
ISSN 1026 261X www.dentalnews.com Volume XVIII, Number II, 2011

















The new KaVo ESTETICA® E50. Simply top of its class.















Experience the feel of perfection and allow visionary details and an intuitive operating system to make your everyday work easier.
Simple to use: user-friendly dentist element thanks to ideal combination of direct buttons and menu control.
Simple to upgrade: state-of-the-art upgrade possibilities and visionary system solutions.
Simply reliable: 100 years experience with highest quality, made in Germany. Simply made to perfection. The new KaVo ESTETICA E50.













The new Programat ceramic furnaces are focussed on you, the user.
The combination of timetested technology and innovation allows you to achieve the best possible firing results.

The range of second-generation furnaces is now complete. All G2 furnaces are equipped with power saving technology and numerous technological innovations.

Volume XVIII, Number II, 2011
EDITORIAL TEAM
COORDINATOR
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat,
Mohammad H. Al-Jammaz
Vanessa Abdelahad
Krystel Kouyoumdjis
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim, Marielle Khoury
Tony Dib
1026-261X
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com
Website: www.dentalnews.com www.facebook.com/dentalnews1
Pr. M.A. Bassiouny BDS, DMD, MSc, Ph.D. Director International Program, Temple University, Philadelphia, USA. Pr. N.F. Bissada D.D.S., M.S.D Professor and Chairman, Department of Periodontics, Case Western Reserve University, USA.
Pr. Jean-Louis Brouillet D.C.D, D.S.O. Chairman, Department of Restorative Dentistry, Aix-Marseille II, France. Pierre Colon D.C.D., D.S.O. Maître de conférence des universités, Paris, France.
Dr. Jean-Claude Franquin, Directeur de l’Unité de Recherche ER116, Marseille, France.
Pr. Gilles Koubi D.C.D., D.S.O. Department of Restorative Dentistry, Aix-Marseille II, France.
Pr. Guido Goracci. University LA SAPIENZA, School of Medicine & Dentistry, Roma, Italia.
Brian J. Millar BDS, Ph.D. Guy’s, King’s, and St. Thomas’ College School of Medecine & Dentistry, London, UK.
Pr. Dr. Klaus Ott, Director of the Clinics of Westfälischen Wilhelms-University, Münster, Germany.
Wilhelm-Joseph Pertot DEA, Maître de conférence, Aix-Marseille II, France.
Pr. Dr. Alfred Renk, Bayerische Julius-Maximilians-University, Würzburg, Germany.
Dr. Philippe Roche-Poggi DEA. Maître de conférence des universités, Aix-Marseille II, France.
Michel Sixou D.C.D., D.E.A. Department of Priodontology, Toulouse, France.
Pr. M. Sharawy B.D.S., Ph.D. Professor and Director, Department of Oral biology, Medical College of Georgia, Augusta, Georgia, USA.
DENTAL NEWS IS A QUARTERLY PUBLICATION DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC. Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.

Orthodontic Camouflage Treatment of a Class II Malocclusion - A Case Report
Dr. Saud A. Al-Anezi, Dr. Manar M. Al-Nouri

Unilateral Subperiosteal Implant
Dr. Haseed Dary
Application of CBCT in Dental Practice A Literature Review
Dr. Mohammed A. Alshehri, Dr. Hadi Alamri, Dr. Mazen Alshalhoub
25th Anniversary, International Meeting of the Egyptian Orthodontic Society
120 Years W&H, Pre-IDS Meeting
International Dental Show 2011 15th Kuwait Dental Association

International Scientific Conference 1st Iraqi Dental Reunion 10th Lebanese Orthodontic Society Meeting
ITI First Middle East Congress Beirut, Lebanon
Product Review




Micro-Series: welcome to a new dimension.
30% shorter and 23% lighter, Micro-Series offers perfect balance, exceptional power and versatility.
The new Bien-Air Micro-Series offers ultra-short contra-angles and straight handpieces combined with the new state-of-the-art MX2 LED micromotor.
With its ultra-compact size, the MX2 offers the same performance as our world leading MX micromotor. This includes power, versatility, and perfect speed control, as well as auto-reverse and torque limitation capabilities ideal for endo.
Micro-Series: welcome to a new dimension.
J
une 15 - 18, 2011
International Association of Pediatric Dentistry 2011 Wednesday, June 15-18, At Athens - Greece Website: www.iapd2011.org/
June 19 - 23, 2011
87th Congress of the European Orthodontic Society
At Istanbul - Turkey. Tel: +90 212 291 1906 Email: cnidus@cnidus.com Website: www.cnidus.com
September 14 - 17, 2011
FDI Annual World Dental Congress Mexico City 2011
At Mexico City - Mexico. Tel: +41 22 560 81 50 Email: congress@fdiworldental.org Website: www.fdiworldental.org
September 21 - 24, 2011
Beirut International Dental Meeting - BIDM 2011
At the Congress Palace, Dbayeh - Lebanon Email: bidm@lda.org.lb Website: www.bidm-lda.com
October 26 - 28, 2011
Egyptian Dental Association
The E.D.A In collaboration with Future University will organize the 15th International Dental Congress. At Cairo City Stars Hotel, Cairo - Egypt Email: eda@internetegypt.com.eg Website: www.eda-egypt.org
January 31 - February 2, 2012
The 16th Edition of the UAE International Dental Conference & Arab Dental Exhibition AEEDC Dubai 2012. At Dubai International Convention & Exhibition Centre (DICEC). Email: vaneza.santos@index.ae Website: www.aeedc.com
ACTEON 67 - A-DEC 25 - ALTURKI 71 - BELMONT 47 - BEYOND 69 - BIEN AIR 7 - BISCO 31 - BLUE X 57 - CAVEX 49 - COLGATE 45 - COLTENE WHALEDENT 9DENTSPLY 23 - DISCUS DENTAL 37 - DR. WILD 4, 5 - DURR 42 - GC 8 - GCOMM 73 - GSK C3, 59 - HU-FRIEDY 61 - INTENSIV 17 - IVOCLAR – VIVADENT 1, C4KAVO C2 - GENDEX 39 - KERR 51, 80 - KOMET 79 - MECTRON 12 - MEDESY 38 - METASYS 65 - MICRO MEGA 10 - MOCOM 55 - MORITA 53 - NISSIN 35 - NSK C1 - PLANMECA 29 - SARATOGA 78 - SIRONA 21 - SOREDEX 33 - SULTAN 18 - ULTRADENT 27 - VITA 6 - VOCO 63 - W&H 41 - ZHERMACK 2 - ZIMMER 76



*Dr Saud A. Al-Anezi BDS, MFD RCSI, DDS , MOrth RCSEd., Dr Manar M. Al-Nouri
*Bneid AL-Gar Specialty Dental Center. - Orthodontic Department - Kuwait
saudalan@gmail.com
Class II division 1 malocclusion is described as the incisal edges of the lower incisors occlude posterior to the cingulum plateau of the upper incisors and the upper central incisors are proclined1 The prevalence of this malocclusion varies amongst different populations but it is reported to be 20% in the UK2. There are a number of features commonly associated with Class II malocclusion including the Class II skeletal pattern and dentoalveolar compensation may mask the severity of the malocclusion but the profile may still be unfavourable. Deep overbite and increased overjet are commonly seen in this malocclusion. Soft tissues can exert an influence on the position and inclination of the incisors. A lower lip trap may procline the upper incisors further and lip incompetence can have an effect on the inclination of the incisors due to imbalance of the pressure on the teeth3. The management of this type of malocclusion will depend on a number of factors including the patient’s age, the severity of the skeletal pattern, the amount of crowding and the overjet. It can be broadly divided into growth modification, orthodontic camouflage or orthognathic surgery involving either one jaw or double jaws. In the following case, orthodontic camouflage was chosen and the reasons for this treatment plan are explained.
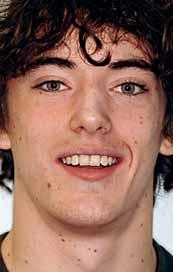
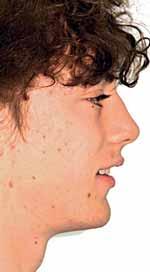
15.7 years old male presented complaining of prominent upper incisors. He had no relevant medical history and there was no history of previous orthodontic treatment.
The patient had moderate Class II skeletal pattern with average Frankfort-mandibular planes angle and lower anterior face height. There was no facial asymmetry and the lips were incompetent with the lower lip trapped at rest behind the upper central incisors (Figure 1).
The oral hygiene was fair but needed improvement prior to orthodontic treatment. All teeth from the left permanent second molar to the right have erupted in both the upper and lower arches. The patient had carious lesions in both upper first molars, upper left second molar and lower left first molar. The maxillary arch was spaced with a midline diastema. Furthermore, there was mild lower labial segment crowding (4mm). The incisor relationship was Class II division 1, the overjet was 12 mm whereas the overbite was increased and complete to the palate


