Journal of Trauma and Orthopaedics

Volume 12 | Issue 02 | June 2024 | The Journal of the British Orthopaedic Association | boa.ac.uk
Kids knee surgery: A new orthopaedic subspeciality p18 Human factors ergonomics in healthcare: How we are influencing change and improving safety p46 Obesity and orthopaedic surgery p22
One



Contact us at sales@ledaortho.com to arrange a consultation and open your personal portal to start planning cases.
your most complex cases with a UK-based, straightforward platform, underpinned by LEDA’s commitment to customer service.
UK-based operation Post-Osteotomy and Correction
Plan
Dedicated
point of contact with clear communication
turnaround of 3D printed guides for osteotomies of: Upper Limb Lower Limb More clinical applications available Distal radius Elbow Clavicle HTO SMO ledaortho.com Powered by Insight Surgery Introducing L3D Osteotomy
and Custom Implants
Rapid
Planning

In this issue...
Guidance on the role of simulation in formal training by the British Orthopaedic Association
Kapil Sugand and Hiro Tanaka
A practical approach to artificial intelligence in trauma and orthopaedics
Andrew Coppola and Vipin Asopa 34 International:
My experience working on Mercy Ships
Rachel Buckingham
38 Trainee:

46 Subspecialty:
The development of regional
Features:
Kids knee surgery: A new orthopaedic subspeciality
Rizwan Arshad, Sheba Basheer, Dominic O’Dowd, Nicolas Nicolaou and Fazal Ali
and orthopaedic surgery
Harriet Lewis, Alexander Dodds and Mark Bowditch

Global surgery ‘the trainees’ perspective’: Ten things we have learnt so far...
Alice Campion, Matthew Arnaouti, William M Nabulyato, James Archer, Alex Schade and James Berwin
42 Medico-legal:
Ownership of removed orthopaedic implants
Devapriyan Johnson, Ahmed Mahmoud, Simon Britten and Samuel Heaton
45 Subspecialty:
Human factors in surgical performance
James Tomlinson
Human factors ergonomics in healthcare: How we are influencing change and improving safety
Sue Deakin
50 Subspecialty:
Ergonomics for the diverse workforce
Roshana Mehdian and Deborah Eastwood
53 Subspecialty:
Behavioural science approaches to enhancing surgical performance
Steven Yule
56 In Memoriam:
John Robson Kirkup










JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 01 3 From the Executive Editor Deborah Eastwood 5 From the President Simon Hodkinson 6-7 BOA Latest News 12 News: Conference Listing 2024 14 News: BOA Annual Congress 2024 15 Features: An update from the International Orthopaedic Diversity Alliance (IODA) 16 Features:
fracture
liaison services
18
Andrew Gray
22 Features:
Obesity
26 Features:
30
Features:
Download the App The Journal of Trauma and Orthopaedics (JTO) is the official publication of the British Orthopaedic Association (BOA). It is the only publication that reaches T&O surgeons throughout the UK and every BOA member worldwide. The journal is also now available to everyone around the world via the JTO App. Read the latest issue and past issues on the go, with an advanced search function to enable easy access to all content. Available at the Apple App Store and GooglePlay – search for JTO @ BOA Did you know that as well as advertising in our Journal publication, we can offer footer banner advertising on the JTO App! For more information please contact Mandy Boyle Email: Mandy@ob-mc.co.uk | Telephone: +44 (0)121 200 7820 Contents Amputation the context T OrthopaedicsT Orthopaedics A Surgical Day Begins Volume 08 Issue 02 Volume 08 Issue 01 Volume 08 Issue 04 Journal of the British Orthopaedic Association The Journal of Trauma and Orthopaedics (JTO) has a dedicated news section, a features section containing interesting articles on various themes, a subspeciality section and a medico-legal section.
We are committed to sustainable forest management and this publication is printed by Buxton Press who are certified to ISO14001:2015 Standards (Environmental Management System). Buxton prints only with 100% vegetable based inks and uses alcohol free printing solutions, eliminating volatile organic compounds as well as ozone damaging emissions. Open Box Media & Communications are proud to be corporate sponsors of Heart Research UK (Midlands)
Journal of Trauma and Orthopaedics
34


Medical 1. Berberich CE, Josse J, Laurent F, Ferry T. Dual antibiotic loaded bone cement in patients at high infection risks in arthroplasty: Rationale of use for prophylaxis and scientific evidence. World J Orthop. 2021;12(3):119-128. doi:10.5312/wjo.v12.i3.119 I 2. Parvizi J, Shohat N, Gehrke T. Prevention of periprosthetic joint infection: new guidelines. Bone Joint J. 2017;99-B(4 Supple B):3-10. doi:10.1302/0301-620X.99B4.BJJ-2016-1212.R1 I 3. Sanz-Ruiz P, Berberich C. Infection Risk-Adjusted Antibiotic Prophylaxis Strategies in Arthroplasty: Short Review of Evidence and Experiences of a Tertiary Center in Spain. Orthop Res Rev. 2020;12:89-96. doi:10.2147/ORR.S256211 I 4. Sprowson AP, Jensen C, Chambers S, et al. The use of high-dose dualimpregnated antibiotic-laden cement with hemiarthroplasty for the treatment of a fracture of the hip: The Fractured Hip Infection trial. Bone Joint J. 2016;98-B(11):1534-1541. doi:10.1302/0301-620X.98B11.34693 I 5. Sanz-Ruiz P, Matas-Diez JA, Villanueva-Martinez M, Santos-Vaquinha Blanco AD, Vaquero J. Is Dual Antibiotic-Loaded Bone Cement More Effective and Cost-Efficient Than a Single Antibiotic-Loaded Bone Cement to Reduce the Risk of Prosthetic Joint Infection in Aseptic Revision Knee Arthroplasty? J Arthroplasty. 2020;35(12):3724-3729. doi:10.1016/j.arth.2020.06.045 12139 EN www.heraeus-medical.com KNOW YOUR PATIENT –AND REDUCE PJI RISK IMPROVED OUTCOMES IN HIGH RISK PATIENTS1 Using dual antibiotic-loaded bone cement as part of set of measures2 in a risk adaptive approach Elective primary hip and knee arthroplasty3 Trauma (FNOF)4 Aseptic revision TKA5 See inside back cover for more information.
JTO Editorial Team
l Deborah Eastwood (Executive Editor)
l Paul Banaszkiewicz (Editor)
l Simon Britten (Medico-legal Editor)
l Karen Chui (Trainee Editor)
l James Tomlinson (Guest Editor)
BOA Executive
l Simon Hodkinson (President)
l Deborah Eastwood (Immediate Past President)
l Mark Bowditch (Vice President)
l Fergal Monsell (Vice President Elect)
l Hiro Tanaka (Honorary Secretary)
l Ian McNab (Honorary Treasurer)
l John Skinner (Appointed Trustee)
BOA Elected Trustees
l Simon Hodkinson (President)
l Deborah Eastwood (Immediate Past President)
l Mark Bowditch (Vice President)
l Fergal Monsell (Vice President Elect)
l Hiro Tanaka (Honorary Secretary)
l Ian McNab (Honorary Treasurer)
l Cheryl Baldwick
l Deepa Bose
l Caroline Hing
l Andrew Price
l Andrew Manktelow
l Andrea Sott
l Paul Banaszkiewicz
l Stephen Eastaugh-Waring
l Vikas Khanduja
l Dominic Meek
l Benjamin Ollivere
l Amar Rangan
Copyright
BOA Staff
Executive Office
Chief Operating Officer - Justine Clarke
Personal Assistant to the Executive - Celia Jones
Policy
and Programmes
Head of Policy and Public Affairs
- Gary Robjent
Head of Education and Programmes
- Alice Coburn
Programme and Committees Officer
- Eliza Heng
Educational Programmes Assistant - Maimuna May
Communications and Operations
Director of Communications and Operations
- Annette Heninger
Marketing and Communications Officer
- Pujarini Basu Nadaf
Membership and Governance Officer
- Natasha Wainwright
Publications and Web Officer
- Nick Dunwell
Finance
Director of Finance - Liz Fry
Finance Assistant - Hayley Ly
Events and Specialist Societies
Head of Events - Charlie Silva
Events Coordinator - Venease Morgan
Events and Fundraising Assistant
- Emma Warwick
UKSSB Executive Assistant - Henry Dodds
Copyright© 2024 by the BOA. Unless stated otherwise, copyright rests with the BOA. Published on behalf of the British Orthopaedic Association by: Open Box M&C
Advertising
All advertisements are subject to approval by the BOA Executive Board. If you’d like to advertise in future issues of the JTO, please contact the following for more information:
Mandy Boyle - Media Manager
Email: Mandy@ob-mc.co.uk | Telephone: +44 (0)121 200 7820 Open Box M&C, Premier House, 13 St Paul’s Square, Birmingham B3 1RB
Disclaimer
The articles and advertisements in this publication are the responsibility of the contributor or advertiser concerned. The publishers and editor and their respective employees, officers and agents accept no liability whatsoever for the consequences of any inaccurate or misleading data, opinions or statement or of any action taken as a result of any article in this publication.
BOA contact details
The British Orthopaedic Association, 38-43 Lincoln’s Inn Fields, London WC2A 3PE
Telephone: 020 7405 6507
How to contact JTO
Email: jto@boa.ac.uk

From the Executive Editor
Deborah Eastwood
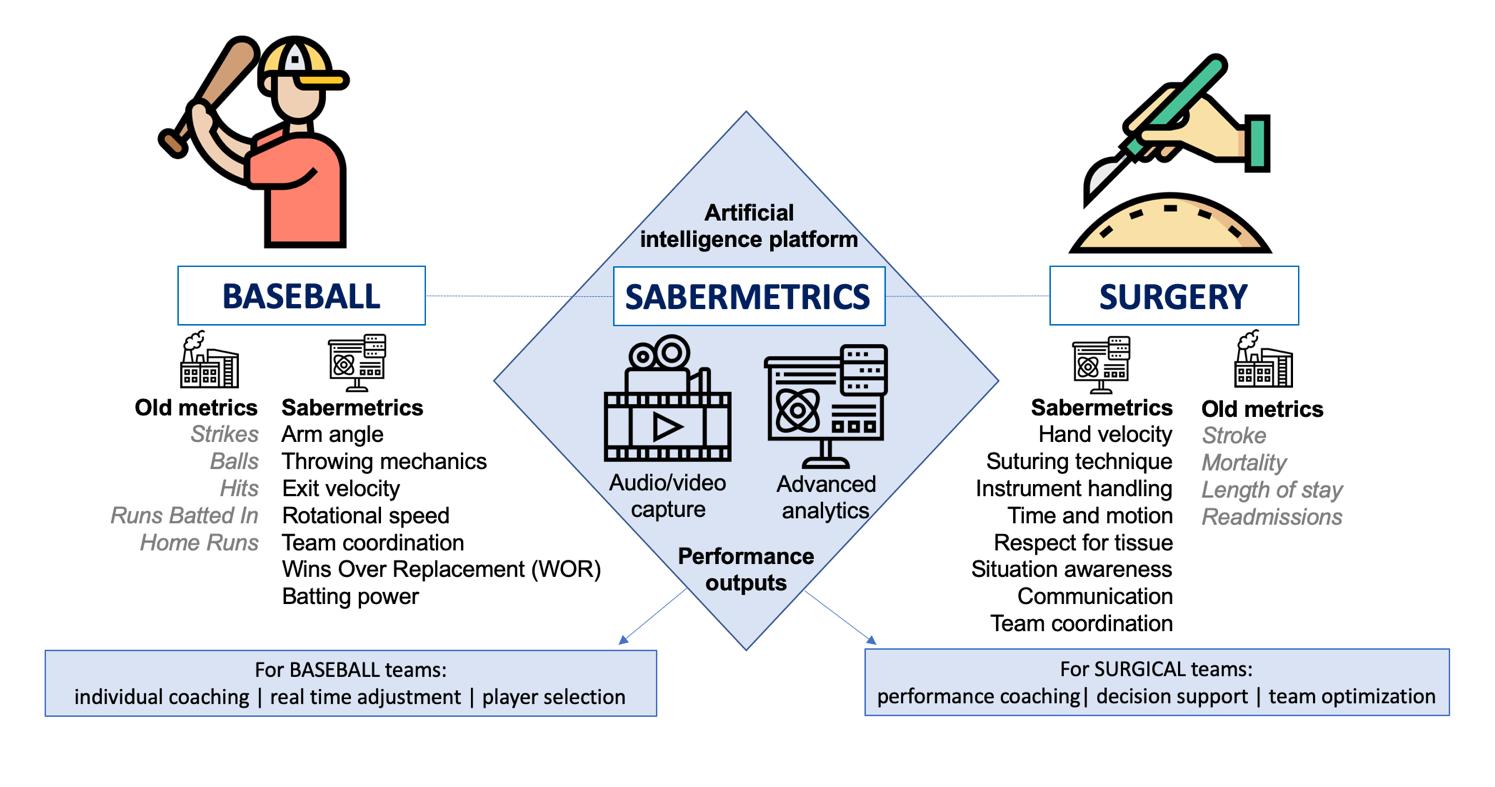
The hard work continues as spring turns into summer and whilst often the thrust of the work is in dealing with numbers: numbers on the waiting list, the percentage theatre utilisation, numbers of overbookings, underutilisation etc., our energy should perhaps be directed to the field of human factors. The complex field of human factors as introduced by James Tomlinson can take up much ‘head space’ as depicted in the cover picture by Chryssa Neo, a ST3 in Edinburgh, but it is a recognition of these factors and their importance that does indeed make us human. An understanding of their relevance makes life safer for our patients (page 46) and for ourselves. An appreciation of diversity in design and the ergonomics of our workplace is also important (page 50) whilst Steven Yule introduces us to a whole new ball game (for me anyway) called surgical sabermetrics (page 53).
If human factors are important at home, they certainly must be so in the different and often challenging environments encountered during global surgery initiatives supported by our impressive trainees (page 38) and whilst running the Mercy Ships orthopaedic missions as described by Rachel Buckingham (page 34).
The kids I treat often ask for their pins and plates to take home with them for ‘show and tell’ at school, and I was interested to read about the current guidance on ownership and/or disposal of removed implants (page 42).
This edition of JTO also includes an introduction to the ‘new’ specialty of kids knee surgery (page 18) and reminds us that obesity must not be an exclusion to care that can transform lives (page 22). Perhaps for both paediatric knee conditions and obesity related problems, prevention is better than cure and certainly the remit of the fracture liaison services is to do just that – reduce the risk of secondary fractures. Andrew Gray comments how he himself is at risk of falls and what the services can do to help him and many of our patients! (page 16).
Teaching and training are always important aspects of our profession but we need to take care that we do not simply jump on each new bandwagon that passes by without evaluating whether or not it is going to be useful. The article by Kapil Sugand and Hiro Tanaka offers us some guidance on the role of simulation in formal orthopaedic training (page 26). Andrew Coppola and Vipin Asopa provide a similarly reasoned approach to the use of AI in Trauma and Orthopaedics and how it is affecting us now.
Remembering where we have come from should always be part of working out where we are headed. So it is fitting what whilst we embrace the excitement of the brave new world of technology that we are participating in, we remember the role of John Kirkup as the BOA archivist for many years as well as an orthopaedic colleague of note (page 56).
Whilst the world does remain in some turmoil, I hope that the summer brings the opportunity for a holiday with friends and family n
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 03
Credits


Workforce and productivity
Simon HodkinsonIt is with great pleasure that I welcome you to this latest edition of the JTO. One hopes by the time this edition drops on your mat we will be experiencing a flaming June but as I write this piece it’s once again pouring here on the South Coast after the obligatory four days of hot weather in May. Our world of orthopaedic surgery is never quiet, as the last few months have shown.
There has been much discussion around the issue of Physician Associates (PAs) and their place in trauma and orthopaedic surgery. The BOA, along with other surgical specialties, has been participating in a process organised by the joint Royal Surgical Colleges to develop a scope of practise for PAs working in surgery. The BOA Council in April considered a paper produced by a BOA short life working group as a basis for the scope of practice for PAs working within T&O surgery.
Currently this document remains confidential whilst it is considered by the Royal College of Surgeons England, but we hope the full scope of practice document – informed by the BOA paper – will be published shortly by the joint Royal Surgical Colleges.
However, as I made clear in a statement published on the BOA website, the BOA will not support any situation where the use of non-medical qualified personnel adversely impacts on the experience and training of our junior colleagues at whatever level.
As many of you are aware, training and trainees are a particular interest and concern of mine. The thread through this year’s Congress will focus on many aspects of training and retention of surgeons within T&O surgery.
I am aware of the main concerns of the British Orthopaedic Trainee’s Association and a BOA short life working group have been formed to evaluate these concerns and to identify solutions. This group will report back at this year’s Congress.
Amanda Pritchard, NHS Chief Executive, a few weeks ago presented NHSE’s latest plans for improving working lives of our junior colleagues. Addressing these issues are an essential part of assuring the future stability of our profession.
At the Royal College of Surgeons of England recently, Amanda Pritchard also told the assembled surgical audience that the government needed more of us. Whilst that means we must retain who we have, we must make a postgraduate career in surgery, T&O in particular, an attractive and viable proposition to all young doctors.
I have met the new National Clinical Director (NCD) for Musculoskeletal (MSK) services, Dr Lesley Kay, Consultant Rheumatologist. We have many shared concerns, and the BOA looks forward to working with her over her tenure as NCD. I would urge you to read the article in this edition on fracture liaison services as she was one of the prime movers in setting this service up but currently only 50% of the UK is covered by such a service.
The BOA is supporting the Royal Osteoporosis Society campaign to secure universal access to fracture liaison services. The BOA has been present at a series of national and local meetings regarding the integration of primary and secondary services for patients with MSK pathology, 20 million in the UK, with 10 million suffering from arthritis in one or more joints.
There are some excellent models of two-way collaboration in the UK many of which have been presented to us but still in many parts of the country there is silo working and this does not help patients. Productivity is a real issue for all of us and if we are to increase the efficiency and effectiveness of available resources across primary, community and secondary care we must have collaboration.
Within our own environment there is a lot we can do to improve productivity, but it does not all rest with us surgeons and we will continue to argue for improvements across the board in theatres and outpatient departments in terms of staffing and facilities.
The best practice pathway for non-ambulatory fragility fractures will have been launched by the time of this edition and the start of the orthopaedic trauma registry is imminent and surgeons will soon receive details of the login process.
Finally, I have had several meetings with the team behind NCIP. The BOA has had some concerns regarding who has access to the data, but it is a valuable tool, and we completely support the process. The team understand the concerns we have raised and have made it clear that NCIP is not a performance management tool. I believe it will become more and more valuable to us all in time and I urge you to look at your data and see what the platform can offer.
Finally, I hope you all have as happy a summer as you can and who knows the sun might shine! n
From the President

Deborah Eastwood elected to the RCS England Council
Congratulations to our Immediate Past President on her election to the Royal College of Surgeons of England Council. She will begin her term this July.
You can read her statement on the RCS England website at: www.rcseng.ac.uk/ news-and-events/news/archive/welcomeelected-council-members-2024
BOA Educational Courses

The BOA runs a wide range of courses under the Education Committee. These courses cater to the educational needs of a wide range of members (and nonmembers in some cases) at all stages of their careers. Upcoming courses include:
Training Orthopaedic Trainers (TOTs)
The underlying premise of TOTs is that if T&O trainers understand how people learn and how the T&O curriculum works, by translating that understanding into action, they should be able to improve their teaching. Much of the work can be done at a time, place and pace convenient to participants, with attendance at live virtual meetings to supplement personal learning. TOTs courses will last for approximately six weeks.
The next Training Orthopaedic Trainers Course (TOTs) is scheduled to begin on Friday 20th September 2024, full course details can be found at: www.boa.ac.uk/TOTs-Friday
Law for Orthopaedic Surgeons
The course covers topics of surgical relevance including consent, clinical negligence, MPTS hearings and the GMC, court etiquette, coroner’s court, confidentiality, data protection and messaging apps, gross negligence manslaughter, and the pitfalls of social media.
The next Law for Orthopaedic Surgeons course is scheduled to take place on Friday 20th September at the BOA Annual Congress in Birmingham. Full details can be found at: www.boa.ac.uk/law-for-orthopaedic-surgeons-Friday
Congratulations to new ASSL Leads
The BOA are pleased to welcome three new Associate Surgical Specialty Leads! Our warmest congratulations to Chris Bretherton (Adult Trauma), Abhinav Singh (Paediatrics) and Luke Farrow (Adult Elective). These new aSSLs will support the activities of the existing Surgical Speciality Leads in Orthopaedic Surgery who are Professor Xavier Griffin (Adult Trauma), Professor Dan Perry (Paediatrics) and (Adult Elective currently under recruitment).
GIRFT NAFF pathway
A webinar discussing the GIRFT’s newly published Non-Ambulatory Fragility Fracture (NAFF) pathway was hosted by Professor Tim Briggs and BOA past President Bob Handley on Tuesday 21st May. This guidance focuses on the importance of ensuring all NAFF patients are given equitable access to care. You can watch a recording of the webinar at: https://youtu.be/gSOeOTVjL9Y
2024 New Year Honours
In the March edition of JTO, we listed those in the orthopaedic community award New Year Honours. We made an omission and would also like to recognise:
Richard Power, Orthopaedic Surgeon, University Hospitals of Leicester NHS Trust, Health Action Leicester in Ethiopia, was awarded an MBE for services to Health in Gondar, northern Ethiopia.
UK and Ireland In-Training Examination (UKITE)
The dates for this year’s UKITE are 6th to 13th December 2024. The UKITE is an online annual assessment that allows trainees of all grades to practice for Part 1 of the FRCS (Tr and Orth) examination, with similar formatted questions based on the UK and Ireland T&O Curriculum. Information on UKITE is available on the BOA website at: www.boa.ac.uk/ukite.
FLP applications
Applications for the next round of the popular Future Leaders Programme are open but will close by 23:59 on Tuesday 18th June 2024.
Further information on the programme and how to apply can be found at: www.boa.ac.uk/FLP-applications
06 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Latest News

King Charles III has retained his Patronage of the BOA
The BOA is delighted to have received confirmation that His Majesty King Charles III has retained his Patronage of the Association. This follows a review of Royal Patronages and the announcement has been made by Buckingham Palace to mark the first anniversary of Their Majesties’ Coronation.
Simon Hodkinson, President of the BOA: “The BOA has been honoured to have the patronage of His Majesty King Charles III for over 30 years. Since its foundation in 1918, the BOA has sought to drive advancements in patient care and we are proud of the recognition by His Majesty of the life transforming difference that trauma and orthopaedic surgery can make. Through professional standards, education, training and research the BOA strives to contribute to the overall medical and surgical knowledge and best practice, leading to faster recovery, increased mobility and an enhanced quality of life”.
New Speciality Standard (SpecS) on PJI published
A new Speciality Standard (SpecS) on Peri-prosthetic Joint Infection by the BOA, BESS, BHS, BOFAS, BASK and BSSH has been published. Initial management is considered in the relevant BOASt and the purpose of this document is to advise on the definitive management, irrespective of anatomical site. The PJI SpecS can be viewed and downloaded at: www.boa.ac.uk/SpecS-PJI
The purpose of BOA Speciality Standards (SpecS) is to compliment the BOASt suite of documents. Whilst the BOASts tend to provide standards on emergent management of critical conditions or key aspects of pathways and processes relevant to the orthopaedic community as a whole, the SpecS provide more specific advice on index conditions over a longer period according to recommendations from appropriate experts. Where feasible, they will be based on existent consensus documents or published literature and are intended to provide an auditable set of standards, but not act as a definitive description of management. SpecS will be the remit of individual specialist societies and will typically run to two to three A4 pages and will be colour coded to ensure that they can be easily distinguished from a BOAST.

