

VENEERS A 2 Ω
digital dentistry meets aesthetic excellence
Presented by Dr Angelo Lazaris
SYDNEY | AUSTRALIA • APRIL 4-5, 2025

Dr Angelo Lazaris is renowned as the doyen of dental veneers... Celebrities, professionals, billionaires and every day Australians seek out Dr Lazaris when they want outstanding aesthetic excellence...
In the ALPHA TO OMEGA OF VENEERS, Dr Lazaris shares his unique, aesthetically-driven protocols and digital workflows as a unified system developed specifically to enhance clinical efficiency and predictability and eliminate any margin for error. Structured in a modular sequence, each topic is delivered as a step in a methodical, reverse-engineering process that maps out a logical pathway to achieving superior treatment outcomes with precision and confidence. Honed through comprehensive critical analysis and evolution, these protocols are universally applicable to every dentist, every patient and every case...
VENEERS are the #1 requested cosmetic dentistry procedure - LEARN TO DELIVER EXCELLENCE!







Dr Angelo Lazaris
BDS (Hons) (Syd), MSc (Aes) (Kings College)
Angelo has developed his own complete digital protocols from inception and design through to delivery and integrated these with biomimetic adhesive dentistry and contemporary restorative materials to create a complete clinical workflow that is equally applicable to single restorations, through to complex full mouth rehabilitations, culminating in outstanding clinical outcomes in a real-world commercial environment. His innovative approach to clinical dentistry is to start at the desired
endpoint, deconstruct complex treatments and develop solutions have made him a sought after KOL, educator and mentor. With appointments including honorary senior lecturer for Kings College London and the University of Sydney, Angelo has recently been assigned as course director for a post graduate diploma and masters degree in digital dentistry; a testament to his expertise and the influence of this discipline in dental practice.

Tips, Tricks and Pitfalls in Implant Dentistry
The specialist perspective on common surgical and restorative quandaries
SYDNEY • MARCH 7-8, 2025
Presented by Specialists Prof. Axel Spahr and Dr Tom Giblin


Professor Axel Spahr
Specialist Periodontist in Private Practice and Head of the Discipline of Periodontics and Program Director of the Doctor of Clinical DentistryPeriodontics post-graduate program at The University of Sydney Dental School.
Doctor Thomas Giblin
Specialist Prosthodontist in Private Practice
President, International Congress of Oral Implantologists, Diplomate ICOI, Board Member of Australian Society of Implant Dentistry (ASID), Member of ADA, ACP, IAG, AARD.
This advanced course is tailored for dentists with prior experience in implant surgery, aiming to further refine their expertise and clinical proficiency. The program is designed to deepen participants’ understanding and enhance their skills in both the surgical and restorative aspects of implant procedures. It emphasizes essential clinical topics to optimise outcomes and success rates, including practical insights into common challenges and solutions.




DAY ONE - FRIDAY MARCH 7
Surgical Considerations
n Patient selection and comprehensive treatment planning.
n The effects of systemic diseases and medications on surgical outcomes, healing and implant success.
n Risk assessment (SAC), and the influence of implant type, material, surface characteristics and implant/abutment connections.
n The use of short and reduced-diameter implants.
n Guidelines for implant planning, key parameters and management of peri-implant tissues.
n Immediate, early and late implant placement strategies.
n One-stage versus two-stage implant surgery techniques.
n Surgical instruments, materials, and common complications.
n Freehand versus guided implant placement methods.
n Implant maintenance to avoid problems.


DAY
TWO - SATURDAY MARCH 8
Prosthetic Considerations
n Evaluating the digital workflow in implant dentistry: practical benefits versus technological novelty.
n Digital shade analysis and lab communication.
n Prosthetic design single / bridge /full arch / removable.
n Restorative materials.
n Impressions vs scanning.
n Optical and biomechanical properties of natural teeth and restorative materials and why it matters.
n Restoration design and preparation geometry.
n Fitting and delivery of indirect adhesive restorations.
n Verification of treatment sequences and outcome validation.
n Breaking down complex cases with novel solutions to restorative dilemmas.
n Practical clinical applications and case studies. Supported by










On the cover...
Digital Dentistry & Dental Technology 2025 is on again on August 1-2 at the newly renovated Novotel Sydney Brighton Beach. Join us for 2 days of the latest and greatest digital dentistry has to offer. Register Now!


68 How “Cheap Charlie” and “Stingy Sarah” achieved their goals
76 Your role in creating a thriving team
78 Dental corporate myth busters: A defence of the most common objections to dental corporates
80 Boost your business: Why a reliable phone system is key to success marketing
82 Why your marketing sucks (and what to do about it)
www.dentalpractice.com.au facebook.com/dentalpracticenow twitter.com/adpmagazine instagram.com/dentevents READ ME


Publisher & Editor: Joseph Allbeury Clinical Editor: Dr David Roessler Technology Editor: Prof. Laurence J. Walsh Infection Control Editor: Prof. Laurence J. Walsh Senior Contributing Editor: Dr Christopher CK Ho
Columnists: Dr Georges Fast, Dr Jesse Green, Garry Pammer, Phillip Win, Dr David Moffet, Graham Middleton, Simon Palmer, Julie Parker, Jayne Bandy, Angus Pryor Design & Production: Jasper Communications Australasian Dental Practice™ ISSN 1445-5269 is printed in Australia and published six times per year by Main Street Publishing Pty Limited ABN 74 065 490 655 PO Box 586, Cammeray NSW 2062 Tel: (02) 9929-1900 Fax: (02) 9929-1999 Email: info@dentist.com.au © 2025 All rights reserved. The contents of this magazine are copyright and must not be reproduced without the written permission of the publisher. Permission to reprint may be obtained upon application. Correspondence and manuscripts for publication are welcome. Although all care is taken, the editor and publisher will not accept responsibility for the opinions expressed by contributors to this magazine, or for loss or damage to material submitted for publication Subscriptions: Australia and NZ: A$99.00 per year includes OralHygiene™ and eLABORATE™ magazines; Overseas Airmail: A$220.00 per year.



102

Immediate FP1 restoration: Next-level digital full arch revolution
108 Shining 3D photogrammetry workflow with Elite intraoral scanner
The Biodentine™ Bio-Bulk Fill technique for deep caries and moderate pulpitis
surgery design 118 Clifton Hill Dental: A seamless transformation by Medifit



infection control 186 Load release - the logic and structure of checking completed loads 192 A-dec sets standard in infection control
MOCOM streamlines sterilisation at Tomaree Dentistry in coastal NSW
Dürr Hygoclave ideal sterilisation solution


By Joseph Allbeury
IDS, DDDT25, etc...
If the year ends in an odd number, then that also means the world’s biggest and best dental event is on again in Cologne, Germany. IDS 2025, being staged from March 25-29 at the Cologne fair grounds, will again showcase everything dentistry has to offer and then some. Plenty of evolution will be on display and no doubt, revolution too. I’m expecting every man and his dog to be touting the benefits of artificial intelligence in dentistry and it’s already making its mark. Expect lots of automation as well and let’s face it, the two go hand-in-hand. Certainly dental laboratories in Australia and New Zealand, where there is a skilled labour shortage, are embracing systems that can automate mundane, tedious tasks and even allow autonomous 24/7 manufacturing without human presence (All good unless you’re a fan of the Terminator movies which may well predict our future). Lucky or not, this will be my 13th “pilgrimage” to IDS and I’ll look forward to catching up with the countless Australians and New Zealanders who likewise make the trip. It is so much more than just a dental exhibition, it really opens your eyes to how massive the industry in which we work actually is. Certainly for anyone who goes by a bucket-list, go to IDS at least once in your life!
Also on everyone’s bucket-list is Digital Dentistry & Dental Technology 2025 which is now being staged on August 1-2, 2025. After looking at many other venues, we’re again back at the Novotel Sydney Brighton Beach. We love the parking. We love the proximity to the airport. And now we love that the hotel will finally have finished their years-long renovation. The brand new ballroom with water views will be available and the reception and lobby are brand new too. There is also a lobby bar and Cocos Beach Sports Bar. There is the new Ammos Greek Restaurant, Ironbark Steakhouse and a new “Pan-Asian/Fusion” Restaurant. This adds to the Sands Terrace Bar and Restaurant that extends outdoors. The pool complex and outdoor areas are now first class. The owner of the property also now owns Luna Park in Sydney and is committed to excellence. So finally we have a true “destination” for DDDT25
Pushing the event back two months to the start of August both avoids the original dates in what has become a very cluttered May calendar and allows many of the new products being released at IDS to make their way to Australia. We’re working with speakers and sponsors and exhibitors now to create an amazing event in what amounts to a new venue. Expect lots on full arch restorations, digital dentures, 3D printing, milling, CAD and CAM software, artificial intelligence, automation, I/O scanning, 3D facial scanning, milling, photogrammetry, materials, smile design, implantology, CBCT, cosmetic dentistry, aligners, ortho and more. So register now and SAVE before the early bird expires! Enjoy the edition...
Joseph Allbeury, Editor and Publisher
Cap Scanbodies for photogrammetry IOS

Shining 3D has further enhanced its newly released Aoralscan Elite intraoral scanner with photogrammetry by providing an additional set of scanbodies designed for immediate loading cases at no additional cost (existing owners have also received a complimentary set). When scanning following tooth extractions, gingival tissue instability can make it hard to capture accurate data using intraoral scanning. Saliva, blood and soft tissue interference can lead to alignment issues between the coded scanbody and the soft tissue. T hat’s where the new Cap Scanbody comes in to save the day! The Cap Scanbody is specifically designed to solve the common challenges faced during immediate loading cases. It ensures precise alignment between the coded scanbody and soft tissue. Once installed and scanned, the Cap Scanbody is recognised by the scanning software, which converts it into standard CAD data. This data is then seamlessly aligned with the CAD data from the coded scanbody,


ensuring perfect alignment of both postoperative gingival tissue and implant positions—completely eliminating any interference from the soft tissue!
For more information on the Shining 3D Aoralscan Elite, contact Fabdent on 1300-878-336 or visit www,fabdent.com.au.
ADVANCED HEMOSTAT WITH WOUNDHEAL®

RRP $15.33 + gst per dressing*
WOUNDHEAL

For topical applications and internal surgical use. Effective in patients using anticoagulants.
• Water soluble, oxidized-etherified regenerated nanocellulose.
• Biocompatible & pH neutral (~7.2).
• Non expanding hemostat, forming sealing clot & reducing pain.
• Tightly woven matrix of plant fibres.
• No animal derived products.
• 100% absorbable without any residue.
• Easy to use, cut, fold or layer and cost effective.
• Sterile, single use packaging. Minimum 3 years expiry.
How BloodSTOP iX Works:
• Adheres to wet/bleeding surfaces.
• Fast acting bleeding control. Actively initiates clotting cascade.
• Creates physiological environment for proliferation of tissue growth and wound healing.
• Transforms into a sticky translucent gel that adheres to and seals the wound.
• Odourless & tasteless. Can be easily removed by irrigation.
13mm x 50mm *Price current at time of publishing (February 2025). Only available in boxes of 24 dressings. Check the website for exact
• Forms protective layer, preventing contamination.
• Enables easy monitoring of the wound.

Uses include: Any intraoral wound | Extraction / ridge preservation | Sutures / flap margins | Donor & recipient sites of gingiva / connective tissue grafts | Mouth ulcers / aphthous ulcerations | Periodontal, oral, implant surgery | Any procedures causing bleeding
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.



By Georges Fast
SOne man’s opinion...
“It appears that a whole industry has been created around this system with medical certificates sometimes being provided after a ‘Telehealth’ consultation sometimes with interstate practitioners certifying that the patient’s request fits into the model required to access superannuation funds...”
tories about the health professions are featuring in the media with increasing frequency.
In NSW, there is a battle between a group of Health Funds and the owners of a large number of hospitals about the fee that is being charged for hospital admissions to members that are not covered by a particular fund, with a demand for copayment from these patients. The issue that should be seen as a “Red Flag” is not the copayment itself, but the fact that this is not required across the board and discriminates against those that choose an insurer that doesn’t have an arrangement with that hospital group.
We need to think how this situation was allowed to develop in what is an essential service dealing with patients when they are at their most vulnerable because of impending hospitalisation.
When Health Funds were in their infancy, they were set up with the aim of a “community” or group to mutually look after each other so that an unexpected health crisis was not accompanied by a financial disaster and the cost was shared across the community. As these funds grew, they engaged financial managers whose catchcry was that they could generate additional “non-subscription” income by investing their funds in property or the stock market and other such instruments rather than collecting bank interest on deposited funds.
An increasing number of funds followed this path. They demutualised by paying a “once only” dividend to their members and as the business aspects increased in importance, their original purpose was pushed further and further towards the back. Profit and return to shareholders had to increase so as to justify increased salaries and bonuses paid to managers. The funds just morphed into businesses that provided profits for shareholders, dividends for directors and employment for managers - all on the back of subscribers’ contributions.
To generate better profits, costs had to be controlled which meant either reducing the benefit paid to those insured with them or obtaining a discount from health care providers, be they medicos, dentists or privately-owned hospitals.
Similarly, when private hospitals that were originally set up by religious groups or charities to attend to the needs of their communities grew and faced increasing regulation and bureaucratic burden, they had to employ professional managers so as not to be overwhelmed. It soon became clear that a whole new industry could be created on the back of this administrative orgy. The cost of running hospitals escalated partly as a result of more complex and improved medical treatment but equally because of newly created regulations generally imposed without a cost/ benefit assessment being done with regards to patient care, but so that it would improve the career path of administrators.
The nett result is that we have the competing needs of health funds attempting to reduce their exposure to the cost of treatment
verses health care providers having to generate ever-increasing profits so as to be able to cover their administrative costs. The patient is copping it from both sides! Waiting lists blow out and unless the patient is in a position to make a substantial financial sacrifice, the level of care and attention that they can expect is clearly in danger of being suboptimal.
The health professions used to be defined by practitioners being expected to place the needs and wellbeing of their patients ahead of their own financial gain. I see a parallel between the situation with hospitals/health funds and a worrying trend developing in dentistry.
As a young dentist when I was at the Eastman Hospital in London, a venerable senior lecturer on his first introduction to us stated that God gave us teeth so that we would be able to eat and not so that dentists would be enriched.
I can’t see anything wrong with charging a sufficiently high fee to ensure that we do our best at all time; we are also entitled to a reasonable income from our practices. I do, however, see a real problem when patients are “sold” invasive treatment that they don’t require for any reason other than having been influenced by social media. The press reports that AHPRA and The Taxation Commissioner are investigating a number of cases where patients have gained access to their Superannuation funds for the purpose of dental treatment; in fact, there are claims that more than 50% of money withdrawn from funds under this scheme was to fund dental treatment.
It appears that a whole industry has been created around this system with medical certificates sometimes being provided after a “Telehealth” consultation sometimes with interstate practitioners certifying that the patient’s request fits into the model required to access funds. There are also businesses that do all the preparation (presumably for a commission) to enable the patient to access their superannuation. I have seen flyers and advertising from dental practices aimed at the general population that informs patients that they can access their superannuation funds in order to fund their dental implants, veneers and other dental treatment.
How did we arrive at this situation? Should we blame the health funds that gave their members financial incentives to change dentists on the basis that attending preferred providers will get them a better rebate? Is it the fault of the corporates that have promoted dentistry as a product rather than a service and thus interfered with patient loyalty? Do we blame the dentists who have never known the traditional practice model and did not expect to care for the dental health of their patients over an extended period of time and whose sole motivation was to increase their income with little consideration of the dental and fiscal damage that their patients will suffer?
Have we as a profession forgotten that the first principle of health care is to “DO NO HARM”?
Works in 3 mins Material compatibility1,2


Removes+ 99.9% of odour-causing bacteria*3-5
Lifts stains, removes discolouration6,7
Helps keep appliances looking clear1,2
Compatible with common dental appliance material1,2
Retainers
Aligners
Night Guards Mouthguards
For more information, visit www. haleonhealthpartner.com/enau/, www.haleonhealthpartner. com/en-nz/ or scan the QR code



By David Moffet
APointless things with no purpose
“It is your duty to your patients and their health to provide them with the necessary treatment they need to restore their mouth to health now. It is not your duty to sell them something useless [like non-functional custom exterior window shutters] that have no working purpose whatsoever...”
ccording to Wikipedia, “exterior house window shutters were originally constructed for light control, privacy, security and protection from the elements. Many areas of tropical Australia, the Mediterranean, Africa and the American South, feature exterior shutters that block the strong sun from windows. Functional shutters hinge on each side of a window or at the top and swing closed when necessary. Fixed and operable louvers shed rain, allow air transfer, filter direct sunlight, protect from small flying debris and provide privacy... Solid panels and board-and-batten shutters are generally used for security or protection during severe weather. Non-functional shutters are merely used to enhance the appearance of a building”.
Another Google search showed that “custom exterior shutters can give a home a polished, unified look when their colours match the existing colour scheme. This is especially beneficial for those seeking to enhance the visual appeal of their residence, as custom shutters can add an individual and distinct touch”. However, custom shutters that are fixed open and are attached permanently to exterior walls of houses and obviously don’t fit the size of the windows they are mounted beside, and are never closed, are pointless, and look ridiculous.
Why would anybody do that?
If you were an auto mechanic and a client brought you a car that needed four bald tyres replaced and also four worn down brake pads replaced, would you allow that client to just fix one tyre and one brake pad now and get the rest done in dribs and drabs sometime next year?
And possibly kill someone or maim them [or themselves] in the meantime?
Just like bald tyres and worn out brakes, dental disease and decay in the mouth does not fix itself... decay does not disappear, pockets don’t heal themselves and nor do chips and cracks get better on their own.
It is your duty as a health care provider to help every patient receive their best dental care now and not allow them to kick the can down the road thinking that things will be OK if they delay...
“If you were an auto mechanic and a client brought you a car that needed four bald tyres replaced and also four worn down brake pads replaced, would you allow that client to just fix one tyre and one brake pad now and get the rest done in dribs and drabs sometime next year? And possibly kill someone or maim them [or themselves] in the meantime?
Just like bald tyres and worn out brakes, dental disease and decay in the mouth does not fix itself...”
It’s like wearing a scarf around your neck, while wearing short sleeves.
It’s incongruous.
In your business...
In your business, are you engaging in practices and processes that are incongruous with function, reality and your goals and visions? Are you practising best practice for your patients, yet dictating their treatment based on their health fund entitlements and benefits, rather than best treatment?
Are you treating their health, or their wallet?
Are your diagnostic processes and treatment plan options aligned with best health practices?
Or are you just telling your patients what you “think” they are wanting to hear, rather than telling them what dentistry they ACTUALLY DO NEED to return their mouth to optimal health?
It is your duty to be a complete practitioner and to be mindful of your responsibility to the patient of letting them know exactly what is going wrong... and what will happen if they don’t get their necessary treatment completed in the time frame that you recommend.
It’s your duty…
It is your duty to your patients and their health to provide them with the necessary treatment they need to restore their mouth to health now.
It is not your duty to sell them something useless [like non-functional custom exterior window shutters] that have no working purpose whatsoever.
About the author
Dr David Moffet is a dentist and a #1 Amazon Bestselling author. He is the inventor of The Ultimate Patient Experience™, a simple to implement patient retention system he used to build and subsequently sell (for several million dollars) his very successful practice [of 28 years] in working class western Sydney. David has now retired from wet-fingered dentistry and spends his time lecturing and coaching private dental clients in the USA, Canada, Great Britain, Europe and Australia and New Zealand on how to improve their practices. David can be contacted at david@theUPE.com or visit www.TheUltimatePatientExperience.com.




Digital Dentistry & Dental Technology is back for a 6th edition in 2025 in Sydney on August 1-2.
The two-day, multistream event is proving as popular as ever with its unique format, allowing delegates to create their own event within an event.
“We’re looking forward to celebrating Digital Dentistry & Dental Technology in August 2025 with the biggest and best event yet,” said Dentevents’ Joseph Allbeury, the organiser and publisher of this magazine. “We’re already working with sponsors and supporters to bring in top international speakers to present alongside the stellar local talent from Australia and New Zealand we always feature.
“We’re also looking forward to the Novotal Sydney Brighton Beach completing all of its renovations to create the destination we’ve been looking for.
“Delegates love the parking and proximity to Sydney Airport but were after more in the way of lifestyle and entertainment within the venue.
“The full refurbishment includes a brand new ballroom with views across Botany Bay to host the exhibition.”
Plus, the upgraded facilities include...
• Upgraded reception and foyer;
• New Ammos Greek Restaurant;
• New Ironbark Steakhouse;
• New Pan-Asian/Fusion Restaurant;
• New Cocos Beach Sports Bar;
• New Lobby Bar;
• New swimming pool complex; and
• Sands Terrace Bar and Restaurant.
The 5th edition of Digital Dentistry and Dental Technology held in 2024 presented delegates with a choice of over 80 education sessions - 70 hours of content - in 6 concurrent streams presented by 39 speakers over two days at the Novotel Sydney Brighton Beach.
Topics covered include 3D printing, intraoral scanning, 3D facial scanning, milling, CAD and CAM software, materials, smile design, digital den
tures, implantology, CBCT, restorative, aligners, orthodontics and more.
“If you’ve never attended before, have been multiple times or attended every event, we would encourage you to take advantage of the early bird discounts.”
For more info or to register for Digital Dentistry & Dental Technology 2025, visit www.dentaltechnology.com.au.










Source: Dr Salvatore Sauro ✔ Unlimited depth of cure (self cure) ✔ Gap-free interface ✔ Only 2 steps: 15 sec prep ✔ High strength ✔ Choose: capsule or automix


STELA GAP-FREE BONDING INTERFACE
A confocal micrograph of a gap-free Stela-dentine interface. Note the penetration depth of Stela Primer (yellow) within the dentine tubules.

dentevents presents...

SYDNEY 1-2 AUGUST 2025
NOVOTEL SYDNEY BRIGHTON BEACH
TWO DAYS OF LECTURES AND WORKSHOPS ON DIGITAL DENTISTRY FOR DENTISTS, SPECIALISTS,
DENTAL TECHNICIANS AND DENTAL PROSTHETISTS






















2025’s Best Digital Dentistry Event

Join us again or for the first time at Digital Dentistry & Dental Technology No 5 for a fun, exciting and fully immersive learning experience with the best of the best in the new age of dentistry. This year’s program will again cover Digital Smile Design • Digital orthodontics • Intraoral scanning • 3D Facial Scanning • Digital implantology • Digital full arch restorations and full mouth rehabilitations • Digital Dentures • 3D Printing • Milling • CBCT • Materials and applications • Software and more with MORE Hands-on Sessions • MORE Advanced Sessions • MORE New Products • NEW Masterclasses... and more!
REGISTRATION FEES
REGISTRATION FEES
$880 inc gst
$880 inc gst
EARLY BIRD PRICING
EARLY BIRD PRICING
$440 before 24 Jan 2024 price increases $110 on the 2nd of every month INCLUSIONS
$440 before 5 apr 2025 price increases $110 on the 2nd of every month
VENUE DETAILS
VENUE DETAILS
INCLUSIONS
Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
Registration fee includes participation in TWO full days of education (12 CPD hours), all catering and Friday drinks. Multiple lectures and workshops are being run concurrently to allow you to build your own program to suit your specific interests. Price is all inclusive.
PROGRAMME DETAILS
PROGRAMME DETAILS
FRIDAY 1 AUGUST 2025
FRIDAY 24 MAY 2024
9.00am - 5.00pm - education 5.00pm - 7.00pm - happy hour
9.00am - 5.00pm - education 5.00pm - 7.00pm - happy hour
SATURDAY 25 MAY 2024 9.00am - 5.00pm - education 12 HOURS CPD
SATURDAY 2 AUGUST 2025 9.00am - 5.00pm - education
Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports Check the website for details of discounted accommodation rates for the conference • Ample parking available at the hotel
12 HOURS CPD
Novotel Sydney Brighton Beach - The Grand Parade, Brighton-Le-Sands NSW 2216 - Close to Sydney Domestic and International Airports Check the website for details of discounted accommodation rates for the conference • Ample parking available at the hotel
by Dentevents™
Inner ergonomics - a practical recipe to career longevity
By Dr Anikó Ball, BDSc (Melb), Dip.Clin.Hypnosis, Adv.Dip. Alexander Studies
Worldwide research shows an alarming incidence of musculoskeletal disorders in dentistry, resulting in early retirement or reduced work hours for many and a career change for some.
Ergonomic research and design have focused on dentists’ work environment - the so-called Outer Ergonomics, overlooking the importance of their efficiency in posture and movement - the Inner Ergonomics.

