











Penn State Health is a multi-hospital health system serving patients and communities across central Pennsylvania. We are the only medical facility in Pennsylvania to be accredited as a Level I pediatric trauma center and Level I adult trauma center. The system includes Penn State Health Milton S. Hershey Medical Center, Penn State Health Children’s Hospital, and Penn State Cancer Institute based in Hershey, Pa.; Penn State Health Hampden Medical Center in Enola, Pa.; Penn State Health Holy Spirit Medical Center in Camp Hill, Pa.; Penn State Health St. Joseph Medical Center in Reading, Pa.; Penn State Health Lancaster Pediatric Center in Lancaster, Pa.; Penn State Health Lancaster Medical Center (opening fall 2022); and more than 3,000 physicians and direct care providers at more than 126 outpatient practices in 94 locations. Additionally, the system jointly operates various health care providers, including Penn State Health Rehabilitation Hospital, Hershey Outpatient Surgery Center, Hershey Endoscopy Center, Horizon Home Healthcare and the Pennsylvania Psychiatric Institute.
We foster a collaborative environment rich with diversity, share a passion for patient care, and have a space for those who share our spark of innovative research interests. Our health system is expanding and we have opportunities in both academic hospital as well community hospital settings.

Benefit highlights include:
• Competitive salary with sign-on bonus
• Comprehensive benefits and retirement package
• Relocation assistance & CME allowance
• Attractive neighborhoods in scenic central Pa.


Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
Gentry Wilkerson, MD, Associate Editor University of Maryland
Alexis M. LaPietra MD, Associate Editor RWJ Barnabus Health-West Orange, New Jersey
Resident Editors
AAEM/RSA
John J. Campo, MD
Harbor-University of California, Los Angeles Medical Center
Tehreem Rehman, MD
Advocate Christ Medical Center
ACOEP
Justina Truong, DO Kingman Regional Medical Center
Section Editors
Behavioral Emergencies
Erin Dehon, PhD University of Mississippi Medical Center
Leslie Zun, MD, MBA Chicago Medical School
Marc L. Martel, MD
Hennepin County Medical Center
Cardiac Care
Fred A. Severyn, MD
University of Colorado School of Medicine
Michael C. Kurz, MD University of Alabama at Birmingham
Sam S. Torbati, MD
Cedars-Sinai Medical Center
Yanina Purim-Shem-Tov, MD, MS Rush University Medical Center
Clinical Practice
Cortlyn W. Brown, MD Carolinas Medical Center
Casey Clements, MD, PhD Mayo Clinic
Patrick Meloy, MD Emory University
Nicholas Pettit, DO, PhD Indiana University
Eric Snoey, MD Alameda County Medical Center
David Thompson, MD University of California, San Francisco
Kenneth S. Whitlow, DO Kaweah Delta Medical Center
Critical Care
Christopher “Kit” Tainter, MD University of California, San Diego
Gabriel Wardi, MD University of California, San Diego
Joseph Shiber, MD University of Florida-College of Medicine
Matt Prekker MD, MPH Hennepin County Medical Center
Edward Michelson, MD, Associate Editor Texas Tech University- El Paso, Texas
Mark I. Langdorf, MD, MHPE
University of California, Irvine School of MedicineIrvine, California
Michael Gottlieb, MD, Associate Editor Rush Medical Center-Chicago, Illinois
Niels K. Rathlev, MD, Associate Editor Tufts University School of Medicine-Boston, Massachusetts
Rick A. McPheeters, DO, Associate Editor Kern Medical- Bakersfield, California
Patrick Joseph Maher, MD, MS, Associate Editor Ichan School of Medicine at Mount Sinai, New York
David Page, MD University of Alabama
Erik Melnychuk, MD
Geisinger Health
Quincy Tran, MD, PhD University of Maryland
Disaster Medicine
Christopher Kang, MD
Madigan Army Medical Center
Gentry Wilkerson, MD University of Maryland
Education
Danya Khoujah, MBBS University of Maryland School of Medicine
Jeffrey Druck, MD University of Colorado
John Burkhardt, MD, MA University of Michigan Medical School
Michael Epter, DO Maricopa Medical Center
ED Administration, Quality, Safety
David C. Lee, MD
Northshore University Hospital
Gary Johnson, MD
Upstate Medical University
Brian J. Yun, MD, MBA, MPH
Harvard Medical School
Laura Walker, MD
Mayo Clinic
León D. Sánchez, MD, MPH
Beth Israel Deaconess Medical Center
William Fernandez, MD, MPH University of Texas Health-San Antonio
Emergency Medical Services
Daniel Joseph, MD
Yale University
Joshua B. Gaither, MD
University of Arizona, Tuscon
Julian Mapp
University of Texas, San Antonio
Shira A. Schlesinger, MD, MPH
Harbor-UCLA Medical Center
Geriatrics
Cameron Gettel, MD
Yale School of Medicine
Stephen Meldon, MD
Cleveland Clinic
Luna Ragsdale, MD, MPH
Duke University
Health Equity
Emily C. Manchanda, MD, MPH
Boston University School of Medicine
Shadi Lahham, MD, MS, Deputy Editor University of California, Irvine School of Medicine- Irvine, California
Shahram Lotfipour, MD, MPH, Managing Editor University of California, Irvine School of Medicine- Irvine, California
Susan R. Wilcox, MD, Associate Editor Massachusetts General Hospital- Boston, Massachusetts
Elizabeth Burner, MD, MPH, Associate Editor University of Southern California
Dan Mayer, MD, Associate Editor American College of Emergency Physicians
Andrew W. Phillips, MD, Associate Editor University of North Carolina-Chapel Hill, North Carolina
Mandy J. Hill, DrPH, MPH
UT Health McGovern Medical School
K. Tom Xu, MD, PhD
Texas Tech University Health Sciences Center
Infectious Disease
Elissa Schechter-Perkins, MD, MPH
Boston University School of Medicine
Ioannis Koutroulis, MD, MBA, PhD
Drexel University College of Medicine
Kevin Lunney, MD, MHS, PhD
University of Maryland School of Medicine
Robert Derlet, MD
Founding Editor, California Journal of Emergency Medicine
University of California, Davis
Stephen Liang, MD, MPHS
Washington University School of Medicine
Injury Prevention
Mark Faul, PhD, MA
Centers for Disease Control and Prevention
Wirachin Hoonpongsimanont, MD, MSBATS
Eisenhower Medical Center
International Medicine
Heather A.. Brown, MD, MPH
Prisma Health Richland
Taylor Burkholder, MD, MPH
Keck School of Medicine of USC
Christopher Greene, MD, MPH University of Alabama
Chris Mills, MD, MPH
Santa Clara Valley Medical Center
Shada Rouhani, MD
Brigham and Women’s Hospital
Legal Medicine
Melanie S. Heniff, MD, JD
Indiana University School of Medicine
Greg P. Moore, MD, JD Madigan Army Medical Center
Statistics and Methodology
Shu B. Chan MD, MS
Resurrection Medical Center
Stormy M. Morales Monks, PhD, MPH
Texas Tech Health Science University
Soheil Saadat, MD, MPH, PhD University of California, Irvine
James A. Meltzer, MD, MS
Albert Einstein College of Medicine
Musculoskeletal
Juan F. Acosta DO, MS
Pacific Northwest University
Neurosciences
Antonio Siniscalchi, MD Annunziata Hospital
Rick Lucarelli, MD Medical City Dallas Hospital
William D. Whetstone, MD University of California, San Francisco
Pediatric Emergency Medicine
Paul Walsh, MD, MSc University of California, Davis
Muhammad Waseem, MD Lincoln Medical & Mental Health Center
Deena Berkowitz, MD, MPH
Children’s National Hospital
Donna Mendez, MD, EdD University of Texas-Houston/McGovern Medical School
Cristina M. Zeretzke-Bien, MD University of Florida
Public Health
Jeremy Hess, MD, MPH University of Washington Medical Center
Jacob Manteuffel, MD
Henry Ford Hospital
John Ashurst, DO
Lehigh Valley Health Network
Tony Zitek, MD
Kendall Regional Medical Center
Trevor Mills, MD, MPH
Northern California VA Health Care
Erik S. Anderson, MD
Alameda Health System-Highland Hospital
Technology in Emergency Medicine
Nikhil Goyal, MD
Henry Ford Hospital
Phillips Perera, MD Stanford University Medical Center
Trauma
Pierre Borczuk, MD
Massachusetts General Hospital/Havard Medical School
Toxicology
Brandon Wills, DO, MS Virginia Commonwealth University
Jeffrey R. Suchard, MD University of California, Irvine
Ultrasound
J. Matthew Fields, MD
Thomas Jefferson University
Shane Summers, MD
Brooke Army Medical Center
Robert R. Ehrman
Wayne State University
Ryan C. Gibbons, MD Temple Health
Official Journal of the California Chapter of the American College of Emergency Physicians, the America College of Osteopathic Emergency Physicians, and the California Chapter of the American Academy of Emergency Medicine




Available in MEDLINE, PubMed, PubMed Central, CINAHL, SCOPUS, Google Scholar, eScholarship, Melvyl, DOAJ, EBSCO, EMBASE, Medscape, HINARI, and MDLinx Emergency Med. Members of OASPA.
Editorial and Publishing Office: WestJEM/Depatment of Emergency Medicine, UC Irvine Health, 333 City Blvd, West, Rt 128-01, Orange, CA 92868, USA Office: 1-714-456-6389; Email: Editor@westjem.org
. 1.1: January 2025
Integrating Emergency with Population Health
Integrating Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
MAAEM
Amin A. Kazzi, MD, MAAEM
Amin A. Kazzi, MD, MAAEM
Gayle Galleta, MD
Gayle Galleta, MD
Beirut,
The American University of Beirut, Lebanon
The American University of Beirut, Beirut, Lebanon
Brent King, MD, MMM University Texas, Houston
Brent King, MD, MMM University of Texas, Houston
Christopher E. San Miguel, MD
Ohio State University Wexner Medical Center
Christopher E. San Miguel, MD Ohio State University Wexner Medical Center
Christopher E. San Miguel, Ohio State University Wexner Medical Center
Daniel J. Dire, MD
Daniel J. Dire, MD University of Texas Health Sciences Center San Antonio
Daniel J. Dire, MD University Texas Health Sciences Center San Antonio
Douglas Ander, MD Emory University
Douglas Ander, Emory University
Emory University
Edward Michelson, MD Texas Tech University
Edward Michelson, MD Texas Tech University
Edward Michelson, Texas Tech University
Edward Panacek, MD, MPH South
Edward Panacek, MD, MPH University of South Alabama
Edward MD, MPH University South Alabama
Francesco
“Maggiore della Carità,” Novara, Italy
Francesco Della Corte, MD Azienda Ospedaliera Universitaria “Maggiore della Carità,” Novara, Italy
Francesco Della Corte, MD Azienda Ospedaliera Universitaria “Maggiore della Novara, Italy
Elena Lopez-Gusman, JD
Elena Lopez-Gusman, JD
California ACEP
California ACEP
Elena Lopez-Gusman, JD California ACEP American College of Emergency
Sørlandet Sykehus HF, Akershus Universitetssykehus, Lorenskog,
Sørlandet Sykehus HF, Akershus Universitetssykehus, Lorenskog, Norway
Sørlandet Sykehus HF, Akershus Universitetssykehus, Lorenskog, Norway
Hjalti Björnsson, MD
Niels K. Rathlev, MD Tufts University School of Medicine
Tufts University School of Medicine
Niels K. Rathlev, MD Tufts University School of Medicine
Scott Zeller, MD
Scott Zeller, MD University of California, Riverside
Scott Zeller, MD University of California, Riverside
Hjalti Björnsson, MD Icelandic Society of Emergency Medicine
Hjalti MD Icelandic Society of Emergency Medicine
Jaqueline Le, MD Desert Regional Medical Center
Jaqueline Le, MD Desert Medical Center
Regional
Jeffrey Love, MD
Jeffrey Love, MD The George Washington University School of Medicine and Health Sciences
Jeffrey Love, The George Washington University School of Medicine and Health Sciences
Katsuhiro Kanemaru, MD University of Miyazaki Hospital, Miyazaki, Japan
Katsuhiro Kanemaru, MD University of Hospital, Miyazaki, Japan
Pablo Aguilera Fuenzalida, MD Pontificia Universidad Catolica de Chile, Región Metropolitana, Chile
Pablo Aguilera Fuenzalida, MD Pontificia Universidad Catolica de Chile, Región Metropolitana, Chile
Pablo Aguilera Fuenzalida, MD Pontificia Universidad Catolica de
Peter A. Bell, DO, MBA Baptist Health Sciences University
Bell,
Peter A. Bell, DO, MBA Baptist Health Sciences University
Peter Sokolove, MD University of California, San Francisco
Steven H. Lim, MD Changi General Hospital, Simei, Singapore
Singapore
Steven H. Lim, MD Changi General Hospital, Simei, Singapore
Terry Mulligan, DO, MPH, FIFEM ACEP Ambassador to the Netherlands Society of Emergency Physicians
Terry Mulligan, DO, MPH, FIFEM ACEP Ambassador to the Netherlands Society of Emergency Physicians
Terry Mulligan, DO, MPH, FIFEM ACEP Ambassador to the Netherlands
Peter Sokolove, MD University of California, San Francisco
University of California, San Francisco
Wirachin Hoonpongsimanont, MD, MSBATS
Wirachin Hoonpongsimanont, MD, MSBATS
Kenneth V. Iserson, MD, MBA University of Arizona, Tucson
The George Washington University School of Medicine and Health Sciences Arizona,
Kenneth V. Iserson, MD, MBA University of Arizona, Tucson
Leslie Zun, MD, MBA Chicago Medical School
Leslie Zun, MD, MBA Chicago Medical School
Rachel A. Lindor, MD, JD Mayo Clinic
Rachel A. Lindor, MD, JD Mayo Clinic
Rachel A. Lindor, MD, JD
Siriraj Hospital, Mahidol University, Bangkok, Thailand
Siriraj Hospital, Mahidol University, Bangkok, Thailand
Robert Suter, DO, MHA UT Southwestern Medical Center
Robert Suter, DO, MHA
Robert Suter, DO, MHA UT Southwestern Medical Center
Robert W. Derlet, MD University of California, Davis
University of California, Davis
Robert W. Derlet, MD University of California, Davis
Rosidah Ibrahim, MD Hospital Serdang, Selangor, Malaysia
Rosidah Ibrahim, MD Hospital Serdang, Selangor, Malaysia
Rosidah Ibrahim, MD Hospital Serdang, Selangor, Malaysia
Linda S. Murphy, MLIS University of California, Irvine School of Medicine
Chicago Medical School Librarian
Linda S. Murphy, MLIS University of California, Irvine School of Medicine Librarian
Langdorf, MAAEM, FACEP
Mark I. Langdorf, MD, MHPE, MAAEM, FACEP
Scott Rudkin, MD, MBA University of California, Irvine
Scott Rudkin, MD, MBA
Scott Rudkin, MD, MBA University of California, Irvine
Staff
American College of Emergency Physicians
American College of Emergency Physicians
Jennifer Kanapicki Comer, MD FAAEM
Jennifer Kanapicki Comer, MD FAAEM
California Chapter Division of AAEM Stanford University School of Medicine
California Chapter Division of AAEM Stanford University School of Medicine
Kimberly Ang, MBA
DeAnna McNett, CAE
DeAnna McNett, CAE
American College of Osteopathic Emergency Physicians
UC Irvine Health School of Medicine
American College of Osteopathic Emergency Physicians
Randall J. Young, MD, MMM, FACEP California ACEP
Kimberly Ang, MBA
American College of Emergency Physicians Kaiser Permanente
UC Irvine Health School of Medicine
Randall J. Young, MD, MMM, FACEP California ACEP
American College of Emergency Physicians
J. American College of Emergency Physicians
Kaiser Permanente
Kaiser Permanente

UC Irvine Health School of Medicine
Mark I. Langdorf, MD, MHPE, MAAEM, FACEP UC Irvine Health School Medicine
UC Irvine Health School of Medicine
Robert Suter, DO, MHA
Robert Suter, DO, MHA American College of Osteopathic
American College of Osteopathic Emergency Physicians UT Southwestern Medical Center
Robert Suter, DO, MHA American College of Osteopathic Emergency Physicians UT Southwestern Medical Center
Shahram Lotfipour, MD, MPH FAAEM, FACEP UC Irvine Health School of Medicine
Shahram Lotfipour, MD, MPH FAAEM, FACEP UC Irvine Health School Medicine
Jorge Fernandez, MD, FACEP
Jorge Fernandez, MD, FACEP
Isabelle Nepomuceno, BS Executive Editorial Director
Isabelle Kawaguchi, BS Executive Editorial Director
Ian Olliffe, BS Associate Editorial Director, WestJEM
June Casey, BA Copy Editor
Visha Bajaria, BS WestJEM Editorial Director
Emily Kane, MA WestJEM Editorial Director
Emily Kane, MA WestJEM Editorial Director
Stephanie Burmeister, MLIS WestJEM Staff Liaison
Cassandra Saucedo, MS Executive Publishing Director
Visha Bajaria, BS WestJEM Editorial Director WestJEM
Stephanie Burmeister, MLIS WestJEM Staff Liaison
Cassandra Saucedo, MS WestJEM Publishing Director
Tran Nguyen, BS Associate Editorial Director, CPC-EM
Nicole Valenzi, BA WestJEM Publishing Director
Sheya Aquino, BS Associate Editorial Director
June Casey, BA Copy Editor
Nancy Taki, BS Associate Editorial Director
Jorge Fernandez, MD, UC San Diego Health School of Medicine
UC San Diego Health School of Medicine
UC San Diego Health School of Medicine
Cassandra Saucedo, MS Executive Publishing Director
Nicole Valenzi, BA WestJEM Publishing Director
Alyson Tsai, BS Associate Publishing Director
Official Journal of the California Chapter of the American College of Emergency Physicians, the America College of Osteopathic Emergency Physicians, and the California Chapter of the American Academy of Emergency Medicine







in Melvyl,
Available in MEDLINE, PubMed, PubMed Central, Europe PubMed Central, PubMed Central Canada, CINAHL, SCOPUS, Google Scholar, eScholarship, Melvyl, DOAJ, EBSCO, EMBASE, Medscape, HINARI, and MDLinx Emergency Med. Members of OASPA. Editorial and Publishing Office: WestJEM/Depatment of Emergency Medicine, UC Irvine Health, 3800 W. Chapman Ave. Suite 3200, Orange, CA 92868, USA Office: 1-714-456-6389; Email: Editor@westjem.org
Editorial and Publishing Office: JEM/Depatment of Emergency Medicine, UC Irvine Health, 3800 W. Chapman Ave. Suite 3200, Orange, CA 92868, USA
Integrating Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
Emergency medicine is a specialty which closely reflects societal challenges and consequences of public policy decisions. The emergency department specifically deals with social injustice, health and economic disparities, violence, substance abuse, and disaster preparedness and response. This journal focuses on how emergency care affects the health of the community and population, and conversely, how these societal challenges affect the composition of the patient population who seek care in the emergency department. The development of better systems to provide emergency care, including technology solutions, is critical to enhancing population health.
1 Substance Use and Addiction Disorders : A Call for Increased Screening and Treatment in the Emergency Department
RG Wilkerson, AM LaPietra
3 Implementation and Evaluation of a Bystander Naloxone Training Course
SG Weiner, SA Goldberg, C Lang, M Jarman, CJ Miller, S Li, EW Stanek, E Goralnick
8 Harm Reduction in the Field: First Responders’ Perceptions of Opioid Overdose Interventions
CE Fockele, T Frohe, O McBride, DL Perlmutter, B Goh, G Williams, C Wettemann, N Holland, B Finegood, T Oliphant-Wells, EC Williams, J van Draanen
18 Pragmatic Emergency Department Intervention Reducing Default Quantity of Opioid Tablets Prescribed
DG Johnson, AY Lu, GA Kim, K Trepka, SC Yang, JCC Montoy, MA Juarez
26 Bystanders Saving Lives with Naloxone: A Scoping Review on Methods to Estimate Overdose Reversals
AT Kinoshita, S Saadat, B Chakravarthy
33 Attitudes, Beliefs, Barriers, and Facilitators of Emergency Department Nurses Toward Patients with Opioid Use Disorder and Naloxone Distribution
C Michels, T Schneider, K Tetreault, JM Payne, K Zubke, E Salisbury-Afshar
38 Improving Healthcare Professionals’ Access to Addiction Medicine Education Through VHA Addiction Scholars Program
Z Basarai, M Celedon, N Dieujuste, J Himstreet, J Hoffman, C Pfaff, J Hsiao, R Malstrom, J Smith, M Radeos, T Jorgenson, M Christopher, C Sasson
43 Initiation of Buprenorphine in the Emergency Department: A Survey of Emergency Clinicians
MM Mroczkowski, JT Walkup, PS Walkup
50 A Novel Use of the “3-Day Rule”: Post-discharge Methadone Dosing in the Emergency Department
JK Nikolaides, TH Tran, E Ramsey, S Salib, H Swoboda
56 Variability in Practice of Buprenorphine Treatment by Emergency Department Operational Characteristics
G Comstock, N Truszczynski, SS Michael, J Hoppe
63 Impact of Emergency Department-Initiated Buprenorphine on Repeat Emergency Department Utilization
RM Skains, L Reynolds, N Carlisle, S Heath, W Covington, K Hornbuckle, L Walter
Policies for peer review, author instructions, conflicts of interest and human and animal subjects protections can be found online at www.westjem.com.
No. 1.1: January 2025
Integrating Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
71 Accessibility of Naloxone in Pharmacies Registered Under the Illinois Standing Order P Quincy Moore, K Ellis, P Simmer, M Waetjen, E Almirol, E Salisbury-Afshar, MT Pho
Integrating Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
This open access publication would not be possible without the generous and continual financial support of our society sponsors, department and chapter subscribers.
Professional Society Sponsors
American College of Osteopathic Emergency Physicians
California American College of Emergency Physicians
Academic Department of Emergency Medicine Subscriber Albany Medical College Albany, NY
Allegheny Health Network Pittsburgh, PA
American University of Beirut Beirut, Lebanon
AMITA Health Resurrection Medical Center Chicago, IL
Arrowhead Regional Medical Center Colton, CA
Baylor College of Medicine Houston, TX
Baystate Medical Center Springfield, MA
Bellevue Hospital Center New York, NY
Beth Israel Deaconess Medical Center Boston, MA
Boston Medical Center Boston, MA
Brigham and Women’s Hospital Boston, MA
Brown University Providence, RI
Carl R. Darnall Army Medical Center Fort Hood, TX
Cleveland Clinic Cleveland, OH
Columbia University Vagelos New York, NY
State Chapter Subscriber
Arizona Chapter Division of the American Academy of Emergency Medicine
California Chapter Division of the American Academy of Emergency Medicine
Florida Chapter Division of the American Academy of Emergency Medicine
International Society Partners
Conemaugh Memorial Medical Center Johnstown, PA
Crozer-Chester Medical Center Upland, PA
Desert Regional Medical Center Palm Springs, CA
Detroit Medical Center/ Wayne State University Detroit, MI
Eastern Virginia Medical School Norfolk, VA
Einstein Healthcare Network Philadelphia, PA
Eisenhower Medical Center Rancho Mirage, CA
Emory University Atlanta, GA
Franciscan Health Carmel, IN
Geisinger Medical Center Danville, PA
Grand State Medical Center Allendale, MI
Healthpartners Institute/ Regions Hospital Minneapolis, MN
Hennepin County Medical Center Minneapolis, MN
Henry Ford Medical Center Detroit, MI
Henry Ford Wyandotte Hospital Wyandotte, MI
Emergency Medicine Association of Turkey Lebanese Academy of Emergency Medicine Mediterranean Academy of Emergency Medicine
California Chapter Division of American Academy of Emergency Medicine
INTEGRIS Health Oklahoma City, OK
Kaiser Permenante Medical Center San Diego, CA
Kaweah Delta Health Care District Visalia, CA
Kennedy University Hospitals Turnersville, NJ
Kent Hospital Warwick, RI
Kern Medical Bakersfield, CA
Lakeland HealthCare St. Joseph, MI
Lehigh Valley Hospital and Health Network Allentown, PA
Loma Linda University Medical Center Loma Linda, CA
Louisiana State University Health Sciences Center New Orleans, LA
Louisiana State University Shreveport Shereveport, LA
Madigan Army Medical Center Tacoma, WA
Maimonides Medical Center Brooklyn, NY
Maine Medical Center Portland, ME
Massachusetts General Hospital/Brigham and Women’s Hospital/ Harvard Medical Boston, MA
Great Lakes Chapter Division of the American Academy of Emergency Medicine
Tennessee Chapter Division of the American Academy of Emergency Medicine
Norwegian Society for Emergency Medicine Sociedad Argentina de Emergencias
Mayo Clinic Jacksonville, FL
Mayo Clinic College of Medicine Rochester, MN
Mercy Health - Hackley Campus Muskegon, MI
Merit Health Wesley Hattiesburg, MS
Midwestern University Glendale, AZ
Mount Sinai School of Medicine New York, NY
New York University Langone Health New York, NY
North Shore University Hospital Manhasset, NY
Northwestern Medical Group Chicago, IL
NYC Health and Hospitals/ Jacobi New York, NY
Ohio State University Medical Center Columbus, OH
Ohio Valley Medical Center Wheeling, WV
Oregon Health and Science University Portland, OR
Penn State Milton S. Hershey Medical Center Hershey, PA
Uniformed Services Chapter Division of the American Academy of Emergency Medicine
Virginia Chapter Division of the American Academy of Emergency Medicine
for Emergency Medicine
To become a WestJEM departmental sponsor, waive article processing fee, receive electronic copies for all faculty and residents, and free CME and faculty/fellow position advertisement space, please go to http://westjem.com/subscribe or contact:
Stephanie Burmeister
WestJEM Staff Liaison
Phone: 1-800-884-2236
Email: sales@westjem.org
Integrating Emergency Care with Population Health
Indexed in MEDLINE, PubMed, and Clarivate Web of Science, Science Citation Index Expanded
This open access publication would not be possible without the generous and continual financial support of our society sponsors, department and chapter subscribers.
Professional Society Sponsors
American College of Osteopathic Emergency Physicians
California American College of Emergency Physicians
Academic Department of Emergency Medicine Subscriber Prisma Health/ University of South Carolina SOM Greenville Greenville, SC
Regions Hospital Emergency Medicine Residency Program St. Paul, MN
Rhode Island Hospital Providence, RI
Robert Wood Johnson University Hospital New Brunswick, NJ
Rush University Medical Center Chicago, IL
St. Luke’s University Health Network Bethlehem, PA
Spectrum Health Lakeland St. Joseph, MI
Stanford Stanford, CA
SUNY Upstate Medical University Syracuse, NY
Temple University Philadelphia, PA
Texas Tech University Health Sciences Center El Paso, TX
The MetroHealth System/ Case Western Reserve University Cleveland, OH
UMass Chan Medical School Worcester, MA
University at Buffalo Program Buffalo, NY
State Chapter Subscriber
Arizona Chapter Division of the American Academy of Emergency Medicine
California Chapter Division of the American Academy of Emergency Medicine
Florida Chapter Division of the American Academy of Emergency Medicine
International Society Partners
University of Alabama Medical Center Northport, AL
University of Alabama, Birmingham Birmingham, AL
University of Arizona College of Medicine-Tucson Tucson, AZ
University of California, Davis Medical Center Sacramento, CA
University of California, Irvine Orange, CA
University of California, Los Angeles Los Angeles, CA
University of California, San Diego La Jolla, CA
University of California, San Francisco San Francisco, CA
UCSF Fresno Center Fresno, CA
University of Chicago Chicago, IL
University of Cincinnati Medical Center/ College of Medicine Cincinnati, OH
University of Colorado Denver Denver, CO
University of Florida Gainesville, FL
University of Florida, Jacksonville Jacksonville, FL
Emergency Medicine Association of Turkey Lebanese Academy of Emergency Medicine Mediterranean Academy of Emergency Medicine
California Chapter Division of American Academy of Emergency Medicine
University of Illinois at Chicago Chicago, IL
University of Iowa Iowa City, IA
University of Louisville Louisville, KY
University of Maryland Baltimore, MD
University of Massachusetts Amherst, MA
University of Michigan Ann Arbor, MI
University of Missouri, Columbia Columbia, MO
University of North Dakota School of Medicine and Health Sciences Grand Forks, ND
University of Nebraska Medical Center Omaha, NE
University of Nevada, Las Vegas Las Vegas, NV
University of Southern Alabama Mobile, AL
University of Southern California Los Angeles, CA
University of Tennessee, Memphis Memphis, TN
University of Texas, Houston Houston, TX
University of Washington Seattle, WA
Great Lakes Chapter Division of the American Academy of Emergency Medicine
Tennessee Chapter Division of the American Academy of Emergency Medicine
Norwegian Society for Emergency Medicine Sociedad Argentina de Emergencias
University of WashingtonHarborview Medical Center Seattle, WA
University of Wisconsin Hospitals and Clinics Madison, WI
UT Southwestern Dallas, TX
Valleywise Health Medical Center Phoenix, AZ
Virginia Commonwealth University Medical Center Richmond, VA
Wake Forest University Winston-Salem, NC
Wake Technical Community College Raleigh, NC
Wayne State Detroit, MI
Wright State University Dayton, OH
Yale School of Medicine New Haven, CT
Uniformed Services Chapter Division of the American Academy of Emergency Medicine
Virginia Chapter Division of the American Academy of Emergency Medicine
for Emergency Medicine
To become a WestJEM departmental sponsor, waive article processing fee, receive electronic copies for all faculty and residents, and free CME and faculty/fellow position advertisement space, please go to http://westjem.com/subscribe or contact:
Stephanie Burmeister
WestJEM Staff Liaison
Phone: 1-800-884-2236
Email: sales@westjem.org
R. Gentry Wilkerson, MD* Alexis M. LaPietra, DO†
University of Maryland School of Medicine, Department of Emergency Medicine, Baltimore, Maryland
†
RWJBarnabus Health, Division of Emergency Medicine, West Orange, New Jersey
Section Editor: Mark I. Langdorf, MD, MHPE
Submission history: Submitted October 24, 2024; Revision received October 24, 2024; Accepted October 24, 2024
Electronically published January 20, 2025
Full text available through open access at http://escholarship.org/uc/uciem_cpcem DOI: 10.5811/cpcem.41808
[West J Emerg Med. 2025;26(1.1)1–2.]
We are very pleased to present the Western Journal of Emergency Medicine (WestJEM) Special Issue on Substance Use and Addiction Disorders. The emergency department (ED) is on the front line in the battle to combat the impact that drugs and alcohol have on the lives of individuals. Each of the articles included in this issue reflects the work and dedication that the authors have devoted to improving the care of patients with substance use and addiction disorders. It is our honor to promote these articles by compiling them under the single banner of a special issue.
According to the 2023 National Survey on Drug Use and Health (NSDUH) 1 released by the US Department of Health and Human Services’ Substance Abuse and Mental Health Services Administration, there are an estimated 48.5 million individuals ≥12 years of age living with a substance use disorder. This is an astounding 17.1% of the population, or more than 1 in every 6 individuals. The NSDUH also found that alcohol use disorder impacts 10.2% of those ≥12. The impact of these disorders leads to high healthcare resource utilization, poor health outcomes, and increased mortality. The average annual number of deaths attributable to excessive alcohol use reached 178,307 during 20202021. 2 Drug overdose deaths have steadily risen every year through 2022 when 107,941 deaths were reported.3 This has largely been driven by opioids. In 2022, there were 82,136 opioid-related overdose deaths.4
The ED bears witness to a multitude of other conditions that are directly related to substance use and addiction disorders. In 2020, there were 11,654 people in the US killed in motor vehicle collisions involving a driver under the influence of alcohol.5 Many more were injured and required care in our EDs. Chronic alcohol use leads to fibrosis and cirrhosis of the liver, which in turn leads to the
development of ascites and esophageal varices. Patients may present critically ill with spontaneous bacterial peritonitis or upper gastrointestinal bleeding. Patients who inject drugs are at risk for development of skin and soft tissue infections, endocarditis, spinal epidural abscesses, HIV, and hepatitis C.
Thanks to pioneers in emergency medicine, our specialty no longer waits for the complications to occur. Rather, we try to reduce the risk of harm related to drug and alcohol use and promote initiation of treatment. In the last decade, it has become common practice for emergency physicians to initiate treatment of opioid use disorder with buprenorphine thanks to the pivotal research showing better retention in treatment when it was initiated in the ED. 6 Many EDs are now using peer recovery coaches and the SBIRT (Screening, Brief Intervention, and Referral to Treatment) process to identify patients with opioid addiction and either initiate treatment in the ED or have a rapid referral to treatment programs.7 In addition to initiating treatment with buprenorphine, EDs are distributing the opioid receptor antagonist, naloxone, to at-risk individuals. The American College of Emergency Physicians has supported increased access to this lifesaving medication since 2015.8
Research is ongoing regarding how to best support patients with substance use and addiction disorders. We hope that this special issue contributes in some way to protecting the health and saving the lives of our patients.
Address for Correspondence: R. Gentry Wilkerson, MD, University of Maryland School of Medicine, Department of Emergency Medicine, 110 South Paca Street, 6th Floor, Suite 200, Baltimore, MD 21201. Email: gwilkerson@som.umaryland.edu.
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. Dr. Wilkerson received research funding from Regeneron Pharmaceuticals, Inc.; Lilly USA, LLC; BioAge Labs, Inc.; Roche Diagnostics; Global Blood Therapeutics, Inc.; Novartis Pharmaceuticals; Egetis Therapeutics AB; EndPoint Health, Inc.; Blade Therapeutics; Janssen R&D LLC; ProvePharma; CSL Behring; Beckton, Dickinson and Company; Pfizer Inc.; Greiner Bio-One North America, Inc.; and the National Foundation of Emergency Medicine (NFEM). He has received research funding from CoapTech, LLC through an NIH/NIDDK grant (R44DK115325). He has received research support in the form of equipment and supplies from Cepheid and Eldon Biologicals A/S. He is a paid consultant for NFEM. The authors disclosed no conflicts of interest.
Copyright: © 2025 Wilkerson et al. This is an open access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) License. See: http://creativecommons.org/ licenses/by/4.0/
1. Substance Abuse and Mental Health Services Administration. (2024). Key substance use and mental health indicators in the United States: Results from the 2023 National Survey on Drug Use and Health (HHS Publication No. PEP24-07-021, NSDUH Series H-59). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. Available at: https:// www.samhsa.gov/data/report/2023-nsduh-annual-national-report.
Accessed September 24, 2024
2. Esser MB, Sherk A, Liu Y, et al. Deaths from Excessive Alcohol Use — United States, 2016–2021. Morb Mortal Wkly Rep. 2024;73(8):154-61.
3. Spencer MR, Garnett MF, Miniño AM. 2024. Drug overdose deaths in the United States, 2002–2022. NCHS Data Brief, no 491. Hyattsville, MD: National Center for Health Statistics. Available at: https://stacks.cdc. gov/view/cdc/135849. Accessed September 24, 2024.
4. The HEALing Communities Study Consortium. Community-based cluster-randomized trial to reduce opioid overdose deaths. N Engl J Med. 2024;391:989-1001.
5. National Highway Traffic Safety Administration (NHTSA). Traffic Safety Facts 2020 Data: Alcohol-Impaired Driving (Report No DOT HS 813 294). Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration, National Center for Statistics and Analysis; April 2022. Available at: https://crashstats.nhtsa.dot.gov/Api/ Public/ViewPublication/813294. Accessed September 23, 2024.
6. D’Onofrio G, O’Connor PG, Pantalon MV, et al. Emergency departmentinitiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. JAMA. 2015;313(16):1636-44.
7. Monico LB, Oros M, Smith S, et al. One million screened: scaling up SBIRT and buprenorphine treatment in hospital emergency departments across Maryland. Am J Emerg Medicine. 2020;38(7):1466-9.
8. American College of Emergency Physicians Policy Statement, Naloxone Access and Utilization for Suspected Opioid Overdoses. Available at: https://www.acep.org/siteassets/new-pdfs/policy-statements/naloxoneaccess-and-utilization-for-suspected-opioid-overdoses.pdf. Accessed September 24, 2024.
ScottG.Weiner,MD,MPH*
ScottA.Goldberg,MD,MPH*
CherylLang,MPH†
MollyJarman,PhD,MPH†
CoryJ.Miller,BS*
SarahLi,BA*
EwelinaW.Stanek,PA-C*
EricGoralnick,MD,MS*
SectionEditor:MarcMartel,MD
*BrighamandWomen’sHospital,DepartmentofEmergencyMedicine, Boston,Massachusetts † BrighamandWomen’sHospital,DepartmentofSurgery,Boston,Massachusetts
Submissionhistory:SubmittedMarch13,2023;RevisionreceivedSeptember26,2023;AcceptedJanuary12,2024
ElectronicallypublishedApril9,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.60409
Introduction: Bystanderprovisionofnaloxoneisakeymodalitytoreduceopioidoverdose-related death.Naloxonetrainingcoursesareavailable,butnostandardizedprogramexists.Aspartofa bystanderempowermentcourse,wecreatedandevaluatedabriefnaloxonetrainingmodule.
Methods: Thiswasaretrospectiveevaluationofanaloxonetrainingcourse,whichwaspairedwithStop theBleedtrainingforhemorrhagecontrolandwasofferedtoadministrativestaffinanofficebuilding. Participantsworkedinanorganizationrelatedtohealthcare,butnonewereclinicians.Thecurriculum includedthefollowingtopics:1)backgroundabouttheopioidepidemic;2)howtorecognizethesignsof anopioidoverdose;3)actionsnottotakewhenencounteringanoverdosevictim;4)thecorrectstepsto takewhenencounteringanoverdosevictim;5)anoverviewofnaloxoneproducts;and6)Good Samaritanprotectionlaws.The20-minutedidacticsectionwasfollowedbyahands-onsessionwith nasalnaloxonekitsandasimulationmannequin.ThecoursewasevaluatedwiththeOpioidOverdose Knowledge(OOKS)andOpioidOverdoseAttitudes(OOAS)scalesfortake-homenaloxonetraining evaluation.WeusedthepairedWilcoxonsigned-ranktesttocomparescorespre-andpost-course.
Results: Twenty-eightparticipantscompletedthecourse.TheOOKS,measuringobjectiveknowledge aboutopioidoverdoseandnaloxone,hadimprovedscoresfromamedianof73.2%(interquartilerange [IQR]68.3%–79.9%)to91.5%(IQR85.4%–95.1%), P < 0.001.ThethreedomainsontheOOASscore alsoshowedstatisticallysignificantresults.Competencytomanageanoverdoseimprovedona fivepointscalefromamedianof2.5(IQR2.4–2.9)toamedianof3.7(IQR3.5–4.1), P < 0.001.Concerns aboutmanaginganoverdosedecreased(improved)fromamedianof2.3(IQR1.9–2.6)tomedian1.8 (IQR1.5–2.1), P < 0.001.Readinesstointerveneinanopioidoverdoseimprovedfromamedianof4 (IQR3.8–4.2)toamedianof4.2(IQR4–4.2), P < 0.001.
Conclusion: Abriefcoursedesignedtoteachbystandersaboutopioidoverdoseandnaloxonewas feasibleandeffective.Weencouragehospitalsandotherorganizationstouseandpromulgatethis model.Furthermore,wesuggesttheconveningofanationalconsortiumtoachieveconsensuson programcontentanddelivery.[WestJEmergMed.2025;26(1.1)3–7.]
Timeisacriticalcontributingfactorinpatientoutcomes inmanyemergencies.IntheUnitedStates,theaverage responsetimebyemergencymedicalservicestoa9-1-1callis sevenminutes.1 Tobridgethisgap,manyeffortshavebeen launchedtoempowerlaypersons,whoaretypically firston thescene,tointerveneandemployskillsrangingfrom cardiopulmonaryresuscitation(CPR)andautomated externaldefibrillator(AED)usetobleedingcontrol interventions.2 BasicLifeSupport(BLS)coursecontentis baseduponrigorousandfrequentlyupdatedconsensus(ie, AmericanHeartAssociation[AHA]GuidelinesUpdatefor CPRandEmergencyCardiovascularCare).3,4 Thesecourses aretaughtinastandardizedfashionbytheAHAandthe AmericanRedCross.Likewise,theStoptheBleed(STB) program,anationalinitiativelaunchedin2015focusedon empoweringthepublicandpublicsafetyprofessionalsto recognizeandcontrollife-threateningbleeding,hasseveral typesofcourses,themostprominentbeingtheAmerican CollegeofSurgeons’ (ACS)BasicHemorrhageControl Course(BCon).5,6
WhileCPR,AEDandSTBtrainingfocusonpreventable deaths,anothersignificantsourceofpreventabledeathsisthe opioidoverdoseepidemic,whichremainsoneofthemost pressingpublichealthissuesofourtime,havingclaimed about1,000,000livesintheUSsince1999.7 Thenumberof overdosedeathshasincreasedgreatlyinrecentyears,with yetanotherrecordnumberin2021,predominantlydueto fentanyl.8 Bystandernaloxoneadministration,whichcanbe usedtoreverseanopioidoverdose,hasbeenintroducedas onepotentialmitigatingfactor.In2018,theUSSurgeon Generalissuedanadvisoryonnaloxoneandopioidoverdose thatencouragescommunitymemberswhocomeintocontact withpeopleatriskforopioidoverdosetoknowhowtouse naloxoneandkeepitwithinreach.9 Likewise,theUS DepartmentofHealthandHumanServices’ overdose preventionstrategyincludesharmreduction,withagoalto widenaccesstoopioidoverdosereversaltreatments.10
UnlikeCPR,thereisnoonestandardizedcoursefor bystandernaloxonetraining.Onlinecoursesareofferedby agenciessuchastheCentersforDiseaseControland Prevention(CDC),11 theAmericanRedCross,12 individual states(eg,Massachusetts13 andNewYork14),andothernonprofits(eg,GetNaloxoneNow15).Thecourseslacka standardizedcorecontent,measuresofeffectiveness,oragreedupondeliverymethods(inperson,hybrid,remote,simulation, didactic,etc).Althoughanecdotesexistoflaypersonuse,we havealimitedunderstandingofaneffective,layperson naloxone-empowermentcurriculum,andgapsremainin knowledgeabouttrainingparametersandstrategies.16
Inthisstudy,weevaluatedanoverdose-responsenaloxone trainingprogramadministeredtolaypersons.We emphasizedthestructureandcurriculumofthecourseand evaluatedefficacywithavalidatedscreeningtool.
Thenaloxonecoursewasdesignedtobeabrief interventionwith20minutesofdidacticsand20minutesof practicalexperiencewithamannequin.Thecoursewas bundledwiththeACSBConcourseaspartofabystander empowermentprogram.Courseinstructorswerethree board-certifiedemergencyphysicians.Thesessiontookplace ataprofessionalofficebuilding.Althoughtheparticipants workedinanorganizationrelatedtohealthcare,allworked asofficestaffandnonewereclinicians.Twoidenticalsessions wereoffered,andbothtookplaceinJune2018during normalbusinesshours.Participantswerenotcompensated specificallyforparticipatingbutattendedinlieuoftheir normalduties.Weadministeredanonymouspre-andpostcourseevaluations.Theprojectwasdeterminedtonotmeet thecriteriaforhumansubjectresearchbytheMassGeneral BrighamHumanResearchOffice.
Createdbythecourseinstructors,thecurriculumincluded thefollowingtopics:1)backgroundabouttheopioid epidemic;2)howtorecognizethesignsofanopioid overdose;3)actionsnottotakewhenencounteringan overdosevictim;4)thecorrectstepstotakewhen encounteringanoverdosevictim;5)anoverviewofnaloxone products;and6)GoodSamaritanprotectionlaws.Content wascreatedby firstsearchingforexistingtrainingresources online,includingtrainingmanualsfromthestatesofNew York(https://www.dhses.ny.gov/naloxone-informationfirst-responders)andTexas(https://txoti.org),andCanadian provinceManitoba(https://www.gov.mb.ca/health/ publichealth/docs/training_manual_overdose.pdf).This informationwasintegratedwithadditionalcontentfrom courseinstructorexpertiseintoadidacticmodulecontaining 30slides(Appendix1),andparticipantswereprovidedwitha hardcopyoftheslides.Thepracticalmoduleentailedsmall groupsaroundasimulationmannequinwithacourse instructor.Participantswereabletopracticewithtwotypes ofnaloxonekits(pre-packagednasalnaloxonesprayandan autoinjector)onthemannequin.Discussionwasencouraged untilallparticipants’ questionsandconcernswereaddressed.
Toevaluatetheefficacyofthecourse,weusedtheOpioid OverdoseKnowledge(OOKS)andOpioidOverdose Attitudes(OOAS)scalesfortake-homenaloxonetraining evaluation.17 The firsthalfofthisvalidatedtool(OOKS)asks objectivequestionsaboutopioidoverdosetoevaluatetrainee knowledge,includingindicatorsofopioidoverdose,howto manageanoverdose,themechanismofactionofnaloxone, anditsdurationofaction.Thesecondpart(OOAS)asks questionspertainingtoperceptionsofcompetenciesto manageanopioidoverdose,concernsaboutmanagingan overdose,andreadinesstointerveneinanopioidoverdose.
Allparticipantscompletedpre-andpost-evaluationson paperforms.Subjectswereaskedtowritethesamerandom four-digitnumberoneachofthetwoevaluationsforpaired analysispurposes.Responsesweretransferredtoa spreadsheet,andasecondinvestigatorconfirmedthe accuracyofthetranscription.TheOOKSscaleisaseriesof true/falsestatements,andthecorrectanswersweresummed, withatotalpossible41points.Wemodifiedtheoriginal 45-pointversionslightly,asmultiplepointswerepossiblefor severalindividualquestions(eg, “Whatisnaloxoneused for?” and “Howcannaloxonebeadministered?”)andwe countedthemonlyasonepointeach.Therewasalsoachoice of “don’tknow” forseveralquestions,andthatwas consideredanincorrectanswerasindicatedinthescoring instructions.TheOOASscaleis28questionsdividedinto threedomainsandmeasuredona five-pointLikertscale (5 = completelyagreeand1 = completelydisagree). Althoughthepost-testOOKSresultsandoneofthedomains ontheOOASwerenormallydistributedasdeterminedbythe Shapiro-Wilktest,theremainderofresultswerenon-normal. Thus,allresults,includingthescalesoneachdomainofthe OOASandtheoverallscoreontheOOKS,aredescribed withmediansandinterquartilerange(IQR)andcompared withthepairedWilcoxonsigned-ranktest.Weanalyzeddata withJMPv16(JMPStatisticalDiscoveryLLC,Cary.NC).
Twenty-eightparticipantstookthecourse.Allcompleted thepre-testandthepost-test,althoughthreeparticipantsdid notanswerallquestionsonthepre-testOOASscale. Therefore,thecorrespondinganswersinthedomainsfor thesethreeindividualsonthepost-testwerenotincludedin theanalysis.TheOOKS,measuringobjectiveknowledge aboutopioidoverdoseandnaloxone,hadimprovedscores fromamedianof73.2%(IQR68.3%–79.9%)to91.5%(IQR 85.4%–95.1%), P < 0.001.ThethreedomainsontheOOAS scorealsoshowedstatisticallysignificantresults. Competencytomanageanoverdoseimprovedfroma medianof2.5(IQR2.4–2.9)toamedianof3.7(IQR 3.5–4.1), P < 0.001.Concernsaboutmanaginganoverdose decreased(improved)fromamedianof2.3(IQR1.9–2.6)to median1.8(IQR1.5–2.1), P < 0.001.Readinesstointervene inanopioidoverdoseimprovedfromamedianof4(IQR 3.8–4.2)toamedianof4.2(IQR4–4.2), P < 0.001.
