2 minute read
FDAU-26 ANTIBIOTICOTERAPIA EN EL TRATAMIENTO DEL ABSCESO ANAL


22 al 26 de noviembre
Advertisement
Almanza, SA1; Chavarría, JE1; González, NS1; Mora, HC1; Rocha, MF1 1 Estudiante de la Facultad de Medicina UAdeC U.T.
RESUMEN
Introducción.
El absceso anal es una patología frecuente que constituye una emergencia para el cirujano. El tratamiento de elección es: drenaje y desbridamiento inmediato. Empero, la antibioticoterapia es requerida cuando existen condiciones que agravan la patología.
Presentación del caso.
Acude al servicio de urgencias paciente masculino de 33 años con diagnóstico presuntivo de absceso perianal.
Antecedentes de importancia.
DM1. Tratamiento: Janumet cada 12 horas. Dislipidemia. Tratamiento: Atorvastatina 40 mg/día
Interrogatorio.
Dolor intenso en región rectal (EVA 10/10). Alérgicos: Ceftriaxona.
Exploración física.
Sistema neurológico y aparato cardiorrespiratorio sin compromiso. Abdomen blando, depresible y peristalsis presente.
Estudios de diagnóstico.
BH, QS y pruebas de coagulación.
Diagnóstico.
Preoperatorio: Absceso anal. Postoperatorio: Fistula anal.
Tratamiento y evolución.
Drenaje del contenido y fistulectomía. Manejo farmacológico. Omeprazol IV 40 mg/día. Ketorolaco IV 30 mg/8 horas alternando paracetamol VO 1 gr/ 8 horas.
Metronidazol IV 500 mg/8 horas.
Elatec VO 1000 mg/8 horas. Contumax 1 sobre por noche. Tramadol IV 50 mg/8 horas.
Justificación del tratamiento utilizado.
El absceso anal frecuentemente se debe a una obstrucción e infección de las glándulas anales por bacterias intestinales. El uso de metronidazol es acertado debido al amplio espectro bactericida contra algunos microorganismos presentes en la patología. Consideraciones éticas: El paciente dio su consentimiento para el uso de su información y recibió una copia del mismo.
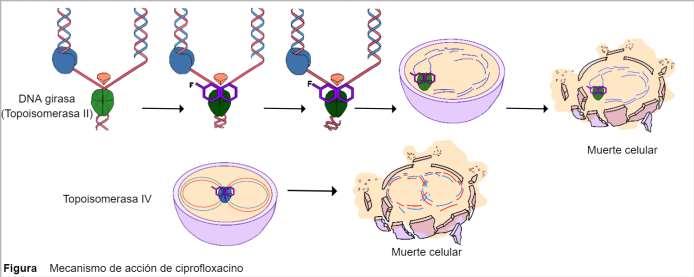
Discusión del mecanismo de acción de un fármaco utilizado en el tratamiento.
El metronidazol ingresa a la célula mediante difusión por bajo peso molecular, la enzima PFOR lo reduce en metabolitos tóxicos que dañan la estructura helicoidal del ADN.
22 al 26 de noviembre
Conclusión.
Identificar tempranamente los abscesos anales debe ser prioridad para el oportuno tratamiento quirúrgico, acompañado de terapia antibiótica adecuada.
ABSTRACT Introduction.
An anal abscess is a frequent pathology that establishes an emergency for the surgeon. The Treatment of choice is drainage and immediate debridement. Nevertheless, antibiotics are needed if conditions that could aggravate the situation are present.
Case presentation.
A 33-year-old man arrives at the emergency room with a presumptive diagnostic: perianal abscess.
Background.
DM1. Treatment: Janumet every 12 hours. Dyslipidemia. Treatment: Atorvastatin 40 mg/day
Interrogatory.
Intense pain in the anal region; (EVA 10/10). Allergic to: Ceftriaxone.
Physical examination.
The neurologic system and cardio-respiratory system were uncompromised. Depressible soft abdomen with active peristalsis.
Diagnostic studies
BB, BQ, and coagulation tests.
Diagnosis
Preoperatorive: Anal abscess. Postoperative: Anal fistula.
Treatment and course.
Abscess drainage and fistulotomy Pharmacological assessment. Omeprazole IV 40 mg/day. Ketorolac IV 30 mg/8 hours alternating with paracetamol O 1 gr/ 8 hours.
Metronidazole IV 500 mg/8 hours.
Elatec VO 1000 mg/8 hours. Contumax 1 sachet per night. Tramadol IV 50 mg/8 hours.
Justification of used treatment.
Frequently, the anal abscess is due to anal glands infection by intestinal bacteria. The metronidazole use is appropriate because of its wide bactericide spectrum against some microorganisms that are present in the pathology.
Ethical considerations.
The patient consented to the use of his information and received a copy of it.
Discussion about the Mechanism of action of one drug used in the treatment.
Metronidazole enters the cell by diffusion due to his low molecular weight. The PFOR enzyme reduces metronidazole into toxic metabolites that damage the DNA helix.
Conclusion.
Identifying anal abscesses must be a priority for the opportune surgical treatment, accompanied with proper antibiotic therapy.