



A step in the right direction Podiatry Review The Institute of Chiropodists and Podiatrists News AUTUMN ISSUE Volume: 79 No: 4 Oct/Nov/Dec 2022 The Institute of Chiropodists and Podiatrists Representing podiatry at the Commonwealth Games - Abid Hussain Pages 41-42 FREE 4 Page CPD Article Principles of Gait: Using the Acceleration Lever System Effectively ATOPIC DERMATITIS –is it just bad luck? Pages 23-26 Pages 10-13 Pages 30-34 Pages 28-29 College of Paramedics: NHS Ambulance Services’ Best Kept Secret Whole body integration using The Flow Motion Model™
Editor: Mr W J Liggins, MA,BSc(Hons), FCPS, FPodA

Academic Editor: Ms B Wright, MSc BSc (Hons), PGCE PGDip, FinstChP
Academic Advisor: David M Holland, CSci, CBiol, FFPM-RCPS(Glasg)
Academic Review Team

Ms B Wright, MSc BSc (Hons), PGCE PGDip, FInstChP
Mr S Miah, CFPodM, MInstChP
Mr W J Liggins, MA,BSc(Hons), FCPS, FPodA
Media and Publicity Contact: Email: media@iocp.org.uk
Medicines and Procedures Panel (MaPP)
Chair: Gaynor Wooldridge, MInstChP, CFPodM
Abid Ali, CFPodM, BSc, MInstChP
Somuz Miah, CFPodM, MInstChP
Martin Harvey, PGCert, BSc, MInstChP, MCPodS
Contents Podiatry Review Autumn Oct/Nov/Dec 2022
Podiatry Review Volume: 79 No: 4 ISSN 1756-3291 Annual Subscription £20 UK / £30 Overseas Published by The Institute of Chiropodists and Podiatrists 150 Lord Street, Southport Merseyside PR9 0NP Tel: 01704 546141 Email: info@iocp.org.uk Website: www.iocp.org.uk
Disclaimer:
CONTACTS 4 IOCP Contacts 5 Editorial ARTICLES 6 5 minutes with your CEO 8-9 Step Ahead Business Club 10-13 ATOPIC DERMATITIS – is it just bad luck? 14 2022 Mid Wales Diary 15-18 Footnotes: Foothealth Practitioner News 20-21 Roy Castle Lung Cancer Foundation 23-26 4 page CPD articlePrinciples of Gait:
the Acceleration Lever System Effectively 28-29 College of Paramedics: NHS Ambulance Services’
Secret 30-34 AiM - Whole body integration using
Flow
36-40 LASERS IN HEALTHCARE - Overview and focus on Photobiomodulation Therapy 40 Podarick 41-42 Representing podiatry at the Commonwealth GamesAbid Hussain 44 Obituary: Lynne Elizabeth Bourgeois COURSES 7 CPD 2023 NEWS 45 Branch News 46 Classified Adverts 47 Diary of Events 10-13 @IOCP_Chiropody @IOCPChiropody Podiatry Review Autumn Issue 2022 | 3 28-29 41-42
© The Institute of Chiropodists and Podiatrists
The Editor and the Institute of Chiropodists and Podiatrists accept no responsibility for any opinions expressed in the articles published in the journal, and they do not accept any responsibility for any discrepancies in the information published. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying or otherwise, without the prior written permission of the publishers.
Using
Best Kept
The
Motion Model™
IOCP Contacts
Executive Committee
President: Mrs C McCartney, MInstChP
Chair Executive Committee: Mr M Harvey, PGCert, BSc, MInstChP, MCPodS
Vice-Chair Executive Committee: Mr A Ali, CFPodM, BSc, MInstChP, BSc
Chair Board of Education: Acting Mr M Harvey, PGCert, BSc, MInstChP, MCPodS
Vice-Chair Board of Education:
Ms B Wright, MSc BSc (Hons), PGCE PGDip, FInstChP
Chair Board of Ethics: Ms B Wright, MSc BSc (Hons), PGCE PGDip, FInstChP
Honorary Treasurer: Mr S Miah, CFPodM, BSc (PodM), MInstChP
Regional Director (Ireland): Mr S Preston, MInstChP
Regional Director (Scotland): Mrs H Jephcote, MInstChP
Regional Director (England North): Mrs C McCartney, MInstChP
Regional Director (England Midlands): Mr W J Liggins, MA, BSc(Hons), FCPS, FInstChP
Regional Director (England South): Mr J Olivelle, MInstChP, AMCPS
Regional Director (Wales): Mrs L Pearson, FInstChP, BSc Pod Med`
Academic Advisor: David M Holland, CSci, CBiol, FFPM-RCPS(Glasg)
Medicines and Procedures Panel (MaPP): Gaynor Wooldridge, MinstChP, CFPodM
Chief Executive Officer: Mr Anthony Hubbard, CSci CChem FRSC
Company Secretary: Miss A J Burnett-Hurst, HonFInstChP Standing Orders Committee: Mr M Franklin, MInstChP Birmingham
Branch Secretary Telephone Email
4 | www.iocp.org.uk CONTACTS
&
& the Shires Kate Harrison 01789 262365 kathrynharrison87@gmail.com Cheshire
North Wales Michele Allison 07766 700027 missminou@hotmail.co.uk Essex Beverley Wright 01702 460890 solespirits@hotmail.com Irish Janette Pegley-Reed 00353 8627 31371 jpegleyreed@gmail.com Leeds and North East Caroline McCartney 07583 934468 hello@chiropodyandfoothealth.co.uk London Sarah Bowen 07790 717833 footwoman@gmail.com North West Alison Marsden 01772 623180 alison.marsden@hotmail.com Sheffield Helen Rawse 07789 025022 hrawse@live.co.uk South Wales & Monmouth Esther Danahar 01656 740772 estherdanahar@yahoo.co.uk Scottish John Stott 0780 135 6485 jls@stottland.com Wolverhampton David Collett 01785 716607 djcollett@hotmail.co.uk
of)
to Mr
as the role of
Director (England
should have been amended in the July issue.
Branch Secretary Contacts (Acting secretary
Apologies
Olivelle
Regional
South)
Throughout her long reign, the Institute of Chiropodists and Podiatrists have always sent loyal greetings to her Majesty on the occasion of our annual general meetings, and this has always been diligently acknowledged by one of the royal staff and such acknowledgement transmitted to the membership.
As an organisation I know that the membership will join the Board, and myself as Chair, in expressing our sincere and heartfelt condolences to her Majesty’s family. In addition however, I believe we are joined by uncounted millions in both the UK and so many countries around the world who are sincerely grateful that HRH Elizabeth Windsor has for so many years been a living symbol of the very best that Britain can offer in personal qualities. Loyalty, dedication to duty, compassion, unswerving devotion and courage are some, but by no means all of those qualities shown by her day after day, year after year and decade after decade.

Rest peacefully your dear Majesty, you have been an inspiration to us all. With respect and grateful thanks,
Martin Harvey FPodM PGC IP BSc DPodM. Chair, Institute of Chiropodists and Podiatrists
Editorial
Wow! What a sizzling hot summer we have had. Whether that meant hunkering down and working in front of a fan in the clinic, or rushing to find an air-conditioned space, while doing those domiciliary visits. I hope you all did your best to survive the heatwave this summer. It is hard to believe that we would even imagine looking forward to some cooler temperatures and rain, but that is among the adventures of the British weather!
We can now look at embracing the Autumn and Winter weather with some self-reflection from the year 2022. Grab a cup of tea or coffee, or something a bit stronger to keep the chill out and settle down for an issue of thought-provoking articles. Hopefully, it will encourage us to think about the challenges ahead, and how we can challenge ourselves in 2023.
There is not just a change in the seasons, but sadly we know there is a change in the economic climate too, where we are all facing a cost-of-living crisis. This could likely impact our practices too. So, there is no better time to think more positively, despite the doom and gloom we hear and read in the news. It is time to think outside the box, and head towards 2023, feeling inspired, motivated, and ready to set some new goals for the New Year. There is nothing like thinking outside the box with some of the inspirational articles written by our colleagues in this issue of the ‘Podiatry Review’. Subjects that may challenge some preconceived ideas around podiatry and foot health. Challenges come in many forms and the work podiatrists have undertaken this year in sport have been incredible. In Abid Hussain’s article, Abid has led his team of podiatrists (half of them IOCP members) working at this year’s 2022 Commonwealth Games. This has certainly been a triumph, and raised the profile of podiatry, as a vital part of sports medicine. It also acknowledges the work podiatrists do and have done to support the athletes who took part in the coveted Birmingham Games this Summer.
Elsewhere, Kirsten Sinclair’s article looks at the use of light therapies and lasers within healthcare in her overview and focus on Photobiomodulation therapy. Gaynor Wooldridge looks through the history and prevalence of atopic dermatology, and its treatments. While there is also the Footnotes section, and some other interesting, events, news, and reviews, in this issue.
To peak our interests further there are some exciting, new continuing professional development (CPD) events coming in October with the UK Roadshows, one already having made its debut this Summer. Ireland too will be hosting meetings and CPD events. All these events will provide support and networking opportunities for chiropodists, podiatrists, and foot health practitioners. With so many exciting ventures to read about, there should be plenty to think about fulfilling aspirations for the future. There are plenty of opportunities to work towards setting new and interesting goals for 2023. Keep positive and happy reading!
All the best Beverley Wright

Guidelines for new and established authors
n

Content of your article should be Podiatry or foot health-related. Podiatry Review is mostly in easy-to-read format, and articles for submission should reflect this. CPD Certificates are issued for Case Studies and Articles. Please ensure that your name and title (ie - FHP, Podiatrist, or other) are included with your article. Please proof-read and spell-check your article before submission.
It would be helpful to the Editorial Committee if you could reference any books or Papers mentioned in your article. If you are not sure how to do this we are happy to assist.
Podiatry Review Autumn Issue 2022 | 5
Hubbard CSci CChem FRSC
Exciting times ahead!
I hope you had a good summer and managed to stay safe and cool in the extreme heat. The prolonged good weather certainly kept our legs and feet on show for longer this year!
Despite the heat and the holidays, it has been a very busy time in the world of podiatry and foot health, with many of you representing your profession at the Commonwealth Games as part of the official medical team. All of your hard work has contributed in raising the profile of podiatry to other professions, athletes and their support staff as well as to the general public, more on this in Abid Hussain’s fantastic article. We’re certainly very proud of all involved.
We are delighted to have welcomed Jill back to Head Office after a short period of absence and have recruited 2 new members to our team. Rae and Sandra join us in administration roles allowing our more established and knowledgeable staff time to progress their work in driving the organisation forward, including our CPD offerings.
As you may be aware, our first ever UK CPD Roadshow will be held this month in Leeds. The event is designed to provide a full focused day of high-quality learning and the opportunity to connect members and
colleagues, as we know so many of you work independently. Unlike our past conferences and other foot and health related conferences we will not have trade stands present, instead we are working with our trade partners to provide clinical speakers for sessions or information on their latest products/ technologies/services to attending delegates via the event goody bags.
Our team in Ireland, led by Stephen Preston and Janette Pegley-Reed, are also holding a CPD event day on the 22nd October, this is their second event of the year after hosting their very first successful conference back in May. Both events have some exceptional speakers, but don’t worry if you couldn’t attend this time, we hope to be holding more of these events throughout 2023.
We also have some new wonderful CPD courses scheduled for 2023 including the new Orthotics course with Andy Horwood and some established favourites such as dermal filler and steroid injection.

Now we are able to increase training activity, more and more podiatrists and FHP’s are visiting our Head Office in Southport. For those of you who have not visited Head Office before we have a fantastic clinical facility. This has now been branded to increase recognition of our organisations.

It is well documented that this winter is likely to be financially difficult on many, including that of businesses. Our Step Ahead Business Club is a members only, confidential, virtual meeting held quarterly. We are a supportive community, there is no right or wrong, there is no stupid question, instead this is your opportunity to share and discuss any concerns, issues, pricing challenges etc, anything relevant to you that you need business support on can be discussed here. You are not alone! The next meeting is being held on November the 2nd and details will be sent to members in advance. We hope to see you there.
Thank you for your support this year, I look forward to meeting more of you in 2023 and wish you, and your families all the best for the remainder of 2022
6 | www.iocp.org.uk ARTICLE
Chief Executive Officer
Anthony
The





5


meet: Maintain an accurate and an up to date record of CPD activities - There is no set format for recording your CPD, it can be as hard copies in a folder or electronically. Demonstrate that CPD activities are a mixture of learning activities relevant to current or future practice Seek to ensure that CPD has contributed to the quality of practice and service delivery Seek to ensure that CPD benefits the service user Upon request, present a written profile explaining how they have met the standards for CPD. It is the aim of the Institute of Chiropodists and Podiatrists to bring you the highest-quality CPD in accordance with HCPC guidelines and to further develop, support and maintain your careers as successful private practitioners.

Podiatry Review Autumn Issue 2022 | 7 COURSES CPD 2023 For full details of our courses or to book your place visit www.iocp.org.uk/courses Dermal Filler Steroid Injection Acupuncture PRP Therapeutic Ultrasound
CPD, is vital in supporting
your
ensuring your
date
ensuring you
to
registration.
NEW for 2023 Laser Therapy with Kirsten Sinclair Orthoses Prescription with Andy Horwood Cadaver with Martin Harvey & William Liggins As well as our established favourites including: ONLINE CPD training via our webinars Full business support with the Step Ahead Business Club
Continued Professional Development –
and developing
career,
skills and knowledge are up to
and
continue
practise safely and effectively. CPD is a requirement of HCPC
HCPC have
standards you must
Step Ahead Business Club
Our Step Ahead Business Club is a IoCP and CoFH members networking group for private practitioners. It is open to all members across the organisations. We meet quarterly to discuss topics raised by yourselves with the aim to offer peer advice and support to your career and business.
Our last meeting was held on 22nd July in which we were joined by accountant Jenny Tobin to discuss the pro’s and con’s of sole-trader vs Limited Company. Below we give an overview of the main differences and share some important questions raised during the meeting. A full recording is available to both IoCP and CoFH members via the secured area of our website.
Sole-trader vs limited company
We’ve completed our healthcare training and know the anatomy and workings of the lower limb inside and out, but whether you are new to this profession or looking to change your career direction, the one thing we all have to do when setting ourselves up as independent practitioners, is have a general understanding of the legal obligations for setting up a business. When setting yourself up to work independently you have 2 options:
1 Sole-trader – self-employed individual responsible for themselves as a business. Simplest legal business structure
2 Limited Company – Creates a business structure. The structure can include shareholders, directors, employees etc, but it can also be just 1 person.
Figures by the Department for Business, Energy & Industrial Strategy list the following statistics on businesses in the UK at the start of 2021 on the Government website:
UK private sector business population comprised 3.2 million sole proprietorships (56% of the total), 2.0 million actively trading companies (37%) and 384,000 ordinary partnerships (7%)
1.1 million companies were employers, as were 221,000 sole proprietorships and 98,000 ordinary partnerships
2.9 million sole proprietorships, 951,000 companies and 286,000 ordinary partnerships did not employ anyone aside from the owner(s)
Sole-trader
Pros
Cons
Easy set-up
Be your own boss
Less admin involved
Funds are not published. Self Assessment required each year
Business structure can always be changed later
Limited Company
Pros
Cons
You are responsible for all legal liabilities including debts
Can be harder to obtain funding/loans from banks, as their preference is often for Limited companies
Business may be less appealing to clients and investors
Less flexibility when it comes to tax
Tax efficiency. More tax benefits are available
Limited Liability. Personal finances are safe. Business would incur any debts
More professionally appealing/attractive
More attractive to clients and investors
Costly to setup
Funds are published via Companies House / Less privacy
More complicated accounts - accounts issues that limited companies need to deal with include payroll, bookkeeping, and tax planning – not to mention tax returns, business expenses, and keeping company accounts up to date. Additionally, failing to fill in tax returns correctly can result in fines & other punishments
Potential issue of ownership – if you have shareholders they have equal say in your business.
8 | www.iocp.org.uk ARTICLE
Q&As
I’ve been advised to stay as a sole-trader to renew my mortgage, why is this?
Currently there is a nervousness from banks to lend. Banks look for consistency, if you are setup as a sole-trader you would have a history as a sole-trader and they will look into that history to find consistency. They want to be sure that you have a secure income whereas if you move to be a limited company your company wouldn’t have that history at that point in time, plus limited companies offer a greater level of flexibility, you may choose to take one income from the business one year and another from the next, the company would pay corporation tax as opposed to you as an individual. It all comes down to consistency and history to ensure lending is secure. There are lenders available who will lend to you as a Limited company but currently that market place is smaller and you may not have access to the best rates available.
Is it better to be a sole-trader in private practice?
Not necessarily. Tax benefits change over the years, if we go back approx. 7 years there was a 0% rate of dividends up to £40,000, that led to a lot of people registering as a Limited Company, after corporation tax you could take up to this amount from the business tax and national insurance free. This then went to 7.5% up to £50,000 and next year we are expecting an increase in corporation tax from 19% to 25%. So there is no set rule on how to set yourself up in private practice, this all depends on your earnings and current tax rates.
Are accountants fees a lot higher for Limited Companies than sole-trader?
Generally they are more expensive because of the level of filings required. It’s not just a set of accounts and a tax return, it usually involves a payroll scheme, corporation tax return, statutory accounts, and other accounts that need filing with companies house and HMRC.
What is Making Tax Digital?
Making Tax Digital (MTD) is a Government initiative to move tax online, the Government says “this will be more effective, more efficient and easier for taxpayers to get their tax right”. This already applies to VAT and is expected in 2 years time on income tax and with the aim to include corporation tax in 2026.
If I’m setup as a Limited Company can I be the only person in that company, i.e. secretary, director, employee etc?
Prior to 2013 this couldn’t be done. Now One person can form a limited company. Whilst the application form requires you to have a minimum of one director and one shareholder, it is commonplace for the same individual to hold both of these positions. This means you can set up a company on your own. There is no longer a requirement to have a company secretary.
Can you employ someone if you are setup as a sole-trader?
Yes but you have to setup a pay as you earn (PAYE) scheme. There are no differences in the rules between sole-trader and Limited Company when it comes to employing someone.
If I move my Limited Company into a dormant state do I still have to pay the £13 annual returns fee?
Yes unfortunately and you will have to file dormant accounts too.
If you work in a private medical practice and you offer a medical procedure and not cosmetic and are HCPC registered, are you exempt from paying VAT?
The subject of VAT is a minefield! It can change quite a lot. Currently healthcare procedures are exempt from VAT. Under the Value Added Tax Act (1994) it states that services are exempt from VAT if “ their primary aim is the protection, preservation or restoration of health”.
Podiatry Review Autumn Issue 2022 | 9
Q Q Q
Q Q Q Q Q
Products & Procedures under the microscope
 With Gaynor Wooldridge Chair of the Medicines and Procedures Panel (MaPP) of the Institute of Chiropodists and Podiatrists
With Gaynor Wooldridge Chair of the Medicines and Procedures Panel (MaPP) of the Institute of Chiropodists and Podiatrists
ATOPIC DERMATITIS – IS IT JUST BAD LUCK?
Introduction
Atopic dermatitis (eczema) is a pruritic, inflammatory skin barrier disease (Koh et al. 2021). It affects approximately 20% of children and 10% of adults in developed countries. An analysis of the 2017 Global Burden of Diseases (Langan et al. 2020), highlighted that atopic dermatitis is the leading contributor of all skin-related disability, affecting approximately 4% of the global population (Laughter et al. 2021). It is a disease that affects people of all ages and ethnicity, and has a significant psycho-social impact on patients and their relatives.
In this article, we will look at the historical precursors to atopic dermatitis (AD), and the reported treatments of the time; a brief comparison of atopic dermatitis and psoriasis; current understanding and treatments of AD; and exciting new discoveries and future treatment pathways.
Old disease, new name
Fred Wise (1881-1950) and Marion Sulzberger (1895-1983) are credited with introducing the term ‘atopic dermatitis’ in 1933 (Kramer et al. 2017). Atopy was actually a term created in 1923 by Arthur Coca (1875-1959) and Robert Cooke (1880-1960), when they recognised an association between allergic rhinitis and asthma (Diaz-Cabrera et al. 2021). The definition, based on ‘atopy’, from the Greek word ‘atophos’ meaning ‘second placed’ (Thomsen, 2014), and dermatitis, again Greek in origin, with ‘derma’ meaning skin, and ‘itis’, inflammation.
However, despite this fairly recent introduction into our medical lexicon, the historical precursors of atopic dermatitis can actually be dated to at least 69-140 AD/CE (Bhattachaya et al. 2016).

