DON’T LOSE SIGHT OF RETINAL DISEASE WHEN VISUALISING OUTCOMES.
CATARACT & REFRACTIVE | CORNEA | RETINA | GLAUCOMA PAEDIATRIC OPHTHALMOLOGY May 2022 | Vol 27 Issue 4
CATARACT

DON’T LOSE SIGHT OF RETINAL DISEASE WHEN VISUALISING OUTCOMES.
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.

Publishers
Publishers Therese Dolan
Therese Dolan
Operations Director ESCRS
Operations Director ESCRS
Barbara Calderwood
Barbara Calderwood
Mark Wheeler
Mark Wheeler
Executive Editor
Executive Editor
Stuart Hales stuart.hales@eurotimes.org
Stuart Hales stuart.hales@eurotimes.org

Editor-in-Chief
Editor-in-Chief
Sean Henahan
Sean Henahan
Senior Content Editor
Senior Content Editor
Kelsey Ingram
Kelsey Ingram
Design Director
Design Director
Kelsy McCarthy
Kelsy McCarthy
Designer
Designer
Jen Basel
Jen Basel
Circulation Manager
Circulation Manager
Vanessa McCourt
Vanessa McCourt
Contributing Editors
Contributing Editors
Cheryl Guttman Krader
Cheryl Guttman Krader
Howard Larkin
Howard Larkin
Dermot McGrath
Dermot McGrath Roibeárd O’hÉineacháin
Roibeárd O’hÉineacháin
Contributors
Contributors
Gearóid Tuohy
Leigh Spielberg
Soosan Jacob
Gearóid Tuohy
Priscilla Lynch
Colour and Print
Soosan Jacob
W&G Baird Printers
Colour and Print
Advertising Sales
W&G Baird Printers
Roo Khan
MCI UK
Advertising Sales
Tel: +44 203 530 0100 roo.khan@wearemci.com
Roo Khan MCI UK
Tel: +44 203 530 0100 roo.khan@wearemci.com
Published by the European Society of Cataract and Refractive Surgeons, Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
Published by the European Society of Cataract and Refractive Surgeons, Temple House, Temple Road, Blackrock, Co Dublin, Ireland. No part of this publication may be reproduced without the permission of the executive editor.
Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS
EuroTimes ISSN 1393-8983
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes ISSN 1393-8983
As certified by ABC, the EuroTimes average net circulation for the 10



The need for ophthalmic support in Ukraine has never been greater. ESCRS is continually monitoring the needs of our Ukrainian colleagues, gathering valuable input from EURETINA and the European Society of Ophthalmic Plastic and Reconstructive Surgery (ESOPRS), and asking our industry partners to help us meet these needs.


In particular, the Lions Eye Institute for Transplantation and Research, Alcon, BVI, and Zeiss have all stepped forward with very generous donations of equipment and material. The first three shipments (FCI products such as PMMA IOLs, orbital implants, silicone oil, Decalin, lacrimal probes, surgical loupes, and eye shields as well as a palette of surgical packs co-donated with Hartmann) from Zeiss have already arrived at our storage in Krakow.
Our storage site in Krakow is ready to receive equipment at any time, and it will then be forwarded to the clinic in Lviv and onwards as quickly as possible to where it is most needed.
Some pieces of equipment cannot be donated by industry, and ESCRS is prepared to use its own funds to purchase these. For example, we are looking at how best to get a phaco-vitrectomy machine for the ophthalmology department of Kyiv military hospital, where that team can use it for up to six operations per day. ESCRS is also covering administrative, transport, and storage costs.
However, more funds are necessary for a range of purposes, including purchasing pharmaceuticals such as eyedrops and, later on, helping with initiatives such as setting up a network of consultants to advise and arranging secondary trauma care at centres across Europe.
To this end, the Society has decided to establish a fund to accept financial donations, which will be directed exclusively to support ophthalmology-related relief efforts arising from the conflict in Ukraine. We can accept donations to the fund from ESCRS members as well as industry partners and fellow societies.
Noel Alpins (Australia), Bekir Aslan (Turkey), Roberto Bellucci (Italy), Hiroko Bissen-Miyajima (Japan), John Chang (China), Béatrice Cochener-Lamard (France), Oliver Findl (Austria), Nino Hirnschall (Austria), Soosan Jacob (India), Vikentia Katsanevaki (Greece), Daniel Kook (Germany), Boris Malyugin (Russia), Marguerite McDonald (USA), Cyres Mehta (India), Sorcha Ní Dhubhghaill (Ireland), Rudy Nuijts (The Netherlands), Leigh Spielberg (The Netherlands), Sathish Srinivasan (UK), Robert Stegmann (South Africa), Ulf Stenevi (Sweden), Marie-José Tassignon (Belgium), Manfred Tetz (Germany), Carlo Enrico Traverso (Italy)
We are able to accept these donations via bank transfer. And, if you are an ESCRS member and wish to contribute, please simply log in at this link (https://appescrs-donations.azurewebsites.net) using your membership details to access information on how to donate, which is a straightforward process.
For industry partners or fellow societies, please email escrs@mcigroup.com for information on how to make your donation. We are especially grateful to both the Hellenic Society of Intraocular Implant and Refractive Surgery and the United Kingdom and Ireland Society of Cataract & Refractive Surgeons for already having made very generous donations to this fund.
As always, our thoughts are with our Ukrainian colleagues, their families, and their patients at this time, and ESCRS shall continue to do all that we can to support them.
Stay safe!
Oliver Findl President of ESCRSAs always, our thoughts are with our Ukrainian colleagues, their families, and their patients at this time, and ESCRS shall continue to do all that we can to support them.


When the Russian Federation’s war against Ukraine began, I had an extreme desire to defend my homeland with weapons in both hands. But my friends convinced me that I could be much more useful in the operating room. Unfortunately, their assumption became real.
Every case of combat eye injury leaves an unhealed impression.


I would like to share a few cases that I will never forget:
The first case was a boy under 22, a very young guy, a civilian. He had been brushing his teeth and looked out the window at the very moment a bomb exploded. The shrapnel has wounded his face, head, and both his eyes. Corneal and scleral wounds were sutured at the battlefront.
When he was brought to our clinic in Lviv, one eye was completely destroyed, and the other had a subconjunctival rupture of the sclera, complete vitreous haemorrhage, and total retinal detachment. Visual acuity of this eye was an incorrect light perception.
The operation lasted more than five hours. At first, it was impossible to distinguish between the blood, the membranes, and the retina. The operation ended with a 360-degree circumferential and radial retinotomy, and an endotamponade with silicone oil. The retina was grey, and I had no hope for him to recover the slightest sight ability. After ten days of recovery, the BCVA was 0.01, and I am happy I could give him back at least some sight.
The fourth case: Military, not young anymore, a strong man. The guy was silent, but I could feel his despair and hopelessness. He had had surgery before coming to Lviv.

His crushing despondency painfully hit me as my own. He was wounded and covered with dirt. One eye was destroyed—very badly injured and with endophthalmitis. The second eye had sutured corneal wound, swollen cornea, hyphaema, iris coloboma, aphakia, and silicone oil tamponade. The fundus could not be ophthalmoscopically examined. Ultrasound examination was unclear. Incorrect light perception. I understood something was wrong inside, and I waited for the cornea to become more transparent before an operation. I removed the epithelium and the silicone oil. There was almost no retina on the temporal side, silicone under the retina. The retina was shortened and shrunken. I straightened it in the best way I could, but there was no central part of the retina. I felt powerless…
Now I am gathering energy for the treatment of other wounded who are defending Ukraine and, therefore, me.
The second case was a young man, a soldier. Blast injury of both eyes. Torn corneal wounds, iris tears, traumatic cataracts, vitreous haemorrhages. When I saw those eyes, I realised there was no other way out—I had to operate on them! But would I manage? I’ve done everything possible: rearrange the sutures to the cornea, sutured the iris, performed cataract extraction and pars plana vitrectomy, implanted an IOL, and sutured it to the sclera. Result: BCVA of the better eye is 0.02; the other has light perception.
The third case was a patient with a traumatic macular hole. But when brought to me, something else struck me—the boy had both his legs amputated. I hoped to restore his sight, but no one could return his legs!



ESCRS Managing Director Tom Ogilvie-Graham met with Dr Dimetro Goriachev and Prof Ihor Novytskyy in Lviv to discuss ESCRS assistance to Ukrainian ophthalmologists.


ET: What a time to become president! As if the COVID pandemic wasn’t enough, you have war to your east in Ukraine, and the planet faces a major challenge in the form of climate change. Let’s start with Ukraine. What is the ESCRS response to the current crisis?
OF: This took us all by surprise. Two or three days after the invasion, we rolled up our sleeves and asked how we could help. We were in continuous contact with our Ukrainian colleagues as we were to hold an ESCRS symposium in Kyiv at the beginning of March. It became clear we should do something as quickly as possible. We reached out to our industry contacts, and they responded quickly. Then the question became logistics, how to get medical supplies into the country.
Our managing director Tom Ogilvie-Graham has some experience in that field. He visited Poland and Lviv and helped set up two warehouses where we keep aid supplies. We also have some contacts with United Nations for transport. Our Ukrainian colleagues have a good network and can anticipate where the supplies will be needed most. This should be well underway by the time this [magazine] goes to print.
In the first days, our colleagues were obviously worried about their families, and there were major efforts to get as many women and children out of there as possible. We got messages and photos from them in bunkers during shelling. The men are staying to help patients. It is difficult for us to understand what is happening. I believe some are filling in as combat surgeons.
ET: What sort of supplies is the ESCRS providing?
OF: Basic supplies such as suture materials, viscoelastics, and instruments needed for ocular trauma surgery. One company donated a small phaco/anterior vitrectomy machine which had been used by military personnel. One company is donating surgical loupes, which can be used if a microscope isn’t available.
We are trying to organise—together with EURETINA and the European Society of Ophthalmic Plastic and Reconstructive Surgery (ESOPRS)—a network of doctors in Europe and North America to

provide 24-hour second opinions and consulting. The goal is to help surgeons in Ukraine who may not be trauma surgeons or vitreoretinal surgeons. This will be done via mobile phone.
ET: Millions of refugees have arrived in Western Europe. How are ophthalmology departments accommodating colleagues and patients?
OF: I received emails from some female Ukrainian ophthalmologists who were able to flee and are now here with their children— even in Vienna. I have met two who arrived in the last weeks. I’m discussing with our hospital management ways to integrate them into our hospital. There are issues with red tape, licensing, language barrier, etc. For starters, we might use them as translators when we are seeing Ukrainian patients, of which there are quite a few in our area. They may have eye problems of all sorts that need to be addressed. Eventually, the doctors may be able to help their fellow Ukrainians directly.
Throughout the EU, the refugees are automatically socially insured. If refugees have been treated before in Ukraine, for example, with intravitreal injections for AMD, that should get continued without a pause. That is something we learned with COVID—intervene quickly to maintain care. So, from that perspective, we may be a little better off than we might have been before the pandemic.
ET: What about our Russian colleagues?
OF: This is a very difficult question for all sides. My belief is that we are all medical doctors, and the highest of our priorities is to take care of our patients. I believe our Russian colleagues feel the same way. That is why we have become doctors. I have been in touch with Russian colleagues. It is very difficult for them: they are locked into their country now and not able to speak freely.
ET: How are things looking for the annual ESCRS Congress in Milan?
OF: We were sad we could not have our winter meeting in Vilamoura in person in February, but that would have been too risky. It looks like COVID is easing up in Europe now. Currently,

we are very confident Milan will take place in person. We have set up a very full programme. For those who cannot attend because they are too far away or their regulations make it difficult, there will also be a hybrid component.
We have substantially revamped the Congress. We realised that, especially for junior doctors, there has been a two-year gap in training. We will have significantly more wet labs and basic courses than we did in Paris, our last full-scale meeting. Amsterdam was a successful hybrid meeting. Milan will be hybrid, but we are really emphasising the face-to-face side.
Of course, there will be a lot of sessions on cataract and refractive surgery. But we will also have a cornea and glaucoma day on Friday and a combined symposium with our paediatric colleagues from WSPOS.



dinner on Saturday, the young ophthalmologists are invited to join us in the disco and have a party.






We’re also organising a new element called iNovation. It takes place Friday, before the ESCRS meeting. It is a meeting of industry partners, key opinion leaders, and start-up companies looking at trends and challenges of ophthalmology. I’m looking forward to it—it will be pretty exciting.










ET: The world is also facing an existential threat in the form of climate change. How is the ESCRS responding?

OF: Even in the midst of COVID and the Ukraine war, we need to address the sustainability issue. Four percent of the world’s total trash is medical waste. And of that, cataract surgery is a key contributing factor. We will be meeting with ASCRS and APACRS to find ways to reduce waste and reduce our carbon footprint in the operating theatre.
This will be a theme at the conference. At the opening ceremony, we’re going to have a young ophthalmologist from the Netherlands who is very involved in sustainability describing the problems and possible solutions we could implement.







