to help improve the health of gingival tissue 4,7 Later, custom fitting night-guard vacuform material was used to carry the carbamide peroxide while placed over teeth This bleaching procedure is initiated without a light source because the reaction is chemical 8 This method is often used at home by the patient and thus is named at-home bleaching
The efficacy of at-home bleaching agents has been well documented in clinical trials 9-11 However, the effectiveness of in-office bleaching has been studied with mixed and controversial results In office bleaching using light activation versus the in-office chemically activated method have been compared with no statistical difference between the two 12 Similarly, when two in-office bleaching methods were tested, one with light and another without light, both resulted in statistically significantly lighter teeth 13 Zekonis on the other hand, found that at-home bleaching resulted in significantly lighter teeth compared to in-office bleaching 14 In contrast, one study found that an in-office product resulted in a 6 shade tab difference with significantly less bleaching cycles compared to at-home 15
In addition to the in-office bleaching method, some systems provide the patient with an extra home bleaching adjunct kit.16
Dental News, Volume XIX, Number III, 2012 22 Comparsi on of Tooth Wh itening Systems
Faraj.
faraj behbehani @yahoo com
Revo-S™, getting to the root of the problem!
MICRO-MEGA®, specializing in endodontics since 1905, has succeeded over the years in providing innovative products, simplified endodontic techniques and outstanding service to worldwide practitioners. Its latest product is a prime example of MICRO-MEGA®’s leadership in endodontic innovation…
Revo-S™ is a unique and innovative high-performance endodontic instrumentation sequence with only three instruments (SC1, SC2 and SU). Revo-S™ is adapted for most root canal anatomies and provides safety and simplicity.
ENDO Revolution!
Revo-S™ instruments have an asymmetrical cross-section that enables a “snake-like” movement of the instrument inside the canal which reduces the stress on the file.
Revo-S™ instruments can be used up to 10 times*. No need to buy an additional endo motor: Simply use your traditional endo handpiece.
Revo-S™ instrument cost is less than 2 ** per canal.
* Check the files after each use and dispose them if they show a sign of fatigue or unwinding.
** Average cost based on 10 uses.



Another new innovation from MICRO-MEGA







Flash this code with your smartphone to discover the Revo-S ™ video.
G-Files™: Glide paths made easy! These new NiTi files create the glide path and secure the passage of root canal preparation instruments. Two instruments are offered:
G1: N°12 - .03% taper - L21, 25 or 29 mm
G2: N°17 - .03% taper - L21, 25 or 29 mm
The G-Files™ can be used in combination with Revo-S™ or any other NiTi system.
54

NEW
G-Files™
MICRO-MEGA®
Tel.: +33 (0)3 81
42 34 mmb@micro-mega.com Join the REVOLUTION at www.revo-s.com
® … Contact
us for further information!
JC.AUGÉ www.jcauge.com
OPERATIVE DENTISTRY
However, only few studies evaluated the effect of this combination on overall bleaching result in comparison with using either of the methods alone 17,18
The most commonly reported side effects of at home and in-office bleaching include gingival and mucosal irritation with tooth sensitivity However, these side effects have been found to be transient 13,15,19,21
Shortcomings associated with bleaching studies:
On reviewing previous studies, it was noticed that the methods used to assess the effect of bleaching varied among different bleaching studies Some investigators used shade tabs solely to measure the effectiveness of the bleaching agents 11,19,22 When using shade tabs, it is important to calibrate the examiners to be able to measure the effectiveness of bleaching methods consistently 19, 23 This calibration is essential to minimize the effect of examiners experience, skills, and fatigue when matching shade tabs to natural teeth
The number of subjects in a study needs to represent the targeted population In a review of in vivo bleach studies, Buchalla 6 noted that the number of subjects in the reviewed studies ranged from 7 to 87 patients The number of subjects in the studies of da Costa 21 and Al Omairi 24 ranged from 20 to 40 respectively
The results obtained from such small samples divided into smaller groups testing different bleaching systems may not be reliable Larger samples are needed to minimize variation and assure representation of the general population
The subjects also need to be void of bias that will skew the results from representing the targeted population In one study 19 dental students were used as subjects 9 This introduces a bias in which the dental students might have been more motivated compared to the general public. Furthermore, the inclusion criteria of some studies can also become a limiting factor Several of the previous bleaching studies included subjects with a minimum shade of D4 or darker according to the Vitapan system 5,9,11,15,24,25 (Vita Zahnfabrik, Bad Säckimgen, Germany) If the sample is skewed toward only those with darker teeth, the effectiveness of the bleaching method could be overestimated
The aims of this study are the following :
1. Report, and compare, the short term effectiveness and major side effects of 4 different bleaching systems in a relatively large sample representing the general public.
2. Investigate if combination treatment (office + home) gives better bleaching effect than using either of the methods alone
3. To assess the patient satisfaction level of bleaching treatments
Material and methods:
Sample: After acquiring the approval of the Ethical Committee at the Health Science Center of Kuwait University, an advertisement was placed on bulletin boards as well as the website of the Health Science Center of Kuwait University, selective private and public dental clinics, and in a local newspaper of the Kuwait University
to recruit patients to participate in a prospective study testing the effectiveness of four different bleaching systems:
As a response to the advertisements, 450 persons volunteered to participate in the study Any individual above the age of 14 who was not medically compromised or mentally challenged and willing to whiten his or her teeth by the method proposed by the researcher, was welcomed to be included in the study Upon our initial clinical examination, 150 participants were excluded due to one or more of the following exclusion criteria:
1. Subjects with active periodontal problems, carious lesion, broken/fractured teeth or restorations, missing anterior tooth, or with restoration covering more than 30% of labial surface of any anterior tooth, or exposed dentin.
2. Subjects with amelogenesis, dentogenesis imperfecta, or other dental anomalies affecting the outer tooth surface
3. Subjects with history of previous bleaching treatment or active orthodontic treatment
4. Pregnant or lactating females
The remaining 300 subjects were consecutively assigned to the following 4 groups with 75 subject in each group
1. Home bleaching (HB) group: (Opalescence 20%, Ultradent Products Inc, South Jordan, Utah USA)
2. Brightsmile (BS) group: Light activated in-office bleaching systems (BRITESMILE 2000, Discus Dental, Culver city, California, USA)
3. Zoom (Z) group: Light activated in-office bleaching systems (Discus Dental, LLC , Culver city, California, USA)
4. Zoom plus home bleaching (Z+HB) group: Light activated inoffice bleaching systems (ZOOM 3) combined with home bleaching system (Day White 9 5%, Discus Dental LLC , Culver city, California, USA)
Dental prophylaxis and scaling were done to all subjects at least one week before starting the bleaching treatment All available anterior teeth, premolars and first molars were bleached All subjects signed an informed consent form before participating in the study which was approved by the Ethical clearance Committee at the Health Science Center of Kuwait University
Bleaching Methods:
Custom trays with bleach reservoir were made for the home bleaching The bleaching tray was made of 0 5mm soft plastic material The subjects who were assigned to (HB) group were instructed to wear the bleaching tray containing the bleaching gel (Opalescence 20%) daily, for 6 hours, for a total of 2 weeks The subjects who were assigned to (Z+HB) group were instructed to start their home bleaching treatment 1 week after finishing the in-office bleaching They were asked to wear their bleaching tray daily for 1 hour for 4 days All subjects were given a dated log form to register their home bleaching time The in-office bleaching was conducted in 4 sessions by applying new bleaching material followed by exposure to light at each session, following the instructions by the manufacturers of BRITESMILE2000 and ZOOM
Dental News, Volume XIX, Number III, 2012 24 Comparsi on of Tooth Wh itening Systems
OPERATIVE DENTISTRY
The session lasts 20 minutes for Britesmile and 15 minutes for Zoom To ensure protection of the maxillary and mandibular gingiva, an isolation material (provided with the bleaching kit) was applied on the gingiva Cheek retractor was used to hold the skin and lips away from the treatment area, and cotton rolls were placed in the cheek vestibules for moisture control Bite blocks were used as a jaw rest Lip balm was applied to the lips The subject and the operatory staff wore an orange-tinted protective eyewear during the light-activated whitening procedures The mixed peroxide gel was applied to the buccal surfaces of all the incisors, canines, premolars, and molars fully to ensure a uniform effect
Clinical Examination:
To avoid the subjective variation and bias, the clinical examination was done by two calibrated dentists (FK and JA) Prior to starting the study, our whitening effect evaluators were calibrated to use the vita shade guide in the following way:
An acceptable kappa score (substantial agreement, 0 61-0.80) was ascertained26 Calibration for the subjective discrepancies regarding the reading of the shade guide was done by making the analyzers read the shade on 18 ceramic tooth models randomly picked The analyzers were provided with the same models a week later and their readings were documented again. The difference between the two trail readings were analyzed and Kappa score was calculated within each examiner and between both examiners This calibration was repeated until accepted kappa score was obtained The intra-examiner consistency by kappa for examiner FK was 0 73 and for examiner JA was 0 98 The inter-examiner consistency kappa between the 2 examiners was 0 80
Whitening effect:
The whitening effect was assessed at the middle third of the labial surface of the upper right central incisor The whitening effect was measured before bleaching (T0), 1 to 3 days post bleaching (T1), and 3 months (+ or – 1 week) after bleaching (T2) The whitening effect was evaluated by the following methods:
1) Self-evaluation by the patient: A 10 cm long Visual analog scale divided into 1cm long segments (scaled form 0 to 10 with 10 as very dark teeth, 5 as normal or acceptable whiteness, and 0 as excellent whiteness) was presented to each subject at each evaluation interval to determine the brightness of the subject’s
Corresponding scores
right upper central incisor (Fig 1). Care was taken to ensure that subject’s lips were not covered with any lip stick at any evaluation time The evaluation was conducted in a well lit room without use of dental chair light The subject would evaluate the shade of his/ her teeth by looking in a non-magnifying hand mirror
2) Clinical evaluation by calibrated dentist: Vita 3D bleached shade guide was used at each evaluation interval to determine the shade of the upper right central incisor The examination was done by two calibrated dentists (FK and JA) The lightest tab of the vita 3D bleached shade guide (0M1) was marked as 0 and the darkest tab (5M3) as 14 (Fig 2).
Side effects:
Patient perception regarding tooth sensitivity and gingival irritation was evaluated by questioning the subjects at T0, T1, and T2 if their teeth were sensitive at all times or sensitive to hot, cold, chewing, or brushing The response of the patient was marked 0 if no sensitivity was present, 1 if mild sensitivity was present, 2 if moderate to severe sensitivity was present Similarly, The subjects were asked if they experienced any gingival sensitivity The response of the patient was marked 0 if no sensitivity was present, 1 if mild sensitivity was present, 2 if moderate to severe sensitivity was present The responses of all questions related to sensitivity of teeth and gingiva were combined and then the mean of the overall responses was calculated
Treatment satisfaction level:
Patient satisfaction level was assessed by questioning the participants at T1 and T2 if they would repeat the bleaching procedure again and if they would recommend the bleaching procedure to a friend The response of the subjects were marked as 0 if their answer was “no”, and 1 if their answer was “yes”
Statistical analysis:
Data management and analysis were carried out using the Statistical Package for Social Sciences Software (SPSS, version 17 0; SPSS Inc , Chicago, Ill , USA) The variables age and whitening scores were examined for normality of data with Kolmogorov-Smirnov test, and descriptive statistics presented as mean and standard error (SE) The whitening effect evaluators were calibrated to use the vita shade guide by kappa values The differences in initial
Dental News, Volume XIX, Number III, 2012 26 Comparsi on of Tooth Wh itening Systems
Fig.1. Visual Analog
0 1 2 3 4 5 6 7 8 9 10 Excellent whiteness Normal or acceptablewhiteness Very dark 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 0M1 0.5M1 1M1 1M1.5 1M2 1.5M2 2M2 2.5M2 3M2 3.5M2 4M2 4.5M2 5M2 5M2.5 5M3 Lighter Shade Lighter Shade Darker Shade Darker Shade VITA 3D shade guide designation
Fig. 2. Vita 3D Bleached Shade Guide

