ESCRS’s vision is to educate and help our peers excel in our field. Together, we are driving the field of ophthalmology forward.
CORNEA
20 Expanding the Keratoconus Treatment Armamentarium
Brandon D Ayres MD
21 Digging Deeper into Fuchs’ Dystrophy
Siyin Liu MBChB, MRes
of Ophthalmology
Malvina Eydelman MD, Marguerite McDonald MD, Priscilla Arnold MD, Bonnie An Henderson MD, and Elizabeth Yeu MD
The Impact of
Angelica Hanna; Joshua C Teichman MD, MPH, FRCSC; and Iqbal ‘Ike’ K Ahmed MD, FRCSC
11 ESCRS IOL Power Calculator Accuracy
Hun Lee MD, PhD and Nahyun Park MD 12 Capsulotomy in Intumescent White Cataract?
Rengaraj Venkatesh MD, Nicole R Fram MD, Vance Thompson MD, and Richard Packard MD
14 A Second Look at the First IOL Implantation
Robert Maloney MD, MA (Oxon)
DIGITAL OPHTHALMOLOGY
18 Smoothing the Way for High Tech Adoption
Kristine Morrill; Georgy Shakirin; Joaquín Fernández Pérez MD, PhD; and Anders Behndig MD, PhD
22 DSO Shows Promise in Treating Fuchs’ Dystrophy
Kathryn Colby MD, PhD
23 AI-Assisted Microbial Keratitis Diagnosis
Mohammad Soleimani MD, FICO
26 Two-Step Procedure Shows Positive Results
Olivier Prisant MD
28 Cataract with Epiretinal Membrane
Amy O’Regan MD
GLAUCOMA
30 Predicting Glaucoma Risk from EHRs
Rohith Ravindranath MS and Sophia Wang MD, MS
32 Future of Trabeculectomy
Andrew McNaught MD, FRCOphth, MB BS, FRCS
33 IOL Selection for the Glaucoma Patient
I Paul Singh MD
34 Lasers vs MIGS
Gus Gazzard MA (Cantab), MD, MBBChir, FRCOphth
RETINA
36 Tackling the Coming AMD Epidemic
Emily Y Chew MD, FARVO
Publisher
Filomena Ribeiro
Executive Editor
Stuart Hales
Editor-In-Chief
Sean Henahan
Senior Content Editor
Kelsey Ingram
Creative Director
Kelsy McCarthy
Graphic Designer
Jennifer Lacey
Circulation Manager
Lucy Matthews
Contributing Editors
Cheryl Guttman Krader
Howard Larkin
Dermot McGrath
Roibeárd O’hÉineacháin
Contributors
Laura Gaspari
Soosan Jacob
Timothy Norris
Colour and Print
CitiPost
Advertising Sales
Roo Khan
MCI UK
Tel: +44 203 530 0100 | roo.khan@wearemci.com
EuroTimes® is registered with the European Union Intellectual Property Office and the US Patent and Trademark Office.
Published by the European Society of Cataract and Refractive Surgeons, Suite 7–9 The Hop Exchange, 24 Southwark Street, London, SE1 1TY, UK. No part of this publication may be reproduced without the permission of the executive editor. Letters to the editor and other unsolicited contributions are assumed intended for this publication and are subject to editorial review and acceptance.
ESCRS EuroTimes is not responsible for statements made by any contributor. These contributions are presented for review and comment and not as a statement on the standard of care. Although all advertising material is expected to conform to ethical medical standards, acceptance does not imply endorsement by ESCRS EuroTimes. ISSN 1393-8983
Looking Back, Looking Forward
Throughout the year, we have been celebrating the 75th anniversary of Sir Harold Ridley’s remarkable idea of implanting a plastic lens in the eye following cataract surgery. The first IOL was implanted in 1949, a pivotal year as the world recovered from the destructive effects of the Second World War. Among the many key events were the founding of NATO, the creation of the People’s Republic of China, and the creation of the Council of Europe—established by 10 European countries to promote democracy, human rights, and the rule of law. The year also saw the creation of the modern British Commonwealth, with Ireland becoming an independent republic.
It was a great year for British scientists. Two technical developments from Cambridge University also presaged massive changes to come—the development of the modem and the creation of EDSAC, a computer with digital storage capabilities. Meanwhile, English astronomer Fred Hoyle coined the term ‘big bang’ to describe the origins of the universe, and George Orwell’s cautionary novel about governmental surveillance and control, 1984, hit the bookshops.
These events provide context as we look back and consider how we got where we are today. The ESCRS returns to Barcelona, a city known for its creative thinking and innovative design, a great location for a conference that will
introduce many new ideas while acknowledging the pioneers who made everything possible. The conference will feature a number of events looking at the development of modern eye surgery since Ridley’s time. This will be balanced with several future-oriented events, starting with the iNovation symposium and continuing with sessions on new technology and how to integrate that technology into your practice.
The anniversary of the first IOL implantation is not just a matter of looking back at sepia-toned photos and marvelling about the early days of going up against a stubborn establishment. It is also a time to reassess and reconsider. As Dr Robert Maloney recounts in this issue, the establishment had plenty of reasons to be sceptical of the new idea. Ridley would not likely have made it past an institutional review board today, considering the lack of preclinical research in vitro or in vivo. Malpractice attorneys would have also had a field day, especially considering some of the poor initial results and the high rate of complications.
Similarly, looking back we can now see obvious examples of inequity and intrinsic bias in many parts of our society. These topics will be addressed in a series of symposia and workshops during the Barcelona Congress.
Can’t make it to the Congress? Don’t worry, EuroTimes will provide comprehensive coverage in coming issues.
EDITORIAL BOARD
Noel Alpins (Australia)
Bekir Aslan (Turkey)
Roberto Bellucci (Italy)
Hiroko Bissen-Miyajima (Japan)
John Chang (China)
Béatrice Cochener-Lamard (France)
Thomas Kohnen Chief Medical Editor
José Güell Medical Editor
Paul Rosen Medical Editor
Oliver Findl (Austria)
Nino Hirnschall (Austria)
Soosan Jacob (India)
Vikentia Katsanevaki (Greece)
Daniel Kook (Germany)
Boris Malyugin (Russia)
Marguerite McDonald (US)
Cyres Mehta (India)
Sorcha Ní Dhubhghaill (Ireland)
Rudy Nuijts (The Netherlands)
Filomena Ribeiro (Portugal)
Leigh Spielberg (The Netherlands)
Sathish Srinivasan (UK)
Robert Stegmann (South Africa)
Ulf Stenevi (Sweden)
Marie-José Tassignon (Belgium)
Manfred Tetz (Germany)
Carlo Enrico Traverso (Italy)
Thank You to the Generous Sponsors of
Our BOSS Initiative
ESCRS is dedicated to creating an environment where everyone—members, sta , and industry partners—feels they are part of an inclusive and open culture.
Join ESCRS in being a part of BOSS (Building Our Sustainable, Inclusive Society). Together we can belong to, feel ownership in, and create a better world for future generations, a world free from conscious and unconscious bias.
Programme Committee Provides Backbone of ESCRS Scientific Content
Congress programme reflects commitment to innovation and expertise.
BY LAURA GASPARI
Meetings as large and important as the ESCRS Annual Congress require thorough organisation and oversight of the scientific programme. This critical task is led by the Society’s Programme Committee, which is composed of experts from across Europe.
“The Programme Committee’s work benefits the ESCRS as a society by keeping the highest standards of scientific and educational content for the Congress and maintaining our reputation as a leading global forum for professional development and knowledge sharing in ophthalmology,” said Filomena Ribeiro MD, PhD, chairperson of the Programme Committee and president of ESCRS.
As the ‘backbone’ of ESCRS scientific activities and events, the Programme Committee selects topics and invites speakers, ensuring the content is innovative, relevant, and of high ethical value. The Congress programme is usually coordinated with the ESCRS Education Committee, and the two committees try to assess all the activities after each Congress to identify opportunities to make improvements the following year.
The 2024 Congress will certainly have plenty of new features. With 2024 marking the 75th anniversary of the first implantation of an intraocular lens, there will be a museum in the exhibition hall illustrating the history of the development of IOLs and expectations for the future. The Congress will also host an EU Trials spotlight session and a Global Refractive Summit in collaboration with other societies. Moreover, many popular activities held at past Congresses will return.
“We will have debates in the arena space focused on presbyopia correction, IOL corneal refractive surgery, and cat-
aract surgery training,” said Professor Ribeiro. “Also, the surgical pearls will be back, as they were very well received last year. The escape rooms we started in Frankfurt will be there, and special space will be given to the Training Lab, especially on cataract surgery, with many educational moments involving digital simulation training for all members and workshops.”
Improvements in outcomes
In addition to overseeing the Congress programme, the Programme Committee is involved in other scientific activities and events the Society organises throughout the year, such as the Winter Meeting. So, what’s next?
“We are developing the Heritage Project, which will be available for all members of the ESCRS on our website,” Prof Ribeiro said. “It will share insights about the development of cataract and refractive surgery and ESCRS as a society.”
Other activities available in the near future include a revamp of the didactic courses and a major development of the World Café—a project launched in Frankfurt, consisting of 20-minute roundtable discussions between delegates. Last but not least, the
committee is currently working on ESCRS guidelines for cataract surgery and refractive surgery, intending to present them next year in the main symposia and workshops of the Congress.
Of the many Programme Committee projects that make her proud, Prof Ribeiro singled out two. “The first one is the museum about the first IOL implantation, and the second one is, of course, the Training Lab,” she said. “We are putting a lot of effort into bringing these special moments to our delegates. Especially for training, we aim at improving our ability to provide the best for our members, with some changes to the skill transfer courses, trying more dry labs or digital labs.”
By providing high-quality scientific content, the Programme Committee benefits ESCRS as well as the field of ophthalmology.
“By delivering cutting-edge research on clinical advancements and best practices to our members and the delegates at the Congress, we make the dissemination of new knowledge and new techniques possible,” Prof Ribeiro concluded. “We promote innovation and support ongoing education, and ultimately, we lead to improvements in patient care and outcomes in our field.”
Congress Symposium to Highlight Practice Management Issues
Creating a culture of collaboration, educating patients to participate in eye care decisions, staying competitive and innovative on a budget, and investing in quality management systems are topics not typically covered in medical school. Ophthalmologists wanting to learn more about them can take advantage of a full-day symposium hosted by the ESCRS Practice Management Committee, Leadership, Business, and Innovation (LBI) on Sunday, 8 September, at the ESCRS Annual Congress in Barcelona.
Comprising four modules, the symposium focuses on practice managers and clinical teams and will include presentations and panel discussions. One module, “Patient Decision Making,” features a pro-con debate by UK surgeons Sheraz Daya and Milind Pande on the correct balance for educating cataract-age patients and will include an audience vote.
The symposium will offer two modules in the morning and two in the afternoon, as follows:
• Team Collaboration and the Culture/Values of an Organisation (8:30 – 10:15), chaired by Vincent Qin
• Patient Decision Making: The path to shared decision making (10:30 – 12:15), chaired by Artemis Matsou
• Marketing: Staying competitive and innovative without breaking the bank (14:15 – 15:45), chaired by Basak Bostanci and David Lockington
• Quality Management Systems: Why they are a great investment in your practice (16:00 – 17:00), chaired by Kristine Morrill Sandwiched between the morning and afternoon modules will be a lunchtime symposium jointly sponsored with the European Society of Ophthalmic Nurses and Technicians (ESONT). The symposium will explore how to successfully implement innovative technology and especially the key factors to consider in evaluating, purchasing, and implementing hightech equipment into your clinic. A boxed lunch will be served to attendees. Registration is required via the Congress website.
Inclusiveness to Feature Prominently at Congress
On Monday, 9 September, a two-hour session combining two ESCRS priorities—leadership and inclusion—will take place starting at 9:00. The session, “Leadership and Mentoring in an Inclusive Society,” will feature presentations on the following topics:
• What we can learn from ESCRS member surveys
• The influence of author gender on the peer-review process in vision science
• How the US National Eye Institute uses internships to reach under-represented communities
• Are we promoting or undermining equity in access to cataract surgery?
• The role of mentorship in inclusiveness
• How industry promotes inclusivity and leadership in their organisations
• Taking the lead on leadership and mentorship: Views from AAO, AUSCRS, ASCRS, and BRASCRS
• What comes next? Inclusiveness, mentorship, and ESCRS plans for the years ahead
The ESCRS inclusivity initiative, BOSS (Building Our Sustainable, Inclusive Society), will present a session on Sunday, 8 September, titled “Combatting unconscious gender bias in ophthalmology, industry, and medicine: An evidence-based and practical course.” The course will present a wide range of perspectives, with speakers from Australia, Ireland, Italy, the United Kingdom, and the United States. The BOSS track will extend beyond the scientific programme, with the BOSS team hosting mentoring sessions at the ESCRS Booth and a brandnew family track. There will also be podcasts and webinars throughout the year.
Session on Clinical Trials to Highlight Industry Views
On Sunday, 8 September, a morning session will allow Congress attendees to hear presentations on clinical trials being conducted on topics such as the safety and efficacy of a new hydrophobic acrylic full-range-of-vision intraocular lens. The session, “EU Clinical Trials Spotlight Symposium,” marks the first time ESCRS has actively solicited abstracts from industry partners.
The session will feature seven presentations. The manufacturers represented in the trials are Bausch + Lomb, Johnson & Johnson Vision, Ophtec, BVI Medical, Hoya, Samsara Vision, and Zeiss.
Rising into Leadership
Accomplished female ophthalmologists offer advice and encouragement.
CHERYL GUTTMAN KRADER
REPORTS
Amain stage session at the 2024 ASCRS spotlighted ‘women leading by example’. Moderating the programme, Malvina Eydelman MD, Director of the US FDA Office of Ophthalmic, Anesthesia, Respiratory, ENT, and Dental Devices, sought insights from the four women who have served as ASCRS president—Marguerite McDonald MD, Priscilla Arnold MD, Bonnie An Henderson MD, and Elizabeth Yeu MD.
The session began with a question about the motivation leading Dr McDonald along her successful career path. She said her interest in serving patients and addressing unmet needs has been her “North Star”.
Asked to comment on the AAO and ESCRS also having female presidents during her 2004–2005 service, Dr Arnold linked this “interesting coincidence” to the large increase in the proportion of women entering medicine approximately 20 years earlier and the length of time needed to build a practice, develop professional relationships, show commitment to professional organisational work, and earn the trust and confidence of colleagues.
