Right to Repair
MedWrench is your online community ask questions and share information about specific medical equipment you work with every day.

medwrench.com THE MEDICAL
SUPPORT NETWORK 2024 DIGITAL MAGAZINE
PRODUCT












ACCOUNTING
THE FACE OF Ben Calibrating
MEDWRENCH is a product focused support network where medical professionals, purchasing administrators, manufacturers, dealers and industry experts can provide opinions, share ideas, and gather relevant information on medical technology and equipment.

Table of Contents 4 COVER STORY Right to Repair 9 EXPOS AND EVENTS Everything You Need in One Place 14 SHOP TALK Q&A from MedWrench Forums Alerts for Medical Equipment Professionals REVOLUTIONIZING HOSPITAL PRESIDENT John M. Krieg VP OF SALES Jayme McKelvey DIGITAL MARKETING Kennedy Krieg Joanna Manjarrez Emma Vitkovitsky SALES Megan Cabot Emily Hise
DEPARTMENT Karlee Gower Taylor Hayes Kameryn King
ART
Diane Costea
MEDWRENCH
MEET OUR TEAM 10 FIELD TESTING ULTRASOUND PROBES Sponsored by Innovatus Imaging MEDWRENCH.COM | DIGITAL MAGAZINE 3
Right to Repair
Right to Repair continues to be a hot topic in healthcare technology management. Recently contacted key stakeholders within the medical device repair industry share their insights on the Right to Repair. Participants in this article are College of Biomedical Equipment Technology President Dr. Richard L. “Monty” Gonzales; MultiMedical Systems LLC Vice President of Operation Nicole Palmer; U.S. PIRG Campaign for the Right to Repair Senior Director Nathan Proctor; Elite Biomedical Solutions CEO and Co-Founder Jeff Smith; Innovatus Imaging Vice President of Sales and Marketing Matt Tomory; and Renovo Solutions Chief Operating Officer Andrew Ulvenes.
Q: WHY IS RIGHT TO REPAIR IMPORTANT FOR HEALTH CARE FACILITIES?
GONZALES: To better address the question of why health care organizations should be concerned about the Right to Repair, we should emphasize that financial stewardship plays a crucial role in health care facilities. I have read many arguments for and against Right to Repair, but it is undeniable that the issue primarily revolves around financial aspects. By limiting health care organizations’ ability to make informed decisions about maintaining their medical devices, arbitrary restrictions can hinder their ability to exercise prudent financial judgment. The same professionals entrusted to make life and death decisions about patients, should be granted control over the maintenance and repair of their medical equipment.
PALMER: We believe when you own equipment you should have the right to access manuals, equipment, parts, tools and diagnostic equipment. This is especially critical in health care when support could be delayed days or weeks. Critical hours can pass while trying to reach tech support and booking an OEM tech to respond. The loss of revenue when some devices are not operable is affecting health care’s bottom line, patient care and patient safety.

