76 | Delaware Journal of Public Health Submission Guidelines
The Delaware Journal of Public Health (DJPH), first published in 2015, is the official journal of the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA).
Submissions: Contributions of original unpublished research, social science analysis, scholarly essays, critical commentaries, departments, and letters to the editor are welcome.
Questions? Contact managingeditor@djph.org
Advertising: Please contact ksmith@delamed.org for other advertising opportunities. Ask about special exhibit packages and sponsorships. Acceptance of advertising by the Journal does not imply endorsement of products.
Any report, article, or paper prepared by employees of the U.S. government as part of their official duties is, under Copyright Act, a “work of United States Government” for which copyright protection under Title 17 of the U.S. Code is not available. However, the journal format is copyrighted and pages August not be photocopied, except in limited quantities, or posted online, without permission of the Academy/DPHA. Copying done for other than personal or internal reference use-such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale- without the expressed permission of the Academy/DPHA is prohibited. Requests for special permission should be sent to managingeditor@djph.org
IN THIS ISSUE
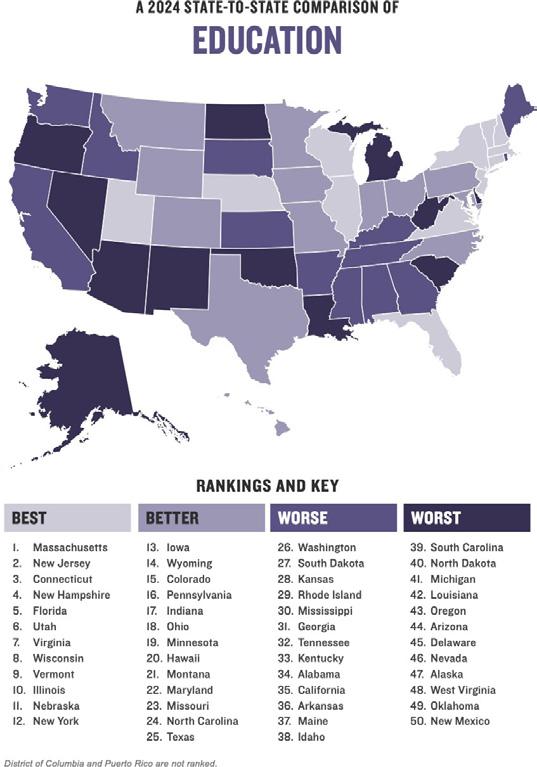
Childhood Development and Education
There is no question that education and health and wellbeing are linked. As a critical yet neglected determinant of health, education is associated with health behaviors, morbidity, and life expectancy, and educational attainment can determine income and employment in the future.1–3 Healthy People 2030 has listed Education Access and Quality as one of its goals (to increase educational opportunities and ensure healthy children and adolescents do well in school),4 and this education starts at an early age. The development of children includes biological, emotional, and psychological changes. These changes happen until the end of adolescence, and there is a growing consensus that early development – including access to education – influences a child’s success later in life.
In this issue, we delve into early childhood education in Delaware, with articles curated by our esteemed guest editors Madeleine Bayard, Senior Vice President at Rodel, and Matt Amis, Director of Communications. Dr. Ross Thompson begins the issue with a level setting article about brain development, and well-known authors throughout the state offer their support for the need for investment in early education in the state. Dr. Annette Pic describes a research study about young children experiencing homelessness, and several authors from the University of Delaware offer a glimpse into the education of our adolescent population.
As always, we welcome your input to the Journal.
REFERENCES
1. Lancet Public Health. (2020, Jul). Education: a neglected social determinant of health. Lancet Public Health, 5(7), e361. Doi: https://doi.org/10.1016/S2468-2667(20)30144-4
2. Tulane University. (2021, Jan 27). Education as a social determinant of health. Retrieved from https://publichealth.tulane.edu/blog/social-determinant-of-health-education-is-crucial/
3. Low, B. J., & Low, M. D. (2006, November 1). Education and education policy as social determinants of health. Virtual Mentor, 8(11), 756–761. https://doi.org/10.1001/virtualmentor.2006.8.11.pfor1-0611 PubMed
4. Healthy People 2030. (n.d.). Education access and quality. Retrieved from https://health.gov/healthypeople/objectives-and-data/browse-objectives/education-access-and-quality
Omar A. Khan, M.D., M.H.S. Editor-in-Chief, Delaware Journal of Public Health
Katherine Smith, M.D., M.P.H. Publisher, Delaware Journal of Public Health
As longtime advocates for early childhood education, it’s an enormous honor to serve as guest editors for this issue of Delaware Journal for Public Health.
Delaware has come a long way since we began working on these issues more than 10 years ago. And, in many ways, our renewed focus on early care and education kickstarted in the 1990s, when medical technology and research confirmed the connection between early brain development and lifelong health and success.
Today, a broader coalition is behind what providers and developmental science tell us: the first few years of a child’s life are filled with critically important milestones that, if missed, can put that child behind the pace of their peers early. If a child does not arrive in kindergarten with essential skills (or does arrive with a developmental delay that hasn’t been caught by educators), they can quickly fall behind in areas like reading. If they are not reading on grade level by third grade, research tells us it’s incredibly hard to get back on track – and more expensive long-term.
Yet, we know early opportunities and long-term outcomes are inequitable and inadequate for the future we want for Delaware and for our own children and grandchildren.
Which is why we’re grateful to the DJPH and the Delaware Academy of Medicine/Delaware Public Health Association for identifying early childhood as a priority for all Delawareans.
We would like to thank the many national and local experts who share their expertise in this edition. This issue features pediatricians, brain researchers, cardiology experts, hospital administrators, community and business leaders, all sharing perspectives on early childhood as a key period in life for public health focus and public investment.
Delaware has made a lot of progress: increasing our investments in doulas, home visiting, high-quality early care and education—including pre-k, developmental screenings, and early intervention.
And our collective “tent” of advocates continues to grow. Thanks to the organizations and individuals active in the First State Pre-K coalition—organizations focused on health, researchers, business groups, early care and education programs, faith groups, parents and more—our message of increased state support for families, children, and providers is also amplified.
We have much more to do to ensure that the future of Delaware—our youngest citizens—get the healthy start we know makes a difference. We hope readers learn from this edition and share it with their family, friends and colleagues. Advancing public health requires collective action, and we can all be a part of advancing the issue by speaking up and speaking out.
We would like to offer a special thank you to the Publisher, Dr. Kate Smith, Delaware Academy of Medicine/Delaware Public Health Association; the Editor-in-Chief, Dr. Omar Khan, President & CEO of the Delaware Health Sciences Alliance; Alejandra Villamares, Rodel Media and Communications Specialist; and Nicole Kennedy, Rodel Research Specialist, for her research and data support for this issue.
Mr. Amis may be contacted at mamis@rodelde.org .
The NATION’S HEALTH
September 2024
The Nation’s Health headlines
Online-only news from The Nation’s Health newspaper
Public health welcomes heat protections for US workers
Kim Krisberg
The Nation’s Health September 2024, 54 (7) 1-6;
Supreme Court decision on ‘Chevron deference’ may bring drastic changes for public health
Mark Barna
The Nation’s Health September 2024, 54 (7) 1-8;
Surgeon general advisory lays out plan to tackle gun violence
Natalie McGill
The Nation’s Health September 2024, 54 (7) 1-14;
Health care remains unequal for many of America’s people, says NASEM report
Sophia Meador
The Nation’s Health September 2024, 54 (7) 1-12;
Healthier behaviors may prevent millions of cancer cases annually
Sophia Meador
The Nation’s Health September 2024, 54 (7) 7;
Q&A: CDC’s Vaccines for Children Program celebrates 30 years
Sophia Meador
The Nation’s Health September 2024, 54 (7) 7;
Keeping your kids safe from the dangers of lead
Teddi Nicolaus
The Nation’s Health September 2024, 54 (7) 16;
APHA 2024 to showcase public health’s biggest, brightest in Minneapolis
Michele Late
The Nation’s Health September 2024, 54 (7) 3;
Council on Education for Public Health marks 50-year milestone
Teddi Nicolaus
The Nation’s Health September 2024, 54 (7) 5;
Newsmakers: September 2024
Sophia Meador
The Nation’s Health September 2024, 54 (7) e8;
Many other articles available when you purchase access
Entire Issue $12
Visit https://www.thenationshealth.org/user
Early Brain Development and Public Health
Ross A. Thompson, Ph.D.
Distinguished Professor Emeritus, Department of Psychology, University of California, Davis
ABSTRACT
Early brain development research is important to public health professionals for understanding early development and strengthening systemic supports for young children’s healthy brain growth. This overview describes basic processes of early brain development, including prenatal development and the “fetal programming” of brain and behavior, neural proliferation and the essential influence of experience in the creation of neural networks, the maturational timing of different brain systems and their behavioral consequences, the myelination of neural pathways and its influence on children’s action and thinking, and the capacity of the brain to create new neural connections throughout life, which contributes to its continuing adaptability to new experiences. The implications of this research for public health and for strengthening support for early brain development are considered throughout this discussion.
ACKNOWLEDGEMENT
This article is an adapted version of chapter 3, “Dispatches from the Laboratory,” from The Brain Development Revolution: Science, the Media, and Public Policy. Figure 1 is also taken from the chapter.
INTRODUCTION
The brain is the most complex biological system in the human body, by far. It consists of billions of nerve cells of different cell types that are interlinked by trillions of connections, organized into distinct neural circuits and located in regions that differ structurally and functionally. Consequently, brain development is a prolonged process, beginning in the first two to three weeks after conception and lasting through early adulthood. This extended maturation derives from the complexity of neurobiological growth, of course, but it is also due to the brain’s continuous incorporation of experience. In other words, the brain’s development is shaped throughout life both by genetic guidance and by experience -- the classic nature-nurture dynamic.
Understanding the early development of the brain is important for public health professionals. It is important not only to inform understanding of early childhood development, but also because the work of public health is crucial to supporting healthy brain development in the early years and preventing and remediating many of the threats that exist. In this article, my goal is to highlight the central processes of early brain development and their relevance to public health.
BRAIN DEVELOPMENT BEGINS EARLY. VERY EARLY.
Because its development is so foundational to the rest of human growth, the brain develops rapidly early in life. Whereas a newborn’s brain is already 26% of its adult weight, by age five, the brain has reached 88% of its adult weight.1 The latter figure helps to account for the well-known claim that the brain is 90% developed by the age of five. That claim is mistaken because brain weight is not a very informative index of its maturation (after all, men’s brains are 10% heavier than women’s). More
important than estimating how heavy the brain has become by various ages is understanding the foundations for life-long functioning that are established by its early growth.
Some of the most important foundations are established prenatally. The nine months of prenatal development witnesses the most rapid growth of the brain. Beginning early in prenatal growth, during the third gestational week, new neurons (nerve cells) and other supportive cells are generated at an astonishing rate -- by some estimates, several hundred thousand each minute -- and then migrate to their eventual destinations in the fetal brain.2 Throughout this process of neural proliferation and migration, neurons continue to develop through gene expression within the cell and by the influence of adjacent neurons. By the 23rd week of gestation, synapses (contacts between neurons permitting the transmission of activation, a.k.a. neural communication) begin to proliferate as the structural organization of the brain begins to form. Before birth, the vast majority of neurons that populate the brain have been created. It is a truism that the more rapid pace of development, the greater the vulnerability of the organism. Consistent with this truism is the vulnerability of prenatal brain development to a variety of hazards, including environmental toxins (such as pesticide and lead exposure), drugs (e.g., alcohol, cannabis), and maternal viral infection (such as influenza and herpes simplex) that can potentially have long-lasting developmental consequences, sometimes because of the epigenetic processes (i.e., changes in gene expression) they trigger.3 Some prenatal influences are hazardous because they provoke developmental adaptations in the fetus that may have negative long-term consequences for health and morbidity. According to the developmental origins of health and disease (DOHaD) theory, certain early influences, such as prenatal undernutrition, can program changes in fetal development in anticipation of the requirements of the postnatal environment.4 In this view, “fetal programming” of physical and neurobiological systems derives from fetal sensitivity to aspects of the intrauterine environment that signal conditions of life outside the womb, and fetal development adapts to enhance the chance of survival after birth.
This was evocatively seen in the Dutch Hunger Winter of 1945, when official rations for citizens in the occupied Netherlands were dramatically cut by Nazi authorities in reprisal for a strike on the Dutch railways. The children born to women who were pregnant during this period have been studied into adulthood to determine the long-term effects of this time-limited period of profound nutritional insufficiency that was followed by the immediate restoration of an adequate diet (when the Allies liberated the Netherlands). Researchers discovered that the children born to mothers who were malnourished early in their pregnancy were at significantly greater risk as adults for a variety of chronic health and mental health problems compared with children of different gestational age or same-sex siblings.5 One explanation is that fetal metabolism, growth rate, and organ system development early and quickly adapted to conditions of limited food intake in preparation for encountering comparably deprived circumstances after birth. Children were biologically unprepared for the conditions of nutritional adequacy into which they were born, however, and this led to a range of physical and mental health problems that endured throughout life.6
Guided by this view, researchers have been concerned not only with nutritional adequacy but also with other prenatal influences, such as the effects of maternal stress on the developing fetus. This concern is warranted given that 15% to 20% of pregnant women experience depression or anxiety symptoms, and these rates increase in the context of other stresses of pregnancy, such as difficult employment conditions, strain in close relationships, and low income.7 Chronic maternal stress has direct effects on the fetal brain: it increases cortisol levels in the brain and contributes to the development of heightened stress reactivity in newborns.8 These consequences may derive from fetal programming, since prenatal exposure to elevated stress hormones is a powerful signal of environmental adversity for which developing biological systems adapt in preparation for birth into a challenging world. One study showed that by six months after birth, the infants of mothers who were prenatally depressed showed weaker connections between the amygdala and the prefrontal cortex, which suggests compromised emotion regulation beginning early in infancy and heightened sensitivity to cues of threat and danger.9 The behavioral effects of fetal exposure to maternal stress can be enduring, and include heightened emotional reactivity and enhanced risk for depression or anxiety as late as adolescence.10
DEVELOPING AN ADAPTIVE BRAIN
Fetal programming shows that from the beginning, the brain incorporates experience into its architecture. This is even more evident in another feature of early brain development: the overproduction and refinement of neural connections. As earlier noted, synapses begin to form prenatally, connecting neurons in communicative networks. Because synapses are a basic means by which the brain develops, they are formed continuously as the brain matures (and, indeed, throughout life). But early in life, the production of synapses is especially rapid, and can be considered (in the technical language of developmental neuroscientists) “exuberant.” By one estimate, more than one million synapses are formed every second in the early years.11 If this seems excessive, it is true: up to 40% more synapses are overproduced early in life than will be retained in the mature brain.12 Consequently, the young brain is a more active and densely packed organ than it will be at maturity.
Overproduction of synapses, which derives from the genetic guidance of brain development, is a good thing. It affords considerable capacity for early growth because synapses can become enlisted into developing and consolidating a potentially expansive range of skills and knowledge. But overproduction has liabilities, including poorer signal-to-noise in neural communication (i.e., lots of incoming transmissions reaching neurons when only a subset is important), and some forms of mental disability are associated with atypical rates of proliferation of synaptic connections.13 Therefore, an important subsequent step in brain development is the progressive reduction and elimination of synapses to increase the efficiency of neural processing.
Experience guides the process of synaptic pruning by strengthening neural connections when they are activated. When the brain responds to stimulation, it activates specific synaptic networks, and these networks become strengthened in the process. By contrast, synapses that are rarely activated eventually wither and disappear. The brain of a Parisian baby overhearing French spoken at home develops consolidated synaptic networks related to the perception of French speech sounds, for example, but synapses for Russian or Chinese speech perception, rarely activated, wither. In this manner, early experiences help to determine the retention of connections in the developing brain (this is the basis for the well-known maxim, “use it or lose it”) and the result is a brain that consolidates skills that are relevant to the world in which the child is living.
In fact, we can observe this process both behaviorally and biologically. Studies have shown that during their first six months, infants can discriminate speech sounds found in languages all over the world, including sounds that their parents cannot differentiate (a young Japanese infant can discriminate, for example, between the sounds /l/ and /r/, even though her parents cannot readily do so). But by the end of the first year, the baby’s speech perception has become more narrowly channeled to the sounds of the home language, and infants can no longer discriminate foreign speech sounds.14 In other words, infants become perceptually fine-tuned to the language system that they are overhearing and preparing to learn. (The same occurs with the child’s own sounds: by 10 months, infants have incorporated the sounds of the home language into their babbling.15) This developmental change can also be observed by neuroimaging brain regions involved in speech perception. One research group found that at seven months, the brain became active in response to speech sounds from different languages. Between seven and 11 months, however, there was an increase in activation to speech in the home language, and by the end of the first year, infants showed neural activation only to sounds of the home language.16
This illustrates the profound adaptability, or plasticity, of the developing brain. Since the fetal brain cannot predict whether it will be born in Paris, Kiev, Tokyo, Los Angeles, or elsewhere, the brain at birth is prepared through the overproduction of synapses to discriminate the sounds of any human language. But months of experience overhearing the language -- or languages -- spoken at home guide the pruning of synapses and reorganization of brain areas governing speech perception to focus on the home language, and the capacity for universal speech discrimination is lost. The benefits of this can be observed a few months later, in the “vocabulary explosion” beginning at 18 months, when the rewired brain is now attuned to this language and new words are acquired at a very rapid rate.
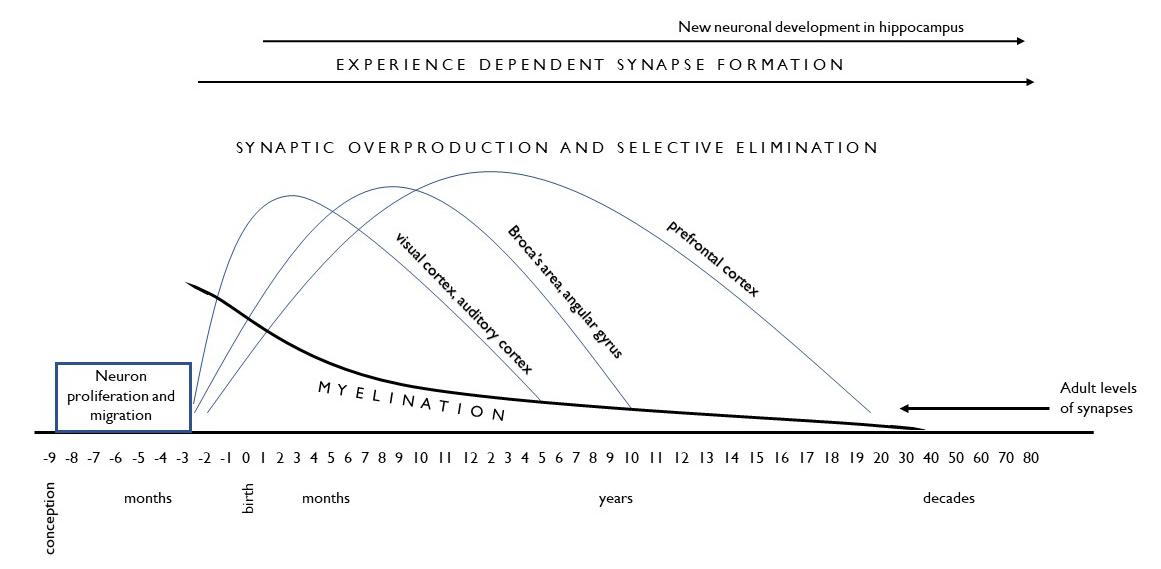
Retaining lots of unneeded synapses is unhelpful, therefore, since the desired developmental outcome is efficient learning. Consequently, the dual processes of exuberant overproduction followed by the experience-guided elimination of synapses occurs throughout the brain to increase the efficiency of neural processing and adapt the brain’s capacities to the world in which the child lives. Importantly, the timing and pace of this process varies for different brain regions, as shown in Figure 1 using three brain regions for illustration. The figure shows that synaptic overproduction begins prenatally in areas relevant to basic sensory skills -- seeing and hearing -- with postnatal experience contributing to the refinement of these connections, completed by early childhood. Language areas of the brain (such as Broca’s area and the angular gyrus) have a more extended period of synaptic pruning as language skills continue to be refined until age 11 or 12. Even longer is the developmental timetable for the prefrontal cortex, an area important to selfregulation, which does not reach maturity until early adulthood (despite the fervent hopes of parents).
Figure 1 illustrates, therefore, that the timing of these dual developmental processes varies for different brain regions and in a manner that accords with what we see behaviorally: young children achieve sensory acuity by kindergarten (a necessary skill for the acquisition of other abilities, such as reading), show a longer timetable for first (and second) language acquisition, and by adolescence are still mastering capacities for self-control in thinking and behavior. Many developmental changes in children’s behavior -- growing motor coordination and fine-motor control, advances in thinking and reasoning, skills in social and emotional understanding -- likewise follow advances in synaptic pruning in relevant brain areas. Note, however, that the figure also illustrates how the first five years witnesses major advances in virtually all of these developmental domains. In this respect, the importance of early childhood is underscored by the neurobiological advances that are establishing a foundation for many developmental achievements that are occurring in childhood and at later ages.
The figure also illustrates another important aspect of early brain development: the myelination of neural connections. Myelin is a fatty protein sheath covering neurons that provides insulation and speeds the conduction of neural activation (in some areas of the brain, over 100-fold).17 Whereas synaptic overproduction and pruning refine the brain’s neural networks, myelination contributes speed and efficiency to them. The timetable for myelination is similar to the one described for synapse development, with earlier advances in sensory and motor regions and much later development in brain regions governing complex information processing and self-regulation. One can observe the effects of myelination in children’s behavior, from the growing speed of coordinated movement to the increased quickness and dexterity of thinking. Although neural transmission can occur in unmyelinated neurons, the efficiency of myelinated neural networks is significantly greater, and it is myelination that significantly advances the efficiency of neural transmission.
NEURAL NETWORKS
Before proceeding further, a clarification. The discussion thus far has referred to neural “networks” because that is how neuroscientists think about brain functioning. Specifically, the brain processes governing most behavior involve connections between neurons that are often widely distributed throughout the brain. This is especially true of the complex behaviors that are most interesting, such as those associated with learning or emotion. The view that the brain functions in neural networks contrasts with the more common locationist view of the brain that attributes specific behaviors to particular brain structures (e.g., the amygdala is where fear responding occurs; the hippocampus is where memory occurs). By contrast with the locationist view, the brain processes involved with emotions like fear network systems associated with sensory evaluation, cognitive appraisal, short- and long-term memory, and other processes that are widely distributed throughout the brain.
Figure 1. Development of the Human Brain
This is important because a view of brain functioning in neural networks not only underscores the amazing complexity of how the brain functions, but also provides greater insight into the development and remediation of behavioral problems. The development of emotion regulation is not, for example, primarily due to maturation of the amygdala, but due to a range of other brain systems we don’t usually see as relevant to emotion, such as areas of the prefrontal cortex that support self-regulation and which take much longer to mature. Understanding the network of brain systems involved in emotion regulation might give parents and practitioners greater patience for understanding the challenges of young children in emotion management, and also provide insights that can help in remedial and therapeutic interventions when problems of emotion management are more severe and enduring.
TWO KINDS OF EXPERIENCE
At this point it is possible to answer a question that is often posed about brain development: why isn’t it all in the genes? In other words, given its importance, why isn’t the entire development of the brain encoded in the human genome?
One reason is that the entire genome is simply inadequate for mapping the trillions of connections in a typical adult brain. Another reason, however, is that a “genetic blueprint” would make brain development inflexible, and render children poorly suited to any of the incredibly diverse environments in which people live. As research has shown, by incorporating experience into the architecture of brain development, individual brains become tailored to the young child’s lived experience in their individual environments.
There are, however, two kinds of “experience” relevant to early brain development.
The first kind of experience contributes to experienceexpectant development. These are experiences that are pervasive in life and, as a consequence, the developing brain “expects” to encounter these experiences as part of its development. Examples include exposure to patterned light, gravity, the sound of human voices and language, touch on skin surfaces, social contact, and others. Although these are common, universal experiences, brain development is built on these exposures occurring when relevant neurobiological systems are maturing. Their failure to occur, or to occur at the right time, can result in the loss of relevant brain capacities. Consequently, experience-expectant development is often viewed in terms of sensitive periods during which certain environmental exposures must occur if brain development is to proceed normally.
Ordinarily there is no reason for concern about this in normal circumstances. But when young children live in profound deprivation early in life, essential experience-expectant exposures may be lacking. When a 13-year-old girl with the pseudonym Genie was rescued by Los Angeles County child welfare authorities in 1970, the authorities were astonished at the grossly neglectful conditions in which she had lived her entire life, lacking normal human contact, language exposure, and even opportunities for normal motor development. Many of her developmental deficits proved to be remediable with therapeutic assistance, but the psychologists assisting in her
care concluded differently with respect to language. Although Genie’s vocabulary development surpassed researchers’ expectations, she never acquired mastery of basic grammar and language pragmatics. Since her rescue occurred when she was at the close of the period of synaptic pruning in regions of the brain relevant to language development (see Figure 1), her irreversible deficits in certain domains of language use were not unexpected.18
The second kind of experience contributes to experiencedependent development. These are experiences affecting the brain that can vary across individuals. Their influence can occur at any age (not just during an early sensitive period) and they can be virtually any kind of experience that leads to the formation of new synapses or modification of existing synaptic connections in the brain. Needless to say, the range of potential experiences contributing to this kind of development is extremely broad: learning how to play the piano, indulging an interest in poetry, joining a support group, or developing deeper understanding of American history are examples. Experience-expectant development constitutes life-long brain plasticity, and helps to account for the increasingly individualized character of brain growth as the years proceed. Although the brain completes its maturation by early adulthood (see Figure 1), evidence that the brain continues to be capable of changing throughout life attests to the lifelong importance of experience-dependent development. Neurobiological studies with adults suggest, for example, that new neurons and synaptic connections develop in the hippocampus, a brain structure important for learning and memory, in response to experiences promoting new learning.19
The profound developmental potential afforded by experience-expectant development is one reason the human brain is such a powerful learning organ, and it helps to account for the astonishingly early and rapid mental advances of early childhood. This developmental potential is one reason that parents who can afford them enlist enrichment experiences for their young children, such as art, music, or other kinds of classes or tutoring, even though there is little or no evidence that such experiences can accelerate early brain development beyond normal limits.20 There is, however, abundant evidence that deprivation and adversity can undermine healthy brain development. Unfortunately, experience-dependent development is undiscriminating with respect to the kinds of experiences affecting the brain’s growth: it incorporates harm as well as enrichment into its developing architecture.21 Deprivation of important supports (such as nurturant care) can also significantly undermine the developing brain through the loss of opportunities that would otherwise strengthen important neural networks.
IMPLICATIONS FOR PUBLIC HEALTH PRACTITIONERS
A quarter-century ago, the American public was rocked by a revolution in their understanding of early childhood development that focused on early brain development and its implications.22 In the years since, developmental science has modified but not fundamentally changed the account that parents and others learned then. Early brain development is foundational to the growth of life-long capacities, and
many of these foundations are established prenatally. Early experiences are important to the development and refinement of neural connections in the early years, although the hazards of adverse experiences are much clearer than are the benefits of enrichment. The brain’s adaptability, or plasticity, is one of its superpowers for tailoring its development to the child’s experience in a specific environment, and this continues to be a strength beyond early childhood as the brain continues to develop in later life. The brain’s adaptability can be a liability, however, when it incorporates into its architecture the effects of abuse, deprivation, and trauma. In light of the brain’s rapid growth, identifying and remediating developmental problems early in life is important before these problems become consolidated, and doing so can be far more cost-effective than trying to remediate them later.
Understanding the implications of developmental neuroscience for parents, practitioners, and policymakers has been as important as understanding the science, and the past 25 years have witnessed slow progress on important science-based initiatives for children, as well as the excesses of overpromising and the liabilities of ignoring important needs.22 For public health practitioners, however, the implications of the science may be self-evident. Improving the prenatal care of expectant mothers, with particular attention to the hazards to fetal brain development of nutritional inadequacy, maternal stress, and toxic exposures. Strengthening the supports for young children within their families, especially in the availability of nurturant relationships, adequate nutrition, safe environments, and learning opportunities. Early intervention when young children’s environments are unsafe or neglectful. Expanding programs to address the multiple threats deriving from childhood poverty, a multisystemic stressor with documented effects on developing children’s brains and behavior.23 Early detection of developmental problems, coupled with stateof-the-science interventions to remediate them. Enlarging the availability of early learning opportunities, but with an important proviso. Early childhood programs to support young children’s learning need to be buttressed by strong primary education opportunities to build on that foundation. The research is clear that early education cannot alone lead to high school graduation and other later achievements.
There are other implications of the research on early brain development. The insights on the developing brain that have been emerging during the past quarter century provide continuing catalysts for the responsibilities of those of us committed to young children’s healthy development. Dr. Thompson may be contacted at rathompson@ucdavis.edu
REFERENCES
1. Dekaban, A. S., & Sadowsky, D. (1978, October). Changes in brain weights during the span of human life: Relation of brain weights to body heights and body weights. Annals of Neurology, 4(4), 345–356. https://doi.org/10.1002/ana.410040410
2. Cowan, W. M. (1979, September). The development of the brain. Scientific American, 241(3), 112–133. https://doi.org/10.1038/scientificamerican0979-112
3. Kundakovic, M., & Jaric, I. (2017, March 18). The epigenetic link between prenatal adverse environments and neurodevelopmental disorders. Genes, 8(3), 104. https://doi.org/10.3390/genes8030104
4. Doi, M., Usui, N., & Shimada, S. (2022, March 15). Prenatal environment and neurodevelopmental disorders. Frontiers in Endocrinology (Lausanne), 13, 860110. https://doi.org/10.3389/fendo.2022.860110
5. Lumey, L. H., Stein, A. D., Kahn, H. S., van der Palde Bruin, K. M., Blauw, G. J., Zybert, P. A., & Susser, E. S. (2007, December). Cohort profile: The Dutch Hunger Winter families study. International Journal of Epidemiology , 36 (6), 1196–1204. https://doi.org/10.1093/ije/dym126
6. Schulz, L. C. (2010, September 28). The Dutch Hunger Winter and the developmental origins of health and disease. Proceedings of the National Academy of Sciences of the United States of America, 107(39), 16757–16758. https://doi.org/10.1073/pnas.1012911107
7. Dunkel Schetter, C., & Tanner, L. (2012, March). Anxiety, depression and stress in pregnancy: Implications for mothers, children, research, and practice. Current Opinion in Psychiatry, 25(2), 141–148. https://doi.org/10.1097/YCO.0b013e3283503680
8. Monk, C., Lugo-Candelas, C., & Trumpff, C. (2019). Prenatal developmental origins of future psychopathology: Mechanisms and pathways. Annual Review of Clinical Psychology, 15, 16.1-16.28.
