Stakeholders debate reimbursement concerns over added expense. ALSO IN THIS ISSUE
Democratised Cataract
Surgery on the Horizon
A new mechanical lens fragmentation and aspiration device offers a phaco alternative.
An Innovative Treatment for Amblyopia
Dichoptic therapy with specialised “brain-training” computer program could improve visual acuity and stereopsis.
ContentsHARMONIZING
Harmonizing
Cataract surgeons in the glaucoma symphony.
Controversies in Anterior Segment Surgery
Fasika A Woreta MD, MPH; Charles Claoué MA (Cantab), MD, DO, FRCS, FRCOphth; Catherine L Chen MD, MPH; and Mor M Dickman MD, PhD
21 Rethinking ACD and Near Add Grzegorz Łabuz PhD
22 Democratised Cataract Surgery on the Horizon
Elizabeth Yeu MD
23 Is FLACS Worth the Cost?
Cedric Schweitzer MD PAEDIATRIC
OPHTHALMOLOGY
24 A New “Ground-breaking” Treatment for Amblyopia
Arthur B Cummings MD, FRCSed, FWRCS
26 Stent-less Glaucoma Surgery
Nir Israeli MBA
27 OCT-Guided Femto-Trabeculotomy
Thomas W Samuelson MD
Sathish Srinivasan FRCSEd, FRCOphth, FACS
28 Better Monitoring with Less Testing
Emer Doolan MB, BCh, BAO, MRSCI
29 Patient Monitoring Post-Laser Capsulotomy
Oscar Chen MD
30 Periocular Cancer Treatment: From Control to Pevention Michèle Beaconsfield MD
32 Controlling Keratoconus Risk Luke C Northey MBBS(Hons), MMed(Ophth Sc), MPH, FRANZCO
34 AI Useful in DME Detection? Cathal Breathnach
Publishers
Carey Earle
Mariska van der Veen
Mark Wheeler
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Nicola Lodge
Contributing
Editors
Cheryl Guttman Krader
Howard Larkin
Dermot McGrath
Roibeárd O’hÉineacháin
Contributors
Soosan Jacob
Timothy Norris
Colour and Print
W&G Baird Printers
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Workshop Hones Medical Writing Skills
Congress programme aims to help researchers get published.
BY STUART HALES, EXECUTIVE EDITOR
Ajourney begins with a first step. A research paper begins with a question—several questions, actually.
“You must first ask yourself, ‘What is my research question?’” says Prof Dr Stephanie Joachim, head of the Experimental Eye Research Institute at the Department of Ophthalmology at Ruhr-University Bochum (Germany). “What was your thesis before you conducted your clinical study or before you conducted the experiment in the lab?”
Dr Joachim addressed this and other questions in a four-hour workshop at the ESCRS Annual Congress on 11
September. Joining her on the workshop faculty were Dr Angeli Yu of the University of Pittsburgh (United States), Prof Dr Ramin Khoramnia of the University of Heidelberg (Germany), Mayank Nanavaty of Brighton and Sussex University Hospitals (United Kingdom), and Kristine Morrill and Faustino Vidal Aroca, both with Medevise (France).
The workshop presented strategies to improve clinical writing and increase publication success rates. Combining a theoretical overview with practical advice, the workshop covered what to prepare before you start writing a paper as well as how to present your data.
You must first ask yourself, ‘What is my research question?’
The faculty presented optimal strategies for creating tables, graphics, and figures and identifying the mistakes
typically made during this process. They also discussed the dos and don’ts of generating a methodology, results, and discussion. Particular attention was given to developing the discussion section and interpreting clinical results.
The time factor
The faculty members were intimately familiar with the publication process, having authored or co-authored numerous research papers and served on editorial boards of leading ophthalmic publications. Notwithstanding their experience, they still ask themselves basic questions before putting pen to paper or fingers to keyboard.
“Before you write a paper, think about the tables and charts you are going to make to present your data,” Dr Khoramnia told workshop attendees. “I always put a lot of time into figures and tables, because when I make a presentation later about my paper, I typically just use the tables and charts for my slides.”
Another factor is the publication you are targeting and the audience you want to reach.
“Always go with a journal that is peer-reviewed,” said Dr Khoramnia. “Also check to make sure that the journal is on PubMed--if it isn’t, probably nobody is going to read your paper.”
One underappreciated factor is time— not just the time needed to write about the research, but the time involved in collecting the data, making revisions, getting approvals, conducting additional experiments or statistical analyses, and so on.
“You need to really be realistic in your timeline,” Dr Joachim said. “Sometimes it might be easier, especially if it’s your first publication, to do a ledger or a case series first before you jump into a big research paper.”
The faculty also stressed the importance of perseverance. “About 70% of the papers I’ve published appeared in the fourth journal I approached,” Navatany told attendees. “So don’t give up. It’s a process.”
999 Shirts, One Mission
Amid the crowd of dark suits and briefcases, a fashion trend could be spotted among attendees at the 2023 ESCRS Annual Congress: a simple white T-shirt.
The shirts were a prize for completing the ESCRS 2023 Mission Zero Challenge, which was designed to create a positive environmental impact. Challenge participants were required to complete the following actions during the Congress and document them with photographs:
• Eating from the climate-friendlier menus at the Congress centre;
• Separating waste carefully into the correct bins;
• Leaving Congress badges and tracking devices at the registration area for re-use when leaving the event; and
• Sharing these sustainability efforts on social media and in person.
The first 999 Congress attendees to document these actions received an ESCRS-branded, organic cotton, fairly-produced and -sourced T-shirt. The shirts were distributed at the sustainability display at the Congress centre, which highlighted several ESCRS initiatives (such as the SIDICS cat pack project) to decrease the environmental impact of ophthalmic surgery and Society events.
“You are a vital part of our goal to host a Congress that sends zero waste to landfills and acts as a role model for social and environmental responsibility,” the display stated. “By taking the Mission Zero pledge, you demonstrate your enthusiasm to join us on this journey and become an active participant who takes care of their environment and will encourage others to do the same.”
2023 Annual Congress Presentations by Topic
CATARACT
CORNEA
DIGITAL/ AI
GLAUCOMA
REFRACTIVE IOLS
SUSTAINABILITY
YOUNG OPHTHALMOLOGISTS
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
The Symphony of AI in Ophthalmology
BY SIYIN LIU MD
Medicine is at a critical inflection point for artificial intelligence (AI). With a whopping 3,327 new AI companies in the mix and a projected $37 billion splurge on AI by 2025, this tech is drastically transforming every industry, including healthcare.
Ophthalmology, with its rich imaging data, presents an ideal setting for training algorithms in image recognition, segmentation, and disease detection. Current focus lies on prevalent ophthalmic conditions like diabetic retinopathy (DR), age-related macular degeneration (AMD), and glaucoma, leveraging large, standardised imaging data sets. The COVID pandemic accelerated the integration of AI into tele-ophthalmology, exemplified by the FDA-approved autonomous diagnostic device for DR, enabling point-of-care diagnosis without human oversight. Challenges exist in AI research for anterior segment diseases due to non-uniform slit-lamp images and limited data sets. Nevertheless, recent advancements demonstrate AI’s potential in the anterior segment, including early detection of keratoconus, post-refractive surgery ectasia screening, and diagnosis of infectious keratitis.
AI in ophthalmology has primarily focused on image-based deep learning. Yet, the adoption of electronic health records has unveiled the untapped potential of unstructured free-text data. Natural Language Processing (NLP) and algorithmic rule-based text extraction techniques have shown promise in leveraging this data to enhance care delivery and for big data analysis, predictive modelling, cohort identification, and stratification. NLP also standardises specialised ophthalmic terminology, facilitating interactions among healthcare providers and patients. With predictions that 85% of customer interactions will be managed without human agents by 2025, NLP-based chatbots hold tremendous potential in triaging symptoms, monitoring treatment adherence, and providing support in areas with limited ophthalmology services.
AI chasm
A core challenge in applying AI is the clinical validation of recently developed concepts and tools. Clinical AI research faces limitations due to retrospective design, leading to biased algorithms “overfitted” to specific data sets. The conventional approach of pitting AI against clinicians may not demonstrate real-world performance, as its realistic application likely involves interaction between clinicians and algorithms. Clinicians, the end users, must grasp AI’s strengths and limitations to foster mutual learning. Envisioning AI’s role in high-risk real-time situations like surgery, where surgeons adapt their approach on the fly, is challenging.
AI regulatory approval is another challenging obstacle. Many algorithms rely on complex and opaque mathematical
More rigorous work is needed to combat the disparity between AI hype and application in healthcare, the so-called “AI chasm.”
models, often referred to as “black boxes.” The lack of transparency raises concerns about data mishandling and understanding of the algorithms’ inner workings. Agencies like the FDA/EMA require extensive transparency in scientific methods, but researchers and companies may hesitate to expose proprietary algorithms publicly due to potential financial risks. Further, without a clear understanding of algorithmic processes, AI may struggle to gain patients’ trust and approval. Would it be worse for patients to be misdiagnosed by a human or a machine? What if the algorithm had demonstrated superior performance in research settings? Ultimately, trust and confidence in algorithmic decision-making play a pivotal role.
Overall, more rigorous work is needed to combat the disparity between AI hype and application in healthcare, the so-called “AI chasm.”
The glass cage
The integration of AI into healthcare runs the risk of stripping medicine of its human touch. With advancing algorithms, we may see clinics where machines take the lead, like a macular clinic where an OCT machine decides on intravitreal anti-VEGF injections for AMD without ophthalmologist involvement. Even with fancy AI voice synthesizers like Siri, the empathy and intuition of the doctor-patient relationship diminishes. After all, to these machines, patients are reduced to mere data points where efficiency and cost-effectiveness are the sole measures of success. Further, overreliance on AI-powered automated diagnosis or treatment decisions may stunt the clinicians’ development of critical thinking and decision-making skills, which may, with time, add them to the list of skills lost due to technology.
Biases embedded in the training data can perpetuate inequalities by providing inaccurate or inadequate recommendations for certain groups or populations. With training data predominantly derived in the Western world, algorithms may struggle to effectively generalise to diverse groups. Unchecked, AI can reinforce and amplify existing disparities in healthcare outcomes. Also, the ethical implications of data
ownership and privacy protection arise in an era of roundthe-clock data collection from gadgets and wearables. Algorithms may exploit this data and stigmatise the chronically ill or those who don’t fit the “healthy lifestyle” mould, potentially leading to unjust financial and health penalties, such as reduced access to insurance.
The rise of AI
We are told AI-powered healthcare is not about replacing ophthalmologists, but rather augmenting their knowledge and expertise. The integration of genomic data, lifestyle factors, and imaging will lead to AI-powered decision support systems that can guide targeted therapies and tailored interventions. Although AI’s current capabilities fall short of the hype, overcoming challenges could unlock its potential in achieving the holy grail of personalised medicine. Yet, the question remains whether the rise of AI lead to the “machinification” of medicine.
THE JOHN HENAHAN WRITING PRIZE
What is the potential role of artificial intelligence (AI) in ophthalmology, and what are the negative implications and caveats?
