




STAY IN THE GAME advance your knowledge, network & skills Missouri Veterinary Medical a ssociation a nnual con V ention January 26-29, 2023 Holiday i nn e xecuti V e c enter 2200 i -70 d ri V e s out H west colu M bia, Mo. 65203 P roceedin G s boo K
2
Table of Contents
Note: Abstracts received as of 12-30-23. Some speakers will use handouts at their lecture.
Companion Animal Presentations
Leah A. Cohn, DVM, PhD, DACVIM (SAIM)
Making Sense of Ehrlichiosis ........................................................................................................................ 9 Insulin: why, when, which, and how ........................................................................................................... 13 What to Do With a Positive 4Dx 19
Ralph Harvey, DVM, MS, DACVAA
Top Ten+ Best Things in Feline Pain Management ................................................................................... 27 Senior Pet Anesthesia & Periop Management – Not Too Old .................................................................. 27 How Can We Help, Unless We Know How They Hurt? – Assessing Acute and Chronic ...................... 27 Feline OA Pain: Suffering in Silence for Too Long and New Therapeutic Options .................................. 27
Jason Gagne, DVM
Nutritional Management of Canine and Feline Obesity ............................................................................ 31 Diet Trials: The Forgotten DiagnosticTool in Your Practice ...................................................................... 41
Natalie Gruchow, CVPM, SHRM-CP, Elite FFCP (Veterinary)
Fear Free Impacts on Patient Care..............................................................................................................51 Fear Free Vaccination Experience ..............................................................................................................51
Equine Presentations
Philip Johnson, DVM, ACVIM
Equine Protozoal Myeloencephalitis .......................................................................................................... 57
Kile S. Townsend, DVM, MS, DACVIM (LAIM)
How and When to Perform a Neurological Examination on the Farm ..................................................... 63 Vitamin E-related Diseases – What do we need to know? ........................................................................ 67
Alison LaCarrubba, DVM, ABVP (Equine Practice)
Care of our Geriatric Horses ...................................................................................................................... 73 Diagnosis and Management of Colic in the field setting ........................................................................... 77
Food Animal Presentations
Celeste Morris, DVM, MBA, MPVM
Bovine Reproductive Problems for the Mixed Animal Practitioner ......................................................... 85 Small Ruminant Pregnancy Diagnosis ........................................................................................................ 95
3
MU-CVM Lectures
Elizabeth A. Giuliano, DVM, MS, DACVO
Enucleation Surgery – Why Does This Seem More Difficult Than the Textbooks Say? ......................... 105
Philip Johnson, DVM, ACVIM
Viral hepatitis in horses (we used to call it Theiler disease) .................................................................... 109
Pamela Adkins, MS, DVM, PhD, DACVIM
Food Animal Neonatal Emergencies ........................................................................................................ 119
Leslie A. Lyons, PhD
Precision Medicine in Dogs and Cats
Owen Skinner, BVSc DECVS DACVS-SA MRCVS, ACVS Fellow
Adrenal Surgery: Don’t They All Die? .................................................................................................... 135
Wellbeing Presentations
Abby Whiting, DVM
The Science of Happy and The Inspired Leader ...................................................................................... 141
4
....................................................................................................... 127
Companion Animal
5
6
Companion Animal
Leah A. Cohn, DVM, PhD, DACVIM (SAIM) Professor, University of Missouri Columbia, Mo.
7
8
Making Sense of Ehrlichiosis
Leah A. Cohn, DVM, PhD, DACVIM (SAIM) Professor, University of Missouri - College of Veterinary Medicine
Ehrlichia, members of the family Anaplasmataceae, are obligate intracellular gram-negative bacteria that are transmitted through feeding of vector ticks. The first recognized disease caused by Ehrlichia, identified in Algeria in the 1930’s, was caused by Ehrlichia canis This potential pathogen is still an important cause of vector borne disease of dogs thoroughly the temperate regions of the world. Since the 1930’s many additional species of Ehrlichia have been recognized. These have different vectors, different cellular tropism, different reservoir and diseased hosts, and different pathogenicity and virulence. Diagnosis of disease and recognition of infection have similarities and differences. Besides supportive care and attention to complicating or co -morbid conditions, the treatment of all Ehrlichial infections usually relies on tetracycline antibiotics.
The three ehrlichial species of most importance for the small animal practitioner to understand are E. canis, E. ewingii, and E. chaffeensis (table 1). Other ehrlichial species occasionally recognized in diseased dogs, such as Panola Mountain Ehrlichia and E. muris eauclairensis will not be further considered here. Virulence of the considered infections depends not only on organism species and strain but also inoculum and host genetic background and immunolo gic status. Co-morbid infections also impact diagnosis, illness, and treatment.
E. canis
The original disease-causing species of Ehrlichia is still the most important as a canine pathogen. Transmitted by brown dog ticks in as little as 3 hours of feeding time, the disease is found in all the temperate regions of the world where the tick is found (essentially everywhere with warm weather other than New Zealand!). Different strains of E. canis may have difference in virulence. Pure bred dogs, especially German Shepherds, often seem to have a more severe clinical course . The disease course in the USA from E. canis seems to be less severe (and less often lethal) than caused by E. canis infections in much of the world.
There are three unique phases to the infection with E. canis. First is an acute infection that can be accompanied by vague febrile illness with or without ocular or neurological signs. In the USA especially, these signs may be quite mild and resolve without therapy. From there, the dog may enter a subclinical phase of infection where there are no discernable clinical signs of illness and all laboratory parameters are normal (resolution of thrombocytopenia typical of acute infection occurs in this phase). This subclinical phase may last for weeks, months, years, or for the life of the infected dog. Some portion of dogs with subclinical infection will go on to develop illness due to chronic canine monocytic ehrlichiosis (CME). The manifestation of illness is again quite variable. Among the more severe consequences are pancytopenia, hyperglobulinemia that can mimic multiple myeloma, bleeding diathesis, weight loss and/or muscle atrophy, uveitis or retinal hemorrhage, neurologic signs, and proteinuria with or without azotemia. Opportunistic infections may also occur.
E. ewingii
9
This pathogen causes granulocytic ehrlichiosis in dogs but is also an important zoonotic pathogen. Transmitted by the lone star tick, this infection is limited to areas in which that tick is endemic. The lone start tick is overwhelmingly the most common tick vector for disease in the state of Missouri. The reservoir for this pathogen seems to be canids, and infection in dogs is often subclinical. In fact, in one study as many as 23% of dogs from mid Missouri tests as a part of a prevalence study were seropositive for E. ewingii. While most infected dogs remain well, a proportion of infected dogs will develop acute clinical signs dominated by polyarthropathy, neurologic disease manifestations, and a febrile illness.
Infection with E. ewingii can be long lasting but the majority of disease manifestations seem to follow infection as an acute illness. There may be chronic infection consequences including renal disease with proteinuria +/- azotemia but this is less well characterized. Luckily, while morbidity of acute infection can be severe mortality is not reported. Disease resolves very quickly with treatment and the severe acute manifestations seem to resolve even without antimicrobial therapy.
E. chaffeensis
E. chaffeensis is predominantly a human pathogen. It is transmitted by the same lone start tick that transmits E. ewingii. This means that is shares geography with E. ewingii and is limited to the southeaster, southern midwestern, and mid Atlantic states. In the same prevalence study that found nearly a quarter of mid Missouri dogs had evidence of E. ewingii infection, 17% had evidence of E. chaffeensis infection. This pathogen has a mononuclear cell tropism like E. canis. It can cause very serious disease, up to and including death, in infected people. Experimental infection in dogs leads to thrombocytopenia but no clinical disease manifestations. Dogs with illness and natural infection have been reported.
Diagnosis
Screening of healthy dogs is a different subject than diagnosis of disease; screening will be addressed in a separate lecture. Routine laboratory tests can demonstrate suggestive findings such as thrombocytopenia (any species of Ehrlichia) or non-regenerative anemia and leukopenia (CME due to E. canis). Recognition of morulae in either mononuclear cells ( E. canis) or granulocytes (E. ewingii) can establish a diagnosis but is very insensitive and is not even entirely s pecific. Morulae are most often visible in the acute disease state so recognition of morulae in dogs with CME is rare. The odds of finding morulae are increased by examination of a buffy coat, and morulae are sometimes found on joint fluid cytology or microscopic examination of cerebrospinal fluid. Granulocytic morulae are identical to the morulae of Anaplasma phagocytophilum but the two infections (which have similar clinical manifestations) can be distinguished by geography , serology, or molecular techniques. Other abnormalities on chemistry profile (eg, hypoalbuminemia, hyperglobulinemia, azotemia) or urinalysis (eg, proteinuria) are important but not routinely identified and not specific. Tests such as bone marrow cytology or serum protein electrophoresi s may have utility in some scenarios more likely to occur with CME than with acute infection.
Serologic antibody testing is the most commonly used diagnostic technique , either using ELISA, IFA, or Western immunoblotting. Like all antibody-based serology, some time is required for seroconversion , meaning that acute infection can occur in seronegative dogs. Serology can be done as a Point-of-Care
10
test such as the extremely sensitive and specific IDEXX 4Dx Plus or as a send-off quantitative titer. Quantitative titers can be useful in looking for a 4 -fold increase in titer compatible with acute infection. Titer in chronic infection is typically stable and sustained and often quite high; high titers can persist despite antimicrobial therapy suggesting that treatment may not entirely eliminate the pathogen. Serology can be more or less specific but there is considerable cross reactivity on the IDEXX 4Dx Plus test. This means that a dog with E. chaffeensis could test positive for Ehrlichia without identifying a specific species type. It is difficult to find a lab offering commercial serology to differentiate between Ehrlichia species causing exposure.
Polymerase chain reaction (PCR) testing can be used to detect these pathogens which can be found in blood cells. PCR testing is most likely to sensitive early in infection with waxing and waning numbers of pathogens in the blood during chronic infection. This means that a negative PCR test cannot rule out infection but a positive PCR confirms the presence of pathogen. Animals with positive PCR for Ehrlichia in tissues such as the spleen or bone marrow can be negative on peripheral blood.
Treatment
Treatment relies on the use of anti-rickettsial antimicrobial therapy and supportive care. In general, acute illness with any of the three species discussed here has an excellent prognosis with a rapid response to treatment with doxycycline or minocycline (10 mg/kg/day, either q 24 h or divided BID). A duration of 2 weeks is likely adequate to address acute illness such as that seen with E. ewingii infection but a more protracted 28-day treatment course is recommended for chronic infection.
Chronic infection can be difficult (or even impossible) to eliminate. Doxycycline and minocycline remain drugs of choice but rifampicin may have utility as well. There is no point in repeating serology after treatment as antibody response can persist, and there is limited utility to PCR because a negative blood PCR does not prove the pathogen has been eliminated. Instead, monitoring of therapy for CME should include monitoring of concurrent issues such as pancytopenia.
Supportive care is often required for dogs with CME. This may include blood transfusion, colony stimulation with drugs such as filgrastim, antibiotics for secondary infections, treatment of proteinuria and/or azotemia, and the like.
Prevention and Public Health
Although work on vaccination is ongoing, the best way to prevent infection is to prevent tick feeding. Stringent ectoparasite control is key and should be used year-round, especially as brown dog ticks prefer to live in buildings (floors, attics, walls) and may thus survive year-round Repeat infections seem to be possible with any or all of the ehrlichial pathogens with no lasting immunity. A second infection could have different more severe consequences than the first.
Blood donor dogs should be screened for Ehrlichia and kept on stringent ectoparasite control programs.
While both E. ewingii and E. chaffeensis are zoonotic infections they cannot be transmitted directly from the dog to a person but require a tick vector. People removing ticks should use caution both to
11
avoid squeezing the tick and injecting additional pathogen in the pet but also to avoid exposi ng themselves. Caution is also suggested with collecting blood or tissues from infected dogs .
Table 1
Species Cellular tropism Vector tick
E. canis Mononuclear Rhipicephalus sanguineous (Brown dog tick)
E. ewingii Granulocytic Amblyomma americanum (Lone star tick)
E. chaffeensis Mononuclear Amblyomma americanum (Lone star tick)
Suggested readings
Zoonotic potential
Canine pathogen (possible very rare human illness)
Canine and human pathogen
Human pathogen (possible rare canine illness)
Beall, MJ, et al. “An Improved Point-of-Care ELISA for the Diagnosis of Anaplasmosis and Ehrlichiosis During the Acute Phase of Tick-Borne Infections in Dogs” Topics in Companion Animal Medicine 51, 2022 https://doi.org/10.1016/j.tcam.2022.100735
Burton, Wade, et al. "Association between exposure to Ehrlichia spp. and risk of develo ping chronic kidney disease in dogs." Journal of the American Animal Hospital Association 56.3 (2020): 159164.
Diniz P, et al “Ehrlichiosis and Anaplasmosis: An Update”. Veterinary Clinics of North America, 52(6):1225-1266, 2022.
Mylonakis, ME., et al. "An update on the treatment of canine monocytic ehrlichiosis (Ehrlichia canis)." The veterinary journal 246 (2019): 45-53.
Rodríguez-Alarcón, Carlos A., et al. "Demonstrating the presence of Ehrlichia canis DNA from different tissues of dogs with suspected subclinical ehrlichiosis." Parasites & Vectors 13.1 (2020): 1 -7.
Sato, Masahiko, et al. "Ehrlichia canis in dogs experimentally infected, treated, and then immune suppressed during the acute or subclinical phases." Journal of Veterinary Internal Medicine 34.3 (2020): 1214-1221.
12
Insulin: why, when, which, and how
Leah A. Cohn, DVM, PhD, DACVIM (SAIM) Professor, University of Missouri
Insulin administration is still the only treatment option for diabetic dogs and is often the best treatment option for diabetic cats. For several decades, people with type I diabetes mellitus (DM) were treated the same way we still treat dogs and cats. Insulins were administered twice a day, causing a decline in glucose over several hours to reach a nadir with a rebound over several more hours. This is no longer the way human diabetics are managed. Typically, humans now either use an insulin pump or administer a basal or “peakless” long acting insulin with multiple additional daily injections of a rapid acting, short duration insulin; this is the basal-bolus model, similar to normal physiology. The basal insulin has a long duration with a constant sustained activity rather than causing a nadir with rebound the way that traditional intermediate insulins work. On top of this sustained basal insulin, multiple additional daily injections of rapid i nsulin are administered based on carbohydrate intake, premeal blood glucose, and anticipated physical activity to mimic what the pancreas would do in health. The frequent monitoring and multiple injections daily is impractical for pet animals. Further, pharmacokinetics/dynamics of the insulins preparations differ between humans vs. dogs and cats with no true basal insulin choices for pets. Insulins vary in source, administration route, potency, concentration, and absorption characteristics, which in turn impact onset and duration of action. The large majority of insulins are now some form of recombinant product similar to human origin insulin. The only commercially available animal derived insulin is Vetsulin® from a porcine source. Insulins in suspension (NPH, Vetsulin, PZI) require thorough mixing prior to use while soluble insulin formulations (most insulins for human use) do not; inconsistent mixing can lead to dosing inconsistencies. Features including binding (eg, zinc, protamine), crystal size, and pH impact absorption after injection. Most insulins are hexamers that dissociate to active monomers and dimers. Other factors that impact absorption include volume, injection site, and local blood flow. Some of the newer basal insulins are more highly concentrated types, which also slows absorption (eg, Insulin glargine U-300).
All of the insulins made for use in long term management of DM are designed for subcutaneous (SQ) administration. It is crucial that pet owners understand insulin syringe size/dosing relationships. Veterinary insulins are made as 40 units per ml because of the small doses used in dogs and cats, while human insulins are typically 100, or even more units per ml for the very concentrated slow absorption types (eg, Toujeo is glargine 300U/ml). If a pet owner uses an incorrect syringe for insulin concentration, over (U-100 given in a U-40 syringe) or under (U-40 given in a U-100 syringe) dosing will occur. However, this syringe/drug matching can also be used to advantage when a pet needs an extremely small dose (or dose change) of a U-40 insulin (eg, Vetsulin) by administering it in a U-100 syringe The U-40 insulin dose can be multiplied by 2.5 to come up with the marking to fill to on the U-100 syringe; for example, if you want to administer 0.5 units of Vetsulin, 0.5 x 2.5 = 1.3, so the owner could pull up enough Vetsulin in a U-100 syringe to come be just beyond the one unit mark. U-100 syringes are available in 0.3,
13
0.5, and 1 ml capacities; it is easier to see the marks per unit using the smaller capacity syringes. Never administer a U-100 insulin in a U-40 syringe due to the risk of overdosing. Most types of insulin should NOT be diluted due to changes in dose and to absorption variability. For many insulins, “pen” administration devices allow the dose to be dialed in. Only VetPens® made for use with Vetsulin have ½ U increments while all pen insulins for humans have 1 unit increments.
Insulin pens
Insulin pens offer major advantages over the use of a needles/syringe and insulin vial. Both inadequate mixing of insulin suspensions (NPH, Vetsulin, PZI) and imprecise dosing lead to dosing errors for the insulins most frequently prescribed by veterinarians to be administered using a needle/syringe and vial of insulin. In fact, when using doses of <5 Units, a >20% error in dosing has been reported to occur >50% of the time. Inaccuracies with use of vial and syringe/needle are especially problematic for pet owners with issues related to vision or manual dexterity, conditions that frequently impact older pet owners.
The only true downside to the use of pens is cost. In essentially every study, insulin pens are more accurate and precise than syringe and vial. Essentially every human recombinant solution insulin can be purchased in a pen form. Pens for use with Vetsulin (VetPen®) can be purchased with ½ unit marks allowing easy administration of tiny doses or tiny dose changes. The human recombinant pens are labeled for storage at room temperature with disposal after about 42 days. Because dogs and cats use much smaller dosages than people, there is a huge amount of insulin left over at the end of this time that would be wasted if disposed of per label instructions. It appears that insulin solution pens can be safe and effective for much longer than 42 days. Many vets will have clients use the pen until empty with two caveats; first, the pen should be kept in the refrigerator to discourage bacterial growth if contaminated, and second, the insulin cartridge should be checked occasionally for discoloration or opacity and disposed of if there is a change in insulin appearance. Another difference in veterinary use of insulin pens has to do with priming the pen. The instructions for human use call for the pen to be primed with 1 to 3 units wasted before each injection. This amount of waste is negligible for human use but would cut the number of dosages available dramatically for dogs and cats. It seems that a first use priming is adequate without ongoing dose wasting for every injection. Skipping the prime does risk “air bubbles” making for inaccurate dosing but if the pen is held with the needle down and pen upright, the air bubbles should rise and not interfere with injection. If bubbles are seen on cartridge inspection, the pen can be held in a way that an additional waste shot eliminates the air bubble. A final consideration for the use of pens is needle size. Needles for human use may be extremely fine and short, but pets have thicker skin and fur. A reasonable size for pen needles for use in animals is a one half inch 29 gauge needle.
Insulin types commonly used in dogs and cats: (U-40) Vetsulin® (Merck Animal Health) is FDA approved for dogs and cats and is the usual “first choice” insulin for diabetic dogs. Vetsulin is a porcine zinc suspension and a lente type insulin. It is considered intermediate acting, with a duration of 8-14 hours in cats and 10-24 hours in dogs. It is typically used twice daily. Nadir is reported to be 2-8 hours in cats and 1-10
14
hours in dogs. It can be given by routine SQ injection by syringe or by use of an insulin pen (VetPen®) with increments of 0.5 U to 1 U (depending on pen size) for ease of delivery. A unique aspect of Vetsulin is that the bottle should be shaken vigorously, while for most insulins shaking is to be avoided. Starting dose: dogs = 0.2 U/kg q 12h, cats = 1U/CAT q 8-12 hr (U-40) PZI (Prozinc®, Boehringer Ingelheim Animal Health) has been FDA approved for cats for many years and was approved for dogs in 2019 . It is considered an intermediate to long acting insulin suspension, with a duration of 8-24 hours and a nadir of 5-7 hours in cats. In dogs, the nadir is reported to be 8-12 hours. PZI is one of two good “first choice” insulins for diabetic cats. Starting dose: dogs = 0.4 U/kg q 12-24h, cats = 1 U/CAT q 12 hr
(U-100 or U-300) Glargine is a long acting insulin made for humans and not FDA approved for pets. Nevertheless, it is often considered a “first choice” insulin for cats in the U-100 formulation and is used occasionally in dogs; in these species it is closer to intermediate action than to a basal or peakless insulin. The duration of U-100 (eg, Lantus®, Semglee®, others) in cats and dogs, respectively, are 12-24 hours and 12-20 hours. In humans, this is a “peakless” or basal insulin type that can be coupled with short or ultrashort acting insulins on a prn basis. However, it is used as a typical intermediate to long acting insulin in veterinary medicine as a stand-alone insulin. In cats the nadir is 12-14 hours, while it is 6-10 hours in dogs. This insulin type comes in a pen with a dial but the demarcations are only in 1 unit increments. The pharmacokinetics of the glargine U-300 glargine (Toujeo®) differ from the U-100, with an even longer duration and more predictable absorption. Due to the more concentrated insulin, administration of the necessary small volume is a challenge in cats so it is used less often than U-100 glargine. It may be useful as a once daily insulin in either dogs or cats, however. U100 (Lantus) Starting dose: dogs = 0.2 U/kg q 12, cats = 1 U/CAT q 12 hr U300 (Toujeo) Starting dose: dogs = 0.4 U/kg q 12-24h, cats = 2 U/CAT q 24 hr (U-100) NPH is an intermediate acting insulin for humans that is not FDA approved for pets. Common brand names include Humulin® N (Lilly) and Novolin® N (NovoNordisk) but it also comes as an inexpensive OTC insulin (ReliON from Walmart) It has been used in dogs with DM for decades and continues to be a reasonable choice in the species The duration and nadir are 4-10 hours and 0.5-8.5 hours, respectively. NPH has a short enough duration in cats that it is not recommended for use The major advantage is that this insulin type is sold over-the-counter (OTC) at a very reasonable price. Owners should be carefully instructed what to ask for if they choose to buy OTC insulin as both regular (short acting) insulin and 70/30 insulin are also sold OTC. Starting dose: dogs = 0.2 U/kg q 8-12, cats not recommended due to need for q 8 hr dosing (U-100) Regular insulin is a rapid acting, short duration insulin. It is not FDA approved for animals but is routinely used for the management of diabetic ketoacidosis in dogs and cats. Duration and nadir depend on route of administration (interestingly, any insulin works quickly and with shorter duration if given IV). Most often, it is administered as a constant rate infusion with near immediate action and extremely short duration, but it can be given by the intramuscular or subcutaneous route once animals are rehydrated. Using the IM/SQ route, the peak is about 0.5 to 3 hours, with a duration of 1 to 4 hours.
15
(U-100) Lispro, Aspart, glulisine insulins are also rapid acting, short duration insulins used in humans on a prn basis (bolus insulins) in addition to a basal insulin They are not FDA approved for animals but can be used for the management of diabetic ketoacidosis in dogs and cats . Because of the extremely short duration of action, they are only suitable for in -hospital management of animals.
(U-100) 70/30 is a mixture of NPH (70%) and regular (30%) insulin. It is not FDA approved for pets and is used only rarely in dogs that have a suitable duration of response to NPH but have a post-prandial glucose increase shortly after feeding and insulin administ ration. It can be purchased OTC.
(U-100) Detemir (Levemir®) is a basal insulin for humans and not FDA approved for pets but it is occasionally used in pets. It binds albumin in a way that prolongs insulin absorption to give a long and steady duration with reduced variability. Due to the fact that it is manufactured with more inulin molecules per unit, it is a very potent insulin in dogs, and they especially require a lower starting dose than for other insulin types. It should be used with caution in small dogs due to possible hypoglycemic episodes. In cats it is slightly more potent than glargine, but is fairly similar and is not particularly potent. Starting dose dogs 0.1 U/kg q 12 h, cats 1 U/CAT q 12 h. (U-100 or U-200) Degludec (Tresiba®) is a basal insulin solution for humans and not FDA approved for pets. In people, it reaches a steady state after several days of use and is truly peakless. Unfortunately, it acts as more of an intermediate insulin in pets and cannot be used once daily in cats but might work once daily in dogs. Though not often used in pets, there are publications demonstrating that this insulin can work well in dogs at least (Miller et al, 2021, Oda et al 2018). Starting dose dog 0.2 U/kg q 24 h, 1 U/CAT q 12 h
For owners where once daily dosing is the only practical option, consider the use of either glargine U300 (Toujeo®) or degludec (Tresiba®) for dogs or glargine U300 (Toujeo®) for cats.
Dose adjustment
It is crucial that pet owners understand that dose adjustment is normal and expected! The single most important determinant of a need for change in dose is how the pet is doing. However, glucose curves can also be helpful, especially when frequent readings are done over several days such as with the flash interstitial glucose monitoring systems. Dose adjustment is beyond the scope of this talk, but attention should be paid to glucose nadir and rate of decline (rapid drop or repeat hypoglycemia should trigger return to starting dose insulin to avoid Somogyi overswing), timing of insulin effect and duration of action, and proportion of time spent in a target glucose range of ~90 to 300 mg/dL. For cats and small dogs an increase of 1 unit at a time is reasonable, while for larger dogs a 10-20% increase is reasonable. It is fine to give a slightly higher dose in the morning than the afternoon when small dose adjustment are necessary.
Suggested reading:
Behrend E, et al. 2018 AAHA Diabetes Management Guidelines for Dogs and Cats. J Am Anim Hosp Assoc 2018; 54:1–21. DOI 10.5326/JAAHA-MS-6822. Updates 2022.
16
Fracassi, Federico, et al. Comparison of lente insulin and NPH insulin therapy for the treatment of newly diagnosed diabetic dogs: a randomised study. Vet Rec 183.8 (2018): 262-262. Gilor C, et al. One hundred years of insulin: is it time for smart? J Sm Anim Pract 63:654-660, 2022.
Hulsebosch SE, et al. Ultra-long-acting recombinant insulin for the treatment of diabetes mellitus in dogs. J Vet Intern Med 36:1211-1219, 2022. DOI: 10.1111/jvim.16449
Miller, M., et al. (2021) Day-to-day variability of porcine lente, insulin glargine 300 U/mL and insulin degludec in diabetic dogs. J Vet Intern Med 35, 2131-2139. https://doi.org/10.1111/jvim.16178
Oda H, et al. Time-action profiles of insulin degludec in healthy dogs and its effects on glycemic control in diabetic dogs. J Vet Med Sci 80, 1720-1723. https://doi.org/10.1292/jvms.170714. 2018.
17
18
What to do with a Positive 4Dx
Leah A. Cohn, DVM, PhD, DACVIM (SAIM) Professor, University of Missouri - College of Veterinary Medicine
Serologic titers detect antibodies or antigen in fluid samples, and these tests have long held an important place in disease diagnosis. In addition to a role in diagnosis, we often employ such tests to screen for infection in apparently healthy animals (e.g., cats for retroviral infections. These screening tests come in a variety of formats and use a variety of technologies; some are “mailed out” and other run as “cage side” tests; some are qualitative, others quantitative . Veterinarians are faced with the choice to screen or not to screen, and if they do screen, they will face questi ons as to how to handle a positive test in a healthy pet. To respond to those questions, they must understand something of the test itself (e.g., antigen vs. antibody, sensitivity and specificity), the pathogen prevalence in the region (which, in turn, effects predictive value), the pathogen behavior (e.g., is there an effective immunologic response, or is there a chronic carrier state?), and the disease caused by the pathogen (e g , is the disease simple or difficult to treat, of high or low virulence?)
Antigen vs. antibody matters to interpretation. Tests that detect antigen (e.g., most serologic heartworm tests, FeLV tests in cats), can prove that a pathogen is present in the sample. When these tests are negative, they cannot prove that a pathogen is absent. For example, cats with heartworm infection usually have very low worm burdens (1 or 2 worms is typical), and the antigen test specifically detects antigen in female worms. If a cat with heartworms has only one male worm, the antigen test will always be negative.
As opposed to antigen tests, antibody tests detect the host’s response to antigen encountered at some point in the past. Antibody formation takes some time. This means that titers may be absent during acute infection/illness, which is the reason that convalescent titers (to demonstrate seroconversion or a 4-fold increase in titer) are often required to confirm acute disease such as leptospirosis or RMSF. On the other hand, antibodies may persist long after an infection has resolved, or at least after any threat of illness due to infection has resolved. For example, dogs infected with E. ewingii may remain well or develop acute illness, but chronic illness is not reported. Yet, chronic infection can lead to chronically increased antibody titers even though the (known) risk of illness is past. Antibodies can be cross-reactive, meaning that a positive test result may be due to exposure/infection not with the pathogen of interest, but with a related, cross-reactive organism (pathogenic or not) . As an example, the pathogen that causes RMSF is cross-reactive with many other Spotted Fever Group organisms, most of which are not pathogenic ; this leads to frequent “false positive” tests . Additionally, certain antibodies may be found after vaccination as well as after natural infection. On occasion, diagnostic tests are designed to “work around” this problem, as is the case with C6 peptide assays for Lyme disease that are positive only after natural exposure to Borrelia burgdorferi and not after vaccination. In fact, all panelists on the ACVIM consensus statement on Lyme borreliosis recommend yearly screening for dogs that have spent time in endemic areas.
19
An additional set of limitations for serologic tests pertains to the likelihood that a given test accurately reflects pathogen/disease presence or absence. Any test, no matter how good, is subject to both false positive and false negative results. These are reflected in the diagnostic sensitivity and specificity of the test. Diagnostic sensitivity refers to the proportion of tests run on infected animals that are positive, while diagnostic specificity refers to the proportion of tests run on uninfected animals that are negative. It is apparent then that to “rule out” a diagnosis, a test with a high sensitivity is desired, while to “rule in” a diagnosis, a test with a high specificity is desired. Generally for screening exams, a test with high sensitivity is preferred over one with high specificity. Even more important to the clinician than a given test’s sensitivity and specificity are the test’s positive and negative predictive values. The positive predictive value is the probability that an animal that tests positive actually has the infection in question, while the negative predictive value is the probability that an animal that tests negative is free of infection. While positive predictive value certainly is related to the sensitivity and specificity of the diagnostic assay, it is also related to the prevalence of disease in the popu lation of animals tested. This means that a positive test result in a population with a low prevalence of disease, even when the test is very sensitive and specific, has a greater chance of being a false -positive than when the same test is applied to a po pulation with a high disease prevalence. As an example, if a diagnostic test has a sensitivity of 95% and a specificity of 90%, the positive predictive value of that test in a population with a 50% pathogen prevalence would be 90%. This means that 1 out of 10 positive tests would be a false positive. On the other hand, for that very same test applied to a population with a 5% prevalence of pathogen, the positive predictive value would be 33%, meaning that 2 out of 3 positive tests might be false positives.
Finally, understanding the disease that might result from the pathogen exposure identified on a screening test impacts reaction to a positive screening test. If the pathogen frequently results in chronic disease, it makes sense to intervene before disease is manifest. This is very true for pathogens such as heartworm infection – a positive screen should prompt treatment. On the other hand, if the pathogen seldom results in chronic disease, a more “watch and wait” approach may be the responsible approach. There will always be both pro’s and con’s to screening healthy dogs for infection. These are summarized here:
Screening Pro’s
• May allow treatment before disease occurs
• Provides regional prevalence information
• May provide sentinel information for both human and animal infections
• Informs ectoparasite control practices
• May reduce pathogen reservoir for some infections
• Alerts to non-tested pathogens carried by the same vectors
Screening Con’s
• False +’s in low prevalence areas are a real issue
• May lead to unneeded treatment
• Infection may never become clinical
• Past infection may be resolved
• Adverse effects; costs; resistance to drugs
20
• Treatment may not “cure” and doesn’t prevent re-infection
• Role of dogs for human infection debatable for some pathogens
So with all this information, what is the optimum response to a positive result on a screening test such as the IDEXX 4Dx in an apparently healthy dog? There is no single answer, but instead all the factors discussed, as well as the owner’s wishes, must be considered. General guidelines are presented here:
Positive Heartworm Screen
1) Evaluate for microfilaria (Knott’s test)
2) Consider confirmatory re -test if microfilaria negative
3) Obtain chest radiographs, CBC, chemistry profile, and UA for disease staging and pretreatment health evaluation. Consider echocardiogram if murmur or cardiomegaly present.
4) Initiate treatment per American Heartworm Society Guidelines using melarsomine (http://www.heartwormsociety.org/veterinary -resources/canine-guidelines.html#8)
5) Initiate heartworm prophylaxis
6) Retest in 6-12 months
Positive Ehrlichia Screen
1) Discuss ectoparasite control with the pet owner. You now have proof their pet was not only bitten by a tick, but that tick transmitted a potential pathogen! Do better on parasite control.
2) Consider geography. In Missouri, it is FAR more likely to be E. ewingii or E. chaffeensis than E. canis causing the positive test. These organisms are far less pathogenic than E. canis.
3) Perform a CBC to look for morulae, thrombocytopenia, anemia, or hyperglobulinemia. If these are identified, antibiotic (doxycycline, minocycline) treatment is indicated.
4) Perform a UA to look for proteinuria. If identified, perform UPC and blood pressure, and consider further evaluation and antibiotic treatment.
5) Perform either a chemistry with creatinine/BUN or an SDMA (much more sensitive) to evaluate renal function. If either are abnormal consider further evaluation and antibiotic treatment .
6) If CBC, renal parameters, and UA are normal, discuss these three options with the owner and let them be part of the decision. The options are:
a. Watch and wait (my preferred option for my own dogs in Missouri)
i. Educate the owner about the signs of disease
ii. Repeat CBC, renal parameters, and UA in one year
b. Investigate further
i. Perform more specific serologic tests to ID species of Ehrlichia (difficult to find lab to run this commercially)
ii. Perform PCR, realizing that a negative test does NOT rule out infection but a positive proves pathogen presence.
c. Treat with tetracyclines
i. Doxycycline 10 mg/kg daily (q 24 hr or divided BID) PO for 28 days (chronic monocytic ehrlichiosis requires longer treatment than acute, or than granulocytic ehrlichiosis) OR minocycline 10 mg/kg PO q 12h for 28 days.
21
ii. Realize there are issues of co st, convenience, and adverse effects (dysbiosis, GI upset, hepatopathy, esophageal stricture [cats esp]) associated with tetracycline use
iii. Realize that antibiotics may not eliminate the pathogen entirely , potentially allowing delayed illness despite treatment.
Positive Lyme Screen
1) The IDEXX SNAP 4Dx will NOT be positive due to vaccination, but some other tests (Osp -based serologic tests) are. The IDEXX test will only be positive after natural infection.
2) Discuss ectoparasite control with the pet owner. You now have proof their pet was not only bitten by a tick, but that tick transmitted a potential pathogen.
3) Perform urinalysis to look for proteinuria. If identified, perform UPC and blood pressure, and consider further evaluation and antibiotic treatment.
4) A quantitative C6 peptide test is available from IDEXX but the ACVIM consensus statement on Lyme borreliosis does not recommend performing the test as there is no proof that the test is predictive of illness.
a. Some panelists on the consensus statement, and t he author, do recommend quantitative C6 peptide. Antimicrobial treatment could be instituted if C6 antibody is >30 U/ml.
b. If treatment is begun after high titer, can repeat quantitative C6 in 4-6 months time to document new baseline for future comparison. Expect titer to decrease by at least 50%.
5) Four of six panelists on the ACVIM consensus statement on Lyme borreliosis do NOT recommend antibiotic treatment for non-proteinuric, healthy dogs with positive screening tests.
i. Watch and wait (Consensus recommendation)
1. Educate the owner about the signs of disease
2. Repeat UA +/- UPC & BP in 3 to 12 months (no consensus on freque ncy)
ii. Treat with antibiotics, especially if C6 >30 U/ml (minority opinion)
1. Doxycycline or minocycline 10 mg/kg q 12 to 24 hr for 30 days
2. Other antibiotics efficacious for Borrelia but not for common coinfection of Anaplasma (amoxicillin, cephalosporins, azithromycine).
3. Realize there are issues of cost, convenience, and adverse effects associated with use of any antibiotic
4. Repeat C6 peptide in 4-6 months to confirm reduced titer resulting from treatment
5. Repeat UA +/- UPC & BP in 3 to 12 months (no consensus on frequency)
6) Discuss pros and cons of Lyme vaccine going forward
Positive Anaplasma Screen
1) Consider geography. In Missouri, a positive test is more likely due to A. platys than A. phagocytophilum.
2) Discuss ectoparasite control with the pet owner. You know have proof their pet was not only bitten by a tick, but that tick transmitted a potential pathogen.
22
3) Perform a CBC to look for morulae, thrombocytopenia or hyperglobulinemia. If these are identified, antibiotic treatment is indicated.
4) Perform a UA to look for proteinuria. If identified, perform UPC and blood pressure, and consider further evaluation and antibiotic treatment.
5) If CBC and UA are normal, discuss the three options with the owner and let them be part of the decision. The options are:
a. Watch and wait (my preferred option)
i. Educate the owner about the signs of disease
ii. Repeat CBC and UA in one year
b. Treat with antibiotics
i. Realize there are issues of cost, convenience, and adverse effects associated with tetracycline use
ii. Realize that antibiotics may not eliminate the pathogen entirely
iii. Doxycycline or minocycline 5 mg/kg PO q 12 hr for 14 to 28 days (ideal therapy little investigated)
Suggested readings
Littman, Meryl P., et al. "ACVIM small animal consensus statement on Lyme disease in dogs: diagnosis, treatment, and prevention." Journal of veterinary internal medicine 20.2 (2006): 422-434.
Diniz P, et al “Ehrlichiosis and Anaplasmosis: An Update”. Veterinary Clinics of North America , 52(6):1225-1266, 2022.
Taber R, et al. “Bartonellosis in Dogs and Cats, an Update”. Veterinary Clinics of North America , 52(6):1163-1192, 2022.
Little, Susan, et al. "Canine infection with Dirofilaria immitis, Borrelia burgdorferi, Anaplasma spp., and Ehrlichia spp. in the United States, 2013–2019." Parasites & Vectors 14.1 (2021): 1-16.
Beall, MJ, et al. “An Improved Point-of-Care ELISA for the Diagnosis of Anaplasmosis and Ehrlichiosis During the Acute Phase of Tick -Borne Infections in Dogs” Topics in Companion Animal Medicine 51, 2022 https://doi.org/10.1016/j.tcam.2022.100735.
23
24
Companion Animal
Ralph Harvey, DVM, MS, DACVAA
Department of Small Animal Clinical Sciences University of Tennessee College of Veterinary Medicine Knoxville, Tennessee.
25
26
1) Top Ten+ Best Things in Feline Pain Management
This is a new era in pain management for cats. New information and products tremendously improve our options and opportunities to address long-standing deficiencies.
Recognition of the benefits of reducing fear/stress/pain
Behavioral and facial grimace scales are validated methods Gentle handling refined and promoted in the AAHA / AAFP / ISFM Guidelines
NSAID therapy - perioperative and chronic uses expanding for cats New opportunities with opioids for cats - emphasis on buprenorphine Anti-NGF mAbs, and so much more
2) Senior Pet Anesthesia & Periop Management – Not Too Old
Although age is not a disease, we see increased co -morbidities and limited resilience in our older patients. Best practices for these animals include using readily available agents and techniques. Increased attention to detail and respect for fragile homeostasis brings clinical success and client appreciation.
Out-patient anesthesia and robust adaptability in our approach are essential Goals include avoiding stress and maintenance of the patient's daily routine These patients and clients are among our best and most valued resource
3) How Can We Help, Unless We Know How They Hurt? – Assessing Acute and Chronic Pain
Recognition and repeated evaluation of pain are essential in veterinary care. Animals often obscure signs of pain, but we have increasingly powerful strategies to assess pain.
Assessment of animal pain is based traditionally and typically on species-specific behaviors Behavioral differences occur in patients removed from their everyday home environments Client/owner input and reassessment after treatment are essential A new medical device provides for objective assessment of acute and chronic pain
4) Feline OA Pain: Suffering in Silence for Too Long and New Therapeutic Options
Osteoarthritis pain in cats is ubiquitous, underdiagnosed , and under-treated. Recognition and assessment of pain in cats have improved significantly in recent years. While NSAIDs are the foundation of treating OA pain in other species, none are US -FDA approved for chronic use in cats. A new therapeutic anti -NGF monoclonal antibody is safe and effective for treating OA pain in cats. Overcoming obstacles to medicalizing cats with OA pain requires improved partnering with clients.
Osteoarthritis pain in cats is ubiquitous, under -diagnosed, and under -treated Adding value with multi-modal management of chronic mal-adaptive pain
A novel therapeutic anti-NGF monoclonal antibody is safe and effective
27
28
Companion Animal
Jason Gagne, DVM
Department of Small Animal Clinical Sciences
University of Tennessee College of Veterinary Medicine Knoxville, Tennessee.
29
30
Nutritional Management of Canine and Feline Obesity Nestlé Purina PetCare
Prevalence and Cost of Obesity
Obesity is an excess of body fat that frequently results in significant impairment of health. Using the ninepoint Purina Body Condition Scoring System,1,2 dogs and cats with a body condition score (BCS) of 6-7 out of 9 are generally considered overweight while 8-9 out of 9 are considered obese 3 Each BCS unit above 5/9 is equal to approximately 10% excess body weight. 4
Obesity is one of the most common diseases encountered by veterinarians and yet, unlike many conditions, can often be prevented altogether. According to a 2018 survey from the Association for Pet Obesity Prevention, 55.8% of dogs and 59.5% of cats are overweight or obese 5 This translates into an estimated 50 million dogs and 56 million cats in the United States in 2018, which reflects a 169% increase in overweight cats and a 158% increase in overweight dogs over ten years 5,6 While the shocking nature of these numbers alone should motivate us to add ress this issue, we also cannot forget that obesity is costly for owners and can negatively impact our patients’ quality of life.
Obese pets are also expensive! In addition to increased food costs, owners of overweight pets are also spending more on veterinary bills. According to pet insurance claim statistics released by Nationwide, $69 million was paid out in claims for diseases related to obesity in 201 7. The most common comorbidity in obese dogs is osteoarthritis, while the most common comorbidity in obese cats is bladder or urinary tract disease.7 The 2017 Banfield State o f Pet Health Report found that over a 4-year period, owners of overweight dogs spent 17% more in healthcare costs and 25% more on medications compared to owners of healthy-weight dogs. Owners of overweight cats also spent 36% more on diagnostic procedures versus owners of healthy weight cats 6
Factors Contributing to Obesity
While many factors contribute to obesity, most can be divided into either pet-related or owner-related factors. Table 1 summarizes these factors. Pet-related factors such as genetics, breed, age, or reproductive status may predispose them to obesity . Neutering is frequently mentioned as a cause of increased body weight and condition in dogs and cats While the exact mechanisms contributing to weight gain after neutering have yet to be conclusively determined, both an increase in food intake and decrease in energy expenditure have been suggested. In one study, a group of adult male cats were neutered in order to examine the effects of neutering on energy expenditure and weight gain. Their results supported the conclusion that there is a period of increase d food intake following neutering.8 Another study paired 11-week-old female kitten littermates and randomly assigned them to either a neutered group (neutered at 19 weeks old) or an intact group. All kittens were offered a dry diet free-choice until they were one year of age. This study observed that post-neutering, the body weight, BCS, and body fat percentage of the neutered kittens continued to increase despite consuming similar amounts of energy to their intact littermates. The authors concluded neutered kittens have a reduced metabolizable energy requirement.9 While these studies observed differing mechanisms, they both concluded that it is essential to feed to maintain an ideal BCS rather than free -choice to prevent post-neutering weight gain.8,9 Common ownerrelated factors include poor compliance to a feeding program, not understanding the seriousness of obesity, overfeeding of food/treats, and not recognizing that a problem exists
31
10-13
Table
1: Factors Relating to Obesity in Pets
Pet-Related
Owner-Related Additional Factors Activity level Genetics/ breed Age
Reproductive status Underlying disease (e.g. hypothyroidism)
Owner compliance Overfeeding Not understanding seriousness Socioeconomic status
Owner age
The Relationship between Obesity and Disease
Meal frequency Single dog household Begging
Adipose tissue is now understood to be an active endocrine organ that results in chronic inflammation, causing oxidative stress and potential secondary health conditions.14 Pro-inflammatory cytokines attract macrophages and immune cell populations may shift. The result is secretion of hormones and inflammatory mediators known as adipokines.14 Table 2 is a brief review of the effects of obesity on select adipokines.
Table
14
2: Select Adipokines in Obesity
↑ TNF-α ↓ Adiponectin ↑ Leptin
Inflammatory mediator Inversely proportional to adiposity Potentiates insulin signaling Less adiponectin = more insulin resistance
Regulates appetite Obese individuals resistant to effects
While many owners may be familiar with the most commonly known health issues associated with obesity, such as musculoskeletal disease or diabetes mellitus, our understanding of the far-reaching impact of obesity on health continue s to deepen. Obesity’s contribution to the progression of osteoarthritis (OA) in patients goes beyond weight-bearing stress. Inflammatory mediators that increase with obesity, such as IL-1 or TNF-α, increase matrix metalloproteases (MMPs) , which are responsible for breaking down cartilage and result in cartilage degradation.14 Oxidative stress can further increase the circulating inflammatory cytokines Common weight related health conditions are reviewed in Table 3.
14,15
Table 3: Common weight related health conditions
Overweight or Obese Cats are
Overweight or obese dogs risk developing 4 times more likely to develop diabetes
Tracheal collapse Nearly 3 times more likely to experience lameness Diabetes More likely to have non-allergic skin problems
Cruciate ligament disease
At risk for urinary tract disease Osteoarthritis Prone to liver disease and failure of the organ Urinary tract disease Likely to experience OA and ligament damage
Intervertebral disc disease
Pancreatitis
Maintaining Ideal Body Condition Can Extend Healthy Years
A groundbreaking 14-year study by Purina researchers showed that feeding dogs to an ideal body condition throughout their lives can significantly extend a dog’s healthy years At the Purina Pet Care Center in Missouri, 48 eight-week-old Labrador Retrievers were paired by sex and litter, then randomly assigned to either a control or restricted-fed group. Dogs in the control group were allowed to eat ad -
32
libitum as puppies and then a consistent amount of food beginning at 3.25 years old. Dogs in the restricted-fed group received 25% less than the amount eaten by their paired littermates. All dogs received the same nutritionally completed and balanced foods (first puppy diets, then adult formulations) throughout the study. Only the amount provided was different. This groundbreaking study demonstrated that feeding dogs to an ideal body condition throughout their lives could significantly extend a dog’s healthy years by a median of 1.8 years. And although the restricted -fed dogs in the study generally developed the same chronic conditions as they aged, the need for treatment of those conditions was delayed. Long-term treatment of osteoarthritis was initiated an average of three years later and treatment for chronic conditions was initiated an average of 2.1 years later in the restricted-fed dogs.16
The Path towards Weight Loss
A five-step approach can be used to help our patients achieve a healthy weight:
1) Identify and assess overweight pets 2) Create a partnership with our clients 3) Make a customized weight loss plan 4) Follow-up
5) Celebrate success!
1) Identify and assess overweight pets
The easiest time to identify overweight pets is during a clinic visit . The body weight, BCS, and muscle condition score should be recorded each visit. Recording and monitoring BCS is essential because while tracking a patient’s body weight can indicate weight loss or gain, it does not determine if a pet is too thin or too heavy for their frame and body type. Full schedules and brief appointments can result in obesity and the diet conversation being overlooked. However, training technical staff on body condition scoring can allow us to leverage their knowledge and help make our time in the exam room as effective and efficient as possible.
2) Create a partnership with our clients
Client commitment is essential to the success of a weight loss program . However, it is often the most difficult component to achieve. Successful weight loss depends on teaching clients how to assess their pet’s body condition, modifying client behaviors, and educating clients about the obesity-associated health risks Purina conducted a study that found that many pet owners may have difficulty accurately assessing body condition in their own dogs. Owners of 201 healthy adult dogs were asked 30 questions about their pets and asked to determine their dogs’ body condition scores, using the Purina Body Condition System as a reference. Independently, a professional skilled in body condition scoring evaluated the same dogs, and the scores were then compared. In this study, only 28% of owners characterized their dogs as overweight, while the expert identified 79% of those same pets as overweight.17 This exercise can be quickly and efficiently reproduced in our exam rooms utilizing BCS charts or posters. It is often more impactful for an owner to reach the realization that their pet is overweight on their own versus quickly being told so during the physical exam.
While conversations about weight may sometimes feel time -consuming or even challenging, our patients depend on us to be their advocates. Some owners may have financial concerns about the cost of therapeutic weight loss diets. A study in Europe found that the cost of feeding a therapeutic weight loss diet is, on average, not significantly different from the cost of feeding a maintenance diet before and during weight loss.18 Furthermore, if we take a moment to explain the specific benefits of a therapeutic weight loss diet as mentioned below, it can increase our client compliance.
33
3) Make a customized weight loss plan
Key Components of a Therapeutic Weight Loss Diet
In humans, the nutritional approach to weight loss focuses on the amount of food intake, the type of food eaten, and the timing of meal consumption.19 In veterinary medicine, the discussion around weight loss has long emphasized caloric restriction. But the issue is more complex; there is no single best approach to weight loss, and having multiple nutritional options allows for individualized care.
We know that modification of certain nutrients can help pets achieve an ideal body weight and condition. For example, fat is a more energy-dense source of calories compared to protein and carbohydrate. Often, limiting the amount of fat in a diet will also lower the total caloric density of the diet
Therapeutic weight loss diets are often high in protein and have a high protein-to-calorie ratio. High protein intake can lead to increased fat loss while preserving lean body mass (LBM) during weight loss A study of overweight adult dogs conducted at the Nestlé Purina Pet Care Center found that feeding a diet with 39% of calories from protein resulted in increased fat loss and reduced loss of LBM during weight loss compared to diets with a lower percentage of calories from protein.20 Results were similar in a study conducted in cats; increased dietary protein in a therapeutic weight management diet results in a greater loss of body fat and greater retention of lean body mass compared to a control diet . 21 LBM is metabolically active and increases energy requirements, stimulates resting energy metabolism, and reduces oxidative stress.
In addition to reduced fat and increased protein, research has demonstrated that isoflavones are beneficial in healthy weight management and are an important additio n to an effective weight loss diet . Isoflavones are natural bioactive compounds found in soybeans and other legumes. Weight management benefits include: increased daily energy expenditure, reduced oxidative stress, reduced weight gain, and reduced fat accumulation (rebound).22-24
A study conducted in 2022 (NPPC Internal Data, St Joseph, MO 2022) evaluated a new and innovative approach to obesity - a diet that aims to help pets lose weight and transform their metabolism. Key features of this test weight loss diet include: 3:1 protein to starch ratio, natural fiber, isoflavones, Lcarnitine, high level of omega-3 fatty acids, and glucosamine. Thirty overweight dogs were enrolled into this 6-month weight loss study, and fed a control diet for 8 weeks to determine their maintenance energy requirement. They were then randomized into two group for the reminder of the 6 -month study: the control weight loss diet or the test diet. Both groups were fed at a caloric restriction of 25% MER for months 1-4, and 40% MER for months 5 -6. Results show overall weight loss was similar in both groups, but there were significant differences in loss of body fat and maintenance of lean body mass. Dogs fed the test diet lost significantly more body fat compared to dogs fed the control diet (Figure 1), and dogs fed the control diet lost significantly more lean body mass where as the test diet actually minimized loss of lean body mass (Figure 2).
34
Figure 1- Change in body fat from baseline (kg) between the test and control


