You’re not just our patient. You’re our neighbor. For more than a century, Orlando Health Orlando Regional Medical Center has been honored to provide nationally recognized care for the Central Florida region we proudly call home. And because it’s your home, too, you deserve trusted healthcare within reach, so we can foster a partnership focused on health and wellness — together. Giving you more reasons to choose well. OrlandoHealth.com/ORMC
4
COVER STORY
Complex neurological treatment plans involving input from multiple disciplines can be frustrating both for patients and their doctors. The complicated quest to keep everyone on the same page can lead to miscommunications and less-than-ideal outcomes.
Those concerns, however, are being erased by the creation of the Orlando Health Neuroscience Institute – Bayfront, which brings an interdisciplinary approach to caring for a wide range of neurological conditions in Pinellas County.
The institute’s Dr. Lowell Dawson, who is a member of Florida Medical Clinic Orlando Health, witnessed the promise of this new approach during a recent meeting involving a young patient and all of his doctors.
“Along with myself – I’m a neurointerventional radiologist – we had a neurologist, a neurosurgeon and a pulmonary critical care physician all in there talking with the family and the patient,” Dr. Dawson said. “To have that congenial working relationship, it definitely yields dividends and benefits.”
The new program brings together highly trained physicians from a number of specialties and practices, creating a full-service patient experience for the neurosciences.
“Interdisciplinary care is the way to go,” Dr. Dawson said. “When you look at any major institution, they treat each patient from an interdisciplinary perspective.”
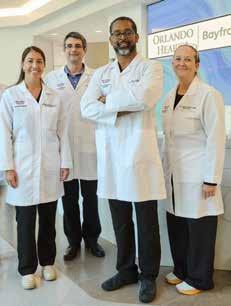
ON THE COVER Orlando Health Neuroscience Institute team members Physician Assistant Jessica Feronti, Dr. Liviu Craciun, Dr. Lowell Dawson and Sr. Nurse Practitioner Tammy Schlatterer at Orlando Health Bayfront Hospital, in St. Petersburg, FL.
Iam pleased to bring you another issue of Florida MD. I can only imagine the emotional and physical trauma that a woman goes through when she has a mastectomy. The procedure affects not only her body, but her mind and her self-esteem. Now add in the inability to not be able to reconstruct her breasts and give that part of her life back, because she’s uninsured or under insured, and it becomes an unthinkable crushing blow. Fortunately there is My Hope Chest to help women who are unable to afford reconstructive surgery. I asked them to tell us about their organization and how you, as physicians, can help. Please join me in supporting this truly wonderful organization.
Best regards,
Donald B. Rauhofer Publisher
MY HOPE CHEST — Making Women Whole Again
In 2010, more than 22,000 uninsured women lost their breasts to cancer and were left disfigured, deformed and feeling “less than whole.” How many years has this figure been growing?
Many organizations raise funds for research, education and “awareness” of breast cancer. Most have no idea there lies a huge gap in assistance for delayed reconstruction and co-pays for survivors wanting this surgery.
My Hope Chest is the ONLY national 501c3 non-profit organization focused on funding breast reconstruction for the uninsured and under insured survivors. Our services “pick up” where other breast cancer organizations leave off… providing the “final step in breast cancer treatment. ”
My Hope Chest is about addressing the needs of survivors now. Through wonderful surgeon partnerships we are able to transform the lives of breast cancer survivors who otherwise have no hope of reconstruction. We hope to hear from you to learn how we can work together to eliminate our wait list and take action to help every woman who desires reconstruction after mastectomy and feel restored in body, mind and spirit. Wish List
• Surgeons to create awareness for My Hope Chest and to identify new clients
• Doctors of Distinction- Surgeon partners nationwide to join our program.
• Corporate partners, interested in Win-Win, Commercial- coventure marketing campaigns promoting their product or service by sharing our vision to make sure there is always coverage for reconstruction surgery.
For additional information on how you can help or refer a patient please go to www.MyHopeChest.org.
ADVERTISE IN FLORIDA MD
For more information on advertising in Florida MD, call Publisher Donald Rauhofer at (407) 417-7400, fax (407) 977-7773 or info@floridamd www.floridamd.com
Email press releases and all other related information to: info@floridamd.com
PREMIUM REPRINTS
Reprints of cover articles or feature stories in Florida MD are ideal for promoting your company, practice, services and medical products. Increase your brand exposure with high quality, 4-color reprints to use as brochure inserts, promotional flyers, direct mail pieces, and trade show handouts. Call Florida MD for printing estimates.
Publisher: Donald Rauhofer
Photographer: Donald Rauhofer / Florida MD
Contributing Writers: John “Lucky” Meisenheimer, MD ,Tara Griffin, DMD Sonda Eunus, MHA, John Meisenheimer, VII, MD;B.S., Daniel T. Layish, MD, FACP, FCCP, FAASM, Akshay Manohar, MD, Tara Griffin, DMD, Frank Ricci, George Haidukewych, MD
Art Director/Designer: Ana Espinosa
Florida MD is published by Sea Notes Media,LLC, P.O. Box 621856, Oviedo, FL 32762. Call (407) 417-7400 for more information. Advertising rates upon request. Postmaster: Please send notices on Form 3579 to P.O. Box 621856, Oviedo, FL 32762.
Although every precaution is taken to ensure accuracy of published materials, Florida MD cannot be held responsible for opinions expressed or facts expressed by its authors. Copyright 2025 Sea Notes Media. All rights reserved. Reproduction in whole or in part without written permission is prohibited. Annual subscription rate $45.
New Orlando Health Neuroscience Institute – Bayfront Provides AllEncompassing Neurological Care
By Staff Writer
Complex neurological treatment plans involving input from multiple disciplines can be frustrating both for patients and their doctors. The complicated quest to keep everyone on the same page can lead to miscommunications and less-than-ideal outcomes.
Those concerns, however, are being erased by the creation of the Orlando Health Neuroscience Institute – Bayfront, which brings an interdisciplinary approach to caring for a wide range of neurological conditions in Pinellas County.
The institute’s Dr. Lowell Dawson, who is a member of Florida Medical Clinic Orlando Health, witnessed the promise of this new approach during a recent meeting involving a young patient and all of his doctors.
“Along with myself – I’m a neurointerventional radiologist – we had a neurologist, a neurosurgeon and a pulmonary critical care physician all in there talking with the family and the patient,” Dr. Dawson said. “To have that congenial working relationship, it definitely yields dividends and benefits.”
The new program brings together highly trained physicians from a number of specialties and practices, creating a full-service patient experience for the neurosciences.
“Interdisciplinary care is the way to go,” Dr. Dawson said. “When you look at any major institution, they treat each patient from an interdisciplinary perspective.”
The institute aims to do just that. It features physicians and clinicians covering a wide range of specialties, including:
• Stroke
• Epilepsy care
• Brain tumors
• Aneurysms
• Head and spinal cord trauma
• Alzheimer’s disease and dementia
• Multiple sclerosis
• Parkinson’s disease
• Chronic pain
• Headaches
COORDINATED CARE FOR PATIENTS
One of the institute’s primary strengths is the way it pulls together a wide range of services and procedures under one roof.
“There are a number of subspecialities in the Orlando Health Neuroscience Institute,” said Jill Benford, senior service line director at Orlando Health Bayfront Hospital. By bringing together all of these specialties, physicians combine efforts to provide individualized care for each patient.”
Current facilities include 38 dedicated beds for neurology care and two neurosurgery operating rooms, along with a neuro ICU. The institute has 24/7 seizure monitoring capabilities and cares for patients throughout their treatment journey – from diagnosis to rehabilitation.
With the institute’s services spanning from treating those suffering from a stroke or a movement disorder like Parkinson’s to headaches and migraines, it is truly an all-encompassing endeavor.
“We felt like it was time to pull all of the different aspects of neurological care together, and I think we’ve been successful in doing that,” said John Moore, president of Orlando Health Bayfront Hospital. “There are a wideranging set of services provided within the neuroscience institute.”
The idea of creating a dedicated neuro institute has been several years in the making, in part due to the al-
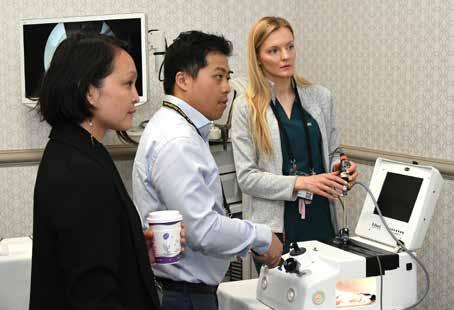
Dr. Passaro and Neuro Diagnostic Supervisor Susan Arriagada of the Orlando Health Neuroscience Institute discuss their findings from a patient’s CT scan and video electroencephalogram (EEG) at Orlando Health Bayfront Hospital.
ready-stellar neuroscience care at Orlando Health Bayfront. The hospital has operated a Level Four Epilepsy Center – the highest accreditation level – for 20 years.