Earlier this year, young ophthalmologists were invited to submit their answer to that question in an 800-word essay for the John Henahan Writing Prize. The competition was open to ESCRS members (including the free membership available to trainees) age 40 or younger on 1 January 2023.
This is the winning essay for the 2023 Henahan Writing Prize. Its author received a €500 bursary and a specially commissioned trophy.
Dr Liu submitted this winning essay to the John Henahan Writing Prize contest. He is Specialty training year 4 at UCL Institute of Ophthalmology, London, UK. siyin.liu@ucl.ac.uk
HARMONIZING EYE HEALTH
Cataract surgeons in the glaucoma symphony.
BY HOWARD LARKIN
Over the past two decades, glaucoma treatments have proliferated with laser and less-invasive surgical options, filling in some of the gap between medical treatment for mild to moderate glaucoma and trabeculectomy to control advanced disease. As a result, ophthalmologists who mainly do cataract surgery now have glaucoma treatment options compatible with phacoemulsification, notably the various minimally invasive glaucoma surgery (MIGS) procedures (see next page).
“The advent of MIGS signifies a change in glaucoma care for cataract surgeons,” Dr Roberto Bellucci said. Though his practice is primarily cataract and refractive surgery, having trained in a glaucoma clinic, he has done more than 2,000 glaucoma procedures—including trabeculectomies before filtering implants were available.
However, while glaucoma and cataract procedures use the same basic surgical skills, glaucoma surgery also typically requires intraoperative gonioscopy and detailed knowledge of angle anatomy.
In addition, glaucoma requires lifelong follow-up to detect and treat progression, which may not fit well with a streamlined cataract practice. Lack of reimbursement for more recent glaucoma devices and procedures, as well as the local out-of-pocket cost of eye drops, are other factors that may affect their uptake.
As a result, adding glaucoma treatment, especially surgical procedures, to a (primarily) cataract practice can be challenging—technically, operationally, and economically. Indeed, between 2016 and 2021, the proportion of respondents to the ESCRS annual Clinical Trends Survey performing glaucoma surgery declined significantly, while a growing proportion offered only medical glaucoma treatment.1
Still, proponents say non-filtering MIGS procedures are a generally low-risk method that may reduce intraocular pressure (IOP) enough to address mild to moderate glaucoma with fewer or no topical medications. Moreover, since they don’t alter the anatomy as much as trabeculectomy, non-filtering MIGS do not preclude later additional MIGS or more invasive procedures, Dr Bellucci said.
Glaucoma specialist Dr Inder Paul Singh noted that five-year data show reduced IOP and medication need—and better quality of life in some cases—with meshwork stenting procedures compared with cataract surgery alone.2
He has used conventional outflow MIGS for select moderate to severe cases to limit fluctuating IOP and delay subconjunctival surgery for those at high risk for complications.
However, glaucoma experts caution that non-filtering MIGS devices may not be suitable, even for patients with mild to moderate glaucoma, if the disease is likely to progress or they need a low-target IOP. And the only way to tell is to follow them for a year or more, said glaucoma specialist Dr Luis Abegão Pinto.
Complicating the issue are inconsistencies in how trials report data and a lack of large randomised prospective trials to determine efficacy of some MIGS procedures. “We need better data to know what really works,” said Dr Pinto, who co-chairs a task force of the European Glaucoma Society that has developed recommendations for uniform data collection in glaucoma studies.
Below are some factors to consider when deciding to treat or refer glaucoma patients in a primarily cataract practice.
What to look for
Since many cataract patients have no contact with ophthalmologists until their vision declines, the preoperative workup goal should be to determine why the patient does not see well, including any comorbidities such as glaucoma, Dr Pinto said. Then, any treatment decision—including medical treatment, MIGS, or filtration surgery—should be driven by the treatment goal, though this can be difficult to establish at the first visit. Dr Singh added glaucoma surgery goals also vary by patient, with some requiring lower IOP regardless of eye drop need.
IOP over 20 mmHg is an obvious red flag. Asymmetry between the optic nerve heads in the two eyes is another, Dr Bellucci said. Optical coherence tomography (OCT) helps spot optic nerve head tissue loss. Visual fields are mandatory when any optic nerve damage is evident on OCT, and gonioscopy should be performed if not previously documented.
Dr Pinto stressed doing a complete diagnostic workup rather than relying on OCT, which cannot be the sole source of diagnosis. Visual fields, he noted, are the best way to detect and track progression.
MIGS procedures:
• Trabecular meshwork bypass, such as the iStent (Glaukos) and Hydrus (Ivantis)
• Trabeculotomy devices such as the Kahook Dual Blade (New World Medical), Trabectome (MicroSurgical Technology), OMNI (Sight Sciences), and gonioscopy-assisted transluminal trabeculotomy
• Viscodilation of Schlemm’s canal devices such as the Visco 360/OMNI, the iTrack microcatheter (Ellex iScience), and the Streamline goniotomy and dilation system (New World Medical)
• Bleb-forming subconjunctival filtration implants such as the Xen gel stent (Allergan), the ab externo EX-PRESS shunt (Alcon), and PreserFlo Microshunt (Santen)
Training for surgeons and staff
As with any new procedure, attend lectures and training, and try MIGS first in wet labs before starting with uncomplicated glaucoma patients, Dr Bellucci said. Learning to accurately identify the trabecular meshwork and where to position bypass devices to be effective is critical, said specialty expert Dr Antonio Maria Fea.
For ophthalmologists out of practise with gonioscopy, fellow specialist Professor Carlo Enrico Traverso recommends first performing intraoperative gonioscopy on a patient who doesn’t need glaucoma surgery. Dr Pinto suggested starting with one or two procedures. “It is impossible to master 10 different technologies with the same proficiency you have in cataract surgery.”
And don’t forget training staff. “There will have to be a certain number of [MIGS] procedures you have to do routinely for the nurse to know the next step to make sure it is as efficient as if you are doing a phaco alone,” Dr Pinto said.
He noted some cataract surgeons are reluctant to adopt even trabecular bypass MIGS because it interferes with cataract surgery efficiency, particularly for those using a superior incision approach. Implanting a stent then requires moving the microscope to a temporal position. “At the end of the day, you’ve probably done two fewer cataracts to account for that time.” Dr Fea added setting aside one day a week for glaucoma patients or moving them to the end of the schedule can help improve efficiency, while Dr Singh said reducing eye drop use with MIGS may save time on follow-up.
Bleb-forming procedures require additional training in managing antimetabolites, ensuring the tube enters the subconjunctival space, and managing complications such as choroidal detachments and fibrosis, Dr Fea said. He recommends following cases closely for the first three to four months after surgery—or even longer if the bleb has to be revised. The period between visits can be extended for uneventful cases, but “I would not leave the patient alone for more than three months for the first two years.”
Treat versus refer
Not all glaucoma patients can be treated without the expertise of a glaucoma surgeon, Dr Bellucci said. He mostly treats patients with early primary open-angle glaucoma who are aware of their condition, but generally refers low-tension glaucoma patients. He also refers patients with significant nerve damage or progression, especially young or myopic patients. Most importantly, he refers advanced glaucoma patients possibly at risk of losing vision permanently due to surgery, known as wipeout syndrome. High myopia, uveitis, secondary glaucoma, and congenital glaucoma, Dr Fea said, should likewise be referred.
Dr Pinto suggests treating patients with whom surgeons have an established relationship. That patient will likely return for follow-up and can be referred if they progress to a glaucoma surgeon with more treatment options, he said.
Combined or separate procedures
MIGS procedures are designed to be used with cataract surgery or alone. But for cases requiring a lower target IOP,
filtration procedures, including trabeculectomy and the filtering implants, are better, Prof Traverso said. For these options, the evidence and consensus are for cataract surgery first, followed three months (or more) later by the glaucoma procedure on a quiet eye, is generally easier and yields better results. However, patients with severe disease and very high IOP that cannot be controlled without immediate filtration indicate combined surgery, he added.
Educating patients
Educating patients on the limitations of glaucoma procedures and the need for lifelong follow-up is essential for good longterm outcomes. Dr Pinto advises having an honest conversation with the patient that does not overpromise or discard the safety concerns. Dr Singh suggests telling the patients, “we are on a journey,” and will use a combination of therapies and technologies to help protect them from losing vision and maintain their quality of life.
“You don’t want to say to the patient that he is cured,” Dr Fea said. “I’ve seen patients who forget everything [after glaucoma surgery] and then come back five years later, and they are miserable.”
Above all, follow the Hippocratic oath: do no harm. Whether slowing progression, lowering IOP, or reducing medication burden, know the goal and only do the procedure if it will help the patient, Dr Pinto said.
Dr Bellucci largely agreed. In patients with early glaucoma without visual field or nerve loss and low IOP, he will use a multifocal lens and femto-cataract surgery. However, for more advanced cases, he does not do anything to risk an IOP spike, avoiding femtosecond lasers, instead opting for advanced fluidics phaco machines. He also will not place a multifocal lens into an eye with contrast sensitivity already reduced due to glaucoma.
For citation notes, see page 40.
Roberto Bellucci MD is an ophthalmologist in Verona, Italy, and a former ESCRS president. roberto.bellucci52@gmail.com
Luis Abegão Pinto MD, PhD is head of the glaucoma unit and assistant professor of ophthalmology at Lisbon University, Portugal. abegao.pinto@chln.min-saude.pt
Antonio Maria Fea MD, PhD is an ophthalmologist, head of glaucoma at the ocular clinic, and aggregate professor at the University of Turin, Italy. antoniomfea@gmail.com
Inder Paul Singh MD is an ophthalmologist at the Eye Centers of Racine and Kenosha, Wisconsin, US. ipsingh@amazingeye.com
Carlo Enrico Traverso MD is professor and chairman of the Clinica Oculistica, Di.N.O.G.M.I., University of Genoa, Policlinico Ospedale San Martino IRCCS, Italy. mc8620@mclink.it; cet@mclink.it
IOLS FOR GLAUCOMA PATIENTS
Selecting an appropriate IOL for cataract patients with glaucoma is challenging, especially given light-splitting lenses reduce contrast sensitivity by 15–20% for multifocal lenses and 7% or so even for extended depth of focus (EDOF) lenses, said glaucoma specialist Dr Inder Paul Singh. He follows these guidelines in selecting IOLs for patients with glaucoma who have or are at risk for contrast sensitivity loss:
• Use any lens for patients with ocular hypertension or stable pre-perimetric glaucoma, though he is hesitant to use multifocal lenses in those likely to progress or need eye drops after surgery.
• Patients with astigmatism may benefit from monofocal toric lenses that do not split light, though capsule tension rings may help those with unstable capsules at risk of rotation.
• For mild open-angle glaucoma with minimal or mild ganglion cell complex GCC loss, monofocal or EDOF lenses are best, with multifocal lenses possibly an option if the patient is fully aware of the risk and stable. If moderate or advanced glaucoma, or mild with significant GCC loss, monofocal is the best choice.