and causing trauma to the palatal mucosa. The centrelines were coincident and the buccal segment relationship was 1/2 unit Class II on both sides (Figure 2).
The Dental Panoramic Tomogram (DPT) confirmed the presence of all permanent teeth including the developing third molars (Figure 3). Root morphology appeared normal. The upper right central incisor had a root canal filling. The upper standard occlusal







radiograph revealed that the upper right central incisor had an adequate root filling with no periapical area. In the cephalometric assessment (Figure 4), the ANB value of 7° suggested a moderate Class II skeletal pattern. The vertical proportions were within normal values. The upper incisors were proclined at 122° and the lower incisors were of average inclination at 94°. The interincisal angle was reduced at 119°. The lower incisor to APo and the lower lip to E line were within normal limits.
This patient presented with a Class II division 1 malocclusion on a moderate Class II skeletal pattern complicated by increased and complete overbite, increased overjet, and mild crowding in the lower labial segment. The genetically inherited skeletal pattern contributed to the presenting malocclusion. Furthermore, the lower lip trapped behind the upper incisor contributing to the

Upper incisor to maxillary plane angle
Lower incisor to mandibular plane angle
Interincisal angle
Maxillary mandibular planes angle
Face height ratio
Lower incisor to Apo line
Lower lip to Ricketts E Plane
increased overjet. Therefore, the main problems in this case were as follows:
1. Moderate Class II skeletal pattern with mild crowding in the lower arch.
2. Increased and complete overbite and increased overjet.
3. Midline diastema and retained upper left second deciduous molar.
4. 1/2 unit Class II left and right molar relationships.
Aims of treatment
1. Camouflage the skeletal pattern with fixed appliances.
2 Relieve crowding and level and align the arches.
3. Reduce overbite and the overjet.
4
. Achieve Class I incisors, canines and full unit Class II molars.
The treatment of the patient was executed in the following order:
1. Scale, polish and oral hygiene instructions session with the dental hygienist.
2. Restoration of the carious lesions and extraction of the upper left deciduous molar by the general dental practitioner.
3. Anterior bite plan to reduce the overbite and bonding the lower arch (Figure 5).
4 Fit a Transplalatal Arch (TPA) with Nance button to reinforce the anchorage.
5. Refer to the general dental practitioner for extraction of upper left and right first premolars.
6. Bonding upper arch.
7. Continue with the fixed appliances to close the space and achieve the treatment aims.
8. Retain with an upper and lower Essix retainers.





The patient’s main concern was the prominence of the upper incisors. Anchorage was a critical issue in this case because of the increase overjet and the planned amount of tooth movement. In addition, after assessing the space requirement, it was necessary to extract teeth in the upper arch to enable the reduction of the overjet. Furthermore, the fact that the crowding in the lower arch was mild and there was increased overbite, it was decided to avoid extraction in the lower arch. It was also planned to use Class II traction during treatment to maximise the anchorage.
The use of headgear to distalise the upper buccal segments and create space to reduce the overjet. However, the patient declined to wear HG and he accepted the extraction of upper premolars approach. Alternatively, Temporary Anchorage Devices (TADs) could be employed to either distalise the upper buccal segments between the upper second premolar and first molar to achieve space closure in order to minimise the mesial movement of the upper buccal segments.
The oral hygiene of the patient and the carious lesions were addressed prior to the start of the fixed appliances treatment. The patient’s compliance was good and treatment progressed without encountering major problems. The reduction of the overbite was achieved initially with the anterior bite plane then a reverse curve of Spee was placed in the lower archwire to control the overbite. A Trans-Palatal Arch (TPA) with Nance button was fitted prior to the extraction of the upper premolars in order to reinforce the anchorage (Figure 6). The treatment continued with the use of Class II traction on both sides and space closure mechanics.
Treatment objectives were achieved and the patient was satisfied with the treatment outcome. The overbite and overjet were reduced, Class I incisors, canines and full unit class II molars were obtained. Overall treatment time was twenty four months
This was a case of camouflaging the underlying Class II skeletal pattern. There was a concern of “damaging” the patient’s profile



with the treatment option adopted that involved the extraction of the upper premolars and space closure. The relation of the profile and extraction of teeth is an ongoing debate in orthodontics.
An investigation carried out a cohort study on two groups of 12 patients, where one group was treated with extractions and the non-extraction 5. They investigated whether any changes occurred in the facial profile three-dimensionally, using an optical surface scanner; and demonstrated that there was no evidence that the extractions resulted in ‘flattening’ of the facial profile.
The authors recognised that the sample size was small and that the findings should be looked upon as a preliminary study and not be extrapolated for the population as a whole. Furthermore, it can be seen from the pre-treatment records (Figure 1) that the patient had a “convex” profile prior to treatment hence retraction of the upper anterior teeth might in theory improve the facial profile. There was a potential risk with the root filled upper right central incisor. Evidence is equivocal as endodonticalLy treated teeth undergo more, or less, root resorption6. However, it is now generally accepted that root treated teeth can be moved orthodontically without the increased risk of root resorption7
The treatment of the case was planned in stages. Stage one consistedof improving the oral hygiene of the patient and management of all carious lesions and assesses the compliance and attitude of the patient towards orthodontic treatment. The next stage involved the reduction of the overbite. The patient presented with a deep overbite that was causing damage to the palatal mucosa (Figure 2). This was achieved with an anterior bite plane removable appliance and bonding of the lower arch. This appliance will free the occlusion of the buccal segment teeth and if worn consistently, will “passively” limit further eruption of the incisors but allow the lower premolars to erupt, thus reduce the increased overbite (Figure 5).
The next phase of treatment involved the fitting of the Trans-Palatal Arch (TPA) and the removal of the upper first premolars. Because of the increased overjet, this was a case of maximum anchorage and any mesial movement of the upper buccal segments was not desirable (Figure 6). It remains equivocal in the literature whether TPA appliances can provide anteroposterior anchorage. In fact, recent evidence suggested the contradictory 8 Alternatively the anchorage issue in this case could have been addressed with a Temporary Anchorage Device. The increase





popularity and use of Temporary Anchorage Devices (TADs) make them attractive in maximum anchorage case. There is an early evidence to suggest that they are effective and safe9
The space closure phase of treatment was conducted carefully in order to prevent anchorage loss (Figure 7). Traditionally, clinicians retract the canines until they are in Class I relationship then the retraction of the incisors is followed. On theoretical grounds, retracting all six teeth together simultaneously would be expected to increase anchorage demands although this increase is not apparent clinically. However, some clinicians choose to retract all six together for two reasons namely simplicity and to avoid retracing steps of tooth movement. It is debatable which method is better but in this case, retracting all six anterior teeth as a block was adopted.
Upon the completion of the space closure stage, some finishing details were carried out. Although some more correction was still needed to be done e.g. the marginal ridge of the upper left second premolar and the palatal root torque in the upper incisors (Figure 9). Furthermore, taking an OPG towards the end of treatment to assess the roots angulation, nonetheless, the patient preferred to have the appliances removed and he was satisfied with the outcome.
Class II skeletal pattern cases can be treated by orthodontics
consider in treatment planning such cases. In this particular case, the skeletal pattern was camouflaged and the treatment involved extraction in the upper arch and anchorage reinforced with Trans-Palatal Arch (TPA). Nowadays, Temporary Anchorage Devices (TADs) can be used with several potential advantages in Class II malocclusion.
I would like to thank all the staff at the Orthodontics Department of the Royal United Hospital, Bath, UK. In particular, Dr Anthony Ireland.
1. British Standards Institutes. Glossary of Dental Terms 1983. BS4492; BSI London.
2. Todd JE, Lader D. Adult DentalHealth 1988; HMSO, London.
3. Lip trap (Turner et al 1997)
4. Houston WJB, Stephens CD, Tulley WJ. A textbook of orthodontics. Wright, Oxford 1992.
5. Ismail S F H and Moss J P. The 3D effects of orthodontic treatment on the facial soft tissues-a preliminary study. BDJ 2001; 192(2): 104-108.
6. Drysdale C, Gibbs SL, Ford TR. Orthodontic management of root-filled teeth. Br J Ortho 1996; 23: 255-260.
7. Costopoulos G, Nanda R. An evaluation of root resorption incidence to orthodontic intrusion. Am J Orthod Dentofacial Orthop 1996; 109: 543-548.
8. Rodkoswski MJ. The influence of transpalatal arch on orthodontic anchorage. Thesis abstract from St Louis University. Am J Orthod Dentofacial Orthop 2007; 132: 562.
9. National Institute for Health and Clinical Excellence. Guidance on Mini/micro implantation for orthodontic anchorage 2007: IPG 238. www.nice.org.uk.


