You’re not just our patient. You’re our neighbor. For more than a century, Orlando Health Orlando Regional Medical Center has been honored to provide nationally recognized care for the Central Florida region we proudly call home. And because it’s your home, too, you deserve trusted healthcare within reach, so we can foster a partnership focused on health and wellness — together. Giving you more reasons to choose well. OrlandoHealth.com/ORMC
Central Florida’s only Level 1 Trauma Center – Orlando Health Orlando Regional Medical Center – has significantly boosted its capabilities and efficiency through a $25 million renovation and redesign of its Emergency Department.
Two years in the making, the project elevates the emergency space to better care for a growing community where traumas are a daily and nightly occurrence. The wide-ranging upgrades increase the center’s capacity, improve patient experience, foster better communication among team members and add new technologies to create better patient outcomes.
“We’ve always served this community from a trauma capacity perspective, but as the Central Florida area is growing, we unfortunately have more and more people in need of our services,” said Kelly Nierstedt, president of Orlando Health ORMC. “The most important thing we want to do is make sure we have everything we need right here in Central Florida, so patients never have to leave their community.”
The renovated Emergency Department – officially unveiled in late January – is a completely reimagined space that emphasizes patient experience and efficiency of care.
Iam pleased to bring you another issue of Florida MD. Sometimes a patient may have the opportunity to participate in a clinical trial. Sometimes a patient may need specialized treatment that is not available in Central Florida. And sometimes there’s no money for that patient to get to those places. Fortunately there is Angel Flight Southeast to get those patients where they need to go. I asked them to tell us about their organization and how you, as physicians, can help. Please join me in supporting this truly wonderful organization.
Best regards,
Donald B. Rauhofer Publisher
ANGELS ON EARTH HELP PATIENTS GET TO LIFESAVING MEDICAL TREATMENT
Everyone knows angels have wings! But did you know in Florida and many parts of the nation they have engines and tails with dedicated volunteers who donate lifesaving services every day? Leesburg, Fla.-based Angel Flight Southeast is a network of approximately 650 pilots who volunteer their time, personal airplanes and fuel to help passengers get to far-from-home medical care. A member of the national Air Charity Network, Angel Flight Southeast has been flying passengers since 1993.
Almost all of its passengers are chronic-needs patients who require multiple, sometimes 25-50 treatments. Passengers may be participating in clinical trials, may require post-transplant medical attention or are getting specialized treatment that is not available near home. Each passenger is vetted to confirm medical and financial need and is often referred to Angel Flight Southeast by medical personnel and social workers.
Angel Flight Southeast “Care Traffic Controllers” arrange flights 24 hours a day, 365 days a year. In the event of a transplant procedure, the Care Traffic Controllers have precious minutes to reach out to its list of volunteer pilots who have agreed to be prepared on a moment’s notice to fly a patient to receive his or her potentially lifesaving organ.
The organization is completely funded through donations by individuals and organizations. A typical Angel Flight Southeast pilot donates $400 to $500 in services-per-trip. In fact, Angel Flight Southeast has earned the Independent Charities of America Seal of Approval as a good steward of the funds it generates from the public. Each $1 donated generates more than $10 worth of contributed services by Angel Flight Southeast.
The charity always seeks prospective passengers, volunteer pilots and donations. For additional information, please visit https://www.angelflightse.org or call 1-888-744.8263.
ADVERTISE IN FLORIDA MD
For more information on advertising in Florida MD, call Publisher Donald Rauhofer at (407) 417-7400, fax (407) 977-7773 or info@floridamd www.floridamd.com
Email press releases and all other related information to: info@floridamd.com
PREMIUM REPRINTS
Reprints of cover articles or feature stories in Florida MD are ideal for promoting your company, practice, services and medical products. Increase your brand exposure with high quality, 4-color reprints to use as brochure inserts, promotional flyers, direct mail pieces, and trade show handouts. Call Florida MD for printing estimates.
Publisher: Donald Rauhofer
Photographer: Donald Rauhofer / Florida MD
Contributing Writers: John “Lucky” Meisenheimer, MD ,Tara Griffin, DMD Sonda Eunus, MHA, John Meisenheimer, VII, MD;B.S., Tabarak Qureshi, MD FCCP, Tara Griffin, DMD, Frank Ricci, Julie A. Tyk, JD, Jaivir S. Rathore, M.D, F.A.E.S & Idha Sood, M.B;B.S
Art Director/Designer: Ana Espinosa
Florida MD is published by Sea Notes Media,LLC, P.O. Box 621856, Oviedo, FL 32762. Call (407) 417-7400 for more information. Advertising rates upon request. Postmaster: Please send notices on Form 3579 to P.O. Box 621856, Oviedo, FL 32762. Although every precaution is taken to ensure accuracy of published materials, Florida MD cannot be held responsible for opinions expressed or facts expressed by its authors. Copyright 2025 Sea Notes Media. All rights reserved. Reproduction in whole or in part without written permission is prohibited. Annual subscription rate $45.
Orlando Health Orlando Regional Medical Center Unveils $25 Million Emergency Department Renovation to Enhance Trauma Care and Community Health
By Staff Writer
Central Florida’s only Level 1 Trauma Center – Orlando Health Orlando Regional Medical Center – has significantly boosted its capabilities and efficiency through a $25 million renovation and redesign of its Emergency Department.
Two years in the making, the project elevates the emergency space to better care for a growing community where traumas are a daily and nightly occurrence. The wide-ranging upgrades increase the center’s capacity, improve patient experience, foster better communication among team members and add new technologies to create better patient outcomes.
“We’ve always served this community from a trauma capacity perspective, but as the Central Florida area is growing, we unfortunately have more and more people in need of our services,” said Kelly Nierstedt, president of Orlando Health ORMC. “The most important thing we want to do is make sure we have everything we need right here in Central Florida, so patients never have to leave their community.”
The renovated Emergency Department – officially unveiled in late January – is a completely reimagined space that emphasizes patient experience and efficiency of care.
The goal was to find ways to make the area more efficient. The A and B sides were combined to create a more cohesive unit, with support spaces down the middle of the department and nursing stations bookending it on each side.
“Everything’s down the middle so it’s easy to find anybody,” said Craig Bullaro, director of project operations for Orlando
Health ORMC. “And then all of the patient rooms essentially go around the perimeter of the department, much like a hotel.”
Of the 44,000 square feet that make up the Emergency Department, more than 40 percent was renovated during the redesign. In addition to being more efficient, the transformation created a more welcoming and comfortable experience for patients.
“It’s going to be very impactful. It’s a much more modern environment. And there’s much better lighting” said Dr. Gary Parrish, chairman of the Department of Emergency Medicine. “It’s a much better experience for our patients.”
Nursing stations were also redesigned to improve communication, two new CT scanners were added, and upgrades were made to Air Care Communications. The ambulance entrance to the Emergency Department was also enlarged.
Individual rooms were redesigned to be more consistent and offer a uniform patient experience. For example, rooms have similar layouts, with supplies and desks kept in the same area.
“We can take care of a sick person really in any bay in the department now,” Dr. Parrish said.
But among the most impactful changes were those made to the Trauma Bay, which was doubled in size to feature six bays that can quickly be surged to 12 when needed.
Four new EMS transfer bays can also be converted to surge trauma spaces for a total of 16 bays, offering 10 more treatment areas than the previous layout.
From improving lighting to layout, exam rooms were redesigned to offer a more modern and uniform patient experience.
Orlando Health ORMC unveiled its $25 million ED renovation to enhance trauma care and community health.
“The doubling of the size and the more than doubling of the number of beds that we have in our Trauma Bay has tremendously increased our capacity to care for patients all at the same time,” said Dr. Tracy Zito, Trauma medical director.
The upgrades are the largest renovation of the Emergency Department in the last 10 years.
LIFE-SAVING UPGRADES
Initial discussions about these upgrades started soon after Orlando was devastated by the Pulse Nightclub Shooting in 2016. All 35 victims who made it to Orlando Health ORMC alive survived their injuries.
“We had seen all of those patients come through our Emergency Department and the team did a spectacular job, but we learned a lot that night,” Nierstedt said. “We learned that we needed to expand our capacity to be able to serve the community if there were ever to be another incident like that.”
Another key goal of the renovation was improving visibility in the Trauma Bay.
The revamped Trauma Bay significantly upgrades Orlando Health ORMC’s capacity to receive and care for trauma patients. An existing corridor and three storage rooms were renovated to become part of the area, with surge capacity significantly increased.
“Our Trauma Bay is absolutely huge now,” Dr. Parrish said.
The number of regular working bays hasn’t changed. But those spaces have been heavily improved upon, with each bay now much larger than its predecessor. They also include enough equipment to care for two patients in each resuscitation care area, creating that surge potential.
“When you have as many as 15 people around a single trauma patient and you have X-ray equipment, ultrasound equipment and EKG machines, the amount of floor space you have is critical,” Dr. Parrish said.
