10:15am – 11:45pm Workshop in Session 11:45pm – 12:45pm Lunch Break Sign-In (CPA Members Only)
12:45pm – 2:15pm Afternoon Sessions Begin 2:15pm – 2:30pm Mid-Afternoon Break (Refreshments Provided) 2:45pm – 4:00pm Workshop in Session 4:00pm Complete Evaluation Forms (Use QR Code Above) & Sign-Out (CPA Members Only)
CERTIFICATES:
• Digital certificates are available for download on the final day for multi-day attendees at: http://registration.jackhirose.com/certificates
CPA MEMBERS
• A new policy requires you to request a form from your on-site coordinator, which must be submitted directly to the association.
• Please sign in after lunch and sign out at the end of the day. Early departures result in the loss of CPA credits.
• Certificates will be updated with CPA credits after form verification (allow 2-4 weeks).
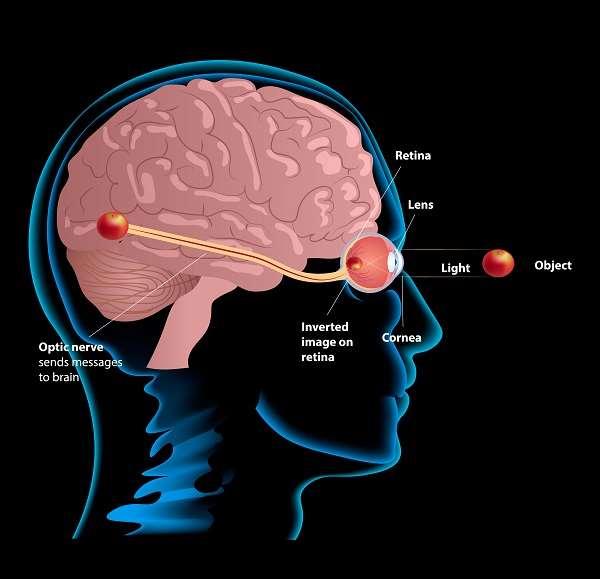
Meaning-Based Therapy in the Treatment of Trauma, Addiction, Anxiety & Depression
Dr. Carissa Muth, Psy.D.
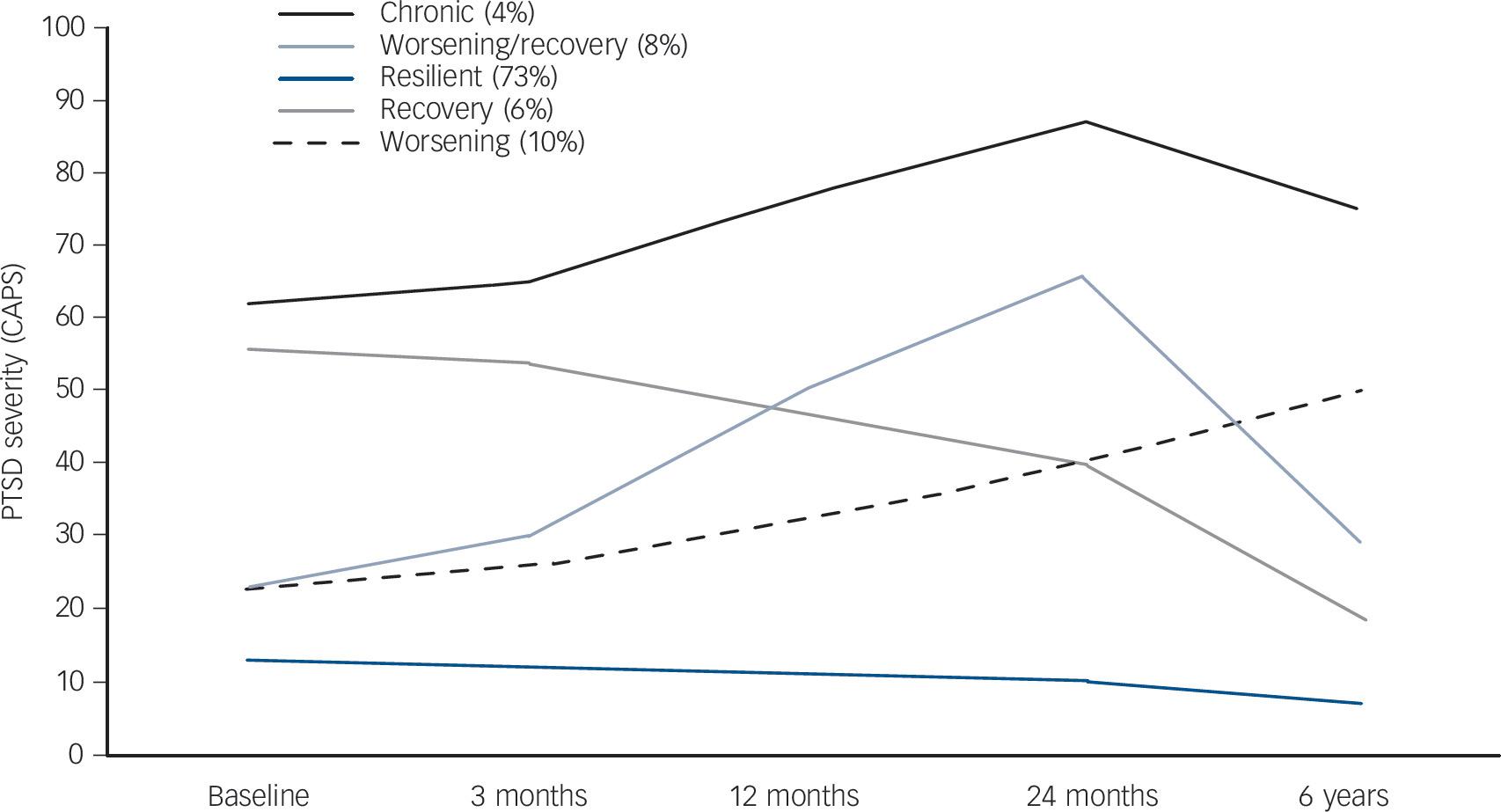
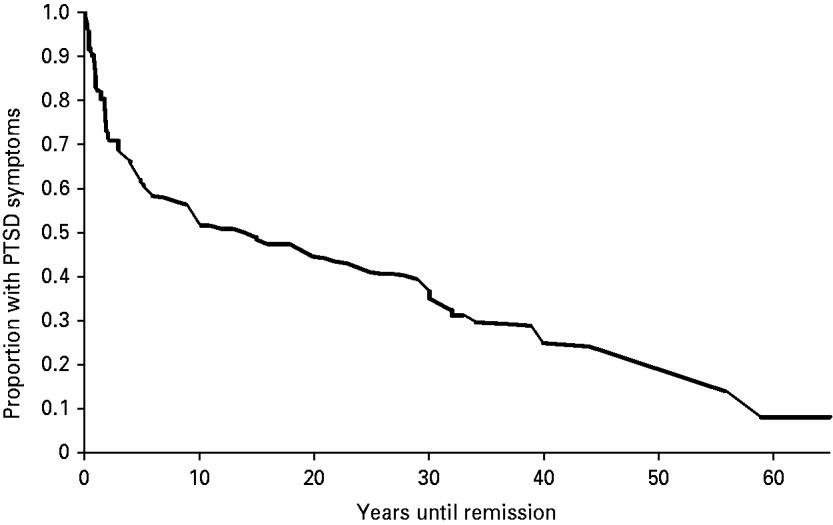
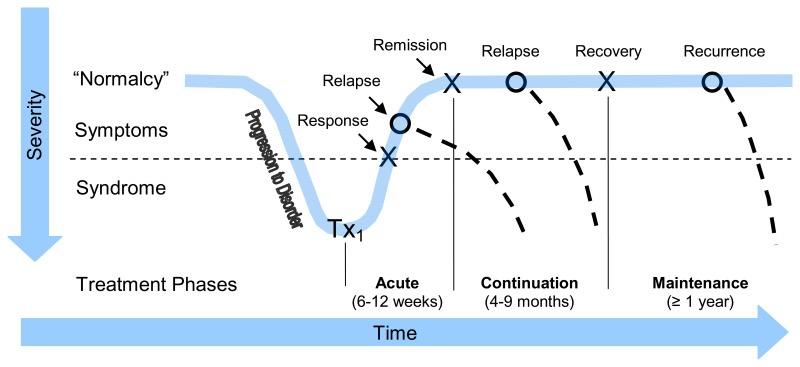
Treatment Resistance
Chapman, C., Mills, K., Slade, T., McFarlane, A. C., Bryant, R. A., Creamer, M., … Teesson, M. (2012). Remission from posttraumatic stress disorder in the general population. Psychological Medicine, 42(8), 1695–1703. doi:10.1017/S0033291711002856
Schlaepfer, Thomas & Ågren, Hans & Monteleone, Palmiero & Gastó, Cristobal & Pitchot, William & Rouillon, Frederick & Nutt, David & Kasper, Siegfried. (2012). The hidden third: Improving outcome in treatment-resistant depression. Journal of psychopharmacology (Oxford, England). 26. 587-602. 10.1177/0269881111431748.
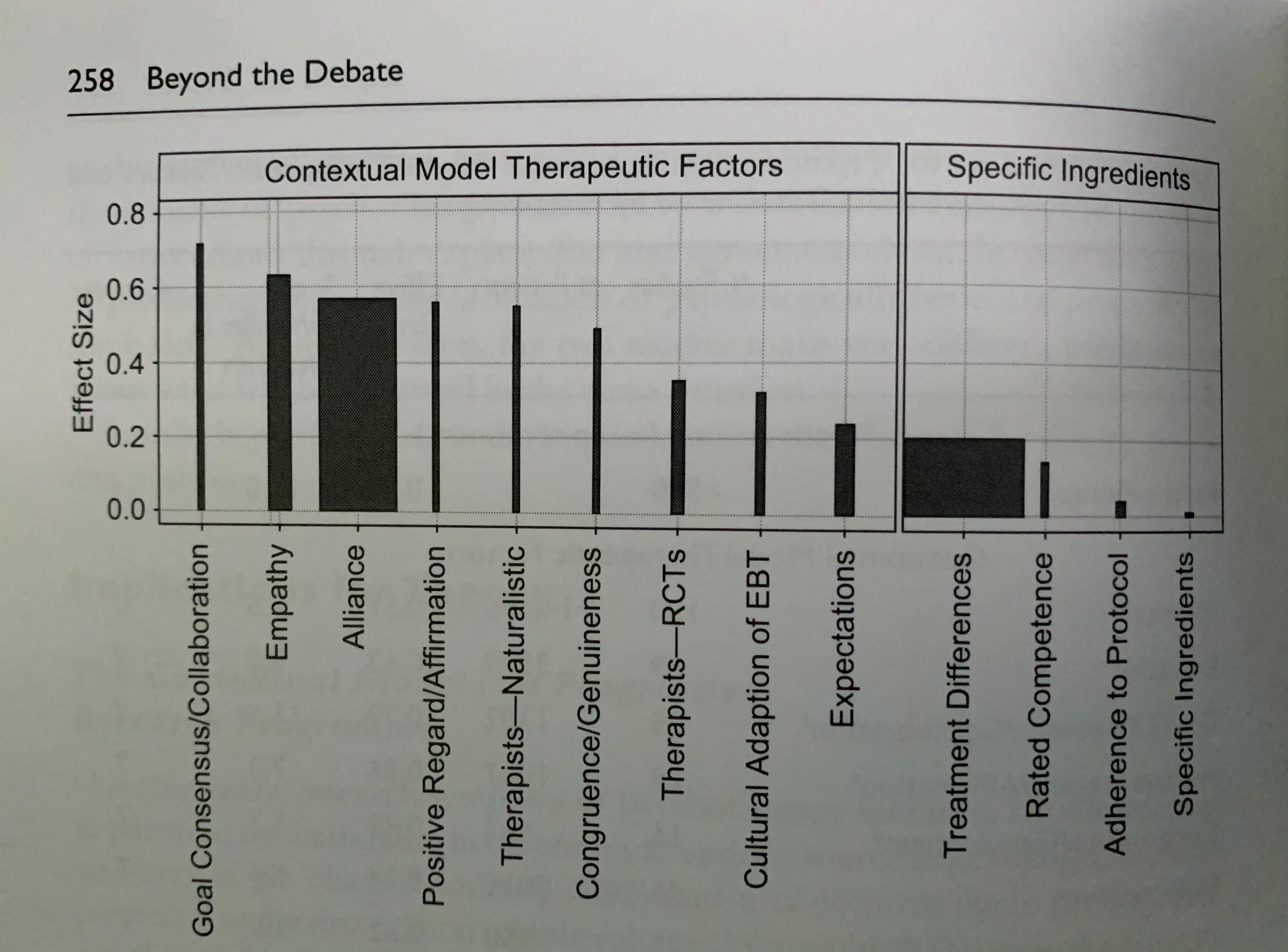
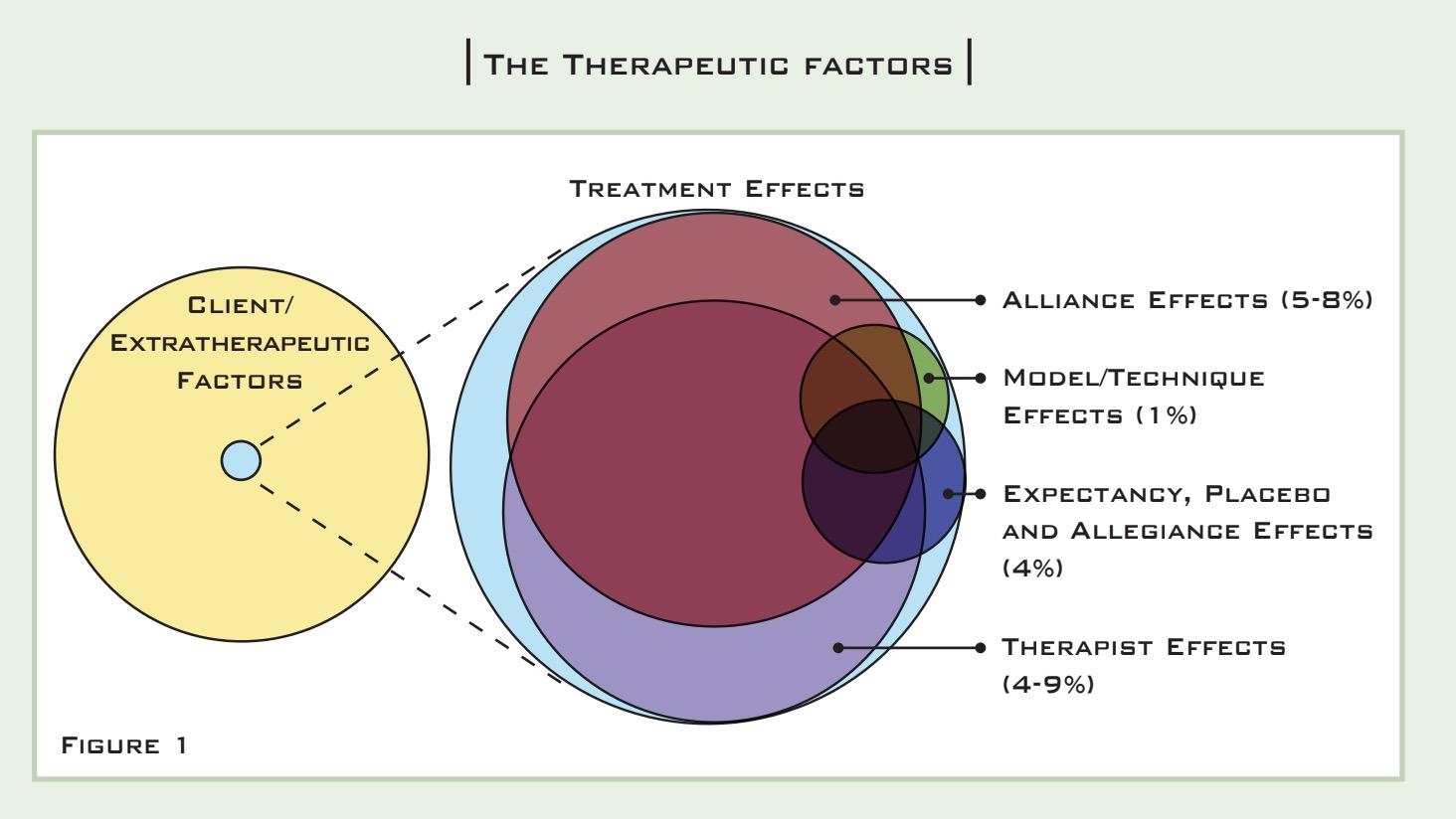
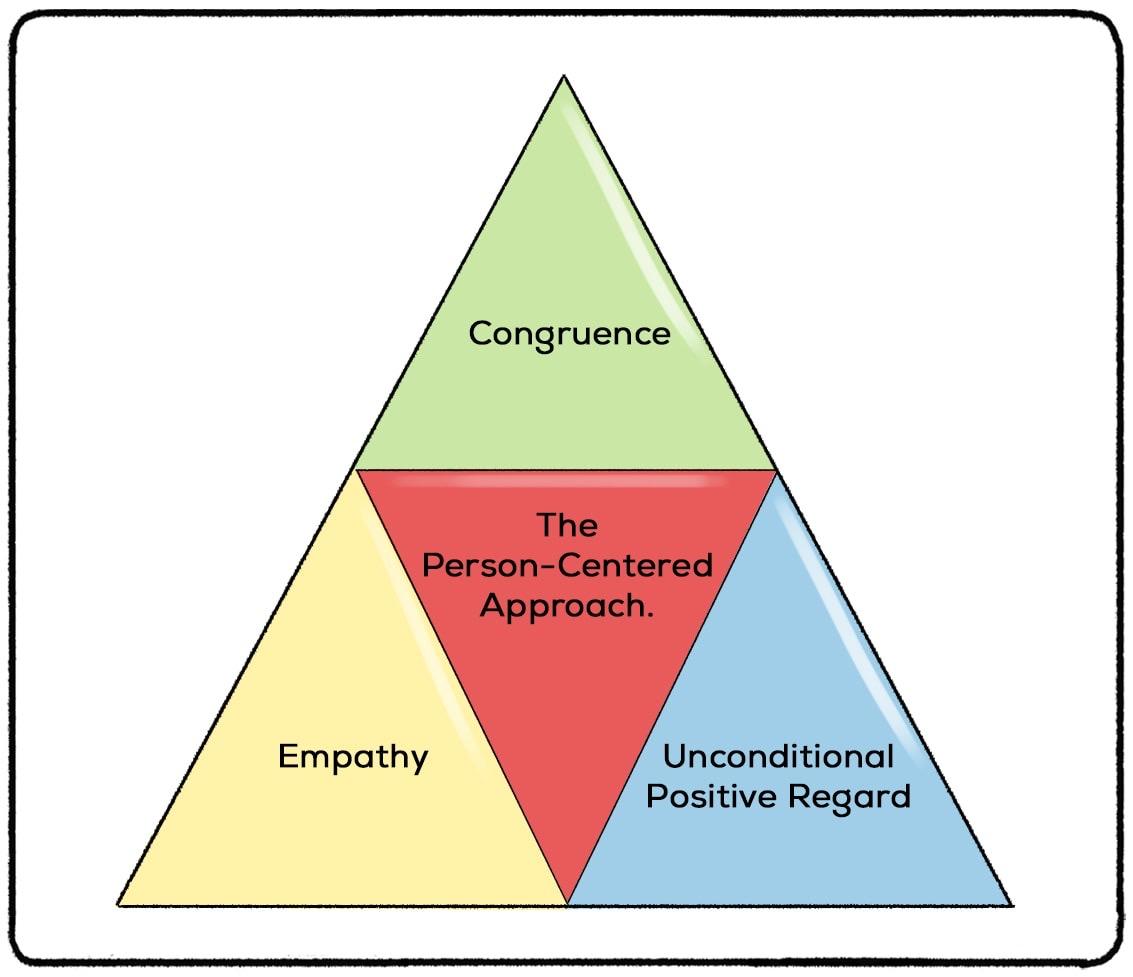