Travelling further back in time, the ancient Greek physician, Hippocrates (c460 BC/BCE - c370 BC/BCE), was to describe the condition of chronically itchy skin. Prevailing thoughts of ‘humors’ guided medical therapy throughout the majority of history, and treating eczema in patients was unpopular (Calvus, 1525). In fact, the oozing often present was thought to be an essential part of the healing process. The term ‘ekzema’ was first used in 543 BC/BCE by the Greek physician Aatius of Amida, and means ‘to boil out’ (Kramer et al. 2017). Ekzema was further described by Girolamo Mercuranali (1572) in his De Morbis Cutaneous, which was the first handbook of dermatological illness at the time.
We had to wait until the mid- nineteenth century for Hebra, the first chair of dermatology in Venice, to describe a recurrent, chronic skin disorder which was characterised by intensely pruritic ‘papules and nodules’ on the skin and trunk. He termed this condition ‘constitutional prurigo’, (Hebra et al. 1866), although many other terms were also used during these times, including eczema rubrum, prurigo diatesique and prurigo’ Besnier (1881).
Moving into the 20th century, the French dermatologist LuisAnne-Jean Brocq (1903) proposed that atopic dermatitis was linked to nerves, and termed it ‘neurodermatitis’. This, bizarrely, was widely accepted by doctors, and the concept that neurodermatitis was a psychosomatic illness flourished (Duncan, 1959). It became the official name for AD for a few decades, and is still a term widely used in America and Germany.

Experts continue to disagree on the appropriate name for atopic dermatitis, and it is clear that this may not be the term that will ultimately be used. The name and condition will continue to change, together with the development of molecular biology and immunology, and with the advances in the aetiology of the disease (Kramer et al. 2019).
Early treatments (if any!)
Throughout history, individuals have had a myriad of dermatologic conditions. The first documented treatments of AD were found on papyrus in Ancient Egypt. Wright and
10 | www.iocp.org.uk ARTICLE
Dermatologist: I can’t decide whether I want to specialise in psoriasis or dermatitis. I don’t want to make a rash decision.
Goldman (1979) found that eczema of the head was treated by painting the broken skin with rotting food, mixed with warm fat, fish oil, rotten cereal and breadmeal, covered with bandages and left over night. The idea of introducing potential pathogens into damaged skin would seem to us now, to be fraught with danger!
der Bogaard et al. found that its use in patients with atopic dermatitis completely restored the expression of major skin barrier proteins, including filaggrin.
Atopic Dermatitis vs. Psoriasis

It can be easy to confuse AD and psoriasis. Both are thought to have a similar cause: an immune system that kicks into overdrive and attacks the body. However, this process is different for each condition. (Gardner, 2018).
https://openpsychometrics.org/tests/ O4TS/1.php
Prior to the 19th century, medical practice was based largely on what the ancient Greeks termed the ‘four humours’. Hippocrates postulated the humoral theory in the 5th Century BC/BCE in his Corpus Hippocraticum. In this vast work, he described multiple dermatologic diseases, with recommendations of spring water, or sea water, baths, and topical application of a fatty substance, as well as treatments using sulphur (Sgontzos et al. 2015).

In 1799, when George Washington (first US president) developed epiglottitis, he was such a proponent of the humoral theory that he insisted on being treated with the established practice of blood letting. He lost an estimated 5-7 pints of blood in less than 16 hours; this proved detrimental to his chances of survival, and he died shortly after (Cohen 2012).
Coal tar is a thick, dark coloured liquid, which is a by-product from coke making, and coal gas from coal (Hamilton, 2015); it was discovered around 1665 (Roelofzen et al. 2007). In a previous Podiatry Review (October, 2021) we examined the history of phenol, and it’s discoverer, Friedlieb Ferdinand Runge (1794-1867). Runge termed phenol ‘ Karbolsaure’ (coal-oil-acid or carbolic acid). This incredible German analytical chemist, who sadly died in poverty, also became the first person to isolate quinine from cinchona bark; he accidentally found that belladonna extract could cause pupils to dilate (after a chance splash in the eye); isolated caffeine from coffee beans; and invented the first coal tar dye (Anft, 1955).
Coal tar began to be used for medical purposes in the early 1800s (Diez and Garcia, 2019), and is still used today. Despite its longstanding clinical use and efficacy, the molecular mechanism is unknown. However, in 2013 Van
In psoriasis, immune system chemicals cause the outer layer of skin cells to go through their life cycle in days, rather than a month. This process causes cells to create a super fast layer to build up on the skin, creating a thick coat of red, silvery scales characteristic of plaque psoriasis (GuttmanYassly et al. 2017). People suffering with eczema tend to have overly reactive immune systems when triggered by a substance (internal or external), which causes inflammation. Research has also shown that some people with atopic dermatitis have a mutation gene which leaves skin more vulnerable to dryness, irritants and allergens (Ballard, 2021). More about this fascinating discovery later in the article.
Atopic dermatitis is approximately four times more common than psoriasis, although it is possible to suffer with both conditions (psoriasis-dermatitis). Both atopic dermatitis and psoriasis can affect people of all ages, but AD typically first appears in babies and children, often between the ages of 15-35. Only 1% of babies suffer with psoriasis (Krupka at al. 2020). Children with AD may find that their symptoms go away or improve as they get older, whilst psoriasis tends to be a lifetime condition.
Current Understanding and Treatment Pathways of Atopic Dermatitis
Most of the current treatments for AD target the immune system with the use of corticosteroids, calcineurin inhibitors
Podiatry Review Autumn Issue 2022 | 11
Which Humor are you? This is an interactive personality test of the ‘Four Temperamants’, an idea from Ancient Greek medicine.
(immunosuppressants) and UVB radiation, with emollients used as an adjuvant to improve skin barrier function. Atopic dermatitis is frequently refractory to topical treatments,and long term treatment with oral immunosuppressive therapy is often required to control the burden of disease, prevent flare-ups and to achieve a better quality of life outcomes (Napolitano et al. 2018).
Standard treatments currently include topical treatments, such as emollients and corticosteroids. If these are not effective, systematic immunosuppressants such as methotrexate, azathioprine and ciclosporin can be added. If there is still no improvement, targeted systemic therapies, such as dupilumab (biologic) and baricitinib (JAK inhibitor) are the next step (Wise, 2022).

Gokaimen (2016) determined that atopic dermatitis was actually a random vestige of evolution. This research included the genomes of more than 2,500 people from around the world. The gene at the heart of the research was the filaggrin gene. Filaggrin, a large protein, was discovered in 1977 by Beverley Dale, but its critical role in skin barrier preservation was not understood until 2006 by Professor Irwin McLeen. The relationship with atopic dermatitis was a significant breakthrough in the understanding of eczema pathogenesis and it was found that patients with atopic dermatitis had loss of function mutations in the filaggrin gene (Brown, 2012). Filaggrin has been shown to be a crucial epidermal protein, vital for the formation of the corneocyte, and the generation of intracellular metabolites (Thyssen and Kezic, 2014); this contributes to the hydration and pH of the stratum corneum. (Filaggrin’s first function is to activate the tenofilaments, hence the name: filament aggregating protein). The faulty epidermal differentiation gene results in the reduced production of filaggrin, and more than 50% of people suffering with atopic dermatitis, have been found to have the faulty gene. In our ancestors, this gene helped ‘natural vaccination’ against small pox and cow pox. This gene has persisted, but modern lifestyles with overuse of detergents on our skin, exposes the weakness and causes AD (Gupta et al. 2020).
Atopic dermatitis can also be caused by a proliferation of staphylococcus aureus on the skin. This displaces helpful
bacteria and disrupts the skin barrier function. This weak barrier function can trigger an immune system response that causes inflamed skin and other symptoms (George et al. 2019). Clausen et al. (2017) suggested that increased staphylococcus aureus colonisation in patients with AD, as well as filaggrin mutations, show how vital host-microbe interactions are. This research was supported by Koh, Ong and Omman (2021) who stated that skin microbiome is a complex and constantly evolving community that interacts across the skin barrier. There is much research regarding the use of bleach (dilute sodium dichlorite/Dakin) for patients with AD. Bleach baths do seem to improve clinical symptoms, and also restore surface microbiome by eradicating staphylococcus aureus (Maarouf and Shi, 2018, and Silverwood et al. 2021).
Emerging New Treatments and Future Therapeutics
Atopic dermatitis is a common, inflammatory, chronic skin disorder with a constellation of symptoms. Currently, there are many therapies, in various phases of drug development, that specifically target the pathogenesis of AD (Edwards et al. 2018). These include oral, injectable and topical novel therapies, all having a diverse range of mechanistic action (Patel and Strowd, 2017).
AD is frequently refractory to topical treatments, and long term treatment with oral immunosuppressive therapy is often required to control the burden of disease, prevent flare-ups and achieve a better quality of life (Napolitano et al. 2018).
JAK inhibitors (janus kinase inhibitors) target several pathways, instead of a single one (Schuttelaar, 2022). Currently, other medications such as Dupilumab, and other human monoclonal antibodies (biologics) thogenesis of AD, are also in the process of being approved for its management (Tameez etal. 2020).
HOW DO JAK INHIBITORS WORK?
•
•
•
•
Several other emerging treatments are expected to play an important role in therapy, and a number of JAK inhibitors (baricitinib, upadacitinib and abrocitinib) have recently been approved by the UK Medicines and Healthcare regulatory agency (MHRA) for atopic dermatitis.
12 | www.iocp.org.uk ARTICLE
Stop activity and response of one or more JAK enzymes
KAK inhibitors block JAK enzymes to halt auto-immune process
Block messages coming from cytokines (proteins that promote inflammation
JAK inhibitors calm over reactive immune systems
Many inflammatory cytokines are involved in the pathogenesis of atopic dermatitis, and these JAK inhibitors would appear to have the potential for a broad therapeutic benefit within dermatology.
However, more robust studies are needed to assess long-term safety, and also to establish future treatment guidelines. JAK inhibitors certainly seem poised to be an important addition for the future treatment of this complex, chronic, very old, skin disease.
TABLES
Table 1: Table created by Gaynor Wooldridge from information provided by research on the four humours.
REFERENCES
FIGURES
Photo of dermatitis to patient’s foot with permission granted 01/08/22
Fig 1: Free image from Shutterstock: http://www.shutterstock.com/imagephoto/four-eggs-eggbox-types-temperaments-sanguine-1040693363
Fig 2: Personal clinic image. Permission granted by patient. Atopic dermatitis vs psoriasis.
Fig 3: Normal skin vs dermatitis. Shutterstock: Designua ID 275935922. Accessed 09 August 2022
Fig 4: Atopic Dermatitis, current treatment pathways. Created by Gaynor Wooldridge based on information provided by research on current treatments.
Fig 5: How do JAK inhibitors work? Created by Gaynor Wooldridge, based on information provided by research on JAK inhibitors.
Anft, B. 1955. Friedlieb Ferdinand Runge: A forgotten chemist of the nineteenth century. J Chen Edu. 32(11): 566 Ballard, A. 2021. JAK inhibitors are coming and they are the biggest eczema development in years. Available at: https://nationaleczemasociety.org/blog/jakinhibitors-research/ Accessed: 09 August 2022 Besnier, EH. 1892. Première note et observations preliminare pour service d’introduction a l’etude des prurigoa diatesique (dermites Multiforms pruringineises chromiques exacerbates et paroxystiquea du type du prurigo’ de Hebra. Amales de dermatologic et de syphiligraphie. Paris. 3: 634-648 Bhattachaya, T et al. 2016. Historical perspectives on atopic dermatitis: eczema through the ages. Pediatr Dermatol. Bozek, A, Zaja, M and Krupta, N. 2020. Atopic dermatitis and psoriasis as overlapping syndromes. Medicines of Inflammation Vol 2020, Article ID 7527859 4 pages Brocq, LAJ, Besnier, E and Jacquet, L. 1900-1904. La pratique dermatologique: traite de dermatologie appliquée. Paris: Masson et Cie Calvus, MF. 1525. Hippocrates (c460-370BC/BCE) attributed to. Octoginta Volumina. The Hippocratic Corpus translated from Greek into Latin by Calvus (c14401527). Rome: Franciscino Minutius Calvus Clausen, ML et al. 2017. Staphylococcus aureus colonisation in atopic eczema and it’s association with filaggrin gene mutations. Br J Dermatol Cohen, J. 2012. A brief history of bloodletting. History Magazine. May 2012.
Dale, BA et al. 1981. Similarities between stratum corneum basic protein and histidine-rich protein 11 from newborn rat epidermis. Biochem Biophys Acta 668, 98-106 Diaz-Carera, NM, Sanchez- Borges, MA and Ledford, DK. 2021. Atopy: a collection of comorbid conditions. The Journal of Allergy and Clinical Immunology in Practice. Vol 9 Iss 11 pp 3862-3866
Diez, MA and Garcia, R. 2019. Coal tar: a by-product in coal making and an essential raw material bin in carbochemistry. Eds: Suarez-Ruiz, I, Diez, MA, Rubiera, F. New Trends in Coal Conversion. Cambridge. Woodland Publishing pp. 439-487 Duncan, MC. 1959. Neurodermatitis -a psychosomatic approach. Med J. 116: 247-54 Edwards, T et al. 2018. Insights into future therapeutics for atopic dermatitis. Expert Opin Pharmacother 19(3): 265-278 Gardner, A. 2018. Key differences between eczema and psoriasis you need to know. https://www.health.com/condition /psoriasis/eczema-psoriasisdifference#:~:text=%E2%80%9C Accessed 3 August 2022
George, SMC et al. 2019. Treatments to reduce infection with the bacteria Staphylococcus aureus in eczema. Cochrane Library Gokaimen, O. 2016. Itchy skin is a random vestige of evolution. Genome Biology and Evolution. Gupta, J et al. 2020. Filaggrin gene mutations with special reference to atopic dermatitis. Curr Treat Options Allergy Guttman-Yassly, E et al. 2017. Atopic dermatitis and psoriasis: two different immune diseases or one spectrum. Curr Opin Immunol 48: 68-73 Hamilton, R. 2015. Coal Tar. Tarascon Pocket Pharmacopoeia. Deluxe Lab Coat Edition. Burlington, Massachusetts. Jones and Bartlett Learning Hebra, FR von. 1866. On diseases of the skin, including the examination. Editor’s: Ferdinand Hebra and Moriz Kaposi. London. The New Sydenham Society. Vol. 3-5 Hippocrates, of Los. c460BC/BCE. Corpus Hippocraticum Koh, LF, Ong, RY, Omman, JE. 2021. Skin mocrobiome of atopic dermatitis. Allergology International Vol 71 Kramer, ON et al. 2019. The history of atopic dermatitis. Clinics in Dermatol Vol 35: Iss 4 pp 344-348 Langan, SM and Irvine, AD. 2020. Atopic dermatitis. The Lancet Vol 396 Iss 10247 pp 345-360 Laughter, MR et al. 2021. The global burden of atopic dermatitis: lessons from the GBD study 1990 to 2017. Br J Dermatol 184: 304-9 Maarouf, M and Shi, VY. 2018. Bleach for atopic dermatitis. Dermatitis 29(3):120-126
Mercuranali, G. 1572. De Morbis Cutaneous, et omnibus corporis humani extrementis tractatus locupletissi. Venice Napolitano, M et al. 2018. Adult atopic dermatitis: new and emerging therapies. Expert Rev Clin Pharmacol 11(9): 867-878 Patel, N and Strowd, LC. 2017. The future of atopic dermatitis treatment. Ader Exp Med Biol 1027: 185-210
Roelofzen, JH et al. 2007. Coal tar in dermatology. J Dermatolog Treat 18(6): 329-34
Sgontzos, M et al. 2015. Hippocrates on paediatric dermatology. Paediatric Dermatology 32(5): 600-603
Silverwood, RJ et al. 2021. Atopic eczema in adulthood and mortality UK population based cohort study, 1998-2016. The Journal of Allergy and Clinical Immunology Vol 147 Iss 5 pp 1753-1763
Schuttelaar, MLA. 2022. A new avenue for the treatment of chronic hand eczema. Br J Dermatol 197(1): 7-8
Tameez Ud Din, A et al. 2020. Dupilumab for atopic dermatitis. The silver bullet we have been searching for? Cureus 12(4)
Thomson, SF. 2014. Atopic dermatitis natural history, diagnosis and treatment. ISRN Allergy 2014: 1-7
Thyssen, JP and Kezic, S. 2014. Causes of epidemal filaggrin reduction and their role in the pathogenesis of atopic dermatitis. Allergy and Clinical Immunology Vol 134 Iss 4 pp 792-799
Van den Boggard, EH. 2013. Coal tar induces AHR-dependent skin barrier repair in atopic dermatitis. The Journal of Clinic Investigation 123(2): 917-927 Wise, J. 2022. NICE recommends three more treatments for atopic dermatitis. BMJ 377 Wright, RC and Goodman, L. 1979. Contact dermatitis: a historical perspective. Int J Dermatol 28(8): 665-8
Podiatry Review Autumn Issue 2022 | 13
Mid Wales Diary
David Holland BSc(Hons) Pod-Med, CBiol, CSci, FFPM-RCPS(Glasg).

