Balkan Beats
Mosaic of Health: Ignite Your Inner Power


Dear readers,
Welcome to the latest 52nd edition of our magazine. We are excited to share this journey with you, exploring what health truly means in our lives. In this issue, we dive into topics from the importance of mental health to the realities of living with cancer, highlighting how our stories and experiences connect us all and reminding us that none of us are alone on this journey. Each chapter brings something different: we will unpack the myths surrounding health, celebrate local habits that make a difference, and share personal stories that inspire resilience. As you read through these pages, we hope you find new insights and ideas that resonate with you. Remember, every small choice we make can lead to healthier futures, not just for ourselves, but for our communities too. Thank you for being part of our family and for taking the time to engage with these important conversations. Let’s create a vibrant community that celebrates health in all its forms.
Warmly, The Editors: Daria, Lilie, Toni, Sheila





by Alexandra Giamouzi
Have you ever thought about how much your mental health can affect your life, especially your physical health? For instance, have you ever had a headache after a difficult day that left you feeling down? Or have you experienced stomach pain when you’re stressed about school or work? These are clear examples of how our mental health impacts on our overall well-being. It’s often said, and rightly so, that there is no health without mental health.
A bout 14% of global diseases are linked to neuropsychiatric disorders, with depression playing a major role. Mental health conditions can not only worsen communicable and non-communicable diseases but can

also increase the risk of both unintentional and intentional injuries.
M oreover, mental health influences much more than just our physical well-being—it significantly affects our relationships and social interactions. People facing mental health challenges often struggle to maintain healthy connections, whether in their personal or professional lives. When stress, anxiety, or depression become overwhelming, individuals may withdraw, feel isolated, or have difficulty communicating. This can lead to loneliness and further deepen mental health struggles, creating a cycle that is difficult to break. Since strong relationships are essential for mental and emotional well-being, maintaining good mental health is crucial for fostering positive social connections.
Now let’s talk about the importance of public health and how it affects the whole system. Despite the undeniable link between mental and physical health, modern societies often focus more on physical health risk factors, frequently overlooking mental health. It’s essential to integrate mental health awareness into all aspects of health planning, social policy, and both primary and secondary health-
care. Mental health must be recognized as a vital component of overall health.
For example, a study conducted by the Texas Department of Health in 2002 revealed that 87.2% of respondents reported good mental health, while 12.8% rated their mental health as poor. However, these figures may have shifted significantly in recent years, especially given the increasing awareness of mental health challenges worldwide. These findings highlight the need for improved public health responses and resources.
A persistent challenge in public health is the misunderstanding of mental health issues. For many years, mental health problems were not viewed as a significant public health concern. However, in recent years, public health agencies have begun to develop strategies that address mental health issues more comprehensively. It’s crucial to distinguish between mental health and mental illness. While those with severe mental illnesses may require medication, housing, and other services, many others experience less severe but still impactful mental health challenges that also require attention and support.
It’s clear that individuals struggling with mental health issues may find it hard to fully engage in their daily lives. Whether it’s a lack of motivation or the inability to participate in routine activities, mental health struggles can limit one’s ability to thrive. As a society, it is crucial to offer support and understanding. With the right government measures, we can
make a meaningful impact on mental health support systems and improve lives.

Mental health is intricately linked to our physical health, relationships, and overall functionality in life. Without good mental health, it becomes increasingly challenging to lead a fulfilling and productive life. Acknowledging the importance of mental health at both the individual and societal levels is key to building healthier, happier communities. Governments, health organizations, and individuals must all take steps to promote mental well-being and offer the necessary support. Only by recognizing mental health as a fundamental aspect of overall health can we truly enhance the quality of life for everyone. Now is the moment to act—whether it’s practicing self-care, raising awareness about mental health, or pushing for policy reforms, each of us can play a role in creating stronger, healthier communities.
by Inna Petrovska
War leaves more than just physical destruction — it profoundly impacts the mental and physical health of those who live through it. Whether civilians or soldiers, the psychological toll of war crosses borders, leaving deep and lasting scars.
ommon
W hen examining the psychological impact of war, it’s crucial to understand that trauma manifests in diverse ways, deeply influenced by an individual’s role and experiences during the conflict. Research shows that military veterans often face unique psychological challenges compared to civilians. However, trauma doesn’t discriminate—civilians can be profoundly affected too, with rates varying based on factors like proximity to conflict and personal experiences.
D espite varying exposure levels, there’s a common thread that binds all those affected by war: the fundamental human response to extreme stress and danger. Whether soldier
or civilian, the brain’s response to trauma involves similar neurological pathways.
According to research by Dr. Steve Sugden, MD, at the Huntsman Mental Health Institute (HMHI), three primary populations are susceptible to war-related psychological trauma:
• Civilians residing in conflict-affected areas
• Military personnel engaged in combat on both sides
• Individuals exposed to war-related content through various media channels
T hese groups can develop similar trauma profiles, with prevalent symptoms including:
• Post-Traumatic Stress Disorder (PTSD)
• Clinical depression
• Chronic anxiety
• Hypervigilance
So, as we can see, the psychological impact of war is not always confined to those directly involved in the frontline, but can cross borders and affect individuals who may be far removed from the physical battleground.
Today, violent conflicts are at their highest since World War II, affecting over 2 billion people globally. The mental health impact of these conflicts spreads like radiation, transcending borders. War-induced anxiety and uncertainty undermine global safety perceptions, demonstrating that mental health issues spread faster across borders than economic crises.
In Ukraine, where the full-scale Russian invasion enters its third year today, feelings of loss, uncertainty about tomorrow, and constant threat of death have become integral parts of many people’s lives. Numerous Ukrainians grapple with profound grief and depression, their emotional difficulties compounded by unresolved loss and the inability of many to return home. These psychological consequences of war create a heavy burden that war survivors carry for a lifetime.
T he weight of this burden often manifests in severe psychological conditions. According to the World Health Organization (WHO), one in five people (22%) who have experienced war in the last decade will face mental health disorders such as depression, anxi-
ety, post-traumatic stress disorder (PTSD), bipolar disorder, or schizophrenia.
According to a comprehensive meta-analysis, the prevalence of war-related mental health disorders is widespread and alarming. Studies show that 28.9% of individuals who have lived through war experience depression , with rates varying between 3.2% and 79.6%, depending on the conflict.
Civilians tend to suffer higher rates of depression compared to military personnel. Similarly, 30.7% of those exposed to war report symptoms of anxiety, with civilians displaying a significantly higher prevalence (38.6%) than military personnel (16.2%). This stark difference can be attributed to the fact that civilians often find themselves unprepared for the chaos and unpredictability of war, while soldiers are trained to cope with high-stress situations, which can mitigate certain anxiety-related responses. The sense of helplessness civilians experience, compounded by the destruction of their homes and threats to their families, fuels their anxiety.
However, it’s essential to recognize that military personnel endure their own set of psychological challenges, distinct from those civilians face. Soldiers may report lower levels of anxiety, but their mental health struggles are far from negligible. They are more likely to suffer from conditions such as moral inju-
ry and survivor’s guilt, which complicate their psychological recovery. These feelings often stem from the traumatic experiences of combat, the loss of comrades, and the ethical dilemmas encountered in war. While civilians and military personnel experience post-traumatic stress disorder (PTSD) at similar rates—25.7% and 21.3%, respectively—the emotional burdens for soldiers are shaped by their direct role in combat and the weight of responsibility, which can be just as debilitating, if not more so.
The psychological toll of war doesn’t just manifest in mental health issues—it also has profound effects on physical health.
Prolonged stress, particularly the type caused by war (distress) , alters our neurobiology and weakens the body’s ability to cope. This distress activates the amygdala, our brain’s “panic button,” making us hyper-reactive to fear and anxiety-inducing stimuli. Constantly being in a state of high alert exhausts the body, leading to the suppression of functions like libido and the immune system. Over time, the depletion of dopamine, a key “happiness hormone,” results in apathy, depression, and emotional fatigue. During war, the cerebral cortex, responsible for regulating behavior and empathy, also suffers, making individuals less tolerant, less able to manage emotions, and more prone to conflict.
T he impact of this stress response extends to chronic physical conditions. The persistent release of cortisol and adrenaline contributes to insulin resistance, raising the risk of diabetes. Simultaneously, stress-induced inflammation can damage arteries, raising the
chances of heart disease, heart attacks, and strokes. War trauma also accelerates blood clotting, further increasing the risk of cardiovascular events.
In the context of the ongoing Russian terror in Ukraine, these health consequences have become particularly severe. The number of patients there with diabetes has increased by more than 20%, heart attacks by over 16% and strokes by more than 10% . The stress and disruption caused by the war have also led to an anticipated surge in neglected cancer cases, as many are unable to access medical care due to displacement, occupation or psychological paralysis. The chronic nature of these conditions, intertwined with mental health issues, creates a vicious cycle, where physical health deteriorates further as mental health worsens, making recovery even more challenging.
To sum-up
There is a complex connection of mental and physical health that underscores the longterm impact of war on both civilians and military personnel. While the statistics may show different mental health outcomes for these groups, the underlying trauma and distress are universal, deeply affecting all who are exposed to the horrors of wars.
by Yelyzaveta Marchenko
Cigarette Labyrinth: The Smoke That Clouds Our Future
Imagine a maze where finding the exit seems impossible. Every turn brings another danger, every step leads into the unknown. Such a maze is created by tobacco, which claims more than 8 million lives globally each year. Cigarette smoke knows no borders; it envelops our lives, obscuring the true consequences of this addiction.
To find a way out, we must focus on the most vulnerable young people, who have not yet fully succumbed to the smoke and still have the chance to choose a healthier future.
Іnvisible Enemy: Why Cigarettes Kill More Than War
Tobacco smoking has remained one of the biggest public health challenges worldwide for decades. It causes one in every eight cancer cases and is responsible for one in every five deaths among cancer patients. Throughout the 20th century, this habit claimed the lives of approximately 100 million people, the majority of whom lived in today’s developed countries.
Tobacco smoke contains over 7,000 chemical compounds, at least 250 of which are toxic, and 69 are known to cause cancer.
B ut the most alarming fact is that tobacco kills not only those who smoke. Secondhand


smoke is deadly for those around them. Every year, approximately 1.2 million people, including children, lose their lives due to the harmful effects of secondhand tobacco smoke.
Smoking on Autopilot: When Life Turns to Ash
Nicotine addiction among children and adolescents is reaching alarming levels, and this age group is particularly vulnerable to the influence of tobacco products. One key factor is that children and teens are in a critical period of personal development, where the influence of social media, advertising, and peer pressure is especially strong. Advertising campaigns that directly or indirectly target youth,
along with the portrayal of smoking as “cool” on social networks, create an environment where tobacco use becomes “normalized,” making it difficult to resist.
Smoking is most prevalent among teenagers aged 16-18. Studies from various countries show that secondhand smoke at home and in public places significantly increases the likelihood that young people will start smoking. In Ukraine, one in eight teenagers (12.1%) started smoking at the age of 14. If healthy habits are not cultivated in children, the number of smokers will rise, and tobacco-related mortality will only increase.
Participants were invited to take part in a survey that included a 48-hour no-smoking challenge. During this time, they were asked to record their emotions, triggers, and replace their smoking habit with healthy activities. The goal was to demonstrate the impact of short-term nicotine withdrawal and help them assess their own habits.
The results showed that most participants reduced the number of cigarettes smoked and noticed improvements in their well-being. The main challenges were physical cravings and stress, but support from friends, physical exercise, and healthy eating helped overcome these difficulties. 60% of participants expressed willingness to continue such practices.
The primary reasons for smoking were social pressure (34.4%) and stress (18.8%). Meanwhile, 46.9% were willing to quit smoking in the future with family support (37.5%) and information on health risks (31.3%).
Additionally, 53.1% of participants felt responsible for secondhand smoke affecting those around them, indicating some awareness of its harm. Participants also suggested that anti-tobacco campaigns focus on real motivations, healthy alternatives, and raising the prices of tobacco products.
Education — The Cornerstone of a Smoke-Free Nation — How Learning Shapes Healthier Generations
Education is a powerful tool in the fight against smoking, especially among young people. It is during school years, when children and teenagers spend most of their time in an educational environment, that their conscious attitudes toward health are formed. Research shows that smoking rates are lowest among
individuals with higher education. This further emphasizes the crucial role that knowledge and learning play in changing behavioral habits.
Nicotine addiction is a challenge not just for the individual but for society as a whole. Each of us can become an agent of change, starting with our own decision to quit smoking and supporting our loved ones in their attempts to break this harmful habit. Schools, universities, and other educational institutions should become active platforms for combating addictions among youth—places where conscious citizens are nurtured, who avoid dangerous habits.
Don’t wait until a harmful habit turns your life or the life of your loved ones to ashes. Take the first step toward health today! Quitting smoking is not just a chance for a longer and better life but also an opportunity to set an example for others. Join the fight against tobacco: support those who are trying to quit, spread awareness about the dangers of smoking, and together we can change the future.