4 DIGITAL MAGAZINE | MEDWRENCH.COM

PROCTOR: Right to Repair is about empowering choice. Not just the ability to choose a repair option that might involve less downtime, or less cost. It’s also about choosing the method of repair that has the best quality. Manufacturers would like us to believe that they offer the best service automatically, but that’s just not true. Sometimes, manufacturers have bought another company, and their servicing quality has taken a hit, but they still charge five times what a local ISO charges, who also does the repair in hours instead of weeks. Meanwhile, the devices fail more often when serviced by this over-stretched OEM. Facing a loss of service revenue, some OEMs would take this opportunity to lock down their service manuals, PM kits, service keys and triple the cost for their trainings – all of which would be aimed at pushing the health care facility to renew a bad service contract. Why shouldn’t the hospital be able to hire the best, fastest, safest option?
Sometimes manufacturers do offer the safest service, and for some equipment a health care facility would never choose any other option given the market options right now. But even in those cases, Right to Repair is a benefit. It keeps the OEM honest, forces them to maintain that quality if they want to keep winning those contracts. This is about creating a system with good
: Medical devices are integral to a health care facility’s ability to provide patient care. Unfortunately, there is shortage of repair technicians in the health care industry, and so hospitals often must outsource device repairs. One significant concern for hospitals focuses on how the Right to Repair fight will impact their ability to repair devices in a timely manner, as OEMs may not be able to repair equipment fast enough or have sufficient available parts. Based on analysis of millions of complaints, a 2018 FDA report concluded that, “the objective
evidence indicates that many OEMs and third-party entities provide high quality, safe and effective servicing of medical devices,” and that “the continued availability of third-party entities to service and repair medical devices is critical to the functioning of the U.S. health care system.” Given the importance of medical devices to patient care, we, as a community, must work together for our country.
TOMORY: The migration to in-house service has been going on for many years and has accelerated due to rising support costs and the increase in competency of HTM staff. With many organizations performing their own service and maintenance, it is critical they have the proper tools and documentation to comprehensively support the equipment they own and operate as well as ensure it is performing as the OEM intends.
ULVENES: Hospitals need very responsive, high-quality and cost-effective solutions for maintaining their medical equipment. They purchase and own their assets and they should have the choice in how they manage their life cycle. Right to Repair creates healthy options for health care facilities that allows them to provide the best patient care and experience to those they care for.
Q: HOW CAN HTM PROFESSIONALS HELP THE RIGHT TO REPAIR CAUSE?
GONZALES: The most important thing that HTM professionals can contribute to the Right to Repair movement is to be well-informed and engaged. Being well-informed includes understanding the fundamental tenants of the argument, the legislative initiatives shaping the fight, and other trends influencing the national debate. Actively participating in trade shows, HTM associations and other professional forums is also important. Lastly, active involvement in the political process, contacting your representatives and
engaging in both public and private discourse on the topic.
PALMER: Ask your local HTM management professionals and follow those working for health care on social media, such as www.prig.org. MMS has worked on initiatives with US PIRG, and many others to raise awareness on this important issue. Write or leave a voice message for your senator or representative. Provide examples of why or how the right to repair affects you and your team and, most importantly, those whom we serve –the patient. We, together as an HTM community, can be a powerful voice!
PROCTOR: I think there are two ways we need more biomeds and HTMs to help. 1) We need your voice. We live in a democracy, where decisions are made by speaking up, and finding others who agree with you. You should join groups like the Medical Device Servicing Community, which aims at fostering a dialog and collaborative community around these topics and other important issues facing HTMs. You can sign our letter and join the more than 500 other biomeds active on this issue. Number 2 is data and facts. I know hospitals track which device servicers are more effective, faster and how much they charge. Lawmakers need to understand this data to make informed decisions. We are working hard to collect data, but we need more people who can share some of their insights with us without violating patient privacy. The FDA 2018 report is the closest we have, but it doesn’t consider downtime, price or how long a repaired device kept working before failing again. I know people track this, and this data tells a very compelling story about why Right to Repair would be common sense.
SMITH: HTM professionals should demand access to the proper manuals/ training/parts needed to safely repair and maintain medical equipment, and OEMs should be made to provide that
MEDWRENCH.COM | DIGITAL MAGAZINE 5
information. Additionally, consumers should reach out to the Federal Trade Commission (FTC) to inform the agency of any concerning practices or statements OEMs may be utilizing, including unsupported statements regarding the safety of third-party parts or when OEMs characterize third-party parts as “counterfeit” parts or “gray market” parts. The FTC has focused on Right to Repair restrictions generally, and the Senate Judiciary Committee’s Subcommittee on Antitrust emphasized the FTC’s continued work combating repair restrictions that allegedly harm consumers, explaining that the FTC is “prioritizing action against business practices that unlawfully restrict consumers’ ability to repair their products, costing them more over the long term.”
TOMORY: The HTM team should be involved in all equipment purchasing processes (in my humble opinion) to provide a post-warranty support perspective. During the purchasing process, critical items such as manuals, software (keys), proprietary test equipment, etc. should be negotiated so the health care provider may partially or fully support after the OEM warranty expires.
ULVENES: There are several things HTM professionals can and are doing to help the cause. One of those is making sure our teams have proper training and skills to repair and support medical devices. In addition, many service providers are ISO (13485 or 9001) certified ensuring that they have quality standards in place.
Q:
CAN YOU SHARE AN EXAMPLE OF A TIME WHEN YOU HAD AN ISSUE WITH A DEVICE THAT RIGHT TO REPAIR COULD PREVENT?
GONZALES: I have a slightly different perspective in my current role as the president of the college and can only speak as an authority to that which I am directly responsible. Nevertheless, it is hardly likely that most technicians within the HTM industry would assert their unfamiliarity with the potential pitfalls that could have been averted had they been
granted the Right to Repair a device.
