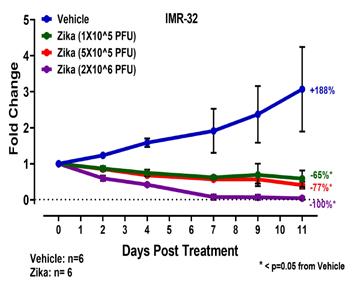
One of the leading causes of death from a pediatric cancer is recurrence of the tumor and its resistance to further chemotherapy. My lab team and I are committed to developing novel treatments to address this issue in order to improve the overall survival of children with pediatric cancers that are challenging to eliminate. Our laboratory recently released a paper in Cancer Research Communications, an American Association for Cancer Research (AACR)journal, which demonstrated a robust survival advantage to mice hosting different forms of neuroblastoma that were treated with the oncolytic Zika virus. Neuroblastoma is a pediatric tumor that develops within the immature nerve cells and can present within the adrenal glands, along the spine, and within the chest or abdomen. It is divided into risk categories with high-risk neuroblastoma having the worst overall five-year survival of 50% even with intense therapy. The focus of this paper is addressing the treatment of high-risk neuroblastoma with Zika virus, which has effectively treated any stage of neuroblastoma. The neuroblastoma tumors were grown subcutaneously in the mice. Initially, we determined the Zika viral dosing and confirmed its effectiveness in high-risk neuroblastoma that had received no therapy. As can be seen in the figure, the neuroblastoma was eradicated within the mouse with the higher Zika viral dose.
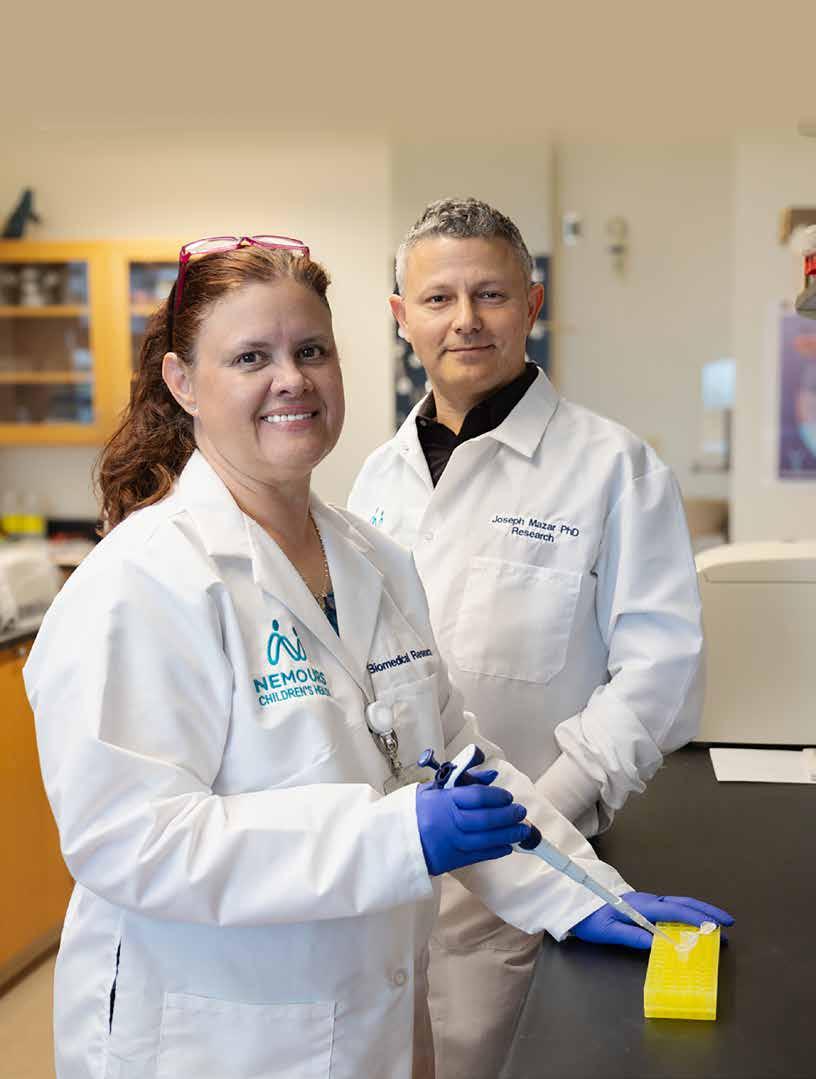
ON THE COVER Pediatric surgeon Dr. Tamarah Westmoreland, MD, PhD and research scientist Joseph Mazar, PhD are studying whether the Zika virus can shrink neuroblastoma tumors at Nemours Children’s Health in Orlando.
Drs. Westmoreland and Mazar and Nemours Children’s Hospital, Florida lab team working on Zika research.
Iam pleased to bring you another issue of Florida MD. Human trafficking is one of the horrors in today’s society. It’s modern day slavery and Central Florida is one of the worst places in the country. I have asked Paving the Way, an organization headquartered here in Central Florida that helps physicians spot signs that one of their patients could be a victim. Please check out their website and help put a stop to human trafficking..
Best regards,
Donald B. Rauhofer Publisher
According to Homeland Security, there are over 300,000 children a year trafficked in the United States. In fact, Florida ranks 3rd in the county for calls to the National Trafficking Hotline and right here in Central Florida, Orange county ranks 2nd in the state for child trafficking case. Sadly, the average age of entry is 11-14.
Those facts can be frightening, leaving most people asking, who am I to do anything about this? More importantly, what can I do?
Paving The Way Foundation was created to provide answers to those questions. We’ve educated over 13,000 youth, parents, teachers, and community leaders about human trafficking, the impact it has on families and the actions to take to prevent it.
A surprising statistic is 88% of trafficking victims reported being in a medical setting for various concerns but did not feel safe enough to ask for help. We can prevent that from happening by training our frontline teams to learn the signs of trafficking, understand grooming and recruitment tactics and how to engage with patients about this silent crime to get them to safety.
Here is one action you can take right now: put the National Trafficking Hotline number in your phone, 888-3737888, you can call 24 hours a day, 7 days a week.
To learn more about what you can do or ways to get involved in ending human trafficking we invite you to join in the fight, please go to our website, www.pavingthewayfoundation.org click on programs for information on what’s available to educate you and your staff or download one of our tool kits. Together we can disrupt the cycle of human trafficking.
ADVERTISE IN FLORIDA MD
For more information on advertising in Florida MD, call Publisher Donald Rauhofer at (407) 417-7400, fax (407) 977-7773 or info@floridamd www.floridamd.com
Email press releases and all other related information to: info@floridamd.com
PREMIUM REPRINTS
Reprints of cover articles or feature stories in Florida MD are ideal for promoting your company, practice, services and medical products. Increase your brand exposure with high quality, 4-color reprints to use as brochure inserts, promotional flyers, direct mail pieces, and trade show handouts. Call Florida MD for printing estimates.
Publisher: Donald Rauhofer
Photographer: Donald Rauhofer / Florida MD
Contributing Writers: John “Lucky” Meisenheimer, MD, Tara Griffin, DMD, Tamarah Westmoreland, MD, PhD,, Daniel T. Layish, MD, Sonda Eunus, MHA, John Meisenheimer, VII, MD, Jaivir S. Rathore, MD, FAES, Idha Sood, MBBS, Omer Abdul Hamid, MD, Tessa Ladd, OTR/L
Art Director/Designer: Ana Espinosa
Florida MD is published by Sea Notes Media,LLC, P.O. Box 621856, Oviedo, FL 32762. Call (407) 417-7400 for more information. Advertising rates upon request. Postmaster: Please send notices on Form 3579 to P.O. Box 621856, Oviedo, FL 32762. Although every precaution is taken to ensure accuracy of published materials, Florida MD cannot be held responsible for opinions expressed or facts expressed by its authors. Copyright 2024 Sea Notes Media. All rights reserved. Reproduction in whole or in part without written permission is prohibited. Annual subscription rate $45.