Increatingandevaluatinganaloxonetrainingprogram forbystanders,wefoundimprovementinbothsubjective attitudesandobjectiveknowledgeaboutopioidoverdose andnaloxone.Thetrainingisrelativelybrief(lastingunder anhour)andeffective.Wehavesubsequentlytaughtthis curriculumseveraltimestolocalcommunityorganizations, includingthosewhoworkwithpeoplewhousedrugs.
Althoughwedidnotmeasureobjectiveoutcomes subsequently,theconceptofbystanderempowerment, teachingbothnaloxoneandSTBskills,hasbeenwell receivedandrepresentsimportantoutreachfromour hospitaltothelocalcommunity.
Onekeyquestionthatremainsiswhetherthistrainingis necessaryforbystanders.Inourpreviousresearch,wefound that49of50bystanderswereabletocorrectlyadminister naloxoneinasimulatedexperienceonapublicsidewalkwith guidancebyasimulated911dispatcher.18 However,not everyonewillhavetheguidanceofadispatcherwhenusing naloxone,andtheremaybeconfusionabouthowtousethe kitandthetimingofaseconddose(ifneeded)withoutthat assistance.Bystandertrainingmayalsobevaluableasaway tofosterself-efficacy,increasingthelikelihoodthata laypersonwillrecognizeandrespondtoanoverdose.Inour course,wealsocoverwhenbystandersshouldadminister naloxoneanddispelmythsaboutanyharmthatcanbe causedbygivingit,aswellashowtoaccessnaloxone.
Naloxoneforbystandersiscurrentlyavailablevia standingorderinseveralstates,meaningthatindividualscan obtainitfrompharmacieswithoutaprescription.19–22 Standingordersareassociatedwithreductionsinfatal overdosesinthecommunity.23 Thecurrentpackagingof prescriptionnasalnaloxonehasa flapthatopensgivingjustin-time(JIT)instructionstothebystander,butthatmaynot besufficient.TheUSFoodandDrugAdministration(FDA) recentlyapprovedmakingnasalnaloxoneanover-thecountermedication,eventhoughitsbriefingdocument describedseveralcasesofincorrectlyadministerednaloxone, includinganindividualwhodidnotplacethetipofthe dispenserfullyinthenostril,someonewhosqueezedthe devicebutdidnotpushtheplunger,anotherwhoplacedthe deviceupsidedownsothattheplungerwasinthenostril,and severalindividualswhodidnotwait2-3minutesbefore administeringaseconddose.24 WhiletheFDAadvisors votedunanimouslytomakenaloxoneavailablewithouta prescription,25 theseerrorsinadministrationindicate theneedforabystandercoursethatcouldfurther improveoutcomes.
Anotherreasontoteachsuchacourseistoaddressstigma, whichispervasivewhenconsideringopioidusedisorder (OUD).26 Arecentstudyofindividualswhodidnotuseillicit opioidsthemselvesbutknewotherswhodidreportedstigma aboutOUDandmisinformationaboutopioid-related risks.27 Naloxone-basedinterventionscanintroducethe conceptofharmreduction,empowerbystanders,and encourageindividualstocarrynaloxoneincasethey encounteranoverdosevictim.28
Althoughnotapartofourstudy,despitethepositive resultsonourobjectiveandsubjectivetesting,wedo encouragethecreationofstandardizedtraining.TheSTB BConportionofourcoursewascreatedandendorsedby theACS,usingstandardizedcontentandcertifiedtrainers.
Asimilarprocesscouldbeusedfornaloxone,eitheraspartof aBLStraining,suchasfromtheAHAorAmericanRed Cross,fromaspecialtysociety,suchastheAmerican AcademyofEmergencyMedicine,theAmericanCollegeof EmergencyPhysicians,ortheAmericanSocietyofAddiction Medicine,orfromanationaladvocacygroupsuchas Shatterproof.Suchbrandingandpromotionmayempower morebystanderstobecometrainedandfurtherreduce stigmaandmisconceptionsaboutOUDamongthe generalpopulation.
WhileCPRtrainingforlaypersonsisthegoldstandard, manygapsinimplementingbystandertrainingremain,and aninvestmentinthestudyoftheeffectivenessoftherelatively simplestepsofnaloxoneadministrationmayhelpuslearn andimprovetechniquesofCPRandSTBtrainingaswell. Forexample,despiteeducationalinitiativesthatbeganinthe 20thcentury,onlyone-thirdofout-of-hospitalcardiacarrest patientsreceivebystanderCPR.Time,location,and durationhaveallbeenperceivedbythepublicasbarriersto CPRclasses.29 BlacksandHispanicsarelesslikelythan WhitestoreceiveCPRathomeorinpublic.30 Inthelast decade,therehavebeenmanyinitiativeswithvariable efficacy,inmostcasesnotmeasured,touseJITtoolslike flashcards,videoortalkingkitstoprovideuserswithrealtimeinstructionsfortheuseofautomatedexternal defibrillatorsorSTBequipment.Whiletheagreementof coursecontentandidentifyingefficacyisa firststep,future workshouldalsofocusondeveloping,trialing,andscaling effectiveJITnaloxone-administrationtools.
Therearelimitationstoourstudy.Wetaughtthiscourse toasmallsampleofadministrativeprofessionalsinasuburb ofMassachusetts,astatewithahighburdenofopioidrelatedoverdose.Itispossiblethatbystandersfromdifferent backgroundsandgeographiclocationswouldhaveanswered thequestionsdifferently.Wealsodidnotcollectany demographicdataaboutourstudyparticipantstoprotect confidentiality.However,thisinformationmighthave determinedthecharacteristicsofindividualswhomaybenefit mostfromthetraining.Thecontentofthepracticalsessionof thecoursewasnotstandardized.Finally,wedidnot measureknowledgeretentionoruseofnaloxonefollowing thecourse.
Abriefcoursedesignedtoteachbystandersaboutopioid overdoseandnaloxonewasfeasibleandeffective.We encouragehospitalsandotherorganizationstouseand promulgatethismodel.Furthermore,wesuggestconvening ofanationalconsortiumtoachieveconsensusonprogram content,delivery,andopportunitiesfordevelopmentofjustin-timetoolstoadministernaloxone.
AddressforCorrespondence:ScottG.Weiner,MD,MPH,Brigham andWomen’sHospital,DepartmentofEmergencyMedicine,75 FrancisStreet,NH-226,Boston,MA02115.Email: sweiner@bwh. harvard.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Outsideofthisresearch,ScottG. WeinerissupportedbyNationalInstitutesofHealthgrant5-R01DA044167,theFoundationforOpioidResponseEfforts,andthe ElevanceFoundation.ScottG.Weinerisanadvisorycommittee memberofVertexPharmaceuticals,Inc.andCessation Therapeutics,Inc.Therearenootherconflictsofinterestorsources offundingtodeclare.
Copyright:©2024Weineretal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.MellHK,MummaSN,HiestandB,etal.Emergencymedicalservices responsetimesinrural,suburban,andurbanareas. JAMASurg. 2017;152(10):983–4.
2.FederalEmergencyManagementAgency.Youarethehelpuntil helparrives.Availableat: https://community.fema.gov/ PreparednessCommunity/s/until-help-arrives?language=en_US AccessedAugust20,2023.
3.AmericanHeartAssociation.2020AmericanHeartAssociation GuidelinesforCPRandECC.Availableat: https://cpr.heart.org/en/ resuscitation-science/cpr-and-ecc-guidelines AccessedAugust20,2023.
4.SoarJ,DonninoMW,MaconochieI,etal.2018InternationalConsensus onCardiopulmonaryResuscitationandEmergencyCardiovascular CareSciencewithTreatmentRecommendationssummary. Circulation. 2018;138(23):e714–30.
5.GoralnickE,ChaudharyMA,McCartyJC,etal.Effectivenessof InstructionalInterventionsforHemorrhageControlReadinessfor LaypersonsinthePublicAccessandTourniquetTrainingstudy (PATTS):arandomizedclinicaltrial. JAMASurg. 2018;153(9):791–9.
6.GoolsbyC,JacobsL,HuntRC,etal.StoptheBleedEducation Consortium:educationprogramcontentanddeliveryrecommendations. JTraumaAcuteCareSurg. 2018;84(1):205–10.
7.CentersforDiseaseControlandPrevention.DrugOverdoseDeaths. Availableat: https://www.cdc.gov/drugoverdose/deaths/index.html AccessedAugust20,2023.
8.NationalCenterforHealthStatistics.ProvisionalDrugOverdoseDeath Counts.Availableat: https://www.cdc.gov/nchs/nvss/vsrr/drugoverdose-data.htm.AccessedAugust20,2023.
9.UnitedStatesHealthandHumanServices.U.S.SurgeonGeneral’s AdvisoryonNaloxoneandOpioidOverdose.Availableat: https://www. hhs.gov/surgeongeneral/reports-and-publications/addiction-
and-substance-misuse/advisory-on-naloxone/index.html AccessedAugust20,2023.
10.UnitedStatesHealthandHumanServices.HarmReduction.Available at: https://www.hhs.gov/overdose-prevention/harm-reduction AccessedAugust20,2023.
11.CentersforDiseaseControlandPrevention.NaloxoneTraining. Availableat: https://www.cdc.gov/opioids/naloxone/training/index.html AccessedAugust20,2023.
12.AmericanRedCross.FirstAidforOpioidOverdosesOnlineCourse. Availableat: https://www.redcross.org/take-a-class/opioidoverdose AccessedAugust20,2023.
13.CommonwealthofMassachusetts.Overdose&NaloxoneTraining Resources.Availableat: https://www.mass.gov/service-details/trainingresources.AccessedAugust20,2023.
14.NewYorkState.CommunityCalendarofOpioidOverdoseTrainings. Availableat: https://www.health.ny.gov/diseases/aids/general/ opioid_overdose_prevention/training_calendar.htm AccessedAugust20,2023.
15.GetNaloxoneNow.Availableat: https://www.getnaloxonenow.org/ #home.AccessedAugust20,2023.
16.Moustaqim-BarretteA,DhillonD,NgJ,etal.Take-homenaloxone programsforsuspectedopioidoverdoseincommunitysettings:a scopingumbrellareview. BMCPublicHealth. 2021;21(1):597.
17.WilliamsAV,StrangJ,MarsdenJ.DevelopmentofOpioidOverdose Knowledge(OOKS)andAttitudes(OOAS)scalesfortake-home naloxonetrainingevaluation. DrugAlcoholDepend. 2013;132(1-2):383–6.
18.GoldbergSA,DworkisDA,LiaoVT,etal.Feasibilityofbystander administrationofpublic-accessnaloxoneforopioidoverdose. Prehosp EmergCare. 2018;22(6):788–94.
19.IjiomaSC,FernándezEV,GatewoodSB,etal.Communitypharmacists inVirginiadispensingnaloxoneunderastandingorder:aqualitative study. JAmPharmAssoc(2003). 2021;61(6):753–60.e1.
20.SugarmanOK,BreithauptJ,WangX,etal.Characteristicsandhealth serviceuseofMedicaid-insuredindividuals fillingnaloxoneundera
standingorderinLouisiana. JAmPharmAssoc(2003). 2023;63(3):904–8.e1.
21.AbbasB,MarottaPL,Goddard-EckrichD,etal.Socio-ecologicaland pharmacy-levelfactorsassociatedwithnaloxonestockingatstandingordernaloxonepharmaciesinNewYorkCity. DrugAlcoholDepend. 2021;218:108388.
22.ChatterjeeA,YanS,XuanZ,etal.Broadeningaccesstonaloxone: communitypredictorsofstandingordernaloxonedistributionin Massachusetts. DrugAlcoholDepend. 2022;230:109190.
23.TaylorM,PradhanA,OgandoYM,etal.Impactofthenaloxonestanding orderontrendsinopioidfataloverdose:anecologicalanalysis. AmJ DrugAlcoholAbuse. 2022;48(3):338–46.
24.UnitedStatesFederalDrugAdministration.JointNonprescriptionDrug AdvisoryCommitteeandAnestheticandAnalgesicDrugProducts AdvisoryCommitteeMeeting.2023.Availableat: https://www.fda.gov/ media/165338/download.AccessedAugust20,2023.
25.AntrimA.FDAAdvisoryCommitteesRecommendNaloxoneBe AvailableOTC.2023.Availableat: https://www.pharmacytimes.com/ view/fda-advisory-committees-recommend-naloxone-be-available-otc AccessedAugust20,2023.
26.FomiattiR,FarrugiaA,FraserS,etal.Addictionstigmaandthe productionofimpedimentstotake-homenaloxoneuptake. Health (London). 2022;26(2):139–61.
27.SlocumS,OzgaJE,JoyceR,etal.Ifwebuildit,willtheycome? Perspectivesonpharmacy-basednaloxoneamongfamilyandfriendsof peoplewhouseopioids:amixedmethodsstudy. BMCPublicHealth. 2022;22(1):735.
28.MillerNM,Waterhouse-BradleyB,CampbellC,etal.Howdonaloxonebasedinterventionsworktoreduceoverdosedeaths:arealistreview. HarmReductJ. 2022;19(1):18.
29.McGovernSK,BlewerAL,MurrayA,etal.Characterizingbarriersto CPRtrainingattainmentusingTwitter. Resuscitation. 2018;127:164–7.
30.GarciaRA,SpertusJA,GirotraS,etal.Racialandethnicdifferencesin bystanderCPRforwitnessedcardiacarrest. NEnglJMed. 2022;387(17):1569–78.
CallanElswickFockele,MD,MS*
TessaFrohe,PhD†
OwenMcBride,MD*
DavidL.Perlmutter,MPH,MSW‡ BrendaGoh,BA‡ GroverWilliams§ CourteneyWettemann§ NathanHolland§ BradFinegood,MA∥
TheaOliphant-Wells,MSW∥ EmilyC.Williams,PhD,MPH‡¶ JennavanDraanen,PhD,MPH‡#
SectionEditor:R.GentryWilkerson,MD
*UniversityofWashington,DepartmentofEmergencyMedicine,Seattle,Washington
† UniversityofWashington,DepartmentofPsychiatryandBehavioralSciences, Seattle,Washington
‡ UniversityofWashington,DepartmentofHealthSystemsandPopulationHealth, Seattle,Washington
§ ResearchwithExpertAdvisorsonDrugUse,Seattle,Washington
∥ PublicHealth – Seattle&KingCounty,Seattle,Washington
¶ HealthServicesResearch&DevelopmentCenterofInnovationforVeteranCenteredandValue-DrivenCare,VeteransAffairsPugetSoundHealthCare System,Seattle,Washington
# UniversityofWashington,DepartmentofChild,Family,andPopulationHealth Nursing,Seattle,Washington
Submissionhistory:SubmittedMarch31,2023;RevisionreceivedOctober24,2023;AcceptedFebruary9,2024
ElectronicallypublishedJune27,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18033
Introduction: RecentpolicychangesinWashingtonStatepresentedauniqueopportunitytopair evidence-basedinterventionswith firstresponderservicestocombatincreasingopioidoverdoses. However,littleisknownabouthowtheseinterventionsshouldbeimplemented.Inpartnershipwiththe ResearchwithExpertAdvisorsonDrugUseteam,agroupofacademicallytrainedandcommunitytrainedresearcherswithlivedandlivingexperienceofsubstanceuse,weexaminedfacilitatorsand barrierstoadoptingleave-behindnaloxone, field-basedbuprenorphineinitiation,andHIVandhepatitisC virus(HCV)testingfor firstresponderprograms.
Methods: Ourteamcompletedsemi-structured,qualitativeinterviewswith32 firstresponders,mobile integratedhealthstaff,andemergencymedicalservices(EMS)leadersinKingCounty,Washington, fromFebruary–May2022.Semi-structuredinterviewswererecorded,transcribed,andcodedusingan integrateddeductiveandinductivethematicanalysisapproachgroundedincommunity-engaged researchprinciples.Wecollecteddatauntilsaturationwasachieved.Datacollectionandanalysiswere informedbytheConsolidatedFrameworkforImplementationResearch.Twoinvestigatorscoded independentlyuntil100%consensuswasreached.
Results: Ourthematicanalysisrevealedseveralperceivedfacilitators(ie,tensionforchange,relative advantage,andcompatibility)andbarriers(ie,limitedadaptability,lackofevidencestrengthandquality, andprohibitivecost)totheadoptionoftheseevidence-basedclinicalinterventionsfor firstresponder systems.Therewaswidespreadsupportforthedistributionofleave-behindnaloxone,althoughfunding wasidentifiedasabarrier.Manybelieved field-basedinitiationofbuprenorphinetreatmentcouldprovide amoreeffectiveresponsetooverdosemanagement,butthereweresignificantconcernsthatthis interventioncouldruncountertotherapidcaremodel.Lastly,participantsworriedthatHIVandHCV testingwasinappropriatefor firstresponderstoconductbutrecommendedthatthisservicebeprovided bymobileintegratedhealthstaff.
Conclusion: TheseresultshaveinformedlocalEMSstrategicplanning,whichwillinformrolloutof processimprovementsinKingCounty,Washington.Futureworkshouldevaluatetheimpactofthese interventionsonthehealthofoverdosesurvivors.[WestJEmergMed.2025;26(1.1)8–17.]
Thepublichealthcrisisofopioidusedisorder(OUD)and opioidoverdosecontinuesunabated,withratescontinuingto rise.1–3 Survivorsofnon-fataloverdosehaveasignificantly greaterriskofrepeatoverdoseandoverdose-related mortalitywithinthefollowingyear,emphasizingthe importanceof firstresponderinterventions.4–7 Thesetrends aremirroredlocallyinKingCounty,Washington,wherethe annual9-1-1callvolumeofprobableoverdosesandother opioiduse-relatedincidentsincreasedbymorethan20% from2018–2021.8 Acriticalwindowforinterventionexists, asapproximately40%ofindividualswhodiedofanoverdose in2018hadatleastoneemergencymedicalservices(EMS) encounterduringtheprecedingyear.9
RecentlegislativechangesinWashingtonStatepresented auniqueopportunitytopairevidence-basedinterventions with firstresponderservicestoaddresstheriseinopioid overdoses.Specifically,inFebruary2021,theWashington StateSupremeCourtstruckdownthestatutethatmade possessionofcontrolledsubstancesaclassCfelony.Thestate governmentrespondedbypassingatemporarylawthat expandedtheroleof firstresponders(eg, firefighters, paramedics,andpoliceofficers)toconnectadultsfoundwith smallamountsofcontrolledsubstancestocasemanagement insteadofthecriminallegalsystem.10 In2023thelegislature rolledbacksomeofthesechangeswithapermanentbillthat increasedcriminalpenaltiesfordrugpossessionandpublic useandmadepre-trialdiversiontotreatmentprograms contingentontheprosecutor’sconsent.11
While firstrespondershavehistoricallyprovided importantreferralstocommunityresources,12 such programshavenothistoricallyofferedharm-reduction resourcesortreatmentinitiation.Specifically,therearethree medicalservicesthatareknowntoreduceoverdosedeath andincreaseaccesstocareforpeoplewhousedrugs:leavebehindnaloxone13,14; field-basedinitiationofbuprenorphine treatment14–19;andHIVandhepatitisCvirus(HCV) testing.20 Theseinterventionshavedocumentedefficacyin emergencydepartments13,15 andcommunityclinics14,20 whiledemonstratingpromisingresultsduringbrief encounterswithstreetmedicineteamsandparamedics.16–19 Inparticular,thedistributionofnaloxonekitsiscost effective21,22 andsignificantlyreducesopioid-related fatalities.23–25 BuprenorphinetreatmentforOUDmay decreaseall-causeandopioid-relatedmortalitybyupto 50%,26–29 andHIVandHCVtestingimprovesaccesstocare forpeoplewhousedrugs.30 However,thereisapaucityof literatureontheimplementationofthesethreeevidencebasedprogramsin firstrespondersystems. Groundedincommunityengagedresearch(CEnR) principles,31 ourteampartneredwiththeResearchwith ExpertAdvisorsonDrugUse(READU),agroupof academicallytrainedandcommunity-trainedresearchers withlivedandlivingexperienceofsubstanceuse,toaddress
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Firstrespondershavenothistoricallyoffered harmreductionservicesthatareknownto reduceoverdosedeathandincreaseaccessto careforpeoplewhousedrugs.
Whatwastheresearchquestion?
Whatarethefacilitatorsandbarriersfor fi rst responderstoprovideharmreductionservices inthe fi eld?
Whatwasthemajor findingofthestudy?
Perceivedfacilitatorsweretensionfor change,relativeadvantage,and compatibility,whilebarrierswerelimited adaptability,lackofevidence,and prohibitivecost.
Howdoesthisimprovepopulationhealth?
Participantsexperiencedatensionforchange andwereactivatedtoimplementleave-behind naloxone, fi eld-basedbuprenorphine,and HIVandhepatitisCvirustesting.
thisgap.Theprimaryobjectivewastoexaminethe facilitatorsandbarrierstotheadoptionofleave-behind naloxone, field-basedinitiationofbuprenorphinetreatment, andHIVandHCVtestingfor firstresponderprograms.The secondaryobjectivewastoinformlocalEMSoverdose responsepolicyandprogramming.
FromMarch–June2022,weconducted32semi-structured interviewswith firstresponders,mobilemedicalclinicians, andEMSleadersworkinginKingCounty,Washington.The studywasapprovedbytheUniversityofWashington InstitutionalReviewBoard.
ThisstudywasinformedbytheConsolidatedFramework forImplementationResearch(CFIR).32 Byprovidinga consistentlyappliedsetofanalyticalcategories,consistingof “constructs” situatedwithin “domains,” theCFIR32 simplifiesprocesses,highlightsbarriers,andidentifies potentialareasofimprovement(Figure).Asdescribed below,thisframeworkprovidedthescaffoldingforthe interviewguides,deductivecoding,andthematicanalysis, whichhighlightedvariousconstructsasperceivedfacilitators
1.Intervention Characteristics
2.Outer
3.InnerSetting
EvidenceStrengthandQuality:Stakeholders’perceptionsofthequality andvalidityofevidencesupportingthebeliefthattheinterventionwillhave desiredoutcomes
RelativeAdvantage:Stakeholders’perceptionoftheadvantageof implementingtheinterventionversusanalternativesolution
Adaptability:Thedegreetowhichaninterventioncanbeadapted,tailored, refined,orreinventedtomeetlocalneeds
Cost:Costsoftheinterventionandcostsassociatedwithimplementingthe interventionincludinginvestment,supply,andopportunitycosts
TensionforChange:Thedegreetowhichstakeholdersperceivethecurrent situationasintolerableorneedingchange
Compatibility:Thedegreeoftangiblefitbetweenmeaningandvalues attachedtotheinterventionbyinvolvedindividuals,howthosealignwith individuals’ownnorms,values,andperceivedrisksandneeds,andhowthe interventionfitswithexistingworkflowsandsystems
Figure. AdaptedConsolidatedFrameworkforImplementationResearch(CFIR)withnumbereddomainsandselectedconstructs.
(ie,tensionforchange,relativeadvantage,compatibility) andbarriers(ie,adaptability,evidencestrengthandquality, andcost).
Ourstudyteamwascomposedofharmreductionists, includingbothacademicallytrainedresearcherswith advanceddegreesinpublichealth,psychology,and medicine,andcommunity-trainedresearcherswithlivedand livingexperienceofdruguseandEMSsysteminvolvement. Together,weembracedCEnRprinciples,31 practiced reflexivity,33 andcenteredtheperspectivesofpeoplewhouse drugsinthestudy’sdesign,execution,andanalyses.Priorto startingdatacollection,weengagedinbidirectionaltraining duringwhichcommunity-trainedREADUmembers educatedtheacademicallytrainedresearchersoneffective outreachstrategiesandexperienceswithpaststudies,while academicallytrainedresearcherssharedknowledgeabout qualitativestudydesignandanalysis.
Participantswererecruitedthroughconvenienceand snowballsampling.Weemailedrecruitmentmaterialsto leadersandadministratorsatavarietyof firstresponder agenciesinKingCountytodisseminateinformationto potentialparticipants,includingparamedics, firefighters, policeofficers,mobileintegratedhealthstaff(ie,corespondingsocialworkersand firefightersengagedin communityparamedicine),andmobilemedicalclinicians (ie,socialworkers,nurses,physicianassistants,andnurse practitionersperformingstreetoutreach).Interested individualscontactedthestudyteamthroughourstudy phoneoremail,andtheywerescreenedforeligibility. Inclusioncriteriaincludedexperienceworkingasa first responder,amobilemedicalclinician,orinamanagement/ leadershippositionina firstresponderorganizationinKing County;beingover18yearsofage;andspeakingEnglish.
Demographicinformationcollectedfromparticipants includedage,gender,raceand/orethnicity,employment,and highestlevelofeducationalattainment.Separatebutrelated interviewguidesinformedbytheCFIR32 frameworkwere developedfor firstresponders,mobilemedicalclinicians,and EMSleaders.Topicscoveredintheinterviewsincluded participants’ perceivedrolewithintheopioidepidemic; perceptionsofservicesprovidedtopeoplewhousedrugs;and theperceivedfeasibility,acceptance,andappropriatenessof leave-behindnaloxone, field-initiatedbuprenorphine,and HIVandHCVtesting.Theinterviewguideswereiteratively refined,andthe finalguidesareincludedasanappendix.An academicallytrainedresearcherwithpriorexperiencein qualitativemethodswaspairedwithacommunitytrained READUmembertoconducteachinterview.
Weusedanintegrateddeductiveandinductivethematic approach34,35 toanalysis.Oncetheinitialinterviewswere completed,wefamiliarizedourselveswiththedata,reviewedthe transcriptsforaccuracy,andnotedinitialimpressionstogether. Wegroupedemergentobservationsintoinductivecodesand situatedtheminourpreliminarycodebookwiththepre-existing deductiveCFIRcodes.32 Weappliedthecodebooktoasingle interviewtranscript,engagedinline-by-linecodingasagroup, andreconciledanydisagreementsincodeapplicationsto finalizethecodebook.Individualteammembersthenprimarily appliedtherevisedcodebooktoeachtranscript,andanother conductedsecondarycoding,addressinganydifferences.
Subsequentsemi-structuredinterviewswereconducted untilthematicsaturationwasreached.Interviewswere recorded,transcribed,deidentified,uploadedtothe qualitativedatamanagementsoftwareDedoose (SocioCulturalResearchConsultants,LLC,Manhattan Beach,CA),andcodeddeductivelyusingexistingCFIR codes32 andinductivelyusingcodescreatedfromreviewinga 5.Process
sampleoftranscripts.36 Wesummarizedcodeddatato identifybarriersandfacilitatorstoadoptingleavebehind naloxone, field-basedbuprenorphineinitiation,andHIVand HCVtestingfor firstresponderprograms,andweextracted prototypicalexamplesofeach.
Weinterviewed32 firstresponders,mobilemedical clinicians,andEMSleaderswhoworkedinsevendifferent citieslocatedinKingCounty,Washington(Table1). ParticipantsincludedBasicLifeSupportprofessionals (ie, firefighter/emergencymedicaltechnicians),Advanced LifeSupportprofessionals(ie,paramedics),policeofficers, nurses,andadvancedregisterednursepractitioners,social workers,andEMSleaders.Ofthe firstresponders interviewed,19(59%)hadbeenintheircurrentroleformore than10years.Participantswere31.3%femaleand12.5% racially/ethnicallydiverse,andmostwereabovetheageof36 withatleastsomecollegeeducation.
ThroughthelensoftheCFIRframework,32 ourthematic analysisrevealedseveralperceivedfacilitators(ie,tensionfor change,relativeadvantage,andcompatibility)andbarriers (ie,limitedadaptability,lackofevidencestrengthand quality,andprohibitivecost)totheadoptionofthree evidence-basedclinicalinterventionsfor firstresponder systems:1)leavebehindnaloxone;2) field-basedinitiationof buprenorphinetreatment;and3)HIVandHCVtesting.
Therewaswidespreadsupportforthedistributionof leave-behindnaloxonewithmanyacknowledgingatension forchangeand findingtheinterventionrelatively advantageousandcompatiblewithinexistingsystems (Table2).Manyintervieweesrecognizedthatnaloxoneisa safe,easy-to-use,indispensablemedicationthatshouldbe accessibletopatients,theirlovedones,andothercommunity responders.Implementationofleave-behindnaloxonewas alsolargelythoughttobefeasiblewithseveralinterviewees explainingthatdistributioncouldbeeffortlesslyintegrated intocurrentworkflows.
Asmallergroupofindividualsexpressedconcernabout potentialbarriers,particularlylimitedadaptability,lackof evidencestrengthandquality,andprohibitivecost.Some policeofficersthoughtthatnaloxonedistributionmay encourageunsafebehaviors(eg,usinglargeramountsor morepotentsubstances)andfeltthatitwasincongruouswith theirdepartments’ currentapproachtocontrollingdruguse throughlegalpenaltiesandincarceration.Otherservice professionalsworriedthatincreasedaccesstonaloxone wouldleadtocommunitymembers,ratherthan first responders,managingmoreoverdoseresponsesand
Table1. Interviewees’ demographicinformation.
Agen(%)
20–252(6.3%)
26–355(15.6%)
36–4511(34.4%)
46–556(18.8%)
56–658(25%)
Gendern(%)
Male20(62.5%)
Female10(31.3%)
Trans,non-binary,orgendernon-conforming2(6.3%)
Raceand/orethnicityn(%)
White28(87.5%)
AsianorPacificIslander2(6.3%)
Hispanic1(3.1%)
Mixedrace1(3.1%)
Employmentn(%)
BasicLifeSupportprofessionals (ie, firefighter/emergencymedical technicians) 8(25%)
AdvancedLifeSupportprofessionals (ie,paramedics) 6(18.8%)
Policeofficers5(15.6%)
Nursesandadvancedregistered nursepractitioners 3(9.4%)
Socialworkers5(15.6%)
Emergencymedicalservicesleaders5(15.6%)
Numberofyearsincurrentrolen(%) <12(6.3%)
1–48(25%)
5–93(9.4%)
10–198(25%) >2011(34.4%)
Highestlevelofeducationalattainmentn(%)
Associate’sdegree8(25%)
Bachelor’sdegree8(25%)
Master’sdegree10(31.3%)
Doctoraldegree2(6.3%)
Unspecified4(12.5%)
consequentlydecreasingthelikelihoodofconnectingpeople totreatmentandotherresources.Lastly,severalinterviewees inleadershipormanagementroleswereskepticalaboutthe relativebenefitofnaloxone,explainingthattheybelieved thereoughttobemoreevidenceontheefficacyofleavebehindnaloxoneprograms.Theyalsoworriedaboutthe resourcesandtrainingrequiredforimplementation.
Table2. Interviewees’ perceivedfacilitatorsandbarrierstoimplementingaleave-behindnaloxoneprogram.
Facilitators
Tensionforchange “AndIthink,yes,certainlythe firedepartmentshouldplayaroleinhavingaccesstothatandbeing abletohanditoutandprovidingeducationonhowtouseitandwhentouseit.” Paramedic(ID#25)
Relativeadvantage “Ithinkthatnaloxonesare[a]lifesavingintervention,andit’srelativelyeasyforpeopletoadministerto theirfriendsorbystanderscanadministertopeopletheydon’tknow.So,Idothinknaloxoneisvery importantanditshouldbeoutthereandthereshouldbeaccesstoit.Andusleavingitbehindwith people,Ithinkisagoodidea.” Paramedic(ID#7)
Compatibility “Ithinkthat’sprobablytheeasiestone WecouldabsolutelygettheNarcan Firstresponders definitelycanprovide[those]asanintervention.” Mobileintegratedhealthsocialworker(ID#20)
Barriers
Limitedadaptability “Ifeellikeit’dbeapsychologicalthingforofficers,especiallyofficerswho’vebeenaroundfor10plus years,whereweusedtoarrestdrugdealersandputtheminjail.Andnowwe’reignoringthecrimes they’recommittingandwe’regivingthemnaloxonesothattheycanfurtherjustcontinuetousedrugs. So,Icanseesomeonewhoismaybenotlookingatthefullpictureorjusthastheirpersonalbeliefs.” Policeofficer(ID#1)
Lackofevidencestrength andquality “Iworrythatwe’rejustput[ting]morepeopleinwithdrawalandsortofmiss[ing]theopportunitiestodo somethingaboutit.” Intervieweeinleadershipormanagementrole(ID#28)
Prohibitivecost “ButIalsohavesomeskepticismthatsortofjustthrowingoutnaloxonekitsisgonnamakeabig difference.I’mnotopposedtoit,butitdoesrequiremoreeffortandtimeandenergy,andthere’sacost toit.Andquitefrankly,wehave[a]limitedbudget,andso,who’sgoingtopayforthosethings?Idon’t know.SoI’mmeasuredinmysupportforthatprogram,butifthere’sevidencethatitsaveslives,then wewillworktowardsthat.” Intervieweeinleadershipormanagementrole(ID#27)
Field-basedInitiationofBuprenorphineTreatment
Despitehavinglessfamiliaritywiththemedication comparedtonaloxone,mostintervieweesrecognizeda tensionforchangeandapprovedoftheimplementationof field-basedinitiationofbuprenorphinetreatment, consideringitevidence-based,appropriate,andrelatively advantageousfortheirsettings(Table3).Manyfelt unpreparedtoaddresswithdrawal,particularlywhena patient’soverdosemayhavebeenfullyreversedwith bystandernaloxone,butbuprenorphinewasseenasa “destigmatizing” toolthatrelievessymptoms,demonstrates compassion,andbuildstrustbetweenpatientsand first responders.Additionally,participantsdescribedhowthe recentuptickinoverdoseresponses,occasionallywiththe sameindividuals,ledtoburnoutandadesiretoaddressthe upstreamcausesofsubstanceuse.Severalhighlightedhow field-basedinitiationofbuprenorphinetreatmentcould bridgevulnerableindividualstoongoingtreatment, potentiallypreventingfutureoverdoses,decreasingoverall callvolumes,andsavinglives.
Thoseopposedwerelargelyconcernedwiththis intervention’slimited adaptability totherapidservice deliverymodelofemergencyservices,emphasizingthatthe timeneededfortheinterventionmayoverburdenanalready overwhelmedsystem.However,otherssuggestedthatthe deploymentofspecializedteams(eg,mobileintegrated healthormobilemedicalclinicteams)dedicatedtotreating thispatientpopulationmaybeawaytooffsetthesedemands. Finally,somepoliceofficersworriedaboutthe evidence
strengthandquality ofbuprenorphine,speculatingthatit couldbedivertedfornon-prescribeduseandcould encourageongoingriskybehaviorsbycurbing withdrawalsymptoms.
Intervieweesobservedthetensionforchangeintheir organizationsandgenerallysupportedincreasingaccessto HIVandHCVtesting(Table4).Somefeltthat first responderencounterscouldserveasrelativelyadvantageous opportunitiestoengageindividualswhomaynotfeel comfortableseekingcareinmoretraditionalsettings. ProvidingHIVandHCVtestinginatrauma-informed mannerwasseentoincreaseeducationaroundprevention andimprovelinkagetocare.
Many,however,wereconcernedabouttheadaptability, appropriateness,andfeasibilityofHIVandHCVtesting duringanEMSresponse.Someworriedthatitwouldbe inconsistentwiththerapidservicedeliverymodelof emergencyservicessincepoint-of-caretestingtakesatleast 20minutestocomplete.37,38 Othersvoicedthattestingmay feelcompulsoryandcoerciveifcompletedimmediatelyafter anunnervingoverdoseevent.Like field-based buprenorphinestarts,someintervieweesalternatively proposedhaving firstrespondershandoffthesepatientstoa specializedteamthatwouldhavemoretimetoconductthe tests,providetheappropriatecounseling,andarrange follow-upasneededforconfirmatorydiagnosis andtreatment.
Table3. Interviewees’ perceivedfacilitatorsandbarriersto field-basedinitiationofbuprenorphinetreatment.
Tensionforchange “Ithinktheopioidissuethatwehaveinourkindofcityrightnow,it’sbigandittakesabigtollon people.AndIthinkthatifthereisevidencethatshowsthatSuboxoneorbuprenorphinecanhelp,and ::: especiallyifwe’refollowinginthefootstepsofanotheragencyoragenciesthathaveuseditand havesomedataonwhatworksandwhatdoesn’t,thenIwouldbeallforit.” Mobilemedical nurse(ID#15)
“Suboxoneisgoodstuff.Ifwe’retrulytryingtohelppeopletransitionoutofaddiction,it’sagreattoolto helpmanagewithdrawals.Asfarasinthe field,Ithinkifwecouldprovidethemaccesstoit, absolutely,Iwouldbe100%behindthat.” Firefighter(ID#4)
“IthinkEMSisoftenthe firstinteractionofaprettytraumaticchainofeventsleadingtotheED.Andso, Ithinkifthatengagementwerepositive,there’dbelesshesitationtocall911,numberone,for overdose.Andthennumbertwo,everychancewecangivesomeonetodecreaseorstoptheiropioid useiswellworthit.Itfeelsalittlemorelikewe’remakingadifferencethangivingthenaloxone,the Narcan,'causehereit’slike, ‘Thisisgoingtohelpyouweanyourbodyoffthisstuff.’" Mobile medicalsocialworker(ID#11)
Relativeadvantage
“Iwouldsay,absolutelyanywaythatwecanexpandourreachtoourcommunityandgetthemmore support,andforaddictionsandforrecovery,Iwouldthinkwouldbeoptimal.AndIthinkthatthe fire serviceisagreatwaytoallowthattohappen ::: I’minfullsupport.Ithinkthatwouldbeadvantageous inourcommunity.” Paramedic(ID#25)
“Anditseemsfarmoreofaviableoptiontomethantheleaveathome[naloxone].Sothe[leave behindnaloxone]wasjustgonnasolvetheproblemintheminute.Butitdoesnottakeawaythenext problem,whichisIneedmore,whereasbuprenorphinedoesaddressthat Butthebetteroption [is]tohowtogetthatmedicinetopeople.” Intervieweeinleadershipormanagementrole(ID#28) Barriers
Limitedadaptability “Thatwouldbepotentiallygood ::: [But]we’re[a]busyunit ::: howmuchoutofservicetimewould thataddtotheunittodothat?” Paramedic(ID#22)
Lackofevidencestrength andquality
“We’vemadelifeeasierforallthese[peoplewhousedrugs]outinSeattle,andithasn’tmadethings better.It’sactuallymadethingsworse.Imean,we’relookingatlike270deathssofarjustinthis first quarter.Thatisfourtimesmorethanthreeorfouryearsago.So,Idon’tknowifgivingsuboxoneis actuallyhelpful.” Policeofficer(ID#1)
EMS,emergencymedicalservices; ED,emergencydepartment.
Table4. Interviewees’ perceivedfacilitatorsandbarrierstoHIVandhepatitsCvirustesting.
Facilitators
Tensionforchange
Relativeadvantage
Barriers
“Thisisoneofthosethingsthatisinourrealmof responsibility.Ourprimarygoalistohelppeoplewith what’shappeningrightnow,butifwecanalsohelpthemoutwithlike, ‘Well,whatisthenextstepfor you?’” Mobileintegratedhealthsocialworker(ID#17)
“Hundredpercentliketheideaofbeingabletohaveanagencythathasacontractthatthisiswhatthey do.Yougoout,andyouprovidesomebodyanHIVtest.Wehavepeoplethatarespeciallytrainedtodeal withalltheramificationsofsomebodywho findsouttheyhaveHIV,'causethat’sgonnabeahorrible feeling.” Firefighter(ID#4)
Limitedadaptability “Thatwouldn’tbesomethingusefulfor firstrespondersbecauseourpriorityisnotnecessarilytestingand tryingtodiagnosewhetherindividualshave[a]specificdisease.” Firefighter(ID#2) “Ijustthinkthat’dbehorribletodotosomebody LikeHIVorhepatitisC,likethosearehugethings.So, youjustdon’twanttojustdropabombonsomebodyontopofthembeing Duringadrugoverdose, forexample.” Paramedic(ID#25)
Workingonthefrontlinesoftheopioidepidemic, first responders,mobilemedicalclinicians,andEMSleadersare confrontedwithskyrocketingoverdoseresponses.Many
wanttoimprovethecareofpatientswhousedrugs,beyond acuteoverdosereversal,butfeeluncertainabouthowto proceed.Peoplewhousedrugshavealsoexpressedaneedfor improvedcarewithmanyrefusingEMStransportfollowing
overdoseduetolawenforcement’spresenceatoverdose scenes, 39 unmanagedwithdrawalsymptoms,andanticipated stigmatizingtreatmentbyEMSandemergencyclinicians.40 OurthematicanalysisinformedbytheCFIRframework32 identifiedseveralperceivedfacilitators(ie,tensionfor change,relativeadvantage,andcompatibility)andbarriers (ie,limitedadaptability,lackofevidencestrengthand quality,andprohibitivecost)totheadoptionofthree evidence-basedclinicalinterventionsfor firstresponder systems:1)leave-behindnaloxone;2) field-basedinitiationof buprenorphinetreatment;and3)HIVandHCVtesting. However,therearefewexamplesofimplementingthese evidence-basedinterventionsin firstrespondersystemswith onenarrativereview findingonly27programsoutofnearly 22,000EMSagenciesnationallydescribedintheliterature, withmanyprovidingnaloxonedistributionandcommunity referralswhilefewfacilitatedlinkagetomedications forOUD.41
Manyrecognizedthetensionforchangeintheir communityandtherelativeadvantageofdistributing naloxonekitsandtreatingOUDwithbuprenorphineinthe field.Leave-behindnaloxoneisacost-effective,21,22 widely accepted42–44 toolthatreducesopioidoverdose-related mortality45,46 anddoesnotincreaseriskydruguse behavior.47 ExistingEMSprogramsdistributingnaloxone kitsdemonstratedfeasibility48 andincreasedconnectionto otherresources.49 Mostintervieweesbelievedleave-behind naloxonewascompatiblewithandcouldbeeasilyintegrated intotheirworkflows,yetseveralhighlightedtheimportance ofsecuringsustainablefundingtoaddresscostsandreceiving additionaltrainingtoaddresstheperceivedlackofevidence strengthandqualitybeforeimplementation.Participants weresimilarlyenthusiasticabouttheprospectoftreating opioidwithdrawalandOUDwithbuprenorphine.In additiontoaninitialcaseseriesdescribingtreating withdrawalfromnaloxoneadministrationwith buprenorphine,18 apilotstudyexaminingprehospital buprenorphinetreatmentforOUDshowed50%retentionin treatmentatsevendaysand36%in30days.19
Notably,participantsworkinginlawenforcementwere moreskepticalofharmreductionthanthoseemployedin healthcareandsocialservices.Someexpressedfrustration withrecentlegislationthatcurtailedcriminalpenaltiesfor drugpossessionandpublicuse.Otherlawenforcement officersexpressedsentimentssimilartothoseofhealthcare andsocialservicesworkersbutquestionedwhattheirrolein addressingtheopioidepidemiccouldbeunderthenewlaws. Importantly,policeofficersstillregularlyrespondtomedical emergenciesinvolvingdruguse,includingoverdoses, highlightingtheurgentneedfortargetededucationonhowto usetheseevidence-basedinterventionseffectively inthe field.
Lastly,themostdiscussedbarriertoallthree interventions,particularly field-basedinitiationof
buprenorphineandHIVandHCVtesting,wasafeelingfrom frontlineprofessionalsthatimplementationhadlimited adaptabilitytotherapidservicedeliverymodelofemergency services.However,othersrecommendedeitherdeployinga specializedteamtothesceneortransportingthepatienttoa diversionfacilitythatcouldprovidewraparoundservices. Localmobilemedicalclinicteamshavesuccessfully integratedharmreductionservicesintotheircareofthose experiencinghomelessness,50 andthecreationofmobile integratedhealthresponseunitshaveexpandedcase managementandreferralsthroughmultidisciplinary collaborationsin firedepartments.51 Withlonger dispatchtimeandtheabilitytodolongitudinalfollow-up, theseteamsmaybewellsuitedtoprovide post-overdosecare.
ThePhiladelphiaFireDepartmenthasanalternative responseunit(“AR-2”)equippedwithAdvancedLife Supportcapabilities,whichislocatedinanareaheavily impactedbyopioidoverdoses.Itrespondstothose resuscitatedwithnaloxonebutwhorefusetransportationto thehospital,andearlydatademonstratesthat84%of patientsacceptedservices,includingtreatmentfacility placement,resources,and/ornaloxonekits.52 Diversion facilitiesofferinglow-barrieraccesstotreatmentandother servicescouldalsooperateasanalternativetoaprolonged EMSresponseoremergencydepartmentvisits;infact,a formerhospitalfacilityinColumbus,Ohio,nowequipped with60bedsdedicatedtoaddictionstabilizationserves astheprimarypost-overdosereceivingcenterfor individualsseekingtreatmentanddeemedmedically stablebyEMS.53
Ourobjectiveinthisstudywastoexaminethefacilitators andbarrierstotheadoptionofleave-behindnaloxone, fieldbasedinitiationofbuprenorphinetreatment,andHIVand HCVtestingfor firstresponderprograms.However,the resultsmayonlybeapplicabletothegeographiclocationof theinterviewees,whichincluded firstresponders,mobile medicalclinicians,andEMSleadersworkinginKing County,Washington.Racialandethnicminoritieswere notablypoorlyrepresentedinourstudy.Becausethereisno publiclyavailabledataonthedemographicinformationof EMSprofessionalslocally,wewereunabletoassesswhether oursamplewasrepresentative.Ourconvenienceand snowballsamplingmayhavealsointroducedbias.Most participantsdescribedbeingintheircurrentroleformore than10years,whichislikelymuchhigherthanthegeneral firstresponderpopulation.Finally,wedidnottrackthe decline-to-beinterviewedrate.
Withoutthetoolstoaddresstheuptickinopioid overdoses, firstresponders,mobilemedicalclinicians,and
EMSleadersinKingCountyexperiencedatensionfor changeandarenowactivatedtoimplementleave-behind naloxone, field-basedinitiationofbuprenorphinetreatment, andHIVandHCVtestingthroughnewEMSprotocols, post-overdoseresponseteams,anddiversionfacilities.Inthis studywetookateam-basedapproachandcenteredthe perspectivesofpeoplewithlivedandlivingexperienceof drugusetoensurethatthisresearchledtoaction.Members ofREADUhighlightedourwork’srelevancetothe communityandframedthese findingstoinformpolicy, particularlywiththerecentchangesinWashington Statelegislation.Futureworksshouldevaluatethe impactoftheseinterventionsonthehealthof overdosesurvivors.
AddressforCorrespondence:CallanElswickFockele,MD,MS, UniversityofWashington,DepartmentofEmergencyMedicine,325 9th Ave.,Box359702,Seattle,WA98109.Email: cfockele@uw.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Thisstudywassupportedbya UniversityofWashingtonImplementationScienceProgramPilot Grant(PIvanDraanen).Therearenootherconflictsofinterestor sourcesoffundingtodeclare.
Copyright:©2024Fockeleetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.KingCountyMedicalExaminer.Overdosedeaths.2022.Availableat: https://kingcounty.gov/depts/health/examiner/services/reports-data/ overdose.aspx.AccessedFebruary23,2023.
2.AdministrationforStrategicPreparedness&Response.Renewalof determinationthatapublichealthemergencyexists.2022.Availableat: https://aspr.hhs.gov/legal/PHE/Pages/Opioids-29Sept22.aspx AccessedonFebruary23,2023.
3.CentersforDiseaseControlandPrevention:NationalCenterforHealth Statistics.DrugoverdosedeathsintheU.S.top100,000annually.2021. Availableat: https://www.cdc.gov/nchs/pressroom/nchs_press_ releases/2021/20211117.htm.AccessedFebruary23,2023.