Developing leadership skills
Discussion continued with Dr Henderson sharing ways women can develop leadership skills. She noted she had taken a course
on leadership in non-profit organisations at Harvard Business School and was struck by hearing that leadership is about looking at innovation, making improvements, and creating change. Leadership also requires staying mindful of “who is at the table” in leadership positions, Dr Yeu noted. She emphasised the importance of diversity and having the face of leadership reflect the demographic makeup of the membership. In that regard, she noted the face of ASCRS leadership has changed in parallel with the changing face of medicine and ophthalmology. Whereas there was a 6:1 ratio of men to women among the ASCRS Executive Committee members and heads of the Clinical Committees in 2014, the ratio in 2024 was just 2:1.
“Staying mindful means looking into the membership and finding opportunities to create equity for members,” Dr Yeu said.
Seek responsibility
The panellists then shared advice for young women entering ophthalmology today. Dr McDonald emphasised the need to “speak up” so others recognise their interest and ability to handle additional responsibilities. “People are not mind readers,” she said, adding speaking up helps overcome any preconceived notions that young women have no time to take on commitments outside of their practice roles.
Dr Arnold dovetailed her advice with Dr McDon ald’s, with a more gender-neutral approach.
“It probably seems self-evident, but I would say that young ophthalmologists need to seek the responsibil ity they want and, when offered the position, do the work,” she said. “That is critical, and it doesn’t always happen. So, [young ophthalmologists should] keep it in mind if interested in moving into a leadership role.”
Know that you have to put in time to develop expertise. It is not going to happen overnight.
The rule of thirds
Dr Henderson shared words of encouragement meant to bolster the fortitude of young ophthalmologists as they pursue their goals in the face of life’s daily challenges. Citing the autobiographical book Chasing Dreams, Befriending Pain, and Other Big Ideas Dr Henderson explained the author, Olympic athlete Alexi Pappas, wrote about the value of accepting the ‘rule of thirds’.
“When Alexi was training for the Olympics, her coach told her that when training for a goal, you are supposed to feel pretty good a third of the time, okay a third of the time, and crappy a third of the time, but if you are within that ratio, you are where you should be,” she said.
“I want to share that idea because, as young oph thalmologists try to balance family and career, it is wisdom to know and accept that life can be hard and overwhelming, and you are not supposed to feel great all of the time.”
Dr Yeu’s advice centred on the importance of creating a layered set of time-focused goals and having patience in pursuing them. Her words stemmed from concern about how the newest generation of ophthalmologists is accustomed to living in an instant-access world.
“Patience is a virtue. Know that you have to put in time to develop expertise. It is not going to happen overnight. Set 1-year, 5-year, and 10-year goals, and live intentionally to achieve them, recognising that it does take time.”
Providing final thoughts, Dr Eydelman highlighted the value of collaboration, advising young ophthalmologists not to be afraid of challenges.
“No matter how complicated or out of the box a problem seems, there is always a way to solve it if you stop, think, and collaborate,” she said. “Involve everybody in the room and outside the room because, jointly, we are much stronger than any of us alone.”
This presentation was made at ASCRS 2024 in Boston, US.
The Impact of Virtual Follow-ups
Phone calls may be as safe as in-person visits—and patients prefer them.
HOWARD LARKIN REPORTS
For uncomplicated cataract surgery, follow-up telephone calls to patients appear to be a safe alternative to in-office visits. Virtual follow-up benefits may include greater convenience and access for patients, according to a literature review.
“The patient doesn’t have to go to the clinic, which can be a really huge advantage, depending on where you are in the world,” said Angelica Hanna. “Some have mobility issues, or they may require a caregiver to take them.”
In addition, phone calls are easier for clinic staff, who don’t have to prepare patients. They also free up office space—not to mention valuable clinician time, added Hanna, a medical student who conducted the review.
The findings are important because guidance on follow-up after uncomplicated cataract surgery varies. For example, the American Academy of Ophthalmology suggests low-risk patients can be seen within 48 hours, whereas the Royal College of Ophthalmologists advises patients with no high-risk ocular comorbidities should not be asked to be seen in clinic following uncomplicated cataract surgery. There is no guidance on the use of virtual follow-up, according to the review.
Diverse study group
Altogether, the review included 7 studies examining virtual follow-up after uncomplicated cataract surgery that contained clinical outcome data. Winnowed from more than 1,700 citations, the studies meeting the screening criteria included 2,113 eyes of 1,994 patients. They came from all over the world, including the Netherlands, the UK, New Zealand, Singapore, the US, and Brazil. Publication dates ranged from 2004 to 2023, with 6 after 2014.
Postoperative follow-up was done through calls from a clinic staff member. These varied from study to study and included clinical assistants, surgeons, trainees, and nurses, Hanna said. Calls were placed between one day and two weeks after surgery, with most within 24 or 48 hours. No other virtual follow-up methods, such as video chats or AI-powered systems, were examined.
Call content varied from study to study, Hanna said. Most included screening questions, asking about the presence of pain and redness, flashes and floaters, and headache or vomiting that might suggest an intraocular pressure spike.
“Patients were advised to call in to be seen in person early if they had any concerns.”
Patient education content—such as reminding patients to take their eye drops on schedule and not take showers— was included in one study, which examined nursing calls. This study found faster recovery among patients receiving the education.
Similar outcomes
Outcomes were similar between telephone follow-up patients and those seen in person. No significant differences were seen in visual acuity or complication rates. No serious adverse events were seen in any of the studies, and rates of emergency room and ophthalmic clinic visits after surgery were also similar, Hanna noted. However, the study does not rule out possible risks, and she cautioned the sample size may not have been large enough to detect them.
One theme that emerged from all the studies was patients preferred the calls and found them more convenient than in-person visits. Telephone follow-up may also make care more accessible for seniors, the review concluded.
Hanna presented a poster at ARVO 2024 in Seattle, US. Poster co-authors included Joshua Teichman MD, and Iqbal ‘Ike’ K Ahmed MD.
Angelica Hanna is a medical student at the University of Toronto, Canada. angelica.hanna@mail.utoronto.ca
Joshua C Teichman MD, MPH, FRCSC is an ophthalmologist at Prism Eye Institute and Trillium Health Partners, and an assistant professor at the University of Toronto, Canada.
Iqbal ‘Ike’ K Ahmed MD, FRCSC is an ophthalmologist at Prism Eye Institute and Trillium Health Partners, director of the University of Toronto Glaucoma and Advanced Anterior Segment Surgery, Toronto, Canada, and a professor at John A Moran Eye Center, University of Utah, Salt Lake City, US.
ESCRS IOL Power Calculator Accuracy
All seven formulas are accurate, but two stand out, study finds.
Measured by conventional discrete accuracy values such as mean and median absolute prediction error, the seven IOL power calculation formulas available from the ESCRS online calculator, plus three incorporated into the IOLMaster 700 (Carl Zeiss Meditec), showed statistically comparable accuracy in a test of normal-length Korean eyes. However, two stood out when evaluated using the Formula Performance Index (FPI), which derives a single total accuracy value by combining several weighted discrete measures, report Hun Lee MD, PhD and Nahyun Park MD.
In a test involving 221 eyes in 221 patients who underwent cataract surgery at the Asan Medical Center in Seoul, Republic of Korea, Drs Lee and Park found that the Cooke K6 and
PEARL-DGS formulas produced FPI scores exceeding 0.700, while the other eight ranged from 0.334 to 0.572. The eight formulas, in descending order of FPI, were Hill-RBF 3.0, Barrett Universal II (two versions from the ESCRS and IOLMaster 700 tested), Kane, EVO 2.0, SRK/T, Hoffer QST, and Holladay 2. Prediction errors were calculated six months after surgery.
Sources of prediction error
The slope of the correlation of prediction error to axial length is one factor incorporated into the FPI. First developed by Dr Wolfgang Haigis, other factors in the FPI are prediction error standard deviation, median absolute error, and the percentage
of eyes with a prediction error within ±0.5 D. Because it is a composite measure, Dr Lee said they could not calculate the statistical significance of differences in the FPI.
Cooke K6 and PEARL-DGS were the only two formulas that did not show a significant correlation with axial length and lens tilt. Dr Park hypothesised this may be because these two formulas use a method developed by Dr David L Cooke for adjusting the axial length value to reduce skewing prediction errors in longer and shorter eyes. Testing this hypothesis is one goal of the team’s ongoing research into IOL formula accuracy with Dr Cooke, she added.
The study also found the SRK/T formula showed a significant keratometry correlation. Prediction error correlated with anterior chamber depth in the Barrett, SRK/T, Holladay 2, and Hoffer QST.
Identifying the source of prediction errors may help guide formula use, particularly in longer or shorter eyes or eyes with unusual anatomy, Dr Lee said. “If there is a correlation, and you are operating [on] extreme eyes, you might get a bigger prediction error.”
Broadening the research
Mean axial length of the eyes tested was 23.82 mm, ranging from about 21.50 mm to nearly 28.00 mm. Drs Lee and Park are extending their study to 1,000 eyes and hope to include a greater sample of shorter and longer eyes for a better idea of how the formulas perform in Asian eyes, which have high rates of myopia. The larger sample may reveal statistically significant differences, Dr Lee said.
The team is also collaborating with Dr Dante Buonsanti, who heads the ESCRS online calculator project, to see if there are any significant differences between Asian and European eye samples. “Comparison of many formulas is very important,” Dr Lee said, even in clinical practice. He routinely uses 10 different formulas to guide lens power selection.
Drs Lee and Park presented at ARVO 2024 in Seattle, US.
Hun Lee MD, PhD is an associate professor of ophthalmology at Asan Medical Center, University of Ulsan College of Medicine, Songpa-gu, Seoul, Republic of Korea. yhun777@gmail.com
Nahyun Park MD is a third-year ophthalmology resident at Asan Medical Center. laurenpark66@gmail.com
HOWARD LARKIN REPORTS
Capsulotomy in Intumescent White Cataract?
Experts express diverse opinions about the best technique.
CHERYL GUTTMAN KRADER REPORTS
Developments in surgical technologies for cataract surgery include new approaches for safely performing capsulotomy in eyes with an intumescent white cataract. Use of these tools, however, depends on access, patient characteristics, and surgeon comfort. Four leading cataract surgeons discussed their preferred technique for confronting these challenging cases.
Rengaraj Venkatesh MD advocated for manual capsulotomy performed with a double rhexis approach.
“There are many publications that establish how easily it can be performed,” he said, contrasting that benefit with the limitations of performing a femtosecond laser-assisted capsulotomy, precision pulse capsulotomy (PPC; Zepto), or selective laser capsulotomy (SLC; CAPSULaser).
Dr Venkatesh noted the femtosecond laser has a large footprint and requires additional staff for operation. Furthermore, the manually created capsulotomy has a smoother and stronger edge than the laser-created capsulotomy.
He said the potential for suction loss is a serious issue using PPC. Although there is evidence both PPC and SLC create a capsulotomy with a stronger edge than manual capsulotomy, Dr Venkatesh noted a lack of long-term data establishing whether the greater tensile strength offers benefit.
The added cost associated with using these automated devices could lead to patients compromising on their IOL choices.
“I think patients are better served having a procedure done by a premium surgeon with a manual capsulotomy and a premium IOL rather than a premium capsulotomy,” he said.
In favour of femtosecond laser
Nicole Fram MD discussed femtosecond laser-assisted capsulotomy. Describing it as “the easiest thing I have ever done to make a complex case routine,” she noted that problems with capsule friability encountered early on with femtosecond laser use have been overcome with new laser platforms containing more optimised settings to deliver less energy and friability of the anterior capsule. She also cited research showing better outcomes were achieved using the laser than a manual technique in shallow anterior chambers and brunescent cataracts.
However, a good outcome still depends on picking the right patient and following a proper docking protocol.
“We can make a complex case more routine using a femtosecond laser, but I think surgeons should consider a manual technique or a femtosecond laser-assisted mini capsulotomy if the anterior chamber is very shallow with a spheroidal appearance of the lens,” Dr Fram said.
Her tips for success using the femtosecond laser included staining the capsule with trypan blue, obtaining a very flat and well-centred dock, and completing the capsulotomy rapidly, ideally within 0.7–0.9 seconds. Dr Fram also suggested having an MST capsulorhexis forceps on hand for better control at capsulotomy completion. Often, an approach through a paracentesis will help avoid anterior chamber collapse and runout of the capsulotomy in an intumescent cataract, she said.
Precision pulse capsulotomy
For Vance Thompson MD, PPC represents the safest way to perform capsulotomy in eyes with an intumescent white cataract.
“The suction cup is easy to put on, and suction is reliably created when the device is connected to the phaco machine. The edge of the capsulotomy is very smooth and strong,” he said. “And one reason I think PPC is the best technology to use in white cataracts is it creates a 360-degree opening in just 0.4 milliseconds.”
In less advanced cataracts, Dr Thompson said he aligns the Purkinje 1 and 4 images for approximating patient fixation to centre the capsulotomy for 360 degrees of capsule overlap so the implant does not tilt or decentre with capsule contraction. He otherwise centres over the pupil in white cataract cases where Purkinje image-guided capsulotomy cannot be performed.
He noted the capsulotomy diameter usually turns out to be smaller in eyes with a white cataract than in those with less advanced cataracts because the capsule in eyes with an intumescent white cataract is under stretch. While he uses a
capsule dye for intraoperative visualisation to avoid nicking the edge intraoperatively, he does not worry about creating tension on the capsule when dialling in a lens.
“We have shown in the laboratory that the capsule edge is quite strong with precision pulse technology,” he said.
Dr Thompson said he tends to avoid doing PPC in eyes with a deep anterior chamber (>3.8 mm) and those with a small pupil—although he noted other surgeons are comfortable using it in those situations.
Selective laser capsulotomy
Richard Packard MD favours SLC in cases of intumescent white cataract.
“The laser has been used in over 20,000 eyes, and none with an intumescent cataract had an Argentinian flag sign,” he said.
Summing up the main reasons for his preference, Dr Packard stated, “The selective laser creates a capsulotomy of consistent size, consistent circularity, and a strong elastic edge in less than 0.3 seconds. Not only does the capsulotomy give 360-degree coverage of the IOL, but the coverage is symmetrical, which is very important for premium and capsulotomy-fixated IOLs.”
The 590 nm laser beam is absorbed selectively by a capsule stained with a microfiltered 0.4% trypan blue solution. Patient fixation is not normally possible with an intumescent cataract, thus making the visual axis—and centration—difficult to determine. The SLC technique overcomes this issue, Dr Packard said.