Controversies in Anterior Segment Surgery
JCRS symposium debates ISBCS and anaesthesia.
HOWARD LARKIN REPORTS
As technology and technique advance, controversies are inevitable in anterior segment surgery. Three current questions were explored in the Journal of Cataract and Refractive Surgery (JCRS) symposium at the 2023 American Society of Cataract and Refractive Surgery annual meeting in San Diego, US. JCRS Editor Dr William J Dupps Jr and Associate Editor Professor Sathish Srinivasan chaired the symposium.
Immediate sequential bilateral cataract surgery (ISBCS): clinical evidence versus economic model
While the merits of ISBCS have been debated for a decade, delayed sequential bilateral cataract surgery (DSBCS) is still dominant in the US, accounting for more than 99% of procedures, despite its safety, lower costs, and greater convenience.
“The main reason for this is economic,” Dr Fasika A Woreta said. The [US] federal Medicare insurance for seniors covers
First author Maartje HM Segers MD (centre), pictured with Sathish Srinivasan (left), and William J Dupps Jr (right), received the JCRS Obstbaum Award for Best Original Article published in 2022 for “Anaesthesia techniques and the risk of complications as reflected in the European Registry of Quality Outcomes for Cataract and Refractive Surgery.” The Obstbaum Award is presented annually in honour of Stephen A Obstbaum MD, co-founding editor of the JCRS.
same-day second eye surgery at only 50%, and anaesthesia for the second eye is not covered, resulting in losses of about $400 per case in ambulatory surgery centres.1
The situation is similar in the UK, where same-day second eye surgery is paid at 25% of the first-eye rate by some private payers, said Dr Charles Claoué, who noted the resulting losses are a major reason why just 0.4% of cases were done simultaneously in 2020.
This begs the question of whether the risk of cataract surgery is actually being increased because of the presence of anaesthesiologists.
Dr Chen and colleagues also found no association between anaesthesia care during cataract surgery and a composite outcome of death, hospitalisation, or systemic complications within seven days of surgery. However, she noted the study of Medicare beneficiaries did not examine cataract outcomes. 7
Further, unpublished registry research suggests patients receiving general anaesthesia or monitored anaesthesia care were more likely to have at least one intraoperative event (mostly hypertension) than those receiving no intravenous sedative or only fentanyl or midazolam, Dr Chen added.
“This begs the question of whether the risk of cataract surgery is actually being increased because of the presence of anaesthesiologists.”
However, one US system paid a flat rate per cataract procedure, reversing the financial incentive, resulting in more than 40% of patients receiving immediate sequential surgery. But, Dr Woreta added, not all patients should receive ISBCS due to ocular comorbidities or previous refractive surgery, complications in the first eye, and surgeon comfort with bilateral procedures.
Fear of lawsuits and blinding patients with bilateral endophthalmitis also limit ISBCS, Dr Claoué said, declaring these fears are overblown.
Adherence to recognised standards of care, which are well-established for ISBCS, limits legal liability, Dr Claoué pointed out. The risk of bilateral endophthalmitis is about 1 in 11.9 million procedures—or 23.8 million eyes—and should it occur, it can be successfully treated. At current endophthalmitis rates, “if there were 3 million cataract surgeries in the US every year, and all were done as ISBCS, one American would not meet driving [visual acuity] standards because of simultaneous bilateral endophthalmitis every 59 years.”
Studies also show ISBCS outcomes are similar to DSBCS, Dr Woreta said.2
The procedure saves about €1,600 per case—including patient travel and aftercare—and can increase surgeon productivity by 30%, Dr Claoué said.3–4
“There is no reasonable doubt that ISBCS is safe, cheaper, and increases productivity,” Dr Claoué said. And patients generally prefer it.5 Both Dr Claoué and Dr Woreta advocated payment reforms to encourage ISBCS in appropriate cases.6
Optimising cataract surgery sedation—is less more?
Cataract surgery anaesthesia is more likely to be administered by an anaesthesiologist or nurse anaesthetist than for many common, low-risk outpatient procedures, at least in the US. Yet cataract surgery has a much lower systemic complication rate than procedures including cardiac catheterisation and bronchoscopy, said Dr Catherine L Chen.
However, Professor Mor M Dickman and colleagues found topical anaesthesia had a significantly higher rate of posterior capsule rupture than general, sub-Tenon’s, or regional anaesthesia, based on a study of more than 4 million case records from the European Registry of Quality Outcomes for Cataract and Refractive Surgery (EUREQUO) from 2008 to 2018.8 This may be due to more eye movement with topical approaches, he said.
Endophthalmitis rates were lower in regional anaesthesia cases than in topical as well—but not significantly different for other approaches, a finding consistent with earlier studies, Prof Dickman said. Over the period, topical anaesthesia use increased from 30% to 75% while regional approaches, including retrobulbar, decreased from 38% to 6% and sub-Tenon’s from 27% to 15%. General anaesthesia and combined topical and intracameral anaesthesia remained steady at about 2% each. More research is needed to better understand anaesthesia risks and optimise procedures for cataract surgery, he concluded.
For citation notes, see page 40.
Fasika A Woreta MD, MPH is Eugene de Juan Professor of Ophthalmic Education at the Wilmer Eye Institute, Johns Hopkins University, Baltimore, US. fworeta1@ jhmi.edu
Charles Claoué MA (Cantab), MD, DO, FRCS, FRCOphth, FEBO, MAE is an ophthalmologist at The Harley Street Eye Centre and head of chambers at Eye-Law Chambers, London, UK. eyes@dbcg.co.uk
Catherine L Chen MD, MPH is an anaesthesiologist and associate professor at the University of California, San Francisco, US. catherine.chen@ucsf.edu
Mor M Dickman MD, PhD is professor of ophthalmology at the University Eye Clinic, Maastricht UMC, Netherlands. m.dickman@maastrichtuniversity.nl
Good Acuity at Near and Far
New presbyopia-correcting lens reveals predictable refractive outcomes.
DERMOT MCGRATH REPORTS
Anew hybrid, acrylic IOL offers a safe and predictable means to correct presbyopia and astigmatism in cataract patients, according to the results of a French study.
“The Precizon Presbyopic NVA lens (Ophtec) is a predictable and safe approach in providing good visual outcomes at all distances with a high level of patient satisfaction,” said Dr Camille Bosc. “Furthermore, the lens is forgiving in cases of tilt or misalignment and can be implanted in more complex cases.”
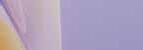
The Precizon multifocal refractive lens is designed with a patented continuous transitional focus (CTF) optic with an anterior surface with multiple segments for far and near.
“It means there is no interruption in the focal point between the far vision and the near vision, and a smooth transition is achieved between the segments,” Dr Bosc explained. “The technology allows for a full range of vision and a continuous transition without visual artefacts.”
The retrospective study included 158 eyes of 79 patients who underwent cataract surgery with bilateral implantation of the Precizon IOL. A toric version of the lens was implanted in 29 eyes.
Refractive outcomes were predictable and stable over time, with 75% of eyes achieving a spherical equivalent of ±0.50 D one month after surgery. The monocular uncorrected distance visual acuity (UDVA) was 0.1 logMAR or better for 79% of eyes, and the binocular UDVA was 0.1 logMAR or better for 96% of eyes. Near vision outcomes were also very good, with 65% of patients requiring additional correction less than 1.0 D and 24% attaining full spectacle independence at near. The binocular uncorrected near visual acuity (UNVA) was Parinaud 3 or better in 86% of eyes.
“The outcomes improved in the series because we adjusted the target refraction over time as we became more familiar with the lens,” Dr Bosc said.
He added the defocus curve showed the lens could provide a visual acuity of 0.16 logMAR or better between defocus levels of +0.50 D to -2.50 D.
What is CTF ?
94%
The overall satisfaction rates were high, with 94% of patients stating they were satisfied with the lens.
66%
66% were very satisfied with the outcome.
“The only correlated prognostic factor preoperatively was the refractive target, which means the lens performance is independent of corneal aberrations, pupil centration, and pupil diameter,” he said.
In quality of life, 71% of patients reported none or only occasional glare, and 11% of affected patients said the discomfort was significant; 66% reported none or occasional halos, with 32% of affected patients reporting significant discomfort from the phenomenon.
“A limitation of the study is that not all patients received the quality-of-life questionnaire at the same time after surgery, and we know halos and glare tend to decrease over time,” Dr Bosc noted.
The overall satisfaction rates were high, with 94% of patients stating they were satisfied with the lens and 66% very satisfied with the outcome. Only 6% of patients said they were dissatisfied with their visual results.
Dr Bosc presented the study at the ESCRS Winter Meeting in Vilamoura, Portugal.
Camille Bosc MD is an ophthalmologist in practice in Nantes, France. camillebosc@hotmail.com
ESCRS Academy in Slovenia
Sessions at the 14th Slovenian Congress of Ophthalmology feature thought-provoking topics.
PROFESSOR SATHISH SRINIVASAN REPORTS
The ESCRS has a tradition of offering educational ESCRS Academy programmes in support of national and sister societies during their regional conferences. ESCRS Committee members attend and present on key topics of interest.
Prof Oliver Findl, Prof Paul Rosen, Prof Sathish Srinivasan, Dr Vladimir Pfeifer, and Dr Alja Črnej were all part of the ESCRS Academy at the 14th Slovenian Congress of Ophthalmology at the very scenic resort town of Bled, Slovenia, in July.
Prof Findl opened the session by highlighting the ESCRS’s many educational activities, including the ESCRS Academy, the ESCRS travelling simulator programme, and the ESCRS charity initiative.
This was followed by a lecture on immediate sequential bilateral cataract surgery (ISBCS) by Prof Sathish Srinivasan, who provided the evidence showing ISBCS is as safe and effective as delayed sequential bilateral cataract surgery (DSBCS). He shared published data on the cost-effectiveness of ISBCS over DSBCS and shared evidence on how and why ISBCS is catching up and becoming more popular in Europe compared to the US.
Next, Prof Paul Rosen gave a lecture on managing postoperative refractive surprises. His very comprehensive lecture detailed all the issues with IOL power calculation, human errors, abnormal eyes, and algorithms on management strategies, including spectacle correction, contact lens, laser vision correction, and IOL exchange.
Local Slovenian expert Dr Alja Črnej shared lots of surgical pearls and videos illustrating several techniques of IOL exchange of single-piece and three-piece IOLs.
Dr Vladimir Pfeifer, one of the local organisers of the congress, spoke very eloquently on surgical techniques of secondary IOL implantation with the Yamane flanged IOL technique. He illustrated the different variations using real life surgical videos, highlighting the advantages and pitfalls of this particular procedure.
Prof Findl closed the session with a compelling talk on reducing waste in the operating room. He detailed
how different manufacturers have varied specifications for making cataract surgical packs and how harmonising this could lead to a massive reduction in the waste and carbon footprint generated by cataract surgeons.
Overall, it was a very enjoyable and thought-provoking meeting in a stunning location of Lake Bled. Although the weather could have been a little kinder to us, the camaraderie and hospitality shown by our Slovenian colleagues easily generated the required warmth and good feelings.