PALMER: It is hard to choose just one. As a national company, MMS works with clients ranging from clinics to hospitals. We see how the Right to Repair affects our clients, especially the critical/rural access hospitals. As well as the smaller, independent health care facilities. Due to the geographical areas, they are delayed much longer than their acute care counterparts. Third-party organizations are restricted even further. Owners not only should have access to the necessary tools and diagnostic equipment, but they should be able to transfer access to their qualified and skilled third-party partners.
SMITH: As a third-party service provider, I can think of multiple examples, but most recently we have learned that our customers have received letters from the OEM informing them that if they utilized third-party parts on the OEM’s devices, the OEM would not repair or upgrade the device unless the customer paid an exorbitant amount of money to remove the third-party parts. I am both dismayed and disappointed in our community of health care professionals that, instead of working together to serve our country’s patient population, they choose to make false accusations and charge significant monetary amounts that may potentially disrupt health care priorities.
TOMORY: As an independent service organization, we engineer solutions to repair OEM MRI coils and ultrasound probes daily so we may serve health care providers, asset management organizations and even several OEMs. We are essentially the forefront of Right to Repair as we partner with these organizations as an OEM supplement or alternative.
ULVENES: In my years I have seen many issues where Right to Repair has unequivocally benefited health care facilities. Supply chain resiliency is one where having multiple sources/options have proved to have better quality and faster turnaround time. In addition,
service responsiveness has been lacking where in-house or third-party service providers have provided instant response because we are onsite allowing continuous operations for health care providers.
Q:
HOW CAN RIGHT TO REPAIR LEGISLATION PROMOTE PATIENT SAFETY?
GONZALES: Right to Repair legislation offers tremendous potential to promote patient safety by fostering collaboration and knowledge sharing among key stakeholders, including original equipment manufacturers (OEMs), healthcare delivery organizations (HDOs), independent service organizations (ISOs) and others. By working together on a more evenly defined playing field, these stakeholders can clarify standards, establish uniform practices, and provide the necessary education and training required to ensure the safe and effective servicing of medical equipment and, ultimately, patient safety.
PALMER: The old saying “Time has a way of showing us what really matters.” Giving the device owner’s control would give them freedom to choose what is right for their facility or health care system. This would also give them the right to choose a qualified vendor who best suits their needs. Delay in service equals time lost. Time lost equals compromised care. Reducing inefficiencies in health care would be a win for all.
PROCTOR: First, I believe that the health care delivery organization has the best and most complete view of patient safety. Right to Repair ensures they have the ability to make choices to repair equipment faster and have more in-house capacity to keep critical devices running. We found that most hospitalbased biomeds have had to delay patient procedures because of equipment downtime, downtime they say would be alleviated through Right to Repair. Secondly, there are a set of important safety issues which are caught in an impasse because they involve a false choice between repair access and safety.
6 DIGITAL MAGAZINE | MEDWRENCH.COM
Manufacturers want to end device alteration, but are pushing for rules which do that by increasing their control on who does repairs. That’s just not going to work. We have a similar fear in the world of cybersecurity which clearly negatively impacts all of us. We need a solution, but one that doesn’t create more control for manufacturers over devices. Once we strike the right balance, we can move forward on all these fronts.
SMITH: The momentum continues to build for the Right to Repair cause. It is my opinion that it is one of the most critical fights for patient safety. As a registered FDA company, Elite consciously chooses to certify to ISO 13485 and ISO 9001, and closely follow the FDA’s 21 CFR Part 820 guidelines. I am absolutely in favor of requirements that demand all OEMs and third-party servicers adhere to the same standards.
TOMORY: HTM staff are already successfully and safely repairing and maintaining their own equipment using a variety of resources. Imagine the increase in efficiency if they are provided the same tools and documentation as the OEM?
ULVENES: Legislation must create an even playing field for medical device service/support in order for health care facilities to deliver consistent patient care. The right equipment, at the right time, for the right patient care is critical for patient safety. Data and evidence exists that shows how delays in care create increased mortality and morbidity. Less choices and options will create patient care delays that increase risks to patients.
Q: WHAT ELSE DO YOU THINK READERS NEED TO KNOW ABOUT RIGHT TO REPAIR?
GONZALES: Ensuring the Right to Repair issue does not become overly polarizing is crucial for fostering positive and necessary change in the health care industry. By allowing individuals and health care providers access to repair, modify, or customize medical devices and equipment, we can enhance patient care, reduce costs, and expand innovation. It is essential to
strike a balance between protecting proprietary information for security reasons and empowering stakeholders with the necessary tools to maintain and repair critical medical technologies. By adopting a collaborative and inclusive approach, we can address concerns from all sides and drive progress that benefits patients, health care providers and the industry.
PALMER: The Right to Repair could enhance not only patient care and patient safety but promote sustainability. Right to Repair could help reduce electronic waste and replacement costs. Legislation could provide cost savings, which is critical in today’s economy. It is especially critical to help our rural hospitals from shuttering. Skilled technicians can be easily trained to maintain and repair these devices just as the OEM techs have been trained. We should never forget that someone’s loved one is counting on this equipment to be working and ready to go 24/7 and 365!
PROCTOR: Right to Repair has passed in six different states for a range of devices ... but so far, not medical devices. If we want that to happen, we need more people to raise their voices.
SMITH: Right to Repair is everyone’s responsibility. It is imperative that we all be accountable and strive for the highest of level of patient safety. That’s why all of us chose this field.
TOMORY: There is always a place for the OEM when developing and supporting a successful in-house program. I believe the best path forward for Right to Repair is cooperation between manufacturers and HTM teams to ensure safe, effective and economical equipment repair and maintenance.
ULVENES: Everyone’s voice is important, and each person can make an impact. I encourage all to get involved and help make sure the Right to Repair effort is supported. We all have the common goal: providing safe and available medical devices for the best patient care. Let’s rally together and make sure we continue to advance this together.
HTM PROFESSIONALS