As part of our educational mission, SLS is providing FREE 2024 membership to Medical Students and Residents* and discounted membership for Fellows* and Affiliated Medical Personnel.
join us at misweek 2024
Register Now to attend the only multispecialty conference for surgeons Master Courses Available
Didactic Master Courses
Hands-on skills courses
REGISTRATION IS OPEN
Become a membeR get discounts for MISWeek and More...
Additional Member Benefits World Class conferences and Resources
Tools and opportunities to advance your career
Publications to keep you at the forefront of your career.
Nemours Children’s Hospital, Florida Research Breakthrough: Oncolytic Zika Virus Shows
Promising Results in Treating Neuroblastoma, Enhancing Survival Rates in Pediatric Cancer Models
By Tamarah Westmoreland MD, PhD, pediatric surgeon, Associate Professor of Surgery at Nemours Children’s Hospital, Florida
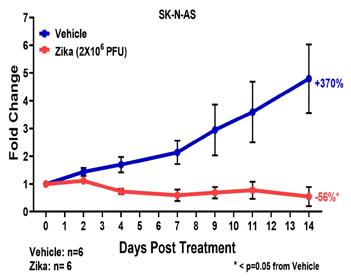
One of the leading causes of death from a pediatric cancer is recurrence of the tumor and its resistance to further chemotherapy. My lab team and I are committed to developing novel treatments to address this issue in order to improve the overall survival of children with pediatric cancers that are challenging to eliminate. Our laboratory recently released a paper in Cancer Research Communications, an American Association for Cancer Research (AACR)journal, which demonstrated a robust survival advantage to mice hosting different forms of neuroblastoma that were treated with the oncolytic Zika virus. Neuroblastoma is a pediatric tumor that develops within the immature nerve cells and can present within the adrenal glands, along the spine, and within the chest or abdomen. It is divided into risk categories with high-risk neuroblastoma having the worst overall five-year survival of 50% even with intense therapy. The focus of this paper is addressing the treatment of high-risk neuroblastoma with Zika virus, which has effectively treated any stage of neuroblastoma. The neuroblastoma tumors were grown subcutaneously in the mice. Initially, we determined the Zika viral dosing and confirmed its effectiveness in high-risk neuroblastoma that had received no therapy. As can be seen in the figure, the neuroblastoma was eradicated within the mouse with the higher Zika viral dose.
Moreover, our research team demonstrated that Zika virus is capable of eradicating multidrug resistance high-risk neuroblastoma in murine models as well. This is well demonstrated in this figure, where the chemotherapy resistant neuroblastoma is almost completely eliminated with a single Zika viral injection. The re-
search team had previously published that the cell surface protein, CD24, is required for Zika viral treatment in neuroblastoma cell culture. The CD24 requirement was confirmed to be true as well in mice. Furthermore, the team found that CD24 is expressed in human pediatric neuroblastoma tumors as well, which is important for the translation of Zika viral treatment into humans.
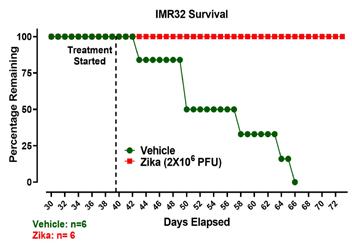
Not only does Zika virus treat with minimal residual tumor, which is confirmed by histology, it also allows the treated mice to outlive those with no treatment. As seen in these survival curves, the mice engrafted with neuroblastoma have a 100% survival when treated with Zika virus compared to the control mice. The neuroblastoma tumor in this experiment had not received any other treatment.
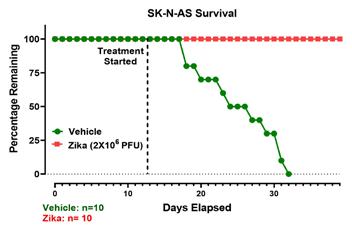
In this experiment, the tumor is a relapsed high-risk neuroblas-
toma that was resistant to chemotherapy. As previously shown, the mice engrafted with the multidrug resistant high-risk neuroblastoma also had a significant survival advantage with 100% survival when treated with Zika virus.
Currently, the Westmoreland research team is expanding the work in neuroblastoma with a goal for translation into a phase 1 clinical trial. A translational murine research study is currently in development to investigate the incorporation of Zika virus into the current Children’s Oncology Group (COG) protocol for high-risk neuroblastoma to determine if earlier treatment with Zika virus will prevent deadly drug resistance and improve overall survival. In essence, Zika virus would serve as a bridge therapy for patients with high-risk neuroblastoma. This is an important step in investigating where Zika virus can incorporate into a human clinical trial.
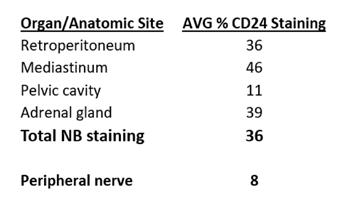
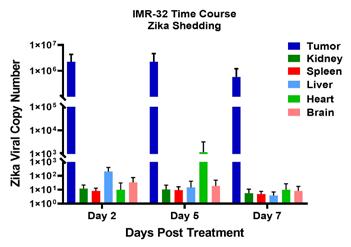
Some may have concern about the use of Zika virus as an oncolytic; however, it is well established that ~80% of Zika viral infections in humans are asymptomatic. The remaining symptomatic cases have low-grade fever, mild conjunctivitis, and rash. These self-limiting symptoms are not associated with long-term sequelae. Furthermore, our team has evaluated the amount of Zika viral shedding to other organs in the mouse and found that there is very little shedding outside of the target tumor as can be seen in the figure. The mice are asymptomatic to the Zika virus. Thus, we predict that wild-type Zika viruses will be well tolerated.
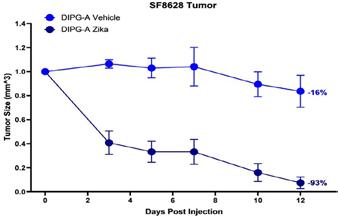
These studies have also been extended to the cancer diffuse intrinsic pontine glioma (DIPG), which is a devastating pediatric brain tumor with virtually no survivors even with intensive chemotherapy and radiation therapy. In our laboratory, we have demonstrated that Zika virus is capable of eradicating greater than 93% of chemotherapy resistant DIPG subcutaneously in mice. This figure illustrates the effectiveness in treating DIPG grown subcutaneously on the mouse and treated with a single Zika viral injection. The research in DIPG is being expanded to translate to a clinical trial. In addition to demonstrating the utility in Zika viral treatment of neuroblastoma, DIPG, and other pediatric tumors, the Westmoreland research team is investigating the underlying mechanism that is allowing the Zika viral sensitivity. The goal of these studies is to advance the treatment of high-risk pediatric tumors with Zika virus to improve overall survival.
PROGRAM OVERVIEW
The Nemours Children’s Center for Cancer and Blood Disorders is not a single place, but a multistate pediatric oncology and hematology program that collaborates on research and developing personalized treatment plans for each patient. When a patient is referred to us, they have the expertise of not only doctors and researchers in Florida and Delaware, but doctors and researchers from across Nemours Children’s multiple specialties. Through this collaboration we ensure that every appropriate step is taken when delivering treatment and care.
Drs. Westmoreland and Mazar and Nemours Children’s Hospital, Florida lab team working on Zika research.
PROGRAM HIGHLIGHTS
• We rank in the top two for enrollment of kids in National Cancer Institute trials.
• We are one of only three National Cancer Institute Community Oncology Research Programs (NCORP) in the country.
• We offer a state-of-the-art infusion center located in our hospital in Orlando.
• Our infusion center offers private rooms for kids who need chemotherapy on an outpatient basis.
