


Growing Doctors from Within
Print is dead, the nay-sayers told me.
I KNEW THEY WERE WRONG, SO I PERSISTED.
I left a high-paying job as an employed physician to pursue a Quixotic calling and became a publisher and founder of a print and online magazine.
It is no secret that medicine is broken.
Costs are high, quality is sub-standard and the focus is increasingly shifting away from the patient. Most concerning is that we have an alarmingly prevalent trend of “physician burn-out” where physicians are choosing to retire early from their professions, or leave completely (some by tragically committing suicide).
“Education by legislation” has become commonplace, resulting in physicians being replaced by lower-cost, rapidly-trained millennial and Gen Y/Z non-physician alternatives who often lack critical thinking skills but who are nevertheless being granted “Full Practice Authority” to practice medicine independently without actually going to medical school or completing a residency.

Physicians (including myself) sadly fell asleep at the wheel, and we have no one to blame but ourselves. It is we who have allowed Hospital Administrators, insurance moguls, and the pharmaceutical mafia to rule the House of Medicine.
We inadvertently relinquished the authority to make decisions about the way our profession should be practiced and how our patients should be cared for, and we need a way to reclaim our voices and share our collective expertise.
I knew that if I launched a platform whose centerpin was a tangible, shareable, concrete periodical I could make a dent, waking up a few doctors who had retreated in defeat.
PhysicianOutlook uniquely engages doctors and patients of ALL ages and persuasions, particularly those who have a healthy aversion to the manipulative powers of social media. They trust us enough to peruse our website (www.PhysicianOutlook. com) to learn more about the stories we highlight and issues we recommend that they participate in calls to action.
Print is NOT dead, especially amongst Baby-Boomers and Gen X’ers.
It’s expensive to produce and distribute a print magazine. It is difficult to make a living in the “medical magazine” world if you refuse to take advertising money from the usual suspects (Big Pharma, Big Hospital, Big Insurance).
overcoming adversity are two of my super-powers.
I am not your typical doctor.
I was born in May of 1963 at Mother Cabrini Hospital in lower Manhattan, blocks away from the sweatshop in the garment district where both of my parents had found employment (and each other).
They had both emigrated to the United States in the early 60’s. My father, to escape Fidel Castro’s Communist Cuba; my mother, to escape the poverty and joblessness that pervaded her Dominican homeland. Neither of them graduated from high school, and both continue to this day to struggle with speaking and completely understanding the English language.
I spent my early years on Tiemann Place in West Harlem, just north of Morningside Heights. There were indents from two bullets that were unable to penetrate the steel door of our 6th floor apartment. Those same bullets killed a neighbor who frantically rang our doorbell as she attempted to seek shelter from her assailant. It was my diabetic grandmother’s obese body habitus that saved her life, or she too may have tragically lost her life to a gunshot wound.
Most of my early healthcare was obtained in the emergency room at Saint LukeRoosevelt Hospital. At 6 weeks of age I was evaluated for bruises all over my tiny body, victim of my teenage mother’s innocent
attempt at cooling me off in front of the high-pressure flow of water from a fire hydrant that the neighborhood kids had uncapped to cool off during a summer heat wave.
The concept of preventive care was foreign to my family. I didn’t have a pediatrician as a baby or toddler. I got my “vacunas” (immunizations) at a free clinic, but otherwise I was a “frequent flyer” at the hospital on 111th and Amsterdam Avenue. I was a few weeks shy of my first birthday when I was taken to the ER for rapid shallow breathing caused by my 8 year old aunt giving me an entire bottle of “caramelitos anaranjados” to entice me to finish my baby food.
She didn’t know that these “little orange candies” (St. Joseph’s Baby Aspirin) were dangerous, and had been left in charge of babysitting me while my parents worked.
Someone with these early childhood experiences doesn’t typically grow up to become a doctor, yet it’s precisely people like me who we need in the profession. If the way to control healthcare costs and improve quality is to focus on prevention and population Health, we need to promote programs such as Hip Hop Health and Harlem Grown, which are “home grown” solutions that help bridge glaring gaps. We need to call out inequities where they exist, and demand that patients across the socioeconomic spectrum have the freedom (and funds) to seek care as they see fit. We need for physicians to not continue to hemorrhage out of the profession in a massive “DrExit” movement because they have become so disillusioned with the hassles of documentation or the corporatization of medicine in general.
The obvious solution is to “grow more doctors.” The place to “grow” them is from within communities at risk. The CUNY “Sophie Davis” program is one way to “homegrow” doctors. The Harlem Hospital 2021 Pediatric Resident cohort is another shining example of an extraordinary group of physicians who are being honored for their impactful contributions to their community. This issue of PhysicianOutlook Magazine is a tribute to those who walk the walk, and talk the talk.

A
magazine that gives physicians a platform to unabashedly tell their stories.
A magazine that is not beholden to complicit conflicted advertisers or sponsors.
A magazine that is not afraid to expose uncomfortable truths and demand transparency.
A magazine that empowers physicians into action and return respect to a profession that is like no other.
A magazine that explores the ways in which we could get back to doing what we like best: Taking care of our patients!




We believe that physicians should own their right to work and move freely.
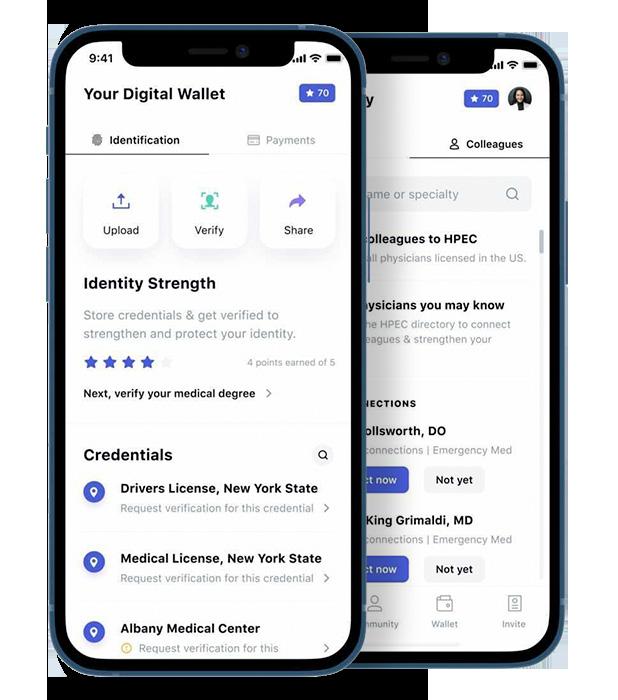
We create this possibility by giving physicians control over their professional digital identity. Our wallet stores your verifiable medical credentials and connects you to a secure and private referral network of other credentialed physicians. We do so through our secure standards based open-sourced technology.
Our patients deserve privacy, and as the practice of medicine becomes more digitized it is clear that it is the physician’s responsibility to adopt secure solutions for communication and identity verification in order to restore that privacy. This is why we are building HPEC.


