30 Matching Technologies to Presbyopic Patient Needs
Gerd Auffarth MD, PhD
32 Knowing Iris Repair: Iris Cerclage
Soosan Jacob MS, FRCS, DNB
40 To Combine or Not to Combine
Thomas W Samuelson MD and Steven R Sarkisian Jr MD PAEDIATRIC OPHTHALMOLOGY
42 Paediatric Cataract Update
Michael Amon MD, FEBO
Publisher
Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin
Dermot McGrath
Roibeárd O’hÉineacháin
Contributors
Laura Gaspari
Soosan Jacob
Timothy Norris
Colour and Print CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review
is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Eyes on the Prize
July and August see the quadrennial return of the Summer Olympics. Athletes from around the world will have prepared for many years and gone through a challenging selection process to represent their nations in their chosen sports. The Olympics have become a metaphor for international cooperation in the common pursuit of excellence, showing the better side of humanity.
In this issue, our first-ever sports issue, we explore how visual health comes into play in competitive sports and the essential role of ophthalmologists. There is really no sport where eye care specialists do not play a key role. Athletes depend on optimal visual acuity, depth perception, peripheral awareness, and eye-hand coordination. Vision accounts for 80% of perceptual input. Routine eye exams, refractive correction, eye protection, and trauma treatment all fall under the purview of the ophthalmologist.
To this end, the International Olympic Committee (IOC) has published a consensus paper on sports-related ophthalmology issues in elite sports, emphasizing the importance of close cooperation among sports physicians and ophthalmologists. Howard Larkin discussed the ways this can happen in an article in this issue.
We also look at the remarkable career of Henry Stallard, who epitomized the scholar-athlete ideal. Stallard competed
in the Paris Olympiad one hundred years ago as part of the British team immortalized in the 1981 film Chariots of Fire He took a bronze medal despite breaking his foot shortly before his race. He later became an influential eye surgeon, developing a sight-saving treatment for retinoblastoma and authoring a key text on eye surgery.
Timothy Norris spoke with noted eye trauma specialist Professor Ferenc Kuhn MD, PhD on the toll boxing takes on the eye, emphasizing the importance of eye protection, a subject also discussed in two related articles on eye protection in young athletes, Paralympians, and participants in the Special Olympics. Norris also discussed with Prof Cosimo Mazzotta MD the potential visual risks young athletes face with keratoconus and keratectasia.
The career of the ophthalmologist parallels that of elite athletes in many respects. The prospective eye surgeon must first demonstrate intellectual ability before committing to many years of training during the prime years of life, aiming at specific goals. Mentors assist in the training, teaching students to learn from failures where there is little margin for error. Potential surgeons also experience personal development, learning to stay focused and handle stress in demanding environments. The reward in this case is not a gold medal—winning comes in the form of satisfied patients.
EDITORIAL BOARD
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)
Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Filomena Ribeiro (Portugal)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)
Thomas Kohnen Chief Medical Editor
José Güell Medical Editor
Paul Rosen Medical Editor
Research. Education. Innovation.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
Global Vision with a Local Flavour
Debates, dry labs, and surgical trainers to highlight 2024 Congress.
BY STUART HALES, EXECUTIVE EDITOR
Aboxing ring is a fitting venue for a spirited debate, but what about a dance hall? If the dance style is flamenco, known for its passion and expressive style, the debaters will certainly feel at home.
That’s the goal of the ESCRS Tablao, a concept that builds on the successful launch of the ESCRS Arena at the 2023 Annual Congress in Vienna. Tablao is a colloquial term for the Spanish word tablado (‘floorboard’) and is also a place where flamenco shows are performed; tablao is also the term for the platform floor on which a flamenco dancer dances. Tablao venues were developed during the 1960s throughout Spain, replacing the cafés cantantes—or cabarets.
The Tablao programme at the 2024 Annual Congress will run from Saturday through Monday (7–9 September) and begin each morning with an 80-minute “Surgical Pearls” presentation on refractive/cornea (Saturday), anterior segment (Sunday), and cataract (Monday). The debates will take place in the afternoon and will be preceded by an animated introduction to flamenco and live presentations of surgical simulators. Each debate will be overseen by a moderator and two judges.
The tentative topics for the debates are as follows:
• Cataract/Refractive Debate: My first option: EDOF IOLs!
• Corneal Refractive Debate: FemtoLasik is the standard procedure!
• Cataract Surgery Training across the World: A simulated curriculum is mandatory!
Each debate will be followed by a panel discussion; the discussion topics are as follows:
• The Surgeon-Industry Exchange: What doctors want to know from industry, and what industry wants to know from doctors
• How should I start refractive surgery?
• Training surgery
• Young ophthalmologists for sustainability
“With Tablao, we are trying to bring a cultural focus to this year’s arena programme and also highlight our Congress as a global model for training and inclusion,” says Filomena Ribeiro, president of ESCRS. “This is something we really want to push for future Congresses as well—to bring more training opportunities to young people and deliver networking moments that can only be experienced face-to-face in a multicultural environment.”
To support these twin goals, the 2024 Congress will feature several other innovations as well. Following are highlights of the Barcelona programme.
Surgical Training Lab
Located in the exhibition hall, the Surgical Training Lab will feature 17 training devices from three manufacturers: Haag-Streit, Alcon, and HelpMeSee. Attendees can register for up to three sessions in the lab, and each session will be guided by a trainer using a curriculum developed by the manufacturer. The sessions are free, and the lab will be open during the hours the exhibit hall is open.
“Having 17 machines will allow us to enrol a large number of participants,” Ribeiro says. “Surgical training is a topic of interest to all attendees, and I expect this will be the highlight of the Congress for many.”
Dry Labs
In addition to its traditional wet labs, the Congress in Barcelona will feature 16 dry lab stations covering 4 different topics (which are still being determined). The dry labs will use model eyes instead of animal material to simulate ocular surgery.
The dry labs will feature Zeiss Stemi microscopes linked to iPads, allowing trainers to watch and record a trainee’s surgery and easily provide feedback about their performance. The majority of the dry labs in Barcelona will be aimed at novice surgeons with little or no prior surgical experience.
“The introduction of digital dry labs will enable trainees to repeatedly practise surgical manoeuvres, such as creating a capsulorhexis, suturing corneal lacerations, and performing steps of penetrating keratoplasty, using high-fidelity model eyes,” says John Ferris, who is coordinating the dry labs with Alja Crnej and Vladimir Pfeifer. “Trainers can observe and record the simulated surgery on iPads, then rewatch the videos with the trainee and provide feedback about their performance.”
Global Refractive Summit
On Friday, 6 September, ESCRS will host a first-ever Global Refractive Summit from 8:00 until 14:00. ESCRS has invited the Brazilian Association of Cataract and Refractive Surgery (BRASCRS) and the International Society of Refractive Surgery (ISRS) to participate in the event.
Congress attendees will have the opportunity to experience the Surgical Training Lab, where they will be guided through a dedicated curriculum on 17 training devices.
The summit will address a multitude of topics, including the following:
• Recent advances in corneal refractive surgery
• Refractive surgery and endothelial disease
• Decision-making processes in refractive surgery based on AI
• New phakic IOL sizing parameters and prediction models
• SMILE for hyperopia outcomes
ESCRS will also host a symposium in conjunction with the American Society of Cataract and Refractive Surgery (ASCRS) and the Asia-Pacific Association of Cataract and Refractive Surgeons (APACRS). That symposium, titled “My Refractive Surgery Path,” will be held Monday, 9 September, from 8:15–10:15 and address topics such as lenticule extraction, LASIK/ PRK boundaries, and refractive lens exchange limits.
Additionally, ESCRS is hosting a mini symposium with the American Academy of Ophthalmology (AAO) on Monday from 9:00–10:00. ESCRS is also inviting presentations of industry abstracts at an EU Clinical Trial Spotlight Session on Sunday from 8:30–10:00.
“We are really delivering a global programme by coordinating with these international societies,” Ribeiro says. “We are also taking a global view of large clinical trials that industry is promoting in the EU. Barcelona is the first time we will present this model, and we are very excited about it.”
75th Anniversary of IOL Implantation
To celebrate the 75th anniversary of the first implantation of an intraocular lens, the Congress will feature a tunnel museum with different rooms to showcase the history behind this groundbreaking event. The museum will explore not only Harold Ridley’s role but also the debates around the procedure, the development of IOL surgery, and what the future holds.
In advance of developing the museum, ESCRS conducted a video clip competition, “My Personal Special IOL Moment.” Ophthalmologists were invited to submit short video clips (maximum 60 seconds) telling their personal IOL story.
“The huge number of submissions we received was amazing,” Ribeiro says. “They will bring a special spirit to this celebration.”
Building our Sustainable Inclusive Society (BoSS)
Building on a leadership session on implicit bias presented at the ESCRS Winter Meeting in Frankfurt, the Congress will feature a symposium, an instructional course, and a workshop on diversity and inclusion. There will also be a mentorship programme and support for families, like a creche and a family-friendly activities programme.
“The digital transformation will bring with it some topics we need to think about, like whether it’s biased or not and, if so, what are the implications of that?” says Ribeiro. “And then we also must try to understand the bias impact on the decision-making process in our field and try to deliver some instruments to deal with these kinds of issues.”
Main Symposia and Lectures
Throughout the Congress, attendees will have their pick of numerous symposia on topics such as:
• Anything new in keratoconus?
• The latest on IOLs
• The future of refractive surgery
• Surgical complications: You make the call
• Telemedicine in ophthalmology
Complementing these symposia will be instructional courses, paper sessions, and workshops, as well as the Heritage Lecture and the Ridley Medal Lecture. The Heritage Lecture will be delivered by Richard Packard, whose presentation is titled “High wire act to the standard of care: Charlie Kelman and the history of phacoemulsification.” Abhay Vasavada will deliver the Ridley Medal Lecture, titled “Late Decentration of IOLs: An Enigma.”
“I think we will have records at this Congress for the number of submissions for free papers, videos, clinical cases, and instructional courses,” Ribeiro says. “There will be lots of reasons to stay for the whole Congress, from the beginning to the end.”
MIGS Masterclass to Offer Grand Rounds and Wet Labs in Barcelona
After a successful debut in 2023, the ESCRS is again offering a masterclass in minimally invasive glaucoma surgery (MIGS) in 2024.
The masterclass, led by Ziad Khoueir, will provide doctors with direct access to world-class mentors, opportunities to learn from online modules and webinars taught by leading faculty, and hands-on instruction through case grand rounds and wet labs.
The goal of the MIGS masterclass (as with all ESCRS masterclasses) is to improve practice patterns and clinical outcomes and significantly increase the number of patients treated. Up to 50 students will be able to participate in the following exclusive activities:
• mentor-guided didactic workshops;
• interactive live webinars;
• in-person case grand rounds at the ESCRS Annual Congress; and
• in-person wet labs at the Annual Congress.
Each participant who completes all of these components and passes the exam will receive a certificate of completion and a credit to apply to future ESCRS registration and membership fees. There is no cost to participate in
the masterclass, although applicants must bear all travel costs.
The MIGS masterclass is targeted towards cataract surgeons who meet the following criteria:
• have practised ophthalmology for more than 5 years post-training;
• conduct at least 200 cataract surgeries per year (preferably have conducted >1,000 cataract surgeries as a primary surgeon);
• see glaucoma patients;
• have begun to implant MIGS devices or intend to start doing so immediately after this masterclass; and
• are based in a surgical facility where MIGS devices are available.
Participants are required to be present and participate in the live components of the masterclass.
New Tool Calculates Patient Travel Carbon Footprint
A new tool available on the ESCRS website will help ophthalmologists understand the carbon footprint associated with patient travel and encourage sustainable practices within the cataract and refractive surgeon community.
The Patient Travel Carbon Calculator assesses factors such as postoperative visits, travel distance, and transportation mode to help
ophthalmologists understand the overall carbon footprint of their practice and make informed decisions. Additionally, the calculator lets doctors estimate the portion (typically about one-third) of the carbon footprint caused by cataract surgery, with the other main portion arising from surgical disposables.