9. Posner, J., Cha, J., Roy, A. K., Peterson, B. S., Bansal, R., Gustafsson, H. C., . . . Monk, C. (2016, November 1). Alterations in amygdala-prefrontal circuits in infants exposed to prenatal maternal depression. Translational Psychiatry, 6(11), e935. https://doi.org/10.1038/tp.2016.146
10 Davis, E. P., & Thompson, R. A. (2014). Prenatal foundations: Fetal programming of health and development. Zero to Three, 34, 6–11
11. Center for the Developing Child. (2024). Brain architecture. Retrieved July 8, 2024 from https://developingchild.harvard.edu/science/key-concepts/brain-architecture/
12. Huttenlocher, P. R., & Dabholkar, A. S. (1997, October 20). Regional differences in synaptogenesis in human cerebral cortex. The Journal of Comparative Neurology , 387 (2), 167–178. https://doi.org/10.1002/(SICI)1096-9861(19971020)387:2<167::AIDCNE1>3.0.CO;2-Z
13. Lepeta, K., Lourenco, M. V., Schweitzer, B. C., Martino Adami, P. V., Banerjee, P., Catuara-Solarz, S., . . . Seidenbecher, C. (2016, September). Synaptopathies: Synaptic dysfunction in neurological disorders - A review from students to students. Journal of Neurochemistry, 138(6), 785–805. https://doi.org/10.1111/jnc.13713
14. Kuhl, P. K. (2004, November). Early language acquisition: Cracking the speech code. Nature Reviews. Neuroscience, 5(11), 831–843. https://doi.org/10.1038/nrn1533
15. de Boysson-Bardies, B., Halle, P., Sagart, L., & Durand, C. (1989, February). A crosslinguistic investigation of vowel formants in babbling. Journal of Child Language, 16(1), 1–17. https://doi.org/10.1017/S0305000900013404
16. Rivera-Gaxiola, M., Silva-Pereyra, J., & Kuhl, P. K. (2005, March). Brain potentials to native and non-native speech contrasts in 7- and 11-month-old American infants. Developmental Science, 8(2), 162–172. https://doi.org/10.1111/j.1467-7687.2005.00403.x
17 Johnson, M. H., & de Haan, M. (2015). Developmental cognitive neuroscience: An introduction (4th Ed.). New York: Wiley-Blackwell.
18 Rymer, R. (1994). Genie: A scientific tragedy (2nd Ed.). New York: Harper Perennial.
19 Erickson, K. I., Voss, M. W., Prakash, R. S., Basak, C., Szabo, A., Chaddock, L., Kramer, A. F. (2011). Exercise training increases size of hippocampus and improves memory. PNAS Proceedings of the National Academy of Sciences, 108, 3017-3022.
20 Tierney, A. L., & Nelson, C. A., III. (2009, November 1). Brain development and the role of experience in the early years. Zero to Three, 30(2), 9–13. https://pubmed.ncbi.nlm.nih.gov/23894221
21. Kim-Spoon, J., Herd, T., Brieant, A., Peviani, K., DeaterDeckard, K., Lauharatanahirun, N., . . . King-Casas, B. (2021, April). Maltreatment and brain development: The effects of abuse and neglect on longitudinal trajectories of neural activation during risk processing and cognitive control. Developmental Cognitive Neuroscience, 48, 100939. https://doi.org/10.1016/j.dcn.2021.100939
22 Thompson, R. A. (2023). The brain development revolution: Science, the media, and public policy. Cambridge, UK: Cambridge University Press.
23 Evans, G. W., Chen, E., Miller, G. E., & Seeman, T. (2012). How poverty gets under the skin: A life course perspective. In R. King & V. Mahalmes (Eds.), The Oxford Handbook of Poverty and Child Development (pp. 13-36). New York: Oxford University Press.
Investing in Delaware’s Early Care and Education to Improve Public Health
W. Steven Barnett, Ph.D.; Karin Garver; Allison Friedman-Krauss, Ph.D. National Institute for Early Education Research (NIEER), Rutgers University INTRODUCTION
The first five years of life are a time of rapid growth and development--physical, social, and cognitive.1,2 How much we invest in those early years as parents and as a society has profound implications for later success in school and work, for citizenship, and even for adult health and longevity.3,4 That makes early care and education an important public health issue. Strong supports for early learning and development—including early care and education—can increase individual success, strengthen communities, and decrease social, economic, and health inequality. Rigorous small-scale scientific studies demonstrated that high quality early care and education programs could produce these outcomes decades ago, and new studies have added contemporary evidence that large-scale high quality preschool increased adult educational attainment and earnings, two outcomes causally linked to civic engagement and health.5–8 The full realization of those gains depends on two conditions: that children have access to programs and that the programs are high quality. Publicly funded universal preschool education is a policy that can promote both access and quality thereby improving the education, development, health, and well-being of future generations.9,10
DELAWARE CONTEXT
For a state with a median family income slightly above the national average, Delaware’s health and education outcomes are surprisingly poor. Delaware ranks 5th highest for spending per person on health care but ranks 29th for longevity with an expected lifespan at birth below the national average.11 Turning to education, in 2022, fourth grade children in Delaware scored far below the national average in reading and math on the National Assessment of Educational Progress (NAEP).12 Delaware scored significantly lower than 39 other states in reading, and just 25 percent of the state’s fourth graders scored proficient or better in reading.12 Eighth grade scores on the 2022 NAEP also were substantially below the national average.12 One reason that Delaware’s test scores are so poor compared to the national averages is that Delaware’s scores have dropped more than the national averages since the onset of the pandemic. However, the downward trend in Delaware’s test scores began before the onset of the COVID-19 pandemic, suggesting that educational decline is not just pandemic related. These current educational outcomes suggest that Delaware’s future health outcomes, including longevity, may decline further below national averages. Of course, these are statewide averages. Although Delaware’s poverty rate is slightly better than the national average, about 1 in 6 children live in poverty and their education and health outcomes are much worse.11
ACCESS TO EARLY CARE AND EDUCATION IN DELAWARE
Clearly, Delaware and its young children could benefit from high quality early care and education. How much access is there currently? Less than half of Delaware’s three- and four-year olds, about 45 percent, attend any kind of preschool program, including part-day preschools and full-day child care, both public and private, and not all of these are high quality.13 Delaware’s preschool enrollment rises with income. From 2018 to 2022, enrollment in preschool was just 33 percent for children in families below 200 percent of the federal poverty level (FPL) while it was 53 percent for children in families above 200 percent of the FPL.13 These percentages are likely to be slightly depressed due to the pandemic, but nationally preschool enrollment has remained low for children in low-income families even as the impacts of the pandemic have receded.14
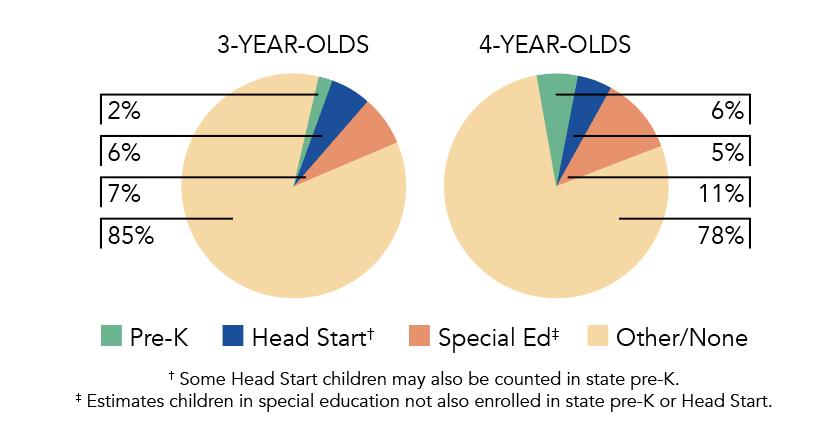
Of course, not all programs are high quality, so the percentage of children receiving a high quality preschool education is even lower. In 2022-23, state-funded pre-K and Head Start combined served just 11 percent of Delaware children at age four, and eight percent at age three. Just seven states serve a smaller percentage of four-year-olds in these two public programs. The percentage of children served rises somewhat when preschool special education for children with disabilities is added, up to 22 percent at age four and 15 percent at age three. The share served by each of these programs is shown in Figure 1. It is remarkable that preschool special education serves about as many young children as do the other state and federally funded pre-K programs combined.
Figure 1 provides a basis for an overall assessment of the extent to which public programs meet population needs. State and federal programs combined do not have the capacity to serve even the 18% of Delaware’s young children in poverty for one year at age four, and reach less than half that at age three.16 As 38% of Delaware’s young children are in families below 200 percent FPL, even serving the low-income population would require a massive increase in state-funded pre-K.16 Moreover, as nearly half of young children in families with incomes above 200 percent FPL do not attend preschool, the full need is even greater. National data indicate that enrollment steadily increases with income, so children in Delaware families with moderate incomes likely have lower preschool enrollment rates than those in families with high incomes.17
The preceding sections establish the need for public policy changes to support increased access to high-quality preschool education. High quality programs could improve Delaware’s dismal educational outcomes. Improving education outcomes would improve long-term health outcomes, as well. Given the disparities in both access to pre-K and current education outcomes, increased access to high quality pre-K could not only improve statewide averages but significantly reduce education inequalities, and thereby, health outcome inequalities. In the following sections we address how this might be accomplished.
DELAWARE’S CURRENT PUBLIC PRESCHOOL PROGRAM
Delaware’s state-funded pre-K program, the Early Childhood Assistance Program (ECAP), was originally modeled after the federal Head Start program and follows the federal Head Start Program Performance Standards (HSPPS). ECAP is administered by the Office of Early Learning within the Delaware Department of Education and is currently offered in all three counties in the state. Programs can apply for ECAP funding, and it is awarded on a competitive basis.
In fall 2022, ECAP enrolled 954 children, including 255 threeyear-olds and 699 four-year-olds.15 ECAP had the capacity to enroll 1,050 children.15 Why the program was underenrolled given the large unserved population is unclear. However, enrollment in most states was down for several years following the onset of the COVID-19 pandemic. As noted earlier, ECAP enrolled just two percent of three-year-olds and six percent of four-year-olds. These percentages have not changed appreciably in the last 20 years.15
Eligibility for ECAP follows the HSPPS, which ties eligibility to income and prioritizes enrollment for children in families living below the FPL.15 Up to 35 percent of children enrolled can come from families between 100 percent and 130 percent FPL, though priority is given to those below 100 percent FPL. Additionally, 10 percent of capacity can be used to serve children with a disability who need not qualify based on income.15 ECAP programs can establish additional enrollment priorities based on community needs that can include low parent education; history of abuse, neglect, or family violence; home language other than English; risk that the child will not be ready for kindergarten; or being born to a teen parent.15
ECAP funds a part-day (3.5 hour) program, five days per week for a total of at least 560 hours per year over 160 days.15 Individual programs can determine their own operating schedule and may choose to use other funding sources to provide a longer school day. ECAP programs in public schools follow the school district operating schedule.
The ECAP program meets 9 of 10 benchmarks that the National Institute for Early Education Research (NIEER) has identified as minimum standards for state policies if large scale public preschool programs are to produce substantive lasting impacts on learning and development.15 These are by no means guarantees, but programs that more closely resemble those that have succeeded in the past should be more likely to succeed in the future.
In 2022-23, Delaware spent $8.8 million on ECAP, an over $2 million increase, resulting in a spending per child of $9,299.15 This marked the first increase in ECAP funding since the program’s inception 20 years ago. Adjusted for inflation, this is a $1,207 per child increase from the year before (15%). However, this increase only partially reversed a long-term decline in ECAP funding per child. More than 15 years ago in 2007, Delaware’s spending for ECAP was over $1,600 per child higher, adjusting for inflation. This is a serious problem and likely affects program performance in more ways than just limiting teacher qualifications. For comparison, per child spending for Head Start in Delaware was much higher at $13,862. This may reflect Head Start’s recent emphasis on providing a full school day schedule as spending per child just a few years earlier was more like Delaware’s spending on ECAP.
The ECAP budget increased to $15.7 million for the 2024-25 school year,18 signaling the potential for significant progress towards the level of funding required to support quality, depending on how many children this level of funding is intended to support. As Delaware continues to expand its access and quality, NIEER recommends looking to meet all 10 benchmarks in a full day program, and providing salary parity for teachers across settings.
IMPROVEMENTS NEEDED IN DELAWARE’S PUBLIC PRESCHOOL PROGRAM
As described above, Delaware’s ECAP program falls short in several respects. If the program is to be worthy of expansion to serve more children, it must be effective. ECAP meets most of NIEER’s ten benchmarks for minimum program quality because it is required to follow standards based on the federal HSPPS
for areas like preschool class sizes and adult/child ratios, child screenings, and comprehensive services.15 Yet, like Head Start, Delaware ECAP does not require all teachers to have at least a four-year college degree. The requirements for ECAP teachers vary depending on where they teach. In public schools, the lead teacher must have at least a bachelor’s degree. In Head Start programs and child care centers funded by ECAP, lead teachers are only required to have an associate’s degree in ECE, following the HSPPS. Requiring a bachelor’s degree for all teachers is a key step toward improving quality and eliminating at two-tier system in which public schools operate at one standard and private ECAP providers at another. Of course, raising teacher qualifications will raise the cost per child, but this is a truly modest step as only about 20 percent of ECAP teachers currently lack a bachelor’s degree.19
If ECAP is to be a highly effective program, it will need to increase funding per child. Requiring all teachers to have bachelor’s degree is just one reason. In addition, ECAP lead and assistant teachers in nonpublic school settings do not have pay and benefit parity with K-3 teaching staff, even when they have the same qualifications. This is a much bigger financial lift. The federal Head Start program recently announced a major initiative to increase compensation to resolve staffing problems.20 To expand, ECAP likely needs to address this problem more rapidly than federal Head Start. Finally, ECAP requires only a half-day schedule which has been found less educationally effective and does not meet the needs of families for child care and likely limits enrollment.21,22
We used a cost modeling tool to estimate the cost per child for a preschool program in Delaware meeting all 10 quality standards benchmarks in a full-day (6 hour) school-year (180 day) program with teaching staff paid comparably to similarly credentialed peers in K-12. Our estimate is about $15,125 per child – roughly $5,800 per child more than the state reported spending in 2022-23. Funding at this level would allow public and nonpublic program providers to meet ECAP standards while also offering families access to a full-day program with bachelor’s-degreed teachers with uniform compensation in all programs that is competitive with K-12.
EXPANSION
To reach even the 38 percent of three- and four-year-old children below 200 percent of FPL would require a program almost 10 times the size of the current program. A truly universal program would be more than 20 times the size of ECAP today. Based on experiences in other states, this could be accomplished in a decade while ensuring quality. Building on the mixed public-private delivery system ECAP already uses can facilitate this expansion while also supporting the broader child care system that serves children birth to age 13. A mixed-delivery system that includes child care, private education, and Head Start, as well as public schools can maximize the use of existing resources including classroom space, program staff, and materials and supplies. Of course, there will be costs to bring all these resources fully up to standards. Facilities may need to be improved. Teaching staff and administrators will need additional education to obtain degrees and specialized preparation in early childhood education. The vast majority of teachers in child care in Delaware do not have a bachelor’s degree and many do not even have basic preparation in early childhood such as that provided by the Child Development Association (CDA) program.19
Additional new facilities and personnel will be required, as well. Many children in Delaware attend no preschool or child care program so expansion is not just a matter of improving what already
exists. This will require planning with higher education for personnel preparation of leaders, teachers, and assistants, both new entrants to the field as well as those currently in the field who need to add to their qualifications. It also will require planning for the development and funding of facilities which might be public or private.
Private providers may be able to acquire facilities more quickly and at lower cost than the public schools, but their ability to do so will be contingent on confidence that Delaware will continue to fund private providers adequately well into the future.23 A state law committing to the expansion, the continued participation of private providers once part of the system (e.g., that private programs meeting quality standards would not be supplanted by public schools in the future) and a funding formula that covers the full cost could instill such confidence.15 Examples of other states’ approaches to this include requirements for minimum percentages of children to be served in nonpublic school settings (e.g., New York and Michigan), New Jersey’s requirement that large districts contract with “willing and able” private providers, direct state to provider contracts (e.g., Alabama) and countywide multi-agency planning (e.g., West Virginia).15
In addition, the state will require additional resources for the infrastructure to administer and support the program. Highly effective programs operate with continuous improvement systems that include supports for strong implementation such as child assessment, classroom quality assessment and in-class coaching, district- and/or county-wide planning, coordination across grades to assure that gains from preschool are built upon in the early grades, and state oversight and support either direct to providers or to intermediaries such as district or county offices.
CONCLUSION
Delaware’s early childhood education problems are so severe that they can be considered a public health crisis. By fourth grade, Delaware’s children score substantially below the national averages and these scores are substantially lower than in the past. Given the relationship between education and health, Delaware can expect the future health and longevity of its population to suffer as a result. Whether or not this problem is due to Delaware’s exceptionally low rates of preschool participation and public preschool provision, increasing access to high quality public preschool programs is one potential remedy. With modest changes, Delaware’s ECAP program could provide the quality needed to improve educational outcomes, especially for the most economically disadvantaged children. It would then need to be massively expanded as it currently serves fewer than one in five children in poverty and very few children in low-income families above the poverty line. For FY 2025, Delaware raised ECAP spending to $15.7 million, an improvement, but just one-quarter of one percent of the state’s more than $6.1 billion budget.18 An adequately funded program to reach all 3 and 4 year old children below 200 percent of poverty would require about $130 million in spending. Reaching that goal could be accomplished by adding another $15 million to funding each year for the next eight years, with adjustments for inflation. To reach all children at this pace of spending increase would require an additional decade. Of course, the state need not fully fund the program. Just as with K-12 some share of the funding could be provided by local government through the public schools, and by integrating Head Start and child care subsidy systems. Two successive years of ECAP funding increases suggest that Delaware is moving in the right direction. The time is now to ensure that ECAP expands with strong program standards that support strong child outcomes. Dr. Barnett may be contacted at sbarnett@nieer.org .
REFERENCES
1. Barnett, W. S., & Frede, E. (2010). The promise of preschool: Why we need early education for all. American Educator, 34(1), 21. https://www.aft.org/sites/default/files/BarnettFrede.pdf
2. Barnett, W. S. (2011, August 19). Effectiveness of early educational intervention. Science, 333(6045), 975–978. https://www.science.org/doi/10.1126/science.1204534 https://doi.org/10.1126/science.1204534
3. Friedman-Krauss, A. H., Bernstein, S., & Barnett, W. S. (2019). Early childhood education: Three pathways to better health. National Institute for Early Education Research. https://nieer.org/sites/default/files/2023-08/nieer-policy-update_ health_2019.pdf
4. Hahn, R. A., & Barnett, W. S. (2023, April 3). Early childhood education: Health, equity, and economics. Annual Review of Public Health, 44(1), 75–92. https://www.annualreviews.org/content/journals/10.1146/annurevpublhealth-071321-032337
5 Campbell, F., Conti, G., Heckman, J. J., Moon, S. H., Pinto, R., Pungello, E., & Pan, Y. (2014, March 28). Early childhood investments substantially boost adult health. Science, 343(6178), 1478–1485.
6. Muennig, P., Schweinhart, L., Montie, J., & Neidell, M. (2009, August). Effects of a prekindergarten educational intervention on adult health: 37-year follow-up results of a randomized controlled trial. American Journal of Public Health, 99(8), 1431–1437. https://doi.org/10.2105/AJPH.2008.148353 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2707464/
7 Akee, R., & Clark, L. R. (2024). Preschool lottery admissions and its effects on long-run earnings and outcomes (No. w32570). National Bureau of Economic Research. https://www.nber.org/system/files/working_papers/w32570/w32570.pdf
8. Gray-Lobe, G., Pathak, P. A., & Walters, C. R. (2022). The longterm effects of universal preschool in Boston. The Quarterly Journal of Economics, 138(1), 363–411. https://academic.oup.com/qje/article-abstract/138/1/363/6701924
9 Cascio, E. U. (2023). Does universal preschool hit the target? Program access and preschool impacts. The Journal of Human Resources, 58(1), 1–42 https://www.nber.org/system/files/working_papers/w23215/w23215.pdf https://doi.org/10.3368/jhr.58.3.0220-10728R1
10 Barnett, W. S., & Jung, K. (2021). Effects of New Jersey’s Abbott preschool program on children’s achievement, grade retention, and special education through tenth grade. Early Childhood Research Quarterly, 56, 248–259. https://www.sciencedirect.com/science/article/pii/S0885200621000478 https://doi.org/10.1016/j.ecresq.2021.04.001
11. Facts, U. S. A. (2023, August). Health in Delaware. Retrieved September 6, 2024 from: https://usafacts.org/topics/health/state/delaware/#how-much-is-spenton-the-health-of-delaware-residents
12 National Center for Education Statistics. (n.d.). NAEP state assessments. Institute of Education Sciences. Retrieved September 7, 2024 from: https://nces.ed.gov/nationsreportcard/state/
13 Kids Count Data Center. (n.d.). Delaware: Statistics on children, youth and families in Delaware from the Annie E. Casey Foundation and KIDS COUNT in Delaware. Retrieved September 7, 2024 from: https://datacenter.aecf.org/data/tables/9010-youngchildren-not-in-school?loc=9&loct=2#detailed/2/9/fal se/2543,2454,2026,1983,1692,1691,1607,1572,1485/any/17975,17976
14 Barnett, W. S., & Jung, K. (2023). Preschool participation in fall 2022: Findings from a National Preschool Learning Activities Survey. National Institute for Early Education Research. https://nieer.org/sites/default/files/2023-08/nieer-plasurvey-fall-2022-report4.5.23-.pdf
15. Friedman-Krauss, A. H., Barnett, W. S., Hodges, K. S., Garver, K. A., Jost, T. M., Weisenfeld, G., & Duer, J. (2024). The state of preschool 2023: State preschool yearbook. National Institute for Early Education Research. https://nieer.org/yearbook/2023
16. National Center for Children in Poverty. (2024). Delaware state early childhood profile. Retrieved September 7, 2024 from: https://www.nccp.org/early-childhood/?state=DE#1
17. U.S. Census Bureau. (2024). Current population survey, school enrollment supplement. Retrieved September 7, 2024 from: https://www.census.gov/data/tables/2022/demo/schoolenrollment/2022-cps.html
18 S325. 152nd General Assembly. (DE, 2024). Retrieved September 7, 2024 from: https://legis.delaware.gov/BillDetail?LegislationId=141569
19. Delaware Department of Education. (2023). Delaware early learning community and workforce needs assessment study 2022-23. State of Delaware. Retrieved September 7, 2024 from: https://education.delaware.gov/wp-content/uploads/2023/07/ECAP_ HB250_Epilogue_Report_2023.pdf
20 Department of Health and Human Services. (2024). 45 CFR Parts 1301, 1302, 1303, 1304, and 1305. Retrieved September 7, 2024 from: https://www.federalregister.gov/documents/2024/08/21/2024-18279/ supporting-the-head-start-workforce-and-consistent-qualityprogramming
21. Atteberry, A., Bassok, D., & Wong, V. C. (2019). The effects of full-day prekindergarten: Experimental evidence of impacts on children’s school readiness. Educational Evaluation and Policy Analysis, 41(4), 537–562 https://journals.sagepub.com/doi/abs/10.3102/0162373719872197 https://doi.org/10.3102/0162373719872197
22. Robin, K. B., Frede, E. C., & Barnett, W. S. (2006). Is more better? The effects of full-day vs half-day preschool on early school achievement. Retrieved September 7, 2024 from: https://nieer.org/sites/default/files/2023-08/ismorebetter.pdf
23 Vincent, J. M., & Monkkonen, P. (2010). The impact of state regulations on the costs of public school construction. Journal of Education Finance, 35(4), 313–330 https://www.jstor.org/stable/40704396 https://doi.org/10.1353/jef.0.0020
Early detection significantly improves female breast cancer survival rates
According to the Delaware Cancer Registry, for the period 2016 to 2020, breast cancer was the most diagnosed cancer and the second leading cause of cancer death (after lung cancer) among women in both Delaware and the United States. For the same period, non-Hispanic Black women (26.8 per 100,000 persons) were more affected by breast cancer mortality compared to non-Hispanic White women (20.3 per 100,000 persons). Also in the period 2016 to 2020, Delaware (20.7 per 100,000 persons) had a higher breast cancer mortality rate compared to the United States (19.6 per 100,000 persons). When caught in the early stages, breast cancer is treatable, and the survivor’s longevity is improved. In 2021, the five-year relative survival rate for female breast cancer in Delaware was 91.2% compared to the United States rate at 91%, according to the CDC’s United States Cancer Statistics: Data Visualizations. In Delaware, for 2021, the relative five-year survival rate for women diagnosed with breast cancer at the localized, most treatable stage was 98.9%; those women lived five years or more after their diagnoses. Survival decreases to 85.4% when breast cancer is diagnosed at the regional stage (when the cancer has spread directly beyond the primary site or to regional lymph nodes) and to 32% when it is diagnosed at the distant stage (when the cancer has spread to other organs or remote lymph nodes).
October is Breast Cancer Awareness Month. The Division of Public Health (DPH) urges women under the age of 40 to perform monthly breast selfexams and report any changes lasting longer than 90 days to their health care provider. Women aged 40 and older should visit their health care provider to determine if a mammogram is needed. Those without insurance or whose insurance does not cover routine cancer screenings may qualify for free screenings through DPH’s Screening for Life program. Visit https://www.dhss.delaware.gov/dph/dpc/sfl_eligibility.html or call 302-744-1040 to determine eligibility
Women without a health care provider or who need help finding an imaging facility may visit https://www.healthydelaware.org/Individuals/Cancer/ Get-Help/Nurse-Navigators to connect with a nurse navigator. Also visit www.healthydelaware.org.
CDC adopts vaccine recommendations
The Director of the Centers for Disease Control and Prevention (CDC) adopted the following recommendations made by the Advisory Committee on Immunization Practices (ACIP): COVID-19
• 2024-2025 COVID-19 vaccines as authorized or approved by the Food & Drug Administration (FDA) in persons 6 months of age or older.
Respiratory Syncytial Virus (RSV)
• A single dose of RSV vaccine is advised for adults aged 60 to 74 years and older who are at increased risk of severe RSV disease, and for all adults 75 years and older
• RSV vaccination is recommended as a single lifetime dose only. Persons who have already received RSV vaccination are NOT recommended to receive another dose.
Influenza (“the flu”)
• Routine annual influenza vaccination is recommended for all individuals aged 6 months and older who do not have contraindications.
• High-dose inactivated (HD-IIV3) and adjuvanted inactivated (aIIV3) influenza vaccines are acceptable options for influenza vaccination of solid organ transplant recipients aged 18 through 64 years who are on immunosuppressive medication regimens, without a preference over other age-appropriate IIV3s or RIV3.
Pneumococcal Vaccines
• PCV21 is an option for adults aged 19 years and older who currently have a recommendation to receive a dose of PCV.
To view all ACIP recommendations, visit https://www.cdc.gov/vaccines/acip/recommendations.html
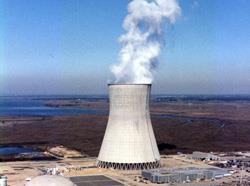
Be prepared for a radiological event
Nuclear accidents and incidents are rare, but learning how to react during a radiological emergency can reduce risks to health and safety.
An Emergency Planning Zone (EPZ) exists within a 10-mile radius surrounding the PSEG Salem and Hope Creek Nuclear Power Generating stations, all located on Artificial Island in Salem County, New Jersey. Eight Delaware ZIP Codes are in the EPZ: 19701, 19734, 19709, 19977, 19730, 19731, 19706, and 19733.
For individuals who live, work, or support people with access and functional needs within the EPZ, it is important to make radiological preparedness part of customized emergency planning Smart 911 registration helps emergency responders locate and safely evacuate EPZ residents who would need transportation in the event of an incident at the power plant. Register for Smart 911 here: https://dema.delaware.gov/onlineServices/index.shtml
To reduce exposure to radiological material resulting from an incident or accident, the Centers for Disease Control and Prevention (CDC) recommend the following general guidelines:
Take Shelter Immediately
• Get inside. A basement is best. Put as much of an interior barrier between you and the outside as possible
• Stay inside. Close windows, secure doors, and turn off any ventilation systems such as air conditioning. If you are in a car, roll up windows, close air vents, and pull off the road to safety
• Stay tuned to emergency alerts and instructions. Protect Yourself After Potential Exposure
• Change clothes and shoes. Immediately put exposed clothing in a plastic bag and close tightly
• Get clean by taking a thorough shower
• Help others and pets with protective actions
• Stay tuned to emergency broadcasting for specific instructions.
Detailed emergency information regarding preparedness and response to a radiological event is distributed to residents within the EPZ in the form of a calendar, which is also online at PrepareDE.org
Hope Creek Nuclear Generating Station #1 in Salem County, New Jersey. Nuclear Regulatory Commission photo
Potassium iodide distribution and siren tests planned for October
In response to a nuclear emergency, state and local officials will issue an Emergency Alert System (EAS) message on local radio and television stations with instructions on how affected residents should react, directions to evacuation routes and emergency reception centers, and when to take Potassium iodide (KI) tablets, if at all. Taking KI is a protective measure outlined in Delaware’s emergency plan.
