Intraoral scanning techniques for full-arch implants
Dr. Christopher R. Resnik
Subperiosteal implants for the rehabilitation of atrophic posterior mandibular regions
Drs. Laurine Birault & Antoine Diss
Management of acute hemorrhage in the anterior maxillary region
Dr. Lanka Mahesh, et al.
The Nation’s Top Implant Practices will be
What if your Doctor, Treatment Coordinator, and Patient Advocate could spend two days in beautiful Orlando, Florida, mastering the best business and clinical strategies to acquire, close, and efficiently produce full-arch cases at scale?
At our Full-Arch Growth Conference, they’ll do just that.
Learn Advanced Strategies to Generate Full-Arch Leads
Quickly Prequalify & Triage Patients Who are Financially Unqualified
Implement Our 10-10-10™ Process to Dramatically Increase Closings
Master Negotiation & Close Price Shoppers Without Cutting Your Fees
Incorporate Digital Workflows to Increase Profits, Predictability, and Quality
Fall 2024 n Volume 17 Number 3
Editorial Advisors
Jeffrey Ganeles, DMD, FACD
Gregori M. Kurtzman, DDS
Jonathan Lack, DDS, CertPerio, FCDS
Samuel Lee, DDS, DMSc
David Little, DDS
Brian McGue, DDS
Ara Nazarian, DDS
Jay B. Reznick, DMD, MD
Steven Vorholt, DDS, FAAID, DABOI
Brian T. Young, DDS, MS
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD
Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
Latest technology benefits patients
From a very early age, I was taught to do my best to help others in any way I could. Sometimes it means doing more for those who have less. During my surgical residency in Chicago, I was frequently faced with this concept. Working in one of the busiest emergency departments in that city, my teammates and I treated emergencies of complex cases without cone beam scanners, reliable electronic medical records, or even digital X-rays. Today, these and countless other innovations in dentistry make it possible for dentists to provide comprehensive and sustainable care to a diverse patient base. Decades ago, we could not recognize the signs of oral cancer as readily as we can today — we intervened in such cases much later than the ideal timing required. That meant more resections and reconstruction, leaving long-term scars but no promise that the cancer would not return.
Today, my team and I are able to utilize the latest in dental technology to serve patients in three very different areas of my home state of New Hampshire. Whether it is the rural southwestern area of Peterborourgh, the state’s fourth-largest city of Concord, or the remote Upper Connecticut River Valley (adjacent to the state’s largest hospital), we provide care for patients representing every social and economic demographic. In a profession where there is heavy influence and marketing in every media, patients are often given confusing information about dental care. Implants, for example, are seen in the public as the most esthetically-pleasing solution, but cone beam and soft-tissue scanning may reveal that implants are not a medical or ideal option. However, our technology and patient relationships help us build treatment plans focused on patients’ long-term economic and medical needs.
Perhaps the biggest challenge to a constantly-evolving dental profession is the dental benefits provider. Labeled commonly as “dental insurance,” such programs are not the same as medical insurance — rather, they are simply limited funds to reimburse patients and dentists for dental procedures. Unfortunately, the disconnect between dental benefit companies and dentists often creates issues regarding treatment and confusion for patients. As an oral surgeon, this fact is particularly evident, when a scan reveals that a patient’s condition requires immediate course correction. In many cases, a lengthy preauthorization is required for reimbursement. Furthermore, as states like New Hampshire build their adult and children’s dental Medicaid programs, third-parties managing these benefits often lag far behind advancements, creating more disconnects.
Dentistry is a constant process of calibration, clinically and in business. Technology has made it easier to do more with less and more for those with less. However, as dentistry expands beyond the clinical setting to include widespread marketing and dental benefits, calibration is a more complex process. Nevertheless, dentists are not the types to shy away from a challenge, particularly when it concerns patient care.
MedMark, LLC 2024. All rights reserved. The publisher’s written consent must be obtained before any part of this publication may be reproduced in any form whatsoever, including photocopies and information retrieval systems. While every care has been taken in the preparation of this magazine, the publisher cannot be held responsible for the accuracy of the information printed herein,
including but not limited to: print and digital distribution by mail, email, and website for industry tradeshows, educational events, including nonpaid bulk copies and/or digital access provided to events, clients and educational institutions. ISSN number 2372-6245
Richard J. Rosato, DMD, attended Saint Anselm College in New Hampshire for undergraduate studies and graduated from Tufts University School of Dental Medicine. He then traveled to Chicago to the University of Illinois Medical Center, Cook County Hospital, Michael Reese Hospital, Mercy Hospital, and the West Side VA for his residency in oral and maxillofacial surgery. He was the New Hampshire Dental Society Council on Government Affairs Chair for 5 years before becoming president. He then served as chair of the American Dental Society Council on Ethics, Bylaws, and Judicial Affairs, the ADA board of trustees as compensation chair, ADA Business Enterprise Inc. as a board member, and a board member of the Innovation Advisory Committee.
Restoring
Cover image of Dr. Richard J. Rosato courtesy of Specialty1 Partners.
Drs. Lanka Mahesh, Gregori M. Kurtzman, Sagarika Shukla, and Zara Dhawan discuss
Dr. Christopher R. Resnik discusses some advances in intraoral scanning devices and acquisition technology
Subperiosteal implants for the rehabilitation of atrophic posterior mandibular regions: A bilateral case report Drs. Laurine Birault and Antoine Diss discuss an innovative concept in custom CAD/CAM implants ............................................24 SERVICE PROFILE
Building success in a competitive market ............................................... 30 SERVICE PROFILE
Why thousands of implant specialists have quietly partnered with IDSOs
Chip Fichtner discusses the benefits of a large silent partner 32
RECEIVE news and event updates in your inbox by registering for our eNewsletter CONNECT with us
“The culture stands out most to me. Egos don’t exist.
are all working together
Dr. Kate Quinlin
Periodontist partner in Chicago, IL
We’re proud to champion Dr. Quinlin and more than 300 elite dental specialists and practice teams in our growing network. Since 2018, we’ve been helping our partners focus on delivering exceptional patient care, while our business experts help lessen the weight of practice management. Find out how our powerhouse community of periodontists, endodontists, and oral and maxillofacial surgeons work together to champion your long-term success. Learn
“By
changing nothing, nothing changes.”
Change is hard — some days it feels like fate is not satisfied with any stable situation that makes us comfortable and secure. Sure, no one can dispute the serenity of “business as usual” in the midst of ever-changing world issues, politics, and everyday craziness. Instead of losing sleep or stomach lining over change, let’s consider the positive aspects of being open to expanding our comfort zones, living in the moment, and having a mindset of “faith over fear.” As the title quote from Tony Robbins suggests, you have to build up some momentum in order to actually get somewhere. Let’s hear from some successful and inspirational people on how change can bring positive movement to our lives.
Lisa Moler Founder/Publisher, MedMark Media
Neurologist and psychologist Viktor E. Frankl said, “When we are no longer able to change a situation, we are challenged to change ourselves.” Some people just need a bigger push to get moving. Taking the easy route and sticking with “the familiar” is only possible until the stress of the known outweighs the fear of the unknown. So, sticking with only the activities or mindsets that are within your safety zone will eventually leave you watching others who have the ambition and confidence to move forward. You don’t want to look around in a few years and see your friends and peers busy and fulfilled with new possibilities that can change your community or your world. There is a lot of competition out there, and being a pioneer or game changer may be a challenge at first, but will head off the future frustration of a stagnating life.
Actress Sarah Parish noted, “Living with fear stops us from taking risks, and if you don’t go out on the branch, you’re never going to get the best fruit.” Overcoming fear of making the wrong decision or failing can feel daunting. But, there are a lot of ways to build your confidence, such as talking to friends, mentors, experts, attending conferences, reading MedMark publications, and listening to those who bring you inspiration. There will be learning curves and maybe even some speed bumps, but most times, innovation will lead to new and exciting ways to grow.
Our fall issue is filled with innovation and information to create productive change. In our Cover Story, Dr. Richard J. Rosato talks about the promise and possibilities of implant dentistry and the wealth of resources for a well-oiled business operation that he has gained as a part of Specialty1 Partners. In our CE, Drs. Laurine Birault and Antoine Diss delve into how CBCTs, CAD/CAM, and patient-specific subperioteal implants bring a more minimally invasive solution to implant dentists, and also Dr. Christopher R. Resnik’s CE looks at full-arch implants and the important part played during treatment by intraoral scanning. Drs. Lanka Mahesh, Gregory M. Kurtzman, Sagarika Shukla, and Zara Dhawan write about how they controlled a hemorrhage during an implant procedure and how imaging technology can avoid this type of complication in the future.
World famous performer Robin Williams said, “No matter what people tell you, words and ideas can change the world.” Don’t leave your success to chance. Change your ideas into action. Innovation will create a happier you, family, and work life. When you embrace change, the benefits will spread throughout your world!
To your best success,
Lisa Moler
Published by
Publisher Lisa Moler lmoler@medmarkmedia.com
Managing Editor
Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com Tel: (623) 340-4373
Marketing & Digital Strategy Amzi Koury amzi@medmarkmedia.com
eMedia Coordinator
Michelle Britzius emedia@medmarkmedia.com
Social Media Manager Felicia Vaughn felicia@medmarkmedia.com
Digital Marketing & Sales Administrator Sharif Rod sharif@medmarkmedia.com
Website Support
Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC 15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260 Tel: (480) 621-8955
Toll-free: (866) 579-9496 www.medmarkmedia.com
www.implantpracticeus.com
Subscription Rate 1 year (4 issues) $149 https://implantpracticeus.com/subscribe/
Dr. Richard J. Rosato
Restoring faith, hope, and implants with the help of Specialty1
Tell us about yourself and your practice.
I am a native of New England, born in Revere, Massachusetts and later raised in the town of Danvers (both just outside of Boston). I graduated from St. Anselm College in New Hampshire, a small, liberal arts college that really imbued in me a sense of community as well as my critical analysis, public speaking, and listening skills (among others). I took the lessons learned from “St. A’s” to Tufts University School of Dental Medicine, which is located in Boston. After graduating from Tufts (where I met my wife, Laurie), I moved to another big city — Chicago — where I completed my residency in oral and maxillofacial surgery, before moving home to New England, first to Rhode Island and finally, the state in which Laurie and I have raised our three children, New Hampshire.
My practice, Capitol Center for Oral and Maxillofacial Surgery, PLLC, is an embodiment of my educational and personal journey. My team is my extended family — we are here for each other in good times and challenging times. Our three offices are there to help the community. The challenges of the pandemic and the workforce shortage have had a great impact on care utilization, causing appointment delays and other issues. Wherever my team and I can help patients — particularly during emergencies — we are ready, willing, and able to step up to lend a hand.
What originally attracted you to the implant specialty?
Dentistry is an integral part of medical art. It inspires great passion in those who practice it even in the most general arenas. But it also stimulates an interest in delving further into that art’s many dimensions. Implant dentistry is one such arena, one that utilizes cutting-edge technologies that were not available even in the last decade. In that regard, for an oral surgeon like me, the promise and possibility of implant dentistry is truly exciting. For me, my initial training in dentistry, coupled with my personal desire to provide care for those who may not otherwise be able to find help, led me to explore implant dentistry and oral surgery on the whole. Some of the patients we see in my practice are far beyond the need for a filled cavity or root canal — they need a full oral rehabilitation. A patient in this situation can become emotionally defeated, knowing that their road back to positive oral health could be a long one. Then again, when the patient sees how the latest in implant dentistry restored their smile and their health, their sense of faith and hope is also restored.
What is your biggest challenge as an implant specialist?
I operate practices in two rural areas (one of which is a dental health professional shortage area) of New Hampshire. The biggest challenge, therefore, is affordability. In New Hampshire, many of our underserved patients are also recovering from addiction, and their mouths are as ravaged as their income. They are aware of the great esthetic promise of implants. However, for many of them, the possibility of a fully restored smile through implants seems a distant reality.
I was taught at an early age that when you believe in something, you find a way to make it happen. I believe in helping my patients, so if implants are not presently affordable, a solution is needed. In New Hampshire — as is the case across the country — our first step has been to work with the state to identify the most vulnerable patients in need of implants. Over 2 decades, I worked with the New Hampshire legislature to pass our first adult dental Medicaid benefit, which came into being just a year ago. Now, we are collecting the data and zeroing in on those patients who need implants so that our state can support their need for care. Meanwhile, most dentists in New Hampshire — even those who do not presently take Medicaid — work with
A clear and well-oiled business operation, such as that which I have built with the help of Specialty1 ... enables me to focus on patient care, including exploring and using the latest in implant technologies.”
veterans, seniors, and recovering addicts to put them on the road to recovery, even if doing so means donating chair time and resources.