Cataract surgery emits roughly 75 kilograms of carbon dioxide (CO2) per surgery, equivalent to the amount of CO 2 absorbed by three trees per year. In Europe alone, cataract surgery is performed about 4.5 million times annually. As physicians, we can make a significant impact by reducing avoidable patient travel through changes in our practice patterns.
Using the Patient Travel Carbon Calculator in combination with the ESCRS SIDICS calculator will provide ophthalmologists with the tools needed to analyse their surgical practices and work towards a more sustainable climate.
Join us in prioritising sustainability and minimising our ecological footprint—calculate your impact today.
Experience iNovation Day
Learn about the hottest topics in ophthalmology!
Building on its success at previous ESCRS Congresses in Milan and Vienna, the ESCRS iNovation® Day programme will introduce delegates to the latest technological developments in the pipeline—along with expert discussion panels on the most urgent clinical needs and barriers to success in anterior segment care. The iNovation programme takes place on Friday, 6 September, at the Fira Barcelona Gran Via, offering a rare opportunity to network with leading researchers, industry CEOs, and financial community leaders. The programme will feature focused panel discussions, up to 20 emerging company presentations, guest speakers, and survey data on attendees’ and ESCRS delegates’ interests, trends, and concerns. The programme includes live voting and commentary, as well as plenty of breaks for socializing and networking. A new session introduced in 2023—‘The Innovators Den’—returns, featuring new proposals developed directly by clinical ophthalmologists and presented before an all-star panel of eminent ophthalmologists and executives.
Rule Number One: Protect the Eyes
Ophthalmologists hold a key role in athlete eye care for all ages and abilities.
BY LAURA GASPARI
Visually impaired individuals can participate in almost any sport, but wearing protective gear for the eyes is crucial to avoid trauma and damage, according to David B Granet MD. This summer, the Paralympic Games in Paris will showcase an astonishing number of athletes with visual impairments and blindness competing in various disciplines, from athletics to football, swimming, and martial arts like judo. Athletes are categorised based on their level of visual impairment, and in some competitions, such as blind football or goalball, wearing eye shades to cover their eyes fully is mandatory to ensure equality in the competition.
Sometimes, these athletes have been visually impaired from a very early age or have lost their sight due to accidents or trauma. Losing sight—or a lack of sight—might seem an obstacle, discouraging participation in activities like sports. In the case of children, ophthalmologists should encourage their parents to let them participate in sports, Dr Granet said. “It’s easy for families with visually impaired children to say no,” he noted. However, the Paralympics demonstrate that everyone can be an athlete, learning resilience, the value of practice, teamwork, and belief in their ability.
“It’s essential for families to see that and recognise their child is differently abled, not disabled,” Dr Granet emphasised.
Security comes first
Protecting one’s eyes is crucial, especially for individuals with visual impairments who engage in sports. They are less able to shield themselves and thus more vulnerable to injuries; sometimes, one eye is in better shape than the other, making it essential to guard the healthier eye.
“In this setting, I always tell families that rule number one is to protect the better-seeing eye,” Dr Granet advised. “Protecting the normal eye is vital to maintain daily activities in life.”
Protective eyeglasses and goggles are made of resistant materials like polycarbonate and must meet international and national standards, such as ISO certification or CE marking in European countries. Scientific societies like the American Academy of Ophthalmology also provide guidelines for this gear (available to everyone) and should be recommended by the ophthalmologist.
It’s essential for families to see that and recognise their child is differently abled, not disabled.
Inclusion and Security
As long as security is taken into account, everyone can participate in sports, even with visual disabilities. Dr Granet recalled some of his patients with visual impairments or blindness could ski in different ways, like using a rope attachment, holding on to someone, and even skiing independently. “There are programmes just for the visually impaired at many mountains,” he said. “Here in California, there’s even a programme for the visually impaired to learn to surf.”
One of his patients competed in the Paralympics in London in 2012 as a rower. “She developed Stargardt’s, which took her vision away as a child, but she did not let it stop her—in sports or in life.”
Visual abilities do not limit athletic capability, but athletic activity can impact vision—making sight important to protect. Ophthalmologists play a key role in preventing damage at every level.
“It should be standard and start from the very beginning with kids participating in sportswear protection. If you are wearing other protective gear anywhere else in your body, you should be thinking about protecting your eyes,” Dr Granet concluded. “With proper protection, everyone can participate in and grow from the joy and value of sport safely.”
However, Dr Granet stressed that not only visually impaired individuals but everyone should wear eye protection during sports, as eye trauma can lead to blindness and disability.
“There is damage occurring after direct contact, called a coup injury, and then there are contrecoup injuries, where the eye bounces around inside the orbit. These are terms borrowed from brain injuries, but the same happens to eyes,” Dr Granet explained. Eye trauma varies from ruptured globes to corneal abrasions and retinal detachments. It is even more crucial when a person has pre-existing conditions like high myopia or previous surgery that can pose an increased risk of visual impairment in case of injury.
Raising Awareness
Unfortunately, eye protection in sports is not yet widespread, although Dr Granet observed things are improving. Some sports, such as football, rugby, boxing, water polo, and baseball, do not require their athletes to wear protective gear and eye injuries—and concussions—are a real concern. Convincing people to wear protection can be challenging, and the only way to raise awareness is to make it mandatory, encourage athletes to wear protection, and have them hear it directly from their ophthalmologist.
“We need to change the attitude that wearing protection is a negative; it doesn’t make you weak or less of an athlete,” he asserted. Fortunately, more professional athletes, sports leagues, and clubs are becoming aware of the issue, introducing more protective gear, especially helmets for the head and goggles for the eyes.
David B Granet MD, MHCM, FACS, FAAO, FAAP is Professor of Ophthalmology & Pediatrics; Vice Chair of the Viterbi Family Department of Ophthalmology; Anne Ratner Chair of Pediatric Ophthalmology; Director, Anne F and Abraham Ratner Children’s Eye Center; and Director, Division of Pediatric Ophthalmology & Eye Alignment Disorders of the Shiley Eye Institute, UC San Diego, US. dgranet@ucsd.edu
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
Collaboration with sports physicians on risk, treatment, and referral advised.
BY HOWARD LARKIN
Vision accounts for about 80% of perceptual input in sports, making close cooperation among sports physicians and ophthalmologists a must. To that end, the International Olympic Committee (IOC) has published a consensus paper on sports-related ophthalmology issues in elite sports.1
Covering everything from blunt trauma to ocular surface conditions, and published in BMJ Open Sports and Exercise Medicine, the statement mainly targets sports medicine practitioners, who are typically the first to see injured athletes. It includes basic information on ocular injury prevention, as well as ocular anatomy, diagnosis, and when to refer injuries and conditions to an ophthalmologist.
However, the relationship between sports and ophthalmology is reciprocal, so ophthalmologists can also learn from the paper—not only regarding physical sports but e-sports as well. Both are affected by vision and can affect vision, said Professor Christophe Baudouin, who contributed to the paper’s section on ocular surface issues.
Ocular surface issues are common
Dry eye or allergy may result from “exposure to light, UV, pollution, and other environmental challenges. It may directly influence comfort, causing more or less severe symptoms,
and more importantly, influence visual capabilities: increased blinking rate and unstable tear film may decrease the quality of vision, which may be very important for high-level and visual-demanding sports,” Prof Baudouin said.
E-sports are a particular concern, especially since they are extremely popular and avid participants have a high incidence of dry eye and other vision strain-related conditions, he added. “The effects of screens on dry eye are well known, and again, dry eye may decrease performance, especially in those sports where visual performance must be very high, like speed, visual field, or reflexes.”
With worldwide e-sport participation in the billions, eye care practitioners have ample opportunities to educate gamers on proper digital hygiene, such as looking away from the screen for 20 seconds at an object 20 feet away every 20 minutes (20/20/20 rule); monitoring vision performance using technologies such as the vision performance index; and treating digital eyestrain, according to the paper.
Assessing ocular trauma
Eye trauma typically results from crashes or contact with an opponent or equipment, the paper says. It characterises sports eye injury risk as high, moderate, or low based on factors such as the use of bats or sticks and the type and intensity of body contact. But while sports-related ocular injuries are relatively rare and most have good visual out-
comes, more severe injuries can involve orbital or intraocular injuries that require emergency attention as well as extensive follow-up and management. Ocular symptoms may also indicate a concussion or other neurologic injury.
The paper outlines sideline evaluation steps for trauma of the orbit, adnexa, and globe. These include noting any lacerations, abrasions, perforations, bleeding, iris damage, or lens displacement and checking visual acuity, pupillary shape, size, and red reflex; diplopia; orbital rim step-off or numbness over the cheek; ex- or enophthalmia; and bradycardia, syncope, or vomiting, which may be signs of extraocular muscle entrapment requiring early surgery. Other conditions requiring immediate referral include lacerations of the medial eyelid, open globe injuries, loss of vision, and lack of ocular motility. CT images indicating orbit fractures are also included, with a warning against MRI imaging due to the possible presence of metallic fragments.
History taking and physical examination are also outlined, as are equipment needed—including penlights, vision charts, direct ophthalmoscope, and hard-shell eye shields—and when and how to use them. Furthermore, it covers visual symptoms of traumatic brain injuries. Because about 90% of eye injuries can be prevented with suitable eye protection, the paper recommends counselling athletes on proper eyewear for their sports.
“In the event of an eye injury, sports medicine physicians must assess whether the athlete can return to the field of play, be substituted with another athlete, be referred to an ophthalmologist, or be immediately transported to the nearest hospital. This decision requires a good
understanding of anatomy, common ocular conditions associated with high-level sports, and knowledge of proper examination techniques by the sports medicine physician. In addition, good eye health is crucial to prevent visual problems in athletes, while regular eye examinations using specialised techniques and equipment allow the early detection and management of visual impairments,” the paper concludes.
Good eye health is crucial to prevent visual problems in athletes.
One weakness of the statement is the lack of prospective studies on the prevalence and severity of eye injuries in sports, the paper says. Until recently, even data collected by Olympic examiners did not distinguish eye injuries from other facial injuries, though it was added to reporting forms as a separate category in 2020. Better data and studies will help inform better prevention and treatment.
For citation notes, see page 46.
Christophe Baudouin MD, PhD, FARVO is professor at Versailles Saint-Quentin en Yvelines University, Versailles, France, chairman of Quinze-Vingts National Ophthalmology Hospital, Paris, and a founder and president of the European Dry Eye Society (EuDES).
Risks to retina increase with every punch.
BY TIMOTHY NORRIS
On the second of August 1980, middleweight Olympic gold medal winner Sugar Ray Seales’ brilliant career was already in peril. Since the tremendous title-ending blow received from Marvin Hagler in 1976, his eyesight in the left eye gradually worsened, exposing him to new and painful jabs, both to the head and his career.
That day, while facing last-minute replacement Jamie Thomas, Seales’ grit was shattered by his opponent’s thumb digging into his right eye, causing a severe retinal detachment, leading to eye surgery. Four months later, Seales was back in the ring, fighting and winning, but things kept getting worse. After defeating Max Hord in 1983, Seales was declared legally blind and, despite undergoing surgery several times, his career abruptly ended, leaving him broke and crippled in debt.
Along with Sugar Ray Leonard, Seales is considered one of the strongest examples of the risks of blindness associated with contact fighting sports. According to a study by Giovinazzo (et al.), two-thirds of boxers show signs of ocular injuries, with almost a quarter with signs of retinal tear.1
The toll boxing takes on the eye is seldom an instant consequence of one trauma but the cumulative effect of several adding up over time, Professor Ferenc Kuhn MD, PhD said. This causes the vitreous gel to break down at a faster pace than a normal eye, increasing the risk of a retinal tear on every hit—eventually leading to retinal detachment. And it is not instantaneous, Prof Kuhn remarked. Some patients could suffer retinal detachment years after they retire.