Twice a year, the Delaware Emergency Management Agency (DEMA) and Delaware Division of Public Health (DPH) distribute free KI tablets to those who live or work within the Emergency Planning Zone (EPZ) surrounding the Salem/Hope Creek Nuclear Generating Stations in New Jersey The next distribution event is October 24 from 11:00 a m to 7:00 p m at the Townsend Fire Company, 107 Main Street, Townsend, Del. 19734.
Individuals allergic to iodine should not take KI. Immediately contact a physician if an allergic reaction occurs. For more information about KI, contact the DPH Office of Radiation Control at 302-744-4546.
Emergency Siren Tests
The next quarterly siren test of the Salem/Hope Creek Nuclear Generating Stations Alert and Notification system is scheduled the morning of October 1, 2024. Delaware State Police, PSEG, and DEMA activate 37 sirens for three to five minutes, followed by EAS messages on radio.
Radiological Drills
DEMA conducts quarterly drills to test response and warning procedures for the Salem/Hope Creek Nuclear Stations Learn more at PrepareDE.org
Reduce the risk of falling by getting screened and taking a balance class
Governor John Carney and Lieutenant Governor Bethany Hall-Long proclaimed September 23 to 27, 2024 as Falls Prevention Awareness Week.
In Delaware in 2023, there were 3,483 falls among individuals aged 65 and older, and 923 of them resulted in a head injury, according to the Delaware Trauma Registry of the Delaware Trauma System of Care
To reduce broken bones, head injuries, and disabilities from falls, the Delaware Coalition for Injury Prevention's Falls Prevention Team asks adults of all ages to get a falls risk assessment, receive regular hearing and vision exams, and review medications with their health care provider and pharmacist. It is important to engage in consistent physical fitness activities and balance exercises. A Matter of Balance classes are held in communities throughout the state. Call Volunteer Delaware 50+ at 302-515-3020 or visit Bayhealth.org/Classes to sign up.
ChristianaCare offers the ThinkFirst to Prevent Falls program which addresses home modifications, medications, balance, and healthy eating to prevent falls. ChristianaCare also offers a “Fall Prevention Education for Caregivers” seminar that educates first time and veteran caregivers how to implement falls reduction strategies in their home and community. The seminar shares medications related to falls, community resources, balance programs, and resources from the National Council on Aging (NCOA) and the Centers for Disease Control and Prevention. Classes are available in person at no cost; contact injuryprevention@christianacare.org
Free fall risk screening is offered at these events:
• September 24, 9:30 a.m. to 10:30 a.m. – MidCounty Senior Center, First Regiment Rd., Sherwood Park II, Wilmington, Del., 19808 Provided by University of Delaware Physical Therapy students and open to the public over the age of 50.
• September 25, 11:00 a.m. to 1:00 p.m. – Modern Maturity Center, 1121 Forrest Avenue, Dover, Del. 19904. Provided by Delaware State University (DSU) Nursing and Master of Occupational Therapy (MOT) students. It is open to the public. A bingo game with prizes begins at 12:15 p.m.
• October 3, 12:00 p.m. to 3:00 p.m. – Milford Senior Center, 111 Park Avenue, Milford, Del. 19963
Provided by DSU Nursing and Master of Occupational Therapy students. It is open to the public, but they must RSVP to 302-422-3385 A bingo game with prizes begins at 12:30 p.m.
Cancer information available at community events
The Division of Public Health’s Cancer Prevention and Control Program will have an information table at these September events:
• “Go Blue” Health Fair at Pedal Away Prostate Cancer, Saturday, September 14, 9:30 a.m. to noon, Eden Hill Medical Center, 200 Banning Street, Dover, Del. 19904.
• Hispanic Heritage Community Health Fair, Saturday, September 21, 10:00 a.m. to 1:00 p.m., Route 9 Library & Innovation Center, 3022 New Castle Avenue, New Castle, Del. 19720.
Public can comment on State Health Assessment and draft regulations
The Division of Public Health (DPH) seeks public comment on the Delaware State Health Assessment through September 20, 2024. Access the report on the State Health Improvement Plan website homepage (https://delawareship.org/) or in the “SHIP Reports” tab. Send comments to info@delawareship.org.
DPH seeks public comment until October 1, 2024 at 4:30 p.m. on proposed revisions to three regulations in Title 16 of the Delaware Administrative Code:
4106 Practice of Non-Nurse Midwifery Regulation – DPH proposes to repeal the regulation governing the practice of non-nurse midwifery
4204 Care and Transportation of the Dead Regulation – DPH proposes new sections, updated definitions, new language regarding natural organic reduction, and technical changes.
4306 Stroke System Regulation – The proposed regulation was previously published in the February 2024, Register of Regulations (27 DE Reg. 567 (02/01/2024) (Proposed)), and was held open for public comment from February 1, 2024 through March 4, 2024. The regulation was substantially revised and is being re-proposed.
Public comment is accepted in written form via email to DHSS_DPH_regulations@delaware.gov, or by U.S. mail to: Vicki Schultes, Hearing Officer, Division of Public Health, 417 Federal Street, Dover, DE 19901. The proposed revisions are available online in the September 1, 2024 Delaware Register of Regulations or by calling DPH at 302-744-4951.
Protect children from lead poisoning
Lead poisoning is a medical condition that occurs when people repeatedly inhale, swallow, or touch lead compounds, even in small amounts.
Lead is toxic, especially in children under the age of six and unborn babies, because it damages the brain and nervous system, causing reduced intelligence, learning disabilities, attention deficit disorders, behavioral problems stunted growth, hearing problems, anemia, kidney damage, and stomach pain. High levels can cause mental retardation, coma, and death.
Delaware law requires the universal testing of all children at ages 1 and 2; however, children can be tested at birth through 72 months. All lead testing results up to age 18 years must be reported to the Division of Public Health’s (DPH) Lead Poisoning Prevention Program. Proof of a blood lead test must be presented for enrollment into a licensed childcare facility and public kindergarten.
The reference level for blood lead testing set by the Centers for Disease Control and Prevention is 3.5 micrograms per deciliter (μg/dL). In Fiscal Year 2023, 694 Delaware children ages 0 to 72 months tested at or above that level (5.9% of the total 11,275 blood lead tests reported, according to the DPH report, Childhood Blood Lead SurveilIance in Delaware, 2023.
A major source of exposure is deteriorating leadbased paint used inside and outside of homes built before 1978. Other dangers are drinking tap water from plumbing fixtures or pipes containing lead or lead solder; working or playing in lead-contaminated soil; and using imported dishes, cosmetics, and plastic or metal jewelry containing lead
Learn how to prevent lead poisoning
National Lead Poisoning Prevention Week (October 20 to 26, 2024) provides opportunities to learn more about this hazard.
Children under the age of 6 and unborn babies are most at risk for lead poisoning, but adults can also be exposed Adults exposed to lead may suffer high blood pressure, fertility problems, nerve disorders, muscle and joint pain, irritability, and memory or concentration problems.
Protect family members from lead hazards by taking these steps:
• If you live in a home built before 1978, hire a certified inspector or risk assessor to check your home for leadbased paint or lead hazards. If renting, ask your landlord to have your home or apartment tested or give you previous test results. When doing renovation, repair, or painting jobs in a pre-1978 home, hire a lead-safe certified contractor who is trained in lead-safe work practices. Find a certified lead-based paint professional using the Environmental Protection Agency’s search tool at https://cdxapps.epa.gov/ocspp-oppt-lead/firmlocation-search, or call the National Lead Information Center at 1-800-424-LEAD [5323]
• Whether or not you live in a pre-1978 home, regularly clean floors and windowsills with wet or damp sponges or cloths to control dust.
• Wipe and remove shoes before entering the home.
• Wash children’s hands often, especially before eating food.
• Do not let small children, especially those who are teething, chew on painted windowsills or eat paint chips.
• Wash toys often.
For more information, visit the Delaware Lead Poisoning Prevention Program at https://dhss.delaware.gov/dhss/dph/hsp/lead.html, where its annual surveillance reports are posted.
The program has two fact sheets. One is about lead poisoning prevention and the other is about program services
Getty Images
It’s Time for Transformational Investments in Early Childhood in Delaware. Help Advocates Make It Happen
Donald Parsons
Retired Vice Chancellor of the Delaware Court of Chancery
Following a long legal career that culminated in serving as a Vice Chancellor on the Delaware Court of Chancery, I became interested in doing what I could to improve the quality of life in Wilmington and beyond.
My goals aligned with those of the Rotary Club of Wilmington, where I have been a member for more than twenty years. The club coalesced around early childhood education as a pivotal ingredient in making Wilmington a world-class city. That was a big vision. We hoped, however, that through education and advocacy, we could help make substantial progress on that ingredient.
Today, I realize there are very few issues that are as impactful for working families as early childhood education, especially for those Delawareans struggling to make a family sustaining income.
Delaware has made progress over the last few years—but progress has been incremental. We’ve slowly bumped up state reimbursement levels for Purchase of Care, the subsidy that helps cover tuition for low-income families. We also have expanded access to state benefits (from 185% of the Federal Poverty Level to 200%). Make no mistake, these are positive developments—but they are not the transformative changes we need to make to support working families and foster a robust and sustainable child care industry.
Why transformational change? As outlined by a generation of doctors, health professionals, and brain science experts, as well as community members found within this journal–early educational experiences are critical to giving children a good start in life. Taken more broadly, early child care and education are essential building blocks for all of Delaware, from the economy and public health, to the wellbeing of young children today and in the future.
In an important election season, Delaware has an opportunity to give kids a strong start, pay early childhood educators equitably, invest in population health, and improve long-term health outcomes and life spans. Transformative investment will yield a transformative return on investment for our state’s economy in the shortand long term. Quality care and education for children from birth to age five not only allows more parents to participate in the workforce and further their careers and education, it also better equips their children to succeed in school and life.
Unfortunately, Delaware lags significantly behind our neighboring states and most other states in making quality early education accessible and affordable to middle class families. Here, a family of four with two adults each making next year’s minimum wage ($15 per hour or $60,000 per year) finally will qualify for state supported child care. A family with any higher income would not. Yet, early child care and education is financially out of reach for many families that make between $60,000 and $100,000.1
It’s time for Delaware to step up, and for each of us to be a part of the growing multitude of advocates. Contact your legislator and other elected officials and ask them how they will expand access to high-quality early care and education in our state.
With help from Rotary, as well as groups like the First State Pre-K coalition, the Delaware Association for the Education of Young Children, and numerous others—the child care message is beginning to spread. We need more people coming to meetings, sending emails, and keeping the pressure on state leaders for true, transformative change.
Mr. Parsons may be contacted at dfparsons2@gmail.com .
REFERENCES
1. Delaware Department of Health and Social Services. (n.d.). Child Care Services. Retrieved from https://dhss.delaware.gov/dss/childcr.html
Parents Across the State Agree: Quality, Accessible, and Affordable Child Care Matters
“We are not able to afford both child care and extended care. We use PTO and have made special arrangements with our employers.”
"The cost of child care makes it impossible to get ahead, let alone pay off debt, or do anything extra outside of daily living."
“I have a good [child care center] but it's costing me quite a bit of money even with [Purchase of Care].”
"My family can only find waiting lists for child care."
“As a full-time school district employee with a self-employed spouse, my entire paycheck goes to child care, but I work so we can have benefits and so my daughters can have quality care that is so important. I hope we can help the families in our community get the same experience my daughters are getting, and provide it so that families do not have to sacrifice to access it.”
"[We are] living in a child care desert so we take it day by day.”
“I stay home because we could not afford bills and child care. Even to stay home I am having to file bankruptcy because we can't even afford this but this was the better option compared to full-time care so I can work. The cost of EVERYTHING is going up but job pay is increasing at a MUCH slower rate.”
PNC’s Commitment to Economic Prosperity Through Early Learning
Greg Miraglia Delaware Market Executive and Wealth Director, PNC Bank
This article originally ran in the July/August 2024 issue of Delaware Business Magazine, published by the Delaware State Chamber of Commerce.
There are many challenges confronting the State of Delaware, Delaware families, and the nation as a whole. To continue to thrive, we must also continue to invest in Delaware’s children, as well as enhance our state’s business climate and quality of life.
This focus on both the present and the future is central to PNC’s 20-year commitment to investing in high quality early education, while simultaneously investing in large and small businesses throughout our state.
Governor John Carney understands the benefits of both and has guided significant investments in early care and education, and encouraged a continued focus on the wellbeing of our state’s families. Last year’s budget increased child care rates for subsidized families and the number of children served in our state pre-K program, further demonstrating that we are headed in the right direction.
We must continue to make progress. Sustained and increased investment to serve more families is needed. A 2023 survey by the First State Pre-K Coalition found that most parents indicated that child care is their biggest monthly expense, with more than 30% saying that it costs more than their mortgage payments or rent. Sixty percent of Delaware families surveyed said they would work more than they do now if they could afford or access child care.
Employees continue to face challenges that hold our companies back in their attendance, productivity, and retention. In recent years, companies across the state have been challenged to address higher than average vacancies/job absence, in part due to child care. We hear that parents face long waiting lists and short supply—in part due to the access provided by the state to only one in five Delaware children, and because child care is expensive and affordable only to upper-middle-income families. Many families earn too much to qualify for state assistance, but still struggle to pay their bills. All of our neighboring states provide access to public programming to more families than Delaware. Our state only covers families earning up to 200% of the federal poverty level, while our neighbors cover those up to 250-300%.
Findings released in the Child Care Is Everyone’s Business: Why Delaware Businesses Should Care About Early Childhood Education report—released by the Federal Reserve Bank of Philadelphia, Delaware State Chamber of Commerce, Rodel, and the Delaware Office of Early Learning—identified that Delaware has insufficient supply to serve the families that need child care and early childhood education, and the state under-invests in child care rates, which limits pay for early educators and accessibility for families.1 The report affirmed these factors are holding back economic growth and workforce participation. High-quality early childhood education programs are essential for young children’s development and school success, and they are critical to recruiting and retaining a competitive workforce. As employers, we’ve been investing in this high-impact area for 20 years.
At PNC, our signature philanthropic initiative, PNC Grow Up Great®, centers on advancing high-quality early education for children from birth to age five. Celebrating its twentieth anniversary in 2024, PNC Grow Up Great® has supported more than 10 million children and their families nationwide, as well as their educators and community partners, to provide innovative opportunities that enhance learning and development in a child’s early years. This investment is a piece of the answer, but employers cannot solve this systemic, collective problem without significant support from the State.
Our state leadership clearly recognizes the growing issues surrounding early childhood education and child care, and we are moving in the right direction. At PNC, we’ve long recognized that these investments will build a legacy for Delaware’s current and future workforce, helping to ensure long-term economic success for all of us across the First State.
Mr. Miraglia may be contacted at Gregory.miraglia@pnc.org
REFERENCES
1. Federal Reserve Bank of Philadelphia. (2022). Child care is everyone’s business. Why Delaware businesses should care about early childhood education. Retrieved from: https://www.philadelphiafed.org/-/media/frbp/assets/communitydevelopment/reports/delawaretoolkit_hi-2_final.pdf
Invest in Early Care and Education to Build Delaware’s Healthcare Workforce of Today and Tomorrow
Colleen Perry Keith, Ph.D. President, Goldey-Beacom College
Brian DiSabatino
President and CEO, EdiS Company; Chairman, Delaware Business Roundtable
As leaders behind a historic business-focused college with a 90% placement rate after graduation and a development company that has reshaped Delaware for generations— we know that the health of Delaware’s population is a critical factor for long-term success. We see the impacts of the workforce shortages on our students, colleagues, and clients. And, we know the health care workforce faces significant challenges, with more than a quarter of Delawareans living in a federally designated health professional shortage area.
One strategy we know is key to attracting and retaining this workforce is quality, affordable child care.
Without access to care, parents and caregivers can’t work or further their education and career. It’s as simple as that.
The Annie E. Casey Foundation found that 13 percent of Delaware’s children had a family member who quit, changed, or refused a job due to difficulty finding and affording child care.1 Today in Delaware, child care costs more than the average mortgage payment and more than the cost of in-state college tuition. These factors hit our local workforce hard. It often makes more financial sense for a parent to stay home with their young child than to further their career. The resulting challenges to families and employers cost Delaware $415 million in lost earnings, productivity, and tax revenue each year.
The Delaware Business Roundtable recently released the 2024 Investment Agenda, designed to set the direction for the state leaders elected this fall.2 The Agenda recommends early care and education as a critical long-term investment for the state:
“Delaware must implement strategies to stabilize and expand access to and affordability of early childhood education.”
One immediate solution, as the Investment Agenda notes, would be to increase income thresholds so more families can benefit from state supported programs. Our neighboring states set family eligibility levels much higher than Delaware (for example, Pennsylvania covers families up to 300% of the federal poverty level, while Delaware only goes up to 200%).
The Agenda notes “a compelling need to invest in this space,” as six out of seven young children in Delaware are unable to access public early childhood education. It also recommends important investments in the early educator workforce and in quality improvement initiatives.
The long-term nature of this investment is critical to the future workforce. Without quality child care, students are less likely to enter kindergarten ready and then less likely to hit other important milestones such as third grade reading, eighth grade math, high school completion, and earning postsecondary credentials. This situation directly impacts the workforce as failure to meet critical milestones along the way to adulthood results in a lesscapable workforce. Quality child care is a key pillar of Delaware’s economic future and long-term health.
Delaware is a small state that knows how to work together. If we can work together to solve child care for families, we will strengthen our economy, workforce, and our communities.
Dr. Keith may be contacted at keithcp@gbc.edu
REFERENCES
1. Annie E. Casey Foundation. (n.d.). Family job change due to child care in Delaware. Retrieved from: https://datacenter.aecf.org/data/tables/11389-family-job-change-due-to-child-care
2. Roundtable, D. B. (2024). Delaware investment agenda. Retrieved from: https://www.dbrt.org/delaware-investment-agenda
Talent and Workforce Recommendations
From the Delaware Investment Agenda
Support equitable investment in early childhood education to increase access and improve outcomes for children in the state.
Ensure wider access to early childhood education by expanding support to families earning over 200 percent of the federal poverty level (FPL) Invest in the early childhood education workforce through apprenticeship models, professional development, support for obtaining professional credentials, and equitable compensation and benefits.
Continue to support evidence-based curricula, screening, and assessments to ensure program quality across early childhood education programs.
The Annie E. Casey Foundation found that 13 percent of Delaware’s children had a family member who quit, changed, or refused a job due to difficulty finding child care. The resulting challenges to families and employers cost Delaware $415 million in lost earnings, productivity, and tax revenue a year.
40 percent of Delaware residents over the age of 16 were not in the labor force, which was the nation’s 10th highest percentage.
% $415M
Early Education is the Civil Rights and Public Health Issue of the Century
Jarrett Royster President and CEO, YMCA of Delaware
Every city and state in the U.S. should measure human capitalization rates (HCR). HCR is a measure of how well a city or state supports, educates and empowers its citizens to meaningfully contribute to society. It is leadership’s job to ensure that investment in education and human capital essential services yield substantial returns in terms of economic growth, social wellbeing, access to healthcare, and overall quality of life.
Our systems should be aimed to lead its citizens to achieve these four outcomes:
1. Economic independence
2. Strong and positive social networks
3. Civic engagement
4. Good health and wellbeing
If, as a nation, we focus on and refine systems toward this goal, we would strengthen our democracy. Our democracy is weakened when we do not have educated, informed and engaged citizens. The rising polarization in our country is a byproduct of growing disconnection, hopelessness, and fear often flamed by social media.
The root cause is our lack of will to prioritize investments in universal systems that lead to improved HCR. This is why I am a staunch advocate for ensuring every child has access to highquality early education, regardless of the zip code they are born into. I believe it is a civil right to be supported to have the tools to fully participate in our democracy.
There is no more important tool or investment that we as a society make than an investment in early education. We have plenty of data and science that tells us of the value of early education and the transformative impact it has on our children. Today, we know the importance of attachment theory—the need for children in the first five years of their lives to have a bond with caring adults that sing, touch, read, feed and protect them. We know that 90 percent of a child’s brain is developed in the first five years of their lives.1 We know that the first 1,000 days of a child’s life is a period of exponential growth.2 We know from science that when we provide children with proper nutrition, healthcare and a supportive environment, it leads to long term benefits for our society.3–5
Dr. James Heckman, esteemed professor at the University of Chicago has proven through research that for every dollar we invest in early childhood education, we get nearly a $16 return as a society.6,7 Despite the overwhelming evidence of the importance of early education and the importance of day care and preschools, in an economy that, for most families, requires the caregivers to work, we woefully under-invest in early education systems across the country.8
Our lack of willingness to make adequate investment is constraining our potential as a nation. Children are being born into poverty, which too often leads to hopelessness and despair.9
Too many children are entering school up to nine months behind the readiness standards for kindergarten. This may result in long-term academic struggles, increased need for special services, behavioral and social challenges, and higher retention rates, among other negative outcomes.10
We know the solution to the problem begins with investing early. Research affirms investing in early learning is the right thing to do, and gives the supports caregivers need. We just need the willingness and coordination to get it done, and the collective understanding that advocating for investment in early childhood education is more than just about providing care for children while their parents work. Advocacy for proper early childhood education is a civil rights issue. It is about protecting our democracy, which requires an educated and informed citizenry— citizens that have the critical thinking skills to discern between misinformation and disinformation; citizens that are civically engaged and push on policymakers for solutions.
As an informed citizen and leader of one of the state’s largest nonprofits, I advocate passionately for adequate funding to ensure every child has access to high-quality learning opportunities. Today at the YMCA of Delaware, we operate three early learning centers, and we are very proud that 92% of the children that attend those centers meet the developmental markers for readiness for kindergarten. All our centers operate on a flexible yet dynamic framework that has four pillars:
1. Inspiring educators and environments.
2. Parents are partners.
3. Diverse and inclusive environments.
4. Holistic curriculum and supports.
At the center of our approach is our commitment to drive continuous improvements.
In the fall of 2026, in partnership with the Community Education Building, we will open a fourth child care center in Wilmington. We plan to make this new center our innovation lab. We will build it with an eye toward encouraging collaboration amongst teachers, piloting emerging practices, codifying them, and taking them to scale not only for our network of YMCAs, but for the entire field. Partnering with the Community Education Building will also allow us to more intentionally and easily provide essential wraparound supports to the children and families. Unique to the YMCA, this investment in early learning is a critical investment in our pipeline of services from cradle to careers. While investing early is important, sustained support over time is even better to ensure transformational impact.
I invite and encourage you all to become more informed on this issue and demand your legislators to adequately invest in early children, because this is the civil rights issue of our century. Our democracy is dependent on it.
Mr. Royster may be contacted at jroyster@ymcade.org
REFERENCES
1. First Things First. (n.d.). Why early childhood matters: The first five years. First Things First. https://www.firstthingsfirst.org/why-early-childhood-matters/the-firstfive-years
2. Brines, J., Rigourd, V., & Billeaud, C. (2022, January 6). The first 1000 days of infant. Healthcare (Basel), 10(1), 106. https://doi.org/10.3390/healthcare10010106
3. Lanigan, J., & Singhal, A. (2009, November). Early nutrition and long-term health: A practical approach. The Proceedings of the Nutrition Society, 68(4), 422–429. https://doi.org/10.1017/S002966510999019X
4 Negussie, Y., Geller, A., & DeVoe, J. E. (Eds.). (2019). Vibrant and healthy kids: Aligning science, practice, and policy to advance health equity. National Academies Press. https://www.ncbi.nlm.nih.gov/books/NBK551489/
5. Donoghue, E. A. (2017, August). Quality early education and child care from birth to kindergarten. Pediatrics, 140(2), e20171488. https://doi.org/10.1542/peds.2017-1488
6 Heckman, J. J. (n.d.). Investing in early childhood development: Reduce deficits, strengthen the economy. The Heckman Equation. https://heckmanequation.org/resource/investing-in-early-childhooddevelopment-reduce-deficits-strengthen-the-economy/
7 First Things First. (n.d.). Investing in early childhood. First Things First. https://www.firstthingsfirst.org/early-childhood-matters/investing-inearly-childhood/
8 The Hamilton Project. (2021). Increasing federal investment in children’s early care and education. The Hamilton Project. https://www.hamiltonproject.org
9 American Psychological Association. (n.d.). Poverty, hunger, and homelessness: Impact on children and youth. American Psychological Association. https://www.apa.org/topics/socioeconomic-status/poverty-hungerhomelessness-children
10 Barnett, W. S., & Friedman-Krauss, A. H. (2016). How much can high-quality universal pre-K reduce achievement gaps? National Institute for Early Education Research. https://nieer.org/research-library/how-much-can-high-quality-universalpre-k-reduce-achievement-gaps
Delaware’s Progress and Potential in Early Childhood
Lynn C. Jones, M.H.A., F.A.C.H.E. President, Rotary Club of Wilmington; President, Delaware Academy of Medicine / Delaware Public Health Association
When leaders of the Rotary Club of Wilmington sat down to consider the top dozen or so attributes that would define a worldclass city, one issue continued to emerge.
The issue was closely aligned with the Rotary’s drive toward service above self and helping the community. It had transformative powers that could alter not only the lives of countless individuals and families, but could also strengthen and heal communities, while boosting our state’s economy. The issue felt tangible enough—and close enough within our grasp—to present an opportunity to truly make an impact.
The issue was early child education and care.
As a longtime practitioner and leader in Delaware healthcare, I’m committed to seeing our local communities thrive in healthy households. After retiring from my 36-year career with Christiana Care, I’ve devoted my time and energy to groups like Rotary, Boy Scouts of America, and the Delaware Academy of Medicine, where I serve as board president. “Retirement” seems like a misnomer in my case—I like to think I’ve graduated onto my postgraduate work.
In these roles, I’ve explored key issues and collaborated with community partners on ways to enrich Delawareans’ lives. And few societal levers hold the potential of child care.
I now know that, as Dr. Ross Thompson tells us in his piece on brain architecture in this issue, the early years are an “exuberant” time for brain development, and set the foundation for human development, beginning prenatally. Without quality early learning experiences, many of these important developmental milestones can be missed or delayed. By the time a child is transitioning into kindergarten, their executive functioning skill set has already been mostly developed.
Experts, educators, and everyone in-between agree that if a child does not arrive to kindergarten with these developmental tools, it becomes very hard to keep up academically. Unless you catch up, a child is unlikely to achieve their potential in school or as an adult. This domino effect that starts so early can eventually lead to lower career earnings, higher healthcare costs, and may even lead to serving jailtime.1
In other words, the early years are critically important. And frankly, Delaware is underserving its youngest citizens and their families. Only about one in five children are enrolled in state-sponsored child care programs, and as a result, a whopping one third of children arrive at kindergarten already behind the curve.2 Working families find it difficult to access state benefits but can’t afford child care tuition, which can cost as much as a monthly mortgage. Caregivers are choosing to stay at home with young children instead of joining the workforce, hurting household incomes and our local economy.3 We know that in many industries, like healthcare and hospitality, workforce shortages have emerged with child care as the primary cause.
The good news is that local leaders, educators, advocates, and many others like me who simply care about the welfare of our state are rallying around this issue and demanding action. And Delaware is responding. Lawmakers have led the charge on historic increases in state-sponsored pre-K and Purchase of Care—the subsidy that covers tuition for low-income families.
But we need to swing for the fences to truly make a transformational change for future generations. Most developed countries have a majority of their children in educational programming before the age of five. It’s time for the U.S. to catch up, and some states are charging ahead. New Mexico, Vermont, and Washington D.C. have provided access to early care and education starting at birth for most families. Delaware still ranks 39th among states for access to state funded pre-K for three- and four-year-olds, behind all our regional neighbors and states like Alabama and Mississippi.4
While Delaware has made substantial and historic progress over the last several years, we’ve mostly been chipping away, rather than undergoing transformational change. To get there, Delaware will need to invest at a level so that every child can access a quality program where educators are paid a familysustaining wage with benefits.
We need everyday citizens—Rotarians, healthcare professionals, scouts, churches, and everyone in-between—to know the facts and make early childhood education a priority.
As our Rotary mantra goes, “Early child education: it’s good for the child, it’s good for the community, and it’s good for the economy.” It’s the future we all want for our state, and one of the best investments we can make for the good of public health.
Mr. Jones may be contacted at lynncjones77@gmail.com .
REFERENCES
1. Vergunst, F., Vitaro, F., Brendgen, M., Larose, M.-P., Girard, A., Tremblay, R. E., & Côté, S. M. (2024, Jan-Feb). Mechanisms and pathways linking kindergarten behavior problems with mid-life employment earnings for males from low-income neighborhoods. Child Development, 95(1), 208–222. https://doi.org/10.1111/cdev.13967
2. Delaware Department of Education. (2023). Delaware Early Learner Survey: Key Findings. Delaware Department of Education. https://education.delaware.gov/wp-content/ uploads/2023/05/DE-ELS-Key-Findings-2020-2023-New-logo-1.pdf
3. First State Pre-k. (November 2023). Delaware Family Survey Results. Rodel Foundation. https://rodelde.org/wp-content/ uploads/2023/11/October-2023-Family-Survey-Results-Draft.pptx.pdf
4. Friedman-Krauss, A., Barnett, W., Hodges, K., Garver, K., Jost, T., Weisenfeld, G., & Duer, J. (2024). The State of Preschool 2023: State Preschool Yearbook. National Institute for Early Education Research. https://nieer.org/sites/default/ files/2024-08/2023_nieer_yearbook_8-9-24.pdf
Dear Medical Provider:
Dear Medical Provider:
The American Cancer Society National Lung Cancer Roundtable (ACS NLCRT), American College of Radiology® (ACR®), and Radiology Health Equity Coalition (RHEC) have partnered once again for the third annual National Lung Cancer Screening Day (“National LCS Day”).
The American Cancer Society National Lung Cancer Roundtable (ACS NLCRT), American College of Radiology® (ACR®), and Radiology Health Equity Coalition (RHEC) have partnered once again for the third annual National Lung Cancer Screening Day (“National LCS Day”).
This year’s National Lung Cancer Screening Day is on Saturday, November 9, 2024 In Delaware, we will be encouraging lung screening during the entire month of November The goal of this event is to reduce disparities, promote access to care, and save lives.
This year’s National Lung Cancer Screening Day is on Saturday, November 9, 2024. In Delaware, we will be encouraging lung screening during the entire month of November. The goal of this event is to reduce disparities, promote access to care, and save lives.