• Early detection through Nemours Children’s Center for Fetal Care. Our program works across specialties to diagnose using ultrasound while the baby is still in the womb.
• We are a member of the Children’s Oncology Group — the most experienced pediatric cancer organization in the world. We work with our colleagues across our system and across specialties to deliver customized treatment plans and deliver excellent patient outcomes.
• We offer proton therapy as part of our collaboration with a community partner facility, one of only a few centers in the United States offering this treatment.
• Neuropsychological assessments are available to assess the cognitive effects of treatment.
REFERRALS
Nonurgent Referrals
407.650.7715
Oncologic or Hematologic Emergencies
855.543.2364
Westmoreland is a member of the Society of University Surgeons and serves on the American Pediatric Surgical Association’s (APSA) Cancer Committee. The mission of the Cancer Committee is to educate the APSA membership on the current approaches to the treatment of children with cancer, as directed by the Children’s Oncology Group (COG), and to update the membership on new COG protocols and changes to existing ones.
Melanoma Makes Me a Real Doctor
By John “Lucky” Meisenheimer, MD and John Meisenheimer, VII, MD
When I was in medical school and revealed to my classmates that I wanted to be a dermatologist, they usually gave me a flabbergasted look and said, “You want to pop zits for a living?” Immediately followed by, “You don’t want to be a real doctor?” I wish the Seinfeld episode, when Jerry was dating a dermatologist, had been released so that I could refer them to it. The Seinfeld episode went something like this:
Jerry was having dinner at a restaurant with his dermatologist girlfriend.
Seinfield - “How’s the life-saving business?
Dermatologist girlfriend - “It’s fine.”
Seinfield - “It must take a really, really big zit to kill a man.”
Dermatologist girlfriend - “What is with you?”
Seinfield - “You called yourself lifesaver. I call you pimple popper M.D.”
A restaurant patron walks up to their table and says, “Dr. Sitarides?”
Dermatologist girlfriend - “Mr. Perry, how are you?”
Mr. Perry - “I just want to thank you again for saving my life.”
Seinfield - “She saved your life?” Jerry has a shocked look on his face.
Mr. Perry - “I had skin cancer.”
Seinfield - “Skin cancer, damn.” Jerry’s face twists in the agony of defeat.
As a Mohs surgeon, I rarely “pop” pimples anymore, not that there is anything disgraceful about helping a patient with a disfiguring skin disease that can leave them permanently scarred. As the Seinfield episode would suggest, laypeople might seem to think unless you are saving lives, you are not a “real” doctor. So, I guess in a sense, melanomas make dermatologists “real” doctors (and let’s not forget squamous cell carcinomas and basal cell carcinomas can also kill you). I know in my practice over the last 30 years, I have found hundreds of melanomas. Even to this day, when I see a melanoma, I quietly give myself a high five. When you catch melanoma in time, you have changed a person’s life for the better, even if they may not realize it. At the same time, I am also grateful that I did not miss that melanoma. There is always a degree of stress when doing a “routine skin exam” there is nothing routine about melanoma or the potential for missing a melanoma.
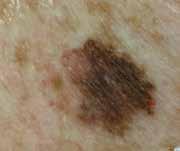
Melanomas come in all different shapes and sizes. They are rarely the archetypal jet black, nodular mole-like growth, in which even a first-year medical student could make the diagnosis. Melanomas may appear elevated, they can be flat, they can be multicolored, and they do not have to have pigment. Some melanomas can persist for very long periods before being discovered, such as lentigo maligna melanoma. Others can grow rapidly and deadly in a few weeks. Melanomas can develop beneath the nails, and even in non-skin areas such as the eye, oral cavity, nasal sinuses, even rectally.
The best guidance for identifying melanomas for non-dermatologists is using the mnemonic ABCDEs of melanoma evaluation, Asymmetry of the lesion, Border irregularity, Color variation, Diameter greater than 6mm and Evolution. However, dermatologists rarely use the ABCDE guide, as most of us know by looking because of intuitive expertise. When a dermatologist observes a suspicious lesion, in our mind, it pops up, “that looks suspicious.” Intuitive expertise is ubiquitous throughout all specialties and comes with experience. The ER doc that walks into a patient room and immediately diagnoses congestive heart failure with only a glance is demonstrating intuitive expertise. Intuitive expertise can be confounding to medical students who need to look up everything online. Still, it is this intuitive expertise we all gain through training and experience that makes us “real” doctors.
Lucky Meisenheimer, M.D. is a board-certified dermatologist specializing in Mohs Surgery. He is the director of the Meisenheimer Clinic – Dermatology and Mohs Surgery. John Meisenheimer, VII is an MD practicing in Orlando.
PHOTO: JOHN MEISENHEIMER, VII, MD
A superficial spreading melanoma.
PHOTO: JOHN MEISENHEIMER, VII, MD
Nodular melanoma.
PHOTO: JOHN MEISENHEIMER, VII, MD
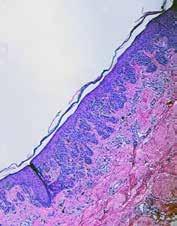
Lentigo maligna melanoma. Pathology of a melanoma.
PHOTO: JOHN MEISENHEIMER, VII, MD
You’re not just our patient. You’re our neighbor. For more than a century, Orlando Health Orlando Regional Medical Center has been honored to provide nationally recognized care for the Central Florida region we proudly call home. And because it’s your home, too, you deserve trusted healthcare within reach, so we can foster a partnership focused on health and wellness –together. Giving you more reasons to choose well. OrlandoHealth.com/ORMC
Chronic Thromboembolic Pulmonary Hypertension
By Daniel T. Layish, MD
There are several categories of pulmonary hypertension. WHO Group I includes patients with idiopathic pulmonary hypertension, familial pulmonary hypertension, drug and toxin related (fen-phen) portopulmonary hypertension, HIV related pulmonary hypertension and pulmonary arterial hypertension associated with connective tissue disorders (such as scleroderma). WHO Group II pulmonary hypertension is often referred to as pulmonary venous hypertension. This includes patients with left ventricular systolic or diastolic dysfunction or valvular heart disease. Essentially, the WHO Group II category includes patients who have an elevated pulmonary capillary wedge pressure and/ or elevated left ventricular end diastolic pressure. WHO Group III pulmonary hypertension consists of patients with COPD, interstitial lung disease, or other conditions in which hypoxia causes vasoconstriction. The remainder of this article will focus on WHO Group IV pulmonary hypertension (chronic thromboembolic pulmonary hypertension or CTEPH). Although WHO Group IV patients are relatively rare, it is crucial to identify them because this is the only type of pulmonary hypertension which is potentially surgically curable.
After acute pulmonary embolism, most patients will recover and have normal pulmonary hemodynamics, gas exchange, and exercise tolerance. It is believed that 1-4% of patients with acute pulmonary embolism will go on to develop CTEPH within two years. It is not clear why some patients with acute pulmonary embolism develop CTEPH. Risk factors include hypercoagulable states, myeloproliferative syndromes, splenectomy and chronic indwelling central venous catheters. Patients with CTEPH present with dyspnea, which can have a gradual onset. Many patients with CTEPH will not have a known previous diagnosis of acute pulmonary embolism. As with other patients with pulmonary hypertension, patients with CTEPH may not show findings on physical exam until pulmonary hypertension is in the late stages. Findings include a right ventricular lift, jugular venous distention, fixed splitting of the second heart sound, hepatomegaly, ascites, and peripheral edema. Patients with CTEPH may have “flow murmurs” heard over the lung fields because of turbulent flow through partially obstructed or recanalized pulmonary arteries. These tend to be accentuated during inspiration.
Acute pulmonary embolism is the trigger for CTEPH. In some patients this triggers a small vessel vasculopathy (for unclear reasons) that contributes to the extent of pulmonary hypertension. This may explain why up to 35 percent of patients who undergo succesful pulmonary thromoendarterectomy can have some degree of postoperative pulmonary hypertension.
