

Traveling Blender, LLC. 10036 Saxet Boerne, TX 78006
PUBLISHER Louis Doucette louis@travelingblender.com
BUSINESS MANAGER: Vicki Schroder vicki@travelingblender.com
ADVERTISING SALES: AUSTIN: Sandy Weatherford sandy@travelingblender.com
SAN ANTONIO: Gerry Lair gerrylair@yahoo.com
For more information on advertising in San Antonio Medicine, Call Traveling Blender at 210.410.0014 in San Antonio and 512.385.4663 in
San Antonio Medicine is the official publication of Bexar County Medical Society (BCMS). All expressions of opinions and statements of supposed facts are published on the authority of the writer, and cannot be regarded as expressing the views of BCMS. Advertisements do not imply sponsorship of or endorsement by BCMS
EDITORIAL CORRESPONDENCE: Bexar County Medical Society 4334 N Loop 1604 W, Ste. 200 San Antonio, TX 78249
Email: editor@bcms.org
MAGAZINE ADDRESS CHANGES: Call (210) 301-4391 or Email: membership@bcms.org
SUBSCRIPTION RATES: $30 per year or $4 per individual issue
ADVERTISING CORRESPONDENCE: Louis Doucette, President Traveling Blender, LLC.
A Publication Management Firm 10036 Saxet, Boerne, TX 78006 www.travelingblender.com
For advertising rates and information Call (210) 410-0014 Email: louis@travelingblender.com
SAN ANTONIO MEDICINE is published by SmithPrint, Inc. (Publisher) on behalf of the Bexar County Medical Society (BCMS). Reproduction in any manner in whole or part is prohibited without the express written consent of Bexar County Medical Society. Material contained herein does not necessarily reflect the opinion of BCMS, its members, or its staff. SAN ANTONIO MEDICINE the Publisher and BCMS reserves the right to edit all material for clarity and space and assumes no responsibility for accuracy, errors or omissions. San Antonio Medicine does not knowingly accept false or misleading advertisements or editorial nor does the Publisher or BCMS assume responsibility should such advertising or editorial appear. Articles and photos are welcome and may be submitted to our office to be used subject to the discretion and review of the Publisher and BCMS. All real estate advertising is subject to the Federal Fair Housing Act of 1968, which makes it illegal to advertise “any preference limitation or discrimination based on race, color, religion, sex, handicap, familial status or national origin, or an intention to make such preference limitation or discrimination.
SmithPrint, Inc. is a family-owned and operated San Antonio-based printing and publishing company that has been in business since 1995. We are specialists in turn-key operations and offer our clients a wide variety of capabilities to ensure their projects are printed and delivered on schedule while consistently exceeding their quality expectations. We bring this work ethic and commitment to customers along with our personal service and attention to our clients’ printing and marketing needs to San Antonio Medicine magazine with each issue.
Copyright © 2024 SmithPrint, Inc. PRINTED IN THE USA

Ezequiel “Zeke” Silva, III, MD, President
Lyssa Ochoa, MD, Vice President
John Shepherd, MD, President-elect
Jennifer R. Rushton, MD, Treasurer
Lubna Naeem, MD, Secretary
John Joseph Nava, MD, Immediate Past President
Woodson “Scott” Jones, MD, Member
Sumeru “Sam” G. Mehta, MD, Member
M. “Hamed” Reza Mizani, MD, Member
Priti Mody-Bailey, MD, Member
Dan Powell, MD, Member
Ana Rodriguez, MD, Member
Raul Santoscoy, DO, Member
Lauren Tarbox, MD, Member
Nancy Vacca, MD, Member
Col. Elisa D. O’Hern, MD, MC, FS, Military Representative
Jayesh Shah, MD, TMA Board of Trustees Representative
John Pham, DO, UIW Medical School Representative
Robert Leverence, MD, UT Health Medical School
Representative
Cynthia Cantu, DO, Medical School Representative
Lori Kels, MD, Medical School Representative
Ronald Rodriguez, MD, Medical School Representative
Victoria Kohler-Webb, BCMS Alliance Representative
Carolina Arias, MD, Board of Ethics Representative
Melody Newsom, BCMS CEO/Executive Director
George F. “Rick” Evans, Jr., General Counsel
Melody Newsom, CEO/Executive Director
Yvonne Nino, Controller
Al Ortiz, Chief Information Officer
Brissa Vela, Chief Membership and Development Officer
Phil Hornbeak, Auto Program Director
Betty Fernandez, BCVI Director
Monica Jacqueline Salas, MD, Co-chair
Jennifer C. Seger, MD, Co-chair
Lokesh Bathla, MD, Member
Elizabeth Clanton, MD, Member
Erika Gabriela Gonzalez-Reyes, MD, Member
Timothy C. Hlavinka, MD, Member
John Robert Holcomb, MD, Member
Soma S. S. K. Jyothula, MD, Member
Kristy Yvonne Kosub, MD, Member
Jaime Pankowsky, MD, Member
George-Thomas Martin Pugh, MD, Member
Rajam S. Ramamurthy, MD, Member
Adam V. Ratner, MD, Member
John Joseph Seidenfeld, MD, Member
Boulos Toursarkissian, MD, Member
Francis Vu Tran, MD, Member
Faraz Yousefian, DO, Member
Louis Doucette, Consultant
Brissa Vela, Consultant
Gabriella Bradberry, Staff Liaison
Trisha Doucette, Editor
Deepthi S. Akella, Student
Moses Alfaro, Student
Victoria Ayodele, Student
Tue Felix Nguyen, Student
Andrew Ta, Student
Alixandria Fiore Pfeiffer, DO, Resident
Elizabeth Allen, Volunteer
Adelita G. Cantu, PhD, Volunteer
Rita Espinoza, DrPH, Volunteer
Natalie Reyna Nyren, PA-C, Volunteer
David Schulz, Volunteer
Ramaswamy Sharma, MS, PhD, Volunteer
By Ezequiel "Zeke" Silva III, President, Bexar County Medical Society (BCMS)
One of my priorities as President is to enhance the strength of BCMS’ partnerships within the community. With a 170-year legacy of representing physicians and medical students in Bexar and surrounding counties, BCMS possesses both the opportunity and the responsibility to collaborate with organizations that are committed to advancing our community. In this column, I will highlight several of BCMS’ community partnerships and the benefits they offer.
BCMS represents a diverse community of physicians who practice across a variety of institutions, stages of their careers and settings. This includes academic centers, military facilities and large healthcare systems, which presents a significant opportunity for meaningful partnerships and representation from these organizations. Our BCMS Board of Directors includes representatives from our two medical schools — UT Health, Long School of Medicine and the University of the Incarnate Word School of Osteopathic Medicine — as well as military medicine from Brook Army Medical Center and the VA system. Additionally, we actively involve medical students and residents on our board, within each of our committees and in our delegation to the Texas Medical Association. Our trainees contribute fresh ideas, valuable experiences and perspectives, and represent the next generation of physician leaders.
Our board members and officers also serve in healthcare systems such as Methodist, Baptist, Christus and University, among others. Each of these healthcare systems is united by a mission to provide the highest quality of care possible to our community. A fundamental


aspect of this mission involves the physicians and medical students who deliver this care. BCMS proudly acts as a conduit, bringing these physicians together to share our challenges, opportunities and strategies for success.
Our city is home to several organizations dedicated to the health and well-being of San Antonio. BCMS maintains positions in several such organizations, and vice versa. For instance, BCMS holds an advisory board position with the San Antonio Medical Foundation, which boasts a rich history of establishing the first medical school and several key hospitals in San Antonio.
We also welcome representatives from the Metropolitan Health District onto our Public Health and Patient Advocacy Committee and have maintained a longstanding partnership with the Southwest Texas Regional Advisory Council (STRAC), particularly during the COVID19 public health emergency. Additionally, as physician practices are businesses, we are members of the San Antonio Chamber of Commerce.
The physicians and medical students in Bexar County are a talented group, and giving back to our community is a natural extension of their abilities. This includes our physicians in large practices and institutions, and our independent physicians. By partnering with local organizations, we help strengthen our city collectively. However, like all meaningful efforts, this requires resources. If you can spare the time and energy, we encourage you to join us in making San Antonio a healthier and stronger community.
Ezequiel “Zeke” Silva III, MD, is the 2024 President of the Bexar County Medical Society. Dr. Silva is a radiologist with the South Texas Radiology Group, Adjunct Professor of Radiology at the UT Health, Long School of Medicine, and Vice-Chief of Staff at Methodist Hospital Texsan. He is Chair of the TMA Council on Legislation and is a TMA Delegate to the AMA. He serves on the AMA Council on Medical Service, and chairs the AMA RVS Update Committee (RUC).
L-R standing: John Pham, DO, UIW Medical School Representative; John Shepherd, MD, President-Elect; Ezequiel “Zeke” Silva III, MD, President; John Nava, MD, Immediate Past President; Melody Newsom, BCMS CEO/ Executive Director
L-R seated: Jennifer Rushton, MD, Treasurer; Lubna Naeem, MD, Secretary; Lyssa Ochoa, MD, Vice President
By Andrew Ta
Dr. John Holcomb’s medical career, spanning over five decades, is marked by a blend of clinical excellence, military service and dedicated advocacy. His contributions to medicine, particularly within the Bexar County Medical Society (BCMS) and the Texas Medical Association (TMA), highlight a commitment to improving healthcare systems and policies.
Dr. Holcomb graduated from medical school in 1971 and began his internship at the University of California at San Francisco. After his internship, he fulfilled a three-year obligation to the Army — a period that profoundly shaped his professional journey. Upon returning to civilian life, he sought to continue his medical training but faced challenges securing a residency position in San Francisco. This led him to the University of Texas Health Science Center at San Antonio (UTHSCSA), where he completed two more years of internal medicine and a pulmonary medicine fellowship. After an additional three years of service, the military funded his final year of fellowship, during which he worked in the ICU at Brooke Army Medical Center (BAMC).
Dr. Holcomb reflects on the stark differences in medical training from his early career to the present. As an intern in San Francisco, he experienced a high degree of autonomy, often managing patients with minimal supervision. He recalls his first rotation at the Fort Miley VA Hospital, where he was responsible for a ward of 40 patients with little guidance from his second-year resident. He was on-call almost every night, and his responsibilities were much less supervised than today. For example, on the oncology ward, he found himself ordering, hanging and giving chemotherapy himself. The mantra “see one, do one, teach one” was true then as ever. In contrast, his residency in San Antonio involved more structured supervision, aiming to support interns better and ensure comprehensive patient care. This shift in training practices highlights the evolving nature of medical education, emphasizing safety and collaboration over the more solitary, trial-by-fire approach of the past.
After completing his medical residency and subsequent military service, Dr. Holcomb started a pulmonary medicine private practice with a partner from residency. The early years of his practice were marked by a lack of guidelines and a more independent approach to medicine. Over time, however, the landscape began to shift towards corporate practice, driven by changes in state regulations and the healthcare market. This transition has had profound implications for the practice of medicine, often constraining physicians’ autonomy and changing the doctor-patient relationship.
Dr. Holcomb’s advocacy work during his presidency at BCMS in 1996 was pivotal. He was actively involved in legislative efforts to allow hospitals to employ doctors, navigating the complex and often restrictive rules around corporate practice in Texas. His tenure saw significant challenges, particularly with the rise of managed care and the acquisition of hospitals by entities like Humana. One of his notable initiatives was a comprehensive survey to understand physicians’ challenges with hospitals and managed care. This effort led to substantial policy changes, demonstrating the power of collective advocacy in shaping healthcare delivery.

Finally, towards the end of our interview, Dr. Holcomb offered crucial advice to future generations of doctors. He emphasized the importance of understanding the business aspects of medicine, which are often neglected in medical training. Many young doctors enter into contracts without fully grasping the implications, leading to dissatisfaction and constraints in their practice. He strongly advocates for seeking legal counsel when signing contracts to avoid unfavorable terms, such as restrictive non-compete clauses. Dr. Holcomb’s experience highlights the need for physicians to be proactive and informed about their professional agreements to protect their interests and maintain the quality of patient care.
Dr. John Holcomb’s career is a testament to his dedication to both his patients and the broader medical community. His work in clinical practice, military service and medical advocacy has left an indelible mark on the field. As medicine continues to evolve, his legacy serves as a reminder of the importance of leadership, resilience and the relentless pursuit of better healthcare for all.

Andrew Ta is a medical student at the Long School of Medicine, Class of 2026. He serves on the BCMS Publications Committee.
By Victoria Kohler-Webb, BBA, MS
The sign says it best! Bexar County Medicine is proud of our Texas Medical Association Alliance President Jenny Shepherd!
What a special year 2024 has turned out to be for her. Not only has Jenny been sworn in as TMAA President, her husband, Dr. John Shepherd, was voted President-Elect for the Bexar County Medical Society and will be installed January 2025. A true power couple that gives tirelessly to their community and to medicine as a whole!
Speaking of power couples, the Alliance Sips & Dips, celebrating Jenny’s installment, was planned and hosted by Alliance Past President Danielle Henkes and her husband, Dr. David Henkes, Past President BCMS, at their beautiful home. A crowd of Jenny fans from both the Alliance and BCMS came together for a fabulous evening to toast her success and celebrate a long tradition of Bexar County leadership and representation on the state board.
The sky’s the limit and we in Bexar County medicine could not be more excited to watch Jenny Shepherd promote her Power of One campaign and strengthen our physician community! Congratulations Jenny — you are truly a DIFFERENCE MAKER!

Victoria Kohler-Webb, BBA, MS Marketing Statistics, is the 2024 Alliance President. She and Ben, an ENT/Head & Neck Surgeon, are proud Aggies and parents to Luke, 15, and four rescue dogs.









For information on the Bexar County Medical Society Alliance, scan the code:


By Rajam Ramamurthy, MD
Olga, the nurse, placed a picture of Our Lady of Guadalupe in a sterile plastic bag and taped it to the incubator in which lay Juan with multiple tubes going into his tiny body; the combined weight of the tubes far exceeding his weight of 800 grams (1 pound, 7 ounces). The grandmother of the baby was silently murmuring a prayer. A very young woman in a hospital gown stood expressionless beside her. This scene is common in present-day hospitals — in the children and adult patient rooms. But this was not always so in medical practice. Many years ago, as my generation was taught medicine, we were indoctrinated into blinding ourselves to religion, language, race and ethnicity of the patient. We did not ask these questions. The healthcare system and the public perceived these considerations to be discriminatory. Biologically based and anatomically focused healthcare created a huge divide between medical practice and the public they served.
The awakening to consider the patients’ illnesses, which is part of the life he or she is living, along with the “disease” that is biologically focused, happened in the 80s and 90s. This is not to say that healthcare providers neglected the difference between the two approaches, but it was not taught in a systematic manner, not role modeled, mostly ignored and sometimes considered discriminatory. A sentence I read during my research of this topic says it succinctly, “It is important to distinguish between stereotyping (the mistaken assumption that everyone in each culture is alike) and generalizations (awareness of cultural norms). Generalizations can serve as a starting point and do not preclude factoring in individual characteristics such as education, nationality, faith and acculturation. Every patient is unique.” I remember an Asian-Indian man who was served a vegetarian meal every time while the patient in the next bed was given chicken noodle soup. The Indian man was a non-vegetarian and believed that chicken
soup would make him strong during his illness. This is “stereotyping” to think that all Indians are vegetarian, whereas, 81 percent of people in India consume some non-vegetarian food. Five percent of the U.S. population is vegetarian.
Cultural diversity in many countries is increasing as global economy, political instability and other factors attract businesses, travel and immigration. The U.S. Census Bureau population estimates as of July 1, 2023 indicate:
with large Buddhist populations such as China, Thailand, Laos and Cambodia, touching someone’s head is an incredibly invasive gesture. A good practice is to just ask, “How should I greet you sir/madam? Is it okay to shake hands?” In India, giving or receiving something with your left hand is considered disrespectful.
Diet: Food is an intro into another culture. I have enjoyed Thai food long before I met a person from Thailand. The fact that someone paid attention to your food will increase the satisfaction and compliance level. A question to the patient would be, “Please tell me, do you have any dietary preference; do you want some food to be brought from home?”
End of life discussions: In some cultures, talking about death is considered a bad omen in that by saying that you are hastening death. In India and many other cultures, diagnosis of a serious disease is first mentioned to the parent, adult children or male spouse before telling the patient. Be mindful of it while at the same time finding compassionate ways to discuss with the patient.
In 2023, Bexar County had a population of 2,087,679, which is a 1.8 percent increase from 2022. This makes Bexar County the 17th largest county in the United States. The county’s population has grown by an average of 2.39 percent since 2009. Medical practice must keep up with this changing demographic.
Cultural competency refers to possessing knowledge, awareness and respect for other cultures. Physicians must respectfully elicit needed information from patients from various cultures to make accurate diagnoses and negotiate acceptable treatment goals. Ethnocentrism, the conviction that one’s own culture is superior, can hinder effective cross-cultural care.
Culture and religion have profound healthcare implications. I have found religious beliefs to be the most difficult areas to negotiate. To utilize this in trying to achieve the best health outcome is more prudent than to try to negate the patient’s beliefs. An interesting experience for me was when an excited nurse came to me and said, “Dr. Rama, Juan’s mom has come with a big pot of water from the Guadalupe shrine. She wants the baby to be immersed in it just once.” I mustered all my compassion training, said a silent prayer and went to the baby. In my limited Spanish and with great help from nurse Olga, my first sentence was, “Mama, we do this in India. I have respect for the holy water.” Grandma’s face lit up; there was an instant bond established. “I want you to help me with some decisions. I want to wait for a few days before completely immersing the baby. In the meantime, let us use a little of the holy water every time we give a sponge bath.” Grandma and mom were happy; they too have contributed to Juan’s care. Here are some things you can consider in navigating the cultural ocean.
Greetings: Most of us learn about greeting people when we visit other countries. Try to learn a few: folded hand with palms together, handshake, a bow. Be spontaneous and authentic.
Touch: In many cultures, men do not touch women on the shoulder and sometimes do not shake hands. In the Indian culture, elders may touch the head of a child as it is considered a blessing. In countries
Death: This is one of the most difficult topics, even when there are no cultural barriers. As a medical team, discuss who will talk to the family, will an interpreter be helpful, and if there is a person of the same cultural background on the team, take him/her with you.
Mental Illness: Mental illness is often kept a secret in the most open cultures and more so in Asian countries. Spend the time to explain if there is definitive treatment, and mention it early in the discussion. Respect privacy.
Cultural awareness training is provided to physicians, nurses and other healthcare workers in many institutions. It must be done in doctors’ offices and private clinics as well. Encourage the trainees in different health professions to learn about other cultures rather than delegate that patient to someone else. Medicine has brought other countries to our doorstep, and it is such an opportunity to learn about another country, the habits and the story of the family.
The physician is revered in many cultures. It behooves us to be extra sensitive to the cultural background of the patients we serve. We must go that extra mile. Juan did get discharged from the hospital after three-and-a-half months. The grandmother held both my hands and Olga’s hands in her shaking shriveled hands. Her eyes teared as she made the Sign of Cross, a blessing. And I did the only thing that comes naturally to me — touched Juan’s head with my right hand. Mom smiled.