I was delighted to read, some months ago, that intelligence may not be pre-determined by our genes after all. This was in the context of a Nobel prize-winner stating, back in 2007, that Africans were less intelligent than Europeans. That theory harkens back to some races supposedly being more intelligent than others. There is absolutely no proof that this is so, and he later suggested he had been misquoted. The information came from an excellent source - the 2019 book A Short History of Humanity - by Professor Johannes Krause, and Thomas Trappe.
A logical extension of this discussion - if intelligence is not pre-determined by our genes, does a fixed intelligence quotient IQ actually exist? Psychologists would say that it does, but they have a vested interest since they ‘discovered” IQ, and monitor IQ testing. If IQ does not exist, then do we, or our children, have the potential to be highly intelligent?
How did our early life experiences - good or bad which would include schooling, affect our understanding, willingness to learn, and ambition?
Johannes Krause is Professor of archaeology and paleogenetics at the University of Tubigen, and Co-Director of the new Max Plank Institute for the Science of Human History in Jena. He is an established international authority in the field of archeogenetics.
Barefoot running is a topic I take professional interest in. Podiatrists in general are not in
favour of barefoot running, largely because of unsubstantiated claims of less running injuries made by Christoper McDougall in his 2009 bookthe “barefoot bible” Born to Run.
Barefoot running by those who choose not to wear shoes, as opposed to habitual barefoot running by indigenous peoples, is not new. Olympic athletes Emil Zatopek, Abebe Bikila, and Zola Budd all ran barefoot - in competition too. They ran barefoot because they were used to it. Not because it was healthier, or would possibly lead to less injuries.
In fact, most of us can run barefoot if we choose to. The fossil record going back over one million years shows that our hunter-gatherer ancestors possessed highly-effective bipedal ability. Surely it seems improbable that evolution would suddenly go into reverse, and drive humans towards less effective bipedalism in which the wearing of footwear became necessary in order to walk and run?
If you or your patients want to try running barefoot (it does feel good) do so by all means, but not on concrete. A mix of supporting surfaces is much better for running - barefoot or shod. Concrete surfaces are hard, and uniformly flat.
Let’s face it - some of our patients need to wear orthotics just to be comfortable on concrete.

14 | www.iocp.org.uk
ARTICLE
Building work has been moving apace at Wyvern - two load-bearing walls knocked out recently, which has meant us living and cooking in one room temporarily. Upstairs is unaffected so we still have bedrooms, “facilities”, and an office - to which I and the dog beat a hasty retreat as soon as the builders arrive - around 8am each day.
Footnotes
Foot Health Practitioners News - Issue 11



Hi everyone.
I hope that this editorial finds you all fit and well. Maybe slightly sunburnt after the wonderful weather that we have had for the last few months. As I write this, it has been raining for the last couple of days, which is perfectly timed, as my holiday starts next Friday. I can always take an umbrella.
On Sunday morning I was getting ready to take my dogs for their morning walk, when the telephone rang, I thought to myself, let the answer machine pick it up. But as I was almost standing next to it, I answered. It was a local Foot Health Practitioner, who over the last few months I have got to know quite well.
As we are both very busy at this time, we refer patients that we can’t accommodate to each other. He was not trained by the IoCP, but I won’t hold that against him.
He started the conversation with the normal “Hello, how are you…” and then a question. “I would like to ask you a favour…” I thought he had a difficult patient who he perhaps wanted me to give him a second opinion, or maybe, he had run out of gloves or something simple like that, but no.
“Ian,” he said,”I have a painful corn on the plantar metatarsal area of my right foot. I have tried to sort it out myself, but I can’t reach it, could you look at it for me?” I said “Yes, of course I can, do you want to pop round in about an hour?” He was very grateful, and the appointment was made.
At this point I started to get a little nervous! What if he had been taught differently to me, would he think I was doing it wrong. Lots of thoughts were running around my head, was I up to the job? My wife, who happens to be a Chiropodist, asked me if I wanted her to do it, but I declined the offer.
I AM an FHP. I deal with things like this every day, why should he be any different? The doorbell rang, it’s him. I took a deep breath and answered the door. We sat down, had a cup of coffee and spoke about some of the patients that we have dealt with, had a very nice chat and lots of laughs. And then the time came. We went through to the surgery, he sat in the chair and I put on my gloves.
It was almost like Martin Harvey was standing behind me, watching. I cleaned his foot with a wet wipe, and there it was, a small Heloma Durum. I had it out in about two shakes of a dog’s tale. (Thanks Martin!) I had never thought about it before, but I suppose Dentists need to see Dentists, Doctors need to see Doctors, so it stands to reason that FHPs need to see each other. I was very worried about treating someone who works in the same profession but at the end of the day my training and experience shone through. For the record, he said his foot felt a lot better, and if you were wondering, no, I didn’t charge him.
I hope you all enjoy what is left of the Summer.
Best Regards
Ian
Podiatry Review Autumn Issue 2022 | 15










16 | www.iocp.org.uk Foot Health Practitioners News - continued
Martin & the Graduation Group
Day JUNE 2022 The podiatry instrument packs given to students are sponsored by Heeley Surgical Erin Congratulations!
Molly
Graduation
For most people, leaving university is the final step forward into their career the beginning of their independent lives. Having entered the working world at 18, it became clear to me very quickly that interacting with a computer screen from 9 to 5; demanding emails and endless spreadsheets was not what I was happy doing until retirement.
But what did make me happy? What gave me purpose? That was something I was still discovering and it was a discovery ultimately made, in the most unlikely way.
Having suffered with painful, ingrown toe-nails for as long as I can remember, (to even touch them was agony), I finally decided enough was enough and booked an appointment with a local podiatrist for surgery. It took some convincing to get me there. The nippers and the anesthetic injections terrified me, but the podiatrist who performed the procedure was excellent at putting me at ease with friendly conversation and a calm approach. As I began to relax, I actually found myself fascinated with the mechanics of the surgery. It’s not often you can describe a visit to a medical professional for a painful procedure as a positive experience, yet as I left the clinic, I could not have been more glad to have gone.
A couple of weeks later, at my follow-up appointment, I was talking to my podiatrist about my new-found fascination and how sympathetic I was to people who were still suffering as I had been. As luck would have it, the podiatrist was looking at expanding the clinic due to high-demand, and offered to let me shadow her in my free time. For the first time in years, I was excited about going into a work-space.
A week later I had signed up to the COFH Foot Health Practitioner course. For the next six months, I shadowed and studied at every opportunity, passing the theory exams, until finally in June the first real test came. My two weeks practical assessment at the College of Foot Health in Southport. Whilst I was initially nervous about the idea of spending two weeks with a dozen strangers, the course had a really welcoming atmosphere (I still keep in touch with the other students) and the tutors were fantastic, showing us the ropes but also trusting us to get in there and get some real experience.
By far my favourite part was working on the real life patients. The practical experience of working on people’s feet, confirmed for me once and for all, that this is what I wanted to do. I feel a great sense of gratification when I can help people by listening to them and giving them the appropriate care that they need. When they leave feeling like they are walking on air that is the best feeling of all.
I am due to start the Podiatry degree at Huddersfield University later this year and I’m incredibly excited to kick start my career and give my patients more advanced knowledge and advice. Since finishing college, I have been working in the local podiatry clinic and have a handful of my own patients to look after now. It’s a surreal feeling to be treating others that were once in my position and I can’t wait for what my future holds.

Podiatry Review Autumn Issue 2022 | 17
Dear readers, my name is Molly Symonds-Hall, and I am honored to share with you my experiences as a young foot health practitioner starting out in the world of podiatry.
I am often asked about how long we need to continue wearing masks or personal protective equipment (PPE) in practice. For health professionals while dealing with patients this is something we all will continue to do as part of our duty of care to patients, if not ourselves. Pre Covid we were able to go mask free, except for certain procedures, including burring nails, surgery, etc.
Many of us have probably suffered less colds or influenza, as well as Covid-19 because of vaccinations and PPE and wearing masks. But mask wearing also has its downfalls with many practitioners having or still suffering from mask acne, but it is a small price to pay to keep yourself and your patients protected from the possibility of contracting Covid-19, or its many variants.
PPE costly, yes, but again a small price to pay to protect yourselves from dust, fluids, etc., during your daily practice. Protecting your clothing and uniforms from collecting and holding onto any viruses that tend to stay in materials for the short-term, until they are washed.
Mask wearing and PPEfor how long?
By Beverley Wright Chair of Ethics and Vice-Chair of Education
It is likely that mask and PPE wear will be more convenient from 31 August 2022. This is because routine asymptomatic testing in England will be stopped across the NHS, adult social care and hospice services, parts of the prison estate and detention and some domestic abuse refuges and homelessness settings.

Free testing for the public stopped in April 2022, while hospitals health care and nursing home settings, etc., could continue to test regularly for free. Testing will remain for those with symptoms of Covid, immunocompromised patients in hospitals, anyone being admitted into care homes and hospices. Particularly, when there are outbreaks in certain high-risk settings such as care homes.
It is interesting that despite the government’s reasons due to falling rates in the number of deaths and hospitalization in England. While also being a government cost cutting exercise. It is a worrying time for the NHS and the public about the safety and resilience of services being provided. Particularly, as there are still about 3 out of 4 individuals with asymptomatic symptoms that will test positive for Covid-19, or its many variants. Although, covid-cases have appeared to fall, the virus has not been eradicated. So, it is important to continue to be vigilant, so that health professionals and their patients are not put at any further risk.
Recently, I lost a patient when a District nurse who contracted covid, came back to work, admitting to and visibly being unwell, visited my two vulnerable patients. A husband and wife, married for over 60 years, both sadly suffering from terminal cancer, days later they contracted covid and were both blue-lighted to hospital. One came home, the other did not having died of covid induced pneumonia.
COVID-19 pneumonia is a horrible way to die. It tends to be more severe than other forms of pneumonia. Studies have shown that ‘Pneumonia caused by SARS-CoV-2, when compared to other forms of pneumonia, including influenza, creates an even more inflammatory type of infection that might be responsible for its severity and prolonged course in some people’. (Grant, Morales-Nebreda, et al).
While we lose government and health resources that have kept us safe, during the Covid-19 pandemic. It is important to keep our own protective procedures in place, as a duty of care to our patients and protecting ourselves.
All the best
Beverley Chair of Ethics and Vice-Chair of Education
REFERENCES
Grant, R.A., Morales-Nebreda, L., Markov, N. S. January 2021. Circuits between infected macrophages and T cells in SARS-CoV-2 pneumonia.
18 | www.iocp.org.uk
- continued
Foot Health Practitioners News
Award of Consultant Fellowship of the IOCP
The Institute of Chiropodists and Podiatrists
Award
Submissions are invited from members or academic fellows of the Institute pursuant to granting them additional recognition as a Consultant Fellow of the Faculty of Podiatric Medicine of the Institute of Chiropodists and Podiatrists (CFPodM). This allows fellows to progress to further advanced training and practice indemnified by the IOCP.
Consultant Fellowship is a clinical award for senior members of the profession, recognising and demonstrating their seniority and an advanced scope of clinical practice. The minimum attainments of individuals seeking the award must be as follows:
• They must be current registrants of the Health and Care Professions Council, in good standing, at the time of application without pending disciplinary action.
• They must be current full members or academic fellows of the Institute of Chiropodists and Podiatrists with current IOCP Option 4 professional indemnity insurance.
• They must have a degree in Podiatry or Podiatric Medicine awarded by a UK university
• They must have Local Anaesthesia (POM-A) and Prescription Medicine (POM - S) annotations recorded on their HCPC registration entry OR have POM-A and Supplementary Prescribing/ Independent Prescribing recorded on their HCPC annotations.
• They must have a minimum of 12 years of clinical practice as a podiatrist.
• They must submit evidence of a pattern of continuing professional development throughout their career to date in subjects appropriate to podiatric medicine.
• They must submit a curriculum vitae, showing their journey through the profession to the date of application and this must demonstrate how they believe themselves to have a scope of practice that merits the title ‘advanced/Consultant’
• They must agree to submit a presentation/lecture to the IOCP Annual Conference demonstrating their advanced knowledge/ practice/research.
The award is via the agreement of the panel of the Consultant Fellowship board of the IOCP who will ensure that all of the minimum standards have been met. Applicants will also be required to successfully undertake an interview and provide two professional references including a statement/sponsor of support. Once the criteria has been met and the appropriate application paperwork submitted to the registered offices of the Institute, the award will then be formally issued upon payment of the nominal administration fee of £150.
Award of Academic Fellowship
The Institute of Chiropodists and Podiatrists
Award
Submissions are invited from members of the Institute pursuant to granting them additional recognition as an Academic Fellow of the Faculty of Podiatric Medicine of the Institute of Chiropodists and Podiatrists (FPodM).
Application is by way of completion of the appropriate paperwork and submission of a 5000 word dissertation containing previously unpublished material on a relevant podiatric subject that meets the approval of the Review Board of the Faculty of Fellows. Such dissertation is to be constructed on sound academic principles and be adequately referenced in an accepted academic style.
For members who have not previously published, the Board is happy to give informal and friendly guidance to members wishing to develop this interesting new area of their professional career. A nominal fee of £100 is payable to cover the necessary administration by Head Office. Certificates of Fellowship will be awarded to successful Fellows and their names recorded on the Roll of Fellows maintained by the Faculty.
Accepted dissertations will be published in Podiatry Review and be added to The Fellows Library which will be an electronic knowledge bank available online to registered members. Such activity is also held to be Continuing Professional Development (CPD) by the IOCP and is suggested as being suitable to record in the event of HCPC audit.
Applications will be accepted from current members who are HCPC registered, annotations such as POMs or LA are not a condition of application as this is an academic award open to all HCPC registered full members of the Institute.
For further information and an application form please contact Head Office by emailing info@iocp.org.uk.
Podiatry Review Autumn Issue 2022 | 19 AWARDS
The Institute of Chiropodists and Podiatrists
As we expand our partnerships and collaborations with other professional bodies and charities we would like to encourage members of both the Institute of Chiropodists and Podiatrists and the College of Foot health to nominate their favourite charity, so we can show our support to their work and commitment in raising awareness of health related conditions and diseases.
The Nominated Charity will be promoted by our organisation for the next quarter featuring in our journal and online.
Please nominate your charity by either writing to Head Office at: The Institute of Chiropodists and Podiatrists, 150 Lord Street, Southport, Merseyside.
PR9 0NP or by email to julie@iocp.org.uk with the subject ‘Nominated Charity’, please include details of your chosen charity, a reason why you have nominated them, please also include your photo as nominee, as this will appear alongside the Charity Nomination Page in our January issue. The chosen Charity for October is the Roy Castle Foundation, see page 22.
The final date for nominations to be received is 5th November, after this date a charity will be chosen at random for the next quarter.