“Centration on the visual axis is aided by having an area of enhanced staining within the capsule centre coincident with the first and fourth Purkinje reflex,” he explained.
To overcome intralenticular pressure, Dr Packard overfills the anterior chamber with a high molecular weight ophthalmic viscosurgical device to flatten the anterior capsule.
Drs Venkatesh, Fram, Thompson, and Packard spoke at ASCRS 2024 in Boston, US.
Rengaraj Venkatesh MD is the Chief Medical Officer of Aravind Eye Hospital, Pondicherry, India. venkatesh@aravind.org
Nicole R Fram MD is the managing partner at Advanced Vision Care, Los Angeles, US. nicfram@yahoo.com
Vance Thompson MD is the director of refractive surgery at Vance Thompson Vision, Sioux Falls, South Dakota, US. vance.thompson@ thompsonvision.com
Richard Packard MD is a senior consultant at Arnott Eye Associates, London, UK. eyequack@vossnet.co.uk
Be the first to get it at the ESCRS: Booth 7. D66
CASIA2
New Brochure!
CASIA2
User Experience
Discover the power of CASIA2 through real-world cases provided by eye care professionals like you. In this brochure, we proudly present a collection of diverse patient experiences that showcase the versatility and clinical utility of CASIA2 Cornea / Anterior Segment OCT.
Dive into the insights, outcomes, and lessons learned from these cases. See firsthand how CASIA2 is transforming ophthalmic care.
at tomey.de
A Second Look at the First IOL Implantation
The traditional hero and villain story might not have a bad guy after all.
SEAN HENAHAN REPORTS
The invention and implantation of the first IOL by Dr Harold Ridley has become the stuff of legend. Every good story needs a villain, and in this case, that role was filled by Dr Stewart Duke-Elder (1898–1978).
But it may be this villain got a bad rap, according to Robert Maloney MD, who recently spent six months on sabbatical at Oxford University researching the early days of cataract surgery. EuroTimes Editor-in-Chief Sean Henahan interviewed Dr Maloney about his work.
This year, we are marking the 75th anniversary of the first IOL implantation by Dr Harold Ridley. You are known to be a historian of ophthalmology—could you tell us about your recent investigations? I pursued a six-month research project on Drs Ridley and Duke-Elder while on sabbatical at Oxford University. I’ve been going through archives at Moorfields Eye Hospital and the UCL Institute of Ophthalmology in London, digging through old records and trying to better understand the invention of the IOL.
What have you found? What was cataract surgery like, implanting the first IOL before phacoemulsification, viscoelastics, even operating microscopes?
You can watch the original video of Ridley’s first IOL implantation on YouTube. The first procedure is mildly terrifying from a modern point of view. It was done with loupes, using a 180-degree corneal-conjunctival section, suture pulling at the cornea, a giant PMMA lens inserted. It makes you want to look away. You don’t know what’s happening to the cornea, don’t know what’s happening to the iris, or where the vitreous is. It is amazing they did as well as they did back then. They didn’t do that well by our modern standards, but they still did pretty well. Some got lucky, with the IOL staying in place, but some didn’t get lucky. This is one area of my research—looking at the complication rates of the early procedures with the Ridley lens.
How was this initial work with IOLs received by the ophthalmology establishment?
Harold Ridley thought up the idea of a lens implant and put it in a patient either in November of 1949 or February of 1950.
There is still some debate about the date. He did 8 patients in 17 months. He then presented his work—a secret until then—at the Oxford Ophthalmological Congress.
Stewart Duke-Elder was the Director of Research at the Institute of Ophthalmology in London and probably the leading ophthalmologist in the world at that time. He refused to look at the two patients Ridley brought to the conference. He allegedly walked out with his acolytes behind him, which, in retrospect, seems petulant and small minded. According to Dr Richard Packard, Duke-Elder threatened a young Peter Choyce (who would become an early pioneer of IOL surgery) that if he helped Ridley with his implant, he would not recommend Choyce for a job.
Duke-Elder is viewed as the evil character here, suppressing a brilliant young inventor who made a world-changing invention. He has really come down through history as the devil in this story. My research has been about who Duke-Elder really was and why he reacted the way he did. I’ve come away with a much more sympathetic view of Duke-Elder than when I started this project. He was the son of a Scottish Presbyterian minister who practised a by-the-book, rules-oriented religion. Duke-Elder was an outsider. His original surname was Duke, but he wanted a hyphenated name to suggest nobility, so he added his mother’s surname to create ‘Duke-Elder.’ He went to London and trained as a surgeon, became the oculist to the royal family (a very high position in ophthalmology), and was knighted at age 35, which is rare.
Duke-Elder worked his way up from modest beginnings by following the rules and doing everything in the right manner. Ridley came along with a clever idea, but he did it with
no animal testing and no lab research. Ridley designed this IOL in the front seat of his Bentley, working with John Pike from Rayner & Keeler—designing a huge IOL the same size and shape as the human lens with no haptics. Ridley implanted the IOL, and the first patient turned out with a refraction of -20 D. He got the IOL power completely wrong because he didn’t research the index of refraction of PMMA and had no idea how to fixate these lenses. He figured if he made the implant the same size as the human lens it might stay there. It didn’t. The PMMA material he used was sterilised with a chemical that resulted in a lot of inflammation. Because Ridley did not do animal testing, patients suffered.
During this time, Duke-Elder ran a research institute with a lab for physiologic optics on the third floor, perfect for determining the power of an IOL. The Institute also had a beautiful set of research facilities for working with rabbits and dogs.
From Duke Elder’s point of view, he saw an invention developed in secrecy and not tested prior to use that caused significant harm to patients. Duke-Elder didn’t have the benefit of hindsight. Who can blame him for saying IOLs were a bad idea? Duke-Elder was not the evil character in this story. In fact, Ridley’s lens implant never really worked. It was the people who came later who invented IOLs with haptics that finally worked. Ridley made a big contribution. Duke-Elder was the person who said there was a more responsible way to develop IOLs.
Did Duke-Elder ever join the IOL camp?
He never came around. At Moorfields in the 1970s, there were two types of eye surgeons: those who put in IOLs and those who took them out. Moorfields was the referral centre for the whole country and saw a significant volume of problem cases associated with early IOLs. This included corneal decompensation, angle closure, and dislocated lenses. It gave the surgeons at Moorfields a slanted viewpoint because happy patients didn’t come in for a second opinion.
Duke-Elder died in 1978. Remember, we didn’t have a safe lens implant until Shearing invented the J-loop posterior chamber lens in 1978. It wasn’t until 30 years after Ridley put in his first lens that we finally had a lens that was safe to use and would become widely accepted.
Robert Maloney MD, MA (Oxon) is a former Professor of Clinical Ophthalmology at the Stein Eye Institute of the University of California, Los Angeles, US. He is the Chairman of the Board of the American-European Congress of Ophthalmic Surgeons (AECOS). He was managing partner of the Maloney-Shamie Vision Institute and Chief Medical Officer of RxSight, the company that developed the light adjustable IOL.
Scan this QR code to watch the video of Ridley’s first IOL implantation.
ISTENT INJECT® W AND SAFETY
“Primum non nocere”, from Hippocrates, is considered Medicine’s first and most important principle. Nevertheless, sometimes, we break this principle involuntarily, namely after glaucoma surgery. Surgery is often needed in glaucoma, but classical surgery, such as trabeculectomy and tubes, presents unpredictable and vision-threatening complications1,2 Consequently, microinvasive glaucoma surgeries (MIGS) were developed to increase the safety of glaucoma surgeries3. I intend to underline the importance of safety in this clinical case.
CLINICAL CASE
I received a lovely 77 year-old female patient with significant cataract in the right eye (with a visual acuity of 0.6) and a progressing moderate primary open-angle glaucoma, with an intraocular pressure (IOP) of 19 mmHg under four medication classes with thin corneas (467 µm), sent for trabeculectomy. She took care of her ill husband and lifted him several times per day. She mentioned that years earlier, he was an athlete and lifted her easily, but the irony of life had inverted the roles, and she accepted it with love and dedication. She didn’t have anyone else to rely on except for one week of vacation of her daughter, so she refused any surgery that would demand more than one week of rest. For this patient, the risks of
a trabeculectomy outweighed the advantages, as a GATT (gonioscopy-assisted transluminal trabeculotomy) or other MIGS.
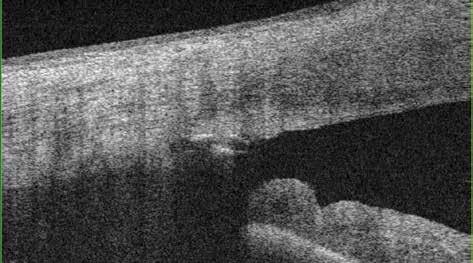
Consequently, I chose the smallest, most well-studied, and probably safest MIGS: cataract surgery combined with iStent inject® W. I discussed the options, respective risks and benefits, and that likely, she would need to continue most or all eyedrops, but the rationale was maximal safety. She accepted with a glint of hope, and the surgery and postoperative period went great. One month after surgery, her IOP remained inferior to 10 mmHg under two classes, allowing me to stop all eyedrops. Two years after surgery, her IOP remained at 12 mmHg under no eyedrops, with stable glaucoma and increased quality of life; her iStents allowed a remarkable outcome.
CLINICAL EVIDENCE
If you don’t trust a clinical case (they are helpful but not sufficient), let’s discuss evidence:
• The iStent technologies are the most studied from all MIGS4, 5 .
• With over 382 published studies (including 14 meta-analyses and 18 randomized clinical trials (RCT))
• And over a million surgeries worldwide.
• RCTs proved its effectiveness even with a baseline IOP higher than 30 mmHg5, its increase in quality of life (more than after
A clinical case
BY ANA MIGUEL, MD PhD FEBO
isolated cataract surgery)6, and its visual field preservation7.
• iStent’s safety is a substantial advantage compared with other surgical techniques.
An RCT stated that the safety of combined cataract-iStent inject® surgery is similar to that of cataract surgery4, and studies comparing the endothelial safety among microstent, Cypass, and iStent inject® showed the superiority of the latter8. The increased safety is probably due to the nature of a trabecular micro-bypass, its small size of 360 µm, and its short learning curve.
“iStent also has the advantage of not extensively
disrupting
the
trabecular meshwork nor the conjunctiva, not occupying too much space, and being the device that disturbs the least when future surgery is needed – this should be considered when choosing a glaucoma surgical technique.”
One should also ponder that cataract surgery has a risk of IOP spike (estimated of 20%9), particularly in glaucoma. Thereupon, performing isolated cataract surgery in a controlled (or worse, uncontrolled) glaucoma patient may aggravate
his glaucoma (and violate the Primum non nocere principle). Alternatively, combining phacoemulsification with MIGS may synergistically decrease the IOP10 (unlike classical filtering surgeries11), decrease healthcare costs12, may reduce IOP spikes, and may help control glaucoma
in the long term (justifying the interventional glaucoma concept13).
In conclusion, there has been a revolution of less invasive glaucoma surgeries that are safer and effective, allowing us to act sooner in glaucoma. We need to
Figure 1. Correct positioning of iStent inject, two years after surgery, as shown by an anterior segment OCT (taken by Christelle Cochet).
Thanks to my Ophthalmology staff and team, particularly to Christelle Cochet, for taking the AS-OCT from figure 1.
identify the best approach for each patient, considering several factors such as the glaucoma damage, the IOP, the age and individuality of the patient, and the safety of the procedures. And sometimes, the best approach is not the strongest but the safest.
ANA MIGUEL, MD PHD FEBO
Fellowship: Glaucoma and Advanced Anterior Segment Surgery, Prism Eye Institute and Toronto University, with Ike Ahmed MD FRCSC, Canada
Ophthalmologue de l'Hôpital Privé de la Baie, Avranches, France
Glaucomatologue au Centre Hospitalier et Universitaire de Caen, France
Financial disclosure: Glaukos sponsored article
References :
1. Dietlein, T.S., [Lessons from 10 years of the Advanced Glaucoma Intervention Study (AGIS)]. Ophthalmologe, 2005. 102(3): p. 227-9. 2. Gedde, S.J., et al., Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol, 2012. 153(5): p. 804- 814 e1. 3. Ahmed, II, MIGS and the FDA: What’s in a Name? Ophthalmology, 2015. 122(9): p. 1737-9. 4. Samuelson, T.W., et al., Prospective, Randomized, Controlled Pivotal Trial of an Ab Interno Implanted Trabecular Micro-Bypass in Primary Open-Angle Glaucoma and Cataract: Two-Year Results. Ophthalmology, 2019. 126(6): p. 811-821. 5. Singh, I.P., et al., Treatment Success Across Different Levels of Preoperative Disease Burden: Stratified Two-Year Outcomes from the Pivotal Trial of iStent inject® Trabecular Micro-Bypass in Primary Open-Angle Glaucoma and Cataract. Clin Ophthalmol, 2021. 15: p. 3231-3240. 6. Samuelson, T.W., et al., Quality of Life in Primary Open-Angle Glaucoma and Cataract: An Analysis of VFQ-25 and OSDI From the iStent inject Pivotal Trial. Am J Ophthalmol, 2021. 229: p. 220-229. 7. Gillmann, K. and D.M. Hornbeak, Rates of visual field change and functional progression in glaucoma following trabecular microbypass implantation of iStent technologies: a meta-analysis. BMJ Open Ophthalmol, 2024. 9(1). 8. Ahmed, I.I.K., et al., Long-Term Endothelial Safety Profile With iStent Inject in Patients With Open-Angle Glaucoma. Am J Ophthalmol, 2023. 252: p. 17-25. 9. O’Brien, P.D., et al., Risk factors for a postoperative intraocular pressure spike after phacoemulsification. Can J Ophthalmol, 2007. 42(1): p. 51-5. 10. Ahmed, JLJMJOI, Cataract Surgery: Advanced Techniques for Complex and Complicated Cases - chapter MIGS in Special Cases. Springer International Publishing, ed. BD. J Alió, R Osher. 2022: Springer. 512. 11. Jampel, H.D., et al., Effect of technique on intraocular pressure after combined cataract and glaucoma surgery: An evidence-based review. Ophthalmology, 2002. 109(12): p. 2215-24; quiz 2225, 2231. 12. Bartelt-Hofer, J. and S. Flessa, Comparative efficacy and cost-utility of combined cataract and minimally invasive glaucoma surgery in primary open-angle glaucoma. Int Ophthalmol, 2020. 40(6): p. 1469-1479. 13. Dubinsky-Pertzov, B. and A. Belkin, [Interventional Glaucoma - a Shift in the Treatment Paradigm]. Harefuah, 2024. 163(5): p. 298-304.
iStent inject® W IMPORTANT SAFETY INFORMATION
INDICATION FOR USE: The iStent inject® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/ PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma. • Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.” • There are no known compatibility issues with the iStent inject® W and other intraoperative devices. (e.g., viscoelastics) or glaucoma medications. • Unused product & packaging may be disposed of in accordance with facility procedures. Implanted medical devices and contaminated products must be disposed of as medical waste. • The surgeon should monitor the patient postoperatively for proper maintenance of intraocular pressure. If intraocular pressure is not adequately maintained after surgery, the surgeon should consider an appropriate treatment regimen to reduce intraocular pressure. • Patients should be informed that placement of the stents, without concomitant cataract surgery in phakic patients, can enhance the formation or progression of cataract. ADVERSE EVENTS: Please refer to Directions For Use for additional adverse event information. CAUTION: Please reference the Directions For Use labelling for a complete list of contraindications, warnings and adverse events.
