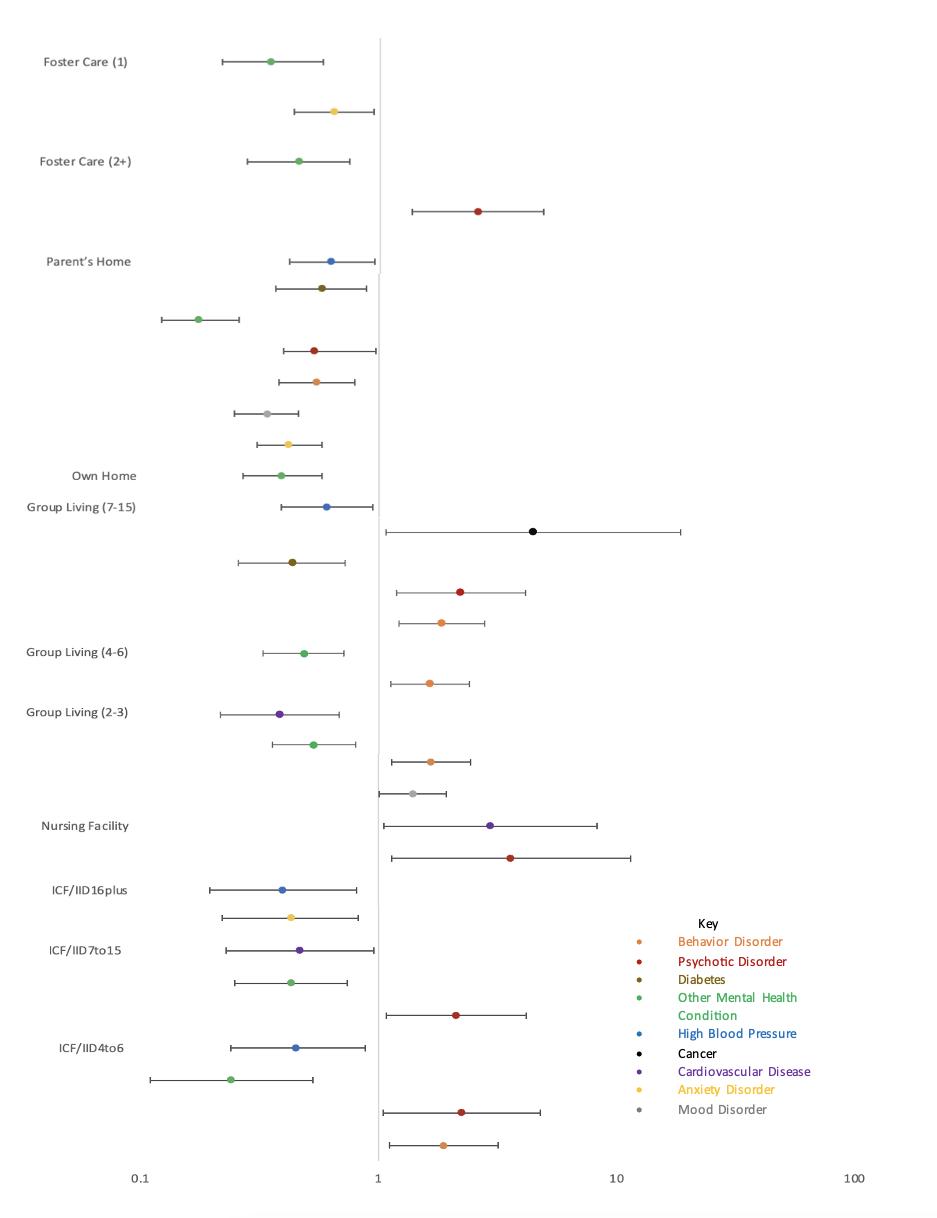
32 | Associations Between Residence Type and Health Outcomes for Individuals with Developmental Disabilities Following the COVID-19 Pandemic: A Quantitative Analysis
Ankita Mohan, M.H.S.
Jody Roberts, Ph.D.
ISSN 2639-6378
42 | Global Health Matters Newsletter September – October 2024
Fogarty International Center
54 | Flipping the Stats: A COVID-19 Success Story
My Healthy Community, Delaware’s Environmental Public Health Tracking Network
60 | Executive Summary of the Delaware State Health Assessment: 2022-2023 Report
62 | Delaware Mini Medical School
An Expeditionary and Health Literacy Program for Youth, Young Adults, and Those Exploring New Career Options
Timothy E. Gibbs, M.P.H.
Nicole Sabine, B.S.
70 | Access to Virtual Care in Behavioral Health: A Social Determinant of Health
Patrick J. Hearle, M.D.
Emily Ann Smith, M.D.
Richard J Caplan, Ph.D.
Ram A. Sharma, M.D.
76 | Index of Advertisers
78 | Delaware Journal of Public Health Submission Guidelines
The Delaware Journal of Public Health (DJPH), first published in 2015, is the official journal of the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA).
Submissions: Contributions of original unpublished research, social science analysis, scholarly essays, critical commentaries, departments, and letters to the editor are welcome.
Questions? Contact managingeditor@djph.org
Advertising: Please contact ksmith@delamed.org for other advertising opportunities. Ask about special exhibit packages and sponsorships. Acceptance of advertising by the Journal does not imply endorsement of products.
Any report, article, or paper prepared by employees of the U.S. government as part of their official duties is, under Copyright Act, a “work of United States Government” for which copyright protection under Title 17 of the U.S. Code is not available. However, the journal format is copyrighted and pages August not be photocopied, except in limited quantities, or posted online, without permission of the Academy/DPHA. Copying done for other than personal or internal reference use-such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale- without the expressed permission of the Academy/DPHA is prohibited. Requests for special permission should be sent to managingeditor@djph.org
IN THIS ISSUE
Rebuilding Public Health and Healthcare Resilience
In late 2019, news coming out of China mentioned whispers of an unknown communicable disease affecting people who had attended a socalled wet market.1 The United States government – and Delaware Public Health leadership – kept an ear out for any news, and soon more and more patients were being affected. Then the disease spread outside of China.
The pandemic (and ensuing lockdowns) made us reimagine the ways healthcare – and education, manufacturing, and any number of other industries – could be provided. Public health was in the spotlight. The Centers for Disease Control and Prevention (CDC) were constantly updating their recommendations, and Dr. Anthony Fauci was the voice of the science behind vaccines. We turned to telemedicine to see patients in their own homes, childhood vaccines were given in parking lots by masked providers, and elective surgeries were cancelled.
But health care centers were struggling to care for sick patients. Many health care providers – citing fatigue, burnout, and overwork – left the industry, and gaps in access to care became prevalent. Access to broadband (for school, for telehealth appointments, to keep in touch with loved ones) became a social determinant of health. Grocery stores held space and time for our older citizens to shop when the store was the cleanest, and churches began to hold worship services on Facebook.
Yet the US as a country did not fare particularly well. Compared with the rest of the world, a disproportionate number of Americans fell ill and died. Vaccines faced a delayed uptake and disinformation was rampant, amid scattershot mask mandates and guidelines between the states.2
With the eventual acceptance of Operation Warp Speed3 and widespread COVID-19 vaccination, the US began to open back up. Masks are now encouraged, especially if someone is sick, but not generally required. Elective surgeries are back in the operating room, and schools are back in session. Some healthcare workers are returning to the field, and some have stayed away. Public health is still in the spotlight, if one not quite as bright, and the social determinants of health continue to affect the health of individuals.
In this issue of the Delaware Journal of Public Health, we invite you to read about how we have researched the strength of the healthcare workforce in our state, how one of our healthcare institutions have used robots to assist the workforce, and how we have incorporated telehealth into primary care. We also highlight how the type of residence affected health outcomes for individuals with developmental disabilities during the pandemic, how switching to virtual classes increased the access to Delaware Mini Medical School for high school students throughout the state, and offer the executive summary of the Delaware State Health Assessment, 2022-2023.
As always, we welcome your feedback and ideas!
REFERENCES
1. World Health Organization. (2020, Jan 5). Pneumonia of unknown cause – China. https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229
2. Nuzzo, J. B., & Ledesma, J. R. (2023). Why did the best prepared country in the world fare so poorly during COVID? The Journal of Economic Perspectives, 37(4), 3–22.
3. Lancet Commission on COVID-19 Vaccines and Therapeutics Task Force. (2021, Jul). Operation warp wpeed: Implications for global vaccine security. Lancet 9, 7e1017-7e1021. https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(21)00140-6/fulltext
Omar A. Khan, M.D., M.H.S. Editor-in-Chief, Delaware Journal of Public Health
Katherine Smith, M.D., M.P.H. Publisher, Delaware Journal of Public Health
Delaware Health Force: A Comprehensive Approach to Addressing Healthcare Workforce and Access Challenges
Nicole Sabine Research Associate, Delaware Health Force
INTRODUCTION
The Delaware Health Force (DHF) initiative1 was presented by Nicole Sabine on behalf of the Delaware Academy of Medicine | Delaware Public Health Association (Academy/DPHA) at the 2024 APHA Annual Meeting & Expo. The healthcare workforce in Delaware faces significant challenges, amplified by a rapidly aging population and increased chronic disease prevalence, particularly in Sussex County, which has become a popular retirement destination. Additionally, the healthcare workforce itself is aging, placing further strain on Delaware’s healthcare infrastructure. With healthcare costs approaching 20% of U.S. GDP,2 the economic burden compounds workforce demands. The Delaware Health Force (DHF) was developed in 2020 to address these challenges comprehensively by supporting workforce retention, improving healthcare outcomes, and fostering a datadriven approach to future policy and resource allocation. DHF is a public-private partnership between the State of Delaware and the Academy/DPHA. Seed funding for DHF was provided by the Delaware Health Care Commission and internal endowments from Academy/DPHA, while major grant funding has been supplied by the State of Delaware’s Department of Labor through the American Rescue Plan Act (ARPA) pandemic relief funds.
DHF’S MULTI-PRONGED APPROACH
Core Workforce Data & Research
To address healthcare workforce challenges accurately, DHF aggregates extensive data to map population trends, provider distribution, and geographic accessibility. Data sources include the Delaware Professional Regulation Online Service (DELPROS),3 Centers for Medicare & Medicaid Services (CMS),4 the Delaware Health Information Network (DHIN),5 and Delaware Health and Social Services (DHSS).6 Using Salesforce, with Agile Cloud Consulting as an integrator, DHF houses all data in a streamlined, accessible format that aligns with the state’s broader data management systems.
The Core Workforce Data & Research initiative provides nearreal-time insights to guide policy and resource allocation. Three main dashboards support this function: Licensed Workforce Charts & Graphs,7 which track licensure status across various specialties; the Delaware Health Force Mapping Explorer,8 offering ZIP Code Tabulation Area (ZCTA)-level data to highlight provider availability per capita; and Employed Workforce Data, Maps & Charts,9 displaying job trends, median salaries, and job postings. Together, these tools enable a dynamic response to evolving workforce challenges.
Graduate Medical Education Expansion
DHF, in collaboration with the Delaware Health Sciences Alliance and ChristianaCare, focused on expanding graduate medical
education (GME) to increase the number of trained healthcare professionals in Delaware. Prioritizing underserved regions such as Kent and Sussex counties, the initiative aimed to fill gaps by creating more training positions for medical residents, advanced practice clinicians, and allied health providers, with an emphasis on behavioral health. At the completion of this arm of the program in 2024, these efforts led to 21 new health practitioners providing care across Delaware. GME expansion also supported additional training in palliative care, dementia care, and education for healthcare providers serving homeless populations. The rapid implementation, made possible by ARPA funding, allowed for an immediate workforce response and improved healthcare service access across Delaware.
Youth Health Literacy & Career Exploration
Youth-focused initiatives are central to DHF’s long-term strategy to build a robust healthcare workforce pipeline. The Delaware Mini Medical School,10 running since 2009, offers a free, sixweek educational series open to students from middle school to undergraduates, although all ages are welcome. Participants gain insight into health topics, diagnostic trends, and emerging fields within healthcare, supporting informed career exploration. Expanding on this model, DHF launched the Delaware Youth Medical Academy (DYMA), a new merit-based program specifically for middle and high school students, offering both virtual and in-person workshops that immerse them in real-world medical experiences and college/career readiness guidance.
Between 2023 and October 2024, the Mini Medical School welcomed over 3,000 registrants across five cohorts, with 63% of attendees indicating that the program positively influenced their career or academic choices. Together, these initiatives are cultivating a future healthcare workforce by engaging Delaware’s youth and encouraging them to consider healthcare career pathways.
Health Care Student Loan Program
The Health Care Student Loan Program is designed to address immediate workforce shortages by providing financial support to healthcare students in Delaware.11 Funded by ARPA, the program offers annual loan amounts between $2,500 and $15,000. The loans are interest-free while students remain enrolled in eligible programs, which include nursing, medicine, behavioral health, allied health, and other healthcare-related degree or certification programs. Repayment options vary by degree type, with certification programs requiring 1-3 years, associate and bachelor’s programs requiring 5-7 years, and doctoral programs requiring 7-11 years. Graduates may qualify for further interestfree repayment if they remain in Delaware, work in an approved healthcare role, and contribute to Delaware’s workforce for a set period. This program incentivizes healthcare students to remain in the state and support underserved communities, addressing both present and future workforce demands.
CONCLUSION
The Delaware Health Force initiative represents a comprehensive, multi-pronged approach to addressing the healthcare workforce challenges faced by Delaware. With a targeted combination of real-time data analytics, expansion of graduate medical education, youth engagement, and financial support, DHF is tackling both immediate workforce shortages and long-term needs. This strategy is particularly responsive to the state’s aging population and the growing demand for healthcare services.
While the use of ARPA funding has enabled rapid implementation of the programs within this initiative, ensuring their sustainability will require continued investment and strategic partnerships. Additional challenges include expanding the scope of the student loan program and further integrating data systems.
Despite these challenges, the effectiveness of the DHF model suggests that it could serve as a replicable framework for other states grappling with similar healthcare workforce and access challenges. With ongoing commitment and collaboration, DHF offers a promising path forward to addressing Delaware’s healthcare workforce needs and ensuring that its residents have access to high-quality care in the future.
Ms. Sabine may be contacted at nsabine@delamed.org .
REFERENCES
1. Delaware Health Force. (2024, October 12). Delaware Health Force. Delaware Health Force - Health Care Work Force Data and Action. https://dehealthforce.org/
2. Centers for Medicare & Medicaid Services’ (CMS) Office of the Actuary. (2024, July 12). CMS releases 2023-2032 national health expenditure projections. www.CMS.gov https://www.cms.gov/newsroom/press-releases/cms-releases-20232032-national-health-expenditure-projections
3. Delaware Professional Regulation Online Service (DELPROS). (n.d.). License Look-Up. eLicense Professional Licensure.
https://delpros.delaware.gov/OH_HomePage
4. U.S. Centers for Medicare & Medicaid Services. (n.d.). NPPES NPI Registry. https://npiregistry.cms.hhs.gov/search
5. Delaware Health Information Network. (2022). Delaware Health Information Network. Dover. https://dhin.org/
6. Delaware Health and Social Services - State of Delaware. (n.d.). Delaware Health and Social Services. https://dhss.delaware.gov/dhss/index.html
7. Delaware Health Force, & Agile Cloud Consulting. (n.d.). Licensed Workforce Charts & Graphs. Delaware Health Force.
8. Delaware Health Force, & Tech Impact. (n.d.). Delaware Health Force mapping (explorer). Delaware Health Force. https://dhf-dashboard.pages.dev/
9. Delaware Health Force, & eImpact. (n.d.). Employed Workforce Data, Maps & Charts. Delaware Health Force. https://delamed.eimpactv3.com/dashboards/273/delamed/del-health
10. Delaware Academy of Medicine & Delaware Public Health Association, & Delaware Health Force. (n.d.). Delaware Mini Medical School. https://delawareminimed.org/
11. Delaware Academy of Medicine & Delaware Public Health Association, & Delaware Health Force. (n.d.). Health Care Student Loan Program. Delaware Academy of Medicine & Delaware Public Health Association. https://delamed.org/student-financial-aid/financial-aid-2023-workforce-initiative/
Improving Postpartum Follow-Up with Telehealth: Did the Pandemic Nudge Us in a Better Direction?
Kathryn Vollum Woodroof, M.D.
Department of OB/GYN, ChristianaCare Health System
Department of OB/GYN, ChristianaCare Health System
Karen Antell, M.D., M.P.H., F.A.A.F.P.
Director of Maternity and Women’s Health Education, Family Medicine Residency, Faculty Physician, Obstetrics and Gynecology Residency, Christiana Care Health
System
Diana Wohler, M.D.
Department of Family Medicine, Warren Alpert Medical School at Brown University
ABSTRACT
Objective: To investigate if a telehealth option as the initial postpartum visit would increase postpartum visit attendance. Methods: This was a retrospective cohort study of women receiving prenatal care through a federally qualified health center, Westside Family Health in Delaware, comparing attendance at a postpartum visit before telehealth was an option (2018) versus after the onset of the pandemic (2021). Representative random samples were taken from one year of deliveries pre- and post-implementation of the telehealth visit option. The primary outcome of this study was attendance of any postpartum visit before and after the option of a telehealth visit.
Results: A total of 700 subjects were enrolled, with 349 subjects pre-telehealth and 351 subjects post-telehealth implementation. Our population was >50% Hispanic/Latina and >40% Spanish- speaking. The post-implementation group had a significantly higher attendance of the postpartum visit (83.95% vs. 90.60%, p-value 0.0092, OR 1.887, 95% CI 1.171-3.043). Conclusion: There was a significant increase in the rate of postpartum visit attendance with the addition of a telehealth visit option. Postpartum depression screening was negatively impacted by the introduction of the telehealth visit. Public Health Implications: The recommendation for all women post-delivery is to see their obstetric provider within the first 3 weeks postpartum. This includes assessing for complications, postpartum wellness and interconception care planning before 12 weeks post-delivery. We found that there was a significant increase in the rate of postpartum visit attendance with the addition of a telehealth visit option. Telemedicine has increased dramatically with the COVID-19 pandemic, and patients are satisfied with telehealth as an option for care. Telemedicine offers the convenience of portable health care. However, those in underserved populations may or may not be able to access care through telemedicine, as telehealth requires reliable internet service, a smartphone or computer, and digital literacy. Lack of access to any of these may create health care disparities, especially in disadvantaged or vulnerable populations.
INTRODUCTION
According to the American College of Obstetricians and Gynecologists (ACOG), “The weeks following birth are a critical period for a woman and her infant, setting the stage for long-term health and well-being… It is recommended that all women have contact with their obstetrician-gynecologists or other obstetric care providers within the first 3 weeks postpartum.”1 Often called the “fourth trimester,” after giving birth, the recommendation for all mothers is a visit with their provider not only for postpartum wellness and assessing for postpartum complications, but also for life course planning and interconception care before 12 weeks post-delivery.1 It is also an opportunity for long-term discussions about interconception planning, contraception, dietary habits, exercise, and risk assessment,2 yet at most only 50-60% of women attend this well-woman office visit.3
Some interventions have been shown to improve the attendance rate of postpartum visits, in particular, programs which foster a sense of connection. One program that created an ongoing education program throughout the prenatal course for low-income, immigrant Latina mothers in 2010 found that the rate of postpartum visits showed a significantly higher number of patients returning for a postpartum clinic visit.4 Family medicine has long been an opportunity to improve postpartum care to the underserved,5 especially in those practices that combine a newborn well-child check with the postpartum visit. Additionally, there are some federal funding assistance programs for qualified health care centers that subsidize healthcare costs on a sliding scale system for patients from underserved populations.6 Another study from 2013 found that women were amenable to postpartum depression screening when bringing their newborns for well-baby office visits, indicating there are many opportunities for increasing
women’s access to care in the fourth trimester,7 as mother and infant care can become fragmented when they are separately addressed by different providers.1 However, these interventions are not widespread.
The COVID-19 pandemic dramatically changed the delivery of healthcare. Telemedicine, while making slow inroads into standard clinical practice over the past 20 years, has become a standard option since the COVID-19 pandemic,8 and patients are satisfied with telehealth as an option for routine care visits.9 The COVID-19 pandemic required many postpartum visits to become virtual initially. A recent study looked at postpartum visit attendance at the onset of the pandemic and noted a 90% increase in postpartum visit attendance when the visit was required to be virtual.10 According to a study by Hirshberg, Downes, & Srinivas, nearly twice as many women attended their primary care visits when the provider allowed for remote contact as opposed to in-person office visits.11At our institution post-COVID-19, we now include telehealth as an option for the postpartum visit, as opposed to a requirement. We aimed to investigate if offering a telehealth visit as the initial postpartum visit would increase the attendance of at least one postpartum visit, and thus care in the fourth trimester.
METHODS AND MATERIALS
We performed a retrospective cohort study of women receiving prenatal care through Westside Family Health (a federally qualified health center with multiple clinics throughout New Castle and Kent Counties in Delaware) to determine how many women attended a postpartum visit before telehealth was a routine option, versus after the onset of the COVID-19 pandemic when low-risk patients were routinely offered the option of either a traditional or telehealth visit for their postnatal care. This study was approved by the ChristianaCare Institutional Review Board and the Westside Family Health Review Board with waiver of informed consent. Westside Family Health is a federally qualified health center in which family medicine providers manage pregnancy and postpartum care for women with low-risk pregnancies. Standard practice for this office is to schedule 2- and 6-week postpartum visits. Prior to the COVID-19 pandemic, all visits were performed in-person. In the initial days of the pandemic, all visits were converted to telehealth; however, as we progressed through the pandemic, telehealth postpartum visits became an option instead of a requirement. Representative random samples were taken from one year of deliveries preimplementation of the option for telehealth postpartum visit (2018) and from one year of deliveries post-implementation of the option for telehealth postpartum visit (2021). We defined attendance of a postpartum visit as any visit discussing postpartum care within 8 weeks of delivery date. Subjects who did not complete their prenatal care with the office were excluded from the study. Based on prior studies, we estimated a 60% rate of attendance of the postpartum visit prior to implementation of the telehealth postpartum visit option. A hypothesized 10% increase in attendance was selected as a likely clinically significant difference. In order to determine this difference with an alpha of 0.05 and power of 80%, 356 subjects would be required per group.
The primary outcome of this study was rate of attendance of a postpartum visit before and after the option of a telehealth visit. The secondary outcomes included postpartum depression screening (defined as completion of a Patient Health Questionnaire-2 (PHQ-2) or Patient Health Questionnaire-9 (PHQ-9)).
Data collected included demographics (including race, ethnicity, and language), labor and delivery information (including parity, gestational age at delivery, mode of delivery, complications including gestational diabetes, hypertensive disorders of pregnancy, intra- or postpartum infection, preterm prelabor rupture of membranes, preterm labor, postpartum hemorrhage, cholestasis, twin gestation, intrauterine fetal demise, 3rd/4th degree or cervical laceration, shoulder dystocia, bladder injury, retained placenta). Ages were compared using t tests, whereas the remainder of the categorical demographic factors were compared using chi-square tests. The primary and secondary outcomes were analyzed using both chi-square tests and multivariable logistic regression.
RESULTS
A random, representative sample from each cohort was selected, with 349 subjects in the pre-implementation group and 351 subjects in the post-implementation group for a total of 700 subjects. Our population was largely Hispanic or Latina (60.7% in 2018 cohort and 56.1% in 2021 cohort) and over 40% Spanish speaking (48.7% in 2018 cohort and 41.9% in 2021 cohort).
The two groups had significantly different demographic data, which can be seen in Table 1. Average age between the groups was statistically, but not clinically, significantly different, at 29.0 and 30.4 in the pre- and post-implementation groups. There were additionally statistically significant differences between the ethnicities, races, and preferred languages, but again, these differences were likely not clinically significant. There was not a significant difference between the gestational age at delivery or the mode of delivery between the cohorts. The post-implementation group had significantly more complications than the pre-implementation group; however, documentation changes were made regarding this aspect of care between the years studied, increasing the available information about pregnancy and delivery complications in the 2021 cohort.
In regard to the primary outcome, Table 2 shows that the post-implementation group had a significant increase in the attendance of the postpartum visit (83.95% vs. 90.60%, p-value 0.0092). The odds ratio between the two cohorts was 1.887 (95% CI 1.171-3.043). Of the post-implementation group, 106 of the 318 subjects that attended a postpartum visit were telehealth visits (33.3%).
The secondary outcome analyzed was the rate of postpartum depression screening (Table 3). In 2018, 95.92% of subjects received a formalized screening for postpartum depression. In comparison, only 64.62% of subjects in 2021 received this screening, which was significantly different (p-value <0.0001). The odds ratio of postpartum depression screening between 2018 and 2021 was 0.065 (95% CI 0.034-0.123).
Table 1. Characteristics and Comparison of Pre- and Post-Telehealth Visit (THV) Implementation Cohorts
1Vaginal delivery includes spontaneous, forceps-assisted, and vacuum-assisted vaginal deliveries, as well as vaginal delivery after cesarean. 2 Complications include gestational diabetes, hypertensive disorders of pregnancy, intra- or post-partum infection, preterm prelabor rupture of membranes, preterm labor, postpartum hemorrhage, cholestasis, twin gestation, intrauterine fetal demise, 3rd/4th degree or cervical laceration, shoulder dystocia, bladder injury, retained placenta.
Table 2. Rate of Postpartum Visit Attendance Pre- and Post-Telehealth Visit Implementation
DISCUSSION
Attendance of the postpartum visit is an essential part of maternal healthcare. Despite this, it has often been shown that attendance of these visits is less than ideal, with as many as 40% of women not attending the recommended postpartum visit.11 Fortunately, in the centers observed in this study, we found that there was a high rate of attendance of at least one postpartum visit within eight weeks postpartum at baseline, with the rate of attendance when only in person visits were available in 2018 of 83.95%. This is likely related to the long-standing goal of family-centered healthcare. Even with this extraordinarily high attendance rate at baseline, after the implementation of the option for a telehealth postpartum visit, we found that there was a significant increase in the rate of postpartum visit attendance. Especially given the extremely high rate of maternal mortality in the United States, this lends credence to adding the convenience of telehealth visits as a welcome addition to optimizing maternal healthcare. Unlike seen in previous studies regarding telehealth postpartum visits, postpartum depression screening was negatively impacted by the introduction of the telehealth visit (Table 4). The post-implementation cohort saw an odds ratio of 0.065 for rate of screening for postpartum depression, with only 65.62% of women being screened as opposed to 95.92% pre-implementation. When looking specifically at the rate of screening for those who had a telehealth postpartum visit, only 10.38% of women received screening for postpartum depression. As the overall rate of postpartum depression of over 10% and absolute risk reduction with screening shown to be approximately 9%, this screening is an important part of the postpartum visit. With maternal suicide as a leading cause of maternal death in the postpartum period, outnumbering hemorrhage and hypertensive disorders, the clinical implication of failure to screen for postpartum depression is significant.12 In this particular set of offices, the responsibility to screen falls on different providers depending on the type of visit. For instance, for in person visits, a medical assistant ensures completion of the questionnaire, whereas for telehealth visits, the provider is responsible for administering the survey. A future direction for quality improvement in this area could include implementation of a pre-visit virtual intake that includes a postpartum depression screening tool to standardize the process and increase the likelihood that patients are being screened.
Telemedicine offers the convenience of portable health care,13 which may be of particular help to new parent, or when transportation is a challenge. However, those in underserved populations may or may not be able to access care through telemedicine. Telehealth requires reliable internet service, a smartphone or computer, and digital literacy. Lack of access to any of these may create health care disparities, especially in disadvantaged or vulnerable populations.14 Demographics associated with lack of technological access may include Black or African American race, rural locations, public or no insurance, limited English proficiency, or immigrant status.14–16 While use of smartphones is fairly widespread, to assume all persons have the ability to conduct a telemedicine visit is at the very least insensitive and at the worst, biased.
Many limitations of this study stem from the retrospective nature of the study. The number of subjects needed to power this study was 356 per arm; this number was close but unfortunately did not meet the desired number of subjects, which does serve as a significant limitation. The change in the documentation between cohorts limited the data that were able to be extracted, making desired study secondary outcomes unavailable for review. As the rate of postpartum visit attendance is already high in this setting likely related to joint mother-baby visits, the inability to determine which women had these joint-visits to determine this as a possible confounder is a limitation. In this study, we only examined telehealth visits in 2021, when this form of visit had been available for approximately onw year. Next steps after this study include comparison of the number of telehealth visits in 2020 and 2022 to see if the rate of postpartum attendance visits correlates with the rate of telehealth postpartum visits. Lastly, we were unable to determine if those that did not attend a visit had missed a scheduled visit or had never scheduled a postpartum visit. A next step could include determining those that had missed a scheduled visit and comparing the rate of missed in-person visits to missed telehealth visits. Another point which merits further investigations would be the difference in new pregnancy visits within two years of the studied delivery: this could be a future direction to examine.
In conclusion, the addition of the option for a telehealth postpartum visit can increase the attendance at the post-delivery visit, but this may come at the expense of postpartum depression screening.