Effective Psychotherapy
Medical Model- characterized by insistence on the correct explanation of a disorder and adoption of the concomitant therapeutic actions that are responsible for the patient benefits
Common factors- aspects of therapy that are common to most psychotherapies, such as hope, expectation, relationship with the therapist, belief and corrective experience
Common factors model understands the therapist as an agent of change and that outcomes are linked to the therapist’s characteristics and relationship with the client
Therapist Effects
• Preponderance of evidence indicates that there are important therapist effects (3-7% of variability)
• Therapist effects general exceed treatment effects
• What are the characteristics and actions of effective therapists?
• Empathy
• Authenticity (real relationship)
• Ability to form strong alliances across the range of clients
• Interpersonal skills (Higher linked to better client outcomes)
• Verbal fluency
• Interpersonal perception
• Affective modulation and expressiveness
• Warmth and Acceptance
• Empathy
• Focus on other
• Reflective about practice
General Effects
• Working alliance
• Healthy, affectionate, and trusting feelings toward the therapist without transference
• Agreement about the goals of therapy
• Agreement about the tasks of therapy
• Bond
• Early symptom change may increase rates of alliance
• Placebo/ Expectation (Hope)
• Desire to feel relief
• Induction of an expectation that treatment can accomplish goal
• Presence of emotional arousal
• Attribution
• Client attributes changes to their own efforts (Self- efficacy increase)
• Acquisition of the belief that one’s efforts are responsible for improvement
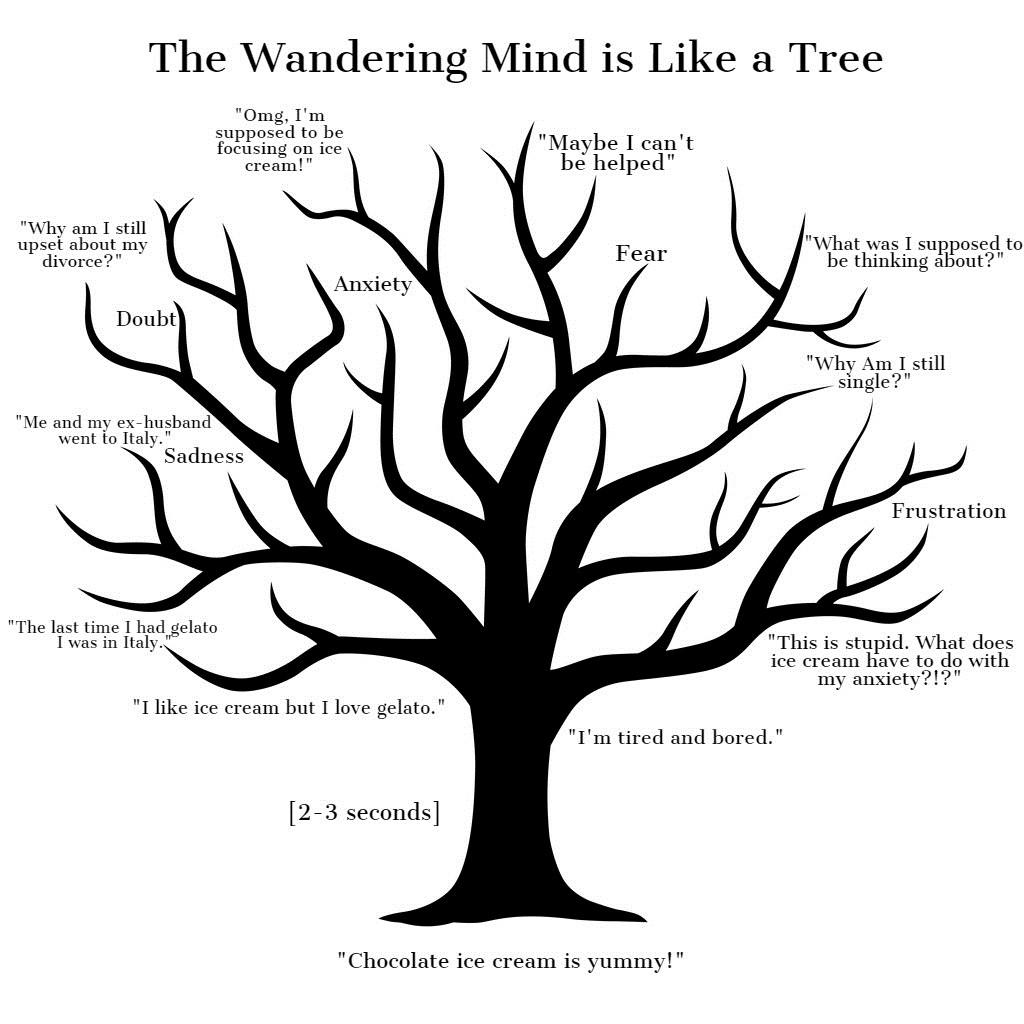
Resistance
Models of Wellbeing
What makes for a Good Life?