HOW a dentist sits on a stool and bends over the dental chair is as important as the stool and chair design. The WAY instruments are held is as important as the shape and the weight of the instrument.
Dental schools don’t provide a “User Guide” on how to bend over patients and what to do with shoulders and arms to ensure career longevity. An understanding of how your body was designed to work, especially during work postures held for prolonged periods, is essential.
OUser Guide for the spine
nce you know that all the intervertebral joints below C2 (just under ear level) are gliding joints, which are not designed for prolonged bending, you will want to avoid work postures that involve bending forward and leaning to the side. Intervertebral discs are distorted when the spine is bent and twisted, resulting in cumulative trauma and a high risk of developing a pain syndrome.
Unless you are using refractive loupes or an operating microscope, you cannot sit upright and see into patients’ mouths without spinal trauma.

Working with nonrefractive loupes or without loupes, you need to pivot your torso slightly forward at the hip joints, without bending the spine and look down by rotating your head at the atlanto-occipital joint (at ear level). As there is only a 10-degree freedom for downward head rotation available at this joint, non-refractive loupe users need an adequate declination angle to avoid compensatory neck bending.
User Guide for shoulders and arms
Most dentists work with a raised non-dominant shoulder and elbow.
The muscles moving the shoulders and arms are designed for a short contraction. Prolonged use of movement muscles to hold up the shoulder, or the arm against gravity when hovering with the mouth mirror without a finger rest, results in cumulative trauma. Always have a finger rest and don’t raise your shoulder or elbow.
Take care of yourself, you are your most precious instrument.
Dr Anikó Ball is the Founder of Optimum Dental Posture. For info, see www.optimumdentalposture.com


Diplomatic Immunity: 6-year
warranty, fixed price service
William Green are taking inspiration from the automotive industry with the launch of its new Diplomatic Immunity deal, offering a 6-year warranty and fixed price service on its full range of Diplomat dental units.
“The Diplomat range are ultra-reliable, fully-featured, high-quality Europeanmade dental units at a variety of attractive price points,” said Ryan Green, managing director of local distributor, William Green Pty Ltd. “However, the Diplomat brand is not as well-known as some in Australia and as a result, buyers may be wary in regard to their reliability and service support.
“So we looked around at other markets and there are a lot of synergies with the automobile industry and the trend towards long warranties and low cost of ownership being used to put buyers’ minds at ease.
“As a result, we’re now reinforcing the Diplomat range with a real 6-year warranty and fixed price servicing during that same period, backed by William Green, the company my grandfather started 78
years ago. In short, trust the brand and we’ll back you 100%.”
Mr Green said that once customers are introduced to the Diplomat range, they are surprised by its ergonomic design combined with lux-level comfort for patients.
“The Diplomat range has a dental unit model suitable for every dental practice – whether you’re on a budget or looking for a fully featured unit with smart connectivity, advanced technology and a full range of options and accessories. There is the perfect unit in the range for every practice.
“And now, Diplomat also has an industry leading ‘real’ 6-year warranty.”
Mr Green said that with most dental equipment being financed, the Diplomatic Immunity deal effectively caps your expenditure over that period. You have the lease payment and the annual fixed price service fee. That’s it. If you’re fitting out a multi-chair clinic, then that becomes even more attractive.
Mr Green said William Green has been selling Diplomat for over a decade and they have hundreds of satisfied customers in Australia already.
Diplomat has been engineering dental units that outlast and outperform the competition for 60 years and are recognised in Europe for superior reliability, advanced technology and award-winning design.
Features include smart handpiece recognition, brushless micromotors with endodontic functions, 3D pneumatic headrests, customisable water, speed and torque controls and a truly open, limitless Smart Display that lets you use any iPad or Android tablet for full access to your imaging software, practice management system, web browsing and even patient education on YouTube.
The Diplomatic Immunity deal is a simple proposition, according to Mr Green.
“Purchase a Diplomat dental unit and commit to the annual fixed price service plan and we will guarantee the product for six years. A fully-featured, high-quality European-made dental unit guaranteed for 6 years… What more could you ask for?”.
For more information on the new Diplomatic Immunity 6-year warranty with fixed price servicing deal, visit www.williamgreen.com.au
fixed price annual service

Introducing NEW! Diplomatic Immunity Deals...
Your guaranteed solution for dental unit reliability across the entire Diplomat range
l Available on the full range of dental units from budget to high-tech ultra-lux.
l 6-year warranty on parts and labour.
l Fixed price annual servicing (required to validate warranty).
l Made in the European Union (Slovakia) by Diplomat (established 60 years).
l Serviced nationwide by William Green Pty Ltd (established 78 years).
l Open, Limitless Smart Display with iPad or Android tablet compatibility (Pro Model).
l Brushless micromotors with endo functions, 3D pneumatic headrest, smart handpiece recognition, customisable water, speed & torque controls and more...
Visit our Sydney showroom to try the Diplomat range before you consider buying any other dental unit for your practice!
William Green Pty Ltd
47- 49 Mary Parade
Rydalmere NSW 2116
Ph + 61 2 8865 0300





A One-Day Intensive Event to Help You Grow Your Implant Skills and Stop Referring Out Too Many Cases
6 CPD Points
Location: Sydney CBD
Date and Time: Saturday, March 29, 2025 9:30 AM - 4:00 PM Pullman Hotel, Hyde Park
Why Attend Implantopia?
If you’re a dentist looking to grow your implant skills, take on more complex cases, and keep more implant work in-house Implantopia is the event you’ve been waiting for.
This one-day, high-impact event is designed to provide you with the practical knowledge and techniques you need to confidently manage more implant cases from start to finish.
Our expert speakers will guide you through the Ps of Implant Success:
Planning:
How to create a detailed, predictable treatment plan for implant cases.
Placement:
Techniques for precise implant placement and minimising complications.
Prostheses:
Strategies for selecting, designing, and delivering implant-supported restorations.

Printing:
The latest in 3D printing for implant prosthetics and workflow integration.
Patients:
You’ve got the skills, now discover how to fill your books with implants patients.
Meet the Speakers:


Adishwar ‘Dish’ Ghose The Rapid Turnaround Dentist
Simple, practical techniques to increase patient case acceptance.


Angus Pryor Practice Growth Specialist
Proven strategies to fill your books with more implants patients faster.
Testimonials:
Dr Yohan shares practical, actionable information that demystifies the implant restoration process. For a structured, step-by-step approach, I highly recommend attending.
– Dr Kerin Jacobs, SA
Yohan Thomas Specialist Prosthodontist
The ‘Prosthodontic Mentor’, renowned for his practical, step-by-step approach to implant restorations.
Angie Papas Laser Dentistry Guru
Cutting-edge techniques for using soft-tissue/hard-tissue lasers in implantology.

Angie is an extremely passionate speaker – lots of knowledge. Loved the little tips, very practical approach. Amazing versatility of use of lasers. Loved it.
– Dr Ankur Sachdeva, TAS
Omid Allan Implant Innovator
Learn groundbreaking techniques for full arch rehabilitation.
Angus is an amazing orator and extremely passionate about what he does. His presentation made me reevaluate everything in my practice.
– Dr Judy Liu, NSW
Includes all meals and refreshments.


A-dec introduces 10-year warranty
New warranty doubled on A-dec core equipment
A-dec has announced the enhancement of its product warranty from five years to ten years. Effective on core equipment invoiced on or after January 1, 2025, the new 10-Year Warranty covers A-dec dental chairs, delivery systems, lights, dental furniture and stools.
A-dec CEO Marv Nelson said A-dec equipment has a longstanding reputation for quality, reliability and performance among dental professionals. “A-dec products are well known for their legendary long life,” he said.
“That’s due to our attention to detail and commitment to quality – what we call the A-dec difference. We’re pleased to offer A-dec customers a warranty that reflects the confidence we have in our equipment’s longevity and high standards of excellence.”
As a family-owned business, A-dec’s focus has always been on meeting the needs of dental professionals with reliable, creative solutions.
Tim Long, A-dec Vice President of Sales and Marketing, said the new, longer warranty will provide another meaningful point of differentiation for practitioners and practice owners considering A-dec for their dental practices.
“Our customers have always been able to rely on A-dec equipment,” he said. “Now they’ll have the extra peace of mind of knowing that A-dec equipment is backed by the best warranty in the business.”
The enhanced 10-Year Warranty is valid on equipment purchased directly from A-dec or an authorised A-dec dealer and covers more than 100 countries worldwide.
For info, see a-dec.com/legal/warranty to see full warranty details, including exclusions or contact A-dec on 1800-225-010 or find your nearest dealer at australia.a-dec.com


Equipment guru celebrates 50 years!
One of Australia’s longest serving and best-known dental equipment technicians, Bill Stoney, has just celebrated an incredible 50 years in the dental industry.
Alldent, Melbourne founder and principal, Bill Stoney, is also one of the longest serving ADIA members, with 50 years’ membership of the organisation. He is also a long time A-dec equipment dealer and installs equipment and assists with surgery design for all leading healthcare builders.
Bill was one of the first dental equipment technicians apprenticed at the Royal Melbourne Dental Hospital (RMDH) back in 1974, making him one of Victoria’s – and Australia’s –most experienced service technicians with five decades in the industry.
Bill says he was the second technician trained at Royal Melbourne Dental Hospital, closely following his former colleague, Peter O’Brien, who retired recently. Both were trained by former naval engineers who were extremely skilled and versatile.
Bill attributes that rigorous training as being invaluable in helping him become an “all-rounder” and a problem solver.
Bill recalls that his trainers were skilled instrument-makers who were highly qualified in electronics but also jacks of all trades and extremely adept in plumbing, fabrication and carpentry. His staff at Alldent are now similarly trained as A-grade electricians.
“When you’re out at sea, literally and something breaks, you have to find a way to fix it as you can’t just drive down the road and buy another one,” he said.
Bill was taught that electrical wire had to be run in a circle around a screwdriver, tin soldered and always placed in a screw with a brass washer.
“Every connection into 3-pin plug had to be soldered for safety. Everything we did had to be done the correct way. If we nicked the insulation when installing a wire, we had to cut off the wire and replace it.”
During his training, Bill worked on not only dental chairs, but all types of equipment from large scale plant room chillers and air compressors to high velocity dry suction motors and separators. He worked closely with engineers who designed some of the equipment and this gave him great insight into the all-important areas of plumbing, electrics and suction systems – all skills that Bill excels in and employs regularly during installations and repairs for his customers across Victoria.
The apprentices and tradesman at RMDH also fabricated a lot of parts and fittings such as clamps for steel flasks.

“We used to make things instead of buying them,” Bill says. “We’d do the drawings, make them out of steel and turn them and cut threads into them on the hospital lathe.”
This early formal training also added to Bill’s own tinkering abilities honed on working on cars and motorbikes from a young age. Oddly enough, after spending 3½ years at Royal Melbourne Dental Hospital, Bill then did a stint at General Motors as an instrument maker prior, to becoming a Registered Electrical Contractor.
From there, Bill worked in various other businesses and electrical companies before finding his way back into the
dental industry in a Gunz technical and sales role. He also worked with the School Dental Service, Commonwealth Dental Supply Co. and Flavell and Ramsay dental companies before going out on his own as a dental equipment technician.
Bill was also involved in a partnership with Bruce Williams and the two ran a dental equipment company together, prior to Bruce later becoming an A-dec Territory manager in Victoria.
Alldent started in a very small way back in December 1988. Growing demand for dental installs in the 1990s led to Bill going full time on this work around 1992–93.
A lot of dentists that knew of Bill insisted that “they only want this bloke to put their equipment in”. There was initially a lot of resistance from suppliers, but when it became apparent that this sort of expertise was in big demand and Bill had a very good reputation for his know-how, reliability, customer service and cost, they started using him.
Bill recalls that A-dec, which had a rapidly growing presence in Australia at that time, was always looking for new recruits to support its equipment in Australia. Former A-dec Technical Manager, Peter Graham, knew Bill from RMDH and sought him out.
If a dentist had a problem, A-dec would call Bill to go and fix problems others couldn’t fix. At times, this took Bill all over the country on major installs and as a trouble shooter, thanks to his sound technical background, natural engineering ability and years of practical experience.
Bill continues to operate Alldent out of Port Melbourne where his skills and knowledge are still highly valued and sought by those who know him.
Alldent has also built a great and highly valued team of specialists, including Paul Petkovski who has been with Alldent for 20 years, key customer support and equipment sales specialist, Fiona Banks who has spent over 10 years at Alldent, electronics whizz, Luke Brundell and Naomi Thomason.
Well done Bill Stoney on an outstanding career in the dental industry and as a great ambassador for A-dec in Australia.
RIVA CEM AUTOMIX

Ideal for cementation of zirconia, PFM and orthodontic bands
Sustained fluoride release BPA free
Study: In vitro properties of different resin-modified glass-ionomer cements
Prof. Dr. Alessandro Loguercio and Alessandra Reis (Brazil)
*Not a registered trademark of SDI.

Enhanced Healing: GEM 21S® is specifically designed to stimulate the body’s natural healing processes, promoting regeneration of bone and gingival tissues.
Enhanced Healing: GEM 21S® is specifically designed to stimulate the body’s natural healing processes, promoting regeneration of bone and gingival tissues.
Enhanced Healing: GEM 21S® is specifically designed to stimulate the body’s natural healing processes, promoting regeneration of bone and gingival tissues.
Innovative Tissue Engineering: Access the full regenerative potential of recombinant human platelet-derived growth factor (rhPDGF), creating an optimal environment for tissue repair and bone growth.
Innovative Tissue Engineering: Access the full regenerative potential of recombinant human platelet-derived growth factor (rhPDGF), creating an optimal environment for tissue repair and bone growth.
Innovative Tissue Engineering: Access the full regenerative potential of recombinant human platelet-derived growth factor (rhPDGF), creating an optimal environment for tissue repair and bone growth.
Proven Effectiveness: Backed by scientific research and clinical studies, GEM 21S® has shown excellent results in hard and soft tissue regeneration, enhancing the predictability of challenging cases.
Proven Effectiveness: Backed by scientific research and clinical studies, GEM 21S® has shown excellent results in hard and soft tissue regeneration, enhancing the predictability of challenging cases.
Proven Effectiveness: Backed by scientific research and clinical studies, GEM 21S® has shown excellent results in hard and soft tissue regeneration, enhancing the predictability of challenging cases.
1C Consistency
1C Consistency
1C Consistency
The first and only off-the-shelf source of purified rhPDGF approved for bone and soft tissue regeneration.
The first and only off-the-shelf source of purified rhPDGF approved for bone and soft tissue regeneration.1
The first and only off-the-shelf source of purified rhPDGF approved for bone and soft tissue regeneration.

How do you predictability? 4C
How do you predictability? 4C
How do you predictability? 4C


A New Benchmark in Regenerative Dentistry!
GEM 21S® Growth-factor Enhanced Matrix is crafted to boost the patient’s naural healing capacity, promoting the restoration of lost bone and gingiva. Extensive in vitro and in vivo studies have demonstrated that rhPDGF-BB is a powerful stimulant of angiogenesis that also stabilises newly formed blood vessels.
GEM 21S® Growth-factor Enhanced Matrix is crafted to boost the patient’s naural healing capacity, promoting the restoration of lost bone and gingiva. Extensive in vitro and in vivo studies have demonstrated that rhPDGF-BB is a powerful stimulant of angiogenesis that also stabilises newly formed blood vessels.
GEM 21S® Growth-factor Enhanced Matrix is crafted to boost the patient’s naural healing capacity, promoting the restoration of lost bone and gingiva. Extensive in vitro and in vivo studies have demonstrated that rhPDGF-BB is a powerful stimulant of angiogenesis that also stabilises newly formed blood vessels.
GEM 21S® is the only dental therapy containing rhPDGF-BB, one of the main growth factors found in the human body and well known for its stimulatory role in wound healing.
GEM 21S® is the only dental therapy containing rhPDGF-BB, one of the main growth factors found in the human body and well known for its stimulatory role in wound healing.
GEM 21S® is the only dental therapy containing rhPDGF-BB, one of the main growth factors found in the human body and well known for its stimulatory role in wound healing.
GEM 21S® increases the amount of PDGF at the grafted site to aid in faster, more bone and better healing. 500+
GEM 21S® increases the amount of PDGF at the grafted site to aid in faster, more bone and better healing.
GEM 21S® increases the amount of PDGF at the grafted site to aid in faster, more bone and better healing.
Promotes rapid healing and new bone formation for oral surgery*
Promotes rapid healing and new bone formation for oral surgery*
Promotes rapid healing and new bone formation for oral surgery*

500+

Affordable A-dec upgrade options




Leading dental equipment supplier, A-dec, is offering Australian dental practices more affordable and novel ways to upgrade their equipment.
Acknowledging the impact of cost-ofliving pressures, A-dec has put together some equipment upgrade options to let you gain the latest technological advancements, while saving thousands compared to buying new equipment.
Don’t replace, refurb!
F or those practices that have existing A-dec equipment that just needs a freshen up, A-dec provides both aesthetic and functional options to make existing dental units look and perform at their best without breaking the bank.
Upholstery upgrades
Colour is a powerful design tool that has an impact on influencing emotion, mood and even physiological reactions. A-dec engaged a colour consultant to devise its latest range of colours to enhance your image and blend seamlessly with your existing décor.
You can update your A-dec chair or stools with A-dec’s new range of upholstery colours in plush sewn or smooth contoured upholstery options for almost any A-dec chair.
Upgrade your accessories
A-dec chairs are built to last 20+ years, but in that time, you might want to refresh your chair’s look and functionality with the latest ancillary instruments to aid diagnosis and treatment options and boost case acceptance by your patients.
A-dec is the perfect platform so you can add new accessories as needed, effectively future-proofing your practice by staying current with technological advancements.
You can choose from:
• Electric Motors;
• Intraoral cameras;
• LED and ultrasonic scalers;
• LED operating lights; and/or
• New delivery systems and touchpads. Depending on the age of your chair, many of these useful tools are ready to bolt straight on to bring your equipment right up to date, enhancing your productivity and making day-to-day dentistry easier for you and your team.
Programmed Maintenance Plan
A-dec’s authorised dealers offers a programmed maintenance plan to swap out those parts and service items that need replacing through normal use, including water reservoirs, O-rings and other minor parts. Regular servicing includes any necessary lubrication and adjustments of your equipment to keep it working at its best.
Just like owning a car, regular maintenance ensures optimum performance and a long service life. This translates into peace of mind without any downtime or cancelled patient appointments from unexpected breakdowns. Services include routine chair maintenance, water quality testing and steriliser validation.
Contact your local A-dec Territory Manager or authorised A-dec dealer to discuss the options... Or fit-out a new practice with the latest class leading equipment from A-dec and its supplier partner Dürr Dental to provide a full range of A-dec dental units, sterilisers and Dürr digital imaging equipment.
Call A-dec on 1800-225-010 or find your nearest dealer at australia.a-dec.com
Driven to perform for your practice
That’s the Avant Advantage

Reliable turnaround times from the lab dentists deserve.
Reliable turnaround times from the lab dentists deserve.
The skeptic’s guide to social media marketing...
Let’s address the elephant in the room: Social media marketing feels like a chore. Everyone’s shouting, “Post more! Go viral! Be consistent!” But is it actually worth the effort, or is this just another trend that marketers are overhyping?
Here’s the truth: social media isn’t magic. It’s not going to solve your business problems overnight. But it’s also not the pointless “time-suck” skeptics think it is. The key is knowing what it can— and can’t—do for you.
What social media can’t do
Print Money: If your product or service sucks, no amount of clever Instagram posts will save it.
Guarantee sales: Followers don’t always translate to buyers. Likes don’t pay the bills.
Work without strategy: Random posts don’t build brands. Sorry, but you can’t just “wing it”.

What
social media can do
Build trust: Sharing your story, wins, and even fails makes you human. People buy from people they trust.
Start conversations: Good social media isn’t about selling; it’s about talking. Engage your audience. Be real. Show up where your customers are: If they’re scrolling, you need to be there too—just don’t interrupt their feed with boring stuff.
The bottom line
If you’re expecting instant results, you’ll hate social media marketing. But if you’re willing to play the long game—building relationships, creating meaningful content and staying consistent—it’s absolutely worth it. Still skeptical? Start small. Pick one platform, focus on quality over quantity and track what works. Who knows? You might just stop hating it. Or at least, hate it a little less.
at dentalmarketingsolutions.com.au

ACCOUNTING & FINANCIAL SERVICES FOR DENTISTS
DON’T RISK SECOND BEST
Synstrat has spent many years collecting data on dental practices. We provide you with the best available knowledge on the performance of your practice relative to others. Our proven service has assisted many dentists Australia wide to create significant wealth. We are able to provide you with business accounting, practice valuation and financial advice services tailored to the dental profession. Buying







When choosing Ampac Dental, your getting More Than Equipment. Your gaining a dependable partner that provides genuine, personalised support, and collaboration in the success of your practice.





CS 9600 CBCT wins its 6th Cellerant
Best of Class Technology Award
In a testament to ongoing innovation and industry-leading technology, Carestream Dental’s CS 9600 CBCT system has earned its sixth consecutive Cellerant Best of Class Technology Award, preserving its place as having won more Best of Class Technology Awards than any other CBCT system. This continued recognition underscores the system’s ability to keep oral healthcare professionals at the forefront of innovation.
The CS 9600’s five-in-one capabilities — including 2D and 3D imaging, object scanning, face scanning and cephalometric imaging — ensure that oral healthcare professionals can tailor their imaging technology to their patients’ specific needs. Its broad FOV options cover a broad range of clinical indications, including implant placement, endodontics, periodontics, oral and maxillofacial surgery, orthodontics, TMJ and airway analysis. So, whether it’s focusing on the intricate details of root morphology
or capturing comprehensive views of the jaws, TMJ and sinuses, the system is engineered to deliver superior, high-quality images. Advanced automation, guided assistance and artificial intelligence (AI) ensure that practitioners capture the right image on the first attempt, reducing the need for retakes and allowing clinicians to focus on diagnosis and patient care.
Part of the CS 9600’s success is its powerful imaging software, like CS Imaging version 8 — a hub that centralises all of a practice’s images.
CS 3D Imaging powers the system with 3D image analysis and AI-powered features to automate tasks.
IO Scanner Link allows for seamless integration with third-party intraoral scanners to further ensure smooth workflows. As dental practices grow, doctors can expand their CS 9600’s capabilities with additional modules to support advanced treatments, like with the Prosthetic-driven Implant Planning module or CS Airway.
“Receiving the Cellerant Best of Class Technology Award for the sixth year in a row is a true testament to the inno-
vation and ease-of-use of the CS 9600 system,” Philippe Maillet, general manager, Imaging, Carestream Dental, said. “We’re committed to providing dental professionals with the advanced tools they need to deliver exceptional patient care and the CS 9600 continues to evolve to meet the growing demands of modern practices.”
The 2024 Best of Class Technology Award was awarded by a panel of distinguished dental technology experts. In addition to the system’s six Best of Class Technology Awards, the CS 9600 has also received accolades such as the 2019 Edison Award in the Medical/Dental Diagnostics category and the Krakdent Medal of the Highest Quality.
For more information on the Cellerant Best of Class Technology Awards, visit cellerantconsulting.com/about-best-ofclass. To learn more about the CS 9600 and Carestream Dental’s innovative solutions, visit carestreamdental.com or contact us at info.apac@csdental.com or call 1800-223-603.

