Delivering a quality patient experience in Guam
Dr. Paul Sauget
Myofunctional therapy for postorthodontic retention
Drs. Ryan Robinson and Carly Jacobs
The importance of maintaining indoor air quality in dentistry







Drs. Tyler Orehek and Troy Roeder
Conservative approach of fortuitously found odontoma in a child with severe autism
Dr. Gabriela Aurora Asensi
Now available! Full custom packaging featuring you, the expert. Only from uLab Systems ™ Visit - ulabsystems.com Summer 2023 Vol 14 No 2 orthopracticeus.com PROMOTING EXCELLENCE IN ORTHODONTICS Bracket & Alignment Systems n 4 CE Credits Available in This Issue*
INNOVATION INSPIRED




At Ormco, orthodontic specialists are at the heart of all we do. From our broad portfolio of best-in-class products that enable greater clinical freedom, to our continuous investment in R&D that leads to breakthrough features, to our education and expert-led events, professional marketing resources, and robust loyalty program that help you grow your practice — you inspire us to innovate every day. So you can continue to improve patients’ lives.




DAMON ULTIMATM SPARK TM ALIGNERS DEXIS™ IS SCANNERS MINI-TWIN TM SYMETRI TM CLEAR AOA ULTIMA TM HOOK 1OrthoPulse® is a registered trademark of Biolux Technology GmbH and is distributed by Ormco. ©Ormco Corporation 2023 MKT-23-0219
GO-ORM.CO/PR-MISSION
BREAKTHROUGH
Technology inspires
Summer 2023 n Volume 14 Number 2
Editorial Advisors
Lisa Alvetro, DDS, MSD
Daniel Bills, DMD, MS
Robert E. Binder, DMD
S. Jay Bowman, DMD, MSD
Stanley Braun, DDS, MME, FACD
Gary P. Brigham, DDS, MSD
George J. Cisneros, DMD, MMSc
Jason B. Cope, DDS, PhD
Bradford N. Edgren, DDS, MS, FACD
Eric R. Gheewalla, DMD, BS
Dan Grauer, DDS, Morth, MS
Mark G. Hans, DDS, MSD
William (Bill) Harrell, Jr, DMD
John L. Hayes, DMD, MBA
Laurence Jerrold, DDS, JD, ABO
Marc S. Lemchen, DDS
Edward Y. Lin, DDS, MS
Thomas J. Marcel, DDS
Mark W. McDonough, DMD
Randall C. Moles, DDS, MS
Elliott M. Moskowitz, DDS, MSd, CDE
Rohit C.L. Sachdeva, BDS, M.dentSc
Gerald S. Samson, DDS
Margherita Santoro, DDS
Shalin R. Shah, DMD
Lou Shuman, DMD, CAGS
Scott A. Soderquist, DDS, MS
John Voudouris (Hon) DDS, DOrth, MScD
Neil M. Warshawsky, DDS, MS, PC
John White, DDS, MSD
Larry W. White, DDS, MSD, FACD
CE Quality Assurance Board
Bradford N. Edgren, DDS, MS, FACD

Fred Stewart Feld, DMD
Gregori M. Kurtzman, DDS, MAGD, FPFA, FACD, FADI, DICOI, DADIA
Justin D. Moody, DDS, DABOI, DICOI
Lisa Moler (Publisher)
Mali Schantz-Feld, MA, CDE (Managing Editor)
Lou Shuman, DMD, CAGS
© MedMark, LLC 2023. All rights reserved. The publisher’s written consent must be obtained before any part of this publication may be reproduced in any form whatsoever, including photocopies and information retrieval systems. While every care has been taken in the preparation of this magazine, the publisher cannot be held responsible for the accuracy of the information printed herein, or in any consequence arising from it. The views expressed herein are those of the author(s) and not necessarily the opinion of either Endodontic Practice US or the publisher.
ISSN number 2372-8396
Whether you’re an early adopter or follow a more conservative approach, it’s an exciting time to be in orthodontics. Fueled by advances in AI and 3D-printing scalability, technology in our industry is evolving rapidly. Just 21 years ago, Align was pioneering sequential aligner treatment using refrigerator-sized SLA machines to make one arch at a time, layer by slow layer. What was cutting edge then would be comparable to a dial-up modem today. We are spoiled by the speed and accuracy of 3D printers that are now available and at a tenth of the cost. The efficiencies gained in the evolution of technology is always inspiring to watch. I must confess I love new technology. When a company asks if I’ll test something, I cannot resist. I’m currently evaluating a novel aligner plastic, a direct print printer and resin, software to help eliminate refinements, and an IDB solution. Working with companies of various sizes, I’ve realized that it is not the amount of money they pump into R&D that makes the difference but rather their fresh approach. Innovation, passion, and nimble company structure give startups an advantage over historical leaders.
If you haven’t implemented them already, you are probably investigating remote monitoring and IDB. Remote monitoring solutions provide greater flexibility for patients and practices, flagging patients for appointments only when necessary. IDB improvements are making the transition between the physical and digital worlds more seamless, and in doing so, facilitating combination treatment. Combining fixed appliances and aligners can result in further efficiencies for the team stemming from fewer attachments as well as reduced appointments and treatment time. Hesitation in combining treatments usually comes with the nuisance of multiple platforms to get the job done. The uLab IDB solution I am currently testing uses the same platform to treatment plan the fixed and aligner phases of my cases, significantly improving my digital workflow. The unique structure of the IDB tray itself is resulting in improved bonding and fewer emergency debonds.
In the next 12-to-18 months, we will see more efficient aligner materials enter the market. These longer-acting aligner plastics will extend the benefit of each stage, resulting in fewer appointments and refinements. I’m eager to see whether these thinner, more comfortable materials also improve compliance.
In 3 to 5 years, the aligner landscape will experience another major shift. Direct printing of clear aligners will be viable when the resin reaches a feasible price point, aligners are produced more rapidly, and the finished product maintains sufficient force. Offices will be able to produce aligners and retainers almost immediately. Aligner biomechanics will change, with orthodontists controlling the regional thickness of plastic, integrating pressure points to maintain or augment force.
Testing new products can take time, but it’s fun and allows me to glimpse the efficiencies on the horizon. These advances will shoulder a greater share of the burden practices are suffering from staffing shortages. Newer technology increasingly allows an office to thrive with a smaller staff, employing tools that enhance their capacity. Once mastered, these tools will make our lives easier.
Eric Wu, DMD, is a Silicon Valley native practicing orthodontics in the San Francisco Bay Area for over 14 years. He is known for state-of-the-art treatment and keeping up with the latest innovations in digital orthodontics. He has extensive experience with 3D printing and has manufactured aligners in-office since 2014. He is an active participant and contributor for several online study groups and orthodontic societies including the Pitts Progressive Study Group. When he isn’t practicing, Dr. Wu enjoys teaching in the orthodontic programs at the University of Nevada, Las Vegas and Roseman University in Henderson, NV. Dr. Wu has two beautiful children with his wife Lisa.
Disclosure: Dr. Wu serves as both an innovation advisor and key opinion leader for uLab systems.

1 orthopracticeus.com Volume 14 Number 2 INTRODUCTION
Delivering a quality patient experience in Guam


Dr. Paul Sauget describes how he takes his experience practicing in the U.S. mainland to the island of Guam and delivers the quality he wants for his patients using the latest technology

2 Orthodontic Practice US Volume 14 Number 2 TABLE OF CONTENTS
approach
fortuitously
odontoma in a
with
autism
CLINICAL Conservative
of
found
child
severe
PERSPECTIVE Be the lotus Lisa Moler, Founder/CEO, MedMark Media............................... 6
MOMENTUM Gone are the days of “spray and pray” marketing for new patients
RDA,
advises practices to get actively involved in their communities 16
VIRAL Is social media placing your personal privacy or your
business at risk?
Pribish offers guidance on
risks of
media ............................................................... 18 8 12
Dr. Gabriela Aurora Asensi discusses treatment of a special needs patient PUBLISHER’S
MARKETING
JoAn Majors,
CSP, CVP,
GOING
small
Mark
minimizing
social
COVER STORY
Cover image of Dr. Paul Sauget courtesy of uLab.
CUSTOMIZE YOUR OFFICE
WITH EFFICIENT & INNOVATIVE PRODUCTS FROM BOYD INDUSTRIES



C600 Exam light Innovative Lighting Technology

Boyd Industries' award-winning operatory equipment for the orthodontic industry is designed to ensure comfort for both patient and doctor. With workplace efficiency and comfort in mind, our new C600 Light is the perfect accessory for your space.
Boyd Industries' C600 Exam Light features cool, power-efficient, and reliable LEDs that emit clear and natural white light for maximum visibility. A front mounter IR sensor allows hands-free operation, light intensity adjustment and switching between light modes.
 M3000LS TREATMENT CHAIR
C600 EXAM LIGHT
M3000LS TREATMENT CHAIR
C600 EXAM LIGHT
r,aeoyd �Industries, Inc. 12900 44th Street North Clearwater, Fl 33762 • 800-255-2693
Drs. Ryan Robinson and Carly Jacobs discuss how myofunctional therapy can help in treating the root cause of some complicated dentitions to minimize relapse






4 Orthodontic Practice US Volume 14 Number 2 TABLE OF CONTENTS CONTINUING EDUCATION The importance of maintaining indoor air quality in dentistry Drs. Tyler Orehek and Troy Roeder discuss the reasons for maintaining diligent air quality standards in the office ...............21 PRODUCT PROFILE Spark™ Clear Aligners & Damon Ultima™ Two systems from Ormco™ designed to meet the needs of orthodontists ............................... 30 INDUSTRY NEWS ....................... 32 BOOK REVIEW All The Best Faces Wear Braces Kyle Fagala DDS, MDS; Neon Canvas: Memphis, Tennessee; 2022; neoncanvas.com............ 33 PRODUCT PROFILE Reduction of patient visits without the expensive lab fee Norris 20/26 System 34 LEGAL MATTERS Anatomy of a dental malpractice action Kristin Tauras, JD, defines the various complex parts of a malpractice claim .......................... 36 FINANCE MATTERS A taxing situation Justin Maxwell offers suggestions for maximizing your tax strategy 39 Connect. Be Seen. Grow. Succeed. | www.medmarkmedia.com READ the latest industry news and business WATCH DocTalk Dental video interviews with KOLs LEARN through live and archived webinars RECEIVE news and event updates in your inbox by registering for our eNewsletter CONNECT with us on social media www.orthopracticeus.com *Paid subscribers can earn 4 continuing education credits per issue by passing the 2 CE article quizzes online at https://orthopracticeus.com/category/continuing-education/ 25 CONTINUING EDUCATION Myofunctional therapy for postorthodontic retention
Performance Reliability Predictability
G&H Orthodontics® wires deliver the predictable forces and movement you want. Benefit from 45 years of craftsmanship that make us the wire leader in orthodontics. Try our most popular and effective options including:


G4™ Nickel Titanium (NiTi)
TitanMoly™ Titanium Molybdenum
Stainless Steel
Get wires that perform for the results you demand at every treatment stage.


Scan the QR code for free samples of G&H Orthodontics’ industry-leading wires.

Be the lotus
In an array of colors, blue, white, purple, red, or pink, lotuses are touted as symbols of peace, beauty, and longevity. I love lotus flowers. Earth.com describes them as extremely strong with the first one estimated to have sprouted millions of years ago. For all of its breathtaking beauty, the lotus flower grows out of the mud, rising above the water. As a result, it also has gained a reputation as a symbol of persistence. What does this flower have to do with anything dental, anyway? Well, like the lotus flower, on our professional and personal journeys, we may have to find the strength to grow out of somewhat messy circumstances or humble beginnings. How do we do it? Persistence, innovation, and constantly reaching for a higher standard.
One way to get out of our rut when we are stuck in the mud is by purging – getting rid of old perceptions, equipment, or materials that hold us back from growing. After freeing up some space, invite future growth by researching and adding new things that can improve life around your office and for your patients. Imaging, 3D printing, AI software, instrumentation – you name it – dental visionaries and entrepreneurs are introducing amazing inventions every day. You just have to find the ones that fit your own space and needs, and maybe even help you grow outside your comfort zone. We hope to be able to help you on your journey.
We have lots of ideas in this issue to help you expand your mind and office. Our Cover Story looks at technology that has made it possible for Dr. Paul Sauget to provide efficient treatment in his Guam-based practice using the latest techniques. uLab has played a significant role in delivering the quality experience that defines his practice philosophy. In our CE, Drs. Ryan Robinson and Carly Jacobs take a look at how myofunctional therapy and orthodontics can be integrated for more successful retention. In our other CE, Drs. Tyler Orehek and Troy Roeder write about how maintaining air quality in the dental office can affect the spread of illnesses. In our Clinical Column, Dr. Gabriela Aurora Asensi discusses conservative treatment of a special needs patient when orthodontic treatment is not feasible.
At MedMark, we don’t want your practices to be stuck in the mud of mediocrity. Ora Nadrich, life coach and mindfulness teacher said, “On the path of self-realization, there is no one big awakening, but many along the way of varying degrees: some small, some big; and each one of them is like the lotus flower, which grows out of muddy waters.” So my message this issue is: No matter how small or big your practice, be a lotus; keep growing, changing, and reaching for whatever it takes to make you blossom.
To your best success,
Lisa Moler Founder/Publisher MedMark Media
Published by
Publisher
Lisa Moler lmoler@medmarkmedia.com
Managing Editor Mali Schantz-Feld, MA, CDE mali@medmarkmedia.com
Tel: (727) 515-5118
National Account Manager Adrienne Good agood@medmarkmedia.com
Tel: (623) 340-4373
Sales Assistant & Client Services Melissa Minnick melissa@medmarkmedia.com

Creative Director/Production Manager Amanda Culver amanda@medmarkmedia.com
Marketing & Digital Strategy Amzi Koury amzi@medmarkmedia.com
eMedia Coordinator Michelle Britzius emedia@medmarkmedia.com
Social Media Manager April Gutierrez socialmedia@medmarkmedia.com
Digital Marketing Assistant Hana Kahn support@medmarkmedia.com
Website Support Eileen Kane webmaster@medmarkmedia.com
MedMark, LLC

15720 N. Greenway-Hayden Loop #9 Scottsdale, AZ 85260
Tel: (480) 621-8955
Toll-free: (866) 579-9496
www.medmarkmedia.com
www.orthopracticeus.com
Subscription Rate
1 year (4 issues) $149
https://orthopracticeus.com/subscribe/
6 Orthodontic Practice US Volume 14 Number 2 PUBLISHER’S PERSPECTIVE
Lisa Moler Founder/Publisher, MedMark Media
A SENSAT NAL & GENTLE CLEAN DESIGNED FOR

SYSTEM INCLUDES:

• Oral-B® iO™ Electric Rechargeable Toothbrush

• Crest® Braces Care Toothpaste (4.1 oz)
• Crest® Braces Care Mouthwash (475 mL)


• Oral-B® Superfloss™ Mint (50 ct.)
Brush head refills include:
• Ultimate Clean • Targeted Clean 3 units/case
FREE downloadable practice management materials also available (simply scan QR code and look in resources tab).
©
ORDER AT CRESTORALBPROSHOP.COM
ORTHO
SUCCESS
P&G ORAL-30446 PWR0024 Brought to you by
2023
Delivering a quality patient experience in Guam
Dr. Paul Sauget describes how he takes his experience practicing in the U.S. mainland to the island of Guam and delivers the quality he wants for his patients using the latest technology

Dr. Paul Sauget is home again. In 2018, he set up practice in the U.S. Territory of Guam and could not be happier to be back on the island with its tropical beaches and welcoming culture.
Returning to this 212-square-mile island to open Future Smiles Orthodontics was no small feat. After completing his undergraduate and dental graduate studies, he served 4 years in the U.S. Navy, helping to make the smiles of Navy pilots and Marines as healthy as possible. He went on to complete his orthodontic residency at Indiana University, and eventually launched various practices in Los Angeles and Sonoma County while associating in Beverly Hills, California.

