6 | Implications of Exposure to Intimate Partner Violence in Childhood
Kelly Oberheim
Janice Barlow, M.P.A.
Erin Nescott, M.S.
10 | It Takes a Village: Moving from Unaligned Action to Collective Impact
Cierra Hall-Hipkins, B.S.
Gwen Angalet, Ph.D.
Dorothy Dillard, Ph.D.
18 | Celebrating Fifty Years of Crime Victims’ Compensation in Delaware
Paige J. Schmittinger, J.D.
24 | Global Health Matters Newsletter March - April 2024
Fogarty International Center
36 | Empowering Victims of Lived Violence: Delaware’s Hospital Violence Intervention Program (HVIP)
David Chen, M.D., M.P.H.
Johanna Rodriguez, M.S.W., L.S.W.
Mishai Pendleton, B.S.
Nichole Johnson, C.M.A.
46 | Understanding the Perception of Place and Its Impact on Community Violence
Dorothy Dillard, Ph.D.
Howard Henderson, Ph.D.
Johnny Rice II, Dr.PH
Amy D. Goldstein, B.A.
Maruice Mangum, Ph.D.
50 | Can Past Psychedelic Use Mitigate the Severity of Opioid Use Disorder? Case Report of a Musician.
Asim Trimzi
Morgan Campbell, M.D.
54 | A Safer Delaware: The Case for a Permit-to-Purchase Policy for Reducing Firearm Violence
Traci Manza Murphy
Sarah Stowens, Ed.D.
62 | Delaware Domestic Violence Coordinating Council Resource Guide
120 | Index of Advertisers
122 | Delaware Journal of Public Health Submission Guidelines
The Delaware Journal of Public Health (DJPH), first published in 2015, is the official journal of the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA).
Submissions: Contributions of original unpublished research, social science analysis, scholarly essays, critical commentaries, departments, and letters to the editor are welcome.
Questions? Contact managingeditor@djph.org
Advertising: Please contact ksmith@delamed.org for other advertising opportunities. Ask about special exhibit packages and sponsorships. Acceptance of advertising by the Journal does not imply endorsement of products.
Any report, article, or paper prepared by employees of the U.S. government as part of their official duties is, under Copyright Act, a “work of United States Government” for which copyright protection under Title 17 of the U.S. Code is not available. However, the journal format is copyrighted and pages June not be photocopied, except in limited quantities, or posted online, without permission of the Academy/DPHA. Copying done for other than personal or internal reference use-such as copying for general distribution, for advertising or promotional purposes, for creating new collective works, or for resale- without the expressed permission of the Academy/DPHA is prohibited. Requests for special permission should be sent to managingeditor@djph.org
IN THIS ISSUE
Violence as a Public Health Issue
Violence is not only a major public health issue, but a root social determinant of so many other health issues. From mental health trauma and physical trauma caused by war, to limited healthcare access due to unsafe neighborhoods, the toll taken by violence is tremendous.
The World Health Organization (WHO) declared violence a major public health issue in 1996, defining it as “the intentional use of physical force or power, threatened or actual, against oneself, another person, or against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment, or deprivation.”1 In 2022, the first World Report on Violence and Health was released, analyzing different types of violence (child abuse and neglect, youth violence, intimate partner violence, sexual violence, etc.).2
The magnitude of what can be considered violence is staggering. It is equally staggering the limited policy responses we have taken in the US against preventable gun violence, which is, shockingly, the leading cause of death among US children.3
This is also a global issue, with ongoing conflicts raging that have destroyed communities and disproportionately affected children.4 The US policy responses in this area are inadequate at best.
In this issue, we continue to bring forward the best thinking about this critical public health topic, in ways which matter to Delaware, and which we hope move forward an agenda of controlling violence locally and globally. We include articles about intimate partner violence, community violence, crime compensation, violence intervention programs, and gun violence, knowing that they are only a drop in the bucket of the ongoing study of violence. Our guest editor, Dr. David Chen, has written several articles about violence and gun violence in previous issues of the journal, and we thank him heartily for the experience and forethought he brings to this issue.
As always, we encourage your feedback, and for you to submit articles about your own work and experiences in this field.
REFERENCES
1. American Public Health Association. (2018, Nov 13). Violence is a public health issue: public health is essential to understanding and treating violence in the U.S. American Public Health Association policy number 20185. Retrieved from https://apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2019/01/28/violence-is-a-public-health-issue
2. Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2022, October). The world report on violence and health. Lancet, 360(9339), 1083–1088. 10.1016/S0140-6736(02)11133-0
3. Firearms are the leading cause of death for American children and teens. Everytown Research & Policy. Retrieved from https://everytownresearch.org/graph/firearms-are-the-leading-cause-of-death-for-american-children-and-teens/
4. B oukari, Y., Kadir, A., Waterston, T., Jarrett, P., Harkensee, C., Dexte, E., . . . Devakumar, D. (2024, February 13). Gaza, armed conflict and child health. BMJ Paediatrics Open, 8(1), e002407. 10.1136/bmjpo-2023-002407
Omar A. Khan, M.D., M.H.S. Editor-in-Chief, Delaware Journal of Public Health
Katherine Smith, M.D., M.P.H. Publisher, Delaware Journal of Public Health
An Introduction to the Violence Issue
David D. Chen, M.D., M.P.H. Institute for Research on Equity and Community Health (IREACH), ChristianaCare Health System
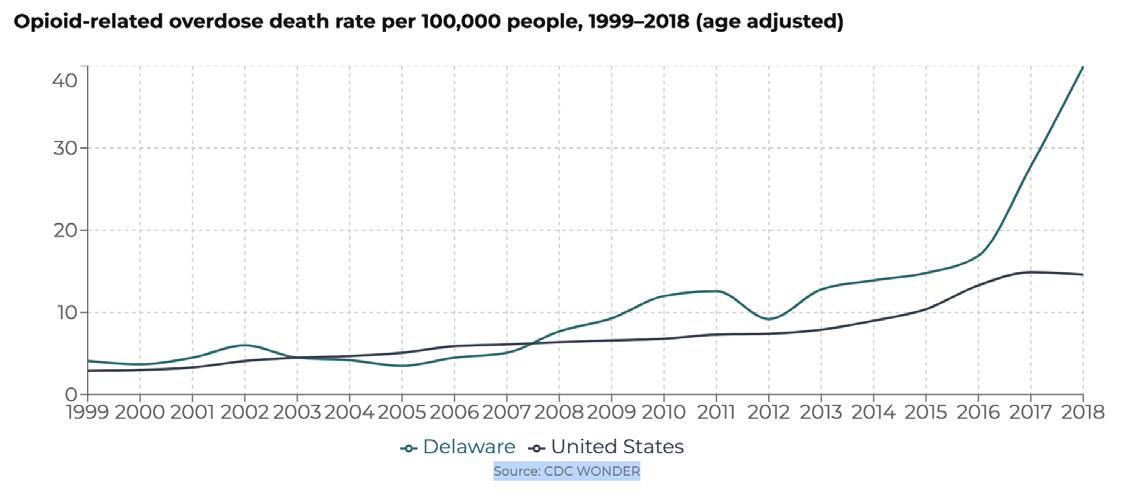
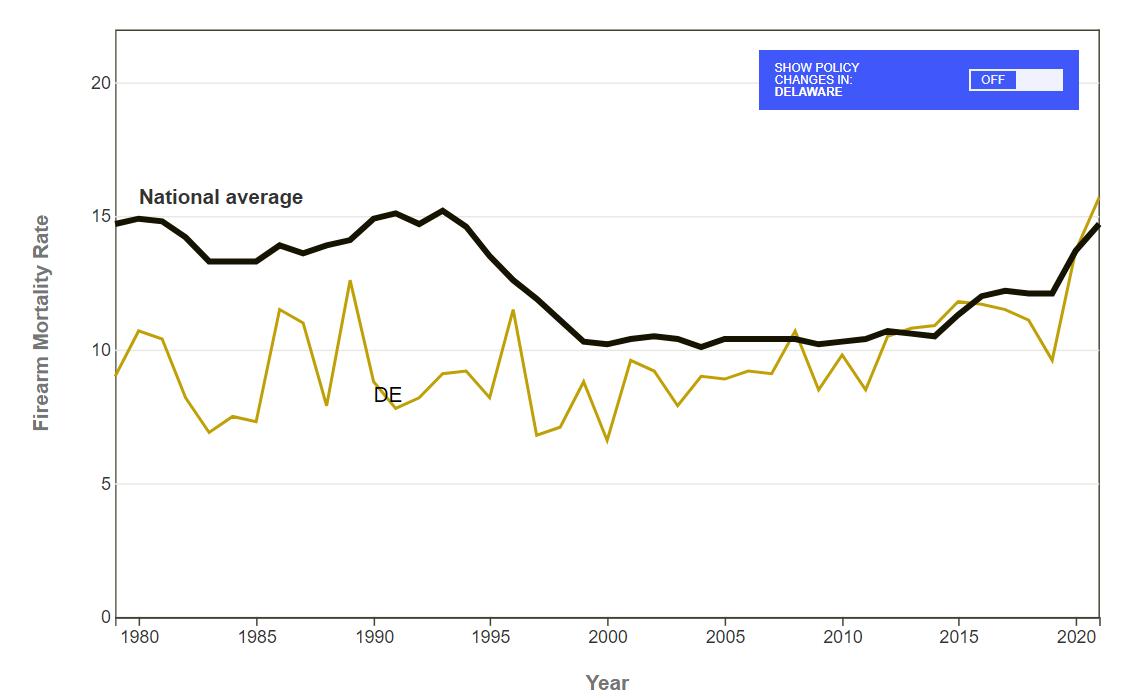
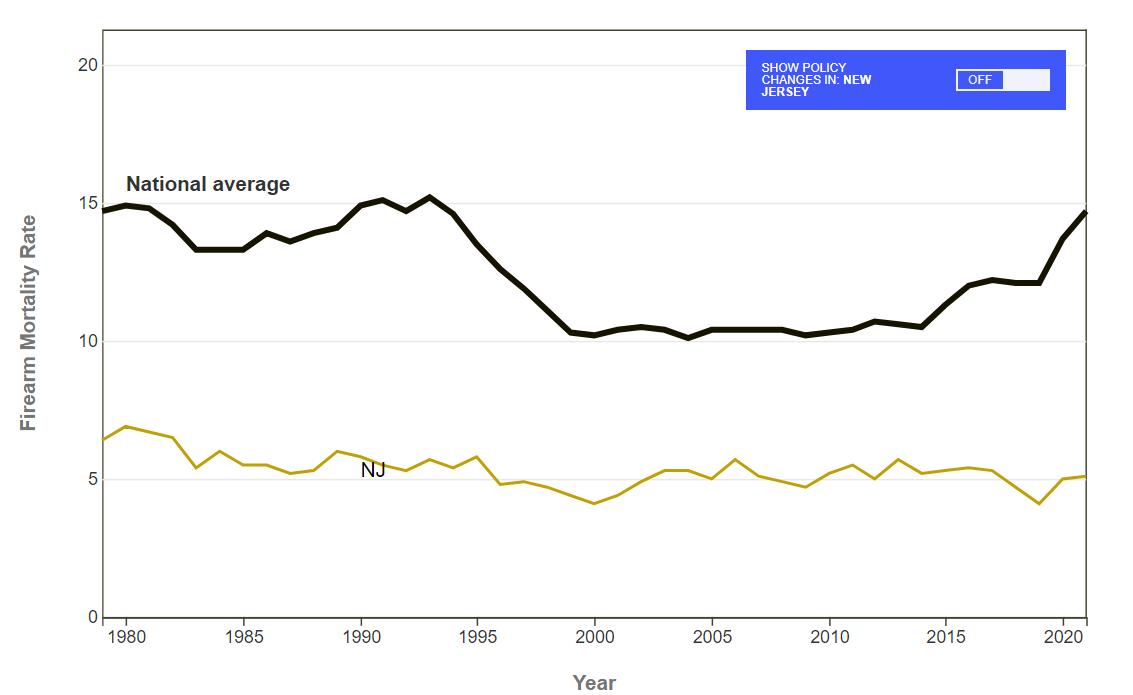
Even though violence affects persons across every demographic, its effects are hardly homogenous or well understood. From the violence that occurs within a household to the broad terror created by incidents highlighted in the media, the use of force to harm is as present in Delaware as anywhere else in the United States. It is a grisly fact that Delaware has been an outlier in elevated firearm homicide rates compared to the rest of the United States, which itself is already an outlier compared to the rest of the world.
Yet though violence has long held recognition as a public health issue, the ways in which it propagates harm between persons and across communities remain vague. Violence –and especially gun violence – is closely intertwined with the deep systemic and structural factors of poverty and racism. This entanglement at the intersection of interpersonal violence with policing, justice, health, social, and political systems makes all forms of observation and intervention highly complex and challenging to interpret. But the past decade has seen a burst in energy and growth in policy, prevention, and interventions within the state. We are pleased to present this issue of the Delaware Journal of Public Health with a focus on violence as a window into emerging landscape shifts and new capacity within academic, healthcare, and policy spaces in the state. Oberheim, Barlow, and Nescott illustrate the nuances in measurement of the childhood exposure to intimate partner violence in Delaware and how
the incorporation of economic justice into policy has led to pragmatic local interventions. A large multicenter qualitative study on gun possession by Dillard, Henderson, Rice, Goldstein, and Mangum gives voice to the lived experiences of young men living in Wilmington, Delaware, and the complementary article by Dillard, HallHipkins, and Angalet widens the scope surrounding this work to describe its place in the evolution of collective action among local community-based organizations. Chen (guest editor), Rodriguez, Pendleton, and Johnson describe their frontline experiences in operationalizing a new Hospital Violence Intervention Program (HVIP) to serve victims of violence after hospitalization. Murphy and Stowens make the case for new legislation in the state to require a permit to purchase handguns (which has since authorship been signed into law, making Delaware the 12th state/district in the USA to do so), while Schmittinger summarizes the fifty year history of implementation of the state’s Victims’ Compensation Assistance Program (VCAP) to help victims begin rebuilding lives after trauma.
This is not a comprehensive description of novel research and programs, but points to areas of future learning and innovation: preventing injury and treating injury, proposals for new policy changes, measures and changes to existing policy, and the path forward in our state to better health.
June 2024
The NATION’S HEALTH
The Nation’s Health headlines
Online-only news from The Nation’s Health newspaper
Stories of note include:
Climate change’s higher temperatures increase suffering at US carceral facilities
Mark Barna
More programs offering low-cost, reliable transportation for health care visits
Teddi Nicolaus
Health care access improving for people with IDD, but gaps remain
Kim Krisberg
Programs train health students to care for people with IDD
Natalie McGill
It’s time to expand equity, inclusion work to include people with IDD
Tia Williams
Mental health issues for people with IDD can be misunderstood
Mark Barna
Personal approach improves oral health care of people with IDD
Mark Barna
Special Olympics initiative to assess ability of health systems to serve people with IDD
Natalie McGill
Health advocacy can help improve access to care for people with IDD
Lawrence Haynes
Dementia rates higher among people with Down syndrome, but condition may be missed in others
Natalie McGill
Living with IDD profile: T.J. Gordon – Advocating for health at the intersection of race and IDD
Natalie McGill
Living with IDD profile: Pauline Bosma — Bringing a voice to people with IDD in the LGBTQ+ community
Teddi Nicolaus
Living with IDD profile: Connie Lewis — Helping people with IDD gain confidence, find independence
Sophia Meador
Living with IDD profile: Ashley Glears — Working toward equity and inclusion
Sophia Meador
Many other articles available when you purchase access
Entire Issue $12
Visit https://www.thenationshealth.org/user
Implications of Exposure to Intimate Partner Violence in Childhood
Kelly Oberheim Undergraduate Research Assistant, KIDS COUNT in Delaware
Janice Barlow, M.P.A.
Policy Scientist, Center for Community Research and Service; Director, KIDS COUNT in Delaware
Erin Nescott, M.S.
Associate Policy Scientist, Center for Community Research and Service
ABSTRACT
The most recent available data show that children were present at 38% of domestic incidents reported throughout Delaware, and analysis of barriers to reporting predict this number to be much higher. Intimate partner violence (IPV) can take numerous forms, such as patterns of physical, sexual, psychological, economic, and reproductive abuse, meaning each situation manifests differently and requires individualized intervention. Children face unique short- and long-term challenges as a result of their witness status within such scenarios. Programming throughout Delaware works to support victims and mitigate the negative ramifications that IPV has on children and their families.
INTRODUCTION
Intimate partner violence (IPV) has long been studied, including the impacts on victims and numerous prevention strategies. Less is known about the impact of IPV on children, especially paired with the ever-increasing understanding of child development. This article explains the prevalence of children witnessing IPV, nationally and in Delaware, and the accompanying short- and long-term challenges.
BACKGROUND
Intimate partner violence (IPV) is a pressing public health issue and a form of gender-based violence that occurs between current or former romantic partners. It can take numerous forms, such as patterns of physical, sexual, psychological, economic, and reproductive abuse, meaning each situation manifests differently and requires individualized intervention. In many cases, perpetrators of IPV will use a combination of these forms of abuse to exert greater power and control over their victims. Nationally, 25% of women and 10% of men report having been victims of IPV in their lifetime, and, though still emerging, recent research indicates that non-binary individuals report higher rates of IPV than women or men.1,2 People from disempowered groups are at an increased risk; abusers may exert control by taking advantage of existing social vulnerabilities. For LGBTQ+ people, abusers rely on existing homophobic and transphobic systems of stigma, discrimination, and lack of education around LGBTQ+ people to increase levels of control.3 When compared to the national landscape, numbers are even higher in Delaware, with 37.6% of women and 32.7% of men having reported victimization in 2020.4 However, there are far more victims of IPV than are captured by incident report statistics. Those who are simply aware of IPV occurring experience lasting physical, mental, and behavioral health consequences, and in most cases these witnesses are children, who are repeatedly exposed to violence before intervention is sought, if at all.
Exposure to IPV is an adverse childhood experience (ACE) that encompasses instances in which the child is physically present at the time violence is committed, as well as those that the child perceives, such as hearing conflict from another room or seeing IPV-related injuries after they have occurred.5,6 In 2023, children were present at 38% of domestic incidents reported throughout Delaware, a figure that has remained relatively consistent over the last five years.7 Still, this data is likely to be undercounted, as broad themes such as “lack of awareness, access challenges, consequences of disclosure, lack of material resources, personal [circumstances], and system failures,” have consistently been found to hinder survivors’ reporting and help-seeking efforts (p. 1279). For example, failure to label behavior as IPV, language barriers, fears of being deported or outed as LGBTQ+, cultural stigma, agency distrust, and lack of housing represent only some of the potential obstacles survivors may encounter in reporting.8 Hence, given the barriers to reporting, it is likely that greater numbers of individuals experience IPV and, consequently, far more of Delaware’s children witness violence than statistics show.
SHORT TERM IMPLICATIONS OF EXPOSURE TO IPV ON CHILDREN
Depending on the child’s age, the implications of IPV will manifest differently in the short term. Preschool aged children may show behavioral regression, meaning that they will resort to behaviors that they engaged in when they were younger, such as bedwetting, thumb sucking, or whining.9 Sleep patterns may also be disrupted at this age, with difficulties falling or staying asleep.9 Research has found associations between witnessing IPV and childhood onset of obesity, asthma, and gastrointestinal problems, with these problems occurring at higher rates than those of nonexposed peers.10,11 Developmentally, preschoolers are beginning to engage in and experiment with prosocial behaviors, but children exposed to IPV may exhibit decreased social competencies and, consequently, struggle to form healthy friendships.12 However, school-aged children (aged 6-12 years) are affected differently than younger children are, namely because of their sophisticated
understanding of themselves, others, and the world in conjunction with influences from peers and formalized education systems.13,14 At this age, children may exhibit difficulties forming and maintaining peer relationships, with many reporting higher levels of conflict with friends, lower self-esteem, and greater levels of loneliness than non-exposed children.15 Initially following violence, it has been shown that children in this age group show higher measures of depression and anxiety, though these measures may decrease as time progresses.16 Physically, school-aged children often experience headaches and stomachaches, and some report bedwetting (35.8%) and weight problems (22.6%) much like preschool aged children do.10,17
LONG TERM IMPLICATIONS OF EXPOSURE TO IPV ON CHILDREN
As child witnesses of IPV age, they are placed at greater risk for physical and mental health conditions, in addition to those afflictions that may persist through childhood such as obesity and low self-esteem. As adults, these individuals are more likely to be diagnosed with depression, anxiety, diabetes, and heart disease.18 Notably, adults who were exposed to IPV in childhood are more likely to be involved in abusive relationships themselves, as either victims or perpetrators of violence.19,20 Preventing or limiting children’s exposure to IPV is an important step in interrupting the cycle of abuse.
IN DELAWARE
Data reveal children were present at 38% of IPV incidents reported in Delaware in 2023, which amounts to nearly 4,000 children.7 This number only includes those conflicts that were disclosed to authorities. Likely, these children have witnessed numerous instances of violence prior to that which was reported. Given this alarming statistic and the observed short- and longterm implications, Delaware must address the issue.
The crux of the public health approach to violence is primary prevention, focusing on stopping violence before it occurs, and effective implementation of this methodology decreases the number of children exposed to and affected by IPV.21 In addition to traditional means of prevention such as teaching healthy relationship skills, another avenue through which violence can be prevented is by incorporating economic justice into policy, as proposed by the Delaware Coalition Against Domestic Violence (DCADV) in their 2022 White Paper, Economic Justice as a Framework for Violence Prevention. Economic justice is defined as “the human right to be compensated a livable wage and benefits equitably, in safe working environments, with the right to choose a job that is fulfilling... [meaning] that everyone has equitable opportunities to be financially self-sufficient and create economically stable lives for themselves and their families.”22 This framework intersects with IPV prevention in that it promotes stable and independent finances, a crucial aspect impacting an individual’s ability to leave an abusive relationship. Notably, economic justice also addresses the gendered component of IPV considering that those victimized by IPV are overwhelmingly female. Implementing fairer and more accommodating workplace practices like lactation-friendly policies, comparable pay, flexible work schedules, and childcare subsidies are especially helpful for women and persons capable of becoming pregnant to achieve financial independence, as these policies and those similar afford survivors of IPV certain flexibilities that their situations demand without compromising their finances nor their careers.22
Strengthening parents’ job stability and financial resources encourages better outcomes for their children, in terms of both their financial ability to provide children with basic necessities and to separate children from violent households. This is the primary mission of INVEST DE, a community workgroup created by the Delaware Coalition Against Domestic Violence that sets out to bolster workplace understanding of economic justice and how the implementation of such policies can reduce the prevalence of IPV throughout the state. However, where primary prevention is not possible, it is necessary to use research and data to inform policy throughout the state to help survivors of IPV and their children.
In New Castle County, the U.S. Department of Housing and Urban Development (HUD) funds CHILD, Inc.’s Rapid Rehousing Program, which creates individualized rehousing plans for clients fleeing IPV based on their unique circumstances and needs. This comes in the form of “assistance in the search for safe and affordable housing, assistance connecting with landlords and finding the best placement options, and monetary assistance for moving costs,” all of which help to stabilize survivors and their families by preventing or interrupting houselessness.23 In 2023, CHILD, Inc. served over 50% more children than adults, with a total of 63 children and 37 adults having received services (p. 38).23 These figures are reasonable considering that individuals seeking services often have and care for multiple children, but they reflect the disproportionate impact that homelessness has upon youth populations. Having and maintaining safe and reliable housing is especially important in creating consistency and security for children who have witnessed IPV, as well as in preventing the negative mental and physical health consequences that accompany housing instability, such as learning difficulties, depression, anxiety, and asthma.24
Receiving therapeutic services after exposure to IPV is important for all individuals, but it is especially important for children, as they are situated amid key developmental stages that make trauma even more impactful on the maturing brain. Traumainformed care is a methodology that centers client experiences in the helping process, acknowledging the distinctiveness of their trauma and providing them with resources, support, and empowerment to work through it. For Kent and Sussex Counties, Turning Point at People’s Place II provides such trauma-informed services to children, and the Helping Children Heal Program by CHILD, Inc. serves children in New Castle County. Across these programs, 83 children and adolescents received services in 2023, and, while this is an abundant success, this figure is far smaller than the aforementioned total number of Delawarean children reported present at instances of IPV throughout the year (p. 46).25
CONCLUSION
Despite mandatory reporting policies, children can be missed when caring for victims of IPV and suffer a wide range of physical, mental, and behavioral health outcomes depending on their age at the time of exposure. Preventing IPV is the surest means of protecting children from the negative health outcomes that accompany witnessing patterns of violence, and prevention can take less traditional forms such as by implementing and updating workplace policies throughout Delaware to be more equitable and economically just. Still, it is important to recognize that prevention is not possible in all cases. Where prevention is unsuccessful, Delaware promotes the well-being of IPV survivors and their children via programming, such as those that exist for housing and trauma-informed therapy.
Ms. Oberheim may be contacted at keo@udel.edu
REFERENCES
1. Gilchrist, G., Potts, L. C., Connolly, D. J., Winstock, A., Barratt, M.J., Ferris, J., . . . Davies, E. (2023, February 13). Experience and perpetration of intimate partner violence and abuse by gender of respondent and their current partner before and during COVID-19 restrictions in 2020: A cross-sectional study in 13 countries. BMC Public Health, 23(1), 316. https://doi.org/10.1186/s12889-022-14635-2
2. National Coalition Against Domestic Violence. (2020). Domestic violence. Retrieved from https://assets.speakcdn.com/assets/2497/ domestic_violence-2020080709350855.pdf?1596828650457
3 Understanding Intimate Partner Violence in the LGBTQ+ Community. Retrieved from https://www.hrc.org/resources/ understanding-intimate-partner-violence-in-the-lgbtq-community
4. National Coalition Against Domestic Violence. (2020). Domestic violence in Delaware. Retrieved from https://assets.speakcdn.com/ assets/2497/ncadv_delaware_fact_sheet_2020.pdf
5. Centers for Disease Control and Prevention. (2023). Risk and protective factors. Retrieved from https://www.cdc.gov/ violenceprevention/aces/riskprotectivefactors.html
6. Child Welfare Information Gateway. (2009). Child witnesses to domestic violence: Summary of state laws. Retrieved from https:// www.ojp.gov/ncjrs/virtual-library/abstracts/child-witnesses-domesticviolence-summary-state-laws
7. KIDS COUNT in Delaware. (2024). Children Present at Domestic Violence Incidents in Delaware. Retrieved from https://datacenter.aecf.org/data/tables/11553-children-present-atdomestic-violence-incidents?loc=9&loct=2#detailed/2/any/fal se/2545,1095,2048,574,1729,37/8145/22757,22758
8. Robinson, S. R., Ravi, K., & Voth Schrag, R. J. (2021, December). A systematic review of barriers to formal help seeking for adult survivors of IPV in the United States, 2005–2019. Trauma, Violence & Abuse, 22(5), 1279–1295 https://doi.org/10.1177/1524838020916254
9. U.S. Department of Health and Human Services Office on Women’s Health. (2021). Effects of domestic violence on children. Retrieved from https://www.womenshealth.gov/relationships-andsafety/domestic-violence/effects-domestic-violence-children
10 Boynton-Jarrett, R., Fargnoli, J., Suglia, S. F., Zuckerman, B., & Wright, R. J. (2010, June). Association between maternal intimate partner violence and incident obesity in preschoolaged children: Results from the Fragile Families and Child Well-being Study. Archives of Pediatrics & Adolescent Medicine, 164(6), 540–546. https://doi.org/10.1001/archpediatrics.2010.94
11 Kuhlman, K. R., Howell, K. H., & Graham-Bermann, S. A. (2012). Physical health in preschool children exposed to intimate partner violence. Journal of Family Violence, 27(6), 499–510. https://doi.org/10.1007/s10896-012-9444-2
12 Hungerford, A., Wait, S. K., Fritz, A. M., & Clements, C. M. (2012). Exposure to intimate partner violence and children’s psychological adjustment, cognitive functioning, and social competence: A review. Aggression and Violent Behavior, 17(4), 373–382. https://doi.org/10.1016/j.avb.2012.04.002
13 Holt, S., Buckley, H., & Whelan, S. (2008, August). The impact of exposure to domestic violence on children and young people: A review of the literature. Child Abuse & Neglect, 32(8), 797–810. https://doi.org/10.1016/j.chiabu.2008.02.004
14 Parker, J. G., Rubin, K. H., Erath, S. A., Wojslawowicz, J. C., & Buskirk, A. A. (2015). Peer relationships, child development, and adjustment: A developmental psychopathology perspective. In Cicchetti, D., & Cohen, D.J. (Eds.), Developmental Psychopathology https://doi.org/10.1002/9780470939383.ch12
15 McCloskey, L. A., & Stuewig, J. (2001, Winter). The quality of peer relationships among children exposed to family violence. Development and Psychopathology, 13(1), 83–96 https://doi.org/10.1017/S0954579401001067
16 Kennedy, A. C., Bybee, D., Sullivan, C. M., & Greeson, M. (2010, April). The impact of family and community violence on children’s depression trajectories: Examining the interactions of violence exposure, family social support, and gender. J Fam Psychol, 24(2), 197–207. https://doi.org/10.1037/a0018787
17. Lundy, M., & Grossman, S. F. (2005). The mental health and service needs of young children exposed to domestic violence: Supportive data. Families in Society, 86(1), 17–29. https://doi.org/10.1606/1044-3894.1873
18 Monnat, S. M., & Chandler, R. F. (2015, September). Long term physical health consequences of adverse childhood experiences. The Sociological Quarterly, 56(4), 723–752 https://doi.org/10.1111/tsq.12107
19 Roberts, A. L., Gilman, S. E., Fitzmaurice, G., Decker, M. R., & Koenen, K. C. (2010, November). Witness of intimate partner violence in childhood and perpetration of intimate partner violence in adulthood. Epidemiology (Cambridge, Mass.), 21(6), 809–818. https://doi.org/10.1097/EDE.0b013e3181f39f03
20. Centers for Disease Control and Prevention. (2021). Risk and protective factors for perpetration. Retrieved from https://www.cdc.gov/violenceprevention/intimatepartnerviolence/ riskprotectivefactors.html
21. Centers for Disease Control and Prevention. (2022). The public health approach to violence prevention. Retrieved from https://www.cdc.gov/violenceprevention/about/publichealthapproach.html
22. Delaware Coalition Against Domestic Violence. (2022). Economic justice as a framework for violence prevention. Retrieved from https://dcadv.org/file_download/inline/3ae71aece683-4e1d-802b-316f0cf9ef27
23. Domestic Violence Coordinating Council. (2023). Annual report: Fiscal year 2023. Retrieved from https://dvcc.delaware.gov/ wp-content/uploads/sites/87/2023/09/FY23-DVCC-Annual-Reportelectronic-version-update-min-9-25-23.pdf
24 Hart-Shegos, E. (1999). Homelessness and its effects on children: A report prepared for the Family Housing Fund. Retrieved from https://shnny.org/uploads/Homelessness_and_Its_ Effects_on_Children.pdf
25. Domestic Violence Coordinating Council. (2023). Annual report: Fiscal year 2023. Retrieved from https://dvcc.delaware.gov/ wp-content/uploads/sites/87/2023/09/FY23-DVCC-Annual-Reportelectronic-version-update-min-9-25-23.pdf
Cierra Hall-Hipkins, B.S.