 Matt Tomory Innovatus Imaging
Nicole Palmer MultiMedical Systems LLC
Nathan Proctor U.S. PIRG Campaign for the Right to Repair
Richard L. “Monty” Gonzales College of Biomedical Equipment (CBET)
Jeff Smith Elite Biomedical Solutions
Andrew Ulvenes Renovo Solutions
Matt Tomory Innovatus Imaging
Nicole Palmer MultiMedical Systems LLC
Nathan Proctor U.S. PIRG Campaign for the Right to Repair
Richard L. “Monty” Gonzales College of Biomedical Equipment (CBET)
Jeff Smith Elite Biomedical Solutions
Andrew Ulvenes Renovo Solutions
MEDWRENCH.COM | DIGITAL MAGAZINE 7


SOLUTIONS We have the key to your success. ISO 13485:2016 certified
exciting
Medical Imaging
Tri-Imaging! We have a world-class hands on training facility
our facility
Madison, TN. 2 WEEKS BMET to Imaging 1 training 2 WEEKS BMET to Imaging 2 training 8 WEEKS Technical Services 12 WEEK APPRENTICE PROGRAM Visit triimaging.com/training/training-program.html to see our Training Calendar! 855.401.4888 Located in Nashville, TN
Become an Imaging Engineer. Start an
career as a
Service Engineer with the Apprentice Program at
at
in
UPCOMING EXPOS AND EVENTS

Bring the heat to AAMI eXchange 2024 this July!
JUNE 14-17, 2024
PHOENIX, AZ
The Americas’ leading medical trade expo and digital platform
JUNE 19-21, 2024
MIAMI, FL


Join NCBA for their annual symposium
AUGUST 19-21, 2024
CHEROKEE, NC
AHRA’s 2024 Annual Meeting
AUGUST 4-7, 2024
ORLANDO, FL
VISIT and AT BOOTH 323 MEDWRENCH.COM | DIGITAL MAGAZINE 9
FIELD TESTING ULTRASOUND PROBES
Ask the Expert: Innovatus Imaging’s Ted Lucidi, CBET, Director of Commercial Operations
We’re often asked, “What are some of the most common failures with ultrasound probes?”. We can confidently say, “It depends”. Many problems are based on the probe type. For example, 60%-70% of all TEE probes are repaired or replaced due to gross fluid invasion (or flooding) of the probe. One of the most common points of failure on standard probes (linear, curved, sector, and endo-cavity) is the acoustic array. A single, accidental, fall to the floor can shatter the fragile piezoelectric elements, resulting in image dropout.
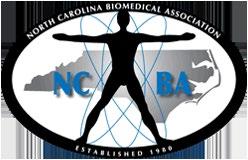
WHAT IS IMAGE DROPOUT?
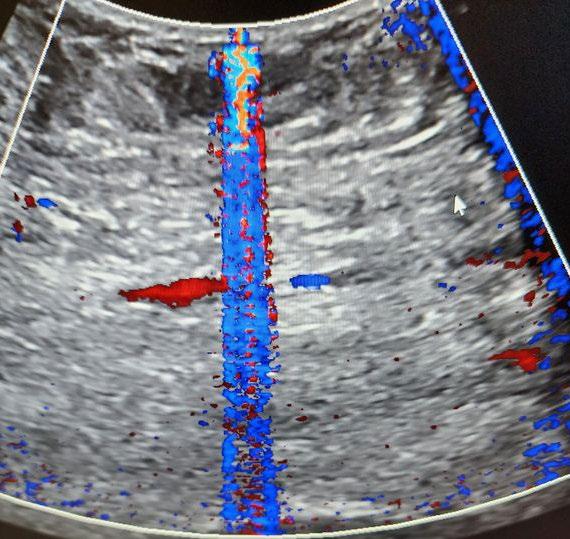
Image dropout is just that…A section of the image that has no information or that has “dropped out” (technically called hypoechoic). Typically, this appears as a black vertical line or shadowy region of the image. Because the acoustic elements are not pulsing (or not working as expected), no information (or erroneous information) is provided to the scanner for display.
WHAT’S THE BEST WAY TO ASSESS PROBE PERFORMANCE IN THE FIELD?
I don’t believe that anyone would argue that the best, first step is to perform a very thorough visual inspection of the probe. Performing with some level of magnification is well recommended. As far as image quality testing, some companies would like to sell you some very precise test equipment for assessing probe performance. Although very comprehensive, these devices just aren’t practical, nor cost-effective, for field work. They are best utilized in acoustic labs, manufacturing divisions, or repair centers, but not the field. Probe testing in the field is best performed using a tissue mimicking phantom. A prior MedWrench Ask the Expert article discusses some basics for image quality testing. It can be viewed here
We’ve also published a “how-to” guide for performing image quality testing. It assists HTM technicians with understanding industry standard testing criteria for assessing probe performance. The guide presents background information on transducer design, detailed testing methods, root cause analysis and troubleshooting techniques. It can be requested via email at training@innovatusimaging.com
WHAT’S ANOTHER COMMON PROBE PROBLEM?
Although grouped together with standard probes, cardiac probes, such as the Philips X5-1 and S5-1, and GE M5S-D experience high failure rates in the wiring harness. It not due to a design flaw or using inferior components, it’s due to the manner in which these