It also operates a stroke program that has earned a DNV-GL Comprehensive Stroke Center accreditation.
VISION BECOMES REALITY
Many of the tools necessary to create an effective institute were already in place, but the vision became a reality after Central Neurology, one of the largest neurology groups in the Tampa Bay region, joined Orlando Health in July.
“That was probably the final piece of the puzzle that allowed us to pull all of this together,” Moore said. “It allows us to offer some of the highest level of treatment in the Tampa Bay market.”
The Neuroscience Institute’s emphasis on interdisciplinary care is evident through its care team, which includes more than 20 clinicians and physicians from numerous disciplines who work in tandem.
The Orlando Health Neuroscience Institute – Bayfront team includes:
• Neurologists
• Neurosurgeons
• Neuro-Endovascular Radiologists
• Neuropsychologists
• Advanced practice providers
• Researchers
The institute also features neuro-trained nurses to ensure that specialized care is available to patients throughout their experience. Considering the amount of time patients interact with nurses during their hospital stays, having nurses with neuro certifications is a key building block in the institute’s treatment plans.
“Nursing care goes beyond addressing the crisis that brings patients to our hospital,” said Tammy Schlatterer, nurse practitioner at Orlando Health Neuroscience Institute – Bayfront. “Neurotrained nurses are empowered with the specialized knowledge patients need to heal and continue their lives in a way that is best for their diagnoses’ needs and challenges.”
Throughout this initiative, Orlando Health Bayfront Hospital has leaned on its physicians to generate ideas and strategies to make the Neuroscience Institute as effective as possible.
“The most valuable asset when you’re putting in an institute is giving the physicians, who are the subject matter experts, a voice,” Benford said. “Having this institute and their own reporting structure allows them to make really good recommendations on investments the organization needs to make and certainly is a great recruitment tool for bringing on the highest talent.”
It hasn’t taken long for physicians and patients alike to see the benefits begin to pay off. The ability to offer stronger disciplinary care has been a game changer.
Subspecialties along the wide spectrum of the neurosciences can now easily communicate, work together toward better outcomes and improve patient care.
Moore was recently stopped in the hallway by a physician who has been with the hospital for nearly 30 years. The doctor wanted to praise the new teamwork approach.
“We are continuing to build on the collaboration of the various specialists,” Moore said.
The institute’s success in unlocking the value of interdisciplinary care has allowed physicians to come together and attack problems with the combined expertise of their various backgrounds.
They can meet with a patient, evaluate them, field their questions together and then go to a conference room to work out the best possible treatment plan. Nothing happens in a vacuum.
“When you have diverse perspectives handling a patient’s care, that only produces better outcomes because we each bring a strength to how we
approach patients’ care,” Dr. Dawson said. “When you have providers sitting at the table and talking about how they would do something, it just really, really results in better outcomes.”
RESEARCH AND INNOVATION KEY
In addition to the upgrades in interdisciplinary care, the Neuroscience Institute also pairs patient services with research and innovation. The institute includes a dedicated research department to provide patients with advanced treatments that may not be available at other hospitals.
This includes new technologies to assist with and improve invasive procedures and new treatment options for patients who are nearing the limit of typical care plans. Neurosciences, like many service lines, are always evolving. There is considerable research is being done in this space, offering hope to patients whose conditions aren’t fully addressed by current treatment strategies.
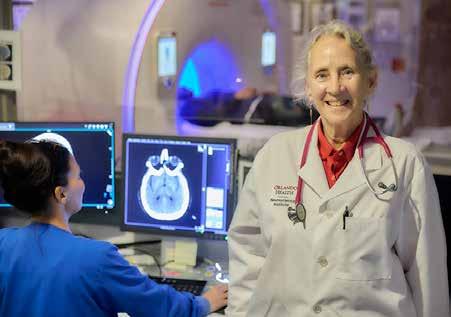
Orlando Health Neuroscience Institute – Bayfront Physician Dr. Carol Pappas accompanies a patient to the CT imaging department at Orlando Health Bayfront Hospital.
“Having a research division in the Neuroscience Institute lays the groundwork for our patients to have access to new emerging therapies,” said Dr. Gregory Scott, Orlando Health Neuroscience Institute – Bayfront. “This offers hope to those who have chronic neurologic disorders where effective treatment is currently inadequate or unavailable.”
That dedication to research is paying off in several big ways. One tool that has already had a huge impact for patients is vizAI, an artificial intelligence tool for a growing number of neuro diseases and conditions, including stroke.
Using pattern recognition to rapidly identify large vessel occlusions and other strokes, the technology saves critical time in situations where every second counts. Stroke patients typically lose 3 million brain cells per minute, making the need for immediate care critical.
The software warns the physician when it identifies early signs of stroke. Among its abilities, it can detect a lack of blood supply or a source of bleeding in the head.
What makes it powerful is its pairing with the institute’s skilled physicians, allowing them to review the information and save precious time. A physician evaluating a patient can receive the information coming from the software and make a judgement of the situation much faster.
Viz-AI also plays key a role in interdisciplinary care.
“In addition to identifying these patients early, we use it as a communication tool,” Dr. Dawson said. “All of the providers, from the emergency staff to the ancillary staff, are on the same page because we’re using it as a communication tool so we can triage patients better. And quicker treatment leads to better outcomes.”
A patient who was treated with the assistance of vizAI recently thanked Dr. Dawson and the stroke team for
their work to successfully remove a blood clot from her brain and restore function to the right side of her body.
“In addition to family members being relieved that she made a full recovery, they specifically mentioned how reassuring it was for me to show them images of their mother’s brain on my phone. They recalled seeing where the clot was, and the most recent scan showing the blood flow restored, as soon as I stepped out of the operating room,” said Dr. Dawson. “I felt honored to bring them relief through understanding. VizAI is a wonderful tool that accelerates the treatment of patients who’ve suffered from a stroke.”
Viz-AI is just one innovation the institute has been able to make use of so far, as it strives to offer next-level neurological care, while harnessing the most advanced technologies available.
The institute’s combination of investing in research and interdisciplinary care has resulted in many examples of new and effective treatments for patients.
Dr. Julia Pfaff, for example, is an ENT with experience performing microsurgery on nerves in the head and neck. She has worked with neurosurgeons and neurologists to implant Vivistim in patients. Once they heal after the surgery, patients undergo six weeks of occupational therapy. “During rehabilitation therapy, the implant provides gentle stimulation to the vagus nerve, improving rehabilitation of the muscles in the hand and arm,” Pfaff said.
This device, which is implanted in the patient’s chest in an outpatient procedure, works as a vagal nerve stimulator for patients with upper extremity weakness after a stroke. The patient uses a
Dr. Julia Pfaff looks on as her patient lifts a weight in physical therapy weeks after she surgically implanted him with a vagal nerve stimulator. He previously had extremely limited use of his right arm, but is now able to perform many tasks with it.
Interior of the Orlando Health Neuroscience Institute - Bayfront’s interventional radiology surgical suite, where physicians perform complex procedures to address the emergent needs of patients.
remote device to initiate stimulation to the vagal nerve when they want to use the affected arm and during rehabilitation therapy. The device increases communication with muscles in the hand and arm. One of Dr. Pfaff’s patients went from having no use of his right arm and hand to being able to turn on lights and help with laundry, in addition to several everyday tasks he struggled with prior to having the device implanted. The makers of the device say it provides two to three times more hand and arm function than conventional rehabilitation.
ABOUT THE ORLANDO HEALTH NEUROSCIENCE INSTITUTE - BAYFRONT
The Orlando Health Neuroscience Institute – Bayfront offers a wide range of services and procedures related to neurosciences. This includes everything from treatments for headaches and migraines to emergency care and complex surgeries.
“We have a number of providers throughout the neurological specialties that are providing excellent, world-class care.” Dr. Dawson said. “The residents of Pinellas County will find they don’t have to go across the bridge, and they don’t have to go very far to get excellent care. That’s what we’re striving to produce.”
The DNV-GL Comprehensive Stroke Center offers 24/7 care and rapid response. Treatment options include surgical operations to repair damage and alleviate issues as well as angioplasty and stent placements and embolizing agents.