Smarter and Better Than Ever. CS 9600 Cone Beam CT
The smart way for your team to capture the high-quality images you need to achieve faster diagnoses and treatment plans. The CS 9600 features multiple advances including video-aided positioning guides and an intuitive SmartPad to enable you and your staff to achieve highquality, precise images on the first try, every time. And intuitive software and innovative metal artifacts reduction tools help you reach a more confident diagnosis.










Design meets efficiency: The new VITA Smart.Fire Advanced
VITA Zahnfabrik presents the next generation of the VITA Smart.Fire furnace: the VITA Smart. Fire Advanced. This extensively developed furnace offers numerous new functions that ensure even greater efficiency in the dental practice, as well as in the laboratory.
Extended range of possible applications and increased flexibility
The VITA Smart.Fire Advanced is equipped with a larger firing chamber, which now also offers enough space for 14-unit bridges, creating even more versatility for laboratories. Linear cooling with object temperature simulation, ensures precise and reliable firing results. The new optional and attachable cooling tables,
along with the new firing tray and firing tray pins (four-finger pins and ceramic pins) expand the range of possible uses for the furnace and make it even more convenient to use. The new firing pins are available separately in single-variety replacement sets, as well as in a mixed basic set.
Proven efficiency and user-friendliness
The VITA Smart.Fire Advanced has retained the intuitive operation, preinstalled programs and space-saving design of its predecessor model. This ensures easy handling and optimum use of space. This furnace has been optimised for chairside applications, as well as for laboratory uses and meets all requirements for efficiency, precision and flexibility.
For info, visit www.vita-zahnfabrik.com
About VITA Zahnfabrik H. Rauter GmbH & Co. KG
VITA Zahnfabrik H. Rauter GmbH & Co. KG is a fourth-generation family business in the dental industry based in Bad Säckingen, in southern Germany. For almost 100 years, VITA has been developing, producing and distributing innovative, high-quality products and restoration solutions for dental technology and dentistry. Worldwide, more than 600 employees work for VITA Zahnfabrik, with the objective of being closer to users and customers than anyone else. Areas of expertise range from analog and digital shade determination, denture teeth and veneering materials, press ceramics and CAD/CAM materials and furnaces and dental materials. With scientific expertise and targeted training programs, VITA supports and advises dental experts from more than 125 countries in their daily work.






GOLD PARTNERS

SCAN DESIGN
MANUFACTURE
As a Shining 3D Dental Gold Partner, Osseo Group provides a seamless Scan-Design-Manufacture workflow and expert support to help you succeed.






BOOK A DEMO AND LEARN MORE
DENTURES
Everything you need to know about fabricating dentures digitally
SYDNEY - JUNE 27-28, 2025






This event is both a lecture documenting why you should choose digital dentures today as the optimal solution for your dental practice or denture clinic together with a LIVE systematic run-through of the process for fabricating both full and partial digital dentures. You will be able to follow Sam Dias as he explains the step-by-step process he uses in his four clinics across Sydney every day.
A demonstration of accurate intraoral scanning and prosthetic design ensures that the outcome won’t be compromised while saving time and money for you and your patient.
The session will conclude with a Q&A session discussing options leading to self-design or aided design as well as the finishing and polishing process.



Abro® Basic and Denture Gingiva Basic Mono Pink resins: New materials for the production of full dentures
Although minimally invasive procedures are becoming increasingly important and their basic idea to preserve as much tooth structure as possible is undisputed among experts, there are still patients who need a complete restoration after total tooth loss. In addition to implant-supported restorations and full dentures are still a tried-and-tested method, especially among the elder demographic.
With the Abro® Basic and Denture Gingiva Basic Mono Pink resins, Zirkonzahn introduces new PMMA-based materials for the production of full dentures. Due to their low residual monomer concentration, they tend to be more biocompatible with the oral environment than conventional heat-cured materials. Abro Basic is available in two different shade variants: monochromatic (Abro Basic Mono) or with a natural colour gradient from dentine to enamel (Abro Basic Multistratum®). The mechanical and optical properties of the Abro resins with regards to their translucency, flexural strength as well as fracture and abrasion resistance make them ideal for the manufacturing of denture teeth. They can also be used for long-term temporaries and superstructures.
The Denture Gingiva Basic Mono Pink is a gingiva-coloured resin with high flexural strength and fracture resistance, which has been developed specifically for the production of denture bases. The Denture Gingiva Basic Mono Pink blanks are also available in Ø 125 mm, allowing dental technicians to manufacture up to two denture bases in a single milling process. In addition, the gingival area of the restorations can be individually characterised with Gingiva-Composites. The colour spectrum of the Gingiva-Composites is based on Zirkonzahn’s ICE Ceramics

articulation using the

Zirkonzahn.Modifier: natural tooth libraries and setup functions for defining tooth placement and alignment
Tissue shades. With the application of the Gingiva-Composites to temporary restorations, both the clinician and patient will have a more accurate indication of what the final restoration may look like.
The following real case illustrates the workflow for a patient who was treated with full dentures in Abro Basic Multistratum and Denture Gingiva Basic Mono Pink.
Treatment plan
T he initial situation presented an edentulous upper jaw and a lower jaw with only the presence of tooth 43. The restorative team opted for two full dentures in Abro Basic Multistratum and Denture Gingiva Basic Mono Pink and a non-invasive zirconia crown restoration for tooth 43 with Prettau® 3 Dispersive®
Digital
PS1 virtual articulator.









PRETTAU® SKIN®
ULTRA-THIN VENEERS FOR THE ANTERIOR REGION IN PRETTAU ® 4 ANTERIOR ® DISPERSIVE ®






- Minimal polishing of the proximal marginal ridges; placement of a retraction cord (000) and acquisition of intraoral scans
- Digital articulation and tooth set-up in Zirkonzahn.Modifier; individualisation of THALIA tooth set from the Heroes Collection library
- Design of the veneers in the Zirkonzahn.Modifier software and immediate creation of the JawAligner models in the Model Maker software module thanks to the Continue Working function; printing with the 3D P4000 Printer
- Milling the structures in the M6 Teleskoper Blank Changer milling unit; sintering with the Zirkonofen 600/V4
- Handover of the fi nal Prettau® Skin® veneers to the dentist after characterisation with ICE Stains 3D by Enrico Steger and minimal layering with Fresco Enamel Fluo; cementation in the patient’s mouth






















Dr. Francisco García Torres – Mexico
DT Alexander Lichtmannegger – Zirkonzahn Education Center Brunico, South Tyrol, Italy



Workflow steps
• Digital acquisition of the patient’s worn prostheses with the Detection Eye intraoral scanner;
• Digital matching and articulation in the Zirkonzahn.Modifier software using the PS1 virtual articulator;
• In the Zirkonzahn.Modifier software: setup and individualisation of tooth shapes with selection from the Heroes Collection rooted tooth library;
• Correct tooth scaling and positioning in occlusion via Plaster Plane; automatic generation of the gingival portion;
• In the patient’s mouth: evaluation of the aesthetic, functional and phonetic aspects by means of try-ins which are then used as impression tray for the final impression;
• Digitalisation of the new aesthetic and functional situation;
• Adaptation of the tooth setup to the new impression;



• Digital design of crown 43 and of two Sinternit crowns (15; 25), which were later gold plated;
• Nesting of the two denture bases in the Denture Gingiva Basic Mono Pink resin blank and of the respective denture teeth in the Abro Basic Multistratum resin blank;
• Milling in the M6 Teleskoper Blank Changer and gingiva layering with Gingiva-Composites;
• Bonding teeth to the denture bases according to the new Polibond procedure; and
• Cementation of the crown on tooth 43 and final insertion of the prostheses in the patient’s mouth.
Zirkonzahn Australia Pty Ltd is located at Unit 57, 6-8 Herbert Street, 2065 St Leonards, NSW 2065. Tel: 0432-446-682 Fax: +45-7022-7158 info.australia@zirkonzahn.com For more information, visit www.zirkonzahn.com
Figure 4a. Before.
Figure 4b. After.

NEW! ABRO® BASIC MULTISTRATUM®
The new Abro ® Basic Multistratum ® resin, with a natural colour gradient and improved material properties, features an extremely low residual monomer concentration and is characterised by excellent translucency values, high flexural strength as well as fracture and abrasion resistance. Specifi cally conceived for the production of denture teeth, this resin is also well suited for long-term temporaries as well as various secondary and tertiary structures.

r.zirkonzahn.com/fcw
NEW! DENTURE GINGIVA BASIC MONO PINK
Gingiva-coloured resin with improved material properties in terms of flexural strength and fracture resistance, specifi cally conceived for the production of denture bases. In addition, the extremely low residual monomer concentration greatly improves biocompatibility The resin blank is available in Ø 125 mm for the manufacturing of up to two denture bases in just one milling process.
POLIBOND
Liquid for bonding Abro ® Basic Mono, Abro ® Basic Multistratum ® and Denture Gingiva Basic Mono Pink resins. It is also suitable for polishing Multistratum ® Flexible and Temp Premium Flexible resins.

r.zirkonzahn.com/6s4















































Miniature Implants:
SYDNEY ON MAY 3, 2025
Presented by Dr Omid Allan
This is an exclusive training course on the BioMiniatures
Miniature Implant system, offering an opportunity to be the first to learn about this innovative system. The course includes hands-on education on the use of Miniature Implants for full and partial arch rehabilitation using a minimally invasive approach. Miniature Implants are narrow diameter implants with a unique self-drilling and self-advancing design which allows placing implants in very narrow alveolar ridges without needing complex and risky bone augmentation procedures.
The course will enable you to restore dentitions in severely atrophic ridges with simplicity and confidence. This will include both surgical and prosthetic procedures.






Dr Omid Allan
DDS, ADC, MFGDP, MSc (Aesthetic Dentistry) (King’s College London), MSc Oral Implantology (Goethe Frankfurt), FICOI
Dr Omid Allan holds a Masters degree in Oral Implantology from Geothe University of Frankfurt and also a Masters degree in Aesthetic Dentistry from King’s College of London. He is the inventor of the miniature implant system and founder of BioMiniatures with extensive knowledge and experience in implant dentistry.






Cologne hosts 41st IDS on March 25-29
From 25-29 March 2025, the International Dental Show is again taking place in Cologne for the 41st time and will once again underline its position as the world’s leading trade fair for dentistry and dental technology. Organised by the GFDI (Gesellschaft zur Förderung der Dental-Industrie mbH) and staged by Koelnmesse, IDS brings the most important players of the dental profession, the dental technology trade, the dental specialised trade and the dental industry together and offers a unique platform for innovations, networking and knowledge transfer.
Intensive marketing and sales activities have particularly been executed in South America, Asia and the USA to further establish IDS as the leading global trade fair. With around 2,000 exhibitors from over 60 countries and a foreign share of around 77%, IDS 2025 is currently demon-
strating its strong international alignment. The most strongly represented countries among the exhibitors are expected to be Korea, Italy, the USA, China, Turkey, Spain, France and Switzerland. The offer is enhanced by numerous country pavilions from all continents. The strong demand from home and abroad shows that as a platform for innovations, market trends and as a central business platform, IDS is the decisive management tool for the global trade.
fair. IDS offers extensive services to make the trade fair experience as pleasant as possible for visitors.

In terms of visitors, IDS also remains a global highlight: In 2023 around 120,000 trade visitors from 122 countries attended the trade fair – IDS 2025 aims to exceed this benchmark.
The newly optimised hall layout with four entrances and an expansive exhibition space spanning 180,000 square metres across multiple halls offers ideal conditions for an efficient visit to the trade
Whilst the presentation of products continues to be of key importance, IDS sees itself as being far more than purely a product show, it considers itself to be an integrative network that promotes an exchange about central industry themes. The focus lies on current challenges such as the promotion of young talents, the lack of skilled labour, sustainability and the implementation of artificial intelligence.
About IDS
The IDS (International Dental Show) takes place in Cologne, Germany every two years and is staged by Koelnmesse GmbH, Cologne. For more information, visit www.ids-cologne.de



Experience the artistry of precision-crafted dentures with Cyberdent. Our specialist team ensures every product meets the highest standards, designed to exceed expectations.

Simplify your workflow with Cyberdent’s seamless case management and fast turnaround. We handle the details, so you can focus on delivering great patient care.
Provide your patients with premium-quality denture solutions. From Valplast to Chrome, trust us to help you deliver outstanding results every time.
Next generation of VITA VACUMAT

VITA VACUMAT furnaces have long been known for their quality and precision. The new VITA VACUMAT 6100 M is continuing this tradition. The new VITA VACUMAT 6100 M combines proven quality standards with innovative technologies. The optimised electronics enable even more precise results, ensuring a consistently high quality of dental work and increased efficiency in the laboratory. The simple operation, the preinstalled programs and the space-saving design have all been retained. These features guarantee easy handling and optimum use of the available space. This makes the VITA VACUMAT 6100 M a clear winner for dental technicians who value reliability, precision and innovation. As a fully automatic furnace with microprocessor-controlled technology, the VITA VACUMAT 6100 M is ideal for use with all dental ceramic firing processes and offers impressive quality and aesthetics. Thanks to its ergonomically optimised design, the furnace only requires a minimal footprint. Two integrated cooling trays support safe storage of fired objects. Innovative materials are used in the combustion chamber of the VITA VACUMAT 6100 M to ensure even more homogeneous heat distribution. The durable firing muffle - made in Germany - and reliable electronics guarantee consistently excellent firing results. The furnace also offers a wide range of monitoring and service programs that maximise working comfort, safety and time savings. One new feature of the VITA VACUMAT 6100 M is the linear cooling with simulation of the object temperature. This function ensures safe and precise firing results by guaranteeing even and controlled cooling. The VITA VACUMAT 6100 M is available now.
For more information on the VITA VACUMAT 6100 M, visit www.vita-zahnfabrik.com
Have you wiped down properly?

Contaminated surfaces in the health care environment have been shown to play an important role in the transmission of common pathogens that cause healthcare-associated infections (HAI). Nosocomial pathogens are commonly found on contaminated high-touch surfaces, where they can remain viable for several months. They are spread when health care workers touch contaminated environmental surfaces and fail to perform hand hygiene before caring for patients. Since contaminated environmental surfaces in the health care setting put patients at risk of acquiring HAI, improved methods of cleaning and disinfection of high-touch surfaces are needed to prevent HAI. A new disinfectant wipe product has been developed (Highlight by Kinnos) with colour-additive technology to help users visualize surfaces that have been cleaned. The wipes produce a transient blue colour on wiped surfaces that fades off after effective cleaning. This enables staff to visually confirm which surfaces have been wiped, and to assess how thoroughly the disinfectant is spread across surfaces. The purpose of this study was to quantify the impact of real-time visual feedback from these wipes on room cleanliness and efficiency. A pre-post comparison was made using Replicate Organism Detection and Counting (RODAC) culture plate counts and room turnaround times, with and without the use of the colour additive. The site for the study was a 160-bed acute care hospital (Griffin Hospital, Derby, CT, USA) over a 5-week period in November to December 2023. The control product was hypochlorous acid disinfectant wipes (Clorox). A total of 400 hightouch surfaces were sampled during the study (200 in the control phase and 200 in the intervention phase), with an average of 26.7 data points collected from each of the 15 designated high-touch surfaces. With the control wipes, a 60.45% reduction in average total bacterial counts (CFUs) was observed, with a reduction in the frequency of high-touch surfaces that were positive before cleaning from 92% to 60%. cleaning. The number of surfaces with very high counts reduced from 5% to 1%. With the coloured test wipes, a 91.33% reduction in average CFU was observed, with a reduction in the frequency of high-touch surfaces that were positive before cleaning from 92% to 31%. The number of surfaces with very high counts reduced from 9% to 1%. Overall, using wipes with colour additive resulted in a 69.2% improvement in room cleanliness, and a 5.9% faster room turnover time. The addition of the colour additive did not impact the microbiocidal activity of the disinfectant itself. Hence, the reduction in microbial contamination was a result of more thorough cleaning technique.
Oremade O et al. The impact of a novel color additive for disinfectant wipes on room cleanliness and turnover time. American Journal of Infection Control 2024;52:1366-1370.





predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy


Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
Biodentine™ saves pulps EVEN with signs and symptoms of irreversible pulpitis*
saves pulps EVEN with signs and symptoms

saves pulps EVEN with signs and symptoms
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:

Bone Grafting
For vital pulp therapy, bulk- lling the cavity with Biodentine™ makes your procedure better, easier and faster:
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
tooth
Biodentine™ brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:

As the first all-in-one biocompatible and bioactive dentin substitute, Biodentine™ fully replaces dentin wherever it’s damaged.
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of
• Vital Pulp Therapy allowing complete dentin bridge formation
brings one-of-a-kind benefits for the treatment of up to 85%** of irreversible pulpitis cases:
Pulp healing promotion: proven biocompatibility and bioactivity
• Minimally Invasive treatment preserving the tooth structure
Reduced risk of failure: strong sealing properties
• Vital Pulp Therapy allowing complete dentin bridge formation

• Minimally Invasive treatment preserving the tooth structure
• Immediate Pain relief for your patients’ comfort
Vital Pulp Therapy allowing complete dentin bridge formation
Only one material to fill the cavity from the pulp to the top
• Immediate Pain relief for your patients’ comfort • Bio-Bulk filling procedure for an easier protocole
• Minimally Invasive treatment preserving the tooth structure
• Bio-Bulk filling procedure for an easier protocole
• Immediate Pain relief for your patients’ comfort

New Biphasic Formulations allowing you to manage the pace of your bone grafting procedures:
Similar mechanical behavior as natural dentin: ideal for bulk filling
Minimally Invasive treatment preserving the tooth structure
Immediate Pain relief for your patients’ comfort
Biodentine™ helps the remineralization of dentin, preserves the pulp vitality and promotes pulp healing. It replaces dentin with similar biological and mechanical properties.
• Bio-Bulk filling procedure for an easier protocole
(80% ß-TCP / 20% Hydroxyapatite)
The final enamel restoration will be placed within 6 months.
Improving on Biodentine the composite onto Biodentine full restoration in a single session
Bio-Bulk filling procedure for an easier protocole
Bio-Bulk filling procedure for an easier protocole
40/60 (40% ß-TCP / 60% Hydroxyapatite)
Innovative by nature
Innovative by nature
Innovative by nature

Please visit our
Please visit our website for more information
www.septodont.com
Please visit our website for more information www.septodont.com








To enjoy the clinical benefits of the first and only dentin in a capsule, ask your dental distributor for Biodentine™.



clinical photography MASTERCLASS
Presented by Dr Angelo Lazaris
SYDNEY

Whether it be creating the WOW in case presentations, communicating with his dental laboratories globally, documenting his work or giving patients the feel good factor after treatment, clinical photography is a well-practised art for Dr Angelo Lazaris and a vital skill for every aesthetic and cosmetic dentist...
Unlike other digital technologies, clinical photography demands a significant degree of user input and technical skill in order to produce photographs that are clinically relevant and diagnostic. This hands-on workshop has been developed to equip participants with the skillsets required to produce high quality, reproducible and clinically relevant photographic records through a standardised workflow that can be implemented in practice with immediate effect.



Dr Angelo Lazaris
BDS (Hons) (Syd), MSc (Aes) (Kings College)
Angelo has developed his own complete digital protocols from inception and design through to delivery and integrated these with biomimetic adhesive dentistry and contemporary restorative materials to create a complete clinical workflow that is equally applicable to single restorations, through to complex full mouth rehabilitations, culminating in outstanding clinical outcomes in a real-world commercial environment. His innovative approach to clinical dentistry is to start at the desired
endpoint, deconstruct complex treatments and develop solutions have made him a sought after KOL, educator and mentor. With appointments including honorary senior lecturer for Kings College London and the University of Sydney, Angelo has recently been assigned as course director for a post graduate diploma and masters degree in digital dentistry; a testament to his expertise and the influence of this discipline in dental practice.