Prof Sathish Srinivasan FRCSEd, FRCOphth, FACS is a consultant corneal surgeon at University Hospital Ayr, Ayr, Scotland, and Professor of Health and Life Sciences at the University of West of Scotland, UK. He is also the Associate Editor of the JCRS
Rethinking ACD and Near Add
Deeper anterior chambers may need more add power in multifocal IOLs.
HOWARD LARKIN REPORTS
Anterior chamber depth (ACD) correlates highly with variations in the add power required to provide patients with an acceptable reading vision distance with multifocal intraocular lenses (IOLs) that fully correct for distance vision. As a result, patients with deeper ACDs may need a higher add power, while those with shallower ACDs may find their reading distance shorter than planned preoperatively, according to Dr Grzegorz Łabuz.
He noted this effect may also partially explain why defocus curves reported in clinical studies vary significantly in patients implanted with the same model of multifocal lenses.
“Although each multifocal lens type has its unique and fixed addition, the position of the secondary visual acuity peak detected in defocus measurements may show high intersubject variability,” he said, adding more research is needed to establish this connection.
Model eyes tested
The ACD, in part, determines the effective lens position after surgery, Dr Łabuz explained. The differences in lens power add needed to achieve a +2.00 D add at the IOL plane varied as much as 0.52 D in a study he conducted on 34 patients scheduled for routine cataract surgery. Variation was more for higher adds and less for lower adds.
The study was designed to predict the add-power shift due to ocular biometry differences in pseudophakic eyes using raytracing simulations in model eyes created for each patient. Each model featured a biconvex lens with radii of curvature adjusted for best distance vision. Then, the team placed trial glasses with a vertex distance of 12 mm. They calculated the
required IOL power change to induce a desirable near-to-intermediate effect relative to the distance power.
“There is a nearly linear relationship between the ACD and the add power demand,” Dr Łabuz reported. The R2 value was 0.96, he said. By contrast, axial length differences show only a low correlation with add power required to achieve a desired reading distance—an R2 value of 0.096—while keratometry differences show no correlation at all.
There is a nearly linear relationship between the ACD and the add power demand.
“When you implant a multifocal lens in a patient with shallower ACD [as in many hyperopes], a lower add power may be required to prevent their reading distance from being too close to the eye,” Dr Łabuz said. “In contrast, a higher power add may be needed in patients with deeper anterior chambers. For instance, in myopes, who are often used to reading at closer distances.”
Dr Łabuz presented his study at the 2023 ASCRS annual meeting in San Diego, US.
Grzegorz Łabuz PhD is senior optical scientist at the David J Apple Center for Vision Research and research fellow at Heidelberg University Hospital, Heidelberg, Germany. grzegorz.labuz@med.uni-heidelberg.de
Materials & Methods
• Each model featured a biconvex lens with radii of curvature adjusted for best distance vision. Then, trial glasses were placed with a vertex distance of 12 mm Material & Methods
Each model featured a biconvex lens with radii of curvatire adjusted for best distance vision. Then, trial glasses were placed with a vertex distance of 12 mm
The required IOL-power change to induce a desirable near/intermediate effect at the spectacle plane was calculated with respect to the far-point condition
• The required IOL-power change to induce a desirable near/intermediate effect at the spectacle plane was calculated with respect to the far-point condition
Democratised Cataract Surgery on the Horizon
Mechanical cataract disassembly device could largely supersede ultrasound.
HOWARD LARKIN REPORTS
For more than 30 years, phacoemulsification has been the dominant cataract extraction method in developed countries. Now a new technology is on the horizon that could largely replace it in wealthy as well as lower- to middle-income countries.
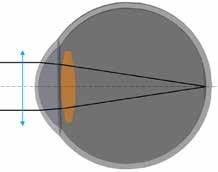
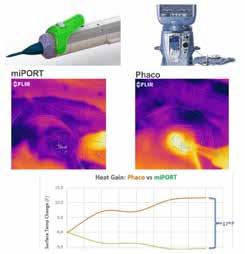
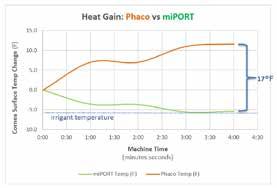
MICOR 700 (Zeiss) is a mechanical lens fragmentation and aspiration device capable of gently removing cataracts without potential tissue damage due to cavitation and heat rise of phaco ultrasound. It uses gentle mechanical agitation for nuclear disassembly and low fluid flow for extraction, maintaining a stable chamber. A blunt tip is more “protective” against capsular bag and iris damage than the traditional phacoemulsification needle tip.
“It reaches a new level of safety with no ultrasound energy,” Dr Elizabeth Yeu said.
All in your hand
The entire low-energy, self-contained device—including its peristaltic pump—fits in hand, requiring only an external fluid connection. The device is controlled entirely by a button on the disposable extractor with no foot pedal required.
Surgeons can use MICOR 700 with the same small incisions as phaco. With its pump just 20 mm from the eye, vacuum changes are instantaneous with virtually no surge, immediately pulling lens fragments into the cutting tip. Enhanced chamber stability allows surgeons more time deeper in the sulcus plane (to even the capsular bag) for nuclear disassembly, said Dr Yeu, who has done more than 200 cases with the device.
In tests and pilot releases, MICOR has demonstrated similar, or better, surgical performance to phaco in nuclear cataracts up to about grade 3.5, Dr Yeu said.
“When you watch the clinical videos, it looks like we’re performing modern, at [its] best, phacoemulsification. … I just didn’t think there was anything that could be more disruptive that does not use ultrasound.”
Lower cost, quicker turnaround
While clinical effectiveness may be similar, MICOR beats phaco in cost and operational efficiency, Dr Yeu said. Because it requires no elaborate console, MICOR requires no periodic capital investment for a phaco console or upgrade and has a smaller operating room footprint. Similarly, maintenance and downtime costs decrease.
The tip of the handpiece is disposable and can be changed in a few seconds, greatly shortening set-up, breakdown, and sterilisation time and costs, Dr Yeu noted. In a test, MICOR set up for surgery in two to three minutes quicker than phaco,
allowing faster OR turnaround between cases. Its disposables and packaging were far less bulky, requiring minimal to no sterilisation and less material waste.
“Our surgical technicians are no longer dishwashers,” she said, adding that combined with reduced nuclear disassembly time, the system shaves upwards of three minutes off each procedure in overall room time.
Such cost and operational efficiency will be of ever greater value in helping a declining supply of cataract surgeons cope with rapidly rising demand, and the rise of immediate sequential bilateral procedures, Dr Yeu said. It will also help democratise small-incision cataract surgery technology by making it more affordable and practical in developing countries.
“This [technology] is absolutely primed for global outreach.”
Dr Yeu described the new device at the Innovators Session of the 2023 ASCRS annual meeting in San Diego, US.
Elizabeth Yeu MD is an ophthalmologist in private practice at Virginia Eye Consultants and an Assistant Professor of Ophthalmology at the Eastern Virginia Medical School in Norfolk, Virginia, US, and President of the ASCRS. eyeulin@gmail.com
The MICOR tip generates no heat The Phaco tip generates heat
MICOR 700 Phaco
Is FLACS Worth the Cost?
Femto laser-assisted cataract surgery compared to PCS may not yet justify reimbursements.
TIMOTHY NORRIS REPORTS
Twelve years since its introduction, femto laser-assisted cataract surgery (FLACS) is still struggling to par with the cost-effectiveness of the reliable and standardised phacoemulsification cataract surgery (PCS), making it difficult to justify funding by private and public healthcare system reimbursements.
Today, many enthusiastic advocates praise the clean, elegant, and precise FLACS, enabling fast and easy high standard capsulotomies and the potential to improve postoperative refractive outcomes. While recognising the undeniable slow adoption rate, many consider FLACS a great option for their future clinical practice. However, the initial promise of replacing PCS as the primary choice worldwide has never really fulfilled, instead placing it at risk of losing the race against its standardised counterpart.
The femtosecond laser-assisted versus phacoemulsification cataract surgery (FEMCAT) study published in 2020 concluded that considering the higher costs, the femtosecond laser-assisted procedure does not provide an advantage over conventional PCS.1
More recently, a preplanned cost-utility secondary analysis of the FEMCAT trial went deeper into the issue of the cost-effectiveness of FLACS on a 12-month time horizon, thoroughly evaluating the micro-costing and utility of both procedures. The authors concluded that in its current state, FLACS is “not cost-effective and should not be reimbursed by healthcare systems,” pointing to investment in research and development as the only worthwhile option for its future.2
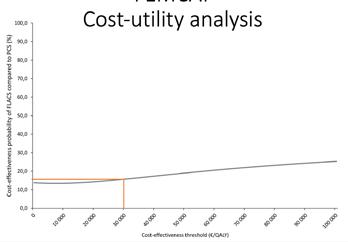
Study results showed that the Institute for Clinical and Economic Review (ICER) of FLACS compared to PCS was not within the €45,000 to €89,000 per QALY range frequently cited as cost-effective, confirming the FEMCAT trial findings.
“We showed in the FEMCAT study that the direct cost of cataract surgery was [more than] €500 in the FLACS group, with only a small health benefit for patients compared to the PCS group,” Dr Cedric Schweitzer, first author of the FEMCAT study, said in an interview for EuroTimes.
“We found the cost-effectiveness priority of FLACS compared with PCS phaco did not exceed 15% for a cost-effectiveness threshold commonly recognised in Europe at €30,000 per QALY gained.”
He reaffirmed more research and development will be required to narrow the gap between the two procedures, improving FLACS’s effectiveness and lowering the costs.
“FLACS is a ground-breaking technology, and despite being still in its infancy stage, it is already at par with its much older counterpart in efficiency. Overall, the results of the FEMCAT trial and secondary cost-utility analysis are not negative for the femtosecond laser-assisted cataract surgery, but the quantitative information on the added benefit for patients and
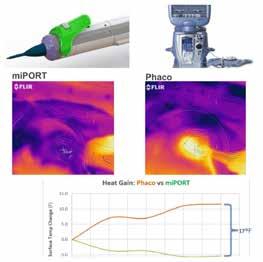
FEMCAT
Cost-utility analysis
Cost-effectiveness acceptability curve, representing the cost-effectiveness probability of FLACS according to cost-effectiveness thresholds ranging from 0 to 100,000 €/QALY The cost-effectiveness probability of FLACS compared to PCS was 15.7% for a cost-effectiveness threshold of 30000 €/QALY and the cost-effectiveness probability of FLACS varies very little: from 14% to 25%
the additional direct and indirect cost of each procedure can be invaluable for all the actors involved,” he said.
“We still need further improvements—both in surgical technology and IOL design—if we want to translate the very precise cut of femtolaser into solid clinical benefit.”
In an invited commentary on the secondary analysis, Professor Oliver D Schein stated that, given the findings of his French colleagues, “it remains unlikely that FLACS in its current incarnation would be funded by federal or private insurers in the US.”3
Ironically, if those insurers did cover it, the rate of FLACS procedures would fall dramatically in the country, he pointed out. “From the perspective of the surgeon, an extra $300 per case would probably not justify the extra time and expense of FLACS, especially in the known absence of clinical benefits.”