Now, Dr. Sauget’s practice, Future Smiles Orthodontics, is bringing the “Hollywood Smile” concept from California to the Western Pacific. He also joins his brother Dr. Earl Sauget of Pacific Smiles Orthodontics as the only Board-certified orthodontists in the region.
It starts with a sound practice philosophy
Quality is a value that I prioritize in my practice. Quality has a lot of facets to it, like a precious stone.
We prioritize complete quality care in my practice, from the smiles we produce to the daily tasks of record keeping. Patient cases should be completed on time and with Board-quality finishes. Cutting corners with patient care is not allowed by anyone on the team; we hold ourselves to the ABO level of care and ensure our patients feel they are getting the best we can offer.
Paul Sablan Sauget, DDS, MSD, a Board-certified orthodontist in Guam, practices at his private practice Future Smiles Orthodontics. Before attending the University of the Pacific School of Dentistry, Dr. Sauget attended Marquette University for his undergraduate degree, where he also played NCAA Division 1 tennis. After graduating from dental school with honors in 2004, Dr. Sauget served in the U.S. Navy as a dental FMF officer at 29 Palms USMC Air Ground Combat Center in the Mojave Desert, then at his own Navy dental clinic at Ops Side NAS Lemoore, where he took care of the fighter squadrons. After 4 years of active duty in the U.S. Navy and Marine Corps, he attended Indiana University for orthodontics residency. Upon graduation, Dr. Sauget associated with his older brother in Guam while also starting practices in Los Angeles and Sonoma County. Prior to opening his solo practice in Guam, he was an associate at a practice in Beverly Hills. Dr. Paul also enjoys flying as a private pilot (with the eventual goal of an ATP license for part-time airline work) and working toward his auto racing license in his spare time.

Quality also means using the most advanced technology and techniques in everything we do. Relying on what used to be the highest standard of care or outdated products is not the experience we want to deliver at our practice.
This also translates into the office presentation. Everything should feel new and should be constantly rejuvenated. The cleanliness and freshness of the office reflects quality to patients; it sets the tone for the level of service they will receive from our facility.
Another facet of the quality value proposition that I strive to deliver is maintaining high morale within my team. We focus on maintaining enthusiasm and energy during patient care days — patients can feel that energy and the welcoming environment the moment they enter. Our team is viewed as a family, which ties into the island culture. We celebrate each other’s accomplishments, and everyone is cross-trained to help whenever a teammate is out of the office. I never want to be viewed as a boss. I am more like a head coach of a championship level team. I empower my staff to be professionals and own their skills and responsibilities. Lunch parties and beach days also help!
8 Orthodontic Practice US Volume 14 Number 2 COVER STORY
Efficient operations are also integral to a quality patient experience. In addition to my dental training, I majored in both biomedical sciences and business administration. My studies in science and business and my military experience running a dental clinic in the Navy gave me a strong foundation in practice operations. Everything must be “squared away” as they say.
How uLab® helps me deliver the quality experience I want
Suppliers play a significant role in delivering the quality experience that defines my practice philosophy. uLab has been an excellent partner in this effort.
Efficiency is a key in delivering cutting-edge orthodontics to today’s patients. As the only two Board-certified orthodontists in Guam, we are very busy. We need to make the most of every appointment and treatment plan. I have noticed my uLab cases require fewer aligners than other systems, by as much as 30-50%. This efficiency in treatment is an advantage both for the practice as well as our patients.

In addition to requiring fewer stages for the treatment, refinements have been more reasonable. In the past, I used to have as many refinement aligners proposed as in the original treatment — sometimes more. How do you explain that to the patient? That can take away from the confidence they have in the modality of treatment or their practitioner. My experience is that there are often far fewer refinements with uLab than with other aligner companies because I have control over the treatment parameters. I can define proper staging so there are no collisions that can push things off course. I can define velocity of the stages and even the trimline I prefer for my patients.
Also, since uSmile aligners can be purchased a la carte, finishing a fixed case with three or four aligners is easy. To do this with the pioneer brand would have been cost prohibitive. By ordering a few aligners, I can avoid repositioning brackets, bending wires, or using tooth positioners to finish a case (though I personally still
love repositioning and bending wire), and the patient is happy to get the wires off and have a removable option for those last few months. They love that I am doing them a huge favor!
Combination treatment is becoming more common in my practice now because uLab has made it more feasible. Combo treatment can save significant treatment time for patients by optimizing the right tool for the right movements and allowing me to think about the best option for that patient with their timeline and goals in mind. The associated pricing structure from uLab means I can affordably integrate aligners in more cases and create a bespoke experience. If a patient wants to remove their braces early and finish treatment with aligners, we can accommodate that; the reduced chair time easily offsets the modest lab fee. I used to treat 10% to 15% of my cases with aligners; now I use them in over half of my cases. With the many military families in Guam, the flexibility to transition patients to aligners to complete their treatment remotely during a deployment or after a transfer has been very helpful.
Making aligners available to a greater percentage of patients enables me to reach that high-quality service ideal that I hold my practice to on every level.

Employing sensible biomechanics reduces IPR and increases efficiency
I am fortunate to have a digital assistant on staff, and we utilize the uAssist™ concierge service from uLab to help with the bulk of the treatment planning. We appreciate receiving treatment plans back within a day or two from the licensed dentists and orthodontists on the uAssist team.1 This resource increases our efficiency by providing individualized treatment plans without compromising quality. They allow our preferences to be the basis for the resulting treatment plans, and they care to ensure we are completely satisfied. With this service, we can review case designs, make the rare minor adjustment ourselves in just a few moments, and order aligners right away.
9 orthopracticeus.com Volume 14 Number 2 COVER STORY
I also appreciate the uAssist team’s approach to biomechanics — the tooth movements make sense logically and are based on best practices gleaned from mechanical principles. Their recommended process of extrusion and intrusion and having relative anchorage around other parts of the arch helps ensure predictable outcomes. When we view the treatment plan animation, my digital assistant and I nod in agreement because the biomechanics are realistic. We can visualize the teeth actually moving the way the animation portrays it.
One example of this that I really like is the choice and placement of attachments for rotations while everything else anchors properly.
In addition, there is minimal round-tripping. Treatment plans from uAssist show excellent biomechanics and logical point A-to-B movements. They create space for de-rotations; we see an obvious demarcation of space opening as the tooth rotates. It’s like an open coil, making the space first so the tooth can turn instead of requiring IPR and rotating into a tight spot. Due to this, I use almost no IPR with my uSmile aligners, saving chair time and providing a superior patient experience.
Logistics
Being in the Western Pacific, you can imagine the challenges we have with shipments from the mainland United States or other major manufacturing centers. We had always accepted long delivery times as inevitable and tolerated it due to our location. Before working with uLab, we waited weeks for aligner delivery. Patients would be impatient to get started with their treatment, and I would hesitate about prescribing aligner treatment when a faster start was needed.
Since starting with uLab, we receive aligners rapidly, which has been a game changer for our operations. uSmile™ aligners are delivered to the island in as little as a week — even Amazon takes longer! There is only one FedEx® aircraft to Guam every week, arriving via Anchorage, Alaska, on Sunday afternoon. If we approve a case by Wednesday morning our time, it is usually manufactured and delivered to our office the following Monday.2 As a result, starting cases is faster. Even converting from
braces or functional appliances to aligners is met with minimal relapse due to faster shipping, improving the patient experience.
Branding
Orthodontists know it is essential to be a part of the community and give back to the people who support their practice. In a tight knit community, this is even more important. Future Smiles Orthodontics supports events and causes throughout the island that help to establish familiarity and trust between the community and our practice.

We take advantage of the custom packaging option for our uSmile aligners, so they arrive in a box printed with the Future Smiles logo. This reinforces our brand and our contributions to the community, highlighting the same logo that flies over our outreach projects; it gives our whole team a sense of pride, enhancing their love for what they do.
Quality is the driving force behind my practice. My team and I strive to provide it in every moment of our patient experience and the outcomes we deliver as planned and on time. We work with our partners at uLab to efficiently offer consistent and predictable results, supporting our standard for treatment excellence. Our patients can feel the difference, too. They can feel it in the welcoming environment they walk into, the streamlined delivery of their aligners, and the efficient treatment they enjoy using the latest technology and techniques, all of which culminates in the smile they see reflected in the mirror.
ENDNOTES

10 Orthodontic Practice US Volume 14 Number 2 COVER STORY
1. Most cases are returned for first review within 3-business days. 2. Delivery times may vary. uSmile aligners are usually delivered within 10 business days after case acceptance. OP
I appreciate the uAssist team’s approach to biomechanics — the tooth movements make sense logically and are based on best practices gleaned from mechanical principles.
–Dr. Kevin
Coastal Orthodontics




Custom packaging is here No need to buy bulk packaging and figure out how to store it in your office. When you order uSmile™ clear aligners from uLab, the packaging is created with your logo on the box, pouches and aligner storage case. Promote your brand every time a patient removes their aligners. To learn more call 866.900.8522 or visit ulabsystems.com © 2023 uLab Systems, Inc. All Rights Reserved. uLab Systems, uSmile, uAssist and uView are trademarks and uLab and uDesign are registered trademarks of uLab Systems, Inc. MAR-0001356 Rev 1 Only from uLab Systems™ How does uLab® deliver aligners in 10-business days already packaged with your logo? That’s a secret. But your logo shouldn’t be. When a patient is presented with a custom-branded package, it reinforces the value of receiveing a high-quality aligner that was designed by somone they know and trust. The patient’s confidence in us and their peace of mind are invaluable.”
Oliviera,
uSmile aligners are made in the USA. uLab recycles over 80% of our aligner molds.
Conservative approach of fortuitously found odontoma in a child with severe autism
Dr. Gabriela Aurora Asensi discusses treatment of a special needs

patient
Abstract
A case of an unexpectedly found compound odontoma discovered while treating a pediatric dental patient with autism during oral rehabilitation under general anesthesia is presented. This odontoma caused impaction of the right central maxillary incisor. This patient shows how an impacted maxillary central incisor with a completely formed root erupted into the mouth after removing its blocking odontoma which took 5 years to complete. Orthodontic extrusion was not achievable due to the patient’s inability to cooperate with orthodontic treatment. Subsequently orthodontic extrusion was not necessary. The conservative approach used with this patient shows how the teeth can erupt on their own. The patient illustrates how a conservative approach can pay off by giving patients with special needs and their caretakers hope when orthodontic treatment is not feasible because of special needs that preclude such treatment.
Introduction
Odontomas are defined as a benign tumor of odontogenic origin.1 They are basically classified into two types, complex and compound.2 Compound odontomas consist of small toothlike structures, and complex odontomas are a conglomeration of dentin, enamel, and cementum.3 Analysis has revealed that compound odontomas, the most common type,4 are usually diagnosed in the second decade of life.5 Their presence causes interferences in tooth eruption including impaction, delayed, and/or ectopic eruption.6 Normally, there is no potential for eruption when the impacted tooth has a completely formed root or when the homologous tooth has been erupted for at least 6 months with complete root formation.7 Orthodontic extrusion is a common way to erupt impacted teeth after odontoma removal if the root is completely formed.8 However, this might not be
Gabriela Aurora Asensi, DMD, MPH, CLC, received her first dental degree from Universidad Central de Venezuela. In 1996, she completed a general dentistry residency program at Miami Children’s Hospital becoming chief resident. In 2000, she also completed the joint residency program of Miami Children’s Hospital and University of Florida. She completed the Doctor of Dental Medicine (DMD) degree at Nova Southeastern University in 2003. Dr. Asensi also graduated from Florida International University (FIU) with a Master in Public Health in 2021. She is a pediatric dentist in private practice in Miami, Florida.
possible with autistic children. Although malocclusions occur more often in physically and/or mentally disabled children, the most severely handicapped patients are those least likely to receive orthodontic treatment due to their uncooperative behaviors.9 This patient shows how the removal of a fortuitously found odontoma in an autistic child treated under general anesthesia by a pediatric dentist allowed an impacted maxillary right central incisor to fully form a root and erupt into the mouth. This tooth found its way into the oral cavity but took 5 years to do so.
Description
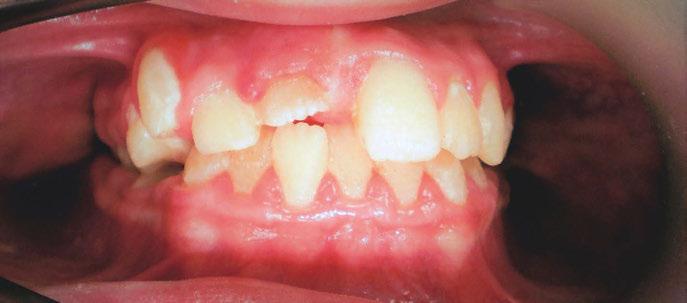
An 8-year-old Hispanic male presented to our private practice in Miami, Florida with the chief complaint of a missing front tooth (Figure 1). Upon review of his medical history, the mother revealed that her son had Autism Spectrum Disorder and confirmed that his condition was severe. This patient did not take

