4 minute read
MISSISSIPPI 2


22 al 26 de noviembre
FDAU-35 Abordaje Farmacológico Y Su Mecanismo De Acción En Paciente Con Síndrome De Hellp Mississippi 2
Advertisement
BORREGO RODRÍGUEZ ROGELIO; DELGADO MARRERO ANDREA; HERNÁNDEZ GARCÍA JESÚS HERNÁNDEZ; SILVA ÁNGEL DE JESÚS
1. Facultad de Medicina. Farmacología sección C.
RESUMEN
Considerado por algunos autores como una complicación de la preeclampsia grave, el síndrome de HELLP se presenta con anemia hemolítica microangiopática, elevación de las enzimas hepáticas y trombocitopenia que afecta al 0.9% de todos los embarazos y se relaciona con elevada morbilidad y mortalidad materna y fetal.
Introducción
Paciente femenino de 38 años con 29 SDG se presenta en urgencias en dos ocasiones con hipertensión arterial, en la segunda ocasión presenta además cefalea y epigastralgia; es diagnosticada con preeclampsia con criterios de severidad clínica.
Presentación del caso clínico
Antecedentes de importancia Tabaquismo positivo desde los 18 años a razón de 6 cigarrillos diarios suspendido durante el embarazo
Alergia a ceftriaxona
2 cesáreas
Interrogatorio Refiere cefalea y epigastralgia, adecuada motilidad fetal y sin pérdidas transvaginales
Exploración física TA 150/100, FC 79/min, FR 20/min, T 36°C. Abdomen globoso por útero gestante, AFU de 27 cm, producto único vivo.
Estudios de diagnóstico Ultrasonido
Perfil pre-eclámptico
22 al 26 de noviembre
Diagnóstico Síndrome de Hellp Mississipi 2
Preeclampsia con criterios de severidad
Embarazo quirúrgico patológico mediato
Tratamiento y evolución Nifedipino 30 mg y Alfametildopa vía oral cada 8 horas
Mejora y egresa con manejo antihipertensivo (Nifedipino y metoprolol) y analgésicos.
Justificación del tratamiento utilizado
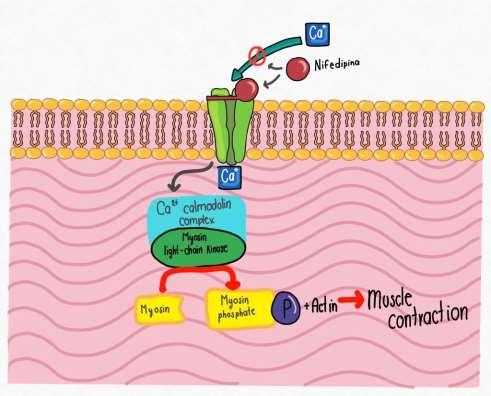
Elegido para disminuir la elevación de cifras tensionales, pues el nifedipino, al actuar bloqueando los canales de calcio, provoca una vasodilatación, logrando el efecto deseado, manteniendo los niveles de la presión arterial.
Consideraciones éticas
Siguiendo los principios de la Declaración de Helsinki y la Ley General de Salud Mexicana, la paciente del presente caso fue informada acerca de sus derechos, confidencialidad y seguridad; aceptó y brindó el consentimiento informado, basado en la Norma Oficial Mexicana NOM-004-SSA3-2012, del Expediente Clínico.
Discusión del mecanismo de acción del fármaco
El nifedipino impide la entrada de calcio a las células de los músculos lisos vasculares, bloqueando el poro del canal de calcio, provocando vasodilatación de arterias coronarias y vasos periféricos; el aumento del flujo incrementa la oxigenación a los tejidos del miocardio, al mismo tiempo que la vasodilatación reduce las resistencias periféricas, la presión arterial sistémica y la postcarga.
Conclusión
Dado que estas elevaciones de cifras tensionales pueden ser muy agresivas para el estado de la madre y el feto, el diagnóstico temprano y el tratamiento oportuno debe ser llevado a cabo con el fin de priorizar la disminución de la mortalidad materna fetal. En casos de elevaciones intensas de transaminasas y DHL con plaquetas disminuidas será necesaria la interrupción del embarazo como alternativa compleja pero con resultados favorables.
22 al 26 de noviembre
ABSTRACT
Considered by some authors as a complication of severe preeclampsia, HELLP syndrome presents with microangiopathic hemolytic anemia, elevated liver enzymes and thrombocytopenia affecting 0.9% of all pregnancies and is associated with high maternal and fetal morbidity and mortality.
Introduction
A 38-year-old female patient with 29 SDG presented to the emergency department on two occasions with arterial hypertension; on the second occasion she also presented with headache and epigastralgia; she was diagnosed with preeclampsia with clinical severity criteria.
Presentation of the clinical case
Important antecedents Positive smoking since the age of 18 years at a rate of 6 cigarettes per day, suspended during pregnancy.
Allergy to ceftriaxone
2 Cesarean sections
Interrogation Headache and epigastralgia, adequate fetal motility and no transvaginal leaks.
Physical examination BP 150/100, HR 79/min, RR 20/min, T 36°C. Globular abdomen due to pregnant uterus, AFU of 27 cm, single live product.
Diagnostic studies Ultrasound
Pre-eclamptic profile
Diagnosis Hellp Mississipi 2 syndrome
22 al 26 de noviembre
Pre eclampsia with severity criteria
Pathologic surgically mediated pregnancy
Treatment and evolution Nifedipine 30 mg and Alfamethyldopa orally every 8 hours.
Improvement and discharge with antihypertensive management (Nifedipine and metoprolol) and analgesics.
Justification of the treatment used
Chosen to reduce the elevation of blood pressure figures, because nifedipine, acting by blocking calcium channels, causes vasodilation, achieving the desired effect, maintaining blood pressure levels.
Ethical considerations
Following the principles of the Declaration of Helsinki and the ‘Ley General de Salud Mexicana’, the patient in the present case was informed about her rights, confidentiality and safety; she accepted and provided informed consent, based on the ‘Norma Oficial Mexicana NOM-004-SSA3-2012, Del Expediente Clínico’.
Discussion of the drug's mechanism of action
Nifedipine prevents calcium entry into vascular smooth muscle cells by blocking the calcium channel pore, causing vasodilation of coronary arteries and peripheral vessels; the increased flow increases oxygenation to myocardial tissues, at the same time that vasodilation reduces peripheral resistances, systemic blood pressure and afterload.
Conclusion
Given that these elevations in blood pressure can be very aggressive for the condition of the mother and fetus, early diagnosis and timely treatment should be carried out in order to prioritize the reduction of maternal and fetal mortality. In cases of intense elevations of transaminases and LHD with decreased platelets, termination of pregnancy will be necessary as a complex alternative but with favorable results.
RESUMEN GRAFICO
22 al 26 de noviembre