“The trauma room that we used to have was very old. It was built before we had computers for our medical records and all the computers were on a back counter at the time,” Bullaro said. “So, physicians’ backs were always to the patients.”
The new design and expanded space include patient-facing workstations to allow the physician in charge to have full command of the room and a view of what is happening in any corner. Each bay’s individual vital monitors are also now duplicated onto larger screens in the work areas.
“Physicians can see exactly what’s going on in each of the bays directly at their workspace,” Bullaro said.
Much like the overall changes to the Emergency Department, the expanded space of the Trauma Bay and its new layout fosters better communication and a more efficient work process.
“When we’re not surged up, there is a complete right side around these beds where we can get all the team members around and step behind the red line to confer on patients if we need to,” Dr. Zito said.
When developing the new design, Orlando Health ORMC leaned on input from other Level I trauma centers from around the country to learn about what has and hasn’t worked to ensure the new setup would be as effective and up-to-date as possible.
This led to seemingly small innovations that make a big difference, such as adding a hydration station to support team members working long shifts.
“We built a little mini refrigerator and hydration station into the trauma bay for all of us who work down there,” Dr. Zito said. “Being able to have bottles of water in approved, designated areas is really important,”
The upgraded layout has helped create a Trauma Bay that can handle a wide array of incidents, ranging from the everyday occurrences of serious car accidents or rushes of patients from large casualty events.
Orlando Health ORMC doubled the size of the Trauma Bay with six bays that can quickly be surged to 12 when needed.
Each trauma bay is equipped with enough equipment to care for two patients creating instant surge potential.
The reimagined space creates a more cohesive unit, including nursing stations redesigned to improve communication.
“It doesn’t take much to have a mass casualty. A bus rolling over on the interstate can be 40 trauma victims coming in and a mass casualty,” Dr. Parrish said. “That’s something that can hit any emergency department at any time and we all plan for.”
DESIGN AND CONSTRUCTION PROCESS PUT PATIENTS FIRST
One of the main priorities of the construction process for the Emergency Department was to ensure that one of the busiest ERs in the country could remain open to patients even while the changes were being made.
“We could’ve shut the whole place down and obviously done it much quicker, but that really wasn’t an option,” Dr. Parrish said. “There was a community standard that we felt the need to uphold.”
To accomplish this, construction was completed in phases and temporary spaces were set up to serve patients as renovations were
implemented. Among the workarounds: An alternate ambulance entrance was built while the main entrance was enlarged. And what became the new EMS transfer bays were used as temporary trauma room space while the Trauma Bay was updated.
“We built the plane as we were flying it,” Bullaro said.
Orlando Health ORMC also decided early on that one of the best ways to improve patient care was to include physicians and other team members in the planning and design process.
“We wanted to change the workflow and make sure that it was the most efficient that it could be,” Nierstedt said. “And it’s really our frontline physicians and team members who can tell us how best to redesign the work.”
The designers worked closely with physicians and team members from the different disciplines of the Emergency Department to make certain that the renovated space would meet their needs. This included taking advantage of virtual reality technology to allow physicians to move through a 3D version of the designs to get a better feel for what the updates would look like. For example, during one consultation, doctors mentioned that a particular column might be in their way during a trauma event or that a monitor should be moved 12 inches to the right.
“This allowed the clinical teams to actually be able to see exactly what it was that the architects were presenting for their ideas,” Bullaro said.
COMMITMENT TO THE COMMUNITY
It’s important to note that this $25 million upgrade was funded entirely through philanthropic efforts, highlighting the special bond Orlando Health ORMC has with the community it serves.
“This expanded Emergency Department, the renovations, our intraoperative MRI, these are just examples of Orlando Health making sure we are investing back in our community so that our community never needs to leave,” Nierstedt said. “They get state-of-the-art health care right in their backyard.”
The changes and updates are set to make a major difference in the care of patients, providing them with a more welcome and pleasing experience, while also better equipping physicians and nurses to handle everything from a mass casualty event to minor scratches and scrapes.
“We are always striving to find ways to take better care of our patients,” Dr. Parrish said. “And we hope we’ll be able to do it better with this renovation.”
INTRAOPERATIVE MRI PROVIDES GAME-CHANGING TECHNOLOGY FOR NEUROSURGERY
In addition to the Emergency Department renovation,
More than 40 percent of the ED was reimagined and renovated to emphasize patient experience and efficiency of care.
Orlando Health ORMC also added another key upgrade to the hospital: a new operating room equipped with an intraoperative MRI, a key technology that can make a massive difference in neurosurgery.
The state-of-the-art equipment, which was added in January, allows for MRI scans to be created while surgeons are removing a tumor in the operating room. Theses valuable images usually can only be taken before or after a procedure, leaving little room for realtime information and course correction.
“Before the intraoperative MRI, we would have a preoperative scan that we would load into our system, and we’d use that for navigation to take out the tumor. But that wasn’t in real time,” said Dr. Robert Hirschl, chairman and medical director of Neurosurgery at Orlando Health. “As you’re taking out the tumor, you don’t know if you got it all or not.”
But intraoperative MRI changes all of that, by allowing the surgeons to evaluate real-time images and assess if they were successful in removing all of the tumor. They can then decide if they need to remove more of it on the spot, instead of having to wait for a postoperative scan. It can all be done without ever leaving the operating room.
‘We can get an image, and we’ll know if the tumor’s completely out or not and that’s a huge benefit for the patient,” Hirschl said. “It really is a state-of-the-art facility and an amazing piece of equipment to help with our neuro oncology program.”
Orlando Health ORMC added a key upgrade to the OR: an intraoperative MRI.
The hospital’s state-of-the-art intraoperative MRI allows for scans to be created while in the OR.
Not All Basal Cell Carcinomas Are Created Equal
By John “Lucky” Meisenheimer, MD and John Meisenheimer, VII
Occasionally a patient will tell me their “doctor friend” recommended that they don’t need treatment for a basal cell carcinoma because it will never hurt you. “Doc, he said it’s only a basal cell carcinoma.” Dermatologists fully recognize this as a genuinely cringe-worthy statement. You don’t need to see too many people missing various parts of their facial anatomy to know this advice is blatantly wrong. Even in this modern time of medical miracles, people still die from neglected basal cell carcinomas. When pressed for the name of their “doctor friend,” it usually comes up as I don’t remember their name, or it ends up being “Doctor Google.”
It is true a superficial basal cell carcinoma on the torso probably would take years and years for it to cause any sort of significant morbidity to a patient. But, on the other hand, even a small basal cell on the torso will continue to grow if left untreated slowly. What might have been a simple, inexpensive procedure now, a decade later, has turned into a monster of aggravation, discomfort, and cost.
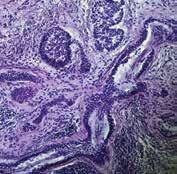
Although metastatic disease risk is low with basal cell carcinomas, it is certainly not zero. Several people die each year from basal cell carcinoma. Even more, patients can have disfiguring bouts with cancer losing various parts of anatomy such as nose, ears, eyes, etc. What a lot of patients and even some physicians are not aware of is that not all basal cell carcinomas are created equal. There are several different histologic growth patterns. These varying histologic types can each behave differently and require different treatment plans.
As mentioned before, a superficial basal cell carcinoma is probably not going to cause a great deal of physical damage unless neglected for long periods. There are other types of basal cell carcinomas; morpheaform and sclerosing basal cell carcinomas with infiltrating growth patterns. These cancers left untreated can cause a significant amount of morbidity in shorter periods measured in months, not years. Aggressive basal cell cancers can also become neurotropic, meaning that they “wrap” around a nerve and can track down its length. Neurotropism can be particularly dangerous, especially if this is on the face and affecting a nerve that happens to pass through a foramen into the brain. Clearly, not a good scenario.
Basal cell carcinomas, limited to the skin, tend to be very amenable to treatment in a variety of different ways. Even as a Mohs surgeon I can think of at least half a dozen different ways that I have treated basal cell carcinomas. Not all basal cell carcinomas need Mohs surgery. Each case of basal cell carcinoma should be evaluated individually and in consideration as to the best method of treatment based on its histologic growth pattern, location, and physical condition of the patient.
The great news about basal cell carcinoma, even though it is the most common type of skin cancer and millions are treated each year, only a tiny percentage of these end up causing death in patients. When someone says I would much rather have a basal cell carcinoma than a melanoma, there is a caveat; if you die from a basal cell carcinoma, you are just as dead as if you were to die from melanoma. Happily, most of the time, with early diagnosis and treatment, you don’t have to die from either. Basal cell carcinoma is called cancer for a reason. Give it its respect that it is due, or otherwise, you may regret saying, “oh, you don’t have to worry about it, it’s only a basal cell carcinoma.”
Lucky Meisenheimer, M.D. is a board-certified dermatologist specializing in Mohs Surgery. He is the director of the Meisenheimer Clinic – Dermatology and Mohs Surgery. John Meisenheimer, VII is an MD practicing in Orlando.