Although VQ scanning has become less commonly used for diagnosis of acute pulmonary embolism this remains the initial imaging study of choice in patients with pulmonary hyperten-
sion to separate “small vessel” variants (Idiopathic pulmonary arterial hypertension) from “large vessel” disease (CTEPH) A normal VQ scan essentially excludes the diagnosis of CTEPH. A scan with one or more mismatched segmental defects is suggestive of the diagnosis. However, it is important to note that VQ scan can often understate the extent of central pulmonary vascular obstruction. Once the VQ scan is found to be abnormal then further testing should be undertaken (such as CT angiogram and/or pulmonary angiography). The angiographic findings in CTEPH are distinct from those of acute pulmonary embolism. They can include pouch defects and pulmonary artery webs. Patients with severe pulmonary hypertension have been found to tolerate performance of angiography as well as VQ scan without significant complication rate.
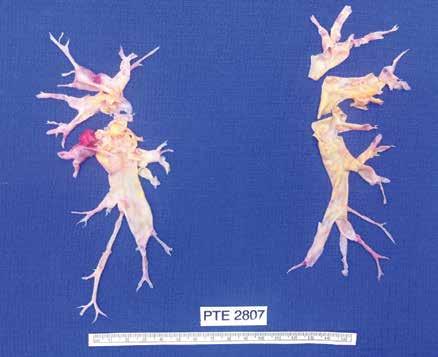
The surgery for CTEPH is quite different from surgical intervention for an acute pulmonary embolism. Surgery for CTEPH is called a pulmonary thromboendarterectomy (PTE), which requires median sternotomy and cardiopulmonary bypass. It requires an often tedious intimal dissection of fibrotic recannalized thrombus from the native pulmonary arterial wall. IVC filter placement is usually recommended before pulmonary thromboendarterectomy. These patients can have a complicated postoperative course and this type of surgery is only done at a few specialized centers in the country. The center which is best known for this type of surgery is the University of California (San Diego). Patients who have undergone PTE are typically maintained on lifelong anticoagulation. To be a candidate for this surgery, a patients must have central, surgically accesible chronic thromboemboli. A significant postoperative complication is pulmonary artery steal, which refers to redistribution of pulmonary arterial blood flow from well-perfused segments into the newly opened segments resulting in ventilation perfusion mismatch and hypoxia. This redistribution of flow resolves over time. Approximately, 30% of PTE patients can develop reperfusion pulmonary edema. The perioperative mortality of pulmonary thromboendarterectomy can be in the range of 2-3% in experienced centers. Outcome is clearly better in high voluime centers (more than fifty PTE surgeries/year). Approximately 5000 thromboendarterectomy procedures have been performed worldwide, 3000 at UCSD alone. Surgery for CTEPH is clearly the best therapeutic option. However, there are some patients with CTEPH who are inoperable or who have persistent or recurrent pulmonary hypertension after undergoing pulmonary thromboendarterectomy. There is now a medical therapy available for these patients. Riociguat (Adempas) was approved by the FDA in October 2013. It is a member of a new class of compounds-soluble guanylate cyclase stimulators. In the multicenter study by Ghofrani et al that was published in the New England Journal of Medicine in July 2013,
261 patients were randomized prospectively to receive riociguat versus placebo. Riociguat was shown to significantly improve exercise capacity and pulmonary vascular resistance. Side effects include systemic hypotension. Prior smaller studies have also shown some benefits to medical therapy in CTEPH (inoperable or with post-operative PH) with oral agents such as bosentan and sildanefil, inhaled iloprost and subcutaneous treprostinil. Medical therapy has also been used as a “bridge” before PTE.
Although relatively rare, CTEPH is an important cause of PH since it is potentially curable with pulmonary endarterectomy. This surgery should only be performed in very experienced, specialized centers. PTE surgery should always be the treatment of choice for CTEPH. However, medical therapy can have a role as a bridge to PTE,in patients who are not surgical candidates or in those who have persistent pulmonary hypertension despite undergoing PTE.
I would like to express my gratitude to Dr. Peter Fedullo (University California San Diego) for his review of this manuscript and providing the photographs.
Daniel Layish, MD, graduated magna cum laude from Boston University Medical School in 1990. He then completed an Internal Medicine Residency at Barnes Hospital (Washington University) in St.Louis, Missouri and a Pulmonary/Critical Care/ Sleep Medicine Fellowship at Duke University in Durham, North Carolina. Since 1997, he has been a member of the Central Florida Pulmonary Group in Orlando. He serves as Co-director of the Adult Cystic Fibrosis Program in Orlando. He may be contacted at 407-841-1100 or by visiting www.cfpulmonary.com.
Example of chronic clots removed during pulmonary thromboendarterectomy.
Example of the large perfusion defects seen on V/Q scan in a patient with CTEPH.
Pulmonary angiogram showing lack of blood flow to the right middle lobe and the right lower lobe from CTEPH.
When The Tremor Isn’t Essential –Parkinson’s Disease: One of the Most Commonly Misdiagnosed Neurological Conditions
By Jaivir S. Rathore, M.D, F.A.E.S & Idha Sood, M.B;B.S
A
COMPREHENSIVE ARTICLE, ON THE OCCASION OF WORLD PARKINSON’S DAY • APRIL 11, 2023
WHAT IS PARKINSON’S DISEASE?
Parkinson’s disease (PD) is the second-most common neurodegenerative disease after Alzheimer’s dementia. More than 10 million people worldwide and nearly one million people in the U.S. are living with PD. This number is expected to rise to 1.2 million by 2030. Nearly 90,000 people in the U.S. are diagnosed with PD each year. The incidence of PD increases with age, but an estimated four percent of people with PD are diagnosed before age 50. Men are 1.5 times more likely to have PD than women. Within the US; Florida has the second highest population of people living with PD. It is a slowly progressive disorder which often first presents with a resting hand tremor. The patient can then develop other cardinal features of bradykinesia, rigidity and postural instability. Autonomic symptoms like constipation, poor sense of smell, excess salivation due to poor swallowing can be present years before the patient develops the classic PD symptoms. In some patients there can be signs of cognitive decline which could be part of “Parkinson’s Plus” or Parkinson’s dementia.
WHAT CAUSES PARKINSON’S DISEASE?
PD results from loss of dopaminergic neurons in the pars compacta of substantia nigra of basal ganglia which is responsible for subcortical control of motor activity. In most cases the exact cause is unknown (Idiopathic Parkinson’s Syndrome, IPS), up to 15% cases may have genetic components, most common being LRRK2, GBA and PRKN (associated with young onset PD). In some cases it has also been linked to exposure to certain pesticides, herbicides, and industrial chemicals. One such compound called MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) accumulates in the mitochondria and generates free radicals, which can cause damage to basal ganglia and hence lead to PD. Latest research is also suggestive of alpha synuclein aggregation playing a role in the pathogenesis of PD. The earliest histopathological changes are hence seen in the myenteric plexus of the gastrointestinal tract, which then progresses to involve the dorsal motor nucleus of the vagus nerve and sleep centers in the ponto-medullary brainstem.
Many known figures in the world history have been affected by Parkinson’s disease including Pope John Paul II, Adolf Hitler, Mao Zedong, Michael J Fox and notably world heavyweight boxing champion Muhammad Ali, in his case repeated hits to his head is considered a risk factor to cause “dementia pugilistica” a neurode generative condition with Alzheimer’s like dementia. Neurode generation is a serious issue for boxing or for any traumatic brain injury for that matter.
WHAT ARE THE EARLY SIGNS OF PARKINSON’S DISEASE?