Figure 2 - Change in lean body mass from baseline (kg) between the test and control diets
Dogs fed the test diet also showed improvement in select metabolic health indicators . Postprandial interstitial glucose was significantly lower in dogs fed the test diet vs control at the 8 -week time point. Fasting serum insulin in dogs fed the test diet was on average 4x lower from baseline after 6 months of weight loss. Fasting serum cholesterol and triglycerides were significantly decreased in dogs fed the test diet over the 6-month study as well. There was a significant reduction in proinflammatory cytokines TNFalpha and IL-6 in dogs fed the test diet at 6 months compared to the control group. Finally, fasting serum leptin levels were significantly reduced compared to control as well.
The Weight Loss Plan
Creating a customized weight loss plan does not have to be difficult or time-consuming. Essential components include a thorough dietary history including the type, amount, frequency of food AND treats, and the pets and people in their household. The World Small Animal Veterinary Association (WSAVA) and the American College of Veterinary Nutrition have each created free diet history forms that can be filled out by owners in the waiting room or at home prior to their appointment.25,26 When reviewing the diet history, it is essential to be specific. A 2010 study found that 59% of owners give table scraps that constitute 21% of the total daily calories of the dogs in the study.27 Additionally, a recent study found that 83% of the owners surveyed indicated that they regularly give 1 to 5 treats per day. 28 There can be a wide range of caloric content in popular treats or diet formulations and asking open -ended questions can encourage our clients to share details they may otherwise neglect to mention. Once we have a more informed idea of what our patient is currently consuming, we can begin to determine a diet recommendation that includes a specific diet and a specific amount , including any treats.
When creating a customized weight loss plan, we must consider that there is a range of acceptable intake for each nutrient. When attempting weight loss in a patient, simply reducing the amount fed of an overthe-counter (OTC) diet can cause a nutrient deficiency. OTC diets are formulated with the correct balance of nutrients for pets that are expected to consume a spec ific amount of food based on their body weight. Therapeutic weight loss diets are formulated with appropriate levels of macronutrients and micronutrients to allow for caloric restriction without creating nutrient deficiencies. Typically, weight loss should be limited to 1-2% of body weight per week in dogs and 0.5-2% in cats
Feeding guide software or calculators, such as the free Nestlé Purina Veterinary Feeding Guide (www.purinafeedingguide.com), can help determine how much to feed of a specific therapeutic diet. Such programs can also incorporate treats as part of a healthy weight loss plan . Another option is to feed 80% of a patient’s current caloric intake using a therapeutic weight loss diet. This method assumes the patient is weight stable at their current caloric intake and that an accurate diet history has been obtained. A third
35
option, if an accurate diet history cannot be obtained, is to calculate resting energy requirement (RER) using the pet’s estimated ideal weight and then feed some percentage of that amount.13 While feeding 80% of RER is often effective and well tolerated, feeding 70% of RER may be required in some cats. RER can be estimated through the linear equation RER = 30 x (BW in kg) + 70. However, this equation is only accurate for pets 2-25 kg Therefore, we recommend use of the exponential equation 70(kg BW)0.75 which is accurate for all sizes. Most calculator apps on smartphones will display the xy exponent function needed to perform this calculation if the phone is turned sideways As an example, the estimated RER for a 30 kg dog is: RER = 70 x (30 kg)0.75 = 897 kcal
Feeding the right amount of food during weight loss is extremely important. There are three common methods of feeding: 1) Free-choice, also called ad libitum 2) Time-limited, which is the amount of food a pet will eat in a given period of time and 3) Portion-limited, which is a measured amount of pet food based on the animal’s daily energy requirements While portion-limited feeding is best, studies have demonstrated that volumetric measurement is often inaccurate 29,30 The best solution to combat this inaccuracy is to use a gram scale, which many clients already have at home. Meals for the day or week can be premeasured and packaged in individual portions to save time later. In addition to feeding the right amount, how often we feed also matters. Dogs that are fed once per day are more likely to be obese than dogs that are fed more than once a day.11 Feeding small, frequent meals can lead to increased energy expenditure due to thermogenesis.11 Modifying how owners are measuring their pet’s food and increasing meal frequency are small changes that may represent an important step towards achieving and maintaining a healthy weight.
While appropriate calorie restriction is still the most critical component of a weight loss plan; exercise can also be important. Not only does exercise increase energy expenditure, maintain RER, and promote maintenance of LBM, it also enhances the human-animal bond. A general recommendation of walking dogs 30 minutes per day is a good place to start, barring any significant physical impairments that may be exacerbated with exercise. In those cases, lower-impact exercises such as swimming are indicated. The idea of increasing activity in cats often feels daunting or even laughable to some owners. However, a 2014 study investigated the effects of feeding frequency and dietary water content on voluntary physical activity and found that increased feeding frequency and dietary water content (without changing energy intake or dietary macronutrient composition) appears to promote physical activity in cats. 31 In addition, Dr. Tony Buffington’s Indoor Cat Initiative website (indoorpet.osu.edu/cats) provides additional ideas to promote physical activity, such as moving the food bowl, leash training cats, or playing with a variety of different toys
4) Follow-up (Overcoming the Obstacles of Weight Loss)
Lastly, it is critical that we follow up. The owner should be called one week after the diet starts to troubleshoot any issues that may arise. A recheck should be scheduled for two weeks after initiating the diet plan, then monthly rechecks conducted thereafter until an ideal body weight is achieved. Many weight loss attempts will fail due to a lack of follow up. By tracking the progress of your patients and making adjustments, you increase the chance of success.
Many dogs and cats will regain weight after weight loss . Researchers found that weight gain occurs more rapidly and at a lower calorie intake than what was originally required to induce obesity. 32 However, the likelihood of regaining weight has been shown to be significantly less if the therapeutic weight management diet is continued during weight maintenance, rather than switching back onto a standard maintenance diet.33 Weight management is a lifelong process and body weight needs to be monitored even after ideal weight has been achieved.
36
5) Celebrate Success
Weight loss alone can often be a potent and effective treatment for some medical conditions. A study of fourteen obese client-owned dogs with clinical and radiographic signs of OA evaluated the effect of weight loss on lameness in obese dogs. The dogs were fed a restricted-calorie diet over a period of 16 weeks that incorporated six follow-up visits. At each visit, body weight was measured and severity of lameness was assessed using a numeric rating scale (NRS), a visual analogue scale (VAS) , and kinetic gait analysis by a single veterinary evaluator. The results indicate that as little as 6.10% reduction in body weight can cause a significant decrease in lameness. The authors concluded that weight loss should be presented as an important treatment modality to owners of obese dogs with OA and that noticeable improvement may be seen after even modest weight loss 34 In addition, weight loss may decrease chronic inflammation. A study that evaluated the effects of weight loss on adipokines and markers of inflammation in 25 dogs before and after a weight loss program found that C-reactive protein, monocyte chemoattractant protein1, resistin, and leptin decreased after weight loss.35
The most notable benefit of weight loss may be an improvement in quality of life. Owners of fifty obese dogs were asked to complete a validated, standardized quality of life questionnaire prior to and following weight loss. Of the 50 dogs that were enrolled in the study, 30 dogs successfully achieved their weight loss goal. As scored by their owners, dogs that failed to complete their weight loss program had lower vitality and higher emotional disturbance scores than those which successfully lost weight. The 30 dogs that achieved their weight loss goals had increased vitality scores (P < 0.001), and decreased scores for both emotional disturbance (P < 0.001) and pain (P < 0.001). The change in vitality score was positively associated with percentage weight loss and percentage of body fat loss. These results indicate that obese dogs that successfully lose weight can achieve a significant improvement in quality of life.36
Be sure to recognize each time the patient loses weight (even a small amount). Adhering to a weight loss plan is not easy and clients will appreciate the praise. Some of the most effective clinic weight loss programs share the successes of their clients and patients. If clients see the successes of others, it will give them encouragement to start a weight loss program for their own pet. Before and after photos can provide a great deal of encouragement
Summary
Obesity is an excess of body fat that frequently results in significant impairment of health. As many as 80% of veterinarians have tried to help their own pet lose weight , as have over 68% of pet owners However, 70% of pet owners have NEVER tried a therapeutic diet. 5 While the battle against obesity may be challenging, a well-designed weight management plan and a therapeutic weight management diet are effective tools in helping our clients significantly extend their pet’s healthy years.
References
1. Laflamme DP. Development and Validation of a Body Condition Score S ystem of Dogs. Canine Pract July/August 1997; 22: 10 -15.
2. Laflamme D. Development and validation of a body condition score system for cats. A clinical tool. Feline Pract 1997;25:13–8.
3. Linder D, Mueller M. Pet obesity management: beyond nutrition. Vet Clin North Am Small Anim Pract 2014;44(4):789‐vii. doi:10.1016/j.cvsm.2014.03.004
37
4. German AJ, Holden SL, Bissot T, Morris PJ, Biourge V. Use of starting condition score to estimate changes in body weight and composition during weight loss in obese dogs. Res Vet Sci. 2009;87(2):249-254. doi:10.1016/j.rvsc.2009.02.007
5. “2018 Pet Obesity Survey Results.” Association for Pet Obesity Prevention, https://petobesityprevention.org/2018, March 12, 2019 Accessed: April 4, 2020.
6. 2017 Banfield State of Pet Health Report. https://www.banfield.com/Banfield/media/PDF/Downloads/soph/2017 -SOPH-Infographic.pdf Accessed: April 4, 2020.
7. “Pet Obesity on the rise for eighth consecutive year.” PR Newswire, https://www.prnewswire.com/news-releases/pet-obesity-on-the-rise-for-eighth-consecutive-year300771328.html, January 2, 2019 Accessed: April 4, 2020.
8. Wei A, Fascetti AJ, Kim K, et al. Early effects of neutering on energy expenditure in adult male cats. PLoS One. 2014;9(2):e89557. Published 2014 Feb 26. doi:10.1371/journal.pone.0089557
9. Alexander LG, Salt C, Thomas G, et al. Effects of neutering on food intake, body weight and body composition in growing female kittens. Br J Nutr 2011; 106 Suppl 1: S19–S23.
10. Kienzle E, Bergler R. Human-animal relationship of owners of normal and overweight cats. The J of Nutr 2006;136, 1947S -1950S.
11. Robertson ID. The association of exercise, diet and other factors influence of diet and other factors with owner-perceived obesity in privately own ed dogs from metropolitan Perth, WA. Prev Vet Med 2003;58,75–83.
12. Brooks D, Churchill J, Fein K, et al. 2014 AAHA weight management guidelines for dogs and cats. J Am Anim Health Assoc 2014;50(1),1-11.
13. Linder D. Weighing in on obesity: prevention, treatme nt and management The Vet Nurse 2012;3(8),502-507.
14. German AJ, Ryan VH, German AC, et al. Obesity, its associated disorders and the role of inflammatory adipokines in companion animals. Vet J. 2010;185(1), 4 -9.
15. Scarlett JM, Donoghue S. Associations betwe en body conditions and disease in cats. J Am Vet Med Assoc 1998;212(11),1725 -1731.
16. Kealy RD, Lawler DF, Ballam JM, et al. Effects of diet restriction on life span and age -related changes in dogs. J Am Vet Med Assoc 2002;220(9), 1315 -20.
17. Singh R, Laflamme DP, Sidebottom-Nielsen M. Owner perceptions of canine body condition score [abstract]. In: Proceedings of the 20th Annual ACVIM Forum ; 2002 May 29–Jun 1; Dallas, TX. Lakewood (CO): American College of Veterinary Internal Medicine; 2002.
18. German AJ, Luxmor e J, Holden SL, Morris PJ, Biourge V. Feeding obese dogs during weight loss is on average cost-neutral. J Small Anim Pract. 2015;56(6):366 –369.
19. Kim JY. Optimal diet strategies for weight loss and weight loss maintenance. J Obes Metab Syndr. 2021;30:20-31.
20. Hannah SS, Laflamme DP. Increased Dietary Protein Spares Lean Body Mass during Weight Loss in Dogs. J Vet Int Med. 1998;12:224.
21. Laflamme DP, Hannah SS. Increased Dietary Protein Promotes Fat Loss and Reduces Loss of Lean Body Mass During Weight Loss in Cats. Int J Appl Res Vet Med. 2005;3:62.
22. Pan Y. Use of soy isoflavones for weight management in spayed/neutered dogs: Nestlé Puri na Research, the FASEB Journal. 2006;20:A854 -A855.
38
23. Pan Y, Tavazzi I, Oberson JM, et al. Effect of Isoflavones, Conjugated Linoleic Acid, and L -Carnitine on Weight Loss and Oxidative Stress in Overweight Dogs. A Supplement to Compendium: Continuing Education for Veterinarians. 2008;30(3A): 69.
24. Pan Y. Soy Germ Isoflavones Supplementation Reduced Body Fact Accumulation and Enhanced Energy Metabolism in Dogs. [abstract]. In: 2012 ACVIM Forum Proceedings ; 2012 May 30–Jun 2; New Orleans, LA: American College of Veterinary Internal Medicine; 2012.
25. WSAVA Global Nutrition Committee Short Diet History Form: https://wsava.org/wpcontent/uploads/2020/01/Diet-History-Form.pdf. Accessed: April 4, 2020.
26. ACVN Small Animal Diet History Form - Complete Version: http://acvn.org/wpcontent/uploads/2020/04/ACVN-Diet-History-Form-2020-FINAL_fillable.pdf Accessed: April 4, 2020.
27. Heuberger R, Wakshlag J. The relationship of feeding patterns and obesity in dogs. J Anim Physiol Anim Nutr (Berl). 2011;95(1):98–105
28. Morelli G, Marchesini G, Contiero B, Fusi E, Diez M, Ricci R. A Survey of Dog Owners' Attitudes toward Treats. J Appl Anim Welf Sci. 2020;23(1):1 –9.
29. Coe JB, Rankovic A, Edwards TR, Parr JM. Dog owner's accuracy measuring different volumes of dry dog food using three different measuring devices. Vet Rec. 2019;185(19):599.
30. German AJ, Holden SL, Mason SL, et al. Imprecision when using measuring cups to weigh out extruded dry kibbled food. J Anim Physiol Anim Nutr (Berl) . 2011;95(3):368 –373.
31. Deng P, Iwazaki E, Suchy SA, Pallotto MR, Swanson KS. Effects of feeding frequency and dietary water content on voluntary physical activity in healthy adult cats. J Anim Sci. 2014;92(3):1271–1277. doi:10.2527/jas.2013-7235
32. Nagaoka D, Mitsuhashi Y, Angell R, Bigley KE, Bauer JE. Re -induction of obese body weight occurs more rapidly and at lower caloric intake in beagles. J Anim Physiol Anim Nutr (Berl) 2010;94(3):287–292.
33. German AJ, Holden SL, Morris PJ, Biourge V. Long -term follow-up after weight management in obese dogs: the role of diet in preventing regain. Vet J. 2012;192(1):65–70.
34. Marshall WG, Hazewinkel HA, Mullen D, De Meyer G, Baert K, Carmichael S. The effect of weight loss on lameness in obese dogs with osteoarthritis. Vet Res Commun. 2010;34(3):241–253.
35. Wakshlag JJ, Struble AM, Levine CB, Bushey JJ, Laflamme DP, Long GM. The effects of weight loss on adipokines and markers of inflammation in dogs. Br J Nutr. 2011;106 Suppl 1:S11–S14.
36. German AJ, Holden SL, Wiseman-Orr ML, et al. Quality of life is reduced in obese dogs but improves after successful weight loss. Vet J. 2012;192(3):428–434.
39
40
Diet Trials: The Forgotten Diagnostic Tool in Your Practice
MANAGING DOGS WITH FOOD ALLERGIES
A balanced diet provides nourishment. However, patients with food allergy develop an aberrant immune response to what typically are common dietary components and may exhibit dermatological and gastrointestinal clinical signs.
In this roundtable, experts in veterinary dermatology and gastroenterology discuss the impact of adverse food reactions, particularly food allergy, on canine health; the challenges of conducting elimination diet trials; and the role of therapeutic nutrition in managing dogs with food allergy.
DEFINING THE CONDITION AND ITS IMPACT
Dr. Jason Gagné: Let’s start by defining some of the terminology we’ll be using. Can you please share definitions for adverse food reaction, allergy and food intolerance?
Dr. Stanley Marks: An adverse food reaction is defined as any abnormal clinical response attributed to the ingestion, contact with or inhalation of a food, its derivatives, or an additive contained in it. Adverse food reactions have been classified according to their underlying mechanisms, including food intolerances, which have no primary immunologic basis; food toxicities; pharmacologic reactions; and food allergies, which have an underlying immunologic basis.
Dr. Craig Griffin: An allergy is a chronic condition involving an immune reaction, called a hypersensitivity, to an ordinarily harmless substance. An allergy can be caused by a food or by an aeroallergen such as a dust mite or weed, tree and grass pollens.
Dr. Alison Manchester: Food intolerance is a type of adverse food reaction and is defined as a non-immune reaction to a wide variety of different dietary components, including carbohydrates, fats or dietary additives. It also includes maldigestion or an idiosyncratic reaction such as a temporary inability to digest a food substance.
Dr. Gagné: What do we know about the prevalence of food allergy in dogs?
Dr. Galia Sheinberg: It depends on who you ask. We see discrepancies between published studies, and dermatologists themselves don’t agree how common it is. Speaking for myself, I estimate that approximately 30% of my atopic patients respond to elimination diets.