Professor Peter Giannoudis awarded an MBE


Former BOA trustee Professor Peter Giannoudis was awarded an MBE in the 2024 New Year’s Honours and we had the pleasure of joining Peter at a reception in April to celebrate the event.
Peter was awarded the MBE in recognition of his services to Trauma and Orthopaedic Surgery. Alongside his work as Professor of Trauma and Orthopaedics, University of Leeds, Peter is Editor in Chief of Injury, Chair of Global Research Commission at the AO Foundation, President of ESTROT Society and President and founder of the charity, Day One Trauma Support. Formed in 2014, with the support of his patients, with the ambition of helping trauma patients through their recovery and to rebuild their lives. Day One has gone from strength to strength with the vision of expanding to major trauma centres across the UK. The BOA is delighted that Peter has been recognised in this way.
UK 5-year action plan for antimicrobial resistance
The UK 5-year action plan for antimicrobial resistance 2024 to 2029 has been published by the UK government. The plan will commit the UK to reducing its use of antimicrobials –such as antibiotics, antifungals and antivirals – in humans and animals, strengthen surveillance of drug-resistant infections before they emerge and incentivise industry to develop the next generation of treatments.
The plan commits to continue to innovate through initiatives such as expanding the world-first ‘subscription model’ for antimicrobials, which was launched in 2019 as a pilot. This will see more companies paid a fixed annual fee for antimicrobials based primarily on their value to the NHS, as opposed to the volumes used. The policy paper can be viewed at: www.gov.uk/government/publications/uk-5-yearaction-plan-for-antimicrobial-resistance-2024-to-2029
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 07 Latest News
BOA Chatterjee travelling fellowship report
Isecured a Major Trauma fellowship at Auckland City Hospital (ACH) under Bruce Twaddle. With the support of the BOA Chatterjee Travelling fellowship, I could make this a reality, bringing my family. I had two aims for fellowship: increase my surgical exposure to trauma, gaining skills and concepts that I could not at home, and to work in an environment comparable to the NHS, to identify solutions to our common problems.
My first words for anyone contemplating an international fellowship is that the orthopaedic surgery will be the easier aspect of your year. Do not underestimate the amount of paper work, medical council interviews, visa applications and of course if you have children, the challenge of getting them to sit quietly on a 30-hour flight!
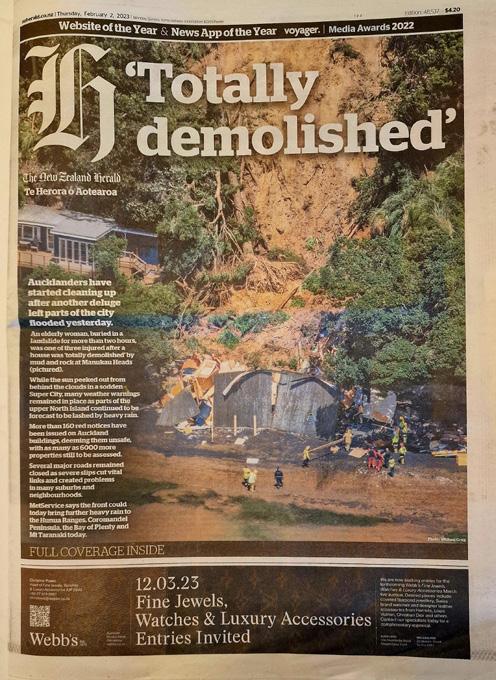
Within my first month, New Zealand and Auckland had endured catastrophic flooding, over a thousand landslides and a tropical cyclone. My first on-call patients were from the aftermath of Cyclone Gabriella and required emergency surgery. The lack of national orthoplastics or open fracture management guidance made me appreciate the resources and guidelines from the BOA and MTN!
 Sabina Barbur
Sabina Barbur

I then undertook a mixed public / private fellowship at the Tauranga and Grace Hospital for a further six months to pursue my subspeciality trauma interests. It was an opportunity to be educated in complex upper limb trauma and lead in a senior role within an orthopaedic department.
The first obvious difference in NZ is the ‘No-fault compensation’ system, allowing freedom for training and independent operating at a more junior level. This independence creates a more effective trauma service. Secondly, Accident Compensation Corporation (ACC), additional to state-funded health care, provides rapid investigations and treatment options for patients as the entire patient pathway can be conducted privately at a pre-agreed ACC price.
My final insight and change which I have taken from 15 months abroad was the need to make medical care more sustainable and the environmental impact the medical industry has on the local land, the loss of biodiversity surrounding hospitals, pollution and the cumulative effect on the climate. This fellowship experience has been worth every effort required to make it happen. n
British Limb Reconstruction Society (BLRS) update
Simon
Britten, BLRS PresidentBLRS members enjoyed another highly successful annual conference in Glasgow in March this year, expertly planned and delivered by our friends and colleagues Bilal Jamal, David Rowland, Chris Crome and David Shields. Outstanding international guest speakers included Steve Quinnan (Miami – cable transport, percutaneous wedge osteotomy for deformity correction and lengthening), Austin T Fragomen (New York – sustained compression nailing for non-union, osteotomies around the knee, management of rotational deformity), and Nando Ferreira (Cape Town – temporary fixation in the traumatised ankle joint). The BOA address to the BLRS conference was kindly delivered by BOA Vice President Elect, Fergal Monsell, who was beamed into western Scotland from south west England. Congratulations to the winners of the best free paper podium presentations – Natasha Brown (first) and Jerry Tsang (second) – and to the two joint best poster prize winners Rebecca Tunbridge and Tareq Tareef.


of the society. We agreed to bring more clarity to the BLRS Trustee role, and consider the possibility of taking on lay trustees to bring specific experience to the table. It was also agreed to look into the development of the currently dormant Honorary Member category, to recognise significant contributions from some of our senior members, who have developed both the sub-specialty of limb reconstruction in the UK and also helped to fashion our society since its inception in 1997.

At the AGM, we agreed to recruit an additional two Members at Large to the Executive Committee, to further widen participation in the decision-making and administration
The BLRS funds research grants via our research committee, headed by Hamish Simpson, soon to hand over the reins to Alex Trompeter. We also fund travel bursaries for consultants, trainees and nursing / AHP members; and we fund two places each year on the BOA Future Leaders programme. We continue to sponsor and badge limb reconstruction courses nationally.
Planning is underway for the BLRS sessions at the BOA Congress in September, including a joint session with colleagues from BOFAS, and we continue to collaborate with BOTA to develop trainee educational sessions in limb reconstruction. The BLRS welcomes applications for members in the following categories – consultant, trainee, nursing / AHP, and overseas. n

08 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
News
Auckland City Hospital
Images with permission from Clockwork Medical
Beard IM Nail Guide Wire Clamp
Designed by David Beard, MD



Designed to help provide quick grasp-and-release of an IM guide wire for positioning and advancement along the length of the guide wire
 Designed by David Beard, MD
Designed by David Beard, MD
Subtrochanteric Femur Fracture Reduction Clamp
Designed with a unique contour, the clamp helps with subtrochanteric and femoral shaft fractures treated with current generation femoral IM rodding systems using external aiming arms/targeting devices


Browner MIS Bone Clamp
by Bruce D. Browner, MDDesigned to help hold a bone or bone plate for fixation, the clamp is inserted anterior to the bone, rotated to wrap around the bone, then screwed into the desired position


Extended Drill Sleeves


Periarticular Reduction






Chandran Double Ball Spike
Designed to help rotate and control a butterfly bone fragment for fixation
 Designed
Designed
Designed by
Prototype Shown
Rama E. Chandran, MD
Designed by Reza Firoozabadi, MD Designed to help reduce fractures when k-wires are passed through, the extra long drill sleeve helps to protect soft tissues and prevent the need for stacking two drill sleeves when pushing a fracture fragment to assist with fracture reduction Sleeve can be used as a reduction aid with placement of a kirschner wire through sleeve Collaborated tips which allow placement of appropriate size drills for lagging by technique — as an example a 2.5 end will fit into a 3.5 drill hole #8027 2.4/1.8 mm #3014-01 2.7/2.0 mm #3014-02 3.5/2.5 mm #3014-03 Set #3014-00 Also Available Individually #3850 #1379 Large #1857 Clamp without Ratchet #3019-01 Medium #1856 Small #1856-01 Guide wire not included. Clamp with Ratchet #3019
Designed for reduction of intraarticular and periarticular fractures Cannulated
Helps to reduce fractures without slipping off the bone, and cannulated to allow the placement of k-wire #8091 FREE TRIAL ON MOST INSTRUMENTS 1.800.548.2362 103 Estus Drive, Savannah, GA 31404 info@innomed.net 912.236.0000 Phone 912.236.7766 Fax Innomed-Europe Tel. +41 41 740 67 74 info@innomed-europe.com © 2024 Innomed, Inc. ISO 13485:2016 www.innomed.net Innomed-Europe Alte Steinhauserstrasse 19 CH-6330 Cham Switzerland Tel: +41 (0) 41 740 67 74 www innomed-europe com UK Distributor: Hospital Innovations Ltd Concept House Talbot Green Business Park Pontyclun UK CF72 9FG Tel: +44 1443 719 555 www hospitalinnovations co uk
Forceps
Fracture Awl
British Society for Children's Orthopaedic Surgery (BSCOS) update
William Guy Atherton, BSCOS PresidentThis year BSCOS is celebrating its 40th birthday! In celebration, Simon Barker, Past President has written, edited and organised publication of an excellent book covering the history of children’s orthopaedics and the formation of BSCOS in 1984. It also includes interesting chapters on the current work of the Society and even a ‘Rogues Gallery’ containing pictures of past and current members.
Each member of BSCOS was given a copy of the book at our Annual Meeting hosted by Laura Deriu and colleagues in Leeds in March this year. The Meeting was based on a theme of the Paediatric Foot and benefitted from an excellent National and International Faculty including Vince Mosca and Jim Wright from North America along with the experiences of Alaric Aroojis and Viraj Singhade from India, attending as part of our new memorandum of understanding with POSI (Paediatric Orthopaedic Society of India). The bar was indeed set high for our visit to Brighton in March 2025!
Other activities this year included a hugely popular revalidation session at the BOA Annual Meeting in Liverpool in 2023. For those who were unable to get in, we have been allocated a bigger room for Birmingham 2024 and will be running a joint session with BESS on upper limb topics crossing between children and adults as well as repeating our ever-popular Trainee’s session with talks on core topics, sawbones stations as well as clinical assessment practice with volunteer children and young people.
Putting that alongside another successful Current Concepts Course, the amazing work of our Education and Research sub-committees and the launch of our new website it is truly an exciting time to be part of BSCOS. Roll on the next 40 years! n

British Hip Society (BHS) update: Shaping the orthopaedic workforce of tomorrow
The British Hip Society (BHS), like many other specialist organisations, recognises the critical role that diversity plays in shaping the future of orthopaedic surgery. Diversity among surgeons transcends mere representation; it is a cornerstone enriching clinical care, enhancing patient outcomes, and driving innovation in surgical practices. Attracting doctors to explore orthopaedic surgery from the outset is vital. Presently, the diversity we observe in medical students does not sufficiently translate to those considering orthopaedics, and consequently hip subspecialisation.

Sustained engagement with medical students is pivotal for fostering long-term diversity. Since the inception of the BHS Culture and Diversity committee, the BHS has always incorporated medical student representation and offers students free membership to the society. This year ongoing efforts culminated in the second BHS Future Hip Surgeons Stream,
developed alongside the British Orthopaedic Medical Students Association, at the annual BHS Congress 2024 in Belfast. We provided 20 medical students sponsored attendance, and the event featured insightful talks, cutting-edge hip arthroscopy and virtual reality workshops. Challenging stereotypes is crucial, and we felt it was important to offer hands-on experience, enthusiasm, and encouragement through mentors and facilitators from diverse backgrounds. New for 2024, the one-to-one speed mentorship stream was an opportunity for students to discuss their aspirations, work-life balance, and gain valuable insights into the brilliance of an orthopaedic career.

This year, the BHS introduces two £750 bursaries to support medical student electives in hip surgery in the UK or abroad. Applications will be open from 1st June to 31st September 2024, with interviews held in October 2024. We urge you to encourage your students to apply for both the bursary and BHS membership. To follow our progress on improving diversity and inclusivity, visit the BHS website (www.britishhipsociety.com), engage with us on social media, and visit us next year at #BHS2025 in Harrogate! n
Naomi Gibbs, BHS Culture & Diversity Chair, and Shivam Kolhe, past BOMSA President10 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk News
The British Society for Surgery of the Hand (BSSH) update
Charlotte Smith, BSSH Secretariat
BSSH 2024 Spring Scientific Meeting
The BSSH Spring Congress took place on 25th – 26th April at the Royal Armouries Museum, Leeds where welcomed our guest society the Scandinavian Society for Surgery of the Hand. The collaborative programme covered operative challenges, socioeconomic aspects of hand and upper limb conditions and current knowledge of nerve injury, repair and regeneration.

BSSH Instructional Course in Hand Surgery (ICHS)

The first course in series 9, Soft Tissue Reconstruction, Burns and Infection is taking place on 7th - 8th June 2024. You can find the full programme and register at: www.bssh.ac.uk/about/events/4697/ichs_91__soft_tissue_ reconstruction_burns_and_infection
Over a three-year period our series of two-day courses cover the entire syllabus in hand surgery. Each course explores a subject area in depth with innovative teaching combining lectures, small group tutorials and simulation.
Date
Course
7th – 8th February 2025 Fractures and Joint Injuries
6th – 7th June 2025 Inflammatory and Degenerative Arthritis
6th – 7th February 2026 Dupuytren’s, Children’s Hand Surgery & Tumours
19th – 20th June 2026 The Wrist
5th – 6th February 2027 Nerve and Tendon
The BSSH wishes to thank our platinum sponsors for this series of courses: Acumed and Sovereign Medical.
The British Association
Aprajay Golash, BASS President
BSave the date: BSSH Autumn Scientific Meeting 2024

Join us on 14th - 15th November 2024 at the International Convention Centre (ICC) in Belfast, Northern Ireland where we welcome our guest society Die Deutsche Gesellschaft für Handchirurgie.
Abstract submission is now open, to find out more visit: www.bssh.ac.uk/ about/events/4622/bssh_autumn_scientific_meeting_2024
Lilongwe Hand Unit
Volunteers from the BSSH and British Association of Hand Therapists (BAHT) are collaborating with staff at the Lilongwe Institute for Orthopaedics and Neurosurgery (LION) in the delivery of treatment for elective and traumatic conditions of the hand in Malawi.


Scan the QR code to find out more about this exciting project.

t General Anaesthetic Operating in Main Theatres. ScrubbedSoren Sjolin (BSSH Orthopaedic Consultant) and Kajal Gohil (BSSH Plastic Surgery Registrar). First stage flexor tendon repairsilicon rod insertion. Observed by four Theatre Staff. n
of Spine Surgeons (BASS) update
ASS had a very successful conference at Bournemouth, 20-22 March 2024, which was organised by the spinal unit at Southampton. This was preceded by a masterclass on Spinal infections. Guest lectures were delivered by well-known international faculty and were well received by the audience. The meeting also provided political updates in relation to spinal surgery. Developing international links is a key focus for the BASS education program. Two international sessions, from the South Korean and Indian Spinal societies, were also held and gave a different flavour to the management of a number of spinal conditions.

BASS is actively involved in promoting women in spinal surgery and focusing on improving diversity in the Spinal community. The Society continues to support development of future leader program and research in spinal surgery. n
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 11 News
Conference Listing 2024:
WOC (World Orthopaedic Concern) www.wocuk.org 7 June 2024, Sheffield
BAJIS (Bone and Joint Infection Society) www.bajis.org.uk
13-14 June 2024, Gateshead
SBPR (Society of Back Pain Research) www.sbpr.info
13-14 June 2024, Aberdeen
BESS (British Elbow & Shoulder Society) www.bess.ac.uk
19-21 June 2024, Aberdeen
BOOS (British Orthopaedic Oncology Society) www.boos.org.uk
27-28 June 2024, Cardiff
OTS (Orthopaedic Trauma Society) www.orthopaedictrauma.org.uk 27-28 June 2024, Nottingham
BIOS (British Indian Orthopaedic Society) www.britishindianorthopaedicsociety.org.uk 5-6 July 2024, Newcastle
BORS (British Orthopaedic Research Society) www.borsoc.org.uk 9-10 September 2024, Sheffield

BOA (British Orthopaedic Association) www.boa.ac.uk
17-20 September 2024, Birmingham
BOSTAA (British Orthopaedic Sports Trauma and Arthroscopy Association) www.bostaa.ac.uk
7 November 2024, Twickenham
BSSH (British Society for Surgery of the Hand) www.bssh.ac.uk
14-15 November 2024, Belfast
BTS (British Trauma Society) www.britishtrauma.com 20-21 November 2024, Bristol
BSS (British Scoliosis Society) https://britscoliosis.org.uk 21-22 November 2024, Birmingham
BOTA (British Orthopaedic Trainee Association) www.bota.org.uk 26-29 November 2024, Manchester
BOFAS (British Orthopaedic Foot & Ankle Society) www.bofas.org.uk
29-31 January 2025, Brighton
BRITSPINE www.BritSpine.com 12-14 March 2025, Manchester

12 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
News
BOA Congress 2024, ICC Birmingham
BESS Annual Conference 2024, P&J Live, TECA, Aberdeen
Joint Action Update
We would like to offer a huge thank you to our TCS London Marathon runners and Ford Ride London riders 2024. Our amazing teams have raised nearly £20k so far for the Joint Action appeal of the British Orthopaedic Association, far surpassing their fundraising target! These vital funds supporting research into musculoskeletal conditions will help transform lives and give people back their freedom and independence.
There are over 20 million people of all ages in the UK living with a musculoskeletal condition and over 20,000 people are impacted by major trauma every year; that’s about one third of the population.
As a charity, we strive to transform the lives of those impacted by musculoskeletal conditions and injuries by funding research and innovation across Trauma and Orthopaedics. Developing a robust clinical research infrastructure goes hand in hand with the BOA mission of Caring for Patients, Supporting Surgeons and our Joint Action appeal provides dedicated funds to achieve this through activities like Clinical Trials and Research Fellowships.
Further information and how you can donate can be found on the Joint Action webpage at www.boa.ac.uk/joint-action






JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 13 News
John McKinley
Treatment Stretcher Discover the newest addition to the QA3 range today. sales@aneticaid.com +44 (0)1943 878647 www.aneticaid.com
Emily Baird
Traceyanne Hughes
Alex Chipperfield
Natalia Mojica
BOA Annual Congress 2024
17th – 19th September, ICC Birmingham
www.boa.ac.uk/Congress

Programme update
The theme for this year’s flagship event will be ‘Recruit, Sustain, Retain: The T&O Work Force’, taking place from 17th – 19th September at the ICC, Birmingham.
The BOA’s Presidential Guest Lecture will be presented by Dr Ann Van Heest, President of the American Orthopaedic Association (AOA) and John McFall, British Paralympic sprinter and ESA Astronaut Reserve, will deliver this year’s Howard Steel Lecture. The Robert Jones Lecture will be delivered by Professor Deborah Eastwood.
We will once again be working closely with the specialist societies to deliver a mix of revalidation and hot topic sessions. The full details of the programme can be found on the Congress website at www.boa.ac.uk/programme
Guest lecturers

Dr Ann Van Heest, Paediatric Orthopaedic Hand Surgeon and President of the American Orthopaedic Association
Dr Ann van Heest is a professor, vice chair of education, and residency program director in the department of orthopedic surgery at the University of Minnesota. She trained at the University of Minnesota for medical school and orthopedic surgery residency, as well as the Harvard hand and upper extremity fellowship.