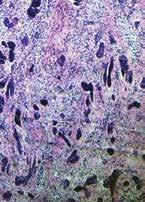
PHOTO: JOHN MEISENHEIMER, VII, MD
Pathology of an infiltrative basal cell carcinoma.
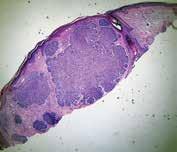
Infiltrative Basal Cell carcinoma of the forehead.
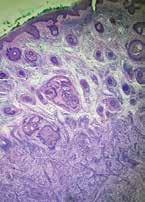
Superficial Multifocal BCC.
Nodular basal cell carcinoma.
Neurotropic basal cell carcinoma.
Sclerosing basal cell carcinoma.
PHOTO: JOHN MEISENHEIMER, VII, MD
PHOTO: JOHN MEISENHEIMER, VII, MD
PHOTO: JOHN MEISENHEIMER, VII, MD
Is Your Online Reputation Costing You Patients?
By Sonda Eunus, MHA, CMPE
What does your online reputation say about your practice? If you have a negative online reputation, you are missing out on new patients every day. Most medical practices now get the majority of their new patients through Google and other search engine queries, such as “Pediatrician in Orlando”. If your practice appears in these searches, the most common next step for a potential new patient would be to check out your reviews – what are other patients saying about your practice? It has been reported that 90% of consumers read online reviews before visiting a business and that online reviews influence 67% of purchasing decisions (Bright Local). For this reason, it is incredibly important to pay attention to the rating and reviews that your practice has on search engines, social media platforms, and local online business directories.
However, despite the importance of cultivating a positive online reputation, only 33% of businesses report actively collecting and asking for reviews (1). One great process to set in place at your practice is asking for patient reviews after each patient visit. It can be as simple as training your front office staff to ask each patient how their visit went while checking them out, and if they receive favorable feedback then they can ask the patient to please leave a review on Google or Facebook about their experience. If they receive negative feedback, this feedback should be taken very seriously, and management should be notified as soon as possible so that the issue can be mitigated before the patient decides to post a negative review.
Setting up an automated text or email campaign that asks each patient for their feedback after their appointment is also a great way to improve your online reputation as well as to correct any issues that may be occurring at your practice. When you receive feedback from patients, you are then able to prompt them to leave a public review on Facebook, Google, Yelp, Healthgrades, or other applicable review platforms. However, you must be aware that legally, you are not allowed to only direct people with favorable feedback to leave reviews, which is known as review-gating – so if you are implementing an automated system like this, just make sure that you are aware of this limitation. There are online reputation management platforms which allow you to customize the messages that people see when they leave negative feedback as opposed to positive feedback, but both of those messages must still offer the option to leave a public review. However, if you create your message in such a way as to communicate to the patient who may leave negative feedback that you are working hard on resolving the issue and that someone will be in touch shortly, that may prevent them from leaving a public negative review.
When you receive a public review on Google, Facebook, or other review sites, make sure that you respond to it – either by thanking them for a good review or by asking them to contact you to discuss how you can improve their experience. Do not argue or try to defend yourself online – try to speak about it with them privately, fix the issue, and ask them to remove the review if possible. When you receive great reviews, make sure to cross-share them on your various social media platforms. You should also create a “Reviews” page on your website and add all great reviews to this page. This instantly adds credibility to your website.
Finally, make sure that when you look over the feedback and reviews that you receive, you are paying attention to what the negative reviews are saying – this is a great opportunity to identify current process challenges and improve your patients’ experience at your practice. Need help managing your practice’s online reputation? Visit www.lms-plus.com to see how Leading Marketing Solutions can help.
Sonda Eunus is the CEO of Leading Marketing Solutions, a Marketing Agency working with Medical Practices and other Businesses to help them identify the best marketing strategies for their business, create a strong online presence, and automate their marketing processes for a better return on their Marketing budget. Learn more about Leading Marketing Solutions at www.lms-plus.com.
What’s New in the Treatment of Mild Obstructive Sleep Apnea and Primary Snoring?
By Tabarak Qureshi, MD FCCP
THE FIRST FDA-AUTHORIZED DAYTIME THERAPY: EXCITEOSA® SNORE... SNORE… SNORE…
We all know of someone who snores, but when people are informed of their snoring, the typical response is denial and disbelief. The truth of the matter is that snoring is extremely common, but most people don’t understand why it happens.
Snoring is generated when the upper airway/pharyngeal muscles relax and as air flows through a relaxed posterior airway. In some people with a crowded posterior airway, these sounds and vibrations result in mild obstructive sleep apnea (OSA), which is identified by having an AHI (apnea hypopnea index) between 5-15 events/hour. The repeated airway obstructions result in sleep disruption, blood pressure swings, and recurrent nocturnal asphyxia and hypoxia resulting in increased sympathetic nervous system activation during sleep. Traditionally, there has not been any significant treatment modality for primary snoring. Mild OSA has been treated primarily with auto-CPAP/PAP or mandibular advancement devices along with lifestyle modifications (weight loss, drinking, and smoking cessation). The most notable change is noted in the upper airway and the genioglossus muscle. This collapsibility is higher in mild OSA compared to primary snoring. In non-snorers, there is an ability to prevent collapsibility of the upper airway and have functional mechanisms that prevent collapse.
The genioglossus is considered the largest muscle of the airway and the most important dilatory muscles during sleep onset. With sleep onset, there is rapid reduction in pharyngeal and tongue muscle contractility. Over time the respiratory stimulus and genioglossus activity progressively increase during stable non-REM sleep. However, a notable number of individuals fail to effectively increase genioglossus activity or achieve inadequate tongue muscle activation to overcome the obstruction prior to the arousal. Therefore, there is a failure of the tongue muscles to generate an appropriate protective response from a neural drive or responsiveness perspective.
The first proof of concept of daytime stimulation of the tongue was presented by Wiltfang in 1999 (28). He demonstrated using a TENS like stimulation during daytime for two weeks resulted in a significantly reduced respiratory disturbance index (RDI), from 13.2/hour to 3.9/hour, oxygen desaturation index improved as did minimum oxygen saturation from 75% to 88%. In another prospective placebo controlled randomized trial of daytime tongue stimulation vs TENS type stimulation the number of snoring epochs decreased significantly (from 63.9±23.1 epochs per hour to 47.5±31.2; P<.05).
EXCITEOSA®:
The eXciteOSA device targets the intrinsic and extrinsic pharyngeal and tongue muscles by delivering neuromuscular electrical stimulation to the tongue with the purpose of increasing muscle responsiveness and preventing excessive relaxation. The device has three components:
1. Washable flexible electrode mouthpiece with an electrode array that fits onto the tongue.
2. Rechargeable control unit that attaches to the mouthpiece via a USB connection.
3. Smartphone App that manages the functions of the device. The mouthpiece is placed in the mouth, on the tongue with the two electrodes located above and two below the tongue. Therapy consists of a series of pulse bursts with rest periods for 20 minutes during the wakefulness state for a period of 6 weeks. With daily use of eXciteOSA, the tongue muscle function improves to prevent the backward collapse of the tongue and hence obstruction of the airway.
CLINICAL TRIALS DATA
The original trial was a prospective multicenter trial of individuals with primary snoring or mild OSA. Snoring was assessed by the bed partner reporting on a visual analog scale-VAS (ranging from 1-10, 10=unbearable snoring). The snorers sleep quality was recording using the Pittsburgh Sleep Quality Index (PSQI) pretreatment (2 weeks before start of therapy), during treatment phase (6 weeks recorded in last two weeks) and post treatment (2 weeks after stopping therapy). 27 individuals completed the trial (8 women and 19 men), average age 44 years (age range 2568 years), BMI 29.7 (range 20.7-35) and AHI 9 (range 2.5-15).
Eight primary snorers and 19 had mild OSA.
Results revealed bed partner reported snoring reduced by 52% (p<0.001) with over 80% declaring a reduction of >40%. The change remained statically significant for primary snores and mild OSA patients (VAS reduction 6.6 to 3.6 p<0,001).
Another multicenter clinical trial was undertaken at London University hospital along with other sites in Europe. The objective was to validate the objective measures and assess the reproducibility of the subjective outcomes of the previous study. This was cohort of mild OSA (HST using WatchPAT®) and primary snorers. Two consecutive night studies were conducted before and after the 6-week period. This was supplemented with partner VAS, Epworth Sleepiness Scale (ESS), and PSQI.
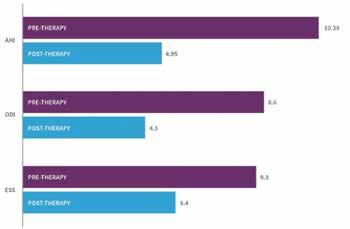
125 patients were recruited and 115 (50 primary snorers and 65 mild OSA patients) completed the trial. The average age was 46 (range 24-79 years), 73 males and 42 females, average BMI 27 (range 20-34). For the study population the mean objective percentage of sleep time snoring at >40dB, reduced significantly by 41% (p<0.001). 90% of the participants recorded an objective reduction in their snoring. Clinically significant reduction in snoring time was also reported at snoring intensities of 45dB and 50dB with an improvement of 52% (p<0.001) and 54% (p<0.001) respectively. In mild OSA, 79% showed an average reduction in AHI of 52% (p<0.001) and the post therapy AHI normalized to 4.95. Statistically significant improvements were noted in ESS and PSQI scores as well (p<0.001).