Smoothing the Way for High Tech Adoption
What is the best way to integrate new technology into the office?
TIMOTHY NORRIS REPORTS
In the digital era, integrating new technology into everyday clinical practice can be challenging. What could be considered a boon for workflow and performance can instead have the opposite effect if the integration process is not optimal, said Kristine Morrill at a recent high tech adoption workshop.
While the clinician may be very enthusiastic about some new tech acquisition, this does not always transmit to the whole clinic team, who might struggle due to a lack of training and support from the manufacturer, she noted.
Morrill added many of the failures in introducing new technology in the field could also be attributed to the industry, from unrealistic expectations regarding clinician needs to proper lack of funding and commercialisation errors. Successfully integrating new technology in clinical practice requires staff engagement and patient communication.
“What is your current situation? What do you want to achieve?”
Adopting a new technology is always gradual: of all the clinicians, only 2.5% will immediately try and adopt an innovation, followed by 13.5% of what are called early innovators. “So, what is stopping a clinician from becoming an early innovator?” asked Carl Zeiss Meditech’s Head of AI, Georgy Shakirin. Surely it is not an easy task—going through all the available evidence just to understand what really works and what does not, he observed.
According to Shakirin, to make it worthwhile both in terms of time and money, it is important first to assess the new technology’s integration and interoperability—asking peers for
feedback and trying to understand how much the workflow can be affected.
A key point is the presence and quality of service and support—which may be essential to guarantee a good integration—and improvement of the clinical ecosystem, Shakirin underlined. Integrating a technology such as AI is especially sensible for these different aspects. It is necessary to understand what kind of data is used, how the model is trained, and if the available computational power is enough. Available cloud storage and all the regulatory aspects also need consideration, he added.
A decision in the making
Patients, regulators, funders, policymakers, and clinicians may all have the best intentions when considering adding a new technology to a practice. This generates a whole ecosystem, with different decision processes that often are poorly coordinated, leading to confusion and lack of decision, Joaquín Fernández Pérez MD, PhD told the workshop.
Adapting to every scenario is then vital to improve this decision-making process. It starts with a Feasible, Interesting, Novel, Ethical, and Relevant (FINER) research question, he observed. Moreover, the question must be based on the PICO-S/T, considering the Patient, Intervention, Control, Outcome, Study Design, and Timeline. Finally, to convert the level of evidence into recommendations, Dr Fernández suggested the GRADE system, a systematic review based on literature. A high level of evidence and randomised controlled trials independent from bias are needed.
Dr Fernández also stressed an evaluation of cost-benefit and cost-consequence as key for a successful health-technology assessment, which he said could improve collaboration and transparency in healthcare decision-making for more inclusive policy development.
ESCRS: monitoring healthcare
When it comes to gathering and analysing data to monitor the quality of European healthcare systems, ESCRS is on the front line—collecting data and analysing and reporting outcomes to identify benchmarks and significant variants, which it hopes will lead to improvements in healthcare quality, Anders Behndig MD, PhD told the workshop.
“We are facing the same problem,” he said. So far, ESCRS has collected data on 4 million cataract surgeries and 13,000 corneal and cell transplantations through different registries, such as EUREQUO and EURECCA, from several EU member states.
“We want to achieve EMR-registry interoperability, to export data from electronic medical records, and cut down the workload,” Dr Behndig said.
The workshop was held at the 2024 ESCRS Winter Meeting in Frankfurt.
Kristine Morrill is Co-founder and President of Medevise Consulting, Strasbourg, France. kristine.morrill@research.escrs.org
Georgy Shakirin is Head of AI of Carl Zeiss Meditech.
Joaquín Fernández Pérez MD, PhD is CEO and Medical Director of the Ophthalmology Department at Qvisión in Vithas Virgen del Mar Hospital, Almería, Spain. JoaquinFernandezoft@Qvision.es
Anders Behndig MD, PhD is President of the Swedish Ophthalmological Society and Professor at Umeå University Hospital, Sweden. anders.behndig@umu.se
GLOBAL REACH
As a renowned authority in the field of cataract and refractive surgery, ESCRS facilitates global connections amongst ophthalmic professionals, fostering collaboration and the exchange of knowledge.
Our events span across continents, providing a platform for pioneering research, advanced surgical techniques, and continuous professional development.
Using the interactive map on our website, we invite you to explore our global presence by viewing upcoming events and academies.
Join us to network with esteemed experts, access the latest advancements, and contribute to the enhancement of eye care on a worldwide scale.
Corneal tissue addition keratoplasty (CTAK) shows promise for improving visual acuity and topography in eyes with keratoconus and may offer a new option to forestall corneal transplantation.
CTAK is similar to corneal allogenic intrastromal ring segments (CAIRS), the modality popularised by Soosan Jacob MD, but CTAK is a branded procedure done using gamma-irradiated, sterilised, preserved, arc-shaped corneal stromal segments and a patient-customised plan for shaping and inserting the inlays provided by a commercial source (CorneaGen). The devitalised stromal tissue has an extended shelf life and is shaped by a femtosecond laser before surgery with a profile based on the patient’s cornea.
CTAK can be used to treat mild, moderate, or severe keratoconus, according to Brandon D Ayres MD. Suitable candidates are patients needing a transplant because they cannot tolerate their rigid gas-permeable contact lens or scleral lens. CTAK could also be considered for patients requiring cataract surgery and tired of wearing a scleral lens, he said.
The surgical procedure takes about 20 to 30 minutes and begins by marking the cornea with the patient seated at the slit lamp. Next, an entry site and insertion channels are cut with customised specifications programmed into a femtosecond laser. The inlays are inserted in the operating room, and proper positioning is verified by overlay of the planning map. Whereas inlay insertion for CAIRS can be facilitated by dehydrating the tissue (i.e., using the “corneal jerky technique”), surgeons performing CTAK may find the insertion step a little more challenging because the tissue tends to “squirt itself back out”. A two-handed technique using the first hand to gradually push the inlay in and coax it along the channel while the second hand holds the segment to prevent backward movement can be helpful, Dr Ayres said.
Implanted around a 4-mm optical zone, the CTAK segments are designed to be pupil-sparing. They do not impede visualisation if cataract surgery becomes necessary and have not been found to impair scotopic vision.
“Only a limited number of CTAK cases have been done so far,” Dr Ayres said. “More experience is needed to develop a better idea of the success and risks of the procedure.”
Rationale
CTAK and CAIRS aim to deliver the benefits of synthetic intracorneal ring segment (ICRS) implantation as a treatment for keratoconus while overcoming the latter procedure’s risks.
“Countless papers show the synthetic ICRS can help patients with keratoconus, but artificial inlays have complications, including exposure, corneal thinning, and infection. What if native tissue could be used instead?” noted Dr Ayres.
He suggested that in addition to having potential safety advantages, the allogenic procedures might offer greater efficacy.
“Because the CTAK and CAIRS inlays are placed more anteriorly, these procedures could result in better corneal flattening and regularisation from epithelial remodelling while avoiding bulging into the posterior cornea,” Dr Ayres explained.
“However, just like with the synthetic ICRS procedures, there have been both miraculous and suboptimal outcomes with CTAK.”
Dr Ayres spoke on this topic at ASCRS 2024 in Boston, US.
Brandon D Ayres MD is co-director of the Cornea Fellowship programme, Wills Eye Hospital, Philadelphia, US. wil-bayres@willseye.org
Digging Deeper into Fuchs’ Dystrophy
Repeat sequences yield clues to Fuchs’ dystrophy pathogenesis.
Research continues to make progress in shedding light on the complex genetic, demographic, and phenotypic correlations underlying Fuchs’ endothelial corneal dystrophy (FECD), according to Siyin Liu.
Although the genetic basis of FECD is complicated and heterogeneous, several causal genes have been identified in recent years, with a region on chromosome 18 responsible for a large proportion of all FECD cases.
First described as an association between FECD and common polymorphisms situated within chromosome 18, studies later confirmed the association came from the transcription factor 4 (TCF4) gene—with genetic and molecular studies implicating an intronic CTG trinucleotide repeat (CTG18.1) expansion as a causal variant in the majority of FECD patients of European ancestry, he said.
“Essentially, you get this CTG sequence that keeps repeating itself, and when it reaches over 50 copies, it becomes pathogenic. Up to 81% of FECD patients harbour one or more alleles with CTG18.1 repeat expansion within the TCF4 gene.”
The rationale behind Dr Liu’s study was to obtain a better understanding of demographic factors, phenotype, and underlying genetic variants in FECD patients.
“When there is a preventative genetic therapy available, understanding the correlations between these factors will be crucial for identifying those individuals who would potentially benefit from these novel approaches before visual impairment and irreversible loss of corneal endothelial cells,” he said.
The researchers collected data from 918 FECD patients at Moorfields Eye Hospital in London and General University Hospital in Prague.
All patients underwent a genome-wide single nucleotide polymorphism (SNP) array, which allowed proband ascertainment and ancestry inference. Some 894 identified probands then underwent CTG.18 genotyping. Those with more than 50 repeat alleles were deemed expansion positive (692 patients), and those with less than 50 (202) were expansion negative. Expansion-negative patients also underwent next-generation sequencing to try to narrow down the potential pathogenic variants.
The results found a higher prevalence of CTG18.1 expansions in European and South Asian patients, which confers a higher risk of FECD.
“Interestingly, a high proportion of South Asian patients within our cohort (64% of 22 patients) can also be attributed to CTG18.1 expansion, which is higher than previously thought,” he said. “Overall, by comparing the European portion of patients to controls, we found that having a CTG18.1 expansion confers a 77-fold greater risk of having FECD.”
Although there is a known female preponderance in FECD, the genetically stratified cohorts in the study showed the
sex-ratio mismatch is primarily driven by factors independent of CTG18.1. “Female preponderance in FECD is driven by CTG18.1-independent factors, possibly environmental, hormonal, or other genetic modifiers, which we need to research further,” he said.
Other findings were that patients who were expansion negative correlated with younger age at first keratoplasty.
“Focusing on the expansion-positive patients, the repeat length of the CTG18.1 also correlates inversely with age at first keratoplasty,” Dr Liu noted. “So, the longer your repeat expansion is, the younger you require keratoplasty.”
From the 150 expansion-negative patients that underwent next-generation sequencing, only 14 potentially pathogenic variants were found within the previously implicated disease-associated genes.
“We know CTG18.1 repeat length is a significant modifier of disease progression, and CTG18.1 expansion dosage also impacts FECD severity and penetrance. Most of the CTG18.1 expansion-negative cases remain genetically unsolved,” Dr Liu said. “The quantification of CTG18.1 somatic instability and interrogation of its link with disease severity must now be prioritised.”
Dr Liu presented at EuCornea 2024 in Paris.
Dr Liu is actively recruiting more patients with FECD and their relatives (including their children). He welcomes collaboration. If you are interested in contributing, please contact him via email or the research coordinator at lin.thaha@nhs.net.
Siyin Liu MBChB, MRes is a Medical Research Council/Fight for Sight Clinical Research Training Fellow and a PhD candidate at the UCL Institute of Ophthalmology, United Kingdom. siyin.liu@ucl.ac.uk
DSO Shows Promise in Treating Fuchs’ Dystrophy
Improved results were seen with no rejection concerns.
Impressive surgical advances have been made in Fuchs’ endothelial corneal dystrophy (FECD) treatment over the past 25 years, with ongoing insights into the biology and genetics of the disease potentially paving the way to an eventual medical therapy of the condition in our lifetime, according to Kathryn Colby MD, PhD.
Speaking at the EuCornea Congress in Paris, Dr Colby focused her presentation on the exciting possibilities of Descemet stripping only (DSO) as a viable treatment for some patients with FECD.
“Over the past 25 years, we have seen a shift in the way we manage Fuchs’ dystrophy surgically,” she said. “We don’t do penetrating keratoplasty anymore, and 2023 was the first year in the United States that Descemet membrane endothelial keratoplasty (DMEK) actually exceeded the numbers of Descemet stripping automated endothelial keratoplasty (DSAEK) procedures for endothelial dysfunction. Since 2014, we have really ushered in the era of modern DSO for treating the disease with results that continue to improve.”
As with every surgical treatment, DSO has its advantages and downsides.
“DMEK is a wonderful surgery with quick visual recovery, but there is still a 6% rejection rate without steroids,” Dr Colby explained. “With DSO, there is no foreign tissue needed and therefore no rejection risk and no risks of long-term steroids. It is a straightforward surgical technique that removes central corneal guttae known to be visually significant.”
On the downside, DSO is not a universal treatment for all FECD cases.
“If the patient has limbus to limbus guttae, they will not do well with DSO. In our original series, we had about a 75% success rate. This was before the era of rho kinase inhibitor (ROCK) supplementation, and some series now approach 100%, but we are not quite there yet.”
Visual rehabilitation and durability of treatment also need to be considered, she said.
“We need to bear in mind that immediately [after] surgery, there will be worse vision after DSO. We remove the endothelium and Descemet membrane, so there will be corneal oedema. The duration of the effect is also not known. The remaining endothelial cells that repopulated the central cornea still have the disease. However, my index patient is now 10 years out from
treatment and is still doing well.”
Dr Colby offered three tips to maximise outcomes from DSO treatments: patient selection, surgical technique, and ROCK inhibitor supplementation.
