TDA
Texas Dental Journal
APRIL 2023
144 Kratom and oral HealtH: WHat a dentist sHould KnoW Dwayne evans, DDs stephen Laman, DDs Gary n. Frey, DDs

CLeveriCk (C.D.) Johnson, DDs, ms Ben F. warner, ms, DDs, mD
146
a ComplianCe protoCol for optimizing response to oral applianCe tHerapy for obstruCtive sleep apnea
JeFF paz DDs, D-aBDsm emet sChneiDerman, phD
162
WHat are tHe etHiCal
Considerations of using video soCial media platforms suCH as tiKtoK in your dental praCtiCe?
kathLeen niChoLs, DDs
138 offiCial Call to tHe 2023 annual session
oF the texas DentaL assoCiation house oF DeLeGates











130 Texas Dental Journal | Vol 140 | No. 3
Anesthesia Education & Safety Foundation
Two ways to register: Call us at 214-384-0796 or e-mail us at sedationce@aol.com Visit us on the web: www.sedationce.com
Two ways to Register for our Continuing Education Programs: e-mail us at sedationce@aol.com or call us at 214-384-0796
OUR GOAL: To teach safe and effective anesthesia techniques and management of medical emergencies in an understandable manner.
WHO WE ARE: We are licensed and practicing dentists in Texas who understand your needs, having provided anesthesia continuing education courses for 34 years. The new anesthesia guidelines were recently approved by the Texas State Board of Dental Examiners. As practicing dental anesthesiologists and educators, we have established continuing education programs to meet these needs.
New TSBDE requirement of Pain Management
Two programs available (satisfies rules 104.1 and 111.1)
Live Webcast (counts as in-class CE) or Online (at your convenience)
All programs can be taken individually or with a special discount pricing (ask Dr. Canfield) for a bundle of 2 programs: Principles of Pain Management
Fulfills rule 104.1 for all practitioners Use and Abuse of Prescription Medications and Provider Prescription Program
Fulfills rules 104.1 and 111.1
SEDATION & EMERGENCY PROGRAMS:
Nitrous Oxide/Oxygen Conscious Sedation Course for Dentists:
Credit: 18 hours lecture/participation (you must complete the online portion prior to the clinical part)
Level 1 Initial Minimal Sedation Permit Courses:
*Hybrid program consisting of Live Lecture and online combination
Credit: 20 hours lecture with 20 clinical experiences
SEDATION REPERMIT PROGRAMS: LEVELS 1 and 2 (ONLINE, LIVE WEBCAST AND IN CLASS)

ONLINE LEVEL 3 AND 4 SEDATION RE PERMIT AVAILABLE!
(Parenteral Review) Level 3 or Level 4 Anesthesia Programs

(In Class, Webcast and Online available):
American Heart Association Advanced Cardiac Life Support (ACLS) and Pediatric Advanced Life Support (PALS) Initial and Renewal Programs

NOTE: ACLS or PALS Renewal can be completed by itself at any combined program
Combined ACLS-PALS-BLS and Level 2, 3 and 4 Program
WEBCASTING and ONLINE RENEWALS AVAILABLE! Live and archived webcasting to your computer in the comfort of your home. Here are the distinct advantages of the webcast (contact us at 214 -384-0796 to see which courses are available for webcast):
1. You can receive continuing education credit for simultaneous live lecture CE hours.
2. There is no need to travel to the program location. You can stay at home or in your office to view and listen to the cou rse.
3. There may be a post-test after the online course concludes, so you will receive immediate CE credit for attendance
4. With the webcast, you can enjoy real-time interaction with the course instructor, utilizing a question and answer format
OUR MISSION STATEMENT: To provide affordable, quality anesthesia education with knowledgeable and experienced instructors, both in a clinical and academic manner while being a valuable resource to the practitioner after the programs. Courses are designed to meet the needs of the dental profession at all levels. Our continuing education programs fulfill the TSBDE Rule 110 practitioner requirement in the process to obtain selected Sedat ion permits.
AGD Codes for all programs: 341 Anesthesia & Pain Control; 342 Conscious Sedation; 343 Oral Sedation
This is only a partial listing of sedation courses. Please consult our www.sedationce.com for updates and new programs.
Two ways to Register: e-mail us at sedationce@aol.com or call us at 214-384-0796
www.tda.org | April 2023 131
Approved PACE Program Provider FAGD/MAGD Credit. Approval does not imply acceptance by a state of provincial board of dentistry or AGD endorsement. 8/1/2018 to 7/31/2022 Provider ID# 217924
NOW Available: In -Office ACLS & PALS renewals; In -Office Emergency Program Live Programs Available Throughout Texas
Dr. Canfield
FEATURES
138 offiCial Call to the 2023 annuaL session oF the texas DentaL assoCiation house oF DeLeGates
144 Kratom and oral HealtH: WHat a dentist sHould KnoW
Dwayne evans, DDs stephen Laman, DDs
Gary n. Frey, DDs CLeveriCk (C.D.) Johnson, DDs, ms Ben F. warner, ms, DDs, mD
146 a ComplianCe protoCol for optimizing response to oral applianCe tHerapy for obstruCtive sleep apnea
JeFF paz DDs, D-aBDsm emet sChneiDerman, phD
162 WHat are tHe etHiCal Considerations of using video soCial media platforms suCH as tiKtoK in your dental praCtiCe?
kathLeen niChoLs, DDs
HIGHLIGHTS
133
160
167
167
170 oral and maxillofacial pathology Case of the month: Diagnosis and management
170 value for your profession: We’re on the precipice of another recession. Here’s how you can maintain control of your revenue.
Editorial Staff
Jacqueline m plemons, DDs, ms, editor
paras B. patel, DDs, associate editor
nicole scott, managing editor
Barbara Donovan, art Director
Lee ann Johnson, Cae, Director of member services
Editorial Advisory Board
ronald C. auvenshine, DDs, phD
Barry k. Bartee, DDs, mD
patricia L. Blanton, DDs, phD
william C. Bone, DDs
phillip m. Campbell, DDs, msD
michaell a huber, DDs
arthur h. Jeske, DmD, phD
Larry D. Jones, DDs
paul a kennedy Jr, DDs, ms
scott r makins, DDs, ms
Daniel perez, DDs
william F. wathen, DmD
robert C. white, DDs
Leighton a wier, DDs
Douglas B. willingham, DDs
the Texas Dental Journal is a peer-reviewed publication. Established February 1883 • Vol 140 | No. 3
texas Dental association
1946 s ih-35 ste 400, austin, tx 78704-3698
Phone: 512-443-3675 • FAX: 512-443-3031
Email: tda@tda.org • Website: www.tda.org
texas Dental Journal (issn 0040-4284) is published monthly except January-February and august-september, which are combined issues, by the texas Dental association, 1946 s ih-35, austin, tx, 78704-3698, 512-443-3675. periodicalspostage paid at austin, texas and at additional mailing offices. postmaster: send address changes to texas DentaL JournaL, 1946 s ih 35 ste 400, austin, tx 78704. Copyright 2023 texas Dental association. all rights reserved. annual subscriptions: texas Dental association members $17. instate aDa affiliated $49.50 + tax, out-of-state aDa affiliated $49.50. in-state non-aDa affiliated $82.50 + tax, out-of-state non-aDa affiliated $82.50. single issue price: $6 aDa affiliated, $17 non-aDa affiliated. For in-state orders, add 8.25% sales tax.
Contributions: manuscripts and news items of interest to the membership of the society are solicited. electronic submissions are required. manuscripts should be typewritten, double spaced, and the original copy should be submitted. For more information, please refer to the instructions for Contributors statement included in the online september annual membership Directory or on the tDa website: tda.org. all statements of opinion and of supposed facts are published on authority of the writer under whose name they appear and are not to be regarded as the views of the texas Dental association, unless such statements have been adopted by the association. articles are accepted with the understanding that they have not been published previously. authors must disclose any financial or other interests they may have in products or services described in their articles.
advertisements: publication of advertisements in this journal does not constitute a guarantee or endorsement by the association of the quality of value of such product or of the claims made.
132 Texas Dental Journal | Vol 140 | No. 3 contents
editor’s
president’s message
member spotlight
Richard “Wick” Alexander
note 135
158
Dr
oral and maxillofacial
Case of the month
pathology
Calendar of events
in memoriam
174 Classifieds 182 index to advertisers
editor’s note
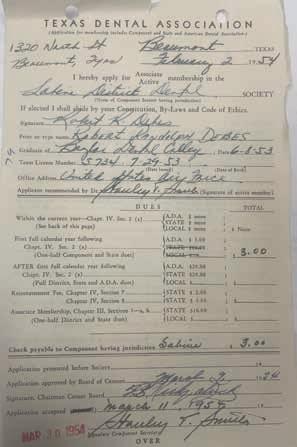
i’ve served as editor of the Journal for almost 1 year now. next month, the tDa house of Delegates will vote on this position, as they do each may. over the years, i’ve seen the association through the eyes of a member, a council and committee representative, as president, and now as editor. in each position, i had the privilege of meeting many of my peers i would not otherwise have been associated. Last week, i was honored to receive a phone call from a member who joined in 1953, Dr robert Debes of houston.
an oral surgeon and clinical professor at ut health school of Dentistry, Dr Debes notably served as the editor of the Journal of the Greater Houston Dental Society in the 1960s. at 95 years young and a tDa member for 70 years, Dr Debes has seen tDa’s journal transform over the years, and he specifically called to comment on its latest new look. he said the Journal is more readable and has a better format. From one editor to another, this is quite the compliment. we love to hear it! thank you, Dr Debes, for your membership and your praises!
 Jacqueline Plemons, DDS, MS
Jacqueline Plemons, DDS, MS

his feedback was a highlight of my month, and i want to hear what you think about our Journal after all, this publication is all of ours, not just mine, or Dr Debes’, or any editor who served the tDa or its components. it is the journal of our association, and we want it to reflect each individual member.
send us your thoughts and feedback and share your ideas. we’d love to hear from you! you may find your comments highlighted in the Journal as well.
this month’s featured topics:
• Increasing compliance in patients using oral appliances in the treatment of obstructive sleep apnea.
• What in the world is kratom, and why is it important for dentists to know?
Dr Robert Debes joined TDA in 1953. Pictured is his membership record, which includes dues of $3.
www.tda.org | April 2023 133 Editorial
JKJ Pathology
Oral Pathology Laboratory
John E Kacher, DDS
¥ Available for consultation by phone or email
¥ Color histology images on all reports

¥ Expedited specimen shipping with tracking numbers
¥ Reports available online through secure web interface
Professional, reliable service
technology solutions
you can better serve your patients. Call or email for free kits or consultation.
jkjpathology.com

281-292-7954 (T)
281-292-7372 (F)
johnkacher@jkjpathology.com
Protecting your patients, limiting your liability
Board of Directors Texas Dental Association
presiDent
Duc “Duke” m ho, DDs 281-395-2112, ducmho@sbcglobal.net
presiDent-eLeCt
Cody C. Graves, DDs 325-648-2251, drc@centex.net
past presiDent
Debrah J. worsham, DDs 936-598-2626, worshamdds@sbcglobal.net
viCe presiDent, southeast Glenda G. owen, DDs 713-622-2248, Dr.owen@owendds.com
viCe presiDent, southwest Carlos Cruz, DDs 956-627-3556, ccruzdds@hotmail.com
viCe presiDent, northwest teri B. Lovelace, DDs 325-695-1131, lovelace27@icloud.com
viCe presiDent northeast elizabeth s. Goldman, DDs 214-585-0268, texasredbuddental@gmail.com
senior DireCtor, southeast shailee J. Gupta, DDs 512-879-6225, sgupta@stdavidsfoundation.org
senior DireCtor, southwest richard m potter, DDs 210-673-9051, rnpotter@att.net
senior DireCtor, northwest summer ketron roark, DDs 806-793-3556, summerketron@gmail.com
senior DireCtor, northeast Jodi D. Danna, DDs 972-377-7800, jodidds1@gmail.com
DireCtor, southeast Laji J. James, DDs 281-870-9270, lajijames@yahoo.com
DireCtor, southwest krystelle anaya, DDs 915-855-1000, krystelle.barrera@gmail.com
DireCtor northwest stephen a sperry, DDs 806-794-8124, stephenasperry@gmail.com
DireCtor northeast mark a. Camp, DDs 903-757-8890, macamp1970@yahoo.com
seCretary-treasurer*
Carmen p smith, DDs 214-503-6776, drprincele@gmail.com
speaker oF the house*
John w. Baucum iii, DDs 361-855-3900, jbaucum3@gmail.com
parLiamentarian** Glen D. hall, DDs 325-698-7560, abdent78@gmail.com
eDitor**
Jacqueline m plemons, DDs, ms 214-369-8585, drplemons@yahoo.com
LeGaL CounseL Carl r. Galant
*non-voting member **non-voting
134 Texas Dental Journal | Vol 140 | No. 3
with high-
so that
DENTIST to DENTIST
Relationship. MentoRship. CoMMuniCation.
i might have aged myself with this last lyric, but hopefully this sentiment is clear: my journey is coming to an end.
throughout my year, my singular focus — in every discussion and every decision, in every planned meeting or chance encounter—was to promote and protect the everyday, practicing dentist while being a positive and welcoming face of the texas Dental association. to accomplish such, i made it my mission to always communicate what our organization is doing for you and your patients. with this curtain call (not including my final address to the house of Delegates), i’d like to look back on what we did well to serve you.
why does your membership matter? Because we offer:
• Personalized Help
• Legislative Advocacy
• Valued Information Resources
• Continuing Education
personalized Help with dental insurance and compliance issues (including the state board or insurance companies)
“ask diane” site (https://www.tda.org/askdiane/question-submission) offers individual, personalized assistance with dental insurance and compliance issues, including with third party payors, our own state Board of Dental examiners, and other regulatory agencies.
legislative advocacy to support bills and laws that safeguard both dentists and patients. impressive for any state, especially given that our legislature meets once every 2 years, our legislative agenda includes:
1. supporting a comprehensive insurance bill (hB 1527) to address retroactive denials, network leasing and disallowable clauses,
2. supporting a clear aligner bill (sB384), which mandates a comprehensive examine prior to starting aligner therapy,
3. increasing medicaid reimbursements (the last increase was in 2007) to support dentists who care for a deserving, underserved community.
valued information resources in all publications and social platforms to keep you informed of valuable resources available or changes in rules or regulations that might affect you.
1. any updates to the state Board rules or regulations can be found on the back page of the TDA Today
2. the progress of any legislation that affects dentistry can be found in the monthly publication The Root, which is shared across multiple platforms.
3. tDa perks’ endorsed vendor erC specialists now has more than $15 million in scheduled refunds to tda members while its other endorsed vendor Cloud dentistry is working alongside member dentists to help fulfill staffing issues and workforce shortages.
Continuing education discounts on Ce courses whether you want to meet in person or in the comfort of your home.
1. may 4-6, 2023, texas meeting in san antonio our state meeting with amazing activities and speakers.
2. July 21, 2023, regional meeting expanding community and education to more remote areas.
3. november 3-5, 2023, dentist symposium at the omni barton Creek resort & spa in austin high-end education and networking.
4. tda dental Concierge tracking your individual state mandated Ce requirements.
your association will continue to do better and be better as we strive to provide meaningful value to your membership. this may be the end of my journey, but it is not the end of the road. i, along with many others, will support our incoming president, Dr Cody Graves, as we work to grow the brand. thank you to everyone who has supported me and the texas Dental association. and as the rest of the song goes, “regrets, i’ve had a few. but then again, too few to mention. i did what i had to do. and saw it through without exemption.”

