5 minute read
FDAU-05: DIABETES MELLITUS TIPO 2


22 al 26 de noviembre
FDAU-05: DIABETES MELLITUS TIPO 2
Advertisement
ALANÍS-PÉREZ, I1; OVALLE-DIOSDADO, AK1; RODRÍGUEZ-DÍAZ, AC1; SERNA-GARCÍA, AS1; SOTO-GARCÍA, XA1
RESUMEN
Introducción
La DM2, no insulino-dependiente, es más común, la glucosa sanguínea aumenta. No se produce suficiente insulina o no se usa adecuadamente. Produce hiperglucemia y complicaciones crónicas.
Epidemiología
Más del 95% presentan de tipo 2. Ocurre más en mayores a 45 años, con antecedentes familiares de diabetes, sobrepeso, obesidad, afroamericanos, hispanos, indígenas estadounidenses, estadounidenses de origen asiático o nativos de islas del Pacífico, predominantemente en mujeres. En México, la Encuesta Nacional de Salud reportó que el 50% con DM2, reconocen su estado, representando al 9.1% de mayores a 20 años, pero se afirma que la prevalencia real es del 18%. Actualmente una de cada 10 personas adultas la presenta.
Etiología
Se involucran varios factores (estilo de vida, genética). Hay mayor probabilidad de desarrollarla con sedentarismo, sobrepeso u obesidad. Comienza con resistencia a insulina, afección en la que músculo, hígado y células grasas no la usan adecuadamente. El páncreas produce más como regulación, después deja de producir suficiente, aumentará la glucosa sanguínea.
Correlación bioquímica (vía metabólica)
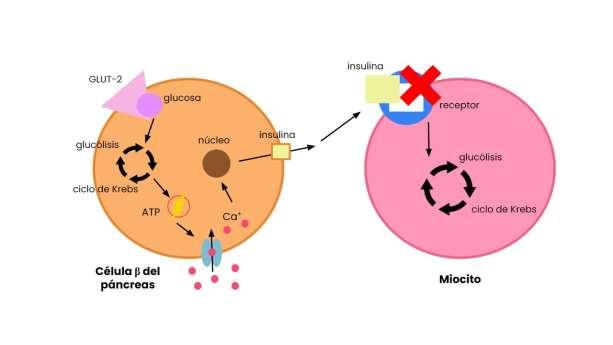
Normalmente, células β de islotes pancreáticos reciben glucosa por GLUT-2 (no insulinodependiente). Entra a glucólisis creando piruvato luego acetil-CoA, entra al ciclo de krebs, sale NADH y FADH2, crea ATP, este activará un transportador de Ca+, el núcleo indica al ARN síntesis y liberación de insulina. No cambia en la DM2, descrito por resistencia a insulina (error de los tejidos a su acción). El páncreas la produce para captar glucosa, manteniendo concentraciones y creando ATP, si no entra, no seguirán los procesos, se necesitarán vías alternativas (beta-oxidación, gluconeogénesis). Sin funcionar, afectaría al organismo, igualmente, células β no mantendrán los niveles, producirán más (hiperinsulinemia compensatoria), se desgastarán. La insulina disminuye la cetogénesis, aumenta la oxidación de ácidos grasos; siendo no tratada, tejidos no responden, aumenta la oxidación y cetogénesis (nivel hepático). Hay agotamiento de carbohidratos transportando ácidos grasos no esterificados. Cuando cuerpos cetónicos se crean y mantienen por largos periodos, aparecerá cetoacidosis (cetonuria y cetonemia). Lleva a disminuir el sistema buffer, como HCO3 , el cual controla. El equilibrio normalmente es por [NAD+]/[NADH] mitocondrial, o sea, estado redox, pues tejidos extrahepáticos los usan como sustratos respiratorios. La gluconeogénesis excesiva da hiperglucemia, por alteración a disminuir con insulina. Es síntesis de glucosa por sustratos (aminoácidos glucogénicos, lactato, glicerol, propionato). En el hígado, resistencia significa incremento de glucosa, causa aumento de insulina, si perdura produce glucotoxicidad y declinación de la función secretora y el número de las células β.