ONLINE CPD CENTRE


Question 1. What has been a major factor contributing to the shortage of dental assistants in Australia over the past five years?
a. Increase in dental school graduates.
b. The COVID-19 pandemic.
c. A decrease in dental insurance coverage.
d. A surplus of dental assistants in other countries.
Question 2. Which technology is highlighted in the article for tracking changes in tooth shade and dental plaque over time?
a. Intraoral cameras
b. Optical Coherence Tomography (OCT)
c. 3D intraoral scanners
d. Fluorescence diagnostics
Question 3. What is one potential benefit of Optical Coherence Tomography (OCT) in dental practice?
a. It uses ionizing radiation for high-resolution imaging.
b. It requires a special laser use license.
c. It has low resolution compared to other imaging technologies.
d. It can replace up to 75% of traditional intraoral radiographs.
Question 4. Which of the following is NOT mentioned as part of sustainable dental practices discussed in the article?
a. Using single-use disposable gowns.
b. Recycling polypropylene surgical wraps.
c. Reducing plastic waste generation.
d. Reusable surgical masks and respirators.
Question 5. What role might dental assistants play in the future regarding sustainability in dental clinics?
a. They will be responsible for diagnosing oral diseases.
b. They will help segregate materials for recycling.
c. They will be in charge of the technological development of dental tools.
d. They will oversee the marketing of sustainable dental products.
INSTRUCTIONS:

Question 6. What is one of the key tasks of staff in the reprocessing area after sterilisation?
a. To inspect the packaging for tampering.
b. To check that the sterilised load meets the required standards.
c. To ensure that all items are properly labeled.
d. To perform the sterilisation cycle again if any errors are found.
Question 7. What can cause a weak seal in paper-plastic pouches used in sterilisation?
a. Using too much paper in the wrap.
b. Not inspecting the load before sterilisation.
c. Overfilling the pouch.
d. Using excessive heat in the steriliser.
Question 8. Why is it important to record the weight of the sterilisation load?
a. To prevent overloading the steriliser and ensure proper sterilisation temperature.
b. To ensure the items fit inside the steriliser.
c. To comply with sterilisation regulations.
d. To track the expiry date of the items.
Question 9. What is the purpose of using chemical indicators is...
a. To determine the weight of the sterilised items.
b. To provide a final check to confirm that steam has reached the wrapped items.
c. To verify the temperature inside the steriliser.
d. To record the cycle number.
Question 10. What should be avoided when cooling sterilised items before storage?
a. Storing the items in plastic containers.
b. Placing the items directly on a flat bench surface.
c. Storing the items in a humid environment.
d. Checking the expiry date of the sterilised items.
By David Petrikas





Question 11. What is the main purpose of A-dec’s end-to-end asepsis program?
a. To improve the speed of dental procedures.
b. To increase patient satisfaction.
c. To provide aesthetic improvements to dental equipment.
d. To maintain the dental units and ensure they do not pose a risk of infection.
Question 12. Which product does A-dec recommend using daily to maintain dental unit water lines?
a. ICX tablets
b. AlphaSan tubing
c. ICX Renew
d. Brass control block
Question 13. How often should water be tested in the dental unit according to A-dec’s guidelines?
a. Once a week.
b. Once a month, or every six months based on results.
c. Once every two months.
d. Only when the water quality seems poor.
Question 14. What is the function of the “Vaporiser” feature in the A-dec Pro delivery systems?
a. It increases the speed of dental handpieces.
b. It disinfects the dental unit water lines.
c. It purges the turbine with a blast of high-speed air to prevent contamination.
d. It reduces the noise produced by handpieces.
Question 15. What does the Pro delivery system’s “auto flush” do?
a. It increases water flow during procedures.
b. It purges all tubing to ensure only fresh water is in the water lines.
c. It cleans the dental unit after each use.
d. It monitors water temperature during treatment.e
Question 16. What is the main advantage of the Shining 3D Aoralscan Elite scanner over other photogrammetry systems in the dental field?
a. It is more expensive than other systems.
b. It is small, lightweight and integrates both intraoral scanning and photogrammetry camera in one handpiece.
c. It requires additional software to complete the scanning process.
d. It only performs photogrammetry, not intraoral scanning.
Question 17. What does the term “hybrid” typically refer to in the context of All-On-X protocols?
a. A restoration base with an aesthetic component on top.
b. A type of implant used for full arch replacement.
c. A dental procedure involving the use of CBCT technology.
d. A method of adjusting the implant placement.
Question 18. What common issue is associated with All-On-X procedures despite meticulous impression techniques?
a. Implant failure due to incorrect materials used.
b. Lack of aesthetic appeal in the final restoration.
c. Misfit between the implant platforms and the prosthesis.
d. Overuse of photogrammetry technology.
Question 19. How does photogrammetry contribute to the accuracy of All-On-X procedures?
a. By improving the aesthetic component of the restoration.
b. By converting 2D photographic data into a 3D spatial model for detailed measurements.
c. By eliminating the need for impressions.
d. By reducing the number of implants required for full arch replacement.
Question 20. What feature of the Shining 3D Aoralscan Elite scanner makes it advantageous for All-On-X procedures?
a. It requires large and cumbersome equipment.
b. It has an built-in photogrammetry camera system.
c. It can only be used for external photogrammetry, not intraoral scanning.
By Terry Whitty
A summary of the latest research
By Emer. Prof. Laurence Walsh AO
Getting close to patients during treatment
Dental health care workers face heightened risks of respiratory infections due to their close proximity to patients’ oral and respiratory tracts, where respiratory infections are predominantly transmitted through close contact, typically defined as being within 1.5 metres. Exposure levels and risks during close contact are closely associated with patterns such as interpersonal distance, contact time, relative facial orientation and relative position. Despite the significance of these interaction patterns, there is a notable lack of research specifically addressing these dynamics between dental HCWs and patients. An observation study was conducted at a hospital in Shenzhen, China, utilising depth cameras (3 frames per second) with machine learning to capture close-contact behaviours of patients with HCWs. Additionally, questionnaires were administered to col lect patient demographics. The study included 200 patients, 10 dentists and 10 dental assistants. Patients had significantly higher close-con tact rates with dentists (97.5%) compared with dental assistants (72.8%, P<0.001). The reason for the visit significantly influenced patient-practitioner (P=0.018) and patient-assistant (P=0.007) close-contact time, with the highest values observed in prosthodontic and orthodontic patients. Furthermore, patient age also significantly impacted the close-contact rate with dental assistants (P=0.024), with the highest rate observed in patients below 14 years old at 85% [range: 70-93%]. These rates were significantly higher than close contact rates in other indoor environments, such as subways during peak hours (42.9%), and working in offices (33.7%). Thus, dental outpatient departments exhibit high HCW-patient close-contact rates, influenced by visit purpose and patient age. When such younger patients are being treated, dental assistants play a crucial role in providing psychological counselling and behaviour control for children and these increase the opportunities for patient close contact with assistants. More intricate clinical processes with prolonged treatment durations cause increased close-contact time with the dentist, thereby augmenting the risk of disease transmission. Enhanced infection control measures are warranted, particularly for prosthodontic and orthodontic patients or those below 14 years old.
Omicron and repeated COVID-19 boosters

The Omicron variant of SARS-CoV-2, which causes COVID-19, is associated with increased transmission and with reduced potency of neutralising antibodies, when compared to other circulating SARS-CoV-2 variants. This study systematically evaluated the effectiveness of currently available mRNA vaccines and boosters for the Omicron variant, based on literature published on PubMed, Embase, Web of Science and preprint servers (medRxiv and bioRxiv). The Omicron variants blunt the potency of neutralising antibodies more extensively than other circulating SARS-CoV-2 variants, making vaccines less effective against these variants. The pooled effect estimate was calculated by the random-effects model. A total of 3,156 publications were screened for eligibility. A total of 34 eligible studies were included in the meta-analysis, including 10 cohort studies, 22 testnegative case-control studies and 2 case-control studies. The majority of studies (22 articles) were produced in the USA. For vaccination protocols with 2 doses, the vaccine effectiveness (VE) against severe infection with any Omicron strain was 63.80% (49.55% for adolescents, 62.80% for adults, 75.83% for the elderly and 64.52% for the general population. For 3 doses, the VE was higher at 87.22% for protection from severe infection (81.18% for adults, 89.89% for the elderly, and 86.80% among the general population). Six months after the last vaccine dose, the protection for the 2 dose protocol declined to 60.43%, while with the 3 vaccine doses, after six months the VE was greater at 73.39%. Hence, the 3-dose protocol continued to provide longer and more effective protection. This was especially so for elderly patients, who are a high risk group for severe complications and death from COVID-19. Many countries have now implemented booster policies for older adults. Moreover, in some countries a fourth dose of BNT162b2 (Pfizer) mRNA vaccine has been implemented to provide additional protection against COVID-19 infection and death in the elderly. Obviously, new strains will continue to emerge over time. The efficacy of the existing vaccines is further reduced due to the immune evasion of the strain. Hence, further attention should be directed to challenge of new strains that emerge as potential threats to health.
Zhao F et al. What influences the close contact between health care workers and patients? An observational study in a hospital dental outpatient department. American Journal of Infection Control 2024;52:1296-1301.
Guo K et al. Effectiveness of mRNA vaccine against Omicron-related infections in the real world: A systematic review and meta-analysis. American Journal of Infection Control 2023;51:1049-1055.
The Solution For Your Retention Issues



• Computer Designed
• Perfect Fit
• Patented Material
• Laser Cut
• Smooth edges
• 3D Printed Model
• Perfect Fit
• Upper &/or Lower
• All scans accepted



Emerging roles for dental assistants over the next decade
By Emeritus Professor Laurence J. Walsh AO

Dental assistants perform an invaluable role in providing safe and effective patient care. Over the past 5 years, in many areas of Australia there has been a developing shortage in dental assistants. Some of this has been attributed to the COVID-19 pandemic and the potential attraction of other forms of employment, in the wider context of a skilled worker shortage across Australia. Of note, there has not been a shortage of dental assistants in the UK over the same period.
A major difference is that dental assistants are registered in the UK under the General Dental Council and this provides a more regimented career structure for them, as well as recognition as part of the health workforce. Undoubtedly this is something that will be explored in Australia over the coming years.
This article focuses on the ways that dental assisting roles may change over the coming decade because of the impact of major forces that are shaping clinical practice, with a particular focus on new technologies and moves to more sustainable practice.
the cutting | EDGE

1. Examples of dental assistant additional tasks for risk assessment. Panel A: Point-of-care saliva-based diagnostics including RAT tests. Panel B: Violet light fluorescence imaging of mature dental plaque biofilm, which appears as red deposits. Panel C: GC Tri-Plaque ID gel showing light blue staining of the biofilm for areas of extreme caries risk.
Patient work-up in the operatory
a.
3D scans
There is growing interest in the use of a range of tools to help assess the risk for oral disease, so that approaches to active treatment and dental maintenance can better be tailored to the needs of the individual patient. Existing technologies such as 3D intraoral scanners can form part of this. Sequential 3D scans can be used to assess changes in hard and soft tissues, to track problems such as non-carious tooth structure loss and gingival recession. In such applications, the use of software and artificial intelligence is paramount because of the need to compare many points across the sequential scans.
3D scans that are taken in colour also provide the opportunity to track changes in tooth shade, including changes due to ageing and discolouration due to endodontic problems.
In a similar way, dental plaque deposits that have been stained with GC TriPlaque ID™ gel can be recorded using colour 3D scans. The colour patterns show whether there is imbalance (dysbiosis linked to acid production and caries risk) in the dental plaque biofilm. Tracking changes in the colour of teeth or in the colour of the stained dental plaque is something that AI software could be very useful for.
Dental assistants already do 3D scans, so there is a nascent opportunity for greater analysis of these scans, to present the clinician with information regarding subtle changes over time.
b. Fluorescence diagnostics
There are many dental devices that use violet light induced fluorescence as part of the diagnostic process, with intraoral cameras being the most widely used of these.
Figure

Figure 2. Initiatives in sustainable dental practice from the World Dental Federation, including a massive open online course, case studies, and practice-level resources.
Analysis of such fluorescent images provides a useful way of tracking the distribution of thick mature deposits of dental plaque biofilm, without the need to use a disclosing dye. These thick deposits have high levels of bacterial porphyrins, giving strong red fluorescence signals when excited by violet light.
Dental assistants can already use an intraoral camera to make recordings or videos of a patient’s intraoral situation, both within the clinic itself as well as in extra-mural settings such as with teledentistry.
Monitoring the distribution of plaque over time can provide valuable insights into a patient’s oral hygiene habits. This would then naturally bridge to the work of dental assistants who have completed a certificate 4 in oral health promotion, who would then be able to provide the patient with oral hygiene advice.
c. Point of care assessment of biological samples
The pandemic has highlighted the usefulness of rapid antigen tests and point-of-care diagnostic devices. These types of technologies can be deployed into clinical practices and applied to samples of saliva, crevicular fluid and microdroplets of blood collected with a periodontal probe from a site with gingival inflammation. Chairside diagnostic devices can undertake more sophisticated analyses, using microfluidic technologies. This can allow rapid analysis of samples of dental plaque for the presence and levels of key pathogenic bacterial species. This is a logical extension of the work that dental assistants already do in assessing samples of saliva for their chemical properties.
Od. OCT imaging
ptical Coherence Tomography (OCT) is used widely in medicine for rapid non-invasive non-ionising imaging of both soft and hard tissues. It provides exceptionally high resolution - in the order of 4 µm - which is similar to histology and superior to other imaging modalities including ultrasound, cone beam imaging and MRI imaging. The technique for using a dental OCT system is almost identical to using a 3D intraoral scanner. In fact, OCT scans provide high resolution surface details that can be used to fabricate various restorations and appliances, eliminating the need for 3D scans as we currently use them. OCT imaging systems use LEDs or very low power diode lasers and no user license is required. Hence, there are no barriers to an OCT scan being done by a dental assistant as part of the patient work-up.
Because of the penetrating nature of the near infrared light used for OCT, it has been estimated that OCT imaging could replace up to 75% of traditional intraoral radiographs, such as bitewings and periapical radiographs. OCT images can assist in almost all types of oral diagnostic procedures and they do not attract concern or alarm from patients because the near infrared light is non-ionising and the light sources used are also eye-safe. This is why ophthalmology is one of the largest users of OCT for the diagnosis of retinal and corneal diseases and conditions. A typical OCT eye scan takes less than 0.5 seconds and existing prototype dental OCT systems can image an individual molar tooth in one second or less. The fact that OCT is a mature technology with many decades of use in medicine will make its adoption into dental practice relatively smooth.

• Any Design
• HD PMMA Milled
• Flexion Milled
• POM Resin Milled
• 3D Print Option
• Perfect Fit
• Upper or Lower
• All scans accepted



the cutting | EDGE

• Take sequential 3D scans and submit to software for evaluation.
• Take violet light fluorescence images and submit to software for evaluation.
• Collect oral samples and process using a point-of-care device.
• Undertake OCT scans of individual teeth and of identified areas of concern.
• Use Nuralyte to induce analgesia immediately before dental procedures.
• Operate washer-dryer unit to reprocess reusable masks and respirators.
• Operate washer-dryer unit to reprocess reusable cloth gowns.
Sustainable dental practice
The second major area of development that is already reshaping dental practice and will affect the working lives of dental assistants in the future are moves to more sustainable dental practice. At the international level, the World Dental Federation (FDI) has led numerous initiatives in this area and likewise, the Australian Dental Association has spearheaded a range of activities to highlight the importance of sustainability considerations. As just one example of this, the 2021 edition of the ADA Guidelines for Infection Prevention and Control were the first national dental guidelines in the world to include specific considerations around sustainability.
As efforts grow to develop additional recycling streams, dental assistants will play an increasingly important role in the segregation of materials. To cite just one example, polypropylene (PP) is a widely used plastic polymer material that forms the foundation of disposable gowns, surgical masks and respirators and nonwoven wrapping materials for sterile instruments sets (such as KimGard™). There has been considerable interest in developing methods for recycling polypropylene. Once in the environment, its remarkable resistance to chemicals and degradation poses long-term issues for waste management. Nevertheless, it can be readily recycled using pressure and temperature to regenerate blocks of polypropylene from items used in healthcare, which can then be reused. Several pilot programs have already been undertaken successfully in Australia to collect polypropylene surgical wraps from operating theatres and these have proven to be highly effective and easy to implement for staff. Similar types of programs will likely be rolled out for small scale producers of polypropylene waste such as dental clinics, over the coming years. How far this thinking could extend into recycling the components of paper-plastic pouches remains to be explored.
At the present time, there is considerable discussion at the international level around measures that reduce plastic waste. Dental assistants can champion initiatives in clinics that reduce plastic waste generation. An example of this would be to convert from using disposable plastic high-volume evacuation tips back to reusable plastic polymer tips or stainless steel suction tips.
Another example of sustainable dental practice is to move from single use polypropylene gowns for nonsurgical dental procedures back to cotton-based reusable gowns. These could be laundered within the practice, using a modern high-efficiency upright washer-dryer unit.
Figure 3. An example of washable reusable masks that withstand 100 cycles of machine washing without performance degradation, from etrema in Canada.
Table 1. Dental assistant activities
The New ELITE Intra Oral
The New ELITE Intra Oral
The New ELITE Intra Oral
Scanner from Shining 3D uses patented Intra Oral
The New ELITE Intra Oral
Scanner from Shining 3D uses patented Intra Oral
Photogrammetry Technology to be the most accurate scanner available.
Scanner from Shining 3D uses patented Intra Oral
Scanner from Shining 3D uses patented Intra Oral

• Edentulous Scanning for Dentures !
• Partial Denture Scanning
• Impression Scanning
• Edentulous Scanning for Dentures !
• Partial Denture Scanning
• Duplicate Denture Scanning
• Impression Scanning
• Scan All On X Cases Accurately
• Duplicate Denture Scanning
• Suitable for all Intra Oral Scanning
• Scan All On X Cases Accurately
• Now Mac or Windows Compatible
• Suitable for all Intra Oral Scanning
• Now Mac or Windows Compatible



A further example is the recent development of surgical masks and respirators which can be washed and reused up to 100 times, such as the eTECH by Etrema in Canada, without degradation in their fluid resistance or their microbial filtration performance. If such products become approved and adopted in Australia, the logic around having a washer-dryer unit located within the dental practice becomes even stronger.
Finally, the activities of dental assistants both within the operatory and also at the “back of house” will likely change as more emphasis is placed on reducing the movement of patients and clinic supplies, since these represent a very large part of the overall environmental impact of a dental clinic, when measured in terms of greenhouse gas emissions.
“The activities of dental assistants both within the operatory and also at the ‘back of house’ will likely change as more emphasis is placed on reducing the movement of patients and clinic supplies, since these represent a very large part of the overall environmental impact of a dental clinic, when measured in terms of greenhouse gas emissions...”
Having longer patient visits where more work is done in a single appointment is a likely direction for the future for some parts of general dental practice. This can be facilitated by technologies such as the Nuralyte™ (from Dentroid in Canberra) that provides rapid onset potent analgesia for dental procedures in different areas of the mouth in the one appointment, without the need for injections of local anaesthetic. This light-based technique does not use a laser and so does not require a laser use license to operate. It is used in the same manner as a traditional curing light, which is a technique already familiar to dental assistants.
Conclusions
As dental practice continues to evolve over time, dental assistants will need to adapt and change. Their tasks may alter, to include new tasks not currently undertaken (Table 1), but the fundamental characteristics that make an excellent dental assistant will remain the same. Those who are eager to learn and take on new tasks will find that the next decade will offer a range of opportunities that invigorate their role.
Recommended further reading for the topics discussed in this article:
Oral diagnostics
1. Walsh LJ. Saliva as the ultimate analyte for the dental professional. Auxiliary 2014; 24(2):22-24.
2. Walsh LJ. Recent developments in chairside diagnostics for dental plaque assessment. Auxiliary 2009; 19(5):28-30.
3. Walsh LJ. Chairside rapid immunoassay testing for Streptococcus mutans: A new tool in caries risk assessment. Australasian Dental Practice 2008; 19(6):118-120.
Fluorescence
4. Walsh LJ. New paradigms for assessing caries risk and lesion activity. Auxiliary 2011; 21(3): 28-33.
5. Walsh LJ. Fluorescence applications in dentistry: current status and future prospects. Australasian Dental Practice 2013; 24(3):62-64.
6. Walsh LJ. Caries diagnosis aided by fluorescence. In: Arkanslan Z (Ed) Dental Caries - Diagnosis and Management. Croatia: InTech Publishers, 2018. Chapter 7, pp. 97-115.
OCT
7. Walsh LJ. New developments in optical imaging: bringing the invisible to light. Australasian Dental Practice 2010;21(6): 50-54.
8. Shakibaie F, Walsh LJ. Optical diagnostics to improve periodontal diagnosis and treatment. In: Manakil J (Ed) Periodontology and Dental Implantology. Croatia: InTech Publishers, 2018. Chapter 4, pp. 73-86.
Sustainability
9. Walsh LJ. Reusable personal protective equipment viewed through the lens of sustainability International Dental Journal 2024; 94 (Suppl 2): S446-S454.
10. Walsh LJ. Current challenges in environmental decontamination and instrument reprocessing. International Dental Journal 2024; 74 (Suppl 2): S455-S462.
11. Walsh LJ. Sustainability in dentistry: Part 1. Plastics and biodegradability. Australasian Dental Practice 2023; 34(3):112-116.
Nuralyte analgesia
12. Kulkarni S, Walsh LJ, Bhurani Y, George R. Assessment of the onset of analgesia and length of analgesia following the use of PBM with different wavelengths: A clinical study. Lasers in Medical Science. 2024; 39(1):236.
13. Sleep SL, Walsh LJ, Zuaiter O, George R. PBM for dental analgesia and reversal from injected local anesthetic agents: A systematic review. Lasers in Dental Science 2024;8:52.
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.