4.BarefootEH,CyrJM,BriceJH,etal.Opportunitiesforemergency medicalservicesinterventiontopreventopioidoverdosemortality. PrehospEmergCare. 2021;25(2):182–90.
5.OlfsonM,WallM,WangS,etal.Risksoffatalopioidoverdoseduringthe firstyearfollowingnonfataloverdose. DrugAlcoholDepend. 2018;190:112–9.
6.StoovéMA,DietzePM,JolleyD.Overdosedeathsfollowingprevious non-fatalheroinoverdose:recordlinkageofambulanceattendanceand deathregistrydata. DrugAlcoholRev. 2009;28(4):347–52.
7.WeinerSG,BakerO,BernsonD,etal.One-yearmortalityofpatients afteremergencydepartmenttreatmentfornonfatalopioidoverdose. AnnEmergMed. 2020;75(1):13–7.
8.PublicHealth Seattle&KingCounty.Non-fataloverdose.2022. Availableat: https://kingcounty.gov/depts/health/overdose-prevention/ non-fatal.aspx.AccessedFebruary23,2023.
9.CarhartE.Abstractsforthe2020NAEMSPScientificAssembly. PrehospEmergCare. 2019;24(1):100–56.
10.WashingtonStateLegislature.SB5476–2021-22:addressingtheState v.Blakedecision.2021.Availableat: https://app.leg.wa.gov/ billsummary?BillNumber=5476&Initiative=false&Year=2021 AccessedonFebruary23,2023.
11.WashingtonStateLegislature.SB5536–2023-24:Concerning controlledsubstances,counterfeitsubstances,andlegenddrug possessionandtreatment.2023.Availableat: https://app.leg.wa.gov/ billsummary?BillNumber=5536&Year=2023&Initiative=False AccessedonOctober3,2023.
12.MarrenR.REACH/EMSpilotstudydesign:vulnerablepopulations strategicinitiative(VPSI)ofKingCountyEmergencyMedicalServicesin partnershipwithREACHandPugetSoundandRentonRegionalFire Authorities.2018.Availableat:~https://kingcounty.gov/depts/health/ emergency-medical-services/vulnerable-populations/~/media/depts/ health/emergency-medical-services/documents/vulnerablepopulations/reach-ems-pilot-study.ashx AccessedonFebruary23,2023.
13.SamuelsEA,DwyerK,MelloMJ,etal.Emergencydepartment-based opioidharmreduction:movingphysiciansfromwillingtodoing. AcadEmergMed. 2016;23(4):455–65.
14.WinhusenT,WalleyA,FanucchiLC,etal.TheOpioid-overdose ReductionContinuumofCareApproach(ORCCA):evidence-based practicesintheHEALingCommunitiesStudy. DrugAlcoholDepend. 2020;217:108325.
15.D’OnofrioG,O’ConnorPG,PantalonMV,etal.Emergencydepartmentinitiatedbuprenorphine/naloxonetreatmentforopioiddependence: arandomizedclinicaltrial. JAMA. 2015;313(16):1636–44.
16.CarrollGG,WassermanDD,ShahAA,etal.Buprenorphine field initiationofrescuetreatmentbyemergencyservices (BupeFIRSTEMS):acaseseries. PrehospEmergCare. 2021;25(2):289–93.
17.CarterJ,ZevinB,LumPJ.Lowbarrierbuprenorphinetreatmentfor personsexperiencinghomelessnessandinjectingheroininSan Francisco. AddictSciClinPract. 2019;14(1):20.
18.HernHG,GoldsteinD,KalminM,etal.Prehospitalinitiationof buprenorphinetreatmentforopioidusedisorderbyparamedics. PrehospEmergCare. 2022;26(6):811–7.
19.HernHG,LaraV,GoldsteinD,etal.Prehospitalbuprenorphine treatmentforopioidusedisorderbyparamedics: firstyear resultsoftheEMSbuprenorphineusepilot. PrehospEmergCare. 2023;27(3):334–42.
20.CalinR,MassariV,PialouxG,etal.Acceptabilityofon-siterapidHIV/ HBV/HCVtestingandHBVvaccinationamongthreeat-riskpopulations
indistinctcommunity-healthcareoutreachcentres:theANRS-SHS154 CUBEstudy. BMCInfectDis. 2020;20(1):851.
21.CoffinPOandSullivanSD.Cost-effectivenessofdistributing naloxonetoheroinusersforlayoverdosereversal. AnnInternMed. 2013;158(1):1–9.
22.UyeiJ,FiellinDA,BuchelliM,etal.Effectsofnaloxonedistributionalone orincombinationwithaddictiontreatmentwithorwithoutpre-exposure prophylaxisforHIVpreventioninpeoplewhoinjectdrugs: acost-effectivenessmodellingstudy. LancetPublicHealth. 2017;2(3):e133–40.
23.BirdSMandMcAuleyA.Scotland’sNationalNaloxoneProgramme. Lancet. 2019;393(10169):316–8.
24.BirdSM,McAuleyA,PerryS,etal.EffectivenessofScotland’sNational NaloxoneProgrammeforreducingopioid-relateddeaths:abefore (2006-10)versusafter(2011-13)comparison. Addiction. 2016;111(5):883–91.
25.WalleyAY,XuanZ,HackmanHH,etal.Opioidoverdoseratesand implementationofoverdoseeducationandnasalnaloxone distributioninMassachusetts:interruptedtimeseriesanalysis. BMJ. 2013;346:f174.
26.LarochelleMR,BernsonD,LandT,etal.Medicationforopioiduse disorderafternonfatalopioidoverdoseandassociationwithmortality:a cohortstudy. AnnInternMed. 2018;169(3):137–45.
27.PearceLA,MinJE,PiskeM,etal.Opioidagonisttreatment andriskofmortalityduringopioidoverdosepublichealthemergency: populationbasedretrospectivecohortstudy. BMJ. 2020;368:m772.
28.SordoL,BarrioG,BravoMJ,etal.Mortalityriskduringandafteropioid substitutiontreatment:systematicreviewandmeta-analysisofcohort studies. BMJ. 2017;357:j1550.
29.WakemanSE,LarochelleMR,AmeliO,etal.Comparativeeffectiveness ofdifferenttreatmentpathwaysforopioidusedisorder. JAMANetw Open. 2020;3(2):e1920622.
30.SimeoneCA,SealSM,SavageC.ImplementingHIVtestingin substanceusetreatmentprograms:asystematicreview. JAssoc NursesAIDSCare. 2017;28(2):199–215.
31.KeyKD,Furr-HoldenD,LewisEY,etal.Thecontinuumof communityengagementinresearch:aroadmapforunderstandingand assessingprogress. ProgCommunityHealthPartnersh. 2019;13(4):427–34.
32.DamschroderLJ,AronDC,KeithRE,etal.Fosteringimplementationof healthservicesresearch findingsintopractice:aconsolidated frameworkforadvancingimplementationscience. ImplementSci. 2009;4:50.
33.JonesRG.Puttingprivilegeintopracticethrough “intersectional reflexivity:” ruminations,interventions,andpossibilities. Reflections: NarrativesofProfessionalHelping. 2010;16(1):122–5.
34.BraunVandClarkeV.Usingthematicanalysisinpsychology. QualRes Psychol. 2006;3(2):77–101.
35.BraunVandClarkeV.Thematicanalysis. JPositPsychol. 2017;12(3):297–8.
36.LyonAR,MunsonSA,RennBN,etal.Useofhuman-centered designtoimproveimplementationofevidence-based psychotherapiesinlow-resourcecommunities:protocolfor studiesapplyingaframeworktoassessusability. JMIRResProtoc. 2019;8(10):e14990.
37.AroraDR,MaheshwariM,AroraB.Rapidpoint-of-caretestingfor detectionofHIVandclinicalmonitoring. ISRNAIDS. 2013;2013:287269.
38.SmooklerD,VanderhoffA,BiondiMJ,etal.Reducingreadtime ofpoint-of-caretestdoesnotaffectdetectionofhepatitisCvirusand reducesneedforreflexRNA. ClinGastroenterolHepatol. 2021;19(7):1451–8.e4.
39.WagnerKD,HardingRW,KelleyR,etal.Post-overdoseinterventions triggeredbycalling911:centeringtheperspectivesofpeoplewhouse drugs(PWUDs). PLoSOne. 2019;14(10):e0223823.
40.BergsteinRS,KingK,Melendez-TorresGJ,etal.Refusaltoaccept emergencymedicaltransportfollowingopioidoverdose,andconditions thatmaypromoteconnectionstocare. IntJDrugPolicy. 2021;97:103296.
41.Champagne-LangabeerT,Bakos-BlockC,YatscoA,etal.Emergency medicalservicestargetingopioiduserdisorder:anexplorationofcurrent out-of-hospitalpost-overdoseinterventions. JAmCollEmerg PhysiciansOpen. 2020;1(6):1230–9.
42.MistlerCB,ChandraDK,CopenhaverMM,etal.Engagement inharmreductionstrategiesaftersuspectedfentanylcontamination amongopioid-dependentindividuals. JCommunityHealth. 2021;46(2):349–57.
43.SealKH,DowningM,KralAH,etal.Attitudesaboutprescribing take-homenaloxonetoinjectiondrugusersforthemanagement ofheroinoverdose:asurveyofstreet-recruitedinjectors intheSanFranciscoBayArea. JUrbanHealth. 2003;80(2):291–301.
44.StrangJ,PowisB,BestD,etal.Preventingopiateoverdosefatalities withtake-homenaloxone:pre-launchstudyofpossibleimpactand acceptability. Addiction. 1999;94(2):199–204.
45.McDonaldRandStrangJ.Aretake-homenaloxoneprogrammes effective?SystematicreviewutilizingapplicationoftheBradfordHill criteria. Addiction. 2016;111(7):1177–87.
46.StrangJ,McDonaldR,CampbellG,etal.Take-homenaloxone fortheemergencyinterimmanagementofopioidoverdose:thepublic healthapplicationofanemergencymedicine. Drugs. 2019;79(13):1395–418.
47.JonesJD,CampbellA,MetzVE,etal.Noevidenceofcompensatory druguseriskbehavioramongheroinusersafterreceivingtake-home naloxone. AddictBehav. 2017;71:104–6.
48.LeSaintKT,MontoyJCC,SilvermanEC,etal.Implementationofa leave-behindnaloxoneprograminSanFrancisco:aone-year experience. WestJEmergMed. 2022;23(6):952–7.
49.ScharfBM,SabatDJ,BrothersJM,etal.Bestpracticesforanovel EMS-basednaloxoneleavebehindprogram. PrehospEmergCare. 2021;25(3):418–26.
50.PublicHealth Seattle&KingCounty.Streetmedicineforpeopleliving unsheltered.2021.Availableat: https://kingcounty.gov/depts/health/ locations/homeless-health/mobile-medical-care/street-medicine.aspx AccessedonFebruary23,2023.
51.ChoiBY,BlumbergC,WilliamsK.Mobileintegratedhealthcareand communityparamedicine:anemergingemergencymedicalservices concept. AnnEmergMed. 2016;67(3):361–6.
52.MechemCC,YatesCA,RushMS,etal.Deploymentofalternative responseunitsinahigh-volume,urbanEMSsystem. PrehospEmerg Care. 2020;24(3):378–84.
53.BurtonWandMartinA.Opioidoverdoseandaddictiontreatment: acollaborativemodelofcompassion,patience,andrespect. JNursScholarsh. 2020;52(4):344–51.
DrakeGothamJohnson,MS° AliceY.Lu,MSL°
GeorgiaA.Kirn, °
KaiTrepka,AM°
YeseniaAyanaDay, °
StephenC.Yang,DDS°
JuanCarlosC.Montoy,MD,PhD
MarianneA.Juarez,MD
SectionEditor:R.GentryWilkerson,MD
UniversityofCaliforniaSanFrancisco,DepartmentofEmergencyMedicine, SanFrancisco,California
°Johnson,Lu,Kirn,Trepka,Day,andYangareco-firstauthors.
Submissionhistory:SubmittedApril1,2023;RevisionreceivedJanuary24,2024;AcceptedFebruary9,2024
ElectronicallypublishedMay20,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18040
Introduction: TheopioidepidemicisamajorcauseofmorbidityandmortalityintheUnitedStates.Prior workhasshownthatemergencydepartment(ED)opioidprescribingcanincreasetheincidenceofopioid usedisorderinadose-dependentmanner,andsystemicchangesthatdecreasedefaultquantityof dischargeopioidtabletsintheelectronichealthrecord(EHR)canimpactprescribingpractices.However, EDleadershipmaybeinterestedintheimpactofcommunicationaroundtheinterventionaswellas whethertheinterventionmaydifferentiallyimpactdifferenttypesofclinicians(physicians,physician assistants[PA],andnursepractitioners).Weimplementedandevaluatedaqualityimprovement interventionofanannounceddecreaseinEHRdefaultquantitiesofcommonlyprescribedopioidsata large,academic,urban,tertiary-careED.
Methods: WegatheredEHRdataonallEDdischargeswithopioidprescriptionsfromJanuary1, 2019–December6,2021,includingchiefcomplaint,clinician,andopioidprescriptiondetails.Datawas capturedandanalyzedonamonthlybasisthroughoutthistimeperiod.OnMarch29,2021,we implementedanannounceddecreaseinEHRdefaultdispensequantitiesfrom20tabletsto12tabletsfor commonlyprescribedopioids.Wemeasuredpre-andpost-interventionquantitiesofopioidtablets prescribedperdischargereceivingopioids,distributionbypatientdemographics,andinter-clinician variabilityinprescribingbehavior.
Results: TheEHRchangewasassociatedwitha14%decreaseinquantityofopioidtabletsper dischargereceivingopioids,from14to12tablets(P =<.001).Wefoundnostatisticallysignificant disparitiesinprescriptionsbasedonself-reportedpatientrace(P = 0.68)orgender(P = 0.65).Nurse practitionersandPAsprescribedmoreopioidsperencounterthanphysiciansonaverageandhada statisticallysignificantdecreaseinopioidprescriptionsassociatedwiththeEHRchange.Physicianshad alesserbutstillsignificantdropinopioidprescribinginthepost-interventionperiod.
Conclusion: DecreasingEHRdefaultsisarobust,simpletoolfordecreasingopioidprescriptions,with potentialforimplementationinthe42%ofEDsnationwidethathavedefaultsexceedingtherecommended 12-tabletsupply.Consideringsignificantinter-clinicianvariability,futureinterventionstodecreaseopioid prescriptionsshouldexaminetheeffectsofcombiningEHRdefaultchangeswithtargetedinterventionsfor cliniciangroupsorindividualclinicians.[WestJEmergMed.2025;26(1.1)18–25.]
Theopioidepidemicisamajorcauseofmorbidityand mortalityintheUnitedStates,includinginCalifornia.1 Opioidprescriptionsinitiatedintheemergencydepartment (ED)andotherclinicalcaresettingscanincreasethe incidenceofopioidusedisorder(OUD)inadose-dependent manner themoretabletsprescribed,thegreatertheriskof futuredevelopmentofOUD.2–4 Inaddition,thepresenceof excessopioidtabletsinthehomeislinkedtodiversionand overdose.5 Decreasingthetotalquantityoftabletsprescribed fromtheEDmayhelpdecreasetheriskoftheseharms.
Manyinterventionsattempttodecreaseandalleviatethe risksofopioidprescriptionsinEDsettings,fromelectronic clinicaldecisionsupportalertstoco-prescriptionofnaloxone, butmostexistingEDinterventionsfocusondecreasing prescriptionratesratherthandecreasingthequantityofopioid tabletsprescribedwhenEDpatientsaredischargedwith opioids.6–8 Priorresearchhasshownthatdecreasingthe defaultquantityoftabletsprescribedintheelectronichealth record(EHR)withoutannouncingthechangetoclinicians candecreasethenumberofopioidsperprescriptiongivenat discharge.Inthesestudies,clinicianswerenotnotifiedof alteredEHRdefaultprescriptionseitherforconvenienceorto testtheeffectofadefaultchangealone,orduetoconcernthat clinicianswouldconsciouslyoverridethedefaults.9–13
BecauseprotocolchangesintheEDarecommonly arrivedatbyconsensusandareusuallyimplemented transparentlyratherthanunannounced,studyingtheeffect ofanannouncedEHRchangemorecloselymirrorsrealworldscenarios.Anannouncementaboutthechangemay havetheaddedbenefitofeducatingcliniciansaboutopioid prescribingguidelines,therisksofprescribingopioids,and signalswhatothercliniciansarethinkingaboutopioid prescriptions.Further,thereisevidencethatnurse practitioners(NP)andphysicianassistants(PA)aremore likelythanphysicianstoprescribeopioidsinprimarycare settings,14 buttherelationshipbetweencliniciantypeand opioid-prescribingbehaviorintheEDsettingremains unknown.Inaddition,priorworkhasnotshownwhether thesedifferenttypesofcliniciansrespondsimilarlytodefaultdirectedattemptstodecreaseopioidprescribing.
Toaddressthesegaps,weimplementedaquality improvement(QI)interventiondecreasingEHRdefault quantitiesofcommonlyprescribedopioidsatalarge, academic,urban,tertiary-carecenter.Ourgoalwasto determinewhetherthisEHRchangewasassociatedwith decreasedopioidprescribingandwhetherthisassociation variedbycliniciantype.
Design
Weimplementedasingle-site,QIinterventionatalarge, academic,urbantertiary-careEDalteringthedefaultquantity ofsixcommonlyprescribedopioids.ThiswasaprospectiveQI
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Emergencydepartment opioidprescriptions increasetheincidenceofopioidusedisorderin adose-dependentmanner,potentially exacerbatingtheopioidepidemic.
Whatwastheresearchquestion?
Thisstudyevaluatedtheimpactofa qualityimprovementinterventiondecreasing defaultopioidquantitiesintheEHRfrom 20pillsto12,onaverageopioidsprescribed atdischarge.
Whatwasthemajor finding ofthestudy?
TheEHRchangewasassociatedwitha14% decreaseinquantityofopioidtabletsper dischargereceivingopioids(P < .001),driven mostlybynursepractitioners ’ andphysician assistants ’ changes.
Howdoesthisimprovepopulationhealth?
Wedemonstrateasimpleinterventionother emergencydepartmentscanimmediately implementtoreducetheburdenopioid prescribinghasontheopioidepidemic.
studywheredatawaspulledfromchartreviewandanalyzed bothduringstudydesignandcontinuouslyduring implementation.Wecollectedpre-interventiondataonallED dischargesreceivingthesesixopioidsatdischargefrom January1,2019–March28,2021,andcomparedthiswith post-interventiondatafromMarch29,2021–December5, 2021.ThisworkwasconsideredQIactivityaccordingtothe UniversityofCalifornia,SanFranciscoinstitutionalreview boardpolicy.Asaresult,therequirementforindividual researchHIPAAauthorizationandsignedconsentformswas waivedforallsubjectsastheresearchpresentednomorethan minimalriskofharmtothesubjects’ privacy.
Wedecreasedthepre-populatedEDdischargedispense quantitiesintheEHRfrom20tabletsto12tabletsforthe followingsixcommonlyprescribedopioids:oxycodone 5milligrams(mg);oxycodone-acetaminophen5–325mg; oxycodone10mg;tramadol50mg;hydrocodoneacetaminophen5–325mg;andhydrocodone-acetaminophen 10–325mg.Changesweremadeatthesystemleveland appliedtoallEDpatientsandclinicians.Cliniciansdecided
forwhomtoprescribeopioidsandcouldchooseanyquantity byalteringthedefaultsetting.CliniciansintheEDwere informedofthestudyandquantitychangesusingtwo communicationmethods:bytwoemailannouncementssent toallphysicians,PAs,andNPs;andbytwoin-person announcementsduringtheweeklyall-staffEDmeetings attendedby10–12totalphysicians,PAs,andNPs.Theemail andweeklyall-staffannouncementsweremadeoveraperiod oftwoweekspriortotheintervention.
WeincludedEDpatientencountersinwhichpatientswere dischargedfromtheEDwithaprescriptionforoneofthesix opioidmedicationsincludedintheintervention.Wealso recordedthetotalnumberofpatientsdischargedfromthe EDeachmonthduringtheperiodofourstudy,regardlessof whethertheyweregivenaprescriptionattheendoftheir visit.Eachencounterwasrecordedasanobservation, regardlessofwhetherthesepatientshadotherEDvisits.
FromallEDencountersthathadanopioidmedication prescribedatdischarge,weextractedthefollowingdatafrom theEHR:dateofvisit;patientdemographics(race,age, gender,insurancetype);acuity(basedontheassigned EmergencySeverityIndexscoreintheEHR),chief complaint,prescribingcliniciantype,opioidmedication prescribedandquantityoftablets.Insurancetypewas categorizedasMedicaid,Medicare,commercial,self-pay,or other.Chiefcomplaintswereclassifiedintothefourmost commonchiefcomplaintsseeninourEDoverthestudy period(backpain,abdominalpain, flankpain,falls),withthe remainingchiefcomplaintsgroupedas “other.” Prescribing cliniciantypeswerecategorizedasphysician,NP,orPA.
Ourprimaryoutcomemeasurewasthedifferenceinmean numberofopioidtabletsprescribedatdischargebeforeand afterourintervention.Oursecondaryoutcomesincluded differencesinthismeasuregiventhepatient’sself-reported raceandself-reportedgender,aswellasprescribingclinician typefortheencounter(physician,NP,PA).Wealsotested thedifferenceinmeanmorphinemilligramequivalents (MME)prescribedatdischargebeforeandafter ourintervention.
WecalculatedMMEsusingtheconversionfactors providedbytheUSCentersforDiseaseControland Prevention(CDC).4 Frequencytablesweregeneratedfor categoricalvariables.Medianandinterquartilerangewere generatedforageandmeans,andstandarddeviationswere calculatedforallothercontinuousvariables.Weperformed twosample t -teststocomparemeanopioidtabletsprescribed beforeandafterourinterventionandcalculated95% confidenceintervals(CI).GiventheeffectoftheCOVID-19
pandemiconthevolumeofEDdischargesduringourpreinterventiondatacollection,weperformedsensitivity analysesrestrictingthestudyperiodtodifferentstarttimes, includingafterthestartoftheCOVID-19pandemic(in March2020).Weperformedchi-squaretestsof independenceforage,race,insurancetype,andacuitybefore andafterintervention,andtheFisherexacttestforgender. Two-wayanalysisofvariance(ANOVA)wasperformedto analyzetheinteractionbetweencliniciantypeand interventiononmeanopioidtabletsprescribed. P values < 0.05werereportedassignificant.Weperformedallanalyses usingPython3(PythonSoftwareFoundation, Wilmington,DE).
Therewere3,575EDdischargeswithanopioidprescribed duringthestudyperiod,ofwhich3,274(91.6%)had prescriptionsforoneofthesixopioidstargetedbyour intervention,including2,666dischargespre-interventionand 608dischargespost-intervention. Opioidsnottargeted byour interventionincludedmorphine(2.5%),hydromorphone (1.4%), oxycodone (1.3%),hydrocodone(<1%),codeine (<1%), tramadol (<1%),methadone(<1%),andfentanyl (<1%).ThepatientpopulationseenintheEDpre-andpostinterventionhadsimilardistributionsofdischargediagnoses, age,gender,self-reportedrace,acuity,insurancetype,and prescribingcliniciantype(Table1).Therewereno statisticallysignificantdifferencesinprescriptionsbetween individualswithdifferentself-reportedraces(chi-squared P = 0.68)orbetweengenders(Fisherexact P = 0.65)before andafterimplementationofourintervention.
ThenumberofEDencountersassociatedwithanopioid prescriptionupondischargewasproportionaltothetotal numberofdischargesfromtheEDthroughoutthestudy period,althoughbothexperiencedaprecipitousdeclineat thestartoftheCOVID-19pandemic(Figure1).
DecreasingtheEHRdefaultquantityofcommonly prescribedopioidswasassociatedwithadecreasefrom14.01 to12.00tabletsperdischargeprescriptionwithopioidsfrom theED,adifferenceof2.01tablets(95%CI1.44–2.58) (Table2).Sensitivityanalysisshowedtherewasastatistically significantdifferenceintabletsprescribedregardlessofhow manymonthswereincludedinthepre-interventiondataset (SupplementalTable1).Thisdecreaseintabletsismirrored byan11.0MMEdecreaseperdischargeprescriptionwith opioids(95%CI5.74–16.22)from94.25to83.27(Table2).
For2,666pre-interventionencountersinthedataset, physicianswrote47.6%ofstudyprescriptions,NPswrote 26.8%,andPAswrote25.6%ofstudyprescriptions.Forthe 608post-interventionencountersinthedataset,physicians wrote50%ofstudyprescriptions,NPswrote24.3%,andPAs wrote25.7%ofstudyprescriptions.Allcliniciantypes prescribedsignificantlyfeweropioidsperencounterafterthe interventioncomparedtoprior,withPAsandNPsaffected
Table1. Patientdemographicsofopioidprescriptionsintheemergencydepartment.
PatientdemographicsAllPrePost
Age,median(IQR)48(27)48(27)48(29)0.88
Gender,n(%)
Female1,707(0.522)1,395(0.5242)312(0.514)
Male1,561(0.478)1,266(0.4758)295(0.486)
Race,n(%)
White1,719(0.525)1,393(0.5225)326(0.536)
Black423(0.129)353(0.1324)70(0.115)
Asian467(0.143)382(0.1433)85(0.14)
Other665(0.203)538(0.2018)127(0.209)
Acuity,n(%)
Emergent286(0.087)243(0.0912)43(0.071)
Urgent2,013(0.615)1,618(0.6071)395(0.65)
Lessurgent947(0.289)781(0.2931)166(0.273)
Non-urgent27(0.008)23(0.0086)4(0.007)
Commercial1,448(0.442)1,172(0.4396)276(0.454)
Medicaid801(0.245)662(0.2483)139(0.229)
Medicare702(0.214)571(0.2142)131(0.216)
Self-pay167(0.051)140(0.0525)35(0.058)
Other156(0.048)121(0.0454)27(0.044)
Physician1,573(0.481)1,269(0.476)304(0.5)
NP862(0.263)714(0.268)148(0.243)
PA839(0.256)683(0.256)156(0.257)
Dischargediagnosis,n(%)
Abdominalpain425(0.130)345(0.129)80(0.131)
Backpain324(0.0990)258(0.0968)66(0.109)
Flankpain292(0.0892)248(0.0930)44(0.0724)
Fall190(0.0580)41(0.0559)149(0.0674)
Other2,043(0.624)1,666(0.624)377(0.620)
IQR,interquartilerange; NP,nursepractitioner; PA,physicianassistant.
themost(Figure2, Table3).Atwo-wayANOVAofthe cliniciantypeandinterventionconfirmedstatistically significanteffectsoftheintervention,cliniciantype,and interactionbetweeninterventionandcliniciantypeonthe numberoftabletsperdischargeprescriptionwith opioids(P < 0.001).
WeimplementedanannounceddecreaseinEHRdefault quantitiesofsixcommonlyprescribedopioidsatalarge, academic,urban,tertiary-careED.Theanalysisofour primaryoutcomeshowedthatthisQIinterventionwas associatedwithastatisticallysignificantdecreaseinopioid
tabletsperdischargeprescriptionwithopioidsfromtheED, from14to12tablets,andacorresponding11-pointdecrease inmeanMMEsprescribed.Whilenostudieshaveprecisely quantifiedtheclinicalsignificanceofthislevelofdecrease, priorliteratureandCDCguidelinesnoteadose-dependent relationshipbetweenprescriptionsandriskofdeveloping OUD,suggestingthateverypillmattersatapopulation level.2–4 Further,giventhatthiscenter’spre-intervention meantabletsperEDdischargeopioidprescriptionwasonly 14,themaximumexpecteddecreasefromadefaultchangeto 12wasonlyadecreaseoftwotabletsperdischarge prescription.However,theseinterventionsmightconfera largerclinicalsignificanceatotherinstitutionswithahigher
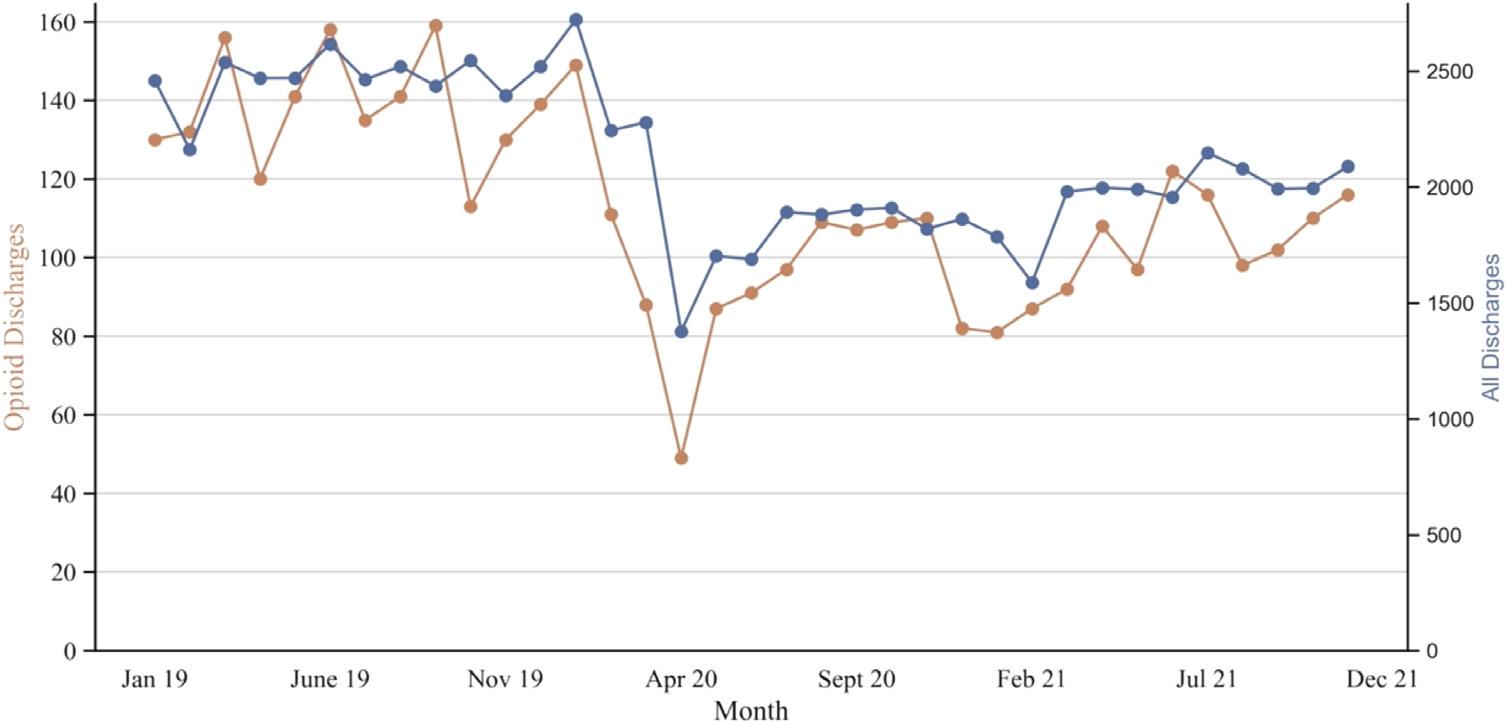
Figure1. DecreasingdefaultopioidquantitiesintheelectronichealthrecordisassociatedwithlowerEDprescriptionofopioidsinthe emergencydepartment.Numberoftotaldischarges(blue)anddischargesinwhichopioidswereprescribed(orange)overthestudytimeline. TheinterventionbeganonMarch19,2021.
Table2. Tabletsandmorphinemilligramequivalentsperdischargeprescriptionwithopioids.
Opioidprescriptions
CI,confidenceinterval; MME,morphinemilligramequivalent.
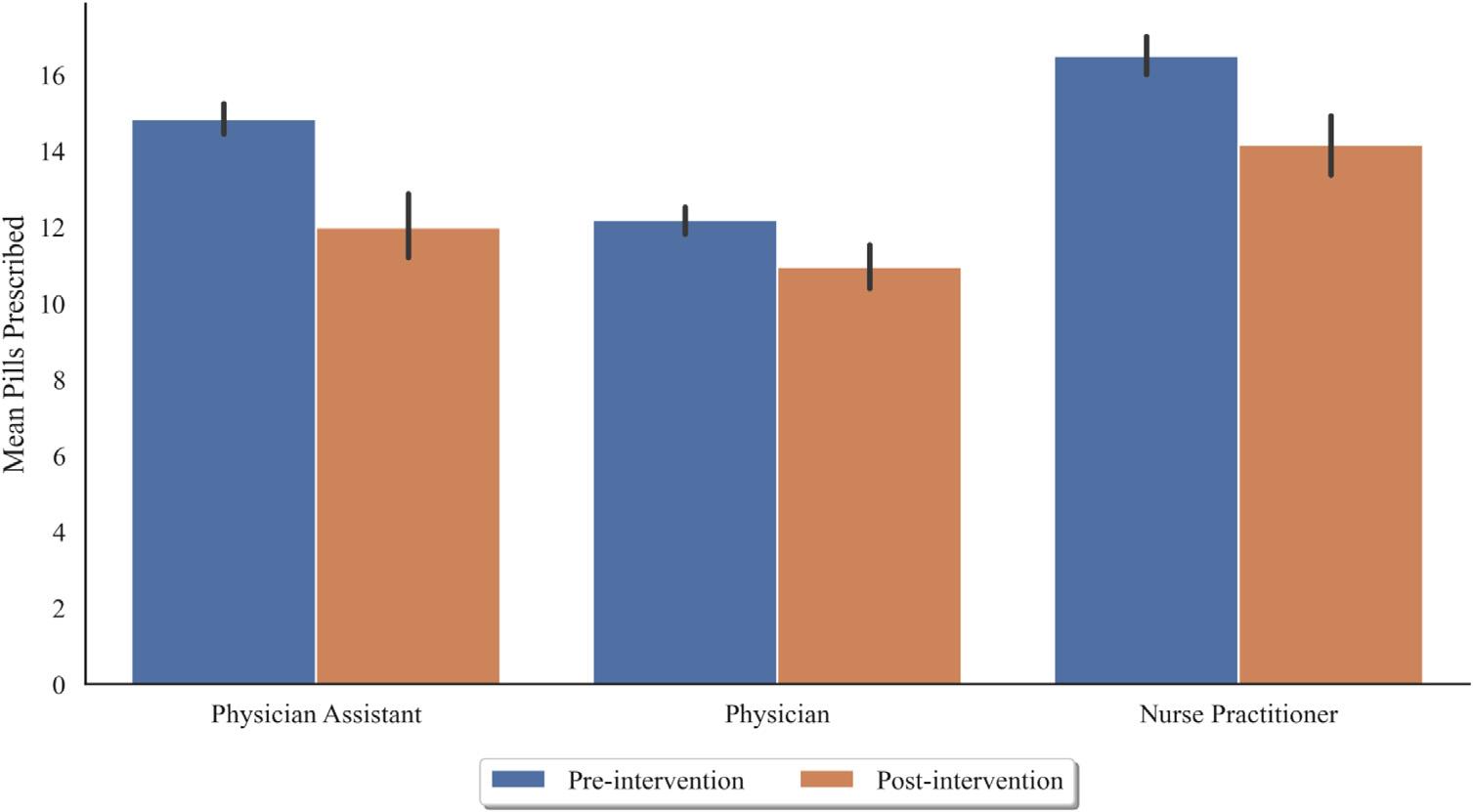
Figure2. Cliniciantypeisassociatedwithopioidprescriptionquantitiesintheemergencydepartment.Averagenumberoftablets perdischargeinwhichopioidswereprescribed,groupedbycliniciantypeandinterventiontime(blue = pre-intervention, orange = post-intervention).
Table3. Numberoftabletsperdischargeprescriptionwithopioids,bycliniciantype.
NP,nursepractitioner; PA,physicianassistant; CI,confidenceinterval.
startingmeantabletsperdischarge.Importantly,we observedthatNPsandPAsintheEDsettingaremorelikely thanphysicianstoprescribehigherlevelsofopioidsat baseline,consistentwithpreviousresultsinprimary caresettings.14
Ourresultssuggestthatauniversaldefaultchangeis associatedwithdecreasedopioidprescriptionsacrossall clinicians,withlargerdecreasesforNPsandPAscompared tothechangeobservedforphysicians.Thehigherratesof opioidprescriptionsamongNPsandPAscouldbeduetoa varietyoffactors,includingdifferencesintheacuityortypes ofillnessesandinjuriesevaluated.Additionally,evenafter theintervention,thehighaverageopioidsprescribedinthe NPgroupwasdrivenbyafewcliniciansstillfarexceedingthe default(SupplementalFigure1).Theexistenceofinterclinicianvariabilityinprescriptionsmayprovide opportunitiesformoretargetedfutureinterventions,suchas NP-orPA-specificinterventionsinconjunctionwithEHRdriveninterventions.
Wechosetoanalyzetheaveragenumberoftablets prescribedperencounterinwhichopioidswereprescribed ratherthanperEDvisitorpermonth.Averagenumberof tabletsalignsmoredirectlywithourintervention,whichwas aimedatreducingthequantityofopioidsprescribedaftera clinicianhadalreadydeterminedaneedforopioidanalgesia. Additionally,thenumberoftabletsprescribedperopioid encounterislessimpactedbytemporalandseasonal variationinprescribingpatternsandvisitacuity,including theeffectoftheCOVID-19pandemic.
Inmostpriorstudies,clinicianswerenotnotifiedofaltered EHRdefaultprescriptionseitherforconvenienceortotest theeffectofadefaultchangealone,orduetoconcernthat clinicianswouldconsciouslyoverridethedefaults.9–13 However,wefoundthatdecreasingdefaultEHRopioid quantitiesto12tabletscoupledwithinformingcliniciansof theEHRchangeresultedinadecreaseinthetotalnumberof opioidsprescribedatEDdischarge.Weobserveddecreases intheaveragenumberoftabletsprescribedperpatientand theaverageMMEoftabletsprescribedperpatient.This suggeststhattransparencywithcliniciansregardingbest practicesinopioidprescribingdoesnotnegatetheeffectof alteringEHRdefaults.Itispossiblethatanannouncementto cliniciansabouttheEHRchangeandtherationalebehindit mayserveasaneducationalfeedbackcomponenttothe
intervention.Clinicianswhoappreciatethepurposeofthe defaultchangemaybemorelikelytousethedefault,golower thanthedefault,orevenwritefewerprescriptionsastheysee fitforeachclinicalscenario,consistentwithpriorwork demonstratingthatauditandfeedbackapproachescan decreaseopioidprescribing.15
Becausepriorworkhasdemonstratedtheexistenceof racialdisparitiesinopioidprescribing,weinvestigated whetherclinicians’ opioidprescribingbehaviordiffered basedonpatientdemographics.16 Ouranalysisshowedthat therewasnostatisticallysignificantdisparityinopioid prescriptionamountsbasedonpatientdemographics, includingage,race,andgender,forboththepre-andpostinterventiondata.
ItisalsoimportanttonotethattheCOVID-19pandemic startedduringourpre-interventionphase,whichresultedin anoveralldecreaseinEDutilization.17 However,our outcomeissomewhatinsulatedfromchangesinEDvolume, astabletsperprescriptionshouldnotbedependentonthe numberofpatientdischarges.TheCOVID-19pandemicmay haveledtoothermoresubtlechangesinprescribingbehavior secondarytochangingpatientpopulationsseen,butthe majorchiefcomplaintsdidnotdifferinthepre-and post-interventionperiod,andtheresultsofoursensitivity analysisconfirmedthattheeffectseenwasstillpresent evenafterrestrictingourdatatoanentirely post-COVID-19timeframe.
Ultimately,werecognizethatopioidsremain fi rst-line treatmentsforcertainindicationssuchasshort-termpain reliefforacutefracturesandcancerpainandareoften necessaryatdischargefromtheED.However,giventhe risksofdiversion,overdose,andOUDassociatedwith dischargingpatientswithlargequantitiesofopioidtablets, itisimportanttoencourageemergencycliniciansto dischargepatientswithaclinicallyappropriateyetsafe quantityoftablets.Itisalsoimportanttousediscretionas opioidsareoftennotindicatedforcertainothercausesof paininpatientspresentingtotheED,includingthe commonchiefcomplaintsofabdominalpainandlower backpain.18 Recommendationsforacutepainsuggest dischargingpatientswithathree-daysupplyofopioid medications,whichcorrespondsto12tabletsorless.19 Our approachisapragmatic,transparent,andscalable interventionthatoffersatoolthatcanbeimplementedin
the42%ofEDsnationwidethatcurrentlyhavedefaults exceeding12tablets.19
Ourstudydesignofasingle-site,pre/poststudydoesnot allowforacausalinterpretationandlimitsgeneralizability. MuchoftheprojectoccurredduringtheCOVID-19 pandemic,inwhichopioidprescribingincreasednationwide; however,patternsforEDdischargeprescriptionshavenot beenstudied.20 Ourdesigndidnotallowustomeasure associatedharmsorbenefits,suchaswhetherpaincontrol wasadequateorwhetherdiversiondecreased.21 Neitherdid ourdesignallowustotestfordifferencesinwhetherpatients wereprescribedopioids,whichisalsoanimportant considerationforopioidstewardship.Additionally,the 12-tabletdefaultquantitywaschosentoapproximatea three-daysupply,butthislengthmayvarybasedonthe frequencyprescribedofagivenopioid,andthereislimited evidencetosupporttheoptimaltimecourseofopioids atdischarge.22
Finally,thestudydesigndidnotallowustomeasurethe precisenumberofclinicianswhowereexposedtothe clinician-facingannouncement,differentiatewhetherthe effectsobservedwereattributabletotheEHRchangesalone, theclinician-facingannouncementalone,oracombination ofthetwo.
Wedemonstratedthataqualityimprovement interventioncouplingdecreaseddefaultopioidquantitiesin theelectronichealthrecordwithinformingcliniciansofthe EHRchangewasassociatedwithadecreaseinthetotal numberofopioidsprescribedfromtheED.Whileall cliniciantypes(NPs,PAs,andphysicians)decreasedtheir quantitiesofopioidsprescribedperdischargefollowingthe defaultchange,NPsandPAsprescribedmoreopioidsthan physiciansinitiallyandexperiencedalargerdecreasein opioidprescriptions.Futureinterventionsseekingtoaddress EDopioidprescribingshouldmeasurethetotalquantityof opioidsleavingtheEDoverlongerperiodsoftime,usea robust,patient-centeredmetricforpainmanagementfollowup,andattempttocorrelateEDopioidprescriptionswith negativeopioid-associatedoutcomesinbothindividual patientsandtheircommunities.
AddressforCorrespondence:MarianneJuarez,MD,Universityof CaliforniaSanFrancisco,DepartmentofEmergencyMedicine,521 ParnassusAvenue,7th floor,SanFrancisco,CA94143.Email: Marianne.Juarez@ucsf.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources
and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.KaiTrepkawassupportedbygrant T32GM007618fromtheNationalInstituteofGeneralMedical SciencesoftheNationalInstitutesofHealth.Therearenoother conflictsofinterestorsourcesoffundingtodeclare.
Copyright:©2024Johnsonetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.SchieberLZ,GuyGP,SethP,etal.Trendsandpatternsofgeographic variationinopioidprescribingpracticesbystate,UnitedStates, 2006–2017. JAMANetwOpen.2019;2(3):e190665.
2.ShahA,HayesCJ,MartinBC.Characteristicsofinitialprescription episodesandlikelihoodoflong-termopioiduse UnitedStates, 2006–2015. MMWRMorbMortalWklyRep.2017;66(10):265–9.
3.HoppeJ,KimH,HeardK.Associationofemergencydepartment opioidinitiationwithrecurrentopioiduse. AnnEmergMed 2015;65(5):493–9.
4.JohnsonDG,HoVT,HahJM,etal.Prescriptionquantityandduration predictprogressionfromacutetochronicopioiduseinopioid-naïve Medicaidpatients.MattieH,ed. PLOSDigitHealth 2022;1(8):e0000075.
5.Kennedy-HendricksA,GielenA,McDonaldE,etal.Medicationsharing, storage,anddisposalpracticesforopioidmedicationsamongUSadults. JAMAInternMed.2016;176(7):1027.
6.DaoustR,PaquetJ,MarquisM,etal.Evaluationofinterventionsto reduceopioidprescribingforpatientsdischargedfromtheemergency department:asystematicreviewandmeta-analysis. JAMANetwOpen 2022;5(1):e2143425.
7.RathlevN,AlmomenR,DeutschA,etal.Randomizedcontrolledtrialof electroniccareplanalertsandresourceutilizationbyhighfrequency emergencydepartmentuserswithopioidusedisorder. WestJEmerg Med.2016;17(1):28–34.
8.DowellD,HaegerichTM,ChouR.CDCguidelineforprescribingopioids forchronicpain UnitedStates,2016. JAMA.2016;315(15):1624.
9.MontoyJCC,CoralicZ,HerringAA,etal.Associationofdefault electronicmedicalrecordsettingswithhealthcareprofessionalpatterns ofopioidprescribinginemergencydepartments:arandomizedquality improvementstudy. JAMAInternMed.2020;180(4):487.
10.CarlsonA,NelsonME,PatelH.Longitudinalimpactofapre-populated defaultquantityonemergencydepartmentopioidprescriptions. JAm CollEmergPhysiciansOpen.2021;2(1):e12337.
11.ZivinK,WhiteJO,ChaoS,etal.Implementingelectronichealthrecord defaultsettingstoreduceopioidoverprescribing:apilotstudy. Pain Med.2019;20(1):103–12.
12.DelgadoMK,ShoferFS,PatelMS,etal.Associationbetweenelectronic medicalrecordimplementationofdefaultopioidprescriptionquantities andprescribingbehaviorintwoemergencydepartments. JGenIntern Med.2018;33(4):409–11.
13.SantistevanJ,SharpB,HamedaniA,etal.Bydefault:theeffectof prepopulatedprescriptionquantitiesonopioidprescribinginthe emergencydepartment. WestJEmergMed.2018;19(2):392–7.
14.LozadaMJ,RajiMA,GoodwinJS,etal.Opioidprescribingbyprimary careproviders:across-sectionalanalysisofnursepractitioner, physicianassistant,andphysicianprescribingpatterns. JGenIntern Med.2020;35(9):2584–92.
15.AndereckJW,ReuterQR,AllenKC,etal.Aqualityimprovement initiativefeaturingpeer-comparisonprescribingfeedbackreduces emergencydepartmentopioidprescribing. JtCommJQualPatientSaf 2019;45(10):669–79.
16.KeisterLA,StecherC,AronsonB,etal.Providerbiasinprescribing opioidanalgesics:astudyofelectronicmedicalrecordsatahospital emergencydepartment. BMCPublicHealth.2021;21(1):1518.
17.VenkateshAK,JankeAT,Shu-XiaL,etal.Emergencydepartment utilizationforemergencyconditionsduringCOVID-19. AnnEmergMed 2021;78(1):84–91.
18.KamperSJ,LoganG,CopseyB,etal.Whatisusualcareforlowback pain?Asystematicreviewofhealthcareprovidedtopatientswithlow backpaininfamilypracticeandemergencydepartments. Pain 2020;161(4):694–702.
19.BlutingerEJ,ShoferFS,MeiselZ,etal.Variabilityinemergency departmentelectronicmedicalrecorddefaultopioidquantities:A nationalsurvey. AmJEmergMed.2019;37(10):1963–4.
20.LeeB,YangKC,KaminskiP,etal.Substitutionofnonpharmacologic therapywithopioidprescribingforpainduringtheCOVID-19pandemic. JAMANetwOpen.2021;4(12):e2138453.
21.DuncanRW,SmithKL,MaguireM,etal.Alternativestoopioids forpainmanagementintheemergencydepartmentdecreases opioidusageandmaintainspatientsatisfaction. AmJEmergMed 2019;37(1):38–44.