Dr. Griffin: I agree that much of what is published is too low, and the reason may be that dermatologists are not always
“Sometimes we lose patients to follow up because they improve. We put them on a hydrolyzed elimination diet, they get better—and they never come back. Because we don’t get the opportunity to challenge these patients, they’re never completely diagnosed.”
Dr. Galia Sheinberg
looking for it, especially partial responders. If you never do a diet trial, you won’t find food allergy very much! Meanwhile, a single diet trial isn’t always enough to rule it out. The prevalence of food allergy could actually be higher than 30%.
Dr. Sheinberg: Another factor is that sometimes we lose patients to follow up because they improve. We put them on a hydrolyzed elimination diet, they get better—and they never come back. Because we don’t get the opportunity to challenge these patients, they’re never completely diagnosed.
Dr. Gagné: What are the perspectives of the gastroenterologists in the group?
Dr. Manchester: As with dermatology, I think it’s difficult to get a true handle on prevalence. It probably varies geographically. Wheat intolerance in humans is much higher in Italy, whereas shellfish intolerance is very common in Japan. I’m sure there is regional variation in our canine populations as well. Week in and week out, I see animals being referred to our academic institution for chronic refractory enteropathies refractory to treatment. When I look through a dog’s history, I see he has been prescribed medications like metronidazole,
41
PAGE 1
problem began years earlier. If you don’t ask owners about ear cleaning, you miss those cases.
Dr. Sheinberg: Patients also slip through the cracks because owners don’t realize that certain behaviors are indicative of allergies. Paw licking is a good example. Owners simply live with their dogs licking their paws and don’t realize it’s a problem. As clinicians, we have to zero in on those signals and ask the right questions if we want to identify patients when they begin showing signs of problems.
Dr. Gagné: Does the location of skin lesions suggest food allergy vs. environmental allergy?

Patients that exhibit subtle signs of allergy, such as paw licking, can be missed if owners don’t realize the behavior is a sign of a problem.

tylosin and prednisone and undergone many fecal PCR panels—with no mention of the diet fed. Whatever diet “trial” he may have had was limited to feeding an easily digestible diet for a week. If the patient wasn’t better by then, the clinician moved on.
Animals like these have often been going to the veterinarian for months to years. I think we need to do a better job of educating the veterinary profession about the significant potential for diet to help these animals.
CLINICAL PRESENTATION OF CANINE FOOD ALLERGY
Dr. Gagné: Let’s move on to clinical presentation and diagnosis. Starting with the dermatologists, what is the typical presentation for dogs with food allergy?
Dr. Sheinberg: Non-seasonal itching and erythema of the skin, mostly along the ventrum, is common in these patients, although it can vary widely. Sometimes we see dogs with otitis or relapsing otitis as the only presentation. Most dogs with food allergy are younger than 1 year of age, although I diagnose senior patients with food allergy, too.
Skin disease that is concurrent with GI manifestations is frequently seen in food allergy patients. When we take a proper history and note that a dog has a host of skin problems and a history of either vomiting, diarrhea, or chronic GI trouble, it is a strong signal that we need to do a food trial.
As the disease advances, we also see chronic skin disease with secondary bacterial or yeast infections.
Dr. Griffin: I see numerous dogs that began getting ear disease when they were 6 months to a year of age; however, the owners learned that if they cleaned the dog’s ears as soon as they started getting dirty, it could prevent ear disease. By the time these dogs are 5 years of age, they are exhibiting clear allergy signs. The owner thinks it is just starting, but in reality, the
Dr. Griffin: There is some evidence in the literature that dogs with food allergy have a bit more dorsal lumbar involvement, but it’s not true for every breed. If the dog’s perianal area looks bad, food allergy typically moves higher on my list of differentials. However, we see perianal signs with both food and non-food allergies, so it’s clear that looking at the pattern of lesions is not enough.
Dr. Gagné: Let’s discuss GI signs. Do these go beyond vomiting and diarrhea?
Dr. Manchester: I try to keep an open mind and see the whole spectrum of GI signs as possibly being secondary to a food reaction. It can range from a loose stool once every two weeks to vomiting after breakfast three times a week to having difficulty putting on weight to constipation.
Dr. Marks: The GI manifestations of an adverse food reaction are broad, and approximately 70% of affected dogs have large bowel diarrhea or mixed bowel diarrhea signs. Vomiting can also be seen in affected dogs. Secondary manifestations of adverse reaction to food can include increased flatulence and borborygmi. Obtaining a complete GI history that includes determining the frequency of secondary GI signs in addition to concurrent pruritic behaviors is extremely important.
We also need to ensure that our questioning about the stool consistency does not lead to an inaccurate response because most pet owners equate diarrhea with a liquid or watery stool. I prefer to show owners a Nestlé Purina Fecal Scoring Chart and ask them to point to the image that most closely matches their pet’s stool over the past week or two to avoid miscommunication.
42
“I…see the whole spectrum of GI signs as possibly being secondary to a food reaction. It can range from a loose stool once every two weeks to vomiting after breakfast three times a week to having difficulty putting on weight to constipation.”
Dr. Alison Manchester
PAGE 2
When food allergy is suspected, a comprehensive diet history that covers well pet and therapeutic diets, as well as treats, can aid in the selection of an elimination diet.
Dr. Gagné: How commonly do dogs with food allergy have concurrent dermatologic and GI signs?
Dr. Griffin: I used to tell people that 50% of dogs that have skin disease and are diet-responsive will have at least some sort of subtle GI sign. I still think that is true. A complicating factor is that by the time a number of dogs with skin disease make it to a referral center, they have already been on antibiotics and other medications; the GI signs are due to the treatments rather than the disease. To sort through this confusion, I ask the client whether there were GI signs in the history of that dog before a veterinarian may have begun using drugs to treat the skin disease.
Dr. Marks: Approximately 20 to 60% of food allergic dogs have concurrent dermatologic and GI signs, and the reason for the wide range is due to the inconsistent incorporation of secondary GI signs (flatulence, increased borborygmi) that are often ignored in the history. We know that the clinical signs associated with the gastrointestinal tract in food-allergic patients can be used as an indirect method for assessing the downstream effect of how the pruritic behaviors may or may not respond to that dietary intervention. If a patient’s diarrhea has resolved within 7-10 days and the animal is still pruritic, I’m more optimistic that the pruritic behavior will be improved or resolved if the diet is continued for another 6-8 weeks.
Dr. Gagné: What do we know about the role of the GI microbiome in these disorders?
Dr. Marks: Without question, the intestinal microbiome plays an important role in early host immunologic development, and the colonization of a diverse microbiota in early childhood is necessary for the induction and maintenance of oral tolerance. In humans, a variety of epidemiological studies have linked environmental factors and intestinal dysbiosis to atopic risk. Examples include children living in rural environments around livestock and children with pets in the household. These
influences in infancy and childhood can have a profound effect on the downstream development of allergic disease involving the skin, respiratory, or gastrointestinal systems. The same is true for administering antibiotics to infants or young children—the intestinal dysbiosis induced by antibiotics shapes the innate and adaptive immune responses, increasing the development of atopy and asthma in adulthood.
Dr. Manchester: It’s exciting that we are looking into this. The microbiome is a very important aspect of gut health, although our understanding is in its infancy. When I ask a student these days for differentials for diarrhea, dysbiosis is often one of the top three things they include. The question is what could have driven that dysbiosis in the first place?
THE INS AND OUTS OF CONDUCTING AN ELIMINATION DIET TRIAL
Dr. Gagné: How do you determine when a patient needs an elimination diet trial?
Dr. Griffin: The dog’s history is critical for me. If a dog has yearround pruritus, pursuing food allergy is worthwhile. If he also has GI signs, it’s foolish not to investigate it promptly. When I see a younger dog with a history of GI disease, I become concerned about food allergy.

Dr. Marks: Most dogs with food-responsive enteropathies are younger dogs with a median age of 3.4 years, with mild to moderate clinical signs and predominantly large bowel diarrhea. If the patient has the above-mentioned features, has a good appetite and has not lost significant body weight, I perform a centrifugation flotation to rule out intestinal parasites and empirically deworm the patient if the fecal is negative. I also start the dog on an elimination diet trial with explicit instructions to feed the diet exclusively with no treats for 10 to 14 days, which reflects the time during which I expect to see a marked improvement or resolution of the animal’s diarrhea. The patient should return for a more comprehensive workup if the diarrhea has not resolved within two weeks following the diet trial.
Dr. Gagné: How do you select an elimination diet? Please discuss the advantages and disadvantages of home-cooked, limited-antigen/novel protein and hydrolyzed diets.
Dr. Sheinberg: A commercial hydrolyzed diet—preferably a vegetarian version—is usually my first choice, because it is a practical, complete, and balanced diet for most patients. Homecooked diets are not my first choice because I find that many owners do not want to cook for their pets. Ensuring the diet is nutritionally balanced can also be challenging, especially with growing dogs. I do use home-cooked diets as a second choice if a pet won’t accept a hydrolyzed diet or the patient was unsuccessful on a hydrolyzed diet.
43
PAGE 3 MANAGING DOGS WITH FOOD ALLERGIES
Evaluating Traditional Diet Options for Elimination Trials
Pros Cons
Home-cooked Diets
• Can be tailored for patients with concurrent disorders
• Appealing to highly committed owners who want to feel involved
• Often unbalanced unless formulated by a Board Certified Veterinary Nutritionist®
• Owner must be committed to diet preparation and strict adherence (no ingredient substitutions)
Novel Protein Diets
• Palatability aids diet acceptance
• Cost may be lower than other options
Hydrolyzed Diets
• Can be fed long-term (complete and balanced)
• Effective and well tolerated
• Available in vegetarian formulas
I tend to stay away from novel protein diets because in Mexico where I practice, novel protein diets are manufactured by over-the-counter food companies and have been proven to be contaminated with other sources. In addition, many clients have already tried several animal proteins or commercially prepared raw diets with multiple animal proteins before they come to me, so we have fewer choices left.
Dr. Griffin: I’ve been in clinical practice for 44 years and I’ve tried them all. Long ago, we recommended home-cooked diets because we didn’t have the commercial options available today. I even promoted homemade vegetarian diets of pumpkin and pinto beans for a time, but I found they weren’t great long-term diets for dogs when clients saw a favorable response and did not follow up to get on a complete and balanced diet.
I’m a big fan of hydrolyzed diets. I haven’t yet found a limited-antigen diet that completely eliminated food allergy, but hydrolyzed diets work in about 90% of cases. While cost can be an issue with these diets, I actually use the expense as an incentive for compliance.
Dr. Manchester: If there is one category of diet I prescribe most frequently to dogs with chronic enteropathy, it would be a hydrolyzed diet. I think it’s important to give the client some direction vs. sending them home with six different diets to try.
Of course, there is no one-size-fits-all approach. A good diet history is so important, because there is a big difference between what I recommend for a dog that has already been on three different over-the-counter diets and four different prescription diets versus a dog that has eaten a single over-thecounter commercial dog food his whole life. It is also important to look at the diet’s formulation, especially the fat content, because chronic enteropathy patients often have a limited
• Can be difficult to find truly novel protein sources for patients with varied diet history
• Cross contamination can be a problem, depending on manufacturer
• Expensive
• Not palatable for all patients
tolerance for dietary fat.
Dr. Marks: It’s worth emphasizing that dietary fat restriction is especially important for patients with certain food-responsive enteropathies such as intestinal lymphangiectasia. These dogs need diets that contain less that 20% fat on a metabolizable energy basis and are digestible and highly palatable. We tend to be less aggressive with dietary fat restriction when managing dogs that are not hypoproteinemic or hypocholesterolemic and have other food-responsive enteropathies.
I initially try to determine via the patient’s diet history whether a limited-ingredient diet might be a feasible option, because these diets tend to be palatable, particularly for small or toy-breed dogs. I typically reserve home-prepared diets for patients with concurrent disorders because there is no single diet that can be used to manage both disorders. Examples include patients with renal disease and a chronic enteropathy, or patients with primary hyperlipidemia and a chronic enteropathy. I strongly advise that these home-prepared diets be formulated by a board-certified veterinary nutritionist.
Dr. Gagné: How long should a practitioner wait to see a decrease in signs with an elimination diet trial?
Dr. Sheinberg: In dermatology, we adhere to an eight-week trial. If I have a severely inflamed dog, I might choose to use prednisone on that patient and try to recheck the dog two or three weeks afterward to see how he is doing and to try to eliminate the prednisone. If I can transition to oclacitinib I will do that to avoid the long-term effects of steroids. I give dogs medication for the first three or four weeks, then take them off of the medication and start measuring the response between four to six weeks. That way, they will be completely off medications once we reach eight weeks.
Dr. Marks: I think veterinary gastroenterologists have one significant advantage in terms of compliance, because GI dietary trials are typically much shorter in duration than those
44
Dr. Gagné: Dr. Manchester and Dr. Marks, what are your thoughts on dietary management of dogs with chronic enteropathies?
PAGE 4
of our dermatologist colleagues. Clinical signs of diarrhea should resolve within 10 to 14 days following the onset of the dietary trial compared to 8 to 12 weeks for patients with pruritic behaviors.
Dr. Manchester: It’s important to stress that success doesn’t have to mean 100% improvement. If I have a patient with really severe signs, I’m happy with 50% improvement. It depends on where you are starting. If an animal is having liquid bowel movements four times a day, improving the consistency and decreasing the frequency will improve the pet’s quality of life.
Dr. Gagné: Knowing that it takes at least eight weeks to resolve dermatological signs, how do you get the patient and the owner to stay compliant on the trial?

Dr. Sheinberg: Choosing the right elimination diet for the patient is critical. You have to consider how the owner feels about the diet you plan to prescribe. If you are going to use a home-prepared diet, are they willing to cook for their dog? If you are going to prescribe a hydrolyzed diet, do they understand the cost? Do they understand what kind of treats are allowed? If a client feels they are being forced to do something they don’t want to do, you won’t be successful.
I have found it useful to have clients keep what I call an “itch calendar.” Starting several weeks before the diet challenge, when we’ve removed medications, the clients ask themselves each night how itchy their dog was that day on a 0-10 scale. Once they start the diet challenge, they are more aware of their dog’s pruritic behaviors and can see changes.
It takes teamwork and good client education to make an elimination diet trial work. If owners lack information or
motivation, they will not do the diet trial correctly or long enough. Follow-up is also important. We usually call clients one week after we prescribe the diet to see how they are doing, if they haven’t already contacted us.
Dr. Griffin: If I have a client whose dog is 100% better and she doesn’t want to challenge, I probably wouldn’t twist her arm. But the vast majority of our cases don’t get 100% better. It may be because the dog has a food allergy and an environmental allergy and the clinical signs are only partially due to the food allergy. If we don’t challenge and recognize that food allergy is part of the problem, we will have trouble using allergenspecific immunotherapy to get clinical signs under control without using other atopic medications. In other cases, we might unnecessarily raise the dose of the medication because we think the lower dose isn’t controlling the environmental allergy, when the problem is that we missed the food allergy.

There are also cases where I do a diet trial and the GI issues clear up, but the owners and I don’t perceive any change in the skin. By re-challenging the dog, we may realize that, in fact, the skin had been improving because now there are areas that flare again within four or five days.
Dr. Marks: Speaking as a gastroenterologist, I would say it is not as important to rechallenge the dog compared to my dermatology colleagues. If a patient is doing well on diet X or diet Y, most owners are relieved that their pet’s diarrhea has finally resolved and are more reluctant to challenge their pet in the event that the diarrhea could recur. Many owners are willing to pay a bit more for a therapeutic diet if the diet is palatable and resolves the diarrhea.
Dr. Manchester: I agree. If the GI signs are better, owners usually want a lifetime supply of the diet. Rather than rechallenge with the original diet, I advise they begin to slowly add new dietary components to the elimination diet. If they want to give the dog a carrot as a treat or a little piece of banana, we let them try it. Assuming we’re successful, A 2-week elimination diet trial is typically sufficient to resolve gastrointestinal signs of adverse food reaction; however, dermatologists recommend an 8-week trial to assess dermatological improvement.
45
PAGE 5
“The dog’s history is critical for me. If a dog has year-round pruritus, pursuing food allergy is worthwhile. If he also has GI signs, it’s foolish not to investigate it promptly.”
MANAGING DOGS WITH FOOD ALLERGIES
Dr. Craig Griffin
Dr. Gagné: Assume a dog has responded to the elimination diet trial. How important is it to rechallenge the dog?
the owner is usually happy to know the dog can have a little more variety.
Dr. Gagné: What if adverse food reaction is ruled out through the elimination diet trial and the diagnostics indicate atopy is the cause of the dog’s clinical signs? How would you approach nutritional management?
Dr. Griffin: Including omega-3 fatty acids in diets for dogs with environmental allergies has been studied for its use in decreasing pruritus. When I talk to veterinarians about diet for allergic dogs, I tell them that all allergic dogs can potentially benefit from a diet. If they are food allergic, they need a diet that eliminates the protein to which they are allergic. If they are not food allergic, a diet that is higher protein and contains a source of omega-3 fatty acids will benefit them and give the atopy medications a better chance of working.
Dr. Sheinberg: Building on that point, I prefer diet over supplements for dogs with atopy. It can be hard enough for clients to bathe and medicate a dog; feeding a dermatological diet in lieu of giving supplements is easier.
Dr. Gagné: What are your thoughts on diagnostic strategies such as intradermal, serum IgE, serum IgG, salivary or hair tests?
Dr. Griffin: There is no alternative test to an elimination diet trial to diagnose food allergy, and some of the alternatives are particularly bad. Even those that statistically correlate to some degree, such as the IgE serum test, don’t always correlate with the exact ingredient.
Dr. Sheinberg: It’s hard when you have an owner who has had a saliva or hair test that they believe has given them a diagnosis, but those tests are definitely not appropriate for diagnosing food allergy. These owners are disappointed to learn they still have to perform a diet trial.