Lung cancer is one of the deadliest forms of cancer and is estimated to claim the lives of over 127,000 Americans this year. Did you know that even though survival rates can be improved significantly by screening, only a small percentage of eligible indivi duals get screened for lung cancer. In Delaware, only 27.9% of those that are eligible reported having a CT scan for lung cancer screening within the past 12 months. Most cases continue to be diagnosed at distant stage, which is harder to treat and decreases survival. In 2015 -2019, 44% of new lung cancer cases were diagnosed at the distant stage.
Lung cancer is one of the deadliest forms of cancer and is estimated to claim the lives of over 127,000 Americans this year. Did you know that even though survival rates can be improved significantly by screening, only a small percentage of eligible indivi duals get screened for lung cancer. In Delaware, only 27.9% of those that are eligible reported having a CT scan for lung cancer screening within the past 12 months. Most cases continue to be diagnosed at distant stage, which is harder to treat and decreases survival. In 2015 -2019, 44% of new lung cancer cases were diagnosed at the distant stage.
Our purpose for this focus in November is to increase screening access for people who cannot take time off during their weekly schedules to get screened for the early detection of lung cancer.
Our purpose for this focus in November is to increase screening access for people who cannot take time off during their weekly schedules to get screened for the early detection of lung cancer.
Support National Lung Cancer Screening Day on 11/ 09/24 by referring your eligible patients for screening . Show them you care about their health. Refer them to a nearby screening center today. We appreciate your support this November.
Support National Lung Cancer Screening Day on 11/ 09/24 by referring your eligible patients for screening . Show them you care about their health. Refer them to a nearby screening center today. We appreciate your support this November.
Together, we can make a difference and create a nation where lung cancer is screened for, detected early, treated effectively, not stigmatized, and conquered!
Together, we can make a difference and create a nation where lung cancer is screened for, detected early, treated effectively, not stigmatized, and conquered!
Let’s work together to save lives!
To easily find a lung screening site near you, click on,
Let’s work together to save lives!
To easily find a lung screening site near you, click on,
For more information visit the National Lung Cancer Roundtable at
A Child’s Health Begins at Pregnancy, Requires Solid Early Investments, and Follows a Child into Adulthood
Priscilla Mpasi, M.D., F.A.A.P. Assistant Medical Director, Clinically Integrated Network, ChristianaCare Health System; Chair, Delaware Maternal & Infant Health Consortium
Imagine being a parent who is faced with the difficult decision of staying home and not working, or sending your child to child care. This is a common discussion in my pediatric practice, where parents ask me about child care resources or affordable child care centers. In particular, I recall one family’s story, a family relatively new to Delaware.
Mom brought all three children, ages 6, 3 and 10 months, for their annual well child visit. As I completed the school paperwork for the 6-year-old boy, I asked mom about any additional paperwork or resources we could provide. After a brief pause, she asked if we had a list of child care centers in the area. When I asked about a specific location or child resources, she replied that she already explored some centers in the area, though the cost for both the 3-year-old and 10-month-old was not affordable with the current household budget. She thought that her husband had a “good income;” however when they learned the daycare rates, they realized they could not afford daycare for two children.
When I mentioned Head Start for the 3-year-old, mom stated that, with the recent move, they missed the application timeline and there was now a long waitlist. Even so, the child care rates for only the 10-month-old were still expensive. Mom also said she desired to return to work within the next one to two years, and that, even with their projected combined income, finances would still be challenging with the child care expense. She expressed both her frustration and sadness that her 3-year-old might not get the learning and social experiences from being in child care, and that she might start behind her peers in preschool next year. She was even more concerned that, even with her second income, they would struggle to pay for child care for her youngest son. At the end of the visit, we had more questions than solutions, and there was no clear path for the family on child care or parent reentry in the workforce.
Many parents do not have to imagine this situation: they are facing similar challenges with accessible and affordable childcare. This story is the reality for many of my families and for even more families across Delaware. With an early start and early investments, together we can write a new story for our families and children.
As a member of the American Academy of Pediatrics and its Council on Early Childhood, as well as the Chair of the Delaware Maternal & Infant Health Consortium—I know that early childhood development starts during pregnancy.
Ensuring that birthing persons are healthy is a great predictor for healthy children. In the field, we think of a child’s first 1,000 days of life: starting in utero and continuing through age two.
I’ve also seen firsthand how the building blocks of prenatal care, early learning experiences, and K-12 education fit together. And all too often, when the first or second piece is missing or insufficient, the rest of the child’s journey is impacted.
The wide achievement gaps we see in Delaware between racial groups can begin startlingly early. And once a child falls behind on developmental milestones, it can be hard to catch up.
In addition to prenatal health, quality early learning experiences are crucial for children’s growth and set the table for kindergarten and beyond. In a child care setting, surrounded by their peers and qualified professionals, a young child’s mind will blossom. They mimic their classmates and providers, learning to speak, to share, to regulate emotions.
On the flipside, when children don’t have the opportunity to develop in a child care setting, they often begin kindergarten at a different academic level than their peers.
Imagine the frustration in a child’s mind realizing they can’t write their letters or pronounce words as their classmates do. How does this frustration manifest in a child? A five-year old can only manifest through their emotions. They may get angry. They may have tantrums. They may want to avoid their work because they know that they’re not at pace with their peers.
And by that stage, things can begin to snowball. A child without child care or intervention for developmental delays often becomes a young student facing school discipline, ADHD diagnoses, or a “problem child” label that will follow them from grade to grade. What should have been an early intervention and need for special resources later on becomes “behavior modification” and punitive measures. That cycle affects parents, too, who now might be even more hesitant for their next children to seek services. It is a downstream effect, and one of the social determinants of health, and one that can literally start from the day the child is born.
In Delaware, too many families are struggling to access and afford quality child care. That is creating a developmental logjam that ripples into our K-12 education system. As a society, we must evolve our thinking around child care. Child care providers are not simply babysitters; they’re trained professionals who guide our young ones through critical developmental milestones in safe and nurturing environments. They’re trained to spot cognitive or social delays, which can necessitate special resources for families.
The full scope of early childhood development should also include affordable housing, livable wages, transportation, and food security. These are all aspects that parents have to consider when they have a child or children that influences the overall development of that child and their outcomes later in life.
As a state, we need to continue to push for these foundational pillars of family life. We need to invest in early childhood education so providers can earn a livable wage and families can have a safe place for their children. We need to ensure pre- and neonatal care, home visiting services, and maternal health are priorities, alongside community prevention programs, and before- and afterschool programs. All of these aspects have to come together to ensure the best chance for a child to live out the life of their dreams.
I always say that education is the great equalizer. Many children are starting in different places, and I truly believe that early education is when you empower a child to learn. If we can make early childhood opportunities equitable, then we can ensure that all of our children are set up for success.
Dr. Mpasi may be contacted at priscillampasi@gmail.com
GLOBAL HEALTH MATTERS
GLOBAL HEALTH MATTERS
Nkengasong
JULY/AUG 2024
JULY/AUG 2024
Defining the genetics behind cleft palate in populations of African descent....p. 5
Defining the genetics behind cleft palate in populations of African descent....p. 5
delivers Barmes Lecture 2024
Nkengasong delivers Barmes Lecture 2024
By Susan Scutti
By Susan Scutti
When asked by NIH Director Dr. Monica Bertagnolli what keeps him up at night, Ambassador Dr. John Nkengasong, presenter of the NIH Barmes Global Health 2024 lecture, answered unhesitatingly: “I fear that HIV fatigue can kick in, complacency can kick in, and if it does, the gains we’ve made may be quickly eroded.” Nkengasong recalled the malaria eradication program the WHO initiated in 1955. It achieved some success though not as much as hoped. The turning point arrived in 1969. “The countries that had made gains saw a resurgence of malaria, and global interest faded.” Financial support dwindled soon after, said Nkengasong.
When asked by NIH Director Dr. Monica Bertagnolli what keeps him up at night, Ambassador Dr. John Nkengasong, presenter of the NIH Barmes Global Health 2024 lecture, answered unhesitatingly: “I fear that HIV fatigue can kick in, complacency can kick in, and if it does, the gains we’ve made may be quickly eroded.” Nkengasong recalled the malaria eradication program the WHO initiated in 1955. It achieved some success though not as much as hoped. The turning point arrived in 1969. “The countries that had made gains saw a resurgence of malaria, and global interest faded.” Financial support dwindled soon after, said Nkengasong.
The Barmes Global Health lecture series was established by the National Institute of Dental and Craniofacial Research (NIDCR) and the Fogarty International Center to honor the late Dr. David Edward Barmes’ lifelong dedication to research aimed at improving health for those in lowincome countries. The 2024 speaker, Dr. John Nkengasong, U.S. Global AIDS Coordinator and Senior Bureau Official for Global Health Security and Diplomacy—a role which includes leading the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR)—highlighted PEPFAR's achievements. In 2012, most PEPFAR-supported African countries reported less than 60% of people living with HIV on ART (antiretroviral treatment); a decade later, many countries are above 80% coverage. AIDS-related deaths have declined
The Barmes Global Health lecture series was established by the National Institute of Dental and Craniofacial Research (NIDCR) and the Fogarty International Center to honor the late Dr. David Edward Barmes’ lifelong dedication to research aimed at improving health for those in lowincome countries. The 2024 speaker, Dr. John Nkengasong, U.S. Global AIDS Coordinator and Senior Bureau Official for Global Health Security and Diplomacy—a role which includes leading the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR)—highlighted PEPFAR's achievements. In 2012, most PEPFAR-supported African countries reported less than 60% of people living with HIV on ART (antiretroviral treatment); a decade later, many countries are above 80% coverage. AIDS-related deaths have declined
68% since their peak in 2004. Overall, the rate of new infections has plummeted, but “we’re not out of the woods,” warned Nkengasong. PEPFAR’s progress, though widespread, is uneven across the globe. “We have a series of countries—Kyrgyz Republic, Tajikistan, Papua New Guinea, and the Philippines—that we
68% since their peak in 2004. Overall, the rate of new infections has plummeted, but “we’re not out of the woods,” warned Nkengasong. PEPFAR’s progress, though widespread, is uneven across the globe. “We have a series of countries—Kyrgyz Republic, Tajikistan, Papua New Guinea, and the Philippines—that we
characterize as ‘epidemics of concern,’ countries where we see incidence increasing.” In all regions, key drivers of transmission include people with undiagnosed HIV, those diagnosed but never treated, and those who interrupt treatment.
characterize as ‘epidemics of concern,’ countries where we see incidence increasing.” In all regions, key drivers of transmission include people with undiagnosed HIV, those diagnosed but never treated, and those who interrupt treatment.
Though hopeful, Nkengasong reminded the audience of the danger that HIV can get pushed to the background whenever other emerging diseases, such as COVID-19 or mpox, arise. Meanwhile, the HIV response is at a crossroads: “We need to think about financing, we need to finish the fight,” said Nkengasong. “If PEPFAR was to stop today, you’d have an almost 400% increase in death rates.”
Though hopeful, Nkengasong reminded the audience of the danger that HIV can get pushed to the background whenever other emerging diseases, such as COVID-19 or mpox, arise. Meanwhile, the HIV response is at a crossroads: “We need to think about financing, we need to finish the fight,” said Nkengasong. “If PEPFAR was to stop today, you’d have an almost 400% increase in death rates.”
Article series focuses on reciprocal innovation
Article series focuses on reciprocal innovation
As part of Fogarty’s Center of Global Health Studies’ Global Health Reciprocal Innovation project, a series of articles has been published as a supplement in BMJ Global Health. Sponsored by Fogarty and U.S. government partners the supplement highlights examples, successes, and challenges in the exchange of innovations between low/middle-income and high-income countries. Links to all articles can be found at go.nih.gov/GHRI_Articles.
As part of Fogarty’s Center of Global Health Studies’ Global Health Reciprocal Innovation project, a series of articles has been published as a supplement in BMJ Global Health. Sponsored by Fogarty and U.S. government partners the supplement highlights examples, successes, and challenges in the exchange of innovations between low/middle-income and high-income countries. Links to all articles can be found at go.nih.gov/GHRI_Articles.
Global health research mentorship today
Global health research mentorship today
We asked nine accomplished investigators about their experiences as global health research mentors and mentees. Each interpreted mentorship in a unique way.
We asked nine accomplished investigators about their experiences as global health research mentors and mentees. Each interpreted mentorship in a unique way.
9
Chia-Chi Charlie Chang/NIH
Ambassador Dr. John Nkengasong presented the David E. Barmes Global Health Lecture, warning of "HIV fatigue" setting over the global response to the epidemic.
Chia-Chi
Charlie Chang/NIH
Ambassador Dr. John Nkengasong presented the David E. Barmes Global Health Lecture, warning of "HIV fatigue" setting over the global response to the epidemic.
Can dismantling stigma reduce HIV rates in Nepal?
Three in 10 of the 11.3% of trans women in Nepal living with HIV do not seek care. This is often due to the stigma of being Hijra, or “the third sex.” The Fogarty-supported Sweekar program aims to increase both HIV testing and treatment adherence by examining and addressing stigma faced by trans women in Nepal.
In ancient Sanskrit texts, Hijra are described as capable of bestowing both blessings and curses. “Every temple you go to you see trans people’s images. They’re seen as mystic and people treat them with both respect and fear,” said Dr. Erin Wilson, senior research scientist, San Francisco Department of Public Health. In rural Nepal, however, most trans people experience exclusion from society and discrimination.
Nepal passed a law in 2007 to recognize those who identify as third gender, yet it hasn’t stimulated much change in societal attitudes.
Regrettably, such stigma can lead Hijra, who are part of the larger trans women population in Nepal, to not seek medical care. Wilson and her colleagues are working on a stigma reduction intervention for Nepal’s trans women community to increase their health care uptake. The project’s name is “sweekar,” which means “acceptance” in Nepali.
Methodology
Wilson believes PhotoVoice, a participatory research tool, can help change attitudes toward trans women at the individual, community, and society levels. Participants take and share pictures of the ways in which they’re not accepted in Nepali society. For example, one trans woman photographed a boy with a water jug and explained that she’d never been permitted to perform this traditional female role (of getting water)—yet this boy was allowed. Wilson said, “It begins with getting the trans women together to talk about their experiences, to share how stigma manifests in their lives and what impact it has, and to find support with one another.”
In addition to building empowerment, these photos will be used to launch a social media campaign aimed at changing
attitudes within the wider society. Wilson and her Nepal research partner, the Blue Diamond Society, are working with the U.S. embassy to garner support from regional thought leaders as well. “Stigma research shows that when leaders have different values, people say, ‘Maybe I should think about that.’ It trickles down to society.”
The Sweekar project also addresses HIV treatment and prevention. Many living with HIV in Nepal can only access a month’s supply of medication at a time. Nepal is small (56,956 square miles, roughly the size of Michigan), but it is mountainous, so traveling is arduous and timeconsuming, observed Wilson. “Every month, they have to travel for hours and then stand in a queue at a hospital and wait for their meds.” Wilson’s team is working with Nepal’s National Center for AIDS and STD Control to facilitate wider access to multi-month dispensation.
“On the prevention side, we’re hoping to implement HIV self-testing so patients can track their (and their partners’) status,” she said. “PrEP is still early in scale-up in Nepal. We need to start with the building blocks of getting and holding onto medications and getting access to testing.”
Social change
Nepal passed a law in 2007 to recognize those who identify as third gender, yet it hasn’t stimulated much change in societal attitudes. Most Nepalese live in multigenerational households and “being excommunicated from the family is traumatic. It’s a collectivist society with no social safety net,” explained Wilson. In Madhesh Province, where Wilson works, many trans women hide their identity to remain within their families; they present as men and have wives, and then travel to India and work as Hijra. “If they identify as third gender, they give up their rights to marriage, their rights to prior education, their rights to inheritance.” Wilson said, “This Fogarty grant gives us the opportunity to understand the stigmatizing attitudes that the general population in Nepal have—can we measure and change those?”
U.S. Embassy, Nepal
An attendee views photos at the Sweekar Photo Exhibit in Kathmandu, Nepal, which features snapshots taken by rural trans women from the Madhesh Province.
When overweight and undernourished live under one roof
Childhood obesity is at an all-time high in the U.S., a trend mirrored across Latin America. The Childhood Obesity Prevention Across Borders project, coordinated by Fogarty's Center for Global Health Studies, brings together researchers from the U.S. and Latin America working on interventions to reverse this trend. Participants shared their results and lessons learned at a recent meeting.
A presentation by Amanda Thompson, professor at University of North Carolina (UNC), Chapel Hill, focused on a pattern seen in roughly 85% of Ecuadorian homes, where a dual burden of being overweight (or obese) and micronutrient deficiencies exists. Examples would be overweight adults living alongside children suffering from undernutrition… or overweight individuals who are also anemic. Studies record a lot of zinc deficiencies as well as anemia in this group, said Thompson. “Ecuador also has high rates of stunting.” (Children are described as “stunted” when their height-for-age is more than two standard deviations below median WHO values.)
Thompson, an anthropologist who specializes in human biology, has worked in the Galapagos since 2014. Her studies dovetail with the Peru-based research of Peggy Bentley, professor emeritus at UNC’s Gillings School of Global Public Health. The two wanted to hear from others working in Ecuador, Peru, and the U.S. Supported by a Cross Borders conference grant, their plans for a live meeting were disrupted by COVID-19 and political unrest in the region, so they hosted a hybrid event with many researchers joining online.
Multiple causes
The dual burden of overweight and undernutrition, though most often seen in middle-income countries, cuts across all nations, whether low-, middle-, or high-income. “There are similar causes and different causes across those contexts,” said Thompson. Lack of access to resources due to inequality is an important consideration. “In Latin America, we tend to see this dual burden focused in rural, lower-income, and indigenous populations. In the U.S., we would see it among racialized minority groups more than other groups,” she said.
Poor diet also contributes to this health problem, though an insufficient diet may not look the same in
all places. Environmental factors are another concern. Minimal access to clean water can lead to diarrhea or recurrent infectious diseases in children, which may, in turn, cause undernutrition, explained Thompson. “In Galapagos, people who are concerned about their water quality are more likely to consume non-water beverages,” said Thompson. Similarly, in the U.S., those who perceive their water quality as poor are more likely to consume sugar-sweetened beverages.
Meanwhile, some low- and middle-income countries are experiencing a surge of socioeconomic growth. “In Galapagos, you have this rapid expansion of the tourism industry, so people have considerably more income than generations before them or families on the mainland,” said Thompson. Greater purchasing power often translates to buying unhealthy processed food. Sometimes rapid urbanization occurs without the necessary infrastructure, noted Thompson. “More people are living in a densely urban environment without improvements in sanitation systems or access to clean water.”
Fresh outcomes
How this dual burden affects childhood development remains “an open question,” said Thompson. A welcome consequence of the conference has been a general desire for more collaborations. Thompson said, “The group in Peru has been doing long-term interventions and we've done a lot of interventions in the U.S. So how can we take what we've learned to think about an intervention that either focuses solely on Ecuador or on both Peru and Ecuador?” A search for appropriate grant mechanisms led the researchers to consider Fogarty training programs. “We’re strongly interested in building capacity.” Meanwhile, Thompson’s group has begun a small pilot study around childhood feeding and household diets. “This formative work with families will help us see the barriers they face, and we’ll work with them to co-create some potential solutions.”
Photo courtesy of Amanda Thompson
People living in remote communities, like the Galapagos, often rely on food that is shipped in.
PROFILE
Empowering women and children from Nepal to the Amazon
Dr. Lisa Labita Woodson’s path to global health research began somewhat by accident. Initially she aspired to be a poet or an ecologist. Her journey took a dramatic turn after she joined the Peace Corps. Assigned as a science teacher to Nepal, she witnessed a tragic joint suicide of one of her students and their partner, which was due to an out-ofwedlock pregnancy. This experience compelled Woodson to seek mental health consultations and reproductive health education for her students.
She was eventually evacuated from Nepal due to civil unrest but went on to pursue a master’s degree in global health at the University of Arizona, where she later earned her PhD. Her experiences in Nepal ignited in her a passion that led her around the world. In Senegal, she studied the feasibility of using potato starch as a dietary supplement during humanitarian crises. In Thailand, she researched HIV/AIDS knowledge among the Hmong tribal community. Later, a Fulbright Fellowship brought her back to Nepal to focus on health messaging from schools to households.
These experiences paved the way for Woodson’s FulbrightFogarty Fellowship during her PhD work in Peru.
“I spent much of my career doing quantitative research, and I wanted to shift to qualitative research to learn something new. The Fulbright-Fogarty Fellowship was a great opportunity to expand my scope,” she added.
Beginning her project in 2022 in the Peruvian Amazon, she aimed to understand the impact of COVID-19 lockdowns on school dropout rates and adolescent pregnancy. Partnering with Mamás del Río, an initiative that works to reduce maternal and infant mortality in remote communities in the Peruvian Amazon led by her mentor and former Fogarty Global Health Fellow and Scholar, Dr. Magaly Blas, Woodson focused on promoting equitable and sustainable access to essential health care for rural communities in the region.
The first phase of Woodson’s project involved interviewing 41 individuals, including adolescents, and asking them, as part of the conversation, to draw their future aspirations. The drawings revealed compelling insights. Pregnant girls
Lisa Labita Woodson, MPH, PhD
Fulbright-Fogarty Fellow: 2022-2023
U.S. institution: University of Arizona
Foreign institution: Universidad Peruana Cayetano Heredia, Lima, Peru
Research topic: The effects of COVID-19 on adolescent pregnancy and educational attainment in the Amazon Basin
Current affiliation: Editor-In-Chief, Beyond Global Health; Principal investigator in sexual and reproductive health research, Mamás del Río
depicted occupations more traditionally held by women such as obstetricians, nurses, or teachers, while nonpregnant girls envisioned a broader range of careers including architect, engineer, and chef. Boys on the whole saw themselves in diverse roles, from doctors to tour guides, not limited to their Amazonian context. Interestingly, adolescents across all groups did not depict themselves as mothers or fathers. “The depth of information from those drawings was truly compelling,” Woodson reflected.
While Woodson and her team are hyper focused on the issues of reproductive education and health, the effects of climate change are simultaneously wreaking havoc on the communities they study, making the roadmap to intervention even more complex. During her time in the Amazon in 2023, Woodson was witness to the one of the most devastating droughts the Amazon has ever seen. This experience was pivotal in refocusing her efforts to understanding climate change as “[it] is affecting everything—women’s health, reproductive health, food security— and is not being gender neutral.”
Today, Woodson and her team distribute in the region informational booklets, tailored to adolescents, that include the data from her study as well as information about reproductive health and contraception. They’re also engaging community leaders and health workers to develop locally viable interventions. Despite the challenges of working in isolated Amazonian areas, she is determined to find effective solutions.
“If we’re moving forward in global health, we need to focus on empowering women, especially marginalized women,” Woodson emphasized. “Focusing on women will change the life trajectories of their children and ultimately make a huge difference.”
Photo courtesy Lisa Labita Woodson
Woodson (left) interviews a woman in the Peruvian Amazon as part of her work with Mamás del Río.
A&Q
AZEEZ BUTALI, PHD
Dr. Azeez Butali is a professor at the College of Dentistry, University of Iowa. After graduating as a dentist from the University of Lagos in 2000, he obtained a PhD in genetic epidemiology in 2010 and completed his postdoctoral training in craniofacial genetics at the University of Iowa. In 2014 he received an NIH Pathway to Independence Award from the National Institute of Dental and Craniofacial Research (NIDCR) to study nonsyndromic clefts in populations of African descent. Today he continues this research as principal investigator at the University of Iowa.
What led you to oral health research?
During my first dentistry internship at the General Hospital in Lagos, Nigeria, the first child I prepared for surgery had a cleft lip and palate. I became very close to that child and their family, which sparked my interest in the causes of cleft lip and palate. While considering my postgraduate studies, I discovered a program at the University of Dundee in Scotland, a WHO Collaborating Center for Congenital Anomalies in Oral Health, which aligned perfectly with my interests. There I focused on the contribution of maternal and environmental factors to cleft lip and palate. Shortly after I transitioned into my PhD, my mentor, Professor Peter Mossey, encouraged me to establish a similar research center in Africa. Recently I ran into that first child I treated for cleft lip and palate again in Nigeria. Now a young man, he expressed to me how happy he was that I had continued to dedicate my career to cleft research and told me about the impact that surgery had on his quality of life.
Tell us about the research centers in Nigeria.
As a PhD student, I set up eleven research centers across Nigeria to collect data and samples from individuals with cleft lip and palate. I trained clinicians to collect DNA samples for genetic analysis, with the plan to send these samples to the University of Iowa, where Professor Jeff Murray, a leading expert in cleft genetics, would analyze them for mutations that could potentially cause clef. I was later invited to Iowa as a visiting scholar where I discovered the first genetic variant for nonsyndromic clefting (a birth defect that occurs when the oral and nasal cavities don't fully divide but there are no other abnormalities) in an African population. During my postdoc, I worked on replicating findings from that first study where I focused on abnormalities in two genes, PAX7 and VAX1, both critical for the normal development of facial features in the early stages of human growth, and confirmed their involvement in clefting using samples from Asian and European populations.
Later, through funding from NIDCR, I expanded my research to Ghana and Ethiopia, allowing me and my colleagues to collect over 3,000 samples for the first genome-wide association study (GWAS) of cleft lip and palate in an African population.
How did you involve the community?
Following the expansion to Ghana and Ethiopia, we began to explore the ethical, legal, and social implications of our genomic studies. Interestingly, most patients wanted their results back, often intending to consult community leaders, religious figures, or others outside the health care system, which told us that we needed to engage with these community gatekeepers, providing them with the necessary education and training to support patients.
This is when we started to understand that many caregivers of children with cleft lip and palate experience significant mental health challenges. To better understand and address these caregivers’ needs, we employed a study design called PhotoVoice. Caregivers took photographs representing their experiences, which they then shared and discussed with us. This method yielded deep insights into their daily struggles and coping mechanisms.
What are the future directions of your research?
Currently we are preparing to share our data on incidental genomic findings, the readiness of health care providers to return genetic results, and the willingness of patients to receive these results. We also plan to publish our mental health study results to inform better support systems for caregivers.
We’re also organizing a photo exhibition in Lagos, as a part of the PhotoVoice project. We hope this exhibition fosters a deeper understanding of the experiences of caregivers of children with cleft lip and palate. We’re hopeful we can also create peer mentoring groups. By supporting caregivers and addressing their mental health needs, we can enhance the overall well-being of both caregivers and their children.
FOCUS
Global health research mentorship today
An important aspect of Fogarty’s mission is training the next generation of global health researchers. Senior researchers routinely work with trainees to help them acquire the skills, knowledge, and experience needed to conduct research that is aligned with the scientific goals of NIH and is relevant to the health priorities of collaborating institutions in low- and middleincome countries. Both teaching and mentoring are necessary aspects of the extensive education they provide.
There’s a difference between teaching and mentoring. The word “mentor” comes from a character in Homer’s Odyssey. Before leaving home to fight the Trojan War, King Odysseus asks his friend, Mentor, to teach and counsel his son, Telemachus, who will remain behind with his mother. While teachers provide instruction usually within a specific timeframe, mentoring is meant to be a longer-term, even life-long relationship.
To learn how mentoring works in the context of global health research, we asked nine accomplished investigators about their experiences. Many common themes emerged, including the bidirectional nature of these special relationships and the need for natural, open communication. Still, each interpreted mentorship in a unique way.
ANNETTE SOHN, MD, PHD
Vice president and director, TREAT Asia program (Therapeutics Research, Education, and AIDS Training in Asia), amfAR (The Foundation for AIDS Research)
Mentors have been incredibly catalytic at different decision nodes in my own life. I had an advisor during residency who had been an officer in the Epidemic Intelligence Service (EIS) program at the U.S. CDC. “You might want to look at it because you’re interested in global health,” he said, so I applied.
To me, a great mentor is someone who makes their mentees feel supported and respected, someone you remember for your lifetime. A mentor is someone without whom—had
we not had that conversation, had they not made that phone call on my behalf—I may not be here doing the work I'm doing now. I’ve had mentors with whom just one conversation lit up my brain. And then there are others who hold your hand along the path. A mentor is responsible for how knowledge that is learned is applied in the professional life of their mentee.
Everybody needs mentors, but the kind of mentors needed differs depending on the stage in our careers. And your relationship shifts over time, with mentees eventually becoming colleagues. How you grow with your mentor is a reflection of the strength of that relationship.
As a mentor, there are a few things that I regularly advise. One is that writing in scientific English is tough, another is that it’s always okay to ask for help. If I'm looking at a group of mentees who are supposed to interact as part of their training, I want them to figure out how to make those relationships as effective as possible. “You want other people to get the best out of you, and you want to get the best out of them.”
DON OPERARIO, PHD
Professor and chair, Department of Behavioral, Social, and Health Education Sciences, Emory University, Rollins School of Public Health
I was always interested in human behavior as it naturally occurs among people in their social, cultural, historical, political environments, and I was also interested in social psychology as a way to understand myself. I grew up in the 1980s and early 1990s, a transformative period in the history of public health as HIV evolved. My Fogarty project aims to promote HIV prevention and testing and is a collaboration with the University of the Philippines, Manila.
Rie Yotsu of Tulane University (standing, middle) reviews data with mentees. “When people approach me for mentorship, I take time to discuss their goals.”
Photo courtesy of Rie Yotsu
FOCUS ON MENTORING
Mentorship is one of the most important components of having a career… and not always easy to come by. It’s bidirectional, a true collaboration.
As a mentor, I must have awareness and sensitivity toward a mentee—their personal circumstance as well as geographic, cultural, economic, and social conditions that shape their professional development opportunities. I take my lead from mentees, while putting effort into learning about them and asking critical questions. My one mantra is: You have to find success on your own terms. Don't let other people—your mentors, advisors, institutions—define success for you. Also, mentorship doesn't have to be all consuming; a person can be a mentor in certain episodic or situational ways. Be open to finding mentors where you don't expect them. The older I get, the more I need mentors.
GABRIEL TRUEBA, DVM, PHD
Professor & director, Instituto de Microbiología, Universidad San Francisco de Quito, Ecuador
A great mentor is someone who changes you fundamentally, helps shape the way you see what making science is all about—how you approach conflicts, frustrations, or even successes that you have. Some of my professors completely changed the way I see all the underlying issues of the scientific work I do. I’ve remained friends with them.