Oral pooling of saliva was most common side effect, with a
small percentage reported tongue discomfort, tooth discomfort, filling sensitivity, gagging, metallic taste and jaw tightness. Prevalence of these symptoms reduced in the six weeks of therapy.
DISCUSSION AND CONCLUSION
Daytime neuromuscular electrical stimulation (NMES) therapy for correction of nighttime airway obstruction is a novel, innovative and probably unconventional therapeutic strategy. The ability to control nighttime sleep disordered breathing without wearing a nighttime device makes this an attractive treatment modality. NMES involves the application of electrical current to induce muscle contractions and has been shown to activate the muscle to a greater extent than voluntary muscle actions. It has
been known to activate motor units that are not otherwise activated. NMES has been shown to change the myofibrillar protein expression to induce a phenotype shift from fatigue prone to fatigue resistant with the strengthening of the cytoskeleton. NMES has been shown to result in metabolic shift from glycolytic to oxidative profiles, increasing intracellular defense against harmful oxygen species, reverse the degeneration of pre and postsynaptic tongue neural morphology associated with ageing and a shift to a higher contractile tension.
eXciteOSA offers a simple and effective method of addressing the above-mentioned process and has been shown to benefit individuals with primary snoring and mild OSA. eXciteOSA provides a targeted retraining tool to stimulate the tongue and the biggest dilatory muscle of the airway – the genioglossus muscle. The clinical trial demonstrated significant reductions in all of the relevant objective measures, 90% of the study population showed reduction in snoring, 79% of the mild OSA population showed a 50% reduction in AHI and ODI resulting in reduction in ESS and PSQI.
Tongue muscle training using eXciteOSA has proven to be effective in reducing multiple indices associated with sleep disordered breathing. Additional studies have been published and accepted for publication and currently underway. eXciteOSA provides a “no nighttime wearable” safe option of therapy for patients and overcomes many of the risks and disadvantages of currently available treatment options.
For more information on this novel daytime therapy option, visit the eXciteOSA website: eXciteOSA.com or email info@signifiermedical.com.
Bibliography available upon request.
Tabarak Qureshi, MD FCCP practices at Central Florida Pulmonary Group. He is Chairman-Division of Pulmonary Medicine at AdventHealth, Director of ICU AdventHealth Altamonte Springs and Director of the Sleep Lab at Central Florida Pulmonary Group.
Regaining Independence: How Advanced Colorectal Care Changed One Patient’s Life
By Robert Michael Dorman, MD
Colorectal conditions like chronic functional constipation can significantly affect a child’s quality of life, limiting their ability to participate in activities and social interactions. At Nemours Children’s, we utilize advanced treatments to help pediatric patients overcome these challenges and live fuller, more independent lives.
Sarah struggled with severe functional constipation for years, leaving her dependent on regular enemas. Exhaustive attempts with traditional bowel management had only delivered limited improvement. As an active 11-year-old, it was becoming a burden on her daily life and independence, and her family began to seek more advanced solutions.
tions independently and confidently helps kids get back to being kids, enjoying the things they previously felt were out of reach.
At Nemours Children’s, we offer a comprehensive, multidisciplinary approach to pediatric colorectal conditions. Our expert team of surgeons, gastroenterologists, advanced practice providers, therapists and nurses collaborate on individualized care plans, working with patients from initial assessment through long-term management and transition to adult care.
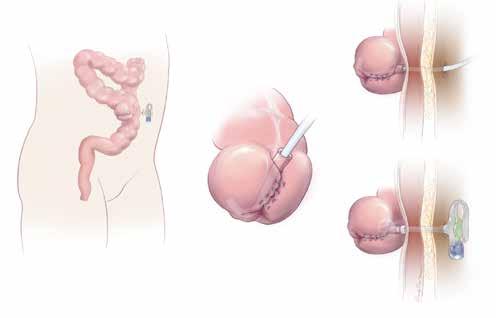
(Illustration of MACE. Source: Wikipedia)
After thorough multidisciplinary assessments, our pediatric colorectal team recommended a-Malone antegrade continence enema (MACE) procedure for Sarah. This surgical procedure creates a small stoma in the abdomen, which enables an enema to be administered directly into the bowel through the appendix (as opposed to a rectal enema). This means Sarah would easily be able to administer enemas on her own.
The surgery was successful and improved Sarah’s condition dramatically. She quickly adapted to her new routine, regaining control over her bowel management. “She doesn’t even let us in the bathroom with her anymore,” her mother tells us, smiling. With her newfound independence, Sarah’s happiness is palpable. She’s now able to participate fully in school, social, and family activities without worry or embarrassment.
Sarah’s experience highlights the transformative impact of advanced colorectal procedures. The ability to manage condi-
To refer a patient or to learn more about our advanced pediatric colorectal care visit Nemours.org/gastrosurgerycenter or call 407.650.7715.
R. Michael Dorman, MD is a board-certified pediatric surgeon at Nemours Children’s Hospital, Florida in Orlando. He provides specialized colorectal surgical services as a member of the coordinated GI surgery center team. Dr. Dorman earned his medical degree at the University of Arkansas, then completed his residency in general surgery at the University of Buffalo in New York. Dr. Dorman’s fellowship trainings include surgical critical care at Children’s Mercy Hospital, Kansas City; general pediatric surgery at the University of Mississippi; and pediatric colorectal surgery at Nationwide Children’s Hospital in Columbus, Ohio. Dr. Dorman is board certified in general surgery, pediatric surgery, and surgical critical care.
At Nemours Children’s Health, our multidisciplinary
• Nationally recognized surgeons
• Experienced specialists across nearly every digestive and GI disorder
• Registered dieticians
• Behavioral therapists and counselors
The Digestive Disorders and Gastrointestinal Surgery Center at Nemours Children’s Hospital, Florida in Orlando is home to an integrated team of experts, working together to help kids with all types of GI conditions achieve a faster, more complete recovery. Our collaborative approach, combined with state-of-the-art robotic procedures and minimally invasive surgical techniques, provides advanced and comprehensive treatment for a wide range of GI disorders, from the common to the most complex.
Early Recognition Can Save Patients’ Hips
By Andrew Carbone, MD
It’s easy for us to imagine the scene. A young adult athlete, such as a hockey goalie or a ballerina, sits with their physician in the examination room reviewing several X-rays on a screen that show an apparently healthy hip.
The physician tells the patient that they have sustained an injury to the joint. The soft tissues will heal with time and the pain can be managed, but arthritis could possibly develop in the future.
While just two decades ago, this may have been the end of the conversation, young adults should no longer accept that arthritis and a deteriorating joint is the inevitable result of a hip injury. Fortunately, a major paradigm shift is underway. Supported by extensive data and increasingly effective arthroscopic techniques, we can recognize the underlying pathologies resulting from hip injuries and treat them now. Such early intervention may possibly delay or obviate the need for total hip replacement in the future and might even prevent the joints from developing arthritis altogether.
THE CHALLENGE –Traditionally, arthritis has been divided into two categories: primary and secondary. Primary arthritis basically means arthritis with no known origin. Secondary arthritis includes arthritic conditions of known medical origin, such as rheumatoid or inflammatory arthritis and infectious or septic arthritis. In the 1970s, 80s and even the 90s, we lacked the diagnostic tools to be more precise than this. But today, with increased awareness, improvements in advanced imaging, better understanding of synovial biomarkers, and other technology available, we can invest greater effort in determining the precise causes of the pre-arthritic condition and treat the underlying pathology.
These pathologies may include femoroacetabular impingement, acetabular labral tears, excessive femoral or acetabular anteversion or retroversion, inadequate femoral head coverage (Acetabular Dysplasia), or hip microinstabiltiy. In some cases, the injury that brings the patient to the physician’s office may reveal another pathology such as generalized ligamentous laxity, or even some connective tissue disorders like Ehlers-Danlos Syndrome.
These conditions may result in an earlier than normal onset of arthritis of the hip if left untreated. Ultimately, the goal is to change the mindset of both patients and providers alike – that osteoarthritis is not a disease, but rather a symptom or side effect of an untreated predisposing hip condition.
THE PARADIGM SHIFT
– The focus of hip preservation is the idea that we don’t treat hip pain patients like pre-arthritic patients; we treat them like they have actual pathologies that need to be treated. A growing body of evidence shows us that early intervention can improve hip function, reduce pain, and possibly delay or even prevent the onset of arthritis.