• Aristippus (435- 356 BCE)- Goal of life is to experience the maximum amount of pleasure and happiness consists of the totality of hedonic moments
• Epicurus (34 BCE)- Goal of life is to obtain a happy, tranquil life, one characterized by peace and freedom from fear and pain
• Aristotle- Goal of life is to achieve “eudaimonia,” which is the pursuit of highest virtue
Hedonic Wellbeing
• 1960s- Life satisfaction and happiness was considered key components of well being
• Wellbeing determined by life satisfaction, positive affect and negative affect
Hedonic Wellbeing
• Factors impacting hedonic wellbeing
• Age (U- shaped trend)
• Satisfaction reaches its lowest point at midlife between ages 30 and 60 and then peaks in older adulthood
• Higher income
• Higher education
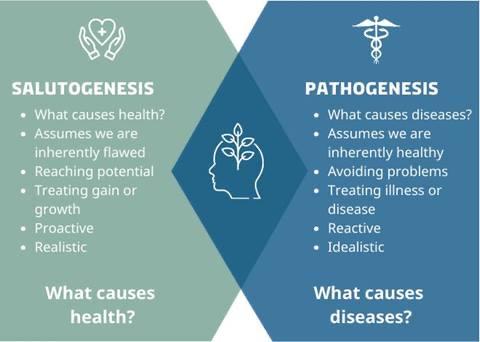
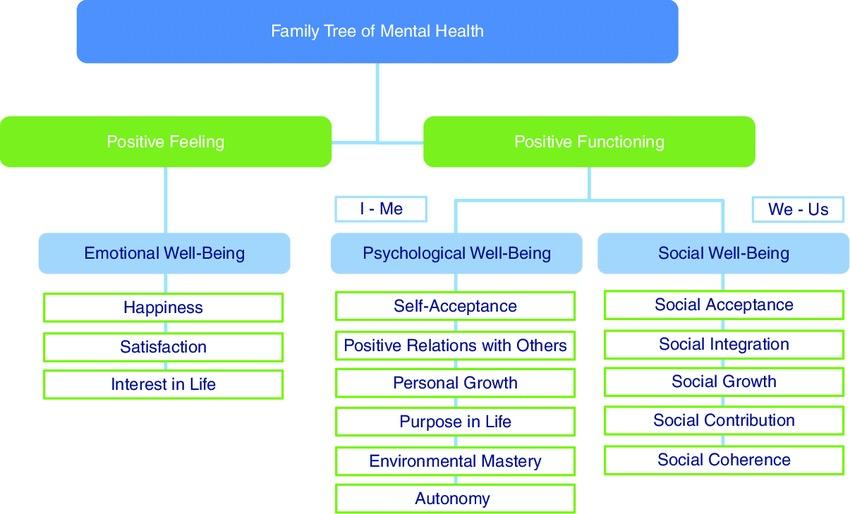
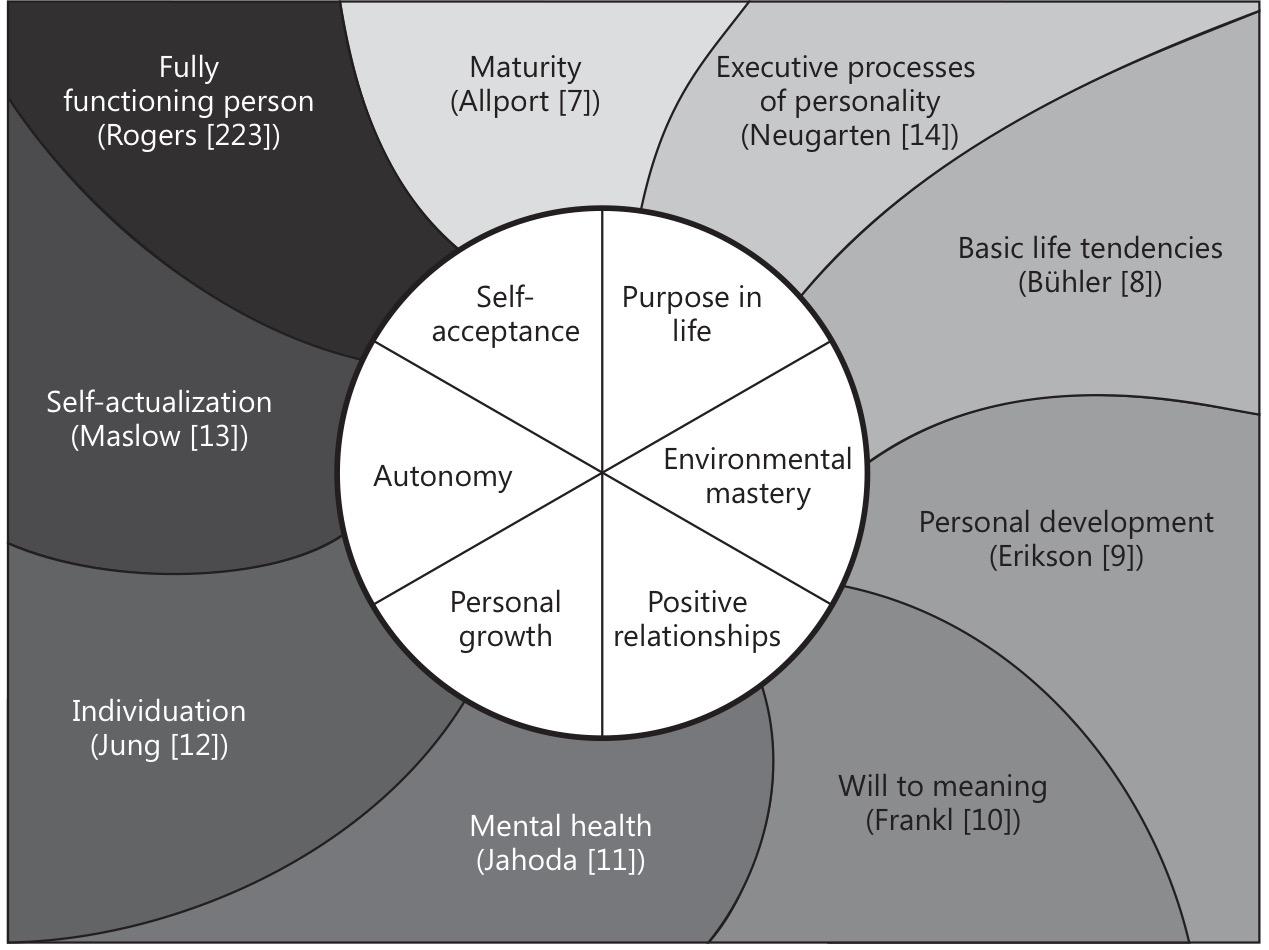
Eudaimonic Wellbeing
• Wellbeing determined by the presence of particular factors rather than by the absence of illness
• Internal rather than external factors
• Self acceptance
• Positive relationships with others
• Environmental mastery
• Autonomy
• Purpose in life
• Personal growth
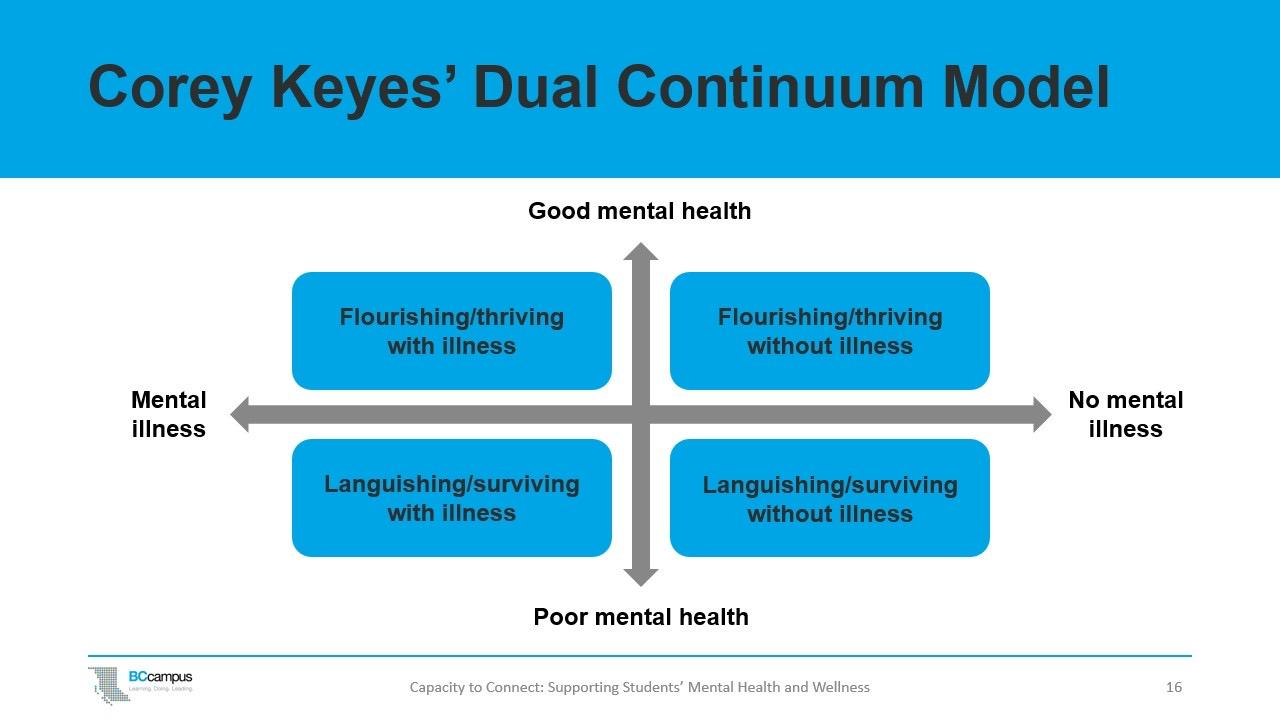
Dr. Corey Keyes
Ryff, C.D (2014). Psychological well-being revisited: Advances in the science and practice of Eudaimonia
Positive Relationships
• Sense of belonging
• Depth of emotional ties
• Warm, satisfying trusting relationships with others; is concerned about the welfare of others; capable of strong empathy, affection and intimacy; understands give and take of human relationships
Purpose in Life
• Has goals in life and a sense of direction; feels there is meaning to present and past life; holds beliefs that give life and purpose; has aims and objectives to living
• “A human being, by the very attitude he chooses, is capable of finding and fulfilling meaning in even a hopeless situation.” (Frankl)
• Principal ways to find meaning (Frankl)
• What they gives to the world in terms of creations
• What they take from the world in terms of encounters and experiences
• The stand they take to their predicament in case they must face a fate which they cannot change
Motivation
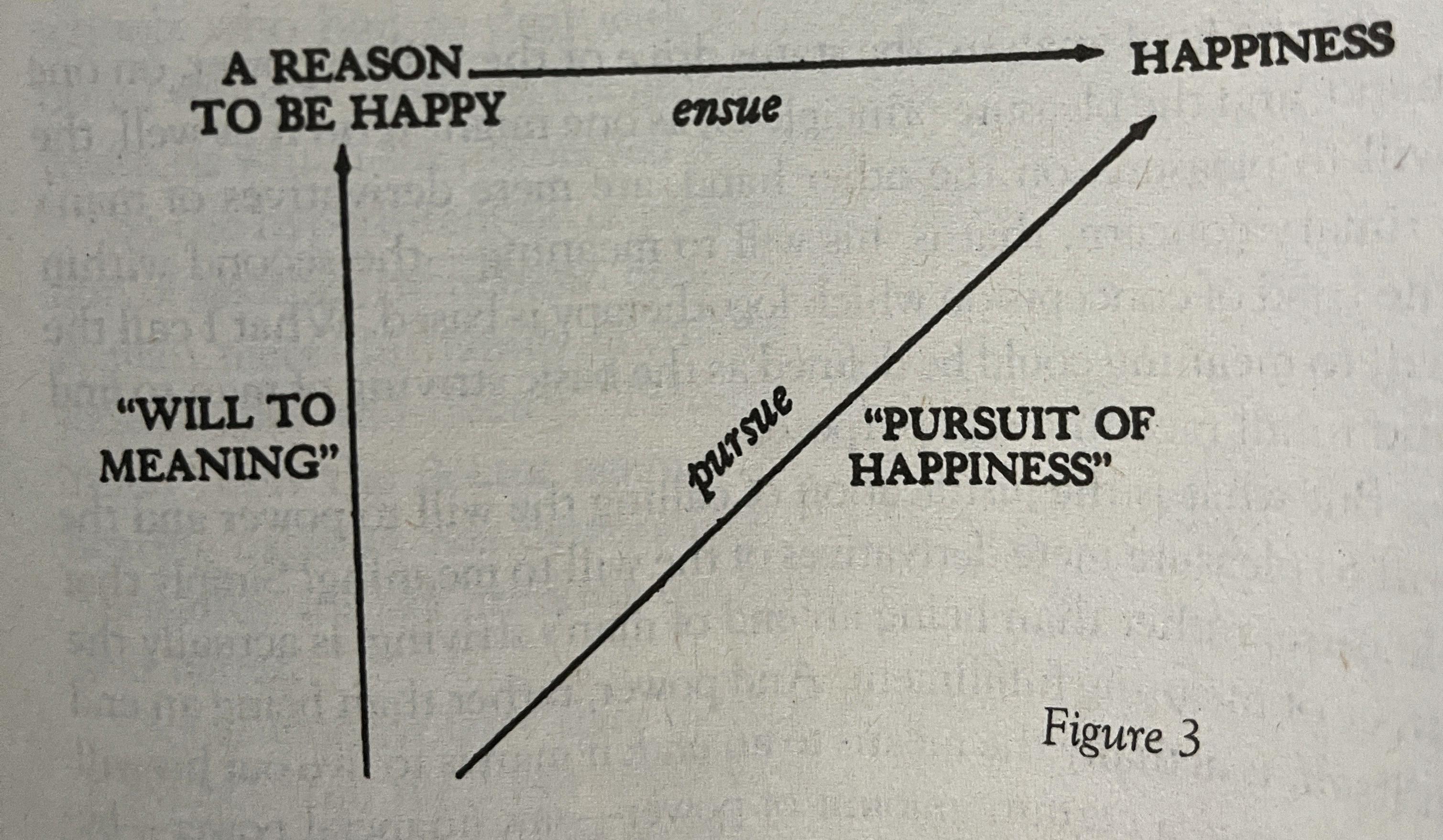
• “Pleasure cannot be attained by directly intending it. But as we now notice, it may well be obtained by a biochemical medium” (Frankl)
• Fulfillment is contingent to the extent to which an individual finds a unique sense of meaning
• “Man is pushed by drives but pulled by meaning” (Frankl)
• “The man who regards his life as meaningless is not merely unhappy but hardly fit for life” (Albert Einstein)
Pain and Suffering
“As soon as a painful fate cannot be changed, it not only must be accepted but may be transmuted into something meaningful, into an achievement” (Frankl)
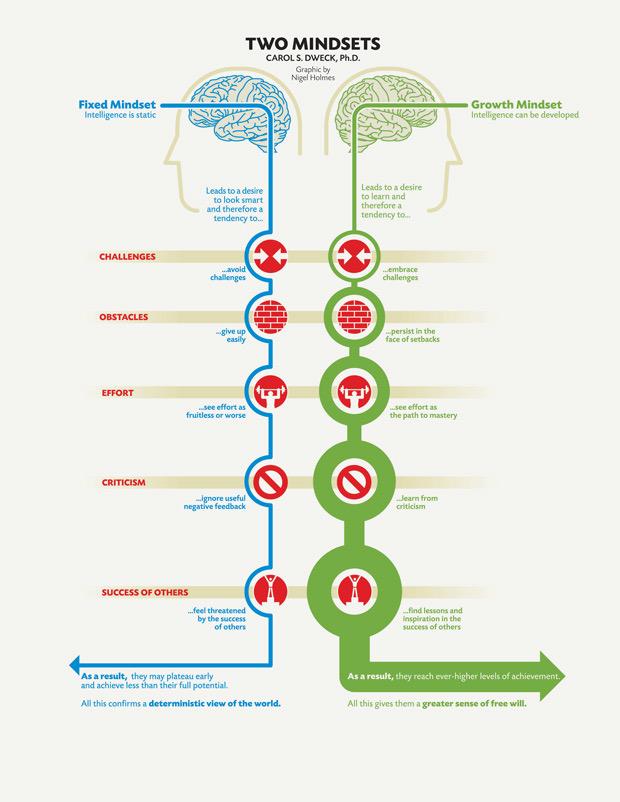
Dr. Carol Dweck
Frankl – The Will To Meaning
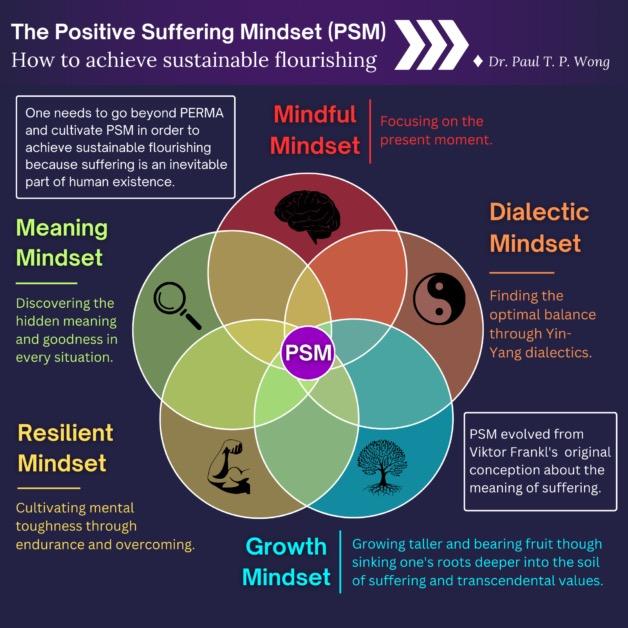
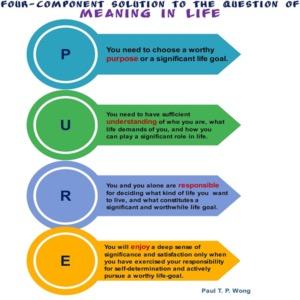
Dr. Paul T. Wong
Dr. Paul T. Wong
Dr. Paul T. Wong
• Difficulties with emotional regulation
• Difficulties with meaning attribution
• Difficulties with taking responsibility for one's wellbeing and future
• Difficulties with relationship skills
• Difficulties with coping resources and skills
• Difficulties with endurance and tolerance of suffering
• Difficulties with life intelligence or existential intelligence
WHAT CREATES PROBLEMS?