Rajam Ramamurthy, MD, is the Professor Emeritus in the Department of Pediatrics, and the President of the Association of Retired Faculty & Associates at UT Health San Antonio. She is a Past President of the Bexar County Medical Society and serves on the Publications Committee.

Interview with Sunil Ahuja, MD, Director of the Veterans Administration Center for Personalized Medicine and Professor of Medicine at UT Health San Antonio; conducted by Amrutha Mummidi and Raavi Chokhawala.
In April 2022, Lucile Randon, a French nun, was recognized by Guinness World Records as the world’s oldest living person. She lived for 118 years and 340 days until her passing in January 2023. Her remarkable life included battling COVID-19, which she overcame in 2021, just weeks before her 117th birthday. Despite the odds, she recovered in about three weeks without significant symptoms. In contrast, UNICEF reported that of the 4.4 million COVID-19 deaths documented as of December 2023, over 17,000 were children and adolescents under 20 years of age. These cases demonstrate the concept of immune resilience, illustrating how different people can experience vastly different outcomes when facing the same disease.
Dr. Sunil Ahuja, head of the Center for Personalized Medicine at VA hospital, and lead author of a paper published in Nature Communications in June 2023, which defined, quantified and demonstrated the efficacy of immune resilience as a marker for immune health, summarized it as “the body’s response to inflammatory stress.”
More specifically, immune resilience tracks the ability of the immune system to effectively respond to and recover from a variety of inflammatory challenges, like infection and other environmental stressors. Immune resilience (IR) is based on the principle that repeated inflammatory exposures are inevitable throughout a person’s life. How the body responds to these exposures represents a patient’s level of immune resilience. In a patient with optimal immune resilience, the body will be able to respond quickly and effectively to antigenic exposure, without launching an excessive inflammatory response, and will be able to return quickly to a baseline state of high immunocompetence, and low inflammation. It is a useful tool for conceptualizing and measuring immune health and predicting health outcomes.
Optimal immune resilience requires a balance between a person’s ability to mount an effective response to inflammatory stressors, or their immunocompetence, and their ability to limit inflammation. To illustrate the importance of maintaining this balance in response to infection, Dr. Ahuja said, “Our study showed that a person’s ability to control inflammation and preserve immunocompetence when they got infected with COVID19 was associated with being asymptomatic. People who don’t get sick when they get infected have a quantifiably better inflammatory response to the infection.” He continued, “It is remarkable that we routinely measure liver and kidney function tests, but infrequently think about assessing immune status even though it is the largest organ system in the body.”
Immune resilience is measured using two peripheral blood metrics — the relative balance between CD4+ and CD8+ T-cell levels, and two gene expression signatures tracking survival-associated immunocompetence and mortality-associated inflammation.
The first metric is Immune Health Grades (IHGs), which uses CD4+ and CD8+ T-cell count to measure IR. IHGs are divided into four categories, I-IV, based on relative proportions of CD8+ and CD4+ T-cells in the peripheral blood. IHG-I and IHG-II track relatively lower CD8+ T-cell counts, while IHG-III and IHG-IV track higher CD8+ T-cell counts. The distinction between IHG-I vs. IHGII and IHG-III vs. IHG-IV is made using CD4:CD8 T-cell ratio, with IHG I and III having a CD4:CD8 ratio ≥1.0, and IHG-II and IV having a CD4:CD8 ratio <1.0. IHG-I is associated with optimal immune resilience. IHG-I is the most common grade in human populations but our capacity to preserve this grade wanes with age. However, as Dr. Ahuja remarked, “These grades are such a simple measure to assess and having the worst grade such as those in grade IV could represent a harbinger of underlying unsuspected immunodeficiency.”
The second metric of IR, survival and mortality predicting gene expression profiles, involves two distinct patterns: The survival-associated signature or SAS-1, and the mortality-associated signature or MAS-1. SAS-1 tracks immunocompetence-related genes, and MAS-1 tracks inflammation-related genes. The optimal SAS-1/MAS-1 profile is SAS-1 high/MAS-1 low, indicating increased immunocompetence and decreased inflammation. IHG-I strongly tracks this gene expression profile, and non-IHG-I grades are strongly linked to SAS-1 low/MAS-1 high. SAS-1/MAS-1 profiles provide context as to how expression of certain genes varies in the face of infection or other stress, including during diseases such as cancer.
Immune resilience is labile. It can change due to a variety of factors. For example, a person’s immune health grade can drop in the acute phase of an illness, and then recover during convalescence. However, IHG does not necessarily drop during the acute phase of an illness, and preservation of IR status can be a predictor of better outcomes. For example, in patients with COVID-19, preservation of IHG-I status during the acute phase of the illness was associated with decreased rates of hospitalization and very low mortality rates, including in older patients. Conversely, presenting with worse grades was associated with increased mortality, regardless of age. But despite this, Dr Ahuja said, “Even if a person starts off with good immune health, I cannot predict if they will do well during an infection. There are no guarantees. That is why monitoring grades during acute illnesses has value and determining whether patients restore their grades to baseline is important.” This is because even if a person has optimal immune resilience prior to the onset of an infection, their IR status can erode rapidly during the course of infection, and may not reconstitute to its original baseline, despite clinical recovery from the illness. It is this residual low-grade immunodeficiency that carries over that worries Dr. Ahuja, as he and his team showed that having lower immune resilience was associated with a shorter lifespan, after controlling for the effects of age.
It is a common notion that a person’s immune status will decrease as they get older due directly to their age. However, the findings presented by Dr. Ahuja and his team illuminate a need to reconsider the current dogma regarding immune health and aging. As Dr. Ahuja explained, “It was traditionally assumed that the only difference in immunity between a young person and an old person is their age, so researchers will often just compare the old versus the young. But
that’s not really true. They might need to compare people with varying degrees of immune health as well as different ages.”
While the researchers did find that immune resilience can erode with age — expression levels of SAS-1 declined with age, and expression levels of MAS-1 increased — they found that this trend was more likely a consequence of the cumulative effects of repeated antigenic stimulation over decades causing erosion of immune resilience in susceptible individuals, than an intrinsic quality of aging per se. Dr. Ahuja explained, “Age is a proxy, albeit imperfect, of cumulative antigenic exposures.” Repeated antigenic stimulation can also cause IR degradation in younger people. For example, it was found that in female sex workers, riskier behaviors (e.g. fewer condoms, more clients) were associated with higher rates of IHG-III and IHG-IV, which were in turn associated with an increased risk of HIV acquisition after obtaining these immune health grades.
In people under 50 years old, IHG-I is the most common immune health grade, while IHG-III and IV are relatively uncommon, with a prevalence of less than 5 percent. While rates of IHG-III and IV are higher in older populations, it is important to note that these grades exist in individuals of every age group, as do IHG I and II. As Dr. Ahuja explained, “While as a group older persons may be at greater risk of getting sick, that risk is disproportionately concentrated to people with worse immune health.” This difference in individuals’ ability to resist erosion of their immune resilience as they age may help explain why some people are predisposed to illness and early death, while others enjoy a longer life and health span.
An individual’s immune resilience can change rapidly, and is linked to their ability to fight infection, as well as to their survival during aging, COVID-19 and immunosuppression (e.g. AIDS), among other conditions. Luckily, there are steps that people can take to maintain and improve their IR and reconstitute their immune health grades. Non-optimal IHGs can recover with risk factor mitigation and treatment of infection. For example, among the cohort of female sex workers discussed above, providing education and interventions for practicing safe sex was associated with IHG-I reconstitution due to lowering CD8+ T-cell counts. And while increased HIV viral load leads to increased rates of IHG-IV, treatment with antiretroviral therapy can lead to reconstitution of IHG-I and IHG-II. Hence, IHGs can serve as benchmark for monitoring immune health deterioration and reconstitution.
Advising patients with poor immune resilience about risk factor mitigation may allow them to reconstitute their IR status. It can also help prevent negative outcomes. To demonstrate this point, Dr. Ahuja offered the following example: “We know that people with poor immune health scores tend to do worse after taking vaccines. If I were talking to one of these people, I would tell them that there is a chance they might not do very well after getting vaccinated.” Preventing antigenic exposure can also help preserve IR status in people who already have optimal IR. So, counseling patients about reducing infection risk has the potential to impact their future health.
Actions that are unrelated to preventing antigenic exposure may also help reconstitute and maintain immune status in certain individuals. For instance, the anti-aging benefits of exercise may accrue the most in persons who with exercise are able to improve their IR status.
Every patient is different. In order to provide the best possible care, clinicians must appreciate these differences and tailor their approach to
fit their patients’ unique needs and physiology. As we move away from reactionary practice of medicine and towards preventative, personalized medicine, knowing patients’ level of immune resilience and understanding how it can impact their overall health is an important part of predicting and preventing negative outcomes, and preserving health.
The concept of immune resilience offers a compelling framework for understanding the varied responses individuals have to infectious diseases and other environmental stressors, illustrated by the contrasting cases of Lucile Randon and the younger population affected by COVID-19. Understanding the myriad interplaying factors that influence a person’s immune resilience could revolutionize our approach to health and disease prevention, offering hope for improving health outcomes across all age groups. As research progresses, unraveling the factors contributing to immune resilience could lead to new strategies for enhancing immune function and extending quality of life, highlighting the need for continued investigation into this fascinating aspect of human health. Furthermore, this research provides individuals with the opportunity to take charge of their own health by giving them the tools to assess their individual health risks and make informed decisions about their health, and enables medical providers to practice personalized medicine, and tailor their care based on concepts such as immune resilience — promoting ethical medical practice and advancing science and medicine as a whole.
References:
• Ahuja, S.K., Manoharan, M.S., Lee, G.C. et al. Immune resilience despite inflammatory stress promotes longevity and favorable health outcomes including resistance to infection. Nat Commun 14, 3286 (2023). https://doi.org/10.1038/s41467-023-38238-6
• Covid-19 confirmed cases and deaths - UNICEF data. (n.d.). https://data.unicef.org/resources/ covid -19-confirmed-casesand-deaths-dashboard/
• Punt, D. (2023, January 17). World’s oldest person, Lucile Randon, dies aged 118. Guinness World Records. https://www. guinnessworldrecords.com/news/2023/1/worlds-oldest-person -lucile-randon-dies-aged-118-733313

Sunil Ahuja, MD, is the Director of the Veterans Administration Center for Personalized Medicine and Professor of Medicine at UT Health San Antonio. He received his infectious disease training at the National Institutes of Health and has received many research accolades, including the NIH MERIT Award, Doris Duke Distinguished Clinical Scientist Award, and the 2023 BioMedSA Award for Innovation in Healthcare and Bioscience. Dr. Ahuja is a member of the Bexar County Medical Society.

Amrutha Mummidi is a sophomore at the University of Texas at Austin pursuing a major in Journalism and Health Reform & Innovation on the Pre-Medical track. She is passionate about the intersection of journalism and healthcare, and is dedicated to exploring how effective communication can drive positive change in the medical field.

Raavi Chokhawala graduated from Tulane University with a BA in Political Science. She is currently a second-year medical student at Long School of Medicine and is interested in pursuing a career in infectious disease.

Despite the challenges that International Medical Graduates face in obtaining licensure in the U.S., they bring with them the knowledge, expertise and diverse cultural perspectives that enhance the quality of healthcare delivery and access.
San Antonio Medicine magazine asked some Bexar County Medical Society members to share their journeys to the U.S., which include commitment, compassion and a little humor.
By Soma Jyothula, MD
July 1, 2024, was a Monday; the start of the week. Upon entering the elevator with my team, we encounter a couple of young doctors with unblemished white, crisply starched doctors’ coats. Memories float back upon realizing this is the first day of residency — the start of the intern year; the rite of passage after medical school to become a practicing physician.
One in five practicing physicians in the United States are born and educated abroad.1 In certain specialties like Family Medicine and Psychiatry, one-fourth of the active physicians are International Medical Graduates (IMG). Per the migration policy institute report based on the 2021 U.S. census, 26.5 percent of physicians and surgeons are immigrants (262,000 out of 987,000).2 Non-U.S. IMGs are more likely to practice in rural, lower income and underserved regions. Beyond the care, they add cultural nuances and complete the kaleidoscope of U.S. healthcare.
Enough with the numbers. Reminiscing with a co-physician who graduated from a medical school in India, we started chatting about our residency experience in the United States and our reflections on the difference in the medical environment compared to our country of origin. The conversation rapidly moved to all the humorous moments we encountered to provide enough material for a standup comedy show by itself and the title was “Curry Docs Run Amok.” I agree that in the current environment of cultural sensitivity, it sounds like reverse racism. Please pardon the author for this brief lapse of judgment. The show starts now.
The acronym deluge: PM&R, IR, PT, OT, PICC … Hailing from an anglophile nation, the sudden barrage of acronyms thrown during rounds in my first month of internship was jarring, to be put mildly. I just wanted to be MIA rather than deciphering them. The look of incredulity on the face of my resident, when I queried about what he meant by that alphabet soup, was priceless. Well, now even EMR spell check does not pick them up (sorry King James version of English). What? Someone performs the blood draws? Being a trainee of the British way of medical education and completing a mandatory one-
year internship as part of medical school, much of my intern time was spent performing phlebotomies on patients. It was the intern’s responsibility to make sure all diagnostic tests were completed prior to rounds. The sense of relief upon realizing I do not have to perform blood draws on the 20-odd ICU patients on my first day of residency and a dedicated phlebotomist is available cannot be put in any other way than “God Bless America.”
“How do I recycle these clamps?” Yours truly asked the bedside nurse after assisting my resident in placing a central line. Coming from a lower middle-income country, every metal medical instrument is autoclaved and recycled for further use. Well, I am sure the thought that popped into the nurse’s mind was, “Yup, fresh off the boat.” Keeping in the spirit of collegiality, she laughed and just said, “We dispose of them in the needle container box, and I hope someone recycles the metal.” All right, well now I know why the carbon footprint of healthcare is high.
Beyond these humorous encounters, healthcare in the U.S. is delivered in a comprehensive multidisciplinary fashion with healthcare professionals from multiple fields. IMGs provide a positive addition to this by bringing unique cultural ethos and making the healthcare experience richer, as in the case above. Namaste!
References:
1. https://www.aamc.org/news/1-5-us-physicians-was-born-andeducated-abroad-who-are-they-and-what-do-they-contribute
2. https://www.migrationpolicy.org/article/immigrant-health-careworkers-united-states-2021