But as with many advances that result in a paradigm shift,
there has been skepticism and resistance in some quarters. I compare this to how arthroscopic surgery was viewed many years ago. For a long time, some physicians considered shoulder arthroscopy to be “an instrument of the devil” by very prominent shoulder surgeons. For example, if you were doing a labral repair arthroscopically, some argued that you were doing harm to the patient and that of course would be a terrible thing. But then our arthroscopy techniques steadily improved. The result has been a total shift away from open surgical labral repairs for shoulder instability. In fact, the role for open shoulder labral repairs is so limited today that the technique is not often taught in surgical residency or fellowship anymore.
With hip surgery, it’s similar. Early articles were published with nearly the same headlines, comparing hip arthroscopy to the “devil’s tool.” Open surgery on the hip for dysplasia, for example, has been around for some time. Whereas hip arthroscopy has been around only since the early 2000s. But now that paradigm has started to change. Now, we are able to combine open surgery with arthroscopic techniques. The results are promising, but they have taken time to gather. Part of this is due to the nature of hip preservation. Unlike surgery to the shoulder or the knee, for example, in hip surgery, the benefits for the patient may not always be immediately clear. Instead, we are trying not only to improve function and reduce pain now, but potentially prevent a disease that’s possible to happen 10 to 20 years from now. Now that we have been doing this work for nearly 20 years, longer term data has begun to demonstrate that hip arthroscopy improves a patient’s pain and function. And while it is likely too early to truly know hip arthroscopy’s effect long term, as we continue to improve our techniques and study our patients, I am confident we will start to see stronger evidence for delayed and possibly reduced rates of hip osteoarthritis.
UNDERDIAGNOSED –
Education is key in hip arthroscopy because many times the underlying pathology goes undiagnosed. For example, often a patient will present with vague groin pain or maybe a tightness they experience when they are trying to stretch out. Sometimes this pain radiates to other areas, such as the buttocks, or the hip. Then it often gets written off as a muscle pull or lower back pain. But unlike those conditions, it never really goes away. The patient gets X-rayed, but the X-ray looks healthy. Eventually, the patient gets frustrated and that’s typically when we are consulted; because, if you are 21 years old, you should not be experiencing hip pain. And if you do, that’s something that needs to be addressed.
Dr. Andrew Carbone is a dual fellowship-trained orthopedic surgeon and sports medicine physician at the Orlando Health Jewett Orthopedic Institute.
At the Orlando Health Jewett Orthopedic Institute, we are seeking to raise awareness among young adult athletes that hip-related pain is not normal and the cause of it should be carefully investigated and identified. And if it is determined not to be a temporary condition, such as a muscle strain, we should review the possible treatment options, which may include arthroscopy. Orlando Health Jewett Orthopedic Institute is the first orthopedic specialty hospital in Florida, and we’ve assembled a team of distinguished experts to address these kinds of cases. When a patient comes here, they aren’t seeing just one doctor and getting just one opinion, they are seeing several doctors and getting several perspectives at once. We form a kind of collective in which we can share our views and challenge each other. In addition to this, we are part of the Academic Network of Conservational Hip Outcomes Research group (ANCHOR). ANCHOR is a multicenter, clinical research group of physicians and scientists who are investigating adolescent and adult hip disorders. We are focused on improving patient care through research, education and mentorship. This collaboration enables us to learn from thousands of data points and patient outcomes.
BOTTOM LINE – If you have a young adult patient who has experienced an injury to their hip or is presenting with unusual pain, don’t dismiss it, investigate it. Find out why this is happening, and let’s get it treated. It might save that patient a lot of pain and difficulty not just now, but many years from now.
Dr. Andrew Carbone is a dual fellowship-trained orthopedic surgeon and sports medicine physician at the Orlando Health Jewett Orthopedic Institute. His expertise is in sports medicine, and he frequently collaborates with athletes across many sports. This includes enthusiasts who play sports in their leisure time as part of an active lifestyle. Dr. Carbone is proficient in a wide array of procedures including:
• Arthroscopic hip labral repair for treatment of femoroacetabular impingement
• Complex primary and revision hip arthroscopy including labral reconstruction for treatment of recurrent labral tears
• Shoulder arthroscopy for rotator cuff tears, shoulder instability and biceps injuries
• Knee arthroscopy for treatment of meniscal and cartilage injuries
• Ligament reconstruction for knee injuries
• Minimally invasive robotic hip replacement
• Minimally invasive treatment of gluteal and hamstring tears
Dr. Carbone stays informed on the latest medical research and science so he can offer his patients the most comprehensive information and care. He takes time to answer all of their questions so they feel comfortable about their treatment options.
DR. CARBONE’S TRAINING
He earned a bachelor’s degree in neuroscience and behavioral biology from Emory University in Atlanta. Dr. Carbone received his medical degree from New York Medical College in Valhalla, where he was inducted into the Alpha Omega Alpha national medical honor society. He then stayed in New York for an orthopedic surgery residency at The Mount Sinai Hospital. He completed a sports medicine fellowship at the Cedars-Sinai Kerlan-Jobe Institute in Los Angeles and another fellowship in hip preservation at the American Hip Institute & Orthopedic Specialists in Des Plaines, Illinois. He received specialized training in open and arthroscopic hip preservation techniques, treatment of gluteal and hamstring injuries, and minimally invasive robotic hip replacement procedures.
ABOUT DR. CARBONE
Dr. Carbone is a member of the American Orthopaedic Society for Sports Medicine, American Academy of Orthopaedic Surgeons, Arthroscopy Association of North America and International Society of Hip Preservation. He is also a peer reviewer for The American Journal of Sports Medicine.
His research has been published on topics including arthroscopic capsular repair, batter’s shoulder, shoulder arthroplasty and femoroacetabular impingement syndrome, a condition in which the bones at the hip joint rub together due to one or both bones being irregularly shaped.
He has a particular interest in the arthroscopic treatment of sports-related injuries of the hip, knee and shoulder. During his medical studies, he spent a year researching the biologic and mechanical pathways involved in tendon to bone healing and how sports-related injuries affect cartilage health and contribute to the development of osteoarthritis.
He constantly reviews the latest research, allowing him to extend to his patients the most comprehensive information and care available to ensure they are comfortable with their treatment options.
An avid sports fan, Dr. Carbone previously served as the assistant team physician for the Los Angeles Dodgers and Los Angeles Angels. He served as the associate team physician for the Anaheim Ducks, Los Angeles Galaxy, Los Angeles Sparks, Pepperdine University and West LA College.
Outside of work, he enjoys spending quality time with his wife and children, playing golf, and exploring new places through travel.
Helping Veterans Treat Obstructive Sleep Apnea
By Tara M. Griffin, DMD, DBDSM, DASBA
As we celebrate Independence Day, it is crucial to remember the brave men and women who have fought for our freedom. Veterans have made countless sacrifices to protect our nation, and it is our duty to ensure they receive the care and support they deserve. One prevalent issue among veterans is obstructive sleep apnea (OSA), a condition that can have serious consequences if left untreated.
A 2019 report estimates that over 1.5 million veterans have been diagnosed with OSA and up to 80% of those diagnosed are not being successfully treated. Continuous Positive Airway Pressure (CPAP) has been the gold standard for treatment for the past 40 years, however, in 2020 after a world-wide recall of CPAP machines, more than 600,000 veterans have been affected and another 600,000 are not compliant with the machines they have been prescribed.
Obstructive sleep apnea is a common sleep disorder characterized by pauses in breathing during sleep, often leading to fragmented sleep and low oxygen levels in the blood. This condition not only affects the quality of sleep but can also have detrimental effects on overall health and well-being. When you experience low oxygen levels in the blood on a regular basis, this creates inflammation in every organ system which leads to chronic debilitating health issues. For veterans, the impact of OSA can be particularly challenging, given the physical and mental toll of their service.
Fortunately, there are effective treatment options available for “managing” and now “resolving” obstructive sleep apnea. While CPAP therapy and surgery are commonly used, most veterans may find these options unavailable and potentially dangerous after recent recalls, uncomfortable and invasive. In such cases, alternative treatments like FDA-approved oral medical devices for sleep apnea can offer a more comfortable and convenient solution.
These custom oral devices are designed to help keep the airway open during sleep, reducing the risk of breathing pauses and improving overall sleep quality. By using these devices, our veterans are experiencing fewer awakenings during sleep, reduced daytime fatigue, improved cognitive function, better overall health and improved quality of life.
Compared to CPAP therapy, studies show that oral medical devices have a compliance rate of over 80% after 5 years of use which is much better than CPAP compliance and just as effective at lowering high blood pressure and reducing cardiovascular risks for patients. Based on recent FDA approved technology, up to 34% of patients may no longer need an oral medical device after 12 months of treatment.
One of the significant benefits of using oral medical devices for sleep apnea is their ability to address not only the physical symptoms and root causes of OSA but also the associated mental health challenges. Many veterans with OSA also suffer from
conditions like post-traumatic stress disorder (PTSD), which can be exacerbated by poor sleep quality and trauma experienced while serving. Over 1.3 million veterans have been diagnosed with PTSD through service-connection with the VA.