The general programme offers a lot to young ophthalmologists. I’m hoping this will be very valuable for young doctors whose training was interrupted. In addition to a YO day and YO symposium, there will be a track with courses and wet labs tailored to their needs. As in the years before, after the President’s
Conferences have a major carbon footprint. My aim is to make our meetings carbon neutral at the latest by next year. We are heading that way in Milan. We are working with a company that focuses on sustainability and congresses. They are helping us understand what we are doing and how we can reduce our carbon footprint. Delegates registering for the meeting will have the option of paying a fee to offset the effect of flying to the meeting; I very much hope that all will participate. I started offsetting all my flights last year.
We will be using more recyclables and placing an emphasis on sustainable food options. My ideal would be for people to take a step towards less red meat, maybe refrain from eating meat altogether during the four days of the meeting.
“Even in the midst of COVID and the Ukraine war, we need to address the sustainability issue. Four percent of the world’s total trash is medical waste. And of that, cataract surgery is a key contributing factor.”
Far from the realms of the cataract surgeon but still crucial to planning and outcomes, appropriate knowledge about retinal diseases is important when contemplating cataract surgery. The goal is to provide a good visual outcome without exacerbating underlying retinal disease or creating any new problems with the retina.
Should cataract surgery be performed in patients with agerelated macular degeneration? As with so much in this field, patient selection is key. The just-published Age-Related Eye Disease Study (AREDS) report #27 concluded patients with AMD benefitted from cataract surgery, with an average gain in visual acuity (VA) persisting for at least 18 months. Eyes with milder AMD or increased severity of lens opacity gained more lines of VA than eyes with advanced AMD or mild lens opacity.
That study also reported similar visual outcomes among advanced AMD sub-types (geographic atrophy/choroidal neovascularization, CNV). There were reports of significant improvement in quality of life after cataract surgery for moderate cataracts with mild-moderate AMD. Patients with geographic atrophy/CNV or mild cataracts with any grade of AMD, on the other hand, did not benefit greatly in vision or QOL.
Reports on the effect of cataract surgery on AMD progression vary, with some reporting an association with early AMD, late AMD, and even both, but not proving causation. However, AREDS2 report #27 clearly states cataract surgery did not increase risk of developing advanced AMD in participants with up to 10 years of follow-up.
Diabetic patients tend to develop cataracts earlier and need good glycaemic and blood pressure control before surgery. The compromised blood-aqueous barrier increases postoperative inflammation. Capsular opacification and contraction are common and compromise retinal monitoring and treatment. Cataract surgery in these patients benefits from the creation of a larger rhexis, complete cortical clean-up, aggressive control of postop-
erative inflammation, and early retinal therapy soon after cataract surgery. Using larger optic IOLs is also recommended.
Decreased lens volume after cataract surgery causes a forward shift of vitreous and release of angiogenic factors and cytokines. The literature reports increased rates of new onset retinopathy and worsening of diabetic macular oedema and existing retinopathy after cataract surgery. The rate of progression can reportedly double in the first postoperative year. The risk is higher with extracapsular cataract surgery and in patients with combined diabetic retinopathy and hypertensive retinopathy.

The ESCRS Prevention of Macular Edema after Cataract Surgery study (PREMED 2) concluded diabetic patients who received a postoperative subconjunctival injection with triamcinolone acetonide had a lower macular thickness and macular volume at 6 and 12 weeks postoperatively than patients who did not. Intravitreal bevacizumab had no significant effect.
A significant improvement in postoperative vision has been found following cataract surgery in patients with retinal vein occlusion (RVO). However, these patients have an increased risk of cystoid macular oedema (CME), even with uncomplicated cataract surgery. Perioperative topical NSAIDs and corticosteroids are beneficial.
“The literature reports increased rates of new onset retinopathy and worsening of diabetic macular oedema and existing retinopathy after cataract surgery.”
Preoperative evaluation and adjunctive therapy such as preoperative laser, intravitreal anti-VEGF, or steroids may be indicated in patients with exudative AMD, diabetic retinopathy, and RVO. Intravitreal anti-VEGF treatment may also be used perioperatively. Rapid regression of new vessels in PDR can cause tractional retinal detachment, so exercise caution in this situation.
Studies have shown roughly 7–8% risk of CME after cataract surgery in eyes with epiretinal membrane (ERM). Vitreous liquefaction and forward movement of the vitreous are known to increase the risk of CME. Epiretinal membranes are more common in diabetics, and these further increase the risk of CME. In addition, the ERM may progress more quickly after cataract surgery necessitating surgery. The decision to combine phacoemulsification with ERM peeling depends on the visual significance of the ERM. Amsler grid distortion and disruption of the outer retinal anatomy on OCT are indications for combined surgery.
Cataract surgery may cause retinal detachment (RD) in the presence of high-risk retinal lesions. Such lesions should therefore be treated prior to surgery. Explain symptoms of retinal detachment and advise the patient to report symptoms immediately.
Pre-existing floaters may become more noticeable after cataract surgery and vitreous liquefaction may induce new floaters. In this case, employ phacovitrectomy or cataract surgery followed by vitrectomy.
Cataract surgery can also induce retinal complications. These range from globe perforation during the peri-ocular block to posterior capsular rent (PCR) with ensuing vitreous loss, nucleus or IOL drop, and/or retained lens fragments. Several factors may increase the risk for CME, vitreous base traction, retinal tears (including giant tears), and retinal detachment. These include chamber fluctuations, PCR or other complications, postoperative inflammation, complex or comorbid eyes, and certain inappropriate surgical manoeuvres. Pseudophakic rhegmatogenous retinal detachment occurs in about 1% of cases, with 50% occurring within the first year of surgery.
Prophylactic topical steroids and NSAIDs are of use in patients at risk for CME. Treatment is also with topical NSAIDs and steroids. For resistant CME, try intravitreal and peri-ocular steroids. Try anti-VEGFs for non-responsive persistent CME. Consider YAG laser vitreolysis, surgical release of vitreous adhesions, and iris capture in select situations.
Hypotony and retinal or uveal damage can cause vitreous haemorrhage. Suprachoroidal haemorrhage and endophthalmitis are two sight-threatening complications that can cause irreversible vision loss.
Various retina procedures can induce cataracts. This will be discussed in a future article.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India, and can be reached at dr_soosanj@hotmail.com.
Monofocal IOLs are preferred in patients with macular pathology or progressive retinal disease as decreased contrast sensitivity and altered macular function degrade multifocal IOL outcomes. Monofocals are also preferred in patients who may need future surgeries or low vision aids who are best served by a simple optical system within the eye.
Toric IOLs do not degrade contrast sensitivity and may be used in this patient group. However, corneal astigmatism induction from possible future surgeries—e.g., telescopic IOLs—may complicate astigmatism management later.
Complete spectacle freedom is not always possible. Set realistic expectations regarding limited visual outcomes and counsel regarding the natural history of the disease.
Silicone IOLs should be avoided in eyes with previous vitrectomy or may require future vitrectomy, as silicone oil sticks to its surface. Additionally, tiny fluid droplets may coat the exposed posterior surface of silicone IOLs during fluid-air exchange, impairing the surgeon’s view. Hydrophobic and hydrophilic IOLs are suitable, with hydrophilic lenses being least prone to oil adhesion. Hydrophobic IOLs are preferred if the corneal endothelium is compromised, as
hydrophilic lenses may opacify following air tamponade used in endothelial keratoplasty. PMMA IOLs are also acceptable.
Three-piece foldable IOLs are easily amenable to closed chamber translocation to glued IOL if progressive zonulopathy causes IOL subluxation/dislocation. In-the-bag, single-piece acrylic IOL may also be refixated using sutured segments or sutureless glued capsular hook technique described by the author. Plate haptic IOLs should be avoided. Large optic IOLs allowing an unhindered view of retina are preferred. Even in high myopes with zero power, IOL implantation is preferred to create a barrier between the anterior and posterior segments as well as provide an ultraviolet barrier.

The role of blue light-blocking IOLs in AMD in decreasing oxidative stress from shorter wavelength high energy blue light is controversial. Recent studies show no advantages in decreasing AMD risk or progression while taking away blue light necessary for optimal mental and physical health as well as scotopic and mesopic vision.
Special IOLs such as the implantable miniature telescope, mirror telescopic IOL, IOL-VIP System, EyeMax Mono, and Scharioth macula lens (SML) have brought new hope to patients with AMD and other macular disorders.

IOL exchange in pseudophakic patients is an option for correcting refractive surprises and changing the optical situation. As an alternative, implanting an add-on IOL in the sulcus offers several advantages—doing so at the time of cataract surgery in a so-called “duet procedure” can also be a valuable approach, said Michael Amon MD, PhD.
“An add-on IOL implanted in a secondary enhancement procedure can be used to correct ametropia in the case of a refractive surprise or to convert a pseudophakic patient with a monofocal IOL to multifocal status. Compared to IOL exchange, implanting an add-on IOL is surgically less demanding and less risky, and the power calculation is more straightforward,” he told a symposium.
He noted implanting an add-on IOL during the primary operation is an attractive adjustable option for children or patients expected to have changing refraction. It is also a reversible option for patients interested in presbyopia correction. The add-on IOL can be more easily explanted than a capsular bag IOL both early or later. Therefore, patients who initially choose presbyopia correction can be changed to monofocal status if they fail to neuroadapt, are bothered by photic phenomena, or develop ocular pathologies such as age-related macular degeneration or diabetic macular oedema that affects their quality of vision.

Performing IOL exchange can present a technical challenge because it involves capsular surgery. Therefore, the exchange procedure is accompanied by a risk of vitreous loss, and that is particularly true in the not uncommon situation where the patient has already undergone Nd:YAG laser capsulotomy, Prof Amon said.
“An add-on IOL implanted in a secondary enhancement procedure can be used to correct ametropia in the case of a refractive surprise or to convert a pseudophakic patient with a monofocal IOL to multifocal status.”
The exchanged IOL will ideally be a posterior chamber lens implanted in an intact capsular bag. A posterior chamber IOL may be placed on capsular remnants or in the sulcus if the ideal is not possible. In some situations, the lens may need to be fixated, which can be done to the sclera or iris using sutures, a tunnelling technique, or flanging of the haptic.

“For IOL calculations with sulcus placement, surgeons will need to take into account the refraction is affected by the change in IOL position,” Prof Amon advised.
The first add-on lenses used in the 1990s were implanted in the capsular bag, either in the primary procedure to correct high hyperopia or myopia, or secondarily to correct pseudophakic ametropia. However, they were associated with several problems and complications, including intralenticular membrane formation, hyperopic defocus, pigment dispersion, inflammation, IOP elevation, and haemorrhage.

“Modern add-on IOLs are designed to avoid these issues. Made of hydrophilic acrylic, they are highly biocompatible with uveal tissue. In addition, they have a large optic diameter providing IOL overlap, a round edge that minimises dysphotopsia, a concave posterior surface to avoid hyperopic defocus, and haptics designed for uveal clearance and stable centration.”
With currently available add-on IOLs (Cristalens Reverso®, Rayner SulcoFlex®, and Medicontur 1stQ AddOn®), surgeons can
choose optic designs that include aspheric monofocal, refractive bifocal, diffractive bifocal or trifocal, toric, and multifocal toric. In addition, there are add-on IOLs used for special indications. They include the Morcher Xtra, which reduces irregular astigmatism and provides extended depth of focus and magnifying lenses (iolAMD Eyemax and Medicontur 1stQ AddOn SML). Although it is off-label and these IOLs have an anterior vault, some surgeons, unfortunately, also use a phakic IOL as an add-on option, Prof Amon said.

IOL power calculation in cases of secondary add-on IOL implantation can be done with the refractive vergence formula that uses data on spherical equivalent, keratometry, and anterior chamber depth. An easier option when the add-on is being used to correct postoperative ametropia ±7.0 D is to multiply the spherical equivalent by 1.5 in cases of hyperopia or by 1.2 in myopia, he said.
Clinical studies reported by Prof Amon and others show the safety and effectiveness of modern add-on lenses.
“We have shown that the add-on lenses are stable in the sulcus and maintain better centration than in-the-bag IOLs, which can change position because of capsular contraction. Studies with toric add-on IOL to correct residual refractive error after primary implantation showed good results, but rotation of the add-on IOL occurred in 10% of cases. In these cases, the sulcus-placed IOL can be easily repositioned. Personally, I prefer to suturefixate the haptic of the add-on IOL in such cases,” he explained. Multifocal add-on IOLs for presbyopia correction have also shown good results.
“Importantly, results from optical bench studies show there are equal reflections beside the additional surfaces, and the optical quality achieved with both the in-the-bag and add-on lens is similar to that associated with a single capsular bag multifocal IOL,” Prof Amon said.
This presentation was made at the ESCRS Virtual Winter Meeting 2022.
Michael Amon MD, PhD is Chair of the Eye Department, Sigmund Freud University Vienna and Academic Teaching Hospital of St John, Vienna, Austria. amon@augenchirurg.com



Every cataract surgeon will sometimes face residual astigmatism after cataract surgery, even with astigmatism correcting options such as toric IOLs. Dr Basak Bostanci gave an informative talk on residual astigmatism correction at a recent conference.