Keywords: Unilateral subperiosteal implant - Insufficient boneBone impression
When the volume of the residual alveolar ridge is insufficient to receive endosteal implants, use of the unilateral subperiosteal implant is one of the treatments of choice.1, 2
This modality of implants has comparable success and survival rates.1, 3, 4 It was specifically developed to treat patients with insufficient available bone in the alveolar ridge; it shouldn’t be used for patients with overabundant bone.1
The surgical protocol in the case presented is comprised of a two-stage surgery, the first of which results in taking a direct bone impression and the second in placing the custom-made implant. The subperiosteal implant is designed to rest on the surface of bone, under the periosteum rather than gaining endosteal support as teeth or most alloplastic implants used in the body, this implant distributes stresses from the prosthesis to large areas of bone in a manner similar to a snowshoe.5
A customized casting made of surgical metal adheres to the bone with a combination of fibrous tissue and direct bone support2, NO OSSEO INTEGRATION.
Permucosal abutment posts and intraoral bars are designed for prosthesis retention.5
So subperiosteal implants are used when there is an insufficient available bone which differs by volume from case to case. That’s why it was classified into four divisions.
In our case there is a deficiency in the height of bone which classify the case under the division C-h available bone
This division of available bone maybe treated by a number of differentimplant approaches. The most common is root form implants of reduced height. The second option is augmentation. Or the third option is the subperiosteal implant5, which is going to be presented in this article.
DIVISION DIMENSION
A (Abundant Bone)
Division A forms soon after the tooth is extracted. Division A corresponds to abundant available bone in all dimensions
B (Barely Sufficient Bone)
Slight to moderate atrophy is used to describe this clinical condition
C (Compromised Bone)
The Division C available bone is deficient in one or more dimensions (width, length, height, angulations, or crownimplant ratio)
D (Deficient Bone)
Long term bone resorption may result in this complete loss of the alveolar process accompanied with basal bone atrophy.
Sever atrophy describes the clinical condition of the Division D ridge.
>5 mm width
>10 -13 mm height
>7 mm length
<30 degrees angulation
C/ I (crown /implant) ratio <1
2.5 – 5 mm width
>10 -13 mm height
>12 mm length
<20 degrees angulation C/ I ratio <1
Unfavorable in:
Width (C-w)
Height (C-h)
Length
Angulations(C-a ) >or = 30
degrees
C/ I ratio > or = 1
Severe atrophy
Basal Bone
Flat maxilla
Pencil thin mandible



The terminology for the subperiosteal implant includes portions of the implant below and above the soft tissue.5
The substructure is the portion of the implant that is responsible for the support of the implant and is located below the periosteum, on top of the bone. It consists of several struts:
Primary struts are the major components of the substructure and can be either peripheral or abutment.
The peripheral struts are the outermost regions of the implant and lay on the most extended areas of the cortical bone.
The abutment struts connect the labial and lingual peripheral struts and a vertical permucosal post on the crest of the edentulous ridge.
Secondary struts help dissipate the forces from the primary abutment struts, improve the rigidity and casting of the substructure, and serve as an additional support mechanism of the implant. (Not used in this case)
The permucosal abutment posts exit through the mucosa, and act as prosthetic retainers.
The superstructure connects the abutment posts designed above the soft tissue. This structure both retains and supports the prosthesis during function and distributes occlusal loads to the substructure below the soft tissue.
Subperiosteal implants heal in the periosteal mode of tissue integration.They are enveloped in a dense fibrous collagenous tissue sheath constituting the outer layer of the periosteum. Functional forces are absorbed by the underlying bone through the periosteum.1, 6, 7
Case report
A 60 years old healthy female came into the clinic asking for a
fixed dental appliance to restore the bilateral edentulous posterior spaces of her own (Kennedy class 1).
There was a missing 6 and 7 on each side with compromised 4 and 5 on each.
The volume of available bone was insufficient to place a root form implant on the site of 7 (C-h available bone) a ridge mapping technique was used and a (C-w available bone) was also encountered.
The use of short implant in this case was not a treatment of choice; the crown - implant ratio is > 1.
A unilateral subperiosteal implant was suggested.
Surgery
A two stage surgical appointment is usually suggested, (Berman introduced the Two-surgery technique in the 1950s8) separatedby at least 6 weeks.5
First surgery
Infiltration was administered with long acting anesthetic (UbistesinTM forte 4%) to anesthetize the residual ridge posterior to the mental foramina from buccal and lingual sides and the lateral aspect of the ascending ramus.
An intraoral and extra oral scrub of the patient is performed with Chlorhexidine.5
Soft tissue reflection
Incision
The incision begins at the retro molar papilla at the base of the retro molar pad to the premolar.
A full thickness incision through the periosteum scores the underlying bone.
Reflections
A full thickness periosteal reflection exposes the underlying residual ridge and lateral regions of the mandible.
Evaluation of the crest
A knife edge ridge was exposed, thin knife like edges resorb shortly after implant insertion, if not before.5
An osteoplasty was performed to recontour the bone so the crest is broad enough to have a blood supply from the underlying trabecular bone. The osteoplasty was performed at the bone impression appointment. In this way the several weeks interval permit initial remodeling.
Impression
Types of Impression Materials
Three major types of elastic materials are used in implant dentistryfor obtaining the direct bone impression: polysulfides, silicones, and polyethers.
The material which was used in this case is addition silicone (GhenesylTM silicone first impression: putty soft. low viscosity).


Making the Impression
A retraction sutures (3-0 atraumatic black silk sutures1) are made to attach the reflected tissues to the mucosa of the cheek – from buccal side – and the lingual side reflected tissues are anchored on the teeth of the contra lateral side, this technique would open a space to take the impression.The gloves are moistened to prevent the impression material from sticking. A small rolled portion of putty was placed into the tunnel of the reflection and molded along the exposed underlying residual ridge no trays are needed in this technique.
After complete setting the impression is gently lifted. Saline irrigations used to rinse and moisten the tissue, and all reflected regions are inspected for remnants of impression material. The direct bone impression is evaluated for all necessary land marks. The retraction sutures were removed and the tissue re-approximated and sutured.
The contra lateral side was treated in a similar fashion.
The subperiosteal implant is fabricated-casted with pure titanium. Laboratories should be members of ASTM (American Society for Testing and Materials) and should not determine their own proceduresand techniques.9
The implant design in this case composed of one abutment connected to the peripheral struts by 4 abutment struts for each implant. One hole was drilled on each implant on a peripheral strut (distal aspect) for the placement of titanium fixation screw. Implants should be thoroughly cleaned and sterilized before placement.







The surgical insertion of the implant is very similar to the direct bone impression surgery but is more rapid and causes less swelling and discomfort to the patient.
After the implant is placed on the ridge a titanium screw is used to fix the implant on the ridge to obtain the primary stability this screw would be of no use after the healing of tissues because the implant would be stable on place by the attachment of the soft tissues to the bone which holds the struts of the implant in between.
The site is then sutured again.
Sutures were removed after 1 week.
After 2 weeks of implant placement the patient came back. A preparation was done to the premolars at both sides and the impression was taken.
4 units bridge was fabricated for each side splinting the implant abutment to the 2 natural teeth of each side.