By improving sleep quality with custom oral medical devices and adjunctive therapies, most veterans we have treated, experience a reduction in PTSD symptoms, fewer headaches, and a decrease in night terrors! Better sleep can have a profound impact on mental health and overall well-being, allowing veterans to lead more fulfilling and productive lives.
For healthcare providers working with veterans, it is essential to consider alternative treatment options for sleep apnea. By offering veterans a comfortable and effective solution for managing or resolving OSA, healthcare providers can help improve the quality of life for those who have served our country.
At Sleep Solution Centers, we are a Community Care Provider for veterans and make it our priority to see our new patients within a week of receiving a referral from the VA. Our motto is, “Our freedom isn’t free but a good night’s sleep can be!”
As we honor our veterans this Independence Day, let us not forget the importance of supporting their health and well-being. By raising awareness about alternative treatments for obstructive sleep apnea and advocating for the use of FDA-approved oral medical devices, we can make a meaningful difference in the lives of those who have sacrificed so much for our freedom. Let us stand together in providing the care and support our veterans deserve!
Tara M. Griffin, DMD, DBDSM, DASBA, graduated from Nova Southeastern University in 2006, with a doctorate in Dental Medicine. She became passionate about helping her patients breathe and sleep better and completed her Diplomate with the American Academy of Dental Sleep Medicine in 2011. In 2015, she completed her Diplomate with American Sleep and Breathing Academy. In 2016, she became a Clinical Advisor with Vivos Therapeutics to help educate and mentor doctors interested in the treatment of OSA with oral medical devices. She owned a private practice focused on sleep, TMD and general dentistry in the panhandle of Florida for 17 years before becoming the co-founder of Sleep Solution Centers in Medical City, Orlando in 2024. She may be contacted at 407-502-0110 or by visiting www.sleepsolutioncenters.com
Negotiating Leases
By Frank Ricci, Healthcare Realty & Development Services LLC
Welcome back to our second in a series about Medical Real Estate. In the first installment we discussed locating property. In today’s chapter, we are discussing leases and important considerations for your practice. If you want to refer back to SESSION 1 in the previous issue of FloridaMD/JanuaryFebruary2024 please contact me at the email address listed below.
Assuming that you and your broker have identified a great property for your practice, the next step is negotiating the lease and the hundreds of potential clauses. We won’t discuss all of them, just some of the more relevant terms and clauses for your practice.
1. RENTAL RATE
Office space is typically quoted on a cost per square foot per year ($/SF/YR) basis. Going into negotiations with the owner or landlord, it is imperative that you have an understanding of the market, including what others are paying for similar space, incentives offered, services included, length of term, escalations, etc.
2. INCENTIVES
Most landlords offer incentives to lease space in the form of “Free Rent” or a “Tenant Improvement Allowance (TIA).” Free rent is usually 1-3 months but is very dependent upon vacancy rates in the area. Tenant improvement allowances vary considerably, depending on the rental rate offered and the condition of the building. For reference purposes, it typically costs around $25/sf to refurbish an office with new paint, carpet, etc. and can run from $80-$150/sf or more to build a new office from a shell condition. In most cases, the owner will provide a TIA but it usually does not cover the entire cost of the improvements. The remaining costs will be financed by your practice as either a lump sum, payments to the Owner or payments to a lender. If the Owner is financing only part of the cost to finish your space, negotiate the terms so that you are paying for the items with the shortest depreciable life, such as flooring and cabinets. This way you can itemize and either write off as an expense or depreciate over a short time period.
3. RENTAL ESCALATIONS
When you lease office space, you are taking a snapshot in time of market rental rates. Historically, those rents have increased over time and to address this, most Owners will incorporate a form of rent escalation. This is negotiable and may be tied to a Consumer price Index (CPI), another basket index or a fixed rate. Discuss this with your broker to negotiate escalations that are fair and appropriate for your situation.
4. LEASE TERMS, EXTENSIONS & CANCELLATIONS
The lease term is the length of the original lease and typically lasts from 5-7 years. Shorter terms are usually available for second generation space and longer terms for spaces requiring extensive
renovations or construction. Extension Clauses allow you to maintain your occupancy past the original lease term while a Cancellation Clause allows you to be relieved of further financial obligation. This can be important for a small practice where a partner dies or falls ill and the practice can no longer sustain the expense.
5. EXPENSES
Your lease should cover all of the expenses that may be incurred in the operation of your office and identify who is responsible for paying them. Here is a partial list of items of expense that should be specified:
1. Common area expenses; cleaning, maintenance, repair, replacement and other expenses to maintain the common areas, parking lot, landscaping, etc.
2. Utilities; water, sewer, trash, electric, etc.
3. Management fees; supervision, accounting, legal, leasing commissions, construction administration
4. Real estate taxes, licenses and legal fees for disputing assessments
5. Future regulatory assessments and impact fees
6. Repair and replacement of major building systems; HVAC, Elevators, roof, windows, etc.
7. Insurance; building, flood, sinkhole, liability, etc.
8. After hours use; Many multitenant buildings charge extra for after hours use and this rate can be substantial.
6. ADJACENT SPACES AND EXCLUSIVITY
A lease is a long-term obligation, especially with renewals, and considering the difficulty involved in moving a practice, it is always advantageous to include a Right of First refusal on adjacent spaces as they become available. This would allow you to expand your practice by adding programs and services without moving. Requesting an Exclusivity Clause is important if a competitor locating within your building would be detrimental to your practice.
7. RESTRICTIONS ON USE AND/OR PROCEDURES YOU MAY PROVIDE (TYPICAL ON A HOSPITAL CAMPUS)
Some professional office buildings may place restrictions on the types of procedures which can be performed on the premises. This typically involves radiology, surgery or laboratory services but can also ban certain procedures such as abortion. Be sure that any procedures necessary for your practice are permitted.
Continued on page 22
Understanding Exculpatory Clauses
By Julie A. Tyk, JD.
An exculpatory clause purports to deny an injured party the right to recover damages from a person negligently causing his injury. Cain v. Banka, 932 So. 2d 575 (Fla. 5th DCA 2006). They are disfavored in the law because they relieve one party of the obligation to use due care and shift the risk of injury to the party who is probably least equipped to take the necessary precautions to avoid injury and bear the risk of loss. Applegate v. Cable Water Ski, L.C., 974 So. 2d 1112, 1114 (Fla. 5th DCA 2008). Such clauses are strictly construed against the party seeking to be relieved of liability. Sunny Isles Marina, Inc. v. Adulami, 706 So. 2d 920 (Fla. 3d DCA 1998). Thus, exculpatory clauses are enforceable, only where, and to the extent, that the intention to be relieved from liability is made clear and unequivocal. Tatman v. Space Coast Kennel Club, Inc., 27 So. 3d 108, 110 (Fla. 5th DCA 2009). The wording must be so clear and understandable that “an ordinary and knowledgeable person will know what he is contracting away.” Id. (quoting Gayon v. Bally’s Total Fitness Corp., 802 So. 2d 420 (Fla. 3d DCA 2001)).
The seminal Florida case on exculpatory clauses is the Florida Supreme Court case of Sanislo v. Give Kids The World, Inc., 157 So. 3d 256 (Fla. 2015). Give Kids the World, Inc. (“GKTW”) provided free vacations to seriously ill children and their families. When applying for the vacation, the Sanislos executed a “wish request” form that contained a waiver of liability, also known as an exculpatory clause. When the parents arrived at the resort village they again signed a liability release form, also an exculpatory clause. The language of the exculpatory clause is reprinted below for reference:
I/we hereby release Give Kids the World, Inc. and all of its agents, officers, directors, servants, and employees from any liability whatsoever in connection with the preparation, execution, and fulfillment of said wish, on behalf of ourselves, the above named wish child and all other participants. The scope of this release shall include, but not be limited to, damages or losses or injuries encountered in connection with transportation, food, lodging, medical concerns (physical and emotional), entertainment, photographs and physical injury of any kind....
I/we further agree to hold harmless and to release Give Kids the World, Inc. from and against any and all claims and causes of action of every kind arising from any and all physical or emotional injuries and/or damages which may happen to me/us....
Sanislo at 258-259.
While participating in a horse-drawn wagon ride, a rear pneumatic lift designed to allow those in wheelchairs to participate failed, and Ms. Sanislo was injured. The Sanislos brought suit and GKTW filed a motion for summary judgment arguing that the signed releases precluded an action for negligence. The Sanislos filed a motion for partial summary judgment against GKTW’s affirmative defense of release. The trial court granted the Sanislo’s
motion and denied GKTW’s motion. The jury found for the Sanislos and GKTW appealed. Id.
The Fifth District reversed, finding the lower court erred in denying GKTW’s motion for summary judgment because the release signed by the Sanislos was unambiguous and did not contravene public policy. It ruled the exculpatory clause barred the negligence action despite the lack of a specific reference to “negligence” or “negligent acts” in the exculpatory clause.