“Patients [need] to have predominantly central guttae with a preserved peripheral endothelial mosaic,” she said. “They [must] be able to tolerate reduced vision for three to six weeks after DSO, and they have to be willing to have an endothelial keratoplasty if the DSO is not successful.”
In surgical technique, Dr Colby advised removing as many of the central confluent guttae as possible but proceeding very gently with the surgery. “If you put a surgical hook into the posterior corneal stroma, you will cause scarring. Additionally, it is best to aim for a smooth-edged tear and to try to centre the descemetorhexis on the visual axis,” she said.
Finally, she advised using a ROCK inhibitor after DSO surgery. “Both ripasudil and netarsudil have been shown to speed corneal clearance and increase final endothelial cell count after DSO in investigator-initiated series.”
Ripasudil has already successfully completed a multinational phase II trial, with patients currently enrolling for randomised phase III trials with the aim of FDA approval.
Looking to the future, Dr Colby suggested DSO might be combined with new therapies for even better outcomes.
“We know the corneal guttae themselves are visually significant. DSO offers a nice option [for combination] with some new therapies that may improve endothelial cell function or reduce the continued dysfunction of the cells,” she said. “In development right now are a bio-engineered fibroblastic growth factor and small molecules which can inhibit the downstream effect of repeat expansion underlying the bulk of FECD.”
Kathryn Colby MD, PhD is the Elisabeth J Cohen Professor and Chairman of the Department of Ophthalmology at NYU Grossman School of Medicine, New York, US. Kathryn.Colby@nyulangone.org
AI-Assisted Microbial Keratitis Diagnosis
Tool in development could enable timely diagnosis and treatment and reduce costs.
HOWARD LARKIN REPORTS
An artificial intelligence (AI)-assisted tool has been shown to reliably diagnose microbial keratitis (MK) and accurately distinguish among bacterial, fungal, and parasitic infections based on slit-lamp photographs. The tool, which is in development, could improve outcomes by enabling preliminary diagnoses sooner, avoiding the complications and extra costs associated with delayed or incorrect treatment.
The technology also could help mitigate health disparities by reducing the expense and high expertise currently needed to diagnose MK and distinguish among infection subtypes, which is critical to guide effective treatment.
“Treatment of bacterial keratitis is very different from fungal keratitis,” as are treatment of acanthamoeba, and of filamentous yeast fungal subtypes, said Mohammad Soleimani MD.
Accurate MK diagnosis now requires specialised cornea experience and expensive equipment, such as confocal scanning microscopes costing about US$75,000 each, which limits access, Dr Soleimani said. Culturing infected tissue samples is also time consuming, expensive, and not always available or reliable. “We need something more affordable and user-friendly, especially in resource-limited settings.”
Deep-learning models
With that goal in mind, Dr Soleimani developed 3 diagnostic models using convolutional neural networks to analyse more than 10,000 slit-lamp images from about 1,400 patients. These included about 2,000 healthy cornea images, 2,000 fungal keratitis images, 4,800 bacterial keratitis images, and 1,400 acanthamoeba keratitis images. About 80% of the images went towards training the deep-learning models and 20% for validation.
The first model, which distinguished between healthy and MK corneas, proved the most accurate, correctly diagnosing more than 99% of cases. The second model distinguished
among bacterial, fungal, and acanthamoeba in about 80% of cases, reaching accuracies of 91%, 80%, and 81%, respectively. The third model successfully distinguished filamentous and yeast fungal subtypes in about 77% of cases, reaching 76% and 78%, respectively.
By comparison, experienced cornea subspecialists correctly differentiate such cases about 50% of the time. Acanthamoeba is particularly hard to diagnose, with accuracy sometimes running around 10%.
Making an app
To strengthen the models’ performance, Dr Soleimani—with collaborators in Germany, the United Kingdom, Canada, the United States, China, South America, India, and the Middle East—are adding images from diverse patient populations. Validation tests in large external data sets are also underway. External validation is critical to ensure reliability before clinical use.
The ultimate goal is to create an AI-powered cell phone app that will allow diagnosis using images from a variety of cameras, including any kind of digital or cell phone camera, Dr Soleimani said. That way, the tool can be used not just by ophthalmologists, but other types of eye care and health professionals.
“It needs to be available and user-friendly so it can be used anywhere in the world” without specialised cornea training or equipment, Dr Soleimani said. He anticipates the app will be clinically available in two to three years.
Dr Soleimani spoke at ARVO 2024 in Seattle, US.
Mohammad Soleimani MD, FICO is a cornea and ocular surface sub-specialist and professor of ophthalmology at the University of North Carolina, US. msolei2@uic.edu
Images beyond
Scheimpflug image
Detect abnormalities at first screening
The best of both worlds
OCULUS Pentacam® Cornea OCT
In a matter of only one second, cornea specialists are provided with a Scheimpflug image of the anterior segment and the ultra-high resolution OCT images of the cornea, all generated in one single measurement process.
Scheimpflug and Cornea OCT simultaneous 360° 3D capture
Ultra High Resolution of 1,9 µm across the entire cornea
Now: Validated Scheimpflug data and OCT image
Groundbreaking. The Pentacam® Cornea OCT.
Two-Step Procedure Shows Positive Results
Study reveals potentially useful prognostic factors in a large cohort of keratoconus patients.
Atwo-step surgical approach combining intracorneal ring segments (ICRS), then topography-guided PRK and cross-linking has proven a safe and effective treatment modality for a large cohort of patients with keratoconus, according to Olivier Prisant MD.
“This approach has already been published but with very small cohorts,” Dr Prisant said. “Whereas at the Clinique de la Vision in Paris, we have a lot of experience with this technique and have now treated 946 eyes with this protocol. Here, we present the three-month follow-up data for 686 eyes using this surgical protocol.”
Dr Prisant’s retrospective single-centre study was carried out at the Clinique de la Vision between 2009 and 2023, with the presenting surgeon operating on all eyes. All patients received either Keraring or Ferrara ring implants followed at least three months later by topography-guided PRK and cross-linking with another three months (minimum) of follow-up. Inclusion criteria were patients with grade 1, 2, or 3 keratoconus, pachymetry greater than 400 microns, and no previous eye surgery. Exclusion criteria included patients with ring explantation.
Ring arc length distribution.
Ring arc length distribution.
Most of the rings were 160° arc length, symmetric or asymmetric (Keraring AS), with 1 or 2 rings implanted.
Most of the rings were 160° arc length, symmetric or asymmetric (Keraring AS) with 1 or 2 rings implanted
Topography-guided PRK was performed using WaveLight Pentacam Oculyzer and WaveLight EX500 Excimer Laser and cross-linking was performed using riboflavin for 10 minutes and exposure to 10 milliwatts of UVA for 9 minutes.
“In terms of the intracorneal rings, the arc length was primarily 160 degrees and either one or two rings, [which] were either standard or asymmetrical rings,” he said. “The surgical technique included marking at the horizontal axis and visual axis. The rings were inserted in a tunnel and performed using an IntraLase femtosecond laser at a depth of 75% minimal pachymetry.”
Dr Prisant said two-thirds of the patients were male. Best-corrected visual acuity significantly improved by an average of 1.0 lines after the ring implantation and 1.3 lines after the topography-guided PRK ablation.
“We achieved a mean improvement of 2.0 lines of BCVA after both treatments. Similarly positive outcomes were obtained for uncorrected visual acuity, which improved by a mean of 3.7 lines after both treatments,” he explained. “Mean
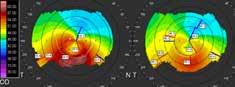
Example of a 25-year-old man who underwent this 2-step procedure. He had ICRS implantation (1 keraring 160°, 250 µm) followed 3 months later by topoguided-PRK with cross-linking. This 2-step protocol improved BCVA from 6 to 10/10, reduced Kmax from 53 to 46.6 D and corrected his ametropia. Topographical flattening effect of ICRS (A) and TG-PRK (B) can be seen on the differential maps.
spherical equivalent reduced by -3.5 D after three months, with most of the regularization achieved by the ring implantation. Refractive cylinder was also reduced by a mean of -3.3 D after both treatments, with the rings again responsible for most of the correction.”
Maximal keratometry was reduced by a mean of almost 7.0 D and most of the flattening effect was obtained with the ring surgery. The complication rate was very low with significant halos in 6 eyes (0.9%), and ring repositioning in 5 eyes (0.7%).
There is a clear rationale for performing the surgical sequence in the order described in the study, Dr Prisant said.
“The logic of the sequence is the ICRS will affect most of the corneal remodelling, which is tissue saving and reduces the need for photoablation. The topography-guided PRK acts as a fine-tuning effect to further improve the visual outcomes,” he said. “Although the aim of this study was to present short-term efficacy and safety results on a large cohort, another study [using] a subgroup of 154 eyes of our cohort with a minimum of three years of follow-up showed good long-term refractive and keratometric stability with this approach.”
The study also found that Kmax and keratoconus phenotypes may be important prognostic factors.
“We found a significant negative correlation between postoperative BCVA and preoperative Kmax, showing that Kmax may be an important prognostic factor. We also studied keratoconus phenotype as a prognostic factor and found decentred keratoconus treated with one 160-degree ring were the eyes that improved the most in terms of BCVA,” he concluded.
Dr Prisant presented at EuCornea 2024 in Paris.
Olivier Prisant MD is an ophthalmologist
in Paris, France. oprisant@gmail.com
Cataract with Epiretinal Membrane
Sequential or combination surgical approach?
TIMOTHY NORRIS REPORTS
Many patients with macular hole or epiretinal membrane have cataract at diagnosis, and many will develop cataract as a side effect of vitrectomy, eventually leading to cataract surgery. For this reason, many surgeons prefer sequential surgery, opting for cataract surgery following vitrectomy.
However, notes Amy O’Regan MD, there is a lack of data in the literature regarding refractive outcomes of patients undergoing phacovitrectomy, with only a meta-analysis published in Ophthalmology1 and only two studies specifically for the refractive outcomes.
This prompted Dr O’Regan to investigate further. With the aid of Professor Dara Kilmartin MD, Dr O’Regan conducted a retrospective review on 25 patients with macular hole or epiretinal membrane and cataract phacovitrectomy over six months. Exclusion criteria were retinal detachment, diabetic-related conditions, and toric IOL implants.
Pre- and postoperative visual acuity were recorded, which was compared from Snellen to logMAR for the analysis. Preand postoperative autorefraction and biometric data such as IOL formula used, axial length, Ks, and predicted refraction
94%
In 18 of the 25 patients, vision improved in 94% by a mean of three lines.
were also recorded. Refractive success was defined as within ±1.00 D of predicted refraction.
Of the 25 cases, 7 had epiretinal membrane (ERM) and 18 macular holes (MH). Mean preoperative visual acuity was 0.43±0.29 logMAR for the ERM group and 0.62±0.16 for the MH group. Mean preoperative astigmatism was about 1.00 D, and only one patient had significant corneal astigmatism. Most patients had an axial length within 22 to 25 millimetres, a very normal axial length.
According to Dr O’Regan, complete postoperative refraction was available for 72% of patients. In 18 of the 25 patients, vision improved in 94% by a mean of three lines: ±0.3 logMAR for the ERM and 0.21±0.15 logMAR for the MH group. Mean deviation of spherical equivalent from target refraction was +0.31 D, slightly hyperopic. Mean postoperative cylinder was similar to preoperative measures, -0.97 D.
SRK/T formula was used in 83% of analysed cases, while the other formulas (Barrett and Holladay 2) showed no significant difference between them, even if numbers were too low for proper comparison, she noted. Cystoid macular oedema occurred in 8% of cases.
Some 33% of patients had an excellent postoperative result with a spherical equivalent within 0.25 D, and 61% had a refractive success within the 1.00 D of the predicted refraction target. Only 6% of cases did not have improved vision.
There appear to be no refractive disadvantages in combining phacoemulsification and vitrectomy, Dr O’Regan said.
“This, however, is a small study, with most patients having an axial length between 22 and 25 millimetres, so we weren’t dealing with very long and less predictable eyes. We need further studies with more numbers, especially if we want to determine which IOL formula is more suited,” she concluded.
Dr O’Regan presented at the 2024 ESCRS Winter Meeting in Frankfurt.
For citation notes, see page 46.
Amy O’Regan MD is a third-year trainee at the University College of Dublin, Ireland. amoregan@tcd.ie
New cataract IOL for Enhanced Intermediate Vision: Precizon Go
Created by Ophtec
Gain extra intermediate vision without compromising the quality of far distance
Precizon Go is the newest addition to Ophtec’s premium line of cataract intraocular lenses (IOLs). This innovative lens represents a significant advancement in enhanced intermediate vision, and closes the gap between traditional monofocal and presbyopic cataract lenses.
Cutting-Edge Design and Technology
The new Precizon Go is a purely refractive lens, precisely engineered with an ingenious technology to provide patients with enhanced intermediate vision while maintaining superior distance vision and visual quality. Its unique optics is characterized by a diopter profile with combined spherical aberrations, which extend the depth of focus without compromising vision quality.
Proven Performance
The new Precizon Go IOL has demonstrated excellent performance both in bench and clinical studies.*
• Modulation Transfer Function (MTF): bench study results show similar MTF curves for both Precizon Go and Precizon Monofocal, confirming the high manufacturing standards of the new design (Figure 1)
• Simulated Defocus Curve: the simulated defocus curve obtained during bench studies demonstrate a clear advantage of Precizon Go within the defocus range of -0.50 D to -2 D (Figure 2)
“The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size.”
Professor Youngsub Eom, MD, PhD
Professor Youngsub Eom, MD, PhD, from the Korean University College of Medicine and Ansan Hospital, performed one of the first surgeries in the clinical marketing study. He remarked, “The aspherical profile of the Precizon Go IOL is a stroke of genius. It provides excellent far and intermediate vision without causing dysphotopsia and corrects the corneal positive spherical aberration according to the pupil size”.
• Visual and satisfaction outcomes: clinical outcomes highlight excellent performance at both far and intermediate distances (CDVA 0,00 ± 0,06 LogMAR, DCIVA80 0,14 ± 0,09 LogMAR & DCIVA66 0,2 ± 0,07 LogMAR), as well as high rates of patient satisfaction with 100% and 94% of patients reporting to be very satisfied or satisfied with far and intermediate vision respectively.
Figure 1. MTF levels of the studied IOLs at the best focus for a 4.5-mm aperture.
Figure 2. Defocus and LogMAR VA simulations as a function of spectacle defocus.