Soma Jyothula, MD, FCCP, is a practicing pulmonary and critical care physician, and is the Chief of Pulmonary Medicine and Lung Transplantation at Methodist Hospital. Dr. Jyothula is a member of Bexar County Medical Society and serves on the Publications Committee.
By Caroline Rebicki, MD, MCSc, PGY2
My medical journey began in the turn of the century, when the Millennium Bug still roamed the planet. I went to medical school in the vibrant city of Curitiba in southern Brazil. Back then, we studied from notes written on paper and photocopied forward until no longer intelligible. Looking back, my fondest memories of those years were the countless hours spent studying with classmates, who became important parts of my support system.
My decision to work as a family physician in a rural primary care clinic was driven by a desire to gain a deeper understanding of primary care in a resource-limited community. The transition from a bustling city to the precariousness of the backcountry expanded my perspective on the political and social drivers of health.
I practiced managing familiar problems like diabetes, anxiety and contraception, but also far more complex problems like injustice, violence, prejudice. Technological resources for the clinic were mere promises. There were no advanced diagnostic tools or specialists readily available. In this service, there were no computers; everything was on paper. I remember when a patient came back for a new prescription shortly after the visit because he inadvertently smoked the script (rolled roped tobacco in it and lit it up). The reality was that to get the job done, I needed to rely on a good base of clinical knowledge, proactivity and empathy.
Without the luxury (or distraction) of tech equipment, the cornerstone of my practice became the patient-physician relationship and interpersonal communication. Active listening was essential: patients often shared what mattered most to them as they told their story. I

learned to listen while paying attention to their choice of words and body language. For one patient who lost one eye in an accident, eye contact during encounters built rapport.
Some of my patients faced the triple burden of chronic illness, poor literacy and loneliness. By showing empathy, patients became more comfortable sharing their concerns and following through with plans. This trust was invaluable in developing therapeutic partnerships.
After a decade in practice and undeniable fulfillment in my work, I was ready for the next peak. I heard the “siren call” for further professional development. The United States, with its advanced medical facilities and diverse patient population, offered the perfect opportunity. I was drawn to residency programs that aligned with my passion for community-oriented and patient-centered care.
San Antonio welcomed me with open arms. The city’s Latin cultural traits made it easier to feel at home. As a resident now, I had access to state-of-the-art facilities and abundant learning opportunities. The diversity of patients fascinates me and has enriched my understanding of the meaning of health or illness through different cultural perspectives.
This Family and Community Residency Program has been an incredibly rewarding experience. It has allowed me to apply and expand upon the skills I developed in Brazil, particularly in patient communication. Every day, I meet patients with unique stories and concerns. Empathy and clear communication remain crucial, however, now I have the benefit of advanced diagnostic tools and specialist support. This combination of technology and interpersonal skills enables me to provide better care to my patients.

Caroline Rebicki, MD, MCSc, PGY2, relocated from Brazil to San Antonio with her family for residency in Family and Community Medicine. She has a master’s degree in Family Medicine from Western University in London Ontario, Canada, and an advanced degree in Health Management from Albert Einstein Education and Research Institute, Sao Paulo.
By Daniela Estrada Gomez, MD, PGY3
Ever since I was a kid, I’ve been fascinated by the world of medicine. My twin sister became my first patient when we played doctor as kids. We pretended to deliver babies and figure out strange illnesses. This sparked my interest in medicine. As I got older, I could not get enough of medical TV shows. Each episode made me want to be a doctor even more.
I started my medical training in my hometown of Medellín, Colombia. My university had a strong focus on working with underserved populations who did not have easy access to healthcare. This made me feel responsible for taking care of those who needed it most, and it shaped what I wanted to do with my career in medicine. After my third year of med school, I came to the United States to work as an au pair. Improving my English was a key goal for me, as I believed it would open up better career opportunities in the future. Additionally, I wanted to experience living independently for the first time, step out of my comfort zone, and embrace new challenges. Working as an au pair also allowed me to travel, explore new places, and engage in cultural exchange. During this time, I decided I wanted to continue my medical education in the U.S.
Trying to get my medical license in the U.S. as a foreign applicant was not easy. There were many hoops to jump through and rules to follow. Even so, in the middle of these hardships, I found deep joy and grew as a person. I got to do rotations at Mass General Hospital in Boston where I participated in medical research and finally started residency as a Family Medicine physician at UT Health San Antonio.

Getting used to a new way of doing healthcare and practicing medicine in another language was hard in its own way. But these problems did not seem as big because my family and husband always had my back. When I wasn’t sure of myself, they cheered me on and kept me going after what I wanted.
My path in medicine shows how powerful passion and determination can be, and how much of an impact crossing cultural and geographic lines can have. It’s taught me that at its core, medicine goes beyond borders and it’s all about caring, being committed, and never giving up on making people’s lives better. Every step on this road has molded me into the doctor I am now, with a goal to help communities and make a real difference in healthcare.
When I think about my own path in medicine, I feel thankful for the chances that have guided my journey so far. My Colombian background and American education have come together to give me a richer view, letting me welcome diversity in patient care and see medicine from a worldwide angle.
In conclusion, becoming a doctor is not just picking a job; it’s a life-changing adventure that goes beyond where you’re from or who you are. It’s a journey fueled by a deep love for healing, a promise to serve, and the strong backing of family and friends. I’m excited to keep going on this path with humility, understanding and a firm commitment to improving the lives of those I’m lucky enough to help.

Daniela Estrada Gomez, MD, PGY3, attended medical school at the Universidad de Antioquia in Medellín, Colombia, and is completing her residency in Family and Community Medicine at UT Health San Antonio.
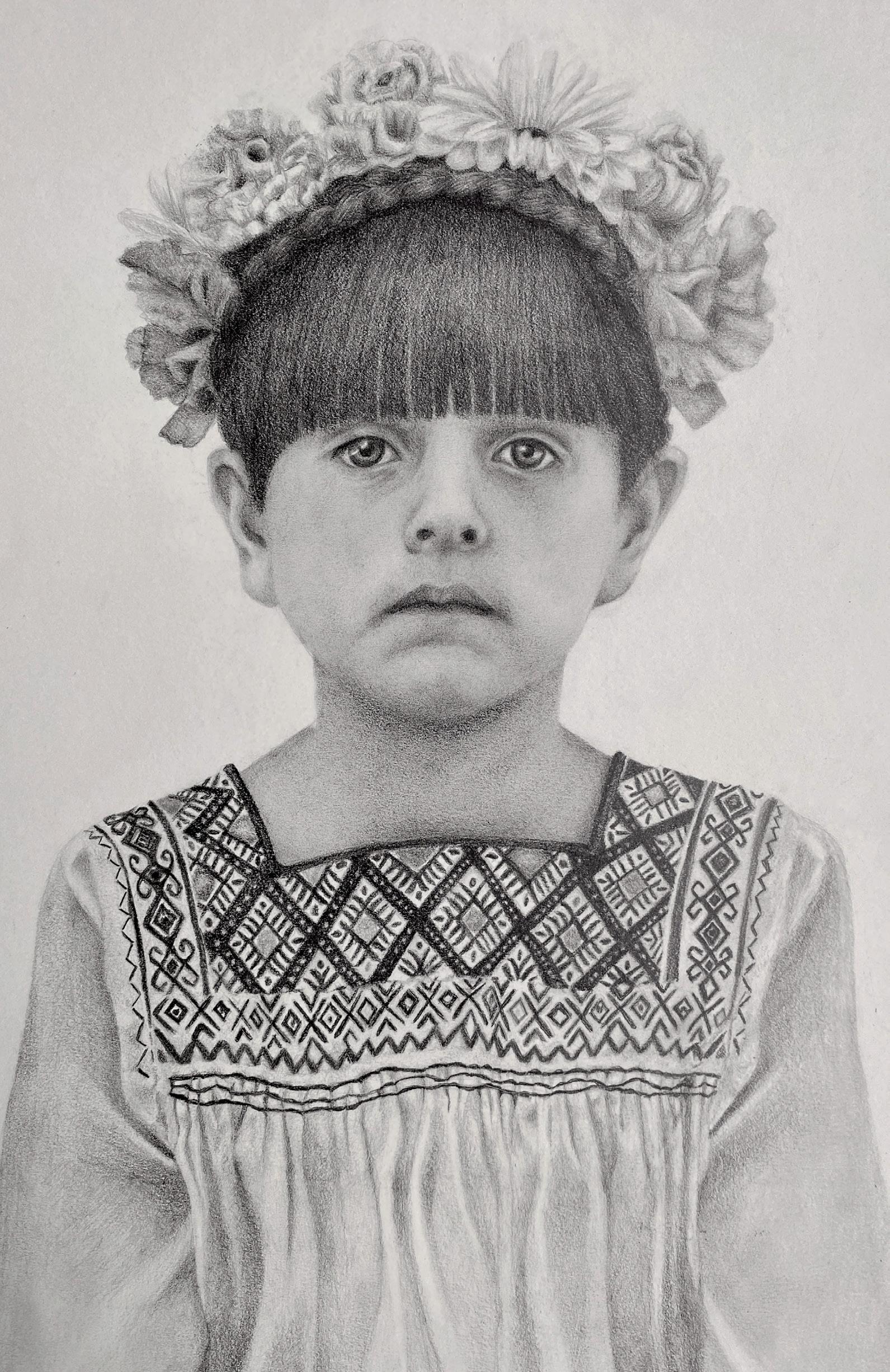
Artist’s Note: This portrait of a young girl was made using graphite. I drew a young girl dressed as Frida Kahlo to depict the unique culture of the city I live in — San Antonio. I am inspired by the diversity of the communities in San Antonio that can be seen during celebratory times like Fiesta and in local markets. The Hispanic patients and families we see in clinic face unique healthcare challenges such as lack of access to care, language barriers and preventative healthcare. I believe that these problems must be addressed along with celebrating the unique cultures that make up San Antonio and South Texas.
Class of 2026
Long School of Medicine UT Health San Antonio
By Trisha Doucette
San Antonio Refugee Health Clinic (SARHC) is one of six student-run free clinics within UT Health San Antonio, developed to address the health and social needs of immigrant refugees living in the northwest region of San Antonio. The weekly acute care clinic, held every Wednesday evening at St. Francis Episcopal Church from 4:00 to 9:00 p.m., is a collaboration of medical, dental, nursing and other health profession students, along with experienced faculty from UT Health San Antonio and the Center for Refugee Services.
“As an interdisciplinary, student-run clinic, we host nursing, dental and medical students on-site weekly. We also conduct a psychiatry clinic on the first and third Wednesdays of each month. Our faculty attendings are integral to the clinic, dedicating several hours each week after their own professional commitments to support patient care and provide educational guidance to our students,” said Moushumi Saha, MS2, volunteer and student leader at SARHC, who says that on average, they see 12-22 patients per day. According to a representative from St. Francis Episcopal Church, 739 patients were seen in 2023.
Since 2011, SARHC has played a crucial role in bridging a significant gap in healthcare access for refugees, regardless of immigration status. Initially, legally resettled individuals and families are supported by time-limited federal and state programs, after which they are minimally supported through local communities’ resources. The primary goal of SARHC is to serve as an initial trustworthy location for refugees to overcome their inhibitions and adequately address their healthcare and social needs. Most patients who visit SARHC have no medical insurance or they do not know how to establish regular care using their new insurance plan.
Clinic volunteers say they see a variety of patients, young and old, mainly from Afghanistan, but also from other countries in Latin America, India, or parts of Africa. “For the first time on my healthcare journey, I was able to translate for a patient who spoke my mother’s tongue, Urdu. As I translated for her, her smile showed me how connected and understood she felt by another woman able to communicate with her amidst all her new experiences in America,” shared volunteer Zainah Siddiqi, MS2.
On-site interpretation services are also provided. Saha said this includes in-person Pashto interpreters and virtual assistance for other languages, effectively mitigating language barriers that may hinder access to care elsewhere. UT Health San Antonio Center for Medical Humanities and Ethics funds 13 interpreters every Wednesday, three of which are females to assist other female refugees when conferring with physicians.
Additionally, representatives from the Center for Refugee Services (CRS) are present during each clinic session, facilitating connections between patients and resources to help them obtain health insurance and physician referrals. Margaret Costantino, MA, LPC, is the Executive Director and Board Member for the Center for Refugee Services, a nonprofit she co-founded 15 years ago. Costantino’s primary role as case worker is to find follow-up services in the community and insurance through the Marketplace when income exceeds Medicaid requirements. She is joined weekly by Dr. Chinar Sediqi, a former general surgeon from Afghanistan, who works closely with physicians, and Dr. Luqman Shah Sultani, a pediatrician from Afghanistan who formerly served with Doctors Without Borders, whose primary role is to connect patients back to the CRS for referrals from doctors.
Costantino explained that the majority of refugees in San Antonio are from Afghanistan, and CRS has registered nearly 6,000 of the estimated 7,000, two-thirds of which are families and the remainder are single men who were unable to get their families out in time. Their primary medical issues include wounds from war and PTSD, or chronic diseases like hypertension or diabetes. “We have identified several patient amputees and partnered with Prescott Bionics to provide orthotic devices. The Center secured a grant to fund prosthetics for four patients. This is where community partners become essential,” she said.
For the student volunteers, their challenges have also been their success stories. Sahu explained that while patients often had access to medications in their home countries, they faced challenges obtaining them during their transition to the United States. Despite the relative availability of these medications here, the interruption during their
relocation negatively impacted their health. Effective management of chronic conditions such as uncontrolled diabetes and hypertension is common, and the clinic addresses the issue by providing the necessary medications through their in-house pharmacy and offers lifestyle counseling to support patients in managing their chronic conditions more effectively.
Siddiqi shared, “A patient who has made an impact on both Moushumi and I had been suffering with epilepsy due to a bombing in Afghanistan as a teenager. It is unfortunate to see that the aftereffects of his difficult past continue to haunt him even now. However, he always wears a smile on our encounters and is kind through his struggles. Due to his labor-intensive job and language barriers alongside his health issues, the patient is unable to stay adherent with medications and doctors’ visits. We have helped him learn to navigate the clock and calendar apps in his phone to remind him of both of these tasks. In addition, we set up a primary care doctor and neurologist for him to regularly see this past week! It has been rewarding seeing his health literacy journey progress.”
It’s a learning experience, both clinically, culturally and compassionately, for the student volunteers as well said Sahu, “Many medical students can relate to the challenge of obtaining hands-on clinical experience during the first two years of their education. I was paired with an upperclassman who guided me in taking comprehensive medical histories and physicals. The faculty mentors at the clinic have been instrumental in my learning process, providing instruction on essential skills such as operating an EKG machine, reading EKGs and interpreting ultrasounds well before these topics were covered in my formal coursework.”

Anna Xu, MS2, and the Follow-up Coordinator for SARHC, added, “Working here, I have learned to appreciate the many barriers’ people face in obtaining healthcare, whether it be from lack of insurance or cost of medical treatments, as well as circumstances such as having to work long hours and lacking adequate transportation to hospitals or outpatient clinics. I have also learned so much about Muslim culture, especially for women and how that can impact their healthcare when there are social expectations that take priority over personal health decisions.”
With services provided once a week, patients cannot always make it to the clinic and if they do, they may not be able to be seen due to the high volume of patients every week. Xu coordinates the follow-up service that runs on an appointment basis right before main clinic. “But even then, getting patients to consistently follow-up is difficult due to their own schedules and busy life making ends meet,” she said.
Sahu explained her initial desire to serve at SARHC, “As the daughter of two immigrants, I have personally witnessed the challenges faced by those who migrate to the United States, including language barriers, significant cultural adjustments, and difficulties in accessing community resources such as healthcare. These experiences initially inspired me to volunteer with organizations supporting refugees during my college years, as I sought to address the struggles my parents encountered.”