The Level Four Epilepsy Center has strong diagnostic capabilities and patient monitoring while also offering epilepsy surgery. Non-epileptic seizures and medical conditions that mimic epilepsy are also treated.
For Alzheimer’s and other forms of dementia, the Neuroscience Institute offers cognitive testing and access to MRI, CT scans and PET scans.
Spinal cord conditions treated at the institute range from spine disorders and deformities to spinal tumors and fractures. Spinal surgery is available in numerous forms depending upon the condition or injury.
Traumatic injuries to the head and spinal cord are also treated both in real time and through rehabilitation programs that include both inpatient and outpatient services.
The Orlando Health Neuroscience Institute – Bayfront offers numerous other procedures and treatments for other conditions, including headaches, aneurysms, chronic pain and movement disorders such as Parkinson’s Disease.
“If it’s you, if it’s your mother, your father, your children, you want to have a comprehensive institute where you can receive the vast majority of the care,” Moore said. “We will have multiple
specialists collaborating, working together which makes it convenient for patients.”
ABOUT ORLANDO HEALTH
The Orlando Health Neuroscience Institute is part of Orlando Health. Orlando Health is a private not-for-profit, integrated academic healthcare system with $12 billion of assets under management, that serves the southeastern United States – including Florida and Alabama – and Puerto Rico. With corporate offices in Orlando, Florida the system provides a complete continuum of care across a network of medical centers and institutes, community and specialty hospitals, physician practices, urgent care facilities, skilled nursing facilities, home healthcare, and long-term and behavioral health care services. Founded more than 100 years ago, Orlando Health’s mission is to improve the health and the quality of life of the individuals and communities we serve. The system provided nearly $1.7 billion in community impact in the form of community benefit programs and services, Medicare shortfalls, bad debt, community-building activities and capital investments in FY 23, the most recent period for which the information is available. For more information, visit orlandohealth.com, or follow us on LinkedIn, Facebook, Instagram and X (formerly Twitter.)
Dr. Lowell Dawson reunites with a patient and her family at Orlando Health Bayfront Hospital, after making a full recovery from a stroke. Dr. Dawson used vizAI to assist him before performing lifesaving treatment that restored function to the right side of her body.
Not All Basal Cell Carcinomas Are Created Equal
By John “Lucky” Meisenheimer, MD and John Meisenheimer, VII
Occasionally a patient will tell me their “doctor friend” recommended that they don’t need treatment for a basal cell carcinoma because it will never hurt you. “Doc, he said it’s only a basal cell carcinoma.” Dermatologists fully recognize this as a genuinely cringe-worthy statement. You don’t need to see too many people missing various parts of their facial anatomy to know this advice is blatantly wrong. Even in this modern time of medical miracles, people still die from neglected basal cell carcinomas. When pressed for the name of their “doctor friend,” it usually comes up as I don’t remember their name, or it ends up being “Doctor Google.”
It is true a superficial basal cell carcinoma on the torso probably would take years and years for it to cause any sort of significant morbidity to a patient. But, on the other hand, even a small basal cell on the torso will continue to grow if left untreated slowly. What might have been a simple, inexpensive procedure now, a decade later, has turned into a monster of aggravation, discomfort, and cost.
Although metastatic disease risk is low with basal cell carcinomas, it is certainly not zero. Several people die each year from basal cell carcinoma. Even more, patients can have disfiguring bouts with cancer losing various parts of anatomy such as nose, ears, eyes, etc. What a lot of patients and even some physicians are not aware of is that not all basal cell carcinomas are created equal. There are several different histologic growth patterns. These varying histologic types can each behave differently and require different treatment plans.
As mentioned before, a superficial basal cell carcinoma is probably not going to cause a great deal of physical damage unless neglected for long periods. There are other types of basal cell carcinomas; morpheaform and sclerosing basal cell carcinomas with infiltrating growth patterns. These cancers left untreated can cause a significant amount of morbidity in shorter periods measured in months, not years. Aggressive basal cell cancers can also become neurotropic, meaning that they “wrap” around a nerve and can track down its length. Neurotropism can be particularly dangerous, especially if this is on the face and affecting a nerve that happens to pass through a foramen into the brain. Clearly, not a good scenario.
Basal cell carcinomas, limited to the skin, tend to be very amenable to treatment in a variety of different ways. Even as a Mohs surgeon I can think of at least half a dozen different ways that I have treated basal cell carcinomas. Not all basal cell carcinomas need Mohs surgery. Each case of basal cell carcinoma should be evaluated individually and in consideration as to the best method of treatment based on its histologic growth pattern, location, and physical condition of the patient.
The great news about basal cell carcinoma, even though it is the most common type of skin cancer and millions are treated each year, only a tiny percentage of these end up causing death in patients. When someone says I would much rather have a basal cell carcinoma than a melanoma, there is a caveat; if you die from a basal cell carcinoma, you are just as dead as if you were to die from melanoma. Happily, most of the time, with early diagnosis and treatment, you don’t have to die from either. Basal cell carcinoma is called cancer for a reason. Give it its respect that it is due, or otherwise, you may regret saying, “oh, you don’t have to worry about it, it’s only a basal cell carcinoma.”
Lucky Meisenheimer, M.D. is a board-certified dermatologist specializing in Mohs Surgery. He is the director of the Meisenheimer Clinic – Dermatology and Mohs Surgery. John Meisenheimer, VII is an MD practicing in Orlando.
PHOTO: JOHN MEISENHEIMER, VII, MD
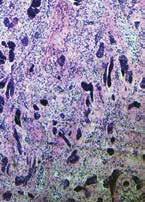
Pathology of an infiltrative basal cell carcinoma.
Infiltrative Basal Cell carcinoma of the forehead.
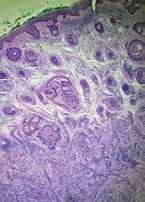
Superficial Multifocal BCC.
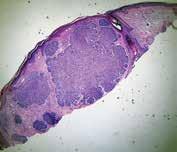
Nodular basal cell carcinoma.
Neurotropic basal cell carcinoma.
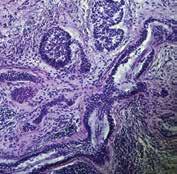
Sclerosing basal cell carcinoma.
PHOTO: JOHN MEISENHEIMER, VII, MD
PHOTO:
Is Your Online Reputation Costing You Patients?
By Sonda Eunus, MHA, CMPE
What does your online reputation say about your practice? If you have a negative online reputation, you are missing out on new patients every day. Most medical practices now get the majority of their new patients through Google and other search engine queries, such as “Pediatrician in Orlando”. If your practice appears in these searches, the most common next step for a potential new patient would be to check out your reviews – what are other patients saying about your practice? It has been reported that 90% of consumers read online reviews before visiting a business and that online reviews influence 67% of purchasing decisions (Bright Local). For this reason, it is incredibly important to pay attention to the rating and reviews that your practice has on search engines, social media platforms, and local online business directories.
However, despite the importance of cultivating a positive online reputation, only 33% of businesses report actively collecting and asking for reviews (1). One great process to set in place at your practice is asking for patient reviews after each patient visit. It can be as simple as training your front office staff to ask each patient how their visit went while checking them out, and if they receive favorable feedback then they can ask the patient to please leave a review on Google or Facebook about their experience. If they receive negative feedback, this feedback should be taken very seriously, and management should be notified as soon as possible so that the issue can be mitigated before the patient decides to post a negative review.
Setting up an automated text or email campaign that asks each patient for their feedback after their appointment is also a great way to improve your online reputation as well as to correct any issues that may be occurring at your practice. When you receive feedback from patients, you are then able to prompt them to leave a public review on Facebook, Google, Yelp, Healthgrades, or other applicable review platforms. However, you must be aware that legally, you are not allowed to only direct people with favorable feedback to leave reviews, which is known as review-gating – so if you are implementing an automated system like this, just make sure that you are aware of this limitation. There are online reputation management platforms which allow you to customize the messages that people see when they leave negative feedback as opposed to positive feedback, but both of those messages must still offer the option to leave a public review. However, if you create your message in such a way as to communicate to the patient who may leave negative feedback that you are working hard on resolving the issue and that someone will be in touch shortly, that may prevent them from leaving a public negative review.
When you receive a public review on Google, Facebook, or other review sites, make sure that you respond to it – either by thanking them for a good review or by asking them to contact you to discuss how you can improve their experience. Do not argue or try to defend yourself online – try to speak about it with them privately, fix the issue, and ask them to remove the review if possible. When you receive great reviews, make sure to cross-share them on your various social media platforms. You should also create a “Reviews” page on your website and add all great reviews to this page. This instantly adds credibility to your website.