How “Cheap Charlie” and “Stingy Sarah” achieved their goals
By Graham Middleton

“Practice owners who are not yet ready to contemplate retirement or practice sale resent being pushed into making premature decisions and this can kill off future opportunity...”
Charlie and Sarah both came from poor families. Each had had a variety of part time jobs from high school onwards including stacking supermarket shelves and working at Maccas. Charlie gained entry to a dentistry course and Sarah to a Bachelor of Commerce. For Charlie, studying dentistry had meant five years of poverty. Sarah fitted a substantial amount of work around her less challenging and shorter course. On completion, she gained a job in a bank. Although modestly paid, it was a substantial jump on what she had been used to. She needed wheels and made an economical choice. Soon after graduation, Charles met Sarah and they began a relationship. He was working two days each in two practices each located in an established mid-income suburb.
BMentoring Charlie
oth practices were introduced to him by a lecturer, a semi-retired successful dentist who had mentored him at dental school recognising his potential and work ethic. His mentor had explained the basis of his own success which was to concentrate on owning four key assets which were his home, his practice, his well-presented premises and his family superannuation fund, keeping his practice free from 3rd party agreements with health funds and that chairside communication skills were as important as clinical skills. Charlie respected his mentor’s success and the formula stuck in his mind.
Saving toward first home
Charlie bought a cheap car and Sarah sourced the finance for him. Years of frugal living had made them careful with money. They rented the most economical but livable flat they could find. Kitchenware mainly came from op shops and furniture from garage sales. Friends had bought flasher cars and some were soon booking exotic holidays. They lived modestly, bought cheap food at a market, ate at home prepared meals, ignored takeaways and saved toward a home.
Sarah proposed a budget and Charlie was keen to improve their finances. They thought about how many ways they could save money, limited driving to save petrol, exercised in the park and used a local library. Their savings grew and HECs debts fell. Having grown-up poor, they were conditioned to frugality.
Reliability and relationships
Charlie quickly moved from sessional payment to commission on the commonly used formula but was in an early learning phase. He steadily improved his clinical skills, gaining confidence. As he improved his chairside manner, patient’s acceptance of follow-up treatment increased. In his first year, both employers, Lewie and Meg were focused on their personal surgeries. He worked diligently, was grateful for appointments but in each practice the pecking order was first the practice owner and then longerterm “lifestyle” dentists but his patient appointments grew tighter with more follow-ons and the beginnings of personal referrals. The receptionists noted that he was prepared to squeeze in the odd extra filling and did not mind finishing later than the others. As they allocated more new patients, his output grew at a healthy rate.
Building fees and cementing relationships
At Charlie’s two-year practice point, Sarah’s salary was now above starting grade but unlikely to match his income potential. They were committed to saving and wanted to be able to buy their first home prior to having a first child. Charlie was working hard and producing more fees per day than the “lifestyle assistant dentists” who limited their hours, often not doing an extra procedure so that they could leave early. He had surpassed them, gaining the second choice of unreferred patients after the practice owners. Receptionists appreciated his reliability and willingness to squeeze in another patient to solve a scheduling issue. He regularly thanked them for their assistance. He was careful to maintain relationships with practice principles Lewie and Meg, greeting each and exchanging the odd piece of dental news gained through his dental study group. He gained a reliable reputation.
practice | MANAGEMENT
First superannuation contributions but retaining focus
Sarah had employer superannuation. Charlie was a dental contractor and a couple of years into practice, his earnings were tipping him into high marginal tax plus Medicare levy territory. He elected to contribute maximum deductible superannuation contributions. Sarah’s tax threshold was lower and she limited her superannuation to her employer’s contributions. Their main focus remained that of buying their first home.
Learning the truth about home loan repayment
By Charlie’s 4th year following graduation, they had amassed a substantial deposit of $250,000 to purchase their first home with a mortgage of $700,000 and an interest rate of 6.25 percent per annum. The bank advised that their loan payments were $4,288 per month on a 30-year loan. A friend advised them to buy a financial calculator and showed them the impact of increasing their monthly home loan payments on reducing the length of their home loan. They pushed calculator buttons utilising various monthly repayments and found that a relatively small increase in monthly payments significantly shortened the period of their loan. They upped their payments to $7,500 per month and their loan payout time shortened from 30 years to 10 years and 8 months. The principle outstanding was reducing quickly and modest increasing real estate values meant that their equity in the home increased rapidly. They learned that in order to make the same after-tax saving, they needed to get a much higher return on a safe investment than they would achieve by simply increasing home loan repayments. Sarah was manic about keeping lifestyle costs down and putting as much spare cash into their housing loan and offset account. Charlie remembered his impoverishment. They kept to a strict budget and further shortened the payout period on their home loan.
In due course, Sarah fell pregnant. She accessed maternity leave and subsequently worked part-time. Charlie had developed his fee base nicely in both practices and they were now thinking toward purchasing a practice within the next
3-4 years. They had placed their home loan with a bank noted for financing dental practice acquisitions which had assured them, that with an impressive record of saving and mortgage reduction, it would be pleased to lend to purchase a practice. Compared to Charlie’s peer group, their lifestyle was austere.
Preparing to purchase a practice
They aimed to put themselves on a financial course to purchase a practice within four years of purchasing their home when Charlie would have been a dentist for eight years; preferably with an option to buy the premises. They intended talking the bank into keeping their interest deductible business loans on the practice on an interest only basis while they accelerated their non-tax-deductible home loan repayments. To enable this, their business loan and their home loan had to be with the same bank lender. Their frugal habits were rapidly improving their financial position.
Hint: On many occasions when advising dentists dealing with banks financing practice purchases, the bank lender has initially been only agreeable to a threeyear interest only period on the business financing loan. But as the interest only period is approaching conclusion, the bank has been persuaded to extend it beyond the period both in the hope of financing a home upgrade and/ or premises purchase or providing significant corporate hire purchase facilities for a major fit out upgrade and equipment purchase. Banks make their money from lending. Good performing loans are assets on a bank’s balance sheet. Efficient profitable dental practices are the source of good recurring business for a bank tuned into the profession.
“Stingy and Cheap” learn about low-cost accounting and cost-effective superannuation strategies
With Sarah’s basic knowledge, they had been able to complete their own tax returns and save fees. When a friend described them as “stingy and miserly”, they delighted in the description. Charlie didn’t mind his peers calling him “Cheap Charlie”. They were well ahead of their friends in building their financial position.
As they approached future practice ownership, they searched for a suitable accountant. They found that a vast majority of accountants were inept at giving business advice, simply pumping out financial and tax returns. They assessed each by asking questions about dental practice, to which they already knew the answers, and found that most were unable to identify the key characteristics of successful practices. Some made naive comments about all businesses having similar characteristics. Accountants at the big end of town demonstrated little knowledge of the characteristics of dental practices, some even confusing them with medical practices which are vastly different, but quoted huge fees. Eventually they found an accountant, Henry, who had a number of dental practice clients, was reasonably priced, was able to give realistic answers to most of their questions and could assist with practice purchase in due course. He advised that the better the presentation and records provided to him, the more economical his fees.
Note: I spent over 33 years as a business and financial adviser mainly to dentists, valued a multitude of dental practices, benchmarked their performance advised on purchase, operation and sale of dental practices and for 26 years was the founding partner of a successful accounting and financial services group. Over those 33 years, I came across a multitude of accountants and realized that while many had signage and web sites proclaiming that they provided business advice, the vast majority were in fact poor business advisers. Most confused completing annual returns with actual business advice and most of what they did was comment retrospectively on last financial years results. Most had little idea as to the relative efficiency of a client’s dental practice and dealt with a jumble of dissimilar businesses. Many had cost their dental clients lots of money due to ill-informed advice or lack of advice.
Henry was able to do super fund returns and advised that the simpler their investments, the lower his and the auditor’s fees. He warned them about complicating their fund with rental property or other unlisted investments or doing lots of trading. He pointed out that certain ETFs and a few long-standing listed investment companies had very low management expense ratios (MERs) and were well diversified.
These were the type of investments that people bought and held long term and hence were not followed by brokers. A few of these investments would provide ample diversification of risk.
Identifying cost effective investments
After an exhaustive search, they settled on two leading international ETFs with very low internal management expense ratios (MERs), the US Standard and Poors 500 Fund (ASX code IVV), holding the top 500 companies listed on the New York Stock Exchange, many of which were international in their operations and the US Total markets Fund which was broadly similar (ASX code VTS).
They explored Australian listed investment funds (LICs) and discarded those with high MERs and any with success fees. They settled on two long standing funds, Argo Investments (ARG) and Australian Foundation Investment Company (AFI) which had very low internal MERs and histories of paying franked dividends. They were each long-term holders of an extensive number of leading Australian companies.
Their 5th choice was Washington H Soul Pattinson (SOL), a combination of an active business and an investment company. It appealed because it had paid a dividend every year since listing on the stock market in 1903.
The five were ignored by brokers since they were mainly purchased and held long term rather than actively traded. This made them appealing to “Cheap and Stingy”.
They started their SMSF by rolling over existing superannuation and adding current years permitted concessional contribution then splitting most of the fund between their five choices. From that point on, they intended to maintain contributions and invest surplus cash into the five choices.
As their fund grew, its administrative cost remained tiny. Perhaps somewhere well into the future they might consider a change of strategy. As they had many years of contributions to come sticking to this strategy, despite fluctuations, was likely to significantly outperform one of investing in interest bearing securities.
Note: After many years of advising professional clients typically with two members and balances in the millions, I concluded that those who tried to actively trade in the stock market, those who bought residential rental properties, those invested in exotic plantation investments or in unlisted companies complicated their funds and their results disappointed. Readers must of course do their own research and seek professional opinions but be beware of adviser’s bias toward inhouse services.
Charlie puts himself in line to buy a practice
Both Charlie’s employers recognised his reliability, wanted to keep him and increase his employment to full-time. In due course, Charlie chose to increase his time at the practice of the older owner, Lewie, to three full days per week and continue his sessions at Meg’s practice at two days. Lewie was closer to likely retirement but he was careful to remain on friendly terms with Meg. While looking toward the future, he did not pressure Lewie as practice owners who are not yet ready to contemplate retirement or practice sale resent being pushed into making premature decisions and this can kill off future opportunity.
He continued to build his follow-on appointments and growing personal referrals while ensuring that his relationships with Lewie, Meg and practice staff remained healthy. He was generating healthy commission income from his work in both practices. Lewie’s longterm receptionist, Katie, who enjoyed his confidence, was urging him to engage Charlie full-time. Lewie himself had reduced to four clinical days per week and was enjoying every weekend being a long weekend.
When another of Lewie’s assistant dentists departed, he asked Charlie to increase his involvement. Lewie was 58 and keen to maintain practice output in the threechair practice. Charlie was significantly out-performing Lewie’s two part-time “life-style” assistant dentists.
As Lewie had initiated the matter, Charlie asked for a discussion about his future plans. He explained that he enjoyed working in Lewie’s practice but was looking to his own future. Before he resigned from Meg’s, he needed assurances.
He asked Lewie whether there was a prospect of purchasing an associateship in his practice. Recognising that Lewie did not want to be pushed into a corner, he asked that if his performance warranted it, he would be offered an associateship in two years when Charlie would have been a dentist for eight years and Lewie would be 60?
Lewie too had to consider the future. While he was aware of corporates offering handsome prices, their offers came with significant conditions. He was not yet ready to sell but was aware that his peak performing years were behind him. He needed Charlie to maintain and improve practice output but knew that it was unlikely that Charlie would sign a contract with a corporate buyer. Lewie did not want the stress of being the lead dentist to a corporate owner when he was slowing down. He knew that Charlie was entering the career point at which there was a risk of losing him to purchase another practice. Practice administration was becoming tiresome and some aspects of the practice were deteriorating. His wife was urging him to slow down and take longer overseas holidays. Katie, their trusted receptionist, recognised the need to engage Charlie fulltime to keep him in the practice and had quietly urged Lewie to cement a deal. Charlie remained polite to all and concentrated on being the most reliable assistant dentist in the practice.
Moving closer to practice ownership
Eventually, an amiable agreement was reached. Charlie would work fulltime in Lewie’s practice and subject to continued performance, would be offered either an associateship or the opportunity (at Lewie’s choice as to which) to buy the whole practice within two years when he would have been qualified for eight years. Commensurate equity in the premises would be offered, with a right to take it up at independent valuation, within four years. The basis of practice valuation was agreed. Lewie would immediately reduce his clinical involvement to seven days per fortnight and take seven weeks leave per year. They would jointly agree on fee reviews and some needed maintenance would occur. They agreed to the basis of valuation on which the practice/associateship sale would occur,
being on a dentist- to-dentist sale, rather than a sale with corporate conditions attached. The practice was to remain a non-preferred provider.
Note: I have seen younger dentists threaten to leave if an older practice owner does not sell to them but often this has backfired. The older practice owner puts up their personal shutters rather than give into pressure and mutual trust evaporates. It usually ends with the younger dentist departing; often to their long-term detriment.
Charlie and Sarah’s home mortgage had now reduced significantly and the value had grown with improvement in house prices. They remained economical in their lifestyle, recognising that to gain the best financial advantage, they needed to achieve practice and premises ownership and gain financial leverage over their assets. Many dentists owning their own practices were far better off financially than those who had chosen careers contracted to dental corporates.
On becoming the full-time assistant dentist in Lewie’s practice, Charlie immediately became its highest fee producer and increasingly the go-to person when treatment issues with part-time assistant dentists arose. He gained autonomy over the structure of his own patient book, working closely with receptionist Katie. As Lewie enjoyed increased leisure, he realised that he needed to sell the whole practice and work for Charlie as an assistant dentist for three days per week rather than take the half way option of first selling an associateship. Corporates were unlikely to buy the practice without having Charlie contracted.
Financing and structuring practice ownership
Charlie and Sarah quickly confirmed their bank finance. The bank included their home in the overall security and as expected, the practice loan was on an interest only basis for the initial three years. They wetted the lenders appetite by mentioning that they intended to buy the premises in due course and mentioned financing some equipment via the bank’s chattel mortgage.
It was music to the banker’s ears as they noted Charlie’s strong position in the practice had effectively negated buyer’s risk.
Note: Bank loans officers lending to professionals improve their own salaries as they grow a profitable client list. Having a successful dental client with home and practice loans, chattel mortgages on equipment and a probability of financing dental premises purchase and possible future home upgrades make them ideal bank clients. Banks make their profit by safe lending to strong clients.
In discussions with Henry, they noted that having several other fee generating dentists in the practice meant that Sarah could be part owner and participate in profits provided that Charlie received an income commensurate with his occupation as a dentist. The option of ownership via a trust was dismissed because a trust was obliged to distribute all of its income on an annual basis. They settled on joint ownership via a simple partnership and elected to “license” the practice to be operated by a company. They did not buy the practice inside a company as doing so would threaten long term capital gains tax concessions on future sale. The company would pay an annual license fee to them to cement the business relationship and would mainly pay them by franked dividends. Henry indicated that this was the critical point to settle on their long-term taxation structure.
As the purchase was made midway through a financial year, they were able to retain several months profit in the company until 1 July, have Henry complete the company’s return early in the new financial year, pay company tax, pay themselves dividends and begin company tax installments. A substantial amount of future practice income would flow to each of them as franked dividends plus license fees, thereby optimising their tax structure. While Charlie maintained his dental income, Sarah’s income jumped substantially and they gained full advantage of her lower tax threshold points. They would each pay and claim the permitted amount of superannuation contribution.
Sarah resigned her external employment as they were expecting their second child. She had done a book-keeping course and henceforth would take responsibility for practice book-keeping, payment of non-professional staff wages, contractual payments to assistant dentists including Lewie and practice bills. She would minimise her presence in the practice, doing most of the book-keeping at home.
They wished to avoid a “boss’s spouse” syndrome situation.
Notwithstanding that their practice acquisition cost about a million dollars, there was a big jump in their joint income. They poured more money into their home mortgage and each paid the allowable tax effective amount into superannuation.
Practice changes
Whereas a typical privately owned and conducted dental practice had a DEBDIT (dental earnings before depreciation interest and taxes of about 57 percent, Lewie had lost the will to drive the practice and DEBDIT was sitting at approximately 51.5 percent. That difference meant that 5.5 percent of gross fees was being lost. Since the percentage of fees retained by dentists remains constant, this inefficiency came off practice profit and had reduced the sale price. Readers should refer to my book Financial Success for Dentists for more detail. In successful practices, the lion’s share of profit is generated in the principal’s surgery but the remainder of a practice can sometimes produce only nominal results for the owner. They were obligated to maintain Lewie as a part time contractor and Charlie continued to discuss challenging cases with him. The two lifestyle dentists each worked at a leisurely pace using significantly more practice resources per dollar of fees than did Charlie. He squeezed their patients into two days each rather than their leisurely 2.5 days each, advising them that he expected timely starts and a lift in their daily throughput. Sarah examined purchasing and by comparing price lists and holding suppliers responsible was able to make economies. Their accounting cost was much lower than Lewie’s had been and with a little coaching by Henry, Sarah was able to maintain book-keeping in good order. They spent a reasonable sum on painting and recarpeting, concentrating on areas seen by patients and financed the replacement of a few aged items of equipment via chattel mortgage and made appropriate fee adjustments. Sarah supervised the trades and negotiated the equipment purchases and chattel mortgage. The practice website was kept simple and gave no hint that Lewie had sold and reduced his presence. Marketing and business consultants promising to do wonders via internet
marketing were ignored. Their emphasis was on serving the practice’s existing substantial patient list which practice records indicated were the source of most new patient referrals. Lewie passed on long standing patients unable to be fitted into his surgery with Katie noting which had significant connection to other patients. They tidied up the patient reminder system and Charlie fine tuned his own patient book. They quickly restored the practice DEBDIT to 57 percent of fees.
Subsequently...
Within a couple of years of practice purchase, they bought the premises with two licensed valuers, one acting for Lewie and one for them agreeing on
“Premises ownership is strategic for dentists because it gains control of fit-out including the hidden plumbing, wiring and air lines. It is hugely expensive to be forced to move a fully quipped dental practice and re-do fit-out...”
a mutually acceptable price. The bank, noting the strong financial performance of the practice, was keen to finance it. They had rapidly reduced their home loan and were looking to upgrade to their long-term family home. Lewie will quietly fade into retirement and they will utilise contacts among dental school’s staff to identify a suitable recent graduate to join the practice and eventually grow into their key assistant dentist. Their lifestyle dentists have had to lift their performance. Firm but friendly control will be maintained over their output.
Note: Premises ownership is strategic for dentists because it gains control of fitout including the hidden plumbing, wiring and air lines. It is hugely expensive to be forced to move a fully equipped dental practice and re-do fit-out.
The content of this article was inspired by a number of successful dentist and spouse couples.
Best wishes to all dentists, Graham Middleton
General Advice Warning
The information contained in this article is unsolicited general information only, without regard to the reader’s individual financial objectives, financial situation or needs. The information contained in this article is general in nature and you should consider whether the information is appropriate to your needs and where appropriate, seek professional advice from an accountant or financial adviser. It is not specific advice for any particular individual and is not intended to be relied upon by any person. Before making any decision about the information provided, you should consider the appropriateness of the information in this article, having regard to your objectives, financial situation and needs and consult your professional adviser. Any indicative information and assumptions used here are summarised, are not a product illustration or quote and also may change without notice to you, particularly if based on past performance. This notice must not be removed from this article.
About the Author
Graham Middleton disposed of his interest in Synstrat group on 30 June 2020 and won’t be starting another business; he spent the later 33 years of his working life advising health professionals on business and financial matters. Dentists were the most numerous of his clients. He is the author of the recently published Financial Success for Dentists.

Dentists may obtain a copy by making a donation of minimum $60 to the Delany Foundation a registered charity which assists schools in Ghana, Kenya and Papua New Guinea then email Graham at graham. george.middleton@ gmail.com. A copy will be sent to you. All proceeds go to the Delany Foundation for its good work. Graham has paid for the printing and mail costs personally.



























*organised in conjunction with the australian dental association in new south wales and victoria
A dental practice is usually one of the most valuable assets in a dentist’s life.
When it comes time to sell, many will do so with little understanding of the value of what they are selling and how to present it effectively to a buyer.
Others delay putting their practice on the market at an optimal time, fearful of what to do next and afraid of a loss of their identity.
This course explains:
• How to prepare your practice for sale to optimise the price, terms and compatibility with a purchaser
• Which exit strategy is right for your practice and why
• When is an optimal time to maximise the return for your asset
• Pitfalls owners fall into that devalue their practice in the final years of ownership
• Steps owners can take to improve the outcome in the final years of ownership
VITAL INFORMATION
for anyone within 5 years of EXITING


Presented by Simon Palmer
With more than 20 years’ experience in dental practice sales, Simon Palmer has extensive knowledge of and insight into the complexities and sensitivities involved in buying and selling dental practices. Simon’s business - Practice Sale Search - sells more than 100 practices per year. He is a regular writer/contributor to dental publications and journals, and is regarded as an expert on dental practice purchases and sales in Australia and New Zealand.
TOPICS INCLUDE
n Exit planning: how do you get your practice ready to sell?
n What are the pros and cons of the exit options/ strategies available to you?
n Succession Planning: What do you need to do now to prepare?
n What is the likely profile of the buyer for your practice and what will they be looking for?
n Valuing Dental Practices: What/ where is the value in your practice?
n How do you handle staff discretion, confidentiality and disclosure?
n Legal agreements
n Effective strategies for transferring patients effectively from seller to buyer
n What to do next post sale: post-sale strategies
n Tax implications and strategies when selling
n Expert finance, legal, accounting speakers


Your role in creating a thriving team
By Julie Parker
As a dental practice management consultant, I frequently hear the same complaint from practice owners and managers: “There are no good people out there”. It’s an understandable frustration - we know it’s tough out there for many professions and industries. But, what if this pervasive issue isn’t entirely about the people you’re hiring? What if the other half of the equation lies with the leadership?
I watched a Simon Sinek video today where he shared a powerful insight.
Simon spoke about his experience at the Four Seasons in Las Vegas, where a barista named Noah stood out for his enthusiasm and authenticity. Simon asked Noah whether he enjoyed his job. Noah responded that he LOVED his job. When Simon probed further and asked why, Noah said “throughout the day, managers will walk past me and ask me how I’m doing and if there’s anything that I need to do my job better”. He said, “not just my manager, any manager”. Simon reflected that Noah then said something magical. “I also work at Caesars Palace. There, the managers are trying to make sure we’re doing everything right. They catch us out when we do things wrong. When I go to work there, I like to keep my head under the radar and just get through the day so I can get my pay cheque”. Noah continued, “Here at the Four Seasons, I feel I can be myself”.
Simon surmised that Noah loved his job because managers at the Four Seasons regularly asked how they could support him, creating a sense of value and trust. In contrast, at his other job at a less supportive workplace, Noah admitted he kept his head down, avoided attention and did the bare minimum. The difference?

Leadership shaped an environment where Noah could thrive in one place and disengage in the other.
This principle applies to dental practices as well. Leaders often focus on finding the “right people” but neglect to ask whether they’ve built the “right environment” to enable those people to thrive.
I have been studying the work of Richard Barrett of late. Barrett is a leadership consultant, author and founder of the Barrett Values Centre, known for his expertise in organisational culture and values-based leadership.
Barrett has a great quote: “If you want to change the culture of your organisation, you must either change your leaders, or your leaders must change”.
Leaders are architects of the environment and the culture they create directly influences how team members show up.
Have you ever considered that you might already have the perfect team, but
they are simply reacting negatively to the conditions you’ve created?
Think about the last time you asked your team members, “What do you need to do your job better?” It’s a simple but transformative question. Often, leaders make assumptions about what’s needed without directly engaging their team, overlooking the practical, day-to-day challenges faced by those on the front lines.
This dynamic is one Charles and I often see in Australian Rules Football (AFL). A promising draft pick might fail to meet expectations and get dropped from their team, only to be picked up by another club where they excel beyond anyone’s expectations. What changed? The player didn’t fundamentally become more talented overnight; they stepped into a different environment, shaped by a different culture and leadership. The right environment allowed their potential to surface and flourish.
practice | MANAGEMENT
Diagnosing the environment you’ve created
If you’re not sure how your leadership style impacts your team, consider starting with these reflective questions:
1. When was the last time I had a one-onone conversation with a team member to understand their challenges?
2. Do I focus more on catching mistakes or celebrating successes?
3. Am I clear about the values and purpose of our practice and do I communicate them effectively to my team?
4. Do I create opportunities for team members to grow and align their work with their strengths?
The answers to these questions can be telling. Practices that cultivate trust and respect find that their teams naturally align with their goals and values. Conversely, practices that operate in a culture of fear or micromanagement find disengagement and turnover to be persistent problems.
A happy and engaged receptionist creates a positive first impression for patients. A supported and appreciated dental assistant ensures smoother proce-
dures and patient comfort. When every team member feels their contribution is valued, the entire practice benefits.
However, a toxic environment - characterised by micromanagement, lack of communication, or misplaced prioritiesleads to disengaged team members who, in turn, deliver subpar patient experiences.
Building a culture of collaboration and growth
The good news is that creating a supportive environment doesn’t require a complete overhaul. Small, consistent actions can lead to significant changes. Here are some practical steps to consider:
• Foster open communication: Implement regular check-ins with team members to understand their needs and address concerns;
• Invest in growth: Offer training and development opportunities that align with team members’ aspirations and your practice’s goals;
• Model your values: As a leader, demonstrate the behaviours and attitudes you want to see in your team; and

SAFety FirSt
Whether you’ve just started working, own your own practice or are considering retirement, Profile Financial Services can help you plan and secure your financial future. Just like good dentistry, in investing, prevention is better than cure! A sound financial plan can help anticipate and avoid risks before they damage your portfolio.
How safe are your investments?

To find out, contact Profile now to book an obligation-free initial meeting: (02) 9683 6422 Or visit our website www.profileservices.com.au
• Celebrate wins: Recognise achievements, no matter how small.
What if you could unlock the potential of your existing team by re-evaluating your leadership approach?
The journey to a thriving practice begins with self-reflection. When you shift your focus from blaming the people to examining the environment, you empower yourself as a leader to create lasting change. Remember, the best teams don’t happen by accident - they are nurtured through intentional leadership.
About the author
Julie Parker is a Dental Practice Management Consultant and Team Educator. At the age of 33, Julie became the first non-dentist to own a dental practice in Australia. Julie is Co-Founder of Julie Parker Practice Success and CoFounder of Dental Business Mastery. Visit julieparkerpracticesuccess.com.au and dentalbusinessmastery.com.au to find how Julie can help your dental practice be more successful through consulting programs, online courses, podcasts and more.