• Only one sterile NiTi instrument per root canal in most cases
• Decreases the global shaping time by up to 40%*
• Reciprocating technology respecting the root canal anatomy
• Single use as new standard of care



(DentoTemp of ITENA) long term temporary cement which is used as a Permanent cementation of implant-retained crowns.
Discussion
In summary, the advantages of subperiosteal implants include: The predictability of the results and the high success rate, the survival and success rates of modern-day subperiosteal implants are equal to or greater than root form implants when placed into C-h bone.5
Noninvasive surgeries are preferred compared to the use of iliac crest bone grafts10, the trauma would be in one site (which is the oral cavity) not in 2 sites. When using the iliac graft the patient would go with pain while he walks out of the operation in addition to the pain in his mouth.
No possibility of parasthesia. This may be the case when nerve repositioning is performed to enhance the bone height to place the root form implants in the mandible.
No bone grafts needed with any possibility of bone graft failure which requires re-grafting of the area with all accompanying trauma and time consumption.
Less expensive procedure when comparing restoring one segment or one side of the arch with bone grafting or sinus lifts and several root form implants to a one subperiosteal implant with 1 or more abutment, the expenses would be way less than the bone grafting procedures.
Disadvantages include the initial complexity of the surgical procedures. This complexity presumes a certain level of experience that the practitioner can obtain only over a long period of time. The procedures require specialized technicians and a titanium melting oven.

Also the disadvantages include the frequent necessity for 2 surgical procedures, this can be overcome by the use of (CAD-CAM)11 but again it’s not considered a mainstream procedure because of technique sensitivity and cost.
Finally, removal of subperiosteal implants, although rarely indicated, can present difficulties.
In a case report under the title REPLACEMENT OF A MANDIBULAR SUBPERIOSTEAL IMPLANT12 the author replaced a subperiosteal implant, which had been in successful service for approximately 15 years. Both the implant and prosthesis had been in service. Although the patient had been given the option of an augmentation using an autogenous iliac crest graft with subsequent insertion of endosteal implants. The importance and potential benefits of subperiosteal implants are undeniable, being at this time the only means of restoring jaws in situations where endosseous implants cannot be placed.
Subperiosteal implants often serve our most troubled patients. For patients who exhibit severe mandibular and maxillary alveolar ridge atrophy, no other treatment options may exist.13
Alveolar ridges with severe atrophy can be reconstructed prosthetically (fixed and removable) with less time compared to bone grafting procedures. Partial subperiosteal implants can be used with endosseous implants and even natural teeth with fixed bridges. The surgical technique and clinical stages are not complicated,generally being mastered by implantologists in general dental practice.
1 Principles and practice of implant dentistry Charles M. Weiss
2 Cranin AN: Posterior region Maxilla: a proven implant alternative, dent implantol update 3:81, 1992
3 Bodine RL, Yanase T, Bodine A: Forty years of experience with subperiosteal implant dentures in 41 edentulous patients, J Prosthet Dent 75:33, 1996
4 Bodine RL, Melros RJ, Grenoble DE: Long-term implant dentures histology and comparison with previous reports J Prosthet Dent 35:665, 1976
5 Contemporary implant dentistry, second edition Carl E. Misch
6 Bodine RL, Mohammed CI: Histologic studies of a human mandible supporting an implant denture.Part I, J Prosthet Dent 21:203, 1969.
7 James RA: Tissue behavior in the environment produced by permucosal dental devices. In McKinney RV, Lemons JE, editors: The Dental Implants, Littleton, Mass, 1985, PSG Publishing.
8 Berman N. An implant technique for full lower denture. Denture Digest.1951;57:438.
9 Leonard I. Linkow, Jon R. Wagner, Manual Chanavaz: Tripodal Mandibular Subperiosteal Implant: Basic Sciences, Operational Procedures, and Clinical data, Journal of Oral Implantology 1998
10 Leonard I. Linkow, Robert Ghalili: Critical Design Errors In Maxillary Subperiosteal Implants journal of oral implantology CLINICAL. 198 Vol. XXIV/No. Four/1998
11 Cranin AN et al: An in vitro comparison of the computerized tomography/CADCAM and direct bone impression techniques for subperiosteal implant model generation, J oral implantol 24; 74, 1998.
12 Robert F. Mansueto: Replacement of a Mandibular Subperiosteal Implant, journal of oral implantology Vol. XXV/No. Three/1999
13 Charles M. Weiss, Terry Reynolds: A Collective Conference on the Utilization of Subperiosteal Implants in Implant Dentistry, journal of oral implantology Vol. XXVI/No. Two/2000
*Dr. Mohammed A. Alshehri, Dr. Hadi Alamri, Dr. Mazen Alshalhoub
*Consultant at the Riyadh Military Hospital dr_mzs@hotmail.com
Abstract: This article presents a review of the clinical applications of cone-beam computed tomography (CBCT) in different dental disciplines. A literature search was conducted via PubMed for studies on dental applications of CBCT published between 1998 and 2010. The search revealed a total of 540 results, of which 130 articles were clinically relevant and were analyzed in detail. CBCT is used in different dental disciplines for numerous clinical applications. The results of this systematic review show the different applications of CBCT imaging in dental practice, which are summarized and categorized under eight different dental disciplines.
Introduction
Two-dimensional (2D) imaging modalities have been used in dentistry since the first intraoral radiograph was obtained in 1896. Since then, significant advances have been made in dental imaging techniques, including the introduction of panoramic imaging techniques and tomography. Advances in digital imaging techniques have led to lower radiation doses and faster processing times without changing the imaging geometry of these intraoral and panoramic technologies.
Cone-beam computed tomography (CBCT) is a new medical imaging technique that generates three-dimensional (3D) data at lower cost and lower absorbed doses than conventional computed tomography (CT). The CBCT imaging technique is based on a cone-shaped X-ray beam that is centered on a 2D detector, and the beam performs one rotation around the object, producing a series of 2D images. The images are reconstructed in a 3D data set using a modification of the original cone-beam algorithm developed by Feldkamp et al. in 198427. CBCT images from the craniofacial region are often acquired at a higher resolution than conventional CT. In addition, these systems are more compact than conventional CT systems, which make them more practical for use in dental offices48
The application of CBCT imaging in different dental disciplines can guide diagnosis, treatment and follow-up.
This article presents a systematic review of clinical applications of CBCT in dental practice.
A literature search was conducted via PubMed for CBCT imaging applications in dentistry published between January 1, 1998 and July 15, 2010 using the keywords “Cone-beam computerized tomography in dentistry”. The search revealed a total of 540 articles, which were all screened in detail. Of these articles, 410 were excluded because they were not relevant to the subject. The systematic review consisted of 130 clinically relevant articles that were analyzed further and categorized according to the discipline of application.
The search revealed 36 articles (27.7%) related to applications in oral and maxillofacial surgery (OMFS), 33 articles (25.4%) relatedto endodontic clinical applications, 22 articles (16.9%) related to clinical applications in implant dentistry, 15 articles (11.5%) related to orthodontic clinical applications, 10 articles (7.7%) about clinical applications in general dentistry, 8 articles (6.2%) about the temporomandibular joint (TMJ), 5 articles (3.8%) related to applications in periodontology, and 1 article (0.8%) about CBCT applications in forensic dentistry.
Table 1. Summary of CBCT application-related articles according to dental specialty
DISCIPLINE
Oral and maxillofacial surgery (OMFS)
Endodontics
Implant Dentistry
Orthodontics
NUMBEROFARTICLES

Review
APPLICATIONSINORALANDMAXILLOFACIALSURGERY
CBCT in OMFS has been used to investigate the exact location of jaw pathology in 3D images3,14, 29, 65, 81, 93, 90,102, 126, to assess impacted teeth (Fig. 1), to assess supernumerary teeth and their relation to vital structures18, 61, 62, 65, 66, 69, 80, 90, 113, 115,123, to evaluate changes in the cortical and trabecular bone related to bisphosphonate-associated osteonecrosis of the jaws12, 29, 57, and to assess bone grafts34. CBCT has also been used to investigate paranasal sinuses6, 65 and to assess obstructive sleep apnea78, 88