Finally, make sure that when you look over the feedback and reviews that you receive, you are paying attention to what the negative reviews are saying – this is a great opportunity to identify current process challenges and improve your patients’ experience at your practice. Need help managing your practice’s online reputation? Visit www.lms-plus.com to see how Leading Marketing Solutions can help.
Sonda Eunus is the CEO of Leading Marketing Solutions, a Marketing Agency working with Medical Practices and other Businesses to help them identify the best marketing strategies for their business, create a strong online presence, and automate their marketing processes for a better return on their Marketing budget. Learn more about Leading Marketing Solutions at www.lms-plus.com.
Eat S***...and Live
By Akshay Manohar, MD
Do you remember that sweet, pungent odor that pierced through your skull as a resident? You wandered through the hallways wondering who on earth managed to convince admin that a skunk qualified as an emotional support animal.
Just then, a seasoned nurse stopped you. The person from the nursing home that was put on “Vanc and Zosyn” for the past six days needed an order for a rectal tube for explosive diarrhea. Standing outside the door, you heard the echo of a strong stream of water filling a plastic basin, and the chatter of three techs in disposable gowns changing the robes and the sheets of the poor individual.
That intense smell wafting off the soiled linen burned itself into your memory. The nurse interrupted your thoughts with her diagnosis that she had come up with using only her olfactory senses.
You ordered the test to confirm, praying that the patient’s hospital stay had not been long enough to set off alarms in the C-suite. “The hospital will be dinged for this! There has never ever been a nosocomial transmission of C. diff here.”
Never.
They put up a sign on the door saying, “Soap and Water”. The convenient alcohol pump lost its power to the hardy spores. You cowered when the result came back positive, but thankfully, nobody came to criticize your decision to test.
You were able to practice medicine. It’s one of the perks of working on a Sunday.
Clostridium difficle is now called Clostridioides difficle. In 2016, a 16S rRNA gene sequence analysis differentiated it from other bacteria in that genus. It was great news for infectious disease doctors like me years before COVID because changing the names of bacteria you read about in school keeps us relevant. Despite our best efforts, the popular abbreviation ‘C. diff’, has not changed, and we still use the term for this gram-positive, spore-forming anaerobic bacillus, cousin of terrible maladies like tetanus, botulism, and the flesh-eating, food-poisoning terror Clostridium perfringens.
I like to think of C. diff as a cowardly school bully whose evil lays hidden only due to fears of standing out in front of the bigger kids (gut bacteria). Most carriers of the bacteria are asymptomatic and it is part of the “normal” flora.
When the competition is wiped out by an antibiotic, however, C. diff rears its head and reproduces at alarming rates, releasing damaging toxins in the colon. If severe enough, it can cause a dangerous condition called toxic megacolon, where sometimes the only chance of survival is a complete resection of the bowel. A less severe, yet complicated scenario is an ileus where oral therapy cannot reach the site of infection. Most people, however, just have diarrhea. Lots of it. Enough to cause dehydration and the need for admission to administer intravenous fluids.
Barely a decade ago, the recommendation was a round or two of treatment with metronidazole. While oral therapy was considered superior, the advantage of this drug is that in an ileus, it can be given intravenously.
Then, the guidelines changed. Oral vancomycin became firstline. The interesting thing about vancomycin is that it does not pass the blood-gut barrier. IV Vancomycin does not enter the gut. Oral vancomycin does not get into the blood. It can a little, but for practical/clinically relevant purposes, let’s say it doesn’t.
More recently, the recommendation for the first line drug was changed to fidaxomicin. This was the cause of much grievance for people involved in budgeting and finances of hospital pharmacies and insurance companies since fidaxomicin was appallingly expensive compared to compounded vancomycin which (depending on the negotiated rate) cost a few cents to a few dollars per dose.
The advantage of fidaxomicin over vancomycin (and the reason for its promotion) was that the rate of recurrence was lower than vancomycin and in 2021 the recommendation was made to give fidaxomicin first for the initial mild to moderate infection.
For fulminant/severe disease where the serum white blood cell count exceeds 15,000/microL, there is a 50% rise in creatinine, or when a “Zar score” that uses factors like ICU admission, age, presence of pseudomembranes, etc., is equal to or greater than 2, vancomycin becomes first line and is sometimes combined with intravenous metronidazole, especially when there is an ileus.
Bezlotoxumab a monoclonal antibody was developed against C. diff Toxin B and it was shown to prevent recurrence.
There is one other way to fight C. diff: biological warfare.
Many years ago, a hospital I was familiar with came up with a protocol. It involved a kitchen blender and a nasogastric (or preferably an extending deep into the jejunum Dobbhoff) tube through which another person’s stool would be administered to the patient. The biggest hurdle I sensed was getting past the fear of litigation.
Stool carries live bacteria, viruses, and parasites. For ID doctors, there is an additional concern of transferring multi-drug resistant bacteria from one person to another.
While everyone was fretting about this, there was a lady with cancer who had debilitating diarrhea from recurrent infection. She was so fed up and miserable that when her daughter made a concoction using her own stool heavily masked in something edible, she drank it out of desperation. That fixed the problem better than everything else her providers had done.
According to OpenBiome, a stool bank that manufactures an FDA approved “poop pill”, the effectiveness of fecal microbiota transplant is 89% compared to 40% with standard antibiotic therapy.
The biggest limitation of transplanting stool is our fear of the unknown, and lack of thorough understanding of the human-microbiome relationship.
We clearly have an ability to determine their fate, but they too have a significant impact in our survival, and perhaps also our personalities. There were two studies where they took stool from people with depression and transplanted it into mice. The mice developed anxiety and depression. The opposite was seen in a case report where a 79-year-old woman with depression showed improvement and was able to stop antidepressants after receiving the stool of her happygo-lucky grandson.
Transplanting microbiota has been shown to cause weight gain, but the golden ticket everyone is trying to find is the bacteria that causes weight loss.
Hopefully, it’s cheap. That way you won’t have to fill out another s**tty prior-auth.
Akshay Manohar, MD, FIDSA is a board-certified infectious disease physician with 7 years of clinical experience. He is a graduate of Kasturba Medical College, Manipal, India, Capital Health’s internal medicine residency in NJ, and the infectious disease fellowship program at SUNY Buffalo, NY, where he did research on a novel drug target for Acinetobacter baumanii and hypervirulent Klebsiella.
In his new clinic, Centaur Medical Center, in Orlando, he strives to create a space for people to be comfortable in what can be an intimidating situation.
He is fluent in English, Tamil, Hindi, Kannada and has an intermediate proficiency in Spanish.
Akshay Manohar, MD, FIDSA • Centaur Medical Center 100 W Gore St, Suite 605•Orlando, FL 32806 (407) 271-4731 • www.CentaurMedical.org
From Risk to Resilience: One Family’s Journey Through Twin-to-Twin Transfusion Syndrome
By Staff Writer
TWIN TREATMENT: AVA AND EMMA’S STORY
Twin girls Ava and Emma have had quite an adventure in their young lives, one that began before they were even born. Their mom, Carly Decker, a Panama City resident was pregnant for the first time. Since she knew she had twins on the way, she didn’t really think twice about any of her symptoms. “I was having pain in my groin and was extremely tired,” explains Carly. “I felt like I was bigger than I should have been … but I just chalked it up to having twins.”
Carly had her first maternal-fetal-medicine (MFM) appointment at Nemours Children’s Health, Panama City. The new clinic reestablished MFM services in the area providing telehealth visits to patients. At 17 weeks, Carly had a consult with Melanie Mitta, MD, FACOG who reviewed the detailed anatomy scans and diagnosed her with stage-3 twin-to-twin transfusion syndrome (TTTS), a serious condition where one twin gets too much blood to the other, leading to abnormal blood flow that can cause significant health risks for both twins.
Dr. Mitta and the perinatal coordinators worked quickly to get mom a consultation for fetoscopic laser therapy the very next day with Emanual Vlastos, MD, an expert in TTTS, at
Orlando Health Winnie Palmer Fetal Care Center. Dr. Mitta helped Carly process the worrying news. “She was compassionate,” says Carly, “and always very calm and throughout my treatment.” Another MFM specialist, Claudia Taboada, DO, also helped Carly. “Both of these doctors took great care of me and made me feel as relaxed as possible in such a scary and uncertain time.”
Carly’s TTTS required surgery while she was pregnant, and Dr. Vlastos performed the fetoscopic laser surgery and amnioreduction, which fixed the blood flow and removed extra amniotic fluid from around the twins.