* The scientific data is the result of research studies conducted to evaluate the performance of the Precizon Go IOL, and/or the outcomes in patients receiving surgical implantation of the IOL. The results are summarized in a compendium and can be downloaded at www.ophtec.com/product-overview/precizon-go
Predicting Glaucoma Risk from EHRs
AI model identifies patients likely to need glaucoma screening from non-ophthalmic health data.
An artificial intelligence (AI) model has shown high accuracy in predicting which asymptomatic patients are at high risk of having or developing glaucoma using only non-ophthalmic demographic and medical data from electronic health records (EHRs). It could help identify which asymptomatic patients may benefit from specialised glaucoma screening, according to Rohith Ravindranath, the data scientist who developed this algorithm with Sophia Wang MD, a glaucoma specialist and principal investigator of the project.1
Although glaucoma is a leading cause of irreversible blindness, and a high proportion of patients with glaucoma are undiagnosed, the US Preventive Services Task Force has recently recommended against general glaucoma screening due to its relatively low prevalence and the need for specialised eye care to screen, Ravindranath explained. Nonetheless, the task force has identified it as a critical need for high-risk patients because of the asymptomatic early stages and irreversible vision loss. Black and Latinx populations are known to be at higher risk.
A method for identifying those most likely to need glaucoma care is necessary to ensure those high-risk patients receive screening, Ravindranath added. His project goal was to develop such a pre-screening tool.
The pre-screening model was developed using data from more than 64,000 patients in the US’s All of Us Research Program who had seen an eye doctor. The programme collects EHR and survey data—including socioeconomic and genomic
information—from a national multicentre cohort representing a cross-section of ages, ethnicities, and socioeconomic backgrounds. Its purpose is to provide raw data for developing guidance for personalised medical care. Of these patients who had seen an eye doctor, about 7,300 were diagnosed with glaucoma and the rest did not have glaucoma. Glaucoma suspects were excluded from the sample.
Non-ophthalmic information was extracted from these records and several algorithms were developed using various approaches to try to predict which patients had glaucoma. The study models considered systemic diagnoses, medications, and lab results, as well as demographic data.
The best performing model was developed using a custom one-dimensional convolutional neural network (1D-CNN) to create dense matrices for diagnoses and medications. These 1D-CNNs are especially good for medical data because they can establish connections among a wide range of factors without much data processing to prepare for analysis, Ravindranath said.
This model proved to have an area under the operating characteristic curve (AUROC) of 0.87 and a balanced accuracy of 75.4%, Ravindranath said. Other models scored AUROCs ranging from 0.69 to 0.82, showing significantly less accuracy. An explainability analysis found that age, race, heart rate, body mass index, and haemoglobin A1c contributed most to the winning model’s predictions.
HOWARD LARKIN REPORTS
Importantly, the sample included a wide mix of races and ethnicities, and the model showed good accura cy across all races and ethnicities, Ravindranath said. AUROCs by racial groups ranged from 0.82 for Asian patients up to 0.89 for white patients.
Pre-screening high-risk patients for glaucoma is possible without ophthalmologic data.
SUPPLEMENT YOUR IOL KNOWLEDGE
“Pre-screening high-risk patients for glaucoma is possible without ophthalmologic data,” Ravindranath said, adding more work is needed to ensure the model is robust across all patient subgroups. In the future, he said it could be tested on a screening population of patients without prior eye care and in a prospective trial.
Ravindranath presented at ARVO 2024 in Seattle, US.
For citation notes, see page 46.
Rohith Ravindranath MS is an artificial intelligence and machine learning data scientist at Byers Eye Institute at Stanford University, Palo Alto, California, US. rohithr@stanford.edu
Sophia Wang MD, MS is the principal investigator on this project and a glaucoma specialist and informaticist at Byers Eye Institute at Stanford University, Palo Alto, California, US. sywang@stanford.edu
Explore IOL solutions and demystify common misunderstandings with insights into a refractive future that offers more improved postoperative outcomes—exclusively on the ESCRS website.
escrs.org/eurotimes/ supplements/
Future of Trabeculectomy
Newer techniques and training styles may bring a renaissance of a classic technique.
ROIBEÁRD O’HÉINEACHÁIN REPORTS
In recent years, the advent of less invasive glaucoma surgery techniques has greatly reduced the popularity of trabeculectomy. Nonetheless, trabeculectomy remains the most reliable method to reduce IOP to single digits, and new training techniques may see its resurgence, said Andrew McNaught MD.
“I think trabeculectomy should not be done away with. Particularly with modern techniques with antimetabolites like mitomycin-C—a key innovation in making the procedure more effective—and adjustable sutures, which are an [essential] safety innovation,” he said.
In addition to the introduction of modern bleb-forming devices, such as the Xen and Preserflo, other factors contributing to the reduction in trabeculectomies performed include the inexperience of modern trainees with 10.0 nylon sutures, since they rarely perform extracapsular cataract surgeries. And as trabeculectomy becomes less common, surgeons have fewer opportunities to practise the technique, potentially making it less safe.
There is also the preference among patients for the new devices—and even among glaucoma surgeons when polled for their treatment choice if they were diagnosed with glaucoma.1 These newer alternatives have a higher reimbursement rate, and the intensive follow-up necessary after trabeculectomy is unaffordable for some glaucoma surgeons.
Newer less invasive techniques, with or without topical medication, may provide sufficient IOP lowering for many glaucoma patients, but a considerable proportion for whom the IOP reduction will be inadequate to prevent disease
progression remains. Moreover, there is abundant evidence in the literature that modern trabeculectomy effectively reduces IOP to single digits2 and doing so will reduce visual field progression in eyes with normal tension glaucoma (NTG).3
A case in point
As an example, he described a patient he recently treated who presented at his clinic with advanced progressive NTG. The patient was a 61-year-old male and a batsman for his local cricket team. His only visual complaint was being unable to see the ball properly. His uncorrected visual acuity was 6/5 in both eyes and his IOP was 20 mmHg in both eyes. However, he had end-stage cupping, with a cup/disc ratio of 0.9 in both eyes.
Medical treatment, first with Ganfort and then with additional brinzolamide, failed to reduce IOP. Professor McNaught next performed trabeculectomy in the patient’s left eye, applying mitomycin-C (MMC) 0.9% for one minute and using adjustable sutures to enable postoperative titration of IOP. At his most recent visit, the patient’s treated eye had an IOP of 0.9 mmHg and retained an uncorrected visual acuity of 6/5. He also reported his vision in that eye had become brighter. A procedure for his second eye is now planned.
Prof McNaught noted that, ironically, the unaffordability of MIGS in low- and medium-income countries—and the introduction of new simulated surgery technology that allows remote training in suturing techniques—has now allowed and encouraged more effective teaching of trabeculectomy.
“Lessons learned from teaching trabeculectomy surgery using simulated surgery eyes in low- and medium-income countries are now being applied to teaching trabeculectomy surgery in the UK and Europe,” he added.
Prof McNaught presented his paper at the 2024 European Glaucoma Society Congress in Dublin.
For citation notes, see page 46.
Andrew McNaught MD, FRCOphth, MB BS, FRCS is based at the Department of Ophthalmology, Gloucestershire Hospitals NHS Foundation Trust, Cheltenham General Hospital, Cheltenham, Gloucestershire, UK. andy.mcnaught@btopenworld.com
IOL Selection for the Glaucoma Patient
Decision-making involves an individualised approach accounting for multiple factors.
CHERYL GUTTMAN KRADER REPORTS
Choosing an IOL for a patient having cataract surgery is becoming more challenging as the options continue to increase, and the task can be even more difficult when the patient has glaucoma. Issues to consider include glaucoma type, stage, and stability; health of the ganglion cell complex (GCC); patient age; and condition of the ocular surface. The selection aims to achieve the ultimate goal of maximising quality of vision to maintain or even improve quality of life, said I Paul Singh MD.
“Glaucoma patients deserve to be 20/happy, including after cataract surgery,” Dr Singh said.
Narrowing down the options
An IOL with a monofocal optic will offer the best quality of vision and is an option for any patient with glaucoma although Dr Singh said he has a low threshold for implanting a monofocal toric IOL in the setting of any visually significant astigmatism.
“Correcting even 0.75 D of against-the-rule astigmatism is important for maximising image quality,” he explained.
A multifocal IOL or extended depth of field (EDOF) IOL can also be considered for some patients with glaucoma, but surgeons must recognise these technologies cause loss of contrast (12%–15% with newer multifocal IOLs, 5%–7% with EDOF IOLs) and will compound existing contrast loss related to glaucoma or comorbid dry eye disease. When deciding whether to offer one of the presbyopia-correcting IOLs, Dr Singh said he looks at the OCT GCC analysis as an indicator of glaucoma-related contrast loss and considers glaucoma stability, patient age, and scotopic vision needs.
“Studies show that even patients with moderately severe glaucoma can function very well with a multifocal IOL. However, I counsel all patients that there are risks going forward, and I am especially concerned about future loss of contrast in younger patients and patients who are driving at night,” Dr Singh said, adding he does not consider a small aperture lens for patients with glaucoma because of its effect on contrast and night vision.
The light adjustable lens (LAL) is a good option for patients with narrow-angle glaucoma or a shallow angle because of the risk of a postoperative myopic shift in such eyes. When deciding on an LAL, however, surgeons should also consider if the pupil can be dilated to at least 5 mm, which is the diameter needed to perform the lock-in procedure.
IOL stability is a concern when a patient has pseudoexfoliation. Consequently, Dr Singh said he tends to use an aspheric lens and has a very low threshold for placing a capsule tension ring if he is implanting a toric, multifocal, or EDOF IOL.
Because dry eye disease affects image quality and the accuracy of biometry data used for IOL calculations, Dr Singh stressed optimising the ocular surface before and after cataract surgery—including by aiming to reduce the need for topical anti-glaucoma medications.
“Being able to take away just one topical medication can have an incredible impact on the ocular surface,” he said, encouraging cataract surgeons not already doing minimally invasive glaucoma surgery to learn a MIGS procedure because of the potential for decreasing topical drop burden.
Dr Singh spoke at ASCRS 2024 in Boston, US.
I Paul Singh MD is President of The Eye Centers of Racine & Kenosha, Ltd, Wisconsin, US. inderspeak@gmail.com
Lasers vs MIGS
Will lasers become so good we’ll stop using MIGS?
ROIBEÁRD O’HÉINEACHÁIN REPORTS
Selective laser trabeculoplasty (SLT) and direct SLT have risen to prominence as first-line alternatives to topical medications, but even as the technology improves in safety and efficacy, it is unlikely to eliminate the need for minimally invasive glaucoma surgery (MIGS), said Gus Gazzard MD.
“Whereas we had meds—then more meds, then trabs—in the past, we are now moving towards SLT and more SLT,” Professor Gazzard said. “I think that group of SLT is going to expand, but I still think there is a role for MIGS before we step into bleb-forming surgery.”
He noted the ideal pressure-lowering procedure should be safe, effective, long lasting if not permanent, and repeatable if necessary. In addition, the treatment’s effect should have a mechanism that uses existing physiological pathways for aqueous drainage rather than creating entirely new channels. Moreover, it should not impair future treatment prospects.
There is now increasing evidence from randomised controlled trials to support the use of primary SLT as a first-line treatment for most glaucoma patients, he said. Examples include a large Swedish study aimed at refining the optimal treatment regimen1 and the LiGHT study, which showed 70% of patients were drop free at six years.2
Research conducted since the 1990s in both primates and humans suggests the underlying mechanism of SLT’s efficacy and longevity of effect is it stimulates the migration of new cells to repopulate the trabecular tissues.
Whilst I think the future for SLT and laser procedures is very bright, I don’t think they are ever going to become so good that we’ll stop using MIGS entirely.
energy transsclerally to the trabecular meshwork without the need for a goniolens. Early reports from the randomised controlled GLAURious trial indicate it has the same efficacy as standard SLT at one year.3
Meanwhile, two new laser technologies have entered the MIGS arena: non-thermal excimer laser trabeculostomy with the Elios Vision device, and ViaLase’s femtosecond laser image-guided high-precision trabeculotomy (FLight) procedure. The latter has the advantage of being performed without opening the eye.
“Whilst I think the future for SLT and laser procedures is very bright, I don’t think they are ever going to become so good that we’ll stop using MIGS entirely—unless you want to broaden out the category of lasers on the horizon, which may allow us to do MIGS surgery with the very lasers themselves,” Prof Gazzard said.
“It might be that SLT is stimulating those stem cells and recovery or reconditioning of the trabecular meshwork might even, in a proportion of patients, head off the development of later pressure rise that would have been inevitable if the eye had been treated medically,” he explained. “Whereas MIGS is doing something different. It is cutting, incising, and really disrupting the anatomy and physiology of that same very delicate and exquisitely evolved trabecular meshwork tissue.”
There have also been technological advances in SLT, notably Belkin direct SLT (DSLT), that deliver the same laser
Prof Gazzard presented his paper at the 2024 European Glaucoma Society Congress in Dublin.
For citation notes, see page 46.
Gus Gazzard MA (Cantab), MD, MBBChir, FRCOphth is Professor of Ophthalmology at University College London and Director of Surgery at Moorfields Eye Hospital, London, UK. g.gazzard@nhs.net
Available as:
• PRELOADED
• TORIC
• 4 LOOP
• C LOOP
By Hanita Lenses
Developed using a patented algorithm
Created for maximum light utilization
Designed to redefine clarity and precision
Join the Hanita Lenses booth talks at the ESCRS 2024!
Benefit from proven technology that minimizes disturbances while maximizing performance, ensuring unparalleled visual outcomes for every patient. SAVE MY SEAT! THE FIRST AND ONLY IOL OF ITS KIND:
World-renowned surgeons will share their experiences and research results with our advanced solutions
ESCRS 2024 6-9 Sept. | Fira de Barcelona, Spain Hall 7 – Booth 7.G41
Tackling the Coming AMD Epidemic
Prevention through healthy diet may be key, but more research is needed.
HOWARD LARKIN REPORTS
Although its incidence has declined in younger generations, overall age-related macular degeneration (AMD) numbers are rising rapidly due to global population ageing. Already the third leading cause of blindness, AMD is predicted to affect about 288 million patients worldwide by 2040, up from about 196 million in 2020.
So, what can the global eye care community do, given it is already beset by labour and other resource shortages? “Prevention, prevention, prevention is really important,” Emily Y Chew MD stressed in her ARVO Proctor Medal Lecture.