Registration
John McFall, Orthopaedic Registrar, Wessex Deanery and ESA Astronaut Reserve
In November 2022, John was selected by the European Space Agency with the aim to become the World’s first astronaut with a physical disability.
Registration is now open (for both BOA members and non-members). BOA members can take advantage of one of their membership benefits and register with a 100% discount on the ticket fee for an extended time period. Full details can be found on the Congress website at www.boa.ac.uk/registration.
Accommodation
Book your exclusive accommodation rates online, through BCD M&E with HotelMap, the BOA Annual Congress 2024’s official hotel booking partners. Find out more at www.boa.ac.uk/accommodation.
BOA App
Make sure to download the BOA App to access the BOA Annual Congress programme, and other event information to make the most of your experience before, during and after the Congress. Available to download from the Apple App Store and GooglePlay.
Please keep an eye on the BOA website over the upcoming months for updates on the programme, speakers, sponsors, travel, accommodation and more, www.boa.ac.uk/Congress
If you have any questions regarding this event, please contact the BOA Events Team, events@boa.ac.uk.
Exhibition and Sponsorship Opportunities
Thank you to all our Industry Sponsors at this year’s exhibition. We are delighted to welcome over 80+ exhibitors, including our Diamond and Platinum sponsors – Heraeus Medical GmbH, IBSA UK, Smith & Nephew, along with our Gold sponsors Getinge, Medacta, Orthofix, Summit Medical IGEA Medical & All Aces Medical Couriers.
Exhibition stand spaces are still available but are selling fast! For further information about our sponsorship and exhibition opportunities please contact our exhibitions team, exhibitions@boa.ac.uk / 020 7406 1754 or visit www.boa.ac.uk/exhibition-sponsorship
Abstract and Innovation Theatre
New for this year, the 2024 selected abstracts will be presented in the Abstract and Innovation Theatre in the Exhibition Hall. With over 800 abstracts submitted, there will be presentations from healthcare professionals from across the UK and overseas on a wide range of orthopaedic topics.
Also, join us in the Abstract and Innovation theatre and discover the latest innovative products and solutions to the market. We have a great line-up planned, with sessions from Bioventus and others. Register and join us! Limited spaces are available and seats are on a first come first serve basis. Visit our website for further details at www.boa.ac.uk/ abstract-innovation-theatre n
14 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk News
#BOAAC24
An update from the International Orthopaedic Diversity Alliance (IODA)

The International Diversity Alliance (IODA) is an international collaboration of surgeons and those working in the industry, with a vision for a global orthopaedic culture in which everyone can thrive, by championing equity, diversity and inclusion in orthopaedics worldwide.
IODA was launched in late 2019 by Australian Surgeon Jennifer Green, who became the second President and is the current immediate Past President. The first President was American Surgeon, Kristy Weber, who is also the ex-President of the AAOS 2019-20. Current President is Mari Thiart, a South African Surgeon and founder of their female orthopaedic surgeon’s society, SAFOSS.
IODA has been involved in various initiatives in the last year, many involving the UK, which are outlined in this update. All our initiatives can be read about in our member newsletters (www.orthopaedicdiversity.org/newsletters).
Membership to IODA is free and open to all in the healthcare sector by signing up at www.orthopaedicdiversity.org/register
IODA’s Charter is a declaration of commitment to promoting DEI in the speciality by developing a strategic plan, regular reporting on progress on set objectives, developing a Board reflective of its strategic goals, developing and providing leadership opportunities and mentorship to under-represented groups, and creating a sense

of belonging in meetings and in teams. The Charter has been signed by 31 signatories to date, including the Bone and Joint Journal, BHS, BOA, BOFAS, BOTA and Scottish Committee for Orthopaedics and Trauma. At the start of 2024, IODA surpassed 1,400 members globally – approximately 30% growth in the last calendar year. It is hoped this trend continues.
Kristy Weber, Past President of IODA and the AAOS, visited the BOA conference in September 2023, alongside then Canadian Orthopaedic Association President Laurie Hiemstra and American Orthopaedic Association President Professor Ann Van Heest. Kristy gave a very insightful and inspirational keynote address and contributed to a panel discussion on diversity.
The National Orthopaedic Alliance (NOA) Conference, sponsored by Stryker, took place in October 2023. IODA Secretary and arthroplasty surgeon, Samantha Tross, contributed in a DEI panel discussion and as judge for Excellence in Orthopaedics Awards in the DEI Category. The conference showcased the Alliance’s commitment to shaping the future of orthopaedics through a diverse range of sessions covering topics such as the NHS England MSK strategy, orthopaedic nursing, the future of the trauma and orthopaedic workforce, motivating patients to move, Model Hospital and much more.
The IODA inaugural Journal Club (youtube.com/ watch?v=y7-jbEiyebg) took place in January 2024 and was entitled ‘The Science of Diversity’. Two articles, ‘The Racial and Sex Disparities in Resident Attrition in Orthopaedic Surgery’ and ‘The Role of Gender in Operative Autonomy in Orthopaedic Surgical Trainees’ were discussed. Deborah Eastwood, Past President of the BOA, Editor of JBJS and current Second Vice President of IODA took part in the discussions.
Jennifer Green, IODA Past President and hand surgeon from Australia, attended the AAOS Annual Meeting in February this year alongside other IODA members – Matthew Schmitz, former Secretary and First Vice President of IODA; Lorraine Boakye, Journal Club Lead and North American regional representative; and Makena Mbogori, who served as African continent Representative. She attended the Stryker Women’s Network Breakfast and met current BOA President Simon Hodkinson and Fergal Monsell Vice President Elect. We are grateful to have Fergal Monsell serving on the IODA Mentoring Committee.
IODA will have a regular biannual feature in the EFORT newsletter. Please continue to engage with us and join our organisation, membership is currently free. If you are part of an orthopaedic subspecialty group, and see the value of DEI, please consider signing the IODA Charter, declaring that your organisation will make efforts to improve diversity, inclusion and belonging. n

 Kristy Weber and Deborah Eastwood. IODA members including Jennifer Green and Simon Hodkinson at AAOS.
Kristy Weber and Deborah Eastwood. IODA members including Jennifer Green and Simon Hodkinson at AAOS.
Features JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 15
Laurie Hiemstra, Samantha Tross and Ann Van Heest.
The development of regional fracture liaison services
Andrew Gray
Andrew Gray is a consultant with a specialist interest in orthopaedic trauma at James Cook University Hospital. He is an active member of the Fragility Fracture Network and is committed to fragility fracture care and its education, to such an extent that he sustained his first, last year, demonstrating that in terms of secondary fracture prevention, he is a falls risk (on skis and whilst multitasking). Over the past four years, he has co-chaired the Fracture Liaison Service Academy Network (FAN) which is committed to making fracture liaison services more effective.
Fracture Liaison Services (FLS) medically and physically optimise patients thus reducing the risk of secondary fracture after fragility related fractures. Any FLS model involves a committed team of individuals from a range of allied specialties who focus on managing osteoporosis and preventing further falls and fractures in at risk patients.
DEXA or FRAX assessments are the commonly used tools that diagnose osteoporosis and identify the likelihood of recurrent falls and fractures respectively. FLSs are important because they identify the treatment gap that often occurs after osteoporotic fractures where there is frequently a lack of investigation and treatment intervention post injury. This results in a higher (and unnecessary) risk of sustaining further fractures with the associated exacerbation of pain, dysfunction and loss of independence.
Any FLS needs to be efficient and cost effective within our financially restricted NHS. The challenge of justifying the funding to key stakeholders is constant. Ideally, the treatment pathway is streamlined and smooth from acute fracture management through to a secondary fracture prevention plan. The Fragility Fracture Network (FFN) in its 2018 global ‘call to action’1 describes this pathway in terms of the ‘four pillars’, (Figure 1). As orthopaedic surgeons we lead and are mostly involved in ‘Pillar 1’ based around acute fracture management, ensuring gold standard surgical care in terms of timing and type that best enables immediate mobilisation. This is concurrent with early orthogeriatric assessment that is essential in minimising the morbidity and early mortality after major osteoporotic fracture. Hip fractures have been central to this in recent years – however they form only 20% of all fragility fractures and therefore these standards of care need to be more universally applied.

Effective rehabilitation after injury is central to ‘Pillar 2’ with secondary fracture prevention the mainstay of ‘Pillar 3’ whilst the key aspects of ‘Pillar 4’ are the management of local and national policies that can influence and improve the fragility fracture pathway.
When setting up an FLS or improving an existing one there is much to consider in terms of standardising and streamlining the service. The original FLS model designed in Glasgow2 was simple and did not over complicate, (Figure 2). It is worth revisiting 25 years after its initiation in 1999. Fractures were referred to the FLS via set routes either through the fracture clinic or the emergency department.
Features
16 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 1: The ‘four pillars' of Fragility Fracture Care.

In-patients with more severe osteoporotic fractures that required hospital admission were also recruited. The patients were then assessed and treated with categories of treatment that involved treatment of osteoporosis and education and falls prevention. Importantly this treatment plan was then communicated effectively back to primary care to implement the recommendations made.
Important aspects to consider with this model were:
1. It was a doctor light service primarily delivered by clinical nurse specialists who worked with pre-agreed, standardised and evidence-based protocols. They identified, recruited, and assessed the patients.
2. Although orthopaedic surgeons were encouraged to engage, the ‘FLS champions’ tended to be the consultant endocrinologists with a proven interest in treating osteoporosis.
3. Critical to success was the establishment of multidisciplinary stakeholder groups representing all hospital specialities, local primary carers, and the regional health authority groups, i.e., the people who controlled finance and had influence.
4. Audit and data capture was complete.
a. In the first 18 months, 4,600 fragility fracture patients were assessed.
b. 20% of that patient cohort were started on osteoporosis treatment without BMD testing.
c. 75% had bBMD testing of which 80% were found to need treatment – a high pick-up rate with good specificity and sensitivity.
5. During the first 10 years, 50,000 consecutive patients were assessed by this FLS. During that time hip fractures were reduced by 7% versus an increase of 17% in other parts of the UK where local health authorities had not implemented an FLS – an improvement in Glasgow, a city that contains some affluent
areas but also some of the poorest and deprived areas in the country.
6. A far higher proportion of wrist and hip fractures were assessed and treated when compared to other areas of the country that did not have a similar service.
7. Cost-effectiveness was demonstrated – for each 1,000 patients managed by the FLS, 18 fractures (11 hip fractures) were prevented with a significant cost saving to the local health authority.
This simple model was successful because there was a defined team and people who knew their specific roles. There was also an accessible and defined population that could be recruited. The FLS goals and objectives were SMART: Specific, Measurable, Achievable, Realistic and Time dependent.
In developing a regional FLS the product needs to be an improvement upon what already exists. It should identify a high proportion of patients who have sustained a fragility fracture and assess them in a cost effective and time efficient manner using DEXA and FRAX only as needed. Effective multi-modality treatment can then be initiated. Importantly it should have the tools and capability to follow-up and monitor patients.
With any clinical service there are key steps to success in terms of setting up and evolving the service. Firstly, you need to know the important steps in your pathway and be able to monitor their relative impact because any pathway is only as strong as its weakest link. For example, an FLS may be strong at identifying and recruiting patients but if the processes are not in place to investigate and treat patients effectively then the system fails.
Harness and use data. Data trumps opinion but do not get swamped by it. Data should be validated but only the relevant, worthwhile information that will influence improvement and change should be presented to the service group.
Welcome change. Processes should evolve and not remain static. Just because something
is working doesn’t mean to say that it cannot be improved upon. Discuss at an early stage with the people who may be affected by a process change and get their input early to keep them on board. Workshops can provide insight into how processes work in practice and allow people to express an opinion. Consider new possibilities, don’t let legacy processes stifle new ideas.
Test, test, and test again. Test before you implement a change to make sure anything introduced operates effectively in practice. Use a sample population to test and realise that change isn’t always smooth.
Automate. Are there opportunities to do this at key steps – the obvious one with regards to an FLS is patient recruitment. Virtual fracture clinics, emergency department screening, fracture clinics, at risk patient groups available on GP databases, better screening and pick up of vertebral fractures. Automation standardises, reduces pressure on the work force, and saves time and money.
Join forces. Establish a multidisciplinary strategy group from the outset. Agree to assessment and management protocols with all stakeholders. Ensure clear and consistent communication between all the multidisciplinary team.
Summary
1. A streamlined FLS service can help to identify osteoporosis patients at risk of fracture and provide them with the necessary care and treatment to manage their osteoporosis and future falls risk.
2. Effective monitoring and data collection to look at outcome allows the service to improve and evolve.
3. In approaching key players in terms of funding and supporting your regional FLS should emphasise the importance of avoiding health inequality in terms of ability to access a gold standard FLS after fragility fracture. n
References
1. Dreinhofer KE, Mitchell PJ, Bégué T, et al A global call to action to improve the care of people with fragility fractures. Injury 2018;49(8):1393-7.
2. McClennan AR, Gallagher S, Fraser M, McQuillian C. The fracture liaison service: success of a program for the evaluation and management of patients with osteoporotic fracture. Osteoporosis Int 2003;14(12):1028-34.
Features
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 17
Figure 2: Simple fracture liason services (FLS) model.

Rizwan Arshad is the current Child, Adolescent and Adult Knee Fellow at Sheffield Children’s and Chesterfield Royal Hospital. He completed his Specialty training in the North Yorkshire Deanery in 2023.
Kids knee surgery: A new orthopaedic subspeciality
Rizwan Arshad, Sheba Basheer, Dominic O’Dowd, Nicolas Nicolaou and Fazal Ali
Who is performing kids’ knee surgery? We can all agree why that is an important question to ask, but the reality is that no one had considered this until the BASK/BSCOS steering committee published their report on the management of paediatric soft tissue knee pathology. In a modern healthcare system,


where there is a constant drive to centralise and subspecialise services to help improve outcomes, it seems quite strange that prior to this report there was very little information available regarding who is treating paediatric knee pathology.
The drive for subspecialists initially began in the post-world war 20th century era, primarily to help improve outcomes for patients with war related injuries1. Subsequently, subspecialisation has shown to significantly improve patient outcomes and has been a good fit for the modern healthcare model. Breadth of practice has been replaced with depth of practice with more emphasis on a surgeon’s outcome with the underlining principle of ‘getting it right first time’. This being said, paediatric orthopaedic practice in the UK has not quite changed in the same manner as other orthopaedic subspecialties. A paediatric orthopaedic surgeon is still expected to maintain a broad practice when arguably the stakes and the need for better outcomes are much greater than in adults. There are specialist centres in the UK where paediatric subspecialists exist, but their main areas of focus are spine, limb reconstruction, hip preservation and foot and ankle reconstruction. In more recent years, particularly in the USA, paediatric sports knee surgery has become its own entity and is now gaining more recognition across mainland Europe. In the UK, treatment of paediatric knee pathology is primarily provided by adult knee surgeons who have less exposure treating the patient with open growth plates. In addition, techniques are not well supported by the literature as there is a lack of good quality evidence in children.
Features
18 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 1: Hand and wrist radiographs for two different patients both which demonstrate discrepancy between the patients chronological age and skeletal age. The image on the left is a radiograph of a 12 year old who has a bone age of 15 by G&P method. The image on the right is a radiograph of another 12 year old who has a bone age of 10 by G&P method.

Sheba Basheer is the current National Paediatric Orthopaedic Fellow at Sheffield Children’s Hospital. She completed her Orthopaedic higher surgical training on the North Yorkshire Rotation and was the Child, Adolescent and Adult Knee Fellow at Sheffield Children’s and Chesterfield Royal Hospital from October 2022 to October 2023.

Dominic O’Dowd is a Consultant Orthopaedic Surgeon at Sheffield Children’s Hospital and Rotherham Hospital, specialising in paediatric and adult trauma, knee surgery, sports injuries and injury prevention. He has worked as a doctor at the British Superbikes, with periods as Club Doctor for West Ham United and Blackpool Football Clubs. Internationally he has worked as a Doctor at the England FA with the U1619 Men’s squads as well as the Senior Women’s 2013 World Cup Qualifying Campaign. He has undertaken prestigious sports and paediatric fellowships in Australia and New Zealand including the first dedicated Paediatric and Adult Knee Fellowship.
The report that was published by the BASK/BSCOS steering committee in 2021 included the results of a survey which had 255 responses from members of both societies. Of note, 85% of all respondents said they performed fewer than 10 paediatric ACL reconstructions in the preceding year, 25% of paediatric orthopaedic surgeons said they treat paediatric ACL injuries compared with 85% of adult orthopaedic knee surgeons and only half of respondents assess skeletal age of patients pre-ACL reconstruction. Interestingly, the vast majority of respondents felt the current way we managed paediatric ACL and meniscal pathology was not the correct way moving forward2
The general problem
Knee pain in the paediatric population is a common complaint. One in three adolescents will present to their doctor with knee pain3 before we even consider sports related injuries or congenital abnormalities.

Clinical photo of a child with fibular hemimelia. Ligament reconstruction is often performed for a variety of clinical reasons. Commonly it is done for patients prior to limb lengthening to prevent knee subluxation. An increasing number of these patients also express a desire to maintain a certain level of activity which we can, in part, help them achieved with ligament reconstruction.
The incidence of paediatric knee injuries are also increasing worldwide with much more participation in elite level sport. Young girls in particular are taking up contact sports at unprecedented rates due to increased inclusion and undoubtedly influenced by the recent success of our national teams. In 2022, a survey by Sport England revealed that there was an increase of 100,000 more young girls playing football compared to five years prior. Along with this we have seen a rise in paediatric sports related knee injuries which has had an impact on the health service globally. A recent UK study reported a 29-fold increase in rates of paediatric and adolescent ACL reconstructions over the last 20 years4. Managing knee injuries in the paediatric patient presents its own unique challenges. Special considerations need to be made right from the initial consultation. Aside from the obvious anatomical differences in children that need to be appreciated, there is a whole host of psychosocial factors and dynamics that need to be addressed throughout their journey. Post-operative physiotherapy engagement is crucial to the success of surgery. Engagement in children can be challenging and requires specialist physios and tailored protocols. The whole service needs to be tailored specifically for children to improve the chances of success.
Knee pathology in children is not just the adult pathology in smaller dimensions, there are a whole host of conditions that predominantly present in childhood. Congenital conditions can present with fixed dislocations of the tibiofemoral and patellofemoral joints, ligament deficiencies and hypoplastic condyles which can alter the geometry of the mechanical alignment. In addition, conditions such as osteochondritis dissecans, which can also affect the adult population, have a different aetiology and natural history in the skeletally immature population. Management is therefore tailored specifically to these patients. Furthermore, specific complications are unique to the paediatric population and can be as result of disease, injury or surgical intervention. Having the experience and training to be able to deal with these complications is an important part of treating children.
The ACL problem
In recent times, more recognition has been given to the importance of ligament reconstruction in the skeletally immature. Historically the consensus was that young children who suffered ACL injuries could wait until they reached skeletal maturity for surgical management. 40% of the respondents from the BASK/BSCOS survey said they have treated paediatric ACL injuries non-operatively. This was mainly driven by the fact there was very little evidence to show what the long-term outcomes were for children with ligament deficient knees. There was also reluctance from surgeons to intervene surgically as they had little or no experience of reconstructions in the presence of open growth plates. Evidence now clearly shows that ACL deficiency increases the risk of meniscal damage and that reconstruction should not be delayed until skeletal maturity has been reached. A recent study by Kolin et al. state there is a 3% chance per week of medial meniscal tear from time of injury to surgery5. Because of the recognised importance of this issue, the BSCOS and BASK joint committee created a report on the management of ACL injuries in the skeletally immature patient which was subsequently published as guidelines by the British Orthopaedic Association Standards for Trauma and Orthopaedics (BOAST) in May 2022. >>
Features
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 19
Figure 2:

Nick Nicolaou is a Consultant Paediatric Orthopaedic Surgeon at Sheffield Children’s Hospital, with an interest in Osteogenesis Imperfecta and the Paediatric Knee. He was the Chair of the BASK/BSCOS steering group for paediatric soft tissue knee injuries, current Chair of the BSCOS/BASK Patellofemoral Steering Group, Honorary Secretary for BOSTAA and current Chair of the EPOS sports study group.

Fazal Ali is Consultant Orthopaedic Knee Surgeon at Chesterfield Royal Hospital & Sheffield Children’s Hospital. He completed his Knee Fellowship in Newcastle upon Tyne and travelling fellowships at HSS in New York and Boston Children’s Hospital. He was appointed as consultant in 2004. He is Vice President of BOSTAA, JCIE Chair of Section 1 Exams for all Surgical Specialities and Chair of T&O Joint Surgical Colleges Fellowship Examinations JSCFE.



Physeal sparing techniques for ligament reconstruction have been well described and are utilised in children where substantial amount of growth remains. Crossing the physis risks growth plate disturbance and this effect is amplified in younger children. Skeletal age is not always akin to chronological age and this can mislead clinicians. There are verified methods that can quantify skeletal age using simple hand and wrist radiographs and this should be used to calculate the amount of remaining growth. The decision to utilise physeal sparing techniques is influenced by these calculations. In addition, the dimensions of the epiphysis should be evaluated to help decide whether an all-epiphyseal reconstruction or an extraphyseal reconstruction is most appropriate.
The physis is not always a hindrance to the paediatric knee surgeon. It can also provide opportunity. Guided growth is the perfect example of how relatively simple it can be to correct coronal malalignment in children that have open physis. In comparison, patients that have reached skeletal maturity would require periarticular osteotomies. Identifying and correcting coronal malalignment early is

much easier and safer. Metaizeau described a technique for guided growth, which involves a cannulated screw rather than an O plate6. This works extremely well in cases where ligaments are being reconstructed in close proximity to the physis as it removes the risk of iatrogenic injury to the ligaments during O plate removal.
The patellofemoral disease problem
Patellofemoral instability is a spectrum and is a significant proportion of the problems treated in children. Symptoms range from anterior knee pain secondary to patella maltracking through to recurrent frank dislocations which can become fixed. Chondromalacia patella and Hoffa fad pad impingement are often described as conditions in their own entity but practically they are signs of patella maltracking. Thus, it is important to address the underlying cause. Instability is multifactorial and could be related to the morphology of the knee joint, coronal malalignment, abnormal rotational profile of the lower limbs or generalised ligamentous laxity. An open physis may limit the amount of planned bony reconstruction. However, there are several well described soft tissue

Features
Figure 3: This is a 13-year-old boy who underwent a transphyseal ACL reconstruction on his right knee. The left X-ray is one year post-op showing a neutral mechanical axis and the X-ray on the right is two years post-op showing valgus arising from proximal tibia secondary to growth disturbance. His bone age was one year behind chronological age.
Figure 4: Intra-operative images showing patient undergoing all epiphyseal ACL reconstruction. Femoral guidewire is inserted using femoral ACL guide.
Figure 6: Clinical photograph of Modified Mcintosh procedure for congenital ACL deficiency. The ITB is harvested and detached proximally. It is then tubularised and passed behind the lateral femoral condyle, through the notch, under the inter-meniscal ligament and anchored to the proximal tibia. Further extra-articular anchorage of the graft to the periosteum at the lateral femoral condyle is also performed.
20 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 5: Arthroscopic images showing complete absence of the ACL in a patient with fibular hemimelia. There is a PCL like structure which is hypoplastic and not anatomical, blending in to the lateral meniscus. This is a likely aberrant and hypertrophied meniscofemoral ligament that has developed.


techniques which give excellent results. Patella instability in children can be a difficult problem to treat but addressing it early may prevent a lifetime of disability for these patients.
The evidence – or lack of it
Currently there are still lots of unanswered questions in kids knee surgery. There are a number of established techniques which are well evidenced in adults but not for paediatric patients. There is no consensus or gold standard for a significant proportion of the pathology we treat in children. The lack of evidence is multifactorial and is in part due to the current approach to paediatric knee surgery in this country. Specialist centres with dedicated paediatric knee surgeons are leading the way with research. The tailored service they provide in conjunction with volume of patients they treat make it easier for these trials to run. Current studies in paediatric knee surgery include the DimE observational study looking at the treatment of discoid meniscus and the PAPI study looking at operative vs non-operative treatment for first time patella dislocations in the skeletally immature. More evidence is needed in paediatric knee surgery and is likely to improve as we adopt a more subspecialist approach.
The solution
So, who should be performing kids’ knee surgery? The BASK/BSCOS survey showed that over 60% of respondents felt that paediatric ACL and meniscal pathology should receive multidisciplinary care and follow-up with both paediatric orthopaedic and adult knee surgeons. Over 30% felt that these patients should be referred to high volume centres. The current approach to kids’ knee surgery in the UK is less than ideal and this is being highlighted by the clinicians that are currently treating paediatric knee pathology.
Having specially trained paediatric knee surgeons ensures that we bridge the gap between the paediatric orthopaedic surgeons
and the adult knee surgeons. Specialist training will allow surgeons to learn soft tissue reconstruction techniques specifically refined for the immature skeleton. It will provide more experience in dealing with the growth plate which will help surgeons prevent and better deal with deformity. Most importantly, it will produce high volume surgeons which is important with regards to patient outcomes and advancing research.
Presently, the only dedicated fellowship in the UK with an emphasis on children’s knee pathology is the Sheffield/Chesterfield Knee Fellowship. This programme was created to address the current issues with paediatric knee surgery. It is important that more of these are developed throughout the country in order to produce the number of surgeons needed to meet the demand. Another strategy that is popular is for surgeons to be double fellowship trained in both adult knee surgery and paediatric orthopaedic surgery.
The biennial International Kids Knee Conference provides a great platform for specialists from all over the world to share their expertise and experience in treating child and

adolescent knee conditions. The popularity of this meeting has demonstrated the increasing importance that this subspecialty is receiving from the orthopaedic community worldwide.
In essence, kids’ knee surgery is an emerging subspeciality within orthopaedics that will hopefully tackle the current challenges associated with treating knee problems in this age group. Its importance is gaining more recognition worldwide as the incidence of knee injuries in children increases along with the demands for better outcomes. n
References
1. Swarup I, O’Donnell JF. An Overview of the History of Orthopaedic Surgery. Am J Orthop 2016;45(7):E434-E438.
2. Nicolaou N, Ajuied A, Ali FM, et al. The BASK/BSCOS steering committee report on the management of paediatric soft tissue knee pathology, Jan 2021.
3. Rathleff MS, Holden S, Straszek CL et al Five-year prognosis and impact of adolescent knee pain: a prospective population-based cohort study of 504 adolescents in Denmark. BMJ Open. 2019;9(5):e024113.
4. Nogaro M, Abram SGF, Alvand A, et al Paediatric and adolescent anterior cruciate ligament reconstruction surgery. Bone Joint J 2020;102-B(2):239-245.
5. Kolin DA, Dawkins B, Park J et al. ACL Reconstruction Delay in Pediatric and Adolescent Patients Is Associated with a Progressive Increased Risk of Medial Meniscal Tears. J Bone Joint Surg Am 2021;103(15):1368-73.
6. Métaizeau JP, Wong-Chung J, Bertrand H, et al. Percutaneous epiphysiodesis using transphyseal screws (PETS). J Pediatr Orthop 1998;18(3):363-9.