“I don’t think that I could have been in better hands,” says Carly. “Dr. Viastos was a rock star from the beginning to the end.” The same could be said of the whole staff at Nemours Children’s, Panama City. Mom required weekly TTTS post therapy follow-ups and evaluation by pediatric cardiologist, Daphney Kernizan, DO for a fetal echocardiogram. “All the nurses and sonographers at Nemours Children’s were absolutely wonderful. I was there once a week (sometimes more), and they were what made every visit a good experience.”The first couple of weeks after Carly’s surgery were the riskiest. That was the time when the chance of complications was highest but luckily there were none. “As I was healing,” says Carly, “I still had over half of my pregnancy to go. My goal was to listen to my body and make sure to rest often. It was scary knowing I still had to make it so far, but I was confident that I would.”
Thanks to the convenient availability and coordinated efforts of both MFM and pediatric cardiology services where she lives, Carly was able to extend her pregnancy to deliver two healthy baby girls in Panama City at our collaborating hospital, HCA FL Gulf Coast, in May of 2024. Her twins Ava and Emma made an early appearance, arriving eight weeks ahead of schedule, but today they’re both happy and healthy.
With a wealth of experience behind her, Carly has helpful
The Decker family: Zach and Carly with twins Ava and Emma.
Mom, Carly Decker, with twins Ava and Emma.
advice for pregnant mothers navigating a similar journey. “Listen to your body and to your doctors,” she encourages. “Have a good support system. The time around the surgery and the following weeks was incredibly scary, but having people by me helped tremendously.” Carly also recommends reading about success stories, which helped her stay uplifted. Finally, she advises remaining positive. “Just know that everything will work out the way that it’s supposed to.”
If you have a patient contemplating a pregnancy or is pregnant during an advanced maternal age, you may consider referring them for a consult with a maternal fetal medicine (MFM) specialist. MFM specialists offer guidance from preconception through pregnancy. Some individuals are referred to a MFM specialist by their obstetrician due to:
• Advanced maternal age
• Maternal history of chronic disease (e.g., lupus, autoimmune disorders, hypertension, diabetes or obesity)
• Multiple gestation (twins, triplets)
• Prior or recurrent pregnancy loss
• Abnormal chromosomes in a prior pregnancy
• Abnormal ultrasound findings in current or prior pregnancy
To learn more or to refer a patient, call 407.567.3000.
Claudia Taboada, DO, FACOOG, is a board-certified maternal fetal medicine specialist. She joined Nemours Children’s from the University of Pittsburgh Medical Center Pinnacle Health where she was the medical director for the department of maternal-fetal medicine. She earned her degree in osteopathic medicine from New York College of Osteopathic Medicine and completed a residency in obstetrics and gynecology at the University of Medicine and Dentistry of New Jersey.
Dr. Taboada is fluent in English and Spanish.
Melanie Mitta, MD, FACOG, is a board-certified obstetrician-gynecologist and fellow of the American College of Obstetricians and Gynecologists (FACOG). She earned her medical degree at the University of Florida (UF) College of Medicine in Gainesville and continued with a residency in obstetrics and gynecology at UF in Jacksonville, Florida. Dr. Mitta’s fellowship in maternal-fetal medicine was completed in Atlanta at Emory University of Medicine.
Dr. Mitta is fluent in English and Spanish.
Daphney Kernizan, DO, is a Medical Director and board-certified pediatric cardiologist with advanced fellowship training in fetal cardiology. She earned her medical degree from NYIT College of Osteopathic Medicine and her residency at Rutgers Robert Wood Johnson University Hospital. Dr. Kernizan has been with Nemours Children’s Health since her clinical fellowship working in pediatric cardiology, prevention, and advance cardiac imaging. Dr. Kernizan has published medical journal articles on rheumatic heart disease in the United States, echocardiographic assessment of ventricular function along with other topics and has lectured on topics such as pediatric heart screening in Haiti.
Dr. Kernizan is fluent in English and French Creole.
Chronic Thromboembolic Pulmonary Hypertension
By Daniel T. Layish, MD
There are several categories of pulmonary hypertension. WHO Group I includes patients with idiopathic pulmonary hypertension, familial pulmonary hypertension, drug and toxin related (fen-phen) portopulmonary hypertension, HIV related pulmonary hypertension and pulmonary arterial hypertension associated with connective tissue disorders (such as scleroderma). WHO Group II pulmonary hypertension is often referred to as pulmonary venous hypertension. This includes patients with left ventricular systolic or diastolic dysfunction or valvular heart disease. Essentially, the WHO Group II category includes patients who have an elevated pulmonary capillary wedge pressure and/ or elevated left ventricular end diastolic pressure. WHO Group III pulmonary hypertension consists of patients with COPD, interstitial lung disease, or other conditions in which hypoxia causes vasoconstriction. The remainder of this article will focus on WHO Group IV pulmonary hypertension (chronic thromboembolic pulmonary hypertension or CTEPH). Although WHO Group IV patients are relatively rare, it is crucial to identify them because this is the only type of pulmonary hypertension which is potentially surgically curable.
After acute pulmonary embolism, most patients will recover and have normal pulmonary hemodynamics, gas exchange, and exercise tolerance. It is believed that 1-4% of patients with acute pulmonary embolism will go on to develop CTEPH within two years. It is not clear why some patients with acute pulmonary embolism develop CTEPH. Risk factors include hypercoagulable states, myeloproliferative syndromes, splenectomy and chronic indwelling central venous catheters. Patients with CTEPH present with dyspnea, which can have a gradual onset. Many patients with CTEPH will not have a known previous diagnosis of acute pulmonary embolism. As with other patients with pulmonary hypertension, patients with CTEPH may not show findings on physical exam until pulmonary hypertension is in the late stages. Findings include a right ventricular lift, jugular venous distention, fixed splitting of the second heart sound, hepatomegaly, ascites, and peripheral edema. Patients with CTEPH may have “flow murmurs” heard over the lung fields because of turbulent flow through partially obstructed or recanalized pulmonary arteries. These tend to be accentuated during inspiration.
Acute pulmonary embolism is the trigger for CTEPH. In some patients this triggers a small vessel vasculopathy (for unclear reasons) that contributes to the extent of pulmonary hypertension. This may explain why up to 35 percent of patients who undergo succesful pulmonary thromoendarterectomy can have some degree of postoperative pulmonary hypertension.
Although VQ scanning has become less commonly used for diagnosis of acute pulmonary embolism this remains the initial imaging study of choice in patients with pulmonary hyperten-
sion to separate “small vessel” variants (Idiopathic pulmonary arterial hypertension) from “large vessel” disease (CTEPH) A normal VQ scan essentially excludes the diagnosis of CTEPH. A scan with one or more mismatched segmental defects is suggestive of the diagnosis. However, it is important to note that VQ scan can often understate the extent of central pulmonary vascular obstruction. Once the VQ scan is found to be abnormal then further testing should be undertaken (such as CT angiogram and/or pulmonary angiography). The angiographic findings in CTEPH are distinct from those of acute pulmonary embolism. They can include pouch defects and pulmonary artery webs. Patients with severe pulmonary hypertension have been found to tolerate performance of angiography as well as VQ scan without significant complication rate.
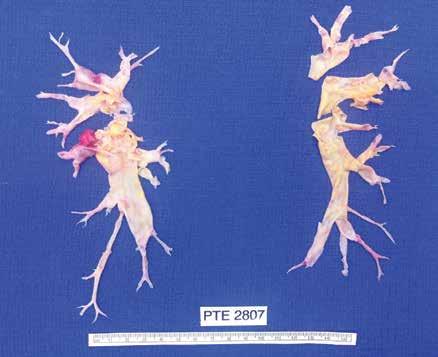
The surgery for CTEPH is quite different from surgical intervention for an acute pulmonary embolism. Surgery for CTEPH is called a pulmonary thromboendarterectomy (PTE), which requires median sternotomy and cardiopulmonary bypass. It requires an often tedious intimal dissection of fibrotic recannalized thrombus from the native pulmonary arterial wall. IVC filter placement is usually recommended before pulmonary thromboendarterectomy. These patients can have a complicated postoperative course and this type of surgery is only done at a few specialized centers in the country. The center which is best known for this type of surgery is the University of California (San Diego). Patients who have undergone PTE are typically maintained on lifelong anticoagulation. To be a candidate for this surgery, a patients must have central, surgically accesible chronic thromboemboli. A significant postoperative complication is pulmonary artery steal, which refers to redistribution of pulmonary arterial blood flow from well-perfused segments into the newly opened segments resulting in ventilation perfusion mismatch and hypoxia. This redistribution of flow resolves over time. Approximately, 30% of PTE patients can develop reperfusion pulmonary edema. The perioperative mortality of pulmonary thromboendarterectomy can be in the range of 2-3% in experienced centers. Outcome is clearly better in high voluime centers (more than fifty PTE surgeries/year). Approximately 5000 thromboendarterectomy procedures have been performed worldwide, 3000 at UCSD alone.