What prompted you to partner with Specialty1 Partners?
All dental practices need to maintain their clinical autonomy while managing financial and business operations. Oral surgeons also have these needs in addition to our own more specialized requirements. However, as a relatively small professional population, oral surgeons do not always have the resources available to meet these needs.
Then again, with Specialty1 Partners, an oral surgeon like me can access a wealth of resources in one place. We are able to obtain information on business operations like marketing, human resources, training, billing, and much more. The best part, for me, is that these resources are gathered by dentists and oral surgeons like me so I know what they offer is what I need.
How has the business side of your practice before and after your partnership with Specialty1 changed?
In a fast-paced and intensive practice like mine, it is critical that our protocols and systems are clearly available for the team and easily accessed. Our partnership with Specialty1 came just as my practice operations expanded, which means new people and new systems. The presence of Specialty1 within my practice helped make this expansion simple and transparent for my entire team. Human resources, training, accounts payable and receivable, and other crucial systems are running smoothly even with new personnel.
What implant platforms or systems do you use?
I use Straumann® BLX, ZimVie, and Astra/Dentsply implant systems.
What is genuinely new in implant dentistry today?
I would say that some of the latest in dental imaging technologies are taking us in new directions with regard to implants. Cone beam imaging, for example, gives us a 3D scan of bone and tissue that is amazingly detailed — it truly enhances our ability to perform implant surgery effectively. Additionally, the increased application of artificial intelligence in implant dentistry has the potential to transform treatment and patient outcomes.
From a bone preparation standpoint, such things as patient-specific bone grafts as well as biologics have created scientifically based, reliable outcomes.
What is the future of implants?
As I mentioned, AI is helping to dramatically evolve implant dentistry. The algorithms employed by these systems could dramatically improve diagnostics, treatment planning, and longterm patient care. Of course, the future of implants is also its affordability. In rural areas like some of those in which I see patients, access to implants has always been a financial challenge, leading to a “haves versus have-nots,” or more precisely, a “dentures versus implants” dynamic. Then again, with the technologies used in implants becoming more readily available and therefore more affordable, it may be possible that more patients will be able to enjoy the long-term benefits of implants.
How
did you first learn about
Specialty1 Partners?
I first learned about Specialty1 through a colleague when I mentioned that as a solo practitioner I was feeling the stress of the administration becoming a burden and creating a level of unhappiness. He mentioned Specialty1 Partners as a dental partnership organization that allows group administration process sharing while maintaining clinical autonomy. This seemed to be exactly what I was hoping for and it turned out to be just so.
Are you concerned about the increasing presence of Dental Service Organizations (DSOs) in the dental market?
Dental Service Organizations (DSOs) are just one of a wide range of diversifying practice modalities. Their structure and “corporate” dynamic is certainly different from the more traditional “brick-and-mortar” private practice, just as is a public health dental clinic, FQHC, or large group practice. To me, a dentist is a dentist — an absolutely essential figure in a patient’s overall health — regardless of where they practice. In New Hampshire, DSO dentists abide by the same ethical standards, practice rules, laws, and license requirements that I do. Dentistry is not the same as medical healthcare — many of us must form and operate small businesses. As a result, the business of dentistry can appear in many forms. There are many positives of each dental practice model, and the future of inclusion in the dental profession will be acceptance of all models and then working to allow the positives of each to span across each model and provide advantages.
Are there any positive developments within the DSO landscape that you find promising?
In my work within organized dentistry — through the New Hampshire Dental Society and the American Dental Association — advocacy is a common ground between the many different dental practice modalities. Every dentist struggles with workforce challenges, dental student debt, continuing education requirements, dental benefit contract issues, and changes to state and federal law. I have found that DSOs are increasingly willing to work with other groups — like the ADA — on advocating in state capitols and Washington DC. With one voice, we are seeing more success in legislatures across the country than we might have with many smaller and disparate voices.
What is your future goal clinically?
I love dentistry. It can be a challenging field in which to work, but the rewards — especially knowing I am helping restore and maintain the oral health of my patients — are immeasurable. Clinically, I want to continue building a network in which I can see as many patients as I can in a state that, frankly, needs oral surgeons. A clear and well-oiled business operation, such as that which I have built with the help of Specialty1, is absolutely essential to that clinical goal. It enables me to focus on patient care, including exploring and using the latest in implant technologies.
What are your hobbies, and what do you do in your spare time?
I am an avid golfer, spending as much time on the links as I can in the warm months. I am also a passionate hockey fan after playing all of my life, rooting for my Boston Bruins — even when they fall short. Above all, I love my family. Spending my free time with my wife, Laurie, my grown kids, and of course, our goldendoodle Roma, keeps me grounded and smiling every day. IP
Management of acute hemorrhage in the anterior maxillary region from an aberrant blood vessel
Drs. Lanka Mahesh, Gregori M. Kurtzman, Sagarika Shukla, and Zara Dhawan discuss management of a surgical complication
Abstract
Implant placement for missing teeth has become a routine procedure to establish functional and esthetics needs of the patient. And just like any surgical procedure, complications like bleeding, infection, etc., can occur during implant placement as well. Bleeding from the alveolar antral artery (AAA) is one such complication which causes bleeding, and any clinician should be prepared for its management. Authors will discuss one such case and the management of this complication. CBCT is a very important diagnostic tool which should be used for every case possible.
Introduction
Implant placement has become a common procedure when one has to rehabilitate missing teeth functionally and esthetically.
Lanka Mahesh, BDS, MBA, completed a bachelor’s degree in dental surgery and a diploma in hospital administration and is currently pursuing a PhD in Integrated Implantology. He has published over 225 articles and authored several textbooks. He practices in a private specialized implant practice at The Specialist Clinic in New Delhi, India and can be reached at drlanka. mahesh@gmail.com.
Gregori Kurtzman, DDS, is in private general dental practice in Silver Spring, Maryland. He is a former Assistant Clinical Professor at University of Maryland in the department of Restorative Dentistry and Endodontics and a former AAID Implant Maxi-Course assistant program director at Howard University College of Dentistry. He has lectured internationally on the topics of restorative dentistry, endodontics and implant surgery, removable and fixed prosthetics, and periodontics. He has over 870 published articles, as well as several ebooks and textbook chapters. He can be reached at dr_kurtzman@maryland-implants.com.
Sagarika Shukla, MDS, has a degree in periodontics with a special interest in facial esthetics. She is in private practice at The Specialist Clinic in New Delhi, India.
With better understanding and advances in technology, many procedures are available to rehabilitate the maxillary arch, and clinicians have many options of bypassing the sinus such as zygoma implants, the All-on-4 technique, indirect sinus lifts or graftless solutions, and short implants. However, each aforementioned technique is not as predictable as a direct sinus lift, especially in cases of a severely atrophic maxilla.1,2 Short implants have less bone-to-implant contact and have more chances of failure in load-bearing areas. In a meta-analysis by Papaspyridakos, et al.,3 authors stated that short implants (≤6 mm) have less predictable survival rates compared to longer implants (>6 mm) after periods of 1-5 years in function. When it comes to an indirect sinus lift, the procedure does not increase the height of maxillary sinus sufficiently,4 leaving a direct sinus lift a predictable treatment choice. However, many patients are anxious about maxillary sinus grafting and the complications which follow the surgery, hence procedures like All-on-4 were developed which can rehabilitate the entire arch along with bypassing the sinus.
Zara Dhawan, BDS, is in private practice at The Specialist Clinic in New Delhi, India. She graduated from the School of Dental Sciences, Sharda University, Uttar Pradesh, India, in 2020.
In this type of clinical situation, knowledge of anatomy and the arterial blood supply becomes paramount. Structure wise, the maxillary sinus (MS) is pyramidal in shape and largest of the paranasal sinuses.5 The anterior wall of the MS is formed by the facial surface of the maxilla and is internally grooved by the canalis sinuosus (which houses the anterior superior alveolar nerve and vessels).5 It receives blood supply via the maxillary artery and its branches. In this article, the artery of interest is alveolar antral artery (AAA), which is an anastomosis of the posterior superior alveolar artery (PSAA) and the infraorbital artery (IOA).6 As the name suggests, it appears on the maxillary facial plate near to or in close approximation with maxillary second premolar and first molar area, a position from where it takes a U-turn, roughly paralleling the sinus floor. Not much has been reported regarding this artery in the literature as it goes undetected, and the clinician only comes to know when it interferes during osteotomy (10%-30% of cases) or any complication.7,8 It has higher detection rates in males due to larger diameters, as well as in narrower maxillary sinuses <14 mm in width. The immediate complication is bleeding, which can be called as the “gateway complication” further leading to a series of complications that impact treatment prognosis and outcome and or abortion of the surgical procedure.6,9
The vertical distance of the artery from the alveolar ridge varies in patients depending upon the resorption of the ridge. Solar, et al.,10 reported a range of 15 mm - 25 mm of vertical
positioning of the artery in alveolar bone in a mixed dentate/ edentulous population. However, a more reliable measurement, which had been found to be mean of 7.66 mm, could be found via CBCT, where ridge resorption would not influence the vertical distance.11 Park, et al.,12 found this height to be between 7.71 mm - 8.01 mm, and suggested a lateral window of 8 mm for visualization, instrumentation, and graft placement if the sinus lift is to be performed. Studies have shown that the artery has an average diameter of 1.5 mm,13 and that a diameter of < 0.5 mm does not indicate any significant bleeding that would interfere with surgery.14 However, Testori, et al.,15 suggested that a small caliber vessel on CBCT may correspond to a much larger caliber vessel clinically.
Case report
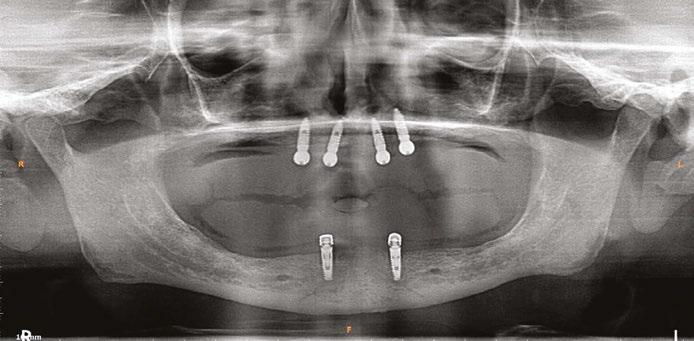
A 59-year-old male reported to the dental office with missing maxillary teeth due to poor oral hygiene. Treatment planning was done for All-on-4 implant placements followed by prosthesis. A complete medical history was obtained and was negative for any significant medical problems. The patient denied being allergic to any medication as well. The patient agreed to the implant placement and was advised to have an orthopantomogram (Figure 1).
On the day of the surgery, before commencing the procedure under strict asepsis, the patient was asked to rinse with 0.12% chlorhexidine gluconate mouthwash (Peridex™; 3M™). Local anesthesia with a vasoconstrictor was infiltrated buccally and palatally into the posterior and anterior maxilla on both the sides using S-blades (straight) (Zabby, India). The incision was made
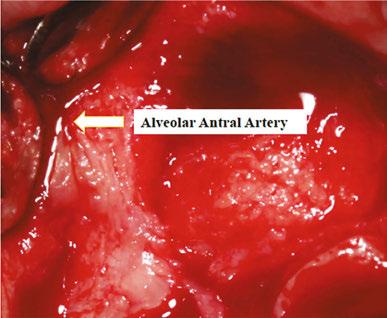
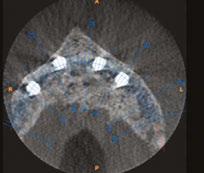
on the crest of the ridge in the region of teeth Nos. 15-25. While creating the incision, bleeding was noticed in the region of tooth No. 15 which intensified during the flap reflection (Figure 2). Bleeding was pulsatile, indicating an arterial bleed. Initially attempts to control bleeding included a pressure pack and ice pack, and the bleeder was isolated and the vessel ligated (Figure 3). The bleeding could be controlled, and the procedure was completed by placing four Bioner implants (Bioner, Spain), size 4/10 mm. Sutures were placed, and patient was kept on basic medication for pain and infection control. Immediately after the surgery, the patient was advised to get a CBCT. As shown in Figure 4, a coronal view and Figure 4B (yellow arrows), the position of the artery can be seen.