FROM THE PUBLISHER
Reap What You Sow
byMarleneWüst-Smith,M.D./p.2
HUMANS OF MEDICINE
Harlem Grown byRoxanneBruce,MBA,DrBA/p.6-7
Education Through Music byAlyssaDean/p.8
Hip Hop Health byYvonneDowner/p.9
Year 6
byUmaruBarrie,M.D./p.11
My Daughter, the Doctor byDanielTorres/p.14
Boricua Badass: Defining Dr. Talia Torres byTaliaTorres,M.D./p.15
Above and Beyond byGuillermoRivera/p.16
¿Hay una Doctora (Talia Torres, M.D.) en La Casa? byMarleneWüst-Smith,M.D./p.17
A Conversation byEliseoRosario,M.D./p.17
THE DOCTOR’S BAG
Capitalizing on Covid byRobinTrimingham/p.12
THE FUTURE OF MEDICINE
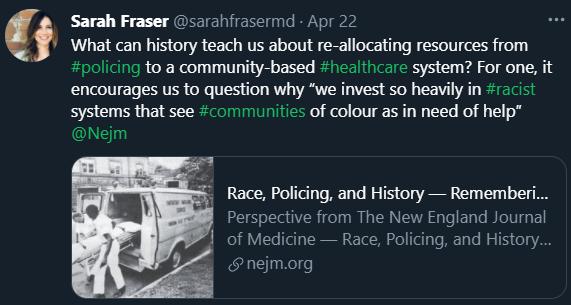
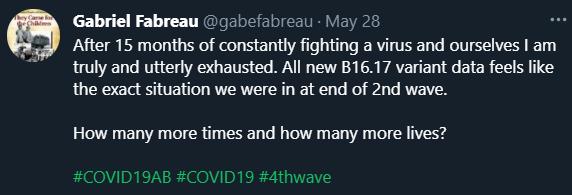
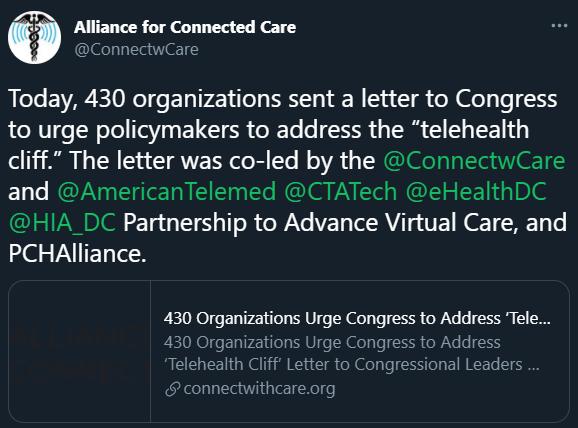
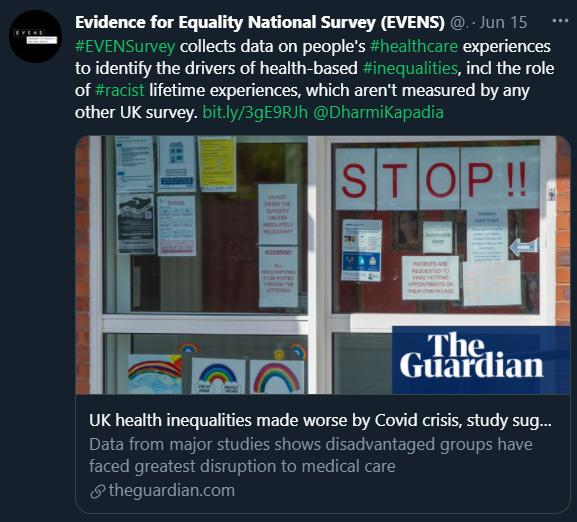
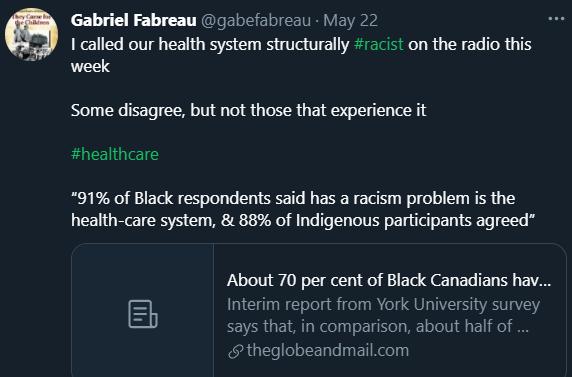
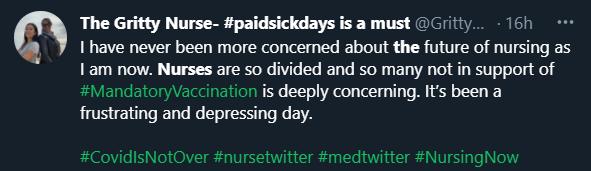
Voices Demanding Change BroughttoyoubyTwitter/p.18-19
Honoring Harlem Hospital’s Pediatricians byLeanneBullian/p.22-23
PLEASURES & PASTIMES
Urban Survival byThomasFarr/p.26-27
Can Examining the Racist Roots of Gun Control Save Lives? byPatrickBruce/p.28-29
THE LAST WORD
Female Activists Have a Higher Price to Pay byDianaLondoño,M.D./p.30
FEATURED ARTIST
Dr. Luke Lin AKA “Luke Dragon” byJackMcGowan/backcover

aren’t
byRoxanneBruce
This question must have been one asked by Tony Hillery, the Founder and CEO of Harlem Grown, a non-profit focused on youth development and urban agriculture. Harlem Grown is leading the way to healthy eating by teaching youth how to grow their own food. The organization is also focused on sustainability by utilizing once abandoned lots and turning them into community farms and gardens.
Imagine living in a city and not experiencing the growth of food from start to finish, then having the opportunity to walk onto an urban farm. Imaging being able to see the plants, smell the tomatoes, taste the fresh picked fruits and vegetables. This is something many children in Harlem have not been able to experience.
Harlem Grown is deeply involved in the Harlem community and has a variety of programs for children like Saturdays on the farm, and farm-based education Tours. For adults there are corporate service projects and adult volunteer days. If that was not enough to make you love this growing organization, you should check out their summer camp. The camp offers kids an opportunity to explore the outdoors, become educated farmers, and taste and love the foods they grow. Harlem Grown’s summer camp is free to all participants and open to children 7 – 14 years old. Former campers are often hired as Counselors in Training for the summer camp which allows them to spend more time with the organization.
There is no better way to teach teens about the difference they can make in the lives of others, than by giving them a chance to work with those in their community.

Now that you have read this far, perhaps you are sitting there wondering how you can help. What can you do to help change this small corner of the world? The answer is easy. You can donate to Harlem Grown online and put your hard-earned dollars where your heart is.
If you want to do more than send in what you can spare, consider the Harlem Grows Employee Matching Gift program. Many employers allow their employees to take a portion of each paycheck and donate that to a non-profit organization doing great work. Here is your opportunity to suggest an organization to your employer that you believe in. Better yet, if you are the employer, reach out to Harlem Grown and give your staff the opportunity to help a growing business change their corner of the world.
To learn more about Harlem Grown, visit them online at www.harlemgrown.org

Written by Roxanne Bruce, MBA, DrBA, along with Harlem Grown
drroxannebruce.com


byAlyssaDean
Hip Hop Public Health (HHPH) is a New York City based organization and collective of community educators, entertainers, and health professionals on a mission to eradicate health disparities—what the Health Resources and Services Administration defines as “population-specific differences in the presence of disease, health outcomes or access to healthcare. Compared to the nation’s population as a whole, most major disparities documented are experienced by African American and other minority groups. For instance, African American adults are 50% more likely to die prematurely from stroke compared to their white counterparts.”
Stroke is a medical emergency caused by a lack of blood supply to part of the brain, preventing brain tissue from getting enough oxygen and nutrients. When someone experiences a stroke, brain cells can die in minutes. Because immediate treatment is very important to reduce the likelihood of brain damage and other long-term complications, Hip Hop Public Health’s founders Dr. Olajide Williams, a neurology physician and director of the stroke center at Harlem Hospital and Doug E. Fresh, the first “human beatbox” partnered back in 2006 with a novel approach to stroke prevention— the Hip Hop Stroke Prevention Program.
Nicknamed Hip Hop Stroke (HHS), the program goes above and beyond as an interactive experience, allowing children to learn
through catchy hip-hop songs and animated cartoon videos. Hip Hop Stroke’s concept is so special because it combines prevention and knowledge in a simple and fun , yet majorly effective way— undoubtedly serving as a creative model for what public health disease prevention should look like.
Research shows that participating HHS children leave with a basic understanding of what stroke is, how it occurs in the body, how to recognize the signs and symptoms, and what to do in a stroke event. This means that as participating HHS children grow-up, they are more likely to have already been engaging in positive health behaviors to reduce the likelihood of experiencing a stroke, as well as know how to identify if a family member or someone close to them were to need help.
The real magic of HHS is in the stories shared about how the Hip Hop Stroke program has saved the lives of children’s parents and grandparents, making themselves a true staple for improving health outcomes. If you would like to find out if your school is eligible for Hip Hop Stroke, or book the Hip Hop Stroke program for a special event, please visit the Hip Hop Public Health website at www.hhph.org. The online portal is also available for schools all around the globe and staff may register their school for the program at any time.
Alyssa Dean is a member of the inaugural Public Health graduating class from St. Bonaventure University. Largely driven by suffering from an autoimmune disease, she has done extensive research rooted in chronic disease and natural healing methods. She is very passionate about educating and promoting wellness and is eager to develop and implement holistic approaches to improve the health of individuals and communities.