It Takes a Village: Moving from Unaligned Action to Collective Impact
Executive Director, Network Connect
Gwen Angalet, Ph.D.
Founder and CEO, GBA Consulting
Dorothy Dillard, Ph.D.
Director, Center for Neighborhood Revitalization and Research, Delaware State University
ABSTRACT
For over two decades, violence has been understood as a public health problem. Despite a well-established and applicable public health framework, progress to address the entrenched violence that plagues many cities has been slow. We believe that progress can be effective only if it fully includes those most impacted by the violence. In this article, we describe an initiative to address one aspect of violence plaguing Wilmington: access to and possession of guns. Our initiative is driven by the lived experience of community members, builds on and expands an established collective impact effort to address gun violence, and focuses on the root causes of gun violence.
INTRODUCTION: UNDERSTANDING GUN VIOLENCE AS A CONTAGIOUS DISEASE
For over two decades, violence has been understood as a public health problem. In 2002, the World Report on Violence and Health,1 jointly produced by the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC), established violence as a global health issue, spurring the development of violence prevention efforts. Shortly thereafter, the CDC embraced and promoted the social ecological model as a framework to address violence.2 This framework emphasizes the multi-dimensional characteristic of violence: individual, relationship, community, and societal. A decade later, Dr. Gary Slutkin provided a clear and compelling explanation of violence as a contagious disease.3 Slutkin used the infectious disease framework, comparing violence in Chicago to cholera in Bangladesh, to demonstrate the population level clustering, spreading, and transmission of violence at the population level. He noted that violence, a behavior, is transmitted through exposure as an observer and/or a victim. This exposure impacts the brain in multiple ways increasing the likelihood that victims of violence become perpetrators of violence. Slutkin further demonstrated the individual level contagious characteristics of violence after exposure, including incubation, latency, carriers state and manifestation. He refers to those exposed to violence as “violence infected.”3
Despite a well-established and applicable public health framework, progress to address the entrenched violence that plagues many cities has been slow. The American Public Health Association’s (APHA) 2018 policy statement accepting violence as a public health problem suggests that the original misdiagnosis of violence as a moralistic problem stalled both research and action. Slutkin explained that the typical reaction to a health crisis is a moralistic diagnosis, essentially blaming the victim as a flawed or immoral person, and that only through scientific examination can the health issue and its effective treatment be developed.3
The lack of progress can be contributed in part to the initial lack of research followed by limited research methodological variation. Several years prior to the WHO and CDC developments promoting violence as a contagious disease, Congress passed the Dickey Amendment as part of the 1997 omnibus spending bill.4 Although the amendment prohibited federal funds from being used to advocate for or promote gun control, it was interpreted much more broadly as prohibiting federal funds to support gun violence research. For the next two decades, research on gun violence essentially came to a halt. The CDC funding for gun violence research decreased by 96% due to the CDC’s fear of being misperceived as advocating for or promoting gun control.5 The CDC’s greatest concern was being penalized financially. Similarly, academic publications on gun violence decreased notably.5 Following the 2012 devastating mass shooting at Sandy Hook elementary school, President Obama directed the CDC to support additional research. It wasn’t until 2018 that Congress clarified and then repealed the Dickey Amendment and allocated funding for gun violence research, albeit a minimal allocation.6 It took another four years before substantial funds, about $25 million to CDC and National Institutes of Health (NIH), were allocated for research to reduce gun deaths and injuries.7
Unfortunately, when research resumed, little of it focused on the most likely group to be both victims and perpetrators of gun violence: young men living in cities marked by high crime and high violence. Additionally, essentially none of the research conducted over the past five years has included the lived experience. Decades of public health research has demonstrated that community engagement in all phases of research is fundamental to properly understanding health issues and to developing effective interventions. Community engaged research (CEnR) is an essential approach to understanding and addressing health issues because it focuses on research participants living in close proximity to each other and sharing similar situational characteristics affecting their health. As such, CEnR is responsive to the centrality of place in addressing health disparities. Thus,
it allows us to understand the context and variations of a health issue. As highlighted in the APHA policy, “[c]ommunity members have unique insight into the local context and often have the credibility to reach those at highest risk and engage in the work of violence prevention.”8
Not only do we need to include those with lived experience in understanding gun violence, we also need to include the community in responding to gun violence. In fact, we believe that the community needs to lead the efforts to understand gun violence as well as lead the response. Community engaged research, when done correctly, stimulates action. And for that action to be effective and sustainable it needs to be inclusive and coordinated. In other words, it needs to be collective. Collective action is commonly understood within a collective impact framework. Collective impact (CI) is defined by five common characteristics: 1) a backbone organization; 2) a common agenda; 3) mutually reinforcing actions: 4) continuous communication; and 5) a shared measurement system. More recently, collective impact has expanded to include equity.9 Creating and fostering equity among traditionally unequal partners within the collective impact framework has become an increasingly important concept. In a review of collective impact projects, Kania and colleagues identified five effective strategies to foster equity: 1) ground the work in data and context, and target solutions; 2) focus on system change in addition to programs and services; 3) shift power within the collective; 4) listen to and act with community; and 5) build equity leadership and accountability.9 As such, CI provides a framework to collaborate with intention and advance clinical and behavioral interventions from transactional to transformational, effecting change at the individual, organizational and system levels. In this article, we describe an initiative to address one aspect of violence plaguing Wilmington: access to and possession of guns. Our initiative is driven by the lived experience of community members, builds on and expands an established collective impact effort to address gun violence, and focuses on the root causes of gun violence. The study that informed the collective impact engaged a community partner, the Center for Structural Equity, steeped in the historical and current issues related to gun violence in Wilmington. The data and, thus, the findings, are grounded in the lived experience of young African American males who are most likely to become victims and perpetrators of violence.
BACKGROUND: COLLECTIVE IMPACT INITIATIVES TO ADDRESS GUN VIOLENCE IN WILMINGTON, DELAWARE
Concerted efforts to address gun violence are not new. In 2009, Newsweek Magazine tagged Wilmington as Murder Capital USA, and city officials recognized the immediate need to address Wilmington’s public health crisis of gun violence, especially among youth, through a public health approach.10 This led the City Council President to propose a City of Wilmington resolution requesting the CDC assist the City in an investigation of gun violence and provide recommendations for preventative action. With the support of the Delaware Department of Health and Social Services (DHSS), the CDC sent scientists to Wilmington to collect both primary and secondary data and to conduct an extensive analysis. The CDC team encountered several challenges obtaining the necessary data to accurately
assess the gun violence crisis. Many of the limitations can be attributed to underdeveloped and uncoordinated data systems; unaligned service systems; and a lack of a cross-system, cross discipline organizing entity. In March 2015, the CDC provided initial findings and three primary recommendations:
1)reach agreement on data sharing;
2) connect data systems to identify potential recipients of targeted services; and
3)establish a Community Advisory Council.
In November 2015, the DHSS released the final CDC report, Elevated Rates of Urban Firearm Violence and Opportunities for Prevention, which looked at gun violence from a public health and social services perspective.11 Based on these recommendations, DHSS created the Wilmington Community Advisory Council (WCAC), formerly known as the CDC Community Advisory Council, with support from the State, City of Wilmington, and New Castle County. In January 2017 the WCAC issued a set of recommendations based on a data analysis of the root causes of the violence grounded in the social determinants and research on the best practices to ameliorate the conditions leading to violence. Since the release of its report, the WCAC, together with its community partners, have advocated and supported the development of policies and programs and explored other opportunities to eliminate the gun violence epidemic, promote positive youth development, help neighborhoods to become more resilient, and improve the quality of life for city residents.
Some of the WCAC’s most noteworthy accomplishments include supporting capacity building in the use of evidencebased programs at community centers such as the Hicks Anderson Community Center and youth-serving organizations. The WCAC also promoted and supported Trauma Informed Practice “train the trainer” training for leadership and staff with community organizations in which 68 participants from 33 organizations were trained as trainers. In 2022, the WCAC also supported the expansion of the City of Wilmington summer youth program in which a total of 304 youth from across the city were employed. In 2023, 369 staff and community members participated in community workshops. The WCAC also contributed to the development of several community programs, including the State’s Community Partner Support Unit to help community organizations and members connect to needed services, the Community Intervention Team which evolved to become the Center for Structural Equity to address youth violence, and the Community Violence Prevention Initiative to help high risk youth to address the challenges they face in school and the community. The WCAC was instrumental in generating $18M in grant awards to community partners for services to youth and their families over six years – Network Connect for the Community Well-Being Initiative, Center for Structural Equity for the Community Violence Prevention Program and COVID outreach, and Department of Education (DOE) for trauma informed practice capacity building and mental health services for underserved youth. The WCAC was an active partner with United Way of Delaware in the launch of the Delaware Racial Justice Collaborative, including championing the creation of the Equity Counts Data Center, a data portal in the Delaware Department of Public Health’s My Healthy Community data portal where data on equity gaps in health,
education, employment, wealth creation, and criminal justice are tracked at the census tract level. When the COVID-19 pandemic struck, the Council mobilized over 35 community organization partners to fight the spread of COVID-19 in the most vulnerable communities in New Castle County through education, testing, vaccinations, and treatment, including advocating for funding to support efforts and addressing health equity among vulnerable community members. The Council also provided strategic support to Network Connect in the development of the Community Well-Being Initiative in the most vulnerable communities in New Castle and Kent Counties aimed at helping community members to address mental health and substance abuse challenges and the social determinants of health. Currently, the WCAC is an active member of Wilmington’s Community Public Safety Initiative, facilitating Public Safety Round Tables in targeted neighborhoods to mobilize community members in efforts to reduce violence and improve safety in their areas.
While the WCAC has addressed gun violence at the system and service levels, many of its member agencies have addressed violence at the community and individual levels. Network Connect, for example, aims to build community capacity by coordinating grassroots and local partners to provide youth and families with social services, education programs, workforce skills, and mental health supports. Through collective impact, Network Connect seeks to break the cycle of Adverse Childhood Experiences in effort to improve the well-being of youth and families. Whether working with youth, families, partners, or organizations, Network Connect provides a culture grounded in community, integrity, partnership, and respect. Blending the organization’s unique culture with pro-social skills and evidencebased practices to support programs and services, Network Connect’s determination, connection, relationships, and sense of collective responsibility motivates the community of practice to strengthen our communities.
In effort to build and maintain a grassroot community of practice, Network Connect has found that the gun violence crisis requires not only a collective approach but one that addresses individual and community challenges within complex macro systems. In 2021, the CDC developed the Youth Violence Prevention Resource for Action, to guide youth violence prevention strategies and approaches.12 Strategies described in this report include investment in early childhood education, mentorship and afterschool programs, health access and coordinated outreach to support adults, increased recreation spaces, and other health and self-sufficiency interventions. The CDC resource guide underscores the interdisciplinary nature of gun violence prevention and emphasizes the necessity of collaborative solutions collaboration across service sectors for youth and adults alike. To this end, Network Connect offers an array of services and interventions.
Within Network Connect, the Future Culture Creators program (FCC) builds individual and group relationships to grow connection, trust, and accountability. FCC provides experiential learning and service opportunities to encourage teens to develop new interests, identities, and purposes. Key FCC experiences like coordinating Teen Town Halls or visiting the New Castle County Hope Center expose teens to different types of community engagement. Network Connect’s partnerships with organizations
like ChristianaCare Health System have launched unique workforce experiences, allowing teens to discover new areas of interest and potential careers. FCC helps youth develop personal mission statements to teach them to live with a purpose greater than oneself.
In 2022, Network Connect became involved in the Community Based Public Safety Collective (CBPSC), a collaborative of nonprofits and community-based organizations focusing on addressing and improving community level safety. The CBPSC conducted a landscape analysis of Wilmington to develop violence prevention strategies.13 The Community Public Safety Initiative (CPSI) was formed and includes four key organizations identified in the landscape analysis: Network Connect, the Center for Structural Equity, Youth Advocate Programs, Inc., and the WCAC. The WCAC hosts bi-monthly roundtable sessions designed to solicit input from community members about safety issues and needs. The roundtables also provide a forum for organizations to share information about their efforts to improve safety in Wilmington. The CPSI also conducts organizational readiness assessments for participating community organizations and assists with building organizational and programmatic readiness. For example, the CPSI provides participating organizations with coaching and training on topics such as financial management, operational protocols, workforce development, relationship/partnership management services to gun violence victims, fundraising, and identifying federal funding opportunities. These efforts aim to strengthen community organizations, particularly grassroots organizations, at the frontlines of the gun violence crisis. Their readiness and resilience are essential to effective gun violence reduction and prevention. The CPSI also facilitates peer learning across selected intervention organizations to share experiential knowledge and best practices, further strengthening readiness and resiliency among its partners.
To date, the CPSI has created one Hub house, located on the Eastside, and has plans for a second one, to be located in Northeast Wilmington, to serve as community resource centers. The Hub houses provide a safe space for community members to get their basic needs met, including receiving food, washing clothes, and attending to personal hygiene. The CPSI has also incorporated wraparound and prevention services when deploying responses to violent incidents and uses trauma informed practices and perspectives to address root causes of community violence.
Network Connect is driven by a mission to ensure that the communities most impacted by violence are at the center of defining and addressing the issues. Network Connect hosts and facilitates two connection circles. Connection Circles are a unique restorative and evidence-based approach. It is Network Connect’s culture to conduct connection circles in the community and internally with our team members. These circles encourage and facilitates the relationship building process used to promote understanding, develop interpersonal capacity, and establish space for all voices. This evidence-based practice has proven to be effective in Network Connects service and culture. The Network Connect Community Partner Connection Circles are designed to provide a space and time to intentionally share updates, needs, data, resources, and ask questions. The exchange during the connection circles builds trusting relationships, reduces siloed interventions, and encourages a collaborative culture among
the local nonprofits within our communities. The Community Partner Connection Circles is fundamental to building equity within the collective impact model and transforming our hierarchical, siloed, competitive approach into a mutually reinforcing, supportive, and aligned collective effort.
Teen Town Halls are one of Network Connect’s efforts to prepare and include young people in community engagement. Teen Town Halls provide a reciprocal learning and development process in which teens learn how to express community level needs and concerns and where community partners and concerned resident learn from the teens. They provide an opportunity for teens to lead civic action, which is critical to crafting relevant and effective interventions. Hosted by FCC participants, teens plan each part of these events. In brief, they select a theme, research the topic, advertise the Town Hall, and facilitate the connection circles. They also report on the different thoughts, ideas, and perspectives shared at the Teen Town Halls, as well as plan activities for follow up action. Topics have included mental health in and out of school settings; gun violence at the local and international levels; systemic racism; community, local and national social environments; community events; teen engagement; social media; and parental relationships. Local community leaders often attend, supporting and learning from tomorrow’s leaders as they present ideas and solutions addressing today’s challenges.
From 2021-2023, Network Connect successfully implemented the Community Well Being Initiative (CWBI) pilot. Key to the success of the CWBI initiative are the Community Well-Being Ambassadors (CWAs). CWAs are community members with social capital who provide guidance and support to individuals, youth, families, and communities using evidence-based and evidence-informed practices. The primary intervention used by the CWA’s is Skills for Psychological Recovery, an intervention designed to assist residents impacted by disasters and found effective for assisting residents living in low resourced communities in need of substance abuse, mental health, housing and/or other services.14 This workforce development model combines social theory with foundational principles of process improvement methodology. The model is based on the belief that those closest to the work, issue, challenge, or in this case community, have the skills, knowledge, and experience to create and implement solutions. In the first full pilot year, Network Connect’s CWA program delivery included more than 4,000 direct points of engagement with community members. Over a thousand (1,079) community members have engaged with Ambassadors since May 2021 with 6,890 total interactions. The interactions underscore the multiple and continuous engagement the CWAs have with individuals as they navigate systems and services necessary to meet their needs. In addition, 880 Naloxone kits were distributed, and 888 community members were trained on the administration of Naloxone. In New Castle County, 91% of Community Members engaged have received at least one SPR skill. Since October 2022, in Kent County, 869 individuals have been engaged for a total of 1,298 interactions. Ninety percent of participants reported living in the 19901 or 19904 zip code. At least one SPR skill was used in 92% of encounters. The collective impact partners and grassroot host site organizations have demonstrated their ability to replicate the model and their ability to be nimble and agile to the services delivery in response to the changing needs of the community.
To be effective, however, the collaborative effort also targets intangibles, such as a sense of safety, emotional regulation, and social norms. The ability to support someone as they expand their individual, social, and community norms becomes the distinguishing feature of effective intervention. Community organizations, including grassroots organizations, are in a unique position to provide guidance and support. Our work requires us to learn how people interact with their environments at all levels, requiring us to collaborate and share insights and information at a deeper level than a “one and done” approach to providing services. We must grow our interpersonal skills to ensure we and our programs are caring, supportive, and understanding of human growth and development. This collective is extremely committed to the community and community-driven work to build capacity and resilience. Together, we are changing how services are coordinated and delivered, making the service delivery system more response to the needs of residents. When the service delivery system includes community organizations working in partnership with each other and government agencies to address the social determinants, the root causes of violence are interrupted and communities become more resilient and thrive.
TRANSLATIONAL & COLLECTIVE ACTION ACTIVITIES: FROM RESEARCH FINDINGS TO ACTION
The Wilmington Community Advisory Council, in partnership with Delaware State University, Center for Structural Equity, Network Connect, MOMS Demand Action, and the Coalition for a Safer Delaware hosted a three-part series on developing collective action solutions to reducing gun violence in Wilmington, Delaware. The effort was grounded in the four-city study examining gun possession among young African American males living in high crime, high violence cities.
The first session of the series focused on a presentation of the study design and findings. The study was coordinated and managed by the Thurgood Marshall College Fund with funding from the National Collaborative on Gun Violence Research. A more detailed description of the study and its findings are presented in the American Journal of Qualitative Research, titled Unlocking Gun-Violence Solutions: The Necessity and Power of Lived Experience15 and summarized in the Dillard et al article, titled Understanding the Perception of Place and Its Impact on Community Violence, included in this DJPH issue. For the collective action presentations, findings specific to Wilmington, Delaware were presented. The presentation included an overview of the study methodology and a description of the Wilmington study group. Ninety-three interviews were completed in Wilmington and responses from 81 were included in the analysis. The average age of respondents was 18 years old with over half (56%) between 15 and 17 years old. Two-thirds of all the respondents and 88% of the juvenile respondents lived with their mother and siblings. Only 12% of those no longer in high school and 80% of all the respondents reported liking school. Few (14%) reported a mental health condition and fewer (9%) reported being in foster care.
All of the young men we interviewed either possessed or had possessed a gun. The majority (86%) were exposed to guns before they were fifteen years old, with 43% younger than ten when they were exposed to guns. A family member or close friend
introduced most (over 90%) of them to guns and 77% were fifteen or younger when they possessed their own gun. Most (94%) knew someone who had been shot and 81% had a family member who had been killed by a gun. For a large majority, the exposure to gun violence occurred before they were 15 years old. The Wilmington respondents described themselves as “smart,” “chill,” and “funny.” They described Wilmington as “rough,” “violent,” and “dangerous.” One respondent said the city is “broken,” and several said it was unsafe for children and not a place to raise a family. Their greatest challenges and pressures were school and money. Most have modest dreams for the future centering around taking care of their family, including having a decent income, a house, and a car. Yet most noted the lack of opportunities to pursue these dreams. The presentation concluded with six recommendations:
1)address systemic inequities;
2)improve police training and community-police relations;
3)increase community involvement in gun research;
4)enact data driven gun law reform;
5)implement behavioral interventions; and
6) increase political will and understanding of the context in which gun violence occurs.
As is frequently the case, there was not adequate time after the presentation to discuss and reflect on the findings. In response to requests for further discussion, the series coordinating group met to discuss the best format to follow up on the study presentation. The follow up offered an opportunity to bridge the research-practice gap by translating the research findings into the community context. Community members’ continued discussion and translation of research findings is fundamental component of community engaged research. Community members, advocates and stakeholders bring deeper meaning to the study findings, adding greater contextual perspective necessary for relevant and effective responses. Without the intentional community guided conversations, solutions for any social issue will have limited impact on individuals and communities at greatest risk.
To meet this goal, the series coordinating group planned for two reflection sessions focused on four of the six recommendations from the gun possession study: improve police training and community-police relations; increase community involvement in gun research; enact data driven gun law reform; and, implement behavioral interventions. Two of the recommendations were not addressed. There was consensus within the coordinating group members that the first recommendation, address systemic inequities, was embedded in the other recommendations and, thus, would be considered across the other recommendations. The coordinating group also agreed that increasing the political will and understanding was beyond the scope of the current effort.
Both reflection sessions were facilitated by Network Connect, using its connection circle model. The first reflection session was designed for community members, allies, and advocates to understand the study findings through the lens of their experiences and providing an opportunity for adult community members and other stakeholders to connect “heads and hearts.” In the connection circles, participants reflected on the study’s recommendations, identified actions already underway and gaps that exist, and brainstormed possible solutions to address the gaps. A second reflection
session focused on teens. It was organized by Network Connect’s Future Culture Creators as a Teen Town Hall and provided an opportunity for the teens to talk about gun violence from their perspective and identify possible solutions. The FCC teens compiled the responses across the connection circle topic discussions and provided the coordinating group with an overview, including recommended actions.
The coordinating group used the results and recommendation from both reflection sessions to guide action. The Wilmington Community Advisory Council convened the partners to translate the findings from the reflections into concrete actions to be taken. Each partner chose the actions they would work on. As of this writing, Network Connect and MOMS Demand Action are implementing a gun safety and safe storage educational awareness campaign with parents, teens, and community members using the curriculum developed by the Be Smart for Secure Gun Storage organization.16 WCAC is working with Network Connect, Minds In Motion, MOMS Demand Action, and the Department of Services for Children, Youth and their Families in developing a community of practice with grassroots organizations to embed and strengthen trauma informed practice within their organizations’ standard operative procedures, conduct on-going professional development with their staff, and work together to hold educational healing experiences for community members. At the community level, the WCAC is working with those partners to implement a trauma education awareness campaign to provide educational and healing experiences through workshops for parents, teens, and other community members on recognizing the signs of trauma, including how parents could talk with their children/teens, how to process emotions, and how to connect to community resources for help. Lastly, the Coalition for a Safer Delaware is working with Network Connect to mobilize teens to advocate for gun law reform through legislation being considered in the Delaware General Assembly.
CALL TO ACTION
To address the multiple and varied factors associated with gun violence reduction and prevention, a collective effort is required. However, implementing a collective impact approach is frequently less clear. In this article, we described one collective action process to address gun violence. This process coupled with other efforts by the partners mentioned and others, Delaware has experienced recent success in reducing gun violence. According to recent statistics, gun violence fell by 20% since 2020 with 300 fewer shootings, with shootings during the summer decreased by almost 40%.17 Collaboration across sectors including legislation, partnerships, funding, education, advocacy, and community programs, have positively impacted Delaware. These improvements highlight the importance of continuing investment in local organizations, including nonprofit service agencies, grassroots agencies, coalition, and partnerships, to ensure programs are innovative, responsive, and flexible to individual, family, and community needs. Community organizations provide vital connections to community members that in turn, instill hope, opportunity, and a belief in a future that drives impact. It is a big lift to change systems, services, values, and culture. It truly takes a village and requires a willingness from all of us to transform.
We must continue to reflect upon the tragedies and traumas that impact our communities. The victims, perpetrators, witnesses, first responders, and others directly and indirectly impacted by the violence provide insight. We must understand how we can improve and expand collaborative strategies and frameworks, and invest in the intangibles, knowing that a sense of hope can lead to impact. There is neither time nor benefits for clinging to territorial and competitive strategies. Change requires persistence, and investment across micro and macro systems. We must commit to this work knowing it affects us all. We must stay involved, capitalizing on opportunities and information to advance our work. As the late statesman John Lewis encouraged us, we must continue to make good trouble to have a collective impact.
Dr. Dillard may be contacted at ddillard@desu.edu
FUNDING ACKNOWLEDGEMENT
This work was supported by the National Collaborative on Gun Violence Research under Grant titled Dangerous Recipe: Ingredients Contributing to African-American Gun Violence.
REFERENCES
1. Krug, E. G., Dahlberg, L. L., Mercy, J. A., Zwi, A. B., & Lozano, R. (2002). World report on violence and health. World Health Organization. https://iris.who.int/handle/10665/42495
2. Dahlberg, L. L., & Krug, E. G. (2002). Violence: a global public health problem. In: Krug, E.G., Dahlberg, L.L., Mercy, J.A., Zwi, A.B., Lozano, R., eds. World Report on Violence and Health. Geneva, Switzerland: World Health Organization, 2002, 1-21.
3. Forum on Global Violence Prevention. (2013, Feb). Contagion of violence: Workshop summary. Washington (DC): National Academies Press (US). Available from: https://www.ncbi.nlm.nih.gov/books/NBK207245/
4. Public Law 104–208, 104th Congress. 110 STAT. 3009. https://www.congress.gov/104/plaws/publ208/PLAW-104publ208.pdf
5. Smart, R., Morral, A. R., Smucker, S., Cherney, S., Schell, T. L., Peterson, S., . . . Gresenz, C. R. (2023, Jan). The science of gun policy: A critical synthesis of research evidence on the effects of gun policies in the United States. RAND Corporation (Third ed.). https://www.rand.org/pubs/research_reports/RRA243-4.html
6. Subbaraman, N. (2020, January). United States to fund gunviolence research after 20-year freeze. Nature, 577(7788), 12. https://doi.org/10.1038/d41586-019-03882-w
7. Consolidated Appropriations Act of 2023, H.R. 2617. (2023) https://www.congress.gov/bill/117th-congress/house-bill/2617
8. American Public Health Association. (2018, November 13). Violence is a public health issue: Public health is essential to understanding and treating violence in the U.S. Retreived from: https://www.apha.org/policies-and-advocacy/public-healthpolicy-statements/policy-database/2019/01/28/violence-isa-public-health-issue
9. Kania, J., Williams, J., Schmitz, P., Brady, S., Kramer, M., & Juster, J. S. (2021). Centering equity in collective impact. Stanford Social Innovation Review, 20(1), 38–45. https://doi.org/10.48558/RN5M-CA77
10. Jones, A. (2014, Dec 9). Murdertown USA (aka Wilmington DE). https://www.newsweek.com/2014/12/19/wilmington-delawaremurder-crime-290232.html
11. Sumner, S., Mercy, J., Hills, S., Maenner, M., & Socias, C. (2015, Nov 3). Elevated rates of urban firearm violence and opportunities for prevention – Wilmington, Delaware: Final report. Retrieved from: https://www.dhss.delaware.gov/dhss/cdcfinalreport.pdf
12. National Center for Injury Prevention and Control, Division of Violence Prevention. (2021, Nov 10). Strategies and approaches to prevent youth violence. Retrieved from; https://www.cdc.gov/violenceprevention/youthviolence/prevention.html
13. Community Based Public Safety Collective. (2022, Aug). Landscape analysis report for city of Wilmington, Delaware. Retrieved from: https://www.wilmingtoncitycouncil.com/wp-content/uploads/2022/09/ Landscape-Analysis-Report-.pdf?mc_cid=b85eedb02c&mc_ eid=2b015dc959
14. Berkowitz, S., Bryant, R., Brymer, M., Hamblen, J., Jacobs, A., Layne, C., . . . Watson, P. National Center for PTSD and National Child Traumatic Stress Network, Skills for Psychological Recovery: Field Operations Guide, 2010. Available on: www.nctsn.org and www.ptsd.va.gov
15. Dillard, D., Henderson, H., Mangum, M., Rice, I. I. J., & Goldstein, A. (2023). Unlocking gun-violence solutions: The necessity and power of lived experience. American Journal of Qualitative Research, 7(4), 182–202. https://doi.org/10.29333/ajqr/13729
17. Mitman, H. (2024, Jan 29). Delaware saw lowest violent crime rate on record in 2023, officials say. NBC Philadelphia. Retrieved from: https://www.nbcphiladelphia.com/news/local/del-officials-say-in-2023state-saw-lowest-violent-crime-rate-on-record/3760140/
PUBLIC HEALTH ESSENTIALS FOR
HEALTH DEPARTMENTS
2024 WEBINAR SERIES
The Public Health Management Corporation (PHMC), in partnership with the Public Health Infrastructure Grant network, National Association of County and City Health Of cials (NACCHO), and the Pennsylvania Public Health Association (PPHA), is offering a series of monthly webinars that will address essential public health concepts, models, resources, and processes. The webinars are developed speci cally for governmental public health departments and their staff to be used as professional development opportunities through the live webinar presentation, but also via leveraging the webinar recording and/or slides (to be shared after the live webinar) as in-house training materials for newly hired staff in health department settings. This series will feature a variety of public health speakers and health department voices. Tune in to learn more about the valuable role of health departments in shaping and supporting their communities.
MARCH
PUBLIC HEALTH FOCUS AND FRAMEWORKS, PART 1
Delve into the foundational concepts of public health and how they link together and support one another. Included are public health de nitions, the social determinants of health, the ten Essential Public Health Services, and Foundational Public Health Services.
