







 Bio f ilm Eraser
Bio f ilm Eraser
POWDER PRO CARE
ABOVE AND BELOW THE GUMS

Bio f ilm Eraser
ABOVE AND BELOW THE GUMS

Dentsply and Sirona have joined forces to become the world’s largest provider of professional dental solutions. Our trusted brands have empowered dental professionals to provide better, safer and faster care in all fields of dentistry for over 100 years. However, as advanced as dentistry is today, together we are committed to making it even better. Everything we do is about helping you deliver the best possible dental care, for the benefit of your patients and practice.
Find out more on dentsplysirona.com


More and more dentists and dental lab technicians rely on IPS e.max, the clinically proven all-ceramic system that offers high esthetics and dependable strength. 100 million restorations placed attest to this. From crowns, inlays, onlays, thin veneers and abutments to bridges – make the choice more dental professionals make... MAKE IT e.max!





Decision-making factors for optimized management of Root fractures in the apical third: About two clinical cases
Dr. Mohamed Rafik Cherif, Dr. Maroua Garma
Dr. Nabiha Douki Zbidi,



Stacey Kirshenblatt, Hui Chen, Marijke Dieltjens, Benjamin Pliska, Fernanda R. Almeida

64. Lebanese Society of Endodontology
June 21 - 22, 2018
Hilton Habtoor Grand Beirut, Lebanon
68. Lebanese Orthodontic Society 16th Annual Meeting
June 22 - 23, 2018
Mövenpick Hotels & Resorts Beirut, Lebanon
73. Byblos Dental Association 25th Summer Dental Meeting
June 23, 2018
Eddésands Hotel & Resort Jbeil, Lebanon
74. Lebanese Society of Pediatric Dentistry
Silver Jubilee’s Convention
June 26, 2018
The Key ApartHotel Beirut, Lebanon
3SHAPE 19
ACE SURGICAL 17
A-DEC 9
BA INTERNATIONAL 35
BIEN AIR 39
BISCO 10
CAMLOG 6
COLTENE 15
DENTSPLY SIRONA C2, 21
DURR 33
EMOFORM 4, 5
FKG 62
GC 25
HENRY SCHEIN 33
HS ORTHO 23
HU FRIEDY 29
IVOCLAR 1, C4
MANI 36
MECTRON 40
MICRO MEGA 65
MORITA 7
NSK C1
ORMCO 31, 69
PLANMECA C3
PROMEDICA 24
SCHEU 20
SDI 27
SEPTODONT 80
ULTRADENT USA 63
VITA 13
VOCO 43
W&H 8, 37
ZHERMACK 2









A dec chair packages offer a bespoke solution tailored to allow you to customise and build your chair specifically for the way you work with your patients. With mix and match customised equipment options and flexible upgrades, you get precisely what you want no more, no less. This is YOUR chair.
Design and configure your very own specification of A‑dec dental chair to meet the needs of your practice. Visit a-dec.com and see for yourself. Alternatively, email international@a-dec.com to find out more.



Volume XXV, Number III, 2018
EDITORIAL TEAM
Alfred Naaman, Nada Naaman, Jihad Fakhoury, Dona Raad, Antoine Saadé, Lina Chamseddine, Tarek Kotob, Mohammed Rifai, Bilal Koleilat, Mohammad H. Al-Jammaz

COORDINATOR
ART DEPARTMENT
SUBSCRIPTION
ADVERTISING
PHOTOGRAPHY
TRANSLATION
DIRECTOR ISSN
Suha Nader
Marc Salloum
Micheline Assaf, Nariman Nehmeh
Josiane Younes
Albert Saykali
Gisèle Wakim
Tony Dib 1026-261X
DENTAL NEWS IS A QUARTERLY MAGAZINE DISTRIBUTED MAINLY IN THE MIDDLE EAST & NORTH AFRICA IN COLLABORATION WITH THE COUNCIL OF DENTAL SOCIETIES FOR THE GCC.
Statements and opinions expressed in the articles and communications herein are those of the author(s) and not necessarily those of the Editor(s) or publisher. No part of this magazine may be reproduced in any form, either electronic or mechanical, without the express written permission of the publisher.
DENTAL NEWS – Sami Solh Ave., G. Younis Bldg.
POB: 116-5515 Beirut, Lebanon.
Tel: 961-3-30 30 48
Fax: 961-1-38 46 57
Email: info@dentalnews.com Website: www.dentalnews.com
www.facebook.com/dentalnews1 www.instagram.com/dentalnews twitter.com/dentalnews
Dental News App








SDM 2018 Sofia Dental Meeting
IADC 2018 International Aesthetic Dental Congress
BIDM 2018
Beirut International Dental Meeting
Middle Eastern Carriere Symposium
AIDC 2018
Alexandria International Dental Meeting
DFCIC 2018 Dental Facial Cosmetic Conference & Exhibition
EPDA 2018
Egyptian Pediatric Dental Association
KDA 2018 Kuwait Dental Association Meeting
SIDC 2019 Saudi International Dental Conference
AEEDC 2019
AIO 2019 International Congress
September 27 - 30, 2018 Sofia, BULGARIA www.sdm.bg
September 28 - 29, 2018 Beach Rotana Hotel Abu Dhabi, UAE www.iadc.ae
October 4 - 6, 2018 Forum de Beirut, LEBANON www.bidm-lda.com
November 2 - 3, 2018 Dubai, UAE www.carrieresymposium.com/dubai
November 6 - 9, 2018 Alexandria, EGYPT www.aidconline.org
November 9 - 10, 2018 Intercontinental Hotel Dubai, UAE www.cappmea.com/aesthetic
November 9 - 11, 2018 Hilton Green Plaza Alexandria, EGYPT www.epdaonline.org
November 25 - 27, 2018 KUWAIT www.kda.org.kw
January 12 - 14, 2019 Ritz Carleton Riyadh, SAUDI ARABIA www.sidc.org.sa
February 5 - 7, 2019 Int’l Convention & Exhibition Centre Dubai, UAE www.aeedc.com
June 13 - 15, 2019
Chia, Sardinia, ITALY www.congressaio.it

Mohamed Rafik Cherif
DDS & Postgraduate Student, departement of Restorative Dentistry & Endodontics, Sahloul Hospital, University of Monastir, Tunisia
Root fractures are among the most complex emergency consultation in our practice; they may involve the cervical, middle or apical third of the root.
Maroua Garma
DDS & Postgraduate Student, departement of medical & surgery, Dental clinic, University of Monastir, Tunisia nabiha.douki@gmail.com
The survival prognosis of the tooth will depend on 3 types of factors referred as pre-traumatic, traumatic and treatment factors by Andreason et al. 1, 2. In this article, we focused on root fractures of
Nabiha Douki Zbidi head of the departement of Odontology. Professor in Restorative Dentistry & Endodontics, Sahloul Hospital, University of Monastir, Tunisia
Root fractures are complex traumatic injury, affecting both hard dental tissues, periodontal and pulpal tissues 3, 4
This type of fracture is rare, between 0.5 to 7% of cases of trauma 3, 5, 6 and occurs most often following a violent shock during an assault, a traffic accident or during sports activities 7 Male patients between the ages of 11 and 20 years old are the most affected 6, 8
The most concerned teeth are mainly the upper central incisors (68%) and the lateral ones (27%) 3. The incidence of radicular fracture of the apical third is 34% compared to 57% in the middle third and 9% in the cervical third 6
The diagnosis may not be straight forward, as clinical signs may be similar to other types of dental trauma, the coronal fragment can be mobile or even displaced
the apical third in order to present the difficulties of their management and to propose a decision making diagram regarding the best course of treatment management, based on the best scientific evidence available and the illustration of two clinical cases.
Key words: Trauma, tooth, fracture, apical third, decision making
mimicking a sub-luxation or luxation respectively. Very often the coronal fragment remains un-displaced with a slight mobility and tender to percussion mimicking a periodontal contusion. Sensitivity tests may give a negative result initially indicating a transient or permanent nerve damage 9.
The diagnosis of radicular fractures of the apical third is essentially based on radiological evaluation. The fracture line is oriented obliquely in the apical-third and middle-third of the root 5 Therefore, these fractures are normally visible only when the central beam is directed in a maximum range of 15 to 20 ° of the fracture plane. Any deviation would show the fracture line as an ellipsoid 10. It is advised that in addition to the conventional periapical radiograph, two additional
From VITABLOCS® to VITA ENAMIC® –high-performance materials for a wide range of indications since 1985


• VITA is the pioneer in the field of dental CAD/CAM materials for practices and laboratories.
• VITA has been offering top-quality materials from a single source for a wide range of indications since 1985.
• Today users in practices and laboratories benefit from numerous proven solutions and trendsetting, innovative materials.
www.vita-zahnfabrik.com facebook.com/vita.zahnfabrik VITA – perfect match.
periapical radiographs should be exposed with a positive and negative angulations of 15° to fracture plane 5 Nowadays, technological advances such 3-D imaging via CBCT (Cone Beam Computed tomography), have made a significant contribution to the diagnosis and the precise localization of the root fracture line.
Particularly, with 3-D image reconstruction that avoid the overlapping of anatomical structures, thus pushing the limits of conventional 2D imaging. The treatment will consist essentially in repositioning the coronal fragment when it is displaced, splinting the tooth for 2 to 4 weeks and establishing regular follow-ups schedule.
The aim of this article is to expose the factors influencing the therapeutic decision-making and prognosis of radicular fractures healing of the apical third in order to put a treatment plan that can be adjusted according to the clinical situation and its evolution during follow-ups. We will review the factors that modulated our thought process in the management of two clinical cases, and finally we will present a summary diagram for decision-making based on a literature review.
According to the work of Andresen et al 1, three types of factors must be taken into account before taking care of a root fracture and establishing a prognosis: (Fig 3)
• The young age of the patient and the root immaturity of the tooth, are the guarantors of a considerable blood
supply containing multi-potent stem cells, immune cells, and growth factors, which favors pulpal and hard tissue healing at the fracture line. This correlation has been widely established in previous studies 11, 12
• The periodontal status is a key factor, as periodontal pocket may cause a communication with the oral cavity exposing the fracture line to bacterial contamination and therefore the tooth is left with a poor prognosis 10. For this factor to be relevant in a root fracture of apical third, probing depth would have to exceed 6 mm.
• The mobility and dislocation of the coronal fragment are conditioned by the severity of the trauma and are the determinant of associated periodontal trauma such as sub-luxation or luxation of the coronal fragment 13
Indeed, a study evaluating the survival prognosis of dislocated permanent teeth has shown that pulpal necrosis was observed in 15% to 55% of subluxation and extrusion cases, respectively 14. On the other hand, if the coronal fragment is not displaced there is not therapeutic interest in splint placement.
• A positive response to pulp sensitivity tests with thermal stimuli during the first consultation would indicate the integrity of the neurovascular system. This sensitivity has been strongly correlated with the increased chances of pulpal healing and healing with interposition hard tissue 11


High flexibility
Extreme resistance to fracture
Centred canal preparation
Regeneration by thermal treatment


• The delay of consultation and treatment of a few hours to a few days does not seem to influence the type of healing compared to immediate management 15, 2
• Adequate repositioning: The chances of pulp healing and hard tissue interposition healing increase significantly, if repositioning of the coronary fragment is optimal for an initial displacement that does not exceed 1mm 2
• The type of splint influences significantly the type of healing pattern observed. A non-traumatic flexible splint is more in favor of pulp healing and hard tissue interposition healing than rigid splint 2
• A period of contention longer than 4 weeks has no therapeutic value. 2
A 49-year-old patient, with non-contributing medical history, reported to the department of conservative dentistry and endodontics of Sahloul state hospital, Sousse, Tunisia, following a trauma on tooth #11 and #21. Clinically the two teeth were mobile and tender to percussion with a 2 mm extrusion of tooth #11, sensitivity test was negative for #11 and positive for #21, and periodontal probing was within normal depth. Also the patient presented a dysfunctional swallowing pattern. The preoperative radiograph (Fig. 1- a) showed, a simple complete and horizontal root fracture at the apical third of # 11 and a widening of the periodontal ligament space of # 21.
The treatment plan was manual repositioning of the coronal fragment which was confirmed clinically by cervical margin and incisal edges alignment and radiologically by coaptation of the two fragments), followed by the placement of a semi-rigid splint for 2 weeks, removal of any occlusal interference with a diamond bur. Immediate root canal therapy (RCT) was performed on the coronal fragment (Fig. 1-b). retro alveolar Radiography Control at 6 months (Fig. 1 -c) shows a healing pattern by the interposition of a connective tissue as described by Andreason and Hjorting-Hansen 1, 11 rounding of edges at the mesial and/or distal aspects of the fracture with no radiolucency near the fracture line. Clinical signs regressed with the persistence of a slight tenderness to percussion and mobility and periodontal probing was within normal depth. Meanwhile, tooth #21 has become negative to cold testing one month later and RCT was initiated. Decision-making

Allografts – Xenografts – Alloplasts Solid



A 20 years old patient, consulting for intermittent and spontaneous pain regarding tooth # 21 with a history of trauma 5 years ago. The tooth was tender to percussion and presented a productive fistula. A preoperative retro-alveolar X-ray with a tracking gutta point (Fig. 2-A) showed a simple, oblique and complete apical root fracture at the apical third, an old filling, and radiolucency at the fracture line level and the apical fragment.
The origin of the fistula was traced back to the level of the fracture line. This is a complication of the initial treatment

by interposition of a granuloma associated to pulpal necrosis of the apical fragment. Non-surgical endodontic retreatment was performed with an apexification of the coronal fragment by a plug of Biodentine ™ which filled the entire canal lumen, followed by surgical removal of the apical fragment, and thorough debridement of necrotic tissue (Fig 2-B, C).
Retro alveolar Control x-ray at 18 months (Fig 2-D) showed complete bone healing. Clinically the tooth was asymptomatic and functional.