Patients typically have constipation, poor sense of smell and REM sleep disorder preceding the motor symptoms by around 10-15 years. Patients most commonly present with the earliest symptom of tremor. The tremor is usually present at rest and sometimes has classic pin rolling features involving the thumb and the index finger; it can disappear for some time while doing a task but returns when the patient is distracted. In cases where PD is not tremor dominant, patients usually present with the cardinal features of “overall slowness” or bradykinesia, mask facies, muffled speech (hypophonia), small handwriting (micrographia) etc. Patients can take a long time to do their usual daily activities and walk slowly. When prompted about mood or sleep issues, patients might elaborate on feeling depressed and can give a history of movements in their sleep, likely REM sleep disorder. Other autonomic features that a patient of PD might have include urinary retention, erectile dysfunction and orthostatic hypotension. Patients with advanced disease can also present with memory decline due to the neurodegenerative changes of the brain.
On examination, patients have the characteristic cog-wheel rigidity which can be elicited by slow rotatory movements of their wrists. Patients can appear to be stiff, they have shortened stride while walking and arm swing is typically reduced asymmetrically. They walk with a stooped posture and have to take multiple short steps to turn around. On pulling them back suddenly, called the posterior pull test, patients take a lot of steps to catch themselves or may even fall.
HOW DOES PARKINSON’S DISEASE PROGRESS?
In classic PD cases, the patient has tremor of one hand in stage 1. This can progress to the other hand in stage 2. Stage 3 is characterized by mild balance problems, which can worsen causing falls in stage 4 needing cane or a walker to walk and if it continues to worsen, in stage 5 patients can be wheelchair or bed bound. Not all patients progress to stage 5 and brain imaging such as (Dopamine Transporter, DaT) scan is not usually a good prognostication tool.
WHAT MIMICS PARKINSON’S DISEASE?
The PD tremor is most commonly mistaken for an essential
tremor and it remains refractory of usual treatment of propranolol, primidone etc. In such situations, emphasis should be put on looking out for other clinical features of PD like bradykinesia and gait disturbances.
Progressive supranuclear palsy (PSP) can have similar features of bradykinesia, rigidity and gait disturbances but patients may also have vertical gaze paralysis and falling en-block while sitting which is not a feature of PD and MRI Brain of PSP patient may show midbrain atrophy which is described as “Hummingbird” sign.
Patients of Lewy Body Dementia (LBD) have many features of Parkinson’s but those symptoms usually tend to occur after dementia symptoms. In contrast dementia is progressively developed later in the course of disease in PD patients due to overall neurodegeneration. In addition, LBD patients have very vivid visual hallucinations along with wide mood fluctuation which are not a feature of PD, however PD dementia patients may get hallucination or psychosis which is treated with pimavanserin. Ischemic or hemorrhagic stroke, mass lesions, hydrocephalus and Wilson’s disease can be excluded using imaging techniques such as MRI brain.
HOW IS PARKINSON’S DISEASE DIAGNOSED?
The diagnosis of PD is primarily a clinical one. A comprehensive examination and proper staging of PD can be done using Unified Parkinson’s Disease Rating Scale (UPDRS) which is a gold standard tool to measure not only the severity and progression of PD but also helpful in monitoring the response to medications. While evaluating the patient it is also imperative to go over their list of medications to exclude the possibility of drug-induced PD. Traditional antipsychotic medications are most implicated in such a condition.
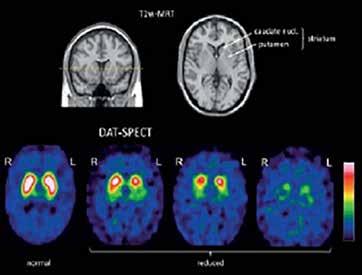
Typical Dopamine Transporter Ligands Single Photon Emission Tomography (DaT-SPECT) scan findings in patients with Idiopathic Parkinson’s Syndrome (IPS) showing reduced striatal DAT availability compared with a normal finding. The reduction is often left/right asymmetrical, usually more pronounced in the hemisphere contralateral to the clinically dominant side. The posterior “tail” of the putamen is almost always most strongly affected. The motor symptoms of IPS manifest only after a DAT loss of about 50% in the putamen. The atypical neurodegen erative parkinsonian syndromes, especially Progressive Supranuclear Palsy (PSP) and Multiple System Atrophy (MSA) of the parkinsonian type show similar patterns of findings on DAT-SPECT as IPS.
In clinically uncertain cases nuclear imaging DAT-SPECT scan may be helpful, however routine use of this test should be discouraged. A clear clinical improvement after levodopa treatment provides the best confirmation of PD.
HOW IS PARKINSON’S DISEASE TREATED?
There is no cure for PD at this time, however since the pathogenesis of PD involves loss of dopaminergic neurons, the primary mode of treatment is replenishing the dopamine levels with medications such as levodopa with carbidopa, which may also be used in combination with other classes of medications including Dopamine Agonists, COMT Inhibitors, MAO-B Inhibitors, and Anticholinergic agents. Treatment is individualized to the patient and adjusted over time based on symptoms, side effects and tolerability. Dopamine agonists like pramipexole, or ropinirole can be used in younger patients with the advantage of lesser side effects. If a patient primarily has tremor only, amantadine or anticholinergics may be used. In advanced stages of PD, patients may have psychosis with visual or auditory hallucinations and delusions. Pimavanserin, a serotonin 5-HT2 receptor antagonist is the only FDF approved treatment for psychosis associated with PD.
Most PD medications provide good improvement in symptoms for the first 3 to 6 years, but with the natural progression of the disease, results can decline with time. Levodopa-Carbidopa can have the “on-off” phenomenon where symptoms may worsen during the “off” periods. Apomorphine, a dopamine agonist, is the only FDA approved medication which can be used for symptom control during the off periods.
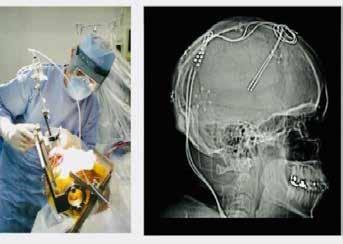
Deep Brain Stimulation (DBS) is a promising and underutilized advanced treatment for people who experience disabling tremors, wearing-off spells, and medication induced dyskinesias.
PD being a multi system disease requires a multi system ap proach. Patients can benefit a lot with physical therapy, like LS VT-BIG (Lee Silverman Voice Treatment), which encompasses physical therapy to improve their gait and balance coupled with speech therapy to address the hypophonia which can be pres ent. Patients should be encouraged to have an active lifestyle.
Continued on page 15
Neuromuscular Clinic at Nemours Children’s Hospital, Florida – Providing Comprehensive Care for Children with Neuromuscular Disorders
By Omer Abdul Hamid, MD
The neuromuscular clinic at Nemours Children’s located in beautiful Lake Nona, a thriving suburb of Orlando, is a specialty clinic supported and certified by the Muscular Dystrophy Association (MDA). Our clinic provides comprehensive medical care by a multi-disciplinary team for children who have neuromuscular disorders.
HOW NEUROMUSCULAR DISORDERS ARE IDENTIFIED
Pediatricians and other healthcare providers identify an abnormality on a child’s exam that may include low muscle tone, not meeting motor milestones, changes in physical function without cause, or regression in motor milestones, prompting them to refer the child to the neuromuscular clinic. The neuromuscular neurologist and advanced registered nurse practitioner meet the families and perform detailed evaluations to determine what diagnostic tools are needed. Common diagnostic measures used to identify neuromuscular conditions are electromyography (EMG) and nerve conduction studies (NCS) to determine the presence and extent of nerve damage, muscle ultrasound which is noninvasive and provides a dynamic way of evaluating the muscles in clinic, or muscle biopsy to have a more detailed look at the muscle fibers. Additional genetic testing is also performed to identify specific gene mutations.