10 DIGITAL MAGAZINE | MEDWRENCH.COM
Image Dropout
specific probes are used in the clinical environment. I would argue that every cardiac probe will need to have its wiring harness replaced sooner versus later in its lifecycle. Innovatus Imaging engineers and fabricates over 100 different replacement cable harnesses to remedy these types of failures.
HOW DO YOU KNOW THAT THE PROBE’S WIRING IS FAILING?
HTM imaging techs will hear reported complaints of heavy static in continuous wave Doppler mode or of color Doppler artifacts. Another complaint is of noise or other performance issues when the cable is moved or when the probe in used is a particular position.
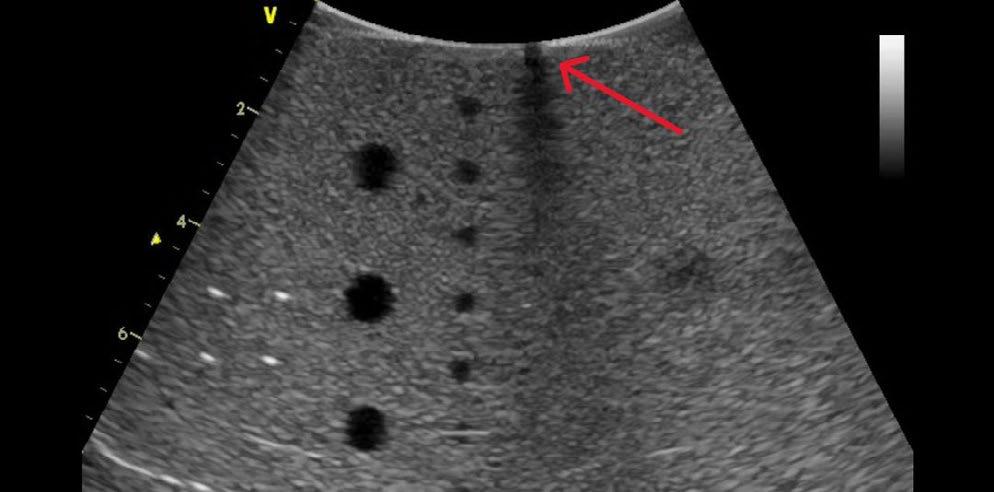
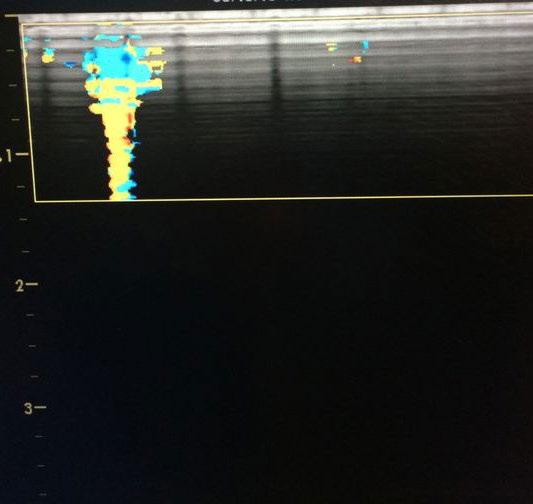
WHAT DO COLOR DOPPLER ARTIFACTS LOOK LIKE?
Well, the term artifact refers to any unwanted and unexpected anomaly in an image. Typically, color artifacts appear as unwanted flashes, vertical streaks, or areas of non-descript color variations in the image. Take a look at the photos.
WHAT ARE SOME CAUSES OF COLOR ARTIFACTS?
There are many root causes, and some lie within the scanner console itself. For this discussion, let’s assume that the scanner is working as expected. One of the most common root causes is worn and intermittent wires in the probe’s wiring harness. As intermittent wires make, and break, contact with one another, the unwanted/unexpected electronic information will be displayed as flashing lines or color streaks in color
Doppler mode. In pulse wave and continuous wave Doppler modes, the same information is expressed as audio static. The exact location of the flashing lines in the image is directly related to one or more intermittent micro-coaxial wires in the wiring harness. One of our most common probe repairs is replacing a worn, intermittent wiring harness.
HOW CAN THE INTEGRITY OF THE PROBE’S CABLE BE CHECKED?
There are several methods of verifying the integrity of an ultrasound probe’s wiring harness. One that lends itself to field-based troubleshooting is below.
1. With the probe connected to and initialized on the scanner, assure that the probe’s lens is clean and dry.
2. On the scanner, enable color Doppler mode.
3. Adjust the size and position of the color box to span the entire width of the image.
4. Adjust the depth of the color box to be less than 5 cm.
5. Adjust the color gain so that there is only very minor background color speckling in the color box.
6. Begin by flexing each strain relief looking for flashing lines or streaks of flashing color, then flex the cable over its entire length.
7. As you flex the cable, focus on any flat sections or areas that may be abraded or scuffed as the cable may have been rolled over.
If any flashes of color appear in the color box, when manipulating sections of the cable, there’s, most-likely, some intermittent wires in the harness. There’s
no method to repair cable intermittencies in the field, so you’ll have to address the problem, either with a repair solution or an exchange. The cable’s integrity will only continue to decline over time.
Innovatus Imaging performs about 400-500 customer repairs on ultrasound probes every month, add to that at least another 200 restoring our loaner inventory. Each probe receives a thorough incoming evaluation, a very comprehensive outgoing quality assessment, and multiple in-process performance inspections. We can confidently say that our evaluation team has performed over 100,000 probe evaluations in the last 5-years. Most-likely, they’ve encountered and troubleshot almost every scenario that you and your clinicians have experienced. We welcome the opportunity to build your comfort with and competence in testing your ultrasound probes. We’re also able to assist in helping you solve any troublesome image quality problems. When the need arises, we’d sincerely appreciate the opportunity to assist you in restoring your probe’s performance back to OEM intent. We have full repair capabilities on over 100 probe models and varying degrees of repairability on hundreds more.

