Changing the Future Landscape of Organ Transplantation with Artificial Intelligence 12 Lead Electrocardiograms Total Lean Medical Record Audit Process via Structured Medical Data ISSUE 01 2023 www.americanhhm.com How U.S. Healthcare Organizations can Leverage Generative Artificial Intelligence
Grow your audience with increased reach, impact and user-friendliness
Rise above geographical boundaries
Generate new business
Gain the strong web presence differentiating yourself from competitors
Connect and engage with your target audience

Give more exposure to industry specific people
Increase your brand profile and share your capabilities with leading industry professionals
2 www. americanhhm.com Let the true “Digital Transformation” be the base of all your marketing campaigns Email: subscriptions@americanhhm.com Tel: +91 40 4961 4567 Fax +91 40 4961 4555 www.americanhhm.com UPGRADE YOUR MARKETING STRATEGY
the webinar as a platform to launch new
Use
products and services
EXCLUSIVE WEBINAR SERVICES Hosting Promotions Lead Generation Engage people to your business Gain Market Confidence Be an Authority
Welcome & Introduction
It is a matter of honour and pleasure for me and my team to announce the launch of the very first issueof American Hospital & Healthcare Management magazine in 2023. I extend my gratitude to my super energetic team, an encouraging panel of advisory board members, and all the subject matter expertswho have contributed their various articles.
We wouldn’t have achieved this milestone without your tenacious efforts and belief.
American Hospital & Healthcare Management is uniquely poised to be a leading industry publication encompassing the healthcare sector, powered by expert insights, trends, an industry forecast, and unbiased data analysis. We envision our publication as relevant, crisp, to the point, and user-friendly for American professionals at all levels in the industry.
We aim to provide you with timely industry news and to be a ready reckoner for American readers regarding industry happenings.
Technology-Enabled Healthcare with Data-Driven Intelligent Diagnostic Systems
We have come a long way from its inception a few decades ago to its rapid proliferation and adoption in the healthcare sector today.AI and ML applications are enabling us to witness giant leaps in sophisticated diagnostics, facilities, patient care, and critical-care medicine.
Artificial intelligence techniques help in critical care and emergency medicine, assisting in diagnosis, patient management, and predictions. Prof. Jean-Louis Vincent, UniversitéLibre de Bruxelles gives a detailed account of how artificial intelligence (AI) will change the critical care medicine scenario and personalize patient care.
Clinical prognostic models assist clinicians in tailoring treatments for changes in the brainbody interface in order to maximize the chances of survival and recovery following an aneurysmal subarachnoid hemorrhage. Benjamin W. Y. Lo from the Department of Neurological Surgery at Lenox Hill Hospital explains how regression analysis, classification, and regression tree analysis, as well as the machine learning technique of artificial neural networks, assist in creating a prognostic decision-making tool for cerebrovascular disorders.
Generative artificial intelligence (GAI) are programmes that allow computers to use data elements such as audio files, images, and text to produce original content. James Gillespie, Addie Bobosky, Sophia Senese from Saint Mary’s College, Notre Dame, Indiana, & LinseyFeit from Optum, Minneapolis, explain how GAI can lead to previously unreached levels of insights into diagnostics, diseases, and treatments.
Deploying artificial intelligence (AI) technology to health records is the next step in the evolution of healthcare. Lorie Morris, senior vice president, clinical, at Prestige Healthcare, explains how AI is helping clinicians move from assessment to intervention faster, speeding up the recovery time.
If you have any views or ideas, or if you want to share your feedback with American Hospital & Healthcare Management, you are more than welcome. You may also connect with us on our social media handles for exquisite stories, articles, and much more.
N D Vijaya Lakshmi Editor
3 www. americanhhm.com
CONTENTS
How U.S. Healthcare Organizations can Leverage Generative Artificial Intelligence

James Gillespie, Faculty, Saint Mary’s College
Linsey Feit, Senior Consultant, Optum
Addie Bobosky, Clinical Specialist, Medical Device Industry
Sophia Senese, Data Analytics Specialist
HEALTHCARE MANAGEMENT
06 Planning Anesthesia Practitioners Staffing To Maximize Their Productivity
Franklin Dexter, MD, Department of Anesthesia, University of Iowa
Richard H. Epstein, MD, Department of Anesthesiology, University of Miami
MEDICAL SCIENCES
12 How Artificial Intelligence will Change Critical Care Medicine
Prof Jean-Louis Vincent, MD, PhD, Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles
17 Current Use of Drug Coated Balloons for the Complex Coronary Artery Disease Patients
Bernardo Cortese, MD, Interventional Cardiologist, President Scientific Committee, Cardiovascular Research and Innovation Foundation
Jegan Sivalingam, MD, Interventional Cardiologist, Hannah Joseph Hospital
22 Let’s Not Put the Genie Back Into the Bottle! Remote Healthcare and Telemedicine
Tom Varghese, Sales and Marketing Manager, Healthcare I Governance, Aceso Health
26 Integration of AI into Healthcare Facilities Uses of AI in Healthcare
Lorie Morris, Senior Vice President Clinical, Prestige Healthcare
32 Total Lean Medical Record Audit Process via Structured Medical Data
Piyanun Yenjit, Founder and Managing Director, APUK Co., Ltd
INFORMATION TECHNOLOGY
45 Artificial Intelligence in Healthcare – Machine Learning for Clinical Outcome Prediction in Cerebrovascular Disorders
Benjamin W. Y. Lo, MD PHD FRCSC, Department of Neurological Surgery, Lenox Hill Hospital
52 Changing the Future Landscape of Organ Transplantation with Artificial Intelligence 12 Lead Electrocardiograms
Smruti Desai, MBBS, Division of Advanced Heart Failure and Transplant, Mayo Clinic
Rohan M. Goswami*, MD, Director of Heart Transplant Innovation and Research, Mayo Clinic
DIAGNOSTICS
57 The Future of Precision Medicine in Healthcare
Mai-Lan Ho, MD, Radiology Professor, Nationwide Children's Hospital, The Ohio State University
63 Cloud Computing in Healthcare
James Doulgeris, Chairman, Population Health Advisory Board, RSDSA
EXPERT TALK
70 Human Centered Care – The Delivery Model of Now
Martie Moore, CEO, M²WL Consulting
74 Impact of Covid-19 on Public Health
Samir Redzepagic, Public Health Officer, Monash Health
4 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
OPERATIONS MANAGEMENT
FACILITIES &
PREVIEW
Interphex Event
Medlab Middle East WEBINAR REVIEW
Digital Health: Using technology to engage with patients
New Care Models and the Future of Healthcare 90 EVENTS LIST 94 NEWS
EVENT
84
86
88
89
38
EDITOR
Vijaya Lakshmi N D

Advisory Board
Thitisak Kitthaweesin
Chief of Phramongkutklao Center of Academic and International Relations Administration, Thailand


Piyanun Yenjit
Managing Director
APUK Co.,Ltd
Thailand
Pinheiro Neto Joao
Chief Executive Officer


Meu Doutor
Angola
Gabe Rijpma
CEO
Aceso Health
New Zealand
Eiman Shafa
Medical Director, Spine Surgery

Abbott Northwestern Hospital
USA
James Doulgeris
Chairman
Population Health Advisory Board, RSDSA

United States
Andrey Andreevich Kapitonov

CEO
Oxygen Technologies LLC
Belarus
Aung Pyae Kyaw
Executive Director Asia Royal Hospital

Myanmar
Wanita Ramnath
CEO
International Pharmacy and Health Care Suriname
Likaa Najuib
Medical Marketing Operational Officer, Alfa Cure Oncology Center
Egypt
EDITORIAL TEAM
Sarah Richards
Debi Jones
Harry Callum
Supraja B R
ART DIRECTOR
M Abdul Hannan
PRODUCT MANAGER
Jeff Kenney
SENIOR PRODUCT ASSOCIATES
Sussane Vincent

John Milton
Peter Thomas
Ben Johnson
PRODUCT ASSOCIATE
Megan John
Ethan Wade
CIRCULATION TEAM
Sam Smith
SUBSCRIPTIONS IN-CHARGE
Vijay Kumar Gaddam
HEAD-OPERATIONS
Sivala VNR
www.americanhhm.com
Ochre Media Group info@ochre-media.com www.ochre-media.com




©Ochre Media Private Limited. All rights reserved. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, photocopying or otherwise, without prior permission of the publisher and copyright owner. Whilst every effort has been made to ensure the accuracy of the information in this publication, the publisher accepts no responsibility for errors or omissions.
The products and services advertised are not endorsed by or connected with the publisher or its associates. The editorial opinions expressed in this publication are those of individual authors and not necessarily those of the publisher or of its associates.
Copies of American Hospital & Healthcare Managemen can be purchased at the indicated cover prices. For bulk order reprints minimum order required is 500 copies, POA.
Magazine Subscribe
LinkedIn
5 www. americanhhm.com
Planning Anesthesia Practitioners Staffing to Maximize their Productivity

Anesthesia staffing refers to daily workforce planning, number of anesthetizing locations, and hours into which cases are scheduled for each such room. Calculations are done to minimize a weighted combination of the costs of too little and too few allocated hours. Managerial epidemiology studies show the value of these methods.
Franklin Dexter
MD, Department of Anesthesia University of Iowa
Richard H. Epstein MD, Department of Anesthesiology University of Miami
Definitions used when making staffing decisions to increase operating room efficiency
Hours worked exceeding allocated hours (i.e., the operating room (OR) hours into which cases are scheduled) are referred to as “hours of over-utilized OR time.” Allocated hours are calculated months before the day of surgery for each combination of service and day of the week, based
6 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
HEALTHCARE MANAGEMENT
upon the historical workload and the total hours of cases, including add-ons and turnovers. Surgical services are functionally defined as groups of surgeons who schedule cases into the same allocated hours (e.g., “general surgery including transplant”). Calculated OR allocations include add-on cases since they contribute to the historical OR workload. OR allocations are needed for staff scheduling, the process that determines which individual anesthesiologists, nurse anesthetists, OR nurses, and others will work each future day.
Staffing is chosen to minimize [(Cost per hour of under-utilized OR time) × (Hours of under-utilized OR time)] + [(Cost per hour of over-utilized OR time) × (Hours of overutilized OR time)]. This is one of the three simultaneous equations for the inefficiency of use of OR time, the other two being for under-utilized OR time and for over-utilized OR time, respectively. With the cost of 1 hour
of over-utilized time to 1 hour of under-utilized time represented by R, (typically 1.5-2.0), the value to be minimized can be expressed in terms of hours: (Hours of under-utilized OR time) + R × (Hours of over-utilized OR time). The solution that minimizes the inefficiency in the use of OR time is insensitive to local experts’ uncertainty in the choice of the value of this parameter. The actual cost per hour is irrelevant to the mathematics, only the ratio of the cost of over-utilized to under-utilized time.
Performing calculations to allocate operating room time
When OR allocations are calculated scientifically, based on OR efficiency, they are categorized by the combination of service and day of the week. That is because the day of the week is the best predictor of a service’s workload. Calculating an OR allocation means determining how many ORs should be staffed

7 www. americanhhm.com
HEALTHCARE MANAGEMENT
daily for each service and, for each of these ORs, how many hours of staffing should be planned (e.g., 8, 10, or 13 hours). Consider all possible staffing solutions for each service, individually. Start with 0 hours and progressively increase staffed hours until additional increases in the staffed hours cause the efficiency of use of OR time to decrease for that service. If shifts of 8, 10, and 13 hours are considered, then the successive choices are 0, 8, 10, 13, 16, 18 hours, etc. Increasing the staffed hours causes the efficiency of use of OR time to increase progressively to a maximum. Further increases in the staffed hours cause the efficiency to decrease, because of the progressively greater hours of under-utilized OR time. The complete enumeration can be constructed such that every series of cases performed by the same surgeon on the same day would be performed in its original sequence and take the same amount of OR time. The only change is in the start times. For example, a surgeon is currently allocated 8 hours of OR time individually on Mondays. The surgeon historically has done 9.0 hours of cases every Monday. The hospital calculates that the expense of one hour of over-utilized time is twice that of one hour of under-utilized time, and inefficiency is expressed in terms of the number of equivalent under-utilized hours. Candidate allocations are 0, 8, 10, and 13 hours. The inefficiency of use of OR time for each potential allocation is determined by using the cost of the under-utilized and over-utilized hours that would have resulted. A 0-hour allocation would have resulted in 9 hours of
over-utilized time, with an inefficiency of use of OR time proportional to 18 hours. An 8-hour allocation would have resulted in one hour of over-utilized time, with an inefficiency of 2 hours. A 10-hour allocation would have resulted in 1 under-utilized hour with an inefficiency of 1 hour. Finally, a 13-hour allocation would have resulted in 4 hours of under-utilized time with an inefficiency of 4 hours. Since the smallest value of the inefficiency of use of OR time was with 10-hours, the surgeon should have been allocated 10 hours of OR time to maximize OR efficiency. The same optimal allocation results if the hospital manager had selected a ratio of the cost of over-utilized to underutilized hours between 1.5 and 4.0.
For example, on 3 Tuesdays, a service performed 12.0, 7.0, and 15.0 hours of cases, including turnover times. There are 8-hour shifts, with overtime scheduled by rotation using a late list. The relative cost of overutilized to under-utilized hours is considered 1.75. If the service were allocated 8 hours of OR time each Tuesday, then the cost of the inefficiency of use of OR time would be proportional to 20.25 hours, where 20.25 = (0 under-utilized + 1 under-utilized + 0 underutilized + 1.75 × [4 over-utilized + 0 overutilized + 7 over-utilized]). If the allocation were two 8-hour ORs each Tuesday, the cost would be proportional to 14 hours, where 14 hours = (4 under-utilized + 9 under-utilized + 1 under-utilized). If the allocation were three 8-hour ORs each Tuesday, the cost would be 38 hours, (12 under-utilized + 17 under-
8 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
HEALTHCARE MANAGEMENT
utilized + 9 under utilized). Therefore, the service should be allocated two 8-hour ORs to maximize OR efficiency. Again, results are insensitive to the cost ratio of over-utilized to under-utilized hours.
Calculated Staffing (Operating Room Allocations) Differ from Those in Current Practice
Although the analytical solution for maximizing the efficiency of use of OR time was first published more than 25 years ago, many OR managers ignore this knowledge. For managers’ efforts to reduce labor costs maximally, they need to focus on OR allocations and case scheduling because almost all anesthesia providers’ costs are labor costs. For 11 of 12 facilities studied, allocating OR time based on OR efficiency achieved significantly lower labor costs than the plans that were being used by the local managers. For 9 of 11 facilities, the statistical method approach resulted in plans that reduced labor costs by at least 10%. The
percentage increases in OR efficiency were larger than 10%. The actual allocations do not match those that maximize the expected efficiency of use of OR time because, frequently, organizations plan the same allocated hours for all ORs (e.g., all services are allocated one OR for 10 hours, or two ORs for 10 hours, etc.).
To appreciate why this is suboptimal, for one day, calculate the standard deviation among ORs at a facility in the workload for elective cases. Among days, for the facility, calculate the mean of the standard deviations. If suitable to use all 8-hour workdays, all 10-hour workdays, etc., then the mean of the standard deviations would be much less than one hour. However, that was not so among 34 hospitals in the United States, Australia, and France.10 All had means of at least 1.5 hours, with many greater than 3.0 hours (Figure 1). Because this variability in the durations of workdays is predictable variability, the allocated hours should be planned to match them, thereby reducing the hours that anesthesiologists, nurse
anesthetists, OR nurses, etc., work late.
N = 34 hospitals
Suppose that anesthesiologists at a hospital report that all of the ORs finish at least an hour or two late every day. To consider the economic irrationality of the situation, suppose that the relative cost of over-utilized to
9 www. americanhhm.com
1.52.02.53.03.54.0 StandardDeviationofHoursAmongEachDay'sORs
HEALTHCARE MANAGEMENT
under-utilized OR time were 2.0. Then, it would be twice as expensive to finish late versus early. Thus, with appropriate OR allocations, the odds for each service and OR to finish early would be approximately chances in.
Two managerial epidemiology studies show that the described matching of staffing to the workload is appropriate for “real-world” practice. Suppose that hospitals and hospital owned ambulatory surgery centers are not limiting surgeons and patients when the cases can be performed safely sometime during a future workday selected by the surgeon. Then, during national surgical meetings, when surgeons are away, there would be fewer cases. However, during anesthesia meetings, the workload would be the same. This was observed among the 121 hospitals in Iowa, 2007 through 2016. The American Society of Anesthesiologists meeting’s Friday to Wednesday periods were compared pairwise with other such periods without holidays during the year. Caseloads were the same (+0.1%, P=0.93). In contrast, fewer general surgery cases were performed during the dates of the American College of Surgeons’ meeting ( 2.5%, P=0.003). Furthermore, fewer joint arthroplasties were performed during the period of the American Academy of Orthopaedic Surgeons meeting (5.9%, P=0.018). As another example, in the State of Florida, among patients with commercial insurance, December had more cases than November (ratio 1.108 [99% confidence
interval 1.092 to 1.125]) or January (1.257 [1.229–1.286]). In contrast, among patients with Medicare insurance (traditional or managed care), December had fewer cases than November (ratio 0.917 [0.904–0.930]) or January (0.823 [0.807–0.839]) of the same year. Comparing December versus November (January) ratios for cases among patients with commercial insurance to the matching ratios for cases among patients with Medicare, years with more commercial insurance cases had more Medicare cases (Spearman rank correlation +0.36 [+0.25], both p < 0.0001). In other words, one set of cases is not negatively limiting the other set of cases.
Matching staffing to the current workload is important because most growth in surgery at hospitals occurs among surgeons who are scheduling so few cases per week that they would not be filling an OR for the day but following another surgeon in a room. All surgeons’ cases were tracked statewide over 2 years. For each surgeon, the increase in their weekly cases was calculated. For each hospital, the percentage increase in overall caseload was calculated from among the surgeons who during the first year averaged only 2 or fewer cases per week. The average hospital in Iowa had the majority of its growth in inpatient and outpatient cases from one year to the next among surgeons who performed N ≤ 2 cases per week in the baseline year (77.0% ± 2.5% [standard error]). The majority of the growth in outpatient surgery Relative Value
10 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
HEALTHCARE MANAGEMENT
Units was among those surgeons (81.9% ± 2.2%). Similar results were obtained for the state of Florida. The average hospital in Florida also had the majority of its growth in inpatient and outpatient cases from one year to the next among surgeons who performed N ≤ 2 cases per week in the baseline year (73.3% ± 1.5%). The majority of the growth in outpatient surgery Relative Value Units was among those surgeons (68.7% ± 0.9%). Finally, these principles of matching staffing to workload is important because there are whole classes of proceduralists who need access to OR time to ensure that
care of their patients but who will not fill an OR for the workday. Hours of daily OR time and cases were calculated among anesthesiologist pain medicine physicians at the University of Iowa and among all such physicians in the state of Florida in 2018. At least 76.6% (95% lower confidence limit) of Florida surgical facilities performing at least one neuromodulation procedure averaged fewer than 1.08 cases per two weeks. At least 89.6% of the facilities averaged fewer than 2 cases per two weeks. At least 96.5% of the proceduralists averaged fewer than 2 cases per two weeks at each facility where they operated.
References are available at www.americanhhm.com
Franklin Dexter, MD PhD FASA, is a Professor in the Department of Anesthesia at the University of Iowa. Several times a year, he teaches a four-day intensive course in the operating room management. He has given more than 190 invited presentations in the United States and abroad. In multiple editorial positions, he has reviewed greater than 7495 papers and grant applications, for 101 different journals over the past 5 years. As Director of the Division of Management Consulting in the Department of Anesthesia, he has performed more than 835 consultations, for more than 235 corporations. He has published more than 640 papers in the fields of operating room management and anesthesia.

Richard H. Epstein, MD, is a Professor of Clinical Anesthesiology at the University of Miami. He is board certified in anesthesiology, pediatrics, and clinical informatics and is the Director of Perioperative Analytics in the department. His research includes clinical informatics, decision support, operating room management, and large healthcare data analytics. He has published more than 250 papers.