Care Eye
Enters Ring the
Prof Kuhn recalled the case of one of his patients, an active professional boxer presenting with retinal detachment. After a vitrectomy and 360-degree laser prophylaxis on both eyes, the patient asked if he could return to boxing. “I could not answer the question at the time, and there was nothing in the literature about it,” he said. Fortunately, the country already had a rule on eye injury preventing the patient from going back to the ring. “However, it should not be up to us to tell a person that his life has to change completely, but rather to prevent this from happening.”
Prevention of retinal detachment is not an easy task, and, as Prof Kuhn underlined, it has no consensus. Data now shows the old approach of frequently treating areas of the peripheral retina at risk may not be sufficient because most of the problems come from those that appear normal at examination.
For this reason, advocating for protection can indeed be the most effective solution. Before Thomas Joseph Pashby CM, a few hundred hockey players went blind every year. Thanks to his advocacy and the introduction of mandatory protection, these cases went down to zero, Prof Kuhn observed, stressing prevention’s efficacy. Everything can happen in a split second, he said, and it is better to be safe than sorry.
For citation notes, see page 46.
Ferenc Kuhn MD, PhD, Helen Keller Foundation for Research and Education, Birmingham, Alabama, US; Department of Ophthalmology, University of Pécs Medical School, Hungary; International Society of Ocular Trauma, Jacksonville, Florida, US. fkuhn@mindspring.com
Weighing the Cornea Ectasia Risks
Many young people with corneas at risk of developing or worsening keratoconus take a cautious path in life, giving up on sports and the prospect of a professional career. According to Cosimo Mazzotta MD, PhD, such important choices should not be dictated by fear of having to deal with a curable, manageable, but still impairing condition such as severe keratoconus.
“Many patients come to my clinic with a whole [host] of concerns, asking me if they should stop doing sports, especially when weightlifting is involved,” he said.
Olympic weightlifting could be considered risky for corneal stability—particularly due to the frequent use of the Valsalva manoeuvre, a breathing technique. How this could be harmful for corneal biomechanics really depends on exercise type, intensity, duration, and recovery.
Available literature demonstrates how an isometric contraction for more than two minutes does not alter the anterior chamber depth, the central corneal thickness, or the maximum corneal curvature, Dr Mazzotta said, pointing out how important this finding is to a better understanding of corneal ectasia prevention and management.
Therefore, he said, using the Valsalva manoeuvre many times a day can still be safe, assuming some preventive measures are in place. Powerlifting, for example, does not represent a risk if spaced out with aerobic activity and appropriate set length and recovery time because a short-term effort does not impact corneal curvature. However, it would not be prudent for high-risk patients to lift more than 30% of their body weight, especially exerting this weight for more than two minutes. Exceeding limits can also be harmful, he warned, as lifting for more than four hours a day, four or five times a week can put stress on the corneal biomechanics and curvature.
These cases do not consider patients with a three- or four-degree keratoconus severity. In that case, Dr Mazzotta said, the maximum lifted weight/body weight ratio must be lowered to 20%; every prolonged isometric contraction needs at least the same recovery time—ideally, two minutes of exercise interspersed with two minutes of recovery. Moreover, patients must be frequently monitored by a specialist.
Yet high-risk athletes are not the only ones at risk. According to Dr Mazzotta, a different culprit could play a stimu-
Athletes should proceed with care with eye protection solutions.
BY TIMOTHY NORRIS
lating role in the onset and progression of corneal ectasias: eye-rubbing in genetically predisposed individuals. A trivial bad habit, he observed, quite common when sweat ends up in the eye, causing burning sensation and involuntary rubbing. This can trigger negative feedback that may change corneal biomechanics in time, which must be stopped as soon as possible, he emphasised.
There are other sports, however, aside from Olympic weightlifting and track and field that may represent a real threat to the progression of corneal ectasias, both aerobic and anaerobic. Full-contact sports, such as boxing and martial arts, can be devastating, he warned, especially when done without some eye protection. There is a strong correlation between ocular trauma and onset of keratoconus, he added.
Even sports featuring eye coverage can pose long-term risks. The suction effect of swim goggles can, in the long run, increase corneal curvature and corneal thinning with an increase in intraocular pressure. Dr Mazzotta advised patients with thin corneas (at high risk of ectasia) and patients with POAG to be aware of the risks and look for a more suitable pair of goggles.
He stressed prevention as the key to avoiding long-lasting dramatic consequences for the athlete’s quality of life and career. As he underlined, ophthalmology should take greater account of sports, both in prevention and research.
“Just like we carefully study pathology in clinical and surgical contexts, we should also pay close attention to sports activities. A lot of people who engage in sports, particularly on a competitive and Olympic level, are obviously young, and we should be able to give them our best and well-informed advice,” Dr Mazzotta said. “We need to solve any lack of information and dispel false myths. So, we need more research, new literature, and whatever it takes to protect the eyesight of young people who want to engage in sport and dream about a future at the Olympics.”
Cosimo Mazzotta MD, PhD, FWCRS is Professor of Ophthalmology at the University of Siena; Anterior Segment Eye Surgeon at Alta Val d’Elsa Hospital; and founder and scientific director of the Siena Crosslinking Centre of Siena, all of Italy. cgmazzotta@libero.it
Limitations Overcoming Visual
Helping every Olympian see what they can do.
BY LAURA GASPARI
Sport is one of those activities that leads people to overcome their limits. This is particularly true when it comes to athletes with physical or mental disabilities. Not only are the Paralympics a great example of professionalism in sport and willpower on the part of people with disabilities—but the Special Olympics also bring extremely positive stories of resilience and inclusivity regarding intellectual disabilities. However, these are athletes who require special care, especially those with ocular conditions.
One such athlete, who competed in several Special Olympics, receives treatment from cornea specialist Elizabeth Lynn Pinney MD. Her patient is an adult woman born with microphthalmos and glaucoma, with light perception vision in one eye and 20/400 in the second eye. Despite this, she is a swimmer who participated in triathlons and many other competitions. According to Dr Pinney, her job as an ophthalmologist is to help this patient maintain her vision as much as possible.
“Our biggest challenge is to maintain the vision that she has left, which we have been able to do for many years,” she recalled. “Our [goal] is keeping her intraocular pressure under control, especially for her swimming, even if she does not engage in deep or scuba diving.”
Luckily, Dr Pinney reported her patient responds well to pharmacological therapy with eye drops for glaucoma to lower IOP and does not require surgery. Also, she always wears appropriate protective goggles in the pool to avoid chemical agents that may irritate her ocular surface or cornea.
To help patients maintain stable vision and carry on with their sporting activities and independence is a wonderful experience, Dr Pinney said. “In ophthalmology, there are highs and lows: patients cannot always be cured, and there are things where there is nothing you can do. It can be really hard because you always want to be able to give as much vision back as you can to every patient.”
Taking an active role in this care at a young age can help ophthalmologists achieve this vision preservation because these younger patients can adapt very well.
“[My patient] adapted very well to her disability and limitations, overcoming them in almost any way and finding workarounds for her low vision like a guide helping her with the biking part of the triathlon,” she noted.
Dr Pinney added having a patient like this is enriching for her as an ophthalmologist and as a human being. “I love to be involved with a patient like this. It is just a blessing for me to see what she can do because it is an incredible thing. I am always impressed by her—she did not let her disability slow her down in any way, shape, or form. She is so happy all the time and does amazing things.”
Elizabeth Pinney MD is a cornea specialist who practices at Kaiser Permanente San Diego Zion and San Diego Medical Center, California, US.
Elizabeth.pinney@kp.org
The Ophthalmologist Olympian
BY SEAN HENAHAN
Henry Stallard’s remarkable career had many milestones.
This year’s Olympiad in Paris marks the centenary of the last time the Games took place in the City of Light. The 1924 Olympics were later made famous in the 1981 film Chariots of Fire, featuring some British athletes’ quest for gold, particularly in running events. Among the select athletes competing for Britain was Hyla (Henry) B Stallard, who would earn a medal in Paris. He would also go on to reach Olympian heights in his chosen field of ophthalmic surgery.
As detailed in an excellent video assembled by Hugh Williams1, Henry Stallard had become one of the fastest middle-distance runners in British history years before the Paris Games. In 1920, he was part of a combined Oxford-Cambridge University team that travelled to the United States for a two-mile relay race against America’s fastest runners. The British team won, setting a new world record in the category. His amateur athletics career continued as a member of the Cambridge University Athletics team. He went on to win the one-mile race against Oxford three years in a row, in 1920, 1921, and 1922. He was also part of the Oxford-Cambridge team that set a world record in the 4×880-yard relay in 1922. His mile record held until Roger Bannister broke the four-minute-mile mark in 1954.
Stallard was selected to run the 800 and 1500 metres at the 1924 Olympics. He injured his right foot in the final of the 800 m, finishing fourth. He then ran in the 1500 m despite having what turned out to be a metatarsal stress fracture in the right foot. He ran against the doctor’s advice, saying famously, “I am going to run tomorrow if I never run again.” He nonetheless received a bronze medal, later apologizing for his “poor show.”
His running career continued alongside his medical training at St Bartholomew’s Hospital and Moorfields Eye Hospital in London. He eventually held positions at both hospitals and maintained a private practice on Harley Street. He was obliged to end his running career in 1928, having suffered recurrent stress fractures of the navicular bone in both feet.
It was at St Bartholomew’s and Moorfields that he became interested in retinoblastoma treatment under the mentorship of Mr Robert Foster Moore. Moore pioneered the use of radioactive radon seeds in treating retinoblastomas in children. Stallard improved on this idea, developing focal radiotherapy, applying a radioactive cobalt 60 plaque to the surface of the eye, overlying the tumour, and giving a measured dose of radiation. Thanks to this research, it became possible to save both the lives and the vision of many children with the disease.
His busy career was interrupted in 1939 by the onset of the Second World War. He served first in Cairo, where he performed more than 600
operations on wounded soldiers and civilians, meticulously logging and describing the injuries and treatments, often with carefully drawn illustrations. He somehow found time to run and climb over the top of the Great Pyramid of Giza, Mr Williams noted.
He was later transferred to Europe, arriving on the beaches of Normandy only days after D-Day, eventually performing eye surgery in France and Belgium. A major in the British Army, he steadfastly refused promotion, fearing he would become more bureaucrat than surgeon.
After the war, he built on his considerable surgical experience, publishing Eye Surgery, the first modern comprehensive guide to eye surgery, which set the standard for ophthalmic surgical training for many years.
The British Journal of Ophthalmology, to which he was a frequent contributor and one-time assistant editor, noted in memoriam: “Stallard’s distinction lay in the quality of his surgical skills and his ability to impart them to others. Every single operation was in fact a research project to be performed as perfectly as possible. He was the complete master. There was a natural reserve, a great humility combined with a high ideal of service and a great compassion which made him an outstanding doctor. [He was] artistic, warm-hearted, and perceptive, with a genial and kindly humour.”2
Stallard is also credited with developing many surgical techniques. As described in a comprehensive article in the Indian Journal of Ophthalmology, this included “partial cyclectomy and its modifications for iris neoplasia, techniques of eyelid reconstruction and partial transplantation (middle third) of levator palpebrae superioris muscle in patients with superior rectus palsy, management of ocular emergencies, and surgeries for epiphora.”3 He also developed several surgical instruments, including a corneal grafting knife, a ptosis spatula, and a non-magnetic foreign body extractor.
“Henry Stallard was an outstanding athlete and gifted surgeon, a truly remarkable man,” Mr Williams noted. “While he had no children of his own, the hundreds of children throughout the world who had their lives and their sight saved and those who will need our help in the future— they are Stallard’s children.”
For citation notes, see page 46.