 Figure 2: A, preoperative retro-alveolar radiography with a locating cone tracing the origin of the fistula to the fracture line at the apical third with bone resorption. B, surgical time; Elimination of the apical fragment and debridement of granulation tissue. C, Postoperative retro-alveolar radiography. D, Control X-ray at 18 months showing complete bone healing.
Figure 2: A, preoperative retro-alveolar radiography with a locating cone tracing the origin of the fistula to the fracture line at the apical third with bone resorption. B, surgical time; Elimination of the apical fragment and debridement of granulation tissue. C, Postoperative retro-alveolar radiography. D, Control X-ray at 18 months showing complete bone healing.
A new scanning solution to excite patients and advance case acceptance

3Shape TRIOS® MOVE allows you to share digital scans and discuss treatment plans with patients, up close and from the comfort of their chair.
Excite patients by creating their future smile in just minutes with TRIOS Smile Design. With just a simple swipe, show them their smile before and after treatment, and boost case acceptance.
Explore more and REQUEST A DEMO at 3Shape.com/TRIOSMOVE
Contact

Decision-making factors for optimized management of Root fractures in the apical third: About two clinical cases






Dental trauma is a real challenge, precise diagnosis and an appropriate treatment plan with regular monitoring are key elements for a favorable prognosis. 17
In the two presented cases, we opted for decisions that we considered the most appropriate, taking into account the different factors and their influence on the final prognosis. For the first case, the coronal fragment was mobile and displaced so it was manually replaced and a flexible splint was placed to allow the healing and reorganization of the periodontal 4 According to the 2012 International Association of Dental Traumatology (IADT) recommendations 9 the cold sensitivity test on a traumatized tooth even in the event of a root fracture can be a false negative up to 3 months and should not indicate immediate endodontic treatment. The period of splinting should not exceed 2 to 3 weeks.
Asiga MAX TM : For the digital workflow in your laboratory. the most compact UV HD 3D printer on the dental market 62 μm resolution
SPS (smart positioning system) for precise printing results fill-quantity monitoring individual support for the complete service life
A minimum follow-up period of one year is necessary. But in our case the age of the patient, complete root edification, the extent of coronal fragment displacement (2 mm) predicted low blood supply and therefore a low repair potential. In addition, the dysfunctional swallowing pattern (tongue taking support on the palatal side upper incisors), would have resulted in the persistence of chronic irritation of the pulp at the level of the fracture line. It is by taking into consideration these factors mentioned that the risk of necrosis was considered high and RCT of the coronal fragment was decided from the outset. The apical fragment retains its vitality in most cases thanks to the neurovascular bundle from the apex and does not require intervention. But regular monitoring is required 4, 9, 18
For the second case:
• Fracture line was oblique so the apical end of the coronal fragment was oval and very large, making the reading of the working length and the fitting of gutta cone difficult. This could explain the failure of the initial endodontic treatment performed by the General practitioner who made a conventional gutta filling by cold lateral condensation.
• Concerns can be raised about the conditions that RCT was carried out: asepsis conditions, use of the dam or not, irrigation protocol used and the density of the canal filling.












V3 Sectional Matrix System









Our Class II Solution™ for a tight marginal seal and efficient aesthetics
Class II restorations are more important to your practice that you may think – they account for nearly half of all direct restorations. Getting them right the first time is the key to happy patients and profitability. Dentsply Sirona’s Class II Solution™ offers a portfolio of products designed to work together to deliver success at the most vulnerable interface – the floor of the proximal box –and achieve aesthetic results. Make your Class II’s count with Dentsply Sirona’s Class II Solution™.
w w w.dentsplysirona.com
Non-surgical endodontic retreatment was decided followed by removal of the apical fragment. The coronal fragment was treated as a non-vital immature permanent tooth.
An apical barrier with a bioactive material was placed, we chose Biodentine™ (Septodont, Saint Maur des Fosses, France) which has an apical sealing ability comparable to mineal trioxide aggregate (MTA) at any apical plug thickness (19).
Also better handling proprieties than MTA as it is presented in pre-dosed capsule with 12 min setting time.
In conclusion we present a diagram that sums up the decision making process in the management of fracture in apical third:
 Figure 4: Decision making diagram for management of apical third root fracture
Figure 4: Decision making diagram for management of apical third root fracture

MIDDLE EASTERN CARRIERE SYMPOSIUM DUBAI, UAE
November 2 - 3, 2018
1. Andreasen JO, Andreasen FM, Mejare I, Cvek M.Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol. 2004 Aug;20(4):192 202.
2. Andreasen JO, Andreasen FM, Meja`re I, Cvek M. Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dent Traumatol 2004; 20: 203–211
3. Von Arx T, Chappuis V, Hänni S Traumatologie des dents définitive s –3e partie: traitement des fractures radiculaires. Rev Mens Suisse Odontostomatol, Vol 117:2/20 07 4. Vania Portela Dietzel Westphalen,Maria Helena de Sousa, Ulisses Xavier da Silva Neto, Luiz Fernando Fariniuk, Everdan CarneiroManagement of horizontal root-fractured teeth: report of three cases Dental Traumatology 2008; 24: e11–e15
5. Y Josna Vinutha, Pavana Sandya Apical Third Horizontal Root Fractures in Anterior Teeth: A Review IJSS Case Reports & Reviews | February 2015 | Vol 1 | Issue 9 page 61-4 6. Caliskan MK, Pehlivan Y. Prognosis of root-fractured permanent inci-
sors. Endod Dent Traumatol 1996; 12:129-36. 7. Andreasen JO, L K Bakland ,M T Flores F M Andreasen L Andreasen : Traumatic Dental Injuries a manual THIRD EDITION 2011
8. Andreasen FM, Andreasen JO, Cvek M. Root fractures. In: Andreasen JO, Andreasen FM, Andreasen L, editors. Textbook and color atlas of traumatic Injuries to the teeth. Kopenhagen: Munksgaard; 2007. p. 337-71. 9. Anthony J. DiAngelis, Jens O. Andreasen and al International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth Dent Traumatol 2012;28:2-12
10. Malhotra, Neeraj & Mala, Kundabala & Acharaya, ShashiRashmi. (2011). A review of root fractures: Diagnosis, treatment and prognosis. Dental update. 38. 615-6, 619. 10.12968/denu.2011.38.9.615.)
Temporary crown & bridge material
• Less than 5 min. processing time
• Paste-paste system on composite basis
• Strong functional load

• Perfect long-term aesthetics
• Excellent biocompatibility
If you are interested in our entire product range and in detailed
11. Cvek M, Andreasen JO, Borum MK. Healing of 208 intraalveolar root fractures in patients aged 7–17 years. Dent Traumatol 2001; 17:53–62.
12. Andreasen FM, Andreasen JO. Resorption and mineralization processes following root fracture of permanent incisors. Endod Dent Traum 1988;4:202–14. 13. Andreasen FM: Pulpal healing after luxation injuries and root fracture in the permanent dentition, Endod DentTraumatol 5:111, 1989. 14. Andreasen FM, Vestergaard Pederson B. Prognosis of luxated permanent teeth – the development of pulp necrosis. Endod Dent Traumatol 1985; 1:207–20. 15. Andreasen JO, Andreasen FM, SkeieA, Hj)rting-Hansen E, Schwartz O. E¡ect of treatment delay upon pulp and periodontal healing of traumatic dental injuries ^ a review article. Dent Trau-


Andreasen JO, Hjørting-Hansen E. Intra-alveolar root fractures: radiographic and histologic study of 50 cases.J Oral Surg 1967; 25:414–26.
Bucher K, Neumann C, Thiering E, Hickel R, Kuhnisch J. Complications and survival rates of teeth after dental trauma over a 5-year period. Clin Oral
Jacobsen I, Kerekes K. Diagnosis and treatment of pulp necrosis in permanent teeth with root fractures. Scand J Dent Res 1980;88:370–6.
Mehmet Bani, Elif Sungurtekin-Ekçi, and Mesut Enes Odabaş, “Efficacy of Biodentine as an Apical Plug in Nonvital Permanent Teeth with Open Apices: An In Vitro Study,” BioMed Research International, vol. 2015, Article ID 359275, 4 pages, 2015. https://doi.org/10.1155/2015/359275.





Dr. Amir Khalid Hassan (BDS, MDSc) QAF, Medical Services, Doha, Qatar. Formerly assistant professor at Dental college, University of Baghdad - Iraq
amiralagidi@gmail.com
Dental abscess is frequently found in oral cavity 1. It is frequently related with badly treated carious tooth and poor oral hygiene. Dental caries and pulp necrosis often ended in extending the infections to alveolar bone and sometimes involving the outer layer of the face (sinus) 1-9
This facial sinus orifice cannot be distinguished easily in its origin, confusing the medical team 2-9
A fistula is an abnormal pathway between 2 anatomic spaces or a pathway that leads from an internal cavity or organ to the surface of the body. A sinus tract is an abnormal channel that originates or ends in one opening. An orofacial fistula is a pathologic communication between the cutaneous surface of the face and the oral cavity.
In the literature, the terms fistulas and sinuses are often used interchangeably. Stedman’s Medical Dictionary defines a sinus as a fistula or tract leading to a suppurating cavity. Orofacial fistulas are not common, but intraoral sinus tracts due to dental infections are common. When infection or neoplasia is involved, immediate treatment is necessary.
Dental infections, salivary gland lesions, neoplasms, and developmental lesions cause oral cutaneous fistulas, fistulas of the neck, and intraoral fistulas.2, 3, 5
Chronic dental periapical infections cause the most common intraoral and extraoral fistulas. These dental periapical infections might cause chronic osteomyelitis, cellulitis, and rarly facial abscesses. Infection can spread to the skin when it is the path of least resistance then causing cutaneous fistulas.
One case report 2 reviewed this occurrence from a periapical infection from the right central mandibular incisor, which drained to the patient’s chin. Because the tooth could not be restored, it was extracted, which resolved the lesion.
Another case with cutaneous manifestations involved a 44-year-old woman with a draining lesion to the skin just lateral to the nasofacial sulcus. Oral antibiotics did not help treating the lesion. The patient had bad oral hygiene, and two periapical radiolucencies of the maxillary right lateral incisor and canine were observed.
The teeth were extracted, which resolved the lesion. Sheehan et al emphasized on the importance of a dental examination and radiographs to rule out infection of dental origin to the cutaneous face or neck.
This case study showed three cases of intra-oral abscess extending through the bone and facial skin.