11 www. americanhhm.com
AUTHOR BIO
AUTHOR BIO
HEALTHCARE MANAGEMENT
How Artificial Intelligence will Change Critical Care Medicine

Artificial intelligence techniques are developing rapidly alongside the increase in big data availability. These methods will have an important place in the future of critical care and emergency medicine, to assist in diagnosis, patient management, and prediction of complications and help as we move toward ever more personalised patient care.
Prof Jean-Louis Vincent MD, PhD, Department of Intensive Care, Erasme Hospital, Université Libre de Bruxelles, Brussels, Belgium
There is no doubt that artificial intelligence (AI) will have an important place in the future of critical care and emergency medicine. The rapid development, availability, and use of less invasive monitoring systems over recent years, alongside increases in computing power and data storage are facilitating the collection and analysis of vast amounts of patient information. Simultaneously, AI technology is
12 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
advancing, such that this “big data” can be used to recognize patterns and associations among variables and outcomes of interest.
AI will have three major applications in the critical care field, to assist in diagnosis, treatment, and prediction of complications.
Machine learning and neural networks
In the medical context, most AI approaches employ machine learning techniques in which algorithms are used to classify or group data or to make predictions about certain outcomes including disease diagnosis and prognosis. Machine learning can be subdivided into two broad methods: supervised and unsupervised machine learning, and reinforcement learning (Figure).
Supervised machine learning is the most widely used method at the present time. Data sets that are already labelled to be associated with a specific event or outcome are used to
“train” computer systems to classify data correctly. Some straightforward examples that have been employed include training computer algorithms to interpret certain types of X-ray, to differentiate cutaneous cancers, and to interpret fundal changes in the eye. Supervised machine learning also enables the computerised system to determine the best therapeutic plan, and predictive modelling can be used to foresee the chances of response to treatment.
Unsupervised machine learning enables the computer algorithm to identify previously unrecognised patterns and clusters within patient populations. This may help to discover previously unknown predictive and/or therapeutic factors; for example, this approach has been used to identify subsets of patients with sepsis and with acute respiratory failure. Latent class and latent profile analysis are the most widely used unsupervised machine learning techniques for this purpose.
Computer science that can analyse complex (medical) data (computers unable to mimic human Intelligence)
Machines trained using artificial networks with multiple layers (artificial neural networkd)
Machines can learn by experience (auto-feeding)
13 www. americanhhm.com
DEEP LEARNING MACHINE LEARNING ARTIFICIAL INTELLIGENCE Supervised Labelled patternsare provided to the machine Unsupervised Algorithms can be developed without human intervention (machine feedling itself) through structured data Reinforcement Trial and error MEDICAL SCIENCES
The limitation of this approach is that the identified groups may not necessarily be clinically meaningful so that some clinical interpretation is needed. The ‘black box’ nature of this approach, in which the reason for the groupings achieved is unknown, can also be concerning.
In reinforcement learning, algorithms are trained by trial and error, with “rewards” being given for decisions giving a positive outcome, and a “penalty” for decisions that have a negative outcome. This approach is particularly suited to optimise the timing, dose, and duration of interventions.
Neural networks are a more complex type of machine learning model designed to identify complex relationships between input variables and outcomes and can be used in both supervised and unsupervised machine learning. Neural networks effectively reproduce layers of artificial “neurons” or nodes with an input layer (which can include a large number of input variables, including physiological or laboratory markers), one or several (so-called deep learning) interconnecting hidden layers, and an output layer. Limitations again include the ‘black box’ aspects of this approach and the difficulty such systems have determining and taking into account clinical priorities.
Therapeutic implications
AI will increasingly help to identify the best therapeutic interventions for each specific situation. There have been many negative randomised control trials (RCTs) in critical
care medicine, showing no impact of the intervention tested on outcomes. The negativity of these trials is largely explained by two factors. The first is the choice of mortality as an end-point. Mortality would initially appear to be a ‘strong’ end-point, but is actually affected by many factors other than the studied intervention, so that the effect of the tested intervention is ‘buried’ among the effects of many other factors. The second is the heterogeneity of the patient populations, meaning that although some patients may benefit from the intervention, others may be harmed; however, it may be difficult to differentiate these two patient populations. One example of this dilemma is the administration of blood transfusions to the critically ill. In some patients, the likely benefit is clear, whereas in others unwanted adverse effects may outweigh any possible (limited) benefits. RCTs on transfusions have provided little help in determining optimal transfusion guidelines because randomisation has largely been based on a haemoglobin threshold, typically 7 versus 9 g/dL. However, the decision to transfuse should
14 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
AI techniques are emerging rapidly and will have an increasingly prominent place in the future of critical care and emergency medicine as we move toward ever more personalized patient care.
be based not only on the haemoglobin levels but also on other elements, such as the presence of associated respiratory distress, coronary artery disease, frailty, and others. Analysis of big data could help better identify those patients who will benefit from a transfusion. The same question may apply to the administration of albumin, as again RCTs have been based on albumin concentrations, whereas other factors, such as risk of further complications, the presence of sepsis, the presence of liver disease, the magnitude of existing oedema, and so on, should also be taken into account. Other therapeutic applications for AI that may be valuable include determining the optimal arterial pressure level that should be targeted in individual patients, as well as the right timing of certain therapeutic interventions, such as vasopressin or corticosteroid administration in septic shock.
AI is now being used to inform clinical decision support systems, based on the big data provided from large numbers of electronic health records (EHRs), which offer information on various aspects of patient demographics, laboratory, and microbiology tests, imaging results, physical examination, progress notes, consultant reports, therapeutic interventions, and so on. An important limitation to the use of such information at present is the lack of common terminology in narrative texts, such as doctors’ notes. For example, some patients may be labelled as ‘septic’ by some physicians but simply as ‘infected’ by others. Similarly, the mode of mechanical ventilation does not always
follow an internationally recognised vocabulary. Natural language processing methods can be used to interpret narrative text and speech and extract in a format appropriate for machine learning.
Prediction of (likely) deterioration
Predictive modelling AI techniques enable the recognition of patterns that are associated with an increased risk of clinical deterioration or development of complications such as sepsis. Importantly, deterioration outcomes should not be restricted to survival or death but include other indications of morbidity such as organ dysfunction (which may or may not eventually result in death in the absence of intervention). These techniques can be used on the regular floor to rapidly identify patients who may need special attention, additional tests, and perhaps admission to the intensive care unit (ICU).
Patients on the regular floor, as in the ICU, are often monitored using several different systems, and the different variables can be

15 www. americanhhm.com
MEDICAL SCIENCES
integrated to create more accurate predictions. It is also important to evaluate trends and avoid the dichotomous separations of the past, in which a single alarm would go off when the heart rate increased, e.g., above 110/min or the systolic blood pressure fell below, e.g., 100 mmHg. Alarms based on single variables may also be limited by artefacts: the most common example of this is the SpO2 signal being altered or cancelled by displacement of the probe. Real respiratory deterioration should be recognised not only by a fall in SpO2 (which never occurs alone), but also by a concurrent increase in heart rate and respiratory rate. Interconnectivity between monitoring systems is still limited today but, increasingly, smart monitors and intelligent systems will combine the different variables and various types of information and be able to continuously update the models as new data become available. The calibration of the models is of paramount importance as we do not want the systems to be too sensitive (with false alarms resulting in so-called ‘alarm fatigue’), but at the same time, we do not want to miss deterioration that should be identified and could be treated if noticed soon enough. The systems tested in hospitals so far have resulted in mixed degrees of enthusiasm. Obviously, there is a long road before they can be reliably applied worldwide.
Will AI replace or assist healthcare staff?
At present, AI systems should not replace the bedside healthcare staff, but are already
Jean-Louis Vincent is a Professor of intensive care medicine at the Université Libre de Bruxelles and a consultant in the Department of Intensive Care at Erasme University Hospital in Brussels, Belgium. He has signed over 1000 peer-reviewed articles and more than 400 book chapters. He is the editor-in-chief of Critical Care, Current Opinion in Critical Care, and ICU Management & Practice.

contributing to enable adequate and early decision-making for diagnosis and treatments. AI is ideally placed to evaluate the multiple possible combinations of patients, diagnoses, and therapies to develop intelligent, individualised patient management plans. In March 2023, a round table conference of experts will be held in Brussels, which will discuss one important aspect of this process, i.e., the identification and recognition of specific patient phenotypes within the loose, heterogeneous entities such as sepsis and acute respiratory distress syndrome (ARDS) on which we currently base diagnosis and treatment.
With the help of AI, the future of intensive care is rapidly moving toward a personalised medicine approach, which will ultimately improve patient outcomes.
16 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
AUTHOR BIO
MEDICAL SCIENCES
Current Use of Drug Coated Balloons for the Complex Coronary Artery Disease Patients
Drug coated balloon plays a very important role in the management of in-stent restenosis and native coronary artery disease, however its role in the treatment of complex coronary artery disease is an interesting and emerging concept. DCB are available for use in Europe and Asia, but not yet in the USA.
 Bernardo Cortese
MD, Interventional Cardiologist, President Scientific Committee, Cardiovascular Research and Innovation Foundation
Jegan Sivalingam
MD, Interventional Cardiologist, Hannah Joseph Hospital
Bernardo Cortese
MD, Interventional Cardiologist, President Scientific Committee, Cardiovascular Research and Innovation Foundation
Jegan Sivalingam
MD, Interventional Cardiologist, Hannah Joseph Hospital
Drug eluting stents (DES) are the mainstay of treatment in a majority of patients with significant stenoses of the coronary arteries. However, the use of DES is associated with various acute and longterm complications such as stent thrombosis, in-stent restenosis (ISR), neoatherosclerosis, and abnormal vasomotion. Moreover, the
17 www. americanhhm.com
MEDICAL SCIENCES
implantation of DES mandates the patient to take dual antiplatelet drugs for a certain duration which is not always feasible in all patients and associated with an inherently increased risk in clinically relevant bleedings. Target lesion failure of DES ranges between 0.8-1% yearly in simple lesion subsets itself, with higher rates in the more complex lesion setting. The long-term results of DES are not optimal in complex coronary artery disease subsets such as chronic total occlusion (CTO), complex bifurcation lesions, long lesions, heavily calcific lesions, small vessel coronary artery disease and also, there are no enough studies available assessing the long-term outcomes of DES in this group. Drug coated balloons were initially developed to address the issue of ISR. Later the usage of DCB in treatment of native vessel coronary artery disease increased as it showed favourable long-term outcomes. The use of DCB in complex anatomy is a boon for the patients
as it decreases the duration of DAPT needed and also works on the principle of the “leave nothing behind” strategy: in fact, no metallic cage is left behind in the arteries which in turn facilitates the vessel remodelling and also avoids the stent related complications. The current status of DCB use in complex coronary artery disease is reviewed in this article.
Drug coated balloon overview
Drug coated balloon works on the principle of transferring an antiproliferative drug to the vessel wall upon inflation of the balloon. Paclitaxel is the drug used in the earlier generations of DCBs with a recent introduction of sirolimus.
Adequate lesion preparation is a prerequisite of any percutaneous coronary intervention (PCI) be it stent implantation or DCB application. The lesion is usually predilated with a semi-compliant or non-compliant balloon sized according to the distal vessel

18 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
reference size in the ratio of 0.8:1 or 1:1. In case of non-yielding lesions further preparation with normal balloons, cutting or scoring balloons may be required. In heavily calcific lesions the use of rotational or orbital atherectomy, or lithotripsy may be required. The aim of lesion preparation is to achieve less than 30% of residual stenosis with TIMI III flow and no flow limiting dissection prior to the application of DCB.
DCB in small vessel CAD
There are various studies which have shown the efficacy of DCB in small vessel CAD. BELLO, BASKET-SMALL 2, RESTORE SVD, and PICCOLETO II are the most important among them. BELLO study compared the angiographic outcomes of 182 patients with small vessel coronary artery disease (SVD) defined as RVD < 2.8 mm, randomized to paclitaxel eluting stent (Taxus, Boston Scientific) vs Paclitaxel coated balloon (In.Pact Falcon, Invatec). The study showed superior angiographic results in paclitaxel coated balloon arm and also lower major adverse cardiovascular events (MACE) at 3 years. A large study, BASKET-SMALL 2, was performed on 758 patients, in which 382 patients were treated with paclitaxelcoated balloon (SeQuent Please, B.Braun), and 376 patients were treated with either the paclitaxel-eluting Taxus Element stent or the Everolimus-eluting Stent (Xience, Abbott Vascular). The rate of MACE after 12 and 36 months were similar between both groups (DCB versus DES: cardiac death 3.1% versus 1.3%, p=0.11; non-fatal MI 1.6% versus 3.5%,
p=0.11; and target vessel revascularisation 3.4% versus 4.5%, p=0.448). In RESTORE SVD trial, 230 patients with RVD between 2.25 mm and 2.75 mm were randomized to RESOLUTE INTEGRITY (Zotarolimus eluting stent) vs RESOLUTE (paclitaxel DCB), at the end of 9 months DCB arm was shown to be
non-inferior to the DES arm in terms of Target Lesion Revascularization (TLR), myocardial infarction, cardiac death and a composite endpoint. PICCOLETO II randomized 232 patients with SVD to everolimus eluting stent vs paclitaxel DCB (Elutax SV, AR Baltic). After a median follow up of 189 days, the in-lesion late luminal loss (LLL) was significantly lower in the DCB group. At 12 months follow up there was no significant differences found in MACE in both groups.
DCB in bifurcation lesions
Bifurcation lesions are encountered in approximately 15-20% of the PCIs. A Bifurcation lesion is defined as a coronary

19 www. americanhhm.com
Drug-coated balloons play a vital role in in-stent restenosis and native coronary artery disease management as they are considered the mainstay of treatment of such diseases.
MEDICAL SCIENCES
artery lesion located at or adjacent to a significant side branch which the operator does not want to lose during the PCI. Treating the bifurcation lesions with stents poses many technical challenges and also carries high risk of stent-related complications due to high metallic load, malapposition, and neo-carina related altered hemodynamics. The Usage of DCB in bifurcation lesions avoids all the above-mentioned problems associated with the DES. In bifurcation lesions, DCB could be applied to both the main vessel and side branch as DCB only treatment or to the side branch alone in case of provisional stenting. Unfortunately, the data available is scarce and the robustness weak. Schulz et al. studied 39 bifurcation lesions with side branch diameter > 2.0 mm treated exclusively with DCB, angiographic follow up was done in 30 out of 39 bifurcation interventions at 4 months and it showed restenosis in 3 (10%), TLR was required in 3 patients corresponding to a MACE of 7.7%. In PEPCAD-BIF trial 64 patients with bifurcation lesions not involving the proximal main branch were randomized to DCB vs Plain Old Balloon Angioplasty (POBA) alone after successful predilation. At the end of 9 months angiogram showed LLL was 0.13 mm in the DCB vs 0.51 mm in the POBA group (p = 0.013). The Restenosis rate was 6% in DCB group vs 26 % in the POBA group. TLR was required in one patient among the DCB group vs three patients among the POBA group.
DCB in CTO lesions
Chronic total occlusion lesions are seen
in around 20% of the patients with CAD. Revascularisation of CTO with DES poses a challenge because there is higher incidence of stent thrombosis and ISR following DES implantation in this setting. Moreover, the distal vessel beyond the CTO grows during the first weeks following the establishment of antegrade flow and potentially leads to late stent malapposition and related complications. There is very scarce literature available regarding the use of DCB in CTO PCI. There are no randomized controlled trials available comparing the DES vs DCB in CTO PCI, only a few observational studies are available.
Philine J Köln et al. studied 34 patients with CTO treated with DCB, the recanalization was considered satisfactory in 79.4% (n=27) and not satisfactory in 20.6 % (n=7) patients. Restenosis occurred in 11.8% (n=4) and re-occlusion in 5.9% (n=2). Out of the 27 patients with a satisfactory initial result, 3.7% (n=1) had re-occlusion and 3.7% (n=1) had restenosis. In the subgroup without satisfactory result (n=7), restenosis occurred in 3 patients (42.9%) and re-occlusion in 1 patient (14.3%). A luminal increase was found in 67.6% (n=23) and mean late luminal gain was 0.11±0.49mm. Angina class improved significantly (p<0.001). There was no death or myocardial infarction.
Eun Jung et al studied 84 patients with de novo coronary CTO lesions (93 vessels).
Patients who had Thrombolysis In Myocardial Infarction (TIMI) flow grade 3 and <50% of residual stenosis following pre-dilatation with balloon angioplasty, and successfully treated with DCB without requiring stent implantation
20 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
were included in the study. Patients had a median follow-up of 720 days (IQR, 406–1,268 days) after the index procedure. Angiographic follow-up was done in 72% of the patients. MACE occurred in 8.3% and 16.7 % of the patients after 1 year and 2 years respectively. This study showed encouraging clinical outcomes of DCB only treatment of de novo CTO at the 2-year follow-up, also the hard endpoints rate were low and MACE rates were acceptable.
DCB in complex CAD - the future
We believe that in 2023 the aim of an interventional cardiologist should be to keep the coronaries free from metal as much as possible and to minimize the very
late adverse events (15). The use of DCB in complex CAD patients appears promising and helps the interventional cardiologist in achieving this goal. Flow-limiting dissections (but not those type A and B with TIMI 3 flow) and acute recoil remain the Achille’s heel of DCB only approach. Proper preparation of the lesion with any available tool and adequate sizing of the balloon, keeping the balloon to artery ratio of 0.8-1.0 is essential for achieving the full efficacy of DCB and also will help in minimizing the acute and long term complications. Further advances in drug delivery and a better understanding of plaque morphology and careful case selection will help in treating the majority of complex CAD patients with DCB.
References are available at www.americanhhm.com
Dr. Bernardo Cortese is an Interventional cardiologist, is one of the pioneers in metalfree interventional cardiology, especially with DCB. He is the owner of DCB Academy. President of the Scientific Committee of Fondazione Ricerca e Innovazione Cardiovascolare based in Milano, Italy. He treats >60% of his patients with DCB, including the very complex lesion setting. He has published >320 peer-reviewed articles indexed in PubMed. www.bernardocortese.com
Dr. Jegan Sivalingam is currently working as Interventional Cardiologist at Hannah Joseph Hospital. He underwent his cardiology training at Christian Medical College, Vellore. He has presented at various national and international cardiology conferences. He is also a fellow of DCB academy. His interest includes complex PCI and structural heart disease interventions.

21 www. americanhhm.com AUTHOR BIO AUTHOR BIO
MEDICAL SCIENCES
Let’s Not Put the Genie Back Into the Bottle!
Remote Healthcare & Telemedicine

Remote healthcare and telemedicine have been a presence across digital healthcare circles for the better part of the last 10 years. It has seen numerous iterations, use cases, and leaders. However, it was the COVID pandemic that helped catapult the field to the forefront of healthcare service delivery in New Zealand. There have been plenty of wins, a few lessons learned, and opportunities missed, but the overarching sentiment is that we must not put the genie back in the bottle.
Tom Varghese Sales and Marketing Manager Healthcare I Governance Aceso Health
The global healthcare system is on the brink of collapse. At the start of 2012, the world's population topped 7 billion. More than half of this total is made up of people under the age of 30. We are enjoying longer lives, but we are also multiplying faster than before. While living longer comes with its own set of healthcare worries, the younger generation
22 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
comes with its own set of specific healthcare red flags. These include rising levels of mental health disorders, obesity, diabetes, and prescription medicine addictions, to name a few.
The current healthcare system is not in disrepair. They are acting in accordance with best practices. However, the system may be overburdened, and it is time to reconsider a number of consequences. Perhaps technology can help make the system more effective and ready for the present and future.
Access to healthcare services has always posed difficulties for healthcare providers. Patients are brought closer to help through a variety of channels, including satellite clinics, virtual health, and mobile healthcare services.
The COVID-19 epidemic highlighted a technology solution that has probably been around for more than a decade. Prior to
the pandemic, less than 10% of the world's population used telehealth services. However, the prolonged isolation caused by lockdowns, combined with an almost bizarre fear of crowds, caused the use of telemedicine services to skyrocket.
The forced move to telemedicine during the epidemic revealed use cases that were previously unknown to us. The global pandemic has had a positive impact on provider behavior and increased investment in telemedicine options.

Human connection is at the heart of healthcare. Telemedicine has a significant impact on improving and supplementing human connections. We arrive at the concept of "digital-enabled care" as a supplement to in-person service provision.
For much of the previous decade, remote healthcare and telemedicine have been a
23 www. americanhhm.com
MEDICAL SCIENCES
presence in digital healthcare circles. It has been through several revisions, use cases, and market leaders. The COVID pandemic, on the other hand, was essential in propelling the field to the forefront of healthcare service delivery in New Zealand. There have been many victories, lessons learned, and missed opportunities, but the overall attitude is that we must not put the genie back in the bottle.
Healthcare workers must embrace innovation not only vertically but also horizontally. Fax machines are still the most popular way of communicating in hospitals worldwide. Instead of focusing on what and how perhaps we should reconsider why.
1. While digitization is imperative, we must not digitize our mistakes. The pace of adoption of telehealth services that we witnessed during and immediately after the first COVID outbreak was driven by a dire need rather than a sequentially staged digital transformation.
The repercussions of the inadequate planning associated with the rapid adoption of this technology are currently being felt. Aligning models and provider/patient behavior management have been obstacles to the use of telehealth on a regular basis, post lockdown.
The lesson to be learned centres around the digitization of prior mistakes. For example, the availability of high-speed internet across the consumer base should not be taken for granted. In addition, the change management journey involved in the introduction and adoption of technology within healthcare workflows should not be underestimated.
2. Adapt your language, not your message the basic tenet of any transaction is trust. Establishing trusted lines of communication between the various actors within the healthcare journey is an essential piece of the adoption puzzle. Understanding the pain points and business requirements of the micro elements that make up the healthcare provider will aid in long-term adoption and growth. Telehealth services across New Zealand were implemented without an accepted level of standardisation. Providers were at the behest of the vendor community, with only a few breaking the mould to provide a better healthcare experience.
3. Understand the business of healthcare the fundamental processes in a healthcare environment have not changed much over the past 50 years: finding a provider, booking a time to see them, receiving health information and referrals, and navigating the healthcare system at large. Many solutions are focused on specific points along this journey and are reluctant to join the dots. A seamless experience along the lines of what the travel and banking industries have achieved is still out of reach for most healthcare consumers. Fixing processes rather than problems should be commonplace in healthcare organisations. Technology is the conduit, not the solution. A succession of clicks, followed by log-ins, backups, and the dreaded system slowdown, is not the promised land of digital wellness.
4. Cohesion through collaboration the creation of an ecosystem through the coalition
24 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
MEDICAL SCIENCES
of the willing will lead to widespread innovation in the healthcare sector.