22.McCarthyDM,KimHS,HurSI,etal.Patient-reportedopioidpill consumptionafteranEDvisit:Howmanypillsarepeopleusing? Pain Med.2021;22(2):292–302.
AndrewT.Kinoshita,MPH* SoheilSaadat,MD,PhD,MPH† BharathChakravarthy,MD,MPH†
SectionEditor:R.GentryWilkerson,MD
*UniversityofCaliforniaIrvine,SchoolofMedicine,Irvine,California † UniversityofCaliforniaIrvine,SchoolofMedicine,DepartmentofEmergency Medicine,Irvine,California
Submissionhistory:SubmittedApril1,2023;RevisionreceivedJanuary26,2024;AcceptedFebruary12,2024
ElectronicallypublishedMay21,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18037
Introduction: Peoplewhousedrugsincommunitysettingsareatriskofafataloverdose,whichcanbe mitigatedbynaloxoneadministeredviabystanders.Inthisstudywesoughttoinvestigatemethodsof estimatingandtrackingopioidoverdosereversalsbycommunitymemberswithtake-homenaloxone (THN)tocoalescepossiblewaysofcharacterizingTHNreachwithametricthatisusefulforguidingboth distributionofnaloxoneandadvocacyofitsbenefits.
Methods: WeconductedascopingreviewofpublishedliteratureonPubMedonAugust15,2022,using PRISMA-ScRprotocol,forarticlesdiscussingmethodstoestimateTHNreversalsinthecommunity.The followingsearchtermswereused: naloxoneAND(“takehome” ORkitOR “communitydistribution” OR “naloxonedistribution”).Weusedbackwardscitationsearchingtopotentially findadditionalstudies. Overdoseeducationandnaloxonedistributionprogram-basedstudiesthatanalyzedonlysingle programswereexcluded.
Results: Thedatabasesearchcaptured614studies,ofwhich14studieswererelevant.Backwards citationsearchingof765referencesdidnotrevealadditionalrelevantstudies.Ofthe14relevantstudies, 11weremathematicalmodels.TenusedMarkovmodels,andoneusedasystemdynamicsmodel.Of theremainingthreearticles,onewasameta-analysis,andtwousedspatialanalysis.Studiesrangedin yearofpublicationfrom2013–2022withmathematicalmodelingincreasinginuseovertime.Onlyspatial analysiswasusedwithafocusoncharacterizinglocalnaloxoneuseatthelevelofaspecificcity.
Conclusion: OfexistingmethodstoestimatebystanderadministrationofTHN,mathematicalmodels aremostcommon,particularlyMarkovmodels.Systemdynamicsmodeling,meta-analysis,andspatial analysishavealsobeenused.Allmethodsareheavilydependentuponoverdoseeducationand naloxonedistributionprogramdatapublishedintheliteratureoravailableasongoingsurveillancedata. Overall,thereisapaucityofliteraturedescribingmethodsofestimationandevenfewerwithmethods appliedtoalocalfocusthatwouldallowformoretargeteddistributionofnaloxone.[WestJEmergMed. 2025;26(1.1)26–32.]
Peoplewhousedrugsincommunitysettingshavetherisk ofafataloverdose,whichcanbemitigatedbynaloxone administeredviabystandersduringoverdoseincidents. Currently,thereissomepublichealthinfrastructureinplace totracknaloxonedistribution.InCalifornia,the DepartmentofHealthCareServices(DHCS)actsasahub
fordisseminationofnaloxonetocommunity-based organizations.1 Theseorganizationsare,inturn,charged withmaintainingdistributionandusedata.However,the DHCSisnottheonlydistributorofnaloxone,nordo programsthatdistributenaloxonehaveanywaytorequire individualstoreportuse.Further,naloxoneinNarcannasal sprayformhasrecentlybeenapproved(inMarch2023)by
theUSFoodandDrugAdministrationforover-the-counter (OTC)distribution.Duetothismultitudeoffactors,itisnot knownhowfrequentlycommunity-distributednaloxoneis administeredtotreatoverdose.
Whilenaloxonedistributionisaneffective,evidencebasedintervention,andOTCformulationsareapproved, thereisstillpushbackagainsthighlyvisibleandavailable naloxonedistributionpointsfrompolicymakersand communitymembersduetothestigmaassociatedwithdrug useand,byextension,thelegallandscape.2,3 Inthisstudywe soughttoinvestigatemethodsofestimatingandtracking opioidoverdosereversalsbycommunitymemberswithtakehomenaloxone(THN)tocoalescepossiblewaysof characterizingTHNreachwithametricthatisusefulfor guidingbothdistributionofnaloxoneandadvocacy ofitsbenefits.
WithPRISMA-ScRprotocolusingthePubMed database,4 weconductedascopingreviewonmethodsto estimateopioidoverdosereversalsbycommunitymembers usingTHN,beforeanypotentialinterventionby first respondersorclinicians.Thedatabasesearchwasfollowed bybackwardscitationsearchingtoidentifyrelevantarticles omittedinthedatabasesearch.PubMed,adatabase providedbytheNationalCenterforBiotechnology InformationattheUSNationalLibraryofMedicine,was usedforthescopingreviewduetoitscoverageof 35millioncitationscontainedwithintheliterature compilationsofMEDLINE,PubMedCentral, andBookshelf.5
SearchStrategy
WeperformedasearchonAugust15,2022,using PubMedto findarticlesthatdiscussedsurveillanceor estimationofTHNadministration.Thesearchwasrestricted toarticlespublishedintheEnglishlanguage,butitwasnot restrictedbyyearofpublication.Thetermsusedforthe searchstrategywereselectedtoensurethatrelevantstudies foundinpilotsearcheswereallincluded.Sincetherehasbeen anevolvinglexiconsurrounding “take-home” naloxone, alternativetermshadtobeincludedinthesearch,even thoughthisdilutedtheproportionofrelevantstudiesinthe finalsearch.Weusedthefollowingsearchterms: naloxone AND( “ takehome ” ORkitOR “ communitydistribution ” OR “ naloxonedistribution ” ) . ArticlesfromthePubMedsearchthatdiscussedTHNand werepossiblyrelatedtosurveillanceorestimationwere sortedintomethodologybucketsforpossiblefurtherreview basedontitleandabstract,orreviewoffullarticleswhere uncertaintyexisted.Thesemethodologybucketsincludedthe following:1)mathematicalmodels;2)meta-analysis; 3)spatialanalysis;4)otherpossiblyrelevantarticles; 5)opioidoverdoseeducationandnaloxonedistribution
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Administrationofnaloxonemitigatestherisk ofafataloverdoseincommunitysettings; however,surveillanceofcommunitynaloxone anditsadministrationisweak.
Whatwastheresearchquestion?
Whatmethodsexistfortrackingorestimating opioidoverdosereversalsbycommunity memberswithnaloxone?
Whatwasthemajor findingofthestudy?
Thescopingreviewyielded14studies:11 mathematicalmodels,onemeta-analysis,and twospatialanalyses.
Howdoesthisimprovepopulationhealth?
Fewmethodshavebeenpublishedtoestimate communitynaloxoneadministration; methodsmustbeadaptedforlocalusebefore informingpolicyoradvocacy.
(OEND)program-basedstudies;and6)otherarticles deemednotrelevant.
Thearticlessortedintothe firstfourbuckets mathematicalmodels;meta-analysis;spatialanalysis;and otherpossiblyrelevantarticles werereadinfullfor confirmationof finalinclusion.Weexcludedfromfurther reviewbucket5(OENDprogram-basedstudies)because thesestudieshavestraightforwardmethodologyandare alreadyawell-knownmethodoftrackingTHN administration,whichisevidencedbythenumberofOEND program-basedstudies(59studiescapturedwithour databasesearchstrategy).TheseOENDprogram-based studiesarediscussedfurtherinthe Discussion section.After selectionofPubMedarticlesfor finalinclusion,we performedbackwardscitationsearchingonthesearticles usingtitles,withabstractsasneeded.Thefulltextofpossibly relevantarticleswasreviewedfor finalinclusion.
Weextractedthefollowingdatausingastandardized table:method(bucket);modeltype;datasources;location (country,location – community);andfundingsources. Methodcorrespondedtothebucketcategoriesdiscussed above.Modeltypewasrelevantforstudiesinbucket1 (mathematicalmodels),andtherecordedmodeltypewas basedonhowauthorsself-describedtheirstudies.Theseself-
descriptionsformathematicalmodelsincludedMarkov modelingandsystemdynamicsmodeling.Datawas synthesizedthroughconceptmapping.
Thedatabasesearchresultedinthecaptureof614studies. Ofthese,108studiesweremarkedaspossiblyrelevantbased ontitlesorabstractsdiscussingTHNprograms,surveillance, orestimation.Usingfullarticlesasneeded,39studieswere categorizedintobucketsofinterest(1–4).Following categorization,fullarticlereviewresultedin14articlesfor finalinclusion.Backwardscitationsearchingofthe765 referencescontainedwithinthe14articlesresultedinthree articlesforfullreview.Allthreewereexcludedfrom final analysisleaving14articlesfor finalinclusion.These14 articleswerefrombuckets1–3. Figure1 presentsa flowchart ofthecapturesandthereviewofliterature.
Theincludedstudiesvariedintheirobjectives.Developing awaytoidentifyhowmuchnaloxonewasadministeredby bystanderswasoftenacontributortotheoverallgoalsofthe studiesinsteadoftheprimaryobjective.Thissectionpresents asynthesisofstudyobjectivesandthemethodsemployedto surveilorestimatecommunitynaloxoneuse.The Table presentsanoverviewofthestudiesbymethod.
Ofthe14studies,11employedmathematicalmodels.Of these,10usedMarkovmodelsandwerepublishedbetween 2012–2022.Markovmodelsdefineseveralnon-overlapping statuses(ie,chronicopioiduse,cessationofopioiduse, overdosing,dead)andrepresenteachindividualwithina simulatedpopulationasamemberofoneofthestatuses.6
Studies identified through database searching. (n = 614)
Abstracts screened. (n = 614)
Abstracts possibly relevant. Categorized into buckets using full text as needed. (n = 108)
Studiescategorized into relevant buckets. Full text reviewed. (n = 39)
Studies included in qualitative synthesis. (n = 14)
Individualstransitionfromonestatetoanother,not necessarilylinearly,basedonprobabilityparametersthat representchangeinindividualstatusesovertime.Thismeans thatmodeloutputofanypriororsubsequentpopulation distributionwithinthesystemcanbederivedfromanygiven populationdistribution.Theoneremainingmathematical modelingstudyusedasystemdynamicsmodelandwas publishedin2022.Systemdynamicsmodelingrepresents differentvariables(ie,population,treatmentavailability, overdosedeaths)withinasystemandtherelationships betweenthem,factoringintemporaldelayasappropriate.7 Thismeansthatthemodeloutputofanysubsequent populationdistributionwithinthesystemmaybebasedon boththegivenpopulationdistributionandthechanges precedingthegivenpopulationdistribution.
Studiesemployingmathematicalmodelsvariedintheir primaryobjectives.FiveofthestudiesemployingMarkov modelsweredesignedtoevaluatethecosteffectivenessof naloxonedistribution.Fourofthesecost-effectiveness studiesusevariationsofthesameMarkovmodel,whichwas originallydevelopedin2013byCoffinandSullivan,who authoredtwoofthefourarticles.8–11 Theoneremainingcosteffectivenessstudy,byUyeietal,wasuniqueinthatitalso investigatednaloxonedistributioninconjunctionwithother interventions,includingpre-exposureprophylaxisfor HIVprevention.12
Oftheremaining fiveMarkovmodelstudies,allmodeled theeffectsofnaloxonedistributiononopioidoverdosedeath rates.Coffinetal(2022)modeledtheUSpopulationusing theMarkovmodeldevelopedpreviouslybyCoffinand Sullivanin2013.13 Irvineetal(2018)andIrvineetal(2019) modeledthepopulationofBritishColumbiausingamodel developedbyIrvineetalin2018.14,15 Irvineetal(2022) modeledtheUSpopulation,andLinasetal(2021)modeled
Titles screened from backwards citation searching using abstracts as needed. (n = 765)
Studies excluded;abstracts not relevant. (n = 506)
Study excluded; bucket not relevant. (n = 69)
Studies excluded; full text not relevant. (n = 25)
Abstract relevant and not duplicate study. Full text reviewed. (n = 3)
Studies included in qualitative synthesis. (n = 0)
Studies excluded; title/abstract not relevant or duplicate study. (n = 762)
Studies excluded; full text not relevant. (n = 3)
TOTAL studies included in qualitative synthesis. (n = 14)
Table. Studycharacteristicsbymethod.
Method (bucket)
Model type First
Mathematical models Markov model
authorYearDatasources
AcharyaM2020Literature, Surveillancedata, Assumption
CoffinPO2022Literature, Assumption
CoffinPO2013Literature, Expertinput, Assumption
CoffinPO2013Literature, Assumption
IrvineMA2018Surveillancedata, Literature, Expertinput, Assumption
IrvineMA2019Surveillancedata, Literature, Expertinput, Assumption
Location country Location communityFundingsources
USUSNotreported
USUSNationalInstitutesofHealth
USUSNationalInstituteofAllergyand InfectiousDiseases(National InstitutesofHealth)
RussiaRussiaOpenSocietyFoundation
CanadaBritish Columbia CanadianInstitutesofHealth Research,NaturalScienceand EngineeringResearchCouncil ofCanada
CanadaBritish Columbia BritishColumbiaGovernment, CanadianInstitutesofHealth Research,NaturalScienceand EngineeringResearchCouncil ofCanada,MichaelSmith FoundationforHealth Research,NationalInstitutes ofHealth
IrvineMA2022Literature, Modified-Delphi panel USUSNationalInstituteonDrug Abuse(NationalInstitutes ofHealth)
LanghamS2018Literature, Assumption UKUKMundipharmaInternationalLtd.
LinasBP2021Surveillancedata, Literature, Assumption USRural,urban Massachusetts NationalInstituteonDrug Abuse(NationalInstitutes ofHealth)
UyeiJ2017Surveillancedata, Literature, Assumption USConnecticutConnecticutDepartmentof PublicHealth,NationalInstitute ofMentalHealth(National InstitutesofHealth)
System dynamics model Stringfellow EJ 2022Surveillancedata, Literature, Expertinput, Assumption USUSUSFoodandDrug Administration
Meta-analysisMcAuleyA2015OENDprogram studies Canada, UK,US n/aNationalHealthService Scotland
SpatialanalysisRoweC2016SurveillancedataUSSanFranciscoNationalInstituteonDrug Abuse(NationalInstitutes ofHealth)
YiG2022SurveillancedataUSBaltimoreNotreported
urbanandruralMassachusettspopulationsalsousingthe 2018Irvineetalmodel.16,17
Theonestudyusingasystemdynamicsmodelwas conductedbyStringfellowetalin2022andinvestigatedthe effectsofdifferentinterventions,includingnaloxone distribution,onopioidoverdosedeathrates.18
Mathematicalmodelsemployedvariousdatasourcesto informtheparametersused.Thesesourcesincluded parametersfrompublishedliteratureandsurveillancedata (ie,publichealthdepartmentrecords,coronerreports, insuranceclaims).Whensourcesofdatawerenotavailable, authorsusedtheirownassumptionsorexpertinput,
includingamodified-Delphipanelinthe2022Irvineetal study.16 Thestudiesdonotapplythemathematicalmodelsto anyspecificcitiesorsmallercommunities,althoughthe2021 Linasetalstudymodelsageneralizedruralcityanda generalizedurbancityinMassachusetts.17 Adoptingthe mathematicalmodelsemployedinthesestudiestoestimate bystandernaloxoneadministrationinaparticular communityofinterestwouldrequiretheinputoflocal parameters,whichcouldbeanintensiveeffortifsurveillance infrastructureisnotestablished.
OnestudybyMcAuleyetal,publishedin2015,consisted ofameta-analysisofnineOENDprogramstudies, synthesizingtheiroutcomesandaccountingforparticipants losttofollow-uptoreporttheproportionofnaloxonekits thatarelikelytobeusedinthe firstthreemonthsafter distribution.19 Thestudiesthatcomprisedthemeta-analysis werefromCanada,theUnitedKingdom,andtheUS. Adoptingameta-analysismethodologytoestimate bystandernaloxoneadministrationinaparticular communityofinterestwouldinvolvesynthesizingdatafrom OENDprogramsinthecommunity.
Twostudies,byRoweetal(2016)andYietal(2022),used geographicsysteminformation(GSI)mappingtechnologyto conductspatialanalysisofnaloxoneoverdoseincidents.The studiesdeterminedtherelationshipbetweenproximityofthe censustractinwhichnaloxonewasadministeredandthe nearestnaloxonedistributionsite.20,21 Roweetalconducted ananalysisofSanFrancisco,California,andYietal conductedananalysisofBaltimore,Maryland.Surveillance datawasusedtoestablishthisrelationship.TheGSI mappingandspatialanalysismethodologyusedinthese studiescouldbeadoptedinotherjurisdictionstoestimate bystandernaloxoneadministrationinaparticular neighborhoodofinterestbasedinpartondistancefrom naloxonedistributionpoints.
LimitedMethodstoEstimateTake-homeNaloxoneUse
Thelimitednumberofstudiescapturedinthisscoping reviewevidencesthelackofsurveillanceandestimation methodsfortheadministrationofTHN,outsideofOEND programrecordsbasedonself-reports.Ofthemethodsused, mathematicalmodelingandmeta-analysisprovideddirect estimationsoftheproportionofdistributednaloxone administered;however,bothmethodswereappliedonlyover largegeographicareas(entirecountries,statesorprovinces, amalgamatingdifferentcitiesaroundtheglobe)or theoreticalcitiesrepresentingalargegeographicarea (“urbancityofMassachusetts”).
Mathematicalmodelingwasthemostpopularformof estimatingadministrationofnaloxonebycommunity members.Further,thepopularityofmodelingincreased relativetotheothermethods.Whilemakingup79%ofstudy methodologiesfoundoverall,itcomprises89%ofstudiesin the fiveyearsfrom2018–2022,asshownin Figure2.Reasons forthepopularityofmathematicalmodelsmaybe convenience,includingtheuseofexpertinputand assumptionsforunknownparameters,andtheabilityto tailormodelstodifferentgeographicareasbyadjusting parameters.Nineofthe11modelingstudiesusedoneoftwo modelbases,CoffinandSullivan(2013)and Irvineetal(2018).9,14
Therelativedisuseofmeta-analysismaybeexplainedby thelowerpracticalvalueofnaloxoneadministrationdata averagedovermultiplelocations,asopposedtoapplying localdatatoinformprogramgrowthandgaugeimpact. Meta-analysisofnaloxoneuseinothercommunitiesmaybe informativeinjurisdictionslackingtheirownsurveillance data,butcaremustbeexercisedinselectingwhich communitiesandprogramstouseasreferences.Thespread ofOENDprograms,however,mayprovideanopportunity formoreapplicablecomparisons.Further,largeproportions offollow-uplossareevidencedinsomeOENDprograms, addinguncertaintytometa-analysisresults;threeofthenine OENDprogramsthatMcAuleyetal(2015)usedintheir analysishadthree-monthfollow-upratesoflessthan70% (eg,34%,30%,23%).19
Spatialanalysisyieldedarelationshipbetweennaloxone administrationanddistancefromnaloxonedistribution point.Bothstudiesincludedinthisscopingreview(Rowe etal2016,andYietal2022)werereliantuponself-reported datafromOENDprograms.Thisdata,whichisneededto constructaGSImap,maybeusefulforidentifying geographicareasforinterventionbutmaybelessusefulfor extrapolationtounreportedTHNuse.Further,onlythe studybyYietal(2022)characterizedtherelationship betweenprobabilityofbystandernaloxoneadministrationat
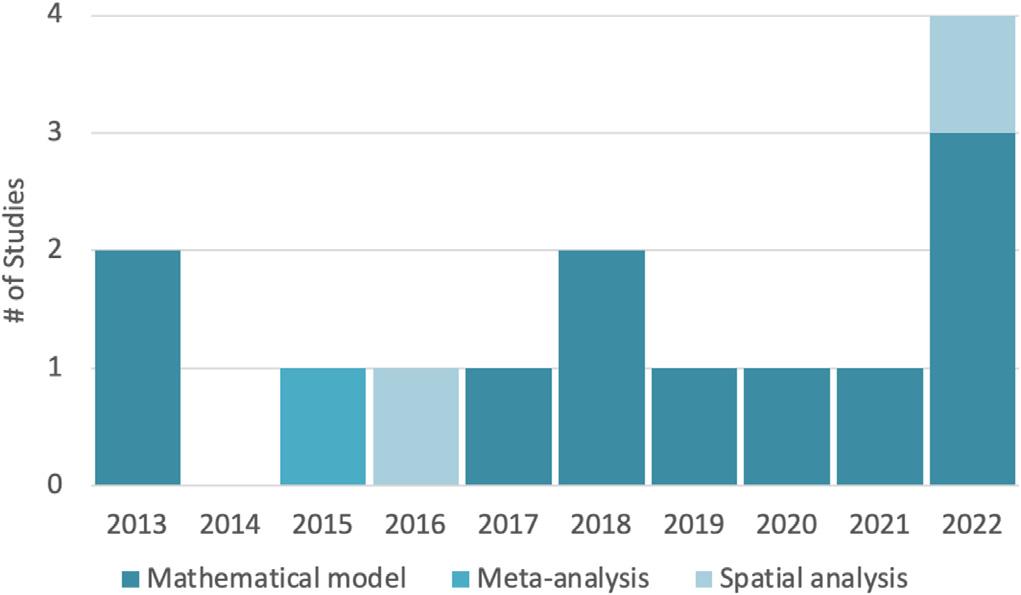
Figure2. Methodsusedovertime.
anoverdoseanddistancefromdistributionpoint.21 Rowe etal(2016)insteadreportedtotalnumberofadministration eventsasafunctionofdistance,furtherlimitingexternal validityoftheresults.20
WhileweexcludedindividualOENDprogram-based studiesfromthisscopingreview,theyareimportantfor discussionandcomprised59ofthecapturedarticlesinthe systematicsearch.Datafromtheseprograms,whetherornot publishedinpeer-reviewedjournals,isthefoundationforthe parametersinmathematicalmodels,thecomponentstudies ofmeta-analysis,andthelocationdataforspatialanalysis. Theaccuracyofallmethodstoestimatenaloxone administrationbybystanderswrapsbackaroundtothe qualityofself-reporteddatafromOENDprograms.When estimationsofTHNuseareputforwardtoinformpolicy,the methodsbehindtheestimatemustbejustifiablybetterthan localOENDdata,ifavailable.Amalgamateddataprovided bygovernmentinstitutionsandnationalcoalitionsmayalso beavailablebutwilllacklocalspecificity.22,23
Therearelimitationstothisscopingreviewandits applicability.Inourstudywedidnotattempttoinclude methodspublishedinthegrayliteratureinourinitialsearch strategy.Thislimitationwasaddressedinpartthrough informalpreliminarysearches,correspondencewithpublic healthpersonnelattheCaliforniaDepartmentofPublic HealthandtheCABridgeprogram,andcitationsearching. Further,itwasnotexpectedthatmethodsforestimationof bystandernaloxoneusewouldexistwithoutbeingpublished inpeer-reviewedjournals.
Arelatedlimitationofthisstudyisthattheinitialsearch forrelevantarticleswaslimitedtothePubMeddatabase. ThisdecisionwasbasedonthePubMedsearchterms comprehensivelycapturingallstudiesidentifiedbyprevious informalpreliminarysearchesandcorrespondencewith publichealthpersonnel.Additionally,thesearchstrategy attemptedtocaptureanypotentiallymissedliterature throughbackwardscitationsearching,andtheabsenceof anynewrelevantarticlessupportedtheparametersofthe initialsearch.
Anotherlimitationtothisscopingreviewisthatitdidnot attempttoascertainthecomparativevalueofmethodsused inestimatingbystandernaloxoneuse.Itispossiblethat preferredmethodsfordeterminingbystandernaloxoneuse willbedependentuponintendeduseoftheanalysisand preferenceforrisk.MethodshighlyinfluencedbyOEND programdatawillinherentlyprovideunderestimation, whileothersmaycauseoverestimation.Finally,the environmentsurroundingharmreductionisconstantly changing.TherecentapprovalofOTCnaloxoneisanew
policythatthestudiescapturedinourreview donotaddress.
Thepresentscopingreviewdescribestheavailable methodsforestimatingbystanderadministrationof naloxone.Mathematicalmodels,particularlyMarkov models,aremostcommon.Systemdynamicsmodeling, meta-analysis,andspatialanalysishavealsobeenused.All methodsareheavilydependentuponOENDprogramdata publishedintheliteratureoravailableasongoing surveillancedata.Overall,thereisapaucityofliterature describingmethodsofestimation,andofthesefewhavebeen appliedwithalocalfocus.Thisisofconcernasharm reductionisstillregardedwithstigma.Further,evenas naloxonedistributionbecomesmorenormalized,both politicallyandsocially,effectivedistributionwillremain importantinalandscapeoffundingandresourcescarcity withcomplementaryinterventionsandcompeting policypriorities.
AddressforCorrespondence:BharathChakravarthy,MD,MPH, UniversityofCaliforniaIrvine,SchoolofMedicine,Departmentof EmergencyMedicine,3800WChapmanAve.,Suite3200,Orange, CA92868.Email: bchakrav@hs.uci.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Thepresentscopingreviewwas researcherfunded.Therearenoconflictsofinterestorsourcesof fundingtodeclare.
Copyright:©2024Kinoshitaetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.CaliforniaDepartmentofHealthCareServices.Naloxone distributionproject.2023.Availableat: https://www.dhcs.ca.gov/ individuals/Pages/Naloxone_Distribution_Project.aspx AccessedMarch22,2023.
2.MartignettiLandSunW.Perspectivesofstakeholdersofequitable accesstocommunitynaloxoneprograms:aliteraturereview. Cureus. 2022;14(1):e21461.
3.CarrollJJ,GreenTC,NoonanRK.Evidence-basedstrategiesfor preventingopioidoverdose:what’sworkingintheUnitedStates. CDC 2018.Availableat: http://www.cdc.gov/drugoverdose/pdf/pubs/ 2018-evidence-based-strategies.pdf.AccessedMarch22,2023.
4.TriccoAC,LillieE,ZarinW,etal.PRISMAextensionforscoping reviews(PRISMA-ScR):checklistandexplanation. AnnInternMed. 2018;169(7):467–73.
5.NationalLibraryofMedicine.PubMedoverview.Availableat: https:// pubmed.ncbi.nlm.nih.gov/about/.AccessedMarch29,2023.
6.SonnenbergFAandBeckJR.Markovmodelsinmedicaldecision making:apracticalguide. MedDecisMaking. 1993;13(4):322–38.
7.WangY,HuB,ZhangY,etal.Applicationsofsystemdynamicsmodels inchronicdiseaseprevention:asystematicreview. PrevChronicDis. 2021;18:E103.
8.AcharyaM,ChopraD,HayesCJ,etal.Cost-effectivenessofintranasal naloxonedistributiontohigh-riskprescriptionopioidusers. Value Health. 2020;23(4):451–60.
9.CoffinPOandSullivanSD.Cost-effectivenessofdistributingnaloxone toheroinusersforlayoverdosereversal. AnnInternMed. 2013;158(1):1–9.
10.CoffinPOandSullivanSD.Cost-effectivenessofdistributingnaloxone toheroinusersforlayoverdosereversalinRussiancities. JMedEcon. 2013;16(8):1051–60.
11.LanghamS,WrightA,KenworthyJ,etal.Cost-effectiveness oftake-homenaloxoneforthepreventionofoverdosefatalities amongheroinusersintheUnitedKingdom. ValueHealth. 2018;21(4):407–15.
12.UyeiJ,FiellinDA,BuchelliM,etal.Effectsofnaloxonedistributionalone orincombinationwithaddictiontreatmentwithorwithoutpre-exposure prophylaxisforHIVpreventioninpeoplewhoinjectdrugs: acost-effectivenessmodellingstudy. LancetPublicHealth. 2017;2(3):e133–40.
13.CoffinPO,MayaS,KahnJG.Modelingofoverdoseandnaloxone distributioninthesettingoffentanylcomparedtoheroin. DrugAlcohol Depend. 2022;236:109478.
14.IrvineMA,BuxtonJA,OtterstatterM,etal.Distributionoftake-home opioidantagonistkitsduringasyntheticopioidepidemicinBritish
Columbia,Canada:amodellingstudy. LancetPublicHealth. 2018;3(5):e218–25.
15.IrvineMA,KuoM,BuxtonJA,etal.Modellingthecombinedimpactof interventionsinavertingdeathsduringasynthetic-opioidoverdose epidemic. Addiction. 2019;114(9):1602–13.
16.IrvineMA,OllerD,BoggisJ,etal.EstimatingnaloxoneneedintheUSA acrossfentanyl,heroin,andprescriptionopioidepidemics:amodelling study. LancetPublicHealth. 2022;7(3):e210–8.
17.LinasBP,SavinkinaA,MadushaniRWMA,etal.Projectedestimatesof opioidmortalityaftercommunity-levelinterventions. JAMANetwOpen. 2021;4(2):e2037259.
18.StringfellowEJ,LimTY,HumphreysK,etal.Reducingopioiduse disorderandoverdosedeathsintheUnitedStates:adynamicmodeling analysis. SciAdv. 2022;8(25):eabm8147.
19.McAuleyA,AucottL,MathesonC.Exploringthelife-savingpotentialof naloxone:asystematicreviewanddescriptivemeta-analysisoftake homenaloxone(THN)programmesforopioidusers. IntJDrugPolicy. 2015;26(12):1183–8.
20.RoweC,SantosGM,VittinghoffE,etal.Neighborhood-levelandspatial characteristicsassociatedwithlaynaloxonereversaleventsandopioid overdosedeaths. JUrbanHealth. 2016;93(1):117–30.
21.YiG,DaytonL,UzziM,etal.Spatialandneighborhood-levelcorrelates oflaynaloxonereversaleventsandserviceavailability. IntJDrugPolicy. 2022;106:103739.
22.WheelerE,DavidsonPJ,JonesTS,etal.Community-basedopioid overdosepreventionprogramsprovidingnaloxone UnitedStates, 2010. MMWRMorbMortalWklyRep. 2012;61(6):101–5.
23.WheelerE,JonesTS,GilbertMK,etal.Opioidoverdoseprevention programsprovidingnaloxonetolaypersons UnitedStates,2014. MorbMortalWklyRep. 2015;64(23):631–5.
CollinMichels,MD*
ThomasSchneider,BS†
KaitlinTetreault,MB‡
JennaMeierPayne,BSN*
KaylaZubke,MSN,RN*
ElizabethSalisbury-Afshar,MD,MPH§∥
*UniversityofWisconsin,SchoolofMedicineandPublicHealth, BerbeeWalshDepartmentofEmergencyMedicine,Madison,Wisconsin
† UniversityofWisconsin,SchoolofMedicineandPublicHealth, Madison,Wisconsin
‡ UniversityofWisconsin,SchoolofMedicineandPublicHealth, DepartmentofBiostatisticsandMedicalInformatics, Madison,Wisconsin
§ UniversityofWisconsin,SchoolofMedicineandPublicHealth, DepartmentofFamilyMedicineandCommunityHealth, Madison,Wisconsin
∥ UniversityofWisconsin,SchoolofMedicineandPublicHealth, DepartmentofPopulationHealthSciences,Madison,Wisconsin
SectionEditor:R.GentryWilkerson,MD
Submissionhistory:SubmittedMarch30,2023;RevisionreceivedJanuary26,2024;AcceptedFebruary16,2024
ElectronicallypublishedMay21,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.18020
Introduction: Asopioidoverdosedeathscontinuetorise,theemergencydepartment(ED)remainsan importantpointofcontactformanyatriskforoverdose.Inthisstudyourpurposewastobetter understandtheattitudes,beliefs,andknowledgeofEDnursesincaringforpatientswithopioiduse disorder(OUD).Wehypothesizedadifferenceintrainingreceivedandattitudestowardcaringfor patientswithOUDbetweennurseswith <5yearsand ≥6yearsofclinicalexperience.
Methods: WeconductedasurveyamongEDnursesinalargeacademicmedicalcenterfromMay–July 2022.AllEDstaffnursesweresurveyed.Dataentryinstrumentsforthenursingsurveyswere programmedinQualtrics,andweanalyzedresultsRusingachi-squaretestorFisherexacttestto comparenurseswith <5yearsand ≥6yearsofclinicalexperience.A P-valueof < 0.05wasconsidered statisticallysignificant.
Results: Wedistributed74surveys,and69werecompleted(93%).Attitudestowardnaloxone distributionfromtheEDwerepositive,with72%ofrespondentsreportingtheywere “very” or “extremely” supportiveofdistributingnaloxonekitstoindividualsatriskofoverdose.Whileattitudeswerepositive, barriersincludedlimitedtime,lackofsystemsupport,andcost.Levelofcomfortincaringforpatientswith OUDwashigh,with78%ofrespondents “very” or “extremely” comfortable.Moreeducationisneededon overdoseeducationandnaloxonedistribution(OEND)withrespondents38%and45% “alittle” or “somewhat” comfortable,respectively.Nurseswith <5yearsofexperiencereportedreceivingmore trainingonOENDinnursingschoolcomparedtothosewith ≥6yearsofexperience(P = 0.03).There werenosignificantdifferencesinreportedattitudes,knowledge,orcomfortincaringforpatients withOUD.
Conclusion: Inthissingle-centersurvey,wefoundEDnursesweresupportiveofoverdoseeducation andnaloxonedistribution.Thereareopportunitiesfortargetededucationandaddressingsystemic barrierstoOEND.Allinterventionsshouldbeevaluatedtogaugeimpactonknowledge,attitudes,and behaviors.[WestJEmergMed.2025;26(1.1)33–37.]
Opioidusedisorder(OUD)isassociatedwitha20-fold riskofearlydeathduetooverdose,infection,trauma,or suicide.1 Nationally,anestimated68,000peoplediedof opioid-relatedoverdosein2020,and2.7millionsuffered fromOUD.2 Theimpactofnon-medicalopioiduseand OUDcanbeseeninmanyhealthcaresettings,includingthe emergencydepartment(ED),asopioid-relatedvisitsinthe EDhadanestimatedcostof$1.47billionperyear between2016–2017.2,3
PatientspresentingtotheEDforopioid-related encounters,includingopioidoverdose,areathighriskfor negativeoutcomes.Emergencydepartment-based interventionssuchasoverdoseeducationandnaloxone distribution(OEND)canhaveasignificantimpacton opioid-relatedmorbidityandmortality.Naloxoneisan opioidreceptorantagonistthatisusedtoquicklyreversethe effectsofopioidoverdose.In2018,theUSSurgeonGeneral recommendedincreasingaccesstonaloxoneforthosewho areatanincreasedriskofanopioidoverdose.4 TheAmerican CollegeofEmergencyPhysiciansalsorecommends providingnaloxoneforpatientsatincreasedriskofopioid overdose,includingthosedischargedfromtheEDafteran opioid-relatedvisitaswellasanypatientwithahistory ofOUD.5
Emergencydepartment-basedtake-homenaloxone programshavebeenaneffectivemeansofdistributing naloxonetopatientsatriskforfutureoverdose6,7;and OENDfromtheEDhasbeenshowntohavepositiveimpact ontrainedlaypersonsinadditiontopatientsandtheirsocial network.8 Large-scaleOENDhasbeenshowntobean effectivepublichealthintervention.9 Patienteducation relatedtooverdosepreventionandnaloxonedistributioncan beprovidedbyEDnurseswhoroutinelyspendmoretime withpatientsthanthetreatingclinician.Clinicalnurse specialist-ledOENDintheEDhavebeeneffectiveacrossan integratedhealthcaresystem.10 Whilemuchisknownabout thebeliefs,attitudes,andbarriersofprescriberstoward naloxonedistribution,includingtime,cost,andclinical decisionsupport,lessisknownaboutnurseperspectivesin theED.6,7,11–15 Wesoughttoevaluatenurseattitudes, beliefs,barriers,andfacilitatorstonaloxonedistributionin anacademicEDintheMidwest.
FromMay–July2022weconductedasurveyofEDnurses ataquaternary-care,academicEDintheMidwestthatsees approximately60,000patientsperyear.Theresearchteam, whichincludedanemergencyphysicianandanaddiction medicinephysician,createdasurveytoolincollaboration withsurveymethodologyexpertsfromtheUniversityof WisconsinSurveyCenter.Mostitemsonthesurveywere developedbytheteam,butthestigmaquestionswere adaptedfromavalidatedmentalhealthstigmasurvey.15–17
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Emergencydepartmentsplayacrucialrolein caringforpatientswithopioidusedisorder (OUD)withinterventionssuchasoverdose educationandnaloxonedistribution.
Whatwasthemajorresearchquestion?
WhatareattitudesofEDnursesrelatedto caringforpatientswithOUD,andtrainingin overdoseeducationandnaloxone distribution(OEND)?
Whatisthemajor findingofthestudy?
EDnurseshavepositiveattitudes(72%) towardnaloxonedistribution.Earlycareer nurses( < 5years)hadmoreOENDtraining.
Howdoesthisstudyimprove populationhealth?
Resultshighlightopportunitiesfortargeted nursingeducation,addressingbarriersand facilitatorstoOENDintheED,thereby improvingcareforpatientswithOUD.
ResearchcoordinatorsintheEDdistributed74paper surveystofullandpart-timeEDstaffnursesatdailystaff huddlesduringthestudyperiod.Eachrespondentwas allowedtocompleteonlyonesurvey.A$5pre-incentivewas includedwiththesurveyatthetimeofdistribution.
Weusedachi-squaretestorFisherexacttesttoassessthe differenceinnurseattitudes,basedonrelativejobexperience (≤5yearsv ≥6years),regardingperception,knowledge,and barriersfornaloxonedistributionandcaringforpatients withOUD.AllanalysesweredoneinRv4.1.12021 (RFoundationforStatisticalComputing,Vienna,Austria). A P -valueof <0.05wasconsideredstatisticallysignificant.
ThisstudywasreviewedbytheUniversityofWisconsinMadisonMinimalRiskResearchInstitutionalReview Boardanddeemedexempt.Noneoftheauthorshaveany financialconflictsofinteresttodisclose.
Surveysweredistributedto74EDnurses,witha93% responserate.Respondentshadabreadthofclinical experience,with60%havingbeenapracticingnurseforsix yearsormore.Ofthatgroup,21%hadbeenapracticing
nursefor ≥16years.ThemajorityoftheEDnursesreported completingtheirnursingtrainingintheMidwest(83%). OtherregionsrepresentedweretheWest(7.6%),Southwest (1.5%),Southeast(4.5),andNortheast(3%).
Overall,theleveloftrainingonOENDduringnursing schoolwaslow,with77%reportingnooralittleeducation received.Nurseswith0–5yearsofexperiencereported receivingmoreeducationcomparedtonurseswith ≥6years ofexperience(P = 0.03).Whenaskedaboutlevelofcomfort providingeducationrelatedtonaloxoneforoverdose preventionimmediatelyfollowingnursingschool,67%felt “notatall” or “onlyalittle” prepared.Despitemorerecent nursingschoolgraduatesreportingmoreeducationin nursingschool,therewerenodifferencesinhowprepared theyfelttoprovideOEND(P = 0.63).
Responsesweremixedwhentheywereaskedaboutthe perceivedeffectivenessofnaloxonekitsasapublichealth intervention,with55%ofallnursesreportingnaloxonekits are “alittle” or “somewhat” effective.However,themajority (66%)feltthatnaloxonekitswouldnotincreasebehavior thatputpeopleatriskforoverdose.Additionalresponsesto questionsaboutattitudes,beliefs,barriers,andfacilitatorsto naloxonedistributionfromtheEDareavailableinthe Table Responsestoallquestionswerecomparedbetweenthenurses with0–5years’ experiencetothosewith ≥6years’ experience, andnostatisticallysignificantdifferenceswereappreciated.
Overallcomfortlevelforcaringforpatientswhousenonprescribedopioidswashigh,with78%ofrespondentsveryor extremelycomfortable.Again,nodifferenceswere appreciatedbetweennurseswith0–5years’ experienceand thosewith ≥6years’ experience.
Barriersandfacilitatorstonaloxonedistributioninthe EDarevariedandrelatedtotime,education,andcost concerns.Staffreportedthemostsignificantbarrierwas limitedstafftime,with47%reportingthiswasan “extremely” impactfulbarrier.Thesearesimilarto previouslydescribedbarriersandfacilitatorsthatprescribers reportfacing;responsesareincludedinthe Table 14–18
Emergencydepartmentnursesarecriticaltothe effectivenessofED-basedOENDprograms.Althoughthere havebeenmultiplestudieslookingatemergencyclinician attitudes,beliefs,barriers,andfacilitatorstonaloxone distribution,littleisknownaboutEDnurse-specificfactors forOEND.Althoughnursesinpracticefor ≤5yearsreported receivingmoreeducationonnaloxoneforoverdose preventionwhileinnursingschool,theadditionaleducation didnotrelatetostatisticallysignificantdifferencesin attitudes,comfort,orperceivedbarriersorfacilitators. Furtherresearchisneededtoprovideabetterunderstanding ofwhyreceivingmoreeducationdidnotleadtoincreased
Table. Responsesofemergencydepartmentnursestoquestionsaboutattitudes,beliefs,barriers,andfacilitatorstonaloxonedistribution fromtheED. NotatallAlittleSomewhatVeryExtremely
AttitudesHowmuchdoyousupportgivingnaloxonekitsto individualswhomightbeatriskforopioidoverdose?
Howeffectiveisgivinganaloxonekittopeoplewho usedrugsasapublichealthintervention?
Howlikelyisgivinganaloxonekittopeoplewhouse drugsgoingtoleadtobehaviorsthatincreaseriskfor overdose,eg,usingmoreopioidsorusingin combinationwithotherdrugs? 41.8%(28)23.9%(16)25.4%(17)9.0%(6)0.0%(0)
ComfortAskingscreeningquestionsaboutnon-prescribed opioiduse?
Caringforpatientswhousenon-prescribedopioids?0.0%(0)1.4%(1)20.3%(14)46.4%(32)31.9%(22) Offeringanaloxonekittobeabletoreversean overdose?
1.4%(1)5.8%(4)33.3%(23)31.9%(22)27.5%(19)
Teachingalaypersontoadministernaloxone?2.9%(2)10.1%(7)27.5%(19)34.8%(24)24.6%(17) Providingcaretoapersonwithanopioiduse disordercomparedtohelpingapersonwitha physicalillness?
Educatingpatientsaboutopioidoverdose prevention?
Educatingpatientsaboutoverdoseresponseand naloxoneadministration?
3.0%(2)4.5%(3)26.9%(18)47.8%(32)17.9%(12)
0.0%(0)5.8%(4)36.2%(25)44.9%(31)13.0%(9)
4.3%(3)15.9%(11)29.0%(20)37.7%(26)13.0%(9)
Educatingpatientsaboutoverdoseprevention?2.9%(2)18.8%(13)30.4%(21)34.8%(24)13.0%(9) (Continuedonnextpage)
Table. Continued.
NotatallAlittleSomewhatVeryExtremely BarriersLimitedstafftime?0.0%(0)4.5%(3)18.2%(12)30.3%(20)47.0%(31)
Lackofsystemssupportingittohappeninatime efficientway?
Lackofclinicaldecisionsupporttoensureconsistent process?
Howmuchofabarriertodispensingnaloxonekits fromtheEDislackofinsuranceorlimitedinsurance coverageleadingtohighcoststopatients?
Concernsaboutbeingabletoidentifypatientsatrisk foroverdose?
Concernsthatalaypersonwon’tbeableto administeritappropriately?
Concernsthatprovidinganaloxonekitwillleadto moreorriskierdruguse?
Concernsthatpatientswillbeoffendedbyitbeing offered?
1.5%(1)4.6%(3)21.5%(14)43.1%(28)29.2%(19)
31.%(2)10.9%(7)25.0%(16)39.1%(25)21.9%(14)
9.4%(6)10.9%(7)17.2%(11)39.1%(25)23.4%(15)
FacilitatorsFundingtoensurepatientsdon’thavetopayco-pays forcostofthenaloxonekit? 3.1%(2)7.8%(5)20.3%(13)32.8%(21)35.9%(23)
Clinicaldecisionsupportthatmakestheprescription anautomatedprocess?
Educationforstaff?1.6%(1)3.1%(2)43.8%(28)35.9%(23)15.6%(10)
Howmuchofafacilitatortodischargingapatient fromtheEDwithanaloxonekitispatienteducation materialstoteachaboutoverdosepreventionand naloxoneadministration?
ED,emergencydepartment.
comfortorknowledgeandwhetherofferingmoretargeted educationcanimprovethesemetrics.Despitereceivingmore education,earlycareernurseshavehadlessexperiencecaring forpatientswithOUD,whichmayhavecontributed totheresults.
Overall,mostrespondentswerecomfortablecaringfor patientswithOUD,includingaskingOUDscreening questions.Slightlylessthanhalffeltnaloxoneisa “ very ” or “extremely” effectivepublichealthintervention,whichisan importantareaforfutureeducationaleffortsandevaluation. Additionalareasforeducationalfociincludetrainingson overdosepreventioneducationandnaloxonetrainingfor patientsandtheirfriends/familywhileintheED.Thisdata providesabaselineunderstandingandcanbere-assessed afterfurthereducationalinitiatives.
Wefoundnursing-identifiedbarriersweresimilarto previouslydescribedprescriberbarriersincludinglimited time,cost,andlackofefficientsystemsupport.18–20 Someof thesebarrierscanbeaddressedwithclinicaldecisionsupport, includingpromptstoordernaloxoneforpatientswith opioid-relateddiagnosticcodes.Providingstandardized, easy-to-followinstructionsonoverdosepreventionand
3.2%(2)7.9%(5)27.0%(17)44.4%(28)17.5%(11)
naloxoneadministrationcanbenefitboththepatientsand thestaffmemberprovidingtheeducation.Although handoutsarehelpful,regulareducationbycontentexperts wouldprovidecontinuededucationtoensureallstaffare comfortablewithoverdosepreventioneducationand naloxoneusemovingforward.
Overall,EDnurseswereopentoreceivingmore education,andmostnursesidentifiedthisasafacilitatorto expandingnaloxonedistributionintheED.Usingbaseline surveysliketheoneourteamusedcanguideEDleadership whendevelopingeducationalandsystemsinterventionsfor nursingstaff.
Limitationsofthisstudyincludeevaluatingasingle, academicLevelItraumacenter;soresultsmaynotapply morebroadlytootherEDs.Wedidnotevaluatefornursing experienceinareasoutsidetheED.Additionally,thenumber ofEDnursessurveyedwassmall(69);soitispossiblethatthe samplesizewastoosmalltoenableustoidentifydifferences betweenthenurseswithlessexperienceascomparedtothose withmoreexperience.
Understandingattitudes,beliefs,barriers,andfacilitators ofnaloxonedistributionamongEDnursesisimportantfor successfulimplementationofoverdoseeducationand preventionprogramming.Emergencydepartmentnurses surveyedweregenerallysupportiveofnaloxonedistribution andcomfortablecaringforpatientswithOUD.Thereare opportunitiesforaddressingsystemicbarriersandproviding targetededucationtofacilitateED-basednaloxone distribution.Theseresultsshowopportunitiestoimprove careforpatientswithOUD,althoughfutureresearchis neededtodeterminewhethereducationimpactsknowledge, attitudes,andbehaviors.
AddressforCorrespondence:CollinMichels,MD,Universityof Wisconsin,SchoolofMedicineandPublicHealth,BerbeeWalsh DepartmentofEmergency,800UniversityBayDr.,Suite310, Madison,WI53705.Email: ctmichels@medicine.wisc.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Thisworkwassupportedbythe UniversityofWisconsinDepartmentsofFamilyMedicineand CommunityHealthandPopulationHealthSciencesaswellasthe UniversityofWisconsinBerbeeWalshDepartmentofEmergency Medicine.Therearenootherconflictsofinterestorsourcesof fundingtodeclare.