CREATING CHANGE
Meaning Therapy assumes that desirable changes depend on:
• Understanding and accepting the true meaning of one’s life situation
• Self and social validation of personal existence as being meaningful and worthwhile
• Pursuit and actualization of valuable life goals
HOW DO YOU FIND MEANING?
• Activity
⚬ Activities that are intrinsically valuable and interesting
⚬ Activities that are instrumental in attaining significant goals
⚬ Activities that are self- transcended and directed at serving others
• Experience - beauty, truth and love joy and wonder
• Attitude - acceptance in suffering
Discovering Meaning
Three types of values whereby one can discover meaning:
• ·Creative- what the person gives to the world
• ·Experiential- what the person receives from the world
• ·Attitudinal- adopting the right attitude of acceptance and taking a stand towards unavoidable suffering
MT GOALS
Develop a deeper understanding of cause- Not just symptoms
Develop a set of positive meanings as foundation upon which to build a fulfilling and productive life
Learn how to overcome internal and external obstacles to attain meaningful life goals
Learn to live productively in spite of certain unchangeable realities of life, such as suffering, aloneness, and anxiety
Improve relationship skills and connection with others
Stess & Trauma
an a%achment-based developmental perspec3ve
Gordon Neufeld, Ph.D.
Clinical & Developmental Psychologist
Founder of the Neufeld Institute Vancouver, Canada
A JACK HIROSE SEMINAR
Healing & Trea,ng Trauma Wounds
Richmond, B.C.
November 25, 2024
Copyright 2024 Gordon Neufeld, Ph.D. All rights reserved.
The handout is intended for registered par?cipants of this seminar only.
Please do notduplicate this document without permission.For more informa?on regarding the Neufeld Ins?tute or Dr. Neufeld and his work, please consult the website.
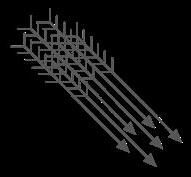
grieving to bouncing back stress Response role of relationship play & playfulness vulnerable feelings optimal functioning sense of safety TRAUMA
fight or flight impact of experience & exposure role of adaptation
tears of futility & sadness sense of strength rest and restfulness emotional defense recovery and healing nature of emotion neural plasticity vasovagal response
Chapter One
THE THREAT: an evolution in understanding Stess & Trauma
WALTER CANNON’S FIGHT-FLIGHT RESPONSE TO THREAT
• Harvard medical professor who studied the effects of physical danger on lab animals and formed his thesis in 1915, published in 1932 in the book “The Wisdom of the Body”
• his focus was on the situaQonal response to a threat to survival but made the mistake of isolaQng animals from their own species to survival
• studied the role of adrenalin and the sympatheQc nervous system in responding to threats to physical survival
FlIGHT
THREAT FIGHT
HANS SELYE’S STRESS RESPONSE (1940’S)
• was seeking a common physiological response that could account for the behaviours that Cannon had observed as a response to threat
• assumed that the FEAR system was the physiological pathway for stress, thus making the mistake that aggression came from fear
• assumed that harm or survival was the essence of threat
• since modified to include a third opQon – FREEZE (immobilizaQon or shutdown mediated by the vagus nerve) if flight or fight are not opQons
STRESs
about Hans Selye and the construct of STRESS
• Selye was a Hungarian-Canadian endrocrinologist who worked at McGill in the 30’s and 40’s and later at the University of Montreal
• popularized the construct of stress (word originates from ‘distress’ meaning coming apart) as a term for the generalized effect of threat on the body
• the term was borrowed from physics and engineering where it was used to describe the force exerted on a physical enQty (like a bridge) that would cause it to snap or come apart
• the term became immediately and immensely popular, influencing the vocabulary and thus thinking in many languages
• the term unfortunately gave the impression that stress was bad, leading to breakdown, something Selye tried in vain to correct
Adversive Childhood Experiences
REDUCE DISTRESSING EVENTS
Self-care is the logical deduction of this understanding if THREAT = STRESS LOAD
MANAGE IMPACT OF STRESS
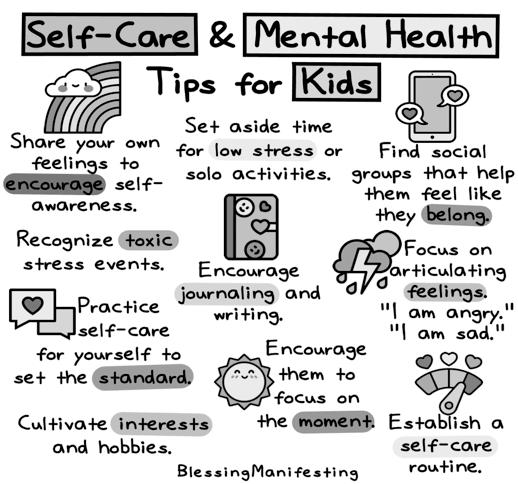
1. When kids pracQce self-care they learn to idenQfy their physical and emoQonal needs and can begin to take care of those needs.
2. PracQcing self-care at a young age allows kids to create a foundaQon that will benefit them as adults.
3. PracQcing self-care allows your child to develop healthy habits that they can benefit from in the future.
4. Your child will be able to become more independent and understand how to take care of themselves.
5. They will develop the skills necessary to keep themselves healthy mentally, physically and emoQonally.
THREAT
FACING SEPARATION = experience of separaSon
SEPARATION is thus the greatest threat
ATTACHMENT = SURVIVAL and is thus our preeminent drive
can’t be with ... not special to ... notunderstoodby... BETRAYED NOT LIKED BY ... feelingunlovedby... replacedby... isolation rejecQon not wanted discounted by ... lack of belonging can’tconnectwith... can’t hold on when apart feelingdifferent losing face not important to ... not recognized by ... threats to identity NEGLECTED NOT HELD ON TO BY ... loneliness not belonging not mafering to ...
Adversive Childhood Experiences
THREAT – an evolution in understanding
threat is to SURVIVAL STRESS itself is the threat
• reduce distressing events
SEPARATION
is the threat
REDUCE SEPARATION
• address issues of safety, food, health, & shelter via naturally developing ...
• manage the impact of stress
... ways to hold on when apart
... viability as a separate being
... resilience in the face of separa3on faced
If FACING SEPARATION is the THREAT,
togetherness is our answer! - and thus CASCADING CARE in the context of togetherness should become our ultimate focus
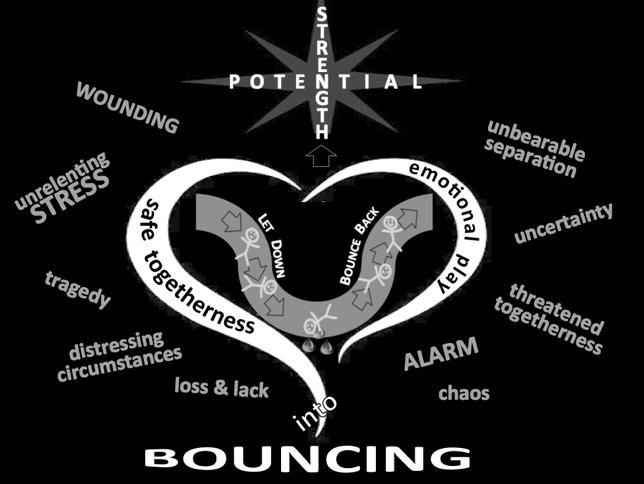
The WISDOM of the stress response Stess & Trauma
Chapter Two
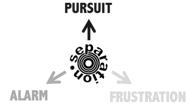
PURSUIT closure
THE STRESS RESPONSE ACTIVATES PRIMAL EMOTIONS cau3on ALARM
FRUSTRATION
separa3on-triggered change
Atachment’s Emergency First Aid Team
OUR MOTTO - “We promise to get emo5onal when holes appear in the fabric of your togetherness”
• gives the STRENGTH and TOUGHNESS needed to funcQon or perform in stressful or wounding circumstances
• instantly CHANGES one to be able to COPE with adversity & SURVIVE distressing circumstances
• taps all available resources to enable one to PERSEVERE in the face of distress and OVERCOME stressful circumstances
Resilience Response
ATTACHMENT’S EMERGENCY RESPONSE TEAM
acQvaQon of (alarm, frustraQon & pursuit)
FEELINGS that would interfere with performing or funcQoning in stressful circumstances are INHIBITED
Feelings that have been inhibited BOUNCE BACK to enable opQmal funcQoning and the full realizaQon of potenQal
SAFETY
THREAT
FACING SEPARATION
STRESS RESPONSE
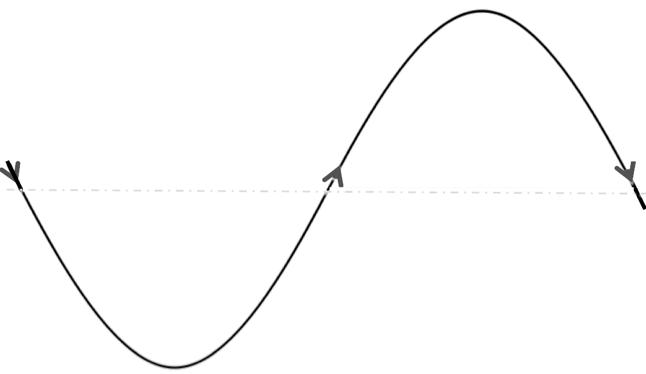
The brain’s naturally evolved emo3onal intelligence
STRESS RESPONSE
STRESS RESPONSE THREAT
RESILIENCE
The brain’s naturally evolved emo3onal intelligence
Is NOT a funcSon of reality NOR is it raSonal in any way; doesn’t even have to be a conscious feeling.
Recovery of feelings REMOVAL OF THREAT
RESILIENCE RESPONSE
The brain’s naturally evolved emo3onal intelligence
STRESS RESPONSE THREAT
RESILIENCE RESPONSE Recovery of feelings REMOVAL OF THREAT
The brain’s naturally evolved emo3onal intelligence
Atachment’s Emergency First Aid Team
OUR MOTTO - “We promise to get emo5onal when holes appear in the fabric of your togetherness”
“We also promise to hang around un5l fu5lity is felt”
When the fixes are fuQle, they need to be FELT as such.
as an afribute
SADNESS brings RECOVERY
HELP THAT IS HELPFUL!!