Don’t wait until a harmful habit turns your life or the life of your loved ones to ashes. Take the first step toward health today! Quitting smoking is not just a chance for a longer and better life but also an opportunity to set an example for others. Join the fight against tobacco: support those who are trying to quit, spread awareness about the dangers of smoking, and together we can change the future.
by Lilie Grosselin
According to the World Health Organisation (WHO), nearly 20 million people are affected by cancer every year. This disease represents a major challenge for society, which has been striving to understand its mysteries since prehistoric times. Evidence of its existence has been discovered dating back more than 76 million years, including an osteosarcoma - a bone tumour - found on the foreleg of a herbivorous dinosaur.
Prehistory
Until -3000 BC
“Our studies show that diseases were already present among our prehistoric ancestors, millions of years before modern industrial societies existed,” reveals palaeoanthropologist Edward Odes.
In 1989, palaeontologists discovered a Centrosaurus leg bone in the Canadian province of Alberta. Initially, they thought that the deformation of this bone was due to a healed fracture. But recent high-resolution tomography
examinations revealed that the apple-sized lump was in fact a cancerous tumour.
Until recently, cancerous tumours were virtually absent from palaeoanthropological studies. The reason for this? Cancer does not only manifest itself in bones: it can affect organs or blood, as in the case of leukaemia, tissues that leave no trace 1 million years after death.
This surprising discovery pushes back the origins of cancer well beyond what was previously thought, anchoring this disease in the depths of prehistory, testifying to its presence from the emergence of multicellular life.
3000 BC to 476 AD
Ancient Egypt (around -3100 BC to 30 BC)
T he ancient Egyptian civilisation left behind not only pyramids, but also a precious legacy of medical texts illustrating their advances in health. The first written document about can-

cer is the Edwin Smith’s papyrus, which details 48 cases of cancer.
The authors of the papyrus admit that there is no treatment for this disease, making it incurable. “They had knowledge, but knew how to recognise its limits”, stresses Dr Edgard Camarós, a researcher at the University of Santiago de Compostela in Spain.
Far from limiting themselves to theories, the Egyptians demonstrated real technical expertise, seeking to unravel the mysteries of malignant tumours. A fascinating discovery, based on the analysis of two skulls over four thousand years old, reveals that they had already attempted to treat cancer using the methods available at the time.
T he use of a sharp metal tool on the skull of a man who lived between 2687 and 2345 BC has been discovered by researchers from
Cambridge University. Letting thought that an operation have been experimented, on the round metastases found in him body. It remains to be seen whether this operation was carried out during his lifetime, in the hope of a cure, or after his death, to gain a better understanding of the disease that afflicted him.
W hatever the case, this discovery sheds new light on the interest of Egyptian civilisations in what we now call cancer, proving that the fight against this disease goes back thousands of years.
Ancient Greece (around 800 to 31 BC)
I n Ancient Greece, although poorly understood and considered incurable, cancer was already attracting the attention of doctors. Hippocrates (460-377 BC), considered to be the father of medicine, was the first to named the disease “karkinos” and “karkino-
ma”, meaning crab in Greek, inspired by the shape of the veins around the tumours, which resembled the animal’s legs.
He classified tumours affecting various organs, including the skin, breast and rectum. According to his theory of the four humours, excess black bile was the main cause of cancer.
Galen (129-216 AD) later developed this idea in his treatise “On Unnatural Tumours”. He attributed the disease to an unbalanced diet that weakened the liver, which produced an excess of black bile, thickening the blood and causing dark veins around the tumours, reminiscent of a crab.
476 to 1492 AD
“ We must now add cancer as one of the main classes of disease that afflicted people in the Middle Ages”, says anthropologist Jenna Dittmar.
A recent study conducted by Cambridge University reveals that between 9% and 14% of

British adults in medieval times would have suffered from cancer. Previous estimations considered around 1% the number of population touched at this period. This difference can be explained by an evolution in the method of analysis “We have looked inside the bones to find hidden cancers” expose the Cambridge anthropologist Piers Mitchell. This proves that a significant proportion of the medieval population was affected by this disease, even thought these figures are four to five times lower than nowaday.
T his analysis, which involved 143 skeletons from six cemeteries in England, was carried out using scanners and X-rays. According to P. Mitchell: “Bones, after being buried for 500 to 1,000 years, are often damaged by environmental factors such as tree roots or rodents”. This is the reason why the researchers focused on skeletons with intact parts, in particular the pelvis, spine and femurs, where metastases are more common. However, it is important to note that these results are not fully truthful “Scans only detect bone cancer in about 75% of cases”, explains P. Mitchell.
1492 to 1789 AD
In the 17th century, cancer was still widely regarded as an incurable and mysterious disease, shrouded in superstition. Fear of an imaginary contagion led to the social exclusion of patients, who were often turned away from hospitals.
However, the progress of medicine thanks to advances in anatomy and the practice of dissection enabled doctors to gain a better understanding of human structure and pathologies, including tumours. Nicolaes Tulp, a Dutch surgeon, contributed to this progress with his detailed descriptions of cancers in “Observationes Medicae”.
T his marked the beginning of a shift in perspective: cancer was no longer seen simply as a general imbalance in the body’s humours, but as a localised condition that could be treated directly, in particular by means of still rudimentary surgery to remove tumours.
This shift in our understanding of cancer, towards a more precise and anatomical approach, marked a turning point in the history of medicine, as it established links between the environment, lifestyles and the onset of disease, and laid the foundations for modern medicine.
In the 19th century, science entered an era of radical transformation with the invention of the microscope which put an end to two centuries of erroneous beliefs, in particular the theory of coagulated lymph.
1858 saw the emergence of Rudolf Virchow (1821-1902), a pathologist who developed the cellular theory of cancer. He introduced the concept of “cellular disease”, asserting that to combat cancer, it had to be attacked at its source: the cells.
T his new vision paved the way for chemotherapy. Even if the effectiveness was not really demonstrated until the 1940s, these discoveries led to the development of the first chemical substances capable of slowing down cell division. Thus becoming the basis of modern chemotherapy.
N owadays, scientists are pursuing in-depth research into the links between cancer and DNA, an idea first mooted by John Hunter (1728-1793). Hunter argued that factors such as heredity, age and even climate played a crucial role in the development of cancer. He estimated that the average age for contracting the disease was between 40 and 60.
Despite centuries of research by palaeontologists, doctors and scientists, cancer remains one of the leading causes of death from disease today. This complex and dreaded illness continues to defy science, despite considerable advances in its understanding and treatment. This persistence invites a significant question is cancer inherent in life, whether human or animal?
by Sheila Wiebe
Flying cars, free healthcare and limitless communication: for most Western countries, the ambitions of the 21st century have only just started to take shape. Things humans could only dream of in the past are now our self-evident reality. Science eradicated smallpox, found a vaccine for polio, and dying from a cold is no longer a fate an average person has to deal with. With this being said, it is more than obvious to everyone who has spared a look at the cause of death in the past centuries that there is an enemy hiding behind this picturesque paradise of Western medicine. The question remains: why has humankind not yet cured cancer?
The historical search to find the answer to this question has been, in many ways, symbolic of the way cancer behaves. Even though breakthroughs in cancer research seem to happen quite frequently, they are merely scratching the surface of a bigger problem. We see researchers as our heroes, Hercules fighting an invisible beast, but what if cancer is like the hydra, a serpentine lake monster with countless heads that regrow two just as one gets chopped off?
Sadly, this is exactly the reality we are dealing with when we look at the dynamic of cancer’s
properties and the search for a cure. To understand why the countless attempts at putting an end to this fight have failed more or less miserably, one has to look at the exceptional characteristics that make cancer tumours such a uniquely challenging opponent. Or, in other words: let us look at the heads that our medical heroes have to cut off.
T he first and most obvious challenge researchers are facing is the sheer range of cancer types. They all indeed share a name, but science describes over 200 diseases under that umbrella term. Although they are all caused by changes in the DNA and spread by uncontrollable cell division (mitosis), each has its quirks and variabilities that create the necessity of treating them separately.
T his pattern of variability continues to make things more complicated as one takes a closer look into microscopic structures. As every human’s DNA is unique, our bodies produce different types of proteins depending on our genes. This also applies to cancer DNA: it has an exceptionally high rate of mitosis, producing countless DNA variants that give each cancer cell distinct characteristics. This state of containing diverse elements in a single organism is labelled as heterogeneity. In practice, it impacts not only the affected individu-
als’ vulnerability to cancer but also their and their tumours’ responses to treatments.
In the lab, treating various tumours - or cutting off these heads of the hydra - leads to an endless cycle of sampling cells, finding out their structure, and developing a treatment that will be obsolete in the unavoidable case that the cells change their integrity. Even in the event in which researchers succeed, another form of variability adds further complexity. Through a trait called clonal heterogeneity, cancer tumours are able to produce mutated sub-clones that differ from the original specimen. These can detach and escape into the circulatory and lymphatic systems of the body. Because of these different types of heterogeneity, only a certain range of cancer cells can be eradicated every time researchers develop a new treatment. The cells with diverging DNA cannot be targeted and therefore remain in a patient’s body. This means that treatment can act as selective pressure, creating a mechanism where only the strongest cancer cells survive. The methods that have been created to act as a remedy unexpectedly have the completely opposite effect of making the cancer more resistant, similar to antibiotic resistance in bacteria.
B esides these properties of multiplication, cancer has additional weapons that make it the invincible hydra we are dealing with. It truly needs them, as it is not only being attacked from the outside, but also from the inside by our immune system. To fight back, cancer has developed strategies to weaken it. Most notably in leukaemia and lymphoma (both types of blood cancer), tumours do this by spreading into the bone marrow, the place where infec-
tion-fighting blood cells are produced. Due to this, cancer patients are often more susceptible to illness, making it harder for their bodies to detect and fight other threats.
In addition to this increased vulnerability, the presence of cancer stem cells plays a crucial role in the disease’s persistence. Being the root of cancer’s unstoppable growth, they have an enhanced ability to invade and migrate. Most importantly, they can resist treatments like chemo- and radiotherapy. Even if the whole tumour is eradicated, a single stem cell could seed the growth of a new one. This makes them one of the main targets that researchers aim at when developing treatments, hoping to eradicate the issue at its source.
W hen looking at cancer treatments, surgery is usually considered as one of the most wellknown, but also the most feared at the same time. The spectrum of possible interventions ranges from taking tissue samples and removing suspicious, superficial skin changes to minimally invasive surgical techniques, in which surgical instruments are used through a small incision, all the way to conventional, so-called open surgery. In the latter, parts of an organ or even the entire affected organ as well as neighbouring tissue affected by the tumour can be removed. But recalling the information we now have about our enemy, we can already predict its reaction: By removing one problem, another one arises. Even the most precise and modern technology is, more often than not, unable to remove all cancerous tissue with absolute precision.
The way experts try to tackle the problem of leftover cells is through methods like chemotherapy and radiotherapy. While surgery tries to be as precise as possible, these therapies have only one goal: to kill as many cells as possible. Though it sounds brutal at first, chemoand radiotherapy can help to eradicate leftover cancer cells during or after other treatments because they are designed to kill fast-growing cells. Nevertheless, the concern is not unfounded. If the tumour shows no vulnerability to them, they attack fast-growing healthy cells that are part of the immune system. This way, our most valuable weapons eventually turn into a self-destructive mechanism: where surgery acts like a dagger in the skin of the hydra, chemotherapy infiltrates the whole lake it lives in, poisoning the beast, but most likely also the other living organisms within.
Given the present limitations and challenges with cancer treatment, the question arises if there even is an effective weapon in our repertoire. The good news is that there are new methods with significant potential. As to not lose the fighting spirit that is vital in this never-ending challenge, let us look at the results of more recent research.
A new approach to cancer treatments is using the body’s immune system to fight cancer from the inside. As already established, the immune system identifies dangerous cells and is able to eradicate them in a precise way. The main obstacle here is that cancer cells have the same structure as body cells, which is why the immune system cannot recognise them as a threat. Therefore, the main objective for re-
searchers is to help the immune system recognise cancer cells as malignant.
T his is possible in multiple ways: Firstly, we have immunotherapy, where cells that are already sensitised to a certain type of cancer are taken from affected organisms and given to patients to strengthen their immune response. Secondly, there is the possibility of cancer vaccines. Some may be surprised by their existence because most people are used to dealing with vaccines in the context of viruses and infections, but they can be applied in a similar way when treating cancer. Genetic information about a patient’s specific tumour is extracted and analysed to find out its unique features. With this information, the immune system can be stimulated to recognise the cancer cells and attack them.
To make this process even more precise, advanced research uses gene manipulation with a technology called CRISPR-Cas9. With this tool, parts of DNA can be altered, added, or removed altogether. As established, the main obstacle in treating cancer is its growth and variability. CRISPR-cas9 can eliminate precisely these characteristics by modifying the genome of immune cells, which in turn attack parts of cancer DNA.
Gene editing could entirely revolutionise the way we treat cancer, but economic challenges make it hard to substantiate. Even if CRISPR-cas9 is very effective, it involves knowing the genetic makeup of the cells that are being targeted. This process is incredibly expensive, especially because it would need to be repeat-
ed numerous times to account for the countless and ever-changing types of cells found in cancer patients. To put it simply, gene editing has a lot of potential for the future, but for now, its complexity makes it way too expensive for it to be profitable for the medical industry.
T his brings us to another significant challenge in cancer research, one that is less about the cancer itself and more about the methods we use to combat it. In clinical research, most cancer treatments are developed using cultures of cancer cells in laboratories. While we possess critical insights about the fundamental biology of cancer using this method, the nature of a tumour in a petri dish differs largely from the complexity that a specimen in a living organism entails. This phenomenon occurs because cancer cells in organisms adapt to their environment, whereas separated ones do not interact with it at all. Accordingly, cures that seem to be effective on lab-grown cells often do not work in clinical trials with real patients. Even animal trials frequently yield ineffective results. A well-known instance showing the insufficiency of animal testing happened in 2006 when the cancer drug Theralizumab was developed. After being created in a laboratory and tested on multiple different animals to ensure safety and efficacy, it was deemed an effective treatment. Following the first infusion of a minuscule dose, all six human volunteers faced life-threatening conditions involving multiorgan failure. This incident reshaped the way clinical trials are
conducted and approved by authorities, but it did not change the fact that, in general, cancer treatments are still developed in animal trials that are insufficient and dangerous for all involved living beings.
Looking at the disillusioning reality, what are the measures that need to be implemented to drive meaningful change? First of all, researchers must find experimental systems that match the complexity of the human body. These should be flexible while the cancer moves and changes depending on its environment to prevent immune suppression.
We need to face the reality that, even if it is an uncomfortable fact, cancer can happen to every one of us. All of the mentioned methods are considerably more successful when implemented in its early stages, which is why prevention is still the most effective cure we have against cancer.
W hile studies about new treatments progress and promising methods are on the horizon, money and time are necessary to extend the research.
H owever, when we talk about cancer, the term includes 200 different types of diseases, meaning that, as an illness, it will not be solved in its entirety. More realistically, some varieties of cancer could be eradicated individually, taking us one step closer at a time to cure the disease.
by Makri Maria
T he diagnosis of cancer is one of the most challenging experiences a person can face, not only physically but also psychologically. How someone copes with cancer and its effects depends on many factors, including the support they receive. In this context, both individual and group therapy play key roles in providing psychological support to patients. But what are the unique characteristics of these types of therapies, and which offers the best outcomes for cancer patients?
Let’s begin with group therapy and how it is conducted. In this setting, there are usually one or two psychologists, who are specialized in this domain, and a small group of individuals who are either battling cancer or are at various stages of their treatment, seeking psychological support. Why might someone choose group therapy? The answer is simple; these individuals may find comfort in sharing their experiences with others going through similar challenges, thereby fostering
a sense of belonging and the realization that they are not alone. Often, many patients feel that no one can truly understand their situation unless they have experienced something similar. Consequently, they may feel overwhelmed when listening to the encouraging phrases from their relatives, who, despite their efforts to support them, do not manage to provide genuine comfort. So, hearing this complain from other patients make them feel less guilty. This need for identification is inherent in human nature, people seek out similar stories to avoid feeling isolated. Additionally, through group therapy, patients come to recognize the importance of having a supportive network.
O n the other hand, the one-to-one session has only one therapist and the patient. Individual therapy allows for the exploration of more personal topics and enables a more thorough approach to the psychological and emotional challenges faced by the patient. It can ad-
dress sensitive issues, such as the concept of death—topics that are neither pleasant nor easy to discuss in front of others. The patient has the opportunity to share their deepest fears and vulnerabilities. It is entirely natural for someone to feel embarrassed to talk about their experiences or even to prefer not to. This should be a matter of personal choice. Furthermore, all attention is focused on a single individual, making it much easier for personal growth to occur and yielding significant results in emotional development and mental well-being.
M oreover, when drawing a comparison between these two aspects,in group therapy, the focus is on shared experiences and mutual support, while individual therapy prioritizes personalized guidance to address specific needs.
In the first option therapy, the focus can promote social exchange and mutual support, in contrast to the second one, which offers more personalized guidance.
Lastly, it is worth mentioning the financial considerations and time management factors, as some individuals may select for the more af-
fordable option of group therapy, which also fosters confidence-building, while others, due to time constraints or a desire for greater privacy, may prefer one-on-one sessions.
Each therapeutic approach has its own benefits, and the choice between personal or group therapy depends on the personal needs of the patient. Either through mindfulness or common experience, the psychological support can contribute essentially into recovery and coping with illness. To whom it may concern, the key is to choose what makes you feel better, allowing you to express yourself and grow, as the journey through illness is already challenging and complex enough without further complications. Find your own way to navigate this path, and whichever option you choose, remember that the most important thing at the end of the day is to feel better and receive the love and support you need.
Despite the health literacy promotion, there are still a lot of false claims about the condition of women’s health and cancer prevention that in the long term may lead to scary consequences. It is high time we debunk them and reveal the truth.
by Larysa Kozak
Background
T hrough centuries, a woman’s reproductive health was falsely claimed to be the most essential aspect of her general well-being and as long as she can successfully perform her reproductive function, she is “healthy”.
H owever, over time the tendency has shifted towards a more neutral approach in terms of female treatment, which contributed to the dispel of a lot of myths.
In spite of that, there are still a lot of stereotypes looming over women’s health for several reasons, and one of them is the deficit of clinical trials and training based on female bodies according to Asha George, professor at the University of the Western Cape.
I n this article, we attempt to focus on the most common misconceptions and why they are untrue.
Myth #1 I should be primarily concerned with my reproductive organs
According to a recent survey by Columbia University, 68% of women tend to perceive their reproductive organs as more significant ones and as far as they are assured those are not threatened, they don’t apply for routine health screening for other organs.
T herefore, there are major campaigns launched by Women’s Health Associates Group to promote the motto that women should not view their general health and the condition of their reproductive function as
equal matters. The female body requires regular check-ups at least once a year, no matter whether she is intended to give birth or not.
M yth 2# I shouldn’t be concerned with having heart disease as it mostly affects men.
It is a common misbelief that men have a better chance of collapsing as a result of cardiovascular disease (CVD) than women. The clinical survey shows that 42% of women experience heart attacks in their 50s in comparison with 21% of men. Even though heart issues are the leading ones among men, sadly, more women than men die from CVD every year.
Myth 3# There are not any possible ways to prevent breast cancer.
Fortunately, going through regular cancer screening and having a healthy lifestyle can help prevent some common types of cancer. Of course, there are those serious types of tumors that will inevitably lead to fatal consequences. However, such procedures as pap smears and colposcopies can help doctors detect and remove precancerous cells in the colon or cervix which can prevent you from cancer.
Myth 4#: There is no breast cancer running in my family so I am safe.
Unfortunately, every woman is at risk of having breast cancer, no matter whether any of her female family members suffered from it or not. Moreover, regular check-ups may help you discover breast cancer at an early stage. Therefore, it is strongly recommended to have
an appointment with your mammalogist at least once a year, as early detection of a tumor and appropriate treatment at a time may lower your risk of dying from breast cancer by 25-30%.
Myth 5#: If I injure my breast, it can cause breast cancer.
If a woman injures her breast it may eventually lead to bruising or even excessive bleeding, however, it cannot provoke the emergence of a cancerous tumor. If a woman had a mammogram following the wounding and was diagnosed with a breast lump, it means the checkup drew attention to a lump that had already been there even before the injury.
L ast but not least, it is important to specify that the new myths are gaining momentum every day, making their way through social media platforms, which makes them even harder to curb.
I n conclusion, there are a lot of other stereotypes about women’s health and cancer prevention that are very common. For this reason, it is extremely important to promote health literacy at school in order to debunk those myths. It is high time we put an extra emphasis on the importance of health and cancer awareness as there are a lot of ways to prevent serious diseases, so we are capable of shifting the current conditions globally by popularizing the general information about our health and bringing more awareness towards people.
Exposing the danger of health myths in popular culture
by Toni Pahlke
“Not brushing your teeth can cause cavities” is one of many beliefs we all know to be true about our health. But some of those beliefs are established not by medical professionals, but by the media spreading and pushing medical myths. When those myths sneak their way into our “common knowledge” they can become very dangerous and stand in the way of you getting the treatment you need.
W hen observing health myths, you can define different reasons for the misinformation to spread and stick in popular culture. We will focus on three of them: trends, stigma and conspiracy theories. Here are a few important example myths within these categories that may have snuck their way into your medical knowledge.
Just like your fashion sense and online presence, your health can fall victim to trends in pop culture. Up until the 1950’s, porcelain skin was a sign of beauty, health and wealth. Now, having a so-called “sun-kissed” complexion is
associated with health and an active lifestyle. Tans are presented as attractive in pictures on social media platforms, fashion magazines offer advice on how to improve your tan and the most good-looking TV-characters have to have glowing, tanned skin.
T he reality however is: there is no such thing as a “healthy tan”. The increase of melanin in your skin, caused by sun-exposure, is always a sign of damage.
It increases your risk of skin cancer, even if your skin doesn’t burn. Unfortunately, 28% of 18- to 26-year-olds don’t believe that tans can cause cancer. The obsession with tans has even produced tanning alternatives that cut the sun out of the equation entirely. While full body spray tans might be an excessive measure to achieve a beauty trend, they at least don’t damage the skin. Tanning beds, on the other hand, are arguably worse than just lying in the sun. Through emitting roughly 12 times more UVA light than sunlight, tanning beds cause significantly more damage to your skin than the sun.
That is a too big price to pay for a fashion trend.
Unprotected sun-exposure is always dangerous for your skin. So even though it’s understandable to want a tan as a souvenir from your beach holiday, consider buying a postcard instead. Keep in mind to wear sunscreen and stay in the shadow as much as possible.
shows a dangerous lack of awareness and unwillingness to confront the issue.
One STD that is heavily affected by stigma is HIV (Human immunodeficiency virus, can lead to AIDS). When HIV spread in the 80’s the medical field demonstrated a lack of care for patients, as the disease primarily affected homosexual men. Because of homophobia, the