Ms. Chichester may be contacted at MLCobnurse@gmail.com
Table 3. Rate of Postpartum Depression Screening Pre- and Post-Telehealth Visit
Table 4. Rate of Postpartum Depression Screening by Type of Visit
REFERENCES
1. American College of Obstetricians and Gynecologists. (2018). ACOG committee opinion no. 736: Optimizing Postpartum Care. Obstetrics and Gynecology, 131(5). https://doi.org/10.1097/AOG.0000000000002633
2 Doret, M. (2015, December). [Postnatal visit: Routine and particularity after complicated pregnancy—Guidelines for clinical practice] Journal de Gynecologie, Obstetrique et Biologie de la Reproduction, 44(10), 1118–1126. https://doi.org/10.1016/j.jgyn.2015.09.018
3 Fabiyi, C. A., Reid, L. D., & Mistry, K. B. (2019, August). Postpartum health care use after gestational diabetes and hypertensive disorders of pregnancy. J Womens Health (Larchmt), 28(8), 1116–1123 https://doi.org/10.1089/jwh.2018.7198
4. Marsiglia, F. F., Bermudez-Parsai, M., & Coonrod, D. (2010, August). Familias Sanas: An intervention designed to increase rates of postpartum visits among Latinas. Journal of Health Care for the Poor and Underserved, 21(3A, Suppl), 119–131 https://doi.org/10.1353/hpu.0.0355
5 Little, S. H., Motohara, S., Miyazaki, K., Arato, N., & Fetters, M. D. (2013, Nov-Dec). Prenatal group visit program for a population with limited English proficiency. J Am Board Fam Med, 26(6), 728–737. https://doi.org/10.3122/jabfm.2013.06.130005
6. HealthCare.gov. (n.d.). Federally qualified health center (FQHC) - glossary. Retrieved April 8, 2023, from https://www.healthcare.gov/glossary/federally-qualified-health-center-fqhc/
7 Walker, L. O., Im, E. O., & Tyler, D. O. (2013, Jul-Aug). Maternal health needs and interest in screening for depression and health behaviors during pediatric visits. J Pediatr Health Care, 27(4), 267–277 https://doi.org/10.1016/j.pedhc.2011.11.008
8 Uustal, M., & Blackmon, L. (2020, December). Telemedicine technology and implications for reproductive office operations. Fertility and Sterility, 114(6), 1126–1128. https://doi.org/10.1016/j.fertnstert.2020.10.049
9. Zimmerman, M., Benjamin, I., Tirpak, J. W., & D’Avanzato, C. (2021, July). Patient satisfaction with partial hospital telehealth treatment during the COVID-19 pandemic: Comparison to in-person treatment. Psychiatry Research, 301, 113966 https://doi.org/10.1016/j.psychres.2021.113966
10. Arias, M. P., Wang, E., Leitner, K., Sannah, T., Keegan, M., Delferro, J., . . . Hamm, R. F. (2022, May). The impact on postpartum care by telehealth: A retrospective cohort study. American Journal of Obstetrics & Gynecology MFM, 4(3), 100611 https://doi.org/10.1016/j.ajogmf.2022.100611
11 Hirshberg, A., Downes, K., & Srinivas, S. (2018, November). Comparing standard office-based follow-up with text-based remote monitoring in the management of postpartum hypertension: A randomised clinical trial. BMJ Quality & Safety, 27(11), 871–877 https://doi.org/10.1136/bmjqs-2018-007837
12 American College of Obstetricians and Gynecologists. (2018). ACOG Committee Opinion No. 757: Screening for perinatal depression. Obstetrics and Gynecology, 132(5). https://doi.org/10.1097/AOG.0000000000002927
13 Rabinowitz, G., Cho, L. D., Benda, N. C., Goytia, C., Andreadis, K., Lin, J. J., Poeran, J. (2023, May-Jun). The telemedicine experience in primary care practices in the United States: Insights from practice leaders. Annals of Family Medicine, 21(3), 207–212. https://doi.org/10.1370/afm.2967
14. Harris, A., Jain, A., Dhanjani, S. A., Wu, C. A., Helliwell, L., Mesfin, A., . . . Ranganathan, K. (2023, March 1). Disparities in telemedicine literacy and access in the United States. Plastic and Reconstructive Surgery, 151(3), 677–685. https://doi.org/10.1097/PRS.0000000000009939
15 Falicov, C., Niño, A., & D’Urso, S. (2020, September). Expanding possibilities: Flexibility and solidarity with underresourced immigrant families during the covid-19 pandemic. Family Process, 59(3), 865–882. https://doi.org/10.1111/famp.12578
16. Wang, Y., Do, D. P., & Wilson, F. A. (2018, November). Immigrants’ use of ehealth services in the United States, national health interview survey, 2011-2015. Public Health Rep, 133(6), 677–684 https://doi.org/10.1177/0033354918795888
DECEMBER 2024
The Nation’s Health headlines
NATION’S HEALTH
Online-only news from The Nation’s Health newspaper
Climate change could worsen dangers of fungal diseases
Kim Krisberg
More kids lacked health insurance in 2023, Census Bureau finds
Natalie McGill
High stress a major problem for US parents, surgeon general says in new advisory
Sophia Meador
Q&A with NCIRD’s Daskalakis: Promoting, providing vaccinations can help prevent “triple-demic” of infectious disease this season
Sophia Meador
Public health on the ballot in states across US in November
Mark Barna
The path to recovery: Healthy healing after injury or illness
Teddi Nicolaus
Creating an advocacy-ready workforce starts with students, task force says Teddi Nicolaus
New APHA book urges systems approach for public health
Mark Barna
Newsmakers: November/December 2024
Sophia Meador
Many other articles available when you purchase access
Entire Issue $12
Visit https://www.thenationshealth.org/user
Virtual Primary Care in a Large Delaware-Based Independent Academic Medical Center: Impact and Opportunity
Darrell C. Dow, M.S.
Corporate Director, Digital Solutions & Analytics, Center for Virtual Health, ChristianaCare
Sarah E. Schenck, M.D., F.A.C.P.
Executive Director, Center for Virtual Health, ChristianaCare
Tracy L. Bell, M.B.A., P.M.P., L.S.S.G.B.
Senior Enterprise Project Manager, ChristianaCare
Stephanie C. Roth M.L.I.S.
Medical Librarian, Flinn Medical Library, ChristianaCare
Omar Khan, M.D., M.H.S.
Enterprise Chief Scientific Officer, ChristianaCare; Professor, Department of Family & Community Medicine, Thomas Jefferson University
ABSTRACT
COVID-19 and related challenges to patient access necessitated the development of new models of care to ensure a healthy patient population. This paper describes the outcomes of a pilot virtual primary care program at a large independent academic health center in Delaware. The preliminary results are encouraging from the perspective of provider and patient satisfaction, as well as the utility of the operational model. A complete cost-benefit analysis was beyond the scope of the paper; thus, future operational research should focus on the metrics of cost and quality as key indicators of model sustainability.
INTRODUCTION
The key to unlocking better health outcomes and an overall better patient experience at a reduced cost is an attainable healthcare trifecta. Global experience has demonstrated effective primary healthcare to be the key driver of this set of outcomes.1 The eminent primary care scholar Dr. Barbara Starfield described the four key elements of effective primary care as: ‘contact, comprehensiveness, continuity and coordination.’2 When patients are more engaged with primary care, they achieve better health outcomes and higher rates of satisfaction at a lower cost to the healthcare system at large.3
The following describes the creation and deployment of a virtual primary care model for covered employees of a large, Delawarebased health system. We believe this to be an opportunity to leverage this model for improves patient access and better, more equitable outcomes.
BACKGROUND
Primary care in general is well-positioned to pilot virtual care. We expanded primary care services to provide virtual (including telehealth) services in a multitude of care settings.4,5 Postpandemic, the convenience that virtual care has proven to provide for both the patient and the provider has resulted in several health systems continuing to expand those services.6
As with other health specialties, there are a variety of ways in which virtual care is delivered in the primary care setting. For virtual visits, patients can be seen synchronously (in real-time by audio or video) similar to the traditional patient visit that mirrors the care given in a ‘bricks-and-mortar’ facility. These synchronous visits can take place in a variety of settings such as the patient’s home, a medical facility, or mobile healthcare unit. Mobile units may provide at-home services or in-home technology such as blood pressure cuffs or digital scales.
By contrast, asynchronous virtual care is delivered through other means, such as secured text messaging, either inbound (from the patient requesting care) or outbound (from the provider who may send standard screening forms and check-ins). The patient receives care on time, but not in real-time.
Virtual primary care has grown tremendously due to the necessities of the COVID-19 pandemic but far from stopping at being a short-term solution, it continues to empower patients and providers with convenience, ease of use, and enhanced access that exceeds pre-pandemic levels.7 Although patients and providers seem positive about the convenience of switching to virtual healthcare, the value proposition of this model is less clear.
Primary care includes several medical disciplines (e.g. family medicine, internal medicine, pediatrics, and geriatrics). It incorporates services including chronic disease management, preventive care, urgent and acute care. The power of primary care lies in the continuity relationship of the patient and provider which can strengthen over time as providers learn the history, values, and goals of patients and families, and caregivers.
Traditionally, this clinical relationship was more formal and took place through scheduled office visits. In a virtual setting, the provider can develop more of a rapport with the patient, as it is not limited by scheduled in-office visits. Since care can now be delivered asynchronously (e.g. texts, emails, messaging) the interaction between patient and caregiver is sometimes more frequent and less formal.
The virtual care model is considered high-frequency, lowintensity care with multiple “mini encounters” over weeks, months, and even years. Patients’ needs are addressed in real-time digitally; without the need to wait for a scheduled visit. When a visit is desired, patients can quickly visit their primary care provider in a real-time video chat. Patients have much broader access as virtual primary care providers are no longer constrained
to scheduled office visits with most care and administrative tasks being accomplished asynchronously. This convenience can provide better health outcomes for the patient.
METHODS
We examined virtual care in the state of Delaware for a limited patient population as part of ongoing monitoring of our program. This is a snapshot of the care received in our region and thus may help evaluate similar programs throughout the state or other regions.
The patients receiving virtual primary care in this sample population were employed by our health system. Data was collected and reported in aggregate using quality improvement indicators to measure care in this setting. This QI project was not considered human subject research.
This population studied was assessed using multiple outcomes: total emergency department utilization, avoidable emergency department utilization, urgent care utilization, patient satisfaction, and provider satisfaction.
Insurance claims data was collected from a period of July 2020 to May 2023; our review included data collected for 683 patients who had at least 12 months of measurable claims activity to before enrollment with virtual primary care as well as 12 months of measurable claims activity after enrolling to create a pre/post comparison. In addition, claims data for the same July 2020 to May 2023 period were collected for a comparison group of 17,825 patients who were attributed to or had visits with one of the traditional primary care offices. Due to claims availability, the population of 683 patients consisted entirely of ChristianaCare employees, spouses, and adult dependents. During the period measured, ChristianaCare benefits were administered by two different payors resulting in two claims datasets that were combined for purposes of analysis. Thus, a weakness in the generalizability of this work is that it examines those employed in a health system population.
Avoidable emergency department visits where individuals sought care in the emergency department for conditions that could have been managed at a lower acuity of care or prevented altogether with appropriate primary care were calculated from claims-based diagnoses compared to the New York University Emergency Department (NYU ED) visit severity algorithm.
Using the guidelines of the 2010 validation study of the NYU ED algorithm,8 avoidable visits were determined using the 50% probability threshold.
Anonymous surveys were sent to all primary care teams in the virtual practice including physicians, nurses, and medical assistants. The survey requested feedback on how well teams worked together, the likelihood to recommend the practice as a place to work, and the likelihood to recommend the practice as a place to receive care. Fourteen of the team members surveyed responded. Clinical quality metrics for all patients were calculated from electronic medical record data, payor claims files, and Health Information Exchange (HIE) data aggregated in Oracle Cerner HealtheRegistries. HealtheRegistries is based on the Healthcare Effectiveness Data and Information Standards (HEDIS®) developed by the National Committee for Quality Assurance (NCQA). The data on clinical quality was then compared to Delaware’s traditional brick-and-mortar practices that opened about the same time as the Center for Virtual Health. Comparison populations not derived internally from HealtheRegistries were found via literature review with sources indicated in the results below.
Note that patient satisfaction survey methodology changed during the analysis period resulting in too few data points to reasonably determine a Net Promoter Score (NPS). However, prior scores were routinely at or above national averages for the healthcare industry.
RESULTS
Data Analysis Results
Claims-Based Utilization
The data collected and analyzed shows that virtual primary care patients experienced a significant decline in utilization at urgent care clinics, emergency departments, and inpatient facilities when compared to utilization a year prior to joining the virtual primary care practice. It was also demonstrated that virtual primary care patients utilized significantly less than the general population of primary care patients who received care at traditional primary care practices.
Of note is the decline in the virtual practice patient population of avoidable emergency department visits. Avoidable visits were observed to be 9% higher than those of patients in traditional practices in the pre-enrollment period but declined to 9% lower than the traditional patient population by 12 months after enrollment with virtual primary care (Table 1).
Table 1. Avoidable Emergency Department Visits
Provider Satisfaction
Care team members in the virtual practice, including physicians, nurses, and medical assistants from both primary care and specialty teams, were surveyed anonymously in May 2023 with respondents giving agreement (8=strongly agree) or disagreement (1=strongly disagree) to the statements as shown in Table 2.
An 8-point scale (1= Strongly Disagree, 8=Strongly agree) was also used to ask the questions in Table 3.
As shown in Table 3, 79% of virtual practice staff responded positively about the virtual environment being safe and effective with 21% remaining neutral on the question Additionally, 71% preferred practicing in a virtual practice as opposed to prior roles in a traditional in-person practice while the remaining 29% were neutral. A total of 71% of team members said they agreed or strongly agreed (responding with a 6-8 on the scale) with the
virtual practice as a place to work while 100% agreed or strongly agreed (6-8 on the scale) that they would recommend the virtual practice to friends or family as a place to receive care.
Clinical Quality Outcomes
As demonstrated in Table 4, virtual primary care results were equal to or better than traditional brick-and-mortar practices in both measures of patient access and measures of clinical quality. These results were gathered in May 2023 via comparison of HEDIS® measure outcomes between Center for Virtual Health patients and deidentified patient data from multiple traditional primary care practices in the State of Delaware. Access particularly stands out as an advantage in the virtual model with new patients having the option to schedule a new patient appointment on the same day that they enroll.
Table 2. Anonymous Virtual Practice Team Member Survey Results
Table 3. Anonymous Virtual Practice Team Member Survey Results, part 2
Table 4. Clinical Quality Outcomes
DISCUSSION
The results from our work demonstrate that, if adequately resourced, avoidable visits to emergency and urgent care settings can be reduced. We also showed a high level of patient and provider satisfaction with this model; this is consistent with literature from across the U.S. following the COVID-19 pandemic.9
While a detailed discussion of the social determinants of health is beyond the scope of this paper, access to care has been studied as a critical determinant of health.10 Virtual primary care has the potential to positively impact this factor. Other related determinants include transportation and even crime and safety, which might render physical access more challenging than a virtual model. While our work was not designed to address these larger societal factors at this time, we are pleased to contribute positively to a mechanism to enhance access and perhaps bypass factors that may impede access, whether a pandemic exists, or not.
It should be noted that there exists a “digital divide” which may create new access barriers for some. The availability of a device with high-speed connectivity as well as audio and video capability may be a barrier as well, and this issue will need addressing if a virtual model is scaled up more broadly.
This project assessed improvements made in healthcare quality and access in a specific patient sample. As such, the results may be generalizable to employees of similar organizations such as large health systems. We cannot yet comment on the generalizability of this model to a statewide population. However, since in Delaware, our employees are demographically representative of the state, it is a reasonable assumption from this pilot study that the methodology could be tested on a larger population level.
An important question concerns the return on financial investment for large-scale virtual programs. The capital investment costs for such programs can be significant, and while our virtual health program was internally funded and expanded out of necessity in the COVID-19 pandemic, future expansions will need to show financial feasibility. Delaware is not unique in considering these issues. Nationwide, models are underway to test telemedicine as a high-quality, reimbursable mechanism for providing primary and specialty care.11 We encourage expanded testing of these models and further exploration into the impact of our model on future use cases in Delaware and beyond. We also encourage a holistic assessment of the benefit, not just in billable hours of care, but of true improvements in population health, patient satisfaction, and provider satisfaction. Our initial results are promising, and further assessments are warranted to validate these on a larger scale.
Dr. Dow may be contacted at darrell.c.dow@christianacare.org
REFERENCES
1. Lewin, S., Lavis, J. N., Oxman, A. D., Bastías, G., Chopra, M., Ciapponi, A., . . . Haines, A. (2008, September 13). Supporting the delivery of cost-effective interventions in primary healthcare systems in low-income and middle-income countries: An overview of systematic reviews. Lancet, 372(9642), 928–939. https://doi.org/10.1016/S0140-6736(08)61403-8
2 Starfield, B. (1979, May). Measuring the attainment of primary care. Journal of Medical Education, 54(5), 361–369 https://pubmed.ncbi.nlm.nih.gov/374735
3 Starfield, B., Shi, L., & Macinko, J. (2005). Contribution of primary care to health systems and health. The Milbank Quarterly, 83(3), 457–502. https://doi.org/10.1111/j.1468-0009.2005.00409.x
4 Etz, R. S., Solid, C. A., Gonzalez, M. M., Britton, E., Stange, K. C., & Reves, S. R. (2023, Jul-Aug). Telemedicine in primary care: Lessons learned about implementing health care innovations during the COVID-19 pandemic. Annals of Family Medicine, 21(4), 297–304 https://doi.org/10.1370/afm.2979
5 Chang, J. E., Lai, A. Y., Gupta, A., Nguyen, A. M., Berry, C. A., & Shelley, D. R. (2021, June). Rapid transition to telehealth and the digital divide: Implications for primary care access and equity in a post-COVID era. The Milbank Quarterly, 99(2), 340–368 https://doi.org/10.1111/1468-0009.12509
6. Shaver, J. (2022, December). The state of telehealth before and after the COVID-19 pandemic. Primary Care, 49(4), 517–530 https://doi.org/10.1016/j.pop.2022.04.002
7. Wosik, J., Fudim, M., Cameron, B., Gellad, Z. F., Cho, A., Phinney, D., Tcheng, J. (2020, June 1). Telehealth transformation: COVID-19 and the rise of virtual care. Journal of the American Medical Informatics Association : JAMIA, 27(6), 957–962 https://doi.org/10.1093/jamia/ocaa067
8. Ballard, D. W., Price, M., Fung, V., Brand, R., Reed, M. E., Fireman, B., Hsu, J. (2010, January). Validation of an algorithm for categorizing the severity of hospital emergency department visits. Medical Care, 48(1), 58–63 https://doi.org/10.1097/MLR.0b013e3181bd49ad
9 Baughman, D. J., Jabbarpour, Y., Westfall, J. M., Jetty, A., Zain, A., Baughman, K., . . . Waheed, A. (2022, September 1). Comparison of quality performance measures for patients receiving in-person vs telemedicine primary care in a large integrated health system. JAMA Network Open, 5(9), e2233267 https://doi.org/10.1001/jamanetworkopen.2022.33267
10. Pratt, C., Taylor, R., & Smith, S. D. (2023, December). Health equity and access to health care as a social determinant of health: The role of the primary care provider. Primary Care, 50(4), 549–559. https://doi.org/10.1016/j.pop.2023.04.006
11 Zhang, X., McJoynt, T., Furst, J. W., & Myers, J. F. (2022, JanDec). Establishing a patient-centered virtual care model across the continuum of care. Journal of Primary Care & Community Health, 13(13), 21501319221088823. https://doi.org/10.1177/21501319221088823
It’s not too late to get your flu vaccine
Protect yourself and others from influenza (“the flu”) by getting the 2024-25 flu vaccine The flu can cause severe respiratory illness, disease, and death. Everyone 6 months and older is eligible to get the flu vaccine, according to the Centers for Disease Control and Prevention Seniors aged 65 and older need a higher dose flu vaccine.
Even though it is December, it’s not too late to get the flu vaccine. It is best to receive the flu vaccine before holiday gatherings, as it takes about two weeks for the body to develop protective antibodies.
The flu is already circulating in the First State. In the week ending November 30, 2024, Delaware had 38 new cases of influenza and no flu hospitalizations, according to the Division of Public Health (DPH). In Delaware, 212,058 doses of flu vaccine (21.6%) had been administered as of November 30
Visit flu.delaware.gov for more information and to find vaccine locations. DPH’s special respiratory viruses newsletter edition can be found at https://www.dhss.delaware.gov/dph/dphbulletins.html
DPH’s health care providers, schools, and workplaces can find free flu prevention marketing items at covidmaterialsde.com.
DPH updates COVID-19 vaccine campaign and shares materials
New posters, fact cards, and social media posts are part of the updated COVID-19 vaccine campaign produced by the Division of Public Health (DPH). The materials educate Delawareans about the COVID-19 vaccine’s benefits and availability.
“Today’s the day to get the updated COVID-19 vaccine” is the tag line on billboards, streaming services, radio, and Facebook, X (formerly Twitter), and Instagram posts.
The campaign reminds individuals that they can get their COVID-19 and flu vaccines at the same time Another message is to visit de.gov/coronavirus to stay informed and find the nearest vaccine location.
Materials are in English and Spanish, with the flyer and fact cards also offered in Haitian Creole. Health care systems, community organizations, schools, and those communicating to the public can save time and money by using these free materials. Order these items and items from other health campaigns at covidmaterialsde.com.
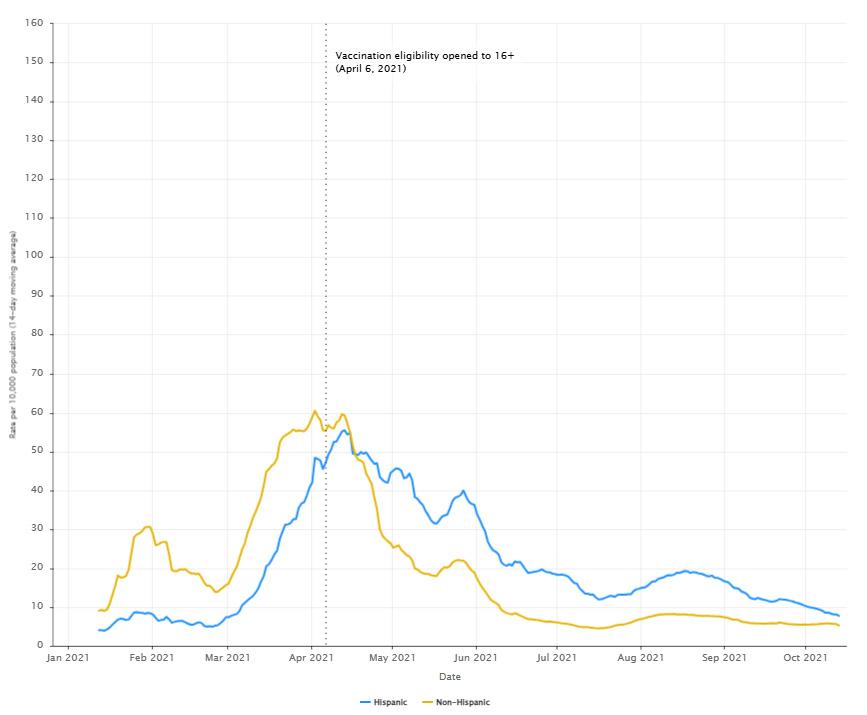
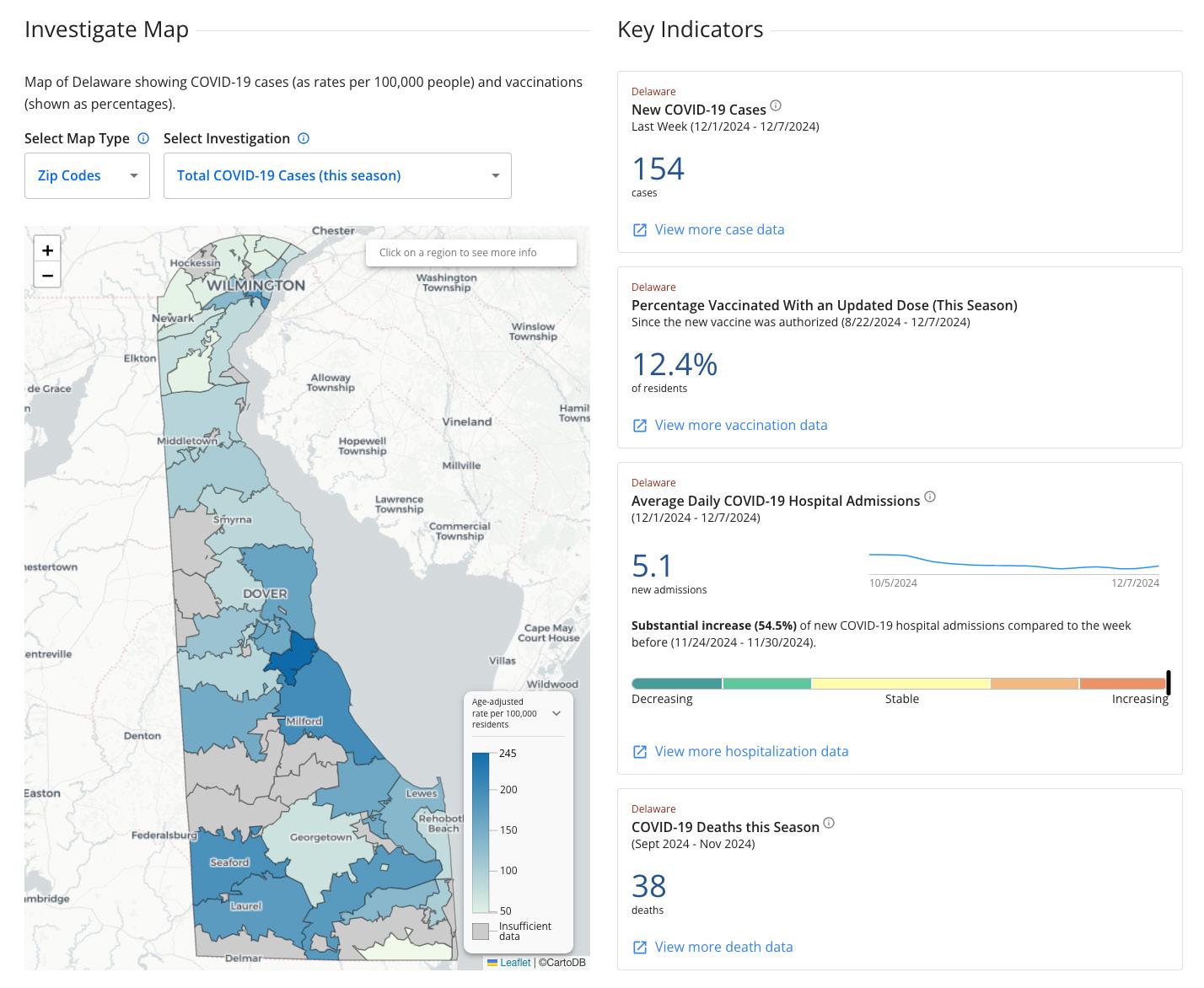
According to DPH, for the 2024 to 2025 winter virus season, the age-adjusted rate of new COVID-19 cases per 100,000 people in Delaware was 12.8 in Sussex County, 5.7 in Kent County, and 6.2 in New Castle County for the week ending November 30, 2024 Since the new COVID-19 vaccine was authorized on August 22, 2024, 12.2% of Delaware residents had received it as of November 30
For Delaware’s COVID-19 data, visit myhealthycommunity.dhss.delaware.gov
Delaware paramedics administer 250th unit of whole blood for prehospital care
Delaware paramedics administered the 250th unit of whole blood as a result of collaboration among county paramedic agencies, the Division of Public Health (DPH) Office of Emergency Medical Services (OEMS), the Delaware Emergency Management Agency, and the Blood Bank of Delmarva
A leader in prehospital care, the state also became the first in the nation that has paramedic agencies in every county providing whole blood for patients before they reach the hospital. Paramedics value whole blood for its components: red blood cells, clotting factors, platelets, and plasma. Their most common application is when patients have suffered traumatic injuries resulting in massive blood loss.
On Nov. 23, New Castle County Emergency Medical Services gave the 150th unit in their county and soon after, the 151st, which became the 250th unit in the state Sussex County also achieved a significant milestone on Nov. 25 when it administered its 100th unit of whole blood Additionally, Kent County EMS delivered their first unit on Nov. 24, which despite the critical nature of the patient’s injuries, provided improvement in vital signs.
The treatment was approved in May 2023 and first used as a pilot program by paramedics in New Castle and Sussex counties. Early success led to statewide adoption for all paramedic agencies, with Kent County currently carrying blood and Delaware State Police paramedics adding blood in early 2025. Nationally, less than 10% of EMS agencies carry and administer whole blood, according to the National Association of State EMS Officials.
Fore more information about OEMS, visit https://www.dhss.delaware.gov/dph/ems/ems.html
Cervical cancer screenings offered at Porter Public Health Clinic January 22
The Division of Public Health (DPH) is offering cervical cancer screenings at the Porter State Service Center in observance of Cervical Health Awareness Month
The Porter Public Health Clinic, located at 509 W. 8th St. #3, Wilmington, Del. is offering cervical cancer screening appointments on January 22 from 8:30 a.m. to 3:30 p.m. except from 12:00 p.m. to 1:00 p.m. DPH’s Screening for Life (SFL) Program is hosting the day for SFL enrolled women aged 35 and older to receive a cervical exam with a Pap test that detects abnormal cells on the cervix. Clients unable to attend on January 22 should select another appointment date without delay
SFL enrolled clients aged 35 and older will be asked if they want to participate in the WISEWOMAN (WellIntegrated Screening for Women Across the Nation) Program during the same office visit. WISEWOMAN assesses clients for risk factors for cardiovascular disease or stroke Women identified with those risk factors are eligible for certain blood tests and access to healthy behavior support services at no cost Women have up to 30 days to get blood work completed.
• SFL enrolled clients who want to make an appointment should call 302-744-1040 (Option 2). Click here to enroll in SFL or for more information.
The Division of Public Health (DPH) published three reports:
• State of Delaware Public Drinking Water Annual Compliance Report and Summary for 2023
• Childhood Blood Lead Surveillance in Delaware, 2023 Annual Report
• Heat-Related Illness Emergency Department Visits in Delaware, 2019-2023
Getty Images
Prepare for hazardous winter weather
Winter weather can bring snow and ice, extreme cold, and power outages. Be prepared with these helpful checklists from PrepareDE.org:
Home
• Assemble a household emergency kit containing water and food for household members and pets.
• Have a warm coat, gloves or mittens, a hat, waterresistant boots, and blanket for every household member. Hypothermia, when the body becomes chilled, can be deadly.
• Stay inside during storms.