• keeping or restoring perspective
• right thinking / being positive
• pursuing happiness
• resisting the ‘let-down’
• acquiring the ‘skills’ of resilience
• pursuing calmness & tranquility
RETIREMENT trauma lossofsibling isolation rejecQon unloved loss of job hospitalization differentness losing face tragedy loss of child threats to identity
FACING DEATH
NEGLECT ABUSE loneliness MORTALITY emptynest not gelng one’s way
te nadir
loss of parent
Strength of DEFENSE Strength of BECOMING
- meant to be situa5onal - - meant to be characteris5c -
potenQal sQll unfolding found needed strength vs
OVERCAME
PERSEVERED
persisted despite distress growth force persists
came through distress seemingly ‘unscathed’
changed to withstand or cope with adversive or distressing condiQons
can funcQon or perform in highly stressful or wounding circumstances
SURVIVED
RESILIENT
ADAPTIVE
HARDY
feelings recover quickly aner Qmes of stress
transformed from inside out by adversity
heart was mended and spirits were revived doesn’t need to be sheltered from stress to preserve growth potenQal
Strength of DEFENSE Strength of BECOMING
- meant to be situa5onal -
potenQal sQll unfolding found needed strength vs
OVERCAME
- meant to be characteris5c -
came through distress seemingly ‘unscathed’
PERSEVERED
persisted despite distress growth force persists
changed to withstand or cope with adversive or distressing condiQons
can funcQon or perform in highly stressful or wounding circumstances
HARDY SURVIVED ADAPTIVE RESILIENT
feelings recover quickly aner Qmes of stress
transformed from inside out by adversity
results from a of feeling results from a of tender feeling
heart was mended and spirits were revived doesn’t need to be sheltered from stress to preserve growth potenQal
Stress Response
Resilience Response
ATTACHMENT’S EMERGENCY RESPONSE TEAM
acQvaQon of (alarm, frustraQon & pursuit)
FEELINGS that would interfere with performing or funcQoning in stressful circumstances are INHIBITED
Feelings that have been inhibited BOUNCE BACK to enable opQmal funcQoning and the full realizaQon of potenQal
SAFETY
as judged by the brain’s innate intelligence
sadness ie, feelings of fuQlity re brain’s emoQonal ‘fixes’
Stress Response
acQvaQon of (alarm, frustraQon & pursuit)
ATTACHMENT’S EMERGENCY RESPONSE TEAM
FEELINGS that would interfere with performing or funcQoning in stressful circumstances
are INHIBITED
TRAUMA is NOT what happens to us but what fails to happen within us in response, ie, the lack of a follow-up resilience response that includes SADNESS
Trauma is not an event but a stuck stress response
STRESS RESPONSE
TRAUMA
The brain’s naturally evolved emo3onal intelligence
Chapter Four Stess & Trauma
Signs of a Stuck Stress Response (ie, trauma)
Missing Key Feelings
Brain’s Backup Defenses
FIVE POINT ASSESSMENT of a STUCK STRESS RESPONSE
Stuck Primal Emo3on
Resilience Response is Lacking
STRESS RESPONSE THREAT
Recovery of feelings REMOVAL OF THREAT
RESILIENCE RESPONSE
- stuck in the WORK MODE
- lacking curiosity - lacking emergent or venturing forth energy
RESTLESSNESS
feltplay feltrest felt ftlit the vital signs of well-being
- past history of ungrieved losses
eg, sadness, sorrow, disappointment, grief
- stuck in fuQle endeavours /unable to let go / brain unable to find work-arounds for impediments
eg, cared for, cared about, caring deeply about, etc
eg, sorry, remorseful, guilty about, bad about
feeling RESPONSIBLE
AGITATION PARANOIA ADRENALIN-SEEKING
feeling ALARMED
feelings re CARE
FEELINGS of ATTACHMENT that may go MISSING ... when facing separaQon
feelings of DEPENDENCE eg, needy, trusjul vulnerable
feelings of ANGER ... when personally mistreated
feeling FULL or EMPTY eg, fulfilled, saQated, missing, longing, afachment ‘holes’ BOREDOM
What BOREDOM is about
When the ‘holes’ in togetherness are NOT sufficiently FELT, it is experienced as BOREDOM.
Boredom-a natural barometer for deficits of feeling - can’t feel the true nature or shape of the hole that exists within -
SIGHT & HEARING
TOUCH & SMELL
feelings of SENSATIONS that may be restricted sensing PAIN sensing BLADDER/BOWEL PRESSURE sensing COLD
& SOILING WETTING
Impact of the
STress Response
- a loss of tnder feeling -
CONFUSING SIGNS OF A WORKING STRESS RESPONSE
the loss of so-called ‘nega3ve’ feelings is typically misinterpreted posi3vely
no longer talks about what distresses or hurt feelings no longer feels unsafe or alarmed no longer reads rejecSon or feels its sSng
be^er able to funcSon or perform under duress no longer given to sadness and disappointment
no longer feels as needy, empty, lonely or dependent no longer is as visibly affected by loss and lack
SIGNS OF AN ACUTE STRESS RESPONSE AFTER A DISTRESSING EVENT
- typically referred to in the ‘disorder approach’ as a post-traumaQc stress syndrome or disorder
Blinded by:
• ‘empathy’ • diagnoses • ‘dysregulaSon’
ALARM
- elevated startle response - flashbacks and nightmares
- avoidance of whatever alarms
- intrusive thoughts & memories
- unable to focus and concentrate
PURSUIT
moreemotionbutlessfeeling
- hyper-arousal and hyper-vigilence
IMPULSIVENESS
FRUSTRATION
- irritability and impaQence
- erupQons of afacking energy - self-afack and suicidal impulses
SIGNS OF STUCK PRIMAL SEPARATION EMOTIONS
- clutching, clinging, possessing, hoarding, acquiring, impressing, pleasing, etc - fragmented fixes & fixaQons with pursuit as the theme – winning, placing, hunQng, chasing, afracQng, demanding, reducing, seeking, enhancing, etc - preoccupaQons with altering self in pursuit of belonging, love or significance
- irraQonal obsessions
- irraQonal avoidance
PURSUIT ALARM
- anxiety reducing behaviour
- an afracQon to what alarms - inability to stay out of trouble - recklessness and carelessness
- afenQon deficits around alarm
moreemotionbutlessfeeling
- preoccupaQons with concealing oneself in pursuit of belonging, love or significance
- anxiety FRUSTRATION
- fits & tantrums
- hilng and fighQng
- obsessions with change
- aggression and violence
- rudeness and meanness
- irritability and impaQence
- chronic agitaQon and restlessness
- erupQons of afacking energy - self-afack and suicidal impulses
THE SEPARATION COMPLEX – A LEGACY OF TRAUMA - the telltale marks of trauma on personality -
- the telltale (but reversable) marks of trauma on personality -
stuck
PURSUIT
stuck in defensive detaching and transference
stuck in defensive alpha or over-dependence
stuck stuck
ALARM
FRUSTRATION
stuck in a defensive flight from feeling & vulnerability (ie, a stuck stress response)
STRESS RESPONSE THREAT
RESILIENCE RESPONSE
Recovery of feelings REMOVAL OF THREAT
Feelings are the mind’s READINGS of emoQonal feedback
depresssion = fla^ened affect
ethreat to attachment can trigger a defensive depressing of emotion m
about defensive detaching
If the separaSon faced is deemed unbearable, the brain can reverse direcSon of the pursuit in an automated a^empt to reduce the threat. The a^achment drive itself cannot be reversed since it is the default and preeminent drive and only increases under threat.
• can be situaQonal or pervasive, physical or emoQonal, parQal or complete
• can involve DEFENSIVE TRANSFERENCE to other persons such as one’s peers and famous figures (includes fantasy afachments)
• can involve the DEPERSONALIZATION of afachment (ie, detaching from persons and afaching instead to pets, groups, objects, naQons, race, ideas, possessions, poliQcs, etc, etc, etc)
• depersonalizaQon can also result in fragmented pursuit – FIXES & FIXATIONS – which are highly addicQng because they cannot fulfill or deliver care
hoarding collecQng
chasing marks clinging clutching possessing achieving
PURSUING PRAISE
WINNING
Some common a^achment-driven where the pursuit is divorced from its relaSonal context: FIXES & FIXATIONS
going for hugs/smiles acquiring seeking status pursuing sameness hunQng for sex PORNOGRAPHY chasing applause
seeking afenQon scoring
placing chasing approval
Stess & Trauma
Chapter Five
The RECOVERY of FEELINGS
Stress Response
Resilience Response
ATTACHMENT’S EMERGENCY RESPONSE TEAM
FEELINGS that would interfere with performing or funcQoning in stressful circumstances are inhibited
Feelings that have been inhibited bounce back to enable opQmal funcQoning and the realizaQon of full potenQal
Provide SAFETY through • RELATIONSHIP • PLAY
RECOVERING FEELINGS
- making it safe to feel -
Where the helper can be ANYONE but preferably a caring adult to whom the child or adult is a^ached or will a^ach
PLAY
RELATIONSHIP helper
acQvaQon of alarm, frustraQon & pursuit applying relaSonal and emoSonal first-aid
• convey a strong CARING ALPHA presence to inspire dependence
• COLLECT to engage and invite dependence
• COME ALONGSIDE emoQonal experience
• support EXISTING ATTACHMENTS with caring adults
• BRIDGE problems and all separaQons
RELATIONSHIP
Helping via Relationship
• convey a strong CARING ALPHA presence to inspire dependence
• COLLECT to engage and invite dependence
• COME ALONGSIDE emoQonal experience
• support EXISTING ATTACHMENTS with caring adults
• BRIDGE problems and all separaQons
RELATIONSHIP
• convey TRUST in their strength to cope (vs over-protecQon)
• provide CARE (including food) in the context of connecQon
• matchmake to embed in CASCADING CARE
We are meant to fit together in hierarchical attachment arrangements of CASCADING CARE
a NATURAL arrangement in harmony with the dynamics of afachment and the principles of development
as opposed to contrived arrangements based on social roles, gender stereotypes, prevailing assumpQons of equality, or parQcular dynamics between parents and children or between partners of a couple or in friendship
Our objective should be to embed in CASCADING CARE as opposed to pushing for independence or promoQng self-care
Helping via Relationship
• convey a strong CARING ALPHA presence to inspire dependence
• COLLECT to engage and invite dependence
• COME ALONGSIDE emoQonal experience
• support EXISTING ATTACHMENTS with caring adults
• BRIDGE problems and all separaQons
RELATIONSHIP
• convey TRUST in their strength to cope (vs over-protecQon)
• provide CARE (including food) in the context of connecQon
• matchmake to embed in CASCADING CARE
• create SAFE SPACES for feelings to bounce back
ADULT
(eg, parent, teacher, therapist)
SPACE FREE : SPACE FREE : wounding teaching problemsolving screens & distractions
(or client)
Create timely spaces for feelings to bounce back
• AFTER times of stress including separation, school, strained interactions, discipline, special performances, wounding, loss, etc
• ideally BEFORE sleep or the passing of time interferes with the ability of the thinking brain to interpret emotional feedback and link to the situations that stirred one up
• FREE of digital pursuit (social or videogames) and other competing activities
• FREE of problem solving, judgment, correction or teaching
• through RITUALS involving safe relationships and/or emotional playgrounds
Through another’s attachment to us, we can BE their ANSWER even when there are no answers:
• BE their HOME
• BE their place of REST
• BE their sanctuary of SAFETY
• BE their SHIELD in a wounding world
• BE their REASON for holding on
• BE their source of WELL-BEING
The answer is in BEING - not in DOING or SAYING or KNOWING the right things – when empowered by the other’s attachment to us.
RECOVERING FEELINGS
- making it safe to feel -
Where the helper can be ANYONE but preferably a caring adult to whom the child or adult is a^ached or will a^ach
• provide MATERIALS to draw, paint, construct, make crans, make music, priming the acQvity where necessary
• sing or hum LULLABY- type songs if possible, to harness their emoQonal and connecQve power
• if defended against closeness, engage in PLAYFUL CONNECTION, providing brief ‘accidental’ experiences of contact that are able to disarm
• engage in the CULTURAL PLAY, ie, the dances, music, art, of their culture of origin
Inviting Instincts & Emotions to Play
• provide opportuniQes to play out ALARM as well as alarming scenarios, while safely in the context of play where it is one step removed and doesn’t count for real
• give residual FRUSTRATION some playful expression via games of construcQon and/or destrucQon
• give SEPARATION- TRIGGERED-PURSUIT safe expression through games or acQviQes characterized by the hunt, the chase, or the find
PLAY
• give ALPHA insQncts safe expression through playing the leader, the boss, the superhero, the rescuer, the one in charge, the one giving the orders
• provide plenty of opportunity for PRETENDING to be someone or something else
• give DEPENDENT insQncts safe expression through playing the baby, the pet, the sick, the wounded, the one in need of care
... in our pursuit of happiness
... in avoiding negaQve thoughts
... in afempQng not to be upset
... in trying to stay in perspecQve
... in afempQng to stay opQmisQc
... in trying to cheer each other up
... in pulng limits on grief and sorrow
... in denying that the glass is half empty
... in trying to change the Eeyores into Tiggers
into the SADNESS whose task it is to facilitate needed endings, strengthen as required, and deliver us back to what happiness exists
Wherewillsit WhoI’llsitwith Weather? Whattimewe’llget back Wherethebathrooms are Bugs? Howmuchwalking? Allergicreaction •Snackbreaks Ifthebuswillbeon time Howbusyit’llbe Howloudit’llbe
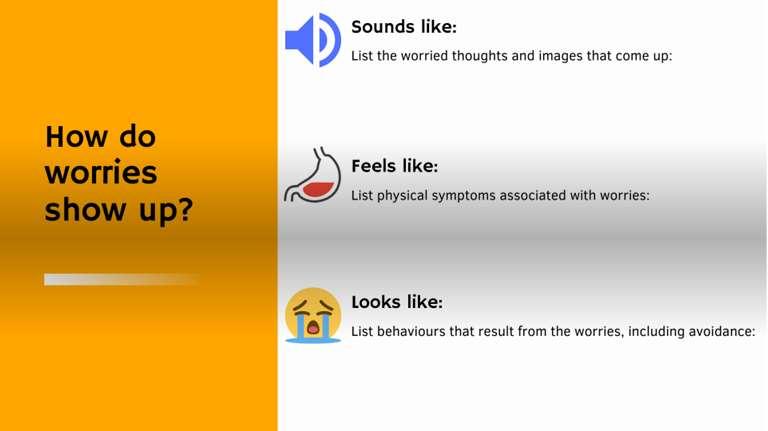
Academic anxiety refers to the feelings of worry, tension, or dread that are associated with academic settings or tasks.