She explained that with-the-rule astigmatism, even up to 1 D, is often easily tolerated by many patients and every patient with residual astigmatism need not be treated. However, surgeons should investigate sources of error to improve surgical technique and future results.
Post-cataract astigmatism has many causes. These include measurement, calculation or transcription errors, and posterior corneal astigmatism. Surgical causes include surgically induced astigmatism; sub-optimal rhexis shape, size, or centration; IOL tilt; subluxation; toric IOL misalignment/ rotation; and capsular bag fibrosis. Wound healing and remodelling and Nd:YAG laser posterior capsulotomy can also play a role.
Using two or more keratometric sources to avoid variability and false measurements and properly marking reference points for toric IOLs are important to prevent postoperative errors. IOL rotation can occur because of retained viscoelastic in the capsular bag, hypotonic or overinflated anterior chamber, or incomplete unfolding of IOL haptics. A ten-degree misalignment leads to a 30% loss of effective power. This is especially important in highpowered IOLs. A 30% rotation leads to 100% loss of effective power. A capsular tension ring is helpful when dealing with a late rotation or in high myopes.

IOL rotation should be delayed until refractive error is stable but is preferred within one to two weeks of surgery before fibrotic adhesions develop. Arcuate keratotomy or limbal relaxing incisions can correct up to 2.5 D of astigmatism but are less predictable and are dependent on age, pachymetry, intraocular pressure (IOP), and corneal rigidity.
Considering risks of capsular-zonular damage, vitreous prolapse, CME, infection, etc., IOL exchange is limited to patients with high SE errors, tilt, decentration, or damage to the IOL. If possible, avoid IOL exchange in patients with Nd:YAG capsulotomy. Newer toric piggyback IOLs have lower risk of pigment dispersion, interlenticular opacity, and increased IOP, but rotational stability still needs assessment.
Small refractive errors not correctable by IOL rotation and eyes with Nd:YAG capsulotomy are best fine-tuned by LVC. Procedures such as LASIK, PRK, and SMILE have proven safety, efficacy, predictability, and stability. Refraction, incisions, and IOL position should be stable before considering LVC. This usually takes three months, though co-existing ocular conditions may delay it further.
“Even though digital imaging modalities and intraoperative aberrometers are available, only 10% of surgeons use these for toric IOL intraoperative alignment,” she noted.


Dr Bostanci suggested the surgeon should start by treating factors contributing to irregular cornea and astigmatism, such as poor ocular surface, dry eye, and even PCO. Nonsurgical approaches include spectacles and contact lenses. Toric IOL patients may be more demanding, and older, infirm patients may find contact lens use challenging.
Lens- or cornea-based surgery may need to be considered. The first step is to calculate spherical equivalent (SE). If the SE is zero or at targeted refraction, rotation of toric IOL or corneal relaxing incisions (CRI) are effective. If not, IOL exchange, laser vision correction (LVC), or even piggyback IOLs may be required. Online calculators www.astigmatismfix.com and LRICalculator. com are helpful in making decisions.
“These patients are in a different age group, often two decades older, and may have tear film abnormalities, a higher refractive index, and lower stromal hydration, all decreasing predictability of LVC. It is also important to remember that LVC creates three competing axes at different locations—axes of refraction, topography, and toric IOL,” Dr Bostanci said.
“Even though digital imaging modalities and intraoperative aberrometers are available, only 10% of surgeons use these for toric IOL intraoperative alignment.”
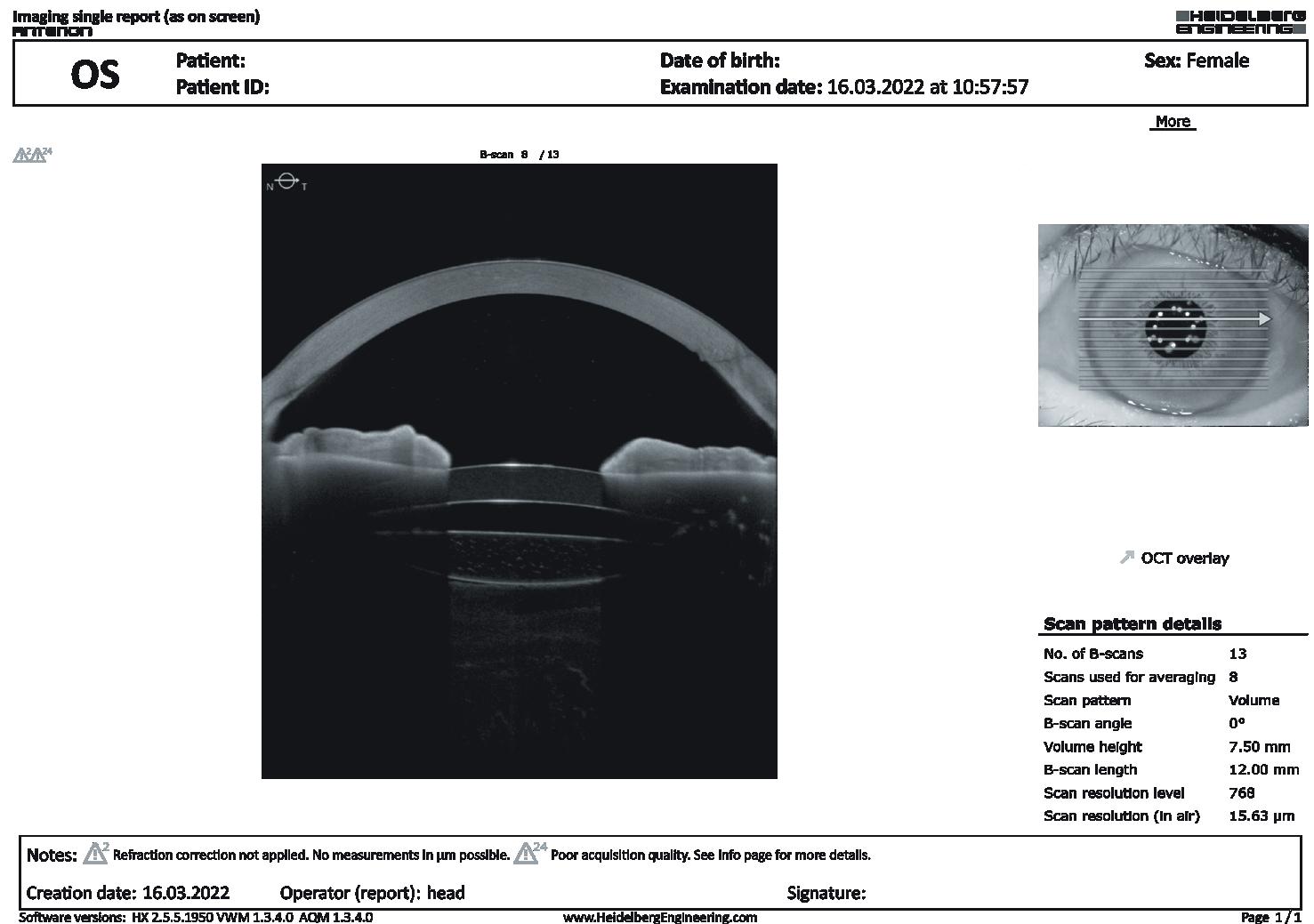
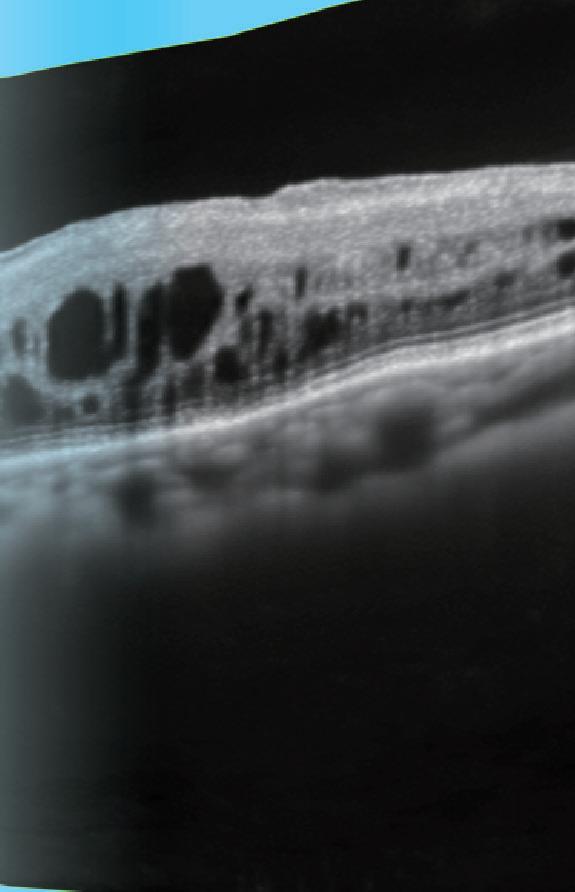
Fundus image acquisition with macula and disc capture in one image on OCT, for enhanced screening and clinical efficiency


Standard model








Widefield image capture in a single shot
High definition OCT image for all scans
Good biometry, optimisation of the ocular surface, and use of a ray tracing IOL power calculation will help to achieve good outcomes after cataract surgery in the challenging and demanding population of patients with a history of keratorefractive surgery, Kjell Gunnar Gundersen MD, PhD told delegates.
“We found that at 5 to 15 years postLASIK, our cohort of patients had a significantly higher prevalence of dry eye disease compared to normal individuals and those who underwent phakic IOL implantation. Optimising the ocular surface preoperatively will reward surgeons with improved refractive accuracy and stability and will also result in improved patient comfort,” Dr Gundersen said.


He explained that due to the altered corneal profile after laser vision correction (LVC), the traditional formulae used for IOL power calculations resulted in errors and outliers. Post-LVC formulae have been developed, but they are based on mathematical averaging and modelling. Ray tracing power calculations are exact calculations, and they are independent of patient history. Instead, they use available data to calculate the best focus for single rays at varying radial distances from the optical axis through the different refractive media of the eye.
A study conducted by Dr Gundersen and colleagues demonstrated the accuracy of ray tracing IOL calculations in post-LVC eyes. The study included 37 eyes of 20 post-myopic LASIK patients and evaluated the refractive predictive error (RPE) resulting from ray tracing calculations (Okulix, Tomey Corporation) done with biometric data from two OCT devices (Anterion®, Heidelberg Engineering, and Casia SS-1000, Tomey Corporation) and traditional post-LVC IOL formulae (Barrett True-K and Haigis-L) incorporating reflectometry data (Lenstar 900, Haag-Streit Diagnostics).

Using the ray tracing program with the Anterion data resulted in the lowest mean absolute RPE and mean arithmetic RPE and the highest percentages of eyes with prediction errors of ±0.25 D (60%), ±0.50 D (88%), and ±0.75 D (100%).
“These outcomes compare favourably with those achieved in virgin eyes,” Dr Gundersen noted.
“Accurate toric correction remains a challenge in these eyes that have asymmetric astigmatism. Nevertheless, implanting a toric IOL is still worthwhile considering the clinical effect.”
















Discussing cataract surgery in keratoconic eyes, Dr Gundersen said ray tracing power calculations can also be used in these cases. In addition, available evidence shows implantation of a toric IOL in eyes with stable keratoconus is associated with good long-term refractive outcomes and excellent improvement in uncorrected visual acuity.
“Accurate toric correction remains a challenge in these eyes that have asymmetric astigmatism. Nevertheless, implanting a toric IOL is still worthwhile considering the clinical effect,” Dr Gundersen said.

He suggested that the “safe” IOL choices for post-LVC eyes and those with keratoconus are monofocal spherical or toric IOLs. Presbyopia-correcting IOLs might be considered for post-LVC patients especially interested in spectacle independence, but these individuals must be informed about the optical compromises.



An alternative for the latter group would be to implant a monofocal spherical or toric IOL in the bag with a sulcus-placed, add-on presbyopia-correcting IOL that offers ease of removal if the patient is dissatisfied. Eyes with keratoconus can also be

managed with a two-step strategy using a monofocal spherical or toric IOL in the bag and a spherical or toric IOL in the sulcus to fine-tune the refractive error, he noted.

This presentation was made at the ESCRS Virtual Winter Meeting 2022.