OPERATIVE DENTISTRY
Table 1: The mean whitening scores in 4 types of bleaching methods by 2 different evaluation methods at T0 and T1
N (Mean whitening scores ±SE )
Evaluation Method Follow-up
p-value (T0 Vs T1)
(T0 Vs T1) 95% CI*
* 95% Confidence Interval of the mean
(6 09 ± 0 13) (3 75 ± 0 17) 0.001 (1 92 - 2 76)
(6 25 ± 0 23) (2 62 ± 0 18) 0.001 (3 04 - 4 22)
(6 09 ± 0 15) (2 90 ± 0 17) 0.001 (2 66 - 3 56)
(6 41 ± 0 22) (3 19 ± 0 19) 0.001 (2 65 - 3 79)
(5 65 ± 0 15) (2 72 ± 0 18) 0.001 (2 46 - 3 40)
(5 71 ± 0 23) (2 29 ± 0 12) 0.001 (2 91 - 3 93)
(6 03 ± 0 13) (3
(6 40 ± 0 24) (2 93 ± 0 17) 0.001 (2 88 - 4 06)
Table 2 : The mean whitening scores in 4 types of bleaching methods by 2 different evaluation methods at T0 and T2
N (Mean whitening scores +SE )
Evaluation Method Follow-up Time
Visual Analog
T2 p-value (T0 Vs T2) 95% CI* (6 09 ± 0 13) (4 49 ± 0 15) 0.001 (1 21 - 1 99) (6 09 ± 0 15) (4 37 ± 0 19) 0.001 (1 17 - 2 11) (5 65 ± 0 15) (4 36 ± 0 21) 0.001 (0 79 - 1 79) (6 03 ± 0 13) (4 28 ± 0 18) 0.001 (1 32 - 2 18)
Vita 3D T0 T2 p-value (T0 Vs T2) 95% CI* (6 25 ± 0 23) (3 29 ± 0 18) 0.001 (2 36 - 3 56) (6 41 ± 0 22) (3 79 ± 0 20) 0.001 (2 01 - 3 23) (5 71 ± 0 23) (3 45 ± 0 17) 0.001 (1 65 - 2 87) (6 40 ± 0 24) (3 43 ± 0 21) 0.001 (2 30 - 3 64)
* 95% Confidence Interval of the mean
values, T0 and subsequent follow up at T1 and T2 were compared using non-parametric Mann-Whitney- or Kruskal Wallis tests The proportional responses on sensitivity to various bleaching methods, and their severity were assessed with Chi-square or normal Z-test The two-tailed probability p value < 0 05 was considered statistically significant
Results:
Whitening effect: Both of the evaluation methods (visual analog and vita 3D) showed that all of the 4 whitening methods (home bleaching - Opalescence 20%, in-office - bright smile, in-office - Zoom, and in-office - Zoom plus home bleaching – Day White
Significant Probablity (p-value) between columns
0.903
0.201
9.5%) were significantly effective at T1 (Table 1) and T2 (Table 2) The p values were all significant at 0 001 There was no significant difference among the 4 whitening methods (home bleaching - Opalescence 20%, in office bright smile, in-office - zoom, and in-office - zoom plus home bleaching – day white 9 5%) used at 3 months post bleaching (T2) The p value was more than 0.2. (Table 2)
Side effects:
Table 3 shows that there was a significant increase in the teeth and gingival sensitivity at T1 (p < 03) However, this sensitivity was transient At 3 months post bleaching (T2), there was no
Dental News, Volume XIX, Number III, 2012 28
Time Home bleaching (HB) Britesmile (BS) Zoom (Z) Zoom + HB (Z+HB) Visual
T0 T1
95%
Analog
CI*
29 ± 0
0.001 (2 34
15)
- 3 14) Vita 3D T0 T1 p-value
Home bleaching (HB) Britesmile (BS) Zoom (Z) Zoom + HB (Z+HB)
T0
Comparsi on of Tooth Wh itening Systems

It’s what’s inside that counts
Sensodyne potassium formulations work inside the tooth to target the source of pain1–4
Your patients can suffer from dentine hypersensitivity at any time. With an advanced formulation and a new fresh flavour, Sensodyne potassium formulations deliver clinically proven relief and 24/7 protection from the pain of dentine hypersensitivity.*1–7 Sensodyne continues to strive to deliver the best solutions for you and your patients with dentine hypersensitivity.





Mean dentine loss shown in situ after 15 days of treatment10
New improved Sensodyne’s formulation is low abrasion§9



§No significant difference observed between brushing with water alone when compared to brushing with a low abrasion toothpaste.
Proven 24/7 protection*1–7
8-10



Sensodyne potassium formulations work within the tooth to withstand daily physical and dietary challenges and provide around the clock protection from dentine hypersensitivity.*1–7
A gentle formulation for exposed dentine


Because exposed dentine is up to 10 times softer than tooth enamel,8 Sensodyne potassium formulations are low abrasion†9 and SLS-free.‡ This can protect vulnerable dentine from further damage and helps preserve the protective smear layer.
**Significant differences observed between brushing with water alone when compared to brushing with a moderate abrasion toothpaste (p=0.0071) and a high abrasion toothpaste (p<0.0001).

Adapted from GSK data on file 2010.10 Randomised, analyst-blind, in situ model involving 29 subjects to evaluate the effect on dentine of low abrasion toothpaste (RDA 60), moderate abrasion toothpaste (RDA 80) and high abrasion toothpaste (RDA 150) compared to water after 15 days of use by contact profilometry.


Sensodyne potassium formulations deliver clinically proven relief and 24/7 protection from the pain of dentine hypersensitivity1–7





*Based on twice daily brushing †Sensodyne Gentle Whitening formula is moderate abrasion ‡Sodium Lauryl Sulphate
References: 1. Jeandot J et al. Clinc (French) 2007; 28: 379−384. 2. Leight RS et al. J Clin Dent 2008; 19: 147−153. 3. Nagata T et al. J Clin Periodontol 1994; 21(3): 217–221. 4. Salvato AR et al. Am J Dent 1992; 5(6): 303−306. 5. Silverman G. Compend Contin Educ Dent 1985; 6(2): 131-136, 136. 6. Silverman G et al. Am J Dent 1994; 7(1): 9–12. 7. Troullos ES et al. 1992. GSK data on file. 8. Pickles MJ. In: Duckworth R M, editor. The Teeth and Their Environment. Monogr Oral Sci. Basel, Karger, 2006; 19: 86−104. 9. RDA: GSK data on file. 2010. 10. Bannon L et al. 2010. GSK data on file. Prepared June 2011 Z-11-202
Water Low abrasion toothpaste Moderate abrasion toothpaste High abrasion toothpaste 15 0 5 10 Mean dentin loss (μm)
** ** *
Low abrasion SLS-free New fresh flavour Think sensitivity,
think
OPERATIVE DENTISTRY
Table 3 : The number of subjects and the tooth sensitivity and gingival irritation for the 4 bleaching methods at T0, T1, and T2
Method
Timepoint
No of patients who turned up at the particular
bleaching (H B)
Britesmile (BS)
Zoom (Z)
Zoom + Home Bleaching (Z + HB)
Table 4 : The number of subjects (%) who were satisfied and would repeat the bleaching procedure or recommend the procedure to a friend, according to bleaching method at T1 and T2
Bleaching procedure
Home bleaching (HB)
Britesmile (BS)
Zoom (Z)
Zoom plus (Z + HB)
Percent of positive response
(71 4)
(83 3)
(72 6)
(75 0)
Repeat again
significant increase in teeth sensitivity and gingival irritation when compared to baseline results at T0 (p 0 425)
Treatment satisfaction level : Patient satisfaction level was high in all of the 4 different bleaching methods used in this study In summary, about 76% of the patients were satisfied with the bleaching treatment and would repeat their bleaching experience in the future And about 86% of the patients would recommend their friends to have their teeth whitened (Table 4) .
51 (82 3) 47 (74 6)
(71 7)
(81 5)
Recommend to a friend
(78 6)
69 (95 8)
(83 6)
(88 2)
(81 0)
(87 1)
(84 9) 47 (87 0)
Discussion:
Modern dentistry has witnessed the emergence of many bleaching methods and materials In pursuit of better shade for vital teeth, bleaching remains one of the most preferred economically viable and conservative treatments4 The manufactures of different bleaching systems claim superior efficacy of their bleaching systems compared to others Since the active ingredients of most bleaching systems is the same, the authors of this study attempt
Dental News, Volume XIX, Number III, 2012 30
Comparsi on of Tooth Wh itening Systems
T2
N(%)
38
44
T1 N(%) 60
50
53
51
214/283 75 60% 180/232 77 60% 245/283 86 60% 197/232 84 90% T2 N(%) 54
51
45
T1 N(%)
55
61
60
Home
timepoint N (%) of negative responses N (%) of positive mild responses p value (T0 )Vs (T1) p value (T0 )Vs (T2) N (%) of positive moderate and severe responses T0 T0 T0 T0 75 75 75 75 65 (86.7%) 66 (88.0%) 66 (88.0%) 70 (93.3%) 8 (10.7%) 8 (10.7%) 5 (6.7%) 4 (5.4%) 2 (2.6%) 1 (1.3%) 4 (5.3%) 1 (1.3%) T1 T1 T1 T1 69 73 73 68 41 (59.4%) 53 (72.6%) 51 (69.9%) 47 (69.1%) 13 (18.8%) 13 (17.8%) 13 (17.8%) 13 (19.1%) 15 (21.8%) 7 (9.6%) 9 (12.3%) 8 (11.8%) 0.001 0.029 0.025 0.001 T2 T2 T2 T2 63 62 53 54 56 (88.9%) 51 (82.3%) 47 (88.7%) 47 (87%) 5 (7.9%) 8 (12.9%) 4 (7.5%) 5 (9.3%) 2 (3.2%) 3 (4.8%) 2 (3.8%) 2 (3.7%) 0.852 0.426 0.906 0.452

Just One Step for Bulk Filling A Giant Step for Dental Technology!

SonicFill is the only sonic-activated, single-step bulk filling system that enables you to go from placement to a polished restoration in less than 3 minutes. The change in viscosity allows perfect adaptation with optimal results and without loss of quality. Over 1,000,000 SonicFill tips have been sold and thousands of dentists are already using SonicFill every day in their practice. Kerr and KaVo innovating the way that dentist do posterior composite restorations!
Go to www.sonicfill.eu and see SonicFill in practice. Or request a demonstration and join the revolution today!