2020 AHA Presidential Advisory on Structural Racism.
Dr. Olajide Williams is a tenured Professor of Neurology and Associate Dean of Community Research and Engagement at Columbia University. He is Chief of Staff of the Department of Neurology at the Columbia University Vagelos College of Physicians and Surgeons and a global leader in health disparities and behavior change in communities of color.
Dr. Williams is Principal Investigator of multiple large NIH investigator-initiated awards and has served on several national panels on health disparities, including the 2021-2026 National Institute of Neurological Disorders and Stroke Strategic Planning Committee. An influential clinician-educator, Dr. Williams is a member of the Columbia University’s Virginia Apgar Academy of Medical Educators and sits on the medical school’s Committee on Education Policy and Curriculum (CEPC).
He is co-Chair of Academy of Community and Public Service, co-Chair of Columbia University’s Medical Campus Anti-Racism Task Force, and co-director of the Columbia University Community Wellness Center. Dr. Williams has authored and co-authored several books and numerous scholarly peerreviewed articles, including the November
Dr. Williams is the founder and board chair of Hip Hop Public Health, an internationally recognized organization that works with iconic Hip Hop influencers to use art, music, and science to promote healthy behaviors, health literacy, and health equity.
He is a board member of the Partnership for a Healthier America whose honorary chair is former First Lady Michelle Obama, where he helps guide health equity related activities.
Dr. Williams is an expert on COVID-19 vaccine acceptance in communities of color and COVID-related health disparities. He has received many prestigious international, national, regional, and local awards. These include the European Stroke Research Foundation Investigator of the Year award, two-time Columbia University Outstanding Teacher of the Year award, American Heart Association’s Trailblazer award, and a National Humanism in Medicine award from the Association of American Medical Colleges.
Dr. Williams has been named on Fast Company Magazine’s 100 Most Creative People list, Root 100’s Most influential Blacks in America list, Advertising Age’s Creative 50 list, and consecutive New York Magazine’s Best Doctors list.
Before joining Hip Hop Public Health as Executive Director and CEO, Lori Rose Benson served as Vice President of Healthy Lifestyles at the YMCA of Greater New York, spearheading all aspects of the preventative health and wellness portfolio for the largest YMCA in the United States with a key focus on health innovation, development of youth fitness programming and scaling chronic disease prevention programs to meet the diverse needs of New York City’s communities. Lori was the principal architect of the award winning Y-MVP Teen Fitness Challenge.
Raised in Brooklyn, Lori attended New York City’s public schools and earned a B.A. from the University of Massachusetts at Amherst in Communications and Graphic Design, and a M.A. in Physical Education from Adelphi University in Garden City, NY, where she is currently an Adjunct Faculty member in the Department of Exercise Science, Health Studies, Physical Education and Sport. Lori personally embraces physical activity and her love of music into her daily life as a yoga enthusiast, an aspiring DJ, and a spinning instructor who still teaches weekly cycling classes at Crunch Fitness in Brooklyn.

educator.






byDr.Barrie
I AM a 6th Year MD/PhD Candidate
Let me say that again, “sigh”
6th year of M.D./PhD
6th year of medical school
I stand before you, today
As a refugee from Sierra Leone
As an immigrant from Guinea
As an American citizen
As a first-generation student
As my ancestor’s wildest dreams
As proof of what Opportunity, Freedom, Hard-work can do for a young man from Harlem
From the trenches to here, today
Blessed Fortunate Driven
Amidst the unspeakable struggles
Amidst the constant obstacles
I embraced my path, I chased my education, I engaged my mentors, I pursued and captured opportunities that many in my neighborhood never had Opportunities that many can only dream of

You see my American dream was never about monetary worth, It wasn’t about getting rich quick
It wasn’t about getting famous
It wasn’t about the materials
Rather, It is about finding ways to contribute to the empowerment and advancement of my community
To have my community on my back
Hood hero, they would say Indeed, we will move forward
To quote Tupac, “Young black males could do anything
If you just give us a shot
Stop trying to beat us down… and to my homeboys, we need to be in control of ourselves”
The marathon continues
The road to becoming a physician-scientist continues
Umaru Barrie, M.D., PhD, is a candidate at University of Texas, Southwestern Medical Center.

what people would do with it once it was accomplished.
Then we had a brief phase affectionately known as the dot.com bubble when all manner of cyber-driven money-making schemes were explored as people struggled to figure out what “the web” was really for. A lot of these early initiatives were good ideas but most of them were ineffectively deployed in that their success hinged on things like cross-border trade agreements, virtual credit card processing systems, and sophisticated fulfillment arrangements that had yet to be invented.
In fact, just prior to the arrival of Covid, at best the internet was largely regarded as a research tool, and at worst as a mindless place to waste the day spreading rumorsand watching endless videos of kittens somersaulting around the kitchen. But what about now?
What if we are only just beginning to stumble upon the real purpose of the internet? What if the internet is not just a shopping mall?
byRobinTrimingham
In recent articles, I have alluded to the fact that the pandemic has opened a door to allow people and business organizations to partner and collaborate in new ways. But what exactly does that mean and how can you position yourself to capitalize on these opportunities?
To answer this, perhaps it’s time to rethink the purpose of the internet itself. To understand why I am suggesting this let’s briefly recap how we arrived at where we are now: Back in the early 1980’s when researchers initially began to assemble the “network of networks” that has evolved into the internet we now take for granted, all of the effort was focused around simply figuring out how to “connect” everyone and little time was spent considering
Then along came a guy with a remarkably simple idea - buy books in bulk, store them in a warehouse and sell them online using an enormous virtual catalogue - and he succeeded in making this work. And everyone went “Aha! The internet is a virtual ordering and fulfillment system,” and rushed to join in without giving the matter much further thought. Overnight everyone and their dog launched a website and then spent many sleepless nights wondering why no one could find them online, or why people balked at the idea of paying shipping charges for something that they could buy faster and more cheaply in a neighborhood store.
Yes, a few people became billionaires, but many more never saw a profit and came to accept that their fancy website was little more than a colorful brochure, and that this was unlikely to change. But then another young upstart from Harvard decided to create a place where people could post information about themselves and even chat with each other and social media was born.
For a time, this looked so harmless and fun that even grannies were joining in and social media begat YouTube and the concept of a life spent almost entirely online was born. And then things got ugly, and people woke up to discover their beloved virtual world had become polluted with computer viruses, malware, cyber bullying, election tampering, ransomware, and fake news.
What if the internet is actually a virtual classroom, a scientific laboratory, a think tank, a live face-to-face marketplace, a telemedicine hub, a global conference room, the world’s largest art gallery, a concert hall, a sport’s arena, a movie theatre, and a place to meet for Sundaydinner all rolled into one?
What if these examples are just the tip of the iceberg?
What if all you need to do to capitalize on the internet in the new reality is to stop fixating on what you do not have and seek out other individuals or companies (regardless of their time zone or postal code) who have skills that add to, or compliment what you are currently doing or trying to build?
What if you stopped merely advertising what you are trying to sell and started letting everyone know what goods, services, skills, and opportunities you are seeking?
What if you were open to collaborating on projects all around the world or trading services in cyber space to create new goods and services and bring them to market?
What if all you had to do to get started was start?
Robin Trimingham is an accomplished international presenter, as well as the Editor of Olderhood.com and co-author of “The Third Journey – Making the Most of Your Life After Work.”
Photo Credits: By Ed Zilch on Pixabay


byDanielTorres
Three years ago, I wrote an article for HispanicOutlook entitled, “TheImpactofa GoodDoctor” and chronicled my daughter’s medical school journey with the hope of inspiring other prospective students on what truly has been an arduous journey for this future doctor.
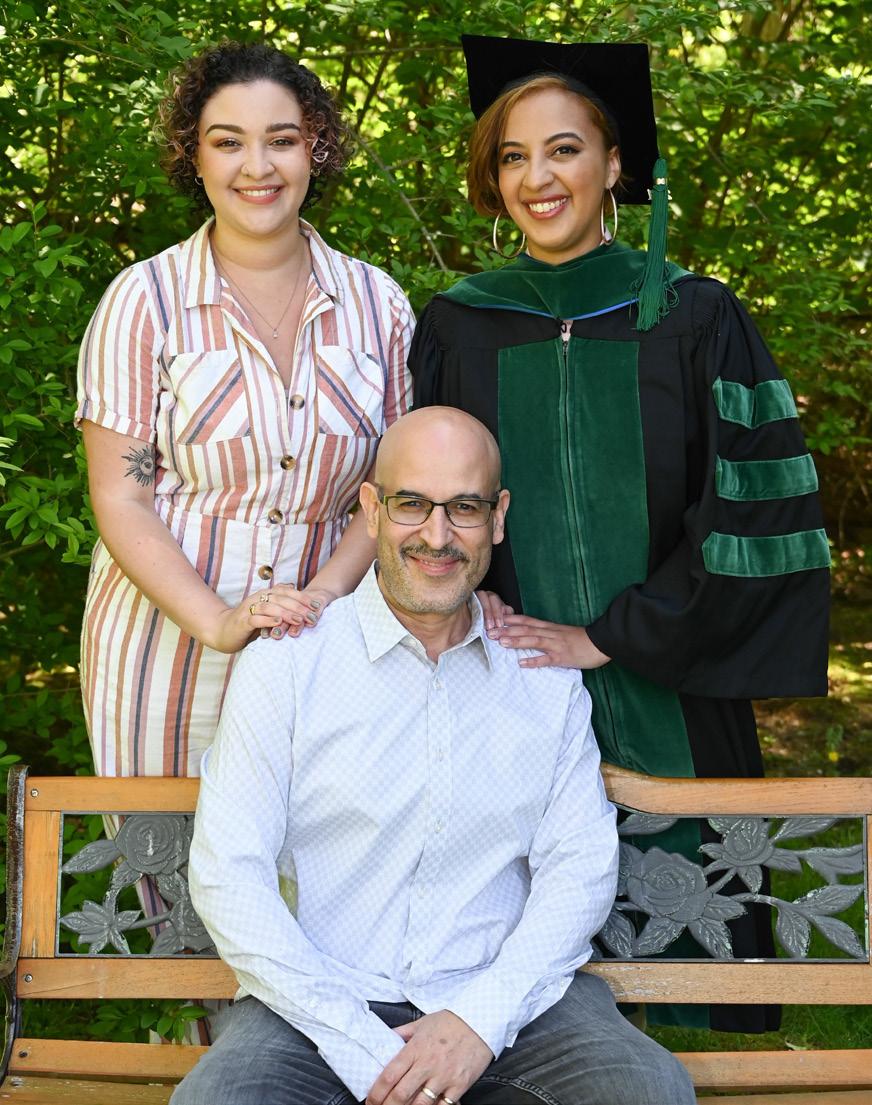
As I reflect on Dr. Talia Torres (which is the FIRST time I’m writing my daughter’s newest prefix in a published article), this has been a surreal moment for an absolutely proud father who the newly christened physician has affectionately called Papi her entire life.