PUBLIC HEALTH FOCUS AND FRAMEWORKS, PART 2
Explore additional foundational concepts of public health and how they link together and support one another. Included are Public Health 3.0, Health in All Policies, and health equity.
PUBLIC HEALTH DEPARTMENT ACCREDITATION: AN INTRODUCTION
Learn the basics of public health department accreditation. Included are an overview of the process, requirements, and bene ts as well as types of required document, tips for preparation, minimum prerequisites, and accreditation preparation best practices.
APRIL
COMMUNITY ENGAGEMENT: HEALTH DEPARTMENTS’ LIFEBLOOD
Examine the “why and how” of health departments’ engagement with their communities. Included are models of the continuum of community engagement, tools and processes to engage with the community, and how a health department can create a department culture that values and practices community engagement.
MAY HEALTH EQUITY
Gain a deeper understanding of the core concepts of health equity, how to incorporate equity into everyday practices, and approaches to facilitating meaningful change in communities and within the public health workforce. This session will present frameworks for using a culturally responsive and racial equity lens in public health practice.
PUBLIC HEALTH ESSENTIALS FOR HEALTH DEPARTMENTS
2024 WEBINAR SERIES
MAY
RESOURCES FOR PUBLIC HEALTH PROGRAM DEVELOPMENT AND DATA
Discover national information resources for the design and development of local public health interventions and programs. Included are governmental and non-governmental national sources for models and examples of programs, and national and state sources of local data.
JUNE
PUBLIC HEALTH 3.0
Engage in the Public Health 3.0 conceptual framework for the future of public health. Included are a discussion of the concept of Public Health 3.0, the importance of the health department being a community health strategist, and recommendations for promoting effective public health agencies.
JULY
COMMUNITY HEALTH ASSESSMENT AND COMMUNITY HEALTH IMPROVEMENT PLAN: FOUNDATIONS OF CREATING A HEALTHY COMMUNITY
Hear how the community health assessment and improvement plan development processes provide the focus and foundation for community partnerships for a healthy community. Included are the importance and value of the process, key elements of the process, the importance of community assets as well as challenges, and the accreditation requirements for these two documents and processes.
AUGUST SOCIAL ISOLATION AND LONELINESS
Enter into a discussion on how isolation and loneliness is a public health issue, the different forms and signi cance of social connections in buffering experiences of loneliness, and evidence-based interventions (both for in communities and within health departments). This webinar will have a special focus on New Jersey’s approach to coordinating public health partners in addressing isolation and loneliness as a public health issue.
Celebrating Fifty Years of Crime Victims’ Compensation in Delaware
Paige J. Schmittinger, J.D.
Executive Director, Delaware Victims’ Compensation Assistance Program
Today, all 50 states, the District of Columbia, Puerto Rico, the U.S. Virgin Islands, and Guam are in agreement that victims of violent crime should have a standardized way of mitigating financial hardships that result from their victimization. This is accomplished through state-sponsored victims compensation programs. The first such program was implemented by California in 1965. Delaware was an early adopter of this notion, legislatively creating its program on July 18, 1974.
Fifty years ago, the Delaware Legislature made clear this law’s purpose was, “to promote the public welfare by establishing a means of meeting the additional hardships imposed upon the innocent victims of certain crimes, and the families and dependents of those victims.”1 Though the organizational form for delivering compensation to these victims has evolved over the past five decades, this mission remains as true now as when it was proclaimed in 1974.
The 1974 legislation created the Victim Compensation Fund and the Delaware Violent Crimes Compensation Board, which began operations in 1975. The Board consisted of five Governor-appointed members and provided tens of millions of dollars in compensation to tens of thousands of victims of crime until 2009. Following a Legislative Sunset Review during fiscal year 2009, the Violent Crimes Compensation Board was restructured into what is now the Victims’ Compensation Assistance Program (“VCAP”). Operations moved to the Department of Justice and the Program is currently staffed by eight full-time employees. This statewide initiative remains an important part of Delaware’s approach to justice by supporting victims of violent crime and their families. By providing financial compensation for crimerelated expenses, VCAP helps victims rebuild their lives and cope with the aftermath of trauma.
VCAP is funded through a mandatory 18% penalty assessment levied on all fines, penalties, and forfeitures imposed and collected by the courts. To supplement its funding, VCAP annually applies for a federal Office of Victims of Crime grant award, which is calculated at 75% of state compensation expenditures from two years prior. In the 2023 fiscal year, VCAP distributed over $2.3 million in compensation.
Victims of crime must actively apply to VCAP and meet specific eligibility criteria defined by state law. Once an application is submitted, it is assigned to one of four Victim Service Specialists to determine if the applicant is an eligible victim of a qualifying crime. Qualifying crimes are determined by state statute, but the rule of thumb is violent crimes are covered and property crimes are not.2 Generally,
to be eligible for victims’ compensation, victims must report the crime to law-enforcement or another appropriate governmental agency within 72-hours of the occurrence, except in instances of domestic violence or sexual assault.3 Additionally, victims must file their application with VCAP within one year of the date of the crime.4 Both of these requirements are waivable at the discretion of the Executive Director. Lastly, victims must give “reasonable cooperation” to state or local-law enforcement.5
Once an application is determined to be eligible for compensation, the Victim Service Specialist works with the applicant to determine what compensation can be provided. VCAP can only provide compensation for pecuniary loss which is defined as “expenses actually and necessarily incurred as a result or personal injury or death resulting from a crime, but it does not include property damage.”6 VCAP cannot provide compensation for pain and suffering. There is a monetary limit of $25,000 per victimization; however, some specific types of compensation have lower monetary caps. The compensation types available are prescribed by state law and include expenses such as medical, mental health counseling, funeral, personal safety property, relocation, and loss of income.6
Recently, there has been a national movement to make compensation programs accessible to more victims of crime. Historically, there have been “bright-line” rules mandating that crime victim compensation applications be denied under certain circumstances. Delaware was no exception. However, in 2021, state legislation was introduced with the goal of eliminating the restrictive requirements and opening up access to the program to a broader population of victims, including victims of human trafficking.7 This legislation was signed into law on October 21, 2021. Simultaneously, there is a national movement toward reducing or eliminating fines and fees for offenders. This delicate balance between funding victim services through fines and fees and protecting offender rights is an ongoing challenge in criminal justice reform. Awareness and legislative support are crucial for the continuation and expansion of VCAP’s services. By understanding and advocating for resources like VCAP, we can collectively enhance the safety net for victims, paving the way for their recovery and empowerment.
Additionally, community awareness is a crucial part of VCAP’s mission. Outreach programs, educational campaigns, and partnerships with community organizations can enhance awareness and understanding of VCAP’s services and eligibility requirements. Initiatives such as enhancing multilingual support and accessibility features in the
application process can ensure that all victims, regardless of background or language proficiency, can access VCAP’s resources. As VCAP works to anticipate the needs of violent crime victims, the integration of innovative partnerships could mark the next chapter in comprehensive victim support. For example, VCAP has partnered with the EVOLV (Empowering Victims of Lived Violence) hospitalbased intervention program at ChristianaCare to ensure violent crime victims who have been treated in the trauma department can successfully access victims’ compensation in a trauma-informed way.
As VCAP commemorates 50 years of service, it stands as a testament to Delaware’s unwavering commitment to supporting victims of crime. Through innovative approaches, community engagement, legislative advocacy, and rigorous evaluation, VCAP will continue to evolve and expand its reach, ensuring that victims receive the support and assistance they need to rebuild their lives and pursue justice.
For more information on the Victims’ Compensation Assistance Program or to download a brochure or application, please visit https://attorneygeneral.delaware.gov/vcap/ Applications can also be submitted through VCAP’s online application portal by visiting https://ccvcde.org.
Ms. Schmittinger may be contacted at paige.schmittinger@delaware.gov
REFERENCES
1. H.B. 127, 127th Gen. Assemb., Reg. Sess. (Del. 1974).
2. Del. Code Ann. tit. 11, § 9002(6).
3. Del. Code Ann. tit. 11, § 9010(5).
4. Del. Code Ann. tit. 11, § 9010(4).
5. Del. Code Ann. tit. 11, § 9010(3).
6. Del. Code Ann. tit. 11, § 9002(10).
7. H.B. 182, 151st Gen. Assemb., Reg. Sess. (Del. 2021-22).
CDC updates recommendations for COVID-19 and respiratory viruses
Recently, the Centers for Disease Control and Prevention (CDC) made several changes to its guidance for COVID-19 and other respiratory viruses. At the end of February, the CDC recommended that adults 65 years of age and older receive an additional updated 2023-2024 COVID-19 vaccine dose if it has been at least four months since their last dose CDC noted that adults 65 years and older are disproportionately impacted by COVID-19, with more than half of COVID-19 hospitalizations from October 2023 to December 2023 coming from that age group Now, those 65+ and people who are immunocompromised are eligible for additional doses to restore protection that might have waned since their last dose and help prevent severe illness. With an updated version of the vaccine expected late this summer or early this fall, now is the time for those eligible to update that protection.
The CDC also made its COVID-19 prevention and isolation guidance consistent with that of all respiratory viruses. The Division of Public Health’s (DPH) messaging aligns with the CDC’s: to get vaccinated; stay home if you are sick and get tested; if you test positive, seek treatment; and consider masking and other extra measures if cases are high or you or someone close to you is at high risk for illness. Sick individuals should stay home for at least 24 hours after they are fever-free and their symptoms improve without fever-reducing medications. Then, for the next five days, they should take added precautions such as masking and distancing in public.
For more respiratory virus-related information, visit DPH’s de.gov/coronavirus and flu.delaware.gov sites.
April is National Donate Life Month
Over 400 Delawareans are awaiting organ transplants, yet less than 50% of Delawareans are registered donors, according to Donate Life Delaware Eight or more lives can be impacted by one organ donor, and hundreds of lives can be impacted by one tissue donor, says the Gift of Life Donor Program, a 501c(3) non-profit organization.
Individuals who apply for or renew a Delaware driver’s license or identification card can sign up to become an organ and tissue donor by submitting a protected online application to the Delaware Division of Motor Vehicles (DMV) Applicants receive a red heart on their license as their driver’s record is updated. The donor designation may not be revoked according to state law. DMV suggests that donors inform their family of their decision to avoid confusion at death.
Each potential donation is considered individually. While some organs or tissue may be compromised by illness or age, others may provide healthy, viable donations. Illicit drug use or overdose death does not prevent someone from being a donor.
Learn more about organ and tissue donation at donatelife-de.org
Governor’s Office seeks nominees for Compassionate Champion Awards
Nominations are open for the State of Delaware Compassionate Champion Awards. The Compassionate Champion Awards recognize individuals, organizations, and educational institutions across the State of Delaware that provide trauma-informed services in a manner consistent with the Delaware Developmental Framework for TraumaInformed Care.
Nominations must be submitted on the Governor’s website by 5:00 p.m. on Friday, April 12, 2024. Award winners and details for the recognition ceremony will be announced at a later date. For award categories and nomination forms in English and Spanish, visit Delaware.gov
April is Cancer Control Month and Minority Cancer Awareness Month
Governor John Carney and Lieutenant Governor Bethany Hall-Long declared April as Cancer Control Month and Minority Cancer Awareness Month. They urge Delawareans to get screened for cancer when advised to do so and encourage health care providers to promote cancer screening as a powerful opportunity to save lives.
Detecting cancer early improves survival rates
According to the Delaware Cancer Registry, for 2016-2020, 22.4% of new cancer cases in Delaware were detected in the distant stage, compared to 48.3% diagnosed at the local stage, when cancer is most treatable. In Delaware, for 2016-2020, breast cancer was the leading cause of cancer death among women, prostate cancer was the leading cause of cancer death among men, and lung cancer was the leading cause of cancer death among men and women, according to the Delaware Cancer Registry.
Only 12% of eligible Delawareans met the U.S. Preventive Services Task Force lung cancer screening recommendations, according to the 2022 Behavioral Risk Factor Survey.
The Delaware Cancer Consortium at the DPH Bureau of Cancer Prevention and Control work to ensure every Delawarean has access to timely cancer screenings and cancer treatment if they cannot afford it. Cancer screenings are covered by insurance or by the State’s Screening for Life (SFL) Program. Delawareans can determine their eligibility for SFL by visiting Healthy Delaware.org or calling SFL at 302-744-1040.
Inequities can be observed in cancer data by race and ethnicity. According to the Delaware Cancer Registry, for 2016-2020, the all-site cancer mortality rate among non-Hispanic Black Delawareans (171.7 people per 100,000 population) was higher than for non-Hispanic White Delawareans (158.9 people per 100,000 population).
For 2016-2020, 28.3% of new breast cancer cases were detected in the distant stage among nonHispanic White Delawareans, compared to 36.7% diagnosed at the distant stage among non-Hispanic Black Delawareans. For the same period, the prostate cancer mortality rate among non-Hispanic Black Delawareans (32.6 people per 100,000 population) was double the rate of non-Hispanic White Delawareans (15.7 people per 100,000 population).
Birth to Three Program accepting public comment on formula grant until May 1
Delaware’s Birth to Three Early Intervention Program invites interested parties to participate in public comment for their FFY2024 grant application to the Office of Special Education Programs (OSEP). The opportunity for public comment on the draft application is available for 30 days from April 1 to May 1, 2024.
Birth to Three helps Delaware families with infants and toddlers, from birth to age 3, by providing early intervention services for eligible children with developmental delays or disabilities. OSEP is dedicated to improving results for infants, toddlers, children, and youth with disabilities ages birth through 21 by providing leadership and financial support to assist states and local districts.
The Individuals with Disabilities Education Act (IDEA) Part C program promotes the development of infants and toddlers with delays or disabilities, enhances the capacity of families to meet the developmental needs of their infants and toddlers, minimizes the need for special education and related services when children enter school, and enhances children’s long-term outcomes.
The IDEA of 2004 authorizes formula grants to be awarded to states annually to support early intervention services for infants and toddlers with disabilities and their families. OSEP reviews and approves state plans and monitors the IDEA C formula grant programs to ensure consistency with federal requirements. Each year, Delaware’s Birth to Three Early Intervention program reapplies for their formula grant. Access this year’s grant application here: www.b23de.org under Part C Reports & Data. Comment by clicking here: Comment Form.
Photo: Birth to Three Program
Advancing Healthy Lifestyles Conference is June
6 in Dover
The Division of Public Health’s Physical Activity, Nutrition, and Obesity Prevention (PANO) Program is hosting its annual Advancing Healthy Lifestyles (AHL) Conference: Engaging Communities to Live Healthy Lifestyles on June 6, 2024. The conference will be held from 8:00 a.m. to 4:00 p.m. in the Martin Luther King, Jr. Conference Center at Delaware State University, located at 1200 N. Dupont Highway in Dover, Delaware
The AHL Conference will provide a platform for cross sectional sharing on national, regional, and local best practices, challenges, opportunities, and success stories. With a focus on engaging communities to live healthy lifestyles and advancing health equity, the conference aims to strengthen efforts to reduce obesity and other chronic diseases. The Conference will provide participants with skills and knowledge in a variety of public health topic areas to bring chronic disease and obesity prevention into their communities.
Participants will have the opportunity to attend presentations from subject matter experts and network with others in the field. The Advancing Healthy Lifestyles Conference will serve as an opportunity to close gaps in health inequities, assess progress, and further strengthen the work of community stakeholders.
The keynote speaker is Jackie Joyner-Kersee, who is known for her athletic achievements in the heptathlon and long jump events. Joyner-Kersee earned six Olympic medals (three gold, one silver, and two bronze) and four World Champion titles over four consecutive Olympic Games. Joyner-Kersee was the first woman in history to earn more than 7,000 points in the heptathlon, and today, over 20 years later, she still holds the world heptathlon record of 7,291 points. She continues to hold the Olympic and national records in the long jump and her 1994 performance remains the second longest in history.
All individuals interested in health disparities, nutrition, chronic illness, and obesity prevention are invited to attend. To learn more and to register, visit the Conference website
U.S. DOT seeks public comment on rule for wheelchair airline standards
The Division of Public Health’s Bureau of Health Equity shared news from Kristin Harvey, Executive Director of the Delaware Developmental Disabilities Council. The U.S. Department of Transportation (DOT) seeks public comments on a new proposed rule designed to ensure airline passengers who use wheelchairs can travel safely and with dignity.
The proposed rule would set new standards for prompt, safe, and dignified assistance; require enhanced training for airline employees and contractors who physically assist passengers with disabilities and handle passengers’ wheelchairs; and specify actions that airlines must take to protect passengers when a wheelchair is damaged during transport. The proposed rule would require airlines to provide two options to repair or replace wheelchairs if mishandled by the airline.
DOT also requests input on two other topics: lavatory size on twin-aisle aircrafts and reimbursement of the fare difference between a flight someone could have taken if their wheelchair fit in the aircraft and the more expensive flight they had to take instead.
An estimated 5.5 million Americans use a wheelchair Many encounter air travel barriers. In 2023, 11,527 wheelchairs and scooters were mishandled by carriers required to report data to DOT.
Comments can be submitted online, by mail or fax, or hand-delivered through May 13, 2024. Read DOT’s press release for a summary of key provisions.
Jackie Joyner-Kersee
Photo: Getty Images
Rights of Crime Victims in Delaware
Delaware has a Victims’ Bill of Rights (Chapter 94 of Title 11 of the Delaware Code) that entitles a victim to be notified of and participate in all major phases of a criminal case. This is a summary of the rights provided victims of crime in Delaware.
When A Crime Is Reported:
At the initial contact with law enforcement , the victim shall be provided:
an explanation of the victim’s rights
information concerning the availability of social service and other victim assistance
a copy of the initial report
notice of available victim services
information about the Violent Crimes Compensation Program that may provide reimbursement or payment of costs associated with being a crime victim
information concerning pre-trial release (bail) of the defendant
an agency contact to allow the victim to check the status of any arrest.
Unless a victim or witness waives confidentiality in writing, or as ordered by a court for good cause, a law-enforcement agency, the Attorney General’s Office, or Corrections Department may not disclose, except among themselves or as authorized by law, the residential address, telephone number or place of employment of the victim or a member of the victim’s family
The Prosecution Process:
A victim shall be notified by the Attorney General’s Office of the schedule of events involved with the prosecution of the defendant.
A victim may be present at the trial and the sentencing of the defendant, unless the judge in the case rules otherwise
The prosecutor assigned to your case must consult with you prior to trial
Court proceedings shall be expedited in cases involving a child victim or witness, particularly in child abuse and sexual abuse cases
The court shall try to minimize the victim’s contact with the defendant, defendant’s relatives, and defense witnesses during court proceedings
A victim’s employer may not discipline the victim for participation in the prosecution process when the participation is requested by the Attorney General’s office
The prosecutor will contact you to discuss any proposed plea agreement
The Attorney General’s office will notify you of the crimes for which the defendant was convicted and the specifics of the sentencing order
A victim shall have any property seized as evidence promptly returned when it is no longer needed for evidentiary purposes, unless it is contraband or subject to forfeiture
A victim has the right to be present at trial and sentencing.
After A Conviction:
If the defendant appeals after being convicted, the Attorney General shall promptly inform a victim of the date, time, and place for any hearing and of the decision once it is made by the court
For a defendant sentenced to prison, a victim must be notified of the release date or any parole hearing
Attempts will be made to locate and notify a victim if a convicted individual applies for a pardon, and a victim may address their position to the Parole Board or Board of Pardons.
GLOBAL HEALTH MATTERS
GLOBAL HEALTH MATTERS
MAR/APR 2024
Studying the risk factors for cancer in Mexico ... p.
Studying the risk factors for cancer in Mexico ... p.
NIH working group issues update on equitable research
NIH working group issues update on equitable research
A new update from an internal NIH working group describes several current initiatives that promote equity across its global health research activities. Among the highlights is Fogarty’s own plan, begun just last year, to provide current grant recipients with additional funding to promote diversity, equity, and inclusion (DEI) in research training programs. Fogarty earmarked more than $1.7 million to distribute to currently funded grants. Recipients have used the funds to support the training of: health workers from the semi-nomadic Turkana tribe in Kenya; indigenous, Quechua-speaking neuroscientists in Peru; women working as junior faculty in trauma and injury research in the Middle East; and junior and mid-career scientists from underrepresented minorities in India.
A new update from an internal NIH working group describes several current initiatives that promote equity across its global health research activities. Among the highlights is Fogarty’s own plan, begun just last year, to provide current grant recipients with additional funding to promote diversity, equity, and inclusion (DEI) in research training programs. Fogarty earmarked more than $1.7 million to distribute to currently funded grants. Recipients have used the funds to support the training of: health workers from the semi-nomadic Turkana tribe in Kenya; indigenous, Quechua-speaking neuroscientists in Peru; women working as junior faculty in trauma and injury research in the Middle East; and junior and mid-career scientists from underrepresented minorities in India.
The NIH Global Health Research Equity Working Group has representatives from nine NIH Institutes and Centers and a mission to encourage and enable global research collaborations grounded in a shared vision among all partners, with equitable input and decision-making throughout the research process. NIH established the group and issued a request for information (RFI) in 2021.
The NIH Global Health Research Equity Working Group has representatives from nine NIH Institutes and Centers and a mission to encourage and enable global research collaborations grounded in a shared vision among all partners, with equitable input and decision-making throughout the research process. NIH established the group and issued a request for information (RFI) in 2021.
Some of the feedback to the RFI included: a lack of training in grants management as a barrier to applying for and administering NIH grants and concerns that NIH's peer review process potentially reflects reputational and
Some of the feedback to the RFI included: a lack of training in grants management as a barrier to applying for and administering NIH grants and concerns that NIH's peer review process potentially reflects reputational and
seniority bias. The Working Group noted a National Institute of Allergy and Infectious Diseases grant program that supports advanced training in NIH grants policy, financial management, and compliance, and highlighted NIH's new Simplified Peer Review Framework, slotted to go into effect in January 2025, which focuses on the scientific and technical merit of grant applications with the investigator's expertise and resources rated solely on whether they are sufficient to conduct the research.
seniority bias. The Working Group noted a National Institute of Allergy and Infectious Diseases grant program that supports advanced training in NIH grants policy, financial management, and compliance, and highlighted NIH's new Simplified Peer Review Framework, slotted to go into effect in January 2025, which focuses on the scientific and technical merit of grant applications with the investigator's expertise and resources rated solely on whether they are sufficient to conduct the research.
The Working Group also acknowledged that equitable global research is an on-going effort. Accordingly, it's been developing next steps to address the barriers and challenges cited in the RFI.
The Working Group also acknowledged that equitable global research is an on-going effort. Accordingly, it's been developing next steps to address the barriers and challenges cited in the RFI.
Barmes Lecture returns June 5
Barmes Lecture returns June
5
The Fogarty International Center and the National Institute of Dental and Craniofacial Research (NIDCR) present the David E. Barmes Global Health Lecture 2024: “Global HIV/ AIDS Response: Then, Now, Future,” by Ambassador John Nkengasong, U.S. Global AIDS Coordinator and Special Representative for Global Health Diplomacy. The lecture will take place on Wednesday, June 5 at 1 p.m. ET (USA) on the NIH campus and virtually. Information can be found at https://go.nih.gov/Barmes2024.
The Fogarty International Center and the National Institute of Dental and Craniofacial Research (NIDCR) present the David E. Barmes Global Health Lecture 2024: “Global HIV/ AIDS Response: Then, Now, Future,” by Ambassador John Nkengasong, U.S. Global AIDS Coordinator and Special Representative for Global Health Diplomacy. The lecture will take place on Wednesday, June 5 at 1 p.m. ET (USA) on the NIH campus and virtually. Information can be found at https://go.nih.gov/Barmes2024.
Fogarty’s G-11 program builds support infrastructure
•Building infrastructure so scientists can focus on research
Fogarty’s G-11 program builds support infrastructure
•Fortifying research ethics at Kinshasa University
•Developing research infrastructure in Nigeria
infrastructure so scientists can focus on research
research ethics at Kinshasa University
research infrastructure in Nigeria
Photo courtesy of Bahare Khodabanda/ Weill Cornell Medicine
In the last four years, two Fogarty mobile health (mHealth) grant recipients have received first-place NIH NTAC awards. The NIH Technology Accelerator Challenge (NTAC), launched by the National Institute of Biomedical Imaging and Bioengineering (NIBIB) in 2020, is a series of prize competitions created to stimulate the design of new diagnostic technologies and accelerate the full development of those products for use in low-resource settings.
Detecting blood disorders with a photograph Dr. Young Kim, professor of biomedical engineering at Purdue University, received a NTAC award in 2020 for his team’s Fogarty-funded project that led to the development of a smartphone application with the ability to detect anemia and sickle cell disease by extracting information about the state of microvasculature and blood hemoglobin from a photo of a patient’s inner eyelid. The algorithm mimics a spectroscope analysis, which detects how hemoglobin absorbs light.
The algorithm was developed over the course of three years through a collaboration with the Moi Teaching and Referral Hospital via the Academic Model Providing Access to Healthcare (AMPATH) program in Kenya. The NTAC award led to the development of HemaChrome, a startup supported by Purdue, which focuses on bringing the technology back to the U.S. for digital health and telemedicine.
principal investigator on a Fogarty-funded project using ML-based mHealth technology to prescreen for malaria among school-age children in Rwanda. If the prescreening tool is successful in this setting, it could provide significant cost savings for mass malaria screenings.
Using AI to monitor postpartum recovery
In 2022, a team led by Dr. Bethany Hedt-Gauthier, associate professor of global health and social medicine at Harvard University and associate professor in the department of biostatistics at Harvard T.H. Chan School of Public Health, and Dr. Fredrick Kateera, deputy executive director of Partners In Health and lecturer at the University of Global Health Equity, Rwanda, won the NTAC Maternal Health award for their Fogarty-funded project.
Since 2016, the team has worked to develop a stand-alone mHealth application for community health workers to monitor postpartum recovery of women who had a cesarean delivery. The tool, recently featured in Science, allows community health workers to provide new mothers with a home-based diagnosis of surgicalsite infections alongside general postpartum monitoring. The app uses computer-vision techniques and AI to detect signs of infection in the photographs of surgical wounds. The team has focused on rural regions of Rwanda, and their machine learning-based algorithms have achieved nearly 90% accuracy in diagnosing infections.
Kim has received additional funding from NIBIB to use machine learning (ML) to assist in spectral recovery, restoring color and light to conventional photos, with a focus on maternal health applications in Kenya. CDC and Kim’s team will soon start a trial using ML photo analysis and mHealth applications to detect fluorosis (overexposure to fluoride) and cavities in the teeth of adolescents. Kim notes that a photograph is more than merely a picture; it contains detailed spectral information that can be used by mHealth applications.
“The initial support from Fogarty triggered a chain reaction of research and I’m so grateful for the ample opportunities that ultimately came from that,” says Kim who is also a
The NTAC award has allowed researchers to flexibly pursue changes needed to scale the application in Rwanda and beyond. Hedt-Gauthier says, “Systems are constantly updating and getting better, so it’s been a learning process for us to understand how we keep up with the pace of that growth.”
Both Kateera and Hedt-Gauthier agree that working in Rwanda over the years has opened their eyes to major gaps in postnatal care, in all settings. The NTAC award has been a great motivation for the team, and, as Kateera says, “it has allowed people to grow and work together around optimizing outcomes for new mothers.”
Purdue University /Vincent Walter
Young Kim (in foreground with his back to the camera) takes a photo with a smartphone of the inner eyelid of study participant.
Fogarty’s impact on display at CUGH 2024
The 15th annual Consortium of Universities for Global Health (CUGH) conference was held March 7–10, 2024, in Los Angeles, California. The conference theme was “Global Health Without Borders: Acting for Impact.”
Fogarty’s first listening session Fogarty hosted its first-ever listening session at CUGH 2024, led by Acting Director Dr. Peter Kilmarx, Acting Deputy Director Dr. Rachel Sturke, and Communications Director Dr. Andrey Kuzmichev. The goal of the session was to gather thoughts and suggestions about global health at NIH going forward. It was also a chance to help Fogarty begin putting together a new strategic plan; the last one was written a decade ago.
Some important topics raised by the group included prioritizing research infrastructure for the health workforce, advocating for research partners in lowand middle-income countries (LMICs), and navigating research in conflict zones.
Creating equitable partnerships in global health In a plenary session centered around how the global health community can work together to balance the playing field between higher- and lower-income countries in all aspects of research, Kilmarx alongside Dr. Patricia García, multiple Fogarty grant recipient and professor at the School of Public Health and Administration at the Universidad Peruana Cayetano Heredia in Peru, Dr. Bethany Hedt-Gauthier, associate professor of global health and social medicine at Harvard University and current Fogarty mHealth grant recipient, Dr. Biraj Karmacharya, director of public health/community programs and global engagement at Dhulikhel HospitalKathmandu University in Nepal, and Dr. Elsie KiguliMalwadde, president of the Fogarty-supported African Association for Health Professions Education and Research (AFREHealth), discussed a broad range of topics including increasing the flow of financial resources to the Global South, restructuring research based on local priorities, elevating the needs of educational institutions in lower-income countries, and advocating for these changes among major global health donors.
Working toward WHO cervical cancer screening goals The National Cancer Institute (NCI) hosted a session on how to integrate the WHO initiative for cervical cancer control into broader global health programs. Dr. Karla Unger-Saldana of Mexico’s National Cancer Institute discussed barriers faced by women in Mexico accessing timely diagnosis and treatment for cervical cancer due to cultural norms prioritizing family needs over their own
health. She also shared how indigenous women often feel disrespected within health care settings, hindering effective care delivery. Another presenter, Dr. Hyo Sook Bae of NCI, noted similar barriers in Korea during her presentation and stated, “Patients have the right to be treated properly, nothing should be preventing them from having proper treatment and living a happy life.”
Studies in implementation science Sturke also led a session about a Fogarty-supported collection of implementation science cases focused on global health and conducted in LMICs, spanning a range of regions and disease areas. Dr. Melisa Paolino of the Center for the Study of State and Society (CEDES) in Argentina presented her assessment of the fidelity of HPV selfcollection tests in low-income areas of that country. While her trial showed that screening and testing for HPV increased from 20 to 85 percent after the introduction of self-screening via community health workers, multiple changes in government administration have made it difficult to implement this strategy on a national level.