Hugh Williams DO, FRCS, FRCOphth is an Honorary Consultant Surgeon, Moorfields Eye Hospital, London. drhpwilliams@yahoo.co.uk
75th Anniversary of the First IOL Implantation
Join ESCRS in celebrating Harold Ridley’s first intraocular lens implantation! There will be infographic spots, an IOL Evolution Timeline Wall, and a tunnel museum featuring selected museum pieces.
ESCRS Arena / Tablao
Following the successful launch of the Arena at ESCRS 2023 in Vienna, this year’s Congress will feature another innovative concept, incorporating the local flavour of Spain into the scientific delivery of content. Don’t miss the ESCRS Tablao!
iNovation® Day 2024
How will the latest technological innovations address the most urgent clinical needs and barriers to success in anterior segment care? Find out at iNovation Day on Friday, 6 September.
Global Refractive Summit
Organised jointly by ESCRS, ISRS, and BRASCRS, the Global Refractive Summit will address recent advances in corneal refractive surgery, refractive surgery and endothelial disease, AI for phakic IOL sizing, and much more!
Medical Writing Workshop
This three-hour workshop will cover what to do before you start writing a paper, how to present your data, and how AI and digital tools affect paper writing today. A special focus will be on developing the discussion section and interpreting the clinical results.
Cornea Day is a concentrated kick-start for your ESCRS visit. It typically ranks as one of the highest-attended events, so come early for a seat—it’s often standing room only!
Sorcha
Ní Dhubhghaill PhD, FEBO, FEBOS-CR
Leadership and Business Innovation Programme
Sunday will feature a day-long programme geared towards practice administrators and clinic teams as well as a lunchtime workshop with ESONT on successfully implementing innovative technology in your practice.
Digital Dry Labs
In addition to its traditional wet labs, the Congress in Barcelona will feature 16 dry lab stations using model eyes instead of animal material. Zeiss Stemi microscopes linked to iPads will allow trainers to watch and record a trainee’s surgery and easily provide feedback.
Plus Regular Favourites … Cornea Day Glaucoma Day Industry Exhibit
Controlling Inflammation after Cataract Surgery
No consensus among leading surgeons regarding whether or how to use a dropless regimen.
CHERYL GUTTMAN KRADER REPORTS
Drops, dropless, steroids? What’s the preferred way to control inflammation after cataract surgery? An expert panel at ASCRS 2024 in Boston tackled this question.
Ehud I Assia MD said a ‘less drops’ approach works better for him. Although he uses intracameral moxifloxacin for infection prophylaxis, Dr Assia prescribes a 1-month course of topical medications for infection control that consists of two medications—a steroid and a nonsteroidal anti-inflammatory drug (NSAID)—each given three times daily.
Providing the rationale for his approach, Dr Assia noted that unless formulated for sustained release, medications administered intracamerally provide only short-term efficacy. While the limited duration of coverage is adequate for preventing endophthalmitis, it is not sufficient to control inflammation.
Short-term efficacy, risk for complications, and/or irreversibility decrease the acceptability of other injectable routes for delivering anti-inflammatory drugs, i.e., subconjunctival injection and approaches for posterior chamber placement. The intracanalicular dexamethasone insert offers reversibility, but available data show it is not more effective than topical steroids, Dr Assia said.
“The ‘less drops’ regimen is effective, reversible, adjustable, and inexpensive,” he asserted.
Support for subconjunctival steroids
Advocating for subconjunctival steroid injection, Neal H Shorstein MD reviewed findings from a recently published study reporting on the effectiveness of subconjunctival triamcinolone acetonide (TA) as a standalone treatment for preventing inflammation after cataract surgery.1 Dr Shorstein noted he and two colleagues at Kaiser Permanente Northern California began an injection-only protocol in 2008 for their cataract surgery medication regimen using an intracameral antibiotic and subconjunctival TA.
“We preferred the subconjunctival route versus a sub-Tenon’s injection for the steroid because, using the subconjunctival approach, we could visualize the needle tip during delivery and the depot postoperatively, allowing us to avoid globe perforation and to excise the depot postoperatively if necessary,” he said.
The steroid regimen was modified over time, transitioning from a 2 mg dose (using TA 40 mg/mL) to 4 mg (using TA 10 mg/mL). Dr Shorstein explained the smaller dose of the higher concentration drug was associated with a significant IOP rise in a very small percentage of patients and was found to be less effective than topical prednisolone plus an NSAID.
The higher dose using a lower concentration of TA was more effective and caused fewer IOP spikes.
The recent study included data from almost 70,000 eyes operated on between 2018 and 2021. They were assessed for development of macular oedema, rebound iritis, and glaucoma-related events occurring from 15 days to 1 year postoperatively. Eyes receiving subconjunctival TA were divided into subgroups by TA dose and concentration. Using multivariate analysis, their outcomes were compared to a reference group receiving topical anti-inflammatory treatment.
Reviewing the results and weighing the benefits and risks, Dr Shorstein and colleagues concluded TA 4 mg (10 mg/mL) was the favoured regimen for preventing inflammation in routine cases. However, they suggested TA 4 mg (40 mg/mL) may be applicable for patients with pre-existing iritis because it further lowered the risks of macular oedema and iritis. However, close follow-up is important because TA 4 mg (40 mg/mL) was associated with higher odds of IOP elevation.
Also considering the risk for increased IOP, Dr Shorstein noted the need to exercise caution using subconjunctival TA in patients with an optic nerve at risk or elevated risk for a steroid response. With safety in mind, he also recommended using the studied product (Kenalog) because different triamcinolone products have different pharmacokinetics, monitoring IOP until the depot is no longer visible and injecting the medication inferiorly versus superiorly.
Sustained release steroid
Seth M Pantanelli MD explained why he uses the intracanalicular dexamethasone insert as his choice for a steroid after cataract surgery.
“The insert has been shown to be safe and effective for controlling pain and inflammation. Insertion is easy and fast—it can be done in less than 15 seconds, and patient perspectives about the insert are overwhelmingly positive,” Dr Pantanelli said.
“Although the insert adds cost for the medical system, the ambulatory surgery centre (ASC), the surgeon, and the patient, it can actually be cost-neutral or even revenue-positive, depending on the comparator.”
Dr Pantanelli reviewed data from premarket approval studies demonstrating the intracanalicular insert was more effective than placebo for controlling inflammation and pain. But he also emphasized results from a retrospective chart review showing it was as effective as topical steroid drops, which is the more relevant
comparator.2 Furthermore, results from two studies in which patients underwent surgery with the insert in one eye and topical drops in the fellow eye showed the vast majority of participants (≥92%) preferred the insert. In one study, 84% of patients indicated a willingness to pay more for the dropless option.3,4
Discussing cost issues, Dr Pantanelli noted that insert use might generate a per-case profit of up to US$35 for the ASC or surgeon.
“We have to consider cost in this world of decreasing reimbursement, and we also have to consider cost to patients with topical drops,” he said.
Drs Assia, Shorstein, and Pantanelli spoke at the 2024 ASCRS annual meeting in Boston, US.
For citation notes, see page 46.
Ehud I Assia MD is Professor of Ophthalmology, Tel Aviv University, Tel Aviv, Israel. assia@eintal.com
Neal H Shorstein MD is an ophthalmologist, researcher, and associate chief of quality at Kaiser Permanente Medical Center in Walnut Creek, California, US. neal.shorstein@gmail.com
Seth M Pantanelli MD, MS is Professor of Ophthalmology, Penn State College of Medicine, Hershey, Pennsylvania, US. spantanelli@pennstatehealth.psu.edu
Bringing PROMs into the Intermediate Vision Equation
Quality of life tools need to consider modern treatment options.
DERMOT MCGRATH REPORTS
With a proliferation of trifocal and extended depth of focus (EDOF) lenses now available, there is a pressing need to accelerate the development of outcome-based quality registries and appropriate tools for patient-reported outcomes for intermediate vision, according to Anders Behndig MD, PhD.
“We do have some tools available to us, but there is still a lack of transparent and standardised outcome data when it comes to patient-reported outcome measures (PROMs) and intermediate vision,” Dr Behndig said. “We know, for instance, that distance visual acuity is poorly correlated with a patient’s total visual functioning.”
The patient’s quality of life and ability to function with daily tasks should be included in any feasible measure, he added.
“Ideally, a decision to perform cataract or clear lens extraction surgery should not be based on visual acuity alone but also consider the impact of the cataract and/or presbyopia on the patient’s quality of life and functioning,” he said. “Preferably, this should include new activities of daily life associated with social change, such as smartphones and laptops, all of which typically require good intermediate vision.”
Ideally, a decision to perform cataract or clear lens extraction surgery should not be based on visual acuity alone.
PROMs provide a direct assessment of a patient’s subjective experience, encompassing aspects such as functional impairment, quality of vision, and overall satisfaction post-treatment, Dr Behndig explained.
In Sweden, for instance, validated questionnaires such as Catquest-9SF have been of considerable value in assessing the impact of cataracts on daily tasks since their introduction in 2007. Nevertheless, the questionnaire has not adapted to capturing the kind of data needed in an era of multifocal and EDOF lenses.
“It is a good gold standard, but one of the disadvantages of Catquest-9SF is its design for cataract with monofocal IOLs for distance vision and near vision corrected with glasses—so it does not really distinguish whether the patient has glasses,” Dr Behndig said. “Furthermore, there are no questions on spectacle independence as it wasn’t designed for that purpose. And while two questions do relate to intermediate vision, it is not possible to extract that data from Catquest-9SF.”
Another assessment tool, the Visual Function Index (VF14), consists of 18 questions covering 14 aspects of visual function affected by cataracts, but again is not really geared to assessing intermediate vision.
“A lot of the questions include phrases such as ‘even with glasses,’ which rules out spectacle independence and intermediate vision,” he said.
The National Eye Institute Visual Function Questionnaire-9 (NEI VFQ-9) is more recent but does not fit Rasch analysis, which rules out any meaningful statistical analysis based on its data. Another tool, the Quality of Vision (QoV) questionnaire, includes 30 items and 10 symptoms and effectively measures subjective quality of vision.
“It is psychometrically robust but very demanding if you want to perform it on a large scale. The Visual Function Index has 18 items and is less demanding—but less psychometrically robust,” Dr Behndig said. “There is also the Near Activity Visual Questionnaire (NAVQ) designed for near-vision functioning in presbyopia—but it does not reflect more recent changes in technology as it was developed in 2008.”
Looking ahead, Dr Behndig said he envisions a future where PROMs are seamlessly integrated into clinical practice through electronic interfaces. Automated data transfer to registries could streamline data collection and analysis, enhancing the efficiency of outcome evaluation.
Dr Behndig presented this study at the 2024 ESCRS Winter Meeting in Frankfurt.
Anders Behndig MD, PhD is Professor of Ophthalmology, Umeå University Hospital, Umeå, Sweden. anders.behndig@ophthal.umu.se
New Trifocal IOL Delivers Positive Outcomes
Seven diffractive rings offer full range of vision.
DERMOT MCGRATH REPORTS
Initial clinical results of a new trifocal IOL (Triva-aXAY, HumanOptics) with a novel diffractive design and a large optic have demonstrated excellent performance in terms of visual acuity and delivering high levels of patient satisfaction, according to Pavel Stodůlka MD, PhD.
“This lens has an innovative and very smooth implantation technique and delivers excellent monocular and binocular visual acuities at all distances,” he said. “Notably, over onethird of patients reported no dysphotopsia at all, while low numbers of patients reported strong halo and glare effects, which is an impressive performance for a trifocal lens.”
Dr Stodůlka said matching the appropriate IOL to the right patient profile is the key to success.
“It is now more than 75 years since the first IOL was implanted, and it is good to see the pace of innovation continues today,” he said. “The properties of this trifocal lens may offer the anticipated level of vision quality sought by individuals with high expectations and a desire for freedom from spectacles.”
Discussing the properties of the Triva-aXAY, Dr Stodůlka explained it is a hydrophilic acrylic lens with a 7.0 mm large optic, seven diffractive rings, near additions of +1.75 D and +3.50 D, and a 3.5 mm diffractive zone. The lens offers built-in powers ranging from +10.00 to +30.00 D in 0.50 D increments.