SonicFill™











KerrHawe SA · Via Strecce 4 · CH-6934 Bioggio Telephone +41 91 610 05 05 · www.kerrdental.eu ™
OPERATIVE DENTISTRY
ed to report if any differences exist among 4 popular bleaching systems with regard to efficacy and major side effects in a relatively large sample Unlike previous studies 5,9,11,15,24,25 which excluded subjects with initial tooth shade lighter than D4, this study did not exclude any patients whose initial shades were relatively lighter on the vita shade guide. We accepted all patients who walked in with dark teeth complaint or with a feeling that their teeth were not as white as they should We believe that including such patients will make our sample more representative to the actual population If the sample is skewed toward only those with darker teeth, the effectiveness of the bleaching methods could be overestimated In order to assure best reliability of the results, 2 evaluation methods were used The patients used 10 cm long visual analog scale divided into 1cm long segments and the dentists used Vita 3D bleaching shade guide in their assessments of the whitening effects Both evaluation methods showed that all of the four bleaching systems were equally effective at T1 and T2 Contrary to what was expected16-18, the combination of in-office bleaching with home bleaching was not more effective than inoffice bleaching alone or home bleaching alone However, this study was limited to short term effectiveness, up to 3 months (+ or – 2 weeks) after the date of the bleaching The sample used in this study will be followed to test if there will be any long term differences in the effectiveness among the 4 bleaching systems, which will be reported in future studies
Confirming the results of the other studies 8, 13 -15, 19-21 there was a significant increase in the tooth and gingival sensitivity immediately after bleaching at T1 The results of this study further reinforces the fact that tooth sensitivity associated with any bleaching method is transient The responses of the subjects to the sensitivity questions at T2 showed no significant differences than their responses to the same sensitivity questions at T0 (Table 3)
The satisfaction level of the patients who participated in this study was assessed by their positive response to the questions about their bleaching or their recommendation bleaching to their friends The significant increase in teeth whitening at T1 and T2 combined with relatively minor and transient tooth and gingival sensitivity seemed to make the majority of the subjects satisfied with the overall tooth whitening results However, it should be emphasized that treatment satisfaction could be influenced by many variables such as the ambience of a dental office and behavior of the staff which could not be controlled in this study
Conclusions:
1) The whitening systems tested in this study are all effective (short term) with no significant difference between them
2) There is transient increase in tooth and gingival sensitivity as a result of tooth whitening treatment
3) The combination of home bleaching with in-office bleaching is not more effective than either alone
4) Patient satisfaction level for tooth whitening procedure is high
Clinical Implications.
Dentists could choose any of the whitening systems which were tested in this study because they are equally effective with self-limiting side effects
Acknowledgement:
The authors wish to thank Fabi Koya for her assistance in clinical investigation and data collection This work was supported by Kuwait University Research Administration grant DI 02/06
REFERENCES
1. CARLSSON GE, WAGNER IV, ODMAN P,.EKSTRAND K,MACENTEE M,MARINELLO C, NANAMI T,.OW RK,SATO H,SPEER C.,. STRUB JR & WATANABE T, “ANINTERNATIONALCOMPARATIVEMULTICENTERSTUDYOFASSESSMENTOF DENTALAPPEARANCEUSINGCOMPUTER-AIDEDIMAGEMANIPULATION”, INTERNATIONAL JOURNALOF PROSTHODONTICS 1998, 11 (3): 246-254.
2.ODIOSO LL, GIBB RD &. GERLACH RW, “ IMPACTOFDEMOGRAPHIC, BEHAVIORAL, ANDDENTALCAREUTILIZATION PARAMETERSONTOOTHCOLORANDPERSONALSATISFACTION”, COMPENDIUMOF CONTINUING EDUCATIONIN DENTISTRY, SUPPLEMENT 29 2000: S35-41.
3.KERSHAW S,NEWTON JT &. WILLIAMS DM, “THEINFLUENCEOFTOOTHCOLOURONTHEPERCEPTIONSOFPERSONAL CHARACTERISTICSAMONGFEMALEDENTALPATIENTS: COMPARISONSOFUNMODIFIED DECAYEDAND ‘WHITENED’ TEETH”, BRITISH DENTAL JOURNAL 2008, 204 (5): E9; 256-257.
4.KIHN PW, “VITALTOOTHWHITENING”,THE DENTAL CLINICSOF NORTH AMERICA 2007, 51(2): 319-331, HTTP://DX DOI ORG/S0011-8532(06)00131-5.
5.TAVARES M.,STULTZ J, NEWMAN M,SMITH V, KENT R, E. CARPINO & J. M. GOODSON, “LIGHTAUGMENTS TOOTHWHITENINGWITHPEROXIDE,” JOURNALOF AMERICAN DENTAL ASSOCIATION 2003, 134 (2): 167-175. 6.BUCHALLA W &. ATTIN T, “EXTERNALBLEACHINGTHERAPYWITHACTIVATIONBYHEAT, LIGHTORLASER ASYSTEMATICREVIEW”,DENTAL MATERIALS 2007, 23 (5): 586-596.
7.. GOLDSTEIN RE &. GARBER DA, COMPLETE DENTAL BLEACHING, QUINTESSENCE PUBLISHING CO 1995, CHICAGO, PP 35-56.
8. HASSON H, ISMAIL AI.&.NEIVA G, “HOME-BASEDCHEMICALLY-INDUCEDWHITENINGOFTEETHINADULTS”, COCHRANE DATABASE SYSTEMIC REVIEWS 2006, ISSUE 4. ART.NO: CD006202.DOI: 10.1002/14651858. CD006202.
9. GIACHETTI L,BERTINI F,BAMBI C, NIERI M.&.RUSSO DS, “A RANDOMIZEDCLINICALTRIALCOMPARINGAT-HOME ANDIN-OFFICETOOTHWHITENINGTECHNIQUES:A NINE-MONTHFOLLOW-UP”, JOURNAL AMERICAN DENTAL ASSOCIATION 2010, 141 (11): 1357-1364.
10.MEIRELES SS, HECKMANN SS,LEIDA FL,. DOS SANTOS IDA S,.DELLA BONA A, &. DEMARCO FF, “EFFICACY ANDSAFETYOF 10% AND 16% CARBAMIDEPEROXIDETOOTH-WHITENINGGELS: ARANDOMIZEDCLINICALTRIAL”, OPERATIVE DENTISTRY 2008, 33 (6): 606-612.
11.BRUNTON PA, ELLWOOD R &. DAVIES R, “A SIX-MONTHSTUDYOFTWOSELF-APPLIEDTOOTHWHITENINGPRODUCTS CONTAININGCARBAMIDEPEROXIDE”,OPERATIVE DENTISTRY 2004, 29 (6): 623-626.
12.AL SHETHRI S.,MATIS BA,. COCHRAN MA,.ZEKONIS R &. STROPES M, “ A CLINICALEVALUATIONOFTWO IN-OFFICEBLEACHINGPRODUCTS”,OPERATIVE DENTISTRY5, 2003, 28 (5): 488-495.
13.. GALLAGHER A,.MAGGIO B,BOWMAN J.,. BORDEN L,.MASON S &. FELIX H, “CLINICALSTUDYTOCOMPARE TWOIN-OFFICE (CHAIRSIDE) WHITENINGSYSTEMS”, JOURNALOF CLINICAL DENTISTRY 2002, 13 (6): 219-224.
14.ZEKONIS R,MATIS BA,. COCHRAN MA,AL SHETHRI SE, ECKERT GJ &. CARLSON TJ, “CLINICALEVALUATIONOF IN-OFFICEANDAT-HOMEBLEACHINGTREATMENTS”,OPERATIVE DENTISTRY 2003, 28 (2): 114-121.
15.AUSCHILL TM.,. HELLWIG E,. SCHMIDALE S,.SCULEAN A &. ARWEILER NB, “EFFICACY, SIDE-EFFECTSAND PATIENTS ’ ACCEPTANCEOFDIFFERENTBLEACHINGTECHNIQUES (OTC, IN-OFFICE, AT-HOME)”,OPERATIVE DENTISTRY 2005, 30 (2): 156-163.
16..KUGEL G,. PERRY RD,. HOANG E &. SCHERER W, “EFFECTIVETOOTHBLEACHINGIN 5 DAYS: USINGACOMBINED IN-OFFICEANDAT-HOMEBLEACHINGSYSTEM”, COMPENDIUMOF CONTINUING EDUCATIONIN DENTISTRY 1997, 18 (4): 378 -383.
17.MATIS BA, COCHRAN MA, WANG G, ECKERT GJ, “A CLINICALEVALUATIONOFTWOIN-OFFICEBLEACHING REGIMENSWITHANDWITHOUTTRAYBLEACHING”,OPERATIVE DENTISTRY 2009, 34-2,142-149.
18.BARGHI N, “MAKINGACLINICALDECISIONFORVITALTOOTHBLEACHING:AT-HOMEORIN-OFFICE”, COMPENDIUMOF CONTINUING EDUCATIONIN DENTISTRY 1998, 19(8): 831-838.
19.. POHJOLA RM,.BROWNING WD,. HACKMAN ST,.MYERS ML &. DOWNEY MC, “SENSITIVITYANDTOOTH WHITENINGAGENTS”, JOURNALOF ESTHETICAND RESTORATIVE DENTISTRY 2002, 14 (2): 85-91. 20.BURROWS S., “A REVIEWOFTHEEFFICACYOFTOOTHBLEACHING”,DENTAL UPDATE 2009, 36 (9): 537-551.
21. DA COSTA JB,MCPHARLIN R, PARAVINA RD &. FERRACANE JL, “COMPARISONOFAT-HOMEANDIN-OFFICETOOTH WHITENINGUSINGANOVELSHADEGUIDE”,OPERATIVE DENTISTRY 2010, 35 (4): 381-388.
22. HAYWOOD VB, “NIGHTGUARDVITALBLEACHING”,DENTISTRY TODAY 1997, 16 (6): 86, 88, 90-81.
23.A. JOINER, “THEBLEACHINGOFTEETH: AREVIEWOFTHELITERATURE”, JOURNALOF DENTISTRY 2006, 34 (7): 412-419.
24..ALOMARI Q & EL DARAA E., “A RANDOMIZEDCLINICALTRIALOFIN-OFFICEDENTALBLEACHINGWITHORWITHOUT LIGHTACTIVATION”, JOURNALOF CONTEMPORARY DENTAL PRACTICE 2010, 11 (1): E017-024.
25.. GURGAN S, CAKIR FY &. YAZICI E, “DIFFERENTLIGHT-ACTIVATEDIN-OFFICEBLEACHINGSYSTEMS: ACLINICAL EVALUATION”,LASERSIN MEDICAL SCIENCES 2010, 25 (6): 817-822, 26.LANDIS JR,KOCH GG. THEMEASUREMENTOFOBSERVERAGREEMENTFORCATEGORICALDATA.BIOMETRICS 1977, 33, 159–174.
Dental News, Volume XIX, Number III, 2012 32
Comparsi on of Tooth Wh itening Systems


Cavex Alginates



Superior in strength, control and balance Cavex ColorChange













Cavex Impressional

















CAVEXYOUR IMPRESSION IS OUR CONCERN Cavex Holland BV, P.O. Box 852, 2003 RW Haarlem, The Netherlands. Tel +31 23 530 77 00 Fax +31 23 535 64 82 dental@cavex.nl www.cavex.nl
5 years shelf life snap-set superior tear resistance
2011 Top Infection Control Product
Cavex Orthotrace
Cavex ImpreSafe
Cavex GreenClean
USE OF GLASS IONOMER CEMENTS IN PAEDIATRIC DENTISTRY: CLINICAL CASES OF APPLICATION IN PRIMARY TEETH
Dr
Elisabeth Dursun,
Dr Lucile Goupy, Dr Frédéric Courson, Dr Jean P ierre Attal elisabethdursun@gmail.com
INTRODUCTION
Successful restoration is linked to various factors: the material, the practitioner and the patient (Donovan et al 2006) The latter characterises the uniqueness of paediatric odontology The patient’s (sometimes limited) co-operation justifies the use of materials that can be easily manipulated and that are favourable to a simple protocol Furthermore, primary teeth are distinguished from permanent teeth mainly by their anatomy and their limited time in the dental arch Consequently, even if the practitioner has the same array of materials for permanent teeth as for primary teeth (composite resins, amalgams, compomers and glass ionomer cements (GICs)), the specificities for the restoration of primary teeth are different After reviewing the uniqueness of primary dentition, a summary of current data in the literature on the longevity of GICs in this clinical indication will then be presented, followed by a discussion of GICs modified by the addition of resin (RMGICs) and packable GICs (pGICs) Finally, the principal uses of these cements, will be illustrated by examples of clinical cases Composites modified by the addition of polyacids (or compomers) will not be discussed in this article because these are more similar to composites than glass ionomers
CRITERIA FOR SELECTING A MATERIAL IN PAEDIATRIC ODONTOLOGY
This section is limited to criteria concerning the characteristics of primary teeth and the types of caries Primary teeth are characterised by a thin layer of enamel consisting of enamel prisms that are directed vertically to the proximal surface In the case of carious lesions, this tenuity can lead to extensive destruction, exacerbated by the fact that the prisms have poor cohesion Dentin forms an equally thin layer and its wide tubules allow bacterial penetration, accelerating the risk of pulp contamination It is therefore important to work with sealable restorative materials The pulp chamber is proportionally much bigger than in permanent teeth and the pulpal horns are prominent A carious lesion can therefore occur rapidly close to the pulp It is therefore important to work with adhesive materials that do not require secondary cavity retention forms that may decay and cause pulpal exposure For the same reason, smooth surfaces in the youngest patients which are affected by linear enamel caries or early carious lesions in the occlusal grooves or proximal surfaces of molar teeth (Psoter et al 2003; Psoter et al 2009) call for minimally invasive adhesive dentistry Owing to their short crown height, marked cervical constriction, relations with adjacent teeth and large gingival papillae, primary
Dental News, Volume XIX, Number III, 2012 34 Using Glass Ionomer Cements In Paediatric Dentistry PEDIATRIC DENTISTRY

Create æ-motion with the composites from GC.
Complete range of highly aesthetic composites for anterior and posterior, with unique injectable composite and 7th generation selective etch bonding. http://www.gceurope.com







