A NEW TOOL: THE AMINO ACID-BASED ELEMENTAL DIET
Dr. Gagné: An amino acid-based elemental diet is a new option for veterinarians in the diagnosis and management of food allergy and other types of adverse food reaction. What does a diet like this have to offer?
Dr. Sheinberg: An amino acid-based elemental diet is something that we as veterinarians have not had available to us. In pediatric medicine, amino acid diets have been used for more than 20 years and are the first choice of many pediatricians for managing allergic gastrointestinal disease in children. I think that being able to have this tool will be very good. Patients that are not doing well with our current diets
and that tend not to respond well to medications are good candidates for using an elemental diet.
Dr. Manchester: I think it will be exciting to have another dietary tool in our armamentarium to combat chronic enteropathy. In human pediatric Crohn’s disease, a high percentage of patients go into complete remission on elemental diets. Not only do their clinical signs go away, but when the patients are re-biopsied, the inflammation is gone. Contrast this to the use of steroids, which have a much greater side effect profile and significant ramifications for growing young children.
While chronic canine enteropathy patients are not the same as Crohn’s patients, the clinical signs associated with both conditions are probably due more to intolerances and aberrant immune responses than food allergens, but they still respond to these elemental or polymeric diets. We have dogs that come in with an acutely insulted, leaky and damaged gut barrier. A diet like this that is very digestible, well-balanced, and non-immune stimulating will definitely be helpful.
Dr. Marks: I think that the introduction of an amino acidbased elemental diet that is complete and balanced, as well as palatable, is long overdue. A diet like this could be used for a plethora of disorders—not just for patients with adverse food reactions, but in patients with short bowel syndrome, critically ill puppies with parvovirus, and in patients with steroidresponsive enteropathies in which the elemental diet might allow a reduction in the dose of immunotherapy (prednisone, chlorambucil, azathioprine, etc.) administered to the patient. When one considers all of the patients we see in the ICU or the critical care setting with severe intestinal disease, this
46
PAGE 6
An amino acid-based elemental diet for use in elimination diet trials and management of gastrointestinal disease is a recent therapeutic diet innovation.
elemental formula could prove to be an invaluable therapeutic modality.
Dr. Gagné: What are your thoughts on the inclusion of a prebiotic in the Purina® Pro Plan® Veterinary Diets EL Elemental diet to alter the microbiome?
Dr. Manchester: It needs to be studied, but I think including a prebiotic is a great idea, especially because so many patients being prescribed this diet will have already had their microbiome wiped out by multiple courses of metronidazole and tylosin. I also think we have a slightly better chance of making a positive impact on the microbiome with a prebiotic that promotes the growth of beneficial bacteria versus just peppering the gut with probiotics alone.
Dr. Gagné: Dr. Sheinberg and Dr. Griffin, having been provided the opportunity to try this diet, how and when do you see yourself using it in practice?
Dr. Sheinberg: I have a particular case of a Labrador-mix dog that had been very difficult to control. She was medicated with long-term steroids, but every time we removed the treatment, she would flare up, get secondary infections and do very poorly. We tried all the hydrolyzed diets on the market as well as a pork and sweet potato diet. She has been on the Elemental diet for almost two months, and her skin is doing really well, with no flares.
Dr. Griffin: I have a case on the diet right now that, in order to initially improve clinical signs, had to be on a homemade unbalanced pumpkin and pinto bean diet. On a blinded challenge, she flared to six different ingredients, then she flared with several different hydrolyzed diets and multiple limited ingredient diets. The only commercial food she has tried that keeps her food allergy controlled is the Elemental diet and she loves it. So do her owners, as they were tired of home cooking and adding supplements to try to balance her diet. She also did not particularly like the homemade diet and would try to steal food and had intermittent flare-ups. She is not only thriving on the Elemental diet but has stopped trying to steal food.
WRAP-UP
Dr. Gagné: What do you see as the primary takeaway of this discussion for practitioners? Is there one piece of advice you would give on helping dogs with allergic and food-responsive conditions?
Dr. Griffin: My takeaway is that foods play a very significant role in allergic skin disease. Because it often isn’t a pure problem, it takes an astute clinician taking a good history to capture all clinical signs—including GI signs—and conduct a good exam to determine what role the food plays.
Dr. Sheinberg: A correct clinical history is so important. It can also be difficult to diagnose food allergy if the dog has another issue, such as a chronic ear infection, that needs treatment. You may have to take care of that before you can evaluate how the elimination diet is working.
Dr. Manchester: Just because one diet didn’t work, it doesn’t mean diet should be given up on. The majority of chronic enteropathy dogs will respond to dietary therapy. Finding the right match for an individual patient may take trial and error.
Dr. Marks: The importance of the dietary history cannot be overemphasized when selecting a diet. In addition, veterinarians should remember to inquire about a pet’s gastrointestinal signs when the pet is presented for dermatological disease, and vice-versa.
MODERATOR:
Jason Gagné, DVM, DACVN, is Director of Veterinary Technical Communications for Nestlé Purina PetCare.

PARTICIPANTS:
Craig Griffin, DVM, DACVD, is a Veterinary Dermatologist in San Diego, California, and Las Vegas, Nevada, with the Animal Dermatology Group. He is also a Clinical Professor of Veterinary Medicine at Western University of Health Sciences.
Alison Manchester, DVM, DACVIM (SAIM), is a Veterinary Specialist and One Health Fellow at the Colorado State University College of Veterinary Medicine.
Stanley Marks, BVSc, PhD, DACVIM (SAIM, Oncology), DACVN, is a Professor of Small Animal Medicine at the University of California Davis School of Veterinary Medicine.
Galia Sheinberg, DVM, DLACVD, is a Veterinary Dermatologist with Dermatología Especializada Centro Veterinario Mexico and practices in Mexico City.
47
PAGE 7 MANAGING DOGS WITH FOOD ALLERGIES
“I think that the introduction of an amino acid-based elemental diet that is complete and balanced, as well as palatable, is long overdue.”
Dr. Stanley Marks
48
Companion Animal
Natalie Gruchow, CVPM, SHRM-CP, Elite FFCP (Veterinary)
Level 3 Fear Free Certified Instructor Animal Health Clinic Fargo, South Dakota
49
50
Fear Free Impacts on Patient Care and Hospital Culture
Description: Would you like to decrease compassion fatigue for your team? Are you having trouble filling vacant job openings? Do you want your patients to receive the best possible care? If you answered yes to any of these questions, implementing a Fear Free culture may be a win-win solution for your patients, clients, & team. This Fear Free overview will provide easy to implement tips from the only Fear Free Certified Practice in the Dakotas, such as effortless facility updates and steps to form a Fear Free Committee. Shifting culture to Fear Free is a change, and even positive change creates uncertainty for employees. To successfully introduce new processes, you need to know how to effectively lead change management. You will leave this session with tools to be a stronger leader that you can use every day!
Abstract:
Fearful pets are more likely to bite and scratch. Veterinary professionals experience greater risk for injury and increased compassion fatigue when medical care is forced on patients that are exhibiting fear, anxiety, and stress. Quality job applicants are increasingly seeking employment at Fear Free hospitals, which is anticipated to increase even more over time, as colleges are teaching these concepts. When an employee works for a Fear Free hospital, it becomes a standard of care they seek in future employers. Becoming Fear Free gives you a competitive advantage and improves clinic culture by aligning values and clarifying company mission. Successful implementation is a team effort, and developing a Fear Free Committee is an effective way to enable the change management process. This session will develop a foundation to enhance leadership skills to affect change (i.e. conflict resolution), define key Fear Free concepts (i.e. gentle control, interpreting patient body language), and implement simple facility changes for a Fear Free experience.
Fear Free Vaccination Experience
Description:
This session will provide a basic overview of Elanco lyme, lepto, and feline leukemia vaccines with the focus on how to clearly explain the benefits to pet owners. There are many lifestyle factors that influence the decision to vaccinate or to not vaccinate, and we must learn to be proactive about addressing potential concerns that may arise. Using Fear Free concepts, we can alleviate fear, anxiety, and stress during the vaccination appointment for the pet and pet owner. Fear Free takes the pet out of petrified and we can keep vaccines serene!
Abstract:
The Fear Free Vaccination Experience looks to the research to understand why some clients are vaccine hesitant. When we understand the deeper emotions (i.e. human fear of needles, anti-vaxx movements, etc.) behind the hesitancy we become more proactive in conflict resolution. The outcome is greater compliance and more protection against disease in our patients. Using the Elanco line of vaccines, we can promote a more comfortable vaccination experience to increase client confidence. A brief overview of how this is achieved (i.e. lower volume, less debris, etc.) will be provided using Elanco approved resources. At the end of this session, attendees will be able to clearly explain vaccination benefits to pet owners, apply Fear Free concepts to safely and comfortable vaccinate patients, and develop skills for successful Fear Free communications with employees and clients.
51
52
Equine
53
54
Equine
Philip Johnson, DVM, ACVIM
Professor of Veterinary Medicine and Surgery
University of Missouri College of Veterinary Medicine Columbia, Mo.
55
56
Equine Protozoal Myeloencephalitis
Philip J. Johnson
Equine protozoal myeloencephalitis (EPM) is one of the more common infectious diseases affecting the CNS of (mostly) adult horses in the mid-west. Recognized in the USA in the 1960s, it was characterized based on its histopathological features as a ‘focal encephalitis-myelitis’. The presence of protozoa in these lesions was subsequently described in the 1970s, whereupon the condition has subsequently been known as EPM.
There are two apicomplexan protozoan parasites that have been implicated in EPM: Sarcocystis neurona and Neospora hughesi. There are still many knowledge gaps regarding the life cycle and pathophysiological significance of N. hughesi and its role as an etiological agent for EPM. The mode of transmission of N. hughesi to horses is not known, but it can be passed vertically (from mare to foal). Much more information is available regarding S. neurona, which is a much more commonly encountered etiological agent for EPM (EPM associated with N. hughesi infection is said to be rare). For its persistence in nature, S. neurona must cycle through two hosts. In the USA, the common opossum ( Didelphis virginiana) is the ‘definitive horse’ for S. neurona (other marsupial species operate as definitive hosts in South and Central America). The protozoa exist in the intestinal tract of the opossum, where they undergo sexual reproduction leading to the genesis of sporozoite-containing sporocysts that are passed into the environment in feces. These sporocysts are infective for the ‘intermediate host’, which is infected by ingesting opossum feces or food/water that has been contaminated by opossum feces. Several mammalian species can play the role of intermediate host for S. neurona, including skunks, raccoons, armadillos, and cats. The protozoa migrate into striated muscles (myocardium, skeletal muscle) of intermediate hosts and develop into cysts (‘sarcocysts’). Continuance of the life cycle requires that the muscle cysts will be ingested by the definitive host, whereupon they will inhabit the opossum intestinal system. The horse is an inadvertent or ‘dead end’ host for S. neurona. In most cases, the horse’s immune system effectively controls the parasite and, albeit that there is an antibody response to the parasite (seroconversion), it is rare that the parasite enters the CNS and results in neurological disease (EPM).
Susceptibility: Having a serum antibody titer against S. neurona indicates that the horse has encountered the parasite (and undergone seroconversion). Immunity against protozoan parasites is complicated and likely more centered on a robust cell-mediated immune response (needing a normal Th1 cell-mediated response, involving both interferon-gamma and interleukin-12). Therefore, demonstration of a positive serum antibody titer is reflective of exposure; positive seroprevalence for S. neurona varies between 1589% of horses with the highest seroprevalence rates being found in those geographical locations with greater opossum populations. Seroprevalence rates for N. hughesi have been reported between 3-34% (but some reporting has employed antibody detection assays that are not specific for this parasite, failing to satisfactorily differentiate it from N. caninum). A satisfactory explanation for the reason that only a small number of S. neurona exposures lead to neurological disease is still lacking. Putative explanations have included idiosyncratic immunosusceptibility of the host, size of infecting inoculum, differences regarding genetic and antigenic features of the parasite (‘virulence’). It has been suggested that exposed horses unable to respond with an adequate interferon-gamma response may be susceptible.
Risk factors from the epidemiological perspective : Neurological disease is more commonly seen in young horses (<4 years of age) and older horses (>13 years). There is a seasonal variance with respect to new EPM encounters –disease is less common in the winter months and more common in spring (X3) and in the fall (X6). Other ‘positive’ risk factors include, as noted above, proximity to opossum populations (geographical variability), proximity to wooded areas, previous encounters with EPM, and various ‘stressful’ criteria (transport, injury, surgery, parturition, heavy exercise, change of management). EPM is more commonly seen in racehorses and show horses (competition stress) but less common in pleasure horses and horses used for breeding. Increased risk has also been reported when vermin (rats, mice) are plentiful and when horses are accommodated at premises in closer proximity to human population centers (wildlife encroachment). Advanced age and PPID are considered to be risk factors (reduced immune effectiveness). Risk of EPM is significantly less if wildlife is denied access to horse feed and if a river or creek runs through the nearby farm/woodland area (opossums less likely to move into closer proximity with horses).
57
Clinical presentation: Often is the case that, without a favorable response to treatment, EPM is characterized as a progressively debilitating disease of the CNS. The clinical chronology may arise as an acute syndrome or a chronic condition with worsening debility. Neuroanatomic localization may reveal focal or multifocal disease affecting either or both the brain and spinal cord. It has been stated that EPM should be (high) on the differential diagnosis list for most equine neurological syndromes. Of note, commonly encountered syndromes of EPM include unusual/atypical lameness (especially those that are difficult to localize), weakness/ataxia, dysphagia, abnormal upper airway function, and focal skeletal muscle atrophy. Other less commonly seen clinical manifestations of EPM include seizures , obtundation (brain involvement), head tilt (brainstem), facial nerve signs (brainstem), integumentary hypalgesia, hyporeflexia, sensory loss, dysuria, and collapse/inappropriate recumbency. Affected horses are often BAR with normal vital signs. It is common that the observed clinical picture is progressive and deteriorates over time. Affected horses are often presented for veterinary diagnosis of lameness. In those cases, lameness is not typically aggravated by limb flexion tests and lameness cannot be ‘blocked out’ with regional/joint anesthesia. Abnormal stanc es, stumbling, and interference may be noticed during the lameness examination and warrant closer scrutiny from the neurological perspective. Movement abnormalities resulting from neurological disease are not typically improved with NSAID treatment and tend to be variable/inconsistent (musculoskeletal lameness is usually consistent) during the examination protocol. In some cases, there may be both a neurological and a musculoskeletal component to observed movement abnormalities. There are three noteworthy c linical features of EPM that are helpful from the perspective of differentiating it from other neurological diseases with ataxia/weakness: EPM signs are often (but not always) asymmetrical; EPM is often (but not always) multifocal in its neuroanatomic diagnosis; there may be areas of focal skeletal muscle atrophy (asymmetrical or symmetrical). If these three neurological characteristics are identified in a patient with neurological disease, it is very likely explained by the EPM diagnosis. During movement evaluation, ataxia, weakness, and dysmetria may be observed in one or more limbs.
Differential diagnosis of EPM should include consideration of the following conditions : cervical vertebral stenotic myelopathy (‘wobbles syndrome’), CNS trauma, viral diseases (herpes myeloencephalopathy, West Nile viral myeloencephalopathy, rabies, etc), polyneuritis equi, motor neuron disease, degenerative myeloencephalopathy/neuroaxonal dystrophy (EDM/NAD), migrating helminth parasite (cerebrospinal nematodiasis), and others.
Diagnosis of EPM: Although diagnosis of EPM may be suspected based on the clinical presentation and outcome of neurological examination, confirmation of diagnosis must be based on both the elimination of other reasonable and qualifying considerations and laboratory testing. For example, signs of symmetrical ataxia that are most evident in the pelvic limbs of a younger horse warrant consideration of cervical vertebral stenotic myelopathy and cervical vertebral radiography/myelography may be undertaken. It is important to emphasize that a diagnosis of EPM is not appropriate in the absence of bona fide neurological signs or in areas of the world (beyond the Americas) where S. neurona is not found. Although a positive serum antibody titer (against S. neurona) is ’supportive’ of an EPM diagnosis, it is not reliable for diagnostic confirmation (especially in Missouri where seroprevalence is quite high). A negative serum antibody titer suggests that EPM may not be present but should be re-tested after 2-3 weeks in acute cases.
Diagnosis of EPM is most strongly corroborated by demonstrating an antibody titer in CSF that is higher than can be explained by diffusion of antibodies from the blood (which is based on the serum antibody titer). Having such a high CSF titer supports the fact that antibodies are being produced within the CSF (intrathecal production) in response to the presence of S. neurona in the CNS. In the past, veterinary diagnosis was established by demonstrating the presence of anti-S. neurona antibodies in the CSF using a Western immunoblot; this diagnostic test is no longer recommended. Presently, using an antibody detecting and quantification ELISA provided by a commercial laboratory (Equine Diagnostic Solutions, LLC, Kentucky, USA), the recommended test involves calculation of a ratio of serum:CSF titers (based on the SnSAG 2, 3, 4 antigens) Diagnosis of EPM resulting from S. neurona infection is supported when the ratio is less than 100. It is also recommended to test for N. hughesi (same laboratory).
58
Some other testing laboratories offer other/different methodological approaches for EPM diagnosis , but validation of those testing outcomes has not been as broadly accepted.
Contact information for Equine Diagnostic Solutions, LLC, Kentucky, USA: https://edslabky.com Telephone: 859-288-5255
Treatment of EPM: Management of EPM entails the administration of an anti -protozoal treatment coupled with one or more adjunctive treatments. Presently, there are three principal anti -protozoal drug approaches: pyrimethamine with sulfadiazine (ReBalance™), diclazuril (Protazil™), and ponazuril (Marquis™). Although treatment of EPM with various other anti-protozoal drugs has also been advocated, published efficacy data are not available. Dietary folate can interfere with the oral bioavailability of administered pyrimethamine, so it is recommended that hay should not be fed 2 hours before or following treatment with ReBalance™. Co-administration of corn oil with the triazine agent ponazuril has been shown to result in higher serum and CSF levels. Other drugs that have been recommended alongside anti-protozoal treatments for EPM have included anti-inflammatory agents (such as flunixin meglumine or dexamethasone for a few days when commencing anti-protozoal treatments to lessen the risk of a ‘treatment crisis’). Several immunomodulator agents (including levamisole, EqStim™, and Equimmune™) have also been recommended upon consideration of the possibility that EPM is more likely in conditions associated with lowered immunity). Vitamin E and other antioxidant substances may be supplemented to ‘preserve’ damaged neurons. In older horses, PPID should be considered and, if present, treated with pergolide.
Prevention of EPM: Although a vaccine that stimulated the systemic production of anti -S. neurona antibodies was briefly introduced some years ago, evidence that it prevented EPM was not forthcoming, and it is no longer available. Metaphylaxis is the term used to describe administration of anti-protozoal medication in the absence of disease intended to control S. neurona in at-risk individuals. To that end, daily treatment with either of the 2 recommended triazines (diclazuril or ponazuril) is sometimes recommended for a period of 7 days, once monthly. This metaphylactic approach is especially recommended for the long-term management of EPM-affected individuals that have responded well to treatment (under the assumption that there is an idiosyncratic susceptibility to EPM) .
References: Available upon request
59
60
Equine
Kile S. Townsend, DVM, MS, DACVIM (LAIM)M
Assistant Teaching Professor of Equine Internal Medicine University of Missouri College of Veterinary Medicine Columbia, Mo.
61
62
How and When to Perform a Neurological Examination on the Farm
Kile S. Townsend, DVM, MS, DACVIM (LAIM)
Performing a neurological examination on the farm is a doable, recommended, and useful skill to develop as an equine practitioner or large animal veterinarian. Horses may often be more relaxed and calmer in their home environment and therefore easier to ex amine from a neurological perspective. Also, some horses with severe neurological deficits are unsafe to load or transport in a trailer, necessitating on farm assessment of neurological status and recommendations for further diagnostic tests or treatments.
The neurological examination of the horse should always be accompanied by complete physical examination and history taking. This should include complete history, signalment, animal’s use, and the time of onset and progression of clinical signs. It is important to determine how long the owner has owned the animal, how long they believe the presenting complaint to be afflicting the horse, and if any other horses or animals on the property or in contact with the horse are displaying any abnormal clinical signs.
Before beginning a neurological assessment of a horse, it is important to gather all necessary items needed for examination. You will need: a bright light (ideally a transilluminator, ophthalmoscope, or small flashlight), a pair of hemostats, a t owel (for blindfolding), and gloves. Also recommended: neurological examination form, pen/paper, laptop/tablet, or video/audio recording. Neurological examination forms can be found online, one such form compiled by specialists in conjunction with Boehringer Ingelheim can be found at: https://docs.boehringer-ingelheim.com/Equine-NeurologicalExam-Long-Form.pdf
There are many ways to systematically perform a neurol ogic evaluation of a horse, but it is important to remember to perform the examination in the same order each time, so as to be thorough, complete, consistent, and predictable. Some general points to remember when beginning a neurological examination include be safe, observe keenly, know what is normal ( i.e., breed/age variations, etc.). You will likely have to tailor your examination to the individual horse (with respect to horse/human safety, horse personality, stability, and facilities being a few limiting factors) and to have to repeat the exam or parts of the exam (not much value in a single test). The examination should occur in two major phases: the static or standing examination and the dynamic or movement examination.
Standing examination (mental status, cranial nerve examination, reflex evaluation) : First, if possible, the horse should be observed in its natural environment without influence of a handler or restraint. Mentation, behavior, posture, and gait can be evaluated by observing interactions in the environment and with the handler (distance examination). The horse should then be restrained in a static position. The overall body condition, musculature, posture, and symmetry of the horse can be observed by walking completely around the horse and observing it from the front, back, and both sides. Observe for areas of patchy sweating or muscle fasciculations during this examination. It is important to move the forelock out of the way to evaluate facial symmetry and to move the t ail to evaluate hindlimb musculature.
The cranial nerve evaluation should then be performed, with special attention being paid to the right vs. left side. There are many ways to perform a cranial nerve examination, but a complete examination should be performed during any neurological examination, if it is safe to do so. See Table 1 (created by Amy L. Johnson, DVM, Diplomate ACVIM -LAIM) for cranial nerves, their functions, and assessment in the
63
horse. It is important to always wear gloves when handling the mouth/tongue of a neurological animal or any animal that has encephalopathic signs or unknown rabies vaccination history to limit exposure. The tongue should be grasped and examined and pulled from each side of the mouth to ev aluate withdrawal and tone. A horse may be fed a small amount of grain/treat/hay during the examination to evaluate prehension and swallowing.
Posture of the head, neck, trunk, tail, and limbs should be observed while standing . Observation of the horse’s posture will give you an idea of the horse’s level of conscious proprioception. Palpation of the head, neck, shoulders, back, rump, and limbs should be performed to assess body mass, symmetry, muscle tone, pain, and changes in skin temperature. The limbs should be flexed and extended manually in the standing horse, if possible. Transrectal palpation of the bladder or distal gastrointestinal tract may be warranted. The strength of the horse can be tested by pulling on the withers or the tail to one side vs the other.
Examination of reflexes in the standing horse are subjective and limited. The reflexes commonly assessed include the cervicofacial reflex (compare right side to left side rather than horse to horse), cutaneous trunci, thoracolaryngeal (“slap test”, best evaluated endoscopically), anal/perianal reflexes, and lordosis/kyphosis of the back when a hemostat is run on either side of the spine and over the rump (evaluate left side to right side)
Moving examination (gait and posture) :
The horse should primarily be evaluated at the walk, unless the neurological deficits are very subtle. It is best to perform the moving part of the neurological examination in a large, enclosed area with relatively flat ground, if possible. An experienced handler should be asked to handle the horse. The handler should be asked to walk the horse in a straight line towards and away the examiner , as well as in a zig/zag fashion and with and without the head elevated. The horse should be made to back up in a straight line and initiate walking forwards after backing. The horse should be walked across different surfaces such as flat hard ground vs soft/deep footing to assess foot placement and adaptation to the different footing. If the farm has pole or Cavalettis, they can be arranged for the horse to navigate through. The horse should be directed into tight circles (while maintaining forward gait) in both directions. If a hill or curb is available, it is practical to walk the horse up and down the hill or curb and do so with and without head elevation. A tail pull can be performed when the horse is walking, and the near hind leg is bearing weight to assess strength, reaction, and limb placement. Ataxia should be graded by scoring each individual limb using the Mayhew grading system Grade 0 -5. The ease with which a comprehensive neurological assessment of a horse’s movements can be undertaken often depends on the extent to which the animal has been trained; neurological assessments are invariably chal lenging in unruly or untrained individuals.
Some clinicians will perform foot-placing tests or conscious proprioception tests (CPs). This can be done by placing the hoof on its dorsum, placing one limb in front of the other, or placing one limb laterally to assess rate of replacement. Although potentially useful in some cases and in smaller animals, these tests are not generally regarded as extremely useful in detecting abnormalities, because neurologically normal horses have widely varied responses, and some well-trained or good-natured horses may be quite slow to replace their limbs. Hopping the horse on one thoracic limb may exacerbate thoracic limb weakness or hyper/dysmetria, but it is often unsafe, impractical, and not lucrative to perform this test. Extensive and careful gait analysis can give the veterinarian the most information regarding ataxia, proprioception, and weakness/paresis. Neurological evaluation is often coupled with lameness
64
evaluation, as the two assess the horse’s gait and can be use d together to diagnose disorders of movement.
Grading System for Ataxia According to Mayhew
Grade 0: Normal strength and coordination
Grade 1: Subtle neurological deficits only noted under special circumstances but mild (e.g., while walking incircles)
Grade 2: Mild neurological deficits but apparent at all times/gaits
Grade 3: Moderate deficits at all times/gaits that are obvious to all observers regardless of expertise
Grade 4: Severe deficits with tendency to buckle, stumble spontaneously, and trip and fall.
Grade 5: Recumbent, unable to stand
Neuroanatomical localization:
The nervous system is generally divided into brain, spinal cord, peripheral nerve, and autonomic nervous system. The brain can be further separated into general areas such as the forebrain (altered mental status, seizures, abnormal behavior), brainstem (altered mental status, cranial nerve deficits, central vestibular disease), and cerebellum (intention tremor, hypermetria, ataxia, menace deficit, shiver s) for localization.

