




FREE Women’s Health
SECTION
15-23 CNYHEALTH.COM OCTOBER 2023 • ISSUE 286 P. 20 P. 6 OCTOBER: THE PERFECT TIME TO TURN OVER A NEW LEAF Orthopedic surgeon in Oneida offers new kind of surgery on knee cartilage. ‘We’re regrowing the patient’s own cartilage cells to repair a cartilage defect that’s causing knee pain,’ he explains P. 4 AI ASSISTED MAMMOGRAMS FEMALE SURGEONS BRING BETTER OUTCOMES FOR PATIENTS P. 2
SPECIAL
PAGES
Female Surgeons Bring Better Outcomes for Patients, Two Studies Show
The field of surgery has long been dominated by men, and still is today.
But two new studies show that if patients want safe, effective longterm results, picking a female surgeon might be key.
In one study involving more than 1 million Canadian surgical patients whose outcomes were followed for a year, “those treated by a female surgeon were less likely to experience death, hospital readmission or major medical complication,” wrote a team led by physician Christopher Wallis, of Mount Sinai Hospital in Toronto.
Another study — this time focused on gallstone removal, one of the most commonly performed surgeries — also found female surgeons outperforming males, on average, when it came to outcomes.
Both studies were published online Aug. 30 in JAMA Surgery.
Why the gender gap?
According to physician Martin Almquist, who wrote an accompanying editorial in the journal, it might come down to differences in attitudes toward risk-taking, the surgeon's ability to collaborate with others, and being “patient-centered” when it comes to making decisions around surgery.
In both studies, female surgeons tended to be more methodical and
compared to their male colleagues, the researchers noted.
“Being accurate and careful most likely beats risk-taking and speed when it comes to consistently achieving good outcomes for the patient,” concluded Almquist, a surgeon at the Skane University Hospital in Lund, Sweden.

Almquist conceded that it’s not yet proven how women outperform men in the OR.
“Perhaps personality traits more common among women contribute to better outcomes?” he said.
Regardless of the reasons, “Surely, the ideal of the surgeon as the [male] ’lonesome cowboy’ belongs to an era long gone," Almquist added.
The surgical profession remains a largely male domain, however.
For example, in the Canadian study — which looked at 25 different types of surgeries conducted between 2007 and 2019 — only about 151,000 of a total of nearly 1.2 million procedures had been conducted by women.
In the study, Wallis and his colleagues tracked 90-day and one-year outcomes for all patients.
Data was first compiled on a “composite outcome” that included deaths, hospital readmissions and/ or complications. According to the study, nearly 14% of patients treated
least one of these events within 90 days, compared to just 12.5% of people operated on by a woman.
At one year post-surgery, 25% of the patients of male surgeons had experienced such an event, compared to just under 21% of those treated by women. When it came to deaths, 2.4% of patients who’d been operated on by a man were deceased by one year post-surgery, compared to 1.6% of those who'd had a female surgeon.
The second study, focused on gallbladder operations, was led by physician My Blohm, a surgeon at Mora Hospital in Sweden.
It focused on more than 150,500 patients who underwent elective or emergency gallbladder surgeries between 2006 and 2019. Patient outcomes were tracked for 30 days after their procedures.
Again, the team found that fe-
time on a surgery — an average 100 minutes for an elective procedure versus an average of 89 minutes for men.
Maybe that extra time and attention paid off for patients: For elective procedures, patients operated on by male surgeons had 28% longer hospital stays and a 66% higher odds for bleeding complications, compared to patients operated on by a female surgeon, Blohm’s team reported.
So why would a surgeon’s gender matter?
“Personal characteristics and attitudes are difficult to study, but probably affect outcomes,” the Swedish group wrote.
“This study’s important finding that female surgeons may perform safer operations and operate more slowly indicates that caution might be a favorable quality," they added.

GET THE UPSTATE ADVANTAGE FOR CANCER CARE Get The Upstate Advantage for cancer care in Syracuse, Onondaga Hill, Oswego, Auburn and now in Verona Our newest state-of-the-art center continues Upstate’s team approach: patients are seen by expert surgeons, medical oncologists, radiation oncologists and other specialists who work together for each patient’s specific treatment and needs UPSTATE.EDU/CANCER Our newest location!
BREAST CANCER AWARENESS MONTH
MORE THAN were diagnosed with cancer last year, according to the American Cancer Society.
250M+ WOMEN
• More than a quarter of a million women in America were diagnosed with cancer last year, according to the American Cancer Society.
• Breast Cancer is the second most common cancer among women in the United States.
• In New York alone, an average of over 14,000 women are diagnosed with breast cancer each year.
• An average of nearly 3,000 lose their battle with the disease each year, according to the New York State Department of Health.
• In Central New York, an average of 865 women are diagnosed with breast cancer each year. Nearly 160 die each year from breast cancer.
LET OUR WOMEN’S HEALTH EXPERTS HELP YOU
Women who get regularly screened for breast cancer have a 47% lower risk of dying from the disease compared to those who don’t. Breast cancer deaths have been declining since 1990 thanks to early detection, better screening, increased awareness, and new treatment options.
 From left to right: Sara DeSanto, Kelly Hart, Phyllis Conte, Melanie Tarolli, Judy Culver
From left to right: Sara DeSanto, Kelly Hart, Phyllis Conte, Melanie Tarolli, Judy Culver
Meet Your Doctor
By Chris Motola
M. Asad Khalid, MD
Q: So it’s more of a sports medicine intervention?
A: Yes, correct.
Q: How are outcomes so far?
A: It’s generally a very good outcome. In my experience, so long as the patients are selected appropriately and they follow up, I’ve seen very good outcomes. It also depends on other factors going on in the knee. The idea is for patients to be able to get to the level of activity that they want to do, whether that’s running or exercise or even just walking and hiking.
Q: I take it these are fairly common sports injuries?
Q: I understand you’re doing a new kind of surgery on knee cartilage?
A: Yeah, it’s called the MACI (matrix-induced autologous chondrocyte implantation). Basically what it is, it’s a way to culture cartilage from someone’s knee. Essentially what happens is that culture is grown into new cartilage cells in a lab and then we come back later and implant those cells into the knee, wherever the cartilage is damaged. So it’s used to treat cartilage defects in active patients. It’s a newer type of procedure. We’re regrowing the patient’s own cartilage cells to repair a cartilage defect that’s causing knee pain in the patient.
Q: What is this procedure replac
ical risk with MACI.
Q: Is the cartilage healthier when you grow it this way?
A: The studies show that it fills in defects pretty well, but it’s still being studied.
Q: Have you found it easier to work with?
A: I think compared to previous generations of this type of procedure, it’s much easier. The surgeries are generally shorter, which means less blood loss, less anesthesia time. I think the technology, at least with this procedure, have taken a jump.
Q: Does it reduce the likelihood that a patient will need a joint replace
A: Yes, cartilage defects can happen on their own. They can be the result of ligament tears, ACL tears, meniscus tears. It’s becoming more and more common as our imaging gets better and better. We start to recognize this more. I’d say we find cartilage damage in around 60% of the patients who undergo knee scopes. So it’s pretty prevalent.
Q: At what point do you consider replacements compared to more conservative treatments?
A: Generally for most patients we try conservative treatments like therapy, activity modifications, bracing, medications, even injections sometimes. Usually when those fail and we’re pretty confident that the source of the pain is the cartilage damage, that’s when we’ll start to take this step.
Q: What put MACI on your radar? Is it common for smaller hospitals like Oneida Health to do procedures like
A: It can be. For me, during my sports medicine training, I trained with one of the pioneers of the MACI procedure, so it was part of my training, so I got extensive experience with that in my sports medicine fellowship. It’s usually performed at bigger academic centers just because of the resources and patient base. This is the first time it’s been done at

Q: Do you specialize in knees?
A: I’d say knees and shoulders are what I treat most commonly, but I also treat hips, ankles, hands, wrist, elbows. But it’s mostly knees and
Q: Do you see a similar use for this
A: Yes. In fact, it’s been done, it’s just not well-studied. It’s not completely approved for shoulder use yet. It was designed for knees, so other joints are pending data for
Q: What got you interested in
A: My father was a team physician and I was an athlete growing up. I played a lot of basketball. I played a lot in college too. For me, this was a way to stay involved in sports, which was my passion, while going down the medicine route. I treat athletes of all ages, from
youth to recreational weekend warriors. I treat all levels of athletes. So it’s a way to stay involved in athletics.
Q: Having been an athlete and having played basketball in particular with all the pressure cutting puts on your knees, have you found that your medical education changes how you approach the game, assuming you still play?
A: I do and it does. I completely changed the way I play. Being a taller guy, I was usually in the post. Sometime in residency, I hurt my back doing that and ended up getting back surgery. After that, I changed the way I play. I don’t really play the post much anymore.
Q: With that in mind, what advice would you give a younger basketball player?
A: Keeping up with your strength and cardio makes a big difference. Stretching after a game to stay flexible. And then also knowing your limitations. You may not want to be dunking at 40 or 50.
Lifelines
Name: M. Asad Khalid, M.D.
Position: Director of orthopedic and sports medicine at Oneida Health
Focus: Sports medicine and general orthopedic surgeon. Specializes in treating injuries of the knee, shoulder, hip, elbow, foot and ankle. Serves as the team physician for the Utica Comets, SUNY Morrisville, Syracuse FC, and multiple local high schools including Oneida and Camden high schools.

Hometown: Houston, Texas
Education: Medical school: University of Texas Health Science Center at Houston; residency: University of Texas Medical Branch at Galveston; fellowship: Ochsner Clinic, New Orleans
Affiliations: Oneida Health
Organizations: American Arthroscopy Association of North America, American Orthopedic Association, American Orthopaedic Society for Sports Medicine
Family: Wife
Hobbies: Basketball, travel
Page 4 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Orthopedic surgeon in Oneida offers new kind of surgery on knee cartilage. ‘We’re regrowing the patient’s own cartilage cells to repair a cartilage defect that’s causing knee pain,’ he explains
‘It’s generally a very good outcome. In my experience, so long as the patients are selected appropriately and they follow up, I’ve seen very good outcomes. ‘
Cost of a Pack of Marlboro Now Around $15
$1 cigarette tax hike projected to save 15,300 New Yorkers’ lives
Beginning Sept.1, New York state’s cigarette tax will be the highest in the nation. The $1 hike is the first cigarette tax increase since 2010 and changes the tax from $4.35 to $5.35 per pack of 20 cigarettes.
A pack of Marlboro in Upstate New York costs an average $14.50. The cost varies from region to region. Research shows a 10% increase in tobacco prices would be expected to decrease tobacco consumption by 4% in high-income countries.
Increasing the cost of cigarettes is one of the most effective ways to pro-
mote smoking cessation and prevent youth initiation.
The American Cancer Society Cancer Action Network projects the impact of the higher tax will save 15,300 New Yorkers’ lives and prevent 14,400 youth under age 18 from becoming adults who smoke.
The latest data from the NYS Department of Health show that one in five high school-age youth uses tobacco products. New York state spends approximately $9.7 billion annually on preventable smoking-related health care costs.
Booming Sales of Legal Marijuana Linked to More Car Crashes
Emergency room visits for injuries related to driving under the influence of cannabis skyrocketed in Canada after the drug was legalized, a new study reports.
In October 2018, Canada became the second country to nationally legalize recreational or nonmedical cannabis for adult use.
While known cannabis-involved emergency department (ED) visits for traffic injuries were still rare, they grew by 475% over 13 years, with a sharper rise in accidents after legalization, the researchers found.
“Our findings highlight a concerning increase in cannabis-involvement in traffic-injury emergency visits over time, with even sharper spikes following the phases of legalization and commercialization,” said lead author Daniel Myran, a post-doctoral trainee at the Institute for Clinical Evaluative Sciences (ICES), and a family physician at the Ottawa Hospital.

“Conversely, alcohol-involvement in traffic injury ED visits did not increase over the study period, which suggests that legalization of cannabis has played an important role in rising rates," Myran said in an ICES news release.
For the study, the researchers
looked at cannabis-involved ED visits for traffic injuries between 2010 and 2021, looking for changes after the October 2018 commercialization of the legal cannabis market, which expanded products and retail stores.
The investigators reviewed data from more than 947,000 ED visits for traffic injuries in the province of Ontario. Annual rates of cannabis-involved visits surged from 0.18 visits per 1,000 total collisions in 2010 to 1.01 in 2021.
Legalizing non-medical cannabis with restrictions was associated with a 94% increase in the rate of cannabis-involved traffic injury ED visits compared to the pre-legalization period.

Later, after commercialization, which overlapped with the COVID-19 pandemic, researchers saw an even greater increase of 223% in rates compared to the pre-legalization period.
Higher rates of ED visits were seen in men, those who lived in lower-income neighborhoods and those aged 19 to 21, as well as for those who had a prior cannabis-related ED visit.
The study findings were published online Sept. 6 in JAMA Network Open.

October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 5
•
A monthly newspaper published by Local News, Inc. 33,500 copies distributed throughout more than 1,000 high-traffic locations, including all Wegmans stores. In Good Health is published 12 times a year by Local News, Inc. © 2023 Local News, Inc. All rights reserved. P.O. Box 276, Oswego, NY 13126 Phone: 315-342-1182 • Fax: 315-342-7776 • Email: editor@cnyhealth.com ONONDAGA, OSWEGO, CAYUGA
No material may be reproduced in whole or in part from this publication without the express written permission of the publisher. The information in this publication is intended to complement—not to take the place of—the recommendations of your health provider. Consult your physician before making major changes in your lifestyle or health care regimen.
Editor & Publisher: Wagner Dotto
Associate Editor: Stefan Yablonski • Writers: Deborah J. Sergeant, Jim Miller, Gwenn Voelckers, Anne Palumbo, Chris Motola, Melissa Stefanec, Eva Briggs
(MD),
Mary Beth Roach, Ernst Lamothe Jr., George Chapman, Tammy
S.
Scott • Advertising: Amy Gagliano, Pam Roe, Tom Bachman Layout & Design: Angel Campos-Toro • Office Manager: Allison Lockwood
& MADISON COUNTIES
Call me to set up in-person or over the phone consultation and let me help you, at no cost!! www.ballardassoc.com • ballardassoc@gmail.com AARON BALLARD President & Owner, Ballard & Associates, LLC. Happy with your Prescription Coverage? Happy with your copays? Do you have extra $$$ set aside for burial expenses? Do you know if you qualify for help paying for your prescriptions? Aaron Ballard is a licensed Insurance broker representing all the top Medicare carriers in CNY & beyond! 315-374-1783 Turning 65 or just confused about Medicare? We do not offer every plan available in your area. Any information we provide is limited to those plans we do offer in your area. Please contact Medicare.gov or 1-800-MEDICARE to get information on all of your options. Discover the path to a fulfilling, in-demand career in Massage Therapy at Northeast College of Health Sciences. Earn your Massage Therapy certificate in just 5 trimesters of weekend classes on our Seneca Falls campus. HEALTH, IN YOUR HANDS Northeast’s certificate program will prepare you to take the NYS Massage Therapy Exam and become a licensed massage therapist (LMT). Pursue your passion for health and wellness today – classes start January 2024. Study Massage Therapy at Northeast College. www.northeastcollege.edu/massage-therapy Northeast College of Health Sciences | Seneca Falls, N.Y. | 800.234.6922
Healthcare in a Minute
By George W. Chapman
Negotiating Drug Prices
Medicare is finally flexing its purchasing power by negotiating the prices it pays for 10 drugs that treat cancer, arthritis, diabetes and heart disease. Why did it take so long?
It took the passing of the Inflation Reduction Act (I.R.A.) to authorize price negotiations of drugs with pharmaceutical companies.
So why did it take, literally, an act of Congress to negotiate drug prices, especially considering that some 80% of us are in favor of Medicare’s ability to negotiate prices?
Well, 20 years ago, then-Presi-
Big Pharma argues that negotiating prices (remember, on a whopping 10 drugs) will lower their profits and thereby negatively impact innovation.
Interestingly, drug manufacturers spend far more on stock buy backs than innovation or research and development.
Several competing drug man ufacturers sell drugs that combat diabetes, cancer, heart disease, etc. The “winner” of the price negotiation or lowest bidder could capture more if not all the market for the drug and thereby actually increase profits.
Big Pharma won’t even use the term “negotiate” as it spins this all as “big government price controls.”
If negotiating a paltry 10 drugs with Medicare will reduce profits, why then do drug manufacturers negotiate prices with just about every country (England, France, Germany, Canada, to name a few) with national or universal healthcare? It’s because those countries have not tied their hands with laws that prevent them from negotiating and employ their substantial purchasing power to keep prices down and lower costs to taxpayers to whom they have a fiduciary responsibility. It should be noted that all the countries listed have a much lower cost of care per capita than the U.S.
dent George Bush signed a law prohibiting Medicare from negotiating drug prices.
That is the penultimate (or maybe worst?) example of the absurd amount of influence Big Pharma lobbyists have on our elected officials. While negotiations are underway, Big Pharma has filed multiple lawsuits to block the government
and a lot of that can be attributed to paying far less for drugs. There is a lot of moaning from both sides of Congress about government spending. So why are we tying the government’s hands when it tries to act like a business?
from implementing this part of the I.R.A. Big Pharma should consider itself lucky to negotiate considering Medicare does NOT negotiate prices with physicians and hospitals. Medicare SETS the prices for providers of care. So much for the AMA and AHA lobbyists. There is plenty of time for the litigation to play out as the prices won’t take effect until 2026.
due to intense Big Pharma lobbying.
You would think it a slam dunk to allow Medicare to negotiate ALL drug prices. We have almost 65 million seniors on Medicare. That exceeds the total population of Canada which is about 38 million. Yet Canada, with far less purchasing power, negotiates all drug prices where it can. If we had a national health plan covering us all, Medicare would be negotiating prices on behalf of 334 million people. Medicare was about 10% ($888 billion) of the federal budget in 2021. 46% comes from general revenues, 34% from payroll taxes and 15% from beneficiary premiums. So, Medicare drug prices affect ALL of us, not just seniors.
The first 10 drugs Medicare chose to negotiate are: Eliquis blood thinner; Xarelto blood thinner, Januvia for diabetes; Jardiance for diabetes; Enbrel for rheumatoid arthritis; Imbruvica for blood cancer; Farxiga for diabetes, heart failure and kidney disease; Entresto for heart failure; Stelara for psoriasis and Crohn’s disease; and Fiasp for diabetes. These 10 drugs account for $50.5 billion or 20% of total part D costs. (Part D drugs are taken at home while Part B drugs are administered in a provider office.)