• Very high fluoride releasing and recharging ability to create more acid resistant restored teeth Ideal dentine replacement material
• Can be bulk filled
• BPA & HEMA free
RIVA® LIGHT CURE AND RIVA® SELF CURE ARE ALSO AVAILABLE IN REGULAR VISCOSITY


• Easy to manipulate and sculpt

• Orange light safe tip prevents premature setting Fabulous aesthetics
• BPA free
• Highest colour stability to tea & coffee

A 20-year-old Yemeni patient visited many doctors only when the abscess came out from her face. Drainage and curettage has been performed by General Physicians as well as laser cauterization by Dermatologist. Lately, it was suspected that it might be of dental origin. The patient was referred to Dental Department. Root canal treatment on upper right first molar has initially been done 3 years ago (2010) but it is not completed. Therefore, she suffered from chronic periapical abscess in which intrapulpal drainage has been made with antibiotics for several times and left open with no further treatment. During the examination it was noticed that the abscess extended to the face and was drained through infraorbital skin area. (pic 1)
Radiographical examination were done by orthopantogram and periapical parallel technique inserting the gutta percha cone inside the facial orifice of the sinus andtrack-


ing the origin of it. These revealed the presence of this abscess and its relation to the suspected tooth.
A case has been discussed fully to the patient, as well as the poor prognosis of the tooth treatment. Full root canal therapy preparation and obturation using protaper system was done through three visits of 10 days interval and under antibiotic coverage of Doxycycline capsule 150 mg twice a day orally systematically. The same antibiotic tablets (3 tabs) were crashed into a chlorohexidine mouthwash and used as irrigant for the root canals along the procedures. (pic 2)
The case has been observed for three months (pic 3, 4), six months (pic 5) and one year without any complaints. The tooth is finally restored with a ceramic crown. The outer scar of the sinus was treated by laser and it is nearly disappeared.



 Figure 1: The facial lesion showing the pus and then the irrigation solution coming out of the facial lesion
Figure 2: Endodontic treatment
Figure 4: After 3 months
Figure 5: After 6 months
Figures 3A, 3B: After 3 months
Fig. 1
Fig. 3A
Fig. 3B
Fig. 5
Fig. 2
Figure 1: The facial lesion showing the pus and then the irrigation solution coming out of the facial lesion
Figure 2: Endodontic treatment
Figure 4: After 3 months
Figure 5: After 6 months
Figures 3A, 3B: After 3 months
Fig. 1
Fig. 3A
Fig. 3B
Fig. 5
Fig. 2




A 22-year-old Pakistani female patient was complaining of recurrent excised skin infection at the neck with purulent discharge from the corner of the mandible. She went to medical physicians many times and ended by surgical excision of the granulation tissue at the neck with many courses of antibiotic with no use.
She attended the facility of Qatar Armed Forces where she was referred to Dental Department for consultation. Full oral examination was carried out, x-ray views using an old technique of inserting gutta percha cone inside

the outer neck skin lesion revealing that its origin is related to the root of lower left 6 (LL 6) which is found badly carious, infected and poor prognosis(PIC 6,7&8). The same method of treatment in case 1 was followed. The skin lesion has subsided and disappeared, leaving a light scar (pic 9-14).
Evaluation for the case were made for one, three months, six months and a year with progressive success. The patient refused to do laser treatment to remove the scar as lesion become shallow and not recognizable.





 Figure 6: Pre-operative OPG showing LL 6 with active and extended periapical lesion
Figure 9: The tooth when oburated.
Figures 7 (A, B, C, D): Photograph showing the clinical features of the facial lesion and the oral status of the affected tooth.
Fig. 6
Fig. 8
Fig. 9
Fig. 7C
Fig. 7A
Fig. 7B
Figure 6: Pre-operative OPG showing LL 6 with active and extended periapical lesion
Figure 9: The tooth when oburated.
Figures 7 (A, B, C, D): Photograph showing the clinical features of the facial lesion and the oral status of the affected tooth.
Fig. 6
Fig. 8
Fig. 9
Fig. 7C
Fig. 7A
Fig. 7B






Just scan the QR code and to get further details.


























A Pakistani female (62 years old) patient had been referred from dermatology clinic suffering from discharging nodule on the right lower nasiolabial fold since more than two months. She took many courses of antibiotics and surface lozenges with no benefits. Patient is diabetic as well as hypertensive and controlled medically.
Oral and dental examination was carried using clinical and radiological investigations, she was wearing a complete fixed prostheses from molar to molar. A (GP) point inserted inside the facial nodule shows clearly that the nodule is related to the apical abscess of the RCF routine.

Work was made through the prostheses to clear the pathological tissue. It was shown during the irrigation procedure of RCF , the solution comes out of the nodule sinus. fucidine cream to cover the facial sinus. Irrigation was made by Doxicycline capsule solved in 500 ml of Saline.
The patient kept monitoring and irrigated every week, for 3 weeks, the facial sinus completely closed, the radioapacity of the periapical area of the specified tooth reduced to minimum, and obturation is done by Gutta Perchas as routine. The patient followed up to after 2 -3 months until successful healing of facial sinus.



 Figure 10: The case after 3 months
Figure 13 (A, B): Clinical appearance and orthopantogram for the case. Note the irregation fluid coming out of the lesion.
Figure 11: The case after 6 months
Figure 12: The case after 12 months
Fig. 10
Fig. 13A
Fig. 13B
Fig. 11
Figure 10: The case after 3 months
Figure 13 (A, B): Clinical appearance and orthopantogram for the case. Note the irregation fluid coming out of the lesion.
Figure 11: The case after 6 months
Figure 12: The case after 12 months
Fig. 10
Fig. 13A
Fig. 13B
Fig. 11





The VistaPano S Ceph is the efficient X-ray solution for jaw orthopaedics and more. It supplies fast Ceph shots (4.1 seconds) with outstanding image quality and low exposure to radiation. At the same time, thanks to S-Pan technology, its 2-D panorama shots provide excellent definition. More at www.duerrdental.com







Some neck or face lesion might confused the physicians in its origin especially if it is dentally involved. A good teamwork treatment is essential to discover such as lesion and even in the treatment to finalize the case properly by cosmetic dermatological treatment using
lazer. The importance of irrigation solution with broad spectrum antibiotic such as doxycycline with chlroheidine mouthwash is equal to proper root canal preparation in the success of treatment of such extensive periapical lesions.
Figure 14 (A-C): The endo treat finished. Figure 15 (A, B): The case finished, followup after 21 days (a) 1 month and (b) 2 months. Fig. 14A Fig. 14B Fig. 14C Fig. 15A Fig. 15B








1. Neville, Brad W. [et al.] (1st ed., 1995). Oral and Maxillofacial Pathology. Saunders. pp. 104–5.
2. Cantatore JL, Klein PA, Lieblich LM. Cutaneous dental sinus tract, a common misdiagnosis: a case report and review of the literature.
Cutis. Nov 2002;70(5):264-7. [Medline].
3. Sheehan DJ, Potter BJ, Davis LS. Cutaneous draining sinus tract of odontogenic origin: unusual presentation of a challenging diagnosis.
South Med J. Feb 2005;98(2):250-2. [Medline].
4. Gound TG, Maixner D. Nonsurgical management of a dilacerated maxillary lateral incisor with type III dens invaginatus: a case report. J Endod. Jun 2004;30(6):448-51. [Medline].
5. Nallapati S. Clinical management of a maxillary lateral incisor with vital pulp and type 3 dens invaginatus: a case report. J Endod. Oct 2004;30(10):726-31.
6. Steffen H, Splieth C. Conventional treatment of dens invaginatus in maxillary lateral incisor with sinus tract: one year follow-up. J Endod. Feb 2005;31(2):130-3. [Medline].
7. Sert S, Bayrl G. Taurodontism in six molars: a case report. J Endod. Aug 2004;30(8):601-2. [Medline].
8. Yasui H, Yamaguchi M, Ichimiya M, Yoshikawa Y, Hamamoto Y, Muto M. A case of cutaneous odontogenic sinus. J Dermatol. Oct 2005;32(10):852-5. [Medline].
9. Gonçalves M, Pinto Oliveira D, Oliveira Oya E, Gonçalves A. Garre’s osteomyelitis associated with a fistula: a case report. J Clin Pediatr Dent. 2002;26(3):311-3. [Medline].
10. Gerhards F, Büttner R, Jänicke S. [Aberrant salivary gland tissue in differential diagnosis of branchiogenic neck cyst]. HNO. Jun 2001;49(6):476-8. [Medline].

»IMPLANT/CRESTAL P«

»IMPLANT/CRESTAL A«

From the makers of the Implantmed –W&H are proud to introduce the all NEW Piezomed.
AUTOCLAVABLE HANDPIECE fhandpiece and cable are thermo washer disinfectable and sterilisable.
INNOVATIVE LED RING shadow-free light and ideal illumination of the operating site.
SPECIAL BOOST FUNCTION to increase the set basic power by 20%.
The new Piezomed offers extremely high performance, yet is gentle on soft tissue. In addition, it includes automatic instrument recognition and LED handpiece illumination. The handpiece with the cable is thermo washer disinfectable and sterilizable!
EFFICIENT COOLING for cooling the operating site extremely efficiently.

AUTOMATIC INSTRUMENT DETECTION protects the instruments against overloading.

FINE TOOTH DESIGN for improved cutting precision.


p1954sa@yahoo.com.au
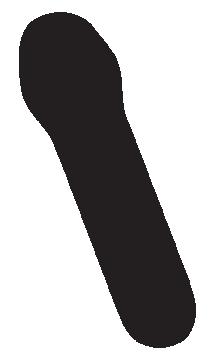
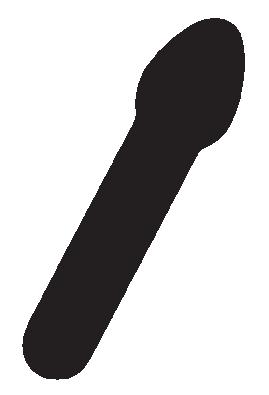
A 49 years old male patient presented to the oral surgery clinic with a history of a plaque like lesion on the right ventral aspect of the tongue. It was of 2 to 3 years duration, yellowish-grey, well demarcated, slightly raised and demonstrated a verrucous surface with no evidence of ulceration (Fig 1). He was medically fit and a non-smoker. Extra-oral examination was non-significant.
A clinical diagnosis of idiopathic leukoplakia was made and option of biopsy was discussed. The patient consented for biopsy and the lesion was excised completely under local anaesthetic. Post-operative phase was uneventful. I have reviewed him during 12 months follow-up with no signs of any recurrence.
Histological examination revealed mucosal verrucous hyperplasia with parakeratosis and collections of foamy histiocytes in the subepithelial stromal papillae (Fig 2).
1
Figure 1: Clinical photograph showing yellowish grey slightly raised well-demarcated area.
These are highlighted in a CD68 histiocytic marker immunoperoxidase stain, confirming the diagnosis of oral verruciform xanthoma (Fig 3). No fungal elements were seen in PAS-stained sections. The features are not those of Fordyce spots. There is no epithelial dysplasia or evidence of malignancy. The differential diagnosis is important as it can clinically resemble malignancy. Differentials include verrucous carcinoma, squamous cell carcinoma, squamous papilloma, verruca vulgaris, condyloma and leukoplakia. The verrucous architecture and exophytic nature of this lesion could mimic malignancy clinically and therefore biopsy becomes mandatory. A reassuring clinical feature is that the lesions tend to be soft on palpation, unlike a malignant process which is firm. The presence of foamy cells is characteristic of VX, which tend to accumulate in between rete ridges in the connective tissue.


Producing the best instruments to simplify the work of practitioners and constantly improve patient comfort. This has been Bien-Air’s mission since its creation in 1959.
Ergonomics, precision and reliability are at the core of the development of every new product. Paying careful attention to professionals every day, Bien-Air has made numerous innovations, always setting the bar higher. A true culture of excellence sitting perfectly with the tradition of Swiss-Made products from the renowned Watch Valley.






mectron s.p.a., Italy, tel +39 0185 35361, www.mectron.com, mectron@mectron.com
Figure 2: H&E stain photomicrograph X 200 showing foamy cells in stromal papillae immediately beneath the epithelium.













→ one device, two indications – easy switch from supra to subgingival air-polishing with a PROPHY to PERIO turn
→ optimal access thanks to 3 available nozzles –90°, 120°and PERIO


















Figure 3: Immunostain photomicrograph X 100 showing foamy cell can be seen darkly stained in the stromal papillae.