GC EUROPE N.V. Head Office Tel. +32.16.74.10.00 info@gceurope.com http://www.gceurope.com
PEDIATRIC DENTISTRY
teeth can cause difficulties in establishing an isolated operative field, rendering the use of hydrophobic materials problematic (Burgess et al 2002) It is therefore important to work with hydrophilic material Proximal caries adjacent to the primary tooth under treatment are common Fluoride-releasing material placed on the proximal surface of the restoration could be advantageous in a favourable environment, in patients with a controlled risk of caries, to reduce the development and progression of caries on the proximal surface of the adjacent tooth It is therefore important to work with bioactive material (Qvist et al 2010) Moreover, the tooth’s sometimes short remaining time in the arch may admit the use of materials compatible with this duration Additionally, as masticatory constraints in children are lower than in adults (Braun et al 1996; Castelo et al 2010; Palinkas et al 2010), materials that are relatively less mechanically resistant may prove to be suitable Thus, while materials with mechanical properties are crucial for permanent teeth, materials with lower mechanical properties may suffice for primary teeth in certain situations This explains why glass ionomers, markedly less mechanically resistant than composites, may have a role in paedodontics Therefore, besides the need for fast implementation related to the patient’s age, restorative material for primary teeth should also be sealable and adhesive to tooth tissues, bioactive and hydrophilic. Glass ionomers meet all of these requirements
LONGEVITY OF RESTORATIVE MATERIALS IN PRIMARY TEETH
A review of the literature concerning the longevity of dental materials used in primary dentition highlights a wide variation in success rates Indeed, numerous factors are involved : the type and brand of the material used, the practitioner’s experience, the site and the depth of the carious lesion, as well as the age and cooperation of the patient Additionally, the life span of restorations in primary teeth is significantly different from that of permanent teeth, regardless of the chosen material (Hickel and Manhart 1999) This emphasises the specificity of the selection criteria for primary dentition material Yengopal and coll. in 2009 (Yengopal et al , 2009) conducted a systematic review of the literature, comparing the outcomes of different materials used for the restoration of primary teeth, in terms of pain relief, durability and aesthetics The study concluded that, from 1996 to 2009, there were only two well-conducted randomised clinical trials evaluating the different restorative materials These trials reported no significant differences between the materials In one of these two trials, Donly and coll. in 1999 (Donly et al , 1999) compared a RMGIC (Vitremer®) with amalgam over a three-year period. However, owing to the high “lost to follow-up” rate, only the 12-month results are reported No significant difference was found In terms of longevity, GICs are therefore materials that may pose an alternative to amalgams or composites for the restoration of primary teeth for a limited period of time At present, two types of GIC are clinically relevant: RMGIC and pGIC However, some studies demonstrate
differences in longevity depending on the type of GIC used and the site (occlusal or proximal) of the cavity
THE TWO MAIN GIC TYPES
Of the different GIC types, two are particularly suitable for paediatric dentistry:
1) RMGICs (resin-modified glass ionomer cements)
Fuji II® LC (GC), Riva Light Cure (SDI), Photac-Fil® (3M-Espe), Ionolux (Voco)
2) pGICs (packable glass ionomer cements)
Fuji IX (GC), Riva Self Cure (SDI), HiFi (Shofu), Ketac Molar (3MESPE), Chemfil Rock (Dentsply) or Ionofil Molar (Voco)
The main differences between these two types of material relate to their mechanical properties and implementation RMGICs demonstrate moderate resistance to wear, but this is sufficient for restorations that have a fixed time in the dental arch Qvist and coll (Qvist et al , 2010) report that the longevity of RMGICs is almost equal to that of amalgams, but is higher than that of pGICs These materials may be indicated for occlusal and proximal restorations in primary teeth, for a remaining period in the arch of around three to four years (Qvist et al 2004; Courson et al 2009)
The implementation of RMGICs is often favoured by practitioners, given the possibility of curing by photopolymerisation Packable GICs have the advantage of single-step placement (particularly attractive property for proximal cavities) and, in certain formulations, have accelerated chemical bonding However, they are not robust in the medium term in proximal areas (Qvist et al 2010) Limiting their use proximally for less than two to three years in the dental arch, and also for their use in small to medium sized cavities, is therefore recommended (Forss and Widstrom 2003) They can also be used for larger multi-sided cavities, but in this case covered with a pre-shaped paedodontic crown (Courson et al 2009) Nevertheless, it is possible that the use of a protective varnish (G-Coat Plus®, GC) may considerably improve durability as shown by a recent study by Friedl et al. in 2011 (Friedl et al 2011), which concluded that these materials could be used for permanent posterior restorations
However, one might question how bioactive fluoride-releasing properties are maintained when a protective varnish is used Finally, it should be noted that a new high-viscosity RMGIC is now available (HV Riva Light Cure - SDI); this is a RMGIC that can be used as a pGIC
EXAMPLES OF CLINICAL CASES
Whatever the clinical situation, an operative field will always be established whenever possible For the following two clinical cases, in which the lesions are not easily accessible, an isolated operative field was established It should be noted that, with or without an operative field, the bioactive nature of GICs, with their fluoride release, gives them an advantage over adhesive materials Without an operative field, the bioactive nature of GICs, with their fluoride release, gives them an advantage over adhesive materials
Dental News, Volume XIX, Number III, 2012 36
Using Glass Ionomer Cements In Paediatric Dentistry
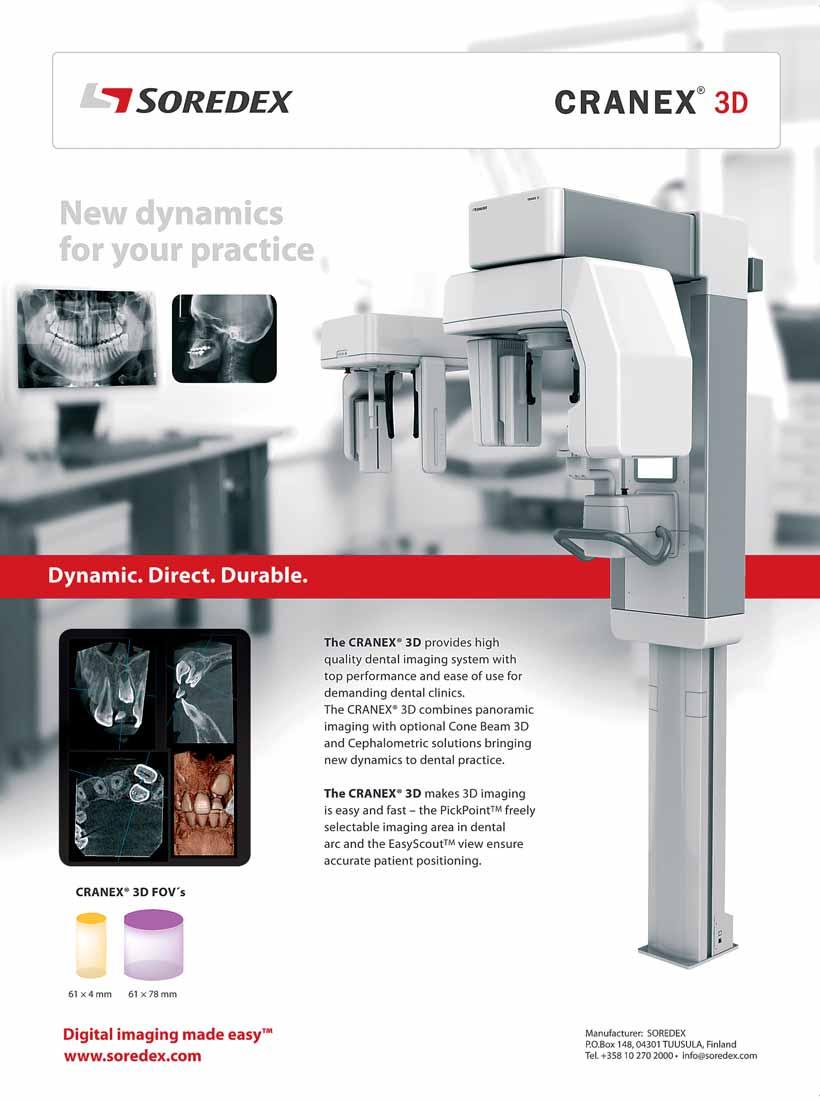
PEDIATRIC DENTISTRY
Clinical case no. 1 (Dr. L Goupy)
Example of the restoration of a proximal and cervical lesion on a primary tooth with a RMGIC: Fuji II ® LC (GC)





Fig 1-a. X-rays of a child aged 8 years taken during the emergency consultation The carious lesion developed under the ring of the band-and-loop space maintainer (75 to 73) Fig 1-b.
Initial clinical view – occlusal view
An IRM® was applied during the emergency consultation Fig 1-c.






Initial clinical view – buccal view Fig 1-d. Initial retroalveolar X-ray (IRM® in place) Fig 1-e. Isolation of the tooth by means of an operative field
Occlusal view Fig 1-f. Bucccal view Fig 1-g. Caries removal and implementation of a matrix. Fig 1-h. Application of polyacrylic acid (10 to 20% for 15 to 20 seconds, followed by rinsing and moderate drying) Fig 1-i. Filling of the coronal cavity with Fuji II® LC Clinical occlusal view Fig 1-j. Clinical buccal view Fig 1-k. Post-operative x-ray taken
* In this case involving a juxta-gingival buccal lesion, RMGIC was the appropriate procedure Admittedly, a composite restoration could have been carried out proximally as the operative field could be established However, for practical reasons, we decided to use the same material so as to avoid having two different protocols to restore the same tooth
Clinical case no. 2 (Dr. L Goupy)
Example of occlusal restoration on a primary tooth with a packable GIC: Riva® Self Cure (SDI)







Fig 2-a: Initial clinical view of tooth 64 (ECC in a child aged 2 years)
Fig 2-b: Initial retroalveolar X-ray
Fig 2-c: Isolation of the tooth by means of an operative field
Fig 2-d: Caries removal
Fig 2-e: Filling of the coronal cavity with Riva® Self Cure Again, the use of the polyacrylic acid surface treatment solution (Riva Conditioner) is recommended (10 to 20% for 15 to 20 seconds, followed by rinsing and moderate drying)
Fig 2-f: Post-operative x-ray taken
Fig 2-g: Clinical view at one week The resistance to wear of the pGIC is well suited to this type of clinical case Moreover, the adhesive properties of the pGIC are very useful, given the architecture of the substance loss
* This second case is entirely different from the first It involved a very young child with early childhood caries The use of GIC material is indicated in this case in point, as the bioactive properties of the material are especially useful
CONCLUSION
The principal characteristics of glass ionomers include the ability to adhere naturally to enamel and dentin, the cariostatic effect of
Dental News, Volume XIX, Number III, 2012 38
Using Glass Ionomer Cements In Paediatric Dentistry
Fig 1-a.
Fig 1-b.
Fig 2-c.
Fig 2-d.
Fig 2-e.
Fig 2-f.
Fig 1-d.
Fig 1-e.
Fig 1-f.
Fig 1-h.
Fig 1-g.
Fig 1-i.
Fig 1-j.
Fig 2-a.
Fig 2-b.
Fig 1-c.

mectron s.p.a., via Loreto 15/A, 16042 Carasco (Ge), Italia, tel +39 0185 35361, fax +39 0185 351374, mectron@mectron.com. www.mectron.com Û IN 1997 WE INVENTED PIEZOELECTRIC BONE SURGERY. IN 2011 WE DIDIT AGAIN. THE NEW MECTRON PIEZOSURGERY® touch Û EXCLUSIVE GLASS TOUCH SCREEN, HANDPIECE WITH SWIVEL-TYPE LEDLIGHT
PEDIATRIC DENTISTRY
fluoride release and moisture tolerance They are therefore particularly worthwhile materials for use in challenging clinical situations concerning uncooperative children or even when isolation is impossible to obtain due to the anatomical peculiarities of the primary teeth In this regard, either a RMGIC or a pGIC would be used when mechanical stress, particularly due to wear, will be great In a future article, we shall discuss the role of compomers in paediatric dentistry in relation to these materials
REFERENCES
BRAUN S, HNAT WP, FREUDENTHALER JW, MARCOTTE MR, HÖNIGLE K, JOHNSON BE. A STUDY OF MAXIMUM BITE FORCE DURING GROWTH AND DEVELOPMENT. ANGLE ORTHOD 1996; 66: 261–4.
BURGESS JO, WALKER R, DAVIDSON JM. POSTERIOR RESIN-BASED COMPOSITE: REVIEW OF THE LITERATURE. PEDIATR DENT 2002; 24: 465-79.
CASTELO PM, PEREIRA LJ, BONJARDIM LR, GAVIÃO MB. CHANGES IN BITE FORCE, MASTICATORY MUSCLE THICKNESS, AND FACIAL MORPHOLOGY BETWEEN PRIMARY AND MIXED DENTITION IN PRESCHOOL CHILDREN WITH NORMAL OCCLUSION ANN ANAT 2010; 192: 23-6.
COURSON F, JOSEPH C, SERVANT M, BLANC H, MULLER-BOLLA M. RESTAURATION DES DENTS TEMPORAIRES [RESTORATION OF PRIMARY TEETH]. ENCYCL MED CHIR, ODONTOLOGIE 2009; 23-410-K-10.
DONOVAN TE. LONGEVITY OF THE TOOTH/RESTORATION COMPLEX: A REVIEW. J CALIF DENT ASSOC 2006; 34: 122-8. DONLY KJ, SEGURA A, KANELLIS M, ERICKSON RL. CLINICAL PERFORMANCE AND CARIES INHIBITION OF RESIN-MODIFIED GLASS IONOMER CEMENT AND AMALGAM RESTORATIONS. J AM DENT ASSOC 1999; 130: 1459-66. FORSS H, WIDSTRÖM E. THE POST-AMALGAM ERA: A SELECTION OF MATERIALS AND THEIR LONGEVITY IN THE PRIMARY AND YOUNG PERMANENT DENTITIONS. INT J PAEDIATR DENT 2003; 13: 158-64.
FRIEDL K, HILLER KA, FRIEDL KH. CLINICAL PERFORMANCE OF A NEW GLASS IONOMER BASED RESTORATION SYSTEM: A RETROSPECTIVE COHORT STUDY. DENT MATER 2011; [EPUB AHEAD OF PRINT]. HICKEL R, MANHART J. ADVANCES IN GLASS IONOMER CEMENTS. GLASS-IONOMERS AND COMPOMERS IN PEDIATRIC DENTISTRY. BERLIN, QUINTESSENCE, 1999. PALINKAS M, NASSAR MS, CECÍLIO FA, SIÉSSERE S, SEMPRINI M, MACHADO-DE-SOUSA JP, HALLAK JE, REGALO SC. AGE AND GENDER INFLUENCE ON MAXIMAL BITE FORCE AND MASTICATORY MUSCLES THICKNESS. ARCH ORAL BIOL 2010; 55: 797-802.
PSOTER WJ, ZHANG H, PENDRYS DG, MORSE DE, MAYNE ST. CLASSIFICATION OF DENTAL CARIES PATTERNS IN THE PRIMARY DENTITION: A MULTIDIMENSIONAL SCALING ANALYSIS. COMMUNITY DENT ORAL EPIDEMIOL 2003; 31: 231-8.
PSOTER WJ, PENDRYS DG, MORSE DE, ZHANG HP, MAYNE ST. CARIES PATTERNS IN THE PRIMARY DENTITION: CLUSTER ANALYSIS OF A SAMPLE OF 5169 ARIZONA CHILDREN 5-59 MONTHS OF AGE. INT J ORAL SCI 2009; 1: 189-95. QVIST V, POULSEN A, TEGLERS PT, MJÖR IA. FLUORIDES LEACHING FROM RESTORATIVE MATERIALS AND THE EFFECT ON ADJACENT TEETH. INT DENT J 2010; 60: 156-60.
YENGOPAL V, HARNEKER SY, PATEL N, SIEGFRIED N. DENTAL FILLINGS FOR THE TREATMENT OF CARIES IN THE PRIMARY DENTITION. COCHRANE DATABASE SYST REV 2009; 2: CD004483.
Dental News, Volume XIX, Number III, 2012 40
YOUR NEW TREATMENT UNIT:
INSPIRED EXCLUSIVELY BY YOUR PERSONAL DESIRES.