www.tda.org | April 2023 135 Editorial
“and now the end is here, and so i face that final curtain.”
—Frank Sinatra, My Way
Duc “Duke” M. Ho, DDS, FAGD TDA President
PROMOTING DENTAL PROVIDER DIVERSITY TO IMPROVE THE



136 Texas Dental Journal | Vol 140 | No. 3 DQ2676 (2.23)
the QR code to learn more about partnering with DentaQuest!
Scan
ORAL HEALTH OF ALL
TO PREVENTISTRY ®
WELCOME





www.tda.org | April 2023 137 Learn more at TXHealthSteps.com Dental CE courses you can put into practice. Join 225,000+ medical professionals who get free CE with Texas Health Steps Online Provider Education. Choose from a wide range of courses developed by experts, for dental experts like you. Courses such as caries risk assessment and dental quality measures are available 24/7. Content on the Texas Health Steps Online Provider Education website has been accredited by the UTHSCSA Dental School Office of Continuing Dental Education, Texas Medical Association, American Nurses Credentialing Center, National Commission for Health Education Credentialing, Texas State Board of Social Worker Examiners, Accreditation Council for Pharmacy Education, Texas Academy of Nutrition and Dietetics, Texas Academy of Audiology, and the International Board of Lactation Consultant Examiners. Continuing Education for multiple disciplines will be provided for some online content. Texas Health Steps is health care for children birth through age 20 who have Medicaid.
Official call to the 2023 Annual Session of the Texas Dental Association
House of Delegates
House of delegates: in accordance with Chapter iv, section 70, paragraph a-1 of the texas Dental association (tDa) Bylaws, this is the official call for the 153rd annual session of the texas Dental association house of Delegates. all sessions of the House will be in the Hemisfair C-3 ballroom of the Henry b. gonzalez Convention Center, 900 e. market street, san antonio, texas. the opening session of the house will convene at 8:00 a.m. on thursday, may 4, 2023. the second meeting of the house will be at 1:30 pm on Friday, may 5, 2023. the third meeting of the house will be at 8:00 am on saturday, may 6, 2023, followed by the fourth meeting at 1:30 pm until close of business.
please see the tDa meeting website for details and additional information (www.tdameeting.com).
Component Societies are urged to certify an accurate list of Delegates and Alternates to fill each of their seats on the floor of the TDA House of Delegates.
referenCe Committee Hearings: reference Committee hearings will be facilitated in the Convention Center on thursday, may 4, 2023, and open to all members who are present (any changes to committee meeting rooms and start times will be posted on the tDa website and announced at the first meeting of the house of Delegates):
• Reference Committee A: 10:00 AM (Room 304A)
Administration, Budget, Building, House of Delegates, Membership Processing
• Reference Committee B: 11:30 AM (Room 303C)
President’s Address, Miscellaneous Matters, Component Societies, Subsidiaries, Strategic Planning, Annual Session
• Reference Committee C: 1:00 PM (Room 304B)
Dental Education, Dental Economics, Health and Dental Care Programs
• Reference Committee D: 2:00 PM (Room 304C)
Legislative, Legal and Governmental Affairs
• Reference Committee E: 3:30 PM (Room 304A)
Constitution, Bylaws, Ethics & Peer Review
the agendas for the committee hearings will be included in the reference Committee section of the Delegate materials.
138 Texas Dental Journal | Vol 140 | No. 3
referenCe Committee reports: reference Committee reports will be made available in pDF format to the members of the house of Delegates (reports may be downloaded from any location with internet access). printed copies will not be provided.
finanCial forum: the tDa secretary-treasurer will facilitate a half hour questionand-answer financial forum open to all members who are present at 10:00 am on thursday, may 4, 2023, in the same meeting room as the reference Committee a hearing.
Candidates forum: the aDa & tDa Candidates Forums will be held on Friday, may 5, 2023, from 10:30 am to 12:00 pm in the Convention Center (room assignment to be posted on the tDa website and announced at the first meeting of the house of Delegates).
divisional CauCuses: Divisional Caucuses (northwest, northeast, southwest, southeast) will be facilitated at 5:30 pm on Friday, may 5, 2023, in the Convention Center and is open to all current members—please see the tDa website for details and additional information (room assignments to be posted on the tDa website and announced at the first meeting of the house of Delegates).
delegate materials: in accordance with tDa Bylaws, the house documents will be available 30 days prior to the annual session of the house of Delegates. the supplements to the house documents, containing the agenda and subsequent reports, will be sent after the april 2023 tDa Board of Directors meeting. the minutes of the tDa Board shall be posted on the members’ side of the tDa website and made available to the general tDa membership once the minutes are approved by the tDa Board of Directors in accordance with policy 26-2018-h. Delegates and alternates will receive all house Documents in pDF format. printed copies of the house Documents will not be provided. Wireless internet access will not be available in the House chamber—please download all House materials on a fully charged laptop or device prior to attendance (charging stations will be centrally located in the meeting rooms).
www.tda.org | April 2023 139
Official call for nominations
OFFICIAL CALL FOR CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT
NOMINATIONS: SPEAKER OF THE HOUSE, SECRETARY-TREASURER, AND EDITOR
OFFICIAL CALL FOR SPEAKER OF THE HOUSE CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of texas Dental association (tDa) speaker of the house may be submitted to tDa secretarytreasurer Dr Carmen p smith for the upcoming 2023 house elections. only an active, life, or retired member in good standing of this association shall be eligible. a curriculum vitae (Cv) must be submitted, and the candidate will also have to sign a conflict of interest statement. nominations are in order at the first meeting of the house of Delegates and remain open until the close of the second meeting of the house of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility may be verified. to become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the house of Delegates. please see the manual on Caucus, Campaigns, nominations and elections at tda.org for full details.
Duties of the speaker of the house are enumerated in the Bylaws and include the following:
1. to serve as an ex-officio member of the Board of Directors without vote or the privilege of proposing resolutions.
2. to serve as an ex-officio member of the executive Committee without vote or the privilege of proposing resolutions.
3. to preside at all meetings of the house of Delegates.
4. to determine the order of business for all meetings, subject to the approval of the house of Delegates, in accordance with section 140B of this chapter.
140 Texas Dental Journal | Vol 140 | No. 3
5. to appoint tellers to assist him/her in determining the result of any action taken by vote.
6. to appoint members of reference committees in consultation with the president, president-elect, and the immediate past president by the Board of Directors’ first meeting of the calendar year.
7. to notify the divisional officers and the Committee on Credentials, rules and order, prior to the annual session, the number of delegates and alternates necessary to constitute a quorum.
8. to meet with the divisional officers prior to the meeting of the divisional caucuses at the annual session to review the rules for Caucus procedures, nominations, and elections.
9. to appoint a parliamentarian pro tem, should it become necessary for the parliamentarian to be absent during a session of the house of Delegates.
10. to serve as presiding officer of the tDa Candidates Forum, unless the speaker is in a contested race, at which time the speaker pro-tem will preside.
11. to be a certified parliamentarian or be in the process of certification
Candidacy announcements are to be mailed to tda secretary-treasurer dr Carmen p smith, texas dental association, 1946 s iH-35 ste 400, austin, texas 78704; or, emailed to tda executive director linda brady: lbrady@tda.org.
(See TDA Bylaws, Chapter IV, House of Delegates—Sections 100 (Officers), 110A (Duties), 150C(3), 150D, Chapter V, Board of Directors—Sections 10 (Composition); TDA House Manual; Speaker Manual).
OFFICIAL CALL FOR SECRETARYTREASURER CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of texas Dental association (tDa) secretary-treasurer may be submitted to tDa secretary-treasurer Dr Carmen p smith for the upcoming 2023 house elections. only an active, life, or retired member in good standing of this association shall be eligible. a curriculum vitae (Cv) must be submitted, and the candidate will also have to sign a conflict of interest statement. nominations are in order at the first meeting of the house of Delegates and remain open until the close of nominations at the end of the second meeting of the house of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility can be verified. to become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the house of Delegates. please see the manual on Caucus, Campaigns, nominations and elections at tda.org for full details.
Duties of the tDa secretary-treasurer are enumerated in the Bylaws and include the following:
1. serve as chair, without vote, of the Budget, assets and Finance Committee.
2. examine the income and expenses of this association and report at each meeting of the Board of Directors.
3. ensure that the minutes of the house of Delegates and the Board of Directors be maintained.
4. to be responsible and perform such other duties as shall be specified by the Board of Directors and the Bylaws.
other duties as secretary include the following:
• Serve as recording officer and custodian of the records of the House of Delegates and the Board of Directors.
• Serve as secretary to the Executive Committee, without the right to vote.
• Serve as secretary to the House of Delegates.
• Serve as the secretary of the American Dental Association Fifteenth Trustee District Delegation.
Candidacy announcements are to be mailed to tda secretary-treasurer dr Carmen p smith, texas dental association, 1946 s iH-35 ste 400, austin, texas 78704; or, emailed to tda executive director linda brady: lbrady@tda. org.
(Ref. TDA Bylaws, Chapter IV, House of Delegates—Sections 70A-B (Notice and Publication-Official Call & Publication of Actions, 110B (Duties); Chapter V, Board of Directors—Sections 10 (Composition), 80B (Officers-Secretary); Chapter VI, Elective Officers—Section 90G (Duties); Chapter VIII, Fifteenth Trustee District American Dental Association Delegates and Alternate Delegates—Section 80 (Delegation Secretary); Board Manual; Secretary-Treasurer Manual).
www.tda.org | April 2023 141
OFFICIAL CALL FOR EDITOR CANDIDACY ANNOUNCEMENTS AND SUBSEQUENT NOMINATIONS
Candidacy announcements for the statewide elective office of texas Dental association (tDa) editor may be submitted to tDa secretary-treasurer Dr Carmen p smith for the upcoming 2023 house elections. only an active, life, or retired member in good standing of this association shall be eligible. a curriculum vitae (Cv) must be submitted, and the candidate will also have to sign a conflict of interest statement. nominations are in order at the first meeting of the house of Delegates and remain open until the close of nominations at the end of the second meeting of the house of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility can be verified. to become a nominee, a delegate must place the name of the candidate in nomination at the first meeting of the house of Delegates. please see the manual on Caucus, Campaigns, nominations and elections at tda.org for full details.
Duties of the editor are enumerated in the Bylaws and include the following:
1. to be editor-in-chief of all journals and publications of the association and exercise full editorial control over such publications, subject only to policies established by the house of Delegates, Board of Directors, and these Bylaws and provided such content is not in conflict with or contrary to the tDa’s established policies, legislative agenda, or advocacy efforts.
2. to control the selection of scientific material published in the Journal the editor may appoint associate editors, with the concurrence of the Board of Directors, to gather and/or review material for publication. such associate editors shall serve as long as the editor deems necessary; but never longer than the term of the editor.
3. to attend all open meetings of the Board of Directors and the house of Delegates of this association, and the annual session of the american Dental association.
4. to hold no other elective office in this association or the american Dental association while serving as editor, except the editor may be elected as delegate or alternate delegate to the aDa house of Delegates from his/her respective division.
5. to cooperate with his/her successor upon termination of the editor’s term of office. should the position of editor become vacant ad interim, the Board of Directors shall appoint an editor to act in the vacated position until such time as an editor is nominated and elected in accordance with Chapter v, sections 40B,b and Chapter iv, sections 30B,b and 150 of these Bylaws.
Candidacy announcements are to be mailed to tda secretary-treasurer dr Carmen p smith, texas dental association, 1946 s iH-35 ste 400, austin, texas 78704; or, emailed to tda executive director linda brady: lbrady@tda.org.
(Ref. TDA Bylaws, Chapter VI, Elective Officers—Section 90I (Duties); Policy Manual).
142 Texas Dental Journal | Vol 140 | No. 3
Official Call for Nominations: Statewide Election of TDA President-elect
Chapter vi, section 30 of the tDa Bylaws state that the president-elect shall be nominated in turn clockwise from and by the members of each of the 4 divisions—southeast, southwest, northwest, and northeast. every third year the president-elect shall be nominated on a statewide basis, which will occur in 2023. the divisional rotation of the president-elect will continue in the intervening years.
announcement of candidacy for the statewide elective office of texas Dental association (tDa) presidentelect may be submitted to tDa secretary-treasurer Dr Carmen p smith for the upcoming 2023 house elections. only an active, life, or retired member in good standing of this association shall be eligible. a curriculum vitae (Cv) must be submitted, and the candidate will also have to sign a conflict of interest statement. nominations are in order at any time until the close of nominations at the beginning of the next to the last meeting of the house of Delegates; however, announcements of candidacy should be made as early as possible so that membership eligibility can be verified.
Duties of the president-elect are enumerated in the Bylaws and include the following:
a. to preside in the absence of the president.
b. to assist the president as requested.
c. to serve as an ex-officio member of the Board of Directors and the house of Delegates.
d. to perform such other duties as may be provided in the tDa Bylaws.
e. to succeed to the office of president at the next annual session of the house of Delegates following his/ her election as president-elect.
f. to serve on the Council of Legislative and regulatory affairs.
Duties of the subsequent position of president are also enumerated in the Bylaws and include the following:
a. to serve as official representative of this association in its contacts with governmental, civic, business, and professional organizations for the purpose of advancing the objects and policies of this association.
b. to serve as an ex-officio member of the Board of Directors of the association.
c. to be presiding officer of the Board of Directors of this association.
d. to be the supervising authority of the executive Director on behalf of the Board of Directors.
e. to annually appoint the parliamentarian for the association who shall serve as the speaker pro-tem of the house of Delegates, should it become necessary for the speaker to be absent.
f. to call special sessions of the house of Delegates and Board of Directors as provided in Chapters iv and v of these Bylaws.
g. to appoint, with approval of the Board of Directors, the members of all committees and such others as may be necessary to the work of the association except as otherwise provided in these Bylaws.
h. to submit an annual report to the house of Delegates at the first session concerning his/her activities during the year and presenting such matters as should be brought to their attention or may require their action.
i. to conduct annually a presidents-presidents-elect conference for component presidents and presidents-elect.
j. to perform such other duties as may be provided in the tDa Bylaws.
nominations are to be mailed to tda secretary-treasurer dr Carmen p smith, texas dental association, 1946 s iH-35 ste 400, austin, tX 78704; or e-mailed to tda executive director ms linda g brady, lbrady@tda.org.
(Ref. TDA Bylaws, Chapter VI, Elective Officers—Section 30, Nominations, and Section 90A,B, Duties of the President and President-elect)
www.tda.org | April 2023 143
The dentist should be informed by their patients if they are taking kratom or any other herbal supplement because it can impact the prescribed dental treatment and overall oral health.