If you consider Big Pharma contributions to the campaigns of our elected officials, you’ll understand why Medicare is limited to negotiating just 10 prices and not ALL prices.
The Senate (100 members) averages about $76,000 per campaign or about $7,600,000 over the course of staggered six-year terms.
The House (435) averages about $36,000 per campaign or about $15,660,000 over the course of staggered two-year terms.
These contributions are why the Inflation Reduction Act barely passed.
Apparently, getting reelected is more important than doing the right thing.
The top 10 elected officials receiving the most money from Big Pharma are from both sides of the aisle.
Newcomer senator Raphael Warnock from Georgia leads the pack at $770,000. He has a commanding lead over the rest. In second place is Cathy Rodgers from Washington at $419,000. The next eight are: Scott Peters, California, receiving $400,000; Catherine Masto, Nevada, $382,000; Tim Scott, South Carolina, $351,000; Patty Murray, Washington, $351,000; Mark Kelly, Arizona, $350,000; our Chuck Schumer at $345,000; Brett Guthrie, Kentucky, $343,000; and Maggie Hassan, New Hampshire, $273,000.
Drug companies can easily afford to pay 1,500 lobbyists and tens of millions to campaigns to protect their profits while hospitals and nursing homes, with little to no cash to spare, struggle to stay open.
Most galling is instead of considering themselves lucky to having to negotiate only 10 drugs while Medicare sets payments to physicians and hospitals, some of the drug manufacturers have decided to sue Medicare for restraint of trade and overreach.

Business negotiations over price are commonplace. Drug companies negotiate prices with all the countries with national health insurance.
billion (with a “b”) outof-pocket last year on just the 10 drugs being negotiated.
Lower prices mean less out-ofpocket. Period.
More savings for taxpayers are on the horizon when Medicare can negotiate 15 prices in 2027-28 and then 20 after that. The severely limited number of prices that can be negotiated and the painfully slow implementation timeframe shows how difficult it was to pass the I.R.A.
No one really knows the price of a particular drug. It depends on whether you’re self-pay or covered by Medicare, Medicaid, or commercial insurance.
Commercial carriers or pharmacy benefit managers negotiate supposed discounts, but often off nebulous inflated prices quoted by the manufacturer. You never know if you’re getting a good deal. Basical ly, there just isn’t price competition among drug manufacturers as there is in most markets. Once Medicare negotiates a price, (which both par ties agree to) it should finally provide the public some price transparency.
But when Medicare flexes its muscle, they sue.
George W. Chapman is a healthcare business consultant who works exclusively with physicians, hospitals and healthcare organizations. He operates GW Chapman Consulting based in Syracuse. Email him at gwc@gwchapmanconsulting.com.

Page 6 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Like us on Facebook!



































October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 7 Your health is as important as ever. ConnextCare is here to help! Say Hello to Healthy! ConnextCare offers highly qualified and accessible providers at several locations throughout Oswego County. Keep you and your family healthy, safe, and happy with convenient, compassionate and comprehensive care right in your neighborhood. • Over 70 dedicated healthcare providers across our network • Acute care treatment with same-day appointments • Services include family medicine, pediatrics, dental, psychiatry, chronic condition treatment, behavioral health, and more. Say hello to the ConnextCare Pulaski team. Call today. Pulaski 61 Delano Street, Pulaski NY 13142 (315) 298-6564 Other Locations Fulton, Mexico, Oswego Parish, Phoenix, Central Square www.connextcare.org
Meet our Pulaski Area Providers
Mary Barbara, PA Physician Assistant Pulaski
Nicole Brubaker, FNP Family Nurse Practitioner Sandy Creek School
Annette Digby, FNP Family Nurse Practitioner Pulaski
Grace Nasri, MD Family Practice Physician Pulaski
Lisa Beagle, PNP Pediatric Nurse Practitioner Lura Sharp School
Mikayla Fox, PA Physician Assistant Pulaski
Heidi M. Kinnally, RN, MSN, FNP-C Family Nurse practitioner Pulaski
Amanda M Pastuf, RN, MSN, FNP-C Family Nurse practitioner Pulaski
Lauren Hehir, AGNP Adult-Gerontology Nurse Practitioner Pulaski
Richard Salvagno, DDS Dentist Pulaski
Jill Brushaber, FNP Family Nurse Practitioner Pulaski
Patrick Carguello, DO Family Practice Physician Pulaski
Miranda King, RN, MSN, FNP-C Family Nurse Practitioner Pulaski
Dean Gardner, FNP Family Nurse Practitioner Pulaski
Brittany Gehrke, RDH Dental Hygienist Pulaski, Sandy Creek School
Anna Gofman, DDS Dental Pulaski, Fulton
Jody Hipple, FNP Family Nurse Practitioner Pulaski High School
Megan Hollister, FNP Family Nurse Practitioner Pulaski
Annalise Isgar, RDH Dental Pulaski
Blaze Fahenstock, FNP Family Nurse Practitioner Pulaski
Kwi Lee, DDS Dentist Pulaski
Melissa Noel, DDS Dentist Pulaski, Fulton
Jessica Overton, RDH Dental Hygienist Pulaski, Fairgrieve School
Megan Pecha, MD Pediatrician Pulaski
Mary Smith, FNP Family Nurse Practitioner Pulaski
Marissa Taber, RDH Dental Hygienist Pulaski
Glenn Thibault, MD Family Practice Physician Pulaski
Dorese Vecchio, RDH Dental Hygienist Pulaski, APW Schools
Jenna Walker, RDH Dental Hygienist Pulaski
Edward G Wolfe Jr., RPA-C Physician Assistant Pulaski
Mary Ellen Xavier Flanagan, FNP Family Nurse Practitioner Pulaski
Live Alone & Thrive
“me time” to meditate and set my intentions for my day.
By Gwenn Voelckers
Practical tips, advice and hope for those who live alone
October: The Perfect Time to Turn Over a New Leaf
Fall is such a special time of year. For me, it means all good things: relaxing in front of a cozy fire, making pumpkin soup on Sunday afternoons, donning my well-worn leather jacket for long walks and turning my attention to all those inside projects I neglected over the summer.
The brilliant colors, autumnal aromas and industriousness that arrive with the falling leaves really appeal to me. But this hasn’t always been the case.
After my divorce, the month of October left me feeling melancholy. I missed sharing the beauty of the season with a special someone. And I missed the sunshine as daylight waned.
Nostalgia and wistfulness would creep in and I just wanted to retreat into myself. For those who live alone, the month of October has unique challenges.
Not one to wallow in a “poor is me” state of mind, I began to develop and employ some strategies to rekindle my love of the fall season. It can be a great time to mix it up, get busy and expand your horizons.
Below are elements of my annual fall “game plan.” Take a look and see if one or more of these suggestions might add a little color to your life palette this fall:
• Tackle indoor projects: Fall is a great time to accomplish all those
nagging indoor projects on your to-do list. I have a long list and I keep it right in front of me — a daily reminder that I have plenty of home improvements to tackle, both large and small.
Too much idle time is not a friend at any time of year, but it can become downright unfriendly when gray clouds appear and the temperature drops. So, let’s get busy: organize your storage space, do some touch-up painting, update your will or clean out your inbox.
There’s nothing like being productive to beat the autumn blues.
Don’t I know it. I just finished coating my flat-roof porch with a sticky tar sealant. Confession: it was messier than it was fun, but still, I’m proud of my accomplishment. It lifted my spirits.
• Get up and get going: Staying active when there’s a chill in the air can be difficult. I can remember many a cold morning when all I wanted to do was hit the snooze button, pull up the covers and stay in bed.
As nice as sleeping in can be from time to time, I don’t recommend it as a steady diet.
In my experience, there's no better way to start your day than to wake early to start your day. In the early morning’s peace and quiet, there is glorious time to reflect and feel gratitude. I use this important
ADHD: What Parents Need to Know
About 6 million kids have been diagnosed with ADHD as of 201
Lots of children and adolescents have the condition known as ADHD, or attention-deficit/hyperactivity disorder.
What should parents know? A number of treatments exist to help with functioning, including medications approved by the U.S. Food and Drug Administration.
Typically, ADHD begins between ages 3 and 6, according to the U.S. National Institute of Mental Health. It can continue into adulthood.
People can experience one of three types of ADHD. They are predominantly inattentive, with trouble focusing, following instructions and finishing tasks; predominantly
hyperactive–impulsive, with behavior of being “constantly on the go,” talking excessively and interrupting others; and a combination of those symptoms.
An increasing number of children are being diagnosed with ADHD. About 10% of children aged 3 to 17 — or about 6 million kids — have been diagnosed with ADHD as of 2019, according to the U.S. Centers for Disease Control and Prevention.
Boys, at 13%, are more likely than girls, at 6%, to be diagnosed with ADHD.
“Boys are also more likely to have the hyperactive-impulsive type. This type of ADHD is easier to spot
As the morning brightens, my energy grows, as does my appreciation for the precious day ahead me.
• Start moving and enjoy the great outdoors: Fresh air, sunlight and even a gentle rain can be invigorating first thing in the morning. I find a sunrise walk boosts my energy and kickstarts my day. Do I always feel like layering up and taking a walk every morning? No. Do I feel better after I make the effort? Yes, without fail.
I love an unhurried solitary walk to clear my head and be mindful. But I also love a walk with my sister, Anne, or good friend, Kate, to enjoy their company and avoid the Siren song of isolation as the days grow short and get colder.
• Learn something new: Going back to school and fall go hand in hand. Who among us isn’t reminded of the nervous excitement associated with returning to school in the fall? It’s a great time to expand your intellectual horizons.
Each fall I identify a new skill or subject to learn. Last year, I researched how to divide and relocate perennials (my irises and peonies); this fall, I’m signing up to learn French on Duolingo, the free language-learning app.
Continuing education opportunities are abundant in this community and online. Check out colleges and universities, community centers, arts and cultural institutions, your local library, and workshop listings for class and workshop offerings.
• Invite people in: Over the years, I’ve discovered a few simple and manageable ways to bring people into my world and into my home. One way is to organize a gathering around a TV show or series — yes, around the TV.
For years, I invited my single friends over to watch “Downton Abbey” with me on Sunday nights. I provided the soup and salad; they provided the good company.
So, what’s your pleasure? Whether it’s football, a favorite weekly sitcom, or “Ted Lasso” on Apple TV — all of these and other TV shows can become reasons to bring friends and family together. The benefits? You’ll hone your cooking skills (boy, do I now have some great soup recipes!) and you’ll connect with people you care about.
What better way to enjoy a nice fall evening.
There are so many wonderful and meaningful strategies to enjoy the fall season and to ward off the blues that can sometimes emerge during this changing time of year. But these strategies require effort — conscious, creative effort.
If you are feeling sluggish, lonely or isolated, try a few of the strategies above. They have stood me in good stead and have reinvigorated my love for the fall season.
If you, too, are ready to turn over a new leaf, October is the perfect time!
Gwenn Voelckers is the founder and facilitator of Alone and Content empowerment workshops for women (now on hiatus) and the author of "Alone and Content: Inspiring, empowering essays to help divorced and widowed women feel whole and complete on their own" To contact Voelckers or purchase her book, visit www.aloneandcontent.com

than the quieter child who is inattentive,” said child psychiatrist Tiffany Farchione, who reviews ADHD drugs at the FDA.
Untreated ADHD can have serious consequences, the FDA warns, including falling behind in school, having difficulties with friendships and experiencing conflicts with parents.
Children with untreated ADHD also have more emergency room visits and are more likely to have self-inflicted injuries. Meanwhile, untreated adolescents are more likely to take risks.
A visit with your child's pediatrician can help determine if your child has ADHD. Also have your child's vision, hearing and anything else that might contribute to inattention checked.
Stimulants and non-stimulants are both approved by the FDA to help reduce symptoms of ADHD in children as young as age 6. Containing various forms of methylphenidate and amphetamine,
stimulants have a calming effect on children with ADHD, Farchione said. They are thought to increase brain levels of dopamine, a neurotransmitter associated with motivation, attention and movement.
Approved non-stimulants are Strattera (atomoxetine), Intuniv (guanfacine), Kapvay (clonidine) and Qelbree (viloxazine).
Some children with ADHD also receive behavioral therapy to help manage symptoms and learn coping skills. Community support groups and schools may also provide some help.
FDA-approved medications have been tested for safety and effectiveness. Clinical trials will now look at their safety and effectiveness in children aged 4 and 5.
“We know ADHD medications are being prescribed for younger children, and we think it's essential that the data from clinical studies reflect the safety and effectiveness for this age group,” Farchione said in an FDA news release.
Page 8 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
General urology, male health, urologic oncology, enlarged prostate, kidney stones At Upstate Urology of Auburn.
















EYAL KORD, MD









urology, treatment of hern as and hydroceles, robotic surger y urinar y trac t infec tions, peni e
abnormalities
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 9 M E E T T H E U P STAT E U RO LO GY T E A M FO R A N A P P O I N T M E N T, C A L L 315.464.1500 Fema e and reconstruc t ve urology urinar y incontinence in women, pelvic oor treatment and neurourology MATTHEW D MASON, MD, FAAP DMITRIY NIKOLAVSKY, MD RYAN SIDEBOTTOM, DO Genera urology male health urologic oncology enlarged prostate, kidney stones At Upstate Urology of Auburn TIMOTHY K BYLER, MD MRI fus on, male health, prostate cancer and k dney stones ZAHI N MAKHULI, MD General uro ogy, andro ogy JC TRUSSELL, MD Male infer t lity erec ti e dysfunc tion andrology genera urology, prosthetics, and Peyronies OLEG SHAPIRO, MD Urologic oncology and endourology, robot c and aparoscop c surger y of prostate kidney bladder and adrenal; kidney stones SCOTT WIENER, MD K dney Stones, M nima ly Invasive Kidney Surger y Enlarged Prostate HANAN GOLDBERG, MD, MSc Urolog c oncology; robotic and laparoscopic surger y of prostate, kidney, bladder and adrenal ANTHONY J TRACEY, MD, MPH, FAAP Pediatric urology treatment of hernias and hydroceles robotic surger y, ur nar y trac t nfec t ons penile abnormalities NATASHA GINZBURG, MD IMAD NSOULI, MD GENNADY BRATSLAVSKY, MD Chairman Urologic oncology; robotic and laparoscopic surger y of prostate, kidney, bladder and adrena STEPHEN BLAKELY, MD ELIZABETH FERRY, MD Genera urology ROBERT FLEISCHER, MD General urology SEETHARAM BHAT, MD, MBBS Urologic oncology; robot c and laparoscop c surger y of prostate, k dney, bladder, and adrenal Reconstruc tive urology; incontinence prosthetics, ur nar y stu a, neurogenic bladder, urinar y diversion Robot c surger y General urology, female and reconstruc tive urology Pediatr c urology treatment of hernias and hydroce es robotic surger y, urinar y trac t infec tions penile abnormalit
care JOSEPH JACOB, MD, MCR Uro ogic oncology;
surger y of prostate kidney bladder and adrenal MAHMOUD CHEHAB, MD General urology, male health,
prostate
, and robotic surger y
es Incontinence, urethral stric ture disease, vesicovaginal stula reconstruc t ve surger y transgender JEFF VILLANUEVA, MD Pediatric
robotic and laparoscopic
uro ogic oncology enlarged
kidney stones
GARRETT SMITH, MD
Urologic oncology; robotic and laparoscopic surger y of prostate k dney , bladder and adrenal
5 Things You Should Know About Asthma
By Ernst Lamothe Jr
The lungs and airways are an important part of the respiratory system that effectively carries and stores oxygen.
A properly functioning respiratory system allows breaths to flow in and out of the lungs and into the airways. This is not always the case for individuals because some suffer from a well-known medical condition called asthma.
One in 13 people in the United States alone has asthma, according to the Centers for Disease Control and Prevention.
“If you are experiencing a breathing problem, make sure you seek help from your primary care provider. Pulmonary function studies may be part of the work up,” said Sherif El Bayadi, a pulmonologist at St. Joseph’s Health.