Copyright:©2024Michelsetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.NationalAcademiesofSciences,Engineering,andMedicine. MedicationsforOpioidUseDisorderSaveLives.WashingtonDC:The NationalAcademiesPress,2019.
2.SubstanceAbuseandMentalHealthServicesAdministration.Key SubstanceUseandMentalHealthIndicatorsintheUnitedStates: Resultsfromthe2020NationalSurveyonDrugUseandHealth. 2022.Availableat: https://www.samhsa.gov/data/sites/default/files/ reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/ 2020NSDUHFFR1PDFW102121.pdf.AccessedJanuary20,2023.
3.WeinerSG,BakerO,BernsonD,etal.One-yearmortalityofpatients afteremergencydepartmenttreatmentfornonfatalopioidoverdose. AnnEmergMed. 2020;75(1):13–7.
4.OfficeoftheSurgeonGeneral.U.SSurgeonGeneral’sAdvisoryon NaloxoneandOpioidOverdose.2022.Availableat: https://www.hhs. gov/surgeongeneral/reports-and-publications/addiction-andsubstance-misuse/advisory-on-naloxone/index.html AccessedJanuary10,2023.
5.DuberHC,BarataIA,Cioè-PenaE,etal.Identification,management, andtransitionofcareforpatientswithopioidusedisorderinthe emergencydepartment. AnnEmergMed. 2018;72(4):420–31.
6.EswaranV,AllenKC,CruzDC,etal.Developmentofatake-home naloxoneprogramatanurbanacademicemergencydepartment. JAM PharmAssoc. 2020;60(6):324–31.
7.EswaranV,AllenKC,BottariDC,etal.Take-homenaloxoneprogram implementation:lessonslearnedfromsevenchicago-areahospitals. AnnEmergMed. 2020;76(3):318–27.
8.DwyerK,WalleyA,LangloisB,etal.Opioideducationandnasal naloxonerescuekitsintheemergencydepartment. WestJEmergMed. 2015;16(3):381–4.
9.WalleyAY,XuanZ,HackmanHH,etal.Opioidoverdoseratesand implementationofoverdoseeducationandnasalnaloxonedistributionin Massachusetts:interruptedtimeseriesanalysis. BMJ. 2013;346:f174.
10.MullennixSC,IselerJ,KwiatkowskiGM,etal.Aclinicalnursespecialistledemergencydepartmentnaloxonedistributionprogram. ClinNurse Spec. 2020;34(3):116–23.
11.LowensteinM,KilaruA,PerroneJ,etal.Barriersandfacilitatorsfor emergencydepartmentinitiationofbuprenorphine:aphysiciansurvey. AmJEmergMed. 2019;37(9):1787–90.
12.HawkKF,D’OnofrioG,ChawarskiMC,etal.Barriersandfacilitatorsto clinicianreadinesstoprovideemergencydepartment-initiated buprenorphine. JAMANetwOpen. 2020;3(5):e204561.
13.EllisK,WaltersS,FriedmanSR,etal.Breachingtrust:aqualitative studyofhealthcareexperiencesofpeoplewhousedrugsinarural setting. FrontSociol. 2020;5:593925.
14.LacroixL,ThurgurL,OrkinAM,etal.Emergencyphysicians’ attitudes andperceivedbarrierstotheimplementationoftake-home naloxoneprogramsinCanadianemergencydepartments. CJEM. 2018;20(1):46–52.
15.KassamA,PapishA,ModgillG,etal.Thedevelopmentand psychometricpropertiesofanewscaletomeasurementalillness relatedstigmabyhealthcareproviders:theOpeningMindsScalefor HealthCareProviders(OMS-HC). BMCPsychiatry. 2012;12:62.
16.EzellJM,WaltersS,FriedmanSR,etal.Stigmatizetheuse,notthe user?Attitudesonopioiduse,druginjection,treatment,andoverdose preventioninruralcommunities. SocSciMed. 2021;268:113470.
17.KellyT,HawkK,SamuelsE,etal.Improvinguptakeofemergency department-initiatedbuprenorphine:barriersandsolutions. WestJ EmergMed. 2022;23(4):461–7.
18.BarbourK,McQuadeM,SomasundaramS,etal.Emergencyphysician resistancetoatake-homenaloxoneprogramledbycommunityharm reductionists. AmJEmergMed. 2018;36(11):2110–2.
19.PenmJ,MacKinnonNJ,LyonsMS,etal.Combattingopioidoverdoses inOhio:emergencydepartmentphysicians’ prescribingpatternsand perceptionsofnaloxone. JGenInternMed. 2018;33(5):608–9.
20.LaneBH,LyonsMS,StolzU,etal.Naloxoneprovisiontoemergency departmentpatientsrecognizedashigh-riskforopioidusedisorder. AmJEmergMed. 2021;40:173–6.
ZahirBasrai,MD*
ManuelCeledon,MD*
NathalieDieujuste,MA†
JulianneHimstreet,PharmD§ JonathanHoffman,PharmD∥ CassidyPfaff,PharmD¶ JonieHsiao,MD*
RobertMalstrom,PharmD# JasonSmith,PharmD**
MichaelRadeos,MD,MPH†† TerriJorgenson,RPh‡‡
MelissaChristopher,PharmD§§ ComillaSasson,MD,PhD†‡
*VAGreaterLosAngelesHealthCareSystem,VeteransHealthAdministration, DepartmentofEmergencyMedicine,LosAngeles,California
† VAEasternColoradoHealthCareSystem,VeteransHealthAdministration, Aurora,Colorado
‡ UniversityofColorado,AnschutzMedicalCampus,Aurora,Colorado
§ VAPharmacyBenefitsManagementAcademicDetailingService, Eugene,Oregon
∥ VAVISN19RockyMountainNetwork,SaltLakeCity,Utah
¶ VISN19AcademicDetailingService,VeteransHealthAdministration, Tulsa,Oklahoma
# VAPharmacyBenefitsManagementAcademicDetailingService, Martinez,California
**VISN19AcademicDetailingService,VeteransHealthAdministration, Denver,Colorado
†† NYCHealth + Hospitals/ConeyIsland,DepartmentofEmergencyMedicine, Brooklyn,NewYork
‡‡ PharmacyBenefi tsManagement,ClinicalPharmacyPracticeOffice, Washington,DC
§§ VAPharmacyBenefitsManagementAcademicDetailingService, SanDiego,California
SectionEditor:R.GentryWilkerson,MD
Submissionhistory:SubmittedFebruary2,2023;RevisionreceivedJanuary26,2024;AcceptedFebruary16,2024
ElectronicallypublishedMay20,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.17850
Introduction: Theseeminglyinexorableriseofopioid-relatedoverdosedeathsdespitethereduced numberofCOVID-19pandemicdeathsdemandsnovelresponsesandpartnershipsinourpublichealth system’sresponse.Addictionmedicineispracticedinabroadrangeofsiloedclinicalenvironmentsthat needtobeincludedinaddictionmedicinetrainingbeyondthetraditionalfellowshipprograms.Our objectiveinthisprojectwastoimplementaknowledge-based,livevirtualtrainingprogramthatwould providecliniciansandotherhealthcareprofessionalswithanoverviewofaddiction,substanceuse disorders(SUD),andclinicaldiagnosisandmanagementofopioidusedisorder(OUD).
Methods: TheVeteransHealthAdministration(VHA)EmergencyDepartmentOpioidSafetyInitiative (EDOSI)offeredafour-daycourseforhealthcareprofessionalsinterestedingainingknowledgeand practicalskillstoimproveVHA-basedSUDcare.Thecoursetopicscenteredaroundthediagnosisand treatmentofSUD,withafocusonOUD.Additionally,traineesreceivedsixmonthsofsupporttodevelop addictionmedicinetreatmentprograms.Evaluationsofthecoursewereperformedimmediatelyafter completionoftheprogramandagainatthesix-monthmarktoassessitseffectiveness.
Results: Atotalof56cliniciansandotherhealthcareprofessionalsparticipatedintheAddictionScholars Program(ASP).TheparticipantsrepresentednineVeteranIntegratedServiceNetworksand21different VHAmedicalfacilities.Nearly70%ofparticipantscompletedtheinitialpost-survey.Thirty-eight respondents(97.4%)felttheASPseriescontainedpracticalexamplesandusefulinformationthatcould beappliedintheirwork.Thirty-eightrespondents(97.4%)felttheworkshopseriesprovidednew informationorinsightsintothediagnosisandtreatmentofSUD.Elevencapstoneprojectsbasedonthe
informationacquiredduringtheASPwerefunded(atotalof$407,178).Twentyparticipants(35.7%) completedthesix-monthfollow-upsurvey.Notably,90%ofrespondentsreportedincreasednaloxone prescribingand50%reportedincreasedprescribingofbuprenorphinetotreatpatientswithOUDsince completingthecourse.
Conclusion: TheASPprovidedhealthcareprofessionalswithinsightintomanagingSUDandequipped themwithpracticalclinicalskills.Thestudentstranslatedtheinformationfromthecoursetodevelop medicationforopioidusedisorder(M-OUD)programsattheirhomeinstitutions.[WestJEmergMed. 2025;26(1.1)38–42.]
Thenationalopioidepidemicisoneoftheleading preventablecausesofmorbidityandprematuredeathinthe UnitedStates.In2017,theUSDepartmentofHealthand HumanServices(HHS)declaredtheopioidcrisisapublic healthemergency.1 TheCOVID-19pandemichas exacerbatedthiscrisiswithanincreasedprevalenceofopioid usedisorder(OUD)anddeathsfromprescriptionandnonprescriptionopioids.2 Veteransareatnearlytwicetheriskof fataldrugoverdosewhencomparedtonon-veterans.3 As partofthe fiveprioritiestocombattheopioidcrisisHHS highlightedtheimportanceofimprovingaccessto prevention,treatment,andrecoverysupportservices.1 However,thereremaincriticalshortagesofhealthcare professionalswhocanprovidetheselife-savingservices.4 Improvingaccesstosubstanceusedisorder(SUD)careat anytime,anyplaceisanimportantpartoftheVeterans HealthAdministration’s(VHA)strategy.Asaresult,thereis agrowingneedfortraininghealthcareprofessionalsoutside thetraditionaladdictionmedicinespecialtyonkey componentsofaddictionmedicineandSUD.
TheVHAisAmerica’slargestintegratedhealthcare system,providingcareat1,298healthcarefacilitiesincluding 171medicalcentersand1,113VHAoutpatientclinics.More thanninemillionenrolledveteransareservedbytheVHA eachyear.5 Despiteitssize,theVHAsystemhasashortageof addictionspecialistsandSUDclinics.Asaresult,the responsibilityofprovidingSUDcarefallsonavarietyof specialties,includingpharmacyandmentalhealth,and primarycareandemergencymedicine.However,the educationopportunitiesforthesepractitionerstoobtain advancedtraininginaddictionmedicineislimited.
Currently,addictionmedicineisnotarequiredgraduate medicaleducationcourseforinternalmedicine,family medicine,oremergencymedicineresidencies.Asaresult, traineesreceivevariableexposuretoSUDcareduring residency,leadingtosuboptimalpreparationmanaging patientswithaddictionwhenpracticingindependently.6,7 Thetraditionalpathwayforaddictionmedicinetrainingisto completea12-monthdedicatedfellowshipatoneofthe90
sitesaccreditedbytheAccreditationCouncilforGraduate MedicalEducation.8 Thissignificantcommitmentlimitsthe abilityforfrontlineclinicianstoobtainfurthertrainingin addictionmedicine.Thereisaneedtocreateaccessible didacticandpracticalclinicaleducationinaddiction medicinetoincreasefrontlinecliniciancomfort.
LackofbasictraininginSUDisasignificantbarrierto physicianengagementofmedicationforopioidusedisorder (M-OUD)programs.9,10 Asaresult,theAddictionScholars Program(ASP)wasdevelopedtoprovideadditionaltraining forphysicianassistants,nursepractitioners,clinical pharmacists,academicdetailingpharmacists,and physicians.Theeducationaltopicsincludedafoundational understandingofthetreatmentofOUD,complexpain,and complexpersistentopioiddependence.Ourobjectiveinthis studywastomeasuretheeffectiveness,immediatelyandat sixmonths,ofahybrideducationalinterventionpairedwith creationofmultidisciplinaryteamsonknowledgeretention andwillingnesstoprescribeM-OUD.
Thiswasapost-implementationstudyoftheASP,anovel hybrideducationalapproachandfacilitated,team-based qualityimprovement(QI)project.Surveyswereperformed attheconclusionofthecourseandatthesix-monthmark. Thesurveysfocusedonthecourse’seffectivenessandthe trainee’swillingnesstoinitiateanaddictionmedicineproject attheirsite.Weuseddescriptivestatisticstointerpretthe resultsofthesurvey.TheEmergencyDepartmentOpioid SafetyInitiative(EDOSI)programwasdesignatedasaQI projectthroughtheOfficeofPharmacyBenefits ManagementAcademicDetailingServicefromthe institutionalreviewboardoftheEdwardHines,Jr.VA HospitalandapprovedbytheRockyMountainRegional VAMedicalCenterResearchandDevelopmentservice.
TheASPisapartoftheVHAEDOSIandwasdeveloped asanintensivecourseforcliniciansinterestedin understandingVHA-basedSUDcare.Frontlineclinicians
andotherhealthcareprofessionalswhowerecurrent employeesoftheVHAwereinvitedtoapplytoattendthe ASP.Fortywereacceptedtoattendtheprogram.Thecourse consistedoffourvirtualsessionsthatwereeachfourhours long.Eachsessioncoveredfundamentalandadvancedtopics ofaddictionmedicineforemergencyandacutecaresettings.
Theentirecoursewasdeliveredvirtuallyusingthe MicrosoftTeams(MicrosoftCorp,Redmond,WA) application.TopicsincludedclinicalmanagementofOUD, opioidoverdosemanagement,buprenorphineinduction, naloxonedistribution,painmanagementinpatientswith OUD,andopioid-inducedchronicpainsyndrome.The programusedacombinationoflecturesandcase-based breakoutsessionstoreinforcekeyconcepts.Lecturerswere selectedbasedontheirexperienceandexpertiseinspecific areasofaddictionmedicine.Interdisciplinarygroupswere strategicallyassembledforthecase-basedbreakoutsessions withmembersfromthesameVHAsiteandVeteran IntegratedServiceNetworks(VISN).Thisallowedfora networkingopportunitywheregroupmemberscouldbuild connectionsthatwouldleadtothedevelopmentofM-OUD programslocallyattheirVHAsiteorattheirVISN.The groupswerepairedwithamemberoftheVHAEDOSIteam whowouldfacilitatediscussionofthecases.
Aftersuccessfulcompletionofthecourse,trainees receivedsixmonthsofsupporttodevelopandimplement addictionmedicinetreatmentprograms.Traineeswerealso encouragedtosubmitcapstoneprojects,whichwereeligible forfundingupto$50,000(uptotwoyears)tohelpimplement addictionmedicineprojectsattheirlocalVHAsite.
Atotalof56individualsparticipatedintheASP,including 32clinicians,10clinicalpharmacypractitioners,and14 academicdetailingpharmacists.Thecliniciansrepresented nineVISNsand21differentVHAfacilities.Theclasswas composedof15physicians,sevennursesandnurse practitioners,31pharmacists,andthreephysicianassistants. Participantsrangedinagefrom30–65(mean46.2years)and hadbeeninclinicalpracticeforanaverageof11years (Table1).Additionally,attendeesrepresentednumerous clinicalserviceareasincludingemergencymedicine,urgent care,primarycare,painmanagement,mentalhealth,and substanceusetreatment.
Ofthe56participants,39(almost70%)respondedtothe initialpost-survey.Thirty-eightrespondents(97.4%) reportedthattheASPseriescontainedpracticalexamples andusefulinformationthatcouldbeappliedintheirwork. Thirty-eightrespondents(97.4%)feltthattheworkshop seriesprovidednewinformationorinsightsintothediagnosis andtreatmentofSUD.Thirty-fiverespondents(89.7%)were veryorsomewhatsatisfiedwiththeASPseries. TwentyindividualswhoparticipatedintheASP respondedtothesix-monthfollow-upsurvey.Themajority
Table1. Scholarcharacteristics.
Scholars(%) (N = 32)
Profession Physician15(46.9) Nursepractitioner6(18.8) Nurse1(3.1) Physicianassistant3(9.4) Pharmacist7(21.9) Yearsoutoftraining
0–5years13(40.6) 6–10years6(18.8) 10+ years10(31.3) Missing3(9.4)
ClinicalArea
Emergencydepartmentorurgentcare6(18.8) Mentalhealth,substanceusetreatment, orpsychiatry 14(43.8)
Painmanagement3(9.4) Primarycare5(15.6) Pharmacy1(3.1) Missing3(9.4)
ofrespondents(85.0%)reportedfeeling “comfortable” or “verycomfortable” initiatingM-OUDsincecompletingthe ASP.Fourteen(70%offollowuprespondents)pursued additionalM-OUDtrainingsincecompletingtheASP.Of the20respondents,fourworkedindepartmentswithoutan activeM-OUDprogram;threeofthefour(75%)are currentlyworkingtodevelopanM-OUDprogram.Eighteen (90%)oftherespondentsreportedincreasednaloxone prescribingsincecompletingtheASP.Ten(50%)ofthe respondentsincreasedprescribingofbuprenorphinetotreat patientswithOUDsincecompletingthecourse(Table2).
AttheconclusionoftheASP,11capstoneprojectswere submittedandawardedatotalof$407,178.Seven(63.6%)of theprojectsfocusedonthedevelopmentofnaloxoneor buprenorphineprograms.Otherprojectswerefocusedon harmreductionwiththedevelopmentofasyringeservice program,theuseoffentanyltestingstrips,developmentofa VISN-widevirtuallearningprogramforSUDtraining,urine point-of-caretestingforcontrolledmedications,andmusicandmovement-basedinterventionstoengagehigh-risk veteransinsubstanceusetreatment.
OurstudydemonstratedtheASPsuccessfullyprovided additionaladdictionmedicinetrainingtocliniciansandother healthcareprofessionalsandthatthereisadesirefor additionaladdictionmedicinetrainingwithintheVHA
Table2. Resultsofinitialandsix-monthfollow-upsurvey.
Initialfollow-up(N = 39)
TheASPseriescontainedpracticalexamplesandusefulinformationthatcanbeappliedintheirwork.38(97.4%)
TheworkshopseriesprovidednewinformationorinsightsintothediagnosisandtreatmentofSUD.38(97.4%)
“Very” or “somewhat” satisfiedwiththeASPseries.35(89.7%)
6-monthfollow-up(n = 20)
“Comfortable” or “verycomfortable” initiatingM-OUDsincecompletingtheASP.17(85%)
PursuedadditionalM-OUDtrainingsincecompletingtheASP.14(70%)
WorkindepartmentswithoutanactiveM-OUDprogram.4(20%)
IncreasednaloxoneprescribingsincecompletingtheASP.18(90%)
IncreasedprescribingofbuprenorphinetotreatpatientswithOUDsincecompletingtheASP.10(50%)
ASP,AddictionScholarsProgram; SUD,substanceusedisorder; OUD,opioidusedisorder; M-OUD,medicationforopioidusedisorder.
system.TheASPwasdesignedasaneducationalprogram withanemphasisonpromotingfacility-levelteambuilding toenhancecross-functionalclinicalcare.These findingsare encouragingas,aftercompletingtheASP,healthcare professionalswithoutformaladdictionmedicinetraining wereabletoadvocateforOUDtreatmentinnon-SUD specialtyclinicalsettingsattheirlocalVHAsite.Successful treatmentofpatientswithOUDrequiresamultidisciplinary approachinvolvingboththeaddictionmedicineserviceand theoutpatientprimarycareteam.Empoweringnon-SUD specialtyclinicswiththeknowledgeandpracticalskillsto treatOUDisessentialinimplementingthe “nowrongdoor” approachtoOUDtreatment.11 Thesupportandnetworking opportunitiesprovidedbytheASPsuccessfullyledtothe developmentoflocaladdictionmedicineprogramsat VHAsitesasevidencedbythe11capstoneprojectsthat werefunded.
ThesuccessoftheASPwasdueinparttotheblended learningstructureofthecourse.Lectureswerecuratedand deliveredbyexpertsinthe fieldandrangedfrombasic addictionmedicinetopicstomoreadvancedtopics.This allowedforengagementofalllearnersregardlessoftheir specialtyorleveloftraining.Thecoursealsoleverageda team-basedlearningapproachthroughthebreakout sessions,whichreinforcedkeycomponentsoftreating complexpatientswithOUD.Team-basedlearninghasbeen showntohavepositiveoutcomesforstudentsintermsof studentexperience.12
Thee-learningplatformalsoallowedforengagementbya wideraudiencethanwouldhaveotherwisebeenpossibleby anin-personcourse.TheASPgaveadditionaladdiction medicinetrainingtothosewhowouldotherwisenothave beeneligibleforafellowshipbythetraditionalpathway.This allowedforengagementofkeystakeholderswhocould implementprogramsatlocalfacilitiesinareasthatare separatefromdedicatedSUDclinics.TheASPisascalable programthatcanbefurtherdevelopedandreplicatedoutside oftheVHAsystem.
Althoughtheprogramdidreceivefavorableratings,itis importanttonotethatattendeesdidself-selecttoattend;asa result,theymayhavebeenmorebiasedintheirratingsofan addictionmedicineprogram.Futureeffortswillbemadeto recruitcliniciansandotherhealthcareprofessionalswhomay beresistantorhesitanttotheadditionofsubstanceuseand opioidsafetymeasuresintheirpractice.Furtherstudiesare neededtoassessactualinterestinadditionaladdiction medicinetrainingthroughouttheVHAsystem.Itshouldbe noted,too,thatthisstudyprovidedonlyasix-monthfollowup,atwhichpointtheparticipants’ surveyresponseratewas low.Additionally,theresultsofthisstudyaresurveybased, andthusthelimitationsthatapplytosurveysalsoapplyhere. Thesurveydidnotcontainknowledge-basedquestionsto assessretentionofknowledge.Futureiterationsofthecourse willcontainknowledge-basedquestionstoassessfor acquisitionofknowledge.Futurestudieswillalsoneedto lookathowtheASPinfluencedthedevelopmentofaddiction medicineprogramsintheVHAsystem.Studieswillalsoneed toexaminehowsuccessfulthemanagementofOUDisin nontraditionalsettingsthatareoutsidetheSUDclinics. Futurestudiescanalsobeconductedtocomparelong-term outcomesforpatientswhosehealthcareprofessionals participatedinASPcomparedtothosewhodidnot.
ThisfeasibilitystudyhasshownthatASPequipped cliniciansandotherhealthcareprofessionalswithan intensiveoverviewofaddictionmedicine.Thestudents translatedtheinformationfromthecoursetodevelop M-OUDprogramsattheirhomeinstitutions.
AddressforCorrespondence:ZahirBasraiMD,VAGreaterLos AngelesHealthCareSystem,VeteransHealthAdministration, DepartmentofEmergencyMedicine,11301WilshireBLVD, LosAngeles,CA90073.Email: Zahir.basrai@va.gov
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.ComillaSassonMD,PhDisemployed bytheAmericanHeartAssociation.Thisworkwassupportedby CARAfundsthroughthePainManagement,OpioidSafetyand PrescriptionDrugMonitoringProgram(PMOP)Office.Thereareno otherconflictsofinterestorsourcesoffundingtodeclare.
Copyright:©2024Basraietal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.HarganED.DeterminationthataPublicHealthEmergencyExists.2017. Availableat: https://aspr.hhs.gov:443/legal/PHE/Pages/opioids.aspx AccessedJanuary18,2024.
2.USCentersforDiseaseControlandPrevention.IncreaseinFatalDrug OverdosesAcrosstheUnitedStatesDrivenbySyntheticOpioidsBefore andDuringtheCOVID-19Pandemic.2020.Availableat: https://stacks. cdc.gov/view/cdc/98848.AccessedApril25,2021.
3.BohnertAS,IlgenMA,GaleaS,etal.Accidentalpoisoningmortality amongpatientsintheDepartmentofVeteransAffairsHealthSystem. MedCare. 2011;49(4):393–6.
4.DepartmentofVeteransAffairsOfficeofInspectorGeneral.OIG DeterminationofVeteransHealthAdministration’sOccupational StaffingShortagesFiscalYear2021.2021.Availableat: https://www. oversight.gov/sites/default/files/oig-reports/VA/VAOIG-21-01357-271. pdf.AccessedJanuary18,2024.
5.USDepartmentofVeteransAffairs.VeteransHealthAdministration. 2008.Availableat: https://www.va.gov/health/ AccessedApril25,2021.
6.MillerNS,SheppardLM,ColendaCC,etal.Whyphysiciansare unpreparedtotreatpatientswhohavealcohol-anddrug-related disorders. AcadMed. 2001;76(5):410–8.
7.PolydorouS,GundersonEW,LevinFR.Trainingphysicians totreatsubstanceusedisorders. CurrPsychiatryRep. 2008;10(5):399–404.
8.AmericanCollegeofAcademicAddictionMedicine.Accredited AddictionMedicineFellowships.Availableat: https://www.acaam.org/ fellowship-training.AccessedApril25,2021.
9.TaylorEN,TimkoC,BinswangerIA,etal.Anationalsurveyofbarriers andfacilitatorstomedicationsforopioidusedisorderamonglegalinvolvedveteransintheVeteransHealthAdministration. SubstAbus. 2022;43(1):556–63.
10.KimHSandSamuelsEA.Overcomingbarrierstoprescribing buprenorphineintheemergencydepartment. JAMANetwOpen. 2020;3(5):e204996.
11.SubstanceAbuseandMentalHealthServicesAdministration. SubstanceUseDisorderTreatmentforPeoplewithCo-Occurring Disorders.2020.Availableat: https://store.samhsa.gov/sites/default/ files/SAMHSA_Digital_Download/PEP20-02-01-004_Final_508.pdf AccessedApril25,2021.
12.BurgessA,vanDiggeleC,RobertsC,etal.Team-basedlearning: design,facilitationandparticipation. BMCMedEduc. 2020;20(Suppl2):461.
ArianaBarkley,MD*
LauraLander,MSW†
BrianDilcher,MD* MeghanTuscano,MPH†
*WestVirginiaUniversity,DepartmentofEmergencyMedicine, Morgantown,WestVirginia † WestVirginiaUniversity,DepartmentofBehavioralMedicineandPsychiatry, Morgantown,WestVirginia
SectionEditor:R.GentryWilkerson,MD
Submissionhistory:SubmittedMarch31,2023;RevisionreceivedFebruary5,2024;AcceptedFebruary16,2024
ElectronicallypublishedJune27,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18029
Introduction: Initiationofbuprenorphineforopioidusedisorder(OUD)intheemergencydepartment (ED)issupportedbytheAmericanCollegeofEmergencyPhysiciansandisshowntobebeneficial.This practice,however,islargelyunderutilized.
Methods: Toassessemergencyclinicians’ attitudesandreadinesstoinitiatebuprenorphineintheED weconductedacross-sectional,electronicsurveyofclinicians(attendings,residents,andnon-physician clinicians)inasingle,academicEDofatertiary-carehospital,whichservesaruralpopulation.Our surveyaimedtoassessemergencyclinicians’ attitudestowardandreadinesstoinitiatebuprenorphinein theEDandidentifyclinician-perceivedfacilitatorsandbarriers.Oursurveytookplaceaftertheinitiation oftheIMPACT(InitiationofMedication,PeerAccess,andConnectiontoTreatment)project.
Results: Ourresultsdemonstratedthelevelofagreementthatbuprenorphineprescribingiswithinthe emergencyclinician’sscopeofpracticewasinverselycorrelatedtoaverageyearsinpractice(R2 = 0.93). X-waiveredcliniciansindicatedfeelingmorepreparedtoadministerbuprenorphineintheEDR2 = 0.93. However,theywerenotmorelikelytoreportorderingbuprenorphineornaloxoneintheEDwithinthe priorthreemonths.Thosewhoreportedhavingafamilymemberorclosefriendwithsubstanceuse disorder(SUD)werenotmorelikelytoagreebuprenorphineinitiationiswithintheclinician’sscopeof practice(P = 0.91),norweretheymorelikelytoobtainanX-waiver(P = 0.58)orreportordering buprenorphineornaloxoneforpatientsintheEDwithinthepriorthreemonths(P = 0.65, P = 0.77). Cliniciansidentifiedavailabilityofpharmacists,inpatient/outpatientreferralresources,andsupportstaff (peerrecoverysupportspecialistsandcaremanagers)asprimaryfacilitatorstobuprenorphineinitiation. Inabilitytoensurefollow-up,lackofknowledgeofavailableresources,andinsufficienteducation/ preparednesswereprimarybarrierstoEDbuprenorphineinitiation.Eighty-threepercentofclinicians indicatedtheywouldbeinterestedinadditionaleducationregardingOUDtreatment.
Conclusion: Ourdatasuggeststhatnewergenerationsofemergencycliniciansmayhaveless hesitancyinitiatingbuprenorphineintheED.Intime,thiscouldmeanincreasedaccesstotreatmentfor patientswithOUD.Understandingclinician-perceivedfacilitatorsandbarrierstobuprenorphineinitiation allowsforbetterresourceallocation.Clinicianswouldlikelyfurtherbenefitfromadditionaleducation regardingmedicationsforopioidusedisorder(MOUD),availableresources,andfollow-upstatistics. [WestJEmergMed.2025;26(1.1)43–49.]
Morethan564,000individualsdiedofopioidoverdosein theUSfrom1999–2020,1 accordingtotheUSCentersfor DiseaseControlandPrevention;morerecent,provisional datasuggeststhatannualoverdoseratescontinuedtorisein 2021.2 Aswouldbeexpected,withincreasedratesof overdose,emergencydepartment(ED)visitsforopioid overdosealsoincreasedin2020.3 Patientswithopioiduse disorder(OUD)arefrequentlyseenintheEDwithboth overdoseandotherlessemergentconditions.Patientsseenin theEDafteranon-fatalopioidoverdosehave >5%one-year mortalityrat.4 TheEDisalow-barrieraccesspointtothe healthcaresystem,andEDvisitsrepresentavaluable opportunitytoengagepatientswithOUDinpotentially lifesavingtreatment.
Buprenorphine,aUSFoodandDrugAdministration (FDA)-approvedmedicationforOUD(MOUD),hasbeen showntobeeffectiveindecreasingoverallopioiduse, reducingriskofopioidoverdose,andreducingbothopioidassociatedandall-causemortality.5 Buprenorphinehasbeen availabletoemergencycliniciansforthetreatmentofopioid withdrawalsince2002,andresearchhasshownthebenefits ofbuprenorphineinitiationintheED.6 Specifically,in comparisontoreferraltotreatmentorbriefEDintervention, initiationofbuprenorphineintheEDresultsinincreased ratesofengagementinaddictiontreatmentat30daysand decreasedillicitopioiduse.7 TheAmericanCollegeof EmergencyPhysicians(ACEP)recommendstheinitiationof buprenorphineinappropriatepatients.Additionally,the ACEPconsensusstates: “Detectingandofferingevidencedbasedtreatmentsforpatientswithopioidusedisorderis alignedwiththegoalsofemergencymedicinetointerveneon high-mortalitydiseaseprocesses.”8
Unfortunately,MOUDsincludingbuprenorphineare largelyunderutilized,andthemajorityofpeoplewithOUD donotreceivedtreatmentwithMOUDs.9 Substanceuse disorders(SUD)areoneofthemosthighlystigmatized medicalconditionsintheworldamongcliniciansandthe generalpublic.10,11 Astudylookingatemergencyphysicians’ attitudestowardpatientswithSUDfoundthatemergency physicianshadalowerregardforpatientswithSUDthan othermedicalconditionswithbehavioralcomponents.12 The MOUDs,includingbuprenorphine,arealsostigmatized, whichimpactstreatmentaccessandprescribingpracticesfor thesemedications.13 Previous findingsidentifythemost significantbarrierstoprescribingbuprenorphineintheED includelogisticalorsystemicfactorsaswellasperceived patientfactors(ie,socialbarriersandlackofinterestin treatment).14 Clinicianlackofknowledge,aswellastheir attitudesandbiases,canimpactwillingnesstoprescribe medicationssuchasbuprenorphineforpatientswithOUD, despiteMOUDbeingawellstudiedandeffective treatment.6,15 NotonlyarepatientsonMOUDstigmatized
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
InitiationofbuprenorphineintheEmergency Department(ED)foropioidusedisorder (OUD)hasbeenshowntobebene fi cial,butis largelyunderutilized.
Whatwastheresearchquestion?
Whatareclinicians ’ attitudestoward initiatingbuprenorphineintheED,andwhat arethebarrierstoprescribing?
Whatwasthemajor findingofthestudy?
Clinicianlikelihoodofinitiatingtreatmentin theEDwasinverselycorrelatedtoyearsin practice.Theprimarybarriertoinitiating buprenorphinewasinabilityto ensurefollow-up.
Howdoesthisimprovepopulationhealth?
Eliminatingbarriersandimprovingclinician readinesstoinitiatebuprenorphineintheED couldincreaseaccesstocareforpatients withOUD.
buttheprescriberswhoprovidethemwithmedicationsare alsostigmatized.16
Topromoteengagementinandreferraltotreatmentfor OUD,ouracademicEDinitiatedtheIMPACTproject (InitiationofMedication,PeerAccess,Connectionto Treatment)in2020.KeyelementsoftheIMPACTproject includedelectronichealthrecord(EHR)promptsandorder sets,peerrecoverysupportspecialistsintheED,and availabilityofinpatientandoutpatientreferral,allofwhich arebarriersidentifiedinpreviousstudies.15,17–18 Additionally,whentheIMPACTprojectwasintroducedto theED,clinicianswereoffereda financialincentivetoobtain aUSDrugEnforcementAdministrationX-waiver.The primarygoalofourstudywastoassessemergencyclinicians’ attitudestowardandreadinesstoinitiatebuprenorphinein theED,aswellasidentifyperceivedfacilitatorsandbarriers toinitiatingbuprenorphinetreatmentinanacademicED, afterimplementationoftheIMPACTprojectandits associatedresources.
ThisstudywaspartofaStateOpioidResponse ImplementationprojectcalledIMPACT.Theprimary objectiveoftheprojectwastointegratepeerrecovery
supportspecialists(PRSS)intheED,toincrease buprenorphineprescribingforpatientswithOUD,andto increaseengagementandreferralstotreatmentforall patientswithSUD.WeextracteddatafromtheEHR regardingpatientdemographics,PRSSinteractionwith patients,andprescribingpracticesoveratwo-yearperiod fromMarch2020–March2022.Amixed-methodsmodelwas usedtoevaluatethedata.Thisprojectwasapprovedbythe institutionalreviewboard.
Weconductedacross-sectionalelectronic-basedsurvey regardingbuprenorphineprescribingintheEDwithall potentialEDprescribersincludingattendingphysicians, residentphysicians,physicianassistants,andnurse practitioners.Wedevelopedthesurvey,adaptingfrom previouslypublishedresearch.15,17–18 Priorsurveyshadbeen conductedinlargeurbanareasbuthadnotbeendeployedin amoreruralsetting.Oursurveywasdesignedtoidentify prescribers’ attitudestowardandreadinesstoinitiate buprenorphineintheEDandidentifyperceivedfacilitators andbarrierstoinitiatingbuprenorphinetreatmentinan academicEDofalarge,tertiary-carehospital,whichservesa ruralpopulation.Cliniciansweremadeawareofthestudy throughaninitialemail,twoemailreminders,aone-time announcementatourweeklydidacticconference,and flyers postedthroughouttheED.Participantswereincentivized,as the first100participantsreceiveda$10giftcard,andall participantswereenteredforachancetowina$100giftcard.
Thesurveycompletedbyemergencycliniciansincluded10 questionsfocusingonyearsinpractice,X-waiverstatus, prescribingpracticesintheEDinthepriorthreemonths, comfortwithtreatmentofOUDandprescribing buprenorphineintheED,andpersonalexperiencewith SUD.TwoadditionalLikert-scalequestionsassessedfor barriersandfacilitatorstoprescribingbuprenorphine.(See AppendixA forfullsurvey).Thesurveywaspublished March23,2022,andclosedMay15,2022.Surveyresponses wererecordedviaQualtrics(Qualtrics,Provo,UT),andthe datawasexportedtoasecureExcel file(MicrosoftCorp, Redmond,WA)foranalysis.Wethenorganizedand analyzedthedatausingSAS9.4(SASInstituteInc,Cary, NC)withchi-squaredorFisherexacttests.Wede-identified andextractedadditionaloperationalpatientdataonthe IMPACTprogramonarollingbasisfromtheEHR.
Atotalof95surveysweredistributedtoallemergency clinicians(attendingphysicians,residents,physician assistants,andnursepractitioners)Therewereatotalof43 respondentsandaresponserateof45%(16/50attendings, 21/30residents,6/15physicianassistantsandnurse practitioners).Threesurveyswerepartiallycompleted.We includedtwothathad >50%ofthequestionsansweredand excludedonesurveywithonlytwoquestionscompletedas thelatterrespondent’sintenttocompletewasinterpretedas
questionable.Ofthosewhoresponded,theiryearsinpractice rangedfrom1-50withanaverageof7.3years.Ofthe43 respondents,31indicatedtheywerefamiliarwiththe IMPACTprojectand12saidtheywerenot.Allthe respondentswhoindicatedtheywerenotfamiliarwiththe IMPACTprojectwereEDresidents.(See Tabl.)Notably, 83%ofallrespondentsindicatedtheywouldbeinterestedin additionaleducationrelatedtomedicationandresourcesfor OUDtreatment.
A five-pointLikertscalewasusedtoassessrespondents’ levelofagreementthatprescribingbuprenorphinewaswithin theirscopeofpractice.While78.6%ofrespondentsagreed thatprescribingbuprenorphinewaswithintheirscope,the levelofagreementwasfoundtobeinverselycorrelatedwith averageyearsinpractice(R2 = 0.93162)(Figure1).Regarding X-waiverstatus,16individualsidentifiedashavingtheir X-waiverand26indicatedtheywerenotX-waivered.When askedwhytheywerenotwaivered,fourindividualsindicated theywere “notinterested,” threesaidcostwasabarrier,seven saidtimewasabarrier,and12responded “other.” Inthe “other” category,tworespondedtheywereunsurehowto obtainthewaiver;twoquestionedwhetheritwasneeded;one said “intheprocess”;threesaid “justhaven’tdoneit” ;one indicatedtheyhadcompletedthetrainingbutwerenotyet licensed;andonesaid “Iknowthedatashowsitworks,butI
Table. Datasummaryofemergencyclinicianswhoparticipatedina surveyregardingED-initiatedbuprenorphine.
CountPercentage
Figure1. Agreementthatbuprenorphineiswithintheemergency clinician’sscopeofpracticeasassessedona5-pointLikertscalein comparisontoaverageyearsinpractice.
stillfeellikeadrugdealer.” Wefoundthatthosewhohadan X-waiver,incomparisontothosewhodidnot,weremore likelytofeelpreparedtoadministerbuprenorphineinthe ED(P = 0.02).
Toenableustodescribeprescribingpractices,prescribers werealsoaskedwhethertheyhadorderednaloxonefor patientsintheEDinthepriorthreemonths;29said “ yes ” and13said “ no. ” Whenaskedwhethertheyhadordered buprenorphineforpatientsintheEDinthepriorthree months,18said “ yes ” and24said “ no. ” Wealsoobserved thatthosewhohadanX-waiverwerenotmorelikely tohavereportedorderingbuprenorphineornaloxone forpatientsintheEDwithinthepriorthreemonths (P = 0.17),(P = 0.51).
Sixty-sevenpercentofcliniciansagreedthattheyfelt preparedtoadministerbuprenorphineintheED,53.7% agreedthattheyfeltpreparedtoprescribebuprenorphineas abridgetooutpatienttreatment,and47.6%agreedthatthey feltpreparedtoprescribebuprenorphineforhomeinduction. Sixty-twopercentofallrespondentsagreedthattheyhadall
theresourcesneededtoinitiatebuprenorphineintheED. Barriersandfacilitatorstoinitiatingbuprenorphineinthe EDareidentifiedin Figure2 and Figure3,respectively. Toassesspossiblepersonalbarriersandfacilitatorsof buprenorphineprescribingthefollowingwasasked: “Have youhad,ordoyoucurrentlyhaveafamilymemberorclose friendwithSUD?” Responsesindicated43%said “ yes ” and 57%said “ no. ” Thosewhoreportedhavingafamilymember orclosefriendwithSUDwerenotmorelikelyto1)agreethat buprenorphineinitiationiswithintheemergencyclinician’ s scopeofpractice(P = 0.91);2)obtainanX-waiver (P = 0.58);or3)reportorderingbuprenorphineornaloxone forpatientsintheEDwithinthepriorthree months(P = 0.65),(P = 0.77).
Overthetwo-yearperiod,1,205patientswereseeninthe EDbyPRSSs,13%ofwhomwerediagnosedwithOUDor opioidwithdrawal.Atotalof377werereferredfor buprenorphinetreatmentbythePRSSswithintheED;168of thosepatientsreceivedbuprenorphinetreatment,and42 weregivenatake-homeprescription.Atthestartofthestudy therewerethreeX-waiveredphysicians;duringthecourseof theproject,12additionalcliniciansobtainedtheirX-waiver, foratotalof15.
Oursurveyaimedtoevaluateemergencyclinicians’ attitudestowardandpreparednesstoinitiatebuprenorphine intheEDaswellasidentifyperceivedfacilitatorsand barrierstoinitiatingbuprenorphinetreatmentafterthe implementationoftheIMPACTprojectanditsassociated resources.Ourresultsshowedthat78.6%ofcliniciansagreed thatprescribingbuprenorphineintheEDwaswithintheir scopeofpractice.Asshownin Figure1,thelevelof agreementthatbuprenorphineiswithintheemergency
Knowledge of available resources
Ability to ensure follow up
Concerned about misuse / diversion
Concerned about safety
Lack of pa ent interest in MOUD
Provides minimal benefit to pa ents
Concerned prescribing buprenorphine is not in my scope of prac ce
Figure2. Clinician-perceivedbarrierstoinitiatingbuprenorphineintheemergencydepartment.Identifiedbarriersweregradedwitha3-point Likertscale:somewhatabarrier,moderatebarrier,significantbarrier. MOUD,medicationforopioidusedisorder.
Pharmacist in the ED
inpa ent referral resources
Outpa ent referral resources
EHR alert re naloxone
EHR alert re buprenorphine
Availablility of PRSS / CM
Figure3. Clinician-perceivedfacilitatorstoinitiatingbuprenorphineintheemergencydepartment.Identi fiedfacilitatorsweregradedwitha 3-pointLikertscale:somewhatafacilitator,moderatefacilitator,significantfacilitator. ED,emergencydepartment; EHR,electronichealthrecord; PRSS,peerrecoverysupportspecialist; CM,casemanager.
clinician’sscopeofpracticewasinverselycorrelatedtoyears inpractice.Anotherstudyfoundthatclinicianswithfewer yearsinpracticeweremorelikelytobelievethatOUDislike otherchronicdiseasesandweremorelikelytoapproveof ED-initiatedbuprenorphine.18 Otherstudieshaveidentified emergencymedicineresidentsasenthusiasticandeagerto incorporatecareforOUDintotheirpractice.17,19 Webelieve theseresultsareencouraginganddemonstratethatnewer generationsofcliniciansmayhavelesshesitancytoward initiatingMOUDtreatmentintheEDsetting.Thischange will,intime,likelyincreaseaccesstocareforthose withOUD.
Sixty-sevenpercentofallcliniciansagreedthattheyfelt preparedtoadministerbuprenorphineintheED.Wesuspect clinicians’ levelofpreparednesscouldbeimprovedwith continuingeducationlecturesandfeedback.Notably,the majorityofrespondentsreportedtheywouldbeinterestedin additionaleducationrelatedtomedicationandresourcesfor OUDtreatment.
WefoundthatthosewithanX-waiver,incomparisonto thosewhodidnothaveanX-waiver,weremorelikelytofeel preparedtoadministerbuprenorphineintheED.Other studieshavefoundthatX-waiveredcliniciansreported higherlevelsofreadinessorpreparednesstoinitiate buprenorphineintheEDincomparisontothosewhowere notX-waivered.14,17 Previously,aneight-hourtraining coursewasrequiredtoobtainanX-waiver;thistraining requirement,andthehassleofobtainingawaiver,was previouslyidentifiedasabarriertoinitiatingbuprenorphine intheED.14,17–18,20 However, findingthatX-waivered cliniciansfeltmorepreparedtoadministerbuprenorphinein theEDmayreflectthevaluethatwasassociatedwiththe previouslyrequirededucationcourse.Notably,wealso foundthatthosewhohadanX-waiverwerenotmorelikely tohavereportedorderingbuprenorphineornaloxonefor patientsintheEDwithinthepriorthreemonths.This finding
potentiallysupportstheideathatsimplyincreasingthe numberofX-waiveredcliniciansdoesnotsignificantly improveaccesstocareifX-waiveredcliniciansarenot activelyprescribingMOUDs.21,22 Notably,ourdatawas collectedpriortotherecenteliminationofthenational X-waiverrequirement.
Whenweaskedwhetherhavinghadafriendorfamily memberwithSUDwouldaffectclinicians’ attitudestoward buprenorphineintheED,wefoundthat42.8%ofclinicians reportedhavinghadafamilymemberorclosefriendwith SUD.Thispersonalrelationship,however,didnotmake cliniciansstatisticallymorelikelyto1)agreethatprescribing buprenorphinewaswithintheemergencyclinician’sscopeof practice;2)obtainanX-waiver;or3)reportordering buprenorphineornaloxoneforpatientsintheEDwithinthe priorthreemonths.Toourknowledge,aprescriber’ s personalrelationshipstoindividualswithSUDhasnotbeen evaluatedinpriorstudies.
Sixty-twopercentofcliniciansindicatedtheyhavethe resourcestheyneedtoinitiatebuprenorphineintheED. WiththeIMPACTproject,asdescribedabove,clinicians haveresourcessuchaspeerrecoverysupportspecialistsinthe ED,EHRprompts,andcloseoutpatientfollow-upavailable. Additionally,ouracademicEDisstaffedwithpharmacists andcasemanagers/socialworkers24/7.Giventhenumberof resourcesavailable,wewouldhaveexpectedthatmore clinicianswouldhavefelttheyhavetheresourcesnecessary toinitiatebuprenorphineintheED.Wesuspectitispossible thatmanycliniciansfelttheydidnothavetheresources necessarybecausetheyweresimplyunawareoftheavailable resources.Notably,lessthan75%ofrespondentswere familiarwiththeIMPACTproject.Allofthosewhowere unfamiliarwiththeIMPACTprojectwereresidents;this highlightsanopportunityforadditionaleducation.
Anumberofstudieshavebeenconductedlookingat facilitatorsandbarrierstobuprenorphineinitiationinthe
ED.14,17–18
Previouslyidentifiedbarrierstoinitiating buprenorphineintheEDincludethefollowing:lackof training/experience;concernsregardingmisuse/diversion/ harm;patientinterest;time/competingprioritiesintheED; concernsregardingfollow-up;concernsregardingincreased EDvolume;andfeelingasifprescribingbuprenorphinewas notwithintheirscopeofpractice.14,17–18
Notably,withtheimplementationoftheIMPACTproject anditsassociatedresources,severalsystemic/logistical barriershavebeeneliminatedasPRSSsareavailableinthe ED,outpatientfollow-upcanbeensured,andtheEHRis equippedwithpromptsandordersetsregardingboth buprenorphineandoutpatientreferrals.