LAUNCH in the spotlight At every CUGH conference, current and former Fogarty Global Health Fellows and Scholars from the Launching Future Leaders in Global Health Research (LAUNCH) Training Program present their work to the global health community. A group of seven program trainees shared their research insights, training experiences, and career trajectories, from treating burn injuries in Nepal to working with cancer survivors in Malawi.
Kilmarx commended the LAUNCH trainees, stating, “We’re so impressed by your commitment, creativity, and the diversity of the work that you're doing all over the world.”
Fogarty International Center
From left: Fogarty's Peter Kilmarx, Rachel Sturke, and Andrey Kuzmichev listen to questions from the audience during a listening session at CUGH 2024.
PROFILE
Preventing mother-tochild HIV transmission in South Africa
Dr. Joan Matji conducted her doctoral research through a joint partnership with Yale University and University of Pretoria, South Africa. She focused on the nutritional status of HIV positive mothers and an assessment of infant feeding practices. She observed that, more often than not, the mothers’ needs were neglected by the research.
“I often found that we were not asking, ‘How is mum doing? How is she coping with her status? How is she doing nutritionally?’” These questions are what motivated Matji’s 2005-2006 Fogarty project that investigated associations among postnatal maternal nutritional status, maternal HIV disease progression, and infant feeding practices. Matji’s team focused on what was happening to the new mothers after they’d delivered. They explored the influence of each mother's psychosocial well-being on how she fed her child and the health implications of these choices.
At that time in South Africa, the general recommendation for prevention of mother-to-child transmission suggested clinicians assess whether formula feeding was affordable, safe, and sustainable for each mother. Women who did not meet the criteria were advised to breastfeed exclusively, while the government provided free infant formula for mothers living with HIV. “It perpetuated discrimination and stigma around mothers with HIV in the region because everyone knew that, if you had [the government supplied] orange-colored tin or formula, you were HIV positive,” said Matji.
To better understand women’s childcare choices, she and her team recruited 317 pregnant women with HIV at 28 weeks of pregnancy and a comparative group of about 53 HIV-negative women at the same stage of pregnancy. Most of the pregnant women living with HIV planned to formulafeed, basing their choice on the shame around breastfeeding when HIV-positive. But later, after giving birth, they changed their minds due to the societal stigma around formula feeding. Matji’s team found that the women living with HIV who ultimately decided to follow through with formula feeding had only done so because they had either been incentivized by free formula or encouraged to do so by their physicians.
Joan Matji, PhD Fogarty Scholar: 2005-2006
U.S. institution: Yale University
Foreign institution: University of Pretoria, South Africa
Research topic: Child and maternal health and nutrition
Current affiliation: UNICEF country representative to Botswana, United Nations Children Fund
The data also showed that about 65% of the mothers were overweight or obese at the end of the study. “This was an interesting finding because, at that time, most people assumed somebody who is HIV positive would be malnourished, even emaciated, but this was not the case among these women.” From these findings, Matji and her colleagues began formulating recommendations for holistic interventions to address the stigma around HIV disclosure and infant feeding practices for mothers.
“My training helped me fine-tune the methodologies and approaches that I could use for this research, which was somewhat clinical in nature,” said Matji. “It was a great refresher and I also learned new terminologies.”
Today, Matji serves as UNICEF's Country Representative to Botswana as part of the United Nations Children Fund. In this role, she manages a staff of 22 focused on developing informed nutritional recommendations and health policies for mothers and children under age 5. The team is developing guidelines to ensure adolescents living with HIV adhere to their treatment regimens and working to prevent violence against children, among many other initiatives. “Because of my Fogarty training, I feel better positioned to critique research findings presented to the organization,” said Matji. “I often ask, ‘What are the implications for public policy?”
In the future, she plans to continue advocating for the mothers and children in Botswana and, one day, to get back into research and academia, potentially as a mentor for up-and-coming researchers. Matji advises those entering Fogarty’s LAUNCH program: “Keep an open mind and take advantage of the networking opportunities afforded to you. The bonds I formed in this program and the work I did as part of it were so beneficial to my career.”
A&Q
MARTIN LAJOUS, MD, SCD
Martin Lajous, a medical doctor and epidemiologist, became a researcher at Instituto Nacional de Salud Pública (INSP), Mexico’s National Institute of Public Health, in 2004. At INSP he helped design and develop the Mexican Teachers’ Cohort (MTC) and now serves as its principal investigator. MTC has since become part of the U.S. National Cancer Institute’s (NCI) Cancer Cohort Consortium. Lajous has conceived and taught courses at INSP on cancer epidemiology, causal inference (methodologies and strategies that allow researchers to draw causal conclusions based on data), and implementation science.
How
did you become aware of aflatoxin exposure in Mexico?
Aflatoxin is a proven Group 1 carcinogen (causing cancer in humans), according to WHO. This toxin comes from two fungi, Aspergillus flavus and Aspergillus parasiticus. Aflatoxin often contaminates crops, including maize, a staple food in Mexico, during harvest, processing and storage. Yet aflatoxin was completely under the radar in Mexico.
Now we knew from an NCI group working in Guatemala, the country with the highest burden of liver cancer on the continent, that aflatoxin was an important factor. So, working with this group and a colleague from Johns Hopkins, we took 100 samples from the Mexican National Health and Nutrition Survey—a representative sample of adults living in Chiapas—and sent them to Baltimore to be evaluated. We found that the prevalence of detectable levels of aflatoxin was 86%. By comparison, using the same technique on NHANES data from the U.S., the prevalence is less than 1%. (The National Health and Nutrition Examination Survey is designed to assess and track the health and nutritional status of adults and children in the United States. This unique survey, which began in the 1960s, combines interviews and physical examinations.)
So, we found that, basically, aflatoxin exposure is commonplace in Mexico likely due to contamination of maize mainly in the form of tortillas. Fortunately, we found the levels were not as high as reported in Guatemala.
What are your other projects in Mexico?
Developing a colorectal cancer screening program in Mexico became one of my career goals. Over the past five years I have collaborated with researchers experienced in colorectal cancer screening program development through the University of California, San Francisco (UCSF)-Mexico Cancer Initiative sponsored by the Global Cancer Program at the Hellen Diller Family Comprehensive Cancer Center. With them, we designed and evaluated the feasibility of a screening program in an integrated health system in
Monterrey in northern Mexico, an area with high colorectal cancer burden.
This brings us to LISTOS—a 5-year, $5 million NCI grant given to UCSF, INSP, the Mexican National Cancer Institute (INCan), and UTHealth Houston. LISTOS (Leveraging Implementation Science To Optimize Strategies) for Cancer Control aims to develop a regional center that will be part of a wider network of implementation science centers funded by NCI in low- and middle-income countries. The center includes two cancer control implementation science research projects, one focused on developing a colorectal screening program, the other focused on speeding up the time between diagnosis and treatment for breast cancer patients.
Tell us about the Mexican Teachers Cohort.
The person who first hired me to work at INSP thought that it was a good time for Mexico to develop a large cohort to study cancer—cancer in general and breast cancer specifically. We focused on teachers for various reasons. The majority of teachers in Mexico had participated in economic incentive programs, which required yearly evaluations, so they’d become very accustomed to filling out bubble questionnaires and could self-report lifestyle and health information.
So, with support from the American Institute for Cancer Research the cohort began in 2006–2008 when 115,000 women responded to our baseline questionnaire. We send questionnaires every three to four years to update their health status and lifestyle factors.
MTC is the largest cancer cohort in Latin America, so it has and will provide important information on a region that's completely understudied. Globally, most cancer cohorts are in European and American populations, with some in Asian populations, so it’s an important addition to NCI's global cadre of cohorts. Our results will likely be informative for Hispanic populations living in the U.S., where there is limited prospective information on cancer risk factors and occurrence.
FOCUS
Fogarty’s G-11 program: Building support infrastructure
By Susan Scutti
Fogarty’s “Infrastructure Development Training Programs for Critical HIV Research at Low-and MiddleIncome Country (LMIC) Institutions” aims to develop educational programs for improving research support in the areas of technical, administrative, and financial management within organizations located in lower revenue nations. Partnerships uniting U.S. and LMIC institutions are considered most capable of cultivating these critical functions.
Program Director Dr. Geetha P. Bansal explained, “Our G-11 program is a mechanism to build infrastructure at institutions that lack adequate support structures—to help them develop an administration office that can help identify research opportunities, submit applications, manage funding, and complete all compliance and post-award activities. The intention is to establish or reinforce common areas of research administrative support, which any investigator within an institution can access,” said Bansal. “The goal is to benefit all researchers, not just one program.”
In particular, the program, which has been around for over a decade, addresses gaps in grants management training, which can become barriers to applying for and administering NIH grants. (Notably, responders to a 2021 NIH request for information on promoting equity in global health research also identified the lack of grant expertise in LMICs as a pain point.) And, while G-11 grants can be used to support administration capacity building efforts, they are intended to augment all ancillary activities crucial to conducting high-level scientific investigations.
Critical functions include but are not limited to: research integrity oversight; ethical review of research for the protection of human subjects; laboratory animal welfare oversight; advanced laboratory instrument services; health sciences library and information services; information and communications technology systems (ICT) for research; biostatistics and data analysis; technology transfer and intellectual property protection; and harassment and
discrimination policy and prevention. Few investigators question the necessity to increase institutional support. “We investigators can’t do the work we do unless our administrators are well-trained, proactive, and really engaged with us,” said Dr. Gregory Aarons of University of California, San Diego (UCSD).
“Research administration is the most important profession you never knew existed,” said Nicole Joyce, a UCSD research administrator. She cited a statistic from COGR, a professional society of research universities, affiliated medical centers, and independent research institutes: Changes in policy and regulations increased 172% over the last 10 years. “Researchers who are focused on their scientific proposals, outcomes, and dissemination don’t have time to understand all of these regulatory changes. By having solidly trained research administrators, researchers can get more proposals submitted and they’ll have better compliance with regulatory changes,” said Joyce.
Dr. Eche Ezeanolue of University of Nigeria Nsukka said the G-11 mechanism “allows you to train the people that you don't see—the people who make investigators that apply for grants successful.” He compared the systemic improvements that can be accomplished with a G-11 grant to erecting a Christmas tree. “If the Christmas tree is there, then everybody can hang their ornament.”
Joyce said, “G-11s are such an important funding instrument because not only are you developing the capacity, the knowledge, the skills, the expertise, but you’re developing the ‘why.’ Why is research important to a country? Why is it important to institutions, communities and individuals?” She believes the more you build awareness and support, the more research will happen.
While she does not have a science background, her profession is critical to research success. “I really believe in science, and I really want to benefit from all the good that researchers do to help society.”
Photo courtesy of Nicole Joyce
Research administrators who have taken part in the training sessions sponsored by UNN and UCSD. From left to right: Joy Udeoma, Pamela Ukeoma, Oge Ojinta, and Amaka Ogidi.
Fortifying research ethics at Kinshasa University
“When I started in global health, we used to search for networks or universities with major research grants in Africa, and now it's very commonplace,” said Dr. Adnan Hyder, who’s been conducting research in sub-Saharan Africa (SSA) for more than 25 years. Today, almost every country has “something going on, so it’s clear the volume of clinical and public health research being done in SSA has really gone up.” World RePORT, an online database of global research investments, supports this perception: the National Institutes of Health funded 1,881 SSA grants in 2016 compared to 3,662 in 2022, while European funder Wellcome Trust supported 110 grants in 2016 compared to 503 in 2022.
This is an advantageous situation, yet difficulties remain. “We found, based on our work in country after country, that, even when clinical trials were being done, one aspect of the research support system—the research ethics system—was very challenging,” said Hyder, a George Washington University (GWU) professor of global health. Dr. Paul Ndebele, a GWU senior research regulatory specialist, identified another stumbling block: “When you look at research ethics committees across Africa, there is a lack of standardization.”
As research proliferates across SSA—and the Democratic Republic of the Congo (DRC) in particular—research ethics systems need continuous reinforcement. “This has been a pain point for Kinshasa University (KU) for years,” said Hyder.
Systems approach
Hyder and Ndebele collaborated with Dr. Paul Lusamba, a professor at Kinshasa University’s School of Public Health (KUSPH), on the proposal, “Strengthening Ethical Review Capacity in DRC.” Their G-11 project, which covered the period from May 2020 through December 2023, aimed to fortify the ethical knowledge and skills of the KUSPH institutional review board (IRB) and improve its efficiency and performance.
They began with a needs assessment. They evaluated the knowledge and skills of research ethics committee members and staff. Next, the team looked at review processes to find pain points. After this, they showed the KUSPH-IRB good examples of efficient systems and then asked, Which systems (or parts of a system) are useful for your context? Hyder explained, “We never impose ideas from outside. It is incredibly important for local professionals, faculty, and staff to determine what is, and isn’t, useful for them.”
While Hyder drove strategy, Ndebele addressed the details, overseeing coursework provided by GWU’s summer institute, various ethics seminars, and several trainee webinars. Additionally, he arranged workshops conducted by GWU educators in Kinshasa and managed technical support. Pulling out all the stops, the team leveraged previous and ongoing ethics capacity building efforts supported by Fogarty to strengthen their influence. Dr. Imran Bari, a GWU senior research associate, who works with the team on a bioethics program in Mali, helped build relationships in the DRC—an intentional dovetailing of two francophone countries, Hyder explained. “We have to use all of our experience. We are currently in Mali, Zambia, and Pakistan.”
Useful tools
On the brink of submitting their final project report, Ndebele noted that KUSPH-IRB’s standard operating procedures have been improved using checklists. Meanwhile, standard disclosure forms and other tools have helped resolve conflicts of interest. Ndebele also provided templates so the IRB can develop management plans and strategies to mitigate any impacts caused by conflicts of interest. Bari noted, “When the project started, KU was hiring new IRB committee members and research committee members. We asked them to aim for greater gender diversity; now almost a third are female.”
Hyder said, “It was clear to us that if we could help local colleagues solve some of this inefficiency, we would help improve the entire research system. In a qualitative, anecdotal manner, we believe that’s what happened.” Since Kinshasa University is a leader in the DRC, this progress will benefit the entire country. Hyder concluded, “The sustainability, energy, enthusiasm of local partners—the local institution—has got to be ultimately responsible for this. The drivers must come from them.”
The School of Public Health building at Kinshasa University
Photo courtesy of Kinshasa University School of Public Health
Developing research infrastructure in Nigeria
A handful of forthright words spurred Dr. Echezona Ezeanolue to reconsider his career. In 2010, he was a Robert Wood Johnson Health Policy Fellow in the office of Kathleen Sebelius, then U.S. Secretary of Health and Human Services. “They were talking about how, despite all the money spent in Nigeria by the U.S., it was one of four countries where HIV testing among pregnant women was less than 20%. So, the secretary turned to me and said, ‘You’re from Nigeria—why can’t you help?’”
At that time Ezeanolue’s appointment was at the University of Nevada, Las Vegas, and all his research was U.S.-based. Yet he left Sibelius’ office determined to work in Nigeria. Soon after, he applied for and received a grant jointly funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), Fogarty and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR) studying mother-to-child HIV transmission.
Community orientation
To work with women on their own terms, Ezeanolue started a community-based intervention in 40 neighborhoods and villages. He decided to offer additional services since he knew HIV/AIDS was highly stigmatized. This way, he’d attract more participants. “We called the pregnant women and asked them what else could we offer them. The first thing they mentioned was nutrition during pregnancy, what could they eat if they couldn’t afford multivitamins?”
“The second thing [the mothers asked about] was sickle cell checkups,” said Ezeanolue, noting Nigeria has the highest number of people in the world born with sickle cell disease. “Then we asked the men what they wanted, since they drive the women to (and pay for) health care.” The men wanted anemia check-ups. “So, we added hemoglobin testing. And, in Nigeria, the number one cause of disability is stroke from undiagnosed and uncontrolled hypertension, so we added blood pressure to our list. Finally, we included depression screening.”
Ezeanolue’s first project in Nigeria yielded 25 publications. “We had data on HIV, anemia, sickle cell, hypertension, and depression.” Since that project, he’s acquired an additional role at University of Nigeria Nsukka (UNN) and conducted several NIH-funded studies in Nigeria, including Strengthening Research Administration Infrastructure for HIV Research, a Fogarty G-11 project that is still underway.
Laying the groundwork for research infrastructure
One of the world’s largest HIV epidemics exists in Nigeria; 1.8 million people there live with HIV. The U.S. government has made substantial investments in HIV care and research in Nigeria, and UNN College of Medicine has implemented multiple projects, but only as a sub-awardee. While 93% of researchers at UNN expressed interest in submitting grant applications, only 28% knew where to get research administration support, a needs assessment found. Ezeanolue’s project, a partnership between UNN and University of California, San Diego (UCSD), aims to further develop, professionalize, and reinforce research administration and management infrastructure at UNN so that it can become a primary grant recipient.
Dr. Gregory Aarons, a professor at UCSD, is a principal investigator (PI) on this G-11 project. “I was doing training on implementation science for Fogarty in sub-Saharan Africa, and I got to meet many researchers, including Eche Ezeanolue,” recalled Aarons. “I became very interested in Eche’s community-based research approach for implementing HIV prevention and treatment for pregnant women.”
Ezeanolue developed his singular research approach following a network meeting organized by Fogarty’s Dr. Rachel Sturke and NICHD’s Dr. George Siberry. In his experience, Nigerian scientists had to go outside the country to learn what’s happening inside the country. Returning to Nigeria, he immediately called all the PEPFARfunded investigators there to discuss forming a platform— an alliance for implementation research.
NISA, an engine for growth
The Nigerian Implementation Science Alliance (NISA) has three main focuses, he explained. First, NISA develops infrastructure to conduct clinical trials and implementation
Photo courtesy of Nicole Joyce
Greg Aarons (left) and Eche Ezeanolue (right) celebrate their partnership in front of the NISA banner.
science. Second, it builds a cadre of well-educated research staff. Third, NISA brings together investigators, policymakers, NGO staff, and others to share ideas and learn what researchers have already done, so they can avoid repeating what hadn’t worked, while adopting and scaling up what had.
Today, NISA rests on four pillars: weekly research-inprogress meetings; monthly webinars; quarterly research sharing weeks; and a yearly conference. Aarons, a NISA conference keynote speaker over multiple years, said, “I was really impressed with the ability of Eche and the UNN team to bring people from across Nigeria and other West African countries to NISA, where people could learn about implementation science.” Aarons also saw how the first-of-its-kind practice-based research network developed from NISA could build on the G-11-funded program in developing research capacity.
Ezeanolue explained, “We selected two sites from each of the country’s six regions and made them what we call ‘implementation laboratories.’ If we implement something in two sites in every region and it works, then each of those sites will become model innovation centers to help scale-up regionally.”
Ezeanolue is director of UNN’s Center for Translation and Implementation Science (CTAIR), the network’s organizing hub. His and Aaron’s G-11 grant, then, aims to strengthen the research administration infrastructure of UNN and CTAIR.
The grant requires training 12 people in research administration. Aarons said, “We cast a wide net to look for who was really poised to be in those administration roles. We didn't want to train people if they weren't going to actually go back and practice.” Then they brought in an additional 12 people, doubling the number of trainees. "Remember the 12 network sites, two in each region?” Ezeanolue asked. “We’re also training one community research engagement officer from each of those sites. These are the people who go to the church, the mosque, the community, and talk about the research we're about to do, why it's important and why people should participate.”
Integrating administration and research training
Nicole Joyce, a UCSD research administrator, had never met Aarons before receiving an email from him in 2020, requesting information about her program. “In our first meeting, it slowly dawned on me that he didn’t want to just send staff to my training—he was asking me to co-develop a capacity building program with UNN.” She immediately felt intimidated. “Administrators don’t cross over to the research side very often.” However,
Joyce’s infectious enthusiasm for research administration was clear to Aarons, who believed this could be a great opportunity for her to make a difference in global health.
Joyce’s training strategy is anchored to the research administration life cycle: “So we look at pre-award activities, post-award activities, compliance activities, and the systems, tools and resources you might need to perform those activities.” Though Joyce began her UNN training in the usual way, she quickly learned to adapt to the realities of Nigeria’s infrastructure. “They commonly have power outages and unreliable Internet. Some trainees didn't have laptops, software, or tech skills.” When they trained on-site in Enugu, Nigeria, the team encountered unexpected hurdles when SAM (the U.S. government system for awards management) couldn’t “talk to” another system. “A little technical challenge around an address character limitation ended up costing us nine months and not being able to pay a sub-awardee.”
Today, NISA rests on four pillars: weekly researchin-progress meetings; monthly webinars; quarterly research sharing weeks; and a yearly conference. “ ”
Nevertheless, the team scored undeniable triumphs. Notably, a National Cancer Institute research grant awarded to Aarons and Ezeanolue alongside the G-11 project helped provide the trainees with much needed real-world experience. Aarons said, “We’re developing a sense of collaboration. Hands-on coaching and mentoring continue during the project’s second year via weekly, sometimes daily calls.” He added, “Through everyone's enthusiasm, it’s going way beyond what we proposed— it’s building not just UNN’s infrastructure but a nation’s infrastructure.”
Stephan Orafa (left), UNN-CTAIR, works with Neil Dutcher, UCSD, to learn how to develop a detailed budget for a proposal submission
Photo
courtesy of Nicole Joyce
DIRECTOR’S COLUMN
GUEST OPINION — By David J. Spiro, PhD, Director, Division of International Epidemiology and Population Studies Fo garty International Center
Charting the evolutionary course of influenza
A recent study in eLife, authored by Drs. Amanda Perofsky and Cecile Viboud from the Fogarty International Center, aims to better understand how antigenic drift—the accumulation of genetic changes—in influenza viruses affects the size and severity of seasonal epidemics each year.
Influenza is a cunning opponent. The flu, short for influenza, is a contagious respiratory illness that affects the nose, throat, and lungs. The viruses that cause the flu continuously accumulate genetic changes to escape detection by your immune system. This process, known as “antigenic drift,” is the reason why you can get sick with the flu each winter, even though you’ve been previously infected or vaccinated.
In theory, flu viruses with increased antigenic drift make people more susceptible to infection, leading to more cases and earlier, larger, or more severe epidemics. However, evidence for this in epidemiological data is unclear. What has been well understood is that two influenza virus types, influenza A and influenza B, routinely co-circulate in humans and cause annual outbreaks in the U.S. One subtype of influenza A, named A(H3N2), experiences the fastest rates of antigenic drift, and causes more cases and deaths than other seasonal flu viruses.
What Perofsky, Viboud and their co-authors discovered is significant: Patterns of genetic changes in broad sets of epitope sites (small regions on the surface of antigens that are recognized by immune system components, such as antibodies or T cells) had stronger, more consistent relationships with different measures of flu epidemic dynamics than the “gold standard” serological assays used to measure how flu viruses change from season to season. These assays, laboratory tests that check for the presence of antibodies or other substances in blood samples, are used to develop yearly flu vaccines.
The authors also looked at how epitope changes in the flu virus’ two major surface proteins—hemagglutinin (HA) and neuraminidase (NA)—could be used to predict things like epidemic intensity and virus transmissibility. They found that genetic changes of H3, the HA antigen of the A(H3N2) virus, were more strongly linked to larger epidemic sizes, higher viral transmissibility, more cases in adults than children, and a greater number of excess deaths caused by the A(H3N2) virus each season than changes in N2, the NA antigen of the A(H3N2) virus. Meanwhile, antigenic drift of N2 was more strongly associated with increased epidemic intensity (“spikier” epidemic curves) and fewer days from epidemic onset to peak incidence, a measure for the speed of an epidemic, than changes in H3.
“ ”
This study provides support for the inclusion of NA in flu vaccines and highlights the importance of monitoring
evolution in both HA and NA to inform vaccine strain
selection and epidemic forecasting efforts.
Importantly, the researchers also discovered that the level of co-circulation of A(H1N1) viruses was more predictive of the size of A(H3N2) epidemics than viral evolution. So, although antigenic drift in both HA and NA contribute to differences in A(H3N2) epidemics across seasons, subtype interference (the co-circulation of different influenza viruses) is more important than viral evolution when it comes to shaping annual outbreaks.
Overall, the study’s authors found that increased susceptibility to flu occurs during seasons with high antigenic drift. This study is also the first to link antigenic drift in NA to the disease burden, timing, and the age distribution of cases. Because HA elicits a stronger immune response than NA, the researchers had expected HA to demonstrate stronger relationships with seasonal incidence, so this outcome surprised the authors. Currently, NA content is not standardized in vaccines, even though anti-NA antibodies lessen the severity of flu infections.
HEALTH Briefs Global PEOPLE
Joshua A. Gordon concludes chapter as NIMH Director
Dr. Joshua A. Gordon will end his tenure as the director of the National Institute of Mental Health (NIMH) on June 14, 2024. He plans to return to Columbia University, as chair of the department of psychiatry, while also serving as director of the New York State Psychiatric Institute.
Former Harvard School of Public Health dean passes
Dr. Howard H. Hiatt, former dean of the public health school (now the Harvard T.H. Chan School of Public Health) died at his home in Cambridge, Massachusetts, in March. In the early 1960s, he collaborated with future Nobel laureates on the identification of messenger RNA.
Krupp granted Fulbright Global Scholar Award
Dr. Karl Krupp, University of Arizona, will use a Fulbright Global Scholar Award to compare how two cities—Mysore, India, and Stockholm, Sweden—support elderly populations. In Mysore, people in their 60s and 70s consume five times more governmentsponsored health care than younger residents; in Stockholm people over 90 have high rates of chronic problems like dementia.
Arlotta wins National Academy of Sciences award
Dr. Paola Arlotta of Harvard University was named the 2024 Pradel Research Award recipient for her work providing insights into the principles that guide development of the cerebral cortex, the portion of the brain responsible for cognition. Arlotta is principal investigator on a Fogarty grant studying molecular principles of neuronal maturation and integration in the adult and aging brain.
Abdellatif wins travel award from IADR
Enas Belal Abdellatif, Alexandria University, Egypt, has won the 2024 International Association for Dental, Oral, and Craniofacial Research (IADR) Newell Johnson Travel Award. Abdellatif aims to help prevent oral diseases, empower those from disadvantaged communities, and minimize oral health inequalities, especially in low- and middle- income countries.
Neurological conditions leading cause of ill health
A March 2024 study published in The Lancet Neurology found a range of neurological conditions collectively represent the leading cause of ill health worldwide. The Global Burden of Disease 2021 Nervous Systems Disorders Collaborators estimated these conditions affected 3.4 billion people and caused 11.1 million deaths in 2021.
TB burden in youth a mixed picture
Among people between the ages of 10 and 24, the toll of tuberculosis (TB) decreased between the years 1990 through 2019, a study published in Pediatrics found. Yet, drug-resistant TB infections increased within that age group during that time span, with South Africa showing the highest increase.
IVI to open Africa office
The International Vaccine Institute (IVI), a nonprofit organization with a mission to discover, develop, and deliver safe, effective, and affordable vaccines, will open its Africa Regional Office in Kigali, Rwanda, this year. The new office is expected to play a pivotal role in providing onthe-ground support and leadership for IVI’s work in Africa.
Antiviral shows promise in treating Ebola Ebola Sudan infections currently have no approved vaccines or treatments. A small study of primates published in Science examined the antiviral drug obeldesivir, a relatively inexpensive pill that can be stored at room temperature. Studies suggest obeldesivir could prove beneficial in fighting all species of Ebola as well as Marburg virus disease.
Intervention speeds up ART adoption
Social work follow-up reduced the time it took for patients hospitalized with HIV in Tanzania to start antiretroviral therapy following discharge. As described in JAMA, Fogarty-funded researchers found that 92% of people in the intervention group attended an HIV clinic by the end of the first month versus 75% in the control group.
Funding Opportunity Announcement Deadline Details
International Bioethics Training
D43 Clinical Trial Optional
R25 Clinical Trial Not Allowed go.nih.gov/BioethicsTraining
Writer/editor: Mariah Felipe Mariah.Felipe@nih.gov
Writer/editor: Susan Scutti Susan.Scutti@nih.gov
Digital analyst: Merrijoy Vicente Merrijoy.Vicente@nih.gov
Designer: Carla Conway
In rare cases when a correction is needed after an issue’s printed version has been finalized, the change will be made and explained in the online version of the article.
All text produced in Global Health Matters is in the public domain and may be reprinted. Please credit Fogarty International Center. Images must be cleared for use with the individual source, as indicated.
SCAN AND READ THIS ISSUE ONLINE
Aug 22, 2024
Aging institute to fund research on US life expectancy gap
The National Institute on Aging (NIA) has issued a notice of special interest (NOSI) on research that examines worsening life expectancies in the U.S. compared to other countries. NIA aims to support projects that examine cross-national and U.S. cross-regional or cross-state differences that may drive poor health outcomes. Projects focusing on other high-income countries as well low- and middle-income countries (LMICs) are welcomed. In fact, research from LMICs is encouraged as these countries often have greater variation and speed of change in policies compared to high-income countries.
After peaking in 2015, life expectancy in the U.S. declined one full year to 78 years of age in 2021. People in many other countries, including those with lower per capita income, live longer than U.S. residents.
A 2021 report led by the National Academies of Science, Engineering and Medicine (NASEM) identified three top causes of death that are higher in the U.S. compared to other countries: substance use, increasing rates of suicide, and poor cardiovascular health. The notice from NIA encourages research that investigates the factors leading to death, disease, and disability uncovered by this report.
More information can be found at: https://go.nih.gov/NOTAG-24-004
Empowering Victims of Lived Violence: Delaware’s Hospital Violence Intervention Program (HVIP)
David Chen, M.D., M.P.H.
Institute for Research on Equity and Community Health (IREACH), ChristianaCare Health System
Johanna Rodriguez, M.S.W., L.S.W.; Mishai Pendleton, B.S. and Nichole Johnson, C.M.A. Department of Community Health, ChristianaCare Health System
ABSTRACT
Hospital Violence Intervention Programs (HVIP) are increasingly implemented across a variety of healthcare-associated contexts to prevent and address violent intentional injury. We describe the establishment of a health system funded HVIP in Delaware and the direct experiences of staff and violence-specialized Community Health Workers.