The Fifth District reasoned that exculpatory clauses are effective if the wording of the exculpatory clause is clear and understandable so that an ordinary and knowledgeable person would know what he or she is contracting away, and that the court had previously rejected “‘the need for express language referring to release of the defendant for “negligence” or “negligent acts” in order to render a release effective to bar a negligence action.’ ” On the public policy argument, the Court said the relative bargaining power of the parties should not be considered because it was outside of the public utility or public function context and the Sanislos were not required to request a vacation with GKTW or go on the vacation. Id.
In affirming the Fifth District’s decision, the Supreme Court wrote that the conflict for the Court’s resolution was “whether an exculpatory clause is ambiguous and thus ineffective to bar a negligence action due to the absence of express language releasing a party from its own negligence or negligent acts.” Id. at 260.
The Florida Supreme Court wrote:
.... we are reluctant to hold that all exculpatory clauses that are devoid of the terms “negligence” or “negligent acts” are ineffective to bar a negligence action despite otherwise clear and unambiguous language indicating an intent to be relieved from liability in such circumstances. Application of such a bright-line and rigid rule would tend to not effectuate the intent of the parties and render such contracts otherwise meaningless. Id. at 270.
The Court found that the GKTW liability release form released GKTW and all of its agents, officers, directors, servants and employees from “any liability whatsoever in connection with the preparation, execution and fulfillment of said wish…” The release then provided that the scope of the agreement included “damages or losses or injuries encountered in connection with transportation, food, lodging, medical concerns (physical and emotional), entertainment, photographs and physical injury of any kind . . . .” The Court found that the release clearly conveyed that GKTW would be released from any liability, including negligence, for damages, losses, or injuries due to transportation, food, lodging, entertainment and photographs. Id.
A B O U T U S
Healthcare Realty & Development Services LLC (HRDS) is pleased to offer this Winter special aimed to create healing environments for you, your staff and your patients. As experts in Evidence Based Design, we proudly present these opportunities to improve your facility aesthetics and operational efficiency. Call today for your free evaluation.
R e f r e s h P a c k a g e
I
F l o o r i n g r e p l a c e m e n t ( c a r p e t , v i n y l , o r t i l e )
W a l l r e p a i r a n d t o u c h - u p s ( e g , p a t c h i n g h o l e s , s m o o t h i n g s u r f a c e s )
M i n o r l i g h t i n g u p g r a d e s ( e . g . , r e p l a c i n g o u t d a t e d f i x t u r e s )
R e n e w a l P a c k a g e ( i n c l u d e s R e f r e s h P a c k a g e )
R e f r e s h P a c k a g e p l u s :
E x t e r i o r p a i n t i n g ( w a l l s , t r i m , d o o r s )
P r e s s u r e w a s h i n g ( s i d e w a l k s , p a r k i n g l o t s , b u i l d i n g e x t e r i o r s )
L a n d s c a p i n g r e f r e s h ( m u l c h i n g , p r u n i n g , n e w p l a n t i n g s )
S i g n a g e D e s i g n a n d I n s t a l l a t i o n ( e x t e r i o r b r a n d i n g , d i r e c t i o n a l s i g n s , o r
A D A - c o m p l i a n t w a y f i n d i n g )
P a r k i n g L o t R e s u r f a c i n g a n d M a i n t e n a n c e ( f i x i n g p o t h o l e s , s e a l i n g c r a c k s , a n d r e s t r i p i n g s p a c e s )
R e n o v a t i o n P a c k a g e ( i n c l u d e s R e f r e s h & R e n e w a l P a c k a g e s )
R e f r e s h & R e n e w a l P a c k a g e s p l u s :
D e m o l i s h i n t e r i o r s / e x t e r i o r s a s n e e d e d
N e w w a l l s , c e i l i n g s , i n s u l a t i o n , e l e c t r i c a l , p l u m b i n g , H V A C , b u i l d i n g s e r v i c e s
C u s t o m M i l l w o r k a n d I n s t a l l a t i o n ( r e c e p t i o n d e s k s , c a b i n e t r y , s h e l v i n g )
D o o r a n d H a r d w a r e U p d a t e s
W i n d o w a n d G l a s s U p g r a d e s ( e n e r g y - e f f i c i e n t w i n d o w s a n d g l a z i n g )
E m e r g e n c y P r e p a r e d n e s s U p d a t e s ( b a c k u p g e n e r a t o r s , e v a c u a t i o n p l a n s , f i r e s u p p r e s s i o n , e t c . )
A r t w o r k a n d f u r n i s h i n g s s e l e c t i o n
C a l l F r a n k R i c c i t o d a y f o r y o u r f r e e e v a l u a t i o n L i c e n s e d R e a l E s t a
When The Tremor Isn’t Essential –Parkinson’s Disease: One of the Most Commonly Misdiagnosed Neurological Conditions
By Jaivir S. Rathore, M.D, F.A.E.S & Idha Sood, M.B;B.S
A COMPREHENSIVE ARTICLE, ON THE OCCASION OF WORLD PARKINSON’S DAY • APRIL 11, 2023
WHAT IS PARKINSON’S DISEASE?
Parkinson’s disease (PD) is the second-most common neurodegenerative disease after Alzheimer’s dementia. More than 10 million people worldwide and nearly one million people in the U.S. are living with PD. This number is expected to rise to 1.2 million by 2030. Nearly 90,000 people in the U.S. are diagnosed with PD each year. The incidence of PD increases with age, but an estimated four percent of people with PD are diagnosed before age 50. Men are 1.5 times more likely to have PD than women. Within the US; Florida has the second highest population of people living with PD. It is a slowly progressive disorder which often first presents with a resting hand tremor. The patient can then develop other cardinal features of bradykinesia, rigidity and postural instability. Autonomic symptoms like constipation, poor sense of smell, excess salivation due to poor swallowing can be present years before the patient develops the classic PD symptoms. In some patients there can be signs of cognitive decline which could be part of “Parkinson’s Plus” or Parkinson’s dementia.
WHAT CAUSES PARKINSON’S DISEASE?
PD results from loss of dopaminergic neurons in the pars compacta of substantia nigra of basal ganglia which is responsible for subcortical control of motor activity. In most cases the exact cause is unknown (Idiopathic Parkinson’s Syndrome, IPS), up to 15% cases may have genetic components, most common being LRRK2, GBA and PRKN (associated with young onset PD). In some cases it has also been linked to exposure to certain pesticides, herbicides, and industrial chemicals. One such compound called MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) accumulates in the mitochondria and generates free radicals, which can cause damage to basal ganglia and hence lead to PD. Latest research is also suggestive of alpha synuclein aggregation playing a role in the pathogenesis of PD. The earliest histopathological changes are hence seen in the myenteric plexus of the gastrointestinal tract, which then progresses to involve the dorsal motor nucleus of the vagus nerve and sleep centers in the ponto-medullary brainstem.
Many known figures in the world history have been affected by Parkinson’s disease including Pope John Paul II, Adolf Hitler, Mao Zedong, Michael J Fox and notably world heavyweight boxing champion Muhammad Ali, in his case repeated hits to his head is considered a risk factor to cause “dementia pugilistica” a neurode generative condition with Alzheimer’s like dementia. Neurode generation is a serious issue for boxing or for any traumatic brain injury for that matter.
WHAT ARE THE EARLY SIGNS OF PARKINSON’S DISEASE?
Patients typically have constipation, poor sense of smell and REM sleep disorder preceding the motor symptoms by around 10-15 years. Patients most commonly present with the earliest symptom of tremor. The tremor is usually present at rest and sometimes has classic pin rolling features involving the thumb and the index finger; it can disappear for some time while doing a task but returns when the patient is distracted. In cases where PD is not tremor dominant, patients usually present with the cardinal features of “overall slowness” or bradykinesia, mask facies, muffled speech (hypophonia), small handwriting (micrographia) etc. Patients can take a long time to do their usual daily activities and walk slowly. When prompted about mood or sleep issues, patients might elaborate on feeling depressed and can give a history of movements in their sleep, likely REM sleep disorder. Other autonomic features that a patient of PD might have include urinary retention, erectile dysfunction and orthostatic hypotension. Patients with advanced disease can also present with memory decline due to the neurodegenerative changes of the brain.
On examination, patients have the characteristic cog-wheel rigidity which can be elicited by slow rotatory movements of their wrists. Patients can appear to be stiff, they have shortened stride while walking and arm swing is typically reduced asymmetrically. They walk with a stooped posture and have to take multiple short steps to turn around. On pulling them back suddenly, called the posterior pull test, patients take a lot of steps to catch themselves or may even fall.
HOW DOES PARKINSON’S DISEASE PROGRESS?
In classic PD cases, the patient has tremor of one hand in stage 1. This can progress to the other hand in stage 2. Stage 3 is characterized by mild balance problems, which can worsen causing falls in stage 4 needing cane or a walker to walk and if it continues to worsen, in stage 5 patients can be wheelchair or bed bound. Not all patients progress to stage 5 and brain imaging such as (Dopamine Transporter, DaT) scan is not usually a good prognostication tool.