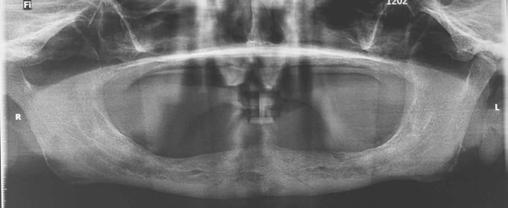
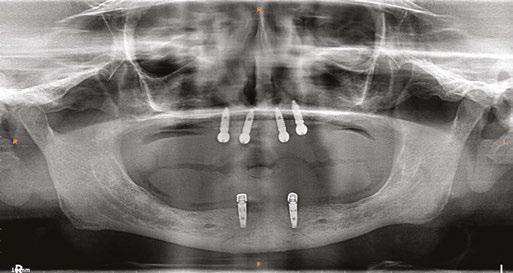
In the follow-up sessions, the patient was comfortable, but did complain of mild swelling which subsided within 4-5 days. A post-op CBCT showed excellent recovery, bone width, and proper implant placement (Figure 5).
Discussion
Encountering an AAA complication during an All-on-4 procedure in the region of teeth Nos. 14 and 15 has not been reported so far, however literature reports bleeding complications from AAA during sinus-lift procedures. Another complication that occurs is infection in about 3% of the cases, and in 1% of the cases loss of graft,16 and this usually happens after hematoma formation. In simple terms, the larger the vessels, the more the bleeding will occur. According to Ella, et al.,17 the risk involving AAA in osteotomies can be >10% whereas according to authors Chan and Wang18 and Elian, et al.,8 it is 20%. Authors Jensen, et al.,19 have reported severe bleeding in sinus elevation surgery through a transcrestal approach, wherein, bleeding led to swelling and consecutive hospitalization for 3 days, after which, normal functioning was regained. Hence management of the complication plays an important part for the clinician.
The first and foremost solution is the application of pressure pack and ice pack to control the bleeding along with topical thrombin. Other products such as SURGICEL® Absorbable Hemostat, SURGICEL™ Powder (Surgicel; Johnson & Johnson Co., Somerville, New Jersey), and bone wax can also be used. Usually because of bleeding at the surgical sight, pinpointing the
Figure 1: Pre-op panoramic radiograph
Figure 2 (left): Alveolar antral artery (AAA). Figure 3 (center): The artery has been ligated with suture. Figures 4A and 4B (right): CBCT post-implant placement and position of the artery coronally (top). 4B. Showing the position of alveolar antral artery (AAA) in relation to implant placement as indicated by the yellow arrows (bottom)
exact bleeding spot becomes difficult, but if that can be isolated, then electrocautery/chemocautery or ligation can be done. As aforementioned, if the vessel is large, and bleeding cannot be controlled, the procedure should be aborted, and patient should be hospitalized.
Use of piezoelectric devices safely bypasses the vessels as it only cuts the bony surface, avoiding any chance of vessel rupture. The only disadvantage is that it is a time-consuming method, but better when it comes to any complication or aborting the procedure. In a surgical double-window technique described by Maridati, et al.,20 an osteotomy is made above and below the vessel, leaving a thin bridge of bone holding the vessel intact. However, this is a difficult technique to follow and does not work in terms of instrumentation, implant placement, and septated sinuses.6 The simplest of the methods to avoid this complication is detection which is best achieved with CBCT, however even with CBCT, AAA can be detected in only 50% of the cases,22 perhaps because the vessel is too small to be detected by CBCT, which does not mean that there is an absent vessel, or anastomosis does not exist. Cadaveric studies have shown that anastomosis is present 100% of the time,23 but it goes undetected or unreported, simply because many clinicians assume that the anastomosis does not exist or use basic radiographic techniques for the implant placement.
In the case discussed here, authors encountered a small vessel wherein the bleeding was easily controlled with pressure packs and ice packs. The site of implant placement is a safe zone, and such a bleeding complication usually occurs during sinus-lift procedures and not in the anterior region. A simple detection could have helped clinicians to plan osteotomy better. Fortunately, the vessel was not big, and the bleeding could be controlled by ligation. Otherwise the implant placement may have had to be postponed. This proves that CBCT is an excellent tool and should be used more often for the case planning and detection of pathologies.21
Conclusion
Dental radiographs are an important tool in accurate diagnosis and treatment planning.21 Imaging is also the most common and important investigation carried out before any dental procedure that requires surgical or corrective intervention.21 Thus, accuracy of the X-ray, whether it is an intraoral periapical radiograph (IOPA) or an Orthopantomogram (OPG) becomes paramount. However, these investigative tools provide a 2D
image of a 3D object and are subject to false positive errors. Also, patients should be counselled and motivated to receive the proper imaging for the procedure. Above all, the surgeon must anticipate and effectively manage complications encountered during the surgery.
REFERENCES
1. Chipaila N, Marini R, Sfasciotti GL, Cielo A, Bonanome L, Monaco A. Graftless sinus augmentation technique with contextual placement of implants: a case report. J Med Case Rep. 2014 Dec 17;8:437.
2. Bedrossian E, Rangert B, Stumpel L, Indresano T. Immediate function with the zygomatic implant: a graftless solution for the patient with mild to advanced atrophy of the maxilla. Int J Oral Maxillofac Implants. 2006 Nov-Dec;21(6):937-942.
3. Papaspyridakos P, De Souza A, Vazouras K, Gholami H, Pagni S, Weber HP. Survival rates of short dental implants (≤6 mm) compared with implants longer than 6 mm in posterior jaw areas: A meta-analysis. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:8-20.
4. Balaji SM. Direct v/s Indirect sinus lift in maxillary dental implants. Ann Maxillofac Surg. 2013 Jul;3(2):148-153.
5. Standring S., ed. Gray’s anatomy: the anatomical basis of clinical practice. 41st ed. London: Elsevier Health Sciences; 2015.
6. Yang D, Lee N. A Simple Method of Managing the Alveolar Antral Artery during Sinus Lift Surgery. Int J Otolaryngology Head Neck Surg. 2021;10(3):131-146.
7. Lee CY. Brisk, prolonged pulsatile hemorrhage during the sinus graft procedure: a case report with discussion on intra-operative hemostatic management. Implant Dent. 2010 Jun;19(3):189-195.
8. Elian N, Wallace S, Cho SC, Jalbout ZN, Froum S. Distribution of the maxillary artery as it relates to sinus floor augmentation. Int J Oral Maxillofac Implants. 2005 Sep-Oct;20(5):784-787.
9. Varela-Centelles P, Loira M, González-Mosquera A, Romero-Mendez A, Seoane J, GarcíaPola MJ, Seoane-Romero JM. Study of factors influencing preoperative detection of alveolar antral artery by CBCT in sinus floor elevation. Sci Rep. 2020 Jul 2;10(1):10820.
10. Solar P, Geyerhofer U, Traxler H, Windisch A, Ulm C, Watzek G. Blood supply to the maxillary sinus relevant to sinus floor elevation procedures. Clin Oral Implants Res. 1999 Feb;10(1):34-44.
11. Varela-Centelles P, Loira-Gago M, Gonzalez-Mosquera A, Seoane-Romero JM, Garcia-Martin JM, Seoane J. Distance of the alveolar antral artery from the alveolar crest. Related factors and surgical considerations in sinus floor elevation. Med Oral Patol Oral Cir Bucal. 2016 Nov 1;21(6):e758-e765.
12. Park WH, Choi SY, Kim CS. Study on the position of the posterior superior alveolar artery in relation to the performance of the maxillary sinus bone graft procedure in a Korean population. J Korean Assoc Oral Maxillofac Surg. 2012;38(2):71-77.
13. Kim JH, Ryu JS, Kim KD, Hwang SH, Moon HS. A radiographic study of the posterior superior alveolar artery. Implant Dent. 2011 Aug;20(4):306-310.
14. Rysz M, Ciszek B, Rogowska M, Krajewski R. Arteries of the anterior wall of the maxilla in sinus lift surgery. Int J Oral Maxillofac Surg. 2014 Sep;43(9):1127-30.
15. Testori T, Rosano G, Taschieri S, Del Fabbro M. Ligation of an unusually large vessel during maxillary sinus floor augmentation. A case report. Eur J Oral Implantol. 2010 Autumn;3(3):255-258.
16. Chiapasco M, Casentini P, Zaniboni M. Bone augmentation procedures in implant dentistry Int J Oral Maxillofac Implants. 2009;24 Suppl:237-259.
17. Ella B, Sédarat C, Noble Rda C, Normand E, Lauverjat Y, Siberchicot F, Caix P, Zwetyenga N. Vascular connections of the lateral wall of the sinus: surgical effect in sinus augmentation. Int J Oral Maxillofac Implants. 2008 Nov-Dec;23(6):1047-1052.
18. Chan HL, Wang HL. Sinus pathology and anatomy in relation to complications in lateral window sinus augmentation. Implant Dent. 2011 Dec;20(6):406-412.
19. Jensen SS, Eriksen J, Schiodt M. Severe bleeding after sinus floor elevation using the transcrestal technique: a case report. Eur J Oral Implantol. 2012 Autumn;5(3):287-291.
20. Maridati P, Stoffella E, Speroni S, Cicciu M, Maiorana C. Alveolar antral artery isolation during sinus lift procedure with the double window technique. Open Dent J. 2014 May 30;8:95-103.
21. Shukla S, Chug A, Afrashtehfar KI. Role of Cone Beam Computed Tomography in Diagnosis and Treatment Planning in Dentistry: An Update. J Int Soc Prev Community Dent. 2017 Nov;7(Suppl 3):S125-S136.
22. Ilgüy D, Ilgüy M, Dolekoglu S, Fisekcioglu E. Evaluation of the posterior superior alveolar artery and the maxillary sinus with CBCT. Braz Oral Res. 2013 Sep-Oct;27(5):431-437.
23. Bernardi S, Mummolo S, Ciavarelli LM, Li Vigni M, Continenza MA, Marzo G. Cone beam computed tomography investigation of the antral artery anastomosis in a population of Central Italy. Folia Morphol (Warsz). 2016;75(2):149-153.
Figure 5: Panoramic radiograph following implant placement
Cool Jaw ® hot/cold therapy
Cool Jaw® has paved the way to postoperative hot/cold therapy through the creation of our exclusive, hands-free patented designed wraps. The hands-free Cool Jaw system reduces postoperative swelling and discomfort and allows patients to recover in a convenient manner. Combine with our extensive variety of hot/cold gel packs to create a post-op recovery solution that best suits your patients.
Our Soft-Sided Round Gel packs are a convenient, post-op cold therapy option for after numerous procedures including implants and cosmetic injections such as Botox. These packs come in a variety of color options to match your office or simply add an element of fun to any procedure. Choose from bright solid colors as well as eye-catching glitters. These reusable gel packs are 4 inches in diameter and remain flexible when frozen, allowing for uniform cold therapy.
Take the Cool Jaw products to the next level, and add customization! Customization is a subtle, yet effective way to promote your practice and enhance your professional image.
Cool Jaw helps you to continue promoting your practice long after the surgery date.
Visit us at the booth, and ask for a free sample!
Visit Cool Jaw at ADA Booth No. 1243 and AAID Booth No. 219
Specialized Dental Partners
Empower your practice. Elevate your care.
As today’s dental specialists look to the future of their practices and careers, more are exploring the trend of practice partnerships — weighing the notion of joining a vibrant culture and community against a lucrative financial opportunity. At Specialized Dental Partners, we know the two go hand in hand. Since 2018, Specialized Dental Partners has championed specialists, building a community of over 330 premier clinicians in 35 states who share our core values and are inspired by our mission. Our culture is about growth in every aspect of our lives — from improving our communication skills to leadership training, to advanced clinical training courses, and beyond. “Specialized Dental Partners offers the chance to become not only a better endodontist, but also a better boss, a better spouse, and a better friend. What we
are building is unique. I’m truly thrilled to be a part of it,” said Dr. Jeremy Young, Director of Partner Engagement. You deserve a champion to support you in designing a future that surpasses expectations. Meet our partners and learn more about the Specialized Dental partnership opportunity at this year’s AAOMS and AAP annual events.