Features
Figure 7: Intra-operative images showing Percutaneous Epiphysiodesis using Transphyseal Screws (PETS) technique described by Metaizeau. This procedure was performed in conjunction with patella stabilisation.
Figure 8: The kids knee team at Sheffield Children's Hospital (from left to right) Nicolas Nicolaou, Fazal Ali, Dominic O'Dowd, Paul Haslam, Rizwan Arshad (Fellow) and Sheba Basheer (Fellow).
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 21
Figure 9: 2022 International Kids Knee Conference held in Sheffield with Faculty members from UK, Japan, Australia, USA, Chile, Brazil and many European countries. Over 200 delegates attended from all over the world.


Obesity and orthopaedic surgery
Harriet Lewis, Alexander Dodds and Mark BowditchAt present 27% of adults in the UK are classified as obese and a further 36% are classified as overweight and this number is likely to increase significantly in the future1. Obesity is estimated to cost the NHS £3.2 billion annually.

The rise in the number of obese patients will have a significant impact on trauma and orthopaedic services in the UK, both in terms of the number of patients being referred, as well as the additional challenges associated with managing patients with obesity. The link between obesity and increased mechanical loading of joints leading to degeneration has been well documented. There are increased demands on the surgical team and provider of resources. In this article, we review challenges to orthopaedic practice with the rise in obesity rates, how obesity can affect operative practice and the use of restrictions on orthopaedic surgery based on body mass index (BMI).
Risks with orthopaedic surgery and raised BMI
Associated medical conditions such as diabetes, hypertension and cardiovascular issues as well as body habitus and venous access may make the anaesthesia more challenging. Regional anaesthetic has been shown to be more likely to fail in obese patients. The anaesthetist may face intra-operative problems due to decreased lung volume, collapse, and decreased chest wall compliance. Surgery in the obese patients will often be more challenging due to the distribution of fat and hence surgical access will be difficult. This in turn, can affect the technical aspects of surgery, such as the placement of pedicle screws in spinal surgery and
implant alignment in knee surgery. Surgeons may need additional retractors for access, and surgery may take longer than normal. There is a link with increased post-operative complications following orthopaedic surgery, including wound infections, thromboembolism stroke and myocardial infarction. Venous thromboembolism risk may also be increased due to poor mobility and altered coagulation profiles. Longer-term, there is some evidence that there is a higher failure rate of orthopaedic implants in patients who are obese2
As with any orthopaedic intervention, the balance between the risks associated with the procedure and the benefits it provides have to be carefully considered and this is no different with obese patients. Despite the increased risks, obese patients with osteoarthritis can still greatly benefit through surgical intervention that still offer significant and effective pain relief and functional improvement. Evidence shows that there is a cost/QALY increase of £1,013 for a patient with a BMI greater of 40 compared to a £3,921 cost/QALY in patients less than 40, yet surgery still remains very cost effective3. Some surgeons will worry about how operating on patients with an increased risk profile could adversely affect their data such as the National Joint Registry (NJR) results. BMI should also be considered in context with other risk factors for surgery such as inflammatory arthropathy, and whilst BMI in itself may not be prohibitive for surgical intervention, it may be when combined with other risk factors.
Body mass index
Body mass index (BMI) is one of the most commonly used measures to assess a patient’s level of obesity. It is defined by weight (kg)
Features
Harriet Lewis is a Trauma and Orthopaedic Registrar, Severn Deanery.
Alexander Dodds is a Consultant Orthopaedic Surgeon, Gloucestershire Hospitals NHS FT Trust.
22 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Mark Bowditch is a Consultant Orthopaedic Surgeon East Suffolk North Essex NHS FT Trust and is the BOA Vice President.

“Whilst central obesity may lead to a rise in a patient’s risk for medical complications, the distribution of fat on the limbs may be more relevant for an orthopaedic surgeon in terms of determining technical operative risk and post-operative complications such as infection.”
Table 1: World Health Organisation
divided by the square of the persons height (m2) (Kg/m2). The World Health Organisation defines obesity as being a BMI of more than 30, (see Table 1). BMI is commonly used clinically as it is a quick and easy way of assessing an individual’s body composition. It has also been used as a research tool, and has been shown to be associated with health issues including cardiovascular disease, diabetes, renal disease and stroke.
Clinicians need to be aware of the limitations of BMI when it is being used to assess a patients risk for surgery. It is unable to distinguish between lean muscle weight and body fat. It also does not give any indication
of the distribution of fat, and this could be critical for the orthopaedic surgeon.
Whilst central obesity may lead to a rise in a patient’s risk for medical complications, the distribution of fat on the limbs may be more relevant for an orthopaedic surgeon in terms of determining technical operative risk and post-operative complications such as infection. The two are different and often not present together. The British Orthopaedic Association has previously stated that BMI should not be used solely as a means to ration procedures such as total hip/knee replacement. This advice has also been given by other organisations including the American Medical Association.
BMI as a cut-off for referral access and surgery
Approximately two thirds of NHS England commissioning groups or integrated care systems have referral guidelines that include obesity limits using BMI. A guideline BMI figure of 40 or less is common but in some areas 35 has been used as a threshold for surgical intervention4. Health optimisation prior to planned surgical care is often indicated and generally beneficial but the reduction of BMI may not be that easy or indeed achieve a significant improvement in the risk:benefit balance. In some cases it may regarded as an inappropriate denial >>
Features
Classification BMI Underweight <18.50 Normal 18.50 to 24.99 Overweight 25.00 to 29.99 Obese >30 Obese Class 1 30.00 to 34.99 Obese Class 2 35.00 to 39.99 Obese Class 3 >40
BMI definition.
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 23

of care. Delaying surgery whilst patients try losing weight may in fact make them less ‘fit’ for surgery leading them to suffer increased pain and disability with further deconditioning. Organisations such as the BOA and RCSEng have stated that commissioning policies should be based on clinical need. Local referral restrictions for orthopaedic surgery based on BMI is not evidenced-based and the variation across the UK could be regarded as a ‘postcode lottery’.
A particular concern with the use of BMI to limit access to orthopaedic surgery is that obesity is associated with health inequalities. Individuals in lower socioeconomic groups are more likely to suffer with obesity, reflected in barriers to healthier food choice, lifestyle and exercise opportunities, and also problems with healthcare access. Using BMI as a measure to restrict access to orthopaedic services may in itself increase these health inequalities. Distribution of fat is linked to genetics, and those of Asian,
Middle Eastern, African or African Caribbean inheritance are more prone to central obesity.
Furthermore, there is a gender difference in adipose tissue distribution, with men more likely to carry adipose tissue centrally. Patients from deprived areas of England and Wales are 69% less likely to have a hip replacement despite clinical need5.
Pre-operative weight loss
One justification for the use of BMI cut offs for access to surgery is that it encourages weight loss in patients. National Institute for Health and Care Excellence (NICE) recognises the importance of a structured approach to preoperative weight management for individuals awaiting arthroplasty surgery.
This may include other surgical interventions including bariatric surgery. A recent study showed that patients who achieved weight loss
pre-operatively showed a decrease reduction in complications including rate of VTE, infection and wound healing problems. The evidence is not clear and other studies have not reached the same conclusions6 Too rapid weight reduction may have adverse effects on surgical recovery.
Summary
Obesity will become a growing problem for trauma and orthopaedic surgery in the future. Surgeons need to be aware and plan for the issues with surgery in this patient group. However, patients will still get reliable improvements in pain and function with orthopaedic intervention. Tailoring surgical management options based on an individual patient characteristic is essential to optimise surgical outcomes. The use of BMI as a sole criterion to limit access to orthopaedic surgery is not evidence-based and should be challenged. Further research and policy revaluation is needed in this area. n
References
1. Johnson W LL, Kuh D, Hardy R. How Has the Age-Related Process of Overweight or Obesity Development Changed over Time? Co-ordinated Analyses of Individual Participant Data from Five United Kingdom Birth Cohorts. PLoS Med 2015;12(5):e1001828.
2. Boyce L, Prasad A, Barrett M, DawsonBowling S, Millington S, Hanna SA, Achan P. The outcomes of total knee arthroplasty in morbidly obese patients: a systematic review of the literature. Arch Orthop Trauma Surg. 2019;139:553-60.
3. Losina E, Smith KC, Paltiel AD, Collins JE, Suter LG, Hunter DJ, et al. CostEffectiveness of Diet and Exercise for Overweight and Obese Patients With Knee Osteoarthritis. Arthritis Care Res (Hoboken) 2019;71(7):855-64.
4. Rooshenas L, Ijaz S, Richards A, Realpe A, Savovic J, Jones T, et al. Variations in policies for accessing elective musculoskeletal procedures in the English National Health Service: A documentary analysis. J Health Serv Res Policy. 2022;27(3):190-202.
5. Wyatt S, Bailey R, Moore P, Revell M. Equity of access to NHS-funded hip replacements in England and Wales: Trends from 2006 to 2016. Lancet Reg Health Eur 2022;21:100475.
6. Seward MW, Briggs LG, Bain PA, Chen AF. Preoperative nonsurgical weight loss interventions before total hip and knee arthroplasty: a systematic review. J Arthroplasty. 2021;36(11):3796-806.e8.
Features
24 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
38th Edinburgh International Trauma Symposium & NEW Edinburgh FRCS(Tr&Orth) Revision Course
EDINBURGH INTERNATIONAL TRAUMA SYMPOSIUM - 14-16 AUGUST 2024
Three-day meeting for orthopaedic surgeons and AHPs
Renowned international and UK faculty
Focus on revalidation and update through short interactive lectures and CBDs
Break out sessions include cadaveric surgical approaches and fixation techniques
Edinburgh FRCS(Tr&Orth) Revision COURSE - 13-16 AUGUST 2024
Four-day intensive revision course
Comprehensive coverage of the syllabus
Viva practice sessions and mock exam
VENUE: SHERATON HOTEL AND EDINBURGH MEDICAL SCHOOL

For more information on booking please visit: www.trauma.co.uk or email: symposium@trauma.co.uk






BOTA DISCOUNT AVAILABLE!! Reduces pain and increases mobility medi. I feel better. www.mediuk.co.uk Tel: 01432 373 500 medi soft OA light knee brace osteoarthritis off-loading knee brace now available on prescription. Intended purpose: medi soft OA light is a knee brace for load relief.
Guidance on the role of simulation in formal training by the British Orthopaedic Association
Kapil Sugand and Hiro Tanaka
AKapil Sugand is a Peripheral Nerve & Musculoskeletal Surgery Fellow at the Royal National Orthopaedic Hospital. He is a member of the BOA Education and Careers Committee.

Hiro Tanaka is a Consultant Foot & Ankle Surgeon, Aneurin Bevan Local Health Board. He is the BOA Honorary Secretary, a member of the BOA Education and Careers Committee and co-directs the BOA Future Leaders Programme.
proposed position has been compiled on the role of simulation in formal training at any stage between medical school to consultancy. The BOA recognises the importance of maintaining a high-quality standard of training and is in the process of becoming the first orthopaedic body to officially release a White Paper on the topic. Proctorship/ apprenticeship still remains the gold standard for training, demonstrating competency and building confidence; but simulation acts as a favourable adjunct to enhance patient safety, which is of utmost priority.
Description of current challenges
The quality of national training has been affected by numerous generational changes as outlined in Table 1.
Definition of simulation
Many definitions of surgical simulation exist. The Society of Simulation in Healthcare defines it as follows:
“A technique that creates a situation or environment to allow persons to experience a representation of a real event for the purpose of practice, learning, evaluation, testing, or to gain understanding of systems or human actions”
(Society of Simulation in Healthcare, 2013)7
A contextualised version includes recreating clinical scenarios in a safe and monitored environment in order for the participant to learn, develop and hone both technical and non-technical clinical skills without
compromising patient safety. As the participant is able to practise a skillset in order to demonstrate competence and confidence to the assessor considered an expert in the field, the assessor, who is is able to evaluate the performance before offering constructive and personalised feedback at regular intervals. The purpose of simulation is self-directed goal-orientated rehearsal. Hence, it ought to be incorporated into regular routine not only to demonstrate continued maturity but to also avoid skills decay. Take heed of 'out of sight, out of mind'.
Possible solutions
1. Learning from other specialist organisations Simulation is both recognised and has become mandated within the curriculum as championed by the General Medical Council8 and other international medical bodies.
Additionally, both the body of work and National Standards Framework are recognised from national organisations such as the Association for Simulated Practice in Healthcare (ASPiH), the Society for Simulation in Healthcare (SSH), Health Education England (HEE) and the Joint Committee on Intercollegiate Examinations (JCIE) as well as the current peer-reviewed literature globally.
Training opportunities (as a result of the European Working Time Regulations)
< 80% decrease in operating training hours to reach consultancy1
National Confidential Enquiry into Patient Outcome and Death (NICEPOD) lists precluding overnight operating lest life or limb threatening2
Clinical activities and training opportunities as a direct consequence of the COVID-19 pandemic3
Operations: > 234 million major procedures / year worldwide4
Musculoskeletal disease: > 1.7 billion people affected globally as the leading cause of disability5
Brain drain: Career intentions of medical students in the UK: a national, cross-sectional study6
Medico-legal / lawsuits / fiscal compensation for iatrogenic errors
Table 1: Altered circumstances in modern training.
Features
Reduced Increased
26 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
2. Working within the BOA
There is an evolving practice of the development, validation and administration of simulation solutions within T&O training through its direct involvement with its diverse membership from medical students through to Consultants. The BOA is also actively collaborating with British Orthopaedic Trainees Association (BOTA) and British Orthopaedic Medical Student Association (BOMSA) in searching for innovative modalities to enhance educational impact. There is also a dedicated section within the Annual BOA Congress highlighting advancements of simulation practice through rigorous research methodologies.
3. Establishing a healthy working relationship with industry partners
Working relationships with industry partners will be forged in order to introduce simulation solutions to its diverse and versatile membership. Opportunities to showcase simulation modalities will be conducted at the annual BOA and BOTA Congresses, discussed at the Simulation section of the Congress through free papers and posters highlighting research on validation of both software and hardware solutions. The BOA will support the showcasing of commercial simulation products and introduce the vendors to its clients. Clients will consist of Training Programme Directors, Deanery Representatives, Consultant Trainers as well as Trainees. The notion of ‘try
before you buy’ concept will be supported while encouraging vendors to offer trial periods to institutions prior to making a sizeable investment into its purchase or hire licensing.
4. Lexicon
The definitions outlined in the Health Education Dictionary compiled by the Society for Simulation in Healthcare (Table 2) is acknowledged. This list is not exhaustive and the entire lexicon can be found on their website (www.ssih.org/dictionary) for further information and definitions.
Other recognised terms are acknowledged in Table 3.
5. Modes of simulation
The following are simulation techniques that are recognised and can be principally categorised as in Table 4.
i. Analogue modalities
Historically, most T&O trainees have experienced some form of simulation; the commonest modality being low-fidelity drybones. This technique is usually for learning procedural steps, obtaining appropriate range of measurements and familiarising with new surgical equipment. Analogue alternatives include drybones with simulated soft tissue envelopes including muscles, tendon, ligaments and neurovascular bundles. Box trainers were able to simulate arthroscopic procedures to
improve
skills as well as manual dexterity including triangulation, economy of movement and pace. Distributed interactive simulation is a combination of analogue modalities that increases the extent of both fidelity, immersion and interaction (Figure 1). Such clinical scenarios may consist of a series of simulation tasks, in various clinical areas and involve multidisciplinary colleagues, thereby reflecting technical and nontechnical skills. Non-technical skills consist of communication, teamwork, interpersonal, clinical decision-making and leadership skills.
ii. Digital modalities
With ever-evolving educational technology, digital simulation solutions have also been commercialised. However, a major limitation to its access is costing. T&O has traditionally been slow to turn to simulation technology compared to other surgical specialities. Options consist of online virtual clinical scenarios that may assess cognitive task analysis for a technical procedure as well as surgical decision-making (Figure 2). Hardware technology has led to the development of simulators using augmented or virtual reality software to simulate operations. With a stake from blue chip companies, holography (Figure 3) in surgery has also become an option to delineate operative steps and visualising abstract concepts in anatomy and physiology. These digital solutions also allows for telepresence where learning can take place in an immersive and interactive virtual setting, regardless of geography and resources for hardware.
iii. Hybrid models
There is also scope for introducing hybrid modalities in order to demonstrate training effect, skills decay and the validation of simulation models. An example would be comparing the educational impact of digital simulation against analogue modalities including reading the operation technique (OpTech), and then having trainees' performance assessed when performing the same procedure on a patient under supervision. >>
Features A G P Actor Gamification Participant Adaptive learning Guided reflection Physical fidelity Artificial Intelligence H Pilot test Assessor Haptic Portable simulator Assessment High-fidelity Procedural simulation Augmented Reality Human factors Prompt Avatar Hybrid Simulation Prop B I R Behavioural skills Immersion Realism Briefing Interactive Reflective thinking C Interdisciplinary / interprofessional Reliability Clinical scenario L Risk management Coaching Learning goal / objective / outcome Role play(er) Cognitive load Low-fidelity S Computer based simulation M Safe learning environment Conceptual fidelity Manikin / mannequin Scenario Cueing Mixed Reality / Methods / Simulation Script D Modality Simulated patient Debriefing Model Simulation • Ethics • Guideline • Standard • Time • Tool • Validity Deliberate practice Moulage Situated learning Distributed simulation Multidisciplinary Situational awareness Dryrun Multimodal T E N Tabletop simulation Educator Negative learning Take-home simulation Environmental fidelity Never event Team-based learning Evaluation Non-technical skills Technical skills F O Technology-Enhanced Health care Simulation Facilitator Objective Structured Clinical Examination Telepresence Feedback Online simulation Telesimulation Fidelity Orientation Trigger Functional fidelity V Validity Virtual • Environment • Patient • Presence • Reality • World
C M Cognitive task analysis Manual dexterity Competence P D Pace Decision-making Proficiency E Psychomotor skills Economy of movements S H Skills decay Hand-eye coordination T L Training effect Learning curve Triangulation Table 3: Other recognised terms acknowledged. Analogue Digital Drybone Online Phantom limbs Altered reality: • Augmented • Virtual Box trainers Holography Distributed interactive simulation Telepresence Instrumentation familiarisation workshops
Table 2: Lexicon adapted from the Health Education Dictionary v 2.1 (Society for Simulation in Healthcare, 2020).
Table 4: Simulation techniques commonly used in Trauma & Orthopaedic training.
probing
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 27


iv. Learning theory
Many theories on adult learning have been posed. However, the unifying hypothesis is for simulation to curb the learning curve. There is also evidence suggesting that the first attempt on a simulator ought to be invalid to account for the learning curve of the familiarisation of hardware or software rather than the performance of the simulation task. Cognitive load of learning a new skill can be reduced by isolating and breaking the tasks into manageable chunks. Cognitive task analysis will allow the learner to understand the streams of decision-making required in order to master a new skillset. Furthermore, the popular adage of ‘seeing one, learning one and doing one’ has now been replaced with teaching and doing many with persistent practice. Simulation is only effective if utilised consistently in order to attain a training effect. Infrequent or disrupted utilisation of simulation will lead to skills decay after a ‘wash out’ period. The Dreyfus model outlines stages of competency and proficiency until a master level is achieved9
6. Invited validation of national courses (CPD)
The BOA is aware of an increasing number of courses run by institutions that offer simulation training, whether that be for learning and acquiring new technical skills, demonstrating competency to be signed off for Intercollegiate Surgical Curriculum Programme (ISCP) core requirements, or preparing for the specialist exams. Both the vetting and validation processes of any course will be supported with a mission to advance T&O training, skillsets and education by offering CPD points upon application. Any such courses will also be featured in an online rolodex once built.
7. Increasing revenue streams
The BOA is a registered charity and relies on various avenues of income. The additional income will go towards supporting our mission, research and advocacy of our membership with




respect to education and training. This proposal, yet to be vetted, aims to introduce further streams of income as follows:
1. Application for CPD points for a course.
2. Introductory commissions between vendors to clients.
3. Encouraging more vendors to attend BOA and BOTA Congresses.
4. Ticket sales from potential Congress dedicated to simulation products –estimated to be held in 2025.
Limitations
This is a preliminary proposal. It has yet to take into account the expert opinions of its representatives and membership. However, this will be an evolving process and our plans have been outlined in the ‘future work’ section. This proposed White Paper has yet to be vetted by EdCar and the BOA as a whole.
Future work
This report will be an evolving body of work that will continuously develop with time and research. Subsequent proposed phases consist of the following:
1. Conducting a national consensus through subspeciality bodies of the BOA to determine the principal objectives and guidance on effective training and the role of simulation. Participants will consist of Consultant trainers as well as Trainee Representatives from undergraduate medicine, Foundation Doctors, Core Trainees and Specialist Trainees. The new evidence will better inform future guidance on simulation-based practice with more consistency in hope of evidence-based standardisation to cater for personalised needs.
2. Expanding categories for the BOA Simulation Award.
3. Collaborating with international orthopaedic professional bodies to increase opportunities for research fellowships.
4. Increasing the number of educational content offerings, including videos on index procedures, screencasts and training videos.
5. Collaborating with industrial partners to validate simulation training programmes.
6. Compiling training toolkits to institutions so that there is a basic level of simulation offered to T&O trainees nationwide which can be incorporated into ISCP work based assessments locally.
7. To foster working relationships with other institutions related and unrelated to orthopaedics for an inter-disciplinary influence to our work. Proposed organisations include the Royal Society of Arts, Science Council, Institute of Science and Technology, Institute of Clinical Research, Institute of Engineering and Technology, AO, SICOT and Royal Society of Public Health, as well as universities.
About BOA Education and Careers Committee (EdCar)
The BOA is the recognised national professional body for all subspecialities under the principal surgical field of trauma and orthopaedics. The EdCar Committee consists of a host of Consultants, Associate Specialists, and Trainee Representatives with a combined experience of simulation methods, training both undergraduates and postgraduates and, stemming from a versatile range of subspecialities. n
References
References can be found online at www.boa.ac.uk/publications/JTO
Features
Figure 1: Distributed interactive simulation scenario consisting of phantom limbs, cardiac monitors, theatre lights and actual theatre draping.
Figure 2: Interaction with the virtual patient; here the participant is gathering information from the primary survey.
28 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 3: Holographic images from a lecture in orthopaedic trauma.. The lecturers are featured behind the Pepper’s Ghost foil as if they were next to the holographic images. This positioning also allows for interaction with the dynamic animations to make the learning experience more immersive and interactive. (Pictured Dr Pedro Campos and Kapil Sugand)

Current and upcoming strategies to prevent and treat metallic implant infections
Innovation impact on BJI (robotics, AI and app)
Large clinical trials in Bone and Joint Infection
Microbial etiology in PJI and new diagnostic techniques
Multi-drug resistant pathogens in PJI: how to deal with this problem?
Open questions in 2-stage exchange
Painful prosthesis, is it really an infection?
Tips for surgery in FRI and PJI
Using local and systemic antibiotics in BJI: a match made in heaven?