Trisha Doucette is the editor of San Antonio Medicine magazine, Cordillera Ranch Living magazine and Rio magazine.
By Marcy Snyder, Fayha Khan and Daniel Zhong
In August of 2021, the United States military withdrew all troops from Afghanistan and the country quickly came under full control of the Taliban. As of this time, more than 76,000 refugees from the country have been relocated to the United States.1 Interestingly, San Antonio has become a site of major relocation for these refugees, accepting more than 6,000 men, women and children as of 2024. Many healthcare providers have noticed increasing numbers of Pashto-speaking families coming into their clinics, emergency rooms and hospitals, and during our time in medical school, we were deeply involved with this population, serving as leaders at the San Antonio Refugee Health Center (SARHC), a free clinic primarily serving migrant populations.
Notably, 46 percent of all foreign-born residents of the U.S. report speaking English less than “very well,” which is substantially lower than the 56 percent of the Afghan population.2 San Antonio has long been viewed as a largely bilingual city with a significant portion of the population being fluent in both English and Spanish. Pashto is the primary spoken language in the Afghan population; however, it is important to note that a provider cannot assume that because a patient speaks Pashto, they are also able to read and write in the language. The UN estimates that around 33 percent of all Afghan refugees worldwide are literate; among women and girls, this number is closer to 8 percent.3 At SARHC, we had success using pictorial explanations of medications as well as color-coded medication bottles, which are given to every patient regardless of whether or not they report being able to read and write. We also continue to use the popular teach-back method through interpreters to ensure that patients understand their medical diagnoses.4
When obtaining family health histories from this population, it is important to consider the state of the healthcare system in their home country. While the healthcare system in Afghanistan has long been strained, things were looking up as recently as 2021. Between 2000 and 2021, the mortality rates for children and adults in the country fell substantially. The under-5 mortality rate was 131.64 per 1,000 5-yearolds in 2000, and fell to 59.61 in 2021.5 The Afghan constitution created in 2004 guaranteed free preventative care to all citizens. Despite real gains made during this time in healthcare access, rural Afghans were much less likely than those living in major cities to have consistent access to medical care. Furthermore, ongoing conflict in the region affected resources like clean water and consistent access to electricity. For these reasons, it is important for practitioners in San Antonio to be aware that Afghan refugees may not know their detailed family histories or be able to share specific diagnoses. Important questions to ask these patients compassionately involve known family deaths, including deaths of children, and what healthcare resources they accessed while in Afghanistan.
We have also noted during our time at SARHC that medication sharing is incredibly common among this community. Patients frequently state that they take medication prescribed to a family member. Asking patients to bring the medications they take with them to the clinic when they schedule appointments or when making referrals is very helpful in this regard.

Finally, it is important to consider strengths of a given community in order to aid them most effectively in a healthcare setting. Afghan refugees are likely to live in large, tight-knit community groups. The Afghan refugees that were evacuated after the Taliban takeover of the country had all served or were the family members of those who served the local military and the American allies in the region.6 Many were translators for the U.S. military and are likely to speak not only Pashto, but several other languages from the region. While it is not necessarily appropriate to use them as translators in clinical settings, they can serve as valuable allies to other vulnerable patients who do not speak English. We hope that providing clinicians with factors impacting the Afghan population’s ability to understand and access care here in the U.S. will help healthcare workers serving them feel more prepared. Personally, our medical education was profoundly impacted for the better by getting to know this population and we are incredibly grateful for the privilege of getting to work with our new neighbors.
References:
1. U.S. Department of State. (n.d.). U.S. Department of State. https://www.state.gov/afghan-arrivals-under-the-u-s-refugee-admissions-program
2. Batalova, J., & Montalvo, J. (2024, February 15). Afghan immigrants in the United States. migrationpolicy.org. https:// www.migrationpolicy.org/article/afghan-immigrants-united-states-2022
3. Jenner, C. (2015, September 14). Education and the future for Afghan refugees. UNHCR US. https://www.unhcr.org/us/ news/stories/education-and-future-afghan-refugees
4. Use the Teach-Back Method: Tool 5. Content last reviewed April 2024. Agency for Healthcare Research and Quality, Rockville, MD. https://www.ahrq.gov/health-literacy/improve/precautions/tool5.html
5. Under Five Mortality Rate-Total. CME Info - child mortality estimates. (2025). https://childmortality.org/all-cause-mortality/ data?sex=_T
6. U.S. Department of State. (n.d.). Afghan Arrivals under the U.S. Refugee Admissions Program. U.S. Department of State. https:// www.state.gov/afghan-arrivals-under-the-u-s-refugee-admissions-program/
Marcy Snyder, Fayha Khan and Daniel Zhong are fourth year medical students at UTHSCSA. They served as medical student clinic coordinators at the San Antonio Refugee Health Center for the year of 2022 and continue to be involved in the clinic. They also conduct research on the needs and demographics of the local San Antonio Afghan refugee population.
By Claire Kowalick, UT Health San Antonio

For the past decade, adolescent mental health disorders have skyrocketed, an issue propelled even further by the COVID-19 pandemic.
Mental health has declined surreptitiously for millions of people in recent years, affecting even the youngest among us. According to the American Academy of Child and Adolescent Psychiatry (AACAP), each year about one in six children aged 6-17 experiences a mental health disorder. Suicide is now ranked as the second leading
cause of death in children aged 10-14. Only about half of children with a diagnosable mental health issue receive treatment.
The rise in mental health concerns is compounded further by a shortage of professionals choosing to work in the public sector, and specifically with adolescent mental health. The AACAP reports a severe nationwide shortage of child and adolescent psychiatrists.1 There are about 11,400 practicing child and adolescent psychiatrists (CAPs) in the U.S. In Texas, there are 853 CAPs, however, 80 percent
of the state’s counties have zero practicing CAPs. Bexar County has 91 CAPs with a ratio of about 18 CAPs per 100,000 children.
To address these chilling trends, child and adolescent mental health professionals and researchers at The University of Texas Health Science Center at San Antonio (UT Health San Antonio) are working toward skillful solutions for diagnosis, treatment and expanded access to care for this vulnerable population.
Treatment of child and adolescent mental health is most successful when there is support from at least one trusted adult. Most children and teenagers do not choose to come to treatment on their own. Often parents, teachers or other adults in the child’s life are the first ones to express concern.
The presence of a caring, genuine adult can make a world of difference in the successful treatment of mental health disorders among children and adolescents. Aside from a family member, a trusted teacher, school counselor or coach can also be a positive figure in a child’s life. Initiatives are underway in many public schools to train educators to identify potential mental health concerns among children and adolescents.
“This is often a key intervention,” said Rene Olvera, MD, MPH, Dielmann Distinguished Professor and Chair of the Department of Psychiatry and Behavioral Science, Joe R. and Teresa Lozano Long School of Medicine, “We don’t expect everyone to be a therapist, but to know what is available and help the family navigate the system.”
The most common child and adolescent mental health conditions are anxiety, depression, attention deficit disorders and severe aggression. While the COVID-19 pandemic magnified mental health concerns, there was already an emerging problem beginning around 2016, Olvera said. The global pandemic only amplified existing issues while piling on potential new stressors like loss of routine, parental death and fear for their safety.
“Developmentally, most teenagers do not sit around worrying about getting sick, and all of the sudden there was a huge intrusion on their lives,” Olvera said.
Adolescents already go through drastic developmental stages and may be dealing with psychosocial stressors such as bullying, relationship breakups, relocation or divorce. The breadth of stressors children and adolescents face only continues to multiply.
Adolescent mental health care is complex, and CAPs are trained to discern how conditions present differently at various ages and developmental levels. Many major psychiatric conditions do not fully express themselves until late adolescence or early adulthood. Some conditions can be treated with non-medication interventions, such as therapy, but others may require a combination of therapy and medication.
One of the most expansive programs in recent years to address child mental health is the Texas Child Mental Health Care Consortium (TCMHCC). This state-funded program was approved during the 86th Legislature and expanded in 2021, through federal funding from the American Rescue Act. The consortium brings together the combined resources of higher education and mental health professionals
to address mental health for children and adolescents throughout the state. 2 Initiatives of the program include the Child Psychiatry Access Network (CPAN); Texas Child Health Access Through Telemedicine (TCHATT); Community Psychiatry Workforce Expansion; Child and Adolescent Psychiatry Fellowships; and research networks like the New and Emerging Children’s Mental Health Research Initiative (NECMHR).
Olvera, who previously served as the chief medical officer with the Center for Healthcare Services, local mental health authority for San Antonio and Bexar County, said one of the best parts of TCMHCC is that it improves access to care by attracting more child psychiatrists to work in the public sector through funding for fellowships, training programs and collaborative networks to encourage more professionals to choose this field.
CPAN is the furthest-reaching portion of the consortium, Olvera said. Since 2019, the network has enrolled more than 12,700 providers and 2,500 clinics that can consult with psychiatrists, request resources or get referrals. Through CPAN, the state’s counties are divided up between 11 medical schools to provide consultation services to pediatricians. Many mild to moderate mental health conditions can be treated by a pediatrician or primary care provider. Through this partnership, Olvera said, Texas pediatricians have become more comfortable treating children and adolescents with mental health concerns, knowing they have the support of the network. For major mental health problems, patients can be referred to a specialist. “Helping pediatricians to feel comfortable treating mental health conditions removes delays in care caused by the shortage of child and adolescent psychiatrists,” Olvera said.
The coordination between the state’s local mental health authorities and academic institutions means less competition for manpower. Instead of a CAP having to choose between working in either the public sector or academia, they can be of service to both. Through the consortium, UT Health San Antonio is contributing to mental health assistance in several South Texas counties, most of which have zero or very few resources for child and adolescent mental health.
Telemedicine expansion has transformed the landscape of what is possible for child and adolescent mental healthcare. Children and their families that did not have the time, money or access to quality mental healthcare are now finding the resources they need through UT Health San Antonio and collaborations like the consortium’s TCHATT program.
Steven Pliszka, MD, professor of psychiatry at UT Health San Antonio is the director of the San Antonio TCHATT. The program works with area school districts to coordinate mental health therapy through telemedicine therapy sessions, all done conveniently at the child’s school and at no cost to the family. Pliszka said they have agreements with districts in Bexar County, throughout the Hill County and as far east as Victoria.
Through TCHATT, if a school identifies a child that may need mental health services, they contact the parent or guardian to discuss possible treatment through telemedicine. With parental consent, the therapist, child and parent/guardian can participate in four to eight
therapy sessions. The child is provided a private room at the school and the session is conducted through video conference with the therapist and parent. If there is a serious mental health issue, or more intensive treatment is recommended, the family will be referred to one of the UT Health San Antonio clinics or a mental health clinic in their area. If a child has a condition that requires medications, they are referred to a nurse practitioner for a medication assessment. “We have seen a wide variety of severities from mild adjustment problems to kids with very significant trauma histories,” Pliszka said.
Having the sessions during the school day minimizes the loss of learning time and the parent can join the virtual sessions without having to leave their home or place of employment. Pliszka said the progress of the program has been phenomenal. So far, the TCHATT program has enrolled several hundred school districts throughout the state and conducted telemedicine sessions for nearly 2,000 students.
Improved access to treatment can’t come soon enough, Pliszka said, as incidents of anxiety and depression in children and adolescents have increased markedly in the past 10 years. “It was already going up preCOVID and we have continued this upward trend,” he said.
UT Health San Antonio honors their commitment of service to the community in part through their continual research into innovative methods of diagnosis and treatment. In the domain of adolescent mental health, university scientists are exploring novel ways to diagnose conditions and personalize care.
Amy Garrett, PhD, associate professor in the departments of Psychiatry and Radiology at UT Health San Antonio, is studying how brain function changes when adolescents receive trauma-focused therapy for post-traumatic stress disorder (PTSD). Garrett is using magnetic resonance imaging (MRI) to measure brain function before, during and after 18 weeks of therapy. In her previous studies, she found that participants in the study showed improvement in their symptoms and that brain function was normalized after treatment. Her current research looks more closely to determine whether therapy leads to brain changes at specific times and, if so, when those changes occur.
Garrett said trauma-focused cognitive therapy is the “gold standard” treatment for trauma, and with research grants from the National Institutes of Mental Health and Baptist Health Foundation, licensed therapists on the research team are providing this therapy to the study’s participants at no cost.
During trauma-focused therapy, an individual works with a therapist to process thoughts, feelings and behaviors associated with trauma. This process can help to reduce the problematic symptoms that sometimes linger for months or years following a trauma.
Unfortunately, there are a great deal of young people in the San Antonio and the South Texas area that have experienced trauma. In this age group, many individuals are undergoing traumas related to domestic violence, sexual abuse and physical assault. Garrett said she is glad that young people are seeking therapy to address trauma because treatment at a young age can be very helpful for their academic and social development.
In July, UT Health San Antonio scientist Jessica Sandoval, MD, associate clinical professor with the Department of Psychiatry, Child and Adolescent Psychiatry Division, was awarded a $300,000 NECMHR grant for a two-year research project. Sandoval will be evaluating the impact of the quality of Spanish-language interpretation during psychiatric evaluation on children’s mental health outcomes. A secondary measure will be how quality of the interpretation impacts trust of the physician. Sandoval’s hypothesis is that quality of the language interpretation will impact patient outcomes and patient trust of their physician. “Hispanic/Latino patients often have unmet mental health needs, with lower access to mental healthcare, underuse of mental healthcare, shorter duration in treatment when they do and treatment disparities. While having an interpreter addresses the language barriers that may exist, we do not know if the quality of that interpretation has any impact on patient outcomes and their ability to form a trusting relationship with their psychiatrist, which can be an important element of treatment,” Sandoval said.
The outcome of this research will inform mental health researchers about an unexplored area that could be contributing to disparities. Interventions may include improved training or interdisciplinary partnerships with interpreters to ensure providers understand the needs of their patients. “Ultimately, we hope it improves linguistic minorities’ ability to communicate with their mental healthcare provider and have equitable care to their English-speaking counterparts,” Sandoval said.
At UT Health San Antonio, medical professionals provide every patient with the same respect and quality care regardless of age, location or financial status. Through rigorous research, strategic collaborations and partnerships with local agencies, we can make a difference in this current crisis of mental health among young people. “We see where we all fit in the system of care, and we all need to work together to succeed. We want every healthcare system here to be healthy because we need everybody, both private and public,” Olvera said.
References:
1. Severe Shortage of Child and Adolescent Psychiatrists Illustrated in AACAP Workforce Maps. https://www.aacap.org/AACAP/ zLatest_News/Workforce_Maps_Illustrate_Severe_CAP_Shortage.aspx
2. UT Health San Antonio, statewide program provides free child mental health services. https://news.uthscsa.edu/ut-health-sanantonio-statewide-program-provides-free-child-mental-healthservices/

Claire Kowalick is a science writer and senior public relations specialist with The University of Texas Health Science Center at San Antonio. She is a graduate of the University of North Texas. As a science writer, she combines her passion for writing with a deep appreciation of biomedical science to tell people about the groundbreaking research and novel discoveries happening at South Texas’ largest academic research institution.
By Kelly LeBlanc, MLA, RD, LDN Food Pyramids courtesy of Oldways, www.oldwayspt.org
The Mediterranean diet, with seven decades of research supporting its benefits, is recommended by physicians far and wide. And yet with patients of color burdened by health inequities and disproportionate rates of diet-related disease, it’s time to take a closer look at the different flavors of what a healthy diet can look like, and help dispel the myth that there’s one “best diet” for everyone.
This May, a groundbreaking new article published in Advances in Nutrition shed light on how other cultural food traditions beyond the Mediterranean diet can also provide high-quality diets that predict low rates of major causes of disability and deaths. By addressing a literature gap on diet and health research beyond its early base in Europe and North America, this research, led by nutrition nonprofit Oldways, emphasizes that foods traditionally consumed in diverse cultures can support guidelines and recommendations that are culturally appropriate. Specifically, the research focuses on Asian Heritage Diets, African Heritage Diets and Latin American Heritage Diets, drawing attention to the common thread of healthful, plant-based foods that emerges throughout these eating patterns.
The elements of traditional Mediterranean, Latin American, Asian and African Heritage diets are depicted in graphic form in Oldways’ Heritage Diet Pyramids, which were developed with a committee of subject-matter experts in nutrition, culinary history and medicine in each of the regions of focus. Because one single plate or diet does not fit all, these pyramids are designed to depict the substantial variation of foods and flavors that exist within these broader dietary patterns. Whether displayed on posters in the office, on handouts and brochures or as “prescription pads,” these visuals can be great conversation starters to help patients reclaim their health by reclaiming their heritage.
“Modern western diets often lose the connection between local ancestral customs revolving around food, the local small-scale production of food products, and a population’s relationship/genetic predisposition towards a set of specific nutrients. Oldways retrieves the best of heritage diets, accessible to all,” said Stephanie Fine, MD, the Director of Breast Surgical Oncology and Assistant Professor in the division of Surgical Oncology at the University of New Mexico Health Sciences Center.