Harnessing the knowledge gained from research such as the Age-Related Eye Disease Studies 1 and 2 (AREDS and AREDS2) and supplementing it with new research into the causes and mechanisms of AMD could help expand prevention beyond the secondary role of adding supplements for patients already diagnosed with intermediate disease. Dr Chew suggested catching and discouraging AMD before it appears or progresses will help relieve the disproportionate burden it creates in later stages for patients, practitioners, and health systems as well.
The role of supplements
Conducted from 1991 through 2001 with follow-up through 2005, AREDS is a landmark in AMD prevention. It examined the impact on AMD of taking daily doses of 500 mg vitamin C, 400 IU vitamin E, 2 mg cupric oxide, 80 mg zinc, and 15 mg beta-carotene.
“Much to our surprise, we found supplements can reduce the risk of AMD progression from intermediate to late disease by as much as 25% in 5 years,” Dr Chew said. A study extension found the effect lasted at least 10 years,
and a 2023 Cochrane review of existing studies that randomised to supplements or no supplements showed supplements reduced progression to late AMD, with neovascular disease risk declining most.
However, beta-carotene increases the risk of developing lung cancer in smokers and former smokers, nearly doubling it in one study. Begun in 2006, AREDS2 found that substituting the carotenoids lutein 10 mg and zeaxanthin 2 mg for beta-carotene reduced the risk of progression to late AMD by about 10% over 10 years compared with the beta-carotene, without raising cancer or other health risks, Dr Chew said. Therefore, smokers and non-smokers are advised to take AREDS2 rather than AREDS supplements. Adding omega-3 fatty acids was found to have no bearing on AMD progression.
New post-hoc data analysis by the US National Eye Institute suggests that in about two-thirds of patients with geographic atrophy, it does not start in the centre of the retina, so it doesn’t have as much impact. Adding AREDS or AREDS2 supplements reduced the risk of central progression by about 36%. “That’s pretty significant,” Dr Chew said. Further investigation is needed to better understand this finding, she added.
Food as medicine
Dietary questionnaires were also included in AREDS and AREDS2, Dr Chew noted. Data from these and other research suggest that eating fish, greens, and other elements of the Mediterranean diet may cut AMD progression by 25–40%, or even prevent it from developing in the first place. For example, patients who reported not eating any greens on AREDS2 had about a 25% greater chance of AMD progression. “Clearly, it has an impact,” Dr Chew said.
Similarly, the Mediterranean diet, which is high in plant-based oils and includes very little red meat or dairy fat, has been shown to cut cardiovascular disease risk by about 30% and slow AMD progression. An analysis of nine diet elements found fish to be especially protective, Dr Chew said. Those who reported eating fish twice a week had about a 30% reduction in risk of progression to late AMD, including geographic atrophy and neovascular disease. For patients with no or early AMD, a Mediterranean diet reduces the risk of devel oping large drusen—a sign of intermediate disease—by about 25%. “Food really is medicine,” Dr Chew said. “It’s never too late to start the Mediterranean diet.”
It’s never too late to start the Mediterranean diet.
A way forward
Better evidence of the preventive effects of treatment and diet, as well as the natural history of AMD and the mechanisms that drive or slow its progression, are needed to expand treatment, Dr Chew said. Animal studies are currently underway to better characterise the effects of the antioxidants on fatty acids in the blood and retina, genetic and metabolic factors that drive AMD occurrence and progression, and how AREDS supplements or other treatments might affect those mechanisms. The effects of the Mediterranean diet are also being studied for a better understanding of how they affect fatty acid signalling, and how this may influence AMD progression. Such research could reveal new treatment targets for drugs and other treatments.
Analysis of blood samples collected during AREDS and AREDS2 may help find genomic, metabolomic, and proteomic markers of AMD risk and progression, Dr Chew added. Developing AI programs that can analyse OCT and other diagnostic images to detect AMD earlier and better track its progression will also help alleviate eye care professional shortages and growing AMD workloads. There is even potential for an AREDS3 investigating prevention and early progression risk reduction, which will also reduce AMD burdens.
“Prevention is indeed very important,” she concluded.
Dr Chew presented the Proctor Medal Lecture at ARVO 2024 in Seattle, US.
Emily Y Chew MD, FARVO is director of the Division of Epidemiology and Clinical Applications, at the US’s National Eye Institute, the National Institutes of Health (NIH), and is an NIH distinguished investigator in Bethesda, Maryland, US. Among other research, she chairs the Age-Related Eye Disease Study 2 (AREDS2) and the eye study of the Actions to Control Cardiovascular Risk in Diabetes (ACCORD) Trial. echew@nei.nih.gov
VJCRS celebrates 40 years of videos
The Video Journal of Cataract, Refractive, & Glaucoma Surgery has hit a major milestone, celebrating its 40th anniversary. The first issue of 2024 is titled “It’s All About Science” and includes nine new videos ranging from Dr Ruth Lapid-Gortzak’s presentation on a novel thermomechanical adjustable IOL to Dr Kansas Veena’s exploration of a model for green cataract surgery.
This brings the journal back to its roots, when the VJCRGS launched in the early 1980s with the singular mission of providing the highest quality of video education for ophthalmic surgeons. Online at vjcrgs. com, the journal is now a free member benefit of virtually every cataract society in the world, including the ESCRS.
Founded by Robert Osher MD in the US, the VJCRGS was the first video journal in medicine, established in the day of videotape, before the internet existed. Each quarterly issue offers at least an hour of the highest quality education for the anterior segment surgeon. The journal is free to all practising ophthalmologists and teaching institutions.
FLACS CONTINUES TO EVOLVE
What is the place of femto in modern cataract surgery?
Femtosecond laser-assisted cataract surgery (FLACS) is a relative newcomer, with the first systems only becoming available in 2008. Since that time, both the hardware and software have continued to evolve. What is the place of FLACS among the options available to ophthalmic surgeons? Which patients are likely to benefit the most? EuroTimes asked Professor Burkhard Dick MD, PhD for an update.
What is your current use of FLACS?
I currently perform femtosecond laser cataract surgery on a wide range of patients. These include uncomplicated cases, people who want good postoperative visual acuity and high safety standards, and patients with complex situations (see below)—even the youngest with paediatric cataracts. We have shown in a number of studies1,2 how safe it is to perform laser capsulotomy in young children—not only anterior capsulotomy but also primary posterior capsulotomy (PPC), which we believe is an absolutely necessary precaution to prevent posterior capsule opacification, which tends to be fulminant in children. The predictability and accuracy of the laser in performing capsulotomies are essential in these patients who require long-term care and monitoring.
What are the known (proven) and potential advantages of FLACS?
In short, it is safe and effective. It has several advantages, although it has to be said that laser cataract surgery (LCS) is always compared to one of the most successful procedures in all of medicine, phacoemulsification. That really is a high bar that does not leave much room for improvement. And yet, the latest meta-analysis suggests that less ultrasound energy results in less corneal tissue damage, which is particularly important in the long term.3 There is greater precision and the prospect of less damage to ocular structures.
Many femtosecond laser platforms now include advanced imaging systems that provide real-time, high-resolution images of the eye to aid precise surgical planning and execution. As cataract surgery today is always refractive surgery, it cannot be overstated that femtosecond laser surgery instils a culture and strategy among surgeons to manage astigmatism. The technology allows precise corneal incisions to correct pre-existing astigmatism. When the astigmatism is not corrected by a corneal procedure but by a lens-based procedure, a perfectly centred and sized capsulotomy allows highly accurate IOL placement, which is invaluable when implanting toric IOLs.
In what situations is FLACS clearly indicated (preferred)? Earlier, I used the term ‘all-comers approach’ to characterise the potential of femtosecond laser-assisted cataract surgery. In my opinion (more than 13,000 procedures later), there is no need to reconsider. The success rate of LCS in uncomplicated cases is convincing. But so are patients with a history of systemic alpha-blockers, zonular instability, or pupils less than 6 mm— to name but a few conditions that can be a nightmare for both patient and surgeon. These challenging cases are probably the patients now thought to benefit most from LCS. It is the much lower impact on the corneal endothelium—compared to the application of ultrasound energy during phacoemulsification—that makes LCS so well suited for eyes with Fuchs’ degeneration and similar conditions.
LCS is not only possible in complex cases—it is often preferable, at least in my experience. Consider mature or ‘white’ cataracts. The often immense pressure inside the capsule (which can lead to an explosive rupture when touched and thus to the dreaded ‘Argentinian flag syndrome’) can be assessed by the laser platform’s OCT. The presence of intracapsular pressure
can convince the surgeon to start the procedure with mini-capsulotomies (which we have performed many times and described in published work)3,4 and thus manage a potentially dangerous situation. In very advanced cataracts (now less common in developed countries), the laser pre-fragments the dense and hard lens, making it easier to remove the fragments with less ultrasound energy.
In patients with relatively dense cataracts and low preoperative endothelial cell counts, a recent meta-analysis has documented the advantages of LCS in terms of lower ultrasound energy, less endothelial cell loss, and, in the safety analysis, a lower incidence of posterior capsule tear with an OR (odds ratio) of 0.29—just to name a few parameters.5
I would also like to mention patients with Marfan syndrome who, like patients with zonular weakness for other reasons such as PEX, have benefited enormously from the precision and reduced ultrasound energy with LCS. Since the femtosecond laser does not require zonular support for capsulotomy and exerts minimal stress on the zonules during reduced ultrasound application, its advantage in treating zonular weakness and subluxated cataracts is obvious.
How would you describe the training and learning curve? Is there a perception that training (and the learning curve) are an obstacle to FLACS uptake?
Not at all. Every first step looks difficult, no matter what you are starting with, and surgical techniques are certainly no exception. As with any other instrument in ophthalmic surgery, a novice needs an experienced teacher and coach to guide them. The learning curve for performing LCS is twofold: the surgeon needs to learn how to use the laser and familiarise themselves with the settings, and they also need to change the way they work. There are steps the surgeon needs to be aware of
Even in the first cases of laser surgery, complications are rare.
as the cortex has been truncated at the capsulotomy edge, and there may also be intralenticular or retro-lenticular gas. Nevertheless, the learning curve is not particularly daunting. In my experience,
ESCRS Academies
Committee representatives of ESCRS organise and present sessions at meetings organised by our national and sister societies. These sessions are typically delivered by a group of speakers on a current topic selected by ESCRS in person or virtually.
These sessions provide useful education as well as collaboration between societies promoting and sharing benefits across both memberships.
and their trainers—in vascular surgery, plastic surgery—in any field of interventional medicine!
Are there recent developments in FLACS technology that address prior limitations not reflected in older studies evaluating its use?
First, it is important to note that the quality of recent cuts has been signifi-
escrs.org/education/academies/
sensitive to room temperature. Smaller, more mobile, and less demanding systems are now available. In addition, some ancillary materials have been developed, such as a special smaller interface for use in paediatric cataract surgery. Treating astigmatism with arcuate incisions is far superior to any form of manual keratotomy—humans can’t control depth and position as perfectly as the laser can. And the ability to make intrastromal incisions is unique to the femtosecond laser.
Having said that, am I happy with the way the technology is developing? Absolutely not. The manufacturers—or, to be fair, some manufacturers—have not contributed to further improvements to the extent I hoped when LCS was introduced.
Are there forthcoming developments that could favour its wider use?
Biomorphometric detection and capsule marker use are being introduced. They are far superior to anything we have seen in the alignment of toric IOLs; there are absolutely no parallactic errors. Alignment can be checked, even months after surgery. Alternatively, the laser can place markers in the cornea to guide the surgeon when making arcuate incisions. Of course, studies without this technology show no difference. Patient safety in these procedures is unsurpassed, and iris recognition makes it almost impossible to treat the wrong eye.
A whole new generation of IOLs is being introduced that would probably not have been developed without LCS. These designs make the most of the perfectly cut and centred capsulotomy the laser performs and can be placed with high accuracy to benefit the patient’s vision. Examples include the bag-in-the-lens (BIL) IOL created by Marie-José Tassignon, the so-called femto IOL, and the lens named after Samuel Masket, who designed it specifically to reduce negative dysphotopsia.
Other innovations we will see include (even) faster laser systems, fully three-dimensional treatment configuration on all systems, advanced iris recognition, and the use of the Helix laser.
Is there anything else about FLACS you want to mention?
Most of the criticism of LCS has not really been directed at its medical performance and documented results. How could this be? LCS is extremely safe, and the rate of posterior capsule rupture (used by some authors as an argument against LCS) is less than 1%, according to recent randomised controlled trials.4,5 Postoperative visual acuity is good, and patient satisfaction is high. The main criticism is the cost of the procedure. There is no doubt LCS is currently more expensive than routine phacoemulsification. There is definitely room for improvement. It can be argued that once the cost of the laser machine and disposables is significantly reduced and accepted into routine practice, it could lead to a new era of refractive cataract surgery and a higher rate of premium lens implantation.
Much has been made of the potential for anterior capsule rupture during or after laser capsulotomy, at the beginning of LCS. This cannot be emphasised enough: The rate of anterior
≤ 1%
ALCS is extremely safe, and the rate of posterior capsule rupture (used by some authors as an argument against LCS) is less than 1%, according to recent randomised controlled trials.4,5
capsule rupture is very low and similar to manual surgery.
What no one talks about, however, is that in the event of a posterior capsule rupture and the need for sulcus implantation, an optimal capsulotomy for the fixation of the optic (optic capture) can be performed perfectly (posteriorly or anteriorly), depending on the situation.
Let me summarise: LCS is now a technology that can be tailored to the individual patient’s anatomy and specific cataract and refractive situation. We have been talking about personalised medicine since we were in medical school. With femtosecond laser-assisted cataract surgery, personalised patient care has become a reality—with functional results that would be the envy of any other medical discipline.
For citation notes, see page 46.
H Burkhard Dick MD, PhD is Professor of Ophthalmology and Chairman, Ruhr University Eye Hospital Bochum, Bochum, Germany. He is also Secretary of the ESCRS. burkhard.dick@kk-bochum.de
NEW TECH FACILITATES VIRTUAL TRAINING
Anovel smartphone-enabled app connected to a slit lamp or microscope allows for real-time simulation of cataract surgery with silicone models, guiding surgeon training through every step of simulated cataract surgery and providing objective feedback.
The app coordinates with Custom Surgical’s MicroREC, an optical system that enables ophthalmologists to connect their smartphone devices to slit lamps and microscopes to capture images or record videos of their clinical findings and procedures, speeding up the process of clinical documentation, the developers say. The system also facilitates sharing of information with colleagues and patients.