Save the date! 26 - 28 September 2024 · Barcelona · Spain Topics 42nd Annual Meeting of the European Bone & Joint Infection Society EBJIS 2024 #EBJIS2024 www.ebjis2024.org
Early
July 2024
registration deadline: 1
A practical approach to artificial intelligence in trauma and orthopaedics

Andrew Coppola is an Orthopaedic Research Fellow at the South West Elective Orthopaedic Centre, Epsom. He holds an MSc in Surgical Innovation from Imperial College, where he focused on predictive artificial intelligence in knee and hip replacements. He has been awarded an NHS Topol Digital Fellowship to advance transformative artificial intelligence applications in orthopaedics.
The concept of artificial intelligence (AI) first emerged in the 1940s. Progress was slow with researchers facing numerous challenges over the years. It was not until the late 1990s and early 2000s, that real-world applications started to appear.
Examples of this include recognition of handwritten postcodes (AT&T, US postal service) and robot pets. The 2010s saw a big leap, with the release of Microsoft’s Kinect, which was able to recognise human gestures and Apple’s voice recognition tool, Siri. A breakthrough occurred in 2012, when Hinton won ImageNet’s image recognition competition, that AI and deep learning was popularised1. His work has formed the basis of computer vision (the application of deep learning to image and videographer recognition) and contributed to the development of large language models that have revolutionised the potential for analysis of unstructured text data.
Although AI is a hot topic in trauma and orthopaedics, commercial applications remain limited. One example is the Sectra Amplifier marketplace AI platform, is BoneView (Gleamer AI), which assists junior doctors in detecting fractures2. Another example is OrthoSensor’s VERASENSE™ technology, which utilises AI to enhance implant positioning during joint replacement surgery3. Interest in the application of AI techniques to managing musculoskeletal problems has grown over the last couple of years due to the realisation that there is a large amount of data available in and outside of hospitals (such as registries). At the 2023 AI in Orthopaedics meeting, hosted by ORUK, several abstracts were presented
covering the application of three main AI/ML disciplines: large language models, computer vision and predictive analytics (identify patterns from past data to predict future events). Since this meeting, numerous projects in these areas are nearing completion and publication or commercialisation.
Examples of the use of large language model (natural language processing) AI to make clinical decisions include making clinical decisions based on radiology reports4 and testing whether it is clever enough to pass the FRCS exam (Turing stated in 1940, that for true intelligence, a machine needs to provide answers to questions that are indistinguishable from human responses)5
Computer vision has been used to produce 3D images from 2D radiographs and to detect and classify fractures6,7. Others have studied quality assurance through the analysis of postoperative radiographs and used image analysis to predict outcomes following joint surgery [personal communication]. Although still at research stage, these papers represent the fast pace at which AI is developing in the trauma and orthopaedic space.
Predictive analytics uses statistical techniques and machine learning to forecast outcomes from historical data. In trauma and orthopaedics, it has been used to predict the duration of surgical procedures in the hope of improving operating theatre scheduling.
The application of AI techniques to clinical problems can include using a variety of techniques such as simple equations to complex deep learning methods (a subset of machine learning). Deep learning is viewed
Features
30 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Andrew Coppola and Vipin Asopa

Vipin Asopa is a Specialist Hip and Knee Surgeon at South West London Elective Orthopaedic Centre, Epsom. His research interests include the use of artificial intelligence to improve patient outcomes following surgery.

“Predictive analytics uses statistical techniques and machine learning to forecast outcomes from historical data. In trauma and orthopaedics, it has been used to predict the duration of surgical procedures in the hope of improving operating theatre scheduling.”
as a black-box because it is not known how the algorithm works although computational techniques can explain some ability of models7,8. Generative AI can be used to create intelligible content from diverse data, for example summarising research publications and clinic letters9.
AI algorithms are developed through training and testing. The broad method of AI applied depends on the question and answer being sought and the data available. For example, computer vision is based on the use of images for analysis. Natural language processing, or handling text is often carried out using large language models. In setting up an AI project, it is important to consider how data will be obtained – for example downloading radiographic images from consented patients. Training requires the use of non-bias data, sometimes using the technique of optimisation and feature selection. Reporting
on algorithms should be transparent (e.g. using the PROBAST and CHARMS frameworks)10. The deployment of a model and how its function will be verified needs to be planned.
The practical considerations of setting up an AI project in an NHS hospital include defining a research project, obtaining ethics / research approval (if indicated), discussing the project with the Caldicott Guardian, obtaining host organisation support and finally, patient consent if needed. AI algorithms can be developed and run on a virtual machine (hosted in the cloud on Microsoft Azure or Amazon Web Services) or a physical computer located within the hospital environment. Cloud machines may be easier to manage, simpler to upscale and do not require physical support services, however they can be costly. Both require consideration of the resources: a powerful central processing, graphics processing unit and fast storage and large memory capacity. >>
Features
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 31
Figure 1: Artificial Intelligence disciplines. This figure illustrates the three main disciplines within AI: Predictive Analytics, Natural Language Processors, and Computer Vision. Each discipline represents a distinct area of AI applications.

“MHRA approval is required before a working AI tool can be safely used in clinical practice. They will only issue a UKCA certificate once the algorithm has gone through extensive testing. Changes to the algorithm after a certificate has been issued will require new authorisation.”
Data security is worthy of consideration along with remote access (VPN) for researchers.
Using and developing AI tools may require an understanding of coding i.e. Python. Examples of computer code are available online. This can be complex and a team-based approach may be appropriate involving university collaboration and/or a data analysist. Once developed, the model will require external validation toassess generalisability.
Governance matters need to be considered. Is consent required to use patient data? Using anonymised data as part of a quality improvement project may negate, but advice should be obtained from research management or the HRA. The Caldicott Guardian should be consulted to ensure patient data is used appropriately.
Access to different data sources is challenging. There is a requirement to improve connectivity between different data sources and software applications within and outside of the hospital environment. Improved connectivity will reduce the need for manual downloading of data and improve the accuracy of algorithms by reducing digital divides13. Standardised APIs to allow connectivity and sharing should be developed instead of aggregating data into large repositories under the control of one company.
Funding for projects may be a concern, but there are organisations that provide funding for research projects relating to musculoskeletal conditions including the Gwen Fish Trust and ORUK (Orthopaedic Research UK). Recent initiatives by the
government are likely to increase the amount of money available for AI research14.
MHRA approval is required before a working AI tool can be safely used in clinical practice. They will only issue a UKCA certificate once the algorithm has gone through extensive testing. Changes to the algorithm after a certificate has been issued will require new authorisation. As a result, there is currently no mechanism for algorithms to continually learn and update themselves with new information11,12
Commercialisation is the step required to obtain large amounts of funding to take promising research projects through further development including obtaining regulatory approval. However, various questions related to intellectual property need to be considered including who does the algorithm belong to when such a product is brought to market? Do the developers get a share? Does the NHS, who provide the data source, control all rights?
Many of the topics in this article will be discussed at the BOA-supported AI in Orthopaedics meeting to be held 19th - 20th December 2024 at the Royal College of Surgeons of England and we look forward to welcoming you at this event! n
References
References can be found online at www.boa.ac.uk/publications/JTO
A more in depth look at this topic is covered in an extended article on Orthopaedics Online. The article titled, Integrating Artificial Intelligence into Trauma and Orthopaedics: History, Current State of AI in Trauma and Orthopaedics and Future Perspectives can be viewed at www.boa.ac.uk/Integrating-AI-into-T&O.
Features
32 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 2: Practicalities of Artificial Intelligence. This figure shows eight key considerations for deploying AI.
Arthrosamid® — The first and only synovial scaffold2,3administered via a single injectable for long-lasting pain relief.4,5


Proven1
Pain relief treatment1

Statistically significant reduction in pain maintained at 3 years.4,5 Learn more about our reproducible results here by scanning the code.


References: 1. Arthrosamid®, Instructions For Use. Release Date March 2022. 10082-003; 2. Christensen, L., et al. (2016). Histological Appearance of the Synovial Membrane after Treatment of Knee Osteoarthritis with Polyacrylamide Gel Injections: A Case Report. Journal of Arthritis. Vol 5: 217; 3. Christensen, L., et al. (2016). Synovial incorporation of polyacrylamide hydrogel after injection into normal and osteoarthritic animal joints. Osteoarthritis and Cartilage. Vol 24(11):19992002. DOI:10.1016/j.joca.2016.07.007; 3. Data on file; 4. Bliddal, H., et al. (2023) A Prospective Study of Polyacrylamide Hydrogel Injection for Knee Osteoarthritis: Results From 3 Years After Treatment. Osteoarthritis and Cartilage. Vol 31(5): 682-683; 5. Bliddal, H., et al. (2024) 3 year follow-up from a randomized controlled trial of intra-articular polyacrylamide hydrogel injection in subjects with knee osteoarthritis. Poster LB-31, OARSI 2024 World Congress on Osteoarthritis.




Contura-Orthopaedics-Ltd Contura Orthopaedics Ltd
information
visit
enquiries@arthrosamid.com
www. arthrosamid .com OUS/ARTHRO/FEB2024/047 Pioneering, proven
@ConturaLtd
For full details about warnings and precautions read the IFU. For more
and the IFU please
www.arthrosamid.com or contact us at
@arthrosamid
pain treatment for knee OA1
2.5 iPAAG
Pioneering
My experience working on Mercy Ships
Rachel Buckingham
Rachel Buckingham is a Children’s Orthopaedic Surgeon in Oxford. She undertook her orthopaedic training in the South West of England followed by a clinical fellowship at the Nuffield Orthopaedic Centre in Oxford.
One warm dusky evening in December 2019, in Dakar, Senegal, West Africa, I climbed up the gangway of an enormous hospital ship, the Africa Mercy to start a two-week voluntary service providing surgical treatment for children with limb deformities. I had never actually walked up a ship’s gangway before, I had never lived and worked on a ship, I had never been to West Africa, and I began to wonder what I had let myself in for.
Mercy Ships is a Christian charity that has provided free surgery for the world’s forgotten poor for over 45 years. This was my ‘trial run’ to see if I might volunteer on a regular basis. I was met at reception by a smiling friendly faced American surgeon, Frank, who was to be my co-consultant. He carried my luggage down to my cabin which turned out to be below the gangway, and next I was given a plate of hot supper. Over the following two weeks, I found myself working with an amazing team of kind and committed people from all over the world, and together we got through a huge amount of work – 39 children with severe limb deformities operated on in ten days of surgery. The kids on the ward lit up each day with their laughter and smiles despite the pain
and anxiety of surgery and entertained us with their races up and down the corridors in post-op plaster casts with miniature Zimmer frames (made by the ship’s engineers) learning to walk again. I was hooked (see Figure 2, 3 & 4).
At the invitation of the host nation, the Mercy Ships dock for ten months bringing everything required to provide much needed surgery apart from fuel, water and waste disposal which are provided as part of the comprehensive agreement. As well as completing thousands of urgent operations onboard our floating hospitals, the Africa Mercy and the Global Mercy, Mercy Ships volunteers also work closely with the relevant Ministry of Health to improve the way healthcare is delivered across the country, by training and mentoring local medical staff, and renovating local hospitals and clinics.
Founded in 1978 by Don and Deyon Stephens, Mercy Ships has worked in more than 55 countries, providing services valued at more than £1.3 billion. By improving healthcare delivery in every country it visits, Mercy Ships is working to eradicate the diseases of poverty and effectively do itself out of a job. Mercy Ships follows the model of Jesus by “bringing hope and healing to the forgotten poor”, helping people of all faiths and none.

International
34 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 1: Mercy Ships Africa.


The Lancet commission on Global Surgery showed that two thirds of people in the world do not have access to safe or affordable surgery, and in sub-Saharan Africa that figure rises to 93%. Furthermore, 32.9% of deaths worldwide are attributable to inability to access timely surgery. That is more than three times the number that die from HIV, TB and Malaria combined.


But while twins like Assanou and Assanne with painful rickets (see Figure 5 & 6) are unlikely to die from lack of surgery, their condition means that they may not be able to attend school, hold down a job or get married, and they are likely to be stigmatised. So, life for them looked pretty bleak. Imagine how their mother’s desperation will have turned to hope when she heard of



the possibility of surgery on board a floating hospital. And what an adventure for them to walk on board a ship for the first time knowing that the next time they set foot on dry land their legs would be straight! (We had to colour code their casts and wrist bands as they liked to trick the nurses by switching beds!).
Sadly, my next trip was delayed due to COVID-19, but in summer 2022 we got things going again and returned to Senegal to complete some surgeries that the pandemic had prevented. After that trip, I was asked to take on the lead orthopaedic surgeon role for the organisation, taking over from Frank Haydon who had pioneered the children’s orthopaedic service over the previous ten years. In March 2023 I found myself back in Senegal, but this time on board the brand new ‘Global Mercy’ which is now the biggest nonmilitary hospital ship in the world. I had the huge privilege of doing the first ever operation on board in the new hospital. Imagine doing an operation where every single instrument is brand new, shiny, and sharp! Imagine doing the first operation whilst being watched and photographed by a thoughtfully non-intrusive comms team… (see Figure 7 & 8)
In addition to paediatric orthopaedics, Mercy Ships also provides plastic, general, maxillofacial, obstetric fistula, eye and dental surgery as well as a palliative care service. >>
International
Figure 2, 3 & 4: Post-operative children learning to walk again.
Figure 5 & 6: Twins Assanou and Assanne.
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 35
Figure 7 & 8: The first surgery on board the brand new Global Mercy, operating with my friend and colleague Andy Wainwright.





Mercy Ships is famous for its Max Fax work due largely to Dr Gary Parker who has worked, lived, and brought up his family on board for over 30 years. Sambany was one of his patients. He was waiting to die until he heard about Mercy Ships, and some of his friends carried him to the nearest road to get transport to take him for his life saving surgery. 14 hours of surgery and 10 units of blood (donated by the crew who are the walking blood bank), and what a result! (See Figure 9 & 10).
I realise I should be sticking to orthopaedics, but I can’t resist telling you about siblings Elodie, Jacques and Marie Grace (See Figure 11 & 12).
Their mother, Amina, had cataract surgery with Mercy Ships in 2001 when she was 13, and 20 years later when she heard the ship was returning to her country, she led her three children to the floating hospital where they all received free cataract surgery on the same day: it is impossible to imagine how Amina felt. It almost makes me want to be an ophthalmic surgeon, but then I wouldn’t get to do cool orthopaedic operations like these pictured (see Figures 13-16).
I now volunteer with Mercy Ships twice per year, once on each ship, doing two to three weeks of surgery each visit. It’s a little different from the day job in Oxford, but parents the world over just want the best for their children, and it’s amazing to be able to provide treatment free of charge, for those who would not otherwise be able to afford it, restoring hope and the possibility of a full life ahead. n
As ortho lead for Mercy Ships one of my jobs is to find the volunteer surgeons to continue this amazing work. If you would like to know more have a look at the website: www.mercyships.org.uk or contact me at rachel.buckingham@ouh.nhs.uk

International
Figure 9 & 10: Sambany before and after life-saving surgery.
Figure 11 & 12: Siblings Elodie, Jacques and Marie Grace before and after cataract surgery.
36 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figures 13-16: Life-changing lower limb orthopaedic procedures.



Alice Campion is an ST5 orthopaedic trainee in the Severn Deanery and is the Global Surgery Rep for BOTA. She has an MSc in Global Health and undertook the Diploma of Tropical Medicine and Hygiene in East Africa. She has worked in various capacities in Uganda, Ethiopia and Malawi. She is Primary Trauma Care (PTC) faculty and outgoing Surgical Rep for GASOC.

Matthew Arnaouti is currently working in the Bone Tumour Unit at the Royal National Orthopaedic Hospital, starting ST3 in the North West London region in October. He is a post-graduate research fellow in Global Surgery and Social Change, at Harvard Medical School – researching trauma systems development and disaster response in LMICs.

William Nabulyato is a Lower Limb Fellow at Barts Health, who completed T&O training in EoE Deanery. He holds an MPhil in Population Health Science from the University of Cambridge, served as a CGHP Global Health Fellow, PTC Educational Research Fellow and has a further clinical fellowship at BOSMC, Brisbane, Australia.
Global surgery ‘the trainees’ perspective’: Ten things we have learnt so far...
Alice Campion, Matthew Arnaouti, William M Nabulyato, James Archer, Alex Schade and James Berwin
Global surgery can be defined as “an area of study, research, practice, and advocacy that seeks to improve health outcomes and achieve health equity for all people who require surgical care”1. The perspectives and insights of trainees have been described as ‘crucial’ in promoting advancements and addressing challenges in global surgery2
As a cohort of trainees from the World Orthopaedic Concern-UK (WOC-UK) network, we wish to share ten key insights from our collective experience in the multifaceted landscape of global surgical practice. We hope these insights offer guidance for navigating the complexities inherent in global surgical endeavours and highlight the role of trainees in shaping the future trajectory of this critical field.
1. Orthopaedic surgeons are urgently required
Nearly a decade after the Lancet Commission on Global Surgery highlighted the extensive burden of musculoskeletal trauma, and its disproportionate impact on low- and middle-
income countries (LMIC), the allocation of healthcare personnel and resources remains inequitable. Traumatic injury results in the premature death of over four million people annually3, and renders millions more either transiently or permanently disabled. This perpetuates a downward spiral of poverty with local, regional and global ramifications4
Analysis of surgical workforce statistics comparing the NHS and data presented at the College of Surgeons of East, Central and Southern Africa (COSECSA) 2023 Conference, reveals a striking discrepancy, with a ratio of 48:1 orthopaedic consultant per million population (Table 1)5,6
The scarcity of orthopaedic consultants encapsulates a critical gap in healthcare provision and underscores the urgent need for collaborative interdisciplinary strategies that bolster surgical capacity, enhance training programmes, and improve access for patients. By fostering partnerships between healthcare institutions, governments and independent organisations, concerted efforts can be made to improve care for all.
Trainee
Number of Orthopaedic Consultants Population Surgeons per 100,000 inhabitants COSECSA, 2022 424 411,000,000 0.103 England, Scotland and Wales, 2022 3,127 65,000,000 4.81
Table 1: Registered Orthopaedic Consultants in the United Kingdom (UK), excluding Northern Ireland 5, and 12 of the 14 member nations of the COSECSA6.
38 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk

James Archer is an ST7 orthopaedic trainee in the West Midlands and the Academic Officer for BOTA.

Alex Schade is an academic orthopaedic trainee in the West Midlands Deanery. His research interests are in conducting health system and cost-effectiveness trials in low-middle income countries. He has previously worked in Uganda and Cambodia and conducted his Wellcome Trust PhD on outcomes of open tibia fractures in Malawi.