Vehicle
• Have a mechanic check antifreeze levels, the battery and ignition system, oil, tires, brakes, windshield wipers and fluid, lights (including hazard lights); and the heater, defroster, and thermostat. It is also important to check for leaks in the exhaust system because carbon monoxide is deadly.
• Keep vehicle gas tanks at least half full in case of emergency and to prevent fuel lines from freezing.
• Before driving, be aware of traffic advisories and restrictions Avoid unnecessary driving during bad weather. Let someone know your destination, route, and when you expect to arrive.
• Keep an emergency kit in your vehicle to keep you safe and alive if your vehicle becomes stuck in a snowdrift or in a lengthy traffic jam.
Know the Evacuation Zones for your residence, workplace, and places where you spend time. Visit https://preparede.org/know-your-zone/#zonefinder Keep your Evacuation Zone where it can be accessed quickly, such as on your cell phone and in your emergency kit.
For more information, visit PrepareDE.org.
Help unhoused people find Code Purple shelters this winter
During extreme cold events in Delaware, Code Purple is activated to shelter homeless individuals and families. Unhoused individuals seeking shelter should call the Delaware Housing Alliance’s Centralized Intake Line at 1-833-346-3233, Monday through Friday between 8:00 a.m. and 5:00 p.m.; send an email to intake@housingalliancede.org; or call a participating shelter listed below.
New Castle County
Pre-register for Friendship House shelters by visiting their Empowerment Centers or calling:
• 720 N. Orange St., Wilmington, Del.: 302-652-8033
• 62 E. Delaware Ave., Newark, Del.: 302-544-0165
• 44 W. Main St., Middletown, Del.: 302-416-0982
Code Purple Kent County
First come, first served. Starts daily between 5:00 p.m. and 8:00 a.m. from December 1 to March 31 unless otherwise stated. Nothing is needed to enter. Hotline: 1-800-733-6816; codepurpledelaware@gmail.com
• Dream4 Foundation Sanctuary shelter (for women and children), Maranatha Life Changing Church, 1203 E. Division St., Dover, Del.: 1-800-733-6816
• 203 E. Division St., Dover, Del.: 1-800-733-6816.
Code Purple Sussex County
Priority is given to those who register in person for the following night.
Hotline: Monday through Friday, 10:00 a.m. to 3:00 p.m., 302-629-7050. Other days and times: 302-519-0024
• Grace Seaford Church (for women), 805 Atlanta Road, Seaford, Del. 19973
• St. Luke's Parish Hall (for men), 202 N. North St., Seaford, Del. 19973
• Georgetown Presbyterian Church (for men), 203 N. Bedford St., Georgetown, Del. 19947
• Milford Church of the Nazarene (for women), 11 N.W. Salevan Place, Milford, Del. 19963
• Avenue United Methodist Church (for men), 20 N. Church Ave , Milford, Del. 19963
• St. Jude The Apostle Church (for men), 152 Tulip Drive, Lewes, Del. 19958
• Lutheran Church of Our Savior (for women), 20276 Bay Vista Road, Rehoboth Beach, Del. 19971.
To connect with Code Purple resources, call or text Delaware 211, use the Delaware 211 mobile app, or visit www.delaware211.org.
Getty Images
National Weather Service revises watches and warnings for cold
As of October 1, 2024, the National Weather Service (NWS) simplified its winter hazard messaging to clarify that cold can be dangerous with or without wind. NWS replaced Wind Chill notifications with Extreme Cold Watch, Extreme Cold Warning, and Cold Weather advisories
weather.gov
An Extreme Cold Watch is issued when dangerously cold air, with or without wind, is possible. Check the forecast and be prepared in case a Warning is issued.
An Extreme Cold Warning is issued when dangerously cold air, with or without wind, is expected with conditions that could lead to frostbite or hypothermia. Avoid going outdoors. If you must go outside, limit time outdoors, dress in layers, cover up exposed skin, and make sure at least one other person knows your whereabouts. Update that person when you arrive safely at your destination.
A Cold Weather Advisory is issued when seasonably cold air temperatures or wind chill values are expected or occurring.
NWS renamed Hard Freeze Watches to Freeze Watches and Hard Freeze Warnings to Freeze Warnings. A Freeze Watch is issued when there is a potential for significant, widespread freezing temperatures within the next 24 to 36 hours.
A Freeze Warning is issued when temperatures are forecasted to go below 32 degrees F for a long period of time. This temperature threshold kills some types of commercial crops and residential plants.
ATSDR report about PFAS includes findings from New Castle, Delaware
A December 10 press release posted to the State of Delaware website Delaware.gov summarizes a health consultation completed by the U.S. Department of Health and Human Services’ Agency for Toxic Substances and Disease Registry (ATSDR) regarding exposure to per- and polyfluoroalkyl substances (PFAS) within 41 residences near the Delaware Air National Guard Base in New Castle, Del. and 51 homes in Westfield, Mass.
The report presents the findings for seven types of PFAS, called “forever chemicals,” in settled household dust samples. According to the report, the U.S. Environmental Protection Agency funded and sponsored the effort, and officials from the Delaware Department of Natural Resources and Environmental Control (DNREC) and the Division of Public Health plan to model methodologies to further study local sources of PFAs and potential exposures to them.
Click here to access the report or read it at the link within the press release. For Delaware’s work on PFAS and links to other reports, visit De.gov/pfas
To lower the risk of PFAS exposure from contaminated household dust, the authors advise to:
• Clean your house on a regular basis.
• Dust with wet cloths.
• Vacuum with HEPA filters.
• Change heating and cooling unit filters regularly.
• Choose furniture and carpets that are not labeled “stain resistant.” Do not apply stain-resistant treatments to items.
• Do not use products with the words “fluoro” and “perfluoro” on the label.
• Replace or remove worn products with newer, PFAS-free items.
DPH regulations available to view
Three sets of Division of Public Health regulations are in the December issue of the Delaware Register of Regulations. They are: 4465 Delaware Radiation Control Regulations and 4466 Radiation Technologists/Technicians (Certification) (both proposed); and 4106 Practice of Non-Nurse Midwifery (final). The regulations are accessible online at http://regulations.delaware.gov or by calling DPH at 302-744-4951.
Public comment is accepted in written form via email to DHSS_DPH_regulations@delaware.gov, or by U.S. mail to: Vicki Schultes, Hearing Officer, Division of Public Health, 417 Federal Street, Dover, DE 19901.
Integrating Collaborative Robots into a Complex Hospital Setting: A Qualitative Descriptive Study
Susan Smith Birkhoff, Ph.D., R.N. ChristianaCare Health System
Paige Merring, M.S.N., R.N., C.C.R.N., N.E.A.-B.C. ChristianaCare Health System
Amanda Spence, B.S.N., R.N.-B.C. ChristianaCare Health System
Wendy Bassett ChristianaCare Health System
Stephanie C. Roth, M.L.I.S. ChristianaCare Health System
ABSTRACT
Objective: To describe the use, activities, and human interactions of cobots as a delivery system for medications, supplies, and equipment within a complex and multi-level 900-bed hospital setting. Integrating collaborative robots (cobots) into existing hospital workflows as a secure delivery transportation system is an early innovation and emerging area to explore. Methods: Guided by the Diffusion of Innovations theory, a qualitative descriptive design was used to build the foundational knowledge required to better understand and describe cobot implementation in the acute care hospital setting. The cobots were observed on all shifts, on different days of the week as they interacted with staff members, clinicians, and visitors while they traveled throughout the hospital completing deliveries. Data were analyzed among the study team members using an inductive coding approach followed by a qualitative content analysis level of interpretation. Results: For seven weeks from November 2022 – December 2022, 33 hours were collected from 23 individual cobot observation sessions. These observations included 89 end-to-end cobot deliveries. After analysis, four major themes emerged: 1) humanization of robots, 2) usability of robots, 3) cobots’ autonomy, and 4) cobots’ functionality within a dynamic hospital environment. Conclusions: Implementing cobots as a semi-autonomous delivery transporter is still in the early innovation phase. The cobots used in this study required human support to function adequately in a complicated and unpredictable environment. To sustainably augment current and future workflows exclusively performed by human, the cobots will need to transition toward greater model of autonomy and less human assistance.
ACKNOWLEDGEMENT
The authors wish to acknowledge ChristianaCare Caregivers and Leaders.
FUNDING
Funding for this research was provided by the American Nurses Foundation Reimagining Nursing Initiative.
INTRODUCTION AND BACKGROUND
Robotic technology has become increasingly integrated into the healthcare landscape. Robots represent a potentially important, even transformative role that started in 1985 through surgical assistance.1 Over the last 40 years, robots have been used in a variety of supportive roles in healthcare such as rehabilitation, surgery, telepresence (i.e. virtual consults), pharmacy, social assistance (i.e. companionship), interventional medicine, radiology imaging assistance, disinfection, radiotherapy, and delivery/transport support.2,3 Robots in healthcare were valued at $4.06 billion in 2022 and are projected to double in value by 2032.4 With the rising demands in healthcare, a limited workforce,
and increasing sophistication of robotic technology, robots are projected to further augment clinical practice that was exclusively human led.5
To meet this evolving need, human-robot collaboration (HRC) has become a critical design principle to ensure robots can safely assist humans in a shared and collaborative workspace.6 A cobot (collaborative robot) incorporates HRC into its functional design6,7 and HRC is important to consider in the inpatient healthcare setting where the environment is complex and unpredictable, and requires rigorous safety measures.5
Cobots are being introduced into the dynamic acute care hospital settings to assist with non-clinical tasks such as completing secure deliveries,2 which in turn may have implications for the healthcare workforce and their work environment. For example, a twowave study design explored whether offloading the delivery of instruments and medical supplies to a robot within an operating room could improve nurses’ job satisfaction and perceived health improvement (i.e., the physical burden of carrying heavy supplies and equipment).8 Their findings supported that amplifying nurses’ focus on their professional tasks increased their overall job satisfaction (p<0.05) and shifting non-professional tasks to a robot improved their perceived health (p<0.05).
Previous research and literature reviews focused on transferring tasks to cobots9–11 and its implications for clinical practice.
Freeman, et al. conducted a proof-of-concept experiment in a simulated intensive care room using a cobot to manually push buttons on an intravenous pump and a call bell, adjust knobs on a ventilator, silence alarms, and turn the dial to increase oxygen delivery.7 Utilizing a cobot to perform these tasks tested whether nurses could enter COVID-19 patients’ rooms less frequently. Findings from this study supported that the use of cobots could reduce the need for clinicians, especially nurses to enter patients’ room to reduce exposure and protective equipment use.7 In another study, Lee et al. surveyed inpatient healthcare professionals to identify needs that could be transferred to cobots. Participants responded they would like cobots to monitor patients and predict safety events such as falls or pressure injuries.11
Kangasniemi et al.’s integrative review identified how robots and automated devices were currently being used in clinical practice.12 Findings revealed robots have mostly been used to deliver medications and monitor patients; outcomes identified included safety, workload, changes in workflow, usability, and satisfaction.
While there is growing literature on cobots in hospitals, research on their use as delivery transporters in acute care is scarce. In one of Delaware’s acute care setting, using robots to innovate hospital workflows offers a new perspective on task management. This study aims to describe the usage, activities, and human interactions of cobots as a secure delivery system in a complex hospital environment.
METHODS
Theoretical Framework
The theory of Diffusion of Innovations (DOI)13 guided this study to describe the innovation stage of integrating this robotic technology into hospital operations and clinical workflows. DOI is a social process that occurs when new technological advancements spread from introduction to adoption.13 The DOI theory consists of four constructs: communication, time, social systems, and innovation.13 Innovation, defined as a practice or object considered to be new,13 was the construct of interest in this study. According to the DOI theory, five factors influence innovation adoption: relative advantage, compatibility, complexity, trialability, and observability.13 Relative advantage is the degree to which an innovation is perceived as being better than what is currently in place and trialability, is the degree to which an innovation is perceived as relatively difficult to understand and use.13 Compatibility is the degree to which an innovation is perceived as consistent with the existing values, past experiences, and needs of potential adopters and complexity refers to the extent to which the environment is ready for a technological innovation.13 Observability is the degree to which the results of the innovation are visible to others.13
Design and Sample
This study received Institutional Review Board (IRB) approval to conduct a qualitative descriptive study14 to observe and take field notes of cobots’ activities, functionality, and human interactions within a dynamic 900-bed inpatient hospital environment. Because of the early innovation of implementing cobots into this complex setting with limited prior knowledge, a qualitative
descriptive design was ideal and appropriate to build the foundational knowledge that will provide the basis for and will inform future in-depth studies.
Using a maximum variation sampling technique,15 the study population included hospital staff members, visitors, and patients who interacted with the cobots on all three clinical shifts (7am3pm, 3pm-11pm, and 11pm-7am). This sampling technique was employed to capture the extensive range of interactions and variation that occurred on each shift among staff, visitors, and the cobots. Prior to cobot deployment, staff members received and were encouraged to watch a brief webinar training via email to learn how to use the cobots. In-person, hands-on training was provided by the Clinical Robot Associates (CRA) when needed at the point of interaction with the hospital staff and cobot. The CRA was a dedicated cobot human operator to support the cobots and/or staff members as needed during the delivery process.
Qualitative data were collected for seven weeks during November 2022 - December 2022, approximately six months after the cobots were operational and making deliveries around the hospital. The cobots were first deployed and operational at the end of April 2022.
Hospital Setting
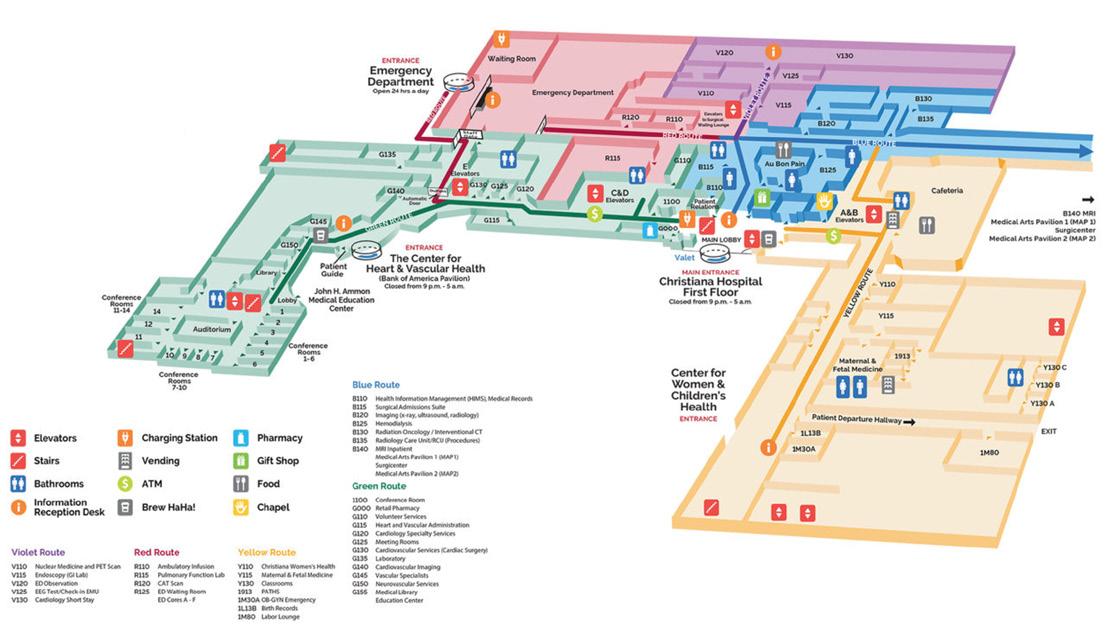
The acute care hospital setting located in suburban Delaware expands 1.3 million square feet with nine floors that includes 31 inpatient units that comprises 900 beds, over 2,000 doors, and 43 elevator bays (Figure 1). This hospital also includes three pharmacies located on the basement, first, and second floor levels. The expansive emergency department has approximately 100 beds.
Cobot Features and Functionality
The two cobots used in this study were approximately 4 feet, 11 inches in height, had a rounded head with digital, blinking eyes that can turn into a heart shape to acknowledge individuals nearby. Other characteristics included a torso, a chest touch screen, and a single robotic right arm that could wave and press door plates to open automatic doors. Their robotic arm was not designed to retrieve items. In addition, the cobots had three different sized drawers (small, medium, large) aligned with the torso to carry supplies. To communicate, the cobots could ‘meep’ and notify clinicians about deliveries through chimes. They could also communicate in a soft, calm feminine voice by saying, “please call me an elevator” when prompted by the CRA at the elevator bays.
To request a cobot-facilitated delivery of medications, supplies, and/or equipment, clinicians and staff could use free-standing iPad kiosks located throughout the hospital in areas such as inpatient care units, equipment rooms, pharmacies, and the front desk. When the cobots received the request, they would navigate to the pick-up location using lidar, cameras, and occasionally the aid of the CRA. The CRA often stayed near the cobots to monitor and observe their functions to ensure successful deliveries especially when elevators and manual doors were involved. The CRAs were required to assist the cobots with elevator ingress and egress, and correct floor location.
Staff would securely load items in one of the cobot’s three identity (ID) badge-accessible drawers. The cobots would then travel to their delivery destination with either supplies, medication, and/
or equipment to be unloaded by staff. The cobots had to navigate an environment of complex and unpredictable elements such as people, closed doors, equipment, and elevators. Because of these contextual circumstances, they sometimes relied on CRA support to make successful end-to-end deliveries.
Data Collection Procedures
Data collection consisted of four study team members who shadowed and observed the cobots from a distance, typically with the CRA, throughout the inpatient hospital settings and on each shift (i.e., day, evening, and night) and on various days of the week, including the weekends. Collecting data on different days and different shifts ensured the research team captured the fluctuations in the dynamic hospital environment that could affect the cobots. For example, dayshift during the week (7am-3pm, M-F) historically is busier and could be more challenging for the cobots to navigate because of the increased number of people and equipment moving around the hallways related to patient care, visitation, and diagnostic procedures. Evening (3pm-11pm) and nightshifts (11pm-7am), and weekends tended to be quieter related to limited patient care procedural activity and visitation. The study team members did not interact with the cobots and/ or any staff, visitors, and patients during observations. Field notes and observations were collected in real time on secure iPads through a Microsoft Teams site to provide a rich, thick description of patients, visitors, and staff’s interactions with and utilization of the cobots. Field notes included reflexive memos15 as the researchers were part of the hospital setting shadowing the cobots.
Data Analysis
Qualitative data were manually analyzed in a stepwise approach after all field notes and observations were collected and organized. Memoing and initial coding was performed
line by line for each observation and field note data entry.16 Data were reviewed several times and analyzed separately by four trained individuals (S.B., P.M., A.S., W.B) on a weekly basis using a content analysis level of interpretation.14 Then the four co-investigators came together to compare and discuss initial codes, code definitions, and segmented texts. Frequently occurring codes were identified, defined, and compared across code books. The emerging themes and subthemes were discussed, labeled, defined, and further refined by merging, adding, and removing redundant themes. This iterative process led to the development of major themes and sub-themes.16 Data saturation occurred when no new codes or themes emerged.
To ensure trustworthiness of the results, codes, code categories, definitions, segmented texts, and themes were reviewed and discussed with consensus reached among the research team (S.B., P.M., A.S., W.B). An audit trail was created and accessible to all study team members in a secure Microsoft Teams site. Study team members discussed their reflexive memos and bracketed any biases that allowed them to refrain from judgement and opinions.16
RESULTS
During seven weeks of data collection, we observed the cobots completing 89 which consisted of traveling from one destination to the next in an expansive hospital setting. At any point during the delivery process, the CRA intervened to support the cobot 107 times of which 72 interventions were related to the elevator assistance. Other CRA assistance rendered to the cobots were related to not being unable to open or navigate through doors
(n=20), difficulty navigating around an obstacle (n=4), staff unsure how to use the cobot (n=7), mislocalization of the destination (n=7), and unable to locate staff to unload the content in the drawers (n=1). People interacted with the cobots totaling 138 times which consisted of 79 positive, 17 negative, and 42 neutral interactions. The cobots were also observed to be ignored or not acknowledged 36 times.
The analytic process yielded 22 initial codes and 12 code categories. From these code categories, four major themes with six subthemes emerged. After collecting and analyzing seven weeks and 33 hours of data, four major themes emerged: 1) humanization of cobots, 2) usability of cobots, 3) cobots’ autonomy, and 4) cobots’ functionality within a dynamic hospital environment (Table 1).
Theme 1: Humanization of Cobots
A prominent theme to emerge in this study was the treatment of the cobots as human beings that included human reactions and emotional responses. Individuals who saw and/or interacted with the cobots typically had an emotional (positive, negative, or neutral) response. Sometimes, individuals had no response upon seeing the cobots. Examples of emotional responses were related to being curious or fearful, such as “Woah, can I take a selfie with
the cobot?” or “That’s crazy, she’s scary” after seeing the cobot roll by. Reactions were mostly positive, but occasionally negative. Examples of positive reactions were, “Wow, it’s a robot” and smiled; and “Hey robot baby. I miss you.” An example of negative reactions was, “we are ruining the cobot’s day with our closed door.” Sometimes, people ignored the cobot rolling by or did not interact with it when they were loading or unloading contents into its drawers.
Theme 2: Usability of Cobots
An important theme to emerge was cobot usability that included subthemes of ease of use and confusion. Staff who used the cobots often were observed loading/unloading items from their drawers with ease. A pharmacy tech stated, “I like using the cobot, it’s easy to use and makes my life easier when I can’t send medications.” Several nurses were observed accessing the cobot without any issues or hesitation. Conversely, some nursing staff demonstrated uncertainty about how to use the cobots to retrieve items in its drawers and/or to interpret its pickup/drop off chimes. For example, one of the nurses did not know how to use her ID badge to unload the cobot’s drawers. She requested assistance from the CRA who demonstrated how to access the cobot’s drawers. Another nurse was observed trying to swipe her ID badge all over
Key Themes Relevant Observations/Quotes
Human responses to the cobots
- Visitor upon seeing the cobot rolling through the hallways began laughing and asked, “Is that your friend?”
- Nursing students after seeing a cobot excitedly stated, “Did you see that?” to one another.
- A visitor said to the patient in the unit, “They have one of those (cobots) at another hospital.”
- A patient was sitting in the hallway and with fascination stated, “That’s crazy.” ”She’s scary.”
- Three staff members walked by and ignored the cobot.
Cobot usability
Perceived cobot autonomy
- One registered nurse opened the cobot immediately without help.
- Another registered nurse attempts to unload the cobot but appears unsure. The CRA walks over to her to demonstrate the draw opening process to her.
- No one at the nurses’ station addresses the cobot upon arrival for delivery. The cobot just silently stands there.
- The cobot did not move through the automatic doors quickly enough and they closed. The CRA had to manually open the automatic doors again for the cobot to go through.
- The CRA uses his remote control to move the cobot onto and off the elevators.
- The cobot is silently waiting by the elevator for the CRA to arrive that will facilitate ingress onto the elevator.
- The cobot automatous travels to the elevators in the basement.
Cobots’ functionality in the hospital setting
- The cobot rolls through the automatic door on the first attempt, stops in its cobot delivery spot on the unit and chimes once to notify staff of its arrival.
- The cobot entered the unit where a yellow caution spill sign was on the floor in the middle of the hallway in proximity to a patient chair. The cobot stopped for approximately 30 seconds to assess the situation and it was able to autonomously navigate through the narrow space with success.
- A bed was partially blocking the hallway. The cobot was able to navigate around the bed with ease and continue down the hallway.
- A bed is blocking the cobots delivery spot. The cobot is silently spinning in circles while people walk by and watch.
- When prompted by the CRA, the cobot will ask, “Can you call for an elevator?” The CRA will push the buttons to call for an elevator.
Table 1. Key themes with Examples from Observations and/or Field Notes
the cobot to open the drawers without any success. In addition to difficulty accessing the drawers on the cobot, clinical staff were observed to be uncertain about whose job it was to address the cobot when it arrived at the patient care unit. For instance, a nurse at the central nurses’ station was observed staring at the cobot rather than badging in to retrieve its contents when it arrived at its delivery spot on the unit.
Theme 3: Cobots’ Autonomy
Cobot autonomy is defined as a robot being able to sense, plan, and act upon that environment, with the intent of reaching a task-specific goal, without external control,17 and this was a major theme to emerge. Cobots in this study often required human support to make successful deliveries within a requisite time of usually 30-60 minutes throughout a complex environment of multiple floors and locations. Clinicians and staff were required to load and unload drawer contents, as the cobots’ arm was designed to open automatic doors and press buttons for navigational purposes. For complex maneuvering such as entering and exiting the elevators, navigating small spaces, or circumventing large obstacles that obstructed their paths, the CRAs intervened with their remote controller to override the cobots.
Cobot navigation within the hospital setting was an autonomy subtheme. The cobots demonstrated a consistent degree of autonomy (i.e., no external or CRA support) when navigating through the hospital basement level where there were less stops and obstacles, as well as between single-level inpatient units. For example, one of the cobots entered a unit with a spill on the floor with a yellow caution sign. The cobot recognized the obstacle and autonomously maneuvered around the spill. In another instance, cobots recognized a bed in the hallway was an obstacle, stopped and assessed its surroundings, then navigated around the bed to complete a delivery. However, the cobots occasionally made navigation errors such as taking a wrong turn or taking a circuitous route to make a delivery. When these errors occurred, the CRA would manually control the cobots to ensure they reached their correct destinations in a timely manner.
Theme 4: Cobots’ Functionality Within a Dynamic Hospital Setting
The last prominent theme to emerge pertained to how the cobots functioned within an inpatient hospital setting. Subthemes included delivery execution, cobot behaviors, and communication abilities. The cobots are designed to be a secure delivery system, yet errors sometimes occurred during the delivery process. For instance, the cobots used their robotic arm to push the door plate to enter a closed-door area; however, sometimes the doors closed too quickly before the cobot could roll through. The cobots would then re-initiate the entire process: reading the door bar code, moving its robotic arm to push the door plate, placing its robotic arm back into position, and then rolling through the doorway. When a cobot could not repeatedly roll through a doorway quickly enough, the CRA would manually push the door plate and override the cobot system to drive it through the doors before they shut.
Cobots also displayed typical robotic behaviors that may be perceived by humans as both expected and unexpected behaviors. Expected behaviors involved stopping to load navigation maps between units, waiting for CRA support at the elevators to manually enter and exit on appropriate floors, stopping when
someone or something was in its path, and waiting for someone to load and unload its drawer contents when it arrived at its designated delivery spots. Unexpected behaviors included spinning around, emitting distressed sounds, and stopping in the hallways for an unusually long time. In one instance, a bed was completely blocking the cobot’s designated delivery location, which resulted in the cobot spinning in circles trying to move into that spot. Another time, one of the cobots emitted a ‘distressed’ sound when it was hit by an automatic closing door that caused it to suddenly stop in the middle of the doorway.
To communicate, the cobots emitted pleasant “meeps” and chimes, and waved its arm. When the cobots arrived at their designated delivery location, they would automatically chime once to alert staff of their presence. While the chimes were automatic, the cobot could meep, wave its robotic arm, or ask for an elevator in a soft feminine voice when prompted by the CRA using a remote handheld control device.
DISCUSSION
Acute care hospitals are dynamic, complex environments where hundreds of people and large volumes of equipment travel daily.18 Deploying cobots to assist in completing deliveries throughout this unpredictable and unstructured environment, with high standards of quality and safety, is a cutting-edge endeavor with unique challenges. Guided by the innovation construct of the DOI theory, this study highlights and describes the use of cobots as artificially intelligent delivery transporters that are still in the early phase of innovation with unique challenges when operating within a complex hospital setting.
Relative Advantage
When hospital staff and clinicians are introduced and expected to use an early-stage innovation such as delivery cobots, they will take into consideration whether the cobots provide an advantage over the current human delivery infrastructure they are already familiar with.19 For example, communication is critically important in the hospital environment because clinicians and staff rely on verbal communication to work in teams.6 We observed the cobots in their current state alerted clinicians and hospital staff of their arrival through emitting a single chime sound yet were not capable of spoken words to explain their purpose or process. This limited communication ability may reduce the perceived advantages of humans providing the same delivery service. Further, the absence of verbal communication meant the cobots were not always quickly addressed after emitting their chime on arrival. This may be related to the important fact that clinicians and staff were working in a busy environment in which they could not hear the single chime without providing additional verbal cues. Clinicians may have grown accustomed to ignoring the cobot too because it could not signify urgency through words like a human could nor does it require respect as a human waiting to receive attention20,21 When these occurrences happened, the CRA would intervene; however, these communication limitations could result in delayed deliveries when these cobot transition to greater autonomy with less CRA oversight. To enhance the perceived relative advantage over the human-only delivery system, better communication is urgently needed6 that would start shifting perspectives that cobots could be part of the healthcare team leading to the adoption of cobots in this setting.18,22
Compatibility
When robotic technology is deployed that requires human support, people will assess its compatibility with their current needs and existing values.23 For example, the intent of these delivery cobots was to offload non-clinical tasks permitting clinicians and staff to focus on higher value, critical thinking patient-centered work. Yet, integrating cobots into the hospital workforce is uniquely different, as it completes delivery tasks previously performed exclusively by humans and requires a level of coordination between human and machine.2 Asking clinicians and staff to embrace these changes may be difficult given the variety of attitudes surrounding technology implementation in healthcare,24 the potential need for more training and expertise,5 and whether cobots fit into their existing working paradigm.23 Shifting tasks from clinicians and staff may also engender uneasiness about job security and possible feelings of competition. Cobots are designed to enhance human abilities, not replace them or their knowledge and experience in healthcare25,26; therefore, an appropriate communication strategy is needed to ensure cobots are not viewed as a threat, but accepted into the workforce.