‘Why AIDS is likely to remain largely a gay disease.’
© Illustration by Lewis Calver for Discover, December 1985. (Paula Treichler, “AIDS, Homophobia, and Biomedical Discourse: An Epidemic of Signification.” October 43 [1987], 38)
A stigma is a set of negative and unfair beliefs that a society has about something. Not only trends, but also the stigma surrounding certain topics can put your personal health at risk.
STDs (Sexually Transmitted Diseases) for one, are one of the most taboo healthcare topics in our culture, which causes a lack of education and therefore a lot of misinformation. For example, 60% of Greek youth report never testing for STDs or only if they notice symptoms. STDs like clamydia, ghonnorea and hepathitis B can be asymptomatic and go unnoticed until they’re passed on to a sexual partner. This
public as well as the medical field distan+ced themselves from the issue. This also put the greater population at risk because they didn’t prepare for the disease affecting heterosexual people as well.
These stereotypes about people with HIV are still heavily spread by the media, but in much more subtle ways than the diagram. In an analysis of 111 TV-characters with HIV, 82.9% of characters were male and 79.3% of characters were gay. This leads to heterosexual people still weighing themselves in a false sense of security regarding HIV, even though homosexual men only make up 41% of
HIV-infections, while heterosexuals make up 29%. There’s only a small difference in infection rates, but a much higher percentage of homosexual men (84%) reports getting tested for HIV in comparison to heterosexuals (49%). This makes it more likely for the disease to be transmitted unknowingly and puts people at risk that don’t believe themselves to be a part of the risk group.
The stigma surrounding STDs, especially HIV, is still very present, even though western societies have progressed to be a lot more sex-positive. The stereotypes about STDs and people that have them are kept alive in the media and popular culture, making medical access and awareness harder for people who defy them.
A s with most conspiracy theories, medical conspiracies most commonly spread due to fear-mongering. They give the believers a “reasonable” explanation for a scary phenomenon that may otherwise be too complex to fully understand. One of the most well-known medical myths is the claim that vaccines cause autism. It is also a prime example for how quickly misinformation can spread and stick in the medical field as well as our culture.
I n 1998, discredited doctor Andrew Wakefield published a study that claims to prove a link between the MMR vaccine and ASD (Autism Spectrum Disorder). The myth caught on incredibly quickly, providing the public with fear-inducing stories of suffering parents and their autistic children. Thousands of studies have since thoroughly disproved this theory, but the idea is still present in our culture: 64% of US-Americans don’t rule out vaccines as a cause for ASD, 21% of Greek people still feel that vaccinations are unsafe. This myth is so
integrated into popular culture that media outlets still present it as fact. One popular piece of media that caused outrage is the US-American show “Eli Stone”. The first episode of this show about a charismatic lawyer has said lawyer win a lawsuit by “proving” a link between vaccines and ASD. To quote Eli Stone’s supposedly convincing argument:
“ Is there proof that [fictional vaccine] causes autism? Yes. Is that proof direct or incontrovertible? No. But ask yourself if you’ve ever believed in anything, in anyone without absolute proof, that’s called faith.”
T his faith is the basis for most medical conspiracies. Just because something is presented as a well known fact, doesn’t mean the claim has any proof to back it up.
This is where faith comes in. Faith in information passed throughout your community or culture. The representation of certain trends or “pop science”, the mischaracterization & stigmatization of diseases and medical misinformation are all spread through television, social media and even news sources.
When the media pushes an idea so thoroughly and consistently, it appears to become a fact.
But nothing about your own personal health is undoubtedly true, unless you receive information from a medical professional. Don’t be tricked by what your brain believes to be a fact. You cannot trace back where that belief came from. It could just be that your perception of health is influenced by trends, stigma or manipulative misinformation, which can ultimately endanger your personal well-being.
by Olha Dziuban
I n my quest to understand common health habits in Greece, I conducted a simple but insightful survey by asking both my Greek friends and passers-by on the streets a few questions related to their health and lifestyle choices. The responses revealed interesting trends, shedding light on how Greeks perceive their well-being, physical activity, dietary habits and relationship with healthcare. Here are the highlights from the survey:
O ne of the first questions I asked was how people rate their overall health on a scale of 1 to 10. Interestingly, most Greeks seem to feel quite positive about their health, with an average rating of around 8. This suggests that, overall, there is a strong sense of well-being among the population. The general sentiment reflected in this number may stem from a combination of active lifestyles
and good dietary habits, which were further explored in the poll.
Physical Activity Varies by Age
W hen it comes to daily activity, the survey showed some generational differences. Younger respondents described themselves as “medium active,” with much of their activity coming from walking. Older Greeks, on the other hand, tend to be less active, largely due to work and family responsibilities, which leave them with less free time for physical exercise.
Despite this, Greeks from all age categories appear to enjoy sports.. There were hiking, swimming, sailing, skiing, and even water polo among the most frequently mentioned activities. However, the clear favorites were running and gymnastics, which are both popular and accessible forms of exercise. These results indicate that sports remain an important aspect
of life among Greeks, even though the level of daily activity may vary.
A particularly encouraging finding was related to food preferences. A significant number of respondents (75%) claimed they prioritize healthy food and actively avoid junk food in favor of nutritious meals. The remaining 25% mentioned balancing between healthy and less healthy choices, but even they emphasized that they include nutritious dishes into their daily ration. Fruit and vegetables, in particular, play a major role in Greek meals. Furthermore, many people also highlighted their preference for home-made food over eating
out. This dedication to proper nutrition reflects the cultural importance of the Mediterranean diet, known for its health benefits.
In terms of smoking, the survey revealed a noticeable difference among various age groups. It seems younger people are less likely to smoke, with many opting for healthier lifestyles. On the other hand, older respondents, especially those in their 30s, are more frequently seen smoking, particularly in coffee shops and restaurants. This trend suggests smoking as a trend is gradually becoming less fashionable among the younger generation, who prefer fitness and wellness over tobacco.