INTRODUCTION
In the United States, the impact of assault injury is significant and widespread; according to 2021 data, homicide (i.e. fatal interpersonal assault) was among the top ten leading causes of death for persons in every age category from 1-54.1 One estimate in 2017 of US adult Emergency Department encounters attributed 1.6% of all visits to violent injury.2 However, there are many categories of violence and though there is increasing recognition of its impact on patients and the healthcare system,3 disentangling the pathways that lead to injury and the recovery journey that follows is complex. In this article, we present an overview of the unique role and structure of Hospital Violence Intervention Programs (HVIPs) and the first-person perspectives of frontline workers describing their roles and contributions.
BACKGROUND
Firearm assault carries the highest morbidity, mortality, and per person cost of care compared to other mechanisms of assault injuries (such as bodily force, blunt object, or sharp object assaults) despite involving a younger population with relatively fewer comorbidities.4 Firearm injury survivors also have worse outcomes related to pain, post-traumatic stress disorder (PTSD), functional limitations, and health-related quality of life even when compared to similarly severe injuries from non-assault mechanisms such as motor vehicle crashes.5 Yet firearm assault and injury have been historically under-researched compared to other leading causes of death in the United States.6 This is especially striking given how much of an outlier in firearm morbidity and mortality the US is compared to other countries; an estimate in 2016 placed Brazil and the United States as collectively contributing to 32% of the world’s estimated number of firearm deaths, and the US firearm homicide rate has been estimated to be 24.9 times higher than for other high-income countries.7,8 These observations point towards the disproportionate burden of firearm violence within the United States as the consequence of structural forces. Gaps in outcomes have also only widened since 2020, which saw an epidemic surge in firearm injuries that made it the nation’s leading cause of death for persons 1-19 years of age with the specific rise in firearm homicide felt most acutely among those already historically most affected: non-Hispanic Black or African American men ages 10-44 with the highest levels of poverty.9,10
Therefore violence, and specifically firearm violence, is one of the most glaring and persistent examples of both severe disparity
and inequity in American healthcare. Recent decades of advocacy and program innovation have sought evidence-based methods to challenge this inequity and among healthcare-based interventions, Hospital Violence Intervention Programs have been the most widely promoted and studied model for reducing related risk for violent reinjury, perpetration, and symptoms of posttraumatic stress.11 However there is wide variation in implementation and measured outcomes for HVIPs.12 In a review of studies, Webster et. al13 summarized this heterogeneity of programs:
Most HVIPs begin with a bedside connection intended to motivate the patient to participate in the program. The initial connection is often made by a “credible messenger,” often someone who has personal prior experience with violence. Some HVIPs employ motivational interviewing techniques to use patients’ own desire for safety and stability to facilitate behavior changes that lower risk for involvement in violence. Most HVIPs are designed to connect patients to needed social services and supports such as assistance with obtaining employment, housing, treatment for mental illness and substance abuse while facilitating postsurgery medical care. Some HVIPs also link survivors to community-based programs specifically designed to prevent revictimization or perpetration of violence such as mentoring or violence interruption programs. HVIPs usually emphasize that the programs are trauma informed and sensitive to the psychological challenges faced by individuals who have suffered serious injuries from violence. In addition to social service supports, some HVIPs provide some form of direct intervention to facilitate nonviolent responses to conflicts and provocations such as a violence prevention curriculum for youth or a support group for adults. In some instances, HVIPs will assist family members of victims, especially when the patient is an adolescent. HVIPs may also be a direct connection to crime victim assistance programs, legal representation, and health insurance for those who are eligible. The types of services and supports offered by HVIPs, of course, depend on their funding. HVIP teams often consist of social workers, nurses, messengers, and surgeons. Despite the considerable needs and the high risks facing gunshot wound survivors, hospitals without HVIPs might offer a social worker to assist with discharge issues, but they rarely offer follow-up supports. (p. 139)
Overall, this review found mixed evidence regarding effectiveness, noting that included studies were primarily limited by underpowered sampling and selection bias. Given that intensive case-management and/or care coordination interventions engage a wide variety of social needs, these findings are neither surprising nor necessarily discouraging. Context, specificity, and fidelity to implementation affect success, and analogous and homologous models show similar variability. Models of intensive case-management interventions for severe mental illness can demonstrate consistent impact for specific measures such as reduction in hospital readmissions and increased retention in care.14 Complex care coordination interventions such as Camden Coalition’s care management program for healthcare “superutilizers” initially showed null effect in a randomized controlled trial testing primary outcomes (hospital readmissions), but did show positive effect on intermediate goals such as increased ambulatory care.15 The Individualized Management for PatientCentered Targets (IMPaCT) model for Community Health Workers (CHWs) serving low-income populations with multiple
chronic conditions found marked improvement across a range of biomarkers and behaviors, improvement in self-rated health measures, and reduction in hospitalizations.16
Delaware experiences high rates of firearm violence as previously studied by the CDC and described in this journal.17,18 Figure 1 depicts this disparity in firearm homicides as calculated by the RAND Corporation’s analysis of CDC epidemiological injury statistics, with Delaware experiencing 26% higher death rate compared to the national average in 2021.19 However, to gain insight beyond statistical descriptions into the implementation of new models of care requires creating spaces within academic arenas to learn from the experiences of frontline CHWs and case workers who provide valuable insight into this complex landscape.20–22 Below, our program staff describe our experiences in Delaware in observing and contributing to the strengths and gaps in patient care, admitting the ways in which we have fallen short and can serve them better, and advocating for the principles and practices that protect their autonomy, dignity, and health.
Figure 1. 2021 Comparison of Firearm Deaths in Total Population of Delaware compared to National Average
MEDICAL DIRECTOR:
DAVID CHEN, M.D., M.P.H.
During my residency training within the state of Delaware, I lived for several years in the Northeast neighborhood of Wilmington, Delaware. My neighborhood experienced some of the highest rates of firearm violence within the city; I regularly heard gunshots in the community and on several occasions was a “streetside responder” in applying direct pressure to treat gunshot wounds for persons injured just outside my home. In the years since, I have continued to live within the city and assess the broad impact of gun violence on our community as well as the role of health systems in intervening both before and after the bullet wound. There have been many advocates and champions for this work within healthcare and the community of Delaware; my primary role has been to build a sustainable implementation of an HVIP and better understand the many ways in which gun violence affects health.
In 2019, ChristianaCare Health System (CCHS) began planning the launch of an HVIP aimed to create a single clinical care team to use two evidence-based synergistic strategies: core HVIP principles and function as articulated by the Health Alliance for Violence Intervention (the HAVI, formerly the National Network for Hospital Violence Intervention Programs/NNHVIP) and the IMPaCT CHW model. This program was proposed to address the “safety/ violence reduction” need identified in the CCHS Community Health Needs Assessment (CHNA) and align with larger organizational goals of ending disparities and simplifying access to care. The program is unusual among surveyed HVIPs, where only 36% have hospital funding, and to the authors’ knowledge is the only program situated and entirely funded by a health system’s Departments of Health Equity and Community Health.20 Despite the extreme challenges faced by acute care health systems during the COVID-19 pandemic, where many institutions were challenged by drawback and reduction of services & staff,23 the program began in February 2021 with the first patient enrollments.
The CCHS HVIP - Empowering Victims of Lived Violence (EVOLV) provides navigation support to patients impacted by community and interpersonal violence. Patients are approached during or directly following an initial hospital encounter for violent injury (including both blunt and penetrating assault) by a program CHW for enrollment. The program serves those ages 14 and older, but due to significant frontline staffing limitations and the preliminary nature of the program, initial inclusion and exclusion criteria focused on several key principles for implementation: focus on patient-centered & identified outcomes, high quality of service navigation and intensive case management, patients with more severe injuries and firearm injuries, and nonduplication with existing services. Consequently, enrollment was initially prioritized for patients with penetrating assault injuries requiring hospitalization, residence in New Castle County, and capacity for independent decision making (and for minors, with parental consent and patient assent). Through a grant funded by the Delaware Criminal Justice Council, this was also later expanded to include all residents of the state of Delaware and with exploratory work pending to expand enrollment for those receiving acute care with similar criteria at Nemours Children’s Health. Relative exclusion criteria are those whose service navigation needs are more specifically met by other similar programs, such as an existing dedicated intimate partner violence/ domestic violence (IPV/DV) CHW program operated by Child Inc. or other CCHS CHW program (e.g. where the needs are primarily related to behavioral health or substance use disorder). In such cases, a “warm handoff” is conducted to introduce other programs and typically the primary choice of service will be at the patient’s discretion; in some cases, such as with the CCHS Food Farmacy program for food insecurity or CCHS Women’s Health, multiple CHW programs will remain engaged.
The focus is on service navigation through working on the patient’s identified needs and addressing social determinants of health (SDoH) barriers. Enrollment involves an SDoH screen but the patient may choose any number of self-determined goals with aim to achieve outcomes within 3 - 12 months (Table 1). Establishment of a primary care clinician for the patient is also considered a standard of clinical care and is an additional primary process measure of success.
Table 1. Screening and Service Categories
During our first 19 months of operation (which included operation with one active frontline worker/CHW and pandemicrelated redeployment of staffing for critical shortages), the CCHS HVIP-EVOLV manually screened over 2,000 patients presenting for acute care from violent intentional injury or maltreatment for eligibility, approached 213 of those with the most critical needs for enrollment, and successfully enrolled 66 patients (30.9%). While program evaluation is ongoing, preliminary process measures compare well with similar established HVIPs; by comparison, a recent evaluation of five-year HVIP performance (2013-2018) for the Boston Violence Intervention Advocacy Program described a 37.4% engagement rate of participants.24 On January 16, 2024, the CCHS HVIP-EVOLV was officially recognized as a Member Organization of the HAVI.
We look forward to next steps in advancing medical care for our vulnerable patients: expanding our inclusion criteria and services, stronger and more specific advocacy for patient needs, and changing structural forces for better healthcare for victims of violence in our state.
PROGRAM COORDINATOR:
JOHANNA RODRIGUEZ, M.S.W., L.S.W.
As a program founded on principles of health equity, we intentionally enter spaces with patients knowing that we will see injustice and disparities in quality of care for our patients injured due to community violence. Preparatory work for, education in, and awareness of systematic oppression does not soften the blow when we witness these moments ourselves. We train our CHWs in bias, advocacy, and patient rights. As liaisons between the patient and the systems they are engaging with, they are not meant to speak on behalf of patients but rather help patients feel confident in taking up spaces where their voice is the most important. Unfortunately, we are often witness to a lack of understanding of how gun violence impacts patients and their continued loss of security.
Administratively, I often see gun violence housed with domestic violence when it comes to victim services. While at times some services may look similar, the experience of violence our patients have is distinct. Even within the world of gun violence, our primary patient population of victims of violent intentional firearm assault injury is not always the focus. Victims of attempted suicide, bystander injury, and domestic or intimate partner violence often have more facilitators to approach in conversation, care, and services. Gun violence as it occurs in Wilmington, Delaware is seen through a different lens, sometimes as a way of understanding nuances and, unfortunately, other times to further ostracize patients impacted. There have been many times where we have engaged with external parties to connect patients to resources only to find that their version of ‘victim services’ rarely includes gun violence survivors.
Negative commentary dominates when it comes to extending services to the “imperfect” patient. In my experience, the patient who is labeled “non-compliant,” “difficult,” or “aggressive” rarely engages with me in the same way. A traditional diagnosis of PTSD is insufficient when we consider the systematic oppression, housing insecurity, community
violence, and inadequate community resources our patients experience. It is hard to describe the feeling of relief and hope when we find a new partner who is excited to hear about our work. Historical distrust in systems meant to care for our patients creates a complicated relationship from the start, and one does not have to search for long to find examples of refusal to engage with “difficult” or “non-compliant” patients, whether by service systems or individuals.
Rather than dissect every negative interaction we’ve had, I’d like to focus on the successes that we’ve had in our threeyear history. We have found partners who not only want to improve their services but repair the broken trust that already exists. We have come to lean into our ability to acknowledge that there is so much more work to be done. It has been encouraging to be welcomed in some spaces with open arms, but it’s important to highlight that it’s often because programming and trusted staff are hard to establish and maintain. The fact that we have been able to serve patients who have placed their trust in us is something that we take extremely seriously.
There are common themes among the staff in our most successful relationships. They are humble. They are patient. And most importantly, they are always building on their self-awareness. What is transformative is the ability to have difficult conversations with partners where we mutually acknowledge our areas for improvement. To be open and honest about our misconceptions and where we fall short in our patient care is essential for creating an environment where our patients themselves can be vulnerable. I admire the leaders that we have engaged with who have been open about negative experiences patients have had with their services in the past. It is uncomfortable to discuss mistakes we have made, but progress cannot be made without a commitment to learning and doing better. Conversations do not end at the acknowledgement. Action must be taken. Our HVIP has begun meeting with partners to share knowledge and experiences to ensure accountability on both ends, especially when we are able to bring our patients directly into these conversations in person or over the phone.
Agencies are made up of humans with an array of lived experiences. We are not robots. Asking our patients to engage with us or perform in ways that we don’t ourselves is unfair and perpetuates power dynamics. I invite our readers to challenge themselves in new ways. Consider ways in which we could have supported our neighbors better or extended kindness to others that we have judged without reason. Often, we make promises that we can’t keep or give patients time frames for something that we miss. Could we have taken an extra minute to ensure our participants felt comfortable asking for clarity? Were there times where we could have ensured a patient understood our conversation before ending a call or a visit? Engage with those difficult conversations and watch yourself when dismissing the imperfect patient as undeserving of your patience. Do not underestimate the power of being a support person for your patient - you never know when you might be the only one by their side.
COMMUNITY HEALTH WORKER:
MISHAI PENDLETON, B.S.
As someone with a background in public service, the decision to apply for this position was by fate. Throughout my career, I’ve dedicated countless hours assessing safety, identifying needs, and creating case plans. I reached a stage in my career where I desired to make a positive impact within the community in a different way. A role within ChristianaCare involving support for victims of violence caught my attention since I hadn’t encountered much discussion on this critical issue. As our senior CHW, I have encountered disparities in the treatment of clients across various circumstances. I have personally made significant progress in understanding how to better support victims of community violence by closely observing clients, providers, and outside agencies.
My initial encounters take place within the hospital environment. I never truly understood the stigma behind gun violence until I witnessed it myself. I remember my first patient’s face and the hopelessness and shame that accompanied this stigma. I engaged in a conversation with a client who has been hospitalized for nearly a month. Upon asking about the patient’s well-being, the patient expressed that he was coping adequately within his confinement, alluding to a prison cell. Clients may experience feelings of isolation in the hospital, exacerbated by the restricted interactions they have with their loved ones. To mitigate this feeling of isolation, I try to see patients as often and consistently as conditions allow, which helps to build rapport and show them that they are not alone. I’ve witnessed patients demonstrate a variety of coping mechanisms while undergoing care for their traumatic injuries throughout their hospital stay. Patients have different ways of expressing their stress and with that in mind, it’s imperative for staff not only to be trauma aware but to display empathy during their patients’ toughest times. I bridge the gap between providers and patients by actively learning from them. As a staff member, I provide clients with a level of autonomy that generates positive relationships and helps them feel empowered to confidently articulate their needs. I initiate difficult conversations with both providers and patients with the goal of building a level of understanding where everyone can be respected.
Throughout my patient-facing interactions, I’ve learned that PTSD and other stress reactions will not always manifest visibly at the bedside. Patients will receive a certain level of care and have their basic needs met in the hospital setting, but once patients are stable for discharge, their social determinants of health needs aren’t necessarily fully attended to. The work within hospitals can be fast-paced and busy, but during quiet hours clients may struggle with thoughts about the incident, their injury, life before and after the event, and how to navigate life after discharge. These stressors, both spoken and unspoken, often go unaddressed. My goal is not to offer clients medical diagnosis, but empathetically connect with them and identify barriers that arise during their journey. We recognize that upon discharge from the hospital, clients often have many tasks necessary for their ongoing healing. However, for many whom were previously physically healthy and had never been hospitalized or treated for serious illness before, it is overwhelming. Many clinicians may not fully understand the initial steps required to begin this process. As a CHW, I identify the needs of clients and help address those barriers so they can
continue their healing journey. No journey is easy, but being someone to accompany them through it is how we can learn and fulfill the role of a true advocate.
Once patients leave the walls of the hospital, there continue to be hard challenges in meeting patient needs. I have witnessed my clients be discouraged and disengage with community partners when their needs are overlooked. While this may be due to structural barriers in systems not designed for our patient population, it is also not uncommon for my clients to encounter other workers displaying a lack of empathy, adequate attention, or provision of accurate information. I act as a liaison when connecting clients with community supports; I also serve as their advocate, assisting them in obtaining the necessary information, collaborating with community partners, and holding everyone accountable. For example, victims of domestic violence can receive certain items such as cell phones to help them stay in communication with their supportive agencies and other personal needs. However, that support is also very important for victims of community violence and other forms of assault. Commonly, individuals are stripped of their cell phones during their initial contact with law enforcement and hospitals, making it unlikely for them to get their phones back due to the circumstances of their injury. Patients may lose track of their devices and on occasion never get them back due to ongoing investigation, and so there is a gap in addressing the need patients have for phones when they return to their communities. This gap directly impacts their ability to contact myself, medical providers, and outside community agencies to start their healing journey. When patients can’t communicate with people with whom they are supposed to follow up, they may be labeled as non-compliant, further worsening stigma associated with violent injury.
Safety is another concern that clients face. It’s likely that clients are injured within their communities and returning home to the same environment poses a threat to their safety once again. There are community agencies that have shelters dedicated to certain populations, but there’s insufficient resources that can help our patients avoid returning to the literal scene of the crime and being retraumatized emotionally as well as physically.
Through my work as a violence-specialized Community Health Worker, I can see how community programs and systems may not be aware of or built to handle differences in needs for patients facing violence. Here, professional development also offers opportunities for advancing care. As an example, while I participated in a conference aimed at assisting victims of violence, I observed that most conversations focused solely on domestic violence. In taking this opportunity to express my role as a CHW and highlight the importance of engaging in these discussions across different spaces including for community violence, not only did I learn more about other community resources but other agencies showed interest in my role and demonstrated openness to incorporating this knowledge into their respective spaces.
Becoming a HAVI recognized Hospital Violence Intervention Program (HVIP) in Delaware marks an initial phase. We have more work to do. I have prioritized empowering individuals who feel marginalized, which is central to my work. Through reflective practices, I have effectively contributed to reducing Emergency Department visits and promoting improved health outcomes. Furthermore, I have empowered clients to advocate for
their healthcare needs and address social determinants of health. Beyond that, I have provided support for clients in pursuing career opportunities and furthering their education. In terms of community involvement, I have stepped into spaces and invite agencies into constructive conversations. Regardless of the nature of individuals injuries or the circumstances surrounding them, I strive to promote the idea that everyone deserves equitable care.
COMMUNITY HEALTH WORKER: NICHOLE JOHNSON, C.M.A.
In both my role as a medical assistant and a community health worker, I have seen the difference in care received by patients depending on their visit reason. I have witnessed firsthand the degree of stigma surrounding a gunshot patient where the preconceived notion that gunshot patients are “bad” individuals or “must have done something wrong” to cause the injury often directly impacts the quality of care. As a Community Health Worker, I advocate for patients who often have the quality of their services impacted by knowledge of the nature of their injury. Sometimes the verbiage and descriptions by healthcare staff – both inside and outside the hospital – paint the picture that the patient is “difficult to engage” or has an “unsavory demeanor.” Often times, my engagement with a patient does not align with the description.
Community Health Workers such as myself often have to buffer communication between partners and our patients. This looks like filling gaps in communication and explaining things in simple terms to ensure that patients feel as though they are just as much a part of the conversation as us and partners. It is important to build trust, ensure understanding, and more importantly advocate when necessary. We want patients to speak for themselves, but sometimes we must step in and present about patient concerns to encourage them in explaining their concerns and explain why a patient may feel uncomfortable. I have seen the difference in how a “normal” acute patient may have access to more visitors for comfort and more family supports, whereas those who are victims of violence have more limited access. While this may be done from a security perspective, it deepens feelings of isolation and reduces support that would need to be in place in the home setting after discharge. I have also seen firsthand barriers with clients who may need physical therapy or rehabilitation services that are “turned down,” possibly due to the nature of the assault injury and the lack of facilities’ knowledge on subject matter.
The individuals we serve often need advocacy, understanding, and someone who knows how to navigate the system while ensuring the patient’s priorities are placed first. While I am privy to knowledge of resources, sometimes this is not enough, and providing support emotionally or physically being there to help bridge gaps and provide understanding for individual clients and needs is necessary. Having broad experience across a diverse caseload allows me to provide timely examples and context that a patient or service provider might not otherwise have noticed. Direct and indirect barriers to care is impacted by both verbiage in charts and the way people speak to and about the patient in general. I feel that it is important for agencies to understand that these are individuals: at the end of the day, although the care may be complex, the need is still the same.
CONCLUSION
These themes affecting victims of gun violence are consistent with other emerging observations within HVIP research literature: stigma within healthcare and social service systems, challenges to recovery in hospitalized settings, social isolation, mental health needs, and the lack of specific services for injuries not related to intimate-partner or domestic violence.5,25,26 Our aim is to give voice and validation to our patients’ experiences, to care for them well with the resources collectively available, and highlight the work needed for future accountability and innovation.
Dr. Chen may be contacted at dchen@christianacare.org
FUNDING ACKNOWLEDGEMENT
Work supported by an Institutional Development Award (IDeA) from the National Institute of General Medical Sciences of the National Institutes of Health under grant number U54GM104941 (PI: Hicks) and the State of Delaware.
REFERENCES
1. Centers for Disease Control and Prevention. (2023). Webbased injury statistics query and reporting system (WISQARS), 2021, All Deaths with drilldown to ICD codes, both sexes, all races, all ethnicities, 2001—2021 with no race. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. https://wisqars.cdc.gov/
2. Monuteaux, M. C., Fleegler, E. W., & Lee, L. K. (2017, November). A cross-sectional study of emergency care utilization and associated costs of violent-related (assault) injuries in the United States. The Journal of Trauma and Acute Care Surgery, 83(5S, Suppl 2), S240–S245. https://doi.org/10.1097/TA.0000000000001525
3. Grossman, D. C., & Choucair, B. (2019, October). Violence and the US health care sector: Burden and response. Health affairs (Project Hope), 38(10), 1638–1645 https://doi.org/10.1377/hlthaff.2019.00642
4 Barry, L. E., Crealey, G. E., Nguyen, N. T. Q., Weiser, T. G., Spitzer, S. A., & O’Neill, C. (2022, June 1). Hospital costs and fatality rates of traumatic assaults by mechanism in the US, 2016-2018. JAMA Network Open, 5(6), e2218496. https://doi.org/10.1001/jamanetworkopen.2022.18496
5 Herrera-Escobar, J. P., de Jager, E., McCarty, J. C., Lipsitz, S., Haider, A. H., Salim, A., & Nehra, D. (2021, December 1). Patient-reported outcomes at 6 to 12 months among survivors of firearm injury in the United States. Annals of Surgery, 274(6), e1247–e1251 https://doi.org/10.1097/SLA.0000000000003797
6 Stark, D. E., & Shah, N. H. (2017, January 3). Funding and publication of research on gun violence and other leading causes of death. JAMA, 317(1), 84–85. https://doi.org/10.1001/jama.2016.16215
7 The Global Burden of Disease 2016 Injury Collaborators. (2018). Global Mortality From Firearms, 1990-2016. JAMA, 320(8), 792–814. https://doi.org/10.1001/jama.2018.10060
8 Grinshteyn, E., & Hemenway, D. (2019, June). Violent death rates in the US compared to those of the other high-income countries, 2015. Preventive Medicine, 123, 20–26. https://doi.org/10.1016/j.ypmed.2019.02.026
9. Goldstick, J. E., Cunningham, R. M., & Carter, P. M. (2022, May 19). Current causes of death in children and adolescents in the United States. The New England Journal of Medicine, 386(20), 1955–1956
https://doi.org/10.1056/NEJMc2201761
10 Kegler, S. R., Simon, T. R., Zwald, M. L., Chen, M. S., Mercy, J. A., Jones, C. M., Dills, J. (2022, May 13). Vital signs: Changes in firearm homicide and suicide rates — United States, 2019–2020. MMWR. Morbidity and Mortality Weekly Report, 71(19), 656–663. https://doi.org/10.15585/mmwr.mm7119e1
11. Purtle, J., Rich, J. A., Fein, J. A., James, T., & Corbin, T. J. (2015, November 3). Hospital-based violence prevention: Progress and opportunities. Annals of Internal Medicine, 163(9), 715–717. https://doi.org/10.7326/M15-0586
12. Monopoli, W. J., Myers, R. K., Paskewich, B. S., Bevans, K. B., & Fein, J. A. (2021, May). Generating a core set of outcomes for hospital-based violence intervention programs. Journal of Interpersonal Violence, 36(9-10), 4771–4786 https://doi.org/10.1177/0886260518792988
13 Webster, D. W., Richardson, J., Meyerson, N., Vil, C., & Topazian, R. (2022). Research on the effects of hospital-based violence intervention programs: Observations and recommendations. The Annals of the American Academy of Political and Social Science, 704(1), 137–157. https://doi.org/10.1177/00027162231173323
14. Dieterich, M., Irving, C. B., Bergman, H., Khokhar, M. A., Park, B., & Marshall, M. (2017, January 6). Intensive case management for severe mental illness. Cochrane Database Syst Rev, 2017(1), CD007906 https://doi.org/10.1002/14651858.CD007906.pub3
15 Finkelstein, A., Cantor, J. C., Gubb, J., Koller, M., Truchil, A., Zhou, R. A., & Doyle, J. (2024, January). The Camden coalition care management program improved intermediate care coordination: A randomized controlled trial. Health affairs (Project Hope), 43(1), 131–139 https://doi.org/10.1377/hlthaff.2023.01151
16. Kangovi, S., Mitra, N., Grande, D., Huo, H., Smith, R. A., & Long, J. A. (2017, October). Community health worker support for disadvantaged patients with multiple chronic diseases: A randomized clinical trial. American Journal of Public Health, 107(10), 1660–1667. https://doi.org/10.2105/AJPH.2017.303985
17. Chen, D. D., & Bolaji, T. (2022, October 28). Firearm violence in Wilmington, DE: An update on 2020. Delaware Journal of Public Health, 8(4), 62–63. https://doi.org/10.32481/djph.2022.10.012
18 Sumner, S. A., Maenner, M. J., Socias, C. M., Mercy, J. A., Silverman, P., Medinilla, S. P., . . . Hillis, S. D. (2016, November). Sentinel events preceding youth firearm violence. American Journal of Preventive Medicine, 51(5), 647–655 https://doi.org/10.1016/j.amepre.2016.08.002
19. RAND Corporation. Gun Policy in America. (n.d.). State Firearm Mortality Explorer. Retrieved May 17, 2024, from https://www.rand.org/research/gun-policy/state-firearm-mortality.html
20 Bonne, S., Hink, A., Violano, P., Allee, L., Duncan, T., Burke, P., Dicker, R. (2022, January). Understanding the makeup of a growing field: A committee on trauma survey of the national network of hospital-based violence intervention programs. American Journal of Surgery, 223(1), 137–145. https://doi.org/10.1016/j.amjsurg.2021.07.032
21. American Public Health Association. (2022, Nov 8). A strategy to address systemic racism and violence as public health priorities: Training and supporting community health workers to advance equity and violence prevention. https://www.apha.org/Policies-and-Advocacy/Public-Health-PolicyStatements/Policy-Database/2023/01/18/Address-Systemic-Racismand-Violence
22 Decker, H. C., Hubner, G., Nwabuo, A., Johnson, L., Texada, M., Marquez, R., Juillard, C. (2020, June 24). “You don’t want anyone who hasn’t been through anything telling you what to do, because how do they know?”: Qualitative analysis of case managers in a hospital-based violence intervention program. PLoS One, 15(6), e0234608 https://doi.org/10.1371/journal.pone.0234608
23 Wical, W., Harfouche, M., Lovelady, N., Aguilar, N., Ross, D., & Richardson, J. B. (2022). Exploring emergent barriers to hospital-based violence intervention programming during the COVID-19 pandemic. Preventive Medicine, 165(A), 107232 https://doi.org/10.1016/j.ypmed.2022.107232
24 Pino, E. C., Fontin, F., James, T. L., & Dugan, E. (2021, March). Boston violence intervention advocacy program: Challenges and opportunities for client engagement and goal achievement. Acad Emerg Med, 28(3), 281–291. https://doi.org/10.1111/acem.14162
25. Hink, A. B., Atkins, D. L., & Rowhani-Rahbar, A. (2022, August). Not all survivors are the same: Qualitative assessment of prior violence, risks, recovery and perceptions of firearms and violence among victims of firearm injury. Journal of Interpersonal Violence, 37(15-16), NP14368–NP14396 https://doi.org/10.1177/08862605211005157
26. Richardson, J. B., Jr., Wical, W., Kottage, N., & Bullock, C. (2020, Nov-Dec). Shook ones: Understanding the intersection of nonfatal violent firearm injury, incarceration, and traumatic stress among young black men. American Journal of Men’s Health, 14(6), 1557988320982181. https://doi.org/10.1177/1557988320982181
The Delaware Healthy Mother and Infant Consortium presented the 2024 Kitty Esterly, MD Health Equity Champion Awards on April 17. From left to right: Dr. Ronald Tello, Estefania Cuellar, and Vanessa Spence accepted The Hispanic American Association of Delaware’s Organization award. Erica Allen, far right, received the Individual award. Photo by Chelsea Manwiller, DPH
2024 Health Champion Awards presented
The 2024 Kitty Esterly, MD Health Equity Champion Awards were presented at the Delaware Healthy Mother and Infant Consortium’s (DHMIC) annual summit on April 17. Dr. Esterly, a pediatrician who specialized in neonatal care, was a visionary who worked to improve health equity.
Erica Allen of Smyrna, Del. was honored for seeking to level the playing field for Black birthing families. Allen is the founder of the Do Care Doula Foundation and the Central Delaware Community Doula and Perinatal Educator Program. She provides free doula training and an avenue for Black women to find a meaningful career in their local community. Allen’s doulas provide free pregnancy, birth, and postpartum care to their clients – thanks to grants, fundraising, and other money-generating efforts that allow these doulas to get paid while providing free services.