“The optic is designed to minimize dysphotopsia, even in larger pupils, and, with only 7 diffractive rings, achieves similar or even better results than traditional trifocal with up to 26 diffractive rings,” he said. “Because the IOL was bigger than other designs, we had some difficulties with implantation with the first models—but our new proprietary implantation technology has resolved this issue and made it very easy and smooth to deliver the lens into the capsular bag.”
One of the novelties of this lens is the plate cut-out haptics are folded underneath the optic at the moment of delivery into the capsular bag.
“We enter with the cartridge inside the eye at the level of the capsulorhexis, and when the optic leaves the cartridge tip, the whole lens unfolds easily in the capsular bag. It is super easy,” Dr Stodůlka explained. “Then we aspirate the viscoelastic and clean up the eye, and we end up with a well-centred large optic with a much lower risk of dysphotopsia coming from the edge.”
Dr Stodůlka’s study included 32 eyes of 16 patients with a median age of 58 years implanted with Triva-aXAY as part of routine cataract surgery. Median IOL power was 23.50 D, and follow-up was set at six months.
“In terms of results, we got what we expected, and the patients were happy,” he noted. “All eyes had corrected
distance visual acuity (CDVA) of 0.1 logMAR or better, and 0.2 logMAR or better was achieved in 78% of eyes for distance corrected intermediate vision acuity (DCIVA) at 80 cm and 97% of eyes for distance corrected near visual acuity (DCNVA) at 40 cm.”
The binocular corrected visual acuity outcomes were also satisfactory, with all patients achieving 0.3 logMAR or better at all distances. The spherical equivalent refractive accuracy showed a slightly myopic outcome with 53% of eyes from -0.14 D to -1.00 D and 75% of eyes within ±0.50 D of target refraction.
“That is a very nice outcome for an initial series,” Dr Stodůlka said.
Regarding dysphotopsia, halo was reported as ‘no or mild’ in 79%, glare as ‘no or mild’ in 64%, starburst in 64%, and 36% of patients reported no photic phenomena at all.
“For a diffractive full range of vision IOL, these are very nice results indeed,” he concluded.
Dr Stodůlka presented at the 2024 ESCRS Winter Meeting in Frankfurt.
Pavel Stodůlka MD, PhD, FEBOS-CR is founder, chief surgeon, and CEO of Gemini Eye Clinics in the Czech Republic and Vienna, Austria. stodulka@lasik.cz
Matching Technologies to Presbyopic Patient Needs
Ever-growing selection of IOLs requires careful screening.
DERMOT
MCGRATH REPORTS
With a vast selection of presbyopia-correcting intraocular lenses now on the market, the key to delivering optimal outcomes still lies in clear communication with the patient and matching their needs closely with the most appropriate technology available, according to Gerd Auffarth MD, PhD.
“The latest generation of presbyopia-correcting IOLs allows us to address specific patients’ needs, and we are seeing a paradigm shift regarding non-diffractive IOL technology,” he said. “With a wide choice of lenses available to us, the key to appropriate IOL selection is to understand patients’ needs and their willingness to compromise and to remember there is no such thing as a ‘free lunch’ in optics.”
In terms of optical performance, Professor Auffarth said any attempt to correct presbyopia, a natural but complex process of physiological insufficiency of accommodation associated with the ageing of the eye, needs to take due account of three interrelated concepts: visual quality, depth of field, and dysphotopsia.
“If we want to increase the depth of field, we will reduce visual quality and increase dysphotopsia,” he said. “We have to play with the aberrations of the eye and other factors to maximize visual quality and balance out a certain amount of depth of focus to achieve our goal.”
There are a lot of aspects to consider in determining patients’ needs, said Prof Auffarth, including medical
condition, refractive status, hobbies, preferences, profession, and personality.
“Patients are more demanding nowadays and it can be difficult to satisfy them. We are not only looking for the right patient for a premium IOL—we also have to look for the right premium IOL for the patient,” he said. “It gets very confusing when we look at the overwhelming number of monofocal plus, extended depth of focus (EDOF), and trifocal IOLs available.”
The most popular presbyopia-correcting IOLs in the ESCRS 2023 Clinical Trends Survey were trifocal (42%) and EDOF lenses (40%).
“However, the patient satisfaction rates for near/intermediate/distance vision struggle to get over 90% if we combine those who say they were ‘very satisfied’ and ‘somewhat satisfied’ with their IOLs,” he said. “So clearly, there is still room for improvement.”
The typical monofocal-plus patient cannot run the risk of experiencing dysphotopsia—pilots or drivers, for example—but would still benefit from the slightly extended depth of focus for intermediate vision and desire some degree of spectacle independence.
EDOF lenses are a popular choice for patients with an active lifestyle who seek reduced spectacle independence for most activities and require good intermediate vision but are risk averse towards visual disturbances.
Hybrid IOLs, which combine aspects of EDOF and multifocal diffractive IOL design, are good for spectacle independence but Prof Auffarth said they also carry a higher risk of dysphotopsia.
Other technologies, such as the small aperture IOL, may be used in compromised corneas, complex cataract cases, or post-LASIK patients. “They are also an option for patients who have previously been successful with monovision or multifocal contact lenses and want to continue without the need for glasses,” he said.
Light adjustable IOLs can be used for reduced dependence on IOL power calculation, post-refractive surgery eyes, customized monovision, anisometropia, long and short eyes, and astigmatism correction.
Prof Auffarth presented at the 2024 ESCRS Winter Meeting in Frankfurt.
Gerd Auffarth MD, PhD is Chairman of the Department of Ophthalmology at the Heidelberg University Eye Hospital and Head of the David J Apple Center for Vision Research, Germany. Gerd.Auffarth@med.uni-heidelberg.de
https://escrs.org/special-interest-groups/yos/
Knowing Iris Repair: Iris Cerclage
Part six in a series on iris repair.
DR SOOSAN JACOB MS, FRCS, DNB
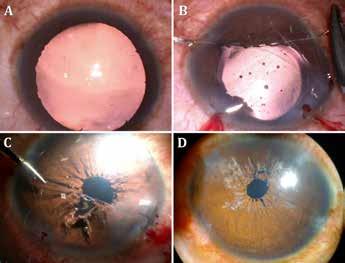
Blunt injury to the eye can result in traumatic mydriasis, secondary to localized or diffuse sphincter tears and can cause glare, photophobia, decreased visual acuity, as well as cosmetic concerns secondary to anisocoria. Both localized and diffuse sphincter damage may be managed with one or more pupilloplasty knots, as described in part two of this series. Diffuse sphincter dysfunction is better managed by iris cerclage, however. This procedure consists of a series of bites taken around the pupillary border in a drawstring fashion so that tightening the two ends of the sutures brings down the pupil size. This is done for a fixed and dilated pupil, generally from post-traumatic pathology or an atonic pupil.
Technique
Very often, the lens is cataractous from the previous trauma and cataract extraction with intraocular lens placement is done prior to iris cerclage. Non-cataractous eyes also require cataract extraction to avoid damage to the crystalline lens during needle passes.
Three limbal paracentesis incisions are made equidistant to each other, and the anterior chamber (AC) is filled with viscoelastic. The dilated iris tissue is pulled inwards gently using microforceps to bring down the pupillary aperture as much as possible. This helps prevent excess stretch and cheese-wiring of the iris later. Pulling the pupil inward is generally possible as iris stroma is relatively healthy in traumatic mydriasis and atonic pupils. With the iris maintained in this position, the AC is refilled with viscoelastic. A double-armed 10-0 Prolene suture with two long, thin, and curved needles (CI-4, Ethicon) on either end is used for iris cerclage.
First needle pass
The first needle is inserted through the paracentesis, taking care to avoid accidentally engaging corneal tissue. The needle is then weaved in and out multiple times close to the pupillary margin, starting from the paracentesis entry site and moving in one direction towards the adjacent paracentesis. The bites are taken such that the needle enters from the anterior stromal side, comes out from the posterior pigment epithelium side, and then similarly moves forward for the next bite—making the needle go around the pupil edge multiple times. This technique requires considerable ambidexterity: the first hand holding the needle needs to be equally assisted by the second hand moving the iris tissue and gently lifting it into position each time to pass the needle from upper side to the underside of the iris and subsequently push the iris bites along the needle to enable more bites.
Once the needle nears the adjacent paracentesis, it is brought out carefully and gently—encouraged by gently pushing the multiple iris bites distally along the needle length
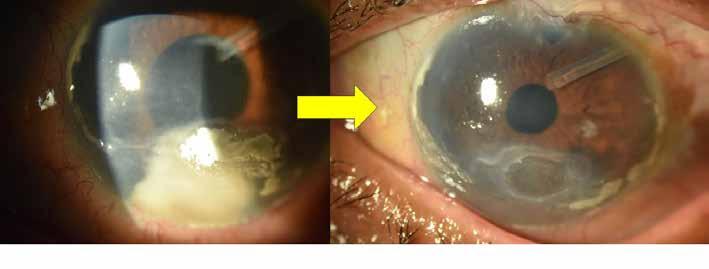
A) Traumatic mydriasis; B) Cerclage sutures; C) Dropped area on tightening suture; D) Cerclage suture tied down. Dropped area repaired with a single-pass, four-throw pupilloplasty knot.
with microforceps to enable the needle to pass through without any cheese-wiring. The needle is brought out by railroading it into a 27-gauge cannula passed through the paracentesis to prevent accidental engagement of corneal tissue at the paracentesis. Care should be taken so none of the above manoeuvres exert excess stress on the iris root to accidentally cause a dialysis. The suture is gently pulled out through the paracentesis before the needle is turned to enter again through the same paracentesis, this time directed toward the third paracentesis with the same procedure repeated carefully to bring the needle out. The AC is replenished with viscoelastic whenever required.
Second needle pass
The second needle of the double-armed suture is now grasped with a needle holder and inserted through the first paracentesis. It is passed multiple times through the pupil border in the opposite direction to the first needle’s path to exit through the third paracentesis. On drawing this needle out, the suture loop enters the AC, and on tightening, the suture encircles the pupil margin from both sides, with both needles having finally exited through the third paracentesis.
Tying the knot
The knot can be tied in one of two ways—using a modified McCannel technique as described by Dr Ike Ahmed, where one end of the suture is cut and looped a few times around a needle holder and tied to the second end. The cut end is then
Figure:
introduced into the AC and grabbed from the opposite paracentesis to cinch the knot. Pulling both ends tightens the drawstring suture around the pupil, thus bringing the pupil size down. Care should be taken not to over-tighten—a pupillary size of 3.5 mm–4.0 mm is ideal for visual purposes and to examine the retina later if required. A second knot may similarly lock the knot and prevent slippage.
The second technique to tie the knot is with the single-pass, four-throw technique, where one needle is internalized and railroaded into a cannula introduced from the opposite paracentesis to come out without taking any iris bite. This gives two sutures in opposite directions, one of which can then be looped out using a Sinskey hook and tied down with a single-pass, fourthrow technique.
Running suture technique
This technique uses a long, thin needle on a polypropylene suture threaded along the iris near the pupillary border and then tied down to complete the cerclage.
Advantages
The iris cerclage suture is useful for diffuse sphincter damage where the iris stromal tissue is still healthy. It creates minimal focal stress on the pupil, avoids over-stretching of iris stroma, and gives a cosmetically appealing, round pupil that can be easily titrated to the desired size. Since the effect of the encerclage is like a drawstring, the pupil is centrally placed and not displaced, as can happen with other pupilloplasty techniques. It also effectively decreases glare and other photic phenomena the patient suffers from and helps improve visual acuity and quality by removing the effects of peripheral aberrations.