Using off-the-shelf toric IOL models does not appear to be inferior to using a fully tailored approach for patients with up to 5.0 D of preoperative astigmatism, a new study suggests.
“The use of off-the-shelf toric lenses with additional opposite clear corneal incisions may improve visual acuity and allow patients to achieve spectacle independence for distance vision. Our preliminary data suggests that it may not be inferior to using fully tailored toric IOLs,” said Khayam Naderi MD.
Explaining the rationale for the study, Dr Naderi said up to 20% of patients undergoing cataract surgery in the National Health Service in the United Kingdom have preoperative astigmatism of more than 1.5 D.
“We know that there are several associated benefits to toric IOLs compared to monocular lenses, including greater rates of spectacle independence, better quality of life scores, and a reduced economic burden for patients. Nevertheless, toric IOLs are only available to a small proportion of NHS hospitals due to their increased associated costs and storage issues. By having a reduced in-house bank of toric lenses, we can potentially reduce these costs, allowing NHS patients routine access to them and their associated refractive benefits,” he said.
Dr Naderi’s prospective single-masked randomised casecontrolled trial compared the visual performance and refractive outcomes of off-the-shelf toric lenses with a set cylindrical correction of 2.0 D or 4.0 D and additional clear corneal incisions as required for a fully tailored approach. The study included 66 patients with pre-existing regular corneal astigmatism of 1.50 D or more, 32 of whom were randomised to the fully tailored treatment group and 34 patients in the off-the-shelf toric IOL group.
LASER VISION CORRECTION RECOVERSThe visual acuity, refractive outcomes, and patient reported outcome measures (PROMs) were comparable between both groups of patients six months after surgery.
“At four weeks and six months of follow-up, there were no differences in the uncorrected visual acuity and best-corrected
visual acuity between the two groups. At four weeks of follow-up, residual refractive cylinder was lower in the off-the-shelf toric IOL group—this levelled off at the six-month follow-up mark. For quality-of-life scores, there were no differences between the two groups at four weeks. However, at six months, patients in the offthe-shelf group had higher CATPROM5 scores,” Dr Naderi said.
Lens stability was also very good for both groups, with no patient from either group needing further surgery to reposition the lens.
Dr Naderi said the preliminary results suggest using the off-the-shelf models might not be inferior to a fully tailored approach for up to 5.0 D of regular astigmatism.
“In the off-the-shelf toric group, 91% and 100% of patients achieved uncorrected visual acuity of at least 0.30 logMAR (6/12) at four weeks and six months respectively. By having a bank of 2.0 D and 4.0 D toric IOLs in-house, we can allow the majority of our public healthcare sector patients with regular astigmatism to have access to them and their associated benefits. Furthermore, bulk production of these lenses could allow manufacturers to supply them at reduced or similar costs to monofocal IOLs,” he concluded.
Dr Naderi presented the study at the ESCRS Virtual Winter Meeting 2022.
Khayam Naderi MD is a clinical research fellow at King’s College London and St Thomas’ Hospital, UK, under the supervision of Professor David O’Brart, Professor of Corneal Science and Consultant Ophthalmologist. david.obrart@ggstt.nhs.uk, khayam.naderi@gstt.nhs.uk

“We know that there are several associated benefits to toric IOLs compared to monocular lenses, including greater rates of spectacle independence, better quality of life scores, and a reduced economic burden for patients.”
LASIK and accelerated CXL safe in myopic diabetic patients. Dermot McGrath reports
LASIK combined with accelerated corneal cross-linking (CXL) appears to offer a safe and effective treatment modality in diabetic myopic patients, according to the results of a study presented at the ESCRS Virtual Winter Meeting.
“Although a longer follow-up is needed to confirm these results, our study indicates LASIK in combination with CXL is safe on the corneal endothelium of diabetic myopic patients,” Mohamed Mahmoud MD told a Cornea Day session.
LASIK is usually considered a relative contraindication in diabetic patients due to the pathologic changes in the cornea of these patients, he said. Furthermore, the immune response is weak, and wound healing is delayed when these patients require more follow-up.

Simultaneous LASIK and accelerated CXL (LASIK Xtra) are now used in many countries around the world on patients at high risk of post-LASIK ectasia and regression, such as those with high degrees of myopia, younger patients, and those with low residual stromal bed thickness, Dr Mahmoud noted.
He next turned to the context of diabetes mellitus (DM), one of the most morbid chronic diseases affecting millions of patients globally. Dr Mahmoud said the disease could reduce endothelial cell density (ECD) and the percentage of hexagonal cells present but also increase the coefficient of variation (CV)—indicating diabetes causes instability in the corneal endothelial cells.
Patients were divided into two groups: group A included 60 eyes of diabetic patients, while group B had 60 eyes of non-diabetic patients. The corneal endothelium was evaluated by specular microscope preoperatively and after three and six months postoperatively. Postoperative treatment was topical antibiotic for one week, a topical anti-inflammatory for two weeks, and topical artificial lubricant for one month or more as needed.
Dr Mahmoud noted the endothelial cell density (ECD) showed statistically significant changes after three and six months postoperatively in group A while group B showed statistically significant changes after three months without significant change after six months. Furthermore, both groups improved close to preoperative density levels, with no significant differences between them, at the end of six months of follow-up.
Corneal endothelial cell morphology—as determined by polymegathism and pleomorphism values—showed a statistically significant difference in diabetic patients after six months, with no significant change evident in the non-diabetic patients.
Dr Mahmoud’s prospective comparative interventional case series included 120 eyes of 60 myopic patients treated with LASIK combined with accelerated CXL. LASIK was performed first with the M-2 microkeratome (Moria, France) to create a 110-micron flap, followed by stromal ablation with the excimer laser. The stromal bed was instilled with 0.1% riboflavin in a 20% hydroxymethyl propyl cellulose solution for two minutes before returning the flap to its original location according to the alignment marks. The cornea was exposed to UVA light for three minutes with a wavelength of 366–374 nm and an irradiance of 30 mW/cm2
Summing up, Dr Mahmoud said LASIK with accelerated CXL seemed to be safe and effective for diabetic patients with myopia, but further studies with longer follow-up are required to confirm his group’s findings.
This study was presented at the ESCRS Virtual Winter Meeting 2022. Mohamed Mahmoud MD, Department of Ophthalmology, Faculty of Medicine, Minia University, Minia, Egypt. Mohamed_Zaki@mu.edu.eg
“Although a longer follow-up is needed to confirm these results, our study indicates LASIK in combination with CXL is safe on the corneal endothelium of diabetic myopic patients.”
“The industry is really working very hard at getting rid of dysphotopsias and improving intermediate vision and enhanced optical quality. We need to understand patient needs and educate them [on] the compromises they may need to make but also show them they can get quite a lot out of these new lenses nowadays,” Professor Gerd U Auffarth MD, PhD, FEBO told an ESCRS symposium.
Prof Auffarth noted that according to the ESCRS 2020 clinical practice survey, presbyopic IOLs represent only 8–10% of IOLs currently implanted. In addition, among respondents to the ESCRS 2021 clinical practice survey, 38% cited loss of contrast visual acuity and 52% cited concerns over problems with nighttime visual quality as reasons for their reluctance to implant presbyopia-correcting IOLs.
The problem with the older, multifocal presbyopia-correcting IOLs is they have two distinct peaks of focus, so a near-focused distant light source creates a halo around the distance-focused image in scotopic conditions. The size and intensity of the halos depend on the degree of difference between the two focal points. However, extended depth of focus lenses (EDOF) do not have two distinct foci.
ENHANCED MONOFOCAL IOLS
“We more or less have to balance out certain things to maximise quality of vision. We can add just a tiny bit of bifocality or depth of focus because we don’t want to decrease quality of vision or increase night vision symptoms. But there is always a certain range that we can take advantage of and give some positive impact on our patients,” Prof Auffarth said.
The first of these new lenses to enter the market is the Tecnis® Eyhance ICB00 (Johnson & Johnson Vision). The IOL is identical in design to the monofocal aspheric Tecnis ZCB00 in terms of basic dimensions and material. However, it differs in having a central, optical area with higher-order aspheric components that increase lens power.
An optical bench study showed the Eyhance has a depth of focus of around -1.0 D to -1.5 D. Researchers confirmed those findings in a multicentre study, which showed an increase of at least one line in intermediate vision and rates of halo, glare, or starbursts very comparable to standard monofocal IOLs.
Other manufacturers have also developed enhanced monofocal designs. One example is the IsoPure 1.2.3 (BVI/Physiol), which features anterior and posterior aspheric surfaces with high-order aspheric terms that extend its visual range compared to a monofocal IOL while maintaining a good far-focus performance. In optical bench tests, the IsoPure 1.2.3 lens performs as well as an aspheric monofocal IOL at defocus of 0.5 D to 0.0 D but exceeds the monofocal IOL’s performance at a defocus of -1.0 D to -1.5 D.

Another of the new enhanced monofocal IOLs, the RayOne EMV (Rayner), uses a totally different approach. This new
range of new enhanced monofocal intraocular lenses (IOLs) may provide a more attractive option than multifocal IOLs to presbyopic and cataract patients who desire increased spectacle independence without loss of visual quality or disturbing photic phenomena.IOL’s optic purposely induces positive spherical aberration to an increasing focus range even in the hyperopic direction. The lens is designed for use in a monovision setup, and optical bench testing shows that with a primary defocus of -1.0 D, it provides defocus up to -2.5 D.
“The industry is really working very hard at getting rid of dysphotopsias and improving intermediate vision and enhanced optical quality.”
NEW ADVANCED TRIFOCALS
There is also the new Tecnis Synergy™ IOL, a hybrid EDOF/ multifocal diffractive lens that combines the diffractive technology from Tecnis® Multifocal and Tecnis Symfony® IOLs with the correction of chromatic aberration to deliver continuous high-contrast vision across its range of focus. It also has a violet light filter to help reduce light-scatter. Similarly, another EDOF/ trifocal diffractive hybrid, the Finevision Triumf (BVI), aims to minimise the dysphotopsias by eliminating chromatic aberration and putting more power into the intermediate focus, Prof Auffarth said.
Dr Auffarth presented the information during a symposium at the ESCRS Virtual Winter Meeting 2022.
Gerd U Auffarth MD, PhD, FEBO works with the International Vision Correction Research Centre (IVCRC), The David J Apple International Laboratory for Ocular Pathology, University-Eye-Clinic Heidelberg, Germany. gerd.auffarth@med.uni-heidelberg.de

Newer technologies and IOL power formulae increase the predictability of cataract surgery outcomes, according to Professor Filomena Ribeiro
MD, PhD, FEBO.Accurate IOL power calculation requires a thorough examination of the cornea, from the tear film to the posterior surface cornea, with multiple measurements and modern IOL calculation formulae, she said.
“Accurate lens power selection demands biometric data validation and a proper IOL power calculation method. One of the golden keys is the preoperative evaluation of all the pathologies that could impact [both] the quality of vision and the probability [of achieving] emmetropia.”
Prof Ribeiro stressed the importance of considering the possibility of ocular surface disease, pupillary abnormalities, and zonular pathology. Regarding the ocular surface, she said to always be sure to treat dry eye before making corneal assessments. Research has shown treating dry eye before making corneal measurements increases the proportion achieving a postoperative refraction within 0.5 D of target by 8% and increases the proportion of patients with 0.5 D or less residual astigmatism from 40% to 75%.
“It is important to recognise the relevance of the corneal dioptric power, which represents two-thirds of the total dioptric power of the human eye’s optical system, and only small changes can be very significant in IOL power calculation.”
She noted that topography is essential to evaluate the regularity of the cornea but also to make sure there is no great difference between the value of the axis between the centre and the more peripheral values. It is also important to always select high-quality images and obtain several measurements (with more than one instrument), if possible.
Prof Ribeiro said the total corneal powers used in classical IOL calculation formulae are based on keratometric values for the anterior cornea curvature and a keratometric index which assumes a constant ratio of 82.2% between the posterior and anterior surface. However, nowadays it is possible to directly measure the posterior surface with Scheimpflug devices like the Pentacam® (Oculus) and optical biometers like the IOLMaster® (Zeiss). Using these measurements, surgeons can calculate the true total corneal dioptric power with Gaussian optics, vector addition, or ray tracing using Snell’s law.
“But these powers cannot be used directly—we need to convert them into equivalent K values because formulae expect keratometric values and there is a systematic difference between keratometric values and directly measured total corneal power.”
Some of the new formulae now have the option to include the directly measured posterior corneal surface values, although it is still under investigation whether using those measurements can improve visual outcomes and refractive accuracy in toric IOLs compared with standard index values. However, research suggests the directly measured total corneal power measurements may improve results in post-LASIK cases and smooth the usual undercorrection of against-the-rule astigmatism.
In the 2021 ESCRS practice survey, optical biometry and Scheimpflug tomography were the primary preoperative
measurements used by 74% and 57% of respondents, respectively. In the same survey, similar proportions of respondents reported using Scheimpflug and optical biometry when making astigmatism power and AXIS decisions when implanting a toric IOL.
In the last decade, many new and better formulae making use of the new biometers, resulting in significant improvements in predicting postoperative refraction. For example, in 2011, 40% of eyes achieved refraction within 0.25 D of target, and 75% did so within 0.5 D of target. By comparison, 2019 respective values were 50% and 80%.
“We can now reach an absolute prediction error of around 0.25 D and with a very good probability of success. And if you use more than one formula, you can have an interval of residual error prediction between two steps of dioptric powers and assess the probability of success in achieving emmetropia,” Prof Ribeiro said.
In addition to the use of directly measured total keratometry values and better IOL calculation formulae, factors contributing to these improvements in predictability include better axial length error correction in long eyes with empirical optimised axial length measurements, sum-of-segment measurements, better effective lens position estimations with more predictive components, and increased computational power that allows for the employment of linear regression and machine learning.
“We need strong preoperative evaluation and validation of all the data. We need to assess the associated pathologies. We need to validate all the measurements, if possible, with more than one instrument, compare the measurements with the population average values, and always do the spherical and toric calculation in every patient. And finally, to optimise outcomes, we need to evaluate our results,” Prof Ribeiro concluded.
This presentation was made at the ESCRS Presbyopia IOL Forum during the ESCRS Virtual Winter Meeting 2022.
Prof Filomena Ribeiro MD, PhD, FEBO is Head of the Ophthalmology Department at Hospital da Luz, Lisbon, Portugal. fjribeiro@hospitaldaluz.pt“It is important to recognise the relevance of the corneal dioptric power, which represents two-thirds of the total dioptric power of the human eye’s optical system, and only small changes can be very significant in IOL power calculation.”
Trifocal IOLs can provide many patients with a full range of spectacle-free vision after cataract surgery, but this implant technology is not without limitations. Therefore, it is necessary to apply rigorous attention to candidate selection for achieving success and patient satisfaction, emphasises Burkhard Dick MD, PhD.
“Patients who will receive a trifocal IOL must have a strong desire for spectacle independence along with realistic expectations, and surgeons must respect the relative indications,” Dr Dick said.