The Hispanic American Association of Del aware (HAAD) was honored for its commitment to promoting health equity beyond providing basic services. HAAD actively addresses the underlying social, economic, and environmental factors that contribute to health disparities. Through tailored programs, collaborative partnerships, data-driven approaches, and community engagement, HAAD demonstrates their dedication to eliminating disparities and creating a more equitable health care system for the Hispanic community in Delaware.
Public invited to Stop the Bleed® Training on May 23 at Legislative Hall
May is National Trauma Awareness Month. Governor John Carney and Lieutenant Governor Bethany HallLong have proclaimed the week of May 19-25, 2024 as Emergency Medical Services Week and Stop the Bleed Day on May 23, 2024
The Delaware Trauma System of Care includes the pre-hospital care of injured patients, the immediate care and transport to an appropriate trauma center, and post-acute care such as patient rehabilitation.
Injury prevention reduces risk and trauma The number one cause of preventable death after an injury is uncontrolled bleeding A person with a severe bleeding injury can bleed to death in less than five minutes unless someone controls the bleeding until first responders arrive. This is why 12 years ago, the American College of Surgeons Committee on Trauma developed the Stop the Bleed® national training program so the public can help save a life when an injured person is bleeding severely.
Delaware Trauma System of Care members invite the public to their May 23 Stop the Bleed® Day training at Legislative Hall, located at 411 Legislative Avenue in Dover, Del. From 9:00 a.m. to 3:00 p.m., on the second floor, Trauma System of Care members will train legislators and the public on tourniquet use and provide tourniquets to those who are trained. There is a limited number of tourniquets. The May 23 training is free and takes less than 15 minutes No registration is required.
The Division of Public Health’s Office of Emergency Medical Services (OEMS) offers Stop the Bleed® training. The training includes a one-hour interactive online course at Training | Stop the Bleed®. The online course is followed by in-person hands-on practice of applying pressure, wound packing, and tourniquet use. To receive this training, call OEMS at 302-223-2700 and ask for the Stop the Bleed® program. For more information, visit StoptheBleed.org.
Elected officials observe Black Maternal Health Awareness Week with action
At the April 17 Delaware Healthy Mother and Infant Consortium Summit, Representative Melissa MinorBrown (RD-15) and Senator Marie Pinkney (SD-13) presented House Concurrent Resolution 107, which they sponsored. The resolution recognized Black Maternal Health Awareness Week (BMHAW), which was celebrated April 11-17, 2024.
The resolution recognizes the work of the DHMIC, the Delaware Perinatal Quality Collaborative, and other stakeholders who promote promising efforts to reduce maternal and infant mortality, morbidity, and disparities. It also calls for improving public and professional awareness of maternal health outcomes, women’s experiences at childbirth, and critical postpartum care, especially for women of color.
During BMHAW, Congresswoman Lisa Blunt Rochester invited DHMIC Vice Chair Tiffany Chalk and Mona Liza Hamlin to a roundtable discussion about decreasing maternal mortality rates for people of color. Chalk chairs the Well Woman/Black Maternal Health (WW/BMH) Committee and Hamlin is the WW/BMH Co-Chair. An article about the meeting can be found here
RECENTLY Published
The DPH Health Systems Protection Section published the Drinking Water State Revolving Fund State Fiscal Year 2022 Annual Report in November 2023.
The Delaware Journal of Public Health published a link to the Impact of Diabetes in Delaware 2023 report and the following two articles in its Chronic Disease in 2024: Diagnosis, Treatment, Prevention issue at https://djph.org/:
1. Lieutenant Governor’s Challenge: Motivating and Honoring Delawareans to Improve Their Health and Well-Being
2. Advancing Healthy Lifestyles: A Multicomponent Initiative to Reduce the Burden of Obesity In Delaware
Gardesey receives gubernatorial tribute
Mawuna Gardesey of the Division of Public Health was honored for his 27 years of State service with a tribute signed by Governor John Carney and Lieutenant Governor Bethany Hall-Long. It was presented at the April 17 Delaware Healthy Mother and Infant Consortium (DHMIC) Summit in Wilmington. Gardesey led the planning of 18 Annual DHMIC Summits.
The Public Health Administrator works for the Center for Family Health Research & Epidemiology within the Family Health Systems Section. He began his service as the State Minority Health Director. His work to reduce infant mortality began when the Infant Mortality Task Force convened in 2004. In 2007, Gardesey was hired as the Center’s Bureau Chief and led a team to support the Task Force and the establishment of the DHMIC and its governance structure. He also led the development of the Healthy Women Healthy Babies Program, the Medical Legal Partnership Program, and the Centers for Disease Control and Prevention’s Pregnancy Risk Assessment Monitoring System. Delaware’s infant mortality rate decreased from 9.3 deaths per 1,000 live births in 2004 to 5.9 deaths per 1,000 live births in 2021, a 37% decrease.
“Mr. Gardesey has exemplified discerning character, empathy, and commitment to promoting the health and well-being of all Delawareans, especially women and children,” the tribute reads. The dignitaries expressed gratitude for his leadership in the areas of public health, health equity, and maternal and child health, and best wishes for continued success.”
Mawuna Gardesey of the Division of Public Health was recognized at the 2024 Delaware Healthy Mother and Infant Consortium Summit for his 27 years of state service. Photo by Alyssa Imprescia, DPH.
Gun violence: a public health crisis
The American Public Health Association calls gun violence a public health crisis and a leading cause of premature death. Gun Violence Awareness Day is June 7, 2024 and #wearorange weekend honors survivors and those working to end gun violence.
In 2021, there were 152 deaths due to firearms among Delaware residents only, according to the Division of Public Health’s Delaware Health Statistics Center (DHSC)
Delaware state law provides for emergency Lethal Violence Protective Orders (LVPO) and nonemergency LVPOs to temporarily prohibit the ownership, possession, control, purchase, access or receipt of a firearm or ammunition by someone who poses physical danger to self or others. The Johns Hopkins School of Public Health says such laws are evidence-informed gun violence prevention policy.
10 Del. Code c. 77 § 7703 permits Emergency LVPOs to be petitioned by law enforcement only, with a Justice of the Peace Court hearing within 24 hours of its filing. The law does not grant the individual to be heard or to be advised that law enforcement is seeking the LVPO.
For a Non-Emergency LVPO, 10 Del. Code c. 77 § 7704 grants law enforcement and family members the right to file an affidavit or verified petition in Superior Court, where the individual has the right to be heard. In both types of LVPOs, the court can prohibit the individual from residing with another person who owns, possesses, or controls firearms or ammunition.
For national data, visit the Centers for Disease Control and Prevention (CDC). Visit the National Extreme Risk Protection Order Resource Center at www.erpo.org for more information about LVPOs.
DHSC provided the following firearm mortality data:
• Among Delaware residents only, assault (homicide) accounted for 51% of the 2021 firearm deaths (78) and intentional self-harm (suicide) accounted for 49% (74).
• In 2021 among Delaware residents only, 87% of the non-Hispanic Black male firearm deaths were due to homicide, compared to 7% of the non-Hispanic White firearm deaths of both sexes from homicide.
• Of the 42 firearm deaths within the 15-24 age group (28%) that occurred in 2021 among Delaware residents only, 18% occurred among non-Hispanic Black males.
Gun violence is preventable with awareness, responsible ownership Awareness, action, and responsible gun ownership reduce firearm injury, disability, and death.
In 2020, the total cost of firearm related injuries and deaths in the U.S. was $493.2 billion, a 16% increase since 2019, according to the American Journal of Preventive Medicine.
Anyone with access to firearms should know how to use them safely. Gun owners can take a variety of gun safety training courses, including firearm basics, concealed carry, and specialized skills training.
Hunters can seek hunter education and training centers in each county. The Delaware Division of Fish and Wildlife manages two shooting ranges: Ommelanden Hunter Education and Training Center, located at 1205 River Road in New Castle, Del.; and Owens Station Shooting Sports and Hunter Education Center, located at 12613 Hunters Cove Road in Greenwood, Del.
Gun safety instructors offer this advice:
• Never point the gun at an unintended target.
• Be sure of the target and what is beyond it.
• Immediately unload firearms when not in use Use gun locks.
• When not in use, store firearms in a safe place such as a locked metal gun safe. Do not store firearms and ammunition together.
• Prevent children and unauthorized adults from accessing firearms and ammunition.
• Regularly clean firearms and have them serviced regularly
• Before or while shooting, never use legal or illegal substances or medications.
• Wear ear and eye protection when shooting For more information about comprehensive gun safety in Delaware, visit the Office of Governor John Carney at de.gov/gunsafety or #gunsafetyDE.
Understanding the Perception of Place and Its Impact on Community Violence
Dorothy Dillard, Ph.D.
Director, Center
for
Neighborhood Revitalization and Research, Delaware State University
Howard Henderson, Ph.D.
Professor of Justice Administration and Director of Center for Justice Research, Texas Southern University
Johnny Rice II, Dr.PH
Associate Professor and Chair of the Department of Criminal Justice, College of Behavioral and Social Sciences, Coppin State University.
Amy D. Goldstein, B.A.
Vice President, Strategy, Thurgood Marshall College Fund
Maruice Mangum, Ph.D.
Professor of Political Science and Chair of the Department of Political Science, Jackson State University
ABSTRACT
In this article, we explore the responses of 357 African American men between 15- and 24-years old living in four high crime high violence cities to better understand their perception of their environment and its impact on community violence. We focus on study participants’ perceptions of their cities, explanations of violence, and their perceived contribution to the level of violence. Respondents describe their cities in grim terms with few opportunities. And, from their perspective, the dangerous environment in which they live necessitates gun possession, potentially perpetuating community violence. Our findings affirm that as with any other public health issue, the perception of place matters in understanding community violence. Further, our findings underscore the importance of seeking and responding to the lived experience of those most likely to be victims and perpetrators of community violence in crafting and implementing interventions
INTRODUCTION
Decades of research has continuously and consistently documented the inextricable relationship between crime and environment. As the public health field developed, the impact of environment on health took a more prominent place. In fact, the socioecological model embraced by the Centers for Disease Control and Prevention (CDC) to address gun violence has its roots in the social sciences. Bronfenbrenner’s1 socioecological theory of human development posits that our development is influenced by a combination of interrelated and varying factors at the personal, community and societal levels. Place or community in the socioecological model (SEM) has become a central component of understanding and addressing public health issues. The Delaware Journal of Public Health issue, Place Matters, demonstrates the many ways in which environment, frequently noted as community or neighborhood, impacts health. In that issue, Phillips2 describes the Vital Conditions Framework, which is a placebased framework and includes safety as a vital condition. Shannon3 introduces a public health intervention designed to reduce school shootings, demonstrating the importance of crafting place specific interventions.
Similarly, the Prevention Institute has compiled a series of fact sheets summarizing findings from the extensive literature on the relationship between health and violence and the impact of environment on both. As captured in the fact sheets, research shows higher rates of chronic diseases, such as asthma, obesity, and diabetes, among children and adults exposed to violence.4 The fact sheets also emphasize worse health outcomes for those living in unsafe neighborhoods compared to those living in neighborhoods described as safe.5
Despite this sound scientific foundation, we continue to focus on individual factors to explain both criminal activity and health outcomes. In turn, we tend to prioritize individual level interventions and fail to address the community level factors embedded in the socioecological public health model. Findings from a recent study6 examining gun possession in four cities characterized by high levels of crime and violence highlights the need to understand how those most likely to be victims and perpetrators of violence view and adapt to their environment. In this article, we further examine the perception of place and its impact on community violence among African American males between 15 and 24 years who possess guns and live in cities marked by high crime and high violence. We discuss how the negative perception of their cities influences their decisions to possess guns. We also examine how they consider their contribution to violence. We then discuss the public health implications.
METHODS
In 2020, Thurgood Marshall College received a grant from the National Collaborative of Gun Violence Researchers to conduct a two phased study on gun possession among African American males between 15 and 24 years old. The study was conducted in four cities experiencing high crime and high violence: Baltimore, Maryland; Jackson, Mississippi; Houston, Texas; and, Wilmington, Delaware. In the first phase of the study, we examined the city characteristics for descriptive and comparative purposes as well as to assess how their characteristics aligned with previous research findings. We found that environmental factors, such as population density, were statistically significant in explaining violent crime rates but not in explaining property crime rates.7
Recognizing that statistical analyses only tell us so much and that they are exponentially more powerful when coupled with qualitative information, we complemented Phase I with a qualitative study exploring the factors associated with gun possession among African American young men. Our qualitative component, Phase II, was based in grounded theory8 and employed community engaged research principles.9 Based on the factors associated with crime and violence identified through previous research, we developed an interview guide comprised of seven broad themes: background (race, ethnicity, age, family, housing); personality, influences and life goals; school, employment and income; arrest and justice system experience; gun exposure and possession, and views on guns, violence, and the city. We vetted the interview guide and research protocol with our community partners.
We aimed to interview 400 study participants, 100 from each city. Eligible participants included African American males between the ages of 15 and 24 years old who possessed or recently possessed a gun. Recruitment varied slightly across sites with the Wilmington site relying exclusively on a grassroots community partner to recruit participants and the other three sites sharing recruitment with community partners. The study sample includes 95 respondents from Baltimore, 86 from Jackson, 100 from Houston, and 93 from Wilmington for a total of 374 respondents or 94% of our target sample size. The sample size for the analysis was 357, excluding 10 of the interviews that could not be used due to audio issues with the taping and seven respondents who did not identify as Black or African American. The respondents were between 15 and 24 years of age, with an average age of 20. About one fifth of the respondents dropped out of high school. Most respondents either graduated from high school or were still in school. We collected information across a broad range of topics which produced an abundance of valuable information to inform policy and practice. In brief, we found that the young men in our study possessed guns because it was necessary to survive in the environment.6 In this article, we explore our respondents’ perception of their city and the violence that characterizes it. We also examine their explanation of the violence and their perception of how they contribute to the violence.
FINDINGS
The findings across all study sites are presented for the interview sections related to perception of place: city description, reasons for high levels of city violence, contribution to city violence, and available positive opportunities. More detailed findings from our respondents living in Wilmington are highlighted.
City Description
Most respondents across the four study sites describe their cities in negative terms. Two-thirds used only negative terms, such as dangerous and violent, to describe their city. In Wilmington, 86% of the respondents described the city negatively and 74% used only negative terms. Wilmington was described as “murder town,” “treacherous,” “crazy,” “chaotic,” and “a war zone” by multiple respondents.
Only 7 (2%) of the respondents described their city in positive terms. None of the Wilmington respondents described the city in positive terms. Only 22 (6%) respondents used qualified positive terms, noting that their city was a mix of good and bad. Among the 87 Wilmington respondents included in the analysis, only three (3%) described Wilmington in qualified positive terms, such as “beautiful but has an ugly side.” Nine (3%) respondents, including one Wilmington respondent, noted that their city had potential.
Reasons for High Levels of Violence
When asked why the level of violence was high, most respondents noted multiple factors. When responses were grouped based on similarity, two categories, negative influences and lack of socialization, emerged as the most common. Negative influences, including music, social media, and peers, was the most common category. About 17% of all respondents but 34% of Wilmington respondents explained the high levels of violence as the result of negative influences. Among the Wilmington group, over half specifically noted “beefing” on social media as a key element fueling violence. As one respondent put it, “There’s so much violence in the city because people be hating. They be beefing over dumb stuff. Over money. They shoot you over females. All sorts of dumb stuff.”
The second most common explanation for the high levels of violence was lack of socialization, such as absent parents and no role models. About 12% of all respondents and one quarter of Wilmington respondents contributed the high levels of violence to the lack of positive socialization. One Wilmington respondent summed it up by saying, “Mothers aren’t raising kids; fathers aren’t around. Not enough money for food. Children aren’t being taken care of.” Another commented, “Violence is all some people know.”
Not surprisingly, easy access to and prevalence of guns was also a common factor in explaining violence. Interestingly, however, less than 10% of the entire sample, including the Wilmington group, mentioned guns as the primary reason for the high levels of violence. More typically, guns were one of many factors, such as crime, poverty, absent parents, and social media, that contributed to violence. Given that all the study participants possessed a gun, we asked them if they thought they contributed to the violence. Only 22 (6%) respondents said they currently contributed to the violence and only 13 (4%) participants noted that they contributed to the violence in the past. In total, only 10% of the young men identified with contributing to the high levels of violence in their city. In Wilmington, 12 (14%) respondents acknowledge they currently contributed to the violence and another 12 (14%) reported that in the past they contributed to the violence. In Wilmington, the proportion of study participants (28%) recognizing their contribution to the violence was almost three times that of the entire study group.
Opportunities
When asked about the opportunities in their cities, less than one fifth (17%) of the young men we interviewed reported that their city had good opportunities. In Wilmington, only 10 (12%) noted that there are positive opportunities and only
five respondents named specific types of opportunities. The types of opportunities identified included sports, school, or jobs. None of them named specific programs or services. For the entire study group, 11% responded that their city offered no opportunities, including about 8% of the Wilmington group. Several of the Wilmington respondents explained that there were no opportunities for them because they were Black, had criminal records, and/or were too young to participate in programs. One Wilmington participant explained the lack of opportunities are the result of a lack of leadership: “Because we have no community leaders. We have no … backbone for the city. We have no one standing up for what’s right and coming here and letting everyone know enough is enough.”
DISCUSSION
The young men we interviewed shared similar perceptions of living in cities characterized by crime and violence. Over two-thirds of our study participants described their cities as a negative social environment with few opportunities. When asked to describe their city, single word responses, such as violent, dangerous, crazy, an in flames, were typical. Wilmington was frequently referred to as “murder town,” referencing the 2014 Newsweek article10 on violence in Wilmington. Similarly, Baltimore was called “a bushel of crabs” by many. The young men told us that the people in the city were “angry and miserable” and comments, such as “if you say the wrong thing, you’re dead and that’s the end of that” underscored the sense of danger that permeates their everyday lives.
In their opinion, surviving this environment required a gun. As we previously described elsewhere,6 all knew where they could easily obtain a gun and two-thirds acknowledged currently possessing a gun. Our study respondents explained that they possessed a gun for safety, and some noted that they needed a gun to protect themselves from enemies and others that they were “beefing with.” The young men were introduced to guns at an early age, typically by friends or family members. Most had handled a gun before they were 15 years old with a few reporting that they were younger than ten years old when they first had access to a gun. Few had been trained to use a gun.
The young men we interviewed painted similar stories about the negative impact of the environment in which they were raised. Socialized in a violent environment and frequently traumatized by that environment, the young men in our study felt that their survival is dependent on possibly perpetuating that violence by carrying a gun. More than once we heard, “Violence is all some people know.” However, few acknowledged their contribution to the violence. When asked why they did not think they contributed to the violence, most respondents did not have a clear reasoning. A few, however, noted that they did not contribute to the violence because they had not killed anyone. Several others explained their response by saying that they possessed a gun for protection and not to hurt others.
Many felt that things could not be changed. Others had a more hopeful outlook as highlighted by responses such as, “I mean, if there was more city events, things like that, the mayor was getting along and participating and things like this and giving back to the communities. I don’t think there would be too much violence…” and “It can be fixed if people came together to stop the bloodshed.”
Practice and experience show us that we can change the environmental factors that fuel violence, crime, and poor health. We can make our schools more inclusive and nurturing environments. We can provide more opportunities in our communities for positive social interaction and growth, recreation, and work force development. We can address the trauma resulting from exposure to the community level violence. We can improve our police community relations. However, we cannot expect sustained violence reduction if we do not solicit and respond to the realities faced by those living in communities marked by violence.
PUBLIC HEALTH IMPLICATIONS
The responses from our study participants remind us that not only does place matter, but perception of place also matters. The public health implication is that we must couple our individual level interventions with community level interventions. In other words, we must address all levels of the socioecological model. If the environmental factors, such as poverty, poor education, limited job opportunities, and inadequate resources, are not addressed the individual level interventions will have limited impact.
Our findings also emphasize that effective public health interventions, including community level interventions, must be informed by the lived experience. The young men in our study knew what they and their communities need to combat gun violence: jobs, better schools, positive social and recreational activities, and inclusion in community planning and events. These match the findings from research.5
Simply increasing opportunities and resources without input from and collaboration with those in need rarely result in the desired effect. Almost 25 years ago, Penchansky and Thomas,11 established that access to resources is a complex issue with interrelated elements related to affordability, availability, accessibility, accommodation, and acceptability. Greater attention to acceptability or the degree to which those in need of the interventions are comfortable with it, requires us to involve not only the victims of violence but also the perpetrators as we design and implement the community level response to violence.
Dr. Dillard may be contacted at ddillard@desu.edu.
FUNDING ACKNOWLEDGEMENT
This work was supported by the National Collaborative on Gun Violence Research under Grant titled Dangerous Recipe: Ingredients Contributing to African-American Gun Violence.
REFERENCES
1. Bronfenbrenner, U. (1992). Ecological systems theory. Jessica Kingsley Publishers.
2. Phillips, K. D. (2022, August 31). Healthy communities Delaware: Accelerating place-based efforts to improve the vital conditions for health, well-being and equity. Delaware Journal of Public Health, 8(3), 10–12. https://doi.org/10.32481/djph.2022.08.004
3 Shannon, K. (2022, August 31). Let it end with us. Delaware Journal of Public Health, 8(3), 102–106 https://doi.org/10.32481/djph.2022.08.017
4 Prevention Institute. (2011, May). Violence and chronic illness [Fact Sheet]. Retrieved from https://www.preventioninstitute.org/sites/default/files/publications/ Fact%20Sheet%20Links%20Between%20Violence%20and%20 Chronic%20Illness.pdf
5. Prevention Institute. (2011, Sep). Violence and health equity [Fact Sheet]. Retrieved from https://www.preventioninstitute.org/sites/default/files/publications/ Fact%20Sheet--Links%20Between%20Violence%20and%20 Health%20Equity.pdf
6 Dillard, D., Henderson, H., Mangum, M., Rice, I. I. J., & Goldstein, A. (2023). Unlocking gun-violence solutions: The necessity and power of lived experience. American Journal of Qualitative Research, 7(4), 182–202. https://doi.org/10.29333/ajqr/13729
7 Smith, S., Ferguson, C. J., & Henderson, H. (2022). An exploratory study of environmental stress in four high violent crime cities: What sets them apart? Crime and Delinquency, 68(11), 2092–2114. https://doi.org/10.1177/00111287211057858
8. Glaser, B. G., & Strauss, A. L. (1968). The discovery of grounded theory: Strategies for qualitative research. Aldine. https://doi.org/10.1097/00006199-196807000-00014
9. Balls-Berry, J. E., & Acosta-Pérez, E. (2017, June). The use of community engaged research principles to improve health: Community academic partnerships for research. [PubMed]. Puerto Rico Health Sciences Journal, 36(2), 84–85.
10 Jones, A. (2014, December 9). Murder Town USA (aka Wilmington, Delaware). Newsweek. https://www.newsweek.com/2014/12/19/wilmington-delaware-murdercrime-290232.html
11 Penchansky, R., & Thomas, J. W. (1981, February). The concept of access: Definition and relationship to consumer satisfaction. Medical Care, 19(2), 127–140. https://doi.org/10.1097/00005650-198102000-00001
Can Past Psychedelic Use Mitigate the Severity of Opioid Use Disorder? Case Report of a Musician.
Asim Trimzi University of Delaware
Morgan Campbell, M.D. State of Delaware
ABSTRACT
Little is known about the association between psychedelic use and substance abuse in the general population. We present a case of an award winning musician with an extensive history of hallucinogen use during his early life and how this impacted his overall wellbeing and opioid experience.
INTRODUCTION
Opioids were involved in 68,630 overdose deaths (74.8% of all drug overdose deaths). More than 932,000 people have died since 1999 from a drug overdose (see Figure 1).1 The majority of substance-use-disorder deaths are attributed to opioid abuse, especially with the highly fatal rise of fentanyl contamination in previous years.1 Current therapies are somewhat helpful, but insufficient because morbidity and mortality of opiate use disorder are increasing. However, psychedelics are beginning to be investigated for the treatment of psychiatric disorders such as substance use disorders or PTSD.
In light of these challenges, our case report explores an unconventional potential therapy: psychedelic drugs. There are studies on the effects of drugs like psilocybin and 3,4-methylenedioxymethamphetamine (MDMA) on individual brain cells2 and their role in rewiring the brain, however, there is little known about the association between psychedelic use and substance abuse in the general population. We present a
case of an award winning musician with an extensive history of hallucinogen use during his early life and how this impacted his overall wellbeing and opioid experience.
BACKGROUND
Illicit opioid use contributes significantly to disease, disability, and death. It strains the healthcare system and burdens the economy. In 2019, opiate use led to 12.9 million global disability-adjusted life years.1 Effective therapies exist, including methadone, buprenorphine, naltrexone, and various support programs, but these therapies are insufficient because the opioid problem continues to grow as opioid-involved overdose deaths rose from 21,089 in 2010 to 80,411 in 2021.1 The risks increase when individuals are unable to break the habit, when they are no longer able to maintain healthy relationships, and when they begin using intravenously.
Hallucinogens are being considered for investigation as potential therapies for opiate use disorder because psychedelic use in
Figure 1. Opioid Death Rate in Delaware Compared to the United States1
naturalistic settings has been found to be associated with reductions in opioid use. A single treatment with the alkaloid ibogaine, from an African root known for its hallucinogenic qualities, was found to reduce withdrawal symptoms and facilitate opioid cessation over a twelve-month period.3 However, despite the promise of psychedelic drugs as therapies, there have not been investigations into the potential prophylactic effect of earlylife use of psychedelics to reduce the severity of opiate use if it develops later in life.
METHODS
This case report centered around a structured patient interview conducted in an outpatient clinic setting. The interview was designed to gather comprehensive information regarding the patient’s drug addiction history, including the onset of drug use, types of substances used, frequency and duration of use, previous attempts at cessation, and any related medical or psychological comorbidities. Prior to the interview, the patient provided informed consent after being assured of confidentiality and the non-judgmental nature of the inquiry. The questions were formulated based on established diagnostic criteria and tailored to elicit detailed responses that could contribute to both the understanding and the treatment of the patient’s addiction.
CASE PRESENTATION:
THERAPEUTIC EFFECTS OF PSYCHEDELICS ON OPIOID USE.
Mr. TF is a 65-year-old married Caucasian male who has been attending an outpatient psychiatric clinic for ongoing management of depression and posttraumatic stress disorder. He has been an exceptional musician all his life who has achieved notable success.
Initial Drug Use
Mr. TF started using psychedelics between the ages of 14 and 20, claiming that it profoundly helped his creativity as a musician. Although he could not perform while under the influence of these psychedelics, they played a key role in his creative process especially when he was brainstorming musical ideas in the course of composition. After this period of psychedelic use, he began using opioids, however, his experience was critically different than most opioid users.
Transition to Opioids
Mr. TF began using opioids after he received a prescription from his physician for pain management, which led him down a spiral of addiction and drug-abuse. He never used drugs intravenously or shared needles and had a shorter duration of use than other opioid users. Although opioids were readily available around him when he was using psychedelics, he never used them. It was after he stopped using psychedelics that he developed severe opioid dependence. Outcomes
This transition underscores a critical period where the absence of psychedelics in his life perhaps left a void, making him more susceptible to the allure of opioids as an alternative means of coping or pain relief. What stands out in Mr. TF’s story is the manner in which he engaged with opioids; despite the severity of his addiction, he maintained certain boundaries—never resorting to intravenous drug use or sharing needles, behaviors often associated with heightened risks of disease transmission and
overdose. Additionally, compared to typical trajectories of opioid addiction, Mr. TF’s period of opioid use was relatively brief. This experience suggests that past hallucinogen use may translate into a less severe opioid experience in the future and could have had a protective effect while he was using opiates.
DISCUSSION
Few and possibly none of the studies on psychedelics have been funded with public money. In light of the dire nature of opioid addiction and promising signals in data on psychedelics with regards to opioid addiction, we hope that more research is undertaken in this area. Because of the growing body of evidence that psychedelics can help with many psychiatric conditions, the question arises why this kind of research does not receive more attention from funding agencies. It has been argued that funding is scarce due to stigma against psychedelics because it is associated with the United States counterculture. It is also possible that there is reluctance to investigate the potential of psychedelics because they are associated with other stigmatized groups, namely indigenous people. These compounds have been used for therapeutic and ceremonial purposes for centuries or perhaps millennia in non-western contexts.4
Linking the therapeutic potential of hallucinogens to the case of a patient with opioid use disorder, such as the mentioned musician, involves understanding the individual’s unique journey through addiction and recovery, and how these substances might facilitate a transformative healing process. In this context, the use of hallucinogens could be seen not just as a method of reducing dependency on opioids, but as a crucial part of a broader therapeutic intervention aimed at addressing the underlying causes of addiction, including emotional pain, trauma, and a lack of connection or meaning in life.
The case suggests that the musician’s previous use of psychedelics may have had a lasting impact on his relationship with substances, possibly contributing to a form of resilience against the more destructive patterns of opioid use. The return to psychedelics, in a therapeutic context, could reinforce this resilience, helping to reduce opioid dependency while addressing psychological distress. Linking the potential benefits of hallucinogenic therapy to a patient’s experience requires a holistic view of addiction treatment, recognizing the complexity of substance use disorders and the multifaceted nature of recovery. For the musician, and indeed for many struggling with opioid use disorder, psychedelics could offer a unique and powerful tool for healing, provided they are used within a carefully structured and supportive therapeutic framework.
PUBLIC HEALTH IMPLICATIONS
Opioid use disorder is a very serious public health problem and it is worthwhile exploring the relationship of opioid use disorder in the context of other substance use disorders, specifically hallucinogens. Drugs with hallucinogenic properties have been found to be useful in many psychiatric disorders.5 In light of our patient TF’s use of psychedelics, which may have protected him from a more serious opioid addiction, we hope that further research may validate whether or not psychedelics indeed have a prophylactic effect if users are subsequently exposed to opioids, and elucidate any mechanisms by which this prophylactic effect occurs.