Disadvantages
It is more difficult to perform and has a longer learning curve. The needle has to travel a long distance, taking multiple bites near the pupillary edge—which can be time-consuming and require considerable manual dexterity. The suture can cheese-wire through the pupillary bites during this long pass or while pulling the needle out, leading to ‘dropped sections’ and areas where the suture traverses the AC between bites and the pupil remains focally dilated. In addition, the pupil is completely ‘locked’ to a particular size and cannot be dilated beyond since the prolene suture encircles it. This contrasts with a repair using two to three Siepser or single-pass, four-throw pupilloplasty knots to bring down the pupil size, leaving the pupil in between the knots untouched and still dilatable to an extent.
Ophthalmic YAG and SLT Laser System / Ophthalmic YAG Laser System
Right on the Mark
"Precision treatments with the YAG/SLT laser"
Exact Targeting
Optics that enhance clarity and contrast
Sharp aiming beam
Precise Treatment
Refined YAG laser delivery with lower plasma threshold
Unique SLT assist function "SLT-NAVI"
Coaxial illumination for better visualization (optional) NEW
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
www.nidek.com
New Approaches for Treating Endothelial Dysfunction
Alternatives to endothelial keratoplasty reduce dependence on graft tissue.
CHERYL GUTTMAN KRADER REPORTS
Endothelial keratoplasty (EK) procedure development has been a major advance for the surgical treatment of corneal endothelial dysfunction, but other approaches are needed to address the global shortage of corneal donor tissue.
Reviewing new and emerging techniques and technologies, Deepinder K Dhaliwal MD said Descemet stripping only (DSO), endothelial cell injection, and insertion of an artificial endothelial layer show promise for reducing future demand for corneal donor tissue.
DSO is a cornea rejuvenation procedure that is an option for eyes with endothelial dysfunction involving only the central cornea. Based on the concept central corneal guttae are a barrier to healthy peripheral endothelial cell migration, DSO removes the diseased tissue to release contact inhibition. Its advantages are it avoids rejection risk, long-term steroid treatment, prone positioning, and the chance of rebubbling. In addition, DSO costs less than EK and has been associated with high patient acceptance and good long-term results. In a retrospective chart review, 10 of 13 eyes (77%) responded and maintained a clear central cornea for at least five years, and 2 others achieved good vision after rescue EK.
A downside of DSO, however, is visual recovery can take up to three months.
“This is a procedure for patients with patience and who have good vision in the fellow eye,” Dr Dhaliwal said. “However, intracameral adjuvant treatment with ripasudil or TTHX1114 (engineered fibroblast growth factor-1) shows promise for accelerating corneal clearing and visual recovery.”
Cell-based therapy
Corneal endothelial cell therapy is being developed as a commercially available procedure by two companies. A technique from Aurion Biotech injects a suspension containing human cultured epithelial cells plus a rho kinase inhibitor into the anterior chamber after polishing the diseased endothelium. The patient recovers in a prone position for three hours, and the cells self-align.
Results from three clinical trials including 130 patients showed similar improvements in corneal thickness and visual acuity with no serious adverse events. The product has regulatory approval in Japan and is under investigation in a phase 1/2 study in the US.
The second approach, developed by Emmecell, couples intracameral delivery of cultured human corneal endothelial cells combined with magnetic nanoparticles with an external magnetic patch application to attract cells to the target location. Favourable results were achieved in a dose-escalation
phase 1 study assessing safety and tolerability, and a randomised, double-masked study currently underway is assessing three doses of cell injection without endothelial brushing of the recipient cornea.
Artificial endothelium
A biocompatible, biostable corneal endothelial prosthesis from EyeYon Medical has received the CE mark, regulatory approval in Israel and India, Green Channel fast-track priority status in China, and breakthrough device designation from the US FDA. Placed on the posterior corneal surface, this synthetic corneal layer serves as an impermeable barrier to aqueous humour transfer into the central cornea while allowing entry of nutrients into the stroma from the periphery. It is considered an option for high-risk patients, such as those with a history of graft failure or previous glaucoma surgery.
“The results have been quite good in eyes that were otherwise considered high-risk or end stage,” Dr Dhaliwal said.
Dr Dhaliwal spoke at 2024 ASCRS Cornea Day, Boston, US.
Deepinder K Dhaliwal MD is Professor of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania, US. dhaliwaldk@upmc.edu
Corneal Cross-Linking for Keratoconus
Ongoing research explores multiple modifications for building on a successful procedure.
CHERYL GUTTMAN KRADER REPORTS
Corneal cross-linking (CXL) performed with the original Dresden protocol has been a revolutionary advance in managing keratoconus, but emerging experiences with modified approaches point to a bright and perhaps better future, according to Michael B Raizman MD.
“CXL based on the Dresden protocol led to a positive sea change in the medical, financial, and social impacts of keratoconus, but the downsides of the epithelium-off procedure leave room for improvement,” said Dr Raizman.
“Although removing the epithelium has been key to the efficacy of CXL because it facilitates delivery of the photosensitising agent, UV light, and oxygen to the stroma, a variety of methods are being developed [aiming to provide] the same efficacy as the Dresden protocol without removing the epithelium.”
In the United States, two companies are pursuing regulatory approval of ‘epi-on’ CXL procedures: Glaukos and Epion Therapeutics. Glaukos is developing an approach that uses a riboflavin solution modified to provide enhanced penetration through the epithelium, increased UV light intensity, pulsed ultraviolet-A (UV-A), and supplemental oxygen delivered via specialised goggles. The Epion Therapeutics approach is being studied as a bilateral treatment. It uses a riboflavin/sodium iodide solution applied with a loading sponge and a proprietary UV-A device.
Technologies used outside the United States or under development include an epi-on technique with a customised approach to UV-A delivery based on the individual’s tomography. Another epi-on procedure uses a scanning spot UV-A diode laser instead of a broad beam delivery system.
Dr Raizman showed the efficacy of the customised light approach with a case example in which irradiation was focused where the cone was steepest. The pre- to post-treatment difference tomography map showed significant cornea flattening at the treated site and a better normalisation of the corneal shape.
“CXL does not just stop keratoconus progression,” Dr Raizman said. “It also changes the shape of the cornea, and I think that may be accomplished more effectively using a customised treatment pattern.”
CXL does not just stop keratoconus progression.
Additional research explores much more: other agents are being looked at as photosensitisers, including oral agents; alternative approaches for irradiation, including the use of UV-emitting glasses or contact lenses; and developing better ways to combine CXL with a refractive procedure, including by using the UV light to induce refractive changes on the cornea.
Implementing new approaches
Dr Raizman observed that if epi-on CXL gains regulatory approval in the United States, clinicians will need to choose between the procedures.
“We can hope epi-on CXL will be as effective as the epi-off technique—then our decision will be easy. But perhaps epi-off CXL will be more effective. Because it is unlikely that large head-to-head trials comparing epi-on and epi-off CXL will be available any time soon, clinicians will need to rely on between-study comparisons to decide if the epi-off CXL procedure should be used for more serious cases or other particular subsets of patients. The good news is that I think we will have multiple options for our patients.”
Dr Raizman spoke at 2024 ASCRS Cornea Day in Boston, US.
Michael B Raizman MD is Associate Professor of Ophthalmology, Tufts University School of Medicine, Boston, US. michael.raizman@tuftsmedicine.org
Treating Fungal Keratitis
Off-label compounded agents serve as alternatives for managing mycotic infections.
CHERYL GUTTMAN KRADER REPORTS
The corneal specialist can represent the final line of defence for helping patients with fungal keratitis avoid painful loss of vision, and fulfilling this role requires maintaining an emergency armoury of antifungal medications for in-office compounding, according to Dean Ouano MD.
“I am sensitive to the realities of medicolegal liability and regulatory issues associated with compounding topical medications, but ultimately, our responsibility is the care of our patients,” Dr Ouano stated. “Safe office preparation of topical antifungals is possible and, I would argue, necessary if we are the last line of defence.”
Outlining the options
Reviewing the agents used for medical fungal keratitis treatment, Dr Ouano noted natamycin 5% is the only commercially available ophthalmic antifungal medication. Its consideration as first-line therapy for infections caused by filamentous fungi is supported by results of the Mycotic Ulcer Treatment Trial, which found it superior to voriconazole monotherapy.1 Natamycin is not available in oral or intravenous forms and cannot be compounded for subconjunctival or intrastromal delivery. Combined use with voriconazole can provide synergistic or additive antifungal activity, according to data from in vitro testing. Voriconazole remains the most widely used compounded antifungal for treating fungal keratitis since it is
reasonably priced, easily formulated, and well-tolerated given topically or when injected into the stroma, anterior chamber, or vitreous. However, fungal resistance to voriconazole and other newer generation triazoles has become a problem secondary to widespread use of triazoles as agricultural fungicides, Dr Ouano said.
Posaconazole, a newer triazole, has been associated with some encouraging results for treating filamentous fungal keratitis when used at a high oral dose. However, this regimen carries a high cost, risks of liver and cardiac toxicity, and the potential for multiple interactions with medications metabolised by CYP3A4.
Amphotericin B is generally regarded as the drug of choice for Candida infections—although Dr Ouano said he prefers not to use it considering its inherent intraocular toxicity, which includes retinal ganglion cell loss, vitreal inflammation, and corneal oedema.
“Lipid-based formulations of amphotericin B are not necessarily less toxic,” he added.
Limited experience shows encouraging results using echinocandin agents to treat fungal keratitis. Caspofungin and micafungin are the two clinically useful drugs in this newest class of antifungals. Caspofungin can be compounded for topical or intraocular administration, but there is limited data on the use of micafungin for intraocular use.
Echinocandins are safer than triazoles because they target fungal cell walls selectively and have fewer drug interactions. In addition, they are fungicidal against Candida, making them more effective than the fungistatic triazoles. The echinocandins are also fungistatic against Aspergillus, albeit less effective than polyenes against Fusarium and Cryptococcus due to their mechanism of action.
Most reports of echinocandin treatment for fungal keratitis involve compounded caspofungin, which can be easily prepared as a solution for topical use at a reasonable price. As another advantage, the preparation remains stable for up to four weeks when kept refrigerated.
Micafungin may be more cost-effective than caspofungin, but there are fewer published reports on its use for treating
fungal ocular infections. However, Dr Ouano cited one case series from Japan describing topical micafungin for treating refractory yeast-related corneal ulcers and reported his own positive experience using it to treat fungal keratitis and fungal-positive donor corneal rims.2
Dr Ouano spoke during ASCRS 2024 Cornea Day in Boston, US.
For citation notes, see page 46.
Dean P Ouano MD specialises in glaucoma, cataract, and cornea surgery at the Coastal Eye Clinic, New Bern, North Carolina, US. ddouano@gmail.com
Meet the Precizon Family: best-in-class IOLs for any cataract challenge. Monofocal, enhanced intermediate vision and full range of vision lenses with patented CTF technology. Regular and Toric. With a natural fit and ingenious optics that deliver extraordinary results. For successful surgery and perfect natural vision.
ophtec.com/precizon-family
Precizon Family
OSD in Glaucoma
Why detection and management of dry eye disease is an essential part of patient care.
CHERYL GUTTMAN KRADER REPORTS
Optimising visual function for patients with glaucoma requires attention to the ocular surface in addition to a focus on controlling intraocular pressure. Chronic use of topical antiglaucoma medications may contribute to dry eye disease (DED), which is commonly found among patients with glaucoma. Left untreated, DED impairs visual performance and quality of life and leads to suboptimal outcomes after cataract surgery. All these issues can underlie patient dissatisfaction with care, explained Laura M Periman MD.
“Managing IOP by choosing preservative-free topical medications, SLT, or performing minimally invasive glaucoma surgery (MIGS) are good options for minimising the ocular surface burden of preservative-containing topical medications,” Dr Periman said.
In addition, she advised delaying, when possible, cataract surgery and incisional glaucoma procedures in cases where the patient presents with significant DED.
“DED reduces the accuracy of preoperative biometry data used for IOL calculations and postoperative visual quality. Furthermore, the wound healing response is already amplified in eyes with DED-related inflammation, leaving them with little functional reserve to recover from a surgical insult,” Dr Periman explained.