There is a renewed emphasis on outcomedriven, customer-centric solutions. Establishing government-level support for proofs of concept should be an expected process rather than an exception. The adoption of telehealth services in New Zealand led the way in this aspect, with the government offering zero-rated data programmes allowing access to health information websites and services. The next step will involve a collaborative effort between public and private enterprises to provide internet access to large sections of the population who are unable to afford it.
Conclusion
The improvement of healthcare services is contingent on communal work by multiple agencies, not restricted to the healthcare sector alone.
There is a sense of urgency among providers to jump on the digital bandwagon. Because of digital Darwinism, an organization's

survival is no longer dependent on strategy or intelligence.
It depends instead on the ability to adapt. Making the journey through a digital transformation is rewarding, but knowing "why" will keep it going.
References are available at www.americanhhm.com
25 www. americanhhm.com AUTHOR BIO
Dr. Tom Varghese is a sales and marketing manager at Aceso Health. His professional background spans clinical orthodontics, strategic business development, and governance. His passions are people, healthcare, and technology, and his goal is to make healthcare better for all.
MEDICAL SCIENCES
Integration
Uses of AI in Healthcare 26 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 FACILITIES & OPERATIONS MANAGEMENT
of AI into Healthcare Facilities
Deploying Artificial Intelligence (AI) technology to health records is the next step in the evolution of healthcare. More must be done with less, and this technology saves time in analysis of volumes of data, helping clinicians move from assessment to intervention faster, speeding up recovery time. Clinicians are utilizing this technology in multiple ways. Diagnosis is at the forefront. Quicker diagnosis leads to faster response times. The patient is the winner with the use of this technology.
 Lorie Morris Senior Vice President Clinical, Prestige Healthcare
Lorie Morris Senior Vice President Clinical, Prestige Healthcare
Artificial Intelligence (AI) is defined as the intelligence of machines, as opposed to the intelligence of humans or other living species. It usually involves a combination of software and hardware. It also refers to situations wherein machines can simulate human minds in learning and in analysis, and it can work at problem solving. This is also known as machine learning (ML).
Technology has evolved quickly over the past decade, making AI feasible in healthcare. It is becoming an integral part of the healthcare continuum. Utilization of AI technology first became apparent in the diagnostic-imaging. Since that time, its uses have spread across multiple areas, likely impacting all healthcare providers and patients. It is being utilized from assessment to evaluation. This technology has sped up the time from onset of first symptoms to resolution.
AI is transformational technology that includes clinical analytics, machine learning, digitized data acquisition, computer analysis, natural language processing (NLP), Clinical Decision Support System (CDSS), machine vision, data mining, motion analysis, and machine perception. This perspective will look at clinical analytics, machine learning, digitized data, computer analysis, NLP, data mining and machine perception.
FACILITIES & OPERATIONS MANAGEMENT
Case Study
Let’s examine how this technology is impacting one patient’s journey to wellness. When a patient first experiences some type of unusual symptom that is concerning to them, they reach out to their medical professional or seek direct medical care through another entry point to the healthcare system. This may include Urgent Care Clinics, Virtual Healthcare, or Emergency care. This is the point when AI technology may first impact this patient’s outcomes. As medical records are becoming more interoperable, medical professionals have access to patient’s health information, and AI technology can quickly scan these records, or other uploaded documents to assist medical provider to determine “how” current symptoms may be related to past known medical information. The provider can also quickly determine what medications, and possible side affects may be related to current symptoms. The fast speed of reading healthcare data helps providers understand “If” current reported symptoms are related, or “If” a new condition or problem has arisen.
AI software can scan for “key words”, speeding up a search if a specific diagnosis, or symptom has been documented before. This type of technology can scan electronic records for pre-selected words. NLP software can also be utilized to read narrative notations in the medical record. Pre-programmed words or phrases assist this technology to scan documents to convert specific information to a summary version quickly.
For this example, let’s use a case study
example of a patient with new onset of symptoms of chest pain. The patient is presented at the hospital’s emergency room. At intake, the provider accesses the patient’s electronic health record (EHR) and obtains medical history. EHR is quickly scanned using AI technology. Within minutes, medical history reveals that the patient has a history of asthma and anxiety. There is no recent history of an accident, or injury. No history of other medical diagnosis is available and all the problems are noted. Patient reports pain in “mid-chest and mid-back”. “It comes and goes and is sharp and burning, but sometimes feels like someone is pushing against me with pressure”.
The Second use of AI technology will be in the diagnostic phase of care. Radiographic testing will likely be ordered for this patient. Radiography is reliant on imaging technology. This technology helps capture high quality images, and helps interpret what the pictures reveal. Without use of AI technology, the diagnostic phase would be slowed considerably. This technology also indicates possible diagnosis, as well as interventions. Increase in usage of radiography for diagnosis is directly related to advances in imaging technology and computerization. These advancements have benefitted patients with diagnosis and treatment.
Radiology technicians have benefitted from advancements in technology to assist them with machine vision and machine perception. It is easier for the technician to determine if a patient is in the best position to obtain accurate results. This technology also speeds up time by reducing the number of images that must
28 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
FACILITIES & OPERATIONS MANAGEMENT
be taken. Ultimately, it reduces the stress and pain that patient experiences by reducing the number of times they must be moved, or repositioned. Positive consequences of AI technology in radiographic examinations are: increased efficiency and throughput with imaging departments. It has increased accuracy of results, while speeding up the time needed from examination to results.
Machine learning in radiography has had positive effects on outcomes for patients. Algorithms are out- performing radiologists in spotting malignant tumors and have assisted with biomarker testing. AI technology has help improve diagnosis to cure rates for multiple conditions. Design, Implementation, and Evaluation of AI enabled solutions have revealed the importance of marrying data science with disciplines, such as incorporation of evidenced based interventions alongside of automated digital identification.
For our patient, the incorporation of radiologic AI technology helps speed up the time to diagnosis, and improves the accuracy of that diagnosis. Let’s assume that the x-ray’s reveal that the lungs do not show any abnormalities. The EKG shows no
abnormalities in the heart. More time is needed for laboratory tests, but preliminary results are back. Lab results show White Blood Cell counts within normal limits. Red Blood Cells are low, as well as the Hemoglobin and Hematocrit. The computer recommends more diagnostic testing. Machine Learning Software indicates that more testing is needed. Since the levels are significantly low, the decision is made to admit the patient to the hospital. While diagnosis is not completed at this point, the patient’s initial symptoms are being managed, and is comfortable. Total time for this case thus far, less than 4 hours. Prior to AI technology, this time to treatment, thus far, could have resulted in many more hours, and more hours of pain for the patient.
Analysis
Clinical Decision Support System (CDSS)’ main objective is to diagnose the disease efficiently by using previous patient data. Features presenting for a patient can be matched to a computerized pre-existed medical dataset. AI technology recommends the diagnosis. Clinicians combine their knowledge with results from the AI software, and are able to make quicker informed decisions.
According to the National Academies of Science, Engineering, “Diagnostic mistakes lead to roughly 10% of patient fatalities, and 6 to 17% of hospital problems. Diagnostic mistakes, according to experts, are caused by: collaboration and integration of health information technology is inefficient (Health IT), com munication breakdown between physicians, patients, and
29 www. americanhhm.com
FACILITIES & OPERATIONS MANAGEMENT
AI is a transformational technology that has become an integral part of the healthcare continuum.
their families, and healthcare work system that is designed to be insufficiently supportive of diagnostic procedures.
AI driven systems have been shown to outperform humans in critical analysis. Improvements in technology have aided in more accurate diagnosis of Cancer, Cardiac Conditions, and in renal conditions. Precision Medicine is the most common use of AI in healthcare. It predicts what treatment protocols are likely to succeed on a patient based on various patient attributes and in the treatment. Machine learning using a “neural network” has been in development since the 1960’s. It is well established in research, and is commonly used to assist in diagnosing and treating many health conditions.
Rule based systems have been in use since the 1980’s. In healthcare, they have been used in clinical decision support purposes over the last couple of decades. Many EHR providers furnish a set of rules with their systems. It allows EHR records to provide analytic information for reporting.
At the time our patient transfers to the inpatient general medical/surgical unit at the hospital, her care is transferred to a new physician, and a new care team. The nurse completes an additional assessment for admission to the hospital. The Machine Learning Technology that uses Natural Language Processing (NLP) tools will transform health information from previous health information records, medical process notes, and laboratory/diagnostic results assists
the nurse to complete the assessment faster, incorporating relevant data into assessment. This information reduces redundancies in repeatedly asking questions. The technology also assists in recommending interventions and developing a care plan.
AI technology assists to transform aggregates of health information into a usable format. Nearly 80% of information kept or “locked” in electronic health record systems is unstructured data. Machine learning in healthcare frequently uses natural language processing (NLP) tools to transform data in to analyzable data.
Conclusions:
AI in healthcare has a significant place in disease diagnosis and prediction, information processing, saving clinician’s time, speeding time to treatment, and in cost savings to patients and providers. The future of AI in Healthcare seems assured. Research and development have moved healthcare further down the road to acceptance of this technology.
The most challenging problems are in:
• Securing acceptance of this technology
• Cost of securing the technology
Outcomes have proven that this technology is playing a critical role in medical management, and that its usage will continue. The benefits far outweigh the barriers.
AI is most often utilized in healthcare for:
• Help with diagnosis
• Administration of healthcare
• Interpretation of health information
30 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
FACILITIES & OPERATIONS MANAGEMENT
Summary
AI technology has had positive impacts on outcomes for patients. It is likely that the progression of this type of technology will continue to expand. Outcomes across multiple disease conditions have shown reduced total dollars spent with reduction in healthcare tests, number of visits, length of stay in the hospital, and targeting specific treatment with higher cure rates. This technology has reduced the number of hours needed for staff, and the results have been mostly for the good. On the diagnostic side, this technology has shown a smaller error rate than historic results, indicating that this technology, when used alongside human knowledge, can improve overall outcomes. References are available at www.americanhhm.com


31 www. americanhhm.com AUTHOR BIO
Lorie Morris, is currently working as a SVP Assessment Coordination at Prestige Healthcare. She is a Registered Nurse with Master’s in Nursing Education from Western Governor’s University and she has received the BSN Degree from Armstrong Atlantic University. She has worked in post-acute care space to include Skilled Nursing, Home Care, and Hospice for 25+ years.
FACILITIES & OPERATIONS MANAGEMENT
FACILITIES & OPERATIONS MANAGEMENT
Total Lean Medical Record Audit Process via Structured Medical Data
Medical record completeness is crucial for patient care, but the audit process still has a lot of waste. The clinical and quality assurance algorithm integration with structured medical record data is the new approach to a completely lean process, a reduction in error, and real-world improvement in patient care.
Piyanun Yenjit Founder and Managing Director, APUK Co., Ltd

Why do hospitals have to audit their medical records regularly, and why is it important?
As we all know, data in medical records plays a crucial role in patient care, process management, and risk management, particularly legal risk management. Moreover, all hospital quality accreditation
32 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
standards, both local—such as Thai Hospital Accreditation (HA)—and global—such as Joint Commission International (JCI) and Global Health Accreditation (GHA)—emphasize the importance of medical record completeness and issue specific auditing guidelines. Not only in the hospital, but external parties such as payors, the government, and the private sector also pay attention to the data in the medical record. Hence, its completeness affects hospital revenue as well.
Although hospital executives and staff fully acknowledge the importance of complete medical records, the comprehensive medical record audit process remains unsatisfactory and needs to be improved. Most hospitals in Thailand still have issues with medical records, as shown below:
• Inadequate audit: All users should receive feedback on their medical records in an adequate number to make improvements. Even though Yamane's, standard sampling calculation formula, is widely used in Thailand, the sampling usually fails to reach the target for several reasons, including selection bias, which is why the auditor prefers to review the medical records of the good data recorders
• Uncertain reliability: An audit result is still questionable, particularly in areas involving complex information, such as clinical assessment. The auditor's qualification is still doubtful.
• Delay in the audit process and feedback: Due to several limitations,
mainly on staff workload and medical record accessibility, an audit process is often carried out a few months later. It may take more than 4-6 months for the feedback to reach medical recorders, or they may never receive it.
• Source of the medical record: Even though medical records are transforming from paper to paperless, it does not mean that medical records will be 100% adequate and reliable. Medical records should be audited on a regular basis with sufficient sampling.
The above pain points come from several reasons, some of which are external and uncontrollable factors, such as unclear and variable audit standards. Most standards identify concepts, e.g., "appropriate" or "sufficient," that need further interpretation. For example, "When appropriate, the family’s educational needs of each patient are assessed and recorded in the patient’s medical record." Therefore, misinterpretation among auditors may occur. Each hospital's quality accreditations and payer standards

33 www. americanhhm.com
FACILITIES & OPERATIONS MANAGEMENT
have similar or different perspectives. If hospitals use many accreditations, some audit items may conflict with each other or become redundant, causing auditing to be unclear or auditors to become confused. However, the following internal factors are possible to control and improve:to control and improve:
• Auditor qualification and availability: Audit standards are complicated and involve multi-specialties, including hospital quality management. The auditor must be skilled, knowledgeable, and experienced in such areas of specialty. However, due to staff shortages, most Thai hospitals' auditors also have to provide daily services, so they cannot fully pay attention and learn about a medical record audit. Apart from that, the attitude of hospital staff, including executives, is a common barrier. A medical record audit seems to be given a low priority and is considered a nonurgent task. The main objective of audit activities is to prepare for hospital quality accreditation, allowing them to undergo an accreditation review just before accreditation. Therefore, the training resource is not sufficiently invested in an audit.
• Medical record quality and accessibility: Poor handwriting and accessibility to medical records are common issues in a paper-based system. Getting a hard copy from the medical records department is complicated and labor-consuming. There are also issues
with keeping it outside the medical record department during non-office hours, which leads to the risk of unavailable data when the patient comes to the hospital. As for electronic medical records (EMR), there are also accessibility issues. Many auditors are required to review the patient's data even if they did not provide service to the patient. The privacy risk control, which restricts access to medical record data to only staff related to specific patient treatment, becomes a barrier to medical record accessibility.
• Analytic capability: Medical record audit data is big data that is highly complicated to analyze. An advanced data analysis feature is needed. Also, a high-performance business intelligence dashboard is preferable. Hospitals unfamiliar with big data handling and analysis are unlikely to fully benefit from audited medical record data.
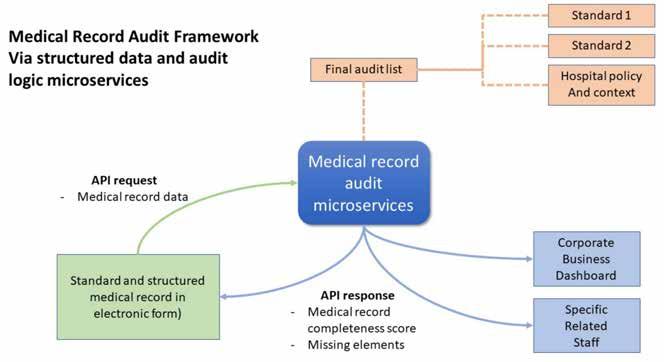
To overcome these challenges, this topic will demonstrate the new approach that totally disrupts the existing medical record audit method, starting from setup to implementing medical record audit logic with IT integration as follows:
1. Standard review: All medical record audit items of all accreditation standards must be reviewed and consolidated by qualified persons who profoundly understand the objectives of the standard. Moreover, knowledge and experience in hospital management, medical care, and hospital context would be helpful. The reviewer must identify which items are
34 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
FACILITIES & OPERATIONS MANAGEMENT
related to the organization and compare similarities across standards; then, the duplicate items must be removed. From this step on, the single list of medical audit items will be ready.

2. EMR field review and audit item mapping: Every EMR screen should be reviewed and mapped with the audit items. This process will be more convenient if the EMR field has identified standard terminology, e.g., SNOMED-CT, Medcin. As for hospitals that use paper-based medical records, the new approach will be impossible. Although HIS in electronic form is already in place, HIS's cooperation is still the biggest challenge. A separate clinical documentation software that already labels standard terminology is a suitable alternative method.
3. Convert a standard into programming logic : If the identified EMR field is a custom code, terminology may be required during an audit of the programming logic conversion. This step is the most challenging because programmers should also have clinical and hospital quality assurance knowledge.
4. User interface development: The audit score, missing element list, and recommendation is helpful for real-time feedback. These could be either pop-ups or links to the full report. The key consideration for the development is "real-time," allowing effective chart review and complete correction before finalizing the document. A fundamental tool for developing these features will likely be available for the modern EMR.
35 www. americanhhm.com
FACILITIES & OPERATIONS MANAGEMENT
5. Monitoring tool development: The dashboard supports executives, the quality management team, and the business unit. It also performs other functions. Committees can access details of the audit results in real-time. The feedback can also reach individual staff, including a doctor, who plays a critical role in medical record completeness. The developer's skill to create a dashboard is not a big challenge because several business intelligence tools are available nowadays. The key success factor is dashboard design. The chart data, type, layout, and analytic design should be done by someone experienced in quality assurance because this is an important part of hospital accreditation. After complete setup and development, as in other new technology implementations, the hospital will face challenges related to changed management and the variety of user skills and knowledge. Effective communication and
training will always be the key success factors. Before everyone recognizes the outcome, like increased medical record completeness, the users will perceive several better experiences, such as:
• Feeling excited by real-time audit results just like playing a game:The structured medical record data will be analysed and the completeness score will be displayed immediately. Most users expected to see a score of 100% and are curious to find the errors when it does not hit the full score. This score is also distributed for hospitallevel indicators, so the turnaround time from complete medical record entry to submitting it to the executive level should be reduced from a few months to a few seconds.
• Completely get rid of the manual process: for well-designed logic, there is no need to process anything manually.
36 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
FACILITIES & OPERATIONS MANAGEMENT
• Everyone will get the same experience: Based on the Yamane solution, the audit coverage increased from 10–30% to 100%. The hospital can ensure that everyone involved receives adequate feedback. Every coin has two sides. This new approach also has some challenges, as shown below:
• Acceptance by related parties: Normally, hospital quality standard organizations, regulators, and payers are familiar with hospitals that follow their standards. So, once hospitals choose to integrate several standards, it will be challenging for some of them.
• Deep understanding of multiple audit standards and integration:Even though some audit items seem similar across standards, only a small portion are exactly the same. Therefore, hospitals need qualified staff to set up custom audit topics based on the hospital's contextual factors.
• Hospital IT capability and Hospital Information System (HIS) integration: Structured data input in the electronic medical
record is the challenging part, as is the programming logic of the audit items.
CONCLUSION
Bangpakok 9 Hospital is an excellent example of successfully implementing this medical record audit approach in a very short period of time. The key success factors are strong governance and management with clear directions that aim to improve the quality of care using lean management. The organizational culture of this hospital also supports consistent electronic medical record usage and user familiarity with digital adoption. Moreover, they wasted no time on audit rule review or logic development. The easiest way to implement this approach is by using ready-to-use microservices for medical record audit that comply with the local standard (hospital accreditation, or HA) and global standard (Joint Commission International, or JCI). With an instantly calculated audit score, the opened chart review percentage increased from 20% to 100%.
References are available at www.americanhhm.com
Piyanun Yenjit is a country manager of HIMSS Thailand and founder of APUK, a healthcare digital transformation consultant and microservices provider, focusing on improvement in patient safety, process efficiency, and business growth. She is also experienced in electronic medical records with structured data implementation compatible with various quality assurance standards.

37 www. americanhhm.com
AUTHOR BIO
FACILITIES & OPERATIONS MANAGEMENT
HOW U.S. HEALTHCARE ORGANIZATIONS CAN LEVERAGE GENERATIVE ARTIFICIAL INTELLIGENCE

The paper examines the potential for generative artificial intelligence (GAI) to positively impact healthcare in the U.S. GAI are programs that allow computers to use data elements such as audio files, images, and text to produce original content. As such, it is artificial intelligence that aims to be creative rather than just to process and synthesize data. GAI has the capability to impact multiple parts of healthcare, including administration, clinical care, and research. This can lead to previously unreached levels of insights into diagnostics, diseases, and even treatments. We also examine the barriers and challenges of GAI implementation.
James Gillespie
Faculty, Saint Mary’s College
Linsey Feit Senior Consultant, Optum
Addie Bobosky
Clinical Specialist, Medical Device Industry
Sophia Senese
Data Analytics Specialist
The Uni healthcare sector is ripe for disruption. In particular, the healthcare technology industry is highly fragmented in the United States, with interoperability challenges (within and between medical organizations) limiting the ability to fully aggregate and analyze data. Fortunately, in terms of data and technology, artificial intelligence (AI) has a particularly large potential to positively impact healthcare across the U.S. health ecosystem. Within the AI domain, a growing field of interest is
38 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
INFORMATION TECHNOLOGY
generative artificial intelligence (GAI), which has the capability to impact multiple parts of healthcare for U.S. provider organizations, including administration, diagnosis, research, and treatment. It can both enhance quality and improve productivity (i.e., attain both effectiveness and efficiency). The integration of AI in certain areas of healthcare, such as medical imaging (e.g., detect cancer on medical scans), is fairly advanced, benefitting greatly from previous research in computer vision, but in many other areas, AI is in the infancy stages of development, testing, and implementation. For example, IBM’s AI-driven supercomputer Watson tried to address a broad set of healthcare challenges, including helping physicians diagnose diseases and recommending participants for clinical trials, but it ultimately has experienced only mixed success. Adopting AI in healthcare will be slow and difficult in the U.S., including with GAI. However, as we discuss, the potential for GAI to positively impact multiple domains in the healthcare ecosystem is tremendous.
Importance of GAI
Generative AI models are sometimes called “foundation models”. In some ways, these models are an entirely new approach to AI, in part because they are able to have a large impact in working with comparatively smaller data sets. Generative AI is currently at a nascent stage, but its impact is likely to grow as new applications continually develop. GAI does have the potential to generate trillions of dollars in economic value in the U.S. and internationally. By 2025, generative AI is projected to account for 10% of all data produced globally. In the long run, there is little doubt that AI will usher in fundamental, world changing innovations.

INFORMATION TECHNOLOGY
GAI is not a new idea, but it has reached a new threshold. Over the past year, machines rather suddenly --or so the pace seemed-became really good at generating completely new images and writing “original” text. Why is this emerging now? There are at least four reasons. First, the corpus of content (i.e., data) continues to increase rapidly, pulling from audio, video, and text sources. Second, there is greater storage capability. Third, processing power (i.e., speed of computation) continues to increase substantially. Fourth, algorithms have gotten considerably better.
Many experts and investors believe generative AI technology will usher in a productivity revolution across various industries, giving birth to massive companies in the process. GAI does hold the potential to eventually transform application software and workflows across many American hospitals and other healthcare organizations. While GAI models have shown rapid innovations over the past couple of years, that does not guarantee continued improvement at the same speed. AI does have a history of overpromising and underdelivering on the investor, practitioner, and societal expectations. For example, self-driving car technology has been promised and promoted for years in Europe and the U.S., but thus far, autonomous vehicles have only been deployed in a few limited pilot programs. However, the impact of GAI on fields such as healthcare is certainly more a matter of “when” not “if”.