Complexity
Understanding the complexity of a hospital environment is critically important to evaluate whether cobots are ready to participate in this work with clinicians and hospital staff. Most hospitals are older facilities that were built for humans, by humans without a future consideration for robotics. Therefore, hallways may be narrow, elevators may be smaller, and end-to-end delivery locations may be a farther distance apart. For example, the inpatient pharmacy in this study was located in the basement, which presented potential navigational difficulties for the cobots to travel long distances to complete deliveries. When these end-to-end point locations are a great distance apart, unique robotic challenges become more apparent because the cobots in this study did not have dynamic awareness of their surroundings similar to what humans possess6,27 or communication abilities. For instance, CRAs must help the cobots enter and exit elevators, navigate manual doors, and override the navigation system in constrained spaces when needed. These unique autonomy challenges reflect the reality of the acute care hospital environment and the current state of cobot capabilities that require a higher level of human dependence depending on the complexity of the physical setting 6,27
Trialability
Deploying this type of robotic technology has the potential to affect hospital workflows by complementing the workforce currently required for deliveries supporting hospital operations and patient care.25 Consistent with previous studies and literature reviews, shifting delivery tasks to cobots could offload these tasks from nurses, clinicians, and staff members, allowing them to work to the top of their training with potential implications for increased job satisfaction and reduced staff turnover.25,28 However, before achieving this workforce goal, this change necessitates human adoption and acceptance.25,29 Our observations indicated that frequent use and familiarity with the cobots influenced trialability (i.e. difficulty to use). Pharmacy technicians who used the cobots often could easily navigate its features while nurses or nursing staff who used the cobot less frequently sometimes
appeared confused about how to open the locked drawers or its purpose on the unit. When these events occurred, the onsite CRA would show staff how to use the cobots. However, being unsure how to use the cobots could affect their trialability, which may hinder their desire to use in the future.29 Therefore, these findings suggest that even though clinicians and staff members were sent basic education, they may require more educational touch points to aid in their adoption.12
Observability
Observing the cobots’ perceived autonomy could influence whether others might embrace this new technology. In our study, people observed the cobots making deliveries with limited to no human interventions. However, when the CRA had to intervene whether for an expected reason, such as for elevator navigation or opening of manual doors, or for an unexpected reason such as obstacle issues or mislocalization of a destination, individuals could witness the cobots requirement of human assistance in certain instances. These observations may influence whether cobots could be adopted with confidence or approached with skepticism.30,31
Individuals could also observe how people interacted with or anthropomorphized the human-like cobots. Anthropomorphosis refers to attributing human qualities to inanimate objects.32 We observed numerous times that when the cobots emitted whimsical beeping sounds, changed their eyes to a heart shape, or waved their robotic hand, many individuals engaged with a smile or an enthusiastic greeting. These human gestures and exchanges were important findings that could foster human-robotic interactions17,33 required to integrate cobots into the healthcare landscape11 especially during the early innovation phase when there could be heightened skepticism. This finding was consistent in a previous study in which the anthropomorphic features were viewed as positive attributes and facilitated ‘liking’ the cobot and viewing it as a ‘cute’ addition to patient care.5 The human aspect of cobots is important to facilitate the adoption of new technology into healthcare because it ensures that the cobots are viewed as useful helpers rather than threats, ultimately leading to a more harmonious incorporation into workflows.25
Limitations
This study sought to explore the clinical phenomena of incorporating cobots in the hospital environment guided by the DOI innovation construct. Because this study design is meant to describe and provide a broad context about cobots, the outcomes did not measure the cobots’ impact on daily workflow, productivity, and/or efficiencies. In addition, this study observed one type of cobot in a 900-bed tertiary care hospital, which may not be representative of all settings and cobots. For example, hospital designs, floors, and number of doors may be different that could affect autonomy, as well as the availability of a delivery tube system to transport medications and supplies among locations. Data collection was limited to a seven-week period of time. A longer data collection period may have encompassed additional diverse observations as the technology improved. Recording field notes has some limitations, such as researcher conscious and/or unconscious biases that may have influenced the notes. To minimize potential biases, the research team engaged in reflexive memoing and bracketing their biases. In addition, the team also regularly participated in open discussions about the assumptions they may have held about the cobots.
CONCLUSION
Integrating cobots into workflows as a secure delivery transportation system is an exciting addition to Delaware’s largest acute inpatient hospital setting, yet there is a pressing need to improve their capabilities if they are they are augment and complement the current hospital workforce. Current state cobots in our setting require human dependency to function adequately in this complicated and unpredictable environment. This initial study was a critical starting point to demonstrate cobots’ potential and future value as they become more sophisticated and integrated into health systems. Currently, cobots may be perceived as an expensive delivery system; thus, smaller, less resourced healthcare systems may not be able to justify the costs of integrating, training, and maintenance.25 However, as the next generation of cobots are created, financial models are expected to evolve toward greater affordability.
This is a promising technology in an early stage of adoption that may offer solutions and possibilities in patient care, not currently realized or imagined.25 The future of cobots assisting with deliveries will need to transition from in-person human task support to a remote presence, which will be an essential step toward consistency and autonomy.2 Further, this innovation has the potential to transforms healthcare delivery in the State and inspire the community to approach the healthcare industry with a renewed sense of excitement.
Dr. Birkhoff may be contacted at Susan.Birkhoff@christianacare.org
REFERENCES
1. Dupont, P. E., Nelson, B. J., Goldfarb, M., Hannaford, B., Menciassi, A., O’Malley, M. K., . . . Yang, G.-Z. (2021, November 10). A decade retrospective of medical robotics research from 2010 to 2020. Science Robotics, 6(60), eabi8017. https://doi.org/10.1126/scirobotics.abi8017
2. Morgan, A. A., Abdi, J., Syed, M. A. Q., Kohen, G. E., Barlow, P., & Vizcaychipi, M. P. (2022). Robots in healthcare: A scoping review. Current Robotics Reports, 3(4), 271–280. https://doi.org/10.1007/s43154-022-00095-4
3. Watson, D., Womack, J., & Papadakos, S. (2020, Jul/Sep). Rise of the robots: Is artificial intelligence a friend or foe to nursing practice? Critical Care Nursing Quarterly, 43(3), 303–311. https://doi.org/10.1097/CNQ.0000000000000315
4 Healthcare Service Robots Market Size, Growth, Trends By 2032. (n.d.). Retrieved January 17, 2024, from https://www.precedenceresearch.com/healthcare-service-robots-market
5. Yoo, H. J., Kim, J., Kim, S., Jang, S. M., & Lee, H. (2022). Development and usability evaluation of a bedside robot system for inpatients. Technol Health Care, 30(2), 337–350. https://doi.org/10.3233/THC-212901
6 El Zaatari, S., Marei, M., Li, W., & Usman, Z. (2019). Cobot programming for collaborative industrial tasks: An overview. Robotics and Autonomous Systems, 116, 162–180 https://doi.org/10.1016/j.robot.2019.03.003
7 Freeman, W. D., Sanghavi, D. K., Sarab, M. S., Kindred, M. S., Dieck, E. M., Brown, S. M., . . . Simon, L. V. (2021, February). Robotics in simulated COVID-19 patient room for health care worker effector tasks: Preliminary, feasibility experiments. Mayo Clinic Proceedings. Innovations, Quality & Outcomes, 5(1), 161–170 https://doi.org/10.1016/j.mayocpiqo.2020.12.005
8 Chang, H.-Y., Lee, I.-C., Chu, T.-L., Liu, Y.-C., Liao, Y.-N., & Teng, C.-I. (2019, September). The role of professional commitment in improving nurses’ professional capabilities and reducing their intention to leave: Two-wave surveys. Journal of Advanced Nursing, 75(9), 1889–1901 https://doi.org/10.1111/jan.13969
9 Carroll, K. (2021, July). Robotics: Considerations for Practice. Nursing Science Quarterly, 34(3), 253–255 https://doi.org/10.1177/08943184211010451
10. Grosso, Silvia, L. J. (n.d.). Prevalence and reasons for non‐nursing tasks as perceived by nurses: Findings from a large cross‐sectional study—Grosso—2021—Journal of Nursing Management—Wiley Online Library. Retrieved November 22, 2023, from https://onlinelibrary.wiley.com/doi/10.1111/jonm.13451
11. Lee, H., Kim, J., Kim, S., Kong, H.-J., Joo, H., Lee, D., & Ryu, H. (2020, May). Usability evaluation of user requirementbased teleconsultation robots: A preliminary report from South Korea. Methods of Information in Medicine, 59(02/03), 86–95. https://doi.org/10.1055/s-0040-1715579
12. Kangasniemi, M., Karki, S., Colley, N., & Voutilainen, A. (2019, August). The use of robots and other automated devices in nurses’ work: An integrative review. International Journal of Nursing Practice, 25(4), e12739. https://doi.org/10.1111/ijn.12739
13. Rogers, E. M. (2003). Diffusion of Innovations (5th ed.). Free Press.
14 Sandelowski, M. (2000, August). Whatever happened to qualitative description? Research in Nursing & Health, 23(4), 334–340 https://doi.org/10.1002/1098-240X(200008)23:4<334::AIDNUR9>3.0.CO;2-G
15. Polit, D. F., & Beck, C. T. (2021). Nursing Research: Generating and Assessing Evidence for Nursing Practice. Wolters Kluwer.
16. Creswell, J. W., & Poth, C. N. (2023, November 8). Qualitative Inquiry and Research Design. SAGE Publications Inc. https://us.sagepub.com/en-us/nam/qualitative-inquiry-and-researchdesign/book246896
17 Beer, J. M., Fisk, A. D., & Rogers, W. A. (2014, July). Toward a framework for levels of robot autonomy in human-robot interaction. Journal of Human-Robot Interaction, 3(2), 74–99 https://doi.org/10.5898/JHRI.3.2.Beer
18. Taylor, A., Lee, H. R., Kubota, A., & Riek, L. D. (2019). Coordinating Clinical Teams: Using Robots to Empower Nurses to Stop the Line. Proceedings of the ACM on HumanComputer Interaction, 3(CSCW), 221:1-221:30. https://doi.org/10.1145/3359323
19. Appio, F. P., Frattini, F., Petruzzelli, A. M., & Neirotti, P. (2021). Digital transformation and innovation management: A synthesis of existing research and an agenda for future studies. Journal of Product Innovation Management, 38(1), 4–20. https://doi.org/10.1111/jpim.12562
20. Reeves, B., & Nass, C. I. (1996). The media equation: How people treat computers, television, and new media like real people and places (pp. xiv, 305). Cambridge University Press.
21. Gambino, A., Fox, J., & Ratan, R. (2020). Building a stronger CASA: Extending the computers are social actors paradigm. Human-Machine Communication, 1(1). https://doi.org/10.30658/hmc.1.5
22. Liu, L., & Miguel-Cruz, A. (2022, May). Technology adoption and diffusion in healthcare at onset of COVID-19 and beyond. Healthcare Management Forum, 35(3), 161–167. https://doi.org/10.1177/08404704211058842
23. Turja, T., Särkikoski, T., Koistinen, P., & Melin, H. (2022). Basic human needs and robotization: How to make deployment of robots worthwhile for everyone? Technology in Society, 68, 101917. https://doi.org/10.1016/j.techsoc.2022.101917
24. von Gerich, H., Moen, H., Block, L. J., Chu, C. H., DeForest, H., Hobensack, M., . . . Peltonen, L.-M. (2022, March). Artificial Intelligence -based technologies in nursing: A scoping literature review of the evidence. International Journal of Nursing Studies, 127, 104153. https://doi.org/10.1016/j.ijnurstu.2021.104153
25. Weerarathna, I. N., Raymond, D., & Luharia, A. (2023, November 21). Human-Robot collaboration for healthcare: A narrative review. Cureus, 15(11), e49210. https://doi.org/10.7759/cureus.49210
26. Johnson, M., & Vera, A. H. (2019). No AI is an island: the case for teaming intelligence. AI Magazine, 40(1), 16–28. https://doi.org/10.1609/aimag.v40i1.2842
27. IJtsma, M., Ma, L. M., Pritchett, A. R., & Feigh, K. M. (2019). Computational methodology for the allocation of work and interaction in human-robot teams. Journal of Cognitive Engineering and Decision Making, 13(4), 221–241. https://doi.org/10.1177/1555343419869484
28. Chang, H.-Y., Huang, T.-L., Wong, M.-K., Ho, L.-H., Wu, C.-N., & Teng, C.-I. (2021, March). How robots help nurses focus on professional task engagement and reduce nurses’ turnover intention. J Nurs Scholarsh, 53(2), 237–245. https://doi.org/10.1111/jnu.12629
29. Riek, L. D. (2017). Healthcare robotics. Communications of the ACM, 60(11), 68–78. https://doi.org/10.1145/3127874
30. Kopp, T., Baumgartner, M., & Kinkel, S. (2023). It’s not Paul, it’s a robot”: The impact of linguistic framing and the evolution of trust and distrust in a collaborative robot during a human-robot interaction. International Journal of Human-Computer Studies, 178, 103095. https://doi.org/10.1016/j.ijhcs.2023.103095
31. Hoffman, G., Kshirsagar, A., & Law, M. V. (2022). Human–robot interaction challenges in the workplace. In The psychology of technology: Social science research in the age of Big Data (pp. 305–348). American Psychological Association. https://doi.org/10.1037/0000290-010
32. Fong, T., Nourbakhsh, I., & Dautenhahn, K. (2003). A survey of socially interactive robots. Robotics and Autonomous Systems, 42(3–4), 143–166. https://doi.org/10.1016/S0921-8890(02)00372-X
33 Formosa, P. (2021). Robot autonomy vs. human autonomy: social robots, artificial intelligence (AI), and the nature of autonomy. Minds and Machines, 31(4), 595–616. https://doi.org/10.1007/s11023-021-09579-2
Members of the Division of Public Health’s Office of Animal Welfare (OAW) team helped spearhead writing House Bill 190, which Governor John Carney signed on Oct. 9 at the Humane Animal Partners’ Stanton/Christiana location. House Bill 190 updates the current law relating to the Spay Neuter Fund so it is easier to administer and conforms with the standards of the Delaware Legislative Drafting Manual. Pictured left to right: Governor Carney, bill sponsor Rep. Kimberly Williams, OAW Director Christina Motoyoshi, bill co-sponsor Sen. Jack Walsh, OAW Deputy Director Joanna Miller, and Spay & Neuter Program Coordinator Melody Purdy. Governor Carney also participated in a ribbon-cutting to celebrate the completion of the facility’s first phase of renovation. Photo by Alyssa Imprescia.
Jones receives Community Health award
The Community Health Worker Association of Delaware (CHWA of DE) announced its 2024 Community Health Worker (CHW) Champion at its October 16 summit at Bally’s in Dover, Del. This year’s winner is Janine Brown, Community Health Coordinator for YMCA Delaware’s Sexual Assault Response Center. Brown is also an advocate for victims of violence and sexual assault.
“I really feel like I can connect with the people in every community that I serve, because I know what it’s like to feel like you don’t have a way out to want to not be a product of your environment,” Brown said in a video shared during the summit. “The help that I’ve given people – there’s nothing more rewarding, nothing else like it.”
The annual award recognizes an individual for their tireless commitment and outstanding work. Twentyeight CHWs were nominated by their peers.
In addition to Brown, these honorees were highlighted during the summit: Brentdy Chavez, Food Access Coordinator with Children and Families First; Denise Ortiz, CHW with Quality Insights; and Gail Plummer, CHW with Beebe Healthcare
Janine Brown, Community Health Coordinator for YMCA Delaware’s Sexual Assault Response Center (at right), received the 2024 Community Health Worker Champion award. At left is Mignaliz Nanny Vega-Morales, Vice Chair of the Community Health Workers Association of Delaware and Bilingual Survivorship Specialist at the Delaware Breast Cancer Coalition. Photo by Sean Dooley
The Delaware Department of Health and Social Services (DHSS), Division of Public Health’s Population Health Bureau helps to support this association in its efforts to bring cohesion and sustainable funding to the workforce.
Click here for more information about CHWA of DE
John Monahan of Lions Club District 22-D accepts the Tina M. Trout, ACSN-BC, CDE Leadership Award at the 22nd Annual Delaware Diabetes Wellness Expo, held in Dover, Del. on November 12. The Lions and the Delaware Department of Education partner with the Delaware Diabetes Coalition to market Lions Empowering School Nurses for Children with Diabetes: A Delaware Partnership, a comprehensive e-learning strategy. Photo by Alyssa Imprescia.
November 21 EpiChat
is “What is One Health?”; HAI is covered December 19
DPH Oral Health screening programs expand students’ access to dental care
The Kindergarten Oral Health Screening Program, created with the passage of House Bill (HB) 83, started this school year. HB 83 requires every public and charter school to provide a dental screening to kindergarten students.
The no-cost screenings are provided by the Division of Public Health (DPH) Bureau of Oral Health and Dental Services (BOHDS) in partnership with the Delaware Department of Education and school nurses. Dental hygienists or dentists inspect the mouths of each child, looking for pain, swelling, infections, decay, or dental sealants. Screenings take two minutes or less. Students receive a dental report card that includes a toothbrush, toothpaste, dental floss, a dental resource guide, and the screening results to take home.
“The passing of HB83 is a momentous step towards improving children's oral health,” said State Dental Director Dr. Nick Conte.
“We can prevent dental issues from developing by prioritizing early dental care, leading to long-term health benefits.
Summer McMenamin provides a dental screening to a kindergartener at Blades Elementary school in Seaford, Del. in October 2024. Photo by Alyssa Imprescia
In addition, the information collected at each school helps to target future public health efforts at schools where children need dental care the most.”
The Division of Public Health Office of Infectious Disease Epidemiology presents the online lecture, “What is One Health?” on November 21 from 12 p.m. to 1 p.m. Registration is required.
The monthly series continues December 19 with “Healthcare Associated Infections” from 12 p.m. to 1 p.m. Registration is required.
Learn more about these EpiChat webinars at www.dhss.delaware.gov/dhss/dph/epi/onehealth.html.
Oral health problems can prevent a child from eating and sleeping, impairing their ability to concentrate and learn. During the 2021-2022 academic year, 45% of Delaware’s kindergarteners had tooth decay in at least one tooth and 22% had untreated tooth decay, according to the Delaware Journal of Public Health article, “A Public Health Update: The Oral Health of Delaware’s Kindergarten and Third Grade Children in 2022 ”
For help finding a dentist for children, insurance questions, and dental screening questions, call the BOHDS Dentist Helpline at 302-318-8850.
Practice food safety during the holidays
This holiday season, follow four steps to food safety, including these from the Centers for Disease Control and Prevention (CDC):
Clean – Wash hands and surfaces often.
• Wash hands before, during, and after preparing food and before eating Always wash hands after handling uncooked meat, chicken and other poultry, seafood, flour, or eggs. Wash hands with warm or cold water and soap. Lather and scrub all surfaces thoroughly for at least 20 seconds
• Wash utensils, cutting boards, and countertops with hot, soapy water after preparing food items.
• Rinse fresh fruits and vegetables under running water.
Separate – Don’t cross-contaminate.
• When grocery shopping and in the refrigerator, keep eggs, raw meat, poultry, and seafood away from other foods. Store raw meat, poultry, and seafood in sealed containers or wrap them securely so juices do not leak onto other foods.
• Use one cutting board or plate for raw meat, poultry, and seafood and a separate cutting board or plate for produce, bread, and other foods that will not be cooked.
Cook to the right temperature.
• Use a food thermometer to ensure foods are cooked to a safe internal temperature. All poultry, including ground chicken and turkey, should be cooked to the internal temperature of 165 degrees F.
Click here for a chart of recommended food temperatures Find turkey cooking tips from the U.S. Department of Agriculture here.
Chill – Refrigerate promptly.
• Never leave perishable food out for more than two hours (or one hour in temperatures above 90 degrees F.
• Keep the refrigerator at 40 degrees F or below and the freezer at 0 degrees F or below. If the refrigerator does not have a built-in thermometer, use an appliance thermometer.
For more information on food safety, visit the Division of Public Health Office of Food Protection at www.dhss.delaware.gov/dhss/dph/hsp/foodsafety.html or call 302-744-4546.
Immunization Coalition of Delaware hosts 2024 summit on December 12
Medical providers are encouraged to attend the 2024 Immunization Summit, set for Thursday, December 12, 2024 from 12:30 p.m. to 5:30 p.m. at the Ammon Education Center, located at Christiana Hospital, 4755 Ogletown-Stanton Road in Newark, Del. The summit is sponsored by the Immunization Coalition of Delaware (a program of the Delaware Academy of Medicine/Delaware Public Health Association) and the Division of Public Health (DPH).
DPH Medical Director Awele Maduka-Ezeh, MD, MPH, PhD, CCHP will present “Immunizations and Refugees.” Andrew Kroger, MD of the Centers for Disease Control and Prevention will give an influenza update. “Vaccines for Pregnant People” will be presented by Matthew Hoffman, MD of ChristianaCare The American Cancer Society and the HPV Roundtable will present “Vaccines for Cancer.” Jonathan Miller, MD of Nemours Children’s Health will speak about vaccine confidence. The event concludes with a vaccine update presented by Marci Drees, MD and Stephen Eppes, MD, both of ChristianaCare
Live registration with Continuing Medical Education (CME) credits is $50. Live registration without CME credits is $40 Medical residents and DPH employees can attend for free by entering promo code dph2024 at checkout.
To register and for an agenda, visit the Immunization Coalition of Delaware at https://immunizedelaware.org/. The registration deadline is December 5.
Stroke System regulation published
The new 4306 Stroke System Regulation became effective November 11, 2024 and is published in the November 2024 Register of Regulations.
CDC.gov
Resilience planning protects structures from hazardous weather events
Resilient structures are better able to withstand high winds, flooding, and other hazardous weather events. Property owners should identify hazard risks and strengthen their structures, according to the Delaware Homeowners Handbook to Prepare for Natural Hazards, Second Edition (2019)
The handbook was published by the Delaware Emergency Management Agency (DEMA), Delaware Department of Natural Resources and Environmental Control, and the Delaware Sea Grant College Program. While its focus is on coastal communities, its advice applies to structures throughout the state.
“While it is never possible to eliminate all damage from a natural disaster, you as a homeowner can take action and implement many small and costeffective steps that could significantly lower your risk,” the introduction reads.
To avoid major damage, the handbook advises building or retrofitting a home to higher standards, following these steps:
• Hire a licensed structural engineer and/or architect contractor to do an assessment. Hire a licensed and insured contractor to retrofit or construct. For guidance, visit The Home Builders Association of Delaware and the Better Business Bureau’s Accredited Business Directory
• Strengthen the roof. Install properly selected and galvanized metal hurricane clips to every rafter to tie the roof to the walls. Add bracing to the trusses and strap down the rafters on the roof’s gable end eaves. Replace old roofs that cannot withstand heavy rains and extreme wind.
First Spouse Quillen Carney champions reading through new children’s book
Delaware First Spouse Tracey Quillen Carney is on a Reading Tour following the publication of her children's book, Books for Blue. The story encourages readers to visit their local library to discover reading.
Books for Blue is available at all Delaware libraries in English, Spanish, and Haitian Creole. This book can be featured at community events through a portable book walk/roll consisting of more than a dozen signs featuring the book’s characters. To request to be an official stop on the First Spouse’s Reading Tour or to showcase the portable book walk/roll at your next community event, contact Emily.hershman@delaware.gov
Casey Family Programs funded the publication of Books for Blue through a founding grant for First Chance Delaware. FEMA.gov
For more information about Delaware Libraries, visit: libraries.delaware.gov.
Cancer program to visit Frankford
• Connect the walls to the foundation, using stronger connectors than required by the building code.
• Install impact-resistant windows and protect them with shutters, storm panels, or fabric windscreens
• Install a wind- and impact-resistant garage door.
• Obtain all required local, county and state permits and approvals before beginning any work. Find the handbook at www.deseagrant.org/coastalhazards and the Wind Retrofit Guide for Residential Buildings (FEMA P-804) at fema.gov/library
The Division of Public Health Cancer Prevention and Control Program will participate in the Frankford Health Fair on Saturday, November 23. Hosted by Beebe Healthcare, the event is from 9 a.m. to 1 p.m. at the Frankford Fire Hall, 7 Main Street, Frankford, Del. 19945.
Screening for Life and Health Care Connection programs can provide eligible Delawareans with cancer screening tests and health care services through a network of providers at reduced cost
To invite the cancer program to a community event, send the information to DHSS_DPH_HealthAccessDE@delaware.gov
Associations Between Residence Type and Health Outcomes for Individuals with Developmental Disabilities Following the COVID-19 Pandemic: A Quantitative Analysis
Ankita Mohan, M.H.S.
Delaware Division of Developmental Disabilities Services, Delaware Department of Health and Social Services; Vanderbilt University
Jody Roberts, Ph.D.
Delaware Division of Developmental Disabilities Services, Delaware Department of Health and Social Services
BACKGROUND
Over the last two decades, there has been a notable shift in residential service models for adults with intellectual and developmental disabilities (ID/DD), transitioning individuals away from institutional settings towards community-based arrangements such as dispersed housing and cluster housing.1–6 It is widely acknowledged that the choice of residential setting has a profound impact on the well-being and outcomes of individuals with ID/DD, encompassing their quality of life, physical and mental health, social integration, and overall satisfaction.7–11
Extensive research has examined these effects, providing valuable insights into the advantages and disadvantages of various residential settings.12–16 Studies have explored outcomes related to physical and mental health, social well-being, adaptive behavior, and overall quality of life.17,18 Additionally, research has identified a variety of contributing factors –including individual, environmental, social, policy, cultural, and familial - that influence the associations between residential settings and these outcomes.19
Further, the COVID-19 pandemic has disproportionately affected individuals with developmental disabilities, particularly those in various residential settings. Research has shown that this population faced heightened risks of infection, severe illness, and mortality due to COVID-19.20,21 The pandemic exposed and exacerbated existing healthcare disparities, with individuals in congregate care settings often experiencing higher infection rates and more severe outcomes.20 Moreover, pandemic-related disruptions to support services, social isolation, and changes in daily routines significantly impacted the mental health and overall well-being of individuals with developmental disabilities across different residential settings.22
The literature has drawn upon theoretical frameworks such as social integration theory, ecological models of disability, and person-centered approaches to better understand these interactions and complexities.23 Collectively, this body of knowledge underscores the importance of understanding the impact of different residential models when considering health outcomes and quality of life for people with disabilities, as we shift from institutional settings.15,24 Collectively, with the shift from institutionalized settings, this body of knowledge highlights the importance of considering the implications of residence type on health outcomes and quality of life for people with disabilities.
Gaps in the Literature
Despite the extensive research on this topic, several gaps and missing links remain:
Mental Health Outcomes: Although some studies have explored aspects of health outcomes, there is still a need for more research specifically focused on mental health, and how different residential settings contribute to these outcomes. A more detailed exploration of specific mental health conditions and interventions is warranted.
Health Outcomes Specific to Intellectual Disabilities: Existing research has mainly focused on well-being and quality of life, with limited emphasis on health outcomes, specific to those with disabilities. Exploring these health aspects in greater detail is crucial, prompting our research goal: assessing the association between residence type and health outcomes for people with developmental disabilities.
Significance of Research
Addressing these gaps is of paramount significance for several reasons:
Enhanced Decision-Making: Filling these gaps will provide a more comprehensive understanding of the effects of residential settings on individuals with ID/DD. This knowledge can inform better decision-making for individuals, families, service providers, and policymakers.
Improved Quality of Life: A deeper understanding of the relationship between residential settings and health outcomes can lead to the development of more effective support systems. This, in turn, can improve the quality of life and well-being of individuals with ID/DD.
Healthcare Planning: Focusing on specific health outcomes related to intellectual disabilities can aid in healthcare planning and the provision of targeted interventions for this population.
Rationale & Hypothesis
The study aims to investigate the associations between different types of residential settings and health outcomes for individuals with intellectual and developmental disabilities using National Core Indicators (NCI) data and STATA for analysis. The rationale for this research lies in the critical need to bridge existing gaps in the literature and to provide a comprehensive understanding of the impact of residential settings on the well-being of this population. This research will build upon previous work by focusing on specific health outcomes,
encompassing both physical and mental health, which remains an underexplored area. This work also adds to the literature by conducting analysis on a larger dataset, encompassing more participants than other studies in this area.
We hypothesize that the choice of residential setting will be significantly associated with the physical and mental health conditions of individuals with ID/DD. Specifically, we anticipate that residential settings where individuals are more emersed in their community will be associated with better mental health outcomes when compared to more restrictive settings.
METHODS
This research employs a quantitative approach to analyze the In-Person Survey (IPS) from the National Core Indicators –Intellectual and Developmental Disabilities (NCI-IDD).25 The study will be cross-sectional in nature, focusing on a single point in time to assess the relationship between residence type and health outcomes.
Data Collection Methods
Data Source: The primary data source for this research is the 2021-2022 In-Person Survey (IPS) from the National Core Indicators (NCI) database. NCI is a well-established program, maintaining the NCI-IDD project, which collects information on the experiences of individuals with intellectual and developmental disabilities. NCI-IDD was initiated in 1996 by the National Association of State Directors of Developmental Disabilities Services (NASDDDS) and the Human Services Research Institute (HSRI). The IPS contains a survey that is conducted in a face-toface setting. Individuals receive annual standardized training to maintain their status as NCI-IDD surveyors. To ensure statistical accuracy, states conduct at least 400 surveys. Data is cleaned and
invalid responses are subsequently dropped. Finally, state data are merged into a national dataset.26 The NCI dataset includes a wide range of variables related to residential settings, health outcomes, and quality of life. Data for the IPS was gathered through direct discussions with the service recipient. Further, background details were predominantly derived from the individual’s records. To ensure that the survey was valid for people with IDD, the survey implemented a two-pronged approach. Responses to Section I inquiries, focusing on personal experiences and necessitating subjective answers, solely came from the service recipient. In contrast, Section II of the survey, encompassing objective queries about the individual’s community engagement, choices, respect, rights, and service access, permitted the involvement of a “proxy” or another informant familiar with the individual, such as a family member or friend. All individuals were given the opportunity to participate in the face-to-face interview portion, and there was no cutoff of answers provided to consider a survey complete. Surveys were excluded from the analysis if 1) no questions were answered or 2) if the individual receiving support did not respond “validly” to the questions in section 1.26 Access to this data was provided by The National Association of State Directors of Developmental Disabilities Services (NASDDDS) via the Human Services Research Institute (HSRI).