The assistance of Associate Professor Hedley Coleman, Senior Staff Specialist, Tissue Pathology & Diagnostic Oncology, Institute of Clinical Pathology and Medical Research, Westmead Hospital, Westmead NSW 2145, Australia, and Dr Peter Cropley, Anatomical Pathologist, Laverty Pathology, 60 Waterloo Road, North Ryde NSW 2113, Australia, in establishing the pathological diagnosis is acknowledged.








1. Byakodi S, Kumar B, Patil S, Shinde S. Verruciform xanthoma of the tongue. Natl J Maxillofacial Surg 2017; 8: 78-80.
2. Harris L, Staines K, Pring M. Oral verruciform xanthoma BMJ Case Rep 2015; doi: 10.1136/bcr-2014-209216.

Fifteen years ago, the composite GC Gradia Direct was first launched on the market. At that time, the indirect composite system GC Gradia was already highly valued by dental technicians all around the world. Dentists noticed that these restorations were blending in with their surroundings very well and they got curious about it. The concept was already there, so why not use it to create a direct composite that dentists could use themselves?
It rapidly became the favourite composite of many dentists, for reasons that are still valid today. The exceptional shade integration, pleasant handling and 15 years of clinical performance need no further explanation.
GC Gradia Direct has a unique multifaceted structure, just like tooth structure. Due to its balanced particle size distribution, the incident light is reflected and dispersed within the material in the same way as in a natural tooth. The result? Imperceptible restorations with invisible transition lines can be created - and in 95% of cases, this can even be accomplished with just one shade. Next to the standard VITA Classical® shades, additional cervical and bleach shades are available. In cases where a multi-shade technique is preferred, the Inside (opaque) and Outside (enamel) Special Shades complete the portfolio to meet all your needs.
The clinical durability of Gradia Direct has been proven in several independent studies 1,2. After 5 or more years, Gradia Direct restorations bonded with G-BOND demonstrated good marginal integrity and a low failure rate. The easy handling of the material allows the dentist to place void-free restorations with an excellent durability.
GC Gradia Direct has been a benchmark in aesthetic restorations ever since it was first created 15 years ago. It’s a classic worth celebrating and we hope you want to join us to make this anniversary memorable.
1. Van Landuyt, K. L., De Munck, J., Ermis, R. B., Peumans, M. & Van Meerbeek, B. Five-year clinical performance of a HEMA-free one-step self-etch adhesive in noncarious cervical lesions. Clin. Oral Investig. 18, 1045–1052 (2014).
2. Van Dijken, J. W. V. A 6-year prospective evaluation of a one-step HEMA-free self-etching adhesive in Class II restorations. Dent. Mater. 29, 1116–1122 (2013).
For more details, go to www.gceurope.com/products/gradiadirect/
Orthodontics

Stacey Kirshenblatt, DDS, MS, FRCD(C) Private practice, Toronto, ON.
Hui Chen, DDS, MS, PhD
Clinical assistant professor, faculty of dentistry, University of British Columbia, Vancouver, BC.
Marijke Dieltjens, MBS, PhD
Associate researcher Faculty of medicine, Antwerp University, Belgium.
Benjamin Pliska, DDS, MS, FRCD(C) Assistant professor, faculty of dentistry, University of British Columbia, Vancouver, BC.
Fernanda R. Almeida, DDS, MSc, PhD
Associate professor, faculty of dentistry, University of British Columbia, Vancouver, BC.
Republished with permission from the Journal of the Canadian Dental Association falmeida@dentistry.ubc.ca
Oral appliances (OAs) are frequently used in orthodontics and for the treatment of obstructive sleep apnea. Because OAs can be inserted and removed by patients themselves, the patient’s cooperation is a major component of effective treatment. In this review, we provide an overview of factors studied in the past that affect adherence to OA use in orthodontics and dental sleep medicine. We also describe future directions in adherence and the use of objective microsensor technology to measure adherence in these patients.
Because removable oral appliances (OAs) can be inserted and removed by patients themselves, their cooperation and adherence to therapy are necessary to achieve success. 1,2
Removable OAs, such as headgear, removable retainers and functional appliances, are used in orthodontics to correct malocclusions. In the field of sleep medicine, removable OAs are increasingly used as an option in the treatment of patients with obstructive sleep apnea (OSA).
The gold standard for the treatment of moderate to severe OSA is continuous positive airway pressure (CPAP); however, adherence to this
treatment has been found to be limited. 3-5 Removable OAs, which reduce upper airway collapse by advancing the mandible, have emerged as a non-invasive treatment option for patients with OSA. These devices are similar in design to functional appliances used commonly for growth modification in orthodontics. They can be inserted and removed by patients, thus, placing responsibility on the patient to follow a prescribed wear schedule.
To date, many scientific publications have addressed the issue of adherence to treatment in orthodontics and dental sleep medicine to determine how to improve and monitor patient compliance.3,6-16 However, there is controversy over the factors that might predict adherence, mainly because, in the absence of objective monitors, information has been limited to self-reported use, which is often false or overestimated. 17
Recently, objective compliance monitoring for removable OAs has become available. 18,19 In this article, we present an overview of the factors that affect adherence to treatment in both orthodontics and sleep medicine.
In addition, we review the use of objective microsensor technology to measure adherence in patients using removable OAs. 17




Factors that are thought to be related to patient compliance and cooperation during therapy with removable OAs in orthodontics and dental sleep medicine include gender, age, socioeconomic status, psychosocial aspects, patient’s family and partner and the interaction between the dentist or physician and the patient. 15,20 This multifaceted system leads to complex interactions in which each individual component as well as the interplay of factors should be studied. 15, 16
Patient gender is a factor commonly cited as a predictor of adherence to orthodontic treatment. Some reports suggest better adherence among female compared with male patients. 21-24 Girls tend to take a more responsible attitude toward orthodontic therapy as they mature earlier than boys. 23 On the other hand, more recent reports have failed to show gender as a significant factor in predicting adherence. 6,22,25-30 Previous findings relied on subjective measures of adherence, such as orthodontists’ judgement, which may be more a reflection of social and gender stereotypes than a valid correlation. 6 Studies using objective measures of adherence during orthodontic treatment, such as electronic sensors, have found no difference in overall wear time between genders. 6,25,29,30
Although many studies in orthodontics have examined these issues, the correlation between gender and adherence has not been thoroughly assessed in OA treatment for OSA. However, long-term discontinuation of this therapy has not been found to be different between genders. 31, 32
Age is also often considered to be an influential factor in adherence to orthodontic therapy. 33 Although some studies have found greater cooperation among younger patients (< 12 years), 6,7,9,28,34-37 others have found no difference. 7,22,25-27,30,38 The variation in reports on the effect of age on adherence may be confounded by variations in children’s individual psychological maturation. Teenage years are often associat-ed with decreased parental influences and cooperation. 7,36,37 Orthodontic studies focus on children, whereas OA therapy for OSA is mainly studied in adults. Although discontinuation of long-term OA therapy by OSA patients has not been found to be dependent on age, the effect of age on OA adherence has yet to be explored in this population. 31,32
The potential influence of a patient’s socioeconomic status on adherence has been addressed and debated in the literature. Patients with higher socioeconomic status have been shown to be more cooperative orthodontic patients. 7,21 A possible explanation is that higher socioeconomic groups perceive dentofacial appearance to be highly important for social and occupational success. 22,39 On the other hand, another study reported greater adherence among patients from lower middle-class families compared with upper-class families.40 This may be attributed to a greater need for social acceptance, higher social aspiration, better child–parent relationships and greater emphasis on value for money seen in these socioeconomic groups. Some studies also report no difference in patient adherence based on socioeconomic status. 22,38
In sleep medicine, patients with lower socioeconomic status are less likely to accept and commence CPAP therapy. 15,41 Sleeping with a spouse or partner has been found to increase adherence as the partner may provide feedback regarding elimination of symptoms, such as snoring, which may increase CPAP use. 42 Although these factors may be similar in OA therapy, this has not been assessed.
Considerable attention has been devoted to the examination of personality characteristics as a method to predict patients’ adherence to orthodontic treatment. 1,2,6,22,25,36,43-46 In general, cooperative patients are characterized as enthu-siastic, energetic, outgoing, self-controlled, responsible and hard working. 33 These patients tend to have better grades and show less deviant behaviour in school. 39 In contrast, uncooperative patients are described as hard headed, independent, temperamental, impatient, individualistic and intolerant of prolonged effort. 33 Based on these findings, a patient’s performance in school may serve as a useful tool in determining adherence. However, children who are of below-average intelligence do not necessarily show poor adherence. 39 Studies showing no correlation between person-ality questionnaires and adherence stated that treatment adherence and orthodontic cooperation is not reflective of a simple, single, monotonous dimension of cooperation, but rather a complex and interactive reaction. 25,22,44,46,47 The use of psychological instruments 44,45 to predict adherence has been shown to be useful, but these tools are not used in clinical practice.

In sleep medicine, OSA patients who display significantly more hypochondriasis and psychopathic deviation, presents a potentially higher rate of discontinuation and lower compli-ance. More specifically, OSA patients with a so-called type D (“distressed”) personality, defined as a combination of negative affectivity and social inhibition, 48,49 show a signifi-cantly higher discontinuation rate for both CPAP and OA therapy. 50,53
There are several approaches to measuring adherence. In orthodontics, the most common method relies on clinicians’ judgement. Typical clinical methods for estimating wear time of devices, such as headgear and removable OAs, include evaluation of patients’ oral hygiene, condition of the appliance, such as a worn-looking neck strap, mobility of molars, ease of patient use and missing or being late for scheduled orthodontic appointments. 21 Unfortunately, these methods are unreliable. For example, adolescent patients brought to the orthodontist’s office by a parent or guardian reflect the punctuality of the parent, not the patient. 2,6,28,52,53 As well, clinicians’ judgement is often influenced by therapeu-tic outcome. This is problematic because it assumes there is a direct link between the clinical outcome and the patient’s adherence to treatment, which is not necessarily the case. 53
Another way to monitor adherence is through patients’ self-reports: interviews, questionnaires or log records. However,thiscanleadtofalseoroverestimatedcompliance, largely because patients wish to appear more compliant than they actually are. 8,29 The best way to assess compliance is by objective measures. Investigators have attempted to provide timers and micro-sensors to record accurate details of patient compliance, and the technology used in manufacturing these microsensors has been improving over many years.
In 1974, Northcutt 10 described the first extraoral orthodontic headgear with a timing mechanism to measure wear. It worked by simultaneously turning on 2 switches triggered by the pull of the strap and pressure on the back of the neck while the headgear is worn. 10,54,55 Banks et al. 56 found that the Northcutt timer was easily circumvented by the patient placing heavy objects on the pressure switch to activate the timer without actually wearing the headgear.
In 1991, Cureton et al. 57 described a micro-electronic approach to measuring compliance using a small ladies’ quartz calendar watch with an accuracy level of 99.9% over 20 days of testing. A limitation of such an external headgear timer is that it is bulky and diminishes patient comfort when it is placed in a neck strap. 58 The patient can also circumvent it by just stretching the band and, thereby, falsifying the wear data.52,59 In addition, many of these devices give only a cumulative overall measure of wear time and provide the orthodontist with intermittent headgear wear information and no easily accessible feedback to patients. 6,53,59,60
The ability to monitor intraoral appliance adherence is even more challenging because of the damaging effects of saliva. One of the first methods used was controlled-release glass discs 60 composed of phosphates, borates and trace elements. A disc was fitted onto the surface of an orthodontic appliance and would dissolve in saline solution indicating wear. Problems with this method included disc separation from the appliance because of poor adhesion, surface grinding of the discs leading to fragmentation and dissolving of discs at different rates. 60
More recently, a compliance indicator was introduced for aligner therapy. A food dye (erioglaucine disodium salt) is embedded in the OA and dissolves from the polymer when exposed to oral fluid. 61,62 The clinician and the patient can evaluate 5 potential colour changes (from dark blue to clear) to obtain a graphic representation of wear time and have instant feedback on adherence. However, the rating on a 5-point scale involves subjective judgement and, thus, does not yield an objective wear time. In addition, the results can be easily falsified by patients, as the dye will fade in various aqueous solutions, for example, when left in the mouth while drinking, stored in water, cleaned with tablets containing oxidizing agents or cleaned in a dishwasher. A large variation in degree of fading was found among patients who strictly adhered to the prescribed wear times. 57
In 1990, Sahm et al. 11,63 created a reed-switch, which was embedded into a bionator functional appliance and was activated by a magnet system bonded to the lingual surface of the mandibular first permanent molar. The main problem noted with this device was its bulkiness and patient discomfort.