Surgery for CTEPH is clearly the best therapeutic option. However, there are some patients with CTEPH who are inoperable or who have persistent or recurrent pulmonary hypertension after undergoing pulmonary thromboendarterectomy. There is now a medical therapy available for these patients. Riociguat (Adempas) was approved by the FDA in October 2013. It is a member of a new class of compounds-soluble guanylate cyclase stimulators. In the multicenter study by Ghofrani et al that was published in the New England Journal of Medicine in July 2013,
261 patients were randomized prospectively to receive riociguat versus placebo. Riociguat was shown to significantly improve exercise capacity and pulmonary vascular resistance. Side effects include systemic hypotension. Prior smaller studies have also shown some benefits to medical therapy in CTEPH (inoperable or with post-operative PH) with oral agents such as bosentan and sildanefil, inhaled iloprost and subcutaneous treprostinil. Medical therapy has also been used as a “bridge” before PTE.
Although relatively rare, CTEPH is an important cause of PH since it is potentially curable with pulmonary endarterectomy. This surgery should only be performed in very experienced, specialized centers. PTE surgery should always be the treatment of choice for CTEPH. However, medical therapy can have a role as a bridge to PTE,in patients who are not surgical candidates or in those who have persistent pulmonary hypertension despite undergoing PTE.
I would like to express my gratitude to Dr. Peter Fedullo (University California San Diego) for his review of this manuscript and providing the photographs.
Daniel Layish, MD, graduated magna cum laude from Boston University Medical School in 1990. He then completed an Internal Medicine Residency at Barnes Hospital (Washington University) in St.Louis, Missouri and a Pulmonary/Critical Care/ Sleep Medicine Fellowship at Duke University in Durham, North Carolina. Since 1997, he has been a member of the Central Florida Pulmonary Group in Orlando. He serves as Co-director of the Adult Cystic Fibrosis Program in Orlando. He may be contacted at 407-841-1100 or by visiting www.cfpulmonary.com.
Example of chronic clots removed during pulmonary thromboendarterectomy.
Example of the large perfusion defects seen on V/Q scan in a patient with CTEPH.
Pulmonary angiogram showing lack of blood flow to the right middle lobe and the right lower lobe from CTEPH.
Helping Veterans Treat Obstructive Sleep Apnea
By Tara M. Griffin, DMD, DBDSM, DASBA
As we celebrate Independence Day, it is crucial to remember the brave men and women who have fought for our freedom. Veterans have made countless sacrifices to protect our nation, and it is our duty to ensure they receive the care and support they deserve. One prevalent issue among veterans is obstructive sleep apnea (OSA), a condition that can have serious consequences if left untreated.
A 2019 report estimates that over 1.5 million veterans have been diagnosed with OSA and up to 80% of those diagnosed are not being successfully treated. Continuous Positive Airway Pressure (CPAP) has been the gold standard for treatment for the past 40 years, however, in 2020 after a world-wide recall of CPAP machines, more than 600,000 veterans have been affected and another 600,000 are not compliant with the machines they have been prescribed.
Obstructive sleep apnea is a common sleep disorder characterized by pauses in breathing during sleep, often leading to fragmented sleep and low oxygen levels in the blood. This condition not only affects the quality of sleep but can also have detrimental effects on overall health and well-being. When you experience low oxygen levels in the blood on a regular basis, this creates inflammation in every organ system which leads to chronic debilitating health issues. For veterans, the impact of OSA can be particularly challenging, given the physical and mental toll of their service.
Fortunately, there are effective treatment options available for “managing” and now “resolving” obstructive sleep apnea. While CPAP therapy and surgery are commonly used, most veterans may find these options unavailable and potentially dangerous after recent recalls, uncomfortable and invasive. In such cases, alternative treatments like FDA-approved oral medical devices for sleep apnea can offer a more comfortable and convenient solution.
These custom oral devices are designed to help keep the airway open during sleep, reducing the risk of breathing pauses and improving overall sleep quality. By using these devices, our veterans are experiencing fewer awakenings during sleep, reduced daytime fatigue, improved cognitive function, better overall health and improved quality of life.
Compared to CPAP therapy, studies show that oral medical devices have a compliance rate of over 80% after 5 years of use which is much better than CPAP compliance and just as effective at lowering high blood pressure and reducing cardiovascular risks for patients. Based on recent FDA approved technology, up to 34% of patients may no longer need an oral medical device after 12 months of treatment.
One of the significant benefits of using oral medical devices for sleep apnea is their ability to address not only the physical symptoms and root causes of OSA but also the associated mental health challenges. Many veterans with OSA also suffer from
conditions like post-traumatic stress disorder (PTSD), which can be exacerbated by poor sleep quality and trauma experienced while serving. Over 1.3 million veterans have been diagnosed with PTSD through service-connection with the VA.
By improving sleep quality with custom oral medical devices and adjunctive therapies, most veterans we have treated, experience a reduction in PTSD symptoms, fewer headaches, and a decrease in night terrors! Better sleep can have a profound impact on mental health and overall well-being, allowing veterans to lead more fulfilling and productive lives.
For healthcare providers working with veterans, it is essential to consider alternative treatment options for sleep apnea. By offering veterans a comfortable and effective solution for managing or resolving OSA, healthcare providers can help improve the quality of life for those who have served our country.
At Sleep Solution Centers, we are a Community Care Provider for veterans and make it our priority to see our new patients within a week of receiving a referral from the VA. Our motto is, “Our freedom isn’t free but a good night’s sleep can be!”
As we honor our veterans this Independence Day, let us not forget the importance of supporting their health and well-being. By raising awareness about alternative treatments for obstructive sleep apnea and advocating for the use of FDA-approved oral medical devices, we can make a meaningful difference in the lives of those who have sacrificed so much for our freedom. Let us stand together in providing the care and support our veterans deserve!
Tara M. Griffin, DMD, DBDSM, DASBA, graduated from Nova Southeastern University in 2006, with a doctorate in Dental Medicine. She became passionate about helping her patients breathe and sleep better and completed her Diplomate with the American Academy of Dental Sleep Medicine in 2011. In 2015, she completed her Diplomate with American Sleep and Breathing Academy. In 2016, she became a Clinical Advisor with Vivos Therapeutics to help educate and mentor doctors interested in the treatment of OSA with oral medical devices. She owned a private practice focused on sleep, TMD and general dentistry in the panhandle of Florida for 17 years before becoming the co-founder of Sleep Solution Centers in Medical City, Orlando in 2024. She may be contacted at 407-502-0110 or by visiting www.sleepsolutioncenters.com
Important Criteria for Selecting Medical Office Space
By Frank Ricci, Healthcare Realty & Development Services LLC
One of the most important investments your practice will ever make is the location of your medical practice. In this article, we will discuss several key elements to consider when selecting medical office space and some of the tools the experts use. In assessing possible locations, it is important to consider the following factors:
1. Accessibility: The location should be easily accessible to patients, staff, and emergency services. This includes convenient access via major roads, public transportation, and ample parking. Building accessibility for people with disabilities is also important as is a covered drop off area, especially here in Florida. In evaluating a potential location, we utilize maps, site plans, and a visual inspection.
2. Visibility and Signage: Depending on your practice, a highly visible location with good signage might attract more patients. High visibility areas are typically those with high foot or vehicle traffic. We use Google Maps and Florida Department of Transportation data to analyze traffic and traffic patterns and Placer AI to analyze foot traffic.
3. Demographics of the Surrounding Area: A thorough understanding of your patients is crucial and matching that information with the markets available is the key to optimizing your decisions. The age, income levels, and healthcare needs of the local community need to align with the services you provide. We use tools like ESRI to research demographic data including age distribution, income levels, and health profiles of a region which we use to identify locations with a high potential patient base.
4. Proximity to Hospitals and Other Providers: Being near hospitals, other medical facilities and other providers can be beneficial for referrals, shared services, and patient convenience, especially for specialists. You should complete an internal survey of your key referral patterns and identify those practices and specialties with which you have symbiosis Use this information in your search and analysis.
5. Competition and Market Saturation: Understanding the level of competition and market saturation in the area is just as important as knowing which referral patterns benefit your practice. A market with too much competition may offer fewer opportunities for growth. Using state health records, you can plot these providers on a map to help delineate areas with the greatest opportunities.