Sample Size: The study sample consisted of 13,559 individuals with intellectual and developmental disabilities, who received services from their state developmental disabilities service system. 453 of those individuals did not respond or responded “don’t know” to their residence type and were subsequently excluded from the study, leaving a total sample size of 13,106. The demographic information and breakdown of participants is detailed in Table 1
Group Living Setting, 2-3 People With Disabilities A group home setting where 2-3 people have a disability.
Group Living Setting, 4-6 People With Disabilities A group home setting where 4-6 people have a disability.
Group Living Setting, 7-15 People With Disabilities A group home setting where 7-15 people have a disability.
Lives in Own Home or Apartment
Parent/Relative’s Home
Foster Care (2+)
Foster care (1)
A participant’s own home which may be owned or rented, or may be shared with roommate(s) or spouse.
A participant’s parent or relative’s home which may include paid services to the family for residential support.
Round-the-clock services provided in a single-family residence where two or more people with a disability live with a person or family who furnishes services.
Round-the-clock services provided in a single-family residence where only one person with a disability lives with a person or family who furnishes services (sometimes called shared living).
Homeless or crisis bed placement: Participant does not have a ‘’permanent” home and is in a crisis bed placement or is experiencing homelessness.
*ICF/IID facilities are Medicare or Medicaid Intermediate Care Facilities for Individuals with Intellectual Disabilities with 4 or more beds that provide “active treatment” (CMS). All 50 states have at least one ICF/IDD.
Table 1. Setting Types
Measures
We utilized a range of variables to investigate the associations between various residential settings and health outcomes among individuals with intellectual and developmental disabilities including the demographic information of age, gender, and race. Age provided insights into the age distribution of the study population while the variable gender categorized participants as “Male,” “Female,” or “Other,” allowing for gender-based analyses. To examine racial disparities in the outcomes, a series of categorical variables indicating race were employed, including “American Indian,” “Asian,” “Black,” Hawaiian,” “White,” “Latino,” and “other,” with each coded as “Yes” or “No” to indicate racial background. Based on records, race was selected, with an opportunity to select “other.”
Our independent variable, residence type, was crucial for characterizing the participants’ residential settings. The data encompassed a wide array of settings including institutional, provider manager, family living, and independent living options (Table 1). Based on records, a residence type was assigned to the individual. These setting types are included in the NCI data.26,27
The outcome variables in our analysis comprised a set of binary variables: “mood disorder,” “anxiety disorder,” “behavior disorder,” “psychotic disorder,” “other mental illness/psychiatric diagnosis,” “cardiovascular disease,” “diabetes,” “cancer,” “high blood pressure,” and “high cholesterol.” Utilizing medical records, “yes” or “no” was selected reflecting if a participant had the health condition of the question. These variables indicate the presence or absence of specific health conditions, which are instrumental in understanding the relationship between residential settings and health outcomes among individuals with ID/IID.
To account for potential confounding factors, in addition to controlling for demographic factors, we also incorporated the categorical variable mobility, which characterizes participants as either “moves self around the environment without aids,” “moves self around the environment with aids, or uses a wheelchair independently,” or “non-ambulatory; always needs assistance to move around the environment.” This covariate is vital for controlling for factors related to mobility in our analysis, therefore avoiding a self-selecting effect in the correlation between residential settings and health outcomes due to mobility restrictions. Overall, these variables collectively form a robust framework for an examination of the complex associations between residential settings and various health outcomes while considering crucial demographic and covariate information to enhance the rigor of our analysis (Table 2).
Data Extraction
Relevant data from the NCI dataset were extracted, focusing on variables related to residential settings (e.g., type of setting), health outcomes (e.g., physical health, mental health), and demographic and other covariates (e.g., race, age, gender, mobility).
Ethical Considerations
This research adhered to ethical guidelines related to the use of the NCI dataset. The study was also deemed “not human subjects research” and “secondary data analysis involving the use of existing de-identified data/specimens, including publicly available data” by the Institutional Review Board (IRB) of Johns Hopkins Bloomberg School of Public Health. Data was stored and analyzed in a confidential manner.
Analysis Methods
Statistical Software: Statistical analysis was conducted using STATA BE 17.0, a statistical software widely employed in social science research.28 STATA provides a range of tools for data management, regression analysis, and hypothesis testing, making it suitable for our study’s quantitative analysis.
Analytical Approach
Our outcome variables were binary categorical variables, and our independent variable was a categorical variable with multiple categories. The categorical variable of residence type was then split into 13 separate dummy variables, allowing analysis of each of the residence types. Based on the variable type and our research question, logistic regression analysis was employed to examine the associations between different residential settings and specific outcomes, such as physical health and mental health. Since the variable of residence type was separated into 13 dummy variables, the reference for each variable was the response “0,” or not living in the residence type. Therefore, for each outcome, the odds ratio of each residence type represents the odds of having the health condition if one lives in the residence type as compared to if they did not. This approach allowed us to identify statistically significant relationships and quantify the magnitude of these associations. In the analysis, statistical significance was determined using a significance level of p < 0.05.
In our logistic regression analysis, we selected covariates to control for a priori. We controlled for the variables gender, age, race, and mobility to account for potential confounding factors.
Rationale for Choosing the Methodological Strategy
The choice of a quantitative methodological approach, along with the utilization of NCI data and STATA, is well-suited for this research for several reasons. First, NCI data is a national dataset that provides a comprehensive view of the experiences of individuals with ID/DD across various residential settings and across nearly every state in the United States. This allows for a robust analysis that can inform broader policy discussions. Second, the quantitative approach provides the means to systematically assess the relationships between residence type and health outcomes. By controlling for potential confounding variables, we can isolate the impact of residential settings on mental health outcomes, thus enhancing the rigor of our findings.
In summary, the methodological strategy chosen for this study aligns with the research objectives and the need to address the identified gaps in the literature. It allows for a comprehensive analysis of the associations between residential settings and health outcomes for individuals with ID/DD, ultimately contributing to improved decision-making, resource allocation, and healthcare planning in this critical area.
RESULTS
The logistic regression analyses were conducted to examine the associations between different residence types and various mental health and physical health outcomes while controlling for potential confounding variables. The models included residence type as the primary independent variable, separated into 13 dummy variables, and adjusted for demographic factors such as age and gender, mobility, and racial/ethnic backgrounds. The associated health factors considered were anxiety, mood,
behavior, psychotic symptoms, other mental health problems, cardiovascular conditions, diabetes, cancer, high blood pressure (HBP), and high cholesterol. Results from the multivariable logistic regression analysis can be seen in Table 3. Odds ratios for each category are compared to the reference group “0” or does not live in the residence type. Statistically significant associations are bolded. Graphical representations of the significant results (< 0.05) can be seen in Figure 1
ICF/IID 4-6: Residents in ICF/IID settings accommodating 4-6 people with disabilities exhibited notable outcomes. They had
significantly higher odds of experiencing behavior disorders (OR=1.88) and psychotic disorders (OR=2.24). However, these residents demonstrated significantly lower odds of other mental disorders (OR=0.24) and high blood pressure (OR=0.45).
ICF/IID 7-15: ICF/IID settings with 7 to 15 residents with disabilities displayed distinct patterns. These settings were significantly more likely to have residents with psychotic disorders (OR=2.12), but significantly less likely to have individuals with other mental disorders (OR=0.43) or cardiovascular disease (OR=0.47).
Table 3. Multivariable Regression Analysis of Predictors of Health Outcomes for People With Developmental Disabilities
ICF/IID 16+: Individuals residing in ICF/IID settings accommodating 16 or more residents with disabilities had specific health outcomes. They exhibited decreased odds of anxiety (OR=0.43), other mental disorders (OR=0.39), and high blood pressure (OR=0.39). However, they displayed significantly increased odds of behavior disorders (OR=4.17).
Nursing Facility: Residents in nursing facilities maintained significantly higher odds of experiencing both psychotic disorders (OR=3.70) and cardiovascular disease (OR=3.02).
Other Institutionalized Facility: No significant findings were observed regarding health outcomes for individuals residing in other institutionalized facilities.
Group Living (2-3): Individuals in group living situations with 2 to 3 people with disabilities experienced distinct odds. They had significantly increased odds for mood disorders (OR=1.41), behavior disorders (OR=1.68), and psychotic disorders (OR=2.64). However, they had a decreased risk of other mental disorders (OR=0.53) and cardiovascular disease (OR=0.38).
Group Living (4-6): Residents in group living arrangements with 4-6 people with disabilities had significantly higher odds of behavior disorders (OR=1.66) and significantly lower odds of other mental disorders (OR=0.48).
Group Living (7-15): Individuals in group living settings with 7 to 15 people with disabilities had distinctive health outcomes. They demonstrated significantly increased odds of having behavior disorders (OR=1.86), psychotic disorders (OR=2.25), and cancer (OR=4.58). Conversely, group living settings of 7 to 15 residents maintained lower odds of individuals with diabetes (OR=0.43) and high blood pressure (OR=0.59).
Own Home: Participants living in their own homes maintained significantly lower odds of experiencing other mental disorders (OR=0.71).
Parent’s Home: Individuals residing in a parent or relative’s home were associated with protective factors. They had significantly lower odds for anxiety (OR=0.40), mood disorders (OR=0.32), behavior disorders (OR=0.53), psychotic disorders (OR=0.52), other mental disorders (OR=0.16), diabetes (OR=0.56), and high blood pressure (OR=0.62).
Foster Care (2+): Individuals living in a foster care setting with 2 or more people with disabilities had distinctive odds. They had significantly higher odds of experiencing psychotic disorders (OR=2.64) and significantly lower odds for other mental disorders (OR=0.45).
Foster Care (1): Individuals residing in a foster care setting with 1 person with a disability demonstrated unique odds. They had significantly lower odds for anxiety (OR=0.64) and other mental disorders (OR=0.34).
Homeless: Individuals experiencing homelessness or in a crisis bed placement did not exhibit any significant odds for the examined health outcomes.
Covariates: While noting that the covariates were directly included in our overall analysis, so findings are in the context of all variables included in the analysis, several covariates emerged as important factors affecting health outcomes. Specifically, individuals identifying as American Indian were at a greater risk for mood and behavior disorders. Black individuals had
increased odds of other mental disorders and high blood pressure, while White individuals had increased odds of anxiety disorders, mood disorders, and cardiovascular disease. Hawaiian individuals exhibited increased odds of other mental disorders, and Latino individuals had increased odds of mood disorders and other mental disorders. In no case did race serve as a protective factor.
Furthermore, age played a significant role in health outcomes, acting as a protective factor for anxiety, behavior disorders, and other mental disorders, but as a risk factor for psychotic disorders, cardiovascular disease, diabetes, cancer, high blood pressure, and high cholesterol. Gender also influenced outcomes, with females at a higher risk for anxiety and mood disorders, but at a lower risk for behavior disorders and high blood pressure. Increased mobility was found to be a protective factor for all examined mental health conditions, as well as for diabetes, high blood pressure, and high cholesterol.
DISCUSSION
Interpreting the Findings
As outlined in the background, the literature emphasizes the multifaceted nature of these impacts, considering various factors such as physical and mental health, social integration, and environmental influences. Our study addresses existing gaps by delving into mental health outcomes and exploring specific health outcomes related to intellectual and developmental disabilities.
The logistic regression analyses unearthed nuanced associations between residence types and health outcomes, shedding light on the complexities of this relationship. Considering the significance threshold of p<0.05, our discussion focuses on statistically significant findings.
Institutionalized Settings
The analysis utilized 13 dummy variables that each represented a residence type. For purposes of the logistic regression analysis, odds ratios were calculated using the value “0” or those who do not live in the residence type as a reference group. Residents in institutional settings accommodating 4-6 individuals with disabilities exhibited heightened odds of behavior and psychotic disorders. However, they demonstrated lower odds of other mental disorders and high blood pressure. Larger ICF/IID settings (7-15 residents with disabilities) displayed elevated odds of psychotic disorders but lower odds of other mental disorders and cardiovascular disease. Residents in nursing facilities had higher odds of psychotic disorders and cardiovascular disease. Based on the analysis, individuals living in these settings, which are classified as “institutions” by the Centers for Medicare and Medicaid Services (CMS), are more likely to experience different mental health disorders. Depending on the specific setting, some of these settings are both risk and protective factors for different physical health conditions. This underscores the need for targeted interventions to address mental and physical health in these settings. However, contrasting findings for these institutionalized settings, residents in larger ICF/IID settings (16 or more residents with disabilities) showed decreased odds of anxiety, other mental disorders, and high blood pressure but increased odds of behavior disorders. This challenges the notion that larger settings universally lead to adverse outcomes and warrants further exploration.
Group Homes
Individuals in group living with 2-3 residents with disabilities faced increased odds of mood, behavior, and psychotic disorders. However, they had lower odds of other mental disorders and cardiovascular disease. Residents in group living with 4-6 individuals with disabilities had higher odds of behavior disorders but lower odds of other mental disorders. Unique health outcomes emerged for participants residing in group homes with 7-15 people with disabilities, with increased odds of behavior, psychotic disorders, and cancer, but decreased odds of diabetes and high blood pressure. All group home settings had increased odds for at least one mental health condition, but all group home settings were also protective for at least one health condition. These dichotomous results prompt further research with specific focus on health outcomes for individuals with developmental disabilities living in different group home settings.
Independent Living
Those living in their own homes exhibited lower odds of other mental disorders. Living in one’s own home was only a protective factor and was not a risk factor for any physical or mental health conditions. This aligns with the understanding that personal autonomy and familiarity with living arrangements contribute to positive mental and physical health.
Parent / Relative’s Home
Residing in a parent or relative’s home was associated with protective factors across various mental and physical health outcomes. This residence type was also only a protective factor and had no risk associated with it related to the mental and psychical health outcome examined. This highlights the role of familial support in fostering well-being.
Foster Care
Individuals in foster care with 2 or more residents with disabilities faced higher odds of psychotic disorders but lower odds of other mental disorders. On the other hand, foster care with 1 resident exhibited protective odds for anxiety and other mental disorders. These findings demonstrate the potential benefits of a more individual level of care, as, as those living as the only individual with a disability in a foster home experienced no risk factors for health conditions, and were at lower odds for two mental health conditions, as compared to those living in a foster home with two or more residents with a disability who were at increased odds for having psychotic disorders.
Homeless
Individuals experiencing homelessness did not exhibit significant odds for examined health outcomes. The transient nature of this setting may pose challenges for comprehensive health assessments.
Covariates Impact
Race emerged as a significant factor, with disparities observed in mental and physical health outcomes. Age played a protective role in certain mental health conditions but acted as a risk factor for others and physical health outcomes. Gender differences indicated varied susceptibility to mental health conditions, emphasizing the need for tailored interventions. Increased mobility consistently emerged as a protective factor, influencing both mental and physical health outcomes.
Limitations
This study, while providing valuable insights into the associations between residence types and health outcomes for individuals with intellectual and developmental disabilities, is subject to several limitations that warrant consideration. Firstly, the crosssectional design employed in this research restricts our ability to establish causation, emphasizing the need for future longitudinal investigations. Further, the reliance on self-reported or caregiverreported health outcomes introduces a potential source of bias or misreporting, particularly concerning the subjective nature of mental health conditions. The study’s primary focus on quantitative measures may overlook the rich qualitative aspects of individuals’ experiences in different residential settings. The categorization of residence types, while providing a broad overview, may oversimplify the diversity within each category, overlooking variations in the quality of care, support, and living conditions. Further, some residence types contained low levels of participants, resulting in difficulty in the interpretation of these results as well as generalizability. Additionally, the study did not delve into specific interventions or support services within each residence type, limiting the understanding of the mechanisms through which these settings influence health outcomes. Finally, the study did not explore potential interactions between residence types and individual characteristics, such as the severity of disability or pre-existing health conditions, which could influence outcomes. Recognizing these additional limitations is crucial for refining future research endeavors and ensuring a more comprehensive understanding of the complexities involved in the relationship between residence types and health outcomes for individuals with intellectual and developmental disabilities.
Overall Findings
Ultimately, individuals living independently, with a parent or relative, and living in a foster care setting as the only individual with a disability were only exposed to decreased odds of having the mental and physical health outcomes examined and experienced no increased odds for any outcome. This highlights the benefits of a smaller, more personalized residence setting. These settings that experienced positive outcomes tend to provide individualized care and potentially a sense of familiarity and comfort for individuals. Results regarding group homes and institutionalized settings were varied, demonstrating the need for further, more focused research on these settings.
Policy Implications
Our findings contribute significantly to the ongoing efforts to rebuild and strengthen public health infrastructure for individuals with developmental disabilities. By elucidating the associations between residential settings and health outcomes, this research provides valuable insights for public health officials and policymakers. These findings can inform the development of more inclusive and responsive public health strategies that account for the diverse needs of individuals across various residential settings. For instance, understanding which residential models are associated with better health outcomes can guide the allocation of resources, the design of health promotion programs, and the implementation of preventive measures tailored to specific living arrangements. This knowledge is crucial for creating a more equitable and resilient public health system that can effectively support individuals with developmental disabilities, regardless of their residential setting, both during
normal times and in the face of public health crises. The following are our policy and research recommendations:
1. Tailored Interventions for Different Settings: Policies should acknowledge the diversity of residential settings for individuals with intellectual and developmental disabilities (ID). Tailored interventions should be designed to address the specific mental and physical health needs of residents in various settings, such as ICF/ IIDs, nursing facilities, group living, independent living, and foster care.
2. Staff Training and Support: Given the varied mental health profiles observed across different settings, there is a need for comprehensive training and support programs for staff working in these facilities. This includes training on recognizing and managing behavior and psychotic disorders, as well as strategies to promote positive mental health outcomes.
3. Holistic Health Assessments: Policy efforts should promote holistic health assessments that consider both mental and physical health outcomes.
4. Support for Independent Living: Policies that support individuals in living in their own homes or with family should be reinforced. Recognizing the protective factors associated with familial support, these policies should aim to empower families and individuals to maintain independence while providing necessary resources and assistance.
Future Research Directions
1. Longitudinal Studies: Conducting longitudinal studies can provide a deeper understanding of how residence types impact health outcomes over time. This would allow researchers to explore the dynamic nature of these relationships and identify potential causative factors.
2. Qualitative Research: Complementing quantitative findings with qualitative research can offer insights into the lived experiences of individuals with IDD in different settings. Understanding the social and environmental factors that contribute to mental and physical health outcomes can inform more targeted interventions.
3. Cost-Benefit Analysis: Conducting cost-benefit analyses of interventions in different residential settings can assist policymakers in allocating resources effectively. Understanding the economic impact of various interventions will contribute to the development of sustainable and efficient policies.
The findings from this study have significant implications for enhancing healthcare resilience for individuals with
developmental disabilities in preparation for future public health crises. By identifying the residential settings associated with better health outcomes, we can develop more robust and adaptable care models. These insights can inform the creation of emergency preparedness plans tailored to different residential settings, ensuring that individuals with developmental disabilities receive appropriate care and support during crises. Moreover, understanding the relationship between residence type and health outcomes can guide the allocation of resources and the development of targeted interventions to strengthen the resilience of vulnerable populations across various living arrangements. By addressing these policy and research considerations, policymakers and researchers can work collaboratively to create evidence-based interventions that improve the overall health and well-being of individuals with intellectual and developmental disabilities across diverse residential settings.
Ms. Mohan may be reached at Ankita.mohan@vanderbilt.edu
REFERENCES
1. Bertelli, M. O., Forte, L., & Bianco, A. (2023, November 1). Updates in the care of youths with intellectual disability and autism spectrum disorder. Current Opinion in Psychiatry, 36(6), 455–460.
https://doi.org/10.1097/YCO.0000000000000901
2. Jarrett, S. (2015, March). The meaning of ‘community’ in the lives of people with intellectual disabilities: An historical perspective. International Journal of Developmental Disabilities, 61(2), 107–112. https://doi.org/10.1179/2047386914Z.00000000094
3. May, P., Lombard Vance, R., Murphy, E., O’Donovan, M. A., Webb, N., Sheaf, G., . . . McCarron, M. (2019, September 20). Effect of deinstitutionalisation for adults with intellectual disabilities on costs: A systematic review. BMJ Open, 9(9), e025736. https://doi.org/10.1136/bmjopen-2018-025736
4. May, P., Lombard Vance, R., Murphy, E., O’Donovan, M. A., Webb, N., Sheaf, G., . . . McCarron, M. (2019, September 20). Effect of deinstitutionalisation for adults with intellectual disabilities on costs: A systematic review. BMJ Open, 9(9), e025736. https://doi.org/10.1136/bmjopen-2018-025736
5. McGinley, J. M. (2016, April). From nonissue to healthcare crisis: A historical review of aging and dying with an intellectual and developmental disability. Intellectual and Developmental Disabilities, 54(2), 151–156. https://doi.org/10.1352/1934-9556-54.2.151
6. Stancliffe, R. J., Tichá, R., Pettingell, S. L., Houseworth, J., & Bershadsky, J. (2023, July). Current services and outcomes of formerly institutionalised and never-institutionalised US adults with intellectual and developmental disabilities: A propensity score matching analysis. J Appl Res Intellect Disabil, 36(4), 859–870. https://doi.org/10.1111/jar.13103
7. Friedman, C. (2019, April). The influence of residence type on personal outcomes. Intellectual and Developmental Disabilities, 57(2), 112–126. https://doi.org/10.1352/1934-9556-57.2.112
8. Lewis, O., & Richardson, G. (2020, Mar-Apr). The right to live independently and be included in the community. International Journal of Law and Psychiatry, 69, 101499. https://doi.org/10.1016/j.ijlp.2019.101499
9. McCarron, M., Lombard-Vance, R., Murphy, E., May, P., Webb, N., Sheaf, G., . . . O’Donovan, M. A. (2019, April 25).
Effect of deinstitutionalisation on quality of life for adults with intellectual disabilities: A systematic review. BMJ Open, 9(4), e025735.
https://doi.org/10.1136/bmjopen-2018-025735
10. O’Doherty, S., Linehan, C., Tatlow-Golden, M., Craig, S., Kerr, M., Lynch, C., & Staines, A. (2016, June). Perspectives of family members of people with an intellectual disability to a major reconfiguration of living arrangements for people with intellectual disability in Ireland. J Intellect Disabil, 20(2), 137–151.
https://doi.org/10.1177/1744629516636538
11. Sheth, A. J., McDonald, K. E., Fogg, L., Conroy, N. E., Elms, E. H. J., Kraus, L. E., . . . Hammel, J. (2019, October).
Satisfaction, safety, and supports: Comparing people with disabilities’ insider experiences about participation in institutional and community living. Disability and Health Journal, 12(4), 712–717.
https://doi.org/10.1016/j.dhjo.2019.06.011
12. Brennan, D., Murphy, R., McCallion, P., & McCarron, M. (2018, March). “What’s going to happen when we’re gone?” Family caregiving capacity for older people with an intellectual disability in Ireland. J Appl Res Intellect Disabil, 31(2), 226–235.
https://doi.org/10.1111/jar.12379
13. Caldwell, J. A., Jones, J. L., Gallus, K. L., & Henry, C. S. (2018, October). Empowerment and resilience in families of adults with intellectual and developmental disabilities. Intellectual and Developmental Disabilities, 56(5), 374–388.
https://doi.org/10.1352/1934-9556-56.5.374
14. Cameranesi, M., Chimney, K., & Shooshtari, S. (2022, December). Changes in the quality of life of persons with profound intellectual and multiple disabilities following community transition: A Canadian study. Research in Developmental Disabilities, 131, 104360.
https://doi.org/10.1016/j.ridd.2022.104360
15. Friedman, C. (2023, April). Moving home: Community transition supports for people with intellectual and developmental disabilities. Disability and Health Journal, 16(2), 101419.
https://doi.org/10.1016/j.dhjo.2022.101419
16. Owuor, J., & Larkan, F. (2017). Assistive technology for an inclusive society for people with intellectual disability. Studies in Health Technology and Informatics, 242, 805–812.
17. Hewitt, A., Emerson, E., & Stancliffe, R. (2013, October). Introduction to the special issue: Community living and participation. Intellectual and Developmental Disabilities, 51(5), 293–297.
https://doi.org/10.1352/1934-9556-51.5.293
18. Neely-Barnes, S. L., & Elswick, S. E. (2016, Apr-Jun). Inclusion for people with developmental disabilities: Measuring an elusive construct. Journal of Social Work in Disability & Rehabilitation, 15(2), 134–149. https://doi.org/10.1080/1536710X.2016.1162122
19. Martínez-Leal, R., Salvador-Carulla, L., Linehan, C., Walsh, P., Weber, G., Van Hove, G., . . . Kerr, M. (2011, September). The impact of living arrangements and deinstitutionalisation in the health status of persons with intellectual disability in Europe. J Intellect Disabil Res, 55(9), 858–872. https://doi.org/10.1111/j.1365-2788.2011.01439.x
20. Landes, S. D., Turk, M. A., Formica, M. K., McDonald, K. E., & Stevens, J. D. (2020, October). COVID-19 outcomes among people with intellectual and developmental disability living in residential group homes in New York State. Disability and Health Journal, 13(4), 100969. https://doi.org/10.1016/j.dhjo.2020.100969
21. Turk, M. A., Landes, S. D., Formica, M. K., & Goss, K. D. (2020, July). Intellectual and developmental disability and COVID-19 case-fatality trends: TriNetX analysis. Disability and Health Journal, 13(3), 100942. https://doi.org/10.1016/j.dhjo.2020.100942
22. Bradley, V. J. (2020, October 1). How COVID-19 may change the world of services to people with intellectual and developmental disabilities. Intellectual and Developmental Disabilities, 58(5), 355–360. https://doi.org/10.1352/1934-9556-58.5.355
23. Verbeek-Oudijk, D., & Eggink, E. (2014). De grens van extramuralisering is nog niet bereikt [The upper-limits of deinstitutionalization not yet reached]. Tijdschr Gerontol Geriatr, 45(4), 188-96. Dutch. doi: https://doi.org/10.1007/s12439-014-0078-0
24. Tichá, R., Hewitt, A., Nord, D., & Larson, S. (2013, October). System and individual outcomes and their predictors in services and support for people with IDD. Intellectual and Developmental Disabilities, 51(5), 298–315. https://doi.org/10.1352/1934-9556-51.5.298
25. National Core Indicators. (2022). Intellectual and Developmental Disabilities (IDD) In-Person Survey. [Data set] Human Services Research Institute.
26. National Core Indicators. (2022). National Core Indicators Intellectual and Developmental Disabilities (IDD) 2021-2022: Overview and Methodology. https://idd.nationalcoreindicators.org/wp-content/uploads/2023/05/IPS21-22-NCI-IDD-Overview-and-Methodology_FINAL5_12.pdf
27 Centers for Medicare & Medicaid Services. (n.d.). Home. https://www.cms.gov/
28 StataCorp 2021 Stata Statistical Software: Release 17. College Station, TX: StataCorp LLC.
GLOBAL HEALTH MATTERS
GLOBAL HEALTH MATTERS
Partnering with innovative modeling group extends Fogarty’s reach....p. 5
Malaria network boosts U.S. government collaboration
Malaria network boosts U.S. government collaboration
By Judy Coan-Stevens
By Judy Coan-Stevens
On June 18, 2024, researchers from across the U.S. government convened for the inaugural meeting of the Federal Malaria Research Network (FMRN). Cofounded by scientists from the National Institutes of Health (NIH) and the Food and Drug Administration (FDA), the network brings together representatives from various U.S.-led malaria efforts. The U.S. government is the single biggest investor in malaria control and prevention in the world. Getting a handle on all that is being done—from basic research in vector biology to malaria vaccine development and anti-vector implementation programs—is no small task. FMRN allows those working in programs across the entire U.S. government to see where investments are being made and how they intersect, leading to collaboration, knowledge-sharing, and amplification of each other's work.
On June 18, 2024, researchers from across the U.S. government convened for the inaugural meeting of the Federal Malaria Research Network (FMRN). Cofounded by scientists from the National Institutes of Health (NIH) and the Food and Drug Administration (FDA), the network brings together representatives from various U.S.-led malaria efforts. The U.S. government is the single biggest investor in malaria control and prevention in the world. Getting a handle on all that is being done—from basic research in vector biology to malaria vaccine development and anti-vector implementation programs—is no small task. FMRN allows those working in programs across the entire U.S. government to see where investments are being made and how they intersect, leading to collaboration, knowledge-sharing, and amplification of each other's work.
collaborations and activities to advance global malaria control and elimination efforts, FMRN plans to convene regularly to share ideas, expertise, and findings pertinent to use-inspired malaria research (research meant for real-world application), from laboratory to field investigations and implementation and impact evaluation. Areas of discussion will focus on novel detection technologies and strategies, vaccines and other preventive and therapeutic interventions, including malaria parasite vector control, as well as new approaches to clinical trial design and monitoring of programmatic impact on malaria morbidity and mortality.
collaborations and activities to advance global malaria control and elimination efforts, FMRN plans to convene regularly to share ideas, expertise, and findings pertinent to use-inspired malaria research (research meant for real-world application), from laboratory to field investigations and implementation and impact evaluation. Areas of discussion will focus on novel detection technologies and strategies, vaccines and other preventive and therapeutic interventions, including malaria parasite vector control, as well as new approaches to clinical trial design and monitoring of programmatic impact on malaria morbidity and mortality.
“We can be good spokespersons for the activities of our sister agencies that are doing amazing work,” said Dr. Patrick Duffy, chief of the Laboratory of Malaria Immunology and Vaccinology at the National Institute of Allergy and Infectious Diseases, and one of the networks’ cofounders. “We can also learn where there are gaps and successes, and how things fit together.” A lot happens between the “upstream" basic research and the “downstream" implementation of malaria control and prevention. By sharing across the entire spectrum, researchers can make connections to their current and future work. If something is not relevant now, “it might be relevant to what’s needed in the future for malaria control and prevention,” added Duffy.