“Culture provides the language for decision-making in the delivery of healthcare especially health services like nutrition. Our culture influences what and when individuals eat,” said Chef Robert Graham, MD, MPH, ABOIM, FACP, Co-Founder of FRESH Medicine and an advisor for Oldways’ Latin American Heritage program. Dr. Graham encourages his patients to share their food story, and emphasizes that “every food culture has nourishing, delicious food, and our food culture deserves to be celebrated.”
There’s an African proverb that says, “If you want to go fast, go alone. If you want to go far, go together.” For too long, physicians incorporating culinary medicine and cultural nutrition have ventured a lonely road. By working together with registered dietitians, community health workers, chefs and community activists, and by scaling existing, evidence-based solutions, physicians can help patients advance farther along on their journey to health.
Given the abundant diversity of global food traditions, it can be overwhelming to know where to begin when trying to offer more culturally inclusive care. A physician’s time is precious, and it isn’t practical to reinvent the wheel with every patient. By scaling solutions that work, providers can make a greater impact on more people. “Instead of worrying about learning everything there is to know about a specific food culture, turn your focus to making sure your patients/clients get the information they need in ways that fit their lives and tastes,” said Dr. Graham.
Emphasizing the cultural aspects of the diet, rather than crafting nutrition programs and policies in more broad terms, can be an especially effective way to generate support for lifestyle interventions. A
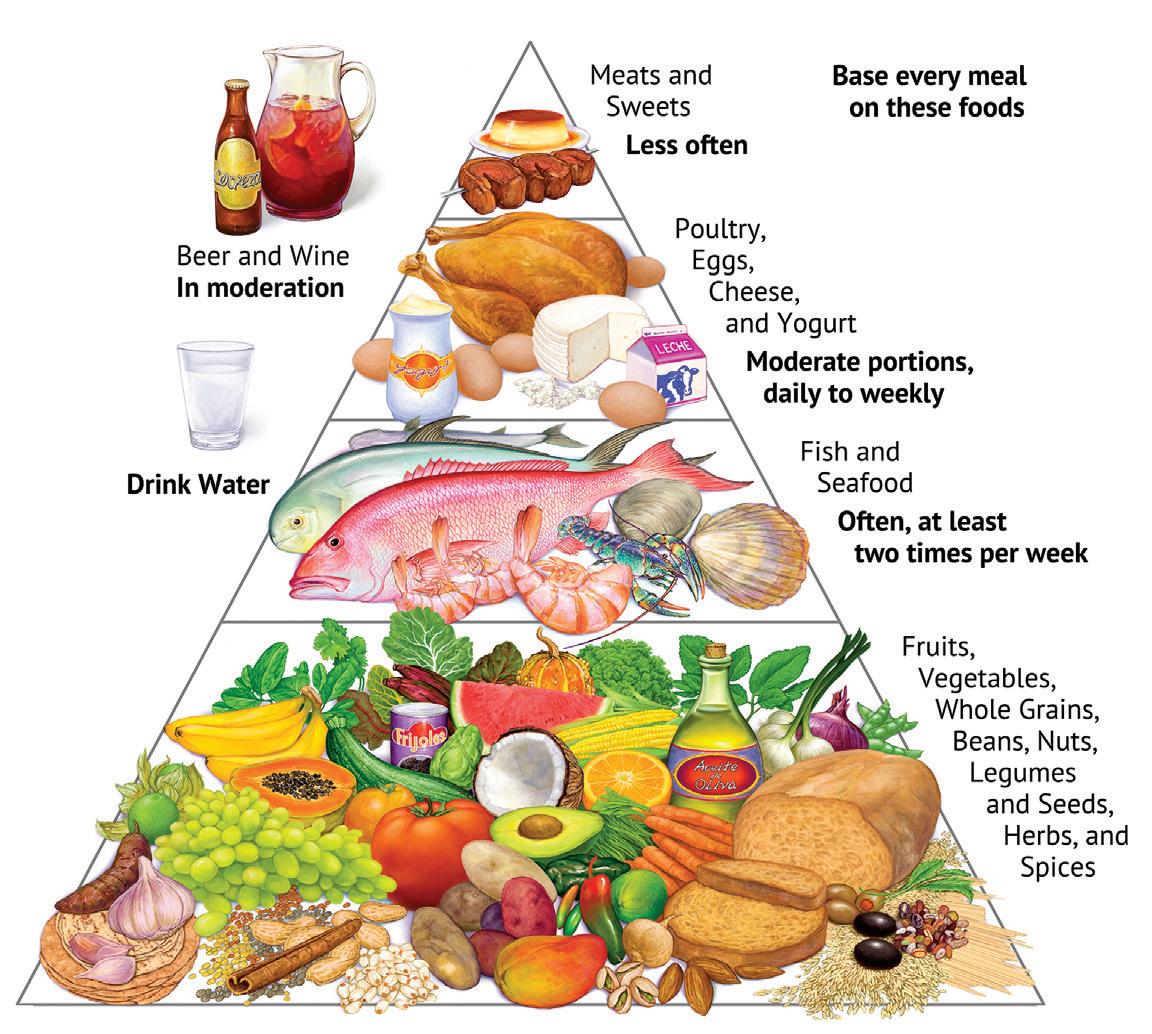
study published in the Journal of Nutrition Education and Behavior found that 98 percent of participants of A Taste of African Heritage, Oldways’ 6-week cooking and nutrition curricula based on plantbased foods from the African Diaspora, indicated that history and heritage were positive motivators for eating and living well. Participants of the program also significantly improved fruit and vegetable intake, weight, waist circumference and systolic blood pressure.
For those immersed in restoring the often-unsung legacy of healthy eating in communities of color, the energy is transformative. “To those of you on the fence, who are considering bringing A Taste of African Heritage to your community … all I can say is DO IT,” shared one of the program’s Chicago-based instructors. “You will be helping yourself and others in the true African spirit of Ubuntu: “I am who I am because of who we are to each other.”
By allowing patients to share their food stories, and by partnering with community-driven initiatives that put culture and tradition first, physicians can lead the way in reducing health disparities. As Dr. Graham shared, “The goal for us is to have a foundation of knowledge and resources that allow us to give equitable care to every patient, regardless of their food culture.”
Kelly LeBlanc, MLA, RD, LDN, is VP of Nutrition Programming at Oldways, a nonprofit nutrition education organization inspiring people to embrace the healthy and sustainable joys of the old ways of eating. To learn more about Oldways’ Heritage Diet Pyramids and culturally tailored resources, visit OldwaysPT.org. Kelly can be reached at Kelly@OldwaysPT.org.
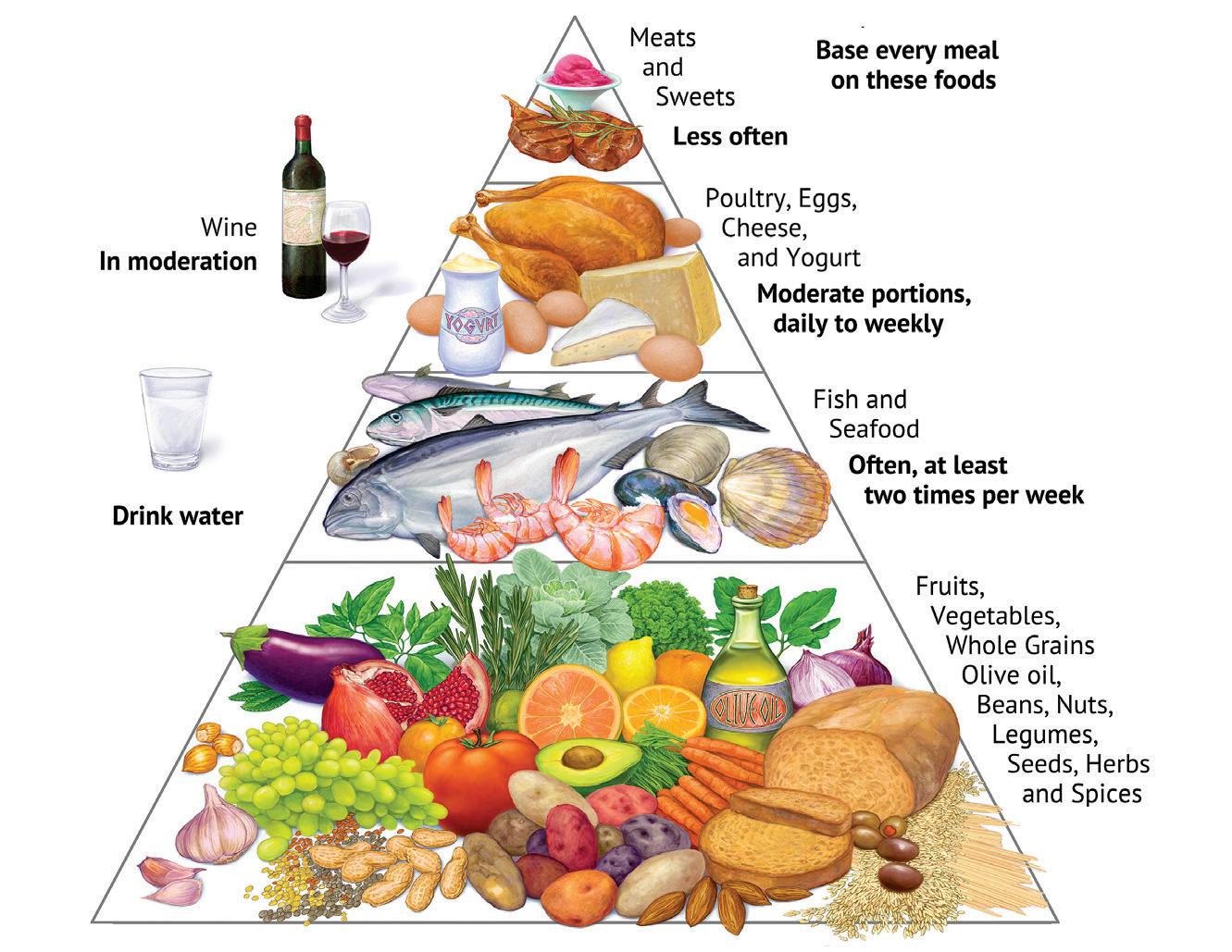
By David Alex Schulz, CIPP
From pho to falafel, San Antonio’s international cuisine has expanded dramatically in kind and venues. Noodle shops, sushi bars, gyros sandwich makers — where one may have served the city in 2000, today it takes a dozen or more. It is transformed by population surging 30 percent in the new Millenium. The non-Mexican foreign-national population has increased both in absolute numbers (app. 33,000 to 75,000) and as a percentage of the whole, growing from three to five percent, leading to a multitude of new, exotic restaurants. But where to get authentic ingredients to replicate recipes at home?
The Medical Center, as in Dallas and Houston, serves as a vibrant hub, attracting and anchoring foreign nationals. To survey the best foreign grocery stores and supermarkets (an ever-changing constellation) called for a “Global Food Availability Tour” using Floyd Curl and Medical as a locus. We searched out exotic ingredients not found in a mainstream supermarket, although H-E-B does contribute essentially to this diversity — more later.
Just as food is integral to health, native flavors are an essential stimulus to appetite. Among new residents, the Asian population was the fastest growing, nearly tripling. Comprising Indian, Filipino, Vietnamese, Chinese and Korean communities as a core, with significant numbers of Japanese, Pakistani, Bangladeshi and Thai residents, each culture adds to our epicurean diversity. Thus, let us begin our tour in the East … a block east of I-10 on Wurzbach Road, behind the H-E-B.
Look closely in the Colony Drive shopping center for Burmese Foods next to a corner lube shop. It’s an easy-to-miss, unvarnished gem, obscured by product signs in windows. Not a supermarket, it’s like a neighborhood grocer in Mandalay: shelves packed with brightly colored packaged goods; beautiful, uncommon vegetables like a truly gnarly looking, spiky leafed vegetable known as Bitter Melon (Momordica charantia), used in stir fry, soups or hollowed out and stuffed like a green pepper; spices and reductions like lime, lemon and ginger powders; and dried fruits, baked delicacies and exotic beverages are all to be found.
Two notes about this store at 3703 Colony Drive: it also caters to Myanmar’s neighbor Thailand, so spices, reductions and specialties in freezers cover both nations’ cuisines; and please don’t be off-put by aisles congested with restocking activities, a common issue since most grocers don’t have large storage areas, so a busy aisle indicates fresh supplies.
Opposite Burmese Foods in both location and approach, Man Pasand International Foods Supermarket is a mainstay of Indian, Pakistani


and Bangladeshi chefs throughout San Antonio. As physically prepossessing as the H-E-B it backs into, Man Pasand presents an alluringly spotless layout with wide aisles and freshly stocked produce; dried grains, beans, peas in sacks small, large and commercial; cheeses, ghee, yogurts and other dairy products; a Halal butchery for freshly prepared meat; and a food court. This is particularly relevant as almost all other grocers and supermarkets are adjacent or close to specialty restaurants while none exist at Colony (the corner curry shop having been replaced by a cocktail lounge.)
Heading west on Wurzbach Road, immediately past I-10, you’ll find an entire block dominated by Middle Eastern cuisine: Za’atar Grill, Pasha Restaurant and Baklava Bakery, all anchored by San Antonio’s mother-ship of pita, Ali Baba International Food Market. Ingredients for cuisines between the Arabian and the Black Seas will be found among Ali Baba’s aisles of olives, chickpeas, tahina, pickled delicacies and kitchen staples like olive oil; binned vegetables and breads; and a Halal butchery for freshly prepared meats. The bread aisle deserves note. Beyond moist and fresh pita in white and whole wheat, sizes large and small, are various flat breads all deserving adoption: Barbari, an oblong-shaped Persian flatbread, particularly associated with Palestinian cuisine; and Manakish, a pizza-like flatbread topped with za’atar, a culinary herb or family of herbs along with toasted sesame seeds, dried sumac and other spices.
Taking the I-10 access road up to Medical Drive, going a mile west to Fairhaven, a brand-new jewel of exotic foods can be found hiding behind the street facing strip, in Des Pardes International Market. Just opened in March, it is setting a new standard for Indian and Pakistani supermarkets in the Alamo City. Spotless, wide aisles are well-stocked with pan-South Asian specialties, with an on-site Halal butchery (in construction). It already features fresh goat and lamb, and all products are priced for fast turnaround. Noteworthy of Des Pardes is that, distinct in its class, it features its own website, despardestx.com, with weekly sales and specials.
Leaving Des Pardes, taking Fairhaven up to Datapoint and following it to Wurzbach puts you at Al Madina Meat Market and Grill, a mainstay of the Halal community that offers grilled skewers of ground meats customized for Iraqi or Turkish tastes, beef or chicken tikka and Afghani and Pakistani specialties. Then, there’s a fusion menu of NY Pizza with beef or chicken shawarma, kafta and other toppings.


With Al Madina’s motto, “Think Halal, Eat Halal, Live Halal,” the Sharia-observant homemaker will find all the ingredients and many more cuts of meat and fresh sausage, immaculately packaged, clearly labeled, and priced to move (according to impressed reviewers.) Dates, figs, nuts and beverages round out the stop, shop and nosh venue. Get some for the road as we head west to Leon Valley for a whole different set of cuisines: African and Caribbean.
Ten minutes down Wurzbach will find you in Leon Valley at the First Choice International Supermarket. Here, you’ll find ingredients inherent in African and Caribbean cuisines, with staples like Mbongo Tchobi spices (for Cameroonian Black Stew), and a good variety of frozen and fresh beef, goat, fish and chicken. Island favorites include jerk seasoning, white yams, coconut milk, Vitamalt (a non-alcoholic, sweet beverage made from malted barley), Milo (an Australian chocolatey-malty drink, iconic in the Islands), tamarind balls, plantain and aisles of snack foods. Spoiler: Fans of the Harry Belafonte song “Jamaican Farewell,” should know that the island’s national dish it describes, “Ackee, rice, salt fish are nice,” uses a fruit prohibited for import to the U.S. and can’t be recreated here. (But, “And the rum is fine any time of year,” is still valid.)
A speedy seven minutes up Bandera Road brings you to the most comprehensive pan-Asian Supermarket, Tim’s Oriental & Seafood Market. A seemingly endless series of aisles are demarked for specialties of Cantonese, Thai, Vietnamese, Japanese and other cuisines. Facing the aisles of bottled and packaged spices, ingredients and savory sauces is a wall of freezers containing every variety of dumpling known to the sub-continent: Chinese jiaozi, Japanese gyoza, Korean mandu and Vietnamese bánh bao were all evident on a recent visit. Equally overwhelming were the types of dried noodle, from Canton wheat noodles to Vietnamese rice vermicelli, in all shapes and forms for pho, wonton, dim sum and spring rolls.
Our visit wasn’t for frozen delicacies or staples, but for the freshest Chinese BBQ Pork, Roast Pork and Roast Duck to be found in San Antonio, every day of the week from about 11:00 a.m. (12:00 p.m. on Sundays) … but show early because like any great barbecue shop, when they run out, they’re out.
Tim’s can be a fitting destination, with the availability of freshly cooked meats to take home, but if you’re still in the mood for something completely different, head to Callaghan Road, and return to the other side of I-10 where you’ll find Sasha’s European Market, tucked inconspicuously in a strip just down from the corner. If that doesn’t sound exotic, think again. You will find pelmeni, pierogi, pickles and soups from Greece, Poland and Russia, blinchiki (Russian pancakes), products from Sweden, the UK, Finland and Ukraine filling aisles with cookies, snacks and preserves; refrigerators with cheeses, yogurts and dairy; and freezers with luscious European and Russian cakes. Crisp or


dense breads like Scandinavian linseed or Westphalian pumpernickel, combined with the selection of wursts, sausage, kielbasa and salami, provide a worthy Continental picnic lunch. Add a bottle of fortified Moldovan wine, and you might imagine yourself in Tsar Peter’s St. Petersburg Summer Garden listening to distant balalaika strumming. These eight are anything but an exhaustive list, nor are all these products limited to these stores. Every neighborhood H-E-B has foods representative of its customers. For instance, the H-E-B at Alon Shopping Center, down the street from the Jewish Community Center, has the best selection of Kosher products, from meats to matzoh, to be found in the city. (Sasha’s is no slouch in this either. Many of the imported noodles, cookies, soups and breads are marked Kosher.)
Another Middle Eastern super-store found up on Babcock near the outer loop, Aladdin International Food Market has its adherents, and down on San Pedro Avenue, Las Americas Latin Market brings us South and Central American produce and products. Minnano Japanese Grocery on Callaghan is a go-to for sticky rice, teriyaki sauces unseen in mainstream stores, shrimp chips and seaweed snacks.