More recently, temperature sensitive microsensors have been used to objectively measure orthodontic OA use. These microsensors record temperature changes, assuming a difference between room and intraoral temperature. Schott and Göz 64 assessed the accuracy of 2 tempera-ture-sensitive microsensors: the Smart Retainer (discontinued production) and the TheraMon microsensor (IFT Handels und Entwicklungsgesellschaft GmbH, Handelsagentur Gschladt, Hargelsberg, Austria) using in vitro testing in a programmable water bath. They reported that the TheraMon microsensor is more accurate, with the Smart Retainer overestimating wear time by 1 h. However, the water bath was programmed to room temperature and oral temperature while not taking into account the time it takes for the water bath to heat or cool.
A year later, in vivo testing of the microsensor was conducted by Schott and Göz58 on patients fitted with upper and lower active plates, functional appliances or retention devices. However, they provide only 1 case report of a patient wearing an upper appliance and no statistical analysis of the accuracy of the device.
In 2013, Schott et al. 30 published a study examining the adherence rate of patients fitted with retainers or functional appliances during the retention phase of their orthodontic treatment. Although patients were instructed to wear the appliances at least 8 h/day, the median wear time was 7 h/day. The report stated that adherence rates were influenced by age, sex and place of treatment, but these differences were not statistically significant.
Using the TheraMon microsensor, Pauls et al. 29 found that orthodontic patients tended to overestimate their OA use by an average of 2.7 h/day. Informing and confronting the patients with their objectively measured OA use led to a more accurate subjective estimation, with an average overestimation of only 0.7 h/day.
The first report on intraoral recording of OA compliance during treatment for OSA was published by Lowe et al.65 This ceramic monitor had a memory system and temperature sensor that would monitor wear time based on temperature measured above 31°C. Several problems with this device were reported, including the damaging effect of saliva, heat intolerance of the electronic components and energy consumption over a long period. 65
Vanderveken et al. 18 were the first to assess the safety and feasibility of the TheraMon microsensor in vivo in dental sleep medicine. In their 3-month prospective clinical trial, they demonstrated that this compliance monitor could be used safely. No adverse effects, including oral burns, lesions or detachment of the microsensor were reported by the participants. Only 1 of 51 sensors was disqualified in this study because of technical problems. Recently, long-term results with the TheraMon microsensor in dental sleep medicine showed relatively high objective OA use on 1-year follow-up. 66
To our knowledge, 3 microsensors that can be integrated into removable OAs for OSA are currently available commercially. These sensors differ in terms of data-recording interval, longevity, form of readout signals, size, weight, storage capacity and availability of a patient station, which permits patients to monitor their own adherence and upload their data remotely. Kirshenblatt et al.67 tested the accuracy of these thermosensitive microsensors in vitro using a water bath (34–37°C) to simulate OA wear time.
The TheraMon microsensor was accurate during both short and long durations of simulated OA wear, whereas the AIR AID SLEEP sensor (AIR AID GmbH & Co. KG, Frankfurt, Germany) significantly underestimated OA use during short durations by 3.67 ± 9.34 min./ day, (mean and standard deviation) and the DentiTrac microsensor (Braebon Medical Corporation, Kanata, Canada) overestimated OA use during both short and long durations by 8.34 ± 3.62 min./day and 3.53 ± 2.42 min./day, respectively. However, these under- and overestimations were considered not clinically relevant.
Adherence to a prescribed treatment modality is of utmost importance in ensuring successful therapy. Lack of adherence can reduce the effectiveness of the best treatment plan and the most promising treatment mecha-nisms.5 This literature review shows that several factors have been thought to affect adherence in the fields of both orthodontics and dental sleep medicine. Studies indicating that adherence may be influenced by gender, age, psychosocial and socioeconomic factors have found wide variation among individuals. 1,25 Other factors may also be found to be important, such as cultural background and severity of


malocclusion/disease. Although the studies have tried to pinpoint which factors are determinants of patient adherence, this review shows that, in reality, it is difficult and challenging for clinicians to predict which patients will be cooperative. This can be explained by the fact that human behaviour is multifactorial and includes complex interactions in which each individual component, as well as the interplay of factors, should be studied. 15
Another important finding is that patients’ adherence significantly increases when there is some objective feedback or when they are aware of being monitored objectively. 10,34,68,69 Because patients are more motivated to change their behaviour when they know it is being monitored, there is a strong need for and interest in an objective compliance monitor for OA therapy in both orthodontics and dental sleep medicine. The use of such monitors alone may improve adherence.
However, the use of such devices is not part of routine daily clinical practice. A major problem with these monitors for removable OAs is accuracy. Besides the technical and functional factors, additional requirements must be met to achieve a high level of product acceptance by patients and health care professionals. Compliance monitors must be safe and small without altering the dimensions of the OA or affecting patients’ comfort; read-outs and monitoring must be easy and fast; and the sensors’ unit price must be reasonable. 70
Microsensors that have recently become available can assist with monitoring patient adherence to orthodontics treatment and OA therapy for patients diagnosed with OSA.19 Such microsensors will give clinicians a better understanding of their patients and will allow them to tailor appointment schedules to best meet patients’ individual treatment needs. These microsensors can be used as a tool to motivate patients. In addition, the availability of objective compliance data will eliminate inconsistencies in patients’ subjective reports if the data prove to be accurate.
Furthermore, it is difficult to compare tolerance to various OA devices based on subjective compliance data without proof that patients are actually wearing them. In the field of sleep medicine, objective monitoring will allow for calculation of mean disease alleviation, which depends on both efficacy and compliance for therapeutic effectiveness. 18 Calculation of real therapeutic effectiveness allows for comparison of
different treatment modalities, such as CPAP therapy, surgery and oral appliances. For example, in the literature, CPAP therapy and oral appliances have been comparable in terms of mean disease alleviation. 18,71 It has been suggested that the greater efficacy of CPAP therapy is being offset by inferior CPAP adherence compared with OA adherence, possibly resulting in equal effectiveness. 72,73
In orthodontics, objective microsensors will increase the strength of evidence from studies comparing various appliances and retainer designs. Future studies using these monitors may also help identify the most appropriate wear pattern clinicians should be prescribing for the most effective treatment results.
Removable OAs are frequently used in both orthodontics and the treatment of OSA. Many of the appliances used in orthodontic practice rely on patients wearing the devices as prescribed. Adherence is of utmost importance in ensuring successful treatment. This literature review shows that, although several factors have been thought to affect adherence, human behaviour is complex and open to multifactorial influences. Therefore, there is a strong need for and interest in objective adherence monitors for OA therapy. The availability of such monitors will allow clinicians to track patient adherence, motivate patients and improve research that compares treatment outcomes.
1. Gross AM, Samson G, Dlerkes M. Patient cooperation in treatment with removable appliances: a model of patient noncompliance with treatment implications. Am J Orthod. 1985;87(5):392-7.
2. Mehra T, Nanda RS, Sinha PK. Orthodontists’ assessment and management of patient compliance. Angle Orthod. 1998;68(2):115-22.
3. Sawyer AM, Gooneratne NS, Marcus CL, Ofer D, Richards KC, Weaver TE. A systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventions. Sleep Med Rev. 2011;15(6):343-56.
4. Hoffstein V. Review of oral appliances for treatment of sleep-disordered breathing. Sleep Breath. 2007;11(1):1-22.
5. Ravesloot MJ, de Vries N. Reliable calculation of the efficacy of non-surgical and surgical treatment of obstructive sleep apnea revisited. Sleep. 2011;34(1):105-10.
6. Bartsch A, Witt E, Sahm G, Schneider S. Correlates of objective
patient compliance with removable appliance wear. Am J Orthod Dentofacial Orthop. 1993;104(4):378-86.
7. Albino JE, Lawrence SD, Lopes CE, Nash LB, Tedesco LA. Cooperation of adolescents in orthodontic treatment. J Behav Med. 1991;14(1):53-70.
8. Cole WA. Accuracy of patient reporting as an indication of headgear compliance. Am J Orthod Dentofacial Orthop. 2002;121(4):419-23.
9. Cureton SL, Regennitter FJ, Yancey JM. Clinical versus quantitative assessment of headgear compliance. Am J Orthod Dentofacial Orthop. 1993;104(3):277-84.
10. Northcutt M. The timing headgear. J Clin Orthod. 1974;8(6):321-4.
11. Sahm G, Bartsch A, Witt E. Reliability of patient reports on compliance. Eur J Orthod. 1990;12(4):438-46.
12. Pelletier-Fleury N, Rakotonanahary D, Fleury B. The age and other factors in the evaluation of compliance with nasal continuous positive airway pressure for obstructive sleep apnea syndrome. A Cox’s proportional hazard analysis. Sleep Med. 2001;2(3):225-32.
13. Rauscher H, Formanek D, Popp W, Zwick H. Self-reported vs measured compliance with nasal CPAP for obstructive sleep apnea. Chest. 1993;103(6):1675-80.
14. Reeves-Hoche MK, Meck R, Zwillich CW. Nasal CPAP: an objective evaluation of patient compliance. Am J Respir Crit Care Med. 1994;149(1):149-54.
15. Shapiro GK, Shapiro CM. Factors that influence CPAP adherence: an overview. Sleep Breath. 2010;14(4):323-35.
16. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-8.
17. Kribbs NB, Pack AI, Kline LR, Smith PL, Schwartz AR, Schubert NM, et al. Objective measurement of patterns of nasal CPAP use by patients with obstructive sleep apnea. Am Rev Resp Dis 1993;147(4):887-95.
18. Vanderveken OM, Dieltjens M, Wouters K, De Backer WA, Van de Heyning PH, Braem MJ. Objective measurement of compliance during oral appliance therapy for sleepdisordered breathing. Thorax. 2013;68(1):91-6.
19. Kirshenblatt SJ, Chen H, Lowe A, Pliska B, Almeida FR. Microsensor technology to monitor compliance with removable oral appliances (Abstract). Sleep Breath. 2013;17:879-94.
20. Bos A, Hoogstraten J, Prahl-Andersen B. Towards a comprehensive model for the study of compliance in orthodontics. Eur J Orthod. 2005;27(3):296-301.
21. Cucalon A 3rd, Smith RJ. Relationship between compliance by adolescent orthodontic patients and performance on psychological tests. Angle Orthod. 1990;60(2):107-14.
22. Nanda RS, Kierl MJ. Prediction of cooperation in orthodontic treatment. Am J Orthod Dentofacial Orthop. 1992;102(1):15-21.
23. Starnbach HK, Kaplan A. Profile of an excellent orthodontic patient. Angle Orthod. 1975;45(2):141-5.
24. Clemmer EJ, Hayes EW. Patient cooperation in wearing orthodontic headgear. Am J Orthod. 1979;75(5):517-24.
25. Ağar U, Doruk C, Biçakçi AA, Büküsoğlu N. The role of psycho-social factors in headgear compliance. Eur J Orthod. 2005;27(3):263-7.
26. Sergl HG, Klages U, Pempera J. On the prediction of dentist-evaluated patient compliance in orthodontics. Eur J Orthod. 1992;14(6):4638.
27. Richter DD, Nanda RS, Sinha PK, Smith DW, Currier GF. Effect of behavior modification on patient compliance in orthodontics. Angle Orthod. 1998;68(2):123-32.
28. Bos A, Kleverlaan CJ, Hoogstraten J, Prahl-Andersen B, Kuitert R. Comparing subjective and objective measures of headgear compliance. Am J Orthod Dentofacial Orthop. 2007;132(6):801-5.
29. Pauls A, Neinkemper M, Panayotidis A, Wilmes B, Drescher D. Effects of wear time recording on patient’s compliance. Angle Orthod. 2013;83(6):1002-8..
30. Schott TC, Schlipf C, Glasl B, Schwarzer CL, Weber J, Ludwig B. Quantification of patient compliance with Hawley retainers and removable functional appliances during the retention phase. Am J Orthod Dentofacial Orthop. 2013;144(4):533-40.
31. de Almeida FR, Lowe AA, Tsuiki S, Otsuka R, Wong M, Fastlicht S, et al. Long-term compliance and side effects of oral appliances used for the treatment of snoring and obstructive sleep apnea syndrome. J Clin Sleep Med. 2005;1(2):143-52.
32. Marklund M, Franklin KA. Long-term effects of mandibular repositioning appliances on symptoms of sleep apnoea.
J Sleep Res. 2007;16(4):414-20.
33. Allan TK, Hodgson EW. The use of personality measurements as a determinant of patient cooperation in an orthodontic practice. Am J Orthod. 1968;54(6):433-40.
34. Brandão M, Pinho HS, Urias D. Clinical and quantitative assessment of headgear compliance: a pilot study. Am J Orthod Dentofacial Orthop. 2006;129(2):239-44.
35. Weiss J, Eiser HM. Psychological timing of orthodontic treatment. Am J Orthod. 1977;72(2):198-204.
36. Colenaty C, Gabriel HF. Predicting patient cooperation. J Clin Orthod. 1977;11(12):814-9.
37. Trulsson U, Linläv L, Mohlin B, Strandmark M. Age dependence of compliance with orthodontic treatment in children with large overjet. An interview study. Swed Dent J. 2004;28(2):101-9.
38. Mandall NA, Matthew S, Fox D, Wright J, Conboy FM, O’Brien KD. Prediction of compliance and completion of orthodontic treatment: are quality of life measures important? Eur J Orthod. 2008;30(1):40-5.
39. Sergl HG, Klages U, Zentner A. Functional and social discomfort during orthodontic treatment — effects on compliance and prediction of patients’ adaptation by personality variables. Eur J Orthod. 2000;22(3):307-15.
40. Dorsey J, Korabik K. Social and psychological motivations for orthodontic treatment. Am J Orthod. 1977;72(4):460.
41. Simon-Tuval T, Reuveni H, Greenberg-Dotan S, Oksenberg A, Tal A, Tarasiuk A. Low socioeconomic status is a risk factor for CPAP
acceptance among adult OSAS patients requiring treatment. Sleep. 2009;32(4):545-52.
42. Weaver TE, Sawyer AM. Adherence to continuous positive airway pressure treatment for obstructive sleep apnoea: implications for future interventions. Indian J Med Res. 2010;131:245-58.
43. Egolf RJ, Begole EA, Upshaw HS. Factors associated with orthodontic patient compliance with intraoral elastic and headgear wear. Am J Orthod Dentofacial Orthop. 1990;97(4):336-48.
44. El-Mangoury NH. Orthodontic cooperation. Am J Orthod 1981;80(6):604-22.
45. Southard KA, Tolley EA, Arheart KL, Hackett-Renner CA, Southard TE. Application of the Millon Adolescent Personality Inventory in evaluating orthodontic compliance. Am J Orthod Dentofacial Orthop. 1991;100(6):553-61.
46. Woolass KF, Shaw WC, Viader PH, Lewis AS. The prediction of patient co-operation in orthodontic treatment. Eur J Orthod. 1988;10(3):235-43.
47. Lee SJ, Ahn SJ, Kim TW. Patient compliance and locus of control in orthodontic treatment: a prospective study. Am J Orthod Dentofacial Orthop. 2008;133(3):354-8.
48. Denollet J. Type D personality. A potential risk factor refined. J Psychosom Res. 2000;49(4):255-66.
49. Denollet J, Sys SU, Stroobant N, Rombouts H, Gillebert TC, Brutsaert DL. Personality as independent predictor of long-term mortality in patients with coronary heart disease. Lancet. 1996;347(8999):417-21.
50. Dieltjens M, Vanderveken OM, Van den Bosch D, Wouters K, Denollet J, Verbraecken JA, et al. Impact of type D personality on adherence to oral appliance therapy for sleep-disordered breathing. Sleep Breath. 2013;17(3):985-91.
51. Broström A, Strömberg A, Mårtensson J, Ulander M, Harder L, Svanborg E. Association of Type D personality to perceived side effects and adherence in CPAP-treated patients with OSAS. J Sleep Res. 2007;16(4):439-47.
52. Lyons EK, Ramsay DS. A self-regulation model of patient compliance in orthodontics: implications for future design of a headgear monitor. Semin Orthod. 2000;6:224-30.
53. Ramsay DS, Soma M, Sarason IG. Enhancing patient adherence: the role of technology and its application to orthodontics. In McNamara Jr JA, Trotman CA (eds.). Creating the compliant patient. Craniofacial growth series, vol. 33. Ann Arbor: Center for Human Growth and Development, University of Michigan; 1997:141-65.
54. Northcutt M. The high-pull timing headgear. J Clin Orthod. 1976;10(12):918-20.
55. Northcutt ME. Updating the timing headgear. J Clin Orthod. 1975;9(11):713-7.
56. Banks PA, Read MJ. An investigation into the reliability of the timing headgear. Br J Orthod. 1987;14(4):263-7.
57. Cureton SL, Regennitter F, Orbell MG. An accurate, inexpensive headgear timer. J Clin Orthod 1991;25(12):749-54.
58. Schott TC, Göz G. Wearing times of orthodontic devices as mea-
sured by the TheraMon® microsensor. J Orofac Orthop. 2011;72(2):10310.
59. Lyons EK, Ramsay DS. Preliminary tests of a new device to monitor orthodontics headgear use. Semin Orthod. 2002;8(1):29-34.
60. Savage M. A preliminary report into the development and use of soluble controlled-release glass timing discs implanted into orthodontic appliances. Br J Orthod. 1982;9(4):190-3..
61. Schott TC, Göz G. Color fading of the blue compliance indicator encapsulated in removable clear Invisalign Teen® aligners. Angle Orthod. 2011;81(2):185-91.
62. Tuncay OC, Bowman SJ, Nicozisis JL, Amy BD. Effectiveness of a compliance indicator for clear aligners. J Clin Orthod. 2009;43(4):2638; quiz 273-4.
63. Sahm G, Bartsch A, Witt E. Micro-electronic monitoring of functional appliance wear. Eur J Orthod. 1990;12(3):297-301.
64. Schott TC, Göz G. Applicative characteristics of new microelectronic sensors Smart Retainer® and TheraMon® for measuring wear time. J Orofac Orthop. 2010;71(5):339-47.
65. Lowe AA, Sjöholm TT, Ryan CF, Fleetham JA, Ferguson KA, Remmers JE. Treatment, airway and compliance effects of a titratable oral appliance. Sleep. 2000;23 (Suppl 4):S172-8.
66. Dieltjens M, Verbruggen AE, Braem MJ, Wouters K, Verbraecken JA, De Backer WA, et al. Determinants of objective compliance during oral appliance therapy in patients with sleep-disordered breathing: a prospective clinical trial. JAMA Otolaryngol Head Neck Surg. 2015 Oct;141(10):894-900.
67. Kirshenblatt SJ, Hui C, Lowe A, Pliska B, Almeida FR. Microsensor technology to monitor adherence with removable oral appliances. Baltimore: American Academy of Dental Sleep Medicine Conference; 2013.
68. Doruk C, Ağar U, Babacan H. The role of the headgear timer in extraoral co-operation. Eur J Orthod. 2004;26(3):289-91.
69. Ackerman MB, Thornton B. Posttreatment compliance with removable maxillary retention in a teenage population: a short-term randomized clinical trial. Orthodontics (Chic). 2011;12(1):22-7.
70. Schott TC, Ludwig B, Glasl BA, Lisson JA. A microsensor for monitoring removable-appliance wear. J Clin Orthod. 2011;45(9):518-20; quiz 516. 71. Grote L, Hedner J, Grunstein R, Kraiczi H. Therapy with nCPAP: incomplete elimination of sleep related breathing disorder. Eur Respir J. 2000;16(5):921-7.
72. Phillips CL, Grunstein RR, Darendeliler MA, Mihailidou AS, Srinivasan VK, Yee BJ, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med. 2013;187(8):879-87.
73. Vanderveken OM, Braem MJ, Dieltjens M, De Backer WA, Van de Heyning PH. Objective measurement of the therapeutic effectiveness of continuous positive airway pressure versus oral appliance therapy for the treatment of obstructive sleep apnea. Am J Respir Crit Care Med. 2013;188(9):1162