Because CBCT images are collected as a combination of several 2D slices, the technique is superior in overcoming superimpositions and calculating surface distances9, 10. This advantage has made CBCT the technique of choice for the investigation of mid-facial fractures8, 41, orbital fracture assessment and management128, and in inter-operative visualization of the facial bones after fracture39, 40 Furthermore, because CBCT is not a magnetic resonance technique, it is the best option for intraoperative navigation during procedures involving gun-shot wounds72, 96
CBCT is largely used in planning orthognathic and facial orthomorphic surgeries, which require detailed visualization of the interocclusal relationship to augment the 3D virtual skull model with a detailed representation of the dental surface. With the aid of advanced software, CBCT facilitates the visualization of soft tissueto allow for control of the post-treatment aesthetics7, 111, 112 and permits the evaluation of lip and palate bony depressions in cases of cleft palate56, 73, 125
The ability of CBCT to detect salivary-gland defects is also under investigation108. In addition, one article has reported a tooth autotransplant case where CBCT demonstrated high accuracy, and the information provided allowed the rapid completion of the transplant operation45
CLINICALAPPLICATIONINENDODONTICS
CBCT is a useful tool in diagnosing apical lesions (Fig. 2a, 2b)13, 17, 19, 20, 23, 25, 31, 64, 83, 84, 92, 115, 120. A few research studies have shown that contrast-enhanced CBCT images can be used to differentiate between apical granulomas and apical cysts by measuring the lesion density (Fig. 3a, 3b)23, 92, 120, 106. Another article describes the
use of CBCT as a tool to categorize the origin of the lesion as endodontic or non-endodontic17




The superiority of CBCT in detecting fractured roots compared to 2D radiographs has been demonstrated by several clinical case reports focused on detecting vertical root fractures17, 77, 89, 92, 106, 115, 120. CBCT is considered superior to periapical radiographs in the detection of fractures in buccolingual or mesiodistal directions35, 36, in the measurement of depth in dentin133 and in the detection of horizontal root fractures17, 92, 115
CBCT is able to detect lesions in cases of inflammatory root resorption, whereas conventional 2D x-rays cannot detect them in early stages24, 115. In other cases such as external root resorption17, 60, 115, 120, external cervical resorption17, 84, 91, and internal resorption17, 84, 115, 120, CBCT cannot only detect the presence of resorption but also its extent.
CBCT can be used to determine root morphology; to measure the number of roots, canals, and accessory canals; and to establish their working lengths and angulations6, 17, 70, 77, 92, 98, 115, 119, 120. CBCT also provides accuracy in the assessment of root canal fillings19, 31, 77, 120, in the detection of pulpal extensions in talon cusps107 and in the detection of the position of fractured instruments118
CBCT is a reliable tool for the presurgical assessment of the proximity of the tooth to adjacent vital structures, the size and extent of a lesion, and the anatomy and morphology of roots through very accurate measurements17, 20, 25, 46, 54, 77, 84, 92, 97, 106, 115, 118, 120. In emergency cases requiring tooth assessment after trauma, CBCT applications can aid in reaching a proper diagnosis to determine the most suitable treatment approach15, 16, 17, 92. Due to its reliability and accuracy, CBCT has recently been used to evaluate canal preparation in different instrumentation techniques74, 76
APPLICATIONSINIMPLANTDENTISTRY
The increasing demand for dental implants to replace missing teeth has necessitated a technique capable of obtaining highly accurate measurements to avoid any damage to vital structures. Previously, such measurements were obtained through conventional CT; however, the ability of CBCT to provide greater accuracy in measurements at lower radiation doses has made it the preferred option in implant dentistry (Fig. 4a, 4b)21, 28, 32, 37, 46, 47, 48, 63, 65, 67, 90, 101, 103, 104 114, 116, 121, 126. Furthermore, the presence of new software to construct surgical guides has further reduced the possibility of structural damage2, 21, 30, 85, 86, 101. Another article describes the interoperative use of CBCT in two cases to guide the insertion of the implant after microsurgical bone transfer38

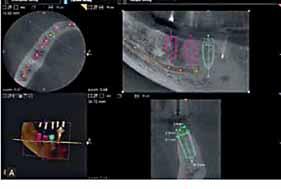
CBCT can be used to measure bone quality4, 37, 46, 47, 78, 90, 109, 110 and quantity37, 103, 109, 116, which has led to a reduction in implant failure because the reliable information provided by CBCT has led to improvements in case selection. CBCT is also used to assess the success of bone grafts and post-treatment evaluations (Fig. 5a to 5d)90, 116
The introduction of new software in orthodontic assessment has enabled the use of CBCT images in cephalometric analysis26, 46, 59, 65, 101 and has led to CBCT becoming the tool of choice for assessing facial growth, age, airway function1, 55, 105, and disturbances in tooth eruption75
CBCT is a reliable tool in assessing the proximity of the tooth to vital structures that may interfere with orthodontic treatment22, 94. In




cases that require the placement of tiny screw implants as temporary anchors, CBCT acts as a useful visual guiding technique for safe insertion of these anchors52, 53, 95 as well as to assess the bone density before, during and after treatment (Fig. 6)33, 99 CBCT incorporates multiple different views of an object in one scan (e.g., frontal, right lateral, left lateral, 45-degree, and submental views), which is an additional advantage of the technique58, 124 CBCT is therefore considered a more accurate option for the clinician because the images are self-corrected for magnification, producing orthogonal images with a 1:1 ratio5
One of the major advantages of CBCT is its ability to define the true position of the condyle in the fossa, which often reveals the possibility of dislocation of the disk in the joint90, 117, 120 and the extent of translation of the condyle in the fossa117. Due to its accuracy, CBCT facilitates easy measurement of the roof of the glenoid fossa51, 68 and provides the ability to visualize soft tissue around the TMJ44, which may reduce the requirement for the use of MRI in these cases.
Due to these advantages, CBCT has become the imaging device of choice in cases of trauma, pain and dysfunction, and fibroosseous ankylosis43, 82, 100, 114, as well as in the detection of condylar





cortical erosion and cysts46. The use of 3D features facilitates the safe application of the image-guided puncture technique, which is a treatment modality for TMJ disk adhesion42
PERIODONTICSAPPLICATIONS
The high measurement accuracy of CBCT with minimal margins of error allows its use in obtaining a detailed morphologic description of the bone120, 122, with measurement accuracy equal to that of direct measurement with a periodontal probe71, 120 CBCT also aids in assessing furcation involvement68, 115,120
CBCT can be used in the detection of buccal and lingual defects49, 120 where conventional 2D radiography shows limitations. CBCT allows accurate measurement of intrabony defects11, 79 as well the ability to assess dehiscence, fenestration defects and periodontal cysts50, 120. CBCT has also proved its superiority in evaluating the outcome of regenerative periodontal therapy49
OPERATIVEDENTISTRYAPPLICATIONS
Based on the data in the available literature, the use of CBCT in detecting occlusal caries is not yet justified because CBCT deliversa higher radiation dose to the patient compared to conventional 2D radiographs with no additional benefit. However, CBCT has proved to be useful in assessing the depth of proximal caries115
Table 2 shows examples of typical radiation doses received from various dental radiological procedures in operative dentistry.
Intraoral (F speed, rectangular collimator)
Intraoral (E speed, round collimator)
Full-mouth set (E speed, round collimator)
Lateral ceph (F speed, rare-earth screen)
DPT (F speed, rare-earth screen)
Cone-beam CT – both jaws
Hospital CT – both jaws
FORENSICAPPLICATIONS
Dental age estimation is considered an important factor in the field of forensic science, and this estimation can be performed non-invasively using CBCT; an estimate of a subject’s age can then be derived from the subject’s pulp/tooth ratio127
Discussion
CBCT scanners represent a significant advancement in dental and maxillofacial imaging. Since their introduction for dental use in the late 1990s129, there has been an increased interest in these devices. The number of CBCT-related articles published per year has increased tremendously over the last few years. We have performed a systematic review of the literature related to CBCT imaging applications in dental practice and summarized the applications of this new imaging technique in different dental specialties. CBCT was used as a keyword in this systematic review. Although
other keywords and terminology were entered into the PubMed search engine (e.g., cone beam volumetric scanning, true volumetric computed tomography, dental CT, dental 3D-CT, and cone beam volumetric imaging), they did not result in additional relevant articles130
The clinical applications of CBCT imaging in dentistry are constantly increasing. The results of this systematic review showed that of the 540 articles published in the last 12 years, 130 were clinically relevant. The most common clinical applications of CBCT were in OMFS, implant dentistry, and endodontics. CBCT has shown limited use in operative dentistry because of the high radiation dose compared to conventional 2D radiography without any additional benefit.
The dental literature on CBCT is promising and indicates that more research is required to explore the benefits of CBCT in forensic dentistry. Although no literature was found on prosthodontic applications of CBCT, the improved standard of care seen in prosthodontic treatment can be attributed to applications of CBCT found in other dental specialties and related to prosthodontic, such as bone grafting, soft tissue grafting, prosthetic-driven implant placement, maxillofacial prosthodontics and Temporomandibular joint disorders. CBCT images are important in special cases that require the assessment of restorability of multiple teeth (Fig. 7a to 7e).
The newest CBCT systems show higher resolution and lower exposure than previous systems, and the new systems are less expensive and more specific for dental use than their predecessors. The flat-panel detectors are less prone to beam hardening artifacts. CBCT also shows disadvantages such as susceptibility to motion artifacts, low contrast resolution, and limited internal soft-tissue visualization capability. Furthermore, due to the distortion of Hounsfield units, CBCT cannot be used for the estimation of bone density.
As far as the radiation dose of CBCT imaging is concerned, it is crucial that a radiation dose as low as reasonably achievable (alara) is respected. Although CBCT imaging will certainly improve patient care, dentists must possess the anatomical knowledge and the experience to interpret the scanned data accurately. Dentists must evaluate whether these imaging modalities add to their diagnostic knowledge and raise the standard of dental care or simply place the patient at a higher risk. Such evaluation requires continuous training, education for dentists and thorough research.
One of the most clinically useful aspects of CBCT imaging is the availability of highly sophisticated software that allows the large volumes of acquired data to be broken down, processed and reconstructed131. This ability makes data interpretation much more user-friendly, particularly if competent technical and educational training is provided to the dentists and technicians.