65
Defects in the spinal cord can be categorized into ‘upper motor neuron’ (signs include exaggerated/hypermetric gait, exaggerated reflexes, increased muscle tone) or ‘lower motor neuron’ (signs include weakness, hypometria/dragging limbs, diminished/absent reflexes, decreased muscle tone). See below (adapted from UC Davis – Neurological Examination in the Horse).
Neurolocalization
C1-C5/6/7 – UMN deficits (normal to exaggerated) of thoracic and pelvic limbs.
C6-T2 – LMN signs of thoracic limbs, UMN of pelvic limbs.
T3-L3 – Normal thoracic limbs, UMN of pelvic limbs.
L4-S1 – Normal thoracic limbs, LMN of pelvic limbs.
S-caudal – Normal thoracic limbs, normal or LMN of pelvic limbs depending on location, and cauda equina signs (e.g., urinary +/- rectal incontinence)
The peripheral nerves can be affected and resulting abnormalities will be specific to the nerves affected (i.e., radial nerve paralysis, tibial nerve paralysis, etc.). Peripheral neuropathies in large animals can often ben attributed to trauma or crush/down animals, but there are a variety of differential diagnoses that could be explored if history does not fit with trauma.
It is important to remember when performing a neurological examination of a horse to document as you go and to repeat tests more than once to demonstrate repeatability. Video documentation can be helpful and can be used to monitor progression or improvement in clinical signs. Neurological examination is a necessary and vital skill to have when working with horses. Remember to take your time and be safe when performing an evaluation, it is never worth risking bodily harm to assess a neurologic patient.
References
Blythe, Linda L. Neurologic Examination of the Horse, Veterinary Clinics of North America: Equine Practice, Volume 3, Issue 2, 1987, Pages 255 -281, https://doi.org/10.1016/S0749-0739(17)30672-7.
Furr M, Reed S. Neurologic examination. In: Furr M, Reed S, eds. Equine neurology. Ames, IA: Blackwell, 2008; 65–76.
Hahn, Caroline. Vet Clin Equine 38 (2022) 155 –169. 2022 Elsevier Inc. https://doi.org/10.1016/j.cveq.2022.05.001
Johnson, Amy L. “How to Perform a Complete Neurologic Examination in the Field and Identify Abnormalities.” Neurology/Ophthalmology. AAEP PROCEEDINGS. Vol. 56 p. 331-337. 2010 https://aaep.org/sites/default/files/issues/proceedings -10proceedings-z9100110000331.pdf
Mayhew IGJ. Large animal neurology. Ames, IA: Wiley Blackwell , 2009;11–46.
Young, Amy. “Neurological Examination in the Horse” Horse Report. Center for Equine Health – School of Veterinary Medicine, University of California, Davis. 1 November 2021. https://compneuro.vetmed.ucdavis.edu/sites/g/files/dgvnsk5376/files/inlinefiles/equine_neuro_exam_0.pdf. Accessed 6 Dec 2022.
66
Vitamin E-related Diseases – What do we need to know?
Kile S. Townsend, DVM, MS, DACVIM (LAIM)
There are several neurological and muscular conditions in horses that are related to vitamin E. In this session, we will particularly focus on three specific vitamin E -related conditions in the horse: Equine Motor Neuron Disease (EMND), Vitamin E Deficient Myopathy (VEM), and Equine Degenerative Myeloencephalopathy/Neuroaxonal Dystrophy (EDM/eNAD).
Vitamin E is a group of fat-soluble compounds found in nature. Vitamin E is broadly known to be essential for neuromuscular function by acting as a potent antioxidant. Vitamin E status is relevant to immune function, reproduction, gene transcription, neuromuscular homeostasis, and exercise . Vitamin E can also modulate gene expression, inhibit platelet aggregation, and stabilize membranes. There are many ways to characterize vitamin E into different subgroups, but the relevant isoform for equine veterinary medicine is known to be RRR-α-tocopherol (it is also the most researched). RRR-α-tocopherol is the most biologically active isoform of vitamin E, and it also is known to have the most potent antioxidant properties. Horses obtain vitamin E solely from dietary intake.
Equine Motor Neuron Disease (EMND)
EMND is a spontaneous, acquired neurodegenerative disease of adult horses that is likened to amyotrophic lateral sclerosis (ALS aka Lou Gehrig’s disease) in human medicine. It usually affects adult horses >9 years of age (median ~ 10 years) but has been known to affect horses as young as 2 years old. It is caused by vitamin E deficiency for ≥ 18 months and has been experimentally induced in animals by denying access to vitamin E for 21+ months. Vitamin E deficiency results in neurodegeneration and the major lesions are present in alpha motor neurons in the spinal cord (ventral horn cells) and brain stem nuclei (V, VII, XII, and nucleus ambiguous). This neurodegeneration is coupled with muscle wasting, most severe in muscles with predominantly type I muscle fibers. It is believed that type I muscle fibers are more affected due to the higher oxidative requirements and are therefore more susceptible to oxidative damage.
Clinical signs of EMND include acute onset trembling, inappropriate or excessive recumbency, shifting of the weight of the hindlimbs, propulsive walking, short-strided gait, weakness, weight loss (often with good appetite), “horse-on-a-ball” posture, low head carriage, and marked muscle atrophy. Beware of mistaking clinical signs of EMND for other common equine afflictions that lead to recumbency, including rhabdomyolysis or colic. Pigment retinopathy is observed upon careful ophthalmic examination in approximately 40% of cases. There is no sex predilection to this disease and Quarter Horses and Thoroughbreds are said to be overrepresented
In order to treat this disease, administration of 5000-7000 IU of water-soluble, natural α-tocopherol/day is recommended and about 40% of horses have shown some clinical improvement within 6 weeks. In order to prevent EMND, horses without access to green forage should be supplemented with 1 U/kg BW/day of vitamin E. The Nutritional Research Council ( NRC) requirements for horses without pasture access is 600–800 IU/500 kg horse/day. Divers et al. have reported that about 40% of horses will stabilize clinical signs with treatment, but these horses remain permanently afflicted. The remainder of horses, treated or not, will continue to deteriorate.
Diagnosis of EMND is supported by low serum vitamin E concentrations and telltale clinical signs, but definitive antemortem diagnosis can be achieved via biopsy of the ventral branch of the spinal accessory nerve (histologic evidence of the degeneration of myelinated axons) or the finding of neurogenic
67
atrophy of predominantly type I muscle fibers in sacrocaudalis dorsalis medialis muscle biopsy. The sacrocaudalis dorsalis medialis muscle biopsy has a sensitivity of approximately 90% but should be examined by a veterinary pathologist with experience evaluating striated muscle . Electromyography can also aid in diagnosis of this disease antemortem. It is important to note that horses on pasture may be affected by EMND and this disease should not be entirely ruled out based on evidence of access to lush grass-based pasture.
Vitamin E Deficient/Responsive Myopathy (VEM)
Horses affected with VEM develop muscle wasting and associated weakness (myasthenia) This condition has been recognized as distinct from EMND because the muscle biopsies from affected horses yielded no evidence of neurogenic atrophy but had a characteristic “moth-eaten” staining appearance of the mitochondria. Some (but not all) horses with VEM also have low serum vitamin E and most horses will have low muscle vitamin E levels.
VEM is typically found in horses with a shorter duration of vitamin E deficiency than those with EMND. Clinical signs include loss of muscle mass, toe dragging, poor performance, muscle weakness, and muscle fasciculations in some cases. There is no known breed or sex predilection and its relationship to EMND is not known at this time
Treatment for VEM consists of vitamin E supplementation (water-soluble, natural form) and in one report all horses recovered completely after vitamin E therapy for several weeks.
Equine Degenerative Myeloencephalopathy/Neuroaxonal Dystrophy (EDM/eNAD)
This disease can be confusing because of the variable and diverse clinical presentations of the disease as well as the nomenclature. Equine NAD (eNAD) is clinically indistinguishable from EDM. Neuroaxonal dystrophy refers to a morphologic abnormality of select neurons and their axonal processes within the nervous system. Equine NAD is considered the underlying basis of EDM, with a high likelihood that the pathophysiology of the two diseases is similar. When classifying these diseases histologically, they both have dystrophic neurons and axons, vacuolization, and spheroid formation, the only (and subtle) difference between the two is the distribution of the lesions within the central nervous system (CNS). Essentially, experts have concluded that eNAD should be considered a localized form of EDM in which degenerative changes in the spinal cord are subtle and easily overlooked.
EDM has been reported in several breeds of equids (Quarter Horse, Arabian, Appaloosa, Thoroughbred, Standardbred, Morgan, Paso Fino, Grant’s zebra, Przewalski horses, and Warmbloods) and clinical signs typically occur in the first 14 months of age. In some Warmblood horses, there is increasing recognition of onset of signs of disease between 5-15 years of age. There is no known sex predilection, and a heritable component is suspected in some breeds.
Clinical signs are classically described as symmetric tetraparesis and ataxia. The onset of this paresis and ataxia is typically within the first 14 months of life. Recently, clinical signs such as topline muscle wasting and a dull haircoat have been reported along with personality changes in the horse. Owners/trainers often report changes in behavior and personality. Some horses appear unusually dull or sedate during examination while others inappropriately spooky or reactive for their level of handli ng/training Dynamic gait evaluation typically reveals proprioceptive deficits and signs of mild-to-moderate ataxia and paresis consistent with a cervical or diffuse myelopathy. Most horses are graded 1 to 2/5 on the modified Mayhew ataxia scale at the time of first evaluation, although some horses show more severe deficits (2.5 to 3/5). Repeated evaluations over months might show a progression of neurologic disease
68
(Johnson, 2021). Some horses are presented for inappropriate behavior under saddle, lameness , or poor performance.
Diagnosis of EDM is difficult and has to be made based on exclusion of other similar candidate diseases. The top differentials include compressive myelopathy, usually due to cervical vertebral stenotic myelopathy (CVSM) or infectious myelitis, usually due to equine protozoal myeloencephalitis (EPM) caused by Sarcocystis neurona CVSM must be ruled out with radiography/myelography and EPM with CSF analysis and serum: CSF antibody titer testing for Sarcocystis neurona. Vitamin E deficiency has been associated with EDM, and vitamin E concentration should be assessed in suspect cases. Low vitamin E concentration (less than 2 ppm or 200 mg/dL) is supportive of EDM diagnosis, particularly when other causes of neurologic disease have been excluded. However, adequate vitamin E levels do not preclude diagnosis of EDM (Johnson, 2021). It has been suggested that vitamin E deficiency in utero may contribute to development of this disease. The use of ‘phosphorylated neurofilament heavy’ (pNF-H) for diagnosis of equine neurologic disease, including EDM, is currently being investigated. Current evidence suggests that abnormally high concentrations of pNF-H in serum and CSF are suggestive of EDM if diseases such as EPM have been excluded. However, pNF-H testing has a low sensitivity for EDM diagnosis, and many confirmed cases have normal pNF-H concentrations in blood, spinal fluid, or both (Johnson 2021). Comorbidities are both possible and probable in some cases and can confuse diagnosis of this disease. In some cases, if neurological evaluations are repeated over months to years, a progression of neurologic disease can be demonstrated
There is no definitive treatment for EDM and horses that are predisposed to EDM or with a clinical diagnosis of EDM should receive oral water-soluble, natural α-tocopherol supplementation. Improvement in clinical signs has been seen in some cases with long-term treatment, but in general, the prognosis for complete recovery is poo r. In a group of Quarter Horses affected with EDM, dietary vitamin E supplementation did not improve neurologic deficit . However, vitamin E administration to pregnant mares appeared to decrease but not prevent disease development among offspring born the following year (Aleman et al. 2011).
Not all horses in which vitamin E deficiency is identified exhibit clinical signs or disease. It is important to supplement vitamin E in at risk horses and serum vitamin E testing is recommended prior to starting supplementation. Some horses require higher levels of supplementation than other (individual variation), so testing baseline vitamin E leve ls is important for monitoring. It is known that healthy horses on pasture maintain a serum vitamin E level of 3-4 µg/mL, so that is the recommended target in the average horse.
Measurement of vitamin E in serum or plasma is the easiest way to determine if a horse ahs vitamin E deficiency. Blood samples should be refrigerated (4°C) and protected from light (wrapped in foil for example) as soon as possible after obtaining a sample. The serum/plasma should be separated via centrifugation as soon as possible. Vitamin E deteriorates rapidly in the samples, so samples should be stored frozen (-70° C). Samples can be sent to the MU-VMDL (https://vmdl.missouri.edu/ ) or other veterinary diagnostic laboratories for analysis (Michigan State University and Cornell University have VMDLs that are often utilized). Reports of vitamin E results usually come with reference ranges/interpretations. Often, laboratories will report vitamin E levels as >2 μg/mL = Adequate, 1.5-2 μg/mL = Marginal, <1.5 μg/mL = Deficient.
69
References
Divers TJ, Mohammed HO, Cummings, JF. Equine Motor Neuron Disease, Veterinary Clinics of North America: Equine Practice, Volume 13, Issue 1, 1997, Pages 97 -105, ISSN 0749-0739, https://doi.org/10.1016/S0749 -0739(17)30258-4
Divers TJ, Mohammed HO, Hintz HF, de Lahunta A. Equine Motor Neuron Disease: A Review of Clinical and Experimental Studies, Clinical Techniques in Equine Practice, Volume 5, I ssue 1, 2006, Pages 24 -29, ISSN 1534-7516, https://doi.org/10.1053/j.ctep.2006.01.005 .
Edwards LA, Donnelly CG, Reed SM, Valberg S, Chigerwe M, Johnson AL, Finno CJ. Serum and cerebrospinal fluid phosphorylated neurofilament heavy protein concentrations in equine neurodegenerative diseases. Equine Vet J. 2022 Mar;54(2):290 -298. doi: 10.1111/evj.13452. Epub 2021 May 9. PMID: 33969539.
Finno, C. and Valberg, S. (2012), A Comparative Review of Vitam in E and Associated Equine Disorders. J Vet Intern Med, 26: 1251-1266. https://doi.org/10.1111/j.1939 -1676.2012.00994.x.
Johnson, Amy. “How to Diagnose Equine Degenerative Myeloencephalopathy in Sport Horses.” HOW-TO SESSION: MEDICAL REASONS FOR POOR PREFORMANCE. AAEP PROCEEDINGS / Vol. 67 / pp.209 -213. 2021.
McGorum, B.C., Mayhew, I.G., Amory, H., et al. Horses on pasture may be affected by equine motor neuron disease. Equine Veterinary Journal, 38: 47-51. 2006 https://doi.org/10.2746/042516406775374207 .
Miller MM, Collatos C. Equine degenerative myeloencephalopathy. Vet Clin North Am Equine Pract. 1997 Apr;13(1):43-52. doi: 10.1016/s0749 -0739(17)30254-7. PMID: 9106342.
Mohammed, H.O., Divers, T.J., Summers, B.A. et al. Vitamin E deficiency and risk of equine motor neuron disease. Acta Vet Scand 49, 17 (2007). https://doi.org/10.1186/1751 -0147-49-17.
Riis, R.C., Jackson, C., Rebhun, et al. Ocular manifestations of equine motor neuron disease. Equine Veterinary Journal, 31: 99 -110. 1999. https://doi.org/10.1111/j.2042 -3306.1999.tb03801.x
70
Equine
Alison LaCarrubba, DVM, ABVP (Equine Practice)
Equine Ambulatory and Equine Internal Medicine Services University of Missouri College of Veterinary Medicine Columbia, Mo.
71
72
Care of our Geriatric Horses
Alison LaCarrubba, DVM, ABVP (Equine Practice)
What do we need to know to best care for our geriatric horses? There are so many facets to horse care and add in age related changes and sometimes things can seem overwhelming. Just like humans, all horses will age differently. Some of this has to do with individual variation, but also there can be breed variation. For example, small and miniature horses are generally known to live a bit longer than are large, heavy breed horses. Also, what do we mean by geriatric? What age horse is considered to be “old” or need extra care? This will certainly vary, greatly in some instances. Generally speaking, it’s safe to say, upper teens and early twenties we will start considering horses entering into their golden years. The average life expectancy of a horse is approx imately 25 to 30 years. We all know horses which have lived many years longer than this. A horse named Old Billy is known to have been the longest living horse in the world, having lived to the age of 62 years. He was from Lancashire, UK.
Perhaps the most important thing we can do for our older companions is to understand the best nutrition practices. For a healthy adult aged horse, the dry matter (hay and grain component) should contain, 12-14% protein, 0.3 – 0.4% phosphorous, 0.6-0.8% calcium. The total intake should be approximately 1.5 – 2% of body weight, or 15-20 pounds per 1,000-pound horse. Many horses can do well on good quality forage, including fresh pasture grass and good quality hay up into their twenty’s, so long as they can maintain adequate body condition. Other horses will start to lose muscle mass and condition and require supplemental grain feeding and/or a complete pelleted feed like equine senior. Equine senior complete feed is a high fat, high forage, easily digestible source of calorie s for our older horses with dental problems, who are unable to utilize hay effectively. These older horses with a body condition score at less than or equal to 4/9 require a diet with approximately 12 -14% protein, 4-7% fat and this should be fed at 0.5 – 1.0% of body weight. It is important to minimize sugars and starches in horses prone to laminitis or diagnosed with insulin resistance. Forage based pellets or cubes or chopped hay can also be used as a supplement. Omega 3 FA play an important role in inflammation. There are benefits to supplementing omega 3FA in horses with lower airway disease and insect hypersensitivity as well as joint disease Fats represent a small amount of overall calorie intake in a normal horse diet at pasture. Fats are necessary as structural components of cells, precursors to hormones, carriers for fat soluble vitamins (A,D,E,K) and to enhance overall body condition in thin horses. Fresh grass, alfalfa and clover are natural, quality sources of omega-3 FA’s, even if at relatively low levels. Cut hay is not a good source of omega-3 FA and once grass is cut and dried most of the activity of the omega -3 FA is diminished. Horses being fed grain and hay diets exclusively would benefit from an omega-3 FA supplement.
One of the reasons geriatric horses have changing nutritional requirements is secondary to dental attrition or dental disease. Horses are designed to live about 30 years, and so are their teeth. Some horses are outliving their teeth and some horses do not have proper dental care over their lifetime and develop dental disease and tooth loss. Geriatric horses may require more frequent dental examinations, where we look for loose or damaged teeth and we can help manage nutritional needs better when we know how effective their chewing/grinding surface is. In horses with significant dental
73
MVMA Proceedings 2022
attrition, the end goal is comfort, so they can chew without pain. There are some common dental abnormalities that can progress over time in the absence of correct dental therapy, resulting in unbalanced dentition, such as wave mouth and excessive hooks. When teeth develop gingivitis and periodontal disease resulting in attachment loss, the tooth becomes loose and painful and will require extraction. Other reasons we extract teeth include tooth ro ot abscesses and fractured or fragmented teeth. Equine Odontoclastic Tooth Resorption and Hypercementosis (EOTRH) is a painful disease of geriatric horses affecting primarily the incisor and canine teeth. Most horses with this disease are in their late teens and twenties. Clinical signs of EOTRH include inability to bite a carrot with the incisor teeth, pain associated with application of the speculum, abnormal eating, fistula in the gingiva around the incisor and canine teeth, infected teeth, periodontal disease, gingival recession, feed packing between teeth, abnormal angulation, and loose or fractured teeth. EOTRH is diagnosed based on history, clinical signs and radiographs – highlighting the resorptive properties of the disease, along with hypercementosis. Currently the only treatment for this disease is exodontia of all affected teeth. Typically we end up removing all maxillary and mandibular incisors and often the canine teeth as well.
The metabolism and endocrine status of each individual horse will be slightly different and this needs to be taken into consideration when feeding older horses. The two most common endocrine diseases effecting horses are Equine Metabolic Syndrome and Pituitary Pars Intermedia Dysfunction (PPID). EMS is not a disease specific to older horses but it can affect older horses and can be what is called a co-morbidity, where horses are affected by multiple different issues which contributes to overall poor health. EMS can in fact complicate other diseases of geriatric horses. Th e hallmarks of EMS include obesity, which can be global or regional adiposity, documented insulin resistance (IR) and laminitis (clinical or subclinical). The predisposition to EMS can be both genetic and environmental. Certain breeds, known to be “easy keepers” seem to struggle more with EMS – ponies, donkeys, Morgan horses, Paso Fino, Arabians, ASB, AQH and TWH are included. Ponies and donkeys have a tendency toward IR. Not all fat is created equal and fat from different areas of the horse, crest of the neck, sheath/inguinal region, tail head, has been shown to be more metabolically active. There is not perfect test to diagnose IR, but we can combine a variety of testing methods. We typically will start with evaluating insulin and glucose levels in the fasted horse, or a horse which was only fed grass hay overnight. The gold standard for proving IR is the CGIT (combined glucose insulin test IV), but this is not practical in the field setting. We do sometimes opt for the oral sugar test, where we feed Karo Syrup to a horse and check insulin glucose at prescribed times after and watch for time to return to normal. This test is less invasive and more physiologic in that it uses the GI tract for absorption, and it can be done on the farm. Any horse diagnosed with EMS will need to be put on a strict weight loss diet, reducing overall calorie intake, removing them from pasture and even soaking hay to reduce sugar content. Thyroid supplementation can be added in the short term to kick the metabolism into gear and allow for more expedited weight loss. If IR is uncontrolled even after dietary changes metformin can be added in an effort to improve insulin sensitivity.
The other common endocrine disease, which is a disease of geriatric horses, is PPID. This typically affects horses over 15 years of age, is slowly progressive and is a result of a lack of dopamine inhibition on the intermediate lobe of the pituitary , secondary to oxidative damage – which results in excessive production and function of certain, specific hormones, such as ACTH. Overproduction of certain hormones (POM-C peptides and cleaved products such as ACTH) can cause the clinical signs associated with PPID as well as resulting in IR. Hypertrichosis is something we think of when di scussing
74
PPID. The pathogenesis of hypertrichosis is unknown, but perhaps related to excess androgens from the adrenal gland, or dysregulation of the thermoregulatory center of the hypothalamus secondary to pituitary compression. Approximately 55 -80% of PPID affected horses will display hypertrichosis and grow a long, thick, curly coat, fail to shed and sometimes are affected by patchy alopecia. This tends to be a sign of later stage disease. The ultimate goal is to diagnose horse s prior to the development of some of the problematic clinical signs. Other clinical signs of PPID include weight loss, PU/PD, pendulous abdomen, muscle loss/weakness/sway back, lethargy, infertility and dermatitis. Some of these clinical signs are a direct effect of IR which is associated with this disease. Endocrine diseases of horses can be difficult to diagnosis accurately and PPID is no exception. Typically, we make a diagnosis based on history, physical examination findings, a baseline ACTH level, which is a screening test. ACTH is a stress hormone so levels can be elevated during times of stress and pain, and all horses have a seasonal elevation during the fall months (July 15 – Nov 15) further complicating the issue. If we suspect disease and our screening tests are normal, we can then move to a TRH stimulation test (thyrotropin releasing hormone) and this has a better ability to detect disease but is discouraged during the fall season as well, as results may vary greatly. Once diagnosed, we manage the disease through the use o f a dopamine agonist, Pergolide. This is not a cure but rather a way to control clinical signs.
Finally, musculoskeletal disease in aged horses can be a long-standing cause of pain which can affect overall quality of life. Diagnosing the exact cause of the pain in order to initiate targeted therapy is important for the long-term comfort of our older horses. Many old horses have varying degrees and locations of osteoarthritis. Arthritis can affect any joint and different breeds and disciplines will have varying predispositions. Laminitis can also be a source of pain, associated with other co -morbidities, such as EMS, PPID, or could be associated with a previous illness or injury. Laminitis can truly affect quality of life and be difficult for owners to manage. Soft tissue injuries include stresses and strains to muscle, tendon and/or ligaments. These can be intense or mild, life threatening or chronic low grade. When we discuss soft tissue injures causing long term lameness issues we think about injury to the suspensory apparatus, ligaments associated with joints, muscle strain and tendon injury or disease. Some breeds are predisposed to a condition called Degenerative Suspensory Ligament Disease (DSLD) which results in chronic breakdown of the suspensory apparatus, loss of support of the fetlock, fetlock drop and associated pain. Neurological dysfunction can be secondary to musculoskeletal pain, when we think about conditions like cervical vertebral instability and cervical arthritis. This can result in pain a s well as neurological dysfunction and ataxia.
Once we understand the cause of the pain, hard tissue, soft tissue, neurological, we can better understand how to treat the horse in order to keep them active and comfortable for as long as possible. There are a variety of diseases and conditions affecting older horses, and this was certainly not a comprehensive list but these are some of the most common conditions we see in horses over 20 years of age. There are many things we can do to help slow the aging process in our older friends and allow them to live not only longer lives, but better quality lives!
75
76
Diagnosis and management of colic in the field setting Alison LaCarrubba, DVM, ABVP (Equine Practice), Associate Teaching Professor
A majority of our after-hours emergency calls involve colic. We know that colic, by definition is abdominal pain associated with the gastro-intestinal system. There are other types of pain associated with the abdomen that can be confused with colic. It is important to do a complete and thorough examination on every colic suspect to determine the cause of pain in order to embark on the correct treatment plan. The vast majority of colic can be managed in the field. Statistically, approximately 80% of horses with colic will resolve with medical therapy. The most common causes of medical colic include spasmodic colic, gas colic and impaction colic.
We need to ask ourselves if this colic is medical or surgical? Does the patient have a surgical option? Is this a large colon problem or small intestinal problem? Do we think the colic is caused by colitis? The answers to these questions will inform our treatment plan.
What are the common clinical signs of colic? Owners will frequently report, inappetence, standing alone, pawing at the ground, flank watching, phlegmon response, kicking at abdomen, getting up and down, sweating, anxiety, distressed appearance, down horse. When examining the horse it is important to rule out other major issues that can result in these similar clinical signs. Horses with fever will often be in-appetent and depressed. It is important to not skip any steps during the examination and to obtain a temperature on all horses when it is safe to do so. Other conditions that may result in distress include esophageal obstruction (choke), urinary obstruction/urethral stone, pneumonia and even dystocia. A down horse can sometimes be difficult to assess and common causes of the down horse include colic, neurological disease, laminitis, and catastrophic musculoskeletal issues, such as a limb fracture.
In order to make an accurate diagnosis a thorough exam will be conducted. This will start with a distance examination which includes behavior – what is the horse doing? What is the body condition? Is the animal emaciated and perhaps this is not something that just started or does the horse appear to be in good flesh and look healthy otherwise? Does the horse have a normal respiratory rate and effort? These are all things that are important and can be assessed before laying hands on the animal. After a distance examination is conducted a thorough physical examination will be next. The importance of a complete and thorough physical examination cannot be overstated! The horse should have a halter and lead rope on and be properly restrained, ideally by a veterinary assistant. Mucus membranes will be assessed for color, moisture and capillary refill time. Information gained from evaluation of mucus membranes is incredibly valuable to understanding the systemic health of the animal. By evaluating the mucus membranes we can begin to rule in or out, shock, endotoxemia, dehydration and determine how severe the immediate situation is. Vital parameters will be important in understanding the severity of the colic as well. Along with this we will evaluate for heart disease , such as an arrhythmia or murmur as well as a thorough auscultation of the lung fields. The abdomen will then be auscultated to evaluate borborygmi - absence or reduction of normal gastrointestinal sounds, increased GI sounds or even sounds that are fluidic and consistent with colitis, which can certainly be a cause of severe colic. During the examination the hair coat will be evaluated, body will be palpated to ascertain accurate BCS and the demeanor of the animal will be assessed.
77 MVMA
2023
Once the physical exam ination is complete, we will continue to hone in the exact cause of the colic and for this we will need to employ further, more invasive diagnostics. Nasogastric intubation is often the best place to start. In some cases this can be done without sedation, but if the horse is anxious or difficult, an alpha-two agonist can be helpful to provide sedation and analgesia. Dosage will vary depending on the patient and severity of the colic. Alpha-two agonists have a significant impact on the cardiovascular system and in a severely compromised patient, this should be avoided, as a significant change in heart rate and blood pressure could compromised the patient. Along these lines, once it has been determined the horse is in fact experiencing a painful colic episode, it is important to administer a non-steroidal anti-inflammatory such as flunixin meglumine to provide comfort. This is best given intravenous and will take approximately 20 minutes to take effect. During this time, if the horse is sedated with an alpha-two agonist, such as xylazine, the sedative effects can help to control the pain until the anti-inflammatory kicks in. Flunixin meglumine is the better choice for visceral pain over phenylbutazone. Buscopan (Hyoscine butylbromide) is an anticholinergic medication used to treat crampy abdominal pain, and esophageal spasms during a choke episode and can be a valuable tool during a spasmodic colic episode. Butorphanol is an opioid partial agonist and will provide short acting but substantial pain relief when administered. For those colics whose pain is difficult to manage butorphanol can be an important tool.
The pain the animal is experiencing may involve gastric di litiation and passing the nasogastric tube early in the process will alleviate pain associated with gastric distention. The goals of passing the tube include gastric decompression, reflux evaluation – present or not and how severe, as well as providing treatment using the administration of cathartics as needed. The tube can be passed, then left in place until further diagnostics are complete, then medications administered as warranted via the tube. If there is no abnormal reflux and medical colic is suspected, the tube can be used to pass water and electrolytes, magnesium sulfate, or less commonly currently, mineral oil. Evidence points to the positive effects or oral electrolyte/water administration in relief of medical colic. A n average 1000 –1200lb horses stomach can hold approximately 6-10 liters. Anything more than 2 liters of net reflux would be considered abnormal and no additional fluid should be added. Treating impaction colic with fluid administration directly into the gastrointestinal tract is recommended. When evaluating reflux it is also important to examine the color, texture and odor.
Examination per rectum can provide important and relevant information. It is important to be safe in order to be effective in this situation. Ideally the horse will be placed in stocks for trans rectal palpation. If this is not possible sedation with an alpha-two agonist and a twitch, situationally dependent, maybe necessary. Safety first for the veterinarian and the horse! Trans rectal examination can provide information on the exact cause of the colic and this can be valuable for further treatment or referral options.
Further diagnostics will be dependent on owner finances, and what is available to the practitioner in a field setting. Abdominal ultrasound is a valuable tool to better discern the exact cause of the colic. This is a more thorough way to examine and evaluate the abdomen than rectal palpation alone. Other important diagnostics that will give us information on the health of the gastrointestinal tract include obtaining abdominal fluid, serum amyloid A (abdominal and systemic) and lactate (abdominal and systemic). When abdominal fluid is obtained, evaluate color, clarity and protein level and this can all be done stall side. Total protein should be less than 2 mg/dL, lactate <2mmol/l and SAA
78
0-20 mg/L. Evaluating total nucleated cell count can be more difficult in the field, when time is of the essence and often is not completed. Normal tncc should be <10,000 cells/l. A significant increase in tncc is indicative of peritonitis which might be caused by a variety of reasons, one of which might be a surgical lesion. Comparing the above parameters – systemic versus abdominal fluid can be helpful as well.
Treatment of colic will depend on the specific findings of the complete work up described, as well as owner finance and specific referral options. For the average field me dical colic, the 80% that respond to medical management, the treatment does not go beyond what has been discussed in the field setting- pain management, rehydration, etc. Other field colics may not be surgical but will require repeat administration of water and/or electrolytes over many hours to days to relieve a persistent impaction. A catheter can be placed in the field and IV fluid administration can be conducted in a field setting. Usually this is done with a single large fluid bolus but depending on th e situation fluids can be administered over many hours. This can be time consuming or impossible given the busy schedule of most equine veterinarians. Leaving a catheter in place or leaving a horse on IV fluid therapy with only an owner is not recommended. Sometimes it is immediately obvious the horse will need surgery and if that is an option then the horse will have the pain managed, nasogastric tube passe and be sent to a referral center immediately. Other times the horse has a surgical lesion that is not immediately obvious and it will require repeated examinations in the field before the horse is sent.
If the horse is refractory to treatment and must be examined multiple times it would be prudent to obtain blood for a serum biochemical profile as well as a complete blood count. If ultrasound was not originally performed it would be important to do so on the follow up visit. If this is not possible a repeat examination per rectum is recommended. Repeat serum lactate and SAA as well as abdominal lactate and SAA.
How do you know when a horse should be referred for surgery or for more extensive medical treatment? The most common reason for referral is that the horse i s refractory to pain management. A horses heart rate consistently over 60 bpm that does not respond to the administration of systemic NSAID therapy can be an indication to refer a horse. Other indications include, positive net reflux, abnormal rectal palpation findings (such as significant impaction, distended SI, severely distended large colon, small colon impaction, displacement, etc.), abnormal abdominal fluid, diarrhea, systemic compromise (muddy or brick red mm, toxic line) .
Although most of our field colics will respond to on farm therapy it is critical to understand when referral is warranted in order to get the horses the help they need in the quickest time frame.
Equine Internal Medicine. Reed SM, Bayly WM, Sellon DC. Elsevier 2018.
Clinical Veterinary Advisor. Wilson DA. Elsevier 2012.
79
80
Food Animal
81
82
Food Animal
Celeste Morris, DVM, MBA, MPVM
Assistant Professor, Food Animal Ambulatory Service University of Missouri College of Veterinary Medicine Columbia, Mo.
83
84
Abstract
Bovine Reproductive Problems for the Mixed Animal Practitioner
Missouri Veterinary Medical Association Convention January 27, 2023
Celeste Morris, DVM, MBA, MPVM
Assistant Professor, Food Animal Ambulatory Service University of Missouri College of Veterinary Medicine c.morris@missouri.edu
Beyond dystocia, there are many other reproductive challenges that can present to veterinarians for treatment. This talk will discuss management of other common reproductive disorders in the bovine, such as freemartins, twins, retained fetal membranes, metritis, pyometra, cystic ovaries, and vaginal and uterine prolapse. It will attempt to propose practical, summary notes on these conditions and the most common and/or easiest routes to diagnosis and treatment.
Key Words: Cystic ovarian disease (COD), twin management, freemartins, uterine prolapse, vaginal prolapse, metritis, pyometra, retained fetal membranes (RFM)
Normal Bovine Reproduction Review
¥ Reproductive anatomy: Bicornuate uterus with a very small uterine body
¥ Estrous cycle
o Non-seasonal, polyestrous
o 21 day cycle (17-24 day range)
o 2-3 waves of follicles
o Estrus length: ~12-18 hour average
o Ovulation 24-30 hours after the onset of estrus (after they go out of estrus, usually)
¥ Gestation: ~280 days (270-292 day range), cotyledonary placentation (convex placentomes)
¥ Normal uterine involution: ~35-45 days
Cystic
Ovarian Disease (COD)
¥ Synonymous terminology: Cystic ovaries, cystic ovarian disease, ovarian cysts, cystic ovarian degeneration
¥ Follicular Cyst Definition (COD): “Presence of a follicle(s) with a diameter of at least 20 mm, present on one or both ovaries in the absence of any active luteal tissue, which clearly interferes with normal ovarian cyclicity” (Hopper, 2021)
o Older definitions require 10 days – not easily known in routine reproductive examinations
o Cystic ovaries can be present with luteal tissue if the cyst is not steroidogenic
¥ Luteal Cyst: Luteal structure that is >20 mm and persistent, interfering with normal cyclicity or known progression of a previously diagnosed follicular cyst
o Differentiation between large/cavitated CL and luteal cyst in one visit can be challenging (based on clinical signs and history, not just presence of a large luteal structure), keep in mind that cavitated CLs are normal
o Often has irregularly filled luteal tissue with cavities or strands (trabeculae) which can help differentiate luteal cyst versus CL
¥ Etiology
o Multifactorial condition
o Individual genetic factors, phenotypic traits, environmental factors, metabolic and cellular factors, and management factors
o Most widely accepted theory is related to LH surge (absent, insufficient, or improperly timed)
o Other likely related factors: Breakdown in estradiol positive feedback loop, loss of progesterone negative feedback, protracted estradiol secretion by the dominant follicle, heat shock protein, high NEFAs
o Leads to follicles that continue to grow and become anovulatory
o Can resolve on their own or continue to re-grow in the same spot even after resolution
85 1
¥ Risk factors: High milk production, calving in summer months, increased parity/age, overconditioning precalving, increased NEFAs, genetics (low heritability, 0.07-0.12), MGA use in beef heifers, genetics
¥ Classification of cysts
o Most common: follicular vs luteal
o Differentiation can be based on degree of luteinization or hormones produced
o Thought to be different phases of the same process: follicular cyst à luteinization à luteal cyst
o Differentiation can require combination of history and physical examination, +/-ultrasound, +/serum progesterone levels
¥ Clinical signs: Anestrus > persistent estrus (nymphomania)
¥ Diagnosis
o Clinical signs
o Transrectal palpation
o Transrectal ultrasound