There was a specific reason behind the above title that shouldn’t diminish the importance of what every medical professional should strive to be in this important occupation. I could have easily selected descriptive words such as extraordinary, exceptional, or phenomenal, but I intentionally chose this particular word in the opening title: Good - which can be defined as acceptable and adequate.
Yet, how do we become great at something? There’s an old adage, “practice makes perfect” but as much as we all wish this was an attainable reality, we must consider our fallibility and accept what we can or cannot control. I’d like to think everyone (especially doctors) want to be considered great.
Nevertheless, the doctor can always strive to improve, but most importantly should never forget to be attentive, be more empathetic, be compassionate, and remember the Hippocratic Oath - to uphold those powerful words they recited during their White Coat Ceremony.
To not only be good. . . but great.
As the father of two adult children, I am exceptionally proud of my daughters but I also know the complexity of becoming a physician first hand when my oldest daughter was faced with an inordinate
amount of exams, lack of sleep, roundthe-clock studying, bombarded with every imaginable roadblock and the questions/ doubts that easily popped into her mind.
Quietly, I’m sure she asked herself if it’s worth it. How much more can I withstand? Am I able to do this? She knew there were many who supported this “rite of passage,” such as her beloved parents, immediate family, close friends, supportive classmates, teachers, mentors, and even doctors who became her biggest and yes. . . greatest “cheerleaders.”
Before you begin to read this heartfelt narrative about my oldest daughter, I’ll never forget what occurred on May 1, 2021. As my immediate family anxiously gathered around a laptop in our home and extended family members and friends watched from afar, I couldn’t believe what I heard during this year’s NorthEast Ohio Medical University’s virtual commencement ceremony.
The School of Medicine finally announced my daughter’s name: Dr. Talia Torres.
And yes. . . she will be a great doctor.

What has your journey through medical school taught you? What kind of hardships did you face?


It has been a few months since I’ve officially become Dr. Talia Marie Torres. It has been 9 years since I have begun this journey. It was non-traditional in every sense. Straight from high school, I started a combined BS/MD program in New York City. This accelerated program forced me to learn quickly, barely passing every class by the skin of my teeth. I somehow made it through unscathed and proceeded to complete my clinical years in Ohio. Being here added new challenges, like driving for the first time as a 23-year-old and moving over 500 miles away from home. Isolated from my support system, I had to try to build new bonds in this foreign place. I wasn’t as lucky this time around.
My motivational quotes app sends me a daily notification, and one of the quotes that resonated with me was, “I survived because the fire inside me burned brighter than the fire around me.” Although I am not familiar with this video game character, Joshua Graham’s quote is the definition of my medical school experience. There were countless obstacles that I faced that I thought were going to end my dream of becoming a doctor.
From failing small exams in undergrad physics to clinical board exams in my third year of medical school to have to repeat that entire clinical year, I felt that failure
was beginning to define me. Imagine being told by a doctor in your desired specialty, “I wouldn’t want you in my program because of your significant lack of knowledge.” Imagine feeling like no one is on your side, except for your family and friends who are 500 miles away. It takes a toll on your mental health when you are isolated and physically not with your support system. Through this arduous journey, I learned that the fire inside of you is what will keep you moving. That fire was my family, friends and the thought of my sweet abuelita telling her doctors, “I want to live to see my granddaughter graduate.” Having faith in the unknown is nearly impossible some days.
Talia Torres, M.D., was born and raised in the Bronx, the elder of two daughters born to a Puerto Rican high school teacher (also a Bronx native) and an African American graphic designer from Long Island City. She chose to become a Family Practice physician so that she can best serve patients from ALL walks of life.

ReflectionsfromCUNY’sAssociate DirectorofAdmissions,GuillermoRivera
How many times in your life do you get to look back and scream to the world how proud you are of a student? As a counselor, and former student myself, I have spoken to many students over my career. What people often forget is that medical school is just one step along the journey to becoming a doctor. Over 25% of students will fail in taking that final step in the journey. Let me share with you a little story about the time I was able to help a family out and watch as their daughter went from college applicant to medical student and then to doctor.
It was a cold day in January about 7 years ago, and I was just getting ready to head home from work. As I was walking down the sidewalk a gentleman, Danny Torres, pulled me aside and asked me, “Do you work here? I need to drop off a letter for my daughter.” The deadline for applications to the City University of New York (CUNY) School of Medicine program, formerly the Sophie Davis BS/MD Program was just days away. His daughter, Talia, had applied to the program but was missing one letter of reference from her application. Danny was there to make sure it got turned in, and his daughter Talia

stood a fighting chance of being accepted. I could see in his eyes how much this meant for him and his family. My own journey from a youth in the Bronx to become the Associate Director of Admissions at the City College of New York had been a long one, full of late nights, hard work and tough decisions. It was the opportunity that I needed to improve my life and I wish that opportunity for everyone. Changing my plans, I escorted Danny over to the office where he needed to go. He thanked me as I left and I wished his daughter good luck; little did I know that was just the beginning.
Danny’s daughter, Talia, was accepted into the medical program and was one of the 72% of students who continue on to become doctors. I was privileged to watch her grow. To be able to wave hello as we passed on campus and to support her family when they needed help navigating the world of college bills. Out of the blue, I was contacted to help find a student worthy of receiving the Herman Badillo Scholarship. This scholarship is reserved for students in the Hispanic community and is a gift that Herman Badillo passed on to CUNY students when he left this world. Right away a name came to my mind, I was able to recommend Talia to the scholarship
committee and they selected her to receive the award.
A few months ago, I received an email from Danny. As I read it, a smile was painted on my face when I saw the words “Dr. Talia Torres” in the message. Talia is a boon for the Latino community and someone that young girls can look up to. Being a father myself, every day I look into my little girl’s eyes and know that one day she could become a doctor too. CUNY has been a life-changing experience for me and for many people that share my story. I started at the bottom, holding three jobs helping in different offices as I was a full-time student as well. One person stepping in to guide your life can change your world; that worked for me so many times at City College. I look forward to watching Talia continue to advance in her career and I am going to make sure to be there for other students like Talia.
More than 50 students from the City University of New York are winners of prestigious national academic awards. Their success reflects the University’s mandate to provide a quality education to students of all backgrounds and socioeconomic circumstances.