WHAT MIMICS PARKINSON’S DISEASE?
The PD tremor is most commonly mistaken for an essential
tremor and it remains refractory of usual treatment of propranolol, primidone etc. In such situations, emphasis should be put on looking out for other clinical features of PD like bradykinesia and gait disturbances.
Progressive supranuclear palsy (PSP) can have similar features of bradykinesia, rigidity and gait disturbances but patients may also have vertical gaze paralysis and falling en-block while sitting which is not a feature of PD and MRI Brain of PSP patient may show midbrain atrophy which is described as “Hummingbird” sign.
Patients of Lewy Body Dementia (LBD) have many features of Parkinson’s but those symptoms usually tend to occur after dementia symptoms. In contrast dementia is progressively developed later in the course of disease in PD patients due to overall neurodegeneration. In addition, LBD patients have very vivid visual hallucinations along with wide mood fluctuation which are not a feature of PD, however PD dementia patients may get hallucination or psychosis which is treated with pimavanserin. Ischemic or hemorrhagic stroke, mass lesions, hydrocephalus and Wilson’s disease can be excluded using imaging techniques such as MRI brain.
HOW IS PARKINSON’S DISEASE DIAGNOSED?
The diagnosis of PD is primarily a clinical one. A comprehensive examination and proper staging of PD can be done using Unified Parkinson’s Disease Rating Scale (UPDRS) which is a gold standard tool to measure not only the severity and progression of PD but also helpful in monitoring the response to medications. While evaluating the patient it is also imperative to go over their list of medications to exclude the possibility of drug-induced PD. Traditional antipsychotic medications are most implicated in such a condition.
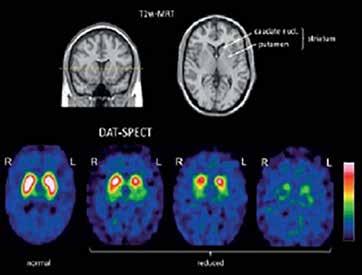
Typical Dopamine Transporter Ligands Single Photon Emission Tomography (DaT-SPECT) scan findings in patients with Idiopathic Parkinson’s Syndrome (IPS) showing reduced striatal DAT availability compared with a normal finding. The reduction is often left/right asymmetrical, usually more pronounced in the hemisphere contralateral to the clinically dominant side. The posterior “tail” of the putamen is almost always most strongly affected. The motor symptoms of IPS manifest only after a DAT loss of about 50% in the putamen. The atypical neurodegen erative parkinsonian syndromes, especially Progressive Supranuclear Palsy (PSP) and Multiple System Atrophy (MSA) of the parkinsonian type show similar patterns of findings on DAT-SPECT as IPS.
In clinically uncertain cases nuclear imaging DAT-SPECT scan may be helpful, however routine use of this test should be discouraged. A clear clinical improvement after levodopa treatment provides the best confirmation of PD.
HOW IS PARKINSON’S DISEASE TREATED?
There is no cure for PD at this time, however since the pathogenesis of PD involves loss of dopaminergic neurons, the primary mode of treatment is replenishing the dopamine levels with medications such as levodopa with carbidopa, which may also be used in combination with other classes of medications including Dopamine Agonists, COMT Inhibitors, MAO-B Inhibitors, and Anticholinergic agents. Treatment is individualized to the patient and adjusted over time based on symptoms, side effects and tolerability. Dopamine agonists like pramipexole, or ropinirole can be used in younger patients with the advantage of lesser side effects. If a patient primarily has tremor only, amantadine or anticholinergics may be used. In advanced stages of PD, patients may have psychosis with visual or auditory hallucinations and delusions. Pimavanserin, a serotonin 5-HT2 receptor antagonist is the only FDF approved treatment for psychosis associated with PD.
Most PD medications provide good improvement in symptoms for the first 3 to 6 years, but with the natural progression of the disease, results can decline with time. Levodopa-Carbidopa can have the “on-off” phenomenon where symptoms may worsen during the “off” periods. Apomorphine, a dopamine agonist, is the only FDA approved medication which can be used for symptom control during the off periods.
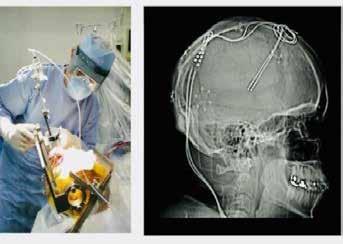
Deep Brain Stimulation (DBS) is a promising and underutilized advanced treatment for people who experience disabling tremors, wearing-off spells, and medication induced dyskinesias.
PD being a multi system disease requires a multi system ap proach. Patients can benefit a lot with physical therapy, like LS VT-BIG (Lee Silverman Voice Treatment), which encompasses physical therapy to improve their gait and balance coupled with speech therapy to address the hypophonia which can be pres ent. Patients should be encouraged to have an active lifestyle.
Continued on page 22
The determination of whether an exculpatory clause is enforceable will be determined by the Judge as the enforceability of a preinjury release is a question of law. The enforceability therefore, will depend on the Judge assigned to the matter. Physicians should not assume that because a patient signed a liability release form the patient does not have a viable cause of action. Physicians should consult with an experienced attorney who can examine the facts of the case and help you determine the best path forward. The Health Care Practice Group at Pearson Doyle Mohre and Pastis, LLP is committed to assisting Clients in navigating and defending medical malpractice claims. For more information and assistance, please contact David Doyle and Julie Tyk at Pearson Doyle Mohre & Pastis, LLP.
Continued from page 20
Julie A. Tyk, JD, is a Partner with Pearson Doyle Mohre & Pastis, LLP. Julie concentrates her practice in medical practice defense litigation, insurance defense litigation and health care law. She has represented physicians, hospitals, ambulatory surgical centers, nurses and other health care providers across the state of Florida. She may be contacted by calling (407) 951-8523; jtyk@pdmplaw.com..
Other features of PD including depression, constipation. REM sleep disorders should also be managed concomitantly.
In long-standing or medically refractory cases of at least 4 years of PD, Deep Brain Stimulation (DBS) of the subthalamic nucleus (STN) or globus pallidus interna (GPI) is a great option to provide relief with disabling symptoms. In summary, early accurate diagnosis by a neurologist experienced in PD along with a multidisciplinary approach should be used for improving the symptoms and quality of life of PD patients.
Dr. Jaivir Rathore, A triple board-certified toprated neurologist trained at the Johns Hopkins and the Cleveland Clinic, Harvard University journal published neuroscientist and the Medical Director of Falcon Advanced Neurology & Epilepsy Freedom Center (FANEFC) in Orlando FL with additional clinics serving the largest retirement community of the world in The Villages FL provides comprehensive neurology care including movement disorders such as Parkinson’s disease. FANEFC is “Care Connected” with the Mayo Clinic, Jacksonville FL for surgical cases including DBS for PD.
Continued from page 17
Negotiating Leases
Leasing space is an important financial and legal transaction and should not be taken lightly. It is important to have an experienced real estate broker and real estate attorney represent you. This combination of professionals provides the greatest protection at the least cost. Based upon their market experience, your broker should handle the preliminary issues, negotiate the rates and terms and prepare the deal points in a “Letter of Intent (LOI).” Once negotiated, a complete legal review should be completed by your attorney before execution. If you address each of these seven issues, you should be able to move forward with confidence in the completion of your lease negotiations and securing your office space for your prosperous enjoyment.
Frank Ricci is president of Healthcare Realty & Development LLC and H R & D Construction Inc. and has over 30 years of medical real estate brokerage, construction and development experience. He can be reached at (407) 947-5074, or FrankR@HealthcareRealtyOnline.com or visit the company website at: www.HealthcareRealtyOnline.com.
JANUARY – Digestive Disorders
Diabetes
2025
EDITORIAL CALENDAR
Florida MD is a monthly medical/business digital magazine for physicians..
Florida MD has been serving the medical community in Florida for twenty years and is currently available as a bimonthly digital edition emailed directly to healthcare providers in Central Florida (Orlando area), Tampa metro and Southeast Florida. Cover stories spotlight extraordinary physician practices, new hospital procedures or facilities, and other professional and healthcare related business topics. Local physician specialists and other professionals, affiliated with local businesses and organizations, write all other columns or articles about their respective specialty or profession. This local informative and interesting format is the main reason physicians take the time to read Florida MD.
It is hard to be aware of everything happening in the rapidly changing medical profession and doctors want to know more about new medical developments and technology, procedures, techniques, case studies, research, etc. in the different specialties. Especially when the information comes from a local physician specialist who they can call and discuss the column with or refer a patient. They also want to read about wealth management, financial issues, healthcare law, insurance issues and real estate opportunities. Again, they prefer it when that information comes from a local professional they can call and do business with. All advertisers have the opportunity to have a column or article related to their specialty or profession.