The Ultradent Premium Class offers treatment units that you can configure as individually as your dream car. We are a modern dental company that flexibly manufactures our products based on your needs. In Germany. With outstanding quality. And absolute perfection. We are the experienced partner of completely satisfied dentists. Providing exceptional reliability and intuitive operation. With the newest technologies and multimedia. Ultradent Premium units will captivate you.

www.ultradent.de
Direct contact: m.murad@ultradent.de, Cell Phone +20 10 69 65 66 66 Ask your participating dealer





ULTRADENT PRODUCES ITS UNITS IN MUNICH UNDER GERMAN SUPERVISION. We are a familyowned and operated company with traditional values and the highest competency. The result: permanent innovation.
ULTRADENT PREMIUM TREATMENT UNITS COMBINE AESTHETICS AND FUNCTION FOR THE MOST DEMANDING NEEDS: The U 1500 and U 5000 models are ideal for your personal treatment concept.
IS THE ULTRADENT PREMIUM CLASS THE PERFECT MATCH FOR YOUR PRACTICE? Your competent dealer for dental products will be happy to assist you. We are delighted about your interest!
latest models. Jaeger & Talente, Munich
about our
GASTRO ESOPHAGEAL REFLUX DISEASE (GERD) AND TOOTH EROSION; STATISTICAL STUDY OF 100 CASES
Dr Ines Kallel, Pr Nab iha Douki, Dr Hajer Turki , Pr Salem el A jmi ineskallel@yahoo
fr
Introduction
Dental erosion was defined as dissolution of tooth by a solution that is low in pH either after the consumption of extrinsic acidic fluids or when gastric fluids come into the oral cavity Gastro esophageal reflux (GERD) is a condition defined as an involuntary passage of gastric juice against the normal flow of digestive tract It can be abnormal phenomena on in newborns and usually disappears with age ; however, in some individuals, its maintenance can be considered a pathological condition 1
The association between acid reflux and dental erosion was first described by Howden in 1971 and was confirmed in other studies later, both in the adult population and in children 2,9,23 This association is commonly observed by dentists, but is given very cursory mention or omitted entirely when describing extra esophageal (supra-esophageal) manifestations of GERD 3
A recent systematic review found a median prevalence of 24% for tooth erosion in patients with gastro esophageal reflux disease (GERD) and a median prevalence of 32 5% for GERD in adult patients who had tooth erosion Therefore, from their observations of tooth erosion, dentists may be the first persons to diagnose the possibility of GERD, particularly in the case of “silent refluxes.” This diagnosis is important, as GERD has increased in prevalence in many countries, and may have severe health effects if not adequately treated Consequently, dentists should be aware of the various manifestations of GERD 4
The aims of the study were to investigate dental erosion prevalence, location and severity and also to determine the effect of oral hygiene level, dietary behavior, dental behavior and GERD related medication and chronic illness in erosion
Patients and methods
This study was conducted at the Departments of Oral Medicine and Gastroenterology of Sahloul Hospital, Sousse Tunisia. The study group consisted of 100 patients with GERD
Inclusion criteria
All patients with GERD for 6 months with typical symptoms (heartburn and/or acid regurgitation, minimum weekly lasting for six months or more), atypical symptoms (epigastria pain, nausea, belching, halitosis, pseudo-angina pain) or with erosive GERD discovered during endoscopic examination (reflux esophagitis) or at the stage of GERD complications (peptic stenosis of the esophagus, Barrett, hemorrhage digestive)
Exclusion criteria
Were excluded from the study all patients treated surgically for GERD or presenting symptoms of GERD less than once a week or presenting undercurrent factors that can cause dental erosion such as; disorders (bulimia, anorexia), professionals exposure to toxic agents (acid fumes and aerosols used in industry) and pregnant women
Diagnosis of GERD
All patients of the study group were new patients seen at the Gastroenterology Department because of symptoms ⁄ signs suspicious of GERD Gastro-esophageal reflux disease was diagnosed by esophagogastroduodenoscopy, 24-h esophageal pH-metry, esophageal manometry
In fact all patients underwent a 24-h esophageal pH-metry to confirm the diagnosis with the exception of those who are carriers of reflux esophagitis (discovered during endoscopic examination) In our series, the characteristics of the disease (GERD), the eventual drug treatment and dietary habits were collected
Dental News, Volume XIX, Number III, 2012 42 GERD And Tooth Erosi on ORAL PATHOLOGY

























































Planmeca ProMax® 3D Unique product family More information www.planmeca.com Planmeca Middle East 306, City Tower 1, Sheikh Zayed Road P.O.Box 28826, Dubai tel. +971 4 33 27 682, mob. +971 50 450 2821, fax +971 4 33 27 684 dariush.vazvan@planmeca-middle-east.com Perfect sizes for all needs 3D X-ray • 3D photo • panoramic • cephalometric Romexis® software completes 3D perfection Romexis® PlanScan ProMax®3D ProFace™ Unique3Dcombination for openCAD/CAM
ORAL PATHOLOGY
Oral involvement assessment
Medical history of potential oral symptoms associated with GERD was carefully collected and the following parameters was evaluated; brushing method, dental erosion, dental sensitivity, loss of dental structure because of abnormal attrition (clenching or bruxing of one tooth surface against another), physical wear by extraneous objects such as toothbrushes, also known as tooth abrasion, alteration of the mucosa
Thus, dental erosion was assessed in all the patients and by a single investigator under ideal lighting conditions, and to standardize this evaluation, patients were assigned a wear Index according to the classification scale erosion of Eccles and Jenkins (table 1)
Tooth sensitivity was ranked on a subjective assessment by the dentist in 4 stages: no sensitivity, low sensitivity, moderate, and severe
Statistics
Data entry and statistical analysis were performed using SPSS software version 11 0, for the descriptive study, we calculated simple and relative frequencies, means, median and standard deviations for the analytical study, we used the Chi 2 test of Person for the comparison of percentages and the Student t test for comparison of means Only P-values <0 05 were considered statistically significant
Results
Distribution of patients: Clinical examination was carried out in 100 patients (Thirty-nine (39%) were men and Sixty-one (61%) were women with sex’s ratio; 0 63% (mean age: 49 4; range: 20–75)
LevelDescription Eccles and Jenkins Repartition of our sample ( n=100) (%)
0 No erosion 1 loss of surface detail; changes are limited to email
Women Men
0-1920-2930-3940-4950-59
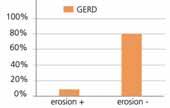
fig1:distribution of patients according to age and sex Prevalence of dental erosion in GERD


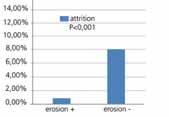
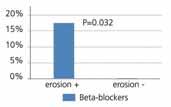