Here are five asthma facts that are essential for sufferers.
1.Causes
Asthma appears in children and some adults who develop the medical condition later in life. Each occurrence in children and adults arises with different symptoms. Asthma may begin in childhood and may ease with age.
Common symptoms can include chest tightness, coughing, wheezing, dark circles underneath the eyes and difficulty eating or, for infants, sucking. These symptoms can range from mild to severe.
“The cause of asthma is a hy-
per reactive airway that is trying to protect the lungs and responds in an exaggerated fashion,” said El Bayadi. “Precipitating factors from the environment cause asthma.”
Individuals can have situational asthma and can experience symptoms with exertion, exercise or during working hours if they have occupational exposures in the workplace. In the younger pediatric population, respiratory infections are a significant cause of asthma triggers, especially viral infections such as viruses of the common cold, flu, RSV or other viruses. Major asthma triggers in individuals with a history of allergies are allergens such as pollen, pet dander, dust mites and others.
2.Air quality
This year we’ve had a number of days that were labeled as poor quality. Smoke from wildfires can contain harmful particles and gases and exposure to these can cause acute respiratory symptoms especially for individuals with asthma.
“The Canadian wildfires caused major air quality concerns, especially among those with asthma. The exposure to the smoke certainly led to worsening symptoms in asthmatics. Avoidance is the best treatment along with usual asthma treatments, depending on how severe the reaction was,” said El Bayadi.
3.Handling asthma
Asthma can be managed
with proper medical treatment, lifestyle and education. It is important to be in tune and recognize our symptoms and understand scenarios that can trigger asthma and this includes identifying and avoiding triggers such as allergens, smoke, pollution and respiratory infections. One should take steps to minimize exposure to these.
“If an asthma attack occurs, there should be an action plan that details how the patient and their loved ones should handle the situation,” said El Bayadi. “This may involve taking a quick-relief short acting beta-agonist. If that does not improve the symptoms, and depending on how severe the symptoms are, the next step would be to seek help at urgent care.”
4.Avoid smoking
Smoking is one of the worst habits for asthma and this includes active smoking as well as exposure to secondhand smoke. These can trigger asthma symptoms and make them more severe. Cigarette smoking is the number one cause of preventable death in the U.S. Cigarette smoke irritates the lungs, causing redness, swelling and more mucus. Your lungs have a natural defense to keep dirt and germs out.
“Smoking is certainly the best example of a bad habit in asthmatics. Other exposures that may be difficult to control include environmental things such as grass, pollen and odors in general. These should be avoided, especially if they precipitate asthma. Precipitating factors for asthma in the work environment should also be kept in mind and avoided as much as possible,” he added.
5.Treatment
Good airway and lung health is important for the respiratory system to function properly. If experiencing asthmatic symptoms, it remains imperative to consult your healthcare provider. Those diagnosed with asthma should visit their physicians annually or more to ensure treatment is effective.
Various medications are in place to reduce inflammation and mucus. These include bronchodilators, anti-inflammatory medications, metered-dose inhalers, nebulizers, allergy shots or other asthma inhalers. In addition to medications, doctors work closely with their patients to identify and reduce interactions with triggers. In some cases, doctors may order a spirometry test to measure airflow through lungs, chest X-rays, blood tests or skin tests.
Hematology Oncology Associates Offers Free Lung Cancer Screening
Event to take place Nov. 4 in Auburn, Syracuse
To celebrate Lung Cancer Awareness month in November, Hematology-Oncology Associates of CNY and CRA Medical Imaging will offer a free lung cancer screening to qualified participants
People interested in getting the test can do so from 8 a.m. to 2 p.m. Nov. 4. at three Hematology-Oncology Associates locations: 5008 Brittonfield Pkwy, E. Syracuse; 4900 Broad Road in Onondaga Hill, Syracuse; and 37 W. Garden St., Auburn.
Who Qualifies
Free screenings are available for individuals aged 50-80 who are heavy smokers (one pack a day for 20 years or two packs a day for 10 years) or are former heavy-smokers who quit in the last 15 years. Those who previously received a free lung cancer screening from HOA are not qualified.
To learn more, call 315-4727504 extension 1301 or visit hoacny.com.

Page 10 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Sherif El Bayadi is a pulmonologist at St. Joseph’s Health.
Hope for Bereaved Celebrates 45 Years
By Tami S. Scott
After three years away, HOPE for Bereaved is returning to the Nicholas J. Pirro OnCenter ballroom on Friday, Nov. 10 to hold its annual Celebration of HOPE fundraiser.
The Syracuse-based nonprofit, dedicated to helping individuals and families through their grief journey, invites you to a night of fun with entertainment, dinner and live and silent auctions.

Proceeds help offset the cost of providing its core services, including support groups, counseling, and a monthly newsletter, that are always free of charge to the public.

This year’s community chairs are John and Robin Katko, and Dan and Danielle Cummings. Co-chairs are HOPE founder Therese Schoeneck, Margie Nye, and Peg Card.
Each year, Celebration of HOPE brings together the community in a shared space and passionate quest to return hope to shattered hearts.
HOPE encourages local businesses and individuals to participate in this special event by considering sponsorship opportunities. Table host, advertising and supporter opportunities are also available and provide a phenomenal occasion to highlight your company’s mission and values.
To review and register, go to https://hopeforbereaved.com for details.
Donations are also appreciated. Consider donating in honor of John and Robin Katko, in honor of Dan and Danielle Cummings, or in memory of a loved one. Donate an auction item in memory or in honor of someone special.

Share your story
HOPE for Bereaved is also seeking people to share their story of how HOPE helped them on their journey.
If you attended a support group, participated in individual counseling, or celebrated in one of its many fundraisers and want to share your experience, the committee would love to hear from you.
“Founder Therese Schoeneck always felt that whenever Hope was in the community, along with raising funds we were bringing awareness of our services, spreading Hope to people that may need help with their journey through grief,” said Margie Nye, event co-chair. “So please share your donations, but also your experience about Hope. It might just be what someone needs to hear to give them the courage to walk through the doors of Hope and get the support that so many people need.”
Your stories can be emailed to pkreisel@hopeforbereaved.com.

HOPE For Bereaved is dedicated to helping grieving children, teens, and adults by providing core services (support groups, monthly newsletter and counseling) at no charge. Founded in 1978, HOPE is an independent nonprofit community organization. Our purpose is to offer support, understanding, coping strategies, friendship and hope to the bereaved, as well as education, consultation and resources for their families, friends, employers, school/ daycare staff, co-workers and invested professionals. The help given by HOPE can add greatly to the physical and mental well-being of the bereaved and therefore to their place of employment and to the community.
St. Camillus Receives Over $6 Million in Grant Funding
St. Camillus recently received $6,431,159 in funding through the New York State Health Care Facility Transformation Grant (phase 2).
The New York State Department of Health announced the availability of funds under the Statewide Health Care Facility Transformation to help health care providers support facility transformation initiatives.
“We are thrilled to announce that St. Camillus was recently awarded the funds to make many critical capital improvements which will directly impact operational efficiencies, functionality, safety, regulatory compliance and support the provision of quality care and services,” said Michael Schafer, president of St. Camillus. “On behalf of our staff, residents, patients and communities in which we serve, we greatly appreciate the support from New York state.”
St. Camillus’s continuum of care includes skilled nursing (long-term care) and sub-acute rehabilitation. In
addition, St. Camillus provides the only New York state-certified brain injury rehabilitation program in Central New York.
The NYS Healthcare Facility
Transformation funds are specifically earmarked for capital improvement projects for the St. Camillus facility and will help support the organization’s initiative to improve the infrastructure and enhance the homelike environment for their residents and patients.
A series of facility upgrades has been launched with the initial primary focus on the roof, flooring, elevators, and parking lot lighting. Construction will occur in phases over a duration of approximately 1.5 years.
Projects include new roof and window on building 1; resident room furniture, HVAC upgrades, third floor lounge expansion, elevator modernization and upgrades to the main entrance, among other upgrades.
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 11
Richard Kim Medicine will be your last stop. This is the call that will change your life! 518-871-9900 Learn from other patients at richardkimmedicine.com MEDICINE THAT MOVES YOU Stop missing life’s greatest moments. Stop planning life around pain. Back Pain should not mean fusion, screws, and lengthy recoveries. Regenerative Medicine is changing how back pain is solved. SUFFERING FAILED BACK SYNDROME? Now I am back to shoveling snow, hiking and looking forward to gardening this spring. Dr. Kim and his staff were great with my questions, friendly and attentive to my recovery. —MARCIA Home Instead is looking for caring and compassionate CAREPros to become a part of our team and join our mission of enhancing the lives of aging adults. Home Instead provides non- medical, in home care to aging adults throughout the Cayuga, Wayne, Seneca and Ontario County communities. Benefits of becoming a CAREPro • Competitive Pay starting at $16.20 per hour • CAREPro Referral Program • Paid Time Off for illness/appointments • Paid training and continued learning 24 hour Administrative support SCAN HERE TO APPLY (315) 252-2354
My Turn
By Eva Briggs, MD


What My New Hobby Has Taught Me About My Hands


Irecently started a new hobby, learning to play guitar.
This requires a lot of hand dexterity and coordination, possible only because of the amazing structures that form our hand.
The framework consists of 27 bones. Eight carpal bones — arranged in two rows in the wrist — lie between the forearm and palm. For the curious, the names of the bones are as follows. In the proximal (closest to the forearm) row, from lateral (pinky side) to medial (thumb side): scaphoid, lunate, triquetrum, pisiform. In the second more distal (closer to the hand) row from lateral to medial: trapezium, trapezoid, capitate, hamate.
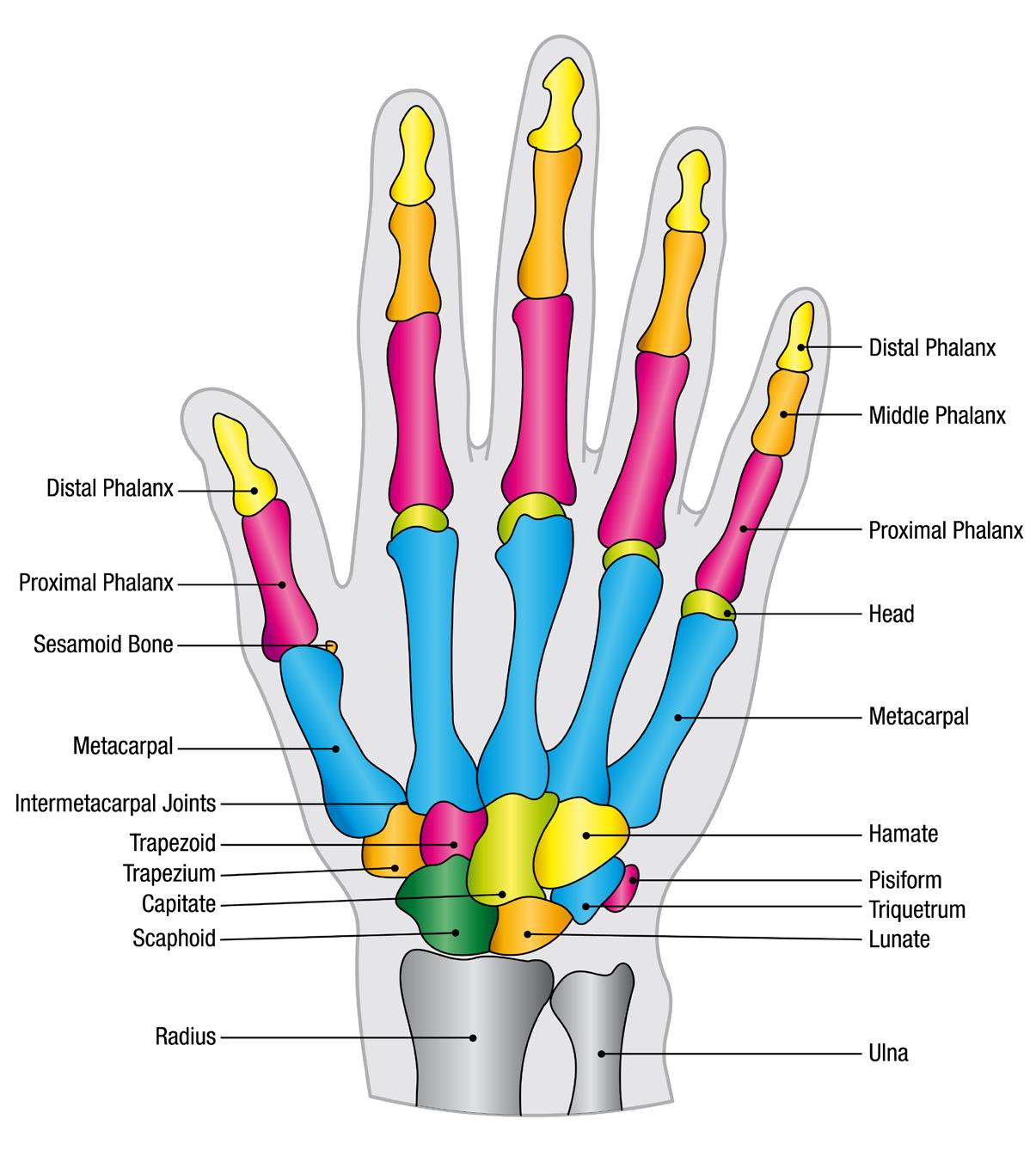
The carpal bones are arranged in an arch. The open side of the arch is connected by a membranous band called the flexor retinaculum forming a space called the carpal tunnel.
The palm of the hand contains five metacarpal bones, one for each digit. They’re numbered 1 (thumb) through 5 (pinky). It turns out this is where guitar playing requires code-switching. Guitarists use numbers 1 -4 starting at the index finger because musicians usually don’t fret with their thumbs.
The fingers contain small bones called phalanges. Two in the thumb and three in each finger. That adds up to 14 more bones.
These bones bend and move with the help of tendons, fibrous cords similar to a rope, which attach bones to muscles. Flexors bend the joints and extensors straighten the joints. Flexor digitorum profundus tendons bend the index, middle, ring and small fingers at the fingertips. A single common muscle divides into four tendons that run through the carpal tunnel, through tendon sheaths, to connect to the fingertip bones. The
word profundus means deep, and these tendons run closest to the bone.
Flexor digitorum superficialis tendons bend the index, middle, ring and small fingers at the middle joint. A single forearm muscle divides into four tendons which travel through the carpal tunnel and then glide inside tendon sheaths. At the level of the fingers, these tendons each split into two separate cords. One attaches on either side of the flexor digitorum profundus tendon that is on its way to the fingertip.
Several extensor tendons straighten the fingers. The extensor digitorum communis tendons originate in the forearm and travel to the index, middle, ring, and small fingers. The small finger has an additional extensor digiti minimi tendon. The index finger too has an additional tendon, the extensor indicis proprius.
The thumb has its own tendons. The abductor pollicis longus tendon pulls the thumb away from the hand. It works alongside the extensor pollicis brevis. When these two tendons become inflamed it’s called DeQuervain’s syndrome. The flexor pollicis longus bends the thumb. The extensor pollicis longus straightens the thumb.
And there are additional tendons that control wrist motions! All those tendons make act like strings of a marionette, but something has to control them. That’s your brain, sending signals through various nerves. The three main nerves are the ulnar, median, and radial nerves.
The ulnar nerve travels from the neck, under the collarbone, through the armpit, and down the inside of the arm to the inner elbow. The ulnar nerve then travels on the inside of the forearm to the hand. It’s near the surface at the elbow and easily bumped,

producing the tingling commonly called “hitting your funny bone.” The ulnar nerve controls many hand muscles and provides sensation to the small finger side of the hand. If the ulnar nerve is cut, the small and ring fingers curl into a claw shape and the hand becomes weak.
The radial nerve runs from the neck, around the humerus (upper arm bone), and down the forearm. Due to the proximity to the humerus, it can be injured if the humerus is broken. The radial nerve straightens the wrist and fingers. If damaged it can cause wrist drop – inability to straighten the wrist. This nerve also provides sensation to the thumb side of the back of the hand.
The median nerve supplies many forearm muscles controlling various wrist movements including bending the wrist as well as powering most of the finger flexors. It passes through the carpal tunnel and if compressed there can lead to carpal tunnel syndrome.
So how can a doctor keep track of all this? Most of us can’t I had to look up what I couldn’t remember to
refresh my anatomy class memories. That’s why there are hand surgery experts: orthopedic surgeons or plastic surgeons with special training. And it takes a lot of training. For orthopedics it’s four years of college, four years of medical school, five years of residency in orthopedics, and one year of fellowship training. That’s 14 years after high school! After that there are both written and oral board exams. Plastic surgeons undergo similar training. As an urgent care physician, part of my job is to recognize when a patient needs the advanced skills of a hand surgeon. Well, time to go practice my guitar now!
Page 12 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Eva Briggs is a retired medical doctor who practiced in Central New York for several decades. She lives in Marcellus.
FREE BFOHEALTH.COM FREE MVHEALTHNEWS.COM OCTOBER 2021 ISSUE 188 ACHIEVING In Good Health publishes unique newspaper editions across 4 Upstate New York markets. Ask your account manager about combination discounts to advertise across multiple markets. Rochester Edition Serving Monroe, Ontario counties Buffalo / W.N.Y. Edition Serving Erie, Niagara counties Central N.Y. Edition Serving Oswego, Onondaga, Madison, Cayuga counties Mohawk Valley Edition Serving Herkimer, Oneida counties Expand your advertising reach to additional markets across Upstate New York GVHEALTHNEWS.COM ISSUE 189 Saying FREE FREE CNYHEALTH.COM SEPTEMBER ISSUE 261 Why Are There More Children with Disabilities? If you get the impression that there are more children with disabilities, the numbers agree with you. But there’s more to the story. P. INSIDE Blind Sport October event in Baldwinsville provides opportunities for with visual impairments participate in sports. P 14 Special Issue on People with Disabilities For inquiries, please email editor@cnyhealth.com
SmartBites
By Anne Palumbo
The skinny on healthy eating
Helpful Tips
Select blemish-free squashes that feel heavy and firm, especially near the stem ends. Delicata’s thin, easy-to-slice skin does not need to be peeled before cooking. Also, this squash holds its shape during cooking, making it an excellent choice for stuffing and baking. As mentioned, whole delicata keep for several months if stored in a cool, dry place.
Boost Your Immune System with Delicata Squash
When I discovered delicata squash a few years ago, I couldn’t stop talking about it. I still can’t! The taste, the texture, the nutrition, the delicate skin…oh, if only it were available year-round.

The good news is, they’re in season now through November. And the even better news is, they can be stored safely for about two to three months in a cool, dry place.
But here’s the best news of all about this striped, pleasantly sweet winter squash: it’s chock full of nutrition, particularly vitamins C and A — two vitamins that boost immune system health. Right now, with flu and cold season bearing down on us, bolstering this all-important system seems wise.