Dental corporate myth busters: A defence of the most common objections to dental corporates
By Lisa Singh and Simon Palmer
As two of the most experienced dental practice brokers in Australia, we remain amazed at the persistence of the scaremongering that occurs surrounding the experience of selling to large dental corporates/aggregators.
In this article, we thought we would address some of the more commonly heard arguments against selling to dental corporates/aggregators.
Argument against dental corporates #1
“I will not consider selling to a corporate. There are horror stories out there from people who sold to them.”
We don’t doubt that these horror stories exist (we have heard some of them), but: 1. Sometimes work conditions deteriorate post sale, due to an incompatibility that emerges between the buyer and the vendor. In our experience, an incompatibility like this is rare and no more or less likely if the buyer is a corporate or a non-corporate buyer.
2. If you heard a dental corporate horror story, the chances are that you only heard one side of the argument... the vendor’s. There could be (and often is) another side of the argument - the buyer’s... or parts of the story that were not told to you by the vendor that may provide a valid justification of why the corporate acted as they did.
3. There are many dental corporates out there. Even if the story you heard was accurate and the corporate in the story was unprofessional/unethical/in the wrong, I don’t think it follows to say that all corporates act unprofessionally or unethically. We have heard plenty of cases where dentist owner-operators have done the wrong thing, yet no one extrapolates from there that all other dentist owner-operators will act the same way.
4. They say that a bad story spreads 10 times faster and 10 times further than a good story. PSS has sold many practices to corporates every year for the past 15 years and I can attest to the fact that there are far more success stories than horror stories. People who are enjoying their post-sale lives just don’t seem to tell people with the same volume and frequency than someone who isn’t.
Argument against dental corporates #2
“Corporates are taking all the good practices off the market, leaving less for owner-operators. It is impossible for an owner-operator to compete with a corporate when buying a good practice, because the corporates have deeper pockets and can afford to pay more.”
I have two main arguments against this myth:
1. Owner operators and corporate/aggregators being interested in the same practice is not as common as you would think.
Dental corporates are only really interested in a very narrow subset of practices that are for sale. They are interested in practices that are:
• General practices (they don’t generally buy specialist practices);
• Having at least 3 chairs (or 2 chairs with room for 3 chairs);
• Grossing well over $1.5M and have a substantial EBITDA (operating profit) of over $300k after paying all expenses (including the principal dentist commission @40%);
• Not key-person dependent (less than 40% patient billings coming from any one clinician); and
• In easily recruitable locations.
There are a huge number of great practices for sale that exist outside of the above corporate criteria.
At the same time, it’s important to note that very few owner-operator dentists seem to have an interest in practices with a justifiable valuation that goes beyond $1.5M. Certainly (with few exceptions), practices with a price tag over $2M seem to be almost exclusively corporate/aggregatorbuyer domain.
Without dental corporates, these practices would either be unsellable or have reduced appraisals. While reduced appraisals may seem good for buyers, I am not sure you would agree if you owned a practice and through hard work and ingenuity were able to grow it to a place far larger and more profitable than others. You would be justifiably upset if you could not get proportionately compensated for what you built.
2. Where you are competing with a corporate, owner-operator buyers have several advantages in negotiations over corporates:
a. Owner-operators can compete on terms. Dental Corporates generally don’t buy practices that allow vendors to exit quickly or pay 100% upfront or without future targets.
b. Owner operators can compete on compatibility. Many vendors prefer the idea of selling to a person, rather than a company.
c. Many practices are worth more as a job than as a business. A corporate will only put a value on the profit of the business after the principal
dentist has been paid for their clinical work. They won’t put a value on the dentist’s high remuneration, good hours, long holidays and many other attributes that would be of interest to a dentist owner-operator.
Argument against dental corporates
#3
“Dental corporates focus on profit to the detriment of the staff and patients.”
Statements like this are the antithesis of the image that any health businesses would want to project to the world.
As much as any dental practice owner tries to project that they are virtuous, community minded and only in it to help people... they are, at the end of the day, owners of businesses that also exist to make money. There are certainly instances out there of practice owners:
• Violating employee rights by short paying, having them work on contracts and under conditions that are not legal and/or not compliant with Australian standards.
• Jeopardising patient safety in practices by not monitoring poor clinical work, or not applying rigorous sterilisation and WH&S protocols.
However, I should add:
1. These types of lapses are extremely rare; AND
2. When they do happen and end up being reported in the newspaper or AHPRA, they are much more likely (in our experience) to have happened with experienced dentist owner-operators who are just running an old or loose ship and cutting corners with compliance, than with dental corporate aggregators trying to maximise profit.
WConclusion
e want to make it clear that we’re not defending all corporate aggregators, or saying that all corporate transactions and their aftermaths are smooth. What we are saying is that corporate acquisition of dental practices:
• Is not the ruthless boogeyman that many will make it out to be;
• That many of the arguments given against dental corporates are arguments that could easily also be said of some privately owned practices; and
• Can be the right choice for some practice owners looking to sell.
About the authors
Lisa Singh has a business degree from Penn State University and is also a qualified Registered Dental Hygienist. Her unique background as both a business coach and hygienist gives her insights into the many factors that contribute to buying, selling and owning a dental practice. Lisa joined Practice Sale Search after many years working for one of Australia’s leading dental corporates, where she held roles as both Regional Manager and Acquisitions Manager, where she was tasked with improving the productivity of both new and existing practices and later identifying, benchmarking and completing the purchase of high-quality dental practices.
Simon Palmer is the Managing Director of Practice Sale Search, Australia’s largest dental practice brokerage. If you’d like more information on practice sales or want to have a confidential discussion about your practice’s circumstances, email Simon Palmer at info@practicesalesearch.com.au or call 1300-282-042.

Boost your business: Why a reliable phone system is key to success
By Jayne Bandy
Iam always shocked to find so many dental offices who have an outdated phone system, yet they have state-of-the-art equipment in their surgery! I get the need to have the latest techniques and ways to provide your patients with the latest technology to create those amazing smiles, but I’m confused why you would not want to have an effective phone system that ensures there are no missed calls coming into your practice.
I’m sure you would agree, it is no secret that the calls coming into your practice are still the main source of New Patients!
Then why are dental offices getting by with a clunky phone system that...
• Does not have multiple lines?
• Does not have an on-hold phone message that won’t put your patients to sleep and cause them to hang up?
• Does not have call recording and tracking set-up, so you know what your patients are saying and what your team are saying to your patients?
It just doesn’t make sense.
Today I want you to have a long and hard look at your phone system and how you have it set up to give you optimum results. If you discover you do have a dinosaur phone system in your practice, then I can guarantee you have a huge, missed opportunity in your business.
The telephone call is absolutely sacred to your business.
Think about this:
• When your patients call you, do you have enough lines?
• Is your phone constantly going to voice mail?
• Are people calling you and having to wait on hold with no message?
• Are people calling your office and having to wait too long while the phone rings, only to then hang up?
• Are people calling your office and then hanging up and calling the other practice down the road?
• Are people calling your office and having to listen to awful guitar music while on hold?

Call Tracking Excellence is not a product IT’S A RESULT!
With Call Tracking Excellence your team will learn the SAME exact processes Jayne used to:
1. Dramatically improve new patient call-in conversions to booked appointments.
2. Retain existing patient appointments
3. Prevent ongoing losses from appointment cancellations. Visit the website to find out how to get started. It’s that easy! www.calltrackingexcellence.com
• Are people calling your office and your team have no idea about customer service and how to convert the call to an appointment?
• Are the calls coming into your office and not being recorded so you can help your team and offer the best customer service training?
I know it’s a lot to take in and think about, but you must.
So many dentists tell me they have been meaning to change and update their phone system but just haven’t got around to it. They also say to me that they want to start recording and tracking the calls coming into the practice but don’t do it because they have an old phone system that won’t let them.
So now is the time to fix this problem. You don’t want to get left behind and be missing out on patients, appointments, production and profits.
To find out how I can teach your team to know what to say and ask your patients, to help them make more kept appointments and prevent cancellations, call me on 1300-378-044 or email jayne@thedpe.com
About the author
Jayne began her career as an educator. After spending several years teaching, she made the jump to practice management, serving as a Practice Manager for a renowned dentist in Sydney for more than 25 years, giving her first-hand experience at what works when it comes to building and maintaining patient relationships, how to convert leads over the phone and most importantly - what it takes to reach your practice goals. As the CEO and Founder of Dental Phone Excellence, Jayne helps practices convert more calls into appointments, reduce cancellations and nurture effective patient communication that will result in increased profitability. Her past experience as an educator combined with her passion for practice management gives her a unique set of skills that allows your team to fully understand and take advantage of the tools she presents.
Oral Health Care


patient-requested whitening brand*






Why your marketing sucks (and what to do about it)
By Angus Pryor, MBA (Marketing)

Let’s be honest—most marketing is boring. Worse than that, it’s annoying. If you’re tired of fluffy advice like “know your audience” or “post consistently on social media,” you’re in the right place.
This isn’t your typical marketing checklist. This is the anti-checklist—a blunt guide to fixing what’s actually broken in your strategy.
1. Stop talking about yourself
No one cares about your business. Harsh? Maybe. True? Absolutely.
Your customers care about themselves. So ditch the “we’ve been in business for 10 years” talk and start answering the one question they have:
“What’s in it for me?”
Pro tip: Go to your website right now. If the first line isn’t about how you solve your customer’s problem, fix it.
2. Your emails aren’t as important as you think
Do you know how many unread emails I have? 3,217. And I’m not opening another one unless it’s worth my time.
Here’s the deal: If you’re sending boring newsletters or spammy sales pitches, you’re getting deleted faster than my gym subscription reminder. Instead, send emails that:
Are short (no one’s reading your essay). Include one clear call-to-action.
Add value—think free tools, insider tips, or something actually helpful.
3. Stop posting for the algorithm
What’s the point of hitting 10,000 views if it doesn’t translate into sales? Forget the vanity metrics and focus on creating content that moves people to act.
Here’s an idea: Post a brutally honest review of your own service. Yes, you read that right. Call out the flaws (every product has them) and explain what you’re doing to improve. People respect transparency.
4. Nobody likes being sold to
Raise your hand if you’ve ever ignored an ad. Exactly. The trick isn’t to sell— it’s to start a conversation. Instead of pushing a product, share a story. Instead of shouting, listen. Build relationships that lead to trust. Trust leads to sales.
5. Don’t be too polished
Perfect marketing is like a perfectly manicured lawn: nice to look at, but no one wants to hang out on it.
Add some grit. Share your fails. Post that video with bad lighting but great content. Be human—it’s more relatable and way more memorable.
6. Do the opposite of what everyone else is doing
If your competitors are all posting “Top 5 Tips” articles, post a “5 Things You’re Doing Wrong” article. If they’re using polished stock photos, post a raw behindthe-scenes video.
The secret to standing out is simple: just don’t blend in.
7. Remember... marketing isn’t just ads
Marketing happens when someone recommends you to a friend. When your business card sparks a conversation. When someone remembers your logo because it’s not boring.
You’re always marketing, whether you realise it or not. So make every touchpoint—big or small—count.
Here’s the bottom line: Marketing doesn’t have to suck. But it does have to feel real.
Forget the “rules,” connect with your audience, and give them something worth paying attention to.
Because at the end of the day, people don’t hate marketing—they just hate bad marketing.
About the author
Multi-award-winning Practice Growth Specialist, Angus Pryor, is an author, marketer and international speaker. He is the #1 Google-ranked dental marketer in Australia. In 2023, Angus’ team at Dental Marketing Solutions received the ADIA’s marketing award. More details are at www.DentalMarketingSolutions.com.au. For a smarter, cheaper solution to finding great team members doing particular tasks, there is a solution. To find out how to unlock the gold in your practice from incomplete treatment plans, reactivations and more (and to access free sources), visit www.DentalStars.com.au.
dentevents presents...
Infection Control BOOT CAMP
29 VIDEOS - 8+ HOURS OF EDUCATION
Presented by Emeritus Professor Laurence Walsh AO BDSc, PhD, DDSc, GCEd, FRACDS, FFOP (RCPA), FFDT (RCS Edin)
8
Learn from Australia’s leading authority on infection prevention and control in dentistry about recent changes in infection control including from the Dental Board of Australia (July 2022), the ADA (4th edition guidelines August 2021 and the ADA Risk management principles for dentistry during the COVID-19 pandemic (October 2021)), the new guidelines from NHMRC (May 2019), Hand Hygiene Australia (Sept 2019) and the CDNA (Dec 2018) as well as recent changes in Australian Standards and TGA regulations that are relevant to infection control. The course provides a summary of how those changes interlink with one another and also covers practical implementation of the new requirements and what it means for everyday dental practice. Hear about the why and the how and keep up-to-date with the changes that are happening.
COURSE TOPICS
This one day course will cover changes in regulations and guidelines from 2018 to 2022 including:
n Risk-based precautions.
n Hand hygiene and hand care practices.
n Addressing common errors in personal protective equipment.
n Biofilm reduction strategies.
n Efficiency-based measures to improve workflow in instrument reprocessing and patient changeover.
n Correct operation of mechanical cleaners and steam sterilisers.
n Wrapping and batch control identification.
n Requirements for record keeping for instrument reprocessing.
n Correct use of chemical and biological indicators.







Laurie Walsh is a specialist in special needs dentistry who is based at the University of Queensland in Brisbane, where he is an emeritus professor. Laurie has been teaching and researching in the areas of infection control and clinical microbiology for over 25 years and was chief examiner in microbiology for the RACDS for 21 years. His recent research work includes multiple elements of infection control, such as mapping splatter and aerosols, COVID vaccines and novel antiviral and antibacterial agents. Laurie has been a member of the ADA Infection Control Committee since 1998 and has served as its chair for a total of 8 years, across 2 terms. He has contributed to various protocols, guidelines and checklists for infection control used in Australia and represented dentistry on 4 committees of Standards Australia and on panels of the Communicable Diseases Network of Australia and of the Australian Commission on Safety and Quality in Health Care.
REGISTRATION
n On-Demand access to 29 Online Learning Videos (Over 8 hours of education).
n Watch and re-watch at your leisure 24/7
n Digital Online Learning Companion.
n Digital Suggested Reading Material.
n Online Questionnaire to earn 8 Hours of CPD.

Load release - the logic and structure of checking completed loads
By Emeritus Professor Laurence J. Walsh AO
This article explores issues around the release of a load from a sterilising cycle. The key concept around this is that the items that have been cleaned, inspected, packaged into a sterile barrier system (SBS) and then sterilised need to be suitable for use in the clinic. Checking the sterilised load conforms to requirements is one of the most important tasks that staff in the reprocessing area will perform as part of their daily work.
TThe sterile barrier system (SBS)
his typically is a paper-plastic pouch, a paper bag or a non-woven polypropylene fabric (such as KimGard™) used as a wrap. Paper-plastic pouches are either self-sealing or are sealed using a heat sealer. The seal must remain intact despite the rigours of the steam sterilisation process, during which pouches and bags expand and contract, expanding to twice their size and collapsing to half their size. These changes put considerable stress on the integrity of the seal. This problem is magnified when pouches are overfilled and when large objects are placed into pouches with limited clearance. With heat sealing, using an insufficient temperature to melt the plastic results in a weak seal.
This is why checking the temperature of the heat sealer and making a test piece to check that the heat sealer is performing properly are important.
A further type of SBS is a rigid container with a replaceable filter. This option is relatively new for office-based dental practice, but is based on a concept developed over 100 years ago by Aesculap, who pioneered fully reusable sterile barrier systems. These are basically rigid containers with replaceable filters. The filters allow the removal of air and the entry of steam. After a sterilising cycle, items inside the container will remain sterile for a specified maximum time, typically up to 30 days. The filter is replaced periodically during the life of the rigid container – which is typically over 2500 cycles.
Data entry prior to initiating the steam sterilisation cycle
Akey part of the record keeping for steam sterilising is the information that is entered before each cycle is commenced by the loading operator (Table 1). The cycle program that is selected and the identification of the loading operator are requirements that carry over from the previous AS/NZS 4185 and 4187 standards. A new requirement which comes from AS 5369:2023 is to have a list of the chamber contents. This is done to provide enough information to be able to retrieve items in the event of a recall from a failed load. The chamber contents list covers what items are present (Figure 1), including how many packages of different types (e.g. instrument sets or kits) as well as unwrapped items (e.g. GIC applicator guns). In the case of sets or kits, recording the number and types is sufficient and it is not necessary to also list the individual contents of each set.
An optional but useful additional piece of information to consider measuring and recording is the weight of the load. This can be measured using scales and can readily be calculated by adding the weight of known instrument sets and items. Each steam steriliser has a weight limit for the load and this varies based on the chamber size and other device characteristics. It will be stated in the steriliser’s operating manual in the specifications section. The manual may give different maximum weight limits for different load types, e.g. solid or porous.
infection | CONTROL

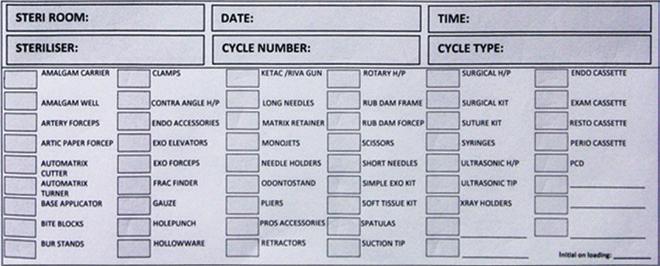
Table 1. Cycle data for steam sterilisation
Entered before the cycle is started...
• Date and time
• Cycle program selected
• Chamber contents
• Loading operator identification
Entered after the cycle prior to release...
• Cycle number/batch identification number
• Check of cycle parameter data (from screen, printout or stored data)
• Check of external Class 1 chemical indicator
• Check of internal chemical indicators (if used)
• Check of packages for SBS integrity (no tears, breaches or broken seals)
• Check of packages for dampness
• Load release authorised based on the above
• Loading operator identification
Figure 1 - Panel B. An example of the part of a cycle record sheet showing the numbers of different kits and items.
Figure 1 - Panel A. The recurring journey of reprocessing, showing with an asterisk the critical control point of load release checks.
If the total weight of items placed into the chamber exceeds the maximum allowed weight, the load will not reach a suitable temperature for sterilisation. A practical advantage of measuring load weight is that it reduces the risk of the chamber being overloaded with items.
Chemical indicators
Prior to sterilisation, each packaged item needs to have a class 1 chemical indicator included. Typically, this is built into the pouch or paper material, or added on in the form of tape. A visual change in this indicates exposure of the wrapped item to steam has occurred. Hence, staff in clinics should always be checking the class I indicator on wrapped items before using the contents. This provides a final control measure should there be an accidental release of a load that has not been sterilised. The use of internal class 4-6 chemical indicators is optional when there has been complete validation of the steriliser using the most difficult load item. The precision of these varies, being 2° for temperature and 25% for time for a class 4 indicator.
chemical indicators, always use the manufacturer’s reference colour as the point of comparison. This is often printed onto the indicator. Some manufacturers also supply interpretation charts. As the colour of indicators changes through different stages, staff need to check that the final colour meets or exceeds the reference colour.
Table 2. Common errors in load release
• Cycle did not commence due to a fault (e.g. low water level or poor quality water)
• Incomplete record keeping
• Printout not checked for key data
• Lack of manual checking of load items
• Dampness of items not checked
• Seal integrity not checked
• Unreadable written records (illegible writing)
• Printout is not retained or is not legible
This improves to 1° in temperature and 15% on time for class 5 and to 1° in temperature and 5% on time for class 6. When internal chemical indicators are essential (e.g. when a loaner steriliser is being used), they should be positioned so that later they can be viewed through any transparent parts of the sterile barrier system, e.g. through clear plastic side and checked as part of load release. There is no requirement to keep any type of internal chemical indicators and moreover, these are not designed for archiving over the long term. During long term storage, the colour of the used indicator can change, causing confusion.
Checking cycle parameter data for completed cycles
This process includes reading the display or printout to verify that cycle parameters were achieved. Staff members need to identify where the key data is located on the printout or on the display and not only look for the words “pass” or “complete”. The information on how data is presented will come from reading the operating manual, paying particular attention to fault codes and their meaning. Cycle parameter data needs to be stored appropriately. While ink printouts can be archived because they do not fade, thermal
copied or scanned to produce a permanent record that can be retrieved at a later date. Staff need to regularly back up the data cards which record cycle information, rather than waiting for these cards to fill up. Data cards in steam sterilisers operate in a hot and humid environment, which means they are more likely to fail than a USB stick or a data card in a smartphone or digital camera.
Checking wrapped items
The key requirements are that the sterile barrier system is completely intact, which includes several elements. First, no instrument ends have pierced through the SBS. Second, the seal, whether from self-sealing adhesive or heat sealing, is completely intact and unbroken. Third, the package is not damp or wet. Labels placed before sterilisation must still be attached and readable.
Checking wrapped items is an important competency requirement and visual inspection requires training so that the routine becomes established. Any nonconforming packages need to be separated so that the items can be re-packaged and re-sterilised, addressing the problems that caused the SBS to be breached in the first place.
Record keeping
The final step in the process of load release is for the loading operator to complete the documentation for the cycle and to verify that all the requirements have been met and enter the cycle

IS EVERYTHING the right one with Hu-Friedy

predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. when it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
EVERYTHING
right one with Hu-Friedy
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right. DENTISTS LOVE OUR STAINLESS STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust



Cooling and storage
number/batch code information into the record book, before transferring the items to the cooling racks where they will sit until placed into storage.
The clinic must use a suitable steriliser cycle record. Commercially produced log sheets do not capture all the required types of information and typically miss all the previously mentioned visual checks that are essential. Many clinics prepare their own hard copy record books or sheets to cover all the required information. Hard copy books are retained (for at least 7 years) or can be scanned and then retained in digital format indefinitely. Regardless of the format, the records need to be legible. That includes clear identification of which staff members completed the records.
Release of items from a steriliser load back into clinical use is a serious decision-making process and staff need to be reminded of their important contribution to the safety of patients when they are doing this task. They need to be alert for trends as they are checking loads. For example, a sudden rise in the number of packages with broken seals indicates either over-loading of those pouches (the most common reason) or a problem with the sealing process itself.
Racks are essential for allowing cooling prior to storage. Items must never be placed directly onto the flat surface of a bench. If this happens, condensation during cooling will make the package wet and this creates a wicking effect by capillary action, bringing contaminants on the bench into the package. After items have cooled, they can then go into a relevant area for storage. Storage processes must factor in the date of sterilising and the expiry date and use a system for cycling through sterile stock. For example, the most recently sterilised stock goes to the back and clinics remove stock from the front. This ensures that the stock is cycled around and items will all be used before their expiry date. The expiry date is used wherever clinics do not have 24/7 air-conditioning for where sterile stock is stored. The expiry date can be printed on a label or written on a package with indelible ink prior to steam sterilisation. Storage areas need to prevent exposure of packages to direct sunlight, dust and splashes of fluid. Cupboards and drawers work well for these purposes. Some clinics use cupboards with clear panels which allows a visual inventory to be taken quickly of the sterile stock on hand (Figure 2).
About the author
Emeritus Professor Laurence J. Walsh AO is a specialist in special needs dentistry who is based in Brisbane, where he served for 36 years on the academic staff of the University of Queensland School of Dentistry, including 21 years as Professor of Dental Science and 10 years as the Head of School. Since retiring in December 2020, Laurie has remained active in hands-on bench research work, as well as in supervising over 15 research students at UQ who work in advanced technologies and biomaterials and in clinical microbiology. Laurie has served as Chief Examiner in Microbiology for the RACDS for 21 years and as the Editor of the ADA Infection Control Guidelines for 12 years. His published research work includes over 400 journal papers, with a citation count of over 20,000 citations in the literature. Laurie holds patents in 8 families of dental technologies. He is currently ranked in the top 0.25% of world scientists. Laurie was made an Officer of the Order of Australia in January 2018 and a life member of ADAQ in 2020 in recognition of his contributions to dentistry.
Figure 2. Panel A: Storage of packaged oral surgery instruments in wall-mounted MaxiBins™. Panel B: A cupboard with sliding glass doors on both sides which provides a visual inventory of sterile stock. In this example, items for use in the clinic are taken from the left side and new items loaded in from the right side to provide proper flow.
With passion for per fection ®
Precision, innovation and reliability

• Crafted from tungsten carbide, these forceps are highly durable and scratchresistant, boasting a Mohs scale number comparable to diamonds
• Hygienic handle design for easy sterilisation.
• Well-balanced weight with ergonomic, targetorientated surface profile permits precise and secure methods of working over long periods or practice time
• Matte surface made to reduce reflections
STO-14052.17 - Forceps, advanced, anatomical TC, 1.3mm, straight stoma® classification
The working tip dimensions of advanced instruments can be categorised as something between classical macro-surgical instruments and microinstrumentation. They allow finely sensitive working methods and mark the changeover to micro-surgical methods.
Stoma® forceps are available in various designs, different-sized working tips and material construction so you can choose the instrument that is perfect for you.