o +/- serum progesterone levels (uncommon in routine practice)
¥ Treatment
o Non-hormonal therapies (not recommended)
§ Ovariectomy
§ Manual crushing
o Hormonal therapy
§
Follicular cyst
¥ GnRH – First line, most common, usually works
o Mechanism: Cause an LH surge exogenously within 2 hours
o Causes luteinization of the follicular cyst and ovulation of a dominant follicle if present
o Resumption of normal cyclicity in 72-85% of cows and return to estrus within 3 weeks if a dominant follicle was present
Follicular Cyst (<3 mm rim, anechoic center)
o Can also follow with prostaglandin in 7-10 days following GnRH to speed up the process
§ Luteal cyst
¥ Prostaglandin
o Mechanism: regression of luteal tissue
o Estrus in 90% of cows by 8 days following treatment
§ Undetermined type of cyst (unable to determine if luteal or follicular, may be transitional): Concurrent GnRH + prostaglandin treatment can be used to elicit response
§ Additional treatments for refractory cysts
¥ hCG
o Mechanism: Should be used only if cyst is refractory to GnRH treatment
o LH like properties cause the cyst to luteinize
o Can also follow with prostaglandin in 7-10 days
o Dose: 10,000 IU IM
o More costly than GnRH, can cause immune reaction, legality?
86 2
Luteal Cyst (>3 mm rim, hyperechoic strands)
Cyst Classification
¥ Progesterone (CIDR Device) +/- prostaglandin +/- ovsynch
o Mechanism:
§ Progesterone “resets” the hypothalamic-pituitary-ovarian axis
§ Reduced LH secretion
§ Regression of the cystic structure
§ New follicular wave after removal
o Dose: One cattle CIDR contains 1.38 g progesterone
Rim Width
Follicular Thin (£3 mm)
Luteal Thick (>3 mm)
Twins & Twin Management
Ultrasound Appearance
Anechoic fluid
Variable - more hyperechoic (luteal tissue), often have trabeculae or echogenic strands
Primary Hormone Secreted
Most common treatment
Estradiol GnRH – synthetic or analog (100 µg IM)
Progesterone Prostaglandin (25 mg dinoprost or 500 µg cloprostenol IM)
¥ Risk Factors: High producing dairy cows, genetic propensity, more common in dairy than beef
¥ Associated challenges: Increased pregnancy loss, especially <60 days Dystocia, periparturient disease, freemartinism, spontaneous regression (may occur without consequences)
¥ Diagnosis
o Suggestive
§
Transrectal palpation: Enlarged horn for stage of pregnancy
§ >95% of twins are dizygotic – examine for 2 corpora lutea
¥ Recommendation to make ovarian examination part of normal pregnancy diagnosis if performed when twin diagnosis is possible to complete examination
§ Ultrasound visualization of “Twin line” (apposing chorioallantoic membranes)
o Definitive
§ Palpation of 2 fetuses
§ Ultrasound visualization of 2 fetuses
¥ Treatment: Current standard is not to reduce twins - no treatment recommended (risks outweigh benefits)
¥ Management recommendations
o Monitor more closely for potential pregnancy loss and dystocia
o Likely will calve early (a few days)
§ If dairy, dry off early to compensate
o Can increase energy in the diet in late gestation
o Monitor for metabolic disease
Freemartins
¥
Definition: Sterile female produced from a twin (male/female) pregnancy
¥ Etiology
o XX/XY chimera produced as a result of anastomosis of placental vessels (day 28-30) before sexual differentiation (mixing of hematopoietic stem cells)
o Female is exposed to AMH and testosterone during sexual differentiation, which results in abnormalities of the normal female reproductive tract (often partial regression of paramesonephric duct products)
¥ Risk Factors: All breeds of cattle are affected
o Remember: If the male twin dies after sexual differentiation, freemartin heifers can appear to be born as singles
¥ Clinical signs
o Enlarged or prominent clitoris
o Elongated clitoral hairs
o Shallow vagina
87 3
o Small or incomplete cervix
o Small, incomplete, or absent uterus
o Small or hypoplastic ovaries
o Otherwise systemically healthy
¥ Presentation
o Heifers that were born co-twin to a male and/or are hard breeders, don’t stand for a bull, or that are open at the end of an appropriate breeding season where others are pregnant
o Abnormal external genitalia
¥ Diagnosis
o Clinical signs and history
o Absence of normal, functional reproductive tract (transrectal palpation and/or ultrasound)
o Measurement of vaginal depth: <1/3 depth of heifers the same age
o Karyotyping (XX/XY Chimera), PCR testing – unusual
¥ Treatment – none, cull if breeding stock
Vaginal Prolapse
¥ Etiology
o Can be vaginal or vaginal and cervical
o More common in bovine than in many other species
o Not related to uterine prolapse
o Usually occurs in late gestation and with increased intra-abdominal pressure
¥ Risk Factors: Genetics (especially Herefords, Charolais, limousine, shorthorns and bos indicus breeds), increased intra-abdominal pressure in late pregnancy, extreme cold weather, overconditioning (perivaginal fat), intake of large volumes of poorly digestible roughage, poor vaginal conformation, increased estrogen influence (late pregnancy, estrus)
¥ Guidelines:
o Retain vaginal and cervical tissue in order to allow delivery and weaning of live offspring
o Perform retention procedure as soon as possible to decrease tissue damage and exposure (try to go within a few hours)
o Cull after job is finished (likely to recur at next gestation/parturition) and do not keep female offspring
¥
Classifications
o Grade I: Intermittent (usually present when animal is laying down)
o Grade II: Tissue prolapsed and continuously visible
o Grade III: Prolapse of the vagina along with cervix (tissue all visible but still healthy/intact), bladder may be involved
o Grade IV: Vaginal mucosa appears necrotic, is fibrosed, or is damaged (with or without cervical involvement)
¥ Short term treatment
o Carefully replace the tissue
§ Apply gentle pressure until replacement can be completed – use palms or fists, not fingers, to avoid traumatizing the tissue
§ Be patient and don’t force it! Finding the location with give is key
§ Hypertonic saline and/or water with sugar can make a hypertonic paste that is easily applied
§ If very edematous, can wrap in a towel and squeeze to attempt to decrease the size of the tissue mass
§ If not making progress with pressure, an occasional twist of the tissue 15-30 degrees can help facilitate slipping back inward
o Buhner Stitch (most common)
§ Supplies:
¥ Caudal epidural anesthesia (2% Lidocaine, 5-10 ml syringe, 18 ga 1.5” needle)
¥ Water
¥ ~2 feet of 3/8” umbilical tape
¥ Gerlach (Buhner) needle
88 4
¥ Optional: #10 blade, betadine solution for soaking umbilical tape, antiseptic solution if needed, obstetrical lubricant
¥ If severe or chronic, can use hypertonic solutions to aid in replacement – see Uterine Eversion (Prolapse) Section for details
§ Directions
¥ Caudal epidural anesthesia
¥ Clean the vulva and surrounding 2-3 inches of tissue with water and/or dilute antiseptic solution if needed
¥ Optional:
o 1 cm stab incision made on midline below the vulva
o 1 cm stab incision midway between anus and top of vulva
o Presenter’s preference is not to do stab incisions and use the needle to make the holes for passage of the umbilical tape – 1 cm apart on midline below the vulva (horizontally) and 1 cm apart on midline above the vulva (horizontally) halfway between the anus and the vulva
¥ Gerlach (Buhner) needle passed starting ventrally below the vulva (if stab incision was made, insert through stab incision) and driven dorsally in the deep musculature lateral to the vulva, exiting the skin halfway between the vulva and the anus (through stab incision if one was made)
o Place non-dominant hand inside the vagina to ensure the needle doesn’t exit through the vaginal mucosa
¥ Thread needle with umbilical tape
o 1/3 on one side, 2/3 on other side (leave a long enough tail that one end can reach along the whole track of the needle)
¥ Pull needle down and out, drawing umbilical tape through track just made lateral to the vulva
¥ Unthread umbilical tape and repeat placement of needle on the opposite side of the vulva
¥ Thread umbilical tape from the dorsal exit of the other incision through the eye of the needle and pull down, threading the same piece of umbilical tape down through the opposite side
¥ Tie ends below the vulva together and tighten until the opening of the vulva is ~2 fingers in width
o Bow +/- knot for late gestation/impending calving
§ Can be opened and retied if necessary, depending on the amount of owner observation that is possible
o Square knot for open animals
¥ The tie should be tucked under the ventral, haired portion of the vulva as not to cause irritation to the opening of the vulva
¥ Need close observation once Buhner stitch is placed if calving!
o Caslick’s – not recommended, often insufficient
o Bootlace technique
§ Directions:
¥ Caudal epidural anesthesia
¥ Eyelets are placed on either side of the vulva in dorsal to ventral line
¥ Umbilical or Buhner tape is used to lace up the vulva (like boot laces)
§ Stronger than a caslick’s
§ Undesirable due to vulvar inversion and extra time and supplies for suture placement
§ Must be loosened prior to calving, need close observation
o Horizontal or vertical mattress
§
Directions
¥ Caudal epidural anesthesia
¥ Needle passed across the top of the vulvar lips in a horizontal line, then repeated from the same side back across with spacing of about 2-3 cm between bites
§ Undesirable due to vulvar edema that frequently develops
89 5
§
Recommend placement with stents or buttons to decrease edema formation
§ Must be loosened prior to calving, need close observation
¥ Long term treatments, secondary methods
o Minchev or modified minchev vaginopexy
o Winkler Cervicopexy
¥ Supportive care
o Antibiotics: only in cases of severe trauma (usually Grade IV)
o Anti-inflammatories: As needed basis
o Steroids: Avoid in late gestation, can induce parturition
¥ Directions following placement
o Monitor animals carefully
§ Untie if signs of calving are seen
§ Retie after calving
§ Monitor for normal urination and defecation
Uterine Eversion (Prolapse)
¥ Etiology
o Usually occurs within 24 hours after calving
o Not related to vaginal or cervical prolapse
¥ Risk Factors: Multifactorial condition
o Reduced uterine contractility following primary or secondary uterine inertia
§ Primary uterine inertia: hypocalcemia, reduced prostaglandin and oxytocin receptors, myometrial defects
§ Secondary uterine inertia: exhaustion, dystocia
o Prolonged recumbency following paralysis or hypocalcemia
§ Increased intra-abdominal pressure
o Extreme weather changes
¥ Guidelines
o True emergency! Uterus becomes quickly traumatized, contaminated, and edematous!
o Do not transport animals if possible
o Handle animals carefully and slowly if they are mobile
o Unlikely to recur, do not need to cull based on occurrence of uterine prolapse
¥ Treatment – Replace!
o Contraindications for replacement
§ Significant trauma
§ Obvious prolapse of abdominal organs
o Cow positioning
§ Cow standing or down depending on the circumstances, experience, or preference
§
§
If down, legs straight behind the animal can help significantly to open space in the caudal abdomen
If standing, can use a towel or a sheet to help support the weight of the uterus
§ Can lift the hind end of the cow if necessary or indicated, but recommended only if absolutely necessary due to potential trauma
o Supplies
§ Caudal epidural anesthesia (2% Lidocaine, 5-10 ml syringe, 18 ga 1.5” needle)
§ Water +/- dilute cleaning solution
§
§
Obstetrical lubricant
Optional: Plastic bag for uterus, hypertonic saline, sugar, towels, dextrose
o Epidural anesthesia
o Clean uterus
o Remove any easily removable fetal membranes (do not tear)
o Large and unruly uterus tips
§ Can place in or on a plastic bag to help with cleanliness and weight/edema
§ If the cow is standing, can “sling” the uterus with a towel or a sheet to decrease worsening dependent edema and help reduce the weight burden
90 6
§
If the cow is down, resting the uterus on your abdomen/chest can be helpful for support
§ If needed, hypertonic solutions (hypertonic saline, sugar, dextrose) can be applied to help decrease edema and facilitate replacement
¥ Use of sugar or other hypertonic solutions can be irritating to the endometrium and are not uniformly supported, but can help in cases of severe edema – they should only be used if replacement without is not possible
¥ Hypertonic saline and/or water with sugar can make a hypertonic paste that is easily applied
o Use gentle, steady pressure (fists or palms only, fingers are likely to puncture the uterus) to gently apply pressure and feel for which part of the uterus has any give toward the vulvar opening
§ If identifiable, try to find the non-gravid horn (slit or small opening) with smaller placentomes to start with steady pressure
o Continue with gentle pressure until replacement can be completed
§ Be patient and don’t force it! Finding the location with give is key
o Fully invert the uterine horns
§ If the end of the uterine horns cannot be reached by hand, the practitioner can use a large bottle (presenter’s preference is plastic, like a soda bottle or hypertonic bottle) in the hand to gently invert the horns inside the cow
¥ Treatment – Amputation – only if no other options (significant trauma to the uterus, untenable size/inability to replace)
o Open
§ Incision in the uterine body to explore contents of the uterus (return any exposed viscera to the abdominal cavity)
§ Fan out the broad ligament on each side and individually double ligate and cut visible vessels
§ Place overlapping mattress sutures across the uterine body and amputate just distal
§ Suture over stump with simple continuous sutures and return the stump
o Closed
§ Salvage procedure and doesn’t take into consideration trapped viscera
§ Ligate the entire organ and leave it to slough
¥ Supportive care
o Anti-inflammatories
o Systemic antibiotics
o Oxytocin (20-30 IU IM, repeat in 30-60 min or 40-100 IU IM or IV once)
o Retention (Buhner) suture?
§ Controversial
§
§
If the cow is standing and responds to therapy (oxytocin) well, unlikely the uterus will evert again
If the cow is down, unable to stand, is still showing significant tenesmus, has other complicating conditions, the uterus may be more likely to re-prolapse
o +/- Calcium therapy (Calcium Gluconate, CMPK)
¥ Directions following replacement
o 18-20% mortality rate after replacement (usually internal hemorrhage from uterine artery) –communicate with clients
o Prognosis for future fertility is usually acceptable as long as replacement was successful and the animal is systemically healthy afterward
o No known heritable component, minimal chance of recurrence
Retained Fetal Membranes (RFM)
¥ Definition: Retention of allantochorion and/or amnion for > 12 hours after calving
¥ Etiology: Abnormal or incomplete placental maturation preventing the usual easy separation and expulsion of fetal membranes
¥ Direct risk factors: Induction of parturition, dystocia, uterine torsion, cesarean section, abortion/uterine infection
¥ Indirect risk factors: intensive stress, twinning, subclinical hypocalcemia, fetal dropsy
91 7
¥ Clinical signs
o Usually visible tissue hanging from vulva >12 hours after calving
o If still present at 36 hours, likely to stay for 6-10 days
o Without smell to malodorous (big range)
¥ Diagnosis
o History, clinical signs
o Visual and physical examination
¥ Treatment
o Condition contained within the uterus (no signs of systemic illness)
§ Monitoring for development of systemic signs (inappetence, lethargy)
§ If the membranes are long, damaged, or dirty, tie them in a knot to prevent further contamination but still allow the weight of the membranes to apply consistent tension to the remaining parts
§ If the membranes are malodorous, but she is otherwise well, no systemic treatment is necessary
o Systemic illness (lethargy, inappetence, fever, etc)
§ Systemic antibiotics (not intrauterine) +/- anti-inflammatories +/- fluid therapy
o Summary
§ Hormonal therapies not shown to help
§ Only treat if systemically affected
§ Do not flush the uterus, administer intrauterine antibiotics, intrauterine antiseptics, or attempt to manually remove the membranes
¥ Can apply light traction in case the membranes are “floating” but do not attempt manual removal
§ Do not manually dilate the cervix
¥ Long term complications
o Delayed uterine involution à increased number of days from calving to first estrus
o Loss of milk production
o Predisposes to metritis (dairy > beef)
Metritis
¥ Definition: inflammation of all of the layers of the uterus (endometrium, myometrium, serosa)
¥ Etiology
o Usually seen within the first 2 weeks (can be diagnosed up to 3 weeks)
o Repeated or overwhelming bacterial contamination of the uterus post-calving resulting in infection
o Organisms: E. coli (early/first week) à Truperella pyogenes (later)
§ Can be complicated by Fusobacterium necrophorum
¥ Risk Factors: Dairy > Beef, dystocia, twins, stillbirth/abortion, retained fetal membranes, negative energy balance (elevated NEFAs), ketosis, immunosuppression
¥ Clinical signs
Color Consistency Smell Time Lochia Bloody to reddish-brown Mucoid Odorless Normal up to 3 weeks
Metritis
Usually brown Watery Fetid <21 days
o Localized infection (contained within the uterus)
§ Fetid discharge
§ May not have any other outward clinical signs
o Acute puerperal metritis/Systemic metritis/Toxic septic metritis
§ Fever, inappetence, lethargy, tachycardia, and/or dehydration
§ Enlarged, fluid filled, flaccid uterus
§ Brown, watery, fetid discharge
¥ Diagnosis
o History and clinical signs
o Physical examination - Uterus may expel fetid fluid upon palpation
¥ Treatment
92 8
o Localized: Monitoring
§ No treatment if not systemically ill
o Acute puerperal metritis/Systemic metritis/Toxic septic metritis
§ Anti-inflammatories
§ Systemic antibiotics
§ +/- fluid therapy, electrolytes (Ca2+), ketosis treatment
o Summary
§ Only treat if systemically affected
§ Do not flush the uterus, administer intrauterine antibiotics or intrauterine antiseptics
§ No known benefits associated with treating with oxytocin or prostaglandin
Pyometra
¥ Definition: accumulation of pus in the uterus in the presence of a CL and a closed cervix
¥ Etiology
o Dairy: Early ovulation when the uterus is still clearing post-calving resulting in a closed cervix and trapping of bacteria within the lumen à results in increased CL lifespan due to increased concentrations of PGE2
o Beef: Tritrichomonas foetus >>> other
¥ Risk factors: Previous diagnosis of reproductive disease (RFM, metritis)
¥ Clinical signs
o Anestrus (no vaginal discharge)
o Not systemically affected otherwise
¥ Diagnosis
o Palpation: Fluid filled uterus in the presence of a CL and no positive signs of pregnancy