The only area where Greeks seem less satisfied is healthcare service. When asked to rate medical services on a scale of 1 to 10, most respondents gave scores between 3 and 4, reflecting general dissatisfaction. While a few people rated it as high as 8, there were also some extreme cases: one respondent rated the service a 1 due to a particularly negative personal experience. These mixed results indicate that the Greek healthcare system, particularly its public hospitals, may need significant improvements to meet the expectation of its population.
One of the more surprising outcomes of the survey was the frequency of the Greeks going for health check-ups. Every single respondent mentioned that they undergo regular health examinations, which is an encouraging trend. The majority stated they have check-ups once a year, while some said they do so every two to three years. Additionally, many respondents emphasized that they also regularly check their bloodwork, a key component of preventive healthcare. While less frequent check-ups can be concerning, the overall commitment to monitoring health is a positive sign.
The poll showed that most of the people in Greece care about their health and are aware
of many dangerous diseases including cancer. They do general health check-ups often enough, but not those specific ones concerning certain vital organs.. As we know the climate and the sun in Greece is really strong, so people must protect themselves from the UVrays in order not to get skin cancer. Despite that, a lot of people don’t consider applying SPF daily is necessary. So, high promotion of health check ups, cancer awareness and sunscreen effect is still really needed in Greece.
This survey provided us with valuable insights into how Greeks approach health in their daily lives. Most people feel good about their health, stay relatively active, enjoy sports and maintain a healthy diet. Smoking rate, while still being a prevalent habit among older generations, is declining among younger people, reflecting broader global trends toward healthier living. However, healthcare services in Greece remain a sore spot, with many feeling that there is a big room for improvement. Despite this, the positive attitude towards regular health check-ups suggests that Greek citizens are proactive about their well-being and committed to maintaining good health.
by Inna Petrovska
Have you ever wondered why all of a sudden you start coughing or experience unexplained headaches during the day/while in the city? The air you breathe might be the culprit.
A ir pollution is a significant environmental challenge in modern cities, affecting both the environment and residents’ health. Thessaloniki, like many large urban areas, faces high pollution levels from various sources, including transportation and industrial emissions. However, some causes and effects aren’t immediately apparent.
T his article explores Thessaloniki’s air pollution levels, the factors behind its fluctuations, hidden contributors to the problem, and ways to protect your health.
Air quality level explained
T he air you breathe directly affects your health and daily life, changing frequently like the weather. The OECD Environmental Outlook to 2050 warns that air pollution will become the leading environmental cause of premature death, surpassing unclean water and poor sanitation.
A djusting your activities on high-pollution days is a key way to protect your health. The Air Quality Index (AQI) can help you easily identify days with clean air and those with harmful pollutant levels.
AQI measures air pollution levels, using ground sensors and satellite data. It indicates health risks from pollutants like ozone, nitrogen dioxide, carbon monoxide, sulfur dioxide, and particulate matter (PM2.5 and PM10).
T he AQI scale ranges from 0 to 500, with six categories:
• Good (0-50)
• Moderate (51-100)
• Unhealthy for Sensitive Groups (101-150)
• Unhealthy (151-200)
• Very Unhealthy (201-300)
• Hazardous (301+).
T he pollutants used to measure air quality include PM2.5, PM10, and ground-level ozone (O3).
PM2.5 are fine particles (2.5 micrometers or smaller) produced by combustion (vehicles, power plants, industry), atmospheric chemical reactions, wood burning, and forest fires. When it comes to PM10, they are slightly larger (up to 10 micrometers), coming from construction dust, road dust, pollen, mold spores, industrial processes, and vehicle emissions, especially diesel engines.
G round-level ozone (O3) is a trace gas in the troposphere, with an average concentration of 20–30 ppbv, reaching up to 100 ppbv in polluted areas.
Greece faces significant air pollution challenges, particularly in urban areas, impacting public health. Its geographic location subjects it to a variety of pollution sources, including mineral dust from Africa and the Middle East, smoke from forest fires, agricultural burning, and pollution from Mediterranean megacities. The National Observatory of Athens (NOA) plays a crucial role in monitoring air quality, operat-

ing national monitoring stations, and participating in European research initiatives to analyze atmospheric composition and forecast pollution levels.
Despite improvements in emissions, pollutant levels frequently exceed EU guidelines. The European Environment Agency (EEA) reported that between 2017 and 2021, around 90% of the urban population was exposed to PM10 and O3 levels above permissible limits. Air pollution significantly contributes to premature deaths, with nearly 10,000 lives lost due to PM2.5 and PM10 exposure, along with additional fatalities attributed to nitrogen dioxide and ozone.
G iven these challenges, Greece requires high-resolution air quality forecasting services to help citizens reduce exposure to harmful pollutants and support efforts to regulate emissions for improved air quality nationwide.
T hessaloniki’s air quality typically fluctuates between “moderate” and “unhealthy for sensitive groups” due to pollutants like PM2.5 and PM10.
R ecent data shows an average AQI in the 60–100 range in Thessaloniki, which is considered “moderate” to “unhealthy for sensitive groups.” However, it’s important to note that there are only a few stations measuring air quality in specific locations within the city, such as the “Aristotle University of Thessaloniki” and “AGIA SOFIA” stations. These stations typically report an average US AQI of 60, though air quality may vary significantly throughout the city, especially for those living near roads. During colder months, these
statistics may increase due to the significant pollution from wood-burning stoves.
While the general public may not be severely affected, these pollutants can have serious health impacts, particularly for individuals with respiratory conditions. These individuals include people with heart or lung diseases (such as heart failure, coronary artery disease, asthma, and chronic obstructive pulmonary disease), older adults (who may have undiagnosed heart or lung conditions), and children.
In order to protect yourself from negative impact, it is recommended:
• Limit outdoor exercise if you’re in a sensitive group or when pollution levels are high
• Keep windows closed to prevent polluted air from entering
• Consider wearing a mask outdoors if you’re part of a sensitive group
• Use an air purifier to improve indoor air quality
• Do regular wet cleaning indoors
This precaution helps minimize exposure to potentially harmful pollutants and protect health.
To sum-up
Since air pollution is a critical issue today, it exposes many to a significant health risks. By identifying the pollutants present in our environment and regularly monitoring air quality in our hometowns, we can take proactive measures to reduce negative aftereffects and protect health over the long term.
by Larysa Kozak
D espite the active promotion of sunscreen and its benefits, the majority remains deluded and fall for a range of disbelieves concerning SPF and its “harm”.
Background
According to the British Cancer Charity Centre, skin cancer has been one of the most prevalent cases for the past few years and the number of affected is swelling uncontrollably. There are several reasons for that including global warming and the protective ozone layer that has weakened gradually since the 1980s. Given this, we are exposed to an even larger amount of direct sunlight than previous generations. Therefore, the formation of sun-protective habits is vital for our well-being. Unfortunately, a substantial number of people still believe in some spurious narratives for not applying SPF and do not intend to follow dermatologists’ recommendations.
I n this article, we attempt to highlight the most common reasons regarding indifference towards skincare and explain why they are untrue.
1# SPF as an anti-age product
S adly, a lot of people don’t understand the primary goal of SPF use. Due to the massive popularization of sunscreen as an anti-age product, people mistakenly view it as another marketing ploy. They fear that unscrupulous entrepreneurs simply seek ways to make money from them, which is partially true, as a lot of skincare brands primarily promoted SPF as an anti-ageing magic pill. Therefore, scientists struggle to articulate the importance of SPF as a cancer prevention product, rather than anti-ageing cream. The truth is ultraviolet radiation does influence our skin which potentially leads to wrinkles and skin roughnesses and SPF may decelerate this process as it
protects us from the UV rays. However, viewing SPF as a substance that may rejuvenate you is utopian.
2#The deficit of vitamin D
Another common misbelief that induces people not to apply sunscreen daily is the claim that SPF inhibits vitamin D. The truth is, however, no matter how much sunscreen you apply, your skin will still experience some sun exposure. Moreover, only 10 minutes in the sun is enough to resupply the amount of Vitamin D your body needs.
3# The lack of cancer awareness
According to a recent questionnaire arranged by the British Cancer Charity Centre, approximately 30% of people rarely use or don’t use sunscreen at all. Additionally, the same number of them were not aware that there are a lot of unbiased surveys constituting the link between skin cancer and daily exposure to sunlight. The absence of knowledge, consequently, resulted in ignorance of SPF use and later prompted skin cancer. One of the reasons why skincare is hard to promote is because skin cancer takes so long to turn up. On average, even if some neglect the daily appliance of sunscreen, they are bound to face the consequences at least in their early 60s. Besides, daily usage of SPF does not provide an immediate effect which does not encourage people to use it.
A s gender preconceptions regarding which behaviour patterns males and females should follow are far from fading away, no wonder a lot of people attempt to correspond to them in order to secure social approval. Among those common stereotypes, there is also the perception of excessive self-care as an exclusively female feature, including daily usage of SPF. In view of this, men prefer not using SPF or using it secretly in order not to be falsely accused of being “too feminine”.
To summarize, there are a lot of reasons why people make a firm decision to avoid sunscreen. The majority of them emerged as a result of different stereotypes and false claims of SPF being either useless or even dangerous. It is high time we debunk those myths as we experience a lot of sunlight daily, more even than our ancestors, which means we have to take good care of our skin in order to prevent some scary consequences.
by Makri Maria, Tzoumaka Anastasia
Women’s health is a topic that is often discussed, but is it being addressed properly? Especially, when gynaecological cancers are concerned , there is still a gap in awareness, so it is natural that early prevention and education are keys to maintain a healthy lifestyle. In a recent interview with a gynaecologist, the significance of prevention in women’s health was emphasised, especially concerning serious illnesses, such as cancer. Information and prevention are fundamental elements to ensure women’s health and promote their general well-being. Regular monitoring by a gynaecologist and attention to symptoms, can indeed make a difference in diagnosis and early intervention.To better understand the importance of this topic, we spoke with Dr. Tona Nerisa, a specialist in obstetrics and gynaecology.
I: Could you introduce yourself and tell us about your background?
T: “My name is Tona Nerisa, I am 39 years old and I am a specialist obstetrician-gynecologist.I maintain my own private office here in Thessaloniki, while also being a research associate at the obstetrics clinic of Ippokrateio
General Hospital. I also have a Master’s degree in high-risk pregnancy.”
I: How did you decide to become a gynaecologist and why in this specific specialty?
T: “When I was a student in Medicine, I knew I wanted to specialise in surgery, but I hadn’t yet decided the exact field. So, when I attended the first birth in university, I was sure I wanted to become a gynaecologist, because I realised that you are able to bring a new life into the world, but you can also save a life.”
I: What are the most common types of gynaecological cancers and from your experience how often do women develop cancer (e.g., 1 in 10 women)?
T: “The most common type of cancer I come in contact with is breast cancer and the second one is cervical cancer. We also have many cases of endometrial and vulvar cancer and lastly the ovarian cancer, which is the most difficult to diagnose in early stages, due to the fact that it doesn’t have symptoms. As for the number of cancer cases we contact, that depends on the working environment. For example, when I was working at an anti-cancer hos-
pital, we had 1 in 8 women with breast cancer, as this is also the general percentage, but here in my private office, I would say that the numbers are around 1 in 20 women.”
I: What is your way to approach a patient when you discover that she has cancer and how would you describe the experience of announcing such news?
T: “In most cases, women have already suspected that they may be diagnosed with cancer, as they have noticed signs that can make them question the state of their health. It’s a very serious issue, and we have to make sure that we won’t use words that will negatively affect the patient’s psychology. In addition, patients have the right to learn the truth about their condition and it’s of great importance to explain to them calmly the details about the steps we are going to take. We should comfort them and reassure them that we will be here from the start until the end, to care about their needs.”
I: What is the most common mistake women make regarding the care of their body and health and how many times, in your experience, has precaution helped to detect something early and prevent it?
T:“I would say lack of prevention. Unfortunately, many women aren’t tested even for the most basic things, like the Pap test and they sometimes are unaware of the procedures themselves. It is also common, for some women, not having a mammography, which should begin in our early 40s, or even earlier when you have a family history with cancer. As for the cases I have encountered, sometimes they didn’t even have the chance to evolve into cancer, because women had their preventive tests and we were able to find the precancerous cells, or the very early stages of cancer. That’s so important and it might be possible that we don’t even have to begin a treatment.”
I: What could you tell us about the HPV vaccine?
T: “Firstly, there are a lot of myths concerning the side effects that the vaccine can cause, but it has been proved that this isn’t true, as the vaccine is absolutely safe. Moreover, people should be vaccinated in adolescence, and before having their first sexual intercourse. It is crucial for boys to be vaccinated as well, because, despite the fact that it’s rare for men to be diagnosed with these kinds of cancer, it is possible for them to be affected by one of the strains of HPV, through sexual intercourse and that can evolve to another type of cancer.”
I: Could you give us more information about the Pap test?
T: “The Pap test is a very simple, painless procedure that every woman should do every year, starting from the age of 21. It can detect a great variety of conditions, from a simple dysplasia or a cervicitis, to cervical cancer.”
I: How does family history influence a woman’s risk of gynaecological cancers?
T: “It depends on the type of the cancer. For example, as far as cervical cancer is concerned, family history isn’t that important. However, breast cancer has a high hereditary component, so women whose relatives were diagnosed with this type of cancer, should be checked earlier and more frequently than the general population and it would be very beneficial, if they had a genetic testing.”
I: Do you believe that most women know how to do in an appropriate way the self -breast examination and what is the correct way?
T: “Many women don’t know how to examine themselves, but they can learn how to do it, as it is very easy. We start from the nipple and we palpate all around, to see if we touch something that is not normal in our breasts,
something that could be rough or look like a little tumour. Then, we check our armpits in the same way.”
I: What are the symptoms that could warn us to get ourselves checked?
T: “Firstly, one symptom can be something alarming we found through our self-breast examination. It could also be a blood or fluid secretion from the nipples. In addition, we should watch out for unexplainable pain in the belly, uncontrolled bleeding outside of menstruation or during menopause, or weird texture and smell in vaginal fluids.”
I: Could you give us some information about cancer during pregnancy?
T: “When a pregnant woman has cancer, the pregnancy is progressing normally, as nowadays, the amount of radiation during treatment is so small that it doesn’t affect the fetus at all. Moreover, it is possible for a pregnant woman with breast cancer to go through a mastectomy and also, it’s a fact that cancer isn’t transmitted from mother to baby.”
I: How accessible are medical examinations for women, in general, based on financial criteria?
T: “Recently, in Greece, the government is running some programs, concerning free mammographies for women over 40 years old and free Pap tests, for women over 21. And regarding the treatments, there is the chance to address a state hospital and conduct the necessary procedures for free.”
I: What advice would you give to women in order to maintain a healthy lifestyle?
T: “Besides prevention, I believe that it’s crucial to adopt a healthy lifestyle, because eating unhealthy food, smoking, drinking, or
experiencing severe stress, can cause detrimental consequences to our health.”
I: Okay, thank you very much for your participation in this interview!
In conclusion, we understand that cancer is a sensitive issue that requires careful handling, highlighting the importance of proper education from both home and schools. From our interview with Dr. Tona Nerisa, it goes without saying that there is a great number of cases, which did not evolve into cancer, only because women conducted their prevented exams. Our conversation served as a heartfelt reminder that women’s health is not just about medical appointments or diagnoses, it’s about understanding, compassion, and empowerment. Women should be encouraged to participate in regular medical examinations and to be informed about the risk factors related to their health. What stands out most is the deep emotional connection between health and selfcare, the courage to ask questions, and the power of early prevention.