1. The Generation of Testers
2. Students are overwhelmed by the pressures to succeed
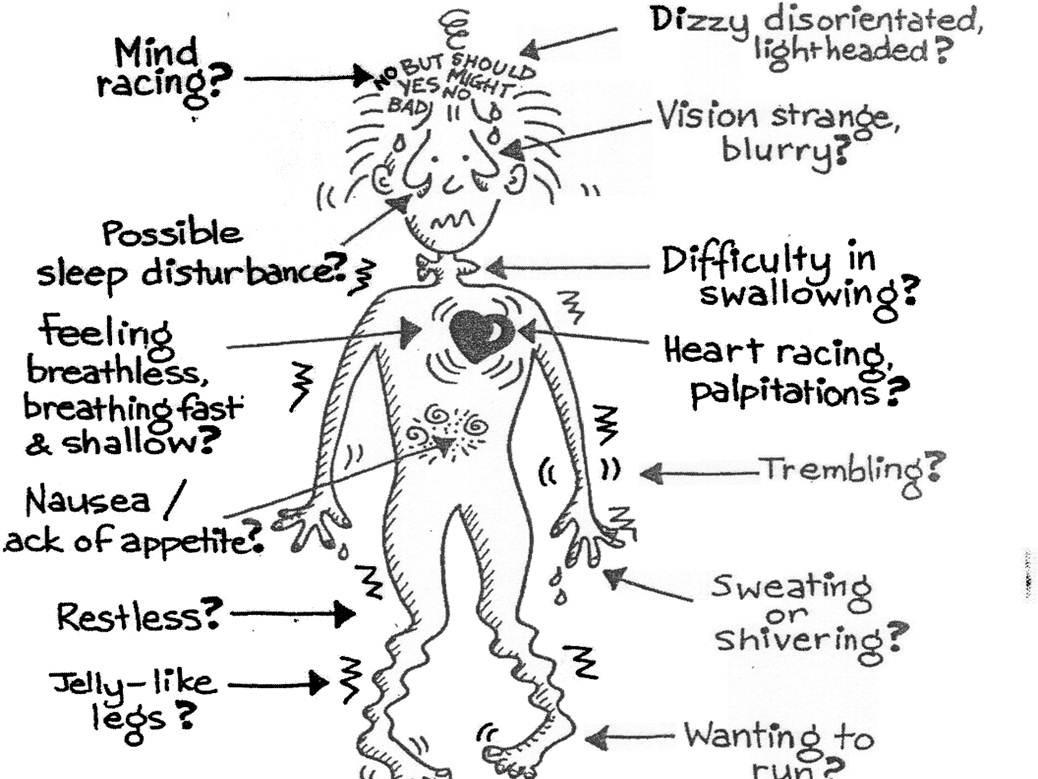
3. What are the Signs? Anxious students may express their fears by:
a. crying or throwing tantrums, seek constant approval or reassurance from others, headaches, stomachaches, racing heartbeat, or difficulty breathing.
4. “In the Pew survey of teens, academic pressure tops their list of stressors: 61 percent say they face a lot of pressure to get good grades.”
5. SINCE COVID - 19 shown an increase in general anxiety in children under 17
Has the potential to negatively impact all aspects of life, including social relationships, academic performance, emotional wellbeing, and future work opportunities
1. Social Media Binging can lead to lower self-esteem and fatigue
2. Social Change
3. Constant notifications, comparisons to others, pictures of events they weren’t invited to, pressure to get comments and “likes”
5. Parents support - empathetic support, structure, reassurance, and boundaries
Shortness of breath
Heaviness in their body/muscle fatigue
Dry mouth
Clammy hands
And more!
Case study: Phoebe
9 Years Old
Mother died from drug overdose
History Of Physical And Sexual Abuse
Living in a Residential Group Home
(No father involved)
1. Deep breathing exercises: Bubble Breaths
2. The power of positive self- talk & Affirmations: “I can do hard things!”
3. Healthy Nutrition & Sleep Schedule
4. Activity focusing on bodily regulation yoga is a great place to start, look into Somatic practices.
5. Understand, don’t invalidate.
6. Positive Interactions
7. Play!
8. Take the pressure off!
9. Co- Regulation Rituals: family dinners, tea time,
10. Parent Groups/Sessions
11. Family/Parent Meetings
12. Modeling self- care, boundaries, assertive communication and self- efficacy
13. Provide Safe Spaces
14. Tools to use:
a. Fidgets
b. Therapy :)
c. Normalize asking for support and recognizing “anxiety tics”
You cannot put your seatbelt on in the middle of a car accident
1. Don’t try to eliminate their anxiety
2. Don’t avoid things just because they make your child anxious
3. Express positive - but realistic - expectations
4. Respect their feelings, but don’t empower them
5. Don’t ask leading questions
6. Don’t reinforce your child’s fear
7. Be encouraging
8. Keep the anticipatory period short
9. Think things through together
10. Model healthy ways of handling anxiety
Draw what scares you
Draw what makes you feel brave DO
● Limit news and images
● Be honest But reassuring
● Say “It will be OK”
● Validate their feelings
● Talk about anxiety
● Talk about other feelings
● Seek professional help, if needed
DON’T
● Avoid the scary things
● Minimize their feelings
● Excessively discuss your own fears
Case study: Rebecca 8 years old:
1. What feelings do you have about (given situation)?
1. What color is that feeling?
1. What shape is it?
1. Where in your body do you feel it?
1. Does it move around or stay in one place?
1. Does that feeling make you do anything?
Safe Place drawing
1. What can you see?
2. What can you hear?
3. What can you smell?
4. What can you taste?
5. What can you feel?
Draw a Heart
1. Turn the paper over to back
2. List 5- 7 feeling
3. Choose a color for each feeling
5. Flip paper back over to the heart
4. Draw how much of each feeling you have right now
1. Draw the Yucky
1. Draw the opposite of the Yucky
1. Imagine that something magical could come along and change the first drawing into the second drawing. What would your magic look like?
Deep breathing exercises 2. The power of positive self- talk & affirmations 3. Healthy nutrition & sleep and daily schedule 4. Activity focusing on bodily regulation
a. Yoga
b. Somatic practices
5. Listen, don’t invalidate.
6. FOSTER RESILIENCE
Start early
Be consistent
Make it part of your routine
1.
Let them Fail
Self Regulation
Self Care
Service to Others
Ask for Help
Act Confident
● Positive physical development
● Academic achievement/intellectual development
● Good coping skills and problem- solving skills
● Engagement and connections in two or more of the following contexts: school, with peers, in athletics, employment, religion, culture
● High self- esteem
● Clear and stable expectations
● Self Efficacy
● Emotional self- regulation
Stick Person Drawing
Something above
Anything else
Holding something
Standing on something
Wearing something
Something beside
Dropping something
Wearing something else
Practice Prevention
Reduce Frustration To Reduce Tantrum Frequency
Don’t give in to Demands
Stay Calm
Humor and/or Distraction
Don’t take it Personally
Differentiate between feelings and behaviors Model appropriate anger management
Establish anger rules
Case Study: Kenji 11 years old
Oppositional Lying Stealing Acting out
Mother died of cancer when he was 5 - living in Japan
Moved in with maternal aunt, and she dies of cancer when he was 7yo
Moved to US to live with maternal Uncle and Aunt
Be consistent Teach healthy coping skills
Consequences when necessary
1. Draw your yucky feeling
2. Use colors, shapes, lines 3. Crumple it up 4. Open it - Say something to it 5. Rip and tear it up
6. Throw half away
7. Write the opposite feeling on the colored papertear into 3 equal parts
8. Give away your opposite feelings
9. Take away someone else’s yucky
10. Collage the parts back together
Play “Freeze!Focus!”
Make Memory Musical
Make the Day a Story
Puzzles and Play
Help children to be in control
Watercolor Paints, blow with straws
Control Breathe
Be intentional
Have fun
Learn to delay gratification - “make future me happy”
● Frequent worrying
● Trouble concentrating
● Skipping activities they used to enjoy
● Difficulty with sleep
● Clinging to caregivers
● Extreme focus on safety and health
● Irritability or edginess
● Shutting down
● Repetitive behaviors
1. Name their feelings
1. Talk about the feeling
1. Identify where in the body those feelings manifest and live
1. Recognize the connection between thoughts and feelings
1. Learn to separate thoughts, feelings and behaviors
● Frequent worrying
● Trouble concentrating
● Skipping activities they used to enjoy
● Difficulty with sleep
● Clinging to caregivers
● Extreme focus on safety and health
● Irritability or edginess
● Shutting down
● Repetitive behaviors
● Delayed Gratification
● Self Restraint
● Trusting the Process
● Encourages Creativity
● Increased Self- Esteem
“Art, like morality, consists of drawing a line somewhere”
- an a%achment-based developmental approach -
Gordon Neufeld, Ph.D.
Copyright 2024 Gordon Neufeld, Ph.D. All rights reserved.
The handout is intended for registered par?cipants of this seminar only.
Please do notduplicate this document without permission.For more informa?on regarding the Neufeld Ins?tute or Dr. Neufeld and his work, please consult the website.
www. neufeldins,tute.org
The Current Crisis of WellBeing
what is happening to our kids?
an a$achment-based developmental perspec3ve
Gordon Neufeld, Ph.D. Developmental & Clinical Psychologist
The current Crisis of WellBeing
- some facts and figures -
• school-aged children suffered an approximate 40% increase in depression, anxiety, irritability and aLenMon problems over the span of the pandemic. Studies indicate these problems are not abaMng.
• during the pandemic, adolescent psych wards were filled, children’s help lines were overwhelmed, and self-reports of anxiety and depression were unprecedented
• suicides and cuTng were increasing before the pandemic, conMnued to do so through the pandemic, and are sMll on the rise
• some studies reported that up to 70% of children experienced harm to their mental health when isolated from their peers (in contrast to about 20% who thrived when sent home from school)
• most experts assumed that being socially isolated from peers must be bad for the mental health of children and so prescribed more peer interacMon as a result
Current Crisis Crisis of WellBeing
ARGUMENT for WELL-BEING being ROOTED in ATTACHMENT
THEORY:
• togetherness is our preeminent drive and as such, has the most profound and widespread impact on emoMonal, mental and developmental processes and dynamics
• togetherness replaces survival as a drive in evoluMon, as survival becomes a natural outcome of togetherness
• the ‘trouble spots’ in our brain have evolved from emoMon extending the reach of insMnct - aLachment being our primary drive
ARGUMENT for WELL-BEING being ROOTED in ATTACHMENT
SOME OF THE EVIDENCE:
• longitudinal study of adolescent health and well-being
• loneliness research which reveals togetherness as the answer to well-being
• happiness research which reveals the key factor as being embedded in caring relaMonships
• marriage research that reveals longevity, health, and well-being as resulMng from being in caring relaMonship
• famous Harvard 2023 study revealing that being embedded in caring relaMonships is the #1 factor in well-being
The most consistent and widespread finding is that those embedded in a context of CARING ATTACHMENTS are found to be less at risk for mental health issues and problems
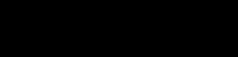
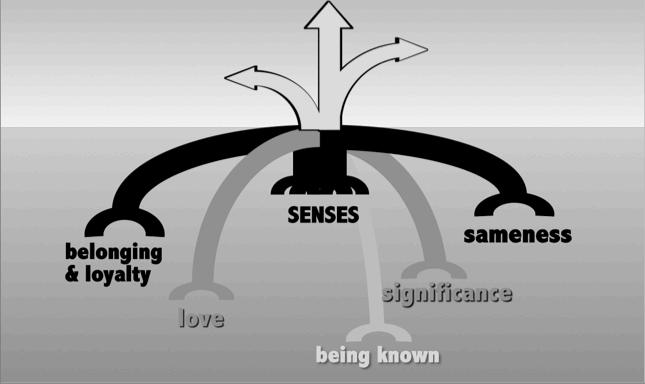
NATURE’S TEMPLATE FOR GIVING AND RECEIVING
Attachments are specifically structured for giving & receiving CARE ... signals ... care
SEEKING CARE
dependent insMncts dependent instincts
• for an invitation to exist
• for contact and connection
• for sameness & belonging
• for safety and comfort
• to get one’s bearings
• for warmth & love
• for recognition
• for significance
• for understanding
• for a relational ‘home’
PROVIDING seeking
PROVIDING CARE
alpha instincts
• for a sense of togetherness
We are meant to fit together in hierarchical attachment arrangements of CASCADING CARE
a NATURAL arrangement in harmony with the dynamics of aLachment and the principles of development
as opposed to contrived arrangements based on social roles, gender stereotypes, prevailing assumpMons of equality, or parMcular dynamics between parents and children or between partners of a couple or in friendship
Our objective should be to embed in CASCADING CARE as opposed to pushing for independence or promoMng self-care
making sense of the
Current Crisis Current Crisis of WellBeing
threats to identity NEGLECT
both parents working
loneliness CHANGE moving school
adopMon daycare DIVORCE facing DEATH RETIREMENT anothersibling
isolation failure being LOST secrets bedtime hospitalization residenMal school disability losing face personal injury loss of loved one
ABUSE
loneliness not belonging not maLering to ...