6. Size and Layout: Your space should be sized to accommodate current needs and allow for future growth. The layout should adhere to the principles of Evidence Based Design for comfort, staff & patient flow, privacy and infection control. Complete a space program analysis to identify required spaces and sizes to determine your space requirements.
7. Infrastructure and Technological Capabilities: Today’s medical offices are able to provide services in-house unheard of even
a decade ago due to advancing technology but in order to use these technologies, adequate infrastructure is required. This will include structural integrity, ample and steady power, reliable internet connectivity and adequate mechanical systems.
8. Building Amenities and Local Services: Facilities such as elevators, security, maintenance, and janitorial services can impact the functionality and perception of your office. Additionally, amenities such as a gift or coffee shop, restaurant, grocery store, personal services, etc. as part of the building or in close proximity offer benefits to both patients and staff.
9. Environment and Atmosphere: A location that offers a pleasant and professional environment can significantly enhance the patient experience. This includes considerations like natural light, noise levels, furnishings and overall aesthetics.
10. Space Terms and Cost: The ownership and financial aspects must be carefully analyzed, including whether to own or lease. Financial details such as sales price, down payment, tax impact, utilities, lease cost, lease terms and the potential for rent increases must be carefully evaluated to ensure they align with your financial plans. A detailed cost/benefit analysis should be performed to determine the financial parameters and risks.
11. Available Properties: A thorough inventory of available properties must be conducted for evaluation. There are a multitude of online searchable databases that list available properties, including Loopnet, CoStar, Crexi, TotalCommercial and many others. Use this as a base from which to start your search but not all property that is available or might be available is accessible through these sites. Actual site and location visits are required to provide an accurate and thorough inventory of prospective sites.
In summary, the selection of medical office space is a multifaceted decision that requires balancing important practical considerations, market opportunities, patient and staff convenience and financial viability. Due to the many variables involved and the tools required, it is often in your best interest to enlist a specialist to help evaluate your needs, analyze the various market opportunities and to help you select the best possible location for your specific practice.
Frank Ricci is a licensed real estate broker and Managing Partner of Healthcare Realty & Development Services LLC based in Winter Park, Florida. Frank has specialized in medical real estate for over 30 years and been involved in the leasing and sales of over $200 million worth of properties. For more information, contact Frank at 407-947-5074, FrankR@healthcarerealtyonline.com or visit healthcarerealtyonline.com
Resolution Revolution: Centering Mental Health to Reframe the Idea of Self-Improvement
By Staff Writer
We know the drill: December winds down and we consider how we want to change. Promises to lose weight, quit smoking, or save money get held aloft as we proclaim, “This year will be different.” Cue the cycle of unmet expectations, self-blame, and frustration. A different approach is needed—one that reinvents self-improvement by focusing on meaningful, lasting progress rather than a wish to start anew.
WHY RESOLUTIONS DON’T WORK
New Year’s resolutions are ineffective because of how we think about them. First, the resolution exists for a reason: the behavior has probably been bothersome for a while. Seeing a resolution through this lens suggests we’ll need to fight to change it, otherwise we would’ve done so already. This practice produces a mindset of opposition, like a boxer entering the ring. Such a mindset also increases the likelihood that we will experience anger when our adversary hits back.
Second, we tend to assume that once we reach our goal, we won’t struggle with that issue. However, nearly all behavior change requires sustained, purposeful effort to maintain. Ask anyone who’s quit smoking for the hundredth time.
These issues suggest we need to shift our focus from outcomes to the process itself. Embracing this mindset not only fosters meaningful progress but also prioritizes mental health. As we are aiming to better ourselves, our first task is developing an evolved view of the change process.
A SCIENCE-BACKED PERSPECTIVE
Research shows that approximately 80% of New Year’s resolutions fail by February. This high failure rate is not due to a lack of willpower, it’s from unrealistic goals, vague planning, and neglecting psychological well-being. A key to breaking the toxic cycle of stress and guilt involves new interpretations about the change process.
Changing must include setbacks, otherwise we won’t develop the tools to overcome them. Evidence suggests that one of the main mechanisms of behavior change involves a feedback loop in the response to setbacks. When we don’t perform as we wish, a series of internal thoughts, assumptions, and beliefs start to unfold and influence whether we continue to try. Because these motivational and cognitive factors are interwoven, we can directly examine these factors to meet our goals.
The Transtheoretical Model offers another valuable framework. It posits that change occurs in stages based on readiness and highlights the importance of connecting to the “why” behind goals. This approach helps sustain motivation and ensures that changes align with personal values.
Creating an ideal roadmap for meeting our behavior change goals – and supporting mental wellbeing in the process – is beyond the scope of a single article; however, taken together, these findings may be able to help us build our own set of skills and strategies to transform the idea of self-improvement.
AN UPDATED APPROACH
1. Lasting change involves new behaviors. We can’t predict obstacles, so we’ll need to keep revising our plan.
2. The only perfect perspective on change is from within. How we talk to ourselves is critically important.
How we plan for change matters. Planning for success is as important as preparing ourselves for setbacks. There are several strategies we can use to plan for change.
The right goal at the right time: Meaningful change happens gradually. We should, therefore, spend our effort building the most realistic and achievable goals first. For example, someone who wishes to better control their diabetes may want to first be consistent with blood sugar monitoring. Small, achievable goals provide early evidence of progress and build confidence for tackling more significant challenges.
Emphasize progress at every turn. Resolutions based on a fixed outcome and unhelpful. “I will get a promotion,” doesn’t considering the process required to get there. One helpful tool involves elevating daily habits and processes that support your overall goal. Instead of “I will get a promotion,” consider “I will consistently seek learning opportunities and communicate effectively with my team.” Research shows that valuing incremental progress enhances motivation and satisfaction.
Specify what will be done – and keep track. Focus on actions within your control. Those who resolve “to lose weight” may forget genetic and biological factors can greatly impact results. It may be smarter to focus on specific behaviors we can impact – such as recording our food intake. Some people are motivated by visual trackers, like coloring in a calendar box each day they complete their goal.
Set and keep boundaries. Early in the change process, enthusiasm can be a hinderance. Overcommitment and unrealistic goals can lead to burnout. Studies confirm that setting boundaries and prioritizing self-care are critical for continued goal pursuit. For example, if your resolution involves increasing productivity, balance it with dedicated time for rest and recreation.
Continued on page 22
Dr. Jonathan Mitchell
A B O U T U S
Healthcare Realty & Development Services LLC (HRDS) is pleased to offer this Winter special aimed to create healing environments for you, your staff and your patients. As experts in Evidence Based Design, we proudly present these opportunities to improve your facility aesthetics and operational efficiency. Call today for your free evaluation.
R e f r e s h P a c k a g e
I
F l o o r i n g r e p l a c e m e n t ( c a r p e t , v i n y l , o r t i l e )
W a l l r e p a i r a n d t o u c h - u p s ( e g , p a t c h i n g h o l e s , s m o o t h i n g s u r f a c e s )
M i n o r l i g h t i n g u p g r a d e s ( e . g . , r e p l a c i n g o u t d a t e d f i x t u r e s )
R e n e w a l P a c k a g e ( i n c l u d e s R e f r e s h P a c k a g e )
R e f r e s h P a c k a g e p l u s :
E x t e r i o r p a i n t i n g ( w a l l s , t r i m , d o o r s )
P r e s s u r e w a s h i n g ( s i d e w a l k s , p a r k i n g l o t s , b u i l d i n g e x t e r i o r s )
L a n d s c a p i n g r e f r e s h ( m u l c h i n g , p r u n i n g , n e w p l a n t i n g s )
S i g n a g e D e s i g n a n d I n s t a l l a t i o n ( e x t e r i o r b r a n d i n g , d i r e c t i o n a l s i g n s , o r
A D A - c o m p l i a n t w a y f i n d i n g )
P a r k i n g L o t R e s u r f a c i n g a n d M a i n t e n a n c e ( f i x i n g p o t h o l e s , s e a l i n g c r a c k s ,
a n d r e s t r i p i n g s p a c e s )
R e n o v a t i o n P a c k a g e ( i n c l u d e s R e f r e s h & R e n e w a l P a c k a g e s )
R e f r e s h & R e n e w a l P a c k a g e s p l u s :
D e m o l i s h i n t e r i o r s / e x t e r i o r s a s n e e d e d
N e w w a l l s , c e i l i n g s , i n s u l a t i o n , e l e c t r i c a l , p l u m b i n g , H V A C , b u i l d i n g s e r v i c e s
C u s t o m M i l l w o r k a n d I n s t a l l a t i o n ( r e c e p t i o n d e s k s , c a b i n e t r y , s h e l v i n g )
D o o r a n d H a r d w a r e U p d a t e s
W i n d o w a n d G l a s s U p g r a d e s ( e n e r g y - e f f i c i e n t w i n d o w s a n d g l a z i n g )
E m e r g e n c y P r e p a r e d n e s s U p d a t e s ( b a c k u p g e n e r a t o r s , e v a c u a t i o n p l a n s , f i r e s u p p r e s s i o n , e t c . )
A r t w o r k a n d f u r n i s h i n g s s e l e c t i o n
C a l l F r a n k R i c c i t o d a y f o r y o u r f r e e e v a l u a t i o n
L i c e n s e d R e a l E s t a t e B r o k e r B K 4 5 4 4 2 8 L i c e n s e d B u i l d i n g C o n t r a c t o r C B C 0 5 9 2 4 4
AI Technology Improving Patient Outcomes, Recovery and Satisfaction in Hip Replacements
By Dr. George Haidukewych/Orlando Health Jewett Orthopedic Institute
In the ever-evolving landscape of medical technology, artificial intelligence (AI) continues to push the boundaries of what is possible in the field of surgery. One groundbreaking development that has captured the attention of the orthopedic community is the integration of AI into hip replacement surgeries, promising enhanced outcomes, reduced recovery times, and improved overall patient satisfaction.