22 al 26 de noviembre
Diagnóstico
No tratada a tiempo significa daños irreparables e irreversibles. Métodos diagnósticos: Hemoglobina glicosilada (A1). Examen aleatorio de glucosa sanguínea. Examen de glucemia en ayunas.
Tratamiento
Basado en control metabólico y prevención: Dieta. Ejercicio. Metformina. Tiazolidinedionas. Inhibidores de alfa-glucosidasas y DPP4 Secuestrador de ácidos biliares. Agonistas del receptor GLP1. Análogos de amilina. Insulinas y análogos (basal y prandial).
Conclusión
La DM2 ocurre por insulinorresistencia o poca secreción, siendo la más común. Se puede desarrollar con sedentarismo, obesidad, o edad avanzada. Exámenes de tolerancia oral a la glucosa, glucemia en ayunas ayudan a diagnosticar antes de que cause daños irreparables. El tratamiento se basa en dieta y ejercicio.
ABSTRACT
Introduction
DM2, non-insulin-dependent, is more common, blood glucose rises. Not enough insulin is produced or it is not used properly. It produces hyperglycemia and chronic complications.
Epidemiology
More than 95% of people with diabetes have type 2 diabetes. It occurs more in people older than 45 years, with a family history of diabetes, overweight, obesity, African Americans, Hispanics, American Indians, Asian Americans or Pacific Islanders, predominantly in women.
In Mexico, the National Health Survey reported that 50% of people with DM2 recognize their condition, representing 9.1% of those over 20 years of age, but it is stated that the real prevalence is 18%. Currently, one out of every 10 adults has it.
Etiology
Several factors are involved (lifestyle, genetics). It is more likely to develop with a sedentary lifestyle, overweight or obesity.
It begins with insulin resistance, a condition in which muscle, liver and fat cells do not use insulin adequately. The pancreas produces more as a regulation, then stops producing enough, blood glucose will increase.
22 al 26 de noviembre
Biochemical correlation (metabolic pathway)
Normally, β-cells of pancreatic islets receive glucose by GLUT-2 (non-insulin-dependent). Enters glycolysis creating pyruvate and acetyl-CoA, enters krebs cycle, exits NADH and FADH2, creates ATP, this will activate a Ca+ transporter, nucleus signals RNA synthesis and insulin release. It does not change in DM2, described by insulin resistance (error of the tissues to its action). The pancreas produces it to capture glucose, maintaining concentrations and creating ATP, if it does not enter, the processes will not continue, alternative pathways will be needed (beta-oxidation, gluconeogenesis). Without functioning, it would affect the organism, likewise, β-cells will not maintain levels, they will produce more (compensatory hyperinsulinemia), they will wear out.
Insulin decreases ketogenesis, increases fatty acid oxidation; being untreated, tissues do not respond, oxidation and ketogenesis (hepatic level) increases. There is carbohydrate depletion transporting unesterified fatty acids. When ketone bodies are created and maintained for long periods, ketoacidosis (ketonuria and ketonemia) will appear. It leads to a decrease in the buffer system, such as HCO3-, which controls. The balance is normally by mitochondrial [NAD+]/[NADH], that is, redox state, since extrahepatic tissues use them as respiratory substrates. Excessive gluconeogenesis gives hyperglycemia, by alteration to decrease with insulin. It is synthesis of glucose by substrates (glucogenic amino acids, lactate, glycerol, propionate). In the liver, resistance means an increase in glucose, causes an increase in insulin, if it persists it produces glucotoxicity and a decline in the secretory function and the number of β-cells.
Diagnosis
Not treated in time means irreparable and irreversible damage. Diagnostic methods: Glycosylated hemoglobin (A1). Random blood glucose test. Fasting blood glucose test.
Treatment
Based on metabolic control and prevention: Diet. Exercise. Metformin. Thiazolidinediones. Alpha-glucosidase and DPP4 inhibitors. Bile acid sequestrant. GLP1 receptor agonists. Amylin analogues. Insulins and analogues (basal and prandial).
Conclusion
DM2 occurs due to insulin resistance or low secretion, being the most common. It can develop with sedentary lifestyle, obesity, or advanced age. Oral glucose tolerance tests and fasting blood glucose help to diagnose it before it causes irreparable damage. Treatment is based on diet and exercise.