plate; this image indicates the teeth to be extracted and the grafting site before implant placement.


The increasing popularity of CBCT has resulted in the manufacture of a large number of CBCT units, numerous presentations at conferences and a significant increase in published articles. These factors have led to an uncontrolled and non-evidence-based reporting of radiation dose values that can be attributed to the limited technical knowledge of medical imaging devices among new users. To counter this uncontrolled exchange, the European Academy of Dental and Maxillofacial Radiology has developed guidelines outlining the basic principles for the use of CBCT in dental applications132; these guidelines are shown in Table 3.
The majority of CBCT applications in the practice of dentistry are found in the specialties of OMFS, endodontics, implant dentistry, and orthodontics. CBCT examinations must not be performed unless they are necessary and unless the benefits clearly outweigh the risks. The images acquired using CBCT must undergo a thorough clinical evaluation of the entire image dataset (i.e., a radiological report should be completed) to maximize the clinical data obtained from these images.
Future research should focus on obtaining accurate data regarding the radiation doses of CBCT systems. These systems have a small detector size, and the field of view and scanned volume are somewhat limited. Due to these factors, ideal CBCT systems for orthodontic and orthognathic surgery are not yet available. CBCT applications in forensic dentistry and prosthodontics require further investigation.
For the references listing please refer to the article on www.dentalnews.com
Table 3. Basic principles on the use of CBCT in dental applications (from eadmft)
1- CBCT examinations must not be carried out unless a history and clinical examination have been performed
2- CBCT examinations must be justified for each patient to demonstrate that the benefits outweigh the risks
3- CBCT examinations should potentially add new information to aid the patient’s management
4- CBCT should not be repeated ‘routinely’ on a patient without a new risk/benefit assessment having been performed
5- When accepting referrals from other dentists for CBCT examinations, the referring dentist must supply sufficient clinical information (results of a history and examination) to allow the CBCT Practitioner to perform the Justification Process
6- CBCT should only be used when the question for which imaging is required cannot be answered adequately by lower dose conventional (traditional) radiography
7- CBCT images must undergo a thorough clinical evaluation (‘radiological report’) of the entire image dataset
8- Where it is likely that evaluation of soft tissues will be required as part of the patient’s radiological assessment, the appropriate imaging should be conventional medical CT or MR, rather than CBCT
9- CBCT equipment should offer a choice of volume sizes, and examinations must use the smallest volume that is compatible with the clinical situation if this provides less radiation dose to the patient
10- Where CBCT equipment offers a choice of resolution, the resolution compatible with adequate diagnosis and the lowest achievable radiation dose should be used
11- A quality assurance programme must be established and implemented for each CBCT facility, including equipment, techniques and quality control procedures
12- Aids to accurate positioning (light beam markers) must always be used
13- All new installations of CBCT equipment should undergo a critical examination and detailed acceptance tests before use to ensure that radiation protection for staff, members of the public and patient are optimal
14- CBCT equipment should undergo regular routine tests to ensure that radiation protection, for both practice/facility users and patients, has not significantly deteriorated 15- For staff protection from CBCT equipment, the guidelines detailed in Section 6 of the European Commission document ‘Radiation Protection 136. European Guidelines on Radiation Protection in Dental Radiology’ should be followed
16- All those involved with CBCT must have received adequate theoretical and practical training for the purpose of radiological practices and relevant competence in radiation protection
17- Continuing education and training after qualification are required, particularly when new CBCT equipment or techniques are adopted
18- Dentists responsible for CBCT facilities who have not previously received ‘adequate theoretical and practical training’ should undergo a period of additional theoretical and practical training that has been validated by an academic institution (Universityor equivalent). Where national specialist qualifications in DMFR exist, the design and delivery of CBCT training programmes should involve a DMF Radiologist
19- For dento-alveolar CBCT images of the teeth, their supporting structures, the mandible and the maxilla up to the floor of the nose (e.g. 8cm x 8cm or smaller fields of view), clinical evaluation (‘radiological report’) should be made by a specially trained DMF Radiologist or, where this is impracticable, an adequately trained general dental practitioner
20- For non-dento-alveolar small fields of view (e.g., temporal bone) and all craniofacial CBCT images (fields of view extending beyond the teeth, their supporting structures, the mandible, including the TMJ, and the maxilla up to the floor of the nose), clinical evaluation (‘radiological report’) should be made by a specially trained DMF Radiologist or by a Clinical Radiologist (Medical Radiologist)


The International Congress of the Egyptian Orthodontic Society was a Joint Meeting with the Cyprus Orthodontic Society, the Greek Orthodontic Society, the Lebanese Orthodontic Society and the South African Society of Orthodontists
On January 21 – 23, 2001, the five Societies joined the International Orthodontic Congress organized by the Egyptian Orthodontic Society, in Alexandria, Egypt. A very successful event organized by Dr. Abbas Zaher, professor in Alexandria University and treasurer of the Egyptian Orthodontic Society.
240 Participants from Egypt and other Societies took part in this event. The largest group came from Greece with 36 persons. 24 local and international companies exhibited at the congress.
18 internationally renowned speakers took the podium to share their clinical and research experiences. Guest speakers for the congress: Eric Liou, Taiwan, Eustaquio Araujo and Varun Kalra, USA, Nasib Balut and Juan Carlos Solorio, Mexico, Arturo Vela, Spain,

Maja Ovsenik, Slovenia, Bakr Rabie, Hong Kong, Christodoulos Laspos, Cyprus, Edmond Chaptini, Lebanon, Athanasios E Athanasiou and Michael Kalavritinos, Greece, Phumzile Hlongwa and Rashid Chamda, South Africa, joined by Walid El Kenany, Yehia Mostafa, Amr Abol Ezz and Abbas Zaher from Egypt.
On Thursday January 20, an opening reception was organized to welcome the attendees and the presidents of the joining societies gave short welcome speeches. Drs. Christodoulos Laspos the president of the Cyprus Orthodontic Society, Dr. Paul Karvelas the president of the Greek Orthodontic Society, Dr. Dayalan Sundrum the president of the South African Society of Orthodontists and Dr. Samir Aboul Azm, the president of the Egyptian Orthodontic Society addressed the congress guests. In addition, Dr. Athanasios E. Athanasiou the immediate past president of the World Federation of Orthodontists and Dr. Maja Ovsenik, the immediate past-president of the European Orthodontic Society were among the guest speakers.