For more information about probe repair and our capabilities, please reach out to Ted Lucidi at TedL@ innovatusimaging.com or visit innovatusimaging.com/ultrasound.
MEDWRENCH.COM | DIGITAL MAGAZINE 11
Click here to view the Ask the Expert Section on MedWrench.com


Regardless of the make, model or field strength, we have the team and infrastructure to get almost any MRI coil back up and running. Quickly With over 35 years of experience and more than 40,000 successful repairs, you can trust your devices to be repaired to their original design. Yes! We can repair your Philips dStream™, GE Air™ coils, and Invivo coils, and we can fully restore your coil’s system cable. All covered by a 6-month warranty. Setup a repair or arrange for a loaner, today 844-687-5100 customercare@innovatusimaging.com Centers of Excellence for Ultrasound Probe and MRI Coil Repair, and Design & Manufacturing When You Are Down... We Can Help You Get Back Up Visit us at the AAMI Exchange at booth 928






visit BOOTH 323 to begin the hunt! Prepare to seek out top MedWrench advertisers at the AAMI eXchange for a chance to win over $2,400 in prizes! medwrench.com AAMI eXchange June 14–17, 2024 Phoenix, AZ JOIN THE HUNT MEDWRENCH.COM | DIGITAL MAGAZINE 13
SHOP TALK

MORTARA ELI 150
Q: When powering up, the LCD screen turns on with a completely dark rectangle. When switching it off, I can see the normal light screen for a second. This happened after I replaced the CMOS battery. Does anyone know why this is happening?
A: Does the keyboard work? I’d double check the keyboard/LCD ribbon cable. There is also the thin ribbon cable from the back of the keyboard to the LCD that may not be seated correctly. Good Luck!
A: Thank you for the feedback.
The keyboard and everything else works. I believe the LCD backlight is not working.
I have changed the ribbon cable from the motherboard to the keyboard and reseated the ribbon cable from the keyboard to the LCD. At a certain angle I am able to see the ECG trace from the ECG simulator. Are there any electronic components I need to check?
A: Problem solved.
With a flash light pointed to the LCD, I was able to adjust the contrast until the sreen became visible.
I believe that on changing the CMOS battery, this configuration was changed for some reason
A: That’s great! Who knew the contrast setting defaults to zero when the CMOS battery is removed. We usually save the flashlight trick for GE MAC 5000, 5500 EKGs. I think you helped me more than I helped you!
A: I believe we helped each other. This is why this forum exists. To exchange ideas and help where we can.
GE OEC 9900 ELITE
Q: I am having an issue with the column not going up or down. I push the buttons and I can hear clicking on the front board, but it does not move. Does anyone know the solution to this problem, or have the service manual for GE OEC 9900 Elite?
A: In the main unit, on the left hand side (remove aluminium cover), is the 220v power supply, its a white box with strange connectors that need a special tool to remove.
A: Thanks for your reply. What should I do with the white box? Should I check if its supply 220V to the column?
Should I replace the white ox?
A: The box is normally replacement only, it could be there is an internal fuse or fusable resistor.
It could be it failed as the customer jammed the unit under operating table or similar.
I woukd try and check if the output is 220v before replacing.
SIEMENS ARCADIS AVANTIC
Q: When I turn on the unit, it does not boot up properly. On the monitor, all I see is an under scroll blinking, and on the C-arm control panel the red lights blink. Also, when I turn off the system, the monitor cart stays the same way with the under scroll blinking and the mouse on but the C-arm turns off. Does anybody know why it does this, and what I should look for to solve this issue?
A: I’m not 100% sure but I believe it comes as a “small parts” box so you get a whole load of bits you will never use.
A: Gen 2.
14 DIGITAL MAGAZINE | MEDWRENCH.COM
TUTTNAUER EZ11 PLUS
Q: My Tuttnauer EZ11 Plus shows no water after starting. I have determined the issue is the water pump. I was wondering if anybody has experience with the water pump delete kit. Just wanted to see if it was worthwhile or replacing it with an OEM water pump is better. Cost is the same. Thanks!
A: Just replace the pump. It’s the easiest way to solve the issue. The delete kit involves flashing the software. If you haven’t done that before don’t. There is a chance you could drop the calibration in the process. If that happens it could take awhile to get it honed back in again. Have had it happen a couple times. Also, this unit is discontinued coming up on 2 years and replacement parts not including water pump are priced crazy.
A: Replace it with the water pump delete kit. It is the same price. New pump converts it to a gravity pump similar to a midmark autoclave. The pump fails often because it is not meant to be used for multiple continuous rounds...water has no time to cool and hot water causes the pump to malfunction. Instructions come with a USB to reflash. I have changed it and its easy. Worst case scenario is youll have a autoclave as a backup.
MORTARA ELI 250
Q: I want to know if the machine stores the records of ECG automatically and how I can send them over to my PC so that I can analyze the signal. Any tips?
A: Which unit do you have. The ELI250 or the ELI250c. The 250c has a blue screen and yellow tracing. If you have the older ELI250, it is obsolete. If you have the ELI250c, the unit does store records and they can be transmitted to a program called ELI Link which can create a PDF or XML file. Contact Baxter who now owns the ELI250c line and the tech support team can help you determine if the unit you have can transmit.