Like other winter squashes, delicata is super low in fat, sodium, cholesterol and calories (only 40 per cup). And while it may have more carbs than some vegetables (10 grams per cup), it is by no means a carb-watcher’s nightmare. As a comparison: 1 cup green beans (7 grams),
— 1 soft pretzel (80 grams).
Delicata’s natural carbs are “complex” and take longer to digest, versus the “refined” carbs found in processed foods, such as sugary drinks, pastries, white bread, most snacks, and many cereals. The good fiber-rich carbs in delicata squash provide longer-lasting energy, more stable blood sugars, and fiber-driven heart protection. The bad fiber-depleted carbs in most processed foods, on the other hand, tend to cause spikes in blood sugar levels, which can trigger hunger and lead to food cravings. Numerous studies support that excessive refined-carb consumption may pave the way for health problems, such as obesity, Type 2 diabetes, and heart disease.
Unlike other hard-skin winter squash, delicata’s skin is edible, adding a nutty deliciousness to an already yummy squash. But that’s not all it adds: its skin is also rich in fiber, vitamins, minerals, and antioxidants. Antioxidants are beneficial molecules that fight free radicals, which, when
PARMESAN-CRUSTED ROASTED DELICATA SQUASH

Serves 4
1 delicata squash, washed and dried
1 tablespoon olive oil
¼ teaspoon kosher salt coarse black pepper, to taste

¼ cup grated parmesan cheese

1. Preheat oven to 425° F. Line a large baking sheet with parchment paper; set aside.
2. Trim the ends off the delicata squash, then slice the squash in half lengthwise and scoop out the seeds. Slice the seeded halves into ½-inch thick slices (half circles) and place them in a large bowl.
3. Drizzle the olive oil, salt, and pepper over the squash slices, tossing well to coat. Transfer
¼ cup whole-wheat panko breadcrumbs
1 teaspoon dried thyme
1 garlic clove, minced
1 teaspoon lemon zest (optional)
to the prepared baking sheet, arranging the slices in an even, flat layer.
4. In a small bowl, combine the parmesan, breadcrumbs, thyme, garlic, and lemon zest.
5. Sprinkle the parmesan mixture over the squash, pressing to adhere.
Roast in the center of the oven until tender and golden brown, about 25 minutes.
– CNY’s Healthcare Newspaper • Page 13
Here are some strategies to help you identify and reduce stress. Work and life can be stressful. But when that stress gets to be too much you can develop burnout. Fortunately, there are tools to help you build resiliency and prevent stress from turning into burnout.








01 02 03 FIND THE POSITIVES PRACTICE SELF-CARE TRY





Look for positives in daily experiences. Current stressors are only temporary. Try to move through a stressful situation with a “can-do” attitude.






Page 14 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023 Cardiovascular Group UPSTATE CARDIOLOGY CONTINUES TO GROW Get The Upstate Advantage for your heart. Our united expertise brings you advanced technology and streamlined care. As the Upstate Cardiovascular Group, we provide connections to research and surgical care. OUR UPSTATE CARDIOLOGY TEAM CONTINUES TO GROW. PHYSICIANS FROM TOP LEFT: OUR OFFICE LOCATIONS 5112 WEST TAFT ROAD Liverpool • 315-701-2170 510 TOWNE DRIVE Fayetteville • 315-663-0500 90 PRESIDENTIAL PLAZA Syracuse • 315-464-9335 208 TOWNSHIP BLVD Camillus • 315-488-2372 102 WEST SENECA STREET Manlius • 315-464-9335 138 EAST GENESEE STREET Baldwinsville • 315-720-1305 Larry S. Charlamb, MD Mark J. Charlamb, MD Jorge Davidenko, MD Christopher A. Nardone, MD Michael Fischi, MD Charles Perla, MD Theresa Waters, DO Andrew M. Weinberg, DO Timothy D. Ford, MD Robert L. Carhart, Jr., MD Debanik Chaudhuri, MD Hani Kozman, MD Sakti Pada Mookherjee, MD Amy Tucker, MD Daniel Villarreal, MD Kiran Devaraj, MD Srikanth Yandrapalli, MD, FACC BUILD RESILIENCY. AVOID BURNOUT.
Calm is an independent company that provides a mobile app for sleep, meditation and relaxation to Excellus BlueCross BlueShield members. Excellus BlueCross BlueShield is a nonprofit independent licensee of the Blue Cross Blue Shield Association Listen to our episode, “Understanding and Avoiding Employee Burnout,” at ExcellusBCBS.com/podcast
CALM
Take time to focus on yourself, away from
away
As our member, you get a free subscription to the Calm app. It can help you manage stress through better sleep, mindfulness and meditation.
work. Find time
from stressors and demands of life.
Breast Cancer Awareness Understanding the Stages of Breast Cancer:
0, 1, 2, 3 and 4
Adiagnosis of breast cancer comes with many tough questions, but one of the biggest is what stage your cancer is.
Millions of women struggle with such questions every year: Breast cancer is the most common cancer in women in the United States, with the sole exception of skin cancers, according to the American Cancer Society. It accounts for roughly onethird of all new female cancers each year.
Once you receive a breast cancer diagnosis, your doctor will determine the stage of your particular cancer using the results of your diagnostic tests. Knowing the specific stage of your cancer helps determine the best treatment options for you, as well as your expected survival rate.

The most common tool physicians use to stage breast cancer is the American Joint Committee on Cancer's (AJCC) TNM system. T stands for the size of the tumor, N for whether the cancer has moved into lymph nodes, and M indicates whether the cancer has spread to other places in the body. Numbers or letters after T, N and M provide more details about each factor. Higher numbers mean the cancer is more advanced.
According to the American Society of Clinical Oncology (ASCO), breast cancer stages are broken down into five levels: Stages 0, 1, 2, 3 and 4. Below you will find expert guidance on each of the stages, along with the associated five-year relative survival rate.
Stage 0 breast cancer
In stage zero (0) breast cancer, also called noninvasive or in situ cancer, the disease is only in the ducts of the breast and has not spread to the surrounding breast tissue (Tis, N0, M0).
Stage 0 breast cancer survival rate is 99%.
Stage 1 breast cancer
Stage IA: In this stage, the tumor is small, but has invaded the breast tissue. There is none in the lymph nodes (T1, N0, M0).
Stage IB: The cancer has spread to the lymph nodes and is larger than 0.2 mm but less than 2 mm. Either there is no sign of a tumor in the breast, or it is 20 mm or smaller (T0 or T1, N1mi, M0).
Stage 1 breast cancer survival rate is 86% (Stage IB) to 99% (Stage IA).
Stage 2 breast cancer
Stage IIA:
• While no evidence of a tumor is found in the breast, the cancer has spread to one to three axillary (under arm) lymph nodes. The cancer hasn't spread to other parts of the body (T0, N1, M0).
• A tumor of 20 mm or less is found in the breast, and the cancer is in one to three axillary lymph nodes (T1, N1, M0).
• While the tumor is larger (greater than 20 mm but not more than 50 mm), it has not spread to the
Excellus BCBS Members Have New Options to a Topselling Drug
Excellus BlueCross BlueShield members living with autoimmune diseases such as rheumatoid arthritis, Crohn’s disease, and plaque psoriasis, and who use Humira to address pain and inflammation, now have additional treatment options covered by the insurer: the biosimilars Cyltezo, and Hadlima.
While Humira remains a preferred treatment option, Cyltezo and Hadlima are also now preferred treatments. They are highly similar to Humira, are approved by the U.S. Food and Drug Administration to treat most of the same conditions, and they can cost less.
Humira is among the biggest-selling medications of all time, with net global sales exceeding $21 billion in 2022. The list price can be several thousand dollars per patient,
per month.
“Biosimilars represent one of the biggest opportunities to improve medication access and affordability for our community,” says pharmacist Mona Chitre, chief pharmacy officer and president of pharmacy solutions at Excellus BCBS.

While most conventional drugs are chemically synthesized, biologics are made from natural and living sources like animal and plant cells, and microorganisms such as bacteria or yeast. They are usually more complex than other drugs and often more complicated to purify, process, and manufacture. Biosimilars are FDA approved to treat most of the same conditions as the biologic in their drug category, and can cost as much as 85 percent less, according to Chitre.
axillary lymph nodes (T2, N0, M0).
Stage IIB:
• The tumor is greater than 20 mm but not larger than 50 mm. It is also found in one to three axillary lymph nodes (T2, N1, M0).
• The tumor is larger than 50 mm but none is found in the axillary lymph nodes (T3, N0, M0).
Stage 2 breast cancer survival rate is 86% to 99%, depending on whether it has spread to the lymph nodes.
Stage 3 breast cancer
Stage IIIA: This stage involves a tumor of any size which has spread to four to nine axillary lymph nodes or to internal mammary lymph nodes, but has not spread to other parts of the body (T0, T1, T2, or T3; N2; M0). This stage may also have a tumor larger than 50 mm which has spread to one to three axillary lymph nodes (T3, N1, M0).
Stage IIIB: The tumor has invaded the chest wall or has caused ulceration or swelling of the breast. There may or may not be cancer in as many as 9 axillary or internal mammary lymph nodes. It hasn't spread
to other parts of the body (T4; N0, N1 or N2; M0). It also may have been diagnosed as inflammatory breast cancer.
Stage IIIC: Any size tumor that has invaded 10 or more axillary lymph nodes, the internal mammary lymph nodes, or lymph nodes under the collarbone. It has not spread to other parts of the body (any T, N3, M0).
Stage 3 breast cancer survival rate is 86%.
Stage 4 breast cancer
This stage involves a tumor of any size. The cancer has spread to other organs, including the bones, brain, liver, lungs, distant lymph nodes or into the chest wall (any T, any N, M1). Metastatic breast cancer found when cancer is first diagnosed only occurs about 6% of the time and may be called de novo metastatic breast cancer. Usually, metastatic breast cancer isn't found until after a previous diagnosis and treatment of early-stage breast cancer.
Stage 4 breast cancer survival rate is 30%.
Excellus BCBS has advocated for the use of biosimilars since 2018 when it first added a biosimilar to the list of drugs it covers. Today, the health plan includes biosimilars in all 10 drug categories in which a biosimilar is available.
Patients typically inject Humira at home using a pen-like device or syringe. Both Cyltezo and Hadlima are citrate-free, which can minimize the pain experienced following injection. In addition, Cyltezo is the only biosimilar that is interchangeable with Humira, which allows a pharmacist to convert a Humira prescription to Cyltezo without first contacting the medical professional who prescribed it.
“Adding Cyltezo and Hadlima to the list of medications covered by our health plan gives members who need this type of drug a choice, which also creates competition among drug makers that can ultimately reduce spending on prescriptions,” says Chitre. “The more we embrace biosimilars, the more we increase our communities’ access to affordable medications.”
The American Journal of Managed Care estimates savings in the
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 15
U.S. from biosimilars from 2021 to 2025 could range from $38 billion to as high as $124 billion.
Breast Cancer Awareness Q & A with Kathy Mezzalingua
 By Mary Beth Roach
By Mary Beth Roach
Q: What is Saint Agatha Foundation and how does it function?
A: It is to assist breast cancer patients in Central New York who have financial need. Laurie, my daughter, had been in the hospital for one of her surgeries and saw that some of her friends, who also had breast

cancer, weren’t able to afford some of the services that she received, some of the medications, surgeries and treatments. The mission of her foundation was to support, comfort and care for breast cancer patients through financial assistance programs. The support allows breast
cancer patients to focus on getting well and not the weight of their bills. That was her vision.
Q: How do patients access the foundation?
A: They can go to the website and there’s a patient access portal. It depends on where they’re being treated because we offer funds to seven counties in Central New York — Onondaga, Cortland, Cayuga, Madison, Oneida, Oswego and Jefferson counties. The best resource for patients is to visit our patient page on the website — saintagathafoundation.org — and submit an inquiry or call 888-878-7900. We are administered by National Philanthropic Trust in Philadelphia.
Q: What are the logistics of accessing that funding?
A: The website will guide them step by step. We work with CancerConnects and the bills are submitted to them. Our contact there does a great job of vetting them to make sure that they’re underinsured or uninsured and then they pay the bills. People have a hard time understanding that we will pay their bills.
Q: Are there certain criteria or parameters that the patients have to meet?

A: Just financial. If they’re uninsured or underinsured, we will take care of them. And it isn’t only their hospital or their medical bills. We will support them while they’re going through chemotherapy with gas money, utilities, mortgage, Wegmans cards. This is Laurie’s dream. She wanted them to be totally free of worry financially so they could just focus on healing.
Q: How many patients have you served since the foundation was established?


A: We have served 8,822 individuals within the counties that we
serve. We’ve given out 232 grant payments to 31 organizations. It isn’t only hospitals, there are other ancillary services. For example, to Legal Aid, for the patients who may have some legal issues. We give to Camp Kesem for the children of breast cancer patients who might be suffering because their mother is going through it. We give to Symphoria. It helps them with music while they’re going through chemotherapy.
Q: How do you keep the monies coming into the foundation? Do you accept donations? Is some of the money invested?
A: Laurie left a significant legacy and she wanted it all to go to Saint Agatha. We have invested it very wisely and it’s actually doubled in the 13 years that we’ve been running this organization. We do accept donations. There’s an opportunity on our website. So many people are so impressed with what we’re doing, they want to help us.
Q: The funding doesn’t go into research. It goes directly to patient care. Is that correct?
A: Absolutely. Laurie was very, very clear about that. She said I don’t want my name on buildings, no endowments, no research. There are other organizations doing that. She was so clear about that, she said: “just help women.”
Kathy Mezzalingua serves as the president and board chair of Saint Agatha Foundation, an organization her daughter, Laurie, established in 2004 to benefit breast cancer patients. Diagnosed with breast cancer when she was 29, Laurie, unfortunately, died in 2009, at the age of 41. Her legacy continues through the foundation.

Page 16 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
President of Saint Agatha Foundation explains how the nonprofit provides financial help to women who undergo breast cancer treatment
NAME ADDRESS CITY/TOWN STATE ZIP 1 YEAR (12 ISSUES) $21.00 $35.00 2 YEARS (24 ISSUES) 4 Riverside Dr., Ste. 251, Utica, NY 13502 Hello. I’d like to subscribe to 55 Plus, the only magazine celebrating life after 55 in Central New York, and have it delivered to my door. Payment is enclosed. Offer valid through August 2022. Offer subject to change without notice. First issue mails within 3 to 6 weeks. 55 Plus is published bi-monthly by Local News, Inc.. Find us online at cny55.com. Issue 107 October-November 2023 For Active Adults in Central New York cny55.com REALLY GOOD PIES P. 52 P. 20 FALL GETAWAYS Stay regional yet get out of town with these nearby autumn escapes P. 38 SPECIAL: HOW TO FIND A DOG THAT FITS YOUR LIFESTYLE The journey of Marlene Parlow of Oneida to baking great pies SELECT CONTENT Fall getaways Why you may want to keep working. basics for the not-so-computer savvy • How to protect from cybercrimes • Friends spend nine days biking around Lake Ontario. Eight steps to writing a great memoir • How to pick a dog that is a good fit. Don’t Miss
We help knock out the financial worries of breast cancer care in CNY.

Chemotherapy. Radiation. Lab work. Transportation. Childcare...
The costs of fighting a breast cancer diagnosis mount quickly. Fortunately, breast cancer patients in CNY with financial need may qualify for financial support from Saint Agatha Foundation.

Through medical and non-medical service providers across seven counties, our support can make the fight against breast cancer a little easier.
If you or someone you love is fighting breast cancer and its financial challenges – OR if you’re a service provider interested in helping breast cancer patients –visit saintagathafoundation.org to learn more!

Let us help you breathe easier with a free lung cancer screening!
November is Lung Cancer Awareness month. As a service to our community, Hematology-Oncology Associates of CNY and CRA Medical Imaging are offering a free lung cancer screening to qualified participants.

Who: Free screenings are available for individuals ages 50-80 who:

- are heavy smokers (e.g., 1 pack a day for 20 years or 2 packs a day for 10 years)
- OR are former heavy-smokers who quit in the last 15 years
- AND have not previously received a free lung cancer screening from us.
Note: Anyone with insurance can contact our office to discuss getting a lung cancer screening at your convenience.
When: Saturday, November 4, 8:00 a.m. to 2:00 p.m.
Where: HOA’s Onondaga Hill, East Syracuse and Auburn offices
To learn more, call 315-472-7504 extension 1301 or visit hoacny.com
This free screening event is co-sponsored by:
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 17
We’re in your corner in the fight against breast cancer
Learn about our Founder ’s inspirational fight with breast cancer
Breast Cancer Drug Could Trigger Dangerous High Blood Sugar
For certain patients with advanced breast cancer, a drug called Piqray (alpelisib) may extend survival. But new research confirms the medication often causes seriously high blood sugar levels.
“This is a very effective drug that we should be using to treat breast cancer, but the problem is that it causes high blood sugar, which also can decrease the efficacy of the medication,” explained study co-author Neil Iyengar. He is a medical oncologist at Memorial Sloan Kettering Cancer Center in New York City.


The findings are not a reason to avoid this drug — but they do indicate that precautions are needed before taking the medication, Iyengar said. “The key is that high blood sugar can be prevented,” he stressed.
Taken as a pill, Piqray is a kinase inhibitor that blocks the signals that cause cancer cells to multiply. It is used along with Faslodex (fulvestrant), a hormone therapy, to combat tumors that express the PIK3CA mutation and are hormone receptor-positive and HER2-negative.
These mutations are found in about 40% of breast cancers, the researchers noted.