A-dec sets standard in infection control
By David Petrikas
When it comes to infection control in the dental surgery, A-dec has you covered.
As one of the world’s most respected manufacturers of dental equipment, A-dec has also developed a comprehensive endto-end asepsis program to make sure your dental units are fully maintained and do not pose a risk of infection to your staff or patients. In keeping with ADA Guidelines, A-dec recommends a three-step “Maintain, Monitor & Shock” approach to keeping water lines clean.
STEP 1: Maintain

A-dec provides the tools to maintain dental unit water lines on a daily basis using A-dec’s convenient ICX tablets. Each time you refill the dental unit water bottle, you simply drop in an ICX tablet directly into the water bottle to ensure the water is effectively treated against microbial contamination.
STEP 2: Monitor
Monitoring requirements will depend on your water quality and the clinic’s individual requirements. Initially, test water once a month. If the results pass your specified action level (i.e. 200 CFU/mL using the ADA guidelines), then reduce the testing protocol to at least every six months.
A-dec’s authorised dealers can offer a digital water testing service to diagnose dental unit waterline quality on the spot. Once treated with ICX Renew and flushed clear, the self-contained dental unit water system is ready for routine treatment with ICX tablets at each refill to maintain water quality.
STEP
3: Shock
Shock when the water quality test results exceed the quality action level to comply with ADA guidelines, as part of your clinic’s infection control. This is especially the case if the dental units have sat idle for an extended period. The most convenient way to do this is with A-dec’s ICX Renew liquid shock treatment.

Asepsis built into A-dec dental units
A-dec builds asepsis right into its chair design, starting with their fully self-contained dental unit water system, using A-dec’s proprietary microbial-resistant AlphaSan tubing and a corrosion resistant brass control block design that prevents water stagnating.
Fresh water circulates through the control block every time you activate a handpiece. See https://australia.a-dec.com/why-a-dec/ optimal-infection-control

Turbines and handpieces
The new turbine “Vaporiser” feature – exclusive to the A-dec Pro delivery systems – purges the turbine with a blast of high-speed air, preventing aerosols and water being drawn back into the turbine head, helping eliminate potential contamination. It also avoids the last drop from dripping onto the patient when the handpiece is removed from the oral cavity.
A-dec’s electric motor, suitable for contra angle and speedincreasing and speed-decreasing handpieces is also favoured by many for its quiet, powerful operation and for greatly reducing the production of aerosols compared to high-speed turbines.
The new A-dec Pro delivery systems also feature a unique “auto flush” function. Activating this operation purges all tubing to ensure only fresh water is in the dental unit water lines.
From beginning to end, the thoughtful design of A-dec delivery systems ensures the highest level of infection control for you, your team and importantly, your patients.
Learn more at australia.a-dec.com

SAFESCRAPER TWIST curve VOLUMIZER
Developed from the long-standing experience of the META SAFESCRAPER family, the NEW VOLUMIZER offers the same proven performance while collecting a larger volume of bone with every scrape.
The Safescraper Volumizer enables rapid and accurate collection of quality autologous cortical bone with many viable osteocytes. The presence of these cells promotes graft acceptance, neovascularisation and bone regeneration.
The gathered bone, now mixed with blood, is prepared for delivery to the surgical site or can be combined with Geistlich Bio-Oss®. Additionally, it may be kept temporarily under sterile conditions within the clear chamber.

20% more volume more info over the page


Double grooves

MOCOM streamlines sterilisation at Tomaree Dentistry in coastal NSW
Tomaree Dentistry in the picturesque Port Stephens region of New South Wales, two and a half hours north of Sydney, is streamlining its infection control practices by utilising innovative solutions from MOCOM that are perfect for small clinics and large. We asked them about their practice and choices...
Q Good morning, please tell us about your practice?
A Of course. Tomaree Dentistry is a long standing practice in Nelson Bay, having provided general dentistry to the local community for 30 years. We focus mainly on the mature, older patient with much of our work involving restorations, crown and bridge work, dentures, implant restorations and oral hygiene. We have 4 treatment rooms currently used by our two dentists and supported by 7 staff.
Q
Describe the infection control workflow - Steri to chair side and back
ATreatment rooms are stocked with instruments that have been processed in the sterilising room each session and as required throughout the day. Before each patient, the chair side is set up with necessary items for the dentist and DA. At the end of treatment, the procedure tray is taken to the sterilising room for processing.
Q What is your sterilisation area like and what equipment do you use?
AWe have a left to right circular flow in our sterilisation room. Treatment trays land in the processing bay ready for reprocessing. Trays are sorted with handpieces going through the MOCOM Thalya Plus handpiece maintenance unit and instruments go into the MOCOM Tethys H10 benchtop washer disinfector. Once both cycles are finished, the handpieces and instruments are moved to the packaging area. We use self-seal bags and once packaged, they go through the autoclave. We have MOCOM autoclaves with printers. Once that cycle is finished, the bags are inspected and a printed label attached.



Instrument reprocessing solutions
Instrument reprocessing solutions
Instrument reprocessing solutions
has revolutionised sterilisation by offering a compact, dedicated line that provides unparalleled performance!
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!
Mocom has revolutionised sterilisation by offering a compact, fully dedicated line that provides unparalleled performance!





Q Are there dedicated staff working in infection control?
AWe have one dedicated staff member in our sterilising room. All assistants and front desk staff are at times required to assist there as well. All staff and dentists participate in infection control training.

Q Regarding the MOCOM Thalya Plus handpiece unit, what was the catalyst for purchasing this?
A Our principal dentist, John Cropley, saw the Thalya handpiece unit at a trade show. He was wanting equipment that not only oiled the handpieces but cleaned internally as well - with the aim to improve the systems in our sterilising protocols. We previously oiled our handpieces in an oiler and staff used a can of spray to clean handpieces internally before processing further. The Thayla Plus provides both procedures during its cycle - we have found it to be a more efficient process and the handpieces are lasting longer than we had experienced prior to installing the Thalya.
Q And why did you choose MOCOM Sterilisers?
A We have two MOCOM autoclaves. These have a reputation for reliability and our previous experience with this brand meant we have stayed with MOCOM. Although we are a small
MOCOM Thalya PLUS
MOCOM Thalya PLUS handpiece maintenance unit treats up to 4 instruments simultaneously including turbines, micromotor handpieces and scalers. The complete Thalya PLUS cycle consists of 6 stages:
n Duct purge
n Internal cleaning
n Internal and external disinfection
n Lubrication
n Excess oil purge
n Drying
The 4 instruments are treated simultaneously and the entire cycle lasts about 12 minutes.
MOCOM Tethys H10 PLUS
MOCOM Tethys H10 PLUS is a compact benchtop, thermal washer disinfector that offers four phases that are all performed in a single, rapid, automatic process:
n Decontamination
n In-depth ultrasound washing
n Effective thermal disinfection
n Forced-draught drying
One cycle eliminates risks for the operator and efficiently completes the four phases that precede instrument packaging and sterilisation in a fast 35 minute cycle.
practice, we are busy and having two machines allows us to keep our treatment rooms well-equipped and allows for efficient and productive days. We find the autoclaves work well and notifications within the system allow us to keep on top of maintenance of the equipment.
QDoes the practice use instrument tracking and if so, how does the MOCOM equipment work in with this.
AThe autoclaves have printers attached. At the end of each cycle, staff check each bag for tears or punctures and then attach a label to each one. Sterilising room forms are then completed so as to keep a record of all loads that are processed and a barcode label is attached here as well. These labels, with barcodes, allow for tracking of instruments from the load and cycle through to the patient they are used on. In the treatment rooms, the barcodes are scanned into the patient’s chart at the time of treatment. Autoclave details are saved and records kept of all cycles.
Q Can you sum up the benefits of using MOCOM equipment in the operation of the practice?
AOur practice uses MOCOM equipment for oiling, cleaning, disinfecting, sterilising and tracking. We have found the equipment has helped us fine tune our infection control procedures within our sterilising room, allowing our staff to work efficiently and feel reassured that standards are being met.


Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes.


Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical. Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Clean. Disinfect. Lubricate. Purge. Dry. In 12 minutes. Replace Manual with Mechanical.
Replace Manual with Mechanical.



Dürr Hygoclave ideal sterilisation solution
By David Petrikas
TThe premium Dürr Hygoclave range provides an optimum solution for small and large practices. Since its introduction to the Australian market by A-dec in 2023, the Hygoclave has been widely adopted and highly regarded in the market. With features like effective sterilisation, fast cycles, reliability and unbeatable ease of use, it’s easy to understand why the Hygoclave autoclave is finding favour in local dental practices.
A-dec Australia’s Product Manager, Dr Wee Teo, said the Hygoclave 40 and Hygoclave 50 have an international reputation for their ease of operation and efficiency, thanks to fast operating cycles and flexible drying programs.
Smart cycles
The Hygoclave can process dental instruments in as little as 30 minutes (including drying time) using the “B Flash” cycle – and does so with minimal water and power use making them “ecofriendly” as well.
The “B Standard” sterilisation program ensures reliable reprocessing of instruments. Being a “smart” machine, drying time is automatically extended according to load size – while additional vacuum cycles can be pre-selected on the Hygoclave 50 using the “B Standard Plus” program to accommodate hard to dry, complex hollow loads. The result is properly processed, dry loads every time with no need for reprocessing.
Feedback from dental practices is that the Hygoclave is a joy to use with next to no training thanks to the intuitive layout of its colour touchscreen display and easy to understand icon-based buttons. Key day-to-day functions are just a simple button-press. Ease of operation is a hallmark of the Hygoclave range. For example, one press on the coloured 5” (125mm) touch screen can select the most recently used sterilisation cycle; produce a batch report; or initiate a test program directly from the home screen without having to go deep into menus to set parameters.

TTraceability
he Dürr Dental Hygoclave steam steriliser takes traceability to new levels – automatically! An automated powered door with locking mechanism and integrated user management system guarantees secure and easy workflows, supporting full traceability, back to an operator and cycle.
The Dürr Hygoclave has a dedicated interface for practice management and hygiene software, as well as internal storage capacity for a massive 100,000 cycles – much more than other autoclaves.
It can also produce barcode labels and batch reports on an optional attached Dürr printer.
The premium Hygoclave 50 is also “future proof” with remote monitoring capability via the Dürr VistaSoft Monitor app and computer software, including remote cycle history backup and downloading of reports to a user’s PC.
The free VistaSoft Monitor program also enables remote service diagnostic ability – which is a bonus especially for remote practices, enabling ease of servicing, together with timely reminders for routine replacement items.
Flexible water supply options
Aunique feature of Hygoclave 50 is its extremely flexible water supply options, making it easy to install in any practice, as well as its built-in automatic water quality test function with alerts.
Hygoclave 50 can be filled manually via the externally accessible tanks with unique top opening “butterfly” doors; via a suction system from a canister of treated water; or from a fully automated Dürr water treatment system for seamless operation.
Hygoclave is manufactured from quality stainless steel and special high temperature and ionised water-resistant plastics for sustained trouble-free operation. It is available with either a 17L or 22L chamber matching the size and throughput of the practice.
The product is also easy to maintain and service-friendly due to its intelligent and modular design which has already won a big thumbs-up from dental equipment technicians in Australia.
The Hygoclave now offers an optional 5-year warranty extension. With this extension, customers can enjoy up to 5 years or 4,000 cycles of protection, whichever comes first.
For more information on the Dürr Hygoclave, contact A-dec Australia on 1800-225-010 or your nearest dealer.
High-performance sterilization- and drying system

5“ high-resolution colour touch display for intuitive navigation
3-fold flexible fresh water supply with integrated quality control
All in view and documented thanks to connection to the practice network



With Hygoclave 50, Dürr Dental and A-dec offers dental practices a professional Class B solution that combines impressive performance with a well thought-out operating concept – for maximum efficiency and exceptional user friendliness designed to cope effortlessly with tough day-to-day working environments. Available with a volume of 17 or 22 litres. More information under www.duerrdental.com
Integrated dust protection filter Scan the QR
ULTRA SAFETY PLUS TWIST



> Protects you and your staff from needle stick injuries
> Complies with latest regulations
> Intuitive device
> Available with either sterile single use or sterilisable handle


Passive or active aspiration: security for the patient
Transparent barrel: aspiration is clearly visible
Sliding protective sheath: protection from needle stick injuries


Two different positions:
first Holding Position (reversible)
final Locking Position (irreversible)



A LONG-PROVEN EFFICACY
OF
EVERYTHING the right one with Hu-Friedy
for you. when it comes to the perfect fit, Hu-Friedy is just right.
A study demonstrated that when introduced in a dental school, Ultra Safety Plus was a the key success factor for avoiding needle stick injuries. With Ultra Safety Plus, needle stick injuries decreased from an average of 11.8 to 0 injuries per 1,000,000 hours worked(1)
STEEL PEDO CROWNS:
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust



case study
Immediate FP1 restoration: Next-level digital full arch revolution
By Dr Joel Teles, DDS (Portugal)
Immediate implant placement and full arch restoration are increasingly recognized as the treatment of choice for both dentists and patients. However, achieving optimal outcomes requires a well-thought-out, evidence-based approach, which involves extensive interdisciplinary collaboration and clinical expertise. This ensures a treatment plan tailored to each patient’s unique needs.
In many modern full arch cases, there is a tendency to remove an excessive amount of bone (FP3), often as a means to simplify the procedure. However, such bone removal should never be performed solely for convenience, as it can significantly increase the risk of complications and failure. Moreover, excessive bone removal may make it difficult to provide follow-up restoration in the event of implant failure.


This case study, presented by Dr Joel Teles from Portugal, demonstrates the comprehensive treatment of a patient utilising an immediate FP1 restoration with TRI matrix implants and TRI ScanBridge, highlighting the importance of preserving bone structure while achieving functional and aesthetic results.
Introduction
A69-year-old female, heavy smoker but in otherwise good health, was referred by a periodontologist due to mobile teeth. She presented with a crossbite. Due to excellent tissue condition and after digital planning and reviewing virtual design options, the decision was made to proceed with immediate FP1 treatment.



Figure 1. Initial situation.
Figures 3-5. Initial situation.
Figure 2. Completed restoration.
Guided Surgery Scan&Smile ScanBridge





DIGITAL SMILE & WAX-UP DESIGN




IMPLANT PLANNING


Figures 9-10. Virtual extraction of teeth.
Figures 6-8. Pre-op intraoral scan of upper and lower jaw plus bite scan.
Figures 11-12. Digital smile design helps create the perfect wax-up on virtual extracted models.
Figures 13-16. Implant planning upper and lower jaw based on digital radiograph, CBCT and wax-up.


Figures 17-18. Upper and lower jaw guide templates set for 3D printing.


Figures 19-20. Templates fixed with fixation pins. Implants placed through the guides.
PRE-OP INTRAORAL SCANS

Figures 21-23. IOS scans with scan bodies, ScanBridge and remaning teeth for accurate matching of pre-OP and post-OP scans.


Figures 24-25. After IOS extraction of final teeth, wide healing collars are inserted during the matching process and 3D printing of temp.

The world’s first implant approved for full digital restorations without abutment
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO ABUTMENT. NO CEMENT. NO LIMITS.
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
www.tri.swiss 0297
www.tri.swiss 0297
IMMEDIATE DESIGN AND 3D PRINTED TEMPORARIES


Figures 26-27. FP1 wax-up design matched with implant position. NOTE: FP1 pontic basal design for immediate adaptation of tissue and papilla.


Figure 28-29. Temporary design STL files ready for in-house printing.
INSERTION OF IMMEDIATE 3D PRINTED PROVISIONAL

Figure 30. 3D-printed and polished FP1 temporaries ready for insertion.

Figure 31-33. Immediate FP1 full arch temporaries in situ.








About the author
Dr Teles graduated from the Faculty of Dental Medicine - University of Porto, Oporto, Portugal and is the clinical director of Medindouro, Peso da Régua, Portugal. He completed a post-graduate degree in Orthodontics at São João Hospital, Oporto; a post-graduate Simplified Straight Wire Technique course with Dr Messias Rodrigues; an implants immersion course with Dr Sérgio Motta; an Advanced Surgery Clinical Residency at CLIVO in Rio de Janeiro and multiple periodontal and implant surgery courses.

Figure 34. Radiograph on day of surgery.
Figures 37-39. 2 months final monolithic restoration in situ.
Figure 36. 45 days post-op 3D printed temporary.
Figure 40. Final restoration.
Figure 35. One week post-op 3D printed temporary.

Shining 3D photogrammetry workflow with Elite intraoral scanner
By Terry Whitty

With the popularity, proliferation and increasing success rates of All-On-X protocols, the procedures are now more widespread and in-demand than ever. The implant placement portion of the procedure, although sometimes challenging, has become more predictable with the rise of CBCT technologies and the adaptation of accurate surgical guide systems.
Unfortunately, the restoration phase is still at loggerheads with what is the definitive way to go and the term “long term temporary” is prevalent. The term “hybrid” usually refers to some type of
restoration base from a supporting structure with an aesthetic component on top.
Why is this so important? Ill-fitting frameworks have been implicated in biological and mechanical complications including screw loosening and fracture, implant failure, bone loss and even framework fracture. It’s all a huge headache as fixed denture wearers often smash prosthetics.
Again, unfortunately, it has been shown that with even the most stringent and meticulous impression techniques, some degree of mis-fit will always exist between the multiple implant platforms and the prosthesis. To go down the analog road takes great skill and patience and requires impressions, timeconsuming verification jig techniques and frankly, just a lot of precise chairside time that could probably be used constructively elsewhere.

Figure 1. Scan the upper provisional in situ. If this is not present just skip this step.

Figure 3. Scan antagonist.


Figure 7. Place Scan bodies on MUA and scan in Photogrammetry mode, this is automatically selected. Note no tissue scan will be taken here it’s purely a photogrammetry scan.

Figure 2. Scan the soft tissue; if during surgery, keep bleeding to a minimum.

Figure 4. Bite scan; the software will automatically match.


Figure 8. Next take a scan of scan bodies again and the software will auto match the position accurately with the soft tissue.
Figure 6. Example of scan bodies in situ.
Figure 5. Example of scan bodies in situ.




Figure 9-12. Select the correct type of scan body from the library. This will be used in the CAD software. If you are using different type/brands of implant in the same situation, this can be accommodated as they can be selected individually.


For years, people have been looking for a digital solution to the All-on-X capture of multiple implant positions with varying degrees of success. We know intraoral scanning alone is just not accurate enough across the arch for the precision of full arch implant-retained prosthetics. Of late, there have been some commendable contenders using a plethora of specialised scan bodies to help capture the exact position and inter relationship, but honestly, they come close but no cigar. The only solution that has succeeded and is amazingly accurate are the ones that have used a technology called photogrammetry.
Photogrammetry is the science and technique of obtaining reliable measurements and detailed information about physical objects or the environment by analysing and interpreting photographs. The photographs captured for photogrammetry are special because they contain not only visual information but also geometrical data about the objects or scenes depicted. In a nutshell, photogrammetry uniquely converts 2D photographic data into a 3D spatial model, enabling detailed analysis of an object or landscape’s size, shape and position.
There are various photogrammetry scanners on the market aimed at dentistry, like the PIC camera, Imetric iCam 4D, BSB Grammee and a few others. They are all excellent systems, however, they all suffer from the same issues - they are extraoral, they are large and cumbersome, they only perform one function and they require other softwares to complete the entire matching task and all are expensive to own and operate.
The Shining 3D Elite scanner differentiates itself as the only intraoral scanner on the market to also have a built-in photogrammetry camera system. To be frank, Shining 3D has done with one scanner what everyone has been asking for for years - small in size, lightweight, easy-to-use and solving the age old problem of scanning full arch implant positions with sub-5-micron accuracy.
Last issue, we reviewed this amazing new Aoralscan Elite from Shining 3D Dental and its tiny size and weight and sheer speed of intraoral scanning should sway even the most skeptical of clinicians. However, the inbuilt photogrammetry scanning function is the groundbreaking inclusion, making the Aoralscan Elite the most advanced scanner on the market.
Figure 14. Completed scans ready for export to CAD software.
Figure 13. Scan bodies in relation to soft tissue scan and temporary.

The New ELITE IntraOral Scanner from Shining 3D uses patented IntraOral Photogrammetry Technology to be the most accurate scanner available.
• Small form factor
• Lightweight 124 grams!
• Ultra fast scanning
• Dual mode IPG scanner
• Complete software suite
• Scan All On X Cases accurately
• Suitable for all IntraOral Scanning
• 3-year Warranty






15-16. The Shining 3D

Elite combines and intraoral scanning with a photogrammetry camera in one handpiece.

Figures 17-18. The Shining 3D Aoralscan Elite is supplied with one set of scan bodies of your choice included in the purchase price. Five scan body kits are currently available covering the majority of popular implant systems. Expect additional kits to be released as uptake of the system increases globally.
While the photogrammetry is definitely pitched at the All-On-X market, the two-in-one device handles all intraoral scanning functions with ease and the speed and precision that arguably leaves everyone else in the dust.
With the Shining 3D Elite scanner, you get a built in photogrammetry scanner and the process of using the photogrammetry function on the Elite is actually straight forward. With every Elite scanner, you receive a High Accuracy Coded Scan body kit. (HICS). These are very different to scan bodies used in other photogrammetry systems for dental as most others are vertical scan bodies. These are horizontal scan bodies and are a breeze to use, screwed down to the MUA. Even when the patient has limited opening capabilities, the nature of the horizontal scan body is advantageous as it requires minimal bite opening.
The scanner, when in photogrammetry mode, picks up all the coded markings for each scan body and matches these to a unique internal library so you will see the scan bodies “appear” in the software and you will know the scan is successful. Afterwards, you can use the intraoral scan function to scan the relationship of

the scan bodies to the soft tissues and all this will be merged perfectly. Finally you can then match the position of the scan body to the virtual scan abutment of your choice ready to export to your favourite CAD software to design your bar, prosthetic, temp or whatever it is you will use.
It’s astoundingly simple and what’s more impressive, is the accuracy and precision that you get from it. Used correctly, you will get results at least equal to or if not better than external photogrammetry dental systems currently on the market. Considering the size, weight and ease of use, not to mention the phenomenal value, the future has definitely arrived.
This article shows a typical workflow using the photogrammetry function of the Shining 3D Aoralscan Elite.
About the author
Terry Whitty is a dental technician and noted commentator and KOL on digital dentistry. He lectures globally on subjects related to digital dentures, 3D printing and orthodontics.
Figures
Aoralscan
The Solution For Perfect Implant Position

Free Case Evaluation Send


All implant surgical guides
• Edentulous Cases
• Scan Appliances
• Free Planning Software


The Biodentine™ Bio-Bulk Fill technique for deep caries and moderate pulpitis
By Dr Sascha Herbst , Dr Chantal Sophie Herbst
Treating deep carious lesions in a time-effective and sufficient manner can be challenging in everyday practice, especially in symptomatic pulpitis.
Methods
In the present case, a pulpotomy was performed in two stages due to an extensive cervical defect on tooth 47.
Discussion
The use of Biodentine™ in the Bio-Bulk Fill technique, combined with a two-step restoration, made it possible to meet the patient’s need for shorter treatment sessions. Bio-Bulk Fill can help to preserve the vitality of teeth and save time.