www.henryscheinortho.com.
The Carriere Motion 3D Appliance: Revolutionizing Class II and Class III Corrections
Dr. Luis Carrière, who invented the Carriere Self-Ligating Bracket and the Carriere Motion 3D Appliance, lectures internationally on these products as well as other topics. Carrière is a member of the editorial review board for the American Journal of Orthodontics and Dentofacial Orthopedics and an invited professor at several orthodontic departments throughout the world. He maintains a private practice in Barcelona.
What features of the Motion 3D Appliance make it so effective?
LC: Its sleek, noninvasive design has allowed it to revolutionize Class II and Class III correction. The appliance attaches to only three teeth, so it’s comfortable and discreet, while it also allows for the use of the progressive “sagittal first” philosophy to correct the AP at the beginning of treatment, when patients are most compliant. It delivers a gentler, more natural force for tooth movement, controlling the movement of the tooth and providing crucial corrections to the bite and tooth alignment, in preparation for treatment with fixed orthodontic appliances such as braces or clear aligners. The appliance provides shorter treatment

times for mixed dentition in adolescents and adults.
How does the appliance fit into Henry Schein Orthodontics’ tenet of airway-friendly orthodontics?
LC: The appliance, based on the action of the human hip ball/socket joint, repositions the mandible forward as a unit for those patients who need it, and controls it with built-in stops for direct molar movement to the ideal position. This prevents over-rotations and unwanted tipping and can be an effective means of increasing a patient’s airway.
It’s been astounding and exciting to watch the progression of airway-friendly ortho-








PROF. ANDREA MOMBELLI, SWITZERLAND
PROF. ANDREA MOMBELLI, SWITZERLAND
Periodontics in the Implant Era...
Periodontics in the Implant Era...


CHRISTIAN
DR. CHRISTIAN MAKARY LEBANON






PROF. CRISTIAN DINU ROMANIA
PROF. CRISTIAN DINU ROMANIA
Guided Bone Regeneration in Simple and Complex Ridge Augmentation
Guided Bone Regeneration in Simple and Complex Ridge Augmentation
Advanced Piezosurgery Techniques: A clinical and Scientific Rationale
Advanced Piezosurgery Techniques: A clinical and Scientific Rationale


DR. DAVIS THOMAS USA
Coming soon
DR. DAVIS THOMAS USA
Coming soon


DR. EDUARDO MAHN CHILE
The Face and Tooth Integration in Modern Dentistry. New Insights
DR. EDUARDO MAHN CHILE
The Face and Tooth Integration in Modern Dentistry. New Insights


DR. CARLOS SABROSA BRAZIL
DR. CARLOS SABROSA BRAZIL
Simple and Reliable Procedures in Modern Restorative Dentistry
Simple and Reliable Procedures in Modern Restorative Dentistry


DR. RAMAN S AULAKH UK

DR. MATTHEW HOLYOAK UK

DR. RAMAN S AULAKH UK
Aesthetic Dentistry and Clear Aligner Therapy
Aesthetic Dentistry and Clear Aligner Therapy
Management of Anterior Tooth Trauma
DR. MATTHEW HOLYOAK UK
Management of Anterior Tooth Trauma

DR. RICCARDO AMMANNATO, ITALY

Advances in Composite Restoration
DR. RICCARDO AMMANNATO, ITALY
Advances in Composite Restoration

DR. MAHMOUD EZZAT GHAZI, EGYPT
DSD Concept in Integration with Facial Analysis
DR. MAHMOUD EZZAT GHAZI, EGYPT
DSD Concept in Integration with Facial Analysis

DR. SYLVIA RAHM GERMANY
All About Esthetic Composite Restoration - Direct and Indirect Procedures
DR. SYLVIA RAHM GERMANY
All About Esthetic Composite Restoration - Direct and Indirect Procedures

DR. MARC LAZARE USA
The Biomimetic Smile Makeover – Conserving and Strengthening Tooth Structure while Transforming a Smile
DR. MARC LAZARE USA
The Biomimetic Smile Makeover – Conserving and Strengthening Tooth Structure while Transforming a Smile

PROF. PAUL TIPTON UK

Influence of Vertical Dimension on Facial Aesthetics
PROF. PAUL TIPTON UK
Influence of Vertical Dimension on Facial Aesthetics