by Tzoumaka Anastasia
Maria’s Interview
I: So, Maria, could you give me some personal information about you first?
M: “Yes, my name is Maria, I am 23 years old and I just graduated from psychology school.”
I: Okay, so what member of your family experienced cancer and when?
M: “It was my mother and she was first diagnosed in 2018. It lasted about a year I think.”
I: How would you describe your relationship with your mother in general?
M: “It was very good, we were actually very close, we discussed many things and did a lot of activities together, like shopping or having lunch.”
I: What was your age when your mother was diagnosed and how was your life at the moment?
M: “I was 18 years old, so I attended the last grade of high school. I had to study hard this
year, because I had to take the national exams, which determined whether or not I would have the opportunity to go to college.”
I: In what way did your mother decide to tell you about cancer?
M : “In the start, she didn’t say something, but I understood that something wasn’t right, because sometimes, she acted a little weird and she made a lot of visits to doctors. I remember that she told us about it, only after she had begun her treatment. Specifically, I was sitting with her in her bedroom and she told me that she found a tumor in her breast, which was alarming and they had to conduct the necessary exams to see if it was needed to receive treatment.”
I: How would you describe your reaction to the news?
M: “I felt angry that she hadn’t told me about it earlier, but I didn’t show it to her, I was calm and I started asking for more informati on, regarding the treatment and in what way we could deal with the situation. Then, I hugged
her and she reassured me that everything will be okay.”
I: During this period, did you notice any changes in her attitude, in her appearance or in her mood?
M: “About her appearance, I didn’t notice anything different, as radiotherapy doesn’t generally have an effect on that part, so I only saw some rashes on her body. But mentally, I noticed many changes, because she seemed more tired and exhausted and also, she was in a way more passive and relaxed, in contrast to what I had known about her character until then, as she used to be more energetic and in control of things.”
I: In what ways would you say that you tried to support her during that period of time?
M: “I think I was the calmest person in the family, so I tried to help her, by viewing things positively, and by using phrases like: everything will be okay, your doctor is a professional and he will help you, you have a thorough plan. So, I focused on supporting her psychologically, as I believed that her mental state had a direct impact on her physical health.”
I: Did you reach out to a mental health specialist for help?
M: “I was already seeing a psychologist, about my anxiety regarding the national exams, so I of course discussed with her my feelings about my mother’s situation and the ways I could use to deal with it better.”
I: Did your mother, during the time of her illness, try to approach you to talk with you about the disease or about your relationship with her?
M: “Yes, she tried to discuss with me things that concerned her cancer, but not our relationship, as she didn’t think that it was affected by the situation, something that is reasonable, as she was tired and focused on overcoming the obstacles she faced.”
I: Would you say that you have concerns in the present that the cancer will resurface?
M: “Yes. Every time that she has to take her medical exams, I am anxious to see if something has resurfaced and I am relieved when I find out that everything’s okay.”
I: Do you fear for yourself sometimes, that because of genetic inheritance, maybe it is possible for you to be diagnosed in the future?
M: “I had some concerning thoughts about this when I was younger, but my mother had the genetic test and we found out that Ι don’t have a predisposition, so there isn’t a reason for me to be afraid in terms of inheriting the disease.”
I: Do you think that your experience with your mother’s illness has changed the way you deal with life?
M: “Yes, because I realized that health problems are the most important thing in life and that they will make you really face your feelings and the way you see life. So, I learnt not to care
a lot about things like my grades, or some personal relationships that aren’t so important to me and to generally try not to care about material goods and rearrange my priorities.”
I: Okay, thank you for your help!
Anestis’s Interview
I:So, Anestis, could you give me some personal information about you first?
A: “Yes, my name is Anestis, I am 29 years old and I have studied Biology, with a master’s in biomedical studies and immunology.”
I: Could you please tell me which member of your family was diagnosed with cancer and when?
A: “It was my mother, in 2012. She was diagnosed with breast cancer at first and then she had some other issues, related to cancer, with her lymph nodes, which led to their removal.”
I: How would you describe your relationship with your mother in general?
A: “I would say it was the classic relationship between a mother and her son. She has taught me many things and shaped my personality in a lot of ways and I have a very close relationship with her.”
I: What was your age when your mother was diagnosed and how was your life at the moment?
A: “I was 17 years old, still in high school and I was preparing for the national exams.”
I: Do you remember the way your mother told you for the first time about her cancer?
A : “At first, she didn’t tell me the truth, that the tumor was malignant, so I thought that it was a benign tumor. I found out the truth later, when we had visited an insurance company, where you had to tell them if it was malignant or not. So, it was there that I connected some things and it was after my mother had completed her treatment.”
I: Did you notice any changes regarding your mother’s mood, acting or physical appearance?
A : “About her physical appearance, I didn’t notice anything changing. But yes, concerning her mood and actions, she was often very tired and especially later, when her lymph nodes were removed, she was even more sensitive to diseases, as her immune system was affected negatively.”
I: Would you say that your relationship with your mother changed after the diagnosis and did she try to approach you, to talk to you about the cancer or your relationship?
A: “No, I think our relationship was the same in general. But, for me especially, some things had changed regarding my mother, because I realized that it is not always sure that your loved ones will be right beside you. I think that maybe we had some conversations, but it’s been many years since then and I can’t remember for sure. ”
I: In what ways would you say that you tried to support her during her illness?
A: “I don’t think I supported her in many ways. I was just anxious about her and I was asking her about how the disease evolved. I believe that mostly, I was a cause of stress for her because I didn’t deal with it well and I also had a stomach crisis because of my anxiety.”
I: Did you happen to visit a mental health specialist during this period to receive help?
A : “No, it didn’t cross my mind, I didn’t think that I needed it.”
I: Do you fear in the present, that the cancer will resurface?
A: “Yes, because when I later studied biology, I learnt how easy it is for the disease to reappear.”
I: Would you say that you fear for yourself, in case you get the same disease in the future?
A : “No, because there aren’t many cases for these types of cancer that affect men, but of course I do my best to take care of myself.”
I: Would you say that your experience with your mother’s cancer affected the way you approach life?
A: “Yes, I always want to have very close contact with my family and my loved ones, in case something happens. I am not so free, so as not to care in which place or city I will be next year, because I want to be near them. And of course, I try not to be stressed about the little everyday problems.”
I: Okay, thank you so much!
After contemplating these interviews, we can, hopefully, understand the perspectives of the
people hiding behind the patients a little better and realize how important their role is, during the evolution of the disease. Both Maria and Anestis, shared their feelings during their family’s experience with cancer, expressing how difficult it was for them to stand by their loved one’s side, while at the same time dealing with their confusing thoughts and questions about this new situation they were facing. Through their personal stories, they emphasize the crucial role of caregivers and as they demonstrate, there is a great need to get resources and care for themselves, in order to manage their own mental health and continue supporting their loved ones.
by Tzoumaka Anastasia, Makri Maria
M ental health, constitutes one of the most crucial parts of our well-being, especially when we face important challenges, like cancer. The power of our mind and soul, is often proved to be of equal significance with cancer treatment procedures, affecting the way that we process the illness. The interview we conducted with psychologist, Dr. Ziliaskopoulou, provided us with valuable information about how cancer affects mental health, and how meaningful emotional support can be, during and after cancer treatment.
I: Could you first give us some personal information, for example your name, age and specialty?
Z : “My name is Despoina Ziliaskopoulou, I am 42 years old, and I am a psychologist, with two Master’s degrees, οn clinical and οn health psychology. I also have a PhD related to cancer and the experience of women with mastectomy. I am currently doing a postdoctoral on breast cancer and I have my own private office, where I offer therapy sessions, as a trained psychotherapist on Cognitive Behavioral approach.”
I: How did you decide to become a psychologist, and why did you choose to specialize in this particular field?
Z: “I first learnt about psychology as a profession, when I was in high school and I decided that I wanted to follow this career, knowing that I was interested only in being a psychotherapist and not working in the research field. I think that I made this decision, because I liked very much to analyze people and to try and interpret their behaviors, and also maybe because of some personal issues that I was dealing with. Then, I specialized in the field of health psychology, as I was very interested in serious diseases and health issues in general and also I liked to work with topics that concerned women. Moreover, when I was a child, my grandmother died from breast cancer, so I saw the difficulties of the disease and how this illness was treated as a taboo and that motivated me as well to learn more about health.”
I: In your opinion, what are the three key things you always take in mind when starting a session with a client?
Z: “At first, I believe that the relationship between therapist and client is a very important part in the process, so there has to be trust, for the client to feel safe. Of course, I put as a priority being a good listener and try to understand the person’s perspective of things. Something else that I consider necessary for the sessions, is to learn as much as I can about the client’s past, because the way in which people deal with the illness is shaped to an extent, from their childhood experiences and the ways they used back then to overcome their problems. For example, if a person is used to being very autonomous and doesn’t ask for help generally, it might be a shock to him/her being in that vulnerable position, needing to ask for support from others.”
I: Which therapeutic approach do you consider to be the most appropriate for people with serious illnesses?
Z : “Many studies have shown that CBT is a very effective way to help people with cancer and from my personal experience, I have realized that it can contribute to the improvement of a client. But that is not always the case, as in CBT we focus a lot on a quality we call “fighting spirit” and we try to work with the person’s resilience. That can be a good thing, as it provides clients with more confidence and trust in their abilities, but it could also pressure people to feel that they must always be strong or hide their fear from others. In some cases, it would be beneficial to work with a more psychodynamic approach, especially if the client isn’t ready to accept the situation and there we can just give them time to express their feelings. In addition, I have noticed that many therapists use the existential approach, as it is more directed towards finding a meaning in your life, and this way, it can help clients to get their own answers about why this has happened to them.”
I: Is there a common element or pattern you notice among cancer patients?
Z : “They usually experience a very strong shock, they have difficulties to realize what is happening to them and they tell me that they are frightened. They also focus at first on the most practical medical issues, for example getting a second opinion from a doctor, beginning their treatment and having their check ups done. Another common pattern I personally noticed, is that when they are under chemotherapy, it is difficult for them to focus on our sessions because of their side effects, so during this period we can’t work so much psychotherapeutically, but acting more as a support system. When this procedure is done, they often try to understand what they had done personally to cause the cancer, so they tell me most times that they think they didn’t take good care of themselves and they were pressured by others. Following this realization, they often state that they will try and use this disease as a chance to change important things in their lives.”
I: How do you handle difficult questions from patients who are facing death or are close to it?
Z:“That is a very hard topic, as I believe that death does not come up easily in a conversation and it’s proved by current studies that we want to act as if death isn’t a part of our lives anymore. Death is considered a failure, a difficulty of the doctor to save the patient’s life and also we, as therapists, are also afraid to some extent. As a result, it is vital that we have addressed these issues ourselves first, in order to be able to endure the pain and fear people face. For these reasons, we might not be able here to understand them completely, but we try to listen as best as possible.”
I: What role does the family play in supporting their loved ones and how do you work with them?
Z: “In general, they say that cancer isn’t a personal disease, but a disease of the whole family, because when someone is diagnosed, that affects the lives of all the family members and his/her loved ones. Families can offer great psychological support to the patients, not by trying to reassure them or pressuring them to be strong, but by being there to listen to them and give them space to express their feelings. I don’t typically invite the family members for a session with them, because I prefer to understand what my client has to say about their interactions with their relatives and then give advice about the way that the patient can alter his/her way of reacting towards their family. However, when I feel that the family interferes or pressures excessively, I might speak with them in a session, in order to help both them and my client as well.”
I: From your experience, do you find one-on-one sessions or group therapy to be more effective?
Z: “In my opinion, this decision lies with the client exclusively. Some people may prefer the extra element that group th erapy has to offer, meaning the sharing of their common experiences and feelings. On the other hand, some clients feel better with the one-on-one sessions, because based on my personal experience, they may feel stressed and frightened to see a person in the group that is in a worse condition than them, so this makes them think that they will reach that stage later and they don’t want to have to deal with this stress. There are times, when I propose some cases, where I would think it would be helpful, to attend a group therapy, but I let the clients decide.”
I: What are some common prejudices or misconceptions that people have about cancer patients?
Z: “Sometimes, people have painted that picture in their minds, that cancer patients are unhappy or miserable, but that isn’t true, because it is very natural for them to experience shock and sorrow, especially in the start, but that doesn’t mean that they don’t work with themselves, or that they are unable to feel happy when good things are happening to them. And of course, we have this main stereotype that cancer means death, so when the public comes in contact with cancer patients, they don’t know how to act, they feel awkward, and that can make the patients distance themselves. As far as women with breast cancer are concerned, there is the prejudice that if they have gone through mastectomy, they aren’t feminine enough, and as a result, a lot of women feel pressured to go through a plastic surgery to improve their breast’s appearance, or they are stressed about if men will find them attractive. Lastly, it is very common for people to believe that patients affected by cancer should be some kind of “fighters”. This could lead to individuals hiding their “negative” feelings, such as the fear for their life, and not being able to express themselves in an authentic way.”
I: In your opinion, how much can resilience help patients throughout their journey and in what extent do you think that resilience comes from our personality or by working to develop it as a trait?
Z: “Some people are more resilient than others naturally and that can contribute to a better and quicker adjustment to the situation. However, one of the main goals of therapy sessions is to help develop this character trait, as the techniques we use, encourage the clients to have more confidence in their personal abilities and help them deal with pain and difficult situations more effectively.”
1. Do you believe that financial factors affect whether people begin or continue therapy sessions?
“As far as psychologists in private offices are concerned, we know that the people who reach out to us for therapy sessions, usually can afford it. But, of course, there is an important percentage of patients that don’t have the financial means to begin therapy privately, so their needs are supposed to be covered by the psychologists working in hospitals, or by the associations created for cancer patients, which offer free psychological support to those who need it. However, I think that the services that are being offered aren’t adequate enough to respond to such a big amount of people and this situation is getting worse, as more and more public clinical settings are getting privatized.”
I: Lastly, have you seen therapeutic sessions resulting in improvements both psychologically and physically?
Z: “That depends on the patients. In some cases, we act more supportingly and not so psychotherapeutically. On the other hand, there are some individuals who want to answer some crucial questions about their situation, to find meaning in their lives, or try to get back to their former activities, before the diagnosis. But, all clients see a big difference compared to the mental state they had when they first asked for help.”
I: What do you think about phrases like “they lost/won their battle with cancer”, which are so commonly used?
Z: “These phrases lead to stigmatization and in recent years we try to avoid using them, because they maintain the viewing of cancer as a taboo issue. We can just say, “They died from cancer”. This is the only way to show that cancer isn’t that frightening anymore and it’s also something that happens in life. And of course,
phrases like “he gave a hard battle with cancer”, are suggested to be avoided, because we can’t evaluate if someone has fighted or not and also because the outcome depends on many factors, and not only by the patient’s attitude.”
I: Okay, thank you very much for your participation in this interview!
To conclude, mental health plays a key role in the process of recovering from cancer. The assistance which a specialized psychologist and a strong social support can provide, have a direct effect on building resilience and help patients to improve the quality of their lives. Our conversation with the psychologist shed light on the deep, emotional layers of mental well-being, especially in times of personal crisis. What truly resonated was the emphasis on the importance of emotional validation and the healing power of being truly heard. It’s not just about solving problems, but about creating a space where people feel safe to express their vulnerability and fears.