Kratom and oral HealtH: What a dentist Should Know
Dwayne Evans, DDS
Assistant Professor, UTHealth Houston School of Dentistry, Department General Practice and Dental Public Health
Stephen Laman, DDS
Associate Professor, group practice director, UTHealth Houston School of Dentistry, Department General Practice and Dental Public Health
Gary N. Frey, DDS
Professor & chair, UTHealth Houston School of Dentistry, Department General Practice and Dental Public Health
Cleverick (C.D.) Johnson, DDS, MS
Professor & Vice Chair, UT Health School of Dentistry; Director, Urgent Care Clinic
Ben F. Warner, MS, DDS, MD
Professor, UTHealth Houston School of Dentistry, Department General Practice and Dental Public Health
144 Texas Dental Journal | Vol 140 | No. 3
Mitragyna Speciosa Korth also known as kratom is derived from the rubiaceae family which grows to 4 to 16 meters high as a tropical tree that is indigenous to southeast asia, the philippines, and new Guinea but now cultivated elsewhere. its leaves have been traditionally used for medicinal and recreational purposes as well as for pain-relieving and mood-enhancing properties. kratom is not commonly known by a specific street name, but it may be referred to by its various strains or colors, such as m Da, Bali, or red vein. while kratom has been used for many years as a traditional herbal remedy, it has gained popularity as a recreational drug and is now being sold in many countries in the form of capsules, powder, and tea. in the united states, kratom is not approved for use by the u s. Food and Drug administration.
the biochemistry of kratom involves the presence of several alkaloids, including mitragynine and 7-hydroxymitragynine, which are responsible for its effects on the body. these specific alkaloids act on the mu opioid receptors in the brain, as well as on other receptors such as adrenergic, serotonergic, and dopaminergic receptors, thus producing a variety of effects which tend to be complex and still not fully understood. while it can produce some beneficial effects, its use carries a risk and should be approached with caution.1
when consumed, kratom can have both stimulant and sedative effects on the body, depending on the dose and strain of the plant. at lower doses, it can act as a stimulant that produces increased energy, sociability, and alertness. at higher doses, it can act as a sedative, producing relaxation, pain relief, and a sense of euphoria. additionally, alkaloids in kratom can also cause constriction of the blood vessels and an increase in blood pressure, which can lead to adverse effects in individuals with pre-existing cardiovascular conditions. as for long-term use of kratom, it can lead to dependency and withdrawal symptoms that include anxiety, irritability, insomnia, and muscle aches as well as a potential for interaction with other medications such as prescription opioids and sedatives causing adverse effects.2
the dentist should be informed by their patients if they are taking kratom or any other herbal supplement because it can impact the prescribed dental treatment and overall oral health. here are some specific reasons why the dentist should know if their patients are taking kratom:3
1. drug interactions: interactions with other medications that are commonly used in dentistry, such as opioids and sedatives. Combining kratom with these medications can increase the risk of adverse effects, such as respiratory depression or sedation.
2. Xerostomia: increases the risk of tooth decay, gum disease, and other oral health problems.
3. Cardiovascular risks: Can be associated with increased blood pressure and tachycardia, which can pose a risk for patients with pre-existing cardiovascular conditions.

4. Cognitive impairment: impaired cognition and coordination, which can be problematic for patients who need to operate machinery or drive after dental procedures.

5. dependence and Withdrawal: Long-term use of kratom can lead to dependence and withdrawal symptoms, which can impact a patient’s ability to undergo dental treatment and manage post-operative pain.
overall, the dentist should be aware and educate the patient on use of kratom to ensure safe and effective dental treatment and to prevent adverse effects.
references:
1. maxwell J. Jentsch, micah m pippin.statpearls publishing: 2023.

2. webmD, kratom uses and more.
3. how Does kratom affect your teeth? a Blog by FFD419/1/05/2023.

www.tda.org | April 2023 145
Dwayne Evans, DDS
STEPHEN LAMAN, DDS
GARY N. FREY, DDS
Cleverick (C.D.) Johnson, DDS, MS
Ben F. Warner, MS, DDS, MD
a Compliance Protocol for optimizing response to oral aPPlianCe tHeraPy for obstructive Sleep apnea
 Jeff Paz DDS, D-ABDSM Adjunct Assistant Professor Department of Biomedical Sciences Texas A&M University School of Dentistry, Dallas, Texas
Emet Schneiderman, PhD Professor, Department of Biomedical Sciences Texas A&M University School of Dentistry, Dallas, Texas
Jeff Paz DDS, D-ABDSM Adjunct Assistant Professor Department of Biomedical Sciences Texas A&M University School of Dentistry, Dallas, Texas
Emet Schneiderman, PhD Professor, Department of Biomedical Sciences Texas A&M University School of Dentistry, Dallas, Texas
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views or positions of the Texas Dental Association.
146 Texas Dental Journal | Vol 140 | No. 3
it is well established that oral appliance therapy (oat) is effective in treating obstructive sleep apnea (osa) of all severities if the patient is compliant.1-4 Despite the availability of recommendations for promoting compliance [5] there are no true guidelines or templates. a suggested protocol is presented here that is intended to maximize compliance. the goal of this oral appliance Compliance protocol (oCp) is not to minimize discomfort or perceived pain but rather motivate the patient to wear the appliance as much as possible during sleep. the elements of the oCp are detailed here and the response to it in 509 patients in a single dental practice is summarized.

www.tda.org | April 2023 147
Initial Consultation
this oCp strategy begins with a referral from a physician who understands oat and has conveyed to the patient a confidence in and an expectation of success with such a dental approach to a medical problem. ninety-nine percent of the patients seen in this practice were referred by a physician.
the clinical assistant (Ca) will bring the patient to the consultation room and ask if any questions can be answered. the patient coordinator (pC) is well versed with physical therapy and with various appliances available to the patient. the pC will discuss reasonable expectations and perhaps draw comparisons to medical procedures such as orthopedic procedures. During the initial consult, the dentist conducts an interactive session with the patient, first reviewing his/her sleep study, then explaining how oat can manage the airway and obstructive sleep apnea. During this phase, the patient is educated on reasonable expectations and the amount of “work” required on his/her part to obtain an acceptable clinical outcome. the patient is then advised that the therapy can only be as effective as their willingness to carry out the oCp this approach can be empowering, as it capitalizes on the patient’s interest in self-healing and promotes ownership of the condition and its resolution. this is a central tenet of oCp
this first phase requires an open discussion of pain, discomfort, and noncompliance. From previous conversations with their sleep physicians, patients will likely be aware of the potential for temporomandibular joint and occlusal change issues and may have notions of their mandibular condyles being “pulled out of
148 Texas Dental Journal | Vol 140 | No. 3
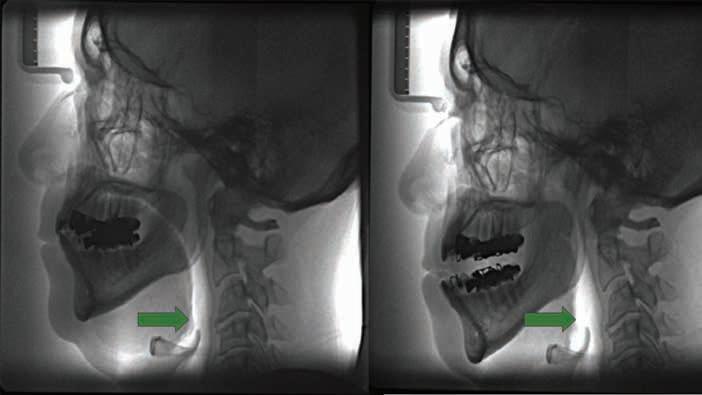
figure 1. Left, patient wearing oral appliance (OA) in neutral position. Right, patient with 2 mm of mandibular advancement. Of interest is the radiographic image of an apparent increase in pharynx size. Courtesy of Dr Trish Braga, AADSM.
their sockets” by an oral appliance. Careful explanations that do not involve contradicting the referring physician are provided. the gradual and nontraumatic advancement of the mandible is emphasized, as well as careful monitoring over a period of months by the dentist, can help reduce anxiety. Diagrams and models are then used to help the patient visualize the anatomy involved in osa and oat (see Figures 1 and 2).
Concurrent with the dentist’s initial consultation with the patient, the patient coordinator (pC) answers any insurance, financial, and clinical questions. the pC addresses misconceptions and focuses on how the patient will play a big role in their oral appliance compliance; empowerment is key. the patient will then be given an opportunity to view our physical therapy videos, oral appliance videos, along with general information regarding sleep apnea and oral appliance therapy.
key to the success of this initial consultation is that the dentist makes no assumptions regarding the patients’ understanding of their sleep breathing disorder; this opens communication during the consult. in addition to the initial oral exam and discussion of the sleep study, the potential benefits of oat for osa, and potential challenges (known risks and side effects) are discussed. the mechanism of action of different oral appliances (oa) is discussed, and all questions are answered. once the patient signs the consent forms, intra-oral scans are performed and sent to the medical manufacturer, for oral appliance fabrication. During the capture of the jaw relation record, the clinical assistant (Ca) will discuss and reinforce reasonable expectations.
the Ca will next break down the myth of the jaw going out of its socket with oat and offer a comparison of “when you bend your knee or straighten your
leg, the knee functions properly in both ways.” an introduction to orofacial physical therapy (Jaw stretching/ isometric exercises) is then provided. Briefly, the posterior portion of the masseter and anterior portion of the temporalis muscles are massaged, once-daily for one-minute. in addition, bilateral retrusion of the mandible also assists the patient in alleviating any tension in the tmJ, tendons, ligaments, and possibly in the lateral pterygoid muscle. this video link is provided as reference: sleep apnea oral appliance Jaw exercises if the patient has no further questions, they will be reminded that they may call your office and discuss any portion of the oCp at any time.
many patients (1) will have only been told that they have a sleep breathing disorder, and (2) will have been sent to another clinic to receive osa treatment using “the mask” or “the mouthpiece” with little explanation. the patient
www.tda.org | April 2023 149
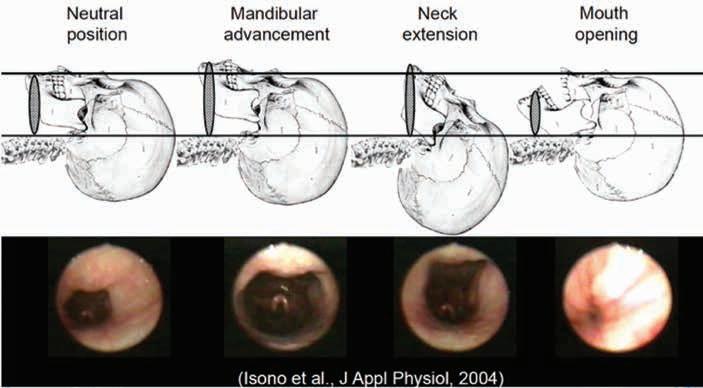
figure 2. Head, neck, and mandible positions, and corresponding airway dimensions.
Many patients (1) will have only been told that they have a sleep breathing disorder, and (2) will have been sent to another clinic to receive OSA treatment using “the mask” or “the mouthpiece” with little explanation. The patient will have had a sleep study that was interpreted and reviewed by a boardcertified sleep physician. Going over key aspects of the study is an opportunity to address questions or misunderstandings about the findings, in the hope of setting patient expectations.
will have had a sleep study that was interpreted and reviewed by a board-certified sleep physician. Going over key aspects of the study is an opportunity to address questions or misunderstandings about the findings, in the hope of setting patient expectations. For example, the dentist may highlight the time their blood oxygen level was below 90%, the nadir (oxygen low point), the apnea hypopnea index (ahi or similar measure), and the sympathetic response (fight or flight) due to difficulty breathing. osa treatment details are further explained: the titration-mechanism of action of the oa, obtaining a subjective “sleep spot” (term used to highlight the patient’s subjective experiences and corresponding mandibular advancement position, or sweet spot). specifically, during their followup appointments, patients will comment on their sleep quality, energy, and snoring levels. the dentist will determine the subjective therapeutic mandibular position and determine if maximum benefit has been achieved. if so, the patient will be referred to their pCp for a titration sleep study and test said sleep spot, where we provide the numerical data that corresponds to the patient’s subjective sleep spot. this is done with a home sleep test (hst, such as the apneaLink, see below) with the oa adjusted at the sleep spot, assuming the pCp and sleep physician deem appropriate. the importance of follow up appointments is also discussed. the need for orofacial physical therapy (jaw stretching/ isometric exercises) is highlighted as these exercises may assist the patient in increasing compliance with oral appliance therapy (oat). how the morning occlusal guide (moG) assists in compliance, and the possibilities for tooth sensitivity and movement are also discussed. this is one of the most critical components for setting the stage for patient compliance and expectations and optimizing clinical outcomes. the preceding information is provided efficiently, in no more than 10 minutes.