VALLEY LAB FORCE FX-C
Q: I am seeing ‘Error 163’ for Valley Lab pop up. Any idea why this is happening?
A: Try disconnecting all accessories from ESU, footswitch and electrodes. Restart the ESU. This happens if a footswitch gets stuck.
Click to visit MedWrench MEDWRENCH.COM | DIGITAL MAGAZINE 15
FDA ALERTS

Two Companion Reports on Medical Device Safety and Innovation
The U.S. Food and Drug Administration’s (FDA) Center for Devices and Radiological Health Center (CDRH) has released two reports on medical device safety and innovation – the core pillars that help protect and promote public health for all. The “CDRH 2024 Safety Report” and the “CDRH 2024 Innovation Report” provide summaries of CDRH’s accomplishments and look ahead to future initiatives.
Fresenius Kabi Recalls Ivenix Large Volume Pump
Fresenius Kabi is recalling the Ivenix Large Volume Pump (LVP), a primary component of the Ivenix Infusion System, because some units have mechanical issues with the Fluid Valve Pins, located inside the pump’s internal housing, causing the pins to not move properly.
CIARTIC Move Self-Driving Mobile C-arm
Siemens Healthineers recently announced the Food and Drug Administration (FDA) clearance of the CIARTIC Move, a mobile C-arm with self-driving capabilities. The system accelerates and standardizes 2D fluoroscopic and 3D cone-beam computed tomography (CT) imaging for surgeons and operating room teams in hospitals and outpatient facilities, bringing consistency to automated workflows and reducing imaging time during operations. Designed to address the needs of orthopedic, trauma, and spine surgery, the CIARTIC Move also can be used in thoracic, vascular, cardiovascular, and general surgery, as well as urology and interventional pulmonology.
Quality Management System Regulation: Final Rule Amending the Quality System Regulation
To ensure medical devices on the market are safe, effective, and of good quality, the U.S. Food and Drug Administration (FDA) issued the Quality Management System Regulation (QMSR) Final Rule.
Syngo Virtual Cockpit Remote Scanning Technology
Siemens Healthineers announces the Food and Drug Administration (FDA) clearance of syngo Virtual Cockpit, a private, secure communication platform for real-time image visualization, acquisition, and collaboration between healthcare professionals across multiple sites. The software enables users to connect to computed tomography (CT), magnetic resonance (MR), positron emission tomography (PET), single-photon emission CT (SPECT), PET/CT, SPECT/CT, and PET/MR scanners from Siemens Healthineers as well as other equipment vendors, regardless of location. syngo Virtual Cockpit is the first and only multi-vendor remote scanning software to receive FDA clearance as a medical product.
For more information on these recalls and more, visit medwrench.com/fda-articles.
MEDWRENCH.COM | DIGITAL MAGAZINE 17

REVOLUTIONIZING HOSPITAL
MAINTENANCE: EMERITUS
At Emeritus, we’re on a mission to transform hospital bed maintenance, setting new standards in efficiency, reliability, and cost-effectiveness. With our nationwide presence and dedication to excellence, we’ve crafted a comprehensive program that not only saves hospitals up to 30% on maintenance expenses but also enhances operational efficiency and ultimately improves patient care outcomes.
1. REIMAGINING MAINTENANCE PROTOCOLS
Emeritus, a service-disabled veteran-owned small business, is not just another maintenance provider. We’ve redefined the approach to hospital bed maintenance, prioritizing quality over quantity and genuine care for our clients. Our Bed Maintenance 2.0 program offers comprehensive coverage for all makes and models of hospital beds, ensuring that every client receives tailored solutions to their unique needs.
2. TECHNICIANS AT THE READY
With Emeritus, you get the benefits of outsourced expertise
with an ‘in-house’ feel. Our Always On-Site program ensures that our highly skilled technicians are readily available to address maintenance issues promptly. Beyond mere repairs, our technicians also provide invaluable training to hospital staff on equipment usage, empowering them to operate efficiently and contribute to improved patient care outcomes.
3. NEAR-ZERO RESPONSE TIME
In critical healthcare settings where every second counts, Emeritus shines with our near-zero response time. By swiftly addressing maintenance issues, we help hospitals maintain a safe and functional environment for both patients and staff. Our rapid response capability prevents equipment failures, ensuring that beds are always available when needed, thus enhancing patient care and satisfaction.
4. COST CONTAINMENT SOLUTIONS
One of the most significant challenges faced by healthcare facilities is cost containment. Emeritus addresses this
18 DIGITAL MAGAZINE | MEDWRENCH.COM
BED
BED MAINTENANCE 2.0 Ask the Expert: Webb Clark, Senior Sales Manager at Emeritus
challenge head-on uncovering the hidden costs associated with hospital bed maintenance, saving hospitals up to 30% on expenses. This significant cost-saving solution allows hospitals to allocate resources more efficiently, invest in critical areas of patient care, and pursue innovative healthcare initiatives for the benefit of their patients.
5. VERSATILITY IN SERVICE
Emeritus takes pride in our ability to service and maintain all makes and models of hospital beds. Whether it’s a specialized bed or a standard model, our bed experts can effectively diagnose, repair, and maintain the equipment to optimal standards. Our unbiased approach ensures our cost saving goals align with the hospitals. This versatility eliminates the need for hospitals to engage multiple service providers, saving them valuable time and resources.
6. STREAMLINED ADMINISTRATIVE PROCESSES
Our ‘one point of contact, one contract’ model simplifies the administrative burden associated with managing multiple service providers. By consolidating all maintenance needs into a single contract, hospitals can efficiently oversee their bed maintenance program without the hassle of dealing with complex paperwork or multiple vendors. This streamlined approach enhances operational efficiency, ensures clear communication channels, and reduces OEM bias.
7. COMPREHENSIVE INVENTORY MANAGEMENT
Emeritus simplifies inventory management and documentation by handling all aspects, from ordering to recording. This comprehensive approach alleviates the hospital’s administrative burden, ensuring seamless tracking of parts and service history. With Emeritus, hospitals can efficiently manage their inventory and documentation, focusing on delivering quality patient care without the hassle of administrative tasks.
FROM AGONY TO JOY: A HOSPITAL’S TRANSFORMATION
Before partnering with Emeritus, hospitals endured the agony of delayed repairs, prolonged downtime, and exorbitant maintenance costs. With Emeritus, however, staff experienced a turnaround of joy and relief. Our at the ready techs, near-zero response time, and cost-saving solutions brought swift resolutions, up to 30% savings on maintenance costs, and expert support for all their equipment needs. With automated inventory and documentation, simplified contracts, and a single point of contact, Emeritus made their experience truly joyful.