Neil Zachs, DMD, MS Periodontist partner in Scottsdale, AZ
“With Specialized Dental Partners, I have access to an
array of top specialists
from all over the country for help, advice, and friendship.”
We’re proud
and
SHOW SPECIAL SECTION
Intraoral scanning techniques for fullarch implants
Dr. Christopher R. Resnik discusses some advances in intraoral scanning devices and acquisition technology
All-on-X implant-supported reconstructions provide an excellent opportunity to restore the function of the dental arch, while improving the quality of lives of our patients. Innovations on the surgical and restorative fronts are evolving at an accelerated rate, facilitating faster, more accurate workflows and results. As the dental industry continues to strive for fully digital solutions, advances in intraoral scanning devices and acquisition technology are widening the disparity between digital and analog methods, favoring intraoral scanning (IOS) as a more viable solution. However, when treating fully edentulous implant cases, there are still inherent inaccuracies associated with conventional intraoral scanning.1
Photogrammetry, at this time, remains the sole validated and most accurate method for digitally recording implant positioning.2 However, drawbacks to photogrammetry include high cost, limited applicability (i.e., full-arch implant impressions), and high demand. Fewer dental offices, therefore, possess photogrammetry units, while many dental offices have access to intraoral scanners. Innovative methods have therefore been developed utilizing intraoral scanners to capture full-arch implant positioning for a fully digital All-on-X workflow.
Intraoral scanners create a 3D virtual model of dentition, soft tissue, and implant position by compiling multiple individual images that are created from a beam of light. For digital implant impressions, a “scan body” is inserted into the dental implant and scanned circumferentially. A virtual model is created, converted to a stereolithography (STL) file, imported into design software, and a restoration is designed. Traditional scan bodies are vertical, with the top one-third of the scan body, termed the “scan region,” being the critical part that must be recorded accurately (Figure 1). Studies have found that for single and multiple
Christopher R. Resnik, DMD, MDS, DICOI, is a prosthodontist in private practice in Winter Park, Florida. He completed his dental degree, prosthodontic residency, and master’s degree in oral implantology from the University of Pittsburgh School of Dental Medicine. Dr. Resnik holds associate faculty positions at the University of Pittsburgh Graduate Prosthodontic Program and Temple University Graduate Periodontics Program. He is a contributing author to multiple textbooks including Avoiding Complications in Oral Implantology, Misch’s Contemporary Implant Dentistry, and Dental Implant Prosthetics.
Disclosure: Dr. Resnik is a faculty member of the Resnik Implant Institute. He reports no other conflicts of interests with the companies mentioned in this article.
Educational aims and objectives
This self-instructional course for dentists discusses innovative methods for utilizing intraoral scanners to capture full-arch implant positioning for a fully digital All-on-X workflow.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Identify several methods for digitally recording implant positioning. Realize some factors that can influence the accuracy of the scans.
• Identify the process of grammetry.
• Observe two Scanbase tracking systems used by the author to facilitate a fully digital workflow for full-arch implant cases.
2 CE CREDITS
implants, intraoral scanning is as accurate or even more accurate than traditional analog impressions.3,4 However, when obtaining full-arch scans, there are several inherent factors that influence the accuracy of the scan.
1. Environmental and intraoral factors: Blood, saliva, and soft tissue (i.e., tongue) create complications and inaccuracies with IOS. Soft tissues can move or deform during scanning, leading to inaccuracies in the final impression.5
Figure 1: Traditional vertical scan body broken into 3 segments. The scan region, top one-third, is the most critical for registering implant positioning
2. Patient factors: Accessibility of the intraoral scanner tip is influenced by its size, the implant location, and the patient’s ability to open. Patient movement also impacts scan accuracy. Full-arch scans take longer to complete, increasing the likelihood of patient movement.
3. Large scan area: Full-arch impressions require scanning a larger surface area compared to single site or partial-arch impressions. Maintaining accuracy over a larger surface is inherently more difficult. Errors can be attributed to the small wand size necessitating subsequent stitching of the fields together and the lack of significant landmarks between scan bodies. Small errors can accumulate over the length of the arch, leading to significant discrepancies in the final digital impression.6
4. Multiple, varying implant angulations: The varying angles and positions of multiple implants can complicate the scanning process. Inconsistencies in capturing the exact orientation and position of each implant can lead to inaccuracies in the final impression.7 Some studies have evaluated the number of implants and found greater accuracy with fewer implants.8
5. Scan body design: The scan body design, shape, material, and alignment influence the outcome of correct acquisition of implant positions.9,10
6. Operator experience: The skill level of the operator significantly impacts the accuracy of IOS. Inexperienced operators may struggle with maintaining consistent scanning techniques, leading to errors.11,12 However, even experienced operators can face challenges with full arch scans due to the increased complexity.
7. Scanning strategy: The pattern and method of scanning (e.g., segmental versus continuous) can influence the precision and trueness of digital impressions. Different scanning strategies may yield varying levels of accuracy, particularly in complex full-arch cases.13,14
8. Scanner limitations: IOS systems have varying capabilities and limitations. Some scanners may perform well in capturing detailed images of smaller areas but may not be as effective for full arch impressions.15 Factors such as the type of scanning technology and the specific algorithms used by the scanner can affect the accuracy and reliability of the impressions.16
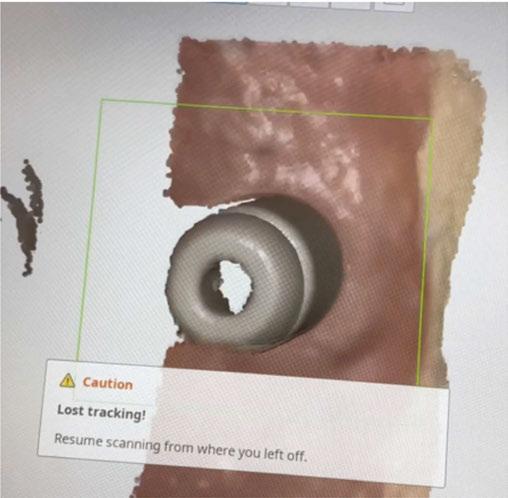
9. Stitching errors: Intraoral scanners only capture a limited area at one time. The final model is generated by stitching images together. For completely edentulous scans, the lack of landmarks, long span of mobile mucosa, and multiple scan bodies may cause the images to be stitched incorrectly and lead to higher deviations9,16 (Figure 2). This is apparent as studies have found increased error with increased interimplant distance.17
Grammetry
Innovative techniques and scan bodies have been developed to help navigate the large scan
areas and stitching inaccuracies involved with traditional, vertical independent scan bodies. Several techniques have been proposed to improve the full-arch digital implant impression accuracy such as the use of fiducial markers,18 auxiliary clips,19 splinting scan bodies together,20 interim prostheses,21 pressure-indicating paste,22 auxiliary geometric appliances,23 and scan powder.24
Grammetry is a method developed that rivals photogrammetry and analog implant impression techniques. Grammetry is the process of capturing a continuous arch scan with an intraoral scanner and a unique ScanBase tracking mechanism, preventing loss of accuracy ensuring scan quality. Utilizing a special Scanbase system, the scan bodies are connected together allowing for a continuous scan with the intraoral scanner, decreasing the chance of stitching errors. Described below are two Scanbase tracking systems that are utilized by the author in private practice. Both techniques provide simplified scanning, improved accuracy, and a fully digital workflow for full-arch implant cases.
Figure 2: Most common error involved with full-arch digital implant impression. The intraoral scanner will become “lost” and unable to stitch together continuous images, leading to inaccuracies
Figures 3A-3B: 3A. Individual scan body with wing-like projection. The projection serves as a way of connecting all scan bodies together. 3B. honeycomb piece that will be luted to the wings of the scan bodies, creating a single jig to be scanned
OPTISPLINT®
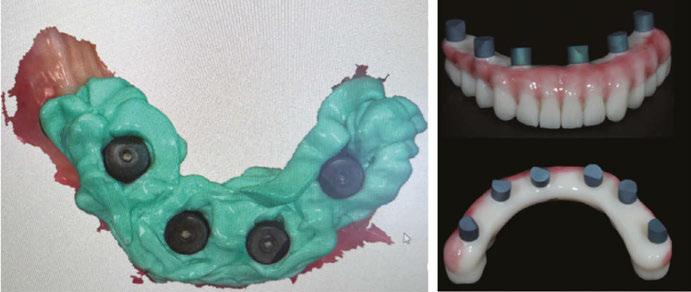
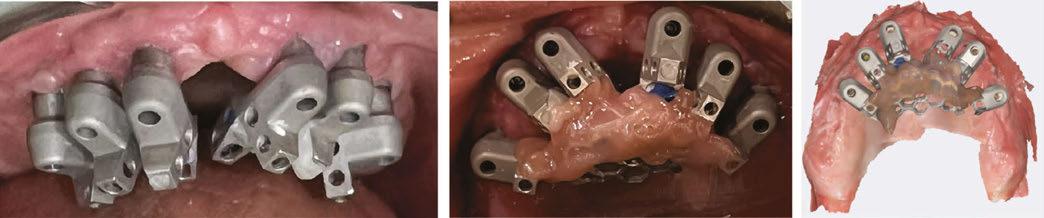
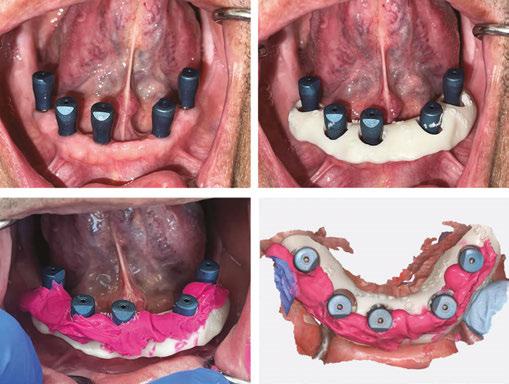
OPTISPLINT, by Digital Arches (https://digitalarches. com), is a dual-purpose implant coping, which serves as an abutment level scan body for fixed complete-arch prostheses as well as an analog verification jig. Individual scan bodies are inserted on each multi-unit abutment individually (Figure 4A). This scan body is unlike a traditional scan body, where a wing-like extension is cantilevered off of the scan region (Figure 3A). A central honeycomb metal frame piece is then placed, adjusted if necessary, within 1 mm-2 mm of wing components of the scan body (Figure 3B). Resin (flowable composite, dual-polymerizing, auto-polymerizing) or acrylic is then added to lute the scan bodies to the central honeycomb metal frame piece (Figure 4B). Once all scan bodies are attached, the OPTISPLINT jig can then be scanned as a single, splinted object, intraorally or extraorally (Figure 4C). If completed extraorally, the patient’s factors (blood, saliva, soft tissue, limited opening) are eliminated. An added benefit of this system is that the OPTISPLINT jig can then be poured in dental stone to facilitate the fabrication of an accurate master cast (Figures 5A and 5B). This is beneficial for checking the passivity of the prosthesis prior to inserting and can aid with the cementation of ti-bases to the interim or final prosthesis.
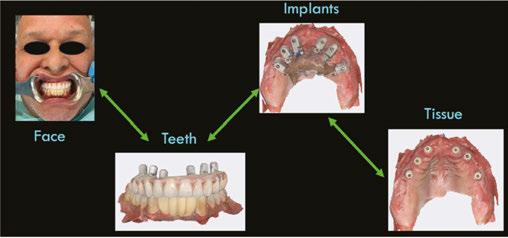
When imported into a design software (e.g., Exocad), the OPTISPLINT scan will produce a digital file of implant positioning. Additional records include facial records, soft tissue records, and tooth/occlusal records (Figure 6).
After all the records are acquired, the scans may then be aligned and the patient’s implant prosthesis can be designed and fabricated (Figures 7A-7F). The OPTISPLINT technique enables clinicians to utilize a fully-digital workflow for a fraction of the cost of other digital methods. Patient factors are able to be eliminated as the OPTISPLINT can be scanned extraorally with the added benefit of acting as a verification jig prior to prosthetic delivery.