Orlando Health Jewett Orthopedic Institute is one of the first in the nation to offer artificial intelligence assistance in hip replacement procedures. I was introduced to the technology by virtue of working with a leading orthopedic company that is developing hip planning simulation and navigated, robotic execution methods. I am part of an international team of experienced hip surgeons working on developing the next generation of hip replacement implants and techniques.
The new simulation modeling allows the orthopedic surgeons to put the hip replacement in with accuracy to the degree and millimeter that is appropriate for the individual patient. We can then apply artificial intelligence to the X-rays taken in the operating room to confirm the placement. The technology provides immediate feedback in the operating room about whether the surgeon hit the target, allowing us unprecedented accuracy and efficiency during surgery. It’s beautiful technology that we’re excited to have at our disposal.
According to the American Joint Replacement Registry 2023 report, more than 3.1 million primary and revision hip and knee arthroplasty procedures have been performed between 2012 and 2022. The data also shows there are 42,228 procedural cases reported by ambulatory surgery centers, which is an 84% increase since 2022. We are seeing more patients, including a younger population, seeking these procedures to improve their daily lives.
When I started operating 25 years ago, patients were sometimes in the hospital for a week after undergoing a hip replacement. With new implant technology and surgical techniques such as robots, as well as advancements in patient care, the length of stay for our patients has continued to decline. The AI technology continues this trend by shortening the procedure and decreasing the amount of time our patient is under anesthesia. Now, our patients can undergo hip replacement surgery in the morning and be home before lunchtime.
We do pre-operative planning to make the hip very specific to patients’ activities, such as yoga or golf. We use computer simulation to tell us where to put the hip, computer-aided navigation to hit our target to the degree, and artificial intelligence in our X-rays on the patient’s anatomy to get their leg lengths just right.
This level of precision has never been available until now. Some of the most common reasons for dissatisfaction with a hip replacement include getting the leg lengths wrong, and poor implant placement resulting in dislocation or premature failure. These are all issues which are prevented by the simulation modeling.
At Orlando Health, artificial intelligence has entered other aspects of care throughout the system. At the Orlando Health Jewett Orthopedic Institute, AI enables us to complete MRI scans rapidly – only taking a few minutes in some cases - and provides sharper images for our radiologists to read. It’s also utilized at the Orlando Health Digestive Health Institute during colonoscopies.
Learning the methods takes professional instruction. Courses are available for interested surgeons. I expect more physicians across the country will begin incorporating AI technology into their practices in the future, though it does not replace our training. We must be able to confirm the information the AI technology produces with our own surgical experience. Used in this fashion, the AI technology is a game changing tool for us to explore and incorporate for the benefit of our patients.
Internationally recognized for joint replacement surgery and trauma, George J. Haidukewych, MD, serves as director of orthopedic trauma, chief of complex joint replacement, academic chairman for the Orthopedic Faculty Practice and professor at the University of Central Florida College of Medicine. He trained at the prestigious Mayo Clinic in Rochester, Minn. Dr. Haidukewych specializes in total hip and total knee replacements as well as orthopedic trauma. He brings extensive experience in the management of failed and infected total hip and total knee replacements and in reconstruction of the joints after trauma.
In the Fall of 2017, Dr. Haidukewych was inducted into the International Hip Society, an exclusive association of joint surgeons from all over the globe that have demonstrated excellence in hip surgery. The society is comprised of top surgeons from various countries who specialize in hip replacement surgery. Members convene at multiple times throughout the year to discuss difficult cases and share best practices. New members must be voted in by current society members. Dr. Haidukewych is the only surgeon in Orlando in the society. He is also an awardwinning researcher, published more than 100 peer reviewed publications and book chapters and has presented hundreds of educational lectures on trauma and hip and knee replacement. Dr. Haidukewych holds several patents and developed multiple innovative implants for fracture fixation and joint replacement.
FloridaMD is the perfect partner to help you increase referrals to your specialty practice.
Resolution Revolution: Centering Mental Health to Reframe the Idea of Self-Improvement
Continued from page 18
Making a declaration that we will turn over a new leaf at the start of a New Year might work better if we consider first that we also have to tend to the tree. This usually involves a resilience and growth mindset. Consider the following strategies:
Aim for a growth mindset. Growth mindsets – the belief that abilities develop through effort – promotes resilience and reduces stress. Redefining setbacks as learning experiences may be challenging, but the more we practice, setbacks themselves become less bothersome. Specific questions we can ask ourselves include: “What lesson did I learn?” or “In hindsight, what else do I need to consider?”
Self-Compassion Over Criticism. Self-compassion involves treating ourselves with the same kindness and understanding as we would a close friend or loved one. We cultivate self-compassion over time by tending to our honest needs. Rather than building expectations for what we “should” achieve, we structure our goals to reflect kindness toward ourselves. For example, instead of “I will lose 20 pounds,” consider “I will prioritize nourishing my body and moving in ways that bring me joy.” This approach acknowledges our needs, regardless of outcome.
Integrate reflective check-ins. Prioritizing mental health requires regular reflection. Just as we track physical health goals, monitoring our emotional status can enhance self-assuredness and reduce burnout. Ask yourself: “Are my goals energizing or overwhelming me?” or “What adjustments can I make to support my emotional wellbeing?” This reflective practice encourages psychological flexibility and responsiveness.
Seek social support and connection. Humans are inherently social beings, meaning support plays a significant role in mental health and goal achievement. We can motivate our own change process by recruiting own friends and family to join in our change or serve as accountability checks. Prioritizing connection over isolation can make the journey toward self-improvement more rewarding and sustainable.
CONCLUSION: A NEW VIEW ON SELFIMPROVEMENT
Self-improvement is more than achieving goals. It involves reimagining how we care for ourselves. By focusing on the process rather than outcomes and practicing self-compassion, we can redefine self-growth.
As we enter a new year, let’s resolve not only to change ourselves but also to nurture our mental and emotional well-being. In doing so, we can embark on a revolution of self-improvement that truly lasts.
*References available upon request.
JANUARY – Digestive Disorders
Diabetes
2025
EDITORIAL CALENDAR
Florida MD is a monthly medical/business digital magazine for physicians..
Florida MD is emailed directly to healthcare providers in Orange, Seminole, Flagler, Volusia, Osceola, Polk, Brevard, Lake and Indian River counties. Cover stories spotlight extraordinary physicians affiliated with local clinics and hospitals. Special feature stories focus on new hospital programs or facilities, and other professional and healthcare related business topics. Local physician specialists and other professionals, affiliated with local businesses and organizations, write all other columns or articles about their respective specialty or profession. This local informative and interesting format is the main reason physicians take the time to read Florida MD.
It is hard to be aware of everything happening in the rapidly changing medical profession and doctors want to know more about new medical developments and technology, procedures, techniques, case studies, research, etc. in the different specialties. Especially when the information comes from a local physician specialist who they can call and discuss the column with or refer a patient. They also want to read about wealth management, financial issues, healthcare law, insurance issues and real estate opportunities. Again, they prefer it when that information comes from a local professional they can call and do business with. All advertisers have the opportunity to have a column or article related to their specialty or profession.