OA Delivery (4-weeks, typical time frame from medical manufacturer)
the Ca seats the patient and solicits questions. the Ca then demonstrates the custom-manufactured oa, verifies initial fit on models, and notes any adjustments accordingly. here the Ca highlights the custom nature of the oa, i.e., this conversation is in stark contrast to the typical durable medical equipment (Dme) provider experience which is very brief and non-individualized. the oa is placed in the patient’s mouth and they are instructed to wear it while sitting for 5 minutes, in the dental chair. once the patient appears reasonably comfortable with oa, the Ca proceeds to demonstrate a modified swallowing technique, and a nasal breathing technique. the goal of these exercises is to reduce the gag reflex by having the patient drink water with the oa in place, 1 hour prior to bed, for 4 nights. the patient may feel overwhelmed with the oa but water will allow the patient to modify their swallowing technique coupled with the calming properties of nasal breathing. again, all in hopes of calming the patient and hopefully increasing patient compliance. the patient is provided with written instructions including how to care for the oa and the possible need for analgesics for four mornings. For oas that restrict mouth opening (see below), patients are advised to use a straw. this helps reduce the amount of salivary flow along with decreasing the chances of over-stimulating the gag reflex.
150 Texas Dental Journal | Vol 140 | No. 3
reassurance is provided. the physical therapy regimen sleep apnea oral appliance
Jaw exercises as recommended by the american academy of Dental sleep medicine is demonstrated.6 this is all done to optimize patient-adaptation to the oa. although significant efforts are made to make the therapy as comfortable as possible, it is ultimately up to the patient to adapt. Lastly, the moG is fabricated; briefly, the thermoplastic material with kevlar, can be purchased from various manufacturers. the moG is heated and formed along the lower anterior teeth. the patient is instructed to bite while the moG polymerizes, typically 1-2 minutes. the patient is to perform this bite check on a daily basis, 1 minute each day. the concept behind the moG is to minimize any shifting or modification of occlusion. Lastly, the patient is encouraged to place and remove the moG followed by the oa using a mirror. the patient then signs necessary paperwork, i.e., confirmation of receipt of moG and oa.
next, the dentist speaks with the patient and verifies the fit and function of the oa and is given encouragement. the patient is reassured that some discomfort and pain is to be expected and can be managed with physical therapy and analgesics for 3 mornings; the patient is told that the latter can be effective for both orofacial pain and tooth sensitivity. the patient is advised to expect a great deal of saliva and to use an old pillowcase, if necessary. thus, drinking of water for 3 nights with the oa in place, 1 hour prior to going to bed, is reiterated. this allows the patient to become comfortable swallowing with the oa and may reduce salivary flow. the 4-week followup appointment is then scheduled.
OCP 4-week Follow Up
the Ca speaks with the patient regarding the subjective component of the therapy. a dialogue is established along the lines of “how are you doing with the appliance… how many nights per week are you wearing it, what is your sleep quality and energy level, and are you snoring?” this is performed to obtain subjective data and work toward further establishing the sleep spot. additional questions may include, “have you experienced any challenges with pt, the moG or elastics” if they are being used. Does the patient require additional elastics (i.e., for bilateral compression and bilateral interlocking oas), and if so, are they assisting in lip competency? is the patient advancing (titrating) in the prescribed manner? are the dental midlines tracking, i.e., mandibular position in the horizontal plane being held constant? For those patients experiencing mouth dryness, depending upon the oa being used, we suggest that they use the mouth-shield (midline traction) or elastics. again, the team emphasizes the importance of pt along with moG. verification of fit and function is also encouraged during the 1st-follow up appointment. prior to the dentist entering the operatory, the Ca measures the titration distance with digital calipers. if needed, an initial conversation regarding how to manage side-effects or other challenges should take place. it is advantageous for the Ca to reassure and focus on positive experiences all the while offering a solution to the challenges of side-effects. the Ca then makes any necessary modifications. the need for a titration sleep study (tss) soon is then discussed.
the dentist reassures the patient by discussing their oa experience regarding the number of nights per week it has been used, sleep quality, energy level, presence of
www.tda.org | April 2023 151
witnessed snoring; simple questions with “improved, same or worsened” as answers are asked. any challenges with pt, the moG or elastics are addressed. the need to increase or decrease titration frequency and/or pt frequency is also discussed. the need for the tss in the near future is also reiterated. this discussion always ends with “have i answered all of your questions today?” Documentation, via a letter, sent to the referring physician regarding treatment status and next office appointment is then completed.
OCP 8-week Follow Up
progress regarding the items discussed at the 4-week follow-up are again discussed between the Ca and the patient, as well as the dentist and the patient. Communication is sent to the referring physician regarding the tss Communication will state perceived “sleep spot” has been achieved as described by the patient (subjective information along with oa titration setting). if deemed to be the case, the dentist communicates to the referring physician that the patient reports that minimization of the chief complaint(s) (e.g., snoring, daytime sleepiness,
disrupted sleep or observed gasping) has been achieved and that it would be worthwhile to compare the tss to the diagnostic sleep study.
the patient is then appointed for an annual compliance appointment. the patient is also encouraged to discuss the tss with the referring physician. results should be made available to the dentist for purposes of documentation. one-week prior to the annual/compliance appointment, the patient will be sent home with a high resolution pulse oximeter or verification of osa management. a copy of the appointment notes coupled with hrpo results are all provided to the referring physician.
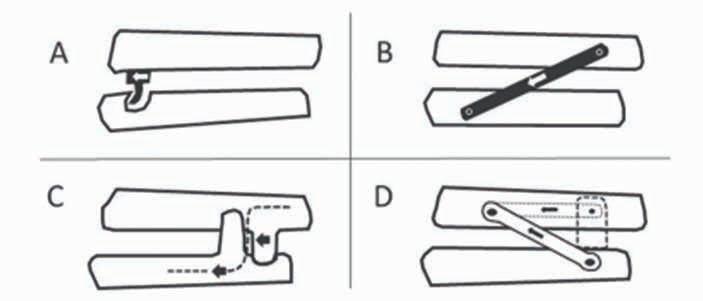
Description of OAs and their Usage
Fifteen mandibular-advancement oral appliances were used from the following companies from 2019-2022 in the practice of Jp/ rBD - owner of practice, richard Drake, san antonio, tx
all the oas were titratable and included the following modes of operation for advancing the mandible:
(a) midline traction, (B) bilateral compression, (C) bilateral interlocking and (D) bilateral traction.
152 Texas Dental Journal | Vol 140 | No. 3
essick et al. part iii oral appliance
september 2016.
therapy for sleep-Disordered Breathing, inside Dental technology,
each was presented and discussed with patients, and then selected jointly based on patient preference and clinical familiarity. except for the tap appliances, all permitted mouth-opening. the manufacturers and the types of oas provided were:
1. tap (airway management inc., Dallas, tx; midline traction)
2. somnoDent (somnomed, plano, tx; bilateral compression, bilateral interlocking).
3. ema (myerson, Chicago, iL; bilateral traction).
4. respire (whole you, new york, ny; bilateral compression, bilateral interlocking).
5. prosomnus (prosomnus, pleasanton, Ca; bilateral compression and bilateral interlocking).
6. Dynaflex, (Dynaflex, st. Louis, mo; bilateral compression, bilateral interlocking.)
7. keller (nDx keller, Fenton, mo; bilateral interlocking).
8. Device masters (Device masters, williamsburg, mi; bilateral compression).
the oa of choice was used for the duration of treatment. participants were instructed to advance their mandibles based on each manufacturer’s guidelines as follows: during the first four-weeks, patients were not to exceed one mm per week. During the 4-week follow up (test-period), patients were asked to report any subjective findings: snoring or osa events observed by bedpartner, daytime sleepiness, energy level and if they experienced any discomfort.
Home Sleep Test
home sleep test (hst) recordings were collected using the night owl (resmed, san Diego, Ca), apneaLink air (resmed, san Diego, Ca), or watchpat (itamar medical, tel aviv, israel). all of the oa devices were used per manufacturers’ recommendations. oxygen saturation (spo2 ) was measured with a finger probe pulse oximeter. all sleep recordings were collected in the patient’s home sleep environment, and each patient received instructions on how to self-apply the sensors. a minimum of 6 recorded hours without artifact was considered acceptable. all apnea and hypopnea events were visually scored using aasm 2007 scoring criteria by a board-certified sleep physician.7