“We can be good spokespersons for the activities of our sister agencies that are doing amazing work,” said Dr. Patrick Duffy, chief of the Laboratory of Malaria Immunology and Vaccinology at the National Institute of Allergy and Infectious Diseases, and one of the networks’ cofounders. “We can also learn where there are gaps and successes, and how things fit together.” A lot happens between the “upstream" basic research and the “downstream" implementation of malaria control and prevention. By sharing across the entire spectrum, researchers can make connections to their current and future work. If something is not relevant now, “it might be relevant to what’s needed in the future for malaria control and prevention,” added Duffy.
With a remit to enhance cross-governmental strategic
With a remit to enhance cross-governmental strategic
FMRN has been inspired in part by a previous entity called the Federal Malaria Vaccine Coordinating Committee. That committee was very focused on vaccine development, while FMRN has a wide interest in a range of issues, interventions and tools relevant to malaria control and prevention. “The genesis of this newer entity, rather than trying to coordinate activities, is to see more broadly across the whole U.S. government malaria effort,” said Duffy, and to “make sure that we’re not working at cross-purposes.” One goal is that, with this network, researchers can speak knowledgeably about the malaria-based work that different U.S. government groups, such as USAID, The U.S. President’s Malaria Initiative, CDC and NIH, are doing in a given country or region.
FMRN has been inspired in part by a previous entity called the Federal Malaria Vaccine Coordinating Committee. That committee was very focused on vaccine development, while FMRN has a wide interest in a range of issues, interventions and tools relevant to malaria control and prevention. “The genesis of this newer entity, rather than trying to coordinate activities, is to see more broadly across the whole U.S. government malaria effort,” said Duffy, and to “make sure that we’re not working at cross-purposes.” One goal is that, with this network, researchers can speak knowledgeably about the malaria-based work that different U.S. government groups, such as USAID, The U.S. President’s Malaria Initiative, CDC and NIH, are doing in a given country or region.
A broader goal is for those working within U.S. government agencies to gain more knowledge about the overall U.S. malaria footprint. “That knowledge can help us get the best return on investment with the research that we're doing,” said Duffy. “It’s really helpful for us to see how we can best direct our resources to near-term needs as well as to future long-term solutions.”
A broader goal is for those working within U.S. government agencies to gain more knowledge about the overall U.S. malaria footprint. “That knowledge can help us get the best return on investment with the research that we're doing,” said Duffy. “It’s really helpful for us to see how we can best direct our resources to near-term needs as well as to future long-term solutions.”
Sickle cell research in Africa yields global benefits
Sickle cell research in Africa yields global benefits
Fogarty-supported research conducted by Dr. Siana Nkya in Tanzania, Dr. Adel Driss in Ghana, Dr. Sophie Kiguli in Uganda, and Dr. Halima Bello-Manga in Nigeria might help patients around the world.
Fogarty-supported research conducted by Dr. Siana Nkya in Tanzania, Dr. Adel Driss in Ghana, Dr. Sophie Kiguli in Uganda, and Dr. Halima Bello-Manga in Nigeria might help patients around the world.
Image courtesy of NIAID
Malaria merozoites (green/purple) invading human red blood cells (red). Merozoites are covered in a fuzzy coating of surface proteins (light blue) that are shed during invasion.
Image courtesy of NIAID
Malaria merozoites (green/purple) invading human red blood cells (red). Merozoites are covered in a fuzzy coating of surface proteins (light blue) that are shed during invasion.
Neuzil engages with AFREhealth on global health
As a new director looking to develop her vision for Fogarty's programs around the world, Director Dr. Kathy Neuzil seized an opportunity to attend the seventh annual African Forum for Research and Education in Health (AFREhealth) Symposium in August to get feedback on barriers to obtaining funding, challenges and opportunities for research, and to establish rapport with its members. Supported by the National Institutes of Health (NIH) and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), AFREHealth is an interdisciplinary society that works with ministries of health, academic and training institutions, and other stakeholders to improve the quality of health care on the continent through research, education, and capacity building. It is Africanfocused and African-led.
As part of the Fogarty strategic planning process, Neuzil and Dr. UnJa Hayes, program officer for AFREhealth and other Fogarty programs, held a break-out session with AFREhealth investigators. Neuzil encouraged attendees “to share as many ideas as we can, openly and transparently.”
Hayes explained how AFREhealth was shaped from the successes the Medical Education Partnership Initiative and the Nursing Education Partnership Initiative, earlier investments by NIH and PEPFAR to improve health care in Africa by strengthening its health and research workforce. Two years later, a Fogarty grant (in partnership with PEPFAR) funded the development of the necessary infrastructure to establish the society, which includes individuals, institutions, associations, and networks from all geographic and linguistic regions of Africa plus external members. “The listening session helps us see where there may be a disconnect—what is generally understood by the community as opposed to what we think we are communicating,” said Hayes.
Research training
Education dominated the thoughts of many attendees. Fogarty currently features a variety of training programs, including bioethics, bioinformatics, infectious diseases, HIV, and trauma and injury research. One attendee noted that research training grants usually “focus on a single disease, but we need some funding that is broad spectrum—that allows people to study various
conditions.” Another attendee commented that caring for patients with noncommunicable diseases becomes an extended responsibility for most families. “In Uganda, someone who is caring for a patient with cancer often ends up with hypertension because of the stress,” she said. “Can we think of a toolkit or policy brief or training of family members to help in that area?” Neuzil and Hayes encouraged innovative research projects that address these real-world challenges.
Fogarty currently features a variety of training programs in bioethics, bioinformatics, infectious diseases, HIV, and trauma and injury research.
Meanwhile, a family physician commented that she’s most “concerned about strengthening the primary health care system because that's the first point of contact that we have and that’s our engagement with the community— that’s where we need grants. What about continuity of care, comprehensiveness, coordination, personcenteredness? Perhaps there are gaps there.”
Grant management
The nuts and bolts of grant mechanisms also took center stage. A research administrator said she’s benefitted “a lot” from NIH YouTube educational videos but sees a gap “in training us—the research managers and administrators—so that we can keep pace with dynamic research and any new requirements.” (Fogarty currently offers funding for infrastructure development training programs for HIV research to help low-and middle-income country institutions build administrative capacity.) She also wondered if Fogarty might fund more studies of African traditional medicine.
In conclusion, Neuzil said, “This has really exceeded all expectations. So many people participated and gave us great ideas. I'm grateful to you all.”
Photo courtesy of AFREhealth
Fogarty Director Dr. Kathy Neuzil leads a listening session at AFREhealth’s seventh annual symposium.
APTI’s third cohort looks toward their second year
The African Postdoctoral Training Initiative (APTI) is a joint effort by the African Academy of Sciences, the Bill & Melinda Gates Foundation and the National Institutes of Health that aims to bolster Africa’s scientific research capacity. Members of APTI’s third cohort of fellows met in September to present their research. We caught up with four fellows as they reflected on their APTI journey.
DR. GILDAS HOUNMANOU
Dr. Gildas Hounmanou studies environmental microbiomes and disease outbreaks in Benin.
Dr. Gildas Hounmanou leads a study in Africa’s largest lake village near Lake Nokoué in Benin exploring the connection between human microbiota and environmental microbiomes. His research focuses on how disease-causing microorganisms persist and spread between humans and the lake’s ecosystem. By examining environmental exposures, seasonal changes, and human activities, the study aims to uncover factors contributing to outbreaks of diseases like cholera, typhoid, and water-related skin diseases, while also considering the impact of climate change on these waterborne epidemics.
Through the APTI program, Hounmanou has gained advanced skills in computational biology, including metagenomics and machine learning, crucial for his goal of establishing a research program on climate-sensitive infectious diseases in vulnerable communities.
DR. VINIE KOUAMOU
Dr. Vinie Kouamou studies HIV drug resistance and mechanisms of HIV persistence in CD4+ T Cells in Cameroon
Dr. Vinie Kouamou credits her interest in HIV research to her late mother who was a laboratory scientist. As part of her APTI project with the National Institutes of Allergy and Infectious Diseases (NIAID), she is investigating how defective HIV-1 proviruses, a form of a virus that is integrated into the genetic material of a host cell but is unable to produce an intact virus, continue to trigger immune responses. This can lead to chronic inflammation among people living with HIV that are on antiretroviral therapy (ART), even though ART suppresses the immune system.
Through the APTI program, Kouamou has learned advanced scientific concepts and methodologies in virology, immunology, and vaccinology, skills vital for her preparation for pursuing independent research in the future. She plans to conduct independent research that contributes to health policies in Africa.
DR. CARINE KUNSEVI-KILOLA
Dr. Carine Kunsevi-Kilola studies HIV and malaria in pregnancy in the Democratic Republic of the Congo
Before joining the APTI program, Dr. Carine Kunsevi-Kilola served as a postdoctoral research fellow at the Reproductive Immunology Research Consortium in Africa (RIRCA), based at Stellenbosch University, where her research focused on investigating the effects of HIV and antiretroviral therapy (ART) on pregnancy outcomes and child development.
Through the APTI program, Kunsevi-Kilola is expanding her research to explore the role of certain proteins on the surface of immune cells (called complement components) in shaping the immune responses to HIV and malaria infections during pregnancy, specifically in the plasma of malaria-infected women.
She says the APTI program has equipped her with valuable technical skills like proteomics and pathway analysis, which will help her reach her ultimate goal of continuing research in reproductive immunology or related fields, focusing on topics like HIV, malaria, and pregnancy outcomes.
DR. AMADOU NIANGALY
Dr. Amadou Niangaly conducts molecular surveillance of malaria in Mali
Dr. Amadou Niangaly started his biomedical research career in the early 2000s, when he received a PhD in parasitology-mycology and medical entomology from the University of Bamako, Mali. He’s currently an associate professor at the University of Sciences, Techniques and Technologies, also in Bamako.
During the first phase of his APTI fellowship, he has been using genomic analysis to understand how the malaria parasite adapts to vaccines, drugs, and monoclonal antibodies. So far, Niangaly has learned critical skills in next-generation sequencing and molecular surveillance, which he plans to apply to infectious disease control in Africa and ultimately establish a genomics laboratory at his institution in Mali.
PROFILE
Monitoring HIV drug resistance in Zimbabwe
Dr. Justen Manasa says he had to “grow up quickly” over the last few years. As a senior lecturer and biomedical scientist at the University of Zimbabwe and director of the University’s Innovation Hub, he watched as COVID-19 took hold in the region and ultimately took the lives of two of his closest mentors, the late Drs. James Hakim and David Katzenstein, both highly regarded in their fields. Manasa says, “These were people whom I admired and looked up to my entire career, and almost overnight, I was thrust into a leadership position to try and fill their shoes.”
Manasa joined the Fogarty Global Health Fellows and Scholars program, now known as LAUNCH, through the Global Health Equity Scholars Program at the University of California Berkeley. Prior to his fellowship, Manasa had received support from Fogarty that allowed him to pursue his master’s degree in molecular virology through a partnership between Stanford Medical School and the University of Zimbabwe. While at Stanford, Manasa participated in SPARK, a translational research program that bridges academia and industry by identifying research products from the academic community that have the potential to be taken to market as therapeutics, diagnostics, or medical devices. Essentially, the program helps the academics who created these products transition to entrepreneurship. While at Stanford, Manasa began to study HIV drug resistance which has been a research priority for him ever since.
In his Fogarty fellowship project, he focused on studying the increase in HIV drug resistance and providing equitable access to diagnostics to improve the effectiveness of treatment for patients. Monitoring HIV drug resistance is essential to determining how to improve treatment outcomes and which antiretroviral (ART) drugs are included in public health treatment regimens. Manasa’s project aimed to leverage the advances in sequencing and bioinformatics technologies to provide increased understanding of HIV drug resistance among patients in Zimbabwe.
Following these experiences, Manasa learned that the University of Zimbabwe planned to transition their educational system to focus not only on teaching research and community service but also on innovation and
Justen Manasa, PhD
Fulbright Fellow: 2016-2017
U.S. institution: Stanford University
Foreign institution: University of Zimbabwe
Research topic: HIV drug resistance
Current affiliation: Senior lecturer and biomedical scientist, University of Zimbabwe
industrialization. Like the SPARK program, the Innovation Hub at the University of Zimbabwe draws from academic research projects to develop products or services that have the potential to improve health. The hub then helps identify funding sources to transition the projects from academia to the market. Manasa knew this would be a natural fit for him.
Today, along with directing the Innovation Hub, Manasa serves as principal investigator for the Enhancing Noncommunicable diseases (NCD) Research and Innovation Capacity or ENRICH program as well as a separate program focused on HIV genomics. With the long-term goal of generating evidence for interventions to improve care for people with NCDs in the region, ENRICH aims to train master’s, PhDs, and postdoctoral candidates in Zimbabwe to be proficient NCD researchers.
Within his many roles, Manasa hopes to incorporate and implement what he learned from Drs. Hakim and Katzenstein. “One of the biggest lessons I learned working with them is that mentorship is key to the flourishing of trainees, and if you have good mentors as a trainee, you will flourish academically and in every other aspect of your life.”
These days Manasa is based in Lesotho, South Africa, where he continues his pursuit of ensuring treatment for HIV remains equitable and accessible for patients throughout southern Africa as well as around the globe. In his free time, he is brushing up on his public health skills by pursuing a master's degree at the Harvard T. Chan School of Public Health. He is also working on a paper highlighting the impact that Fogarty programs have had on the research infrastructure in Zimbabwe.
A&Q
KAIYUAN SUN, PHD
Dr. Kaiyuan Sun earned a PhD in physics at Northeastern University. Dr. Sun’s dissertation focused on complex system modeling of infectious disease dynamics. He joined Fogarty in 2018 as a postdoctoral visiting fellow and has worked as an in-house research scientist in the Division of International Epidemiology and Population Studies (DIEPS) since 2021. He has studied pathogens that cause global public health emergencies, including Ebola, Zika, and SARS-CoV-2, and is particularly interested in using mathematical models to translate findings of epidemiological studies into population-level impact and to inform public health decision making.
Why focus on infectious disease modeling?
If you think about infectious disease, it’s kind of like a perfect system to reflect biological complexity. There’s the human population (host) and a pathogen, and there’s this arms race between the two, right? The pathogen will infect us and then it will evolve to evade immunity and to find as many ways to infect as many hosts as possible. From the human perspective, we can mount an adaptive immune response to a pathogen, and that either lessens the severity of response to the pathogen (disease) or prevents infection altogether. Humans also have the advantage of the invention of vaccination, so we can start the arms race even before pathogens infect us!
What are the findings from your recent Nature Medicine paper?
This study is unique because we’re looking at immunity induced by prior infections—not immunity induced by vaccines—and how that might protect us in the future. We're also using a “correlate of protection,” which is an immune biomarker that can reliably predict the extent of protective immunity. For example, seeing neutralizing antibodies in your blood indicates that you’ve already been exposed to an infection; and higher titers should mean better protection against a future infection.
We did this study when two SARS-CoV-2 variants—delta and omicron—were circulating in South Africa. So, we measured the neutralizing antibody titers prior to the delta wave and prior to the omicron wave and then we looked at how those titers potentially protected against reinfection. Our study confirms that neutralizing antibody titers correlate with protection against SARS-CoV-2, just as previous studies of vaccine-derived immunity showed.
The more interesting finding, however, is that the neutralizing antibody titer levels don't explain the majority of protection. For the delta wave, they explain just one third of the protection, while for the omicron wave, they explain even less: just 10%.
What does this mean?
This raises the question, What provides the remaining protection and what immune markers correlate with that? We need to look at other compartments of adaptive immunity and how they protect us against SARS-CoV-2 instead of focusing exclusively on neutralizing antibodies. For example, recent flu studies show immune markers like T cell response or innate response correlate with protection independent of neutralizing antibodies.
What’s PHIRST? Why is it so special?
Our study of infection-induced immunity would not be possible without the groundbreaking design of PHIRST— the Prospective Household cohort study of Influenza, Respiratory Syncytial virus, and other respiratory pathogens community burden and Transmission dynamics in South Africa. The PHIRST studies are the genius of Dr. Cheryl Cohen's team at NICD (National Institute for Communicable Diseases), South Africa.
To understand the transmission of respiratory viruses, Cohen’s team set up cohorts of people who get twice weekly PCR testing for influenza and RSV, irrespective of symptoms. In an early PHIRST study of influenza, Cohen’s team found that asymptomatic influenza infection and transmission are much more common than we previously thought.
When the SARS-CoV-2 pandemic hit, they swiftly adapted their preestablished cohort infrastructure and protocol to create the PHIRST-C study (where “C” represents “COVID-19”).
What’s next for you?
A priority is to share my knowledge and expertise in mathematical modeling with my brilliant South Africa colleagues. I’m working closely with Dr. Jackie Kleynhans, a scientist on the PHIRST team, to model the impact of influenza vaccine and the potential impact of introducing pediatric vaccines to reduce influenza transmission.
FOCUS
Sickle cell research in Africa yields global benefits
More than 100 million people worldwide are living with sickle cell trait. Between 2000 and 2021, the number of babies born with sickle cell disease (SCD) surged by 13.5%, with increasing rates reported in nearly every nation studied. According to the Global Burden of Disease Study 2021, the highest SCD disability burden was concentrated in western and central subSaharan Africa and India.
SCD is a genetic mutation that causes red blood cells, which are typically round, to form more like crescent moons. Round red blood cells move quickly through the blood vessels, but these sickle-shaped cells can impair blood flow and result in blood clots and poor oxygen levels, leading to chronic, acute pain syndromes, severe bacterial infections, and tissue death. Someone who is a carrier of sickle cell trait does not suffer from SCD; however, they will likely pass that gene on to their children, who may potentially suffer from SCD as a result.
Between 2000 and 2021, the number of babies born with sickle cell disease (SCD) surged by 13.5%, with increasing rates reported in nearly every nation studied .
Currently, there are several treatment options available for SCD. In 2023, the U.S. Food and Drug Administration approved two new gene therapies to treat SCD that can either add a modified gene to the body or make changes to a gene that is already in the body. The existing and new therapies reveal the scientific advances that have been made, yet they can be cost-prohibitive for many patients in high-income countries—and even more so in low- and middle-income countries.
Tanzanian research
Dr. Siana Nkya of Tanzania, a senior lecturer at Muhimbili University of Health and Allied Sciences (MUHAS) and president of the Tanzanian Human Genomics Organization (THGO), studies the genomic determinants of SCD in
sub-Saharan African populations. Nkya, a former Fogarty Global Health Fellow, has spent the last 15 years of her career studying the effects of fetal hemoglobin decline among infants with sickle cell disease, a key factor in modifying the severity of sickle cell disease.
She recently completed a five-year project through an Emerging Global Leader Award funded by both NIH and Fogarty. This project involved establishing a birth cohort of more than 250 infants to study the natural decline of fetal hemoglobin in both sickle cell and non-sickle cell infants. The study tracked the hemoglobin levels of these infants from birth up to 3 years of age, providing critical insights into how fetal hemoglobin declines more slowly in infants with SCD compared to those without it. This delayed decline, or “delayed switch,” is vital for understanding how to develop effective interventions, such as the timely administration of hydroxyurea.
Nkya’s work has not only contributed to a better understanding of SCD but also laid the groundwork for future research and policy development in genetics across Africa.
Recently, the National Human Genome Research Institute (NHGRI) published a study highlighting that genetic carriers for sickle cell trait are prevalent across diverse human populations, including those of Mediterranean, Indian, and Middle Eastern ancestry, not just those of African origin. Other recent studies have also shown a marked increase in SCD prevalence birth rates in Latin America and the Caribbean. Fogarty-supported research in genomics and other disciplines conducted by Dr. Adel Driss in Ghana, Dr. Sophie Kiguli in Uganda, and Dr. Halima Bello-Manga in Nigeria also might contribute to the knowledge base that helps patients with SCD around the world.
Nkya said, “The more we support research in Africa, it’s not just for Africa. It benefits the globe.”
Health care workers monitor the blood pressure of a person with sickle cell disease.
Photo courtesy of Badru Katumba/WHO
Probing the interaction of sickle cell disease and malaria resistance in Ghana
Sickle cell disease (SCD) is a genetic condition caused by a mutation in one of the genes that controls hemoglobin, the protein in red blood cells that transports oxygen. People with sickle cell trait— those who carry one mutated allele of the sickle cell gene—are protected against severe malaria. This unusual interaction between a genetic disease and a parasitical infection transmitted by mosquitoes intrigued Dr. Adel Driss during his 2014 Fogarty Global Health Fellowship.
His fellowship at the Noguchi Memorial Institute for Biomedical Research in Ghana led to his Fogarty International Research Scientist Development Award (IRSDA) project, which investigated the molecular factors underlying the complex relationship between SCD and malaria resistance.
Molecular deep dive Driss, an assistant professor at Morehouse School of Medicine, split his IRSDA project time between field research in Ghana and performing lab experiments and data analysis in the U.S. The relationships he established as a fellow helped him in his immersive investigation. Specifically, he investigated how microRNAs, small molecules in the blood that regulate gene expression, may play a role in protecting individuals with sickle cell trait from severe malaria. This study involved collecting blood samples from individuals with various sickle cell genotypes to examine whether microRNA levels fluctuate during malaria infection. (“Sickle cell genotype” refers to the specific abnormal hemoglobin gene a person inherits— there are a few different types.) Driss also conducted lab experiments and mouse model studies to explore how microRNAs affect malaria parasites in red blood cells. “For example, if we increase the expression level of a specific microRNA, will that enhance or inhibit malaria parasite growth?” he explained.
His project, scheduled to run from September 2016 to August 2021, was extended to March 2022 due to COVID-19 disruptions. The early years were productive, with almost 900 samples collected and progress made on the study’s objectives. Later, pandemic restrictions prevented travel and fieldwork in Ghana and limited lab access in the U.S. Despite challenges, he and his colleagues achieved key milestones. Their findings included identifying
differences in microRNA expression across various hemoglobin genotypes. They also showed that malaria parasites in red blood cells derived from donors grew at different rates (in petri dishes) depending on the donor’s hemoglobin genotype.
“Additionally, we identified miR-451a, a microRNA, as a potential new player in the pathogenesis of malaria and SCD,” said Driss. Though he’s still preparing final results for publication, six articles have already been published in high impact journals. Overall, his findings enhance the understanding of the relationship between microRNAs, SCD, and malaria. Possible long-term outcomes of this work include development of new therapies, interventions, and diagnostic tools aimed at preventing severe malaria and improving the health of individuals with SCD.
Why Ghana?
Dr. Adel Driss’ findings enhance the understanding of the relationship between microRNAs, SCD, and malaria.
Conducting research on SCD in Ghana was essential to his study because it is a malariaendemic country with SCD affecting approximately 2% of newborns, said Driss. (Sickle cell allele prevalence among Ghana’s general population is reported to be 25%.) The West African nation’s rich genetic diversity allowed him to investigate a variety of distinct sickle cell genotypes and their interactions with malaria. His project, a collaboration between Morehouse School of Medicine and the Noguchi Memorial Institute for Medical Research, has benefited the local population and also informed resource allocation in the region. “We’ve trained students and early-career researchers in both Ghana and the U.S.,” said Driss.
Previously, Driss studied muscular dystrophies in Tunisia, France, and Japan. He’s also conducted research on cancer at Emory University. “Since grad school, I’ve been involved in research all over the world, which is amazing and the best part of my work. I’ve collaborated with various institutions in different countries and trained different students at different career levels.”
Photos courtesy of Adel Driss
Sickle Cell researchers keep pace with patients as they grow beyond childhood
Until recently in Uganda, most children with sickle cell disease (SCD) never celebrated their fifth birthday—only 30% lived past this milestone. This low survival rate was mainly due to inadequate health care interventions for these children, plus lack of widespread newborn screening, explains Dr. Sarah Kiguli, a professor at Makerere University College of Health Sciences. Things are different today. Over the past decade, the East African nation has instituted a policy of screening newborns while strengthening strategies to manage their health. This means more children with SCD are growing into adolescence and adulthood.
Challenges still exist, says Kiguli. For example, the community and district facilities where many Ugandan children are born cannot provide comprehensive services, including newborn screening. Another issue: the risk of SCD complications in the kidneys, lungs, heart—in almost all organs—grows higher as patients grow older, yet scientific research in Uganda hasn’t caught up with the reality of these longer lives. As a result, teens and adults with SCD don’t get “the care they deserve,” says Kiguli.
“It’s very painful for us pediatricians to see our patients encounter challenges and problems when they transition to adult care.”
Renewed research focus
Despite years devoted to children’s health, Kiguli believes it’s time to prioritize studies exploring appropriate SCD management for teens and adults. “We need solutions that address all the patient needs, including reproductive health, as they transition out of childhood.” She’s spearheaded a multidisciplinary research training program for researchers focused on the needs of people with SCD at all ages: Enhancing Research capacity for Sickle Cell Disease and related NCDs across the Lifespan in Uganda (ENRICH).
“Among our PhDs, we don't have anyone from pediatrics— and that's fine,” says Kiguli. “We have someone looking at mental health in adolescence, sickle cell in pregnancy, bioinformatics, and epidemiology of malaria in SCD.”
Importantly, the researchers are trained as a group to emphasize the benefits of multidisciplinary collaboration. “We’ve been working in silos—pediatricians alone, physicians alone, social scientists alone—that won’t help us
Dr. Sarah Kiguli of Makerere University leads the Fogarty-funded program: Enhancing Research capacity for Sickle Cell Disease and related NCDs across the Lifespan in Uganda (ENRICH)
to address the comprehensive needs of these patients.”
Methodology has also been considered. “We provide both individual and team mentorship from the beginning,” said Kiguli. Monthly meetings help trainees develop personal development goals and career path plans in the hopes they will continue in the field. The program also provides research training to health professionals, such as medical doctors, laboratory personnel and nurses, who are not necessarily doing degree programs—“so those who manage patients routinely might also benefit,” said Kiguli.
South-to-South unity
For the project, Makerere University has partnered with Busitema University, located in eastern Uganda, where “prevalence of the sickle cell trait is as high as 20%,” says Kiguli. (This contrasts with about 13% prevalence elsewhere in the country.) Studying the disease in a high burden locale is highly relevant, with results likely to influence policy and treatment guidelines.
Kiguli has other reasons for collaborating with Busitema University, which is less than 15 years old. “We want to build capacity at this young institution since our colleagues there have less chance of doing research than we do.” Working and supervising trainees together will give Busitema’s faculty much-needed experience, while providing faculty at both universities opportunities to learn from each other. Kiguli also hopes the new collaboration will advance progress made by their past partnerships. “Capacity must be built in a sustainable way,” says Kiguli. “It’s important to work collaboratively and not competitively—this is just as important for Makerere University as it is for Busitema University.”
Photo courtesy of Sarah Kiguli
This Nigerian hematologist established an SCD stroke prevention program in the community
Sickle cell anemia (SCA) is the most severe form of sickle cell disease, an umbrella term for all disorders caused by the various sickle gene variants. Annually, more than 300,000 children worldwide are born with this inherited disease. Nigeria accounts for more than 50% of these babies. Before they reach their 20th birthday, about 11% of children with SCA will have suffered a devastating complication—stroke. As they grow older, stroke risk will increase, reaching about 24% by age 45.
In 2016, Dr. Halima Bello-Manga, a hematologist and associate professor at Kaduna State University, worked as a site investigator for a National Institutes of Healthfunded clinical trial: The primary stroke prevention in children with SCA in Nigeria (SPRING). Later, she established a stroke prevention program for children with SCA at Barau Dikko Teaching Hospital, an academic facility affiliated with her university. These projects planted the seed for her ongoing Fogarty Emerging Global Leader Award study: Primary Prevention of Stroke in Children with Sickle Cell Anemia in Nigeria: Community vs Teaching Hospital.
Implementing evidence-based care
More than 20 years ago, scientists found that children who are at highest risk for stroke can be identified by measuring the velocity of blood in their cerebral vessels using Transcranial Doppler (TCD) ultrasound. Simply, high velocity corresponds to high risk. “Now, we routinely test children between the ages 2 and 16 because high-risk children can benefit from an intervention,” said BelloManga.
An NIH-funded clinical trial compared dosing levels of hydroxyurea for stroke prevention and found an effective lower dose, which the American Society of Hematology (ASH) also endorsed. The study also showed that twiceyearly blood tests to check for unwanted effects from this potent (and potentially toxic) drug are sufficient. BelloManga said, “These studies prove that it’s possible to use lower dose of hydroxyurea for stroke prevention and to administer fewer lab tests. That's a huge benefit to families because the financial burden is less.”
The three factors combined—TCD screening, hydroxyurea dosage levels, and frequency of lab testing—represent “the backbone of my project,” said Bello-Manga. She’s hoping to prove a community hospital can do as good a job as
Dr Halima Bello-Manga with two children (siblings with SCA) who suffered strokes before her prevention program was established.
an academic hospital in correctly identifying high-risk children and managing their stroke prevention care.
Assistance from mentors
In Nigerian academic centers, stroke prevention teams are led by physicians, TCD is performed by radiologists, and hydroxyurea is prescribed by pediatricians or hematologists. “In our community hospital, we don’t have physicians or specialists, so we had to identify the right personnel and task-shift,” said Bello-Manga. She established guidelines so that prescribing responsibilities could be transferred to medical officers and then organized workshops—with educational videos created by her advisor, Dr. Lori Jordan of Vanderbilt University—to train nurses to perform TCD.
Her reorganization of duties proved successful, but Bello-Manga has not yet completed a feasibility study (or “non-inferiority trial”) to confirm that the community site is equal to the academic site in managing stroke prevention risk. COVID-19 disrupted her progress. “I'm behind by about one year.” Still, she’s pleased with her accomplishments so far—especially the publication of several papers.
She’s also proud to have had a profound impact on many patients’ lives. For her community program, children with SCA and stroke risk receive hydroxyurea free from the state government. Her wish is to see this replicated in all parts Nigeria and other LMICs with high burden of SCA.
As she nears completion of her project, Bello-Manga speaks with confidence about the importance of conducting sickle cell research in Nigeria. “There is nothing more interesting than observing or doing research on a certain condition in the natural space of that condition. Every patient has a different presentation and it's not what you read in books,” she said. “Our clinics are encyclopedias.”