DR. RASHIDA JUZAR ALI VAJIHI, UAE
Digital Occlusion and Neuromuscular Paradigm

DR. RASHIDA JUZAR ALI VAJIHI, UAE
Digital Occlusion and Neuromuscular Paradigm
dontics in our industry. Orthodontists everywhere are realizing how they’re able to provide patients with more than just beautiful smiles—they also can provide the opportunity for patients to live healthier, happier lives, which is a strong aspect of HSO’s culture.
How does the appliance shorten treatment time?
LC: Class II or Class III correction takes place at the beginning of the orthodontic treatment, when there are no competing forces in the mouth caused by brackets or other appliances. This is also when the patient is the most
Dr. John Graham is an innovator and educator who lectures internationally to both doctors and orthodontic staff on orthodontic treatment philosophies. He holds faculty appointments at the University of the Pacific Arthur A. Dugoni School of Dentistry and the University of Rochester Eastman Institute for Oral Health. Graham sits on the editorial board for Orthotown and is a contributing editor for the Journal of Clinical Orthodontics and a reviewer for Orthodontics: The Art and Practice of Dentofacial Enhancement. He lives in Salt Lake City.
The Carriere Motion 3D Appliance fits into the HSO tenets of airway-friendly orthodontics, shorter treatment times and the “sagittalfirst” philosophy. Explain how it’s used in your practice, and the results you’ve seen.
JG: The “sagittal-first” philosophy using the Motion 3D Appliance is a real paradigm shift in the way orthodontists treat patients. It helps me reduce patient treatment times—sometimes by up to one year. It’s so rewarding to offer this treatment concept because I no longer receive hesitation from patients, especially adults, about moving forward with treatment. I get to explain that they won’t be making a commitment to wearing braces for two years—most likely, it will be around a year or less.
How do the appliances work with clear aligner therapy?
JG: The orthodontist and the patient don’t have to make
motivated and compliance is at its highest. Treating to the Class I platform is made simple and usually completed in three to four months.
Each Motion 3D Appliance addresses its intended sagittal dimension to reduce the need for extractions or surgery, and also helps reposition the jaws in better relation to one another, balancing the relationship between the nose, upper and lower lips, and chin for facial harmony. Both are biomimetic in function and consist of a small single-part design. This offers patients considerable freedom of movement for significantly greater comfort than traditional AP correctors.

a decision between braces or aligners before the patient starts treatment—we can think about it while the AP is being corrected.
This new treatment method allows me to treat more cases with clear aligners. The Motion 3D Appliance allows me to easily turn complex Class II patients into Class I patients; previously, a complex case would not be suitable for aligner treatment. Also, using the appliance allows you to empower patients to be compliant. As you watch them through the AP correction, you can see if they’re a good fit for aligners.
How did you get your staff on board with this shift?
JG: For an orthodontist to succeed with any new treatment philosophy, you need to have buy-in from your staff. The great thing for me when I introduced the “sagittal-first” concept to my staff is that it made total
sense to them that the heaviest lifting we do in ortho, which is generally the AP correction, should take place at the beginning of treatment, rather than after the patient has already been in braces for a year or longer.
Which benefits does the Motion 3D Appliance offer that haven’t been previously experienced?
JG: I’m able to confidently tell my patients that their treatment time should take a year or less.
Henry Schein Orthodontics’ mission is to provide stateof-the-art orthodontic products and innovative clinical solutions that enable its customers to offer exceptional patient care while expanding the scope and profitability of their practices.
The company continues to grow as a global orthodontic solutions provider by not only providing high-quality products but also going beyond the typical supplier/client relationship, instead cultivating partnerships with its customers so they can deliver positive patient outcomes and maintain healthy, successful businesses.
HSO’s wide array of orthodontic offerings include brackets and bands, intraoral appliances, elastomerics, archwires and temporary anchorage devices. Other solutions include innovative orthodontic products and progressive continuing education opportunities to help fuel the growth and success of orthodontic practices in more than 75 countries.
With the “sagittal-first” philosophy, I am able to achieve AP correction on average in just three months! AP correction used to take a year and at the end of treatment, when no patient was interested in being compliant anymore. Also, because the Motion 3D Appliance is so discreet, patients don’t think of themselves in treatment even though they are.
You’re able to get patients to commit to being cooperative at the beginning of treatment, when they are excited about the impact braces will make on their lives.
For more than 40 years, Henry Schein Orthodontics has manufactured most of its products in the United States, including at its 65,000-square-foot corporate building in north San Diego. Among its offerings is the Carriere System, which incorporates the latest advances in orthodontic technology with gentle forces that work with natural physiology to correct a bite at the beginning of treatment. By utilizing the Carriere Motion 3D appliances in the beginning stages and then transitioning into Carriere SLX Self-Ligating Brackets to complete treatment, the total time in treatment is greatly reduced when compared with other traditional approaches.
“Shifting to the Carriere Motion 3D Appliance has been one of the most significant treatment advances I have implemented during the past five years,” says Ron Maddox, a San Dimas, California-based orthodontist. “I’ve been able to reduce the overall treatment time and significantly reduce the time that my patients are in braces.”


CAD/CAM supported restoration of single teeth using the fine-structure feldspar ceramic VITABLOCS Mark II and the polychromatic, layered VITABLOCS TriLuxe and TriLuxe forte variations (VITA Zahnfabrik) has become established in numerous dentist practices worldwide.
The clinical procedure has been tested and proven over many years. The success of this all-round ceramic material in the area of single tooth restorations is based on the combination of numerous advantageous properties, which, among others, include profitability, esthetics and flexibility. In the following, some clinical cases are used to demonstrate these advantages.
Figure 1A and 1B:
A core buildup and acrown were used to restore the root-treated tooth 12; the partially damaged toot 11 was restored with a veneer. VITABLOCS Mark II was used in both cases. Perfect matching of shades could have hardly been accomplished with different materials. Complex fabrication processes and temporary restorations were avoided thanks tochairside treatment in a single appointment.
Compared to other types of dental restorations, such as reduced and veneered substructures, fully anatomically designed, mono-ceramic CAD/CAM restorations ensure high profitability.

When using the overpressing technique andwhen fabricating sintered crowns, each unit requires much more time and higher manufacturing costs. The VITABLOCS Mark II ceramic enables fully anatomical restorations and reduced structures, which can be individualized later on.
In cases of a crown restoration on a tooth and a veneer on an adjacent tooth, it is not possible to achieve an identical visual appearance using different materials. In such cases a material should be selected which can be used for both indications (fig. 1a and 1b).
Since the feldspar ceramic blocks VITABLOCS Mark II, TriLuxe and TriLuxe forte are suitable for all single tooth restorations (table 1), they ensure perfect combination and harmony of materials, which is desired for esthetic reasons.
 Fig. 1A
Fig. 1A

















Today “smooth” designs without stress-causing edges and corners are recommended for the preparation of all-ceramic restorations 1. More and more dentists prefer the round diamond instrument instead of the classic fissure bur. Adhesive cementation of the restorations is mandatory to achieve permanent resistance to stress comparable to zirconium oxide crowns fixed with glass ionomer cement 2, 3, 4
In cases of epigingival (not subgingival) preparation margins, drying, intraoral scanning and final cementation can be completed without any major problems. Since the silicate ceramic provides an excellent chameleon, the preparation margin can no longer be seen after adhesive cementation, grinding and polishing of the restoration. In cases of deeper preparation margins, surgical lengthening of the clinical crown is recommended. Subgingival margins are difficult to control so that – in many cases – a supragingival position is obtained due to periodontal recession.
Naturally, there are also situations in which subgingival preparations margins are required.
Such cases, however, can also be treated with a chairside or semi-chairside sandwich crown (VITA YZ + VITABLOCS Mark II) prepared in a single appointment.
VITABLOCS Mark II blocks are available in ten VITA SYSTEM 3D-MASTER and in three VITA classical A1-D4 shades. In addition to the monochromatic VITABLOCS Mark II, there are also the polychromatic block types VITABLOCS TriLuxe and TriLuxe forte with three and four harmoniously matched shade layers.
VITABLOCS TriLuxe can be used to fabricate restorations which simulate the higher cervical chroma and the increased incisal transparency of natural teeth (fig. 2).
Treatment can be completed chairside in a single appointment. Time-consuming and complex subsequent thermal treatment and staining are not required. Glaze firing to achieve characteristic shade effects can, but does not need to be, carried out.
Table 1: The entire range of single tooth ceramic restorations is covered with the fine-structure feldspar ceramic of VITABLOCS Mark II, TriLuxe and TriLuxe forte. Depending on the requirements, the restorations can be fabricated chairside, semi-chairside and labside. Subsequent thermal treatment is not required; glaze firing can be carried out. The ceramic exhibits excellent processing characteristics and problems of chipping have hardly been reported.

Fig. 2: When using VITABLOCS TriLuxe and TriLuxe forte, the restoration can be placed individually in the polychromatic block using the milling preview.
Not highly demanding cases but examples of daily routine work are listed below for documentation purposes. The examples given are limited to anterior restorations.
1. Tooth 21 was simply restored with VITABLOCS TriLuxe and manual polishing was carried out subsequently. In this case, less emphasis needs to be put on the esthetic appearance. The target was to fabricate a favorably priced restoration for the patient (fig. 3a, 3b.)


3a and 3b:
2. The result, which features esthetic and natural shade, shape and surface structure, was achieved by reworking in the dental laboratory and subsequent glaze firing performed chairside. Digital shade measurement confirms the good visual impression of the restoration made from VITABLOCS TriLuxe (fig. 4a - 4c).



4a to 4c: A perfect shade and surface structure were achieved.
Fig. Efficient solution: manually polished crown made from VITABLOCS Mark II. Fig. Fig. 2 Fig. 3A Fig. 3B Fig. 4B Fig. 4C Fig. 4A3. Light colors (Tetric Color, Ivoclar Vivadent) were applied to the severely discolored, prepared teeth to add the desired color depth (see also contrast photo) to the translucent ceramic (VITABLOCS TriLuxe) with a basic shade of 2M2. Perfect imitation of the shades of adjacent teeth is achieved by the slightly yellowish color of the cervical areas - obtained with glaze material (fig. 5a to 5f).





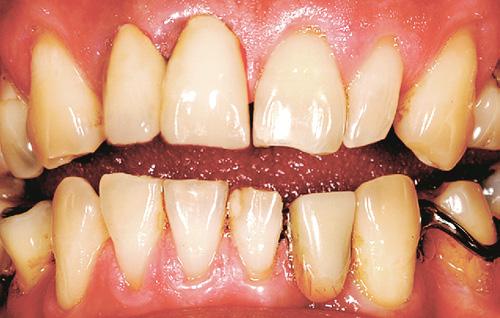
Fig. 5a to 5f: The crowns made from VITABLOCS TriLuxe exhibit natural color depth and are harmoniously integrated into the dentition. The restorations were fabricated and fitted in a single appointment in a way to ensure high profitability.
Fig. 5A Fig. 5B Fig. 5C Fig. 5D Fig. 5E Fig. 5FThe feldspar ceramic VITABLOCS from VITA Zahnfabrik is an all-round ceramic since it is suitable for all types of single tooth restorations. With more than 16 million restorations, the material has proven its clinical suitability all over the world. The fine structure features an abrasion behavior identical to that of natural enamel.
Thanks to the homogeneous type of structure, the VITABLOCS ceramic can be easily polished and milled in a way to reduce tool wear. The high translucency of the ceramic ensures perfect integration into the residual tooth substance.
1. Arnetzl, G.; Arnetzl, V.: Präparation für vollkeramische Restaurationen. Universitätsklinik für Zahn-, Mund- und Kieferheilkunde, Graz (2008).
2. Frankenberger, R.: Adhäsivtechnik 2009 – Neuigkeiten, Tipps und Trends. In: Quintessenz, 60(4); 415-423 (2009).
3. Hämmerle C. et al.: Dentale Keramiken, Aktuelle Schwerpunkte für die Klinik. Universität Zürich, (2005).
4. Zahran, M.; El-Mowafy, O.; Tam, L. et al.: Fracture Strength and Fatigue Resistance of All-Ceramic Molar Crowns Manufactured with CAD/CAM Technology. In: J Prosthodont., Mar 17 (2008).