THE CHAMPIONS OF OUR NEMOURS NEUROMUSCULAR CARE TEAM
Our neuromuscular care team is led by a pediatric neurologist and advanced registered nurse practitioner who specialize in neuromuscular conditions and aid in the diagnosis, treatment, and follow-up care for children with neuromuscular conditions. The team also consists of a physical and occupational therapist who assess patients’ strength, range of motion, coordination, mobility, self-care skills, and adaptive equipment needs to make recommendations for community therapies and assist in maximizing independent function. The therapists also complete all necessary performance testing required for medication authorizations. The registered dietitian nutritionist (RDN) provides evidence-based nutrition counseling to help children with neuromuscular disorders get the nutrients they need to provide favorable growth and nutrition balance for optimal health. Another important member of the team is the licensed clinical social worker who provides support for children and families to manage the emotional and financial challenges that come along with having or raising a child with a neuromuscular disorder. A neuromuscular program coordinator and neuromuscular RN support the team and families with coordinating care, prior authorizations, scheduling, insurance forms, and more.
UTILIZING A TEAM APPROACH TO MANAGEMENT OF NEUROMUSCULAR DISORDERS
Neuromuscular disorders are complex conditions and can affect a child’s physical, cognitive, and emotional development. At Nemours Children’s, we recognize that to provide comprehensive care for the children in our neuromuscular clinic, the entire team must collaborate and coordinate with healthcare professionals who have considerable expertise in a variety of areas. These often include cardiologists, pulmonologists, endocrinologists, physiatrists, gastroenterologists, psychologists, psychiatrists, geneticists, and orthopedists. Multidisciplinary care is essential, so our neuromuscular clinic works diligently with the other specialists to develop and provide a comprehensive treatment plan that ensures each child is receiving the best possible care.
IMPROVING THE LIVES OF CHILDREN WITH NEUROMUSCULAR DISORDERS
There is no cure for most neuromuscular disorders, but there are a variety of treatments available today that can help improve a child’s quality of life. There are medications that can be prescribed to help improve muscle strength, reduce pain, and manage other symptoms of a neuromuscular disorder. Physical, occupational and speech therapies are often recommended to assist children with their physical and cognitive functions and increase their potential to interact with the environment around them. Nutrition counseling by an RDN can help children maintain a balance with nutrient intake to promote optimal growth and wellness. In some cases, surgery may be required to correct an orthopedic deformity and improve pain, posture and overall function.
In addition to traditional treatments, there is ongoing research to develop medications that can impact the root cause of some neuromuscular disorders. We are committed to conducting research and has been involved in several research trials, some of which have led to the development and FDA approval of treatments for spinal muscular atrophy and Duchenne muscular dystrophy. These treatments now offered to Nemours Children’s patients include exon skipping medications for children with Duchenne muscular dystrophy, gene transfer therapies to provide healthy copies of the SMN1 gene to children with spinal muscular atrophy (SMA), antisense oligonucleotides to reduce, restore, or modify protein expression helping produce more SMN protein in children with SMA, and immune modulating medications to help children with myasthenia gravis and chron-
ic inflammatory demyelinating polyneuropathy (CIDP) improve their muscle strength.
THE IMPORTANCE OF NEUROMUSCULAR CARE TEAMS
As one of only of only three pediatric MDA Care Centers in the State of Florida, our clinic supports patients from the entire Southeast region of United States (Florida, Alabama, Georgia, South Carolina) to Central and South America (Ecuador, Trinidad, Puerto Rico). With over 10 years of experience as a recognized MDA clinic, we have a long-established neuromuscular program. Our team has a deep understanding and efficient processes in place to diagnose, treat, and manage care for these rare plus complex diseases. The neuromuscular clinic at Nemours Children’s is also registered with the state of Florida as a newborn screening treatment center for SMA. This allows us to diagnose and treat babies quickly to minimize loss function that occurs quickly at an early age.
CASE STUDY
One of our patients was born in Florida and had a positive newborn screening for SMA. The family decided to pursue treatment
When The Tremor Isn’t Essential –
Continued from page 13
and care at Nemours Children’s Hospital, Florida in Orlando. The patient was started on Spinraza at 2 weeks of age then dosed with Zolgensma at 7 months after his titers decreased to allow treatment. Now at 9 months old, he continues to not have any observable symptoms of SMA with good vigorous movements of all his limbs, good strength throughout and normal reflexes without tongue fasciculations.
The family meets regularly with our neurologist in person, via telehealth, and over the phone. The patient completes regular functional testing with our neuromuscular therapists to track his milestones, strength, and progress. He is monitored by our dietitian to ensure appropriate weight gain and nutritional intake. Our RN is in regular contact with the family to ensure labs are completed appropriately and in a timely manner. The program coordinator has managed the prior authorizations for his expensive treatments. The social worker met with the family to offer support, asses for resource needs, provide health insurance benefit information, and offer emotional support.
To learn more about our clinic, visit Nemours.org/services/ neuromuscular-disorders.
Other features of PD including depression, constipation. REM sleep disorders should also be managed concomitantly. In long-standing or medically refractory cases of at least 4 years of PD, Deep Brain Stimulation (DBS) of the subthalamic nucleus (STN) or globus pallidus interna (GPI) is a great option to provide relief with disabling symptoms. In summary, early accurate diagnosis by a neurologist experienced in PD along with a multidisciplinary approach should be used for improving the symptoms and quality of life of PD patients.
Dr. Jaivir Rathore, A triple board-certified top-rated neurologist trained at the Johns Hopkins and the Cleveland Clinic, Harvard University journal published neuroscientist and the Medical Director of Falcon Advanced Neurology & Epilepsy Freedom Center (FANEFC) in Orlando FL with additional clinics serving the largest retirement community of the world in The Villages FL provides comprehensive neurology care including movement disorders such as Parkinson’s disease. FANEFC is “Care Connected” with the Mayo Clinic, Jacksonville FL for surgical cases including DBS for PD.
The Benefits of Pelvic Floor Therapy and Why It’s Important to Talk to Patients about this Sensitive Topic
By Tessa Ladd, OTR/L
For someone experiencing pain in their knee, the journey to wellness is simple. They’d make an appointment to discuss it with their primary care provider or a specialist. They certainly wouldn’t feel uncomfortable discussing their knee with family members or in casual conversations with friends.
Unfortunately, the same is not always true for women dealing with pelvic floor issues and the life challenges they create.
Despite affecting about one third of all women, pelvic floor dysfunction and its symptoms often go unreported by patients. Women may feel hesitant or even be ashamed to tell their physician about urinary incontinence, urinary urgency, bowel dysfunction or pain with intimacy.
Women often assume these conditions are simply a side effect of childbirth or a natural element of getting older and that there are no real solutions for the problem. Fortunately, that isn’t true. There are several treatment options available, including pelvic floor therapy, which can have a major impact.
They key is understanding that the pelvic floor is a part of the core and these muscles are something that women can gain control over. Despite lingering myths and stigmas that say otherwise, pelvic floor muscles don’t stop working after childbirth or gradually with age.
Pelvic floor dysfunction is a problem that can create profound changes in how patients live their day-to-day lives. Specific therapies vary based on symptoms, but pelvic floor therapists work with patients on areas such as diaphragmatic breathing, core strengthening, pelvic floor muscle recruitment, and body mechanics to help them regain more control over their lives.
It’s not so much about what patients do every day but how they do it. Pelvic floor therapy teaches them to identify, engage and strengthen the muscles in their core. They also learn proper body mechanics, such as better ways to pick up a toddler, for example.
Treatment starts under the supervision of a therapist, but patients will also be instructed on how to do exercises at home.
Many of my patients have noticed improvements almost right away. With urinary urgency, for example, patients often report things are getting better after just one week of therapy. For most patients, 10 weeks of therapy will put them in a much better place, with little or no leakage problems.
It’s difficult to overstate the value of this therapy for patients suffering from pelvic floor dysfunction. They often arrive at therapy, feeling broken or depressed. It is understandably difficult to adapt to a world where you can no longer rely on your body’s
ability to control urinary or bowel functions. It can threaten to take over your life.
