December - January 2023
 Dr M. Mark Melin
Dr M. Mark Melin
 M Health Fairview Wound Healing Institute, University of Minnesota Physicians Minneapolis MN, United States
M Health Fairview Wound Healing Institute, University of Minnesota Physicians Minneapolis MN, United States

December - January 2023
Dr M. Mark Melin
M Health Fairview Wound Healing Institute, University of Minnesota Physicians Minneapolis MN, United States
Lymphedema is a major global condition defined as progressive swelling of the body part which is in part due to disruption of the lymphatic system. This article is going to discuss the pathophysiology of lymphoedema, the demographics of the condition and its management. There will be a deep overview of the importance of the endothelial or Calix layer as well as the importance of the starling model of capillary fluid change. A detailed look at the lymph circulation including the capillaries and lymphatic endothelial cells and its relevance to lymphedema. There will also be a focus on hyperglycaemia and diabetes in lymphoedema In this article. The role of albumin and glycocalyx as well as sodium are explored. The clinical characteristics and management will also be analysed.
Lymphedema affects 140-300million patients worldwide. It is defined as the progressive swelling of a body part, usually an extremity following developmental (primary lymphedema) or acquired (secondary lymphedema) disruption of the lymphatic system resulting in lymph accumulating in the interstitial space.1 This article discusses the pathophysiology of lymphedema, demographics of this condition and its management.
In 1894, Starling proposed a model of capillary fluid exchange, based on hydrostatic and oncotic pressures in the blood capillaries and interstitium, with the capillary acting as a semiporous membrane, through which fluid moves freely in and out.2 In 1940, Danielli introduced the concept of a protein-based lining of vessels which played a vital role in fluid filtration, and in 1966, Luft visualised this layer using electron microscopy.2 The “endothelial glycocalyx layer” (EGL) was then recognised as controlling the movement of proteins and fluid across the blood capillary wall, through dynamic and complex processes.2
The endothelial glycocalyx is a complex carbohydrate-rich gel-like layer lining the luminal surface of blood vessels functioning as a barrier between the blood and vessel wall.3 The glycocalyx layer is composed of membrane-bound proteoglycans, secreted glycosaminoglycans (GAGs), sialic acidcontaining glycoproteins, and glycolipids
associated with the endothelial surface.3 The main proteoglycans of the endothelial glycocalyx are membrane-spanning syndecans and glycosylphosphatidylinositol-linked glypicans which carry the two main GAGs, heparan sulphate and chondroitin sulfate.3
In 2010, it was demonstrated that there was no net resorption of fluid back to the venous side of the blood capillaries and there is only diminishing net filtration across the capillary bed.2 Capillaries and venules can only resorb fluid in extreme situations.2 An acute reduction of transendothelial pressure, for example caused by precapillary vasoconstriction, post-capillary vasodilation, haemorrhage or hypovolaemia will allow transient venous absorption preserve blood volume.2 This challenges the previously accepted view regarding Starling forces.2
Acting as a complex molecular sieve, the EGL precisely regulates fluid and protein movement through the capillary wall into the tissues and prevents movement of proteins and fluid back into the venous side of the capillaries, even when interstitial tissue hydrostatic pressure is increased, or capillary oncotic pressure is higher than the tissue oncotic pressure (Figure 1).2,4 All fluid and blood proteins moving into the interstitium each day must be removed via reabsorption through the lymphatic capillaries alone.2 Thus, all oedemas fall on a continuum of lymphedema, and can lead to chronic inflammation and tissue thickening caused by accumulation and degradation of proteins.2
Glycocalyx and endothelial cell damage occur in several clinical situations including ischemia–reperfusion injury, hypoxia/reoxygenation,
inflammation, sepsis, haemorrhagic shock, hypervolemia, hyperglycemia, excessive shear stress and coronary artery bypass surgery.3 These injuries determine pathological changes in the endothelial glycocalyx such as impaired mechanotransduction, increased egress of leukocytes, loss of coagulation control, loss of anti-oxidant defence, loss of deposited growth factors and increased vascular permeability, which is of vital importance in lymphedema.3