Available trifocal IOLs include the Acriva Reviol Tri-ED, AcrySof® IQ PanOptix® (Alcon), AT LISA® Tri 839MP (Zeiss), FineVision POD F GF, and Versario® MF 3F (Bausch & Lomb). The clinical registration trials conducted for these lenses enrolled only patients with healthy eyes other than for the cataract, and there are limited studies involving eyes with more complex constellations. Therefore, decisions on trifocal IOL implantation in the latter eyes are more challenging.
The manufacturers’ product labelling lists the various contraindications, precautions, and warnings. Dr Dick reviewed his considerations.
Humphrey 24-2 VF can be completely normal. Moreover, simultaneously performed 10-2 and 24-2 VF demonstrate a superior topographic structure–function relationship when compared with them separately,” he said.
Trifocal IOLs may be considered for patients with a history of laser vision correction. Evaluation to identify good candidates should include topography and tomography. The surgeon should consider the type of ablation because it bears on selection of the optic design (aspheric, neutral, or spherical) and should check the functional optical zone size and centration.

Dr Dick said he excludes patients who had correction of more than 6.0 D of myopia or more than 4.0 D of hyperopia as well as those with elevated higher order aberrations (total >2.0 µm, coma >0.32 µm, trefoil >0.4 µm), although there are only weak data regarding the impact of preoperative corneal aberrometry on outcomes.

The preoperative workup should also include measurement of angle alpha and angle kappa. Dr Dick said caution and further evaluation are needed if either value is 0.3 to 0.5 microns while values >0.5 mm lead to patient exclusion. It is also important to perform dynamic pupillometry, as it confirms the photopic pupil is >2.5 mm in diameter.
He recommended against trifocal IOL implantation in eyes with a history of radial keratotomy where postoperative visual performance is likely to be poor. He also excludes patients with severe dry eye disease if the ocular surface cannot be optimised. The presence of corneal pathology—including epithelial and endothelial dystrophies, stromal scars, or opacification—is also a contraindication because of loss of contrast and increased risk of dysphotopsia.
A trifocal IOL may be considered for eyes that are glaucoma suspect or have early disease without obvious visual field loss, but not if the glaucoma is moderate to advanced because the implant will further reduce already decreased contrast sensitivity. In eyes with mild glaucoma, surgeons need to be aware that subtle central scotoma is more common, Dr Dick said.
“I recommend also doing a 10-2 visual field test (VF) in these cases to exclude early central fixation involvement because the
He also recommended the ASCRS calculator for IOL power calculation, as well as ray tracing analysis. He suggested checking recent publications on IOL power calculations in eyes with previous corneal refractive surgery.1–2
Careful candidate selection and thorough consultation facilitate good outcomes.
Cheryl Guttman Krader reports
“Patients who will receive a trifocal IOL must have a strong desire for spectacle independence along with realistic expectations, and surgeons must respect the relative indications.”
Dr Soosan Jacob MS, FRCS, DNB reports
The Main Symposium on “IOL Fixation in the Absence of Capsular Support” at the Winter ESCRS conference— chaired by Professor Jorge L Alió and Professor David J Spalton—was an enlightening one with well-known speakers giving valuable insights into their procedure of choice.
Dr Richard Packard began by discussing the reasons behind the checkered past of anterior chamber IOLs (ACIOLs). This type of lens appeared in the early 1950s. It was popular because placement was easy, non-traumatic, and stable and its power calculations were similar to those for contact lenses—an advantage in the absence of ultrasound and other technologies.
However, all early ACIOL models failed. Nordeholm reported in 1975 that Barraquer had to remove 250 of 493 of these IOLs. In 1979, Drews examined half of these explanted IOLs and found poor manufacturing and rough edges, resulting in endothelial compromise, UGH syndrome, iris bombe, iris tuck, etc.
Rigidity was also thought a contributor to the poor performance, resulting in many flexible loop designs, almost all failing except for the Kelman Quadriflex. This was further modified as Kelman Multiflex by incorporating Peter Choyce’s findings on correct sizing of footplates and plano-convex optics, serving as the standard since 1980.
Dr
Three studies (Bellucci et al, 1996; Everiklioglu et al, 2003; Donaldson et al, 2005) comparing ACIOLs with sutured PCIOLs found no significant differences in outcome. For ACIOLs, Dr Packard said there was a clear need for proper education regarding accurate measurement of white-to-white (WTW) and incision size.
He also noted the importance of proper IOL sizing (WTW+1 mm), the need for an IOL bank with three sizes for each IOL power, and the need to recalculate for correct A-constant (115.3). WTW can be measured on a table with standard callipers, Stahl caliper, Kelman dipstick, or intraoperative anterior segment OCT. Other essentials include using Miochol®-E to constrict the pupil, a Sheets lens glide to assist implantation, and cohesive viscoelastic.
He advised using a gonio lens to check proper haptic positioning and the absence of iris distortion. PCIOL placement in the anterior chamber should be strictly avoided because of the high incidence of endothelial cell loss.
Dr Packard said the current design has stood the test of time, with results comparing favourably with scleral fixation IOLs pro-
vided basic rules of measurement and insertion are applied. It offers a simple, straightforward, and quick implantation technique in a compromised eye, thus not prolonging an already long procedure.
Dutch innovator Jan Worst developed the iris clip IOL (ICIOL) in the early 1970s. That lens comes in two models: aphakic, a non-foldable, rigid, single-piece PMMA requiring a 5.5–6.0 mm incision that needs suturing; and phakic, the modern version being three-piece with foldable acrylic optic and PMMA haptics that hold on to iris tissue.
The aphakic model can be used for anterior chamber (AC-ICIOL) or retropupillary (RP-ICIOL) enclavation. Professor Sorcha Ní Dhubhghaill offered her perspective on the ICIOL she preferred as her first choice if bag or sulcus placement were not possible. Poor candidates for the ICIOL include those with insufficient iris tissue, uveitis, and ischaemic vitreoretinopathies (diabetic retinopathy or vascular occlusions), as the iris may also be involved, she noted.
An interesting report by Sarioglu [et al] used two ICIOLs for both anterior and posterior enclavation in the same eye for a case of nanophthalmos. At Prof Ní Dhubhghaill’s hospital, among 492 IOL explantations, 28% had received ICIOL, with 5% AC-ICIOLs and 23% RP-ICIOLs. AC-ICIOL and RP-ICIOL seemed to have equivalent visual outcomes, although RP-ICIOLs performed slightly better with some IOP reduction and lesser CME. Data showed endothelial loss to be the same for both positions as AC-ICIOLs are at a more posterior plane in aphakic eyes than in phakic eyes.
Though enclavation is easier with RP-ICIOL, it needs additional dexterity and vitrectomy to avoid vitreous incarceration while enclavating. Haigis, Holladay 1, and SRK/T formulae work well, but it should be remembered A-constant is lower for AC-ICIOL and higher for RP-ICIOL, Prof Ní Dhubhghaill cautioned.
Complications include pupillary peaking and ovalization, IOL drop with unstable RP-ICIOLs, and endothelial decompensation with AC-ICIOLs. Prof Ní Dhubhghaill concluded that ICIOLs were reliable, stable, and technically simple with no major issues with tilt. Disadvantages include large incisions, hard material, scleral tunnels, incisional sutures, difficulty in enclavation (especially in post-vitrectomised eyes), and ordering these IOLs beforehand.
SCLERAL FIXATED IOLS
Several speakers discussed different techniques of scleral fixation.
Sutured SFIOL:
Dr Mayank Nanavaty demonstrated the sutured SFIOL technique by showing intravitreal triamcinolone acetonide-assisted anterior vitrectomy, followed by scleral IOL suturing and 9-0 Prolene suture anchoring under partial-thickness scleral flaps. He also showed variations such as sclerally sutured aniridia IOLs and combined surgery with customised DSAEK lenticule.
Intrascleral haptic fixation (ISHF):
Advantages of intrascleral haptic fixation include a sutureless standardised technique, minimal contraindications, standard PCIOL, minimal uveal contact, easy centration, and indepen-
Packard said the current design has stood the test of time, with results comparing favourably with scleral fixation IOLs provided basic rules of measurement and insertion are applied.
dence from angle and iris. Dr Gabor Scharioth gave important tips such as making symmetrical sclerotomies 180 degrees apart and 1.5–2.0 mm post-limbal, using AC or pars-plana infusion for globe stabilisation, performing vitrectomy and capsulectomy, using handshake technique, and creating a peripheral iridectomy in eyes with floppy or sticky iris. Dr Scharioth emphasised the importance of proper instrumentation (e.g., Scharioth forceps, DORC), proper IOLs (e.g., AR40e Sensar® IOL), exchanging instead of refixing a dislocated and damaged IOL, and suturing sclerotomies in case of leaks. He also reported on his use of single-piece AcrySof® platform IOLs and even the PanOptix® IOL for ISHF when powers more than 30 dioptres or multifocals were desired—but found that after two years, nearly 50% of cases showed scleral atrophy with extrusion of haptic tip into the subconjunctival space. Though revision with haptic trimming and scleral suturing over haptic showed good intermediate results, he concluded this was not the ideal technique yet.
Flanged
The Yamane technique has advantages of a minimally invasive transconjunctival approach, sutureless surgery, weathertightness, and the ability to perform under topical anaesthesia with some subconjunctival infiltration near tunnels. Dr Vladimir Pfeifer said the biggest challenge was docking, and hence many variations have been introduced. He demonstrated his own technique that included marking entry points 2.2 mm behind limbus, limbus-parallel tunnels to avoid lens tilt, 45-degree bend for the first needle, and 80–90 degrees for the second needle. He mounted the thin wall 30 g needles on a syringe for better control while docking and then dismounting using pean forceps, resting and stabilising the first needle on the iris after docking to prevent needle tip proximity to retina. Docking the second haptic is performed through the main 3 mm incision using Eckardt forceps again. Both haptics are externalised, pulling needles simultaneously out of tunnels. Flanges are performed and partially buried into the scleral tunnels under conjunctiva. Dr Pfeifer said advantages include the ability to perform even with small pupils, adding surgeons need to take care to avoid haptic damage and consequent tilt. His tip is to hold the Eckardt forceps in the same way as a fencing foil.
The informative session included discussion breaks where session chairs Professor David J Spalton and Professor Jorge L Alió gave valuable insights. Prof Spalton summarised that most fixation types work well if surgeons follow the proper technique. Since all techniques have a learning curve, surgeons with no prior experience may find it daunting to suddenly implant them in complex and complicated eyes in an atmosphere of surgical stress. Training, therefore, goes a long way in helping handle these situations, but if in doubt, it can be better to leave the eye aphakic and come back to do the implant as a planned secondary procedure in a more relaxed situation for both the surgeon and the patient.
Prof Spalton noted vitrectomy skills, a bimanual approach, and specialised instruments were necessary for most iris and scleral fixation techniques whereas iris clip IOLs had a lower learning curve.
Prof Alió discussed the Gore-Tex suture’s disadvantages of being thick and ropy, forming chunky, difficult-to-bury knots as well as the need to obtain them from the cardiac theatre. He said the Alcon MA60 IOL was his first choice for sulcus placement, iris suture, scleral suture, and even ISHF, but it ran a risk of the embedded haptic coming loose. His second choice was the Zeiss CT Lucia three-piece IOL. Lastly, he discussed the advantages of scleral flaps and tissue glue in preventing postoperative hypotony. The session concluded by stressing the need for stratification of techniques based on ease of performance and surgeon experience.
At the end of the symposium, the audience voted on what they thought was the “best buy” technique. All techniques had their supporters, but iris clip IOLs came out as the winner.
Dr Soosan Jacob is Director and Chief of Dr Agarwal’s Refractive and Cornea Foundation at Dr Agarwal’s Eye Hospital, Chennai, India. dr_soosanj@hotmail.com.
Richard B Packard MD, DO, FRCS, FRCOphth: eyequack@vossnet.co.uk
The Carlevale IOL is a single-piece foldable IOL specially designed for sutureless intrascleral fixation. It has a closed haptic design acting like a spring and damper to adjust to different sulcus widths and a T-shaped terminal end to haptics for anchoring under scleral flaps. Dr Matteo Forlini emphasised that contraindications for scleral fixation included connective tissue disorders and scleromalacia. UBM evaluation in a study by Mularoni [et al] showed a low incidence of horizontal or vertical optic plate tilt. ASOCT showed secure intrascleral haptic fixation. The study also described a special case where surgeons used the closed-loop haptic design to confine silicone oil to the posterior segment. Advantages include easy and fast implantation, foldable and “elastic” IOL, nature, and a minimal learning curve. Dr Forlini advised caution to avoid excessive pulling, which could break or rupture the haptic or the T-plug.