Introduction
The treatment of deep carious lesions is often complex and time-consuming in practice, especially in the case of acute complaints.
Reconstructing cervical marginal areas at the subgingival to epicrestal level, with adequate dental dam placement, presents a challenge even for experienced practitioners.1 It can help to divide the treatment over two appointments, especially if pulp involvement is expected.
Figure 1.
Figure 2.






Case report
Clinical findings
A23-year-old female patient presented to the Department of Oral Diagnostics, Digital Dentistry and Restorative Research at Charité Centre 03 for the first time in August 2021 with acute, throbbing pain in tooth 47. Clinically, the tooth exhibited an inadequate composite restoration along with a localised enamel fracture (Figure 1), as well as increased sensitivity to cold.
Pulpotomy and indirect capping are methods of preserving vitality in order to avoid root canal treatment.2
Subsequently, the teeth are typically restored with time-consuming composite restorations in the same session, resulting in extended treatment times. A radiograph showed secondary caries that had extended into the pulp (Figure 2).
The Biodentine™ Bio-Bulk Fill technique can initially seal cavities after pulpotomy or indirect pulp capping in a bacteria-proof and time-saving manner so that a planned, definitive restoration can be carried out in a second step.3
How long have you been using Biodentine?
In my clinical practice, I have employed Biodentine™ for an extended period of six to seven years.
Why do you use the Bio-Bulk Fill procedure with Biodentine? What are the main advantages for you?
This technique enables clinicians to simplify direct posterior restorations, including both direct and indirect pulp capping, through the utilisation of a bioactive material
Diagnosis
The clinical and radiological findings suggested moderate pulpitis.
Clinical procedure
Due to the extension of the carious lesion, a non-selective caries excavation
such as Biodentine™, as a dentine substitute. Indeed, the placement of a protective barrier over exposed or unexposed pulp induces the formation of a dentinal bridge and maintains its vitality and function. The combination of Biodentine™ and a resin-based composite for cavity filling ensures a safe outcome, preserving pulp vitality within a single visit.
When do you use the Bio-Bulk Fill procedure?
I use it mainly in very deep cavities as a protective base, or for vital pulp therapy, both for indirect and direct pulp capping.
with pulpotomy was planned. The old filling was removed under local anaesthesia and dental dam. After excavation, an epicrestal cavity floor was revealed (Figure 3). At this point, the patient already showed limited compliance with regard to sufficient mouth opening time, which is why the treatment steps had to be prioritised. The goals for the first treatment session were defined intraoperatively:
Dr Herbst on Biodentine...
Figure 3.
Figure 6.
Figure 4.
Figure 7.
Figure 5.
Figure 8.


1. Restoration of the epicrestal cavity margin; and
2. Removal of the caries-exposed pulp and capping of the healthy pulp tissue.
The final restoration with composite was planned for the second session.
In the first step of the first session, the caries at the mesial cavity margin was removed non-selectively and a sectional matrix was adapted with Teflon. The mesial cavity margin was then elevated with composite (Filtek Supreme, Solventum).
Non-selective caries removal was then performed in the area of the pulp with the opening of the pulp chamber. A complete pulpotomy was performed using sterile diamond and haemostasis was achieved within five minutes using a foam pellet and 3% NaOCl (Figure 4). In the final step, the pulp tissue was capped with Biodentine™ (Septodont) using the Bio Bulk-Fill technique (Figure 5).
In the second session two weeks later, the patient appeared recovered and symptom-free for the final composite restoration. The Biodentine was partially removed under rubber dam so that a remaining layer of 2-3 mm could be ensured (Figure 7). The restoration was then restored with Scotchbond Universal SE and Filtek Supreme A2 (both Solventum; Figure 8) and a radiological control was carried out (Figure 9).
Follow up
In April 2023, the patient appeared for a follow-up check of the pulpotomy at tooth 47 after 20 months. The patient was symptom-free and radiographic examination revealed physiological apical conditions (Figure 10).
UDiscussion
tilising Biodentine™ in the Bio-Bulk Fill technique eliminates the setting time and the necessity for the permanent restoration in a single session.
This approach supports the effective implementation of vital pulp therapy in even sophisticated treatments.
Such measures, once frequently relegated to root canal treatments, can now be efficiently managed.
In the area of pain treatment, the number of treatment steps that can be carried out may be limited by the patient’s co-operation.
The opportunity to streamline the treatment phase of pulp capping has enabled the intricate reconstruction of the cervical area to be conducted during the initial session.
In this case, this led to an increase in patient comfort, as the treatment could be spread over two sessions and the pulp could be preserved.
Utilising Biodentine within the BioBulk Fill technique, coupled with a two-step restoration process, facilitates an optimal alignment with the patient’s pain management needs.
This treatment approach ensures that treatment quality remains uncompromised, even within time-constrained scenarios such as this.
Conclusion
Pulpotomy and capping with Bio-Bulk Fill and subsequent restoration in a two step procedure can be a good clinical solution for deep defects.
This, in turn, can lead to increased patient co-operation.
About the authors
Since 2024, Dr Chantal Sophie Herbst has been Assistant Professor at the Department of Conservative Dentistry and Periodontology - University Hospital - Ludwig-Maximilians-University Munich - Munich, Germany. Prior to this, she worked in private practice.
Since 2024, Dr Sascha Herbst has been Deputy Head of the Department of Conservative Dentistry and Periodontology - University Hospital - LudwigMaximilians-University Munich - Munich, Germany. Prior to that, he was Deputy Head of the Department of Oral Diagnostics, Digital Health and Health Services, Research Center for Dental and Craniofacial Sciences - Charité - Universitätsmedizin Berlin - Berlin, Germany. He was also Co-Head of the Dental Trauma Board Charité - Universitätsmedizin Berlin - Berlin, From 2016 - 2020, he was Assistant Professor in the Department of Operative and Preventive Dentistry, Center for Dental and Craniofacial Sciences - Charité - Universitätsmedizin Berlin - Berlin, Germany.
References
1. Eggmann F, Ayub JM, Conejo J, Blatz MB. Deep margin elevation-Present status and future directions. J Esthet Restor Dent. 2023 Jan;35(1):26-47.
2. By ES of E (ESE) developed, Duncan HF, Galler KM, Tomson PL, Simon S, El-Karim I, et al. European Society of Endodontology position statement: Management of deep caries and the exposed pulp. International Endodontic Journal. 2019;52(7):923-34.
3. Koubi G, Colon P, Franquin JC, Hartmann A, Richard G, Faure MO, et al. Clinical evaluation of the performance and safety of a new dentine substitute, Biodentine, in the restoration of posterior teeth - a prospective study. Clin Oral Investig. 2013 Jan;17(1):243-9.
Figure 9. Figure 10.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. it comes to the perfect fit, Hu-Friedy is just right.
predictable outcomes for your littlest patients with Hu-Friedy Stainless Steel Pedo Crowns. discover why dentists favor our impeccable fit. Perfect for your patients. Easy for you. comes to the perfect fit, Hu-Friedy is just right.
Septanest : the first choice of dentists with over 150 million injections per year, provides you high quality you can trust

Clifton Hill Dental: A seamless transformation by Medifit
In the heart of north Melbourne, Clifton Hill Dental has been a cornerstone of the community for over 30 years, providing exceptional dental care under the leadership of Dr Nick Malamas. Recently, the practice underwent a significant transformation to expand its capacity and modernise its facilities, a project successfully completed by Medifit Design & Construct. The result is a state-of-the-art dental practice that balances functionality with a welcoming aesthetic, perfectly meeting the needs of both patients and staff.
Dr Malamas had a clear vision for the future of Clifton Hill Dental: to expand the practice from three to five surgeries and to enhance the staff amenities to accommodate a growing team. With limited space in an older building, the challenge was not just to add more surgeries but to do so without disrupting the daily operations of the practice. “We had quite limited space, an old building and our goal was to be able to complete the project without losing too much work time,” Dr Malamas said. “Within the 8 months that the project took, they managed to only close us up for about 6 to 7 days in the whole process.”
The ambitious project required meticulous planning and execution and Medifit Design & Construct delivered on every front. Known for their expertise in dental fit-outs, Medifit ensured that the practice remained operational throughout the construction period, a feat that speaks volumes about their commitment to client satisfaction and project efficiency.
The redesigned Clifton Hill Dental practice now covers 156 square metres of ground-floor space, with an additional 56 square metres on the first floor. The ground floor houses five fully-equipped surgeries, a central sterilisation and lab area, a plant

room and a spacious waiting and reception area. Upstairs, the first floor accommodates two offices, a staff room that doubles as a training area with and shower and toilet facilities, ensuring that the team has everything they need for a comfortable and productive working environment.
The design aesthetic throughout the practice is a blend of modernity and professionalism. Light, neutral tones create a calming atmosphere, while accents of turquoise and blue, drawn from the practice’s logo, add a touch of vibrancy. The careful use of light timber textures further enhances the natural feel of the space, contributing to an overall ambience that is both inviting and professional.





surgery | DESIGN

The execution of the project was as impressive as the design itself. Dr Malamas was particularly pleased with Medifit’s approach to problem-solving and their ability to plan ahead, ensuring minimal disruption to the practice’s operations.
“What Medifit did particularly well was number one, any issue we had, they’ll get onto it straight away and sort it out immediately,” he remarked. “They planned the whole process for minimal inconvenience. There was never a time where we had to wait for them to get back to us if an issue happened.”
The quality of workmanship was another standout aspect of the project. Medifit’s attention to detail is evident in every corner of the practice, from the seamless integration of new equipment to the flawless finishes on the walls and floors.
Dr Malamas summed up his experience with Medifit by highlighting their reliability, responsiveness and exceptional planning. “They created a result which blended both form and function for any dental practice and I can’t recommend them highly enough.”
With the completion of this project, Clifton Hill Dental is wellpositioned to continue serving the community for many more
Summary
The Practice
The Practice Clifton Hill Dental
Principal Dr Nicholas Malamas
Type of Practice General
Location Clifton Hill, Melbourne, Victoria
Size 212 square metres
No of chairs 5
The Team
Design Medifit Design & Construct
Construction Medifit Design & Construct
Equipment
Dental Units Dentsply Sirona Sinius and Dentsply Sirona Intego Pro
Autoclaves Mocom Futura B22
Imaging Orthophos and Axeos with Progeny
Compressor Cattani K300S
Suction Cattani C2A
years to come. The expanded capacity allows for more patients to be seen, while the enhanced facilities provide a better working environment for the growing team. The practice’s new look also reinforces its reputation as a modern, professional dental clinic where patients can feel confident in the care they receive.
For Medifit Design & Construct, this project is another example of their ability to deliver tailored solutions that meet the unique needs of their customers. Their expertise in managing complex renovations within operational settings ensures that clients like Clifton Hill Dental can achieve their goals with minimal disruption and maximum impact.
In conclusion, the transformation of Clifton Hill Dental is a testament to what can be achieved when vision, expertise and craftsmanship come together. Medifit Design & Construct have not only met the brief but exceeded expectations, delivering a dental practice that Dr Malamas and his team can be proud of. The future is bright for Clifton Hill Dental and the practice is ready to continue its legacy of exceptional care in a space that truly reflects its commitment to excellence.

Practices that work with you
Since 2002, Dentists and Dental Specialists all around Australia have trusted Medifit to create state of the art practices with individual interior designs that boost productivity and enhance levels of care.
Whether it’s your first practice or your latest, we’ll help you create a dental practice that reflects your personal style and complements the way you work - and we do it with a friendly, no fuss approach using proven best practices.
Contact Medifit today for a no obligation consultation and experience our award winning service.
• SITE ASSESSMENTS
• LEASE NEGOTIATION
• FEASIBILITY STUDIES
• COUNCIL SUBMISSIONS
• ARCHITECTURAL DESIGN
• INTERIOR DESIGN
• BUILDING CONSTRUCTION
• PRACTICE FIT-OUTS
• RENOVATIONS / REFRESHES
• BRANDING & MARKETING





Portside Dental offers ambience and functionality
Adecision to “go it alone” and establish their own dental practice has paid off for Dr Meredith Metin, co-founder of Portside Dental, Newport, Melbourne and her practice manager partner, Rachael Jones.
This stylish practice goes well beyond any conventional “drill and fill” dentist to offer a range of treatments from oral surgery, including bone grafting, sinus lifts and dental implants, sleep dentistry and all-on-X surgery to dermal fillers for a complete face makeover.
Despite its clinical excellence, Portside Dental stands apart for its aesthetically pleasing and comfortable ambience, along with the gentle touch and reassuring manner of its highly skilled team who put patients at ease.
Principal dentist, Meredith, jokes that after working for over 20 years in other practices, that she had an “epiphany” and decided to establish her own practice so she could do things her way, both clinically – and also by providing the type of stylish setting that she would like to work in and would also be attractive to patients.
By David Petrikas
Partnering with colleague and friend, Rachael Jones, they found an ideal building in an area they know had an opening for more dental services. As one of the few modern shopfronts in the area, the building was a virtual blank canvas, fitted out by Rite Space.
Meredith said this resulted in a very specific design brief which made the fit-out company’s job very clear and straight-forward.
“We were quite specific with our brief and had quite a good idea of what we wanted. We even visited the PolyTec showroom looking at laminates.”

The overarching theme is “luxe” which is reflected in premium finishes, such as fluted marble tiles on the curved reception counter and complementary corrugated wall panelling behind.
Entering the waiting room, which is bathed with soft natural light, reveals sumptuous, upholstered waiting room chairs, a tropical palm and striking original abstract paintings in bright pastels. Other artworks feature in the surgeries.
The cleverly themed “Portside Dental” glass signage features a discreet graphic within the logo referencing the landmark chimney from Newport Power Station. This is echoed by other artworks within the practice featuring the Melbourne skyline captured from across Port Phillip Bay as well as a poster of Newport featuring the same chimney stack and also the Westgate Bridge.


The premium feel is continued in the surgeries, which feature natural-look bleached timber laminate finishes to the below-bench cabinets, brass cabinet and drawer handles throughout and contrasting “Hamptons” accents such as the deliberately chosen charcoal A-dec chair upholstery.
The rest of the practice is finished in off white shades which extends to the galley style sterilisation room cabinetry and out to the staff kitchen with its large dining setting finished in white with a natural timber tabletop and matching white highbacked chairs.
Meredith points out that the décor is not the most important element, with her choice of equipment deliberately being designed to make her work easier and patients more comfortable.


Having worked with a range of brands, Meredith consulted with A-dec Melbourne Territory Manager, Mindy Green, to find equipment which would deliver the quality, comfort, reliability and ergonomics she was looking for.
This is a practical consideration given the length of some of the more involved procedures which makes patient and dentist comfort paramount.
“I was looking for the ‘Rolls Royce’ of dental units and Mindy convinced me that the new A-dec 500 ‘Continental’ unit was the way to go,” Meredith said.
She then spoke to equipment sales specialists, Michelle De Blasis and Luke Williams from dental equipment dealer, Presidental, who supplied the A-dec chairs and assisted her equip the rest of the practice and provide ongoing support with servicing.
Portside Dental has another A-dec 500 chair and an A-dec 300 chair used mostly by the Oral Health Therapists. However, Meredith says the Continental style delivery system was a bit of a revelation compared to the chairs she’s previously worked on.
“I imagine it’s a bit like flying first class or business class; once you’ve experienced it, you don’t want to go back to economy and
while I’ve got other chairs in the practice, I find I can’t go back to them after using this one.”
She said among the benefits of the Continental system were the support of the instruments by the soft rubber whip arms and tubing, which made the instruments very light in the hand.
It also means that you don’t have to take your eyes off the patient to return an instrument to the control head, along with a reduced risk of dropping an instrument or needle stick injuries as the burs aren’t facing upwards like on traditional delivery units.
The Continental delivery system glides easily into position and stays in place without drifting, thanks to the inbuilt touch-sensitive brake which activates automatically when you release the grab handle. It can also be positioned low to work on wheelchair patients.
Special provision also had to be made to provide direct street access from the main surgery to comply with additional regulations concerning medical anaesthesia. The surgery is also wheelchair friendly throughout.
Meredith says she moves the delivery system to the side of the patient to provide a better patient experience than working right over the patient which may feel a bit claustrophobic to them. The delivery system is also left- or right-handed compatible.


She said you can swing the delivery system away to allow the patient to get on or off the patient chair and move it out of the way while talking to the patient.
The delivery system is equipped with a compact A-dec electric motor, high speed turbines and an inbuilt intraoral camera.
Other important equipment considerations include the latest A-dec 500 dentist’s and assistant’s stools designed for optimum ergonomics, including an orthopaedically designed seat cushion and base which provides maximum support without restricting blood flow to the legs.
The cohesive design of the A-dec stool and patient chair work together to provide market-leading comfort for the user and practitioner and also unparalleled patient access.
The tilt design of the seat also helps distribute body weight through the chair and legs to maintain correct posture and reduce fatigue from hours of sitting. The assistant’s stool has an adjustable integrated torso support, providing an elevated position for the dental assistant while supporting the upper body to reduce back strain and the risk of long-term musculoskeletal injury.
Summary
The Practice
The Practice Portside Dental
The Principals Dr Meredith Metin & Rachael Jones
Practice Type General
Location Newport, Victoria
Size 133 square metres
No of chairs 3+1
The Team
Design Owners, McKibbin Design
Builder Rite Space
Project Manager Ben Bampton, Rite Space
Installer Presidental, Melbourne
Equipment
Dental Units A-dec 500 Continental, A-dec 300 A-dec 572 Chair Mount LED Light
Sterilisation Melag Vakuclav 44B+
Imaging Acteon X-Mind X-ray unit
Dürr VistaScan PSP scanner
Compressor Cattani K400
Suction Cattani Turbo SMART
Software CareStack
The practice caters to mostly female patients with complementary treatments such as cosmetic injectables as well as a full range of restorative and cosmetic dental treatments.
A visiting oral surgeon and medical anaesthetist also work from the practice to provide sleep dentistry, advanced oral surgery and implant procedures.
The practice is open six days a week and the team has been kept busy since the new practice opened, indicating an unmet demand for comprehensive dental treatments in the portside suburb.



A - dec® 30 0 Pro: Fit s today. Flexible tomorrow.
We took the modular, compact design of the A-dec 300 and made it even better. Now, with enhanced features, and the option of A-dec+ digital connectivity, you’ll have all the powerful performance you need for the way you practice today. With more functionality, more versatility, and even more possibilities for tomorrow.
LEARN MORE
Information contained in this section is provided by the manufacturers or distributors. Australasian Dental Practice does not assume responsibility for the accuracy of the data.
HART process challenge device

Air Removal Test - is manufactured to ISO 11140-6:2022 in the “helix” style to demonstrate the air removal and steam penetration efficiency for hollow items in small steam sterilisers. The HART is built to ISO11140-6, a more rigorous test for air removal and steam penetration (ARSPT) than previously man-
ufactured “Helix Devices” to EN867-5. It is not the fault of the device. The device is, in fact, proving that the cycle choice is unable to remove all air from the chamber, a fundamental requirement for effective sterilisation of a hollow item. The test is fit for purpose and doing its job, highlighting this fundamental issue. ISO11140-6 sets a standardised approach to the design of Hollow PCD’s and all benchtop sterilisers designed to EN13060 should pass any brand of device manufactured to ISO11140-6. The device comes with 250 strips.
Available: STS Professional Tel: (08) 9244-4628 orders@sts-group.com.au www.stspro.com.au
Shining 3D Aoralscan Elite

The Aoralscan Elite is the world’s first device to integrate both intraoral scanning and photogrammetry into a single unit. The device functions as a standard intraoral scanner (IOS) for capturing images of dentulous cases, allowing for detailed scans of teeth and oral structures. Additionally, it serves as a photogrammetry system, which is used to accurately record the position of dental implants in edentulous cases. This dual
functionality makes it versatile for both traditional dental work and advanced implant procedures. This groundbreaking innovation allows for comprehensive dental imaging and precise implant positioning, setting a new standard in dental technology.
Available: Fabdent Tel: 1300-878-336 www.fabdent.com.au
BloodSTOP iX haemostatic dressing


BloodSTOP iX with WoundHeal adheres to wet/bleeding surfaces to form a protective layer to prevent contamination. It is highly adhesive and fast acting while controlling bleeding and accelerating the clotting cascade. It transforms into a sticky translucent gel that adheres to and seals the wound. BloodSTOP iX creates a physiological environment, encouraging the proliferation of tissue growth and wound healing. It is odourless and tasteless and can be easily removed by irrigation. It is designed for any oral surgery or dental procedures causing bleeding. BloodSTOP iX is biocompatible and 100% absorbable without any residue.
Available: TRI Dental Implants ANZ Tel: (02) 8355-2200 info@tri-implants.com.au www.tri-implants.com.au
GEM 21S® Growth Factor

GEM 21S ® Growth-factor
Enhanced Matrix is crafted to boost the patient’s naural healing capacity, promoting the restoration of lost bone and gingiva. Extensive in vitro and in vivo studies have demonstrated that rhPDGF-BB is a powerful stimulant of angiogenesis that also stabilises newly formed blood vessels. GEM 21S® is the only dental therapy containing rhPDGFBB, one of the main growth
factors found in the human body and well known for its stimulatory role in wound healing. GEM 21S increases the amount of PDGF at the grafted site to aid in faster, more bone and better healing.
Available: Geistlich Pharma Tel: 1800-776-326 info@geistlich.com.au www.geistlich.com.au

48hr ALIGNERS

Tru-line® Invisible Orthodontics celebrates 20 years of Australian made clear aligners with the last innovation - Tru-Line X-tra 48 hour ALIGNERS™
s Precision CAD designed and CNC manufactured, Laser Cut
s Free case evaluation
s Free online training course
s Free viewing software
s Realistic treatment setupsNo Cartoonodontics!



Mention this ad for 50% off your first case
s Free Click retainers
s 48 hour turnaround on request
s Trusted experience, Australia’s first established Aligner brand in 2004
s Satisfaction guaranteed
s 100% value




The world’s first implant approved for full digital restorations without abutment
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation. NO ABUTMENT. NO CEMENT. NO LIMITS.
The world’s first implant approved for full digital restorations without abutment
The matrix® is the first-ever dental implant connection that has been specifically designed for the new digital manufacturing technologies such as CAD/CAM milling or 3D printing. The implant concept allows to plan the restoration directly on the implant without the use of the abutment and without manual cementation.
www.tri.swiss 0297
www.tri.swiss 0297























