12 Orthodontic Practice US Volume 14 Number 2 CLINICAL
Figure 1: Face of 8-year-old patient at initial consultation


Monitor your patients Open up chair time. “Using DentalMonitoring on braces patients helped me eliminate unnecessary appointments and triage emergencies. I optimized my scheduling with 24.5% fewer physical visits to the practice.” - Dr. Paolo Manzo Master Smart Orthodontics. Create your future. Contact us today. *Dr. Paolo Manzo. The benefits of using DentalMonitoring in fixed appliance orthodontic therapy: Improved efficiency, early detection, and management of emergencies. DentalMonitoring, SmileMate and Vision are products designed and manufactured by Dental Monitoring SAS, under the DentalMind branding for Health Care Professionals (HCPs). They are also used by patients under the mandatory supervision of Health Care Professionals (HCPs). DentalMonitoring and SmileMate are designed to assist HCPs with remotely observing intraoral situations (and monitoring orthodontic treatments for DentalMonitoring). Refer to your HCP and/or the Instructions for Use before use. DentalMonitoring product is a medical device (in Europe only), registered as such and holding the CE mark. Vision simulations are generated using artificial intelligence, they are not contractual and may differ from the final results of the patient’s treatment. Product availability, claims and regulatory status may differ across countries depending on local regulations. Contact your local representative for further information. AD_MON_AD_ ad_100_01_rd_H_MF_en.
any medications, was nonverbal, avoided eye contact with any staff member including the treating pediatric dentist, did not sit in the dental chair, and was constantly tapping his ears. No dental radiographs were obtained due to his uncooperative behavior. For the dental exam, the mother agreed and consented with placing him in a passive restraining device. With a limited visualization of his oral cavity, a mixed dentition was noted. The maxillary right permanent central incisor was absent. No significant pathology was found in his oral soft tissues. Dental caries was found on both primary and permanent molars. A decision was made to complete dental treatment using general anesthesia as a behavior management technique at the local children’s hospital.
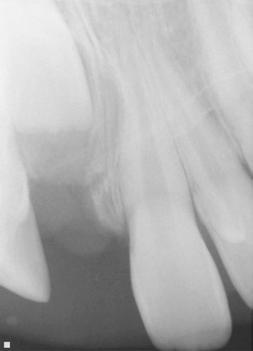
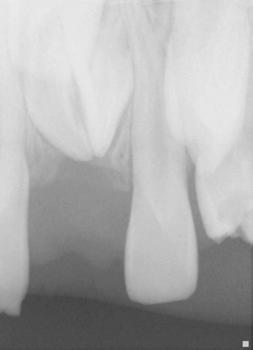
The following procedures were accomplished under general anesthesia on an outpatient basis — full mouth dental radiographs and a comprehensive oral exam. A complex odontoma was found to be the etiology of the noneruption of the maxillary right permanent central incisor (Figure 2). Since dental caries also was diagnosed, a full-mouth prophylaxis was completed. Dental caries was controlled, and teeth were restored. A 5 mm incision was made on the gingiva over the impacted maxillary right permanent central incisor, and two tooth-like structures were extracted from the right maxillary incisor area. A postoperative periapical radiograph was taken to confirm complete odontoma removal (Figure 3). Three interrupted sutures using 3-O chromic gut were placed.
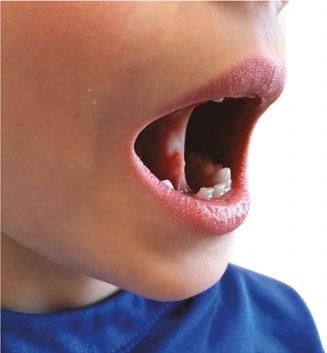
At the postoperative consultation with the mother, we told her the tooth’s complete root formation might prevent its eruption. Orthodontic extrusion of the incisor was ruled out due to his behavior. A conservative approach with observation only was elected as treatment modality. This patient returned for follow-up appointments at ages 10, 11, 12, and 13. During all these visits, the maxillary right permanent central incisor had not erupted. At age 14, due to recurrent dental caries, the patient was taken to the local children’s hospital for dental rehabilitation again. During this second hospitalization, we noticed that the right maxillary central incisor was partially erupted into the oral cavity (Figure 4).
Discussion
It is well known that autism is a serious developmental disorder that impairs the ability to communicate and interact with others. Children with autism pose a challenge in terms of behavior management in the standard dental setting. Comprehensive orthodontic treatment offers clinicians even more of a challenge with these patients.
Every patient needs to be evaluated individually because a great deal of cooperation and time is required for orthodontic treatment. Parents need to understand that in severely autistic children, orthodontic treatment might not be a viable solution. Communication is paramount, and realistic expectations ought to be communicated with these children’s caretakers. This patient illustrates that a conservative approach consisting of odontoma removal was enough to allow eventual eruption of the incisor.
Conclusion
Pediatric dentists, by training and expectation are primarily therapists, but with this patient, minimal therapy produced a good outcome.
REFERNCES
1. Odontoma. Dorland’s Illustrated Medical Dictionary. Philadelphia: Elsevier Health Sciences; 2011:1313.
2. Satish V, Prabhadevi MC, Sharma R. Odontome: A Brief Overview. Int J Clin Pediatr Dent. 2011 Sep-Dec;4(3):177-185.
3. Katz RW. An analysis of compound and complex odontomas. ASDC J Dent Child. 1989 Nov-Dec;56(6):445-449.
4. Budnick SD. Compound and complex odontomas. Oral Surg Oral Med Oral Pathol. 1976 Oct;42(4):501-506.

5. Suri L, Gagari E, Vastardis H. Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004 Oct;126(4):432-445.
6. Kjær I. Mechanism of human tooth eruption: review article including a new theory for future studies on the eruption process. Scientifica (Cairo). 2014;2014:341905.
7. Review Article. Mechanism of Human Tooth Eruption: Review Article Including a New Theory for Future Studies on the Eruption Process Scientifica Volume 2014 (2014), Article ID 341905, 13 pages
8. Strategies for treating an impacted maxillary central incisor. International Orthodontics Volume 8, Issue 2, June 2010, Pages 152-176
9. Behaviour management needs for the orthodontic treatment of children with disabilities. The European Journal of Orthodontics 22(2):143-9 · May 2000.
14 Orthodontic Practice US Volume 14 Number 2 CLINICAL
Figures 2 and 3: 2. Periapical radiograph of involved area taken in the operatory during initial dental rehabilitation under general anesthesia (left). 3. Periapical radiograph of involved area taken in the operatory during initial dental rehabilitation under general anesthesia immediately after odontoma removal (right)
OP
Figure 4: Photograph of area at 14 years old during second rehabilitation under general anesthesia


Gone are the days of “spray and pray” marketing for new patients
actively involved in their communities
JoAn Majors, RDA, CSP, CVP, advises practices to get


Since my career in dentistry has spanned nearly 4 decades, I’ve seen many things change in the realm of marketing for new patients. Gone are those days when we could honestly “spray something out and hope it stuck” regarding how we thought marketing for new patients worked. Early in my career, I worked with a unique and talented orthodontist who was very involved and President of the Houston District Dental Society and the Southwest Orthodontic Society. He was an incredibly creative mind who loved coming up with ideas for us to grow his two locations. He semi-created the concept, and I executed it! This was a time when the referring GPs were loyal, and we focused on them for our growth. It worked well at that time. We could literally spray some new events, food, and swag out there, and something would stick for just about all our referrals. I mean no disrespect; just making a point of how drastic the times have changed marketing strategies for orthodontics.
Fast forward, and now we are in a time when that strategy no longer works. Nowadays, more GPs and pedodontists are training and doing much more than interceptive orthodontics. With the emergence of the clear aligner market and their powerful marketing to practices other than orthodontics, you need an excellent, purposeful marketing plan now more than ever — a plan that can be measured and expectations set for clear understanding. (We want to do XYZ and expect ABC results by this date.) Expectations have changed as much as the actual marketing, partly due to the publicity around social media and reviews.
In one of our practices, an orthodontist rented our office located in a “bedroom community” about 35 minutes from the
JoAn Majors, RDA, CSP, CVP, has spent the last two decades focused on the soft skills that create greater connections and impact with every relationship individuals have within dentistry. She is the author of four books and published in over 25 magazines and newsletters. Her platform voice and writing voice are authentic to her storytelling style, and she has a passion and expertise for inspiring team members to their greatest potential. She has earned the highest designation of a Professional Speaker (CSP) Certified Speaking Professional from the National Speakers Association and is a member of multiple organizations in and out of dentistry. She is on the advisory board for Dental Entrepreneurial Women Magazine (DeW Life).
JoAn and her dentist husband co-founded The Soft Skills Institute, LLC., a nationally recognized AGD PACE provider. A content creation specialist, her speaking and training are augmented by her online curriculum (available to lease) for greater adoption, scalability, and ease of implementation. To see her in action or learn more, visit www.joanmajors.com.
city. He always reminded me of the gentleman I had worked for with his creative ideas. This practice’s involvement in the community made his group a household name, literally. I’m positive some of his patients were third-generation in a family. He did the general things like sports and cheerleader calendars for the schools, but he had a fantastic team of happy individuals who were a big part of the culture created in the practice. They sponsored a newsworthy clip called “A Reason to Smile.” People from the area could submit their pictures online, and their story and photo, if picked a winner, would be featured on the morning and evening news, accompanied by a fantastic gift. They received pictures of everything you can imagine from babies, anniversaries, birthdays, and trips that would bring a smile! It was “a thing” that everyone remembered or knew about. It was also great for featuring a broad community of people on social media and driving traffic to their website from others.
Community-wide involvement can be incredible, and it’s magical with a great team to help. I worked with a client who rented an entire theater for two dates at the matinee and encouraged his patients to invite a friend. The group shared the upcoming event with patients and parents and promoted the “bring a friend” part. It was an expensive endeavor, but it became “a thing,” and the group became known for the “Summer Movie Party.” Whatever the big new summer movie was, it worked. Patients had to register for the tickets by calling the practice, and of course, they collected the invitee’s names and a parent email for safety and perhaps a little follow-up marketing with the parents. The team was at the curb of the theater, opening doors and greeting those attending. You would have thought celebrities were in town with the red carpet (literally) and smiles. The
16 Orthodontic Practice US Volume 14 Number 2 MARKETING MOMENTUM
Jurassic World series and films like this functioned well for so many age groups; it was perfect. However, it is more than hosting significant events or sending Donut Dolly around with treats today. It combines many action items and how you use them to drive the results you expect.
Recently, I reached out to Ian McNickle, MBA, Co-Founder and Partner at WEO Media (Voted 4 times Best in Class Award) to get his input on what they know to be true about community involvement and sharing this type of news as a marketing tool. Here is what he had to say.
“Based on our experience of having marketed for hundreds of dental and specialty practices, we generally find practices with a continuous dose of new online reviews each month in combination with a great website and active social media engagement perform well above average for new patient growth. Orthodontic practices who are actively engaged in the community would do well to highlight this activity on their social media and websites in order to increase Google rankings and local awareness.”

To sum up — today, you’ll need a combination of specific solutions for a successful marketing plan. The first orthodontist I worked with wasn’t concerned about social media or Google reviews. That was then; this is now! Many who read this will now call your providers for these services and rethink your plan, investment, and expectations. If you are one of the lucky
ones who are geographically desirable and don’t need as much structure in your marketing, consider yourself blessed. When I speak, I often write and share with my audiences; we are in a connection economy. Today people want connection, and they trust based on that connection. There was a time when degrees and specialties drove the trust factor. It’s just not so these days. Now, if you listen to patients or potential patients and connect with them, they will trust you.
Remember, it’s an individual preference, and you and your team (if you choose) should meet and discuss what might work best in your community. What could you do differently? Your team likely has family and perhaps teens in their household who have specific places they congregate or hang out. How can you meet them where they are? Be creative, or let those creative team members weigh in. Lastly, who is the professional in your circle of solutions you can turn to for insight on these critical issues today?
17 orthopracticeus.com Volume 14 Number 2 MARKETING MOMENTUM
We are in a connection economy. Today people want connection, and they trust based on that connection. If you listen to patients or potential patients and connect with them, they will trust you.” OP
Is social media placing your personal privacy or your small business at risk?
Mark Pribish offers guidance on minimizing risks of social media

Some critics of social media say our addiction to apps in general and social media (in particular) open ourselves up to privacy risks. My question to app and social media users is, “When was the last time you read the terms and conditions or adjusted the privacy settings of your app or social media accounts?”
While apps and social media offer convenience, entertainment, and networking opportunities — cyber thieves and ID-theft criminals are leveraging social networks and apps to do their dirty work.