Sorcha Ní Dhubhghaill MD, PhD, MRCS(Ophth), FEBO: nidhubhs@gmail.com
Gabor Scharioth MD, PhD: gabor.scharioth@augenzentrum.org
Vladimir Pfeifer MD: oefpv@icloud.com
Matteo Forlini MD: matteoforlini@gmail.com
David Spalton FRCS, FRCP, FRCOphth: profspalton@gmail.com
Mayank A Nanavaty MBBS, DO, FRCOphth, PhD: mayank_ nanavaty@hotmail.com
Jorge Alió MD, PhD, FEBOphth: jlalio@vissum.com
Since all techniques have a learning curve, surgeons with no prior experience may find it daunting to suddenly implant them in complex and complicated eyes in an atmosphere of surgical stress.
Even in the current era of lamellar corneal transplantation, there remain timeless indications for performing penetrating keratoplasty (PKP), notes Professor Berthold Seitz MD.
Addressing the question “Should we still do PKP?” at a recent conference, Prof Seitz answered, “Of course.” He described situations where a full-thickness transplant is indicated and reviewed technical details for preventing complications and optimising success after PKP.
“The principal indications for PKP include optical grafts in eyes at normal risk for rejection but especially in highrisk optical grafts and therapeutic grafts,” Prof Seitz said.
His list of indications for PKP included post-PKP eyes with high astigmatism (with and without endothelial decompensation), those with advanced keratoconus, aphakia, and eyes with an unstable cornea (e.g., post-radial keratotomy, descemetocele, or perforated ulcer), among others. In addition, PKP is indicated in eyes with all types of infectious keratitis.

Although eye banks apply established criteria when accepting corneal tissue for grafting, the requirements did not consider curvature abnormalities present in eyes with keratoconus or a history of laser vision correction. Therefore, Prof Seitz and colleagues introduced sterile donor tomography using anterior segment OCT as a screening tool for detecting corneal tissues with refractive anomalies.
Prof Seitz also discussed the use of excimer laser trephination and metal masks with “orientation teeth”, which he said reduces astigmatism, improves surface regularity, and results in better visual acuity. In addition, this technique has practical advantages for the surgeon that includes enabling the exact positioning of the second cardinal suture.
“Recently we introduced the use of the Amaris® 1050RS excimer laser (Schwind) for trephination with a pseudoring profile that improves the results,” he added.
Other tips mentioned included making an open-sky iridotomy at 12 o’clock peripherally to prevent the so-called UrretsZavalia syndrome and using the Homburg cross-stitch marker (Geuder) to support precise localisation of double-running cross-stitch sutures.
“Using sterile donor tomography in the eye bank to measure the front and back radii of curvature and corneal thickness, we can optimise donor selection and prevent refractive surprises after PKP. Donor corneas that should not be used for PKP or deep anterior lamellar keratoplasty because of curvature issues may still be suitable for Descemet membrane endothelial keratoplasty or Descemet stripping automated endothelial keratoplasty,” he explained.
Prof Seitz said that with safety in mind, PKP is typically performed under general anaesthesia with controlled arterial hypotension and maximal relaxation. However, he cautioned against using mivacurium as the muscle relaxant because it is associated with an increased risk of vis-a-tergo.
He emphasised the importance of horizontal positioning of the head and limbal plane to avoid decentration, vertical tilt, and horizontal torsion that could lead to high and/or irregular astigmatism.
“The double-running cross-stitch suture is preferred as long as Bowman’s layer is intact since it results in higher topographic regularity, earlier visual rehabilitation, and lessens the risk of suture loosening and consequently the rate of resuturing,” he said.
“Using the Homburg cross-stitch marker for placing the double-running sutures allows even inexperienced surgeons to achieve good results.”
Prof Seitz presented his findings during the ESCRS Virtual Winter Meeting 2022.
Berthold Seitz MD is Professor and Director of the department of ophthalmology at Saarland University Medical Centre, Homburg/Saar, Germany. berthold.seitz@uks.eu

“Using the Homburg cross-stitch marker for placing the double-running sutures allows even inexperienced surgeons to achieve good results.”Six months after excimer laser-PKP (8.0/8.1 mm) for keratoconus with continuous double-running cross-stitch suture according to Hoffmann.
Descemet membrane endothelial keratoplasty (DMEK) results in superior visual acuity rates with quicker recovery compared to Ultrathin Descemet stripping automated endothelial keratoplasty (UT-DSAEK). However, UT-DSAEK has a more favourable complication profile, particularly regarding lower rates of rebubbling, according to a systematic review and meta-analysis presented by Daire Hurley MB, MCh.
“Both are valuable options in [treating] corneal endothelial disease, and choice of procedure may depend on surgical expertise,” Dr Hurley said.

Dr Hurley conducted a comprehensive search on Medline, Embase, and Cochrane Library databases to identify studies reporting comparative results of UT-DSAEK versus DMEK. Of 135 studies reviewed, seven met the inclusion criteria for the meta-analysis, namely, best-corrected visual acuity (BCVA), endothelial cell density (ECD; cells/mm2), central corneal thickness (CCT), and complications.
Altogether, a total of 306 patients were included in the analysis, 161 of whom underwent UT-DSAEK and 147 DMEK. Their average age was 71 years, and 68.9% were female. For 90% of cases, Fuchs’ endothelial dystrophy was the indication for surgery. The baseline visual acuity, endothelial cell density, and central corneal thickness were similar in the two cohorts. The average donor graft thickness in the UT-DSAEK group was 80.7 microns.
The study showed patients who underwent DMEK had significantly better BCVA than those who underwent UT-DSAEK at three months (logMAR 0.13 versus 0.23) postoperatively and one year postoperatively (logMAR 0.10 versus 0.19), roughly a difference of one line of BCVA.
“DMEK resulted in superior visual acuity rates with quicker recovery compared to UT-DSAEK. This is likely due to improved restoration of anatomy in the DMEK procedure because of the use of a thinner graft with no lamellae and the lack of a stromato-stroma graft interface,” Dr Hurley said.
Patients undergoing DMEK also had significantly greater reductions in CCT, with an average reduction at one year of 117.3 µm (18%) compared to a reduction of only 50.4 µm (7.8%) in the UT-DSAEK groups. The one-year postoperative CCT values were also significantly higher in the UT-DSAEK group (592.0 µm versus 524.8 µm).
There were no significant differences between the DMEK and UT-DSAEK groups in terms of postoperative ECD at one year, which were 1,705.3 cells/mm2 and 1,673.8 cells/mm2, respectively. Nor was there any significant difference between the two groups in terms of endothelial cell loss, which were 36.7% and 38.6%, respectively, at one year.
On the other hand, UT-DSAEK resulted in significantly lower total complications (23.2% versus 57.3%, p = 0.0001) and rates of rebubbling (11.0% versus 33.7%). The most common complication was the need for rebubbling, which occurred in 30 patients in the DMEK group compared to only 10 patients in the UT-DSAEK group. Raised IOP was the next most common complication, which occurred in seven eyes in the UT-DSAEK group and eight in the DMEK group. There was one graft failure in each group.
“Previous studies have shown DMEK to have less rejection compared to traditional DSAEK. As UT-DSAEK uses less donor tissue, this may result in rejection rates closer to those of DMEK,” Dr Hurley added.
Dr Hurley presented the study during the ESCRS Virtual Winter Meeting 2022.
Daire Hurley MB, MCh is a Senior House Officer in the Department of Ophthalmology, Mater Misericordiae University Hospital, Dublin, Ireland. dairehurley@gmail.com
Better visual outcomes with DMEK than UT-DSAEK, but more rebubbling with DMEK. Roibeárd O’hÉineacháin reports
Topical application of azithromycin may provide an acceptable alternative to systemic doxycycline in patients with meibomian gland dysfunction (MGD), a recent study suggests.

“Our study showed that systemic side effects were less common with azithromycin compared to systemic doxycycline without losing any efficacy in terms of improving the signs and symptoms of ocular surface disease (OSD) in patients with MGD,” reported Andreas Schlatter MD.
MGD is a major cause of ocular surface disease, with treatment strategies including but not limited to lid hygiene for mild cases and anti-inflammatory treatment for more severe cases.
Although both topical azithromycin and systemic doxycycline have been found effective in MGD, the effect of both therapies on tear film thickness (TFT) remains unclear. The efficacy of topical azithromycin for the treatment of MGD has been attributed to its anti-inflammatory and antibacterial properties, which may suppress MGD-associated posterior blepharitis and bacterial growth on the eyelid.
In Dr Schlatter’s study, 23 patients with MGD were randomised to either receive 15 mg/g topical azithromycin twice daily in both eyes for two days, then once daily for 26 days, or 100 mg oral doxycycline twice daily for six weeks. In total, four study visits at intervals of two weeks were scheduled.
were no significant changes in LLT, tear film osmolarity, conjunctival staining, or Schirmer I test. Systemic adverse events were more frequent in the doxycycline group, while mainly local adverse events occurred in the azithromycin group.
“The adverse events in the azithromycin group were mainly eye related, with burning eyes the main symptom identified. Two patients discontinued treatment as a result. Headache and gastrointestinal symptoms were the most frequent adverse events for patients treated with systemic doxycycline, with one patient discontinuing treatment as a result,” Dr Schlatter said.
Summing up, Dr Schlatter said the study showed both treatment regimens improved TFT in addition to signs and symptoms of OSD.
“The increase observed in tear film thickness can probably be attributed to an increase in the thickness of the aqueous layer. There were [fewer] systemic adverse events in the azithromycin group, and the treatment can therefore be considered a viable alternative to systemic doxycycline,” he said.
Dr Schlatter added that larger sample sizes and a longer observation time would be needed in future studies to confirm these initial findings.
The main study outcome was a change in tear film thickness as measured with ultra-high resolution optical coherence tomography (UHR-OCT). Ocular Surface Disease Index (OSDI), OSD composite sign score, lipid layer thickness (LLT), tear film osmolarity, conjunctival staining (as assessed with Lissamine green), and Schirmer I test served as secondary outcomes.
TFT significantly increased in both groups with no statistical difference between them. Additionally, OSDI score and OSD composite signs significantly decreased in both groups. There
He presented the results of the study at the ESCRS Virtual Winter Meeting 2022.
Andreas Schlatter MD is a research associate at the Medical University of Vienna, Austria, and the Vienna Institute for Research in Ocular Surgery (VIROS), Austria. andreas.schlatter@meduniwien.ac.at
“Our study showed that systemic side effects were less common with azithromycin compared to systemic doxycycline without losing any efficacy in terms of improving the signs and symptoms of ocular surface disease (OSD) in patients with MGD.”
Anovel therapeutic contact lens that increases the overall contact time of antimicrobial drugs in the eye may speed up corneal healing in cases of infectious keratitis, help address compliance issues, and reduce the treatment burden for patients.
“The concept of using a novel drug repository contact lens is effective in prolonging corneal antimicrobial availability and drug contact time over the lesion and has demonstrated faster corneal healing in this study, which may affect the overall outcomes in bacterial keratitis,” said Lional Daniel Raj Ponniah MD. There is an unmet need for more effective treatments for infectious keratitis in India and elsewhere, he stressed.
“Up to 5% of all blindness is due to infections, and in our part of the world, the prevalence of microbial keratitis is as high as 11.3 per 100,000 population. Although topical antibiotic eyedrops in loading dose are currently the preferred treatment option, the precorneal factors and anatomical barriers negatively affect the bioavailability of topical formulations at the lesion.”
The proprietary contact lens in Dr Ponniah’s study is designed with dual base curves, resulting in a central reservoir and fenestrations to enable the capture of topical antimicrobial.
“The aim is to retain the drug in the precorneal space using the contact lens to generate a central antimicrobial lake rather than employing a drug with sustained release properties,” he explained.
Dr Ponniah’s randomised controlled study compared the efficacy of the therapeutic contact lens with conventional topical antibiotic treatment in 40 patients with bacterial keratitis, using moxifloxacin 0.5% as the antimicrobial of choice. Ulcer size and depth, anterior chamber reactions, corneal haze, and pain were evaluated at 12 hours and days 1, 3, 5, and 14.
The results showed pain relief and resolution of the bacterial keratitis was faster in patients treated by contact lens.
Significantly better early visual acuity gains were also observed in the contact lens treated group in the early phase of treatment up to three days. Anterior chamber reaction and corneal haze also resolved faster within three days in CL-treated patients.
A separate drug retention study of the contact lens using triamcinolone acetonide showed drug availability in the central reservoir peaked immediately on instillation and was detected in the precorneal space for up to four hours, favouring an extended drug-corneal contact time. By contrast, most current treatment protocols require hourly application of topical agents in the early stages of infection.
Summing up, Dr Ponniah said using a drug repository contact lens may reduce the regimen of antibiotics, decrease treatment burden on the medical staff, improve patient tolerance, and reduce toxicities, effectively bypassing the loading dose concept.
“The resolution of corneal infiltration was usually observed before the third day. We recommend the treating physician remove the lens after a significant healing response has been noticed, usually around the three-day mark,” he said.
The study was presented at the ESCRS Virtual Winter Meeting 2022.
Lional Daniel Raj Ponniah MD is a researcher at Dr Agarwal’s Eye Hospital and Research Institute, Tirunelveli, India.
drlionalraj@gmail.com, drlionalraj@dragrawal.com
Young ophthalmologists are invited to write an essay on “What can the field of ophthalmology do to meet the pressing challenges of climate change, sustainability and social equity?”
The winner of the prize will receive a €500 bursary and a specially commissioned trophy. The prize will be awarded during the ESCRS Video Competition Awards ceremony during the 40th Congress of the ESCRS in Milan, Italy in September.
Descemet membrane endothelial keratoplasty (DMEK) has changed the approach to managing corneal endothelial pathologies—particularly Fuchs’ endothelial corneal dystrophy (FECD), for which keratoplasty is being performed more often and earlier, according to Marc Muraine MD.