Ourcliniciansidentifiedinabilitytoensurefollow-up, limitedknowledgeofavailableresources,andlackof education/preparednessasthetopthreebarrierstoinitiating buprenorphineintheED.AlthoughtheCOAT (comprehensiveopioidaddictiontreatment)clinichasa standingappointmentforEDreferrals,andPRSSsworkto facilitatetheseappointments,andevenaccompany patientstotheseappointments,concernregardingfollow-up wasstilltheprimarybarrieridentifiedbyclinicians. Arecentstudyvalidatedtheseconcernsasitfoundthat lessthan30%ofpatientswho fillbuprenorphine prescriptionsfromtheED fillsubsequentbuprenorphine prescriptions.23 Currentlywedonothavedataregarding EDfollow-upratesorratesofsubsequentbuprenorphine refills;however,thisisanareaofinterestforfuture investigationtobetterevaluatetheeffectivenessofour IMPACTprogram.
Previouslyidentifiedfacilitatorstobuprenorphine initiationintheEDincludeabilitytoensurefollow-up; supportstaff – PRSSs/socialwork/caremanagers;department protocols;EHRordersets;pharmacistconsultation;and feedbackonpatientexperiences.14,17–18 Ourclinicians identifiedavailabilityofpharmacistsandofbothinpatientand outpatientresources,andthepresenceofPRSSsand caremanagersasprimaryfacilitatorstobuprenorphine initiationintheED.Thefactthatcliniciansidentified pharmacistavailabilityasasignificantfacilitatorlikely highlightsunderlyingcliniciandiscomfortwiththe pharmacologyofbuprenorphineandagainhighlightsan opportunityforongoingeducationandexperience.Notably, timewasnotaprimarybarrieridentifiedbyourclinicians,and thismaybeduetothepresenceofadditionalsupport staffintheED.
Ourstudyhasseverallimitations.Overallwehadasmall samplesize,andourrespondentsallworkatthesame academiccenter.Additionally,nearlyhalfofrespondents wereresidentswithfewerthanthreeyearsinclinicalpractice. Ourdatawascollectedpriortotheeliminationofthe X-waiverrequirement.Itispossiblethatthisnewlegislation
hassinceinfluencedprescribers’ attitudestoward buprenorphineaswellasprescribingpractices.Results relatedtofacilitatorsandbarriersmaynotbegeneralizable tocommunity-based,non-academicEDsthatdonothave similarresources.Additionally,ourresultsmaynotbe generalizabletoacademicEDsinurbanareas.
Theresultsofoursurveyidentifiedthefollowing: 1)agreementthatbuprenorphineiswithintheemergency clinician’sscopeofpracticewasinverselycorrelatedtoyears inpractice;2) >80%ofclinicianswereinterestedin additionaleducationregardingMOUDsandresourcesfor OUDtreatment;3)thosewithanX-waiverweremorelikely toreportfeelingmorepreparedtoadministerbuprenorphine intheEDincomparisontothosewhowerenotX-waivered; and4)clinicianswhoreportedhavinghadafamilymember orclosefriendwithSUDwerenotmorelikelytoagreethat buprenorphineinitiationiswithintheemergencyclinician’ s scopeofpractice,norweretheymorelikelytoobtainan X-waiverorreportorderingbuprenorphineornaloxonefor patientsintheEDwithinthepriorthreemonths.Wealso identifiedclinician-perceivedbarriersandfacilitatorsto initiatingbuprenorphineintheED.Ourcliniciansidentified inabilitytoensurefollow-upasaprimarybarriertoinitiating buprenorphineintheED.
Moreresearchisneededonretentionintreatmentfollowing EDreferraltoidentifywhatfactorsareassociatedwith successfultransitionsofcarefromED-initiatedMOUDto community-basedtreatment.Education/preparednesswas alsoidentifiedasasignificantbarrier.Weplantoaddressthis withadditionaldidacticsandprogramupdates.Timewasless ofabarrier,likelysecondarytotheavailabilityofpharmacists, supportstaff,andinpatientandoutpatientresources, whichwereidentifiedasfacilitators.Abetterunderstandingof facilitatorsandbarriersallowsforbetterresourceallocation.
Ourresearchwassupportedbyagrant(G230766)from theSubstanceAbuseandMentalHealthServices AdministrationthroughasubcontractfromtheWest VirginiaDepartmentofHealthandHumanResources BureauforBehavioralHealth.
AddressforCorrespondence:LauraLander,MSW,WestVirginia University,DepartmentofBehavioralMedicineandPsychiatry,930 ChestnutRidgeRd.,Morgantown,WV26505.Email: llander@hsc. wvu.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Thispublicationwassupportedbya grant(G230766)fromtheSubstanceAbuseandMentalHealth
ServicesAdministrationthroughasubcontractfromtheWest VirginiaDepartmentofHealthandHumanResourcesBureaufor BehavioralHealth.Therearenootherconflictsofinterestorsources offundingtodeclare.
Copyright:©2024Barkleyetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.USCentersforDiseaseControlandPrevention.Opioiddataanalysis andresources.2022.Availableat: https://www.cdc.gov/opioids/data/ analysis-resources.html#anchor_data_sources AccessedSeptember19,2022.
2.USCentersforDiseaseControlandPrevention.Drugoverdosedeaths intheU.S.top100,000annually.2021.Availableat: https://www.cdc. gov/nchs/pressroom/nchs_press_releases/2021/20211117.htm AccessedSeptember19,2022.
3.SoaresWE,MelnickER,NathB,etal.Emergencydepartmentvisitsfor nonfatalopioidoverdoseduringtheCOVID-19pandemicacrosssixUS HealthCareSystems. AnnEmergMed. 2022;79(2):158–67.
4.WeinerSG,BakerO,BernsonD,etal.One-yearmortalityofpatients afteremergencydepartmenttreatmentfornonfatalopioidoverdose. AnnEmergMed. 2020;75(1):13–7.
5.LarochelleMR,BernsonD,LandT,etal.Medicationforopioiduse disorderafternonfatalopioidoverdoseandassociationwithmortality:a cohortstudy. AnnInternMed. 2018;169(3):137–45.
6.NationalInstitutesofHealth.Initiatingbuprenorphinetreatmentinthe emergencydepartment.2022.Availableat: https://nida.nih.gov/ nidamed-medical-health-professionals/discipline-specific-resources/ emergency-physicians-first-responders/initiating-buprenorphinetreatment-in-emergency-department.AccessedSeptember19,2022.
7.D’OnofrioG,O’ConnorPG,PantalonMV,etal.Emergencydepartmentinitiatedbuprenorphine/naloxonetreatmentforopioiddependence:a randomizedclinicaltrial. JAMA. 2015;313(16):1636–44.
8.HawkK,HoppeJ,KetchamE,etal.Consensusrecommendationson thetreatmentofopioidusedisorderintheemergencydepartment. Ann EmergMed. 2021;78(3):434–42.
9.U.S.DepartmentofHealthandHumanServices.Keysubstanceuse andmentalhealthindicatorsintheUnitedStates:R=resultsfromthe 2019nationalsurveyondruguseandhealth.2020.Availableat: https:// www.samhsa.gov/data/sites/default/files/reports/rpt29393/ 2019NSDUHFFRPDFWHTML/2019NSDUHFFR090120.htm AccessedSeptember19,2022.
10.vanBoekelLC,BrouwersEPM,vanWeeghelJ,etal.Stigmaamong healthprofessionalstowardpatientswithsubstanceusedisordersand
itsconsequencesforhealthcaredelivery:systematicreview. Drug AlcoholDepend. 2013;131(1–2):23–35.
11.RoomR.Stigma,socialinequalityandalcoholanddruguse. Drug AlcoholRev. 2005;24(2):143–55.
12.MendiolaCK,GalettoG,FingerhoodM.Anexplorationofemergency physicians’ attitudestowardpatientswithsubstanceusedisorder. J AddictMed. 2018;12(2):132–5.
13.BozinoffN,AndersonBJ,BaileyGL,etal.Correlatesofstigmaseverity amongpersonsseekingopioiddetoxification. JAddictMed. 2018;12(1):19–23.
14.LowensteinM,KilaruA,PerroneJ,etal.Barriersandfacilitatorsfor emergencydepartmentinitiationofbuprenorphine:aphysiciansurvey. AmJEmergMed. 2019;37(9):1787–90.
15.MoranGE,SnyderCM,NoftsingerRF,etal.(2017). Implementing Medication-assistedTreatmentforOpioidUseDisorderinRuralPrimary Care:EnvironmentalScan.Rockville,MD:AgencyforHealthcare ResearchandQuality;2017.
16.Dickson-GomezJ,SpectorA,WeeksM,etal. “You’renotsupposedto beonitforever”:medicationstotreatopioidusedisorder(MOUD) relatedstigmaamongdrugtreatmentcliniciansandpeoplewhouse opioids. SubstAbuse. 2022;16:117822182211038.
17.HawkKF,D’OnofrioG,ChawarskiMC,etal.Barriersandfacilitatorsto clinicianreadinesstoprovideemergencydepartment-initiated buprenorphine. JAMANetworkOpen. 2020;3(5):e204561.
18.ImDD,CharyA,CondellaAL,etal.Emergencydepartmentclinicians’ attitudestowardopioidusedisorderandemergencydepartmentinitiatedbuprenorphinetreatment:amixed-methodsstudy. WestJ EmergMed. 2020;21(2):261–71.
19.WhitesideLK,D’OnofrioG,FiellinDA,etal.Modelsforimplementing emergencydepartment–initiatedbuprenorphinewithreferralfor ongoingmedicationtreatmentatemergencydepartmentdischargein diverseacademiccenters. AnnEmergMed. 2022;80(5):410–9.
20.MartinA,KunzlerN,NakagawaJ,etal.Getwaivered:aresident-driven campaigntoaddresstheopioidoverdosecrisis. AnnEmergMed. 2019;74(5):691–6.
21.DuncanA,AndermanJ,DeseranT,etal.Monthlypatientvolumesof buprenorphine-waiveredcliniciansintheUS. JAMANetwOpen. 2020;3(8):e2014045.
22.GordonAJ,KennyM,DunganM,etal.AreX-waivertrainingsenough? Facilitatorsandbarrierstobuprenorphineprescribingafterx-waiver trainings. AmJAddict. 2022;31(2):152–8.
23.SteinBD,SalonerB,KerberR,etal.Subsequentbuprenorphine treatmentfollowingemergencyphysicianbuprenorphineprescription fills:anationalassessment2019to2020. AnnEmergMed. 2022;79(5):441–50.
JennaK.Nikolaides,MD,MA*†
TranH.Tran,PharmD*‡
ElisabethRamsey,LCSW*
SophiaSalib,MSW,MPH*
HenrySwoboda,MD§
*RushUniversityMedicalCenter,SubstanceUseInterventionTeam, DepartmentofPsychiatryandBehavioralSciences,Chicago,Illinois
† RushUniversityMedicalCenter,DepartmentofEmergencyMedicine, Chicago,Illinois
‡ ChicagoCollegeofPharmacy,MidwesternUniversity,DownersGrove,Illinois § Queen’sUniversity,DepartmentofEmergencyMedicineandAddictions Medicine,Kingston,Canada
SectionEditor:PierreBorczuk,MD
Submissionhistory:SubmittedMarch31,2023;RevisionreceivedFebruary9,2024;AcceptedFebruary16,2024
ElectronicallypublishedJune11,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18030
Introduction: Methadoneisamedicallynecessaryandlifesavingmedicationformanypatients withopioidusedisorder.Toadequatelyaddressthesepatients ’ needs,methadoneshouldbeoffered inthehospital,butbarriersexistthatlimititscontinuationupondischarge.Thecodeoffederal regulationsallowsformethadonedosingasaninpatientaswellasoutpatientdispensingfor uptothreedaystofacilitatelinkagetotreatment.Asaqualityinitiative,wecreatedanewwork fl ow fordischargingpatientsonmethadonetoreturntotheemergencydepartment(ED)for uninterrupteddosing.
Methods: Ouraddictionmedicineteamchangedhospitalmethadonepolicytobetterallow hospitalizationasawindowofopportunitytostartmethadone.Thisnecessitatedthecreationofawarmhandoffprocesstolinkpatientstomethadoneclinicsifthatlinkagecouldnothappenimmediatelyon discharge.Thus,ourteamcreatedthe “EDBridge” process,whichusesthe “3-dayrule” todispense methadonefromtheEDposthospitaldischarge.Wethenfollowedeverypatientwedirectedthroughthis workflowasanobservationalcohortforoutcomesandtrends.
Results: OfthepatientsforwhomEDbridgedosingwasplanned,40.4%completedallbridgedosing andanadditional17.3%receivedatleastonebutnotallbridgedoses.Establishedmethadonepatients madeup38.1%ofsuccessfullinkages,and61.9%werepatientswhowerenewlystartedonmethadone inthehospital.
Conclusion: Improvingmethadoneasatreatmentoptionremainsanongoingissueforpolicymakers andadvocates.OurEDbridgeworkflowallowsustoexpandaccessandcontinuationofmethadonenow usingexistinglawsandregulations,andtobetterusehospitalsasapointofentryintomethadone treatment.[WestJEmergMed.2025;26(1.1)50–55.]
Therearemanyregulatorybarrierstoinitiating medicationsforopioidusedisorder(MOUD)intraditional healthcaresettings.Sincetreatmentwithmethadone,an opioidagonist,orwithbuprenorphine,apartialopioid agonist,remainsthestandardofcareforpatientswithopioid
usedisorder(OUD),therehasbeenmuchfocusrecentlyon easingorcircumnavigatingbarrierstofacilitatelinkageto treatment.Whilethepassageofthe2023Consolidated AppropriationsActremovedtheX-waiverrequirementfor buprenorphineprescribing,1 methadonedispensingremains restrictedtoopioidtreatmentprograms(OTP).Giventhese
restrictionsonprescribingandotherlegalconsiderations, manyhospitalsareoftenhesitanttostartandtitrate methadoneforinpatientswithOUD.
Everyyeardrug-relateddeathscontinuetoincrease,and in2021over80,000peoplediedofanopioidoverdose.2 UnderuseofMOUDiscommonamongpatientsseeninthe hospitaldespiteevidencesupportingemergencydepartment (ED)andinpatientinitiationasbeneficialopportunitiesto starttreatment.3,4 Toaddressthisdeficit,ourtertiarymedical centercreatedtheSubstanceUseInterventionTeam(SUIT) in2018.5 TheSUITiscomprisedofemergencyphysicians whoaredual-ortriple-boardedinmedicaltoxicologyand/or addictionmedicine,psychiatricnursepractitioners,social workers,arecoverysupportspecialist,andapharmacist; SUITisavailableduringbusinesshours,Mondaythrough Friday.Theteamisacomprehensiveaddictionmedicine consultservice,workingtowardincreasingtherecognition, treatment,andlinkagetooutpatientcareforallsubstance usedisorders.TheSUIToffersallformsofMOUD, includingbuprenorphineandmethadone.Forpatientswho requestedorpreferredmethadone,thedosetitrationwas guidedbythe2019versionoftheCalifornia[CA]Bridge in-hospitalmethadonestartprotocol,6 tailoredtoeach patient,withthemostaggressivepossibletitrationbeing 40milligrams(mg)onday1,50mgonday2,and60mgon day3,atwhichpoint,thedosewasnotincreaseduntilevery fivedays.
Startingmorepatientsonmethadonenecessitatedthe craftingofnewpoliciesandproceduresatourcenterthat wouldallowawarmhandofftomethadoneOTPs.TheCode ofFederalRegulationsTitle21restrictsthedispensingof methadonetoOTPsandspecifiesthatmethadonemaybe administeredforthreedaysinahealthcaresettingforthe purposeofalleviatingwithdrawalwhilearrangementsare madetorefertotreatment.6 Itdoesnotlimittreatmentto threedays;however,ifthepatientisinthehospitalfor reasonsotherthanwithdrawal,MOUDcanbeused “to maintainordetoxifyapersonasanincidentaladjunctto medicalorsurgicaltreatmentofconditionsotherthan addiction.”7 Therefore,methadone,ifstartedwhilean inpatient,canbecontinuedfortheentiretyofthestay.Prior toSUIT’screation,ourtertiarymedicalhospitalhadan internalpolicythatifmethadonewasstartedforapatientnot previouslyenrolledinanOTP,thepatienthadtobeweaned priortodischargebecauseoftheprescribinglimitation. Becauseweaningwithoutfurthermaintenancetreatment onlyaddressesthephysicaldependenceintheshortterm whileneglectingthechronicdiseaseofOUD,itincreasesrisk ofrelapse,fataloverdose,andall-causemortality.8–11 This policy,althoughcompliantwiththelaw,wasnotevidencebasedbestpractice.
TheSUITcreatedanewpolicyandworkflowthatallowed thestartofaninpatienttitrationofmethadoneforpatients notpreviouslyenrolledinanOTP,arrangedlinkagetoOTPs
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
FederalregulationsallowEDstodispense methadoneforopioidusedisorder, andhospitalscanusethe3-dayruleto assistwithlinkagestomethadone maintenanceprograms.
Whatwastheresearchquestion?
WelookedatthefeasibilityofusingtheEDas apost-acutecarelandingsitetobridge patients ’ methadonetreatmentindischarging hospitalizedpatients.
Whatwasthemajor findingofthestudy?
Fortypercentofpatients(21/54)completed allbridgedosing,ofwhom62%werenewly initiatedonmethadoneinthehospital.
Howdoesthisimprovepopulationhealth?
Thiswork fl owisanoveluseofthe3-dayrule toexpandaccesstomethadoneviatheED.
whilestillinpatient,andavoidedweaningpriortodischarge; ifpatientscouldnotimmediatelybetreatedatanOTPupon discharge(duetogapsintreatment,includingweekendor holidayclosures),theEDisusedasapost-dischargesetting forcontinueddosingunderthethree-dayruletocompletea warmhandoff.Thisworkflowwasreviewedbyourhospital’ s pharmacy,compliance,andlegaldepartments,allofwhich agreedthatitcompliedwithexistinglawsandhelpedusenact thechangeinhospitalpolicy.Oncethisprocesswasbuilt,our teamrealizedthatitwasalsohelpfulforthosepatientsin establishedOTPswhoweredischargedonweekendsor holidaysandcouldn’treturntotheirOTPfordosinguntilthe nextbusinessday.
HavingtheEDasapost-acutecarelandingsitefor methadonecontinuationhelpedavoiddisruptionof establishedMOUDaswellasnewlyinitiatedMOUD. Becausethenew-startmethadonetitrationwasmore aggressivethanatypicaloutpatientinitiationofmethadone, whenpatientsreturnedtotheED,thedoseadministeredwas theirdischargedoseandwasnottitratedintheEDtokeep thematsteady-stateandtoavoidaneedforobservationin theEDafterdosing.Duringthetimeframethisworkflowwas builtandused,theOTPsinourcityindependentlyunderwent changes.OneOTPinparticularagreedtohonorhospital titrationsonday1intheirclinicifthepatientbrought dischargepaperworkwiththem.Theprogrambecamea
preferredoptionforthisworkflow,althoughmanypatients eitheralreadyusedorrequestedotherOTPs.
Thisarticleservesasaproofofconceptandan observationalcohortofallpatientsthatSUITdirectedto returntotheEDformethadonedosing.
Thesettingofthisstudywasourtertiaryurbanmedical center.Patientsidenti fi edasbeinginneedofan “ED bridge ” wereincludedinthisstudyiftheywereseenbythe SUITconsultservice;iftheywereidenti fi edaseither alreadyinamethadoneOTPornewlystartedon methadoneduringthehospitalizationandinneedof enrollmentinanOTP;andiftheprimaryteamdetermined thattheywouldbedischargedonadaywherethepatient wouldnotimmediatelybeabletogetoutpatientmethadone dosingbutwithaplaninplaceforlinkingtoanOTPwithin 72hoursofdischarge.Thisidenti fi cationusuallyhappened onaThursdayorFridayinanticipationofaweekend dischargeorfornewmethadonestartswhenanOTP appointmentcouldnotbemadeforthedayafterdischarge. SocialworkersontheSUITteammadeclearfollow-up plansbycontactingcooperatingOTPsaheadoftime. Patientswereexcludedfromthestudyiftheyendedupnot dischargingasplannedandtheEDbridgewasnolonger required,orifpatientsdeclinedtoreturn.Thesepatients weremanuallytrackedbychartreviewtodetermine whethertheyreturnedtotheEDfordosingovertheperiod fromJuly2019 –July2022.
The “EDbridge” processconsistedof1)instructingthe patienttoreturntotheEDeverydaystartingthemorning followingthedayofdischargeformethadoneadministration untilthedayofplannedOTPintakeorreturn(maximum threedays);2)writingacareplannoteinthechartnotifying theEDofthedosingplan,daysofdosing,andpolicy; 3)enteringanexpectedarrivalnotificationontheEDtrack board;and4)triagingthepatientonarrivaltoalow-acuity partoftheEDformethadonedosingandimmediate dischargeaslongastheydidnotappeartobeintoxicatedor haveanothercomplaint.
Atemplatednoteforthe “EDbridge” careplan (Appendix1)wasapprovedbythehospital’sPharmacyand TherapeuticsCommitteetoprovideconsistencyforthe process.Itincludedadotphraseforanotetemplatethatthe emergencycliniciancouldalsousewhenthepatientreturned. Theelectronichealthrecord(EHR)usedinourhospitalis Epic(EpicSystemsCorporation,VeronaWI).Ourhospital’ s methadonepolicywasamendedtoincludetheEDbridge pathwayandapprovedbyourhospital’scomplianceand legaloffices.Thepharmacydepartmentdisseminated hospital-widenotificationaboutthepolicyupdatesand providededucationaboutthenewprocesstoprescribers, pharmacists,nurses,andclinicalstaff.Thisstudyreceived institutionalreviewboardapproval.
Theprimaryoutcomemeasurementswerethepatient returnratetotheEDfordosingandthenumberofdoses completed.AnEDbridgewasconsideredsuccessfulifthe patientcamefordosingonallplanneddays;partially successfuliftheycamefordosingonsomeoftheplanned daysbutmisseddaysofdosing;andunsuccessfuliftheydid notcomeforanyoftheplanneddaysofdosing.Outcomes anddemographicdataareexpressedbydescriptivestatistics.
Therewere53plannedEDbridgessetupfor47unique patients.OneEDbridgewasexcludedafterthepatient stayedthroughtheweekendanddidn’trequireit.Several patientsusedtheEDbridgeworkflowmorethanoncedueto repeatedhospitalizations:threepatientsusedittwice,and onepatientuseditthreetimes.Demographiccharacteristics ofthe52plannedbridgesaresummarizedinthe Table. AllthepatientswithOUDwhousedthisworkflowwere usingheroin.
Ofthe52plannedEDbridges,21patientscompletedall necessarybridgedoses(40.4%).Ninepatients(17.3%) returnedtotheEDforatleastonedaybutdidn’tpresentfor allplanneddays.Theremainingplanswerenotsuccessful because22patients(42%)eitherdidnotreturntotheEDor lefttheEDbeforereceivingonedose.Intotal,94visitsfor methadonedosingintheEDwereplannedviatheEDbridge workflow,and40visitsactuallyoccurred.TheaverageED lengthofstay(LOS)fromtriagetodischargewas120 minutes,witharangeof36-682minutes.Sixofthe40visits requiredfullevaluationsforadditionalcomplaints. Excludingthesesixvisits,theaverageEDLOSwas89 minutes.Ofthe52plannedEDbridges,theaveragenumber ofdaysrequiredtocompletelinkagetotreatmentwas1.8 days.Forpatientswhosuccessfullycompletedallnecessary bridgedoses,theaveragenumberofdaysforlinkagewas 1.3days.
Patientswerelinkedtooneof10methadoneclinics,allof whichacceptedpatientswithMedicaid.Eightpatientswho werealreadyestablishedinamethadoneclinicaccountedfor 38.1%ofsuccessfullinkages.
Forthepurposesofthisstudy,apatientwasdefinedasa “ new ” methadonepatientiftheywerenotenrolledinaclinic priortotheiradmissiontothehospitalandasan “established” patientiftheywere.Theterms “ new ” and “established” werenotdescriptorsofstabilityintreatment becauseoccasionallyevenestablishedpatientsneededtobe newlyrestartedonmethadoneduetomissingdosesattheir establishedOTP,andtheoutcomesofwhethertheycomplied withtheEDbridgeplanwereessentiallysimilarbetweenthe twogroups.Becauseourprojectlackedfollow-upwith patientsatalatertimepoint,wewereunabletodiscernthe reasonforpatientsnotreturningtotheED.
Table. Characteristicsofparticipantsintheemergencydepartmentbridgeprogramforpost-dischargemethadonedosing.
Characteristics(attimeofEDbridge)
Age
Average(years)44.647.945.140.5
Range(years)29 – 6929 – 6931 – 6129 – 64
Housingstatus
,emergencydepartment.
“Success” wasdefinedasthepatientreturningforall planneddays.Theredidn’tappeartobeanydemographic factorthatcorrelatedwiththesuccessofthebridge,although thisstudywasnotpoweredtolookforanystatisticaltrends. Theclearestexplanationfromthedatawewereabletocollect isthatifabridgeplanwasshorter,itwasmorelikelytobe successful.Onaverage,patientsreturnedforapproximately oneday.Planslongerthanonedaywerelesslikelytobe successful.Nearlyhalfofthe10unsuccessfulbridgeplans occurredwithinarelativelyshortfour-monthtimespan (September–December2021).Emergencydepartmentwait timesandtheCOVID-19pandemicmayhavecontributedto thishighrateofunsuccessfulbridgedosesduringthattime.
PriortoinstitutingtheEDbridgeprocessinourcenter,we wouldroutinelyholdpatientscommittedtotreatmentinthe hospitaltoensurelinkagetoamethadoneclinicwithno misseddosestodecreasethepatients’ riskofrelapse,
overdose,anddeathupondischarge.TheEDbridgeprocess allowedgreater flexibility:patientswhowerecommittedto treatmentbutwerereadyfordischargeotherwisecouldleave andcomebackfordosing;patientswhoweregettingplaced inpost-acutecaresettingsbutneededtotransportfor methadonecouldnowtransportbacktotheEDfordosing, therebyallowingweekenddischarges;andevenpatientswho wereleavingagainstmedicaladvicewereofferedthe opportunitytodoseintheEDtoreinforcethemessagethat MOUDisapriority.Whileitisdifficulttodeterminewhether everyEDbridgeplandecreasedLOS,thefactthat40visitsto ourEDformethadonedosingdidoccurviatheEDbridge processsuggeststhatwediddecreaseinpatienthospitaldays andthatthismitigatedtheincreaseduseofEDresourcesfor thesevisits.
InstitutingtheEDbridgeworkflowwasanadjustmentfor theEDstaff.Sincetherewasnopop-upintheEHR,the
triagenursesattimesneededtoberemindedtolookforan expectedarrivalnoteandtoberemindedthatthesepatients couldbetriagedtothelowacuitypartoftheED.Most clinicianswrotestandardEDnotesanddidnotusethepreformedtemplatednoteforamethadonevisit.Ittooksome timeforallstaffmemberstogetusedtothenewworkflow, whichlikelyexplainedtheaverageLOSbeingapproximately 1.5hourswhenafullevaluationwasnotrequired.TheLOS alsoaccountedfortimespentinthewaitingroomand cliniciansorderingmethadoneandprovidingdischarge instructions.Itwasnot1.5hoursofobservationafterthe dosewasgiven.Basedonourteam’sexperienceswith teachingtheworkflow,itappearedthattheEDstaffwas receptivetotheoverallidea,inpartbecauseourinstitution hadgottenusedtothecultureoftheemergencyphysician-led SUITteam.DuringtheCOVID-19pandemic,therewasalso turnoverintheEDnurseworkforcethatnecessitatedretrainingsontheworkflow,whichcouldhavealsocontributed tothewidevariationinLOS.
Thisstudytookplaceinalargeurbanenvironmentfrom 2019–2022,aperiodthatnotonlyencompassedtheCOVID19pandemicbutalsothecontinuedworseningoftheopioid epidemic.Duringthattime,thereweresignificantand evolvingchangestohowOTPsfunctionedduetoCOVID-19 emergencyconditionsandtothedesiretoreducebarriersto treatment.TheOTPschangedtheirintakeprocess, sometimesseveraltimesthroughoutthatperiod,at firsttobe morerestrictive12 andthenlatertoallow flexibility.Priorto thisperiod,atypicalOTPhadspecificdaysdesignatedfor intakeappointments.Intakescouldtakeapproximatelyone hour,andapatientmaynothaveactuallystarteddosing onthatday.Patientswereofteninstructedtoreturnafew dayslatertothenmeetwiththecliniciantostarttheir methadonetitration.
ThetypicalinitialdosingscheduleisdailydosingMonday throughSaturdaywithatake-homedosedispensedon SaturdayforuseonSundaywhentheOTPwasclosed. InitiallyourSUITprogramwasabletohelppatients completephoneintakeswhilehospitalized;however,this protocollaterevolvedtomatchthechangesinOTPs,which developedexpandeddaysforwalk-inintakes.SeveralOTPs alsochangedtheirworkflowsregardingdayofintakeand dayof firstdose,andsometimeswehadtouseourEDbridge protocoltokeepdosingpatientsduringthegapbetweenthe dayoftheirintakeandthedayoftheir firstdose.Duringthis period,OTPsalsopermittedmoretake-homemethadone doses,sometimesswitchingtoMonday-Wednesday-Friday dosingscheduleswitheveryotherdaytake-homedoses, weeklydosingscheduleswithsixdaysoftake-homedoses,or evenmonthlydosingwith27daysoftake-homedoses.This allowedpatientstonothavetogototheOTPasoften, facilitatingsocialdistancing,butitalsoledtogreateraccess todivertedmethadone.Thegoalofour “EDbridge” workflowwastodecreasedosedisruptionbyprovidingaway
forpatientstoobtainmethadonesafelywhilecomplyingwith dispensingrestrictions.Itispossiblepatientsobtained methadonethroughothermeansand,thus,didnotreturnfor theEDbridge.
OneOTPinoururbanareadecreasedthebarrierstoentry significantlyoverthistimeperiod:theyexpandedintakesto MondaythroughFriday;alloweddosingevenbeforefull completionofintake;didnotrequirephotoIDaslongasthe patienthadidentifyingpaperwork(includinghospital dischargepapers);andacceptedallformsofgovernment insurance.ThisOTPendedupbecomingthedefaultoption thatwecouldrelyonwhensettingupourEDbridgeplans, eventhoughwestilldidusetheworkflowforlinkingtoother OTPsaswell.Inareasofthecountrywithmorelimitedand restrictiveaccesstomethadoneOTPs,ourthree-dayED bridgemodelmaynotbeasfeasible.
Thisstudytookplaceinanurbanareawithfederaland statesupportforOTPs.WedidnotlookatpatientfollowthroughforOTPintakesorretentioninlong-termtreatment. AnotherlimitationisthatfeedbackfromEDstaffonthis newworkflowwasnotcollectedtofullyassessattitudes andbarriers.
Expandingaccesstomethadoneremainsanissuefor policymakersandadvocates.Ideassuchasmobileclinics, newguidelinessuggestinglimiteddispensing,andproposals toallowstandardcommercialpharmaciestodispense methadoneareallongoingconsiderations.13 OurEDbridge workflow,however,allowsustoexpandaccessand continuationofmethadoneusingexistinglawsand regulations,andtobetterusehospitalsasapointofentryinto methadonetreatment.
AddressforCorrespondence:JennaKNikolaides,MD,Rush UniversityMedicalCenter,SubstanceUseInterventionTeam, DepartmentofPsychiatryandBehavioralSciences,1611W Harrison,Suite106b,Chicago,IL60612.Email: Jenna_Nikolaides@ rush.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.TheSUITservicesweresupportedinpartbyacontracttoRushUniversityMedicalCenterfromtheIllinois DepartmentofHumanServices,DivisionofSubstanceUse PreventionandRecovery,aspartoftheIllinoisOpioid-State TargetedResponse(STR)Grant(TI-080231)andIllinoisState OpioidResponse(SOR)Grant(TI-081699)fromtheSubstance AbuseandMentalHealthservicesAdministration.Thecontentis solelytheresponsibilityoftheauthorsanddoesnotnecessarily
representtheofficialviewsoftheNationalInstitutesofHealth, AgencyforHealthcareResearchandQuality,SubstanceAbuseand MentalHealthServicesAdministrationortheIllinoisDepartmentof HumanServices.Therearenootherconflictsofinterestorsources offundingtodeclare.
Copyright:©2024Nikolaidesetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.SubstanceAbuseandMentalHealthServicesAdministration.Waiver elimination(MATAct).2023.Availableat: https://www.samhsa.gov/ medications-substance-use-disorders/removal-data-waiverrequirement.AccessedMarch30,2023.
2.AhmadFB,CisewskiJA,RossenLM,etal.Provisionaldrugoverdose deathcounts.2024.Availableat: https://www.cdc.gov/nchs/nvss/vsrr/ drug-overdose-data.htm.AccessedMarch30,2023.
3.RosenthalES,KarchmerAW,Theisen-ToupalJ,etal.Suboptimal addictioninterventionsforpatientshospitalizedwithinjectiondruguseassociatedinfectiveendocarditis. AmJMed. 2016;129(5):481–5.
4.D’OnofrioG,ChawarskiMC,O’ConnorPG,etal.Emergency department-initiatedbuprenorphineforopioiddependencewith continuationinprimarycare:outcomesduringandafterintervention. J GenInternMed. 2017;32(6):660–6.
5.TranTH,SwobodaH,PerticoneK,etal.Thesubstanceuseintervention team:ahospital-basedinterventionandoutpatientclinictoimprovecare forpatientswithsubstanceusedisorders. AmJHealthSystPharm. 2021;78(4):345–53.
6.CaliforniaBridgeProgram.Methadonehospitalquickstart.2019. Availableat: https://www.acep.org/siteassets/sites/acep/media/ equal-documents/ca-bridge protocol methadone-hospitalquick-start nov-2019.pdf.AccessedOctober12,2023.
7.DrugEnforcementAdministration,DepartmentofJustice.21CFR 1306.07:Administeringordispensingofnarcoticdrugs.Availableat: https://www.ecfr.gov/current/title-21/part-1306/section-1306.07 AccessedMarch23,2023.
8.BaileyGL,HermanDS,SteinMD.Perceivedrelapserisk anddesireformedicationassistedtreatmentamongpersons seekinginpatientopiatedetoxification. JSubstAbuseTreat. 2013;45(3):302–5.
9.DavoliM,BargagliAM,PerucciCA,etal.Riskoffataloverdoseduring andafterspecialistdrugtreatment:theVEdeTTEstudy,anationalmultisiteprospectivecohortstudy. Addiction. 2007;102(12):1954–9.
10.CornishR,MacleodJ,StrangJ,etal.Riskofdeathduringandafter opiatesubstitutiontreatmentinprimarycare:prospectiveobservational studyinUKGeneralPracticeResearchDatabase. BMJ. 2010;341:c5475.
11.CousinsG,BolandF,CourtneyB,etal.Riskofmortalityonandoff methadonesubstitutiontreatmentinprimarycare:anationalcohort study. Addiction. 2016;111(1):73–82.
12.JoudreyPJ,AdamsZM,BachP,etal.Methadoneaccessforopioiduse disorderduringtheCOVID-19pandemicwithintheUnitedStatesand Canada. JAMANetwOpen. 2021;4(7):e2118223.
13.CongressionalResearchService.H.R.6279-OpioidTreatmentAccess Actof2022.Availableat: https://www.congress.gov/bill/117thcongress/house-bill/6279?s=1&r=64.AccessedMarch31,2023.
GrantComstock,MD*
NataliaTruszczynski,PhD
†
SeanS.Michael,MD,MBA‡ JasonHoppe,DO
§
SectionEditor:R.GentryWilkerson,MD
*MedicalCollegeofWisconsin,DepartmentofEmergencyMedicine, DivisionofMedicalToxicology,Milwaukee,Wisconsin
† UniversityofColoradoSchoolofMedicine,Aurora,Colorado
‡ UniversityofColoradoSchoolofMedicine,DepartmentofEmergencyMedicine, Aurora,Colorado
§ UniversityofColoradoSchoolofMedicine,DepartmentofEmergencyMedicine, DivisionofMedicalToxicologyandPharmacology,Aurora,Colorado
Submissionhistory:SubmittedMarch30,2023;RevisionreceivedDecember27,2023;AcceptedFebruary28,2024
ElectronicallypublishedJune11,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.18019
Introduction: Wesoughttodescribeemergencydepartment(ED)buprenorphinetreatmentvariability amongEDswithvaryingoperationalcharacteristics.
Methods: Weperformedaretrospectivecohortstudyofadultpatientswithopioidusedisorder dischargedfrom12hospital-basedEDswithinalargehealthcaresystemasasecondarydataanalysisof aqualityimprovementstudy.Primaryoutcomeofinterestwasbuprenorphinetreatmentrate.We describedtreatmentratesbetweenEDs,categorizedbytertileofoperationalcharacteristicsincluding annualcensus,hospitalandintensivecareunit(ICU)admissionrates,EDlengthofstay(LOS),and boardingtime.SecondaryoutcomeswereEDLOSand30-dayreturnrates.
Results: Therewere7,469uniqueEDencountersforpatientswithopioidusedisorderbetween January2020–May2021,ofwhom759(10.2%)weretreatedwithbuprenorphine.Buprenorphine treatmentrateswerehigherinlargerEDsandthosewithhigherhospitalandICUadmissionrates. EmergencydepartmentLOSand30-dayEDreturnratedidnothaveconsistentassociationswith buprenorphinetreatment.
Conclusion: RatesoftreatmentwithEDbuprenorphinevaryaccordingtotheoperationalcharacteristics ofdepartment.Wedidnotobserveaconsistentnegativerelationshipbetweenbuprenorphinetreatment andoperationalmetrics,asmanyfeared.Additionalfundingandtargetedresourceallocationshouldbe prioritizedbydepartmentalleaderstoimproveaccesstothisevidence-basedandlife-saving intervention.[WestJEmergMed.2025;26(1.1)56–62.]
Theopioidcrisisisaworseningpublichealthemergency, withover80,000opioid-involvedoverdosedeathsintheUS in2021,anditisunlikelytoabateintheabsenceofeffectively implementedharmreductionandtreatmentstrategies.1 Buprenorphineisaneffective,evidence-basedtreatment resultinginincreasedabstinencefromillicitopioiduseand decreasedopioid-relatedmortality.2,3 Emergency department(ED)buprenorphinetreatmentisanevidencebasedpracticeandhasbeenassociatedwithincreasedfollowupandreducedillicitdruguseandmedicalcosts.4,5Although buprenorphineprescribingfromEDshasincreasedinrecent years,prescribingstilllagsfarbehindtheapparentneed,with disparitiesbypayerstatus,race,andethnicity.6,7
Improvedimplementationreliesonidentificationand removalofbarriers,providingresourcesforpatientsand clinicians,anddispellingstigmaandmisperceptions.8 Emergencydepartmentoperationalconsiderations,
includingperceptionsofinsuf ficienttimeandincreasedED returnvisits,arecommonlycitedasperceivedbarriersto implementation. 9 However,thereal-worldinterplay betweenEDbuprenorphineinitiationandEDoperationsis notwelldescribed.UnderstandingtheimpactofED buprenorphinetreatmentonEDclinicaloperational outcomescaninformdecisionsonresourceallocationfor EDbuprenorphineprogramdevelopment.Conversely, barrierstoimplementationlikelyvarydependingonthe baselineoperationalperformanceofthedepartment. Identi fi cationofoperationalcharacteristicsofEDswith lowerbuprenorphinetreatmentrateswouldallowfor targetedinterventions.
WesoughttodescribetheknowledgegapregardingED buprenorphinetreatmentvariabilityandoperational barrierstoimplementationby1)quantifyingtreatment ratesbetweenhospitalEDswithdifferentbaseline operationalcharacteristics,and2)measuringtheimpactof EDbuprenorphinetreatmentonoperationalmetrics.
Weperformedaretrospectivecohortstudyofadult(age ≥18)EDpatientswithopioidusedisorder(OUD)discharged fromanyoftheacademic(one)orcommunity(11)hospitalbasedEDswithinalargehealthcaresystembetweenJanuary 2020–May2021.Thestudywasapprovedbyour institutionalreviewboardforsecondarydataanalysisofa completedqualityimprovementproject.
ToidentifyEDpatientswithOUDwhomaybenefitfrom buprenorphinetreatment,weappliedanelectronichealth record(EHR)computablephenotypepreviouslydevelopedand validatedbyChartashetal.10 Datawereextractedbyquerying anEDanalyticsdatamartpopulatedbyanightlyextractfrom theEpicClarity(EpicSystemsCorporation,Verona,WI) database.PatientswereidentifiedbysearchingfromphenotypespecificdiagnosiscodesandEDchiefcomplaints.Pertinent codesincludedInternationalClassificationofDiseases,10th Rev,ClinicalModification(ICD-10)diagnosticcodesrelating toopioiduse(T40.0*,T40.1*,T40.2*,T40.3*,T40.4*,T40.6*, andF11*)codedbyeitherthetreatingclinicianorsubsequently byamedicalcoder.Weadditionallyincludedpatientsnot identifiedbyICD-10diagnosticcodeEDchiefcomplaints relatingtoopioiduse.Chiefcomplaintdataisenteredintothe EHRattimeofEDencounterfromaprepopulatedlist,limiting ourselectionofsearchterms.Withinthelimitsofourdatabase, inclusionofencounterscontaining “opioid” or “naloxone” mostcloselyreflectedoriginalphenotypeterminology.Per phenotype,patientswiththeterms “benzodiazepine” or “alcohol” intheirEDdischargediagnosiswereexcludedto limitfalsepositiveinclusion.
Encounter-leveldataextractedincludedthefollowing: patientdemographics;chiefcomplaint;disposition;ED lengthofstay(LOS);dosesofmedicationsadministeredand prescribed;andfollow-upinformation,including30-dayED
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue? Understandingtheimpactofemergency department(ED)buprenorphineon operationscaninformresourceallocation decisionsforEDbuprenorphine programdevelopment.
Whatwastheresearchquestion?
HowdoesEDbuprenorphineimpact operations?HowdoEDoperational characteristicsimpacttreatmentrates?
Whatwasthemajor findingofthestudy?
Asmallnumberofpatientswithopioduse disorderwereprescribedbuprenorphine(2.5%in smallhospitals,11.6%inlargehospitals).ED lengthofstayand30-dayreturndidnotdiffer basedonbuprenorphinetreatment.
Howdoesthisimprovepopulationhealth?
DepartmentalleadershipcanprioritizeED buprenorphineprogramdevelopmentwithout fearofnegativeoperationalimpactto increaseaccesstolifesavingtreatment.
returnrateandnumberofdaysuntilEDreturnwithinthe samehealthsystem.Alldatawasdeidentifiedforanalysisby theresearchteam.
TheprimaryoutcomeofinterestwasEDbuprenorphine treatment,definedaspercentageofpatientsadministered buprenorphineduringand/orprescribedbuprenorphineas partoftheEDvisitamongallpatientswithOUDidentifiedby theEHRphenotype.Afterconsultingwithkeyadministrative leadersandsystemstakeholders,wepartitionedEDsbasedon operationalcharacteristicsincludingannualEDcensus; hospitalandintensivecareunit(ICU)admissionrates;median EDLOS(timefromEDarrivaltoEDdeparture);andmedian boardingtime(timefromadmissionorderplacedtoED departure).Hospitalsweredividedintotertilesforeach characteristic.Asnopowerorsensitivityanalyseswere performed,andourgoalwasdescriptiveandhypothesisgenerating,wedidnotperformhypothesis-testing comparativeanalyses.Statisticalanalyseswereperformed usingRStudioversion4.0.5(RStudioPBC,Boston,MA)and IBMSPSS26(SPSS,Inc,Chicago,IL).
The2021annualcensusforthe12EDsrangedfrom8,934 to103,381patients.Among541,962totaluniqueED
Table1. Characteristicsofcohortofpatientswithopioidusedisorder.
EDbuprenorphinetreatment
YesNo
Totalencounters541,9627596,710
Gender
Male243,961(46.9)436(57.4)3,528(52.6)
Female286,504(52.9)323(42.6)3,182(47.4)
Notreporting1,497(0.3)00
Race
Black55,975(10.3)91(12)610(9.1)
White374,736(69.1)537(70.8)5,094(75.9)
Anotherrace111,251(20.5)131(17.3)1,006(15)
Insurancestatus
Self-pay62,124(11.5)3(0.4)22(0.3)
Medicare/Medicaid307,513(56.7)589(77.6)4,955(73.8)
Otherinsurer163,489(30.2)162(21.3)1,648(24.6)
VA8,836(1.6)5(0.7)85(1.3)
Averagebuprenorphinedose(mg)
AdministeredN/a76.28N/a PrescribedN/a103.42N/a
EncounterswithnaloxoneprescriptionN/a268(45.5)1,041(21)
*Percentagesnotedinparentheses
ED,emergencydepartment; VA,VeteransAdministration; mg,milligrams.
encountersacrosssitesfromJanuary1,2020–May31,2021, 7,469(1.4%)visitswerephenotypepositiveandconstituted ourstudypopulation,representing5,637uniquepatients, withameanof622visitsperEDsite(range51–2,547). Phenotype-positivepatientswerepredominantlyWhite (75.4%)andmale(53.1%)(Table1).Aminority(759,10.2%) weretreatedwithbuprenorphineduringtheEDencounter, 695ofwhom(91.6%)receivedbuprenorphineadministered intheED,301(40%)receivedabuprenorphineprescription, and237(31.2%)receivedboth.
BuprenorphinewasadministeredintheEDmore frequentlythanitwasprescribedatdischarge,irrespective ofoperationalcharacteristics.Largerhospitalsandthose withhigherhospitalandICUadmissionrateshadhigher buprenorphinetreatmentrates(Table2).EDsexperiencing longerboardingtimesalsotrendedtowardhigherrates oftreatment.
MedianEDLOSwassimilaramongpatientstreatedwith buprenorphineversusnottreated,althoughconfidence intervalswerewide(Table3).Loweradmissionrate,smaller EDsize,andsmallervolumewereassociatedwithlongerED LOSforpatientstreatedwithbuprenorphine.Proportionof patientsreturningtotheEDwithin30daysandtimetoED returndidnotdifferconsistentlybasedontreatment withbuprenorphine.
Withinthissinglehealthsystem,weobservedthatED buprenorphinetreatmentratesvariedaccordingtothe baselineoperationalcharacteristicsoftheED,whichmay beaproxyfortheprogressivenessorphilosophical approachofagivenED’ slocalchampionsandleadership team.Weobservedlowerratesofbuprenorphinetreatment inEDswithsmallerannualcensusandloweracuity(as measuredbyoverallandICUadmissionrates),whichare presumablypracticesettingswheretheremaybeless perceptionofinsuf fi cienttime.However,smallerEDsare lesslikelytohavemultipleprescribingcliniciansworking simultaneously.Priorstudieshavesuggestedthatpractice variationportendslowerqualitycareandinequitiesin accesstoeffectivetreatmentforOUD. 11 ,12 Ourdata supportstheneedforinterventionsdesignedtopromote buprenorphinetreatmentinsmaller,loweracuityEDsto narrowthisvariation.
Buprenorphinetreatmentdidnotappeartohavea consistentassociationwithEDLOS,incontrastto commonlycitedbarriers.9 Thirty-dayreturnratesandtime toEDreturnweresimilarbetweenpatientswithOUD, regardlessoftheirtreatmentwithbuprenorphine,afarcry fromcitedfearsofEDsbecoming “ overrun ” bypatients seekingbuprenorphinerefills.13
Table2. Buprenorphineadministrationandprescription,categorizedbyemergencydepartmentoperationalcharacteristics.