The winning charity would be contacted to let them know that they have been nominated as our charity of the quarter, for their logo and information, and we will publish their information along with a link to where members and subscribers of Podiatry Review can donate to.
Hi Julie,
Lung cancer remains the main cause of death in the U.K. Roy Castle Charity helps and support not only in research, screening program in association with the NHS, treatments, with a view to improve life expectancy and quality of life. They also provide a global education element to the public, patients and their family affected by lung cancer. They aim to support people who are diagnosed with financial help, group counselling, and specialist nurse.
A talk was given at our branch meeting by Mrs Angela Massey who is the community fundraising Manager, which was excellent. I have contacted the members who were present at that meeting, the Vice-Chair and the Treasurer, and for all the reasons and points given above, we would like to bring Roy Castle our support.
I have for some years been a volunteer in one of their shops to help raise money which I found most rewarding.
 Michèle Allison
Michèle Allison
20 | www.iocp.org.uk
NOVEMBER
5th
Roy Castle Lung Cancer Foundation
 By Simon Malia
By Simon Malia
Lung cancer is the UK’s biggest cancer killer- every 15 minutes, someone in this country dies of it. It kills more people than breast, prostate and pancreatic cancers combined. Lung cancer is also a major health threat for women; it kills more women than breast and ovarian cancers combined.
So, why does this happen? There is a complex mix of reasons. Around 75% of people with lung cancer are not diagnosed until it is too late to offer curative treatment. Too few of us recognise and understand the key signs and symptoms of the disease, and often people have misconceptions about it. There is one basic fact to bear in mind: if you have lungs, you can get lung cancer. Many people still believe smoking is the only cause, whereas other factors include air pollution, expose to toxic chemicals, radon gas, and genetic changes. For many decades, lung cancer received far less funding for dedicated scientific research than other cancers.
These are the key challenges for the only one UK charity dedicated entirely to supporting people with all forms of lung cancer, Roy Castle Lung Cancer Foundation. It has its roots in an idea first put forward in 1990 by Professor Ray Donnelly, a thoracic surgeon at Liverpool’s Broadgreen Hospital. Prof Donnelly, heartsick of seeing patients with inoperable, incurable lung cancer, set up a charity known initially as the Lung Cancer Fund. One of its earliest achievements was to fund the first-ever dedicated lung cancer support nurse. Now, Lung Cancer Nurse Specialists are key members of lung oncology teams worldwide.
In 1993 Prof Donnelly proposed that the charity should aim to build to the world’s first centre dedicated specifically to lung cancer research. The following year, the much-loved entertainer Roy Castle learned he was dying of lung cancer. Roy selflessly dedicated his final few months to raising funds for the research centre project. The public response to his immense courage was astounding. Following his death, the charity was renamed in his honour, and in 1997 the Roy Castle building was opened in Liverpool.
Nowadays, lung cancer research is carried out in laboratories and institutes worldwide, with data and resources from the Liverpool centre making significant contributions to this global effort. The charity now funds research projects across the UK, chiefly seeking ways to improve early detection of lung cancer or to improve the overall experience of patients affected by it.
Sadly, lung cancer remains the leading cause of cancer deaths across the UK. Each year, it claims just under 35,000 lives - more than the total number lost to by breast, prostate and pancreatic cancers combined. Therefore, the work of Roy Castle Lung Cancer Foundation remains vitally important.
Lung cancer can affect anyone at any time. While smoking remains the major causal risk factor, around 28% of all cases are not related to smoking. Anyone with lungs can get lung cancer. Survival rates remain stubbornly poor, mainly because
the disease is too often detected at a point when curative treatment is no longer an option. Early diagnosis is the key to improving outcomes. Screening by means of low dose computed tomography (LDCT) can shift detection to an earlier stage and reduce lung cancer mortality in high-risk individuals.
Roy Castle Lung Cancer Foundation aims to see the introduction of a full national lung cancer screening programme, and the charity is working with the NHS to ensure this happens. A community project funded by the charity helped pave the way for the NHS Targeted Lung Health Check programme now being rolled out across England. This is designed to detect lung cancer even before symptoms appear, and will play a key part in the recovery from the impact of the COVID-19 pandemic across the entire lung cancer pathway.
The charity also funds essential research into early detection so people can be diagnosed at the earliest opportunity. New treatments mean people are living well for longer with incurable lung cancer, so the charity campaigns for more people to have access to life-lengthening treatments.
The charity is represented on both the National Institute of Health and Care Excellence (NICE) and Scottish Medicines Consortium (SMC), the bodies whose job is to determine which new treatments are made available to NHS patients. There are other key roles too. Being diagnosed with lung cancer can be both worrying and confusing. So, the charity provides a wide range of practical, emotional and financial support for everyone with lung cancer.
The Foundation offers first-class independently audited information and support services for patients and families. It campaigns on behalf of people with lung cancer and to protect public health; raising awareness of the disease, its signs and symptoms, and issues that surround lung cancer, It also offers a free nurse-led helpline for people with lung cancer, an online quit-support service for people who want to stop smoking, and being a major presence within the online lung cancer community via ‘Health Unlocked’,
Roy Castle Lung Cancer Foundation is the only UK charity that offers such a complete range of services, dedicated to helping and supporting all those affected by all forms of lung cancer. Those were its founding principles in 1990, and they remain firmly in place today.
If you would like to make a donation, please go to https://roycastle.org/donate/
Podiatry Review Autumn Issue 2022 | 21 ARTICLE
If you have lungs, you can get lung cancer
28%
of all cases are not related to smoking

Essentials of Biomechanics

Principles of gait: Using the Acceleration Lever System Effectively
By Andy Horwood Visiting Lecturer & Fellow Staffordshire University Product Designer & Research at Healthy Step Ltd

INTRODUCTION
Levers are simple machines that can be used to move loads. Every lever system needs a relatively solid beam that can rotate around a fulcrum, which in biomechanics, means an instantaneous joint axis. Remember joint axes change position with joint motion for they are not stable points of rotation but momentary and instantaneous, constantly moving with changing joint positions. Long bones make perfect levers for animal motion, as they form a single long, narrow structure that provides good rigidity with very limited compliance to permit bending deflection. The more deflection within a beam, the more effort power lost within the lever system. For a beam to move or resist motion it requires effort. In biomechanics this derives from muscular contractions that are usually interacting with gravitational forces to create or resist motion. Finally, there is the resistance or load to move. For lower limb motion, this consists of either proximal or distal body masses, derived from either segments within the lower limb or above it from the head, arms, and trunk. Most levers used within the lower limb consist of long bones acting as beams within class three lever systems to create flexion or extension motions at low metabolic costs, and yet they are using lever arm mechanics that compromise mechanical efficiency. Heel lift is different for several reasons.
Complications in Using the Foot as a Beam
The foot does not make a simple beam. This is because it is constructed from multiple bone components between the ankle and metatarsal phalangeal (MTP) joints, only five being long bones (metatarsals). Thus, to function in a beam-like manner requires the use of soft tissues to create stability across the foot’s articulation. A disproportionate amount of metabolic energy is used during the acceleration phase compared to other periods of human gait (Gottschall and Kram, 2003; 2005). This tells us that heel lift and early terminal stance is energetically more costly and therefore more difficult to perform compared to loading response, midstance weight transfer, or swing phase.
There could be a good reason for this. Using a single long bone, such as the femur or tibia, to replicate a beam is relatively easy as these are biologically stiffened structures ideal for the purpose. Under loading, long bones are subjected to bending moments, which tends to focus different stresses to different surfaces. When beams are bent downwards a deformation occurs, known as ‘sagging’ deflection. This causes tension forces to focus on the inferior surface of the beam, while compression forces focus onto the superior surface. In the middle will be a neutral zone where neither tension nor compression exists. When beams are deflected upwards, known as ‘hogging’, forces reverse with tension now focused onto the superior surface (see figure 1 overleaf). Having a highly erect posture, human lower limb long bones avoid most of these sagging and hogging deflections because they are primarily loaded in a vertical superior-inferior direction, more like a column than a beam. However, this tends to lead to anterior-posterior and medial-lateral bending stresses instead.
Podiatry Review Autumn Issue 2022 | 23 CPD 4 page article
Figure 1: When a beam is loaded horizontally it will either bend downwards (sagging deflection left image) or deform upwards (hogging deflection right image) depending on the direction of the load. This deflection direction effects where compression and tensional forces are concentrated.

Image from the upcoming text ‘Clinical Biomechanics in Human Locomotion: Origins and Principles’, with permission of www.healthystep.co.uk).
The foot is not made of a single long bone beam. Modelling the foot as a solid structure dramatically underestimates the power dissipated within the foot and overestimates the power derived from the foot during gait (Farinelli et al, 2019). This is important because it tells us that a structure with twenty-eight bones (remember the two sesamoids) is not going to be rigid at any point during gait. Indeed, it is important that the foot can dissipate energy passing through it by permitting deformation and motion within it. As a structure supplied with (usually) twenty-five articulations (from ankle to the MTP joints), some ten extrinsic muscles, around nineteen intrinsic muscles, and an extensive network of strong ligaments and fascia, the foot certainly possesses the capacity to provide structural property adaptability.
For the application of acceleration power, the foot needs to behave as much as it can as a single rigid structure running from the ankle to the MTP joints. During late midstance and at heel lift, the foot is lying horizontally over the support surface, with body weight driving down above and under the influence of the ankle dorsiflexion moment. Therefore, it is subjected to sagging deflection at the all-important heel lift boundary. Thus, the dorsum of the osseous foot is subjected to compression while the plantar foot is exposed to tension strains before and as the heel starts to lift. How well it copes and resists the sagging deflection depends on how stiffened the foot is at heel lift, remembering that the healthy foot is going to be in some degree of a semi-rigid state, never totally rigid.
How Heel Lift Occurs in the Healthy Foot
Let us consider how the foot is behaving towards the heel lift boundary during the normal compliance-stiffness cycle of the walking stance foot. During late midstance, the midfoot starts to stiffen due to the fall under gravity of the body’s mass over the foot at the ankle as part of the inverted pendulum’s motion (Horwood, 2021). As forces on the foot start to rise as a percentage of body mass, the foot stiffens exponentially (Stolwijk et al, 2014; Bjelopetrovich and Barrios, 2016; Takabayashi et al, 2020). Forces at heel lift tend to peak at around 120% (1.2x) of body weight. This exponential stiffening under higher loading is the classic behaviour of a viscoelastic structure. These are properties which all biological tissues constructed from collagen conform to.
However, both intrinsic and extrinsic plantar muscle become increasingly active throughout late midstance (Ferris et al, 1995, Kokubo et al, 2012, Murley, et al, 2014; Farris et al, 2019), providing effort that is compressing the midfoot articulations together. This active stiffening compliments the passive connective tissue stiffening to create an adaptable level of stiffness across the vault of the foot in all three orthogonal planes.
The foot reaches its peak of pronation-induced vault depression (sagging deflection / lowest profile) at the heel lift boundary (Hunt et al, 2001). This should have induced maximal passive stance phase vault stiffness. Foot stiffening muscular actions of tibialis posterior and peroneus longus (Kokubo et al, 2012) also reach their peak activity at the heel lift boundary (Murley et al, 2014).
24 | www.iocp.org.uk CPD 4 page article Principles of Gait: (continued)
Thus, the mobile midfoot should achieve a semi-rigid state so that it can act as an acceleration beam to induce heel lift via energy applied from the Achilles, rather than providing a zone of mobility that dissipates plantarflexion power. During late midstance, the Achilles has become increasingly loaded with energy derived from the breaking activity of triceps surae acting on the body’s centre of mass (CoM) while it is rotating forward under gravity via ankle dorsiflexion. This action in turn has been increasingly moving the centre of the ground reaction force (CoGRF) to the forefoot, while applying a dorsiflexion moment across the midfoot. The ankle and midfoot dorsiflexion moments are forcing the vault to depress under sagging deflection, stretching and widening connective tissues such as the plantar ligaments and plantar aponeurosis. This process should stiffen the foot vault to help resist this sagging deflection passively, while the plantar muscles assist in an adaptable manner. As energy storage rises within the Achilles, a point is reached where the elastic power inside the Achilles is greater than the body mass keeping the heel on the ground. At that point, the heel ‘pops’ off the ground under the elastic recoil power of the Achilles, generating a powerful ground reaction force (GRF) under the forefoot (see figure 2).
Figure 2: Heel lift uses a biomechanically rare class two lever-like system to initiate acceleration. The effort (E) is further from the fulcrum (F) than the resistance (R). This is probably because myofascial fibre shortening occurs via elastic recoil, rather than via active muscular contraction, which would be metabolically expensive. The ankle plantarflexion effort provided by Achilles tendon elastic recoil requires midfoot stiffness and ankle and midfoot plantarflexion, to apply power to the forefoot as a large ground reaction force (black arrows). The upper body’s centre of mass (CoM-black circle) falls forward under gravity and the centrifugal forces of the swing limb, but heel lift adds extra momentum to opposite heel contact. Loss of midfoot semirigid stability loses any semblance of an efficient class two lever at heel lift.
Image from the upcoming text ‘Clinical Biomechanics in Human Locomotion: Origins and Principles’, with permission of www.healthystep.co.uk).