 Drs. Bakr Rabie, Yehia Mostafa, Walid El Kenany and Khaled Aboul Azm
Dr. Edmond Chaptini delivering his lecture
Dr. Abbas Zaher delivering his presentation in the congress
The Exhibition floor
Drs. Bakr Rabie, Yehia Mostafa, Walid El Kenany and Khaled Aboul Azm
Dr. Edmond Chaptini delivering his lecture
Dr. Abbas Zaher delivering his presentation in the congress
The Exhibition floor


As in other IDS years, W&H presented many new products and innovations to the special guests from around the world during the weekend prior to the IDS.
In small groups, the visitors had the opportunity to see the latest product such as the class-B Lina sterilizer and the new water treatment system Multidem. Also to see the actual brightness of LED+ in reality, understanding the new instruments and technologies, watch how to use professional new treatment techniques and the use of digital media as well as hands on use - W&H staff was proud to guide customers through the world of W&H.
Also captivating was the unique and passionate lecture during the lunch break by Thomas Bubendorfer - alpine extreme athlete. He showed that achieving unprecedented levels of success through passion, joy, self-motivation, responsibility and learning is for both parties a philosophy - for professional climbers as well as W&H. Because People have Priority.
Emotional evening
In the evening, the guests went to a wonderful gala dinner with a show and an upbeat video on W&H journey through the 120year history since 1890 in Berlin right up to the present day. The evening was also full of emotion due to the retirement of Dr. Bernd Rippel and Michel Paten, who took leave of our partners and were surprised to be presented with gifts.
Dr. Rippel again officially passed over the sales portfolio to his successor - Rudolf Flieger and Dr Rippel, thanked all the partners for their loyalty and cooperation, which he hopes will continue for W&H.


 Distributors from around the world during the presentation
Distributors from around the world during the presentation


The world's leading dental trade fair IDS came to a close with an extremely upbeat mood and outstanding results after five days in Cologne. "We've succeeded in making the International Dental Show even more attractive, both domestically and internationally. The strong increase in international participants especially shows that IDS is the world's leading dental trade show," says Dr. Martin Rickert, Chairman of the Association of German Dental Manufacturers (VDDI).
Once again, IDS offered a whole range of new products and excellent opportunities to exchange information, communicate with partners and place orders. That's why exhibitors, visitors and media representatives alike were all delighted with the trade fair.
Not only the exhibitors but also trade visitors report that the trade fair was a great success. This is confirmed by initial responses to the visitor survey. Altogether 95 per cent of respondents indicated that they were satisfied or very satisfied with IDS. In addition, 93 per cent would recommend a visit to IDS to a close business associate.
Feedback from exhibitors:
Klaus Rübesamen, Managing Director, Komet/Gebr. Brasseler
"As far as Komet is concerned, IDS 2011 was a great event. In fact it even exceeded our expectations. Once again, we were

able to present ourselves to a broad specialist public as an innovation leader when it comes to dental instruments and tools. The many customers we met from Germany and abroad were very positive about our innovations. As a result, we are optimistic about the future."
Jost C. Fischer, Chairman & Chief Executive Officer, Sirona Dental Systems
"The trade fair was very successful as far as we're concerned. The number of visitors was amazing. In fact, all of our employees were involved in discussions around the clock. You could clearly see that the economy had picked up again. As a result, the atmosphere at the fair was extremely positive. In my opinion, it was the best IDS ever."
In my opinion, it was the ever best IDS “ ”




















lanoisnemiD ilibatS t y Dimensional Stabili t y 5days




5 years shelf life superior tear resistance
snap set
Cavex has been producing alginate impression materials for more than 55 years. As a result all our alginates have been developed to perfection. In September 2007 Cavex ColorChange has been awarded the highest rating “excellent” by THE DENTAL ADVISOR. Cavex ColorChange was used by 27 consultants and received a 96% clinical rating. 71% of consultants would switch, and 76% would recommend Cavex ColorChange to colleagues.











The easiest solution for creating a perfect contact point
•Integrated tensioning and opening device
•Easy creation of contact point
•No additional tools needed

Kuwait Radisson SAS– 9 - 11 April 2011


Honorable guests,
I am pleased to welcome you all, to this scientific event which takes place in the State of Kuwait “the land of friendship and peace” under the patronage of the Minister of Health H. E. Dr. Hilal M. Al-Sayer. My dear colleagues, conducting such an event habitually and continuously is a pride and credit for the dental association. Today, in this conference, we have adopted a new slogan “Invitation to the World of Dentistry” which intended to reflect the KDA’s Board of Directors extent and the keenness towards the importance of developing the scientific and professional training for dentists. We consider this is to be a turning point that thrust our brothers’ and sisters’ professional standard by means of the scientific and educational vision that sustained through scientific and interdependence exchange among the dentists in the State of Kuwait and other countries as well. We deem that this will motivate all our colleagues to work together and strive to provideall that is new in dentistry for a better future of this beloved country. In the meantime, we also take this opportunity to congratulate all of you and us on the occasions of celebrating the 50th anniversary of the independence of the State of Kuwait, the 20th anniversary of the Liberation and the 5 years of the succession of his Highness the Amir of Kuwait Sheikh Sabah Al – Ahmed al – Jaber Al Sabah. Finally, I wish for my all doctor brothers and sisters and participants from outside the State of Kuwait, a pleasant stay in their second home. Dr. Ebrahim Esmail Taqi, President of the Kuwait Dental Association


















La Droguerie Tamer membre de G. Tamer Holding rafle trois trophées à l’ « International Dental Show » (IDS).


L’équipe de la Droguerie Tamer membre de G.Tamer Holding s’est rendue à l’International Dental Show (IDS) qui s’est tenu à Cologne. Cette exposition internationale la plus importante dans le domaine dentaire attire chaque année plus de 120.000 visiteurs des quatre coins du globe et présente les technologies récentes des marques les plus connues.

Droguerie Tamer qui représente sur le marché libanais et régional des marques importantes (comme A-Dec, NSK, Septodont, Bego, Biomet 3i, Discus Dental et Ivoclar Vivadent, Dentsply, Coltène Whaledent, Sunstar-Gum, Waterpik), fut représentée par Tarek Skaff (directeur général), Diaa Khreich (directeur Tamer Levant), Carlos Abillama (directeur 3i Mena) et Wael Houry (directeur des ventes),pour recueillir trois trophées: le premier trophée fut décerné par la société Adec en commémoration de son 20e anniversaire de partenariat et en reconnaissance de son soutien aux ventes et services des produits dentaires Adec. Les deux autres trophées furent décernés respectivement par les sociétés NSK et Bego en appréciation du résultat remarquable des ventes accompli par le groupe en 2010.


 Tarek Skaff, Gaby Tamer, David Halimi (V.P. Septodont) Diaa Khreish, Wael Houry
Stephen Lawry, Tarek Skaff, Gaby Tamer et Scott Parrish (Président de A-Dec)
L’équipe Tamer: Carlos Abillama, Diaa Khreish, Gaby Tamer, Tarek Skaff, Wael Houry
Wael Houry, Diaa Khreish, Eiichi Nakanishi Président de NSK, Gaby Tamer, Tarek Skaff, Hiroki Kano
Gaby Tamer, Alex Al Dahi, Tarek Skaff sur le stand BegoStand Biomet 3i
Tarek Skaff, Gaby Tamer, David Halimi (V.P. Septodont) Diaa Khreish, Wael Houry
Stephen Lawry, Tarek Skaff, Gaby Tamer et Scott Parrish (Président de A-Dec)
L’équipe Tamer: Carlos Abillama, Diaa Khreish, Gaby Tamer, Tarek Skaff, Wael Houry
Wael Houry, Diaa Khreish, Eiichi Nakanishi Président de NSK, Gaby Tamer, Tarek Skaff, Hiroki Kano
Gaby Tamer, Alex Al Dahi, Tarek Skaff sur le stand BegoStand Biomet 3i

With the same spirit of G. Tamer Holding in the MENA region, and since day one in Iraq, Tamer Levant decided to take the level of dentistry in Iraq to a higher position by listening closely to the dental community needs and investing more in the education and support of the Iraqi dentists and above all believing in them.
With top international brand names in dental industry Tamer Levant was among the first gold sponsors of the 1st Iraqi Dental Reunion IDR meeting held in Erbil last April. More than 1200 participants from the different provinces of Iraq, Ministers of Health, Deans, Professors, Dentists and Dental Technicians had the opportunity to reunite and see closely the latest in dentistry. Tamer Levant through its supplier DENTSPLY, offered 2 lectures followed by a workshop presented by a highly professional lecturer from the Saint Joseph and the Lebanese University in Beirut Dr Karim Corbani who lectured on: "Direct Posterior Restorations" and "Achieving Consistent Results with Direct Anterior Composite". And Dr. Edward Rizk, lectured on "Winning the Challenge of Mechanical Shaping of Narrow and Curved Canals". While the workshops were prepared to receive a maximum of 20, 250 dentists were striving to get these places.
“The Exhibition was a great success. It gave us the opportunity to be at the service of the Iraqi dentist in both Governmental and private sector” said Diaa Khreish Managing Director of Tamer Levant in Iraq.
In addition to the presence of the President and CEO of G.Tamer Holding Mr Gaby Tamer, and the General Manager, Mr Tarek Skaff, Technical Manager Mr Antoine Eid, and the Managing Director of Tamer Levant Mr Diaa Khreish, top supplier were among the attendee from A-dec Mr Steven Lawry Territory Manager, from Dentsply Dr Harika Gokcesu Regional Director of Dentsply UK export, Dr Ghada Bassil Sales and Professional Services Manager in addition to the team of Tamer Levant in Iraq.
Tamer Levant will keep on investing into education, training and will continue to provide the finest products and services for all the dental communities in Iraq through its direct offices in Erbil and Baghdad and its chain of distributors in the rest of the cities of Iraq.
Tamer Levant represents the following leading brands in Iraq: Dentsply , Dentsply Maillefer, A-dec, NSK, Biomet 3i,Tecnogaz, MGF, BlueX , Nordent.