§ Wall of the uterus is often thickened
§ Variable in size, can be in one horn or both
§ Can confirm with ultrasound – variable echogenicity, from anechoic with speckles to highly cellular
¥ Treatment
o Dairy or non-infectious: Most cows will respond to a single dose of prostaglandin
§ Can treat twice 14 days apart if non-responsive
§ Will need at least one heat cycle following luteolysis to increase the chances of successful conception after complete uterine clearance of debris
o Beef or suspected infectious: If CL present, can still treat with prostaglandin, BUT consider below
§ If several cows present with pyometras and the herd also has low pregnancy rates overall, suggest testing the pyometra fluid and/or bull for Tritrichomonas foetus
§ Recommend culling these animals due to overall disease risk and decreased reproductive efficiency for this season
§ Tritrichomonas regulations (State of Missouri): https://agriculture.mo.gov/animals/health/disease/trich.php
§ 2021 Disease Map: https://agriculture.mo.gov/animals/pdf/PositiveTrichomoniasisMap2021.pdf
General Reminders
¥ Epidural anesthesia:
o Dose: ~1 ml 2% Lidocaine/200 lbs (Adult bovine rule of thumb: 4-8 ml)
o Caudal epidural (Sacral/coccygeal space)
o 18 ga 1.5” needle
93 9
Pyometra
¥ Estradiol prohibited for use in food animal practice (If not sure about legalities of medications, submit a FARAD request or visit the site for guidance)
¥ Oral progestogens not for use in livestock species
¥ Consider the job of the animal you’re treating and let that help you make treatment decisions
o Don’t forget withdrawal periods, even on pets
¥ Antimicrobials approved for use in adult lactating dairy cattle (also for lactating goats, sheep where there is human consumption of dairy products):
o Oxytetracycline (LA200) - Follow labeled route, dose, frequency (ELDU Permitted)
o Penicillin (PPG) - Can dose at 3-5 ml/100 lbs (label dose is 1 ml/100 lbs) (ELDU Permitted)
o Ampicillin (Polyflex or ampicillin sodium) - Follow labeled route, dose, frequency (ELDU Permitted)
o Ceftiofur (Naxcel, Excenel, Excede) - Follow labeled dose, route, frequency, duration (Can change indication but nothing else, ELDU Restricted)
¥ Always educate and include the producer
¥ Call us if you have questions!
Bovine Medication Table
Anti-Inflammatories
Trade Name Drug Name Route Dose+ Meat withdrawal* Milk Withdrawal* Special Notes
Banamine Flunixin meglumine IV 1.1-2.2 mg/kg or 1-2 ml/100 lb
4 days 36 hours q24 hr, consult FARAD if multiple doses Topical 3 ml/100 lbs 8 days N/A Not for dairy
- Meloxicam PO 0.5-2 mg/kg Approx. 30 days, consult FARAD
- Dexamethasone IM or IV 0.1-0.15 mg/kg Approx 6 days, consult FARAD
Trade Name
Approx. 14 days, consult FARAD
Approx 3 days, consult FARAD
q24 hr
Avoid in pregnant animals
Reproductive Hormones
Example Drug Name Route Dose+ Meat withdrawal* Milk Withdrawal* Special Notes
Estrumate Cloprostenol IM 500 µg 0 days 0 days
Lutalyse Dinoprost IM 25 mg (5 ml) 0 days 0 days Pyometra, luteal cysts; caution with Lutalyse HC (half dose)
Cystorelin Gonadorelin IM 100 µg IM 0 days 0 days Follicular cysts - Oxytocin IM or IV 20-100 IU 0 days 0 days Can repeat if given smaller doses or just give once
*If going off label or giving multiple doses, always extend your withdrawals and submit a FARAD request
+ Always refer to medication label for dosing information
Sources
¥ Bovine Reproduction; Hopper, R.M., Ed.; 2nd Edition.; Wiley & Sons, Inc: Hoboken, NJ; ISBN 9781119602361.
¥ Current Therapy in Large Animal Theriogenology; Elsevier, 2007; ISBN 9780721693231.
¥ Veterinary Reproduction and Obstetrics; Elsevier, 2019; ISBN 9780702072338
94 10
Small Ruminant Pregnancy Diagnosis
Missouri Veterinary Medical Association Convention January 27, 2023
Celeste Morris, DVM, MBA, MPVM
Assistant Professor, Food Animal Ambulatory Service University of Missouri College of Veterinary Medicine c.morris@missouri.edu
Abstract
This talk includes methods for and timing of pregnancy diagnosis in small ruminants. It will compare and contrast transrectal and transabdominal ultrasonography, discuss fetal counting, pregnancy staging and blood pregnancy testing.
Key Words: Small ruminants, pregnancy diagnosis, transabdominal ultrasound, transrectal ultrasound, pregnancy associated glycoproteins (PAGs), fetal counting, pregnancy staging
Normal Small Ruminant Reproduction Review
Species Estrous Cycle Length Estrus Length Ovulation
Puberty Age* Gestation Length CL Dependency Sheep 17 days (14-19) 30 hours (15-45 hr) Final 1/3 of estrus (21-45 hrs after start of behavioral estrus)
Cycling @ 7-8 months
145-150 days CL dependent days 0 to ~75, then placenta Goats 21 days (18-22) 36 hours (24-72 hr) Variable, 9-37 hours after onset of estrus Cycling @ 6-8 months
150 days (147-155) CL Dependent throughout pregnancy
¥ Seasonally polyestrous (short day breeders)
o Deepest anestrus is in April and May
o Seasonality varies significantly by breed
o Can be manipulated with hormonal protocols
¥ Pregnancy checking often performed from late summer to late winter, but can be year-round depending on the breed and management style of the owner
¥ Classic breeding season is October to December, but can range from August to March
More Seasonal Less Seasonal Goats Nubians Boers Kiko
Sheep Southdown Hampshire Hair Sheep (Equator breeds)
¥ Reproductive anatomy: bicornuate uterus with small uterine body
¥ Gestational anatomy: concave placentomes
Methods of Pregnancy Diagnosis
Methods Not Recommended
¥ Presumptive
o Non-return to estrus
Nigerian Dwarf Goats
TN Fainting Goats
Dorset Merino Rambouillet
§ This may be a good producer tool to help monitor animals and get used to detecting estrus; however, it should not be used for pregnancy diagnosis alone. There are a variety of reasons animals may not come back into estrus (including incorrect owner observations) and some animals can show signs of estrus even if they are pregnant.
95 1
¥
o Enlargement of abdomen
§ Again, this may be a good tool for owners to monitor for general health and well-being, but it should not be used for pregnancy diagnosis. In goats especially, it is not uncommon for them to have a protruding, pendulous abdomen as part of normal anatomy.
o Development of mammary glands
§ This can be used by owners to help monitor progression of mammary tissue, pregnancy, and an indicator of overall health; however, it should not be used for pregnancy diagnosis on its own. Mammary tissue can change significantly in some animals in the absence of pregnancy, and even males can develop seasonally affected mammary tissue (galactorrhea, inappropriate lactation syndrome)
o Ballottement
§ This method has been popular in the past and can be relatively useful in those that are experienced; however, if access to more definitive methods is possible, it should not be used on its own for pregnancy diagnosis. A fetus can easily be mixed up with gastrointestinal contents for an inexperienced examiner and also does not give any information about the health of the pregnancy.
Hormone testing
o Estrone sulfate
testing
§ This is a pregnancy specific hormone produced by the placenta; therefore, presence is almost 100% indicative of pregnancy. It can be performed after day 50 of gestation. It is not recommended because few labs perform it and it can be expensive. PSPB (discussed below) is less expensive, more widely available, and can be done sooner.
o Progesterone testing
§ Progesterone is not a pregnancy specific hormone and only indicates that there is a corpus luteum present. Although progesterone is produced by the CL of pregnancy, progesterone testing alone doesn’t distinguish between progesterone from a CL of a normal estrous cycle versus a CL of pregnancy. Progesterone testing is better suited for detecting nonpregnant animals and is effective for this purpose.
¥
Special case – Radiography
o Many veterinarians are often comfortable using radiography in general and for pregnancy diagnosis and evaluation in small animals; however, it is not the best method for pregnancy diagnosis in small ruminants.
o Finances: Due to financial concerns, it is often not practical for large numbers of animals.
o Practicality: If in a clinic, radiography is often easily accessible but it can be challenging in the field and many clinics do not have portable radiography equipment.
o Interpretation: Visualization of fetuses, evaluation of fetal and gestational health, and identification of fetal remnants can be difficult due to being superimposed by a large rumen
o Timing: If this is the preferred method by the veterinarian, fetal skeleton is radiopaque by day 65 but best to wait until 90 days to avoid false negatives.
Recommended methods
¥ Pregnancy specific protein B (PSPB), a pregnancy associated glycoprotein (PAG)
o Method: PSPB is produced by the placental binucleate giant cells and is produced throughout gestation. It can be detected in blood samples and is pregnancy specific.
o Sample: Serum or clotted blood
o Timing: 28+ days goats, 35+ days sheep
o Idexx kit: ~99% sensitivity, ~93% specificity
o Cost: $5-10 depending on the lab, widely available
o Challenges:
§ Can be positive up to 60 days after lambing/kidding
§ Doesn’t account for fetal viability, health of the pregnancy, or numbers of fetuses
¥ Higher amounts of PSPB frequently means multiple fetuses, but delineation of the amount of PSPB per fetus or counting based on PSPB levels has yet to be established
o How to integrate:
§ Offer as an option for clients that don’t want to pay for ultrasound (better than nothing).
96 2
§
For clients that know how to draw blood, offer as a way to separate pregnant and nonpregnant animals, and then use a follow up ultrasound examination to perform more advanced services (fetal counting, fetal health evaluation, etc, pregnancy confirmation).
§ Educate clients on how this can help but also the limitations and integrate it in your offerings as another option for management tools
¥ Ultrasonography
o General Guidelines
§ Bladder is your reference point
§ Better to wait until at least 42 days to increase chances of fetal survival (or recheck if done early)
§ Method(s) and timing will change from client to client –need to adapt
§ Coupling media –methylcellulose (transrectal), alcohol or ultrasound gel (transabdominal)
o Ultrasound specifics
§ Transrectal: linear or curvilinear 5 or 7.5 MHz probe
§ Transabdominal: Microconvex, 3.5 to 5 M
ugh, 2021
¥ Can also use convex, linear, or transrectal probe depending on goals of examination
o Transrectal method
§ Be gentle, use lots of lubricant
§ May need to evacuate rectum (fingers)
§ Can purchase or make an “introducer” to allow more control of the transrectal probe while inside the rectum
¥ Can be made from PVC pipe with probe taped in, just ensure the edges are smooth
§ Make sure you know where the probe is pointed at all times
§ Can apply gentle downward pressure to increase visibility
§ Useful in overconditioned and large small ruminants for whom transabdominal ultrasound may be challenging
§ Timing: Most appropriate for early pregnancy (~28-60 days) because the pregnant uterus in mid and late gestation moves more ventral and cranial, further away from the rectum, and may be obscured by gastrointestinal contents.

o Transabdominal method
§ Scan from the right side rather than the left to minimize rumen gas interference
§ Many probe types depending on goal
¥ Microconvex > linear, convex, transrectal
§ Stand next to (on the right) or behind the animal and hook the probe in the right inguinal area, underneath the inguinal skin flap by the stifle
¥ Can clip small area of hair (~2”x2”) in goats (this is not necessary in sheep and may not be necessary in all goats, always ask owners first)
§ Scanning in inguinal area starting pointed backward toward the bladder
§ Scan cranially from bladder to find uterus
§
Timing: 30 + days through end of gestation
97 3
Recommended Methods for Small Ruminant Pregnancy Diagnosis
Method Ideal Days Gestation Additional Days Gestation

Blood (PAGs) 40+ Can perform as early as: 28 days goats 35 days sheep
Transrectal Ultrasound 25 - ~60 Can technically perform at any time beyond 28 days

Transabdominal Ultrasound ~30 – end Fetal counting days ~ 42-58
Fetal Staging
¥ Fetal age determination
o Crown-rump length: Measurement from one end of the fetus (most rostral tip of the head that can be identified, the crown) to the opposite end (rump)
o Biparietal across the head from the caudal margin of across to the caudal margin of the opposite eye s not measure the this measurement.
¥ Fetal sexing
o Timing: 55
o Male: The genital t become the glans pen will be identified near the (the location animal)
o Female: T become the cl be identified of the cli
98 4
DesCôteaux,
2010
Fetal Counting
¥ Method:
o Count either heads or heartbeats – not both
o Perform when the fetus is smaller than your probe
o Follow all loops of uterine fluid until they join together and then slowly narrow and disappear
§ If they disappear abruptly, it is likely that you “fell off” the uterus, rather than that you reached the end of the uterine horn to be scanned
¥ Client expectations
o Communicate with client that it’s an estimate
o Seek feedback for improvement
¥ Timing: Microconvex probe – preferred ~42-58 days (range 42-90 days)
o In later gestation, give the information you see but set client expectations
¥ Purpose: Use to guide feeding programs (pregnancy toxemia)
Abnormal Reproductive Findings
¥ Hydrometra: Primarily anechoic fluid distending uterus, no placentomes
o Treat with prostaglandin, 10 mg dinoprost or 250 mcg cloprostenol
¥ Pyometra: Primarily hyperechoic or mixed echogenicity fluid distending uterus
o Treat with prostaglandin, 10 mg dinoprost or 250 mcg cloprostenol
¥ Mummies: Fetal bones visible with little or no fluid surrounding
¥ Dying/dead/macerated fetuses
o Non-viable fetuses (anatomic abnormalities, no heartbeat)
o Abnormal appearing fluid
o Fetuses of different sizes
o Placentome/fetal size mismatch
Small Ruminant Reminders
¥ Some small ruminants (goats > sheep) may exhibit signs of estrus during pregnancy, which is normal
¥ Most common reason for non-cycling small ruminants is pregnancy
¥ Do not induce >5-7 days before due date if viable offspring are expected
¥ Colostrum is ESSENTIAL – no nutrients are passed across epitheliochorial placentas
o 10-15% of body weight within 24 hours
Sources
¥ Current Therapy in Large Animal Theriogenology; Elsevier, 2007; ISBN 9780721693231.
¥ Practical Atlas of Ruminant and Camelid Reproductive Ultrasonography; Wiley-Blackwell, 2010; ISBN-13: 9780813815510.
¥ Sheep, Goat, and Cervid Medicine; Elsevier, 2021; ISBN 9780323624633.
99 5
100
MU-CVM Lectures
101
102
MU-CVM Lectures
Elizabeth A. Giuliano, DVM, MS, DACVO
Professor, Department of Veterinary Medicine and Surgery Section Chief, Comparative Ophthalmology University of Missouri College of Veterinary Medicine Columbia, Mo.
103
104
ENUCLEATION SURGERY – WHY DOES THIS SEEM MORE DIFFICULT THAN THE TEXTBOOKS SAY?
Elizabeth A. Giuliano, DVM, MS, DACVO
Professor and Section Chief of Ophthalmology, MU-VHC University of Columbia, Missouri
The author would like to begin by thanking The MVMA for their kind invitation to participate in this year’s continuing education program. I recognize that there are many individuals who work hard to put together MVMA’s meeting each year. It is my sincere pleasure to share with you my passion for veterinary comparative ophthalmology. In almost 25 years of lecturing experience, I aim to teach what is practical, immediately applicable to the small animal general practitioner, and helpful to our patients’ welfare. Thank you for joining me!
OVERVIEW OF THE ISSUE
Many practitioners, particularly new graduates, often do not feel comfortable removing a blind, painful eye that warrants enucleation. This lecture will provide an overview of this procedure and provide some useful tips to making each procedure a more comfortable experience for both patient and veterinarian alike.
LEARNING OBJECTIVES OF THE PRESENTATION
1. Define the following 3 surgical procedures and list their indications: evisceration/prosthes is, enucleation (either subconjunctival or transpalpebral), and exenteration.
2. Describe the key steps in a subconjunctival enucleation.
3. Why do all removed eyes merit being submitted for histopathologic examination?
4. According to Dr. Giuliano, how many layers at a minimum should be used to close an enucleation in a dog or a cat?
5. List the advantages and disadvantages of various surgical material used to close an enucleation surgery.
ESSENTIAL INFORMATION
Enucleation is performed for the follo wing reasons: intraocular neoplasia, severe perforating ocular trauma with disruption and loss of ocular contents, uncontrollable endophthalmitis or panophthalmitis, intractable ocular pain (especially in glaucomatous eyes), or an owner’s inability or unwi llingness to give long-term treatment to a blind eye to keep it comfortable. This author uses a subconjunctival approach to the majority of her enucleations in dogs, cats, and horses. The steps as discussed in lecture are as follows:
• A retrobulbar, regional eyelid, and 4-point peritomy block is performed using Bupivicaine with epinephrine (see additional information below).
• A lateral, 1- to 2-cm canthotomy is performed and the eyelid margins and a bordering area of skin 2- to 3-mm wide so as to include the meibomium glands are removed from the lateral to the medial canthus.
• The conjunctiva is grasped near the limbus with toothed forceps, and a 360 -degree perilimbal incision is made posterior to the limbus, leaving sufficient conjunctiva to grasp throughout the remainder of the procedure.
• The sclera is separated from the conjunctiva, Tenon’s capsule, and extraocular muscles with curved Stevens scissors (Metzenbaum or Mayo scissors can also be used) to the optic nerve. The extraocular muscles are severed near their insertion on the sclera.
105 Page 1 of 5
• No effort to visualize the optic nerve is made before it is severed with scissors: Traction must not be placed on the nerve lest damage the optic chiasm occur causing blindness in the remaining eye (this is especially a concern in cats).
• The remaining conjunctiva, third eyelid, and gland are carefully removed to avoid the formation of an orbital cyst postoperatively.
o Note that Dr. Giuliano will now routinely remove the eyelids and third eyelid PRIOR to removing the globe and the residual fornix conjunctiva.
• The eye should be placed in formalin and submitted for histopathologic evaluation. Closure (recommended suture sizes are for dogs or cats):
• The deep fascia and periorbita is closed with a simple conti nuous suture of 3/0 or 4/0 absorbable material (I typically use Vicryl in all my closure layers, including the skin) .
• The subcutaneous tissue is closed with a simple continuous suture of 3/0 or 4/0 absorbable material followed by closure of the skin with simple interrupted or simple continuous sutures of 4/0 or 5/0 nylon or polypropylene (Prolene)
• Application of a cold pack to the surgical site while the animal recovers from anesthesia may help to reduce post-operative swelling.
• Postoperative analgesia with an oral nonsteroidal anti-inflammatory drug or opiate or narcotic is often recommended for 3 -5 days following surgery.
LOCAL ANESTHESIA IN VETERINARY OPHTHALMOLOGY
Local anesthetic (LA) techniques can provide an invaluable adjunct to general anesthesi a. Addition of local anesthesia to a general anesthetic protocol has many benefits, including:
• minimal equipment required
• minimal systemic effects when delivered peripherally
• reduced inhalational/ intravenous anesthetic requirement
• reduced sympathetic response to surgical stimulation
• improved post-operative analgesia
Local anesthesia is commonly used for retrobulbar blocks prior to enucleation and to provide eyelid akinesia when examining/treating horses. Retrobulbar anesthesia provides excellent extrao cular muscle akinesis. Additionally, it has the benefit of providing local analgesia that may help reduce the need for perioperative administration of systemic analgesics such as opioids or non-steroidal anti-inflammatory drugs. Finally, without the specific need for a mechanical ventilator (as is often needed with the use of systemic non-depolarizing neuromuscular blocking agents commonly used in veterinary ophthalmology), additional monitoring equipment, and associated personnel, the overall operative cost of commonly performed ophthalmic procedures may be reduced. Retrobulbar blocks are also used by some veterinary ophthalmologists prior to cataract surgery.
POTENTIAL APPLICATIONS AND TECHNIQUES
Retrobulbar block
When performing a retrobulbar block, the practitioner should have a thorough understanding of orbital and ocular anatomy. The target cranial nerves when performing a retrobulbar block include CN III, IV, V, VI and the ciliary ganglion. Local anesthetic may be placed eithe r internal or external to the retrobulbar muscular cone. Injection into the intraconal space is preferred, as it will result in the most rapid and consistent analgesic effect with the least volume of drug(s) required. Extraconal injection is considered safer by some ophthalmologists because the needle is not as close to the globe as with intraconal injections, however this technique requires a higher volume of anesthetic to be used with
106 Page 2 of 5
multiple injections and typically has a longer onset of action. Regardless of what technique is employed, the practitioner should be cognizant of possible complications, including retrobulbar hemorrhage, intravenous injection, globe perforation, damage to the optic nerve, extraocular muscle myopathy, and intrathecal injection with possible seizure or cardiorespiratory arrest. Despite the risks associated with retrobulbar injection, it can be argued that these risks may be less than the effects of inappropriate ventilation secondary to the use of systemic neuromuscular blockers without adequate monitoring or attempting ophthalmic surgery on eyes not centrally rotated and paralyzed.
There is no real consensus among veterinary ophthalmologists about the optimal approach to local anesthesia for various ophthalmic procedures and the technique that is employed is largely surgeon preference. One study has determined that the most reliable technique to obtain an intraconal distribution of local anesthetic material is the inferior-temporal palpebral approach (this author’s preferred technique in the small animal patient). For this technique, a 20-degree angle is created by mechanical bending at the midpoint of a 1.5 inch (3.81 cm), 22 gauge spinal needle. The needle is then positioned at the inferior orbital rim and inserted through the inferior lid at the junction of its middle and the temporal third and advanced until a slight “popping” sensation is noted. This indicates that the needle tip has pierced the orbital fascia. The needle is then directed slightly dorsally and nasally towards the apex of the orbit and advanced approximately 1 -2 cm. Using this technique with lidocaine, the authors successfully induced changes that were favorable for ophthalmic surgery such as pupil dilation, central rotation of the eye, inhibition of globe movement and no significant effects on intraocular pressure. The duration of effect is approximately 2 hours at the reported anesthetic dose (2 ml of 2% lidocaine hydrochloride; see table below for additional doses) and was sufficient for a variety of commonly performed ophthalmic procedures.
Perilimbal injection
Local infiltrative anesthesia is also useful when administered prior to enucleation to facilitate hemostasis during surgery and a smooth recovery during the postoperative period. In this technique, a subconjunctival perilimbal injection around the circumference of the globe can be made using a mixture of bupivicaine and lidocaine. When used in conjunction with a retrobulbar block prior to enucleation, the analgesic effect may last for several hours after surgery and, in this author’s opinion, remarkably improves post-operative comfort.
Eyelid surgery
This author has found local / regional anesthesia, commonly administered via a “line block”, to be extremely useful after eyelid surgery in the small animal patient. Common surgeries in which this technique is useful include the Hotz-Celsus, wedge resection, and lateral canthotomy. Benefits include improved comport post-operatively and a “space occupying effect” useful for those entropion ca ses with a significant spastic component to their entropion.
DOSE:
This author as described using equal parts 2% Lidocaine mixed with 0.5% Bupivicaine, although more commonly I now only use Bupivicaine with epinephrine for all my local -regional anesthesia.
107 Page 3 of 5
108
Caution: Do not exceed the maximum IV dose for Bupivicaine in any patient (I do not exceed 1 mg/kg). If maximum IV dose is exceeded, it may potentiate arrhythmias and seizures. Delayed wound healing has been reported as a complication with large volumes; however I have not found this to be a problem with the volume of drug I administer to my ophthalmic patients.
PHARMACOLOGY REVIEW
Local anesthetics are classified as esters and amides. The local anesthetics used in veterinary practice (lidocaine, bupivicaine, mepivicaine) are amides. Local anaesthetics are predominantly metabolised by the liver.

Recommended dose (mg/kg) Toxic dose (mg/kg) Onset time (mins) Duration (hours) lidocaine 5 10 – 20 10 – 15 1 – 2 mepivicaine 5 15 - 20 1.5 - 3 bupivicaine 2 3.5 – 4.5 20 - 30 2.5 - 6 ropivicaine 2 4.9 20 - 30 2.5 - 6
Agent
AMINO ESTERS – procaine, 2-chloroprocaine, tetracaine
AMINO AMIDES – lidocaine, mepivicaine, ropivicaine, bupivicaine
Clinical differences between the ester and amide LA’s involve their potential for producing adverse effects and the mechanisms by which they are metabolised Half-life of esters is only a few minutes, and of amides is a few hours Esters are metabolised by para-amino benzoic acid (PABA). Patients with reduced cholinesterase activity (newborn and pregnant) may have increased potential for toxicity from ester LA’s. Amides are mainly metabolised by the liver – so risk with severe hepatic disease Block nerve conduction through two mechanisms – by impairing propagation of the action potential in the axon; by interacting directly with specific receptors on the sodium channe l, inhibiting sodium ion influx
Esters and amides differ with respect to their chemical stability, biodegradation and allergenicity. Esters have short shelf lives and are degraded in plasma by pseudocholinesterases. Amides are very stable and are metabolised by hepatic microsomes. The potential allergenicity of the
109 Page 4 of 5
ester LA’s is a result of production of PABA as a primary product of biotransformation. Amides aren’t broken down to PABA, so that allergic reactions are very rare.
KEY LEARNING POINTS:
• The sub-conjunctival enucleation can be used in dogs, cats, and horses and affords several advantages over the trans-palpebral approach.
• After an enucleation and as clots within the orbit break down, bloody fluid may drain via the nasolacrimal duct and appear at the nostril (usually on the third to fifth day after surgery; most noticeable in horses).
• The emotional resistance of the owner to enucleation should be evaluated prior to surgery, and, when appropriate, globe sparing alternatives such as evisceration and intrascleral prosthesis may be considered.
• All enucleated globes should be submitted for histopathologic examination to establish a definitive diagnosis that may alter management of the remaining eye (glaucoma, lens luxation) and to rule out an unsuspected disease process such as neoplasia, systemic mycoses, septic endophthalmitis, etc.
Additional references available upon request
110 Page 5 of 5
MU-CVM Lectures
Philip Johnson, DVM ACVIM
Professor of Veterinary Medicine and Surgery
University of Missouri College of Veterinary Medicine Columbia, Mo.
111
112
Viral hepatitis
in
Philip J. Johnson
horses (we used to call it Theiler disease)
At the outset of the twentieth century, Sir Arnold Theiler originally described outbreaks of an acute fatal liver disease in horses following administration of antisera, being developed for protection of horses against African Horse Sickness. He also reported that in-contact horses also developed severe liver disease, albeit that those horses had not received the antiserum. Theiler was a Swiss veterinarian working in what is now South Africa. Prior to his significant observations regarding the risk of ‘seru m hepatitis’ in horses treated with antiserum, he had been celebrated for success in the production of a vaccine to combat an outbreak of smallpox that afflicted miners in the Witwatersrand. He was appointed as the state veterinarian for the Zuid-Afrikaansche, where he worked throughout the Anglo-Boer war (1899-1902). He also developed a vaccine against the contagious bovine disease, rinderpest. Acute fatal hepatitis following administration of antiserum (any disease) has subsequently been known as Theiler’s disease.
Fatal hepatitis (Theiler disease) outbreaks have arisen in the context of administration of antisera (and other equine biological treatments) since the time of Theiler. Deployment of antisera against Western Equine Encephalitis (WEE) to protect horses in the western USA (1930s) also led to substantial death from severe hepatic disease. Antisera against various other diseases (EEE, anthrax, tetanus, botulism, clostridiosis, strangles, EHV1, influenza) have also been implicated. The use of allogeneic stem cell therapy for orthopaedic injuries and the administration of plasma/serum products to horses have also resulted in Theiler disease (it is not restricted to the use of antiserum products per se). Moreover, the fact that in-contact but untreated horses also sometimes develop hepatitis has been well known. Therefore, the ‘idea’ that Theiler disease results from an infectious contagion has long been suspected. Attempts to cultivate viral pathogens using traditional virus isolation methods from the liver of affected individuals failed and the ‘etiology’ of Theiler disease has, for so many years, been consigned to that ‘last chapter’ in veterinary medical textbooks dedicated to diseases of unknown etiology.
Theiler’s disease in horses is an example of a situation in which molecular tools have enhanced our understanding of etiology. Using PCR-based massively parallel sequencing technology with subsequent nucleic acid-based screening, Chandriani and coworkers (2013) first described a previously unknown and highly divergent member of the Flaviviridae family in horses that developed Theiler’s disease after being treated with botulism antiserum. This candidate virus was designated “Theiler’s disease-associated virus” (TDAV) and could be demonstrated in both blood obtained from affected horses and from the equine antiserum product that had been administered to the horses. Only RNA viral metagenomic analysis was performed in that study, resulting in limited results. TDAV (flavivirus) is no longer thought to cause Theiler disease
In further pursuit of a putative viral etiology for Theiler’s disease, the employment of modern molecular PCR-based diagnostic methods (unbiased amplification and high-throughput sequencing of serum and tissue samples) led to the identification of three additional candidate viruses that infect horses (another two RNA viruses and one DNA virus) since 2013. Of importance, two of these novel viruses have been shown to cause liver disease. One is a non-primate hepacivirus (NPHV) also called equine hepacivirus or hepacivirus A, the closest homologue to hepatitis C virus (HCV) infecting humans, and the other has been designated equine parvovirus-hepatitis (EqPV-H). Results of a prospective study showed that EqPV-H virus could be identified in the blood and/or liver of 18 cases of Theiler’s disease that occurred 4–12 weeks following administration of an equine-origin biologic product (usually tetanus antiserum). In many of those cases, presence of EqPV-H was also demonstrated in antiserum that had been administered to affected horses. Subsequent experimental EqPV-H infections showed that biochemical evidence for hepatitis correlated with peak viremia and initial EqPV-H antibody detection. Interestingly, retrospective testing of archived frozen samples (blood and antisera) from the first Theiler’s disease outbreak, in which TDAV was discovered, showed that all of those samples were also positive for EqPVH.
Presently, increasing evidence points to EqPV-H as being the responsible etiological agent in Theiler’s disease. The equine hepacivirus (NPHV) is now more strongly associated with the syndrome that had
113
previously been characterized by its histopathological features, chronic active hepatitis. There have been some reports in which both EqPV-H and NPHV have been identified in cases of Theiler’s disease, suggesting that co-infection may play a role, at least in some cases , but further work is needed to better explore the relationship between these viruses in the face of liver disease in horses. Infection with EqPVH has also been demonstrated in horses affected with Theiler’s disease but that did not receive treatment with an equine-origin biologic product
In the past, veterinarians had to acknowledge risk of potentially fatal Theiler’s disease whenever there was a call for administration of equine-origin biological products, especially if antiserum was needed to provide protection against tetanus in wounded horses that had not been actively vaccinated and/or boosted. It is now possible to screen donor horses for both of these hepatitis viruses, thus significantly reducing the risk of both Theiler disease and chronic active hepatitis. PCR testing of blood for both EqPVH and NPHV is now available to veterinary diagnosticians at the Animal Health Diagnostic Center at Cornell University. Moreover, the USDA Center for Veterinary Biologics now requires that all licensed equine blood products must test negative for EqPV-H. Modern PCR technology has facilitated identification of two potential viral etiologies for serum hepatitis and, secondly, has enabled screening for these viruses in candidate horses potentially used to produce equine-origin biological products thus significantly impacting equine veterinary practice.
Of further note, an additional three viral agents (equine kirkovirus, equine hepatitis B virus, equine circovirus) have been more recently identified in the context of hepatic disease in horses. It remains to be seen whether these viruses represent important considerations in the USA context or whether they are rare/uncommon findings. That said, it is clear that both the parvovirus and the hepacivirus are endemic in the USA.
Viral hepatitis: parvovirus (EqPV-H):
Infection with EqPV-H (DNA virus) may result in mild or subclinical hepatitis or massive liver necrosis with attending signs of liver organ failure. This parvovirus (EqPV-H) has been identified in the blood of a substantial number of unaffected (ostensibly healthy) horses around the world. It is not known why some horses develop severe disease (classic Theiler disease) following infection with EqPV-H and others do not. It is likely that, as with most infectious diseases, contributory factors include the size of the infecting inoculum, the state of the host’s immune system, and differences in viral genotype/antigen characteristics. Signs of acute hepatitis include inappetence/anorexia, lethargy, jaundice, photodermatitis, edema, colic, encephalopathy and death. The case fatality rate for severe Theiler disease exceeds 80%. Milder forms of hepatitis may include inappetence/anorexia, lethargy, and biochemical evidence of hepatic disease. Fever is not typically reported. The DNA prevalence of EqPV-H has been estimated at 3.2-17% in the USA (seroprevalence 15-34.7%). Many healthy horses are positive for this virus in the blood. It has been suggested that 98% of infections occur subclinically (no clinical signs and biochemical evidence not investigated absent clinical disease). Early work suggests that there is no biochemical evidence of hepatitis following experimental exposure in approximately 10-15% of cases. The route of transmission is not completely understood but is believed to be via fecal-oral or respiratory routes (no longer believed to be via an insect vector). The number of ‘classic’ cases of Theiler disease has dropped very significantly since the USDA imposed viral screening for commercial products (such as tetanus antiserum). Infection with EqPV-H tends to cause individual hepatocyte necrosis with lymphocytic clustering. Some larger hepatocytes may be observed, making the histopathological characterization potentially similar to that for pyrrolizidine alkaloid toxicosis (megalocytic hepatopathy). Viral specificity at (hepatic) histopathology can be assured via both immunohistochemistry and in situ hybridization. Following infection, liver damage (as detected through plasma biochemistry) appears to coincide with the point of immune control (seroconversion), suggesting that it is the horse’s immune response to the virus that determines the severity of clinical disease. When provoked, evidence for hepatitis (example elevated GGT), even when mild, lasts up to 12 weeks. Detectable viremia (even at low levels) can last months and years. Chronic disease (fibrosis, cirrhosis) has NOT been reported with EqPV-H infections. Diagnosis of EqPV-H hepatitis cannot be based simply on demonstration of the virus in clinical cases as there are too many healthy horses in which the virus circulates, absent signs of disease. Diagnosis of EqPV -H viral hepatitis is based on demonstration of liver disease (plasma biochemistry), viremia (high viral titer), and
114
histopathology (biopsy, necropsy). Presence of EqPV-H in the context of hepatic lesions is important (quantitative PCR, ISH, IHC) in these regards. There is some evidence that disease severity is related to viral load in liver tissue, more so than the level of viremia. Disease resulting from EqPV-H can be fatal or self-resolving. There are no presently recommended anti -viral drugs for this infection. Questions arise regarding the biosecurity implications for this virus. It is generally recommended that isolation of affected horses is impractical. It is suggested that a vaccine against EqPV-H may be possible in the future.
Viral hepatitis: hepacivirus (EqHV): Also, worldwide distribution for this RNA virus (flaviviridae). Low genetic variability. RNA prevalence 1.4 –41.2% Seroprevalence up to 80%. Mode of transmission is being actively studied; EqHV can be transmitted vertically. As with parvoviral hepatitis, subclinical infections appear to be much more common than infection that results in disease. Disease associated with EqHV appears to be significantly less common than disease resulting from EqPV-H. Current thinking suggests that EqHV may be the etiological agen t for ‘chronic active hepatitis’, a disease of the equine liver that has traditionally been regarded as ‘idiopathic’. ‘Chronic active hepatitis’ is diagnosed when clinical signs of hepatitis have been associated with specific hepatic histopathological features, that include fibrosis. Clinical signs associated with EqHV hepatitis are nonspecific and may include inappetence, weight loss, photodermatitis, HE, and (sometimes, but not commonly) fever. Clinical hepatitis associated with EqHV infection appears to be less common than that associated with EqPV-H. There have been instances in which both EqPV-H and EqHV are identified in the context of hepatitis. As with the parvovirus, the onset of clinical evidence of disease (including circulating biomarkers) appears to coincide with the time of seroconversion. Hepacivirus also causes hepatitis with lymphocytes but there is also a chronic component to this disease (fibrosis). Most (~80%) of infected horses can ‘clear’ the virus but some (~20%) develop hepatitis that, in some cases, can lead to cirrhosis eventually (slowly progressive disease with a diffuse distribution of lesions, including micronodular fibrosis). If infected during foal hood, it is more likely that viral tolerance will occur, and the animal will remain infected into the long term (years). There is currently no USDA ruling about screening donors for purposes of sale of equine-derived biologicals. Although there is one report of disease in a 4-year-old horse, most EqHV infections that progress with disease have been seen in teenage horses; fewer females are affected. This equine EqHV is, in many respects, similar to human hepatitis C. There is some anticipation that research regarding the equine virus may lead to vaccine development for HEP C -affected human patients (there is not presently a vaccine for the human hepatitis C virus as it mutates too quickly; interestingly, the equine EqHV virus is much slower in that regard). Similar to parvoviral hepatitis, diagnostic confirmation of EqHV hepatitis cannot be based simply on demonstration of the virus in clinical cases as there are too many healthy horses in which the virus circulates, absent signs of disease. Diagnosis requires demonstration of liver disease (plasma biochemistry), viremia (higher viral titers are more significant), and histopathology (biopsy, necropsy). Presence of EqHV in the context of hepatic lesions is important (quantitative PCR, IHC) in these regards but in situ hybridization is not (presently) available for this pathogen. The prognosis for EqHV hepatitis is difficult to gauge. Prognosis should be based on repeated clinical examinations (including hepatobiliary biomarkers, viral titers). If the plasma GG T activity continues to increase, it is possible that ‘bridging fibrosis’ is occurring; ‘bridging fibrosis’ is always considered a sign of an unfavorable prognosis in hepatobiliary disease, regardless of the cause. Histopathological conclusions for EqHV hepatitis can (confusingly) include all of the following: cholangiohepatitis, toxic insult, viral hepatitis, or even sometimes as suspected pyrrolizidine alkaloid toxicity Co-infection with EqPV-H is not uncommon and in situ hybridization at Cornell AHDC can clarify if parvovirus is the primary pathogen.
Treatment considerations for viral hepatitis:
Supportive treatments for liver function; control abnormal behavior (alpha2 agonists; avoid benzodiazepines)
Reduce dietary protein, increase carbohydrate (sorghum, milo, beet pulp are good sources of branch chain amino acids); add molasses to promote palatability
Decrease GIT ammoniagenesis (oral neomycin (or metronidazole), lactulose, mineral oil ) IV glucose to support liver function
Plasma for clotting, if needed
Vitamin E (RRR-stereoisomer)(natural form)
Anti-fibrotics (colchicine, pentoxifylline, benazepril (minimal equine evidence for efficacy)
115
Corticosteroids? Controversial (use in later stages, palliative)
Anti-oxidants: S-Adenosyl-L-methionine (also called S-adenosyl methionine, S-adenosylmethionine, SAMe, or SAM-e in the United States or ademetionine in Europe, and also often abbreviated as SAM and AdoMet
Milk thistle extract. Silybin™. Good reputation in human medicine (not much studied in horses, poor oral bioavailability)
Hepatalyte™: B-Vitamins B1, B2, B6, B12, and vitamin E, generous levels of Milk Thistle Sofosbuvir for EqHV? (in silico evidence)
Ursodiol™ Bile acid formulation with anti-inflammatory properties (very positive reputation) – more recommended for cholangiohepatitis
References available upon request
116
MU-CVM Lectures
Pamela Adkins, MS, DVM, PhD, DACVIM
Assistant Professor of Food Animal Medicine and Surgery
University of Missouri College of Veterinary Medicine Columbia, Mo.
117
118
Pamela R. F. Adkins University of Missouri