What is GAI?
GAI are programs that allow computers/ machines to use data elements such as audio files, images, and text to produce content. As such, it is artificial intelligence that aims to be creative rather than just to process and synthesize data. Generative AI can be used to produce original content on behalf of healthcare organizations. For instance, a GAI application looks at 100,000 samples and then aims to create the 100,001st sample itself. Generative AI is one of the most promising advances in the AI ecosystem in the past decade. GAI results in the creation of higher quality outputs as the machine self-learns from every data set. This permits the computer to comprehend, evaluate, and leverage new abstract, conceptual, and ideational principles. Unsupervised learning allows AI to more quickly acquire adaptable transferable skills that increase accuracy, effectiveness, and speed relative to typical human efforts where little employee training is required. As such, this technology has the
40 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
INFORMATION TECHNOLOGY
capability to be tremendously beneficial for U.S. healthcare, life sciences, and medical organizations.
Generative AI creates new content by powerfully utilizing existing content. It references AI techniques processing data (text, image, audio, and video), utilizing them to create new original content that preserves similarities to original data. GAI models can pull from almost all available information on the internet, a data resource that obviously continues to grow rapidly, roughly doubling in size every two years. For example, text-oriented GAI models can examine thousands of digital books and trillions of words on the internet. GAI can enable machines to automatically control and regulate environments by taking action to accomplish definable goals. It can even create neural networks that imitate and mimic human brain activity. These capabilities are growing at a steady pace, including learning complex patterns in a repetitive nature similar to the human brain.
Leveraging state-of-the-art generative technology that learns new patterns, structures, and variations automatically using existing data, the industry is now developing realistic simulations and representative synthetic data at scale. Also, via video synthesis technology, GAI companies are implementing innovative visual content creation that reduces cost, improves quality, and lowers language barriers. GAI can leverage unsupervised learning algorithms to build new plausible content based on existing content, allowing machines
to understand patterns in the input content and then generate similar content. Typically, during the training, GAI models are provided with limited parameters; this allows the model to yield its own conclusions about the most essential characteristics of the data. In theory, which makes GAI more capable of creating results free of the normal biases attendant to human comprehension, experience, and thought processes. In contrast, many traditional AI learning models have proven vulnerable to becoming discriminatory and skewed.
Generative AI can train neural networks even without access to all the training examples. Instead, we can provide the network with sufficient examples to learn the underlying structure of a problem. Then, after the model has learned this structure, we can generate more samples leveraging this knowledge. GAI can be taught to generate fake examples of underrepresented data that help develop and educate the model. Overall, one primary aim of generative intelligence is to identify new cases before they materialize, while also developing a recommended course of action.
Healthcare Applications
Artificial intelligence, including GAI, can be used to disrupt the healthcare industry. In terms of healthcare specifically, how are and how will U.S. healthcare organizations leverage GAI? These can be placed into five large buckets: (i) clinical, (ii) privacy/security, (iii) administrative, (iv) fraud detection, and (v) drug discovery.
41 www. americanhhm.com
INFORMATION TECHNOLOGY
First, from a clinical perspective, generative AI can help enhance patient treatment. GAI-powered applications enable computers to produce new content based on existing information, so they can be used to create fake cases for underrepresented data, which substantially enhances development and training of the model. For example, in the case of X-ray images, it can supply various additional “fake” angles to visualize potential tumor growth outcomes, or it can be utilized to contrast the image of healthy organs with affected ones to help detect malignant developments. In the case of retinopathy diagnosis, this can be leveraged to create new medical images for diagnosis and testing (e.g., helping detect malignant developments by contrasting images of healthy organs from the databank to the affected one or to visualize possible tumor expansion by computing different angles of an x-ray image). GAI can also enable early detection of certain conditions for effective treatment options.
Second, GAI can strengthen privacyprotecting applications. Data de-identification is a significant problem for healthcare analysts. The reversal process can compromise sensitive and valuable patient records as it can lead to full identification. GAI provides a potentially promising solution. It can strengthen privacy and security for patients. It can help secure the reversal process to make it more penetration-proof and less susceptible to data de-identification. Also, generative AI avatars can be used to protect the identity of patients
in the virtual care setting, particularly for patients who may not be fully comfortable with disclosing their identities in certain cases. GAI holds significant potential for American healthcare organizations to enhance the privacy and security of patient data.
Third, GAI can help with the administration and management dimensions of healthcare organizations. Primary care physicians spend twice as much on administrative and clerical tasks, including EHR entry, as direct patient care. Leveraging GAI-based technologies, (e.g., natural language processing and voiceto-text transcription), administrative and clerical activities such as completing EHR notes, filling prescriptions, and ordering tests can be substantially automated. This would also help improve physician satisfaction and reduce burnout rates. It would be particularly advantageous if one could leverage computer vision sensors and microphones hardware, coupled with a deep learning model software, to automatically and simultaneously convert patient-physician conversations into clinical documentation. Relatedly, healthcare
42 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
INFORMATION TECHNOLOGY
Generative AI models are sometimes called “foundation models” as they can impact various parts of healthcare and can work with comparatively small data sets.
organizations can use GAI to create new patient records that are then inserted into the system to enhance accuracy. In the business development domain, some companies are using AI to help automate highly repetitive tasks such as blog posts or sales emails. Thinking even more ambitiously, GAI can use audio synthesis to generate a computer voice very similar to a human voice, which can be used for communicating with patients and narration for videos.
Fourth, GAI can be used to help organizations detect the significant fraud, waste, and abuse that afflicts the U.S. healthcare ecosystem, as it does globally. GAI can automate fraud analysis to detect fraudulent transactions leveraging predefined algorithms. According to an analysis of one healthcare market from McKinsey & Company, nearly three-fourths of received health claims are flagged as unusual for manual review via audits, but only about one-tenth of these cases are successfully investigated. GAI can be used to identify and isolate malevolent activity.
Fifth, GAI can play a crucial role in drug discovery. By 2025, it is estimated that half of drug development initiatives will rely on generative AI. GAI is able to create molecular structures of drugs employed in curing certain indications. The treatment of new diseases can be accelerated when GAI is used to perform a rapid database search of compounds applicable for utilization. GAI can also be used to create organic molecules and prosthetic limbs from scratch with 3D printing. GAI can also help
with drug development. For example, GAI was used to research antimicrobial peptides (AMP) to find drugs for Covid-19. Over the long-term, this means GAI has the power to improve the quality and speed of drug development, which has positive implications for both providers (who are the entities that tend to administer clinical trials and prescribe drugs) and pharmaceuticals (who are the entities that tend to design and pay for clinical trials).
Challenges
While the overall future is exceptionally bright, GAI does present several challenges for full adoption by American health leaders and managers. First, because of their underlying complexity, GAI models can sometimes be unstable and difficult to control – often leading to unexpected, unexplainable outputs. This stochastic element is conducive to creativity and originality, but the healthcare environment generally prefers controllable, expected, explainable, and stable outputs. Thus, there will be an ongoing challenge for healthcare institutions in the U.S. who adopt GAI to resolve this inherent tension of creativity/ originality versus unpredictable/unexpected.
Second, a significant amount of training data is needed to train GAI, so it is more expensive to implement given the requirement of significantly greater processing power. Third, while GAI can create new content by combining data provided in new ways, it cannot create completely new things. Machines struggle to comprehend highly abstract concepts
43 www. americanhhm.com
INFORMATION TECHNOLOGY
encountered in real and virtual healthcare environments. Fourth, just as it can be a force for good, GAI can also be used by bad actors for untoward purposes such as generating fake news stories, developing sophisticated fraud schemes, and violating patient privacy. Fifth, artificial intelligence applications in healthcare, including GAI, can seem like a “black box” and thus untrustworthy to patients and providers. Thus, over time, a lack of trust by patients and providers will likely be a key roadblock to achieving greater use of AI across the healthcare ecosystem.
Conclusion
The future of generative artificial intelligence in the U.S. healthcare ecosystem is indeed promising. The most compelling use case for Generative AI-powered applications is original content creation based on existing information. GAI programs can use deep learning techniques to train themselves on massive amounts of data from actual patients and then generate new images based on those patterns. This technique allows GAI to create new data sets that humans could never have developed within any limited space and time. To further improve accuracy, the apps can then compare generated content against real-world data, allowing them to analyze huge quantities of data quickly and efficiently. In turn, this can lead to previously unreached levels of insights into diagnostics, diseases, and even treatments. GAI can be the basis for many applications in healthcare, and as the technology continues to develop and evolve, it will be finetuned to integrate more advanced applications.
AUTHOR BIO
James Gillespie is a faculty member in business administration and global studies at Saint Mary’s College, Notre Dame Indiana. His education includes Northwestern University, PhD, MS; Harvard University, JD; Princeton University, MPA; and Massachusetts Institute of Technology, BS.

Linsey Feit is a Senior Consultant at Optum, part of UnitedHealth Group, where she leverages innovative technology to solve problems faced across all facets of healthcare. Her other ventures include pro bono efforts surrounding digital healthcare transformation, diversity and inclusion, and improving the accessibility of healthcare as Co-Founder of LIKE Ventures.
Addie Bobosky is a graduate from Saint Mary’s College, Notre Dame Indiana. She currently works as a Clinical Specialist for Regional Anesthesia.


Sophia Senese is a thirdyear business student at Saint Mary's College, Notre Dame Indiana. She has expertise in data analytics.

44 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
INFORMATION TECHNOLOGY
Artificial Intelligence in Healthcare – Machine Learning for Clinical Outcome Prediction in Cerebrovascular Disorders
Clinical prognostic models help clinicians tailor treatments for alterations in the brain-body interface to maximize chances of survival and recovery after aneurysmal subarachnoid hemorrhage. This article uses regression analysis, classification and regression tree analysis, as well as machine learning technique of artificial neural networks to create a prognostic decision making tool for cerebrovascular disorders.
Benjamin W. Y. Lo
MD PHD FRCSC Department of Neurological Surgery Lenox Hill Hospital
Clinical outcome prediction model was created using the 3551-patient Tirilazad database to investigate clinical factors that influence outcome in patients with ruptured brain aneurysms ( Figure 1). Dependent variable used for statistical analysis is the dichotomized Glasgow Outcome Score (GOS) at three months post aneurysmal subarachnoid hemorrhage. Good outcome represents functional independence (GOS 5 or 4). Poor outcome represents functional dependence (GOS 3), persistent vegetative state (GOS 2) or death (GOS 1).
45 www. americanhhm.com
INFORMATION TECHNOLOGY
Regression Analysis
The main effects logistic regression model confirmed the significance of neurological grade, age, stroke, and time to surgery in outcome prognosis in aneurysmal SAH ( Table 1).
This study also demonstrates that the odds of poor neurological outcome is increased by a factor of 4 in aneurysmal SAH patients who develop post-admission strokes (OR: 4.03, 95% CI: 2.11–7.69, p < 0.01). Cerebral infarction after aneurysmal SAH may occur early after aneurysmal rupture or in a delayed manner.
7-REPERFUSION
Factors associated with the development of cerebral infarction include admission neurological status, treatment related complications, and occurrence of symptomatic vasospasm.
In addition, we make the observation that development of cerebral edema, in the context of history of hypertension and liver disease, has a significant impact on neurologic outcome deterioration in aneurysmal SAH. By itself, the development of cerebral edema may predispose the aneurysmal SAH patient to poor neurological outcome. Examination of systemic
8-MICROCIRCILATORY THROMBI & SPASM
6-PERILESIONAL & CORTICAL SPREADING ISCHEMIA
2-INCREASED INTRACRANIAL PRESSURE
SPECTRUM
3-ANAEROBIC METABOLISM & LACTIC ACIDOSIS
9-IMBALANCE BETWEEN OXYGEN SUPPLY & DEMAND
10- NEURONAL MEMBRANE DYSFUNCTION & RELEASE OF EXCITATORY NEUROTRANSMITTERS
5-INCREASED OSMOTIC PRESSURE
4-CEREBRAL EDEMA
12 - CELL-MEDIATED APOPTOSIS
11 - DEOXYHEMOGLOBIN DECREASED NITRIC OXIDE OXYHEMOGLOBIN INCREASED ENDOTHELIN-1 REACTIVE OXYGEN SPECIES CALCIUM INFLUX
46 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
PRIMARY INJURY SECONDARY INJURY
INFORMATION TECHNOLOGY
1-ANEURYSM RUPTURE
factors revealed that aneurysmal SAH patients with a history of hypertension and development of cerebral edema have 2.7 fold increased odds of poor neurologic outcome (OR: 2.66, 95% CI 1.59–4.45, p< 0.01). Patients with a history of hypertension are prone to defective cerebral autoregulation. When disrupted cerebral autoregulation is present after aneurysmal SAH, brain engorgement can occur as plasma proteins leak from capillaries with increased permeability. Extracellular vasogenic edema may follow as a result of increased hydrostatic pressures, with a predilection for posterior cerebral circulation territories.

This study also makes the observation that development of cerebral edema in aneurysmal SAH patients with a history of liver dysfunction markedly increases likelihood for poor outcome (OR: 5.47, 95% CI: 1.13–26.46, p = 0.03). Similar to patients with hypertensive history, patients with chronic liver disease have been shown to have altered cerebral autoregulation and cerebral blood flow with decreased cerebral blood flow in the anterior
cingulum and increased blood flow in the basal ganglia and occipital lobes at baseline. In acute states of ruptured cerebral aneurysms, these patients’ blood brain barriers become disrupted with marked increased cerebral blood flow secondary to luxury perfusion, thus, predisposing them to development of vasogenic edema. In addition, cytotoxic osmoregulatory mechanisms are involved whereby astrocytes swell secondary to the toxic effects of ammonia and glutamate. The end result is a vicious cycle of neuronal swelling and death, a marked increase in cerebral blood flow (cerebral hyperemia), and cerebral edema. It is important, therefore, to prevent the development of hepatic encephalopathy and monitor for cerebral edema in aneurysmal SAH patients who have chronic liver dysfunction.
Seizures increase mortality after cerebral aneurysmal rupture. In this study, we observed that seizures in the clinical setting of post–admission fever and background history of myocardial infarction significantly increase morbidity and mortality. The epileptic aneurysmal SAH patient who develops post–admission fever is predisposed to poor outcome (OR: 2.39, 95% CI: 1.86–3.06, p< 0.01). Fevers increase cerebral metabolic rate and can exacerbate the secondary injury. Early onset fevers can be secondary to dysfunction of temperature regulation centers in the hypothalamus whereas late onset fevers are more likely to be infectious, but can include fevers secondary to central damage, drugs, deep venous thrombosis andpulmonary embolism.
47 www. americanhhm.com
INFORMATION TECHNOLOGY
Exogenous and endogenous pyrogens increase the propensity for fevers and seizure development. In febrile states, inflammatory cytokines increase neuronal excitability via temperature sensitive ion channels leading to the increased likelihood of synchronized neuronal activity. Not only is it essential to monitor, prevent and treat both seizures and fevers themselves, it is also important to search for underlying etiologies, including infections, venous thrombosis and pulmonary embolism, drug-drug interactions and delayed strokes which may alter seizure thresholds in the febrile aneurysmal SAH patient.
Lastly, our regression analysis makes the observation that seizures in the setting of a history of myocardial infarction increase the odds of poor outcome by a factor of 3.05 (95% CI: 1.35–6.87, p = 0.01). Repetitive autonomic stimulation can occur in the actively seizing aneurysmal SAH patient in a lock-step phenomenon, which can trigger the development of cardiac ictal arrthymias. Continuous cardiac sympathetic discharges
and cortical epileptiform activity can occur in a synchronized time-locked manner. These repetitive synchronized autonomic sympathetic discharges lead to cardiac ischemia and structural damage to the myocardium. In aneurysmal SAH, patients with pre-existing coronary artery disease and seizures, the propensity of cardiac ischemia is increased, along with potentially fatal multi-systemic complications, including development of neurogenic pulmonary edema and respiratory suppression associated with fatal cardiac tachyor brady-arrthymias, or cardiac asystole. Multi-system critical care cardiovascular and respiratory supports, therefore, are essential in these epileptic aneurysmal SAH patients in order to maximize their chances of survival.
Aneurysmal Subarachnoid Hemorrhage
Prognostic Decision Making Algorithm using Classification and Regression Tree Analysis
Clinical prediction tools facilitate the process of prognostication and clinical decision making for both clinicians and patient families. In the 3551-patient Tirilazad database, unfavorable
48 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 Variable Terms Odds Ratios 95% Confidence Intervals p value Neurological grade 2.06 1.83-2.32 <0.01 Age (per year) [For every ∆5 years] 1.06 [1.28] 1.05-1.07 [1.22-1.42] <0.01 Time to surgery (hour) 1.01 1.00-1.02 0.02 Stroke 4.03 2.11-7.69 <0.01 Seizures by fever on day 8 2.39 1.86-3.06 <0.01 Brain edema by hepatic disease 5.47 1.13-26.46 0.03 Brain edema by hypertension 2.66 1.59-4.45 <0.01 Seizures by myocardial infarction 3.05 1.35-6.87 0.01
INFORMATION TECHNOLOGY
outcome (functional dependence, persistent vegetative state, and death) at three months after aneurysmal rupture was observed in 1061 (30%) of patients. Our current classification and regression tree makes use of the two most frequently retained clinical
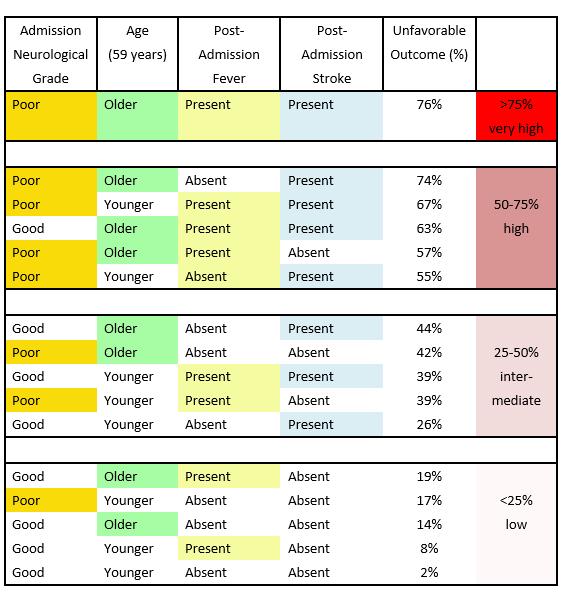
outcome, namely, neurological grade and age. It also demonstrates the significance of both post-admission stroke and fever in outcome prediction (Table 2).
In the present study, the occurrence of post-admission stroke increases the
49 www. americanhhm.com
INFORMATION TECHNOLOGY
proportion of unfavorable neurologic outcome in aneurysmal SAH patients originally presenting with favorable admission neurological grades by 30%. Patients experiencing vasospasm are at an increased risk of post-admission strokes. In addition, several secondary injury cascade events may predispose these patients to post-admission strokes, including: (1) microthrombi formation, (2) cortical spreading depression, (3) microvascular constriction, (4)
proliferation of pro-inflammatory cascade, (5) presence of blood–brain barrier disruption, and (6) inadequate collateral circulation.
Fever is often a clinical indicator of neurological deterioration because it also triggers events in the secondary cascade of neurological injury. The various causes of post-admission late onset fevers, including nosocomial infections, central neurological injury, thromboembolic events, and drugdrug interactions, can lead to neurological
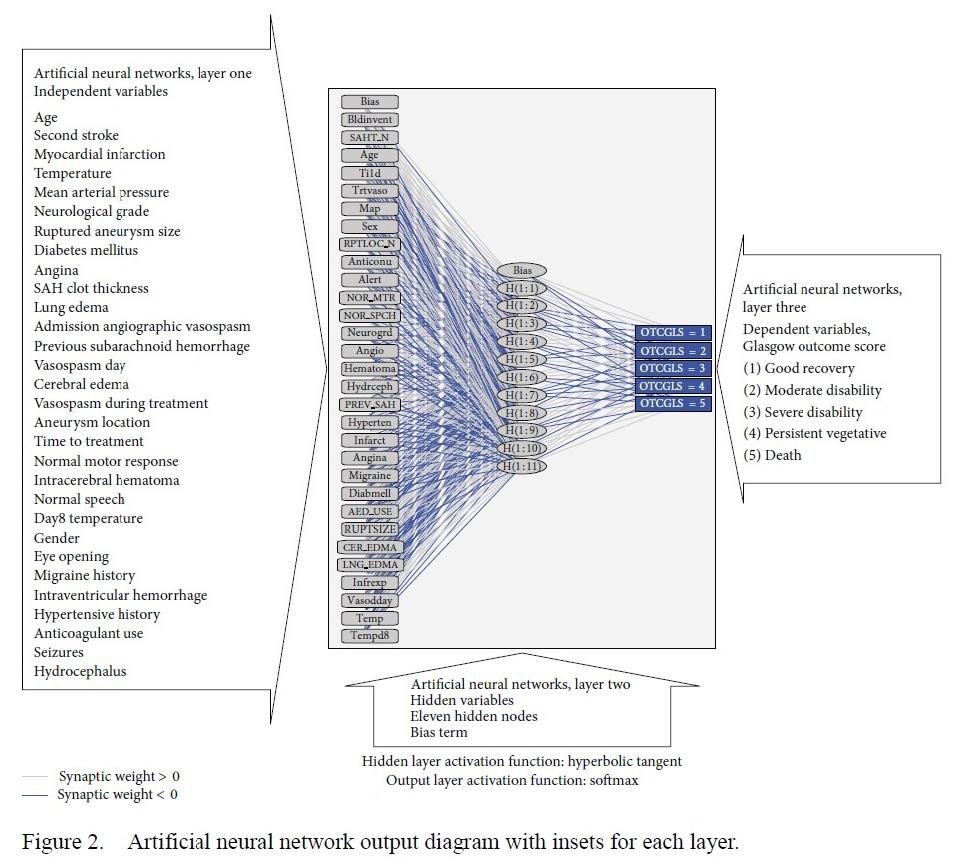
50 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
INFORMATION TECHNOLOGY
complications, including increased intracranial pressures, cerebral edema, and post-admission strokes. Aggressive symptomatic control and rigorous search for underlying etiology are, therefore, warranted.
Clinical Outcome Prediction in Aneurysmal Subarachnoid Hemorrhage using Machine Learning Techniques
Exploratory analysis using artificial neural networks reveals the complexity of brain-body interactions in aneurysmal subarachnoid hemorrhage ( Figure 2). In addition to the aforementioned variables, other variables, not directly measured, also influence clinical outcomes in aneurysmal subarachnoid hemorrhage patients. These include:
1. Disrupted cerebral autoregulation contributing to both ischemia and cerebral edema after subarachnoid hemorrhage.
2. Biochemical markers of brain injury predisposing to cortical spreading depression.
3. Cellular markers demonstrating physiologic dysfunction (such as mitochondrial dysfunction as reflected by the imbalance of oxygen supply and consumption).
4. Genetic factors affecting the outcome (such as inheritance of genetic markers predisposing to micro-thrombotic events in the cerebral microvasculature disrupting cerebral blood flow).
5. Multiple drug-drug interactions, especially in the elderly aneurysmal subarachnoid hemorrhage patient population with multiple pre-existing comorbidities, and
6. Multi-organ systemic dysfunctions, including interactions between the central nervous system and neuro-endocrinologic, metabolic homeostasis, hematologic, hepatic and splenic systems.
Conclusion
Using clinical prognostic models, the clinician can tailor individual specific treatment efforts to prevent and treat various alterations in the brain-body interface in order to maximize the chances of survival and recovery after aneurysmal subarachnoid hemorrhage.
References are available at www.americanhhm.com
W Y Lo is a Neurosurgeon and Neuro-ICU specialist. His clinical focus is cerebrovascular disorders. His research focus characterizes brain-body interactions in Neurocritical care patients with cerebrovascular disorders. Dr. Lo’s qualifications include FRCSC certification in Neurosurgery (2009), FRCSC certification in critical care medicine (2011), and MSc and PhD degrees in clinical epidemiology and biostatistics from McMaster University, Canada. His clinical experience includes working as a neurosurgeon and neuroICU specialist at St. Michael’s Hospital, University of Toronto; Montreal Neurological Institute & Hospital, McGill University; and Northwell Health Lenox Hill Hospital, Manhattan, New York.