¿Hay
byDr.Wüst-Smith
The best thing about being the “founder” of PhysicianOutlookMagazine is that I get to tell MY story, and the story of others that have had a great impact on my life.
It’s no secret that we have a shortage of physicians in the United States, and we have an even greater shortage of physicians of diverse backgrounds. As we experienced during the COVID19 pandemic, diverse patient populations were disproportionately harmed by the virus because of a combination of factors (higher rates of obesity, hypertension, poverty, multiple generations living together, poor access to care, and employment as underpaid essential workers, among many other contributing circumstances).
It has been well documented that patients’ health improves when care is delivered by someone who is culturally similar. So the obvious solution to overcoming our nations’ shortages of culturally competent and diverse physicians?
It’s not rocket science: the solution is obvious. We need to “grow” more doctors, and we need to cultivate them from within the very communities that need medical care and preventive education the most.
Thanks to the generosity of a female entrepreneur and philanthropist by the name of Sophie Davis, a program that does just that was born at the City
University of New York. The accelerated degree program created a path to medicine for economically disadvantaged students who promise at least two years of primary care service in an underserved community. Although graduates are no longer called “Sophies,” the program’s goals and commitment remain the same: to produce broadly educated, highly skilled physicians of African American, Hispanic/ LatinX, and other ethnic backgrounds who have historically been under-represented. The graduates of this program excel as healthcare advocates and role models for future generations.
The story of Dr. Talia Torres is a very special one for me, because she is the first of my pediatric patients who has literally “followed in my footsteps” and career path to become a doctor. You can read more about her-story in The Hispanic Outlook on Education. When Talia was born, I was a young, fresh-faced, eager new Attending Pediatrician at the
New York Hospital-Cornell Medical Center (now NY-Presybeterian), working for the famous Dr. David Israel Smith, whose office was across the street from the hospital.
Dr. Smith’s practice was the medical home for many of New York City’s “famous families.” We saw our fair share of celebrities and their children, but what I loved most about working for Dr. Smith is that we also saw a lot of “regular, normal folk.” Talia and her parents did not fall into the “rich and famous” category in the traditional definition, but they have filled my life with the sort of currency that money can’t buy.
I am beyond proud of Dr. Talia Torres, as it is in her reflection that I see a promising future.
Marlene Wüst-Smith, M.D., is the publisher for PhysicianOutlook magazine, and a practicing pediatrician.

“T,” come here.
I need to talk to you.
As you are entering your residency, one essential chapter is ending.
However, the bulk of the book is yet to be written!
Remember that medicine is just a part of who you are, a significant part, no doubt, but only a part.
You will need to discover and nurture your other personas.
Unbeknownst to you, they will grow in importance for maintaining the balance necessary in all our lives.
You’ll need to guard against the doctor smothering the other aspects of your being.
The passion that brought you to medicine should also fuel all parts of your world.
Trust me; it will impact everything.












Sundari Periasamy, M.D.
A proud graduate of the very program she is now in charge of, Dr. Periasamy loves that she is able to play an important role in shaping future pediatricians’ careers. She is dedicated to the teaching and development of the residents who put their trust in the program, much like parents put their trust in the doctors they choose to care for their children.

Mary Marron-Corwin, M.D.
Dr. Corwin started her medical career as a pediatric nurse but after a few years realized that her true calling was to become a physician. She is a humble Servant Leader, who describes her job as a neonatologist and Department Chair at a public hospital both a privilege and an honor.

Aracelis D. Fernandez, M.D.
Dr. Fernandez completed her Pediatric Infectious Disease fellowship at Cornell Medical Center in 2000, and returned “home” 15 years later. She describes herself as truly blessed to be able to work with an “amazing group of colleagues, residents, nursing staff, clerical staff and medical students as they care for awesome patients and their families.”
Caring for children and growing our future doctors
byLeannBullion
Physician Outlook chose to highlight the graduates of Harlem Hospital’s Pediatric Residency class of 2021 in this issue because of their dedication to the medically underserved children of Central Harlem and the South Bronx, and their long journeys to becoming pediatricians. This extraordinary group of doctors (who hail from all corners of the world) truly connected with the community and with one another in ways that will have long-lasting impact.
Dr. Aracelis Fernandez told us the story of how one of the chief residents was able to earn the trust of a notoriously non-compliant young adult patient who was overdue for a recommended medical procedure. Being able to successfully engage patients in taking care of their own health is just one of the ways that we can eliminate structural racism and health disparities.
Harlem Hospital is affiliated with the Columbia University College of Physicians and Surgeons. We congratulate this amazing group of pediatricians for a job well done!



Gurtej Sangha, M.D., grew up in Edmonton, Alberta and graduated from Ross University Medical Center. His decision to become a pediatrician was inspired by the resilience and happiness that children display. He served as Chief Resident for the Harlem Pediatrics program after completing his 3 year residency, and has returned to his native Canada to work as a general pediatrician in Vancouver.
Audrie Lazaga, M.D., received her Medical Doctorate in the Philippines and came to the US to pursue a residency at Harlem Hospital, where she was honored to serve as Chief Resident during her third year. Her family was the greatest influence in her life’s path. She loves Harlem so much that after completing her residency, she remains at Harlem Hospital as the Associate Program Director for the residency and as an Attending Physician.
Xinming Wu, M.D., grew up in the Hubei province of China and graduated from the Wenzhou Medical University before coming to Harlem Hospital to become a pediatrician. He is interested in caring for critically ill or injured children and has stayed on in Manhattan to complete a Pediatric Critical Care Fellowship at the Mount Sinai School of Medicine.
Su Mon Thwe, M.D., was born and raised in Southeast Asia in Myanmar, where she obtained her Medical Degree at the University of Medicine in Yangon. “My passion has always been working with and caring for children.” Emerging from a country with a weakened healthcare infrastructure was one of the primary catalysts for choosing the Harlem Hospital program for her residency. She has moved across the country to serve as a primary care pediatrician in an underserved area of San Bernardino, California.
Ravi Bhavsar, M.D., was born in Mumbai, India but spent his early childhood in a different country (Brunei). Growing up in two different countries contributed positively to his “cultural quotient.” He returned to Mumbai for college and med school (he obtained his M.D. from the DY Patil School of Medicine). Dr. Bhavsar reports that it has been a privilege to be able to train in NYC, especially at Harlem. “There is so much history within the walls of the hospital.” He is currently pursuing his Fellowship at the University of Kentucky’s Neonatal and Perinatal Medicine program but would love to return to work at Harlem.
Daniel Caicedo Proano, M.D., attended the Universidad Internacional del Ecuador. As a child his mother served rural communities as a dentist, and it inspired him to become a pediatrician so that, he too, could make a difference. He started his Pediatric Cardiology Fellowship at the University of Mississippi after completing his residency at the Harlem Hospital program.
Shivraj Vishwanath Savadkar, M.D., graduated from the Mysore Medical College in India. He and his fellow residents feel very fortunate to have trained under wonderful mentors like Dr. Fernandez, Dr. Marron and Dr. Periasamy, who have gifted them with “lessons for life.” His life goal is to become a pediatric cardiologist (he is currently at the University of Mississippi Medical Center doing his fellowship) so he can help the healing process of children suffering from conditions that afflict them through no fault of their own.
Motoki Yasuda, M.D., graduated from the Keio University School of Medicine in his native homeland. A physician treating him for a pneumothorax as a youngster left an indelible mark on his own career path and inspired him to become a pediatrician. Japan has no formal training programs for Pediatric Emergency Medicine, which is what prompted Dr. Yasuda to come to the United States. After completing a 3 year residency in general pediatrics at Harlem, he is now in his first year of 3 at the Virginia Commonwealth University Pediatric Emergency Medicine Fellowship.




You can learn more about the Harlem Hospital residents at www.physicianoutlook.com


Podcasts are a useful and entertaining way of dispensing information related to all kinds of topics. In fact this technology has made it easier for content creators to talk on any niche of their choosing It’ s no wonder that the popularity of podcasts in general keeps increasing
Over the last year or so, it has been especially exciting to see physicians create more and more podcasts addressing various aspects of physician life.
That’ s where Doctor Podcast Network comes in...
Founded in June 2020 by Dr. David Draghinas, a Dallas-based anesthesiologist Ryan Inman a fee-only financial planner for physicians, and Desiree Leos a sole proprietor of her own content development and podcast production company Doctor Podcast Network was created for the purpose of helping physicians feel supported throughout their podcast journeys
Simultaneously, “DPN” brings together in one location many quality podcasts that are essential listening to physicians and their families
Dr. Draghinas and Ryan are both podcasters Desiree built their teams to help support them and others to consistently produce content All three knew how challenging that was to do in the midst of busy schedules competing priorities unpredictable monetary compensation, and fluctuating motivation
Physician podcasters are there for the doctors and healthcare providers that make up their podcasting audience But “this can be a tough and lonely journey for the podcast creator ”
Doctor Podcast Network is there for the physician podcaster It’ s a place where they can come together learn from, collaborate, and confide in one another as well as facilitate the monetization of their shows
Having soft launched with 15 founding members in October 2020 and formally launching in January 2021 with 17 shows the network has shown its capability of creating the community and environment that podcasters need to thrive
Doctors Unbound is a podcast created for doctors who are busy with unique side passions outside of their normal schedule. Dr. David Draghinas shares their stories of triumph, learned lessons, and, ultimately, their humanity
Financial Residency is geared toward early-careered physicians looking for practical ways to manage their finances. Ryan Inman is usually found nerding out over phoned-in questions by his listeners asking about student debt, investing, insurance, and balancing budgets
The Physicians Guide to Doctoring is hosted by Dr Bradley B. Block where he seeks to answer the question, "what should we have been learning while we were memorizing Kreb's cycle?" His podcast is a practical guide for practicing physicians and other healthcare practitioners looking to improve in any and all aspects of their lives and practices.
O U R M I S S I O N :
W E ’ R E A B O U T T O B R E A K I T D O W N
T H E F O L L O W I N G A R E A F E W W A Y S