James Berwin is doing his post-CCT fellowship in lower limb arthroplasty, revision arthroplasty and trauma at the Royal Prince Alfred Hospital, Sydney. He co-founded the Bahir dar Orthopaedic Network and Exchange with Severn (BONES), a teaching partnership between Severn Deanery and Bahir Dar, Ethiopia. He is the PTC lead for Ethiopia.
2. Meaningful clinical work is possible but needs to be conducted carefully
At the WOC-UK 2022 Conference, four ‘pillars’ of global surgery were discussed: Clinical, Advocacy, Research and Education (CARE). These pillars must be actualised within a Specific, Measurable, Attainable, Realistic and Time-bound (SMART) framework, to ensure transparent and accountable goal-completion7. Clinical work is often the fire that ignites long-term personal investment in global surgery, but to be conducted meaningfully, careful preparation is required. This should be guided by the department hosting the initiative, with appropriate oversight. At all levels, trainees should strive to positively affect and foster sustainable health-system collaboratives.
The British Orthopaedic Trainees Association (BOTA) and WOC-UK strongly support orthopaedic trainees who wish to pursue clinical opportunities in low-resource settings, and contribute to a number of trainee bursaries every year8. There are many excellent partnerships that trainees have been involved with, including the British Society for Surgery of the Hand’s partnership with the Lilongwe Institute of Orthopaedics and Neurosurgery in Malawi9, and the Kadoorie Senior Orthopaedic Fellowship in Cambodia10. Other trainees have engaged with collaborations within their local trusts, such as the ‘Cambridge Global Health Partnerships Fellowship’ scheme11 and the ‘Poole-Africa Link’12; or with international organisations such as the ‘Primary Trauma Care Foundation’13 and ‘Mercy Ships’14.
We believe that a bidirectional transfer of knowledge and skills benefits both the trainee and host institution. Trainees across the UK describe their experiences working in low-resource settings as incredibly valuable, sharing innovation, developing leadership skills and nurturing international relationships with overseas peers.
3. Working in global surgery can count towards training
As seen in other medical specialties, and parallel orthopaedic training programmes in other high-income countries, surgical placements in low-resource settings are rightly becoming increasingly formalised – and in some cases, count towards a ‘Certificate of Completion of Training’. Surgeons previously trailed behind our anaesthetic and emergency medicine colleagues, but fortunately the Speciality Advisory Committee (SAC) guidelines, not only state that trainees are permitted to take up to two-weeks of study leave for orthopaedic projects in lowresource settings, but that longer periods may be undertaken as an ‘Out of Programme Experience’ (OOPE). They have stipulated that this may be considered towards achieving
training competencies15. There is a growing recognition that clinical work in low-resource settings is valuable and can contribute towards achieving curriculum competencies.
Global surgical volunteering is supported by the Academy of Medical Royal Colleges16 and all four home nations17. The BOTA survey demonstrates a strong interest in global surgery experiences amongst UK orthopaedic trainees, which is largely supported by Training Programme Directors (TPD)18. Trainees have previously worked in low-resource settings for Out of Programme Research (OOPR), and currently, there is one trainee who is working overseas as part of Out of Programme Training (OOPT), rather than taking time out for an OOPE. We hope this will gain momentum with time, making it easier for trainees to benefit from valuable learning opportunities, and for TPDs to support them.
4. Clinical work is an ethical minefield –volunteer but don’t ‘voluntour’
As clinical work in low-resource settings becomes possible within training, a comprehensive understanding of ethical practice is a prerequisite for any trainee seeking to engage in international global surgery development work. It is essential to embrace a model of regulated professional partnerships, where those involved are governed by minimum standards, discarding outdated practices such as ‘voluntourism’19 Trainees must take conscious steps to mitigate any pressure to act beyond their current competencies. Furthermore, basic requirements should not be overlooked, such as ensuring clinicians are licensed to practise within the host nation and obtaining patient consent for treatment or clinical photography. Trainees can be placed in difficult situations, nevertheless, ethical standards must be adhered to at all times20
5. Advocacy needs to occur at every level
Along with its ethical challenges, the field of global surgery is unfortunately marred by a lack of regulatory mechanisms and evidencebased interventions21. Seemingly well-meaning projects are often driven by donor agendas, rather than those of beneficiaries22. Care must be taken not to undermine the integrity and capabilities of local institutions, where solitary interventions – which do not form enduring partnerships with the host country – risk creating parallel health systems that do not address LMIC healthcare objectives23-25 They significantly hinder sustainability and should be consciously avoided.
Whilst trainees are in a position to advocate for the right type of partnerships, they are also vulnerable to inadvertently perpetuating ineffective and potentially damaging practices. In order to prevent this, trainee- and studentled advocacy groups have been formed >>
Trainee
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 39
– including the ‘Global Anaesthesia, Surgery and Obstetrics Collaboration’ (GASOC)26 and the ‘International Student Surgical Network’ (InciSioN)27 – which facilitate responsible and impactful engagement of trainees, within global surgery education, research and fieldwork. Additionally, through providing educational resources, such as courses and conferences – they serve as platforms for uniting highand low-income trainees and promoting interdisciplinary collaboration. Following the Lancet Commission’s recommendation that trainees should develop broad competencies in global surgery, these groups are working towards its inclusion in medical school curricula nationally28,29
6. Listen and be accountable
In developing partnerships, actively listening to stakeholders in emerging economies is crucial30. Consensus meetings can be utilised to derive agendas that align with those of local health systems, ensuring that interventions are led by colleagues in host nations31. Without investment from local teams, courses and interventions are unlikely to be valued or sustained. Shortterm programmes can be worthwhile, but demand huge amounts of planning, specialised skill sets, and consecutive visits – wherein previous work is continued32. Further research into their cost-effectiveness is crucial. We have a responsibility to ensure accountability of engaged parties and ensure sustainable practice with explicit objectives and robust follow-up plans32
7. Promote equitable engagement in research
Our colleagues in low-resource settings face myriad barriers to conducting research. Academics from emerging economies are subject to marginalisation by major journals and are under-represented amongst editorial boards. They also face practical issues, such as fewer research facilities, greater clinical burdens, and limited protected time for research33.
Huge changes are required to decolonise global health34, and whilst the goal may be ‘local people writing about local issues for local audiences’, challenging the disproportionate imbalance in power in global health academia, and advocating to remove expensive article processing fees should continue33.
Trainees have a great potential to contribute to research collaborations with LMIC colleagues whilst advocating for high quality, ethical practices. The days of high-income country surgeons ‘data mining’ in low-resource
settings, and publishing their work as first author, are over. Research priorities should be driven by local stakeholders, facilitating policy and funding into areas that are important to local teams35
8. Perhaps the best way to be involved in global surgery is not through clinical work
Work in advocacy, training and research roles is achievable for trainees, and can provide sustained benefits which should be championed. For example, the Northwest Orthopaedic and Trauma Alliance for Africa (NOTAA) started an annual research methodologies course, at the request of trainees in Ethiopia. A collaboration between multiple organisations, it is freely available and globally accessible. They also help to run a ‘Residents’ Day’ which showcases work undertaken by Ethiopian residents, and collaborative projects with UK-based trainees, to improve clinical practice through audit and research. This pioneering initiative highlights how UK-based trainees can get involved with global surgery, without travelling overseas36
The trainee-led podcast ‘Global Scalpels’, showcases particular individuals who are contributing to the field of global surgery in innovative and inspiring ways37. Whilst online events hosted by ‘Cambridge Global Health Café’, provide trainees with the opportunity to gain exposure to diverse perspectives and evidence-based approaches to patient care interventions, as well as critical insights regarding participation.
Collaborative initiatives, such as the partnership between the Guyana Orthopaedic Training Programme and the Birmingham Orthopaedic Training Programme, exemplify a model for engaging in mentorship, regular virtual teaching sessions, and developing open-access educational resources38. These roles represent potent mechanisms for fostering enduring relationships that enhance innovation, mutual support, camaraderie, and ultimately the potential for positive outcomes that transcend national boundaries.
9. Involvement in global surgery is self-investment
It is clear that our involvement in global surgery as trainees strengthens our own professional skills and competencies –enabling us to develop skills to communicate across professional cultures and learn about the processes required to enact and sustain change23,39. Bidirectional learning and overseas volunteering facilitates access to novel approaches to healthcare delivery.
Healthcare volunteers often report having a greater confidence to challenge and change established practice in their trust based on their experiences, as well as having exposure to a wider variety of clinical conditions29,40 Research shows that involvement in overseas partnerships results in improved enthusiasm, better staff morale, reduced rates of sick leave, and reduced workforce attrition41.
10. Working towards equity in global surgery is a marathon not a sprint
Quick solutions to complex problems rarely exist. As with any area of medicine, sustained engagement and commitment is required to ensure the success of international collaborations. Trainees who become involved in global surgery early on in their careers can identify areas of interest and tailor their experiences to strengthen existing skills. Ongoing participation, rather than transient contributions, is required to collectively work towards establishing equitable surgical care32.
Conclusion
We are grateful to many orthopaedic consultants who inspire and mentor us, and we are delighted that our educational bodies now support trainees wishing to pursue experiences working in low-resource settings. We recognise the importance of avoiding surgical colonialism and facilitating equitable engagement in research33,42. As we progress through our careers, we hope to meet the goals of high-quality, professional, and ambitious partnerships, by consolidating and strengthening existing schemes. We aim to improve collaboration, at regional and national levels, in all four pillars of Global Surgery: Clinical, Advocacy, Research and Education (23).
If you are reading this and want to get involved in global surgery, the WOC-UK Annual Congress serves as an excellent opportunity to engage with many different projects. Many alternative global surgery based conferences exist, most of which are accessible virtually. There are also a number of relevant surgical courses available, which can lead to further opportunities. See the World Orthopaedic Concern UK webpage for more details (https://wocuk.org ), follow us on twitter(@Orthoconcern), or contact globalsurgery@bota.org.uk for more information. n
References
References can be found online at www.boa.ac.uk/publications/JTO
Trainee
40 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk


fitting Corail ® (Depuy Synthes) Quadra ® (Medacta) Optimys (Mathys) Precise, safe and bone-saving swiss quality Official Distributor for the UK Judd Medical Unity House, Buntsford Park Road, Bromsgrove, Worcestershire B60 3DX Tel. +44 (0)15 27 55 90 10, sales@judd-medical.co.uk, www. judd-medical.co.uk www.gomina.ch J ig-guided hip revisions
Ownership of removed orthopaedic implants
Devapriyan Johnson, Ahmed Mahmoud, Simon Britten and Samuel Heaton
Patients occasionally express a desire to retain their removed medical implants. However, there is confusion amongst surgeons and other staff due to lack of clarity regarding ownership, cleaning and packaging of implants before returning them to patients.
Some staff refuse to return orthopaedic implants denying the patient requests, possibly due to infection control concerns. This hesitation is understandable in view of absence of clear guidance. We looked into existing national guidelines and local guidance revealing the complexities surrounding this issue. Additionally, in order to explore the


baseline understanding within a group of health professionals regarding retention of removed implants, we carried out prospective questionnaires. We have provided suggestions for adaptions to enable legal compliance and patient satisfaction.
Literature on the possible journey of removed orthopaedic implants
Implant removal is a common orthopaedic procedure1,2. In adults, removal indications include local pain, soft tissue irritation and infection, while in children, the practice also aims to prevent conflicts with the growing skeleton.
Opinions among orthopaedic departments vary, with assumptions that all metal implants are treated as ‘sharps’ and disposed of in a sharps bin, while others even believe that hospital trusts may monetise removed materials through recycling2. If removal is for infection the implant may be sent for microbiological assessment while anecdotally they sometimes become collector items for medical professionals.
In limb reconstruction practice implants are occasionally returned to the manufacturer for investigation if there has been early implant failure. Although returning them seems sensible for biomechanical evaluations and assessments of material properties, these practices are rarely undertaken3. The possibility of sterilising removed implants in low-resource hospitals raises concerns of the potential risks of infections2
Due to the absence of standards, the handling of removed implants varies based on the discretion of the local healthcare providers. In most hospitals orthopaedic devices are not sent to pathology or returned to the patient but rather disposed of, much like sharps, through local aggregation and eventual incineration.
Medico-legal
Devapriyan Johnson is a LAS registrar at Yeovil District Hospital. He is the President of UK Future Surgeons (UKFS), a society providing regular teaching and training for foundation and core trainees.
Ahmed Mahmoud is a speciality doctor in Trauma and Orthopaedics at Somerset NHS Foundation Trust.
42 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 1: An 85-year-old lady sustained a periprosthetic fracture of the proximal femur with a broken stem. Before revision hip replacement, she requested to keep her removed implants. Post-operatively, the removed implants were washed and given to the patient in a clear sample bag.

Simon Britten is a Consultant Trauma and Orthopaedic Surgeon specialising in lower limb reconstruction. He is the current President of the British Limb Reconstruction Society and Chair of the BOA Medico-legal Committee.

Sam Heaton is a consultant orthopaedic surgeon at Somerset Foundation Trust and is Trauma lead at Yeovil District Hospital.
Perspectives within our orthopaedic department
We conducted a questionnaire-based survey within our department. Using opportunistic cohort sampling, we elicited insights from 37 participants, including orthopaedic consultants, junior doctors, theatre staff, ward and clinic nurses. Participants shared their perspectives on the handling of orthopaedic implants post-removal.
When asked about their knowledge regarding what happens to orthopaedic implants after removal, 90% believed they were disposed of, 8% thought they were retained by the health organisation, and 2% suggested they could be given back to the patient. Notably, 57% proposed that patients should not be allowed to keep the removed implants, while 43% were in favour of patients retaining them.
Whilst exploring the ownership of the removed implant, 60% presumed that the health organisation where the implant was applied or removed owns it. 38% believed it belonged to the patient, and the remaining group considered ownership linked specifically to the party who paid for the implant.
Opinions varied regarding the processing of implants before handing them to the patient. 43% advocated sterilisation, 30% preferred decontamination with antiseptic agents, and 27% suggested washing it under a sink would suffice. Overall, the results indicated a prevailing belief that removed implants are disposed of, with a majority presuming that hospitals own these implants. Respondents also revealed a preference for processing implants under sterile conditions before handing them to the patient.
National Regulatory Guidance: Insights from MHRA
The Medicines and Healthcare Products Regulatory Agency (MHRA) is an executive agency of the UK Department of Health and Social Care. The MHRA plays a pivotal role in ensuring the effectiveness and safety of medicines and medical devices.
According to advice received from MHRA, guidance on implant ownership stems from Health Notice HN (83)6, issued by the Department of Health and Social Security in 1983. Section 3 of this notice states that upon implantation, an implant becomes the property of the person in whom it has been implanted, retaining this status even if subsequently removed. Section 5 addresses potential disputes regarding the right of health authorities to retain an implant for
examination. To navigate such situations, a form of consent has been produced by the MHRA, ideally agreed with the patient and signed before surgery or soon after the implant’s removal when the patient regains consenting capacity4
The MHRA confirmed that no updates have been made to the guidelines or consent form since 19835. The law regarding consent has shifted over the last 40 years, away from paternalism to a patient autonomy-based model. This favours the concept of returning the implants to patients who requested them, if they are not required for microbiological investigation (infection) or return to the manufacturer for assessment (early or unexpected failure).
Local guidance: Coordinated approach to implant handling
We sought guidance from our hospital’s infection prevention control team and microbiology consultants. They advised a pragmatic approach, suggesting that metal implants could be washed with soap and water before being handed over to patients who wished to take them home. They emphasised clinicians to inform patients that the items were washed and not sterilised.
Further insights were gained through our interaction with the trust-wide surgical safety analyst team. They provided a comprehensive theatre standard policy form specifically designed for instances where patients express a desire to take away removed implants. The form includes patient demographic details, a section completed by medical staff detailing the type of implant, date and time of removal, surgeon and speciality information. Patient consent is a crucial component, acknowledging that the removed implant has been washed but not subjected to any specific decontamination process. The patient also accepts full responsibility for removing the implant from the Trust premises. This local guidance ensures a systematic and transparent approach, balancing patient preferences with infection control measures.
Adaptations to practice
Integrating insights from both the MHRA and our local infection prevention team, we proposed a pragmatic departmental policy for the handling and processing of removed orthopaedic implants. The policy highlights three options based on the preferences: the patient’s desire to receive the implant, the institution’s wishes to retain it for investigation or education, or if neither party wishes to keep the implant. >>
Medico-legal
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 43

If a patient wishes to receive the implant, our suggested practice involves completing a form for the removal of the implant. Subsequently, the implant is washed with soap and water and handed over to the patient. The completed document is then kept in the patient’s medical records.
In cases where the institution wishes to retain the removed implant, the proposed practice involves signing the MHRA consent form specifically designed for retaining implants. Conversely, if neither the patient nor the institution wishes to retain the implant, appropriate disposal methods are followed. This adaptive approach ensures a systematic and transparent process in line with both MHRA guidelines and local guidance, balancing patient preferences and clinical needs.
Summary
Foreseeing where the frequency of fracture fixations, joint replacements and subsequent implant removals continues to rise, it is important to navigate the complexities of implant handling postremoval. Our exploration into the perspectives within our orthopaedic department, complemented by insights from national and local bodies, emphasises the need for a standardised approach.
As per current MHRA national guidelines, the implants belong to the patient and
should be returned to the patient if they request ownership. The MHRA’s longstanding health notice, untouched since 1983, suggests an opportunity for re-evaluation 40 years on through either the MHRA or a new BOAST (British Orthopaedic Association Standards for Trauma) guideline. We recommend a collective consensus and consideration of new formal guidelines in the handling and processing of removed orthopaedic implants. Meanwhile, explore and adhere to any pre-existing local guidelines in your local hospitals.
The proposed adaptations in practice offer orthopaedic surgeons in our department a framework for managing patient expectations and improving their overall satisfaction. Balancing patient choices, institutional needs, and infection control, this approach not only streamlines implant handling but also advocates patient-centred care.
Key learning points
1. Contrary perhaps to popular belief, the patient owns any implanted and then removed surgical implants
2. The law and MHRA guidelines governing this go back to the early 1980s, well before any semblance of consent law based on patient autonomy and patient rights
3. 40 plus years on, we suggest that the issue should be revisited with the MHRA and the Department of Health and Social Care.
4. Individual trusts should have in place guidelines to facilitate safe provision of removed implants to patients if they request them, provided they are not required for microbiological or other analysis in cases of early or unexpected failure. n
References
1. Böstman O, Pihlajamäki H. Routine implant removal after fracture surgery: a potentially reducible consumer of hospital resources in trauma units. J Trauma 1996;41(5):846-9.
2. Walley KC, Bajraliu M, Gonzalez T, Nazarian A. The Chronicle of a Stainless-Steel Orthopaedic Implant. The Orthopaedic Journal at Harvard Medical School. 2016;17.
3. Hothi H, Bergiers S, Henckel J, et al. Analysis of retrieved STRYDE nails. Bone Jt Open 2021;2(8):599-610.
4. Hemming J. Metal-on-metal hip replacements - who owns your implant? Bevan Brittan [website], 2012. Available at: www.bevanbrittan.com/insights/ articles/2012/metalonmetalhipreplacements.
5. Department of Health and Social Security. Health services management ownership of implants and removal of cardiac pacemakers after death. London: Health Notice HN(83)6, 1983.
Medico-legal
44 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 2: Flowchart demonstrating our recommendations bringing together all the guidelines and infection control advice.
Human factors in surgical performance
James Tomlinson
James Tomlinson is a Consultant Spinal Surgeon in Sheffield, UK. He has an interest in surgical education and training, and is an Associate Medical Director for Education and Deputy Director of the Faculty of Surgical Trainers, RCSEd. He teaches nationally and internationally on surgical non-technical skills and human factors.
“Yes but what’s the ODEP rating...?” You have probably all overheard a conversation like this in the theatre coffee room, on more than one occasion. When was the last time you heard someone discuss instrument design, or the ideal image intensifier position for optimal operative workflow?
We talk a lot about the implants we use, but we spend less time thinking about the environment we deploy them in, or the optimal operative conditions for the surgeon using them. Human factors and ergonomics offer a wealth of opportunities to think about how we work within our environment, in the most effective ways, to deliver the highest standards of care for our patients.
Healthcare is increasingly complex and collaboration between different specialties, or even subspecialties is more and more common, and part of our normal working patterns. This issue’s articles explore the roles that ergonomists, psychologists, engineers and our industry partners can play in helping improve the work environment, and ultimately help us to improve patient care. Clinical academic research and multi-centre research studies are now well established in our specialty. In time, I would hope we will see similar studies exploring
surgeon performance and workplace design. This offers the opportunity to advance patient care, and help us ensure our colleagues can enjoy long and fulfilling careers.
We have three articles exploring this topic from different perspectives. Sue Deakin has written an eye-opening and uniquely personal piece through learning from an adverse event. Her article offers insights into the multiple factors that contribute to adverse events, and the opportunities for learning and system change. It also offers insights into the benefits a trained ergonomist can bring to an NHS Trust, and the opportunities to make improvements in working conditions for all surgical staff.
The second article written by Roshana Mehdian and Professor Deborah Eastwood, explores the importance of ergonomics in the operating theatre and other clinical environments. Increasing workforce diversity is vital to ensure we represent the populations we care for, and to ensure we select the very best future colleagues. It is critical then that we have surgical instruments and safety equipment suitable for all of our workforce; their article explores some of the challenges this brings, and some of the ongoing collaborations in the field.
Our final article brings a psychology and sports perspective to surgeon performance. Professor Steven Yule explores surgical non-technical skills and the emerging field of surgical sabremetrics. It is a timely exploration of current evidence to support non-technical skills training, and the opportunities that technology offers to understand how we optimise surgeon performance, and ultimately patient outcomes.

I hope you enjoy reading the articles. Our authors have all suggested opportunities for further reading and learning. The BOA continues to host a Non-Technical Skills (NOTSS) half-day course (pre-registration essential) on the Friday of BOA Congress. It would be great to see some of you there and continue the discussions in this fascinating field of work. n
Subspecialty
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 45
© Non-technical skills of surgeons (NOTSS), RCSEd.
Human factors ergonomics in healthcare: How we are influencing change and improving safety
Sue Deakin
Sue Deakin is a Consultant Trauma and Orthopaedic Surgeon at West Suffolk NHS Foundation Trust specialising in trauma, paediatric orthopaedics and foot and ankle surgery, and she is the Clinical lead for Human Factors. She is Vice President of AO UK and Ireland and a member of the British Orthopaedic Association wellbeing Steering Group.
Ideveloped an interest in human factors ergonomics in 2011, when after eight years as a consultant orthopaedic surgeon, our team during a routine Wednesday afternoon operating list, somehow managed to operate on the wrong ankle in a patient with bilateral ankle instability and the anaesthetist managed to block the wrong leg.
Thankfully, it was not the only functioning kidney, eye, ear or lung – but what if it had been? This possibility affected the whole team from clinic to ward to theatre. As I write this article 13 years on, I still get palpitations!
I needed to understand what, why and how this could happen with an experienced and technically capable team. It became apparent that there were multiple contributory factors to this ‘Never Event’.