can’t be with ... not special to ... notunderstoodby... BETRAYED NOT LIKED BY ... feelingunlovedby... replacedby... isolation rejecMon not wanted discounted by ... lack of belonging can’tconnectwith... can’t hold on when apart feelingdifferent losing face not important to ... not recognized by ...
threats to identity NEGLECTED NOT HELD ON TO BY ...
cau$on ALARM
closure separa$on-triggered change
PURSUIT
FRUSTRATION
Stress Response
Resilience Response
PRIMAL SEPARATION EMOTIONS ARE ACTIVATED
Feelings that have been inhibited bounce back to enable opMmal funcMoning and the realizaMon of full potenMal
FEELINGS that would interfere with performing or funcMoning in stressful circumstances are inhibited the recovery of feelings requires a sense of SAFETY
TIME (ideally the end of the day or end of the week at most)
EMOTION IS AT THE HEART OF THE MATTER
• emoMon is in charge of managing the brain, including development, prioriMes, aLenMon, and memory
• the stress response is emoMonal in nature
• emoMonal processes precede and undergird mental processes – in evoluMon, in development, and in everyday funcMoning
EMOTION NEEDS TO MATTER TO US
• most problems in learning, aLenMon, and maturaMon are rooted in emoMon
• adaptaMon (including healing & recovery) is an emoMonal process
• mental processes are primarily derivaMves of emoMon, rather than the other way around
• almost all troubled thinking and behaviour (including diagnoses) are found to have roots in emoMon
• emoMons need to be resolved to reduce symptoms as well as to effect deep and lasMng change
EMOTION IS STILL DISCOUNTED & ECLIPSED
EMOTION IS AT THE HEART OF THE MATTER
STILL MISREAD & MISINTERPRETED
• emoMon is in charge of managing the brain, including development, prioriMes, aLenMon, and memory
• the stress response is an emoMonal process
• emoMonal processes precede and undergird mental processes – in evoluMon, in development, and in everyday funcMoning
EMOTION NEEDS TO MATTER TO US
MORE CONCERNED WITH MANAGING EMOTIONS THAN UNDERSTANDING THEM MOST MEDICATIONS NUMB EMOTION WITH LITTLE PROTEST FROM SO-CALLED EXPERTS STILL CONSIDERED INFERIOR TO REASON
• almost all troubled thinking and behaviour (including diagnoses) are found to have roots in emoMon
MEDICAL DIAGNOSES STILL ECLIPSE THE ROLE OF EMOTION
• most problems in learning, aLenMon, and maturaMon are rooted in emoMon
WOMEN & CHILDREN STILL BLAMED FOR BEING TOO EMOTIONAL
MORE CONCERNED WITH ‘CALMING DOWN’ THAN MAKING ROOM TO BE ‘STIRRED UP’
• adaptaMon (including healing & recovery) is an emoMonal process
• mental processes are primarily derivaMves of emoMon, rather than the other way around
STILL ECLIPSED BY THEIR EFFECTS ON COGNITION & BEHAVIOUR
• emoMons need to be resolved to reduce symptoms as well as to effect deep and lasMng change
KEY INSIGHTS REGARDING E M O T I O N
• there is PURPOSE to emoMon - it is Nature’s way of moving us and taking care of us
• each emoMon has specific WORK to do (ie, emoMons are Nature’s workforce)
• emoMons need sufficient REST in order to do be effecMve in their work
• emoMons seek RELIEF through expression but this will be thwarted if working aLachments are threatened
• emoMons need to be RESOLVED in some way or another or they will get stuck
• the emoMonal system needs to DEVELOP for opMmal funcMoning but can only do so if condiMons are conducive
• the emoMonal system begins in the ‘EITHER OR’ mode and is meant to mature into ‘THIS AND’ funcMoning where inner conflict is felt
• emoMons need to be FELT for opMmal funcMoning and for children to flourish
Stress Response
PRIMAL SEPARATION EMOTIONS ARE ACTIVATED
FEELINGS that would interfere with performing or funcMoning in stressful circumstances are inhibited
The core emo3onal condi3on underlying mental health problems is
Resilience Response
Feelings that have been inhibited bounce back to enable opMmal funcMoning and the realizaMon of full potenMal
the recovery of feelings requires a sense of SAFETY
MOREEMOTIONBUTLESSFEELING
TIME (ideally the end of the day or end of the week at most)
The Continuum of ALARM Problems
ANXIETY problems (obsessions & compulsions)
feel unsafe but alarm not linked to the separa$on faced
alarm is displaced alarm is perverted alarm is dysfunc;onal
AGITATION, ATTENTION, & DISCIPLINE problems
driven by alarm that is not felt
ADRENALIN SEEKING problems
devoid of feelings of alarm, fu$lity & vulnerability
including cuVng & burning
The Continuum of Aggression Problems
EXISTENCE of attacking impulses
ERUPTIONS of attacking energy
VIOLATING aggression problems
not feeling the fu$lity of changing the frustra$ng circumstances
including suicidal impulses
devoid of feelings of alarm, fu$lity & vulnerability
Stress Response
Resilience Response
PRIMAL SEPARATION EMOTIONS ARE ACTIVATED
FEELINGS that would interfere with performing or funcMoning in stressful circumstances are inhibited
Feelings that have been inhibited bounce back to enable opMmal funcMoning and the realizaMon of full potenMal
the recovery of feelings requires a sense of
SAFETY
TIME (ideally the end of the day or end of the week at most)
More Wounding in today’s world
SAFETY
interac3on
scrip3ng & supervision
The experience of SAFETY required for the recovery of feelings is ...
... NOT a func3on of reality, percep3on or cogni3on
... an inherent wired-in state of the brain when in one of two basic modes
1. the a$achment drive in the dependent mode where closeness is experienced and seems secure
2. the play drive where emoMons are at play attachment-based safety play-based safety
less empathy
more bullying
ADULT
CHILD
more social interac3on
less scrip3ng & supervision
less empathy
more bullying
ADULT
We must HAVE their hearts before we can protect their hearts
CHILD
more social interac3on
less scrip3ng & supervision
less empathy
more bullying
ADULT
We must MATTER MORE than those who are wounding the child
CHILD
more social interac3on
less scrip3ng & supervision
NOT work NOT for real expressive PLAY
Feelings are recovered when emotions are at play!
The current Crisis of WellBeing
Why are today’s kids not receiving the CARE they need, nor experiencing the SAFETY they require for the spontaneous recovery of their feelings? what is happening to our kids?
1. They are NOT depending upon the adults who care.
2. The proximity in their aLachments is constantly threatened, depriving them of the SAFETY required to recover their feelings.
3. They are NOT engaging in the kind of play that provides the SAFETY required to recover their feelings.
Our children are losing their play, especially their emo$onal play:
• although play is a natural insMnct & primary drive, it is not demanding and so requires space, as well as protecMon from compeMng acMviMes
• SPORTS PLAY has become organized and outcome-based, compeMng with ‘play for play’s sake’
• creators of DIGITAL SCREEN GAMES primarily harness the more robust aLachment drive (eg, winning, dominaMng, placing) which is outcome-based, highly addicMve in this depersonalized form, and takes the place of the kind of play that children truly need
• ENTERTAINMENT has become universally accessible, replacing and suffocaMng the more fragile expressive play children require
• PARENTS now seek acMviMes to help their children ‘GET AHEAD’, at the expense of the play children need to get ahead developmentally
• SCHOOLS are becoming more OUTCOME DRIVEN, reducing the playful acMviMes that are required for healthy development to occur
The current Crisis of WellBeing
what is happening to our kids?
Why are today’s kids not receiving the CARE they need, nor experiencing the SAFETY they require for the spontaneous recovery of their feelings?
Because they are NOT depending upon the adults who care, their aCachments are con;nually threatened, and they are NOT engaged in true play.
WHY is this so?
Their ATTACHMENT INSTINCTS are AWRYPEER ORIENTATION
PEER ORIENTATION
Children taking their cues from each other as to how to act, what to do, how to talk, what to wear, how to express oneself, what is valued, what is expected, what is right and what is wrong The compe3ng nature of most peer a$achments today (ie, can’t be close to both peers and adults simultaneously) pulls children out of orbit from around the adults responsible for them.
THE PROBLEMS WITH PEER ORIENTATION
• does NOT serve survival as children were not meant to take care of each other
• destroys the natural context for raising & educaMng children
• robs adults of the power they need to parent, teach and treat
• breeds ALPHA children and fosters DEPERSONALIZATION
• fuels a preoccupaMon with digital devices and social media, which further compete with family
• the more peers maLer, the more separaMon to be faced, resulMng in escalaMng emo3onal distress
• robs children of the shielding and protecMon they need to live in an wounding world
• is not conducive to feeling, as the vulnerability is too much to bear
• can result in chaoMc polarizaMon & tribaliza3on which in turn can create a ‘lord of the flies’ scenario
positive polarity negative polarity shies away from resists contact alienates looks down upon ignores & disregards mocks & mimics disowns opposes & betrays holds in contempt ridicules and derides spoils things for discounts as not ma$ering annoys and irritates eschews loathes keeps secrets from or creates secrets about
seeks to be with makes contact endears looks up to a$ends & listens to imitates & emulates possesses is loyal to holds dear a$empts to find favour makes things work for seeks to ma$er to seeks to please befriends loves shares secrets with or keeps the secrets of
society is not structured to facilitate peer togetherness
The PEER-ORIENTED ...
SUFFER more WOUNDING ...
eleva3ng the separa3on-triggered emo3ons of alarm, frustra3on and pursuit ...
while losing the very feelings that would lead to their resolu3on.