Reflecting on this shift, Dr Muraine noted a need for more information on long-term outcomes after DMEK.
“We all know that visual results after DMEK are impressive from the first postoperative week. Results at five years are excellent as well and help explain the increased number of transplanted patients. However, is it the best option to graft patients with FECD very early when they are just 50 to 55 years old?” he asked.
could be transplanted more easily and therefore were undergoing surgery earlier in the evolution of the pathology. But if patients are undergoing transplantation with DMEK at an earlier age, it is absolutely necessary to know the long-term survival rate of DMEK in FECD so we can prepare them for the possibility of needing one or more transplants in the future.”
Discussing the literature on this topic, Dr Muraine said most published reports on postoperative results after DMEK are based on follow-up that does not exceed two years. Available studies published by Melles [et al] and Weller [et al] estimate that graft survival is between 90% and 95% at five years. The first studies with longer term follow-up are being published, but as Dr Muraine reviewed, the series suffer from high dropout rates.
The reports include a study by Weller and Kruse in which 66 patients were followed for at least eight years after DMEK. For this population that included 60 patients with FECD, the investigators reported an 80% graft survival rate at 10 years and mean endothelial density of 729 cells/mm3
“These good results should not make us forget that 20% of patients had to be regrafted and only 32% of the patients reached the 10-year visit as many were lost to follow-up,” Dr Muraine cautioned.
Melles and colleagues reported findings from a retrospective study that included 100 eyes operated on after the surgeons completed the DMEK learning curve. The results for 10-year graft survival and endothelial cell density in this study were similar to those reported by Weller and Kruse, but 52% of patients were lost to follow-up after six years.
“The first results from a series with follow-up [up] to 10 years are becoming available, and they are good. But they show 20% of patients need a regraft, and many of the grafted patients were lost to follow-up. We need to know the long-term survival of a regraft. Let us not forget that a failed graft for Fuchs’ patients means they will have visual acuity much lower than the preoperative level. Therefore, management decisions need to be individualised.”
Early questions surrounding DMEK related to its technical difficulty. Therefore, for several years after DMEK’s introduction, several surgeons developed methodological variations aiming to increase surgical ease. In addition, developed techniques for eye banks to provide preloaded DMEK grafts take the risks of graft preparation out of surgeons’ hands and make the procedure faster and safer, Dr Muraine explained.
“Current debates about DMEK are no longer about the surgical technique itself. Different methods are used by surgeons and eye bank technicians and are more or less equivalent,” he noted.
The developments in DMEK surgical technique and the advent of preloaded DMEK grafts underlie rising numbers of DMEK procedures—a phenomenon demonstrated in various temporal analyses. For example, data from the French eye bank in Paris showed an exponential increase in the proportion of corneal grafts used for DMEK from 15% in 2015 to 60% in 2020.
Particularly interestingly are data on indications for keratoplasty procedures showing that as soon as surgeons perfected the DMEK technique in 2015, the number of surgeries for FECD exploded. Whereas there were only 60 procedures for FECD in 2010, the number rose to 150 in 2015 and reached 550 in 2020, Dr Muraine reported.
“It is as if we were facing an epidemic, but the incidence of FECD was not increasing. The main explanation is that patients
In a retrospective study including 150 eyes that underwent DMEK for FECD or bullous keratopathy, Beşek [et al] reported that only 60% of grafts performed in eyes with FECD remained clear at seven years. Dr Muraine noted, however, that the cases in this study included those done during the surgeons’ learning curve.
Finally, in a series reported by Montesel [et al], the graft survival rate for endothelial keratoplasty cases was only 85% at five years, and it dropped steeply after seven or eight years.
“Thirty percent of the surgeries were for endothelial dystrophy, and only 40% of grafts were clear at 10 years,” Dr Muraine said.
results lead to rapid uptake, cautious optimism on long-term outcomes. Cheryl Guttman Krader reports
“It is as if we were facing an epidemic, but the incidence of FECD was not increasing. The main explanation is that patients could be transplanted more easily and therefore were undergoing surgery earlier in the evolution of the pathology.”
Do you have ideas for any stories that might be of interest to our readers?
Small, large, floppy, or damaged irides complicate cataract and glaucoma surgery. Gayle C Howard MD, PhD offered pearls for getting them under control at the American Glaucoma Society 2022 annual meeting.

Small or poorly dilating pupils can result from medications, older age, or inflammatory or neovascular membranes—though 25% occur with no known risk factors. Intraoperative floppy iris syndrome often results from taking tamsulosin or other beta blockers. Bleeding with dilation and sphincter tears are other causes of erratic iris behaviour. All increase the risk of complications such as capsular rupture, retained fragments and CME, and increase surgery time and surgeon anxiety, Dr Howard said.
For cataract surgery, the iris sometimes can be stretched with a second instrument, such as a Kuglen iris hook or collar button. When this does not allow sufficient room for surgery or prevent iris tissue from occluding the phaco tip, she advises deploying other techniques.
through another corneal incision midway between the suture insertion and exit points and allowing the knot to retract back into the eye.
The process can be repeated to achieve the desired pupil size, Dr Howard said. The Siepser suturing technique is similar but uses slip knots to pull the iris together, eliminating the need for a third incision. Videos and schematics of both techniques can be found online.
For microincision glaucoma surgery, Dr Howard cautioned avoiding engaging iris tissue in the angle or when entering or leaving the eye. Using cohesive viscoelastics and pupil constriction medications can help.
Iris hooks are one, though these require additional corneal incisions and are time consuming to insert and remove. Malyugin rings have the advantage of easier insertion and no extra incisions. Non-device options include Omidria® (Omeros), and while this prevents miosis and maintains iris tone, it is expensive.
When membranes prevent dilation, peeling them in segments can help, though this may involve some bleeding. If peeling is not effective to allow a larger pupil, hooks or a Malyugin ring may also be needed.
In the case of traumatic mydriatic pupils, a McCannel suturing technique can reduce pupil size. This involves running a suture through a pair of corneal paracenteses, then through two points in the iris, drawing the suture points together by tying a knot
She also said plugging the shunt or device with iris tissue or tearing the iris root can be avoided in trabeculectomy or tube surgery by determining the correct angle for insertion and positioning. A second instrument can push the iris out of the way—or viscoelastic can deepen the chamber and push the iris posteriorly.
For cyclophotocoagulation, too much power can lead to permanent mydriasis, Dr Howard noted. Power should be reduced and not applied at the three and nine o’clock positions to avoid this problem.
“Dealing with the iris is just like Goldilocks—not too small, not too big, and not too soft or floppy. Use devices, medicines, and suturing to get it just right,” Dr Howard said.
C Howard MD, PhD practices in Chula Vista, California, USA. gchoward1@yahoo.com“Dealing with the iris is just like Goldilocks—not too small, not too big, and not too soft or floppy. Use devices, medicines, and suturing to get it just right.”
Emerging diagnostic techniques should help detect and track glaucoma progression, reports Felipe
 A Medeiros MD, PhD.
A Medeiros MD, PhD.
Optical coherence tomography angiography (OCTA) is one promising technology. OCTA allows mapping of blood vessel density in the retina, which decreases as glaucoma progresses, Dr Medeiros explained.
In one study with a mean follow-up of 14 months, OCTA showed faster loss of macula vessel density in eyes with primary open-angle glaucoma than healthy eyes without evidence of change in conventional macular thickness measures.i
A second OCTA study found a relationship between the decline in macula vessel density and faster future visual field loss.ii
“The relationship was somewhat higher than you would see with the ganglion cell complex thinning but still not very strong at an R2 of 0.07,” Dr Medeiros noted.
While OCTA is a promising technology that may help clarify pathogenetic mechanisms in glaucoma, there is currently no clear evidence of additional benefit for detecting progression compared with conventional OCT studies, such as peripapillary retinal nerve fibre layer thickness.
Applying artificial intelligence to imaging data may help detect glaucoma progression, Dr Medeiros said. Working with colleagues, he recently trained a deep learning algorithm to replicate the work of glaucoma specialists, who graded progression based on OCT scans. It replicated the work of glaucoma experts well, with a score of 0.935 in the area under the Receiver Operating Characteristic (ROC) curve.
“The combination of multiple sources of imaging with AI is likely to improve our detection of change in the near future,” said Dr Medeiros, adding there are still challenges related to how to train and validate these models.
Detection of apoptosing retinal cells (DARC) involves fluorescently marking phosphatidylserine—an early marker of apoptosis—and imaging it with confocal scanning laser ophthalmoscopy.
AI is useful for interpreting these images as well. A baseline DARC
was able to predict progression seen 18 months later on OCT with an accuracy of 0.88 for the area under the ROC curve.iii
“You see more apoptotic cells in the eye that was progressing,” Dr Medeiros said.
Adaptive optics OCT is another promising technology that may allow for detecting progressive loss of ganglion cells in glaucoma. AI can help automate the quantification of ganglion cell damage in this technology, Dr Medeiros said. This may eventually find a way into clinical practice. For the present, however, the technology may be more useful for research, such as in early-stage drug trials.
Lastly, Dr Medeiros considered head-mounted perimetry systems for detecting progression but noted that none has yet been validated in a longitudinal study.
“They may enable more frequent testing, which would be a very welcome addition. But they still need validation as tools for detection of progression.”
i American Journal of Ophthalmology, 2017; 182: 107–117.
ii JAMA Opthalmology. Online Feb 24, 2022. doi:10.1001/jamaophthalmol.2021.6433
iii Expert Review of Molecular Diagnostics, 2020 Jul 1; 20(7): 737–748.
Felipe A Medeiros MD, PhD is Joseph Wadsworth Distinguished Professor of Ophthalmology, professor of electrical and computer engineering, professor of biostatistics and bioinformatics, and vice-chair (technology) at Duke University, Durham, North Carolina, USA. felipe.medeiros@duke.edu
New technologies and AI may soon better detect progression. Howard Larkin reports from the American Glaucoma Society 2022 annual meeting
“The combination of multiple sources of imaging with AI is likely to improve our detection of change in the near future.”
It’s well known that Blacks have a higher risk of primary open-angle glaucoma (POAG) than the general population. But racial identity is less important for addressing disparities in glaucoma than other factors, said M Roy Wilson MD, MS in the AGS Lecture at the American Glaucoma Society 2022 annual meeting. Other more relevant factors include ancestry of geographic origin, and economic and social circumstances.
Since Dr Wilson wrote a commentary on the subject in a 1989 issue of JAMA asking “Glaucoma in Blacks: Where Do We Go from Here?”, much progress has been made in defining race and the use of race in scientific studies and medical practice. He discussed these developments as well as the way forward, including the importance of better understanding social and individual determinants of health.
In 2022, race is defined differently than in 1989, Dr Wilson said. “Today it is accepted that race is a social construct.”
To illustrate, Dr Wilson used a personal example. While he identifies as Black, 51% of his genes are of Japanese origin, while 29% are West African. Similarly, he displayed genetic maps of two Caucasians who each shared more genes with an Asian man than they did with each other.
“There is tremendous variation within a population group.”
Yet race isn’t entirely irrelevant. Studies going back to the early 2000s show significantly higher glaucoma prevalence among Blacks and the associated clinical differences, Dr Wilson said. Structural differences include thinner central corneal thickness and larger disc area in Blacks than in other populations. Visual function is reduced and the burden of disease is higher.