Mr. Trimzi may be contacted at trimziasim@gmail.com
REFERENCES
1. Centers for Disease Control and Prevention. (2023, Aug 22). Drug overdose deaths. Centers for Disease Control and Prevention. https://www.cdc.gov/drugoverdose/deaths/
2. Ly, C., Greb, A. C., Cameron, L. P., Wong, J. M., Barragan, E. V., Wilson, P. C., . . . Olson, D. E. (2018, June 12). Psychedelics promote structural and functional neural plasticity. Cell Reports, 23(11), 3170–3182. https://doi.org/10.1016/j.celrep.2018.05.022
3. Noller, G. E., Frampton, C. M., & Yazar-Klosinski, B. (2018). Ibogaine treatment outcomes for opioid dependence from a twelve-month follow-up observational study. The American Journal of Drug and Alcohol Abuse, 44(1), 37–46 https://doi.org/10.1080/00952990.2017.1310218
4 Yaden, D. B., Yaden, M. E., & Griffiths, R. R. (2021, May 1). Psychedelics in psychiatry-keeping the renaissance from going off the rails. JAMA Psychiatry, 78(5), 469–470. https://doi.org/10.1001/jamapsychiatry.2020.3672
5. De Gregorio, D., Aguilar-Valles, A., Preller, K. H., Heifets, B. D., Hibicke, M., Mitchell, J., & Gobbi, G. (2021, February 3). Hallucinogens in mental health: Preclinical and clinical studies on LSD, psilocybin, MDMA, and ketamine. The Journal of Neuroscience : The Official Journal of the Society for Neuroscience, 41(5), 891–900 https://doi.org/10.1523/JNEUROSCI.1659-20.2020
Delaware Journal of
Public Health
Upcoming Issues
Each year, the Delaware Journal of Public Health publishes five different theme issues. Article submissions are accepted on a rolling basis, and the editorial board considers all submissions, both those connected directly to a theme issue, and non-thematic submissions. The editorial board reserves the right to include non-thematic submissions in each issue.
The working publishing calendar and thematic issues for 2024 are as follows:
Issue Submission Publication
Chronic Disease February 2024 March 2024
Violence April 2024 May 2024
Cancer & the Power of Preventive Screening June 2024 July 2024
Childhood Development & Education August 2024 September 2024
After COVID - Rebuilding Public Health & Healthcare Resilience October 2024 November 2024
If you have questions about submissions, ideas for an article, or suggestions for a future theme issue, please email Kate Smith: ksmith@delamed.org
All submissions can be submitted via the online submission portal: https://www.surveymonkey.com/r/2DSQN98 Submissions guidelines can be found at: https://djph.org
Tuesday, October 29, 2024 Hosted
Delaware Healthcare Association
1280 South Governors Avenue, Dover DE 19904
Phone: 302-674-2853 | Fax: 302-734-2731
Web Site: www.deha.org
Primary Forum Contact: Yasmine Chinoy E-Mail: yasmine@deha.org
Sponsorship Opportunities Available!
A Safer Delaware: The Case for a Permit-to-Purchase Policy for Reducing Firearm Violence
Traci Manza Murphy Executive Director, Coalition for a Safer Delaware
Sarah Stowens, Ed.D. Senior Manager, Government Relations and Strategy, ChristianaCare
INTRODUCTION
Recently, in guest lecturing at the University of Delaware, a group of students were asked how far apart they should stand from someone to avoid contracting COVID-19. “SIX FEET!” Every student knew the answer, instantly. It’s an excellent example of public health messaging - everyone knew the answer, they knew it was the right answer, and they were able to recall the answer quickly.
By contrast, a landmark survey in 2023 by the Kaiser Family Foundation estimates that only 49% of Americans know that gun violence has recently become the leading cause of death for those under 20, even though 84% have “taken at least one precaution to protect themselves or their families from the possibility of gun violence.”1 Despite being a small state of just over one million residents, Delaware is not exempt from the crisis of gun violence. We are a state of neighbors, a state where everyone knows everyone, or seems to.
So why is our lingering national reputation that of “Murdertown, USA”?2,3 Why are our rates of gun violence higher than those of so many states perceived to be far more dangerous?
According to 2021 data from the Centers for Disease Control (CDC), Delaware ranked 28th for gun safety, far behind our safest neighbor New Jersey (3rd) and still significantly behind other neighbors Pennsylvania (20th) and Maryland (22nd).4 What lessons can we learn from our safest neighbors to help us build a safer Delaware?
First, let’s look at what is driving Delaware’s dismal gunrelated fatalities: disproportionately high rates of community violence. Figures 1 and 2 are a visualization derived from CDC epidemiologic data.5
Why? Nearby Pennsylvania and New Jersey have far lower rates of community violence, even with more densely populated cities experiencing similar root causes, including educational outcomes, poverty, insecure housing.4 So, if our root causes are similar, why are the outcomes so vastly different?
Delaware Attorney General Kathy Jennings has said, “Straw purchasing is a major means of firearms getting into the hands of violent people who intend to kill others, who intend to rob others and who intend to commit firearm crimes, drug trafficking, et cetera.”6 Firearms trace data from 2022 in the state of Delaware from the Bureau of Alcohol, Tobacco, and Firearms (ATF) shows where guns that were found to be used in crime came from (Figure 3).7
Recently released ATF data from 2023 continues to show “the majority of guns used to commit crimes in Delaware were bought in Delaware.”8
Are Delaware federally licensed firearm dealers (FFLs) particularly nefarious? No. FFLs are following the law and guidelines, but their goal is to sell firearms,9 and recent research points to this disproportionately affecting communities with concentrated disadvantage.10,11 Delaware has served as a linchpin for easy access to guns along the I-95 corridor - the iron pipeline - for years.12 And in order to change it, a strong policy shift is needed.
CATEGORIES OF FIREARM LAWS
There are a few distinct categories of laws currently regulating firearms. First, regulations on the kinds of weapons that can be sold to civilians. In Delaware, we have banned the sale and transfer of assault-style weapons, large capacity magazines, auto-sears, bump stocks, and ghost gun kits. These policies are designed to limit the firepower of any one person – but these laws do nothing to regulate who can own weapons.13–16
That takes another category: regulating who can purchase firearms In Delaware, we have universal background checks and we do not sell firearms to those under 21 or those prohibited from ownership due to specific mental health concerns or criminal histories.17–21 Third, Delaware has specific parameters of where and how firearms can exist in society. Delaware prohibits firearms at polling locations, in schools and on school grounds, in courthouses and requires a Concealed Carry of a Deadly Weapon permit to carry firearms concealed anywhere in the State. Delaware also requires “secure storage” of firearms when children or persons prohibited are present.22–25
A PERMIT-TO-PURCHASE POLICY
The most recent significant legislative proposal to reduce gun violence in Delaware is a permit to purchase policy. Implementing permit to purchase or firearm purchaser licensing requirements adds an additional layer of scrutiny to firearm transactions, ensuring that only individuals who pass a thorough background check and meet specific criteria are permitted to buy firearms. This process typically involves a comprehensive background check, completion of a firearm safety course, and obtaining a permit from law enforcement or a designated authority before purchasing a gun. Permit to purchase laws have shown effectiveness in reducing firearm-related homicides and suicides by preventing individuals with a history of violence or mental illness from obtaining firearms legally.26–28 Permit to purchase requirements act as a proactive measure to identify and prevent high-risk individuals from accessing firearms. By establishing stringent criteria and mandatory safety training, these laws promote responsible gun ownership while safeguarding public safety. Furthermore, permit systems enable authorities to track firearm transactions, aiding law enforcement in investigations and reducing the illegal trafficking of firearms.
1.
per 100,000 by State from 1979-2020 in Delaware
Figure
Firearm Homicides
Figure 2. Firearm Homicides per 100,000 by State from 1979-2020 in New Jersey
Top 15 Soure States for Firearms with Delaware Recovery
January 1, 2022 – December 31,2022
NOTE: An additional 23 states and Puerto Rico accounted for 45 other traces. The Source state was identified in 1,369 total traces.
Just this year, Delaware’s General Assembly passed a permit to purchase bill, but with an 18-month stand-up period, Delaware won’t see gun violence reductions as a benefit for several years.29 In fact, while Delaware has passed a number of policies in the past 4 years with respect to gun violence prevention, the expected benefits of those policies won’t be experienced over night for any of them
RECOMMENDATIONS FOR THE WORK AHEAD
As we work towards a safer Delaware, is our hope that together, these policies – when implemented properly –weave together a tight safety net that has the potential to truly deliver that promise our neighbors, friends, children deserve. Of course, with the need for safer communities imminent it is our duty to continue to evaluate the impact of the policies passed to ensure successful implementation. To ensure comprehensive analysis, the state agencies responsible for the policy implementation should continue to work with community organizations and hospital violence intervention programs to:
1. Engage in critically needed research that illuminates how policies can influence the intersections between access to firearms and the misuse of them;
2. Study how those data collected may support the combination of policies has impact on lowering suicide and homicide rates;
3. Use data to identify evidence based ways to mitigate “upstream” factors in community and gun violence prevention.
Ms. Murphy may be contacted at tracimurphy@decagv.org
REFERENCES
1. Schumacher, S., Kirzinger, A., Presiado, M., Valdes, I., & Published, M. B. (2023, Apr 11). Americans’ experiences with gun-related violence, injuries, and deaths. KFF. https://www.kff.org/other/poll-finding/americans-experiences-withgun-related-violence-injuries-and-deaths/
2. Jones, A. (2014, Dec 9). Murder town USA (aka Wilmington, Delaware). Newsweek. https://www.newsweek.com/2014/12/19/wilmington-delaware-murdercrime-290232.html
3. Payne, Y. A., Hitchens, B. K., & Chambers, D. L. (2023). Murder town, USA: Homicide, structural violence, and activism in Wilmington. Rutgers University Press.
4. Davis, A., Kim, R., & Crifasi, C. (2023). A year in review: 2021 gun deaths in the U.S. Johns Hopkins Center for Gun Violence Solutions. Johns Hopkins Bloomberg School of Public Health. https://publichealth.jhu.edu/sites/default/files/2024-01/2023-june-cgvsu-s-gun-violence-in-2021-v3.pdf
5. RAND Corporation. (n.d.). Gun Policy in America. Changes in State Firearm Mortality. Retrieved from https://www.rand.org/research/gun-policy/longitudinal-firearmmortality.html
6. Barrish, C. (2022, Feb 17). ‘Real evil of straw purchases’ revealed in Delaware firearms cases. WHYY. https://whyy.org/articles/real-evil-of-straw-purchases-revealed-indelaware-firearms-cases/
7. Bureau of Alcohol. Tobacco, Firearms and Explosives. (2023, Sep 27). Firearms trace data: Delaware—2022. https://www.atf.gov/resource-center/firearms-trace-data-delaware-2022
8. Edelman, H. (2024, Feb 16). 5 Delaware stores made list of shops that sold most guns used in crimes, new data shows. Delaware News Journal. https://www.delawareonline.com/story/news/crime/2024/02/16/ crime-gun-sales-in-delaware-highest-at-5-stores-atf-datashows/72613370007/
9. Glasser, N. J., Pollack, H. A., Ranney, M. L., & Betz, M. E. (2022). Economics and public health: Two perspectives on firearm injury prevention. The Annals of the American Academy of Political and Social Science, 704(1), 44–69. https://doi.org/10.1177/00027162231168738
10. Semenza, D. C., Stansfield, R., Steidley, T., & Mancik, A. M. (2023). Firearm availability, homicide, and the context of structural disadvantage. Homicide Studies, 27(2). https://doi.org/10.1177/10887679211043806
11. Semenza, D. C., Griffiths, E., Xu, J., & Stansfield, R. (2022). Firearm dealers and local gun violence: A street network analysis of shootings and concentrated disadvantage in Atlanta. Journal of Research in Crime and Delinquency, 59(5), 627–658.
https://doi.org/10.1177/00224278221077626
12. Enos, S. L. (2012). “Iron Pipeline”. In Carter, Gregg Lee (ed.). Guns in American Society: An Encyclopedia of History, Politics, Culture, and the Law. Santa Barbara, CA: ABC-CLIO, 440–44. ISBN 9780313386701.
13. Del. Code tit. 11, § 1466
14. Del. Code Ann. tit. 11, § 1469
15. Del. Code Ann. tit. 11, § 1444
16. Del. H. 125 (2021)
17. Del. Code Ann. tit. 11, § 1448B
18. Del. Code Ann. tit. 11, § 1448
19. Del. Code Ann. tit. 11, § 1445
20. Del. Code tit. 10, § 3930
21. Del. Code Ann. tit. 24, §§ 901, 903
22. 11 Del. C. Chapter 5, Section 1457B
23. 20 U.S.C. §7961 and 11 Del.C. §1457
24. 11 DE Code § 1442 (2012 through 146th Gen Ass)
25. 11 DE Code § 1456 (2023)
26. Crifasi, C. K., Buggs, S. A. L., Choksy, S., & Webster, D. W. (2017). The initial impact of Maryland’s firearm safety act of 2013 on the supply of crime handguns in Baltimore. RSF: The Russell Sage Foundation Journal of the Social Sciences, 3(5), 128–140. https://muse.jhu.edu/pub/207/article/677236
27. McCourt, A. D., Crifasi, C. K., Stuart, E. A., Vernick, J. S., Kagawa, R. M. C., Wintemute, G. J., & Webster, D. W. (2020, October). purchaser licensing, point-of-sale background check laws, and firearm homicide and suicide in 4 US states, 1985–2017. American Journal of Public Health, 110(10), 1546–1552. https://doi.org/10.2105/AJPH.2020.305822
28. Webster, D. W., McCourt, A. D., Crifasi, C. K., Booty, M. D., & Stuart, E. A. (2020). Evidence concerning the regulation of firearms design, sale, and carrying on fatal mass shootings in the United States. Criminology & Public Policy, 19(1), 171–212. https://doi.org/10.1111/1745-9133.12487
29 Goggin, C. (2024, March 15). “Permit to purchase” handgun bill passed by lawmakers in Delaware; governor to sign into law. 6abc Philadelphia. https://6abc.com/delaware-gun-bill-permit-to-purchase-senate-govjohn-carney/14529228/
Prepare people with access and functional needs for hurricane season
Now is the time for people with access and functional needs and their caregivers to prepare for the 2024 hurricane season, which officially began on June 1.
Everyone, especially those with special needs, should have an emergency plan Build a plan for people with access and functional needs with these tools from the Delaware Department of Health and Social Services: Preparedness Buddy, Travel Buddy, and the Disaster Shelter brochure, located at https://dhss.delaware.gov/dhss/dph/php/preparednes sbuddy.html
To increase your chance of survival during a hurricane, the National Weather Service (NWS) advises knowing what actions to take before the hurricane season begins, when a hurricane approaches, when the storm is in your area, and after a hurricane leaves your area. Plan ahead with accurate information:
• Sign up for Delaware Emergency Management Agency (DEMA) Emergency Alerts and SMART 911 at https://de.gov/dens
• Know your flood risk and whether you live, work, or travel in Evacuation Zones. Evacuation Zones encompass low-lying areas susceptible to flooding and storm surge. Visit DEMA at https://preparede.org/know-your-zone.
• Learn the evacuation routes where you live and work at https://de.gov/evacroutes
• Only use trusted sources for accurate storm information, such as from DEMA, NWS, local news, and The Weather Channel. Visit https://preparede.org/stay-informed/#tune-in-to-media
Emergency personnel cannot respond until it is safe to do so, as hurricanes can bring flood waters, high winds, blocked roads, and dangerous conditions.
For more information, visit https://www.samhsa.gov/dtac/disasterplanners/special-populations
Customize emergency kits for special needs
In the event that a natural or man-made emergency should occur, the most empowering thing Delawareans can do is to be prepared.
People with access and functional needs and those who support them regularly know best what they need to survive in an emergency.
The U.S. Department of Homeland Security (DHS) recommends creating an emergency kit that is customized to an individual’s or family’s specific support needs. An emergency kit should include the basics to survive for at least three days. Consider different ages of household members, dietary needs, medical needs including prescriptions and equipment, pets or service animals, and anything else needed to survive. Learn more about building a customized emergency kit at https://www.ready.gov/disability#kit.
Learn how to prepare for severe weather, flooding, and wildfires by visiting DHS’s Federal Emergency Management Agency at https://www.ready.gov/
More recommendations from DHS are:
• Individuals with a communication disability should carry printed cards or store information on their devices to inform first responders.
• Plan how to protect assistive technology devices so they will not be harmed during an evacuation.
• The U.S. Department of the Treasury advises those who depend on Social Security or other regular federal benefits to sign up for electronic payments before disaster strikes. Visit Go Direct® at https://godirect.gov/gpw/
The website www.ready.gov/toolkits offers toolkits for people with access and functional needs, youth, pet owners; types of disasters; and preparedness campaigns.
Getty Images
Getty Images
RespondDE honors
1,700 volunteers
RespondDE Medical Reserve Corps volunteers prepare for and respond to public health emergencies and disasters and promote health education throughout the state. In 2023, they assisted with public health emergencies, including sheltering and recovery centers for coastal flooding and tornado response.
On April 23, the Delaware Department of Health and Social Services (DHSS), Division of Public Health (DPH), Emergency Medical Services and Preparedness Section (EMSPS) hosted an appreciation event to thank the 1,700 RespondDE volunteers for their hard work and generous time they gave to Delawareans in 2023. In the last three years, RespondDE volunteers contributed over 15,000 hours with an economic impact of over $600,000 by assisting with public health emergencies and providing outreach education.
The Volunteer of the Year Award for 2023 was presented to Joyce Junious of Felton, Del. Junious is Kent County’s RespondDE Representative. She volunteered the most hours last year, and participated in four events. In 2023, Junious attended multiple trainings and contacted all pending volunteers to welcome them. She also assists with administrative tasks and volunteer outreach for pending volunteers.
Beatrice Gale of Camden, Del. received the Shining Start Award for her participation in three 2023 outreach events. A 15-year member of the Medical Reserve Corps, Gale also volunteers for RespondDE’s Interpreter Corps.
To learn more about RespondDE or to become a volunteer, visit https://www.dhss.delaware.gov/dhss/dph/php/vohome.html
On May 23 (Stop the Bleed Awareness Day), Delaware Trauma System of Care members offered tourniquet training at Legislative Hall in Dover, Del. Above, Niki Morris of Beebe Healthcare, at left, instructs Jazmine Gibbs of the Division of Public Health how to save a life during a bleeding emergency Photo by Sean Dooley.
This spring, the Division of Public Health (DPH) Cancer Prevention and Control Bureau provided skin cancer outreach sessions to 450 Delaware Department of Transportation (DelDOT) staff, focusing on outdoor workers. The Bureau gave attendees sleeves and wide-brimmed hats constructed of sun protection fabric Clockwise, from top left: During the May 20 session, Teresina Jensen, PA-C of Dermatology Partners of Wilmington provides a courtesy skin check. Water Resources Engineer Stephen Wright of DelDOT models SPF50 sleeves that protect arms from ultraviolet light. Public Health Treatment Program Administrator Paulette Robinson-Wilkerson, MS presents Photos by Donna Sharp.
Joyce Junious Submitted photo
Protect your skin to save your life
To urge Delawareans to protect their skin to prevent skin cancer, Governor John Carney and Lieutenant Governor Bethany Hall-Long proclaimed May 2024 as Skin Cancer and Melanoma Awareness Month. According to HealthyDelaware.org, people at higher risk for skin cancer:
• Have a history of frequent sunburns (especially before age 20)
• Have light-colored skin, freckles, light hair, and/or blue or green eyes However, people of color also get skin cancer and should take precautions
• Have a family or personal history of malignant melanoma
• Are exposed to excessive ultraviolet (UV) light from the sun, tanning lamps, or tanning beds
• Have many moles (particularly abnormal ones).
Follow this sun safety advice:
• Limit time in the sun, especially between 10:00 a.m. and 4:00 p.m., when UV rays are strongest.
• Use a water-resistant sunscreen with a Sun Protection Factor (SPF) level of 30 or higher, and reapply it every two hours or more often if swimming or sweating.
• Wear a wide-brimmed hat and sunglasses that block 99% or more of UV light. Wear UV protective clothing.
• Wear lip balm and makeup products with an SPF of 30 or higher.
• Self-examine skin for changes If at high risk, visit a health care provider for regular skin exams People of color should pay particular attention to their palms, soles, and nails of the hands and feet
Melanoma skin cancer – the sixth most common newly diagnosed cancer type in Delaware – can be deadly when it attacks other organs. Delaware (27.1 people per 100,000 population) has a higher melanoma cancer incidence rate than the U.S. (22.4 people per 100,000 population) and currently ranks tenth among the states for 2016-2020, according to the Delaware Cancer Registry. Also for 2016-2020, Delaware males (35.0 people per 100,000 population) have a higher melanoma cancer incidence than Delaware females (21.0 people per 100,000 population).
For more information, visit HealthyDelaware.org Health care providers can also visit cdc.gov/skin-cancer
Prevent Lyme disease; avoid ticks
Lyme disease is the most common tick-borne disease in Delaware with over 300 cases reported each year, according to the Division of Public Health’s (DPH) Office of Infectious Disease Epidemiology.
Lyme disease is spread by the bite of an infected blacklegged tick, also known as a deer tick, if it is attached for 24 hours or longer. In some cases, a bull’s eye rash will appear near the bite site. If an expanding rash with a diameter of more than two inches appears or flu-like symptoms occur over a 30-day period following a tick bite, individuals should contact their health care provider immediately.
To remove an attached tick, use tweezers to grab it as close to the skin’s surface and pull upward.
Prevent tick bites by following these precautions:
• Avoid wooded or brushy areas with high grass and leaf litter. Stay to the center of trails.
• Treat clothing with products containing 0.5% permethrin or use Environmental Protection Agency (EPA)-registered insect repellents containing products like Diethyltoluamide (DEET). Always follow label instructions.
• Perform tick checks on people and pets after being outdoors.
• Shower within two hours of coming indoors and tumble dry clothes in a dryer on high heat for 10 minutes to kill ticks.
• Keep pets up to date on tick prevention products.
• At home, place a three-foot-wide barrier of wood chips or gravel between lawns and wooded areas and around patios and play equipment. Maintain a nine-foot-wide barrier between the wood chips and high-use areas. Keep grass short in high-use areas and keep leaves raked.
For more information about Lyme disease and tips for preventing tick-borne illnesses, visit the DPH Lyme disease webpage at https://www.dhss.delaware.gov/dhss/dph/epi/lyme.html For additional information, visit Delaware’s Lyme Disease Education Oversight Board’s webpage at https://www.lymediseaseeducation.org/.
A wide-brimmed hat with front and back flaps made of sun protective material DPH photo.
Lyme disease can present as a bull’seye rash. CDC photo.
Prevent drownings with water safety
Spending time at the beach, pool, or favorite swim spot is a fun summer activity, but there are risks associated with water-related activities Alarmingly, drowning is the leading cause of death in children in the United States. More children ages 1-4 die from drowning than any other cause, according to the Centers for Disease Control and Prevention (CDC).
The American Academy of Pediatrics advises to teach children how to swim, to never let children dive into water unless an adult has first checked its depth, and to never swim in canals or fast-moving water. Water safety is especially important for children and adults with autism because they are drawn to water, and some are unable to understand its dangers.
Prevent drowning and increase safety in and around water by following these guidelines from the CDC:
• Learn basic swimming and water safety skills and Cardiopulmonary Resuscitation (CPR).
• Never swim alone and swim only in areas where lifeguards are on duty
• Swimmers and adults supervising them should pay attention and avoid distractions. Unlike television and movies, drownings are often silent.
• Wear brightly colored swimsuits that are more visible
• Know the risks of natural waters such as oceans, rivers, lakes, and creeks
• Take additional precautions for medical conditions and prescription medications
• Follow boating safety laws summarized in the Handbook of Delaware Boating Laws and Responsibilities on the Delaware Department of Natural Resources and Environmental Control’s Boating Safety page, which also lists recommended boating safety courses.
For more detailed information on water safety, visit: https://www.cdc.gov/drowning/prevention/index.html https://www.safekids.org/poolsafety
Delaware’s public swimming pool regulations ensure health and safety
Safe Kids Delaware and the Delaware Coalition for Injury Prevention recommend following local requirements for fences and barriers. Safe Kids Delaware and the Coalition advise that private pools and non-locking hot tubs should have a fence that is at least 48 inches tall, have no openings larger than 4 inches, and remain locked when not in use.
Public swimming pools must follow the State of Delaware Public Swimming Pool regulations within 16 Del. Code § 4464. Every year throughout the summer months, the Division of Public Health (DPH) conducts routine inspections of all public swimming pools to ensure compliance with the regulations. This includes verifying that they have required emergency equipment such as ring buoys, rescue tubes, and backboards. DPH also investigates complaints.
The Public Swimming Pool regulations do not require a lifeguard to be on duty at any pool of any motel, hotel, or private campground. Therefore, adults should supervise swimmers of all ages.
Access to public swimming pools for disabled persons must conform to American Disabilities Act standards. Public pools with diaper-aged bathers must have a diaper changing station and an operational hand wash sink
Regarding security, all outdoor public swimming pools must be enclosed by a fence that is at least four feet high everywhere (six feet is recommended). All pool fences must have a locking gate which must be locked when the pool is closed. The entrances to indoor public swimming pools must be locked when the pool is closed.
All public swimming pools drain covers must comply with the Virginia Graeme Baker Pool and Spa Safety Act, which is federally mandated Slides in public swimming pools are prohibited unless a variance has been obtained.
Every public pool must be monitored at least weekly by a qualified operator, who must document the visits and have them available for DPH review. Any patron or DPH representative must be able to view the certificates that DPH issues to qualified operators.
Read the complete set of regulations at: https://dhss.delaware.gov/dph/hsp/poolsandspas.html
For more information, contact the Environmental Health offices in each county:
• New Castle County: 302-283-7110
• Kent County: 302-744-1220
• Sussex County: 302-515-3302
Getty Images
RESOURCE GUIDE
TABLE OF CONTENTS
Resources
Hotlines
by Type
Domestic Violence
Rape and Sexual Assault
Counseling, Mental Health, and
Advocacy
Sexual Assault Nurse Examiners
Police and Department of Corrections
Advocacy
Prosecution
Restorative Justice and Victim-
Offender Mediation
Abusive Partners'
Intervention/Batterers' Intervention
j.Civil
k.Family Visitation Centers
l.Human
1.A: HOTLINES
CASTLE COUNTY
KENT & SUSSEX COUNTIES
NEW CASTLE COUNTY
LATIN AMERICAN COMMUNITY CENTER
MENTAL HEALTH SERVICES: 302-295-2169
DOMESTIC VIOLENCE SERVICES: 302-295-2173
The LACC provides mental health services, short- and long-term case management, substance abuse prevention, advocacy for victims of crime, and more.
Student Wellness and Health Promotion provides services to victims of sexual assault, harassment, stalking, dating, and domestic violence.
CHILD, INC. DOMESTIC VIOLENCE SERVICES
OFFICE: 302‑762‑8989
HOTLINE: 302-762-6110
CHILD, Inc. provides crisis shelter, counseling, assistance with protection from abuse orders, family visitation centers, abusive partners' intervention/batterers' intervention services, and more.
YWCA DELAWARE, HOME-LIFE
MANAGEMENT CENTER
OFFICE: 302-658-7110
This Center is an innovative residential program designed for emergency and transitional housing. The program provides supportive services for women and men with children and two-parent families who find themselves destitute.
DELAWARE CENTER FOR JUSTICE FOR JUSTICE ADULT VICTIMS SERVICE PROGRAM
OFFICE: 302-658-7174 EXT.12
The Adult Victims Services program supports adults who are at least 50 years of age who are victims of crimes, including domestic violence
KENT & SUSSEX COUNTIES
PEOPLE'S PLACE II, INC. TURNING POINT
OFFICE: 302-424-2420
Turning Point offers an abusive partners' intervention/batterers' intervention program, as well as individual counseling and support groups for both children and adults.
LA ESPERANZA
OFFICE:
302-854-9262
La Esperanza provides trauma-based counseling and support services for victims of domestic violence and sexual assault. Mental health counseling and support services.
DOVER AIR FORCE BASE FAMILY
OFFICE: 302-677-2711
CRISIS LINE: 302-213-3508
Active-duty Air Force members and civilian employees (including contract employees) will report all incidents of known or suspected family maltreatment immediately to the Family Advocacy Program. The Program also offers abusive partner's intervention/batterer's intervention.
PEOPLE'S PLACE II, INC.
SAFE PROGRAM
HOTLINE: 302-422-8058
The SAFE Program provides safety planning, support, emergency shelter, domestic violence information and referrals.
1.C: RAPE AND SEXUAL ASSAULT RESOURCES DELAWARE
SURVIVORS OF ABUSE IN RECOVERY, INC.
NEWARK: 302-655-3953
WILMINGTON: 302-655-3953
DOVER: 302-422-3811
GEORGETOWN: 302-645-4903
SOAR is a statewide non-profit recovery program which provides counseling, referral, and education services to adult, adolescent and child survivors of sexual abuse and assault, their non-offending partners, and non-offending family members; in addition, SOAR also provides outreach programs to community organizations and businesses.
HOTLINE: 800-656-4673
RAINN sexual assault hotline staff can provide crisis intervention and referral services via phone, mobile app, or webpage chat.
NEW CASTLE COUNTY
YWCA SEXUAL
ASSAULT RESPONSE CENTER (SARC)
HOTLINE: 1-800-773-8570
SARC provides complete, free and confidential rape crisis victim service to sexual assault survivors aged 12 and older and their non-offending family members, friends and partners throughout the State of Delaware.
OFFICE: 302-831-3457 HOTLINE: 302-831-1001
PRESS 1 Student Wellness and Health
Promotion provides services for victims of sexual assault, harassment, stalking, dating, and domestic violence.
KENT & SUSSEX COUNTIES
DELAWARE STATE UNIVERSITY RAPE CRISIS
HOTLINE: 302-420-5751
Delaware State University's hotline provides victim services and crisis support.
YWCA SEXUAL ASSAULT RESPONSE CENTER (SARC)
HOTLINE: 1-800-773-8570
SARC provides complete, free and confidential rape crisis victim service to sexual assault survivors aged 12 and older and their non-offending family members, friends and partners throughout the State of Delaware.