According to the second quarter 2022 Brand Phishing Report from Check Point Research, which “highlights the brands that were most frequently imitated by cybercriminals in their attempts to steal individuals’ personally identifiable information (PII) or payment credentials over the quarter,” LinkedIn remains the most impersonated brand by phishing campaigns.1
As most know, LinkedIn is not only a social media site but also the world’s leading professional networking site. Hackers have imitated brands in business sectors such as social media (LinkedIn), technology (Microsoft), shipping/courier services (DHL), and online shopping (Amazon) and highlights the ongoing risks facing users of trusted business platforms.
I have listed below from the Check Point Research Brand Phishing Report the top-ranked brands by their overall appearance in brand phishing attempts.2
These imitation phishing scams of leading brands are effective and lucrative for cyber thieves and ID-theft criminals because both consumers and business executives are more likely to click on a well-known name/brand.
But sometimes it’s more than just the hacker you must worry about. Consumers and business executives need to know that apps and social media can track your search engine history, purchasing habits, geographical location, and even investigate your files and contact list — all without your knowledge and sometimes without your permission.
For example, when you install an app, most apps will require you to “accept” their terms and conditions — but did you read and really understand the type of information that is being collected and the kind of privacy threats you now are exposed to?
How bad can these “privacy threats” be? Just imagine an app vendor or third-party marketer collecting and selling your smartphone’s unique device ID, phone’s location, phone number, your age, gender, likes, dislikes, search engine habits, emails, usernames, and more to data brokers. And then imagine how these data brokers collect, analyze, and package your most sensitive personal information in a unique profile and sell it over and over again — without your knowledge.
But it gets worse as The Federal Bureau of Investigation (FBI) released its Internet Crime Complaint Center (IC3) 2021 Internet Crime Report and accompanying 2021 State Reports last March.3 The FBI reported 847,376 complaints of suspected Internet crime in 2021, a 7% increase from 2020 that resulted in losses exceeding $6.9 billion. This is happening even though small and big businesses along with state and Federal governments spend billions of dollars to fight daily cybersecurity attacks.
18 Orthodontic Practice US Volume 14 Number 2 GOING VIRAL
1. LinkedIn (45%)
2. Microsoft (13%)
3. DHL (12%)
4. Amazon (9%)
5. Apple (3%)
6. Adidas (2%)
7. Google (1%)
8. Netflix (1%)
9. Adobe (1%)
10. HSBC (1%)
Mark Pribish is the Practice Leader, Identity Theft and Data Breach Solutions at Scottsdale, Arizona-based Vero, LLC. He has authored hundreds of articles and is frequently interviewed by local and national media as an identity theft and data breach risk management expert. He is a member of the Identity Theft Resource Center Board of Directors and is a graduate of the University of Dayton.

© 2023 Align Technology, Inc. Align, Invisalign, and Vivera, among others, are trademarks and/or service marks of Align Technology, Inc. or one of its subsidiaries or affiliated companies and may be registered in the U.S. and/or other countries. A004525 Rev B 1 Data on File at Align Technology as of January 13, 2022. Keep your patients smiling long after treatment with Vivera retainers. Learn more at Invisalign.com/provider Vivera retainers are at least 30% stronger and twice as durable than other leading clear retainer materials such as Essix Plus, Essix Ace, Essix C+, Invisacryl A.1 Shift happens. Prevent it with Vivera™ retainers.
Microsoft is an example of a large and sophisticated technology company with annual revenue of $168 billion that spends about $2 billion annually to respond to current and future cybersecurity challenges and threats. At the same time, hackers focusing on Microsoft vulnerabilities have successfully beached Microsoft 4 times, creating four significant data breach incidents that have exposed customer data and placed clients at risk during the last 12 months.4
In addition, the FBI Internet Crime Report stated that of the more than 30 crime types reported, the top three cybercrimes were phishing scams, non-payment/non-delivery scams, and personal data breach, closely followed by identity theft and extortion.
The reality is that small- and mid-sized businesses such as dental and medical practices are viewed as easy targets because of limited resources and poor information security best practices.
The fact is that cyber thieves and ID theft criminals love the trail we leave on social media. Specific to individual consumers and small business employees, here are my five tips to help you minimize your social media privacy risks:
1. Limit and/or eliminate sharing your personal information online.
2. Increase your privacy awareness by reviewing and adjusting your privacy settings.
3. Be aware that some apps reset your privacy settings during major upgrades.
4. Learn more about how your personal information is used and for what purposes.
5. Consider using “privacy assistant or automation software” to help keep your privacy preferences current.
Specific to small (and big) businesses, no one company can ever prevent itself from ever experiencing a data breach event — especially with how apps and social media can place a small business at risk. Some of the most notable data breaches in 2021 and 2022 include CNA, Experian, Facebook, GEICO, Instagram, LinkedIn, Marriott, Microsoft, Tesla, and Twitter.
The irony to these data breaches is that these businesses pride themselves on safeguarding PII, and these businesses have more financial and information technology resources than most other business. Yet they still cannot prevent a data breach event from happening.
The reality of data breaches is that they occur almost every day — whether it is an accidental release (which is a polite phrase for carelessness or incompetence) or malicious intent (with the insider threat a common focal point, although the media heavily focuses on IT and hacking events).
The Verizon 2021 Data Breach Investigations Report can help both consumers and small businesses be proactive in mitigating their exposure to identity theft and data breaches. Last year’s Data Breach Investigations Report (DBIR) highlights the reality of data breaches that can support a cyber-risk management strategy for all businesses in general but small business in particular, including these findings.5
• Social engineering is the most successful attack.
• 85% of breaches involved a human element.
• Older vulnerabilities that haven’t been patched are being exploited by attackers.
• Credentials remain one of the most sought-after data types, followed by personal information.
• Employees continue to make mistakes that cause incidents and breaches.
• Business email compromises were the second most common form of social engineering.
• Most social engineering incidents were discovered externally.
This year’s 2022 Verizon Data Breach Investigations Report highlights “the importance of building a culture of cybersecurity vigilance,” including these findings.6
• There are four key paths leading to your estate: credentials, phishing, exploiting vulnerabilities, and botnets.
• All four are pervasive in all areas of the DBIR, and no organization is safe without a plan to handle each of them.
• This year ransomware has continued its upward trend with an almost 13% rise — an increase as big as the past 5 years combined.
• The human element continues to drive breaches. Whether it is the use of stolen credentials, phishing, or simply an error, people continue to play a large part in incidents and breaches alike.
• Error continues to be a dominant trend, and the fallibility of employees should not be discounted.
Whether you are an individual consumer, employee, or a small business owner, you need to be aware that social media can place your personal privacy and/or small business at risk. Be aware of the latest social engineering trends including apps and social media where hackers imitate leading business brands.
As for receiving links of well-known brands on social media, my recommendation on receiving notifications from LinkedIn, Facebook, or any other social media is to ignore the links or attachments. If a social media notification is legitimate, you will receive it again, and then you can go to the social media network login page to retrieve it directly.
REFERENCES
1. 2022 Brand Phishing Report from Check Point Research. LinkedIn remains the most impersonated brand by phishing campaigns. Accessed August 16, 2022.
2. 2022 Brand Phishing Report from Check Point Research. https://www.securitymagazine.com/articles/98046-linkedin-remains-most-impersonated-brand-by-phishing-campaigns#:~:text=Below%20are%20the%20top%20brands,DHL%20(12%25). Accessed August 16, 2022.
3. FBI Internet Crimes Report. https://www.ic3.gov/Media/PDF/AnnualReport/2021_ IC3Report.pdf. Accessed August 16, 2022.
4. Microsoft Data Breaches: Full Timeline Through 2022. https://firewalltimes.com/microsoft-data-breach-timeline/. Accessed August 16, 2022.
5. 2021 Verizon Data Breach Investigations Report. https://www.verizon.com/about/ news/verizon-2021-data-breach-investigations-report. Accessed August 16, 2022.
6. 2022 Verizon Data Breach Investigations Report. https://www.verizon.com/business/resources/reports/2022/dbir/2022-data-breach-investigations-report-dbir.pdf. Accessed August 16, 2022.
20 Orthodontic Practice US Volume 14 Number 2 GOING VIRAL
OP
The importance of maintaining indoor air quality in dentistry



Drs. Tyler Orehek and Troy Roeder discuss the reasons for maintaining diligent air quality standards in the office
Three years into the COVID-19 pandemic, most industries and professions have undergone significant long-term changes. As more Americans resume their lives, each with a different definition of normalcy, all industries must adapt. New safety protocols, guidance, and equipment are the bare necessities for those looking to thrive in a post-pandemic world.
The dental industry is no stranger to these changes. A report from the National Library of Medicine explored how the industry must adapt to the challenges presented by the pandemic, namely through masking, sanitizing, and most importantly, indoor air purification.1 The prevalence of SARS-CoV-2, a highly contagious airborne virus, means that indoor air purification is crucial in any dental space. This is critical not only for patients who are unable to mask during cleanings and procedures, but for the dentists, hygienists, assistants, and office staff who spend hours of their days in these environments.
For dental offices, simply masking is not enough. During dental treatments, aerosols that may contain blood, saliva, oronasal secretions, microorganisms, filling particles, and tooth particles, are produced. Aerosols are created and spread through the air as a result of various devices used such as turbine handpieces, ultrasonic scalers, air and water syringes, polishing procedures, and surgical lasers. Given that most dental treatments involve the use of many of these instruments, the potential for viruses and infections to spread throughout a dental space is incredibly high.
Tyler Orehek, DC, MSc, CIEC, began his professional career in 2003, and he owned and operated a multidisciplinary practice in midtown Manhattan, serving as the primarycare physician and portal-of-entry healthcare practitioner, with a special emphasis on the treatment of pulmonary and neuromusculoskeletal conditions. Dr. Orehek has been an indoor air quality specialist since 2007. He is also a Council-Certified Indoor Environmental Consultant (CIEC), board-awarded by the American Council for Accredited Certification (ACAC).
Troy Roeder, DDS, is a general dentistry practitioner with over 30 years of experience based in Moline, Illinois. Dr. Roeder attended The University of Iowa, with studies in Biology and Chemistry, before completing his dental training at The University of Iowa College of Dentistry. Dr. Roeder’s dental practice provides both general and cosmetic dental treatments as well as orthodontics for teens and adults.
Disclosure: Dr. Orehek is the President of Airgle Corp., and Dr. Roeder employs Airgle air purification units at his dental practice.
Educational aims and objectives
This self-instructional course for dentists aims to discuss the importance of maintaining indoor air quality in dentistry.
Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can: Identify the primary causes of airborne pathogens in dentistry.
• Recognize the role that dental tools play in spreading aerosols and airborne pathogens.
• View the most effective tools to combat aerosols and airborne pathogens.
• Identify various strategies that can be put in place to maintain air quality.
• Observe how air purification units work to eliminate aerosols and airborne pathogens.
2 CE CREDITS
A recent study demonstrated that saliva may have a significant role in the virus’ ability to spread through airborne transmission.2 A patient infected in the early stages of COVID-19, potentially before they’re even aware of the infection, could have high viral loads in their saliva, and cases with multiple symptoms often
21 orthopracticeus.com Volume 14 Number 2 CONTINUING EDUCATION
correlate with higher viral loads. These viruses can spread very far, quickly, and remain suspended in the air for very long periods of time.
Asymptomatic patients are also at risk of spreading high viral loads, as many can be unaware of their asymptomatic infection. Respiratory droplets are produced quickly, and heavier droplets can spread within 6 feet of the source in seconds. However, coughing and sneezing can produce even smaller droplets, which can linger in the air up to 20 feet from the source, hours after initially being produced and creating a hazardous environment for patients and dentists.3 Additionally, HVAC systems with poor specifications and efficiency can further contribute to the spread of such droplets.
Furthermore, dentists work in small, tight rooms, making it easy for infections to spread. This has forced the industry to become leaders in infection control in the past, and a similar opportunity presented itself over the past few years during the COVID-19 pandemic.
The pandemic forced dental practices to close for months in March 2020, providing yet another opportunity for the industry to reassess how to improve indoor air quality. For example, while high-volume evacuation (HVE) equipment is effective in sucking up aerosols, the smallest viral particles will often be able to escape, necessitating a more comprehensive solution. Alternative methods are required to improve air quality in dental offices, while also reducing the spread of airborne particles. The following are a few examples of the ways that the dental industry can prioritize indoor air quality, creating a safer environment for patients and practitioners alike.
Negative pressure rooms
One option for practices is to convert operatories into “negative pressure rooms,” which are typically found in hospitals. Designed to combat airborne infections, negative pressure rooms ideally undergo between six to 12 air changes per hour (ACH) and must have air pressure that is lower than the external air pressure. However, while negative pressure rooms protect those outside of the room, they do not provide additional protection to those inside. Additionally, this is a costly conversion, and out of reach for many practices.
HVAC and filtration
Another option is to modify existing HVAC systems, such as through adding high efficiency particulate air (HEPA) filtration. Unfortunately, older HVAC systems often use rudimentary filter stages and are also incapable of sustaining adequate air exchange. These systems are not as robust nor efficient in exchanging air as compared to stand-alone, medical-grade air purifiers, and the difference can be critical. One way to modify these systems is by incorporating UV light into existing HVAC systems, which works if microorganisms are consistently exposed to the UV light. However, this is far from a guarantee, and the modifications can be costly.
Oftentimes, HVAC systems are set to “auto” mode, which adversely affects indoor air quality as it turns off from time to time. This allows contaminants to remain in the air for longer periods of time. By switching the setting to “on,” HVAC systems can work more effectively, relatively speaking, by promoting constant air flow.
Medical grade air purification units
Ultimately, air purifiers are one of the most effective ways to improve indoor air quality. However, the quality and specifications are critical to examine when determining the kind of professional-grade air purifier to implement. While consumer-grade air purifiers are more economical, allowing numerous units to be installed throughout a practice, they are typically less effective than medical-grade air purification systems for a host of reasons. Lesser systems are often underpowered and have smaller cubic feet per minute (CFM) ratings compared to medical-grade purifiers. CFM represents how much air can be drawn into a system per minute. Dental operatories necessitate high CFM to be truly impactful. Additionally, consumer-grade purifiers cannot provide high ACH as compared to medical-grade systems. Lastly, many do not remove ultra-fine particles as small as the SARSCoV-2 virus, which is incredibly small, with an average diameter of only 0.1 microns.
High efficiency, medical-grade air purification systems are one of the most effective ways to combat this issue. Standalone, medical-grade air purification systems are far more effective than HVAC systems in filtering out pollutants as well as airborne viruses, bacteria, and mold. Medical-grade purifiers have the highest rate of CFM, meaning they purify more of the air in the same amount of time as compared to other methods of purification. This helps mitigate the potential risk of transmission between doctors, patients, and other staff. Medical-grade purifiers effectively draw aerosolized particles away from operatories and trap them within its filter media. Studies have found that exposure to droplets and contaminants dropped 80% to 95% when air purifiers were used in dental offices.4
Air purification systems must be engineered to combat airborne pathogens (including CoV-2), ultra-fine particulates, and volatile organic compounds (VOCs). For example, Airgle air purification systems utilize a cleanroom-grade cHEPA filter with a capture threshold down to 0.003 microns, which is 100 times more discriminating than traditional HEPA, to capture the smallest of ultra-fine airborne particulates and microbial con-
22 Orthodontic Practice US Volume 14 Number 2 CONTINUING EDUCATION
Air purification systems are the only solutions that have discriminating enough filtration, the necessary CFM of delivered air, and the vitally important air changes per hour, resulting in the cleanest possible air in the shortest amount of time.
taminants. Medical-grade purifiers also have more adept cubic feet per minute (CFM), a critical consideration for dental practices. As aerosols linger and remain suspended in operatories for longer periods of time, the risk for cross-contamination can increase exponentially.