High blood sugar, or glucose, levels occur when the body has too little insulin or can’t use insulin properly, and it sets the stage for diabetes.
“You can start working on your [blood sugar] status a year or more in advance if you know you are a candidate for this medication,” Iyengar said. Doctors can do genomic testing of the breast cancer when you are diagnosed. “The first line of therapy usually lasts for a year, so you have time to get your blood sugar under control before starting Piqray,” he explained.
The study included 147 people who were treated with Piqray. Of these, more than 80% developed high blood sugar (hyperglycemia), and about 40% developed serious hyperglycemia. Another 100 people were treated with Piqray as part of a clinical trial, and the rates of high blood sugar were lower in this group. This is likely because participants in studies tend to be healthier and are monitored more closely, Iyengar said.
Most people developed high blood sugar within 16 days of starting the medication, the study showed. The risk was higher among those who had elevated hemoglobin A1c before starting the drug. (Hemoglobin A1C provides a snapshot of blood sugar over the past two or three months.) Among those who developed high blood sugar, two-thirds received treatment, most commonly with the diabetes drug metformin.
Piqray blocks insulin in cells, which leads to higher circulating levels of blood sugar, Iyengar explained.
Now, researchers are looking at how various diets or diabetes drugs can affect blood sugar levels among patients taking this medication, he said.
Alpelisib is the only U.S. Food and Drug Administration-approved PI3K inhibitor. “There are several newer mutation-specific PI3K inhibitors that are currently in clinical trials which do not cause hyperglycemia, but it is unknown whether they are as effective,” Iyengar said.

The findings confirm Piqray’s effect on blood sugar, said Natalie Klar. She is a medical oncologist and assistant professor of medicine at NYU Langone Cancer Center in New York City.


Page 18 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023 All In One Location www.craimaging.com For an appointment, call 315-234-4680 Breast MRI through MDR of CNY 3D Mammography Joint Injection, Port Insertion, and Paracentesis and Thoracentesis Breast Ultrasound NEW! Ultrasound-Guided Breast Biopsy
5000 Brittonfield Parkway, E. Syr., NY 13057
Breast Cancer Awareness Medicare Insurance Specialist/Licensed Independent Agent 315-727-4933 • tcangemi@RetirementHPMS.com www.RetirementHealthPlansMadeSimple.com “Commissions Paid by the Carriers, Not Fee Based” Theresa Cangemi, CSA, CLTC Retirement Health Plans Made SimpleTM Medicare Advantage • Medicare Supplement • Prescription Drug (Part D) Plans Long Term Care (CLTC) • Life Insurance • Final Expense (Burial) • Dental Plans Travel Insurance Coverage Serving New York State’s medicare eligible population since 2008! DO YOU & YOUR PARENTS HAVE PROPER MEDICARE INSURANCE COVERAGE? FIND OUT. Personalized Consultation & Enrollment Services* *Not a government entity *Formally Medicare Made Simple, LLC.







October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 19 VISIT ONLINE NUNNSHME.COM PROUDLY SERVING LADY JANE CUSTOMERS! Certified Mastectomy Fitters on Staff ROME 1340 Floyd Avenue Rome, NY 13440 (315) 339-4084 SYRACUSE 817 E Genesee Street Syracuse, NY 13210 (315) 475-5181 Your Best Choice for a Sleep Therapy Provider! TWO CONVENIENT LOCATIONS to make a difference? Scan this code or visit hoacny com for important safety and lab/test information. Or call 315-472-7504 to see if Galleri is right for you! early enough With Galleri™ multi-cancer early detection from HOA, you can! a simple blood draw is all it takes to screen for 50+ types of cancer not commonly screened for no referral required not covered by insurance, but does generally qualify for HSA and FSA reimbursement What if you found cancer
Breast Cancer Awareness
that AI-assisted mammograms may be an important tool to help radiologists detect breast cancer,” said Susan Brown, RN, senior director of health information and publications at Susan G. Komen headquarters in Dallas. “It is hoped that AI-assisted mammograms will increase accuracy and efficiency.”
Brown noted that false positives and false negatives could be an issue with AI-read mammograms but hopes that additional research will confirm the early studies on AI assisted mammograms.
Nancy Wayne, marketing administrator at Elizabeth Wende Breast Care headquartered in Rochester, wants to see additional research to show that AI plus a radiologist is just as good as two radiologists.
AI Assisted Mammograms
Study: Radiologists using AI detect 20% more cancers than those read only by radiologists without AI help
By Deborah Jeanne Sergeant
Astudy published by Swedish researchers in August indicates that artificial intelligence (AI) can safely augment and even improve radiologists’ work in detecting breast cancer.
The study is the first trial that compares AI-assisted mammogram readings with human-only mammogram readings. The radiologist using AI detected 20% more cancers than those read only by two radiologists without AI help. Using AI did not appear to increase the number of false positive mammograms, which is when an abnormality is noted but not actually present.
In addition to greater efficacy, using AI also reduces the workhours needed to read mammograms by 44% because AI replaces the work
of one radiologist (some hospitals require that two radiologists are required to read each mammogram). This can be particularly helpful in health systems with few radiologists, such as in rural areas.
According to the American College of Radiology, 82% the 20,970 radiologists providing patient care are age 45 and older and 53% are age 55 and older. The demand for radiologists is rising as the aging Baby Boomers require more care. The Bureau of Labor Statistics states that the need for new radiologists is expected to rise by 6%, “faster than average” between 2022 and 2032 compared with all other occupations. Enlisting the help of AI can help mitigate this rise in demand.
“Early research appears to show
More American Men Now Opting for Vasectomy
Vasectomies are becoming more common in the United States, with rates surging by more than one-quarter during the past decade, a recent study reveals.
The U.S. vasectomy rate increased by 26% between 2014 and 2021, according to an analysis of commercial health claims data.
“All areas in the United States except the Northeast showed increased vasectomy rates,” said senior researcher and physician Omer Raheem. He is an assistant professor of surgery-urology with the University of Chicago School of Medicine.
Overall numbers remain low, with roughly 4% of men having undergone vasectomy, the researchers noted.
But doctors expect the demand for vasectomy will continue to increase following the 2022 Supreme Court decision that abolished the
national right to abortion.
“After the Roe v Wade overturn, there has been a significant increase in Google searches for vasectomy, as well as an uptick in vasectomy consultations and procedures,” physician Stanton Honig, division said chief for reproductive and sexual medicine at Yale School of Medicine.
“This recent study points to the fact that men are taking more of a role in reproductive health and family planning, especially when they are finished having children,” continued Honig, who was not involved with the new research.

For the study, Raheem and his colleagues gathered health insurance claims data to calculate the annual vasectomy rate among privately insured men in the United States, aged 18 to 64.
The percentage of all male patients undergoing vasectomies in
“AI is a wonderful tool,” she noted. “We’re still early on in the development of AI. There are multiple products out there currently. We’re still not quite able to say one product fits all. There are multiple companies with proprietary products. We’re hopeful where at some point the AI has to fulfil certain criteria to be appropriate. I’m not sure at this point we’re there. It is promising.”

A form of AI has been used for a long time; however, the current use “learns” from past mammograms, honing its ability to detect cancers that humans might miss.
“AI is everything in imaging,” said Avice O’Connell, director of the University of Rochester Medicine breast imaging program. “But it’s not going to take our jobs. AI is something we’ve been using for more than 20 years in mammography. In 1998 the first computer aided detection, the computer scanned images and highlighted things that could be cancer. There’s still that kind of computer aided detection. There are usually four marks on every exam, so a human still has to look at it. It’s just an aid to make sure we’re not missing things.”
O’Connell views AI as a means to screen the “easy” cases more quickly
so radiologists can pay more attention to more challenging cases. But in either, a human must be involved; AI is only a tool but doesn’t make any decisions about health.
“The patient makes the ultimate decision whether or not to have the biopsy,” O’Connell said. “We’d still follow up the patient in six months.”
O’Connell sees machine learning as the next threshold of mammography advancement, meaning that AI technology reads more and more mammograms, it becomes more skilled at catching abnormal findings. She also thinks that AI-assisted mammography will help in areas of the world where few specialists exist.
“The vast majority of breast imaging around the world is not read by breast experts,” she said. “AI has huge value in every country.”
a given year increased from about 0.43% in 2014 to 0.54% in 2021, the investigators found.
The relative increases were greatest in men with no children (61%), men with an older wife (41%), single men (41%), and young men 18 to 24 (37%).
Vasectomy also remained a popular option for men with two or more children, the results showed.
Rural areas experienced greater
increases in vasectomy rates than urban areas, the researchers added.
“Given the political landscape, some men are leaning in and taking more responsibility to prevent unintended pregnancy,” said physician Monica Dragoman, system director of the complex family planning division in the department of obstetrics, gynecology and reproductive science at Mount Sinai School of Medicine in New York City.
Page 20 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Susan Brown is a registered nurse and the senior director of health information and publications at Susan G. Komen. “It is hoped that AI-assisted mammograms will increase accuracy and efficiency.”
Breast Cancer Awareness
Breast Cancer ‘Overdiagnosed’ Among Older Women
Study: Some women over 70, if diagnosed with breast cancer, need to weigh if pursuing treatment is the right course
By Deborah Jeanne Sergeant
Arecent study of 54,635 women ages 70-plus by Yale School of Medicine indicates that 31% of women ages 70-74 and 47% of those 75-84 were possibly “over-diagnosed” with breast cancer.
The term means that they were found to have a kind of breast cancer that is slow growing and that treatment would likely not extend their lives or improve their quality of life.
In fact, pursuing treatment such as lumpectomy, mastectomy or chemotherapy would dramatically decrease quality of life.
“There is no exact age at which women should stop getting mammograms,” said Susan Brown, registered nurse, senior director of Health Information and Publications at Susan G. Komen headquartered in Dallas. “Breast cancer risk increases with age, and mammography doesn’t appear to be less effective in women 70 and older. However, there are risks of mammography in older women, including over-diagnosis and over-treatment, when a cancer that would not have caused problems if untreated is treated and the person is subjected to side effects without receiving any real benefit from the treatment.
“Many major health organiza-
tions recommend women ages 70 and older continue to get regular mammograms as long as they are in good health and could benefit from treatment if breast cancer were found.”
She added that poor health may cause some women may stop routine breast cancer screening, as would the presence of other health issues that would take precedent. The organization’s stance is that women should be able to access regular screening mammograms as long as they and their providers think they should.

When to stop mammography— and when to start—relies upon many health factors.
Robert Smith, physician, vice president of Early Cancer Detection Science for the American Cancer Society, said that women at high risk may start with annual mammograms earlier than other women, typically around age 30.
“Some women with a first-degree relative like a mother or a sister who was diagnosed at a young age have been advised to begin screening ten years before the age that relative was when she was diagnosed,” Smith said. “Women who receive regular mammograms are more likely to have breast cancer diagnosed earlier,
Saint Agatha Foundation Launches Awareness Effort
Nonproft provides financial support to qualified breast cancer patients across seven CNY counties
Saint Agatha Foundation, a nonprofit organization providing financial assistance for unmet financial needs of CNY breast cancer patients, recently announced it will leverage October’s National Breast Cancer Awareness Month to raise awareness of the disease and kick-off its own campaign focused on raising awareness of its mission.
Founded in 2004 by Laurie Mezzalingua, taken by breast cancer in 2009 after a years-long battle with the disease, Saint Agatha Foundation has provided $17.5 million in financial support to over 10,000 breast cancer patients in Central New York to date; funds are distributed to patients via both medical and non-medical service providers who apply on behalf of their patients or clientele.
“Saint Agatha Foundation joins many other institutions in Central New York in recognizing National
Breast Cancer Awareness Month as a way to draw attention to the continuing and critical fight against breast cancer,” says Kathy Mezzalingua, chairwoman of the Foundation and Laurie’s mother. “We’re also taking this opportunity to spotlight our unique mission of providing financial support to breast cancer patients in our community, to focus on overcoming their diagnosis instead of worrying about unmet financial stress they may be facing.”
Mezzalingua added that bills the foundation can assist with, once insurance has done its part, can include everything from clinical items like lab tests, infusion, radiation therapy, doctor’s appointments to non-medical items like child care, transportation, household and legal expenses.
The foundation’s new awareness campaign will include advertising, public relations, social media,
less likely to need aggressive treatments, and more likely to be cured. However, mammograms are not infallible; they may miss some cancers, and even when issues are found in an initial screen, further testing may be needed to confirm the presence of cancer.”

Those who are 55 and older may choose to switch to every other year. But Smith said those who are 75 or older can continue annual screening as long as they remain in good health and expect to live at least another 10 years.
Onondaga County Health Department Medical director James Alexander, physician, said that most organizations currently state that through age 75 is reasonable as for how long to receive mammography.
“After that, it comes down to ‘shared decision making,’” he said. “You sit down with the patient and talk about their desire to continue breast screening and what would they do if they had a positive. Do all the women and their family live to be 100 with healthy, active, productive lives? That 75-year-old is different
grassroots presentations to community groups, and outreach to – and training for – providers seeking to apply for funds to assist their patients in need. Additionally, Saint Agatha Foundation will participate in a range of breast cancer awareness month activities in October.
• Saint Agatha Foundation Community Partner Convening will be held Oct. 11 at the Crowne Plaza Hotel and Conference Center in Syracuse. This event served as an opportunity for medical care and other service providers to learn more about Saint Agatha Foundation and how the organization assists breast cancer patients in Central New York; connect with other partner organizations; and share ideas and feedback with the foundation. This meeting is intended for those who work with breast cancer patients directly, such as breast cancer patient navigators, social workers, financial counselors, among others. For more information reach out saintagathafoundation@nptrust. org by Oct. 2
• Saint Agatha Foundation will be a lead sponsor at the American Cancer Society Making Strides Against Breast Cancer walks in Syracuse at Clinton Square on Oct. 15 and in Utica at Mohawk Valley Community College on Oct. 22.
– Those wishing to register
from one who doesn’t have those great genetics of longevity. You have to really consider also the general health status of the patient and incorporate that into your shared decision making.”
He said that a woman who is 75 and not well, who has advanced heart disease is not as likely to continue to seek mammography.
“As you get older, they’re going to find more breast cancers present, but maybe they wouldn’t be aggressive or advance quickly,” he said. “It maybe won’t be life threatening. What we need to figure out is what is the appropriate intervention in that case and how much screening do we continue?”
The treatment of a tumor at this stage in life might be progesterone for a slow-growing tumor rather than aggressive treatment with surgery or chemotherapy, which would decrease the quality of the life the woman likely has left. Alexander calls this a “risk-based analysis” to decide about the appropriate care on an individual basis rather than stating that a certain age is a hard-and-fast cutoff.
and participate in the October 15 walk should visit: https://secure. acsevents.org/site/STR?pg=entry&fr_id=105628
– Those wishing to register for Oct.22 walk should visit: https://secure.acsevents.org/site/STR?pg=entry&fr_id=105631.
– Those attending either event are encouraged to visit the Saint Agatha Foundation team at each event’s check-in area or Survivor Tent.
• Saint Agatha Foundation is also a presenting sponsor at the E-Race Cancer Half Marathon and 5-K in Bridgeport on Oct 22 in support of the foundation’s valued partner, CancerConnects. To find out more or sign up, interested parties should visit: E-Race Cancer Half Marathon, 10K & 5K (runsignup.com) For more information, visit www. saintagathafoundation.org.
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 21
Laurie Mezzalingua
Oral Contraceptive to Be Available Without Prescription Early in 2024
New drug, Opill, offers a 98% rate of effectiveness in preventing conception
By Deborah Jeanne Sergeant
The FDA recently approved Opill (norgestrel) as an over-thecounter oral contraceptive.
Typically, oral contraceptives require a physician’s exam and prescription. Opill was first approved with a prescription in 1973. When taken as directed — one pill daily at the same time each day — Opill offers a 98% rate of effectiveness in preventing conception.
“Opill will improve access, which is always an issue for young women,” said Mustafa Awayda, physician and medical director at Rahma Health Clinic in Syracuse. “They may not go get an appointment to get a prescription. I think it will be very effective if used correctly.”
He does wonder what the cost will be, as prescription contraceptives are typically covered by insurance plans. Awayda said Opill may cost $30 to $50 for a month’s supply, which could negate its availability to some women. But Opill may be used more as a “bridge” for patients who want contraceptives but are between doctors or insurance plans. It is still important for patients to seek routine PAP smears as part of their routine healthcare regardless of to any contraception chosen.
“There may be concerns about taking it long-term without physician oversight,” Awayda added. “It might create health concerns.”
Opill is considered safe for people who smoke, who have a history of blood clots, stroke or bleeding disorders.
“This pill can be used very safely,” said Onondaga County Health Department Medical Director James Alexander, a physician. “They’ve had it in France for a while. This oral contraceptive is progesterone-only as opposed to estrogen and progesterone. The latter is much more broadly used.
“Progesterone-only is effective, but not as effective as the combined pill. The combined pill is associated with more irregular bleeding. Bloating and breast tenderness and acne are associated with progesterone-only pills. To the extent that it’s expanded access to birth control, it’s wonderful. It’s fantastic.”
He viewed the lack of patient counseling about when to stop and start the pill as a drawback to Opill. It also lacks the other advantages associated with a combined pill, such as regulating bleeding.
The FDA’s website states that women who have or who have had breast cancer should not take Opill. Other contraindications include women who are pregnant or who think they might be pregnant, along with another birth control pill,
vaginal ring, patch, implant, injection or an intra-uterine device, or as an “emergency contraceptive,” also known as a “morning-after pill.” Men should also not take Opill.
Dual-hormone contraceptives typically warn that’s it’s not recommended for women 35-plus. However, Opill has no such contraindication. Its safety has been established for women as young as 15. Sale of Opill will not be limited by age, however.
Opill has the typical oral contraceptive side effects. The FDA listed irregular bleeding, breast tenderness, headaches, nausea, dizziness, abdominal pain, increased appetite and bloating.