Data collected with MicroREC can be uploaded to the cloud-based platform MicroREC Connect, allowing instant access to cross-platform compatible surgical information. Major clinics and hospitals around the globe already use this service. The company founders aim to further improve this service by involving big data and artificial
intelligence to enhance precision and help doctors better track their patients’ conditions over time. The first steps are already in motion with the integration of an automatic segmentation tool in the MicroREC Connect platform to guide clinicians in anatomical structure analysis—facilitating ocular pathology diagnosis and treatment.
Professor Wolfgang J Mayer MD and Daniel R Muth MD have developed a novel application called Augmented Reality MicroART. This didactic software can be attached to the MicroREC hardware adapter for real-time simulation of cataract surgery with silicone models, guiding surgeon training through every step and providing objective feedback thanks to the use of a responsive AI algorithm.
The process of digital transformation is a paramount principle for the Munich-based start-up Custom Surgical, according to its founders, Federico Acosta and Fernando Benito. Established in 2019, the start-up aims to facilitate and optimise diagnostics in
clinical practice by implementing new technological solutions that promise to revolutionise eye disease detection and tracking and combat avoidable blindness worldwide.
According to Acosta and Benito, the system revolves around the deployment of Computer-Aided Diagnosis (CAD) tools, apps, and web-based services that foster the broad availability of high-performance smartphones—offering worldwide access to timely diagnostics for every patient, regardless of location or financial resources.
While openness to innovation and a keen eye for cutting-edge technology and digitalisation are common among all fields of medicine, ophthalmology has always been very inclined to innovate, often implementing new solutions for a better, faster, and safer practice. In this landscape of constant evolution, digital transformation may represent one of the greatest hotspots, not only for new solutions for clinicians but for a broader democratisation of healthcare access, Dr Mayer noted.
ESCRS Educational Forum is supported by multiple industry partners to provide independent didactic education on selected therapeutic areas. The platform combines presentations from ESCRS Winter and Annual Congresses, selected EuroTimes articles, videos, and webinars to provide an in-depth overview on current clinical outlooks.
Education Forum
escrs.org/education/forum/
Nidek’s new preloaded IOL injection system received CE mark
NIDEK has received a CE mark for the NP-1/NP-1C Preloaded IOL Injection System, preloaded with the hydrophobic acrylic Aktis SP IOL. The lens has a 90-degree haptic design (Anchor Wing Loop) to increase the contact area with the capsular bag and optimise its stability and centration. The company reports implanting the lens with the system is a simple two-step process of filling the viscoelastic material and pressing the plunger. nidek.com
EMA refused marketing authorisation for Syfovre
The European Medicines Agency (EMA) has recommended the refusal of marketing authorisation for pegcetacoplan (Syfovre®, Apellis), a complement inhibitor for geographic atrophy treatment. The EMA based its decision on the lack of clinically meaningful benefits for patients in the OAKS and DERBY trials—despite a reduction in the growth of geographic atrophy lesions. apellis.com
Breakthrough designation for new cell therapy
The US FDA has granted Breakthrough Therapy (BT) and Regenerative Medicine Advanced Therapy (RMAT) designations to Aurion Biotech’s AURN001, an investigative allogeneic cell therapy designed to treat corneal oedema secondary to corneal endothelial disease. AURN001 is composed of neltependocel, derived from allogeneic human corneal endothelial cells and Rho-kinase inhibitor Y-27632 and designed for a one-time intracameral injection. aurionbiotech.com
FDA clearance granted for vitreoretinal and cataract surgery systems
Alcon has received FDA 510(k) clearance for its Unity Vitreoretinal Cataract System (VCS) and Unity Cataract System (CS). Unity VCS combines vitreoretinal and cataract surgery capabilities, and both systems are designed to improve workflow efficiencies over Alcon’s existing systems. alcon.com
Neurotech granted priority review for encapsulated cell therapy
The FDA has granted priority review of Neurotech Pharmaceuticals’ biologic license application (BLA) for NT-501 (revakinagene taroretcel), an investigational encapsulated cell therapy for treating macular telangiectasia type 2 (MacTel). NT-501 is a semi-permeable capsule filled with proprietary allogeneic RPE cells which, when implanted in the vitreous, delivers sustained therapeutic doses of ciliary neurotrophic factor (CNTF) to the retina, promoting photoreceptor survival and maintenance. The FDA’s priority review means the license application is sufficiently complete to permit a review and aims to act within 6 months, compared to 10 months for standard review. neurotechpharmaceuticals.com
New cryopreserved amniotic membrane product launched
BioTissue has launched a new hydrated, shelf-stable cryopreserved amniotic membrane product called the CAM360 AmnioGraft, intended to treat mild to moderate dry eye and other ocular surface disorders. CAM360 is ringless and does not require refrigeration. The graft has adhesive properties to ensure it stays in place under a bandage contact lens. biotissue.com
SIGNIFICANT
DIFFERENCES BETWEEN SEXES IN OCULAR BIOMETRY
Including gender as a parameter in IOL calculation may improve predictive accuracy, according to a retrospective single-centre observational study. The study included 34,589 eyes of 20,004 cataract patients and showed significant differences between the sexes for most biometric variables. Women’s eyes were shorter than those of men by an average of 0.53 mm. Women also had steeper anterior keratometries but showed no difference in anterior astigmatism magnitude, although there was a different orientation. The distribution of IOL power also differed between sexes, with the interquartile range shifting 1.0 D toward more powerful lenses in women. The difference in lens thickness was minimal, although statistically significant, and central corneal thickness differed barely by 5 µm.
M Jiménez-García, et al. “Biometric description of 34 589 eyes undergoing cataract surgery: sex differences,” 50(7): 668–675.
ESCRS ONLINE CALCULATOR PERFORMS WELL FOR PAEDIATRIC EYES
In paediatric patients, using the refined IOL constants that are provided by the online ESCRS IOL calculator seems to improve postoperative residual refraction predictability according to a retrospective, consecutive case series. The study included 60 eyes from 47 patients with a mean age of 6.5 years, phacoemulsification, and IOL implantation (AcrySof SN60AT) due to congenital or juvenile cataract. The authors compared the prediction error of formulas provided by the online ESCRS IOL calculator with the SRK/T formula. The median absolute prediction error (MedAE) was lowest in the SRK/T formula, which performed significantly better than Hoffer QST and Kane, followed by BUII, Pearl DGS, EVO, Hoffer QST, and Kane. The SRK/T also resulted in the highest proportion of eyes within ±0.5 D of the target refraction, followed by BUII, EVO, and Pearl DGS. The lowest number was found using Kane and Hoffer QST. Some formulas had a significantly higher rate of eyes within ±0.5 D when eyes without optic capture were excluded.
C Lwowski, et al. “Intraocular lens calculation using the ESCRS online calculator in paediatric eyes undergoing lens extraction,” 50(7): 676–681.
MUSIC RELIEVES PATIENTS’ ANXIETY DURING CATARACT SURGERY
Playing patient-selected music during cataract surgery is an effective way to decrease anxiety, according to a prospective, randomised, controlled clinical trial. The study included 107 patients with a mean age of 71.2 years who were randomised to undergo cataract surgery with their chosen genre of music or cataract surgery without music. Those in the music group had significantly lower total self-reported anxiety (mean 5.98) than the control group. Moreover, patients exposed to music reported feeling significantly less frightened, nervous, and confused during surgery. There was no significant difference between the groups in the number and dosage of sedatives given.
P A Rivera, et al. “Music during cataract surgery: effect on anxiety,” 50(7): 688–692.
the leading community and trusted source for SCIENCE, EDUCATION & PROFESSIONAL DEVELOPMENT in the fields of cataract and refractive surgery.
Cited in this Issue
Cataract with Epiretinal Membrane
Page 28
1. Daud F, et al. “Combined versus Sequential Pars Plana Vitrectomy and Phacoemulsification for Macular Hole and Epiretinal Membrane,” Ophthalmology Retina, 7(8): 721–731. doi: 10.1016/j.oret.2023.03.017.
Predicting Glaucoma Risk from EHRs
Page 30
1. Ravindranath R and Wang S Y. “Development of Artificial Intelligence Models to Identify Patients at High Risk for Glaucoma Using National Electronic Health Records,” Investigative Ophthalmology & Visual Science, 65(7): 1505–5. https://iovs. arvojournals.org/article.aspx?articleid=2794075
Future of Trabeculectomy
Page 32
1. Chang TC, et al. “Glaucoma surgery preferences when the surgeon adopts the role of the patient,” Eye (Lond), 2019; 33(10): 1577–1583.
2. Schultz S, et al. “Achieving Single-Digit Intraocular Pressure Targets with Filtration Surgery in Eyes with Progressive Normal-Tension Glaucoma,” Journal of Glaucoma, 2016 25(2): 217–222.
3. Naito T, et al. “Effect of trabeculectomy on visual field progression in Japanese progressive normal-tension glaucoma with intraocular pressure < 15 mmHg,” PLoS One, 2017 Aug 29; 12(8): e0184096.
Lasers vs MIGS
Page 34
1. Dahlgren T, et al. “Optimal Performance of Selective Laser
Trabeculoplasty: Results from the Swedish Optimal SLT Multicenter Randomized Controlled Trial,” Ophthalmology Glaucoma, 2024, 7(2): 105–115.
2. Gazzard G, et al. “Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial,” Lancet, 2019, 393(10180): 1505–1516.
3. Belkin M, et al. “GLAUrious, a multicentre, randomised, controlled study of direct selective laser trabeculoplasty in open angle glaucoma,” 2023 ARVO Annual Meeting Abstract, June 2023. https://ivos.arvojournals.org/article.aspx?articleid=278925
Newsmaker: FLACS Continues to Evolve
Page 38
1. Alio JL, Dick HB, Osher RO. Cataract Surgery. Advanced techniques for complex and complicated cases. Springer, Cham (Switzerland), 2022.
2. Dick HB, Gerste RD, Schulz T. Femtosecond Laser Surgery in Ophthalmology. Thieme (New York), 2018.
3. Chen DZ, Chee SP. “Femtosecond laser-assisted cataract surgery for complex cataracts – A review,” Indian J Ophthalmol, 2024; 72(5): 629–936.
4. Levitz LM, Dick HB, Scott W, et al. “The Latest Evidence with Regards to Femtosecond Laser-Assisted Cataract Surgery and Its Use Post 2020,” Clinical Ophthalmology, 2021;15: 1357–1363.
5. Pichardo-Loera NS, Corredor-Ortega C, Castro-Monreal MA, et al. “Femtosecond laser-assisted cataract surgery versus conventional phacoemulsification: A meta-analysis of randomized controlled trials,” Eur J Ophthalmol, 2024 Jan 30: 11206721241229129. doi: 10.1177/11206721241229129
ESCRS iLearn is an online learning platform, free for ESCRS members.
Visit elearning.escrs.org to access over 30 hours of interactive, assessed, and accredited e-learning content, including surgical videos, diagrams, animations, quizzes, and forums.
https://escrs.org/special-interest-groups/yos/
Upcoming Events
September 6–10
2024 ESCRS Congress
Barcelona, Spain
September 6
ESCRS iNovation Day
Barcelona, Spain
September 26
2nd International TOA Retinopathy of Prematurity Course Istanbul, Turkey
September 27–29
19th Symposium of the CroCRS Split, Croatia
October 18–21
American Academy of Ophthalmology Chicago, United States
November 20–24
The 58th TOA National Congress Antalya, Turkey
November 28–29 UKISCRS
75th Anniversary of the IOL London, United Kingdom
6 Sept
27 Sept 26 Sept
28 Nov
ESCRS IN A SNAPSHOT
We are a society of surgeons who specialise in improving vision and restoring clarity. Since 1991, ESCRS has promoted the education and research of implant and refractive surgery. With more than 7,500 members from 130 countries worldwide, ESCRS is a vital global platform for the field of ophthalmology.
YOU DON´T WANT TO MISS THIS!
Saturday 7th and Sunday 8th
Join Our Experts Panel
and learn about iStent inject® W, a PROVEN SAFE technology for an early intervention preserving Patients’ Functional Vision1 and Quality of Life2
SCAN THE QR CODE TO ACCESS THE FULL PROGRAM
1- Gillmann K, Hombeak DM. BMJ Open Ophth 2024;9:e001575.doi:10.1136/bmjophth-2023-001575.
Hands-on Experience
Daily with iStent inject® W Trabecular Micro-Bypass a PROVEN Truly Tissue-Sparing Procedure
SCAN THE QR CODE AND BOOK YOUR SESSION NOW!
2- Samuelson, Thomas W., et al. “Quality of life in primary open-angle glaucoma and cataract: an analysis of VFQ -25 and OSDI from the iStent inject ® pivotal trial.” American Journal of Ophthalmology 229 (2021): 220-229.
iStent inject ® W IMPORTANT SAFETY INFORMATION INDICATION FOR USE: The iStent inject ® W, is intended to reduce intraocular pressure safely and effectively in patients diagnosed with primary open-angle glaucoma, pseudo-exfoliative glaucoma or pigmentary glaucoma. The iStent inject ® W, can deliver two (2) stents on a single pass, through a single incision. The implant is designed to stent open a passage through the trabecular meshwork to allow for an increase in the facility of outflow and a subsequent reduction in intraocular pressure. The device is safe and effective when implanted in combination with cataract surgery in those subjects who require intraocular pressure reduction and/or would benefit from glaucoma medication reduction. The device may also be implanted in patients who continue to have elevated intraocular pressure despite prior treatment with glaucoma medications and conventional glaucoma surgery. CONTRAINDICATIONS: The iStent inject ® W System is contraindicated under the following circumstances or conditions: • In eyes with primary angle closure glaucoma, or secondary angle-closure glaucoma, including neovascular glaucoma, because the device would not be expected to work in such situations. • In patients with retrobulbar tumor, thyroid eye disease, Sturge-Weber Syndrome or any other type of condition that may cause elevated episcleral venous pressure. WARNINGS/PRECAUTIONS: • For prescription use only. • This device has not been studied in patients with uveitic glaucoma.
• Do not use the device if the Tyvek® lid has been opened or the packaging appears damaged. In such cases, the sterility of the device may be compromised. • Due to the sharpness of certain injector components (i.e. the insertion sleeve and trocar), care should be exercised to grasp the injector body. Dispose of device in a sharps container. • iStent inject ® W is MR-Conditional; see MRI Information below. • Physician training is required prior to use of the iStent inject ® W System. • Do not re-use the stent(s) or injector, as this may result in infection and/or intraocular inflammation, as well as occurrence of potential postoperative adverse events as shown below under “Potential Complications.”