Safe Heel Lift
Vault depression (pronation) during single-limb support of midstance achieves three primary roles: that of increased contact surface area and thereby reducing peak plantar pressures (the mobile adaptor), that of energy dissipation and storage via tissue deformation, and that of passive foot stiffening. By passively stiffening the foot under increasing loads during late midstance, while also providing energy dissipation and storage, the foot vault creates a highly energetically efficient way of supplying a number of essentials roles for safe gait. Muscle activity allows this process to be adaptable, permitting increased energy dissipation or providing more energy storage for acceleration, as each step’s kinetics and kinematics requires it. Adaptability, not consistency, is the most important capability of the foot and lower limb.
A number of factors need to come into play for a safe heel lift to provide efficient acceleration. Requirements in any give step will reflect the spatiotemporal parameters (gait angle, step length, gait speed, etc.) of each step. The contralateral swing limb should be applying maximal centrifugal forces during late swing and be entering its terminal swing just before ipsilateral heel lift. The heel of the swing foot should be around 1 cm above the ground at ipsilateral heel lift.
Podiatry Review Autumn Issue 2022 | 25
Safe Heel Lift (continued)
The centrifugal forces of the swing limb help accelerate the CoM of the body towards the next step. As part of this swing limb positioning, the bulk of body mass should be placed anteriorly to the MTP joints before heel lift so that excessive body mass over the single support limb does not delay or overloading heel lifting power. Heel lift itself is a single-limb support event, although it should rapidly be followed by the start this foot’s terminal double-stance phase.
At heel lift, the foot must be rigid enough that plantarflexion power derived from the Achilles (aided by that derived from other plantarflexing extrinsic muscle’s tendons) can be applied to the forefoot to make a stable acceleration platform. Most of this acceleration power arises from soleus, especially at slower walking speeds, because soleus provides most of the anterior tibial rotation braking moment during midstance (McGowan et al, 2008; Orselli et al, 2017). Foot stiffening allows the foot to act as a linear spring with the Achilles, rotating the foot and the lower limb mass around the MTP joints, passively driving digits into extension. The activity of tibialis posterior and peroneus longus are essential to this process, for together they profoundly influence the setting of foot stiffeness properties (Kokubo et al, 2012). Setting stiffness correctly for each step allows the plantarflexion power stored within midstance to be converted to acceleration power without excessive energy dissipation across the potentially very mobile midfoot.
SUMMARY
Acceleration power and energy stored across the vault of the foot during late midstance can only be utilised effectively if the foot is stiffened into a semi-rigid beam before heel lift. The position of the body mass, the centrifugal forces of the swing limb, and vault posture all play an important part in permitting safe and efficient heel lift. If performed well, heel lift should release stored energy for acceleration power and mild energy dissipation to prevent injury, while using relatively little muscular activity during acceleration. Efficient heel lift provides significant momentum into the next footstep that greatly improves gait energetics (Ruina et al, 2005).
In the next issue we will consider the length of the acceleration lever arm and what happens if the foot is too compliant to form a beam at heel lift.
REFERENCES:
Bjelopetrovich A, Barrios JA. (2016). Effects of incremental ambulatory-range loading on arch height index parameters. Journal of Biomechanics. 49(14): 35553558.
Gottschall JS, Kram R. (2003). Energy cost and muscular activity required for propulsion during walking. Journal of Applied Physiology. 94(5): 1766-1772. Gottschall JS, Kram R. (2005). Energy cost and muscular activity required for the leg swing during walking. Journal of Applied Physiology. 99(1): 23-30.
Farinelli V, Hosseinzadeh L, Palmisano C, Frigo C. (2019). An easily applicable method to analyse the ankle-foot power absorption and production during walking. Gait & Posture. 71: 56-61.
Farris DJ, Kelly LA, Cresswell AG, Lichtwark GA. (2019). The functional importance of human foot muscles for bipedal locomotion. Proceedings of the National Academy of Sciences of the United States of America. 116(5): 1645-1650.
Ferris L, Sharkey NA, Smith TS, Matthews DK. (1995). Influence of extrinsic plantar flexors on forefoot loading during heel rise. Foot & Ankle International. 16(8): 464-473.
Horwood A. (2021). Essentials of Biomechanics. Principles of gait: the inverted pendulum model. Podiatry Review. 78(4): 29-32.
Hunt AE, Smith RM, Torode M, Keenan A-M. (2001). Inter-segment foot motion and ground reaction forces over the stance phase of walking. Clinical Biomechanics. 16(7): 592-600.
Kokubo T, Hashimoto T, Nagura T, Nakamura T, Suda Y, Matsumoto H, et al. (2012). Effect of the posterior tibial and peroneus longus on the mechanical properties of the foot arch. Foot & Ankle International. 33(4): 320-325.
McGowan CP, Neptune RR, Kram R. (2008). Independent effects of weight and mass on plantar flexor activity during walking: implications for their contributions to body support and forward propulsion. Journal of Allied Physiology. 105(2): 486-494.
Murley GS, Menz HB, Landorf KB. (2014). Electromyographic patterns of tibialis posterior and related muscles when walking at different speeds. Gait & Posture. 39(4): 1080-1085.
Orselli MIV, Franz JR, Thelen DG. (2017). The effects of Achilles tendon compliance on triceps surae mechanics and energetics in walking. Journal of Biomechanics. 60: 227-231.
Ruina A, Bertram JEA, Srinivasan M. (2005). A collisional model of the energetic cost of support work qualitatively explains leg sequencing in walking and galloping, pseudo-elastic leg behavior in running and the walk-to-run transition. Journal of Theoretical Biology. 237(2): 170-192.
Stolwijk NM, Koenraadt KLM, Louwerens JWK, Grim D, Duysens J, Keijsers NLW. (2014). Foot lengthening and shortening during gait: A parameter to investigate foot function? Gait & Posture. 39(2): 773-777.
Takabayashi T, Edama M, Inai T, Nakamura E, Kubo M. (2020). Effect of gender and load conditions on foot arch height index and flexibility in Japanese youths. Journal of Foot & Ankle Surgery. 59(6): 1144-1147.
26 | www.iocp.org.uk
CPD 4 page article
Principles of Gait: (continued)
The motives of authors of peer-reviewed or professional journal articles are always difficult to pin down, sometimes even for the authors themselves. Many authors use article publications to announce their presence in the field of research, often as part of a quest for further research funding. Others use them as a means of disseminating information in an attempt to direct a professional or scientific community towards specific subject areas they believe may reveal more evidence-based data, and thereby might encourage others to perform further research in those specific areas. Another reason to publish may be to promote an up-coming book or an education programme by which they may profit. All of these represent perfectly good publishing motives. However, whatever their motives may be, authors must always publish their sources of information by way of supporting citations. This well-established process allows readers to critique the quality of the knowledge presented to them and it avoids ‘belief’ being expressed where ‘science’ is required. It is also true that ‘bad science’ can cause considerable problems, as has recently been confirmed in relation to the model based on abnormal serotonin levels being proposed as the reason for the use of antidepressants (Ang et al, 2022; Davies et al, 2022; Read and Moncrieff, 2022). The key is that ‘good science’ in time reveals ‘truth’ whereas ‘bad science’, and ‘bad medicine’, incurs unnecessary costs and patients to risk their health. While the recent articles in Podiatry Review by Gary Ward have been interesting (Ward, 2022a, 2022b), the authors of this letter have long studied the concepts discussed within them and have consequently found many questions that must be asked of them. The articles seem to propose yet another new clinical model/technique referred to as ‘Anatomy in Motion’ or AiM. This concept implies that in contrast to other techniques, something new and advantageous is being offered in the studying of motion/examination of patients. The articles make such claims without any references to support them, despite extensive critiques of clinical examination techniques being widely available in the literature. Today, the ‘Foot Posture Index’, the ‘arch height index’ and ‘arch height flexibility’ (also known as the arch flexibility index) seem to be the foot examination techniques most supported by the literature (Gates et al, 2015; Zifchock et al, 2019; Cen et al, 2020). However, they are not included as ways of assessing the foot in the AiM foot assessment article (Ward, 2022b). Claiming the foot is a tripod based on the stability of three bones is not a new model. As a concept, it demonstrates a long and well-established history in the medical/orthopaedic literature (Dowie, 1865; Scholl, 1915; Dickson and Diveley, 1953; Kapandji, 1987: pp.218-219) but does not stand up well in the face of research. The 1st and 5th metatarsals offer greater mobility at their respective tarsometatarsal joints than do the 2nd and 3rd metatarsals (Lundgren et al, 2008; Wolf et al, 2008) and this fundamentally undermines the ‘foot as a tripod’ concept. These evidence-based metatarsal mobility findings help explain forefoot energy-dissipation mechanisms, but not tripodal foot stability. Pointing out that the triangle is the most stable structure to achieve ‘balance’ without recourse to citations is again unhelpful. This is a concept that is tied into engineering where a triangulated structure is greatest at resisting shear (a highly damaging strain within animal tissues) and is also tied into concepts of biotensegrity (Levin, 1995; Scarr, 2010, 2011, 2020).
The concepts of pronation creating only mobility within the foot and supination being required before the foot can become a rigid lever are both old ideas that have not stood up to scientific research. The semi-rigidity achieved in the foot occurs at the heel-lift boundary when the foot is most prone or flat (Hunt et al, 2001), and this semi-rigidity seems to derive primarily as a result of muscular function and changes within the transverse vault (arch) profile (Ferris et al, 1995; Kelly et al, 2012; Kokubo et al, 2012; Farris et al, 2019, 2020; Venkadesan et al, 2020). We could go on, but here is not the place.
The AiM articles seem to be based on foundational statements that are incorrect, making everything else that follows open to question. If the author were able to cite recent papers that challenge our understanding of foot function and support the articles, then we would be pleased to investigate, reflect, and reassess our present understandings. The field of clinical management of the foot in particular is already littered with functional models that do not appear to be supported by scientific research. Adding more unsupported models will not help. Let us all try to publish ‘truth’ as we have researched it, for there is still much to be learned. However well-intentioned, the inadvertent misleading of colleagues through the publication of unsubstantiated “alternative perspectives” must be avoided.
Yours
sincerely, Andy Horwood & William Eric Lee
REFERENCES:
Ang B, Horowitz M, Moncrieff J. (2022). Is the chemical imbalance an ‘urban legend’? An exploration of the status of the serotonin theory of depression in the scientific literature. SSM - Mental Health. 2: 100098. doi: 10.1016/j.ssmmh.2022.100098.
Cen X, Xu D, Baker JS, Gu Y. (2020). Association of arch stiffness with plantar impulse distribution during walking, running, and gait termination. International Journal of Environmental Research and Public Health. 17(6): 2090. doi: 10.3390/ijerph17062090.
Davies J, Cooper RE, Moncrieff J, Montagu L, Rae T, Parhi M. (2022). The cost incurred by the NHS in England due to the unnecessary prescribing of dependency-forming medications. Addictive Behaviors. 125: 107143. doi: 10.1016/j. addbeh.2021.107143.
Dickson FD, Diveley RL. (1953). Functional Disorders of the Foot. 3rd edition. J.B. Lippincott Co., Philadelphia.
Dowie J. (1865). On the Motions of the Human Feet and the Means of Preserving Them Unimpaired; Being the Philosophy of Shoemaking. Robert Hardwicke, 192, Piccadilly, London.
Farris DJ, Kelly LA, Cresswell AG, Lichtwark GA. (2019). The functional importance of human foot muscles for bipedal locomotion. Proceedings of the National Academy of Sciences of the United States of America. 116(5): 1645-1650.
Farris DJ, Birch J, Kelly L. (2020). Foot stiffening during the push-off phase of human walking is linked to active muscle contraction, and not the windlass mechanism. Journal of the Royal Society: Interface. 17(168): 20200208. doi: 10.1098/rsif.2020.0208.
Ferris L, Sharkey NA, Smith TS, Matthews DK. (1995). Influence of extrinsic plantar flexors on forefoot loading during heel rise. Foot & Ankle International. 16(8): 464-473.
Gates LS, Arden NK, McCulloch LA, Bowen CJ. (2015). An evaluation of musculoskeletal foot and ankle assessment measures. Working Papers in the Health Sciences. 1: 11. www. southampton.ac.uk/assets/centresresearch/documents/wphs/ LGAn%20evaluation%20of%20musculoskeletal%20foot.pdf Hunt AE, Smith RM, Torode M, Keenan A-M. (2001). Intersegment foot motion and ground reaction forces over the stance phase of walking. Clinical Biomechanics. 16(7): 592-600.
Kapandji IA. (1987). The Physiology of the Joints. Volume 2: The Lower Limb. 5th edition. Churchill Livingstone Inc., New York, NY. Kelly LA, Kuitunen S, Racinais S, Cresswell AG. (2012). Recruitment of the plantar intrinsic foot muscles with increasing postural demand. Clinical Biomechanics. 27(1): 46-51.
Kokubo T, Hashimoto T, Nagura T, Nakamura T, Suda Y, Matsumoto H, et al. (2012). Effect of the posterior tibial and peroneus longus on the mechanical properties of the foot arch. Foot & Ankle International. 33(4): 320-325.
Levin SM. (1995). The importance of soft tissues for structural support of the body. Spine: State of the Art Reviews. 9(2): 357-363.
Lundgren P, Nester C, Liu A, Arndt A, Jones R, Stacoff A, et al. (2008). Invasive in vivo measurement of rear-, mid- and forefoot motion during walking. Gait & Posture. 28(1): 93-100.
Read J, Moncrieff J. (2022). Depression: why drugs and electricity are not the answer. Psychological Medicine. 52(8): 1401-1410.
Scarr G. (2010). Simple geometry in complex organisms. Journal
of Bodywork and Movement Therapies. 14(4): 424-444.
Scarr GM. (2011). Helical tensegrity as a structural mechanism in human anatomy. International Journal of Osteopathic Medicine. 14(1): 24-32.
Scarr G. (2020). Biotensegrity: What is the big deal? Journal of Bodywork and Movement Therapies. 24(1): 134-137.
Scholl WM. (1915). The Human Foot: Anatomy, Deformities and Treatment; a Volume Containing a Complete and Comprehensive Description of the Anatomy of the Foot. Normal and Abnormal Conditions, Deformities of the Foot, Their Cause and Mechanical Treatment. Special Chapters on Shoe Fitting and Its Allied Branches, Including Historical Footwear. A Text Book for the Student and Practitioner. Foot Specialist Publishing Company, Chicago.
Venkadesan M, Yawar A, Eng CM, Dias MA, Singh DK, Tommasini SM, et al. (2020). Stiffness of the human foot and evolution of the transverse arch. Nature. 579(7797): 97-100.
Ward G. (2022a). Beyond podiatry: an introduction to the principles of anatomy in motion (AiM). Podiatry Review. 79(2): 30-34.
Ward G. (2022b). Part 2 The foot (AiM). Podiatry Review. 79(3): 30-34.
Wolf P, Stacoff A, Liu A, Nester C, Arndt A, Lundberg A, et al. (2008). Functional units of the human foot. Gait & Posture. 28(3): 434-441.
Zifchock R, Parker R, Wan W, Neary M, Song J, Hillstrom H. (2019). The relationship between foot arch flexibility and medial-lateral ground reaction force distribution. Gait & Posture. 69: 46-49.
Podiatry Review Autumn Issue 2022 | 27 Dear Editor
Letter to the Editor
NHS Ambulance Services’ Best Kept Secret
By Mark Mearns MCPara, Specialist Paramedic, Urgent & Emergency Care, Isle of Wight Ambulance Service.


When most of us think about NHS ambulance services in England, we naturally think of the 10 remaining Ambulance Trusts established in 2006. In most cases, England’s coastal islands are the responsibility of the nearest mainland trust, however, the Isle of Wight stands out as the only NHS ambulance service in the country that is part of a wider NHS Trust.

Located just off the south coast of England, the Isle of Wight is England’s largest island with an area of 147 square miles. Popularised as a holiday destination by Queen Victoria, the Island’s population of just over 140,000 swells to around 250,000 at peak times during the summer.
Isle of Wight NHS Trust provides all NHS services to the Island’s community and visitors and is unique in being the only integrated NHS Trust in the country that is responsible for acute, community, mental health, and ambulance services together. It would be easy to assume that a small island’s ambulance service might be a little behind the rest of the country but this couldn’t be further from the truth; this selfcontained ecosystem creates a wide variety of opportunities such as our pioneering sepsis care that simply cannot exist in a large Ambulance Trust.
Our close-knit frontline ambulance service is made up of just 104 staff and responds to around 24,000 emergency calls each year. The family feel where everybody knows everybody is in
stark contrast to mainland Ambulance Trusts and new faces always receive a warm welcome. It’s no surprise then that the Isle of Wight Ambulance Service had the best national scores in seven out of the nine elements measured in the 2021 NHS Staff Survey.
The Island is served by St. Mary’s Hospital in Newport, a 245bed facility that includes major services such as an emergency department, intensive care unit, maternity department and special care baby unit. In June 2022, our average hospital handover time for all conveyed cases was just 12.5 minutes making St. Mary’s Emergency Department one of the best performing nationally.
28 | www.iocp.org.uk
ARTICLE
Having our own Emergency Operations Centre on the hospital site complete with dual-trained 111 and 999 call handlers means that we can process all of the Island’s emergency calls in one place. Clinicians of all grades are supported by both our Clinical Support Desk and the recently established Specialist Paramedic Desk.
Like everywhere else in the country, interfacility transfers take place in order for patients to receive care at specialist centres, but the body of water between the hospitals makes this a little less straightforward. The Island’s Patient Transport Service conveys routine transfers where safe to do so, and most days, a paramedic crew will transfer more acute patients by ferry in emergency ambulances.
In cases of acute myocardial infarction (AMI) the Island does not have access to primary percutaneous coronary intervention (pPCI) so direct referral is made to Queen Alexandra Hospital in Portsmouth. Patients suffering AMI are conveyed by road to Ryde where they then travel to Southsea by hovercraft in a 10-minute journey with the initial responding paramedic crew escorting them. The patient’s onward journey is then facilitated by South Central Ambulance Service. Should the hovercraft not be available, HEMS will usually undertake the transfer either from scene or rendezvous with the crew at St. Mary’s. If neither are available, pre-hospital thrombolysis is delivered on scene with later transfer to pPCI.
Since 2013, frontline ambulance crews have delivered prehospital IV antibiotics to patients with signs of sepsis after taking blood cultures for laboratory analysis on scene. Whilst this may seem like an easy intervention that could be provided by any ambulance service, different receiving hospitals are
likely to have differing antimicrobial policies and the universal approach we are able to adopt cannot simply translate into mainland services.
The Isle of Wight Ambulance Service also operates two specialist paramedic services. Our urgent care service is focused on lower acuity 999 calls that can be managed in the community with the extended skillset of the Specialist Paramedics while also undertaking out of hours GP visits, managing end of life care in the community, and carrying out advanced wound care. The team comprises of experienced paramedics who are undertaking their full MSc in Advanced Clinical Practice funded by the Trust, with those who are not yet independent prescribers supplying a wide range of medicines under patient group directions including analgesia, antibiotics, and end of life anticipatory medicines.
Our newly-created critical care service is also staffed by experienced paramedics who are continually extending their scope of practice. Working closely with the service medical lead who is both an emergency department consultant and HEMS doctor, the team offers senior clinical support and enhanced care in serious medical and trauma cases across the Island, again with a wide range of patient group directions to support their practice.
I’m sure you’ll agree that there is a lot more to Britain’s smallest NHS ambulance service than you might expect, and that’s without mentioning our NQP programme, major incident exercises involving hovercrafts and helicopters, hospice work, and the many other interesting facets that come with working in an isolated island community.

Podiatry Review Autumn Issue 2022 | 29
Whole body integration using The Flow Motion Model™
Introduction
By Gary Ward Founder of Anatomy in Motion
OOur previous articles discussed the AiM rules, philosophy and an interpretation of the human foot in motion and in closed chain biomechanical terms. This article will explore how the foot is much more than just a foundation in the gait cycle – it can also provide us with clues to restrictions elsewhere in the body.

As a quick recap, AiM’s philosophy sets out that: Joints act: muscles react Muscles lengthen before they contract and The body moves around its perceived centre.

AiM’s Flow Motion ModelTM is a description of the journey taken by every single bone and joint in the human body through a single footstep taking into account all 3 planes of motion (the sagittal, frontal and transverse planes) in closed chain biomechanics (weight bearing). It is observed that an inability to access its three dimensional movement potential creates an environment for dysfunction and symptoms to arise.

By observing the foot and its movement through the gait cycle, the response in the rest of the body through the kinetic chain can be determined. This article will discuss how the Flow Motion Model™can identify: a) which movement in the body and foot is not occurring and b) provide whole body movement exercises to re-educate the body to move more efficiently through improved joint motion. This will allow the patient to access the positions outlined in the model (for simplicity’s sake we will focus on a frontal plane element of the model).
The Flow Motion Model™
The gait phases:
STRIKE - Initial contact SUSPENSION Foot flat
TRANSITION - Mid-stance
SHIFT - Early heel rise PROPULSION Toe off (almost)
As described in Article One, the Flow Motion Model™is broken down into phases. Each phase represents a snapshot in time in the gait cycle and describes the position that the whole body adopts at each of these key moments. The model has identified 8 postural shapes that the body adopts through the five phases in order to minimise stress and strains on the joints and the surrounding tissue. To be in a position to access each phase of the model, your body needs to be capable of accessing all joint ranges in all three planes of motion.
This is a highly unlikely scenario for the vast majority of people. When tasked with simple movement or exercise drills, the majority will favour one joint range over another. This naturally shows up in their gait cycle.
For example: The person may prefer to laterally flex their spine left Perhaps the quality of spinal lateral flexion is better to the left or It hurts when they laterally flex right Either way if they favour left lateral flexion, they will avoid or struggle to access the movement to the right. Let’s explore in greater detail a scenario of a patient who can access more lateral flexion of the spine to the left and is experiencing strain in the left lower back . The AiM Flow Motion Model will demonstrate how to guide the patient into reintegrating the reduced right lateral flexion and reduce the stresses being placed on the back. The model predicts the impact on the joints and structures occurring throughout the kinetic chain in these whole body positions.
30 | www.iocp.org.uk ARTICLE
Scenario: Patient with limited lateral flexion
Symptom:
Patient attends the clinic predominately complaining of left lower back pain, some left achilles pain and right side groin/ psoas pain. They may have a history of experiencing right medial knee pain or right ankle sprain in the past (which lead to them to lead predominantly with their left foot)
Observation of the patient:
predominantly laterally flexes to the left. experiences persistent closure of the vertebrae on the left hand side of the vertebral column persistent opening of the vertebrae on the right.
This creates a habitual shortening of the tissues and a compression between the joints on the left and a lengthening of the tissues and a gapping of the joints on the right.