An air purifier’s ability to contain airborne contaminants such as pathogens and mold, in addition to volatile organic compounds and ultra-fine particulates, is primarily determined by the type of filter used. An air purification system’s effectiveness is largely correlated to the quality, specifications, and integrity of the purification filter media used within a system.
Putting it into practice
When treating patients, it is critical to keep operating rooms as clean and safe as possible, with a focus on removing aerosols. Installing two medical-grade air purification systems, one at each side of the chair in the main operating room, can ensure a
healthy and safe space for patients. These units also incorporate germicidal UV lights and a high number of air changes per hour, ensuring that rooms are as clean and safe as possible for patients and staff.
While it was standard operating procedure to employ standard screening questions and take patient and staff temperatures when re-opening, patients were looking for more preventative measures. They wanted assurances that every action possible was being taken to make the air safe to breathe. Employing air purification units that filter out the smallest particles gave patients peace of mind when visiting the dental office. In fact, it would serve patients well to have high quality air purifiers in their own home and workplace.
Four main takeaways to highlight, both from personal experience and published studies on the matter:
1. The pandemic is here to stay. Americans are starting to return to their pre-pandemic lives, and many are looking for assurance that they’ll be safe from being exposed to CoV-2 when doing so.
2. Dental practices have a unique challenge. Operating rooms are small, tight areas, where potentially hazardous aerosols can linger for hours if not properly purified and ventilated. This is why dental practices are consistently leaders in public safety.
3. Not all methods of air purification are equal. HVAC systems are effective, but are often unable to combat the smallest of airborne particles like SARS-CoV-2. Consumer-grade air purification systems can be economical, but frequently do not possess the more discriminating filter media, nor the necessary CFM and ACH rates required to keep operatories as safe as possible. Negative pressure room conversions are also an option, but are often too costly for the average dental office to afford.
4. Medical-grade air purifiers are imperative. Air purification systems are the only solutions that have discriminating enough filtration, the necessary CFM of delivered air, and the vitally important air changes per hour, resulting in the cleanest possible air in the shortest amount of time. Purifiers are the most appropriate approach for targeting and capturing the SARS-CoV-2 virus.
The time is now for dental offices to make adjustments if they have not done so already, and medical-grade air purification is the best way to ensure safety for dentists and patients alike.
REFERENCES
23 orthopracticeus.com Volume 14 Number 2 CONTINUING EDUCATION
1. Ancuta G, Sandu D, Tatarciuc M, Luchian I. The Impact of the COVID-19 Pandemic on Dentistry and Dental Education: A Narrative Review. Int J Environ Res Public Health. 2022 Mar; 19(5):2537.
2. Carrouel F, Gadea E, Esparcieux A, Dimet J, Langlois ME, Perrier H, Dussart C, Bourgeois D. Saliva Quantification of SARS-CoV-2 in Real-Time PCR From Asymptomatic or Mild COVID-19 Adults. Front Microbiol. 2021; 12:786042.
3. Xie X, Li Y, Sun H, Liu L. Exhaled droplets due to talking and coughing. J R Soc Interface. 2009 Dec 6;6 Suppl 6(Suppl 6):S703-714.
OP
4. Chen C, Zhao B, Cui W, Dong L, An N, Ouyang X. The effectiveness of an air cleaner in controlling droplet/aerosol particle dispersion emitted from a patient’s mouth in the indoor environment of dental clinics. J R Soc Interface. 2010 Jul 6;7(48):1105-1118.
Operating rooms are small, tight areas, where potentially hazardous aerosols can linger for hours if not properly purified and ventilated.
Continuing Education Quiz
The importance of maintaining indoor air quality in dentistry
OREHEK/ROEDER
1. A report from the National Library of Medicine explored how the industry must adapt to the challenges presented by the pandemic, through ________.
a. masking
b. sanitizing
c. indoor air purification
d. all of the above
2. During dental treatments, aerosols that may contain __________, microorganisms, filling particles, and tooth particles are produced.
a. blood
b. saliva
c. oronasal secretions
d. all of the above
3. Aerosols are created and spread through the air as a result of various devices used such as turbine handpieces, ultrasonic scalers, air and water syringes, polishing procedures, and surgical lasers.
a. True
b. False
4. Respiratory droplets are produced quickly, and heavier droplets can spread within ________ of the source in seconds.
a. 6 feet
b. 10 feet
c. 12 feet
d. 14 feet
5. However, coughing and sneezing can produce even smaller droplets, which can linger in the air up to _________ from the source, hours after initially being produced and creating a hazardous environment for patients and dentists.
a. 20 feet
b. 30 feet
c. 35 feet
d. 40 feet
6. Designed to combat airborne infections, _____________ ideally undergo between six to 12 air changes per hour (ACH) and must have air pressure that is lower than the external air pressure.
a. positive pressure rooms
b. negative pressure rooms
c. high particulate rooms
d. auto-mode HVAC rooms
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 130
Date Published: June 29, 2023
Expiration Date: June 29, 2026
2 CE CREDITS
7. By switching the setting to ______, HVAC systems can work more effectively, relatively speaking, by promoting constant air flow.
a. “on”
b. “off”
c. “auto”
d “professional”
8. ___________ represents how much air can be drawn into a system per minute.
a. Pressure per minute (PPM)
b. High-volume evacuation per minute (HVEM)
c. Cubic feet per minute (CFM)
d. none of the above
9. Standalone, medical-grade air purification systems are far more effective than HVAC systems in filtering out pollutants as well as _________.
a. airborne viruses
b. bacteria
c. mold
d. all of the above
10. Studies have found that exposure to droplets and contaminants dropped when air purifiers were used in dental offices.
a. 25%-34%
b. 46%-53%
c. 65%-76%
d. 80%-95%
To provide feedback on CE, please email us at education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
24 Orthodontic Practice US Volume 14 Number 2 CONTINUING EDUCATION
Myofunctional therapy for postorthodontic retention
Drs. Ryan Robinson and Carly Jacobs discuss how myofunctional therapy can help in treating the root cause of some complicated dentitions to minimize relapse

Introduction
The history of myofunctional therapy in conjunction with orthodontic treatment dates to as early as 1906 with the publication of American orthodontist Alfred Rodgers’ “Living Orthodontic Appliance.” Rodgers presumed that muscle alone would correct a malocclusion.1 To further this claim, Edward Angle theorized that “every malocclusion has a myofunctional cause.”2 Angle’s contribution to myofunctional therapy relied primarily on fixed orthodontic appliances (Figure 1). However, the myofunctional component of orthodontics with fixed appliances fell out of favor when relapse occurred in a high percentage of patients coupled with time-consuming techniques to achieve results. Hence, tooth-centered orthodontics with extractions or self-ligating brackets without the need for extractions grew in popularity (Figure 2). Nevertheless, post-orthodontic relapse was still problematic, requiring permanent retainers. As George Hahn once wrote in his publication “Retention — The Stepchild of Orthodontia,” Irrespective of the length of time a tooth is held in its new position … upon release, it will seek a place where it is in balance.”3 Myofunctional therapy has made significant strides in using specifically designed exercises to bring oral, facial, and
Educational aims and objectives
This self-instructional course for dentists discusses incorporating myofunctional therapy into orthodontic treatment planning to reduce post-orthodontic relapse.

Expected outcomes
Orthodontic Practice US subscribers can answer the CE questions by taking the quiz online at orthopracticeus.com to earn 2 hours of CE from reading this article. Correctly answering the questions will demonstrate the reader can:
• Recognize the benefits of incorporating myofunctional therapy into orthodontic treatment planning. Recognize the role dentists can play in identifying and treating orofacial disorders treatable by myofunctional therapy.
Identify orofacial disorders that benefit from myofunctional treatment options for long-term post-orthodontic retention.
• Realize myofunctional therapy’s potential to reduce post-orthodontic relapse and overall patient health.
2 CE CREDITS
Ryan P. Robinson, DDS, Delaware’s sole triple-boarded doctor in Craniofacial Pain and Dental Sleep Medicine, is dedicated to enhancing the overall health and well-being of his patients. Recognizing the significant impact of addressing the airway on patients’ health, he founded The Pain and Sleep Therapy Center. With extensive knowledge gained from over 1,000 hours of continuing education and mentorship by renowned airway clinicians, Dr. Robinson prioritizes identifying root causes instead of relying on temporary fixes. His passion extends to all age groups, as he helps adults improve their quality of life and children overcome lifelong issues. Beyond his profession, Dr. Robinson enjoys family time, travel, golf, and volunteering, including contributions to the blood cancer research department at Alfred I. DuPont/ Nemours Hospital.
Carly M. Jacobs, DMD, a compassionate and dedicated dentist, found her true passion in dental sleep medicine after witnessing the transformative effects of treating sleep-related breathing issues. With extensive training and mentorship from top chronic pain and sleep providers worldwide, she takes pride in relieving facial pain, headaches, TMD, and airway obstructions. Driven by a patient-centric approach, she aims to find customized solutions for each individual, rejecting a one-size-fits-all model. Collaborating with Dr. Robinson, she expands the reach of The Pain and Sleep Therapy Center, focusing on patients in the Main Line and greater Philadelphia, Pennsylvania region. Beyond dentistry, Dr. Jacobs enjoys traveling, cooking, tennis, and Broadway shows.

cervical muscles into balance to reduce the need for permanent retainers.
Myofunctional therapy (MFT) can be defined as exercising facial and cervical muscles to improve tone, function, and mobility, often referred to as neuromuscular re-education of muscle function.4 The scope of the exercises is designed to correct and maintain orofacial abnormalities such as mouth breathing, lip incompetence, tongue thrust habits, and parafunctional oral
25 orthopracticeus.com Volume 14 Number 2 CONTINUING EDUCATION
Figure 1: A fixed orthodontic appliance
habits such as thumb sucking and bruxism, among others (Figures 3A-3C).5 These orofacial disorders increase the degree of difficulty in treating and retaining orthodontic conditions. Combining MFT with orthodontics produces stable maxillary arch development and resolves lower anterior crowding with little mechanical effort. In a systematic review of the effectiveness of myofunctional therapy with orthodontics conducted by Homem, et al., patients presenting with irregular movements of the tongue and malocclusions can be treated with both forms of treatment.6 The same study concluded that orofacial dyskinesis and anterior open bite treated with a combination of myofunctional therapy and orthodontics result in a more successful outcome for treatment and retention.6 An additional study concluded that closure of anterior open bite treated with a combination of MFT and orthodontics minimized relapse (0.48 mm-0.8 mm ortho and MFT; 1.3 mm-3.8 mm ortho only) (Figure 4).7 These studies and more represent ways MFT and orthodontics can be integrated to benefit the patient and provider through more successful treatment and retention of orthodontic abnormalities.
Identifying myofunctional abnormalities
Several types of dysfunctional areas of the oral cavity can be identified through pre-orthodontic treatment planning. As orthodontists, the qualifications and skills to determine the cause and treat orthodontic maladies are already established; thus, integrating MFT would be effortless. Typically, an evaluation of treatment options for the patient includes a combination of radiographs, dental impressions, and clinical observations. Adding diagnostic assessments of the oral, facial, and cervical muscles would identify areas in which post-orthodontic retention may be negatively affected. Myofunctional therapy can then be integrated into the treatment plan for a more comprehensive approach to treatment planning. However, using myofunctional therapy with the mechanical approach to minimize relapse has yet to be entirely accepted within the orthodontic community.
According to the American Dental Association, the primary justification for orthodontic treatment is malocclusion or teeth or jaw misalignment. The core issues that result in malocclusion or jaw misalignment are tongue thrust, narrow palate, bruxism, and lip incompetence, where myofunctional therapy can increase stability post-orthodontic treatment (Figure 5). The root cause of these abnormalities rests with the muscle tone of the tongue, mouth breathing, or tongue-tied situations (Figure 6). Evaluating these scenarios can seem obvious; however, there are unique cases that often are not completely evident. For instance, a tongue tie can create a speech impediment, mouth breathing habit, and/or a tongue thrust. Sounds that require the tongue to


utilize the roof of the mouth, such as s, t, j, th, etc., or arch of the floor, such as r, c, etc., are difficult to pronounce.8 In addition, mouth breathing can lead to upper lip incompetence, narrow upper arch, retroposition of mandibular incisors, increased anterior face height, narrow (V-shaped maxillary arch), or expanded



26 Orthodontic Practice US Volume 14 Number 2 CONTINUING EDUCATION
Figure 2: Traditional tooth-centered brackets and wire orthodontics
Figure 4: Open bite after palatal expander due to low resting tongue posture, tongue tie, and tongue thrust
Figures 3A-3C
mandibular plane.9 Finally, a tongue thrust is among one the most difficult to treat and retain in orthodontics successfully. A tongue thrust identified by Dixit, et al., presents a” forward tongue posture, tongue thrust, during swallowing, contraction of the perio muscle, excessive buccinator hyperactivity, and swallowing without the momentary tooth contact normally required.”10 As a result, prolonged tongue thrust leads to open bites, high proclination of upper anterior teeth, high or narrow maxillary arch, and Class 11 Div. 1 Malocclusion (Figure 7).10,11 In addition, lisping or impaired speech has also been linked to tongue thrust. Myofunctional therapy would aid in treating the root cause of these particular abnormalities to minimize relapse.
Orofacial Myofunctional Therapy exercises
Orofacial Myofunctional Therapy (OMT) can include exercises to strengthen, reposition, and improve coordination of the mouth and throat muscles. Ideally, these exercises can achieve the optimal posture of lips, tongue, and teeth with the tongue resting on the roof of the mouth, the teeth touching or slightly apart, and the lips together without strain.4 The benefits of using these exercises that can minimize post-orthodontic relapse, as described by Dr. Krishana Acanta, include:
• Improving tongue elevation and tongue movement strength
• Correcting resting posture of the tongue, lips, and cheeks
• Improving tongue motility