by Tzoumaka Anastasia
S erious diseases like cancer, are often followed by a great deal of other obstacles, including the extremely limited amounts of available blood, which is necessary to perform the surgeries needed, to help the patients recover. Therefore, it is of major importance for every one of us to donate blood and to do our part in assisting the patients and the medical health professionals, who fight tirelessly to save people. In order to understand the importance of the topic better, I spoke with Sophia and Savvas, members of a blood donating organization located in Ptolemaida, Greece. Below, we can find these very interesting interviews.

Sophia’s Interview
I: Sophia, when did you decide to donate blood for the first time and how long did you consider it before actually going through with it?
S: “I actually considered it for the first time a year ago, when the most recent blood donation took place, but I wasn’t yet an adult, so I didn’t have the ability to do it, as it isn’t generally permitted. But when I learnt about the next donation event and I was finally of legal age, I decided I needed to do it and I didn’t have to think twice about it”.
I: How would you describe your feelings before, during and after the procedure?
S: “In all the three circumstances you referred to, my feelings were pretty much the same. So, before the donation, I wasn’t anxious or fearful, because I don’t generally fear needles or doctors and I felt happy, both before and after giving blood.”
I: How would you describe the treatment you received from the members of the association and the medical staff, regarding it as your first experience with blood donation?
S : “The members of the association were surprised at first, as I just turned 18, but they were pleasantly surprised and told me that it was great that a new member joined the club. They first thought that I came because of my dad, as he has been a member there for years, but it was my personal desire to do it. As for the medical staff, the doctor told me
bravo for my decision and the nurses were very supportive.”
I: How did you first hear about this blood giving organization and how do you feel about their cause?
S: “I heard about it first from my father, as he was a member of the club for many years and later he also became the president, so you know it’s not only the posters they make, that inform you about the association. For their cause, I feel grateful, because with this initiative a whole village donates blood and I think that we are the first village in the region to develop something like this. So, I feel that we have the ability to save lives and bring happiness to people and I wanted personally to do the same.”
I: Did you share the information and feelings you had about your first experience with your friends and if you did, what was their feedback?
S: “Yes, I described my experience to my two closest friends, like the papers I had to fill and the medical exams I took in order to donate blood and they said that they felt proud for me and happy.”
I: How would you describe the percentages of the organization, regarding the participation of young people and women in the initiative?
S: “I would say that around 70% of the members are men and 30% women. As for young
people, there weren’t a lot of people of my age group, I only saw a 19 year old guy the day I went to donate. Also, about the 20-30 year olds, there are many of them, but the greatest percentage consists of 40 years old and above.”
I: So you, as a young girl, would you suggest some ways to get more women and youngsters to participate?
S: “A good way, in my opinion, would be to talk to them and educate them about the benefits of volunteering and also explain to them how important their contribution to the cause would be, as the population of our village is getting older, meaning that because of the rule that you can’t donate blood if you are above 65 years old, only the young people could help to support the initiative.”
I: Okay, for the last question, I would like to ask you if you think that you gained something new about the procedure or if you learnt things you didn’t know before?
S: “I learnt about how strict the requirements of giving blood are, because they tell you the exact rules of who can and who cannot participate, and I thought there were a great number of them. I don’t find them wrong, but I learnt new criteria, as I knew about the restrictions they have concerning blood transmitted diseases, like AIDS, syphilis or hepatitis, but I hadn’t heard about some others.”
I : Okay, thank you so much for your participation!

Savvas’s Interview
I : For the first question, I wanted to ask you when was the association founded first, where is it facilitated and what was the motive for beginning creating this club?
S: “Our blood giving association was founded in 2015, it is based in our village, called Foufas, near the city of Ptolemaida in Greece and the motive for beginning was a simple conversation among friends, where we decided to start donating blood. Also, a common friend of ours was in need of blood and we learnt that the necessary blood for surgeries is very difficult to find, so we decided to help.”
I: Okay, so could you tell what the requirements are for a person, in order to be able to donate blood?
S: “Concerning the procedure itself, it’s necessary to bring your social security number and your I.D and of course you need to be healthy. More specifically, it’s important that you don’t take medication for serious health issues and not to be affected by AIDS, syphilis and hepatitis. You must be above 50 kilos and to have a normal blood pressure, because they conduct medical exams before the procedure. In addition, you have the ability to donate blood until a certain age limit, 55-60 years old, depending on your health condition.”
I: Can you tell us some ways that you use to promote your association?
S: “We usually put up some posters in our village and in nearby cities and we organize events in which doctors inform people about blood giving, because many individuals don’t have the knowledge about these things and as a result they are hesitant to go through with it. We also have given interviews in local and national channels, like West and ERT and we post on our social media all the events that are being organized and information about the blood donations.
I: Okay, what could you tell me about the diseases that affect the patients you send the blood to?
S: The greatest percentage goes to cancer patients, but it’s also directed to renal failure cases. And we also organize the donations when something urgent comes up. For example, when the train accident at Tempi took place, we sent blood immediately for the victims.”
I: Concerning the health professionals, would you say that they provide you with adequate support in these procedures?
S: “Yes, they have helped a lot from the start, each one of them with the knowledge they offer us. For example, an orthopedic and an urologist came to educate the people in our village about the benefits of donating blood and now we also think that it would be a great help for the women in our team to bring a gynecologist, in order to perform the necessary preventive exams for free. In addition, we have a great number of staff trained in first aid, and as for the procedure of donating blood, we collaborate with the same people each time, including our cardiologist, 2 nurses, a blood donation supervisor, who is responsible for all the necessary papers and of course a paramedic with an ambulance, in case of an emergency.”
I: So, moving to a more personal level, what was your personal motive for beginning donating blood?
S: “For me, it was the help I wanted to offer to people.”
I: Would you say that by participating in the organization you learnt some things about the procedure and the medical aspects of donating blood that you didn’t know before?
S: Of course. For example, I learnt about how the blood is being analyzed after the procedure, how it is decided if it’s suitable for donating and to what kind of patients it’s used for.”
I: How did you decide to become the president of the association and how would you evaluate this experience?
S:“I had a strong desire to try harder for the improvement of the organization and I was glad that I was elected, as that proves the trust that people have on me.”
I: Have you shared your experience about the blood donation and the association with your family and friends and what was their feedback?
S: “Yes, I have shared some information and my feelings with them and they were surprised and very eager to try it themselves.”
I: Okay, that’s all, thank you for agreeing to this interview!
By speaking with these two people, I gained a very good insight about the experience of donating blood and I left with a content feeling, knowing that there is such a willingness in humans to help each other, whenever it’s needed. The fact that a very small village, with a population of only 300 people, has achieved such a great percentage of blood donors, is an inspiration for all of us to remind ourselves that offering to others isn’t something difficult that requires hard work, but only our good will and a little bit of our time. Blood donation is one of the greatest forms of taking care of our fellow humans and I strongly believe that we should all at least give it a try!

by Makri Maria, Tzoumaka Anastasia
It is widely known, that medical procedures and frequent health appointments, are vital and unskippable steps, when it comes to cancer treatment. However, in such cases, healthy diet and exercise creates a powerful synergy, which can boost the immune system, reduce stress and even prevent the development and recurrence of cancer cells. With that being said, Christina, Panagiotis and Marialina, specialists in the fields of nutrition and gymnastics, shared with us their professional opinions, regarding the role of eating healthily and exercising and offered us their unique perspectives and the knowledge they have acquired from their experience with cancer patients.
Christina’s interview
I: Christina, can you tell me first some personal information about you, regarding your age, your specialty and the years of your experience in your domain?
C: “My name is Christina, I am 33 years old and I am a nutritionist-dietician. I also have a Bachelor’s degree in biology, and I have been working as a nutritionist for 6 years.
I: How did you decide to become a nutritionist?
C: “I would say that I wanted to satisfy a personal need, because I was always concerned about my body and my weight, but by working in this field, I realised that I was born for it, as it’s a very beautiful thing helping people to achieve their goals.”
I: What do you think about the relationship between a balanced diet and health in general?
C : “Studies have shown that nutrition and health are inextricably linked, but also on a personal level, we can see the truth in it. For example, if someone is consuming junk food for a month, he/she will definitely notice problems with their digestive system, their concentration and their mental state.”
I: Could you tell me which factors do you take in mind when you need to make a nutrition plan for a person who faces a serious disease, like cancer and if the client participates in the making of this plan in some way?
C: “We need to take in mind many factors, like the weight, the height and the age of the person, without forgetting to check their blood tests and of course their personal food preferences. Definitely, the client always participates energetically in the making of the diet plan, as the approach I follow is very human-centred.”
I: What are the food groups that prevail in a diet plan for a cancer patient and which are the ones that should be avoided?
C: “In these cases, we focus on adequate protein intake, to avoid excessive weight loss. It’s important to consume fish, eggs, white meat and legumes. In addition, good fats are very beneficial, as they have anti-inflammatory action and they can be found in olive oil, nuts and avocado. At last, it is crucial to include fruit and vegetables, because they contain dietary fibers, vitamins and minerals. On the other hand, there are some food groups that