51 www. americanhhm.com
AUTHOR BIO
INFORMATION TECHNOLOGY
CHANGING THE FUTURE LANDSCAPE OF ORGAN TRANSPLANTATION WITH ARTIFICIAL INTELLIGENCE 12 LEAD ELECTROCARDIOGRAMS

The increased use of artificial intelligence (AI) in medicine has not yet permeated the field of organ transplantation. Our current capabilities of predicting patient survival or organ rejection remain limited and require invasive biopsies. Using AI to improve outcomes with non-invasive standard testing through 12-lead electrocardiograms (ECG) has allowed us to predict outcomes after heart transplantation. We continue to expand the research and utilization of this capability in the fields of liver and kidney transplantation.
The explosion of artificial intelligence (AI) in healthcare over the past decade has increased exponentially year over year. Continued advances have made it easier for data-minded and clinically oriented providers to efficiently utilize data with automated research and product development tools. Organizations are now understanding the value of big data and using machine learning (ML) algorithms and other cognitive technologies in the
MBBS
Division of Advanced Heart Failure and Transplant
Mayo Clinic
Rohan M. Goswami
MD
Director of Heart Transplant Innovation and Research
Mayo Clinic
52 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
Smruti Desai
INFORMATION TECHNOLOGY
medical setting to diagnose diseases and improve treatment pathways for patients –on the heels of implementing these solutions for billing and revenue capture.
Feeding large amounts of patient data and other linked information through a data analytics platform, helping them to learn independently, and developing a unique algorithm that can recognize hidden or complex patterns for the benefit of patients and institutions is taking shape in many areas across the US and the world.
A key stumbling block, however, has been the development of clinically relevant platforms to help create processes and workflows. Over the past few years, ML has complemented clinical practice in the settings of automated image interpretation and data extraction from electronic health records (think CMS audit) and now begins to enter the realm of precision medicine. Companies have developed and validated ML algorithms and translated them into commercially available tools approved or cleared by the Food and Drug
INFORMATION TECHNOLOGY
Administration (FDA) for use in clinics. Based on currently available information from the FDA and recently published data, most of these devices and applications remain within the radiology and cardiovascular clinical spaces. However, exponential growth and adoption in the healthcare industry will surely change that over the next decade.
Within the United States and abroad, cultural trends have also highlighted the role of the merger of healthcare and artificial intelligence technologies, namely the Apple Watch and its integration of ML technology to interpret your heart rhythm and record a single-lead electrocardiogram (ECG) to assess for atrial fibrillation. The broader utilization of ML in cardiovascular medicine has been established in multiple settings. In the recent era, ECG analysis has been the most developed machine learning algorithm in cardiology.
A key reason for the continued growth of AI techniques used in cardiology can be directly associated with heart failure. New heart failure patients are diagnosed at a staggering rate of nearly 550,000 per year in the US. Admissions and readmissions have continued to increase, despite programs focused on decreasing them from 2010 – 2017 between 18 and 31%. Despite expanding the use of ML in cardiac diseases – end-stage heart failure and organ transplantation have not been a critical priority. Artificial intelligence in predictive medicine has not yet blossomed within the field of organ transplantation. As such, the progression of disease burden is not
something intervenable by AI, at least not yet. Considering this and the extensive use of AI and ECG, we at Mayo Clinic in Florida have used this to optimize outcomes of the sickest patients – those necessitating heart transplantation. Understanding the nuanced interactions of the neurohormonal cascade, environmental factors, and patient-specific genetic mutations remain out of reach for many practitioners, data sets, and ML capabilities.
Our unique position at Mayo Clinic, with large data sets, blood banks, and genomic information, allow us the capability to develop new and innovative models. The current practice for predicting organ rejection after heart transplantation remains barbaric. We are utilizing catheters with ‘jaws’ on the end to sample donor heart tissue as the standard of care. Novel methods of cell-free DNA from blood work exist but are in infancy, without significant adoption when looking at highvolume transplant centers. Using AI to improve outcomes with non-invasive standard testing through 12-lead ECG has allowed us to begin to understand what is involved in predicting,
54 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
Using AI to improve outcomes with non-invasive standard testing through 12-lead electrocardiograms (ECG) has allowed us to predict outcomes after heart transplantation.
INFORMATION TECHNOLOGY
with some accuracy, outcomes after heart transplantation.
Our preliminary proof of concept data, published and presented at the 2022 International Society of Heart and Lung Transplantation (ISHLT), demonstrated the utilization of ECG after heart transplantation to establish for the first time a new parameter –Physiologic (Heart) Age (7). Based on this and the recipient’s chronologic age, we determined high-risk or low-risk patient clusters for potential rejection based on our retrospective data. As this is a hypothesis-generating study, the results of which are helping future providers assess for risk of potential post-transplant rejection – future studies comparing ECG prediction and biopsy results will shed light on the possible use of this in real-time; for example – imagine your patient using a 12-lead hand-held or Apple watch based ECG, remotely transmitted to an on-call provider – enabling the highly accurate prediction of potential rejection based on patient symptoms and the initiation of upstream management of medical therapy and interventions – a possibility in the not so distant future!
Moreso, the pathway forward is not only prolonging life, but early intervention to prevent organ failure. End-organ damage after progressive heart failure is a cascade that continues to topple over time. Machine learning interventions using patient data have allowed us to understand the potential for temporary mechanical circulatory support devices (tMCS, e.g., Impella, ECMO, and
TandemHeart) and the potential for both cardiac and non-cardiac organ recovery. Cardio-renal syndrome, a large swath of patients with progressive renal failure after heart failure, is a crucial area for this technology to be applied. Renal replacement therapy with dialysis allows for increased survival for some but significantly decreases the quality of life.
Early patient-based real-world case series from our center demonstrates the ability for tMCS in six patients with end-stage heart and kidney failure awaiting heart transplantation to exhibit renal recovery – not requiring heart and kidney, but only heart transplantation – which is known to affect their short- and long-term survival. Understanding clinical factors that may not have previously been elucidated with conventional research highlights a standout characteristic of ML in medicine.
Increased access to data with collaborative partnerships remains the last mountain to climb. Understanding the benefit of multiInstitutional data, varied populations, and increased diversity within similar disease states will only help underscore common trends –
55 www. americanhhm.com
INFORMATION TECHNOLOGY
detected through machine learning – applicable to all patients. These new diagnostic criteria may allow us to evolve beyond those factors that, as providers, we use today to predict diagnoses and therapeutic responses.
Limitations in increasing the survival of patients beyond that of currently available traditional medicine drive the field of organ transplantation and regeneration towards a future that has the potential to break the barriers of current survival while maintaining
AUTHOR BIO
both quality and quantity of life. Artificial intelligence integration within the practice of transplant medicine can potentially optimize post-transplant survival. Further translational projects continue to progress toward the demonstration of validity and safety in the clinical setting. Financial burdens of innovation, ethical considerations, and regulatory organization policies will hopefully navigate this future in a way that can create an equitable application of artificial intelligence for both diagnostic and therapeutic applications – while keeping the innovation fires burning as more and more promising results are seen – impacting both patients and providers alike.
References are available at www.americanhhm.com
Dr. Goswami is a Transplant Cardiologist practicing at Mayo Clinic in Florida. He is a graduate of the American University of the Caribbean School of Medicine and completed his internal medicine residency at Columbia University College of Physicians and Surgeons – Stamford Hospital, a cardiology fellowship at The University of Tennessee Memphis, and a Transplant Fellowship in 2017 at Mayo Clinic in Florida. He has a keen interest in clinically focused artificial intelligence research to improve outcomes in patients with advanced heart failure. He has published articles in the field of both heart transplantation and artificial intelligence, as well as presented at Ai4 in 2020 on the future impact of AI in healthcare and invited lectures at the International Society of Heart and Lung Transplantation in both 2021 and 2022. He looks forward to one day utilizing AI integration to prevent organ failure.

Dr. Desai was born in Gujarat, India, and raised in Troy, Michigan. She is a graduate of the Surat Municipal Institute of Medical Education and Research. She is currently a Research Fellow at the Mayo Clinic in Jacksonville Florida’s Division of Advanced heart failure and Transplantation. She looks forward to a promising career as a cardiologist in the future as she hopes to begin her Residency training in internal medicine in 2023.

56 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
AUTHOR BIO
INFORMATION TECHNOLOGY
The Future of Precision Medicine in Healthcare
Precision health involves individualized approaches to patient risk screening and prevention, earlier and more accurate disease diagnosis, and personalized treatment decisions. The future of precision medicine involves population data collection and artificial intelligence approaches to integrate multi-omic information from electronic health records to improve health care quality, safety, and value.
Mai-Lan Ho
MD
Radiology Professor Nationwide Children's Hospital
The Ohio State University
Multi-omics and Theranostics
The Precision Medicine Initiative was established by the United States government in 2015 to better customize patient health care delivery based on unique genetic, environmental, and lifestyle characteristics. These goals are commonly summarized as “P4”: predictive, preventive, personalized, and participatory. In other words, precision health seeks
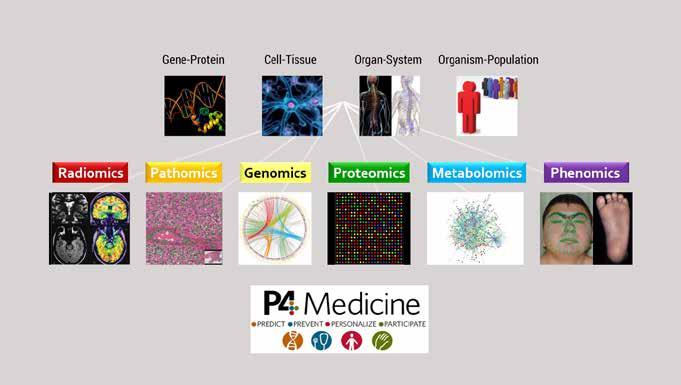
57 www. americanhhm.com
DIAGNOSTICS
to achieve better risk screening and disease prevention, earlier and more accurate patient diagnosis, personalized care and treatment regimens, and fully participatory decision making among patients and clinicians.
In current practice, most precision medicine efforts are based on individual genomic information: prediction of disease risk; drug, chemotherapy, and radiation susceptibility; enzyme replacement and gene therapy for single-gene disorders; and molecular therapy, immunotherapy, and cell therapy for oncologic diseases. On a larger scale, tremendous progress has been made in systems medicine, which integrates biochemical, physiologic, and environmental information on multiple scales to understand the mechanisms of health and disease. The “bottom-up” approach utilizes “omics” technologies—such as
genomics, transcriptomics, proteomics, metabolomics, metagenomics, and phenomics—to collect and synthesize large volumes of molecular data. The “top-down” approach models organisms as complex mathematical systems in order to reproduce specific biological functions or phenotypes.
Theranostics is an emerging field that combines diagnostics and therapeutics. Recent updates by the World Health Organization emphasize the concept of oncologic “layered reporting” with integrated diagnostic information from genomics, pathology, and radiology. Sequential diagnosis and treatment are also becoming a reality with cutting-edge technologies such as molecular imaging and nanotherapeutics; image-guided interventions; and real-time biosensors and biofeedback.
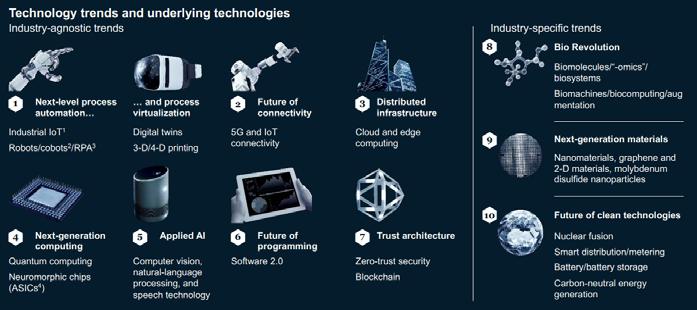
58 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
DIAGNOSTICS
Artificial Intelligence
A key requirement for precision medicine is the ability to share, curate, and aggregate large quantities of data for analysis. Given the vast heterogeneity of clinical practice, there must be stringent governance standards to protect patient privacy and security, as well as systems interoperability to facilitate access, deidentification, and sharing of electronic health records. Many novel informatics platforms and digital health innovations are being driven by partnerships among academic, government, industry, and public stakeholders. These parallelsocietal technology trends including automation, virtualization, interconnectivity, and artificial intelligence (AI).
AI solutions are rapidly transforming medicine due to massive gains in computing power and infrastructure, as well as the innovation pressures of the COVID-19 pandemic. Like all disruptive technologies, AI follows a “hype cycle” with unrealistic initial hopes followed by inevitable disappointments, recalibration of expectations, and a return to steady progress. Current AI algorithms are “narrow,” meaning that they are designed to perform specific tasks such as language translation, data processing, and image recognition. Machine learning (ML) has been utilized for decades, with small amounts of structured data that require less processing power. Deep learning (DL) is a more recent development,
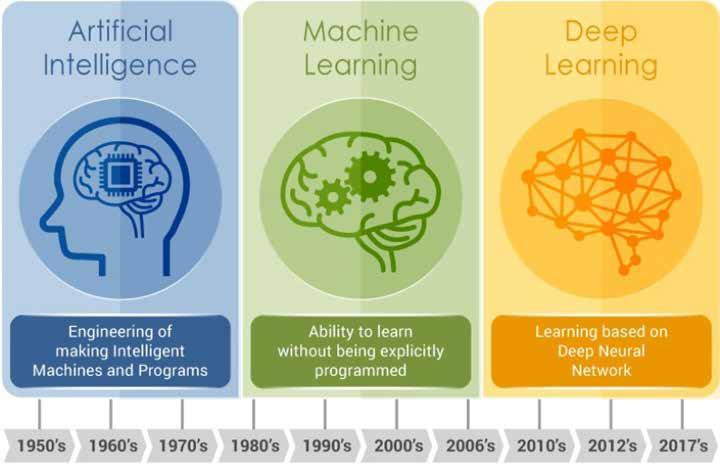
59 www. americanhhm.com
DIAGNOSTICS
based on neural networks mimicking the human brain in order to learn patterns from large volumes of unstructured data with minimal supervision. However, DL is data-hungry, requiring hundreds if not thousands of training cases to achieve high model performance.
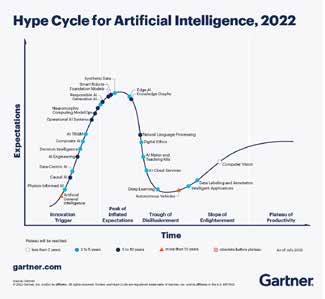
In health care, it is prohibitively expensive and impractical to acquire and maintain comprehensive datasets of patient information. Even within large organizations, data for a specific patient group or disease process can be sparse, low-quality, missing, or biased. During COVID-19, prior training data were simply not available, and situations evolved rapidly with strong geographic dependencies. As a result, institutions shifted away from big data to “small and wide”: lower-volume but diverse datasets offering greater value to local stakeholders. Recent AI advances with promise for medical applications include few-shot, transfer, federated, and attention learning. The overall challenges for health care include scalability, generalizability, and explainability. As we continue to evaluate informatics solutions,
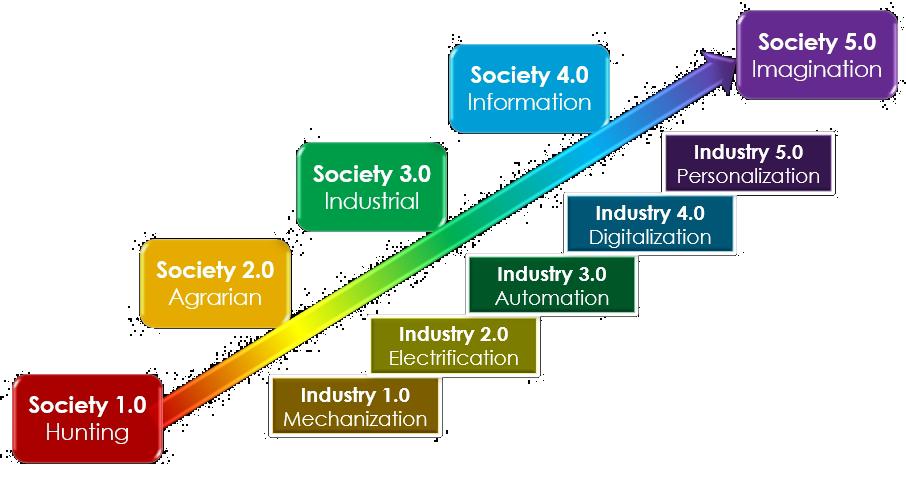
60 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
DIAGNOSTICS
we must ensure efficient, operational, and responsible algorithms that can optimize, accelerate, and democratize healthcare delivery.
Internet of Things
We are well into the 4th Industrial Revolution, with widespread automation, digitalization, and interconnectivity transforming our society in novel and innovative ways. Machines are beginning to perform routine daily tasks and replace traditional human work. Given the profound global workforce shortages, we have a unique opportunity to reimagine human/machine collaborations in order to maximize collective
productivity, creativity, and sustainability. Such strategies are already being employed with remote patient monitoring, cobots (collaborative robots), and telemedicine appointments. At this time, AI solutions show particular promise for workflow optimization including ordering, scheduling, triage, patient notes, decision support, results communication, productivity metrics, and revenue cycle management. End-to-end automation will help free up physicians and staff time to consult with patients, interact with other departments, and maximize added value.
The Internet of Things (IoT) refers to physical objects that collect and exchange
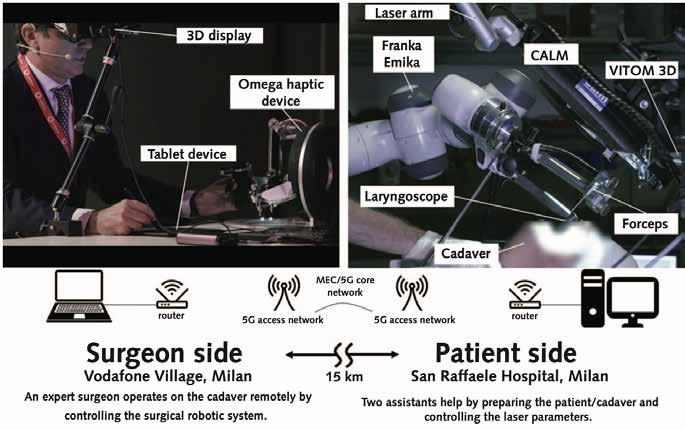
61 www. americanhhm.com
DIAGNOSTICS
data over networks, including smart devices, mobile sensors, and wearable clothing/ accessories. These technologies enable real-time tracking of location, vital signs, physical activity, and other biometric data. Interfacing with smartphone apps or remote devices enables point-of-care evaluation and action plans, such as scheduling physician appointments, requesting medication refills, or activating emergency alert systems. The Addition of sensory (optical, haptic) feedback can provide an immersive experience (extended reality, metaverse) that facilitates social interactions such as telehealth, telerehabilitation, and teletherapy.
Digital health strategies are poised to democratize healthcare delivery across the globe. With the advent of population-level monitoring, socioeconomic determinants of health can be better characterized, thus informing public health interventions for disease prevention and risk minimization. Furthermore, global informatics solutions can be deployed to improve patient access with automated triage and decision support, expert consultations, and standardized medical education. Even more futuristic, the feasibility of robotic telesurgery has recently been demonstrated over wireless 5G networks, with exciting implications for remote interventions.
By leveraging advances in systems biology and information technology, we can vastly improve health care delivery by aiding consumers to make lifestyle changes;
addressing underlying causes and risk factors; accelerating disease detection and diagnosis; and developing targeted treatment plans to optimize outcomes. These combined approaches will encourage the development of high-value, cost-effective systems that provide best quality care to patients across the world.
References are available at www.americanhhm.com
Mai-Lan Ho is an internationally recognized radiology leader, scientist, and educator with experience at multiple institutions and practice models across North America. She trained in chemical engineering at Stanford University and Massachusetts Institute of Technology, medical school at Washington University in St. Louis, and radiology at Beth Israel Deaconess Medical Center / Harvard Medical School and the University of California, San Francisco. Dr. Ho’s academic specialization includes translational advanced imaging and precision medicine with an emphasis on interdisciplinary clinical care, research, and teaching. She is the author of 95 articles, 27 grants, 4 books, 14 chapters, 74 abstracts, 18 technical reports, 5 multimedia works, and nearly 300 invited lectures.
62 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 AUTHOR BIO
DIAGNOSTICS
Cloud Computing in Healthcare