It's important to understand the interests of the mentee. What is the main goal in their lives? When I mentor, I try to get them to understand the difficulty of becoming a PhD and a scientist. I also teach them about research ethics. The main difference when mentoring in the global health space (compared to other fields) is bioethics, working with human subjects. I spend a lot of time on bioethics—the respect you must have for the people involved in the studies and the responsibility of the data you're producing.
Mentees often don’t understand the amount of failure involved when doing experiments—that’s striking for many people. They always think that everything you do, you publish. That's not it. You have to do many trials until there is something that could be published. And then they are confronted by the response from journal editors, the response from reviewers—that is also shocking for some.
JAY GRAHAM, PHD, MBA, MPH
Associate professor in residence, environmental health sciences, and program director, Master of Public Health Program, University of California Berkeley
Some of my mentorships have lasted a long time—I still talk with my first MPH student from nearly fifteen years ago. Others I only hear from when they need a letter of recommendation. When I mentor someone, I always think, I could one day be working for them, so I try to create a level of respect.
I’ve had some awesome mentors. Dr. Joao Ferreira-Pinto, a behavioral health scientist, helped me think empathetically about other populations and focus on what I wanted with my life. When I got to Berkeley five years ago, we started a group called The Surf Club— just a random name. We were a bunch of junior faculty who’d meet and just talk, maybe problem solve, and sometimes invite speakers to come talk to us. Mentorship is about a network. You’re not going to get everything you need from one mentor, so you need to devise a group of people that you're pulling from.
Culture and context affect mentoring, so you need awareness. Maybe you come from a high-income country, they’re from a low- or middle-income country, and they feel the pay gap is unfair—which it is. Navigating those issues and being honest is important. You need to know your own weaknesses—what you’re not catching. What could I do to improve my mentoring? What would you have liked more of? I may not be as aware as I think I am.
RIE YOTSU, MIPH, DTM&H, PHD
Associate professor, Tulane School of Public Health & Tropical Medicine, Tulane University
At the beginning of my career, I was a general surgeon. I always thought of doing surgeries as having skills, while dermatology was more about knowledge. But having knowledge is also a skill, I realized over time. I have been fortunate to have different types of mentors at various stages of my career, each fitting perfectly that particular career stage. During my dermatology training, I had a great mentor who pushed me to complete my dermatology license,
FOCUS ON MENTORING
even though I was inclined towards global health. Having expertise in a specific field is crucial—I cannot imagine what path I would have taken without his guidance.
When people approach me for mentorship, I take time to discuss their goals. I look for three qualities. First, do they have respect? For example, if I wait in the Zoom meeting room but the mentee doesn’t show up, that's not showing respect. Without respect, it won’t work; I’ve tried but it doesn’t work. The second quality I look for is passion. Some medical students in the U.S. just want to have a global health project to put on their CV. That’s not enough. Third, I look for open communication. There was one student at Nagasaki University. Her English was poor, requiring me to edit almost all of her work initially, but she had these three qualities: respect, passion, and open communication. She's still working with me.
GRACE JOHN-STEWART, MD, PHD, MPH
Professor (epidemiology, medicine, pediatrics, & global health), University of Washington I went to medical school and really loved clinical medicine, loved seeing patients, and then I applied for an infectious diseases fellowship. My mentor at the time thought I should become involved in this HIV project and maybe get an MPH. Actually, I was a little reluctant! As part of the fellowship, I went to Kenya to do research. It really hit home how population health impacts your understanding of transmission and ways to prevent it. I ended up doing a PhD in epidemiology and now all my work is in population health and clinical research.
The mentorship I received had a profound impact on me. My primary mentor during my infectious disease fellowship, Dr. Joan Kreiss, was meticulous and detail-oriented and taught me how to build careful research and how to think about research. She saw something in me that I didn't see in myself; this was very valuable to me and encouraged me to choose this path.
How you're mentored affects how you mentor others. Mentoring is quite different than teaching in that you get to work one-on-one. You have to understand your mentees to help facilitate their vision of what their next step will be. You might bring some experience or some wisdom, but they bring new ideas, so it’s a catalytic and synergistic process.
I encourage my mentees to meet with me so we can form a closer relationship because nothing will happen without that. Some mentees are polite and don't want to
“waste time,” but mentorship only works when people feel comfortable coming and just brainstorming. Culture can affect the level of engagement.
CAREY FARQUHAR, MD, MPH
Professor (medicine, epidemiology) and acting chair, Department of Global Health, University of Washington When I did my fellowship in infectious diseases at the University of Washington, I had my first great research mentor, Dr. Grace John-Stewart. Grace was critical as a mentor and shaped the way I currently do my research. She insisted on rigor and, more importantly, inspired a love of science, of asking the questions that matter, and of figuring out how to ask the questions that matter. Grace was living in Kenya, and she built friendships and bonds with her Kenyan colleagues and encouraged me to always do the same.
I’ve also been fortunate to have career mentors, where I say, I’ve been offered this dean’s office position, should I take it? I tell my mentees: Get a whole bunch of mentors, because each will have a different perspective or meet different needs.
A mentor needs to believe in their mentees and care enough to prioritize their development and provide the time needed. Competence and commitment must be there, and also the ability to communicate in a way that is encouraging. Someone who’s about my age was just telling me that 40% of NIH grants had been funded when he started, and now it’s just 8%. Encouragement is needed now, more than ever. Mentoring others is a way that those of us who have worked hard and been fortunate can amplify our impact and bring along the next generation. By mentoring we can help carry the torch.
ILYA RASKIN, PHD
Distinguished Professor, Rutgers, The State University of New Jersey
Mentoring, particularly in the international arena, is a two-way street. It’s based on our ability to learn from and enrich each other and adapt to individual culture, traditions, beliefs. The mentor’s personality becomes very important. Role modeling becomes important. It’s long-term; you not
FOCUS
only care about your students passing an exam, you care about their whole professional lives.
As a mentor, you need to understand the culture and whom you’re mentoring. It’s very important, particularly in the developing world, to make mentees comfortable.
This educational hierarchy where professors are gurus is very powerful. So first, you need to behave as a human being. You need to talk about yourself and ask them about their family, ask them about their lives. This icebreaking takes much longer in other cultures than here in the U.S.
You also need to understand what has been done there scientifically, the publications coming from the country. The internet totally revolutionized how we work internationally. I remember when we were shipping journals to Eastern Europe, when it was still under the Soviet Union. Those people had no access. There was this enormous informational gap. That has been nearly erased; now you can listen to lectures from Harvard, Yale, and MIT online… for free!
Do I think everyone needs mentorship? Frankly that’s like asking, Does everyone need parents? We learn by example, even if it is subconscious.
Mentoring others is a way that those of us who have worked hard and been fortunate can amplify our impact and bring along the next generation. By mentoring we can help carry the torch.
CHARLES WOOD, PHD
Professor, Department of Interdisciplinary Oncology, LSU Health New Orleans
When I was at University of Miami, I met a Fogarty fellow, Dr. Ganapati Bhat, a pediatrician at the University of Zambia. We started talking about HIV and cancers, and he told me about the cases of Kaposi’s sarcomas he’d seen in children. This led to a collaboration in Africa in 1995. We wrote grants and were fortunate to receive funding from Fogarty and NCI—the first ever D43 HIV cancer research and training grant awarded.
When I was an undergraduate at the University of Kansas, a top scientist at Abbott Laboratories, the late Dr. Arthur Hirata, decided to join academia and I did my honors thesis project with him. We had lunch together every day and talked about science and life. He recommended me to the top lab in immunology at Columbia University and later for a postdoc in Switzerland with a top molecular biologist.
I believe mentorship is a one-to-one relationship. As a mentor, you have to have the mentee’s best interests in mind and they have to be able to come to you for anything, either personal or professional. When mentees first start working with me, I watch over them and design everything for them. In the end, I expect them to know so much that they become my mentors. I tell them, Only then will you really be ready to go out on your own. Learning is never finished—new technologies, computers, AI—we need mentoring in each area.
Four concentric circles show the systems of interaction between the mentor and mentee in this visualization from a 2019 supplement to the American Journal of Tropical Medicine and Hygiene.
First circle (at center)
MESOSYSTEM. Interpersonal interactions. Alignment of goals and objectives. Contains mentee and mentor.
MACROSYSTEM. Sociopolitical movements. Cultural factors: Hierarchy, Gender roles, Individualism, Uncertainty avoidance, Time perspective. National economy.
Fourth (outer) circle
SUPRA-MACROSYSTEM. Global politics, Global economy.
SOURCE: Image adapted from Figure 1 of the publication, “Conceptual Framework of Mentoring in Low- and Middle-Income Countries to Advance Global Health.” Courtesy Prasad et al.
DIRECTOR’S COLUMN
By Kathleen
Reflecting on My First 90 Days as Fogarty Director
It’s hard to believe that I’ve already passed the 90-day mark as director of the Fogarty International Center. These first three months have been demanding, humbling, energizing— and most of all inspiring. Every day, I see tangible evidence of the impact of our work and the dedication of our staff, partners, and trainees. I feel privileged to be part of this incredible community.
I want to take a moment to thank Dr. Peter Kilmarx for his exemplary leadership over the past year. His tenure as acting director didn’t just maintain operations: it expanded our networks and advanced and promoted Fogarty’s mission for collaboration. His expertise, experience and compassion have been key to my onboarding, and I am grateful for his past and current service to our mission.
I was told before I came onboard that Fogarty is a special place, and that has proven to be true. I’ve learned so much in these first few months, and this has only reinforced my commitment to supporting research in low- and middleincome countries (LMICs) and training the next generation of scientists around the globe. In my view, the Fogarty mission has never been more relevant, and global scientific partnerships have never been more important, than in today’s interconnected world. A diverse scientific work force and strong partnerships will be needed to combat the health challenges of our time and to ensure a resilient future.
Research Training Program) orientation. LAUNCH is our flagship program for predoctoral students (scholars) and postdoctoral fellows. At the event, I met the grant recipients and mentors that run the seven individual consortia that participate in the program as well as program alumni and new U.S. and LMIC trainees. The excitement was palpable!
A recurring theme I’ve noticed among everyone I’ve met—trainees, partners, and Fogarty staff—is the hard work and sacrifices they’ve made that have led to Fogarty’s success. This was especially evident during my visit to Kenya this August for the annual AFREHealth Symposium. AFREhealth is an interdisciplinary health professional group, supported by Fogarty/NIH, that seeks to improve the quality of health care in Africa through research, education and capacity building. At the University of Nairobi, I met with bright, energetic trainees. Their passion was contagious as they described projects spanning mental health, maternal-fetal health, and HIV and aging, among others.
While my time at Fogarty has already taken me around the world, I’m grateful that this move to NIH has allowed me to stay in my home state of Maryland. As Harriet Tubman, a great Marylander, once said, “Every great dream begins with a dreamer. Always remember, you have within you the strength, the patience, and the passion to reach for the stars to change the world.”
In July, I had the pleasure of participating in my first LAUNCH (Launching Future Leaders in Global Health
In these first few months, I’ve seen firsthand how Fogarty has changed the world, and I’m confident we will continue to do so.
Neuzil, Director, Fogarty International Center
Neuzil (second from right) attended her first LAUNCH program orientation this summer. Pictured from left are former and current fellows: Evelyn Hsieh, Valeria Navarro-Galarza and Carla Villanueva.
Fogarty International Center
HEALTH Briefs Global PEOPLE
Kallings, founding president of IAS, is mourned
Dr. Lars Olof Kallings, a pioneer in the global response to HIV, passed away on June 17th. Kallings founded the International AIDS Society in 1988 and served in key roles at WHO. His impactful career included leadership in infectious disease control and advisory roles for global AIDS initiatives.
Dhakal receives human rights award
Manisha Dhakal, executive director of Blue Diamond Society, Nepal’s first and largest LGBT rights organization, was awarded the Elizabeth Taylor Human Rights Biennial award at the 2024 International Aids Society meeting. The Blue Diamond Society has partnered on several Fogarty grants to reduce HIV stigma in Nepal.
Taylor named ASTMH president
Dr. Terrie E. Taylor of the University of Michigan, a longtime Fogarty Global Infectious Disease grant recipient, was named president-elect of the American Society of Tropical Medicine and Hygiene. Taylor has studied malaria for over 30 years and founded the Blantyre Malaria Project in Malawi.
Former Fogarty Fellow elected to NAS
Dr. June Kwon-Chung was elected to the National Academy of Sciences in April 2024 for her discoveries about both benign and disease-causing fungi. Kwon-Chung began her NIH career as a Fogarty International Fellow in 1966 and has studied diseasecausing fungi at the NIH intramural program for over 50 years.
IAS names new leadership team
The International AIDS Society (IAS) recently named Beatriz Grinsztejn from Brazil as IAS President and Kenneth Ngure from Kenya as President-Elect.
Grinsztejn, a leading infectious disease physician-researcher, cofounded FIOCRUZ HIV/AIDS Service, and has served as director of the HIV/AIDS Clinical Research Unit at FIOCRUZ for 25 years.
Ngure, a former Fogarty trainee from Kenya, is also an HIV prevention expert. He is co-lead on a randomized trial that evaluates how HIV self-testing might support PrEP delivery among men and women in Kenya.
Oropouche virus may cause stillbirths
Oropouche virus, which is transmitted by a pinhead-sized midge found throughout the Americas, may cause stillbirths and neurological defects in babies infected in the womb, reported the Brazilian health ministry. The Pan American Health Organization has asked other countries to watch for similar cases caused by the virus.
New test detects HIV strains in Africa
A multinational team led by Weill Cornell Medicine investigators developed a test to measure the persistence of HIV in people affected by viral strains found predominantly in Africa. Most HIV research has focused on strains circulating in Western countries. The study, published in Nature Communications, could help researchers achieve a globally applicable cure.
Chad eliminates threat of trypanosomiasis
Chad has eliminated the gambiense form of human African trypanosomiasis as a public health problem, according to the WHO. “Sleeping sickness” can cause confusion, sleep cycle disturbances or even coma, often leading to death. This is the first neglected tropical disease to be eliminated in Chad.
UNICEF, partners launch child health dashboard
Currently, 4.9 million children under 5 years old die every year; based on current trends, 59 countries will miss the UN’s Sustainable Development Goal target for under-5 deaths. An updated global dashboard will shed light on various issues to help policymakers track progress on critical factors influencing children’s health.
Trial confirms efficacy of twice-yearly PrEP Lenacapavir, a long-acting HIV pre-exposure prophylaxis (PrEP), was found safe and 100% effective among cisgender women in Uganda and South Africa in a Phase 3 clinical trial, according to the National Institute of Allergy and Infectious Diseases. Lenacapavir, developed by Gilead Sciences, Inc., is administered by injection every six months.
Writer/editor: Mariah Felipe Mariah.Felipe@nih.gov
Writer/editor: Susan Scutti Susan.Scutti@nih.gov
Digital communications specialist: Merrijoy Vicente Merrijoy.Vicente@nih.gov
Designer: Carla Conway
In rare cases when a correction is needed after an issue’s printed version has been finalized, the change will be made and explained in the online version of the article.
All text produced in Global Health Matters is in the public domain and may be reprinted. Please credit Fogarty International Center. Images must be cleared for use with the individual source, as indicated.
Dec 9, 2024
Fogarty to host meeting on humanitarian health & climate change
Are you a researcher studying health in humanitarian crises? Interested in how that intersects with climate change? Fogarty, Canada's International Development Research Center, and Elrha are collaborating to convene the second Global Forum on Humanitarian Health Research: GFH2R 2025.
GFH2R 2025 will include a series of public webinars starting in August 2024 and an in-person meeting in May 2025 in Nairobi, Kenya. The Forum seeks to bring researchers and humanitarian organizations (including NGOs, local policymakers, and international agencies) together to share experiences and promote collaboration around health research in humanitarian settings. The theme for GFH2R 2025 is Health Research at the Nexus of Humanitarian Crises and Climate Change.
The May 2025 meeting will be built around case study presentations by researchers from regions of the world affected by humanitarian crises. The Forum prioritizes the participation of researchers from low- and middle-income countries (LMICs), encourages networking and mentoring, and creates a venue for open and inclusive discussions.
Information on how to apply to attend the May 2025 meeting can be found online at: go.nih.gov/GFH2R
Families and Businesses in Delaware Share a Common Challenge: Child Care
Michael J. Quaranta President, Delaware State Chamber of Commerce
It’s long been an issue for working parents who struggle with finding access to the affordable and quality child care that enables them to participate in the workforce. So, let me share some data with you.
Families in Delaware pay an average of 20 percent of their median household income on one child’s care per year.1 And yet, one study estimates that 25% of people in Delaware live in a child care desert. The total licensed capacity across Delaware—the number of children providers have space for—is 53,640. This falls short of the estimated number of children aged zero to nine in Delaware, 109,075.2
You’ve heard the phrase “the numbers don’t lie.” Delaware’s child care issues cannot be overlooked. The supply cannot meet the demand. The numbers don’t work.
The struggle for employees to find child care is a top concern in the business community. According to a national U.S. Chamber Foundation study, absences and employee turnover cost employers anywhere from $400 million to $3 billion a year.3 More and more employers are recognizing child care is not just a social issue, it’s a workforce barrier.
The issue of affordability also stands out. Here in Delaware, families pay an average of $11,000 in child care per child per year.4 A 2023 survey by the First State Pre-K Coalition found that most parents indicated that child care is their biggest monthly expense, with more than 30% saying that it costs more than their mortgage payments or rent.5
And just as thousands of low-income Delawareans receive state assistance to afford housing, food, utilities, health care, and more, many families and providers rely on a state subsidy for child care tuition. But the state’s eligibility threshold is incredibly narrow compared to national rates. A family of four would need to make no more than $60,000 a year to qualify for publicly funded child care.6 If Delaware adopted neighboring states’ policies, many more families could access child care.
Recently, some employers reported that some of their lower paid employees, when faced with promotion opportunities and the potential for higher income, refuse the promotions and better wages because that raise will make them ineligible for some of the state services they have used to cover household or family expenses. This reaction is quite logical. If you make $35,000 a year and were offered a $6,000 raise to $41,000, you might lose some of the state subsidies you had relied upon before and now must finance yourself because you are financially ineligible for further benefits. Welcome to the benefits cliff.
And as Delaware continues to age—in 2019 the share of Delaware’s population aged 55 or older was 32%; in 2023 it was 37%7—we could have a serious labor shortage in high-need industries like healthcare. Health-related occupations are projected to grow faster than all other occupations in Delaware through 2032,8 yet these workers simply won’t be there if they don’t have child care. Far too many working middle-class families are stuck between a rock and a hard place in Delaware—unable to afford quality care, but earning
too much salary to qualify for state help. Families suffer, schools suffer, and business suffers.
Families face tough choices. Providers are struggling to survive. Our state’s youngest citizens are caught in the middle.
So, the question is, “how do we fix the system?”
We must first recognize that child care is a valuable and integral component of a strong and vibrant economy. Child care is important to recruiting and retaining a competitive workforce. And decades of research show that high-quality early learning experiences can generate huge returns on investment for Delaware’s economy.
We at the Delaware State Chamber of Commerce have been engaged in discussions that could lead to the reimagining of child care in the First State. In 2022, we released a report with partners that summarizes what we’ve heard from business and community leaders up and down the state, through focus groups and survey responses.1 With the proper knowledge and resources, we can lead in solutions to meet the needs of our workforce, today and tomorrow. This challenge in front of us is one we can solve. Together, we can make a difference.
Mr. Quaranta may be contacted at mquaranta@dscc.com .
REFERENCES
1. Federal Reserve Bank of Philadelphia. (2022). Child care is everyone’s business. Why Delaware businesses should care about early childhood education. Retrieved from https://www.philadelphiafed.org/-/media/frbp/assets/communitydevelopment/reports/delawaretoolkit_hi-2_final.pdf
2. ChildCare Aware. (n.d.). Delaware child care supply by legislative district: 8 September 2024. Retrieved from https://ccaoa.maps. arcgis.com/apps/dashboards/4568932af0bf468881a77405be6d7ea7
3. Ferguson, S. (2024, Jun 26). Understanding America’s labor shortage: The impact of scarce and costly childcare. U.S. Chamber of Commerce. https://www.uschamber.com/workforce/ understanding-americas-labor-shortage-the-scarce-and-costlychildcare-issue
4. Tootris. (n.d.). Average cost of child care in Delaware. Retrieved from https://tootris.com/edu/blog/parents/cost-of-child-care-in-delaware-abreakdown-for-2023/
5. First State Pre-K. (2023, Feb). Delaware family survey results. Retrieved from https://rodelde.org/wp-content/uploads/2023/01/2023Parent-Survey-Results-Draft.pdf
6. Delaware Department of Health and Social Services. (n.d.). Child care services. Retrieved from https://dhss.delaware.gov/dss/childcr.html
7. Ipums, U. S. A. (n.d.). U.S. census data for social, economic, and health research. Retrieved from https://usa.ipums.org/usa/
8. Delaware Department of Labor. (n.d.). Projections. Retrieved from https://lmi.delaware.gov/Projections/
The Delaware Healthcare Association Presents:
The 28th Annual Delaware Healthcare Forum on Tuesday, October 29, 2024, 8:30 AM To 4:30 PM At Bally’s Dover Casino Resort, Dover, Delaware
The Delaware Healthcare Forum is the only event attended by all of Delaware’s hospitals and health systems, from CEOs to department managers.
Sponsor Opportunities:
You don’t want to miss this opportunity to showcase your products and services to decision-makers in the healthcare industry. Sponsor participation, over the years, has been greatly appreciated, both by us and by the forum attendees. We are sure you, too, will benefit from the exposure your company receives through these events. With your sponsorship, the Delaware Healthcare Association can provide healthcare education at a reasonable cost.
Registrations:
Registrations for some members are being coordinated by one staff person – please send your registration information to the designated person as follows:
Beebe Healthcare – Becky Roberts (reroberts@beebehealthcare.org).
TidalHealth Nanticoke – Kim Mitchell (Kim.mitchell@Tidalhealth.org) Nemours Children's Health - Doreen Albert (Doreen.albert@Nemours.org).
Employees of all other organizations not listed above should register individually in accordance with their customary internal processes for attending educational events.
ACHE Education Credits
The Forum offers Continuing Education Credits to attendees:
Bayhealth - Nursing Contact Hours
Bayhealth is approved as a provider of Nursing Continuing Professional Development by the Maryland Nurses Association, an accredited approver by The American Nurses Credentialing Center’s Commission on Accreditation. (MNA#4003178).
Register online at https://deha.org/Resources/Forms/Annual-Delaware-Healthcare-Forum-Registration
Our Partners:
Providers:
Navigating Life: Delaware Families Experiencing Homelessness with Young Children
Annette Pic, Ph.D.
Delaware Institute for Excellence in Early Childhood, University of Delaware
ABSTRACT
Objective: This study explored the lived experience of Delaware families residing in homeless shelters and motels with young children. We focused on their daily experiences to gain understanding about their day-to-day living to foster understanding about optimal supports that can facilitate more permanent housing arrangements. Methods: We used qualitative approaches to obtain descriptions about the daily lives of families experiencing homelessness with young children. Semi-structured interviews were conducted between November 2022 and February 2023. This study analyzes data from three families using open and thematic coding methods. Results: Families experiencing homelessness with young children discussed their struggle to locate housing, attend to day-to-day tasks, and maintain and obtain employment. Having access to conveniently located affordable and available child care and reliable transportation were discussed across the themes. Conclusions: Evidence building through gathering pertinent qualitative information is a critical step toward understanding the needs of families experiencing homeless. Findings from this study can inform state-level policy and state and non-profit agencies’ practices.
Policy Implications: Current policies that support family homelessness could be adjusted to better address connecting families to resources (e.g., direct connection to landlords), transportation (e.g., increasing allotted bus passes, providing a “free” monthly bus pass), and child care (e.g., co-located care – shelter plus child care, funding enrollment slots left “open” specifically for families experiencing homelessness).
ACKNOWLEDGEMENTS
We (the authors) would like to express our deepest appreciation and gratitude to the families who shared their experiences and trusted us with their story. A special thank you to the community partners who helped foster connections to families experiencing homelessness. We would also like to thank Dr. Grace Whitney for her expertise and review of this work. No funding was received for this work.
INTRODUCTION
Family homelessness is a traumatic experience that significantly impacts the health and well-being of caregivers and children.1 Yet U.S. housing policies primarily focus on single adults. Families with children compromise roughly 30% of the U.S. homeless population with an average size of 3.2 people for sheltered families.2 This does not include families staying in rapid rehousing programs, permanent supportive housing programs, and unsheltered families that may be difficult to identify, like those sleeping in backyards or vehicles used for transportation. The 2024 Delaware Point-In-Time Count reported 19% of Delaware households experiencing homelessness were households with children under 18. Shockingly, children under 18 accounted for the largest age group experiencing homelessness (26%) followed by people ages 35-44 (17.6%).3 Additionally, between 10/2/22 and 9/30/23, data in Delaware’s Community Management and Information System (CMIS) indicated that 16% of those tracked were children under the age of five.4 The CMIS data included anyone who was enrolled in a street outreach,
National data finds families experiencing homeless with children are more likely to be female-headed with children under the age of six.1 Family and child age level data specific to Delaware are not available at this time. Americans experiencing homelessness who identify as Black or African American account for almost 40% of the homeless population; a rate disproportionate to the national population.2 The disproportionality is a product of past and current racial inequities in housing, education, and healthcare constructed to protect the status quo of White Americans.5,6 The homeless population in Delaware is also disproportionately minority families. Black or African American residents account for 22% of the state’s population but comprise 59% of the people experiencing homelessness.3
Understanding these families’ experiences is vital to creating and implementing policies that provide actionable and necessary support to promote family stability, health and wellbeing. Conversing with families to understand their needs and desires is imperative for the process, and can yield a wealth of knowledge from a small number of people. This study gives rise to the voices of Delaware families experiencing homelessness through documenting day-to-day experiences of living in homeless shelters and motels with young children.
Housing stability is associated with better health outcomes for adults and children such as improved mental health and decreased delays in seeing a doctor.7 Stable housing also provides a foundation for participating in the economic and social
life of a community. Locating housing can be challenging for under resourced families like those experiencing homelessness. Families experiencing homelessness encounter stressors at higher rates than their low income housed peers – including multiple moves, neighborhood dislocation,8,9 lack of food preparation areas,10 and unpredictable daily life.11 Co-occurring stressors negatively affect health and wellbeing12 and disrupts early childhood development13 affecting physical, emotional, and social development.14 Stressors also inhibit family functioning altering time spent together and parenting practices.11,15,16
Early childhood is a critical developmental period that affects future health and education outcomes. Adverse experiences, such as homelessness, negatively affect child development while supportive and stable environments offer protective factors that foster optimal developmental outcomes.17 The chaotic nature of homelessness does not support day-to-day stability. Likewise, shelters and motels often lack safe floor space for children to play and learn to crawl, and frequently do not have separate sleeping areas for children.18
Parenting can be stressful under the best circumstances; parenting while experiencing the loss of permanent housing -creates additional stress. The sudden loss of permanent housing removes people from their community, support networks, friends, family, and the majority of their possessions often leaving them with a diminished sense of security.18 Parents report the experience of parenting while homeless makes them feel judged and viewed as incompetent.19 They describe a phenomenon referred to as public parenting where they feel added pressure and stress to change their style of parenting to adapt to the loss of privacy and autonomy experienced in sheltered living.10 These experiences impact parental mental health and self-efficacy. In turn, parental mental health affects family relationships and child development.1
We explore the experiences of families living in homeless shelters and motels with children age eight and younger and draw on in depth interviews to answer the question: What are the experiences of families experiencing homelessness with young children?
METHODS
Data were collected as part of a larger study that explored the use of early care and education services (child care, early intervention, child care subsidy) among families experiencing homelessness with young children in New Castle, Kent, and Sussex Counties.20 Homelessness was defined according to the McKinny-Vento Homeless Assistance Act.21
The larger study employed semi structured interviews and an inperson survey conducted at the conclusion of the interview. Ten families participated in the study. Participants received a $25 gift card and a daily bus pass. Interview recordings were transcribed verbatim. University Institutional Review Board (IRB) approval was received prior to data collection and necessary procedures were followed to protect human subjects, confidentiality of data, and consent procedures, as outlined by the Ethical Principles of Psychologists and Code of Conduct.22 Participants were assigned a pseudonym to protect the participants’ identity.
This study is an in-depth exploration of larger study data that primarily resulted from the interview question, “I understand that you are experiencing a lack of stable housing for you and your family. During this time, what do you consider your greatest
need?” and two follow up probes, “How would addressing (your greatest need) help you and your child?” and “How do you feel you could obtain (your greatest need)?”
Three participant interview transcripts were selected to represent mothers’ and fathers’ experiences, rural and urban locations, and residing in motels and shelters. The transcripts were imported into Dedoose qualitative coding software23 and coded using open and thematic coding to gain understanding about families’ daily lived experiences. Three themes emerged 1) locating housing; 2) navigating day-to-day life; and 3) maintaining and obtaining employment. Table 1 describes the codebook.
To increase reliability of study findings, analytic memos drafted during initial data collection were used during this analysis to support data interpretation.24,25 To maintain trustworthiness and credibility, and decrease researcher bias, the coding and analysis for this study includes triangulation and construction of a detailed code book. An audit trail was maintained to reduce research bias and increase transferability.24,26
Table 1. Coding themes and descriptions Code Definition
Locating housing Experiences with locating stable housing such as downpayment, child care, availability
Daily life (day-to-day life) Experiences with daily life tasks and responsibilities such as work, child rearing, meal preparation
Maintaining and obtaining employment Experiences with maintaining employment and/or obtaining employment such as transportation, child care, or searching for work
Sample
The unit of analysis was the family.27 Family was defined as at least one adult 18 years of age or older caring for one or more child(ren) while experiencing homelessness. Specific details about the participant and their family are provided below. The primary language spoken by the three participants and their family members was English. This was the first experience of homelessness for each family. The duration of their homelessness experience at the time of their interview ranged from five to eighteen months
Participant 1 (“Aaliya”), is a single mother of three children ages 4 months, 2 years, and 3 years. She is 19 years of age and self identifies as Black. She resides in a motel due to a domestic violence situation. For safety reasons, Aaliya and her children had recently moved to a different motel. The move required her to shift her work location so that she could walk to work because she could no longer maintain her car. Aaliya works two service industry jobs to pay the $72 nightly motel fee. The motel fee was previously covered by the COVID hotel motel voucher program funded Delaware Department of Health and Social Services. Her older two children were enrolled in child care before and at the start of their first hotel stay. As a result of the move, the distance to the child care program was too far because she was reliant on public bus service with limited service. Aaliya now relies on a disabled family member and the children’s fathers’ family to provide child care while she works. Most days, the children receive care separately by different family members.