Patients end up making decisions like not drinking water in the morning because they have plans to leave the house later in the day. Or they obsess over whether they will have access to a bathroom whenever they are out. These issues have resulted in patients choosing to miss important family events like graduations or outdoor gatherings.
The goal of therapy is to help patients return to a place where they can trust their bodies again. It’s easy to imagine the liberation they feel when they go about their daily lives without constantly worrying about having an accident. They can jump on a trampoline with their toddler, go jogging with friends or watch a funny movie with the family.
Physicians and other medical providers may be able to help more patients address this issue by making it a more common conversation during patient visits.
First, you have to find out whether your patient has any symptoms of pelvic floor dysfunction. From there, you can further identify the problem. Does leakage happen as the result of sneezing, laughing and coughing? Or is it because they can’t make it to the bathroom on time? Do they have generalized pain in the pelvic area, with or without a bowel movement?
Ask if your patient needs to strain a lot to have a bowel movement. Do they feel any bulging, pressure or heaviness in the pelvic region? These can be signs and symptoms of prolapse.
Also ask if they have any pain during sexual intimacy. Some women believe it’s natural for intimacy to become painful after pregnancy or as a result of aging. But in reality, this is a red flag for pelvic floor dysfunction, and it can be addressed and treated.
Another issue to consider is diastasis recti, the separation of the abdominal muscles during and after pregnancy. It’s a common problem for postpartum women, though many people are unaware of it. While it’s a typical part of pregnancy progression, there are things that can be done both during pregnancy and postpartum to minimize its impact and improve the recovery phase.
Asking about these topics can help uncover pelvic floor dysfunction in women. Pelvic floor therapy patients range from teenagers struggling with pain from endometriosis, to new mothers and women in their 80s.
While this may be obvious, it’s worth considering again the Continued on page 18
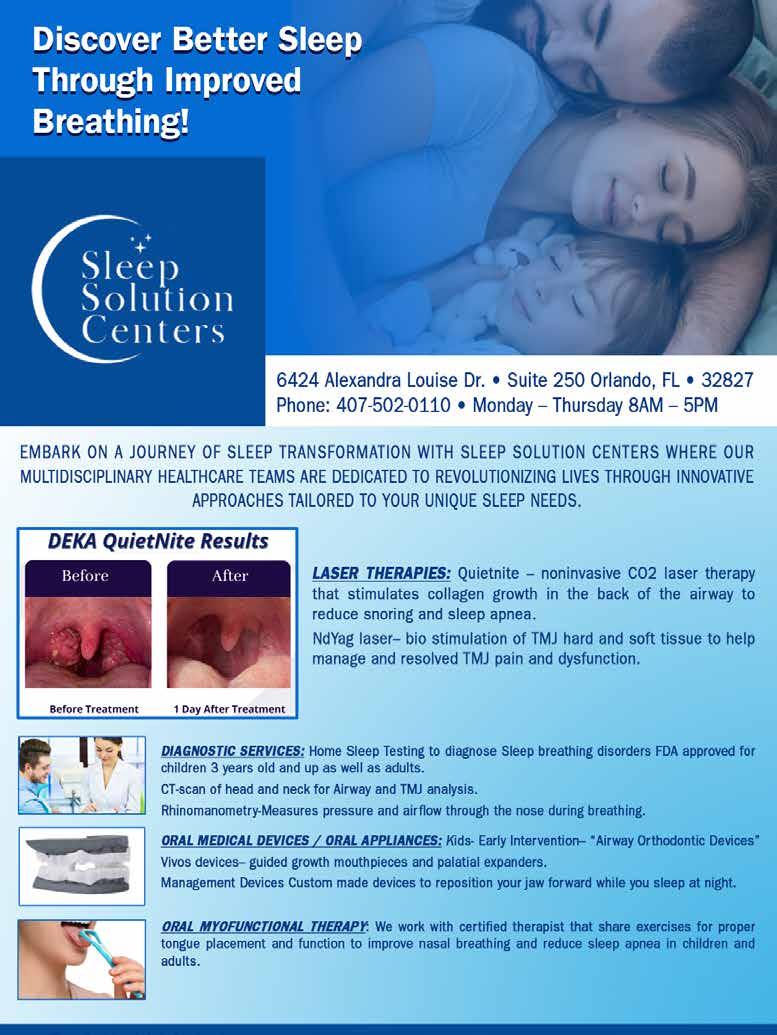
Innovative Treatment for Children with Obstructive Sleep Apnea: Transforming Care with Dental
Guided Growth Devices
By Tara M. Griffin, DMD, DBDSM, DASBA
Pediatric obstructive sleep apnea (OSA) is a significant health concern affecting a growing number of children worldwide. As healthcare providers, it is crucial for us to stay abreast of the latest advancements in the field to ensure optimal care for our children of today. One such innovation that holds promise in the treatment of pediatric OSA is the use of dental guided growth devices. These modalities not only address the symptoms of OSA but also contribute to the growth and development of the upper and lower jaws and airway, offering a holistic approach to resolve this condition for most children.
SYMPTOMS OF PEDIATRIC SLEEP APNEA AND SLEEP DISORDERED BREATHING
Identifying and diagnosing pediatric sleep apnea is essential in providing timely intervention. Children with OSA may exhibit a range of symptoms, including ADD/ADHD, loud snoring, gasping or choking during sleep, restless sleep, bedwetting, daytime fatigue, irritability, speech problems, behavioral issues and poor academic performance.
When children are properly screened, 9 out of 10 children have more than one of these symptoms and may be at risk. These children are struggling to breathe at night and often have a narrow long face, small jaws, crowded teeth or lack of spacing with their primary teeth. These are often the kiddos that crawl into bed with mom and dad at night.
At Sleep Solution Centers, we offer FDA approved home sleep tests as a screening tool for children 2 years old and up. It’s best to diagnose and treat this condition as early as possible because they are in their developmental stages of life.
Children today are being medicated for ADD/ADHD symptoms at an alarming rate! In 2012, Dr Karen Bonuck from Einstein University performed a population based cohort study of 11,000 children and her results showed that behavior issues and sleep breathing disorders are very difficult to differentiate. At Sleep Solution Centers, our motto is “Don’t Guess, Just Test!” Before medicating anyone for ADD/ADHD or behavior issues, take a simple home sleep test to rule out a sleep breathing disorder and avoid mis-diagnosing the patient.
Left untreated, OSA can lead to serious health consequences such as cardiovascular problems, neurobehavioral issues, systemic and pulmonary hypertension and growth restrictions, only to name a few conditions. Recognizing these symptoms and referring patients for further evaluation is vital in ensuring the overall well-being of children with OSA and sleep breathing disorders.
TREATMENT FOR PEDIATRIC SLEEP APNEA WITH DENTAL GUIDED GROWTH DEVICES
Current medical guidelines developed over 25 years ago for pediatric OSA involve surgical removal of tonsils and adenoids and continuous positive airway pressure (CPAP) therapy as first and second line of treatment. While these interventions may be effective in some cases, they may not be well-tolerated by all children, they are invasive and do not address the root cause of the problem. Many parents today are looking for a root cause solution for their child’s health. Studies show that dental guided growth devices focus on a child’s developmental growth and offer a noninvasive, root cause approach for resolving OSA and sleep breathing disorders in most pediatric patients.
The American Academy of Dental Sleep Medicine and other likeminded organizations are now collaborating with the FDA with recent clinical trials and with the American Academy of Pediatrics to provide new data with this innovative technology to revisit and hopefully revise these guidelines to offer better root cause, non-invasive solutions.
These custom-made guided growth devices work by training the tongue to rest on the roof of the mouth, stimulating proper nasal breathing. They stabilize the jaw and tongue to prevent airway obstructions during sleep, promoting better airflow and reducing the incidence of apnea episodes. By addressing underlying anatomical issues such as narrow arches, retruded jaws, and enlarged tonsils, guided growth devices can help optimize the growth and development of the airway in children.