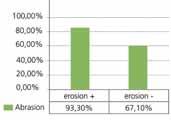

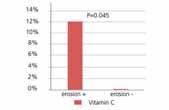
fig 2: Prevalence of dental erosion in GERD The Predilection sites are the palatal surfaces of maxillary incisors followed by palatal surfaces of maxillary molars
fig (3 a,b) and the occlusal surfaces of lower molars (protected by the tongue and saliva),fig 4
Fig 3 (a,b): dental erosion in palatal surface of maxillary incisors and molars.
Fig 4: erosion in occlusal surfaces of lower molars. A significant association was found between grade of erosion related to GERD and dental sensitivity (p=0.009)
A statistically significant associations between dental erosion related to GERD and the presence of abrasion or attrition was found (p<0.001) (fig5, fig6 ,fig7).
Fig 5: Significant associations between dental erosion related to GERD and the presence of abrasion.
Table 1: Repartition of our data according to the classification scale erosion of Eccles and Jenkins.
Fig 6: Significant associations between dental erosion related to GERD and the presence of attrition.
Fig 7: Associations between dental erosion related to GERD and pathologic attrition
Dental News, Volume XIX, Number III, 2012 44 GERD And Tooth Erosi on
65%
exposure on less than a
15% 3dentine exposure on more than one
20%
2dentine
third of the crown of the tooth
third of the crown of the tooth
1 5 2 40 30 16 2 4
Fig 1
Fig 2
Fig 3a
Fig 3b
Fig 4
Fig 5
Fig 7
Fig 6
Fig 9
Fig 8
(bruxism). Horizontal brushing was found to affect dental erosion in our series (p = 0.02). Concerning dietary hygiene we found a positive correlation between soft drink consumption and stage of erosion related to GERD (p=0.009) unlike the alcoholic beverage. About factors related to medical antecedent; History of the presence of treated ulcer disease was significantly related to the presence of dental erosion (p=0.01). On the contrary, no significant association was found between dental erosion related to GERD and diabetes (p =0.917) in our series The use of vitamin C and Beta-blockers: predisposes to dental erosions with a respective p 0.032 and 0.045 (fig8, fig9).
Fig 8: Significant associations between dental erosion related to GERD and the use of Beta-blockers.
Fig 9: Significant associations between dental erosion related to GERD and the use of vitamin C. In contrast the effect of anti-reflux therapy (proton pump inhibitor) reduced the percentage of erosion (p=0.038). On the other hand we found statistically significant association between the age of the symptoms of GERD (≥12 months), the average number of episodes of GERD (mean 6.68 / week) , the prevalence of nocturnal GERD symptoms and the presence of erosion with a value of p=0.027; 0.001 and 0.028 respectively.
Discussion
Lazarchik and Filler (1997), Groen and Smount (2003) revealed that dental erosion is the major lesion of GERD supraglottic.2
In fact research on tooth wear and related factors has received great interest in recent years The present study recorded the prevalence, location, severity and also to determine the effect of oral hygiene level, dietary behavior, dental behavior and GERD related medication and chronic illness in dental erosion
According to the present results, dental erosion is a common disease with a prevalence that falls within the reported rates observed in previous studies 8, 10
However, no clear definitive data are available regarding the real prevalence of dental erosion in patients with GERD and prevalence varies widely among different studies This can be explained by several factors such as frequency of regurgitation, duration of untreated disease, buffering properties of saliva, diet, friction caused by tongue on teeth during mastication, deglutition, phonation, diagnostic difficulty of erosion at the early stage, lack of description of diagnostic criteria.5,9,16,17,18
The most affected dental surfaces were found to be the maxillary anterior teeth, a finding which is in agreement with other studies 14, 8, 6, 11 On the other hand, lower rates of erosion were found in the mandibular teeth, especially in their lingual surfaces, and this may be attributed to the protective effects of the saliva produced by submandibular and sublingual glands3, 4, 5, 19 ,these findings are in accordance with those reported by Magdalini and co-workers 8
The present study has recorded a significant association between erosion related to GERD and dental sensitivity this finding is on contrast with the result found by Di Fede and al who found that dental hypersensitivity was present in both sample and control group at the same prevalence 5
In our study the coexistence of attrition in these lesions was important as well as abrasion; which is in agreement with other studies wich explain the aggravating role of these lesions on the erosion linked to GERD8, 10 ; some experimental findings support these observations and indicate that tooth wear under bruxism
ORAL PATHOLOGY
and gastric acid conditions can occur at an alarming rate, thus these findings point to the need for early preventive strategies 3 Tooth brushing is an important factor, in our series horizontal brushing was found to potentiate dental erosion, in fact it should be done carefully, using a soft tooth brush and a low-abrasive high sodium fluoride containing dentifrice not immediately after acid regurgitation, it should be avoided for approximately 2 h after a regurgitation episode to allow for the re-establishment of salivary pellicle and subsequent tooth surface remineralization 3
A positive correlation between soft drink consumption and stage of erosion related to GERD was found in our patient in fact this relationship was also quoted in the literature unlike the alcoholic beverage 4 , this can be explained by the majority of women in our sample
In fact alcohol consumption may increase gastric acid secretion, delay gastric emptying and cause incompetence of the lower esophageal sphincter
Thus patients should be advised to avoid such acidic foods and beverages and instead rinse their mouths either with water, milk, sodium bicarbonate solutions or sodium fluoride mouth rinses after each acid regurgitation episode 3, 8
As regards to medical history, the presence of treated ulcer disease was significantly related to the presence of dental erosion in our sample, the same observation has been cited by Frank Z 26 this observation could be explained by the restoration of a normal acid secretion after eradication of the bacterium (Helicobacter pylori ) unlike the study of Munoz et al 27
For diabetic patients has not found a correlation with GERD in our sample in contrast to the literature 28,29
In our study we found that the use of vitamin C and Beta-blockers predisposes to dental erosions this finding is in accordance with the literature in fact physicians should be aware of any drugs or medicines consumed by patients that may cause or exacerbate hypo salivation and lead to xerostomia or being itself acid, in some instances, saliva substitutes may be prescribed or recommended.3,8
This fact is in accordance with the findings of Al-Malik et al who found that the use of vitamin C supplements is a predictive factor for dental erosion 22
In contrast anti-reflux therapy reduced the percentage of erosion; it is a protective factor, Tantbirojn and colleagues have the same finding in their study where he observed a faster increase in the loss of tooth surface in patients in whom acid reflux is not controlled 4,10,24
In our study we found a significant correlation between the severity of dental erosion and the duration of the disease, frequency of regurgitation and the prevalence of nocturnal GERD symptoms which is in agreement with literature 1, 3
The potential for erosive damage during sleep-related GERD can be explained by the fact that the anti reflux protective mechanisms present during the waking period like increasing salivary flow and swallowing mechanisms and localized
Dental News, Volume XIX, Number III, 2012 45
GERD And Tooth Erosi on
ORAL PATHOLOGY
esophageal peristalsis to buffer the acid and facilitate volumetric clearance are decreased during sleep.4
As regards the effect on the mucosa, in the literature GERD was recently reported to be associated with erythematous lesions on soft and hard palate mucosa and uvula.5
Some microscopic alterations in the palatal mucosa, such as epithelial atrophy and increased fibroblast numbers was found; thus attention should be paid to mucosal inflammation in GERD patients on dental check-up 15,12,5 but in our sample no such lesion was found
As a result special attention must be given to prevention to avoid the loss of substance and alteration consecutive to GERD as well as on the soft and hard tissue of the oral cavity the principal method is to eliminate the primary cause requiring a close relationship with the patient’s medical practitioner From the dental practitioner’s perspective, preventive measures may involve the stimulation or substitution of salivary secretions, providing dietary advice, placement of any physical barrier between the tooth surfaces and the endogenous acid like “metal ion” fluorides such as SnF, AgF, TiF4, and FeF3; the mechanism of action is probably not by the fluoride ion itself, but by the metal ion precipitate that forms a physical barrier to the acid. Other dental products can be used as, often, temporary physical barriers like resin-based viscous varnishes, resin-based dentin bonding agents, glass-ionomer cement, sealant 3,4,30
Conclusion
According to many research publications, the association of tooth erosion and GERD is stronger than generally perceived by physicians Dental practitioners should also determine whether a patient has erosive tooth surface loss and, if present, try to identify the cause If the tooth surface loss is the result of acid reflux, the practitioner should advise the patient to see his or her family physician or internist for diagnosis and treatment of GERD or of another illness related to acid regurgitation In addition, dental practitioners should educate their patients about the damage that acid reflux can cause to their teeth and ensure prevention of further tooth wear involving local prevention, restorative and maintenance phases
As a result, collaboration between gastroenterologist and dentists is strongly advocated to prevent or ameliorate possible adverse oral effects from endogenous acid.
REFERENCES
1.RENATA O. GUARE´ , MARIA C. D.FERREIRA,MARIANA F.LEITE1, JONAS A.RODRIGUES,ADRIAN LUSSI,MARIA T.B.R.SANTOS:DENTALEROSIONANDSALIVARYFLOWRATEINCEREBRALPALSYINDIVIDUALSWITHGASTROESOPHAGEAL REFLUX; J ORAL PATHOL MED (2012) 41: 367–371
2.DENA A.ALI;RONALD S.BROWN;LUCIANO O.RODRIGUEZ,; EDWARD L.MOODY;MAHMOUD F.NASR,B.DENTALEROSIONCAUSEDBYSILENTGASTROESOPHAGEALREFLUXDISEASE; JADA, VOL. 133, JUNE 2002
3.SARBIN RANJITKAR,ROGER J. SMALESAND JOHN A.KAIDONIS:REVIEW ORALMANIFESTATIONSOFGASTROESOPHAGEALREFLUXDISEASE; JOURNALOF GASTROENTEROLOGYAND HEPATOLOGY 27 (2012) 21–27
4.SARBIN RANJITKAR, JOHN A.KAIDONIS, AND ROGER J. SMALES:REVIEW ARTICLE GASTROESOPHAGEAL REFLUX DISEASEAND TOOTH EROSION; INTERNATIONAL JOURNALOF DENTISTRY VOLUME 2012, ARTICLE ID 479850, 10 PAGES
5.OLGA DI FEDE, CHIARA D LIBERTO, GIUSEPPE OCCHIPINTI,SERGIO VIGNERI,LUCIO LO RUSSO,STEFANO FEDELE,LORENZO LO MUZIO, GIUSEPPINA CAMPISI :ORALMANIFESTATIONSINPATIENTSWITHGASTRO-ESOPHAGEALREFLUXDISEASE: A SINGLE-CENTERCASE–CONTROLSTUDY; J ORAL PATHOL MED (2008) 37: 336–340
6. JUANLI GUO, GLENN RESIDE,LYNDON F. COOPER:FULL-MOUTH REHABILITATIONOFA PATIENTWITH GASTRO ESOPHAGEAL REFLUX DISEASE:A CLINICAL REPORT; JOURNALOF PROSTHODONTICS 20 (2011) S9–S13
7.A PALI S HUNGINA,ANAN SRAGHUNATHAAND INGELA WIKLUNDB:BEYONDHEARTBURN: ASYSTEMATICREVIEWOFTHEEXTRA-ESOPHAGEALSPECTRUMOFREFLUX-INDUCEDDISEASE ;FAMILY PRACTICE AN INTERNATIONALJOURNALJULY2005
8.MAGDALINI MANTONANAKI , HAROULA KOLETSI-KOUNARIAND ELENI MAMAI-HOMATA & WILLIAM PAPAIOANNOU: DENTALEROSIONPREVALENCEANDASSOCIATEDRISKINDICATORSAMONGPRESCHOOLCHILDRENIN ATHENS, GREECE; CLIN ORAL INVEST 2012
9. JOEL J. HEIDELBAUGH , ARVIN S. GILL , R. VAN HARRISONAND TIMOTHY T.NOSTRANT:ATYPICAL PRESENTATIONS OF GASTROESOPHAGEAL REFLUX DISEASE;AMERICAN ACADEMYOF FAMILY PHYSICIANS: 2008;78(4):483-488.
10.DARANEE TANTBIROJN,MARIA R. PINTADO,ANTHEUNIS VERSLUIS, CAROL DUNNAND RALPH DELONG :QUANTITATIVEANALYSISOFTOOTHSURFACELOSSASSOCIATEDWITHGASTROESOPHAGEALREFLUXDISEASE : A LONGITUDINALCLINICAL STUDY; JADA 2012;143;278-285
11. GENG-RU WANG, HUI ZHANG , ZHONG-GAO WANG, GUANG-SHUI JIANG ,CHENG-HAO GUO :RELATIONSHIP BETWEENDENTALEROSIONANDRESPIRATORYSYMPTOMSINPATIENTSWITHGASTRO-ESOPHAGEALREFLUXDISEASE ;JOURNAL OFDENTISTRY38(2010)892-898
12. HIROO YOSHIKAWA , KENJI FURUTA , MAYUMI UENO , MASAYOSHI EGAWA , AYA YOSHINO , SEIJI KONDO , YOSHIKI NARIAI , HIROAKI ISHIBASHI , YOSHIKAZU KINOSHITA , JOJI SEKINE : ORALSYMPTOMSINCLUDINGDENTALEROSIONINGASTROESOPHAGEALREFLUXDISEASEAREASSOCIATEDWITHDECREASEDSALIVARYFLOWVOLUMEANDSWALLOWING FUNCTION ; J GASTROENTEROL (2012) 47:412–420
13.ROBERT P. BARRON,ROBERT P. CARMICHAEL,MARGARET A.MARCON, GEORGE K.B.SÀNDOR: ÉROSIONDENTAIRE ETREFLUXGASTRO-OESOPHAGIENPATHOLOGIQUE ; J CAN DENT ASSOC 2003 ; 69(2) :84-9
14. WIEGAND A,MULLER J, WERNER C, ATTIN T: PREVALENCEOFEROSIVETOOTHWEARANDASSOCIATEDRISKFACTORSIN 2-7-YEAR-OLD GERMANKINDERGARTENCHILDREN.ORAL DIS 2006, 12:117–124
15.SILVA MAGS,DAMANTE JH, STIPP ACM,TOLENTINO MM, CARLOTTO PR,FLEURY RN. GASTROESOPHAGEALREFLUXDISEASE: NEWORALFINDINGS ORAL SURG ORAL MED ORAL PATHOL. 2001;91:301–10.
16.SILVA MA,DAMANTE JH, STIPP AC,TOLENTINO MM, CARLOTTO PR,FLEURY RN. GASTROESOPHAGEALREFLUX DISEASE: NEWORALFINDINGS.ORAL SURG ORAL MED ORAL PATHOL ORAL RADIOL ENDOD 2001; 91: 301–10. 17.MOAZZEZ R,BARTLETT D,ANGGIANSAH A.DENTALEROSION, GASTRO-OESOPHAGEALREFLUXDISEASEANDSALIVA: HOWARETHEYRELATED? J DENT 2004; 32: 489–94.
18. GREGORY-HEAD BL, CURTIS DA,KIM L, CELLO J. EVALUATIONOFDENTALEROSIONINPATIENTSWITHGASTRO ESOPHAGEALREFLUXDISEASE. J PROSTHET DENT 2000; 83: 675–80.
19.TAJI S,SEOW K,TOWNSEND G, HOLCOMBRE T (2010) A CONTROLLEDSTUDYOFDENTALEROSIONIN 2- TO 4-YEAR-OLDTWINS. INT J PAEDIATR DENT 20:400–409
20.BARTLETT DW, EVANS DF,ANGGIANSAH A,SMITH BGN.A STUDYOFTHEASSOCIATIONBETWEENGASTROOESOPHAGEALREFLUXANDPALATALDENTALEROSION.BR DENT J. 1996;181:125–31.
21.BARTLETT DW, EVANS DF,SMITH BGN.THERELATIONSHIPBETWEENGASTRO-ESOPHAGEALREFLUXDISEASEAND DENTALEROSION. J ORAL REHABIL. 1996;23:289–97.
22.AL-MALIK MI, HOLT RD,BEDI R (2001) THERELATIONSHIPBETWEENEROSION, CARIESANDRAMPANTCARIESAND DIETARYHABITSINPRESCHOOLCHILDRENIN SAUDI ARABIA. INT J PAEDIATR DENT 11:430–439
23.F. PACE,S. PALLOTTA,M.TONINI,N. VAKIL AND G. BIANCHI PORRO, “SYSTEMATICREVIEW: GASTRO-ESOPHAGEALREFLUXDISEASEANDDENTALLESIONS,”ALIMENTARY PHARMACOLOGYAND THERAPEUTICS, VOL. 27, NO. 12, PP 1179–1186, 2008
24. C. H. WILDER-SMITH, P. WILDER-SMITH, H. KAWAKAMI-WONG, J. VORONETS,K.OSANN, AND A.LUSSI, “QUANTIFICATIONOFDENTALEROSIONSINPATIENTSWITH GERD USINGOPTICALCOHERENCE TOMOGRAPHYBEFOREANDAFTERDOUBLE-BLIND, RANDOMIZEDTREATMENTWITHESOMEPRAZOLEORPLACEBO,”THE AMERICAN JOURNALOF GASTROENTEROLOGY, VOL. 104, NO. 11, PP. 2788–2795, 2009.
25. VAN PINXTEREN B,SIGTERMAN KE,BONIS P, LAU J, NUMANS ME.SHORT-TERMTREATMENTWITHPROTONPUMP INHIBITORS, H2-RECEPTORANTAGONISTSANDPROKINETICSFORGASTRO-ESOPHAGEALREFLUXDISEASE-LIKESYMPTOMSAND ENDOSCOPYNEGATIVEREFLUXDISEASE. COCHRANE DATABASE SYST.REV. 2010; (11): CD002095.
26.FRANK ZERBIB L’INFECTIONPAR H.PYLORIOUSONÉRADICATIONJOUENT-ELLESUNROLEDANSLEREFUXGASTROOESOPHAGIEN ?GASTROENTEROLOGIE CLINIQUE BIOLOGIQUE 2003 ;27 :427-431
27.MUNOZ JV,HERREROS B,SANCHIZ V .DENTALANDPERIODONTALLESIONSINPATIENTSWITHGASTRO-ESOPHAGEAL REFLUXDISEASE;DIGESTIVE LIVER DISEASES 2003;35(7):461-467
28.BARTLETT DW,EVANS DF,ANGIANSAH A,SMITH BG.A STUDYOFTHEASSOCIATIONBETWEENGASTROESOPHAGEAL REFLUXDISEASEANDPALATALDENTALEROSION;BRITISH DENTISTRY JOURNAL2006;181:125-131
29. G CAMPISI,LLO RUSSO,CDI LIBERTO,FDI NICOLA;SALIVAVARIATIONSINGASTRO-ESOPHAGEALREFLUX DISEASE;JOURNALOFDENTISTRY36,2008,268-271
30.B.T.AMAECHIAND S.M. HIGHAM, “DENTALEROSION: POSSIBLEAPPROACHESTOPREVENTIONANDCONTROL,” JOURNALOF DENTISTRY, VOL. 33, NO. 3, PP. 243–252, 2005.
Dental News, Volume XIX, Number III, 2012 46
GERD And Tooth Erosi on
Brilliant
light, the new A-dec LED light combines

For information on what to look for in quality dental lighting, visit a-dec.com/LED to learn more.
Chairs Lights Cabinets
Maintenance
The Esthetic Anterior Restoration
Dr Mayada Jemâa, Pr Ne ila Zokkar dr.jemaamayada@gma il.com
Summary:
Today, the demand for esthetic restorations is increasing. Thus, the use of composite resins is clearly growing. It is therefore our duty to perform high quality restorations that combine science, art and technology of high performance 3 The increasing demands of patients in terms of aesthetics and the character of micro- invasive restorative materials placed directly on anterior teeth is at the heart of current concerns A thorough knowledge of color characteristics of natural teeth and restorative materials combined with a careful analysis of operative techniques and the sequence of stratification allow the clinician to obtain highly functional, aesthetic and predictable results 8 The composite resins have reached a high degree of excellence and are now utilized with predictable results in restoring the anterior dentition. (Fahl N Jr and al, 1995)
In our work, we are going to present 3 clinical cases of anterior stratification with composite resin Opallis® (FGM) that we have treated in our department of conservative dentistry
Key Words : Esthetic, stratification, composite, opallis ®
Introduction:
Direct bonding is one of the most commonly used form of restoration for the conservative esthetic improvement of anterior teeth 6,8 Recent developments in adhesive technologies, the design of composite resin materials, and contemporary placement techniques have revolutionized the delivery of minimally invasive direct restorations Indeed, the aesthetic demands of patients for the restoration of anterior teeth have prompted the doctors to see the tooth as one entity: a smile and gingiva and its components through the development of clinical procedures and techniques for restoration The stratification technique of composite resin
shades is the most appropriate way to achieve a final restoration with a very natural appearance (Kose and Dourado Loguercio, 2009) Manufacturers have sought to improve more and more biomechanical and optical properties of composite resins The evolution of composite resins is based on the dimensions of the charges Turn, has classified the macrofilled, the microfilled, hybrid and currently nanohybrids composite resins 8 Opallis is a microhybrid composite resin indicated for direct restoration of anterior and posterior teeth It provides a complex and perfect balance between the masses of dentin and enamel as they have different levels of translucency and opacity (Sanzio Marques, 2009) Two optical phenomena are indispensable : *fluorescence and, **opalescence the composite resin Opallis presents these features as well as many other advantages (Sanzio Marques, 2009) The mechanical and physical-chemical properties of this composite guarantee stability and longevity for anterior and posterior restorations Opallis restorations match the patients’ smiles gathering esthetic, functionality, longevity and patient’s satisfaction (Walter Dasch et al 2009)
*Fluorescence: an optical property of a material capable of absorbing ultraviolet light (non visible to the naked eye) and emitting light in a visible wavelength in response (white and blue). Therefore, when irradiated by ultraviolet light, fluorescent bodies increase their brightness and opacity (Walters and al, 2009).
**Opalescence: a material property related to the capacity of an object to present a bluish color when observed under direct light and look reddish orange when observed under indirect light (Walters and al, 2009).
Dental News, Volume XIX, Number III, 2012 48 The Esthet ic Anteri or Restorat i on
RESTORATIVE DENTISTRY