entry of proteins, fluids, macromolecules, small molecules and immune cells.4 The lymphatic capillaries coalesce into progressively larger lymphatic collectors which are formed by one layer of lymphatic endothelial cells supported by a more organized basal membrane containing lymphatic muscle cells, connective tissue and fibroblasts.4 The directional flow of lymph is maintained through a series of unidirectional valves, positioned along the collectors, which open and close in synchrony with the vessel contraction.4 Contraction from the more distal lymphangion toward the one closer to the lymph node, in synchrony with directional valve closure, allows unidirectional lymph transport and prevents backflow, enabling the collectors to work as pumps.4
Increased lymphangiogenesis has been observed in primary and secondary lymphedema, acute and chronic inflammation and cancer, related to the increased production of different vascular endothelial growth factors released by immune and stromal cells and nuclear factor-κB up-regulates the transcription factor Prox1 that promotes lymphatic endothelial cell proliferation.4
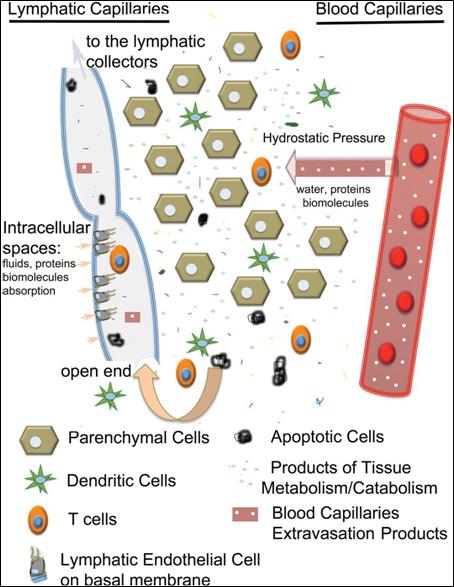
All parenchymal organs, with the exception of the brain, contain a network of openended lymphatic capillaries, which collect the interstitial fluid.4 The capillaries are formed by a single layer of lymphatic endothelial cells which function as one-way valves to facilitate
In response to hyperglycaemia, the thickness of the glycocalyx on blood vessel endothelia is significantly reduced, leading to loss of protective functions and other deleterious changes, including increase in risk of lympoedema.5 A study showed that acute hyperglycaemia in healthy subjects was associated with a ~50% reduction in glycocalyx volume which was likely to be due to damage by reactive oxygen species (ROS) generated under hyperglycaemic conditions, because infusion of the antioxidant N-acetylcysteine (NAC) could prevent this reduction.5-6 Both the systemic glycocalyx volume and the directly measured glycocalyx thickness are reduced by 50–86%
“In response to hyperglycaemia, the thickness of the glycocalyx on blood vessel endothelia is significantly reduced, leading to loss of protective functions and other deleterious changes, including increase in risk of lympoedema.” 5Figure 1: Schematic of lymph formation.4
in type 1 diabetic patients relative to normal controls.5 Hyaluronan (HA) is an important component of the glycocalyx and is affected in diabetes - hyaluronidase activity and circulating levels of HA are both elevated in the serum of diabetic patients, suggesting that hyaluronidase activity may contribute to the degradation of the endothelial glycocalyx in diabetes.5
Albumin has a net negative charge, but its amphoteric nature promotes tight binding to the glycocalyx which results in reduced hydraulic conductivity across the vascular barrier, resisting glycocalyx degradation (i.e., protecting against shedding) and thereby contributing to maintenance of vascular integrity and normal capillary permeability, and facilitating transmission of shear stress.3 Under physiological conditions, the concentration of intravascular albumin is the major determinant of plasma colloid osmotic pressure.3
Exposed thiol groups on the albumin molecule act as a scavenger for reactive oxygen species (ROS) such as superoxide and hydroxyl radicals and reactive nitrogen species, e.g., peroxynitrite radicals.3 Albumin has an additional antioxidant effect through binding to free copper ions (Cu2+) which accelerate the production of free radicals.3
Studies illustrate the multifunctional nature of albumin including maintaining glycocalyx integrity and partially restoring impaired vascular permeability via release of sphingosine-1-phosphate (S1P) from red blood cells, anti-inflammatory and anti-oxidative effects, improvement of the microcirculation and hemodynamics following hemorrhagic shock or endotoxemia, and acting as an effective plasma volume expander.3 Compared with saline, albumin improves skin endothelial cell function, improving microcirculatory blood flow, and this maybe independent of the oncotic
properties of albumin as neither cardiac output nor skin blood flow differed between albuminand saline-treated patients in these studies.3