Photo Courtesy of Halima
Bello-Manga
DIRECTOR’S COLUMN
By Kathleen Neuzil, Director, Fogarty International Center
Vaccines: Potential tools for health equity
On September 9, 2024, I had the honor of (virtually) delivering the Edward Jenner Lecture for the 18th Vaccine Congress in Lisbon. Edward Jenner was an 18th century physician, who is often referred to as the “Father of Vaccinology.” He pioneered the use of vaccination to control an infectious disease—specifically, he used a cowpox virus inoculation to protect against smallpox. What Jenner understood is that the two viruses, though distinct, come from the same orthopoxvirus family, and so immunization with one would protect against the other. In a treatise describing his work, Jenner wrote, “…the annihilation of the smallpox, the most dreadful scourge of the human species, must be the final result of this practice.”
I received a smallpox vaccine as a child, more than a hundred and fifty years after Jenner delivered his first inoculation. Many of you reading this blog didn’t receive a vaccine, because you didn’t need one. Smallpox was eradicated worldwide in 1980.
My plenary talk, “Vaccines as tools for health equity,” discussed the phenomenal impact of vaccination programs. Over the past half century, in addition to eradicating smallpox, vaccines are estimated to have averted 154 million deaths and saved 9 billion years of life. Here in the U.S., routine immunizations have prevented more than one million deaths and conserved an estimated $540 billion dollars over the past 30 years.
for more than a decade. This has coincided with decreased population immunity following the discontinuation of smallpox vaccines. In 2022, mpox spread around the world and was declared a Public Health Emergency of International Concern (PHEIC). A new strain of mpox is now widely disseminated in parts of Africa, leading the WHO to declare a second mpox PHEIC in August.
Fogarty-funded public health scientists are among those leading the charge to raise awareness about mpox and to combat the outbreak in Africa. In an article published on the same day as my lecture, Fogarty grant recipient Dr. Jean Nachega and his colleagues delineate the multiple reasons why Africa, once again, must confront a public health emergency: Poverty, population displacement, lack of diagnostics, lack of vaccines… in summary, a general lack of political will. To contain the mpox outbreak, Nachega and colleagues called for long-term research investments, a leveraging of Africa's post-COVID-19 mRNA vaccine manufacturing hubs, and equitable access to diagnostics, vaccines and therapeutics. We at Fogarty are committed to scientific training and capacity building, understanding that the development of a scientific work-force will be key to preventing future pandemics and other health emergencies, while enabling a more resilient future.
Unfortunately, and paradoxically, global childhood immunization levels stalled in 2023. Armed conflicts and the inability to reach children are the primary cause of this drop in vaccinations. Remarkable scientific advances have catalyzed the development of new and better vaccines, yet such challenges mean that too many people do not benefit. Vaccine misinformation, vaccine hesitancy, and lack of access to vaccines have likewise contributed to the declines.
The mpox virus is an orthopoxvirus in the same family as smallpox. Mpox infections have been increasing in Africa
Though the WHO declared an emergency in August, vaccines only reached the Democratic Republic of Congo in September, while vaccination programs only began on October 5. In contrast, mpox vaccines were widely available in the U.S. and other high-income countries during the 2022 outbreak.
I can’t help but be reminded of this famous painting, “Jenner: Smallpox is Stemmed,” painted by Robert A. Thom. Here, Dr. Jenner is depicted inoculating a young boy to prevent smallpox, a disease that had immense impact on children in his time. Despite the outsized effect of mpox on African children today, there’s no similar picture of a child receiving a life-saving vaccine.
I can only hope that soon—more than two centuries after Jenner advanced his own dream of health equity—that new picture will be available.
Edward Jenner, an English physician, performed the first vaccination against smallpox in 1796.
Image courtesy of the National Library of Medicine
HEALTH Briefs Global PEOPLE
Abdool Karims receive Lasker Award
Quarraisha and Salim Abdool Karim have received the prestigious 2024 Lasker-Bloomberg Public Service Award. The Abdool Karims were honored for illuminating key drivers of heterosexual HIV transmission; introducing life-saving approaches to prevent and treat HIV; and statesmanship in public health policy and advocacy.
The couple helped build South Africa’s scientific infrastructure and cultivated the next generation of infectious disease experts via CAPRISA (Centre for the AIDS Program of Research in South Africa), which they founded with Fogarty funding in 2002.
NIH names new AIDS research director
Dr. Geri Donenberg has been named the NIH associate director for AIDS research and director of the NIH Office of AIDS Research (OAR). She brings over 25 years of experience with a focus on factors that influence HIV transmission. In this role, she will lead efforts to coordinate and advance HIV/AIDS research across NIH.
Hotez to receive Winslow Award
Dr. Peter Hotez, a renowned vaccine researcher, will receive the 2024 Winslow Medal from the Yale School of Public Health for his leadership in global health, particularly his work in developing vaccines for neglected tropical diseases and codeveloping a low-cost COVID-19 vaccine, and his fight against vaccine misinformation and promoting scientific literacy.
Remembering Kawango Agot
Former Fogarty trainee and long-time grant recipient Dr. Kawango Agot has passed away. As the founder of Impact Research and Development Organization and the Nyanza Initiative for Girls’ Education and Empowerment, she led nearly 60 studies and programs that shaped HIV policies in Kenya focused on women and girls living with HIV.
Tengiz Tsertsvadze dies at age 76
Dr. Tengiz Tsertsvadze, founder of the HIV/AIDS service in Georgia and general director of the Center for Infectious Pathology, AIDS, and Clinical Immunology, has died at the age of 76. Tsertsvadze, a former Fogarty trainee, was one of the main initiators of Georgia’s hepatitis C elimination program.
NIAID updates mpox research priorities
The National Institute of Allergy and Infectious Diseases (NIAID) has revised its priorities for mpox research as part of the overall U.S. government. The agenda includes research into the biology of all clades (strains) of the virus; evaluating current vaccine dosing regimens; and supporting strategies for detecting the virus.
Natural antimicrobial could treat cholera
Researchers at the University of Texas at Austin explored a class of natural antimicrobials called microcins, which are produced by bacteria in the gut, and identified one that targets the bacteria that causes cholera. Microcin could potentially remove unwanted bacteria without disturbing the healthy balance of the gut microbiome.
CDC describes imported Oropouche virus infections
The U.S. Centers for Disease Control and Prevention (CDC) reported 21 imported Oropouche virus cases. Since late 2023, Oropouche virus has spread beyond the Amazon where it is endemic to new areas of South America and the Caribbean. Scientists are working to see if U.S. midge and mosquito species can carry the virus.
Marine sponge provides insights into TB Researchers at Australia’s Peter Doherty Institute for Infection and Immunity discovered a bacterium in a marine sponge with striking similarity to Mycobacterium tuberculosis, the pathogen that causes tuberculosis. They say their findings could inform future research and lead to the development of new TB treatment strategies, including potential vaccines.
High-risk HPV may affect male fertility
The potential effects of human papillomavirus (HPV) in men and boys are unknown. Researchers at Universidad Nacional de Córdoba in Argentina found High Risk (HR) HPV-positive men had significantly lower counts of leukocytes (a type of white blood cell) in their semen, suggesting that HR-HPV positive men could have impaired fertility.
SUBSCRIBE: fic.nih.gov/subscribe
Funding Opportunity Announcement Deadline Details
Global Brain Disorders Research R01 Clinical Trials Optional R21 Clinical Trials Optional go.nih.gov/FogartyBrainResearch
Global Brain Disorders Research
R01 Clinical Trials Optional (AIDS Research)
R21 Clinical Trials Optional (AIDS Research)
HIV-associated NCDs at LMIC Institutions
Nov 15, 2024
Dec 9, 2024
go.nih.gov/FogartyBrainResearch
R21 Clinical Trials Optional go.nih.gov/HIV-NCDs
For more information, visit www.fic.nih.gov/funding
Global Health Matters
September/October 2024
Volume 23, No. 6 ISSN: 1938-5935
Fogarty International Center National Institutes of Health Department of Health and Human Services
Writer/editor: Mariah Felipe Mariah.Felipe@nih.gov
Writer/editor: Susan Scutti Susan.Scutti@nih.gov
Digital communications specialist: Merrijoy Vicente Merrijoy.Vicente@nih.gov
Designer: Carla Conway
In rare cases when a correction is needed after an issue’s printed version has been finalized, the change will be made and explained in the online version of the article.
All text produced in Global Health Matters is in the public domain and may be reprinted. Please credit Fogarty International Center. Images must be cleared for use with the individual source, as indicated.
Dec 9, 2024
Reframing stressors of Syrian refugees
Researchers at American University of Beirut propose an innovative model for conceptualizing stressors and their impact on the mental health of Syrian refugees. Their study, funded by Fogarty and the National Institute of Environmental Health Sciences, was published in Frontiers in Public Health earlier this year.
The number of individuals forcibly displaced has doubled over the past decade. More than 14 million Syrians have fled their homes since the beginning of the war in 2011. Adult Syrian refugees are up to 10-fold more likely to develop post-traumatic stress and other disorders than the general population of host countries. Post-displacement stressors, which include financial, political, and social components, impact Syrian refugees, sometimes “exerting a more substantial influence on mental health than warrelated stressors,” writes senior author Dr. Rima Habib and her colleagues. Their new study proposes a conceptual framework for how these different types of stressors contribute to survivors’ outcomes.
For example, “interventions targeting one stressor can reduce the occurrence and intensity of other stressors and contribute to better mental health,” state the researchers. This framework could serve as a foundation for policymakers and practitioners interested in the health and well-being of all displaced people, no matter their origins.
Migrants walk on the railway tracks between Bicske and Szar, about 40 km west of Budapest, Hungary.
Photo courtesy of Freedom House
Flipping the Stats: A COVID-19 Success Story
My Healthy Community, Delaware’s Environmental Public Health Tracking Network
Editors’ Note: The following text is taken from Delaware’s MyHealthyCommunity website: https://myhealthycommunity.dhss.delaware.gov/stories/vaccination . Please visit the page to see the figures and data that accompany this story.
Hispanic Delawareans were hit hard during the pandemic’s early months—and slow to be vaccinated. Now they outpace the vaccination rates of non-Hispanic Delawareans.
What Happened?
The answer appears to be a uniquely Delaware story blending immigration trends, the poultry industry, and grassroots efforts of community leaders and organizations.
At the pandemic’s outset, the portion of Hispanic residents testing positive for COVID-19 exceeded the non-Hispanic rate almost every day (see Figure 1).
Reasons were multiple and overlapping.
• Many Hispanics live in dense multigenerational (or multi-family) households, prime conditions for a respiratory illness like COVID-19 to spread.
• Language and cultural barriers hindered messaging around handwashing, masks, and social distancing.
• Identification requirements at some test sites dissuaded some Hispanics from testing.
Figure 1. Daily Rate of New Positive COVID-19 Cases by Hispanic Origin, Delaware, March 2020-October 2021
Another factor was poultry processing facilities. Delaware is home to some of the largest broiler chicken facilities on the Eastern Seaboard.1 The heart of the industry is the farmland of Sussex County, where processing plants from Milford to Georgetown to Selbyville can employ upwards of 1,000 people at a single facility. In recent decades, poultry plants have attracted significant numbers of Hispanic workers, including many immigrants from Guatemala and Mexico who settled in pockets of Sussex County.
Upon COVID-19’s arrival in the US, public health authorities recognized the heightened vulnerability of poultry and meat facility workers nationwide—who often could not afford time off unpaid—and observed a disproportionate impact on minorities.
In the pandemic’s early months, case hotspots flared around poultry facilities and across the adjacent census tracts where the percentage of Hispanic residents is higher than the state and county percentage.
Fast Forward to Vaccination Roll-Out
Delaware, following Centers for Disease Control and Prevention guidance, classified poultry and other food processing employees as “frontline essential workers” – a priority group for COVID-19 vaccination in early 2021. By then the virus was widespread, afflicting all corners of the state. And, Delaware-wide, going into 2021, Hispanic persons continued to test positive for COVID-19 at rates higher than non-Hispanics.
Despite early distribution efforts, including onsite clinics and poultry facilities, Hispanic Delawareans across the state were vaccinated at a slower pace than non-Hispanics during the first months of vaccine availability until early April 2021, when all residents 16 years and older became eligible for vaccination.
At that point, the tables turned.
Going forward and into fall, the daily portion of Hispanic Delawareans getting vaccinated exceeded that of non-Hispanic residents nearly every day (Figure 2).
Figure 2. Daily Rate of New COVID-19 Vaccinations by Hispanic Origin, All Ages, Delaware, January – October 2021
The trend appears particularly pronounced among older Delawareans. As under-50 year-olds became eligible, Hispanic persons 50 and older continued seeking vaccinations at rates higher than non-Hispanics of the same age (Figure 3). The belated surge in Hispanic vaccination rates is consistent with an observation from health officials during the first six months of vaccine availability: Hispanic Delawareans were arriving at vaccination sites not just individually, but as households.
Some Possible Explanations?
• Close-knit families may have preferred getting vaccinated together rather than according to the age groupings of the eligibility schedule.
• Older generations possibly postponed until younger, English-fluent relatives could accompany them to clinics.
• A single, all-family appointment may simply have been the easiest logistical solution for a large household juggling childcare and frontline or other jobs.
Health officials also saw community-level efforts making a difference. Faith and community figures relayed information from Lieutenant Governor Bethany Hall-Long’s “Latino Community Leaders” meetings, disseminating accurate, myth-busting vaccine information. Communication was two-way, with local leaders conveying to officials the barriers to successful testing and vaccination, including the imperative of providing services at locations convenient to, and already frequented by, Hispanic residents. Despite some of the most troubling initial positive case rates of any demographic in Delaware, 65 percent of Hispanic residents had at least one COVID-19 vaccination dose by midJanuary 2022, a rate exceeding non-Hispanics by roughly ten percentage points.
The latest figures can be found at My Healthy Community’s Coronavirus Vaccine Tracker.2
Figure 3. Daily Rate of New COVID-19 Vaccinations by Hispanic Origin, Age 50 and Older, Delaware, January – October, 2021
REFERENCES
1. U.S. Poultry and Egg Association. (2020). The chicken industry creates jobs in Delaware. National Chicken Council. Retrieved from: https://www.dcachicken.com/facts/docs/DE%201%20Congress%20 Impact%20Report.pdf
Updated regularly to give an overview of the cases, vaccinations, hospitalizations, and deaths in Delaware attributed to COVID-19.
myhealthycommunity.dhss.delaware.gov
Protect against respiratory diseases
The Division of Public Health (DPH) follows the vaccination recommendations from the Centers for Disease Control and Prevention (CDC). Vaccination can prevent severe disease, hospitalization, and death, including from the following
The flu vaccine is needed every year. The CDC recommends that individuals 6 months of age and older get the 2024-25 flu vaccine Seniors aged 65+ need a higher dose flu vaccine.
Flu vaccinations are recommended for those who live or work with infants under 6 months of age and who live or work in settings with many people, such as multi-family households, apartments, schools, offices, and correctional facilities. Vaccination is important for health care workers, especially those who work in long-term care facilities or who live with or care for people at highest risk.
The CDC recommends that everyone aged 6 months and older get the 2024-2025 COVID-19 vaccine, regardless of whether you received a vaccine in the past, have had COVID-19, and have long COVID That is because vaccine protection decreases over time. There are additional specifications for children and those who are moderately or severely immunocompromised In addition, the CDC recommends that adults aged 65 and older receive a second dose of the 2024-2025 vaccine six months after their first dose.
https://www.cdc.gov/covid/risk-factors/
The COVID-19 vaccine is needed every year.
Respiratory syncytial virus (RSV)
The CDC recommends one dose of adults aged 75 and older and adults aged 60 to 74 who are at increased risk for severe RSV. The CDC recommends all babies be protected from severe RSV by one of two immunization options: a maternal RSV vaccine given to the mother during weeks 32 through 36 of pregnancy or an RSV antibody given to your baby. details and specific recommendations.
How to prevent respiratory diseases
• Get and keep up with your recommended vaccinations.
• Avoid close contact with sick people.
• Cover coughs and sneezes with a tissue, or cough or sneeze into your inner elbow.
• Wash hands often with soap and water for 20 seconds or use hand sanitizer.
Do not touch your eyes, nose, and mouth.
Clean and disinfect frequently touched surfaces.
• If sick with flu-like illness, stay home until you are fever free without using feverreducing medication for 24 hours A fever is a measured temperature of 100.4 degrees Fahrenheit or greater. If symptoms worsen, call your doctor.
Find flu, COVID-19, and RSV vaccines
Flu and COVID-19 vaccines are available for all Delawareans, regardless of insurance status
Uninsured individuals and those on Medicaid or Medicare may receive flu and COVID-19 vaccines at DPH clinics and Federally Qualified Health Centers
Those with insurance can get flu, COVID-19, and RSV vaccines at pharmacies or participating medical providers Vaccination sites are listed at de.gov/getmyvaccine
Health care providers give RSV vaccines. Tell the vaccinator if the person getting the vaccine:
• Has had an allergic reaction after a previous dose, or has any severe, life-threatening allergies.
• Has a chronic medical condition such as heart or lung disease, a weakened immune system, or certain other underlying medical conditions.
Lives in a nursing home or long-term care facility.
Increasing age, especially those over 60. Having an underlying medical condition such as obesity, diabetes, asthma or chronic lung disease, heart disease, blood disorder, immune disorder, and/or another genetic, neurologic, or
Having a rare medical condition. Being from a racial and ethnic minority group. Having a physical, cognitive, developmental, or
Having a weakened immune system, such as when undergoing cancer treatment.
Respiratory diseases spread when droplets from an infected person’s cough or sneeze contact your eyes, nose, or mouth. They also spread by touching a surface that has the virus on it, such as a doorknob, counter, or table, and then touching your face before washing your hands.
The U.S. government approves vaccines U.S. vaccines are reviewed by the U.S. Food and Drug Administration’s Vaccines and Related Biological Protects Advisory Committee. Vaccine composition is updated as needed to best match the viruses that research indicates will be most common.
Division of Public Health Director Steve n Blessing received his 2024-2025 flu vaccination on October 30 at the James Williams State Service Center in Dover, Del. Krystal Peterson, Supervisor of Nurses for the DPH Mobile Health Units, administered the vaccine. The CDC recommends that everyone 6 months of age and older get a flu shot every year. Photo by Sean Dooley.
Seniors 65+ need higher-dose flu vaccine
For adults aged 65 years and older, the CDC preferentially recommends one of three higher dose or adjuvanted flu vaccines: Fluzone High-Dose influenza vaccine, Flublok recombinant influenza vaccine, and Fluad adjuvanted influenza vaccine. If these are not available, people aged 65 and older should get a standard-dose unadjuvanted inactivated flu vaccine instead.
For more information about higher dose flu shots recommended for adults aged 65 years and older, visit https://www.cdc.gov/flu/highrisk/65over.htm
Visit DPH at flu.delaware.gov or call 1-800-2828672. Or, visit the CDC at cdc.gov/flu
Click here for the difference between cold and flu.
Visit DPH at coronavirus.delaware.gov/vaccine or call 1-800-282-8672. Or visit the CDC at https://www.cdc.gov/covid/vaccines/stay-up-todate.html
Talk to your health care provider or call DPH at 1-800-282-8672.
Getty images
Executive Summary of the Delaware State Health Assessment: 2022-2023 Report
The Delaware Department of Health and Social Services, Division of Public Health (DPH) completed a state health needs assessment (SHA) of the state of Delaware with support from the University of Delaware Epidemiology Program and the Partnership for Healthy Communities (UD EPI/PHC). The assessment was designed to compare Delaware’s health to the health of the nation. The intent of the SHA was to determine the health needs of Delaware’s residents. To determine the needs of the state, survey data was collected to analyze the current health of Delawareans. In addition, community members and stakeholders across various sectors and all counties of Delaware were selected to gather further information about access and barriers to health and well-being using the framework of the vital conditions. The vital conditions of health and well-being framework guide the major determinants of health, factors necessary to producing health and well-being, and the discussions surrounding the areas of need in the state. The SHA also highlights the factors that contribute to the challenges across the state and if existing resources can be mobilized to address them. Delaware undertakes a full statewide SHA every five years, with the last report being completed in 2017.
Since the last SHA, Delaware has made progress on several important measures:
• Excessive drinking decreased from 18.9% to 14.3% of adults between 2019 to 2021.1
• Flu vaccination rates among adults increased from 38.2% in 2018 to 49.8% of adults in 2021.2
The 2022-2023 SHA (September 2022-June 30, 2023) appraised community health needs through a multi-pronged approach by using interviewer-administered surveys, hosting community conversations, and forming a statewide partnership coalition. Secondary data, including statistics from federal, state, and local sources about various health indicators (i.e., education, poverty, and health care services) were also gathered and assessed throughout the assessment period. The methods used to accomplish the assessment were established by the Public Health Accreditation Board.3
The vital conditions for health and well-being framework were used to create an equity-driven assessment by producing a meaningful and broad portrayal of factors that most impact the health of Delawareans.4
DPH, UD EPI/PHC, and its partners will use the findings from this assessment to identify a set of health priorities. This will be the focus of the State Health Improvement Planning (SHIP) process. The SHIP will provide opportunities for communities and other stakeholders to work together to improve health outcomes and health equity for all Delawareans. To read the full SHA, please visit the Delaware SHIP website (https://delawareship.org/).
ACKNOWLEDGEMENTS
We want to acknowledge the following individuals for their support and contributions to the SHA: Leanne Fawkes, DrPH, MPH, Noel Duckworth, Paulette Hussey-Kasten, Matt Simon, Braulio Florentino Benitez, Alexander Burris, MPH, Christiana Oyekanmi, MPH, Sarah Scales, PhD, MPH, Danielle Whyte, Keyonna Austin-White, and various reviewers at the Delaware Division of Public Health.
REFERENCES
1. America’s Health Rankings. (2022a). Excessive Drinking in Delaware. https://www.americashealthrankings.org/explore/measures/ExcessDrink/DE
2. America’s Health Rankings. (2022b). Explore Flu Vaccination in Delaware. https://www.americashealthrankings.org/explore/measures/flu_vaccine/DE
3. Public Health Accreditation Board. (2022). Standards & Measures for Initial Accreditation Version 2022. https://phaboard.org/wp-content/uploads/Standards-Measures-InitialAccreditation-Version-2022.pdf
4. The Rippel Foundation. (n.d.). Vital Conditions for Health and Well-Being. Retrieved July 29, 2024, from https://rippel.org/vital-conditions/
Delaware State Health Assessment
2022–2023 REPORT
October 2023
Delaware Mini Medical School
An Expeditionary and Health Literacy Program for Youth, Young Adults, and Those Exploring New Career Options
Timothy E. Gibbs, M.P.H. and Nicole Sabine, B.S. Delaware Health Force, Delaware Academy of Medicine/Delaware Public Health Association
INTRODUCTION
Delaware Mini-Medical School (DMMS) is a free, six-week series designed for individuals who want to gain a deeper understanding of the world of healthcare – from dentistry and medicine to public health and research. This series is designed for middle, junior, high school, and undergraduate students, though all are welcome to attend. Attendees learn about trends in diagnosing and treating illness and general health topics. Faculty provide in-depth lectures and allow time for questions to enhance the experience. DMMS complements many other local programs targeting differing age groups and disciplines, encouraging and preparing students for a career in the health sciences. Unlike many of the other programs, there are no tests and grades to enter the program or to obtain a certificate of attendance. This is consistent with our goal to remove as many barriers as possible to engagement.
HISTORY
DMMS has been operating continuously since 2009. When the COVID-19 pandemic occurred, we migrated the series from in-person to online presentations and shifted the focus to more of an upstream intervention to engage youth and young adults considering careers in the healthcare and biosciences fields—both areas already experiencing workforce shortage stresses.
Anesthesia
Anxiety - types, identification, and treatment
Athletic Training
Bariatric Surgery
Behavioral Health
Cardiology
Dentistry
Emergency Medicine
Family Medicine
From Nurse to Nurse Practitioner
Gene Editing
Health Informatics
Heart & Circulatory Health
Hospice and Palliative Care
DMMS is currently a funded component of the Delaware Health Force initiative. For this article, the statistics and information presented start with the infusion of American Rescue Plan Act (ARPA) funding from the State of Delaware in 2023, which supported the significant expansion of this program.
Where DMMS used to be presented once a year in the spring, we expanded to present four times a year, two series in the spring, and two in the fall.
TWO YEAR CURRICULUM SCOPE
Table 1 below shows the topics covered by DMMS during the ARPA funding period.
TWO YEAR SCOPE OF PRESENTER TYPES
Consistent with our workforce-building strategy, degree representation has been present over the past two years (Table 2). For all degrees shown below, there are workforce shortages. Our practice is to expose the cohort to a range of provider types who talk about their own educational journey and how they got to where they are now in their careers. We do this to provide transparency regarding the pathway individuals took and allow the participants to consider this in relation to their own aspirations and life goals.
Immunization and Public Health
Interventional Cardiology
Neuro-Interventional Surgery
Neurology
Pediatric Nursing
Physical Therapy
Prenatal Care and Childbirth
Primary Care
Primary Care in Special Populations
Psychiatry
Radiology
Stroke
Women’s Health
Working with Addictions
Table 1. Delaware Mini Medical School Presentation Topics
Table 2. Degree Types Represented in Delaware Mini Medical School
ABPP Rehabilitation Psychology
BS RT(T) Bachelor of Science in Radiologic Technology
BSN Bachelor of Science in Nursing
CHW Community Health Worker
CNM Certified Nurse Midwife
DMD/DDS Dentist
DNP Doctor of Nursing Practice
DPT Doctor of Physical Therapy
EDD Doctor of Education
STUDENT CHARACTERISTICS
Since starting this pattern of two series in the spring and two in the fall in 2023, we have had a total of 3,058 students. Several of those students (720) have returned to take the series again, as each one is unique in content and degree representation. Adjusting for duplicates, we have engaged with 2,338 unique students. Equitable access to the program through all communities, including communities of color, is a fundamental goal of DMMS. Since 1994 it has been observed that patient satisfaction and resulting health outcomes are better when the patient and provider share racial/ethnic similarities.1 The overall race and ethnic distribution of Delaware (figure 1) and that of the DMMS student cohort (figure 2) are shown below. DMMS have succeeded in representing non-white minorities in the cohort beyond their representation statewide as based on US Census Data. Regarding gender, figure 3 shows the prevalence of female participants (81%), followed by male (17%) and non-binary / non-conforming and blank or prefer not to answer at 1% each.
With respect to age demographics, we use reported grade level
LCSW
MD/DO
Licensed Clinical Social Worker
Medical Doctor
MPH Master in Public Health
MSN
Master of Science in Nursing
NP Nurse Practitioner
PhD Doctor of Philosophy
PsyD
Doctor of Psychology
PT Physical Therapist
RN Registered Nurse
as our proxy and find the following distribution (figure 4). While there is a concentration of DMMS students in ninth, tenth, eleventh, and twelfth grades, there is also even younger engagement as early as the fifth grade (the youngest class eligible to participate).
There is also a healthy and even distribution throughout undergraduate school, and a small but significant showing in graduate school.
Adult learners represent an essential component (41.9%) of the cohort, and many of them are the parents or caregivers of younger students. While we do not directly report on their age, rather we make the correlation based on identical addresses and other metrics as well as self-reporting during the series.
Other adult learners report informally, that they are in the process of mid-career redirection, and we welcome them to the class as well. A reality of population growth is that we cannot rely only on youth to supply the necessary numbers to address the retiring portion of the provider population, nor the continued population growth.
Figure 1. Delaware Racial and Ethnic Diversity
Figure 2. DMMS Student Cohort Racial and Ethnic Diversity
TOP 30 EDUCATIONAL INSTITUTIONS REPRESENTED
Students report an association with 318 academic institutions from middle school to graduate schools (Table 3). A complete list of these schools is available at https://dehealthforce.org or https://delawareminimed.org . Notably, DMMS students are mostly from Delaware institutions, followed by those from surrounding states, and a small number from other states. DMMS has even reached students in Canada, France, Indonesia, Iran, Turkey, and the United Kingdom. This geographic range is only possible through the adoption of an online webinar format for the series. Parents have indicated strong support for this format as it frees them from transportation challenges with their children. Adult learners report they enjoy the ability to log in remotely from the comfort of their home or other location.
A major goal of the addition of ARPA-funding was to bring the series to communities across the state. We have found the best success in engaging local healthcare institutions to support DMMS by arranging for their staff to act as our instructors. We have been pleased to partner with ChristianaCare, Bayhealth, La Red Health Center, Beebe Healthcare, and several independent practitioners. We are also working with Nemours Children’s Health for one of the two spring 2025 series.
We engaged the Sussex County Health Coalition (SCHC), which operates in Kent and Sussex counties, as our partner in central and southern Delaware. The SCHC is well known and established, and this has proven to be a significant programmatic partnership. All of these strategic decisions have led to even representation from all three counties in Delaware.
DEFINITIONS OF SUCCESS
Today, DMMS is based loosely on an expeditionary teaching model.3 This model is frequently applied to adventure, outdoor, environment, or experiential education, and is well suited to our own methods and goals. In addition, health literacy is a key component of our efforts.
In the absence of tests and grades, there are limitations in assessing knowledge uptake, thus assessing health literacy improvement is difficult.
From the perspective of exposing the cohort to a variety of disciplines and types of healthcare professionals, our proxy for achievement is the number of sessions attended within any given series. For students attending all sessions, there is a physical, signed certificate of attendance which is mailed to them. For students who attend fewer than the total number of sessions, they must complete a short satisfaction survey, and are then directed to a fillable pdf which they can download and complete for their records. Figure 5 shows aggregate attendance across the last two years by percent.
For any number of reasons, 15.1% of students who initially registered may not be able to attend the series due to other academic, sports, or family obligations. For that portion of the cohort, we encourage their attendance in a future series through follow up. Another 24.2% of the cohort attended four or fewer sessions. Encouraging results can be seen in the 39.6% of students who attend five sessions and 21.1% who complete the series.