Chronic disease accounts for well over 80 percent of the cost of care, costing tens of millions of lives every year. The primary culprit is uncoordinated, fragmented care. Cloud computing promises to solve this problem by consolidating health information in one place and allowing easy, secure access to every provider.
James Doulgeris Chairman Population Health Advisory Board RSDSA
Mike Sutten, the former Chief Technology Officer at Kaiser Permanente and the Central Intelligence Agency, and today’s CTO of healthcare tech heavyweight Innovaccer weighs in on why Innovaccer took the bold strategic leap to create a comprehensive healthcare cloud. As the retired CEO of the physician based Accountable Care Organization Osler Health, I believe the healthcare cloud represents the most important clinical management tool of our generation. Here’s why:
63 www. americanhhm.com
DIAGNOSTICS
Iasked Mike Sutten what three key decision points led him to change Innovaccer’s business model to cloud based information and data accumulation, informatics and analytics. The response was pretty much what I expected about an industry segment he says will grow from $9.5 billion in 2020 to $39.9 billion by 2025, at a compound annual growth rate of 33.2%.
“ SCALABILITY: One of the key decision points that led Innovaccer to adopt a cloudbased model was the ability to scale our services as needed. As a health tech company, we needed to be able to handle large amounts of data and process it quickly, which is something that a cloud-based infrastructure allows us to do. With cloud-based services, we can easily add more resources as needed, ensuring that we can always meet the demands of our clients.
SECURITY: Another key decision point was the need for a more secure infrastructure. With sensitive patient information being handled, security is a top priority for Innovaccer. A cloud-based model allows us to take advantage of the latest security technologies and best practices, ensuring that our clients' data is always protected.
COST-EFFECTIVENESS: A cloudbased model also allows us to be more costeffective. We no longer have to invest in expensive hardware and software, and we can take advantage of pay-as-you-go pricing models. This allows us to keep our costs low and pass those savings on to our clients.”
“Overall, a cloud-based model is the future for health tech companies like Innovaccer. It allows us to be more scalable, secure, and cost-effective, which ultimately leads to better outcomes for our clients.”
From a business perspective, and as the former CEO of a large physician based accountable care operator, the business case is rock solid. Mr. Sutten went on to add something much more important to all of us as providers and consumers alike: “Also, it is estimated that the use of cloud-based services can help to reduce healthcare costs by up to 30% over the next five years.”
That would be over $1.35 trillion dollars and compounding for years to come. Sutten ended the interview with that bombshell almost as if it was a throwaway. I not only fully agree, I believe that it is the lead story about the healthcare cloud because it represents the most important clinical management tool of our generation. Here’s why:
In 2017, chronic diseases; heart disease, cancer, diabetes, rare diseases, over 7,300 in all, cost $3.5 trillion of the total $4.1 trillion in direct medical costs in the United States. The breakdown then was 76 percent of the cost before age 65 and 96 percent after age 65. It has only gotten worse since then.
The overall cost to the economy is more than double the direct cost, a problem exacerbated because the cost of healthcare in the U.S. is twice the cost of the next most expensive system in the world while the
64 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
DIAGNOSTICS
results measured in health status linger near the bottom of the twenty-six most developed nations.
Far more sobering, chronic disease is the leading killer and disabler according to the Centers for Disease Control. Eventually, it kills virtually everyone not killed by trauma, crime, or accident.
By example, there are over 7,000 rare diseases. While each one affects less than 200,000 people, they add up, and each one, by definition, is, in the parlance of physicians, a zebra lost in a herd of horses. Rare diseases also impact one in seven people in the U.S.
The direct cost of rare diseases alone was $418 billion in 2019 according to a study by the Lewin Group leading to a cost to the U.S.
economy of nearly one trillion dollars. And that is just rare disease.
Why is our management of chronic diseases such a costly and deadly failure?
We have not managed to put patient health information in one place and give doctors access to it.
Why is having a single patient record with all their information so important?
Without it, our care is fragmented. It is discontinuous. It is disrupted. Early diagnosis of chronic disease, so critically important to slowing, stopping, or reversing its progression over a lifetime is delayed, often for years.
Despite all our technology, electronic medical record systems, Clinically Integrated

65 www. americanhhm.com
DIAGNOSTICS
Networks, Accountable Care Organizations and so on, doctor’s notes, treatment records, pharmacy records, test results and so much more disparate data and information remain disassociated.
The present trend, particularly in the United States, of focusing on episodic and acute care through freestanding walk-in clinics in pharmacies, urgent care centers and emergency rooms wreaks havoc on the diagnosis, treatment, and continuity of care for chronic disease. Private insurers, Medicare Advantage and Managed Medicaid programs with preferred provider and closed networks all competing with one another to encourage annual change further silo patient health information into discrete, competitively closed compartments.
Add the common practice of employers changing commercial third-party administrators with their separate networks on average every 2.3 years or so to different

networks through competitive bidding and it is not hard to conclude that by the time people reach Medicare age at 65, the cost of chronic care skyrockets from just over 75 percent to over 96 percent.
For example, if a patient sees multiple providers, but none of them have access to all the patient's test results and medical history, it is nearly impossible to get a complete picture of the patient's health status and to make an accurate diagnosis. Without access to a complete patient record, the risk of harmful drug interactions, under medication and overmedication is not only amplified, it is totally unnecessary, a systemic forced harm on society.
Conversely, under continuous care, a person with diabetes will see a doctor, properly care for their diet, weight, exercise and take medication that will keep the disease in check for the long term. If that cycle is broken, which it most often is, the disease
66 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
DIAGNOSTICS
will progress leading to other diseases called comorbidities. These complications lead to an exponential decline in the patient’s health status – and increase in their cost of their care and inevitable disability and death.
Inadequately managed chronic disease caused by uncoordinated, fragmented care is complicated by siloed, closed access health information, among other factors. These are generally accepted to be the leading causes. Cloud computing promises to solve this problem by consolidating health information in one place allowing easy, secure access to every provider.
With a single patient record on the cloud, healthcare providers have the complete patient medical history, including test results, medications, and treatment history, however, this is also a massive amount of data and information. Tools embedded in electronic medical record systems such as Navina’s Patient Portrait, Innovaccer’s One Note and Epic’s
Storyboard use AI to pick relevant data and information for physicians and consolidate it into a single, consumable page.
With great promise come daunting challenges in adoption, collaboration, cooperation, and deployment. I asked Mr. Sutten, as an electronic medical record (EMR) provider in competition with Epic, Cerner and other large-scale systems, how does having a cloud-based system provide an advantage? Do your cloud services enhance the Epic’s and Cerner’s of the world, or do they resist cooperation with third party cloud services?
“As a cloud based EMR provider, Innovaccer offers several advantages over traditional, large-scale systems like Epic and Cerner. One of the main advantages of a cloud-based system is that it allows for more flexibility and scalability. Our cloud based EMR system can easily adapt to the changing needs of healthcare organizations, whether that be an increase in patients or new regulations.
Additionally, our cloud-based system is built with an open API structure, allowing for seamless integration with other systems like Epic and Cerner. Our approach is to promote building on top of our platform, rather than replacing it. This allows healthcare organizations to take advantage of the features and capabilities of their existing systems, while also adding new features and capabilities that our cloud-based system offers. This approach enables healthcare organizations to get the best of both
67 www. americanhhm.com
DIAGNOSTICS
It is estimated that the use of cloud-based services can help reduce healthcare costs by up to 30% over the next five years.
worlds and helps to bridge the gap between traditional systems and new technologies.”
Sutten concludes with, “Innovaccer's cloudbased system provides an advantage over traditional, large-scale systems like Epic and Cerner by offering more flexibility, scalability, integration capabilities, realtime data access and analysis, and a robust security infrastructure.”
Nonetheless, I asked, with so many competing clinical providers, EMR companies, closed provider networks, third party networks, Preferred Provider Networks, Clinically Integrated Networks and others, for many of whom clinical data represents a competitive advantage, how do you encourage and secure their cooperation and participation? More importantly, with the solution to managing chronic disease being a single patient record accessible to all providers, how does your system help to reach that goal?
“At Innovaccer, we understand that clinical data is a valuable asset for healthcare providers, and we work hard to earn their trust and cooperation. We believe that our unique approach to data management and analytics is what sets us apart from other platforms in the market.
First, we prioritize data privacy and security. We understand that clinical data is sensitive and must be protected, which is why we have invested in industry-leading security measures to ensure that our clients' data is always safe and secure.
Second, we are committed to providing value to our clients. We believe that by working together, we can help providers to improve patient care, reduce costs, and streamline operations. We work closely with our clients to understand their needs and tailor our services to meet those needs.
Third, we are transparent and open about how we use data. We believe that our clients should have control over their data and understand how it is being used. We provide clear explanations of our data use policies, and we are always available to answer any questions our clients may have.”
It did occur to me that, since the control of clinical data is not up to vendors and with the goal of a single, comprehensive patient record accessible to everyone being so important, was there something that you and others like you to become a catalyst or enabler? And yes:
“…We are open to collaboration and integration with other systems. We understand that healthcare providers may have existing systems in place, and we work to seamlessly integrate our platform with theirs. Our open API structure allows for easy integration with other systems, enabling providers to take advantage of the features and capabilities of our platform, while also preserving the features and capabilities of their existing systems.
Overall, at Innovaccer, we strive to be a trusted partner for healthcare providers, and we believe that our approach to data management, analytics, and integration sets
68 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
DIAGNOSTICS
us apart from other platforms in the market. We are dedicated to working closely with our clients to improve patient care, reduce costs and streamline operations.” That leaves three tall barriers, which require the consensus of the three primary stakeholders who are also the three primary beneficiaries:
1. GOVERNMENT: HIPAA (the Health Insurance Portability and Accountability Act of 1996) served its purpose to protect patient privacy twenty-five years ago and serves as a bureaucratic barrier to sharing Personal Health Information (PHI) today. This will require bilateral and bicameral consensus in the U.S. Congress. A tall ask in today’s
polarized political environment.
2. PROVIDERS: Every vendor is required to commit to protect their client’s data to the detriment of their own patients’ wellbeing. Government and payer intervention may be the only solution and is already in play, not by force, but by transferring risk from themselves to providers, which has resulted in consolidation to big healthcare. While consolidation itself represents its own concerns, it may be the lesser of the evils.
3. The American People Themselves: There is strong resistance to a national patient ID identifier or national ID of any kind. That leaves arrangements between health systems, who will ultimately forge agreements for data sharing on a system by system basis, and will likely want to monetize that sharing as well. It may be a small price to pay for such big gains since they will be the primary beneficiaries of cost savings.
Conclusion:
Clearly there is a long way to go but the effort is well worth it in time, treasure, quality of life and our lives themselves.
Since medically retiring after 35 years in CEO roles in hospitals and value-based care providers, James Doulgeris stays active by advising healthcare companies and systems in the AI and analytics spaces, and as a healthcare journalist and novelist. He also volunteers to develop analytic tools to create actionable information to improve care and treatments for the rare disease community.

69 www. americanhhm.com AUTHOR BIO
DIAGNOSTICS
Times are changing, and healthcare is in the vortex of change. Human centered care is a blueprint to guide the transformation healthcare needs to meet/ exceed the demands/ desires of consumers and families. Healthcare systems are design for the human experience will see lower cost, safer care and higher performance.
Martie Moore CEO, M²WL Consulting

Human Centered Care – The Delivery Model of Now
1. Why are healthcare delivery systems so significant?
If you look at the definition of system, it is “a set of things working together…as parts of an interconnecting network”. The basic premise of a healthcare delivery systems is just that, “working together and interconnection”. When
healthcare delivery systems fail in doing such, healthcare harms and hurts the very individuals that have entrusted them. That is the significance of healthcare delivery systems. They must be interconnected not by computers, but by synergy of the very people who are the interconnectors within the system. Human centered healthcare is designed to maximize synergy.
2. What were the most significant impacts of the COVID-19 pandemic on the business during this period of transformation?
What didn’t the pandemic impact? The Supply chain, delivery and standards of care, revenue streams, workforce, every operational system, and everybody associated has been impacted, and still are being impacted. The impact has caused a tsunami of changes, some not for the betterment of healthcare. That cause and effect has led to what I believe is the most significant of impacts, trauma. Trauma is a lasting emotional response that results from living through a distressing event. Human beings, who are the business of healthcare have lost trust, and belief in the system of care because of all they have witnessed or experienced. Leaders must focus not only on business recovery, but also recovery of trust.
3. What are the two main objectives of a healthcare delivery system?
Reading any health systems document, you will see strategic statements committed to quality, patient safety, excellence, care, compassion, and stewardship of resources. When you distill
the words written it comes down to two main objectives:
Perform to grow and maintain revenue streams. Do no harm.
Do no harm, is the hardest objective for healthcare delivery systems to meet and exceed. Healthcare is one of the most highrisk complex industries with a million or more points of failure that contribute to error. Do no harm must be the top objective of delivery systems with the engagement of all involved to strive to protect those who seek care and treatment from medical errors. Leaders must strive for human centered care.
4. From your perspective, what does excellence in healthcare mean to patients?
Excellence is defined as the quality of being outstanding or extremely good. What quantifier(s) do you use then to measure the quality of being outstanding? Measurements of outcomes such as reduction of infections, adverse outcomes from procedures or treatments, management of chronic disease states, individual & family experiences and other metrics is typically used to define excellence. I would argue that metrics are just statistics. Healthcare has built its reputation on metrics and grades. While those are part of the equation of excellence, it is not the total definition. The total definition must include organizations/leaders who remain committed, curious, and willing to continually elevate performance, engagement, and connectivity of human centered design and care. It is the
71 www. americanhhm.com
ExpertTalk
experience of care that matters the most to patients.

5. What, according to you, are the major challenges in healthcare delivery, and how can we avoid them?
Chaos theory describes the qualities of the point at which stability moves to instability, or order moves to disorder. Every system in healthcare has been disrupted by events of the past few years. The challenge is moving healthcare out of instability to capability of adaptation to meet the emerging demands of a new era for healthcare. I would flip the question of how can we avoid the challenges, to how can we best use the challenges to create what healthcare should be in this new era? The creative energy that was needed during the pandemic to meet needs with constraints is what must be channeled now towards a human centered designed health system.
6. Could you provide us with the five major sectors of the healthcare delivery system?
Healthcare delivery systems are typically defined as acute, senior living/ long term, community/home, technological and products/ retail sectors. I would argue that instead of thinking of healthcare in sectors, think of it as a series of circles interconnected, such as a spiral. There is no sector that can function without some form of connectivity of other sectors. When you analyze sectors using systems theory methodology, the degree of intertwined systems throughout sectors shows the magnitude of interdependence. For example, think of the
system of getting healthcare products to the point of care. Typically called supply chain as it is a series of interlocked circles connect to assure delivery. Think about what happened when supply chained fail. That is the point of interconnection.
7. Can you describe how challenges with medicine regulation affect patients’ access levels?
Certainly, within some countries, tightened regulations and payment have caused providers to leave underserved areas, or healthcare all together. Statisticians were projecting a global provider (Doctor/Nurse/Therapist/Pharmacist) shortage prior to the onslaught of the pandemic. When examining access issues, the level of complexity shows in the data. Woven into regulation issues is disparity of race, social economics and other determents that drive access availability. I believe access is one of our top priorities for healthcare.
72 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
Martie Moore, MAOM, RN, CPHQ is the CEO of M²WL Consulting. Moore is an award-winning healthcare executive with outstanding knowledge and skills in advancing research, implementation science, cultural transformation, and patient safety. Moore is a global presenter and author. She holds patents and trademarks for healthcare innovations and leadership models.
8. What role can the healthcare industry play in the establishment of a robust medicine regulation system?
Regulations come about for two reasons, an event or events have occurred and the only way to assure it will not happen again is through rules. The second reason is to control costs. Healthcare industry must play a leadership/partnership role with others in the development and revision of regulatory systems. Healthcare must be aware of biases deeply embedded into their systems of care. Example of bias driven care is assigning a diagnosis based upon age, versus remaining curious and exploring causations. My father fell and hit his head, knocking him unconscious. He was sent home with the diagnosis of edematous ligaments. Several days later he was having urinary retention, the urologist put him on a medication to help his urine flow. I argued that this was new onset since his fall. The urologist stated he was an 89-year-old male, urinary retention is normal for his age. He had fractured his neck when he fell. The bias of ageism harmed my father through misdiagnosis and unnecessary medications/treatments.
9. What are your hopes for future collaboration and innovation in the healthcare space?
Healthcare must collaborate to innovate or be left behind as others bring disruption to this space. I have heard no one who states that healthcare is fine in its current
state. Healthcare is typically described as costly, fragmented, complex, inaccessible, high risk, and antiquated. Investors are loving disruptive innovative ideas within the healthcare space and are salivating at the possibilities. My hope is that these disruptions use the principles of human centered design, making healthcare affordable, connected, and safe.
10. What would success look like for you in a few years’ time?
Success is defined as the accomplishment of an aim or purpose. My aim or purpose is simple, healthcare needs to be safer and affordable. Healthcare is not designed for the consumer; it is designed for the system itself. Healthcare must morph and transform to emerge to meet the demands of the future.
11. What is your final message to our readers around the world?
Embrace human centered design which will transform your health systems towards human centered care. Do not lean into past performance as your standard, be curious and willing to implode systems and processes to design for the future. Lean into your customers, team members, and fresh outside perspectives to help you envision what can be, what should be and what will be. Healthcare is at a bifurcation, one road is filled with sinkholes of the past, the other road promotes change and transformation. Do not let yourself fall into a sinkhole.
73 www. americanhhm.com
ExpertTalk
Impact of Covid-19 on Public Health
An Australian public health reflection from Monash Health on lessons learned from the Covid-19 pandemic. We discuss the public health strategies to help stop the “infodemic”, crucial elements for a health programme to be successful, Australian national Covid-19 response framework and what the very important lessons are learned from our own experiences fighting the pandemic. With an uncertain future short and long term priorities are addressed.
Samir Redzepagic, Public Health Officer, Monash Health
1. Please describe your extensive background in the medical field and at Monash Health.
First of all, I would like to thank the editorial office of the AmericaHHM Magazine for inviting me to this editorial interview which covers this very current and still challenging topic of Covid pandemic. I studied medicine both in US and Europe after which I entered general surgery and cardiothoracic surgical residency in Berlin, Germany. Additional training in heart and lung transplant with German Heart Institute in Berlin where I spent my initial 2 years working as a consulting surgeon before moving to the Alfred Hospital Cardiothoracic and Transplant Services in Melbourne, Australia. Spent considerable time in research as well, mainly associated with transplant surgery and basic science. Further interests in minimally invasive cardiac procedures, aortic surgery and surgery for heart
arrhythmias. Always had interest in public health and epidemiology which I treated as my hobby in medical domains. As the Covid pandemic hit in early 2020, I decided to step aside and join Victorian Department of Health in a public health officer and mentor role. It was a very challenging period for myself and all my much more experienced colleagues at the Department. I used that period to additionally advance and educate myself in Public Health and Medical Administration and commenced MBA with La Trobe University as well. After spending 18 months with Department of Health Victoria in Melbourne, I was offered a public health role at the newly formed Monash Health Public Health Unit in Oct 2021, which covers the whole south east of Melbourne approx. 3.5 million residents. I am currently involved in developing strategies and management of residential age care facilities in this area.
74 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
2. How could a public health strategy help stop the infodemic?
It’s a very difficult question which we all in public health and wider are trying to tackle, but in my opinion it starts from every individual and everyone counts. I would have few suggestions for your readership.
1. As individuals be critical when you look at social media and talk to reliable sources in the area.
2. Don't spread false information through your online networks. If you encounter false information, please politely ask the person who shared it to remove it.
3. Report false information to the platform administrators without any hesitations and delays.
4. Verify and check the shared information whenever you're in doubt.
5. Make more noise than people who share fake news or false information.
6. If you are part of the health provider services please discuss regular media briefings with scientific and confirmed facts