Average valueper quantile(SD) OUD visits (n = 7,469)
AnnualED censusvolume Patients
Small(n = 4)11,424 (±2,413)
Buprenorphine administered (n = ,%) Buprenorphine prescribed (n = ,%)
Administered and prescribed (n = ,%) Any buprenorphine (n = ,%) No buprenorphine (n = ,%)
2456(2.4%)1(0.4%)1(0.4%)6(2.5%)239(97.6%)
Middle(n = 4)29,351.5 (±5,715) 1,24561(4.9%)2(0.2%)2(0.2%)61(4.9%)1,184(95.1%)
Large(n = 4)69,739 (±30,656)
EDnumberof beds Beds
5,979628(10.5%)298(5%)234(3.9%)692(11.6%)5,287(88.4%)
Small(n = 4)10.25(±2.5)2456(2.4%)1(0.4%)1(0.4%)6(2.5%)239(97.6%)
Middle(n = 4)21(±4.34)1,24561(4.9%)2(0.2%)2(0.2%)61(4.9%)1,184(95.1%)
Large(n = 4)49.5(±17.23)5,979629(10.5%)298(5%)234(3.9%)692(11.6%)5,287(88.4%) Hospital admissionrate Rate
Low(n = 4)7.90% (±4.7%) 52726(4.9%)1(0.2%)1(0.2%)26(4.9%)501(95.1%)
Middle(n = 4)16.98% (±1.8)
High(n = 4)27.41% (±3.2%)
ICUadmission rate Rate
1,745115(6.6%)6(0.3%)4(0.2%)117(6.7%)1,628(93.3%)
5,197554(10.7%)294(5.7%)232(4.5%)616(11.9%)4,581(88.2%)
Low(n = 4)0.2%(±0.4%)2456(2.5%)1(0.4%)1(0.4%)6(2.5%)239(97.6%)
Middle(n = 4)1.8%(±0.3%)2,027135(6.7%)6(0.3%)4(0.2%)137(6.8%)1,890(93.2%)
High(n = 4)3.1%(±0.6%)5,197554(10.7%)294(5.7%)232(4.5%)616(11.9%)4,581(88.2%) EDlengthofstayMinutes
Short(n = 4)106.3(±8.6)2456(2.5%)1(0.4%)1(0.4%)6(2.5%)239(97.6%)
Middle(n = 4)149.8(±4.7)4,216587(13.9%)287(6.8%)225(5.3%)649(15.4%)3,567(84.6%)
Long(n = 4)160.5(±2.1)3,008102(3.4%)13(0.4%)11(0.4%)104(3.5%)2,904(96.5%) MedianED boardingtime Minutes
Short(n = 4)59.5(±10.2)2456(2.5%)1(0.4%)1(0.4%)6(2.5%)239(97.6%)
Middle(n = 4)78.4(±4.6)1,43791(6.3%)2(0.1%)2(0.1%)91(6.3%)1,346(93.7%)
Long(n = 4)110.5(±24)5,787598(10.3%)298(5.2%)234(4%)662(11.4%)5,125(88.6%)
ED,emergencydepartment; ICU,intensivecareunit; OUD,opioidusedisorder.
Supportfromkeydepartmentalstakeholdersisa repeatedlyidentifiedfacilitatorforimplementingED buprenorphineprograms,andourobservationscorroborate this finding.13 IfLOSandEDreturnratearerelatively unaffectedbyEDbuprenorphinetreatment,thishas importantimplicationsthatmightallowdepartmental leaderstopromotegreaterresourcingandmitigatesomeof
theirapprehensionstofacilitatebuprenorphinetreatment withoutfearofnegativeoperationalimpacts.
Ourstudyintentwasdescriptiveandshouldbeconsidered hypothesis-generating.Theuseofsecondarydatalimitedour abilitytopowerthestudy,and95%confidenceintervalswere
Table3. EmergencydepartmentoperationaloutcomesbyEDoperationalcharacteristics.
EDOUDlengthofstay(minutes)30-DayEDOUDreturnvisitsDaysbeforeEDOUDreturn
Buprenorphine95%CI
AnnualEDcensusvolume
Small(n = 4)264(148.2,379.8)181.6(159.4,203.8)1(0.1%)81(1.2%)7N/a8.5(6.8,10.3)
Middle(n = 4)250.4(211.8,289)263.7(251.1,276.3)14(1.8%)318(4.7%)8.7(4.7,12.8)11.2(10.2,12.2)
Large(n = 4)238(216.9,259.1)275.6(268.4,282.7)203(26.8%)1525(22.7%)11.5(10.2,12.67)11(10.6,11.5)
EDnumberofbeds
Small(n = 4)264(148.2,379.8)181.6(159.4,203.8)1(0.1%)81(1.2%)7N/a8.5(6.8,10.3)
Middle(n = 4)250.4(211.8,289)263.7(251.1,276.3)14(1.8%)318(4.7%)8.7(4.7,12.8)11.2(10.2,12.2)
Large(n = 4)238(216.9,259.1)275.6(268.4,282.7)203(26.8%)1525(22.7%)11.5(10.2,12.7)11(10.6,11.5)
Hospitaladmissionrate
Low(n = 4)258(212.4,303.7)245.2(225.1,265.3)6(0.8%)156(2.3%)7.8(4.7,11)10.4(9.1,11.8)
Middle(n = 4)266(224.9,306.1)287(276.1,297.9)33(4.4%)461(6.9%)9.3(6.3,12.2)10.2(9.4,10.9)
High(n = 4)233.4(210.7,256.1)266.8(259.1,274.6)179(23.6%)1307(19.5%)11.7(10.4,13)11.3(10.8,11.7)
ICUadmissionrate
Low(n = 4)264(148.2,379.8)181.6(159.4,203.8)1(0.1%)81(1.2%)7N/a8.5(6.8,10.3)
Middle(n = 4)264.1(228.8,299.5)289.2(278.9,299.6)38(5%)536(8%)9.1(6.5,11.7)10.5(9.8,11.2)
High(n = 4)233.4(210.7,256.1)266.8(259.1,274.6)179(23.6%)1307(19.5%)11.7(10.4,13)11.3(10.8,11.7)
EDlengthofstay
Short(n = 4)264(148.2,379.8)181.6(159.4,203.8)1(0.1%)81(1.2%)7N/a8.5(6.8,10.3)
Middle(n = 4)225.8(205.2,246.3)279.7(271.6,287.9)187(24.6%)1059(15.8%)11.3(10.1,12.6)11.1(10.6,11.6)
Long(n = 4)321.7(261.8,381.6)265.5(255.8,275.3)30(4%)784(11.7%)11(7.9,14.1)11(10.4,11.6)
MedianEDboardingtime
Short(n = 4)264(148.2,379.8)181.6(159.4,203.8)1(0.1%)81(1.2%)7N/a8.5(6.8,10.3)
Middle(n = 4)285.9(242.6,329.2)300.6(285.8,315.4)27(3.6%)370(5.5%)9(6,12)11.4(10.5,12.3)
Long(n = 4)232.6(211,254.1)266.2(259.3,273.1)190(25%)1473(22%)11.6(10.3,12.9)11(10.5,11.4)
ED ,emergencydepartment; ICU ,intensivecareunit; OUD ,opioidusedisorder.
oftenwide.Treatmentratesmaybefalselyloweredbythe presenceofpatientsalreadyontreatmentand,therefore,not offeredED-basedbuprenorphine,althoughthiswouldbe unlikelytoimpactcomparisonbetweensites.Ourdatasetis alsolimitedbysizeandconfinementtoasinglehealthsystem aswellaslackofpatientdiversity,whichmaylimit generalizability.Importantly,unmeasuredoperationaland culturalfactorsmaypromptanygivenED’sleadershipteam tosupportbuprenorphinetreatment,andmanyofthose samefactorslikelyinfluencethegeneraloperational characteristicsoftheED.
WhilethishealthsystemoperatesonacommonEHR, cliniciansareallemployedbythehealthsystem,and incentivesatallsitesaretiedtorelativevalueunits,thereisa strongelementoflocalcontrolovertheoperationsofeach localED,withlittleadmixingofstafforoperational processesbetweenthem.Nevertheless,cliniciansmayhave movedbetweensitesorworkedatmultiplesites.Theremay beunmeasuredtemporaltrendsduringthestudyperiod,and aminorityofmoreprogressiveEDs(includingonlyone academicED)mayhavecontributeddisproportionatelyto our findings.Finally,ourpartitioningofEDsby organizationalmetricswasbasedoninternalcomparisons specifictoourhealthcaresystem.Attemptstousenational benchmarkingdatafromtheAcademyofAdministratorsin AcademicEmergencyMedicineorEmergencyDepartment BenchmarkingAlliancewereunsuccessful,asnationalmean andmedianmetricscreatedseverelyunevengroupsizes. Whileourapproachmaylimitgeneralizabilitytoother healthcaresystems,itstillmayhaveimplicationsforfuture hypothesis-testingresearch.
TheevidencesupportingthesocietalbenefitofED initiationofbuprenorphineforpatientswithopioiduse disorderisclear,butEDoperationalleadershipand stakeholderbuy-iniskeytoincreasingimplementation. Basedonourstudyresults,wehypothesizethatED buprenorphinetreatmentratesvariedbasedonoperational characteristicsofEDs,withlowertreatmentratesatsmaller, loweracuityfacilities.Wedidnotobserveconsistent differencesinlengthofstayorreturnvisits.Futureresearch willallowdepartmentalleadershiptocontinueprioritizing theevidence-basedpracticeofEDbuprenorphinetreatment todecreasevariabilitywhileimprovingqualityofcareand accesstolife-savingtreatmentforpatientswithOUD.Thisis particularlyimportantgiventherecentremovalofthe X-waiverrequirement.
AddressforCorrespondence:GrantComstock,MD,Departmentof EmergencyMedicine,MedicalCollegeofWisconsinHubfor CollaborativeMedicine,8701WatertownPlankRd,Milwaukee,WI 53226.Email: gcomstock@mcw.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Thedataforthisstudywereabstracted fromapreviouslycompletedqualityimprovementprojectfundedvia the2021EMF/NIDAMentor-FacilitatedTrainingAwardinSubstance UseDisordersScience.Therearenootherconflictsofinterestor sourcesoffundingtodeclare.
Copyright:©2024Comstocketal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.AhmadFB,CisewskiJA,RossenLM,etal.Provisionaldrugoverdose deathcounts.2024.Availableat: https://www.cdc.gov/nchs/nvss/vsrr/ drug-overdose-data.htm.AccessedJanuary5,2024.
2.MattickRP,BreenC,KimberJ,etal.Buprenorphinemaintenance versusplaceboormethadonemaintenanceforopioiddependence. CochraneDatabaseSystRev. 2014;(2):CD002207.
3.LarochelleMR,BernsonD,LandT,etal.Medicationfor opioidusedisorderafternonfatalopioidoverdoseand associationwithmortality:acohortstudy. AnnInternMed. 2018;169(3):137–45.
4.D’OnofrioG,O’ConnorPG,PantalonMV,etal.Emergencydepartmentinitiatedbuprenorphine/naloxonetreatmentforopioiddependence:a randomizedclinicaltrial. JAMA. 2015;313(16):1636–44.
5.BuschSH,FiellinDA,ChawarskiMC,etal.Cost-effectivenessof emergencydepartment-initiatedtreatmentforopioiddependence. Addiction. 2017;112(11):2002–10.
6.StevensMA,TsaiJ,SavitzST,etal.Trendsanddisparitiesinaccessto buprenorphinetreatmentfollowinganopioid-relatedemergency departmentvisitamonganinsuredcohort,2014–2020. JAMANetwOpen. 2022;5(6):e2215287.
7.HollandWC,LiF,NathB,etal.Racialandethnicdisparitiesin emergencydepartment-initiatedbuprenorphineacross fivehealthcare systems. AcadEmergMed. 2023;30(7):709–20.
8.WakemanSEandRichJD.Barrierstomedicationsfor addictiontreatment:howstigmakills. SubstUseMisuse. 2018;53(2):330–3.
9.ZuckermanM,KellyT,HeardK,etal.Physicianattitudeson buprenorphineinductionintheemergencydepartment:resultsfroma multistatesurvey. ClinToxicol(Phila). 2021;59(4):279–85.
10.ChartashD,PaekH,DziuraJD,etal.Identifyingopioidusedisorderin theemergencydepartment:multi-systemelectronichealthrecordbasedcomputablephenotypederivationandvalidationstudy. JMIR MedInform. 2019;7(4):e15794.
11.BrothersTD,MosselerK,KirklandS,etal.Unequalaccesstoopioid agonisttreatmentandsterileinjectingequipmentamonghospitalized patientswithinjectiondruguse-associatedinfectiveendocarditis. PLoSOne. 2022;17(1):e0263156.
12.AmiriS,McDonellMG,DenneyJT,etal.Disparitiesinaccesstoopioid treatmentprogramsandoffice-basedbuprenorphinetreatmentacross therural-urbanandareadeprivationcontinua:aUSnationwidesmall areaanalysis. ValueHealth. 2021;24(2):188–95.
13.RosenbergNK,HillAB,JohnskyL,etal.Barriersandfacilitators associatedwithestablishmentofemergencydepartment-initiated buprenorphineforopioidusedisorderinruralMaine. JRuralHealth. 2022;38(3):612–9.
RachelM.Skains,MD,MSPH*†
LindyReynolds,MSGH*
NicholasCarlisle,JD‡
SonyaHeath,MD§
WhitneyCovington,MPH,MLS*
KyleHornbuckle∥
LaurenWalter,MD*
*UniversityofAlabamaatBirmingham,HeersinkSchoolofMedicine,Department ofEmergencyMedicine,Birmingham,Alabama
† BirminghamVAMedicalCenter,DepartmentofEmergencyMedicine, Birmingham,Alabama
‡ UniversityofAlabamaatBirmingham,SchoolofPublicHealth,Departmentof HealthBehavior,Birmingham,Alabama
§ UniversityofAlabamaatBirmingham,HeersinkSchoolofMedicine,Department ofInternalMedicine,Birmingham,Alabama
∥ UniversityofAlabamaatBirmingham,HeersinkSchoolofMedicine, Birmingham,Alabama
SectionEditors: AlexisLapietra,MD,andR.Wilkerson,MD
Submissionhistory:SubmittedMarch30,2023;RevisionreceivedSeptember26,2023;AcceptedSeptember27,2023
ElectronicallypublishedNovember8,2023
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem DOI: 10.5811/westjem.60511
Introduction: Recentstudieshavedemonstratedthepromiseofemergencydepartment(ED)-initiated buprenorphine/naloxone(bup/nx)forimproving30-dayretentioninoutpatientaddictioncareprograms forpatientswithopioidusedisorder(OUD).WeinvestigatedwhetherED-initiatedbup/nxforOUDalso impactsrepeatEDutilization.
Methods: WeperformedaretrospectivechartreviewofEDpatientsdischargedwithaprimarydiagnosis ofOUDfromJuly2019–December2020.Characteristicsconsideredincludedage,gender,race, insurancestatus,domicilestatus,presenceofcomorbidDiagnosticandStatisticalManualofMental Disorders,FifthEdition(DSM-5)diagnosis,presentingchiefcomplaint,andprovisionofabup/nx prescriptionand/ornaloxonekit.PrimaryoutcomesincludedrepeatEDvisit(opioidornon-opioidrelated) within30days,90days,andoneyear.Statisticalanalysesincludedbivariatecomparisonand Poissonregression.
Results: Of169participants,themajorityweremale(67.5%),White(82.8%),uninsured(72.2%),andin opioidwithdrawaland/orrequesting “detox” (75.7%).Ninety-one(53.8%)receivedED-initiatedbup/nx, whichwasindependentofage,gender,race,insurancestatus,presenceofcomorbidDSM-5diagnosis, ordomicilestatus.Naloxonewasmorelikelytobeprovidedtopatientswhoreceivedbup/nx(97.8%vs 26.9%; P < 0.001),andbup/nxwasmorelikelytobegiventopatientswhopresentedwithopioid withdrawaland/orrequested “detox” (63.3%vs36.7%; P < 0.001).Bup/nxprovisionwasassociatedwith decreasedEDutilizationforopioid-relatedvisitsat30days(P = 0.04).Homelessnessandlackof insurancewereassociatedwithincreasedEDutilizationfornon-opioid-relatedvisitsat90days (P = 0.008and P = 0.005,respectively),andagainatoneyearforhomelessness(P < 0.001).When controllingforageanddomicilestatus,theadjustedincidencerateratioforoverallEDvisitswas0.56 (95%confidenceinterval[CI]0.33–0.96)at30days,0.43(95%CI0.27–0.69)at90days,and0.60(95% CI0.39–0.92)atoneyear,favoringbup/nxprovision.
Conclusion: Initiationofbup/nxintheEDsettingwasassociatedwithdecreasedsubsequentED utilization.Socioeconomicfactors,specificallyhealthinsuranceanddomicilestatus,significantly impactednon-opioid-relatedEDreuse.These findingsdemonstratetheED’spotentialasaninitiation pointforbup/nxandhighlighttheimportanceofconsideringthesocialriskandsocialneedforOUD patients.[WestJEmergMed.2025;26(1.1)63–70.]
AccordingtotheSubstanceAbuseandMentalHealth ServicesAdministration,nearly5.6millionresidentsofthe UnitedStateshadopioidusedisorder(OUD)in2021, accountingfor2%oftheUSpopulation.1 From2020to 2021,therewereanestimated1.8millionnewusersof prescriptionpainrelieversand26,000newheroinusers,or nearly5,000newopioidusersperday.1 Correspondingly,the USCentersforDiseaseControlandPreventionobserveda recordhighdrugoverdosemortalityin2021,withover 107,000drugoverdosedeathsintheUS,morethan80,000of whichinvolvedopioids.2
ThestateofAlabamahasbeenparticularlyaffectedbythe opioidepidemic.Since2014,Alabamahasledthenation withthehighestrateofopioidprescriptionsinthecountry (80.4prescriptionsforevery100personsin2020), approximatelytwofoldgreaterthanthenationalaverage.3 JeffersonCounty,thestate’smostpopulouscounty,hadthe highestnumberofopioidoverdosedeathsinAlabamain 2021,with342confirmedopioidoverdosedeaths,a44.7% increasefrom2020.4 Theopioidepidemicisanongoing, significantpublichealthemergencyasevidencedbytherising incidenceofopioidmisuse,OUD,andopioid-relateddeaths intheUS.
Emergencyphysiciansareuniquelypositionedtohelp combatthegrowingopioidcrisisbyscreeningandinitiating careforpatientspresentingtotheemergencydepartment (ED)withOUD.Opioid-relatedEDvisitshaveincreased, representingnearlyonein80EDvisits,andescalated dramaticallyduringthecoronavirusdisease2019(COVID19)pandemicwhennon-opioid-relatedEDvisits decreased.5,6 Importantly,screeningforopioidmisuseand dependenceintheEDhasbeenproventopositivelyaffectthe prognosisofthesepatients.Inalandmarkrandomized clinicaltrialin2015,D’Onofrio andcolleaguesdemonstratedthatEDscreening,brief intervention,andreferraltotreatment(SBIRT)forOUD, includingED-initiatedmedicationsforOUD(MOUD)with buprenorphine/naloxone(bup/nx),significantlyincreased 30-dayretentioninoutpatientaddictiontreatment, decreasedtheuseofopioids,anddecreasedutilization ofinpatientaddictionservices.7 AsMOUDhasbeen recognizedasaneffectivetreatmentoptiontoreduce mortality,overdose,andcost,EDsareincreasinglyengaged inOUDtreatmentinitiation.8–14 Further,arecent community-basedstudybyLeetaldemonstrateddecreased subsequenthealthcareutilizationat12monthsafter initiationofMOUDintheED.15
MostED-initiatedMOUDstudieshavefocusedon treatmentretentioninlarge,urban,academicmedicalcenters outsidetheSoutheastorsubsequenthealthcareutilizationin communityhospitals.7,11,12,15,16 Ourlarge,urban,academic EDintheSoutheastoffersauniqueperspectiveontheimpact
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Emergencydepartment(ED)-initiated buprenorphine/nalox one(bup/nx)improves 30-dayretentioninoutpatientaddiction programsforopioidusedisorder(OUD).
Whatwastheresearchquestion?
DoesED-initiatedbup/nxforOUDalsoimpact acutehealthcareutilization,specificallyrepeat EDvisits,forOUDpatients?
Whatwasthemajorquantitative finding ofthestudy?
Bup/nxdecreasedEDutilizationat30days (37.5%vs.62.5%,P < 0.05).Homelessness andlackofinsuranceincreasedEDutilization at90days(P < 0.01).
Howdoesthisimprovepopulationhealth?
FindingsshowtheED ’ spotentialasan initiationpointforbup/nxandhighlightthe importanceofsocialriskandneedfor OUDpatients.
ofED-initiatedMOUDonhealthcareutilizationina resource-limitedregioncharacterizedbypersistentMedicaid non-expansion,highpovertyrates,andhealthcareaccess challenges.13 Inthisstudy,weinvestigatedwhetherEDinitiatedbup/nxalsoimpactsacutehealthcareutilization, specificallyrepeatEDvisits,forEDOUDpatients.
Weconductedaretrospectivechartreviewofpatientswho presentedtooururbanacademicmedicalcenterEDatthe UniversityofAlabamaatBirmingham(UAB)andwere dischargedfromtheEDwithadiagnosisofOUD,using InternationalClassificationofDiseases,10th Revision,(ICD10)codedocumentation.17 WeobtainedUABInstitutional ReviewBoardapproval.Our48-bed,tertiarycareED evaluatesover75,000patientsannually.TheUABHospital has1,157licensedbedsandservesastheprimaryhospitalfor north-centralAlabamaandsurroundingareas.Weselected thestudyperiodJuly2019–June2020becauseitmarkedthe inauguralyearofthehospital’sED-initiatedOUDprogram, wherepatientswithadiagnosisofOUDweretobedischarged withabridgebup/nxprescription,naloxonetake-homekit, andreferraltooutpatientaddictiontreatment.However,
emergencyclinicians’ uptakeandutilizationofthebup/nx prescriptionwasnotuniversalduringthat firstyear.Priorto July2019,bup/nxwasnotroutinelyprescribedfromtheED.
TheprimaryoutcomesofinterestwererepeatED utilizationwithin30days,90days,andoneyearoftheinitial EDvisit.RepeatEDvisitswerefurtherclassifiedaseither opioid-relatedornon-opioid-related,asdefinedbyICD-10 documentation.17 Whenanalyzingopioid-relatedEDvisits andnon-opioid-relatedEDvisitsseparately,weconsidered outcomesateachtimepointasbinaryvariables.Thenumber ofopioid-relatedrepeatEDvisitswasaddedtothenumberof non-opioid-relatedEDvisitswithin30days,90days,andone yeartoobtainthecompositeoutcomeoftotalrepeatED visitsateachtimepointofinterest.Weusedcompositevalue forPoissonregressionanalysis.Theprimaryexposureof interestwaswhetherthepatientwasdischargedwith abup/nxprescription,whichwasabinaryvariablecodedas yesorno.
Othervariablesintheanalysisincludedage,gender,race, healthinsurancestatus,domicilestatus,provisionofa naloxonekit,comorbidDiagnosticandStatisticalManualof MentalDisorders,FifthEdition(DSM-5)diagnosis,and presentingchiefcomplaintattheinitialEDvisit.Agewas measuredinyearsandwasexaminedasacontinuous variable.Genderwasdeterminedbydatarecordedinthe electronichealthrecord(EHR)atthetimeofED registration,typicallydictatedbyavailablelegal identification(eg,driver’slicense)orself-reportedinabsence ofID.Genderwasanominalvariableclassifiedasmale, femaleorother,perEHRlimitations.Racewascategorized asWhiteorBlack.(Otherracialcategorieswerenot consideredduetolownumbers.)Healthinsurancewas definedasprivate,public(Medicareand/orMedicaid),or self-pay(uninsured).Domicilestatuswasabinaryvariable andclassifiedaseitherhomelessornothomeless.The provisionofanaloxonekitupondischargefrominitialvisit wasincludedasadichotomousyesornovariable,aswasthe presenceofacomorbidDSM-5mentalhealthdiagnosis. Concomitantmentalhealthdiagnosiswasdeterminedby presencein “pastmedicalhistory” duringchartreview.Chief complaintattheinitialEDvisitwasnotedandwasmanually classifiedbyreviewersasopioidwithdrawal/detoxification (“detox”)request,opioidoverdose,psychiatriccomplaint,or medicalcomplaint.
WecarriedoutallanalysesusingSAS9.4(SASInstitute, Cary,NC),and P < 0.05wasconsideredstatistically significant.18 Frequenciesandproportionsweretabulatedfor categoricalvariables,whichincludedgender,race,health insurance,naloxonekitprovision,buprenorphine prescription,comorbidDSM-5diagnosis,andEDchief
complaint.Wecalculatedmeanandstandarddeviationfor age,whichwastreatedasacontinuousvariable.Chi-square andFisherexacttestswereusedtocomparethecategorical demographicandmedicalcharacteristicsofthosewithvs thosewithoutarepeatopioid-relatedEDvisitwithin30days, 90days,oroneyear.Weused t -teststoassessdifferencesin agebyoutcomestatus.Identicalmethodswereusedforthe non-opioid-relatedEDvisitoutcomes(at30days,90days, andoneyear).CrudeandadjustedPoissonmodelswere constructedtoestimatechangesinthenumberoftotalrepeat EDvisitsaswellastheassociated95%confidenceinterval (CI)betweenthosewhowereprescribedbup/nxandthose whowerenotattheindexEDvisitforeachofthetime periods(30days,90days,andoneyear).Separate modelsweregeneratedforeachoutcome.Althoughno overdispersioninthe30-daymodelwasobserved, overdispersioninthe90-dayandone-yearmodelswas detectedandwasaccountedforbyscalingbythedeviance. Secondaryanalysesexaminedwhethertheassociation betweenbup/nxprescriptionandtotalnumberofrepeatED visitsvariedbasedonwhetherthepatientalsoreceiveda naloxonekitattheirinitialEDvisit.Toaccomplishthis,we includedaninteractiontermbetweenbup/nxprescription andnaloxonekitineachofthemodels.Alladjustedmodels includedageanddomicilestatusascovariates.
Thisstudyincluded169OUDpatients.Ofthese, approximately67.5%weremaleand82.8%wereWhite. Mostpatientsdidnothavehealthinsurance(72.2%),and27 (15.9%)werehomeless(Tables1, 2).Additionally,over75% ofpatientspresentedtotheEDattheirinitialvisitinopioid withdrawalorrequesting “detox.” Ninety-onepatients (53.8%)receivedED-initiatedbup/nx(suboxone),and110 (65.1%)weregivenanaloxonekittotakehomeattheirinitial EDvisit.Abup/nxprescriptionwasmorelikelytobegivento patientswhopresentedinopioidwithdrawaland/or requested “detox” (63.3%vs36.7%; P < 0.001),butbup/nx prescriptiondidnotshowsignificantassociationswithage, gender,race,insurancestatus,presenceofco-morbidDSM-5 diagnosis,ordomicilestatus.Analoxonekitwasmorelikely tobeprovidedtopatientswhoreceivedbup/nx(97.8%vs 26.9%; P < 0.001).
At30days,32patients(18.9%)hadarepeatopioid-related EDvisit(Table1).Nosignificantdifferencesemergedin termsofage,gender,race,healthinsurancestatus, homelessness,EDchiefcomplaint,orcomorbidDSM-5 diagnosisrates.However,bup/nxprescriptionandnaloxone kitprovisionwereassociatedwithdecreasedEDutilization foropioid-relatedvisitsat30days(P = 0.04and P < 0.001, respectively).By90days,30.2%ofthestudysamplehada repeatopioid-relatedEDvisit.Inthistimeframe,male patients(P < 0.05)andthosewhodidnotreceiveanaloxone kit(P = 0.001)weremorelikelytohavearepeatvisit;
Table1. Comparisonofpatientcharacteristicsbywhetherthepatienthadarepeatopioid-relatedemergencydepartmentvisit.
Variables 30-DayrepeatEDvisit90-DayrepeatEDvisit1-YearrepeatEDvisit
Gender,n(%)
Female49(35.8)6(18.8)0.0644(37.3)11(21.6) <0.05*35(34.3)20(29.8)0.54
Male88(64.2)26(81.2)74(62.7)40(78.4)67(65.7)47(70.2)
Race,n(%)
White113(83.7)27(84.4)0.7997(83.6)43(84.3)0.6486(86.0)13(19.4)0.33
Black22(16.3)5(15.6)19(16.4)8(15.7)14(14.0)54(80.6)
HealthIns,n(%)
Private18(13.1)2(6.2)0.4915(12.7)5(9.8)0.8614(13.7)6(9.0)0.43
Public23(16.8)4(12.5)19(16.1)8(15.7)18(17.6)9(13.4)
Self-pay96(70.1)26(81.3)84(71.2)38(74.5)70(68.6)52(77.6)
Homeless,n(%)
No117(85.4)25(78.1)0.31103(87.3)39(76.5)0.0890(88.2)52(77.6)0.07 Yes20(14.6)7(21.9)15(12.7)12(23.4)12(11.8)15(22.4)
Naloxonekitgiven,n(%)
No39(28.5)20(62.5) <0.001*32(27.1)27(52.9)0.001*28(27.4)31(46.3)0.01* Yes98(71.5)12(37.5)86(72.9)24(47.1)74(72.6)36(53.7)
BuprenorphineRx,n(%)
No58(42.3)20(62.5)0.04*51(43.2)27(52.9)0.2445(44.1)33(49.2)0.51
Yes79(57.7)12(37.5)67(56.8)24(47.1)57(55.9)34(50.8)
ComorbidDSM-5Dx,n(%)
No116(84.7)28(87.5)0.6898(83.0)46(90.2)0.2384(82.4)60(89.6)0.20
Yes21(15.3)4(12.5)20(17.0)5(9.8)18(17.6)7(10.4)
EDchiefcomplaint,n(%)
OpioidWD/detoxrequest102(74.4)26(81.2)0.5288(74.6)40(78.4)0.2377(75.5)51(76.1)0.30
OpioidOD21(15.3)2(6.2)19(16.1)4(7.8)15(14.7)8(11.9)
Psychiatriccomplaint9(6.6)2(6.2)8(6.8)3(5.9)8(7.8)3(4.5)
Medicalcomplaint5(3.7)2(6.2)3(2.5)4(7.8)2(2.0)5(7.5)
Raceinformationwasmissingfortwopatients.
ED,emergencydepartment; Detox,detoxification; DSM-5,DiagnosticandStatisticalManualofMentalDisorders,5thEdition; Dx,diagnosis; Ins,insurance; OD,overdose; Rx,prescription; WD,withdrawal.
*Denotesstatisticalsignificancewhere P < 0.05.
however,ED-prescribedbup/nxwasnolongersignificantly associatedwithhavingarepeatvisit(P = 0.24).
Withinoneyear,67patients(40.0%)hadarepeatopioidrelatedEDvisit.Inthistimeframe,theonlyvariableshowing asignificantassociationwithrepeatEDvisitwasnaloxone kitprovision(P = 0.01).Ofthosewhoreceivedanaloxone kit,32.7%hadarepeatvisit;however,amongthosewhodid notreceiveakit,52.5%hadarepeatvisit.Thus,naloxonekit provisionwasassociatedwithdecreasedEDutilizationfor opioid-relatedvisitsat30days,90days,andoneyear (P < 0.001, P = 0.001,and P = 0.01,respectively).Ofthe169 patients,only11(6.5%)hadanon-opioid-relatedrepeatED
visitwithin30days(Table2),comparedwith32(18.9%)who hadanopioid-relatedrepeatEDvisitinthatsametime frame.Increasingagewasassociatedwitharepeatnonopioid-relatedvisitat30days(43.8 ± 8.9yearsvs36.3 ± 9.2years; P = 0.009).Atthistimepoint,nosignificant differencesemergedintermsofgender,race,health insurance,homelessness,naloxonekitprovision, bup/nxprescription,comorbidDSM-5diagnosis,orED chiefcomplaint.
By90days,thenumberofpatientswithanon-opioidrelatedrepeatEDvisitincreasedto23(13.6%).Thosewitha repeatvisitwereolder(P = 0.004),morelikelytobe
Table2. Comparisonofpatientcharacteristicsbywhetherthepatienthadarepeatnon-opioid-relatedEDvisit.
Variables 30-DayrepeatEDvisit90-DayrepeatEDvisit1-YearrepeatEDvisit
Gender,n(%)
Female53(33.5)2(18.2)0.5150(34.2)5(21.7)0.2343(34.4)12(27.3)0.39
Male105(66.5)9(81.8)96(65.8)18(78.3)82(65.6)32(72.7)
Race,n(%)
White130(83.3)10(90.9)0.75121(84.0)19(82.6)0.83103(83.7)37(84.1)0.70
Black26(16.7)1(9.1)23(16.0)4(17.4)20(16.3)7(15.9)
Healthins,n(%)
Private18(11.4)2(18.2)0.6817(11.6)3(13.0)0.005*15(12.0)5(11.4)0.36
Public25(15.8)2(18.2)18(12.3)9(39.1)17(13.6)10(22.7)
Self-pay115(72.8)7(63.6)111(76.0)11(47.8)93(74.4)29(65.9)
Homeless,n(%)
No134(84.8)8(72.7)0.39127(87.0)15(65.2)0.008*112(89.6)30(68.2)0.001* Yes24(15.2)3(27.3)19(13.0)8(34.8)13(10.4)14(31.8)
Naloxonekitgiven,n(%)
No55(34.8)4(36.4)0.9246(31.5)13(56.5)0.02*41(32.8)18(40.9)0.33
Yes103(65.2)7(63.6)100(68.5)10(43.5)84(67.2)26(59.1)
BuprenorphineRx,n(%)
No73(46.2)5(45.4)0.9664(43.8)14(60.9)0.1358(46.4)20(45.4)0.91 Yes85(53.8)6(54.6)82(56.2)9(39.1)67(53.6)24(54.6)
ComorbidDSM-5Dx,n(%)
No134(84.8)10(90.9)0.58123(84.2)21(91.3)0.53108(86.4)36(81.8)0.46
Yes24(15.2)1(9.1)23(15.8)2(8.7)17(13.6)8(18.2)
EDchiefcomplaint,n(%)
OpioidWD/detoxrequest118(74.7)10(90.9)0.62109(74.7)19(82.6)0.2993(74.4)35(79.6)0.32
OpioidOD22(13.9)1(9.1)21(14.4)2(8.7)20(16.0)3(6.8)
Psychiatriccomplaint11(7.0)0(0.0)11(7.5)0(0.0)8(6.4)3(6.8)
Medicalcomplaint7(4.4)0(0.0)5(2.4)2(8.7)4(3.2)3(6.8)
Raceinformationwasmissingfortwopatients.
ED,emergencydepartment; Detox,detoxification; DSM-5,DiagnosticandStatisticalManualofMentalDisorders,5thEdition; Dx,diagnosis; Ins,insurance; OD,overdose; Rx,prescription; WD,withdrawal.
*Denotesstatisticalsignificancewhere P < 0.05.
uninsured(P = 0.005),morelikelytobehomeless(P = 0.008),andlesslikelytohavereceivedanaloxonekitatthe initialvisit(P = 0.02).Byoneyear,44patients(26%)hada repeatnon-opioid-relatedEDvisit.Again,patientswitha repeatvisitwereolder(P = 0.003)andmorelikelytobe homeless(P < 0.001),althoughinsurancestatusand naloxoneprovisionnolongershowedasignificant association(P = 0.36).
Next,thetotalrepeatall-causeEDvisitswereconsidered. Within30daysoftheirindexEDvisit,23.1%ofpatientshad atleastonerepeatall-causeEDvisit(range1–4visits).By90
days,thispercentageincreasedto35.5%(range1–12visits). Atoneyearfromtheinitialvisit,50.3%ofpatientshada repeatvisit(range1–36visits).Intheunadjustedmodels, bup/nxprescriptionprovisionwassignificantlyassociated withareductioninthenumberofrepeatall-causeEDvisits at90days(butnot30daysoroneyear)(Table3).Giventhat significantassociationwasalsoobservedbetweenolderage andhomelessnessandall-causerepeatEDvisits,thebup/nx association findingswerere-evaluatedafteradjustingforage anddomicilestatus.Afteradjustingforageanddomicile status,astrongerassociationemergedbetweenbup/nx
Table3. Countratiosand95%confidenceintervalsfortheassociationbetweenbuprenorphine/naloxoneprescriptiongivenandnumberof all-causerepeatemergencydepartmentvisits.+
RepeatEDvisitwithin30daysRepeatEDvisitwithin90daysRepeatEDvisitwithin1year
Overall
Nobup/nxRefRefRefRefRefRef
Bup/nxgiven0.60(0.35–
Nonaloxonekitgiven
0.56(0.33–0.96)0.48(0.29–0.79)0.43(0.27–0.69) 0.66(0.42–1.05) 0.60(0.39–0.92)
Nobup/nxRefRefRefRefRefRef
Bup/nxgiven0.95(0.13–6.97)1.10(0.15–8.13)0.37(0.03–4.88)0.50(0.04–5.68)0.39(0.03–5.66)0.52(0.04–6.54)
Naloxonekitgiven
Nobup/nxRefRefRefRefRefRef
Bup/nxgiven1.73(0.52–5.78)1.50(0.45–5.07)3.46(0.75–15.97)2.67(0.63–11.28)2.38(0.76–7.44)1.85(0.63–5.44)
+Estimatesofcountratioand95%CIsgeneratedfromPoissonmodels.
*Boldfacefont indicatesstatisticalsignificancewhere P < 0.05.
1Adjustedforageanddomicilestatus.
ED,emergencydepartment; CI,confidenceinterval; bup/nx,buprenorphine/naloxone; ref,reference.
prescriptionprovisionandrepeatall-causeEDvisits,with bup/nxprescriptionbeingassociatedwitha44%reductionin thenumberofrepeatall-causeEDvisitsat30days(adjusted incidencerateratio[IRR]:0.56,95%confidenceinterval[CI] 0.33–0.96),a57%reductionat90days(adjustedIRR0.43, 95%CI0.27–0.69),anda40%reductionatoneyear (adjustedIRR0.60,95%CI0.39–0.92)(Table3).
ThisstudyhighlightstheimpactofOUDandtheopioid epidemicingeneralontheED.Overhalfthepatients includedinthisstudyhadarepeatEDvisitwithinoneyear. Thishighlevelofutilizationislikelydue,inlargepart,tothe overlappingsocialriskandsocialneedexperiencedbythis cohort.Thegeneraldemographiccharacteristicsofthisstudy populationaresimilartothenationalopioidepidemic landscape,predominantlyWhite(82.8%)andmale (67.5%).19 However,whenconsideringsocialfactors,suchas insuranceanddomicilestatus,ourOUDpopulationwas disproportionatelyaffectedbynegativesocialdeterminants ofhealth(SDoH).MorethansevenintenOUDpatients wereuninsured,comparedwiththeaverageuninsuredrateof 12.7%innon-expansionstatesin2021.20 Further,16%were homeless,whichisnearly100timesthenationalrate.21 Homelessnessandlackofinsurancewereindependently associatedwithincreasedEDutilizationfornon-opioidrelatedvisitsat90days(P = 0.008andp = 0.005, respectively),andagainatoneyearforhomelessness (P < 0.001).Thisunderscoresthecomplexsocialcontextof theEDOUDpopulation.Ifco-occurringSDoHdomainsare notaddressedduringtheEDvisit,MOUDmaynotbe successfulindecreasingsubsequenthealthcareutilization.
AtUABHospital,EDsocialworkersandcasemanagersare available24/7toprovidehousingandhealthcareaccess resourcestounderservedpatients;however,referralsto assistanceprogramsarenotconsistentlydocumentedin theEHR.
Althoughbup/nxprovisionwasassociatedwithdecreased EDutilizationforopioid-relatedvisitsat30days(P = 0.04), only53.8%receivedED-initiatedbup/nx.Further,bup/nx wasmorelikelytobegiventoOUDpatientswhopresented inopioidwithdrawaland/orrequesting “detox” (63.3%vs 36.7%; P < 0.001).Therearemanyplausibleexplanationsfor why46.2%ofOUDpatientsdidnotreceivebup/nxatthe initialEDvisit,althoughthispercentageismuchlowerthan arecentlypublishednationalretrospectivecohortstudy where91.5%werenotprescribedbuprenorphineafteranED visitforopioidoverdose.22 First,inJuly2019(studyperiod startdate),theUABDepartmentofEmergencyMedicine hadjustinitiatedtheDrugAddictionTreatmentAct of2000(DATA2000) “X-waiver” trainingrequirement tolicenseemergencycliniciansforMOUDprescribing bup/nxthroughanincentiveprogram,whichwas stronglyencouragedbutnotmandatedforallclinicians.23 Further,MOUDprogramuptakewasnotuniversaldue toseveralknownbarrierstoMOUDintheED,including lackoftrainingandexperienceinSBIRT,lackofavailability ofcloseoutpatientfollow-upinaddictiontreatmentcenters, andlimitedcliniciantimeinabusyED.24 Finally,notevery OUDpatientpresentingtotheEDwasacandidatefor MOUDwithbup/nxduetolackofmotivationtoseekand engageinoutpatienttreatment,concomitantuseofillicit depressiveagents,hypersensitivityreaction,andconcernfor diversion.25 ItisstandardpracticeattheUABEDfor
patientsreceivingED-initiatedMOUDtobereferredto communitytreatmentprograms;however,outpatient follow-upratesarenoteasilymeasuredwithinour currentsystem.
WhileroughlyhalfofthepatientsreceivedMOUDatthe initialEDvisit,nearlytwo-thirdsreceivedatake-home naloxonekit,which,atthetimeofthestudywasprovidedto patientsfreeofchargewithanemergencyphysician(EP) orderviaacollaborativeprojectwiththeJeffersonCounty HealthDepartment.Importantly,naloxonekitprovision wasassociatedwithdecreasedEDutilizationforopioidrelatedvisitsat30days,90days,andoneyear(P < 0.001, P = 0.001,and P = 0.01,respectively)andnon-opioid-related visitsat90days(P = 0.02).Naloxoneisapotentiallylifesaving,easy-to-useand,inthisinstance,freeintervention. Severalfactorsmighthavecontributedtoincomplete provision:1)ThenaloxonekitrequiredaspecificEPorderto bedispensed,whichmaynothavebeenprioritizeddueto competingdemandsforphysicianfocusandtime;2)EPsmay havehadmisperceptionsoftime-consumingcounseling accompanyingnaloxoneprovision;and3)EPsmayhave beenunawareoftheavailabilityofnaloxoneprovidedasa take-homekitratherthanaprescription.
Ingeneral,therewassignificantcollinearitybetweenbup/ nxandnaloxonekitprovision.Analoxonekitwasmorelikely tobeprovidedtopatientswhoreceivedbup/nx(97.8%vs 26.9%; P < 0.001).Further,bup/nxwasmorelikelytobegiven topatientswhopresentedinopioidwithdrawaland/or requested “detox:(63.3%vs36.7%; P < 0.001).However, patientswhopresentedinthemostsevereformofOUD,an acuteoverdose,werenotmorelikelytoreceivebup/nx.This maybeduetotheEP’sfocusonresuscitationofacute decompensationandrespiratorydepression,ratherthan engagementofabriefinterventionforMOUDtoassessa patient’smotivationtowardbehavioralchange.
OurstudyisuniqueinassessingwhetherED-initiatedbup/ nximpactssubsequentacutehealthcareutilization,while alsoevaluatingtheimpactofSDoH,suchashealthinsurance anddomicilestatus.Ourresultsshowedthatwhen controllingforageandhomelessness,initiationofbup/nxin theEDsettingwasassociatedwithdecreasedsubsequent all-causeEDutilization.Further,socioeconomicfactors, specificallyinsuranceanddomicilestatus,appeartohave significantimpactonnon-opioid-relatedEDreuse.These findingsdemonstratetheED’spotentialasaninitiationpoint forOUDtreatmentandhighlighttheimportanceof consideringsocialriskandsocialneedforOUDpatients intheED.
Thisstudyhadseverallimitations.First,thestudydesign wasaretrospectivechartreview,whichpreventsabstractors frombeingblindedtothestudypurposeanddrawing conclusionsofcausality.However,tominimizebias,
establishedemergencymedicinechartreviewstudymethods wereadheredto.26 Further,thestudypopulationwas obtainedfromasinglesite,whichlimitsgeneralizability. RevisitstoEDsinoutsidehealthcaresystemswereunableto betracked,preventingcompletecapture.However,UAB Hospitalisthecatchmenthealthcaresystemforthestateof Alabamaprovidinghealthcareaccesstounderserved populations,includingtheCharityCareProgram, EqualAccessBirminghamfreeclinic,ProvidingAccess toHealthcareclinic,andaComprehensiveUrban UnderservedandRuralExperienceprogram.Finally, EDvisitratesforopioidoverdoseincreasedbyover25% in2020duetotheCOVID-19pandemic,despiteadecline inoverallEDvisits.27 Thus,expandedcommunity-and hospital-basedMOUDinterventionswereneededtosupport OUDpatientsduringtheCOVID-19pandemic;however, manycounselingandtreatmentclinicswereunavailable duringthattime.
Initiationofbuprenorphine/naloxoneintheEDsetting canresultindecreasedsubsequentEDutilization. Socioeconomicfactors,specificallyhealthinsuranceand domicilestatus,alsoappeartohaveasignificantimpacton EDreuse.These findingsdemonstratetheED’spotentialas aninitiationpointforprescribingmedicationforopioiduse disorderandhighlighttheimportanceofconsideringsocial riskandsocialneedforOUDpatients.
AddressforCorrespondence:RachelMSkains,MD,MSPH, UniversityofAlabamaatBirmingham,HeersinkSchoolofMedicine, DepartmentofEmergencyMedicine,17202nd Ave.South,GSB238, Birmingham,Alabama352494.Email: rskains@uabmc.edu
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Theprojectdescribedwassupportedby GrantNumber1H79T1081609-01fromtheSubstanceAbuseand MentalHealthServicesAdministration(SAMHSA).Itscontentsare solelytheresponsibilityoftheauthorsanddonotnecessarily representtheofficialviewsoftheSAMHSA.Therearenoconflictsof interesttodeclare.
Copyright:©2023Skainsetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.KeysubstanceuseandmentalhealthindicatorsintheUnitedStates: Resultsfromthe2021NationalSurveyonDrugUseandHealth(HHS PublicationNo.PEP22-07-01-005,NSDUHSeriesH-57).Centerfor BehavioralHealthStatisticsandQuality,SubstanceAbuseandMental
HealthServicesAdministration.Availableat: https://www.samhsa.gov/ data/report/2021-nsduh-annual-national-report.PublishedDecember 2022.AccessedMarch13,2023.
2.SpencerMR,MininoAM,WarnerM.DrugoverdosedeathsintheUnited States,2001–2021.NCHSDataBrief,no457.Hyattsville,MD:National CenterforHealthStatistics.2022.Availableat: https://www.cdc.gov/ nchs/data/databriefs/db457.pdf.AccessedMarch13,2023.
3.U.S.opioiddispensingratemaps.CentersforDiseaseControland Prevention.Availableat: https://www.cdc.gov/drugoverdose/ rxrate-maps/index.html.PublishedNovember10,2021. AccessedMarch13,2023.
4.Annual2021ReportJeffersonCountyCoroner/MedicalExaminer’s Office.Availableat: https://www.jccal.org/Sites/Jefferson_County/ Documents/Coroner_Medical%20Examiner%20Office/2021% 20annual%20report.pdf.AccessedMarch13,2023.
5.HallGT,CruzDS,LankPM,etal.Opioid-relatedemergencydepartment visitsduringCOVID-19inalargehealthsystem. JAddictMed 2021;15(4):345–8.