Participant 2 (“Shaunae”), is a single, divorced mother of two children ages 11 months and 8 years. She is 34 years of age and self identifies as Black. She resides with her children in a homeless shelter due to a domestic violence situation. She was employed as a warehouse worker when she and her children began residing at the shelter. Her abrupt move to shelter resulted in the loss of child care that was provided by a family member who resided at the residence she left. She was subsequently terminated from her employment due to the inability to maintain consistent child care. She has her own car. Each weekday morning she drives her older child to school from the shelter.
Participant 3 (“Jamel”), is a father of four; two biological children ages 22 months, 3 years and two “adopted” children ages 6 years and 7 years. He resides in a shelter with his partner and their four children. Jamel is 28 years of age and self identifies as Black. He and his partner were laid off during the COVID-19 pandemic. Shortly thereafter they lost their housing and moved into the home of a family member. They also lost this housing arrangement when the family member suddenly passed away. Prior to arriving at the homeless shelter, they lived in two different motels funded by the Delaware DHSS. He is currently employed as a warehouse worker and his partner works in housekeeping at a hotel. They rely on public transportation. His partner was present at the interview and she responded to some of the questions and added details to the experience shared by Jamel.
FINDINGS
The three main themes that emerged from data are discussed below. Although each theme is discussed separately, they are interdependent. For example, taking time to locate housing takes time away from managing daily life and working to save money takes time away from locating housing.
The Reality of Locating Housing
Locating stable and permanent housing was the top priority and most pressing need for all three families. Each family struggled to locate housing even though they felt they were taking the necessary steps to pay for housing or qualify for subsidies (finding employment, establishing a bank account, fixing their credit score). The conversation about housing became overwhelming at times for the families, but they choose to continue to share their stories.
Families expressed feeling constant pressure to obtain housing quickly while simultaneously managing their daily lives and ensuring the health and safety of their children. They shared their frustration with not being able to locate housing which they attributed to a lack of effective resources and the lack of time.
Families expressed feeling overwhelmed, frustrated and confused because even though they followed the steps needed to prepare, they still could not locate housing. Jamel shared, “We open up a bank account. Then they told us um, try to fix our credit score and we did that.”
Aaliya and Jamel spoke about saving money and opening back accounts for the downpayment and proof of income required by landlords. To save as much money as possible, Aaliya shared that she pulls a lot of double shifts and will go back for second shift on the same day. She explained that she does this because,
“when you try to get a house or apartment, they gonna look at them paystubs and how much you got.”
Families felt the root of the problem (not finding housing) was the lack of effective resources (e.g., case manager to help fill out housing applications) and adequate information (e.g., list of landlords who accept vouchers). Aaliya commented. “Delaware barely has any resources…because finding housing is very, very, what do you call it? Difficult. So, like I say, like resources that actually help.” Aaliya also felt resources should include both mental health services, “I have anxiety so like mental health, or like ah just like a counselor, or (pause) yeah somebody keep me like motivated, like don’t give up you got it type of thing” and child care in concert with supportive housing, “I wish like some child care…support sheltering because you have kids. Cause now a days, especially in Delaware you cannot be like homeless with kids.”
Jamel expressed the need for hands-on support and more specific guidance,
“They (housing staff) should be callin’ landlords for us…they should be knowin’ landlords…this is our first time rentn’. We don’t know nothin’ about this. This is like dropping us in no man’s land and tryin’ make us figure out…Like I got scammed already twice.”
He also shared, “(I spoke to) plenty of landlords and they say it sound like you got your head on straight. I would love to take a chance with you but to be honest with you, I got better candidates then you.”
The need for available, affordable, and accessible child care was mentioned as a necessary for locating housing and providing daily stability. According to Jamel,
“If we have somebody to take these kids (child care) and us to really handle business like say if we want to go out and look for a house…Not even enough time to really even look for housing cause we do that like on the fly. Like we on the bus like we lookin’ for a house while we got time…if it’s Saturday or Sunday when one of us is off we are lookin’ for housing. We don’t really have time to do what you really want to do or what you be able to do if you already was stable (housed).”
Families shared that their inability to locate housing after completing the required steps took an emotional toll on them. They expressed feelings of frustration, disbelief, guilt, and a loss of faith with the process. Shaunae shared,
“I’ve been on my own for 11 years…I maintained for 10 years of my life…We didn’t have this problem… We had a roof over our head…They (shelter staff) say that they have resources to help us along the way. I don’t know what type of resources that they offer. How can I put this, they’ve offered me resources that I, there’s stipulation that I have failed… So, I’m just a little confused… If it wasn’t for them (her two children), I feel like I don’t have a purpose…I have just so many emotions, so many mental like, but I’m okay. I’m mentally sane, trust me. I pray.”
Jamel expressed,
“If getting a house was that easy, you’d see a lot of people leave out fast (no longer homeless)…It’s a lot and it’s been very hard to be honest with you, very hard because if you don’t meet the requirements that they want you to do you’ll be homeless again. Then we’ll be starting over. I mean she would lose her job. I would lose my job and we’ll be homeless again and the kids wouldn’t be in school so then that mean most likely the kids will be taken from us. So, we don’t want none of that to happening you know. It’s just you gotta keep a good head and do what you supposed to do. They say believe in God, that’s what we do.”
The Reality of Managing Daily Life
Managing day-to-day life without permanent housing, reliable transportation, and child care was complex for these families. Families described the experience of completing day-to-day tasks while being homeless. In the words of Jamel, “it’s really a learning process…If you’s already stable, then you have, you would know how your day would go. You get what I’m saying, we’d plan it out already. This is like everything is like on the fly.” Similarly, Shaunae stated it’s “a whole new ballgame…I am just figuring out and relearning because now I’m at the bottom.”
Day-to-day tasks were difficult to manage with the persistent fear of being on the streets with their children. Families shared how the daily stress to secure/safeguard their nighttime sleeping arrangement was extremely difficult. The fear of not having a place to sleep weighed heavily on them. All three expressed fear of losing their children if they did not maintain a roof over their heads, “DFS will take your children from you in a heartbeat. They do not play around” (Aaliya). Jamel shared their experience about accepting a roof, any roof, over their head. He described in detail his families experience with two motels,
“I asked them…can we move, cause where we was livin’ (first motel) was like…when I say drug infested I’m meaning like people doing “duz” right outside the door it just wasn’t a good place at all for the kids to be raised…my kids saw people who die…We comin’ outside early in the morning to take them to school and there’s a person that OD, overdosed outside right in front of the door… It was like a no choice. We didn’t have no choice…First day we got in there (second motel), bed bugs literally crawling. We stayed up the whole - when I say we stayed up the whole night, we couldn’t sit down, we were standing up like the whole entire night. 24-hours we stayed up even the kids, like couldn’t let them stay down, sleep nowhere…but they did get us out that room the next morning, got us to a way better room that didn’t have bed bugs and then we slept a little bit better.”
Families discussed attending to daily activities such as getting themselves ready for work, helping their children get ready for school (washing their face and ensuring they brush their teeth), taking care of sick children, eating meals together,
and taking public transportation or walking to work, stores, and the bank. Jamel expressed his frustration with being reliant on the public bus for all their day-to-day activities, “Transportation, that’s the key. It’s key to people who is homeless or don’t have a car…Every time I get the bus I gotta pay. I gotta do multiple busses like two busses going there (work) and two busses going back…$8 to $10 every day.” Aliya shared a similar sentiment about traveling between work, child care, and the motel, “I don’t have transportation…be far to get there-there-there and in the bus. Buses don’t run in (name of neighboring town). They run like here or (name of another town), like highways type of thing.”
Mealtime, a main day-to-day activity was discussed at several points during the interviews. Families expressed the desire to have a place to prepare and share meals. Aaliya expressed, “I don’t want to be in a hotel anymore or even a shelter…so she (daughter) can have her own room you know and I could finally cook a meal.” The absence of food preparation and storage areas evoked emotional stress and the desire for the past. Shaunae shared,
“My daughter she’s havin’ me feeling real bad cause she said, ‘Mama I want breakfast, I want French toast and eggs, scrambled eggs’, and I’m like okay, um let me order it from a diner, and she’s like ‘no, I don’t want it from a diner, I want your cookin’. I want your home cookin’’. It’s one of those ahh moments. You know like, I know I need to get it together but, ohh no, (breaks down in tears -pauses- resumes talking through tears). Now those are moments that I have that I’m like how did I get here? I’m just wrapped up with all types of different emotions, feelings, everything, you know, it’s just a big old difference for me.”
Mealtime was also talked about as family bonding time. Jamel and his partner described how they located places to share meals together as a family by watching out the bus window as they travel to and from work,
“We took ‘em to dinner…and we sat down and ate dinner. Showin’ ‘em that we love ‘em, and we can spend our time occupied on what they want us to do for them…We only know the (restaurant name) because it’s on our work route. So now we know when to get to like, sit down, and eat pizza and have a family dinner.”
Families expressed that managing daily life was overwhelming and short on time without access to child care and child care subsidy (Purchase of Care, POC). Shaunae shared, “(Child care) would be real nice cause…I can’t leave my kids nowhere. I got to take them everywhere I go.” Aaliya mentioned how she cobbles together child care to work her two jobs that require her to work various shifts. Due to the lack of transportation and child care hours of operation she no longer uses center-based care. Therefore, she cannot receive POC and now pays out-ofpocket for care, “They’re not in daycare so Purchase of Care isn’t paying…I give (relative’s name) like a few dollars…here and there…whatever I can just like (a) thank you, you know.”
The Reality of Maintaining and Obtaining Employment
Families in this study were working or had recently worked. Maintaining and obtaining employment was fostered by key supports like child care and reliable transportation. However, families identified housing as the most important factor for employment because it provided stability and predictability. Jamel shared, “If we had a stable home…A lot of stuff is not stable enough (without housing) so if daycare call us…you gotta pick ‘em up or anything like that, we can’t leave work…We gonna get fired from the jobs that we have.
Aaliya and Jamel and his partner work between 5 and 7 days per week. Shaunae had employment when she entered the shelter but due to a domestic violence situation, her local child care arrangement was no longer an option. She began driving to a relative’s home in a neighboring state in order to maintain her employment, “I would go all the way out that way, that’s what I was doin’ when I was working…I was driving all the way to (name of town) and then coming all the way back here to come to work…I was doing a lot of drivin’…you know oil changes every two months instead of every 4 months.” Currently to provide income for her and her children, Shaunae mentioned she works on the weekends doing hair for friends and family. She sets up three appointments and is able to bring the children with her. She stated that she uses the money to “get by” until she finds a job.
Child care was also mentioned as a key support for obtaining and maintaining their employment, “I came here with a job… now I’m not working ‘cause I can’t get daycare for her right now” (Shaunae). Jamel expressed that child care would make their lives easier,
“It will be way much easier if we can have all of them…two gone (referring to child care for the two youngest children) and them two (two oldest children) in an afterschool program. And we would work longer…basically it’s that like one hour that one hour missing right there that one of us need to be here.”
Shaunae’s process of locating new employment was inhibited by her POC denial,
“They denied me. I have to go up there after I’m done with you to see exactly why. Like I said, that’s what makes me feel like I’m on Candid Camera. If you all sendin’ my literature to the (shelter), why did I get denied? Cause the first reason why I was eligible, makes me eligible is that I’m in a homeless shelter.”
To maintain employment without child care, Jamel and his partner coordinated their schedules. Without an understanding manager, the arrangement would likely be insufficient.
“I have to tell my uh manager that I’m gonna be little be late because… She get off when I supposed to go to work... I don’t get to arrive until 5:30 or 5 o’clock…She get off at 5. I supposed to be at work at 4:30 already… the (two older) kids don’t get off the bus until 4:20 so I’m already late right there just from them two…and they really get out at what I think 3:30 but they the last kids on the bus.”
DISCUSSION
Families shared details of their lives revealing their experiences regarding locating housing, navigating day-to-day life, and maintaining and obtaining employment. Families conveyed their lived experience clearly. They were acutely aware of their needs and identified support that would help them obtain housing. Families articulated that stable housing was their number one need. Stable housing was perceived as the main resource that would have a positive effect on every aspect of their lives and the lives of the children by providing stability and reducing their daily stress. Over time, chronic stress negatively affects the nervous, cardiovascular, endocrine, and immune system.12
Families described experiencing compounding stressful situations like substandard housing conditions that impact health and emotional wellbeing such as bed bugs28 and living in high stress environments.17 Families recognized their housing situation directly affected their mental health and suggested supportive services should include mental health counseling. They also identified transportation and child care as a support and a barrier to these three aspects of their lives.
Locating housing for these families went beyond searching for an available apartment or home to rent. Families stated that locating housing meant they needed to have employment, obtain a voucher, open a bank account, clean-up their credit score, save money for a downpayment, find a landlord willing to rent to them, and ensure the location had access to transportation and was located in a safe environment to raise their children. This process was described as stressful and difficult to manage while working and caring for the needs of their children.
An approach to reducing some of the stress experienced during the process of locating housing, is to connect families experiencing homelessness with landlords who accept vouchers and have availability. However, the Delaware affordable housing market is tight, likely making the process challenging for these families even with connections to landlords. Thinking creatively about ways to encourage landlords to accept vouchers and builders to convert existing dwellings or incorporate more units into affordable housing is necessary. Steps to increase the number of landlords accepting vouches could entail providing incentives such as assistance with building repairs or assuring them that families will receive ongoing services to enhance stability (e.g. financial counseling, enrollment in Head Start). Conversations about housing systems and supports are currently occurring across Delaware; these conversations should include hearing directly from families experiencing homelessness.
The experience of homelessness undermines parents’ ability to protect their children leaving them feeling guilty.29 However, positive parenting can support resilience among children experiencing homelessness.30 Mealtime was conveyed as positive family time and a guilt inducing interaction. Parents described scouting out and memorizing restaurants on bus routes as they traveled to and from work. The additional effort to create family mealtime opportunities was intentional to create space and time to build relationships with their children and spend time together as a family. Conversely, the lack of personal space and a kitchen to prepare homecooked meals requested by their children injected stress and negative feelings about their parenting into mealtimes. Supporting families’ ability to eat together fosters the opportunity for positive parenting and reducing parental stress.
Families expressed that obtaining child care was a key pressing need to locate housing, complete day-to-day activities, and obtain and maintain employment. Child care programs allow parents with young children to work and promote early childhood development.31 Enrollment in child care programs offer protective factors against the risks of homelessness by providing stable and enriching early care environments.
Child care in conjunction with subsidy facilitates access to affordable, high-quality child care. Programs such as Early Head Start and Head Start prioritize enrollment for families experiencing homelessness and reduce barriers to enrollment (e.g., longer time periods for immunization record submission), yet we know that families experiencing homeless are less like to engage in such programs.32 Providing families experiencing homelessness with low barrier access to highquality early care and education services such as child care and child care subsidy can help provide stability and foster optimal early childhood development.
An identified child care barrier in this work is the denial of POC while residing in shelter. In Delaware, families experiencing homelessness are given presumptive eligibility for 90 days. Denial of POC for a family experiencing homelessness warrants further inquiry into the implementation of the POC policy and how families interpret housing questions on the POC application. The denial of POC for this family experiencing homelessness in Delaware was not unique. Prior work found several instances of POC denial while living in shelter.20
Family homelessness is complex and multifactored; reducing barriers to early care and educations services is not sufficient. Additional consideration must be given to housing programs and Delaware’s Child Care Resource and Referral (CCR&R) agency connecting families directly to accessible, affordable, and available child care. In 2020, a summary report on early learning opportunities for young Delaware children experiencing homelessness was submitted to the Delaware Department of Education.33 The report details the strong interest in Delaware to increase enrollment and participation of children experiencing homelessness in early education programs such as child care. Additionally noted is the need for better data to understand the prevalence of young children experiencing homelessness in Delaware. Robust data can help us identify families experiencing homelessness, thus providing support by fostering direct access to the resources necessary to address their unique needs. Support could entail finding available and affordable open child care slots within walking distance or near parent’s places of employment. The previously mentioned Delaware report outlines several recommendations including strengthening partnerships with partner agencies. Working collaboratively across organizations and agencies to connect families to simultaneously to affordable, accessible, and available child care and stable housing is vital ensuring the youngest Delawareans are provided the opportunity to reach their optimal development.
Families in this study lived their day-to-day lives in the context of enduring the daily stress of homelessness and they lived in fear of losing their children. Yet, families demonstrated perseverance and resolve in navigating through systems to locate housing, live their day-to-day lives, and maintain or obtain work. Families repeatedly emphasized that stable housing would reduce their stress, help them in their day-to-day life, and support their ability to work. Child care access, subsidy, and reliable transportation were identified as needs that would help them obtain stable housing.
IMPLICATIONS
This study supports the value of research that includes the voices of those with the lived experience of homelessness when considering policy and practice changes and implementation.34 Their stories reveal the added complexity of experiencing homelessness while caring for young children. This study adds to the information known about the experience of homelessness while caring for young children even though it is limited by a small sample. Although our work does not capture the full scope of experiencing homelessness with young children it provides an in-depth description of many aspects of their daily lives and adds to what is known about family homelessness. Families described how their health and wellbeing were negatively impacted by the lack of stable housing.
Insights gleaned from this work can inform policy and practice to create a multi-pronged approach to stable housing. Reasonable actions can be taken to begin to address the identified needs. Embedding housing case managers/housing navigators within housing programs could enhance wraparound services to facilitate families’ direct access to landlords. Providing monthly “unlimited rides” bus passes to families experiencing homelessness can support their continued employment. Fully implementing federal child care, Head Start and public school policy options could include connecting families experiencing homelessness directly to child care programs and subsidy.
Navigating housing and child care systems is complex and overwhelming. A strategy to support families experiencing homelessness with young children navigating these systems is to create an ongoing partnership between the CCR&R agency, the Delaware Department of Health and Social Services (POC administrator), and the housing system using designated case managers. Designated case managers would facilitate connecting families experiencing homelessness to available child care, POC, and housing and can also support families in child care with housing supports when needed.
Dr. Pic may be contacted at ampic@udel.edu .
REFERENCES
1. Bassuk, E. L., Hart, J. A., & Donovan, E. (2020, April 2). Resetting policies to end family homelessness. Annual Review of Public Health, 41, 247–263. https://doi.org/10.1146/annurev-publhealth-040119-094256
2. de Sousa, T., Andrichik, A., Prestera, E., Rush, K., Tano, C., & Wheeler, M. (2023). The 2022 Annual Homelessness Assessment Report (AHAR) to Congress: Part 1: Point-intime estimates of homelessness. Department of Housing and Urban Development. https://www.huduser.gov/portal/datasets/ ahar/2023-ahar-part-1-pit-estimates-of-homelessness-in-the-us.html
4 Stucker, R. (2024, June 6). Homelessness in Delaware—Setting the context. Homelessness in Delaware: New Ideas and Directions. Newark Delaware. http://www.udel.edu/0012179
5 Trounstine, J. (2018). Segregation by design: Local politics and inequality in American cities. Cambridge University Press.
6 Wilkerson, I. (2020). Caste: The origins of our discontents. Random House.
7. Carnemolla, P., & Skinner, V. (2021). Outcomes associated with providing secure, stable, and permanent housing for people who have been homeless: An international scoping review. Journal of Planning Literature, 36(4), 508–525. https://doi.org/10.1177/08854122211012911
8. Balfanz, R., & Byrnes, V. (2012). Chronic absenteeism: Summarizing what we know from nationally available data. Johns Hopkins University Center for Social Organization of Schools. https://new.every1graduates.org/wp-content/ uploads/2012/05/FINALChronicAbsenteeismReport_May16.pdf
9 Perlman, S. M., Shaw, S. H., Kieffer, C. H., Whitney, G. C., & Bires, C. (2017). Access to early childhood services for young children experiencing homelessness. In: M. Haskett, (Eds) Child and Family Well-Being and Homelessness. Springer Briefs in Psychology. Springer. https://doi.org/10.1007/978-3-319-50886-3_5
10 Mayberry, L. S., Shinn, M., Benton, J. G., & Wise, J. (2014). Families experiencing housing instability: The effects of housing programs on family routines and rituals. The American Journal of Orthopsychiatry, 84(1), 95–109 https://doi.org/10.1037/h0098946
11. Fraenkel, P. (2020). Time as a source of struggle and resilience in homeless families. Time & Society, 29(2), 581–603. https://doi.org/10.1177/0961463X20908082
12 Schneiderman, N., Ironson, G., & Siegel, S. D. (2005). Stress and health: Psychological, behavioral, and biological determinants. Annual Review of Clinical Psychology, 1(1), 607–628 https://doi.org/10.1146/annurev.clinpsy.1.102803.144141
13 Herbers, J. E., Cutuli, J. J., Jacobs, E. L., Tabachnick, A. R., & Kichline, T. (2019). Early childhood risk and later adaptation: A person-centered approach using latent profiles. Journal of Applied Developmental Psychology, 62, 66–76 https://doi.org/10.1016/j.appdev.2019.01.003
14. Murran, S., & Brady, E. (2023). How does family homelessness impact on children’s development? A critical review of the literature. Child & Family Social Work, 28(2), 360–371. https://doi.org/10.1111/cfs.12968
15. Anthony, E. R., Vincent, A., & Shin, Y. (2018). Parenting and child experiences in shelter: A qualitative study exploring the effect of homelessness on the parent–child relationship. Child & Family Social Work, 23(1), 8–15. https://doi.org/10.1111/cfs.12376
16 Knitzer, J., & Lefkowitz, J. (2005). Resources to promote social and emotional health and school readiness in young children and families: A community guide. National Center for Children in Poverty, Columbia University, School of Public Health.
17 Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighborhoods: The science of early child development. National Academy Press.
18. Friedman, D. H. (2000). Parenting in public: Family shelter and public assistance. Columbia University Press.
19 Swick, K. J., Williams, R., & Fields, E. (2014). Parenting while being homeless. Early Childhood Education Journal, 42(6), 397–403 https://doi.org/10.1007/s10643-013-0620-7
20 Pic, A. (2023). Exploring access and utilization of early care and education services among families experiencing homelessness with young children. ProQuest Dissertations & Theses. https://doi.org/10.13140/RG.2.2.35110.91204
21. McKinney-Vento Homeless Assistance Act of 1987, Pub. L. 100–628, 101 Stat. 482, 42 USC §§ 114301. 1987.
22. American Psychological Association [APA]. (2002). Ethical Principles of Psychologists and Code of Conduct. American Psychologist, 57(12), 1060 1073. https://psycnet.apa.org/doi/10.1037/0003-066X.57.12.1060
23 Silver, C., & Lewins, A. (2014). Using software in qualitative research: A step-by-step guide (2nd ed.). SAGE.
24. Charmaz, K. (2008). Grounded theory as an emergent method. In S.N. Hesse-Biber & P. Leavy (Eds), Handbook of emergent methods (pp. 155-170). The Guilford Press.
25 Lareau, A. (2021). Listening to people: A practical guide to interviewing, participant observation, data analysis, and writing it all up. University of Chicago Press.
26 Gibbs, G. R. (2018). Analyzing qualitative data. Sage (Atlanta, Ga.) https://doi.org/10.4135/9781526441867
27. Smith, S. R., & Hamon, R. H. (2012). Exploring family theories. Oxford University Press, Inc.
28 Sheele, J. M. (2021, May 14). Associations between bed bugs and mental illness among emergency department patients. Cureus, 13(5), e15024–e15024. https://doi.org/10.7759/cureus.15024
29 Paquette, K., & Bassuk, E. L. (2009, July). Parenting and homelessness: Overview and introduction to the Special Section. The American Journal of Orthopsychiatry, 79(3), 292–298. https://doi.org/10.1037/a0017245
30 Cutuli, J. J., & Herbers, J. E. (2014). Promoting resilience for children who experience family homelessness: Opportunities to encourage developmental competence. Cityscape (Washington, D.C.), 16(1), 113–140
31 Burchinal, M., Whitaker, A. A., & Jenkins, J. M. (2022). The promise and purpose of early care and education. Child Development Perspectives, 16(3), 134–140 https://doi.org/10.1111/cdep.12463
32. Yamashiro, A., McLaughlin, J. (2021). Early childhood homelessness state profiles: 2018-19. U.S. Department of Education, Office of Planning, Evaluation and Policy Development, Office of the Chief Data Officer. https://www2.ed.gov/rschstat/eval/disadv/homeless/early-childhoodhomelessness-state-profiles-2021.pdf
33. Whitney, G. (2022). Early learning opportunities for young children experiencing homelessness in Delaware. Delaware Department of Education and Delaware Head Start State Collaboration Office.
34 Morgan, A., & Ziglio, E. (2007). Revitalising the evidence base for public health: An assets model. Promotion & Education, 14(2, Suppl 2), 17–22. https://doi.org/10.1177/10253823070140020701x
The “Missing Middle:” Delaware’s Working Families Can’t Afford Child Care but Don’t Qualify for
State Programs
2024 Eligibility for Purchase of Care by State
Neighboring states provide child care to more families than Delaware
**Delaware Purchase of Care is at 215% and ECAP is at 135%.
These numbers reflect exit eligibility—the most you can make before you lose benefits. Entry requirements range from 135 – 200%.
Source: NWLC. 2024. TWO STEPS FORWARD ONE STEP BACK STATE CHILD CARE ASSISTANCE POLICIES 2023. https://nwlc.org/wp-content/uploads/2024/06/NWLC-State-Child-Care-Assistance-Policies-2023.pdf
A Family of Four Can Make No More Than $60,000 to Qualify and $62,400 to Keep Publicly Funded Child Care
If Delaware adopted neighboring states’ policies, many more families could access and keep child care benefits
Benefits phase out up to $67,080.
Source: Office of the Assistant Secretary for Planning and Evaluation. 2024. Poverty Guidelines. https://aspe.hhs.gov/topics/poverty-economic-mobility/poverty-guidelines
Eligibility
Source: Children's Funding Project. 2022. A fraction of those eligible are able to navigate state processes, find openings and get off waiting lists, and afford co-pays associated with POC.
These families are NOT eligible in Delaware.
Quit Your Job or Afford Child Care?
Delaware Families in Tough Financial Spot
is working, they would need to make $44.33 an hour (Delaware minimum wage is currently $13.25).
https://www.epi.org/resources/budget/
Source: Economic Policy Institute, Family Budget Calculator. A survival budget includes: housing, food, child care, transportation, health care, other necessities and taxes. These numbers were calculated for one adult and one child. To see more scenarios, visit EPI’s Family Budget Calculator.
Child care—per child—costs nearly as much as, if not more than, housing and healthcare.
Care Expenses for two children under four years old Other household expenses
These numbers were calculated for two adults and two children. To see more scenarios, visit EPI’s Family Budget Calculator.
Source: Economic Policy Institute. Family Budget Calculator. & United States Census Bureau American Community Survey. https://www.epi.org/resources/budget/
At what point do families fall off the benefits cliff—or 215% of Federal Poverty Level— and when can they afford child care again? $130K
Many dual-income, working families do not qualify and cannot afford it in their budget
At 417% of FPL, this family is ineligible for state-funded pre-K (ECAP) or subsidized child care (Purchase of Care) and can afford the basics + child care.
At 387% of the FPL, this family is ineligible for state-funded pre-K (ECAP) or subsidized child care (Purchase of Care) and can afford the basics + child care.
At 292% of the FPL, this family is ineligible for state-funded pre-K (ECAP) or subsidized child care (Purchase of Care) and cannot afford the basics + child care.
At 234% of the FPL, this family is ineligible for state-funded pre-K (ECAP) or subsidized child care (Purchase of Care) and cannot afford the basics + child care.
Source: Rodel & The Public Policy Center of Conference Board. (2024). Child Care Affordability by Occupation. https://rodelde.org/child-care-affordability-by-occupation/
Delaware Ranks 45th Nationally in Education Outcomes: Measuring Academic
Success and
Improving Educational Outcomes for Delaware’s Youth
Kelly Oberheim
Undergraduate Research Assistant, KIDS COUNT in Delaware
Janice Barlow, M.P.A.
Policy Scientist, Center for Community Research and Service; Director, KIDS COUNT in Delaware
ABSTRACT
Delaware’s ranking as 45th in the nation for education outcomes highlights the multifaceted challenges and influences affecting children’s development and education in the state. This paper explores how student success is measured in Delaware and the impact social determinants of health have on youth outcomes, including chronic absence, homelessness, nutrition, poverty, and adverse childhood experiences. By addressing these interconnected issues, Delaware can work towards closing achievement gaps and improving educational experiences for all students. Findings underscore the necessity for comprehensive support systems within schools informed by empirical evidence to foster a conducive learning environment and improve student outcomes. By addressing the social determinants of health driving educational challenges, policymakers can take a comprehensive approach to enhance the well-being and academic success of all children in Delaware.