“If you have the luxury of waiting before doing cataract surgery, take time to manage the ocular surface first.”
Insights on DED management
Dr Periman noted chronic use of glaucoma medications impacts all components of the lacrimal functional unit, including goblet cells. The effect on goblet cells is important because they are critical for maintaining immunoregulatory function, a normal tear film, and a healthy ocular surface. The available immunomodulatory drugs (cyclosporin and lifitegrast) for treating DED increase goblet cell density.
Discussing the use of immunomodulators, she added, “I also want everyone to disabuse themselves of the notion immunomodulatory drugs take too long to work. We know that is not the case because, in phase 4 studies of patients with DED needing cataract surgery, improvements were seen within 28 days after starting treatment with lifitegrast and cyclosporin products. So, initiate immunomodulatory treatment early and give the ocular surface a chance to develop the functional reserve to respond appropriately to your surgical insult.”
If you have the luxury of waiting before doing cataract surgery, take time to manage the ocular surface first.
When evaluating patients for DED, Dr Periman reminded her colleagues about using the ASCRS Look, Lift, Push, Pull approach for performing the external examination to detect various DED risk factors, including floppy eyelid syndrome, rosacea, and Demodex blepharitis (among others).1 In addition, she discussed her retrospective chart review research (presented at ARVO 2024) that demonstrates the positive predictive value of the presence of dermal collarettes on the nose and facial skin (‘the Periman Alpenglow Sign’) during the slit-lamp exam as a predictor of microscopic evidence of Demodex blepharitis in patients who have characteristic Demodex symptoms with or without visible eyelash collarettes.
“We are about to begin a prospective study to confirm if this novel, rapid clinical finding can assist in the detection and management of Demodex blepharitis,” she said.
Identifying Demodex, rosacea, inflammation, and other DED risk factors provides a construct for efficient and targeted management using existing and emerging therapies. Further information can be found in a 2016 paper by Baudouin (et al.).2
“This is a [Wikipedia] version of how to manage ocular surface disease and make it less overwhelming,” she said.
Dr Periman spoke during a symposium on optimising refractive outcomes in the glaucoma patient at ASCRS 2024 in Boston, US.
For citation notes, see page 46.
Laura M Periman MD is in private practice in Seattle, Washington, US, where she specialises in dry eye disease. dryeyemaster@perimaneyeinstitute.com
To Combine or Not to Combine
Is phacoemulsification alone or combined with MIGS the preferred procedure?
CHERYL GUTTMAN KRADER REPORTS
Phacoemulsification can effectively lower intraocular pressure (IOP) in eyes with ocular hypertension or primary open-angle glaucoma (POAG), but a combined approach including a minimally invasive glaucoma surgery (MIGS) procedure may provide greater benefit, leading glaucoma surgeons agree.
Participating in a point-counterpoint discussion on this topic, Thomas W Samuelson MD was assigned to defend the position that phacoemulsification alone is effective for IOP control while Steven R Sarkisian Jr MD argued phacoemulsification plus MIGS is the way forward.
Both speakers presented data from prospective randomised clinical trials confirming the IOP-lowering effect of phacoemulsification alone. Reviewing results from five MIGS studies, Dr Samuelson showed an IOP reduction averaging about 5.3 mmHg achieved in eyes undergoing phacoemulsification alone while the groups assigned to phacoemulsification plus MIGS benefited ‘incrementally’ with an additional 1.0 to 2.0 mmHg reduction in IOP.
“The level 1 evidence that phacoemulsification lowers IOP is overwhelming,” Dr Samuelson said. “Phacoemulsification is not a cure for glaucoma, nor does it reduce IOP in all patients. And while the effect is modest in most patients, it is a [success] in many, especially in eyes with POAG acquired later in life presenting with a higher preoperative IOP.”
Using an American football analogy to illustrate the difference between phacoemulsification alone and the combined procedure, Dr Samuelson explained, “I have always considered high-quality phacoemulsification the very foundation of the combined MIGS-phacoemulsification procedures. In fact, I think we can say cataract surgery is the touchdown because it lowers IOP by approximately six points (rounding up) while a MIGS procedure is the extra point or two-point conversion.”
Discussing the mechanism of the IOP-lowering effect of phacoemulsification, Dr Samuelson revisited an explanation
he and co-authors put forth in a paper published in 2008 in which they proposed a causal relationship between the natural lens and OAG.1
“Perhaps the more intriguing question is not if cataract surgery lowers IOP but if the reverse is true—does cataract formation cause OAG in susceptible individuals?” he asked. “We accept that angle-closure glaucoma can be phacomorphic, but perhaps phacomorphic glaucoma can occur with an open angle.”
He further explained the natural age-related increase in crystalline lens thickness causes anterior displacement of the lens and iris diaphragm with effects on the scleral spur and trabecular meshwork microanatomy and function that could lead to reduced aqueous outflow even if the angle remains optically open.
“IOP autoregulates in most patients, but in those with marginal outflow reserve, it increases. Replacing the 4.0- to 5.0-mm thick cataractous lens with a 1.0-mm thick IOL in the latter patients helps to reduce IOP,” he said.
Making sure the local surgeons do high-quality phacoemulsification is an essential and important step in the management of glaucoma.
Considering the IOP-lowering effect of phacoemulsification in the context of glaucoma being a leading cause of blindness in developing countries, Dr Samuelson emphasised its quality. “Making sure the local surgeons do high-quality phacoemulsification is an essential and important step in the management of glaucoma.”
Nevertheless, he concluded his presentation with a concession to Dr Sarkisian by admitting, “[In my practice], I
virtually always perform phacoemulsification plus MIGS in patients with cataract and glaucoma requiring treatment.”
In favour of combined surgery
Advocating for performing MIGS with phacoemulsification, Dr Sarkisian cited the summary from a recent review article as evidence of a growing consensus that combined surgery is the preferred procedure in patients with POAG.2 He also presented results from multiple studies showing the advantages of the combined procedure, including statistically significant reductions in IOP and medication need. It additionally offers greater durability and a clinically relevant positive impact on protecting against glaucoma progression and improving quality of life.
“We know from the Advanced Glaucoma Intervention Study that in treating glaucoma, lower IOP prevents visual field loss,” Dr Sarkisian said. “And, by reducing medication dependence [and the adverse effect of medication on the ocular surface], adding MIGS to phacoemulsification may improve quality of life by reducing ocular symptoms and vision-related activities.”
Dr Sarkisian noted that earlier in the history of MIGS, this category of procedures was being referred to by some surgeons as MEGS—minimally effective glaucoma surgery. The renaming was based on the belief phacoemulsification
explained the reduction in IOP achieved when the two procedures were done together.
“That idea is absurd in the face of the available evidence. Now, no one can say with phacoemulsification plus MIGS that the phaco is doing most of the IOP lowering, making no need for the MIGS,” Dr Sarkisian said.
“In my mind, when patients with treatable ocular hypertension or mild-to-moderate POAG need cataract surgery, it is indefensible to recommend phacoemulsification without offering MIGS.”
Drs Samuelson and Sarkisian spoke during ASCRS 2024 in Boston, US.
For citation notes, see page 46.
Thomas W Samuelson MD specialises in glaucoma management and ca taract and refractive surgery. He is a founding partner, Minnesota Eye Consultants, Bloomington, Minnesota, US. twsamuelson@mneye.com
Steven R Sarkisian Jr MD specialises in cataract and glaucoma surgery. He is the founder and CEO of Oklahoma Eye Surgeons, Oklahoma City, US. research@ okeyesurgeons.com; drsarkisian@okeyesurgeons.com
OCULUS Myopia Master ®
Paediatric Cataract Update
Special consideration required in the biometry and IOL selection in children with cataracts.
ROIBEÁRD O’HÉINEACHÁIN REPORTS
Paediatric cataract surgery presents many unique challenges, and timely intervention is necessary to prevent blindness and amblyopia, said Michael Amon MD at an ESCRS e-Connect Webinar.
“Cataract is the most common cause of blindness in children,” he said. “We don’t need to do surgery before six to eight weeks, but in unilateral cataracts, there will be irreversible amblyopia if we don’t intervene before the third or fourth month.”
He noted children have smaller eyes than adults, and their ocular tissues behave differently. In addition, wound closure generally requires suturing and posterior capsulorhexis and vitrectomy are often necessary. Furthermore, infants’ eyes are more prone to complications, including inflammation, secondary cataract, and glaucoma.
Also to be considered is eye growth. The greatest proportion of growth occurs in the first year of life, during which the axial length increases by around 4 mm to 5 mm. Axial length continues to grow substantially up to six years old and is largely complete by age eighteen to twenty. Changes in the cornea’s optics partially compensate for the increase in axial length but not entirely.
Biometry is also more complicated and less precise in paediatric patients than in adults. Instead of laser interferometry and corneal tomography performed as an office procedure, biometry in children often requires general anaesthesia, handheld keratometry, and ultrasound biometry.
There are no specific IOL calculation formulas for children’s eyes, so Professor Amon recommended using modern formulas. The most important factor is the postoperative refraction. Effective lens position will depend on whether the lens is placed in the capsule, the sulcus, or with scleral fixation. In unilateral cataracts, the contralateral eye’s refraction must be considered to avoid anisometropia.
Algorithms to prevent high myopia in the eye as it matures include undercorrecting. One algorithm suggests reducing the IOL power by 20% in patients younger than two years and 10% in patients two to five years of age. IOL exchange is one option for cases of myopic shift. But add-on IOLs represent an interesting, reversible option for refractive adjustment during the period of the dynamic change of eye length.
Prof Amon said that in children zero to one year with amblyogenic cataracts, he generally performs a 25-gauge dry vitrectomy and iridectomy and leaves the eye aphakic, providing their parents or guardians will be able to adequately supervise spectacle or contact lens use. Otherwise, he may implant an IOL, but with a high undercorrection.
He generally performs posterior capsulorhexis, a 25-gauge dry vitrectomy, and implants a neutral aspheric IOL with or without posterior optic capture in cataract patients one to five years old. In children older than six, he implants a neutral aspheric IOL, but posterior capsulorhexis is optional as the patient will be able to undergo YAG laser capsulotomy.
Options for eyes without capsular support include glasses and contact lenses until the eye is grown, at which point a scleral fixated lens may be implanted. Prof Amon noted he no longer implants anterior chamber or iris-fixated IOLs but prefers flanged scleral fixation of IOLs. He also postulated some concerns about fixating IOLs in a scleral pocket because of the risk of scleral thinning over the long term.
Prof Amon presented this information at the ESCRS e-Connect Webinar “Update on pediatric cataract.”
Michael Amon MD, FEBO is based at the Academic Teaching Hospital of St John and Sigmund Freud University, both of Vienna, Austria. Amon@augenchirurg.com
ESCRS IN A SNAPSHOT
We are a society of surgeons who specialise in improving vision and restoring clarity. Since 1991, ESCRS has promoted the education and research of implant and refractive surgery. With more than 7,500 members from 130 countries worldwide, ESCRS is a vital global platform for the field of ophthalmology.