David Alex Schulz is certified in HIPAA privacy and security compliance, serves on the BCMS Publications Committee and is a contributing writer to San Antonio Medicine magazine.
1st Choice Int. African Caribbean Market 5712 Wurzbach Rd, 210-465-9692
Al Madina Meat Market and Grill 9218 Wurzbach Rd, 210-949-0430
Aladdin International Food Market 15503 Babcock Rd, 210-695-4444
Ali Baba International Food Market 9307 Wurzbach Rd, 210-691-1111
Burmese Foods
3703 Colony Dr, 210-467-5808
Chacha Bedoy Donuts and Bakery 1723 Babcock Rd, 210-515-4886
Des Pardes (International Market) 4081 Medical Dr, 210-254-9073
Himalayan Bazar 8466 Fredericksburg Rd, 210-614-8600
JB African/Habesha International Grocery Store 1634 Babcock Rd, 210-429-2627
Las Americas Latin Market 6623 San Pedro Ave, 210-340-2747
Man Pasand Indian International Food Market 3727 Colony Dr, 210-455-2888
Minnano Japanese Grocery 7460 Callaghan Rd, 210-340-7900
Sasha’s European Market 8023 Callaghan Rd, 210-348-7788
Tim’s Oriental & Seafood Market 7015 Bandera Rd, 210-523-1688
By John D. Rodriguez, MD
The primary care crisis is in full swing. Issues such as the shortage of primary care physicians, the lack of interest in the profession, as well as poor payor reimbursement and dissatisfaction amongst current providers has created a healthcare disaster. By the year 2034, there will be an expected shortage of between 17,800 to 48,000 primary care physicians as reported by the Association of American Medical Colleges.
This dissatisfaction with the healthcare system is also reflected amongst patients where, in a Harris poll, 70 percent of U.S. adults feel the healthcare system is failing to meet their needs. In the primary care setting, this unhappiness is exacerbated by the long wait times for appointments, shortened time with the provider and the lengthy time spent in the waiting room. These are just a few of the many hurdles patients have to jump through to get the care they need.
An important issue to consider is the decrease in private, independently owned primary care practices. A study commissioned by the Physician Advocacy Institute in 2022 showed that three-quarters of all physicians (74 percent) now are employed by a hospital, health system or a corporate entity. Contrast that with only 28 percent in 1988. This shift is mainly driven by the difficulties, financial and otherwise, in running a private practice. The safety of employment within a large healthcare system can provide some peace of mind but not without its challenges and struggles.
One solution to help generate interest in primary care as a profession to be appreciated and financially viable is to look at the “Marcus Welby” model of care delivery. For some of you who are not familiar with “Marcus Welby, M.D.,” this was one of the first TV medical series, which aired from 1969 to 1976. It portrayed a family physician who officed out of his home and employed only one staff member, his nurse/manager Consuelo Lopez. What you did not see in his practice was a crowded waiting room or four exam rooms where patients were being shuffled in and out by as many as four to five full time staff members so as to maximize revenue. I think some of us who have worked under this model realized there was a point of diminishing returns. Marcus Welby did not need to support an overhead, which in today’s numbers can run as high as 70 to 80 percent of collections. Roughly speaking, approximately 10 to 15 patients/day need to be seen to cover overhead. This is before the provider can take home a salary.
What Marcus Welby had in today’s vernacular would be a “micro practice.” His overhead consisted of mainly his home mortgage, nurse’s salary and some supplies. I suspect his medical life was much less chaotic compared to what we see today, where providers have to see between 20 to 25 patients/day. Having to follow up with all ordered lab/x-ray tests, review consults, answer emails/phone calls and refill prescriptions are just a few of the items dealt with by today’s providers. By drastically reducing overhead such as fewer staff and smaller space,
a provider can see a fraction of the usual patient volume. Despite seeing fewer patients in a day, a provider can still make or exceed an income seen in an employed position while reducing the overall burden of running a practice. This slower practice style can improve one’s quality of life while giving the patient a better care experience.
Numerous primary care providers across the U.S. have adopted this primary care model of “micro practice.” They report incomes that meet or exceed an employed provider’s salary while giving them the independence and quality of life they have been looking for. This care model does ask that the provider do more of the work that used to be delegated to employees, but with today’s EHR systems utilizing patient portals, much of this work can be handled by the provider. Your patient volume is half of a traditional practice so managing this practice is possible.
Marcus Welby did it right: smaller is better and with “micro practice” medicine, and we can again generate interest in and showcase a sustainable primary care model that will serve patients for years to come. Yes, there are some risks, but done properly, your chance of success is almost guaranteed in a society where primary care is in high demand.

John D. Rodriguez, MD, is board certified in Internal Medicine and has a passion for primary care. He is the owner of Parvus Medical Suites, and Chief Medical Officer and Co-founder of Healthcare2u LLC. Dr. Rodriguez is a member of the Bexar County Medical Society.
Parvus Medical Suites is a Platinum Member of the BCMS Circle of Friends program.
By Ayomide D. Akinsooto
The Student National Medical Association (SNMA) at UT Health Science Center San Antonio organized the inaugural Sickle Cell Walk and Health Care event on September 30, 2023. This collaborative effort with the Sickle Cell Association of Texas (Marc Thomas Foundation), Be The Match and the South Texas Blood & Tissue Center strove to bring attention to sickle cell disease, educate the San Antonio community, and create a supportive network for those affected by this condition.
Our mission was threefold: to educate the public about sickle cell disease, support those living with the condition, and empower individuals through increased visibility and access to resources. By offering health screenings and educational sessions, we sought to increase the community’s understanding of sickle cell disease and promote early detection and management.
The significance of such events cannot be overstated. Sickle cell disease is a genetic disorder that affects hemoglobin, leading to severe pain, anemia and potential complications such as stroke and organ damage. Despite being the most common inherited blood disorder in the United States, affecting approximately 100,000 individuals, sickle cell disease remains underrecognized and underfunded in research compared to other genetic disorders.
Recent advances in sickle cell disease research and treatment have shown promise in improving the quality of life and outcomes for patients. One of the most groundbreaking developments occurred recently as the FDA approved the first gene therapies to treat patients with sickle cell disease. Casgevy and Lyfgenia are cell-based gene therapies approved for treating sickle cell disease in patients aged 12 and older.1 These therapies treat recurrent vaso-occlusive crises, which occur when sickled red blood cells restrict the flow in blood vessels and limit oxygen delivery to the body’s tissues, leading to severe pain and organ damage. Casgevy, the first FDA-approved therapy using CRISPR/Cas9 technology, modifies hematopoietic stem cells to increase fetal hemoglobin (HbF) production, preventing red blood cells from sickling. Lyfgenia uses a lentiviral vector to genetically modify stem cells to produce HbAT87Q, a hemoglobin similar to normal adult hemoglobin, reducing the risk of sickling. Both therapies involve collecting patients’ stem cells, undergoing myeloablative conditioning, and reinfusing the modified cells. Early clinical trials have demonstrated that gene therapy can potentially cure sickle cell disease by enabling the body to produce healthy red blood cells. Long-term studies are being conducted to evaluate their safety and effectiveness. Another significant advancement is the development of new drug therapies. Voxelotor (Oxbryta), has been approved by the FDA to reduce the risk of hemolysis and improve hemoglobin levels in patients with sickle cell disease.2 This medication works by increasing the affinity of hemoglobin for oxygen, thereby reducing the sickling of red blood cells. Addition-
ally, Crizanlizumab (Adakveo), an FDA-approved monoclonal antibody, has been shown to reduce the frequency of pain crises in patients with sickle cell disease.3 This therapy targets P-selectin, a molecule that plays a key role in the adhesion of sickle cells to blood vessels, thereby preventing vaso-occlusive episodes.
The promise of these treatments offers hope to many, but accessibility and awareness remain critical challenges. This is where community events like our Sickle Cell Walk and Health Care Event play a crucial role. By informing communities and educating the public, we can increase support for research funding and improve access to these life-changing treatments.
Our event was not only about enhancing the knowledge surrounding sickle cell disease but also fostering community engagement. We believe that building a supportive community for those affected by sickle cell disease is essential for improving their quality of life. Through partnerships with organizations like Be The Match and the South Texas Blood & Tissue Center, we aimed to highlight the importance of blood and bone marrow donations, which are vital for many patients with sickle cell disease.
The success of last year’s event has inspired us to make it an annual occurrence. This year’s walk and health fair is scheduled for September 7, 2024, at Gold’s Gym San Antonio Medical Center. Our goal is to expand our reach, attract more participants, and continue building a strong support network for the sickle cell community.
References:
1. FDA (2023). FDA approves first gene therapies to treat patients with sickle cell disease. U.S. Food and Drug Administration. https://www.fda.gov/news-events/press-announcements/fda-approves-first-gene-therapies-treat-patients-sickle-cell-disease
2. FDA (2021). FDA approves drug to treat sickle cell disease in patients aged 4 up to 11 years. U.S. Food and Drug Administration. https://www.fda.gov/drugs/news-events-human-drugs/fdaapproves-drug-treat-sickle-cell-disease-patients-aged-4-11-years
3. FDA (2019). FDA approves first targeted therapy to treat patients with painful complication of sickle cell disease. U.S. Food and Drug Administration. https://www.fda.gov/newsevents/press-announcements/fda-approves-first-targeted-therapy-treat-patients-painful-complication-sickle-cell-disease

Ayomide D. Akinsooto is a medical student at the UT Health San Antonio Long School of Medicine, Class of 2026.

By Daniel A. Deane, MD
The links to the updated South Texas Asthma Coalition (STAC) Asthma Action Plan (AAP) and Provider Tip/Instruction Sheet and School Nurse information were provided by Mandie Alice Tibball Svatek, MD, Associate Professor, Pediatrics, Division of Inpatient Pediatrics, Joe R. and Teresa Lozano Long School of Medicine. Dr. Svatek is chair of STAC and Medical Director of SA KIDS BREATHE (SAKB).1 I have been on the SAKB Advisory Board and have followed SAKB and the STAC development over several years. Her leadership, along with diverse input from many sectors of the local, state and national pediatric healthcare community and Metro Health, has provided a free resource, SA KIDS BREATHE. SAKB allows Primary Care Physicians, allergists or pulmonologists to improve their outpatient management of children with Difficult-to-Control or Not-Well-Controlled Asthma. Every family of an asthmatic child must have an Asthma Action Plan, as well as every caretaker outside the family and the school nurse. Unfortunately, only 24 percent of students with asthma have a plan to deal with an emergency.2 The Asthma Action Plan is an emergency action plan for all caretakers. The STAC Asthma Action Plan should facilitate implementation in the school.
“The STAC AAP was approved for all San Antonio area school districts back in 2009 with extensive outreach provided to PCPs and school nurses. The 2024 STAC AAP has now been updated to incorporate the 2020 NHLBI 2020 Focused Updates to the Asthma Management Guidelines | NHLBI, NIH3 and GINA Asthma SMART guidelines 2024 GINA Main Report — Global Initiative for Asthma.4 The STAC Asthma Action Plan can be uploaded for use on the SAKB website,” said Dr. Svatek.
Provider Tip/Instruction sheet: There is an instruction sheet for the provider to review before filling out that explains the modifications that have been made to the STAC AAP.5
For School Nurses: There is a flyer that you can use to print and give to a child if they need the STAC AAP (noted under AAP Flyer) from their doctor. We ask that you please print this and give this to a child
that you think needs the STAC AAP. The QR code is included on the flyer — a quick and easy way for the doctor to access the website where the STAC AAP is housed. *Spanish version pending.
On average, 150 children die yearly from asthma in the U.S.6 On average, 10 children die of asthma in Texas.7 These deaths are preventable. As a Pediatric Pulmonologist, no child should die from asthma. It is important to understand the SAKB referral guidelines. Referral requires at least one of these five criteria. Subspecialty referral should be considered as well. These children should be considered at risk for a life-threatening asthma exacerbation when compared to the EPR3 risk factors, indicated in parentheses below. See the Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma, EPR3.8
• One hospitalization in the past year (Two or more hospitalizations in the past year per EPR3 page 377, Figure 5-2a. Risk Factors for Death from Asthma)
• Two or more emergency, urgent care or acute care visits in the past year, virtual or in-person (Three or more ED visits per EPR3 page 377, Figure 5-2a. Risk Factors for Death from Asthma)
• Two or more documented steroid bursts within the past year — not-well-controlled8
• Two or more unscheduled school treatments in the past week — not-well-controlled8
• Missing 10 percent or more of school days in the past year (asthma one of the leading causes of school absenteeism).9
The EPR3 states: “patients who had ≥2 exacerbations requiring oral systemic corticosteroids in the past year may be considered the same as patients who have not-well-controlled asthma, even in the absence of impairment levels consistent with not-well-controlled asthma.” (EPR3 page 345.) “44.0% of children with current asthma had uncontrolled asthma. The percentage with uncontrolled asthma was higher among boys (49.9%) than among girls (36.2%) (sex at birth).”10
STAC provides the evidence-based pediatric asthma therapeutics. SAKB implements this expertise with in-home asthma education for the at-risk asthmatic child.
STAC will be conducting extensive outreach in 2024 to clinics and hospitals about the updated 2024 AAP. Mandie Tibball Svatek, MD, Chair of STAC, is happy to receive your feedback on the AAP or answer any questions. She can be reached through SA KIDS BREATHE.