Oral appliance treatment details
all appliances were adjusted/titrated to the participant’s maximal comfortable protrusive position/and or active movement by the patient in the wake state and/ or until the ahi was reduced to less than 10 events per hour. 8 the starting position was determined by the patient at a comfortable position but not less than 40% of maximum active advancement as determined by the horizontal sliding ruler. “Comfortable” is defined as no report of ongoing discomfort or pain. patients were instructed to advance their appliances based on each manufacturer’s guidelines and, during the first 4 weeks, not to exceed 1 mm per week. During the 4-week follow up, patients came to the clinic and discussed the following symptoms: snoring, observed osa events, daytime sleepiness, energy level and discomfort. patients were invited to have a clinical assistant help in the titration process; due to complexities of
www.tda.org | April 2023 153
scheduling and limited availability, most patients self-titrated. patients were given an hst kit and asked to advance their oas 1 mm every night until the ahi dropped below 10 or until they found it intolerable. once perceived maximum medical benefit was obtained, the patient was referred back to the referring provider for a titration sleep study.
each patient was custom-fitted for a morning occlusal guide to be used for up to 20 minutes. some patients used the moG immediately upon awakening while others wore it after pt regardless, all patients performed pt at least once daily for 40 seconds; this assisted in returning to habitual occlusion.
Overall Performance of the OCP
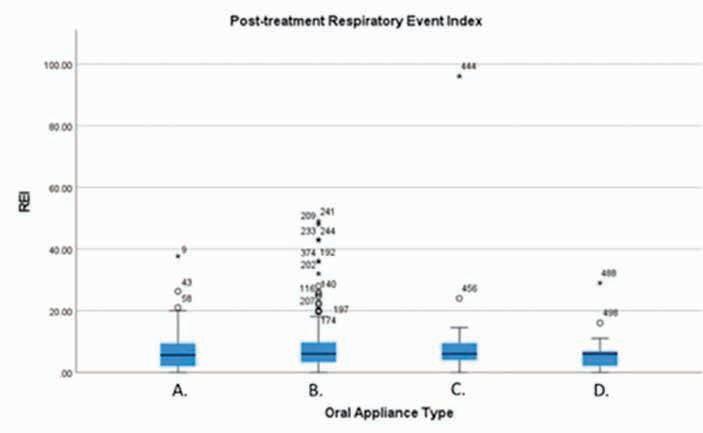
the 15 different appliances were grouped into 4 categories of similar mandibular advancement mechanisms. the respiratory event index (rei) was used to characterize the patients’ sleep disturbed breathing before and after treatment; it is widely accepted and is a more appropriate measure for hst than the apnea hypopnea index (ahi) for this private practice setting. the latter requires overnight polysomnography (psG) performed in a sleep lab where the exact duration of sleep time is measured; the former uses the time that the device is worn. the rei was measured prior to oat and again 8 to 12 weeks after the initiation of treatment.
the overall response to oat across appliance designs was substantial over this time: the median values (and their interquartile ranges, iQr) for pre- and post-treatment respiratory event index obtained from the hsts were 23 (13.25,38.35) and 6 (2,8) respectively (n = 509); the difference between these before and after medians is highly significant (wilcoxon signed rank test, p < 0.001, figure 3). in other words, on average, patients experienced 6 respiratory events per hour after treatment with the oCp, and the most typical 50% of these patients (those falling within the iQr) had reis between 2 and 8 events per hour. there were no significant differences in post-treatment rei among the 15 individual oas models nor among the 4 types (kruskal-wallis p > 0.20, Figure 3). the performance of the different oa designs was remarkably similar when the oCp was followed. these statistical results, regarding variability, sex, osa severity, and other factors, are detailed and are considered in light of other comparative studies of oa designs in a separate report.
the oral appliance Compliance protocol presented here may be somewhat more involved than what is used in many dental sleep medicine practices. it is believed that this protocol holds the patient accountable for adapting to the appliance and not having the appliance adapt to the patient. with this protocol, it is also believed that it provides reasonable clinical outcomes, excellent documentation and physician communication—all the while being able to reduce most clinical oa side effects. it is evident that if reasonable parameters are set and provided/reinforced to patients by the whole team, these clinical outcomes should be duplicated in most Dsm practices. ultimately, it is the trust and reassurance that allows us to care and help participate in osa management. all the while, patients are aware that they can call and schedule an appointment with the treating dentist for an adjustment—this relationship along with the physical therapy is important to obtaining these results.
154 Texas Dental Journal | Vol 140 | No. 3
With this protocol, it is also believed That it provides reasonable clinical outcomes, excellent documentation and physician communication— all the while being able to reduce most clinical OA side effects.
figure 3. Box plot of responses to oral appliance therapy across the four different types of devices in 509 patients. Types are: A, midline traction (N=109); B, bilateral compression (N=319); C, bilateral interlocking (N=53); D, bilateral traction (N=28). Thick black lines represent median (50th percentile) respiratory event index (REI); blue boxes represent the interquartile range, that is, the span from the 25th to 75th percentiles. The individual data points are outliers. Note the similarity of responses among the groups.
this study used de-identified data collected solely for therapeutic reasons and was determined to be “not human subjects research” by the texas a&m university school of Dentistry institutional review board (protocol irB#2023-0164).
references
1. haviv y, Bachar G, aframian D, almoznino G, michaeli e, Benoliel r. 2015. a 2-year mean follow-up of oral appliance therapy for severe obstructive sleep apnea: a cohort study. oral Dis. 21(3):386–392.
2. schneiderman e, schramm p, hui J, wilson pD, moura p, German z, mcCann a, newton m randomized trial of 2 self-titrated oral appliances for airway management. Journal of Dental research. 100(2): 155-162, 2021.
3. venema Ja, rosenmöller Br, De vries n, de Lange J, aarab G, Lobbezoo F, hoekema a mandibular advancement device design: a systematic review on outcomes in obstructive sleep apnea treatment. sleep medicine reviews. 2021 Dec
1;60:101557.
4. Labarca G, sands sa, Cohn v, Demko G, vena D, messineo L, Gell L, hess L, white Dp, wellman a, azarbarzin a. mouth Closing to improve the efficacy of mandibular advancement Devices in sleep apnea. annals of the american thoracic society. 19(7): 1185-1192, 2022.
5. radmand r, Chiang h, Di Giosia m Defining and measuring compliance with oral appliance therapy. J Dent sleep med. 2021;8(3).
6. american academy of Dental sleep medicine (aaDsm). February 8, 2023. sleep apnea oral appliance Jaw exercises. youtube. https://www.youtube.com/ watch?v=xBoe7rcQrLa&t=115s
7. Berry rB; Budhiraja r; Gottlieb DJ; Gozal D; iber C; kapur vk; marcus
CL; mehra r; parthasarathy s; Quan sF; redline s; strohl kp; ward sLD; tangredi mm rules for scoring respiratory events in sleep: update of the 2007 aasm manual for the scoring of sleep and associated events. J Clin sleep med 2012;8(5):597-619.
8. wee Jh, Lim Jh, Gelera Je, rhee Cs, kim Jw. Comparison of success criteria based on longterm symptoms and new-onset hypertension in mandibular advancement device treatment for obstructive sleep apnoea: observational cohort study. BmJ open. 2018 may 8;8(5):e021644. doi: 10.1136/bmjopen-2018-021644. pmiD: 29739785; pmCiD: pmC5942426.
www.tda.org | April 2023 155
DENTAL
less chairside, more income
Are you a Dentist who is becoming tired of working chairside, near the end of your career, or merely looking for supplemental income? Dental Expert Witness work could be the answer for you!
Until now there have been no lectures and no instruction available on what it is, what it takes, and how to market yourself as an Expert Witness. Our exclusive workshop is the first ever of its kind!
Using their 30 years of experience, Dr. Boeke DDS & Dr. Krueger DDS/JD have created a 2 day workshop on the beautiful Texas A&M-Commerce campus, that will teach you the ins and outs of becoming an Expert Witness in a way that is informative, effective, and fun.
- what it is to BE a Dental Expert Witness




- how it helps serve your peers and community
- how it generates additional income outside of the chair

-how to market yourself as an Expert Witness.
- Dr. Krueger’s firsthand records and depositions of trials past
- mock testimonies based on those trials, complete with testimony from a witness stand

- end your day with a Texas BBQ experience on Dr. Boeke's Ranch
For an exclusive experience, our program is limited to 10 seats per sessio n!
$2,895.00
For more information, class dates, and to reserve your seat, please visit www.drbradboeke.com
Oral and Maxillofacial Radiology Interpretation Service


*Comprehensive, clinically oriented radiology reports
*Reassurance for exclusion of occult pathology
*Annotated images of relevant findings
*In-depth assessments aiding patient understanding
*Easy to use, HIPAA compliant image sharing portal
*2-4 day business day turn around time
156 Texas Dental Journal | Vol 140 | No. 3
EXPERT witness training
DAY ONE - learnDAY TWO - experience -
346-221-0316


www.tda.org | April 2023 157 MCNA Dental is a provider-centered organization committed to helping dentists serve Medicaid and CHIP enrollees. We provide dentists with leading-edge technology and superb customer service support to reduce missed appointments and encourage patients to seek timely dental care. Visit our website at www.MCNATX.net for more information.
SPOTLIgHT
Each Member Has a Story
Dr Richard “Wick” Alexander of Arlington
is likely a household name among orthodontists for his profound influence on this branch of specialty. he created the alexander Discipline, a philosophy of orthodontic treatment utilizing a specific bracket system that he designed, which is used by dentists around the world.
But, it’s in amarillo, texas, that a mentee of Dr alexander keeps his memory alive through an old american elm tree. on the 1-year anniversary of Dr alexander’s passing (april 21, 2022), Dr phil Corbin shines the tDa member spotlight on his close friend.
Dr Corbin says that Dr alexander made every person feel cared for and special. “his passion was excellent, patient-focused orthodontics with an emphasis on long-term stability.”
Drs Corbin and alexander both grew up in amarillo and graduated from amarillo high school, 12 years apart. they both attended texas tech university from which Dr alexander graduated, and Dr Corbin finished at west texas a&m university. they both continued on to the university of texas Dental Branch. “he was an outstanding orthodontist,” Dr Corbin says. “he developed a treatment philosophy that i personally used in my practice for over 40 years!”
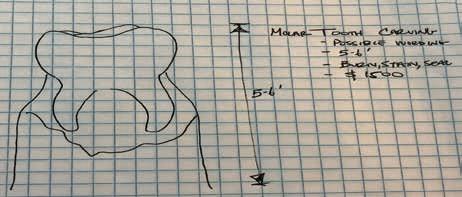
“All our wisdom is stored in the trees.”
Dr alexander’s approach to orthodontic treatment had such an impact on Dr Corbin that he created a very special memorial in his honor. “i had a 70-yearold, 80-foot tall american elm tree in my backyard that died last year,” says Dr Corbin. From this unconventional blank canvas grew an idea.

Dr Corbin hired a chainsaw sculpture company from Lubbock to carve a lower right first molar out of the 10-foot tree trunk. he then commissioned a former patient to construct a brace, identical in scope to the american orthodontics alexander Lts system molar band, to fit the tooth sculpture.
Complete with a scaled replica of an alexander signature lip bumper tube, the dead elm tree had a new lease on life. “ the brace was fabricated with the exact specifications as to what Dr alexander had designed and patented in his appliance,” explains Dr Corbin.
158 Texas Dental Journal | Vol 140 | No. 3 member
― santosh kalwar, nepalese poet
Pictured are Drs Wick Alexander and Phil Corbin.
Dr Phil Corbin used his 70-year-old American elm to create a memorial for his friend and mentor Dr Wick Alexander.
he says the tree’s bracket has a -6° tip back, -10° lingual crown torque, and 8° distal rotation. it even has a .017x.025 archwire (with a tie back hook) that is placed into the bracket and held in place with bungee cords that look like rubber bands to keep the teeth consolidated and the wire from shifting around and poking the “cheek!”
Dr Corbin says Dr alexander’s wisdom influenced the treatment mechanics and motivational techniques of orthodontists from around the world. he would often refer to the k i s s principle (keep it simple, sir), says Dr Corbin. “he felt that the type of treatment that is easier and more convenient for the patient will also
reduce stress on the orthodontist and staff and shorten treatment time. he also felt that the patient’s time was as valuable to them as his time was to him.”
and, if all our wisdom is stored in the trees, as the nepalese poet santosh kalwar says, Dr alexander’s influence lives on for years to come in the elm tree in Dr Corbin’s backyard and as treatments advance.

“Dr alexander would often say, ‘if your only tool is a hammer, everything looks like a nail,’ which meant that orthodontists need to individualize their treatment mechanics and not let the newest appliance or fad dictate the type of treatment the patient receives.”

www.tda.org | April 2023 159
Dr Corbin’s sketch of the memorial for Dr Alexander.
The final product of the memorial with exact specifications to Dr Alexander’s bracket system.
Dr Corbin hired a company to carve a tooth sculpture out of the 10-foot stump of the dead elm tree.
ORAL
and maxillofacial pathology case of the month
AUTHORS CLINICAL HISTORY
ida ann varghese, bds, dds

Department of Diagnostic and Biomedical Sciences, The University of Texas Health Science Center at Houston, School of Dentistry, Houston, Texas
nadarajah
vigneswaran, bds, dmd, dr med dent

Department of Diagnostic and Biomedical Sciences, The University of Texas Health Science Center at Houston, School of Dentistry, Houston, Texas
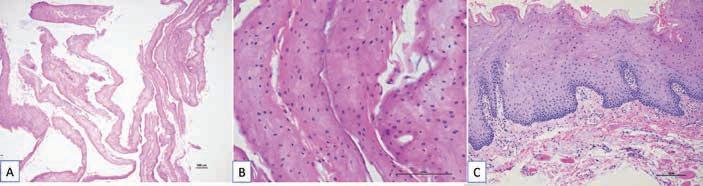
a 62-year old african-american female presented with a chief complaint of “my skin inside my mouth is peeling.” the patient had experienced sloughing of the oral mucosa for 2 months, which occasionally caused discomfort while talking and eating (Figure 1a-C). she brought with her a petri dish with small whiteish-tan colored pieces of tissue that she collected from her mouth (Figure 1D). the patient denied taking any new medications preceding the mucosal sloughing and denied pain or a burning sensation to spicy or acidic food or beverages. she also denied having a dry mouth or altered taste. the patient reported that the mucosal sloughing occurs continuously throughout the day. her medical history included hypertension, hypercholesteremia, overactive bladder and osteoarthritis. she reported taking lisinopril, Crestor, solifenacin (vesicare™) and otC-multivitamins. the patient’s surgical history was significant for appendectomy, C-section, hysterectomy and left coronoidectomy for temporomandibular joint (tmJ) osteoarthritis. she reported no allergies to medications, foods, metals or cosmetics, and her family history was significant for hypertension and diabetes. she had no history of cigarette smoking and rarely consumes alcohol. the patient had limited mouth opening, 2-fingers width due to previous tmJ surgery. Bilaterally, the buccal mucosa, along with the mandibular and maxillary buccal vestibule, ventral tongue, and floor of the mouth (nonkeratinized oral mucosal sites) showed a diffuse white homogeneous film/tissue-like surface covering which easily peeled away (Figure 1). the sloughed mucosal surfaces were non-painful and appeared normal in color without erythema, erosion or ulceration. the remainder of the oral soft tissue examination was unremarkable. the patient’s salivary flow was within normal limits. an incisional biopsy was taken from the left buccal mucosa adjacent to an area of mucosal sloughing.
What are your differential diagnoses?
Biopsy findings
microscopic examination of the biopsy specimen revealed a hyperparakeratinized stratified squamous epithelium and detached strips of desquamated parakeratin layers (Figure 2 a-B). the underlying lamina propria was composed of fibrovascular connective tissue which was devoid of inflammation (Figure 2C).
What is your most likely diagnosis?
See page 168 for the answer and discussion
160 Texas Dental Journal | Vol 140 | No. 3

www.tda.org | April 2023 161
Figure 2. An incisional biopsy of the irritant contact stomatitis reveals strips of detached parakeratin (A and B), hyperparakeratosis of the epithelial surface and the lack of inflammation in the underlying lamina propria (C).
Figure 1. Irritant contact stomatitis resulting from frequent use of Listerine mouthwash. White tissue-paper like peeling and sloughing of the buccal mucosa and labial sulcus (A & B). Detached desquamated and degenerated strips of keratinocytes coat the tongue surface (C), which was collected and brought by the patient in a petri dish (D).
ethics corner
tDa Council on ethics and Judicial affairs
What are the ethical considerations of using video social media platforms such as TikTok in your dental practice?