• Improving maxillary constriction




• Improving sleep and breathing disorder patterns12
Exercises that improve the oral stability of the tongue, lips, and cheek muscles aid in preventing relapse (Figure 8). However, many challenges exist in incorporating OMT into the treatment phase of orthodontics. A few of them include the need for OMT training, the availability of a myofunctional therapist, and the shortage of time in a busy orthodontic practice. Ideally, an in-office myofunctional therapist or a referral to another certified myofunctional therapist for collaboration would make this transition easier, especially in complex cases. However, in less complicated cases, a few simple exercises taught in the office could benefit post-orthodontic retention. Incorporating OMT into pretreatment treatment planning, either with an MFT in-office or through collaboration outside of the office, would reduce some of these post retention challenges. Examples of OMT exercises compiled by Shah, et al., are as follows:
Lip Exercises
Lip closure and competency exercise: The child holds an ice cream stick between tightly closed lips for 5 seconds. Repeat 5-10 times.
27 orthopracticeus.com Volume 14 Number 2 CONTINUING EDUCATION
Figures 5A and 5B: Narrow palate before palatal expansion and developed palate after expansion and myofunctional therapy
Figures 7A-7C: Tongue thrust causing labial tipping of central incisors and open bite
Figure 6A-6C: 6A-6B. Tongue tied patient showing inability of tongue to elevate to the palate. 6C. Lip tie showing thick attachment of labial frenum restricting maxillary growth and development
Lip Puffing exercise: The child is asked to force air between lips and teeth, puffing out the lips as much as possible.
Lip movement: The child is asked to repeat the “OO-EE” sound.
Bubble-blowing exercise: The child blows bubbles through a toy with the help of the lips.
Tongue Exercises
Tongue clicks: The child places the tongue at the roof of the mouth, snapping it down.
Touch nose exercise: Protrude the tongue to touch the nose for 10 seconds. Repeat 10 times.
Touch chin: Protrude the tongue to touch the chin for 10 seconds. Repeat 10 times.
Touch sideward movement: Protrude the tongue and move from side to side, holding for 10 seconds. Repeat 10 times.
Teeth counting exercise: Count each tooth with the tongue.
Cheek Exercise
Roll tongue from side to side.
Fish face exercise: Puff the cheeks with air and blow a fish face. Repeat 10 times.
Yawning exercise: Yawning helps cheek and throat muscles. Repeat often throughout the day.
Jaw Exercises
Open the jaw wide and say AHH hold for 3-5 seconds. Massage jaw gently toward and away from the lips.
Breathing Exercises
Balloon blowing: blow a balloon while breathing through the nasal cavity. Balloon blowing can also assist with lip competency.
Hold water in the mouth while breathing through the nasal cavity.13
One of the key factors in using myofunctional therapy is ensuring muscle compensation in other areas is not utilized. Therefore, treatment should be done routinely until the patient understands the correct technique, and then monitored for several weeks afterward until the patient demonstrates proper habituation of the right function.
Conclusion
It is essential to note that oral myofunctional therapy exercises alone are not intended to alter skeletal changes or move teeth but rather work as an integrated approach to comprehensive orthodontic treatment for a better long-term retention strategy. Therefore, assessing muscle dysfunctions included with standard orthodontic treatment planning would achieve better stability and retention results. Ideally, the earlier these dysfunctions can be identified in a patient’s life, the better the chances of positive results. However, it could also be considered in adult patients to minimize relapse post-orthodontics. As the orthodontic community realizes the benefits of myofunctional therapy on retention and overall patient satisfaction, it will soon become part of traditional orthodontic treatment planning.
REFERENCES
1. Rogers AP. Living orthodontic appliances. International Journal of Orthodontia, Oral Surgery and Radiography. 1929;15(1):1-14.
2. Hawley CA. A removable retainer. International Journal of Orthodontia and Oral Surgery (1919). 1919;5(6):291-305.
3. Hahn GW. Retention–The Stepchild of Orthodontia. The Angle Orthodontist. 1944;14(1):3-12.
4. Swaroop AK. Oral Myofunctional Therapy: Breaking Detrimental Habits. iCliniq. Published https://www.icliniq.com/articles/dental-oral-health/oral-myofunctional-therapy. December 30, 2022. Accessed April 10, 2023.
5. Vollmer E. What is Orofacial Myofunctional Therapy. Therapy Works. https://therapyworks.com/blog/language-development/what-is-orofacial-myofunctional-therapy/. Published October 21, 2021. Accessed April 10, 2023.
6. Homem MA, Vieira-Andrade RG, Falci SG, Ramos-Jorge ML, Marques LS. Effectiveness of orofacial myofunctional therapy in orthodontic patients: a systematic review. Dental Press J Orthod. 2014 Jul-Aug;19(4):94-9. doi: 10.1590/2176-9451.19.4.094-099.oar.
7. Smithpeter J, Covell D Jr. Relapse of anterior open bites treated with orthodontic appliances with and without orofacial myofunctional therapy. Am J Orthod Dentofacial Orthop. 2010 May;137(5):605-14.
8. Reddy N, Marudhappan Y, Devi R, Narang S. Clipping the (tongue) tie. Journal Indian Soc Periodontol. 2014;18(3):395-398.
9. Zhao Z, Zheng L, Huang X, Li C, Liu J, Hu Y. Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis. BMC Oral Health. 2021 Mar 10;21(1):108.
10. Dixit UB, Shetty RM. Comparison of soft-tissue, dental, and skeletal characteristics in children with and without tongue thrusting habit. Contemp Clin Dent. 2013 Jan;4(1):2-6.
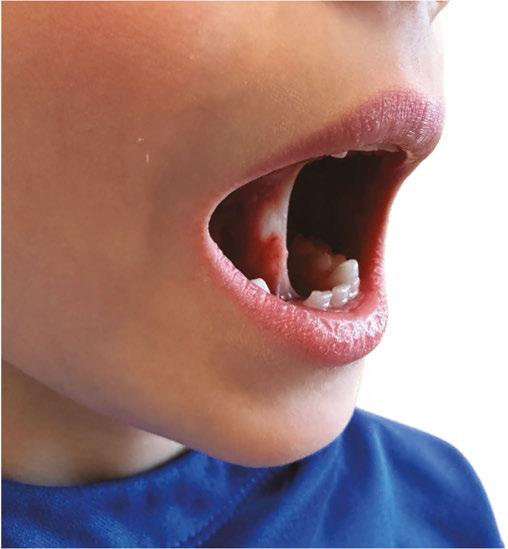
11. Cayley AS, Tindall AP, Sampson WJ, Butcher AR. Electropalatographic and cephalometric assessment of tongue function in open bite and non-open bite subjects. Eur J Orthod. 2000 Oct;22(5):463-74.
12. Mason R. Lip Incompetence. 2019. Orofacialmyology.com. https://orofacialmyology.com/wp-content/uploads/2019/08/orofacial-myologist-lip-incompetence.pdf. Accessed April 10, 2023
13. Shah SS, Nankar MY, Bendgude VD, Shetty BR. Orofacial Myofunctional Therapy in Tongue Thrust Habit: A Narrative Review. Int J Clin Pediatr Dent. 2021 Mar-Apr;14(2):298-303.
28 Orthodontic Practice US Volume 14 Number 2 CONTINUING EDUCATION
OP
Figure 8: Patient practicing lingual palatal suction to strengthen, tone, and improve range of motion of the tongue
Continuing Education Quiz
Myofunctional therapy for post-orthodontic retention
ROBINSON/JACOBS
1. Myofunctional therapy (MFT) can be defined as exercising facial and cervical muscles to improve __________, often referred to as neuromuscular re-education of muscle function.
a. tone
b. function
c. mobility
d. all of the above
2. ________ produce(s) stable maxillary arch development and resolves lower anterior crowding with little mechanical effort.
a. Combining MFT with orthodontics
b. Orthodontics alone
c. MFT alone
d. Extractions
3. In a systematic review of the effectiveness of myofunctional therapy with orthodontics conducted by Homem, et al., patients presenting with can be treated with both forms of treatment.
a. Excessive dental caries
b. Irregular movements of the tongue and malocclusions
c. Supernumeraries
d. Impacted third molars
4. Typically, an evaluation of treatment options for the patient entails _________.
a. radiographs
b. dental impressions
c. clinical observations
d. all of the above
5. Prolonged tongue thrust leads to open bites, high proclination of upper anterior teeth, high or narrow maxillary arch, and Class 11 Div 1 malocclusion.
a. True
b. False
6. Ideally, Orofacial Myofunctional Therapy (OMT) exercises can achieve the optimal posture of lips, tongue, and teeth with the ________, the teeth touching or slightly apart, and the lips together without strain.
a. tongue resting on the floor of the mouth
b. tongue resting on the roof of the mouth
c. tongue curled back inside the mouth
d. none of the above
7. An example of lip closure and competency exercise is: The child holds
Each article is equivalent to two CE credits. Available only to paid subscribers. Free subscriptions do not qualify for the CE credits. Subscribe and receive up to 16 CE credits for only $149; call 866-579-9496, or visit https://orthopracticeus.com/ subscribe/ to subscribe today.
n To receive credit: Go online to https://orthopracticeus.com/continuingeducation/, click on the article, then click on the take quiz button, and enter your test answers.
AGD Code: 370
Date Published: June 29, 2023
Expiration Date: June 29, 2026
an ice cream stick between tightly closed lips for _______. Repeat 5-10 times.
a. 5 seconds
b. 30 seconds
c. 45 seconds
d. 60 seconds
8. An example of tongue exercises is: Touch sideward movement Protrude the tongue and move from side to side, holding for 10 seconds. Repeat ________.
a. 5 times
b. 10 times
c. 20 times
d. 30 times
9. An example of a cheek exercise is: Fish face exercise: and blow a fish face. Repeat 10 times.
a. With your face muscles, pull the cheeks inward
b. Using only the muscles on one side of the face, pull your mouth towards one side of the face
c. Puff the cheeks with air
d. Keep your mouth closed, clasp your lips together firmly
10. Treatment should be done routinely until the patient understands the correct technique, and then monitored for afterward until the patient demonstrates proper habituation of the right function.
a. a few days
b. several weeks
c. 8 months
d. 1 year
To provide feedback on CE, please email us at
education@medmarkmedia.com
Legal disclaimer: Course expires 3 years from date of publication. The CE provider uses reasonable care in selecting and providing accurate content. The CE provider, however, does not independently verify the content or materials. Any opinions expressed in the materials are those of the author and not the CE provider. The instructional materials are intended to supplement, but are not a substitute for, the knowledge, skills, expertise and judgement of a trained healthcare professional.
29 orthotpracticeus.com Volume 14 Number 2 CONTINUING EDUCATION
2 CE CREDITS
Spark ™ Clear Aligners & Damon Ultima ™

Two systems from Ormco™ designed to meet the needs of orthodontists

Spark™ Clear Aligner System
Designed for the needs of orthodontists, the Spark Clear Aligner System offers the latest innovations in aligner material and digital orthodontics.
For treatment planning, efficiency, and effectiveness, Spark’s Approver software is designed to give orthodontists start-to-finish control. CBCT integration lets orthodontists import and visualize CBCT patient data, while posterior Bite Turbos can be added to address complex cases.*
Spark’s superior force retention and surface contact of the Spark aligner is due to its manufacturing technology. Compared with the leading aligner brand, Spark’s advanced technology enables more sustained force retention and better surface contact with the tooth, and Spark Aligners are made with 80% better printing resolution and a more uniform surface texture.*
Spark’s beveled attachments conform to the surface of each tooth to provide a more uniform active attachment surface.* As a result, there is need to resort to optimized attachments — doctors can still obtain optimum results!
Spark’s proprietary CBCT features
• Root visualization provided on all cases (not only on those submitted via CBCT)
• Skin, Translucent Skin, and Bone and Soft Tissue preset views
• Clipping plane available in axial, coronal, and mesialdistal views
• Ability to continue to work on the prescription form while uploading the DICOM file, avoiding delays
• Spark Advanced, Spark 20, and Spark 10* are available on all Spark products for increased control and flexibility
Please visit https://ormco.com/spark to learn more
The Damon Ultima™ System
As is the first true full expression* orthodontic system with a proprietary integrated wire and slot design that virtually eliminates play for faster and more precise finishing,* the Damon
Ultima™ System is designed with a unique and patented technology that provides orthodontists with earlier and precise control of rotation, angulation, and torque.* The signature Damon™ Smile is the result of the full expression with lighter forces. Orthodontists can treat in less time and fully express the patient’s prescription with fewer wire bends.* With this system, 98.9% of cases were determined to have first-order rotations corrected with the first round-sided rectangular wire, and full expression is achieved with the second.* After all rotations are corrected, the wire/bracket interface returns to a passive state while maintaining the desired rotational alignments throughout the remainder of treatment with the .0275” dimension wires.*
Options for enhanced torque control
For enhanced torque control, the Damon Ultima brackets are available in the neutral, retrocline, and procline options.* When needed, larger size and different material Damon Ultima archwires are available for more torque control.
Introducing — The Ultima™ Hook
For doctors who value performance and want to provide patients with healthier1 oral treatment and more comfortable experience, the Damon Ultima System now includes the Ultima Hook, the only re-positionable hook2, designed to save time.*
To learn more about the Damon Ultima System, please visit https://ormco.com/products/damon-ultima-system/ or https://ormco.com/ultimahooks. *
30 Orthodontic Practice US Volume 14 Number 2 PRODUCT PROFILE
Data on file. ** Source article: https://www.mdpi.com/1198216 1. When used as a stop.
OP
2. Using the Ultima™ Hook Repositioning Instrument. This information was provided by Ormco.
Spark™ Clear Aligners
The Ultima™ Hook
Damon Ultima™ Bracket







UNLEASH YOUR SUCCESS WITH THE ULTIMA JOURNEY. Faster, more precise finishing. Better control. Less chair time*. Damon Ultima™ delivers all this, and more. By joining the Ultima Journey you’ll stay connected to: • Leading experts who share techniques for maximum results •Discounted admission to education events •Exclusive product discounts
System Key Expert
Dr. Michael Bicknell
Damon Ultima™
Ultima™ System Key Expert
Dr. Matias Anghileri
Damon
Expert
Dr. Stuart Frost
Damon Ultima™ System Key
Expert *Data on file.
are paid consultants for Ormco. The opinions that are quoted in this material are those of the doctors. Clinicians should use their own judgment in treating their patients. MKT-23-0355 ©2023 Ormco Corporation Driving the Future of Orthodontics SIGN UP TODAY! go-orm.co/OrthoPracticeUltimaJourney
Dr. Todd Bovenizer Damon Ultima™
System Key
Drs. Bicknell, Anghileri, Frost and Bovenizer
Urbanek TMJ device announces launch of commercial operations