The glycocalyx covering the luminal surface of the vascular endothelium also plays an essential role in the regulation of sodium homeostasis.7 When the volume of the endothelial glycocalyx is reduced or its integrity is impaired, its capacity to bind and buffer sodium diminishes.7 As previously discussed, several clinical conditions are known to damage the endothelial glycocalyx, but with respect to sodium homeostasis, the acute sodium/volume loading appears to be the most relevant.7 In response to salt loading, the barrier function of the glycocalyx diminishes and more sodium reaches the luminal surface of endothelial cells, where it induces and activates epithelial sodium channels, which results in increased sodium uptake by the cells, stiffening of the cortex of the cells and a reduction in the generation of endothelial NO which elevates vascular tone.7 As a mechanotransductor, the glycocalyx mediates flow-dependent vasorelaxation by stretching the glycocalyxlipid bilayer cytoskeleton system and increases NO production though the activation of transient receptor potential (TRP) channels.7
The endothelial glycocalyx functions as a sodium buffer and first-line barrier to protect endothelial cells against increased sodium influx when exposed to excess circulating sodium.7 In clinical conditions characterized by a decreased sodium binding capacity of the glycocalyx, more sodium enters into the cells, causing impaired NO generation, elevated vascular resistance, and hypertension.7 The sodium load would increase unbound, osmotically active sodium, resulting in water retention, volume expansion, and a increase in blood pressure.7
“The glycocalyx covering the luminal surface of the vascular endothelium also plays an essential role in the regulation of sodium homeostasis.” 7
The most common cause of lower extremity lymphedema is chronic venous insufficiency (CVI), followed by cancer-related lymphedema, primary lymphedema and lipedema with secondary lymphedema.8 Patients are most commonly female, white, obese with bilateral involvement.5 Surgery, particularly total knee replacements and trauma are associated with worsening lymnphoedema.8
There is no definitive cure for lymphedema, but management options that have been used include physical therapy, drugs and surgical options.9 Physical treatments include massages, lymphatic drainages, the application of different kind of compression garments, and intermittent pneumatic compression.9 Natural compression can be simulated by intermitted pneumatic compression devices, which use a sequential airflow to inflate special hoses and, therefore, applying positive pressure on the tissue, and these have been shown to be an effective treatment in those with secondary lymphedema.9 A novel therapeutic approach that uses the application of negative pressure (representing a pulling/opening force) has been described and whilst this approach has already been used in the field of wound healing, its use in lymphedema has not yet been fully investigated.9 Another form of negative pressure uses kinesiology tapes which are used to decongest lymphatic fluid that accumulates under the skin.9 Kinesiological methods have been shown to improve quality of life and a reduction in volume, but these are not seen as superior compared to other treatments.9
Diuretics, benzopyrones, ketoprofen and tacrolimus have all been suggested for the management of lymphedema but are not generally recommended.9 Surgical methods have been investigated, which can be divided
in to physiological and excisional procedures.9 Physiological procedures are aimed at promoting fluid flow properties, either by redirecting the lymphatic flow directly into the venous system or by providing new pathways.9 Excisional procedures involve the removal of affected tissue parts.9 In lymphvenous anastomosis (LVA) surgery, a connection between the lymphatic structures and blood vessels is established.9 Patients report improvements following this surgery, which is more effective in upper than lower limbs, but compression garments are still required post-surgery.9 Vascularized lymph node transfer (VLNT) is performed in more advanced stages in lymphedema patients in which lymphatic vessels are dysfunctional and/ or lymph nodes are not present.9 The proposed mechanism of action of this is that accumulated fluid in the close area is absorbed by the nodes and VEGF-C induced lymph angiogenesis by vascularized lymph nodes.9 LVA and LVNT have both shown promising outcomes in clinical studies in terms of limb volume reduction and reduced episodes of cellulitis but no beneficial effect in reducing fibrosis has been observed.9 In cases of fibroadipose hypertrophy, as can often be found in chronic lymphedema, suction assisted lipectomy (SAL) can be the surgery of choice, but lifelong compression bandages are required to prevent recurrence.9