W E H E L P P H Y S I C I A N S G R O W :
by building a community for physicians to connect & network with others on social media (join FREE networking FB group) by providing an organized space for doctors online to be found by readers, members of media, conference organizers, and anyone else who could use an expert online voice (look at our Databank!) by providing unique forums to discuss interesting topics by providing tools needed to leverage the healthcare social media space of today
I A M A D O C T O R !
List your profile in our Databank so that readers, journalists, producers, conference organizers and others can all find you and link into your work for a fitting gig
Consume engaging written and video content on social media
Find platforms that connect you with like-minded peers across ALL social media platforms
Find online resources to grow your business and yourself (through courses, platforms and other unique ways)
Get inspired with ideas we are chock full of 'em!
Scroll through our unique Databank of vetted online physicians to:
Find a physician whose message and work you enjoy, and link in to follow their online work! (as a reader)or find sources for your article, recorded/televised appearance, or speaking engagement (as a journalist, producer, or event organizer)you can also select a physician based on their specialty! or consume content we create (like articles & videos) that pose questions about various social media & healthcare topics, share to start a discussion, or tag us to get our attention
Board-certified internist who took on the world of entrepreneurship headon looking to grow SoMeDocs into the hub where both physicians and readers can congregate, connect, and form relationships that successfully take off from there

Will You Make It Out Alive?
byThomasFarr
When looking at survival skills, the first thing everyone thinks about is getting lost in the woods and needing to stay alive until help arrives. While this is true, urban areas are continuing to grow and the need-to-know urban survival skills are important.
Knowing how to get through natural disasters and man-made incidents in the dense urban environment is crucial. Rural or remote skills do transition over into the urban setting but urban survival skills have some unique skill sets of their own. This includes preparing for an incident by taking classes to learn the skills to survive, so you can keep yourself and your loved ones safe. These classes not only give you the basics you need but can help build confidence, improve your everyday skills, and allow you to meet new people.
There are skills some of us have and use every day and some you might say “I have never considered doing that in the city.” These topics or skills will be broken down more as we go but the basics include procuring food and water, situational awareness, navigation, and
personal safety including finding or making a shelter and dealing with injuries. These skills are crucial for your survival!
Situational awareness is a skill that we use every day, without even knowing it. When driving we keep an eye on our surroundings and that is situational awareness, BUT, do you use situational awareness when walking around or when out at the mall shopping?
Situational awareness is a skill I never thought I would teach but people do not seem to know what is going on around them. Next time you are in a store take the time to look for the exits, fire extinguishers, who is near you, or just try to read people.
Reading people is a big part of situational awareness and more so in the urban setting where there could be large crowds. In a way you will be profiling people to determine who could be helpful and who could be a threat.
This can make the difference of making it out of an incident, whether it is a fire,
or an active shooter situation. Looking, remembering, and knowing how to read a person or group before a situation arises will help you be better prepared to survive.
Being situationally aware, like so many other skills, is more of a state of mind.
When there is an incident, food and water might be difficult to find and this makes it essential to have foraging skills. It will be important to have a form of purification for your food and water source because drinking water from a stream, pond, or lake can carry diseases or parasites like giardia and improperly prepared food can transfer parasites or cause illness. Many commercial filters are available but simply boiling the water will make it potable and cooking food helps too.
We live in a prepackaged fast-food world and learning how to forage, scavenge, and cook meals is an essential skill that can be used on a weekend camping trip or in a time of emergency.
Knowing what plants are edible and where to find them, and what to avoid will help you be successful. Another important part of foraging for food is knowing what areas to avoid. This is important because some edibles will absorb chemicals from their surroundings and turn an otherwise safe food source against you. This brings us to the next step, and that is food prep.
Do you have the skills to start a fire so that you can safely and deliciously prepare your foraged foods? There are many ways to start a fire, but keeping matches readily available would be the easiest. Some alternate fire-starting methods include bow drills, ferro rods, and steel. These skills can be learned very easily in classes, and YouTube is a great resource for how-to videos.
First aid is valuable, and includes the basics of stopping the bleed, how to bandage small wounds, signs and symptoms of illnesses that include environmental issues like hypothermia and heat related illness. Many times it is the most basic skill that saves someone, not the more advanced ones.
As a paramedic, the most advanced skills would not save someone if we did not do the basics first. Having a first aid kit with you even on a simple day hike can make a difference, and having the right tools in that first aid kit make all the difference in the world.
A uniquely urban skill is dealing with and surviving riots or large protest. This again starts with situational awareness and reading the crowd. Never move against the crowd in these situations. Move with them or on an angle through them. Once you get to a safe area you can make your way out of the area. Do not start shouting or yelling to draw attention, keep quiet and moving. If approached, it is safer and easier to comply with what the individual or crowd is demanding.
Property can be replaced, but your life cannot be.
Navigation is important in everyday life! We use landmarks and personal knowledge of the area that we live in to find our way to the places we frequent. This, however, can be an issue if all of a sudden, the mode of transportation is interrupted by a natural disaster or any kind of incident including fires, law enforcement activity, and/or weather related problems such as flooding.
Knowing how to find your way home from work using alternate routes or by alternate means of transportation including walking is a great first step. This includes the use of situational awareness for standing water in the road and the saying “turn around, don’t drown.” Remember, navigating does not always mean a map and compass, however those skills are also useful if the need to evacuate the area arises.
The final skill that can be important and has a unique twist in the urban environment is shelter building. This is looking for a building or shelter for the purpose if survival. In the urban setting, this is probably not building a shelter out of fallen trees, but instead abandoned cars, buildings, or even dumpsters. The use of an abandoned building presents some issues. The first is how structurally sound the building is, and the second is can you protect yourself from others in the space, as others will want to take shelter there as well?
This last skill is more of a lifestyle, and I call it Urban Homesteading. This means simply growing some of your own food in vertical gardens, canning and preserving food that you can purchase locally like vegetables, jelly making, and even dehydrating meat into jerky. Safe foodhandling practices need to be followed, and many places offer canning classes. This is a great skill to learn!
It is not just for emergencies, but for everyday life. Eating healthy is a bonus.
Learning these skills and other survival skills, will not only help you in a time of need or emergency, but it will also offer you the chance to think outside of the box and try something new. Taking a class to learn these skills helps you meet new people, improve on skills you might already have, and most importantly improves self-esteem. These skills transfer to many different settings from walking in the park, to taking the weekend camping trip for vacation. So, learn new skills and TRAIN LIKE YOUR LIFE DEPENDS ON IT, because some day, it might.
You can learn more about Thomas Farr online at: www.farrsecurity.org