The FDA encourages women to discuss Opill with a healthcare provider or pharmacist if they currently take a prescription for drugs to treat seizures, tuberculosis, HIV AIDS, or pulmonary hypertension or take an over-the-counter supplement containing St. John’s Wort. Opill may interact with these drugs or become less effective. Opill can also affect the efficacy of emergency contraceptives.
The Centers for Disease Control and Prevention states on its website that “all women are at risk for gynecologic cancers and risk increases with age.”
It’s vital that women seek preventative exams on the schedule their care provider recommends, even if they use Opill.
Women taking Opill should take it for seven days prior to relying on it for contraception to better ensure its effectiveness. For many years, doctors have routinely prescribed oral contraceptives for controlling patient’s abnormal bleeding, period pain and other similar issues. But the FDA has not approved Opill for these uses. It’s vital that women seek a provider’s care for such symptoms and not try to self-diagnose and hope Opill will take care of it.
The active ingredient in Opill concerns the Rev. Jim Harden, CEO of CompassCare, which offers reproductive counseling and sexually transmitted infection testing and treatment services in Rochester, Buffalo and Albany and statewide via telehealth.
“Peer-reviewed medical articles and the World Health Organization state that this exposure to steroidal contraception increases risks of cancer,” Harden said.
Harden writes extensively on medical ethics. His book “Ethical Theory and Pertinent Standards in Women’s Reproductive Health” was endorsed by the late Edmund D. Pellegrino, a physician, former chair of the President’s Council on Bioethics;
senior research scholar at the Kennedy Institute of Ethics, and professor emeritus of Medicine and Medical Ethics at Georgetown University.
Hardin noted the National Institutes of Health’s statement about progestin-only oral contraceptives as “at least comparable to the risk of combined oral contraceptives” which the NIH said, “increase the risk of breast cancer” as a “group 1 carcinogen for breast cancer, as well as for cervical and liver cancer.”
The FDA’s website states that “each Opill tablet contains 0.075 mg. of a single active steroid ingredient, norgestrel, a totally synthetic progesterone.”
Harden believes that the side effects of Opill have not been clearly communicated to patients and that once it’s available without a prescription, many women, particularly younger women, will take it without reading any of the package warnings or without knowledge of it side effects.
“It appears this drug is wildly unsafe under normal circumstances, say nothing of giving access without physician oversight,” he said. “Once this is available over the counter, you’re eliminating the safety net that is so important to medicine.”
He believes that over-the-counter access to Opill would mean that women may try to take Opill off-label as emergency contraceptives, a use for which Opill has no FDA approval.
Colt Wasserman, a physician, views Opill as lowering barriers for people who face barriers in obtaining contraceptives. “It provides another way of obtaining contraceptives,” he said. “I feel really excited for patients.”
Wasserman is chief medical officer for Planned Parenthood of Western and Central New York,
which includes offices in Syracuse, Rochester, Canandaigua, Batavia, Buffalo and Niagara Falls.
Every county’s health department offers free condoms, as do many other organizations.
Wasserman feels that “contraception is not a one-size-fits-all decision. It’s really important for each patient to have lots of different resources to plan their future. I’m excited about barrier methods and condoms being widely available, but an over-thecounter contraceptive is only going to increase the number of choices people have.”
The cost for Opill is not yet known. If it follows the pattern of emergency contraception, which costs about $88, then Opill would not reduce barriers to contraception for people with a low income.
Opill will likely not have an age minimum for purchasing it. Youth who are too young to buy over-thecounter cough syrup will be able to purchase Opill once it’s available in the first quarter of 2024. As for concerns about teens taking Opill without parental supervision, Wasserman doesn’t see a problem.
“We know that teenagers and youth can understand how to use contraception safely and effectively,” he said. “Requiring some kind of ID proof of age can disproportionally affect those who don’t have access to an ID. When this was issued, it was decided to make it generally available.”
He also does not believe that greater availability of contraception will increase the rates of teens becoming sexually active. Wasserman wants parents to try to maintain open conversations about matters such as sex and “establish themselves as safe people in their youth’s lives to be able to provide guidance,” he said.
Page 22 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
HEALTH
OMEN'S
PebbleKranz
Hormone Replacement Therapy Can Ease Menopause Symptoms

As if night sweats, mood swings, mid-section weight gain, low libido and vaginal dryness weren’t bad enough, menopause can also raise the risk of cardiovascular disease, autoimmune disorders and osteoporosis
By Deborah Jeanne Sergeant
Ever since prescribing hormones for menopausal symptoms— known as hormone replacement therapy (HRT)—was correlated with increased risk of blood clots, stroke and cancer, fewer doctors have offered hormone replacement as an option.
However, Onondaga County Health Department Medical Director James Alexander, a physician, said that low-dose HRT is an example of one of the “much safer approaches to using hormone therapy. We’ve modified the medication and combinations and doses, all in the interest of maximizing relief and minimizing symptoms.”
He added that many primary care providers don’t recommend hormone replacement therapy because it’s not within their area of expertise. And many women don’t seek it because once they’re done having babies, they don’t see an OB-GYN anymore.
“A very effective way to mitigate many of those [menopausal] symptoms is to give women back estrogen and progesterone, whether in the form of a birth control pill for younger women to regulate the fluctuations, and in women who are over the traditional age of menopause, low dose hormone replacement therapy,” Alexander said. “Both are really quite effective in mitigating most of the symptoms of the menopausal transition.”
He also recommends vaginal medication to help with dryness, improve sleep and reduce hot flashes.
Instead of oral medication, patches and creams can provide relief that’s more targeted and doesn’t require the liver to filter it, thus reducing risk of blood clots.
Maintaining hormone levels isn’t only about pesky symptoms. James Woods, an, OB-GYN with University of Rochester Medical Center, said that balanced hormones can also help
SENIOR CITIZEN HOUSING
reduce inflammation and promote the body’s ability to support bone density. In younger women, the bones are in a constant state of building new cells and breaking down old cells. But an inflammatory response of the body disrupts that process, so the bones become softer.
Hot flashes are more than a nuisance. Woods said that they can indicate a higher cardiovascular risk. The hypothalamus in the brain signals the body to develop at puberty.
“Right next to that group of two neurons is the heat center,” Woods said. “When you’re younger, you didn’t realize you have half a degree that your body temperature could fluctuate and it would send a signal that you’re hot. You lose that half a degree and it sends a signal to the brain that you’re hot.”
The body sweats as a response to move that heated blood near the surface of the skin to cool.
“It’s a cardiovascular risk,” Woods said. “If it’s not treated and stopped, those women will be at more risk of cardiovascular damage and death. It’s not just an inconvenience.”
Weight gain also affects many women between 45 and 65. Woods said that the lack of estradiol causes inflammation of the lining of the intestines and upsets gut bacteria. In turn, the body’s metabolism slows down so that it stores more fat, increasing risk of cardiovascular disease, diabetes and more.
Depression and anxiety can also increase the risk of cardiovascular disease. These mental health struggles can stem from health issues, as well as what Woods calls the “chronic stress window” of caring for aging parents, working full time at the busiest part of her career, and bearing the majority of household chores and child rearing responsibilities.
“At that stage many women realize life didn’t work out,” Woods said.
“Domestic violence, divorce and kids who could be in trouble add to the stress.”
Woods said that compared with women of the same age who lack these stressors, their immune system is different from those subjected to chronic stress.
He said that the best time to begin hormone replacement is around 48, as the levels begin to dip and before inflammatory damage begins. Woods also counsels about other, non hormonal treatments that may help.
“The story about the risks of HRT have been confusing for both women and their medical providers over the last 20 years after the press around the Women’s Health Initiative study in the early 2000s leading to a generation of patients and clinicians terrified about HRT generally,” said Pebble Kranz, a physician, assistant professor of clinical family medicine and obstetrics and gynecology at University of Rochester and medical director of the Rochester Center for Sexual Wellness. “We now know that many of the findings from that study need to be evaluated in context and with more nuances.
“For most people younger than 65, HRT is not harmful and can be beneficial regarding heart, bone, sleep, mental, and sexual health. Meanwhile, the current guidelines are that HRT should be used for bothersome symptoms of menopause — hot flashes, sleep disruption, vaginal symptoms and others — not for prevention of health issues of aging. As with so much in medicine, the benefits and risks of HRT should be an individualized conversation with a qualified healthcare provider.”
She wishes more providers would seek more up-to-date information about menopause care from organization such as The Menopause Society.
SIMEON DEWITT
150 E. 1st St. Oswego, NY 13126 315-343-0440
TOWPATH TOWERS
100 Rochester St. Fulton, NY 13069 315-598-4700
SPRINGBROOK APARTMENTS
4920 N. Jefferson St. Pulaski, NY 13142 315-298-6101
The following services are included in your rent
• Trash Collection • Free Wi-Fi
• Bus for shopping/groceries
• Heat, Electricity & Hot Water
• Snow Removal & Lawn Care
• Planned Activities
• All repairs & maintenance
Applications are now being accepted! 62+ No smoking! Preference given for veterans & spouses of veterans.
Enjoy reading In Good Health newspaper? The paper is free to you but very expensive to produce and distribute. Keep the publication going. Consider supporting it. If you are a reader, please become a paid subscriber (see coupon in this issue). If you’re a nonprofit, a medical practice or organization, consider advertising. You will get a great deal of exposure since the paper is everywhere for the entire month. We will even design your ad at no charge. For more information, send an email to editor@CNYhealth.com —
Type “Support” on the subject line.
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 23 OMEN'S
HEALTH
Equal Housing Opportunity Supervised by NYS DHCR
WORTH SUPPORTING It’s YOUR SUPPORT
Parenting
By Melissa Stefanec MelissaStefanec@yahoo.com
What’s in a Team?
Our society is obsessed with superheroes. When it comes to idolization, many adults (and children alike), put superheroes on pedestals. We look to them for inspiration. We look to them to light the fires within us. We elevate them to places we think we cannot go.
Most of these modern-day idols don’t wear capes. Our modern superheros often wear sneakers, cleats, helmets, spandex or goggles. That’s because our society is obsessed with sports and we make the players into heroes and structure much of our lives around admiring them.
Whether it’s college or professional teams, we pack the venues and buy expensive streaming packages so we can indulge our idolization. Similarly, we pack children’s lives with teams, leagues, travel teams and elite squads. Sports are a mighty presence in our lives.
That’s totally cool. But what if I told you that there was more? For many kids and adults, sports offer an outlet and a way to grow. For other kids, sports have no allure. In fact, sports actually make some kids feel bad. And, strangely enough, many adults make kids feel bad for not
making sports a part of their formative years. Some folks think that without athletic competition, childhood is lacking in some way.
I think we can do better than that.
First, I want to acknowledge there are many benefits to children who participate in sports. From physical fitness to collective problem solving to self-betterment, overcoming challenges and learning how to achieve as a team — group athletics have a lot to teach our children about life.
However, there is so much more to life than sports. We owe it to our children to recognize this simple fact. It’s time parents put equal stock in activities outside of sports and recognize how non-athletic activities can enrich our children as they grow into adulthood.
Here is a list of activities that teach as many life lessons as sports do. I encourage other parents to nurture their children in these activities. These hobbies are no less or greater than athletics, they are just a different outlet and an alternative basis for self expression. These activities deserve the same respect and investment from parents and communities alike.
ARTS, CULTURE ENTERTAINMENT EVENTS!



• Chorus, band or orchestra
Few teams work harder to refine their individual abilities and collective efforts than a chorus, band or orchestra. Kids in these activities have to practice their personal craft for the betterment of a team. Their coach is a conductor, and the conductor leads them to become something better than they could ever be on their own.

• Drama or theater
To be part of a theatrical production, you have to understand the strengths and weaknesses of everyone around you. You have to work on yourself and figure out how to combine forces with others. Each performance is a production, and if you don’t do your part, no one gets to shine.

• STEAM competitions

For some kids, their brains work harder than any part of their bodies. But kids who participate in team STEAM activities quickly learn that one brain isn’t enough. A lone brain has blindspots and oversights. It takes a team to build a holistic force. Together, these kids learn they can do more together than they ever could alone.
• Community involvement

Kids who want to give back to their communities have learned a lesson many adults have failed to — there are things more important than ourselves. These kids understand that together we rise and divided we fall. Kids who choose community over self deserve respect. They deserve to be backed and cheered like the hometown team at the homecoming game.
• Lifeguarding/counseling
There are many children who have come to understand that you’re never too young to build up
the younger generation. Kids who choose to be counselors or lifeguards understand that we can work together to protect and nurture each other. They know that teams can lead us when we feel lost and save us when we’ve gone off course.
• Writing
Writing is one of the most robust empathy exercises a child can participate in. On its surface, writing may not feel like a team event, but to write is to understand oneself and others. Writing is at once an act of empathy and compassion. It’s an act of awareness and recognition of others’ experiences. It takes a team mentality, even if it happens as a solo effort, until the workshop rolls around.
• Art
Some of the best art makes people feel things they didn’t know they needed to feel. To be an artist means that you can create something that others find meaning in. Art brings self awareness and peace to many people. When you’re an artist, you’re on team human.
So the next time we ask ourselves, “What’s in a team?”, I suggest we broaden our proverbial horizons. Teams come in many outfits and varieties. Sometimes, after hours of practice. a team takes to the field in perfectly matched uniforms. They run plays in the hopes of besting their opponent. Other times, after hours of practice, a team takes the stage, assembled to move emotional mountains with song. Both of these teams deserve admiration and demand much of their players. Both of these teams are something children should aspire to and something adults should support and nurture.

Page 24 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
FOR MORE INFORMATION CHECK OUT CNYARTS.ORG/EVENTS DISCOVER THIS SEASON’S MOST EXCITING & SCAN HERE
CNY Arts programming is made possible by the New York State Council on the Arts with the support of the Office of the Governor and the New York State Legislature.
Women’s Services at
Because women deserve the quality care they strive to provide everyone else.

In most households, women are the managers of their families’ health care needs.* Combined with the challenges associated with juggling child care and workplace demands – it can be a struggle to ensure women, quite literally, take care of themselves. FCMG can help. Available across CNY’s widest network of general practitioners and specialists – with short wait times, convenient hours and family-friendly offices – we make it easy to access a wide range of women’s care options, including:
• Reproductive health care and gynecology, including ultrasound exams
• Heart health, cholesterol management, and treatment of high blood pressure
• Type 1 and Type 2 Diabetes
• Chronic care and pain management
• Nutrition
• Dermatology
• Bone density, including diagnosis and care of Osteoporosis
• Among others
To learn how FCMG can address women’s health care needs – for women of all ages – contact us today. New patients and families are welcome!

care for yours!

October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 25
* Kaiser Women’s Health Survey (2017) indicated that 79% of the time, women are the one who take charge of health care responsibilities such as choosing their children’s provider; that 77% of the time, women take children to appointments; and that 77% of the time, women follow through with recommended family care.
Let
family
315-472-1488 •
our
fcmg.org
Crouse. As individual as you are. crouse.org/women BREAST HEALTH | CARDIAC CARE | WEIGHT-LOSS SURGERY | UROLOGY | PELVIC PHYSICAL REHAB | GYN | GYN ONCOLOGY LOW & HIGH-RISK OB | REGIONAL NICU | LACTATION CONSULTANTS | PERINATAL ANXIETY & MOOD DISORDER | SPIRIT OF WOMEN No two women are alike. At Crouse, we believe you want — and need — healthcare that puts a continual focus on what matters most — you. Our hospital was founded by women, and more than a century later, services for infants and women of all ages remain at the heart of Crouse Health. Partner with women’s wellness providers who discover your individual needs by listening more closely and caring more deeply — and treating you with the respect and dignity you deserve.
Domestic Abuse Recovery
By Deborah Jeanne Sergeant
Surviving domestic abuse requires not only escaping the reach of the perpetrator to achieve physical safety, but also recovering emotionally and mentally.

“Those mental, psychological, emotional [components] last longer, even if the person is safer,” said Grace Puchalski, licensed clinical social worker and owner of Walk with Grace in Liverpool. “They need a lot of support to deal with the aftereffects. Of course, trauma is a common reaction. The person may be in a safe place but acting like they’re not. The power and control are that far reaching. Just imagine the adrenaline when you’re nearly hit by a car. It settles down in a few minutes but for someone in domestic violence, they can’t settle down that fight or flight response even when safe.”
For a long time, the survivors of domestic violence have denied their own thoughts, wishes, and needs to fulfill the perpetrator. Some survivors were dominated by an abuser so long that they no longer know how to make decisions or even what they want anymore, from choices as trivial as what to eat for dinner choices as important as who to date. This can place them in danger of becoming trapped in another abusive relationship again.
Puchalski likens it to the processing required for grief and loss. The stages are not necessarily linear, and it takes time to work through it, as victims have been conditioned to live under the perpetrator’s control over every area of their lives for months and typically years. Before diving into another romantic relationship, it’s vital to recover first.