Sensodyne Repair & Protect
Presenting a new layer of protection






Sensodyne Repair & Protect harnesses advanced NovaMin® technology to help build a robust hydroxyapatite-like layer over exposed dentine and within dentine tubules.1–5 With Sensodyne Repair & Protect, you can do more than treat the pain of dentine hypersensitivity – you can repair and protect your patients’ exposed dentine.
Think beyond pain relief and recommend
Sensodyne Repair & Protect


 References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; 21(3): 72-76. 3. West NX et al. J Clin Dent 2011; 22(Spec Iss): 82-89. 4. Earl J et al. J Clin Dent 2011; 22(Spec Iss): 62-67. 5. Efflandt SE et al. J Mater Sci Mater Med 2002; 26(6): 557-565. Prepared December 2011, Z-11-516.
References: 1. Burwell A et al. J Clin Dent 2010; 21(Spec Iss): 66–71. 2. LaTorre G, Greenspan DC. J Clin Dent 2010; 21(3): 72-76. 3. West NX et al. J Clin Dent 2011; 22(Spec Iss): 82-89. 4. Earl J et al. J Clin Dent 2011; 22(Spec Iss): 62-67. 5. Efflandt SE et al. J Mater Sci Mater Med 2002; 26(6): 557-565. Prepared December 2011, Z-11-516.
RESTORATIVE DENTISTRY
Objectives:
- To present the stratification technique with composite resin Opallis ®
- Acknowledge the contribution of the composite resin in terms of better esthetic results, smoothing surface, saving time and easy manipulation
Clinical case1:
Age : 21 years
Reason for consultation : restoration of the 31 with an abnormal structure
Therapeutic decision : restoration of 31 by stratification technique with the resin composite Opallis ®



Fig 1: Initial clinical view
Fig 2: Shade selection and elimination of the colored structure and the tooth was prepared for Placement of composite resin Opallis ®
Fig 3: Final aspect of the restoration after the stratification procedure
Clinical case 2:
Age : 17 years
Reason for consultation : restoration of the 11, 12 and 21 traumatized since 1 month.
Therapeutic decision : restoration of the 11, 12 and 21 which are vital with stratification by composite resin.





Adjustment of the silicone guide helps in construction of the palatal enamel
Then elaboration of the incisal opaque halo with Opallis A1 enamel, the composite resin A2 dentin was employed to reconstruct the area corresponding to dentin, translucent enamel placed between dentinal mamelons and the layering of the restoration was finished with composite resin A1 enamel

Fig 6: Plaster model and mock-up (after shade selection)
Fig 7: Elaboration of silicone guide
Fig 8: Adjustment of the silicone guide (verification of the adaptation and the retention)
Fig 9: Elaboration of the palatal enamel (A1 opallis®)
Fig 10: Final aspect of the restoration after complete mimicry of the esthetic natural characteristics of the teeth
Fig 11: After 3 months
Clinical case 3:
Age : 23 years
Reason for consultation : restoration of the 11 fractured
Therapeutic decision : restoration of 11 (vital) by stratification technique with the resin composite Opallis ®




Dental News, Volume XIX, Number III, 2012 50
Fig 1
Fig 2
Fig 3
Fig 4
Fig 5
Fig 8
Fig 9
Fig 10
Fig 12
Fig 14
Fig 13
Fig 4: Preoperative Facial view showing the fractured maxillary right and left central incisors and the maxillary right lateral
Fig 5: Palatal view
Fig 11
The Esthet ic Anteri or Restorat i on Fig 6 Fig 7 Fig 15






RESTORATIVE DENTISTRY



Fig 12: Initial aspect (the tooth is vital)
Fig 13: The field was first isolated with a rubber dam after shade selection
Fig 14: A 0.5-mm scalloped bevel was placed with a long-tapered diamond
Fig 15: After the preparation of the surface
Fig 16: Acid etching with 37% phosphoric acid (30 seconds on enamel, 15 seconds on dentin)





Fig 17: After (adhesive was applied to the cavity surfaces with an applicator tip and air dried, palatal enamel was constructed with composite resin Opallis A1 , the incisal opaque halo with Opallis A2 dentin, Dentin reconstruction with increments of Opallis A1 Dentin, enamel was placed (in marginal ridges and the last increment) with Opallis A1
Fig 18: Adjustment of the incisal edge morphology finishing procedure with abrasive disks to impart a high luster while maintaining the existing texture and surface anatomy
Fig 18, 19, 20, 21: Superficial polishing with diamond past (Excel diamond ®) applied with felt disks
Fig 22: Occlusal adjustment of the restoration.
Fig 23: Premature occlusal contacts should be removed
Fig 24: Postoperative appearance reflects the harmonious integration of composite resin with natural tooth structure.
Clinical case 4:
Age : 14 years
Reason for consultation : restoration of the 11 and 22 fractured after a trauma.
Therapeutic decision : restoration of 11 and 22 (both tooth are vital) by stratification technique with the resin composite Opallis ®



Fig 25: initial view



Fig 26: Isolation of the field with a rubber dam
Fig 27: Elaboration of the palatal enamel
Fig 28: Dentin reconstruction
Fig 29: The final aspect of restoration after stratification procedure
Fig 30: Natural integration of the restoration
Discussion:
These cases presentations demonstrate restoration of fractured incisors taking aesthetic consideration of the anatomic variations of the adjacent teeth to produce a direct composite resin in harmony with the surrounding dentition
The major challenges is selecting the composite that have an adequate strength as well as provide lifelike optical properties that render the restoration functionally sound and esthetically pleasing.6 The results we have obtained in the three clinical cases, make us reconsider this type of restoration with composite resin quite satisfactory with an optimal esthetic results (Surface, polishability, wear resistance ).
Therefore, we can integrate these restorations as aesthetic solutions to long term durability since opallis composite, under wet conditions, reached the highest fatigue limit values.1
Of course, provided they are carried out in good conditions and combined with regular annual clinical inspections
To optimize the physical and optical characteristics of the natural tooth, Ardu S and al (2006) proposed the combination of microfilled composite with a microhybrid composite and the biomimetic composite restoration could be an interesting alternative to ceramics, minimizing invasiveness, chair time, and costs for patients
To obtain a functionally successful and esthetic natural appearing direct composite restoration, the clinician must have a comprehensive knowledge of adhesive dentistry, including
Dental News, Volume XIX, Number III, 2012 52 The Esthet ic Anteri or Restorat i on
Fig 19
Fig 20
Fig 21
Fig 22
Fig 23
Fig 16
Fig 17
Fig 18
Fig 25
Fig 26
Fig 27
Fig 28
Fig 29
Fig 30
001182

COMPONEER ™

Surprise your patients with a new s ile –in onl one session!




Innovative. Time-saving. Surprisingly easy. COMPONEER is the Direct Composite Veneering System used for quick, easy and save restorations of single or multiple teeth. This offers new perspectives for you and your patients. So both of you have a reason to smile. www.componeer.info









SMILE TO GO.







COMPONEER benefits:





www.coltene.com/contact

No laboratory required | One session | Naturally aesthetic corrections using freehand technique | Easy application with prefabricated composite veneers | Brillant result | Attractive added value






001182 THE
RESTORATIVE DENTISTRY
the properties of composite resins, proper tooth preparation techniques, and an understanding of the primary and secondary optical properties of the natural tooth and their relationship to anatomical morphology 8
Conclusion:
As contemporary modes of treatment continue to evolve, manufacturers and scientists are leading the way with new advances in restorative materials and adhesive technology These techniques and concepts from clinicians, scientists, and technicians around the world are the spark that ignites the reaction Nevertheless, it is the clinical experience and judgment that is the true catalyst of the reaction that creates form, function, aesthetics, longevity and more predictable options for direct treatment protocols
«The provision of high-quality restorative dentistry depends upon the dentist» Peter Jacobsen
- Making an accurate diagnosis
- Devising a comprehensive and realistic treatment plan
- Executing the treatment plan to a high technical standard
- Providing subsequent continuing care
REFERENCES
1. WALTER DASCH,ULRICH LOHBAUER,ANDREA WAGNER, JOHANNES EBERT,R.FRANKENBERGER,MATTHIAS PELKA, LISA SCHEUERMEYER,GUDRUN AMBERGER, GIRIT STEIN,MARTINA RÖDEL, HERBERT BRÖNNER
COMPOSITEFORANTERIORANDPOSTERIORTEETH. WHATEXPECTFROM OPALLIS: ESTHETICRESULTS, OPTIMALBALANCEOF
PROPERTIESSPECIALSHADES, 4 DEGREESOFTRANSLUCENCY
MAGAZINE FGMNEWS- EDITION 2- OCTOBER 2009
2. CARLOS KOSE,ALESSADRO DOURADO LOGUERCIO
COMPOSITERESINLAYERINGINANTERIORTEETH- CLINICALCASEREPORT
MAGAZINE FGMNEWS- EDITION 2- OCTOBER 2009
3.SANZIO MARQUES
MIMICKINGTHENATUREWITHOPALLISCOMPOSITE
MAGAZINE FGMNEWS- EDITION 2- OCTOBER 2009
4. PETER JACOBSEN
RESTAURATIVEDENTISTRY:ANINTEGRATEDAPPROACH
SECOND EDITION 2008
5.FAHL N JR,DENEHY GE, JACKSON RD. PROTOCOLFORPREDICTABLERESTORATIONOFANTERIORTEETHWITHCOMPOSITERESINS
PRACT PERIODONTICS AESTHET DENT. 1995 OCT;7(8):13-21; QUIZ 22.
6.FAHL N JR
ACHIEVINGULTIMATEANTERIORESTHETICSWITHANEWMICROHYBRIDCOMPOSITE
COMPEND CONTIN EDUC DENT SUPPL. 2000;(26):4-13; QUIZ 26.
7.ARDU S,KREJCI I.
BIOMIMETICDIRECTCOMPOSITESTRATIFICATIONTECHNIQUEFORTHERESTORATIONOFANTERIORTEETH
QUINTESSENCE INT. 2006 MAR;37(3):167-74.
8.MAUD CONTI
LASTRATIFICATIONDESRÉSINESCOMPOSITESSURDENTSANTÉRIEURES
THÈSEDEDOCTORATEN MÉDECINEDENTAIRE, 2010
UNIVERSITÉ HENRI POINCARE-NANCY1



The Power. The Silence. The new Tornado Super Silent


























Tornado – the new generation of compressors from Dürr Dental
Dürr Dental, the inventor of oil-free dental compressors, presents an unbelievably quiet and powerful compressor for dentistry in the form of the new “Made in Germany“ Tornado.
▪ Oil-free, dry, and hygienic
▪ One of the quietest of its kind
▪ Dust- and Sandresistant
▪ Antibacterial inner tank coating
▪ Low-maintenance thanks to membrane-drying unit
Duerr Dental Middle East, P.O.Box: 87355, Al Ain - U.A.E., Mobile: +971 (0) 50 - 550 84 12, Fax: +971 (0) 3 767 - 5615, email: koll.m@duerr.de

COMPRESSED AIR SUCTION IMAGING DENTAL CARE HYGIENE
8
Beauty. Versatility. Performance.





VersaCOMP™ Flowable Composite VersaCOMP™ Universal Total Etch Adhesive VersaCOMP™ Universal Hybrid Composite Sultan Healthcare introduces VersaCOMP™ , a complete line of restorative materials that offers easy handling, versatility and clinical performance…all at a great price. The result is the ideal combination of performance and value. BEFORE AFTER INTRODUCING





Bienvenue à tous
Après beaucoup de travail, toujours dans la bonne humeur et l’enthousiasme, nous voici parvenus aujourd’hui au bout de nos peines. C’est enfin la séance inaugurale de notre congrès qui se tient chaque deux ans sur le campus des sciences medicales. Mon propos sera axé aujourd’hui autour de deux points: Notre but a toujours été de faire évoluer et de revaloriser notre profession en lui rendant son attractivité. Ce congrès est une mise à jour pour tous les praticiens, y compris les responsables de stage de la Faculté. Je remercie vivement les conférenciers étrangers parmi lesquels plusieurs libanais expatriés de longue date, anciens de la Faculté avec qui nous entretenons toujours des relations amicales et chaleureuses. Je remercie également les doyens des Facultés de chirurgie dentaire du monde arabe, qui malgré la situation critique que traverse la région, ont bien voulu participer à notre Assemblée générale.
Je tiens à remercier tous les membres du comité d’organisation et son président le Pr Antoine Khoury qui ont accepté courageusement et généreusement la responsabilité scientifique et logistique de cet événement. Pour terminer, je voudrai vous dire ma joie de vous accueillir en si grand nombre, le plaisir de vous connaître, de partager des idées et de construire, peut-être des projets avec certains d’entre vous.
À toutes et à tous, je souhaite un excellent congrès!