For those students attending five sessions, they are afforded the opportunity to make up the missing sixth session; however,
Table 3. Top Educational Institutions Represented in Alphabetical Order
Appoquinimink High School
Aspira High School
Cab Calloway School of the Arts
Caesar Rodney High School
Cape Henlopen High School
Charter School of Wilmington
Delaware Technical Community College
Delcastle Technical High School
Delaware State University
Dover High School
Georgetown Middle School
Hodgson Vocational Technical High School
Howard High School of Technology
Lake Forest High School
Laurel High School
scheduling conflicts and other academic pressures are reported as reasons they do not take advantage of the offer. In addition, certain topics are of no interest to a given portion of the cohort in any given series, which may significantly contribute to missing one session.
Email addresses for all attendees are collected, and program staff follows up with as many students as possible over time. Although it is currently too early to understand the long-term impact of DMMS in directing students toward a career in healthcare or biosciences, results from a follow up survey with past DMMS students since 2009 showed that those who responded did indicate that their participation in the series had an impact on their career decision-making.
Mr. Gibbs may be contacted at tgibbs@delamed.org
REFERENCES
1. Saha, S., Komaromy, M., Koepsell, T. D., & Bindman, A. B. (1999). Patient-physician racial concordance and the perceived quality and use of health care. Archives of Internal Medicine, 159(9), 997–1004. 10.1001/archinte.159.9.997
2. State of Delaware. (n.d.). The Delaware pulation consortium. Retrieved from https://stateplanning.delaware.gov/demography/dpc.shtml)
3. ElEducation. (n.d.). Educating for a better world. Retrieved from https://eleducation.org/
Middletown High School
MOT Charter High School
Newark Charter High School
Newark High School
Odessa High School
Padua Academy
Saint Mark’s High School
Salem County Vocational Technical School
Smyrna High School
Sussex Central High School
Sussex Academy of the Arts and Sciences
Tower Hill School
University of Delaware
William Penn High School
Wilmington University
Figure 5. Attendance Expressed as Percentage of Sessions Attended
Longest-running DPH program, Delaware WIC, reaches 50 years
Since 1974, the National and Delaware Women, Infants and Children (WIC) Programs have championed access to healthy food, breastfeeding support, health screenings, and referrals. On September 12, the Delaware WIC Program within the Division of Public Health (DPH) celebrated its 50th anniversary with a fun family event on Legislative Mall in Dover, Del. Delaware WIC supports 15,000 to 18,000 families every year
Photos, clockwise, from top: Lieutenant Governor Bethany Hall-Long, center, presents a tribute. (From left to right: DPH Director Steven Blessing, First Spouse Tracey Quillen Carney, Delaware WIC Program Director Joanne White, former WIC director Deborah Clendaniel, Lt. Governor HallLong, former WIC director Beth Freeh, Dr. Patty Bennett, Regional Administrator, Food and Nutrition Service, Mid-Atlantic Region, and Christine Berberich, Branch Chief, Supplemental Food Programs.) The First Spouse reads her children’s book, Books for Blue. Spiderman danced. WIC Nutritionist Natasshia Nealous, left, and Social Service Technician Julia Toalongo greet attendees. Photos by Alyssa Imprescia, DPH
DPH publishes cancer data report
Delaware's cancer mortality rate continues to decline, according to the latest data from the Division of Public Health (DPH)
According to the DPH report, Cancer Incidence and Mortality in Delaware, 2017-2021, Delaware and U.S. mortality rates dropped by an average of 1.8% and 1.5%, respectively, between 2007 and 2021. In the 2024 report, which looked at the 2017-2021 time period, Delaware ranked 16th among the states for highest all-site (i.e., all cancer types) cancer mortality, with lower rankings indicating cancer mortality rates.
“The decrease in cancer deaths in Delaware reflects earlier cancer detection, prevention, and better access to timely care and quality of life among cancer survivors,” said Governor John Carney. “Thanks to the Delaware Cancer Consortium and the Division of Public Health, our cancer mortality rate has declined because they have worked diligently to prevent cancer, primarily through cancer screening.”
Key findings include:
• Between 2007 and 2021, mortality rates for allsite cancer decreased among non-Hispanic White males, non-Hispanic White females, and non-Hispanic Black males year over year. Allsite cancer mortality rates were stable among non-Hispanic Black females, Hispanic males, and Hispanic females in Delaware.
• Delaware has a lower prostate cancer mortality and a lower colorectal cancer mortality rate compared to the U.S.
• Uterine cancer is the fifth most diagnosed cancer in Delaware, followed by melanoma as the sixth most diagnosed cancer in Delaware.
“DPH is developing innovative approaches to reduce disparities in cancer outcomes,” said DPH Director Steve Blessing. “It is our mission to continue to reduce preventable cancers, make sure all people get the right screening at the right time and that we support cancer survivors in living longer, healthier lives.”
Read the report by visiting DPH’s Bureau of Cancer Prevention and Control at https://dhss.delaware.gov/dhss/dph/dpc/cancer.html.
Lung cancer screenings offered Saturday, Nov. 9
To reduce disparities, improve access to care, and save lives, the Division of Public Health (DPH) Screening for Life (SFL) Program is promoting lung cancer screening throughout the month of November. SFL will join its Delaware partners to commemorate National Lung Cancer Screening Day on Saturday, November 9, 2024.
Delaware Cancer Treatment Program helps over 2,000 people in 20 years
The Delaware Cancer Treatment Program (DCTP) is celebrating its 20th year ensuring that those diagnosed with cancer can access necessary medical care without the burden of overwhelming treatment costs Since its inception in 2004, DCTP has served 2,088 people as of September 25, 2024.
This partnership, established by the American Cancer Society, asks health care providers to open their doors on the second Saturday in November to give low-dose CT lung screenings (LDCT) to referred individuals. For screening locations, visit the American College of Radiology’s Lung Cancer Screening Locator Tool.
“Delaware is proud to support National LCS Day, as this proactive approach is vital in saving lives and reducing the burden of lung cancer on families and communities within our state,” said Dawn Hollinger, chief of the DPH Bureau of Cancer Prevention and Control. “Screenings are used to find cancer early when it is more treatable and even curable. Through this collaborative effort, we hope to increase awareness about the lifesaving benefits of lung cancer screening and encourage individuals at risk to take action.”
Lung cancer is one of the deadliest forms of cancer According to the Cancer Incidence and Mortality in Delaware, 2017-2021 report, lung and bronchus cancer accounted for 28% of all new cancer deaths in the First State in the 2017-2021 time period. Lung and bronchus cancer was the second most common type of cancer after female breast cancer. Regarding incidence, of the 23 site-specific cancers analyzed during the 2017-2021 time period, lung and bronchus cancer accounted for 14% of all newly diagnosed cancer cases in Delaware after female breast cancer, which accounted for 17% of all new cancer cases. For information about lung cancer screening, visit www.healthydelaware.org/individuals/cancer/lung#intro or https://www.cancer.org/cancer/types/lungcancer/detection-diagnosis-staging/detection.html
For SFL eligibility guidelines for Delaware adults, visit https://www.dhss.delaware.gov/dph/dpc/sfl.html
Follow DPH Facebook and DPH Instagram for screening events, educational materials, and more.
DCTP works with health care providers across Delaware to ensure high-quality care is provided to Delawareans Its financial assistance covers timely medical intervention, including doctor visits, medications related to treatment, and supportive care. Dependent upon enrollment status, it can provide up to two years of free cancer treatments, such as chemotherapy, radiation therapy, surgery, and other medically necessary treatments.
DCTP enrollees diagnosed with any type of cancer must meet specific benchmarks, including income eligibility, being uninsured, and being ineligible for Medicaid. Individuals who have insurance but face substantial out-of-pocket costs may also qualify for assistance.
To be considered for this program, applicants must submit the DCTP application within one year of their cancer treatment start date.
DCTP offers peace of mind during this major life challenge. It extends informative resources and counseling to help Delawareans know their treatment choices and direct patients through complex cancer care.
For more information about DCTP and to access application forms in English and Spanish, visit HealthyDelaware.org. Delawareans can also call 1-302-844-245-9580 to apply and 2-1-1 (toll-free) for more information.
Join
the 22nd Annual Delaware Diabetes Wellness Expo on Nov. 12
The Delaware Diabetes Coalition proudly presents the 22nd Annual Delaware Diabetes Wellness Expo, an event that unites health care providers, businesses, and diabetes-related organizations in a celebration of wellness and resilience.
The Expo will be held on Tuesday, November 12, 2024 from 9 a.m. to 3 p.m. at Delaware Technical Community College in the DEL-ONE Conference Center, located on the Terry Campus at 100 Campus Drive, Dover, Del. 19904.
The Delaware Diabetes Wellness Expo is a beacon of hope and empowerment for those affected by diabetes: individuals living with diabetes, caregivers, and those eager to learn more about prevention and management. Attendees will experience a day filled with inspirational educational sessions on managing diabetes, nutrition, and physical activity.
From health screenings to interactive exhibitor booths, attendees will discover practical tools for thriving with diabetes. With plenty of giveaways and demonstrations, it is a vibrant space for learning, networking, and taking the first step toward a healthier future.
Admission and lunch are free. Pre-register at https://www.dediabetescoalition.org/ to skip the check-in line.
Vendors have the chance to showcase their offerings at one of Delaware’s most impactful health events. Vendor registration closes on November 5, or once spaces are filled. Click here for the online vendor registration form.
The
The Delaware Diabetes and Heart Disease Prevention and Control Program (DHDPCP), located within the Division of Public Health, is sponsoring this event. For more information about diabetes, including materials and classes, click here or call 302-7441020.
DPH accepting public comment
The Division of Public Health (DPH) DPH seeks public comment until November 1, 2024 at 4:30 p.m. on proposed revisions to the following two regulations in Title 16 of the Delaware Administrative Code:
4103 Inherited Metabolic Disorders – DPH proposes to repeal the regulation because DPH no longer has designated funding for formula and cannot guarantee formula availability.
4470 State of Delaware Marijuana Code –Proposed revisions include, but are not limited to:
• Allowing health care providers to make the determination of whether a patient has a diagnosed medical condition for which the patient would receive therapeutic or palliative benefit from the use of medical marijuana
• Allowing patients aged 65 and older to selfcertify their qualification for a Medical Marijuana Registry Identification Card without a written certification from a health care provider
• Authorizing the Department of Health and Social Services to issue Medical Marijuana Registry Identification Cards with 1-, 2-, or 3year expiration dates
The proposed revisions are available online in the October 1, 2024 Delaware Register of Regulations, accessible online at http://regulations.delaware.gov or by calling DPH at 302-744-4951.
Public comment is accepted in written form via email to DHSS_DPH_regulations@delaware.gov, or by U.S. mail to: Vicki Schultes, Hearing Officer, Division of Public Health, 417 Federal Street, Dover, DE 19901.
Written comments on proposed amendments to 4465 Delaware Radiation Control Regulations and 4466 Radiation Technologists/Technicians (Certification) were reviewed by DPH, including amending the definition of “licensed practitioner” to be consistent with Title 16 of the Delaware Administrative Code. The proposed amendments became effective October 11, 2024
DPH received one comment on the proposed new 4306 Stroke System Regulation and determined that no changes will be made. The proposed regulation will become effective November 11, 2024.
Division of Public Health provides helpful resources at the annual Delaware Diabetes Wellness Expo. DPH photo
Cancer information available at community events
The Division of Public Health’s Cancer Prevention and Control Program will have an information table at these public events:
• Monster Mile Walk for A Cure, Saturday, October 19, 10 a.m. to 2 p.m., Homestead Gardens, 5580 Dupont Highway, Smyrna, Del. 19901.
• Multi-Cultural Community Wellness Fair, Saturday, October 19, 10 a.m. to 2 p.m., Lulu M. Ross Elementary School, 310 Lovers Lane, Milford, Del. 19963.
Information will be provided about Screening for Life and Health Care Connection programs that can provide eligible Delawareans with cancer screening tests and health care services through a network of providers at reduced cost .
November 21 Working4Equity lecture spotlights antimicrobial stewardship
The Division of Public Health offers the virtual Working4Equity Lecture Series through its Health Equity Institute of Delaware and in partnership with the Medical Society of Delaware (MSD). The lectures are designed for working physicians and clinicians, and may appeal to scholars, practitioners involved in public health and health disparities work, community members, and for-profit businesses.
Jasmine Riviere Marcelin, MD, FACP, FIDSA will present “How Antimicrobial Stewardship Can Influence Health Equity” on November 21 at 6 p.m.
Dr. Marcelin is an Associate Professor of Infectious Diseases at the University of Nebraska Medical Center. She is Vice Chair for Equity & Inclusiveness Excellence, Department of Internal Medicine, Associate Medical Director of the Antimicrobial Stewardship Program, and Co-Director, Digital Innovation & Social Media Strategy, Division of Infectious Diseases.
The lecture is free. Registration is required at https://reg.planetreg.com/AntimicrobialStewardship.
View all lectures at MSD Events. Accredited continuing Medical Educational credits are available from MSD at nominal cost.
The Division of Public Health’s Health Systems Protection Section published two reports:
• State of Delaware Public Drinking Water Annual Compliance Report and Summary for 2023
• Childhood Blood Lead Surveillance in Delaware, 2023 Annual Report
DPH’s Health Promotion and Disease Prevention Section published the report, Cancer Incidence and Mortality in Delaware, 2017-2021
DPH staff co-authored three cancer articles published in the August 2024 issue of the Delaware Journal of Public Health (DJPH), Cancer and the Power of Preventive Screening (Volume 3, Issue 3):
• “Development of Sub-County Cancer Reporting Zones in Delaware and Example Use Case for Targeted Interventions”
• “Sustaining Improvements in Colorectal Cancer Across Delaware: A Look at Racial Disparities a Decade Later”
• “Evaluating Quality of Cancer Care in Delaware using Commission on Cancer (CoC) Quality Measures, 2018-2019.”
DJPH published the Cancer Incidence and Mortality in Delaware, 2016-2020 report in the same issue.
Assistive technology devices available Amplified phones, ergonomic computer equipment, and Smart home technology are provided by the Delaware Assistive Technology Initiative (DATI).
Individuals who can benefit from such AT tools can contact DATI at 800-870-3284 or dati-ud@udel.edu. They can visit the New Castle or Kent/Sussex Assistive Technology Resource Centers to borrow AT tools to test in real-life settings. Transportation services to the resource centers can be provided. This program is available through 2024 at no cost to Highmark Health Options members referred by their Long Term Services and Supports case manager, care coordinator, or service coordinator.
Access to Virtual Care in Behavioral Health: A Social Determinant of Health
Patrick J. Hearle, M.D.
Sidney Kimmel Medical College
Emily Ann Smith, M.D.
Department of Psychiatry, ChristianaCare
Richard J Caplan, Ph.D.
Institute for Research on Equity and Community Health (iREACH), ChristianaCare
Ram A. Sharma, M.D.
Department of Psychiatry, ChristianaCare
ABSTRACT
Objective: In the wake of COVID-19, the use of virtual modalities to provide healthcare has increased significantly. While virtual care services, particularly for behavioral health encounters, have become commonplace in many healthcare systems, there is limited data describing to what extent access to virtual care is affected by social determinants of health. The present study aims to characterize the utilization of virtual (video, phone) and non-virtual (in—person office visits) behavioral health care encounters among differing socioeconomic and demographic populations in two campuses served by a tertiary care center in Delaware to identify trends and potential barriers to these services. Methods: A dataset of 19500 behavioral health visits among 3420 patients in the Christiana-Care health network at sites in Newark, DE and Wilmington, DE was analyzed using Kruskal-Wallis test results for continuous variables and chi-squared tests for categorical variables. Results: Patients utilizing virtual (video, phone) visits tended to be younger and have a lighter burden of economic inequality than patients seen in-person. Metrics such as access to a computer, internet connection, and median income were directly correlated with increased use of virtual modalities. Conclusion: The findings indicate that access to and utilization of virtual care may be a social determinant of health. Future research should assess access to telehealth and its impact on health outcomes.
ACKNOWLEDGMENT
Work was supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number U54GM104941 (PI:Hicks) and the State of Delaware. This research received no external funding.
INTRODUCTION
The COVID-19 pandemic has had profound and lasting changes on the provision of healthcare worldwide. In the US, virtual care has seen tremendous growth,1 where telehealth visits (0.32 visit per person) accounted for 23.6% of all interactions in 2020 compared with 0.3% of contacts in 2019.2 Furthermore, behavioral health encounters were far more likely than medical contacts to take place virtually (46.1% vs 22.1%) in 2022.2 In the aftermath of COVID-19, telehealth has established itself as a powerful tool to expand access to care in the current era. Despite its utility, there are concerns that as health systems increasingly focus on technically advanced modalities such as virtual care, they may enhance disparities in access to and outcomes of care.3,4 In the setting of this new healthcare paradigm, there is a need to further characterize both users and nonusers of virtual care and the barriers they face. Relationships among race, income inequality and social resources are complex and have been implicated in predicting negative health outcomes, which became particularly apparent during the
pandemic. Tan et al demonstrated that income inequality within US counties was associated with more cases and deaths due to COVID-19 in the summer months of 2020.5 Currently there is limited research regarding how social determinants of health impact access to virtual care. With proper implementation, virtual care may enable providers to improve overall health through identification and provision of care to at-risk populations and underserved geographical areas.
The present study aims to characterize users and non-users of virtual care among behavioral health patients of one of Delaware’s largest health systems and to thus provide insights into trends of virtual care use among patients of differing socioeconomic and demographic backgrounds, with the goal of identifying potential barriers to access to virtual care. We conducted a retrospective cohort study to analyze users of virtual and in-person care at behavioral health outpatient clinics at the ChristianaCare health network from January 2020 to September 2021. Patient visits were analyzed temporally, and grouped based on visit type (office, phone, or video), demographics, geographical location, and diagnoses.
METHODS
Institutional review board approval from ChristianaCare was granted for this study. We extracted behavioral health visit subtypes and demographic information from the electronic health records data warehouse for patients seen for outpatient behavioral health visits at Wilmington and Newark campuses
of ChristianaCare, a tertiary care center in Delaware, during January 2020 through September 2021. A limited data set as per institutional review board definition was used. Informed consent was waived by the Christiana Care institutional review board in accordance with the Office for Human Research Protections regulations 45 CFR 46.116(d). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines relevant to our study were followed. All patient visits occurred in outpatient behavioral health offices in the ChristianaCare Health System between January 1, 2020, and September 30, 2021. Visit data were collected via an electronic health records data warehouse maintained by ChristianaCare. Additionally, data from the 2018 United States Census Bureau Community Survey were merged with these data to provide demographic information, with census tract of residence used as a unifying datapoint.
Data were grouped by service location between Wilmington and Newark campuses within the ChristianaCare network. The Wilmington campus serves a primarily urban population within Delaware’s most populous city, while the Newark campus, in a suburban area of Delaware, serves more suburban residents. Encounters were subdivided by visit type: office, phone, or video. These subdivisions were analyzed by Kruskal-Wallis test results for continuous variables and chi-squared tests for categorical variables to determine statistically significant differences between means of various datapoints, including unemployment rate, access to broadband internet connection, percentage of individuals with a vehicle, primary payor, gender, and median household income by census tract.
RESULTS
19500 visits were analyzed from 3420 patients (table 1). 7846 visits occurred in Wilmington, DE among 1569 patients, and 11654 visits occurred in Newark, DE among 1851 patients. The average age of all participants was 42(±19.2) years old. 85.7% of participants were under the age of 65, and 14.3% were age 65 and above. 47.9% of participants had commercial insurance, 25.6% were insured by Medicaid, 25.8% were insured by Medicare, and 0.7% had self-pay insurance. 64.8% of patients were classified as female per the EMR, and 35.2% of patients were classified as male.
The Wilmington and Newark campuses had comparable proportions of office visits during the study period, however in Newark phone and video visit percentages were similar (33.7%, 39.3%) as compared with less than half as many phone visits compared to video visits (19.3%, 51.8%) in Wilmington (table 2).
The most common visit type among all male participants was video (44.0%), followed by office (31.6%) and phone (24.4%), whereas among females the most common visit type was video (44.5%) followed by phone (29.7%) and office (25.7%).
A greater proportion of video and phone visit users tended to have computers, internet connection, higher income, and own a vehicle compared with office users. GINI coefficient, which is an international measure of wealth and income inequality, was lower in video and phone users than in office visit users.
Visits were divided into Wilmington and Newark campuses and sub-divided into office, phone, and video types (table 3). On average, outpatient behavioral health clients served
(standard deviation)
Table 1. Unique Patient Demographics
Row statistics ** column statistics
Table 3. Patient Visits with Census Tract Characteristics Split by Location
by the Wilmington outpatient clinic had less computer ownership, less access to an internet connection, greater unemployment, fewer vehicles, lower income, and a higher GINI coefficient compared to patients served by the Newark campus. In Wilmington, video visit users on average had less unemployment, more vehicles, greater income, and a lower GINI coefficient than office visit users. These differences are less apparent in Newark residents, who have a similar GINI coefficient across all visit modalities and less variance among other census points.
A temporal trend (figure 1) of visits by type reveals a sharp increase in phone visits in early 2020, followed by a gradual replacement by video visits and a return of office visits during and in the latter half of 2021. When split by location, Wilmington clinical sites (figure 2) maintained a majority of video visits through 2021, whereas Newark sites returned to predominantly office visits by September 2021 (figure 3). Visit types subdivided among individuals age 65 and older (figure 4) shows a preference for phone visits in early 2020 and in-person visits in late 2021. The census tract characteristics of this sub-group were also summarized (table 4).
Figure 1. Visits Over Time, by Type
Figure 2. Wilmington, Visits Over Time by Type
Figure 3. Newark, Visits Over Time by Type
Figure 4. Age 65+ Visits Over Time by Type
Table 4.
DISCUSSION
As evidenced by its higher GINI coefficient, lower median income, and greater unemployment, the region of Wilmington, DE has higher measurements of inequality than Newark, DE. These differences in socioeconomic status are also correlated with distinct patterns in the usage of virtual versus in-person healthcare encounters between the two regions. In Newark, an area with a lower burden of socioeconomic challenges, differences among groups of video, phone, and office users were of lesser magnitude than in Wilmington. In Wilmington, users of in-person office visits tended to face greater barriers to health such as a lower median income, less access to a vehicle, and greater unemployment than video users. In addition, these users reported less computer availability and less broadband internet access. Differences among video, phone, and office users via measures of income inequality were significant for the overall cohort and this was primarily driven by Wilmington as opposed to Newark.
In terms of overall usage, however, Wilmington patients used video visits to a far greater extent than Newark residents. It appears that in Wilmington, an area with greater economic diversity, more affluent residents tended towards video visits while others opted for phone or office visits. This trend was less pronounced in Newark, a location with less variance in measurements of inequality such as the GINI coefficient. Rates of video visits were higher among patients with commercial insurance and lower in those with Medicaid. These trends suggest multiple barriers to providing virtual care to differing populations depending on their socioeconomic status, with individuals of lower socioeconomic status tending to opt for in-person encounters.
On temporal analysis the rates of video use by Wilmington patients remained the most popular visit type through September 2021, while in Newark office visit rates increased and eventually overtook other visit modalities in
2021. Among patients aged 65 and older, in-person visits became the most popular option in 2021 once quarantine measures from COVID-19 subsided. This supports the finding that video visit usage rates were proportionally lowest among patients with Medicare. The Newark sample also had a higher proportion of patients 65 and older, suggesting that the trend in Newark towards in-person visits may have been attributable to this population. Census data for the 65 and older cohort did not demonstrate relative socioeconomic inequality or access to virtual care compared with the overall cohort, suggesting that this trend toward in-person visits was likely due to a generational and cultural preference for in-person care among older individuals. This preference may represent a barrier to virtual care in older patients for whom virtual visits may be optimal, for example due to limited mobility or heightened risk of infection due to other health conditions. Approximately two-thirds of the study cohort were female, and approximately one third were male. This result is reflective of established literature demonstrating gender differences in utilization of healthcare services in the United States.6
PUBLIC HEALTH IMPLICATIONS
In conclusion, these findings uncovered significant variations in usage of virtual and non-virtual visits among individuals with respect to age, gender, location, and economic conditions. Patients from groups that experience greater income inequality, higher unemployment, and greater housing insecurity are disproportionately infrequent users of virtual care modalities. Thus, these metrics can be interpreted as potential barriers to equitable access and utilization of virtual care in vulnerable populations. Future studies should examine this trend’s impact on health outcomes to determine whether access to virtual care is itself a social determinant of health.
Dr. Sharma may be contacted at: Ram.a.sharma@christianacare.org .
REFERENCES
1. Zachrison, K. S., Yan, Z., Sequist, T., Licurse, A., Tan-McGrory, A., Erskine, A., & Schwamm, L. H. (2021, June). Patient characteristics associated with the successful transition to virtual care: Lessons learned from the first million patients. Journal of Telemedicine and Telecare, 29(8), 621–631. https://pubmed.ncbi.nlm.nih.gov/34120506/
2. Weiner, J. P., Bandeian, S., Hatef, E., Lans, D., Liu, A., & Lemke, K. W. (2021, March). In-person and telehealth ambulatory contacts and costs in a large US insured cohort before and during the COVID-19 pandemic. JAMA Network Open, 4(3), e212618. https://pubmed.ncbi.nlm.nih.gov/33755167/
3. Thomas-Jacques, T., Jamieson, T., & Shaw, J. (2021, November). Telephone, video, equity and access in virtual care. NPJ Digital Medicine, 4(1), https://pubmed.ncbi.nlm.nih.gov/34795356/
4. Dang, S., Muralidhar, K., Li, S., Tang, F., Mintzer, M., Ruiz, J., & Valencia, W. M. (2022, April). Gap in willingness and access to video visit use among older high-risk veterans: Crosssectional study. Journal of Medical Internet Research, 24(4), e32570.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9034417/
5. Tan, A. X., Hinman, J. A., Abdel Magid, H. S., Nelson, L. M., & Odden, M. C. (2021, May). Association between income inequality and countylevel COVID-19 cases and deaths in the US. JAMA Network Open, 4(5), e218799. https://pubmed.ncbi.nlm.nih.gov/33938935/
6. Vaidya, V., Partha, G., & Karmakar, M. (2012). Gender differences in utilization of preventive care services in the United States. Journal of Women’s Health, 21(2), 140–145.
https://pubmed.ncbi.nlm.nih.gov/22081983/
The flu vaccine:
THE REASON FOR A SEASON.
There are so many things to do and see this season. Make sure you can enjoy them all by making time for a flu vaccine.
Everyone 6 months and older is eligible. To find locations, scan the QR code or visit flu.delaware.gov.
Public Health Delaware Journal of Submission Guidelines
updated March, 2024
About the Journal
Established in 2015, e Delaware Journal of Public Health is a peer-reviewed electronic publication created by the Delaware Academy of Medicine/Delaware Public Health Association. e publication acts as a repository of news for the medical, dental, and public health communities, and is comprised of upcoming event announcements, past conference synopses, local resources, peer-reviewed content ranging from manuscripts and research papers to opinion editorials and personal interest pieces, relating to the public health sector. Each issue is largely devoted to an overarching theme or current issue in public health.
e content in the DJPH is informed by the interest of our readers and contributors. If you have an event coming up, would like to contribute an Op-Ed, would like to share a job posting, or have a topic in public health you would like to see covered in an upcoming issue, please let us know.
If you are interested in submitting an article to the Delaware Journal of Public Health, or have any additional inquiries regarding the publication, please contact the managing editor at managingeditor@djph.org, or the publisher at ksmith@delamed.org.
Information for Authors Submission Requirements
e DJPH accepts a wide variety of submission formats, including brief essays, opinion editorials pieces, research articles and ndings, analytic essays, news pieces, historical pieces, images, advertisements pertaining to relevant, upcoming public health events, and presentation reviews. Additional types of submission not previously mentioned may be eligible, please contact a sta member for more information.
e initial submission should be clean and complete, without edits or markups, and contain both the title and author(s) full name(s). Submissions should be 1.5 or double spaced with a font size of 12. Once completed, articles should be submitted via the submission page at https://djph.org/submissions/submit-an-article/ Graphics, images, info-graphics, tables, and charts are welcome and encouraged to be included in articles. Please ensure that all pieces
are in their nal format, and all edits and track changes have been implemented prior to submission. To view additional information for online submission requirements, please refer to the DJPH website: https://djph.org/submissions/submit-an-article/
Trial registration information is required for all clinical trials and must be included in the nal article and/or abstract.
Abstracts
Authors must submit a structured or unstructured abstract along with their article. Abstracts will have a maximum of 200 words, including headings. Structured abstracts should employ 4-5 headings, and may include Objectives, Methods, Results, and Conclusions. A fth heading, Policy Implications, may be used if relevant to the article. All abstracts should provide the date(s) and location(s) of the study if applicable, as well as any trial registration information.
Submission Length
While there is no prescribed word length, full articles will generally be in the 2,500-4,000word range, and editorials or brief reports will be in the 1,500-2,500-word range. If there are any questions regarding the length of a submission or APA guidelines, please contact a sta member.
Copyright
e journal and its content is copyrighted by the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA). e contents are licensed under Creative Commons License – CC BY-NC-ND (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Images are NOT covered under the Creative Commons license and are the property of the original photographer or company who supplied the image.
Opinions expressed by authors of articles summarized, quoted, or published in full within the DJPH represent only the opinions of those authors and do not necessarily re ect the o cial policy of the Academy/DPHA, the DJPH, or the institution with which the authors are a liated.
Con icts of Interest
Any con icts of interest, including political, nancial, personal, or academic con icts, must be declared prior to the submission of the article, or in conjunction with a submission. Con icts of interest are any competing interests that may leave readers feeling misled or deceived, and/or alter their perception of subject matter. Declared con icts of interest will be published alongside articles in the nal publication.
Nondiscriminatory
Language
Use of nondiscriminatory language is required in all DJPH submissions. e DJPH reserves the right to reject any submission found to be using sexist, racist, or heterosexist language, as well as unethical or defamatory statements.