6.LangabeerJR,StottsAL,BobrowBJ,etal.Prevalenceandchargesof opioid-relatedvisitstoU.S.emergencydepartments. DrugAlcohol Depend.2021;221:108568.
7.D’OnofrioG,O’ConnorPG,PantalonMV,etal.Emergencydepartmentinitiatedbuprenorphine/naloxonetreatmentforopioiddependence: arandomizedclinicaltrial. JAMA.2015;313(16):1636–44.
8.SordoL,BarrioG,BravoMJ,etal.Mortalityriskduringandafteropioid substitutiontreatment:systematicreviewandmeta-analysisofcohort studies. BMJ.2017;357:j1550.
9.WakemanSE,LarochelleMR,AmeliO,etal.Comparativeeffectiveness ofdifferenttreatmentpathwaysforopioidusedisorder. JAMANetw Open.2020;3(2):e1920622.
10.FairleyM,HumphreysK,JoyceVR,etal.Cost-effectivenessof treatmentsforopioidusedisorder. JAMAPsychiatry 2021;78(7):767–77.
11.ReuterQR,SantosAD,McKinnonJ,etal.Long-termtreatmentretention ofanemergencydepartmentinitiatedmedicationforopioidusedisorder program. AmJEmergMed.2022;55:98–102.
12.KaucherKA,CarusoEH,SungarG,etal.Evaluationofanemergency departmentbuprenorphineinductionandmedication-assistedtreatment referralprogram. AmJEmergMed.2020;38(2):300–4.
13.WalterLA,LiL,RodgersJB,etal.Developmentofanemergency department-basedinterventiontoexpandaccesstomedicationsfor opioidusedisorderinaMedicaidnonexpansionsetting:protocolfor engagementandcommunitycollaboration. JMIRResProtoc 2021;10(4):e18734.
14.MelnickER,NathB,DziuraJD,etal.Usercenteredclinicaldecision supporttoimplementinitiationofbuprenorphineforopioidusedisorder intheemergencydepartment:EMBEDpragmaticclusterrandomized controlledtrial. BMJ.2022;377:e069271.
15.LeT,CordialP,SankoeM,etal.Healthcareuseafterbuprenorphine prescriptioninacommunityemergencydepartment:acohortstudy. WestJEmergMed.2021;22(6):1270–5.
16.EdwardsFJ,WicelinskiR,GallagherN,etal.Treatingopioidwithdrawal withbuprenorphineinacommunityhospitalemergencydepartment:an outreachprogram. AnnEmergMed.2020;75(1):49–56.
17.OwensPL,WeissAJ,BarrettML.Hospitalburdenofopioid-related inpatientstays:metropolitanandruralhospitals,2016.2020May26. In:HealthcareCostandUtilizationProject(HCUP)StatisticalBriefs [Internet].Rockville(MD):AgencyforHealthcareResearchandQuality (US);2006Feb-.Table2,ICD-10-CMdiagnosiscodesdefiningopioidrelatedinpatientstays.Availableat: https://www.ncbi.nlm.nih.gov/ books/NBK559382/table/sb258.tab4/.AccessedMarch13,2023.
18.SASInstituteInc.2016.SAS® 9.4LanguageReference:Concepts, SixthEdition.Cary,NC:SASInstituteInc.
19.Racial/ethnicdifferencesinsubstanceuse,substanceusedisorders, andsubstanceusetreatmentutilizationamongpeopleaged12orolder (2015–2019)(PublicationNo.PEP21-07-01-001).Rockville,MD: CenterforBehavioralHealthStatisticsandQuality,SubstanceAbuse andMentalHealthServicesAdministration.Availableat: https://www. samhsa.gov/data/sites/default/files/reports/rpt35326/ 2021NSDUHSUChartbook.pdf.AccessedMarch13,2023.
20.Healthinsurancecoveragestatusandtypebygeography:2019and 2021.Availableat: https://www.census.gov/content/dam/Census/ library/publications/2022/acs/acsbr-013.pdf.AccessedMarch13,2023.
21.DeSousaT,AndrichikA,CuellarM,etal.The2022Annual HomelessnessAssessmentReport(AHAR)toCongress.Part1:PointIn-TimeEstimatesofHomelessness.TheU.S.DepartmentofHousing andUrbanDevelopmentOfficeofCommunityPlanningand Development.Availableat: https://www.huduser.gov/portal/sites/ default/files/pdf/2022-AHAR-Part-1.pdf.IssuedDecember2022. AccessedFebruary12,2023.
22.ChuaKP,DahlemCHY,NguyenTD,etal.Naloxoneandbuprenorphine prescribingfollowingUSemergencydepartmentvisitsforsuspected opioidoverdose:August2019toApril2021. AnnEmergMed 2022;79(3):225–36.
23.FosterSD,LeeK,EdwardsC,etal.Providingincentiveforemergency physicianX-waivertraining:anevaluationofprogramsuccessand postinterventionbuprenorphineprescribing. AnnEmergMed 2020;76(2):206–14.
24.KimHSandSamuelsEA.Overcomingbarrierstoprescribing buprenorphineintheemergencydepartment. JAMANetwOpen 2020;3(5):e204996.
25.MackeyK,VeazieS,AndersonJ,etal.Barriersandfacilitatorstotheuse ofmedicationsforopioidusedisorder:arapidreview. JGenInternMed 2020;35(Suppl3):954–63.
26.KajiAH,SchrigerD,GreenS.Lookingthroughtheretrospectoscope: reducingbiasinemergencymedicinechartreviewstudies. AnnEmerg Med.2014;64(3):292–8.
27.SoaresWE3rd,MelnickER,NathB,etal.Emergencydepartmentvisits fornonfatalopioidoverdoseduringtheCOVID-19pandemicacrosssix UShealthcaresystems. AnnEmergMed.2022;79(2):158–67.
P.QuincyMoore,MD*†
KaitlinEllis,MD‡
PatriciaSimmer,MD§
MweyaWaetjen,BA∥
EllenAlmirol,MPH,MA¶
ElizabethSalisbury-Afshar,MD,MPH#**
MaiT.Pho,MD,MPH††
*PermanenteMedicalGroup,Oakland,California
† KaiserPermanenteOaklandMedicalCenter,Departmentof EmergencyMedicine,Oakland,California
‡ BrownUniversity,DepartmentofObstetricsandGynecology, Providence,RhodeIsland
§ UniversityofChicago,DepartmentofMedicine,Chicago,Illinois
∥ UniversityofChicagoPritzker,SchoolofMedicine,Chicago,Illinois
¶ UniversityofChicago,ChicagoCenterforHIVElimination, Chicago,Illinois
# UniversityofWisconsin-Madison,SchoolofMedicineandPublic Health,DepartmentofFamilyMedicineandCommunityHealth, Madison,Wisconsin
**UniversityofWisconsin-Madison,SchoolofMedicineandPublic Health,DepartmentofPopulationHealthSciences,Madison,Wisconsin
†† UniversityofChicago,DepartmentofMedicine,SectionofInfectious DiseasesandGlobalHealth,Chicago,Illinois
SectionEditor:R.GentryWilkerson,MD
Submissionhistory:SubmittedMarch16,2023;RevisionreceivedJanuary24,2023;AcceptedFebruary9,2024
ElectronicallypublishedMay21,2024
Fulltextavailablethroughopenaccessat http://escholarship.org/uc/uciem_westjem
DOI: 10.5811/westjem.17979
Introduction: Toexpandaccesstonaloxone,thestateofIllinoisimplementedastandingorderallowing registeredpharmaciestodispensethedrugwithoutanindividualprescription.Toparticipateunderthe standingorder,pharmacieswererequiredtooptinthroughaformalregistrationprocess.Inourstudywe aimedtoevaluatetheavailabilityandpriceofnaloxoneatregisteredpharmacies.
Methods: Thiswasaprospective,de-identified,cross-sectionaltelephonesurvey.Trainedinterviewers posedaspotentialcustomersandusedastandardizedscripttodeterminetheavailabilityofnaloxone betweenFebruary–December,2019.Theprimaryoutcomewasdefinedasapharmacyindicatingit carriednaloxone,currentlyhadnaloxoneinstock,andwasabletodispenseitwithoutan individualprescription.
Results: Of948registeredpharmacies,886(93.5%)weresuccessfullycontacted.Ofthose,792(83.4%) carriednaloxone,659(74.4%)hadnaloxoneinstock,and472(53.3%)allowedpurchasewithouta prescription.Naloxonenasalspray(86.4%)wastheformulationmostcommonlystocked.Chain pharmaciesweremorelikelytocarrynaloxone(adjustedoddsratio[aOR]3.16,95%confidenceinterval [CI]1.97–5.01, P < 0.01)andhavenaloxoneinstock(aOR2.72,95%CI1.76–4.20, P < 0.01),butnomore likelytodispenseitwithoutaprescription.Pharmaciesinhigherpopulationareas(aOR0.99,95%CI 0.99–0.99, P < 0.05)andruralareasadjacenttometropolitanareas(aOR0.5,95%CI025–0.98, P < 0.05) werelesslikelytohavenaloxoneavailablewithoutaprescription.Associationsofnaloxoneavailability basedonotherurbanicitydesignations,overdosecount,andoverdoseratewerenotsignificant.
Conclusion: AmongpharmaciesinIllinoisthatformallyregisteredtodispensenaloxonewithouta prescription,theavailabilityofnaloxoneremainslimited.Additionalinterventionsmaybeneededto maximizethepotentialimpactofastatewidestandingorder.[WestJEmergMed.2025;26(1.1)71–78.]
Theriseofopioid-relatedoverdosehashadadevastating effectoncommunitiesacrosstheUnitedStates.In2020alone, over68,000peoplediedfromopioid-relatedoverdose,ofwhich almost3,000occurredinthestateofIllinois.1,2 Therapidly evolvingdrugmarket,withtheintroductionoffentanyl, fentanylanalogues,andxylazineintotheillicitdrugsupply,has contributedtotheincreasingopioidoverdosefatalityrates, with64%ofUSdrugoverdosedeathsduringMay2020–April 2021involvingillicitlymanufacturedfentanyl.3–5
Inresponsetotheopioidoverdoseepidemic,amultiprongedapproachhasbeenenactedtoreducemorbidityand mortality.Amongtheseareseveralharmreduction strategies,includingsyringeserviceprograms,infectious diseasescreening,drugchecking(eg,fentanyltest-strip distribution),supervisedconsumptionsites,anddistribution ofnaloxone.Multiplestudieshavedemonstratednaloxone’ s abilitytobeusedeffectivelyandappropriatelybypeople withnoformalmedicaltraining.6 Forexample,Enteenetal foundthatofthe24%ofpatientswhoreturnedfornaloxone refillsoverasix-yearperiod,11%ofthosereportedusing naloxoneduringanoverdoseevent,withan89%successrate ofoverdosereversal.7 Further,studieshaveshownthat naloxonedistributiondoesnotleadtoincreasedopioid consumptionandmayevenleadtodecreaseduse.7,8 Recognizingitssafetyandefficacy,theUSSurgeonGeneral issuedanadvisorynoticein2018encouragingitsuseand availability.9 Despitewidespreadsupportbyleading healthcareorganizationsandfederalagencies,naloxone accessremainslimited,andopportunitiestohelpindividuals atriskforoverdosearefrequentlymissed.10,11
Asof2017,all50stateshadpassedlegislationexpanding publicaccesstonaloxone.12 Inadditiontolegislation protectingagainstcivil,criminal,orprofessionalliabilityfor bothprescribersandlayadministratorsofnaloxone,some stateshaveintroducedpoliciestoincreasetheaccessibilityof thelife-savingdrug.Studieshavedemonstratedthat pharmacistsarewillingtoprovidenaloxonetothepublic underastandingorderorothersimilarprocess(Stewartetal, 2018;Nielsenetal,2016;Greenetal,2017).Toexpand accesstonaloxone,theIllinoisDepartmentofPublicHealth (IDPH)implementedastatewidestandingorderin2017 (PublicAct99–0480),allowingregisteredpharmaciesto distributenaloxonetopatientswithoutanindividual prescriptionintheirname.ToregisterundertheIllinois NaloxoneStandingOrder,licensedpharmaciesmust participateinapre-approvedtrainingandagreetoreport anydispensednaloxonetotheIllinoisPrescription MonitoringProgram.13
Illinoisisnowoneof49statesthatallowpharmaciststo dispensenaloxonewithoutapatient-specificprescription fromaclinician,44ofwhichuseastandingorder.14 Despite this,studiesfromotherstateshaveshownlimiteduptakeof
PopulationHealthResearchCapsule
Whatdowealreadyknowaboutthisissue?
Moststatesoffernaloxoneatpharmacies withoutaprescription,butuptakeislimited.
Whatwastheresearchquestion?
Whichpharmaciesregisteredunderthe IllinoisNaloxoneStandingOrder hadnaloxoneavailablewithout aprescription?
Whatwasthemajor findingofthestudy?
Only53.3%ofregisteredpharmacies(1/8 th of allIllinoispharmacies)hadnaloxoneinstock andavailablewithoutaprescription.
Howdoesthisimprovepopulationhealth?
Statewidestandingordersareanimportant butinsuf fi cientsteptowardwidespread naloxonepossession.Moreeffortisneededto improveparticipation.
thesenewprotocolsandwidevariationsinavailabilityof naloxoneatregisteredpharmacies.15–22 Inthiscrosssectionalstudyweaimedtoevaluatetheaccessibilityof naloxoneatpharmaciesregisteredunderthestatewide standingorderbydeterminingwhichpharmaciesreported routinelycarryingnaloxone,whichpharmacieshad naloxonecurrentlyinstock,whichpharmacieswerewilling todispensenaloxonewithoutaprescription,which formulationswerecarried,andtheout-of-pocketcostof naloxone.Ourprimaryoutcomewastodeterminewhich pharmacieshadnaloxoneavailablewithoutaprescriptionon thedayoftheinquiry.Wefurthercomparedpharmacies’ naloxoneavailabilitybypharmacytype(chainvsnon-chain), urbanicity,populationofZIPCode,andopioidoverdose ratesinthepharmacies’ surroundingregion.Thisstudy expandsontheexistingliteraturebyusingasamplethat includedallpharmaciesthatoptedintoregisteringunderthe IllinoisNaloxoneStandingOrder.Wealsoanalyzedfactors thatmayaffectthelikelihoodthatapharmacyhadnaloxone availablewithoutaprescription,whichwasrarelydonein previousstudies.
Aprospective,anonymous,cross-sectional “secretshopper” telephonesurveysamplingallIllinoispharmacies
thathadregisteredunderthestate-levelstandingorderwas performedbysixtrainedcallers.Thelistofpharmacies registeredunderthestandingorderwasaccessedon February17,2019(Chicago)andMay23,2019(remainder ofIllinois)viatheIDPHOpioidDataDashboard.2 Thelist ofpharmacies,theircities,andtheircontactnumberswere transposedfromthedashboardintoanExceldocument (MicrosoftCorp,Redmond,WA)fortrackingpurposes.For eachpharmacy,weobtainedaZIPCodeandevidenceof continuedoperationviaGooglesearches.Ifapharmacywas foundtonolongerbeinexistence,thepharmacywasmarked asunabletocontact.
Sixstudypersonnel(oneattendingphysician,oneresident physician,threemedicalstudents,andonemaster’slevel researchassociate)underwentthreehoursoftraining consistingofreviewingthecallscript,discussingthelogic behindeachquestion,discussingspecificlanguagetouse,and conductingatleastthreepilotcallstopharmaciesnot includedinthestudysample.Pilotcallsweredebriefedas agroup.
Thecallersposedaspotentialcustomersanduseda standardizedscripttoasktargetedquestions.Callers followedautomatedpromptsorrequestedtobeconnectedto thepharmacy.Callersspokewithwhicheverpharmacystaff firstansweredthecallandcontinuedtousethescriptifthe callwastransferredtootherpharmacystaff.Ifplacedon hold,thecallerwaitedupto10minutesbeforeterminating thecall.Ifthecallwasinterruptedorthepharmacywas unreachableontheinitialattempt,thepharmacywas contacteduptotwoadditionaltimes.Ifapharmacywas unreachablethreetimes,itwasconsideredinactiveandnot includedinouranalyses.Callswerecompletedfrom February–December2019.Datawascollectedeitherdirectly intoREDCap9.5.35LTS(ResearchDataCapturehostedat UniversityofChicagoMedicine)orintoMicrosoftExceland latertransposedintoREDCap.
Thescriptforthecallswascreatedusinganiterative processbythegroupofinvestigators.Wedesignedthescript toaddressthestudyquestionswhilemaintainingthe appearanceofalaycaller.Thegenericnameofthe medication(naloxone)wasusedinitially.Ifstaffseemed uncertainofthemedicationinquestion,thebrandnameof Narcanwasusedafter firstrepeatingthegenericname.See Appendix1forthescriptforthesecret-shoppertelephone surveyofpharmaciesthatareregisteredundertheIllinois NaloxoneStandingOrder.
Wecollectedcharacteristicsforeachpharmacybasedon pharmacytype,urbanicity,populationofpharmacyZIP Code,andtheoverdoserateinthepharmacyZIPCode. Pharmacieswereclassifiedas “chain” iftheyhadfouror
morelocationsundersharedownership,and “non-chain” if theyhadfewerthanfourlocations.15,16 Wedefined urbanicityusingtheUSDepartmentofAgriculture2013 Rural-UrbanContinuumCodes(RUCC)thatassign countiesascoreonascaleof1-9basedoncountypopulation sizeandadjacencytoametropolitanarea.17 Ascommonly practicedelsewhereintheliterature,wedividedthis continuumintothreegroups:1)urban;2)ruraladjacenttoa metropolitanarea;and3)ruralandnonadjacenttoa metropolitanarea.
WeusedZIPCodescorrespondingtoeachpharmacyto analyzethedatausingoverdoseratesandpopulation. Numberofcombinedfatalandnon-fatalopioid-related overdoseeventsin2018byZIPCodewasobtainedfromthe IDPHOpioidDashboard.2 WeobtainedpopulationbyZIP Codefor2018fromtheUSCensusBureau.18 Usingthe populationsizeandthenumberofoverdoses,wecalculateda 2018rateofcombinedfatalandnon-fatalopioid-related overdoseper10,000peopleforeachZIPCodeinoursample.
Weperformedbivariateanalysestodeterminewhether differencesinnaloxoneavailabilityonthedayofthecallwere significantlydifferentbasedonthefollowingcovariates: pharmacytype;urbanicityusingRUCCcode;populationof pharmacyZIPCode;andthe2018overdosecountand overdoserateper10,000residentsinthepharmacyZIP Code.WeanalyzeddatausingSTATAMPv17statistical softwarerelease15(StataCorp,LLC,CollegeStation,TX). ThisstudywasreviewedbytheUniversityofChicago InvestigationalReviewBoardanddeterminedtobeexempt fromreview.
Weidentified948pharmaciesregisteredundertheIllinois NaloxoneStandingOrderandsuccessfullycontacted886 (93.5%)(Figure1).Ofthe886pharmaciesthatwere successfullycontacted,806(91.0%)werechainpharmacies and80(9.0%)werenon-chain.Ofthe886contacted pharmacies,807(91.1%)werelocatedinurbanZIPCodes, 57(6.4%)inruralZIPCodesadjacenttoametropolitanarea, and22(2.5%)inruralZIPCodesthatwerenonadjacenttoa metropolitanarea.Additionally,ofthecontacted pharmacies,792(89.4%)reportedcarryingnaloxone,with 659(74.4%)reportingthemedicationtobeinstockatthe timeofthecall,and472(53.3%)respondingthatthecaller didnotneedaprescriptionfromadoctortopurchasethe naloxone.The472pharmacies(53.3%)thatcarried naloxone,hadnaloxoneinstock,andofferednaloxone withoutrequiringaprescriptionwereconsideredpositivefor theprimaryoutcome.Pharmacycharacteristicsare summarizedin Table1
Figure2 displaysthecascadeofnaloxoneavailabilityby pharmacytypeandRUCC.PharmaciesinurbanRUCC
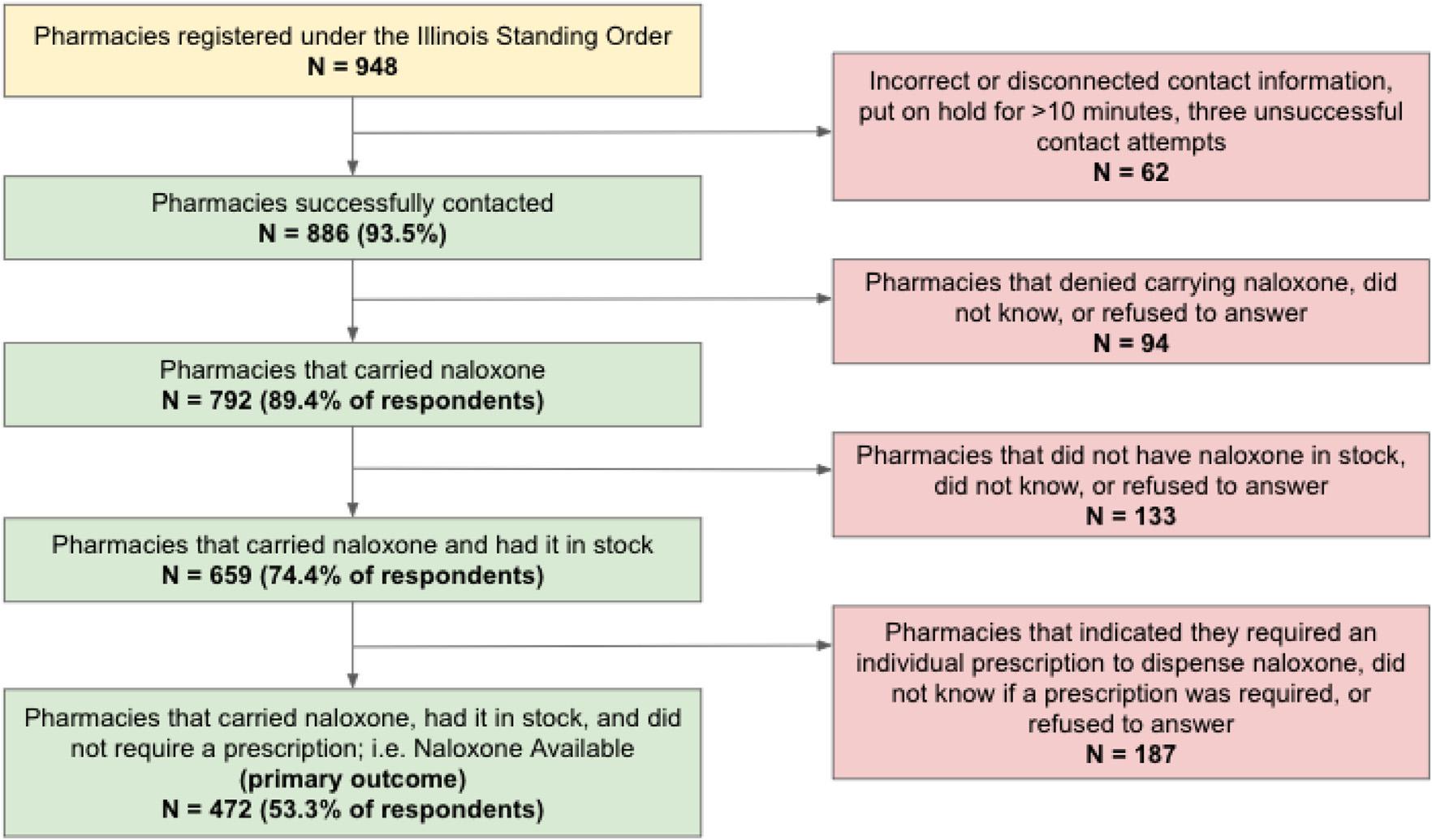
Figure1. AvailabilityofnaloxoneandneedforaprescriptioninIllinoispharmaciesregisteredundertheIllinoisNaloxoneStandingOrder.
Table1. Pharmacytype,urbanicity,andnaloxoneavailabilityofpharmaciesregisteredundertheIllinoisNaloxoneStandingOrderthatwere successfullycontacted(n = 886).
Successfully contacted, n = 886(Col%)
Carry Naloxone n = 792(Row%)
CarryNaloxone, instock n = 659(Row%)
Naloxoneavailable withoutaRx, n = 472(Row%)
Pharmacytype
Chain(CVS,Walgreens)806(91.0%)728(90.3%)611(83.9%)432(70.7%)
Non-chain(Independent)80(9.0%)64(80.0%)48(75.0%)40(83.3%)
RUCC
Urban807(91.1%)720(89.2%)599(83.2%)433(72.2%)
Ruraladjacenttoa metropolitanarea
57(6.4%)52(91.2%)43(82.7%)28(65.1%)
Ruralandnonadjacenttoa metropolitanarea 22(2.5%)20(90.9%)17(85.0%)11(64.7%)
Rx,prescription; RUCC,Rural-UrbanContinuumCodes.
codeshadthehighestnaloxoneavailabilitywithouta prescription(63.7%).Alargerproportionofchain pharmaciescarriednaloxone(90.3%)comparedtononchainpharmacies(80.0%)(P < 0.01).Ofthe772pharmacies thatstockednaloxoneandprovidedaresponsetothetypeof naloxone,624(78.8%)carriednaloxonenasalspray (see Table2).
Intheadjustedanalyses,wefoundthatchainpharmacies hadgreateroddsofcarryingnaloxone(adjustedoddsratio [aOR]3.16,95%confidenceinterval[CI]1.97–5.01, P < 0.01) andhavingnaloxoneinstock(aOR2.72,95%CI1.76–4.20,
P < 0.01)comparedtonon-chainpharmacies(Table3). However,therewerenodifferencesbetweenpharmacytype andnaloxoneavailabilitywithoutaprescription.With regardtoRUCC,ruraladjacenttoametroareahadlower oddscomparedtourbanareasofprovidingnaloxone withoutaprescription(aOR0.50,95%CI0.25–0.98, P = 0.05).WealsoobservedthatmoredenselypopulatedZIP Codeswerelesslikelytohavenaloxoneavailablewithouta prescription(aOR0.99,0.99–0.99, P < 0.01).Neither overdose(OD)countnorODratewereassociatedwith naloxoneavailability.
Figure2. Pharmacytype,countyurbanicity,andnaloxoneavailabilityofpharmaciesregisteredundertheIllinoisNaloxoneStandingOrder thatweresuccessfullycontacted. Rx,prescription.
Table2. Ofthosewhocarrynaloxone,availableformulationsof naloxoneandmedianprice.
Naloxone types N = 722 (%) Medianprice [IQR]
Naloxone nasalspray
624(86.4)$135.99[$89.99,$4,500]
IMvials71(9.8)$39.50[$21.99.$239.00]
Naloxone autoinjector
27(3.8)$4,000[$399.59,$6,000.00]
IQR,interquartilerange; IM,intramuscular.
Standingordersareanimportantsteptowardreducing opioid-relatedmortality,butour findingssuggestthis legislationhasnothadthedesiredeffectinstateresidents’ accesstonaloxone.In2019,twoyearsafterthe implementationoftheorder,therewasanaverageof3,861 licensedpharmaciesstatewide.19 Ofthese,only948(24.6%)
wereregisteredunderthestandingorderatthetimeofour study.Wesuccessfullycontacted91%oftheregistered pharmaciesandfoundthatjustoverhalf(53.3%)had naloxoneavailableonthedayofcontactandappropriately offereditwithoutrequiringaprescription.Giventhatall pharmaciesonourcontactlistunderwentpre-approved trainingtoregisterwithIDPHasanaloxonedistributionsite underthestandingorder,our findingsindicatethereis substantialroomforimprovement.
Studiesfromotherstateswithcomparablestatewide naloxoneaccesspolicieshaveshownlimiteduptakewith widevariationsinavailabilityofnaloxone.Across California,Texas,Pennsylvania,Massachusetts,andNew York,theproportionofpharmaciesthathadnaloxonein stockrangedfrom23.5–70%,withsomevariationbasedon stateandthespecificsampleofpharmaciesstudied.20–24 Few studieshaveanalyzedspecificcharacteristicsthatmayaffect anindividualpharmacy’slikelihoodofhavingnaloxone available.22,25 InPennsylvania,Gravesetalfoundthatchain
Table3. Associationbetweenpredictorsandcarrynaloxone,instock,andnoprescriptionneeded.
Pharmacytype
Non-chain RefRefRef
Chain 3.16(1.97,5.01) <0.012.72(1.76,4.20) <0.01 0.45(0.20,1.00)0.05
RUCC
Urban RefRefRef
Ruraladjacenttoametroarea1.77(0.79,3.98)0.171.27(0.69,2.36)0.44
0.50(0.25,0.98)0.05
Rural,nonadjacenttoametroarea1.16(0.41,3.30)0.781.15(0.47,2.82)0.750.48(0.17,1.36)0.17
PopulationbyZIPCode1.00(0.99,1.00)0.611.00(0.99,1.00)0.40
0.99(0.99,0.99)0.003
ODcount1.00(0.99,1.00)0.741.00(0.99,1.00)0.420.99(0.98,1.00)0.09
ODrate0.99(0.98,1.00)0.160.99(0.99,1.00)0.360.99(0.98,1.00)0.27
Bold, P ≤ 0.05;Adjustedanalysesincludecontrollingforpharmacytype,RUCC,andpopulationbyZIPCode. Rx,prescription; aOR,adjustedoddsratio; CI, confidenceinterval; RUCC,Rural-UrbanContinuumCodes; OD,overdose.
pharmaciesweremorelikelytocarrynaloxone,butODrate andurbanicitydidnotinfluencenaloxoneavailability.22 In Indiana,Meyersonetalfoundthatchainpharmacies, pharmacieswithmorethanonefull-timepharmacist,and thosewherepharmacistshadreceivednaloxone-related continuingeducationwereassociatedwithincreased likelihoodofstockingnaloxone.25
Asystematicreviewofthetopicfoundthata heterogeneousgroupof30studieshadwide-ranging findings, butoverallone-thirdofpharmaciesauditeddidnotcarry naloxoneandalmosthalfdidnotoffernaloxonewithouta prescription.26 Whilepreviousstudieshaveexploredthe availabilityofnaloxoneunderastandingorderindifferent states,analysisoffactorsthatmaycontributetothe likelihoodthatapharmacyhasnaloxoneavailablewithouta prescriptionremainslimited.Ourstudyisalsouniqueforits highresponserateaswellasouruseofasampleincludingall pharmaciesthatoptedintoformalizedtrainingand registrationunderthestandingorder.
Improvedaccesstonaloxonethroughcommunity pharmaciesmaycomethroughmultipleapproaches.First, withlessthanaquarterofpharmaciesregistered,our findings highlighttheneedformorewidespreadparticipationinthe IllinoisNaloxoneStandingOrder.Itappearsthatthepublic goodandthe financialincentivesattachedtoincreased dispensingofnaloxoneareinsufficienttoincentivize pharmaciestotakethestepsnecessarytoregisterunderthe standingorder.Ofnote,IllinoisMedicaidplansarerequired tocoveratleastoneformulationofnaloxone,withthe intranasalformulationthemostcommonlycovered formulation.IllinoisMedicaiddoesnotchargeacopayfor receiptofnaloxone.Additionalincentivesmaybenecessary tomobilizegreaterpharmacyparticipationstatewide.
Ruralareasappearedtohaveparticularlypooraccessto naloxonethroughcommunitypharmacies.While11.5%of Illinoisresidentsliveinruralareas,wefoundthatonly22 (2.3%)ofthepharmaciesregisteredunderthestandingorder wereinruralareas.27 Whiletherewasnosignificant differenceintheprimaryoutcomeinruralvsurban pharmacies,theoverallpaucityofregisteredpharmaciesin ruralareashighlightsalackofaccessthatmayputrural peoplewhousedrugsathigherriskofdeathfromoverdose. Thismayfurtherexacerbatethedisproportionateimpactof theopioidcrisisonruralareas.28,29
Oftheregisteredpharmacieswecontacted,our findings highlightspecifictrendsthatmayinformeffortstoimprove accesstonaloxone.Wefoundthatchainpharmacieswere morelikelythannon-chainpharmaciestocarrynaloxone andhaveitinstockbutwerenomorelikelytohaveitinstock withoutaprescriptionrequired.Thissuggeststhatthereare policiesuniquetochainpharmaciesthatfacilitateregistering underthestandingorderandstockingnaloxone,butthat perhapstrainingforcustomer-facingstaffhasbeen inadequate.Thisledultimatelytosimilaroutcomestonon-
chainpharmacieswhenitcametocustomersseekingto purchasenaloxonewithoutaprescription.These findings havesomeconsistencywithonePennsylvaniastudy,which foundchainpharmaciestobemorelikelytocarrynaloxone andanswerquestionscorrectlyaboutthestandingorderfor naloxone.22 Chainpharmaciesmayhavemorestandardized trainingprogramsforcertainstaffmembers,maintain robustsupplychainsfornaloxone,orhaveastronger responsetopublicpressuretocontributetoreducingopioidrelateddeaths.
Therewasnostatisticallysignificantassociationbetween thenumberorrateofODsinaZIPCodeandlikelihoodof naloxoneavailability.This findingsuggeststhattheremaybe additionaloutreachorincentivesnecessarytoencourage pharmaciesinareaswiththehighestratesofODtoincrease accesstonaloxoneviathestandingorder.
Costandavailableformulationmayhaveasignificant impactonhowlikelyacustomeristoobtainnaloxone.Inour sample,bothcostandformulationwerevariable.The majorityofpharmaciesthathadnaloxoneinstockcarried thenasalnaloxonespray(brandnameNarcan)foran averagecostof$135.99foratwo-pack.WhileIllinois Medicaidplanscoveratleastoneformulationofnaloxone withoutcopay,privateinsuranceandMedicarePartDplans havevariablecopaystructuresandformulationcoverage. Foruninsuredindividuals,thosewhodon’twanttousetheir insuranceto fillthismedication,orthoseforwhomnaloxone isnotacoveredmedication,theout-of-pocketcostmaybea significantdeterrenttoobtainingnaloxone.Vialsof naloxone,whichcanbeusedwithaneedleandsyringeand injectedintramuscularly,orwithanatomizerfornasal administration,hadalowermedianpriceof$39.50;however, only9%ofpharmacieshadthisformulationinstock,andthe availabilityandcostofothernecessarysuppliessuchas syringes,intramuscularneedles,and/ornasalatomizerswas unclear.Wedobelievethatsomeofthehighpricesthatwere reportedbypharmacystaffareinaccurateandforthisreason wepresentthemedianprice,whichwebelieveaccurately reflectswhatmostconsumerswouldpayoutofpocket. Ourstudyhighlightstheneedforadditionalstrategiesto maximizeaccesstonaloxone.Giventhatruralareasareless likelytohavecommunity-basednaloxonedistribution(often aserviceofferedatharmreduction/syringeservice programs),thisneedisparticularlygreatinruralareas.30–32 Futureresearchisneededtounderstandwhethernaloxone availabilityinpharmaciesisassociatedwithincreased utilizationand,ifso,howtoincreaseavailabilityofnaloxone viastandingorderinretailpharmacies.Possible considerationscouldincludethefollowing:publiceducation campaignsthatwouldworktoincreasedemandfornaloxone inpharmacies,therebyencouragingpharmaciestoregister andstocknaloxone;offering financialincentivesorother publicrecognitionforpharmaciesthatregisterforthe standingorderandstocknaloxoneformulations;and
improvedpublichealthoutreachandeducationalprograms (eg,academicdetailing)toincreaseawarenessamong pharmacies,pharmacists,andpharmacystaffaboutthe purposeofandevidencebaseofnaloxoneasitrelatesto reducingopioid-relatedmortalityatthecommunitylevel.
Researchhasfoundthatpharmacists’ discomfort dispensingnaloxonetocustomersremainsanimportant barrierandoftenresultsfrominadequatetraining(Green, 2017;Thornton,2017;Rudolph,2018).AsofNovember20, 2017,only19stateshadmandatednaloxoneeducationfor pharmacists(Roberts,2019).33 Illinoisregulationrequires participatingpharmaciststocompleteanIllinois DepartmentofHumanServices-approvedtrainingmodule orto “understandtheNaloxoneStandardizedProcedures” andwatchtwotrainingvideos(IDPHNaloxoneFAQ),butit isunclearhowmuchofthistrainingispassedalongtostaff whodirectlyinteractwithcustomers.Onestudycomparing trainingmaterialprovidedbystatesfoundthatwhilemost materialcoveredthepurposeanduseofnaloxoneaswellas thestandingorderlegislation,fewprovidedthorough educationonhowtocommunicatethisinformationto customers(Carpenter,2018).Overall,whiletherehasbeen anincreaseinnaloxonedispensedacrossallstateswith expandedaccesspolicies,retailpharmacynaloxone distributionisstillunderusedandvariesstateby state(Xu,2018).
Ourstudyhasseverallimitations.Wedidnotclarifythe roleofthestaffmemberwithwhomwewerespeaking.Itis possiblethatifwehadaskedtospeakdirectlytothe pharmacist,wewouldhaveobtainedmoreaccurate information;however,wefeltitwasmostusefultomimica morenaturalconsumerinteraction.Itispossible,however, thatresponseswouldvarybetweenstaffmembersatan individualpharmacy.Informationmayalsohavebeenmore accuratehadweidentifiedourselvesasacademicresearch staff.Fiveofsixcallershadatleastsomemedical background,butwebelievethatotherstudiescouldachieve thesamegoalinananalogousstudyusingstaffwithno medicalbackground.
Wedidnotcallpharmaciesthatwerenotlistedonthe IDPHwebsite;sofutureresearchmayincludeanalysisofthe percentageoftotalpharmaciesindifferentregionsthatoffer naloxone.Wecollectedonlyinformationaboutout-ofpocketcost,whichislikelyonlyrelevanttopatientswithout insurance,thosewhodon’twanttouseinsurancewhen receivingnaloxone,orthosewithoutnaloxoneincludedin theirpharmacybenefit.Lastly,andperhapsmostrelevantto futureresearch,werecognizethatavailabilityofnaloxonein retailpharmaciesmaynotdirectlycorrelatewithincreased utilizationbypeoplewhousedrugs(PWUD).Futurestudies shouldincorporateinputfromPWUDtodelineate preferencesinsourcesofnaloxone.
Wefoundthattwoyearsafterimplementationofthe IllinoisNaloxoneStandingOrder,onlyone-eighthofall pharmacieshadnaloxoneinstockandavailablewithouta prescription.Withinthisgroup,chainpharmaciesweremore likelytocarrynaloxoneandhaveitinstockbutwerenomore likelytoprovideitwithoutaprescription.Pharmaciesin moredenselypopulatedZIPCodesandthosewithaRuralUrbanContinuumCodereflectingruralareasthatare adjacenttometroareaswerelesslikelytohavenaloxone availablewithoutaprescription.Overdoseratesinthe surroundingcommunityhadnoeffectonnaloxone availability.Ourstudyillustratesauniquesampleofall pharmaciesstatewidethathavegonethroughformaltraining andregistrationunderthestandingorder.
Increasedaccesstonaloxoneinretailpharmaciesin Illinoiswillrequireimprovedeffortsrelatedtoawarenessand implementationofthestandingorder,aswellasfurther investigationintothereasonsthatapharmacythathasgone throughtheprocessofapplyingtobeabletousethestanding orderdoesnotreliablystocknaloxoneandmakeitavailable withoutprescription.Specificattentionshouldbe giventoareaswherethereislimitedaccesstonaloxone throughcommunity-baseddispensingprograms andwhereratesofoverdoseandpotentialforimpact arehighest.
AddressforCorrespondence:P.QuincyMoore,KaiserPermanente OaklandMedicalCenter,DepartmentofEmergencyMedicine,3600 Broadway,Oakland,CA94611.Email: paul.q.moore@kp.org
ConflictsofInterest:Bythe WestJEMarticlesubmissionagreement, allauthorsarerequiredtodiscloseallaffiliations,fundingsources and financialormanagementrelationshipsthatcouldbeperceived aspotentialsourcesofbias.Noauthorhasprofessionalor financial relationshipswithanycompaniesthatarerelevanttothisstudy. Therearenoconflictsofinterestorsourcesoffundingtodeclare.
Copyright:©2024Mooreetal.Thisisanopenaccessarticle distributedinaccordancewiththetermsoftheCreativeCommons Attribution(CCBY4.0)License.See: http://creativecommons.org/ licenses/by/4.0/
1.NationalInstituteonDrugAbuse.Drugoverdosedeathrates.2023. Availableat: https://nida.nih.gov/research-topics/trends-statistics/ overdose-death-rates.AccessedJanuary19,2022.
2.IllinoisDepartmentofPublicHealth.IDPHdata.Availableat: https://dph. illinois.gov/topics-services/opioids/idph-data-dashboard.html AccessedJanuary19,2022.
3.O’DonnellJ,TanzLJ,GladdenRM,etal.Trendsinandcharacteristicsof drugoverdosedeathsinvolvingillicitlymanufacturedfentanyls-United States,2019–2020. MorbMortalWklyRep.2021;70(50):1740–6.
4.KariisaM,PatelP,SmithH,etal.Notesfromthe field:xylazinedetection andinvolvementindrugoverdosedeaths-UnitedStates,2019. MorbMortalWklyRep.2021;70(37):1300–2.
5.ChhabraN,MirM,HuaMJ,etal.Notesfromthe field:xylazine-related deaths-CookCounty,Illinois,2017–2021. MorbMortalWklyRep 2022;71(13):503–4.
6.WalleyAY,XuanZ,HackmanHH,etal.Opioidoverdoseratesand implementationofoverdoseeducationandnasalnaloxonedistribution inMassachusetts:interruptedtimeseriesanalysis. BMJ 2013;346:f174.
7.EnteenL,BauerJ,McLeanR,etal.Overdosepreventionandnaloxone prescriptionforopioidusersinSanFrancisco. JUrbanHealth. 2010;87(6):931–41.
8.BazaziAR,ZallerND,FuJJ,etal.Preventingopiateoverdosedeaths: examiningobjectionstotake-homenaloxone. JHealthCarePoor Underserved.2010;21(4):1108–13.
9.OfficeoftheSurgeonGeneral.U.S.SurgeonGeneral’sAdvisoryon NaloxoneandOpioidOverdose.2018.Availableat: https://www.hhs. gov/surgeongeneral/priorities/opioids-and-addiction/naloxoneadvisory/index.html.AccessedJanuary1,2020.
10.GuyGPJr.,HaegrichTM,EvansME,etal.Vitalsigns:pharmacy-based naloxonedispensing UnitedStates,2012–2018. MorbMortalWkly Rep.2019;68(31):679–86.
11.FollmanS,AroraVM,LyttleC,etal.Naloxoneprescriptionsamong commerciallyinsuredindividualsathighriskofopioidoverdose. JAMA NetwOpen.2019;2(5):e193209.
12.TheNetworkforPublicHealthLaw.Legalinterventionstoreduce overdosemortality:naloxoneaccesslaws.2021.Availableat: https:// www.networkforphl.org/wp-content/uploads/2021/05/NAL-Final-4-29. pdf.AccessedJune7,2022.
13.IllinoisDepartmentofPublicHealth.IDPH-NaloxoneStandingOrder Form.Availableat: https://idph.illinois.gov/Naloxone/ AccessedJune7,2022.
14.PrescriptionDrugAbusePolicySystem(PDAPS).Availableat: http:// www.pdaps.org/datasets/laws-regulating-administration-ofnaloxone-1501695139.AccessedJune7,2022.
15.SchommerJC.APhAcareerpathwayevaluationprogramforpharmacy professionals2012.2013.Availableat: https://aphanet.pharmacist. com/sites/default/files/files/Profile_06%20Chain%20pharmacy% 20Final%20071713.pdf.AccessedJanuary19,2022.
16.HatemiPandZornC.IndependentpharmaciesintheU.S.aremoreon therisethanonthedecline.2020.Availableat: https://www.pcmanet. org/wp-content/uploads/2020/03/FINAL_Independent-Pharmaciesin-the-U.S.-are-More-on-the-Rise-than-on-the-Decline.pdf AccessedJanuary19,2022.
17.U.S.DepartmentofAgricultureEconomicResearchService.RuralUrbanContinuumCodes.2020.Availableat: https://www.ers.usda.gov/ data-products/rural-urban-continuum-codes/documentation/ AccessedJanuary19,2022.
18.U.S.CensusBureau.Availableat: https://www.census.gov/ AccessedJune7,2022.
19.SmithSteven.IllinoisDepartmentofFinancialandProfessional Regulation.PublishedonlineFebruary1,2023.
20.PuzantianTandGasperJJ.Provisionofnaloxonewithoutaprescription byCaliforniapharmacists2yearsafterlegislationimplementation. JAMA.2018;320(18):1933–4.
21.EvoyKE,HillLG,GroffL,etal.Naloxoneaccessibilitywithouta prescriberencounterunderstandingordersatcommunitypharmacy chainsinTexas. JAMA.2018;320(18):1934–7.
22.GravesRL,AndreyevaE,PerroneJ,etal.Naloxoneavailabilityand pharmacystaffknowledgeofstandingorderfornaloxonein Pennsylvaniapharmacies. JAddictMed.2019;14(4):272–8.
23.StopkaTJ,DonahueA,HutchesonM,etal.Non-prescriptionnaloxone andsyringesalesinthemidstofopioidoverdoseandhepatitis Cvirusepidemics:Massachusetts,2015. JAmPharmAssoc(2003) 2017;57(2S):S34–44.
24.CorrealA.Overdoseantidoteissupposedtobeeasytoget.It’sNot. 2018.Availableat: https://www.nytimes.com/2018/04/12/nyregion/ overdose-antidote-naloxone-investigation-hard-to-buy.html AccessedJanuary1,2020.
25.MeyersonBE,AgleyJD,DavisA,etal.Predictingpharmacynaloxone stockinganddispensingfollowingastatewidestandingorder,Indiana 2016. DrugandAlcoholDependence.2018;188:187–92.
26.LaiRK,FriedsonKE,RevelesKR,etal.Naloxoneaccessibilitywithout anoutsideprescriptionfromU.S.communitypharmacies:asystematic review. JAmPharmAssoc(2003).2022;62(6):1725–40.
27.U.S.CensusBureau.2010CensusofPopulationandHousing, PopulationandHousingUnitCounts,CPH-2-15.2012.Availableat: https://www2.census.gov/library/publications/decennial/2010/cph-2/ cph-2-15.pdf.AccessedFebruary2,2023.
28.JenkinsRA,WhitneyBM,NanceRM,etal.TheRuralOpioidInitiative Consortiumdescription:providingevidencetounderstandthefourth waveoftheopioidcrisis. AddictSciClinPract.2022;17(1):38.
29.BergoCJ,EpsteinJR,HoferkaS,etal.AVulnerabilityassessmentfora futureHIVoutbreakassociatedwithinjectiondruguseinIllinois, 2017–2018. FrontSociol.2021;6:652672.
30.WhiteHouseOfficeofNationalDrugControlPolicy(ONDCP).Vermont DrugControlUpdate.Availableat: https://obamawhitehouse.archives. gov/sites/default/files/docs/state_profile_-_vermont_0.pdf AccessedJune7,2022.
31.BuerLesly-Marie. RXAppalachia:StoriesofTreatmentandSurvivalin RuralKentucky.Chicago,IL:HaymarketBooks;2020.
32.OstrachB,BuerLM,ArmbrusterS,etal.COVID-19andruralharm reductionchallengesintheUSsouthernmountains. JRuralHealth 2021;37(1):252–5.
33.LegislativeAnalysisandPublicPolicyAssociation.NaloxoneAccess: SummaryofStateLaws.2020.Availableat: https://legislativeanalysis. org/wp-content/uploads/2020/10/Naloxone-summary-of-state-lawsFINAL-9.25.2020.pdf.AccessedFebruary3,2023.