People can both experience tension based symptoms or compression based symptoms on either side of the spine. In this scenario, it can be observed that where the tissues are short and the joints are compressed, the patient is experiencing compression based discomfort on the left side of their lower back.
In order to relieve pressure on the system, the patient needs to be taught how to laterally flex their spine to the right, open the closed joints on the left and encourage those tissues to come out of their persistent shortened state.
How do we do this?
Step 1 : Observation of patient’s posture in ourselves:
Before discussing solutions to this patient’s presentation, it is important that we can experience the patient’s position for ourselves. This is so we can feel the tissue tensions and pressures on certain joints. We will also be able to experience what moves more freely and what feels restricted. This can help us, as clinicians, understand our patient’s symptoms better. Try this at home by following a few simple options to check anyone’s capacity to access this particular shape. Firstly, stand in a split stance with one foot forward, no more than a stride’s length apart and bend your knee on your front foot - compare your left with your right:
Check in with yourself Observational Comments
Is there a natural difference in comfort or ability to be in this position?
Is the pressure under your front foot the same on both sides?
Is it easier to commit forwards toward one foot more so than the other?
Is it easier to commit sideways toward one foot more so than the other?
Now stand with feet hip width apart:
Check in with yourself Observational Comments
Bend one knee keeping the other knee straight, your hip should hike up (laterally tilt) on the straight leg side. Which side feels easier to do this?
Keeping the knees soft, can you laterally flex your spine evenly to the left and right? Or do you favour one side?
Can you laterally flex your neck left and right evenly? Or do you favour one side?
It’s likely that the side you find easier to commit to, both forwards and sideways is the same as the side on which you are more comfortable hiking the pelvis up (and adducting the hip). The foot on this side will likely be the more pronated. This could well be the side you laterally flex more easily towards, thus compressing that side of the lower back and increasing tension in the opposite side lower back tissues. Spending a prolonged amount of time in this position could lead to the tension in the tissues or the compression in the joints becoming problematic as they rarely have the experience of shortening from their lengthened position or decompressing via oppositional movements. With this in mind, what muscles do you feel working when you do your personal check in?
Observation of our patient
It’s clear that a right lateral flexion is necessary for this particular client. In the Flow Motion model, right lateral flexion occurs when the foot is flat on the ground and pronating.
Could how well the foot pronates predetermine how well the spine can move? Or is the limited lateral flexion affecting the foot’s potential? The interconnectedness of the body suggests it could be either. To create a foundation for the right lateral flexion, the right foot must be capable of accessing a tripod stance position (1st and 5th met heads and heel on the ground), as discussed in article 2, in order to achieve a good foot pronation.
Podiatry Review Autumn Issue 2022 | 31
B
This creates the environment for a pronating leg. Foot pronation should occur in gait when the foot is in front of us in the stride. Foot supination should occur as the foot passes beneath us and behind us.
A pronating leg incorporates: a flexed valgus knee an internally rotating femur which creates the environment for an anterior tilting pelvis a hiked (Laterally tilted) pelvis on the same side as the pronating foot and a pelvis that is rotating away from the pronating foot All while making sure that the skull keeps its eyes on the horizon to keep us balanced when upright.
When a pelvis is hiking up on the same side as the pronating foot, the hip must be adducting. The angle of the pelvis establishes a foundation for the spine that is no longer level. In order for it to maintain the eyes on the horizon at the skull level, it must laterally flex back towards the skull, in the direction of the pronating foot.
In the absence of a right lateral flexion in the spine: the hike of the pelvis would be compromised on the right side of the body right hip adduction will be limited the Centre of Mass (COM) will be drawn towards the left due to the left hip adduction weight bearing increases on the more pronated foot. the patient is established in a dominant left weight bearing versus right weight bearing pattern. Could this global position explain my patient’s symptoms?
Greater weight bearing on the left foot = larger amounts of ankle dorsiflexion and increased tension in the achilles
Perpetual abduction in the right hip due to the weight bearing increases tension in the TFL/ITB & persistent left hip hike pulls tension into the right adductor muscle
The pelvic hike creates an environment for a left laterally flexing spine which adds a compression into the left low back area.
As a result, this person is spending more time on their left foot than their right. The dominant left lateral flexion means the body struggles to get back to the right. This causes a lack of right foot pronation as well as right pelvic hike and right hip adduction. All of these things can be construed as “missing” in the habitual and unconscious way of walking for this person.
Step 2: Find what’s missing?
Movement, walking, is a learnt and habitual behaviour. People only access movements they can access and avoid those they cannot. Our goal is simply to restore motion that is missing using movement, specifically movement highlighted
by the Flow Motion Model and deemed as necessary for key moments in the gait cycle.
A foot that does not follow the guidelines for a good foot pronation could be considered as ‘missing’. Rather than focus on eliminating pronation or indeed strengthening this foot with supination exercises, the foot needs to be taught how to pronate correctly. AiM teaches the bones how to experience the movement of pronation. This was covered in the previous article.
The specific focus may not be the foot, but could be the pelvis or the spine, the movements of which are equally ‘missing’ and yet may be influencing the foot. We look for the cause in the system. If the spine is influencing the foot instead of the other way around, our focus would be placed on the spine. Improvements in spinal motion will then give permission to other parts of the body to function better. AiM then uses the whole body position to integrate the movements of the missing parts, in this case, foot, pelvis and spine. All of the integrated motions work together in some way to create efficient movement. The model highlights these patterns to us at each stage of the footstep.
Step 3: How would we use the Flow Motion Model to address such a case?
IIn the Flow Motion model, foot pronation occurs in the Suspension phase of gait. It is the one chance we have in the cycle to generate a healthy pronation. In suspension phase, it allows the body to eccentrically load (lengthen) the supinator muscles of the foot. These are then responsible for contracting our foot into a supination shape. It gives the foot the potential to contract, shorten into a rigid lever and power us forwards into the next footstep. Feet that continue to pronate beyond Suspension phase are taking too long to eccentrically load up these extensors and generate a sub-optimal forward propulsion. This causes us to flex at the hip and drag our leg forward rather than experience an effortless propulsion push off moment. Suspension phase (Frontal Plane) The frontal plane in Suspension phase must follow these rules: Weight bearing in the front foot with COM sitting on top of the foot. Foot pronates, tripod stance valgus knee adducted hip hiked pelvis spine laterally flexes towards front foot the cervical spine laterally flexes away from front foot (to keep the eyes on the horizon) Pelvis, ribcage and skull in line (on axis)
Notice that this whole body position is compromised if any of the following is challenging: Hip adduction
Foot pronation Lateral flexion of the cervical spine to the right An inability to access any of the joint motions required for this moment in time would compromise the phase.
M
32 | www.iocp.org.uk ARTICLE (continued)
From our observation it appears that our client is stuck in left Suspension phase and struggles to get out of this position to access the right Suspension phase. In order to get out of this position, the muscles must be able to contract from their lengthened position. This means they have to improve their ability to access left Suspension.
Suspension phase muscle loading: Foot pronation loads the supinators
Valgus knee loads knee extension
Hip adduction loads the abductors
Hip flexion / Anterior tilt loads the hip extensors
As the foot pronates better on its tripod and the body begins to move more easily into the position of Suspension phase. It will begin to newly eccentrically load the extensor chain and develop the capacity to start to move its mass out of the left foot and across to the right foot.
Then to access the opposite position, right foot forward, the joints must now become capable of accessing the opposite motions. The patient’s body must be taught how to access right suspension phase correctly.
Flip the image around and notice the skeleton is accessing its right foot forward shape in Suspension phase. We already know that this person cannot right laterally flex their spine nor hike the pelvis on the right. There is a good chance the rest of the joint motions you see are also challenging. We can now use this global position to re-educate the body to access joint motions it has not been able to for a long time. Teaching a hip to hike on a pronating foot with a spinal column that is laterally flexing toward it, introduces the person and their brain to a whole new position in space.


Ultimately this teaches the closed joints on the left to open, the abducted right hip to adduct and the foot that avoids weight bearing to bear weight, thus taking pressure off the left achilles, right adductor and left lower back.
Somewhere in between these two moments in time (right and left suspension) is the moment we should meet a neutral posture in all three planes in our gait cycle. This moment is close to mid stance as the non-stance leg is swinging through the midline in the sagittal plane.
If the whole body shape is unable to equally access the shape when each foot is weight bearing, the neutral shape can not be achieved when required in mid-stance. Instead, it can be observed that a person laterally flexes left when the left foot is forward and be neutral (or upright-ish) when the right foot is forward. This is a gait with limited movement and altered
timings. In order to be able to access both of these shapes, a person must be able to move all of their joints in all directions and in each plane.
Failure to be able to do that leads to: an imbalance in any of the structures in the body, the aggregate outcome of which is to favour one side of your gait cycle more than the other directly affect the potential for foot function. To be able to hike their pelvis on both sides, a person must have the capacity to both pronate their foot as the pelvis hikes; and supinate their foot as the pelvis drops. The model shows us that when the left leg is in Suspension phase, the right leg is in Propulsion phase, powering us forwards into our next step. Suspension phase is when the foot pronates as a mobile adaptor. Propulsion phase is when the foot should achieve its rigid lever. These two extremes of movement in the feet must occur at the exact same moment in time, one on the left and one on the right. One feeds the other. And in the absence of being able to achieve one, you compromise the ability to access the other and thus compromise the whole moment in time.
The realisation is that people need to be taught to access both pronation and supination movements in their feet. Foot pronation becomes harder the more pronated (e.g no tripod load) we are and a rigid lever becomes all but impossible for a foot that is beginning the foot step in an overly pronated position.
By paying attention to the feet, you have the opportunity to set the foundations for efficient and effortless movement throughout the whole body. Here AiM wedges are utilised to promote the movements of foot pronation.
Step 4: AiM wedges
AAiM wedges are foam wedges designed with specific degree angles to encourage directional movement in the bones of the feet. They are used in movement to guide the foot to experience its ‘missing’ movements. The goal is to influence movement in the foot using a wedge and then make use of the movement when walking without the presence of the wedge.
They can be placed medial, lateral or posterior to the rearfoot and medial, lateral or anterior to the forefoot in order to encourage the motions in the foot bones that were discussed in article 2, for instance position a wedge lateral to the rearfoot to promote eversion and generate a directional movement.
A wedge can also fill space between where the tripod is not in contact with the ground, thus bringing the ground up to meet the met head. For instance a patient might find themselves with more weight in the big toe on the left foot and more lateral border on the right foot.

Podiatry Review Autumn Issue 2022 | 33
If we used a wedge to support the 5th met head on the left and the first met head on the right, this would even out the tripod and create more opportunity to access the whole body movement. Just standing on these wedges alone may even improve the pelvic hike and/ or the lateral flexion of the spine in a bilateral stance.
Once the base has been set and is able to access more of the pronation movement, we can build the frontal plane shape into the body. This includes: knee flexion pelvic hike ensure mass on top of the foot lateral flexion of the spine toward the newly pronating foot keep eyes on the horizon- to manage the cervical structures of the spine.
Joint Motion gives muscle something to do
In the absence of joint motion, muscles have less and less to do. As we promote a higher quality of joint motion, the body can begin to place more and more demand on the surrounding soft tissues, including muscle, tendon and ligament. The closer the body is able to access these global movement postures: the more balanced the joint system will be
the more active the muscle system is the more organised the position and potential of the whole body. This creates an opportunity for an efficient, effortless and energy conserving movement known as Flow.
Conclusion
Working with the Flow Motion Model gives a great insight into what factors may be causing the problems your patient is asking you to work with. In the patient example above, a complaint of lower back and groin pain is less about treating the symptoms and more about getting weight out of the left foot and into the right foot. Adding a system based approach to our symptom-lead thinking widens our toolbox and greater possibility of finding solutions for our patients, and in ourselves too.
If you have enjoyed this series of articles on Anatomy in Motion and Gary Ward’s Flow Motion Model and you would like to learn more along these lines, you can find out more about his online programmes and live classrooms on the website www.findingcentre.co.uk. A great place to start is his book What The Foot?, videos on You Tube and follow Gary on instagram @GaryWard_aim or www.facebook. com/anatomyinmotion to see his perspective on bunions and all things whole body movement.

34 | www.iocp.org.uk ARTICLE (continued)
HJ sock Review by the Institute of Chiropodists and Podiatrists
A product review team, made up of 4 podiatrists at The Institute of Chiropodists and Podiatrists, were asked to review the HJ Hall sock products, these included socks from the following ranges; HJ HALL™ HJ703 – Mountain Comfort Top, HJ640 – HJ643 Men’s Comfort Tops, HJ530, 531, 532, 533, 534, 535, 540, 541, Ladies Comfort Tops and HJ607 – Garden Sock.
After assessing these products by material and finish, comfort, support, design and fit, we are delighted to recommend and endorse these ranges from the long-established and reputable HJ Hall Socks. Our review team noted the great comfort from the soft materials used, with the walking range providing extra padding for greater comfort on long walks and could help reduce blisters. The well stitched toe areas form a properly shaped toe section allowing the toes to be unrestricted. The soft grip comfort top is designed to prevent marking or tightness, this design and the overall well-structured design of the socks ensure the tops do not crumple holding the sock nicely around the foot without being too tight or leaving an indented impression around the ankle and leg. All of our review team members noted that the socks washed very well and there was no depreciation in the quality of the materials used or the soft tops, even after repeated washing. The price of the socks may be more expensive than an average pair of cotton socks, but you pay for what you get!

Podiatry Review Autumn Issue 2022 | 35
The HJ Hall range of socks are of superior design, comfort and quality!
LASERS IN HEALTHCARE – Overview and focus on Photobiomodulation Therapy
Kirsten Sinclair, BSc, Podiatrist & Clinical Trainer in MLS® Laser