Finding an agreement between stakeholders about direct and indirect costs may very soon become necessary to avoid such a negative scenario.
“By measuring the cost of each surgical procedure, we provided valuable information [available] to develop a suitable economic model for this technology,” Dr Schweitzer said.
With the results of these studies, “each company and decision maker can play on the price of each part of the surgery to narrow the gap and make FLACS a better choice than PCS,” he concluded.
For citation notes, see page 40.
Cedric Schweitzer MD is a professor of ophthalmology at the University of Bordeaux, France. cedric.schweitzer@u-bordeaux.fr
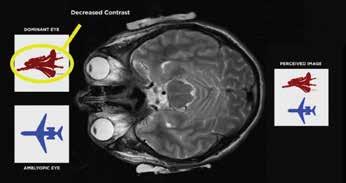
A New “Ground-Breaking” Treatment for Amblyopia
Dichoptic therapy could improve visual acuity and stereopsis. PRISCILLA LYNCH REPORTS
Aspecialised “brain-training” computer program has emerged as a highly effective treatment for correcting amblyopia and improving vision, even in adult eyes, according to Dr Arthur Cummings.
“Dichoptic therapy for amblyopia is absolutely game-changing,” he told EuroTimes. “The way it works is fascinating yet very simple, but it is a very big paradigm shift for people to understand.”
The company Bynocs, for which Dr Cummings is an advisor, has created a vision therapy software programme (AmblyGo) to treat amblyopia in the form of tailored computer games. The patient plays the games with both eyes open while wearing special 3D anaglyph glasses (with different colour lenses) for 30 minutes over 30 sessions.
“We’ve seen remarkable results not only in improving vision in the lazy eye, but also in the brain using both eyes together,” he said.
How it works
Traditional treatment for “lazy eye” involves patching the “good eye” in younger children for months or years. Atropine drops are another means of occlusion therapy. A landmark study by the Pediatric Eye Disease Investigator Group (PEDIG) showed as little as two hours of patching a day, or atropine drops during the weekend, were as effective as more intensive therapy.1
Until now, untreated or unsuccessfully treated adults with amblyopia had no option to improve vision in either eye, as procedures like laser eye surgery remained unavailable due to the risk of damaging vision in the dominant eye, Dr Cummings noted.
However, this is no longer the case with the advent of dichoptic treatment—a visual training process involving the presentation of simultaneous and separate visual stimuli to both eyes.
We’ve seen remarkable results not only in improving vision in the lazy eye, but also in the brain using both eyes together.
The Bynocs vision therapy software presents the contrast-adjusted images to the two eyes, with the dominant eye receiving an image of lesser contrast than the amblyopic eye. For possibly the first time ever, the brain receives an equal image from the two eyes during the therapy, encouraging it to use both eyes at the same time.
This contrast differentiation removes the interocular suppression in the ocular dominance columns in the amblyopic eye, resulting in a sustained visual gain. The neuroadaptive treatment is non-invasive, safe, and very effective, Dr Cummings said.
Research data
Dr Cummings outlined the results of 45 amblyopia patients treated in his clinic with dichoptic therapy, with an age range of 13 to 65 years, noting this age group would not have had any therapy or treatment available to them previously.
Visual acuity and stereopsis were measured before and after a six-week duration of dichoptic treatment.
Of the 45 patients, 20 had anisometropic amblyopia (the category of amblyopia that does best with dichoptic therapy)—13 had no stereopsis prior to therapy and 11 developed stereopsis during. Seven patients had some stereopsis before therapy, and all improved their stereopsis. Patients gained between 3 and 5 lines of CVDA in the amblyopic eye.
The results show dichoptic therapy is very effective in improving visual acuity and stereopsis in adult amblyopia, especially when caused by anisometropia, Dr Cummings said.
“It is very exciting. Ideally, within 10 to 15 years, this will be the definitive treatment for amblyopia in children, too, once the success in adults becomes more common knowledge. Why would a child not rather play a video game than wear a patch?”
Dr Cummings presented his findings at the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
For citation notes, see page 40.
Arthur B Cummings MD, FRCSed, FWRCS is Medical Director at the Wellington Eye Clinic, Dublin, Ireland. ABC@WellingtonEyeClinic.com
Stent-less Glaucoma Surgery
Expanded indications sought for minimally invasive technology.
Aminimally invasive device that creates a stent-less aqueous drainage channel into the subconjunctival space for treating moderate to severe glaucoma is now under development for two new indications; rescuing failed trabeculectomies in severe glaucoma and opening passages to Schlemm’s canal for mild cases.
Successfully launched at the 2023 ESCRS Congress, the Sanoculis Minimally Invasive Micro Sclerostomy® (MIMS) device is now available in several countries, including Germany and Spain.
“The market reception was great,” said Nir Israeli, who is now working to set up a clinical trial for US approval by the Food and Drug Administration (FDA).
Performed through the anterior chamber, MIMS involves injecting viscoelastic into the sub-Tenon’s space to expand a gap for the instrument to protrude into and create a channel for aqueous to drain into the nasal subconjunctival space, where it is absorbed by surrounding blood vessels.
The MIMS instrument is then inserted into the anterior chamber through a side port to the angle, where a trephine extends about 2.5 mm, cutting a drainage channel through to the subconjunctival space, and withdraws automatically, along with the cylinder of sclera-corneal tissue removed. The procedure takes two to three minutes.
IOP and meds reduced
Israeli presented three-year follow-up data on 120 MIMS cases, including 20 combined with cataract surgery. Mean IOP reduced from 27.9 mmHg at baseline to 17.3 and 17.4 mmHg at one and three years, respectively, for a 38% reduction. Over the same periods, the mean number of topical glaucoma medications used declined from 1.80 at baseline to 0.27 at one year for an 85% reduction and 0.53 at three years for a 71% reduction.
The percentage of MIMS patients seeing IOP reductions of at least 20% without increasing medication use, which is the FDA’s success threshold, was 81.1% at one year and 57.1% at three years. By contrast, trabeculectomy achieves 72.7% success
at one year and 64.4% at two years, and the PreserFlo stent (Glaukos) 54.7% and 50.6% at one and two years, respectively.
The results suggest drainage channels remain patent for at least three years without a stent, and OCT imaging bears that out. Israeli showed scans of a patient with 32 mmHg at baseline, reduced to 14.0 mm at one year and 14.5 mm at three years with no topical medications. The drainage channel and subconjunctival bleb are clearly visible on OCT scans at both follow-ups.
Expanded indications
For treating failed trabeculectomies, the sclerostomy and bleb are positioned inferonasally. When used experimentally to create channels to Schlemm’s canal, a procedure dubbed “MINT™” for minimally invasive nasal trabeculostomy, the Sanoculis device trephine extends about 0.5 mm to cut five holes in the trabecular meshwork.
An interim analysis of an ongoing study involving 82 MIMS inferonasal patients showed mean IOP reduced by 23% and medication use by 34% from baseline at nine months follow up, Israeli reported. In 66 patients receiving standalone MINT, IOP was reduced by 30% and meds by 82% at nine months, which compares favourably with competing stent solutions.
“The two new indications expand our market to address all glaucoma patients who need surgery with the same stentless technology for all indications—from mild to severe,” Israeli concluded.
Nir Israeli presented at the Eyecelerator event at ASCRS 2023 in San Diego, US.
Nir Israeli MBA is co-founder and CEO of Sanoculis LTD, Kirat Ono, Israel. nir@sanoculis.com
HOWARD LARKIN REPORTS
OCT-Guided Femto-Trabeculotomy
Laser system provides clear angle view for non-invasive precision incisions.
HOWARD LARKIN REPORTS
Anew laser system now in development promises a non-invasive and more precise way to create trabeculotomy incisions without damaging adjacent tissues.
The ViaLase FLigHT (Femtosecond Laser High-precision Trabeculotomy) procedure combines the micron accuracy of optical coherence tomography (OCT) imaging guidance with the precise cutting of a femtosecond laser to non-invasively create trabeculotomy incisions near collector channels in all four quadrants of the angle. The system also incorporates a novel high-definition camera and illumination arrangement to clearly visualise the trabecular network, covering 360 degrees without a traditional gonioscope lens.
“It gives some of the best imaging we’ve seen to help guide surgery,” said Dr Thomas W Samuelson.
The device is docked to the eye using a single-use disposable curved lens that minimises cornea applanation, increasing patient comfort and physician visibility, Dr Samuelson added. It also allows the surgeon to cut several precisely sized channels without redocking.
It gives some of the best imaging we’ve seen to help guide surgery.
The visualisation and OCT system may also be used in other glaucoma surgeries to find outflow channels for placing stents and teaching residents, said Dr Richard A Lewis.
Reduced IOP
First-in-human studies show the incisions remain patent without signs of scarring or other tissue reactions visible on either the system’s on-board camera or OCT 24 months after surgery, Dr Samuelson said.1 The initial 18 patients receiving a single channel treatment of 500 x 200 microns showed a mean reduction in intraocular pressure (IOP) of 34.6% at 24 months with no serious adverse events at any point after surgery. Overall, 82% of eyes achieved more than 25% IOP reduction, and 53% achieved 25% or more.
“The 24-month first-in-human trial demonstrates excellent safety and durable IOP reduction,” Dr Samuelson said.
Asked how the FLigHT procedure outcomes might compare with selective laser trabeculoplasty (SLT) as an office-based glaucoma treatment, Dr Samuelson said the technology would have to show better efficacy to justify its use.
82%
Overall, 82% of eyes achieved more than 25% IOP reduction.
“It’s going to be a high bar to overcome SLT as the initial procedure since SLT is a step less invasive, but this is an incredibly non-invasive way to cut 500 x 200-micron channels.”
The initial registration plan is to standardise the technology on a single channel. Tests to determine the efficacy of cutting more than one channel are underway, but he said the numbers are too small to tell for sure if it increases efficacy.
ViaLase is conducting studies to register the FLigHT procedure and its related devices for both the European CE mark and US FDA clearance.
Dr Samuelson presented at the Eyecelerator at the 2023 ASCRS annual meeting in San Diego, US.
For citation notes, see page 40.
Thomas W Samuelson MD is an ophthalmologist at Minnesota Eye Consultants and associate professor at the University of Minnesota, both in Minneapolis, US. twsamuelson@mneye.com
Richard A Lewis MD is an ophthalmologist in Sacramento, California, US, who pioneered minimally invasive glaucoma surgery (MIGS) and is a past president of ASCRS and the American Glaucoma Society. He also works part-time as the Chief Medical Officer for ViaLase. rlewiseyemd@yahoo.com
Better Monitoring with Less Testing
Drive-through IOP monitoring clinic proves successful alternative to in-hospital visits.
PRISCILLA LYNCH REPORTS
A“drive through” intraocular pressure (IOP) screening clinic used during the COVID-19 pandemic proved an effective and safe method of monitoring glaucoma patients and has provided the evidence to support more efficient patient monitoring using less testing.