kathleen nichols, DDs
Qsome of my colleagues are using social media platforms like tiktok to create short videos to appeal to a larger patient population, to build their practice bases, and to educate patients. some of these videos can be shared in the form of duets whereby other dentists can opine on the post. so, if 1 dentist posts a video of their treatments, a second dentist can repost the video and comment if this feature is enabled by the content creator, giving their “professional” opinion, without the full knowledge of the patient’s dental history, consent, or specific case details. these “ tiktok Dentists” are providing generalized treatment recommendations and have no specifics of the patient in question. i do not want to be left behind, but i wonder what the ethical considerations of this social media platform are in the world of modern dentistry.
162 Texas Dental Journal | Vol 140 | No. 3
This article is a reprint of a previously published article. For citation purposes, please use the original publication details; Nichols K. What are the ethical considerations of using video social media platforms such as TikTok in your dental practice? The Journal of the American Dental Association (JADA). 2022; 153(12):1191-1192. https://doi.org/10.1016/j.adaj.2022.08.010.
Asocial media video applications offer free and potentially viral forms of communication that appeal to everyone, from Generation z to baby boomers. in addition to reaching new audiences with generalized and viral video content, this form of communication also allows users to duet other content creators’ videos and share their own opinions or advice on the topic. when videos on platforms like tiktok are liked or viewed, the platform’s algorithm fills the user’s feed with similar videos based on the topics with which they have interacted.1 For example, if you are an avid reader and watch videos about book reviews, you will be targeted with content created by creators who also love books. some users dub these genres as Booktok, Dentaltok, and so on, depending on the topic of videos viewed regularly.
social media is used widely among both patients and providers. tiktok, in particular, seems to be gaining momentum and, like other forms of social media use, presents both risks and opportunities. in recognition of that, consideration of some of the ethical parameters of dentists using tiktok are worthy of consideration. the introduction to the american Dental association principles of ethics and Code of professional Conduct (aDa Code) states that “the profession makes a commitment to society that its members will adhere to high ethical standards of conduct.”2 Furthermore, the preamble to the aDa Code states that “dentists should possess traits of character that foster adherence to ethical principles. Qualities of honesty, compassion, kindness, integrity, and fairness, help to define the true professional.”2 although these sections were developed long before the advent of tiktok and other social media applications, the message they convey is still applicable and relevant.
the aDa Code section 1 addresses patient autonomy (“self-governance”), including the patient’s privacy and confidentiality of their information. “the dentist has a duty to respect the patient’s rights to self-determination and confidentiality.”2 Dental care professionals who post videos that are meant to influence and educate patients about particular treatments without knowing the patient’s history or specific information about the patient may be unduly influencing patients in their decision making and therefore interfering with true self-determination. Care also must be taken to protect the confidentiality of patients when using a case history or patient’s images in these videos. in fact, in sharing this information, the dentist must be aware of not only potential ethical implications but legal implications as well, including applicability of the health insurance portability and accountability act and any relevant state laws regarding patient privacy.3
Furthermore, section 2 of the aDa Code, nonmaleficence (“do no harm”), states, “ the dentist has a duty to refrain from harming the patient.”2 specifically, section 2.G., personal relationships with patients, may apply when a dentist posts a video that includes a particular patient. this may “risk the possibility of exploiting the confidence placed in them by a patient” if the dental care professional posts videos in instances that could be considered unprofessional or questionable or that might portray the patient in an unfavorable light.2 again, the dentist, if using a video regarding a specific patient, must be sure that the patient has provided their informed consent in adherence with the principle of patient autonomy. the dentist also must be mindful of not potentially harming other patients. when the information in the video is used in a generalizable way, without sufficient acknowledgment that each patient’s circumstances may differ, it is potentially harmful to other patients. the dentist
viewing the tiktok should be mindful that although the material may have some educational benefit to how they might manage a similar situation, what is presented on tiktok is general and should not replace sound professional judgment.
section 3, Beneficence (“do good”), is also applicable. “ the dentist has a duty to promote the patient’s welfare.”2 this directive may support use of social media platforms if the information is educational. these types of social media platforms could be used to provide a community service such as encouraging dental health, dental education, or overall community service. the aDa Code obligates dentists to “use their skills, knowledge and experience for the improvement of the dental health of the public.”2 however, we must always keep in mind that “dentists in such service shall conduct themselves in such a manner as to maintain or elevate the esteem of the profession.”2 so, when using a platform like tiktok, the dentist should be careful to be accurate, truthful, and protective of individualized patient information.
the principle of Justice (“fairness”) obligates dentists “to treat people fairly.”2 this obligation of dentists is not only toward patients but peers and the dental team as well. section 4.C., Justifiable Criticism, might be applicable in the context of dueting. any dentist commenting on or responding to the recommendations and work of another dentist should be careful to not disparage another dentist publicly. “Dentists issuing a public statement with respect to the profession shall have a reasonable basis to believe that the comments made are true.”2 if critical of the work of another dentist, airing that criticism in a public forum such as tiktok may not be appropriate without
www.tda.org | April 2023 163
first addressing the concern with the dentist in question or, if necessary, discussing with one’s constituent or component society.
Finally, section 5, veracity, addresses issues related to “truthfulness”: “ the dentist has a duty to communicate truthfully.”2 specifically, dentists are responsible for “communicating truthfully and without deception, and maintaining intellectual integrity.”2 For example, making unsubstantiated recommendations would be considered unethical as would any type of advertising or marketing that is false or misleading.
social media platforms are here to stay. they are an effective method of communication for existing and prospective patient engagement. a 2021 article by zenone and colleagues acknowledges that “public health is served by paying urgent attention to the potential health-related implications and opportunities of tiktok” and suggests “a research agenda to inform decision-makers, health providers, researchers and the public.”4 Dentists should be mindful of these questions. the ethical dentist and, by extension, auxiliary dental staff members must take measures to ensure adherence to the aDa Code in day-to-day practice as well as when engaging in social media in their professional capacity. although giving generalized oral health care tips may be beneficial to social media users, specific treatment recommendations should be made only once a dentist-patient relationship has been established. in addition, dentists engaging with the social media of another dentist must be sure to avoid unjustifiable criticism of peers, protect patient privacy, and maintain the integrity of the profession as a whole.
https://doi.org/10.1016/j.adaj.2022.08.010
Copyright ª2022 American Dental Association. All rights reserved.
This article was reprinted with permission from The Journal of the American Dental Association (JADA) and published in JADA, Vol 153, Issue 12, Kathleen Nichols, DDS, What are

the ethical considerations of using video social media platforms such as TikTok in your dental practice?, pp 1191-1192, ©2022 American Dental Association (ADA). Reprinted with permission from the ADA. All rights reserved.
Dr Nichols practices general dentistry in Lubbock, Texas, and is a member of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs. Address correspondence to the American Dental Association Council on Ethics, Bylaws and Judicial Affairs, 211 E Chicago Ave, Chicago, IL 60611.
Disclosure: Dr Nichols did not report any disclosures.
Ethical Moment is prepared by individual members of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs (CEBJA) or guests of CEBJA, in cooperation with The Journal of the American Dental Association. Its purpose is to promote awareness of the American Dental Association Principles of Ethics and Code of Professional Conduct. Readers are invited to submit questions to CEBJA at 211 E Chicago Ave, Chicago, IL 60611, email ethics@ ada.org.
The views expressed are those of the author and do not necessarily reflect the opinions of the American Dental Association Council on Ethics, Bylaws and Judicial Affairs or official policy of the ADA.
references
1. hermann J. how tiktok is rewriting the world. new york times. march 10, 2019. accessed september 8, 2021. https://www.nytimes.com/2019/03/10/ style/what-is- tik-tok.html
2. american Dental association. american Dental as- sociation principles of ethics and code of professional conduct, with official advisory opinions revised to november 2020. accessed september 8, 2021. https:// www.ada.org/en/ about-the-ada/principles-of-ethics-code- ofprofessional-conduct
3. health insurance portability and accountability act, 42 usC § 201 et seq. (42 u s.C. 1320d-2) (1996).
4. zenone m, ow n, Barbic s tiktok and public health: a proposed research agenda. BmJ Global health. 2021;6:e007648.
164 Texas Dental Journal | Vol 140 | No. 3
The ethical dentist and, by extension, auxiliary dental staff members must take measures to ensure adherence to the ADA Code in dayto-day practice as well as when engaging in social media in their professional capacity.
Your practice is one of your most important assets. DO YOU KNOW WHAT IT’S WORTH?

While no one likes to think about it, things do happ
While no one likes to think about it, do happen and it’s always important to be prepared.
Knowing your practice’s value can make the differe your value can make the difference between selling your practice or having it become unsellable. That your or it become unsellable. That is why practice owners should have an up-to-date practice valuation.
A Henry Schein Dental Practice Transitions valu Schein Dental Practice Transitions valuation considers both tangible and intangible assets of th considers both tangible and intangible assets of the practice and can provide the many key factors which influence the p the many key factors which influence the practice’s value.
To get started on your practice valuation or schedule a complimentary, confidentia confidential consultation, contact me or scan the QR c me scan code!
 Kristi Eisel
Kristi Eisel
Transition Sales Consultant Transition 405-590-9694
Kristi.Eisel@henryschein.com

www.henryscheinDPT.com
CBCT AND IMAGING SERVICES:

• Comprehensive structured reports for all scans, with images
• We can also perform scans for your patients at several resolutions based on your diagnostic task
• iCAT, Morita Accu-i-tomo, CS9000 CBCT units
• HIPAA compliant image upload


• 24-hour turnaround time for all reports (business days)
• Provide interpretation service for all specialties
• Three board-certified radiologists with a combined experience of 55 years and several thousand scans
• Neuroradiology consult as needed at no additional cost
• Liability coverage for reports through Texas A&M University Imaging Center at School of Dentistry, Dallas
• Critical incidental findings reported immediately via phone, with recommendations for follow-up
• The only IAC accredited CBCT imaging facility at a dental school in the State of Texas that accepts medical insurance.
CHECK US OUT:
The Imaging Center
Tel: 214|828|8479
Email: codimagingcenter@tamu.edu
Radiologists in the Imaging Center:
Dr. M. K. Nair DMD MS Lic.Odont.(Sweden), PhD, Dipl ABOMR, Professor & Director
Dr. Hui Liang DDS MS PhD, Dipl ABOMR, Professor
Dr. Mehrnaz Tahmasbi-Arashlow DDS, Cert (OMR), Dipl ABOMR, Clin Asst Professor
Ms. Crystal Malek: Clinic Coordinator, Imaging Center Imaging Center

www.tda.org | April 2023 165
© 2023 Henry Schein, Inc. No copying without permission. Not responsible for typographical errors.
n C C n n B Y
Free Dental Practice Valuation Take the 1st step in selling your dental practice. Contact us to receive a free practice valuation.
469-222-3200
Terry Watson, D.D.S. Jeremy Brown, J.D. Frank Brown, J.D., LL.M.
Calendar of events
TDA Meeting May 4-6, 2023 • San Antonio (tdameeting.com)
tmom 2023 events
tmom abilene: July 14-15, 2023
tmom edinburg: september 15-16, 2023
Due to COVID-19, please check each meeting’s website for up-to-date information related to cancellations or rescheduling.
the TExAS DENTAL JOURNAL’S CaLenDar will include only meetings, symposia, etc., of statewide, national, and international interest to texas dentists. Because of space limitations, individual continuing education courses will not be listed. readers are directed to the monthly advertisements of courses that appear elsewhere in the Journal.
Those in the dental community who have recently passed
r Jeffrey Colquitt
Dallas
9/29/45–5/8/22
Good Fellow: 1998
Life: 2010
Fifty year: 2022
bobby W
Holland
Fort worth
4/6/35–1/31/23
Good Fellow: 1989
Life: 2000
Fifty year: 2014
James
Cundiff ii
Dallas
2/7/34–3/13/23
Good Fellow: 1984
Life: 2000
Fifty year: 2010
Dallas, Texas
Comprehensive Dentistry at Texas A&M University School of Dentistry invites applications for the Director of the Advanced Education in General Dentistry (AEGD) Residency Program. This is a full-time tenure track or tenure review upon hire, 11-month academic appointment beginning as quickly as possible. Responsibilities include coordinating clinical activity, supervising patient care, evaluating resident professionalism, clinical progress/performance, counseling residents. Position includes clinical and didactic teaching in ALL areas of comprehensive dentistry. Salary and academic rank commensurate with qualifications and experience of selected applicant. Interested individuals should have a strong commitment to teaching and service. Opportunity for extramural private practice is available.
Learn more and or apply at https://faculty.tamu.edu/Positions
www.tda.org | April 2023 167 in memoriam calendar
Texas A&M University is an Equal Opportunity/Affirmative Action/Veterans/Disability employer committed to building a culturally diverse educational environment. Applications from veterans, individuals with disabilities, women, minorities, and members of other underrepresented groups are strongly encouraged.
ORAL
and maxillofacial pathology diagnosis and management—from page 169
Diagnosis: Irritant contact stomatitis also known as dentifrice induced desquamation
Discussion
upon further questioning, the patient reported that she started using Listerine oral rinse frequently because of the limited mouth opening and difficulty in brushing her teeth. she also acknowledged that the mucosal sloughing began after she started rinsing her mouth with Listerine. Complete resolution of the mucosa sloughing was achieved once she discontinued the mouth rinse.
irritant contact stomatitis (also known as oral mucosa peeling, oral sloughing, oral mucosal desquamation) is clinically analogous to contact irritant dermatitis which is the most common form of contact dermatitis.1,2 irritant contact stomatitis is less prevalent than irritant contact dermatitis, the most common type of occupational skin disease.2,3 irritant contact stomatitis is caused by disruption of the mucosal barrier by chemical agents resulting in direct cellular toxicity followed by activation of innate immune responses. mouthwashes and toothpastes containing anionic sodium lauryl