should be avoided, like those who are rich in saturated fats and those which contain palm oil and seed oils. Of course, patients should try to avoid overconsumption of sugar.”
I: Are there some dietary supplements that could also help?
C: “If we have to deal with patients that aren’t nourished adequately, we can propose some dietary supplements, in collaboration with a doctor. It is common for these clients to have vitamin D deficiency, or to experience symptoms, such as vomiting or diarrhea, so we give the suitable supplement, depending on the personal needs.”
I: How do you deal with a client who has a loss of appetite because of the disease?
C : “I try to give clients some simple advice, such as consuming small and frequent meals, eating their favourite food and being in a pleasant environment, maybe with music during eating. However, if the patients aren’t able to get the necessary calories, we suggest hyper caloric solutions.
I: How can family members support the dietary needs of a loved one facing the disease?
C: “They could try to support their loved ones, by not keeping in the house junk food and also by not pressuring them to eat if they face a loss of appetite, as this could lead to the opposite result.”
I: Do you think that apart from diet monitoring, it is needed to support the client psychologically as well and have you ever needed to consult with a psychologist to help you with a patient?
C: “I think that because I see a psychologist myself, I sometimes take some elements from her and use them when a client tells me that he/she is feeling frustrated, in order to support them mentally, but I haven’t felt the need to ask my psychologist for advice, concerning a certain client.”
Panagiotis’s interview
I: What is your name, age, and specialty?
P: “My name is Panagiotis Antoniadis, I am 31 years old and I am a gymnast, specifically instructor of basketball, martial arts, Pilates, but mainly of Kangoo jumps and a personal trainer.”
I: How did you choose to become a trainer?
P: “When I was a little kid, it was my dream to become a basketball player, but because of a lot of factors I could not make it. After that, I noticed that something that was a big part of my daily life was exercise. I wanted others to succeed and of course to help them, and me financially. In addition, friends of mine were asking me to train them or to come with me to the gym.”
I: How do you choose which workout programs are best suited for each of your clients?
P: “Firstly, I take the medical history, the age, the weight and the personal goals of each client. For example, someone may want to focus on changing his or her appearance and others do it only for medical reasons.”
I: How do you approach someone with a diagnosis, whether it’s pathological or psychosomatic?
P: “It depends on the case. For example, I had a client who had depression and obesity. That
kind of combo needed a little bit more of a reward and that helped her with confidence and achieving small goals each day, until she lost 30 kilos.”
I: From your experience, have you noticed changes in your clients, either psychological or physical?
P: “Usually those things come together, even though sometimes the psychological changes come first.”
I: Could you provide an example of a client who had a serious issue initially and has made significant progress?
P: “The one that I mentioned before with depression. She started telling me that she is not getting tired easily and she can clean her kitchen in 3 hours. A simple example that others take for granted, but for her was really important. Also another 45 years old client, who had cancer. When I met her, she had just finished her treatment, so because we were talking a lot, the psychological progress came first and then the physical. She was telling me that she felt stronger in her daily life.”
I: Can you mention some of the psychological and physical benefits of exercising for those with cancer?
P: “First things first, gymnastics helps restore functional range of motion , as it can help with everyday tasks such as putting on a shirt. Additionally, it strengthens the muscular system overall and improves psychological well-being. Exercise itself can serve as a distraction and help one clear their mind.”
I: For someone who is currently dealing with cancer, what kind of workout would you recommend?
P: “It depends on the type of cancer they have and how tired they are or if we are before or after starting the treatments. We could start with a more conservative kind of work out, but as we are going forward the level would be upgraded.”
I: Would you feel comfortable working with a client who has this illness?
P: “Yes, of course I had worked with cancer patients before, but also there is fear, so I am

trying to keep myself updated about the recent working out programs related to cancer.”
I: What kinds of activities would you recommend to help prevent cancer and promote physical fitness?
P: “If you ask a kid, he or she won’t tell you that he/she is working out, but that they are playing. If most of us view exercising as a game, as a safe space of playing, we will be more willing to work out. Because gymnastics does not only mean lift gains, but also dancing or boxing.”
I: Okay, thank you very much for your participation in this interview!
Marialina’s interview
I: What is your name, age, and specialty?
M: “My name is Marialina Papadopoulou, I am 31 years old and I am a pole dancer.”
I: How did you choose to become a pole dancer?
M: “To be honest, pole dancing was random. Even as a kid, I enjoyed gymnastics and dancing, but in my hometown, I did not find a dance school that I trusted, so I was on and off. Only when I came to Thessaloniki to study, I found a dance school that offered pole dancing as a choice. I tried it and I liked it. I have danced the last eleven years, but I have worked as a teacher, the last five to six.”
I: How did you decide to train in this specialty, and what kind of clients do you work with?
M: “I decided to focus on this specialty, because it has the acrobatic part of the dance and I think it suits me best. Time proved me right! As far as the kind of clients I work with is concerned, there is no restriction. For example, if
you do not have strength, confidence or flexibility, you will build it with dancing. It has happened in the past to work with cancer patients or with neurological conditions and those that carry the HIV virus. The collaboration with them made me realise that the disease did not stand as an obstacle for them to dance.”
I: How do you choose which workout programs are best suited for each of your clients?
M: “Well, firstly I want to say that pole has different kinds of dancing. Now, I will say that I will choose the best kind of pole for my clients, depending on their interests, their mental and physical health and if they were working out before.”
I: How do you approach someone with a diagnosis, whether it’s pathological or psychosomatic?
M: “Definitely by discussing with them. Personally, I think the pathological element has probably more possibilities to be dealt with, rather than the psychosomatic or the psychological one, such as depression.”
I: From your experience, have you noticed changes in your clients, either psychological or physical?
M: “Of course, I noticed that they have more confidence and their body is changing for the better. My own clients confirm that, because they are coming on their own to tell me this.”
I: For someone who is currently dealing with cancer, what kind of workout would you recommend?
M: “Any kind of workout would be great, it depends on someone’s interests and with the appropriate preparation, everything is possi-
ble. I would like to give a few examples, such as aerobics, lifting weights, Pilates and of course pole dancing.”
I: Would you feel comfortable working with a client who has this illness?
M: “Yes, I am comfortable with this idea, I have already worked with those people, but I want to keep myself updated on their medical history, in order not to push them harder than they can.”
I: Okay, thank you very much for your participation in this interview!
Given the information that these three experienced specialists provided us, we can state now with certainty that nutrition and exercise are some of the most effective ways to maintain good health during cancer treatment. Aside from that, a balanced diet in combination with gymnastics, are great weapons for promoting prevention, and as the professionals stated in their interviews, these two acts can work miracles in patients’ mental health as well.

Cancer survivors provide their tips to keep healthy and aware
by Makri Maria
Cancer is not just a diagnosis; it represents a complex journey filled with challenges, growth, and resilience.It is widely known that cancer refers to a group of diseases characterized by the uncontrolled growth and spread of abnormal cells. These cells can form tumors or infiltrate healthy tissue. With over 200 types of cancer affecting different parts of the body, such as the lungs, breast, colon, and skin, the challenges faced by patients are immense.
P eople who have experienced cancer often end up identifying themselves solely as patients or survivors. Are we defined by our illnesses, or do they reveal the strength we already possess?
A better insight will be provided by cancer survivors who are willing to share their experiences. They will offer detailed accounts of their difficulties, emotions, and advice on coping with an illness like this, while also trying to enjoy life as much as possible.
Interview with anna
I: Would you be comfortable sharing your name, age, and a brief overview of your educational background? (or we can keep it anonymous)
A: “Yes, my name is Anna, I am 58 years old and I studied History Archaeology “
I: Do you have a family?
A: “Yes, I have 2 children, one boy and one girl and of course my husband. “
I: How old were you when you found out about the cancer?
A: “I was 47 years old, when I found out about the cancer”
I: How long were you ill?
A: “The first time I was diagnosed, was July of 2012 and the second time, February of 2013 and approximately it lasted one year both times.”
I:What type of cancer did you have?
A: “The first one was breast cancer and the second one lymph node cancer in the neck”
I: How did you discover it?
A: “The first one, I discovered through my annual checkup and the second one also in the same way, but I had also Hashimoto’s disease and that’s why I looked into it more “
I: How did you feel when the doctor told you about the diagnosis?
A: “I felt the ground fall out from under me”
I: What were your first thoughts?
A: “That I would die and I would leave my kids behind all alone “
I: How did you cope with it?
A: “At first with panic, meaning crying a lot, being angry and disappointed, and of course fear. After that I took my time to process it and after I got the first results from the treatment, which were good, I started getting encouraged. I was praying a lot too. My hope was back. The second time I got cancer I was calmer, because the type of cancer that I had, was easier to deal with”
I: How did others treat you after your illness started?
A: “I had emotional support from friends, especially from my best friend Soula was coming with me in doctor’s appointments and my son’s godfathers, who were calling me every day to see how I was. My husband was supportive as well, but he was scared and lost too. My children did not know at the beginning about the disease, they found out five years later, when based on the protocol a doctor is feeling safe about his patient, that the cancer is definitely gone. Even though my older son might had suspected something.”
I: How was life during the cancer journey, what changed?
A :“I was feeling everything in half, I was insecure and in constant fear. I was looking through my window the sky, the sun and I thought if I will ever have the chance to view it again, to be together with my family for Easter holidays.”
I: What was the side effects of the treatment?
A: “I was constantly tired, without energy, I could not sleep well”.
I: Did you seek help from a specialist, such as a psychologist or a priest? If yes, who and why?
A: “I wanted really badly, but the cost of the treatment was so big, that I could not afford a psychologist as well, so that is why I did not go to therapy. I went to a priest, but only before each radiation therapy, so as to pray to God.”
I: Once it was treated, how did you feel? What did you do after it?
A: “I felt relieved and happy when it was cured and I was setting small goals, like watching my kids finish the school or graduate.”
I: Has this experience changed your perspective on life and how you view things in general?
A: “Even though everyone says that after that traumatic experience they change their way of thinking or daily lives, I still continued to think the same way as before, with anxiety and agony for things. My perspective did not change at all.”
I: What advice would you give to your past self and to those who are still struggling with this illness?
A: “Each case and type of cancer is unique, so I cannot give a general advice, but as far as I am concerned, I would tell to my past self not to be so afraid, because everything worked out at the end and I should have been calmer. Those kinds of difficulties, need to be handled with patience and calmness.”
I: How is life after the cancer, are you afraid that will appear again?
A:“Always, even when I am getting the flu, my mind goes there, I learned to analyse the facial expressions of the doctors, during reading my results of examination.”
I: What advice or thoughts would you offer to people who are stressed by the difficulties of everyday life?
A: “Not to put pressure in themselves about meaningless issues.”
I: Okay, thank you very much for sharing your experience with me in this interview!
Interview with anonymous
I: Would you be comfortable sharing your name, age, and a brief overview of your educational background? (or we can keep it anonymous)
A: “I would like to keep my anonymity, but I will share my age, I am 25 years old and I study Tourism Management, in which I did a gap year, during my illness. “
I: Do you have a family?
A : “Yes, it is my mother and I. Oh and our three dogs! “
I: How old were you when you found out about the cancer?
A: “I was 24 years old, when I found out about the cancer.”
I: How long were you ill?
A : “The time I was diagnosed, was May of 2023 and approximately it lasted six months.”
I: What type of cancer did you have?
A: “I had Hodgkin’s Lymphoma, a type of cancer that affects the lymphatic system, which is part of the body’s immune system.”
I: How did you discover it?
A: “I discovered it through my beard care, I felt something strange, like a lump near my throat and that’s why I decided to look into it more.
At first, I thought it was related to my dental health or skin issues., but then I did some more detailed exams and a surgery to remove this lump. The doctor who took over my case, did a biopsy and then announced to me that I had cancer. The whole process took 1 month and a half, until we found out. “
I: How did you feel when the doctor told you about the diagnosis?
A : “To be honest, I did not feel anything at all. I knew something was off the minute that I started to do the examinations. When the doctor made the announcement, I felt as if my soul left my body and I was watching, what was happening as a third-party observer.”
I: What were your first thoughts?
A:“As I said before, I did not have any thoughts or feelings. It was like, this is not happening to me. I could not feel. “
I: How did you cope with it?
A: “I do not know if I cope with it the right way. I just thought that I have to suck it up, as we say, meaning to endure the process until it was over, since I already knew it would only last for 6 months.”
I: How did others treat you after your illness started?
A: “I had emotional support from friends, especially from my best friends, they handled the situation really well, with discreetness. Of course, my mother was really supportive as well, which was really difficult for her, as we have lost my dad from a different type of cancer, who ironically was treated at the same hospital as me. This made me more worried about her.”
I: How was life during the cancer journey, what changed?
A: “It was definitely hard, I was going to my chemotherapies two times per month and every time I was coming back home even more tired, but I had my dog with me. It really helped me to keep me sane and it was as if he knew that something was off. My perspective changed at some degree, I became calmer and decided to prioritize myself more.”
I: What was the side effects of the treatment?
A: “I was mostly tired, had dizziness, nausea and I could not eat easily. Fortunately, I did not have so much hair loss as it was expected in most cases”.
I: Did you seek help from a specialist, such as a psychologist or a priest? If yes, who and why?
A: “I did not think that I needed one, even though I had a few call sessions with my therapist from time to time, like three calls in three months. He suggested to me, to start sessions more regularly, but I did not think it was essential.”
I: Once it was treated, how did you feel? What did you do after it?
A: “Of course, I felt happy, but to be honest I did not feel like it has ended yet. I have not realized it.”
I: Has this experience changed your perspective on life and how you view things in general?
A: “As I said before, yes definitely in most things. It made me realise the importance of life.”
I: What advice would you give to your past self and to those who are still struggling with this illness?
A: “Each case and type of cancer is unique, so I cannot give a certain piece of advice. In my opinion, those diseases are not something that you can not give advice for. Even to my
past self I could not, because of the fact, that it was not the verbal consolation that helped me, such as <<you can do it, you are a fighter>>, but the facts.”
I: How is life after cancer, are you afraid that will appear again?
A: “It is not like that, maybe because I have not realized it yet. Of course, I made some changes in my life, about priorities.”
I: Okay, thank you very much for sharing your experience with me in this interview!
To conclude, the stories shared by cancer survivors in our interview reveal the remarkable strength of the human spirit in the face of overwhelming challenges. The psychological and physical resilience required to confront such a serious illness is evident in each case. Despite the physical struggles, doubts about the effectiveness of treatments, and the inevitable psychological pressure, these individuals sought out small glimpses of light in their daily lives. They found strength in their loved ones and in their own capacity to endure. Their experiences highlight the crucial importance of psychological and emotional support, of holding onto hope, and the need to care for one’s physical health. It emphasizes that battling cancer is not just about medical treatment, but also about mental well-being. This serves as a powerful reminder that even in the darkest of times, life can remain full of hope and meaning. As Dumbledore wisely said in Harry Potter once, “Happiness can be found even in the darkest of times, if one only remembers to turn on the light.”

by Camille Prod’homme
I didn’t trust any doctor
To their words I closed the door
Escaping examination room
Postponing the “soon”
To a far away, which I hoped could last a long time
In this way,
I would have protected my mind.
From stress, fears of having a problem.
A woman’s one, I though “another, again”.
Campaigns and flyers gave me information
I have to check if there is a deformation, Nipple discharge or any mark
Something which seems particular
I didn’t find anything special
But prevention is elemental
When he says yes, or positive
What he said? I wanted to leave
My brain stopped listening I guess
In my head, beginning of a mess
My femininity involved on it
Is breast cancer can kill it?