Adding genetics has helped refine the concept and made it more clinically relevant. For example, cytochrome P450 and CPY2C9 polymorphisms are associated with metabolism of about 15% of prescription drugs, and their distribution falls roughly along racial lines, with Asians often poor metabolisers and Caucasians extensive metabolisers. However, the correspondence is far from perfect. One of the genetically mapped Caucasians Dr Wilson presented was a much more extensive metaboliser than the other.
Also, finding differences by race of POAG-associated genes can be challenging. It wasn’t until the late 2010s that genetic studies identified a gene, ENO4, uniquely associated with POAG in people of African descent. Previously, 16 genes associated with POAG had been identified, but all in Caucasian or Asian populations.
“There’s a lot more work to be done in this area,” Dr Wilson said.
Adding geography or ancestry of origin also helps refine the concept. In one study of Latinos Dr Wilson highlighted, the ancestry of origin ranged from 90% European to more than 90% Native American, showing once again the need to study the large genetic variations within ethnically identified populations. However, there is some correlation between racial and ethnic identities, genes, and geographic origins, Dr Wilson noted. People intuitively understand this and reject the notion there is no connection between biology and race.
“To say that race is biologically meaningless is really not correct,” he said.
But because it is so subjective, neither is race biologically important, Dr Wilson added. He cautioned against race-based medicine.
For example, using racial modifiers for kidney filtration studies also distorts results and leads to less treatment for Black patients.
“Race-based medicine perpetuates the false narrative that race is an essential, biological variable and translates it into clinical practice,” Dr Wilson said.
As such, it inhibits the need for finding more precise biomarkers underpinning disparities as well as the overwhelming importance of social determinants of health.
Glaucoma in Blacks: Where Do We Go From Here?
• Race increasingly less relevant in medicine

• Genetic admixture
• Shift from clinical trials and surveys to real world, big data analysis (AAO IRIS)

• Evolution of personalized medicine: NIH All of Us 1
Dr Wilson noted that the life expectancy of a Black man in Bethesda, Maryland— located just northwest of Washington, DC, and the most affluent community in the USA—is 19 years longer than a Black man in Suitland, a poor neighbourhood 19 miles southeast on the other side of Washington. Dr Wilson attended high school in Suitland and later worked in Bethesda at the National Institutes of Health.
“For every mile … you lose a year of life,” dramatically demonstrating the impact of socioeconomic circumstances on health.
Such disparities are also evident in clinical glaucoma data. For example, one study found visual field loss much higher at initial presentation for affluent patients than less affluent patients.i Similarly, patients with public insurance received less care—including fewer visual fields, optic imaging, and fundus photos—than patients with private insurance, regardless of race or ethnicity.ii
Race is not irrelevant in medicine, Dr Wilson said. “Racism at both the individual and systems level is alive and well.”
However, race is increasingly less relevant and researching other factors is essential to better understand and address disparities in glaucoma and all of medicine. The advent of big data studies and personalised medicine will help focus medicine away from arbitrary measures of race and towards the specific needs of individuals, he concluded.

i Eye, 2009; 23: 1038–1044.
ii Opthalmology, 2017; 124(10): 1442–1448.
M Roy Wilson MD, MS is a glaucoma specialist and epidemiologist and president of Wayne State University, Detroit, Michigan, USA. president@wayne.edu
2022 ESCRS Clinical Research Awards

Microbiological profile of infectious keratitis unchanged during COVID-19 pandemic. Dermot McGrath reports
The long-term use of face masks does not seem to promote significant changes in the microbiological causes of infectious keratitis, a recent Portuguese study concludes.
“Most of the microorganisms identified in our study are known commensals of the upper respiratory tract or pathogenic agents associated with respiratory infections. However, our results did not significatively differ from the ones previously published in 2019 regarding the microbiological profile of infectious keratitis in our tertiary centre in Porto, Portugal, from 2009 to 2018,” said Mário Lima Fontes MD.
Microbial keratitis (MK) is the most common non-surgical ophthalmic emergency ocular infection. Its potential causes are bacteria, fungi, viruses, or parasites and can rapidly progress, causing irreversible sight loss.
patients were included, with a 43% culture-positive rate. The mean age at diagnosis was 49 years, and 54% of the patients were female.
Bacteria accounted for 83% of all positive scrapes (61% were Gram positive and 35% were Gram negative), fungi for 12%, and acanthamoeba for 4%. The most frequent Gram-positive agent identified was Corynebacterium macginleyi (23%), followed by staphylococcus aureus (17% each) and streptococcus pneumoniae (8%).
Discussing the study’s background, Dr Lima Fontes noted the COVID-19 pandemic introduced profound changes in daily habits, including the frequent use of face masks. There have been observations of an increasing number of patients presenting with dry eye symptoms among regular mask users with no history of ocular surface pathology.
“Numerous reports from around the world pointed to an increase in dry eye symptoms due to an upwards route of the exhaled air over the ocular surface. Therefore, we speculated this mechanism could have led to a change in the microbiological profile of infectious keratitis,” he said.
Dr Lima Fontes and co-workers carried out a retrospective study based on a survey review of electronic medical records of all patients with presumed infectious keratitis between March 2020—when the first cases of COVID-19 were identified in Portugal—and October 2021.
A total of 194 samples from the same number of
The Gram-negative bacteria pseudomonas aeruginosa was found in 17% of cultures. Various strains of candida comprised the main fungi identified in 12% of cases, followed by acanthamoeba in 3.5%.
The most common ophthalmologic risk factors identified were the use of contact lenses (41%), previous ocular trauma (12%), and history of corneal ulcers (9%). Diabetes (8%) and poor systemic status/multiple comorbidities (5%) were the most frequent systemic associations.
Summing up, Dr Lima Fontes said while most of the organisms identified in the study were known commensals of the upper respiratory tract, there was no evidence that the widespread use of face masks during the pandemic had significantly altered the root causes of infectious keratitis.
“The long-term use of face masks does not seem to promote significant changes in the microbiological causes of infectious keratitis,” he said.

“The long-term use of face masks does not seem to promote significant changes in the microbiological causes of infectious keratitis.”

10 Issues per year. 6 Subspecialties. 25 Years. 169 Countries.
A European focus. A global perspective.
EUROTIMES.ORG/SUBSCRIBE

STAAR Surgical Company announced USFDA approval for its EVO/EVO+ Visian® Implantable Collamer® Lens for the correction of myopia and myopia with astigmatism. The company reports more than one million EVO lenses have already been implanted by doctors outside the US, and 99.4% of EVO patients in a survey stated they would have the procedure again. The lens is indicated for use in phakic eye treatment in patients 21–45 years of age:





• for the correction/reduction of myopia in patients with spherical equivalent ranging from -3.0 D to -20.0 D at the spectacle plane
• for the correction/reduction of myopic astigmatism in patients with spherical equivalent ranging from -3.0 D to -20.0 D with cylinder of 1.0 D to 4.0 D at the spectacle plane
• with an anterior chamber depth (ACD) of 3.00 mm or greater, when measured from the corneal endothelium to the anterior surface of the crystalline lens
• and a stable refractive history (within 0.5 D for one year prior to implantation)
staar.com



Johnson & Johnson received USFDA approval for ACUVUE® Theravision™ with Ketotifen contact lens. The daily wear, daily disposable contact is designed to release ketotifen to ease allergic conjunctivitis symptoms. It is indicated for the prevention of ocular itch due to allergic conjunctivitis and correction of refractive ametropia (myopia and hyperopia) in phakic and/ or aphakic patients who do not have red eye, are suitable for contact lens wear, and do not have more than 1.00 D of astigmatism.
cloud.inform.jnj.com/ acuvue-theravision-withketotifen
Paris-based Luneau will now be known as Visionix. Visionix will produce and provide diagnostic, OCT, refraction, and finishing solutions. The product lineup includes the OptoVue line of imaging devices. www.visionix.com








Patients who undergo implantation with a foldable iris-fixated phakic intraocular lens (PIOL) to correct myopia or astigmatism appear to have a progressive myopisation over time, a new study suggests. The prospective case series involved 481 eyes of 277 patients with a mean age of 39.8 years and a preoperative mean manifest refraction spherical equivalent (MRSE) of -8.98 D. One year after undergoing implantation of a foldable iris-fixated PIOL, the mean MRSE was -0.19 D. However, at the five-year follow-up, MRSE was -0.35 D. Likewise, mean uncorrected distance visual acuity declined significantly, from logMAR 0.02 at one year to logMAR 0.05 at five years. SMR Jonker et al, “Changes in visual outcomes and ocular morphometrics after foldable myopic and toric intraocular lens implantation: 5-year results”, 48(4): 393–400, April 2022.

IOL calculations based on measurements with the Anterion (Heidelberg Engineering) anterior segment optical coherence tomographer will result in significantly larger refractive prediction error in the myopic direction than those with the IOLMaster® 700 (Zeiss), the findings of a retrospective observational study suggest. In 150 eyes of 150 cataract patients who underwent preoperative measurement with the two devices, the arithmetic means of refractive prediction errors for the Anterion and IOLMaster were 0.06 diopters (D) and 0.02 D, respectively, when using the SRK/T formula; 0.23 D and 0.08 D, respectively, when using the Haigis formula; and 0.02 D and 0.11 D, respectively, when using the Barrett Universal II formula. Y Kato et al, “Refractive prediction error in cataract surgery using an optical biometer equipped with anterior segment OCT”, 48(4): 429–434, April 2022.
A polynomial regression formula, WeOptimeye2nd (WO2nd), developed using a machine-learning algorithm, appears to provide significantly more accurate IOL calculations for second eye surgery than SRK/T and Barrett Universal II formulae, a new study suggests. The study’s authors retrospectively calculated predicted refraction in a multicentric dataset of 722 patients with WO2nd, SRK/T, and Barrett Universal II formulae as well as three other constant factors (CFs) second-eye refinement methods (CF0.38, CF0.35, and CF0.5). They found that WO2nd yielded the highest percentage of eyes within 0.5 D of the predicted refraction, and the difference was statistically significant compared to the SRK/T and Barrett Universal II formulae but not compared to CF0.38, CF0.5, or CF0.35. E Klein et al, “New polynomial regression formula to improve second-eye refractive outcomes in sequential bilateral cataract surgery”, 48(4): 435–442, April 2022.
European Registry of Quality Outcomes for Cataract and Refractive Surgery
European Cornea and Cell Transplantation Registry
European Registry for Childhood Cataract Surgery
Accountability. Benchmark. Patient Care. Research. Outcomes & Risks.
15th European Glaucoma Society Congress
4 – 7 June
Athens, Greece
EUCornea

25 – 26 June
Athens, Greece
EURETINA
1 – 4 September
Hamburg, Germany
40th Congress of the ESCRS
16 – 20 September
Milan, Italy

Belong to something inspiring. Join us.
Visit escrs.org for information about membership & benefit
The 2022/2023 ESCRS Systematic Review Award (“SRA”) is a new initiative sponsored by the ESCRS to produce a high quality body of research aimed to prepare, collate, analyse, synthesise and report medical research.

Applications now open:
escrs.org/about-escrs/ESCRS_Systematic_Review_Award.asp
Friday 16th September 2022
A safe environment for in-person interaction
Networking opportunities with 500 clinical and business experts
Learn about the latest developments in the European commercial and capital markets, projected 2023 innovations, regulatory changes, and reimbursement trends