sulphate (sLs), pyrophosphates, or essential oils disrupt the mucosal protective barriers resulting in epithelial desquamation.3 toothpastes with high sLs content and Listerine are the most frequently cited oral care products causing irritant contact stomatitis.3 irritant contact stomatitis appears as grey to white thin films of oral epithelium that sloughs easily. most often irritant contact stomatitis is asymptomatic and, therefore, patients may not even be aware its presence in the mouth. hence, irritant contact stomatitis is frequently diagnosed as an incidental finding during a periodic oral examination. the most frequently involved areas are the oral vestibule, buccal mucosa and gingiva. treatment for irritant contact stomatitis includes obtaining a careful history to identify the offending agent followed by discontinuing its use. a systematic review documented that resolution of symptoms occurred between 24 hours to 3 weeks after discontinuation of the offending toothpaste or mouthwash with accompanying use of an alternative biologically inert dentifrice.3
allergic contact stomatitis, on the other hand, results from type iv delayed-type hypersensitivity reactions involving both innate and acquired immune responses. the offending allergens are often smaller molecular weight chemicals (haptens) that penetrate and combine with oral epithelial proteins to form the antigenic allergen. after the initial exposure to an allergen, a pro-inflammatory mucosal change occurs without clinical signs or symptoms. allergic contact stomatitis develops during subsequent exposures following the activation of antigenspecific effector and memory t cells. exposure to the offending allergen most commonly occurs through the topical contact route, typically occurring on the buccal mucosa and lateral surfaces of the tongue and often as a result of cinnamon flavored drinks, chewing gum, and candy. Figure 3 illustrates a case of allergic contact stomatitis caused by cinnamon flavored nicorette gum. the patient is a 65-year-old female who presented with oral burning, pain, and white patches with focal erythema involving the buccal mucosae and lateral surfaces of the tongue bilaterally (Figure 3). the patient had experienced symptoms for more than 1 year. her primary care physician and dermatologist diagnosed her condition as oral candidiasis and treated her with multiple courses of antifungal medication without resolution of her symptoms. an incisional biopsy of the red and white patch from her left buccal mucosa revealed a histologic diagnosis
168 Texas Dental Journal | Vol 140 | No. 3
Figure 3. Allergy contact stomatitis resulting from the use of cinnamon flavored Nicorette gum: Diffuse white patches with focal erythema involving the buccal mucosa (A and B) and lateral surface of the tongue (C).
of lichenoid mucositis with perivascular lymphoplasmacytic infiltrate suggestive of allergic contact stomatitis (Figure 4). Further questioning revealed that the patient had been using cinnamon flavored “nicorette chewing gum” as an aid for smoking cessation. the patient was treated with a course of corticosteroids and was advised to discontinue the cinnamon flavored nicorette gum. she reported complete resolution of her symptoms after completing treatment and substituting cinnamon-flavored nicorette gum with non-flavored nicorette gum. Critical differences in the etiology, pathogenesis and clinical findings between irritant contact stomatitis and allergic contact stomatitis are listed in table 1.
other differential diagnoses for contact irritant stomatitis include leukoedema, pseudomembranous candidiasis/ thrush, mucosal burns, and oral lichen planus. Leukoedema, often an incidental finding on oral examination, is asymptomatic and is considered a variation of normal. it occurs symmetrically in the buccal mucosa as a diffuse grayish-white milky surface which dissipates with stretching of the mucosal surface. pseudomembranous candidiasis (thrush) is an acute candidal
Figure 4. An incisional biopsy of the allergic contact stomatitis reveals hyperparakeratosis, acanthosis with elongated rete ridges, and lichenoid
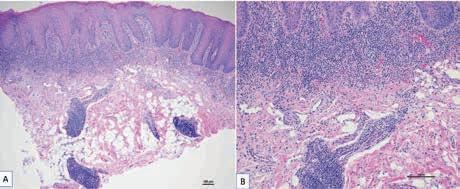
infection presenting as diffuse soft white plaques that can be wiped away leaving a painful erythematous and eroded surface.4 a mucosal burn is caused by the topical application chemicals such as aspirin or other caustic agents including phosphoric acid-etching solution or gel. Chemical burns, resulting from coagulative necrosis of the mucosal surface, present as a white sloughing membrane that can be wiped away leaving a denuded and erythematous surface. Lichen planus is one of the most common immune mediated oral mucosal inflammatory diseases and presents as asymptomatic diffuse white patches/plaque with striations (reticular form) or red patches with fine white striae, and focal erosions/ulcerations (erythematous or atrophic form).4 Lichen planus affects surfaces lined by stratified squamous epithelium including the skin, oropharynx, esophagus, and vulvovaginal mucosa.4
references:
1. tosti, a., B.m piraccini, and a m peluso, Contact and irritant stomatitis. semin Cutan med surg, 1997. 16(4): p. 314-9.
2. scheinman, p.L., et al., Contact dermatitis. nat rev Dis primers, 2021. 7(1): p. 38.
3. wang, D. and s.B. woo, histopathologic spectrum of intraoral irritant and Contact hypersensitivity reactions: a series of 12 cases. head neck pathol, 2021. 15(4): p. 1172-1184.
4. vigneswaran, n. and s. muller, Diagnosis of oral mucosal inflammatory and ulcerative diseases. Clinical Dentistry reviewed, 2020. 4(1): p. 17.
irritant contact stomatitis allergic contact stomatitis
etiology
Chemicals that exert irritant cytotoxic effect small reactive chemicals (haptens), modify proteins and induce immune responses
Common causative Listerine mouthwash, toothpastes with high sodium Cinnamon flavored gums, mint flavored agents lauryl sulfate (sLs) content; tartar control toothpaste gums, amalgam
pathogenesis
Direct cytotoxic effect the surface epithelium t-cell mediated delayed hypersensitivity reaction susceptible individuals all a minority areas affected topically at the contact site initially at the contact site, but extending later to adjacent sites
Clinical signs mucosal sloughing, peeling; white plaques, sensitive and painful white plaques chemical burn, minimal erythema and pain with erythema, surface erosions
histopathology hyperparakeratosis with superficial epithelial surface epithelial spongiosis, exocytosis of degenerative changes. minimal inflammation neutrophils and lymphocytes, interface mucositis in the lamina propria with perivascular lymphocytic infiltrate in the lamina propria
treatment identification and elimination of causative agent identification and avoidance causative allergen, topical corticosteroid treatment
www.tda.org | April 2023 169
mucositis with deep perivascular lymphoplasmacytic infiltrate.
Table 1: Comparison of irritant contact stomatitis with allergic contact stomatitis
It always seemed like an injustice to me to represent revenue in just a few simple lines, given there are so many inputs to those numbers. Revenue reflected is the result of patients entering your facility, receiving treatment, and you getting paid for the work.
Seems pretty simple, right?
Except there are so many decisions that go into that equation.
We’re on the precipice of another recession.
 By Nicholas Partridge, President; Five Lakes Dental Practice Solutions
By Nicholas Partridge, President; Five Lakes Dental Practice Solutions

170 Texas Dental Journal | Vol 140 | No. 3
Here’s how you can maintain control of your revenue.
Provided by: PERKS p r o G r a m value
for your profession
there is much talk about inflation and a slowing economy, interest rates are significantly higher, and Big tech has been laying off employees en masse. pundits agree, we’re seemingly on the precipice of another downturn in the economic cycle. Fear mongering ensues. yet through good times and bad, humans have teeth—thus the need for dentistry endures!
instead of worrying about things we can’t control (i.e., interest rates, russian aggression, or where all the Ftx money went), devote yourself to what you can control: your business!
i understand some of us have developed rather robust abilities to spend (i-Cats and a new website, or tuition payments and porsches, maybe?); but managing expenses is pretty straightforward for most (save the us Congress): don’t spend more than you earn. in this article, let’s underscore the importance of earning, because earning power is a dentist’s greatest asset!
specifically, we’ll unpack some of the many levers at your disposal to drive revenue for your practice, recession be damned.
A profit and loss (P&L) statement, simplified
to start, open the profit and loss (p&L) statement your accountant sent you. your p&L has 3 sections: revenue, expenses, and what’s left over.
the top part of the report is revenue—i.e., money, which has many names like collections, production, etc. For all your toil, revenue is captured with only a few lines. the second part of the report is expenses—money out, exposing all your spending habits or obligations, summarized nicely in a long list of categories. the final section—operating income, simply reflects the math illustrating how well you did earning versus spending.
Your revenue is controlled by a series of levers
it always seemed like an injustice to me to represent revenue in just a few simple lines, given there are so many inputs to those numbers. revenue reflected is the result of patients entering your facility, receiving treatment, and you getting paid for the work.
seems pretty simple, right? except there are so many decisions that go into that equation.
• Where is your facility?
• What hours are you choosing to be available?
• How does your business communicate with the people in your community to attract patients?
• How do you differentiate yourself from the dentist across the street?
• What services are you offering?
• What are you referring out?
• How do you communicate the need for treatment? who will perform the work?
• How are you getting paid? At what rate?
the point is, revenue is the result of hundreds of decisions you make as a business owner; levers you can adjust up or down to drive desired outcomes. mastering control of these levers will give you the gift of predictability which will assuage concerns about the economy.
Let’s unpack the last 2 of these levers.
How are you getting paid?
will you collect payment in full from a patient or accept assignment of benefits from a policy holder?
nearly every dental practice i’ve encountered accepts assignment of benefits to ease financial considerations for a patient. when a patient has a dental benefit, accepting assignment of benefits allows the payer to pay you as a provider directly. thus, if a patient completes treatment for $500 and the benefit will pay $400, the patient is only responsible for $100; and the provider then collects $400 from the insurance company.
if you don’t accept assignment of benefits, the patient is responsible for the $500 and bears responsibility for collecting the balance from the insurance company. if that’s the case, do you collect the patient portion at the time of service or bill later?
www.tda.org | April 2023 171
value for your profession
while some offices will file the claim for the patient, the implication is this: the more difficult you make it for the patient, the less likely new patients will choose your practice and the more likely existing patients may look elsewhere.
this leads to even more questions.
• Do you offer an in-house membership plan for uninsured patients?
• Do you offer in-house payment plans?
• Financing options like CareCredit?
• Who’s sending statements and how (via email, text, snail mail)?
• Who’s calling on open accounts receivable? How often and for how long?
• Do you use a collection agency?
• Do you keep a credit card on file for balances?
• Do you take online payments?
• If you are appealing to a younger demographic, do you take Apple Pay, Venmo or zelle? keep in mind most 27-year olds aren’t carrying around checkbooks.
in the last few paragraphs, there are at least 12 decisions you make as a business owner about just one aspect of revenue. there are costs to using a billing service, collection agency, online payment platforms, accepting payments via zelle, or getting paid through CareCredit. have the goal of understanding how the many options before you affect patient revenue—and what your return on investments are—before you make the decisions.
At What Rate Are You getting Paid?
pricing services in your practice should reflect your business model, community, and target market. Consider the differences between nordstrom and target. they have different target customers and different product offerings, but they both sell clothes and they both make money.
however, the most common method for establishing your usual, customary, and reasonable (uCr) fees is doing so based on competition in the market. very few dental practices have performed a detailed cost accounting of each procedure and then added a mark-up accordingly.
• How will you collect and store for review competitive pricing?
• Will you buy benchmark data for your community? If so, from which source?
• How often will you review and update pricing?
• Should you participate with insurance companies? if so, what are your contract rates? how long since you last revisited them?
• What is your practice’s policy on discounting?
these are more decisions you must make that will affect patient attraction, patient retention, case acceptance, and ultimately practice revenue.
understanding, learning, and ultimately mastering the levers of your business that lead to revenue growth and predictability are key to long-term success. so, instead of worrying or getting caught up in the latest macroeconomic distraction, go to work on your business!
TDA Perks Program-endorsed Five Lakes Dental Practice Solutions can help your practice maximize reimbursements and manage your entire credentialing process. Five Lakes can also help you optimize your revenue and improve your patients’ experience. Learn more about Five Lakes at tdaperks.com (Insurance, Dental Benefits, and Marketing) or call Five Lakes at 440-490-3118.
172 Texas Dental Journal | Vol 140 | No. 3
Continued