CONnX Scan System
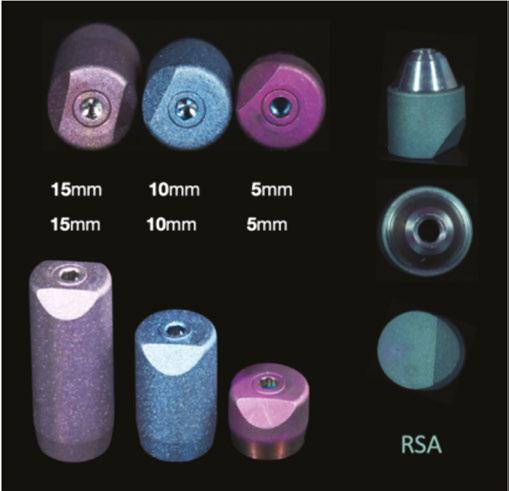
Another type of grammetry method is the CONnX Scan system, by Synergy Dental Lab (https://www.synrglab.com/). The CONnX Scan system utilizes individual scan bodies and connects them together with a tracking material. Individual scan bodies are available in different sizes (5 mm, 10 mm,15 mm depending on the height of the gingival tissue) and with a
Figures 7A-7F: 7A. Alignment of facial record to teeth, to aid in smile design and tooth setup. 7B. Detecting implant position via scan region of OPTISPLINT jig. 7C. Alignment of patient’s teeth to soft tissue, to allow tooth setup at correct vertical dimension. 7D. Alignment of implant position to soft tissue. 7E. Digital design of patient’s prosthesis. 7F. Final prosthetic delivery
Figures 5A-5B: 5A. Multi-unit analogs inserted into the OPTISPLINT jig. 5B. Stone verification jig created to aid in checking the passivity of the prosthesis
Figure 6: Summary of records acquired that will be aligned in CAD software
Figures 4A-4C: 4A. Individual scan body inserted into the multi-unit abutments. 4B. Central honeycomb piece attached to the scan bodies intraorally. 4C. Intraoral scan of OPTISPLINT jig
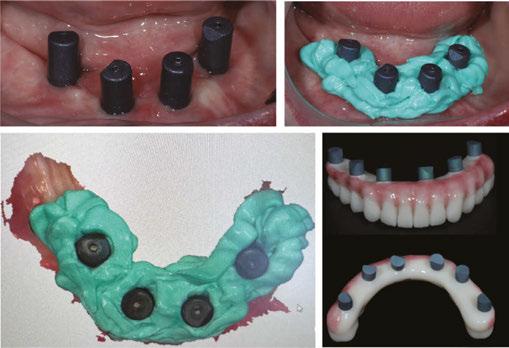
reverse scan body analog that can be inserted into a prosthesis (Figure 8). Individual scan bodies are placed on the multi-unit abutments, then through two different methods, are connected together allowing for a continuous scan. One method involves placing ScanLink (Rigid Bite Registration Material) around the scan bodies to connect them together, leaving 5 mm of the scan body exposed to allow capturing of the scan region (Figures 9A-9D). The ScanLink allows the intraoral scanner to capture the scan regions continuously. The second method involves placement of a ScanBase around the scan bodies. The ScanBase is a
printed composite material that is custom made for each patient (Figure 10). Specific geometrical shapes are present on the ScanBase which allow the intraoral scanner to pick up details that aid in stitching. If needed, ScanLink may also be added to the ScanBase to allow for easier scanning.
By connecting the scan bodies together with the CONnX Scan system, the area the scanner needs to travel between the scan regions of neighboring scan bodies is decreased, thereby improving accuracy and stitching capability. The final digital file of the intraoral scan will then be uploaded into the CAD software. Similar digital records also acquired include facial records, soft tissue records, and tooth/occlusal records.
All of the digital files are then exported to the dental lab for fabrication of the full-arch implant prosthesis, utilizing a fully digital workflow (Figures 11A-11D). ScanLink and ScanBase
Figures 9A-9D: 9A. Individual scan bodies inserted into the multi-unit abutment. 9B. ScanLink utilized to connect all scan bodies together, leaving 5 mm atop for scanning. 9C. Intraoral scan of scan bodies with ScanLink. 9D. Reverse scan analogs inserted in prosthesis to generate tooth position and vertical dimension
Figures 10A-10D: 10A. Individual CONnX scan bodies inserted. 10B. ScanBase inserted around scan bodies.This ScanBase is custom made for the patient and has geometrical shapes that will aid in continuous scanning. 10C. ScanLink is added to fill in the voids to aid the intraoral scanner in completing a full-arch scan. 10D. Intraoral scan of scan bodies completed within seconds
Figure 8: Individual scan bodies are color coded based on the size and also come with a reverse scan analog. All scan bodies will have same scan region at the top
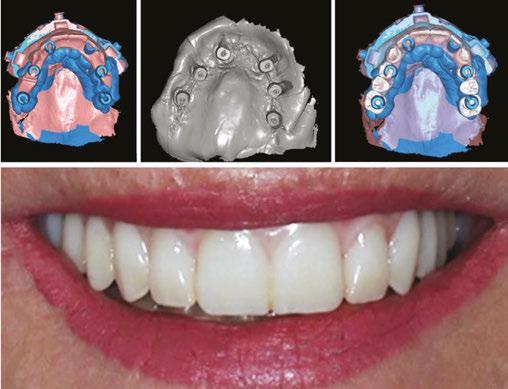
Figures 11A-11D: 11A. Intraoral scan of scan bodies with ScanLink and ScanBase. 11B. Soft tissue record. 11C. Alignment of all data including patient’s tooth positioning, occlusion at correct vertical dimension. 11D. Delivery of immediate fixed prosthesis
allow the intraoral scanner to capture the scan regions more accurately, with less stitching errors compiling the various images. The option for multiple sizes of scan bodies with the same scan region accompanied with a reverse scan analog allows easier alignment of digital data and a smoother transition to the prosthetic manufacturing.
Summary
While intraoral scanning offers many advantages, such as patient comfort and digital integration, it faces significant challenges when utilized in full-arch implant impressions. The large surface area in edentulous cases, lack of stable reference points, lack of teeth or keratinized mucosa, and the similarities in scan body morphology make it difficult to distinguish and stitch together multiple images accurately. Innovative scanning techniques and scan body systems have strived to overcome these challenges. Grammetry, through utilization of a scan base system, allows the intraoral scanner to continuously capture data which has led to improved accuracy in full-arch digital implant impressions. OPTISPLINT and the CONnX Scan system are two types of these scan base systems that connect the scan bodies together, thus limiting stitching difficulties. With these techniques, the everyday clinician is able to utilize their intraoral scanner for a fully digital All-on-X workflow.
We are at a time in implant dentistry of rapidly evolving products, techniques, and workflows. The Resnik Implant Institute has implemented these digital methods into their surgical, prosthetic, and hands-on curriculums. Attendees receive didactic and hands-on training with photogrammetry, intraoral scanning techniques, and alignment of all data to allow for the ultimate experience in prosthetic digital designs. Teaching these contemporary methods, as well as the foundation of implant dentistry, helps doctors understand and appropriately implement these updated technologies and workflows into their practices.
REFERENCES
1. Kim KR, Seo KY, Kim S. Conventional open-tray impression versus intraoral digital scan for implant-level complete-arch impression. J Prosthet Dent. 2019 Dec;122(6): 543-549.
2. Resnik C. The use of photogrammetry for the fabrication of full-arch immediate prostheses. Implant Practice US. Fall 2023;16(3):26-30.
3. Albanchez-González MI, Brinkmann JC, Peláez-Rico J, López-Suárez C, Rodríguez-Alonso V, Suárez-García MJ. Accuracy of Digital Dental Implants Impression Taking with Intraoral Scanners Compared with Conventional Impression Techniques: A Systematic Review of In Vitro Studies. Int J Environ Res Public Health. 2022 Feb 11;19(4):2026.
4. Schmidt A, Wöstmann B, Schlenz MA. Accuracy of digital implant impressions in clinical studies: A systematic review. Clin Oral Implants Res. 2022 Jun;33(6):573-585.
5. Mangano FG, Admakin O, Bonacina M, Lerner H, Rutkunas V, Mangano C. Trueness of 12 intraoral scanners in the full-arch implant impression: a comparative in vitro study. BMC Oral Health. 2020 Sep 22;20(1):263.
6. Gehrke P, Rashidpour M, Sader R, Weigl P. A systematic review of factors impacting intraoral scanning accuracy in implant dentistry with emphasis on scan bodies. Int J Implant Dent. 2024 May 1;10(1):20.
7. van der Meer WJ, Andriessen FS, Wismeijer D, Ren Y. Application of intra-oral dental scanners in the digital workflow of implantology. PLoS One. 2012;7(8):e43312.
Grammetry,
through utilization of a scan base system, allows the intraoral scanner to continuously capture data which has led to improved accuracy in full-arch digital implant impressions.”
8. Gherlone EF, Ferrini F, Crespi R, Gastaldi G, Capparé P. Digital impressions for fabrication of definitive “all-on-four” restorations. Implant Dent. 2015 Feb;24(1):125-129.
9. Meneghetti PC, Li J, Borella PS, Mendonça G, Burnett LH Jr. Influence of scanbody design and intraoral scanner on the trueness of complete arch implant digital impressions: An in vitro study. PLoS One. 2023 Dec 19;18(12):e0295790.
10. Mizumoto RM, Yilmaz B. Intraoral scan bodies in implant dentistry: A systematic review. J Prosthet Dent. 2018 Sep;120(3):343-352.
11. Pesce P, Bagnasco F, Pancini N, Colombo M, Canullo L, Pera F, Bressan E, Annunziata M, Menini M. Trueness of Intraoral Scanners in Implant-Supported Rehabilitations: An In Vitro Analysis on the Effect of Operators’ Experience and Implant Number. J Clin Med. 2021 Dec 16;10(24):5917.
12. Flügge T, van der Meer WJ, Gonzalez BG, Vach K, Wismeijer D, Wang P. The accuracy of different dental impression techniques for implant-supported dental prostheses: A systematic review and meta-analysis. Clin Oral Implants Res. 2018 Oct;29 Suppl 16:374-392.
13. Hardan L, Bourgi R, Lukomska-Szymanska M, Hernández-Cabanillas JC, Zamarripa-Calderón JE, Jorquera G, Ghishan S, Cuevas-Suárez CE. Effect of scanning strategies on the accuracy of digital intraoral scanners: a meta-analysis of in vitro studies. J Adv Prosthodont. 2023 Dec;15(6):315-332.
14. Ma J, Zhang B, Song H, Wu D, Song T. Accuracy of digital implant impressions obtained using intraoral scanners: a systematic review and meta-analysis of in vivo studies. Int J Implant Dent. 2023 Dec 6;9(1):48.
15. Di Fiore A, Graiff L, Savio G, Granata S, Basilicata M, Bollero P, Meneghello R. Investigation of the Accuracy of Four Intraoral Scanners in Mandibular Full-Arch Digital Implant Impression: A Comparative In Vitro Study. Int J Environ Res Public Health. 2022 Apr 13;19(8):4719.
16. Zhang YJ, Shi JY, Qian SJ, Qiao SC, Lai HC. Accuracy of full-arch digital implant impressions taken using intraoral scanners and related variables: A systematic review. Int J Oral Implantol (Berl). 2021 May 12;14(2):157-179.
17. Di Fiore A, Meneghello R, Graiff L, Savio G, Vigolo P, Monaco C, Stellini E. Full arch digital scanning systems performances for implant-supported fixed dental prostheses: a comparative study of 8 intraoral scanners. J Prosthodont Res. 2019 Oct;63(4):396-403.
18. Saaedi TMASE, Thabet YG. Customized scan bodies to facilitate intraoral scanning for full arch implant prosthesis: A dental technique. J Prosthodont. 2024 Mar;33(3): 297-300.
19. Etxaniz O, Amezua X, Jauregi M, Solaberrieta E. Improving the accuracy of complete arch implant digital scans by using auxiliary clips for intraoral scan bodies: A dental technique. J Prosthet Dent. 2024 Feb 27:S0022-3913(24)00066-0.
20. Retana L, Nejat AH, Pozzi A. Effect of splinting scan bodies on trueness of complete-arch implant impression using different intraoral scanners: an in vitro study. Int J Comput Dent. 2023 Feb 24;26(1):19-28.
21. Papaspyridakos P, Bedrossian A, Kudara Y, Ntovas P, Bokhary A, Chochlidakis K. Reverse scan body: A complete digital workflow for prosthesis prototype fabrication. J Prosthodont. 2023 Jun;32(5):452-457.