Daniel A. Deane, MD, graduated from LSU Medical School in 1980 with a pediatric residency in Charity Hospital in New Orleans. He is board certified in Pediatrics, Pediatric Critical Care and Pediatric Pulmonary Medicine, and was a Pediatric Pulmonologist at the Medical College of Georgia (Augusta), Texas Children’s Hospital (Houston), Cleveland Clinic, Christus Children’s Hospital (San Antonio) and private practice, among others. Dr. Deane retired in 2016 after 36 years in Pediatric Medicine. He is a member of the Bexar County Medical Society.
References:
1. SA KIDS BREATHE. www.sanantonio.gov/Health/HealthServices/Asthma
2. Individual Medical Emergencies Occurring at School, Policy Statement AAP. https://publications.aap.org/pediatrics/article/150/1/e2022057987/188345/Individual-Medical-Emergencies-Occurring-at-School?autologincheck=redirected
3. 2020 Focused Updates to the Asthma Management Guidelines | NHLBI, NIH. https://www.nhlbi.nih.gov/health-topics/asthma-management-guidelines-2020-updates
4. 2024 GINA Main Report - Global Initiative for Asthma. https:// ginasthma.org/2024-report/
5. Guide to Using the AAP Form. https://www.sanantonio.gov/ portals/0/files/health/healthservices/asthma/AAP-Guide. pdf?ver=2024-05-10
6. Asthma Quick-Look – The National Center for Fatality Review and Prevention. https://ncfrp.org/center-resources/quick-looks/ asthma-quick-look/
7. https://www.dshs.texas.giv/asthma
8. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma | US EPA. https://www.epa.gov/asthma/ expert-panel-report-3-guidelines-diagnosis-and-management-asthma
9. Asthma | Healthy Schools | CDC. https://www.cdc.gov/healthyschools/asthma/index.htm
10. Uncontrolled Asthma Among Children With Current Asthma, 2018–2020 | CDC Archive. https://archive.cdc.gov/#/ details?url=https://www.cdc.gov/asthma_stats/uncontrolled-asthma-children-2018-2020.htm
By Blair Ortmann, CFRE

In Bexar County, Child Advocates San Antonio (CASA) has profoundly impacted the healthcare outcomes for children in foster care. By providing targeted medical advocacy, CASA ensures that these vulnerable children access the essential services they need, significantly reducing long-term health issues and associated costs.
Children in foster care encounter unique challenges, especially in accessing consistent and comprehensive healthcare. CASA offers a proactive approach to these challenges, ensuring these children receive the medical attention they need, which supports healthier developmental outcomes.
The primary reasons for child removal in Bexar County include neglectful supervision and, increasingly, sexual abuse, with the highest incidence among children under three years old. The need for consistent medical care is thus critical. CASA advocates work to ensure that children in foster care maintain continuity of care amidst frequent relocations. By reviewing medical records quarterly and coordinating with healthcare providers, CASA advocates uphold the health needs of these children, ensuring routine check-ups and specialized services are timely and effective.
Through CASA’s advocacy, 95.3 percent of children in foster care promptly receive the necessary health services, a critical factor in preventing the escalation of mental health issues like PTSD, depression and anxiety. This approach not only aids in the immediate well-being of the children, but also presents substantial economic benefits. For every child who receives the services they need, CASA saves the community $5,917, based on cost avoidance from escalating health issues.
In August 2023, CASA, in collaboration with Jewish Family Services and Thru Project, launched the Project Launch pilot program. This initiative focuses on providing consistent mental health therapy to children in foster care who are likely to age out of the system. By addressing this significant gap, Project Launch ensures these youths have access to stable mental health support, which is crucial for their successful transition out of foster care.
The initiatives led by CASA in Bexar County represent a successful model of integrated medical advocacy within the foster care system. The measurable improvements in healthcare access and outcomes highlight the effectiveness of CASA’s approach. These efforts not only enhance the immediate health of children in foster care, but also contribute to broader community health and economic stability.
Beyond medical advocacy, CASA plays a crucial role in ensuring the overall well-being of children in foster care. This includes educational support, emotional development, and preparation for independent living. Each advocate is trained to address the multifaceted needs of these children, providing a stable and supportive presence in their lives.
The Bexar County medical community plays a pivotal role in the success of CASA’s programs. Pediatricians, mental health professionals and specialists contribute by providing expert care and by participating in CASA’s training programs. This collaboration enhances the quality of care provided to children in foster care and ensures that medical practitioners understand the unique challenges these children face.
CASA’s integrated advocacy approach has established a robust support system for children experiencing foster care in Bexar County, demonstrating significant improvements in healthcare access and quality of life. The community’s involvement and support are vital in continuing this positive trajectory.
For those interested in making a profound difference in a child’s life, becoming a CASA advocate is a powerful and rewarding way to contribute to the community. Visit www.casa-satx.org to learn more about how you can get involved and help continue the mission of providing essential support to children experiencing foster care in Bexar County.
Blair Ortmann, CFRE, is the VP of Mission Advancement for Child Advocates San Antonio, which recruits, develops and leads court-appointed volunteer advocates who provide support for children and youth who have experienced abuse and neglect.
Courtesy of Eleos
San Antonio’s healthcare sector is at a tipping point. Provider burnout and staff shortages are intensifying, threatening the quality of care for the city’s diverse and growing population. Yet, amidst this crisis, there is a beacon of hope: Eleos Virtual Healthcare Solutions.
Imagine nearly half of all healthcare providers in Bexar County feeling emotionally exhausted, depersonalized and unaccomplished. It’s a grim reality that leads to more errors, dissatisfied patients and a higher turnover rate among providers. The COVID-19 pandemic has only worsened this situation, pushing an already strained workforce to its limits.
The numbers are stark: Texas saw a 16 percent increase in its patient population from 2010 to 2023, yet nearly 25 percent of healthcare jobs remain unfilled. Texas also boasts one of the highest provider burnout rates in the country at 49 percent. This shortage means longer wait times for patients, reduced access to care and, ultimately, poorer health outcomes.
Eleos Virtual Healthcare Solutions steps in as a game-changer. With a team of highly trained, qualified and educated Virtual Healthcare Associates, Eleos handles essential non-patient-touching tasks remotely. From front and back-office duties to Revenue Cycle Management (RCM), administrative medical assistance, value-based care measures and comprehensive physician scribe support, Eleos covers it all. This partnership allows healthcare facilities to fill hard-to-find, high-turnover positions, streamline workflows, and boost efficiency — all while costing less than hiring regular full-time employees. Though Eleos offers ready-made solutions in their current product line, they also create customized solutions catering to the individual needs of their clients whenever possible.
By integrating seamlessly with HR teams, Eleos brings bilingual physicians from Honduras to collaborate with San Antonio-based doctors in real-time, handling chart preparation, live documentation and workflow enhancement. This collaboration frees up two to three hours daily for providers, reducing burnout, enhancing patient care, and promoting a healthier work-life balance. This newfound efficiency also translates into increased revenue for healthcare facilities. Additionally, their ability to tailor services to the specific workflows and needs of each facility ensures that every client receives the precise support they require to maximize operational efficiency.
Eleos focuses on building workforce resilience. Their virtual support and efficient staffing solutions distribute workloads more evenly, mitigating burnout risks and fostering a supportive and sustainable work environment. Providers can now focus on what they do best: delivering high-quality patient care without the overwhelming administrative burden.
Real-World Scenario: Dr. David Johnson’s Transformation with Eleos
Picture Dr. David Johnson, a dedicated family physician in San Antonio, who had always been passionate about patient care. However, the relentless administrative tasks began to take a toll on him. Working late into the night to complete chart notes and struggling to keep up with the demands of his growing practice, Dr. Johnson felt burnout creeping in. The joy he once found in his work was overshadowed by the never-ending paperwork and the stress of not having enough hours in the day.
When Dr. Johnson was introduced to Eleos Virtual Healthcare Solutions, he was skeptical but willing to try anything to reclaim his work-life balance. Eleos paired him with a Virtual Clinical Optimizer, a highly trained physician in Honduras who completed his chart prep in advance and managed live documentation during patient visits. This increased efficiency allowed Dr. Johnson to close his chart notes faster, giving him a sense of accomplishment at the end of each day. His patients noticed the difference, too; with more time and energy to focus on them, the quality of care improved, leading to higher patient satisfaction scores. The transformation was nothing short of revolutionary for him.
Eleos didn’t just help Dr. Johnson; it helped his entire clinic retain one of their most valuable assets — a passionate and dedicated physician who was once on the brink of burnout. By providing the support he needed, Eleos enabled Dr. Johnson to rediscover his love for medicine and continue serving his community with renewed vigor.
In conclusion, while the challenges of provider burnout and staff shortages in San Antonio are daunting, they are not insurmountable. Eleos Virtual Healthcare Solutions offers innovative, practical solutions that promise a more resilient and efficient healthcare system. By partnering with Eleos, healthcare organizations can secure the qualified staff they need, ensuring the well-being of both providers and patients. Eleos is ready to transform San Antonio’s healthcare landscape, one partnership at a time.

choice.
www.eleosvhs.com
Virtual
Solutions is a Silver Member of the BCMS Circle of Friends program.
(Note: Dr. David Johnson is a fictional character created to illustrate the positive impact of Eleos on reducing provider burnout).
Courtesy of Baptist Health System
Westover Hills Baptist Hospital officially opened on July 30 to serve the fast-growing community and those in far west San Antonio and beyond. With more than 500,000 residents and the largest school district (Northside ISD) in San Antonio, Westover Hills experiences a growth rate six times the national average. With an investment of more than $300 million, Baptist Health System saw and answered the community’s need for hospital care and programs specifically tailored to the Westover Hills community. The hospital’s first patient was an ED visit on day one, and the first baby born at the hospital came a few days later on August 1.
Brady Phillips is the Westover Hills Baptist Hospital CEO. “As a hospital system, we are committed to the health and well-being of our patients and the communities we serve,” Phillips said. “Hospitals are anchors in the community and we are especially proud that not only are we bringing advanced healthcare to the residents here, we are incredibly proud of the team of caregivers we have assembled for this community. Our physicians, nurses, techs and ancillary staff are all dedicated to providing high quality, compassionate care and a great experience for every patient who walks through our doors.”
At more than 350,000 square feet and sitting on 72 acres, the five-story hospital offers emergency and cardiac care, maternity and a surgical services, imaging, lab and vital inpatient services. The hospital opened with 92 beds and additional floors set for rapid expansion if needed to serve the growing community. The hospital features a spacious Emergency Department with separate entrances for walk-ins and ambulances, modern procedure suites and surgical technology, six large operating rooms, two cardiac cath labs, two C-section suites, fully private pre- and post-surgical rooms, advanced minimally invasive robotic surgery equipment to support general surgery, urology, gynecology and orthopedics, and a dedicated women services floor with more than 50,000 square feet of floor space for women's and infants’ healthcare needs. A 90,000-square-foot medical office building, adjacent to the hospital, brings physician offices and a variety of healthcare services for Westover Hills and surrounding areas. The economic impact of the new hospital in Westover Hills included 700 jobs during construction and more than 500 permanent jobs at opening.
Matt Stone, group CEO for Baptist Health System, is a native San Antonian who is passionate about ensuring the health and well-being of all residents throughout the city. “Baptist Health System has been caring for San Antonio for 121 years. We are thrilled that the Westover Hills community now has access to the same, high quality, compassionate care our system delivers at all of our hospitals across San Antonio and the surrounding area,” Stone said.
Much thought and planning has gone into the common spaces and outdoor environment around the hospital. The hospital courtyard is designed to connect visitors, patients and the community to a walking trail and a peaceful pond. Hospital leaders ensured native trees on the property were preserved and incorporated into the design and landscape of the multi-acre public space between the hospital and the medical office building.
“Paths from inside the hospital lead visitors, patients and staff into a tranquil courtyard,” Phillips said. “This will be our ‘Central Park’ where
employees can also benefit from enjoying the greenery and trees from the time they arrive at work and park in the parking lot, to the time they enter the building, and throughout their entire day. It’s a beautiful place where they can take breaks between their busy shifts,” he added.
Hospital leadership thoughtfully worked to preserve and enhance existing native trees and green spaces around the facility. Research studies have shown that exposure to hospital green spaces has been associated with a range of positive health outcomes, including improved mental health, reduced anxiety, improved blood pressure, and faster recovery from illness or surgery. (Source: National Institutes of Health).
Westover Hills Baptist Hospital is proud to continue contributing to the well-being of San Antonio by bringing our Community Built on Care, professional careers, community service partnerships and many new vital resources for the far west side community it will serve.
Westover Hills Baptist Hospital is the seventh Baptist Health System acute care hospital, the others being Baptist Medical Center downtown, Mission Trail Baptist on the south side, North Central Baptist Hospital in Stone Oak, Northeast Baptist Hospital on the city’s northeast side, St. Luke’s Baptist Hospital in the Medical Center, and Resolute Baptist Hospital in New Braunfels.
The hospital is located at the corner of Wiseman Boulevard and Highway 1604 (3011 W. Loop 1604 N. San Antonio, Texas 78251), in the heart of the Westover Hills community.
For more information, go to: http://www.baptisthealthsystem. com/westoverhills



We encourage you to use our friends of medicine businesses whenever you or your practice need supplies or services.

Sol Schwartz & Associates P.C. (HHH Gold Sponsor)
Sol Schwartz & Associates is the premier accounting firm for San Antonio-area medical practices and specializes in helping physicians and their management teams maximize their financial effectiveness.
Christopher Davis, CPA 210-384-8000, ext. 118 CDavis@ssacpa.com www.ssacpa.com
“Dedicated to working with physicians and physician groups.”

Aspect Wealth Management (★★★ Gold Sponsor)
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Michael Clark President
210-268-1520
MClark@aspectwealth.com www.aspectwealth.com
“Your wealth. . .All aspects”

Broadway Bank
(HHH Gold Sponsor)
Healthcare banking experts with a private banking team committed to supporting the medical community.
Thomas M. Duran
SVP, Private Banking Team Lead 210-283-6640
TDuran@Broadway.Bank www.broadwaybank.com
“We’re here for good.”
Texas Partners Banks (HHH Gold Sponsor)
Our private banking team specializes in healthcare banking and will work with you to craft and seamlessly integrate financial solutions for you and your practice, including practice loans, lines
of credit and custom local lockbox solutions headquartered in San Antonio. Maria Breen 210-807-5562
Maria.Breen@texaspartners.bank www.texaspartners.bank

Lone Star National Bank (HHH Gold Sponsor)
Established in 1983, Lone Star National Bank has provided banking services to communities in South Texas for the past 41 years. LSNB is an independent and locally owned bank subsidiary of Lone Star National Bancshares-Texas, Inc with consolidated assets of $3 billion (12/31/23) and 36 full-service banking centers throughout Starr, Hidalgo, Cameron and Bexar counties. Aside from personal and business banking, LSNB offers investments, wealth management & trust along with property and casualty insurance, health insurance and supplemental coverage.
Summer L. Reyes Banking Officer 210-479-4716
ReyesS@lonestartnationalbank.com
Ivan Corona Molina
Assistant VP 210-479-4713
MolinaI@lonestartnationalbank.com www.lonestarnationalbank.com
“We do what the Little Banks can’t, and the Big Banks won’t!”
Amegy Bank of Texas (HH Silver Sponsor)
We believe that any great relationship starts with five core values: Attention, Accountability, Appreciation, Adaptability and Attainability. We work hard and together with our clients to accomplish great things.
Robert Lindley
SVP | Private Banking Team Lead 210-343-4526
Robert.Lindley@amegybank.com
Denise Smith
Vice President | Private Banking 210-343-4502
Denise.C.Smith@amegybank.com
Scott Gonzales
Assistant Vice President | Private Banking 210-343-4494
Scott.Gonzales@amegybank.com www.amegybank.com
“Community banking partnership”
Synergy Federal Credit Union (HH Silver Sponsor)
Looking for low loan rates for mortgages and vehicles? We've got them for you. We provide a full suite of digital and traditional financial products, designed to help physicians get the banking services they need.
Synergy FCU Member Services 210-750-8333
info@synergyfcu.org www.synergyfcu.org
“Once a member, always a member. Join today!”

Genics Laboratories (HHH Gold Sponsor)
Genics Laboratories offers accurate, comprehensive and reliable results to our partners and patients. Genics Laboratories is committed to continuous research, ensuring our protocols are always at the peak of current technology.
Yulia Leontieva
Managing Partner, Physician Liaison 210-503-0003
Yulia@genicslabs.com
Kevin Setanyan Managing Partner 210-503-0003
Kevin@genicslabs.com
Artyom Vardapetyan Managing Partner 210-503-0003
www.genicslabs.com
“Accurate results in record time.”
Livingston Med Lab (HH Silver Sponsor)
High Complexity Clia/Cola accredited Laboratory providing White Glove Customer Service. We offer a Full Diagnostic Test Menu in the fields of Hematology, Chemistry, Endocrinology, Toxicology, Infectious Disease and Genetics.
Robert Castaneda CEO 210-316-1792
Robert@livingstonmedlab.com www.livingstonmedlab.com/home
“Trusted Innovative, Accurate and STAT Medical Diagnostics”

American Health Imaging (★★★ Gold Sponsor)
American Health Imaging (AHI) has 5 state-of-the-art imaging centers in San Antonio, TX with industry- boardcertified subspecialized radiologists delivering precise, reliable results. Easy scheduling and prompt report turnaround times, serving both physicians and their patients. Imaging at AHI is priced up to 60% less than hospitals and in-network with 99% of health plans with competitive rates to save patients money. AHI has an additional 37 best-in-class diagnostic imaging facilities in Alabama, Florida, Georgia, Texas and South Carolina.