• stuck in the aLachment drive resulMng in developmental arrest and loss of playfulness
attaching to PARENTS and other adults responsible for the child
emergence into PERSONHOOD
PEERS
able to relate to PEERS without loss of individuality or loss of adult attachment
The current Crisis of WellBeing - some facts and figures -
• during the pandemic, adolescent psych wards were filled, children’s help lines were overwhelmed, and self-reports of anxiety and depression were unprecedented
• suicides and cuTng were increasing before the pandemic, conMnued to do so through the pandemic, and are sMll on the rise
• most experts assumed that being socially isolated from peers must be bad for the mental health of children and so prescribed more peer interacMon as a result
Reversing peer orientation should be a top priority in the support of our children’s well-being
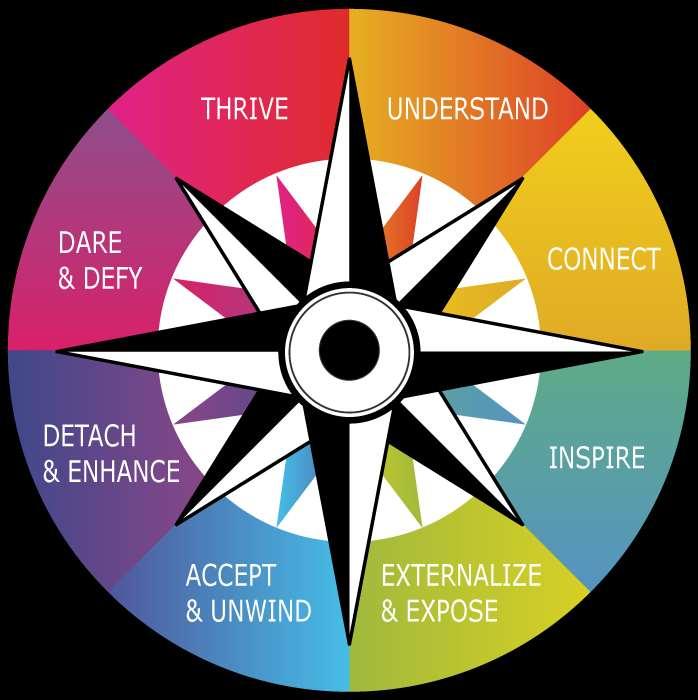
• a COMPASS POINT to orient by (regarding what’s happening but especially regarding their strengths, uniqueness & contribuMons)
• a HOME BASE, GUIDE or COMFORTER if needed
• for NURTURANCE – offering a ‘TOUCH OF PROXIMITY’ to hold on to
- a sign of belonging, or something special that belongs to us
- a likeness or similarity, something held in common
- a touch of loyalty – that we will come to their side and alongside
- a sign of significance, something beyond the role expectaMons
- a touch of warmth or delight, something that suggests liking
- a sign that we truly get them or understand them
- some sign of being welcomed and invited into our presence
Three Common ATtachment Disorders
... and how they impact received care and recovered feelings
1. PEER ORIENTATION
3. DEPERSONALIZED ATTACHMENT
Typical manifesta;ons of alpha children
bossy, controlling or demanding
compelled to take over or take charge
difficulty with taking direcMon or asking for assistance
obsessed with winning or being seen as the best
can be driven to dominate or show superiority
seeks to be on top or take front stage
driven to trump interacMon, to have the last word
may need to be in the know / can act as a know-it-all
Typical manifesta;ons of alpha children
bossy, controlling or demanding
compelled to take over or take charge
difficulty with taking direcMon or asking for assistance
can be driven to dominate or show superiority
- is part of the ATTACHMENT drive which is Nature’s answer to SURVIVAL for birds and mammals
- it’s ulMmate purpose is to take CHARGE of the CARE of one’s dependents
- is meant to create a LEAD in the aCachment dance, inspiring trust and dependence in response
seeks to be on top or take front stage
driven to trump interacMon, to have the last word
may need to be in the know / can act as a know-it-all
obsessed with winning or being seen as the best an alpha complex has formed when these aQributes characterize their personality or their rela$onships with adults who care for them
- requires extensive taming and development to turn the raw displacement insMncts into an effecMve ALPHA CARING RESPONSE
- should never be characterisMc of an individual, only an aLachment DANCE with a ‘dependent’ in need
- successful development requires ample PRACTICE in a context rich with FEELING,
- if characterisMc of a child, can seriously INTERFERE with development and being taken care of, including being parented or taught
FEELINGS convert raw displacement into ALPHA CARING
- unites primi;ve displacement ins;ncts with their ul;mate care-taking
PURPOSE
feelings of CARING & RESPONSIBILITY
- develops the capacity for CONSIDERATION - necessary to make caring effec;ve
feeling CONFLICTED
(can begin between 5-7 years but only if condi;ons are conducive)
feeling the FUTILITY of controlling & domina3ng
- soHens and prunes displacement ins;ncts to where they become sensi;ve to context and in the service of caring and community
DEVELOPING THE CARING ALPHA RESPONSE
“neurons that FIRE together WIRE together”
DIVERSE MANIFESTATIONS of UNTAMED ALPHA
moved to exploit the vulnerable & needy (the bully response) unrelenMng drive to dominate & displace
narcissism
chronic resistance or opposiMonality
drive for superiority and supremacy
obsessed with winning, placing, status, coming out on top
fuels the impulse to ‘lord it over’
driven to be the centre of aLenMon
compeMng with spouse or children for care
authoritarianism, racism, imperialism, and colonialism unable to depend, submit or take direcMon
Caring
The Continuum of Troubling Alpha Behaviour
common alpha syndromes perversion of alpha ins;ncts
bossiness ea3ng problems BULLYING
lacking feelings of dependence and neediness
devoid of feelings of caring and responsibility
HOW ELEVATED DISPLACEMENT INSTINCTS IMPACT LEARNING AND THE CLASSROOM
- CANNOT COMMAND their aLenMon or orchestrate their behaviour
- they do not accept their teachers as authoriMes and are NOT RECEPTIVE to instrucMon
- tend to be fraught with ALARM problems (eg, anxietybased, agitaMon-based and adrenalin-based)
- their peer relaMonships are oqen fraught with CONFLICT, or they can develop significant followings that draw students away from their teachers
- tend to be fraught with FRUSTRATION problems (aLacking energy, impulses & behaviour)
- tend to be fraught with ADAPTATION problems as not able to feel the fuMlity encountered (eg, sadness & grief)
ATTENTION ISSUES - cannot command their aLenMon / elevated alarm scaLers aLenMon / must be the centre of aLenMon
FRUSTRATION ISSUES - aggression, violence and self-aLack including suicide
EATING ISSUES - anorexia & food issues of all kinds
LEARNING PROBLEMS - literacy problems, dysfuncMon due to learning disabiliMes, difficulMes with seeking assistance
COMPLIANCE ISSUES - resistance & opposiMonality
ENTITLEMENT ISSUES - self-evident to them that they are most important
PEER ISSUES - conflict, bullying, dominance, and supremacy issues
the making of the bully response highly moved to displace Lacking feelings of caring & responsibility the BULLY response to perceived vulnerability, neediness, threat or weakness
- to assert dominance by exploiting vulnerabilityRenders today’s children increasingly UNSAFE and highly ALARMED, whether peer-oriented or not
ATTENTION ISSUES - cannot command their aLenMon / elevated alarm scaLers aLenMon / must be the centre of aLenMon
FRUSTRATION ISSUES - aggression, violence and self-aLack including suicide
EATING ISSUES - anorexia & food issues of all kinds
LEARNING PROBLEMS - literacy problems, dysfuncMon due to learning disabiliMes, difficulMes with seeking assistance
The alpha problem has been totally ECLIPSED by misinterpreMng alpha as ‘independence’, by our aversion to the construct of ‘hierarchy’, by our lack of understanding of the nature & purpose of aLachment, and by the lack of any supporMng language – rendering the symptoms unexplained and resul$ng in a fu$le baQle against them
COMPLIANCE ISSUES - resistance & opposiMonality
ENTITLEMENT ISSUES - self-evident to them that they are most important
PEER ISSUES - conflict, bullying, dominance, and supremacy issues
FACTORS CONTRIBUTING TO BEGETTING ALPHA CHILDREN
- schools tend to generate PEER ORIENTATION which, in turn begets alpha children
- many parents and teachers think they are being forward thinking by PUTTING CHILDREN IN THE LEAD
- today’s adults use behaviour management methods that make it UNSAFE TO DEPEND, evoking alpha by defense
- parents have LOST THEIR CONFIDENCE in being their children’s ‘answer’, presenMng as weak or inadequate, and thus evoking alpha by default
- today’s adults are increasingly seeking answers as to HOW TO parent and teach, puTng them in the ‘dependent’ mode
- decades of veneraMng independence has made us BLIND to the problems of children who resist dependence because of being stuck in the alpha mode
PEER ORIENTATION, the ALPHA COMPLEX and MENTAL HEALTH
- the perfect storm - peer orientaMon creates CONTRIVED hierarchies devoid of care and safety
DEPENDENT peer-oriented children, having lost their adult shields, suffer significant WOUNDING at the hands of their peers
increasing numbers of ALPHA peer-oriented kids who are devoid of taming feelings, evolve into BULLIES who make life unsafe for EVERYONE
the lack of received care and recovered feelings results in escalaMng and pervasive MENTAL HEALTH PROBLEMS
Reversing runaway alpha should be a top priority in the support of our children’s well-being!
Children need to be deeply & personally attached in the dependent mode to the adults responsible for them ... for the delivery of care
to empower the adults to fulfill their roles to shield from wounding for the regular recovery of feelings for the transmission of culture to make flourishing possible to activate and direct their desire to be good for the unfolding of human potential to activate caring and develop empathy to properly purpose their shyness & counterwill to support wellness & mental health
Take ALPHA INSTINCTS to PLAY
• use controlled games of compeMMon and conquest to safely vent the quest for dominance and supremacy
• use stories, imaginaMon, drama, role play and theatre to invent or idenMfy with alpha characters who always come out on top
• provide playful acMviMes where there is plenty of opportunity for leading, direcMng, or orchestraMng
• use playful games and acMviMes where children and students get to displace the adults in charge – eg, being the boss, having the last word, giving the orders, making the demands, making up the rules
• encourage or support alpha caring play, where alpha insMncts are used to take care of others
• provide ample access to emoMonal playgrounds where there is more chance for the alpha insMncts to awaken the impulse to care
School-Based Practice – developing the vertical dimension
STUDENT-TEACHER RELATIONSHIPS
EMOTIONAL PLAYGROUNDS
CASCADING CARE RELATIONSHIPS
FAMILY RELATIONSHIPS
Embed in CASCADING CARE
• our aim should be to shield students at risk by fostering an aLachment with a safe caring adult who is willing to serve that role
• matchmake by presenMng one as the ANSWER to the other
• use playful acMviMes to matchmake students to teachers and across the grades and the ages
• our aim should also be to matchmake students hierarchically so that every student experiences being both cared for and in charge of taking care of
• matchmake the more mature students with those in need, to serve as HOME BASE as needed
• uMlize the ‘house system’ if possible, to foster cascading care across the grades and ages
Assume a caring alpha lead in order to ...
1. INSPIRE the DEPENDENCE necessary in order to fulfill one’s responsibiliMes and to foster healthy development
2. Render students RECEPTIVE to your instrucMon and MOTIVATED to be good for you, thus OPTIMIZING their learning as well as their behaviour
3. Possess the POWER to SCRIPT the behaviour of the immature
4. Serve as the ATTACHMENT IN COMMON in one’s class in order to keep children from revolving around each other and maLering too much to each other
5. FuncMon as a SHIELDING aLachment as needed (for wounding that may come from others including peers, siblings, parents or other adults)
6. Bring the followers of charismaMc ALPHA STUDENTS under your control and influence
Mastring te Lead in te dance of atachment
• assume the posture and demeanor of the ALPHA in charge, concealing one’s own needs and insecuriMes
• perceive the student(s) as being IN NEED of you, as an ANSWER to their aLachment needs
• INVITE dependence and make it SAFE to depend
• convey CARING and find a way to get the message across that you will take care of them
• be GENEROUS - providing more than is pursued
• seize the lead by ANTIPICATING ‘demands’ and geTng there first
• READ the needs & take the lead (don’t ask too many quesMons)
• WIN the alpha baLles you can, but avoid the rest
• invite the INEVITABLE to preserve one’s alpha and convey that the relaMonship can take the weight
• ARRANGE scenarios where there is no choice but to depend upon you
• for an invitation to exist
• for contact and connection
• for sameness & belonging
• for safety and comfort
• to get one’s bearings
• for warmth & love
• for recognition
• for significance
• for understanding
• for a relational ‘home’
• INSPIRE dependence by taking a strong caring alpha LEAD
• INVITE dependence by gestures of CARE
• make it SAFE to depend, never using their rela$onal needs against them
• be GENEROUS with one’s care, providing more than is pursued
• DON’T BE FOOLED by the myriad illusions of independence
• for a sense of togetherness
Three Common ATtachment Disorders
... and how they impact received care and recovered feelings
1. PEER ORIENTATION
2. ALPHA COMPLEX in a dependant
about the defensive DEPERSONALIZATION of a$achment
If a$aching is sensed as leading inevitably to unbearable separa3on or wounding, the a$achment brain can reverse the direc3on of the pursuit to reduce the vulnerability involved. The a$achment drive itself cannot be reversed since it is the preeminent/default drive and only increases under threat.
- depersonalized aLachment cannot fulfill so the drive remains unabated and any experienced proximity becomes addicMve
- depersonalized aLachment cannot deliver care or safety, but competes with personal aLachments that could
- can involve the defensive transference to non-personal enMMes: objects, pets, groups, categories, ideas, religion, race, poliMcs, naMons, etc (fuels racism, sports obsessions, and all the ...ISMs)
the DEPERSONALIZATION of attachment
Sarah Matthew Genevieve Rorie Scott
Ms.Kerr Kendall Sherry
the PURSUIT of PROXIMITY with a PERSON ATTRACTING WINNING MEASURING UP DEMANDING IMPRESSING HELPING BEING NICE BEING CHARMING SEEKING STATUS the the to be to be to be to be to be to be to be ATTENTION APPROVAL VALUED SPECIAL ESTEEMED IMPORTANT LIKED LOVED RECOGNIZED of of by to by to by by by
the DEPERSONALIZATION of attachment
The Depersonaliza3on & Fragmenta3on of Pursuit
the PURSUIT of ATTRACTING WINNING MEASURING UP DEMANDING IMPRESSING HELPING
BEING NICE
BEING CHARMING
SEEKING STATUS
The depersonaliza3on and fragmenta3on of a$achment-based pursuit in the face of threatened connec3on
Some common a$achment-driven where the pursuit is divorced from its rela3onal context:
Reversing defensive depersonalization should be a top priority in the support of our children’s well-being
Right Relationships & Emotional Playgrounds
ENCOUNTERS WITH FUTILITY
REST RECOVERY RESILIENCE RENEWAL
HELP THAT IS HELPFUL!!
• keeping or restoring perspective
• right thinking / being positive
• pursuing happiness
• resisting the ‘let-down’
• acquiring the ‘skills’ of resilience
• pursuing calmness & tranquility
Do NOT allow the popular construct of ‘mental health’, thrice removed from a working reality a) a euphemised spin on mental illness which is b) itself an instrumental analogy vs evidence-based reality, and c) an indirect ‘fruit’ versus useful point of intervenMon - to thus ECLIPSE its developmental ROOTS in ATTACHMENT and EMOTION
MISDIRECTING and thus EXHAUSTING our valuable resources and energy with regards to the emo;onal well-being of our beloved children and youth.
Diagnosing syndromes and Battling against Symptoms
vs
- crusades against bullying, meanness, discriminaMon, violence, insensiMvity, injusMce, intolerance
- prosocial programs aimed at children being nice and kind
- discipline approaches aimed at teaching a lesson, socializa3on approaches aimed at declaring hurrul interacMon unacceptable, and legal approaches punishing the violators
- mental health advocacy and literacy programs as well as selfcare programs
Cutivating the Conditions for Well-Being
RIGHT RELATIONSHIPS WITH CARING ADULTS
... that can deliver CARE and provide safe sanctuary for FEELING
PLAYGROUNDS for EMOTION
... so that emo;on can find REST, working aCachments can be PROTECTED, vulnerable feelings can be RECOVERED, and the CARE that has been delivered via trus;ng dependence to caring adults can be FELT
Through a child’s attachment to us, we can BE their ANSWER even when there are no answers:
• BE their HOME
• BE their place of REST
• BE their sanctuary of SAFETY
• BE their SHIELD in a wounding world
• BE their REASON for holding on
• BE their source of WELL-BEING
The answer is in BEING - not in DOING or SAYING or KNOWING the right things – when empowered by the other’s attachment to us.
The Current Crisis of WellBeing
what is happening to our kids?
an a$achment-based developmental perspec3ve
Gordon Neufeld, Ph.D. Developmental & Clinical Psychologist