byPatrickBruce
GUN CONTROL IS RACIST! There, I said it. It’s also elitist, xenophobic, and more. Can addressing this issue help our emergency medical professionals? The history of gun control in the United States is a history of racism. This isn’t limited to just the past, though. Right now, minorities, those who are not politically connected and or wealthy, young adults under 21, and immigrants, are subject to these discriminatory and unconstitutional laws and policies. Even though the phrase “except whites’’ has been removed, the effects remain to a large degree.
To be clear, I am also biased. Biased against gun control. Though I wasn’t always so. I believe after a full review of the facts, the conclusions I’ve drawn will be clearer as well as my reasoning. The Merriam – Webster Dictionary defines racism as; “a belief that RACE is the primary determinant of human traits and capacities and that racial differences produce an inherent superiority of a particular race AND racial prejudice or discrimination” (Dictionary, n.d.). While quoting statistics is often misused by both sides of the gun control issue, history cannot be misquoted so easily, so let’s look at some examples.
This first one is from before we were even a country. Virginia, in 1640, “Prohibiting negroes, slave and free, from carrying weapons including clubs.” (The Los Angeles Times, “To Fight Crime, Some Blacks Attack Gun Control,” January 19, 1992).
Not long after the emancipation proclamation, the Mississippi Statute of 1865 prohibited black individuals not in
the military, “and not licensed so to do by the board of police of his or her county” from keeping or carrying “fire-arms of any kind, or any ammunition, dirk or bowie knife.” [reprinted in 1 Documentary History of Reconstruction: Political, Military, Social, Religious, Educational and Industrial, 1865 to the Present Time, p. 291, (Walter L. Fleming, ed., 1960.)] (GLJ, p. 344). Notice how this law incorporates the police as arbitrators as well as licensure. This will become more important with this next example as context.
In debating what would become 42 USC Sec. 1983, today’s federal civil rights statute, Representative Butler explained “This provision seemed to your committee to be necessary, because they had observed that, before these midnight marauders [the KKK] made attacks upon peaceful citizens, there were very many instances in the South where the sheriff of the county had preceded them and taken away the arms of their victims. This was especially noticeable in Union County, where all the negro population were disarmed by the sheriff only a few months ago under the order of the judge...; and then, the sheriff having disarmed the citizens, the five hundred masked men rode at nights and murdered and otherwise maltreated the ten persons who were in jail in that county.” [1464 H.R. REP. No. 37, 41st Cong., 3rd Sess. p. 7-8 (20 Feb. 1871)].
Now we can introduce another couple phrases of control into the discussion, namely “Saturday Night Special.” This phrase came from “Suicide Special” which was the initial derogatory term used to describe handguns. In more modern times it is used to describe “cheap,” meaning inexpensive handguns. The supposed goal of laws was that such inexpensive handguns and imports were poorly constructed, and therefore dangerous. The purpose, though, was merely to keep arms

from the poor. These poor are statistically minorities in the areas these laws are or were, though not exclusively so.
In 1870 Tennessee, the first “Saturday Night Special” economic handgun ban passed. In the first legislative session in which they gained control, white supremacists passed “An Act to Preserve the Peace and Prevent Homicide,” which banned the sale of all handguns except the expensive “Army and Navy model handgun” which whites already owned or could afford to buy, and black individuals could not. (“Gun Control: White Man’s Law,” William R. Tonso, Reason, December 1985) Upheld in Andrews v. State, 50 Tenn. (3 Heisk.) 165, 172 (1871) (GMU CR LJ, p. 74) “The cheap revolvers of the late 19th and early 20th centuries were referred to as ‘Suicide Specials,’ the ‘Saturday Night Special’ label not becoming widespread until reformers and politicians took up the gun control cause during the 1960s.
The source of this recent concern about cheap revolvers, as their new label suggests, has much in common with the concerns of the gun-law initiators of the

post-Civil War South. As B. Bruce-Briggs has written in the Public Interest, “It is difficult to escape the conclusion that the ‘Saturday Night Special’ is emphasized, because it is cheap and being sold to a particular class of people.”
The name is sufficient evidence. The reference is to “****** Town Saturday Night.” (“Gun Control: White Man’s Law,” William R. Tonso, Reason, December 1985. The Racist Origins of US Gun Control Laws Designed To Disarm Slaves, Freedmen, And African-Americans by Steve Ekwall, pg.7). The 1911 Sullivan Act of New York City was crafted to go after immigrants and political opponents. The proposed gun control measure would prove to be corrective and salutary in a city filled with immigrants and evil communications, floating from the shores of Italy and Austria-Hungary.
New York police reports frequently testify to the fact that the Italian and other south Continental gentry here are acquainted with the pocket pistol, and while drunk or merrymaking will use it quite as handily as the stiletto, and with more deadly effect. It is hoped that this
treacherous and distinctly outlandish mode of settling disputes may not spread to corrupt the native good manners of the community.” (January 27, 1905, New York Times Editorial). Unless you are politically connected, and/or mega rich, there are no rights for you in NYC.
Now moving forward on the racism timeline, we get to 1968. With the passage of the 1968 Gun Control Act (1968 GCA) our country firmly planted itself among other countries that passed weapon laws based on race. While many purely racist gun control measures existed in the United States prior to the 1968 act, this marked the first time the Federal government passed gun control which it said was for purely public safety reasons; not associated with race. However, the evidence and history say otherwise.
During the years preceding the 1968 act there was great unrest in the country as black people fought for racial equality. This, coupled with the assassination of Rev. Dr. Martin Luther King and President John F. Kennedy, gave the extra push needed to pass gun control. Prior to the act being passed it was possible to order firearms through the mail and import inexpensive military surplus firearms from overseas. The real motivations for the 1968 act are much more insidious than one would like to imagine.
Robert Sherrill, the strongly anti-gun author of “The Saturday Night Special” (1973), declared after investigating the background of the 1968 GCA, “The Gun Control Act of 1968 was passed not to control guns but to control blacks …”. The 1968 GCA restricted mail order sales of firearms and cheap import firearms. These arms were typically what was within economic reach of black individuals who tended to be of poorer economic power. In this instance, the how is the same as the why. The reason for this is as simple as to where the inspiration for the 1968 Gun
Control Act came from. The framework for it was obtained from the 1928 and 1938 Law on Weapons from Nazi Germany. Evidence of this exists in the form of a letter from the Library of Congress to Senator Thomas J. Dodd who had provided a personally owned copy of the Nazi law to be translated. It should be noted for context that the late Senator Dodd served as part of the prosecution in the Nazi War Crimes Trials and therefore would have had access to Nazi laws and documents. It is worthwhile to note that during the period of 1933 - 1945, Nazi Germany had some of the most severe gun control measures in effect. (Law on Firearms & Ammun., 1928 Weapon Law, March 18, 1938, Regulations against Jews, 1938) These were used to systematically target the Jews and others deemed “undesirable.”
In seeking truth, we must be open to any conclusion that is based on fact. Like many myths and lies, gun control is based on fear and a desire to control. My belief is that to understand gun control is step one. Next, is to dispel the idea that solving misuse of guns in crimes, suicides, and accidents is not a simple two-step solution such as passing a law, and the desired result happens. Fear of minorities, immigrants, and other groups have been the basis for our gun control laws and its history. Now fear of the firearm itself is pushed forward politically as the basis for proposed regulation, yet history proves otherwise. Empirically this should be the opposite. Training in what firearms are and what our rights are, regardless of what color or group you belong, should be the foundation of solutions to these issues. These ideas compliment the idea that there would be less stress placed on emergency medical professionals and society at large if we used knowledge and facts vs. fear and mistrust, as a foundation for solutions to these issues. We have tried it one way and it has not worked. Let’s try knowledge, training, and rights instead.
byDr.Londoño
It is said that visionaries don’t see what everyone else sees. That they see what others can’t. That it takes courage to see what others cannot, and that they hold on to that vision no matter what others say or think. This is usually used to describe entrepreneurs. Yet, activists are just the same.
An activist will see an injustice that others cannot see, and they will hold on to this, and fight for it regardless of the stakes involved. They will pursue their vision and goal even when they are faced with personal attacks, intimidation, retribution, physical pain, or hunger because their belief is unshakable.
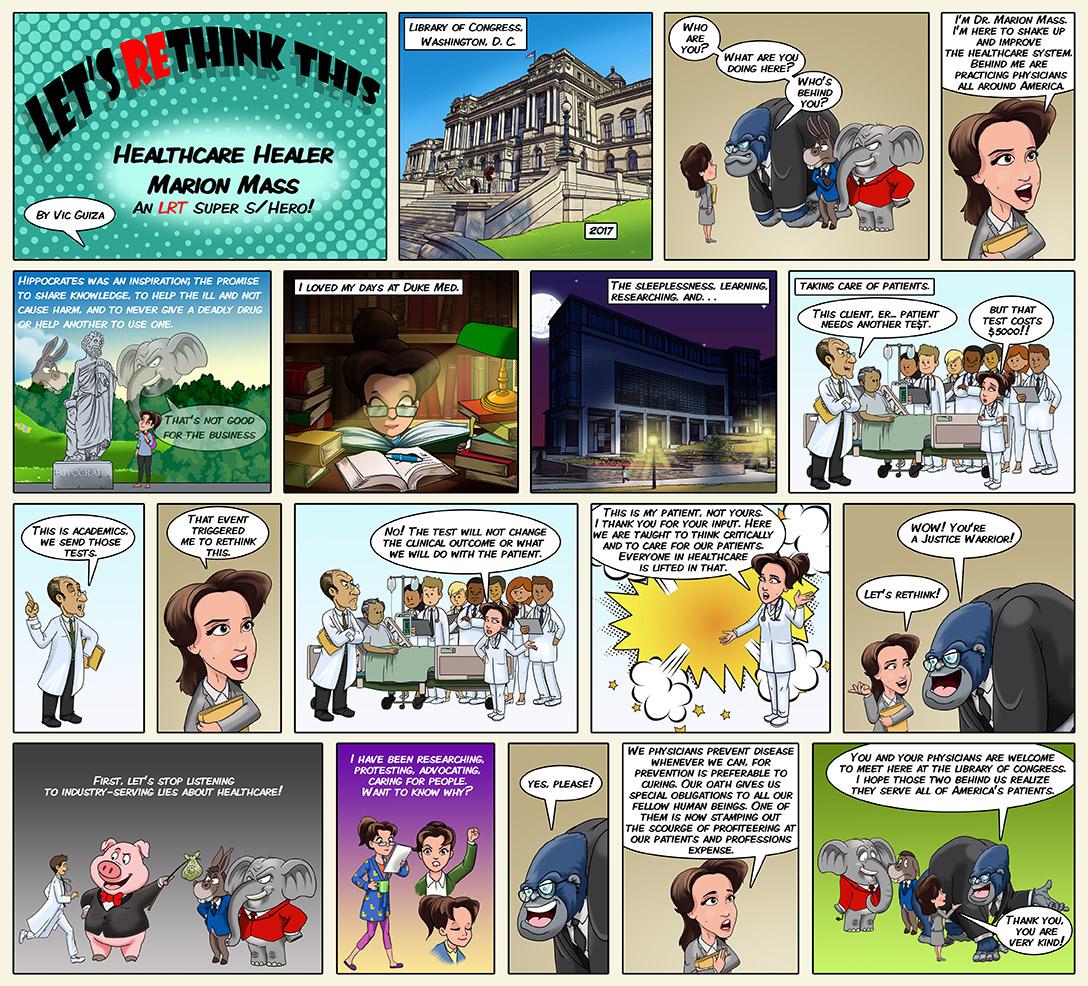
I recently saw an interview with Dr. Marion Mass who is an advocate for patient protection in which they asked her how she became an activist. She described how she thought of some things she was observing. She said, “Why are you letting this happen? I just can’t let things go…I mean, it’s like, I’m not built that way… I’m like built for justice and this didn’t seem just because it wasn’t going to help patients.”
It is the vision of being able to see something so clearly that others are too unconscious about, too tired, too scared, too indifferent to take any action for. Yet, an activist and a leader who is a visionary, will continue and will not falter despite the toll it takes. And every activist will state that no matter what the personal retribution is, they will do it again because it matters: humans matter. What activists fight for is not a bigger paycheck or a bigger mansion, it’s about equality, humanity, and people.
The stakes are not small when women speak up. Female physicians will be called “insane, needing psychiatric evaluation, conspiracy theorists.” We will be gaslighted and told: “gender discrimination cannot truly be there,” “this is just a matter of perspective,” “this is how older generations see things,” “it is not that bad,” and “no others have ever spoken about this before you,” etc.
It is no surprise that in academic medicine, a study from the New England Journal of Medicine in 2018 found that less than 10 % of women ever report any injustice they experienced. The stakes are high. Women physicians will be burned at the stake twice, just like Joan of Arc was in 1431.
We will fight for the injustice to then have our reputation, our credentials, our promotion, our job stripped away. At the same time our sanity will be called into question. It is no coincidence that the word “hysterectomy” or surgical removal of the uterus that was coined in 1881, comes from the Greek word hystera or uterus. So that when women were thought of as having hysteria or neurosis, this was due to a problem caused by the womb or uterus. Thus, to fix the dysfunction of the hysteria, a “hysterectomy” had to be performed.
I wonder if these ideas and definitions which trace back to the Greeks continue to influence our thoughts. There is an implicit bias in which we may not be aware of how our subconscious thoughts are affecting our conscious thoughts, opinions, or actions we have daily. They manifest in all aspects of life. Whether you come to see me for a surgical consultation and when you walk into the room you think to yourself, “She is too young to be a doctor, too pretty to be smart, too feminine to be a good surgeon.” Before a word has been uttered by me, you have already decided a narrative in your head. It is instant, unconscious, but it is there. It is just running in the background, like the music in the elevator that brought you to the office. Or like the air
conditioner that keeps you cool, but you are not aware of it until you are conscious of the music, or too uncomfortable and hot.
This implicit bias will affect how women are judged when we speak up. There are countless examples of courageous women who have stood up for what they believed and paid an unimaginable price. You can google Dr. Abby Rosenberg and her KevinMD article, “Questions of a cancelled whistle-blower.”
Read about the prolonged legal battles in which Dr. Diana Blum spoke up about policies pressuring physicians in Sutter Health to increase productivity or prescribe medications which were possibly inferior and not indicated to save costs. It then used unlawful practices to wrongfully terminate those that disagreed with them. In turn, Sutter Health sued her for $1.3 million in legal fees.
Another example is how The Regents of University of California were sued and the verdict awarded $13 million to Dr. Lauren Pinter-Brown at UCLA for disability discrimination claim which was then moved to a mistrial. Most recently, Dr. Brytney Cobia an Alabama hospitalist who stated in a local newspaper article how she was sorry, “but it’s too late” to vaccinate those dying of COVID because they had refused a lifesaving vaccine as 70% of her state is unvaccinated. Her voice brought about intimidation, personal threat to life, being called a “murderer”, and many other expletives as her story went viral.
All these women have an unwavering courage despite the toll it takes on them personally, to their families, their patients, and to their neighbors. We can take a moment and be grateful for the courage of these visionaries and leaders, and whether privately or publicly, support them. Injustice is ubiquitous, but our humanity, empathy, and support for each other can be as well.
Diana Londoño, M.D., is a skilled surgeon, who specializes in urology, treating men and women.