7. Promoting health strategies in education from kindergartens to tertiary academic institutions.
8. Going proactively in the communities, especially diverse and disadvantaged. Attracting community leaders to join the discussions and advocate for their base.
9. Inversing in new platforms-especially social media before they are taken over by deniers.
The new Delphi Covid consensus, which was just published, the volume and velocity of information during the COVID-19 pandemic has made it difficult for individuals to evaluate the accuracy of any given piece of information. When public health officials' communications fail to accurately reflect the reality that SARSCoV-2 transmission is largely airborne, they
ExpertTalk
regrettably contribute to the spread of incorrect information. Additionally, governments have handled erroneous information in the COVID-19 pandemic context in an inconsistent manner. There are undoubtedly a lot of places where misleading information may be found, which weakens the social cohesiveness required for effective public health responses. The public health officials had engaged populations with low levels of immunity ineffectively as the pandemic was starting to spread.
3. What are the crucial elements required for a public health programme to be successful?
This is just a slide that represents these crucial
elements for an effective and successful public health program and was developed by Australian Federal Department of Health with our collaboration from Melbourne and Victoria. I am always using it as a starting point.
It only took few months early in the Covid-19 pandemic 2020 to develop this very simple and flexible plan that proved to be very successful over last few years.
As you can see the very essence of this framework is the fundamental base level strategies in community settings, individuals at higher risk, business sector, and high risk settings being accordingly
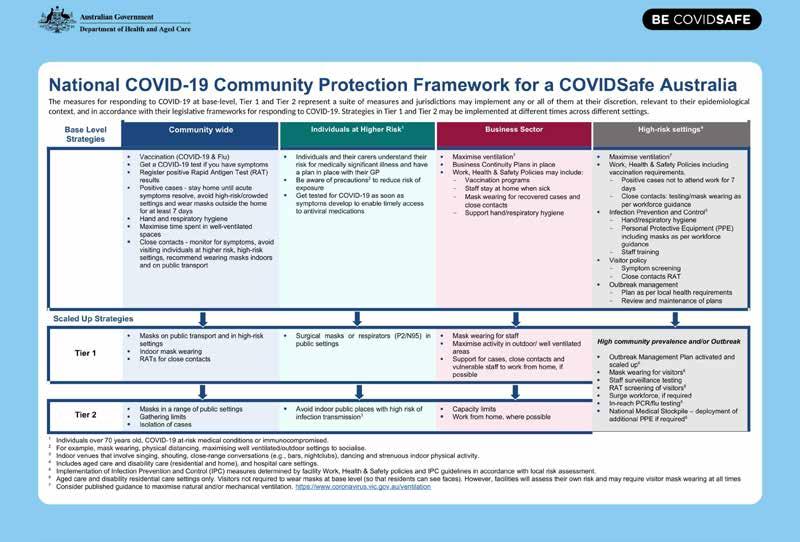
adjustable in Tier 1 and 2 scaled up options when required.
So having a national community based framework not only to deal with the current Covid-19 pandemic but for all the potential future pandemics and crisis situations is one of the crucial elements for a public health response and programme to be successful.
Further to that I would like to emphasize that health systems are continuing to face enormous staffing shortages mainly to do with the mental and physical health impacts on their workers from the pandemic. Healthcare workers continue to experience unaddressed mental health issues due to protracted working hours and increased risks in healthcare settings. Governments have not always addressed the high out-ofpocket expenditure to consumers for some pandemic control measures (for example, testing) and personal protective equipment (for example, facemasks). The COVID-19 pandemic continues to reveal vulnerabilities in the global supplychain framework for essential public health supplies. The COVID19 pandemic has catalysed opportunities for rapid innovation in digital health solutions throughout the care continuum.
During public health emergencies like the global Covid-19 outbreak, managing regional economies of scale and scope using internationally pooled procurement can unquestionably assist health services in enhancing access to necessary medications and supplies.. Community-based interventions
and services to address pandemic-related issues continue to be underused by healthcare providers in many countries.
As recent research has indicated that when the risk of harm to others is increasingly prevalent, the authorities may determine that the right of all citizens to good health overrides the autonomy of any one individual who chooses not to be involved in the vaccination program. As we are aware that medical autonomy acknowledges that every person who has decision-making capacity has the right to make decisions regarding their treatments and immunization, even when their decisions may contradict their health providers’ recommendation and support. Despite the availability of immunization services, vaccine reluctance—which can range from postponing to outright rejection—remains a significant obstacle to managing the COVID-19 pandemic as a hazard to public health in every nation.
4. What have we learned about public health from the pandemic?
The main emphasis of future responses should concentrate on how to improve and strengthen our public health systems and collaborate accordingly not only on a local level but much wider to easier exchange and disseminate the critical scientific data flow. These are some of the facts learned through the pandemic which I will further elaborate on.
Healthcare providers and systems have experienced wide-ranging challenges throughout the Covid pandemic, from periods
77 www. americanhhm.com
ExpertTalk
of relative calm and control to periods of struggle and near collapse. Although many healthcare systems will continue to be at risk of being overtaken by the new waves, the unanimous agreement among the Covid Delphi consensus panellists strongly implies that those risks may be addressed and mitigated. The absence of an evidence-based data, a globally accepted platform of minimal COVID-19 pandemic response recommendations and standards is one of several factors that endanger health systems in a structural manner. While the community transmission of SARS-CoV-2 still continues to havoc around the world and create risks to health systems, especially through variants of concern, robust virological surveillance should be implemented in all areas.
Given the persisting uncertainties regarding the prevalence, virulence, severity, and duration of post-COVID-19 morbidity due to extended Covid, pertinent public health strategies should better account for the possible longterm implications of undetected transmissions of COVID-19. In order to deliver improved public health and clinical targets relating to the COVID-19 pandemic, all member nations should give the World Health Organization (WHO) the go-ahead. This endeavour should focus especially on cases, immunisation rates, morbidity, and mortality. Massive economic impact, particularly expenditures borne by consumers and businesses, raises the stakes for the health care system.
Removing financial obstacles to COVID-19 tests, personal protective equipment, medical
treatment, and patient care are just a few of the risks that should be addressed with strong structural and economic recommendations. There should also be a clear plan to support the establishment of local and regional production hubs for COVID-19 supplies, medications, and vaccines, as well as the necessary legislative and regulatory changes and reforms to address market weaknesses and risks. Authorities and healthcare professionals should think about using a flexible approach in nations where access to PCR or fast antigen tests is inadequate or constrained. The duties of primary healthcare should be enhanced and properly supported in order to lessen the impact and load on hospitals, and the physical, mental, and social wellbeing of the healthcare workforce should also be improved.
The recommendations should stimulate expanding IT infrastructure expenditures, further modifying and enhancing user interfaces, and efforts to widen access, especially for vulnerable demographic groups and individuals. Digital health will play an additional significant role. Investing in the development of applications and platforms to identify the best digital health solutions Relevant public health policies should better take into account the potential long-term effects of undiscovered COVID-19 transmissions given the ongoing uncertainties surrounding the prevalence, virulence, severity, and duration of post-COVID-19 morbidity caused by extended Covid. All members should grant the World Health Organization (WHO) the go-ahead in order to meet better public health and clinical
78 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
ExpertTalk
aims related to the COVID-19 pandemic. Particular attention should be paid to cases, immunisation rates, morbidity, and mortality in this endeavour.
Significant economic impact raises the stakes for the healthcare system, especially when it comes to costs incurred by consumers and corporations. In order to address all of these issues, strong structural and economic recommendations should remove financial barriers to Covid-19 tests, personal protection equipment, medical treatment, and patient care. They should also have a well-defined strategy for how ideas may be quickly expanded and supported.
5. What has been the recent trajectory and current state of healthcare in Australia, and what is the role of drug suppliers?
So besides the traditional issues like an ageing population and increasing demand on health services. Increasing rates of chronic disease. Costs of medical research and innovations the Australian health landscape has been immensely affected by covid-19 pandemic since early 2020. Although Australian health system is considered one of the best in the world, the covid pandemic has exposed number of deficiencies and gaps in the system and just confirmed that even with the best planning, vulnerabilities are very hard to foresee, especially when you are dealing with a very novel and invisible enemy.
In terms of medication and pharma supply issues, Australia imports approximately 90%
of its medicines from China and India, while the locally produced medications and their producers have traditionally had to compete with offshore companies on costs and logistics, raising recent concerns that Australia is ‘dangerously dependent’ on global supply chains. NPS Medicine Wise has estimated more than nine million Australians are being prescribed daily medications, which means that medical providers need to more closely and frequently follow up patients’ health conditions considering the current shortage of medications on our market.
The TGA (Therapeutic Goods Administration) stipulates that many disruptions can’t be avoided, admitting that the issue of drug supply shortages is not unique to Australia. Further factors contributing to short supplies include manufacturing problems, difficulties in procurement, overseas political instability, global market crises, the current pandemic, and natural disasters in other regions. It’s just unfortunate that the current situation leaves patients with no alternative but to pay additional costs for essential medication or adjust their dose until they can be provided with their correct medications, with shortages at local pharmacies being a daily struggle. That means marked-up prices on generic brand medications, and pharmaceutical companies ringing overseas suppliers to outsource critical medications. Luckily these issues and concerns have been already dealt with in Australia and the local supply chains have been increasingly popping up and covering the existing gaps in manufacturing domains.
79 www. americanhhm.com
We can only see the global surge on local supply and manufacturing capabilities in the next decade, that’s where significant investments are being diverted.

6. What are the teams' strengths and weaknesses in your area?
Many of us through the Covid pandemic have admitted that we all have recognized and unrecognized weaknesses, but resilience and adaptability emerged as one of our main strengths. With recognized weaknesses, it’s much easier to deal with and plan, or do risk management modelling. While the main burning issues might be different elsewhere, I see and recommend to other healthcare systems and providers to try and recognize what potential team weaknesses might be in their setting and environment. Running regular assessment modellings for a specific health provider or area is one of the tools available. We certainly think that further improvements in essential medical infrastructure and resource checks can be very challenging but are necessary. As we have experienced that despite the fact that the healthcare system in normal conditions, providing general medical services, and lacking Covid trained staff and appropriate PPE equipment, including doctors, nurses, and other emergency staff, but with proper plan and management and the use of enthusiastic young and skilled healthcare workers, was able to maintain treatment management indicators, such as doctor and nurse-to patient ratios,
and more importantly ventilator-to-population ratio, almost close to our standards. With appropriate use of hospital capacities space, additional number of beds, and necessary equipment were also created in the main Covid wards.
Additional capacities to treat Covid patients were also created in other healthcare settings and emergency departments. With good communication and team building strategies like regular meetings, motivation team huddles, and peer support of the healthcare management teams in the fight against Covid19 we have been able to address and deal with our weaknesses, becoming stronger, and more resilient and ultimately improving our response to the pandemic. For the leadership teams the importance of regular weekly meetings, brainstorming of ideas to improve the response, further discussing operational plans in various areas of health were usually held with the presence of hospital administrators, public health officers and other decision-makers to evaluate the implementation of newly developed protocols and strategies.
80 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
7. Where is Monash Health looking to make investments? Do you have a distinct vision for the direction the business will take?
Primary directions for Monash will be governed by our mid and long term plan which has that flexibility in the case of need. As we see the very turbulent economic crisis at the moment, war in Ukraine and lots of challenges managing covid-19, I think that future investments will be in local manufacturing of essential medical consumables, strategic stockpiling, relying on local energy resources and transitioning to self sufficient health systems which will be able
8. How did you deal with the many deferred surgeries and procedures in the early years?
That was very tough as most health providers in Australia had to completely cancel or reschedule even life-saving surgeries and procedures. We obviously had to adapt quickly and develop strategies with the collaborative approach with our inter state and federal colleagues and health providers. So re assessing all our lists on regular basis and involving the primary health care providers who played an amazing role as well. Between the initial restrictions and free periods we increased the number of procedures to compensate for the periods lost, emergency and high priority patients were never cancelled and we always found the solutions necessary to get the things done. The resilience played a great role and the general population was very understanding a tolerable considering the situation, lots of going into the communities and talking to them.
to survive longer periods of time on their own resources. Further transition to health digitalisation and patient communication platforms, digital public health systems and teaming up with start-ups in relevant domains. Vaccine production facilities like the current collaboration between Monash Health, Moderna and Victrian Department of Health to support the production facility in Melbourne. So I see a lot of new changes in a very short future, further collaborations between the healthcare providers globally will be of huge financial benefits.
9. What are your short- and long-term priorities?
We learned on the job what our short and longterm priorities are through the initial support and recommendations of The Australian Commonwealth government postulated healthrelated actions during the primary response to the Covid-19 pandemic: provides national leadership in managing external borders and protecting residents of aged care facilities and approves, procures, and rolls out multiple vaccine options.
The initial short-term priorities were very effective and could be always readily re-implemented again. Our state governments were responsible for determining what public health measures are appropriate, adopting emergency response legislations and implementing them promptly— with managing the border quarantine arrangements and the required Covid
81 www. americanhhm.com
ExpertTalk
ExpertTalk
testing, tracing, and isolation protocols, with additional management of healthcare and hospital response. As it has been over three years of fragmented but coordinated global and national responses, we can certainly advocate noting that three of the highestranked recommendations call for the adoption and implementation of whole-of-society and whole-of-government models, while proven prevention measures using an Covid-19 immunization approach that incorporates a wide range of public health and financial support measures to additionally compliment the vaccination programs. Long term priorities would be to monitor the situation and develop more flexible public health response strategies as we really don’t know when the next pandemic may hit back and please remember that it may not be related
to Covid or one of its variants. Obviously we have learned a lot and probably desire more credit than we realize. We were very vulnerable initially but resilient and quicky learned to adapt as a society on a global level. I still have to acknowledge the positive role Chinese healthcare workers played at the very start of the pandemic, it’s sad that they are not properly recognized as they were at the forefront and only took them few weeks to share the genomic sequence of the Covid-19 virus. This has been unfortunately politicized a lot around the world, precious time was lost and some countries are still talking about it.
10.What do you hope to accomplish for Monash Health in the next five years?
An internationally recognised cardiothoracic surgeon and public health officer who joined the Covid19 public health response in Melbourne, Australia. After having spent initial 18 months of pandemic, working with Victorian State Department of Health he joined Monash Public Health Unit which took over the Covid-19 management in southeastern Melbourne suburbs.
It’s very hard to foresee the future and especially with Covid-19 being so adaptable and variant prone virus. For myself personally I do intend to further contribute to public health and stay in some capacity at Monash Health, although my next endeavour might be in research and clinical work, so I will try to be involved on multiple fronts of challenging medical and public health issues. I look forward to complete the necessary transitions of public health response in age care facilities which at the moment take most of my time. We should be a better and safer place in 5 years from now and I can see the changes and improvement literary on a daily basis. Hopefully we can say that for many other regions in the world as well. Who knows we may touch base again in 5 years and reflect? Time will only tell.

82 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023

83 www. americanhhm.com TWO POWERFUL DOSES PER YEAR Every issue of AmericanHHM magazine is a powerful dose of information and knowledge – filled with original and undiluted content. Written by the best brains in hospital and healthcare industry, the magazine offers timely business insights and articles on cutting-edge technologies. Subscribe now to get your doses regularly. Email: subscriptions@americanhhm.com Tel: +91 40 4961 4567 Fax +91 40 4961 4555 www.americanhhm.com
84 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
EVENT PREVIEW
Experience science through commercialization
April 25 - 27, 2023 at New York, NY, USA
The International Pharmaceutical Expo (INTERPHEX), the premier event in the USA dedicated to pharmaceutical and biotechnological innovation from development to marketing, is scheduled to take place at the end of April at the Javits Center in New York, NY.
INTERPHEX is the leading global event that fuses industry innovation with expert-led technical conference. It’s where the newest ideas are shared, technology is unveiled, and the power of science through commercialization comes to life. No matter where you are in the pharmaceutical supply chain, INTERPHEX delivers relevant solutions through curated education sessions, networking and over 500 global suppliers to source quality products and services. The future of pharma, through the power of experience.
Who can attend?
Industry professionals from pharmaceutical, biotech and device facilities and service providers involved in specifying, recommending or purchasing technologies/products/services for the develop and manufacture of cost effective, quality products.
Benefits of attending INTERPHEX –
• Find new, more cost-effective alternatives to existing processes and procedures
• Discover highly efficient new technologies to increase productivity
• Meet partners who can provide instant access to cutting-edge technologies
• Acquire new skills and insights from qualified experts
• Evaluate the full range of competing solutions in every product category
• Learn from industry experts who share effective strategies to maximize efficiency, enhance product quality, and ensure regulatory compliance and more
• Upgrade your skills, your knowledge and your on-the-job effectiveness
• Network with peers from across the country and around the world
• Hear free keynotes by industry thought leaders and innovators
Registration includes access to:
INTERPHEX exhibit hall and technical conference badge offers access to the latest in technology, innovation, device development and manufacturing to:
Learn
• 3-Day technical conference
• Interphex live
• Keynote series with pharmaceutical technology and biopharm int’l
• Ips technologies tours
• Contract-specific sessions
Discover & explore
• 3-Day access to exhibit hall
• New exhibitor zone
• Contract services pavilion
• Interphex exhibitor award winners
• Access to leading suppliers
• Technology launches
• Poster hall
• New! Innovatech gateway pavilion
Network
• Technology-based networking events
• Conference recommendations
• Exhibitor recommendations
• New exhibitor networking happy hour
• Ips reception
• Exhibitor in-booth events
Interphex 2023
Date: April 25 - 27, 2023
Location: Javits Center, NYC, USA
Website: https://www.interphex.com/
Email: inquiry@interphex.com
85 www. americanhhm.com
EVENT PREVIEW
EVENT PREVIEW
Medlab Middle East 2023
Paving the way for technological advancements and sustainability in laboratory medicine
Navigate through the exhibitor profiles, negotiate deals and schedule meetings to discuss your needs with over 700+ participating companies at Medlab Middle East LIVE & in-person.
6-9 February 2023 Live-in-person at Dubai World Trade Centre
Online – 16 January – 9 March 2023
OVERVIEW
Conference Overview
The 22nd edition of Medlab Middle East Congress - the region’s only multi-disciplinary congress will take place both live, in-person & online featuring 12 CME accredited tracks from 6-9 February 2023 at the Dubai World Trade Centre; with the online-only track, ‘Future of Lab’, taking place online from 13-14 February 2023.
700+ exhibitors from 40+ countries will showcase the latest laboratory innovations and technologies across 8 product categories. From global manufacturers to established laboratory suppliers, all the biggest names in the industry are gearing up to interact, network and conduct business with you across four fantastic days. Featuring 130+ world-class laboratory champions under one roof, the 6-day intensive congress programme aims to continue to empower every medical professional with advanced knowledge and skills as clinical laboratories transform and evolve rapidly.
Medlab Middle East brings to you innovations by the dozen with products and services from
regional and international suppliers falling under these main product categories:
• Disposables
• Healthcare/General Services
• Imaging
• Infrastructure
• IT
• Laboratory
• Medical Equipment
• Orthopaedic Devices
• Physiotherapy/Rehabilitation/Mobility
• Pharma/Nutrition
Benefits of Visitor Registration:
By completing the registration form, you will get your FREE visitor badge that gives you access to:
• The exhibition halls and all exhibiting companies
• Innovative sessions at Labpreneur
• Workshops and product launches on the show floor
• Access to the Village, a perfect networking place for you and your clients
• FREE online tool to explore products, companies and setup meetings in advance of the live show days (available from 16 January 2023)
• Your Visitor badge will be digital - available to you through the Medlab Middle East Mobile App (when live) and will be emailed to you in the days before the in-person event.
Exhibitors can register for 2024!
Medlab Middle East returns in 2024 from February 5th-8th. Booking is already available to exhibitors. Secure your place at the heart of healthcare and book your stand today.
We cannot wait to welcome you back in February 2024!
Join the community of global clinical laboratory manufacturers with healthcare specialists, procurement professionals, dealers and distributors.
Tom Coleman, Group Exhibition Director, Informa Markets Healthcare, said: “It has been an incredible year of growth for the medical laboratory
86 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
industry and Medlab Middle East. This year we will welcome 650 exhibitors from 180 countries, many of whom are making their debut at the event by highlighting the latest technological advances on the market.
“We are also welcoming back several of our Asian counterparts who have been unable to travel due to restrictions in their home countries as well as stalwarts of the event Abbott, Biomerieux, Beckman Coulter, Randox, illumina, bioMérieux, Randox and Mindray, amongst others.”
ABOUT THE ORGANISER About Informa Markets
Informa Markets, the global exhibitions division of Informa PLC, enables communities

across the globe to engage, experience and do business by providing them with powerful platforms to connect across key regions and market verticals. Industry insight, coupled with an innovative and customer first approach, provides Informa Markets’ customers and partners with the opportunity to create business advantage and access markets, both digitally and face-toface, 365 days of the year.
Medlab Middle East 2023
Date: Live-in-person – 6-9 February 2023
Online – 16 January – 9 March 2023
Location: Dubai World Trade Centre
Website: https://www.medlabme.com/en/home.html
Email: medlabme@informa.com
87 www. americanhhm.com
EVENT PREVIEW
Digital Health: Using technology to engage with patients
This webinar was presented by Anurag Saxena from IQVIA. Emphasising on the need for a universal healthcare management approach that blends with solutions from different suppliers – this webinar takes you to a journey that introduces newer frameworks and operations protocols for universal healthcare.