Perpetrators do more than hit. Abuse can also include intentional and persistent mental, emotional, spiritual and sexual abuse. Mental abuse includes intimidation, mind games, gaslighting and manipulation. Emotional abuse can take the form of “love bombing” followed by withdrawal, threats, cruelty, and completely withholding love and affection. Spiritual abusers may restrict or force participation in particular worship and spiritual expression and use ever-shifting rules about spiritual practice to control the victim. Sexual abuse involves using sexual practice for manipulating the victim, such as forcing or withholding intimacy or demanding unwanted types of sexual activity. The foundation of all abuse is consistently using means to control and dominate the other person.
In addition to the brainwashing aspects of abuse, survivors suffer the loss of their relationship (difficult though it was) and often their home, pets, work, friends and possessions. Numerous areas of their lives change in a flash.
“A community of support who just listen and not give solutions is helpful,” Puchalski said. “It could just be a person who’s sharing. Someone may sense something is going on. Just being there and listening. Minimizing, discounting, justifying, and giving false hope is not effective. This person is just trying to heal. Everyone heals differently. If the person is open, the hope is they’ll seek professional support.”
Caring friends can also help provide support in rebuilding a sense of self-worth and confidence. Often-
Fertility Treatments Up Stroke Risks
Scientists have spotted an elevated risk of stroke in women who became pregnant after fertility treatments.
Although the absolute number of strokes reported in the new study were low, women seeking fertility treatment should be made aware of the increased risk, said senior study author, Cande Ananth, chief of epidemiology and biostatistics at the Robert Wood Johnson Medical School in New Jersey.
Ananth offered possible explanations for the link, including that infertility procedures can cause physiological changes because women receive large amounts of estrogen during the treatments. This can lead to increased clotting, which is a strong risk factor for stroke.
“We know that women who receive infertility treatment have certain vascular complications, typically an increased risk of preeclampsia and placental abruption,” Ananth told the
New York Times.
“People who receive the treatment receive it for a reason. Perhaps there are different biological characteristics,” among women seeking treatment, Ananth added.
In the study, researchers analyzed the cases of 31 million patients who had a hospital delivery between 2010 and 2018 in 28 states. This included more than 287,000 women who had infertility treatments.
They found that women who had undergone the treatments faced twice the risk of bleeding in the brain, known as hemorrhagic stroke. They also had 55% greater risk of ischemic stroke, when blood supply to the brain stops.
About 37 women were hospitalized for stroke for every 100,000 women who had fertility treatment.
About 2% of U.S. births involved fertility treatments, such as intrauterine insemination, assisted reproductive technology, use of a surrogate
times, survivors are more gracious to others than themselves. Treating themselves as they would treat others can help them build better skills for navigating relationships, whether friendships or romantic relationships. For example, affirming that they’re worthy of love, respect and healthy relationships. Survivors need to learn how to set personal boundaries that are neither too permissive nor too restrictive.
Most abusers damage the survivor’s relationships with others as isolating the victim helps keep the abuse secret and prevent supportive friends and loved ones from helping. Becoming involved in group settings with a hobby or other activity can help rebuild friendships and build new friendships.
“Having connections to healthy outlets whether social, recreational or spiritual is important,” Puchalski said, “as is being around in a normal, natural state. Being in a domestic violence state is not normal.”
She said that self-care can also help in recovery, such as taking care of medical, spiritual, and physical
needs. Puchalski also suggested becoming involved in a beloved hobby that was dropped or to try something completely new.
Some people find that practicing martial arts provides a supportive community of new friends, a physical activity that is both mentally and physically engaging, and practical skills that can boost their confidence.
and fertility preservation procedures.
Some studies have linked the treatments to increased risks during a pregnancy, though they are generally considered safe, the Times reported.
While this study, published Aug. 30 in the journal JAMA Network,
Page 26 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Expert: mental, psychological and emotional components of abuse last longer, even if the person is in a safe situation
found these risks, another study of women in Scandinavian countries published earlier this month in the journal JAMA Cardiology did not. That study included 2.4 million women.
CNY Medicare/Insurance Symposium
October 10, 2023
9am - 1pm
CNY Regional Market — E Shed
2100 Park Street, Syracuse, NY
By Jim Miller

How Seniors Can Save on Prescription Drug Costs

Dear Savvy Senior,
I take several medications for multiple health conditions and the prices keep going up, even with my Medicare prescription drug insurance. Can you recommend any tips that can help cut my costs?
Tapped
Out Tina
Dear Tina,
The high cost of prescription drugs is an ongoing problem that stings everyone, but it usually affects seniors more because they have a greater need for medications and because Medicare doesn’t cover all their drug costs.
While the Inflation Reduction Act, that was signed into law last year, will help seniors save on their medications by negotiating lower drug prices and capping out-of-pocket spending at $2,000, it will be a few years before the law is fully enacted. In the meantime, here are some different strategies that can help reduce your costs so you can afford what you need.

• Talk to your doctor: A good first step is to review your medications once a year with your doctor to find out if any of them can be stopped or reduced. If you’re taking any brandname drugs check to see if they are available in a cheaper generic form. Also, for any drugs you’re taking long-term ask your doctor for a cheaper three or six-month prescription, versus a one month. And find out if any of the pills you’re taking can be cut in half. Pill splitting allows you to get two months’ worth of medicine for the price of one. If you do this, you’ll need to get a prescription for twice the dosage you need.
• Review your insurance: Carefully review your drug coverage during the open enrollment period, which runs Oct. 15 – Dec. 7 for Medicare beneficiaries. Make sure all your regular medications are covered in the plan’s formulary; that your current pharmacy is in the plan’s network; and that your plan covers additional medication coverage in the gap. To shop and compare Medicare prescription drug plans go to Medicare. gov/plan-compare.
• Pay cash: Not using insurance for prescriptions seems counterintuitive, but in some cases, it may save you money. For example, many chain pharmacies and big-box stores like Walmart and Costco have their own prescription savings programs that may be lower than your insurance copayment. Or you can use coupons through GoodRx.com or RxSaver. com that can save you up to 80% off
the list price of generic and some brand-name drugs in certain pharmacies.
• Shop online: You can also save on regularly used medications by having them sent to you from a mail-order pharmacy. Check with your health insurer or regular pharmacy to see whether it will get you a better deal. If not, check online pharmacies like CostPlusDrugs.com or HoneybeeHealth.com. With these, you may spend less in some cases than you might with insurance.
• Buy from Canada: Because prescription drugs are often much cheaper north of the border, many Americans have chosen this option for years. While this is technically illegal in most states, the Food and Drug Administration generally does not stop people from doing it. If you want to explore this option use PharmacyChecker.com, an online tool that will help you identify reputable Canadian and international online pharmacies.
• Get more help: If your income is limited, you may also be able to get help through Medicare’s Extra Help program (Medicare.gov/basics/ costs/help/drug-costs), your state pharmaceutical assistance program (Medicare.gov/plan-compare/#/ pharmaceutical-assistance-program/ states) or patient assistance programs (Medicare.gov/pharmaceutical-assistance-program). Visit each website to see if you’re eligible and to apply.
Door prizes and giveaways
Stop out with your questions about Medicare or another kind of insurance. We will have experts from major carriers, non-profits, and brokers. We will also have speakers on an array of insurance topics.

SAGE Upstate Serves
Older Lesbian, Gay, Bisexual, & Transgender People in CNY

Get active, share history, learn about health issues, write or knit or crochet, join others for a meal, gather with other Trans folks, gather with other Veterans, share a dish at a potluck, talk to our Neighborhood Advisor about resources to help you age healthy and strong ... and more.
sageupstate.org
315-478-1923
SAGE Upstate Center:431 E. Fayette St, Syracuse
Find us on Facebook
SAGE Upstate Serves Older Lesbian, Gay, Bisexual, & Transgender People in CNY Health Programs, Social Gatherings

October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 27
Send your senior questions to: Savvy Senior, P.O. Box 5443, Norman, OK 73070, or visit SavvySenior. org. Jim Miller is a contributor to the NBC Today show and author of “The Savvy Senior” book.
M E E T I N G Y O U W H E R E Y O U A R E
e geSa Upstate gather
us on Facebook
geSa Upstate
Neighborhood Advisor sageupstate.org 315-478-1923 431 E. Fayette St, Syracuse Find
e
Find
Park
Independent
Independent Living at the Oaks

18 Arbor Lane, Syracuse
18 Arbor Lane, Syracuse
Live independently and give loved ones peace of mind knowing help is always available. Spacious 1 & 2 bedroom apartments, fine dining, 24-hour security, free Wi-Fi, social/cultural activities and much more!
Live independently and give loved ones peace of mind knowing help is always available. Spacious 1 & 2 bedroom apartments, fine dining, 24-hour security, free Wi-Fi, social/cultural activities and much more!
Live independently and give loved ones peace of mind knowing help is always
Live independently and give loved ones peace of mind knowing help is always available. Spacious 1 & 2 bedroom apartments, fine dining, 24-hour security, free Wi-Fi, social/cultural activities and much more!
The Social Security Office
Ask From the Social Security District Office
Minimizing The Risk of Financial Abuse For People Living With Dementia

 By Warren Beck Social Security District Manager in Syracuse.
By Warren Beck Social Security District Manager in Syracuse.
4101 East Genesee Street, Syracuse
Assisted Living at the Inn Hodes Way, 4101 East Genesee Street, Syracuse
Way, 4101 East Genesee Street, Syracuse
Assisted Living at the Inn Hodes Way, 4101 East Genesee Street, Syracuse


Live independently and give loved ones peace of mind knowing help is always available. Spacious 1 & 2 bedroom apartments, fine dining, 24-hour security, free Wi-Fi, social/cultural activities and much more! Over time we all need help. The Inn provides superior accommodations and a dedicated team. Furnished apartments, all meals in beautiful dining areas, housekeeping, social programming, personal care, nursing staff and much more!
Over time we all need help. The Inn provides superior accommodations and a dedicated team. Furnished apartments, all meals in beautiful dining areas, housekeeping, social programming, personal care, nursing staff and much more! Let
Financial crime against older Americans is a growing problem. People living with dementia are at an especially high risk of becoming victims. That’s why we’re committed to combatting fraud.
Over time we all need help. The Inn provides superior accommodations and a dedicated team. Furnished apartments, all meals in beautiful dining areas, housekeeping, social programming, personal care, nursing staff and much more!
Over time we all need help. The Inn provides superior accommodations and a dedicated team. Furnished apartments, all meals in beautiful dining areas, housekeeping, social programming, personal care, nursing staff and much more!
As their memory and other thinking skills decline, people with dementia may struggle to make financial decisions. They may not remember or report the abuse — or understand that someone is taking advantage of them. This abuse can occur anywhere — including at home or in care settings.
Victims of fraud who are 80 years and older lose an average of $39,200 every year. Studies show that financial exploitation is the most common form of elder abuse. However, only a small fraction of these incidents is reported.
You can help protect others by learning to recognize common signs of financial exploitation and abuse, including:
• Unopened bills.
• Unusual or large purchases.
• Utilities being shut off due to unpaid bills.
• Money given to telemarketers or soliciting companies.
• Unexplained withdrawals from the person’s bank account.
There are also many simple things that caregivers can do to reduce the risk of financial abuse for
Q&A
Q: I worked for many years before I became disabled, but I didn’t have enough recent work to receive Social Security Disability (SSDI) payments. Instead, I receive SSI. Will I ever receive Social Security payments?

A: It depends. If you have at least 40 quarters of coverage, you can be eligible for Social Security retirement payments beginning at age 62. Additionally, if you are performing some work while you are on SSI, you may become currently insured for disability payments in the future. There are other ways you could become eligible for Social Security benefits, including benefits through a spouse or a divorced spouse. For more information, call 1-800-772-1213 (TTY 1-800-325-0778) or contact your local Social Security office.
Q: My husband has been in poor health for some time and doctors have recently diagnosed him with amyotrophic lateral sclerosis (ALS)–commonly referred to as Lou Gehrig’s Disease. I’ve heard





people with dementia and similar conditions, like Alzheimer’s. Do your best to make sure they’re involved in deciding which safety measures to put into place.
Some options include:
• Agreeing to spending limits on credit cards.
• Signing up for the “Do Not Call” list at DoNotCall.gov.
• Setting up auto-pay for bills instead of paying them by check.
• Signing up to receive automatic notifications for withdrawals from bank accounts or large charges to credit cards.
• Requesting electronic bank and credit card statements and watching for unusual purchases or changes in how the person typically spends money.
• Asking credit card companies to stop sending balance transfer checks and opting out of future solicitations.
• Creating a separate account where you can keep a small, agreed-upon amount of money that the person can use for recreational activities, meals with friends, etc.
To learn more about combating elder abuse, visit our blog at https://blog.ssa.gov/world-elder-abuse-awareness-day-combating-injustice/.
Please share this with those who may need it.
Social Security has a “fast track” for some people who are disabled. Would you tell me about it?
A: We have two processes to fast track applications for disability benefits. Our compassionate allowances initiative allows us to fast track certain cases of individuals with very severe disabilities. There are dozens of different types of disabilities that qualify for this expedited decision, including ALS, and that list continues to expand. Learn more about compassionate allowances and see the full list of conditions at www.ssa. gov/compassionateallowances.
Another way we speed up decisions is with our quick disability determinations initiative, which uses technology to identify applicants who have the most severe disabilities and allows us to expedite our decisions on those cases. Read more about quick disability determinations at www.ssa.gov/disabilityresearch/ qdd.htm.
Page 28 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Find Your Level of Comfort And Well-Being at Menorah
Let us help you plan your move. Call Lisa at 315-449-3309 Ask about our Summer Move-In-Special! SUMMER SPECIAL Ask about our Summer Move-In-Special! SUMMER SPECIAL 5 Find Your Level of Comfort And Well-Being at Menorah Park
Living at
the Oaks
Assisted Living at the Inn Hodes Way,
us help you plan your move.
Lisa
Ask about our Summer Move-In-Special! Ask about our Summer Move-In-Special! 5 www.M enorah Parkof C n Y. C o M Find Your Level of Comfort And Well-Being at Menorah
Call
at 315-449-3309
Park Independent Living at the Oaks 18 Arbor Lane, Syracuse
Let us help you plan your move. Call Lisa at
Ask about our Summer Move-In-Special! SUMMER SPECIAL Ask about our Summer SUMMER SPECIAL 5 www.M enorah Parkof C n Y.C o M
315-449-3309
Your
And Well-Being at Menorah Park Independent Living at the
Living at
Hodes
Level of Comfort
Oaks 18 Arbor Lane, Syracuse Assisted
the Inn
Let us help you plan your move. Call Lisa at 315-449-3309 Ask about our Summer Move-In-Special! SPECIAL about our Move-In-Special! SPECIAL 5 www.M enorah Parkof C n Y. C o M Find Your Level of Comfort And Well-Being at Menorah Park Independent Living at the Oaks 18 Arbor Lane, Syracuse Assisted Living at the Inn Hodes
Way, 4101 East Genesee Street, Syracuse
1 & 2 bedroom apartments, fine dining, 24-hour security, free Wi-Fi, social/cultural activities and much more! Over time we all need help. The Inn provides superior accommodations and a dedicated team. Furnished apartments, all meals in beautiful dining areas, housekeeping, social programming, personal care, nursing staff and much more! Let us help you plan your move. Call Lisa at 315-449-3309 Ask about our Summer Move-In-Special! SPECIAL Ask about our Summer Move-In-Special! 5 www.M enorah Parkof C n Y. C o M FALL SPECIAL FALL SPECIAL Ask about our Fall Move-In-Special Ask about our Fall Move-In-Special Not a Subscriber? FREE Meet Your Doctor DAVID LANDSBERG, M.D. Another Reason to Hate Higher Risk for Severe Heart Attacks P.7 New chief medical officer oversees all care provided at Crouse Hospital — still sees patients at the hospital’s ICU and finds time to volunteer as firefighter. P. 4 Move Over Prunes, It’s Kiwi Time p.12 CNYHEALTH.COM JULY 2023 ISSUE 283 DRUG SHORTAGE LEAVES LOCALSCRAMBLINGPHARMACISTS THINGS THAT MAY HELP YOU LOSEWEIGHT FREE P. 10 P. 6 Habits That Could Lengthen Your Life 8 GOLDEN YEARS SPECIAL ISSUE Starts on page 19 CNYHEALTH.COM SEPTEMBER 2023 • ISSUE 285 SOLO TRAVEL: THE HIDDEN JOYS AND BENEFITS LIVE ALONE & THRIVE water consumption — too much can kill some people with certain heart conditions — her relationship with local patients and the movies she has produced for Netflix P. 4 Q&A with SANDRA SEABROOK LOOK WHO’S BACK! COVID-19. HERE’S WHAT YOU SHOULD KNOW P. 11 NAME ADDRESS CITY/TOWN STATE ZIP 1 YEAR (12 ISSUES) $21.00 $35.00 2 YEARS (24 ISSUES) Clip and Mail with payment to: In Good Health P.O. Box 276, Oswego, NY 13126 Subscribe today and get In Good Health: CNY’s Healthcare Newspaper right to your home or office!
available. Spacious
New COO announced at Auburn Community Hospital
Joshua Alexander has been ap
pointed chief operating officer (COO) at Auburn Community Hospital (ACH), effective Sept. 12
years, has been named to Becker’s
Hospital Review’s 2023 list of 84 top academic medical center CFOs to know. This is not the first time Wright has landed on this list. He made the list most recently in 2022 and 2019.
Joshua
Alexander
He joins the leadership team of Auburn Com munity Hospital after serving at New York–Presbyterian Hospital/Weill Cornell Medical Center as the manager of business administration for the nursing department. In this role, he managed business operations for 32 inpatient nursing units.

His expertise includes business development, procurement, capital proposals and growth strategy for hospital-wide programs. Additionally, he oversaw an annual operating budget of $25 million and a salary budget of $310 million. Before joining New York-Presbyterian, he was a physician practice manager for the Rochester Regional Health System, where he was responsible for the day-to-day operations of a multidisciplinary primary care practice.
Alexander earned his bachelor’s degree in economics and a minor in business from Loyola University in Maryland. He continued his education and received a Master of Business Administration from the University of North Carolina Kenan-Flagler Business School in Chapel Hill, North Carolina.

The COO is responsible for optimizing the hospital’s overall efficiency, organization and fiscal operations. In this new role, Alexan der will report to the ACH president, executing the hospital’s strategic and operational plan. He will work to ensure alignment with enterprise objectives while addressing the needs of the local Auburn community and its patients. Alexander will collabo rate closely with the leadership team to maintain high levels of productiv ity, enhance consumer access, foster patient retention, and uphold excep tional quality and service standards.
“We are thrilled to have someone with Josh’s business caliber and ex perience as our new chief operating officer. This is a critical role for the hospital as we continue to grow and expand services for our community,” said Auburn Community Hospital President & CEO Scott Berlucchi.
chief financial officer of Upstate University Hospital for more than 15
Stuart Wright
As CFO, Wright oversees all financial functions for the hospital as well as patient access services, utilization management and retail-contract pharmacy operations.
Among Wright’s accomplishments during his tenure as CFO is his role in facilitating and driving the growth of the enterprise from $500 million in annual revenues to more than $1.6 billion. Part of this growth was related to his key role in the successful acquisition and integration of Community General Hospital. He also led an organization-wide re-engineering of revenue cycle processes, facilitated the growth of our retail pharmacy operations to over $170 million in revenues in five years, and drove a paradigm shift in the organization toward financial disciplines, which has resulted in the hospital earnings profits in nine of the past 10 years.
During the COVID-19 pandemic, Wright was instrumental in monitoring hospital finances, ensuring funding for needed resources to fight the pandemic and working closely with the state and federal governments to address the financial implications of COVID-19 on hospitals and promoting appropriate methodologies for
Prior to joining SOS, Quinzi completed a fellowship in adult reconstruction surgery at the Rothman Institute in New Jersey. He completed his residency at the University of Rochester Medical Center and received his medical degree from Upstate Medical University in Syracuse. Quinzi received his bachelor’s degree from Cornell University, graduating with distinction. He has already been published in several peer-reviewed journals, book chapters, and presented at many conferences.
“Dr. Quinzi is great asset to our joint replacement team, and we are excited to have him join SOS,” said Mike Humphrey, CEO of Syracuse Orthopedic Specialists. “We welcome him back to Syracuse and know his expertise will benefit many patients in Central New York.”