INTRODUCTION
Delaware has ranked 45th in the nation for education outcomes in the 2024 KIDS COUNT Data Book, an annual, 50-state report that assesses data on 16 indicators in four domains -- economic wellbeing, education, health, and family and community factors -- to determine how children across the country fare in comparison to one another. Based on the latest figures, Delaware ranks 8th in economic well-being, 25th in child health, 32nd in family and community, and 31st in overall child well-being.1 While there is room for improvement in each of these domains, the greatest opportunity for growth exists in education. Some shortcomings can be attributed to post-pandemic difficulties and those issues exacerbated by it, such as chronic absenteeism and poverty. However, educational struggles have existed and been of concern for Delaware – and, more broadly, the United States -- prior to 2020: a decade ago, Delaware ranked 23rd in education and had already fallen to 26th by 2019.2–4 Because education is impacted by broader societal factors and individual experiences, advocates can reframe intervention efforts to also target these needs and conditions in conjunction with educational reform
MEASURING SUCCESS IN DELAWARE
Delaware’s ranking in the education domain is based on four criteria: the proportion of young children (ages three and four) not enrolled in school (55%), fourth graders not proficient in reading (75%), eighth graders not proficient in math (82%), and high school students not graduating on time (20%) (Figure 1).1 Two of the four measures in this indicator rely on students’ scores on the National Assessment of Educational Progress (NAEP) tests in reading and mathematics. Standardized testing scores such as these are one common tool for understanding how well students understand core concepts in reading, writing, and mathematics. Yet, while reflecting on students’ scores is helpful, experts in the field caution against using test scores as the sole metric of success.
Figure 1. A 2024 State-to-State Comparison of Education1
Existing research emphasizes test scores’ correlation with positive outcomes later in life such as higher earnings, greater work experience, choice of occupation, and less participation in illegal activities.5,6 While these findings are notable, they are not causal: unmeasured, confounding factors such as students’ intrinsic motivation; their relationships with family, teachers, and faculty; and the communities in which they live are a few of many possible components influencing later life outcomes.7 For this reason, looking exclusively at test scores is limiting and falls short of capturing a complete picture of the competencies of students, teachers, and schools.8 Currently, Delaware uses multiple tools and measurements in an effort to fully understand its students’ academic performance and growth opportunities.
The Delaware School Success Framework (DSSF) is a statewide tool for measuring school success and communicating it to the public, evaluating schools in key areas like academic achievement, academic progress, school quality, student success, graduation rates, and English language proficiency.9 Since 2014, academic metrics have been based on students’ scores on the Delaware State System of Assessments (DeSSA) and the Smarter Balanced Assessments in Mathematics and English Language Arts/Literacy, the newest in a series of testing systems that have been utilized by the state.10 Schools with low scores according to the DSSF can then be identified and supported via comprehensive support and improvement (CSI) or targeted support and improvement (TSI), which often results in funding increases.9 While the DeSSA and DSSF are used as evaluative systems within the state, the National Assessment of Educational Progress (NAEP) serves a similar function on a national scale. The NAEP is administered to a random selection of schools and students in grades 4, 8, and 12, whose results are used to inform decisions on educational reform in the country.11 The NAEP and DeSSA are two testing measures that Delaware’s children are evaluated on, but non-test measures such as those incorporated into the DSSF are a promising focus of emerging research on how to better measure and define student success.
Best Practices: What Experts Support
Ongoing debate surrounds the best ways to measure student success. Test scores have long been a part of the American education system and have become a convenient way for educators to communicate student progress. The system largely revolves around a proficiency binary, with those deemed proficient also deemed successful. This metric is simple to convey to parents and other interested parties, as it solely involves meeting a threshold or falling below it rather than weighing multiple, qualitative factors to first define what success is and then whether a child is reaching expectations. However, those who favor incorporating more qualitative measures into student achievement acknowledge that the task is not simple; instead, they value the measures’ intricacies as a more comprehensive way of acknowledging nuances that influence schools and students. Academicians, educators, school administrators, policymakers, parents, and the public all hold varied opinions about what is best for children based on their own observations, beliefs, and roles within a child’s educational journey. Hence, defining best practices is challenging given the subjectivity that experts in different domains may abide by.
Still, regardless of where individuals stand on divisive topics like using test scores to measure student and school success, experts recommend abiding by certain guiding principles in all situations. First, and most importantly, discussions on student success should be framed by relevant empirical evidence. Data serve as a starting point to have informed conversations and, eventually, to make informed decisions on educational policy. Moreover, experts recommend that individuals familiarize themselves with the basics of data and statistics to better understand a measure’s own inherent strengths and weaknesses. Depending on the context in which they are used, some measures’ predictive validity could appear stronger than others. For example, where test scores show strong predictive validity, one must consider whether nontest measures such as school climate, attendance, and leadership quality may factor into the outcome observed.12
Societal Drivers of Poor Outcomes
The pandemic resulted in a considerable amount of lost learning, the true extent of which is only now becoming apparent. COVIDspecific challenges such as school closures, distance learning, sick days, and changing school policies are partially responsible for declining test scores and student proficiency, but the ways in which the pandemic impacted existing societal drivers of poor outcomes is noteworthy.
Social determinants of health (SDOH) are “nonmedical factors that influence health outcomes,” and are organized into five key categories: health care access and quality, neighborhood and built environment, social and community context, economic stability, and education access and quality (Figure 2). They are impacted by larger forces and systems such as socioeconomic status, geographic location, political structures, and social norms, creating a wide network of interconnected and often bidirectional influences. In addressing disparities in SDOH, progress is made toward health equity, “a state in which every person has the opportunity to attain their highest level of health,” regardless of age, gender, race, ethnicity, or zip code.13 These factors existed long before the pandemic and have been correlated with poor educational outcomes over time.14 That said, COVID-19 compounded upon families’ existing hardships and underscored the impact of SDOH on public health as Delaware saw educational inequities widen.
Chronic Absenteeism and Homelessness
More than one-fourth (27%) of Delaware’s children were chronically absent in the 2021 to 2022 school year.15 A student is considered chronically absent when not present for 10% or more of school days, though many school districts throughout the state do not distinguish between chronic absence and truancy despite the important differences that exist between these two situations. Chronic absence encompasses absences for any reason – both excused and unexcused – such as chronic illness, lack of reliable transportation to school, housing insecurity, and student disengagement. Truancy, however, includes only those absences that are unexcused and often seeks to remedy the situation through penal measures.16 Put simply, “children cannot learn if they don’t attend school,” and the more encompassing measure of attendance is chronic absence.1
Research has found that attendance is often a stronger predictor of academic success than test scores.17 Online learning was a necessary adaptation that schools made during the peak of the
public health emergency, but in-person attendance has not yet caught up with pre-pandemic levels. Some question if the pandemic has permanently altered the way that children and their families view education, now thinking of school as an obligation that can be completed distantly, or even as a non-obligation altogether. However, the importance of in-person instruction should not be understated. Attending class in-person, on time, and ready to learn as often as possible not only ensures that children extract the most that they can from each given lesson and are meeting age-appropriate academic benchmarks, but also allows children to form relationships with teachers and peers, establish routines, build social-emotional intelligence, and access school services and extracurriculars.18 When a child misses school, they are missing valuable instruction time and time spent refining skills that will help them be successful adults and employees.
Yet not all missed instruction time is because a child does not want to physically be in school – often, children face barriers to attending school that are out of their control and even their parents’ control. For example, chronic and mental illnesses, unsafe commutes to school, bullying, poverty, and homelessness are a few of many reasons a child may be chronically absent. Each issue is challenging to address, but homelessness presents unique hardships that are deeply intertwined with attendance. Homeless children are more likely to be chronically absent from school, as well as to move schools and have lower academic achievement than securely housed children.19 Absences can often be attributed in part to an unhoused child’s lack of necessities like access to nutritious food, clean clothing, school supplies, and reliable transportation. Systemic inequities built into school policies also contribute to homeless children’s difficulties, such as enrollment policies that require documentation homeless families do not have, or a lack of properly informed staff and resources within schools.20 Racial equity is of concern as well, with Black families more likely to experience homelessness than any other racial or ethnic group.21 Understanding and addressing this reality is especially relevant as the number of homeless students as identified by the McKinney-Vento definition is on the rise in Delaware; since 2019, the number of homeless students has increased by 21% throughout the state, totaling a startling 1,878 students in the 2021-2022 school year.22
Poor Nutrition
A balanced diet is essential for children’s brain development and peak academic performance. Attending school hungry or undernourished interferes with children’s ability to learn, negatively impacting their cognitive functioning and causing inattention. The preoccupation that accompanies sourcing their next meal not only diverts children’s focus on learning, but also does lasting harm to their mental health and relationships with food.23 Research has indicated that, “moving in and out of food security as well as experiencing persistent marginal food security or food insecurity contributes to adverse child development outcomes across cognitive and behavioral domains,” which poses challenges for educators (pp. 14-15).24 Food insecurity exists along a spectrum, and multiple loci within this range contribute to negative educational outcomes for children that must be addressed by schools and staff. The issue is then further complicated if poor nutrition is not identified as the root cause of a child’s academic or behavioral difficulties, delaying proper intervention or unnecessarily expending school resources on alternative solutions.
Initiatives to address children’s nutritional needs such as SNAP, WIC, and School Nutrition Programs (SNP) have been increasingly utilized during and since the pandemic, both in Delaware and nationwide. Temporary increases to SNAP benefits significantly decreased food insecurity throughout the state, but since benefits were returned to pre-pandemic levels in 2023, Delaware has seen a surge in demand at organizations like the Food Bank. This demand is largely serving Delaware’s youth, given that children under 18 are more likely to be food insecure than adults across all three of the state’s counties (Figure 2). In total, 14.4% of youth in Delaware lack consistent and/or sufficient access to food, and those who are of school age are more likely to experience the negative educational outcomes associated with inadequate nutrition.8
Poverty
Socioeconomic status (SES) is known to be correlated with children’s academic success, and some studies have found that SES is over “three times more important than race in predicting [academic] outcomes.”25 Notably, a student’s success is also impacted by the economic well-being of their peers’ families. Just as children are shaped by other students’ language or behavior in their classes, “there are likely a variety of mechanisms by which peers can either negatively or positively influence individual student achievement,” including their classmates’ own socioeconomic standing.26 Intuitively, this finding makes sense: wealthier families are more likely to have disposable income that can be used to make investments in their communities and schools, and all children educated in well-resourced schools are more likely to fare favorably regardless of their families’ own financial standing. But even more, school funding is structured in a way that perpetuates inequities between districts because of the disparities that persist in housing. About 92% of public schools’ funding is derived from state (47%) and local (45%) sources, and the funding from local communities is almost
Figure 2. Children Are More Likely to Experience Hunger than Adults8
entirely from property taxes in the district.27 Homeownership is the primary means through which Americans amass wealth, but historically exclusionary policies have prevented families of color from obtaining mortgages and purchasing homes.28 Consequently, predominantly white areas are better resourced because district lines tend to be drawn in ways that create pockets of concentrated wealth, or “small affluent islands of well-funded schools within larger poorer areas that serve mostly students of color.”29 This results in widening wealth and educational gaps that then become racialized because of the systems that perpetuate them.
Around 13% of Delawarean children live at or below the federal poverty level, a figure slightly lower than the national average (16%). In total, 26,000 children across the state face not only the academic challenges directly associated with attending school in under-resourced districts, but also those challenges that poverty makes more likely.30 Living in poverty limits access to healthcare, safe housing, and a balanced diet, each of which can affect a child’s educational success by negatively impacting their attendance, cognitive functioning, and mental health. In short, it is not only poverty itself that can harm children’s achievement, but also the conditions poverty creates.
Lack of Individualized Services
In addition to their many other responsibilities, schools are also tasked with providing resources to students that require additional assistance, such as tutoring and mental health supports. Despite individualized instruction being among the most effective educational interventions and a source of mentorship, access to tutoring services is unequal across class and racial lines. In the past, federally funded tutoring programs such as America Reads were not sustained nationally due to a “lack of central funding, data collection, guidance, and structure,” and those that did succeed were able to do so because of exceptional leadership and/or local funding.31 Public schools also provide safe spaces for children to seek mental health support or confide in trusted adults. When children are mentally well and cared for, school climate improves alongside individual outcomes. Still, public schools often lack adequate funding for mental health and counseling services, particularly within rural communities.32
Adverse Child Experiences (ACEs)
Adverse childhood experiences (ACEs) are traumatic events experienced by children under 18 that are correlated with negative long-term outcomes. This can include experiences such as parental incarceration; witnessing intimate partner violence or violence within the community; a family member’s death by or attempted suicide; witnessing or experiencing child abuse or neglect; and living in a household with substance misuse or mental health problems, among others. In 2022, it was reported that 43% of children in Delaware experienced at least one ACE. Of non-Hispanic Black/African American children, 51% experienced one or more ACE as compared to only 36% of non-Hispanic white children, underscoring the racial disparities that exist among children experiencing ACEs.33 Not only do ACEs impact one’s adult outcomes, but adolescents with an ACE history are more likely to be chronically absent, have lower academic achievement, be suspended from school, and have lower educational aspirations.34 Adversity in childhood is not only of public health and safety concern, but also of developmental and educational concern.
IMPROVING DELAWARE’S EDUCATIONAL OUTCOMES
Addressing the social determinants of health that contribute to poor educational outcomes allows Delaware to fare better on a national scale. Ensuring that children perform their best in primary school promotes future economic stability because it creates the foundation for a healthy, prosperous workforce that can be drawn upon. It is worth noting that a tension exists between prioritizing individual and structural factors among experts, but both are valuable and worthy of addressing in education reform. Peak performance starts at an individual level, with each child arriving at school on time, ready to learn, and having had enough food and sleep prior. Meeting individual students’ needs appears more manageable than confronting the complexities of contributors like chronic absenteeism, poverty, and homelessness, but approaching larger, structural issues has far-reaching impacts in domains outside of that which is the primary focus. Regardless of which route policymakers favor, taking any steps to make education more equitable is an ongoing process that often calls for incremental changes, and any recognition and disruption of inequities in SDOH is beneficial.
CONCLUSION
Children’s achievement is determined by far more than what they are taught in the classroom or how they score on a test. Emphasizing education’s role as a social determinant of health allows advocates to look deeply at the various contributors to poor academic outcomes and focus their attention on the root causes of Delaware’s shortcomings. In reducing disparities in housing, healthcare, and economic security, education outcomes can be equalized, nurturing an environment in which all children are provided the opportunity to grow and thrive regardless of their class, gender, race, ethnicity, or zip code. With proper investment, attention, and intervention, Delaware can change its educational landscape from one that ranked 45th in the nation to one that reflects the full potential of the state’s students and educators. Ms. Oberheim may be contacted at keo@udel.edu
REFERENCES
1. Annie E. Casey Foundation. (2024). 2024 KIDS COUNT Data Book: State Trends in Child Well-Being. Retrieved from https://assets.aecf.org/m/resourcedoc/aecf-2024kidscountdatabook-2024.pdf
2. National Center for Education Statistics. (2020). International comparisons: Reading, mathematics, and science literacy of 15-year-old students. Condition of Education. U.S. Department of Education, Institute of Education Sciences. Retrieved from https://nces.ed.gov/programs/coe/pdf/coe_cnu.pdf
3. Annie E. Casey Foundation. (2014). 2014 KIDS COUNT Data Book: State Trends in Child Well-Being. Retrieved from https://assets.aecf.org/m/resourcedoc/aecf-2014kidscountdatabook-2014.pdf
4. Annie E. Casey Foundation. (2019). 2019 KIDS COUNT Data Book: State Trends in Child Well-Being. Retrieved from https://assets.aecf.org/m/resourcedoc/aecf-2019kidscountdatabook-2019.pdf
5. Hanushek, E. (2009). The economic value of education and cognitive skills. In Sykes G., Ford T., Plank D., Schneider B. (Eds.), Handbook of Education Policy Research (pp. 39–56). New York, NY: Routledge.
6. Heckman, J., Stixrud, J., & Urzua, S. (2006). The effects of cognitive and noncognitive abilities on labor market outcomes and social behavior. Journal of Labor Economics, 24(3), 411–482. https://doi.org/10.1086/504455
7. Tienken, C. (2017). Students’ test scores tell us more about the community they live in than what they know. Retrieved from http://theconversation.com/students-test-scores-tell-us-more-about-thecommunity-they-live-in-than-what-they-know-77934
8 KIDS COUNT in Delaware. (2024). 2024 FOCUS: On Public Policy. Retrieved from https://udspace.udel.edu/items/7463483e47eb-45bb-8a34-bdc4fcb34f91
9 Delaware Department of Education. (2024). Measuring school performance. Delaware Department of Education. https:// education.delaware.gov/educators/school-operations/measuring_ school_performance/
10. KIDS COUNT in Delaware. (2020). 2020 Fact Book: Now & Then. Retrieved from https://udspace.udel.edu/items/c2d7487103e2-4509-b7d4-5d4c74a3bd8d
11 Delaware Department of Education. (2024). National Assessment of Educational Progress (NAEP). Delaware Department of Education. Retrieved from https://education. delaware.gov/educators/academic-support/standards-and-assessments/naep/
12. Goldhaber, D., & Özek, U. (2019). How much should we rely on student test achievement as a measure of success? Educational Researcher, 48(7), 479–483 https://doi.org/10.3102/0013189X19874061
13 Centers for Disease Control and Prevention. (2024). Social determinants of health (SDOH). Retrieved from https://www. cdc.gov/about/priorities/why-is-addressing-sdoh-important.html
14 U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion. (n.d.). Education access and quality. Retrieved from https://health.gov/healthypeople/ objectives-and-data/browse-objectives/education-access-and-quality
15. Attendance Works. (2023). State trend chart 2017-2022. Retrieved from https://www.attendanceworks.org/rising-tide-ofchronic-absence-challenges-schools/
16 Delaware Department of Education. (2019). Chronic absenteeism: A resource guide for Delaware districts and charter schools. Retrieved from https://education.delaware.gov/ wp-content/uploads/2020/02/190829_chronic_absenteeism_resource_ guide_final.pdf
17. Baltimore Education Research Consortium. (2011). Destination graduation: Sixth grade early warning indicators for Baltimore City Schools. Retrieved from https://baltimore-berc.org/destination-graduation/
18 U.S. Department of Education. (n.d.). Supporting students during the COVID-19 pandemic: Maximizing in- person learning and implementing effective practices for students in quarantine and isolation. Retrieved from https://www.ed.gov/coronavirus/supporting-students-during-covid-19-pandemic
19. U.S. Department of Education. (2016). Supporting the success of homeless children and youths. Retrieved from www.ed.gov
20. School House Connection. (2024). The education of children and youth experiencing homelessness: Current trends, challenges, and needs. Retrieved from https:// schoolhouseconnection.org/article/the-education-of-children-andyouth-experiencing-homelessness-current-trends-challenges-and-needs
21 U.S. Interagency Council on Homelessness. (2018). Homelessness in America: Focus on families with children. Retrieved from www.Usich.gov
22. The McKinney-Vento Homelessness Act. (n.d.). Retrieved from https://nche.ed.gov/legislation/mckinney-vento/
23. Melchior, M., Chastang, J. F., Falissard, B., Galéra, C., Tremblay, R. E., Côté, S. M., & Boivin, M. (2012). Food insecurity and children’s mental health: A prospective birth cohort study. PLoS One, 7(12), e52615 https://doi.org/10.1371/journal.pone.0052615
24 Gallegos, D., Eivers, A., Sondergeld, P., & Pattinson, C. (2021, August 26). Food insecurity and child development: A stateof-the-art review. International Journal of Environmental Research and Public Health, 18(17), 8990. https://doi.org/10.3390/ijerph18178990
25. Battle, J., & Lewis, M. (2002). The increasing significance of class: The relative effects of race and socioeconomic status on academic achievement. Journal of Poverty, 6(2), 21–35 https://doi.org/10.1300/J134v06n02_02
26 Caldas, S. J., & Bankston, C. (1997). Effect of school population socioeconomic status on individual academic achievement. The Journal of Educational Research, 90(5), 269–277. https://doi.org/10.1080/00220671.1997.10544583
27 Irwin, V., Zhang, J., Wang, X., Hein, S., Wang, K., Roberts, A., Parker, S. (2021). Report on the condition of education 2021 (NCES 2021-144). U.S. Department of Education. Washington, DC: National Center for Education Statistics. Retrieved from https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2021144
28. Urban Institute. (2024). Nine Charts about wealth inequality in America. Urban Institute. Retrieved from https://apps.urban.org/features/wealth-inequality-charts/
29 American University. (2020). Inequality in public school funding: key issues & solutions for closing the gap. American University. Retrieved from https://soeonline.american.edu/blog/inequality-in-public-school-funding/
30 KIDS COUNT in Delaware. (2024). Children in poverty in Delaware. KIDS COUNT Data Center. Retrieved from https://datacenter.aecf.org/data/tables/43-children-in-poverty
31. Kraft, M. A., & Falken, G. T. (2021). A blueprint for scaling tutoring and mentoring across public schools. AERA Open, 7. https://doi.org/10.1177/23328584211042858
32 Shelton, A. J., & Owens, E. W. (2021, January). Mental health services in the United States public high schools. The Journal of School Health, 91(1), 70–76 https://doi.org/10.1111/josh.12976
33. Population Reference Bureau analysis of data from U.S. Department of Health and Human Services, National Survey of Children’s Health
34. Stewart-Tufescu, A., Struck, S., Taillieu, T., Salmon, S., Fortier, J., Brownell, M., . . . Afifi, T. O. (2022, September 14). Adverse childhood experiences and education outcomes among adolescents: Linking survey and administrative data. International Journal of Environmental Research and Public Health, 19(18), 11564. https://doi.org/10.3390/ijerph191811564
Each year, the Delaware Journal of Public Health publishes five different theme issues. Article submissions are accepted on a rolling basis, and the editorial board considers all submissions, both those connected directly to a theme issue, and non-thematic submissions. The editorial board reserves the right to include non-thematic submissions in each issue.
The working publishing calendar and thematic issues for 2024 are as follows:
Issue
Chronic Disease February 2024 March 2024
Violence April 2024 May 2024
Cancer & the Power of Preventive Screening June 2024 July 2024
Childhood Development & Education August 2024 September 2024
After COVID - Rebuilding Public Health & Healthcare Resilience October 2024 November 2024
If you have questions about submissions, ideas for an article, or suggestions for a future theme issue, please email Kate Smith: ksmith@delamed.org
All submissions can be submitted via the online submission portal: https://www.surveymonkey.com/r/2DSQN98 Submissions guidelines can be found at: https://djph.org
Rebecca McColl, M.A.
Youth Mental Health in the Wake of the COVID-19 Pandemic
Associate Policy Scientist, Center for Community Research & Service, Joseph R. Biden, Jr. School of Public Policy and Administration, University of Delaware
Erin Nescott, M.S.
Associate Policy Scientist, Center for Community Research & Service, Joseph R. Biden, Jr. School of Public Policy and Administration, University of Delaware
ABSTRACT
Objective: In this article we examine the current state of youth mental health across the United States and in Delaware, and discuss the impact of the COVID-19 pandemic on the mental health and well-being of children and adolescents. Methods: We review available literature detailing the short- and long-term effects of the COVID-19 pandemic on youth mental health and discuss the resultant programmatic and legislative efforts in Delaware and nationally. Results: The COVID-19 pandemic had a severe impact on the mental health of young people. The prevalence of depression and anxiety among children and adolescents, which was already increasing pre-pandemic, spiked after the pandemic’s onset. Even as public health precautions have lifted, young people continue to struggle with mental health in conjunction with lower levels of educational achievement, hindered social development, increased screen time, diminished access to effective mental healthcare, and economic instability. The negative impact of the pandemic will continue to have ramifications on the health and wellbeing of young people for years to come. Conclusions: Compiling evidence examining mental health trends is an important first step to understanding the impact of the pandemic on child and adolescent mental health and developing effective solutions. Policy Implications: Although the official state of emergency is over, the effects of the COVID-19 pandemic are far-reaching and long-lasting. It is imperative that legislators and program administrators in Delaware and nationally work to ensure that young people and their families have access to affordable, high quality mental healthcare.
INTRODUCTION
It has been more than four years since the COVID-19 virus began to spread in the United States and one year since the federal public health emergency expired. Efforts to mitigate the spread of the virus included stay at home orders, school closures, and shutdowns of many public spaces nationwide. In addition to the deleterious impact on physical health, much of the population also experienced negative impacts on mental health. Young people are particularly vulnerable to these disruptions in development and have continued to experience the mental and social ramifications of the pandemic more acutely than older adults.1
Pre-pandemic, mental health was already declining among young people, with feelings of hopelessness or sadness increasing by 40% among high school students between 2009 and 2019.2 The pandemic heightened these issues: according to one survey, 71% of parents reported the pandemic took a mental health toll on at least one of their children, and 64% believed the pandemic will have lasting developmental impacts.3 More than two years into the pandemic, 40% of parents said they were extremely worried about their child struggling with anxiety or depression.4
In the months following March of 2020, emergency department visits for mental health reasons and suspected suicide attempts increased among young people nationwide, and these visits remained elevated through the pandemic’s second year.5 At Nemours Children’s Hospital in Delaware, the
number of patients over 12 reporting suicidal thoughts and requiring observation more than quadrupled during the first year of the pandemic.6
As a result of this public health crisis, the American Association of Pediatrics declared a national state of emergency in child and adolescent mental health and the U.S. Surgeon General issued an advisory on protecting youth mental health.7,8 In May 2022, several government agencies including the Centers for Disease Control and Prevention (CDC), the Centers for Medicare & Medicaid Services (CMS) and the Administration for Children and Families (ACF) released a joint letter on children’s mental health encouraging states, tribes, and jurisdictions to prioritize mental well-being of children.9
In this paper, we explore how the ramifications of COVID-19 —social isolation, increased screen time, threats to physical health, economic instability, and reduced access to care— impacted the mental health and wellbeing of young people nationwide and in Delaware.
SOCIAL ISOLATION
Many children and young people have networks of friends, classmates, and adults outside of their immediate family that they rely on for socialization and support. Lockdowns, mandatory isolation after exposure to the virus, and fewer activities outside of the home removed children from these extended support networks. Although individuals of any age may experience the harmful effects of social isolation, research
suggests that children and adolescents are more susceptible to experiencing depression and anxiety during enforced isolation and after it ends.10 In one survey, more than half of parents reported that a lack of socialization during the pandemic compromised their child’s mental health.3
Periods of social isolation often go hand in hand with loss of routine and missed milestones by reducing the necessary interactions that form a child’s social development. Incidences such as this may have a major impact on the health-related quality of life (HRQoL) of young people, which involves an individual’s perception of their own mental and physical health functioning.11 When considering interventions to address the mental health challenges faced by young people, it is imperative to consider the ways in which mental and physical health intersect.
REMOTE LEARNING AND EDUCATIONAL ACHIEVEMENT
To keep students, teachers, and staff safe during the pandemic, school systems in Delaware and nationwide adopted remote or hybrid learning models. In addition to the challenges of a new learning environment, many students struggled with the resultant isolation from their peers and teachers. Although students made overall gains during and after the onset of the pandemic, these gains—and overall achievement levels—have remained lower than expected.12 Students of color and students at high-poverty schools are disproportionately impacted by this achievement gap. Delaware students in grades 4-8 achieved 56% of expected growth in 2023, with low-income students experiencing the least amount of growth (52%).13 Although some recovery has been made, students are still catching up to learning missed during the pandemic.
Remote learning led many students to feel isolated from their school communities. During the 2020-2021 school year, more than one in five students reported feeling disconnected from their classmates and school community, and 29% felt disconnected from school adults.14 This disconnect can negatively impact mental well-being, as students who feel connected to people at school are less likely to experience poor mental health and persistent feelings of sadness and hopelessness.15 A survey of parents from October and November 2020 found that children in a virtual learning environment experienced greater negative impacts on physical activity, time outside, time spent with friends in-person, and physical and mental health than children in hybrid or in-person learning environments.16
Educational staff and administrators had to make many challenging but necessary decisions throughout the pandemic to keep school communities safe. It is necessary to emphasize the importance of remote learning as a public health tool for mitigating the spread of COVID-19, and to note that not all students have negative experiences with remote learning environments.17 As Delaware moves forward in continued recovery from the COVID-19 pandemic, it’s important for leaders in education to consider the benefits and risks of educational approaches for each student’s individual learning style.
SCREEN TIME
As remote learning and virtual socialization peaked in the early stages of the pandemic, the overall screen time for adolescents, including time spent on computers, phones, televisions, or video games, drastically increased. Children were more likely to experience an increase in screen time than adults, especially children aged 6-10 who had the highest increases in total screen time out of any age group during the pandemic.18 Older children experienced similar increases in screen time, and data from May 2020 show that 12- and 13-year-old adolescents spent 7.7 hours a day on non-school related screen time, which is more than double the pre-pandemic estimate.19
Screen time has continued to remain high even as public health precautions have been lifted.20 In 2023, 23% of fifth graders in Delaware spent more than five hours a day in front of a computer, phone, or television screen, not counting screen time needed for school.21 These high levels of screen time can have adverse effects on young people. Research has shown that excessive screen time for children and youth is associated with a variety of physical and mental health issues including unhealthy diet, depressive symptoms, and perceived stress.22 These findings emphasize the importance of mitigating unnecessary screen time and encouraging participation in alternative activities, such as in-person socialization and time outdoors. Promisingly, interventions to decrease children’s time spent in front of screens—particularly those involving the components of goalsetting and self-monitoring—have shown effectiveness in screen time reduction.23
HEALTH AND WELL-BEING CONCERNS
Children are less likely to become severely ill with COVID-19 than adults, representing just under one in five COVID cases since the beginning of the pandemic.24 However, severe cases are still possible, particularly for children with comorbidities including chronic respiratory and cardiovascular diseases.25 The fear of catching the virus, or dealing with the impact of illness in themselves or family members, can be a stressor for young people. During the pandemic, more than half of adolescents aged 13-19 reported heightened levels of concern about their own or their families physical and mental health.14 In one survey of public schools, 20% of schools reported that students with, or in families with, a high-risk medical condition were more likely to seek out mental health services.26 Dealing with the anxiety of getting sick, or the loss of a loved one, may critically impact a child’s mental and emotional well-being.
ECONOMIC INSTABILITY
Many young people have either experienced or witnessed family and friends endure a myriad of economic challenges during the COVID-19 pandemic. Financial instability can have lasting effects, as adolescents from families experiencing greater economic hardship are more likely to suffer from long-term impacts to mental health as a result of the pandemic.12
To combat widespread economic hardship during the pandemic, many safety net measures supporting families and children were expanded during the public health emergency. The free school meal program made meals available to all children through the 2023 school year,27 the
Supplemental Nutrition Assistance Program (SNAP) provided an emergency allotment to expand families’ food budgets,28 Temporary Assistance for Needy Families (TANF) increased cash benefits,27 and Medicaid expanded eligibility, enabling recipients to stay enrolled even if they did not meet previous guidelines.29 However, all of these increased benefits ended between February and June 2023, leaving many families without supports they had come to depend on. The unwinding of these program expansions may mean that many families are experiencing increasing food and financial insecurity, which can be a major stressor for adults and children alike.