Are you ready to experience the difference with Emeritus’ Bed Maintenance 2.0?
Contact Webb Clark at Webb.Clark@ emerituscs.com or visit emerituscs.com/ hospital-bed-repair/ for more information.
Click here to view the Ask the Expert Section on medwrench.com/ask-the-expert.

MEDWRENCH.COM | DIGITAL MAGAZINE 19
All webinars, podcasts, and product demos are eligible for 1 CE credit from the ACI.

LEARN, GROW, AND BE INSPIRED.
ON-DEMAN D LIVEWEBIN A R S PODCASTS TOOLS OF THE TRADE LIVE DEMO webinarwednesday.live


BEN C. Photo Contest
Monthly Prize is a $25 Gift Card
Since 2010, the face of MedWrench is Ben Calibrating or Ben C. for short. While he may just be a small Lego figure, you can find him all over the world.
• Is he helping to fix broken equipment at your facility?
• Is he fighting off sharks at the beach?
• Is he crowd surfing at a concert?
The possibilities are endless! How does Ben C. do these amazing things? That’s where you come into play. MedWrench has an ongoing photo contest to see where Ben Calibrating is traveling and what he is up to.
HOW DO I GET A BEN C. AND ENTER THE CONTEST?
Follow MedWrench on Facebook and LinkedIn and checkout the Expos and Events section of the Bulletin Board on MedWrench.com to find us at an upcoming show!
Post your pics on Facebook or LinkedIn using #BenC and tag @MedWrench. Follow Ben C. on Instagram at @BenCMedWrench.
Each month, we will announce a winner on social media, with a prize of a $25 Amazon gift card!
BEN C. PHOTO WINNERS:









MEDWRENCH.COM | DIGITAL MAGAZINE 23
• A niche job board for the HTM and imaging communities powered by TechNation.
• 3,000+ actively looking biomedical and imaging professionals.
• Completely FREE and confidential registration and application process.
• The fastest growing HTM talent network in the country.
• 400+ open opportunities throughout the United States.
• A variety of posting options ranging from single-job postings to 12-month unlimited memberships.

htmjobs@mdpublishing.com for posting inquiries
htmjobs.com to register today
YOUR DREAM JOB AWAITS HTMJOBS IS THE FUTURE HTMJOBS IS THE FUTURE HTMJOBS IS THE FUTURE NICHE JOB BOARDS **HELP WANTED**
Have PM Tips to Share? Send Them In!
Submit your preventative maintenance and other industry tips today
Take your time! Even though it can be hard with everything else going on, it is worth it.
- Derrick Adams
They told me that the device should be turned on with your “T-Tubes”, which attach between the SimCube and your BP test cuff, NOT connected to the NIBP hose or even the SimCube itself, until you see the zeroes. Sometimes, when turning on the device with the hose connected to the SimCube, but not the NIBP hose, it can be hard to clear those lines. In that case, take your thumb, put it over the connection to the test cuff and put it over the opening a couple of times. If that doesn’t work, try powering it on without the T-hose connected to the device.
- Deanna Wilkinson
Best practice for the use of any pressure measurement device is to start-up/zero the device with NOTHING connected. This eliminates the possibility of the device self-calibrating to a false (not quite) zero.
- Jim Munro
“ “Service your equipment like it will be put on your family tomorrow.
- Fred Jamarillo
Click here to submit your PM Tip
- Tony Cody
At MedWrench, our mission is to be the go-to resource for the medical equipment industry. This starts with sharing tips with each other! PM Tip Form online.
“
“ “
“ “
Sumbit Yours Now!
“ “
MEDWRENCH.COM | DIGITAL MAGAZINE 25







THE MEDICAL PRODUCT SUPPORT NETWORK Have a question about medical equipment? We Have Answers! Share ideas and information with other medical equipment professionals in our live Q&A forums. medwrench.com/ask-a-question