Introduction
Historically light has been used as medicine for thousands of years with the ancient Greeks, Romans and Indians utilising the power of natural sunlight. Light therapy is used in a variety of ways to either treat or destroy tissues in the body. There are now lasers for hair removal, surgical cutting, ablation, tattoo removal and tissue healing amongst many other uses.
The word laser is an acronym for ‘Light Amplification by Stimulated Emission of Radiation’, describing an optical device that produces an intense, monochromatic, coherent beam of light. The worlds first laser was built and patented in 1960 by the physician Theodore Maiman. In 1967 Endre Mester discovered photobiomodulation (PBM) whilst attempting to cure tumours in rats but instead noted an increase in hair growth and healing times.
Lasers of numerous types are now present in clinics, hospitals and medical centres across the globe. This article will focus primarily on PBM.
Principles of Medical and Therapeutic Laser Mechanisms
Laser therapy, also called Photobiomodulation therapy (PMBT) works by delivering light to tissues where it interacts via one or a combination of biological effects. These include photothermal (heat delivery), photochemical (alterations to chemical processes), and photomechanical (non-destructive distortion of cells). Some lasers, used for removal of tissue, rely heavily on the photothermal effect to cause tissue ablation. However most of the research in PBMT has concentrated on the photochemical effect.
The photochemical effect relies on photoreceptors within cells and tissue (also known as chromophores) absorbing light and triggering a cellular response (Sutherland, 2002) and subsequent physiological changes. Research has demonstrated several photochemical effects at cellular and molecular levels. The most widely reported effects include: effects on cellular metabolism, ATP production, and mitochondrial membrane potential (Bayat et al 2005, Monici et al 2013). The absorption of light by chromophores such as cytochrome c oxidase affects production of reactive oxygen species and nitrous oxide, leading to an increase in ATP production (Hamblin, 2017) and modulation of the inflammatory response reducing inflammation, improving cellular metabolism and increasing the natural healing response of the body. PMBT can reduce the permeability of mitochondrial membranes leading to lowering of the
action potential and reduced speed of neural transmissions contributing to an analgesic effect [Chow, David and Armati, 2007].
There are a large number of suggested additional cellular and molecular effects of PBM, with research continuing to reveal new mechanisms and further explore existing knowledge [Hamblin and Liebert, 2022].
Properties of laser and their importance Wavelength
Laser light is monochromatic which means it consists of a single wavelength. This enables lasers to be designed and used for a specific function. Wavelength is the primary factor in determining where the light is absorbed and therefore how well it can penetrate into tissue. The depth to which the light penetrates and its subsequent ability to reach the target area is key to carrying out effective treatments
The wavelengths of light used in PBMT have different absorption rates by the various chromophores that exist in tissue. There are certain chromophores (namely H2O, haemoglobin and melanin) that exist in high concentrations in superficial tissue and can absorb these wavelengths of light and therefore reduce the penetrating ability of the beam. By selecting a wavelength that is absorbed least by these chromophores, the % of light which reaches the target tissue can be maximised.
WAVELENGTH PENETRATION DEPTH
600 - 700nm 0.5 - 1cm
700 - 800nm 1 - 3cm
800 – 970nm 3 - 4cm
970 – 990nm* 1 - 2cm
990 – 1200nm 4 - 5cm
*there is more absorption by water and haemoglobin at these wavelengths
In photobiomodulation therapy (PBMT) the ‘therapeutic window’ is often referenced. This is an absorption spectrum of wavelengths covering from approximately 600nm up to 1200nm. The specific wavelength selected will depend on the depth of penetration required for the desired clinical outcome of the device.
36 | www.iocp.org.uk ARTICLE
IMAGE: Sommer et al (2001)
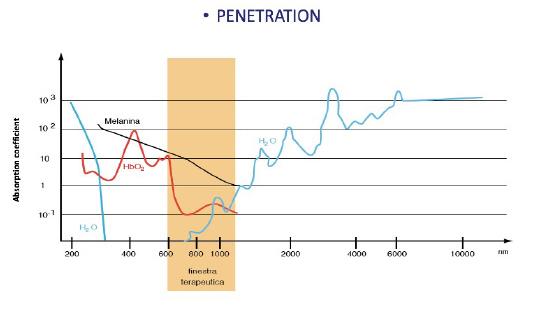
IMAGE: ASA Laser
Additional Parameters For Consideration
Whilst wavelength is a key factor in laser treatment, there are other important parameters to consider. These include energy density (Jcm2), power (W), spot size, pulse frequency (Hz) and treatment protocol.
The energy density or dosage, measured in Jcm2, is important in determining the cellular effects of the treatment. Dosage is calculated by Energy Density (J/cm2) = Power Density (W/cm2) x Time (s). Taking into consideration the Arndt-Schultz graph of photobiological stimulation it can be deduced that there is a peak dosage to stimulate cellular activity and that higher dosages may inhibit rather than stimulate (Sommer et al 2001).
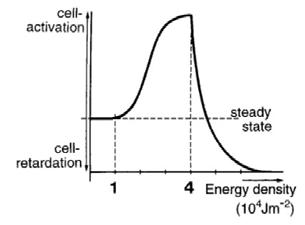
Many therapeutic lasers deliver pulsed waves at varying frequencies. Pulse rate can influence the cellular response achieved. Pulsed wave is reported to be more effective for healing, analgesia by enhancing ATP synthesis in mitochondria (effective range between 10 and 8k Hz) with specific cellular effects at specific frequencies (Kim et al 2017).
Because the most effective treatment outcomes for specific conditions are based on a number of key parameters and many of these vary greatly between devices, laser companies often have integral pre-set parameters or a guide to suggested settings with their equipment to allow practitioners to get the best results from that particular machine. These settings can then be adjusted as required to allow for customised treatments for individuals.
PBMT has a cumulative effect with each treatment building upon the effects of the last. For this reason, it is important to carry out a course of treatment at regular intervals with most manufacturers suggesting that treatments be carried out at a rate of a minimum one per week, with 2-3 sessions weekly often suggested.
Laser classification and nomenclure
Lasers are classified for safety purposes with 4 main classes and a number of subclasses. Most lasers used in healthcare are class 3B or class 4 devices.
CLASS REASON FOR CLASSIFICATION
Class 1 Safe under reasonably foreseeable conditions of operation. Users of Class 1 laser products are generally exempt from optical radiation hazard controls during normal operation.
Class 1C Designed explicitly for contact application to the skin or non-ocular tissue. Ocular hazard is prevented by engineering means.
Class 1M Products that produce beams with a large diameter. Safe for the naked eye under reasonably foreseeable conditions of operation.
Class 2 Limited to a maximum output power of 1 milliwatt or one-thousandth of a watt (abbreviated to mW) and the beam must have a wavelength between 400 and 700nm. Natural protection provided by blink response.
Class 2M Beams with a large diameter beam in the wavelength range 400 to 700nm.
Class 3R Maximum output power of 5mW. Exceed the MPE for accidental viewing and can potentially cause eye injuries.
Class 3B Power output power of up to 500mW. May have sufficient power to cause an eye injury, both from the direct beam and from reflections.
Class 4 Class 4 laser products have an output power greater than 500mW. Capable of causing injury to both the eye and skin from direct exposure and reflections also may be hazardous. Class 4 laser beams also present a fire hazard.
Laser classification sources: https://www.gov.uk/government/publications/laser-radiation-safety-advice/laser-radiation-safety-advice https://warwick.ac.uk/services/healthsafetywellbeing/guidance/lasers/appendix1classification/
Podiatry Review Autumn Issue 2022 | 37
There have been over 70 different terms used to describe the use of near infra red light to cause change in tissues with some referring to specific classifications. Some of the more common terms are listed here:
General terms
• Photobiomodulation (PBM/T)
• Photobiostimulation
• Laser therapy
• Monochromatic light therapy
Laser therapy using class 4 lasers and surgical lasers
• Low-level laser therapy (LLLT)
• Low level light therapy (lllt)
• Low- intensity laser therapy
• Cold laser therapy
Laser therapy using class 2 and 3b lasers
• Class IV laser therapy
• High intensity
In addition to the varying nomenclature and classification of laser there are also different types of laser devices with specific applications for each.
LASER WAVELENGTH (nm) APPLICATION
CO2 10, 600 Surgery / Dermatology
Er:YAG 2, 940 Dermatology
Ho:YAG 2, 060 Urology
Nd:YAG 1, 064 Opthalmology / Dermatology / Surgery /Therapeutic
Alexandrite 755 Cosmetic / Dermatology
Diode 630 - 1470 Therapeutic / Dermatology / Surgery / Research
Dye 550 - 600 Surgery / Dermatology
Argon 514 Opthalmology
Excimer 193 Opthalmology
Safe use of laser
Resource: BMLA Core of Knowledge course
It is important for practitioners to understand the safety implications of laser and how to ensure their practice is safe for them and their patients. As noted in the laser classification table, class 3 and 4 lasers are potentially harmful to eyes and skin, and must therefore be used in a careful and controlled manner. The light you can see being emitted from some therapeutic lasers is a guide light as opposed to the actual functional wavelength which may be invisible to the naked eye. Optical harm can occur even though the light cannot be seen or felt until it is too late.
Points for consideration for safe operation include controlled access to rooms where laser is being used, window coverings, reflective surfaces in the room, warning signs on doors, flammable chemicals in the vicinity of the laser equipment and knowing the optical hazard zone of your laser. The MHRA (2015) document suggest daily, weekly and annual/bi annual checks and tasks which can be carried out such as checking condition of eyewear and the functionality of warning lights etc.
Each clinic using laser should appoint a Laser Protection Officer (LPO) who is a nominated person, usually a member of staff, who is responsible for ensuring health and safety standards are being met. For additional help, a Laser Protection Adviser (LPA) can be employed to help a clinic ensure risk assessments have been properly completed and that all guidelines and standards are being met.
THERAPY LASERS: Indications for use
The primary effect of PBMT is to reduce pain, inflammation and swelling and to encourage the healing process (Bayat et al 2005, Monici et al 2013). Therefore, the number of potential applications is huge. Currently there is strong evidence for the use of laser to treat musculoskeletal (MSK) pain in both chronic and acute and to aid in muscle recovery, stamina and strength. The NICE guidelines already recommend PBMT for the treatment of oral mucositis. There is also evidence to suggest PBMT is an appropriate treatment for wounds, in cases of lymphedema and neuropathies. There is ongoing research at the Limburg Oncological Laser Institute looking into the use of laser as both a preventative and a treatment for post-operative cancer care for issues including lymphedema and chemotherapy induced peripheral neuropathy as well as other undesirable side effects. Podiatric use of PBMT is most commonly in wound care and for MSK conditions such as tendinopathies, plantar fasciitis, haematomas, bursitis and arthropathies. There are specific devices on the market for the treatment of fungal nail infection and verrucae.
38 | www.iocp.org.uk ARTICLE (continued)
Subdermal haematoma after a traumatic injury: x4 sessions of PBM over 2 weeks.
Image Source: Pure Movement Clinic
Non healing neuropathic ulcer: x12 sessions over 6 weeks, treatment in conjunction with dressings, offloading etc.
Non healing neuropathic ulcer: x12 sessions over 6 weeks, treatment in conjunction with dressings, offloading etc.


When using PBMT as a treatment in MSK patients in particular, it is important to note that the laser forms part of an overall treatment plan. A full and proper assessment is essential to allow an accurate diagnosis and appropriate adjacent treatment interventions which will ensure the root cause of the issue is also addressed. The function of PBMT in these cases is primarily to rapidly reduce pain and inflammation to allow the patient to carry out any rehabilitation exercises and to return to activity as quickly as possible.
Adding value in Private Practice with Therapeutic Laser
Investing in equipment can be daunting and clinic owners need to know that it will be worth their while. Adding therapeutic laser to the range of treatment options could add value for patients, practice and practitioners.
Value For Practices
Adding a laser to your clinic has potential to bring value to a clinic in a number of ways:
• It could open up a wider selection of patients. It may allow clinicians to offer treatments for conditions which they currently do not treat such, as arthropathies, attracting new patients as a result.
• It aids clinics in standing when compared to competitors. Patients may choose to visit due to the option of laser therapy when others in the vicinity do not offer it.

• It can generate word of mouth referrals.
• It allows clinicians to offer treatment to those patients who have tried many other interventions.
• Introducing laser into your clinic gives you great potential to make a return on your investment.
Please see the examples below:
Single Podiatrist + Physio = £1356.27 pm average = £16, 275.25 pa potential
Multi Pod Clinic with x2 lasers = £3107.40 pm average = £37, 288 pa potential
Single Pod Clinic = £1066 pm average = £12, 800 pa potential
Value For Patients
Feedback is generally that patients love laser therapy. Some reasons are:
• It is generally painless.
• It could speed up recovery time.
• It could reduce discomfort quickly therefore makes rehabilitation easier.
• Patients love tech! A laser treatment appeals to many patients and gives them a story to tell their friends.
• Extremely low risk of side effects.
Value for Practitioners
Introducing laser can make daily practice more enjoyable. It may help clinicians to:
• Attract a new type of patient. For example, it may encourage more athletes or MSK patients to a clinic.
• Save hard worked hands! Many manual therapists have described how they use the laser to soften/ relax tissue to “save” their hands and allow manual work.
• Great feedback from patients gives a feel good factor. Clinicians do what they do to help people and there’s nothing more satisfying that hearing that patient to achieve their treatment goals.
SUMMARY
* It’s a business expense and so goes against your tax
Light as a therapy has been utilised for hundreds of years and its potential continues to be recognised and researched. In Podiatry there is a huge scope for therapeutic laser covering MSK conditions, wound care and more. Excellent clinical skills, an accurate diagnosis and implementation of appropriate treatment plans alongside a full understanding of treatment parameters and appropriate dosage is important so as to achieve the best possible treatment outcomes. Proper training to ensure safe and effective use of laser devices is paramount.
Adding laser into private practice can add a variety of benefits for patients, practitioners and for the business itself.
The use of light in healthcare, specifically in the field of photobiomodulation is a hugely exciting area to be involved in as indications for use and the research into its efficacy continues to grow.
Podiatry Review Autumn Issue 2022 | 39
Images Source: Adam Smith Podiatry
page
References for this article can be found at the bottom of
40
PODARICK NAILS
IT!
Podarick can you help me?
I have had my first bad review (one star) on my social media site after decades of podiatry service and hundreds of very happy customers. The customer’s review was harsh and stated, ‘I will not go back there’, as if I had caused them a real problem. I was shaken by the review, having given good service and treatment, as I do for all my customers. I am not much of a media user, but I know bad reviews can upset practices, as well as bad feeling.

Podarick says:
Any negative reviews can hurt and are often cruel. It is natural to get upset about a negative review, but it’s important not to get overly upset, lose your cool or retaliate. Remember you are a professional, and any reviews good or bad should be responded to in a calm and professional manner.
We are aware that any negative feedback can damage a practice’s online reputation. Patients who see negative reviews, may think to look elsewhere for their foot healthcare needs. But patients realise that no-one can be 100% perfect all the time. What they do expect is for practitioners to take responsibility when things go wrong. Many people develop a healthy scepticism towards a string of five-star positive reviews all the time, because they may potentially be fake reviews. It is wise to focus on a few moderate to bad reviews, where patients can hope for a more realistic picture of you and your service. It is, however, important to respond to the reviews you do receive. Particularly, as a large percentage of people searching for services, will look at how you responded to a bad review. In other words, there are always two sides to a story and your side matters. A good response to a negative review can do a lot of damage control. It’s an opportunity for you to show you are a caring practitioner, with a chance to make things right. It can also win over other readers who may come across your online reviews.
There are many principles to respond to a bad review. This is not an exhaustive list, but here are a few: Balance - a positive response to the negative; Change a chance to reflect; Concession and Empathy; Gratitude - for the feedback; Objectivity – being calm; Reasoning – justifying the apology; Responsibility – ownership of the issue; Solution offering a concession; and Speed timely responses puts the patient first.
Perhaps, one of the easiest ways to remove a bad review is to impress your dissatisfied/ complaining patient with how you manage the complaint. If your patient is happy about your response and solution/s you offer, they may delete the bad review on their own terms.
Send your Nail Clippings to Podarick: email: info@iocp.org.uk
REFERENCES for article on pages 36 -39
Bayat M, Vasheghani M, Razavi N, Taheri S, Rakhshan M (2005) ‘Effect of lowlevel laser therapy on the healing of second- degree burns in rats: a histological and microbiological study’, Journal of Photochemistry and Photobiology, 78, pp.171–177. Available from: https://www.sciencedirect.com/science/article/abs/ pii/S1011134404001472?via%3Dihub [Accessed 11 May 2022]
Chow, R., David, M., Armati, P. (2007) ‘830 nm laser irradiation induces varicosity formation, reduces mitochondrial membrane potential and blocks fast axonal flow in small and medium diameter rat dorsal root ganglion neurons: implications for the analgesic effects of 830 nm laser’, Journal of the Peripheral Nervous System, 12(1), pp. 28-39. Available from: https://onlinelibrary.wiley.com/ doi/10.1111/j.1529-8027.2007.00114.x [Accessed 8 July 2022]
Hamblin, M. (2017) ‘Mechanisms and applications od the anti-inflammatory effects of photobiomodulation’, AIMS Biophysics, 4(3), pp. 337-361. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5523874/ [Accessed 8 July 2022]
Hamblin, M., Liebert, A. (2022) ‘Photobiomodulation Therapy Mechanisms Beyond Cytochrome c Oxidase’, ‘Photobiomodulation, Photomedicine and Laser Surgery, 40(2). Available from: https://www.liebertpub.com/doi/10.1089/photob.2021.0119 [Accessed 8 July 2022]
Kim, H., Baik, K., Choung, PH., Jung, J. (2017) ‘Pulse frequency dependency of photobiomodulation on the bioenergetic functions of human dental pulp stem cells’, Scientific Reports, 7. Available from: https://www.nature.com/articles/ s41598-017-15754-2 [Accessed 8 July 2022]
MHRA (2015) “Lasers, intense light source systems and LEDs guidance for safe use in medical, surgical, dental and aesthetic practices”. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/ attachment_data/file/474136/Laser_guidance_Oct_2015.pdf )[Accessed 18 July 2022] Monici, M., Cialdai, F. Ranaldi, F., Paoli, P., Boscaro, F., Moneti, G. and Caselli, A. (2013) Effect of IR laser on myoblasts: A proteomic study. Molecular BioSystems. 9, 1147. Available from: https://www.researchgate.net/publication/235385528_ Effect_of_IR_laser_on_myoblasts_A_proteomic_study [Accessed 10 May 2022]
Pascu, M. (2000) ‘Laser Physics Elements to Consider for Low Level Laser Therapy’, Laser Therapy, 13(1). Available from: https://www.researchgate.net/ publication/228575343_Laser_Physics_Elements_to_Consider_for_Low_Level_ Laser_Therapy [Accessed 8 July 2022]
Sommer, A., Pinheiro, A., Mester, A., Whelan, H., Franke, RP., ‘Biostimulatory Windows in Low Intensity Laser Activation: Lasers, Scanners and NASA’s LightEmitting Diode Array System, Journal of Clincal Medicine Laser & Surgery, 19(1), pp. 29-33. Available from: https://www.researchgate.net/publication/11799260_ Biostimulatory_Windows_in_Low-Intensity_Laser_Activation_Lasers_Scanners_ and_NASA%27s_Light-Emitting_Diode_Array_System [Accessed 8 July 2022]
Sutherland, J. (2002) ‘Biological effects of polychromatic light’, Photochemistry and Photobiology, 76(2), pp. 164-170. Available from: https://pubmed.ncbi.nlm.nih. gov/12194212/ [Accessed 8 July 2022]
ARTICLE 40 | www.iocp.org.uk
Representing podiatry at the Commonwealth Games
- Abid Hussain
The privilege to be the Sport Podiatry Team lead at the Birmingham Commonwealth Games 2022 was bestowed upon me. This is following in the footsteps of one of my mentors and inspirations within podiatry, Professor Nat Padhiar who was the Sports Podiatry Team Lead at the London Olympics 2012. I feel it is not possible to discuss sports podiatry without recognizing the huge efforts of Professor Padhiar in terms of promoting sports podiatry as well as designing and implementing a podiatric sport specific PGc and MSc at Queen Marys University, London.