www.tda.org | April 2023 173 CONTACT YOUR LOCAL DENTAL SUPPLY FOR THE E-VAC TIP The Original E-VAC Tip • Inexpensive • Disposable • Non-Toxic • 100 Tips/Pk PROTECT YOUR PATIENT FROM PAINFUL TISSUE PLUGS • PROTECT YOUR EQUIPMENT FROM COSTLY REPAIRS E-VAC INC.© Phone: (509) 448-2602 • EMAIL:kenevac hotmail.com Made in USA FDA Registered • Representation Before the Texas State Board of Dental Examiners • Medicaid Audits and Administrative Hearings • Employment Issues—Texas Workforce Commission Hearings • Administrative (SOAH) Hearings and Counsel • Professional Recovery Network (PRN) Compliance • Employment/Associateship Contract Reviews • Practice Acquisition and Sales • Business Organizations, PAs, PCs, and PLLCs • Civil Litigation 2414 Exposition Blvd., Suite A1 • Austin, Texas 78703 • Phone: 512-477-6200 • Fax: 512-477-1188 • Email: mhanna@markjhanna.com Not Board Certified by the Texas Board of Legal Specialization Mark J. Hanna JD
General Counsel, Texas Dental Association LAW OFFICES OF MARK
HANNA EXPERIENCED LEGAL REPRESENTATION FOR TEXAS DENTISTS
Former
J.
classifieds
opportunities online at tDa.org and printed in the texas dental Journal
Classifieds information
DeaDLine
Copy text is due the 20th of the month, 2 months prior to publication (ie, January issue has a due date of november 20.)
monthLy rates
print: First 30 words—$60 for aDa/tDa members & $100 for non-members. $0.10 each additional word.
onLine: $40 per month (no word limit). online ads are circulated on the 1st business day of each month, however an ad can be placed within 24 business hours for an additional fee of $60.
suBmission
ads must be submitted, and are only accepted, via www.tda.org/member-resources/tDaClassified-ads-terms. By official tDa resolution, ads may not quote specific incomes or revenues and must be stated in generic terms (ie “$315,000” should be “low-to-mid-6 figures”).
Journal editors reserve the right to edit and/or deny copy.
PRACTICE OPPORTUNITIES
all teXas listings for mClerran & assoCiates. austin-nortH (id #572): 100% FFs, state-of-the-art office in north austin featuring a modern buildout with 7 equipped operatories, a CBCt, a digital scanner, and a CereC milling unit in over 2,600+ sq ft. the office is ideally located in a high visibility retail shopping center with easy access to the surrounding community. austin-nortH (id #575): GD practice in the killeen/harker heights/Copperas Cove area. 4 operatories with recently purchased chairs, digital x-rays, intraoral cameras, and paperless charts. 1,800+ active patients, 40+ new patients per month, revenue of mid-6 figures with 30-35% of total production derived from hygiene procedures, and excellent profitability. austin-nortH (id #580): established GD practice and real estate in a growing community between austin and waco. Located in a 2,184 sq ft professional building with additional space for future expansion, 5 fully equipped operatories, digital x-ray units, a pano, and a digital scanner. the office serves a large, FFs/ppo patient base
174 Texas Dental Journal | Vol 140 | No. 3
(over 3,400 active patients seen in the last 24 months) with 35+ new patient visits per month which supports a strong hygiene recall program (40% of total revenue). austin, ortHo (id #581): rare opportunity to purchase an orthodontic practice and real estate in a highly desirable area just 15 miles west of downtown austin. the turn-key facility is located within a free-standing building in a high-traffic retail center. the practice has strong profitability, and the facility includes four chairs, a digital pan-Ceph, itero element digital scanner, and paperless charts. the owner is available postsale to assist the buyer with a transition period. austin (id #588): FFs/ppo GD practice in the heart of austin. Located in a spacious condo, it has 4 fully equipped operatories, computers throughout, digital radiography, digital scanner, CaD/Cam, intraoral cameras, paperless charts, and has realized revenue of over seven figures with external marketing activities and most specialty procedures being referred out. the real estate is also available for purchase. el paso (id #591): ppo/FFs GD practice in el paso with 4 fully equipped operatories plumbed for nitrous,
digital radiography, digital pano, computers in all ops, Cerec digital scanner + CaD/Cam, intraoral cameras, and paperless charts. this practice boasts a healthy active patient base, great reputation, and long-standing presence in the community. Houston-soutHWest (id #565): Large, comprehensive GD practice in sw houston. spacious 3,200+ sq ft retail location, 7 fully equipped ops, digital radiography, computers in operatories, a digital scanner and CBCt. revenue of over 7 figures with over 40% profitability. this is a great opportunity for a highly trained clinician or group that is looking for a large office that they can continue to grow into. Houston-nortH (id #568): turn-key GD practice in a rapidly growing suburb of houston. FFs/ppo office, modern build out, 3 equipped operatories, computers in ops, digital radiography, intra oral cameras, paperless charts, and a digital pano. this is an ideal opportunity for a buyer who is interested in a start-up and is ready to take an office that is primed for growth to the next level! HoustonnortHWest (id #589): 100% FFs GD practice in northwest houston. Located in a highly visible retail center, the practice features 4 fully
www.tda.org | April 2023 175
classifieds
equipped operatories (with an opportunity to equip a 5th), computers in ops, digital radiography, intraoral cameras, and paperless charts. this is a turn-key practice with strong growth potential. Houston-soutHeast (id #592): Legacy practice in a growing suburb southeast of houston, large, multigenerational, ppo/FFs patient base, and annual revenue of 7 figures. Located in a high visibility retail location that contains 5 fully equipped operatories, digital radiography, and computers throughout. with many specialty procedures being referred out, little to no external marketing or advertising, and robust hygiene recall, this practice offers significant upside potential. the real estate is also available for purchase. nortHeast teXas (id #584): 100% FFs general dentistry practice in a desirable town in northeast texas with seven figures in revenue and strong net income. the turn-key practice features 4 fully equipped operatories with digital radiography, intra oral cameras, paperless charts, CBCt, and a digital scanner. san antonio (id #582): well-established, ppo/FFs family practice in Central san antonio in a high visibility building. 4 fully equipped
ops, digital radiography, a digital pano, intraoral cameras, and computers in all ops. Large active patient base and a robust hygiene recall program with no website and minimal external marketing efforts and significant growth potential by way of expanding services to include endodontics, implant placement, ortho, and oral surgery. san antonio (id #583): 100% FFs, high-tech practice in nw san antonio. 2,000+ sq ft, 6 operatories, digital radiography, CBCt, milling machine, 3D printer, porcelain and zirconia ovens, computers in ops, and a digital scanner. the practice has high six figures of annual revenue, solid monthly new patient flow, a fantastic web presence and a stellar online reputation that the seller has built up over several years. if you enjoy cosmetic dentistry and placing implants with a focus on using state of the art technology, this is the practice for you! soutH teXas (id #585): majority ppo/FFs GD family practice in south texas. 1,900 sq ft office, 3 fully equipped operatories, computers in all operatories, digital radiography, digital pano, intraoral cameras, digital scanner, and paperless charts. strong active patient base, an average
176 Texas Dental Journal | Vol 140 | No. 3
monthly new patient count of 45+ (over past 12 months) on limited external marketing efforts, healthy hygiene recall program (20% of annual production) and primed for continued success and future growth. to reQuest more information on mClerran & assoCiatesí listings: please register at www.dentaltransitions.com or contact us at 512-900-7989 or info@dentaltransitions.com.
Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com. houston: (sharpstown area). GeneraL (reFerenCe “sharpstown GeneraL”). motivateD seLLer well-established general dentist with high6 figure gross production. Comprehensive general dentistry in the southwest houston area focused on children (medicaid). very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. over
beaumont: GeneraL (reFerenCe “Beaumont”) small town practice near a main thoroughfare. 80 miles east of houston. Collections in 7 figures. Country living, close enough to houston for small commute. practice in a stand-alone building built in 1970. the office is 1,675 sq ft with 4 total operatories, 2 operatories for hygiene and 2 operatories for dentistry. Contains reception area, dentist office, sterilization area, lab area. majority of patients are 30 to 65 years old. practice has operated at this location for over 38 years. practice sees patients about 16 days a month. Collection ratio of 100%. the practice is a fee-for-service practice. Building is owned by dentist and is available for sale.
www.tda.org | April 2023 177 www.dentaltransitions.com McLerran & Associates is the largest dental practice brokerage firm in Texas. When it’s time to buy or sell a practice, we’ve got you covered. DSO C S PRACTICE SALES Email: texas@dentaltransitions.com PRACTICE APPRAISALS Austin 512-900-7989 DFW 214-960-4451 Houston 281-362-1707 San Antonio 210-737-0100 South Texas 361-221-1990
classifieds
1,200 active patients. 20% medicaid, 45% ppo, and 35% fee-for-service. 30% of patients younger than 30. office open 6 days a week and accepts medicaid. Contact Christopher Dunn at 800-930-8017 or christopher@ ddrdental.com. houston (Baytown area)GeneraL (reFerenCe “Baytown GeneraL”) motivateD seLLer well-established general practice with mid-6 figure gross production. Comprehensive general dentistry in Baytown on the east side of houston. Great opportunity for growth! 1,400 sq ft, 4 operatories in single story building. 100% collection ratio. 100% fee for service. practice focuses on restorative, cosmetic and implant dental procedures. office open 3.5 days a week. practice area is owned by dentist and is available for sale. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com. west oF austin: orthoDontiC (reFerenCe “hiLL Country ortho”). Located in a rapidly growing small town, this practice is in the heart of the texas hill country. this practice serves the youth of the area. there are 4 operatories in the practice. the practice is 100% fee for service. orthodontic care is the only service provided
at this office. 1300 sq ft. open 4 days per week. Digital x-rays and pano and Cloud9ortho software. the practice has excellent visibility and is located near a hospital. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com.
Houston, College station, and lufKin (ddr dental listings). (see also austin for other DDr Dental listings and visit www. DDrDental.com for full details. LuFkin: GeneraL practice on a high visibility outer loop highway near mall, hospital and mature neighborhoods. Located within a beautiful single-story, free-standing building, built in 1996 and is aLso available for purchase. natural light from large windows within 2,300 sq ft with 4 operatories (2 hygiene and 2 dental). includes a reception area, dentist office, a sterilization area, lab area, and break room. all operatories fully equipped. Does not have a pano but does have digital x-ray. production is 50% FFs and 50% ppo (no medicaid), with collection ratio above 95%. providing general dental and cosmetic procedures, producing mid-6 figure gross
178 Texas Dental Journal | Vol 140 | No. 3
collections. Contact Christopher Dunn at 800930-8017 or Christopher@DDrDental.com and reference “Lufkin General or tx#540”. houston: GeneraL (sharpstown). well established general dentist with high-6 figure gross production. Comprehensive general dentistry in the southwest houston area focused on children (medicaid). very, very high profitability. 1,300 sq ft, 4 operatories in single building. 95% collection ratio. over 1,200 active patients. 20% medicaid, 45% ppo, and 35% fee-for-service. 30% of patients younger than 30. office open 6 days a week and accepts medicaid. Contact Chrissy Dunn at 800-9308017 or chrissy@ddrdental.com and reference “sharpstown General or tx#548”. Houston: GeneraL (pearLanD area). GeneraL located in southeast houston near Beltway 8. it is in a freestanding building. Dentist has ownership in the building and would like to sell the ownership in the building with the practice. one office currently in use by seller. a 60 percent of patients age 31 to 80 and 20 % 80 and above. Four operatories in use, plumbed for 5 operatories. Digital pano and digital x-ray. Contact Christopher Dunn at 800-930-8017
or christopher@ddrdental.com and reference “pearland General or tx#538”. houston: peDiatriC (north houston). this practice is located in a highly sought-after upscale neighborhood. it is on a major thoroughfare with high visibility in a strip shopping center. the practice has three operatories for hygiene and two for dentistry. nitrous is plumbed for all operatories. the practice has digital x-rays and is fully computerized. the practice was completely renovated in 2018. the practice is only open three and a half days per week. Contact Christopher Dunn at 800-930-8017 or christopher@ddrdental.com and reference “north houston or tx#562”. west houston: motivateD seLLer medicaid practice with production over $600,000. three operatories in 1200 sq ft in a strip shopping center. equipment is within 10 years of age. has a pano and digital x-ray. Great location. if interested contact chrissy@ddrdental.com. reference “ west houston General or tx#559”.
soutHeast Houston: above mid 6 figures of adjusted net production and almost full collection (97%). Fee-for-service and ppo
www.tda.org | April 2023 179
classifieds
practice, highest-net income. the total collection over total production is about 90%. 4 days / week, free weekends. no medicaid, no hmo/Dmo, no in-network and no hassle. this practice has been in this area for over 40 years; the current practice location was built in 2006 in a new building with all new equipment. 4000 square feet, 5 fully equipped operatories, and 5 additional operatories plumbed. CBCt with pano and digital x-ray with a phosphor-plate scanner require little to no maintenance. we have a few digital sensors too. microscopes and Fotona Lasers are available. Doctors over 70 years of age are ready to retire. instead of using a broker, we are willing to provide a discount equal to the broker fee. interested parties can contact us by calling or texting our personal cell number 346-754-9643. email: smile.office@proton.me. principals only. sales agents and buyers bonded to the broker, please don’t contact this sales poster. Do not contact us with unsolicited services or offers.
Watson broWn praCtiCes for sale: practices for sale in texas and surrounding states, For more information and current listings please visit our website at www. adstexas.com or call us at 469-222-3200 to speak with Frank or Jeremy.
interim serviCes
Have mirror and eXplorer, Will travel: sick leave, maternity leave, vacation, or death, i will cover your general or pediatric practice. Call robert zoch, DDs, maGD, at 512517-2826 or drzoch@yahoo.com.
180 Texas Dental Journal | Vol 140 | No. 3
www.tda.org | April 2023 181

182 Texas Dental Journal | Vol 140 | No. 3 PRN Helpline (800) 727-5152 Visit us online www.txprn.com YOUR PATIENTS TRUST YOU. WHO CAN YOU TRUST? If you or a dental colleague are experiencing impairment due to substance use or mental illness, The Professional Recovery Network is here to provide support and an opportunity for confidential recovery. anesthesia education & safety Foundation, inc... 131 Choice transitions ........................... inside Back Cover Dental expert witness training............................... 156 DentaQuest ............................................................... 136 e-vaC inc .................................................................... 173 henry schein Financial services ............................. 165 JkJ pathology .............................................................. 134 Law offices of mark J. hanna .................................. 173 mcLerran & associates............................................. 177 mCna Dental ............................................................. 157 penumbra Diagnostics ............................................. 156 princess Dental staffing .............................. Back Cover professional recovery network .............................. 182 southwest sedation education ............................... 157 tDa perks ......................................... inside Front Cover texas a&m school of Dentistry ................ 165 and 167 texas health steps ................................................... 137 watson Brown ........................................................... 166 ADvERTISERS








VISIT PRINCESSDENTALSTAFFING.COM. Lorem psum ! DENTAL STAFFING Lorem I psum LQuestions Call us at 1-844-700-JOBS rem psum THAT COMES WITH 5-STAR RE VIE WS.