Through the use of these custom devices, treatment aims to create more space in the oral cavity, promote nasal breathing, and enhance overall airway patency. This proactive approach not only supports the treatment of pediatric OSA but also contributes to long-term oral and systemic health benefits.
Dental guided growth devices for pediatric growth and development are designed to be adjustable, allowing for optimal fit and function as a child grows. When the jaw and airway are restricted and underdeveloped, devices can be used to expand the jaw and airway and align the teeth to prevent future need for costly braces.
Starting treatment at a young age such as 2 to 8 years old can save a parent many thousands of dollars. Guided growth devices focus on improving the function and structure of the upper airway to facilitate better breathing and overall health.
Continued on page 18
feelings of patients suffering with pelvic floor dysfunction. Whether they feel shame or embarrassment, it can be incredibly challenging for them to talk openly about it. This is where you as a provider can play a key role by initiating the subject yourself and asking basic screening questions.
Women who opt for pelvic floor therapy finish their course of treatment saying they wish they had done it much sooner, or that they can’t believe how long they lived with issues for which there were solutions.
A few simple questions on a sensitive topic can be all it takes to help patients find their way to this life-altering therapy.
Tessa Ladd is an occupational therapist who specializes in pelvic floor therapy at Orlando Health. She has a passion for the postpartum population and is a Pregnancy and Postpartum Corrective Exercise Specialist.
Innovative Treatment for Children with Obstructive Sleep Apnea
Continued from page 15
INCORPORATING GUIDED GROWTH DEVICES IN PEDIATRIC OSA TREATMENT
As physicians, it is essential to collaborate with experienced dental professionals who have advanced training in the treatment of pediatric OSA with guided growth devices. By working together, we can offer comprehensive care that addresses the multifaceted nature of this condition. Through a multidisciplinary approach, we can combine medical management with dental interventions to provide personalized treatment plans tailored to each child’s unique needs. Referring our patients to experts in utilizing dental devices for pediatric growth and development can lead to improved outcomes and enhanced quality of life for children with OSA and sleep breathing disorders.
CONCLUSION
At Sleep Solution Centers, we have over 14 years of experience treating children with guided growth devices. Innovative treatment modalities are reshaping the landscape of pediatric OSA and sleep disordered breathing resolution. By incorporating these therapies into our practice, we can offer our patients from birth to their last breath, effective and non-invasive solutions for addressing their sleep-related breathing disorders. Embracing a collaborative and holistic approach to pediatric OSA care can help optimize treatment outcomes and promote better overall health and well-being for children with this condition.
Let us continue to stay at the forefront of pediatric sleep medicine and explore the possibilities that dental guided growth devices and adjunctive therapies offer in transforming the lives of our young patients with obstructive sleep apnea and sleep disordered breathing. Remember, the key to success lies in early identification, timely intervention, and comprehensive, patient-centered care. Collaboration Cures!
Tara M. Griffin, DMD, DBDSM, DASBA, graduated from Nova Southeastern University in 2006, with a doctorate in Dental Medicine. She became passionate about helping her patients breathe and sleep better and completed her Diplomate with the American Academy of Dental Sleep Medicine in 2011. In 2015, she completed her Diplomate with American Sleep and Breathing Academy. In 2016, she became a Clinical Advisor with Vivos Therapeutics to help educate and mentor doctors interested in the treatment of OSA with oral medical devices. She owned a private practice focused on sleep, TMD and general dentistry in the panhandle of Florida for 17 years before becoming the co-founder of Sleep Solution Centers in Medical City, Orlando in 2024. She may be contacted at 407-502-0110 or by visiting www.sleepsolutioncenters.com
Is Your Online Reputation Costing You Patients?
By Sonda Eunus, MHA, CMPE
What does your online reputation say about your practice? If you have a negative online reputation, you are missing out on new patients every day. Most medical practices now get the majority of their new patients through Google and other search engine queries, such as “Pediatrician in Orlando”. If your practice appears in these searches, the most common next step for a potential new patient would be to check out your reviews – what are other patients saying about your practice? It has been reported that 90% of consumers read online reviews before visiting a business and that online reviews influence 67% of purchasing decisions (Bright Local). For this reason, it is incredibly important to pay attention to the rating and reviews that your practice has on search engines, social media platforms, and local online business directories.
However, despite the importance of cultivating a positive online reputation, only 33% of businesses report actively collecting and asking for reviews (1). One great process to set in place at your practice is asking for patient reviews after each patient visit. It can be as simple as training your front office staff to ask each patient how their visit went while checking them out, and if they receive favorable feedback then they can ask the patient to please leave a review on Google or Facebook about their experience. If they receive negative feedback, this feedback should be taken very seriously, and management should be notified as soon as possible so that the issue can be mitigated before the patient decides to post a negative review.
Setting up an automated text or email campaign that asks each patient for their feedback after their appointment is also a great way to improve your online reputation as well as to correct any issues that may be occurring at your practice. When you receive feedback from patients, you are then able to prompt them to leave a public review on Facebook, Google, Yelp, Healthgrades, or other applicable review platforms. However, you must be aware that legally, you are not allowed to only direct people with favorable feedback to leave reviews, which is known as review-gating – so if you are implementing an automated system like this, just make sure that you are aware of this limitation. There are online reputation management platforms which allow you to customize the messages that people see when they leave negative feedback as opposed to positive feedback, but both of those messages must still offer the option to leave a public review. However, if you create your message in such a way as to communicate to the patient who may leave negative feedback that you are working hard on resolving the issue and that someone will be in touch shortly, that may prevent them from leaving a public negative review.
When you receive a public review on Google, Facebook, or other review sites, make sure that you respond to it – either by thanking them for a good review or by asking them to contact you to discuss how you can improve their experience. Do not argue or try to defend yourself online – try to speak about it with them privately, fix the issue, and ask them to remove the review if possible. When you receive great reviews, make sure to cross-share them on your various social media platforms. You should also create a “Reviews” page on your website and add all great reviews to this page. This instantly adds credibility to your website.
Finally, make sure that when you look over the feedback and reviews that you receive, you are paying attention to what the negative reviews are saying – this is a great opportunity to identify current process challenges and improve your patients’ experience at your practice. Need help managing your practice’s online reputation? Visit www.lms-plus.com to see how Leading Marketing Solutions can help.
Sonda Eunus is the CEO of Leading Marketing Solutions, a Marketing Agency working with Medical Practices and other Businesses to help them identify the best marketing strategies for their business, create a strong online presence, and automate their marketing processes for a better return on their Marketing budget. Learn more about Leading Marketing Solutions at www.lms-plus.com.
JANUARY – Digestive Disorders
Diabetes
2024
EDITORIAL CALENDAR
Florida MD is a monthly medical/business digital magazine for physicians..
Florida MD is emailed directly to healthcare providers in Orange, Seminole, Flagler, Volusia, Osceola, Polk, Brevard, Lake and Indian River counties. Cover stories spotlight extraordinary physicians affiliated with local clinics and hospitals. Special feature stories focus on new hospital programs or facilities, and other professional and healthcare related business topics. Local physician specialists and other professionals, affiliated with local businesses and organizations, write all other columns or articles about their respective specialty or profession. This local informative and interesting format is the main reason physicians take the time to read Florida MD.
It is hard to be aware of everything happening in the rapidly changing medical profession and doctors want to know more about new medical developments and technology, procedures, techniques, case studies, research, etc. in the different specialties. Especially when the information comes from a local physician specialist who they can call and discuss the column with or refer a patient. They also want to read about wealth management, financial issues, healthcare law, insurance issues and real estate opportunities. Again, they prefer it when that information comes from a local professional they can call and do business with. All advertisers have the opportunity to have a column or article related to their specialty or profession.