ACCESS TO CARE
Although mental health issues among young people have risen throughout the course of the pandemic, many parents and children have faced challenges accessing the care they need. As the U.S. healthcare system struggled to meet demand at the start of the pandemic, some services were unavailable or halted completely. Between February and October 2020, the number of child Medicaid/CHIP beneficiaries receiving mental health services dropped by 50%.30
Concerns about access to effective mental healthcare have continued to persist several years into the pandemic. In an April 2022 survey, 70% of public schools stated that the rate of students seeking mental health services has increased during the pandemic, though just 56% agreed that they are able to effectively provide mental health services to all students in need.28 Barriers to access for mental healthcare can include availability to appropriate providers, cost, parental reluctance, long waiting lists, lack of insurance coverage, and cultural stigma.28,29,31 While telehealth visits may reduce some of these barriers, in-person visits are important for many children who may not have the private space or quality of internet access necessary to have a virtual visit with a mental healthcare provider.
Specifically for youth who identify as LGBTQ+, a 2022 survey by The Trevor Project of young people ages 13 to 24 showed that many desired mental health care but did not access it. Factors limiting access included fear of discussing concerns, worries around obtaining permission to access care, fear they wouldn’t be taken seriously, affordability issues, concern their identity would be misunderstood, and a lack of transportation.32 It is imperative that mental health supports meet the needs of all adolescents, regardless of race, ethnicity, sexual or gender identity, or economic status.
DISCUSSION
As schools have resumed in-person learning, educators and administrators have recognized the need for increased mental health services among school aged children, resulting in programs and legislation to expand existing and new infrastructure. Nationwide, schools are working towards acknowledging and adapting to student challenges. Twelve states currently allow students to take a certain number of mental health days as excused absences.33 Additionally, teachers across the country are working to better understand the signs of mental distress among their students and establishing regular check-ins as part of their classroom routines.34
Policymakers in Delaware have continued to work towards increasing access to youth mental health services. The state passed House Bill 301, requiring the establishment and implementation of statewide mental health educational programs for each grade, kindergarten through grade 12, in each school district and charter school in this State.35 Moreover, Governor Carney has signed bills expanding access to school counselors.36
While mental health services are vital to ensuring the needs of children and adolescents are met, it is necessary to note the importance of security in all areas of life for young people. For many adolescents, meeting basic needs such as security of family relationships, a safe and stable home environment, the availability of nutritious food, and financial stability, can majorly impact their overall wellbeing.13 Children experiencing adverse childhood experiences (ACEs)—which include forms of abuse, neglect, and household instability—at home during the pandemic were significantly more likely to have poor mental health or a suicide attempt in the past year than children without ACEs.37 In order to address the mental health crisis, Delaware must continue to focus on increasing the overall quality of life for children throughout the state.
CONCLUSION
The ramifications of the COVID-19 pandemic will continue to impact children’s health and development for years to come. With this in mind, is important to have tools in place to track the experiences of families and youth so their needs can be met. Tools such as the Household Pulse Survey38 will continue to collect data to quantify family experiences during the coronavirus pandemic, with data reported close to real-time. The National Survey of Children’s Health39 works to capture detailed health data, with trends to analyze before, during, and throughout recovery from the COVID-19 pandemic, and the Youth Risk Behavior Survey (YRBS) captures a variety of mental and physical health data from students in Delaware and nationally.40
The data from these surveys and research tools are vital in order to formulate effective services to aid young people in their continued recovery from the COVID-19 pandemic. Providing children and their families with the mental, physical, and emotional support they need is paramount to ensuring the well-being of Delaware’s children throughout the public health crisis and beyond. Ms. McColl may be contacted at bmccoll@udel.edu
REFERENCES
1. Kaiser Family Foundation. (2023, Mar 20). Latest federal data show that young people are more likely than older adults to be experiencing symptoms of anxiety or depression. https:// www.kff.org/mental-health/press-release/latest-federal-data-show-thatyoung-people-are-more-likely-than-older-adults-to-be-experiencingsymptoms-of-anxiety-or-depression/
2. Centers for Disease Control and Prevention. (n.d.). Mental health among adolescents. https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/dash-mental-health.pdf
3. Lurie Children’s Hospital of Chicago. (2021, May 27). Children’s mental health during the COVID-19 pandemic. https://www.luriechildrens.org/en/blog/childrens-mental-healthpandemic-statistics/
4. Minkin, R., & Horowitz, J. M. (2023, January 24). Parenting in America today. Pew Research. https://www.pewresearch.org/social-trends/2023/01/24/parenting-inamerica-today/
5. Yard, E., Radhakrishnan, L., Ballesteros, M. F., & Sheppard, M. Gates, A., Stein, Z., …, Stone, D.M. (2021). Emergency department visits for suspected suicide attempts among persons aged 12-25 years before and during the COVID-19 pandemic. Morbidity and Mortality Weekly Report, 70(24), 888-894.
8. U.S. Department of Health and Human Services. (2021, Dec 7). U.S. Surgeon General issues advisory on youth mental health crisis further exposed by COVID-19 pandemic. https://www.hhs.gov/about/news/2021/12/07/us-surgeon-generalissues-advisory-on-youth-mental-health-crisis-further-exposed-bycovid-19-pandemic.html
9. U.S. Department of Health and Human Services. (2022, May 25). Joint letter on children’s mental health. Retrieved from: https://www.hrsa.gov/sites/default/files/hrsa/about/news/2022-jointletter-childrens-mental-health.pdf
10. Loades, M. E., Chatburn, E., Higson-Sweeney, N., Reynolds, S., Shafran, R., Brigden, A., . . . Crawley, E. (2020, November). Rapid systematic review: The impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. Journal of the American Academy of Child and Adolescent Psychiatry, 59(11), 1218–1239.e3. https://doi.org/10.1016/j.jaac.2020.05.009
11 Liu, C. H., Zhang, E., Hyun, S., Wong, G. T. F., & Hahm, H. C. (2021, August). Health-related quality of life among US young adults during the COVID-19 pandemic: Psychiatric symptoms and emotional experiences to target within clinical practice. Ann Clin Psychiatry, 33(3), 232–240. Retrieved from: https://par.nsf.gov/servlets/purl/10322708
12. Di Pietro, G. (2023, May). The impact of Covid-19 on student achievement: Evidence from a recent meta-analysis. Educational Research Review, 39, 100530 https://doi.org/10.1016/j.edurev.2023.100530
13 Kids Count in Delaware. (2024). KIDS COUNT in Delaware 2024: Focus on Public Policy. https://udspace.udel.edu/items/7463483e-47eb-45bb-8a34-bdc4fcb34f91
14 Flanagan, S. K., Margolius, M., Pileggi, M., Glaser, L., Burkander, K., Kincheloe, M., & Freeman, J. (2021). Where do we go next? Youth insights on the high school experience during a year of historic upheaval. Research for Action & America’s Promise Alliance. https://www.researchforaction.org/wp-content/uploads/2021/06/ gradnation-final.pdf
15 Jones, S. E., Ethier, K. A., Hertz, M., DeGue, S., Le, V. D., Thornton, J., Geda, S. (2022, April 1). Mental health, suicidality, and connectedness among high school students during the COVID-19 pandemic - adolescent behaviors and experiences survey, United States, January-June 2021. MMWR Supplements, 71(3), 16–21 https://doi.org/10.15585/mmwr.su7103a3
16 Verlenden, J. V., Pampati, S., Rasberry, C. N., Liddon, N., Hertz, M., Kilmer, G., Ethier, K. A. (2021, March 19). Association of children’s mode of school instruction with child and parent experiences and well-being during the COVID-19 pandemic – COVID Experiences Survey, United States, October 8-Novermber 13, 2020. MMWR. Morbidity and Mortality Weekly Report, 70(11), 369–376 https://doi.org/10.15585/mmwr.mm7011a1
17. Abramson, A. (2021). Capturing the benefits of remote learning. Monitor on Psychology, 52(6), 46. Retrieved from https://www.apa.org/monitor/2021/09/cover-remote-learning
18. Trott, M., Driscoll, R., Irlado, E., & Pardhan, S. (2022, June). Changes and correlates of screen time in adults and children during the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine, 48, 101452. https://doi.org/10.1016/j.eclinm.2022.101452
19 Nagata, J. M., Cortez, C. A., Cattle, C. J., Ganson, K. T., Iyer, P., Bibbins-Domingo, K., & Baker, F. C. (2022, January 1). Screen time among US adolescents during the COVID-19 pandemic: Findings from the adolescent brain cognitive development (ABCD) study. JAMA Pediatrics, 176(1), 94–96. https://doi.org/10.1001/jamapediatrics.2021.4334
20 Hedderson, M. M., Bekelman, T. A., Li, M., Knapp, E. A., Palmore, M., Dong, Y., Ferrara, A., & the Environmental Influences on Child Health Outcomes Program. (2023, February 1). Trends in screen time use among children during the COVID-19 pandemic, July 2019 through August 2021. JAMA Network Open, 6(2), e2256157
21 The Annie E. Casey Foundation. (n.d.). Television or online 2020-2023 in Delaware. KIDS COUNT Data Center. https://datacenter.aecf.org/
22. Stiglic, N., & Viner, R. M. (2019, January 3). Effects of screentime on the health and well-being of children and adolescents: A systematic review of reviews. BMJ Open, 9(1), e023191.
https://doi.org/10.1136/bmjopen-2018-023191
23. Jones, A., Armstrong, B., Weaver, R. G., Parker, H., von Klinggraeff, L., & Beets, M. W. (2021, September 16). Identifying effective intervention strategies to reduce children’s screen time: A systematic review and meta-analysis. The International Journal of Behavioral Nutrition and Physical Activity, 18(1), 126. https://doi.org/10.1186/s12966-021-01189-6
24 American Academy of Pediatrics. (2022). Children and COVID-19: State-level data report. https://www.aap.org/en/pages/2019-novel-coronavirus-covid-19infections/children-and-covid-19-state-level-data-report/
25. Tsankov, B. K., Allaire, J. M., Irvine, M. A., Lopez, A. A., Sauvé, L. J., Vallance, B. A., & Jacobson, K. (2021, February). Severe COVID-19 infection and pediatric comorbidities: A systematic review and meta-analysis. Int J Infect Dis, 103, 246–256. https://doi.org/10.1016/j.ijid.2020.11.163
26 Institute of Education Sciences. (2022). 2022 school pulse panel. https://ies.ed.gov/schoolsurvey/spp/#tab-7
27. Delaware Department of Education. (n.d.). School nutrition programs. https://education.delaware.gov/educators/whole-child-support/nutrition/snp/
28 Delaware Division of Social Services. (n.d.). Important changes to benefit programs in response to COVID-19. https://dhss.delaware.gov/dhss/dss/covid19.html
29 Medicaid.gov. (n.d.). Unwinding and returning to regular operations after COVID-19. https://www.medicaid.gov/resources-for-states/coronavirus-disease2019-covid-19/unwinding-and-returning-regular-operations-aftercovid-19/index.html
30. Panchal, N., Kamal, R., Cox, C., Garfield, R., & Chidambaram, P. (2021, May 26). Mental health and substance use considerations among children during the COVID-19 pandemic. Kaiser Family Foundation. https://www.kff.org/coronavirus-covid-19/issue-brief/mental-healthand-substance-use-considerations-among-children-during-the-covid19-pandemic/
31 Lu, W., Todhunter-Reid, A., Mitsdarffer, M. L., MuñozLaboy, M., Yoon, A. S., & Xu, L. (2021, March 8). Barriers and facilitators of mental health service use among racial/ ethnic minority adolescents: A systematic review of literature. Frontiers in Public Health, 9, 641605. https://doi.org/10.3389/fpubh.2021.641605
32 The Trevor Project. (2022.) 2022 national survey on LGBTQ youth mental health. www.thetrevorproject.org/survey-2022
33 Bruce, G. (2022, June 10). More states are allowing students to take mental health days off. NPR.
35. An act to amend Title 14 of the Delaware code relating to mental health educational programs, House Bill 301, 151st General Assembly of Delaware, 2021-2022 session. (2022). https://legis.delaware.gov/BillDetail/79144
36. An act to amend Title 14 of the Delaware code relating to free public schools, House Bill 100, 151st General Assembly of Delaware, 2021-2022 session. (2021). https://legis.delaware.gov/BillDetail?LegislationId=48362
37. Anderson, K. N., Swedo, E. A., Trinh, E., Ray, C. M., Krause, K. H., Verlenden, J. V., . . . Holditch Niolon, P. (2022, October 14). Adverse childhood experiences during the COVID-19 pandemic and associations with poor mental health and suicidal behaviors among high school students – Adolescent Behaviors and Experiences Survey, United States, JanuaryJune 2021. MMWR. Morbidity and Mortality Weekly Report, 71(41), 1301–1305. https://doi.org/10.15585/mmwr.mm7141a2
38. United States Census Bureau. (n.d.). Household Pulse Survey (HPS). https://www.census.gov/data/experimental-data-products/householdpulse-survey.html
39 Data Resource Center for Child & Adolescent Health. (n.d.). National survey of children’s health (NSCH). https://www.childhealthdata.org/learn-about-the-nsch/NSCH
40 University of Delaware Center for Drug and Health Studies (n.d.). Youth risk behavior survey. https://cdhs.udel.edu/seow/school-surveys/youth-risk-behavior-survey-yrbs/
•
•
•
Early Investments Yield Long-Term Health and Community Returns
David A. Tam, M.D., M.B.A., C.P.H.E., F.A.C.H.E.
President & CEO, Beebe Hospital; President, Delaware Board of Directors, American Heart Association
E. Thomas Harvey, III
Chairman & CEO, Harvey, Hanna & Associates; Delaware Board of Directors, American Heart Association
Megan Tucker
Senior Director, Field Advocacy, Eastern States Region, American Heart Association
Stephanie Scarmo, Ph.D., M.P.H.
National Senior Policy Analyst, American Heart Association
ABSTRACT
As leaders in the healthcare and business sectors, members of the Delaware Board of Directors for the American Heart Association, and advocates for cardiovascular health and well-being, we know that supporting Delaware’s youngest children promotes public health and thriving communities.
INVESTING IN OUR WORKFORCE
We have witnessed firsthand the workforce challenges facing the healthcare and business sectors in our state. Healthcare is one of Delaware’s largest employers and is facing major shortages. Our workforce is contingent upon families and caregivers having access to quality child care and early education programs. Investments in these areas are vital to filling existing job openings, recruiting highly skilled workers, and attracting new companies to grow our economy.
A September 2023 online survey conducted by Rodel, the Delaware Association for the Education of Young Children (deaeyc), YMCA of Delaware, Delaware Readiness Teams, St. Michael’s School and Nursery, and the First State Pre-K coalition found that working families in Delaware struggle to afford quality early care and education programs, including many who earn too much money to qualify for state-funded programs.1 Hundreds of Delaware families with children ages 0-12 responded to the survey. These families continue to face limited supply and high costs for child care. Forty-four percent of respondents said they cannot find a program that has room, cannot find a program that meets the needs of their schedule, and cannot afford to send their child to a program. The findings also point to child care challenges as a hindrance to Delaware’s economy and workforce participation. Sixty percent of respondents said they would get a job and/or pick up more hours or move from part-time to full-time employment if they could afford/access child care.
A 2014 White House report on the Economics of Early Childhood Investments reported that access to high-quality care for young children can help parents increase their employment, which strengthens their attachment to the labor force and increases their earnings potential. Higher labor force participation and earnings have potential benefits for children, such as lower healthcare expenditures, higher education spending, more consistently nutritious food, and reduced household budgeting stress.2
More recent data from 2023 show that the infant-toddler child care crisis costs families, businesses, and taxpayers in the U.S. a total of $122 billion in lost earnings, productivity, and revenue.3 According to the U.S. Chamber of Commerce Foundation, investments in high-quality child care result in wide-ranging positive business outcomes, including increased employee performance, improved recruitment and retention, and future organizational growth.4
SUPPORTING CHILDREN’S HEALTH, WELL-BEING, AND PUBLIC HEALTH
As Board members and staff for the American Heart Association, we know that access to affordable, high-quality early care and education offers a range of benefits for children, both in the short and long term.
In the first few years of life, a child’s brain develops rapidly, building an important foundation for future learning, behavior, and health.5 Research shows that high-quality early care and education programs promote children’s school readiness by supporting cognitive, social-emotional, and behavioral development.6 Early care and education may affect children’s health directly via access to health screenings, healthcare, improved nutrition, or other health-promoting activities; and indirectly via increasing household resources resulting from increased parental employment or earnings.6
A growing body of research also supports the long-term health effects of participation in high-quality early care and education programs. Children who participate in early childhood programs may be more likely to, as adults, be healthy and have higher earnings, and may be less likely to commit crime and receive public assistance (Figure 1).7 Other studies show improvements in blood pressure, reductions in smoking, and improved self-reported health in adolescence and adulthood.6 Yet, stark disparities in young children’s access to, experience in, and outcomes during and after early learning vary drastically based on a child’s race and ethnicity, where they live, what languages they speak, and where they are from.8 The most impacted families are those facing systemic barriers while navigating public programs, including immigrants, families
with low income, families with children who have disabilities (developmental delays or needs), and families who do not speak English as their primary language.9 Delaware has made important investments in quality early care and education programs. We must build on that foundation to shore up this essential sector and public health contributor. If we prioritize all children and families, we will support the workforce and ensure a strong child care and early education system for Delaware’s future.
CONCLUSION
The American Heart Association is proud to work alongside Rodel, deaeyc, and the First State Pre-K coalition to increase state funding for vital programs including Purchase of Care (POC) and the Early Childhood Assistance Program (ECAP). Together, we can ensure quality early care and education programs are accessible and affordable for all Delaware families.
Dr. Tam may be contacted at dtam@beebehealthcare.org
REFERENCES
1. Rodel. (2023, Nov). Delaware family survey results. November 2023. Retrieved from: https://rodelde.org/wp-content/ uploads/2023/11/October-2023-Family-Survey-Results-Draft.pptx.pdf
2. Executive Office of the President of the United States. (2014, Dec). The economics of early childhood investments. December 2014. Retrieved from: https://obamawhitehouse.archives.gov/sites/default/files/docs/the_ economics_of_early_childhood_investments.pdf
3. ReadyNation. (2023). $122 billion: the growing, annual cost of the infant-toddler child care crisis. Retrieved from: https://strongnation.s3.amazonaws.com/documents/1598/05d917e29618-4648-a0ee-1b35d17e2a4d.pdf
4. U.S. Chamber of Commerce Foundation. (2023, Oct). Employer roadmap: childcare solutions for working parents. Retrieved from:
5. Harvard University. (2016, May). From best practices to breakthrough impacts: a science-based approach to building a more promising future for young children and families. Center on the Developing Child. Retrieved from: https://developingchild.harvard.edu/wp-content/uploads/2016/05/ From_Best_Practices_to_Breakthrough_Impacts-4.pdf
6. Morrissey, T. (2019). The effects of early care and education on children’s health. Health Affairs Health Policy Brief. Retrieved from: https://www.healthaffairs.org/content/briefs/effects-early-care-andeducation-children-s-health doi: 10.1377/hpb20190325.519221
7. Robert Wood Johnson Foundation. (2014, Aug). Early childhood experiences shape health and well-being throughout life (Issue Brief). Retrieved from: http://www.rwjf.org/content/dam/farm/reports/issue_briefs/2014/ rwjf414926
8. Children’s Equity Project. (2021, Dec). Start with equity. 14 priorities to dismantle systemic racism in early care and education. Retrieved from: https://childandfamilysuccess.asu.edu/sites/default/files/2021-12/14priorities-equity-121621.pdf
9. Center for Law and Social Policy. (2018, July). Equity starts early: addressing racial inequities in child care and early education policy. Retrieved from: https://www.clasp.org/wp-content/uploads/2022/01/Equity-StartsEarly-Executive-Summary.pdf
Figure 1. Potential Impacts of Affordable, High-Quality Early Care and Education Programs on Children’s Development and Lifelong Health
Creating the Healthiest Generations of Children: How Nemours Children’s Health is Increasing Accessibility to Health Education
Adrienne Palmer, C.L.S.
Community Health Education, Nemours Children’s Health
Erica Singleton, M.P.H., C.H.E.S.
Community Health Education, Nemours Children’s Health
Can you think of an opportunity your child has had to learn about stress management? The signs of an unhealthy relationship? How to communicate with others in a clear and healthy way? This is where health education comes in. Health education is defined as “learning experiences on health topics, to provide people with knowledge, skills, and tools to live healthier lives.”1 These topics can range from mental and emotional health to food and nutrition; subjects that may not necessarily be covered at home or at school. Health educators have a unique opportunity to fill these gaps and increase health equity for everyone in our community.
WHY HEALTH EDUCATION IS IMPORTANT
The Centers for Disease Control and Prevention notes the relationship between health education and adolescent behaviors:2
• Youth behaviors and experiences set the stage for adult health.
• Health behaviors and experiences related to early sexual initiation, violence, and substance use are consistently linked to poor grades and test scores and lower educational attainment.
• Providing health education as early as possible can help youth to develop positive well-being, academic success, and healthy outcomes into adulthood.
Health education also improves health literacy, which empowers people to make better-informed decisions regarding their health. Increased health literacy is positively associated with people seeking out preventative healthcare, decreased unnecessary emergency room visits, better management of chronic conditions, and improved quality of care and health outcomes.3
WHAT NEMOURS CHILDREN’S HEALTH IS DOING
Meeting our community members where they are is not just a phrase but a call to action. In 2023, Nemours Children’s Hospital in Delaware established a Community Health Education (CHE) team, where our health educators work to break down accessibility barriers to health information by collaborating with community organizations all over the state to provide prevention education. As a children’s healthcare system, our health educators build curricula that are not only age-appropriate, but also evidence-, research-, and medically-based. We then offer to bring these
educational opportunities to children and their families throughout Delaware and the Delaware Valley via schools, community programs, and family organizations. This allows us to work toward our goal of improving health outcomes and reducing health disparities.
In addition, we partner with other departments within Nemours Children’s Health such as our school-based health centers, community engagement, and dental outreach teams, to find additional ways we can enhance care outside of our walls. Our various program offerings are a vehicle for children to have access to health education where they live, study, and play. This is essential because it provides early prevention and awareness, while also empowering children to think critically so they can make informed decisions about their own health. Our programs aim to increase health literacy and encourages children to become advocates for health in their families and peer groups.
LOOKING FORWARD
Nemours Children’s is founded on several strategic pillars to guide the organization in achieving its aspirational vision of creating the healthiest generations of children. One of those pillars focuses on the equitable delivery of health in the community. The Community Health Education team is reinforcing that goal by meeting children and families where they are, providing essential health education services, and helping ensure that every child in Delaware has access to the tools and skills that will help them maintain healthy behaviors throughout their lives.
Ms. Palmer may be contacted at Adrienne.palmer@nemours.org
REFERENCES
1. Rural Health Information Hub. (2024). Health education. https://www.ruralhealthinfo.org/toolkits/health-promotion/2/strategies/ health-education
2. Centers for Disease Control and Prevention. (2023). Health education.
Nemours Children's Health Community Health Education Team
Mission of the Team:
To develop and provide preventative health education to vulnerable populations in the Delaware Valley and improve health outcomes and health equity.
Health Education Topics:
Asthma, Nutrition and Healthy Living, Mental and Behavioral Health, Substance Use Prevention, Childhood Safety, Vaping Prevention, Healthy Relationships, Vaccine Education, and more!
If you are interested in having the Nemours Children's Health Community Health Education team attend or host an event at your location, scan the QR cod e below or please email us at chede@nemours.org
Early Head Start (EHS) programs serve infants and toddlers under the age of 3, and pregnant women. EHS programs provide intensive comprehensive child development and family support services to low-income infants and toddlers and their families, and to pregnant women and their families.
Delaware Association for the Education of Young Children
https://www.deaeyc.org/
The Delaware Association for the Education of Young Children (deaeyc, pronounced “day-see”) is an affiliate of the National Association of the Education of Young Children (NAEYC), the leading membership association for those working with and on behalf of children from birth to age eight. Founded in 1969, deaeyc serves and acts on behalf of the needs, rights, and well-being of all young children and their families in Delaware.
The CCR&R is dedicated to serving the child care community through information and referrals, training, advocacy, and education. CCR&R’s goal is to be the primary resource for the child care community and to assume a leadership role in supporting children, families, child care providers, employers and the public to ensure that quality child care takes its place as an integral part of society.
Delaware Purchase of Care Subsidy
https://dhss.delaware.gov/dss/childcr.html
This service provides support for families with children to enable the caretaker to hold a job, obtain training or meet special needs of the parent or child. Child care may also be provided in child abuse cases to help protect the child.
The Delaware School Success Framework (DSSF) outlines the accountability standards by which all Delaware public schools are measured. This state- and school-level data helps identify each school’s needs and determine how best to support students across the state.
First State Pre-K Coalition
https://www.firststateprek.com/
First State Pre-K is a coalition of partners focused on expanding access to publicly funded high quality early care and education in Delaware.
Head Start
https://www.acf.hhs.gov/ohs/about/head-start
Head Start programs support children’s growth from birth to age 5 through services centered around early learning and development, health, and family well-being. Head Start staff actively engage parents, recognizing family participation throughout the program as key to strong child outcomes.
The 35th edition of the Annie E. Casey Foundation’s KIDS COUNT® Data Book examines the unprecedented declines in student math and reading proficiency brought on by the COVID-19 pandemic’s effect on education.
The National Office of Policy & Prevention is an embodiment of Nemours Children’s commitment to enabling the healthiest generations of children, within our service areas — and nationally. The National Office’s Practice & Prevention team collaborates with other health systems and other sectors around the country to spread “what works” for improving health outcomes for children and their families — including programming, policy and systems change strategies.
National Institute for Early Education and Research
https://nieer.org/
Improving the learning and development of young children through research that transforms policy and practice.
PNC Grow Up Great, a $500 million, multi-year, bilingual initiative, helps prepare children from birth to age 5 for success in school and life.
Rodel
https://rodelde.org/
We believe a great education changes everything—from the life of a young person to the health and vibrancy of a community. A great education opens up worlds of opportunities, strengthens economies, and promotes civic engagement. It changes everything. At Rodel, we’re working to build an excellent and equitable public education system that supports all Delawareans to achieve success in school and life.
Rotary clubs bring together people across generations who wish to create lasting change in the world, in their communities, and in themselves. Rotary and Rotaract members around the world strengthen their connections to friends and neighbors taking action through service.
Index of Advertisers
Public Health Delaware Journal of Submission Guidelines
updated March, 2024
About the Journal
Established in 2015, The Delaware Journal of Public Health is a peer-reviewed electronic publication created by the Delaware Academy of Medicine/Delaware Public Health Association. The publication acts as a repository of news for the medical, dental, and public health communities, and is comprised of upcoming event announcements, past conference synopses, local resources, peer-reviewed content ranging from manuscripts and research papers to opinion editorials and personal interest pieces, relating to the public health sector. Each issue is largely devoted to an overarching theme or current issue in public health.
The content in the DJPH is informed by the interest of our readers and contributors. If you have an event coming up, would like to contribute an Op-Ed, would like to share a job posting, or have a topic in public health you would like to see covered in an upcoming issue, please let us know.
If you are interested in submitting an article to the Delaware Journal of Public Health, or have any additional inquiries regarding the publication, please contact the managing editor at managingeditor@djph.org, or the publisher at ksmith@delamed.org.
Information for Authors Submission Requirements
The DJPH accepts a wide variety of submission formats, including brief essays, opinion editorials pieces, research articles and findings, analytic essays, news pieces, historical pieces, images, advertisements pertaining to relevant, upcoming public health events, and presentation reviews. Additional types of submission not previously mentioned may be eligible, please contact a staff member for more information.
The initial submission should be clean and complete, without edits or markups, and contain both the title and author(s) full name(s). Submissions should be 1.5 or double spaced with a font size of 12. Once completed, articles should be submitted via the submission page at https://djph.org/submissions/submit-an-article/ Graphics, images, info-graphics, tables, and charts are welcome and encouraged to be included in articles. Please ensure that all pieces
are in their final format, and all edits and track changes have been implemented prior to submission. To view additional information for online submission requirements, please refer to the DJPH website: https://djph.org/submissions/submit-an-article/
Trial registration information is required for all clinical trials and must be included in the final article and/or abstract.
Abstracts
Authors must submit a structured or unstructured abstract along with their article. Abstracts will have a maximum of 200 words, including headings. Structured abstracts should employ 4-5 headings, and may include Objectives, Methods, Results, and Conclusions. A fifth heading, Policy Implications, may be used if relevant to the article. All abstracts should provide the date(s) and location(s) of the study if applicable, as well as any trial registration information.
Submission Length
While there is no prescribed word length, full articles will generally be in the 2,500-4,000word range, and editorials or brief reports will be in the 1,500-2,500-word range. If there are any questions regarding the length of a submission or APA guidelines, please contact a staff member.
Copyright
The journal and its content is copyrighted by the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA). The contents are licensed under Creative Commons License – CC BY-NC-ND (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Images are NOT covered under the Creative Commons license and are the property of the original photographer or company who supplied the image.
Opinions expressed by authors of articles summarized, quoted, or published in full within the DJPH represent only the opinions of those authors and do not necessarily reflect the official policy of the Academy/DPHA, the DJPH, or the institution with which the authors are affiliated.
Con icts of Interest
Any conflicts of interest, including political, financial, personal, or academic conflicts, must be declared prior to the submission of the article, or in conjunction with a submission. Conflicts of interest are any competing interests that may leave readers feeling misled or deceived, and/or alter their perception of subject matter. Declared conflicts of interest will be published alongside articles in the final publication.
Nondiscriminatory Language
Use of nondiscriminatory language is required in all DJPH submissions. The DJPH reserves the right to reject any submission found to be using sexist, racist, or heterosexist language, as well as unethical or defamatory statements.