22. Mizumoto RM, Yilmaz B, McGlumphy EA Jr, Seidt J, Johnston WM. Accuracy of different digital scanning techniques and scan bodies for complete-arch implant-supported prostheses. J Prosthet Dent. 2020 Jan;123(1):96-104.
23. Iturrate M, Eguiraun H, Solaberrieta E. Accuracy of digital impressions for implant-supported complete-arch prosthesis, using an auxiliary geometry part-An in vitro study. Clin Oral Implants Res. 2019 Dec;30(12):1250-1258.
24. Donmez MB, Çakmak G, Dede DÖ, Küçükekenci AS, Lu WE, Schumacher FL, Revilla-León M, Yilmaz B. Effect of scan powder and scanning technology on measured deviations of complete-arch implant supported frameworks digitized with industrial and intraoral scanners. J Dent. 2023 Nov;138:104736.
Continuing Education Quiz
Intraoral scanning techniques for full-arch implants RESNIK
1. _____, at this time, remains the sole validated and most accurate method for digitally recording implant positioning.
a. Photogrammetry
b. Intraoral scanners
c. Tomographs
d. Panoramic radiographs
2. Intraoral scanners create a _______ by compiling multiple individual images that are created from a beam of light.
a. 2D black and white image
b. 3D virtual model of dentition, soft tissue, and implant position
c. holograph
d. physical model
3. For digital implant impressions, a _________ is inserted into the dental implant and scanned circumferentially.
a. “scan body”
b. “fiducial marker”
c. “auxiliary marker”
d. “geometric appliance”
4. Traditional scan bodies are vertical, with the top _______ of the scan body, termed the “scan region,” being the critical part that must be recorded accurately.
a. one-third
b. one-fourth
c. one-half
d. two-thirds
5. ________ create complications and inaccuracies with IOS.
a. Blood
b. Saliva
c. Soft tissue (i.e., tongue)
d. all of the above
6. Full-arch scans ___________, increasing the likelihood of patient movement.
a. are more painful
b. take longer to complete
c. are very short and complicated to capture
d. are short but uncomfortable
7. When capturing a full-arch scan, the scan body design, shape,
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: August 31, 2024
Expiration Date: August 31, 2027 2 CE CREDITS
material, and alignment influence the outcome of correct acquisition of implant positions.
a. True
b. False
8. _______ is the process of capturing a continuous arch scan with an intraoral scanner and a unique ScanBase tracking mechanism, preventing loss of accuracy ensuring scan quality.
a. Photogrammetry
b. Stitching
c. Grammetry
d. Auxiliary geometric imaging
9. Utilizing a special Scanbase system, the scan bodies are connected together allowing for a continuous scan with the intraoral scanner, ________.
a. decreasing the chance of stitching errors
b. complicating the scanning process
c. reducing accuracy
d. creating a partially digital workflow
10. The large surface area in edentulous cases plus ________ make(s) it difficult to distinguish and stitch together multiple images accurately.
a. lack of stable reference points
b. lack of teeth or keratinized mucosa
c. similarities in scan body morphology
d. all of the above
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Subperiosteal implants for the rehabilitation of atrophic posterior mandibular regions: A bilateral case report
Drs. Laurine Birault and Antoine Diss discuss an innovative concept in custom CAD/CAM implants
Introduction
Subperiosteal implants, more recently called AMSJI (Additively Manufactured Subperiosteal Jaw Implants) by some authors,1 are an innovative concept in custom CAD/CAM implants. They perfectly match the ridge anatomy of patients with insufficient bone volume to receive endosteal implants traditionally used in axial implantology.
Dr. Gustave Dahl first described the concept of subperiosteal implants in 1940. However, the first implants, made of cobalt-chromium and using a direct bone impression from wide-flap surgery, were not very successful. Their poor fit, lack of stability, and inability to osseointegrate resulted in an excessively high failure and complication rate.
With the advent of digital tools, it is now possible to perfect implant design using materials such as titanium. This advancement considerably improves fitting accuracy. As a result, subperiosteal implants have increased success rates and are becoming a relevant treatment option that deserves our attention.
Dr. Laurine Birault is a Doctor of Dental Surgery graduated from the University of Nice Sophia-Antipolis. She is in private practice in Nice, as a Doctor of Dental Surgery. She practices Periodontology and Implantology at Cabinet Arénas Dentistes in Nice and is a trainer for the Génération Implant association. Dr. Birault also holds a University Diploma in Implantology from the Université D’evry Val d’Essonne and a specification in Periodontology from the Université de Nice Sophia-Antipolis. Her professional journey includes contributions to dental literature, such as her work on the integration of facial scanning in surgical planning and on immediate loading.
Dr. Antoine Diss is a Doctor of Dental Surgery and holds a University Diploma in Implantology from the Faculté de Chirurgie Dentaire de Nice. He is in private practice in Nice, as a Doctor of Dental Surgery, Doctor of Odontological Science (PhD). He is the Founder and President of the Génération Implant association, a former Scientific President of the Société Française de Parodontologie et d’Implantologie Orale de la Côte d’Azur and holds a Doctorate in Odontology Sciences. Dr Diss has made significant contributions to dental education as a former professor of periodontology at the Faculté de Chirurgie Dentaire de Nice, and to dental research, particularly on platelet-rich fibrin (PRF), its evaluation, effects, and healing.
Educational aims and objectives
This self-instructional course for dentists discusses an innovative concept in custom CAD/CAM implants.
Expected outcomes
Implant Practice US subscribers can answer the CE questions by taking the quiz online at implantpracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Define subperiosteal implants.
• Realize some history leading up to modern subperiosteal implants.
• Identify various treatment solutions for the posterior mandibular region.
• Realize various approaches that can compensate for certain anatomical constraints.
• Observe a procedure for subperiosteal implants. 2 CE CREDITS
Complexity of the posterior mandibular region
Treatment of atrophic posterior mandibular regions has long been a challenge in our rehabilitation procedures. The various treatment solutions depend on a number of parameters:
• Removable solutions are rarely accepted due to their initial bulkiness. Moreover, their instability leads to functional and esthetic limitations. In the most severe cases, they can even cause pain when chewing due to the compression of the inferior alveolar nerve.2
• Implant solutions face several anatomical limitations. On one hand, there is a concomitant lack of height and width of the alveolar ridge, making vertical augmentation particularly difficult to achieve. On the other hand, the superficialization of the inferior alveolar nerve considerably increases the risk of postoperative nerve disorders. Finally, resorption of the bone surface leads to a reduction in the surrounding soft tissue, thus limiting the survival rate of the joint prosthesis.3
Various approaches have been developed to compensate for these numerous anatomical constraints:
• Several bone reconstruction techniques are used to restore sufficient crestal volume to allow the placement of endosteal implants. These methods include expansion, bone distraction, guided bone regeneration procedures using specific protocols such as the “sausage technique” or the use of titanium mesh, bone blocks, or mandibular framework.4,5
• In direct contrast, basal implantology by definition consists of anchoring implants of specific design (disc, blade, plate, oblique, etc.) in the basal bone of the maxilla without the need for bone grafts.6
• Finally, subperiosteal implantology offers another treatment solution, as it requires neither bulky reconstruction nor bone anchorage. These implants are specially designed to adapt to residual bone and are positioned under the periosteum.
Newer patient-specific implants use modern CBCT and patient scanning technology to create custom-milled patient specific subperiosteal implants. The authors selected Panthera Dental as their partner to design and manufacture this patientspecific subperiosteal implant. Nevertheless, other companies like Bone Easy® and KLS Martin also provide similar implants.
Procedure for subperiosteal implants
1. Planning and designing Panthera implants
After a patient with no contraindications to oral surgery is selected, these implants are designed after collecting three pre-implant data:
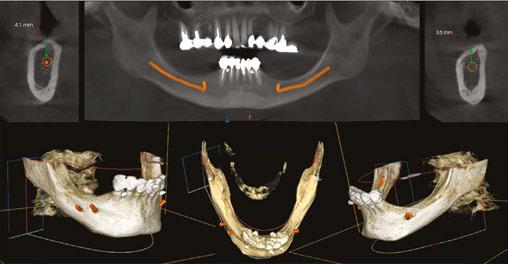
• A cone beam scan exported in DICOM format. The success of the treatment depends largely on the accuracy and quality of the CT data. It is therefore advisable to opt for a large acquisition field, covering the entire mandible up to the posterior ascending ramus. In addition, the highest possible image resolution and the use of metal artifact reduction tools (such as the CS “MAR” — Metal Artifact Reduction) are essential to ensure optimal implant adaptation (Figure 1).7
• An optical impression of the dento-mucosal surfaces.
• This is all combined with a digital wax-up, a preview of the future prosthetic project which will be exported in STL or PLY format. In the case of a limited number of residual teeth, radiopaque markers can be used to help combine the three types of data (Figure 2).8,9
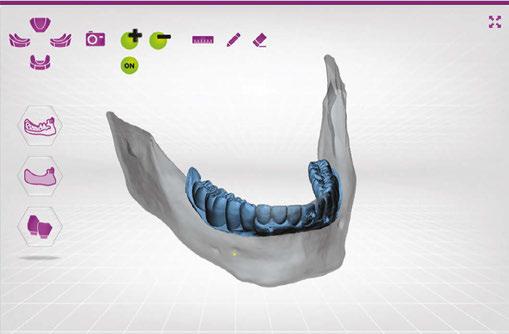
DICOM and STL files are transferred to the Panthera online platform. Once the order has been placed, a viewer allows you to follow and validate the implant creation stages (Figure 3).
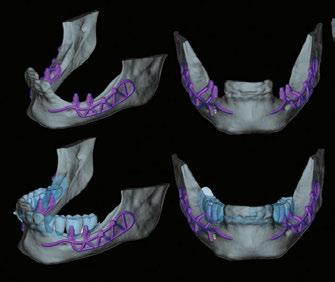
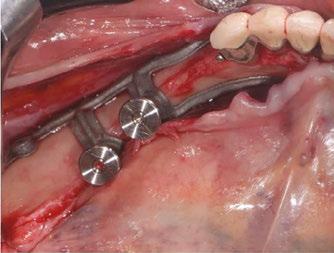
Implant modeling is performed by the company’s designers using their proprietary software, adapting to the clinical case and respecting a common structure. At the vestibular level, the exoskeleton bypasses the chin (mental foramen) foramen, while osteosynthesis screws positioned more posteriorly stabilize the implant on the cortex of the external oblique line. A loop extends and completes the structure on the lateral surface of the ascending branch.
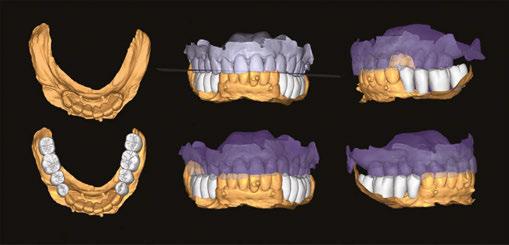
Figure 2: Optical impression (Primescan – Densply Sirona) and prosthetic project based on the antagonist arch (Design4me)
Figure 3: CBCT, optical impression, and digital wax-up uploaded to the Panthera platform dashboard
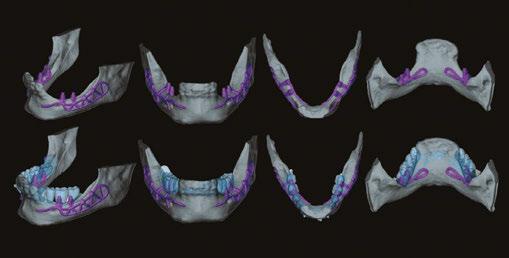
Figure 4: Subperiosteal implant design on the Panthera Dental platform. (Vestibular, frontal, occlusal, and lingual views)
Lingually, the framework forms a loop in the retro-symphyseal region and stops at the most distally located abutment, remaining coronal to the mylohyoid line (Figure 4).