I had been involved for 12 months before the games with logistics, recruitment and providing extensive hands-on training to the younger podiatrists, which is something I really enjoyed.
Being part of the Games was a huge honour and something that myself and my fellow podiatry colleagues immensely enjoyed. We had three polyclinics operating in three athlete villages; Birmingham University, NEC and Warwick, with podiatrists on duty from 7am to 11pm on 8-hour shift patterns. As you can imagine it was challenging but hugely rewarding, as working within a multi-disciplinary team of physiotherapists, osteopaths, chiropractors, sport medicine doctors, GPs, pharmacists, dentists, sport massage therapists, paramedics and radiologists was amazing.
The atmosphere inside the polyclinics was absolutely fantastic with sports podiatrists working closely primarily with physiotherapists, sports medicine doctors and radiologists. I have spoken to many members of the podiatry team since the conclusion of the games and they have all agreed that it was an incredible learning opportunity to work closely with a leading multi-disciplinary team. It was interesting and equally fascinating to observe how different medical specialities assess and treat the same foot and ankle condition. Many of the younger podiatrists on our team found this experience invaluable as we had Ultrasound, X-ray and MRI on site and the team had the opportunity to be part of the athlete’s journey and had to ask the radiologist, as well as the sports medicine doctor, detailed questions.
We primarily treated athletes from nations that did not have the same level of medical support as our home nations. In fact many of the athletes did not know what a podiatrist was, which provided an opportunity to discuss the role, scope and importance of the profession. These conversations also extended to many of our multi-disciplinary team colleagues which led to the promotion of the role and scope of sports podiatry.
The Birmingham 2022 Commonwealth Games was also the first games to have a fully integrated para sport schedule which enabled the team to manage injuries that are specific to para-athletes.

Podiatrists assessed and treated athletes from around the world with a variety of foot, ankle and lower leg sporting injuries including ligamentous, tendonous and muscular injuries to bone stress reaction injuries along with nerve entrapments. Most injuries were overuse and acute injuries with the predominance being overuse injuries. Some of the athletes had travelled to the UK with a pre-existing injury as the Commonwealth Games was a once in a lifetime opportunity.
The most injured athletes were from the discipline of athletics however the sports podiatry team have treated athletes from many disciplines including beach volleyball, squash, basketball, aquatics, hockey and gymnastics to mention a few.

Many injuries come to mind, however, a few injuries that I took a particular interest in, include:
• nerve entrapment in a sprinter with an enlarged abductor hallucis muscle
• an isolated calcaneofibular ligament tear in a hockey player (which is actually quite rare)
• superficial peroneal nerve entrapment in a long distance runner and
• tenosynovitis of the Knot of Henry which is the superficial crossing of the flexor digitorum longus tendon obliquely over the flexor hallucis longus tendon in the midfoot in a hockey player.
Podiatry Review Autumn Issue 2022 | 41 ARTICLE
Bone stress reaction injuries especially to the head of the 2nd metatarsal and Achilles pathologies were common place; not so common place is a Lisfranc injury. I personally assessed and managed two such injuries confirmed on MRI on the same shift as well as a plantar fascia tear; you could say it was an eventful shift!
Looking back, the one injury that intrigued me the most, as it felt like a medical Sherlock Holmes mystery, was a 200m sprinter who firstly went to a chiropractor colleague for right side lower back pain, the athlete then mentioned she actually had right side gluteus medius pain so a physiotherapy colleague was called to assess. This then led to a discovery that the proximal symptoms actually started from the right foot, so I was called into the room as the on-duty sports podiatrist, a real time multi-disciplinary team effort to assess an athlete! The athlete had pain and reduced range of motion in the first metatarsal phalangeal joint which when in the starter blocks and an explosive start led functionally to proximal symptoms.
Addressing the first metatarsal phalangeal joint symptoms resolved all proximal symptoms which enabled the athlete to get through to the next qualifying heat and qualify.
Without mentioning specific names of athletes, the sports podiatry team in all three polyclinics helped athletes to compete and gain medals at the games which is hugely rewarding.



Treatments that sport podiatrists could offer were limited as the polyclinics were not equipped with shockwave or class 4 laser however; we did provide taping of injuries, mobilization techniques, padding, providing off the shelf orthotics with modifications, evidence-based rehabilitation prescriptions and a few of the more experienced sports podiatrists were able to perform image-guided injections. Skin and nail pathologies presented very rarely, however, we did have the occasional blister and ulcer in para wheelchair athletes.
Treating athletes at a major international sporting event is very different to how we would manage our clinical patients. It is primarily the clinical rationale of ‘fire fighting’ with a multi-disciplinary team which focusses on getting the athletes through to the next round or heat of their respective event and not necessarily providing a long-term rehabilitation and treatment plan as this will be initiated in the athlete’s home country.
In conclusion this was a once in a lifetime experience for myself and the team which we all enjoyed immensely. Working alongside experienced multi-disciplinary teams raised the profile of sports podiatry and our profession as a whole. For me, it was a tremendous honour and privilege to be leading such a fantastic team of sports podiatrists at the Commonwealth Games in my home city.
Abid Hussain, Consultant Podiatrist
MSc, PGC, BSc (hons), MInstChP, CFPodM, MFPM RCPS(Glasg), MRCPod
42 | www.iocp.org.uk ARTICLE (continued)

The
and Podiatrists are
offer our members comprehensive, market
support and
insurance packages,
your needs! Including insurance
colleagues
we’ll
you stranded! Join our growing podiatry familybecome a member Run by members for the members! We are a truly democratic organisation where your voice is heard. We strongly believe in working together to build a stronger future for podiatry • Quarterly issues of Podiatry Review, contributing to your Professional Development Support
Continuing Professional Development Support – Guidance and assistance with the members continuing professional development portfolio for HCPC audits & 20% discount on Elsevier academic books
Business Support and special discounts from our trade and advice partners
Access to the members area of the Institute website including a private discussion forum
Member rates on all our CPD courses and access to our free
Join
to
search
events
Access our
advice service,
our
Student membership available! Allowing you to practice when you have completed year 2, as you learn, plus special rates once fully qualified PLUS… Podiatry Review Podiatry Review Autumn Issue 2022 | 43
Institute of Chiropodists
proud to
leading
unrivalled
tailored to suit
to
in the Republic of Ireland,
never leave
•
•
•
•
CPD webinars! •
the IOCP ‘Find a practitioner’ service
promote your business to members of the public finding the IOCP website through
engines. • Network through local member branches, situated throughout the United Kingdom and the Republic of Ireland for peer support and CPD
•
confidential
including advice from the IOCP medicines and procedures panel (MaPP) on the use of drugs and therapeutics as well as appropriate podiatric procedures. Head to
website: www.iocp.org.uk or contact our team: info@iocp.org.uk
Lynne Elizabeth Bourgeois
16 February 1948 – 31 July 2022
Lynne passed away on Sunday 31 July 2022 from a brain tumour that had been devastatingly diagnosed in November 2018 and given a prognosis of three months without surgery and possibly an extra six months following surgery. Lynne bravely underwent the surgery which could not remove all the tumour and which needed a plate fitting and she also had chemotherapy sessions and as a result had three precious years being cared for and supported by her devoted husband, Jean-Pierre and sons Paul and Richard and their families. The chemotherapy sessions she eventually, bravely, discontinued as the after effects left her feeling very unwell for some time and she wanted to live every precious minute she could without suffering very badly from the after effects.
Lynne was educated at Melton Mowbray Grammar School and from there had gained a place at Loughborough choosing to study fashion and in particular Millinery and opened a small shop in Melton Mowbray mainly selling ladies hats and gloves. Whilst still at school, aged 14, she had a French pen-pal, Jean-Pierre, an exchange student programme run by the school, and they continued to write to each other and over time they met and fell in love and were married on 16 August 1969. Such was the local interest in the dashing Frenchman from Fontainebleau and the beautiful local girl that the press took wedding pictures and wrote a feature on the happy couple. Lynne became interested in Chiropody whilst working for a friend in Loughborough Chiropody Clinic and deciding to change careers she qualified as a Chiropodist in 1970 and then joined the Institute where she was a dedicated and committed member for over 50 years. In various moves around the country, with Jean-Pierre’s engineering work, Lynne took Branch positions as Secretary in the Sussex Branch and Chair at Leicester/Northants, Treasurer at Nottingham Branch and latterly serving for some years as a Nottingham Branch Auditor and was always involved with the organisation of Branch seminars and CPD events. Having professional membership of the Institute was very important to Lynne and her years of commitment helped support our Association.
When Nottingham Branch hosted the AGM and Conference at Eastwood Hall in 2010 both Lynne and Jean-Pierre were visible both days working together on some of the stands and meeting members.
All the qualities one would hope for in a friend and a colleague Lynne possessed in heaps! She was a very practical and professional person with a kind and compassionate heart and that was evident when early in her career she agreed to hold a regular session at the Blind Institute locally as it couldn’t find a willing practitioner to arrange sessions to trim toenails.
Lynne had an open mind and didn’t discount the benefits of alternate therapies and was interested and knowledgeable about herbal remedies. Knowing a friend had trouble sleeping Lynne, in her practical and helpful way, produced some bags of Lavender she had grown, dried, and prepared herself which she said would be helpful if the bags were placed near the pillows as Lavender had long usage as a wellknown remedy to aid sleep! A typical gesture of Lynne’s help and care to others. She was a terrific person, kind and caring and even though she had such a consuming illness to cope with she was interested to hear of others and when she could no longer attend Branch meetings would always ask how friends and Branch members were and were they well.
Lynne will be sadly missed by her friends and colleagues and greatly by her husband Jean-Pierre and her sons Paul and Richard and their families who were supported by the British Red Cross Crisis Intervention Community Support Services, Nottingham, and whose help enabled Lynne to be cared for at home and to where donations made in memory of Lynne were directed.
We offer her family our heartfelt condolences and sympathies. Lynne will always be remembered by friends and colleagues for the virtuous person she was and of her long-time commitment and dedication to our professional body.

Vivit Post Funera Virtus.
Valerie Dunsworth, Nottingham Branch Secretary/Treasurer
Lynne had a rare ability to put people at ease, along with a mischievous sense of humour and fun. Always on hand for advice and help.

I will miss her dearly. A true friend.
Tony Eaton, Past Branch Member
It has been a pleasure over the years to have known Lynne. A true friend and colleague.
She will be fondly remembered.
Heather McCance and Anne Rockley, Nottingham Branch Members.
I knew Lynne, initially as a Committee Member, when I joined the Institute but it was quite obvious what a lovely person she was. Sensible, knowledgeable, but most of all so friendly and approachable – and always with a lovely warm smile.
From the moment she was diagnosed with her illness Lynne carried on regardless, she was so strong and you couldn’t do anything but have the utmost respect for her. She fought her illness with such dignity.
The Institute has sadly lost a dedicated and valuable member! My sympathies go to her family as I know they will miss her terribly. Rest in Peace Lynne.
Anne Sparkes, Nottingham Branch Minute Secretary.
I worked with Lynne as a Branch Auditor with both of us in previous years having served as the Branch Treasurer. Lynne was a reliable and conscientious colleague and had a very good sense of humour as well as being a kind, caring and professional member.
Mark Humphries, Nottingham Branch Auditor
OBITUARY
Irene Huskisson and I had a marvellous opportunity to visit the Roy Castle research laboratory based in Liverpool. Doctor Michael Davies looked after both of us along with 4 members of Roy Castle Head Office.




It started with a presentation on the considerable work done in finding treatments and to try to understand how lung cancer develops. For some years, they have created and have a considerable bank of tissues, malignant, benign, blood all kept in these huge freezers at -80 degrees. All catalogued carefully, a library of diverse tissues.
People, who have been selected and have agreed to be on the panel, give their blood, which is studied then preserved in these freezers. From that moment, these people are closely monitored and if at any time, they are diagnosed with lung cancer, then the scientists look back at their blood and the changes in the present bloods. It enables them to try to understand and see what has changed in their blood. They also test DNA from healthy and sick people.
During our visit, we were surrounded by very sophisticated machines, some are able to give them a rapid response compared to the ones in the past. Absolutely fascinating!
Dr Davies stressed the fact that they share their findings and data with Belgium, who are very proactive in lung cancer research and with America.
At the William Henry Duncan building, there are other departments research ing for other cancers and they exchange their findings. Clatterbridge Centre across the road also send tissues of tumours, obviously with the agreement of families or patients to be studied.

The Roy Castle research lab is the only one in that building which is solely funded by the Charity. Hopefully we will find a cure soon.
Members who regularly attend meetings with the Cheshire, North Wales branch have been invited to visit the lab in the near future.
 Allison Branch Secretary
Allison Branch Secretary
Podiatry Review Autumn Issue 2022 | 45 BRANCH NEWS
Michele
Cheshire, North Wales Branch News
Please note: all products advertised in the Podiatry Review and on the Website are accepted by the Institute of Chiropodists and Podiatrists on the basis of a commercial advertising service and purchasers should carry out their own assessment as to the suitability of such products for their own specific needs. Acceptance of the advertisement by the Institute does not imply our endorsement or approval of the product.
SVTS Chiropody Drill repair and sales
We offer an excellent competitive and efficient repair service for all makes of Podiatry/chiropody Nail drills. Berchtold, Hadewe, Suda, Footman, Podiacare, Podo Tronic and Podo Pro EVO-30,40&50 drills. We sell Berchtold S35/ S30, Hadewe, EVO 30,40.50 Dust Bags from £1.25 – £2 each. WE ALSO BUY UNWANTED DRILLS.
Unit 255 Stratford Workshops, Burford Road, London E15 2SP Contact us on 0208 5190044 or www.chiropodydrillrepair.co.uk
Chiropodist/ Podiatrist required in Heswall, Wirral
We are situated in Heswall, Wirral. We are a busy multi-discipline clinic in the heart of a thriving village.
Our clinic is exceptionally busy with five chiropodists and full-time reception staff. The position is offered with hours to suit applicant. The successful candidate must be personable, not afraid of being busy and have great attention to detail. In return they can earn £200-300 per day. This is a self-employed position and payment is on a fee sharing basis. Tel: 01513 429665 for further information
Experienced Chiropodist/Podiatrist required for busy Bristol clinic
Immediate start to join long established friendly practice on a self-employed fee sharing basis
Hours
to suit applicant
For further information call Jon on 07885 102112
Associate required in Bromley area
Associate required in Bromley area. FHP or podiatrist for busy multidisciplinary Clinic. We cover nursing homes, professional football clubs and private residences. We also offer shock wave, swift, microwave, 3D scanning and other innovative treatments.
Inhouse training can be provided as we have 2 former podiatry lecturers with doctorates working at our Clinic. Contact number 0208 467 1910 or email chislehurstclinic@aol.co.uk and ask for Tony or Liz.
CLASSIFIED ADVERTS 46 | www.iocp.org.uk
To place an advert here or for more information please email julie@iocp.org.uk Diabetic Foot Module Course 10th – 14th October 2022 At The Wellcome Collection Euston Road, London Intensive update course for specialist practitioners. For more information, please email diabeticfootmodule@gmail.com
2022
3 Leeds Branch Meeting
IOCP CEO Anthony Hubbard will be attending to chat to members & answer any questions re the IOCP & the COFH. At St Mary’s Social Club, Melton Street, Batley. WF17 8PT. Contact Caroline on 07583 934468 or email hello@ chiropodyandfoothealth.co.uk
6 UK Regional CPD Roadshow
Novotel Hotel in Leeds City Centre
The event will be a highlyinformative, intimate, interactive, full day of CPD! Offering members the chance to network with friends, colleagues and peers as well as many members of the IoCP support team including CEO Anthony Hubbard, President and Regional Director (North England) Caroline McCartney. Book your place at iocp.org.uk/ course/uk-cpd-roadshow/
9 Wolverhampton Branch Meeting and AGM
10am at the Reading Rooms, Market St, Penkridge, Staffs. ST19
5DH Speaker to be arranged Contact: David on 01785 716607 or email djcollett@hotmail.co.uk
22 Ireland CPD day
The Ireland team have a wonderful line up for attendees including midfoot tendinopathies, Padding and Strapping and Laser Therapy in Podiatry.
Speakers include Sean Savage, Gareth Hicks, Michael Radcliffe and Kirsten Sinclair. As usual we promise to have plenty of opportunities to network, we hope to have some of our wonderful leadership team in attendance and plenty of vendors.
Contact Janette on jpegleyreed@gmail.com for further information
26 London Branch Meeting
7.30pm via Zoom.
Contact Sarah on 07790 717833 or email footwoman@gmail.com
NOVEMBER 2022
6 Leeds Branch Meeting
9am fora 9.30am start & finish 12.30 -1pm latest.
Steve McGowan will be giving a lecture on a new dressing product plus a fresher re Emtrix and his wife Caroline will be there to give a talk on Flexitol.
At St Mary’s Social Club, Melton Street, Batley. WF17 8PT. Contact Caroline on 07583 934468 or email hello@ chiropodyandfoothealth.co.uk
10 Sheffield Branch Meeting
At 7.30pm Via Zoom. Contact Helen on 07789 025022 or email hrawse@live.co.uk

DIARY OF EVENTS
JANUARY 2023
8 Wolverhampton Branch Meeting & AGM
At 10am at the Reading Rooms, Market Street, Penkridge, Staffs. ST19 5DH.
Contact: David on 01785 716607 or email djcollett@hotmail.co.uk
25 London AGM Meeting
At 7.30pm via Zoom.
Contact Sarah on 07790 717833 or email footwoman@gmail.com
SOUTH WALES AND MONMOUTH BRANCH
Meetings are taking place via Zoom, members who would like details of the next meeting and wish to attend please contact Esther on 01656 740772 or email estherdanahar@ yahoo.co.uk
or via Zoom etc.
Podiatry Review Autumn Issue 2022 | 47
OCTOBER
Please email julie@iocp.org.uk with information about Branch Meetings whether face-to-face
Keep your Branch members up to date so they can attend.