The multiple contributory factors
1. Distractions in an overbooked clinic.
2. The patient could not decide which side to have operated on first and said she would make a decision on the day.
3. On the paper prescription for surgery at the time, there was no mandatory field for ‘side of surgery’ so no patient side appeared on the operating list.
4. An overworked nurse on the ward responsible for giving the patient her antiembolism (TED) stocking put the stocking over the mark on the correct leg for surgery.
5. The registrar and anaesthetist did not recheck the mark in the anaesthetic room at sign-in.
6. The scrub nurse prepped the unmarked, incorrect leg, whilst we scrubbed to be more efficient.
7. The newly introduced WHO checklist was not designed, at that time, to ensure another check of the mark just prior to knife to skin at time out.
8. The scrub nurse not rechecking the consent form (which was accurate.)
It was a problem with teamwork, tasks, design of equipment/tools and culture.
In the aftermath of this Never Event, l explored and discovered a discipline called human factors ergonomics. Why had I not learnt about this earlier you might ask. I could not believe it myself. This episode and my learning from it, have now transformed my surgical practice. >>
Subspecialty
46 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Figure 1: Proxies for Work as Done.
A just culture guide
This guide supports a conversation between managers about whether a staff member involved in a patient safety incident requires specific individual support or intervention to work safely. Action singling out an individual is rarely appropriatemost patient safety issues have deeper causes and require wider action.
The actions of staff involved in an incident should not automatically be examined using this just culture guide, but it can be useful if the investigation of an incident begins to suggest a concern about an individual action. The guide highlights important principles that need to be considered before formal management action is directed at an individual staff member.
An important part of a just culture is being able to explain the approach that will be taken if an incident occurs. A just culture guide can be used by all parties to explain how they will respond to incidents, as a reference point for organisational HR and incident reporting policies, and as a communication tool to help staff, patients and families understand how the appropriate response to a member of staff involved in an incident can and should differ according to the circumstances in which an error was made. As well as protecting staff from unfair targeting, using the guide helps protect patients by removing the tendency to treat wider patient safety issues as individual issues.
Please note:
• A just culture guide is not a replacement for an investigation of a patient safety incident. Only a full investigation can identify the underlying causes that need to be acted on to reduce the risk of future incidents.
• A just culture guide can be used at any point of an investigation, but the guide may need to be revisited as more information becomes available.
• A just culture guide does not replace HR advice and should be used in conjunction with organisational policy.
• The guide can only be used to take one action (or failure to act) through the guide at a time. If multiple actions are involved in an incident they must be considered separately.
Recommendation: Follow organisational guidance for appropriate management action. This could involve: contact relevant regulatory bodies, suspension of staff, and referral to police and disciplinary processes. Wider investigation is still needed to understand how and why patients were not protected from the actions of the individual.
3a. Are there agreed protocols/accepted practice in place that apply to the action/omission in question?
Are there indications that other individuals from the same peer group, with comparable experience and qualifications, would behave in the same way in similar circumstances?
Was the individual missed out when relevant training was provided to their peer group?
Did more senior members of the team fail to provide supervision that normally should be provided?
Supported by:


Subspecialty
END HERE
2b.
2c.
3b. Were the protocols/accepted practice workable and in routine use? 3c. Did the individual knowingly depart from these protocols? Start here - Q1. deliberate harm test Yes Recommendation: Action directed at the individual may not be appropriate; follow organisational guidance, which is likely to include senior HR advice on what degree of mitigation applies. The patient safety incident investigation should indicate the wider actions needed to improve safety for future patients. Yes Recommendation: Follow organisational guidance for appropriate management action. This could involve individual training, performance management, competency assessments, changes to role or increased supervision, and may require relevant regulatory bodies to be contacted, staff suspension and disciplinary processes. The patient safety incident investigation should indicate the wider actions needed to improve safety for future patients. Supporting consistent, constructive and fair evaluation of the actions of staff involved in patient safety incidents Recommendation: Action singling out the individual is unlikely to be appropriate; the patient safety incident investigation should indicate the wider actions needed to improve safety for future patients. These actions may include, but not be limited to, the individual. END HERE
1a. Was there any intention to cause harm?
Are there indications of physical ill health?
Are there indications of mental ill health?
if
all go to next question - Q3. foresight test If No to any Recommendation: Action singling out the individual is unlikely to be appropriate; the patient safety incident investigation should indicate the wider actions needed to improve safety for future patients. These actions may include, but not be limited to, the individual. END HERE
if Yes to all go to next question - Q4. substitution test If Yes to any 5a.
if No to all go to next question - Q5. mitigating circumstances if No Recommendation:
needed
if substance abuse could have been recognised
addressed earlier. END HERE END HERE END HERE 2a.
No go to next question - Q2. health test Yes Recommendation: Follow organisational guidance for health issues affecting work, which is likely to include occupational health referral. Wider investigation is still needed to understand if health issues could have been recognised and addressed earlier. END HERE Yes Based on the work of Professor James Reason and the National Patient Safety Agency’s Incident Decision Tree improvement.nhs.uk
2: NHS ‘A just culture guide’. JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 47
No to
4a.
4b.
4c.
Were there any significant mitigating circumstances?
Follow organisational substance abuse at work guidance. Wider investigation is still
to understand
and
Are there indications of substance abuse?
Figure
“The scientific
discipline
concerned with the understanding of interactions amongst
humans
and other elements
of the system, and applies theory, principles, data and methods to DESIGN in order to optimise human wellbeing and performance and overall system performance”. (Chartered institute of Ergonomics and human factors definition).


What is human factors ergonomics?
Put simply, it is ‘Making it easier to do things well or right, or harder to do things less well or wrong’.
Two recognised definitions of human factors/ ergonomics are:
“Enhancing clinical performance through an understanding of the effects of teamwork, tasks, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings”. (NHS Quality board definition).
“The scientific discipline concerned with the understanding of interactions amongst humans and other elements of the system, and applies theory, principles, data and methods to DESIGN in order to optimise human wellbeing and performance and overall system performance”. (Chartered institute of Ergonomics and human factors definition).
What did I do?
I produced a trust wide business case for a human factors approach to patient safety and quality of care in my role as the divisional director of surgery.
I read copiously, spoke to human factors experts, consulted the Clinical Human Factors group advice on our website on “‘How to’ Guide to Human Factors” – Volume 1 and 2 (https://chfg.org/how-to-guideto-human-factors-volume-1). The Clinical Human Factors group is a charity founded in 2007 by Martin Bromiley after the loss of his late wife during a routine operation.
I set up and facilitated training of a human factors faculty of interested clinicians of all types to deliver free, multidisciplinary, one-day Human Factors workshops, mainly focussing on team resource management skills. We now include faculty from the patient safety team.
We have trained over 900 people from all specialties in various roles, including porters, receptionists, clinicians, managers and leaders and we continue to do so.
I was aware that no matter how useful the skills picked up during these courses were, we needed a more systems thinking approach to make it easier for staff to do the right thing.
I wrote a business case and a job description for a fulltime human factors practitioner trained via the Chartered institute of Ergonomics and Human factors to get involved in using human factors science in enabling improvement of safety, efficiency and wellbeing.
Subspecialty
Figure 3: Basic needs at work framework.
4 | SEIPS quick reference guide and work system explorer
Figure 3. SEIPS work system explorer questions
Figure 4: System Engineering Imitative for Patient Safety (SEIPS) explorer questions NHS England. SEIPS is a framework for understanding outcomes within complex socio-technical systems. It describes how a work system (or socio-technical system, left) can influence processes (work done, middle), which in turn shapes outcomes (right). The SEIPS framework acknowledges that work systems and processes constantly adapt.
48 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
The role is not part of the management hierarchy. Their job is to help make it easier for us to do our work by casting a human factors ergonomics lens on WORK AS DONE. Not work as imagined /described/ prescribed by others far removed from the frontline (see Figure 1).
Examples of how we can apply the lens of human factors ergonomics to our work
Culture and looking after staff
At West Suffolk NHS Foundation Trust, we are involved in connecting with our HR team and organisational culture team casting a human factors lens on ways of supporting our staff.
We encourage them to think about how the NHS ‘A just culture guide’ ensures system factors are taken into account (see Figure 2). We encourage them to address work hygiene issues such as being paid on time, badges and logins are all in place to relieve unnecessary additional stress from colleagues’ shoulders. We asked them to look at practical ways of enabling psychological safety so that staff can raise concerns, suggestions and feel able to bring their whole selves to work.
We encouraged the implementation of 24/7 access to hot nutritious food for all staff. Our junior doctors now have this provided in the doctors’ mess. We are working to make this available to all staff.
We pushed for and achieved calm rooms during the COVID-19 pandemic so that staff could find a quiet non-clinical space to recover /rest from work pressures.
We are hoping to introduce the basic needs at work framework (Figure 3).
Patient safety improvement
At West Suffolk, we facilitated the training of patient safety investigators to use a human factors tool, System Engineering Imitative for Patient Safety (SEIPS), to consider systems factors in their safety investigations, see Figure 4. SEIPS is a tool now used in the newly implemented Patient Safety Investigation Response Framework (PSIRF). It ensures consideration of all the below in a patient safety investigation or after action review and it is now being incorporated into debriefing huddles, now known as swarm huddles immediately after an event.
SEIPS is a framework for understanding outcomes within complex socio-technical systems. It describes how a work system (or socio-technical system, left) can influence processes (work done, middle), which in turn shapes outcomes (right). The SEIPS framework acknowledges that work systems and processes constantly adapt. (Figure 4)
Our human factors practitioner (the HFP) is now a valuable link between our patient
safety team and the improvement teams in our trust. Many trusts have a gap between insight gleaned from patient safety incidents and implementation of the recommendations.
The HFP is working with our theatre leads to introduce National Safety Standards for Invasive Procedures (NatSSIPs 2.0), (Figure 5), to not only look at the steps and how we should do our implant checks, but to ensure implants are stored and labelled in a way to make it easier for us to get it right.
Proactive work on the environment we work in We have ensured a human factors ergonomist perspective is considered in the design of our proposed new hospital due to be built by 2030. They used their knowledge to translate what our co-production teams were suggesting to the architects.
For instance, the workflow in the path labs is easier and more efficient if the equipment is placed in a way that makes it easier in terms of ‘traffic flow’ to get tasks done.
Ensuring that we do not have ‘mirrored’ theatres as this makes it harder for anaesthetists. For example, it is not universally appreciated that all anaesthetic machines are now designed to only work on one side of the patient. This example highlights how seemingly inconspicuous changes in design can significantly affect system efficiency and safety.
Procurement of equipment tools and IT Within our Trust, we are ensuring there is collaboration with our procurement team to ensure that the equipment we buy has had human factors usability assessment declared and ideally tested in situ by those using it, for example, syringe drivers, operating tables, instruments should have been assessed to ensure they suit all types of user.
We are influencing our IT team to reconsider the electronic discharge summary template ergonomics to make it easier for discharge summaries to be completed with greater accuracy and efficiency. Negotiations are being led and influenced by feedback from those on the ‘ground’, namely the doctors doing the work, not those managing the system.
Observing and using human factors tools to analyse the challenges of doing drug rounds using a scan for safety drug administration system. Looking at drug storage, ordering, drug locker access, IT issues, scanning failure rates etc.
Service redesign
We are doing proactive work with the surgical operational team in the way we move an element of our elective orthopaedic work to an elective orthopaedic hub in our ICS. Using the SEIPS tool to ensure all aspects are considered with the input of staff.
Proactive work with the virtual ward leads continues to encourage optimisation of the system for both patients and staff alike.
Why should you as an orthopod take an interest in human factors ergonomics?
It will improve your own and your team’s wellbeing. It will improve your ability to provide safe quality effective care to your patients.
How can you be involved/learn more?
If you have a human factors ergonomics team in your trust, ask them to help – it is what they are there to do. If you have not asked, ask yourself why not? There are always points to learn.
Attend or become faculty on Non-Technical Skills for Surgeons (NOTSS) courses or Multidisciplinary Team Resource management courses.
Join the Clinical Human Factors Group –free membership lots of resources and advice on the website www.chfg.org
Visit the Chartered Institute of Ergonomics & Human Factors website at https://ergonomics. org.uk for courses from PGCert, MSc or PhD. n

Subspecialty
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 49
Figure 5: National Safety Standards for Invasive Procedures (NatSSIPs 2.0).

Roshana Mehdian is a trauma and orthopaedic registrar in south London. She worked for the HMG department of international trade in Washington DC, USA as the health and health technology specialist working closely with industry. She is Chair of the Healthcare Workers Foundation and a member of the BOA Diversity Working Group. She is a mum and a long time advocate for diversity and culture change in surgery.

Deborah Eastwood is UCL Professor of Paediatric Orthopaedic Surgery at Great Ormond Street and the Royal National Orthopaedic Hospitals. Deborah is Immediate Past President of the British Orthopaedic Association (BOA), a former council member of BSCOS (British Society for Children’s Orthopaedic Surgery) and current Board Member for EPOS (European Paediatric Orthopaedic Society).
Ergonomics for the diverse workforce
Roshana Mehdian and Deborah Eastwood
The 'Oxford English Dictionary' defines ergonomics as the ‘study of working conditions, especially the design of equipment and furniture, in order to help people work more efficiently’. Whilst ‘Ergonomics for Dummies’ defines this as ‘the study of how the human body interacts with the workplace’.
Let us put aside for the moment, that it is not uncommon to use a bin as a chair in the NHS, and ask ourselves which ‘human body’ are we talking about? Caroline Criado-Perez’s best-selling book ‘Invisible Women’ leaves little uncertainty that most commonly, the ‘human body’ is the male of the species whether it be in the design of car restraints or town planning and public transport routes, the historical data standard used has been that of ‘the average man1’.
The issue of ergonomics in surgery is gaining widespread recognition due to a surge in musculoskeletal injuries reported by surgeons in various specialties. Orthopaedic surgery is a physically demanding surgical specialty that puts enormous pressure on the musculoskeletal system via forceful and repetitive manoeuvres.
Predominant musculoskeletal (MSK) injuries reported involve the neck and lower back, followed by upper extremity injuries, including shoulder and rotator cuff disease, lateral epicondylitis, tendinitis and carpal tunnel syndrome. The career prevalence of MSK disorders in junior doctors ranges from 37% to 97%2. It is also recognised that the risk of injury may be higher in orthopaedics than in other surgical specialties due to unique ergonomic challenges of orthopaedic procedures.
It is true that trauma and orthopaedic surgery has historically been dominated by men and that there has been reason to use the ‘average man’ for workplace ergonomic consideration, however with the increase in female orthopaedic surgeons and greater ethnic diversity in the profession, there is a pressing need to revisit this standard.
This revisit ranges from tools to rota and service design. It follows that to fairly diversify the workforce we must design the workplace to meet the needs of this workforce, a significant undertaking.
When the price we pay is not only with efficiency, but also with our health, these considerations need to be taken seriously. Gone should be the days that these should be considered an occupational hazard when we now have the awareness, data and scientific capabilities to radically improve ergonomics in the workplace. All we need now is the will to make change happen or at the very least the eradication of our corporate willful blindness to these issues. Improvements in these areas for diverse surgeons will benefit all surgeons. The advocacy for diversification of ergonomics needs to come, from both surgeons and their employing trusts.
Inclusive orthopaedics
The British Orthopaedic Association Diversity and Working Group Committee, in recognising the need for updating of workforce ergonomic considerations, launched the Campaign ‘Inclusive Orthopaedics’ appealing to Orthopaedic Medical Devices Industry partners to set a new standard in tool design to meet the diversifying workforce. The letter
Subspecialty
50 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk


recognised the legacy of dynamic innovation in the orthopaedic industry and sought to galvanise its use in this new direction of travel.
The average glove size is around 7.5 for men and 6.5 for women. A significant number of surgeons self-report that hand size could be the cause of physical discomfort in their hands. Women have a smaller glove size, on average, and studies have shown that ill-fitting instruments are associated with greater difficulty and injury. The correct sizing could improve excess ulnar and radial deviation, ring handle pressure on fingers, and pressure on the thenar eminence that leads to better operation ergonomics2. In post menopausal women, both grip and pinch strength reduce making some tasks more difficult or impossible.
It is not only women who would benefit from an alternative approach to the design of tools. This approach could help others who have had to adapt to the one-size fits all approach, for example left handed surgeons, those with disabilities, or those that generally struggle with heavy weight power tools. There is evidence that power tools may present difficulties even in those they are ideally designed for, with problematic levels of vibration and wrist torque identified in previous studies3.
Surgeons who are not of average body size and shape may find it difficult to fit into a lead grown, and there is some evidence that gowns may increase levels of back pain and abnormal forefoot loading3
Tools
Repetitive use of heavy hammers, drills, and heavy equipment including jigs and instruments may account for high rates of occupational injury. Using appropriately sized instrumentation may reduce hand and forearm pain, as well as using lighter equipment to lessen the peak forces on upper extremities.
Table height
Table height plays a significant role in decreasing strain on back muscles, minimising neck flexion and reducing leaning and reaching over. The table height should also vary based on the nature of task performed. Performing a precise task such as soft tissue dissection or mobilising critical structures requires the table height to be about 5 cm above the level of your elbow (elbow height). For light work such as screw
“The British Orthopaedic Association Diversity and Working Group Committee, in recognising the need for updating of workforce ergonomic considerations, launched the Campaign ‘Inclusive Orthopaedics’ appealing to Orthopaedic Medical Devices Industry partners to set a new standard in tool design to meet the diversifying workforce.”
insertion or suturing, the table height should be approximately 5–10 cm below the elbow height. When performing heavy tasks, and downward forces are needed, such as drilling or impacting a component with a mallet, table height is recommended to be 20–40 cm below the elbow height. Diversity in design concepts might encourage a foot control to be used by the surgeon to adjust the table height - this would make it much more likely that adjustments were made as the surgical team would not be reliant on other staff to adjust the table height.
Non-musculoskeletal work-related injuries
Orthopaedic surgeons also face a higher incidence of nonmusculoskeletal work-related injuries. These include the risks of radiation exposure from using intraoperative C-arms; infections from accidental skin punctures by drills, saws, Kirschner wires, and bone shards; >>
Subspecialty
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 51
Figure 1: Ergonomics in the workplace.
inhaling surgical smoke and encountering chemicals like polymethylmethacrylate (PMMA) and isocyanate; as well as the risk of hearing damage due to the high decibel levels from power tools and intense suction device. Orthopaedic surgeons also experience cardiovascular and mental stress during procedures with higher mean blood pressure and heart rate on operating days3.
The strain brought about by poor work-place ergonomics is likely exacerbated by altruistic attitudes among surgeons, with many surgeons prioritising the health and safety of their patients whilst neglecting their own comfort and well-being.
Ergonomic solutions
Three categories of ergonomic solutions should be considered to reduce MSI risks:
1) Engineering controls (changes to the environment).
2) Administrative controls (workforce or human changes).
3) Personal protective equipment (PPE).
Engineering controls are changes that can be made in the operating theatre environment; these include structural changes such as bed height and equipment changes, such as the use of floor mats. Administrative controls are workforce or human changes. These include taking short breaks during prolonged operations and ergonomic training. PPE are tools individual staff may use, such as lighter lead aprons or body support equipment. Orthopaedic device companies are exploring instrument design through ergonomic research in collaboration with engineers.
Koshy et al. evaluated the literature on interventions currently used to minimize MSI in surgeons and reported that 69.9% of surgeons noted improvement in symptoms after implementing ergonomic solutions3
One difficulty is that despite recommendation and guidance on ergonomics there is a lack of data on the logistics of designing and executing ergonomic training programmes and how these programmes impact on surgeon outcomes. A study by Franasaik et al. utilised a brief surgical ergonomics programme within a group of robotic surgeons to demonstrate proper positioning and strategies to avoid robotic strain4. The programme consisted of a slideshow presentation and an in-person training session on how to set up the robotic console. They found that 88% of participants made changes to their operative practice
after taking part in the programme, and 74% reported reduced robotic associated strain because of the training.
With the drive for national teaching programmes, there is a clear opportunity to incorporate surgical ergonomics training into higher surgical training programmes so surgeons can understand the potential risks and how to mitigate them.
PPE and X-ray protection
The most high profile case of poor ergonomics is that of PPE, coming to light as the COVID-19 pandemic struck, with high rates of fit test failure amongst women and nonCaucasian ethnicities6. Ill-fitting PPE in surgery is a common frustration amongst the diverse workforce with, for example, surgical gowns often being too long, too small or too large, and limited options available at any one trust.
Disposable surgical gowns also carry a significant environmental cost and there is a need for surgeons to be more involved in gown design and procurement.
Most recently, PPE specific to surgeons exposed to ionising radiation by theatre based C-arms/X-ray has been found to be inadequate at protecting women. Exposure has been linked to increased incidence of breast cancer in female health workers. Studies have shown that current gown designs, during certain specific operative procedures, risk exposing the upper outer quadrant of breast tissue to excess irradiation. This is the area of the breast which is most likely to develop the disease.
A UKHSA/BOA study dosimetry study is currently underway to quantify the amount of exposure to ionising radiation of the chest wall versus the axilla. This study hopes to provide important evidence on the relative exposures to irradiation for surgeons of all grades over a three-month period.
Irrespective of the study results, there is clearly a requirement for trusts to provide lead gowns, thyroid shields and eye guards that are appropriate for their diverse staff to use comfortably and safely. Such diversity includes factors such as age, size, shape and specialty interest. Heavy, poorly fitting gowns also contribute to MSK occupational problems affecting agility and stamina and causing pain and stiffness.
There is also a need for both research and training on image intensifier positioning and use in theatre, to ensure that radiation use is minimised, with careful thought to the positioning of key personnel in theatre when
using it. Orthopaedics will always be an X-ray dependent specialty but a starting point must be to minimise its use.
If it is a requirement that office workers in the NHS are assessed for appropriate desk and chair heights and shape for example (see figure 1), it must surely also be a requirement that PPE fits the person wearing it.
In summary, the research of improving the ergonomics of operating and reducing musculoskeletal injury in surgeons has been gaining widespread recognition. It is hoped that with improvements in the design of the operating environment and the use of tools that elevate user comfort while improving safety, performance, and efficiency this will enhance work performance and reduce the incidence of work-related musculoskeletal injury. An increasingly diverse workforce, with rising retirement ages means there is an urgent need to increase our understanding of surgical ergonomics and ensure the long-term health of our workforce and patients. n
References
1. Perez, C. C. (2019). Invisible Women: the Sunday Times number one bestseller exposing the gender bias women face every day. Random House.
2. Tran M, Kortz MW, Johnson B, Janis JE. Operation-related Musculoskeletal Injuries among United States Surgeons: A Genderstratified National Survey. Plast Reconstr Surg Glob Open. 2022;10(2):e4142.
3. Vasireddi N, Vasireddi N, Shah AK, et al. High Prevalence of Work-related Musculoskeletal Disorders and Limited Evidence-based Ergonomics in Orthopaedic Surgery: A Systematic Review. Clin Orthop Relat Res. 2024;482(4):659-71.
4. Koshy K, Syed H, Luckiewicz A, et al Interventions to improve ergonomics in the operating theatre: A systematic review of ergonomics training and intra-operative microbreaks. Ann Med Surg (Lond) 2020;55:135-42.
5. Franasiak J, Craven R, Mosaly P, Gehrig PA. Feasibility and acceptance of a robotic surgery ergonomic training program. JSLS 2014;18(4):e2014.00166
6. Shelton C, El-Boghdadly K, Appleby JB. The ‘haves’ and ‘have-nots’ of personal protective equipment during the COVID-19 pandemic: the ethics of emerging inequalities amongst healthcare workers. J Med Ethics. 2021;48:653-7.
Subspecialty
52 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Behavioural science approaches to enhancing surgical performance
Steven Yule
Steven Yule is Professor of Behavioural Sciences at the Usher Institute, University of Edinburgh where he leads the Surgical Sabermetrics Laboratory and MSc in Clinical Human Factors and Patient Safety. He is also Director of NonTechnical Skills for the Royal College of Surgeons of Edinburgh. Steve is an academic psychologist with 20 years’ experience studying team performance and non-technical skills in high risk/high reliability industries (surgery, healthcare, energy, transportation, space exploration).
In the realm of surgery, proficiency extends beyond mere technical prowess; it involves a nuanced understanding and application of non-technical skills (NOTSS) that are indispensable for optimal performance1. Recognised as pivotal components in surgical practice, NOTSS encompasses a range of abilities including situation awareness, decision-making, communication, teamwork, and leadership. These skills are fundamental in successful navigation of the complex and dynamic surgical environment, where split-second decisions and effective collaboration can mean the difference between success and failure. Non-technical skills constitute the bedrock upon which surgical proficiency is built for professional life, complementing technical skills to ensure optimal performance, patient care and team well-being in the demanding environment of the operating room. As such, cultivating and refining these skills is imperative for surgeons seeking to excel in their practice and enhance the quality and safety of surgical interventions. In this article, I will describe the evidence base for non-technical skills in surgery, introduce surgical sabermetrics and data-science approaches to measuring operative performance, and suggest future implementation of NOTSS in surgical training and practice for all.
Situation awareness lies at the core of NOTSS, enabling surgeons to maintain a comprehensive understanding of the evolving picture during a procedure. This entails not only recognising the current state but also anticipating future developments and potential complications. Decision-making, another crucial aspect, involves the ability to evaluate various options swiftly and effectively under pressure, often with incomplete information.
Communication serves as the linchpin of teamwork in the surgical setting. Clear and concise communication among team members facilitates coordination, enhances efficiency, and mitigates errors. Moreover, effective communication extends beyond verbal exchanges to encompass non-verbal cues and active listening, fostering mutual understanding and trust among team members. Teamwork, in conjunction with leadership, forms the basis of collaborative efforts in surgery. A cohesive surgical team, characterised by mutual respect, shared goals, and distributed leadership, can enhance patient outcomes, and mitigate adverse events. Leadership within this context involves not only directing and coordinating team activities but also fostering a culture of safety, accountability, and continuous improvement. It is important to emphasise that leadership is action, rather than position – and although surgeons are often thought of as the leader in the operating room, other team members can provide leadership during different phases of the procedure.
Surgical sabermetrics
Sabermetrics involves the systematic analysis of video footage and performance data to glean actionable insights and facilitate informed decision-making. While traditionally associated with sports such as baseball, its application in fields like trauma and orthopaedic surgery holds immense promise for enhancing patient care and refining surgical techniques (Figure 1). Sabermetrics involves a multidimensional examination of performance factors, encompassing individual skills, team dynamics, system resources, and patient variables, such as surgical techniques, non-technical proficiencies, >>
Subspecialty
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 53