Thanks to the evolution of materials, the development of digital tools, and the improvement of production techniques, Panthera is able to manufacture subperiosteal implants in grade 23 6AL 4V ELI titanium discs using 5-axis milling machines with a precision of 5 mm. Finally, the surface finish is sandblasted in areas in contact with bone and the periosteum to promote bone regeneration.10.11
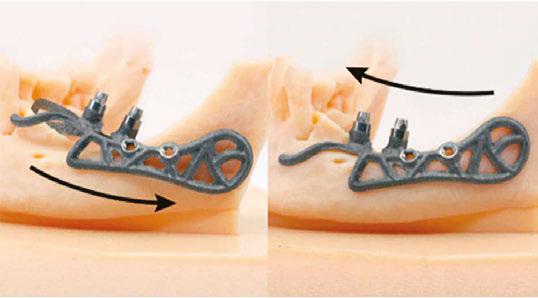
Implants are supplied with a 3D resin model of the jaw. This model is used to check that implants fit perfectly before they are inserted. It also helps the operator find the ideal insertion axis, which should be achieved by distal translation followed by mesio-lingual rotation. This movement may differ slightly from one patient to another (Figure 5).
2. Surgical protocol
The procedure is performed under local anesthetic and lasts between 1 and 1-1/2 hours per side.
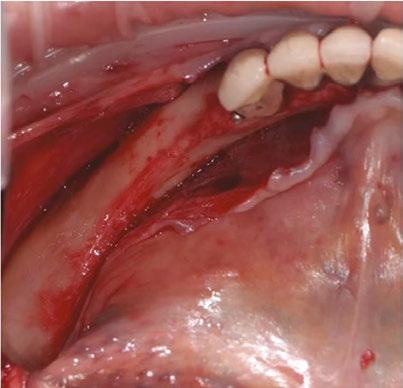
The first step is to raise a flap wide enough to allow adequate access to the surgical site. The crestal incision is made so as to evenly distribute the attached gingiva on either side of the future abutments. It extends to the anterior teeth via an intrasulcular incision and ends along the anterior edge of the ascending ramus.
The aim is to create full-thickness flaps to expose the chin foramen and protect the inferior alveolar pedicle (nerve) on the vestibular side. The detachment should then continue beyond the external oblique line to the basal margin of the mandible, then to the insertion of the buccinator muscle without detaching it.
On the lingual side, it is also important to push back the sublingual compartment by lifting, still in full thickness, to the medial oblique line posteriorly and apically up to the anterior digastric fossa, avoiding effraction of the mylohyoid muscle and mental spines (Figures 6 and 7).12
Some clinicians may choose to use a technique for one-piece subperiosteal implants. However, the author notes that one-piece bilateral subperiosteal implants are more difficult to insert, making surgery more complex. The surgery
Subperiosteal
implants have increased success rates and are becoming a relevant treatment option that deserves our attention.”
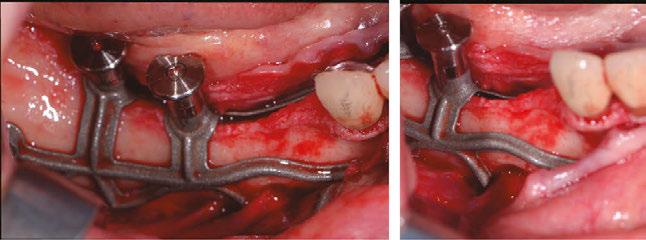
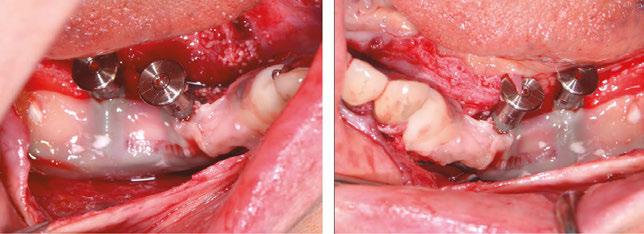
Figure 8 (left): The Panthera SUB implant is gripped to facilitate insertion without damaging it. Figure 9 (right): Positioning the implant and checking its fit (occlusal view)
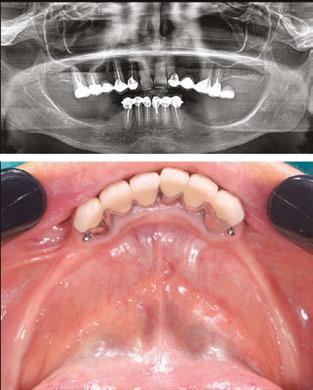
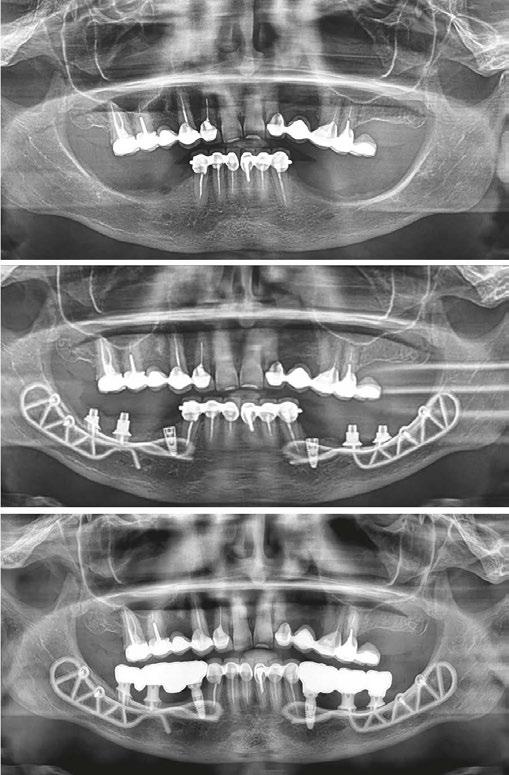
Figure 6 (left): Preoperative situation, panoramic radiograph and intraoral photo. Figure 7 (right): Incisions and flap detachment
Figure 5: Ideal insertion axis for Panthera implants created on the 3D model
time while the flaps are detached is longer with a one-piece bilateral subperiosteal implant, increasing the risk of complications, infections, pain, edema, and discomfort for the patient. If there are minor or major complications, it’s easier to manage them when there are two unilateral subs. Finally, thanks to the large bone/implant contact surface, there is great stability even with a unilateral sub implant, making no difference between a bilateral or two unilateral.
Before inserting the implants, a “soft brushing” technique can be used to relax the flaps and thus allow tension-free closure of the site while preserving the periosteum. The bone is then scraped to ensure that any residual fibrous tissue is removed.
The implant is inserted along the recommended axis, validated beforehand on the resin model. It is advisable to leave the healing abutments in place and use hemostatic forceps to facilitate gripping of the implant, while remaining clear of the subgingival portion during the placement procedure (Figures 8, 9, and 10).
Once the position and fit have been carefully checked, the implant is stabilized using two osteosynthesis screws. A drilling guide is also provided to facilitate the procedure (Figure 11). In this specific case, two endosteal implants are placed simultaneously in positions 34 and 44.
PRF membranes are positioned to optimize gingival healing (Figure 12). Finally, the flaps are sutured tension-free using apical and crestal mattress stitches.
3. Prosthetic steps
After 4 months of osseointegration, the second surgical stage uncovers the buried implants, and a 15-day gingival maturation period around the healing abutments will be observed before proceeding with the prosthetic steps (Figure 13).
Transgingival abutments for subperiosteal implants are similar to those used for endosseous implants. These are tapered abutments designed for a fixed, screw-retained prosthesis.
The steps involved in using prostheses are the same as for conventional techniques:
• physical impression using the pick-up technique (Figure 14)
• fitting mock-ups to validate the prosthetic project (Figure 15)
• final screwing of permanent prostheses (Figure 16)
Figure 10: Positioning the implant, checking its fit, and highlighting the chin foramen (vestibular view)
Figure 11: Drilling guide and implant retaining screws
Figure 12: Covering implants with PRF membranes
Figure 13: Second surgical stage after 4 months of osseointegration and placement of healing abutments
Figure 14: Physical impression
Conclusion
The rehabilitation of atrophic posteromandibular areas is a major surgical challenge. In certain clinical situations, the limits of implant and bone reconstruction therapies may be reached.
Thanks to the evolution of CAD/CAM technologies and the improved accuracy of CBCTs, the subperiosteal technique is becoming a genuine treatment alternative.
Thanks to their unique surgery with no bone contribution, subperiosteal implants are a minimally invasive approach. Postoperative recovery and the risk of complications are thus reduced. Healing times prior to prosthetic rehabilitation are also reduced for the patient.
First developed over 80 years ago, this solution is now more sophisticated and biocompatible than its historical counterpart, with reliable and promising results.
2. Le Bars P, Kouadio AA, Niagha G. Prothèse amovible et pertes de substance des maxillaires: une association incontournable. (Removeable prosthesis and loss of jawbone substance: an essential association.) Paris, France: Editions CdP; 2012;160.
3. Keller Pierre, La gestion des tissus mous après les augmentations osseuses, (Management of soft tissues after bone augmentation) Paru dans Réalités Cliniques n° 3 – September 2018: 205-213. https://www.information-dentaire.fr/formations/ la-gestion-des-tissus-mous-apres-les-augmentations-osseuses/.
4. Urban IA, Nagursky H, Lozada JL, Nagy K. Horizontal ridge augmentation with a collagen membrane and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: a prospective case series in 25 patients. Int J Periodontics Restorative Dent. 2013 May-Jun;33(3):299-307.
5. Khoury F, Hanser T. Three-Dimensional Vertical Alveolar Ridge Augmentation in the Posterior Maxilla: A 10-year Clinical Study. Int J Oral Maxillofac Implants. 2019 Mar/ Apr;34(2):471-480.
7. Davidowitz G, Kotick PG. The use of CAD/CAM in dentistry. Dent Clin North Am. 2011 Jul;55(3):559-570, ix.
8. Janeva NM, Kovacevska G, Elencevski S, Panchevska S, Mijoska A, Lazarevska B. Advantages of CAD/CAM versus Conventional Complete Dentures - A Review. Open Access Maced J Med Sci. 2018 Aug 4;6(8):1498-1502.
9. Truitt HP, James R, Boyne P. Noninvasive technique for mandibular subperiosteal implant: a preliminary report. J Prosthet Dent. 1986 Apr;55(4):494-497.
10. Cohen DJ, Cheng A, Kahn A, Aviram M, Whitehead AJ, Hyzy SL, Clohessy RM, Boyan BD, Schwartz Z. Novel Osteogenic Ti-6Al-4V Device For Restoration Of Dental Function In Patients With Large Bone Deficiencies: Design, Development And Implementation. Sci Rep. 2016 Feb 8;6:20493.
11. Claffey N, Bashara H, O’Reilly P, Polyzois I. Evaluation of New Bone Formation and Osseointegration Around Subperiosteal Titanium Implants with Histometry and Nanoindentation. Int J Oral Maxillofac Implants. 2015 Sep-Oct;30(5):1004-1010.
12. Poitras Y. Diagnotic et plans de traitement (Diagnosis and treatment plans) [Internet]. Canadian Implant Institute. 2021. Available at: https://www.youtube.com/watch?v= y3oNPMEk9Dg
Figure 17: Pano pretreatment (top), during treatment (center) and posttreatment (bottom)
Figure 16: Permanent prostheses screwed in
Figure 15: Fitting mock-up
Continuing Education Quiz
Subperiosteal implants for the rehabilitation of atrophic posterior mandibular regions: A bilateral case report
BIRAULT/DISS
1. Subperiosteal implants, more recently called __________ by some authors, are an innovative concept in custom CAD/CAM implants.
a. AMSJI (Additively Manufactured Subperiosteal Jaw Implants)
b. Zygomatic implants (ZI)
c. Ridge expansion implants (REI)
d. Titanium Manufactured Implants (TMI)
2. first described the concept of subperiosteal implants in 1940.
a. Dr. Gustave Dahl
b. Dr. Per-Ingvar Brånemark
c. Dr. Leonard Linkow
d. Dr. Paulo Maló
3. The first implants, made of and using a direct bone impression from wide-flap surgery, were not very successful.
a. nickel-titanium
b. stainless steel
c. cobalt-chromium
d. zirconium-oxide
4. Subperiosteal implantology offers another treatment solution, as it requires neither bulky reconstruction nor bone anchorage.
a. True
b. False
5. Newer patient-specific implants use to create custommilled patient specific subperiosteal implants.
a. modern CBCT
b. patient scanning technology
c. titanium mesh
d. both a and b
6. The success of the treatment depends largely on the accuracy and quality of the _______.
a. CT data
b. extensive 2D radiographs
c. impression material
d. osteosynthesis screws
7. For the surgical protocol, the aim is to create full-thickness flaps to expose the chin foramen and protect the inferior alveolar pedicle (nerve) on the vestibular side.