Unified Health Interface - An Open network for digital health services embodies the design principle of universal health coverage ecosystem. As a case study this webinar gives a detailed walk-through of a system in place that has used the unified health interface principles. The various frameworks and technology stack that are being developed at federal level or from private sector players are easily interoperable and achieve seamless sharing of data across various healthcare hubs. This would also provide for hassle-free migration of patient from one facility to another.
Another important factor while designing the system was to keep a patient centric approach within the frameworks. This would ensure that the data is secured at the patient's end and shared by patient only.
Inclusivity within system would encourage that people from all levels of the socio-economic sphere can benefits of this universal system.
Anurag Saxena
Designation: Principal & Head - Digital Health Consulting and Solutions for Payers, Providers & Government (South Asia)
Organization: IQVIA, India
Anurag is a Principal at IQVIA and leads teams in India and South Asia focusing on Digital Health Consulting as well as Products and Solutions for Payers, Providers and Government. He is spearheading some of the largest transformation projects in Digital Health in the region for IQVIA. He is also driving Digitization of Healthcare systems for some of the largest Providers in the region. Prior to joining IQVIA, he has worked with organisations like Ernst & Young, Deloitte, SAP, NEC Corporation and HCL Technologies in leadership roles. Anurag has been involved in some of the world's largest Digital Transformation projects in the areas of Digital Health, Digital Identity, Digital Government and Digital Payments in Advisory and Program Management roles. He has also advised several boardrooms for formulation and execution of Go-tomarket strategy for Technology businesses in India and South Asia.
Get direct access by scanning the QR Code

88 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 WEBINAR REVIEW
New Care Models and the Future of Healthcare
The healthcare ecosystem consists of those who pay, those who benefit and those who are responsible. New Care Models are helping to align these interests and share capacity across the ecosystem, all enabled by a modern digital infrastructure.
Varian is a Siemens Healthineers company driving progress in cancer care. It is using software and automated processes to help oncology professionals collaborate and develop more precise and holistic cancer treatments, making cancer care easier to manage and deliver.
Kenneth Daniel Tan from Varian explains the importance of network care in Oncology care space which would guarantee standardised clinical decision making protocols like centralised telediagnostic radiology and centralised treatment planning. It also renders the capability to streamline workflows with the treatment providers that would reduce the need for human effort.
The benefits of network care among many are standardised high-quality care, shared knowledge base optimised infrastructure and decreased reliance on human intervention. He further goes into the various network care models and gives insights on their pros and cons.
Designation: President, Asia Pacific & Japan
Organization: Varian Medical Systems

Kenneth Tan is the President of Asia Pacific and Japan at Varian Medical Systems. He joined Varian in January 2017. Varian is a global leader in solutions for advancing cancer treatment; specialising in radiotherapy, radiosurgery, proton therapy, brachytherapy and oncology informatics software.
Kenneth has 20 years of experience in healthcare; having held Commercial leadership roles in Varian, Medtronic, Covidien, Boston Scientific and Novartis. More than 14 years are in the implantable, disposable medical devices, capital equipment and managed services; covering various Global markets and regions in Asia Pacific. He has deep experience in developing and executing strategic growth plans in China, Japan, India, and South-East Asia.
Kenneth has held various leadership roles in Sales, Marketing, Strategy and P&L Management. In recent years, he has built his success around driving complex strategic shifts through organisations; in areas of business strategy and organisational transformation. The hallmarks of his tenure are growth acceleration, business-model innovation and a strong leadership team.
Get direct access by scanning the QR Code
Kenneth obtained his BBA from the University of South Australia and a diploma in Biotechnology (Medical Technology) from Singapore Polytechnic.

89 www. americanhhm.com
WEBINAR REVIEW
Kenneth Daniel Tan
Sanctuary of Endovascular Therapies
February 16-18, 2023
Kiawah Island, South Carolina
https://setmeeting.org/
About Event: The Sanctuary of Endovascular Therapies (SET) has established itself as one of the premier endovascular meetings. The Symposium provides vascular surgeons, interventional radiologists, cardiologists, podiatrists, and allied health professionals a unique interactive program with the most current information and treatment options for endovascular disease.
Listed Under: Medical Sciences
Pan Arab Interventional Radiology Society Annual Congress, 2023

February 11 to 14, 2023
Dubai
https://pairscongress.com/
About Event: PAIRS 2023 the largest endovascular and interventional radiology conference in the region featuring a four-day comprehensive program with more than 150 speakers that presents highlevel scientific content, live and recorded cases, workshops, ePosters & Oral presentations, interactive education and innovative discussions, cutting-edge technology and image-guided therapy providing both clinically relevant updates as well as hands-on educational activities.
Listed Under: Diagnostics
Imaging Informatics for Healthcare, Research, and Applications
February 19-23, 2023
United States
https://spie.org/mi/conferencedetails/imaginginformatics?SSO=1
About Event: Medical Imaging is the meeting where information is shared about image processing, physics, computer-aided diagnosis, perception, image-guided procedures, biomedical applications, ultrasound, informatics, radiology, digital pathology, and more.

Listed Under: Diagnostics
HIMSS23 Nordic Delegation
April 17-21, 2023
USA
https://www.himss.org/events/himss23-nordicdelegation
About Event: HIMSS offers a unique depth and breadth of expertise in health innovation, public policy, workforce development, research and digital health transformation to advise leaders, stakeholders and influencers across the global health ecosystem on best practices.
Listed Under: Information Technology
90 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 EVENTS LIST
International Conference on Surgery & Anesthesia | ICSA-2023
April 20-21, 2023
France
https://www.phronesisonline.com/surgeryanesthesia-conference/
About Event: ICSA-2023 provide a unique platform to bring together worldwide distinguished academicians in the field of Various Surgeons, Anaesthesiologists, Doctors, Medical Professionals, Surgical tool technicians, Pharmaceutical Industrialists, business professionals, scientists, industry researchers and scholars to exchange about growing research and technologies.
Listed Under: Surgical Speciality
2nd World Congress on Cardiology and Cardiovascular Diseases (WCCD 2023)

April 20-21, 2023
France
https://phronesisonline.com/cardiology-congress/
About Event: WCCD 2023 will provide the opportunity for a comprehensive overview of the new information on risk factors for different cardiac diseases and breakthrough emerging therapies and technologies.

Listed Under: Medical Sciences
disease recovery and prevention and on new analysis of innovation within the field of cardiac specialty.
Listed Under: Medical Sciences
Medical Fair India
April 27-29, 2023
India
https://www.medicalfair-india.com/
About Event: Medical Fair India is to Explore how the latest digital technologies and new approaches shaping healthcare.
Listed Under: Technology, Equipment & Devices
Digital Health 2023
May 16-17, 2023
California
https://events.reutersevents.com/healthcare/digitalhealth-usa
3rd World Congress on Heart
April 24-25, 2023
Switzerland
https://heart.euroscicon.com/
About Event: Heart 2023 Conferences will be an examination of the newest successions in heart
About Event: Digital Health hosts 300+ digital leaders over two intensive days of learning, idea sharing, collaborating, and networking to help accelerate the transformation that our consumers desire and our care teams deserve.
Topics Covered: Interoperability and Health Data, Automation in healthcare, Change Management, Cybersecurity, Virtual and Remote Care.
Listed Under: Information Technology
91 www. americanhhm.com EVENTS LIST
International Conference on Nursing Care and Patient Safety
May 25-26, 2023
Dubai, UAE
https://www.nursingcare. scientexconference.com/
About Event: The conference theme is "Exploring advanced technology practices in Nursing care and Patient safety" with the goal of educating attendees on the most recent challenges in nursing care, illuminating the most recent trends, and analyzing the future of Patient safety and Healthcare science.
Listed Under: Medical Sciences
International Conference on Neurology and Brain Disorders
Hybrid Event | May 25-26, 2023
Dubai, UAE
https://www.neurology.scientexconference.com/
About Event: Neurology 2023 is up with an excellent opportunity for Neurological experts in the field of Medicine, Industry, Pharma, Surgery, Teaching, and Learning Practices
Listed Under: Medical Sciences
International Conference on Neuroscience and Neurology
Hybrid Event May 25-26, 2023
Dubai, UAE
https://www.neuralscience.scientexconference.com/
About Event: The International Conference on Neuroscience and Neurology welcomes all the ingenious neurologists, neuroscientists, neurosurgeons, psychologists, psychiatrists, and Allied health professionals for developing consensus in contentious areas in Neuroscience and Neurology
Listed Under: Medical Sciences
International Conference on Cardiology and Cardiovascular Research
Hybrid Event | May 18-19, 2023
Dubai, UAE
https://www.cardiology. scientexconference.com/
About Event: Cardiology 2023 conference features more compelling presentations in 27 scientific session categories that point up basic, clinical, and translational sciences as they progress toward a better understanding of stroke pathophysiology with the aim of developing more effective remedies
Listed Under: Medical Sciences

92 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 EVENTS LIST
Neuroscience and Brain Disorders Forum
March 27-28, 2023
United Kingdom
https://scholarsconferences.com/ neuroscience/
About Event: Neuro Forum 2023 is the leading meeting dedicated to Neurosurgeons and Neurology researchers to discuss "Emerging Perspectives in Neurology and Brain Research".

Listed Under: Surgical Speciality
World Congress on Heart and Cardiovascular Diseases
Hybrid Event | May 18-19, 2023
Dubai, UAE
https://www.heartcongress.scientexconference.com/
About Event: The Cardiology 2023 Conference provides a stimulating chance for the developing generations engaged in numerous cardiac research projects to advance their expertise in the field of cardiovascular diseases. It will also share scientific knowledge and experience, giving people the chance to learn about various cardiac disorders and cardiovascular treatments.
Listed Under: Medical Sciences
Nursing and Advanced Healthcare

July 12-13 2023
France
https://nursingworldcongress.com/
About Event: Nursing World 2023 aims to foster and conduct collaborative interdisciplinary research in state-of-the-art methodologies and technologies within Nursing & Advanced Healthcare. It provide invaluable opportunities to extend and strengthen the Nursing and Healthcare community
Listed Under: Healthcare Management
Medlab Asia
July 5-7, 2023
Bangkok
https://www.medlabasia.com/en/home.html
About Event: Medlab Asia 2023 will be welcoming world-class suppliers and industry leaders as well as top-of-the-line buyers to explore the APAC market.
Listed Under: Technology, Equipment & Devices

93 www. americanhhm.com EVENTS LIST
PRODUCT LAUNCH
December 13th 2022
Stryker launches Citrefix™ Suture Anchor System
Featuring award-winning Citregen biomaterial designed to support bone regeneration and the natural healing process.
Citrefix is a disposable suture anchor system that features a resorbable biomimetic anchor body. It is made with Citregen, an elastomeric material made from a citrate polymer specially designed to mimic bone chemistry for controlled resorption without chronic inflammation.1 These unique chemical and mechanical properties are designed to help grafted tissue heal and healthy bone to grow when used in orthopaedic surgical applications.2 The sterile-packed set includes a cartridge with preloaded implant and eyelet, a drill bit, a drill guide and pre-assembled inserter.
“By leveraging Citregen’s unique material properties, Citrefix introduces design features that greatly increase its pull-out strength compared to other suture anchors,” said Wayne Berberian, M.D., orthopedic surgeon at the Ankle & Foot Institute in Maywood, N. J. “At the same time, the Citregen material benefits patients’ recovery since it is more easily accepted by the body, so they heal without suffering from the chronic inflammation that may occur with other bioresorbable suture anchors.”
PRODUCT LAUNCH
December 19th, 2022
Abbott launches the world's smallest implantable, rechargeable spinal cord stimulation system for chronic pain

Abbott today announced the U.S. Food and Drug Administration (FDA) approval of the company's Eterna™ spinal cord stimulation (SCS) system –the smallest implantable, rechargeable spinal cord stimulator currently available on the market for the treatment of chronic pain. Eterna SCS utilizes Abbott's proprietary low-dose BurstDR™ stimulation, the only SCS waveform technology with the highest level of clinical evidence, proven to reduce pain 23% more than traditional waveform technology approaches.
After the successful launch of Citrelock last year, Citrefix is the second product in Stryker’s expanding portfolio using the material, with additional products expected in 2023. Citregen was awarded the 2022 Technology Innovation and Development Award by the Society for Biomaterials earlier this year.
Read the complete post
"Abbott's low-dose BurstDR stimulation is clinically proven to reduce pain, improve people's ability to perform everyday activities, and reduce emotional suffering associated with pain,"^8 said Timothy Deer, M.D., DABPM, president and chief executive officer of the Spine and Nerve Centers of the Virginias in Charleston, W.Va. "Until now, it wasn't available on a rechargeable device that was this small, and that only needs to be charged a few times a year. This makes a big difference in comfort for many patients who now can have access to the best of both worlds – a small, best-in-class rechargeable device with superior stimulation therapy."
Read the complete post


94 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023 NEWS
BREAKTHROUGH
December 6th 2022
Ultromics receives FDA Clearance for its Breakthrough Device EchoGo® Heart Failure
An AI-based platform that enables precision detection of heart failure with preserved ejection fraction.
Read
Ultromics’ EchoGo® Heart Failure, an AI solution for echocardiography with the potential to revolutionize the diagnosis of heart failure with preserved ejection fraction (HFpEF), has received US Food and Drug Administration (FDA) clearance. The news puts EchoGo® Heart Failure in the 7% of devices that have gone on to obtain full marketing authorization after being awarded FDA breakthrough status.
The clinical and technological breakthrough was developed by echocardiography and AI experts from Ultromics, a spin-out of the UK’s University of Oxford, in collaboration with Mayo Clinic. The device uses AI to accurately detect HFpEF from a single echocardiogram image, which accounts for 50% of the 64 million cases of heart failure worldwide and has overtaken heart failure with reduced ejection fraction (HFrEF) as the most prevalent form of the deadly disease.
This development marks a huge leap forward from traditional diagnostic algorithms for HFpEF, a heterogeneous syndrome that can be challenging to identify, and is missed in up to 75% of cases.4 Current approaches include time-consuming and often inconclusive diastolic function assessment, and require a highly specialized, increasingly rare skillset, and often invasive testing. To counter this, EchoGo® Heart Failure has a vital role to play in the future HFpEF landscape.


FDA APPROVAL
December 12th 2022
Agilent Resolution ctDx FIRST Receives FDA Approval as a Liquid Biopsy Companion Diagnostic Test for Advanced Non-small Cell Lung Cancer
Agilent Technologies Inc. announced today that the U.S. Food and Drug Administration (FDA) has approved Agilent Resolution ctDx FIRST as a companion diagnostic (CDx) to identify advanced non-small cell lung cancer (NSCLC) patients with KRAS G12C mutations who may benefit from treatment with KRAZATITM (adagrasib).
This is the first liquid biopsy NGS assay approved by the FDA as a CDx for the newly approved KRAZATI in advanced NSCLC and was developed in collaboration with Mirati Therapeutics. ctDx FIRST has also been approved by the FDA for tumor profiling of the epidermal growth factor receptor (EGFR) gene for use by qualified healthcare professionals in accordance with professional guidelines in oncology patients with NSCLC.
The ctDx FIRST assay uses novel propriety technology to detect genomic alterations in circulating tumor DNA (ctDNA) from plasma. This minimally invasive approach is preferred by 90% of cancer patients compared to more invasive tissue biopsy tests. In addition, liquid biopsy overcomes some limitations encountered with tissue-based methods providing a notably faster turn-around time to potentially accelerate treatment decisions.
95 www. americanhhm.com
NEWS
the complete post
Read the complete post
ACQUISITION
December 20th 2022
Olympus to acquire pioneering cloud-AI endoscopy startup, Odin Vision, signifying strategic next step in the company’s broader digital strategy
Read
Acquisition enables Olympus to provide advanced AI-powered solutions and data-driven insights that transform patient care and improve clinical and procedural workflows.
The acquisition is a strategic component of Olympus’ broader digital strategy to improve patient care by transforming clinical and procedural workflows. Olympus plans to utilize procedure and clinical data collected and analysed in real-time to provide care professionals with digital solutions that reduce administrative burden, assist point of care clinical decision-making and empower them to deliver the best possible care.
The acquisition complements the company’s Digital Endosuite vision, which envisions the use of AI and other digital technologies to extend the reach of endotherapy and improve patient care pathways. The company aspires to lead the future of digital health by establishing a platform with a broad range of cloudconnected software solutions built by both Olympus and a strong ecosystem of third-party development partners.
Peter Mountney, CEO of Odin Vision commented, “Together with Olympus, we are embarking on an exciting journey to bring the next generation of cloud and AI healthcare applications to patients.”
APPOINTMENT
December 19th 2022
Cardinal Health Names Aaron Alt Chief Financial Officer
Read


Cardinal Health (NYSE: CAH) and its board of directors announced that Aaron Alt will become the company's new chief financial officer (CFO). Alt will succeed interim CFO, Trish English and will report to CEO, Jason Hollar, as a member of the company's Executive Committee effective Feb. 10.
In his capacity as CFO, Alt will lead financial activities across the enterprise, including Financial Strategy, Capital Deployment, Treasury, Tax, Investor Relations, Accounting, and Reporting. Additionally, he will lead the Corporate Development team.
"We're pleased to welcome Aaron as the new CFO of Cardinal Health," said Jason Hollar, CEO of Cardinal Health. "He's an exceptional talent with a breadth of experience across complex organizations that will position him well for this critical companywide role. I'd also like to thank Trish for her contributions as interim CFO and her commitment to help with this transition."
Aaron holds an M.B.A. from the J.L. Kellogg School of Management at Northwestern University, a J.D. from Harvard Law School and a B.A. in History and Political Science from Northwestern University.
96 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
the complete post
the complete post
NEWS
EXPANSION
December 8th 2022
New facility in Hangzhou, China helps pharmaceutical and biotechnology customers more quickly deliver patient therapies
FDA APPROVAL
December 14th 2022
FDA Grants Emergency Use


Authorization for Thermo Fisher Scientific’s Monkeypox Test

Thermo Fisher Scientific, the world leader in serving science, announced the U.S. Food and Drug Administration (FDA) has granted Emergency Use Authorization (EUA) for its Applied Biosystems TaqPath Monkeypox/Orthopox Virus DNA Kit, a polymerase chain reaction (PCR) test designed to detect non-variola Orthopoxviruses, including monkeypox virus, in approximately three-and-a-half hours.
Thermo Fisher Scientific, the world leader in serving science, is opening a new facility in Hangzhou, China, as part of its global effort to help companies provide therapies to patients more quickly. The site can address the needs of organizations in China, as well as those outside that country, for biologics and steriles development and manufacturing capabilities in the Asia-Pacific region.
The site incorporates stringent quality control processes that meet or exceed regulatory guidelines established by the China National Medical Products Administration (NMPA), the U.S. Food and Drug Administration, and authorities in Europe and elsewhere.

The TaqPath Monkeypox/Orthopox Virus DNA Kit is also designed for identification of other nonvariola Orthopoxvirus DNA. While positive results are indicative of the presence of DNA from monkeypox virus or other non-variola Orthopoxvirus, clinicians must correlate PCR results with patient history and other diagnostic information to determine infection status.
The Hangzhou site is representative of the global scale of Thermo Fisher’s comprehensive end-toend, contract development and manufacturing capabilities. With this facility and Thermo Fisher’s
“Ensuring that all U.S. laboratories have access to monkeypox PCR testing is a critical part of the response to this public health emergency,” said Manoj Gandhi, senior medical director for Genetic Testing Solutions, Thermo Fisher Scientific. “This helps expedite availability of results so that current capabilities in clinical packaging and logistics, the company can now offer a seamless end-to-end solution from molecule development through the accelerated delivery of critical medicines to patients.
patients can receive the appropriate treatment quickly. Authorized testing also enables public health agencies to stay one step ahead of the virus by monitoring viral spread and addressing affected populations accordingly.”
97 www. americanhhm.com
Read the complete post Read the complete post
NEWS
EXPANSION
December 9th 2022
Siemens Healthineers opens new Ultrasound manufacturing facility in Košice, Slovakia

Siemens Healthineers opened a new Ultrasound manufacturing facility in Košice, Slovakia, its first in Europe, with an initial capacity of up to 120 systems per week. The company will use this new facility to expand manufacturing capabilities for its ultrasound products, including the Acuson Sequoia and the Acuson Redwood. These products can have a significant impact on how clinicians treat and monitor their patients.
The facility in Košice will manufacture some portion of all general imaging and cardiovascular ultrasound systems and will supplement additional manufacturing facilities in Asia and the United States. The additional manufacturing facility will allow for a reduction of carbon emissions by more than 90 percent by ground shipping products to customers in Europe instead of via air freight from Asia.
“The great advantage of Acuson Redwood is primarily its versatility, easy handling and mobility. It offers superior imaging capabilities for specialist departments as well as general radiology within a single hospital. From the patient’s point of view, there is also a benefit in its quiet operation and in reducing the need for invasive procedures,” says prof. MUDr. Gabriel Valočik, PhD, Head of the 1st Cardiology Clinic at the Faculty of Medicine UPJŠ and ESICD in Košice.
EXPANSION
December 13th 2022
Trinity Health Michigan has begun construction on a US $238.2 million hospital in the USA
Introduction: Trinity Health Michigan has started construction of a new US $238.2 million replacement hospital in Livingston County, USA.
Features: The 174,000-square-foot hospital will expand patient access and offer an integrated campus of medical and surgical treatment, at its current medical facility in Brighton. The four-story facility will be able to accommodate eight licensed operating rooms, 18 existing short-stay unit beds, and 56 acuity adapted beds.
Additionally, renovations will be made to the current medical centre facility.

The upcoming facility, which is scheduled to open in 2025, will bring top medical specialists and services to Livingston County and the surrounding areas. This will provide a continuum of care in one place.
As a result of the newly designed acuity-adaptable patient rooms, patients will not have to be transferred to different care units.
Acuity-adaptable rooms will provide medical, surgical, and intermediate care in one room throughout the duration of the patient's hospital stay, from admission to discharge. The proposed hospital will offer medical services such as primary care, gynaecological surgery, general medicine, cardiology, orthopedics, and urology, among others.
98 AMERICAN HOSPITAL & HEALTHCARE MANAGEMENT ISSUE 01 - 2023
the complete post
the complete post
Read
Read
NEWS

99 www. americanhhm.com Introducing Advent of NEW-AGE HEALTHCARE REPORTING From the house of Ochre Media: Automotive-technology.com | Defence-industries.com | Hospitals-management.com | Packaging-labelling.com Pharmaceutical-tech.com | Plantautomation-technology.com | Plastics-technology.com | Pulpandpaper-technology.com Sportsvenue-technology.com | Steel-technology.com | Asianhhm.com | Pharmafocusasia.com Aspiring to be leading journals in the B2B landscape of Healthcare-Industry covering Medical Science, Business & Technology and all the latest innovations. Introducing a group of highly focused magazines for the American and European markets. Poised for bi-annual issuance, our new magazines bring a fresh outlook towards insightful and pragmatic Healthcare-Industry reporting. Scan to check websites Scan to check websites www.ochre-media.com