Dr Emer Doolan discussed the results of a study she and her colleagues conducted to assess the outcomes of glaucoma patients who attended the drive-through clinic.
“We found that once we extracted the patients [needing urgent care], a huge volume was very stable and absolutely fine in terms of their IOP,” she said. “For monitoring them going forward, we could save a lot of man-hours by just doing a simple IOP measure at every visit rather than the whole range of tests at every visit.”
An Irish hospital launched the drive-through IOP monitoring clinic as an alternative to in-person visits for glaucoma patients during the pandemic. Suitable glaucoma patients from the Royal Victoria Eye and Ear Hospital (RVEEH), Dublin, were invited to attend the drive-through clinic for an IOP measurement with an iCare tonometer while they remained in their cars.
We found that once we extracted the patients [needing urgent care], a huge volume was very stable and absolutely fine in terms of their IOP.
522
A total of 522 glaucoma patients attended the drivethrough clinic over one year.
92%
Of this cohort, 479 (92%) have since attended review at RVEEH.
Results
A total of 522 glaucoma patients attended the drive-through clinic over one year, from August 2020 to July 2021. Of this cohort, 479 (92%) have since attended review at RVEEH.
In a subgroup of 208 patients originating from the virtual glaucoma clinic, 14 (7%) had visual field progression recorded, 24 (12%) required a change in topical treatment, 4 (2%) required laser treatment, and 2 (1%) required surgical intervention.
Comparatively, a similar cohort attending the virtual glaucoma clinic in 2019 had visual field progression in 3%, required a topical treatment change in 5%, laser intervention in 1%, and surgical intervention in 1%.
In summary, the study shows a drive-through IOP monitoring clinic was a safe alternative to hospital attendance during the COVID-19 pandemic, Dr Doolan said. There has been a low rate of visual field progression and a need for surgical intervention in attendees, with the latter comparing favourably with a typical year of attendance for stable glaucoma patients. Where urgent intervention was required, these patients were identified early due to the efficient use of electronic medical records and timely review of results.
Staff also recorded results from a short patient questionnaire, including subjective issues with their eyes and compliance with current treatment. Ophthalmologists then reviewed the results in the electronic medical records before deciding the appropriate follow-up.
The follow-up clinic visit noted a Goldmann IOP (GAT), presence of visual field progression, and any management changes. A subgroup of stable glaucoma patients who ordinarily attend the “virtual” glaucoma clinic (an in-person clinic where a nurse records GAT, visual fields, and disc photographs, later interpreted by an ophthalmologist) was analysed and compared to a cohort of patients attending the same service pre-pandemic.
Based on the findings, she suggested monitoring stable patients’ IOP with iCare instead of GAT may be suitable in the virtual clinic setting, so nurses and technicians would not need training to carry out GAT. This way, more stable patients would be seen in the virtual clinic, alleviating the burden on service overall.
Dr Doolan presented her research during the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
Emer Doolan MB, BCh, BAO, MRSCI is an ophthalmology trainee at the Royal Victoria Eye and Ear Hospital, Dublin. emerdoolan@gmail.com
Patient Monitoring Post-Laser Capsulotomy
Study supports deferring follow-up for most patients.
CHERYL GUTTMAN KRADER REPORTS
Only select patients with glaucoma may warrant follow-up after Nd:YAG laser capsulotomy for a check of their intraocular pressure (IOP), advised Dr Oscar Chen, based on the findings of a recent retrospective study.
The study investigated rates of post-capsulotomy complications and potential risk factors in a contemporary cohort of 1,214 patients seen at an academic teaching clinic or attending a private office within 90 days after capsulotomy. The results showed that sight-threatening complications were rare. Elevation in IOP, defined as a change in IOP from <21 mmHg pre-capsulotomy to >25 mmHg post-capsulotomy, was the most common complication (0.82%). Further analysis showed the risk of developing a post-procedural IOP elevation increased significantly among patients with glaucoma.
“Although Nd:YAG laser capsulotomy is a safe and effective procedure, complications can occur. Available studies on this topic, however, are mostly outdated and have generated some conflicting results. Furthermore, there appears to be heterogeneity among providers in post-procedural monitoring,” said Dr Chen.
“Based on our findings, we recommend that patients with glaucoma warrant a post-procedure IOP measurement. Otherwise, considering Nd:YAG laser capsulotomy is associated with a low rate of complications, we believe most patients can be counselled about the signs and symptoms of post-procedural complications and told to contact their physician if they have any concerns.”
The study methods involved a chart review to extract clinical data in addition to the complications, including patient demographics, prior ocular history, visual acuity, IOP, and refractive error. Information was also collected on Nd:YAG laser settings (number of spots applied, energy used) and training level and practice location of the individual performing the capsulotomy.
The analyses showed no significant change in refractive error after capsulotomy. Aside from elevation in IOP, the recorded complications included cystoid macular oedema (0.65%), anterior uveitis (0.58%), macular hole (0.33%), corneal oedema (0.25%), retinal detachment (0.16%), and retinal tear (0.08%).
“There were no statistically significant associations between any of the latter complications and training level of the proceduralist, clinic, patient sex, or laser parameters,” Dr Chen observed. “The rates of retinal detachment and tear in our study were lower than those associated with cataract surgery.”
Economic and access implications
Dr Chen told EuroTimes he was motivated to conduct the study, in part, because of his interest in healthcare economics.
“One topic that I am passionate about is eliminating unnecessary healthcare expenditures and streamlining clinical practices. Healthcare expenditure is a huge problem in the US for payers, providers, and patients. One approach that can help to address this issue is to remove routine visits that benefit neither the patient nor the clinic,” he said.
“By eliminating routine post-Nd:YAG laser capsulotomy appointments that require a dilated fundus exam, we decrease the burden on patients and the healthcare system and thereby open up appointment times for patients in need of ophthalmic care.”
Dr Chen presented his research at ARVO 2023 in New Orleans, Louisiana, US.
Oscar Chen MD is a resident in the department of ophthalmology, Rush University Medical Center, Chicago, Illinois, US. oscar_chen@rush.edu
Periocular Cancer Treatment: From Control to Prevention
Confronting the enormous burden of eye cancer.
DR CLARE QUIGLEY REPORTS
An enhanced understanding of the aetiology of common eye cancers is leading to new treatments and diagnostic techniques, according to Dr Michèle Beaconsfield, who delivered the inaugural Richard Collin Lecture at the European Society of Ophthalmology (SOE) meeting in Prague.
“Of course, we’ve known about skin cancer as long as we’ve been alive,” Dr Beaconsfield said. “The first written documentation of skin cancer [was in] Egyptian papyri from around 2500–3000 BC.”
She observed how basal cell carcinoma (BCC), the most common skin cancer, was first described in 1827 by Arthur Jacob—an Irish ophthalmologist who coined the term “rodent ulcer” to illustrate the slow-growing cancer. Jacob had written in the journal Dublin Hospital Reports that a rodent ulcer has characteristic features of “slowness of its progress, the peculiar condition of the edges and surface of the ulcer, the comparatively inconsiderable suffering produced by it, its incurable nature unless by extirpation, and its not contaminating the neighbouring lymphatic glands.”
Noting the current European incidence of nonmelanoma skin cancer approaches 150 per 100,000 annually, she said, “The European incidence of nonmelanoma skin cancer is enormous. The health burden on health systems is enormous. Clinicians like us have warned that this is getting worse.
“Eighty percent of basal cell carcinomas occur on the head and neck, and 20% of those are palpebral, so overall, of the [most common] cancer worldwide, we look after about 16%.”
Surgery remains the gold standard for eradication, Dr Beaconsfield said. Basal cell carcinoma presentations at an advanced stage or in patients unfit for surgery present difficul-
ties—even today. However, alternative treatment approaches, previously limited to radiation therapy or palliation, have recently become available, thanks to progress in the understanding of the dysregulated growth pathways and immune surveillance that may lead to skin cancer development.
One important growth pathway is the Hedgehog signalling pathway (Hh). Experiments with drosophila flies led to an understanding of the importance of this pathway in body segmentation during development. Dr Beaconsfield explained how the Hh pathway in adults regulates growth and repair in response to tissue injury. The Hedgehog pathway can be used in cancer cells to contribute to abnormal cell overgrowth.
This same growth pathway is associated with basal naevus syndrome, also known as Gorlin syndrome, a rare autosomal disorder characterised by the development of multiple basal cell carcinomas from a young age.
“In the majority of cases, it is a defect in this particular gene—chromosome 9q—and does not produce a normal Patched protein,” Dr Beaconsfield said.
The normal inhibitory action of Patched is missing from the Hedgehog pathway, leading to an abnormal overgrowth signal to cells, which she said results in unrestrained growth of basal cell carcinomas. Thus, the pathway presented a potential target for molecular inhibition of basal cell cancer development.
Wildflower and dying lambs
Our understanding of cancer’s molecular basis has not always progressed in a straightforward, stepwise manner. Dr Beaconsfield explained initial scientific interest in the Hedgehog pathway involved targeting it in cancer, which, regrettably, was unsuccessful. Finally, a breakthrough came
from a report in veterinary science. Unfortunate freak events were recurring in Idaho, United States, in the 1950s. Lambs were born with severe, often deadly, congenital deformities. The lambs had cyclopia, in addition to other cranial defects, that caused feeding and respiratory problems. In-depth investigation, including by federal authorities, revealed the ewes had consumed Veratrum californicum while pregnant. Analysis of the wildflower found it contained the alkaloid chemical cyclopamine.
Researchers subsequently discovered cyclopamine mediated teratogenic effects in the lambs by downregulating the Hedgehog pathway before finally uncovering a naturally occurring antagonist to the Hh pathway. Unfortunately, it was too toxic for clinical use. Further refinement of cyclopamine ultimately led to the development of vismodegib and sonidegib. These groundbreaking medications reversed basal cell carcinoma growth and caused tumours to shrink, though they carry a significant side effect profile. They are not active against all basal cell carcinomas, as different growth pathways may be active in different tumours.
Dr Beaconsfield emphasised the importance of immunosurveillance in cancer cell inhibition, as cancer cells can escape the immunosurveillance by host immune cells
through various means. Augmenting the immune response to cancer has become a major therapeutic target, particularly in deadly melanoma.
She added more and more drugs are coming online “to the extent that in the last five years alone, 2,000 agents have come on the market for investigation.” Combining different drugs can have an additive effect, especially useful in metastatic melanoma.
But ideally patients should not get to the stage of having advanced metastatic disease—rather, diagnosis should be at the earliest asymptomatic stages.
“The Galleri test is about to come on the market now,” Dr Beaconsfield said. “It detects early cancers.”
This intriguing device, predicted to come on the market in 2024, will detect about 50 cancers at their very earliest preclinical stages via liquid biopsy (i.e., a blood draw). The test is not perfect but represents a further progression in cancer management.