NEW CASTLE COUNTY
CHRISTIANA CARE BEHAVIORAL HEALTH
OFFICE: 302-320-2100
Christiana Behavioral Health offers psychiatry and therapy services to children, adolescents, and adults. They also specific services for those with substance abuse issues.
JEWISH FAMILY SERVICES
WILMINGTON OFFICE: 302-478-9411
AMANACER
COUNSELING & RESOURCE CENTER
OFFICE: 302-576-4136
Amanacer provides mental/behavioral health care services from licensed, bilingual (Spanish/English), culturally competent professionals. Services are available for children, adolescents, and adults.
TRANSITIONS
DELAWARE, LLC OFFICE: 302-440-6737
Jewish Family Services provides family counseling, individual counseling, and psychiatric services to children, adolescents, and adults.
Transitions Delaware provides counseling for folks within the LGBTQ+ community and for other members of the community.
KENT AND SUSSEX COUNTIES
DOVER BEHAVIORAL HEALTH SYSTEM
OFFICE: 302-741-0140
The Dover Behavioral Health System has inpatient and outpatient services for adults and adolescents. They also offer outpatient services for children ages 9 to 11. They offer specialized care for current and former military members and their families.
LA RED
OFFICE: 302-855-1233
JEWISH FAMILY SERVICES OF DELAWARE LEWES OFFICE:
302-827-6040
Jewish Family Services provides family counseling, individual counseling, and psychiatric services to children, adolescents, and adults.
La Red provides behavioral health services including counseling for children and adults, medication management, substance abuse recovery groups, treatment services for chronic mental illness, psychiatric evaluations, and more.
Sexual Assault Nurse Examiners (SANEs) can see patients who have been victims of sexual assault or intimate partner violence. They can collect evidence, provide medical treatment, and initiate crisis intervention. Nemour's Children's Hospital sees victims of child abuse.
FACILITIES
NEMOURS
1.F: PROSECUTION
DELAWARE
ATTORNEY GENERAL'S OFFICE
VICTIM/WITNESS UNITS: 1-800-870-1790
NEW CASTLE COUNTY: 302-577-8500
KENT COUNTY: 302-739-4211
SUSSEX COUNTY: 302-856-5353
BILINGUAL (SPANISH/ENGLISH): 1-877-851-0482
Delaware's Attorney General, the State's chief law enforcement officer has broad responsibility to combat crime, safeguard families, fight fraud, and protect consumers in the First State. The Criminal Division of the Department of Justice is responsible for the prosecution of criminal cases throughout the State from misdemeanors to murders. The Family Division is responsible for areas relating to violations committed by juveniles, as well as protecting children in vulnerable situations and enforcing child support orders.
FEDERAL
OFFICE: 302-573-6170
1.G: RESTORATIVE JUSTICE AND
VICTIM-OFFENDER MEDIATION
DELAWARE
VICTIM'S VOICES HEARD, INC.
OFFICE: 302-697-7005
Victims’ Voice Heard, Inc.
NEW CASTLE COUNTY
DELAWARE CENTER FOR JUSTICE COURT OF COMMON PLEAS/VICTIM
1.G: RESTORATIVE JUSTICE AND VICTIM-OFFENDER MEDIATION SERVICES
Offers victims and survivors of violent crime the opportunity to meet with their offender faceto-face in order to facilitate the healing recovery process. Victims’ Voices Heard acts as an advocate on behalf of the victim, helping them through the process and arranging a safe and secure environment for the meeting to take place.
RESTORATION & COMMUNITY CONFERENCING PROGRAM
OFFICE: 302-658-7174
The Conferencing Program offers those who have been harmed (victims) the opportunity to address those who have caused them harm (offenders) in a safe, structured setting, with the goal of directly holding an offender accountable for their actions while providing important assistance to the victim.
PEOPLE’S PLACE II, INC.
CENTER FOR COMMUNITY JUSTICE
OFFICE: (302) 424-0890
The Conferencing Program offers those who have been harmed (victims) the opportunity to address those who have caused them harm (offenders) in a safe, structured setting, with the goal of directly holding an offender accountable for their actions while providing important assistance to the victim.
KENT & SUSSEX COUNTIES
PEOPLES PLACE II, INC.
TURNING POINT
OFFICE: 302-424-2420
Turning Point at People's Place II, Inc. has an abusive partners' intervention/batterers' intervention program certified by the Delaware Domestic Violence Coordinating Council.
DOVER AIR FORCE BASE
FAMILY ADVOCACY
PROGRAM
OFFICE: 302-677-2711
The Family Advocacy Program at the Dover Air Force Base has an abusive partners' intervention/batterers' intervention program certified by the Delaware Domestic Violence Coordinating Council.
1.I: CIVIL LEGAL SERVICES & LEGAL ADVOCACY
(DVLS)
DVLS assists clients with problems relating to Protection from Abuse, divorce and custody cases involving domestic violence, guardianship, housing, Landlord/Tenant, wills, government benefits, home ownership and consumer issues.
NEW CASTLE COUNTY OFFICE: 302-575-0660
KENT COUNTY OFFICE: 302-674-8500
SUSSEX COUNTY OFFICE: 302-856-0038
CLASI provides free legal services to people with disabilities, older citizens (60 and over), victims of housing discrimination, people living in poverty, victims of domestic violence and immigrant victims of crime, abuse and neglect.
SUSSEX
1.M: CHILD ABUSE
DELAWARE
CHILD ABUSE AND NEGLECT REPORT LINE
REPORT LINE: 1-800-292-9582
All suspected child abuse and neglect must be reported to the 24-hour Division of Family Services (DFS) Child Abuse and Neglect Report Line or online. You may also call any Law Enforcement Agency or 911, but not in lieu of contacting DFS. You are not required to provide proof. Anyone who makes a good faith report based on reasonable grounds is immune from prosecution
CHILDREN’S ADVOCACY CENTER OF DELAWARE
NEW CASTLE COUNTY OFFICE: 302-485-7088
KENT COUNTY: 302-741-2123
SUSSEX COUNTY: 302-854-0323
The mission of the Children’s Advocacy Center (CAC) is to reduce the devastating long-term effects that child abuse has on children, their families and society through immediate, coordinated, child focused services, education, and advocacy. They provide crisis intervention, forensic interviews, court testimony, and more.
COURT APPOINTED SPECIAL ADVOCATES
WILMINGTON: 302-255-1730
DOVER: 302-672-1125
GEORGETOWN: 302-856-5720
Court Appointed Special Advocates (CASAs), a program in the Office of the Child Advocate, serve as a voice for Delaware’s abused and neglected children. CASAs provide quality representation for children who have experienced abuse and neglect.
2.A:
CHILDREN’S ADVOCACY CENTER OF DELAWARE
NEW CASTLE COUNTY OFFICE: 302-485-7088
KENT COUNTY: 302-741-2123
SUSSEX COUNTY: 302-854-0323
The mission of the Children’s Advocacy Center (CAC) is to reduce the devastating long-term effects that child abuse has on children, their families and society through immediate, coordinated, child focused services, education, and advocacy. They provide crisis intervention, forensic interviews, court testimony, and more.
COURT APPOINTED SPECIAL ADVOCATES
WILMINGTON: 302-255-1730
DOVER: 302-672-1125
GEORGETOWN: 302-856-5720
Court Appointed Special Advocates (CASAs), a program in the Office of the Child Advocate, serve as a voice for Delaware’s abused and neglected children. CASAs provide quality representation for children who have experienced abuse and neglect.
DELAWARE SCHOOLBASED HEALTH CENTERS
OFFICE: 302-608-5730
School-based wellness centers or student wellness centers are a type of health care delivery model that provides school-aged youth with comprehensive physical, behavioral, and preventive health services delivered by qualified medical and behavioral health providers in school settings. Every public high school in Delaware, as well as some other schools, have a School-Based Health Center.
CHILDREN & FAMILIES FIRST
OFFICE: 302-658-5177
OFFICE:
302-652-3948
Delaware Guidance Services provides counseling and psychiatric services for children and adolescents ages 2 to 18.
This nonprofit provides services to pregnant persons, Head Start education, nutrition assistance, adoption counseling, family therapy, parenting classes, and childcare referrals. Their Adolescent Resource Center provides counseling, puberty education, and reproductive medical services.
MOBILE RESPONSE AND STABILIZATION SERVICES (UNDER 18)
HOTLINE: 1-800-969-4357
Call this number to receive crisis intervention for minors experiencing a mental health or substance use emergency.
NATIONAL LOVE IS RESPECT NATIONAL TEEN DATING VIOLENCE HOTLINE
HOTLINE: 1-866-331-9474
TEXT HOTLINE: 800-787-3224
A project of the National Domestic Violence Hotline, love is respect offers 24/7 information, support, and advocacy to young people between the ages of 13 and 26 who have questions or concerns about their romantic relationships. They also provide support to concerned friends and family members, teachers, counselors, and other service providers through the same free and confidential services via phone, text, and live chat.
CHILD, INC.
SERVICES FOR CHILDREN AND TEENS
NEW CASTLE COUNTY OFFICE: 302-762-8989
CHILD, Inc. offers counseling for children who were exposed to intimate partner violence. They offer anger management for youth. Kids Place is a community center for children and youth in the Sparrow Run community.
CHILD, INC.
RUNAWAY AND HOMELESS YOUTH PROGRAM
24 HOUR RUNAWAY AND HOMELESS YOUTH HOTLINE: 302-762-6373
CHILD, Inc. operates a Runaway and Homeless Youth Program with counseling, emergency housing, and other services. They welcome LGBTQ+ youth and have experience serving that population.
NEW CASTLE COUNTY
AMANECER OFFICE: 302-576-4136
Amanacer provides mental/behavioral health care services from licensed, bilingual (English/Spanish), culturally competent professionals. Services are available for children, adolescents, and adults.
WEST END NEIGHBORHOOD HOUSE
CAMP W.E.S.T.
OFFICE: 302-658-4171
Camp W.E.S.T. programs include childcare, before care, after care, a virtual learning support center, summer camp, as well as other camps aligning with school breaks.
KENT & SUSSEX COUNTIES
PEOPLE'S PLACE II, INC. - TURNING POINT
OFFICE: 302-424-2420
Turning Point offers support groups and individual counseling for children ages 4-17 who have been affected by domestic violence.
LA RED
OFFICE: 302-855-1233
La Red provides therapy services for children ages 3 and older. They also provide psychiatric evaluation and medication management services for ages 7 and older.
NATIONAL
2.B: LGBTQ+ RESOURCES
SAGE: ADVOCACY AND SERVICES FOR LGBTQ+ ELDERS
HOTLINE (SPANISH/ENGLISH): 877-360- 5428
SAGE provides advocacy, services, and resources for aging and elderly LGBTQ+ persons.
THE TREVOR PROJECT
HOTLINE: 1-866-488-7386
TEXT HOTLINE: TEXT "START" TO 678-678
The Trevor Project provides educational resources on LGBTQ+ and mental health issues, virtual community spaces, and virtual crisis intervention services.
NEW CASTLE COUNTY
CHILD, INC. RUNAWAYAND HOMELESS
YOUTH PROGRAM
24 HOUR RUNAWAY AND HOMELESS YOUTH HOTLINE: 302-762-6373
CHILD, Inc. operates a Runaway and Homeless Youth Program with counseling, emergency housing, and other services. They welcome LGBTQ+ youth and have experience serving that population.
WEST END NEIGHBORHOOD HOUSE
LIFELINES PROGRAM
OFFICE: 302-658-4171
The Life Lines Program serves current and former foster care youth, unaccompanied youth, as well as those who identify as LGBTQ+ between the ages of 16-18 for those in foster care and 18-23 years of age for all youth.
OFFICE: 302-440-6737
Transitions Delaware provides counseling for folks within the LGBTQ+ community and for other members of the community.
KENT & SUSSEX COUNTIES
DELAWARE AGING AND DISABILITY
RESOURCE CENTER
PATHWAYS TO EMPLOYMENT
DELAWARE DISABILITY HUB
OFFICE: 302-739-4553
Delaware Disability Hub provides resources and toolkits for teens and young adults with disabilities who are in the transitional years.
THE ARC OF DELAWARE
NEW CASTLE COUNTY
OFFICE: 302-996-9400
KENT AND SUSSEX COUNTIES OFFICE: 302-736-6140
The Arc of Delaware engages in advocacy work and provides direct services to people with disabilities. They provide housing, employment, outreach, and social and recreational services.
INDEPENDENT RESOURCES, INC.
OFFICE: 302-765-0191
Independent Resources, Inc. is a nonprofit that provides quality services to people with disabilities, assisting them to achieve and to maintain an independent lifestyle. They offer referrals, peer support, living skills training, and transition life skills workshops.
COMMUNITY LEGAL AID SOCIETY, INC.
(CLASI) ELDER LAW PROGRAM
NEW CASTLE COUNTY: 302-575-0660
NEW CASTLE COUNTY: 302-575-0696 (TDD)
KENT COUNTY: 302-674-8500 (INCLUDES TDD)
SUSSEX COUNTY: 302-856-0038 (INCLUDES TDD)
The Elder Law Program (ELP) of Community Legal Aid Society, Inc. provides limited legal assistance to Delawareans aged 60 years or older. The services provided by ELP are free of charge.
COMMUNITY LEGAL AID SOCIETY, INC.
(CLASI) DISABILITIES LAW PROGRAM
NEW CASTLE COUNTY: 302-575-0690
NEW CASTLE COUNTY: 302-575-0696 (TDD)
KENT COUNTY: 302-674-8500 (INCLUDES TDD)
SUSSEX COUNTY: 302-856-0038 (INCLUDES TDD)
The Disabilities Law Program (DLP) is a special project of CLASI, which is designated by the Governor as the Protection and Advocacy agency in Delaware. The DLP provides advocacy services to Delaware residents with physical or mental disabilities.
NEW CASTLE COUNTY
FREEDOM CENTER FOR INDEPENDENT
LIVING
OFFICE: 302-376-4399
The Freedom Center for Independent Living (FCIL) provides services that are consumer-controlled, community-based, cross-disability, nonresidential. FCIL is a nonprofit agency that provides referrals, independent living skills training, peer support, and transition assistance for those moving out of long-term facilities.
DELAWARE CENTER FOR JUSTICE FOR
JUSTICE ADULT VICTIMS SERVICE PROGRAM
OFFICE: 302-658-7174 EXT.12
The Adult Victims Services program supports adults who are at least 50 years of age who are victims of crimes, including domestic violence
2.D: RESOURCES FOR IMMIGRANTS DELAWARE
ATTORNEY GENERAL'S OFFICE - OFFICE OF
IMMIGRATION ASSISTANCE
OFFICE: 302-577-8390
The Office of Immigration Assistance provides counseling services and assistance for residents of Delaware applying for citizenship and/or immigration benefits. Establishes case files and follows up with federal agencies to determine status. Serves as the liaison between residents of Delaware and the US Citizenship and Immigration Service.
JEWISH FAMILY SERVICES - REFUGEE
INTEGRATION SUPPORT EFFORT (RISE)
OFFICE: (302) 478-9411
JFS is the only refugee resettlement agency in Delaware. Through intensive, culturally sensitive case management, they help refugees and other immigrants integrate and make a home in their new communities, obtain and retain employment, and establish and maintain healthy lifestyles to achieve self-sufficiency.
COMMUNITY LEGAL AID SOCIETY, INC.
(CLASI)
NEW CASTLE COUNTY OFFICE: 302-575-0660
KENT COUNTY OFFICE: 302-674-8500
SUSSEX COUNTY OFFICE: 302-856-0038
CLASI can help clients understand whether they are eligible to apply for legal immigration status under the several federal programs that provide protections for legal or undocumented immigrants who have been victims of crime. CLASI also assists immigrants who are victims of crime, trafficking or domestic violence, and juvenile immigrants who are in long term foster care or who have been declared dependent.
CATHOLIC CHARITIES OF WILMINGTON
NEW CASTLE COUNTY OFFICE: 302-655-9624
KENT COUNTY OFFICE: 302-674-1600
SUSSEX COUNTY OFFICE:302-856-9578
Catholic Charities, Diocese of Wilmington, provides comprehensive and reliable immigration counseling to assist individuals and families in negotiating immigration and naturalization processes. Catholic Charities is fully recognized by the U.S. government’s Board of Immigration Appeals (BIA).
JUSTICE FOR OUR NEIGHBORS OF THE DELAWARE VALLEY
OFFICE: 215-925-7788
Justice for Our Neighbors is a community run non-profit. The Delaware Valley office provides immigration legal services in Pennsylvania, New Jersey, and Delaware. They assist clients with preparing immigration forms and applications, counsel clients about their rights, and litigate cases before the U.S. Department of Justice and U.S. District and Appellate courts.
The Latin American Community Center (LACC) offers a citizenship program for clients who are in the Naturalization process or who are about to start it. Participants must have a lawful permanent resident card. N E W C A S T L E C O U N T Y
LATIN AMERICAN COMMUNITY CENTER - CIVICS/CITIZENSHIP CLASS
OFFICE: (302) 655-7338
KENT & SUSSEX COUNTIES
LA ESPERANZA
OFFICE: 215-925-7788
La Esperanza provides immigration counseling, assistance processing documentation for citizenship, and community information sessions
NATIONAL
U.S. IMMIGRATION CITIZENSHIP AND IMMIGRATION SERVICES
CALLING FROM WITHIN THE U.S.: 800-375-5283
CALLING FROM WITHIN THE U.S. (TDD): 800-767-1833
CALLING FROM OUTSIDE THE U.S.: 212-620-3418
USCIS is the government agency that oversees lawful immigration to the United States.
3.: POLICY, INFORMATIONAL, AND FUNDING RESOURCES
DELAWARE
DOMESTIC VIOLENCE COORDINATING COUNCIL (DVCC)
OFFICE: 302-255-1700
The DVCC is a state agency legislatively created to improve Delaware’s response to domestic violence and sexual assault. The DVCC brings together all stakeholders including service providers, policy-level officials and community partners to eradicate domestic violence. The DVCC is committed to leading the nation through innovative legislative action, community education and an outstanding coordinated system response to violence in families and the community.
DELAWARE COALITION AGAINST DOMESTIC VIOLENCE (DCADV)
OFFICE: 302-658-2958
The DCADV works with its member organizations and allies to support the empowerment of victims of domestic violence and their children through access to services and legal remedies. DCADV also seeks to change the societal conditions that support sexism, racism, homophobia, and other oppressions and which contribute to the continued presence of domestic and sexual violence in intimate relationships.
DELAWARE ALLIANCE AGAINST SEXUAL VIOLENCE (DAASV)
OFFICE: 302-468-7731
The DAASV is tasked with building a community among service providers, developing statewide best practices, identifying and addressing gaps in services to survivors of sexual violence, and providing technical assistance and training to law enforcement, court systems, and medical professionals, anyone that may interact with survivors.
SAFE + RESPECTFUL
OFFICE: 302-658-2958
Safe + Respectful is a collaborative initiative coordinated by DCADV to provide resources and information focused on adolescent relationship abuse (teen dating violence).
Safe + Respectful strives to provide young people access to information, resources and services designed specifically for them.
REAL RELATIONSHIPS
REAL Relationships, a program of Turning Point at People’s Place, seeks to engage youth to make changes in their local communities and schools to help promote relationships that are full of respect, equality, acceptance, and love.
DELAWARE ANTI-TRAFFICKING ACTION
COUNCIL
The Delaware Anti-Trafficking Action Council was established to coordinate the State's response to human trafficking; support victims; collect and evaluate data; coordinate training and promote public awareness.
CHILD PROTECTION ACCOUNTABILITY COMMISSION (CPAC)
OFFICE: 302-468-7731
CPAC's overall statutory mission is to monitor Delaware's child protection system to ensure the health, safety, and wellbeing of Delaware's abused, neglected, and dependent children.
CRIMINAL JUSTICE COUNCIL (CJC)
OFFICE: 302-577-5030
The CJC is an independent body committed to leading the criminal justice system through a collaborative approach that calls upon the experience and creativity of the Council, all components of the criminal justice system and the community.
DEVELOPMENTAL DISABILITIES COUNCIL (DDC)
OFFICE: 302-739-3333
The DDC is authorized by Public Law 106-402 to address the unmet needs of people with developmental disabilities through system-wide advocacy, planning and demonstration projects. The DDC funds projects that promote system change, facilitates culturally competent services, educates the public and policy makers, and holds agencies accountable.
MENTAL HEALTH ASSOCIATION OF DELAWARE
OFFICE: 302-654-6833
The Mental Health Association of Delaware promotes improved mental well-being for all individuals and families in Delaware through education, support and advocacy.
THE NATIONAL COALITION AGAINST DOMESTIC VIOLENCE (NCADV)
OFFICE: 303-839-1852
NCADV's mission is to lead, mobilize and raise our voices to support efforts that demand a change of conditions that lead to domestic violence such as patriarchy, privilege, racism, sexism, and classism. NCADV is dedicated to supporting survivors and holding offenders accountable and supporting advocates.
THE OFFICE ON VIOLENCE AGAINST WOMEN (OVW)
OFFICE: 202-307-6026
OVW provides federal leadership in developing the national capacity to reduce violence against women and administer justice for and strengthen services to victims of domestic violence, dating violence, sexual assault, and stalking.
THE OFFICE FOR VICTIMS OF CRIME (OVC)
OFFICE: 202-836-6998
OVC, a part of the U.S. Department of Justice, oversees programs and grants for service providers and other professionals who assist victims of crime.
THE ADMINISTRATION FOR CHILDREN AND FAMILIES (ACF)
REGIONAL OFFICE: 215-861-4000
ACF, a division of the U.S. Department of Health & Human Services (HHS), promotes the economic and social well-being of families, children, youth, individuals and communities with funding, strategic partnerships, guidance, training and technical assistance.
FUTURES WITHOUT VIOLENCE
OFFICE: 415-678-5500
For more than 30 years, FUTURES has been providing groundbreaking programs, policies, and campaigns that empower individuals and organizations working to end violence against women and children around the world.
WOMEN OF COLOR NETWORK (WOCN), INC.
OFFICE: (844) 962-6462
The purpose of WOCN, Inc. is to work in and beyond the fields of domestic violence and sexual assault to address a broad range of violence affecting communities of color such as human trafficking, police brutality and over-incarceration.
LOVE IS RESPECT
HOTLINE: 1-866-331-9474
TEXT HOTLINE: 800-787-3224
A project of the National Domestic Violence Hotline, love is respect offers 24/7 information, support, and advocacy to young people between the ages of 13 and 26 who have questions or concerns about their romantic relationships. They also provide support to concerned friends and family members, teachers, counselors, and other service providers through the same free and confidential services via phone, text, and live chat.
CENTERS FOR DISEASE CONTROL –
4.: TRAINING RESOURCES
DELAWARE
DOMESTIC VIOLENCE COORDINATING COUNCIL (DVCC)
OFFICE: 302-255-1700
The DVCC provides trainings for a variety of groups including law enforcement, healthcare providers, clergy, educators, counseling professionals, and healthcare professionals. The DVCC collaborates extensively with community partners statewide by participating in public outreach events such as health fairs, faith-based workshops, and interactive resource tables.
DELAWARE COALITION AGAINST
DOMESTIC VIOLENCE (DCADV)
OFFICE: 302-658-2958
DCADV is recognized as a leader in domestic violence training for advocates, criminal and civil justice personnel, and social service staff, reaching over 4,000 participants each year. Training initiatives include an annual conference, a semi-annual DV101 training, and issue-specific workshops.
OFFICE OF THE CHILD
ADVOCATE (OCA)
WILMINGTON:
302-255-1730
GEORGETOWN:
302-856-5720
The OCA and the Child Protection Accountability Commission (CPAC) are responsible for developing and providing quality training to Delaware's child welfare professionals and other professionals working with children.
CRIMINAL JUSTICE COUNCIL (CJC)
OFFICE: 302-577-5030
One of the goals of the CJC is to increase the availability of local training for victim services professionals. The CJC offers an annual Delaware Victims Services Conference. The CJC also provides interdisciplinary, evidence-based training through the Delaware Victim Assistance Academy (DVAA).
SAFE AND TOGETHER INSTITUTE
OFFICE: 860-319-0966
The Safe and Together Institute is a resource for domestic-violence informed trainings, systems consultations, and tools. The Institute uses a perpetrator pattern-based framework, provides training on practical skills, and takes a strengths-based approach. N A T I O N A L
TRAINING INSTITUTE ON STRANGULATION
PREVENTION
OFFICE: 888-511-3522
The Training Institute on Strangulation Prevention is a program of Alliance for HOPE International. The Institute provides training, technical assistance, web-based education programs, a directory of national trainers and experts, and a clearinghouse of all research related to domestic violence and sexual assault strangulation crimes.
NATIONAL CENTER ON DOMESTIC VIOLENCE, TRAUMA, & MENTAL HEALTH
312-726-7020 | TDD: (312) 726-4110
The National Center on Domestic Violence, Trauma, and Mental Health enhances agency- and system-level responses to survivors and their families through comprehensive training and technical assistance, research and evaluation, policy development, and public awareness. Their Online Training & Resource Center (OTRC) is designed to increase access to their resources, training, and technical assistance.
NO MORE
The NO MORE Foundation is dedicated to ending domestic violence and sexual assault by increasing awareness, inspiring action, and fueling culture change. NO MORE is a groundbreaking, global initiative comprised of the largest coalition of nonprofits, corporations, government agencies, media, schools and individuals addressing domestic violence and sexual assault.
ONELOVE
OFFICE: 1-844-832-6158
OneLove educates young people about healthy and unhealthy relationships, empowering them to identify and avoid abuse and learn how to love better.
BEAU BIDEN FOUNDATION
The Beau Biden Foundation works to prevent child abuse by educating adults and children, developing the next generation of child welfare professionals, and strengthening child protection laws. They offer workshops, training, and the Shield of Protection certification for organizations.
DARKNESS TO LIGHT
OFFICE: 843-965-5444
HOTLINE: 866-FOR-LIGHT
Darkness to Light empowers adults to prevent, recognize, and react responsibly to child sexual abuse through awareness, education, and stigma reduction. They provide training for those working or volunteering with youth, educators and guidance counselors, health professionals, parents and caregivers, corporations, and any other concerned adults.
INTERNATIONAL ASSOCIATION OF CHIEFS OF POLICE (IACP)
OFFICE: 1-800-THE-IACP
IACP, as the world’s largest and most influential professional association for police leaders, is committed to advancing the safety of communities worldwide. They provide leadership development training, training for the creation of police facilities, and a women's leadership institute. They also offer trainings and resources on a variety of policing topics, including victim services, mental health, and criminal justice
Index of Advertisers
Date
Recruiters
Public Health Delaware Journal of Submission Guidelines
updated March, 2024
About the Journal
Established in 2015, The Delaware Journal of Public Health is a peer-reviewed electronic publication created by the Delaware Academy of Medicine/Delaware Public Health Association. The publication acts as a repository of news for the medical, dental, and public health communities, and is comprised of upcoming event announcements, past conference synopses, local resources, peer-reviewed content ranging from manuscripts and research papers to opinion editorials and personal interest pieces, relating to the public health sector. Each issue is largely devoted to an overarching theme or current issue in public health.
The content in the DJPH is informed by the interest of our readers and contributors. If you have an event coming up, would like to contribute an Op-Ed, would like to share a job posting, or have a topic in public health you would like to see covered in an upcoming issue, please let us know.
If you are interested in submitting an article to the Delaware Journal of Public Health, or have any additional inquiries regarding the publication, please contact the managing editor at managingeditor@djph.org, or the publisher at ksmith@delamed.org.
Information for Authors Submission Requirements
The DJPH accepts a wide variety of submission formats, including brief essays, opinion editorials pieces, research articles and findings, analytic essays, news pieces, historical pieces, images, advertisements pertaining to relevant, upcoming public health events, and presentation reviews. Additional types of submission not previously mentioned may be eligible, please contact a staff member for more information.
The initial submission should be clean and complete, without edits or markups, and contain both the title and author(s) full name(s). Submissions should be 1.5 or double spaced with a font size of 12. Once completed, articles should be submitted via the submission page at https://djph.org/submissions/submit-an-article/ Graphics, images, info-graphics, tables, and charts are welcome and encouraged to be included in articles. Please ensure that all pieces
are in their final format, and all edits and track changes have been implemented prior to submission. To view additional information for online submission requirements, please refer to the DJPH website: https://djph.org/submissions/submit-an-article/
Trial registration information is required for all clinical trials and must be included in the final article and/or abstract.
Abstracts
Authors must submit a structured or unstructured abstract along with their article. Abstracts will have a maximum of 200 words, including headings. Structured abstracts should employ 4-5 headings, and may include Objectives, Methods, Results, and Conclusions. A fifth heading, Policy Implications, may be used if relevant to the article. All abstracts should provide the date(s) and location(s) of the study if applicable, as well as any trial registration information.
Submission Length
While there is no prescribed word length, full articles will generally be in the 2,500-4,000word range, and editorials or brief reports will be in the 1,500-2,500-word range. If there are any questions regarding the length of a submission or APA guidelines, please contact a staff member.
Copyright
The journal and its content is copyrighted by the Delaware Academy of Medicine / Delaware Public Health Association (Academy/DPHA). The contents are licensed under Creative Commons License – CC BY-NC-ND (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Images are NOT covered under the Creative Commons license and are the property of the original photographer or company who supplied the image.
Opinions expressed by authors of articles summarized, quoted, or published in full within the DJPH represent only the opinions of those authors and do not necessarily reflect the official policy of the Academy/DPHA, the DJPH, or the institution with which the authors are affiliated.
Con icts of Interest
Any conflicts of interest, including political, financial, personal, or academic conflicts, must be declared prior to the submission of the article, or in conjunction with a submission. Conflicts of interest are any competing interests that may leave readers feeling misled or deceived, and/or alter their perception of subject matter. Declared conflicts of interest will be published alongside articles in the final publication.
Nondiscriminatory Language
Use of nondiscriminatory language is required in all DJPH submissions. The DJPH reserves the right to reject any submission found to be using sexist, racist, or heterosexist language, as well as unethical or defamatory statements.