Marketing authorisation for home OCT device
The FDA has granted de Novo Marketing authorisation for Notal Vision’s SCANLY Home OCT device, intended for patients with wet AMD. The AI-powered device allows patients to perform daily retinal imaging at home and captures spectral-domain OCT images in a 10 x 10-degree area centred on the fixation point. The proprietary Notal OCT Analyzer segments and estimates the volume of hypo-reflective space, a key biomarker of neovascular AMD, enabling ophthalmologists to monitor disease progression and treatment efficacy remotely.
notalvision.com
New aflibercept biosimilars gain FDA approval
Two new biosimilar aflibercept biosimilars—Biocon Biologics’ Yesafili® and Biogen’s Opuviz®—have received US FDA approval for the treatment of neovascular age-related macular degeneration, retinal vein occlusion, and macular oedema. The FDA approval is based on comparative clinical data, which confirmed their similarity in structural and functional features and clinical efficacy to the reference drug aflibercept.
bioconbiologics.com; biogen.com
Clearance for new goniotomy device
New World Medical was granted US FDA clearance for an expanded indication for its KDB (Kahook Dual Blade) Glide. The expanded indication allows KDB Glide use in performing goniotomy for primary open-angle glaucoma during cataract surgery or as a standalone procedure. The device’s design includes tapered sides and a rounded heel to ensure an optimal interface with Schlemm’s canal. In addition, its dual blades and proprietary ramp allow for a clean excision, the company says.
newworldmedical.com
Positive results reported with new anticomplement treatment
Annexon’s new anticomplement therapy, ANX007, provided statistically significant time and dose-dependent protection from vision loss in patients with geographic atrophy, according to new data from phase II ARCHER trial presented at the ARVO annual meeting in Seattle. The study showed that, compared to sham-treated patients, those receiving ANX007 were significantly less likely to lose 15 or more letters of best-corrected visual acuity and have greater preservation of low luminance visual acuity. The study showed no difference in choroidal neovascularisation rates between the treated and sham arms and no incidents of retinal vasculitis.
ir.annexonbio.com
Recruitment completed for new anti-VEGF phase 3 trial
Opthea Limited has completed patient enrolment in the COAST phase 3 pivotal clinical trial of sozinibercept (OPT-302), the treatment of wet age-related macular degeneration. Sozinibercept is a soluble form of vascular endothelial growth factor receptor 3 (VEGFR-3) and functions as a ‘trap’ fusion protein, targeting the inhibition of VEGF-C and VEGF-D. COAST phase 3 enrolled 1,984 patients and will assess the safety and efficacy of sozinibercept in combination with standard anti-VEGF-A therapies. The company expects to report results by mid-2025.
opthea.com
FLACS SAFER THAN CONVENTIONAL PHACO
Femtosecond laser-assisted cataract surgery (FLACS) can significantly reduce phacoemulsification time, surgical time, and endothelial cell loss compared with conventional phacoemulsification when treating dense cataracts, according to the findings of a prospective, randomised, comparative study. The study involved 100 eyes of 100 patients with cataracts grade 3.0 or above in the Lens Opacities Classification System III. They were randomly assigned to undergo either FLACS with customised nuclear fragmentation with the LENSAR Laser System or conventional phacoemulsification (CPS). The study showed the average total phacoemulsification time was 8.03 seconds in the FLACS group compared to 11.17 in the CPS group and the effective phacoemulsification times were 4.42 seconds and 6.14 seconds, respectively. The overall surgical time in the FLACs and CPS groups were 8.18 minutes and 7.11 minutes, respectively. In addition, on the first postoperative day, the CPS group had significantly higher mean scores for corneal oedema and central corneal thickness. Moreover, at the six-month mark, the mean endothelial cell density loss was 12.80% in the FLACS group, compared to 16.08% in the CPS group. Additionally, three cases in the CPS group experienced wound burns of varying degrees.
S Ganesh, et al. “Changes in endothelial cell density after conventional phacoemulsification and FLACS in eyes with dense cataracts,” 50(6): 572–577.
STEEPNESS THRESHOLD FOR HYPER-
OPIC LASIK CALLED INTO QUESTION
The findings of a new retrospective study indicate the commonly recommended 49-dioptre threshold of postoperative corneal steepness following hyperopic LASIK may require re-evaluation. The study included 1,703 eyes of 1,703 consecutive patients who underwent hyperopic LASIK between January 2013 and December 2019. The study showed that patients with postoperative keratometry greater than 49 D had significantly worse logMAR corrected distance visual acuity (CDVA) than those with values less than 49 D (0.07 vs 0.04). After adjusting for baseline differences and spherical treatment, no significant differences were observed in postoperative logMAR CDVA. The factors associated with poorer postoperative CDVA included higher spherical treatment and preoperative CDVA.
R Sella, et al. “Hyperopic LASIK and postoperative corneal steepness: revisiting the 49-dioptre limit,” 50(6): 550–557.
EPITHELIAL COMPLICATIONS FOLLOWING KLEX
GENERALLY RESOLVE WITHOUT SURGERY
Most cases of epithelial membrane basement dystrophy (EBMD) following keratorefractive lenticule extraction (KLEx) respond well to nonsurgical treatment with good clinical results. A minority have long-term complications such as corneal scarring and decreased CDVA, a retrospective single-centre study suggests. Among 26 eyes of 16 patients who exhibited signs of EBMD after KLEx, the complications were first observed within one week postoperatively in 22 eyes (84.6%). They included epithelial defects in 6 eyes (23.1%), subepithelial corneal opacity in 10 (38.5%), diffuse lamellar keratitis in 5 (19.2%), and epithelial ingrowth in 1 eye (3.9%). At three months postoperatively, 21 eyes (80.8%) showed no specific findings on slit lamp microscopy after medical treatment, but 2 (7.7%) showed subepithelial corneal opacity, 2 (7.7%) showed corneal scars, and 1 eye (3.9%) showed epithelial ingrowth.
B K Kim, et al. “Clinical outcomes of epithelial basement membrane dystrophy after keratorefractive lenticule extraction,” 50(6): 558–564.
GLOBAL REACH
As a renowned authority in the field of cataract and refractive surgery, ESCRS facilitates global connections amongst ophthalmic professionals, fostering collaboration and the exchange of knowledge.
Our events span across continents, providing a platform for pioneering research, advanced surgical techniques, and continuous professional development.
Using the interactive map on our website, we invite you to explore our global presence by viewing upcoming events and academies.
Join us to network with esteemed experts, access the latest advancements, and contribute to the enhancement of eye care on a worldwide scale.
escrs.org/meetings-and-events/global-reach/
Cited in this Issue
Olympic Committee Targets
Sports-Related Ophthalmic Issues
Page 14
1. BMJ Open Sport Exerc Med, 2023; 9(3): e001644. DOI: 10.1136/ bmjsem-2023-001644.
Eye Care Enters the Ring
Page 16
1. VJ Giovinazzo, et al., “The Ocular Complications of Boxing,” Ophthalmology, 94(6): 587–596.
The Olympian Ophthalmologist
Page 22
1. Museum, The Royal College of Ophthalmologists. www. rcophth.ac.uk/about-the-college/museum
2. Bullock JD, Henry B, Stallard MD. “The 1924 Paris Olympics, and Chariots of Fire,” Survey of Ophthalmology, 2011; 56: 466–71.
3. Mrittika Sen, et al. “Hyla Bristow Stallard: Citius, Altius, Fortius,” Indian Journal of Ophthalmology, 2021 Sep; 69(9), 2252–2255.
Controlling Inflammation after Cataract Surgery
Page 26
1. Shorstein NH, McCabe SE, Alavi M, Kwan ML, Chandra NS. “Triamcinolone Acetonide Subconjunctival Injection as Stand-Alone Inflammation Prophylaxis after Phacoemulsification Cataract Surgery,” Ophthalmology, 2024 Apr 4: S01616420(24)00206-9. Epub ahead of print.
2. Lu AQ, Rizk M, O’Rourke T, et al. “Safety and Efficacy of Topical vs Intracanalicular Corticosteroids for the Prevention of Postoperative Inflammation after Cataract Surgery,” J Cataract Refract Surg, 2022; 48(11): 1242–1247.
3. Donnenfeld ED, Hovanesian JA, Malik AG, Wong A. “A Randomized, Prospective, Observer-Masked Study Comparing Dropless Treatment Regimen Using Intracanalicular Dexamethasone Insert, Intracameral Ketorolac, and Intracameral Moxifloxacin versus Conventional Topical Therapy to Control Postoperative Pain and Inflammation in Cataract Surgery,” Clin Ophthalmol, 2023; 17: 2349–2356.
4. Gira JP, Sampson R, Silverstein SM, et al. “Evaluating the Patient Experience after Implantation of a 0.4 mg Sustained Release Dexamethasone Intracanalicular Insert (Dextenza™): Results of a Qualitative Survey,” Patient Prefer Adherence, 2017; 11: 487–494.
Treating Fungal Keratitis
Page 36
1. Prajna NV, Krishnan T, Mascarenhas J, et al; Mycotic Ulcer Treatment Trial Group. “The mycotic ulcer treatment trial: a randomized trial comparing natamycin vs voriconazole,” JAMA Ophthalmol, 2013; 131(4): 422–429.
2. Matsumoto Y, Dogru M, Goto E, Fujishima H, Tsubota K. “Successful topical application of a new antifungal agent, micafungin, in the treatment of refractory fungal corneal ulcers: report of three cases and literature review,” Cornea, 2005; 24(6): 748–753.
OSD in Glaucoma
Page 38
1. Starr CE, Gupta PK, Farid M, et al.; ASCRS Cornea Clinical Committee. “An algorithm for the preoperative diagnosis and treatment of ocular surface disorders,” J Cataract Refract Surg, 2019; 45(5): 669–684.
2. Baudouin C, Messmer EM, Aragona P, et al., “Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of meibomian gland dysfunction,” Br J Ophthalmol, 2016; 100(3): 300–306.
To Combine or Not to Combine
Page 40
1. Poley BJ, Lindstrom RL, Samuelson TW, Schulze R Jr. “Intraocular pressure reduction after phacoemulsification with intraocular lens implantation in glaucomatous and nonglaucomatous eyes: evaluation of a causal relationship between the natural lens and open-angle glaucoma,” J Cataract Refract Surg, 2009; 35(11): 1946–1955.
2. Sabharwal J, Garg AK, Ramulu PY. “How much does cataract surgery contribute to intraocular pressure lowering?,” Curr Opin Ophthalmol, 2024; 35(2): 147–154.
Need a quick introduction or refresher about a surgical procedure? Have a tip to share about a technique or approach you use that makes surgery easier?
The ESCRS 100 is the place to go. It’s a library of short (roughly 100 seconds), high-quality instructional videos about all fields of cataract and refractive surgery.
More than a dozen videos have already been created, and additional videos are being uploaded each month. Current videos include the following topics:
• Phaco rolling
• LASIK: Lifting the flap
• Descemet membrane stripping
MAKE EVERY SECOND COUNT
—PUT THE ESCRS 100 VIDEO SERIES ON YOUR LIST OF MUST-WATCH EDUCATIONAL RESOURCES !
Upcoming Events
September 6–10
2024 ESCRS Congress
Barcelona, Spain
September 6
ESCRS iNovation Day Barcelona, Spain
September 26
2nd International TOA Retinopathy of Prematurity Course Istanbul, Turkey
September 27–29
19th Symposium of the CroCRS Split, Croatia
October 18–21
American Academy of Ophthalmology Chicago, United States
November 20–24
The 58th TOA National Congress Antalya, Turkey
November 28–29
UKISCRS
75th Anniversary of the IOL London, United Kingdom
6 Sept
27 Sept 26 Sept
28 Nov
STOP! Glaucoma Disease Progression
iStent ® technologies have been proven to stabilize visual fields loss and glaucoma disease progression with a favourable risk-benefit ratio1
+3 YEARS FOLLOW-UP
15 STUDIES ON ISTENT TECHNOLOGIES
1,115 EYES
26.6 % MEAN IOP REDUCTION WAS SUFFICIENT TO ACHIEVE THIS FUNCTIONAL EFFECT
-0.024
DBS/YEAR MEAN RATE OF PROGRESSION SIMILAR TO THAT REPORTED IN NONGLAUCOMATOUS EYES
INTERVENE EARLIER WITH ISTENT INJECT ® W TO PRESERVE PATIENTS’ FUNCTIONAL VISION AND QUALITY OF LIFE
1. Gillmann K, Hombeak DM. BMJ Open Ophth 2024;9:e001575.doi:10.1136/bmjophth-2023-001575.
iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATION FOR USE: The iStent inject ® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject ® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject ® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS:
• For prescription use only.
• This device has not been studied in patients with uveitic glaucoma.
• Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject ® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject ® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.”