Dr Beaconsfield has had a long career in oculoplastic surgery. She set up the eyelid oncology service in Moorfields Eye Hospital, London, where she first took up a consultant oculoplastic surgeon post in 1991. mb@consultan tsee.co.uk
The Gamechanger for ophthalmic surgeons
Thanks to the streamlined measurement workflow and application-oriented overview screens you further improve your time efficiency. Plus, with tons of studies and a huge user community to support data validity, you are always on the safe side. Optimized workflows, satisfied patients and best possible clinical results are all achieved quickly and reliably and without long training periods.
No risk, just fun – the Pentacam® AXL Wave
www.pentacam.com/axl-wave
Controlling Keratoconus Risk
Study suggests risk reduction strategies may help stabilise disease.
HOWARD LARKIN REPORTS
Risk factor control—including avoiding eye rubbing and high-risk sleep positions—and treating allergic eye disease may be an effective primary intervention in reversing or stabilising keratoconus, according to a small study conducted by Dr Luke C Northey, Dr Tanya Trinh, and Dr Greg Moloney.
The retrospective non-consecutive case series study involved 11 eyes of 7 patients observed to have disease stabilisation or improvement after conservative intervention focusing on risk factor control.
After an assessment to identify risk factors, patients were counselled on changing behaviour to avoid mechanical factors such as daytime eye rubbing and sleeping prone or on their sides. Patients unable to avoid side or prone sleeping were prescribed protective eyewear or modified pillows for use when sleeping. Patients were also treated for allergic eye diseases to reduce eye rubbing due to itching and watering.
Eligibility criteria included a keratoconus diagnosis based on clinical examination and corneal tomography followed for at least six months. Patients underwent serial clinical examination, visual acuity (VA) assessment, and Scheimpflug corneal tomography as part of their follow-up. The study recorded changes in best corrected visual acuity (BCVA), thinnest corneal thickness (TCT), steep keratometry (K2), Kmax, and Kmean. Mean patient age was 28.1 ± 12.8 years; 6 were male—5 were affected on the right eye and 6 on the left.
Eye rubbing was the most common risk factor, affecting 6 patients—3 slept prone, 1 on the side, and 5 had allergic eye disease or atopy.
Stabilisation
At baseline, mean BCVA was 0.26 ± 0.35 logMAR with a median of 0.06, ranging from 0 to 1. Mean TCT was 427.64 ± 67.88 microns, ranging from 295 to 505 microns. Mean K2 was 55.93 ± 14.32 D, ranging from 45.10 to 77.10 D; mean Kmean was 57.03 ± 13.24 D, ranging from 44.00 to 75.90 D; and mean Kmax was 63.43 ± 16.35 D, ranging from 46.60 to 87.80 D.
At 6 and 12 months, there was no significant decline in mean BCVA, Dr Northey reported. Mean TCT decreased slightly at both intervals but not significantly. Mean K2, Kmean, and Kmax also declined slightly but not significantly at 6 months and appeared to stabilise between 6 and 12 months.
Study limitations included a small, non-consecutive sample with no control group, a limited follow-up period, and instrument repeatability at high K values, Dr Northey said, adding the results also may not hold for higher keratoconus severity.
Still, modifying and managing risk factors is important in stabilising appropriate patients, Dr Northey concluded.
“We encourage people to further investigate the effect of risk factor control on keratoconus management.”
Dr Northey presented at the 2023 ASCRS annual meeting in San Diego, US.
Luke C Northey MBBS(Hons), MMed(Ophth Sc), MPH, FRANZCO is an ophthalmologist at the Sydney Medical School of the University of Sydney, Australia. luke.northey@sydney.edu.au
TABLE. Visual acuity and corneal pachymetry outcomes
We are a society of surgeons who specialise in improving vision and restoring clarity. Since 1991, ESCRS has promoted the education and research of implant and refractive surgery. With more than 7,500 members from 130 countries worldwide, ESCRS is a vital global platform for the field of ophthalmology.
AI Useful in DME Detection?
Deep learning algorithm performed well in early study.
PRISCILLA LYNCH REPORTS
An artificial intelligence (AI) deep learning algorithm has proven “very accurate in the detection of diabetic macular oedema (DME)”, which could have implications for screening programmes worldwide, an Irish researcher said.
“The key message [from my research] is we can apply AI in OCT [optical coherence tomography] scan analysis, and it works very well. It could be used in triage, an automated screening setting, or other community-based settings to get the most urgent cases into hospital,” said medical student Cathal Breathnach. “Eye clinics are very busy places—they are overcrowded, and some referrals do not need to be there. Using OCT and applying this type of automated AI-driven software in DME screening, we could streamline the most urgent referrals and hopefully deliver more efficient care to patients.”
DME is reliably detected using OCT, and deep learning algorithms can successfully detect retinal pathology from OCT scans. Breathnach and colleagues tested the feasibility of using such a deep learning algorithm for DME detection.
Anonymised OCT images were retrospectively obtained from 950 patients at University Hospital Galway in Ireland. Taken at the foveal level, a consultant ophthalmologist graded the images to classify the DME level present on a novel scale (Normal, DME not affecting the foveal contour, and DME affecting the foveal contour).
A deep learning algorithm was validated using cross-validation and then evaluated on an additional test data set. A second ophthalmologist graded the test set for comparison.
In detecting the presence of DME, the algorithm achieved an average accuracy of 94.34% on cross-validation and an accuracy of 92.5% on the test data set, compared to the first
ophthalmologist. The algorithm detected DME with an accuracy of 87.9% compared to the second ophthalmologist.
When detecting the DME class, the algorithm achieved an average accuracy of 89.3% on cross-validation and an accuracy of 86.6% on the test data set compared to the first ophthalmologist. The algorithm detected the DME class with an 80.0% accuracy compared to the second ophthalmologist.
This study showed promising results for deep learning use in detecting DME, particularly for those with the most severe, sight-threatening disease, Breathnach said. Further data, an increased number of graders, and model refinement may further increase the performance, he added.
The study adds to the increasing body of knowledge on AI use in ophthalmology, which is important to ensuring a robust evidence base and gaining patient trust in this technology, Breathnach said.
“AI programs are going to be a very useful future tool for ophthalmologists in making the best clinical decisions,” he said. “It will not replace us—it will assist and ultimately lead to more efficient patient care. There is a lot of development happening—it is a very exciting time—but there is still a considerable amount of work before we have it fully regulated and integrated into practice.”
This research was presented during the Irish College of Ophthalmologists 2023 annual conference in Killarney, Ireland.
Cathal Breathnach is a final-year medical student at the University of Galway, Ireland. breathnach.cathal@gmail.com
https://escrs.org/special-interest-groups/yos/
FS-LASIK FOR THE TREATMENT OF MODERATE TO HIGH HYPEROPIA
In the latest episode of the ESCRS Eye Journal Club, Dr Artemis Matsou and Dr Myriam Boehm discussed a JCRS study by Alió del Barrio (et al.1) with guest speakers Professor Paolo Vinciguerra and Dr Florian Kretz, who provided valuable insights on managing moderate to high hyperopia with femtosecond LASIK (FS-LASIK).
Despite the advancements in FSLASIK and modern excimer laser platforms, LASIK for hyperopia up to +7.00 dioptres (D) remains underutilised among refractive surgeons. One reason is the technically more challenging technique required to correct such high hyperopic prescriptions (larger peripheral ablations, necessitating larger flaps on smaller diameter corneas). Also, there is a lack of consistent scientific evidence supporting LASIK for this range of hyperopia, with varying outcomes across different excimer laser platforms. In addition, managing latent hyperopia to minimise the risk of postoperative ciliary spasms and patient dissatisfaction is a considerable challenge, making refractive lens exchange (RLE) with multifocal intraocular lens implantation for young nonpresbyopic hyperopic patients the commonly preferred and recommended method for this group.
In this retrospective single-centre study, the authors included 92 eyes of 64 patients who underwent FS-LASIK for moderate to high hyperopia (≥3.50 D and ≤6.50 D), using a Visumax 500 kHz femtosecond laser and an Amaris 750 excimer laser. The study reported favourable outcomes for FS-LASIK with an efficacy index of 0.91 and 0.90 at 6 months and 36 months, respectively.
The safety index was 1.00, showing a low incidence of complications. Impressively, 72% of patients achieved UCVA of 20/20 or better, and 80% had a postoperative spherical equivalent within 0.50 D. However, researchers observed a slight but significant regression at 36 months. At this point,
21.73% of patients required a flap lift for laser enhancement, and 11.95% needed orthoptic visual rehabilitation for self-resolving accommodative spasms not resolving on their own.
Prof Vinciguerra commented on the study’s robust design, highlighting its strength in using a laser platform capable of tracking the visual axis versus the pupil. This feature is particularly important in hyperopic patients with a large angle kappa, as tracking the visual axis minimises the risk of decentred ablations that can lead to high-order aberrations, coma, and suboptimal vision. Large optic zones (average 6.76 ± 0.22 mm) enabled the correction of high hyperopic prescriptions, contributing to the study’s overall success. These underscore the significance of advanced laser technology in optimising outcomes of FS-LASIK for moderate to high hyperopia.
Dr Kretz also stressed the importance of large-diameter flaps and optic zones in achieving favourable outcomes in hyperopic LASIK, sharing his preference for even thinner femto-flaps, around 90 microns, as he has seen a lower incidence of microfolds that would require early flap replacements (3.26% of patients in this study). He also noted RLE still exhibits a higher degree of safety for hyperopic patients, particularly in retreatment rates. In Dr Kretz’s experience, retreatment rates after RLE in young hyperopic patients are significantly lower compared to that reported for FS-LASIK, which the study authors also mentioned.
Potential risks associated with flap lifting during retreatments, such as epithelial ingrowth, should be taken into consideration and discussed with patients. Both speakers emphasised the risk of epithelial ingrowth is higher when the ablation area is very close to the flap edge (which can happen in hyperopic treatments), where a portion of the treatment often extends directly onto the edge of the flap.
Regarding the laser retreatment rates in this study, Prof Vinciguerra observed the corneal curvature gradient plays a pivotal role in determining regression outcomes. When the corneal curvature gradient exceeds 5.00 D/mm, he said to expect some degree of regression. High regression rates in this cohort are also attributed to more aggressive epithelial remodelling of the peripheral ablated zone in high hyperopic treatments, Dr Kretz said.
He also noted the number of patients in the study requiring orthoptic treatment after the procedure—due to treatment of a varying degree of latent hyperopia— which patients are not used to. Such patients may take up to six months to adapt to a reduced need for accommodation, underscoring the need for careful counselling, as it aids in managing patient expectations and facilitating a smoother adaptation period.
If the difference between cycloplegic and manifest refraction is more than 1.50 D, both Prof Vinciguerra and Dr Kretz provide patients with contact lenses or spectacles matching that prescription to assess their adaptability and simulate the visual experience post-treatment. For patients who struggle to cope, they advise slight undercorrection, initially maintaining a degree of hyperopia and discussing the future need for retreatment once adaptation occurs. It is essential to clearly communicate the potential risks to the patient, ensuring their full awareness.