 Tamer Levant Stand
Dr. Karim Corbani
Endo hands-on by Dr. Edward Rizk
Dr. Edward Rizk, Wissam Shedid, Dr. Ghada Bassil, Diaa Khreish, Gaby Tamer, Steve Lawry, Dr. Karim Corbani, Dr. Harika Gokcesu, Tony Eid, Tarek Skaff
Tamer Levant Stand
Dr. Karim Corbani
Endo hands-on by Dr. Edward Rizk
Dr. Edward Rizk, Wissam Shedid, Dr. Ghada Bassil, Diaa Khreish, Gaby Tamer, Steve Lawry, Dr. Karim Corbani, Dr. Harika Gokcesu, Tony Eid, Tarek Skaff



It’s our pleasure and honor to welcome you to our 10th scientific Meeting and we are deeply grateful to your presence today in the opening ceremony.
We thank the Lebanese Dental Association for its continuous support, the world Federation of Orthodontics for its invaluable help and the Luxembourg Orthodontic Society for having made this event a real success.
We have tried to focus through this meeting on basics as well as on recent advancements and new developments in orthodontics in order to bring to our colleague “Orthodontics after year 2000”.
The main objectives were:
First: To honor our teacher, our friend, our colleague Professor Pierre Rizkallah who passed away. Multi-talented man, honest and passionate who left a major print on the field of orthodontics in Lebanon.
Second: To bring the latest developments in orthodontics through pre- and post-congress Courses dealing with 3D Imaging and Lingual Orthodontics. and Third: To open the door for multidisciplinary interaction with Oral Radiology and Human Anthropology. All this, without forgetting the basic clinical teaching as well as Evidence Based Orthodontics. Topics which will be developed by different experts in their fields.
The success of the event is due to a highly motivated group of people who worked hard as a solid team, I would like to thank every one of them from the bottom of my heart.
We hope that this meeting will be remembered and this occasionwill be an annual appointment to see and learn from each other.









ThenewPiezotome2andImplantCenter2combinedunitsfor bonesurgerydonotjustofferthebestofSatelec ® knowhow... Theyarethreetimesmorepowerfulthanthepreviousgeneration!The extrapowerofPiezotome2,togetherwithanexcellentsurgicalmotor, willguaranteeyoushorter,betterorganizedtreatmentsintotalsafety andcomfortforthepatientthankstotheprecisionandselectivecut procuredbyultrasonics.








With the ongoing enhancement of the premium treatment units U 1500, U 5000 S and U 5000 F, dental manufacturer ULTRADENT has created a modern class of unit that provides the highest possible quality in the compact treatment unit segment. ULTRADENT’s special modular design makes it possible to equip units in line with dentists’ individual requirements and specifications. Extremely high standards are also set in terms of design, construction and quality of workmanship.
The 2011 models have some interesting new features.The 19-inch flatscreen monitor and the completely reworked spittoons are particularly striking. The assistant’s control console now has a new holder, making it even more ergonomic. The design of the dental assistant’s unit and tray table have been adapted to fit in with the overall concepteven more optimally.
Various details, such as the new touch-screen display,an optional wireless foot control, replaceable controlvalves, and a non-drip filter system, make treatmenteasier and promote dental practice hygiene. The supersoft chair upholstery, which is available in 12 colors and includes an individual headrest system with magnetic supports, ensures comfort. Movable armrests make it easier to get into the chair. The exclusive comfort padding with air conditioning or massage function is another feature developed by ULTRADENT.















Thank you for subscribing at

The winner of the W&H LED Contra - Angle Handpiece (ALEGRA WE - 56 LED G) is Dr. Marwan Qasem from al Bireh
The Result were also posted on the Dental News Facebook Page (www.facebook.com/dentalnews1)


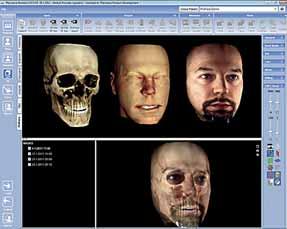
The Planmeca ProMax 3D ProFace unit acquires patient’s facial 3D photo in a radiation-free process giving the medical or dental professional opportunity to plan operations and document the follow-up images.
Planmeca is first to introduce an integrated 3D unit producing a realistic 3D face photo in addition to traditional digital maxillofacial radiography. One single scan generates both a 3D photo and a CBVT volume. Alternatively, the 3D photo can be acquired separately in a completely radiation-free process: the lasers scan the facial geometry and the digital cameras capture the colour texture of the face.
The 3D photo visualises soft tissue in relation to dentin and facial bones, providing an effective follow-up tool for maxillofacial operations. As Planmeca ProMax 3D ProFace acquires both a CBVT image and a 3D photo in single scan, the patient position, facial expression, and muscle position remain unchanged, resulting in perfectly compatible images. Careful preoperative planning, where the medical professional can study the facial anatomy thoroughly using Planmeca Romexis software, facilitates a detailed operation and enhances the aesthetic results.
“This new product clearly demonstrates our groundbreaking R&D and best practices in imaging. Planmeca provides the most advanced tools – 3D imaging units and software – for visualising patient anatomy making treatment planning and follow-up for orthodontic, maxillofacial and aesthetic surgeries more precise, faster and safer,” explains Ms Helianna Puhlin-Nurminen, Vice President of Digital Imaging at Planmeca Oy. helianna.puhlin@planmeca.com










The CP-ONE PLUS is the latest addition to the dental unit range from TEKARA BELMONT. The CP-ONE PLUS succeeds in taking the concept of the CP-ONE and improving it with advanced technology and comfort. The CP-ONE PLUS was designed by incorporating dentists’ requirements and desires one by one, from the treatment space all the way down to minute details that will be recognized through dentists’ fingertips. An ideal treatment environment, the CP-ONE PLUS is a “think-all” dental chair and unit, the answer to dentists’ aspirations.
The CP-ONE PLUS is a comfort ergonomically designed folding leg-rest chair and base-mounted unit enabling patients to access to the chair either from front or from side with ease. It can be put in a 6-o’clock faceto-face treatment. Standing directly in front of the patient gives the doctor an accurate picture of the patient’s jaw and bite.
To provide true comfort for all patients including children, the elderly and those with limited mobility, the CP-ONE PLUS is designed with abundance of new innovative features. The folding leg-rest chair with low initial height of 40mm secures easy access.
The redesigned instruments holder is adjustable horizontally and vertically, which ensures that the dentist always has his tools within easy reach. The newly developed foot controller (electric control) is controlled by either pressing and/or turning the disk, which provides precise instruments control. Furthermore the newly-developed LED dental light equipped with 10 white LED modules is coming soon as an extra option.


Compothixo™ is a unique generation in composite placing and modelling instrument suitable for all class restorations.
The new Compothixo™ technology optimizes the thixotropic properties of composites by changing viscosity only, without altering the chemical and mechanical characteristics of the material.
•Better wettability
•Superior adaptation of composite to cavity walls
•Reduction of air bubbles
•Precise application
•Layer thickness control
•Improved sculptability
•Reduced stickiness
Nowfeaturing a fill-levelindicator

Economical– around 120applicationsper VivaPen
Click & Bond® with theV ivaPen ® Fluoride-releasing, selfetching all-in-oneadhesive
Significantlyimproved adhesion toenamel