The Urbanek TMJ Device and Protocol announced today the official launch of its commercial operations in North America, offering dentists a new way to treat the 10+ million TMD/TMJ sufferers in the United States. Developed by an oral maxillofacial surgeon with over 40 years of experience, The Urbanek Device and Protocol is the only non-surgical, custom CADCAM, 3D-printed resin device that alleviates the inflammation of the TMD joint. Unlike a nightguard, this FDA-cleared medical device was specifically designed to treat the root cause of TMD. CEO and Founder Dr. Anthony Urbanek noted that his mission in creating the device was to provide dental care professionals with a system to safely eliminate TMJ/TMD for their patients without surgery or medications.
For more information, visit www.UrbanekTMJ.com or register for Dr. Urbanek’s CE webinar here: https://bit.ly/3WHfb2W.
Introducing Ultracare™ Topical Anesthetic Gel

Ultradent has announced the return of Ultracare™ topical anesthetic gel — a delightfully flavored 20% benzocaine oral gel formulated for rapid, profound topical anesthesia. Dental professionals can administer Ultracare gel directly on a cotton swab for increased patient comfort. The gel’s trio of benefits include 20% benzocaine for effective numbing, as well as rapid onset — numbing tissues in 15–20 seconds. Last, Ultracare gel comes in a delicious dye-free Walterberry flavor with no bitter aftertaste. For more information, call 800-5525512 or visit ultradent.com.
Introducing a revolutionary CAD/CAM and 3D-printed guided technology for precise IPR
DynaFlex® introduces second generation precision aligner buttons for clear aligners


DynaFlex has announced the release of the second generation Precision Aligner Buttons specifically designed for use with clear aligners, offering orthodontists a reliable and comfortable solution for attaching rubber bands. The buttons have a wide range of clinical applications, including Class II and Class III elastic patterns, crossbite elastics, and posterior vertical elastics. Several key features set them apart. The shape of the base pad is meticulously tailored to fit the aligner cutout windows, ensuring a precise fit. The maximized surface area of the base pad prevents detachment, delivering a reliable bond strength. In addition, the buttons are engineered for gumline placement, matching the shape of the tooth at the gingival third. The enhanced button head facilitates easy attachment of elastics of different sizes, enhancing patient compliance and comfort. Furthermore, the dimple on the button face allows for precise positioning using an explorer or scaler.
The second generation of the Precision Aligner Buttons come in three variations: G2 METAL, Designed to fit the cutout windows of upper and lower molars; G2 CLEAR, ideal for the cutout windows of upper and lower canines and premolars; and the new METAL MINI Precision Button, specifically created for second molars or partially erupted first molars.
For more information, visit www.precisionbuttons.com.
Viax Dental Technologies introduces an innovative CAD/ CAM and 3D-printed guided technology for precise interproximal reductions. Developed in collaboration with Dr. Lou Shuman, CEO of Cellerant Consulting Group, this solution guarantees consistent and highly accurate IPR through a simplified and efficient process. Traditional IPR methods can present significant challenges. They require not only determining the appropriate amount to be removed but also mastering the art of maintaining point contacts. Viax Dental Technologies has leveraged the power of 3D-printed guides and specially crafted burs to make IPR a straightforward and hassle-free task for clinicians. The guided IPR solution empowers clinicians to replicate required reductions with total accuracy and precision, seamlessly integrating into digital orthodontic treatment plans. The user-friendly technology requires minimal training, allowing clinicians to effortlessly incorporate it into their practice. Moreover, the streamlined process enhances overall patient experience and satisfaction levels.
For more information about the guided IPR solution and to explore how this technology can benefit your dental practice, please visit www.viaxdental.com.
32 Orthodontic Practice US Volume 14 Number 2 INDUSTRY NEWS
All The Best Faces Wear Braces
Kyle Fagala DDS, MDS
Neon Canvas: Memphis, Tennessee 2022; neoncanvas.com
In this book, Dr. Kyle Fagala waxes poetic about some patients with pretty diverse dentitions — one has teeth like gummy bears, one has three rows of teeth, and one is a snowman with a case of “frostbite.” They all have different reasons for visiting the orthodontist, but they all have one self-esteem boosting characteristic in common — all the best faces wear braces.
Once upon a time, kids were subjected to nicknames like “Brace Face,” or “Metal Mouth.” It was hard to smile or eat in the school cafeteria while trying to keep one’s mouth closed. But thankfully, times have changed with new types of options for straightening teeth and, with this book, a mindset that makes braces cool. For example, one page boasts of an Internet influencer on Facebook, TikTok, Instagram, and Twitter, who “gained followers in such an impressive amount, the braces got their own account.”
Dr. Fagala’s new book of orthodontic-inspired children’s rhymes was developed in coordination with Neon Canvas, the digital-marketing company he cofounded in 2016 with Alex Rasmussen, and illustrated by nationally syndicated cartoonist Greg Cravens. Dr. Fagala said that he wrote the book as a celebration of the unique individuals who choose to be patients at his practice, Saddle Creek Orthodontics. Then he decided to expand the book’s reach. “This was too good of an idea for us to keep all to ourselves,” said Dr. Fagala. “We debuted the book at the AAO meeting, and it’s already getting a tremendous response.”
Pages have large colorful illustrations and large, readable font. Dr. Fagala and Neon Canvas created the book to be customizable to other orthodontic practices. Available in paperback or hardcover (with silver foil braces on the cover), the customized book can include the doctor’s name on the cover, logos in multiple spots, customizable practice information, and even a custom caricature of the doctor(s). Distribution is limited to one per market.
Dr. Fagala invites orthodontists to learn more about the book at neoncanvas.com/book. The Memphis-based orthodontist is a frequent public speaker about orthodontic social media and digital marketing, a course director and lecturer at the University of Tennessee Health Science Center, host of “The Digital Orthodontist: Live” video podcast, and drummer for Relapse, a band made up entirely of orthodontists that recently performed in front of an audience of 2,000 at the American Association for Orthodontists annual meeting in Miami.
“All the Best Faces Wear Braces is a celebration of the unique individuals who choose to be patients of our practice,” notes Dr. Fagala. He wants his patients to love their faces whether they are in braces, or afterwards when they flash their new spectacular smiles.
OP
Review by Mali Schantz-Feld
33 orthopracticeus.com Volume 14 Number 2 BOOK REVIEW
Reduction of patient visits without the expensive lab fee
Norris 20/26 System
As orthodontists strive for clinical excellence with fewer patient visits, customizable braces have emerged as a popular solution. However, many of these platforms come with an unavoidable lab fee, reducing profits for doctors. And, for those who prefer the efficiency of self-ligating brackets, a customizable bracket is not an option. So, what is the alternative that may provide a better ROI and be a better fit for your practice?
A bracket slot that better fits the wires you want to use
For doctors who love the PSL workflow, but want an easier time finishing in a 19x25 wire, the .020 x .026 slot allows clinicians to pick up torque control earlier in treatment and maintain optimal 3-dimensional control of the teeth throughout the finishing phase. With this slot dimension, there is no need to implement uncommon wire sizes. You and your staff can use three common wire sizes from start to finish: 014, 18x18 and 19x25.

Bracket manufacturing and slot play

There are slight inaccuracies that occur in injection molding or milling brackets. (https://europepmc.org/article/med/34002705). Manufacturers have consciously made the slot a little larger so it’s not too small for wires to fit. However, those slight inaccuracies result in a major loss of torque and rotational control and unpredictable tooth movement. This has been compensated for in various ways from specifying additional degrees in programming, to continuous repositioning and wire bending. DynaFlex
includes an additional proprietary manufacturing step to ensure that the slot dimension is remarkably precise. That manufacturing process, combined with the .020 x .026 dimension, provides unbelievable control with precise tooth movement and superior case finishing.
Minimize chair time with the most advanced PSL door technology
If a bracket door breaks, becomes jammed from plaque, or self-opens, then the benefits of self-ligating are eliminated. A self-ligating door needs to be user friendly for staff, it needs to be sturdy, and it must be dependable throughout treatment. All three can be achieved with engineering and design. The Norris 20/26® door employs the most advanced door technology with a dependable, audible click. This ensures doctors and clinical teams will love its reliability from start to finish.
ROI
The Norris 20/26 System delivers unbeatable value. Unlike other systems that come with hefty lab fees and possibly a steep learning curve, this system offers a cost-effective solution that won’t break the bank. You can achieve clinical excellence and reduce patient visits without draining your resources. Visit www.dynaflex.com/norrissystem/ to learn more or schedule a demo.
34 Orthodontic Practice US Volume 14 Number 2 PRODUCT PROFILE
This information was provided by Dynaflex.
OP
Torque Control In 2nd Wire 18 x 18
Nickel-Free Alloy
• More Comfortable Button Head
• Maximized Base Precisely Matches Molar Curvature
• Lower Profile Stem For Patient Comfort
Nickel-Free Alloy
• Ideal For 7’s Or Partially Erupted 1st Molars
• 15% Smaller Base Pad
• Same Precise Base Shape For Superb Retention



“My team and my patients love the Precision Aligner Buttons®. The large bonding pad, ease of use, and the shape make it a perfect match for my aligner patients and a perfect match for my practice. They truly are rockstar buttons!”
Dr. Dovi Prero Beverly Hills, CA


• More Retentive Base Pad
• Sturdier Button Stem With Less Breakage
• Lower Profile Stem For Patient Comfort
“The Precision Buttons® have allowed me to use what I want - orthodontic buttons - without the headaches of frequent breakage and it has really changed the way I practice. The low profile and smooth corners provide spectacular comfort”
G2 METAL #10-PAB10210 NEW! METAL MINI #10-PABMINI G2 CLEAR #10-PABCLR2 The Only Bondable Buttons Designed Specifically For Clear Aligners www.dynaflex.com | 866-346-5665 052223 © 2023 DynaFlex®, Lake St. Louis, MO 63367. Printed in U.S.A. Clear: Design Patent (USD910,191) Metal: Design Patent (USD859,663) Utility Patent (US11,564,778) Purchase Today!
Dr. Bryan Lockhart Charlotte, NC
2 ND GENERATION
Anatomy of a dental malpractice action
Kristin Tauras, JD, defines the various complex parts of a malpractice claim
Today’s reality is that most dental and medical providers have a high probability of being sued. Below is a primer on the “anatomy” of a dental malpractice case. Lawsuits are controlled by state and federal law, but the basic anatomy of the lawsuit is the same in each state and follows the same general timeline.
The term used in the lawsuit may be “professional malpractice” or “dental malpractice,” but this article encompasses all professional negligence claims against dental specialists, including dentists, cosmetic dentists, pediatric dentists, prosthodontists, periodontists, endodontists, oral and maxillofacial surgeons, and orthodontists. It also encompasses the liability of the dental specialist(s) staff who assist with the dental treatment and may be named in the dental malpractice lawsuit, including dental hygienists, dental assistants, nurses, anesthesiologists, and other dental care providers.
Parties
There are at least two parties to a lawsuit: the plaintiff and the defendant.