The standard therapy of choice is a form of physical therapy that is known as complete/ complex decongestive (physio-)therapy (CDT).9 This form of treatment is not curative for lymphedema, but mainly aims at reducing fluid volume as well as preventing the disease from progression.9 It can generally be separated into two phases: Phase one involves manual lymphatic drainage (MLD), usage of multilayered compression bandages, carrying out physical exercises, and meticulous skin care.9 Phase two mainly focuses on self-care via elastic sleeves or compression stocks application as well as continuous exercise.9
“There is no definitive cure for lymphedema, but management options that have been used include physical therapy, drugs and surgical options.” 9
Main Components of CDT:
• Manual Lymphatic Drainage (MLD) is performed to enhance lymphatic outflow. Lymph therapists use specific hand movements (rhythmic, flowing or stirring) in a frequency that mimics the intrinsic frequency of the lymphangion, starting in the area of healthy tissue and then expanded into adjacent areas where the obstructed vessels are located
• Compression bandages are applied, aiming at increasing interstitial pressure and therefore, to decrease capillary filtration leading to a decrease in accumulated fluid/ volume
• Physical exercise such as ergometry, aerobic exerciseand/ or resistance exercise as well as associated respiratory movements which are believed to assist in increasing lymphatic flow, in reducing swelling and in improving muscle strength as well as quality of life in lymphedema patients
• Skin care and skin restauration
• Psychological support
• Educational seminars on skin care or nutrition.9
MPFF has been demonstrated in rats to have dose dependent anti-oedema properties°. In humans, a study demonstrated that treatment with MPFF resulted in an increase in the number of functional lymphatics and reduction of the diameter of lympathic capillaries and of the intralymphatic pressure. A recent study found a significant improvement in
lymphoscintigraphic parameters and also observed a tendency in favour of MPFF in patients with more severe lymphedema°. A Cochrane review of benzopyrones (including MPFF) for lymphedema acknowledged the difficulties about studies in this area, especially as lymphedema is frequently distributed unevenly, so volume calculation based on circumference measurement becomes inaccurate and chronic lymphedema needs long periods of treatment, long follow-up, and standardising decongestive therapy is difficult.
An understanding of the pathophysiology of lymphedema, and in particular the glycocalyx, is important when considering the management of this condition. Glycocalyx and endothelial damage occur in a number of clinical situations, and an understanding of the role of sodium, albumin and hyperglycaemia in the function of the glycocalyx is vital. There is no cure for lymphedema, but a multifaceted approach is used in its management.
1. Lymphedema. BMJ Best Practice. Last updated 8/2/22 https://bestpractice.bmj.com/ topics/en-gb/610
2. Bjork R, Hettrick H. Endothelial glycocalyx layer and interdependence of lymphatic and integumentary systems. Wounds International 2018. 9 (2): 50-55
3. Aldecoa Cet al. Role of albumin in the preservation of endothelial glycocalyx integrity and the microcirculation: a review. Ann Intensive Care. 2020 Jun 22;10(1):85.
4. Kirk Cet al. Lymph formation, composition and circulation: a proteomics perspective, International Immunology. 2015. 27(5): 219–227
5. Shakya S et al.Hyperglycemia-Induced Changes in Hyaluronan Contribute to Impaired Skin Wound Healing in Diabetes: Review and Perspective. International Journal of Cell Biology. 2015
6. Nieuwdorp Met al. Loss of endothelial glycocalyx during acute hyperglycemia coincides with endothelial dysfunction and coagulation activation in vivo. Diabetes.2006. 55 (2): 480–486
7. Sulyok Eet al.Tissue Sodium Accumulation: Pathophysiology and Clinical Implications. Antioxidants (Basel). 2022. 11(4):750
8. Dean SMet al. The clinical characteristics of lower extremity lymphedema in 440 patients. J VascSurg Venous LymphatDisord. 2020 8(5):851-859.
9. Brix, Bet al. Biology of Lymphedema. Biology 2021, 10, 261.
“There is no cure for lymphedema, but a multifaceted approach is used in its management.”