Figure 1: Surgical sabermetrics applies baseball-inspired data science to provide new insights into operating room performance that enhances patient safety and saves lives. [Reproduced with permission from Elsevier, original reference: Yule S, Janda A, Likosky DS. Surgical sabermetrics: Applying athletics data science to enhance operative performance. Annals of Surgery Open [Internet]. 2021;2(2):e054.
and clinical outcomes2. By harnessing datadriven methodologies, surgeons can deepen their understanding of surgical intricacies, pinpoint areas for enhancement, and enact tailored interventions to optimise patient results. Integrating sabermetrics alongside conventional surgical metrics may unveil additional insights into patient outcomes, bolstering patient safety, quality of care, and educational endeavours through personalised training, performance feedback, team refinement, and real-time clinical guidance.
Sabermetrics leverages surgical data science, an interdisciplinary field that involves extracting insights and knowledge from structured and unstructured data through various methods, including statistics, machine learning, and data visualisation. Surgeons can utilise data science to enhance their performance and patient outcomes by leveraging data-driven approaches. They collect and analyse surgical data, such as operative times, complication
Decision-making Spinal fusion: Involves complex decisionmaking regarding the selection of fusion levels, instrumentation, managing intra-operative challenges, and reviewing decisions.
Communication ACL reconstruction: Demands clear communication among surgical team members regarding graft selection, tunnel placement, and post-operative care instructions.
Teamwork Total knee replacement: Relies on effective collaboration among surgeons, anaesthetists, nurses, and other team members for efficient intra-operative workflow and patient safety.
Leadership Fixation of femoral shaft fracture: Requires strong leadership to coordinate the surgical team, prioritise tasks, and manage unexpected complications during the procedure.
1: Example NOTSS skills and sabermetrics data for orthopaedic surgery.
• Video-based scenarios
• Virtual reality simulations
• Observation assessments
• Case-based discussions
• Decision-making exercises
• Reflective practice activities
• Communication skills assessments
• Simulated surgical team interactions
• Debriefing sessions
• Team-based simulations
• Peer evaluations
• Surgical team observation assessments
• Leadership role-play exercises
• 360-degree feedback assessments
• Crisis scenarios simulations
rates, and patient outcomes, to identify patterns, trends, and areas for improvement. Through predictive modelling, surgeons can anticipate potential complications or optimise surgical techniques tailored to individual patient characteristics. Additionally, data science enables surgeons to track their performance over time, receive personalised feedback, and engage in continuous learning and improvement. By integrating data science and sabermetrics into their practice, surgeons can make more informed decisions, enhance patient safety, and ultimately improve the quality of surgical care. Examples of non-technical skills and sabermetrics data relating to several orthopaedic surgical procedures are illustrated in Table 1.
In laparoscopic bariatric surgery, peer evaluations based on video footage assessing technical skills, such as suturing movements and instrument handling, have yielded valuable performance insights predictive of outcomes3. The advent of artificial intelligence-enabled video analysis holds promise for transformative advancements in surgery, promising reduced errors, improved patient care, and enriched professional growth for clinicians. The integration of computer vision and machine learning in automating operative phase detection is paving the way for real-time clinical decision support systems, revolutionising surgical safety and quality4
Subspecialty
Non-technical skills category Illustrative orthopaedic surgical procedures Potential sabermetric data sources for formative assessment Situation
during the
awareness Total hip replacement: Requires awareness of anatomical landmarks, implant size availability, potential complications, and patient positioning
procedure.
Table
54 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk
Nevertheless, individual proficiency alone does not guarantee consistent success. A significant portion of surgical outcomes hinges on team dynamics, communication, situational awareness, adaptability, and decision-making. Consequently, emerging sabermetric-like capabilities for team performance analysis are gradually finding application in surgery. Crowd-sourced video platforms equipped with taxonomies for assessing technical and non-technical skills across surgical teams, including surgeons, anaesthetists, and scrub practitioners, are harnessing embedded artificial intelligence to uncover previously unseen practice patterns, signalling an imminent revolution in surgical sabermetrics.
Improving your own non-technical skills
Several options are available to surgeons at all career levels who are interested in enhancing performance through dedicated non-technical skills training:
1. Simulation-based training: This offers surgeons a safe environment to practice and refine their non-technical skills. Through realistic scenarios that mimic surgical situations, all trainees can enhance their communication, teamwork, and situation awareness. Senior trainees and consultants can hone decision-making, and leadership abilities. These simulations may involve virtual reality platforms, high-fidelity mannequins, or standardised patients. By immersing themselves in simulated surgical experiences, learners can develop confidence, practice new skills, improve performance, and learn how to navigate challenging situations. Instructors provide structured feedback and debriefing sessions after each simulation, offering valuable insights and allowing learners to identify strategies for continual improvement.
2. Structured debriefing: Debriefing sessions are a critical component of both simulationbased training and real clinical experiences. Structured debriefing involves a systematic review of the simulation or clinical encounter, focusing on both technical and non-technical aspects of performance. Trainees reflect on their actions, decisions, and communication strategies during the scenario. Facilitators guide the discussion, encouraging trainees to identify strengths, weaknesses, and areas for development. Through open dialogue and constructive feedback, trainees gain valuable insights into their non-technical skills and learn how to apply lessons learned to future practice.
3. Peer observation and feedback: This is a strategy that can be enacted without any equipment or technology, providing trainee surgeons with an opportunity to learn from their colleagues and receive valuable insights into their nontechnical skills. Trainees can observe each other during simulations, surgeries, or clinical interactions, paying attention to communication patterns, teamwork dynamics, and leadership behaviours using a validated framework such as the NOTSS taxonomy5. Afterwards, peers provide feedback on observed strengths and areas for improvement. This reciprocal process promotes a culture of continuous learning and collaboration, fostering mutual support and professional growth. Instructors also often learn new strategies from participants which can be passed on to others, enriching the learning experience.
4. Surgical coaching: Mentorship relationships often extend beyond technical proficiency to encompass broader professional development and career guidance, further enriching the learning experience for trainee surgeons. This is different from surgical coaching, a recently adopted method for skill enhancement and patient safety improvement, drawing from business and sports coaching techniques that emphasise adult learning principles. Unlike teaching and mentorship, it prioritises surgeons becoming agents of change. Various coaching programmes for surgeons exist worldwide, such as the Surgical Coaching for Operative Performance Enhancement (SCOPE) programme from Ariadne Labs in Boston6. SCOPE defines coaching as a collaborative partnership between two surgeons aimed at pursuing self-identified goals through joint analysis, feedback, and peer learning support. It focuses on continuous development of intraoperative performance, covering technical skills (e.g. tissue respect, exposure, instrument handling) and non-technical skills (e.g. situation awareness, decisionmaking, communication). The programme follows four principles: self-identified goals, collaborative analysis, constructive feedback, and peer learning support. Current questions regarding how best to train peer coaches, coach-coachee matching mechanisms, and optimal metrics for evaluating surgical coaching are being investigated. As surgical coaching evolves, it presents an avenue to enhance skills and patient safety throughout surgeons’ careers.
The technological future of surgical performance
As we look ahead to the future of surgery, the convergence of advanced technologies and innovative methodologies promises a new era of excellence and precision in patient care. With continued integration of artificial intelligence, virtual reality, and augmented reality into surgical practice, surgeons could have access to real-time feedback, personalised training, and predictive analytics, revolutionising the way surgeries are performed and outcomes are optimised. As surgical sabermetrics and data science become increasingly sophisticated, the operating room of tomorrow will be a dynamic ecosystem where decisions and action are informed by data-driven insight, ensuring that every patient continues to receive the highest standard of care, every time. n
References
1. Yule S, Gupta A, Gazarian D, Geraghty A, Smink DS, Beard J, et al. Construct and criterion validity testing of the Non-Technical Skills for Surgeons (NOTSS) behaviour assessment tool using videos of simulated operations. Br J Surg. 2018;105(6):719-27.
2. Howie EE, Ambler O, Gunn EG, Dias RD, Wigmore SJ, Skipworth RJ, et al. Surgical Sabermetrics: A Scoping Review of Technology-Enhanced Assessment of NonTechnical Skills in the Operating Room. Ann Surg. 2024 Jan 23; [Online ahead of print].
3. Birkmeyer JD, Finks JF, O’Reilly A, Oerline M, Carlin AM, Nunn AR, et al. Surgical skill and complication rates after bariatric surgery. N Engl J Med. 2013;369(15):1434-42.
4. Hashimoto DA, Rosman G, Witkowski ER, Stafford C, Navarette-Welton AJ, Rattner DW, et al. Computer Vision Analysis of Intraoperative Video: Automated Recognition of Operative Steps in Laparoscopic Sleeve Gastrectomy. Ann Surg. 2019;270(3):414–21.
5. The Royal College of Surgeons of Edinburgh [Internet]. [cited 2024 May 12]. Non-Technical Skills for Surgeons (NOTSS). Available from: www.rcsed.ac.uk/professional-supportdevelopment-resources/learning-resources/ non-technical-skills-for-surgeons-notss.
6. Pradarelli JC, Yule S, Panda N, Lowery KW, et al. Surgeons’ coaching techniques in the Surgical Coaching for Operative Performance Enhancement (SCOPE) program. Ann Surg 2022;275(1):e91-e98.
Subspecialty
JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk | 55
John Robson Kirkup
17th March 1928 – 17th March 2024
Obituary by Ian Stephen
John Robson Kirkup was born on 17th March 1928 at Chester-le-Street, County Durham. His mother was a schoolteacher, and his father was a tenant farmer, supplying food to nearby coal mines, but later working as a blast furnaceman in Corby. John attended Kettering Grammar School and was initially intent on joining the Merchant Navy. However, his headmaster suggested studying medicine and he gained a place to read natural sciences at Emmanuel College, Cambridge. He then went to St Mary’s Hospital in London, where he was taught bacteriology by Alexander Fleming. He qualified in 1952.
During his house jobs, he found that he had a talent for fracture manipulation and decided on a career in orthopaedics. He did his National Service in the Royal Navy and was a Surgeon-lieutenant in the Naval Dockyard in Malta where he saw all sorts of traumatic injuries. On return to civilian life, he was surgical registrar at the Norfolk and Norwich Hospital, where he was taught by Ken McKee, and then a senior registrar at the Bath and Wessex Orthopaedic Hospital. He was appointed as a consultant in Bath in 1964.







We specialise in casing and packaging solutions for orthopaedic implants, medical equipment and have supplied many of the world’s leading medical organisations.
We specialise in casing and packaging solutions for orthopaedic implants, medical equipment and have supplied many of the world’s leading medical organisations.
Our flight cases are made in our 70,000 sq ft factory in the UK using the highest quality materials to ensure that your vital
Our flight cases are made in our 70,000 sq ft factory in the UK using the highest quality materials to ensure that your vital equipment is fully protected in transit.

During his long career as an orthopaedic surgeon working in the Bath Clinical Area, John specialised in lower limb surgery, with a particular interest in children’s leg lengthening after polio. Later, he specialised in foot and ankle surgery, particularly the surgical treatment of rheumatoid arthritis, and developed the Bath and Wessex ankle joint replacement. He retired from active practice in 1988. He was a long-standing fellow of the BOA, serving on Council, and he was appointed as Honorary Archivist in 1980. He was in this post for twenty years, longer than any of his predecessors since it was inaugurated in 1953. He also acted as President of the British Society for the History of Medicine and of the History of Medicine Section of the Royal Society of Medicine.
He developed an interest in medical history, particularly the evolution of surgical instruments. He had gained a Diploma in Medical History from the Society of Apothecaries in London in 1979 and later acted as Lecturer in Surgical History to the Diploma Course. He was an Honorary Curator at the Royal College of Surgeons of England in London, where he helped to identify and catalogue the surgical instrument collection and made many contributions to the development of the Hunterian Museum. He had a large personal collection of medical antiques and donated many of them to the Museum of Medicine and Health in the Manchester Medical School. He founded the Historical Medical Equipment Society in 1996 and acted as chairman until 2004.
He published three important reference books: The Evolution of Surgical Instruments (2006), which is considered perhaps the most prominent work on the evolution of surgical instruments yet published: A History of Limb Amputation (2007) and An Illustrated History of Hip Joint Surgery: from Hippocrates to Charnley (2014). He also wrote many papers and book chapters on surgical instruments, including 31 articles in the Journal of Medical Biography, and presented many eponymous lectures. He was awarded the Sir Arthur Keith medal and an MBE for services to medical heritage in 2011.
John was married to Pierrette Léger, a French teacher and artist from Bordeaux and they had four children. His wife and children all survive him. He died on his 96th birthday, 17th March 2024. n
equipment is fully protected in transit. We design and manufacture cases to your exact specification. A range of pull-out drawers, shelves, lift-out trays, doors and shutters can be integrated into the case. With an in-house design team and advanced computer aided design and CNC routing facilities, we can produce custom foam interiors to
house implant samples, instruments and any other equipment.
We design and manufacture cases to your exact specification. A range of pull-out drawers, shelves, lift-out trays, doors and shutters can be integrated into the case. With an in-house design team and advanced computer aided design and CNC routing facilities, we can produce custom foam interiors to house implant samples, instruments and any other equipment.
Trifibre Ltd 17 Boston Rpad
Trifibre Ltd 17 Boston Rpad Gorse Hill Industrial Estate Leicester LE4 1AW
Telephone: 0116 232 3166
Email us: info@trifibre.co.uk
Web: www.trifibre.co.uk
Gorse Hill Industrial Estate Leicester LE4 1AW
Telephone: 0116 232 3166
Email us: info@trifibre.co.uk
Web: www.trifibre.co.uk




Download the App


The Journal of Trauma and Orthopaedics (JTO) is the official publication of the British Orthopaedic Association (BOA). It is the only publication that reaches T&O surgeons throughout the UK and every BOA member worldwide. The journal is also now available to everyone around the world via the JTO App. Read the latest issue and past issues on the go, with an advanced search function to enable easy access to all content. Available at the Apple App Store and Google Play – search for JTO @ BOA
In Memoriam 56 | JTO | Volume 12 | Issue 02 | June 2024 | boa.ac.uk

Preventing PJI in arthroplasty patients
Know your patient – and reduce PJI risk!
A tremendous challenge in arthroplasty
Periprosthetic joint infection (PJI) is a frequent, severe, and costly complication following total joint arthroplasty, accounting for up to 2% in primary surgery and 4% after revision.1 Potential complications can range from superficial skin infections to more serious problems such as loss of limb or amputation which can be caused by deep PJI. Implant infections can result in substantial morbidity, mortality, and health care costs and have a negative impact on patients’ quality of life and psychological well-being. Treatment of PJI usually requires surgical intervention and prolonged intravenous or oral antimicrobial therapy.2
Despite many advances in research and clinical practice over the last decades, prevention and management of PJI remain challenging not only for the orthopaedic team, but also for the patient.
Take your patients’ risk into consideration
Not all patients undergoing total joint arthroplasty are equally at risk of developing post-operative infections. Identifying and addressing associated risk factors prior to surgery is essential in reducing PJI after surgery. Risk factors can be both patientrelated or treatment-related.
Some patient-related PJI risk factors are: older age, diabetes, cardiovascular disease, obesity, previous infection, smoking and revision surgery.3-5 According to a clinical risk
score established by Sanz-Ruiz & Berberich, a high risk of PJI is defined by the presence of two or more of the above-mentioned risk factors in knee arthroplasty patients and three or more in hip arthroplasty patients.3 Based on results obtained with this score approximately 60% of patients aged 65 years or older are at higher risk for infection.3
An integrated and effective preventive approach to reduce the risk of infection in patients with risk factors is essential. In this respect, individually tailored measures for infection prevention may include optimisation of surgical procedures, such as skin preparation and wound irrigation, improved peri-operative blood management, pre-operative optimisation of patient risk factors and comorbidities, normothermia and adequate oxygenation as well as systemic peri-operative antibiotic prophylaxis. Last but not least, the addition of high-dose antibiotics to bone cement can be implemented as part of a risk-adapted approach.3,5-8
Dual antibiotic-loaded bone cement: effective in various clinical prevention settings
In particular, using dual instead of single antibiotic-loaded bone cement such as COPAL® G+C can provide a viable option within the set of preventive measures.3,7 Clinical trials have demonstrated effectiveness of high-dose gentamicin- and clindamycin-loaded COPAL® G+C bone cement in common clinical settings such as in primary and revision hip and knee arthroplasty as well as in trauma.
In elective primary hip and knee arthroplasty dual antibiotic-loaded bone cement has been shown to reduce PJI frequency from 3.7% to 2.5%;3 in fractured neck of femur, PJI frequency was reduced from 3.5% to 1.1%;9 and in aseptic revision knee arthroplasty a reduction from 4.1% to no PJI was shown.10
Furthermore, dual antibiotic-loaded bone cement appears not only to be more effective but also more cost-efficient than a single antibiotic-loaded bone cement in aseptic knee arthroplasty.10
Lower PJI burden – now!
Due to demographic aging, arthroplasties such as hip replacement surgery are projected to be performed in a growing number of patients. The number of PJI-related implant failures and the need for revision surgeries associated with PJI are, consequently, expected to further increase. Accordingly, it is essential to lower the high burden of PJI faced by clinicians, institutions, and patients.11,12
Clinical evidence shows that arthroplasty patients can benefit from an integrated and risk-stratified preventive approach.3 In particular, elderly high-risk patients obtain advantages from prevention measures that may include the use of high-dose dual antibioticloaded bone cement for implant fixation.8 n
References available upon request.
SPONSORED CONTENT www.heraeus-medical.com

My patient was desperate. Having tried lifestyle changes and other treatment options for his debilitating hyperhidrosis and blushing, he wanted a sympathectomy.
Two years after the surgery I received a letter that set my heart racing. It was from the patient’s solicitors, requesting a copy of his medical records. Chronic compensatory sweating had led to severe depression, and he deeply regretted the operation.
Medical Protection were immediately there for me. My medicolegal consultant concluded that I’d undertaken a thorough consent process, and was in a strong position to defend an allegation of negligence. The patient’s solicitors agreed, and thankfully no further action was taken.
This has reaffirmed two things for me: the importance of a detailed consent discussion and the support I get from Medical Protection. They know exactly what to do and always have a plan for doing it. As well as helping with legal advice, they offer risk reduction courses to prevent problems happening. I’ve always known I needed protection. Now I fully appreciate the value of everything my membership gives me.
I’m a consultant and... I was facing a possible negligence claim Always there for you medicalprotection.org/case5 The Medical Protection Society Limited (“MPS”) is a company limited by guarantee registered in England with company number 00036142 at Level 19, The Shard, 32 London Bridge Street, London, SE1 9SG. MPS is not an insurance company. All the benefits of membership of MPS are discretionary as set out in the Memorandum and Articles of Association. MPS® and Medical Protection® are registered trademarks. For information on MPS’s use of your personal data and your rights, please see our Privacy Notice on our website. This case is based on a real scenario, with some facts altered to preserve confidentiality. *Cost shown is the annual membership price for a UK Medical Consultant working exclusively in the NHS. Subject to protection requirements and underwriting approval.
£549* Get protection you can depend on from just