The plaintiff is usually the patient or the parent/guardian of a minor patient. The lawsuit may be brought by the estate of a deceased or incapacitated plaintiff.
The primary defendant is the treating dental specialist, but there may be multiple defendants. Defendants may include any individual involved in the patient’s care and treatment leading up to and through the alleged malpractice event, including consulting dental specialists, nurses, radiologists, surgeons, dental hygienists, and even the medical malpractice insurance companies in some states. The lawsuit may also name the practice group, corporation, or limited liability company that employs the dental specialist(s).
Pleading stage
A dental malpractice lawsuit begins with a pleading or complaint that is filed with the court. It is the story the patient wants to tell the jury of what the dental specialist(s) did wrong and why the jury should award the patient money. The complaint must set forth that there was a patient and dental specialist(s) relationship, the dental specialist owed a duty of care to the patient, the den-
tal specialist(s) violated the duty of care, and that the violation of the dental specialist(s) duty to the patient proximately caused the patient’s injuries, and the patient (or patient’s estate) suffered damages.
Twenty-eight states have the additional requirement to file a certificate of merit for a dental malpractice claim to move forward.
The complaint must be served on each defendant. The date of service of the complaint on the defendant governs the timing of when the defendant must respond to the complaint. The defendant typically has 21 to 28 days to respond to the complaint. The response may either be an answer to the complaint (admitting, denying, or claiming insufficient information with respect to the allegations), or a motion to dismiss the complaint for technical errors or substantive reasons why the dental professional is not liable.
The pleading stage is also where the defendant may want to file a third-party action against another entity to bring them into the suit. While most attorneys will advise against filing a thirdparty action against another dental treater so that they can bring a unified defense, there may be an occasion to file a third-party suit against the manufacturer of a faulty instrument that caused or contributed to the problem. Most dental malpractice claims do not have third-party actions.
Respondents in discovery
Some states allow for complaints to be filed against an individual, but not name the individual as a defendant. Called a Respondent in Discovery, these individuals are named for discovery purposes only. A Respondent in Discovery may be converted to a direct defendant so long as the plaintiff follows the rules of the state for converting the Respondent in Discovery to a proper party defendant.
Notifying the insurer
The dental specialist(s) must notify their insurance company at the time they know of a claim or are served with a lawsuit. Every insurance policy contains a duty to notify the insurance
36 Orthodontic Practice US Volume 14 Number 2 LEGAL MATTERS
Kristin Tauras, JD, is a partner in the law firm of McKenna Storer in Chicago, Illinois. She has a litigation practice in the areas of employment law, insurance coverage, and professional malpractice. McKenna Storer is a fullservice law firm providing legal services to individuals and small-to-midsize companies, including defending professional malpractice negligence lawsuits and Illinois Department of Professional Regulation investigations, as well as advising dental and medical professionals regarding business and employment matters.
company upon learning of the potential claim when served with a lawsuit. If the dental specialist(s) fails to notify the insurance company, the insurer may refuse to defend and indemnify the claim.
Notice of the claim allows the insurance company to assign the dental specialist(s) an attorney, direct them on what records to keep, and how they should proceed. Some policies allow the dental specialist(s) to choose their own counsel.
Immediately retain documents and preserve evidence
Upon knowing of a claim and/or being served with a lawsuit, it is imperative that the dental specialist(s) retain all medical and dental records, notes, bills, x-rays or other imaging, correspondence with the patient, and machines used in the treatment of the patient, essentially “preserving” all evidence of the alleged malpractice. Your attorney and/or the insurance company will advise you what they need you to retain and send to them to defend the case as well. If you do not, or if you destroy relevant evidence, some states will allow a “spoliation of evidence” claim to be filed against you, which may include a putative finding of liability with just damages to be assessed.
Discovery stage
After the answer is filed or the motion to dismiss is resolved, the case will enter the discovery phase.
Discovery is broken down into three types: fact written discovery, fact oral discovery, and expert discovery.
Written discovery
All parties may issue written discovery against the other parties. Where there are multiple defendants, each plaintiff may issue discovery against each defendant, and each defendant may issue discovery against the plaintiff, as well as against each of the other defendants.
Written discovery is divided into four types: Interrogatories, Requests to Produce, Third-Party Subpoenas, and Requests to Admit.
Interrogatories are questions submitted to the other parties. The plaintiff’s Interrogatories to the defendant(s) will include requests for information such as the identity of all treaters (both dental and non-dental), dates of treatment, types of treatment, types of tests done prior to the treatment, cost of the treatment, and information regarding the insurance. The defendant(s) Interrogatories will include the basis for the negligence allegations, identify the claimed negligent treatment, damages (including alleged injury, days off work, cost of alleged repair or further treatment, as well as pain and suffering and disfigurement), and identity of witnesses.
The Requests to Produce are written requests for documents. The plaintiff’s Requests to Produce will usually include the patient’s dental records, bills, x-rays or other imaging, correspondence, as well as the office policies and procedures. The defendant’s Request to Produce will usually include the plaintiff’s dental and medical records, bills from additional treatment, and proof of damages such as time off work.
The parties may also issue Subpoenas to other entities not involved in the lawsuit, including other medical and dental treaters who have treated the patient both in the past and with respect to the claimed malpractice.
The parties may also issue Requests to Admit. These are statements that the parties must either admit or deny or set forth a reason they can neither admit nor deny the statements. Depending on the state law, these Requests to Admit may become binding on the parties at the time of trial.
Oral fact discovery
Discovery also includes non-expert testimony from the plaintiff, defendant(s), and any other fact witness.
The patient’s deposition is usually the first deposition taken in a case. If the patient is unable to testify, such as when the patient is a minor or the patient is disabled or deceased, the family members or next of kin who brought the lawsuit may testify about the patient’s treatment and injuries.
The defendant(s) depositions then take place. The defendant(s) include the dental specialist(s) sued in the case, as well as the other individuals in the office that took part in the care. The depositions of the defendant(s) usually center around the issues of informed consent, care provided to the patient, policies and procedures of the office, and the dental specialist(s) training and experience to perform the procedures that form the basis of the lawsuit.
After the defendant(s) depositions are taken, the parties will take the depositions of the other dental and medical treaters who have seen the patient.
Additional fact witness(es) depositions may also be taken. These fact witness(es) may include the office manager(s) to testify regarding bills and the office policies and procedures, and family members that can testify to the condition of the patient before and after the procedure.
Expert discovery
In all states, almost without exception, the plaintiff must have dental specialist(s) testify to the standard of care and whether the care deviated from that standard. While technically the defendant(s) may be qualified to testify to the standard of care and alleged deviation, standard of care experts are usually paid experts who evaluate the patient’s records and testify regarding their expertise. Expert testimony may be excused when it is readily apparent that malpractice occurred (such as inexcusably removing the wrong tooth) and that an expert’s testimony might be redundant. Many trials rise and fall on the strength of the dental specialist(s) expertise.
Other experts may also testify regarding damages, including financial experts who testify about the financial harm the plaintiff suffered because of the sub-standard care.
37 orthopracticeus.com Volume 14 Number 2 LEGAL MATTERS
Under most insurance policies, the dental specialist has the ultimate right to make all decisions regarding settlement.
Dispositive motions
Most states have a mechanism for filing a dispositive motion, such as a motion for summary judgment or summary decision, after the close of discovery. The dispositive motion requests that the judge review the law and the facts to see if there is an issue of fact that requires that the matter be tried. Usually, this motion is filed by the defendant(s), alleging that the plaintiff cannot prove a required element of their case.
Settlement
While settlement discussions can happen at any time during the case, most parties will engage in settlement discussions after the close of discovery or before the trial begins. In dental cases, there is the notion that the case is either in a “settlement posture” or a “trial posture.” Nevertheless, many cases do settle on the eve of trial. Under most insurance policies, the dental specialist(s) has the ultimate right to make all decisions regarding settlement.
Trial
Many dental malpractice cases go to trial. A trial date is usually set between 18 months to 36 months after the date the lawsuit was filed. The dental specialist(s) should sit at counsel’s table through the duration of the trial.

Professional malpractice trials are long, lasting a week or longer. The first day is usually a “pretrial conference.” The judge will attempt to settle the case and then rule to either admit or exclude evidence from trial (called the motions in limine), and review jury instructions.
Day 2 and Day 3 are spent with jury selection. Jury selection is heavily individualized by the judge who presides over the case. The judge may ask the jury questions or let the attorney ask the questions.
Once the jury is empaneled, the trial begins. The attorneys will give their opening statements, explaining to the jury what they believe the evidence will show. After that, the plaintiff will present their case in chief, and the defendant(s) will then present their case in chief.
At the end of the evidence phase, the judge will instruct the jury on the law, and the deliberation process begins. The jury will deliberate until either they reach a decision, or they inform the court that they are unable to reach a decision.
Motion to overturn the verdict or appeal
After the jury reaches its verdict, the jury foreman will read the verdict. This does not end the proceedings. The parties in all states have the right to file a motion to contest the jury verdict and/or file an appeal from the jury’s verdict.
If the jury verdict is affirmed by the appellate court, and the appellate process is exhausted, the matter ends. If the jury verdict is overturned by the judge and/or the appellate courts, then it is possible the matter will be retried.

Reporting
Some states require that any settlement or an adverse judgment be reported to the state licensing board. In that case, the dental specialist(s) should retain defense counsel to assist with the defense of the dental license. OP
38 Orthodontic Practice US Volume 14 Number 2 LEGAL MATTERS
3 REASONS TO SUBSCRIBE • 16 CE credits available per year • 1 subscription, 2 formats – print and digital • 4 high-quality, clinically focused issues per year 3 SIMPLE WAYS TO SUBSCRIBE • Visit www.orthopracticeus.com • Email subscriptions@medmarkmedia.com • Call 1-866-579-9496 Orthodontic Practice US 1 year $149 / 1 year digital only $79 Visit-ulabsystems.com Summer2023 Vol14 No2 orthopracticeus.com ORTHODONTICS Bracket&AlignmentSystems n 4CECreditsAvailableinThisIssue Myofunctional TherapyforPostOrthodonticRetention Drs.CarlyJacobsandRyanRobinson Theimportanceof maintainingindoor airqualityindentistry Drs.TylerOrehekandTroyRoeder Conservativeapproach offortuitouslyfound odontomainachild withsevereautism Dr.GabrielaAuroraAsensi Deliveringaquality patientexperience inGuamDr.PaulSauget
A taxing situation
Justin Maxwell offers suggestions for maximizing your tax strategy


Senators, CPAs, and tax attorneys have long stated that most American small business owners pay more tax than is legally required. In fact, as a successful orthodontist, you have probably felt that you pay too much to the government in taxes. An independent study proved them right — they found that per $250,000 of income the average American business owner will pay about $11,000 more per year than is legally required in taxes.
Over 20 years, that’s an additional $220,000 paid to the government on top of what you are already paying them, and 100% of it is unnecessary. Fortunately, this problem is fixable, and there is a way to legally and ethically pay less tax that doesn’t require you to become a tax attorney or spend hours and hours doing something outside of your genius. In this article, we will explore one simple fix that can drastically improve or eliminate any and all unnecessary tax payments.
Whenever new orthodontists begin their business journey, one consistently offered piece of advice is: “find a good CPA.” While this advice is something every orthodontist should follow, it lacks a critical component that leads to the overpayments mentioned above. Instead, the recommendation should be to find a good tax TEAM. This is the simple fix that every orthodontist can implement today. Find a tax team versus a tax person.
The tax code is a behemoth. When you include all supporting documents, it contains over 80,000 pages. Expecting one person or one company to be an expert in all the nuances and available options is a mistake that will result in paying more taxes than is legally required.
Who then should be on this accounting team, and what roles should each team member fill?
Tax filer
The tax filer is responsible for complying with the ever-changing tax rules and regulations. These team members will compile all of your data, help you report what was made to the IRS, and tell you how much you owe in taxes. They will help you understand what is the best entity to be set up under for your given situation. They may also assist in bookkeeping, audits, providing accurate numbers as to what is going on in your business, and being a valuable resource for tax advice.
39 orthopracticeus.com Volume 14 Number 2 FINANCE MATTERS
Justin Maxwell is a wealth and tax strategist at Big Life Financial. He received a Master of Science degree from the University of Utah. He and his business partner join forces with dental and medical professional accounting teams across the country to help professionals implement effective business strategies. He can be reached at justinm@biglifefinancial.com.
Table 1
Cost segregation
Paying your kids
Tax-advantaged investing
Augusta Rule
Tax-advantaged insurance
Special entity structuring
Maximize your charitable giving
Tax credits and incentives
An owner of commercial or single family rental real estate can accelerate the depreciation taken. Most of the time, an engineer is a required member of the team.
Depending on the age of the child, entity type, and a few other factors, a business owner can potentially pay children who work in the business tax-free.
The US government incentivizes individuals to invest in specific industries/markets. The incentive they use is giving tax deductions, which at times can be quite large. A registered investment advisor who specializes in these areas must be a member of the team.
Leveraging a rule that allows an individual to rent out their personal residence up to 14 days a year tax-free and turning it into a business expense.
There are ways to save income tax and payroll tax by using a variety of insurance offerings, including health, commercial and life insurance. These are extremely niche and require a specialist to set up.
There are ways to strategically create and pair entities together (corporations and trusts) to build tax favorable environments.
Donating provides tax deductions, but there are ways to increase the tax deduction by donating to specific things or utilizing certain strategies. For example, you can create an arbitrage where you donate $1 but save $2 in taxes.
The tax code contains a variety of tax credits and incentives that may or may not be applicable, but unless a specialized tax credit professional looks at it, you can’t say for sure. These include things like the R&D, ERC, WOTC, SALT, and more.
Tax-advantaged accounts
Tax-deferred accounts
Pay the tax now, but the growth of the account is tax free. These are vehicles like the Roth IRA, cash value life insurance, etc.
Delay the tax today, but pay taxes on what you put in and the growth that occurs when you use it down the road. These are vehicles like 401K, traditional IRAs, etc.
Most people go to the “tax filer” to get their taxes done. While this team member is a vital component of the team, they should not be the only member of the team. The tax filer is what we call a tax historian, meaning they can take what has happened and tell you how it will be taxed, but unless this person is paired with a proactive tax planner, there will always be unnecessary tax payments.
Tax strategists
The tax strategists are the most often missed member of the team. These team members will be a combination of specialists, tax attorneys, and third-party administrators. However, to ensure your time is maximized, it will need to be spearheaded by one quarterbacking person or group. This quarterbacking person will bring all the needed players to the table. The tax strategist’s job is to provide quality, proactive strategy that accesses more of the tax code and focuses on lowering the tax bill. The tax filer and strategist work hand-in-hand. No decision moves forward without the consent of the other. When both parties work together, you get a tremendously powerful approach that results in using more of the tax code and paying less tax.
The tax strategist will help you as the business owner navigate through and implement the tax strategies that are most
applicable to your situation. These include but are not limited to strategies found in Table 1.
If you were going through this table and thinking:
“My tax person tells me they do tax planning, but I’ve never had anyone talk to me about all these options, or why is that I have only had a conversation about one or two items on the list?”
Then it’s time for you to upgrade your team. When people hear that, they automatically assume they should dump their old accountant. But if you go and only hire a tax filer again, you will be in a very similar situation just with a new person. The simple fix is NOT hiring a new accountant; the simple fix is creating a tax team of both a tax filer and a tax strategist. This combination results in you having the best chance of reducing your tax bill to its legal minimum.
One of the biggest problems is that most people don’t even realize that an accounting team is something they are entitled to and that these tax savings options actually exist. Yet, throughout this article, we discovered that most business owners pay more taxes than is legally required, that there is a difference between a tax filer and a tax strategist, and that there are many more legal ways to pay less tax. Most importantly, we realized that the solution is not nearly as complicated as we think it should be. The simple fix is to create a tax team filled with both tax filers and tax strategists. When action is taken on this solution, you will find your tax bill goes down. OP
40 Orthodontic Practice US Volume 14 Number 2 FINANCE MATTERS
Eliminate Airborne Threats
Air Quality Guard is a Clean Air System Designed for the Unique Challenges of Dental Practices



Air quality is CRITICAL to your practice. Contaminants are everywhere: Pathogens, Pollutants, Viruses, Bacteria & Fungi all threaten our air quality and quality of care.
Benefits of Air Quality Guard:
• Arm and ceiling intakes capture aerosols at the source and move them away from occupants
• Contaminated air is filtered through a 3 layer system, removing greater than 99.99% of all contaminants
• Reduces the spread of COVID-19 and reduces sick leave
• Negative pressure airflow cycle ensures that contaminants are captured before they can circulate
• Quietly and efficiently filters & replaces up to 100% of air with pure, clean air
• Power ful enough to replace all the air in the room every 7 minutes*
Pre-Filter Gas Phase Media Filter HEPA Filter Directional Airflow design
contaminants are removed at the source and replaced by fresh, clean air. Clean air returned to hallway Aerosols collected at source
ensures
on recommended system design principles. Customization may increase or decrease this value. Learn More and Request a Consultation Today! (800) 210-9768 | support@airqualityguard.com | www.airqualityguard.com
*Based