US Radiology Physician Number 210-572-1211
Casey Allen
Regional Sales Director | San Antonio US Radiology Specialists 210-846-0606
Casey.Allen@usradiology.com
Jasmine Mendoza
Jasmine.Mendoza@usradiology.com
Jaime Zamora
Jaime.Zamora@usradiology.com
Sydnie Caradec
Sydnie.Caradec@usradiology.com
Sarah McMindes
Sarah.Mcmindes@usradiology.com
Scott Roberson
Scott.Roberson@usradiology.com
Ryan Denman
Ryan.Denman@usradiology.com
www.americanhealthimaging.com (main site)
www.americanhealthimaging.com/ physician-resources/ (Physician Resources to refer to American Health Imaging)

Bexar Credentials Verification, Inc. (HHHH 10K Platinum Sponsor)
Bexar Credentials Verification Inc. provides primary source verification of credentials data that meets The Joint Commission (TJC) and the National Committee for Quality Assurance (NCQA) standards for healthcare entities.
Betty Fernandez Director of Operations 210-582-6355
Betty.Fernandez@bexarcv.com www.bexarcv.com
“Proudly serving the medical community since 1998”

Oakwell Private Wealth Management (HHH Gold Sponsor)
Oakwell Private Wealth Management is an independent financial advisory firm with a proven track record of providing tailored financial planning and wealth management services to those within the medical community.
Brian T. Boswell, CFP® , QKA
Senior Private Wealth Advisor 512-649-8113 Service@oakwellpwm.com www.oakwellpwm.com
“More Than Just Your Advisor, We're Your Wealth Management Partner”
Elizabeth Olney with Edward Jones (HH Silver Sponsor)
We learn your individual needs so we can develop a strategy to help you achieve your financial goals. Join the nearly 7 million investors who know. Contact me to develop an investment strategy that makes sense for you.
Elizabeth Olney Financial Advisor 210-858-5880
Elizabeth.Olney@edwardjones.com www.edwardjones.com/elizabeth-olney "Making Sense of Investing"
Aspect Wealth Management (HHH Gold Sponsor)
We believe wealth is more than money, which is why we improve and simplify the lives of our clients, granting them greater satisfaction, confidence and freedom to achieve more in life.
Michael Clark President 210-268-1520
MClark@aspectwealth.com www.aspectwealth.com
“Your wealth. . .All aspects”

Hancock Whitney (HHH Gold Sponsor)
Since the late 1800s, Hancock Whitney has embodied core values of Honor & Integrity, Strength & Stability, Commitment to Service, Teamwork and Personal Responsibility. Hancock Whitney offices and financial centers in Mississippi, Alabama, Florida, Louisiana and Texas offer comprehensive financial products and services, including traditional and online banking; commercial, treasury management, and small business banking; private banking; trust; healthcare banking; and mortgage services. www.hancockwhitney.com
John Riquelme
San Antonio Market President 210-273-0989
John.Riquelme@hancockwhitney.com
Larry Anthis Corporate Banking, Relationship Manager 210-507-9646
Larry.Anthis@hancockwhitney.com
Serina Perez
San Antonio Business Banking 210-507-9636
Serina.Perez@hancockwhitney.com
Erik Carrington
Texas Regional Wealth Management Manager 713-543-4517
Erik.Carrington@hancockwhitney.com

UT Health San Antonio
MD Anderson Cancer Center (HHH Gold Sponsor)
UT Health provides our region with the most comprehensive care through expert, compassionate providers treating patients in more than 140 medical specialties at locations throughout San Antonio and the Hill Country.
UT Health San Antonio Physicians
Regina Delgado Business Development Manager 210-450-3713
DelgadoR4@uthscsa.edu
UT Health San Antonio
MD Anderson Mays Cancer Center
Laura Kouba
Business Development Manager 210-265-7662
NorrisKouba@uthscsa.edu https://uthscsa.edu/
Appointments: 210-450-1000
UT Health San Antonio 7979 Wurzbach Road San Antonio, TX 78229
Healthcare Administration Consultants
(HH Silver Sponsor)
Our mission is to help healthcare organizations small or large to achieve sustainable growth and success by providing them with expert healthcare administration consulting services.
We focus on key factors such as: revenue, supply chain visibility, and aligning operations to save time so that your team can focus on improving the patient’s health and well-being. We transform patient care outcomes and employee working experiences while driving brand and revenue growth.
Dr. Reshma Beherry, DHA
Doctor of Healthcare Administration 210-602-6905
RB@administrative-consultants.com https://administrative-consultants.com/
SERVICES

Equality Health
(HHH Gold Sponsor)
Equality Health deploys a wholeperson care model that helps independent practices adopt and
deliver value-based care for diverse communities. Our model offers technology, care coordination and hands-on support to optimize practice performance for Medicaid patients in Texas.
Cristian Leos
Network Development Manager 210-608-4205
CLeos@equalityhealth.com www.equalityhealth.com
“Reimagining the New Frontier of Value-Based Care.”
(H Bronze Sponsor)
We were founded to meet a need: helping business owners succeed by giving them simple, quality, affordable U.S.-based contact solutions. In only a few years, our focus on nurturing client relations and building trust not only helped our customers grow their businesses, but helped us stake our claim in the highly competitive TAS industry as one of the most well-regarded and referred. Our 50 years of collective experience are the driving force behind our clients’ satisfaction.
Rachel Caero Managing Partner
844-554-3473
Rachel@dialops.net
Insperity
(HH Silver Sponsor)
Insperity’s HR solutions offer premium service and technology to facilitate growth by streamlining processes related to payroll, benefits, talent management and HR compliance. We provide the tools to help you lighten your administrative load, maximize productivity and manage risks – so you can focus on growth.
Fran Yacovone Business Performance Advisor 210-558-2507
Fran.Yacovone@insperity.com
Dayton Parker Business Performance Advisor 210-558-2517
Dayton.Parker@insperity.com www.insperity.com
“Insperity’s mission is to help businesses succeed so communities prosper”

(HHHH 10K Platinum Sponsor)
TMA Insurance Trust is a full-service
insurance agency offering a full line of products – some with exclusive member discounts and staffed by
professional advisors with years of experience. Call today for a complimentary insurance review. It will be our privilege to serve you.
Wendell England Director of Member Benefits 512-370-1746
Wendell.England@tmait.org 800-880-8181
www.tmait.org
“We offer BCMS members a free insurance portfolio review.”

Texas Medical Liability Trust (HHHH 10K Platinum Sponsor)
With more than 20,000 healthcare professionals in its care, Texas Medical Liability Trust (TMLT) provides malpractice insurance and related products to physicians. Our purpose is to make a positive impact on the quality of healthcare for patients by educating, protecting and defending physicians.
Patty Spann Director of Sales and Business Development 512-425-5932
Patty-Spann@tmlt.org
www.tmlt.org
“Recommended partner of the Bexar County Medical Society”

The Bank of San Antonio Insurance Group, Inc.
(HHH Gold Sponsor)
We specialize in insurance and banking products for physician groups and individual physicians. Our local insurance professionals are some of the few agents in the state who specialize in medical malpractice and all lines of insurance for the medical community.
Katy Brooks, CIC 210-807-5593
Katy.Brooks@bosainsurance.com www.thebankofsa.com
“Serving the medical community.”
MedPro Group
(HH Silver Sponsor)
Rated A++ by A.M. Best, MedPro Group has been offering customized insurance, claims and risk solutions to the healthcare community since 1899. Visit MedPro to learn more.
Kirsten Baze, RPLU, ARM
AVP Market Manager, SW Division 512-658-0262
Fax: 844-293-6355
Kirsten.Baze@medpro.com www.medpro.com

LASO Health Telemedicine and Rx App (HHH Silver Sponsor)
LASO Health is the industry’s only solution that makes healthcare services accessible, cost-transparent and convenient. Its mission is to reinvent “healthcare” in the United States by empowering every individual and employer, insured or uninsured to have easy, timely, predictable, cost-effective care. LASO combines an intuitive, mobile superapp with a marketplace of virtual and in-person health services to give customers a one-touch, onestop-shop, comprehensive health solution.
Ruby Garza, MBA 210-212-2622
RGarza@texaskidneycare.com www.lasohealth.com

Parvis Medical Suites
(HHHH 10K Platinum Sponsor)
Parvus Medical Suites offers a new way to start your own private clinical practice, either full-time or part-time, at a much lower cost than a traditional clinic. We take care of providing well-qualified employees, so that you can focus solely on delivering high-quality patient care. Our turn-key practice spaces in San Antonio and New Braunfels are available for short- and long-term lease options, and come complete with all amenities. Micropractice medicine is revolutionizing independent clinical care.
John Rodriguez, MD Chief Medical Officer 210-632-3411
DrJohn@parvussuites.com www.parvussuites.com
Henry Schein Medical (HH Silver Sponsor)
From alcohol pads and bandages to EKGs and ultrasounds, we are the largest worldwide distributor of medical supplies, equipment, vaccines and pharmaceuticals serving office-based practitioners in 20 countries. Recognized as one of the world’s most ethical companies by Ethisphere.
Tom Rosol
Field Sales Consultant 210-413-8079
Tom.Rosol@henryschein.com www.henryschein.com
“BCMS members receive GPO discounts of 15 to 50 percent.”

Equality Health (HHH Gold Sponsor)
Equality Health deploys a wholeperson care model that helps independent practices adopt and deliver value-based care for diverse communities. Our model offers technology, care coordination, and hands-on support to optimize practice performance for Medicaid patients in Texas.
Darby Rodriguez Regional Client Executive 281-753-3565
D.Rodriguez@eleosvhs.com www.equalityhealth.com “Reimagining the New Frontier of Value-Based Care.”
Healthcare Leaders of San Antonio (HH Silver Sponsor)
We are dedicated to nurturing business connections and professional relationships, exchanging knowledge to enhance leadership, and creating career opportunities for healthcare and other industry leaders in a supportive community.
David Neathery President 210-797-8412
HealthcareLeadersSA@gmail.com
Gary Meyn, LFACHE
Vice President 210-912-0120
GMeyn@vestedbb.com https://healthcareleaderssa.com/ “Come, Learn, Connect!”
The Health Cell (HH Silver Sponsor) “Our Focus is People” Our mission is to support the people who propel the healthcare and bioscience industry in San Antonio. Industry, academia, military, nonprofit, R&D, healthcare delivery, professional services and more!
Kevin Barber President 210-308-7907 (Direct)
KBarber@bdo.com
Valerie Rogler Program Coordinator 210-904-5404
Valerie@thehealthcell.org www.thehealthcell.org
“Where San Antonio’s Healthcare Leaders Meet”
San Antonio Medical Group Management Association (SAMGMA) (HH Silver Sponsor)
SAMGMA is a professional nonprofit association with a mission to provide educational programs and networking opportunities to medical practice managers and support charitable fundraising.
Jeannine Ruffner President info4@samgma.org www.samgma.org
Oakwell Private Wealth Management (HHH Gold Sponsor)
Oakwell Private Wealth Management is an independent financial advisory firm with a proven track record of providing tailored financial planning and wealth management services to those within the medical community.
Brian T. Boswell, CFP® QKA Senior Private Wealth Advisor 512-649-8113 Service@oakwellpwm.com www.oakwellpwm.com
“More Than Just Your Advisor, We’re Your Wealth Management Partner”

Favorite Healthcare Staffing (HHHH 10K Platinum Sponsor)
Serving the Texas healthcare community since 1981, Favorite Healthcare Staffing is proud to be the exclusive provider of staffing services for the BCMS. In addition to traditional staffing solutions, Favorite offers a comprehensive range of staffing services to help members improve cost control, increase efficiency and protect their revenue cycle.
Mike DeQuattro
Director of Operations - Texas & New Mexico 210-918-8737
Mike.DeQuattro@favoritestaffing.com
“Favorite Healthcare Staffing offers preferred pricing for BCMS members.”
Eleos Virtual Healthcare Solutions (HH Silver Sponsor)
Empowering physicians for a Balanced Future. Our virtual health associates alleviate administrative burdens in the evolving healthcare landscape, combatting burnout. Join us in transforming healthcare delivery, prioritizing your wellbeing and patient care.
Chris Stansbury SVP Growth 816-309-9991
CStansbury@eleosvhs.com www.eleosvhs.com


"The Lexus GX550 is a true testament to Lexus' commitment to luxury, performance and off-road capability. It's a versatile SUV that effortlessly transitions from city streets to rugged trails, while providing unparalleled comfort and refinement for its drivers and passengers. The new GX is in very high demand and we at North Park Lexus are proud to offer this exceptional vehicle to our loyal and new customers."
— Jose Contreras,
Vice President/General Manager of North Park Lexus
North Park Lexus San Antonio and Dominion are thrilled to introduce the all-new 2024 Lexus GX550, a vehicle that embodies the perfect fusion of luxurious comfort and unparalleled off-road capability. This comprehensive redesign marks a new era for the GX series, boasting an array of cutting-edge features and a striking aesthetic that commands attention.
The 2024 GX550 makes an immediate statement with its bold, boxy exterior, a deliberate departure from its predecessor. Its sculpted lines, wider stance and aggressive grille exude confidence and hint at the vehicle’s off-road prowess. The available 18-inch wheels and all-terrain tires further enhance its rugged appeal.
Inside, the GX550’s cabin is a sanctuary of modern luxury. Premium materials, meticulous craftsmanship and thoughtful design elements create an inviting atmosphere for both driver and passengers. The spacious interior comfortably accommodates up to seven occupants (luxury plus edition), with ample legroom and headroom for all.
The GX550 is equipped with the latest in Lexus technology, designed to elevate both comfort and convenience. The standard 14-inch touchscreen infotainment system serves as the command center, offering intuitive access to navigation, entertainment and vehicle settings.
For audiophiles, the available Mark Levinson® Premium Surround Sound system delivers an immersive audio experience, while the stan-
dard Lexus Safety System+ 3.0 suite of advanced safety features provides peace of mind on and off the road.
Under the hood, the 2024 GX550 is powered by a robust 3.4-liter twin-turbocharged V6 engine, delivering an impressive 349 horsepower and 479 lb.-ft. of torque. This powertrain, paired with a 10-speed Direct-Shift automatic transmission, ensures smooth acceleration and effortless highway cruising.
For off-road enthusiasts, the GX550 offers a full-time four-wheel drive system with a Torsen® limited-slip center differential and a twospeed transfer case. This combination, along with the available Crawl Control and Multi-Terrain Select systems, allows the GX550 to conquer even the most challenging terrain with confidence.
The 2024 Lexus GX550 represents a bold step forward for the Lexus brand, blending refined luxury with rugged capability in a way that few vehicles can match. Whether navigating city streets or venturing off the beaten path, the GX550 is poised to deliver an exceptional driving experience.
North Park Lexus invites you to experience the all-new 2024 Lexus GX550 firsthand. Visit our San Antonio or Dominion locations to explore this remarkable vehicle and discover why it’s the perfect choice for your next adventure.







11911 IH 10 West San Antonio, TX 78230
Coby Allen 210-696-2232
Northside Honda
9100 San Pedro Ave. San Antonio, TX 78216
Jaime Anteola 210-744-6198
Kahlig Auto Group
Audi Dominion 21105 West IH 10 San Antonio, TX 78257
Anthony Garcia 210-681-3399
14610 IH 10 West San Antonio, TX 78249
Tim Rivers 832-428-9507
Northside Chevrolet 9400 San Pedro Ave. San Antonio, TX 78216
Domingo Saenz 210-341-3311
Land Rover San Antonio 13660 IH 10 West San Antonio, TX
Cameron Tang 210-561-4900
North Park Lincoln 9207 San Pedro San Antonio, TX
Sandy Small 210-341-8841
North Park Subaru at Dominion 21415 IH 10 West San Antonio, TX 78257
Phil Larson
877-356-0476
Mercedes Benz of Boerne 31445 IH 10 West Boerne, TX
James Godkin 830-981-6000
Mercedes Benz of San Antonio 9600 San Pedro San Antonio, TX
Chris Martinez 210-366-9600
Auto Group
Bluebonnet Chrysler
Dodge Ram 547 S. Seguin Ave. New Braunfels, TX 78130
Matthew C. Fraser 830-606-3463
Northside Ford 12300 San Pedro San Antonio, TX
Marty Martinez 210-477-3472
North Park Lexus 611 Lockhill Selma San Antonio, TX
Jose Contreras 320-308-8900
North Park Lexus at Dominion 25131 IH 10 W Dominion San Antonio, TX
James Cole 210-816-6000
9455 IH 10 West San Antonio, TX 78230
Jordan Trevino 210-764-6945
North Park Subaru 9807 San Pedro San Antonio, TX 78216
Raymond Rangel 210-308-0200
Cavender Toyota 5730 NW Loop 410 San Antonio, TX
Spencer Herrera 210-581-0474
North Park Toyota 10703 Southwest Loop 410 San Antonio, TX 78211
Justin Boone 210-635-5000