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://implantpracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://implantpracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 690
Date Published: August 31, 2024
Expiration Date: August 31, 2027
a. True
b. False
2 CE CREDITS
8. The author notes that one-piece bilateral subperiosteal implants are _______.
a. easier to insert
b. the preferred choice
c. more difficult to insert, making surgery more complex
d. eliminate the risk of complications
9. Before inserting the implants, a technique can be used to relax the flaps and thus allow tension-free closure of the site while preserving the periosteum.
a. “metal artifact redactor”
b. “soft brushing”
c. “oblique technique”
d. “Dahl technique”
10. After of osseointegration, the second surgical stage uncovers the buried implants, and a 15-day gingival maturation period around the healing abutments will be observed before proceeding with the prosthetic steps.
a. 1 month
b. 2 months
c. 3 months
d. 4 months
To provide feedback on CE, please email us at education@medmarkmedia.com Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
Mastering the art of dental implant marketing and strategic sales training
Building success in a competitive market
When choosing a practice for life-changing dental implants, patients have options — and they’re going to weigh them. So, how do you make sure they choose your practice and not someone else’s? At Progressive Dental Marketing™ and The Closing Institute™, two of the nation’s foremost dental marketing and sales coaching authorities, we provide the tools, tactics, strategies, and know-how to encourage patients to choose you.
Competition among practices for full-arch implant cases has skyrocketed in recent years. To maintain or capture market share, you need an experienced dental marketing team and a sharp in-office team with a well-defined system, strategic plan, and the capability to execute effectively on all fronts. When both teams are in place, you will turn your practice into a thriving, life-changing destination for implant excellence.
There’s power in our process, and it begins with marketing. Progressive Dental Marketing is a full-service agency that has helped thousands of implant practices reshape their routine and raise their ROI by continually analyzing market trends, consumer behavior, and competitive landscapes to develop strategies that drive leads. From brand identity and dynamic websites, to customized content and award-winning videos and beyond, we provide you with proven, lead-generating tactics that will scale your practice and grow your brand.
The next step focuses on mentorship. Once your marketing is up and running, and the leads are coming in, we don’t leave you to figure it out on your own. We support you with the training, techniques, scripting psychology, and know-how to immediately increase your closing percentages and case acceptance with The Closing Institute, a division of Progressive Dental.
The Closing Institute is the only business and mentorship course of its kind in the dental industry, and is an accredited ADA CERP and PACE Program provider. Moreover, we are an immersive sales and coaching program designed to empower, train, and equip doctors and their key team members to sell and close more full-arch implant cases with:
• Our proprietary 10-10-10™ process
• 1:1 personalized sales coaching
• Consultation critiques with our CEO, Bart Knellinger
• In-person and virtual events
• Monthly power sessions
• Continuing Education credits and tiered certification program
• 24/7 access to online learning resources
This ensures your team can efficiently manage and prequalify high lead volumes, streamline scheduling, reduce no-shows, empower treatment coordinators as consultation leaders, simplify the consultation process for patient comfort and trust, close price shoppers, and ensure perceived value matches cost for all patients.
Being an amazing clinician isn’t enough. To be more effective, impactful, and profitable, you need knowledge beyond implant dentistry. You must know how to elevate your brand, attract qualified leads, make critical decisions, and have compassionate conversations. Because empathy and personalized care are key components of what we do, ensuring your patients feel understood and valued, which as a result, fosters loyalty and enhances treatment outcomes. Emphasizing these elements, your sales and marketing efforts not only attracts new patients but also solidifies your brand reputation for exceptional patient care.
Each day, a patient is deciding whether to trust you or someone else with their dental implants. If you want it to be you, let’s talk. Scan the QR code to schedule your free consultation today!
How to submit an article to Implant Practice US
Implant Practice US is a peer-reviewed, quarterly publication containing articles by leading authors from around the world. Implant Practice US is designed to be read by specialists in Periodontics, Oral Surgery, and Prosthodontics.
Submitting articles
Implant Practice US requires original, unpublished article submissions on implant topics, multidisciplinary dentistry, clinical cases, practice management, technology, clinical updates, literature reviews, and continuing education.
Typically, clinical articles and case studies range between 1,500 and 2,400 words. Authors can include up to 15 illustrations. Manuscripts should be double-spaced, and all pages should be numbered. Implant Practice US reserves the right to edit articles for clarity and style as well as for the limitations of space available.
Articles are classified as either clinical, continuing education, technology, or research reports. Clinical articles and continuing education articles typically include case presentations, technique reports, or literature reviews on a clinical topic. Research reports state the problem and the objective, describe the materials and methods (so they can be duplicated and their validity judged), report the results accurately and concisely, provide discussion of the findings, and offer conclusions that can be drawn from the research. Under a separate heading, research reports provide a statement of the research’s clinical implications and relevance to implant dentistry. Continuing education articles also include three to four educational aims and objectives, a short “expected outcomes” paragraph, and a 10-question, multiple-choice quiz with the correct answers indicated. Questions and answers should be in the order of appearance in the text, and verbatim. Product trade names cited in the text must be accompanied by a generic term and include the manufacturer, city, and country in parentheses.
Additional items to include:
• Include full name, academic degrees, and institutional affiliations and locations
• If presented as part of a meeting, please state the name, date, and location of the meeting
• Sources of support in the form of grants, equipment, products, or drugs must be disclosed
• Full contact details for the corresponding author must be included
• Short author bio
• Author headshot
Pictures/images/tables
Illustrations should be clearly identified, numbered in sequential order, and accompanied by a caption. Digital images must be high resolution, 300 dpi minimum, and at least 90 mm wide. We can accept digital images in all image formats (preferring .tif or jpeg).
Ensure that each table is cited in the text. Number tables consecutively, and provide a brief title and caption (if appropriate) for each.
Disclosure of AI use
Authors must disclose any AI used in researching, writing, or creating their articles. This includes a language model, machine learning, or similar technologies to create or assist with this submission. If AI was used, please provide a description of the AI-generated content and the name, model or tool used, and manufacturer. If AI was used, please confirm that you take responsibility for the integrity of the content that you are submitting.
References
References must appear in the text as numbered superscripts (not footnotes) and should be listed at the end of the article in their order of appearance in the text. The majority of references should be less than 10 years old. Provide inclusive page numbers, volume and issue numbers, date of publication, and all authors’ names. References should be submitted in American Medical Association style. For example:
Journals: (Print)
White LW. Pearls from Dr. Larry White. Int J Orthod Milwaukee. 2016;27(1):7-8. (Online)
Or in the case of a book: Pedetta F. New Straight Wire. Quintessence Publishing; 2017.
Website:
Author or name of organization if no author is listed. Title or name of the organization if no title is provided. Name of website. URL. Accessed Month Day, Year. Example of Date: Accessed June 12, 2011.
Author’s name: (Single) (Multiple) Doe JF Doe JF, Roe JP
Permissions
Written permission must be obtained by the author for material that has been published in copyrighted material; this includes tables, figures, pictures, and quoted text that exceeds 150 words. Signed release forms are required for photographs of identifiable persons.
Disclosure of financial interest
Authors must disclose any financial interest they (or family members) have in products mentioned in their articles. They must also disclose any developmental or research relationships with companies that manufacture products by signing a “Conflict of Interest Declaration” form after their article is accepted. Any commercial or financial interest will be acknowledged in the article.
Manuscript review and extra issues
All clinical and continuing education manuscripts are peer-reviewed and accepted, accepted with modification, or rejected at the discretion of the editorial review board. Authors are responsible for meeting review board requirements for final approval and publication of manuscripts. If additional issues are desired, they must be ordered from the publisher when the page proofs are reviewed by the authors. The publisher does not stock back issues. Reprints can be purchased after the issue is published.
Proofing
Page proofs will be supplied to authors for corrections and/or final sign off. Changes should be limited to those that are essential for correctness and clarity.
Articles should be submitted to:
Mali Schantz-Feld, managing editor, at mali@medmarkmedia.com
Why thousands of implant specialists have quietly partnered with IDSOs
Chip Fichtner discusses the benefits of a large silent partner
Over the last 5 years, hundreds of single implant and full-arch focused practices have partnered with Invisible Dental Support Organizations (IDSO). An IDSO becomes a doctor’s silent partner by buying 51% to 80% of a practice for cash up front at today’s low tax rates. Doctors remain as owners, with their brand, team, and full autonomy for years or decades. Practice performance can be enhanced, and the upside in a doctor’s retained ownership can be far greater than competing alone.
IDSO partner practices benefit from the resources of a larger silent partner to reduce the administrative burdens of banking, payroll, accounting, compliance, credentialing, tax, and legal. Doctors can also access 30% lower costs on supplies and implants. And many practices today benefit from their partner’s professional, full-time recruiting and marketing teams.
While there are now almost 1,000 IDSOs and DSOs in the U.S., in the last 3 years, several new implant-only IDSOs have been created. They are competing with multispecialty and GP IDSOs for great practices nationally. In an LPS, process values are achieving new records, often with six or more eager, qualified bidders from which doctors can choose the right partner.
Tens of thousands of practices have quietly partnered with IDSOs over the last 35 years in all 50 U.S. states. Some may have only a few practice partners and others over 700. Their size also
gives them leverage in payer negotiations and lower team benefit costs not available to independent dentists.
IDSOs are eager for growing practices with at least $1.8 million in collections, and the younger the doctor, the more valuable the practice. In LPS’ $1.0 billion of completed IDSO partnerships in the last 24 months, over $150 million have been for doctors in their 30s.
The IDSOs act as a doctor’s silent partner. Their goal is to support a practice, not to micromanage it or homogenize a practice to meet some corporate standard. Doctors retain full autonomy, not just clinically, but also in how they hire, fire, and lead their teams. Supply, lab, and payer decisions are made by the owner doctor, not the IDSO.
Ultimately, the IDSO can also provide doctors with a known exit strategy for retirement, years or decades in the future. Thousands of doctors have experienced dramatic increases in the value of their retained ownership over time. Some have experienced equity increases of 300%, 500%, 1,000%, or more when they selected the right IDSO partner.
Doctors today should understand the potential value of their practice in an IDSO partnership. Values achieved by LPS are often twice or more than what a practice might achieve in a doctor-to-doctor sale or associate buy-in. Doctors who own their real estate also have two great options. They have an AAA credit tenant for decades, or due to their new IDSO tenant, the value of the real estate increases in a sale to a Real Estate Investment Trust (REIT) now or in the future.
Chip Fichtner, co-founder of Large Practice Sales which completed over $1.0 billion of IDSO partnerships in 2022 and 2023. Over the past 40 years, he has built, bought, and sold public and private companies in a variety of industries, and has been featured in numerous media outlets. His tolerant wife of 34 years allows him to live on his airplane visiting clients every week. IP
To learn more about IDSOs and receive a confidential, no cost, no obligation practice valuation, doctors can contact Large Practice Sales at 844-577-1057, implant@largepracticesales. com, or by visiting www.LargePracticeSales.com. This information was provided by Large Practice Sales.
Silent Partners Buy Part of Your Practice - IDSOs purchase 51% to 80% of practices for cash now at low tax rates. Doctors retain ownership and have significant upside in the equity value. Some LPS clients have achieved 3x to 7x equity returns in only three to five years.
Long-Term Wealth Building Partnership - Doctors continue to lead their practice with their brand, team and strategy for years or decades. Practices benefit from the resources of a larger, silent partner, but are not micromanaged or homogenized.
Six or More Choices in Partnership - LPS clients often have 6 to 10+ qualified bidders. LPS is the largest advisor which enables our clients to achieve record values that the little advisors cannot match.
Your Value in Today’s Consolidation Frenzy - You should understand the value of your practice in an LPS-advised process. Doctors who deal directly with IDSOs often leave millions on the table and do not get to consider ALL of their options.
Large Practice Sales (LPS) is the largest transaction advisor to GP and specialty dental practices in the U.S. and completed over $1 Billion of Invisible Dental Support Organization (IDSO) partnerships in the last 24 months.
“I am ecstatic! You guys got me DOUBLE the best offer I could get on my own! Have any doctor call me and I’ll tell them you can’t go wrong with LPS. Use my name. I am referring all my friends.”