Let’s Rethink This is a specialized social media platform, a content delivery system, and an impact engine. We are building online communities and families of like-minded individuals interested in rethinking solutions to today’s biggest challenges in addition to our real-world impact work as we: Searchlight, Spotlight, and Ignite!
Publisher: Marlene Wüst-Smith, M.D. Editor in Chief: Alicia Roselli Managing Editor: Roxanne Bruce, MBA, DrBA, VP of Advertising: Pamela Ferman Director of Art and Production: Tobias Sarrio Marketing/Copyright Editor/Journalism/Social Media Interns: Samantha Petzold, Riley Snowden, and Madison Smith, Pennsylvania State University and Molly Matthews, Hobart and William Smith Colleges Contributing Authors: Roxanne Bruce, MBA, DrBA, Alyssa Dean, Yvonne Downer, Umaru Barrie, M.D., PhD, Robin Trimingham, Daniel Torres, Talia Torres, M.D., Guillermo Rivera, Marlene Wüst-Smith, M.D., Eliseo Rosario, M.D., Leann Bullion, Thomas Farr, Patrick Bruce, Diana Londoño, M.D. Cover Art: Luke Lin, M.D.
Published by “PhysicianOutlook Publishing” (ISSN 2768-6019) Editorial policy: PhysicianOutlook magazine is a national magazine dedicated to empowering physicians and their patients to improve the world of medicine together. Editorial decisions are based on the editor’s judgement of the quality of the writing, the timeliness of the content, and the potential interest to the readers of the PhysicianOutlook magazine. The magazine may publish articles dealing with controversial issues. The views expressed herein are of the authors and/or those interviewed, and may not reflect the official policy of the magazine. PhysicianOutlook neither agrees, nor disagrees with those ideas expressed, and no endorsement of those views should be inferred, unless specifically identified as officially endorsed by the magazine. “Letters to the Editor” email: rbruce@physicianoutlook.com Information on advertising, subscriptions, and job board email: hello@physicianoutlook.com “PhysicianOutlook” is a registered trademark.


Dr. Luke Lin (aka Luke Dragon) is currently pursuing an Emergency Medicine Fellowship at Arrowhead Regional Medical Center after having completed his residency at the New York Presbyterian Hospital in Queens, New York. He practices by the philosophy of “work hard, play hard,” and Emergency Medicine is the perfect “lifestyle specialty” for him. During his spare time, Luke enjoys creating artwork, with acrylic paint and spray paint. Medicine is both a science and an art. In addition to explaining medical concepts to patients, a physician has to be skilled in communicating with patients on an emotional and spiritual level. That’s why you can find Luke at the patient’s bedside with a pen and paper, sketching anatomical diagrams for patients with compassionate care.
In the world of street art, he goes by the name “Luke Dragon.” In 2015, Luke founded a non-profit organization called Dragon School in Oakland, California which curated public murals by the local community and overseas artists. Many of Luke Dragon’s personal murals can be found along Grant St. in San Francisco Chinatown. Although the Dragon School project is no longer active, Luke continues to pursue aerosol art. He is currently working with the Museum of Urban Art to create a series of stylized anatomical diagrams. You can follow Luke on Instagram @LukeDragon911 for updates.