From anterior restorations to mock-ups, the reusable Uveneer direct composite template system allows you to work smarter and faster with predictable, beautiful results.
Use for

TEMPORARIES




June 21 - 22, 2018
Hilton Habtoor Grand Beirut, Lebanon
 DR EDWARD RIZk, PRESIDENT OF THE LEBANESE SOCIETY OF ENDODONTOLOGY
DR EDWARD RIZk, PRESIDENT OF THE LEBANESE SOCIETY OF ENDODONTOLOGY



Dr. Philippe Sleiman, inventor of SP pluggers Hu-Friedy, cryotherapy technique in RCT, sequence of irrigation, apiectomy, coinventor of TF instrument and has a book about ultrasonics. Prof. Walid Nehme, one of the team developing 2 Shape and one flair from MicroMega.
Prof. Roger Rebeiz leader in the field of education and developing instruments. Prof. Rebeiz is
Prof. Issam Khalil Past President LSE developer of MMTA and BioMM a new bioceramic Material. Prof. Edmond Koyess Past President LSE involved in education since 30 years and actual director of
Prof. Rola Abiad vice Dean of BAU and also involved in Endodontic Education and worked on Laser Doppler flow meter. Prof. Charbel Allam pioneer in the endodontic surgery field and developer of surgical techniques and instruments. Dr Allam is a reference to all endodontists in this field.
Prof. Edgard Jabbour leader in the world of endo surgery and in extraction and direct implantation in case of failed root canal treatment and also in complex cases of bone grafting .
Dear all, you have been exemplary for the coming endo generations with your devotion, knowledge, expertise and the way of teaching and in transmitting the bug of endo which leads to
We at the LSE, have also trusted our dreams and each year we try to challenge ourselves and upgrade our event, as we have one main goal ahead of us which is to deliver to our endodontic and dental community the best of knowledge and science through lectures, workshops, exhibition and
Welcome again to our rich event, Enjoy!
Edward Rizk
President, Lebanese Society of Endodontology
PICTURE FROM THE OPENING CEREMONY
Safety
Quality of cleaning

P ropri e tary H eat Tre a tm e n t p ro ces s
Inc reas e s flex i b i lit y Mini m iz e s th e ris k o f i nstrumen t fra c tu re



Usability
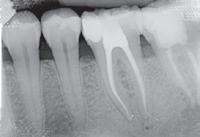


PR ROGER RBEIZ RECEIvING HIS TROPHY FROM DR MARC kALOUSTIAN


PR GHASSAN YARED RECEIvING HIS TROPHY FROM LSE PRESIDENT DR EDWARD RIZk
DR FILIPPO SANTARCANGELO TALkING ABOUT THE ANATOMICALLY GUIDED SHAPING

L TO R: DR EDWARD RIZk, PR JOSEPH SADER, PR HRANT kALOUSTIAN, DR MARC kALOUSTIAN

PR PHILIPPE SLEIMAN TALkING ABOUT THE ROLE OF IRRIGATION IN ENDO


DRS: EDGARD JABBOUR, EDMOND kOYESS, CARLA Z MOUBARAk

CARLA
PHOTO FROM THE ExHIBITION DR ZGHEIB MOUBARAk, PR STEPHEN NIEMCZYk
R,

L TO R: WALID NEHME, LAURENT BATAILLARD, GHADA BASSIL,



With Tunisian Association of Research & Studies in Orthodontics
June 22 - 23, 2018
Mövenpick Hotels & Resorts
Beirut, Lebanon


DR MONA SAYEGH GHOSSOUB
PRESIDENT OF THE LOS

founded Carthage in the 12th Century BC. Thus, this empathy could have been generated from these shared ancestors.
I would like to recognize the hard work of all previous Lebanese Orthodontic Society Presidents and all committees and individuals for their precious contributions to establish a solid base on which we will continue to build in order to achieve all the aforementioned goals.
And now I declare opened the Lebanese-Tunisian congress which coincides with the 16th Annual Meeting of the Lebanese Orthodontic Society.















DR JOSEPH GHOUBRIL, PRESIDENT OF THE SCIENTIFIC COMMITTEE

DR ROY SABRI LECTURING ABOUT MANAGEMENT OF DENTAL TRAUMA

DR GILBERTO SAMMARTINO RECEIvING THE CERTIFICATE FROM DR ADEL BEN AMOR

L TO R DRS: ADEL BEN AMOR, SAAD NAFAA, FADI GAITH, CHAFIC TABBARA

DR NAJI ABOU CHEBL TALkING ABOUT THE ROTATION OF THE OCCLUSAL PLANE

DR BACHAR REDA RECEIvING THE CERTIFICATE FROM DR ZOUHAIR SkAF AND ANTOINE DARAZI

DR MOHAMED SALAH kHALFI RECEIvING THE CERTIFICATE FROM DR MONA SAYEGH

PR DIRk WICHMANN ExPLAINING LINGUAL ORTHODONTICS

DR SAMIR TOBJI TALkING ABOUT THE DYNAMICS OF THE BRACkETS

TROPHY DISTRIBUTION TO DR. JOSEPHINE BOUERY

DR FAYEZ SALEH LECTURING ABOUT THE CORRECTION OF THE GUMMY SMILES


TROPHY DISTRIBUTION TO DR. CARLA DAOU

TROPHY DISTRIBUTION TO DR.

TROPHY DISTRIBUTION TO DR. CORINE









3D agility_ The One to Shape your Success
3D anatomical root canal preparation
Exclusive Adaptive Core™ Technology
Remarkable cyclic fatigue resistance
3D efficiency_
Optimal Cleaning while Preserving Dentine
3D cleaning and biofilm removal
Enhanced irrigation and debridement
Unique expansion capacity
25th Summer Dental Meeting
June 23, 2018
Eddésands Hotel & Resort Jbeil, Lebanon

L TO R: DR. ELIE ROUPHAEL, PROF. CARLOS kHAIRALLAH, DR. MARTIN BAkHOS (LABD), PROF. TONI ZEINOUN
View More Pictures On facebook.com/dentalnews1


Under the patronage of the Lebanese Dental Association represented by its president Prof. Carlos Khairallah, the Byblos Dental Association (BDA) and the Lebanese Association of Dentists graduated from Belgian Universities (LADB) held their 25th Summer Dental Meeting on Saturday June 23, 2018 At é Byblos Hall - Eddésands Hotel & Resort - Jbeil.




 DR. RAWAD SAMARANI
DR. ZIAD SALAMEH
DR. RAWAD SAMARANI
DR. ZIAD SALAMEH

June 26, 2018
The Key ApartHotel Beirut, Lebanon




conventions year after year since 1992. Every past president increased the standard of communication between all pedodontists and even among other societies abroad. We will follow that pathway for the three years to come and work hard for an optimal level and make sure that we will be chapters in other professional societies to make us more scientifically exposed ”

 Dr. Bechara Al Asmar President, Lebanese Society of Pediatric Dentistry
PHOTO OF PAST AND ACTUAL BOARD COMMITTEE MEMBERS OF THE LEBANESE SOCIETY WITH THE FOUNDER PROF. ELIA SFEIR AND PAST PRESIDENTS
Dr. Bechara Al Asmar President, Lebanese Society of Pediatric Dentistry
PHOTO OF PAST AND ACTUAL BOARD COMMITTEE MEMBERS OF THE LEBANESE SOCIETY WITH THE FOUNDER PROF. ELIA SFEIR AND PAST PRESIDENTS








MR. MATTIAS FINZELBERG, CREATOR & DEvELOPPER OF kIDDY-CAPS

PROF. ELIA SFEIR, SPEAkER


L-R: PRESIDENT PROF. ROULA DIB, DEAN PROF. TONY ZEINOUN, PROFS: NADA MCHAILEH, AMINE EL ZOGHBI, MONA NAHAS, JEAN-CLAUDE ABOU CHEDID

PROF. SAMIA ABOU JAOUDEH, PROF. AMINE EL ZOGHBI (REP. PRES. LDA), DR. BECHARA AL ASMAR

PROF. MONA NAHAS, DR. GEORGE ABI HATEM, DR. HITAF NASSEH
DR. HASSAN BACHO, SPEAkER

L-R: MR. JOSEPH NADER, MR. CHAWkI HACHEM, MR MATTIAS FINZELBERG, PROFS: TONY ZEINOUN, AMINE EL ZOGHBI, SAMIA ABOU JAOUDEH, DR.

PROF. NADA MCHAILEH (REP. DEAN MAkHZOUMI), DR. TONI DIB, PROF. SAMIA ABOU JAOUDEH

L-R: DR. MAYA AYOUB, PROF. NADA CHEDID, PROF. ROULA DIB, DR. HITAF NASSEH
MICHEL SALAMEH

DR. SANDRA DAGHER (vICE PRESIDENT LSPD), DR. GUITTA ABI NASR (GENERAL SECRETARY LSPD)


 L-R: DR. CAMILLE SAMNEH, PROFESSORS: NADA MCHAILEH, ROULA DIB (PRESIDENT LDA NORTH), SAMIA ABOU JAOUDEH, AMINE EL ZOGHBI, DEAN TONY ZEINOUN, DRS: GUITTA ABI NASR, MOHAMMAD EZZEDDINE, SANDRA DAGHER, PROF. JEAN-CLAUDE ABOU CHEDID, DR. MICHEL SALAMEH
L-R: DR. CAMILLE SAMNEH, PROFESSORS: NADA MCHAILEH, ROULA DIB (PRESIDENT LDA NORTH), SAMIA ABOU JAOUDEH, AMINE EL ZOGHBI, DEAN TONY ZEINOUN, DRS: GUITTA ABI NASR, MOHAMMAD EZZEDDINE, SANDRA DAGHER, PROF. JEAN-CLAUDE ABOU CHEDID, DR. MICHEL SALAMEH

Osstell, the developer of the ISQ diagnostic technology (Implant Stability Quotient), now presents the next leap in the evolution of implant diagnostic instrumentation: The Osstell BeaconTM, an innovative and highly intuitive tool designed to guide implant treatments for more predictable results.
Osstell’s patented technology allow clinicians working with implants to make decisions based on reliable and objective stability values when determining the course of treatment for each patient. The procedure can be used to measure primary implant stability, observe osseointegration based on secondary stability readings and determine the best possible time for loading the implant, thereby helping to prevent failures, shortening healing time and ensuring high quality.
The dental implant market has changed over the past few years. There are now more dentists with less experience within implantology and a generation shift with different expectations is coming.
Clinicians are facing more complex decisions as there is an increase in patients with risk factors as well as increasing demands for shorter treatment times. Digital planning and workflows are redefining protocols and techniques.
There is thus a need for objective tools to increase efficiency, and to guide and optimize the implant treatment for both complex and more straight-forward cases, making ISQ diagnostics a necessary and objective key value to help improve outcomes and quality.


“We have listened to our users who need advanced technology in the form of an easy-to-use and intuitive complete product concept for the Osstell approach. Accordingly, we have developed a complement to the more comprehensive Osstell IDx to meet the needs from both large University clinics and small private practices. For clinicians that are new to this method and technology, the feedback from the color coding, which essentially is an extract of all the scientific data that the Osstell ISQ scale is based on, will provide a guide as to when to load the implant.”
- Stefan Horn, VP Product Development, Osstell.
In the industry today, there is a lot of talk about connectivity, Internet of Things and big data. With this comes a strong need to, not only capturing the data, but also to be able to provide context to the numbers, to turn it into something useful and insightful. That’s why we are continuously focusing on enhancing connectivity and Osstell Connect, our online service where you can analyze your data and get relevant insights of your implant treatment performance.
We believe this will only become more and more valuable for the clinicians.”, continued Mr. Horn. Both the Osstell Beacon and the Osstell IDx give you access to Osstell Connect.
“Osstell’s innovative and patented technology allow dentists around the world to make dental implant treatments even safer and more predictable, and thereby helping clinicians improve patient confidence and comfort. We always aim to serve our customers and users with even better products and services as well as helping them to provide best practice services to their customers – the patients. Patients’ well-being is always the top priority.
With this – the Osstell Beacon – being newest addition we take another important major step towards making our technology, products and our approach even more accessible”, says Mr Jonas Ehinger, CEO of Osstell.

From 14 - 17 November 2018






High-quality composites for esthetic anterior and posterior restorations