119 12/16/2022 1
Animal Neonatal Emergencies
Food
Outline Common diseases and species differences Weak neonate Calf diarrhea Sepsis Floppy kid syndrome Hyperosmolar syndrome in crias Updates and considerations Weak neonate Dam • Mismothering • Poor udder confirmation • Lack of colostrum Neonate • Dystocia • Premature • Injury Environment • Inclement weather • Overcrowding • Mud Any stress can interfere with nursing and optimum GI absorption Weak Neonate Calves born with little energy reserve Liver glycogen stores used within 4-6 h Depletion of brown fat within 1-6 d Weak Neonates Why is this an emergency? • Hypoglycemia Hypothermia Starvation Outcomes: Failure of passive transfer Emaciation Death Requires quick response to resolve presenting problem and then investigation to determine the underlying cause Weak Neonates • Hypoglycemia • Hypothermia • Starvation Hypothermia is an adaptive response, allowing survival during prolonged periods of hypoglycemia by reducing metabolic requirements Buchanan et al., 1991 Highly related 1 2 3 4 5 6
Severe Hypoglycemia
Associated clinical signs:
• Severe depression
• Recumbency
• Loss of suckle reflex
• Hypothermia
• Poor body condition
• Hyperemic mucous membranes
• Convulsions
• Opisthotonus
Associated lab findings:
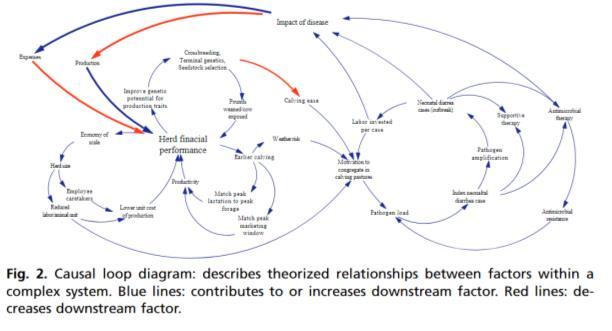
• Higher plasma L-lactate
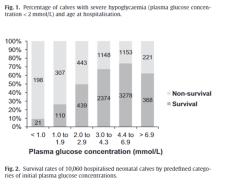
• Lower serum protein
• Lower leukocyte counts
• Coma Trefz et al., 2017
Severe Hypoglycemia
• Most common during first 2 days of life
• More likely to be diagnosed with sepsis
High risk of non-survival
• Neonatal diarrhea more likely normoglycemic Trefz et al., 2017
Calf Diarrhea
Calf Diarrhea
• Risk factors:
• Earlier calving season
• Poorly drained ground in the nursing areas Calves born to heifers

• Herds that calve heifers and cows together
• High stocking density Longer calving season
120 12/16/2022 2
Leading cause of calf morbidity, mortality, and antimicrobial usage during the first three weeks of life – dairy and beef Rivero et al., 2022 Digestive 70.5% Respiratory 32.6% Multisystemic 24.2% CNS 17.9% Urogential 16.8% Cardiovascular 6.3% Muscoskeletal 12.6% Other Known 11.6% Hemolymphatic 7.4% Number of Calves (95) with Lesions Identified within each System (n = 190)
Clark, 2022 Clark, 2022 Clark, 2022 Related to: High dystocia rates Reduced labor per cow Need to treat calves 7 8 9 10 11 12
Diarrhea – treatments considerations

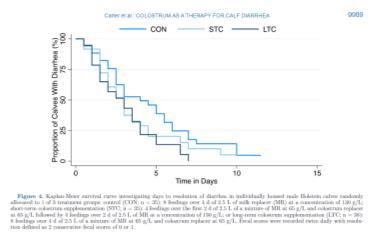
• Colostrum?

•
Sepsis
•
Floppy Kid Syndrome
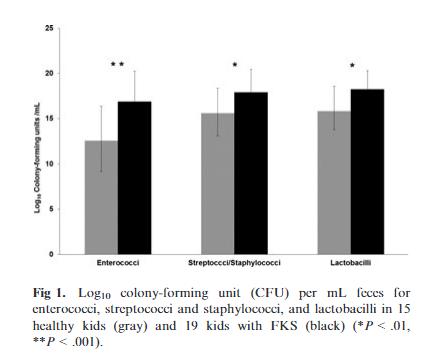
•
•
•
•
Diarrhea
considerations

Failure of Passive Transfer
•
•
• MU Study
Floppy Kid
•
121 12/16/2022 3
Resolves diarrhea sooner and improves growth levels Further studies needed Carter et al., 2022
– treatments
App-guided fluid therapy plans more closely aligned with best practice. Zduoba et al., 2022
of lesions in necropsied calves at MU: digestive, respiratory, multisystemic (sepsis)
Majority
MU prospective study: 4/23 sick calves were bacteremic All bacteremic calves died/euthanized
suckle
quality, heart rate, neutrophile count, and GGT concentration
• Predictors of mortality:
reflex
• Acute phase proteins? Jaramillo et al., 2022
NOT an emergency – but important contributor to health/disease
22-29% of beef calves had FPT (Irish study)
3 times more likely to become ill
• 4 times greater risk of mortality
• 7/12 (58%) of sick beef calves had FPT Todd et al., 2018
Disease
goat kids – 4 to 30 days old
of
Wobbly
knuckling forelimbs with progressive listlessness
gait,
somnolence
Eventually
Coma
• Death
diarrhea or
• Kids do NOT have
sepsis
Diagnostics: metabolic acidosis in the absence of diarrhea
Syndrome
Caused by increased Dlactate concentrations Mechanism: bacterial fermentation of carbohydrates in the GI tract Bleul et al., 2013 13 14 15 16 17 18
Sick crias
Sick crias
Sick crias



122 12/16/2022 4
• Not always the same as calves and foals
Prematurity and dysmaturity have not
wit poor
in crias Opposite is true for calves and foals
Example:
been associated
prognosis
Common diagnoses for sick crias At least 1 congenital defect Choanal atresia* • Ocular malformation (cataracts, blindness, microphthalmos) Bone deformation (deformity of the appendicular skeleton) Vulvar malformation Cardiac malformation (tetralogy of Fallot, PDA, VSD) *Associated with nonsurvival Bertin et al., 2013)
• Common diagnoses for sick crias Ophthalmic lesions (most common: ulcerative keratitis) GI lesions (most common: meconium impaction, peritonitis, diarrhea) Respiratory disease (aspiration pneumonia) Neurologic disease (hypoxic ischemic encephalopathy, septic meningitis) Bertin et al., 2013)
• Hyperglycemia is initiated by glucocorticoids Stressful event • Premature birth Sepsis Trauma Shearing Iatrogenic Insulin response = normal for a camelid but Low baseline insulin Compromised pancreatic function? • Access to water = limited Hyperosmolar Syndrome in Crias Hyperglycemic • Stress, iatrogenic (glucocorticoid, dextrose fluids) • Inadequate insulin response Hypernatremic • > 170 mEq/L • Inadequate water intake • Glucose diuresis Hyperosmolar • ECF >300 mOsm • Major serum solutes: Sodium, Chloride, Glucose, Urea
• Clinical Signs: • Lethargy Weakness • Anorexia • Head tremor • Base-wide stance in hind • Seizure activity • Coma • Death • Diagnosis: Glucosuria • Serum Chemistry • Severe hyperglycemia Severe hypernatremia Metabolic acidosis Azotemia Buchheit et al. 2010 19 20 21 22 23 24
Hyperosmolar Syndrome in Crias
Hyperosomolar Syndrome in Crias
Hyperosmolar Syndrome in Crias
Hyperosmolar Syndrome in Crias




123 12/16/2022 5
Calculating plasma osmolarity: [2 x sodium concentration] + [glucose concentration/18] + [BUN concentration/2.8] = ___ mOsm/L Normal (270-320 mOsm/L)
• Treatment Goals Restore normal blood osmolarity Avoid cerebral edema Monitor sodium and glucose closely • Treatment includes: IV fluids Oral hypotonic fluids Insulin CRI • Treatment of concurrent diseases Buchheit et al. 2010 Summary • Unique emergencies within each species you evaluate • Important to address the underlying management issues Please join us for our free vi rtual C E program, which offers sessions from 1 2- 1 pm t he s econd Tuesday of every m onth The goal of our VET ECHO program is to share evidence-based knowledge and build a community for discussing important t op cs n l vestock m ed cine Each session includes a short topic presentation by a leader in the field and is followed by a case presentation. All session are interactive and focus on group discussion. Each month is a new topic, and all topics are sele cted from recommendations given to us by our local veterinarians. All sessions are worth 1 hour of CE through the University of Missouri, College of Veterinary Medicine. You can get more information and register to receive email reminders and zoom links at: https://showmeecho.org/clinics/veterinary-education-training/ If you have questions about the program, please contact Dr. Pamela Adkins at adkinsp@missouri.edu Free Food Animal C ontinuing Education! Questions? adkinsp@missouri.edu 25 26 27 28 29
124
MU-CVM Lectures
Leslie A. Lyons, PhD
Gilbreath-McLorn Endowed Professor of Comparative Medicine University of Missouri College of Veterinary Medicine Columbia, Mo.
125
126
MVMA Lyons Proceeding 2023
Disclosure: Dr. Lyons studies are periodically supported by donations to the 99 Lives project, the NIH, pet food companies, the EveryCat Foundation and Royal Canin provides food for her cat research colony. Dr. Lyons has strong interactions with the UC Davis Veterina ry Genetics Laboratory and will assist any commercial laboratory seeking counseling and information for their improved commercial services. These activities have no influence on Dr. Lyons ’ research or scientific presentations.
One form of Precision Medicine is the use of genetic testing. The first genetic tests for the domestic cat were developed over 25 years ago. Presently, 167 different mutations affecting 101 genes have been identified, producing interesting phenotypes and traits but also diseases and other health concerns. Current genetic and genomic technologies can be employed to test nearly all the known mutations in one assay (parallel genotyping) using DNA arrays, mass spectroscopy or genotyping-by-sequencing. Unlike in human medicine, where tradit ionally a physician had to request a genetic test, the owner of a pet can directly purchase genetic tests from a company, i.e., direct – to – consumer testing (DTC). DTC of large panels of DNA variants developed for humans and are now easily available for cats and dogs as DTC tests. Thus, no longer are genetic tests only available from the researcher who identified the mutations or a laboratory associated with a veterinary / research facility. Private companies now offer genetic tests at lower costs by using the massively parallel genotyping, however, provide little genetic counseling and education to the owner, breeder or veterinarian. These large panel tests generally do not have documented sensitivities and specificities for the mutation being tested.
How to use Direct to Consumer Testing (DTC)
Veterinarians should consider using genetic testing, either submitted by the veterinarian or by the client, to support clinical diagnoses. Note that genetic tests are only one aspect of a diagnosis and only a part of the overall healthcare of the patient. Hopefully, the genetic test may lead to a more appropriate treatment plan and prognosis. Genetic testing should be considered once other environmental factors, including nutrition, toxic and viral exposures have been considered. A genetic test will not be useful if the condition is not genetic. Most genetic testing is limited to Mendelian traits, i.e., traits with simple autosomal or X -linked dominant or recessive modes of inheritance. Environment can influence the presentation, including age-at-onset and severity of genetic conditions. If a condition is genetic, likely a veterinary specialist may need to be consulted.
Once a tentative diagnosis has been established and a genetic test may be supportive, use the Online Mendelian Inheritance in Animals (//OMIA.org) to see if this condition has been previously documented and if a genetic test is available. Provided below is a table of the genetic tests for disease variants in domestic cat breeds in which many companies provide genetic testing, including research universities. But also, several genetic service laboratories provide genetic tests for DNA variants that were originally identified in a random bred cat. The rediscovery of these variants is extremely rare but can occur. The OMIA website lists all the DNA variants that are associated with diseases in companion animals. This site also collates the scientific information and publications associated with the disease and will list the year of the variant discovery as well as the researchers involved. Researchers are often keen to be of assistance and realize the genetic implications may not be familiar to the veterinarian. Thus, don’t hesitate to ask the researcher first for advice on genetic testing as they may perfor m the testing within their own laboratory! The published manuscripts often have the email address for the
127
corresponding author of the publications. Otherwise, preferably use a DTC laboratory associated with a research university, which will be invested in the science, provide the best education, genetic counseling and customer service.
Pros & Cons / Dos & Don’ts of DTC
Large panel DTC tests allow an effective screening method for many diseases and traits. No one technology can accurately genotype all the various different types of mutations that cause diseases, thus, look for services that can use a second method, or use a secondary service, which are generally associated with research universities.
Many tests are not valid in different breeds, which is not generally divulged by some services. Thus, conversations with the researcher who made the discovery will help clarify the risks.
While some services work towards scientific standardizations, others are more profit oriented. The World Small Animal Veterinary Association (WSAVA) and other groups are working towards standards that will help clarify genetic testing results. The WSAVA Hereditary Disease Committee can be contacted for assistance.
Don’t make health & neutering decisions based on results from large panel DCT testing. Request a single gene test for a second opinion. Use the overall health indications of an animal.
Where to find genetic testing?
• Use OMIA to find the researcher who found the variant – ask the researcher first! (google them!) See instructions below.
• Preferably use a laboratory associated with a research university – invested in the science! These labs will have the best customer services and most thorough counseling!
• Various canine registries sites have lists of genetic tests
• The Orthopedic Foundation of America (OFA) has phenotypic and genetic test information
• The World Small Animal Veterinary Association (WSAVA) has genetic information
Precision / Genomic (P4) Medicine
If a genetic test has a negative result – consider whole genome sequencing (WGS)
Precision Medicine is an emerging approach for disease treatment & prevention that takes into account individual variability in genes, environment, and lifestyle. Precision medicine is used to understand the complex mechanisms underlying a patient’s health, disease, or condition, and to better predict which treatments will be most effective – not the average or average for an ethnic group!
DNA testing is a form of Precision Medicine. Large panel genetic testing is an improvement and further facilitates the use of genetics for diagnoses and potentially treatment of health concerns. Whole exome and whole genome sequencing of a patient is a larger scale effort to even further advance precision medicine. Genome and exome sequencing projects are available for cats and dogs and these techniques are becoming common place for the identification of mutations that
128
cause heritable diseases and traits. Generally, if a result is negative for genetic test, the patient may have a novel genetic cause for their presentation. WGS and WES help to find novel causes. Genetic testing only confirms the presence or absence of an already known DNA mutation for a disease or trait. Precision Medicine hence incorporates discovery, which hopefully will lead to diagnosis and more precise treatment. Only a few research laboratories are equipped to conduct WGS and WES sequencing for companion animals on a Precision Medicine basis. The University of Missouri, laboratories of Dr. Gary Johnson and Dr. Leslie Lyons (99 Liv es Cat Genome Sequencing Consortium), are discovering new disease-causing DNA variants for dogs and cats, respectively. Many of the researchers involved with DNA discoveries should also be able to suggest contacts for WGS / WES. As costs lower and data pro cessing becomes cheaper and more streamline, genome sequencing can become a commercial service for veterinary diagnostics and be used by the everyday practitioner.

Different laboratories and different species use different methods for DNA collection. Talk to the laboratory to find the most efficient means for DNA submission for genetic testing or for whole genome sequencing.
How to use the OMIA website
1) Go to the OMIA website: https://omia.org
2) Select the “likely causal variants” for your species
a. Example: Dog = 477 and Cats = 167
3) Scroll through the list of diseases for your species and select the “OMIA Phene Species - ID” that you think might be your disease
4) Read through the provided information. A list of published articles regarding the disease and DNA variant are present. Select the publication for the discovery of the variant.
5) Contact the investigator from the provided contacts in the publication OR Google them!
129



130
Common inherited diseases in domestic cat breeds (i.e., genetic tests to consider).
Disease / Trait (alleles)
OMIA Entry (-9685) MO‡
Phenotype (Breeds affected)* Gene
Acrodermatitis Enteropathica 000593 AR Turkish Van SLC39A4 ALPS - Autoimmune lymphoproliferative Disease 002064 AR non-neoplastic lymphoproliferative disease (British Shorthair) FASL
Centronuclear myopathy 001508 X Neurological (Maine coon) MTM1 Chediak-Higashi Syndrome 000185 AR Storage disorder (Persian) LYST
Craniofacial Defect 001551 AR Craniofacial Defect (Burmese) ALX1 Cystinuria 002023 AR (MCC, Sphynx, Siamese) SLC7A9
Ehlers-Danlos 002165 AR Stretchy skin (Bengal, Bombay) COL5A1 Factor XI Deficiency 000363 AR Bleeding disorder (Maine Coon) F11 Gangliosidosis 1 000402 AR Lipid storage disorder (GM1) (Korat, Siamese, S.E. Asia) GLB1
Gangliosidosis 2 01462 AR Lipid storage disorder (GM2) (Burmese) HEXB
Gangliosidosis 2 01462 AR Lipid storage disorder (GM2) (Korat) HEXB
Glycogen Storage Disease Type IV 000420 AR Glycogen storage disorder (GSD) (Norwegian Forest Cat) GBE1 Hermansky-Pudlak syndrome-5 002161 AR Ocular albinism (Donskoy) HPS5
Holoprosencephaly 002366 AR Forebrain malformation (Toyger) GDF7 HCM 002316 AD Cardiac disease (Sphynx)) ALMS1 HCM 000515 AD Cardiac disease (Maine Coon, Ragdoll) MYBPC
Hypokalemia 001759 AR Potassium deficiency (HK) (Burmese) WNK4
Hypotrichosis 001949 AR Hairless, early death (Birman) FOXN1 Hypothyroidism 000536 AR Small size, low T4 (British) TPO
Progressive Retinal Atrophy 001244 AR Late onset blindness (rdAC) (Abyssinian) CEP290
Progressive Retinal Atrophy 000881 AR Rod-cone dysplasia (Abyssinian) CRX
Progressive Retinal Atrophy 001613 AR Mid onset blindness (Bengal) KIF3B
Progressive Retinal Atrophy 001222 AR Early onset blindness (Persian) AIPL1 Polycystic Kidney Disease 1 000807 AD Kidney cysts (PKD) (Persian) PKD1 Polycystic Kidney Disease 2 002525 AR Polycystic kidney disease (Siberian) PKD2
Pyruvate Kinase Deficiency 000844 AR Hemopathy (PK Deficiency) (Abyssinian, Siberian, MCC) PKLR Skeletal dysplasia 002485 AR Skeletal dysplasia (British) LTBP3
Spasticity 001621 AR Congenital myasthenic syndrome (CMS) (Devon Rex) COLQ
Spinal Muscular Atrophy 000939 AR Muscular atrophy (SMA) (Maine Coon) LIX1- LNPEP
131
‡ Mode of inheritance of the variant allele (disease-causing allele). *The breed affected represents the breed in which the DNA variant was identified. Other breeds may be affected if they have common ancestry, especially other breeds in a breed family. In reference to the variant allele, AD implies autosomal dominant, AR implies autosomal recessive, co-D implies co-dominant, X implies X-linked. OMIA: Online Mendelian Inheritance in Animals (http://omia.org) entries provides links to citations and clinical descriptions of the phenotypes and the diseases.
132
MU-CVM Lectures
Owen Skinner, BVSc DECVS DACVS-SA MRCVS
Assistant Professor of Small Animal Surgical Oncology
University of Missouri College of Veterinary Medicine Columbia, Mo.
133
134
ADRENAL SURGERY: DON’T THEY ALL DIE?
Owen Skinner, BVSc DECVS DACVS-SA MRCVS, ACVS Fellow - Surgical Oncology
The adrenal gland consists of the medulla, a modified sympathetic ganglion that secretes catecholamines, and the cortex, with strata that produce mineralocorticoids, glucocorticoids, and sex hormones. Adrenal tumors can arise from any of these components and tumors may or may not be functional. If functional, they can cause substantial morbidity through their endocrine effects. In addition, adrenal masses can pose a risk of sudden death through hemorrhage, thrombotic events, or arrhythmias. Each patient must be carefully assessed to determine the functional status and extent of the tumor. Low dose dexamethasone suppression tests are used to assess for tumors producing cortisol, electrolytes can provide an indication of tumors producing aldosterone, and urine metanephrine/normetanephrine may help identify some pheochromocytomas. We recommend CT for staging (primarily in assessment of the primary tumor and potential vascular invasion) in all dogs where adrenalectomy may be considered. Metastasis, while possible, is rare, and dogs managed with adrenalectomy that survive the perioperative period typically do well long-term. Perioperative mortality is variable, ranging from approximately 3% in dogs with small adrenal tumors without vascular invasion, resected via laparotomy by experienced surgeons, to 20-25% for dogs with caval invasion. It is important to consider that risk is not evenly distributed, and dogs with small foci of caval invasion are unlikely to experience a mortality rate as high as 25%, while dogs with highly extensive lesions may be at higher risk or not considered surgical candidates. Experience and a multi-disciplinary approach are essential to minimize risk.
135
136
Wellbeing
137
138
Wellbeing
Abby
Whiting, DVM
Emergency Veterinarian Veterinary Specialty Services St. Louis, Mo.
139
140
MVMA January 2023 Convention
Wellness track :
Presenter Abby Whiting: Chair of wellbeing Task Force
The Science of Happy: What advances in positive psychology can offer veterinary medicine
● Definitions : positive psychology, predictors of success, markers of joy ○ Utilization of positive psychology allows us to increase our innate “happiness” above our previous genetic set point. The result is an increase in educational, productivity, and healthcare outcomes; as well as increased sustainability of the healthcare team.
● An Evidence based exploration of the data ○ A team is 31% more effective and profitable if they describe themselves as “happy” vs neutral or unhappy.
■ Who doesn't want to be 31% more profitable? ○ Yale and Harvard both have PHDs in happiness ○ Data from fortune 500 companies, military units, local, state, and national governments.
● What companies and industries have already utilized this ○ US Military, Google,Meta, Starbucks, Virgin Atlantic, Orlando Trauma Center
■ Aristotle project: the superstar problem ○ What we can learn from their experience and wealth of data
● Using the evidence to increase productivity and profitability
● Using the evidence to reduce burn out, staff turnover and toxic employees.
● Whiting’s Voodoo Magic for increasing joy and happiness ○ How a team can use these tricks to become a highly functional unit.
The Inspired Leader: leading the Veterinary Team of the Future: Shifting from managing to coaching.
● Classic team management vs servant leadership ○ Managing: Getting people to do things that need to be done. ○ Coaching: Getting people to WANT to do what needs to be done. ○ Getting “buy in” from all team members on the common goal and ethos
■ Managing large personalities in team sports
● Phil Jackson vs Bobby Knight (NBA) ○ Kobe Bryant vs Micheal Jordan ○ Applying this in veterinary medicine; don’t reinvent the wheel
● Moving our average to the right of the bell curve ○ Aiming for exceeds expectations ○ Why does the bell curve matter?
■ The “set points’ are movable!
● Integration of gratitude, communication, and belonging into the veterinary practice ○ Exercises that increase cohesion and team success - measurably (data)
141
○
The habits and conscious decisions that predict happiness/ profitability/sustainability.
■ Whiting’s Voodoo Magic for increasing joy and happiness
● Roadblocks to coaching ○
The Emotional terrorist ○
Fear of crucial conversations ○ Lack of communication training
142
143
Missouri Veterinary Medical Association
2500 Country Club Drive • Jefferson City, MO 65109 573-636-8612 • www.movma.org • mvma@movma.org

144