Quinzi has a patient-specific orientation when it comes to patient care. “Every patient has a life story to share. They aren’t just a hip or a knee to me. I get to know the patient, not just their surgical needs.”
Quinzi said that nearly 40% to 50% of his orthopedic fellowship was training with new robotics technolo gies. “This technology can be useful for more complex cases, those with preexisting hardware or different challenges,” says Quinzi.
At SOS, Quinzi has access to the CORI Surgical System for robotic-as sisted joint replacement surgery and is certified with the MAKO for robot ic assisted total knee, partial knee, and hip replacement.
Rebecca Kindon named director of Health Sciences Library

Rebecca H. Kindon has been
named director of the Upstate Medical University Health Sciences Library effective immedi ately. Kindon had served as interim director since March 2023.
utive boards. She currently serves on the executive advisory board of the National Network of Libraries of Medicine, Region 7, and the executive board of the Upstate New York and Ontario Chapter of the Medical Library Association, where she is a previous executive chair and the recipient of the 2018 Katy Nesbitt service award.
Kindon holds a master of library and information degree from Syracuse University and undergraduate degrees from Le Moyne College and Cazenovia College. She resides in Fabius, with her spouse John and children Adelina and Abigael.
Crouse Medical Practice welcomes new PA
Physician assistant Jacqueline
Barkley has recently joined Crouse Medical Practice. Barkley completed her physician assistant training at LeMoyne College and received an undergraduate degree in biology from Penn State University.

She is currently seeing new patients at CMP in Camillus.
Upstate New York Poison Center has new clinical director
Jeanna Marraffa has been named
clinical director of the Upstate New York Poison Center.
he is joining the SOS joint replacement program, known as one of the nation’s best with more than 3,000 surgeries performed annually.
Rebecca Kindon
Kindon joined the Upstate Health Sciences Library in 2005 as an instruction and outreach librarian. She has served in numerous roles with the library, including as coordinator of library instruction, information resources manager, assistant director for customer services and associate director of libraries.
During her tenure at Upstate, Kindon has restructured the information literacy program; coordinated library instruction to learners in the colleges of medicine, nursing, health professions, and graduate studies; taught expert searching skills to residents; participated in assessment and strategic planning activities; and coordinated the library’s current continuity of service agreement with partnering health sciences libraries across the country. She has also served on numerous university and faculty committees, including the faculty council.
Kindon is active with many professional associations and exec-
Marraffa, who has served as assistant director since 2017, succeeds Christine Stork. Marraffa originally joined the poison center as a fellow in 2002 and became one of its toxicologists in 2004.

As clinical director of the Upstate New York Poison Center, Marraffa oversees the clinical activities of the department specifically ensuring that its poison information specialists are up-to-date on any new information to ensure the best quality care for the patients and communities served. Marraffa also serves as a clinical professor in the department of emergency medicine at Upstate Medical University and teaches emergency medicine residents, medical students, and pharmacy students on the clinical toxicology rotation. She also teaches in the College of Medicine and works with the College of Nursing on the opioid and substance use disorder (OSUD) program for family nurse practitioner students.
Marraffa is active with many professional associations and is currently the president-elect of the American Academy of Clinical Toxicology (AACT).
Marraffa received her doctor
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 29
Health News
David Quinzi
Jacqueline Barkley
Jeanna Marraffa
of pharmacy degree from Albany College of Pharmacy and a master’s degree in public health from University at Albany. She is a diplomate of the American Board of Applied Toxicology and a fellow of the American Academy of Clinical Toxicology.
The Upstate New York Poison Center manages more than 50,000 calls from healthcare providers, 911 operators, hospitals, industry, schools, and the general public in in its 54- county service area.
Christopher Community has new HR director
Christopher Community, Inc. has
both human resources management and recruitment and has specialized training in various topics including meticulous hiring and supervisor effectiveness.
Torrice is married to husband, Seth, and they have three children, Ryan, Matt and Hadley. She enjoys swimming, family vacations, and crafting.
St. Joseph’s Physicians announces new personnel
St. Joseph’s Physicians has an
nounced the following professionals have joined its team:
attending Queens University.
• Nurse practitioner Nikki D. Ramos has joined St. Joseph’s Health Primary Care Center, west. In her new role, Ramos will support her patients’ individual health as a member of an integrated primary care team.
Ramos returns to Syracuse following several years in the Columbus, Ohio area where she practiced as a registered nurse specializing in primary care, diabetes education, endocrinology, gastroenterology, and nephrology.

“I’m very excited to join St. Joseph’s Health primary care team,” said Ramos. “I look forward to serv ing this community and becoming an integral part of my patients’ health care team.”
tions for inpatient, outpatient adult, outpatient youth, school-based, and assertive community treatment services. In addition, he will establish goals, budget, plan, organize, implement, and coordinate all mental health programs and collaborate with the local governing unit and senior leadership team to ensure that psychiatric needs are being met for the community.
Michelle Rockwood promoted at Oswego Health
and CEO Justin Rudgick. “Erin’s background and experience will be of tremendous benefit to our employees and Christopher Community, and we look forward to her joining our executive team.”
Torrice will be responsible for overseeing the management and operations of the human resources department, adhering to organizational policies and procedures, and ensuring compliance with HR laws and regulations. Furthermore, her role will be to implement Christopher Community’s mission and strategies, drive organizational change, and foster organizational culture including communication amongst executives, management, and staff.
She was most recently the human resources manager, regional recruiter and recruiting strategy manager for Cintas for the past eight years. She started in the human resources industry as an HR generalist with Loretto.
A resident of Baldwinsville, Torrice received her bachelor’s degree from Nazareth College in Rochester in 2010, a Master in Business Administration degree from UMUC in 2013, and her PHR certification in 2014.
She has won PEAK awards for
• Physician Madison Healey has joined St. Joseph’s Health Hospital in a dual role as a hospitalist and primary care provider. A board-certified physician, Healey completed her residency at St. Joseph’s Health Hospital where she will continue to provide quality care.


In the hospitalist role, Healey oversees the care of hospitalized patients with a wide variety of diseases and high degree of acuity. Providing this level of continuity in patient care contributes to an increase in patient satisfaction, reduced hospital lengths of stay and reduces the possibility of the patient being readmitted.
Healey is also seeing patients at St. Joseph’s Physicians Primary Care in Liverpool. In that role, she is establishing relationships and providing healthcare for patients who see her for their regular health checkups.
Healey earned her medical degree from Ross University School of Medicine, Dominica, and her undergraduate degree in psychology from Queen’s University, Kingston, Ontario. She completed her family medicine residency at St. Joseph’s Health Hospital where she served as chief resident for two years. A passion for teaching and mentoring future physicians, Healey will join the St. Joseph’s Health Family Medicine residence faculty. Her teaching experience further includes SUNY Upstate Medical University, and teaching grades 7-12 students and undergraduates while
Hematology-Oncology Associates receives specialtypharmacy accreditation
Hematology-Oncology Associates of CNY (HOA) has recently achieved a three-year accreditation for specialty pharmacy with a distinction in oncology through the Accreditation Commission for Health Care (ACHC).

This accreditation applies to the practice’s patient-centered, on-site medication services offered in each of its clinical locations in East Syracuse, Auburn and Onondaga Hill.
Accreditation by ACHC reflects HOA’s dedication and commitment to meeting standards that facilitate a higher level of performance and patient care. ACHC is a nonprofit organization that has stood as a symbol of quality and excellence since 1986.
ACHC is ISO 9001:2015 certified and has CMS (Centers for Medicare & Medicaid Services) deeming authority for home health, hospice and durable medical equipment, prosthetics, orthotics and supplies.
“This accreditation further highlights HOA’s commitment to provide patients with the best and most convenient personalized care,” said Maryannn Roefaro, CEO. “The close collaboration between our providers and pharmacists to insure our patients have the right medicine at the right time helps lower patient costs and minimize medication waste.”
HOA is a private community cancer center established in 1982 with a mission provide the highest level
Ramos earned her master’s de gree in nursing, family nurse practi tioner from Mount Caramel College of Nursing in Columbus, Ohio. She holds a Bachelor of Science degree in nursing from Utica College and Bachelor of Science in chemistry from SUNY Oneonta. Ramos is board-cer tified by the American Academy of Nurse Practitioners.
Ramos enjoys spending time with her husband and 1-year-old son. Having grown up in Manlius, she likes to travel and hike.
New mental health director appointed at Oswego
Oswego Health recently wel comes Clark Sargeant as its new executive director of mental health and wellness.
Sargeant is a family face to Oswego Health as he previously worked in the medical surgical unit as a senior RN from 2012-2018. Since then he has worked throughout Central New York including as a nurse manager at Crouse Hospital from 2018-2020 and then in his most recent position as director of primary care operations and integrated health for Liberty Resources.
Sargeant earned his Master of Business Administration in healthcare from Jack Welch Management Institute in Virginia in 2022, his BSN from Utica University in 2017, and his Associate of Science in nursing from Crouse Hospital College of Nursing in 2012.
As executive director of mental health and wellness for Oswego Health, Sargeant will oversee opera-
recent promotion of registered nurse Michelle Rockwood to director of women’s services.
Rockwood graduated with a Bachelor of Arts in public justice from SUNY Oswego in 2008 before pursuing healthcare career. In 2015, she graduated with an Associate in Applied Science in nursing from Crouse College of Nursing.
Rockwood has held a variety of positions in healthcare including as a critical care technician at Northern Oswego County Ambulance and also at Menter Ambulance. She previously worked at Crouse Hospital before joining Oswego Health in 2016. Since then she’s worked in the women’s services department caring for women and newborns and assists families as they transition into their new roles.
“I have the utmost confidence in Michelle, and she is perfect for this leadership role,” said director of nursing, Melissa Purtell. “Michelle is very passionate about patient advocacy, education, and staff empowerment. We are so proud of her accomplishments at Oswego Health and thankful she’s a part of our team!”
Oswego Hospital’s maternity center is staffed 24 hours a day by experienced registered nurses, 24-hour breastfeeding support during the postpartum period and after discharge, and a neonatal nurse practitioner on duty for newborn care after delivery.
of quality care in a healing environment for the mind, body and spirit of patients dealing with cancer and blood disorders. A member of the
Page 30 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • October 2023
Erin Torrice
Nikki Ramos
Michelle Rockwood
Community Oncology Alliance, HOA has offices in Auburn, Camillus, East Syracuse and Onondaga Hill.
Pharmacy team at Hematology-Oncology Associates. From left: Bethany Joss, Debra Duquette, Nicholas Bouchard, Danielle Maciorowski and David Wilson.
ConnextCare, a comprehensive health care provider with seven main locations and eight school based health centers in Oswego County, offers medical, mental health, dental and substance abuse disorder services in Fulton, while its ongoing focus is building close-knit relationships with its patients and communities, while maintaining a “small practice” feel, according to Tricia Peter-Clark, ConnextCare president and CEO. Fulton Mayor Deana Michaels, back row center, is joined by staff members of ConnextCare’s Fulton Health Center following a recent tour. To her immediate left is pediatrician Faranza Chaudhary; and to her right is family practice physician Michael Miller.
ConnextCare Health Center in Fulton Offers Wealth Health Care Services
ConnextCare, a comprehensive health care provider with seven main locations and eight school based health centers in Oswego County, offers medical, mental health, dental and substance abuse disorder services in Fulton.
Its ongoing focus is building close-knit relationships with its patients and communities, while maintaining a small practice feel, according to Tricia Peter-Clark, ConnextCare president and CEO.
“Connecting with the patients we serve, and with the people in the communities in which we are locat-

St.
Joseph’s
ed, is at the core of our mission,” Peter-Clark said. “At our Fulton health center, we’re continually expanding our network of connections, while receiving tremendous support from emergency medical services, and Oswego Health’s labs and urgent care. We will see any patient regardless of their ability to pay for the care they need. In 2022, we had more than 4,300 unique patients in the Fulton office alone. Across all sites we served nearly 30,000.”
“We are so very fortunate to have ConnextCare in our community,” said Fulton Mayor Deana Michaels.
Health Receives
“Since 2013, when they acquired the Oswego County Opportunity primary care offices in Fulton and Oswego, they have enriched the health care resources in our city and helped thousands here in the process.”
Located at 510 S. 4th St., in the Fulton Urgent Care building, ConnextCare also has health centers in Central Square, Mexico, Phoenix, Pulaski, Oswego and Parish. It operates school-based health centers with dental services at Fairgrieve Elementary in Fulton, as well as health centers at schools in Mexico, Altmar-Parish-Williamstown, Pulaski, and
Sandy Creek which offer medical, dental and mental health services to enrolled students. In addition, they operate dental offices in Fulton and Pulaski, and they have been providing family-oriented health care for 50 years.
“We maintain great relationships for patient referrals from Oswego County Opportunities and Catholic Charities of Oswego County in our communities as well,” Peter-Clark said. “Our services are often part of a custom package these agencies put together to help the individual needs of the clients they serve.”
$750,000
to Address for its ‘Food Farmacy’ Program
St. Joseph’s Healthwill continue and expand its Food Farmacy program through Mother Cabrini Health Foundation funding. The funds will expand activities related to food Insecurities, chronic conditions, and social determinants of health throughout Syracuse.
In 2021, St. Joseph’s Health launched the Food Farmacy program to support patients with uncontrolled Type 2 diabetes who were also experiencing food insecurity.
Utilizing lessons learned from the Food Farmacy’s pilot, St. Joseph’s Health expanded the program’s scope in 2023 by increasing from one to three Food Farmacy sites found at Primary Care Centers Main and West, and Outpatient Behavioral Health.
“We are honored by the gener-
osity of the Mother Cabrini Health Foundation, for their continued support to addresses the pressing social and health needs of our communities,” said Meredith Price, senior vice president of hospital operations at St. Joseph’s Health. “With aligned missions to serve at risk or underserved populations, the new Food Farmacy structure is key to address unique obstacles faced by our patients and will work to optimize care, increase community benefit, and program access through collaboration.”
The program now accepts patients with at least one chronic health condition who are also experiencing food insecurity. Program participants work directly with a registered dietitian and a community health worker to receive medical nutrition therapy and other nutrition education. Meals
are also provided, helping to improve the availability of healthy food options. Also, the community health worker assists program participants with identifying and accessing social care resources.
Another feature of the enhanced Food Farmacy program is occurring outside the brick-and-mortar walls of St. Joseph’s Health, where a network of community-based organizations serves the residents of Syracuse.
St. Joseph’s Health is partnering with Brady Market, Dunbar Association, Syracuse Northeast Community Center and Westcott Community Center to identify at-risk individuals and support those with chronic health conditions by screening for food insecurity, providing social support, and assisting with transportation needs, unemployment, and other social determinants of health. Network partners will place community health workers at strategic sites for improved access for residents who live in pockets of poverty.
“St. Joseph’s Health understands the need to address health inequities and social determinants of health, as they are root causes of many chronic
diseases,” said Brian Fay, executive director, Syracuse Northeast Community Center. “The enhanced Food Farmacy program and our partners are working together to address the largest factors that impact health including social and economic factors, physical environment, and healthy behaviors, such as job status, physical activity, and nutrition.”
“We are excited to be a part of this important community program,” said Joan Royle, Executive Director from Westcott Community Center. “The proven link between a poor diet and poor health outcomes is often made worse by fast foods and less-nutritious corner store options that are common in food deserts where it is difficult to access affordable, healthy foods. This program will not only help address food insecurity, but it will also offer education for participants who might benefit from more nutritious meals that impact chronic conditions sensitive to the quality of foods they consume.”
To learn more about the Food Farmacy at St. Joseph’s Health, call 315-448-6470.
October2023 • IN GOOD HEALTH – CNY’s Healthcare Newspaper • Page 31


Acupuncture Center USA 7th Generation Rui Wang, LLC Northeast Medical Center, Suite 209 4000 Medical Center Dr., Fayetteville, NY 13066 Tel1: 585-358-6186; Tel2: 315-378-5556; Tel3: 607-372-2082 Ancient Wisdom Integrated with Modern Medicine LIFE CHANGING MEDICINE, MOVING MEDICINE FORWARD ONE OF THE BEST ACUPUNCTURE CENTERS IN THE WORLD Acupuncture is a general practice alternative medicine, it can help a wide range of health problems at different extents. Ask for professional, confidential, personalized evaluation / consultation appointment before starting any treatment Balance Immune System Build Stronger Immunity www.AcupunctureCenterUSA.com 7th Generation Medical Acupuncture Rui Wang, MD of China, L.Ac. Featuring RUI Anti-Inflammatory Acupuncture, Medical Oncology Acupuncture, and Neuromedicine Acupuncture Experienced in both Western Medicine & Traditional Chinese Medicine Experienced in both Academic & Private Practice Experienced in both Basic Science & Clinical Science Experienced in Cancer Research at Major Medical Centers in USA THE WORLD’S GREATEST TREASURE OF MEDICINE Integrative, Regenerative, Personalized Pain Management Treat the Root of Diseases Underlying Pain Relieve Pain and Inflammation Improve Functions *Do Not Stop Your Conventional Western Medicine Care during the Acupuncture Care, since Acupuncture Is Only Part of Your Comprehensive Care 靈樞止痛