Both guests felt that there is not yet enough evidence to argue FS-LASIK should be a first-line treatment instead of RLE for this extent of hyperopia, as the paper concludes. To truly ascertain the superiority of one approach over the other, a prospective randomised study with long-term follow-up comparing RLE and FS-LASIK with modern laser platforms is essential. For now, when deciding whether FS-LASIK or RLE is the correct choice, a very customised approach considering long-term outcomes and individual patient needs and preferences is required.
For citation notes, see page 40.
Right
on the Mark
"Precision treatments with the YAG/SLT laser"
Exact Targeting
Optics that enhance clarity and contrast
Sharp aiming beam
Precise Treatment
Refined YAG laser delivery with lower plasma threshold
Unique SLT assist function "SLT-NAVI"
Coaxial illumination for better visualization (optional) NEW
Ellex laser recall
Ellex has issued a voluntary recall of 57 Integre Pro and Integre Pro Scan photocoagulation lasers due to problems reported with radiation control. The issue came to light in the UK as a single event during a device servicing, with no report of any patient injuries. The cause was traced to an incorrectly assembled submodule in the laser cavity system. The company said using a laser indirect ophthalmoscope as the laser’s delivery device may result in a scattered laser beam inside the laser cavity system exiting through the slit lamp output port and emitting from the objective lens. Ellex said it would fix the defect at no charge. For questions, contact your local Ellex-Lumibird representative or email eservice@ellex.com.
www.ellex.com
New dry eye treatment
Novaliq GmbH has announced that the European Medicines Agency (EMA) has accepted the marketing authorisation application (MAA) for CyclASol (cyclosporine ophthalmic solution) for regulatory evaluation. CyclASol is a new investigative drug for dry eye disease (DED) treatment in patients who do not respond to tear substitutes, composed of cyclosporine and an innovative, water- and preservative-free excipient. CyclASol is delivered in a unique 10-microlitre small drop. Based on efficacy in treating DED in two pivotal registrational studies—ESSENCE-1 and ESSENCE-2—the US FDA granted approval of the new drug under the name VEVYE™ on May 30, 2023. www.novaliq.com
Milestone for RayOne IOL
Rayner, the manufacturer of the world’s first IOL, celebrated the successful implantation of their 4 millionth RayOne IOL last month. Introduced in 2016, RayOne is Rayner’s fully preloaded IOL system with an intuitive two-step injector and a 1.65-mm nozzle diameter. It is available in nine optical designs, including monofocal, toric, enhanced monofocal, and trifocal options. This milestone follows the recent achievement of 10 million IOL implantations made from Rayacryl, Rayner’s glistening-free hydrophilic material. The RayOne was also honoured with The Queen’s Awards for “The Queen’s Awards for Enterprise (Innovation)” in 2020. Dr Nathan Radcliffe of New York Eye in the US had the distinction of performing the implantation.
rayner.com
The leading community and trusted source for SCIENCE, EDUCATION & PROFESSIONAL DEVELOPMENT in the fields of cataract and refractive surgery.
NO ADDITIONAL RISK WITH OFFICE-BASED LENS SURGERY
The rate of adverse events for office-based cataract or refractive lens surgery is similar to or less than the reported rate for modern cataract surgery in an ambulatory surgery centre setting, the findings of a retrospective multicentre study suggest. The analysis included case records of 18,005 consecutive patients who underwent office-based lens surgery for visually significant cataract, refractive lens exchange, or phakic intraocular lens (IOL) implantation between August 2020 and May 2022 at 36 participating sites across the US. The study showed rates of postoperative endophthalmitis, toxic anterior segment syndrome, and corneal oedema were 0.028%, 0.022%, and 0.027%, respectively. Unplanned anterior vitrectomy was performed in 0.177% of patients.
L Kugler, et al., “Safety of office-based lens surgery: U.S. multicenter study,” 49(9): 907–911.
SIMILAR RESULTS WITH TWO ENHANCED MONOCULAR IOLS
The Tecnis Eyhance ICB00 (Johnson & Johnson Vision) and the ZOE Primus-HD (Ophthalmo Pro GmbH) enhanced monofocal IOLs appear to provide excellent monocular and binocular uncorrected distance visual acuity and similar and satisfactory spectacle-independent intermediate vision, according to the findings of a comparative study. Included in the non-randomised trial were 100 eyes of 50 cataract patients—half underwent bilateral implantation of the Eyhance ICB00, and half underwent bilateral implantation of the ZOE Primus-HD. At six months follow-up, all patients achieved a corrected distance visual acuity CDVA of 0.1 logMAR or better, and none reported needing spectacles for distance. In addition, more than 70% of patients in both groups achieved a binocular uncorrected intermediate visual acuity of 0.1 logMAR or better. Regarding defocus curves, visual acuities with both lenses were better than 20/25 up to -1.0 D of defocus level, beyond which they dropped to lower values.
E Corbelli, et al., “Comparative analysis of visual outcomes with 2 enhanced monofocal intraocular lenses 49(9): 929–935.
Research Education Innovation
ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
2. Dickman MM, et al. Cochrane Database Syst Rev. 2022 Apr 25; 4(4): CD013270.
3. Leivo T, et al. JCRS, 2011; 37(6): 1003–1008.
4. Moti, et al. S African Ophthalmol J, 2019; 14(4): 23–26.
5. Arsenault R, et al. JCRS, 2023; 49: 184–153.
6. Woreta FA, et al. JAMA Ophthalmol, 2021 Aug 1; 139(8): 885–886.
7. JAMA Intern Med, 2022; 182(11): 1171–1180.
8. Segers MHM, et al. JCRS, 2022; 48(12): 1403–1407.
Is FLACS Worth the Cost?
Page 23
1. Schweitzer C, Brezin A, Cochener B, Monnet D, Germain C, Roseng S, et al. “Femtosecond laser-assisted versus phacoemulsification cataract surgery (FEMCAT): a multicentre participant-masked randomised superiority and cost-effectiveness trial.” Lancet, 2020 Jan 18; 395(10219): 212–224. doi: 10.1016/ S0140-6736(19)32481-X.
2. Bénard A, Sitta R, Brezin AP, et al. “Cost Utility and Value of
Information Analysis of Femtosecond Laser-Assisted Cataract Surgery.” JAMA Ophthalmol., Published online May 18, 2023. doi:10.1001/jamaophthalmol.2023.1716
3. Schein OD. “Femtosecond Laser-Assisted Cataract Surgery— Conclusive Evidence of Lack of Incremental Value.” JAMA Ophthalmol., Published online May 18, 2023. doi:10.1001/jama ophthalmol.2023.1828
A New “Ground-breaking” Treatment for Amblyopia
Page 24
1. Repka MX, Beck RW, Holmes JM, et al., Pediatric Eye Disease Investigator Group, “A randomized trial of patching regimens for treatment of moderate amblyopia in children,” Arch Ophthalmol., 2003; 121(5). 603–611.
OCT-Guided Femto-Trabeculotomy
Page 27
1. Nagy ZZ, et al., “First-In-Human Safety Study of Femtosecond Laser Image Guided Trabeculotomy for Glaucoma Treatment: 24-Month Outcomes,” Ophthalmology Science, 2023; 3(4). https://doi.org/10.1016/j.xops.2023.100313.
FS-LASIK for the Treatment of Moderate to High Hyperopia
Page 36
1. Alió del Barrio JL, Milán-Castillo R, Canto-Cerdan M, Molina-Lespron A, Alió JL. “FS-LASIK for the treatment of moderate-to-high hyperopia.” J Cataract Refract Surg., 2023 Jun 1; 49(6): 558–564.
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
Upcoming Events
October 5–8
2023 EURETINA Congress Amsterdam, Netherlands
October 7-8
ESCRS Leadership, Business and Innovation Weekend Frankfurt, Germany
Oct 28–Nov 1
German Society of Ophthalmology Berlin, Germany
November 3–6
American Academy of Ophthalmology
San Francisco, United States
November 24–26
Italian Society of Ophthalmology Rome, Italy
February 15–18
2024 ESCRS Winter Meeting Frankfurt, Germany
Oct 5
Nov 3
Oct 28 Nov 24
POWERFUL PREDICTABLE PROVEN
EARLIER WITH ISTENT INJECT® W DELAYING GLAUCOMA DISEASE PROGRESSION1-8 40+ PUBLICATIONS DEMONSTRATE ISTENT TECHNOLOGIES PROTECT AGAINST VISUAL FIELD LOSS † 81% OF PATIENTS BELOW 15MMHG AFTER 5 YEARS FOLLOW-UP2 97% OF 778 PATIENTS IN A METAANALYSIS OF STANDALONE ISTENT INJECT EYES DID NOT REQUIRE SECONDARY INCISIONAL SURGERY DURING FOLLOW-UP6
† Data on file.
1. Berdahl, J., Voskanyan, L., Myers, J. S., Katz, L. J., & Samuelson, T. W. (2020). iStent inject trabecular micro-bypass stents with topical prostaglandin as standalone treatment for open-angle glaucoma: 4-year outcomes. Clinical & Experimental Ophthalmology, 48(6), 767-774. 2. Hengerer, Fritz H., Gerd U. Auffarth, and Ina Conrad-Hengerer. “iStent inject Trabecular Micro-Bypass with or Without Cataract Surgery Yields Sustained 5-Year Glaucoma Control.” Advances in Therapy (2022): 1-15. 3. Ferguson, Tanner J., et al. “iStent trabecular micro-bypass stent implantation with phacoemulsification in patients with open-angle glaucoma: 6-year outcomes.” Clinical Ophthalmology (Auckland, NZ) 14 (2020): 1859. 4. Ziaei, Hadi, and Leon Au. “Manchester iStent study: long-term 7-year outcomes.” Eye 35.8 (2021): 2277- 2282. 5. Salimi, Ali, Harrison Watt, and Paul Harasymowycz. “Long-term outcomes of two first-generation trabecular microbypass stents (iStent) with phacoemulsification in primary open-angle glaucoma: eight-year results.” Eye and Vision 8.1 (2021): 1-12. *Consistent cohort. 6. Healey, Paul R., et al. "Standalone iStent trabecular micro-bypass glaucoma surgery: A systematic review and meta-analysis." Journal of Glaucoma 30.7 (2021): 606-620. 7. Samuelson TW, on behalf of the iStent inject Pivotal Trial Study Team. Three-Year Effectiveness and Safety of 2nd-Generation Trabecular MicroBypass (iStent inject). Paper at the Annual Meeting of the American Academy of Ophthalmology (AAO). Virtual Meeting: November 13-15 2020. 8. Samuelson, Thomas W., et al. "Prospective, randomized, controlled pivotal trial of an ab interno implanted trabecular micro-bypass in primary open-angle glaucoma and cataract: two-year results." Ophthalmology 126.6 (2019): 811-821. iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATION FOR USE: The iStent inject ® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject ® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject ® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations.
• In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS:
• For prescription use only.
• This device has not been studied in patients with uveitic glaucoma.
• Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised.
• Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject ® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject ® W System.
• Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.”