58
Pr Nada Naaman Dean St Joseph University Dental School
Reverend Chamussy Rector of St Joseph University
Pr Fouad Khoury lecturing on the latest in implantology
Dr Friedrich Pape from Germany
Pr Antoine Khoury President of The Congress
Pr Khaldoun Rifaie and Pr. Nuhad Rizk presiding the session





PICTURES FROM THE EXHIBITION






 Picture of the Deans of the Dental Schools from the Arab countries at the St Joseph University Dental School
Picture of the Deans of the Dental Schools from the Arab countries at the St Joseph University Dental School
For extra protection from the effects of Acid Wear...
...Recommend the Pronamel combination regime
IndividuallyPronamel DailyToothpaste and Pronamel Daily Mouthwash are proven to reharden acid-softened enamel comparedtostandard options7,8
Figure1: Insitu rehardening microindentation study following treatment with dentifrices7

Adapted from Hara AT et al. Bovine enamel specimens were subjected to an erosive challenge. This was followed by fixation to palatal appliances and a 4-hour intra-oralphase in 58 human subjects.



Figure2: Invitro laboratory rehardening (mean) microindentation study following treatment with fluoride mouthwashes8
Adapted from Young M and Willson R. 6 human enamel specimens were subjected to an erosive challenge in vitro. This was followed by a mean rehardening microindentation study after treatment with fluoride mouthwashes.




contributor to tooth wear.1–5 Acid Wear is a widespread and growing condition, affecting both adults and children,6 but in its early stages can be difficult to identify. *based on clinical data with 450ppm Pronamel Daily Mouthwash and 1450ppm Pronamel



But used in combination, provide 80% more protection from the effects of Acid Wear than brushing with Pronamel DailyToothpaste alone 9*



Oral Sci 1996;104:191–198. 3. Bartlett DWet al. Int Dent J 2005;55:277–284. 4. Zero DT.Int Dent J 2005;55:285–290. 5. Zero DTet al.J Clin Dent 2006;17 (Spec Iss):112–116. 6. Deery Cet al. Pediatr Dent 2000;22(6):505–510. 7. Hara ATet al. Caries Research 2009;43:57-63. 8. Young Mand Willson R. GSK data on file. 2008. 9. Maggio Bet al. J Dent 2010;38(53);537–544. Prepared October 2011, Z-11-404.
100 60 45 30 15 0 Mean percentage surface microhardness recovery Pronamel (1450ppm NaF) A leading toothpaste (1450ppm NaF) Placebo (oppm F) P<0.001
Pronamel Daily Mouthwash 160 140 120 100 80 Enamel microhardness relative to initial etched / % FluorigardListerine coolmint Water
2010. Original study design contained 5 test cells;
one not included here is a fluoride-free dentrifice plus water. 0 -5 -10 -15 -20 -25 -30 -35 The smaller the negative value the better the products have performed. Mean % net erosion resistance Pronamel Daily Toothpaste (1450ppm NaF) and Pronamel Daily Mouthwash (450ppm NaF) Pronamel Daily Toothpaste (1450ppm NaF) and water Competitor toothpaste (1450ppm NaF) and water -2.88 -14.54 -29.48 Fluoride-free Toothpaste and Pronamel Daily Mouthwash (450ppm NaF) -3.76 Extra protection from theeffects of Acid Erosion Giveyourpatients80%moreprotectionfromtheeffectsofAcidWear,comparedto PronamelDailyToothpaste alonebyrecommendingthePronamelcombinationregime Figure3: Insitu erosive resistance after treatment with a dentifrice and mouthwash regime9 FMCG /11/11/21 Modern
the exposure
tooth enamel to
acid
can lead to Acid Wear (erosive tooth wear), the biggest
Daily Toothpaste References: 1. Lussi A. Erosive Tooth Wear – a Multifactorial Condition. In: Lussi A, editor. Dental Erosion – from Diagnosis to Therapy. Karger, Basel, 2006. 2. Lussi A. EurJ
Sensoydne Pronamel is a registered trademark of GlaxoSmithKline Group of companies. Further information is available upon request from GlaxoSmithKline Health care, P.O. Box 23816, Dubai, UAE. For adverse event reporting, please send us an email on OAX84543@gsk.com Consumer Healthcare
Adapted from Maggio B et al.
the
eating and drinking habits increase
of
dietary
that

EuroPerio7 was a great success.
More than 7800 colleagues from all over the world participated in this magnificent event in Vienna. Here are some pictures from the sessions as well as general congress impressions




 Picture of a Group of Lebanese Implantologists by the Danube River
Picture of a Group of Lebanese Implantologists by the Danube River





PICTURES FROM THE EXHIBITION










09-10 November 2012 Jumeirah Beach Hotel Dubai UAE 4th Edition WhereScienceMeetsTheArtofBeauty Dental - Facial Cosmetic International Conference CME 14 Hours Tel: +971 4 3616174 | Fax: +971 4 3686883 | Mob: +971 50 2793711 Email: info@cappmea.com www.cappmea.com/aesthetic2012
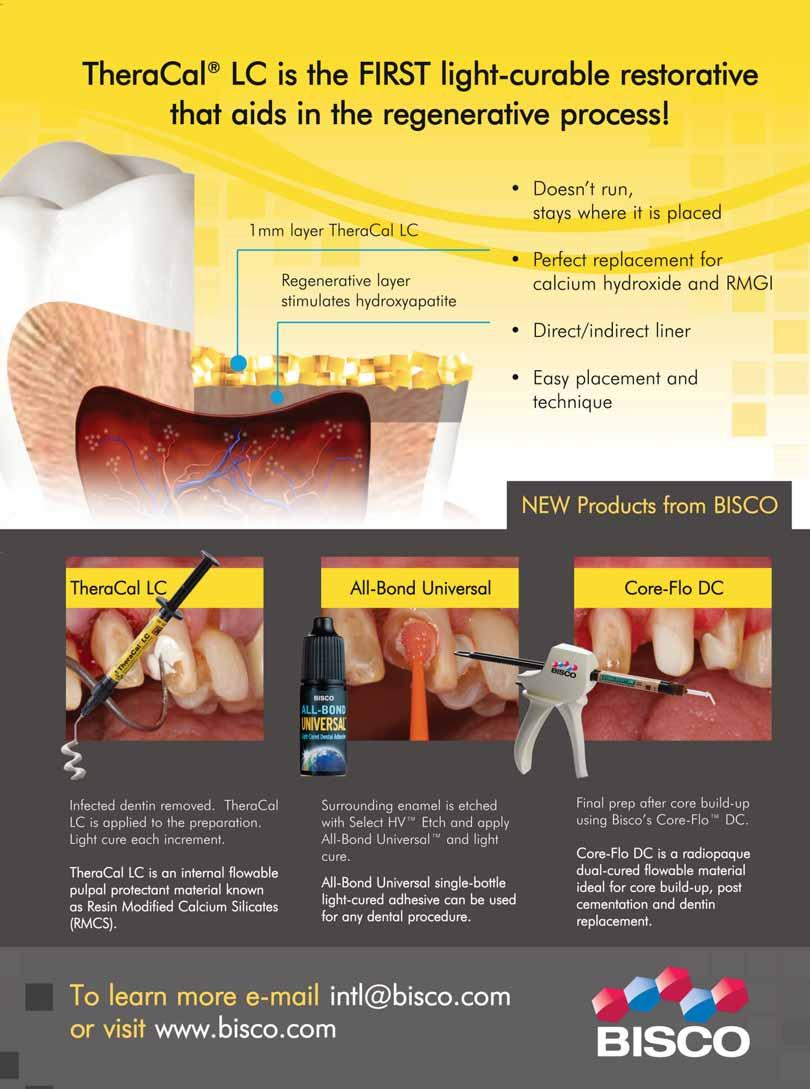

















a herbal alternative in gum problems no discoloration of the teeth no change of the sense of taste Melaleuca alternifolia (tea tree oil) antimicrobial fungicidal antiviral antiseptic Dr. Wild’s Mideast Regional Office: Actco, P.O. Box 40746, Larnaca 6306, Cyprus, Tel.: (24) 623515 / 654252, Fax: (24) 623844 E-Mail: joeissa@yahoo.com Dr. Wild & Co. AG, CH-4132 Muttenz/Switzerland www.wild-pharma.com Swiss made
Special toothpaste and mouthbath with Ems salts for sensitive teeth and denuded toothnecks, irritations of the gums, plaque



Swiss made
desensitizes teeth and denuded toothnecks
firms up the gums and combats dental plaque neutralizes acids harmful to the teeth

Special toothpaste and mouthbath for sensitive teeth and denuded toothnecks, caries prophylaxis and gum care






Swiss made
desensitizes teeth and denuded toothnecks
caries prophylaxis stimulates salivation
Alcoholfree
Alcoholfree
Dr. Wild & Co. AG, CH-4132 Muttenz/Switzerland www.wild-pharma.com
Bahrain: Awal Pharmacy, East Riffa, Bahrain. Egypt: Sesic, Alexandria. Jordan: Nairoukh Drugstore, Amman Kuwait: Al-Maseela Pharmaceutical Co , Safat Lebanon: A.M.G. Medical.Jdeideh-Azur Center Oman: Ibn Sina Pharmacy L.L.C., Muscat Qatar: Ahmed Khalil Al Baker & Sons, Doha Saudi Arabia: Depot Pharmaceutique du Moyen Orient, Jeddah Sudan: Pharma Care Co, Khartoum United Arab Emirates: Al Hayat Pharmaceuticals, Sharjah Yemen: Al Rawdha Trading Group, Sana’a












I am the Zimmer ® Trabecular Metal™ Dental Implant, the first dental implant to offer a mid-section with up to 80% porosity—designed to enable bone INGROWTH as well as ONGROWTH. Through osseoincorporation, I harness the tried-and-true technology of Trabecular Metal Material, used by Zimmer Orthopedics for over a decade. I add ingrowth to implant dentistry.... and I am Zimmer.
Visit TrabecularMetal.zimmerdental.com to view a special ingrowth animation and request a Trabecular Metal Technology demo.
www.zimmerdental.com
Trabecular M e tal Material Osseoinc o rporation
l a r bone Theprocess of ingrowth
Trabecu
THEIMPLANT FOR OSSEOINCORPORATION Artistic Rendering











SOLE BA steam sterilizing system B CLASS SAFE QUALITY 36 MONTHS GUARANTEE BEST PRICE edoo WIEDOO is a trade mark of Trident S.r.l. via Verdi, 20 - 20090 ASSAGO - ITALY www.trident-dental.com - info@trident-dental.com






The winner of the W&H LED Contra - Angle Handpiece (ALEGRA WE - 56 LED G) is Dr. Marwa Ghanem from Egypt
The Result were also posted on the Dental News Facebook Page www.facebook.com/dentalnews1

Thank you downloadingfor Dental News App
Dr.
Winner of the W&H Hand Piece
Marwa Ghanem
Dedicated to dental imaging
WHO CARES?
SWISS PRECISION AND INNOVATION
The Thommen Implant System represents superior precision, sophistication and functional design
Our products have been developed to meet the needs of the clinician through a combination of experience, expertise, and an ongoing commitment to innovation Our in-house R&D and manufacturing allow for the creation of superior products that exceed patient expectations and simplify your daily office life Tune in to Swiss precision and innovation
More information : www thommenmedical com
Evolution in shade measurement : VITA Easyshade Advance
Thanks to its groundbreaking software, the new VITA Easyshade Advance allows especially simple, fast and highly accurate determination of the basic shade of natural teeth and restorations
The results ensure reliable reproducibility since they cannot be impaired by external influences such as ambient light or the user Moreover, the precisely defined measurement data can be clearly interpreted and hence guarantee trouble-free communication between dental practices and laboratories to leave no room for misunderstandings Accurate shade determination and communication with the state-of-the-art VITA Easyshade Advance enables perfect reproduction of the shade and hence contributes to minimizing the number of errors Time-consuming and expensive adjustments or even remakes can be avoided and patients will receive a perfect shade result at one go – regardless whether restorations are fabricated using conventional procedures or CAD/CAM technology
www.vita-zahnfabrik.com
SOLE BA B CLASS steam sterilizing system
74 possibility to set the drying time under vacuum cannulas, etc ) Porous materials; Textiles; Enveloped materials; (Single envelope, double envelope, box etc);Unwrapped solid materials
www trident-dental com






Dental News, Volume XIX, Number III, 2012
CARESTREAM DENTAL CARES
We consider it vital that we have remained focused on dental imaging. By drawing on a century of experience, leadership and continued learning, we can provide oral health professionals the world over with the very best imaging and diagnostic solutions, which enhance their workflow and optimize patient care.
We used to be known as Kodak Dental Systems, now we’re Carestream Dental – the global leader in dental imaging.
visit
Flowable AND stable : Honigum, DMG’s innovative impression material
DMG’s precision impression material based on A-silicones combines exceptional mechanical values with a previously unachieved rheological behaviour Honigum provides an exceptional form of stability by still providing incomparably good flow properties under light pressure –due to its innovative rheological matrix. Exact details even in areas below the preparation are precisely imprinted Honigum is available in several application forms and material types With Honigum-Heavy, Light and -Mono it offers a solution for every indication With Automix and MixStar cartridges it is possible to mix Honigum automatically and thus to obtain a homogeneous and bubble-free consistency www dmg-dental com







Dental News, Volume XIX, Number III, 2012
carestreamdental.com