I didn’t trust any doctor
But on this day, I had to, for Myself, my health, my future
Ourself, research, start a cure
Now I understand
The problem is not being ill
It’s when you stand
And we are ignoring the hill
Everything can be overcome
We just need support to get home.
by Charlyne Fransioly
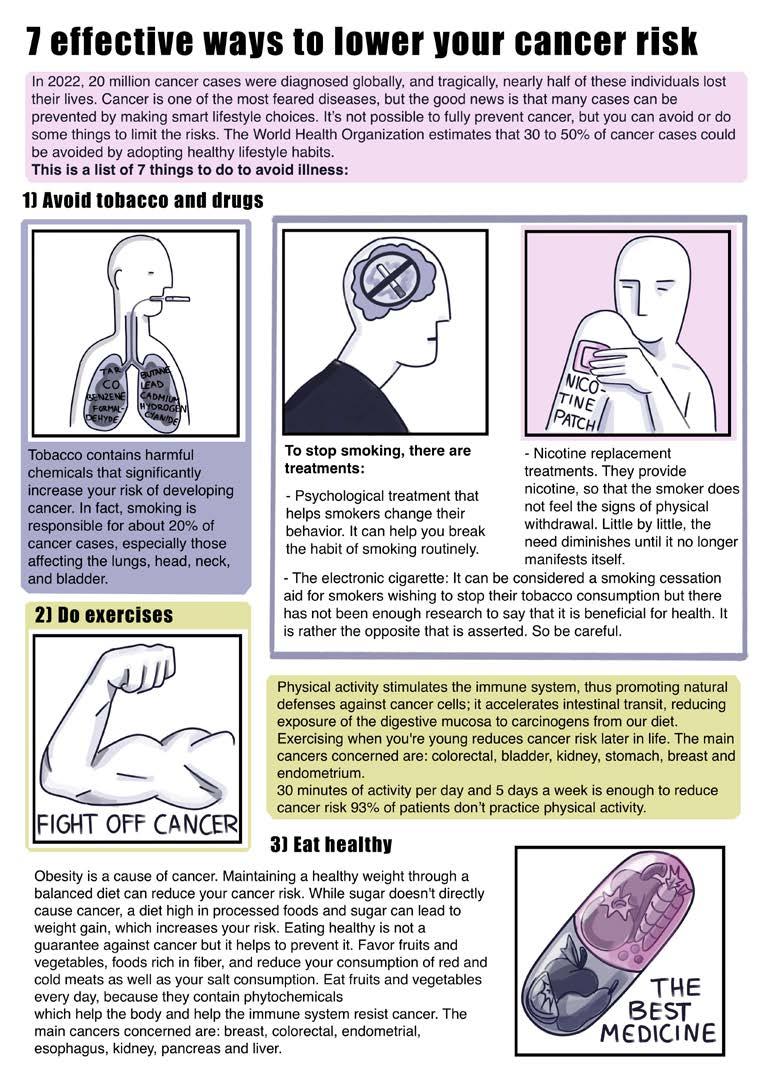
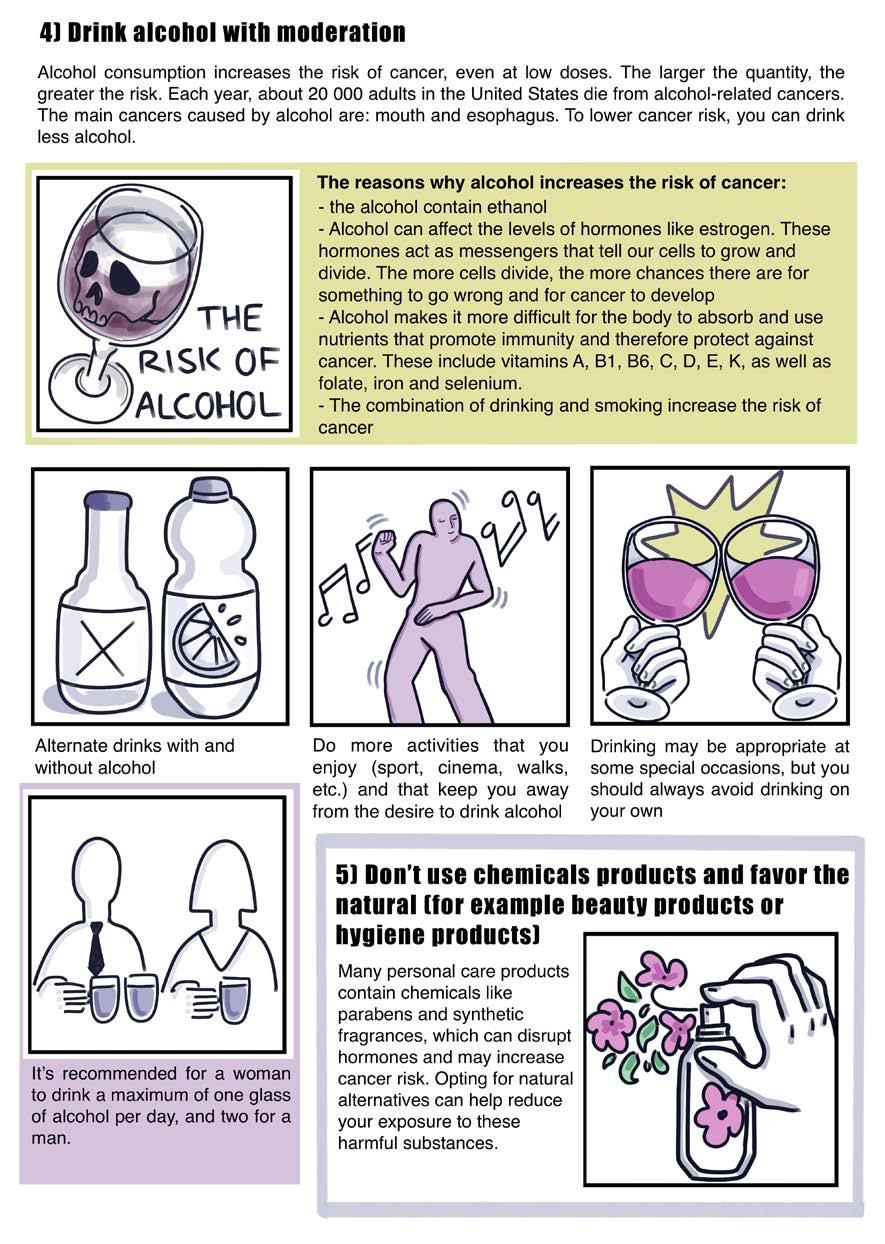
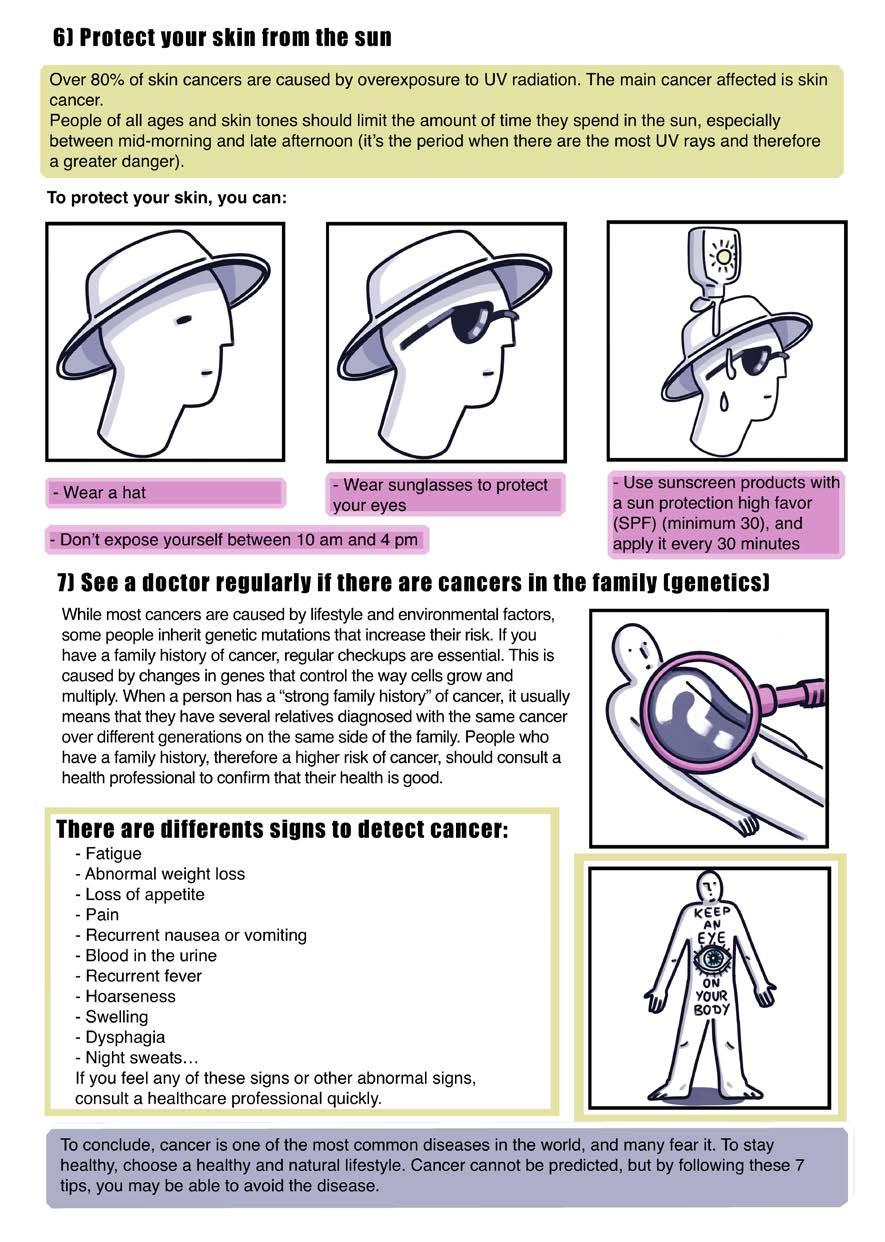
by Inna Petrovska













© Inna Petrovska

















United Societies of Balkans is a Non Governmental Organization, founded in Thessaloniki in 2008, by a team of active young people. The organization was created as a response to the pressure of constant changes in the Balkan and Eastern European region and under the need for the creation of a better social environment. Key areas of the organization’s activities concern the defense of human rights, the organization of youth exchanges and training courses, which will bring young people from Balkans and Europe together, the organization of local educational seminars and multimedia production (webradio, videos, documentaries).
Main goals of the organization
To promote the values of non formal le- aring,volunteering, active citizenship and democracy for the creation of a better future for European youth.
To promote human rights, solidarity and respect for diversity.
To build healthy cooperation bridges between countries of the Balkan area and that of Eastern Europe with the rest of Europe.
To locate and multiply the special cultural attributes of our societies.
The break down of prejudices and stereo- types between Balkan countries.
Property of Balkan Beats
The United Societies of Balkans, NGO, does not necessarily share the opinions expressed in Balkan Beats. It is illegal to reproduce any part of this publication without referring to the source.
Balkan Hotspot is the ESC (European Solidarity Corps) project of “United Societies of Balkans”, a NGO founded in Thessaloniki in 2008 by a team of active young people.
The Balkans and Eastern Europe are geographical regions with many cultural features which offer a broad spectrum of actions and youth involvement initiatives. The organiza -
tion was created as a response to the pressure of constant changes in the Balkan and Eastern European region and under the need for the creation of a better social environment.
Key areas of the organization’s activities concern the defense of human rights, the organization of youth exchanges and training courses, which will bring young people from Balkans and Europe together, the organization of local educational seminars and multimedia production.
The volunteers responsible for this publication are hosted in Greece in the framework of the European Solidarity Corps. This project has been funded with support from the European Commission. This publication [communication] reflects the views only of the authors, and the Commission can not be held responsible for any use which may be made of the information contained therein.
This magazine is distributed free of charge.
General Directors: Aristodimos Paraschou | Christian Cibba
Editors:
Daria Bondarenko | Lilie Grosselin | Toni Pahlke | Sheila Wiebe
Graphic Designer: Anna-Maria Diamantidou